Allegheny County Medical Society

Allegheny County Medical Society
Editorial
• Spring Nourishment
Deval (Reshma) Paranjpe, MD, MBA, FACS
Membership
• Q&A with Dr. Kirsten Lin
ACMS News
• Meet the Therapists
Foundation News
• ACMS Foundation Breakfast Membership
• Skin Deep Recap
Foundation News
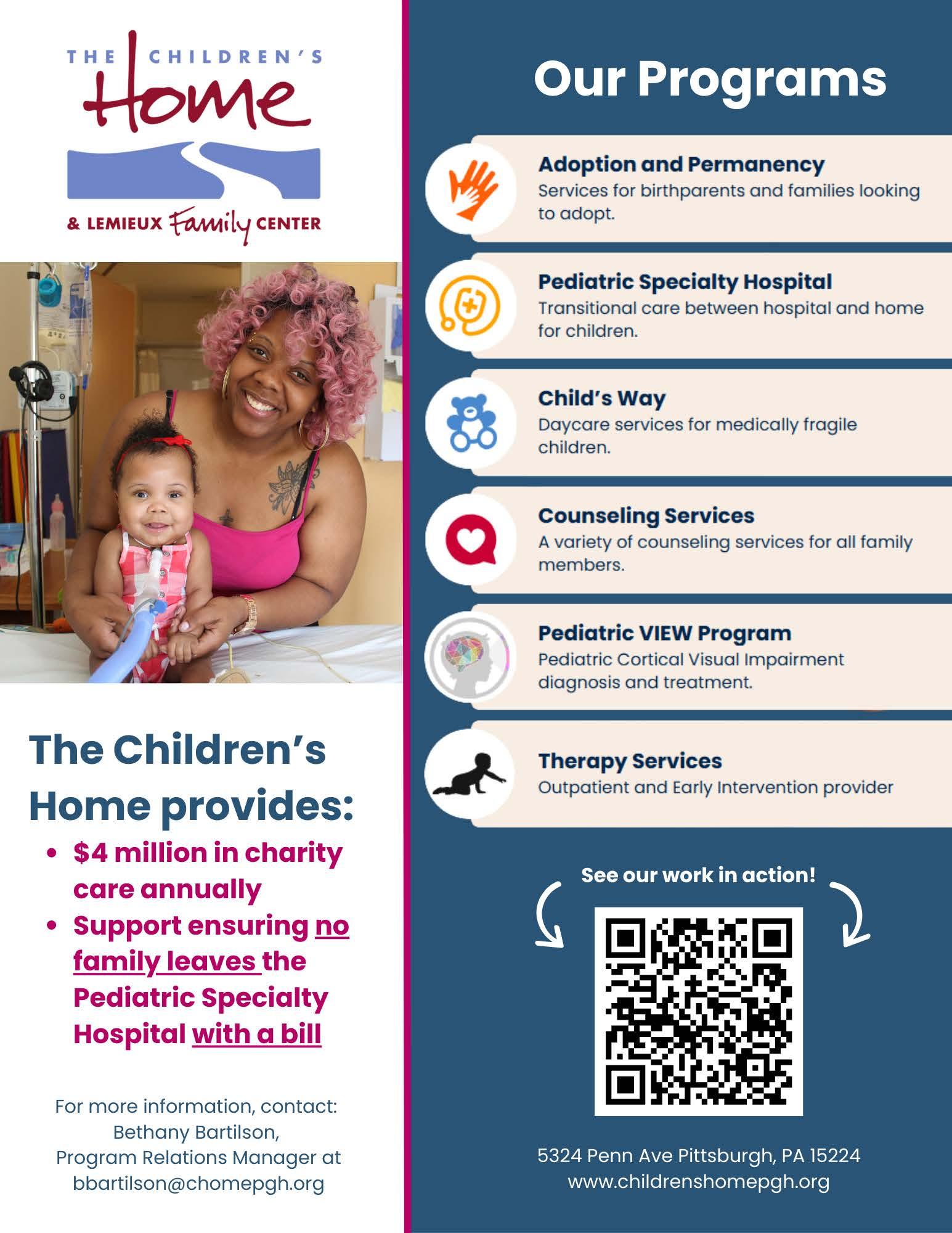
• Children's Home Feature
ACMS News
• Specialty Group Updates
ACMS Staff: Nadine

Popovich, Melanie Mayer and Haley Thon
Advocacy
• This Will Cost Lives
Raymond Pontzer, MD
Advocacy
• Interview with Dr. Julia Vann MJ Lerma
Article
• Stay Ahead of Colon Cancer Kojo-Frimpong Awuah, MD; Kaitlyn Gernhard, DO; Kingsley Ozongwu, MD; Oyepeju Abioye, MD; Kriti Dhamija, MD; Alexandra Johnston, DO
Materia Medica
• Sotagliflozin, That Don't INPEFA™ Me Much
Jason Timothy Fine, PharmD and Taylor Thompson, PharmD, MBA, BCPS

2025
Executive Committee and Board of Directors
President
Keith T. Kanel, MD
President-elect
Kirsten D. Lin, MD
Secretary
Richard B. Hoffmaster, MD
Treasurer
William F. Coppula, MD
Board Chair
Raymond E. Pontzer, MD
Board of Directors
Term Expires 2025
Anuradha Anand, MD
Amber Elway, DO
Mark A. Goodman, MD
Elizabeth Ungerman, MD, MS
Alexander Yu, MD
Term Expires 2026
Michael M. Aziz, MD, MPH, FACOG
Michael W. Best, MD
Micah A. Jacobs, MD, FIDSA
Kevin G. Kotar, DO
Jody Leonardo, MD
Term Expires 2027:
David J. Deitrick, DO
Sharon L. Goldstein, MD
Prerna Mewawalla, MD
Raymond J. Pan, MD
Nicole F. Velez, MD
James Latronica, DO, DFASAM
Richard B. Hoffmaster, MD
Finance
William F. Coppula, MD
Nominating
Kirsten D. Lin, MD
Women’s Committee
Prerna Mewawalla, MD & Meilin Young, MD
Managing Editor
Sara C. Hussey, MBA, CAE
ACMS Executive Director shussey@acms.org
Medical Editor
Deval (Reshma) Paranjpe, MD reshma_paranjpe@hotmail.com
Bulletin Designer
Victoria Gricks victoria@thecorcorancollective.com
2025 Bulletin Editorial Board
Richard Daffner, MD, FACR
Robert Howland, MD
Anthony Kovatch, MD
Charles E. Mount, MD, FAAD
Alexandra Johnston, DO
John P. Williams, MD
Executive Director
Sara Hussey shussey@acms.org
Vice President - Member and Association Services
Nadine M. Popovich npopovich@acms.org
Manager - Member and Association Services
Haley Thon hthon@acms.org
Operations CoordinatorACMS & ACMS Foundation
Melanie Mayer mmayer@acms.org
Manager - Operations and Finance
Elizabeth Yurkovich eyurkovich@acms.org
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
EDITORIAL/ADVERTISING
OFFICES: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212; (412) 321-5030; fax (412) 321-5323.
USPS #072920. PUBLISHER: Allegheny County Medical Society at above address.
The Bulletin of the Allegheny County Medical Society is presented as a report in accordance with ACMS Bylaws.
The Bulletin of the Allegheny County Medical Society welcomes contributions from readers, physicians, medical students, members of allied professions, spouses, etc. Items may be letters, informal clinical reports, editorials, or articles. Contributions are received with the understanding that they are not under simultaneous consideration by another publication.
Issued the third Saturday of each month. Deadline for submission of copy is the SECOND Monday preceding publication date. Periodical postage paid at Pittsburgh, PA.
Bulletin of the Allegheny County Medical Society reserves the right to edit all reader contributions for brevity, clarity and length as well as to reject any subject material submitted.
The opinions expressed in the Editorials and other opinion pieces are those of the writer and do not necessarily reflect the official policy of the Allegheny County Medical Society, the institution with which the author is affiliated, or the opinion of the Editorial Board. Advertisements do not imply sponsorship by or endorsement of the ACMS, except where noted.
Publisher reserves the right to exclude any advertisement which in its opinion does not conform to the standards of the publication. The acceptance of advertising in this publication in no way constitutes approval or endorsement of products or services by the Allegheny County Medical Society of any company or its products.
Annual subscriptions: $60
Advertising rates and information available by calling (412) 321-5030 or online at www.acms.org.
COPYRIGHT 2025: ALLEGHENY COUNTY MEDICAL SOCIETY POSTMASTER—Send address changes to: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212. ISSN: 0098-3772

By:
A weekend full of sunshine not too long ago brought a burst of energy back to Pittsburghers that will sustain us with hopeful anticipation of Spring as we navigate the remainder of the grey days ahead. And like Punxsutawney Phil pulled from his cozy den, we’re about to be thrust back into the bright world after months of hearth, hygge, and home cooking. Naturally, delicious treats should be waiting to lure us from our burrows.
Nanxiang Soup Dumplings
South Side Works
2773 Sidney Street 412-707-8888
Mon-Thurs 11am-10pm; Fri-Sat 11 am 11pm; Sun 11am-9pm.
Run, don’t walk, to this newly opened outpost of the famed NYC eatery. Featuring authentic and exquisite dim sum with a wide range of buns and dumplings, a variety of delicate and delicious soup dumplings, filling noodle soups, tasty stir-fried noodles, hot and cold appetizers, chef’s specials and fried rice, wonton soups, breakfast specialties and desserts. The soup dumpling selection is terrific; all contain some pork, except for the chicken soup dumpling. Options include the House dumpling, crab, truffle, scallop, gourd luffa with shrimp, sea cucumber, abalone, and ham. You can try a sampler of the first six (Lucky Six) or the last three (Three Treasures). As with traditional dim sum/yum cha establishments, you mark your choices on order sheets as you go and pay your tab at the end. Bring friends—you’ll want to try everything, which will take multiple visits. I especially
enjoyed the Lucky Six soup dumplings (the luffa dumpling had a delicate melon flavor), the Shanghai Siu Mai, and the seaweed with spicy garlic. Nearby diners had meatballs, scallion pancakes, black pepper beef, and crispy noodles—all of which looked and smelled divine.
I tried Nanxiang on a Saturday at 11:30 am, and the spacious, elegant restaurant was already packed, with a line forming soon after. Try to make reservations. Parking is expensive but readily available in nearby garages; street parking may be easier during off-hours.
Fet-Fisk
Bloomfield
4786 Liberty Avenue
Thurs-Mon 5-10pm, closed Tue-Wed. Reservations via Resy
Fet-Fisk means “greasy fish,” but you don’t have to order any to have an excellent meal. The restaurant has risen from the ashes of the classic Lombardozzi’s, keeping its dark, romantic décor. The clientele is young and sophisticated. Reservations are essential unless you arrive at exactly 5 pm and grab a bar seat, which was my modus operandi. Surprisingly, babies seem welcome (not at the bar), as long as they are sophisticated too.
The cocktails are lovely; I recommend the Aromatic. Small, elegant plates abound, some smaller than others. Highlights: the Ora King Salmon Gravlax with cultured butter and egg yolk (luscious and not greasy), the Hasselback Potatoes (the best I’ve ever had), and the Fried Sunchokes, which
impersonate steak in a bordelaise sauce but are better. The scallop crudo is ethereal and consists of one lonely scallop finely sliced in a delicate sauce; however it is more of a large amusebouche than an appetizer. The pickled mackerel is an interesting take on mackerel, but still failed (despite the server’s hearty assurances) to make me like mackerel. Your mileage may vary; you may adore it, as many do. For the less seafood-inclined, roast chicken and strip steak are also on the menu and looked great at nearby tables. A perfect date-night spot.
Bloomfield
4744 Liberty Avenue Tues, Thurs-Sat 5pm-10pm. Closed Sun, Mon, Weds.
If you are in the mood for little things to nosh on that are pure comfort food, this is your place. They serve strawberry pretzel salad and pistachio fluff alongside homemade chips, dip, and fries. They have a satisfying selection of hearty, homey, delicious sandwiches including includes roast beef, turkey, steak, mortadella, ham, and vegetarian options. Entrees include steak frites, vodka rigatoni, and leek and pancetta pappardelle, as well as a rotating selection of similarly comforting dishes. Tuesday is wing night, with a tasty selection of favorites. Take a load off, relax, and settle into a meal that feels like a hug. May your Spring be delicious!
When your patients need specialty care, AHN has physicians with world-class expertise — like our new reproductive endocrinology and infertility specialist.
Dr. Lewis uses cutting-edge techniques to help diagnose and treat both male and female infertility.
To refer your patient, call (412) DOCTORS.
Terrence D. Lewis, MD, PhD, FACOG
Reproductive Endocrinology and Infertility
Location: AHN Center for Reproductive Medicine
200 Quinn Drive, Suite 120 Pittsburgh, PA 15275
Specialties :
Skilled in diagnosing and treating both male and female infertility, offering advanced procedures such as artificial insemination, in vitro fertilization (IVF), and the use of donor oocytes or sperm to help patients conceive
Clinical interest in managing conditions like polycystic ovarian syndrome (PCOS), endometriosis, recurrent pregnancy loss, and implantation failure


By: Raymond E. Pontzer, MD – ACMS Board President
As you are all aware, the course of public health and clinical medicine has taken a sharp turn, impacted by recent policies and leadership changes that have been set in motion by the current federal administration. The ACMS leadership, including our officers, board of directors and administrative staff, are quite concerned with newly implemented policies and budget cuts. There is indeed great trepidation that these measures will result in a marked detriment to the health and well-being of our nation.
First, there is concern with the credibility and experience of the leaders who have been installed to direct the various health organizations, including HHS, CMS, FDA and CDC. As an infectious diseases specialist, I am especially concerned about Robert Kennedy, Jr. as the Secretary of Health and Human Services (HHS). His promotion of vaccine misinformation and public-health conspiracies, including the scientifically disproved claim of a causal link between vaccines and autism, threaten to dimmish the herd immunity necessary to prevent many preventable diseases. As an example, he has been hesitant to recommend measles vaccination to curb the current outbreak in Texas and New Mexico, which may further encourage parents not to have their children properly vaccinated.
The projected funding cuts targeting the National Institutes of Health (NIH) are also worrisome, causing immediate and long-term adverse effects in the realm of scientific research. As the NIH is the primary funding engine for medical research at more than 2500 institutions across the U.S., NIH funded research is integral to vaccine development
and the availability of new drugs. NIH funding contributed to research for roughly 99 percent of drugs approved between 2010 and 2019. Also, the rapid development of COVID-19 vaccine in 2020, estimated to prevent 15 to 20 million deaths worldwide, was a direct result of work performed by NIH based scientists. Here in Pittsburgh, several hundred jobs are supported by the NIH. The University of Pittsburgh receives the sixth highest amount of NIH grants and could lose an estimated $183 million. CMU also is projected to lose several million dollars from their grants. Another worrisome event is the recent sudden unexplained cancellation of the FDA annual flu vaccine advisory committee meeting. This threatens next season’s vaccine planning and could lead to unnecessary illness and loss of life. The U.S. sudden withdrawal of financial and strategic support of the World Health Organization is of particular concern in view of recent increasing frequency of global epidemics and pandemics -- avian influenza, Ebola, Mpox and other disease outbreaks currently ongoing across the globe. The CDC has also been ordered to cease communication, again for unexplained reasons, with the WHO, blinding both organizations to potentially critical information regarding the spread of these and other diseases that may pose a risk to us in the U.S. and globally. The dismantling of U.S.A.I.D. is a major blow to crucial health efforts around the world, including the elimination of another early detection system for epidemics.
The planned draconian slashing of federal CMS funds is projected to cut
$880 billion from the Medicaid budget. This will have an immediate devastating impact on the health and well-being of a large proportion of the U.S. population, including here in western Pennsylvania. This cut will necessitate action at the state level to hopefully soften the blow to this high-risk population. Additional hot burner issues at the Pennsylvania state legislature impacting medical care include scope of practice for nurse practitioners/physician assistants, addressing noncompete contractual clauses and the change in venues for malpractice cases.
As you can see, this is a turbulent era for all of us. We at ACMS continue to closely monitor the rapidly changing health care environment and look for ways that our medical society can safeguard the health and wellbeing of our region. The sudden policy changes impacting healthcare appear to be diametrically opposed to our vision here at ACMS – “A healthy region with compassionate medical care.” Each individual member of our society can make an impact on how the government’s role in health care evolves. First, I recommend that each of you personally contact your state and federal legislators to let them know how these changes are impacting you and your patients. Legislators inform us that hearing reports of how patients have been adversely impacted can make a difference. Secondly, the aggregate impact of ACMS advocacy at local and state levels is important to educate and influence our legislators. We appreciate the support of each of you, our members, in this time of crisis. Thank you and keep up the fight.


Friday, September 26th, 2025
Omni William Penn Hotel, 530 William Penn Pl, Pittsburgh, PA 15219
AHN Women Physician’s ERG
Allegheny General Hospital
Allegheny County Medical Society
Prerna Mewawalla, MD Associate Professor Hematology & Cellular Therapy
Maria Gioia, DO Clinical Associate Professor Family Medicine

Scan or Click Here to register
Please contact Samantha Kunvatanagarn in the CME office at samantha kunvatanagarn@ahn org for more information
Dr. Kirsten Lin, ACMS PresidentElect, is a dedicated family physician and advocate for patient-centered care. A Pittsburgh native, she resides in the North Hills with her family. She earned her B.S. in Biochemistry and Molecular Biology with a minor in Human Development and Family Studies from Penn State University before obtaining her M.D. from the University of Pittsburgh School of Medicine. She then completed her internship and residency in Family Medicine at UPMC St. Margaret Hospital.
After 12 years working within large health systems, Dr. Lin felt constrained by administrative pressures that limited her ability to provide the level of care she believed her patients deserved. In October 2017, she founded Direct Care Physicians of Pittsburgh, opening its first location in Hampton Township. Her practice follows the Direct Primary Care (DPC) model, which allows her

to provide affordable, personalized healthcare without the restrictions of insurance-driven systems.
Beyond her clinical work, Dr. Lin is an educator and advocate, frequently lecturing and appearing on radio programs to inform both healthcare professionals and the public about the benefits of Direct Primary Care. She is deeply involved with ACMS, serving as Chair of the Nominating Committee and Co-Chair of the Membership Task Force, in addition to her role as President-Elect. Through her leadership, she continues to support physician advocacy, mentorship, and engagement within the medical community.
Q: CAN YOU SHARE A LITTLE ABOUT YOUR BACKGROUND AND WHAT LED YOU TO A CAREER IN MEDICINE?
A: There are no other doctors in my family. I was inspired by my pediatrician, the late Dr. Bernie Michaels, whose mural is in the new Children's Hospital of Pittsburgh in Lawrenceville.
Q: WHAT INSPIRED YOU TO PURSUE YOUR SHIFT INTO INDEPENDENT PRACTICE?
A: I practiced for 12 years in large health systems, where administrators pressured me to see more patients. This led to a feeling that I wasn't providing excellent medical care for my patients, and I didn't have enough time
for my own self-care. As an independent physician, I have the autonomy to decide how much time I spend with patients,and I can carve out time every day to care for my own nutrition, fitness, sleep, and mental health.
Q: CAN YOU TELL US ABOUT YOUR CURRENT ROLE AT DPC AND WHAT A TYPICAL DAY OR WEEK LOOKS LIKE FOR YOU IN DIRECT PRIMARY CARE?
A: I own a DPC practice in Allison Park, PA, where the entire care team consists of myself and an executive assistant. We have a small patient panel of 300. On a typical day, I see about 4–6 patients in the office and respond to around 20 patient emails. I typically spend an hour with each patient. Occasionally, we have a medical student or resident rotating with us. We have a lot of fun!
Q: HOW DID YOU FIRST GET INVOLVED WITH THE ALLEGHENY COUNTY MEDICAL SOCIETY?
A: After residency, my ACMS membership lapsed for many years. When I decided to leave big-box healthcare, I needed help setting up a practice, and I turned to ACMS for mentorship and support. A few years later, during the COVID-19 pandemic, I was able to secure vaccines earlier than most other medical practices in the area. ACMS helped me assemble a team of volunteers and find a large enough

space to vaccinate approximately 3,000 healthcare workers. Once I recognized the value of membership, I never left!
Q: WHAT HAS BEEN THE MOST REWARDING ASPECT OF BEING AN ACMS MEMBER?
A: Honestly, it's the camaraderie with other local physicians. I enjoy spending time with colleagues who share similar career experiences. It’s wonderful to interact with both more experienced and younger physicians—I find myself in the role of both mentor and mentee. The events are fun and educational, and ACMS has provided me with leadership and advocacy opportunities.
Q: ARE THERE ANY ACMS INITIATIVES OR EVENTS THAT YOU ARE PARTICULARLY PASSIONATE ABOUT?
A: I am particularly interested in exploring the idea of physician unionization. With over 80% of physicians in our county being employed, it is important to provide organization for collective bargaining with large health system employers.
Q: WHAT DO YOU THINK IS THE BIGGEST CHALLENGE FACING HEALTHCARE TODAY?
A: Many challenges stem from health insurance companies, which now cover even the more affordable parts of healthcare, such as primary care. This is akin to car insurance covering gas purchases. Along with lack of pricing transparency, this has led to astronomical healthcare costs and contributed to lower-quality care.
Q: HOW DO YOU SEE YOUR FIELD EVOLVING IN THE NEXT 5–10 YEARS?
A: I hope to see the direct care movement continue to take flight, bringing affordable primary and specialty care, as well as surgical services, to all.
Q: WHAT ADVICE WOULD YOU GIVE TO MEDICAL STUDENTS OR EARLYCAREER PHYSICIANS?
A: Consider independent practice! Don’t buy into the myth that doctors don’t know enough about business. You are intelligent and hardworking—you can do it!
Take ownership of every patient. Don’t just "clock in and clock out." Make time for self-care every day.
Q: OUTSIDE OF MEDICINE, WHAT ARE YOUR HOBBIES OR INTERESTS?
A: Our family enjoys travel, exercise, and musical theater. In the past few years, I’ve loved seeing my kids perform on stage in productions like Matilda the Musical, The Little Mermaid, Into the Woods Jr., Finding Nemo Jr., and Phantom of the Opera.
Q: HOW DO YOU MAINTAIN A WORKLIFE BALANCE?
A: I build it into my schedule. A few years ago, I read Indistractable by Nir Eyal, which helped me learn time blocking.
Q: DO YOU HAVE A FAVORITE BOOK, PODCAST, OR RESOURCE THAT HAS INFLUENCED YOUR CAREER?
A: Start with Why by Simon Sinek.
Q: WHAT’S ONE PIECE OF WISDOM YOU’D LIKE TO SHARE WITH FELLOW ACMS MEMBERS?
A: Physicians are stronger together. Let’s be involved in our local medical society, on social media, and engage with politicians about issues that matter to us and our patients.
Q: IF YOU COULD HAVE DINNER WITH ANY HISTORICAL OR CONTEMPORARY FIGURE IN MEDICINE, WHO WOULD IT BE AND WHY?
A: Elizabeth Blackwell, the first modern female physician. I’d love to hear her story—what inspired her to pursue this career when most women didn’t work outside the home? How did she manage to get into medical school at a time when women couldn’t even vote? She must have had incredible determination, which I admire.
Q: HOW CAN FELLOW ACMS MEMBERS CONNECT WITH YOU OR SUPPORT YOUR WORK?
A: I love collaborating with other physicians. If any ACMS members are interested in learning more about the direct care model, I’m always available for a phone call or a coffee chat.


By: MJ Lerma – MPH Candidate Policy/Administrative Intern at ACMS
The Allegheny County Health Department (ACHD) offers valuable opportunities and resources for physicians, students, and the community, with a strong focus on public health and community engagement. Dr. Iulia Vann, ACHD Director, brings an interdisciplinary perspective as both a physician and public health professional. In this interview, she discusses the department’s priorities, collaboration, and the impact of health policy in Allegheny County.
Questions and responses have been edited for clarity.
What are the Allegheny County Health Department’s top public health priorities this year?
I believe my predecessors and our leadership team have done an excellent job setting a path forward for the health department, especially post-COVID. Our top priorities include community engagement, air quality, substance use disorder, and opioid prevention initiatives. With the new County Executive, we've emphasized datadriven strategies and collaboration with community-based organizations, particularly on infant mortality prevention and maternal health. These priorities are backed by clear data, reinforcing their importance.
Since stepping into this role last August, I’ve been grateful for the groundwork already laid. That foundation has allowed me to focus on additional areas, such as improving how we communicate our work to the community. Effective communication means ensuring our reports and materials are accessible to both
professionals and community members, meeting people at their level of expertise. We serve both professionals and community members, so our messaging should be accessible across that spectrum.
Another key focus is increasing visibility through events and social media. We recently hired a communications public health information officer to develop a strategy for better outreach and storytelling. We do a lot of meaningful work, but we need to be better at sharing our impact.
Community engagement is also a personal and professional priority for me. I've always focused on the idea that we cannot do things to the community, we have to do things with the community. To that end, we’ve created a community engagement coordinator position to help us be more strategic in outreach. People want to share their voices, and we need to ensure there’s space for that.
Additionally, as someone new to this community, I’m prioritizing relationshipbuilding with partners. Allegheny County has a strong network of organizations, and I want to strengthen those connections to be a valuable resource for our partners. Lastly, I’m focused on understanding the local public health ecosystem. While I have over 12 years of experience in public health, every community is unique. My goal is to learn, listen, and support the department’s work in a way that respects and enhances existing efforts.
How does the Allegheny County Health Department support physicians and students, and where do
opportunities for further collaboration exist?
The Allegheny Health Department is highly collaborative in engaging physicians, the medical community, and students across various disciplines. We work closely with universities in Allegheny County and support physicians seeking to expand their knowledge in public health. For example, I recently spoke with the Dean of Pitt’s Public Health School about a medical physician in the MPH program eager to engage with the department— opportunities like these are truly exciting.
While practicing as a physician in family medicine, I did not have the opportunity to engage very closely with the public health system. I now recognize the critical role of public health in supporting physicians in the community. We provide internships, shadowing experiences, and placement refer interested individuals to federally qualified health centers. While we don’t offer primary or maternity care, our clinical services—such as STI/ HIV testing, communicable disease treatment, immunizations, and referrals—are unique and essential.
There is always room for further collaboration, whether through expanded training programs, stronger university partnerships, or new initiatives that bridge clinical practice and public health.
How do you think the current federal administration will impact the Allegheny County Health Department, physicians, and public health?
We've been navigating a whirlwind of information in recent weeks, working to
understand the implications of federal policies and what to anticipate. It's clear that federal public health policies and funding have a significant impact on the work we do at the county level, making advocacy and collaboration essential.
Local public health departments are on the front lines, directly serving communities. Historically, we've had strong partnerships with federal agencies, helping to elevate the realities of on-the-ground public health work. This ensures that higher-level decisions are informed by local needs, and I hope we can continue fostering that collaboration.
At the same time, local public health has the advantage of jurisdictional autonomy. While federal policies are influential, we can still take action independently within Allegheny County. Our county administration, particularly under the County Executive, has prioritized public health, and my team feels well-supported in our mission. Ultimately, public health professionals will continue advocating for what’s right for our communities. Our work is not at the individual level but at the community level, and we've always been resourceful in finding ways to sustain our programs. Allegheny County is fortunate to have strong relationships with philanthropic organizations, foundations, and businesses that support public health, giving us a solid infrastructure to rely on should challenges arise. We are staying positive, and we know how to pivot if needed.
We've already weathered two vastly different approaches to the COVID-19 pandemic, proving public health’s resilience and determination. That same grit drives us forward—we won’t back down. I’m the kind of person who won’t let go—like a dog with a bone. I’m committed to doing everything I can to support the incredible team at the health department as they provide vital services to our community. My pledge is to use every resource at my disposal to advocate for and strengthen our community. I don’t back down easily."
Which resources and reports on the Allegheny County Health Department’s website do you believe would be most beneficial to physicians?
Our website offers a wealth of resources for physicians and medical professionals, including the Community Health Assessment and the Plan for a Healthier Allegheny. These reports provide valuable insights into public health trends that can inform medical decision-making and help physicians better understand the health challenges their patients may face.
We also have a variety of data dashboards covering environmental health, the environmental justice index, communicable diseases, and other key community health indicators. These tools can help medical professionals incorporate data-driven approaches into their practice.
Additionally, we host quarterly calls with physicians, pharmacists, and other healthcare professionals to provide updates on health department initiatives. We encourage the medical community to engage with us through town halls and roundtables, sharing their insights and helping us improve our outreach efforts.
Physicians can also support public health efforts by promoting our initiatives—keeping health department flyers in their offices, informing patients about surveys and community programs, and collaborating with us to enhance public awareness. Together, we can strengthen the connection between clinical care and public health in Allegheny County.
Get involved
See the event form on the Allegheny County Health Department website.

Iulia Vann, MD, MPH Director of the Allegheny County Health Department
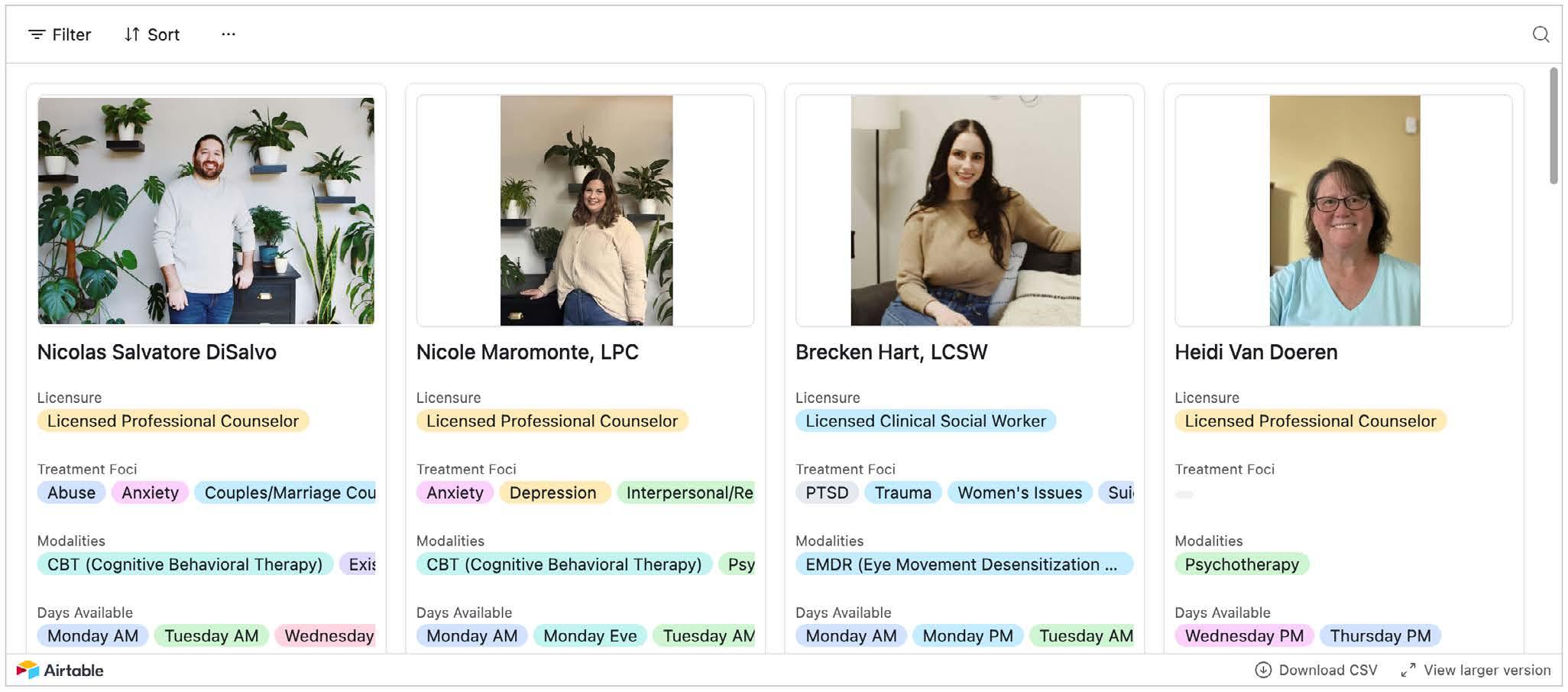
Welcome to the first installment of our "Meet the Therapists" series, where we introduce you to the dedicated professionals behind the Allegheny County Medical Societys (ACMS) Physician Wellness Program. This month, we are excited to feature half of our esteemed therapists who are committed to supporting the mental health and well-being of physicians in Allegheny County.
About the Physician Wellness Program
The ACMS Physician Wellness Program is designed to address the urgent issue of physician burnout and mental health challenges. Supported by The Physicians Foundation and the Allegheny County Medical Society
Foundation, this program provides confidential counseling services tailored to the unique needs of physicians. Our goal is to eliminate barriers to accessing mental health services and empower physicians to seek the resources they need to thrive both personally and professionally. How to Use the Program Participating in the Physician Wellness Program is simple and confidential:
1. Visit the ACMS Website: Navigate to the Physician Wellness Program section on the ACMS website.
2. Book an Appointment: Choose a therapist from our list and book an appointment directly through the website.
3. Confidentiality Assured: Your participation is voluntary and confidential. No medical diagnosis is recorded, and no insurance billing is involved.
4. Flexible Scheduling: Appointments are available within one to two weeks, with options for weekend and evening telehealth sessions.
Stay tuned for next months article, where we will introduce the remaining therapists who are part of this invaluable program.
For more information and to book an appointment, please visit the ACMS Physician Wellness Program at www. acms.org/physicianwellness.
WHAT IT LOOKS LIKE ON OUR WEBSITE

ANITA BARNHART, LCSW
Specialties: Anxiety, anger management
Approach: Cognitive Behavioral Therapy
Location: Telehealth
Contact: anita@ijcpgh.com
Availability: Monday AM, Monday PM
Quote: "At some point, we can all benefit from what therapy offers: an opportunity to be deeply known and understood. Starting with a warm and collaborative therapeutic relationship, I work from the understanding that meaningful change is possible."

GILLIANNE DEFONE, MD
Specialties: Burnout, anxiety, insomnia
Approach: Coaching, narrative therapy
Location: Telehealth
Contact: gillianne@thetimemd.com
Availability: Flexible and variable
Quote: "My passion is helping individuals navigate their personal and professional challenges to achieve a balanced and fulfilling life."

NICOLAS DISALVO, LPC
Specialties: Abuse, anxiety, couples/marriage therapy
Approach: Cognitive Behavioral Therapy
Location: Telehealth
Contact: nic@ijcpgh.com
Availability: Monday AM
Quote: "I specialize in helping individuals and couples overcome their struggles and build healthier relationships."

BRECKEN HART, LCSW
Specialties: PTSD, trauma
Approach: Eye Movement Desensitization and Reprocessing (EMDR)
Location: In-Person, Telehealth
Contact: brecken@ijcpgh.com
Availability: Monday AM, Monday PM
Quote: "I specialize in trauma-informed care and am dedicated to helping individuals heal from their past experiences."

Introduction
By: Kojo-Frimpong Awuah, MD; Kaitlyn Gernhard, DO; Kingsley Ozongwu, MD; Oyepeju Abioye, MD; Kriti Dhamija, MD; Alexandra Johnston, DO
Colorectal cancer (CRC) is the third most common cancer diagnosed in both men and women in the United States¹. It is the second leading cause of cancer-related deaths, following lung cancer¹. Approximately 70% of sporadic CRC cases develop through the chromosomal instability pathway, leading to the formation of adenomatous polyps, while the remaining 25–30% arise from sessile serrated lesions². Screening modalities include colonoscopy, sigmoidoscopy, CT colonography, and stool-based testing methods³. These screenings aim to detect both CRC and its precursor lesions early, allowing for endoscopic removal of polyps, which significantly reduces CRC incidence and mortality³. Since the mid-1980s, there has been a steady decline in CRC incidence rates by approximately 1.7% per year and mortality rates by about 3.2% per year, largely attributed to increased screening and advancements in treatment modalities⁴.
Importance of Colon Cancer Awareness/Young-Onset Trends
Thanks to the widespread use of screening colonoscopy, the overall prevalence of CRC has been decreasing over the past two decades. However, the incidence has been increasing in people younger than 50 years, with a 63% increase between 1988 and 2015⁵. Sullivan et al. concluded that risk factors for young-onset colorectal cancer (YOCC) include a family history of CRC, hyperlipidemia, obesity, alcohol consumption, and obesity5. YOCC is more frequently located on the left side and in the rectum and generally
presents at an advanced stage compared to late-onset CRC6. When adjusted for stage, YOCC patients had a survival benefit compared to those diagnosed at ages 50–55 years, HR = 0.95, p-value < 0.001, as calculated by Cheng et al. in an NCDB-based study7. Hence, the guidelines for screening must account for YOCC.
Screening Guidelines: USPSTF vs. ACG
CRC screening is essential for early detection and prevention, with varying guidelines across medical societies. The ACG recommends screening for average-risk individuals from ages 45–75, with personalized decision-making for those older than 758. The USPSTF provides a Grade A recommendation for screening adults 50–75 and a Grade B recommendation for ages 45–499. There is a Grade C recommendation for CRC screening in patients aged 76–85 based on health status and prior screening history9. These recommendations apply to average-risk individuals and exclude those with personal history of CRC, inflammatory bowel disease, or a genetic predisposition⁹. For individuals with a family history of CRC or advanced polyps in a first-degree relative before age 60—or in two or more first-degree relatives at any age—ACG recommends colonoscopy starting at age 40 or 10 years before the youngest affected relative’s diagnosis, whichever is earlier8
Screening Modalities (Sensitivity and Specificity)
There are multiple methods for CRC screening, each with its own advantages and limitations. The ACG recommends colonoscopy or annual
FIT testing as primary methods8. Colonoscopy has a nearly 95% sensitivity for detecting CRC, allows for polyp removal, and reduces CRC incidence⁹. Disadvantages are that it is invasive, requires sedation, and carries a small complication risk (4–8 per 10,000)⁹. FIT (fecal immunochemical test) is non-invasive, done at home, and has 79% sensitivity and 94% specificity, but requires annual testing and follow-up colonoscopy for positive results⁹. Flexible sigmoidoscopy has 90–100% sensitivity for distal CRC, is less invasive, but requires repeat screening every five years, with full colonoscopy for positive findings⁹. Other options include CT colonography (every five years, 89% sensitivity, 88% specificity⁹), stool DNA-FIT (every 1–3 years, 92% sensitivity, 89% specificity⁹), and FOBT (yearly, 70% sensitivity, 92% specificity⁹). Unlike the ACG, the USPSTF does not endorse a specific test but emphasizes shared decision-making to determine the best screening approach.
While colonoscopy remains the gold standard for CRC screening, newer blood-based tests offer a less invasive alternative. In July 2024, the FDA approved Guardant Health’s Shield™ blood test as a primary screening option for CRC in average-risk adults aged 45 and older10. A recent study in The New England Journal of Medicine demonstrated that Shield detects CRC with 83% sensitivity and 90% specificity, though its sensitivity for precancerous lesions remains low at 13%11
The appeal of blood-based screening lies in its accessibility and ease of use, which may improve adherence, particularly among individuals hesitant to undergo colonoscopy. However, its lower sensitivity for precancerous lesions means it can't replace colonoscopy, the only method that allows detection and removal of precancerous polyps. Instead, these tests may serve as an additional tool to increase screening rates and reach underserved populations.
Reaching a joint decision with your patient regarding the appropriate screening options is important. CRC screening can be divided into a onestep test vs. a two-step test. One-step tests include colonoscopies, while two-step tests (stool-based, colon capsules, CT colonography) require follow-up colonoscopy after a positive test. For most average-risk individuals, it is appropriate to recommend colonoscopies every 10 years and FIT testing every year. Patients who are unable or unwilling to undergo either colonoscopy or FIT have options such as flexible sigmoidoscopy or CT colonography, which require more frequent surveillance and a follow-up procedure if the test is positive. With an increased risk of CRC in patients with affected relatives, patients must be screened with colonoscopy as opposed to stool tests. Colonoscopy allows for better surveillance, especially for sessile serrated lesions, which can be missed with stool-based modalities.
Access to Colonoscopy and Disparities in Screening
Significant disparities in CRC screening exist across multiple demographic groups. African Americans, followed by American Indians and Alaska Natives, experience disproportionately higher CRC incidence and mortality compared to other races and ethnic groups9. Geographic variation and socioeconomic status further
complicate access issues, particularly in rural areas with limited healthcare infrastructure. Emerging research indicates that inequitable access to, utilization of, and quality of CRC screening and therapeutic interventions, rather than genetic factors, are the key drivers of these disparities12,13. Of note, health systems with equal access to the screeningdiagnosis-treatment care continuum demonstrate significant reductions in these disparities14. Both the ACG and USPSTF recommend targeted interventions, including culturally appropriate outreach, increased access to diverse screening modalities, and systemic healthcare delivery improvements to address these disparities8
Conclusion/Call to Action
As healthcare providers, we play a critical role in the fight against CRC. Despite the availability of effective
screening options, many eligible patients remain unscreened. This Colon Cancer Awareness Month, we must prioritize patient education, address barriers to screening, and advocate for early detection. Whether through colonoscopy, stool-based tests, our goal is to tailor guideline-based screening to each patient’s needs and preferences. By fostering informed discussions and emphasizing the lifesaving impact of early detection, we can improve adherence and reduce CRC mortality. Let’s use our platform to drive awareness, encourage screening, and ultimately save lives.

28, 2025



The ACMS Foundation hosted a networking breakfast for our 2024-2025 grant recipients, fostering collaboration, idea-sharing, and impactful discussions. The ACMS Foundation is proud to support organizations making a difference in Allegheny County. A special thank you to Babb, Inc. for hosting us in their historic ballroom.




7. Group Discussion and Networking



The ACMS Women in Healthcare Committee hosted a successful skincare lecture on March 5, 2025, at Ritual House in Downtown Pittsburgh. Dr. Nicole Velez covered skincare essentials, while Dr. Charles Mount discussed melanoma detection and advanced imaging. Guests enjoyed dinner, networking, and sponsor engagement with Johnson & Johnson, Revance, SkinCeuticals, and Evolus. Stay tuned for the Women in Healthcare Summer Social date, and mark your calendar for the AHN Women Physicians’ Wellness Conference on September 26, 2025.





By: Jason Timothy Fine, PharmD and Taylor Thompson, PharmD, MBA, BCPS
Background
Sotagliflozin, INPEFATM, is a novel inhibitor of both sodium glucose like transporter 1 and 2 (SGLT1 and SGLT2) approved in May of 2023. Although it was only studied in patients with type 2 diabetes mellitus (T2DM), sotagliflozin is indicated to reduce the risk of hospitalizations for heart failure (HHF), cardiovascular (CV) death, and urgent heart failure (HF) visits in patients with HF or patients with T2DM, chronic kidney disease (CKD), and other CV risk factors.1 SGLT are proteins found in the proximal tubules of the nephron and in the brush-border of the gastrointestinal tract.2 In the nephron, SGLT2 proteins are responsible for the majority of glucose reabsorption from the filtrate.2 SGLT1 is expressed in both the brushborder of the intestines and in the renal tubule.2 In addition to the inhibition of glucose reabsorption from the filtrate mediated by SGLT2, sotagliflozin delays glucose absorption in the intestinal brush-border mediated by SGLT1.1,3,4
The 2022 American Heart Association, American College of Cardiology, Heart Failure Society of America Guideline for the Management of Heart Failure recommends using SGLT2 inhibitors to reduce HHF. They are now one of the medication classes included in guideline-directed medical therapy (GDMT) for HF in patients with HF with a reduced ejection fraction (HFrEF), and to reduce HHF in patients with HF with a mildly reduced ejection fraction (HFmrEF) and HF with a preserved ejection fraction (HFpEF).6 Sotagliflozin is administered starting at 200 mg once daily and titrated to 400 mg once daily as tolerated.5
Treatment-emergent adverse effects leading to death were lower in the sotagliflozin group than in the placebo group (8.4% vs 8.8%) in the Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure (SOLOIST-WHF) trial.3 Adverse events leading to amputation were observed to be lower in the sotagliflozin group than in the placebo group (32/5291 vs 33/5286).4
Listed warnings and precautions for diabetic ketoacidosis in patients with type 1 diabetes mellitus (T1DM), volume depletion, urosepsis and pyelonephritis, hypoglycemia with concomitant use of insulin or insulin secretagogues, necrotizing fasciitis of the perineum, and genital mycotic infections included in the package insert for sotagliflozin.1 These warnings are shared with other SGLT2 inhibitors (canagliflozin, dapagliflozin, and empagliflozin) with the exception of the diabetic ketoacidosis risk specifically in patients with T1DM.7-9
Sotagliflozin is not recommended during the second or third trimester of pregnancy based on animal studies, and insufficient data exists to evaluate drug-associated fetal harm.1 Safety of sotagliflozin in patients under the age of 18 has not been established, and its use is not recommended in patients with Child Pugh B or C.1
Sotagliflozin has been studied in the Sotaglifozin in Patients with Diabetes and Chronic Kidney Disease (SCORED) trial in patients with CKD and an estimated glomerular flow rate (eGFR) as low as 25 mL/min/1.73 m2 4 Use of sotagliflozin in patients with mild kidney
impairment, classified as eGFR 60 to <90 mL/min/1.73 m2, and moderate kidney impairment, classified as 30 to <60 mL/min/1.73 m2, was associated with a 70% and 170% increase in drug exposure, respectively, after a single 400 mg dose.1 There are no recommendations for dose adjustment in these patients, despite the increased drug exposure.1 The safety and efficacy of sotagliflozin was not assessed in patients with eGFR <25 mL/min/1.73 m2.3, 4 In these studies, patients were discontinued from the trial if their eGFR fell below 15 mL/min/1.73 m2 or were initiated on chronic dialysis.3, 4 Patients that are concomitantly taking sotagliflozin and digoxin must undergo monitoring of digoxin levels due to the increased Cmax and AUC of digoxin observed in patients taking sotagliflozin 400 mg daily.1
The SOLOIST-WHF and SCORED trials showed that sotagliflozin is associated with more volume-related adverse events (e.g., hypotension, dizziness) in patients with an eGFR < 30 mL/min/1.73 m2 as compared to placebo, (6.0% vs. 4.6%) and (2.6% vs. 1.9%) in SOLOIST-WHF and SCORED, respectively.3, 4 The most common side effects observed with sotagliflozin were urinary tract infection (11.5%), diarrhea (8.5%), and volume depletion (5.3%).3 Sotagliflozin administered to healthy humans at two and five times the recommended daily dose (800 mg or 2000 mg) did not exhibit any increase in QT corrected for heart rate (QTc).1
Efficacy data was derived from clinical trials investigating its use in
patients with T2DM and HF or CKD.3, 4
Patients with T2DM who were recently hospitalized for worsening HF were randomly assigned to receive either sotagliflozin or placebo in the SOLOIST-WHF trial.3 Eligible patients were 18-85 years old with a diagnosis of T2DM, had been hospitalized due to HF, had an elevated B-type natriuretic peptide or pro-B-type natriuretic peptide level, and received intravenous diuretics. Patients with end-stage HF or recent acute coronary syndrome, stroke, percutaneous intervention (PCI), coronary artery bypass graft (CABG), or those with an eGFR <30 mL/min/1.73 m2 were excluded from the study.3 1,222 patients underwent randomization and were followed for a median of 9 months. The primary end point was the composite of the total number of deaths from CV causes, hospitalizations and urgent visits for HF. Patients randomized to the sotagliflozin group received 200 mg daily before or within 3 days of hospital discharge. The rate of primary outcome in the sotagliflozin group was 51.0 per 100 patient-years, and 76.3 per 100 patient-years in the placebo group (HR, 0.67; 95% CI 0.53 to 0.85; p<0.001).3
The SCORED trial was a multicenter double-blind trial that enrolled 10,584 patients 18 years and older with a glycated hemoglobin level of 7% or greater, CKD (defined as an eGFR 25 to 60 mL/min/1.73 m2), and at least one major CV risk factor (or two minor CV risk factors if age 55 or greater) randomized 1:1 to sotagliflozin and placebo.4 The coprimary end points were the first occurrence of a major adverse CV event (MACE, defined as death from CV causes, nonfatal myocardial infarction, or nonfatal stroke), and the first occurrence of death from CV causes or HHF. The coprimary endpoints were later changed to be the composite of deaths from CV causes, HHF, and urgent visits for HF due to the early closing of the trial and the fewer than anticipated number of events. Rates of total primary end-point events were
5.6 and 7.5 events per 100 patientyears in the sotagliflozin and placebo groups respectively (HR 0.74; 95% CI, 0.63 to 0.88; p<0.001).4 The secondary end points included the coprimary endpoints individually. The significance of the primary outcome was driven by the significance of the total number of HHF and urgent visits for HF (HR 0.67; 95% CI, 0.55 to 0.82; P<0.001). There was no significant difference between sotagliflozin and placebo in total deaths from CV causes (HR 0.90; 95%CI, 0.73 to 1.12; p=0.35).4
Price
INPEFATM is supplied in packages of 30 and 90 tablets of 200 mg strength. Each 200 mg tablet has an average wholesale price of $23.92.10 INPEFATM is available at most pharmacies for a cash price of $735 for a month supply of 200 mg tablets, and $1,430 for a 30 day supply of 400 mg (administered as two 200 mg tablets).11
Simplicity
Sotagliflozin is a once daily oral medication for the reduction of risk of CV death, HHF, and urgent heart failure visits in patients with HF or patients with T2DM, CKD and other cardiovascular risk factors. Sotagliflozin is approved for patients without T2DM; however, the two phase-three clinical trials only studied the medication in patients with T2DM. As an SGLT2 inhibitor, it is one of the medication classes indicated for the GDMT of HFrEF, as well as to reduce HHF in patients with HFmrEF, and HFpEF.6 Currently there are no direct head-to-head trials comparing sotagliflozin and other SGLT2 inhibitors.
Bottom Line
Sotagliflozin is a novel SGLT2 inhibitor with SGLT1 inhibitory properties indicated for heart failure, regardless of ejection fraction. Like other SGLT2 inhibitors, it has been shown to reduce morbidity associated with heart failure. In two randomized controlled trials, sotagliflozin was associated with a statistically significant reduction in HHF in patients with comorbid T2DM.
Jason Timothy Fine, PharmD is a PGY1 Pharmacy resident at UPMC St. Margaret and can be reached at finejt@upmc.edu. Taylor Thompson, PharmD, MBA, BCPS is a Clinical Assistant Professor at West Virginia University, School of Pharmacy. Heather Sakely, PharmD, BCPS, BCGP, the Director of Clinical Pharmacy Services and PGY2 Geriatric Pharmacy Residency, served as editor and mentor for this work and can be reached at sakelyh@upmc.edu.
References
1. INPEFATM [package insert]. The Woodlands, TX: Lexicon Pharmaceuticals, Inc.; 2023.
2. Wright EM. Renal Na(+)-glucose cotransporters. Am J Physiol Renal Physiol. 2001;280(1):F10-8. doi: 10.1152/ ajprenal.2001.280.1.F10. PubMed PMID: 11133510.
3. Bhatt DL, Szarek M, Steg PG, Cannon CP, Leiter LA, McGuire DK, et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N Engl J Med. 2021;384(2):117-28. Epub 20201116. doi: 10.1056/NEJMoa2030183. PubMed PMID: 33200892.
4. Bhatt DL, Szarek M, Pitt B, Cannon CP, Leiter LA, McGuire DK, et al. Sotagliflozin in Patients with Diabetes and Chronic Kidney Disease. N Engl J Med. 2021;384(2):129-39. Epub 20201116. doi: 10.1056/NEJMoa2030186. PubMed PMID: 33200891.
5. Fadiran O, Nwabuo C. The Evolution of Sodium-Glucose Co-Transporter-2 Inhibitors in Heart Failure. Cureus. 2021;13(11):e19379. Epub 20211108. doi: 10.7759/cureus.19379. PubMed PMID: 34925982; PubMed Central PMCID: PMC8654149.
6. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/ American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e895-e1032. Epub 20220401. doi: 10.1161/cir.0000000000001063. PubMed PMID: 35363499.
7. INVOKANA® [package insert]. Titusville, NJ Janssen Pharmaceutical Inc.; 2013
8. JARDIANCE® [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; 2021.
9. FARXIGA® [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2014.
10. Sotagliflozin. Lexi-Drugs [database online]. Lexi-Comp, Inc.; Accessed October 23, 2023
11. Inpefa. GoodRx. Available at: https://www. goodrx.com/inpefa. Accessed October 23, 2023.
By: Nadine Popovich, Melanie Mayer and Haley Thon
Allegheny County Immunization Coalition (ACIC) — 2024-2025 Chair - Patrick Hussey, PharmD, MBA: The Allegheny County Immunization Coalition (ACIC) invites you to participate in our 2025 General Membership Meetings, held at the AIU Building and via Zoom from 9:00 AM –11:00 AM on March 20th featuring Dr. Victor Rullan, the epidemiologist for the Delaware County Department of Health. With 40 years of public health experience, Dr. Alós-Rullán will discuss vaccine hesitancy.
Allegheny County Immunization Coalition membership is free and funded by our grants. All healthcare professionals with an interest in vaccination are welcome. See our website for full details on membership and how to volunteer at our community events: www.immunizeallegheny.org
American College of Surgeons Southwestern Pennsylvania Chapter (ACS-SWPA) — 2025 President – Richard Fortunato, DO, FACS: The Southwestern PA Chapter of the American College of Surgeons continues to advance its initiatives for 2025. Planning is underway for the March 26th Resident Event, "Debates and Dilemmas," at the Kimpton Hotel Monoco. This is the first in our 3 part Resident Series. Please save the date for our next one “Most Interesting Cases” on May 28th. If you are a surgeon or surgical resident interested in attending, please visit https://lp.constantcontactpages.com/ ev/reg/da7dvnz or email Melanie Mayer at mmayer@acms.org.
Pennsylvania Geriatric Society Western Division (PAGS-WD) — 2025 President - Heather Sakely, PharmD,
BCPS, BCGP: Registration is live for 33rd Annual Virtual Clinical Update in Geriatric Medicine. https://cce.upmc. com/33rd-annual-clinical-updategeriatric-medicine.
We invite you to join us for the 33rd Annual Virtual Clinical Update in Geriatric Medicine on April 24-25, 2025! This year, we’re excited to introduce a fresh format focused on Fostering Age-Friendly Care through the 5Ms: Mentation, Medication, Mobility, What Matters Most, and Multi-Complexity.
Attend from the comfort of your home or office and engage in an outstanding lineup of lectures and panel discussions. This AGS award-winning course is a collaborative effort between The University of Pittsburgh, the AGS state chapter, and leading healthcare organizations.
Visit pagswd.org to view the course brochure. Register by April 11 to secure your spot—a $50 late fee applies after this date, and registration closes on April 19, 2025.
For questions, please contact Haley Thon, Administrator, at hthon@acms. org. We look forward to seeing you there!
Spring Newsletter planning is underway. For content submissions please contact Haley Thon, Administrator, at hthon@acms.org.
Chandler Grant Glaucoma Society
— 2025 President – Peter A. Netland, MD, PhD: Over 90 members attended the Chandler Grant Glaucoma Society (CGGS) Annual Meeting on February 27 at the Cosmos Club in Washington, D.C. The evening began with a reception, followed by remarks from outgoing President Joshua Stein, MD, MS, and

incoming President Peter Netland, MD, PhD. A highlight was Dr. Joel Schuman’s traditional "Glass of Wine with Chandler and Grant" toast, honoring the society’s founders.
Leon Herndon, Jr., MD, was confirmed as President-Elect and will assume the presidency in 2027. Special acknowledgments included Lisa Praeger, MD, of Alcon, who spoke on collaborations through the David Epstein Clinician-Scientist Grant. Rithambara Ramachandran, MD, MSc, was named the 2024 David Epstein Clinician-Scientist Award recipient.
Andrew Pittner, MD, of Virginia Eye Consultants and EVMS, delivered the annual guest lecture, "How to Catch a Fish on Your First Cast," tying Dr. Chandler’s love of fishing to insights on expertise and timing. His story of reeling in a 750-pound tuna with a visually impaired partner left a lasting impression.
The CGGS includes several local glaucoma specialists, many of whom practice or trained in the region. The Allegheny County Medical Society provides administrative support for
society, strengthening its ties to the local medical community. Featured in the photo are Bushra Usmani, MD, Sarah Ullah, MD, Andrew Williams, MD, Julia Polat, MD, Tom Wajda (Alcon), and Ian Conner, MD, PhD.
The Pittsburgh Ophthalmology Society (POS) — 2024 President - Pamela P. Rath, MD: Pittsburgh Ophthalmology Society Hosts February 6 Meeting Featuring Dr. Mark Westcott
The Pittsburgh Ophthalmology Society (POS) welcomed a robust audience of 70 physicians to its February 6 meeting, featuring distinguished guest speaker Mark Westcott, MD, FRCOphth, Adjunct
Professor in Ophthalmology, University of Pittsburgh; Consultant at Moorfields Eye Hospital, University College London and St. Bartholomew’s Hospital, London, UK.
Dr. Westcott, a globally recognized expert in uveitis, inflammatory eye disease, and glaucoma, delivered two insightful lectures: "The Challenge of Ocular TB – What Have We Learned from the COTS Study, and Its Relevance to North America" and "Tips and Tricks in Getting the Diagnosis in SightThreatening Uveitis – How to Get It Right." His presentations were met with enthusiasm, sparking engaging discussions among attendees.
With over 22 years of experience as a Consultant Ophthalmologist at prestigious institutions, including Moorfields Eye Hospital and St. Bartholomew’s Hospital, Dr. Westcott brought a wealth of knowledge to the evening.
The February meeting concludes the POS 2024-2025 Monthly meeting series. Planning for the 2025-2026 series is underway. Members will receive notification in May which will include the dates of each meeting and the guest presenter.