Allegheny County Medical Society

Allegheny County Medical Society
September
Editorial
• Back to School
Deval (Reshma) Paranjpe, MD, MBA, FACS
Editorial
• The Ageing Athlete
Richard H. Daffner, MD, FACR
ACMS News
• Election Report
ACMS News
• ACMS Night at the Pirates Game August 2024
ACMS News
• WIHC Summer Social August 2024
ACMS News
• Specialty Group Updates
ACMS Staff: Nadine Popovich, Eileen Taylor, and Melanie Mayer
Article
• Breaking Barriers
Dr. Sarahgene Gillianne DeFoe
Article
• Time: Our Most Precious Resource
Dr. Emily Scott, DO, CAQSM
Article
• Acne Revisited
Nicole F. Velez, MD
Article
• Non-Competes
Adam Appleberry, Esq. & Michael Cassidy, Esq.


2024
Executive Committee and Board of Directors
President
Raymond E. Pontzer, MD
President-elect
Keith T. Kanel, MD
Secretary
Kirsten D. Lin, MD
Treasurer
William F. Coppula, MD
Board Chair
Matthew B. Straka, MD
Directors
Term Expires 2024
Douglas F. Clough, MD
David J. Deitrick, DO
Jan B. Madison, MD
Raymond J. Pan, MD
G. Alan Yeasted, MD, FACP
Term Expires 2025
Anuradha Anand, MD
Amber Elway, DO
Mark A. Goodman, MD
Elizabeth Ungerman, MD, MS
Alexander Yu, MD
Term Expires 2026
Michael M. Aziz, MD, MPH, FACOG
Michael W. Best, MD
Richard B. Hoffmaster, MD
Micah A. Jacobs, MD, FIDSA
Jody Leonardo, MD
G. Alan Yeasted, MD, FACP
2024 Board Committees
Bylaws
Kirsten D. Lin, MD
Finance
William Coppula, MD
Nominating
Keith T. Kanel, MD
Women’s Committee
Anu Anand, MD & Tiffany DuMont, DO
Managing Editor
Sara C. Hussey, MBA, CAE ACMS Executive Director shussey@acms.org
Medical Editor
Deval (Reshma) Paranjpe, MD reshma_paranjpe@hotmail.com
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
Term Ending 2024
Richard Daffner, MD; Anthony Kovatch, MD; Andrea Witlin, DO, PhD
Term Ending 2025
Robert Howland, MD; John Williams, MD; Alexandra Johnston, DO; Charles Mount, MD
Executive Director
Sara Hussey shussey@acms.org
Vice President - Member and Association Services
Nadine M. Popovich npopovich@acms.org
Manager - Member and Association Services
Eileen Taylor etaylor@acms.org
Operations CoordinatorACMS & ACMS Foundation Melanie Mayer mmayer@acms.org
Part-Time Controller Elizabeth Yurkovich eyurkovich@acms.org
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
EDITORIAL/ADVERTISING
OFFICES: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212; (412) 321-5030; fax (412) 321-5323.
USPS #072920. PUBLISHER: Allegheny County Medical Society at above address.
The Bulletin of the Allegheny County Medical Society is presented as a report in accordance with ACMS Bylaws.
The Bulletin of the Allegheny County Medical Society welcomes contributions from readers, physicians, medical students, members of allied professions, spouses, etc. Items may be letters, informal clinical reports, editorials, or articles. Contributions are received with the understanding that they are not under simultaneous consideration by another publication.
Issued the third Saturday of each month. Deadline for submission of copy is the SECOND Monday preceding publication date. Periodical postage paid at Pittsburgh, PA.
Bulletin of the Allegheny County Medical Society reserves the right to edit all reader contributions for brevity, clarity and length as well as to reject any subject material submitted.
The opinions expressed in the Editorials and other opinion pieces are those of the writer and do not necessarily reflect the official policy of the Allegheny County Medical Society, the institution with which the author is affiliated, or the opinion of the Editorial Board. Advertisements do not imply sponsorship by or endorsement of the ACMS, except where noted.
Publisher reserves the right to exclude any advertisement which in its opinion does not conform to the standards of the publication. The acceptance of advertising in this publication in no way constitutes approval or endorsement of products or services by the Allegheny County Medical Society of any company or its products.
Annual subscriptions: $60
Advertising rates and information available by calling (412) 321-5030 or online at www.acms.org.
COPYRIGHT 2024: ALLEGHENY COUNTY MEDICAL SOCIETY POSTMASTER—Send address changes to: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212. ISSN: 0098-3772

By:
When we were children, September meant going back to school, with a new classroom, a new teacher, some new friends, and perhaps a new you. You were suddenly more sophisticated because you had moved up in the K-12 hierarchy, and you may have wanted an image to match. This change often included new outfits, a new backpack to replace a worn one, and new shoes because we were all growing like weeds. Maybe a new lunchbox—would it be Davey Crockett, Scooby Doo, Wonder Woman, G.I. Joe, or Jem and the Holograms? Maybe Rugrats or The Simpsons (and there my pop culture knowledge stops, but you get the idea).
Perhaps you wanted to try on a different persona. Perhaps you tried out being a prep, or a jock, or an artist, or a goth. Maybe you dyed your hair green and drove your parents crazy. Maybe you finally got out of braces and glasses and jaws dropped when you walked down the corridor that first day.
Although the spectacle we chose to present didn’t affect our grades, we learned that image mattered. It shaped how we were treated and perceived, influencing our teachers and adults alike. Our appearance either reflected who we were or masked teenage angst, insecurity, and fear.
It turns out that these concepts apply equally well once you’re a middleaged adult buckling down for literal or metaphorical September in your life, The pandemic saw a huge increase in plastic surgery and cosmetic procedures—since meetings were on Zoom during Covid and cameras didn’t always have to be on, recoveries could be discreet and easy. This
cosmetic boom has continued now that pandemic precautions are no longer commonplace, with both women and men signing up for changes.
Looking younger is a defensive action in an inherently ageist society. Our medical world can be terribly ageist. I saw my fellowship mentors transform themselves when I was a fellow; they were smarting from patients and colleagues asking them when they were going to retire. For men, it seems to be relatively straightforward process— significant weight loss, a new wardrobe, some hair dye, and a good moisturizer, perhaps with a blepharoplasty and brow lift thrown in for good measure.
And then… stay that way.
For women physicians, it can be far more complicated. Sometimes it’s as easy as a few new clothes for school, but more often, it can be Botox, fillers, nip this, tuck that, but not so obviously that anyone might notice. It’s the constant maintenance of hair and nails and waistline. Ozempic? Ozempic! The need to look competent and in control but not flashy; stylish but not obsessed to the point where people think you think more about your look than your work. Thin but not too thin. Healthy but not overweight. Looking put-together enough so that everyone thinks you’re coordinated in every aspect of your life and yet simple enough that you look relatable and comforting to all your patients. And then there’s the image we try to project to administration and colleagues: wise but still energetic, exuding gravitas but still flexible, experienced but still young and vital. The famous America Ferrera speech from the Barbie movie comes to mind.
These are impossible standards to meet, even if you didn’t have a career and family to worry about.
Recently, I’ve wandered into several Women Physicians’ Style Groups on Facebook. There are groups for high fashion brand lovers, bargain hunters, liberals, and conservatives. Some are obsessed with the latest purse or trendiest shoes, none of which you can take to work without risking a tib-fib fracture on polished hospital floors.
I've also met women physicians who stopped dyeing their hair and embraced their natural gray during the pandemic, never looking back. Some have embraced comfortable work-fromhome clothes, swearing off structured suits, makeup, and heels for good.
I’ve met male physicians who worry about looking over the hill, debating between a combover or hair transplant, wondering if a trendy shirt with contrasting patterned collars and cuffs will make them look hipper, or if a fun new car will do the trick. I’ve come across male physicians who just shave their heads and embrace going bald.
Is any of this important to our ability to practice good medicine, no matter our gender? Not at all.
Whatever we look like and whatever we wear, it’s our brains that matter.
Scrubs and school uniforms, the great equalizers that they are, have always helped prove this point. They—and you— are fine, as long as they—and you—are clean and professional.
The moral of the story? Do, wear, and be what makes you feel your best.
You are enough. You are still enough. You always were enough.
When your patient needs a world-class specialists, AHN delivers experts like our new neurology physician.
Dr. Samples provides high-quality neurological care to meet each patient’s individual needs.
Department Chair of Neurology
Neurology
Locations:
AHN Neurology
AHN Allegheny General Hospital 320 East North Avenue
Hemlock Building, Third Floor Pittsburgh, PA 15212
2315 Myrtle Street, Suite L90 Erie, PA 16502
Specialties :
Skilled at headache and migraine, as well as diagnosing and treating diseases of the brain, spinal cord, and nerves
To refer your patient, call (412) DOCTORS.

Provides patient-centered care for neurology
The Allegheny County Medical Society conducted its election from September 2, 2024September 9, 2024. The following are the official results of the election:

Chair / Immediate Past President
Raymond E. Pontzer, MD




Treasurer
MD
Three-Year Term (Term Expires in 2027)
David Deitrick, DO
Sharon Goldstein, MD
Prerna Mewawalla, MD
Raymond Pan, MD
Nicole Velez, MD
Two-Year Term (Term Expires 2026)
Kevin Kotar, DO
Term Expires in 2025
Anuradha Anand, MD
Amber Elway, DO
Mark Goodman, MD
Elizabeth Ungerman, MD
Alexander Yu, MD
Term Expires in 2026
Michael M. Aziz, MD
Michael Best, MD
Jody Leonardo, MD
Micah Jacobs, MD
Matthew Straka, MD (Chair)
Peter Ellis, MD
Patricia Bononi, MD
*A member of the Peer Review Board cannot be an active member of the ACMS Board of Directors.
Elected – Two-Year Term 2025-2026
Michael M. Aziz, MD
Vint Blackburn, MD
Douglas Clough, MD
Molly Fisher, MD
Geoffrey Lim, MD
Michael McDowell, MD
Charles Mount, MD
Alexander Yu, MD
Currently Serving (Not Up for Election)
Holly Appleberry, MD
Alexandra Johnston, DO
Kevin Kotar, DO
Stacie McKnight, DO
Devon Ramaeker, MD
Dillon Stein, DO
*Listed in Order of Votes Received*
Amber Elway, DO
Richard Hoffmaster, MD
Anthony Kovatch, MD
Rasha Abdulmassih, MD
William Coppula, MD
Elected – One Year Term 2025
The ACMS Nominating Committee and 2024 Board of Directors congratulate all the newly elected officers, board members, and delegates. We look forward to your active participation as we continue our mission for the Society. Thank you for your dedication to our profession.
— Keith T. Kanel, MD, Chair, Nominating Committee
Keith T. Kanel, MD Nominating Committee Chair
Amber L. Elway, DO
Jody Leonardo, MD
Jan Madison, MD
Raymond Pan, MD
G. Alan Yeasted, MD


By: Emily Scott, DO, CAQSM
When thinking about healthy aging, the first theme that comes to my mind is time. No, not how long we’re going to live, but rather, the limiting factor between us and the things that we want to do to take care of ourselves.
In the realm of primary care sports medicine, my goal isn’t just to improve my patients’ lifespans, but to maximize their healthspans. How can I keep my patients moving, eating, sleeping, and living well for as long as possible, all while trying to keep myself moving, eating, sleeping, and living well? It’s an imperfect balance that’s ever evolving, and more often than not feels like an unobtainable goal for most of us in the current healthcare climate.
In a perfect world not burdened by writing notes, responding to patient messages, keeping up with CME, etc., I’d imagine that most of you reading this would do a multitude of other things to take care of yourself: run or walk more, lift more weights, take up yoga, spend more time with your family, volunteer in your community, practice guitar, get more sleep…the list could go on.
In my first year of running a direct primary care practice, balancing life has become tougher, and exercise is often the first to go. It's easy to let workouts slip while managing a growing business, but excuses are always there if you allow them.
We have all learned motivational interviewing in medical school, but have you ever motivationally interviewed yourself? Ask yourself, are you doing the things you want to do? How would you get started? Do you see yourself getting back into it soon? What are some barriers that are keeping you
from it? How can you overcome those barriers? Why do you want to do it in the first place?
How do I keep myself on track? I continue to work on it, but the biggest driving force is focusing on my “why.” Why do I want to exercise? In the short term, I know that several areas of my life are improved when I exercise regularly, including my mood, focus, sleep, strength, self-esteem, relationships, and sense of community. In the long term, it is reducing my risk of cardiovascular disease, insulin resistance, Alzheimer’s, cancer, osteoporosis, falls/frailty, sarcopenia, and improving not just my lifespan but also my healthspan. There’s also evidence that shows when parents live active lifestyles, their children life active lifestyles, too, and I want to instill in my children the importance of movement. I want to do everything in my power to be an active participant in my family and my community for as long as I can. I want to live long, but I really want to enjoy those extra years.
If you’re looking for a “why,” consider this; the average lifespan in the US is 78 years old (74.5 for men, 82 for women), whereas the average health span is only 62! The average age of retirement for men is 65 and for women 63. People are working hard, saving their money, and then are too sick to enjoy it. They also end up using their savings for healthcare costs in their later years.
Setting boundaries for your "nonnegotiables" and scheduling protected time allows you to recharge and be your best self. It's okay to be a little selfish for self-care. What’s also beautiful to observe is when those habits become
part of your life, it’s easier to keep them as a part of your life. However, protecting your time often means saying "no" to social events or work committees, which can be challenging for early-career physicians.
To me, the key to healthy aging is protecting your time to focus on the fundamentals of longevity: movement, nutrition, sleep, stress management, community, and purpose. I often remind my patients, and I'll remind you too, that supplements, saunas, fancy lasers, or fad diets won't fix a poor lifestyle.
I won’t claim to be the timemanagement guru, because it’s far from the truth. But I know if we don't prioritize ourselves, no one else will. Neglecting our "non-negotiables" leads to poorer physical and mental health. Find your why, schedule time, and take care of yourself—you deserve it.
Dr. Scott practices direct primary care and sports medicine with Direct Care Physicians of Pittsburgh in Shadyside. When she is not practicing medicine, she enjoys spending time with her husband Paul, their dogs Cece and Pickle, and their family and friends. She also enjoys running, cycling, cross country skiing, yoga, and gardening.
References:
1. Rodrigues, D., Padez, C., & Machado-Rodrigues, A. M. (2018). Active parents, active children: The importance of parental organized physical activity in children’s extracurricular sport participation. Journal of Child Health Care, 22(1), 159–170. https://doi. org/10.1177/1367493517741686
2. Harvey A. Friedman Center for Aging (2017). Healthspan is more important than lifespan, so why don’t more people know about it? Washington University in St. Louis Institute for Public Health. https://publichealth. wustl.edu/heatlhspan-is-more-important-than-lifespanso-why-dont-more-people-know-about-it/

By: Dr. Sarahgene Gillianne DeFoe
As a practicing physician and physician life coach, I am deeply passionate about mental health and wellness in the medical community. With National Physician Suicide Awareness Day approaching on September 17th, 2024, we must highlight the challenges we face. According to the American College of Emergency Physicians, an estimated 300 to 400 physicians die by suicide each year in the United States1. By bringing these issues to light, we can develop meaningful interventions that improve our well-being and fulfillment in our profession and enhance the care we provide to our patients.
Physician burnout remains a significant issue within the medical community. In 2021, at the height of the pandemic, burnout among U.S. physicians soared to 62.8%, up from 38.2% in 20202, 3. Although the burnout rate has dropped below 50% this year4, these statistics underscore the persistent challenges physicians face and highlight the critical need for effective strategies to address this issue. Contrary to belief, burnout is caused by excessive demands from our jobs coupled with inadequate resources and support and is not an individual problem triggered by personal limitations. Simply telling physicians to practice better self-care and be more resilient does not work, as this puts the blame solely on us to fix a systemic problem.
The Stigma Surrounding Mental Health in Medicine
The stigma surrounding mental
health in the medical community is a significant barrier to physician wellness. One proposed way of destigmatizing "mental health" is to replace it with the term "mental wellness." Despite the name change, many physicians hesitate to seek mental health care due to fears of being perceived as weak or unfit for our demanding roles. This stigma is compounded by the intrusive language used in credentialing and licensing processes, which often require physicians to disclose any mental health treatment. Such disclosures can lead to concerns about career repercussions, including potential restrictions on our medical licenses and/or hospital privileges.
Additionally, the culture within our medical community often emphasizes resilience and self-sacrifice and is quick to exalt us to superhero status at the risk of denying us our humanity. Thus, it is no wonder that we do not admit to mental health struggles. The fear of judgment from colleagues and the potential impact on our professional reputation further deters us from seeking help.
Achieving a healthy work-life balance is particularly challenging for physicians due to several factors. For example, we work long, unusual hours at nights, weekends, and holidays, which encroach on our personal time and family commitments. The highstress nature of the job, along with the emotional toll of patient care, leads to increased stress and fatigue. Additionally, the administrative burden
of paperwork, electronic health records (EHR), and staying current with medical advancements adds to our workload.
We are often under pressure to meet patient expectations and maintain high standards of care, further complicating the pursuit of balance. These factors combined make it challenging for physicians to find time for relaxation, hobbies, and family life—essential components of a healthy work-life balance.
Healthcare organizations and systems have an ethical responsibility for addressing burnout amongst their physicians, but there is also a strong business case. It costs organizations $ 500 K to $ 1 million to replace a physician who retires early or leaves to pursue other career opportunities.5 Many healthcare institutions have already recognized the role of promoting physician wellness and have instituted resources such as Employee Assistance Programs (EAP), physician peer coaching, and workshops on physician well-being. Although with good intent, these programs can fall short of their goals in improving physician well-being when institutions fail to prioritize policies that support a culture of wellness, such as flexible working schedules, paid sick and parental leave, and ensuring adequate staffing.
Allegheny County Medical Society (ACMS) recognizes how policies can impact a culture of wellness and is working with key stakeholders to address the removal of intrusive
language in licensing and credentialing applications that stigmatize those with mental health issues.
In addition, the ACMS Foundation has launched the ACMS Physician Wellness Program (PWP), which aims to break down barriers for physicians seeking mental wellness care. This initiative breaks down barriers by providing free, confidential, one-on-one therapy or coaching sessions for any M.D. or D.O. within Allegheny County. Securing a session with a licensed therapist or certified coach is as easy as clicking a button. Your sessions with your coach or therapist can be done from the comfort of your home through a virtual portal (if you choose). Since our schedules are often unpredictable, flexibility in scheduling is available at night and on weekends. Finding the right fit for you is easy since the PWP committee has vetted all coaches and therapists, and they are all acutely aware of the unique nature of our profession and the challenges we face.
I am excited to be part of the ACMS PWP initiative as a member of the committee and as a coach within the program. As a physician coach, I witnessed the impact that burnout can have on our ability to enjoy the careers we have worked so hard for. Burnout can lead to feelings of overwhelm, shame, and anxiety, which can affect our ability to sleep, focus, and our interactions with our patients, peers, and those we love. A coach or therapist can provide you with tools to feel more in control of your life. By working with a PWP therapist or coach, you can quickly implement time-saving techniques that can allow you to achieve a worklife balance that you can only dream of. Just imagine not doing Electronic Health Record (EHR) charts in your P.J.s and instead spending quality time with your kids or curling up on the couch with a good book. I coach physician clients who are burned out simply because their goals are not matched with their values, and we work to get them in alignment, which often results in clients going after and getting that
promotion and still having space on their calendar to breathe something they never thought was possible. Should I Choose a Coach or Therapist?
Within PWP, you have the option of a coach or a therapist. Therapy tends to focus on the past, while coaching tends to be more future-focused. Therapy uses tools such as Cognitive Behavioral Therapy (CBT) to address psychological disorders and to get individuals from non-functioning to functioning. For example, a therapist may be best for you if you are feeling so overwhelmed that you are struggling to cope with everyday tasks. A coach uses tools to get clients from coping to thriving. For example, you are getting by ok, but you want to change a specific behavior such as procrastination- to finally write that book! I also work with clients on leveling their time management skills so that they spend less time at work and more time doing other things they love. Many physician clients see me simply because they are experiencing intense emotions such as anxiety and overwhelm, and I can teach them how to manage their brains the second that these emotions show up. Do not let the decision of whether you need a coach or a therapist be the reason for not signing up for this amazing program. Pick someone based on their specialty, and whoever you choose will help guide you and ensure you have the right fit. While addressing the challenges to physician well-being requires systemic changes, we must also take personal responsibility for our well-being. To create a culture of wellness within the medical community, we must learn to prioritize ourselves, show compassion to colleagues who may be struggling, and resist the rhetoric in medicine that often dehumanizes us. When we prioritize physician wellness, we create a healthier, more resilient healthcare community that benefits everyone.
References:
1. Physician suicide. Accessed September 6, 2024. https://www.acep. org/life-as-a-physician/wellness/ wellness/wellness-week-articles/ physician-suicide/
2. Physician burnout rate spikes to new height. American Medical Association. Accessed August 27, 2024. https://www. ama-assn.org/press-center/pressreleases/physician-burnout-rate-spikesnew-height
3. American Medical Association. Pandemic pushes U.S. doctor burnout to all-time high of 63%. American Medical Association. Published September 15, 2022. Accessed August 27, 2024. https://www.ama-assn.org/practicemanagement/physician-health/ pandemic-pushes-us-doctor-burnoutall-time-high-63
4. American Medical Association. Physician burnout rate drops below 50% for first time in 4 years. American Medical Association. Published July 2, 2024. Accessed August 27, 2024. https://www.ama-assn.org/practicemanagement/physician-health/ physician-burnout-rate-drops-below-50first-time-4-years
5. Noseworthy J, Madara J, Cosgrove D, et al. Physician Burnout Is A Public Health Crisis: A Message To Our Fellow Health Care CEOs. Health Affairs Forefront. doi:10.1377/ forefront.20170328.059397
Dr. DeFoe is a Clinical Assistant Professor of Radiation Oncology and Certified Physician Coach. Her passion is helping physicians end the burnout cycle and find joy in medicine and their personal lives. You can learn more about her at www.thetimemd.com

By: Nicole F. Velez, MD
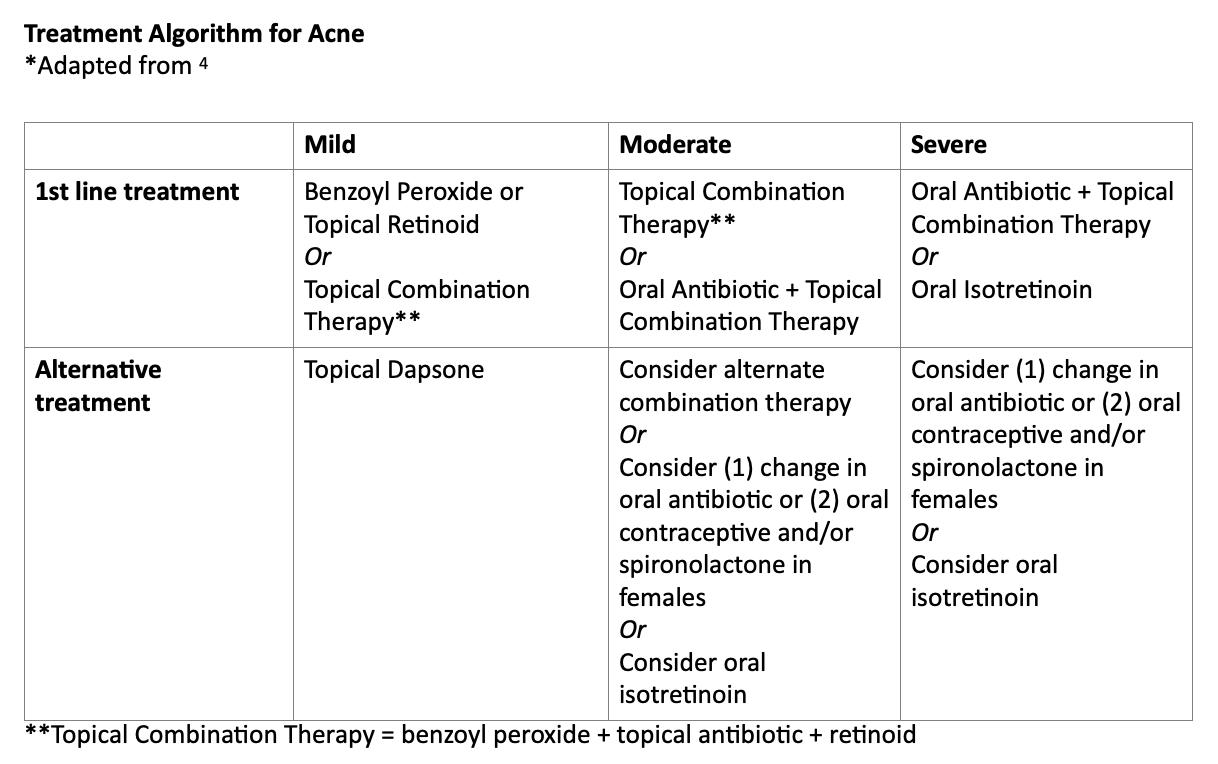
Regardless of your medical specialty, you have probably been approached at some point by patients or friends with questions about acne management. Acne vulgaris affects 9.4% of the global population and is the eighth most prevalent disease globally.1 In the US, acne accounted for $846 million in medical costs and $398 million in lost productivity in 2013.2 Studies show that the health-related quality of life impact of acne is similar to that of other chronic conditions, such as asthma and arthritis.3 Fortunately, there have been many advancements in our understanding of acne, as illustrated by the latest Guidelines on Acne published this year in the Journal of the American Academy of Dermatology.4 While this is not meant to be a comprehensive review, here are some updates that may be of interest to you no matter your field of practice:
Combination therapy is best. When using topical treatments, multimodal therapy is best. By incorporating multiple mechanisms of action, combination therapy optimizes efficacy and reduces the risk of bacterial resistance.4 A typical regimen might include a benzoyl peroxide product (often over the counter), a topical antibiotic and a topical retinoid. Vitamin A derivatives, retinoids are a mainstay in acne management and should be a part of most treatment plans. Retinoids work at the level of the keratinocyte nucleus to provide comedolytic and anti-inflammatory effects as well as to help improve discoloration and scarring. Counseling regarding amount and frequency of use is important when prescribing a retinoid so that
patients do not develop irritation and discontinue use prematurely.
Spironolactone is a safe and effective treatment. While not FDAapproved for acne, oral spironolactone has been used for decades in female acne due to its anti-androgen properties. Especially as we aim to reduce oral antibiotic use (current guidelines recommend no more than 3-4 months of oral antibiotics a year), spironolactone has been shown to be an effective alternative. The first multi-centre, randomized controlled study of spironolactone vs doxycycline was published this year and showed that spironolactone outcomes (lesion count and quality of life) were better than doxycycline at both month 4 and 6.5 Concerns regarding tumorgenicity and hyperkalemia have contributed to underutilization of spironolactone in the past. However, in a retrospective study this year, spironolactone exposure was not associated with gynecologic or other common malignancies.6 Additionally, no association between spironolactone use and breast cancer recurrence was found among patients with a history of breast cancer. Unless a patient has risk factors for hyperkalemia (i.e. older age, medical comorbitidies, or other medications), potassium monitoring has been shown to be of low usefulness and is no longer recommended.7
There are treatment options in pregnancy. Fortunately, many topical medications are safe in pregnancy, including benzoyl peroxide, azelaic acid, clindamycin, erythromycin and metronidazole. Certain retinoids, such as tretinoin and adapalene (over
the counter), were also shown to be safe in pregnancy in large studies with no increased risk of congenital malformations. When oral antibiotics are needed, there is clinical date to support the use of cephalexin, cefadroxil, amoxicillin, azithromycin or erythromycin. Doxycycline, however, should not be used in pregnant patients. Vascular laser, intralesional steroid injections and low dose courses of prednisone can also be helpful. Isotretinoin can help in refractory mild to moderate acne. While traditionally considered for nodulocystic acne, isotretinoin is being used increasingly for patients with mild to moderate acne that is resistant to oral antibiotics. By reducing the size of sebaceous glands, and normalizing keratinocyte development, isotretinoin has long term disease modifying potential. Recent studies show that laboratory abnormalities are seen in <1% of patients. Guidelines now recommend only checking alanine aminotransferase and triglycerides prior to initiation and at peak dose.4 More research has also emerged regarding concerns of isotretinoin and psychiatric side effects. A 20 year retrospective study, showed suicide rates among patients treated with isotretinoin were lower than the national average.7 In a recent study, authors found that treatment with isotretinoin was not associated with an increased incidence of neuropsychiatric diagnoses (ie: mood disorders, anxiety) when compared to treatment with oral antibiotics.9 In fact, multiple studies suggest that isotretinoin may improve quality of life and decrease symptoms
of anxiety.4 Still, isotretinoin is often prescribed to the adolescent population which is at higher risk for depression and appropriate screening is indicated. Diet can play a role. The pathogenesis of acne is multifactorial and related to follicular changes, hormones, microbial colonization and genetics. We know that a high glycemic diet can contribute to acne. Whereas, a Mediterranean diet, rich in omega-3-fatty acids, has been shown to improve acne in small studies. More data is also emerging about the role of probiotics (both oral and topical) to help treat acne, alone and/or in conjunction with prescription medications. This is an evolving field and hopefully will continue to expand in the future. In the meantime, we have many more options for acne now than we did even a decade ago. By taking a multimodal and personalized approach, we should be able to make a difference for our patients with acne.
References
1. Hay RJ, Johns NE, Williams HC, et al. The global burden of skin disease
in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol.2014;134:1527-1534.
2. Lim HW, Collins SAB, Resneck JS Jr, et al. The burden of skin disease in the United States. J Am Acad Dermatol. 2017;76:958-972.e2.
3. Cresce ND, Davis SA, Huang WW, et al. The quality of life impace of acne and rosacea compared to other major medical conditions. J Drugs Dermatol. 2014;13:692-697.
4. Reynolds RV, Yeung H, Cheng CE, et al. Guidelines for the management of acne vulgaris.. J Am Acad Dermatol 2024;90:1006.e1-30.
5. Dreno B, Nguyen JM, Hainaut E, et al. Efficacy of Spironolactone Compared with Doxycycline in Moderate Acne in Adult Females: Results of the Multicentre, Controlled, Randomized, Double-blind Prospective and Parallel Female Acne Sprionolactone vs doxycycline efficacy (FASCE) Study. Acta Derm Venereol 2024 ;104 :26002.
6. Hill RC, Wang Y, Shaikh B, et al. No increased risk of breast or gynecologic malignancies in women exposed
to spironolactone for dermatolgic conditions: A retrospective cohort study. J Am Acad Dermatol 2024; 90(6):13021304.
7. Han JJ, Faletsky A, Barbieri JS. New Acne Therapies and Updates on Use of Spironolactone and Isotretinoin: A Narrative Review. Dermatol Ther 2021;11(1):79-91.
8. Rau A, Keri J, Murase JE. Management of Acne in Pregnancy. Am J Clin Dermatol 2024;25(3): 465-471.
9. Paljarvi T, McPherson T, Thompson C, et al. Neuropsychiatric diagnoses after isotretinoin initiation in pediatric acne patients : A retrospective cohort study. J Am Acad Dermatol 2024. May 23 :S0190-9622.
Dr. Nicole F. Vélez is a board certified dermatologist and Mohs surgeon at Pittsburgh Skin: Dermatology & Mohs Surgery, with offices in Shadyside and Cranberry, PA. She can be reached at nvelez@pittsburghskin.com.

By: Richard H. Daffner, MD, FACR
“I was getting by with experience more so than I was with athletic talent.”
-- Johnny Davis, former NBA player, on his retirement
Tom Brady won several Super Bowl Championships and continued his football career at age 45. Jaromir Jagr, winner of two Stanley Cups, is still playing ice hockey professionally in his native Czechia at the age of 52. Hockey Hall of Famer Gordie Howe retired from the game at age 52, after playing professionally in the World Hockey Association and the NHL with his two sons Mark and Marty. And George Blanda retired from the NFL after 26 seasons at age 48. How were these ageless sports icons able to perform at the highest levels of competitive play long after most of their peers stepped back from the games they loved?
I was fortunate to have been able to play competitive hockey and softball well into my 40’s before arthritis caused my “retirement”. I had played hockey since my youth, but once I went to medical school, then the Air Force and residency, I took a long leave of absence, before making a comeback at the “ripe old age” of 32. In 1973 a new sports complex that featured a fullsized hockey rink opened just outside of Louisville, KY, where I had my first job after residency. The new facility allowed us to establish a youth hockey program, an amateur adult program, as well as serving as a home for the semipro Louisville Blades. I was involved in all three programs, being a founder of the youth association and playing in the adult program. Although I never played for the Blades, I was their team
physician and practiced with them. And it was with the Blades that I made my first observations on how ageing athletes adjusted to the changes that “Father Time” had placed on them.
Most of the Blades players were in their 20’s. Two, however, Tony Fargnoli and Grant Morton were 39 and 42, respectively. Both had played professionally in the minor leagues. Both were slower than their younger teammates. However, they were never out of position and were among the leading scorers on the team. What I observed was that they (and other older athletes) traded speed and physicality for a more mental approach to the game. Instead of skating all over the ice, they anticipated where the puck would go and positioned themselves accordingly. In addition, they were able to immediately speed up whenever necessary, conserving their energy.
When I returned to Duke in 1976, I continued playing in an adult league as well as a player/coach for the Duke Hockey Club. Our adult league played by “Old-timer Rules” - no checking and no slapshots. With those two elements of rough play removed, the games became one of skill. We had only four teams in our “league”, and we rapidly learned most of our opponents’ moves. By the time I moved to Pittsburgh in 1983, the four teams had achieved parity and the outcomes of our games depended on what kind of night the goalies had. Our team had the two oldest players, one of whom was 52 (Rick) and the other (Cliff) was 62. Cliff was a slow skater who had an uncanny sense of where to position himself. Our game plan was to get the puck to Cliff, who, incidentally, was the
highest scorer in the league.
Adjusting
So how do older players do it?
Recently, Pittsburgh Penguins head coach Mike Sullivan commented on Jeff Carter, who, at 39 was the team’s oldest player and was still effective. Sullivan said that older players train the right way, have good off-ice habits, have good nutrition habits, and strive to control everything within their power to set themselves up for success. Avoiding major injuries also helps.
I have observed the adjustments older athletes make to how they play, both at the amateur and professional levels. The two most important adjustments are conservation of energy and relying more on their brain power and less on their muscle power. Older athletes tend to be slower than their younger counterparts. In hockey, nothing is more tiring than the sudden starting and stopping that occurs in the corners of the rink or in the sudden bursts of speed needed for a breakout from one’s defensive zone. Older players glide slowly when the action is not immediately in front of them, saving their energy for a sudden transition from defense to offense. An old joke illustrates this. A young bull and an old bull were standing on top of a hill looking at a herd of cows below. “Let’s run down the hill and get us a cow,” the young bull said. The old bull snorted and replied, “Let’s walk down there and get them all.”
Sometimes, a change in the player’s position will help the older athlete conserve energy. For example, in my younger hockey-playing days, I was a forward, necessitating skating the full
length of the ice at times (because of having to help the defensemen). When I played in Louisville, my coach told me I’d be better as a defenseman, where I’d only have to skate 2/3 of the length of the rink (goal line to offensive blue line). Fortunately, I quickly learned the nuances of my new position.
Similarly, in softball, which I participated in a weekly pick-up game for twenty years, I also adjusted. In my younger days, when my arm was strong, I played outfield. However, once I passed the magic age of 40 and could no longer throw the ball from deep in the outfield to one of the bases, I moved to the infield, playing at first and second bases.
The most important adjustment, however, is mental. Humans are creatures of habit. As both a hockey player and a softball player, I began observing the moves the members
of the opposing teams were making. In sports parlance this is known as “getting a book” on the player (like the “tells” poker players exhibit). This allowed me to position myself to defend against the opposition by anticipating what they would most likely do. I, for example consistently hit the ball within five feet of third base. My goal was to hit the ball over the head of the third baseman. However, try as I might, there was nothing I could do to change the direction of where I hit the ball.
Two examples of adaptation by older players stood out. One of the men I played softball with had the gift of being able to hit a ball anywhere he wanted. He would look at the field and would consistently hit the ball to any place he perceived a weakness on the opposing team. Looking at his “tells” (for example, a right-handed batter who put his right foot behind him indicated that he was
planning to hit the ball to right field) was not useful. That was what using his brain instead of his brawn was all about. Another man in his early sixties was ambidextrous. This allowed him to pitch two games in a row. He alternated pitching one inning right-handed, and the other using his left hand. By the way, he brought two softball gloves with him.
Age need not necessarily end one’s playing career. Physical fitness and proper warm-up exercises help. I did note, however, that the aches and pains I suffered after a hockey game took longer to resolve as I grew older. Eventually, though, I retired from the games I loved when my body told me it was time.
Dr.Daffner is a retired radiologist.


Over the last several months, there has been a significant amount of discussion surrounding non-compete agreements and the extent to which employers may enforce them. Whether it was the proposed legislation in Pennsylvania that restricted noncompete agreements for healthcare practitioners in the state or the passing of the Federal Trade Commission’s rule that would ban non-compete agreements nationwide, one of the most common questions we have received recently has been “is my noncompete agreement still enforceable?” Now seemed like as good a time as any to lay out the current status of noncompete agreements, both from a state perspective and at the national level.
In April, the Pennsylvania State House passed H.B. 1633, introduced by state Representatives Dan Frankel and Arvind Venkat, MD. The initial bill that passed the House prohibited medical employers from using restrictive noncompete agreements that prevent doctors, nurses, and other medical professional who leave a job from practicing elsewhere. This bill moved to the Pennsylvania State Senate, where it was amended and returned to the House for consideration in July. On July 17, 2024, Governor Josh Shapiro signed the Fair Contracting for Health Care Practitioners Act into law.
As it stands now, the Fair Contracting for Health Care Practitioners Act is the law that governs non-compete agreements for medical doctors, doctors of osteopathy, registered nurse anesthetists, registered nurse practitioners, and
By: Adam Appleberry, Esq. & Michael Cassidy, Esq.
physician assistants in Pennsylvania. Under this law, healthcare employers are restricted from enforcing noncompete agreements that are greater than one year in length or if the healthcare practitioner was terminated by the employer; non-compete agreements that are not greater than one year in length and where the healthcare practitioner departs on his or her own volition remain enforceable. Additionally, employers are still authorized to recover reasonable expenses from a healthcare practitioner for expenses “related to the relocation, training, and establishment of a patient base,” but these expenses can only be recovered if the healthcare practitioner leaves on his or her own volition and was not terminated or dismissed by the employer. Finally, any non-compete agreements related to the sale of an ownership interest or the sale of all or substantially all of the assets of a practice are not subject to the restrictions of the Act.
The Act is far less restrictive than the original H.B. 1633 passed by the House, but it still provides some protections for healthcare practitioners in Pennsylvania, especially if terminated by their employer.
In April, the Federal Trade Commission (FTC) voted to approve a final rule to ban non-compete agreements for for-profit businesses, with an anticipated effective date of September 4, 2024. Under this new rule, the FTC acknowledged that much of the healthcare industry operates under a non-profit tax status, meaning that many healthcare entities would
not be subject to the new rule. In the days immediately following the final rule’s approval, businesses around the nation challenged the FTC’s rule, claiming that the FTC overstepped its authority and that the rule violates the Administrative Procedure Act and the U.S. Constitution. Most notably were the challenges in the Eastern District of Pennsylvania and the Northern District of Texas.
In the Eastern District of Pennsylvania challenge, a local tree service company claimed that the FTC exceeded its authority beyond Congress’s intent. In July, the court denied the company’s request for a preliminary injunction and a stay of the effective date, ruling that the company failed to show that the rule would cause irreparable harm.
Conversely, in the Northern District of Texas, the court ruled that the FTC’s rule is unlawful and cannot be enforced. In this challenge, several businesses claimed that the FTC exceeded its statutory authority and that the FTC’s actions were arbitrary and capricious. The court issued a preliminary injunction in July that prohibited the enforcement of the rule against the plaintiffs. On August 20, 2024, the court set aside the rule, agreeing with the plaintiffs by concluding that the FTC lacks statutory authority to issue the rule and that the rule is arbitrary and capricious. This ruling applies nationwide and to all employers.
As it stands now, because of the Texas court’s decision, the rule did not go into effect as planned, and the FTC is now blocked from enforcing the rule. The FTC is considering an appeal
to the Texas court’s ruling and has until October 19, 2024, to appeal this decision. As of the time this article was written, no appeal has been filed.
Conclusion
Although there was a significant amount of legislative and regulatory action over the past several months, the only changes to non-compete agreements as it relates to healthcare practitioners in Pennsylvania are what were set forth in the Fair Contracting for Health Care Practitioners Act. Visit

Tucker Arensberg Lawyers Have Experience in All Major Healthcare Law Issues Including:
• Compliance
• Reimbursement
• Mergers & Acquisitions
• Peer Review and Credentialing for Physicians
• Employment Contracts and Restrictive Covenants
• Tax & Employment Benefits
For additional information contact any of the following attorneys at (412) 566-1212
• Mike Cassidy - Compliance; Contracts, Peer Review, Stark/AKS
• Jeremy Farrell - Labor & Employment and Commercial Litigation
• Adam Appleberry - Mergers & Acquisitions and Physician Contracts
• Jerry Russo - Criminal Defense and Investigations
• Paul Welk - Mergers & Acquisitions










On August 24, ACMS members, along with their families and friends, had a fantastic time at the Pittsburgh Pirates game. Attendees enjoyed the pre-game Happy Hour at the Babb, Inc. Blitzburgh Tailgate Room, with a special event sponsored by Axias Wealth Advisors. Although the Pirates didn't come out with the win, the fireworks show definitely made up for it! Thank you to everyone who joined us for a night of baseball, camaraderie, and fun!





3.
4. Attendees enjoying the tailgate!
5. Our junior members having pre-game snacks.
6. Pre-game Tailgate
7.
8. Fireworks to end the



The Women in Healthcare Committee Summer Social was held on August 22 at the Longue Vue Club. Attendees were able to connect with incredible female physicians and they heard from Dr. Kristen Sandel, MD, FACEP, FAAEM - President of Pennsylvania Medical Society.





3.
4.
5.
6.
7. Isabella
8. Event Sponsors Brianne Laffey and Bethany Shreckengost - both from Vertilocity - with ACMS President-Elect, Keith Kanel, MD
By: Nadine Popovich, Eileen Taylor and Melanie Mayer
Allegheny County Immunization Coalition (ACIC) — 2024 Chair - Patrick Hussey, PharmD, MBA: The Allegheny County Immunization Coalition has several fall events planned. On September 24, join us for a fun and educational Immunization Awareness Bingo Night at the Pitt CEC in Homewood.
On September 19, our General Membership Meeting will feature Dr. Kyle Dipaola, PharmD, BCPS, BCPPS, presenting "Nirsevimab for the Prevention of RSV in Infants."
Registration is now open for the ACIC Annual Immunization Conference on November 6, 2024! Titled "Strengthening Vaccine Confidence," the event is open to all and features keynote speaker Dr. Richard Zimmerman, MD, MPH, FAAFP, FIDSA. The conference will focus on vaccine updates and offer continuing education credits. Visit www.immunizeallegheny. org for details and registration. This event is FREE for students and only $40 for ACIC members (by the way, ACIC membership is FREE).
For more on ACIC activities, membership, and upcoming events, visit our website and get involved in promoting immunization and public health in Allegheny County!
American College of Surgeons Southwestern Pennsylvania Chapter (ACS-SWPA) — 2024 President –Richard Fortunato, DO, FACS: Don’t miss our annual Resident Surgical Jeopardy competition and dinner scheduled for Wednesday, October 2nd at Eddie Merlot's. This event features resident teams from Allegheny Health Network, Conemaugh, UPMC Mercy, and
UPMC Presby. The event also offers a fantastic opportunity to challenge your surgical knowledge and network with fellow surgeons in a fun, competitive atmosphere. The registration fee is $25.00 for Members of the ACSSWPA, $75.00 for Non-Members of the ACS-SWPA, and free for students and residents. You may register here –https://acs-swpa.org/event-5764108 For any questions or membership inquiries, please contact Eileen Taylor, Chapter Administrator, at 412-321-5030 x105 or etaylor@acms.org.
Pennsylvania Geriatric Society Western Division (PAGS-WD) — 2024 President - Heather Sakely, PharmD, BCPS, BCGP: We are delighted to share the latest news from the Pennsylvania Geriatrics Society Western Division. Our commitment to providing exceptional educational and networking opportunities for geriatric healthcare professionals continues to flourish. We are thrilled to announce our Fall Program, set for Wednesday, November 6th. This event is a prime opportunity to explore the latest advancements in geriatric care and connect with colleagues dedicated to enhancing the health and well-being of older adults. We will also recognize the 2024 Teacher of the Year Awardees and David. C Martin Award Recipients at our Fall Program. More details will be available soon. Be sure to visit our PAGS-WD website (www.pagswd.org) regularly for the latest news and updates on upcoming events. For any questions or to join the society, please contact Eileen Taylor, Chapter Administrator, at 412-321-5030 x105 or email etaylor@acms.org.
Greater Pittsburgh Diabetes Club — A Message From Noah Lubowsky, MD President, GPDC: The GPDC Board has decided with regret to disband the current iteration of the Greater Pittsburgh Diabetes Club. We did not take this decision lightly. We all agree that the GPDC is a wonderful networking and learning opportunity for those in the diabetes treatment community of Western PA. We also hope that at some point that the GPDC can be revived in some form.
If you paid dues for 2024 and would like the money refunded, please e-mail Melanie Mayer (mmayer@acms.org) in September. After September, we plan to donate any remaining funds in our account to diabetes-related charities that serve Western PA.
From all of us on the GPDC Board, we thank you so much for your support over the last decade, and we thank the ACMS for their support as well. We hope that this is not a goodbye to the GPDC, but just a temporary pause.
The Pittsburgh Ophthalmology Society (POS) — 2024 PresidentPamela P. Rath, MD — September 12 Meeting Recap: The Pittsburgh Ophthalmology Society (POS) kicked off its 2024-2025 monthly meeting series on September 12, 2024, at the PNC Champions Club at Acrisure Stadium. This venue offered a distinctive atmosphere, allowing members to connect for collegial fellowship, and engage in high-quality continuing education sessions led by esteemed speakers.
The Society was honored to welcome Lisa Feulner, MD, PhD, Founder of Advanced Eye Care &
Aesthetics in Bel Air, MD. Dr. Feulner is a board-certified comprehensive ophthalmologist specializing in cataract, glaucoma, and ocular surface disease management. Notably, in 2016, she was recognized as one of the Premier Surgeon 300—a list of leading refractive cataract surgeons identified by Ocular Surgery News for their innovation in refractive cataract surgery.
Dr. Feulner delivered two exceptional lectures The Ocular Surface: Critical for Refractive Cataract Surgery and Advanced Technology Lenses in Complex Corneas, which were appreciated, as evidenced by the many insightful questions asked by the audience.
Additionally, Samyuktha Melachuri,
October, as the American Academy of Ophthalmology's national conference will be held from October 18-21.
Looking ahead, we are excited to welcome Christopher Glisson, DO, MS, FAAN, on November 7, 2024. Dr. Glisson serves as the Medical Director of Warren Clinic Neurology and the Warren Neuroscience Institute at Saint Francis Health System in Tulsa, OK. He is a specialist in adult and pediatric neuroophthalmology and adult neurology. Prior to his current role, Dr. Glisson was the inaugural medical director of the neuro-ophthalmology program and co-founding program director of the neurology residency at the Hauenstein Neuroscience Center in Grand Rapids, MI. He also held the position of assistant professor of neurology