A monthly update covering people, events, research, and key developments
Editor’s Note:
Welcome to fall hiring season! Whether you're searching for a job or searching for new employees this is always the busiest time of the year. This month's job listings prove that the market is starting to turn around with lots of new opportunities. Make sure you take a chance to review all of them.
Following up on last month's interest in our Autism article, we've brought you a fresh perspective from north of the border in the form of a piece that investigates the increase in Autism diagnoses and the possible origin. We've also got an opinion piece on COVID and, for those of you shopping for the holidays, a special book for the 9-12 set that helps them understand what epidemiologists do. Finally you'll find a piece on routine vaccinations with a look back at history along with another piece that questions whether you should quit or keep your current job.
LAST CALL - Annual Event Calendar
As you know, our December issue is always dedicated to publishing a calendar of industry events offered worldwide. If you have a conference, meeting, short course, winter/summer program, or other event that you think would be of interest to our readers please send them to us at events@epimonitor.net and make sure you include contact information so we can get back to you with questions in order to list your event correctly.
Summer Programs
2026 is right around the corner and the time to start planning your summer schedule is right now. In the Marketplace you'll see our summer program sponsors are starting to advertise. Take a look and book a seat early. If you are in a position where you run a summer program we would be happy to talk to you about advertising options that will allow our readers to consider your offerings. Our annual summer program issue will be published in February.
As always, we continue to provide you with our popular monthly word game feature, Notes on People, an overview of what we are reading from the public media, and a listing of upcoming events. Ask us about the sponsorship opportunities for these standard monthly features - it offers you great exposure for your event, institution, book or other item of interest to our readers!
Until next month - stay safe and enjoy the holiday season!
In This Issue
-3- Rethinking Autism's Origins - Beyond the Genome
-6- Covid Revisionism to Public Health Intelligence
-10- Explaining Epidemiology to Middle Schoolers - "The Disease Detective"
-14- Routine Vaccinations, Sanitation, and a Look Back at History
-20- The Job Hunt: Should I Stay or Should I Go?
-23- Resources: More Free Books
-24- Winter Programs 2026
-25- Monthly Word Game -26- What We're Reading -28- Notes on People -31- Near Term Event Calendar -32- Newly Listed Public Health Jobs
-36- Marketplace - Sponsored Jobs & Events
Did you miss last month’s issue? Read it here: https://tinyurl.com/ettxsd97 or here: https://tinyurl.com/48pp3yek
Rethinking Autism's Origins Beyond the Genome
Author: Bruce Lanphear, MD, MPH
NOTE: This article was originally published on March 25, 2025 by Plagues, Pollution & Poverty on Substack.
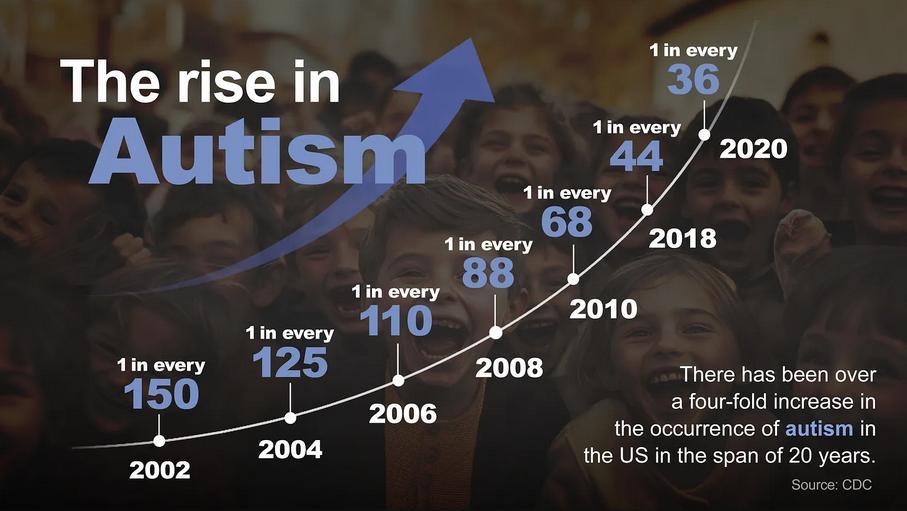
The spike in autism over just one generation is hard to ignore. In 2000, the rate among 8-yearold children was 1 in 150 children in the US. In 2022, the incidence among 8-year-old children is 1 in 32. That spike can’t be fully explained by changes in diagnosis, growing awareness or genetics; genes evolve slowly on the scale of hundreds to thousands of years. Those factors matter—but they don’t tell the whole story. Something else is happening, and we need to look harder at the world around us.
For 30 years, I’ve studied how toxic chemicals lead, air pollution, pesticides affect children’s brain development. My wife, a developmental pediatrician, works with children with behavioral conditions, including autism. Like many people drawn to this field, we have a personal stake: our granddaughter has autism.
The Limits of Genetics
Most autism research has focused on genes. Twin studies are often cited: identical twins are more likely to both have autism than fraternal twins. From that, people often say autism is “80 percent genetic.” It sounds like genes are the main cause but that’s a misunderstanding. The number doesn’t mean genes cause autism in 80 percent of cases. It means that, in today’s world, genes help explain who develops autism. Change the
environment, and that number could change too.
If everyone is exposed to the same stew of chemicals, then genes appear to matter more than environment. But most children who are genetically vulnerable only show symptoms when exposed to certain environmental triggers.
This is where most genetic studies fall short. They rarely ask how genes and environment interact. It’s like listening to only one half of a conversation and calling it a full story.
And yet, the genome has remained an alluring place to search for answers. Rare genetic mutations account for only 5 to 10 percent of autism cases. More common variants may raise the risk, but if they’re so common, why doesn’t everyone develop autism? The answer: genes don’t act alone.
A child may inherit a vulnerability, but whether it is expressed depends on what the developing brain is exposed to during development. That’s where genes and environment meet and where we should be looking.
A Toxic World
We’ve learned some hard lessons from environmental disasters. Lead, mercury, PCBs were once considered safe. Now we know they can damage the developing brain in ways that lasts a lifetime.
Today, we’re all exposed to hundreds of synthetic chemicals. Some of them pesticides, - Autism cont'd on page 4
air pollution, flame retardants, PFAS (so-called “forever chemicals”) are known to interfere with brain development.
Over the past two decades, scientists have discovered troubling links between prenatal exposure to toxic chemicals and autism.
Take air pollution. Numerous studies have found that children with the highest prenatal exposure especially from traffic are more
likely to have autism. One study found that children with the highest prenatal exposure were twice as likely to be diagnosed with autism. Pollutants like nitrogen dioxide and polycyclic aromatic hydrocarbons can inflame the developing brain and alter its chemistry.
Pesticides tells a similar story. Chlorpyrifos, once widely used in homes and still used in agriculture, harms the developing nervous system. Children born to mothers living near
fields sprayed with chlorpyrifos and glyphosate had higher autism rates.
Phthalates, found in plastics and personal care products, disrupt hormones and are particularly risky during fetal development. Higher prenatal exposure, especially in boys, has been linked to autistic traits.
Different chemicals, same pattern: exposures to toxic chemicals during critical stages of brain development appear to raise the risk of autism.
Folate: A Line of Defense
Amid the risks, one protective factor stands out:
folate, or vitamin B9. It’s essential for DNA synthesis and brain development. Women who take folic acid before conception or early in pregnancy lower their child’s risk of autism.
Many forces can block folate or make it less available. Maternal diabetes or infection which increase the risk for autism—stress the body and make it harder to use folate efficiently. Some genetic variants reduce the body’s ability to process folate. Some chemicals interfere with how folate works. Valproic acid (an anti-seizure drug which was linked with autism), tobacco
- Autism cont'd on page 5
smoke, and arsenic can block or deplete folate. When these factors combine, the risk of autism rises sharply.
A Wider Lens
When studies examine both genes and environment together, the signals grow stronger. When a high-risk genotype met a highrisk exposure—like air pollution or no prenatal vitamins the risk of autism rose threefold to sevenfold. That’s the kind of gene-environment interaction we should be studying more closely.
But most studies aren’t designed that way. We’ve been searching for autism triggers with a microscope; we need a wider lens.
Enter the exposome the total sum of environmental exposures we experience throughout life, starting before birth. Chemicals transfer across through the placenta and shape the brain in ways we are just beginning to understand.
Maybe we’ve been looking in the wrong place. Maybe what’s “hidden” isn’t deep in the genome it’s in the space between our genes and the world we’ve made.
Asking Better Questions
The real mystery isn’t whether the environment matters. It’s why we’ve been so reluctant to study it seriously. Genes feel safe—impersonal, fixed, beyond our control. The environment is messier. It forces us to ask harder questions about responsibility. It leads us to industry practices, weak regulations, and who should be held accountable.
If we want to understand autism in all its complexity, we need to ask better questions. What’s in our air? Our water? Our food? Our
homes? Our bodies? Who bears the greatest burden of exposure and who gets to avoid it?
The next chapter of autism research must begin at the intersection of biology and chemistry, where genes meet the chemical world.
We don’t need to wait for perfect knowledge to act. We already know enough to reduce the risk or severity of autism, ADHD, and other brainbased conditions:
► Start folic acid or folate supplements before or early in pregnancy
► Avoid tobacco and alcohol
► Minimize exposure to traffic pollution
► Use HEPA air cleaners in the home
► Choose organic foods when possible
► Limit pesticide use around your home
► Avoid heavily processed foods and plastic packaging
Of course, not every family has equal access to these choices. And even people like me who study toxic chemicals can’t protect our grandchildren. That’s why personal action must be paired with public policy. We need to modernize chemical safety laws, tighten pollution limits, and invest in safer alternatives. We need to treat early brain development as both a public health priority and an issue of environmental justice.
We’ve spent decades fixated on genes. It’s time we turn our attention to the environment—and how it interacts with those genes to understand what’s really going on and what we can do to change it. ■
For more content like this, please visit Plagues, Pollution & Poverty on Substack.
Author: M.A. Soto, PhD
November 10, 2025
Reader Opinion COVID Revisionism to Public Health Intelligence
Five years after the start of the pandemic, In Covid’s Wake: How Our Politics Failed Us by Stephen Macedo and Frances Lee compellingly argues that the American political system failed to take collective actions in response to COVID that balance the benefits and harms of public health interventions. This analysis has gotten a lot of attention, for instance in the New York Times Daily podcast, where the focus became "Were COVID-19 lockdowns worth it?" (their answer was “no”). To some, this book has come to define the conventional wisdom about public health: “intellectual malpractice and authoritarian impulses infecting governmental, scientific, academic and media institutions.”
Macedo and Lee’s revisionist history, however, is seriously biased. While their analyses have a kernel of truth, the public health science side is not clearly presented. This is unfortunate because their larger point about how the challenges of developing public health policies and some thoughtful solutions they propose may be lost to epidemiologists and public health scientists.
Summarizing, updating, and expanding on my detailed analysis of In Covid’s Wake, this commentary addresses the problems in the book, but also proposes a public health strategy to implement Macedo and Lee’s call for a policy process that recognizes uncertainty, respects evidence and its limits, and acknowledges legitimate differences in values and preferences.
Did non-pharmaceutical interventions work?
Macedo and Lee argue that U.S. policymakers abandoned evidence that non-pharmaceutical interventions (NPIs) did not work and implemented widespread lockdowns without consideration of the social and economic costs. Nowhere in the U.S., however, were restrictions as severe as in China or Italy, and the most severe restrictions were eased by the summer. Moreover, the NPI literature did recognize that well-chosen combinations of NPIs could limit the speed with which a pathogen spreads through the community and discusses the practical feasibility of implementing NPIs and their potential social and economic side-effects.
The authors provide a simple statistical analysis to show that lockdowns (their shorthand for all NPIs) did not work. However, the global literature now shows that stringent implementation of combinations of NPIs were effective in some countries in reducing the transmission of COVID-19. In the U.S., approximately 300 thousand deaths could have been averted before February 2021, when vaccines became widely available. This suggests that public health interventions – generally short of lockdowns – did save many American lives. State-level disparities in mortality rates are shaped by multiple variables ranging from demographic, socioeconomic, and racialethnic characteristics to access to health care and the prevalence of health behaviors and preexisting conditions but these calculations
- Covid cont'd on page 7
show that partisan choices made by state policymakers and the public are likely to have contributed to substantially higher mortality during the pandemic.
Did public health policymakers ignore social and economic consequences?
Macedo and Lee’s argument about the failure of the American political to adequately consider the harms of public health interventions is largely based on the response to the Great Barrington Declaration. This document emphasized the harms of lockdowns and called for a “focused protection” strategy emphasizing the most vulnerable, but offered no concrete plans for implementing these ideas. According to Macedo and Lee, a consensus emerged among Blue state policymakers and opinion leaders against those who argued for greater attention to the costs of businesses and school closures and hardened into dismissal of dissent. The authors maintain that Blue state policymakers and opinion leaders gave little consideration to these costs, in some cases hardening their positions into dismissal of dissent.
It is true that intemperate language from some government officials can be cited. But the response to the Declaration cannot fairly be characterized as a broad dismissal of the costs of NPIs or as a “jeremiad” against its authors. Rather, public health officials and scientists explicitly recognized the social and economic costs. Moreover, their position papers critiqued the Great Barrington Declaration on scientific and practical grounds, making the case that limited restrictions – not “lockdowns” – could reduce transmission rates until a vaccine was available.
I closely followed the experience of several states and local areas as well as universities in developing responses to the pandemic. In
Available on Amazon https://a.co/d/j0qU1Qy
contrast to Macedo and Lee’s contentions, Blue state policymakers and opinion leaders seemed acutely aware of the harms of restrictions on social gatherings and sought to identify the least restrictive policies that would meet public health goals. They also sought to address the inequities that were amplified by the pandemic. The Trump White House, on the other hand, seemed to be concerned only with social and economic costs.
Macedo and Lee do have a compelling case when it comes to schools, which were slower to re-open in Blue states and cities. The authors attribute this to Democratic politicians and the undue influence of teachers’ unions, but the scientific and general literature published in the summer of 2020 is remarkably well balanced, with the likely harms and limited public health benefits both clearly identified. And survey data suggest that while Democrats were slightly more concerned than Republicans about academic and social harms, they were far more concerned about their children getting sick while attending in-person school and supportive of online learning. It is also easy to understand that Democrats might not trust a White House that consistently downplayed the
threat of COVID-19, and promoted horse medications and bleach. In other words, decision makers were trying to balance of benefits and harms in the face of uncertainty, just as they should.
Declining trust in public health
What could explain the partisan difference in perceived risks Leonhardt documents when the actual risks could not have been substantially different? One possibility is that, starting in the summer of 2020, rather than facing up to the challenges of choosing public health policies that balance benefits and harms, some Republican leaders gave more credence to experts who minimized the risks of COVID-19 and questioned the efficacy of NPIs and later vaccines. It was easier, for instance, to say that “masks don’t work” than “the inconvenience does not justify the benefits.” Or that vaccines are ineffective and unsafe rather than the benefit to the community is not worth the loss of “freedom.” Experts who supported mask requirements or vaccine mandates were not to be trusted.
As Francis Fukuyama wrote at the beginning of the pandemic, when confronted with a novel virus for which there is no treatment or vaccine, the most effective way for a government to protect its citizens is by convincing them to take measures to protect themselves and one another. Compliance with government guidance depends on citizens’ confidence that the government is trustworthy, that it knows what it is doing and is acting for the common good, and that public health programs will be administered fairly and competently. But as the pandemic progressed, we argued about the science rather than facing up to value choices, undermining trust in science and public health.
In support of this hypothesis, Oreskes and Conway note that the public's level of
confidence in science has been falling slowly for decades, with Republicans and Democrats having similar attitudes. During the first years of the pandemic, however, the parties diverge sharply. This suggests that conservative hostility toward science is rooted in conservative hostility toward government regulation of the marketplace, which has morphed in recent decades into conservative hostility to government across the board. Science – particularly environmental and public health – became the target of conservative antiregulatory attitudes. Distrust of science therefore, is mostly collateral damage, spillover from carefully orchestrated conservative distrust of government.
Since the pandemic, the view of public health captured in Macedo and Lee’s book has been used to justify efforts to dismantle public health agencies and limit their authority, sometimes with words far harsher than anything uttered against the Great Barrington Declaration.
From “follow the science” to public health intelligence
Macedo and Lee are right that “we must not forget the deepest values of liberal democracy: tolerance and open-mindedness, respect for evidence and its limits, a willingness to entertain uncertainty, and a commitment to telling the whole truth.” Going forward, policy makers and public health officials need to better communicate the need for collective action and develop processes to engage with the community about the value tradeoffs involved, especially when the benefits and costs are unequally distributed. Public health scientists must understand that “follow the science” is not enough.
Beyond differences in values, however, public
health policy design should also reflect uncertainty about transmission risks (e.g aerosol vs. droplet transmission) or intervention efficacy (masks) and differences in the epidemiological context (New York City vs. Idaho in March, 2020, or nursing homes vs. schools). Optimal policy, therefore, requires better “public health intelligence.”
There is always uncertainty about how a pathogen is transmitted, the efficacy of control strategies, their social and economic costs, and other factors, and how these facts change over time. However, during the pandemic, we spent far too much time and energy arguing about whether SARS-CoV-2 was transmissible through aerosols, whether masks and vaccines “worked,” and the potential benefits and harms of control policies. The lingering uncertainty created an opportunity to argue about the science rather than address the balance of benefits and harms, or how they were distributed. To address this problem, public health agencies should be more proactive in creating and updating risk assessments to clarify what is known and unknown. And rather than simply analyzing existing studies, or waiting until uncertainties subside, they should conduct or commission laboratory and epidemiologic studies to fill in gaps.
Furthermore, the Centers for Disease Control and Prevention (CDC) should work with state health departments, hospitals, and others to provide accurate, standardized surveillance systems for outbreak detection and situational awareness. In addition to better integrating existing data, this effort should include developing and fostering systematic implementation of population surveys, wastewater surveillance, and other new systems to track both epidemiologic trends and social and economic consequences.
Public health intelligence requires resources and perhaps enhanced legal authorities. Monitoring the avian influenza now circulating in America’s poultry flocks and dairy herds, for instance, demands more than voluntary case reporting; public health agencies must have the authority to survey agricultural workers as well as conduct bulk testing of milk. This will not be easy to achieve in the current political environment, but reframing public health as an information agency rather than a policymaking body might provide a path forward. Although this shift in emphasis will not convince everyone, at least it might lead to better informed policy decisions for those who recognize the need for better intelligence. ■
Michael A. Stoto, PhD, is a Professor Emeritus in the Department of Health Management and Policy, School of Health, Georgetown University. He is also an adjunct professor of biostatistics at the Harvard T. H. Chan School of Public Health. Dr. Stoto has an AB from Princeton University and a PhD from Harvard University, both in statistics. A statistician, epidemiologist, and health services researcher, his research focuses on public health systems, especially with regard to emergency preparedness, infectious disease policy, drug and vaccine safety, and global health security. During the COVID-19 pandemic, his research has focused on surveillance and data systems and other aspects of public health policy and practice from the local to global level. Dr. Stoto also worked with the European Centre for Disease Prevention and Control (ECDC) and the University of Bologna on the assessment of public health emergency capabilities during the COVID-19 pandemic and the implications monitoring and assessment of public health emergency preparedness.
Explaining Epidemiology to Middle Schoolers
"The Disease Detective"
Editor's Note:
If you're shopping for the holidays and have a 9-12 year old on your list this might be a gift to consider. In story format the author explains what epidemiologists actually do.
"Rosie Franklin loves a good mystery but never expected one to hit so close to home.
The day after Brown Intermediate's annual field day festival, three of Rosie's classmates are out sick. The next day, three more students are missing from class, and then another the following day. While the rumors fly, nobody knows what is making the students sick.
Luckily for Rosie, her Aunt Liv is an epidemiologist-a disease detective. Rosie learns that unraveling the mystery gets more difficult as time passes and the stakes grow higher. It is up to Rosie to grab her best detective fedora, lean into her curiosity superpower, and join forces with friends (and an arch-nemesis) to reveal the illness' true identity.
We follow Rosie to school, a disastrous softball game, and even a public health laboratory as she learns more about both epidemiology and herself on her first adventure as a disease detective." - Amazon.com
Available on Amazon in Kindle & Paperback https://a.co/d/6qGUIGf
While the journey to becoming an epidemiology novelist is unlimited in scope and experience, a fairly essential starting point includes believing you have something publication-worthy to say. If you read nothing else in this article, I hope you leave with the renewed sense that we all have worthwhile stories to tell.
Author: Elyse Fritschel
I can't imagine a more fitting way to begin an article about writing than by quoting one of the most celebrated modern authors (and one of my father's personal favorites), Stephen King:
"There's a saying – 'Write what you know.' It's bad advice if you take it as an unbreakable rule, but good advice if you use it as a foundation."
As a brief personal introduction, I am an epidemiologist and Director of Infection Prevention at Tufts Medical Center. As of October 2025, I also became a published middle-grade epidemiology mystery author. Like many of my Millennial cohorts, I do not remember receiving much, if any, formal education around epidemiology until my postsecondary years as a Biology major at the University of Texas. While efforts to improve scientific literacy in the field of epidemiology
- Detective cont'd on page 11
have increased in the last few decades (and have received an enhanced focus in the wake of the COVID-19 pandemic), it is still an emerging topic of interest in public school settings. As the needle slowly moves from essentially no epidemiology education to punctuated pilot modules or a topic to integrate in other core subjects (e.g., science, math) to more substantial/standalone course content, I can't help but think about other ways of introducing the field to younger generations.
Epidemiology professionals are no strangers to navigating health communication nuances to the public. We often distill complex scientific processes into accessible and actionable content which is sensitive to the lived experiences of diverse communities. Fiction, though typically seen as a separate domain from public health communication, can be an equally powerful vehicle for engagement. Stories allow readers to imagine themselves in roles they may not have considered before. For the purpose of my story, the mystery genre lent itself well to the process of guiding young readers through the basics of disease transmission, outbreak investigation, and evidence-based reasoning. Fiction does not replace formal education, of course, but it plants the seeds of curiosity. Perhaps for some children, exposure to a compelling fictional protagonist is at least as influential as exposure to formal classroom content.
Before I learned about epidemiology in college, I was transfixed by Richard Preston's The Hot Zone in middle school. I also loved stories with smart, independent female protagonists, like Anne Shirley and Nancy Drew. While performing some cursory research for this article, I learned that since 1930, Nancy Drew and her deductive reasoning skills have been inspiring readers like Hillary Clinton, Judy Blume, Oprah Winfrey, and Supreme Court Justices Sonia Sotomayor and
Ruth Bader Ginsburg. In the words of Billie Jean King, "If you can see it, you can be it." As I thought about the desire to get younger generations curious about epidemiology, I considered the potential impact it could make on children if epidemiology had its own Nancy Drew. What if more epidemiology professionals could discover their calling earlier in life?
Shortly before the pandemic started, I was inspired to write the contemporary epidemiology mystery novel I wished had been available when I was younger. I knew I wanted to focus on an infectious disease with gastrointestinal symptoms since children seem rather universally fascinated by poop and associated bathroom humor. After witnessing the societal burnout that followed from the COVID-19 pandemic (and experiencing a little of it as a healthcare leader), I'm considerably relieved I didn't change course during the writing process.
Crafting the protagonist was equally important. I wanted a character who was relatable, curious, and resilient. Someone who approached problems with tenacity rather than genius-level giftedness. I drew inspiration from the bright, determined, unapologetically strongwilled girls and women in my life who embody the type of protagonist I would have gravitated toward as a young person. Rosie, my main character, became a touchstone for many narrative decisions, guiding the tone, pacing, and emotional authenticity of the story. Balancing creativity with scientific accuracy posed its own set of challenges. Epidemiology, particularly at the middle-grade level, required careful calibration. Too much jargon and the narrative became inaccessible; too little, and the story lost a bit of its educational value.
I spent time thinking through the mechanics of clues, how to embed realistic (but simplified) versions of case investigations, and how to show epidemiological reasoning without overwhelming young readers.
While balancing a more-than-full-time job during the pandemic, it took me approximately one year to finish writing my 84-page middlegrade mystery novel. Al though the operational demands of healthcare Infection Prevention left relatively little energy for creativity, writing became a source of grounding for me. I made the wise decision to include family, friends, and children in the middle-grade age range as reviewers, and I paid for an editor before I knew whether I would self-publish. Although I ultimately signed a contract with a traditional publishing company with editors of their own, this is a decision I would repeat every single time. I began the querying process to find a publisher who might be interested in the book and able to work with an agent-less author in December 2022 and ultimately signed a contract in early 2024. While this process certainly varies in duration for authors, it's important to prepare for rejection and keep track of sent/received communication. After the contract was signed, it took over a little over 18 months for the book to be published. I am currently in the marketing phase, so it is certainly a labor of love and a journey that never truly ends.
In an effort to demystify the process of publication, I find it interesting to reflect on the volume of literature being churned out worldwide. The United Nations Educational, Scientific, and Cultural Organization (UNESCO) estimates that approximately 2.2 million books are published each year, or a little over 6,000 books per day. While Amazon's Kindle Direct Publishing (KDP) limits the number of daily
published titles to three in order to manage the volume of low-quality and AI-generated books, there is a wealth of content available from a wide array of sources. Furthermore, unless an author publishes their book through a large traditional publishing agency, they will likely encounter several system-level barriers in retail and marketing access. Authors who self-publish or publish under smaller agencies generally need to hustle locally to obtain retail shelf space since it is difficult to project their demand. Large publishing agencies have publicists with media relationships, established influencer and reviewer networks, and advertising budgets. Without access to those resources, authors can find themselves paying for ads, running their own social media, and cold contacting media personally. While this is all technically achievable, it is considerably more laborintensive and expensive for the author. Books published via large publishing agencies benefit from source credibility bias as well. Some prestigious literary awards will exclude indie/self-published book titles from consideration entirely (e.g., Pulitzer, Booker, Newbery, Caldecott, etc.).
These realities are not meant to discourage but to contextualize. While this may not be the case for everyone, understanding the current landscape of the book industry helped me manage my expectations and prioritize my time on the elements of publishing and distribution that mattered to me personally. I do not expect to become a full-time novelist; I identify as an epidemiologist so strongly that I can't imagine pivoting too much at this stage in my life. I've focused my efforts on marketing to local bookstores, libraries, and schools and remain open to adjusting my plan as needed.
- Detective cont'd on page 13
My hope for the book (and for any future epidemiology-focused fiction) is that it encourages readers to view public health not as an abstract institutional entity but as a dynamic, exciting, human-centered field filled with problem-solvers, investigators, and advocates. Additionally, representation profoundly matters. When young readers see characters who investigate disease mysteries, use evidence to solve problems, and engage with their communities constructively, they may begin to imagine themselves capable of the same.
For epidemiology professionals or enthusiasts interested in writing, I encourage you to explore the narrative potential of your own experiences. Epidemiology certainly offers no shortage of compelling stories. When you reach the publication finish line, do not hesitate to reach out to fellow colleagues to review or otherwise amplify your message. Accurate and engaging science communication is incredibly important, and epidemiology thrives on collaboration. ■
Elyse Fritschel is an epidemiologist who was raised in Texas and currently works at Tufts Medical Center as the Director of Infection Prevention. With over ten years of experience in non-profit academic medical center and public health settings, she has developed a well-rounded skillset in preparing for and managing public health emergencies, developing strategic communications, building strong relationships with area stakeholders, and utilizing data-driven strategies to address complex issues and achieve meaningful change. Her former role as the Mishap Program Manager at the NASA Jet Propulsion Laboratory broadened her understanding of emergency management at the federal level as well. When she isn't working, she can generally be found hiking, playing pinball, searching for the best desserts wherever she goes, or spending quality time with her cat, Merlin.
Do You Have A Book You Want To Publish?
Publishing & Communications, Inc. can assist in all phases of the process. Whether you need an editor, want to market your book, need to convert it to a digital format, understand how to print copies and sell on Amazon or just determine if there's a market for your work - we can help. For more information please contact:
Routine Vaccinations, Sanitation, and a Look Back at History
Authors: Katelyn Jetelina, PhD, MPH
Kristen Panthagani, MD, PhD
Editor's Note: This article was originally printed in Your Local Epidemiologist on October 2, 2025. To read more content from this source subscribe to Your Local Epidemiologist (YLE): https://tinyurl.com/47494ms4
There are many great questions as well as confusion and doubt swirling around routine vaccinations. We’re seeing things like: I know vaccines have saved many lives, but does everyone really need them now?
In many ways, vaccines are victims of their success. Given the drama and polarization surrounding vaccines, it can be hard to find answers that aren’t simplistic, defensive, or angry. And, as everyone discovered during the
pandemic, disease risks are often not uniform.
Here are a few of your top questions answered!
Note: Paid subscribers can download a PDF of the top 14 FAQs on routine vaccinations at the bottom of this email. I co-created it with grassroots MAHA leaders. Print it, share it, or just doodle on it your call.
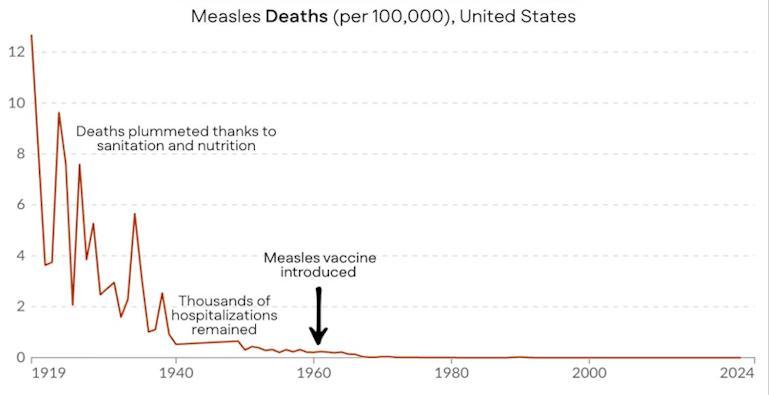
“Did sanitation and nutrition decrease measles, or was it vaccination?”
It’s true that measles deaths fell dramatically before the vaccine was introduced. Improvements in sanitation, education, nutrition, and advances in medical care made a real difference in public health over the past century, and we shouldn’t minimize that. But this graph of measles deaths alone tells only part of the story.
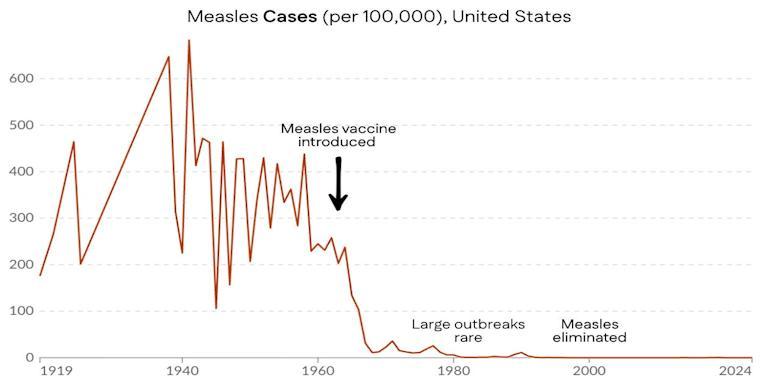
While measles deaths plummeted during the first half of the 20th century before vaccination, measles infections did not. But once the measles vaccine was introduced, cases declined precipitously.
Data: Our World In Data; Annotated by Your Local Epidemiologist
That’s because measles is different from viruses like flu or Covid-19. The virus hasn’t changed much since the 1960s, and it replicates slowly and deep in the body. This makes the vaccine uniquely powerful: it doesn’t just reduce the risk of severe disease, but prevents infection itself.
This is important because the infection has profound effects, even if you survive: hospitalizations, hearing loss, immune amnesia (i.e., wiping your immune system memory of all viruses), and other long-term consequences. Death is not the only outcome we want to avoid.
We were reminded of this in a heartbreaking way just last week. A child who caught measles at 12 months old too young to be vaccinated died years later from SSPE, a rare but devastating brain disease caused by the virus.
So, sanitation and nutrition did make a big impact on reducing measles mortality, but they didn’t do the whole job. When the vaccine was invented, it allowed us to eliminate measles from the U.S. Thankfully, we don’t have to choose between appreciating the historical impacts of sanitation, nutrition, and vaccination. In public health, they’re all important.
“Why are vaccines mandated for diseases that aren’t endemic, like rubella?”
Rubella is the “R” in the MMR vaccine. It’s caused by a virus that spreads in airborne droplets from coughing or sneezing. It’s not endemic in the United States anymore. So yes, the risk is extremely low. Yet the vaccine is required for schoolchildren in all 50 states (soon to be 49 states, with news from Florida). Why?
Think of population immunity like a dam built to prevent flooding. Once it’s built, we won’t have flooding anymore. But if the next generation comes along and says, “Hey, there’s not flooding anymore do we really need this dam?” and decides to get rid of it, the flooding would return quickly.
Rubella is still alive and well in other parts of the world. In the U.S., we have rubella cases yearly, but only from international travelers. However, outbreaks don’t happen often in the U.S. because population immunity an invisible shield stops them in their tracks. In other words, vaccination is the reason rubella isn’t endemic.
Once a virus is eliminated from the planet and poses no risk of returning such as smallpox we stop vaccinating against it.
“Currently in the U.S. the probability of
getting measles is very low. If we consider that, do the vaccine’s benefits still outweigh risks?”
Yes, because fighting against infectious diseases is a team sport.
Individual decisions to get vaccinated changes the risk-benefit calculation for everyone. In other words, your probability of encountering measles is low because so many people around you are vaccinated.
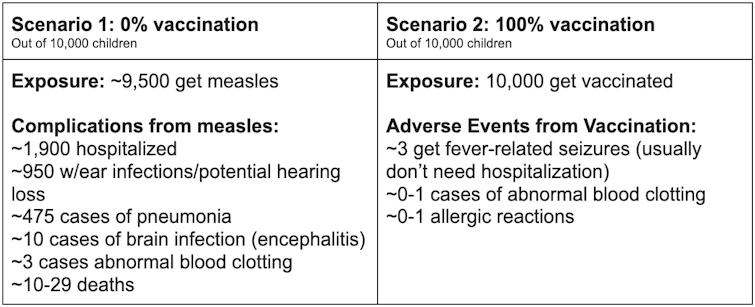
But you’re right the risk of exposure makes a difference. Let’s look at two scenarios: nobody vaccinated and everybody vaccinated. Before the measles vaccine, nearly every child in the U.S. got measles by age 15, because it’s so contagious. So risk of exposure was near 100% (to be conservative, say 95%). At 100% vaccination, the risk of measles goes to zero. Here’s what we get after accounting for exposure risk during childhood:
- History cont'd on page 17
Is there a situation where the probability of an individual getting a complication from measles infections roughly equals the likelihood of an adverse event from a vaccination? The math to calculate this is really tricky it depends on not just vaccination coverage, but the risk of an outbreak, the density of the population, the size of an outbreak, etc. Even if this scenario happened, the average vaccine side effect isn’t equivalent to the average measles outcome for example, fever-related seizures, while understandably scary to watch, fortunately often don’t require hospitalization or result in long-term problems.
At the community level, the benefits of measles vaccination far outweigh the risks.
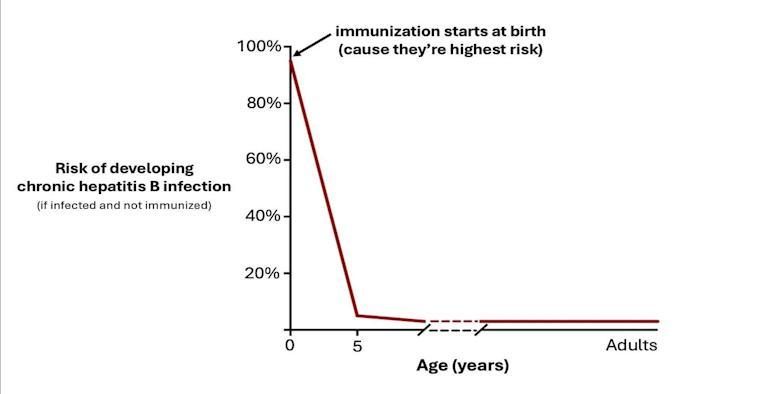
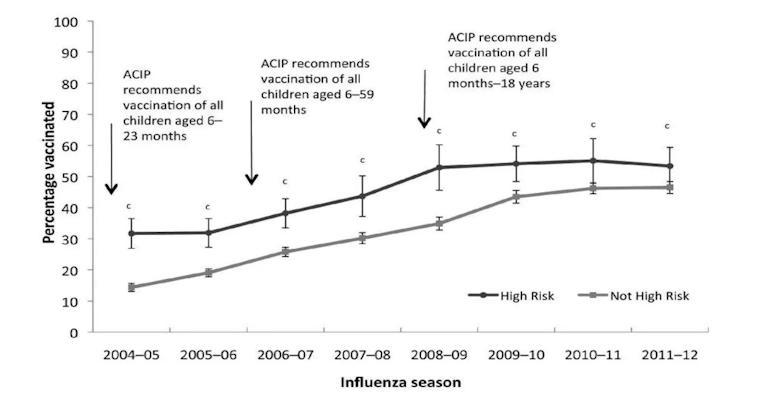
“Could you comment on babies getting the hep B vaccine even if they aren’t high risk?”
The highest risk factor for Hep B (or HBV) is a history of sexually transmitted infections or multiple sex partners. So, if you’ve only had one partner for a decade, is this even applicable to your baby?
Yes, because the hep B virus is a tricky booger:
1. “High risk” routes aren’t the only way of catching it. IV drug use and sexual contact aren’t the only ways hepatitis B spreads. Over a quarter of new hepatitis B cases detected in 2022 had no known risk factor or exposure. This virus is very stable in the environment (can stay infectious for days on surfaces) and only a very tiny dose is needed to cause infections (which means it can be shared through casual contact, like sharing a toothbrush).
2. Many people who are infected don’t
2. know it. If we rely on moms to self-report hepatitis B infection, we will miss many cases. It’s estimated about half of people in the U.S. with hepatitis B don’t know they have it.
3. Screening isn’t a perfect tool. While screening moms for infection during pregnancy is highly recommended, inevitably, not every mom is screened (and some may catch it after screening), leading to missed infections. About 12% of mothers with commercial insurance and 16% of mothers with Medicaid aren’t screened appropriately, not to mention mothers who don’t have insurance for prenatal appointments.
4. Transmission from mom isn’t the only way babies get it. Some reports suggest that infants may catch it from other family members, such as fathers who carry the virus. Family members aren’t routinely screened, so these infections would be missed.
5. The outcomes can be severe. Mother-tobaby transmission at birth is the most common cause of chronic HBV infection, which can lead to liver cancer, liver failure, and death. If babies contract hepatitis B disease near birth, 95% develop the chronic form. Importantly, moving out the hepatitis B vaccine to 4 or 12 years old (instead of the historical recommendation of infants), misses the window of risk.
- History cont'd on page 18
from You Can Know Things
The HBV vaccine induces protective immune responses in nearly everyone (80-100%). The vaccine risks are extremely low: the only safety signal found is rare allergic reactions (1 severe allergic reaction for every 2-3 million doses).
So, all babies have been recommended to get the vaccine at birth. In the 1980s, before the universal birth dose was recommended in 1991, about 18,000 children under age 10 were infected with hepatitis B each year—half of them at birth. Today, thanks to universal vaccination, CDC reports fewer than 20 cases per year (though modeling suggests the true number is still several hundred).
“Why does the U.S. have sweeping recommendations when other countries have more targeted vaccine recommendations?”
It’s fair to wonder why. We are all high-income countries. We all have the same vaccines. We are all looking at the same data. How could public health officials come to different
conclusions across countries?
Three main reasons:
1. Behavioral. Universal vaccination recommendations work better than targeted vaccinations because of convenience and increased awareness. The U.S. used to have targeted hep B vaccine recommendations, but uptake was poor. After a universal recommendation, there was a big decline in disease, and many lives (and livers) were saved. The same thing happened with the flu vaccine; universal recommendations increased uptake among high-risk groups.
- History cont'd on page 19
Figure
2. Financial. Many countries’ governments pay for vaccines, so the cost-benefit analysis is a big consideration when making policy decisions. For some countries, it would be too expensive for the government to vaccinate everyone, so they try to find where the money will have the biggest impact.
3. Safety net. The U.S. has much less wiggle room because of worse health care access, social support, health care capacity, and health. Casting a larger net through universal vaccine recommendations is more critical than in other countries. I’ve covered this in another YLE post.
Bottom line
The effect of vaccines is often invisible infections prevented, childhood deaths that never happened. It’s essential to remember why we do what we do. Improved sanitation, pasteurization, nutrition, and other advances in medical care (like the development of antibiotics) also made a huge impact in reducing childhood mortality during the 20th century. Thankfully, we don’t have to choose only one!
■
Kristen Panthagani, MD, PhD is an emergency medicine physician completing a combined residency and research fellowship focusing on health literacy and communication. She is the creator of the newsletter You Can Know Things and a regular YLE contributor. Views expressed belong to KP, not her employer.
The Job Hunt Should I Stay or Should I Go?
Author: Public Health Hiring Help
NOTE: This article was originally published on October 6, 2025 by Public Health Hiring Help on Substack.
Well, we’ll address the elephant in the room we’re starting the week still in the midst of a government shutdown.
It’s yet another moment of frustration, of challenge, of fear, of doubt in the landscape of public health.
Up until now, I’ve had many conversations with friends, colleagues, and peers about the “viability” of entering the public health job market and workforce. I still say it is, even now. Heck, this page was created with the idea that despite all obstacles making a difference in public health IS possible.
It’s easy to be discouraged by current events and the rhetoric surrounding them. It’s easy to feel like your public health dream is now a pipe dream. But let me be clear it’s not.
But don’t just take my word for it! We’re back with The Public Health Burnout Coach, Marissa McKool, MPH, to discuss the fear, doubts, and voices in your head trying to tell you that using your public health knowledge isn’t possible.
How do we conquer them? How do we change our mindset? How do we charge forth, even in spite of the setbacks? Marissa McKool has the answers!
PHHH: Let’s get right into it. I think the question on so many folks’ minds as of late is “Do I stay in public health?” What do you tell clients who ask you that?
MM: The first thing I say is: that’s only a question you can answer. Everyone will have opinions, but you’re the one working those 40 hours each week. Some powerful questions to reflect on are:
If I knew public health would improve in a year, what would I do today?
If I knew I could love my job in either public health or another sector, what would I choose and why?
What am I hoping to achieve by making this decision?
I also remind my clients that burnout and challenges exist in every sector. If you’re leaving public health just to escape stress, you’ll be disappointed because challenges show up everywhere. Instead of running from your current stress, the best investment you can make is learning how to reduce your current stress and face your challenges with less overwhelm. That requires tools we were never taught in school, but they’re learnable. If you’re leaving public health for reasons other than stress, that’s valid. But if stress is the only reason, changing jobs won’t solve that problem. You have to solve that problem by learning how to reduce your stress no matter the external challenges.
- Job Hunt cont'd on page 21
PHHH: I think, for a lot of folks considering transitioning out of traditional public health to private sector gigs, there’s this stigma/guilt around being a “sell-out”, but that’s so far from the truth. How do you remind clients that it’s okay for change in any direction?
MM: The “sell-out” narrative is unfair and outdated and thankfully, it’s starting to shift. I remember in grad school hearing people joke, “You’re going to the dark side.” But the truth is, the private sector has a lot to offer. They excel at marketing, communication, and strategy— skills we can learn from. These roles often come with valuable growth opportunities and new perspectives.
Transitioning to the private sector, tech, consulting, or any other space doesn’t erase your passion for public health. You can still make an impact on the world, often in new and innovative ways. Many clients find their skills transfer beautifully and create fresh opportunities to serve. Change is part of growth. Giving yourself permission to pivot doesn’t diminish your commitment to service it expands it.
Back by popular demand, Marissa McKool chats all things uncertainty and doubt and building the confidence and irrepressibility to combat them.
PHHH: From your perspective, where are these folks going? What do these positions look like?
MM: A lot of the roles look very similar to traditional public health jobs just with different titles. For example:
An epidemiologist in a state health department might become a principal researcher at a pharma company.
A project officer at a federal agency might become an implementation manager at a sustainability tech firm.
Health equity leads, strategy consultants, communications managers, and community engagement specialists are all in demand across tech companies, foundations, consulting agencies and the private sector. The skills and experience are the same. What often changes is the language. Adjusting your search terms and tailoring your resume to match the sector can make those opportunities much more visible.
PHHH: On the flip side, there are also folks who can’t see themselves doing anything else besides working at the state or local level or doing public health research, but they worry that this path just isn’t realistic right now. How can we encourage them to stick to it, despite the obstacles?
MM: First, notice the “all or nothing” thinking that can creep in. It’s easy to believe public health is disappearing, but that’s not true. Public health has traditionally resisted change and moved slowly, which can create fear when shifts do happen. But public health isn’t going anywhere it’s evolving.
If your heart is in government, research, or academia, you can absolutely stay. The key is adaptability. That means building resilience, embracing change, and taking ownership of your experience. Instead of falling into the “there’s nothing I can do” mindset, shift into “I have agency and influence over my path.” Learn to navigate challenges without letting anxiety or overwhelm take over. That’s what allows you to sustain your calling in the long term.
- Job Hunt cont'd on page
PHHH: There sometimes feels like so much finality with the choice to stay or not to stay right now, since the skills and experiences on your resume play a big role in your career and career journey. Like if I jump to a clinical research associate role in Pharma, for example, it’s going to be easier for me to stay in Pharma going forward than jump to another health-related field. Is that mindset limiting or is it just realistic? How do we make the best decisions today to help us down the line?
MM: Often, when we say “I’m just being realistic,” it’s a sign we’re limiting ourselves. Yes, certain career paths or sectors may seem more straightforward or linear and right now, they might even feel easier. But things can change quickly. Instead of focusing on what feels “most realistic,” put your energy into building your adaptability muscle. That’s what will keep you open to opportunities no matter how the landscape shifts.
The first step is accepting that the workforce is changing rapidly—and it’s not slowing down. The future of work is moving away from deep specialization in one narrow skill and toward generalization and adaptability. With AI and other forces reshaping the job market, what’s most valuable now are strong problem-solving skills, creativity, flexibility, and the ability to learn quickly. A great resource on this is The
Adaptation Advantage by Chris Shipley and Heather E. McGowan, which explains the four workforce revolutions and the one we’re in today. The takeaway: being adaptable and willing to grow matters far more than locking yourself into a single path.
PHHH: Obviously, this decision and all the other decisions involved in the job hunt— bring a lot of anxiety and frustration. Do you have any other words of advice to those tackling this, especially those so early in their careers?
MM: If you’re experiencing anxiety and frustration in the job search, now is the perfect time to learn how to manage those emotions. We often believe the job market causes our stress, but in reality, it comes from how we think about the job market.
Learning how to reduce the intensity of negative emotions will help you shift more quickly into confidence, calm, and focus. And it’s a skill you can carry with you wherever you go. Remember, a job search is just another problem to solve just like the challenges you’ll face in your next job. The problems themselves don’t create our emotions; our thoughts about them do. Once you know how to manage your mindset, it becomes much easier to solve the problems in front of you. ■
Marissa McKool, MPH The Public Health Burnout Coach is a coach, speaker, and trainer dedicated to helping women in public health do meaningful work without sacrificing their well-being. Drawing on 15+ years of leadership experience and her own journey through burnout, Marissa equips public health professionals with the tools to thrive while protecting their energy and health. Her unique approach combines evidence-based strategies, feminist coaching principles, and lived experience to create sustainable change.
Resources
More FREE Books!
Editor's Note:
In a recent issue we printed a list of books that were available online that was sent to us by a long time reader. When that article appeared another reader sent us the list below. Based on the interest the first list received we would like to continue printing lists like this. If you are aware of books others would benefit from, please send us a link so that we can publish that for everyone to be able to have access.
We are also interested in publishing book reviews. If you have a new book that you have read or written that you believes deserves to be seen by a wider audience please send us the information you have on it. If you're interested in reviewing books for the EpiMonitor, just drop us a line and we'll start a discussion to see what we can work out.
Causal Inference What If (2020) by MA Hernan and JM Robins
Survival Analysis using SAS, 2nd Ed (2010) by PD Allison
Exercises in Epidemiology, Applying Principles and Methods, 2nd Ed (2017) by NS Weiss
The Little SAS Book, A Primer, 6th Ed (2019) by LD Delwiche and SJ Slaughter
Resources
Winter Programs 2026
Editor's Note:
Looking for something to do this January or February? Looking for ski weather or beach weather? Want to study online? Want a change of venue - maybe even a different country? Regardless of what you want there's a winter (or summer if you're in Australia) program to meet your needs.
January 1 - 16
Title: Johns Hopkins Winter Institute
Sponsor: Johns Hopkins Bloomberg School of Public Health
Location: Baltimore, MD and Online
Website: https://tinyurl.com/5n7f5spu
January 19 - 24
Title: Swiss Epidemiology Winter School
Sponsor: Institute of Social & Preventive Medicine - Bern
Location: Wengen, Switzerland
Website: https://bit.ly/3qunYrg
January 19February 13
February 9 - 13
Title: Summer Program 2026
Sponsor: Australian Consortium for Social & Political Research
Location: Melbourne, AU and online
Website: https://tinyurl.com/y2xpcak5
Title: Winter School in Clinical Epidemiology
Sponsor: UMIT
Location: Tirol, Austria
Website: https://bit.ly/3lRZeDf
What's In A Title?
It's hiring season so this month's words come to us from our job listings. Good luck - don't let the easy words fool you!
For an interactive online version go to: https://tinyurl.com/yp9sz6xf
Words
1. Administrator 2. Analyst
3. Biostatistician
4. Coordinator
5. Data Specialist
6. Department Chair
7. Division Chief
8. Emeritus Prof
9. Epidemiologist
10. Faculty Member
11. Fellow
12. Intern
13. PostDoc
14. Professor
15. Program Director
16. Researcher
17. Scientist
What We're Reading This Month
Editor's Note: All of us are confronted with more material than we can possibly hope to digest each month. However, that doesn't mean that we should miss some of the articles that appear in the public media on topics of interest to the epi community. The EpiMonitor curates a monthly list of some of the best articles we've encountered in the past month. See something you think others would like to read? Please send us a link at info@epimonitor.net and we'll include it in the next month
Washington DC Chaos
♦ Working at the CDC Is a Living Hell - Gaslighting, surveillance, and layoffs under the RFK Jr. regime. (NY Magazine)
https://tinyurl.com/3vshjbbr
♦ Harvard’s Funds Are Back. Can Its Scientists Trust the Government Again? (Harvard Crimson)
https://tinyurl.com/yc8hfms2
♦ Epidemiologists Are Running for Office (The Atlantic via AppleNews)
https://tinyurl.com/yfhu7u3j
Public Health Topics
♦ New form of bird flu hospitalizes Washington state resident (LA Times)
https://tinyurl.com/2ep59eyk
♦ The Americas, led by Canada, are on the brink of losing measles-elimination status (STAT) https://tinyurl.com/mdjf4nyv
♦ Saskatoon epidemiologist calls to strengthen public trust as Canada loses measles elimination status (The StarPhoenix) https://tinyurl.com/yw7h7c25
♦ Officials declare health emergency as disease sweeps through major city: 'If we fail to act now, the situation could spiral' (The Cool Down)
https://tinyurl.com/hhw7e35s
- Reading cont'd on page 27
What We're Reading This Month
[Type a quote from the document or the summary of an interesting point. You can position the text box anywhere in the document. Use the Text Box Tools tab to change the formatting of the pull quote text box.]
- con't from page 26
Public Health Topics, cont.
♦ How a childhood virus can contribute to dementia later and what you can do (WAPO via AppleNews)
https://tinyurl.com/km5xcrfk
♦ No Evidence of Link Between Tylenol and Autism or ADHD, Study Confirms (Time)
https://tinyurl.com/mr4b9ptm
♦ Yellow fever and dengue cases surge in South America as climate crisis fuels health issues (The Guardian)
https://tinyurl.com/538umc93
♦ This virus infects almost everyone and it may lead to lupus (NatGeo via AppleNews)
https://tinyurl.com/mr4ausaj
♦ The states where more people are likely to die before turning 65 (WAPO via AppleNews)
https://tinyurl.com/mww6e2fj
♦ VIDEO Genetically engineering mouse DNA could be key to curbing Lyme disease (CBS 60 Minutes)
https://tinyurl.com/bdhsuufz
♦ Highly contagious virus experiencing resurgence in US... posing risk to food safety (Daily Mail)
https://tinyurl.com/bddzepf3
Notes on People
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Honored: Evelyn O. Talbott, Dr.P.H., M.P.H., professor of epidemiology at the University of Pittsburgh School of Public Health, received the prestigious John Snow Award from the American Public Health Association (APHA) and the Royal Society for Public Health in England.
Honored: Dr. Judith Rijnhart, assistant professor in the Department of Epidemiology at the USF College of Public Health (COPH), has been honored with the 2025 Early Career Epidemiologist Award from the American College of Epidemiology (ACE). Inspired by the mentorship she received, Rijnhart cofounded the Causal Inference in Public Health Research (CIPHR) Lab in January 2024. The lab provides students with opportunities to develop methodological skills and collaborate on research projects.
Honored: Dr. Matthew Mimiaga, professor in the UCLA Fielding Department of Epidemiology, was recognized in September with The Alumni Award of Merit - the highest honor presented by the Harvard T.H. Chan School of Public Health Alumni Association - which recognizes alumni whose careers reflect a lifetime of impact, organizers said.
Appointed: ColoradoSPH is pleased to announce the new chair of its Biostatistics & Informatics department, David Conti, MS, PhD. Conti comes from the University of Southern California, where he was a professor and the associate director of Data Science Integration.
An overarching aim of his research is the investigation of diverse populations and the factors driving differences in disease incidence. His specific research covers both applied genetic and environmental epidemiology and statistical methods development, with a focus on integrated multi-omic data analysis and Bayesian approaches.
Notes on People, con’t
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Honored: The University of Arizona's Dr. Justin Starren, director of the Center for Biomedical Informatics and Biostatistics, has been named a distinguished fellow of the ACMI. His research career has focused on the challenges that occur at the boundaries between different domains and on creating new methods that address unmet needs, including exploring the ethical issues involved with technology-enabled research data collection during clinical encounters.
Honored: The University of Arizona's Dr. Jose Fernando Florez-Arango, associate director for education and training at the Center for Biomedical Informatics and Biostatistics has been elected a fellow of the American College of Medical Informatics. He has focused his career on global health equity and implementation of innovative health information technologies. He is a physician, educator and health informatics expert with experience in implementing digital health technologies in low-resource settings across Latin America, South Asia and beyond.
Honored: The University of Arizona's Vignesh Subbian, interim director of the BIO5 Institute, has been elected a fellow of the American College of Medical Informatics. Subbian, associate professor of biomedical engineering in the College of Engineering, is a collaborative health systems scientist and informatician who uniquely leverages systems engineering, human factors and computational methods to address sociotechnical issues and opportunities in biomedicine and learning health systems
Retiring: Berkeley's epidemiology legend Arthur L. Reingold, is retiring this year after 40 years at UC Berkeley, leaving a profound public health legacy. He mentored countless students, investigated major outbreaks—including a norovirus-linked custard pie case and helped launch the NIH AIDS Training Program and California Emerging Infections Program. His leadership shaped COVID vaccine safety oversight and global infectious disease policy.
from page 29
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Retired: The University of Utah has announced the retirement of 4 epidemiology faculty members with a combined total of 100 years of service to the division. The were celebrated for that service and their contribution to research throughout their careers.
Your Ad Should Be Here
Do you have a job, course, conference, book or other resource of interest to the epidemiology community? Advertise with The Epidemiology Monitor and reach 35,000 epidemiologists, biostatisticians, and public health professionals monthly.
For more information please contact: Michele Gibson / 770.309.7937 / michele@epimonitor.net
L to R: Karen Curtin, Alun Thomas, Matt Samore (Division Chief), Lisa Cannon-Albright, and Molly Leecaster
Near Term Epidemiology Event Calendar
Every December The Epidemiology Monitor dedicates that issue to a calendar of events for the upcoming year. However that often means we don't have full information for events later in the upcoming year. Thus an online copy exists on our website that is updated regularly. To view the full year please go to: http://www.epimonitor.net/Events The events that we are aware of for the next month follow below.
December 1-2
Type: Conference
December 2025
Web: https://tinyurl.com/vbwk6s7z
Title: 14th Annual Conference on Tropical Medicine and Infectious Disease
Sponsor: Conference Series Location: Rome, Italy
LAST CALL
2026 Worldwide Event Calendar
Every December the EpiMonitor publishes a calendar of events happening throughout the world in the coming year. This includes summer / winter programs, short courses, conferences, meetings and any other event that is at least one day long. To be included we need the following information from your organization:
Event Name / Sponsor(s) Date(s) / Location
Website / Contact Information
Event advertising opportunities exist in this digital publication, on our website and social media pages, and in our Epi-Gram emails if you desire.
For more information please contact: Michele Gibson / 770.309.7937 / michele@epimonitor.net
Open Public Health Positions
What it means and why it matters
The list below has been compiled by Public Health Hiring Help the new Substack column that has been created to help individuals in the public health community find positions in the midst of the chaos that is now impacting governmental agencies and grant recipients. This list represents the most current positions PHHH has been able to identify. We thank PHHH for their permission to reprint these listings.
Baystate Health, Research Coordinator I (Springfield, MA)
$59–81k + benefits, Education: Bachelor’s min (EPI)
AstraZeneca, EHS Intern Public Health Alignment: EH
What it means and why it matters
US Chamber of Commerce, Policy Intern Public Health Alignment: HPM
US Chamber of Commerce, Global Development Intern Public Health Alignment: GH, HPM
GA Dept of Health, Health Policy Intern Public Health Alignment: HPM
US Green Building Council, Health Schools Research Intern Public Health Alignment: EH, BSHES, HPM
Blue Shield of CA, Digital Health Record Intern Public Health Alignment: HPM
BJC Healthcare, Epidemiology Intern Public Health Alignment: EPI
King County, Fatal Overdose Surveillance Intern Public Health Alignment: BSHES, EPI
FleishmanHillard, Health and Life Sciences Intern Public Health Alignment: HPM, BIOS, EPI
Gilead Sciences, HEOR Intern Public Health Alignment: EPI, BIOS, HPM
American Heart Association (HQ), Research/Grants Administration Intern Public Health Alignment: HPM, GH
Takeda, Global Regulatory Project Management/Strategic Planning Intern Public Health Alignment: HPM, GH
Gilead Sciences, Nonclinical Safety/Toxicology Intern Public Health Alignment: EH
AZ Dept of Health, Maternal and Child Health Systems Intern Public Health Alignment: GH, HPM, BSHES
Open Public Health Flexible Positions
City of Savannah, Equitable Growth Program Coordinator (CT)
Public Health Alignment: BSHES, GH, HPM
What it means and why it matters
Avenir Management Partners, Global Health and Life Sciences Analyst (PT)
Public Health Alignment: GH, EPI, HPM
World Economic Forum, Early Careers Programme (CT)
Public Health Alignment: ANY
Birth in Color, Policy Fellowship
Public Health Alignment: BSHES, HPM, GH
Malaria No More, Communications Manager (PT)
Public Health Alignment: BSHES, GH
DC Dept of Environment, Environment and Sustainability Fellow
Public Health Alignment: EH, HPM
MA Appleseed, Policy and Education Intern
Public Health Alignment: HPM, BSHES, GH
City of Forth Worth, Sr. Consumer Health Specialist (PT)
Public Health Alignment: EH, HPM, BSHES
Hudson Mohawk Area Health Education Center, Program Coordinator (PT)
Public Health Alignment: BSHES, EH
Pueblo Dept of Health, Emergency Preparedness/Response Generalist (PT)
Public Health Alignment: EPI, BSHES, GH
Westat, Population Assessment for Tobacco and Health Interviewer (PT)
Public Health Alignment: BSHES, GH, EPI
IA State Univ, Program Specialist I (PT)
Public Health Alignment: BSHES, GH, EPI
Prince George County, Disease Control Specialist I/II (PT)
Public Health Alignment: EPI, BSHES, EH
George Washington Univ, Digital Health Literacy Educator (PT)
Public Health Alignment: BSHES
For Full Information on jobs: http://www.epimonitor.net/JobBank
The EpiMonitor offers a variety of plans for you to advertise your job opening, event or other item of interest to our readers. The basic advertising options are:
Web Only
This provides you with a full page on our website along with banner ads in appropriate places for what you are advertising (e.g. our Job Bank or Events pages). In addition, these ads are also featured in our monthly email blast. Web ads normally appear on our site within 2-3 hours of your order.
Web + Digital Print
This option provides either a full or half page digital print ad in this publication monthly along with all of the services included in the "Web Only" option.
Social Media
Starting in January 2026 we will also have social media add-on options for our web and print advertising programs.
Your Ad Should Be Here
Do you have a job, course, conference, book or other resource of interest to the epidemiology community? Advertise with The Epidemiology Monitor and reach 35,000 epidemiologists, biostatisticians, and public health professionals monthly.
Advertising opportunities exist in this digital publication, on our website and social media pages, and in our Epi-Gram emails.
For more information please contact: Michele Gibson / 770.309.7937 / michele@epimonitor.net
Open Rank Faculty - Environmental Epidemiology
The Department of Epidemiology and Biostatistics in the Arnold School of Public Health (ASPH) at the University of South Carolina (USC) invites applications for a full-time, open-rank faculty position in environmental epidemiology. Research expertise in all areas of environmental epidemiology will be considered. This recruitment is part of a campus-wide strategic effort to expand the University’s leadership in advancing research and educational excellence in environmental health. The cluster will broaden expertise across disciplines to foster innovation and address the complexity of environmental health challenges through multidisciplinary scholarship. This initiative focuses on determining the impact of chemical, physical, behavioral, biological, and social environmental stressors across the lifespan, and emphasizes designing, testing, and scaling programmatic and policy interventions that address these stressors.
All applicants must hold a doctoral degree in epidemiology or a related field by their start date. At the assistant professor level (tenure-track), candidates should demonstrate excellence in research and the potential to secure external funding, teach graduate courses, and collaborate with public health and biomedical researchers. At the associate- or full-professor level (tenureeligible), candidates must also demonstrate an established record of top-tier publications and competitive grants, a proven track record of supervising graduate students, and leadership in curriculum development, junior faculty mentoring, and crossdisciplinary collaboration. The successful candidate will maintain an active research program in environmental epidemiology, engage with cross-disciplinary research teams on topics related to environ-mental health, mentor graduate students, and teach graduate-level environmental epidemiology courses.
USC is a comprehensive Carnegie University of High Research Activity and Community Engagement. USC has five Health Science Units in addition to ASPH: 1) School of Medicine in Columbia, 2) School of Medicine in Greenville, 3) College of Nursing, 4) College of Pharmacy, and 5) College of Social Work. ASPH was founded in 1975. Among public universities in the US, the ASPH ranks second in overall enrollment and fourth in NIH funding. ASPH consists of six departments and several research centers that address topics such as disease prevention, nutrition and physical activity, cancer, health services and policy, rural health, HIV/AIDS, aging, and health disparities. For more information about ASPH and the department, please visit www.sph.sc.edu.
The Department of Epidemiologyand Biostatistics is home to 35 full-time faculty members,12 in the Biostatistics Division and 23 in the Epidemiology Division. The faculty’s robust research portfolio includes funding from a broad spectrum of federal agencies (e.g., NIH and CDC) and non-profit organizations. The department has a rich tradition of producing outstanding trainees. Currently, 112 students are enrolled in our master’s and doctoral degree programs. The department, school, and university provide a strong collaborative environment for cross-disciplinary team science across the public health research continuum.
Columbia, SC, enjoys more than 300 days of sunshine annually and has ready access to pristine beaches, lakes, and mountains. The city boasts a range of historical and cultural attractions, festivals, performing arts, sporting events, and many outdoor recreation areas, including Congaree National Park and Lake Murray.
Toapply: Applications must include: 1) application letter, 2) curriculum vitae, 3) research statement, 4) teaching statement, and 5) contact information for three references. Submit your application at the following link:
https://uscjobs.sc.edu/postings/196750
Application review will begin by November 1st, and the search will continue until the position is filled. The anticipated start date is August 16, 2026. For additional information, please contact Janine Rominger at janiner@mailbox.sc.edu or (803)-777-7666. The University of South Carolina does not discriminate in educational or employment opportunities or decisions for qualified persons on the basis of age, ancestry, citizenship status, color, disability, ethnicity, familial status, gender (including transgender), gender identity or expression, genetic information, HIV/AIDs status, military status, national origin, pregnancy (false pregnancy, termination of pregnancy, childbirth, recovery therefrom or related medical conditions, breastfeeding), race, religion (including religious dress and grooming practices), sex, sexual orientation, veteran status, or any other bases under federal, state, local law, or regulations.
USC offers a robust benefits package described at: http://www.sc.edu/about/offices_and_divisions/human_resources/benefits/index.php
Postdoctoral Scholar in Cancer Epidemiology
The Department of Public Health Sciences at the University of Chicago is seeking a highly motivated postdoctoral scholar to join a dynamic research team focused on molecular epidemiology and health disparities in multiple myeloma. Our research integrates diverse large-scale datasets, including GWAS data, tumor and cell-free DNA methylation profiles, clinical and epidemiological data, and biological samples. As a postdoctoral scholar, you will play a leading role in analyzing these data and preparing manuscripts that investigate the roles of epigenetics, lifestyle influences, environmental factors, and social determinants of health on myeloma risk and outcomes. The post-doc scholar will also contribute to consortium-based research initiatives, participate in liquid-biopsy and epigenetic biomarker analysis, and have opportunities to initiate new projects and develop grant proposals.
Qualifications
Successful candidates will have:
1. A PhD or equivalent graduate degree in epidemiology, biostatistics, data-science, or a related field.
2. Strong expertise in epidemiology, biostatistics, genetics, and epigenetics.
3. Proven experience with programming and data analysis using R, SAS, or STAT
4. Excellent written and oral communication skills.
Candidates with experience in survival analysis, machine learning, and applying advanced biostatistical techniques will be highly regarded. As a postdoctoral scholar, you will work closely with dedicated mentors in a collaborative and multidisciplinary environment, with opportunities to pursue career development activities, develop independent research projects, and apply for grants (e.g., K99/R00).
Start date: 1/5/2026 (flexible)
Application process
Please send a letter including a statement of research interests and future goals, curriculum vitae, and names/addresses of 3 references to: Dr. Brian Chiu (mmepi@health.bsd.uchicago.edu). Application review will begin immediately but will continue until the position is filled.
Application information
This position is benefits-eligible, and information regarding benefits can be found at: https://clients.garnett-powers.com/pd/uchicago/
Additional information for postdocs in the University of Chicago Biological Sciences Division can be found at: https://bsdpostdoc.uchicago.edu/. Compensation in the Biological Sciences Division follows the NIH NRSA Stipend scale.
All University departments and institutes are charged with building a faculty from a diversity of backgrounds and with diverse viewpoints; with cultivating an inclusive community that values freedom of expression; and with welcoming and supporting all their members.
We seek a diverse pool of applicants who wish to join an academic community that places the highest value on rigorous inquiry and encourages diverse perspectives, experiences, groups of individuals, and ideas to inform and stimulate intellectual challenge, engagement, and exchange. The University’s Statements on Diversity are at: https://provost.uchicago.edu/statements-diversity
The University of Chicago is an Affirmative Action/Equal Opportunity/Disabled/Veterans Employer and does not discriminate on the basis of race, color, religion, sex, sexual orientation, gender, gender identity, national or ethnic origin, age, status as an individual with a disability, military or veteran status, genetic information, or other protected classes under the law. For additional information please see the University's Notice of Nondiscrimination.
Job seekers in need of a reasonable accommodation to complete the application process should call 773-834-3988 or email equalopportunity@uchicago.edu with their request.
Faculty Positions - Epidemiology & Biostatistics
The Washington University School of Public Health is seeking applications for tenure-track faculty positions at the rank of Assistant, Associate, or Full Professor in Epidemiology and Biostatistics who are accomplished, curious, intellectually courageous, and committed to excellence in population health science and scholarship.
As a research-intensive institution, the school provides a supportive, collegial, and intellectually engaged environment for faculty to pursue leading-edge, grant-driven scholarship. We encourage applicants who are enthusiastic about conducting interdisciplinary work across a breadth of disciplines.
Position: Tenure-Track Faculty Positions in Public Health
Location: St. Louis, Missouri
Position Overview:
The successful candidate will be expected to develop an extramurally funded research program, teach and mentor graduate students, and contribute to the service missions of the WashU School of Public Health and University. The candidate should demonstrate a commitment to excellence in research, teaching, and service, and have a strong desire to contribute to the advancement of public health.
Key Responsibilities:
►Develop and maintain an independent, innovative, and extramurally funded research program in epidemiology and/or biostatistics.
►Teach graduate courses in epidemiology, biostatistics, and related public health disciplines.
► Mentor and advise students at the master's and doctoral levels.
► Participate in school, community, and university service activities.
► Collaborate with faculty colleagues and promote interdisciplinary research initiatives.
Qualifications:
►A doctoral degree (PhD, DrPH, ScD, or equivalent) in Epidemiology, Biostatistics, or a closely related field.
► A strong record of scholarly achievement and evidence of, or potential for, securing extramural research funding.
► Demonstrated excellence in teaching and mentorship in the field of public health.
► Strong communication and interpersonal skills.
Application Procedure:
► Candidates are encouraged to apply through Interfolio. Applications will be accepted until the positions are filled. A complete application package must include:
► A cover letter specifying the position(s) being applied for and detailing the candidate's qualifications.
► A curriculum vitae.
Equal Employment Opportunity Statement
Washington University in St. Louis is committed to the principles and practices of equal employment opportunity and especially encourages applications by those underrepresented in their academic fields. It is the University’s policy to provide equal opportunity and access to persons in all job titles without regard to race, color, age, religion, sex, sexual orientation, gender identity or expression, national origin, protected veteran status, disability, or genetic information.
Specific inquiries about these positions may be directed to Debra Haire-Joshu, Associate Dean for Faculty Affairs, WashU School of Public Health at the SPHFacultyAffairs@wustl.edu
We look forward to reviewing your application and thank you for your interest in joining our academic community.
YLE can be found here: https://yourlocalepidemiologist.substack.com/
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, wife, and mom of two little girls. YLE reaches more than 305,000 people in over 132 countries with one goal: “Translate” the ever-evolving public health science so that people will be well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members.
To support the effort, subscribe or upgrade your existing subscription: https://yourlocalepidemiologist.substack.com/
The Epidemiology Monitor ISSN (2833-1710) is published monthly by Monitor Publishing & Communications, Inc.
All material in this publication is subject to copyright. For possible reprint permission please contact us at michele@epimonitor.net
Advertising options include but are not limited to:
Website only ads or website ads combined with digital print ads in this publication. Sponsorship for features in this newsletter or for the newsletter issue itself
Ads are accepted for open positions, events, programs, books, merchandise and other items of interest to our readers.
Subscriptions to this publication are free. Go to http://epimonitor.net/Subscribe.htm