A monthly update covering people, events, research, and key developments
Editor’s Note:
We hope you will appreciate this month's issue and all that it includes but at the same time, we are already looking ahead to future issues and several of them include features where we need your help. In fact, we can't build these specific issues without your help
2025 - 2026 Salary Survey
One of our most popular features pre-Covid was the annual salary survey so this year, in partnership with Public Health Hiring Help, we are bringing it back. If you are the dean or chair of a school or department of public health / epidemiology / biostatistics you will soon be receiving an email from us requesting information so that we can build this year's report. For the first time we will be breaking information down into subsets so you can understand the differences in salary for epidemiologists, biostatisticians, and public health faculty. We also hope to be able to quantify the number of projected job openings (or reductions) for the 2026-2027 academic year. If you'd like to get a head start on the process, please email us at salarysurvey@epimonitor.net and we will send you the necessary forms required to submit your data. Assuming everyone responds in a timely fashion, we hope to publish the data at the end of January but again, it is up to you to provide us the data.
Annual Event Calendar
As you know, our December issue is always dedicated to publishing a calendar of industry events offered worldwide. If you have a conference, meeting, short course, winter/summer program, or other event that you think would be of interest to our readers please send them to us at events@epimonitor.net and make sure you include contact information so we can get back to you with questions in order to list your event correctly. While we do a comprehensive search for events and find most of them, the only way to ensure that your event is included in the calendar is to send it to us with all the pertinent details (dates, location, price, topics, sponsors, etc).
This month's issue takes a look at the trauma faced by the employees at CDC during the recent shooting and another article about which science we're follow in our work. We also have a profile of a biostatistician from the University of South Carolina that you'll find quite interesting. On top of that we've got some tips on the job search process and a list of free epidemiology books that you can download.
As always, we continue to provide you with our popular monthly word game feature, Notes on People, an overview of what we are reading from the public media, and a listing of upcoming
miss
In This Issue
Did you miss last month’s issue? Read it here: https://tinyurl.com/3acrn433 or here: https://tinyurl.com/av95kbcy
Public Health in the Face of Trauma and Violence
Authors: Katelyn Jetelina, PhD, MPH
Kristen Panthagani, MD, PhD
Megan Ranney, MD, MPH
NOTE: This article was originally published on August 13, 2025 by Your Local Epidemiologist on Substack.
It’s been a struggle to process what happened at the CDC just a few days ago [August 8, 2025]. The facts are coming in: one officer died, 500 rounds fired, 200 bullets made contact with 6 CDC buildings, hundreds of staff sheltered in place for hours. The intention is undeniable: this was an attempted massacre.
The state of the world feels unrecognizable. We are living headline to headline, tragedy to tragedy. The bar for shock has been set so high that there are ten other stories deemed more urgent, more outrageous, than hundreds of bullets hitting a federal building. So many people don’t even know this happened. That’s not normal. Our world is swallowed whole by the endless churn of violence and crisis we’ve come to accept as ordinary. We are drowning in the abnormal, yet forced to carry on our “normal” lives, living in a constant state of cognitive dissonance.
It feels deeply unfair. Unfair as members of the public who feel completely powerless over the systems that continue to fail us and, at times, betray us. As parents trying to navigate through the noise and uncertainty, as concerned citizens watching our nation go numb to violence and death, as workers mourning both a loss of life in the case of
Officer Rose and a loss of any semblance of safety at work.
It’s exhausting. The public health field has been the punching bag for six straight years, yet some of us are the very ones who are trying to change and reimagine the systems. Many of us are choosing listening over judgment seeking to build bridges and understand those who have felt marginalized by health policies. To extend empathy and then be met with bullets feels demoralizing, to put it mildly.
It’s deeply angering. Watching those who fan the flames ignore the consequences when hostile rhetoric turns to physical violence. Words matter. From statements from public officials to casual posts on Facebook, language of hate, vitriol, and the vilification of an entire professional field have contributed to this moment.
And it’s lonely. The silence. The absence. The indifference. Without genuine acknowledgment or visible solidarity from federal leadership, the weight of this moment feels even heavier and, at times, permissive.
Trauma doesn’t move at the same pace for everyone. For those closest to it, the moment freezes in time—every sound, every detail etched in memory. A step further out, people feel the shock and recognize the pain, but find words clumsy and insufficient. Beyond that, the world either moves on quickly or never even realizes it happened. That dissonance between the depth of the experience and how fast it fades from public consciousness can make the loss feel
even heavier, the isolation even sharper. The sheer volume of trauma is such that everyone cannot fully empathize with every event. Never in human history have we had so much realtime access to tragedy, and it overloads people. People can only bear so much.
For us in public health, where do we go from here?
Those of us in public health signed up for one overarching mission: to help people. We show up every day to analyze data, predict disease patterns, inform policy, or treat patients to improve the health of our communities not to figure out how to respond to violent attacks on our workplaces. It’s absolutely not fair. And it’s not normal.
But it’s also the time we find ourselves in, and we all have to decide how we’re going to respond. (Gandalf said it better here.) The first step is to pause, grieve, and process. That’s what we did on Sunday night here on Substack Live (see recording above). It’s ok to not be ok, and it’s critical that we take the time to process what is happening. And then, in solidarity with our community, we act with each other, for each other.
To the public, what can you do?
We received a lot of comments during this Substack Live, and the most common question was ‘what can we do to help?’ We partnered with Nelba Marquez Greene (licensed therapist, Yale scholar, and mother of Sandy Hook victim) and put our heads together for you, and this is where we landed:
1. Support the family of the fallen officer. A law enforcement officer gave his life protecting CDC employees that day. If
you’re able, contribute directly to his family through the CDC Foundation.
2. Write in to support public health workers.
For this post, we turned on the comments section for everyone. Drop a note in there, and I will compile for CDC employees. Another option is a handwritten note or heartfelt email. It can mean more than you think. We created a template to make it easy you can adapt it, sign it, and send it to someone who has shown up for your community.
3. Understand and acknowledge secondhand trauma.
Learn the steps you can take as an individual and/or in the workplace to mitigate the impact of secondary trauma.
4. Humanize healthcare workers, public health workers, and scientists. Share a story of a public health success in your community, or highlight the person behind it. Maybe we even need someone to jumpstart a campaign like Hero and Human to highlight the fact that health workers are both, while demanding systems change.
5. Learn the warning signs and tools for crisis prevention.
Educate yourself about Extreme Risk Protection Orders (ERPOs) and other tools to intervene when someone poses a danger to themselves or others.
6. Resist dehumanizing the “other side.”
There’s nothing quite as dehumanizing as violence actions that say “your life doesn’t matter.” As humans, when we’re under attack, it’s so easy to respond by treating our attackers as a twodimensional villain. This may feel justified in the moment, but ultimately, it can continue the cycle that drives polarization and violence even more. Refusing to dehumanize our attackers (both physical and verbal) breaks the cycle. This doesn’t mean pretending things are ok, tolerating mistreatment, or not responding but it does mean treating people with dignity in our responses, even when they aren’t affording us the same treatment. This does two things: 1. It stops escalation, and 2. It shines a brighter light on the reality of their mistreatment, because it’s contrasted with our response demanding dignity and respect for all humans.
Even in the middle of this grief and exhaustion, resilience is everywhere. We’ve seen colleagues show up for each other in ways that matter.
Some outside of the “public health bubble” have also spoken out, including a grassroots leader of the MAHA Movement and a former U.S. Surgeon General (from the first Trump administration). These may feel like small acts and certainly haven’t been a chorus, but they are seeds. And history tells us that seeds can grow into movements. Every action, no matter how small, helps build a culture where violence has no place and the public’s health can thrive.
Bottom line
The 500 bullets that hit the CDC were aimed at more than buildings. It is heartbreaking, deeply angering, lonely, and, unfortunately, unsurprising. It will require all of us taking action so that the next generation inherits a country where directing bullets at health workers is unthinkable. ■
This article was originally printed in Your Local Epidemiologist. To read more content from this source subscribe to Your Local Epidemiologist (YLE): https://tinyurl.com/47494ms4
Do you want to read more content like this? This piece was reprinted from Substack. YLE can be found here: https://yourlocalepidemiologist.substack.com/
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD an epidemiologist, wife, and mom of two little girls. YLE reaches more than 305,000 people in over 132 countries with one goal: “Translate” the ever-evolving public health science so that people will be wellequipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members.
To support the effort, subscribe or upgrade your existing subscription: https://yourlocalepidemiologist.substack.com/
"Follow the Science"
Or Just the Convenient Parts?
Author: Bruce Lanphear, MD, MPH
NOTE: This article was originally published on August 19, 2025 by Plagues, Pollution & Poverty on Substack.
We Keep Ignoring the Warnings at the Cost of Lives—and Trust
“Follow the Science”—
But Which Science?
“Follow the science” became a rallying cry during the pandemic. It was painted on protest signs, invoked in political speeches, and deployed in countless social media posts. At its best, the phrase calls for humility: let evidence, not ideology, guide our decisions. At its worst, it becomes a slogan without substance an empty reassurance that what’s being done is backed by reason, even when crucial evidence is ignored.
The problem isn’t science itself. The problem is which science we choose to follow—and which science we choose to ignore.
Science is not a set of commandments. It’s a method a way of asking questions, gathering evidence, and testing ideas against reality. It’s neutral in the sense that it can be used for noble or destructive ends. The same chemistry that gave us antibiotics also gave us nerve gas. The same industrial ingenuity that created clean drinking water systems also produced PFAS, “forever chemicals” that now contaminate those systems. The same scientific principles that led to life-saving statins were also behind the invention of tetraethyl lead, a fuel additive that poisoned entire generations.
The problem isn’t science itself. The problem is
which science we choose to follow and which science we choose to ignore.
When Science Serves Power Instead of People
Throughout the 20th century, we saw a pattern that should have been impossible to miss. Industrial breakthroughs were hailed as triumphs of human ingenuity. Years or decades later, those same breakthroughs turned out to be environmental disasters.
Tetraethyl lead reduced engine knock but unleashed a neurotoxic metal that lowered IQs and increased crime rates. Asbestos made buildings fire-resistant but left workers and residents with mesothelioma. DDT wiped out mosquitoes but devastated bird populations and elevated the risk for breast cancer. PFAS made cookware non-stick and firefighting foam more effective—but now they’re in the blood of nearly every American, linked to cancer and immune dysfunction.
In each case, the hazards were known early. Scientists warned about lead’s toxicity before it was added to gasoline. Evidence of asbestos disease existed decades before the bans. Studies on PFAS health risks date back to the 1960s. Yet regulation lagged far behind the science not because the evidence was unclear, but because corporate and political power worked to suppress, delay, or discredit it.
We’re seeing the same pattern with plastics. They’re more than waste in our oceans plastic chemicals are a mix of polymers and thousands
- Follow cont'd on page 6
of additives, from phthalates to flame retardants. Many disrupt hormones, harm the brain, or strain the heart. Studies now link everyday plastic exposures to falling fertility, heart attacks, and ADHD. Microplastics have turned up in blood, placentas, and even the brain, raising urgent questions about their longterm effects. Yet international talks to curb plastic production have stalled, with industry steering the focus to recycling—an inadequate fix that leaves unchecked the rising tide of new plastic.
The Science We Cherry-Pick
When leaders say “follow the science,” they often mean the science that supports immediate action on a politically palatable problem developing vaccines, improving storm forecasts, launching Mars rovers. They rarely mean following the science that challenges entrenched industries, questions long-standing public health practices, or calls for costly regulation.
Consider air pollution. We have known for decades that it causes premature death, heart attacks, and lung cancer. We can quantify how many lives would be saved by tougher standards. And yet, regulatory action is slow, often stalled by legal challenges from polluting industries.
Consider fluoridation. The policy was adopted in the mid-20th century to prevent cavities, based on the best evidence at the time. Today, new studies show that fluoride impairs brain development in children at levels found in fluoridated communities. But questioning fluoridation is still treated as heresy in much of the public health establishment. Following the science here would mean re-evaluating old assumptions not because we’ve “changed sides” but because the evidence has changed.
How Ignoring Science Breeds Distrust
When science that threatens powerful interests is ignored, the public notices even if they don’t know the details. Communities living near chemical plants, fracking sites, or leadcontaminated water supplies can see the gap between official assurances and lived reality. They learn, sometimes the hard way, that the government is not protecting them from industrial harms.
This breeds not just cynicism, but anger. And in a political climate already primed for grievance, that anger can be redirected. People who have seen their health ignored or sacrificed may come to believe that all institutions are corrupt, all expertise is suspect, and that the only truth is the one that confirms their own tribe’s beliefs. It’s not a big leap from there to the distrust and defiance we’ve seen among some MAHA followers. If the “official” science failed to protect your child from autism or your community from toxic waste, why would you believe it now about vaccines or climate change?
The irony is that ignoring inconvenient science doesn’t just harm public health it erodes the very trust needed to mobilize public health measures in the future.
Following All the Science
If “follow the science” is to mean anything, it must mean following all the science not just the parts that make for good headlines or fit neatly into our political comfort zones. It means:
- Follow cont'd on page 7
Acting on hazards we’ve known about for decades, not just the newest threats.
Asking hard questions about long-standing practices, like fluoridation, even when they’re cherished by the establishment.
Funding and protecting research that challenges powerful industries, knowing that suppression of inconvenient findings is a recurring hazard.
Treating prevention with the same urgency we treat treatment because preventing harm is usually cheaper, kinder, and more effective than repairing it.
And it also means adopting the precautionary principle. The default should be to protect the public from plausible hazards while we gather more evidence, not to wait for proof beyond all doubt before acting.
The Real Test
Following the science isn’t tested in the moments when science confirms what we want to believe. It’s tested when the evidence forces us to rethink, to disrupt profitable industries, or to admit we were wrong.
In the case of PFAS, the science told us early on that these chemicals were persistent and bioaccumulative. We didn’t follow that science. In the case of lead, we had clear toxicology a century ago. We didn’t follow that science. In the case of asbestos, the link to fatal disease was undeniable decades before bans. We didn’t follow that science.
Instead, time and again, we allowed the economic interests of a few to outweigh the health of the many. The result is not just a legacy of environmental damage, but a corrosive loss of public trust.
A Stronger Standard
The next time you hear “follow the science,” ask: Which science? Who decided which evidence counts? And what happens to the science that doesn’t make the cut? Because the science we ignore is often the science that matters most for protecting health.
If we truly want to follow the science, we need to make it harder to bury inconvenient findings, easier to act on early warnings, and unacceptable to treat prevention as optional. We need to admit that our track record—on regulating toxic chemicals, on confronting environmental hazards, on acting in time is abysmal. And we need to understand that every time we fail, we deepen the distrust that fuels not only public health crises but political ones.
Following the science must mean more than chasing innovation. It must mean controlling environmental hazards, asking uncomfortable questions, and protecting the public even when it’s inconvenient, costly, or unpopular. That’s the kind of science worth following and the only kind that can rebuild the trust we’ve squandered. ■
This article was originally printed on Substack in Plagues, Pollution & Poverty. To read more content from this source subscribe to Plagues, Pollution & Poverty: https://tinyurl.com/3rfeuama
Profiles in Public Health
Assistant professor uses biostatistics to advance neuroscience and wearable device research
[Editor's Note: Parts of this article were originally published by the University of South Carolina and we thank them for their reprint permission.]
Interviewer: Staff
The advent of physical activity trackers, respiratory, temperature, and sleep sensors have transformed the possibilities of modern health care, but we have biostatisticians like Beniamino Hadj-Amar to thank for bridging the gap between data and impact. The assistant professor of biostatistics at the University of South Carolina is one of the essential scientists working behind the scenes to make the most of wearable devices and the lifesaving neuroscience and neuroimaging information they provide.
Can you tell us a bit about where you're originally from and how your childhood influenced your career choices?
I was born and raised in Italy, living in both Rome and Genoa, in a family of five supported by a single income. My mother is Italian and my father is Algerian, and growing up in that environment gave me both resilience and perspective. We didn’t have much, but that experience imparted in me a strong determination to improve my circumstances and, at the same time, to do something meaningful for others. From a young age, I found that mathematics came naturally to me, and I loved the clarity and challenge it offered. I also had a strong drive to approach everything with determination and persistence, whether it
Hadj-Amar
Asst Professor, University of South Carolina
was learning a musical instrument, playing sports, or developing new skills. That combination of passion for mathematics and determination to create impact ultimately set me on the path that led to my career in biostatistics and scientific research.
When you went to university was it always your plan to study statistics or did you have a different plan and, if so, what changed your mind?
In my last year of high school, I discovered how much I enjoyed solving integrals. I thought it was genuinely fun. That made me realize I wanted a career where I could apply mathematics to real-world problems. At the same time, I had the intuition that software and coding would also be important, though I was
- Profile cont'd on page 9
Beniamino
still uncertain about the exact path. So, I first tried to enter a program in Computer Science and Engineering. For some reason, I didn’t pass the preliminary admission exam. I remember taking it personally and feeling disappointed. But soon after, I discovered a program called Mathematical Statistics and Data Management. It immediately felt like the right fit: a perfect combination of statistics, probability, computing, and real-world applications. Looking back, it was the best choice I could have made. When one door closed, another, much bigger, door opened! That experience taught me an important lesson. From there, I was fortunate to win a studentship to pursue a master’s degree in the UK, and more opportunities kept opening.
You were educated overseas and have since done postdoctoral work at both Rice University and the University of Minnesota. Can you speak a bit about the differences in education between the US and Europe? Do you find American students approach their studies differently?
I’ve been fortunate to experience university life in Italy, the UK, and the US. While the UK and US share a more comparable structure, Italy offers a very different model.
In Italy, the system felt more relaxed and with less pressure. Something that can be both positive and negative. Public education makes university highly accessible, and while exams are scheduled at specific dates, you have the option to postpone them. If things don’t go well, you can retake the exam as many times as needed until you’re satisfied with your result. For some students, that flexibility works very well, though others may find it easy to fall behind. Personally, I had a wonderful experience, with excellent teachers and mentors for whom I’m very grateful. One aspect of the Italian system that I think is particularly
mentors for whom I’m very grateful. One aspect of the Italian system that I think is particularly strong is the method of assessment. Most exams involve both written and oral components. Being asked questions on the spot can be intimidating, but it really pushes you to master the material and demonstrate deep understanding.
In the UK, where I did both my master’s and PhD, I found the system more structured and with higher expectations. There was more pressure compared to Italy, and assessments were usually based on written assignments and projects rather than oral exams. This required me to present my knowledge in a different way, with more emphasis on written clarity and technical reporting.
In the US, I noticed even more structure, particularly in coursework, assignments, and assessments. The expectations are very clear, and there’s a continuous flow of feedback through regular homework, projects, and exams. At the same time, the pressure can be significant—partly, I think, because of the high cost of education. That financial dimension influences both the intensity of the programs and the way students approach their studies. Overall, though, I’ve been impressed by how well-defined and organized the system is, and I’ve found students here to be very motivated and engaged.
At the EpiMonitor we keep close tabs on the job market for epidemiologists, biostatisticians and public health professionals overall. It has become clear over the last year that there are many more job openings for biostatisticians than
- Profile cont'd on page 10
epidemiologists both in academia and industry. Do you find that phenomena is encouraging students to consider biostatistics as a career or perhaps to switch their concentration?
That’s a very interesting observation, and I don’t doubt it’s true. From my perspective, I can’t say I’ve seen a clear shift myself, but I do think students are increasingly aware of how valuable statistical skills are. So even if they don’t formally switch to biostatistics, they’re looking for ways to strengthen their quantitative background.
With the massive cuts to research grants in the US over the last 8 months, outside funding is becoming even more important. What do you see as the outlook for external funding for biostatistics research?
While it’s true that we are experiencing a difficult moment with the recent cuts to research grants in the U.S., I remain optimistic. The demand for innovative biostatistical methods continues to grow, and that will sustain the need for investment, whether through traditional funding sources or through new partnerships. Challenges are inevitable, but I believe they also bring opportunities. The landscape will continue to evolve, and our role is to adapt and make the most of the resources available to drive meaningful impact.
What interested you in the University of South Carolina?
The University of South Carolina’s emphasis on translational science and community impact resonates strongly with my own research goals developing statistical methodologies that are both rigorous and directly relevant to real-world health challenges. I was first introduced to
these challenges as a student at the University of Warwick and the University of Oxford, where my Ph.D. program in Statistics placed a strong emphasis on methodological innovation. During that time, I became increasingly drawn to biomedical and biological applications, particularly those with broad public health implications. At USC, I saw an exciting opportunity to build on that foundation. The university hosts outstanding groups working on wearable devices and neuroscience two areas where my interest has grown significantly in recent years — and I felt that this environment would be an ideal place to contribute and collaborate.
What also drew me to USC was the extremely welcoming and collegial environment. From the beginning, I felt a sense of peace and a healthy atmosphere to work in, and the longer I am here, the more grateful I am for this choice. The university also offers an incredible amount of resources from the Propel Research Mentorship Program for grant development, to the Center for Teaching Excellence, and many more initiatives that foster growth and success. I truly feel part of a supportive and inspiring community, and that has made USC a unique and rewarding place to carry out my research and teaching.
USC highlighted your work with wearable sensors in their original article but what other areas of research are you involved in?
My expertise lies at the intersection of statistics, machine learning, and scientific application, with a particular focus on Bayesian methods for analyzing complex time-series data. While wearable sensors and circadian health are an important part of my work, my research more
- Profile cont'd on page 10
broadly addresses statistical modeling challenges in biomedical and neuroscience applications. At the heart of this research is a central question: how can we detect and interpret changes over time — in a brain, a body, or a population when the signals are noisy, sparse, or hidden?
Methodologically, I develop flexible Bayesian models that capture dynamic structure in data. This includes hidden Markov and semiMarkov models to infer latent states in neural and physiological signals; time-varying graphical models to map evolving networks of interactions; spectral and frequencydiscovery methods to identify rhythms in EEG, actigraphy, respiration, and temperature signals; and Gaussian processes and changepoint models to track smooth but evolving biological patterns. I also work on Bayesian variable selection and shrinkage priors to handle high-dimensional data where identifying key drivers is essential.
In terms of applications, my research spans several domains. I have worked on neuroscience, studying dopamine and norepinephrine release in conscious humans and dynamic connectivity in fMRI; on epilepsy and circadian rhythms, modeling daily sleep–wake cycles and their disruption; on respiratory research, identifying sleep apnea recurrence. While my main applications have been in these areas, the modeling tools I develop are broadly applicable across public health, where scientists frequently face the same challenges of noisy, complex, and timedependent data.
How is AI impacting your work and what do you see as the future of that tool in your research?
has greatly enhanced my research productivity and efficiency, especially for tasks that used to take a considerable amount of time. For example, generating clean code for visualizations, checking grammar, or debugging algorithms can now be done in minutes rather than hours. I also find it to be a valuable learning platform, e.g. helping me quickly summarize papers, clarify complex concepts, brainstorm new ideas, or learn unfamiliar coding tools. When used wisely and at the right stage of one’s career, AI can be a tremendous asset that boosts both research and creativity.
At the same time, I recognize that it is a doubleedged sword, particularly for students just beginning their academic journeys. A critical part of my own training was struggling with difficult problems and finding my way out of them a process that built intuition, resilience, and independence. With generative AI, there is a risk of shortcutting that process, relying too quickly on an easy answer rather than pushing through the challenge. That balance is difficult to define, but it is essential.
For me, I am grateful to be able to use AI now, while also being grateful that I completed my Ph.D. in an era before it was available. That combination gives me perspective: I can embrace AI as a powerful tool in my current work, while still valuing the formative experiences that shaped my development without it.
Let's talk about wearable sensors
I am fascinated by the rich and complex datasets that wearable sensors now allow us to collect. Actigraphy, for example, provides continuous measurements of rest–activity
- Profile cont'd on page 11
cycles across days or weeks, offering unprecedented insight into sleep–wake patterns and circadian rhythms. These data open enormous scientific opportunities, from understanding how daily rhythms are disrupted in epilepsy patients to quantifying how demographic, psychological, or medical factors shape sleep and activity patterns. Yet they also pose significant methodological challenges: the signals are noisy, highly dimensional, and often nonstationary, with rhythms that can shift over time or under different conditions.
To meet these challenges, I have developed Bayesian statistical frameworks that extract meaningful information from such data. Hidden semi-Markov models allow us to reconstruct unobserved daily states, such as sleep, quiet rest, or activity, while explicitly modeling their durations. Covariate-dependent circadian models capture how amplitude and phase of rhythms vary across individuals and respond to clinical or demographic factors. Bayesian spectral methods and change-point models identify periodic components that may appear or disappear over time, from circadian cycles to ultradian oscillations in respiration and temperature. Together, these tools provide interpretable markers of circadian health such as rhythm regularity, stability, and timing — which can be directly linked to questions in neurology, psychiatry, and personalized medicine.
Let's talk about your other
areas of research
Another strand of my research focuses on graphical models and high-dimensional data. In fMRI, for example, we want to know not just how one brain region behaves but how networks of regions interact and change over time. To capture this, I’ve developed sparse switching graphical models that reveal evolving connectivity patterns, while accounting for
uncertainty and avoiding overfitting. In simple terms, these models let us track which brain regions are “talking” to each other, when those connections change, and how those shifts relate to tasks or disorders.
More broadly, my methodological work develops flexible Bayesian tools for analyzing complex signals. For instance, I’ve worked on autoregressive switching processes for multivariate time series. These models use past information to predict the future, but they also allow for sudden shifts. This is useful in practice because biological or behavioral systems don’t always change smoothly they may jump from one state to another, like a person moving abruptly from rest to intense activity or a brain network switching from focus to distraction.
I’ve also designed Bayesian spectral models that search for oscillations in noisy data, distinguishing true rhythms from background variability. Think of this as trying to pick out the steady beat of a drum in the middle of a crowded concert hall we want to separate meaningful cycles, like daily circadian rhythms, from random fluctuations that don’t carry biological meaning.
In the context of wearable and physiological signals, I have built Gaussian process frameworks to model smooth but dynamic processes and to detect transitions or circadian disruptions. These are flexible models that don’t assume a fixed pattern, so they can capture gradual changes in sleep–wake cycles or detect when a person’s daily rhythms suddenly shift — for example, due to illness, stress, or treatment.
Finally, I’ve contributed to Bayesian variable selection techniques including shrinkage priors and sparsity-inducing approaches — that identify the key drivers of high-dimensional data while quantifying uncertainty in those decisions. In practice, this means helping scientists figure out which factors really matter for instance, which among hundreds of genetic, behavioral, or clinical variables are actually influencing health outcomes while also being honest about how confident we are in those findings.
Together, these methodological advances form a coherent toolkit for uncovering hidden structure in dynamic systems, whether the data come from the brain, the body, or broader public health applications. ■
Thank you for participating in this interviewwe look forward to hearing more from your campus in the future!
Your Ad Should Be Here
Changing Your Job Hunt Outlook
How to fight the 'doom and gloom' and keep going
Interviewer: Public Health Hiring Help
NOTE: This article was originally published on September 22, 2025 by Public Health Hiring Help on Substack.
A couple weeks ago, PHHH brought you the guidance of The Public Health Burnout Coach, Marissa McKool, MPH, for all things networking. With the great feedback we received from this collaboration, we have decided to explore other topics related to our mental and emotional interactions within the job hunt. After all, the job hunt isn’t as simple as dragging and dropping resume after resume. It’s taxing, timeconsuming, and turbulent.
Today’s topic is a biggie how do we maintain perspective, clarity, and drive when there is so much anxiety and uncertainty swirling around us? How do we keep the present moment in mind without letting it become all-consuming and totally demoralizing?
These are tough questions. Each day, there seems like there is some new setback in public health echoing in the abyss of social media, breaking our hearts just a little more. You have the experience necessary to make a difference but it can seem like the job market is no longer a hospitable place for public health knowledge, skills, and abilities.
While it has been a uniquely hard year for public health, maybe not all hope is lost. Maybe that’s just what’s being shouted the loudest. Marissa McKool, the Public Health Burnout Coach, is back to guide us in how to find balance and positive self-talk in today’s public health landscape.
PHHH: What has it been like being the Public Health Burnout Coach this year? What are common themes you’ve seen and talked about with clients?
MM: This year has been both heavy and hopeful. Public health professionals are carrying enormous stressors layoffs, funding cuts, political instability, and the constant pressure to serve under impossible conditions. A theme I hear again and again is people questioning whether they can stay in public health, and if so, for how long. It’s such a painful question, because so many are deeply passionate about this field and don’t want to leave. At the same time, I’ve witnessed incredible community, advocacy, and resilience. People are coming together to support one another—creating public health–specific job boards, like PHHH, offering free services, and finding ways to lift each other up in the midst of uncertainty.
The most common challenges I’m working through with clients are: setting boundaries at work when there’s always more to do with fewer resources, processing the anger, fear, and anxiety about what’s happening (and what might come next), and learning how to truly “shut off” from both work and the political landscape. As hard as it is, we have to rest and recharge so we can keep going and keep trying.
PHHH: How does the media—both the news and social platforms like LinkedIn—play into the ‘doom spiral’ we feel trapped in?
Most people don’t know that our brains have a built-in negativity bias constantly scanning for what could go wrong. Thousands of years ago,
- Hunt
that kept us alive. It was far more important to remember which berry could kill us than which one tasted good. Survival depended on noticing danger.
Fast forward to today: most of us aren’t fighting to literally survive each day, but that part of our brain is still running. And media outlets whether news or social take full advantage of it. That’s why the content that gets published, shared, and goes viral is overwhelmingly negative. It can start to feel like the world is crumbling, when in reality, your feed is just skewed. It’s like receiving a community needs assessment that only includes negative data while leaving out the neutral and positive. You’re not getting the full picture.
That’s why I always recommend being intentional about who you follow and what news sources you consume. Positive, hopeful, change-driven stories are happening every day but you won’t see them unless you deliberately seek them out.
The same is true on LinkedIn. The platform often amplifies scarcity and comparison, even unintentionally. Think about it: most people who post are at one end of the spectrum either celebrating a promotion or new job or sharing about being laid off and struggling to find work. What we don’t see are the vast majority of people in the middle those who are steady, doing meaningful work, but not posting about it.
In fact, less than 1% of LinkedIn users post at all.
So when you scroll, remember: your feed is not reality. It’s a highlight reel. It’s a tiny slice of a much bigger picture.
PHHH: So who do you follow to get a good dose of empowerment and hope in the
midst of so much turmoil? What helps you stay hopeful?
MM: It’s less about who you follow and more about how you engage. Creating a balanced news and social media feed takes intention.
Here’s what I do:
If I see ads or posts that are fear-mongering, I click “not interested.” If I see positive or empowering content, I interact with it—like, comment, or share. The great thing about algorithms is that they feed you more of what you engage with. You actually have the power to shift your own feed by choosing what you say yes to and what you say no to.
I’m also not afraid to unfollow people. It’s never personal it’s about protecting my focus. That doesn’t mean I bury my head in the sand; it means I’m creating balance between the hard realities and the hopeful stories. I also make sure to contribute by posting or reposting positive things myself. For example, when someone shared that Colorado has seen the lowest teen suicide rates since 2007, I reposted it so more people could see that good news.
And while it might sound like something I’d say just because I’m a coach, it’s the truth: I stay hopeful by staying grounded in the tools I teach. I use them every single day because they work. They don’t prevent me from ever feeling stress, anxiety, or fear but they keep me from getting stuck there.
One of my favorites is something I call “The Pride Jar”. It started as a daily practice of writing down one thing I was proud of to train my brain to notice the positive. Over time, it evolved into my “Celebration Jar”. Now I write down
- Hunt cont'd on page 15
something worth celebrating—sometimes it’s a huge client breakthrough, sometimes it’s a contract I secured, and sometimes it’s something happening in the world. It’s a small ritual, but it keeps hope alive. I have a whole podcast episode that walks you through how to use this tool (listen here).
PHHH: But, obviously, we can’t just surround ourselves with only positive content, right? What does balance look like?
MM: Exactly. Toxic positivity isn’t helpful either. Balance is about being intentional. I set limits on my media consumption, but I don’t avoid reality. I want to stay informed, I just don’t let every headline hijack my nervous system.
For me, that looks like giving myself 10 minutes in the morning to scan the top headlines then I’m done for the day. Not much changes in 24 hours, and if something truly earth-shattering happens, I’ll hear about it organically through others or my feed. On social media, I intentionally look for both updates and positive stories so I’m not only consuming one side of the picture.
I like to think of it like nutrition: if you eat only junk food, your body feels it. But if you eat only kale, you’re also missing vital nutrients. Balance is making sure you’re consuming enough reality to stay grounded, and enough hope to keep going.
PHHH: At least from my observations, there feels like two major demoralizing “agents” in public health. There’s the broader challenges what we see in the news but there are also the personal experiences, like rejections. In fact, a question I’ve been asked several times is ‘What am I doing wrong in my job hunt?’ How can we shift
our individual internal monologues to give us more patience and grace during a long, frustrating job hunt?
MM: This is such an important question. First, we have to acknowledge that the public health job market has shifted dramatically: fewer positions, more competition, and constant uncertainty. That doesn’t mean you’re doing anything wrong, and it certainly doesn’t mean it’s impossible to land a job. Just in the past few months, I’ve had clients secure Executive Director roles and Faculty positions.
Like I said in our chat about networking, getting a job is about selling yourself. And, again, I know many public health professionals cringe at the word “sales,” thinking it’s manipulative. But sales isn’t that at all it’s simply helping someone get what they need. For example, if I want a minivan, and someone helps me find the right one, that’s sales. If they try to push a sports car on me, that’s not.
In the job search, it’s the same principle. You are helping an organization get what they need: a person who can do the job they’re advertising well. But here’s the key: if you don’t believe you’re capable of doing the job, you’ll struggle to convince anyone else. You have to sell yourself first on your abilities, then sell the organization on why you’re the right fit.
That means shifting your focus from “I need a job” to “What does this organization need, and how can I deliver it?” When your mindset is about meeting their needs with confidence, rejections don’t sting as much, and they don’t make you want to quit. Rejection hurts when we tie it to our self-worth. Have confidence in your value before the organization validates it. Then,
rejection becomes data to help you sell yourself better, not proof that you’re not enough.
PHHH: I also think it’s easy to measure progress in rejections, interviews, and job offers. But that seems to miss so much else of what is happening in job applicants’ efforts, right? How can we reframe our perspective on progress to better represent our efforts while also angling towards the ultimate goal?
MM: If you focus only on long-term outcomes and think in binary terms “Did I get the job or not?” you’ll end up feeling disappointed for the entire job search. It’s like asking, “Did we do a good job addressing COVID?” and only measuring success by whether there were zero cases. You’d miss so much: reduced transmission rates, lower death rates, and the valuable lessons learned along the way. In public health, we know the importance of evaluating multiple outcomes: short-term, medium-term, and process measures.
The same principle applies to job searching. Measure progress beyond just the final outcome. Process measures might include how many applications you submitted, how many networking events you attended, or how many informational interviews you scheduled. Short- and medium-term outcomes could be qualitative: how much your cover letters improved, how your outreach skills developed, or how your confidence grew in connecting with others.
By broadening your definition of success, you give yourself credit for the work you’re actually doing, feel better because of it, and build momentum toward the ultimate goal.
PHHH: Any last words of advice about selftalk and perspective in the job hunt?
MM: Burnout in the job search and burnout on the job share one key factor: both happen when we believe our success is out of our control.
You can focus on posts about people struggling to get a job and let that convince you that you won’t succeed. Or, you can focus on the incredible value you can bring to an organization. You can let 10 rejections convince you that you’ll never get a job—or you can stay excited about every opportunity you apply for.
What you focus on grows. When you fixate on things outside your control, you feel powerless. When you focus on your skills, your experience, and the possibilities ahead, you create momentum and opportunity.
Use your focus and energy wisely! ■
Marissa McKool, MPH —The Public Health
Burnout Coach is a coach, speaker, and trainer dedicated to helping women in public health do meaningful work without sacrificing their wellbeing. Drawing on 15+ years of leadership experience and her own journey through burnout, Marissa equips public health professionals with the tools to thrive while protecting their energy and health. Her unique approach combines evidence-based strategies, feminist coaching principles, and lived experience to create sustainable change.
Resources
Free Epidemiology Books
Author: Staff
[Editor's Note: One of our valued readers took our request to heart and forwarded a list of epidemiology texts available for free in digital format. We would love to publish more content about free resources of value to our readers - please forward any information you've got to: info@epimonitor.net for inclusion in future issues.]
Statistical Methods in Cancer Research Volume II: The Design and Analysis of Cohort Studies, Breslow NE, Day NE IARC Scientific Publication No. 82, 1986 Free PDF copy: https://tinyurl.com/bdzdmpnd
Statistical Methods in Cancer Research Volume I: The Analysis of Case-Control Studies, Breslow NE, Day NE IARC Scientific Publication No. 32, 1980. Free PDF copy: https://tinyurl.com/39p9rn2z
Basic Epidemiology 2nd Edition, Bonita et al, https://tinyurl.com/22ctcc6k
CDC's Principals of Epidemiology in Public Health Practice 3rd Edition, https://tinyurl.com/2nfcexra
Gordis Epidemiology 6th Edition, Celentano and Szklo https://tinyurl.com/3pzn2ar9
Clinical Epidemiology - The Essentials, 5th Edition, Fletcher et al https://tinyurl.com/2utkkzh6
Epidemiology, Charlotte Baker https://tinyurl.com/y3ss39fy
Foundations of Epidemiology, Marit L. Bovbjerg https://tinyurl.com/23cj8k4w
An Introduction to Epidemiology for Health Professionals, Olsen et al, https://tinyurl.com/5bbbh3fx
We are looking to list other resources of interest to epidemiologists, biostatisticians, and public health professionals. They do not need to be free or low cost but that does make them more attractive. In addition to books, we would like to list online courseware, software programs, and other similar items. Please forward your lists to: info@epimonitor.net so that we can add them to future issues and to our website. Thank you!
From Our Archives
What We Knew About COVID-19 / Early Fall 2020
What it means and why it matters
EDITOR'S NOTE: As we have now reached the 5th anniversary of the initial days of our awareness of COVID19, it seemed appropriate to begin looking back at what we knew, when we knew it and how our thoughts evolved over the early months of the pandemic. Accordingly, we will be reprinting our articles from that period over the next few months. We welcome your comments and suggestions about what you would like to see.
Projections By The Institute For Health Metrics And Evaluation
Reveal We Are Nowhere Near The End
Widespread Availability And Uptake Of Vaccine Appear To Be Many Months Away
The epidemic in the US is far from complete and, even in the optimistic scenario of herd immunity kicking in after 40% rather than 6070% cumulative infection, the country would be less than halfway through the pandemic even three months from now on January 1, 2021, according to the Institute for Health Metrics and Evaluation (IMHE).
Likewise, IMHE estimates the epidemic globally is also very incomplete and the larger world will be less than one quarter through the pandemic on January 1, 2021. In short, we have seen only a fraction of the burden of disease to be experienced from this pandemic unless drastic change through vaccination or treatment is brought about.
Fatigue
Even the social distancing and other mitigation activities we have that are known to work may become less effective through decreased use. There is concern that fatigue with nonpharmaceutical control measures is setting in the US and elsewhere and that erosion of public support may lead to adoption of more hands-off approaches. These would potentially
create herd immunity to eventually slow or halt the spread of the pandemic virus, however, letting nature take its course would extract a heavy price in terms of morbidity and mortality. This is because relatively low percentages of the populations in the world, with few exceptions such as Ecuador and Mexico City, have been infected.
Herd Immunity
Recently, unproven claims that herd immunity may occur at much lower levels such as 40% or even 20% have appeared on social media, according to IHME. The reasons cited for a lower threshold are the role of superspreaders, non-random mixing in less dense populations, non-overlapping social networks, and some prior coronavirus immunity. The fatigue with control measures is coming just at a time when more robust social distancing measures would be called for in the Northern Hemisphere to counter the anticipated upsurge in cases by January 1, 2021. For example, another lockdown is being urged for the United Kingdom where cases are doubling.
-
Toll With Herd Immunity
Even assuming herd immunity could kick in at 40% in the US, IMHE’s analyses of seroprevalence data and infection fatality ratios suggest the US would eventually experience over 800,000 deaths to get to that point. This projected number increases to over 1,000,000 deaths if herd immunity requires 50% seroprevalence and approximately 1,300,000 deaths if 65% seroprevalence is required. These numbers of deaths are approximately 2-7 times larger than the number of deaths that have already occurred in the US.
Global Toll
Globally, making similar calculations for herd immunity predicts the world would see 10-13 million deaths before the pandemic extinguishes itself. Currently, just under 1,000,000 deaths have been recorded worldwide. Needless to say, both sets of projections could be reduced considerably with widespread use of effective vaccines or new treatments. However, as we read less about when a vaccine or vaccines might be “available” and more about but when a vaccine or vaccines might be in “widespread distribution”, the return to normalcy may be months or even years away globally, and this will be reflected in a sustained number of excess deaths when compared to the years just prior to 2020.
End of the Pandemic?
A recent article in The Atlantic made this point forcefully by asserting that “the sublime postpandemic period that so many are longing for will likely not arrive at once like a clock striking midnight on New Year’s Eve….As a matter of epidemiology, there’s no clear cut criterion that
determines a pandemic is over. You can’t sign a treaty with a virus, so we have to settle for a kind of cease-fire, Columbia epidemiologist Stephen Morse told the Atlantic.
Near Term Projections
The IMHE has lowered its projection of US deaths by January 1, 2021 from 415,000 to 378,320 because of steeper than expected declines in deaths in several states. Daily deaths have been steadily declining reaching 650 per day recently, but COVID remains the second leading cause of death in the United States. And with the expected seasonal surge later this year, IMHE anticipates over 3,000 deaths per day by the end of December.
Preventable Deaths Now
Approximately 180,000 additional deaths are projected to occur between now and January 1, 2021 with almost two-thirds of these (115,000) able to be prevented if mask use could increase to 95%. Such an achievement appears unlikely since global mask use defined as the percentage of the population that reports always wearing a mask when leaving home remains constant globally at about 60% and is below 50% in the US.
Global Near Term Projections
IMHE believes it is likely that global deaths will increase from approximately 5,000 per day now to over 30,000 deaths per day in December. Hundreds of thousands of lives could be saved with increased mask use worldwide just over the next few months, that is, preventing approximately 43% of the deaths expected between now and the end of the year. ■
- Covid cont'd on page 20
Epidemiology Group Wants To Speed Up Rather Than Slow The Spread Of SARS-CoV-2 To Reach Herd Immunity More Quickly
Harms Of Current Strategy Outweigh Benefits They Believe
A group of medical and public health professionals led by Sunetra Gupta, Oxford University Professor of Theoretical Epidemiology, has concluded that the harms being caused by COVID control measures outweigh the benefits, and a new strategy called“ focused protection” is being proposed.
Furthermore, they question the feasibility and efficacy of testing and tracking that are part of current efforts to slow the spread of SARS-CoV-2 and note that suppressing the virus in not a viable or permanent solution.
The Harms
In a joint statement called the Great Barrington Declaration (GBD) after the name of the town where it was signed by Gupta and Harvard University’s Martin Kulldorf, and Stanford University’s Jay Bhattacharya, the co-authors note that “Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice. Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.”
In addition, a recent report from Oxfam asserts that travel restrictions and other control measures are causing breaks in the food supply that threaten thousands of starvation deaths in some food problem “hotspots”.
New Strategy
The new strategy seeks to exploit the fact that older persons have a higher risk of mortality from COVID and that an “age-stratified” approach could be implemented that protects the elderly and the high risk while allowing free circulation of the virus in the younger age groups. According to the authors of the GBD, their strategy provides the quickest path to herd immunity which would keep infections low enough for all age groups to return to normal living. What is not stated in the GBD is the level of past infections in the population needed to achieve herd immunity. Gupta and colleagues in previous reports estimate that level to be as low as 10-20% of the population. Most experts disagree and give estimates significantly higher in the range of 50-70%. A recent Lancet study found that less than 10% of the US population has a history of COVID infection at this point in the pandemic, suggesting 50-70% herd immunity is still a long way off and highlighting the importance of having effective vaccines as soon as possible.
Alternative Harms
The GBD authors provide no estimates of the number of preventable deaths likely to be caused by allowing free circulation of the virus until an adequate level of herd immunity is achieved. It was just such alarming estimates about the number of deaths that initially moved epidemiologists and public health professionals to recommend lockdowns and other restrictive measures. In one of several interviews given by Gupta, she acknowledged that a certain number of potentially avoidable deaths would occur, thought it could be a “low fraction,” but said these deaths are a burden that we have to accept, given the alternative. She does not believe that the occurrence of a larger number of persons with residual effects of COVID (so called long-haulers) should be an argument against the herd immunity approach.
A recent article in the NY Times reports that the White House supports the herd immunity strategy being promulgated by Gupta and colleagues.
Iceland Example
The current thinking about the importance of lockdowns and restrictions was on display recently in Iceland where the Chief Epidemiologist gave a public briefing in early October in which he stated “no country in the world is even close to achieving herd immunity to the SARS-CoV-2 and he noted that his country’s health care system would be completely overwhelmed if social restrictions were lifted and the virus was left to circulate freely.
Death Projections
In fact, the Institute for Health Metrics and
Evaluation continues to project an estimated 2.5 million total global deaths from COVID by February 2021 using current strategies and an even larger number of 3.7 million deaths if there is an easing of restrictions. These numbers and the differential would be even larger if projections were extended out to the anticipated date when herd immunity was achieved several months from now either through vaccination or natural infection.
When IHME issued its first set of global projections for COVID in early September 2020, the Director Christopher Murray criticized those who call for allowing the COVID virus to circulate by easing restrictions. He said “This first global forecast represents an opportunity to underscore the problem with herd immunity, which essentially ignores science and ethics, and allows millions of avoidable deaths,” Murray said. “It is, quite simply, reprehensible.” This approach however does not appear to be what Gupta and others are calling for which does include restrictions that protect the older adults and other high risk persons.
Another Criticism
In a British Medical Journal account of the “focused protection” strategy, Johns Hopkins University’s Stefan Baral acknowledged that COVID control measures such as lockdowns were causing harms, however, he remained unpersuaded about the new strategy. It would require real programs to protect the vulnerable and these were not spelled out in the declaration. For such a strategy to work, according to Baral, society would have to provide easy access to health care for everyone, sick pay for those not able to work because of - Speed Up cont'd on page 22
COVID, and housing for people in multigenerational households. These types of resources were available in Sweden which is often cited as a country where allowing freer circulation of virus has been the goal since the outset of the pandemic.
Gupta Expands
In an opinion piece in The Telegraph, Gupta notes that the pandemic has highlighted many of the inadequacies in our social systems and that we should use the opportunity to close the gaps that have been revealed. Such reforms are unlikely to take place in the near term and thus the kind of safety nets that would be necessary to implement a “focused protection” strategy are not present in many societies. To read the full Great Barrington Declaration, visit https://gbdeclaration.org/
One Goal
The goal of the current social distancing
strategy and of the focused protection strategy is the same—namely, to minimize mortality and social harm until we reach herd immunity. Perhaps what was not foreseen as clearly as experience has shown are all of the social and public health harms caused by social restrictions. Societies are still struggling to map out and follow a middle course which implements restrictions in such a way that some modified version of normal activities can take place. And according to Gupta and colleagues, their principal aim in making the GBD has been to put the topic of COVID strategy “on the table” for discussion. Gupta said the number of signatories to the GBD now exceeds several thousands so the co-authors are not alone in seeing the burden of current approaches. ■
Your Ad Should Be Here
Do you have a job, course, conference, book or other resource of interest to the epidemiology community? Advertise with The Epidemiology Monitor and reach 35,000 epidemiologists, biostatisticians, and public health professionals monthly.
Advertising opportunities exist in this digital publication, on our website and social media accounts, and in our Epi-Gram emails.
For more information please contact: Michele Gibson / michele@epimonitor.net
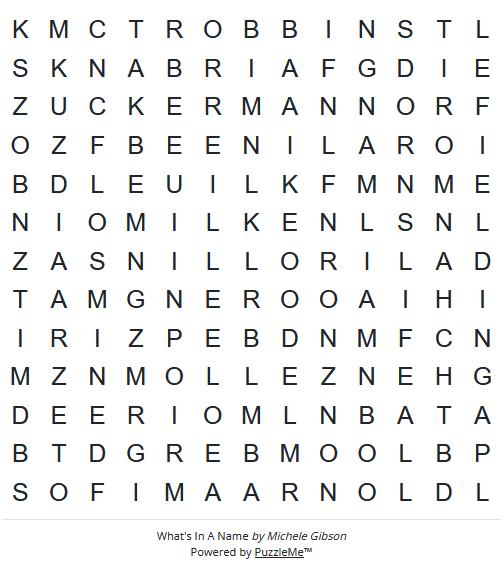
What's In A Name
We know fall is incredibly busy for our readers so this month, instead of a long crossword, we are bringing you a short word search. Good luck - don't let the easy words fool you!
For an interactive online version go to: https://tinyurl.com/2pvvsnh9
Words to find:
1. Gillings
2. Stempel
3. TH Chan
4. Rollins
5. Dornslife
6. Mailman
7. Zuckerman
8. Arnold
9. Boozman
10. Fairbanks
11. Zilber
12. Bloomberg
13. Fielding
14. Milken
15. Robbins
16. ODonnell
What We're Reading This Month
Editor's Note: All of us are confronted with more material than we can possibly hope to digest each month. However, that doesn't mean that we should miss some of the articles that appear in the public media on topics of interest to the epi community. The EpiMonitor curates a monthly list of some of the best articles we've encountered in the past month. See something you think others would like to read? Please send us a link at info@epimonitor.net and we'll include it in the next month
Washington DC Chaos
♦ West Coast governors unveil coalition to establish their own immunization guidelines (OregonLive)
https://tinyurl.com/4fphzfuw
♦ HHS, CDC Announce New ACIP Members (HHS)
https://tinyurl.com/2wxyz529
♦ Amid CDC turmoil, Pennsylvania joins Northeastern states in regional public health coalition (WHYY.org)
https://tinyurl.com/aw6ftzh9
♦ Gen Z Is Losing Trust in Public Health. Can You Blame Them? (MedScape)
https://tinyurl.com/bde7sdmt
♦ Public Health Associations Call on RFK Jr. to Resign as HHS Secretary (Health Innovation Group)
https://tinyurl.com/3yw77ybn
Public Health Topics
♦ Ebola outbreak is declared in the Province of Congo (NYT)
https://tinyurl.com/58twzh26
♦ Passengers Reportedly Quarantined Over Fear of Contagion After New York-Bound Flight Diverted to Canada (People Magazine)
https://tinyurl.com/3zbr6h5m
♦ A flesh-eating parasite is at our borders. What happens if it spreads? (Vox)
https://tinyurl.com/5n72yzpb
What We're Reading This Month
[Type a quote from the document or the summary of an interesting point. You can position the text box anywhere in the document. Use the Text Box Tools tab to change the formatting of the pull quote text box.]
- con't from page 24
Public Health Topics, cont.
♦ Ancient disease makes a comeback (NPR)
https://tinyurl.com/mry7b2ax
♦ Seeking answers in women’s health: A research agenda for the coming decade (Harvard SPH)
https://tinyurl.com/a9wxp6sn
♦ Guiding epidemic interventions through a fog of noisy data (MedicalXpress)
https://tinyurl.com/bdh4bfrx
♦ How genetically modified mice could save a Massachusetts vacation town from a disease outbreak (The Independent via AppleNews)
https://tinyurl.com/r2pd5dee
♦ This growing fungal disease outbreak spreads through dust and dirt (USA Today) https://tinyurl.com/43twwf5u
♦ Measles outbreak growing in parts of Arizona and Utah, health officials say (NBC News) https://tinyurl.com/mt3ymjvx
♦ 2 experts explain the true role of slavery and racism in the history of public health policy –and the growing threat ignorance poses today
https://tinyurl.com/vb3ksmfc
♦ Navy and Marine Corps Force Health Protection Command Epidemiologists Enhance Force Health Protection Through Improved Medical Surveillance Capabilities (DVIDS) https://tinyurl.com/2w5uk437
♦ Madison County reports first-ever human case of EEE, an extremely deadly mosquitoborne virus (Syracuse.com)
https://tinyurl.com/97k5bhs8
Join EpiMonitor on our Facebook page at: https://bit.ly/2U29gUA on Twitter at: @theEpimonitor on Instagram at: @epimonitor
Notes on People
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Named: Greta Massetti has joined the Georgia State University School of Public Health as Professor and Chair of the Department of Population Health Sciences. Massetti comes to Georgia State from the Centers for Disease Control and Prevention, where she was Principal Deputy Director of the National Center for Injury Prevention and Control. Prior to joining CDC, Massetti was an assistant professor at the University of Buffalo with a joint appointment in the departments of psychology and pediatrics.
Named: Jeffery Talbert, PhD has been named the inaugural chair of the newly created Department of Artificial Intelligence and Health at the Medical College of Georgia at Augusta University. Talbert has spent the last two decades of his career in various leadership positions at the University of Kentucky, including chief of biomedical informatics in the Department of Internal Medicine and director of the Institute for Biomedical Informatics.
Honored: Dr. Karl E. Peace, a renowned biostatistician and professor, has been awarded an Honorary Doctorate (Doctor Honoris Causa) by Vlore University in Albania, recognizing his significant contributions to the field of biostatistics and public health. Dr. Peace is a Senior Research Scientist and Professor of Biostatistics in the Jiann-Ping Hsu College of Public Health (JPHCOPH) at Georgia Southern University (GASOU). He is the architect of the first degree (MPH) program in Biostatistics and the Founder of the first college of public health (JPHCOPH) in the University System of Georgia (USG).
Honored: Dr. Todd Miano, has been named the 2025 recipient of the American College of Epidemiology’s Early Career Epidemiologist Award. This award recognizes an early career epidemiologist who has made major contributions to the field in methods development, etiologic research, or applied epidemiology. Dr. Miano was recognized for his work in the field of acute care pharmacoepidemiology.
Notes on People,
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Honored: Marco Carone, a professor of biostatistics at the University of Washington School of Public Health and holder of the Norman Breslow Endowed Faculty Fellowship, has received the prestigious 2025 Myrto Lefkopoulou Distinguished Lectureship from the Harvard T.H. Chan School of Public Health. Carone was recognized for his work in advancing the fields of causal inference, survival analysis, and the development of robust statistical methodologies for analyzing complex observational data.
Honored: Bryan S. Blette, PhD, assistant professor of Biostatistics at the Vanderbilt University Medical Center, was awarded an Early Career Award by the Association of Clinical and Translational Statisticians (ACTStat) at the organization’s annual meeting in August.
The Early Career Award is given to recognize meritorious works and achievements of an early-career individual providing substantial support to team clinical and translational science through the practice of statistics.
Honored: Daniel T. Lackland, Dr.P.H., FAHA, professor of epidemiology and neurology at the Medical University of South Carolina, will receive this year’s Population Research Prize at the American Heart Association’s Scientific Sessions 2025. Dr. Lackland is a global leader in hypertension research, stroke prevention and efforts to address gaps in cardiovascular disease outcomes. He directs the Division of Translational Neuroscience and Population Studies and the Master of Science in Clinical Research Program at Medical University of South Carolina in Charleston, South Carolina. A fellow of the American Heart Association and the American College of Epidemiology, he is internationally recognized for his population-level research on hypertension and cardiovascular disease, with a special focus on differences among various communities.
Notes on People,
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Resigned: Iowa Department of Health and Human Services Director Kelly Garcia has resigned, the governor’s office announced. Garcia served as head of the department for six years after Gov. Kim Reynolds appointed her to head the then-Department of Human Services in 2019. Garcia took on the role of interim director of the Iowa Department of Public Health in June 2020 during the COVID-19 pandemic, and the two departments were officially merged in 2022 under her leadership.
Resigned: Seven years after announcing the founding of his new peerreviewed journal, Global Epidemiology, in the EpiMonitor; editor-in-chief George Maldonado along with half of his board have resigned from the [currently] Elsevier owned publication. The resignations were prompted by actions by Elsevier that the individuals felt were not compatible with the highest standards of peer review.
Passed: J. Michael (Mike) Bowling, Ph.D., 71, of Chapel Hill, NC passed away peacefully on Friday, August 15, 2025. Mike was a respected scholar and educator whose career at the University of North Carolina at Chapel Hill spanned decades of impactful research, teaching, and service. As a professor in the Department of Health Behavior and the Department of Biostatistics at the Gillings School of Global Public Health, Mike authored numerous scholarly publications that advanced the fields of health behavior, tobacco control, and injury prevention. He also held leadership roles in university centers and initiatives, including the Injury Prevention Research Center (Associate Director) and the Carolina Survey Research Laboratory (Assistant Director). His greatest professional joy was teaching biostatistics to graduate students, winning the McGavran Award for Excellence in Teaching in 2003. He encouraged his students to “embrace” biostatistics and celebrated their success by serving his famous homemade cheesecake at the end of each semester. Following Mike’s transition to Professor Emeritus status in 2016, the focus of his professional career was serving as Chair of the Survey Review Committee of the CDC Global Adult Tobacco Survey. https://tinyurl.com/4puxka6p
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Passed: Professor John Patrick Vaughan, Professor Emeritus of Epidemiology and Public Health at the London School of Hygiene and Tropical Medicine (LSHTM), and inaugural Chair of BRAC UK’s (now BRAC Europe) Board of Trustees. Patrick passed away on 26 July in London at the age of 87, following a courageous battle with cancer. Patrick was a dedicated educator and a public health expert. His long career in international health and health systems research spanned the globe.
Much of his career in epidemiology was spent working in low and middle income countries. He served with government health services in Papua New Guinea (PNG); helped start a medical school at the University of Dar es Salaam, Tanzania; and spent three years researching diarrhoea in Bangladesh. In 1985 he was among those consulted by the organisers of Live Aid on how best to spend the estimated £150m raised by the UK and US concerts.
He authored more than 120 academic papers and 22 books over his career. As a lockdown project he co-edited Practical Epidemiology: Using Epidemiology to Support Primary Health Care (2021) with Cesar Victora and Mushtaque Chowdhury, both of whom he had mentored when they were doctoral students. https://tinyurl.com/3uxjrt5c
Near Term Epidemiology Event Calendar
Every December The Epidemiology Monitor dedicates that issue to a calendar of events for the upcoming year. However that often means we don't have full information for events later in the upcoming year. Thus an online copy exists on our website that is updated regularly. To view the full year please go to: http://www.epimonitor.net/Events The events that we are aware of for the next month follow below.
October 5-9
Type: Conference
Title: 65th ISI World Statistics Congress
October 2025
Web: https://tinyurl.com/2e3kt9zd
Sponsor: International Biometric Society Location: The Hague
October 12-14
Type: Conference
Title: AHIMA 2025 Conference
Web: https://tinyurl.com/5n9ad3uy
Sponsor: American Health Information Management Association Location: Minneapolis, MN
October 14-18
Type: Conference
Web: https://tinyurl.com/4yjxtumy
Title: American Society for Human Genetics 2025 Annual Meeting
Sponsor: ASHG Location: Boston, MA
October 19-22
Type: Conference
Title: ISPE Annual Conference
Sponsor: Multiple Location: Atlanta, GA
October 23-25
Type: Conference
Title: 5th International Vaccines Conference
Web: https://bit.ly/3uYKFES
Web: https://tinyurl.com/muyzzc9t
Sponsor: Magnus Group Location: Orlando, FL & Virtual - Calendar con't on page 27
2026 Annual Event Calendar
We are just starting to build our annual calendar issue. If you have a conference, short course, meeting, or winter/summer program of interest to our readers we need information about your event so it can be included in this calendar when it is issued in December.
November 2-5
Type: Conference
Title: APHA Annual Meeting & Expo
November 2025
Web: https://tinyurl.com/bdfkhrv3
Sponsor: American Public Health Association Location: Washington, DC
November 11-14
Type: Conference
Title: 18th European Public Health Conference
Sponsor: EPH Location: Helsinki, Finland
November 15-16
Type: Conference
Web: https://bit.ly/3jcNVcY
Web: https://tinyurl.com/2j6pbbfa
Title: Biostatistics in the New Era of Data-Driven Sciences
Sponsor: HTHealth Houston Location: Houston, TX
November 18-21
Type: Short Course
Web: https://tinyurl.com/7tcjta6b
Title: Leadership Development to Advance Equity in Healthcare
Sponsor: Havard University Location: Virtual
November 18-21 Type: Conference
Web: https://tinyurl.com/ukxk929m
Title: 17th International Conference on Molecular Epidemiology and Evolutionary Genetics of Infectious Diseases
Sponsor: Elsevier Location: Kolkata, India
November 24-25
Type: Conference
Title: Infectious and Chronic Disease Conference
Sponsor: Pharmaweb Location: Dubai, UAE
Nov 30 – Dec 3
Type: Conference
Web: https://bit.ly/31SL1ln
Web: http://bit.ly/2K5CCm0
Title: 10th Intl Conference on Infectious Disease Dynamics
Sponsor: Elsevier Location: San Diego, CA
2026 Annual Event Calendar
We are just starting to build our annual calendar issue. If you have a conference, short course, meeting, or winter/summer program of interest to our readers we need information about your event so it can be included in this calendar when it is published in December. For more information please contact: Michele Gibson / michele@epimonitor.net
Open Public Health Positions
What it means and why it matters
The list below has been compiled by Public Health Hiring Help the new Substack column that has been created to help individuals in the public health community find positions in the midst of the chaos that is now impacting governmental agencies and grant recipients. This list represents the most current positions PHHH has been able to identify. We thank PHHH for their permission to reprint these listings.
PATH — Epidemic Preparedness Intern Public Health Alignment: EPI, GH
What it means and why it matters
City of Minneapolis — Public Health Pathways Intern Program Public Health Alignment: ANY
Mayo Clinic Healthcare Health Intern Public Health Alignment: ANY
Walworth Co Health and Human Services Intern Program Public Health Alignment: ANY
Duke Cancer Institute Clinical Research Intern Public Health Alignment: EPI
Mayo Clinic Computation Pathology and AI Intern Public Health Alignment: BIOS, EPI
IBM AI Healthcare and Life Sciences Intern Public Health Alignment: BIOS, EPI, HPM
Voloridge Investment Management LLC Health Research Analyst Intern Public Health Alignment: EPI, BIOS, HPM
Orlando Health Idea Generation Intern Public Health Alignment: ANY
Sanofi Biostatistics Evidence Generation Intern Public Health Alignment: BIOS, EPI
APCO Health Communications Intern Public Health Alignment: BSHES, GH, HPM
Dairy Farmers of America EHS Intern Public Health Alignment: EH
Agiliti — Environmental Intern Public Health Alignment: EH
American Cancer Society Outreach and Advocacy Intern Public Health Alignment: BSHES, GH, HPM
Multiple Open-Rank Faculty - Epidemiology
The O’Donnell School of Public Health and the O’Donnell Brain Institute at UT Southwestern Medical CenterDallas, TX are seeking exceptional epidemiologist candidates for multiple tenured or tenure-track faculty positions preferably at the associate or full professor level. Both the School and the Brain Institute are undergoing significant expansions, and an outstanding startup package, along with opportunities for program development, will be provided.
We encourage applications from exceptional scholars with a national reputation in epidemiological and population research on Alzheimer’s disease and other dementias, stroke and cerebrovascular disorders, Parkinson’s disease, or other neurological disorders. Qualified candidates should hold a doctoral degree (Ph.D., D.Sc., Dr.PH., or equivalent) in Epidemiology or an MD with additional training in Epidemiology or Clinical Investigation (M.S., M.P.H., MSc., or Ph.D.). Candidates must demonstrate a successful, impactful research career with a strong record of securing external funding (e.g., NIH, CDC, AHRQ, PCORI, etc.). Experience in academic leadership, program development, teaching, and fostering multidisciplinary collaboration is highly desired.
OPEN RANK FACULTY - EPIDEMIOLOGY DEPARTMENT
Appointment rank will be commensurate with academic accomplishment and experience. Consideration may be given to applicants seeking less than a full-time schedule.
Candidate Requirements:
♦ Ph.D., M.D., Sc.D., DrPH, or equivalent doctoral degree in a relevant discipline
♦ Demonstrated ability to conduct scholarly research and capacity to obtain peer-reviewed funding
♦ Highly self-motivated individual, enthusiastic about scientific discovery and able to collaborate closely and effectively with other members of multidisciplinary research teams
♦ Desire to partner with healthcare systems, public health agencies, and/or community organizations to conduct research aimed at enhancing the health of the people of Texas and beyond
Apply Here: https://tinyurl.com/4yt4ytjd
OPEN RANK FACULTY - EPIDEMIOLOGY BRAIN HEALTH RESEARCH
Appointment rank will be commensurate with academic accomplishment and experience. Consideration may be given to applicants seeking less than a full-time schedule.
Candidate Requirements
♦ Ph.D., D.Sc., Dr.PH., or equivalent in Epidemiology or an MD with additional training in Epidemiology or Clinical Investigation (M.S., M.P.H., or Ph.D.)
♦ Candidates must demonstrate a successful, impactful research career with a strong record of securing external funding (e.g., NIH, CDC, AHRQ, PCORI, etc.).
♦ Experience in academic leadership, program development, teaching, and fostering multidisciplinary collaboration is highly desired.
Apply Here: https://tinyurl.com/3rdj676f
CARDIOVASCULAR DISEASE EPIDEMIOLOGY AND PREVENTION POSTDOCTORAL FELLOWSHIP
The Division of Epidemiology & Community Health of the University of Minnesota has a current opening and is seeking candidates for a postdoctoral training fellowship in cardiovascular disease epidemiology and prevention.
Fellowship Experience Training emphasizes research methods in the epidemiology and prevention of cardiovascular disease. Training can include formal coursework in epidemiology, biostatistics, clinical research, nutrition, physiology, data science, and behavioral science.
Graduates gain competency in designing, administering, and analyzing cardiovascular population studies or preventive programs. The Division provides a rich and collaborative environment for the investigation of cardiovascular disease and related areas, in one of the largest Academic Health Centers in the U.S. Current Division research in cardiovascular epidemiology includes a robust blend of observational studies (e.g., ARIC, MESA, CARDIA, DISCOVERY), pharmacoepidemiology and interventional investigations (e.g., mGlide hypertension control RCT, Stand & Move at Work group randomized trial) aimed at improving public health and engaging a multidisciplinary integration of epidemiology, biology and behavioral science.
Benefits The program provides a stipend, tuition and fees for an MS or MPH degree, if desired, during the fellowship. This paid 2-3 year fellowship is sponsored by the National Institutes of Health.
Eligibility Candidates must have either an MD or a PhD degree and must be either a U.S. citizen or have permanent residency status.
Apply Interested applicants will complete an online application https://tinyurl.com/4e7yzp4c
Questions, please contact: Jim Pankow, PhD, MPH panko001@umn.edu or Pamela Lutsey, PhD, MPH lutsey@umn.edu Co-Directors of CVD Epi Training Program
YLE can be found here: https://yourlocalepidemiologist.substack.com/
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH
PhD an epidemiologist, wife, and mom of two little girls. YLE reaches more than 305,000 people in over 132 countries with one goal: “Translate” the ever-evolving public health science so that people will be well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members.
To support the effort, subscribe or upgrade your existing subscription: https://yourlocalepidemiologist.substack.com/
The Epidemiology Monitor ISSN (2833-1710) is published monthly by Monitor Publishing & Communications, Inc.
Mailing Address
663 Landing Drive
Aiken, SC 29801
info@epimonitor.net
Manager michele@epimonitor.net
All material in this publication is subject to copyright. For possible reprint permission please contact us at michele@epimonitor.net
Advertising options include but are not limited to:
Website only ads or website ads combined with digital print ads in this publication. Sponsorship for features in this newsletter or for the newsletter issue itself
Ads are accepted for open positions, events, programs, books, merchandise and other items of interest to our readers.
Subscriptions to this publication are free. Go to http://epimonitor.net/Subscribe.htm