monthly update covering people, events, research, and key developments
Editor’s Note:
We hope you will appreciate this month's issue and all that it includes but at the same time, we are already looking ahead to future issues and several of them include features where we need your help. In fact, we can't build these specific issues without your help.
This month's issue takes a look at epidemiology and the law. The first piece discusses the cost of testifying in legal cases. We've pulled two other piece from our archives that talk about being an expert witness and how the law influences public health. As the first piece discusses a lawsuit over the Tylenol / Autism connection we've also included a piece that discusses that possible connection.
Next you'll find a piece by Gideon about what is keeping public health teams up at night these days. That is followed by a piece about the newly updated John Snow website hosted by UCLA. This month's job hunt column talks about leveraging LinkedIn as an effective tool in your job search.
2025 - 2026 Salary Survey
One of our most popular features pre-Covid was the annual salary survey so this year, in partnership with Public Health Hiring Help, we are bringing it back. If you are the dean or chair of a school or department of public health / epidemiology / biostatistics you will soon be receiving an email from us requesting information so that we can build this year's report. If you'd like to get a head start on the process, please email us at salarysurvey@epimonitor.net and we will send you the necessary forms required to submit your data. Assuming everyone responds in a timely fashion, we hope to publish the data at the end of January but again, it is up to you to provide us the data.
Annual Event Calendar
As you know, our December issue is always dedicated to publishing a calendar of industry events offered worldwide. If you have a conference, meeting, short course, winter/summer program, or other event that you think would be of interest to our readers please send them to us at events@epimonitor.net and make sure you include contact information so we can get back to you with questions in order to list your event correctly.
As always, we continue to provide you with our popular monthly word game feature, Notes on People, an overview of what we are reading from the public media, and a listing of upcoming events.
Ask us about the sponsorship opportunities for these standard monthly features - it offers you great exposure for your event, institution, book or other item of interest to our readers! As you'll see this month, we can also tie our monthly word game to one of the articles in the issue.
Finally, don't miss the Job Bank offerings this month both here and on our website. We have some interesting opportunities - thankfully things are starting to slowly pick back up.
In This Issue
-3- The Price of Testimony - When Scientists Enter the Courtroom
-6- Epidemiology and the Law - Reflections on Serving as an Expert Witness
-8- Understanding the Role of Legal Frameworks in Shaping Public Health
-11- What's Keeping Public Health Teams Up At Night?
-19- Tylenol and Autism: What Parents Deserve to Know
-24- The Job Hunt: Beef Up Your LinkedIn Strategy
-27- Resources: UCLA Expands Its John Snow Website
-32- Monthly Word Game
-33- What We're Reading
-35- Notes on People
-39- Near Term Event Calendar
-40- Newly Listed Public Health Jobs
-43- Marketplace - Sponsored Jobs & Events
Did you miss last month’s issue? Read it here: https://tinyurl.com/5n6w3trc or here: https://tinyurl.com/ys47msmm
The Price of Testimony
When scientists enter the courtroom; money, credibility & justice collide
Author: Bruce Lanphear, MD, MPH
NOTE: This article was originally published on September 25, 2025 by Plagues, Pollution & Poverty on Substack.
Courts as Public Health Battlegrounds
Imagine being asked to compress years of scientific nuance into a simple yes-or-no answer for a jury. That was the dilemma Dr. Andrea Baccarelli faced when he testified in lawsuits over acetaminophen and autism and it is the same dilemma many scientists will face as the courtroom, rather than the regulator’s office, becomes the frontline of public health.
A New York Times article put Dr. Andrea Baccarelli a respected scientist at Harvard squarely in the spotlight. The story focused on his role as a paid expert witness in lawsuits over acetaminophen and autism.
As reported by the New York Times, Dr. Baccarelli wrote in his 2023 expert report for the lawsuit that “substantial evidence supports a strong, positive, causal association between acetaminophen” and neurodevelopmental disorders, particularly autism and A.D.H.D. That statement was enough to ignite a storm after Trump’s announcement that acetaminophen was linked to autism.
The controversy isn’t just about one scientist or one chemical. It raises a broader, uncomfortable question: should scientists testify in court cases at all?
When Courts Outpace Regulators
If we look honestly at the last half-century of public health, many of the most important victories did not come from regulators. They came from courts.
I was personally involved in litigation against the paint and pigment industry in California, where ten cities and counties ultimately secured a $305 million settlement to clean up lead hazards in housing. Regulators had stalled for decades while millions of children were exposed to dangerous levels of lead paint. It was the courts that finally broke through.
The pattern has repeated itself. Earthjustice went to court to force the EPA to strengthen rules protecting children from lead hazards in their homes. Years of administrative dithering and industry lobbying had left the standards badly outdated. Only when the agency was sued did it move. Chlorpyrifos, a widely used pesticide that can damage children’s brains, remained in circulation long after the science was clear. Litigation rather than regulation finally forced its removal from agriculture, though a subsequent court case left it available for certain select applications.
It may sound hyperbolic to say that nothing seems to happen in public health without the courts, but experience makes it hard to conclude otherwise. The courtroom has become the place where evidence collides with power, where delay gives way to decision, and where the hidden toll of toxic chemicals finally becomes visible.
- Testimony cont'd on page 4
The Tension for Scientists
And yet, the courtroom is not the laboratory. Science traffics in probabilities, confidence intervals, and cautious caveats. Courts demand clarity. Judges and juries want yes-or-no answers. When a scientist steps into that environment, the tension is palpable.
Money complicates it further. Dr. Baccarelli was paid $150,000 for his testimony. That is a substantial sum by any measure, even for
a tenured professor at an Ivy League university. We know from decades of research on conflicts of interest that financial incentives shape judgment. They may not buy opinions outright, but they bend perception in ways that scientists themselves may not recognize. Why else would journals demand disclosures, why else would advisory committees set strict financial thresholds, why else would we impose rules on clinical trials?
"It is difficult - perhaps impossibleto remain fully objective when large payments are on the line. Scientists know this. The public knows this. And when the sums are large, trust erodes."
It is difficult perhaps impossible to remain fully objective when large payments are on the line. Scientists know this. The public knows this. And when the sums are large, trust erodes.
What Happens If Scientists Stay Silent
Still, here is the dilemma: if scientists refuse to testify, public health falters.
Take paraquat, a herbicide strongly linked to Parkinson’s disease. Litigation has uncovered internal documents suggesting manufacturers knew more than they revealed. Without scientists to explain the biology to juries, those cases would wither. Atrazine, another pesticide, contaminated aquifers across wide swaths of the country. The courtroom revealed its spread
and its risks long before regulators were willing to act. The sprawling settlements over PFAS “forever chemicals” that taint water supplies across the United States—would never have materialized without scientists translating the complex toxicology into terms a judge could understand.
I could add asbestos, benzene, vinyl chloride, diesel exhaust. The pattern is the same. Regulators move slowly; industry lawyers sow doubt; and public health languishes until litigation forces the issue. If scientists walk away, the only experts left are those who hire themselves out to industry to manufacture uncertainty. The absence of credible scientific
- Testimony cont'd on page 5
testimony doesn’t make cases more objective— it tilts the scales decisively toward those who profit from pollution.
How to Balance Ethics and Engagement
So what should scientists do? The answer cannot be to retreat. The stakes are too high. But we also cannot ignore the corrosive effect of money.
I believe scientists should serve as expert witnesses, but they must do so with care. They should choose cases where the evidence is strong enough to support their testimony and where the litigation has broad implications for public health. I avoid individual cases that hinge on personal injury alone. My focus is on lawsuits that can shape entire populations cases that change housing codes, force cleanup of water supplies, or establish precedents that protect millions.
And the financial side must be handled differently. When I work with advocacy groups, I often provide my services pro bono. I served as an unpaid expert in the recent fluoride case, Food & Water Watch v. EPA, where the question of neurotoxicity and water fluoridation was at stake. When I collaborated with the Natural Resources Defense Council to help Pittsburgh deal with its lead service lines, I did so without charging a fee.
In instances where payment for my service is warranted, I direct it to my university. The funds support research or teaching, but they do not buy me a personal computer, a vacation, or a car. By drawing a bright line, I protect myself and science from the perception that my testimony is for sale.
For Dr. Baccarelli, the path forward seems similar. He should continue to serve as
an expert witness when the science is sufficient and when the case has implications for public health. His voice matters. But he should not pocket the money. Redirecting those funds to a nonprofit organization or to a university account for research and teaching would not only safeguard his reputation but strengthen the credibility of the work itself.
The Bigger Picture
This debate is not really about one scientist, one drug, or one deposition. It is about the relationship between science and the law, and about how public trust is earned or squandered. If the public comes to believe that scientists are merely hired guns, then science loses its power in the courtroom and, by extension, in society.
At the same time, if scientists retreat entirely, industry voices dominate. Cases stall, exposures continue, and preventable disease spreads. The courts have become the frontline of public health. From lead paint to pesticides to PFAS, the evidence is clear: litigation often does what regulation cannot.
Public Health Over Personal Gain
Scientists should not abandon the courtroom. On the contrary, they must be there precisely because the stakes are so high. But they should be there on different terms terms that prioritize public health over personal enrichment. That is how science can serve justice without selling its soul.
This article was originally printed on Substack in Plagues, Pollution & Poverty. To read more content from this source subscribe to Plagues, Pollution & Poverty: https://tinyurl.com/3rfeuama
From our Archives Epidemiology and the Law
Reflections on Serving as an Expert Witness
Author: David Savitz, PhD
For many, perhaps most, epidemiologists, engaging in legal disputes as an expert witness is unappealing. These impressions may be based on past legal decisions that run counter to an informed interpretation of the epidemiologic evidence, an aversion to being drawn into advocacy for fear of damaging one’s reputation as an objective scientist, or a distaste for being tormented by opposing attorneys in depositions or trial cross-examination. None of these are without merit, but there are ways to mitigate the negative aspects and enhance the positive aspects of serving as an epidemiology expert on legal matters.
For epidemiologists who are motivated to bring scientific rigor and knowledge to bear on societal decisions, court cases provide perhaps the most direct opportunity to do so. In contrast to the sometimes-meandering pipeline of scientific discoveries influencing public policy or individual decisions, legal disputes are direct and relatively rapid: a decision will be made, epidemiologic evidence is relevant, and providing accurate interpretation of the evidence should lead to a more just outcome. While there are legitimate reasons to question whether legal disputes are the best means of reaching decisions, they are an important aspect of the way society operates.
The adversarial nature of the legal system seems counter to an objective, dispassionate assessment of the evidence by informed experts to reach a decision, as is generally the case for expert committees charged with assessing evidence. Attorneys are advocates
for their clients, and when they engage epidemiologists, it is with the belief that the experts will contribute to winning the case. Epidemiologists need to maintain clarity regarding their role (and integrity) as experts and accept that the attorneys who engage them will be seeking ways to use their expertise to the benefit of their client.
Maintaining objectivity is critical not just for the reputation of the epidemiology expert but ultimately for the attorney’s client and even for the justice system itself. I have been approached by attorneys who indicate need for an epidemiology expert who will provide the opinion that helps their client, and my routine response is to indicate that I need to review the evidence in order to provide an informed, defensible opinion but until I do so, I don’t know what my opinion will be. Sometimes I have been engaged for an initial assessment that suggests my views will not be beneficial to their case, but at minimum it provides a preview of what they can expect to face from the opposing side. A colleague summarized the need for objectivity succinctly: don’t say anything in court that you would not say to your colleagues. The way to engage without becoming a biased advocate is to be vigilant and consistent in striving for objectivity.
There can be challenges to managing the schedule by which legal cases evolve, with crises and long hiatuses, but attorneys are generally able to buffer experts from the vicissitudes of the legal calendar. And facing the opposing
- Witness cont'd on page
attorney in depositions and testimony can be stressful and tiring, responding to the challenges ranging from nitpicking to misunderstanding. But so long as the evidence and basis for interpretation of the evidence are clear, the epidemiology expert is explaining rather than arguing. The information needs to be presented in a way that is accessible to nonexperts and simplified without misrepresenting the evidence or the relevant methodologic issues.
Attorneys involved in cases that draw on epidemiology are often quite knowledgeable about how epidemiologic research is done and what study results mean. Based on my experience with attorneys who were seeking a deeper understanding of epidemiology, I collaborated with an attorney for whom I had consulted to write a book which has just been published, “Epidemiology and the Law.” The purpose of the book is to provide a brief tutorial on epidemiology that is accessible to nonexperts and relevant to those who are drawing on epidemiology in legal cases. While it was challenging to be accurate without “dumbing it down,” to a large extent, epidemiology can be made intuitive. The book’s focus is on the connection between the epidemiologic research and making inferences about causality, which is at the heart of legal matters. Topics that are particularly prone to misinterpretation such as statistical significance testing and the interpretation of negative studies warranted their own chapters, as well as several chapters that address the legal context in which epidemiology operates.
Serving as an expert witness may not be appealing for all epidemiologists, but our profession would be better served by having more epidemiologists willing to engage in legal disputes. The alternative to having informed, objective epidemiologists serve is for attorneys
Available on Amazon in hardcover format. https://tinyurl.com/2yf538t8
to engage “hired guns,” those who will predictably support their side. Such experts predictably find that the agent of concern is harmful (for plaintiffs) or always find that it is not harmful (for defendants). In fact, the evidence often falls close to the fence for issues that make their way to court since definitive evidence generally leads to rapid settlements since there is a reputational incentive to being receptive to mix work as an expert or defendants and plaintiffs.
There are several underappreciated benefits to engaging as an expert. It may provide an opportunity to dig deeply into a controversial issue of societal relevance and get a firm grasp on the body of research. Being called upon to make a judgment and defend it sharpens practical skills in causal inference. And beyond applications in court, improving our ability as epidemiologists to communicate with those outside the field is generalizable to other audiences that stand to benefit from a deeper appreciation of what epidemiology has to offer.
■
Understanding the Role of Legal Frameworks in Shaping Public Health
"Legal Epidemiology: Theory and Methods"
Author: Alexander C. Wagenaar, PhD
Epidemiology and related fields conducting scientific evaluations of the population health effects of public policies typically report studies with major limitations. Studies are often atheoretical, without a clear articulation of the underlying theory on the expected mechanisms of effect between a legal change and health outcomes. When random assignment to treatment conditions is not possible, studies often do not include a full complement of other important research design elements available to strengthen causal inference. Finally, studies often pay little or no attention to measurement consistency, reliability and validity, especially for independent variables designed to measure changes in laws or policies.
Legal Epidemiology: Theory and Methods, a [new] text published by Wiley, advances science by directly addressing the above limitations.
Edited by Alex Wagenaar, Rosalie Liccardo Pacula and Scott Burris, a team of 23 distinguished scholars from a diverse set of public health and social science disciplines deliver a thorough primer addressing issues that arise specifically in legal epidemiology the scientific study and deployment of law as a factor in the cause, distribution, and prevention of disease and injury in a population.
Law is critical as a mechanism of influence on the public’s health, well-being, and equity. In shaping physical and social environments, and in shaping individual and social behaviors, law
serves as a systemic intervention one we saw clearly during the height of the recent COVID-19 pandemic. Law can also serve as a barrier to systemic interventions, as we have seen with harm reduction efforts related to opioids. A holistic consideration of legal environment therefore is important for addressing the ongoing challenges around the social determinants of health and most other areas of research in epidemiology. Law is at the root of most major public health advances, and yet we have historically not paid sufficient attention to improving its scientific assessment.
The book’s first two chapters provide a framework for situating the field of legal epidemiology within the broader field of public health. Then six chapters lay out theories relevant for understanding mechanisms of legal effect from public health, sociology, criminology, social psychology, and economics, closing with a chapter integrating concepts and mechanisms from diverse disciplines. Part three of the book lays out specific practical steps for the measurement of legal variables, ensuring reliable and valid indicators required for highquality scientific studies. The final major section of the book focuses on research design considerations that are central for making causal inferences concerning effects of law on the public’s health, including RCTs, controlled time-series trials and natural experiments, as well as qualitative and cost-benefit studies of public health policies.
The text is particularly helpful to PhD students, post-docs, and career scientists interested in the social determinants of health, and studying effects of regulations, laws and other public policies on population-level health outcomes.
Contents
Foreward to the First Edition: Michelle A. Larkin
Forward to the Second Edition: Sandro Galea
Preface
PART ONE: Frameworks for Legal Epidemiology
Editors:
ALEXANDER C. WAGENAAR, PhD, is Research Professor at the Emory University Rollins School of Public Health and Professor Emeritus at the University of Florida College of Medicine.
ROSALIE LICCARDO PACULA, PhD, holds the Elizabeth Garrett Chair in Health Policy, Economics & Law in the Sol Price School of Public Policy at the University of Southern California.
SCOTT BURRIS, JD, is Professor of Law and Public Health at Temple University, where he directs the Center for Public Health Law Research, and Professor in Temple’s College of Public Health.
1. A Framework for Research in Legal Epidemiology
Scott Burris, Alexander C. Wagenaar, Jeffrey W. Swanson, Jennifer K. Ibrahim, Jennifer Wood, and Michelle M. Mello
2. Law in Public Health Systems and Services Research
Scott Burris, Glen P. Mays, F. Douglas Scutchfield, and Jennifer K. Ibrahim
PART TWO: Understanding How Law Influences Environments and Behavior
3. Perspectives from Public Health
Kelli A. Komro and Alexander C. Wagenaar
4. Law and Society Approaches
Robin Stryker
5. Criminal Theories
Wesley G. Jennings and Tom Mieczkowski
6. Procedural Justice Theory
Tom R. Tyler and Avital Mentovich
Frameworks
6. Procedural Justice Theory
Tom R. Tyler and Avital Mentovich
7. Economic Theory
Frank J. Chaloupka and Rosalie Liccardo Pacula
8. The Theory of Triadic Influence
Marc B. Schure, Kazi Faria Islam, and Brian R. Flay
9. Integrating Diverse Theories for Public Health Law Evaluation
Scott Burris and Alexander C. Wagenaar
PART THREE: Identifying and Measuring Legal Variables
10. Picturing Public Health Law Research: The Value of Causal Diagrams
Jeffrey W. Swanson and Jennifer K. Ibrahim
11. Measuring Statutory Law and Regulations for Empirical Research
Evan D. Anderson, Sue Thomas, Ryan D. Treffers, and Alexander C. Wagenaar
12. Coding Case Law for Public Health Law Evaluation
Mark Hall
PART FOUR: Designing Legal Epidemiology Evaluations
13. Randomized Trials in Legal Epidemiology
Harold Pollack, Alida Bouris, and Scott Cunningham
14. Natural Experiments: Research Design Elements for Optimal Causal Inference Without Randomization
Alexander C. Wagenaar and Kelli Komro
15. Qualitative Research Strategies for Public Health Law Evaluation
Jennifer Wood
16. Using Cost-Effectiveness and Cost Benefit Analysis to Evaluate Public Health Law
Rosalie Liccardo Pacula
17. The Future of Research in Legal Epidemiology
Scott Burris, Rosalie Liccardo Pacula, and Alexander C. Wagenaar
What's Keeping Public Health Teams Up At Night
5 Battles in the Age of Information
Author: GIDEON (Global Infectious Disease and Epidemiology Online Network)
Overview
Public-health teams face rising expectations, data quality challenges, and shrinking budgets. In particular, five issues now loom large:
● A murky information environment
● Climate-linked health risks
● Antimicrobial resistance
● Fragmented data
● Uneven outbreak preparedness and equity
How do public health teams and epidemiologists navigate these challenges?
1. Misinformation as an operational hazard
Health departments now compete with a flood of misleading content that directly undermines their work. When social media posts promoting unproven treatments go viral faster than official health alerts, it affects whether people seek appropriate care or follow public health guidance.
A 2024 review found that post-pandemic misinformation has become so pervasive that monitoring and response must be embedded into routine health operations. The impact extends beyond emergency response. Analysis of nearly 1,000 social media posts about popular medical tests revealed that benefits were mentioned far more often than risks or potential for overdiagnosis. This
promotional content, often from influencers with no medical training, drives demand for unnecessary services and creates confusion about evidence-based care.
The World Health Organization (WHO) now considers “infodemic” management a core public health function, requiring the same systematic approach as disease surveillance. Their framework includes four pillars: listening to community concerns, promoting understanding of risk, building resilience to misinformation, and engaging communities to take appropriate action.
What this means for public health
Misinformation directly interferes with outbreak control when false cures spread faster than prevention messages. Health departments must now budget for social media monitoring just as they do for laboratory testing. Staff need training not just in epidemiology but in rapid response communications.
Every delay in correcting false information translates to preventable illness and death. Traditional press releases and weekly reports cannot compete with viral posts that reach millions in hours. Public trust, once lost to misinformation, takes years to rebuild.
2. Climate-related health risks
In October 2025, mosquitoes were discovered in Iceland for the first time in recorded history. The country had been one of only two mosquitofree places on Earth. However, as Iceland warms at four times the global average, even this last
refuge has fallen to expanding disease vectors.
Climate impacts on health are now measurable and severe. Heat-related mortality among adults over 65 has increased 167% since the 1990s, with 2023 recording the highest levels yet. These deaths translate directly into predictable surges in emergency services and hospital admissions during heat waves.
Disease vectors are expanding their reach. The climate conditions suitable for dengue transmission have increased dramatically over the past decade. For Aedes albopictus mosquitoes, suitable areas expanded by 46%, while Aedes aegypti territory grew by 11%. These shifts mean dengue can now spread in new regions and during previously safe seasons.
What this means for public health
Health departments must prepare for diseases in places they've never been before and heat emergencies outside traditional summer months. Budget cycles based on historical patterns no longer match reality.
Communities without experience managing dengue now need diagnostic capacity, clinical guidelines, and vector control programs. Emergency departments designed for typical seasonal variation face overwhelming surges during extended heat events.
The populations most vulnerable to the impact of climate change often have the least access to healthcare and preventive services, widening existing health inequities.
3. Fragmented data
Today's outbreak intelligence arrives through a chaotic mix of channels. A cluster of unexplained pneumonia cases might surface
first on social media, followed days later by a ProMED alert, then eventually appear in WHO bulletins.
Health officials monitor everything from Twitter posts to news reports to faxed laboratory results, each with different verification standards and time lags.
The fundamental problem isn't just volume but incompatibility:
● Official surveillance systems weren't designed to integrate with media reports or social media alerts
● Different countries use different case definitions
● The same outbreak gets reported under multiple names across various platforms. What appears to be three separate events might be one outbreak reported differently, or three distinct emergencies requiring immediate action
This fragmentation paralyzes decision-making. During the critical early hours of an outbreak, epidemiologists spend more time reconciling conflicting reports than analyzing transmission patterns. Some platforms work to consolidate these streams.
GIDEON (Global Infectious Diseases and Epidemiology Online Network), for example, maintains a comprehensive database of global health events, and a list of 2-week epidemiological events updated daily with verified information.
- Night cont'd on page 13
What this means for public health
Every hour spent verifying duplicate reports is an hour not spent containing disease spread. Border control decisions rely on whatever incomplete information arrives first. Resource allocation becomes guesswork when officials cannot distinguish signal from noise.
Most critically, the absence of standardized reporting across systems forces each country to build its own surveillance picture from scratch.
While jurisdictions duplicate each other's verification efforts, outbreaks cross borders undetected, turning manageable local clusters into international emergencies.
Platforms like GIDEON offer verified and
comprehensive infectious disease data in one place, making it easier for officials to get the information they need, faster.
4. Antimicrobial resistance (AMR): a silent pandemic
In 2019, bacterial antimicrobial resistance (AMR) directly caused 1.27 million deaths and contributed to 4.95 million deaths globally. Lower-respiratory infections accounted for the largest share of deaths, particularly in low- and middle-income countries.
Methicillin-resistant Staphylococcus aureus (MRSA) exemplifies the crisis, killing more than
- Night cont'd on page 14
100,000 people in 2019 alone. But MRSA is just the beginning. In Greece, 59% of Klebsiella pneumoniae infections now resist carbapenems, once considered last-resort antibiotics. In Italy, the crisis has deepened: among patients whose infections already resist carbapenems, 43% also resist colistin. Since colistin was the final fallback drug, when both drugs fail, no available antibiotics may work.
Data on bacterial AMR reveals an evolving threat:
● In 2021, overall AMR deaths decreased slightly to 1.14 million, yet mortality patterns shifted dramatically by age
● Deaths among adults 70 and older increased by over 80% since 1990, even as under-5 mortality declined
Future projections paint a dire picture: 300 million premature deaths over the next 35 years and global economic losses of 60-100 trillion USD by 2050.
Additionally, a WHO 2025 report captured 23 million lab-confirmed infections across 104 countries. One in six infections showed resistance to standard antibiotics. Resistance increased in over 40% of pathogen-antibiotic combinations since 2018.
What this means for public health
Standard treatment protocols increasingly fail because they rely on outdated resistance patterns. Patients require longer hospitalizations and more expensive secondline drugs.
Outbreaks once routine to manage now strain resources. Resistant strains spread more easily and require intensive containment efforts. When common antibiotics fail, doctors turn to
toxic older drugs or experimental treatments. Even these options are rapidly disappearing.
5. Preparedness, governance, and equitable access
The global health security framework shifted significantly in 2024. WHO Member States adopted critical amendments to the International Health Regulations that took effect in September 2025, emphasizing information sharing, financing mechanisms, and health equity.
Yet implementation remains uneven. Some countries have filed reservations or outright rejections, creating a patchwork of compliance that undermines coordinated response.
The numbers reveal why preparedness fails. WHO data show that in 2021:
● 4.5 billion people lacked full coverage for essential health services
● Two billion face financial hardship from healthcare costs
● One billion experiencing catastrophic health expenditures that can bankrupt families. This coverage gap has widened since 2015, not narrowed.
Preparedness cannot exist without basic healthcare infrastructure. Countries with weak primary care systems, understaffed laboratories, and fragile supply chains cannot suddenly scale up during emergencies. The COVID-19 pandemic proved this definitively. Nations with robust primary care detected cases earlier, traced contacts more effectively, and distributed vaccines more equitably.
- Night cont'd on page 15
Comprehensive infectious disease databases like GIDEON, which track disease patterns across 230+ countries and territories with daily updates help health departments understand their vulnerabilities before crises hit.
With outbreak data spanning from 1338 to present, epidemiologists can identify historical patterns of disease emergence in their regions and prepare for similar threats.
What this means for public health
Outbreak preparedness built on inequitable foundations will inevitably collapse under pressure. The communities most vulnerable to disease outbreaks are precisely those excluded from basic healthcare.
When surveillance systems miss these populations, diseases spread undetected until they reach wealthier areas with better healthcare access. By then, containment becomes exponentially more difficult and expensive.
True preparedness requires closing equity gaps before emergencies strike, not promising to address them during crisis response when resources are already stretched beyond capacity.
How GIDEON
helps address public health challenges
Tackling today’s complex health threats is everyone’s problem. Government agencies, clinicians, educators and researchers all play a part.
For over 30 years, GIDEON (Global Infectious Disease and Epidemiology Online Network)
has been a vital resource for public health professionals, educators, researchers, clinicians, and epidemiologists. It provides up-to-date reliable data, evidence-based updates, diagnostic tools, therapeutic data, and data visualization features to help turn infectious disease trends into actionable insights.
GIDEON exists to advance the global effort against Infectious Disease. Here’s how.
1. Countering misinformation with verified data
In an age where false information spreads faster than official updates, GIDEON serves as a verified, evidence-based counterweight.
Its continuously updated database consolidates information from more than 20,000 trusted sources, including ministries of health, peerreviewed journals, and international surveillance systems.
Each entry undergoes an editorial review by infectious disease specialists to ensure accuracy and relevance.
GIDEON delivers consistent, evidence-based outbreak data and curated summaries, helping health departments communicate clearly and in a timely manner.
2. Mapping disease outbreaks
As climate change drives new disease patterns, GIDEON allows users to observe these shifts through frequently updated visuals.
Interactive maps and customizable epidemiological charts can help officials
- Night cont'd on page 16
analyze trends and compare them to changes in temperature or rainfall. This can shed light on connections with vector- and water-borne disease outbreaks.
Health departments can compare regional data, identify potential hotspots, and adapt preparedness plans as environmental conditions evolve. This way, GIDEON helps officials anticipate disease emergence in new regions.
3. Bringing structure to fragmented data streams
Outbreak information today arrives through through multiple, often disconnected sources. GIDEON integrates these verified reports into one comprehensive resource.
Instead of piecing together social-media mentions, ProMED alerts, and health-ministry bulletins, users can access curated, cross-
checked data through a single platform.
Plus, GIDEON’s Epidemiological Events page provides a two-week rolling summary of global health reports updated frequently, while historical records span centuries. This structure saves time, prevents duplication, and gives officials confidence that they are working with validated and timely information.
4. Comprehensive disease intelligence
Understanding infectious disease patterns requires access to integrated data on diseases, pathogens, and therapeutic options.
GIDEON consolidates these critical elements into a single platform for evidence-based clinical and epidemiological decision-making.
- Night cont'd on page 17
● Extensive disease database: GIDEON maintains clinical and epidemiological information on more than 370 infectious diseases, including their global distribution, prevalence surveys, and historical outbreaks. This context allows users to study where infections occur and how they spread.
● Robust drug reference system: The anti-infective drugs module catalogs over 30,000 trade names and allows users to search and compare medications by class, spectrum, toxicity, or interactions. These tools support informed prescribing decisions and help clinicians select appropriate treatments based on local availability and clinical guidelines.
● Detailed pathogen profiles: GIDEON provides phenotype data on 3,000+ medically important bacteria, mycobacteria, fungi, parasites, viruses, and yeasts for organism identification and characterization. The database includes 2,000+ bacterial and mycobacterial entries with relevant synonyms and diagnostic images.
● Global and regional insights: The GIDEON platform incorporates 25,000+ country-specific notes and 100,000+ prevalence and seroprevalence surveys, providing localized context for disease burden and treatment practices. Users can easily download or share findings to facilitate collaboration across departments and institutions.
By bringing together pathogen profiles,
therapeutic data, and disease patterns in one platform, GIDEON streamlines how healthcare teams access critical information.
With GIDEON, users get credible infectious disease data at their fingertips to help develop public health strategies, clinical, epidemiological, and public health needs.
5. Strengthening preparedness and equity
GIDEON’s global datasets offer an evidence base for assessing outbreak preparedness and response capacity.
By visualizing disease trends and case distribution across 230 countries and territories, agencies can identify surveillance gaps before they become crises. Outbreak records span from 1338 to the present, offering historical depth to modern risk assessment.
Final thoughts
Public health has always faced complex threats, but today's landscape brings unique challenges:
● Misinformation now spreads at digital speed
● Climate change drives diseases into regions with no immunity or infrastructure to manage them
● Surveillance data arrives through hundreds of channels simultaneously
● Antimicrobial resistance leaves doctors with fewer options for effective treatments
● Outbreak preparedness is hindered by inequitable access to healthcare
- Night cont'd on page 18
These challenges demand new approaches. Verified databases now organize what once took days to cross-check. Historical outbreak data reveals patterns that help predict future risks. Global networks enable rapid information sharing between countries facing similar threats.
The transformation is already underway. Platforms like GIDEON convert centuries of outbreak data into practical intelligence for today's decisions. Expert verification promotes reliability. Regular updates keep pace with evolving situations. Health departments that once worked in isolation now benefit from collective knowledge.
The path forward is becoming clearer. When public health officials can access comprehensive data quickly, compare patterns across regions, and base decisions on evidence rather than assumptions, they shift from reactive to proactive response. Resources flow where data shows they're needed most.
The scale and speed of modern threats require tools that match their complexity. Fortunately, such tools now exist and continue to improve. By embracing verified data and global collaboration, public health teams can anticipate emerging threats rather than chase them. The future of public health depends on making smart use of these advances today. ■
Your Ad Should Be Here
Tylenol and Autism
What Parents Deserve to Know - Nuance & Empowerment Instead of Underestimation
Authors: Katelyn Jetelina, MPH, PhD and Kristen Panthagani, MD, PhD
Editor's Note: This article was originally printed in Your Local Epidemiologist on September 25. 2025. To read more content from this source subscribe to Your Local Epidemiologist (YLE): https://tinyurl.com/47494ms4
On Monday [September 22, 2025], RFK Jr.’s autism “report” landed. This was supposed to be the culmination of RFK Jr.’s months-long promise to “finally uncover” the cause of autism by September.
But no report was published, no new science was unveiled, and no fresh data was presented. Instead, we got an X post, a press conference, and politicians coming to far-reaching conclusions from data that obstetricians, pediatricians, and scientists have already spent decades studying.
As an epidemiologist, I could see the falsehoods spewing out like a firehose with a few kernels of truth mixed in. But as a mom, the aftermath was visceral. My DMs and texts lit up with worry. Even the faint suggestion of blame haunts pregnant women and parents, piling more weight on shoulders already carrying enough. Being told to “toughen up”, without regard for the confusion, doubt, and guilt that are placed on us far too often these days.
This is where I believe this “report” is making a grave mistake. They are underestimating the power of parents. Parents don’t need fearmongering or false certainty they want accurate information, context, and respect. Not
chaos, but clarity. Not underestimation, but empowerment with the best evidence at their fingertips to help them make the best decisions for themselves and their families.
What happened earlier this week is far, far from this. And parents deserve better.
Bottom line up front
Scientists have been working to uncover autism for decades. This is ongoing, but for now, the balance of evidence shows this: There is no causal link between Tylenol use and autism.
To all the mothers out there, you are doing amazing.
Where did this claim come from?
The idea that Tylenol (acetaminophen) use during pregnancy could be linked to autism has been investigated by the scientific community for more than a decade. Some scientists have wondered if Tylenol might affect a baby’s brain during pregnancy by stressing cells or changing certain chemical pathways. These hypotheses primarily originate from laboratory and animal studies at high doses.
There have also been many, many human studies.
- Autism cont'd on page 20
The paper behind many of the headlines this week is a Harvard/Mount Sinai study that reviewed over 46 studies evaluating the associations between Tylenol and neurodevelopmental disorders, including autism and ADHD, with six studies focusing specifically on autism. They found a mix of conclusions:
27 studies found a positive link (Tylenol in pregnancy is correlated with neurodevelopmental disorders)
9 studies found no link
4 studies showed a negative link (Tylenol is correlated with fewer neurodevelopmental disorders)
These authors found a pattern consistent with rat studies: Tylenol, particularly during third trimester, was associated with higher risk. Also, they found a dose-response relationship: the more Tylenol someone had during pregnancy, the greater the associated risk. Importantly, the overall increased risk they found in these correlative studies was quite small.
BUT. These were not randomized controlled trials (the gold standard), because it would be unethical to assign pregnant women to take or avoid Tylenol (the risks of untreated fever are real). Instead, each of these individual studies had to rely on observational methods. And observational studies can be tricky. They’re always vulnerable to confounding variables (what caused moms to take Tylenol in the first place?) or other factors (like genetics or environmental exposures) that may explain the pattern.
In 2024, a major study from Sweden took the evidence a step further. Researchers there did something clever: they compared siblings. One child had been exposed to Tylenol during pregnancy, the other had not. This kind of
“natural experiment” is powerful because it controls for what siblings share, including genetics and family environment. We know autism has a strong genetic component, so studies like this, controlling for genetics, are critical.
The Tylenol–autism link disappeared when comparing siblings.
When the researchers examined the data without sibling comparisons, they reproduced the same association that older studies had found. That means the study was strong enough to detect the association but also strong enough to show it evaporated once they controlled for genetic and other environmental factors.
In other words, this evidence leans heavily toward correlation, not causation. (Tylenol is not the cause.)
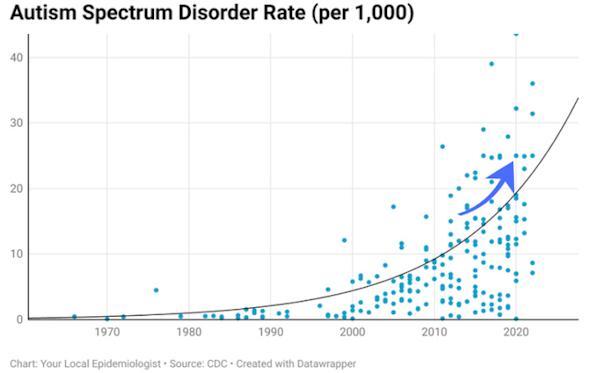
What else could explain changes in autism prevalence numbers?
Many epidemiologists do think there is a rise in autism due to improved recognition and diagnostic criteria, but not at the dramatic rate that the “report” insinuated. (Read more here for a deep dive into the data trends.)
Autism is rooted in brain development. While neuroscience is still being mapped, we do know that some autistic brains show differences in neuron growth and connectivity differences that originate in utero, when the brain is forming.
- Autism cont'd on page 21
So why do some developing brains take this path while others don’t? Research shows that it’s highly genetic—85% of the risk is attributed to your genes. But genetics haven’t changed over time. Therefore, if there is an increase, it’s
likely that environmental exposures.
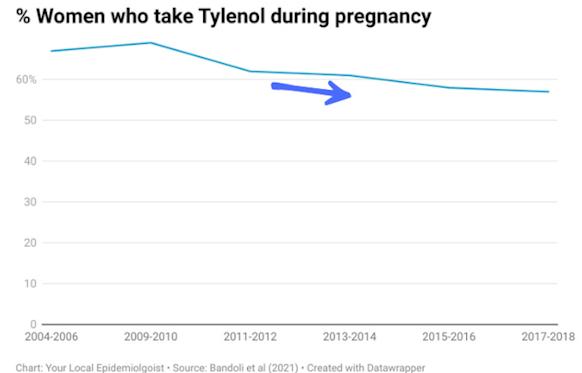
Tylenol use has decreased over time. So, again, another sign this isn’t leading to a dramatic rise in autism.
- Autism cont'd on page 22
Other hints include:
Advanced parental age. Many studies suggest that both advanced paternal and maternal age are risk factors for autism, as the likelihood of spontaneous mutations in sperm and eggs increases as people get older. However, one 2016 study even suggested that younger mothers (those under 20 years old) are at increased odds of having a child with ASD.
Premature births are more likely to be diagnosed with autism.
Maternal inflammation. Infections, high fevers, or immune activation during pregnancy may play a role.
And other factors, including folic acid deficiency, obesity during pregnancy, and air pollution.
So what do parents do with this?
All medications have risks and benefits, and that includes Tylenol. For pregnant moms trying to wade through the headlines, here’s where we’re at:
Possible risk: Inconsistent signals in observational studies, with some suggesting a correlation between Tylenol and autism. These studies cannot prove causation, and the strongest sibling study showed no causal link.
Known benefit: Tylenol is one of the few pain and fever relievers considered safe during pregnancy; all other options have shown risks (not just potential). And treating fever during pregnancy is important, as fever is associated with increased risks birth defects (and has even been associated with increased risk of autism in small studies).
So, here’s how I would think about it:
Not one medicine or one exposure causes autism. All evidence points to a constellation of factors with a strong genetic component.
The data to date have not demonstrated a causal link between Tylenol and autism. The American College of Gynecologists and Obstetricians recommends pregnant women use Tylenol if needed, for fever or significant pain.
Remember context. The risk signals we’ve seen are small, inconsistent, and likely explained by confounding factors. The risks of untreated high fever in pregnancy are clear.
Oversimplifying science
If you’ve watched RFK Jr.’s scientific claims over the last several decades, his claim that a commonly prescribed medicine is causing autism comes as no surprise. He has a long history of pointing fingers at medications Tylenol, vaccines, you name it as the root of health challenges. It’s a convenient scapegoat.
This taps into a common fallacy he often defaults to: the idea that “natural” is always good and “chemical” is always bad. This “appeal to nature” fallacy is seductive because it feels intuitive but it isn’t evidence-based. Reality is more complex. Plenty of natural things are harmful (arsenic, poison ivy), and plenty of manmade medicines save lives.
Some diseases are naturally occurring. Some conditions like autism are part of the natural spectrum of human diversity. Pretending
- Autism cont'd on page 23
otherwise doesn’t just mislead; it actively harms families by piling on stigma and misplaced blame and providing empty solutions instead of support and real answers.
Bottom line
The “report” made a grave mistake: it underestimated parents and placed an undue
burden of anxiety and guilt on them instead of empowering them to make informed decisions. Science is ongoing, but for now, the balance of evidence shows this: There is no causal link between Tylenol use and autism.
To all the mothers out there, you are doing amazing. ■
YLE can be found here: https://yourlocalepidemiologist.substack.com/
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD an epidemiologist, wife, and mom of two little girls. YLE reaches more than 305,000 people in over 132 countries with one goal: “Translate” the ever-evolving public health science so that people will be well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members.
To support the effort, subscribe or upgrade your existing subscription: https://yourlocalepidemiologist.substack.com/
The Job Hunt
Beef Up Your LinkedIn Strategy!
Author: Public Health Hiring Help
NOTE: This article was originally published on July 11, 2025 by Public Health Hiring Help on Substack.
Are You Really Using LinkedIn to Its Fullest?
“Who are even getting these jobs?!”, a subscriber remarked in my LinkedIn DMs. He had applied for dozens of jobs and had received rejection after rejection, despite meeting the posted qualifications.
It’s a valid question, and one I’ve grappled with too. How can you meet all the qualifications maybe even be OVERqualified—and still receive an auto-rejection? You cast a wide net, you got your resume and cover letter reviewed and tailored them for the kinds of jobs you apply to, you added folks on LinkedIn nonstop and commented on posts about openings what more could you be doing?
Wait. Rethink that last one. ‘You added folks on LinkedIn nonstop.’ And?
I can’t remember who asked me this simple question to challenge this strategy, but thank goodness for them.
What are you doing with those connections? Just adding them isn’t enough. Recall that LinkedIn, before becoming the professional social media it is today, was a networking platform first. Networking isn’t just amassing connections or followers or dropping one-off comments declaring “interest”; it involves direct conversation and interpersonal exchange. See where I’m going with this?
Just adding connections on LinkedIn and commenting on posts here and there, more often than not, will not lead to much—you just become one of many faces on someone’s feed. So how do you stand out?
It’s time to bolster your LinkedIn strategy.
Like I often say, I practice what I preach and beefing up my approach has yielded more interviews. Those I’ve networked with also say it shows intention, initiative, and confidence three things employers ADORE! I’m not a professional career counselor by any means, but those I look to for mentorship also swear by this approach.
Let me be clear this approach isn’t novel. In fact, it’s actually putting together pieces of networking advice you’ve probably gotten over the years and making it into an actionable set of steps.
Without further ado…
7. Apply to a job you are 1) actually interested in and 2) a strong fit for maybe you have a lot of relevant experience, maybe your academic background aligns with the skillset needed, maybe you have coursework or projects directly connected to the topic whatever the reason/s, this job wouldn’t be a reach. It’s on target.
1. NOTE: I still believe you should cast a wide net, but, realistically, the time needed for this strategy likely means you can’t do it for every single job you apply to. Like I’ve always said, be discerning! Pick your best ones!
4. Go to the company’s LinkedIn page, then go to the People tab. Buckle up we’re using our resources and the tech skills being Gen Z/Millenials gave us!
5. You’re looking for folks who fit any of the following:
1. You’re already connected to them (IDEAL!)
2. You have mutual connections (designated with ‘2nd’ on LinkedIn)
3. You have something in common. Think same city, same educational institution, same past employer, same core interests, SOMETHING!
1. NOTE: Why prioritize folks fitting into any of these three buckets? They are more likely to respond to someone they don’t deem as a random stranger, or someone they actually have a CONNECTION to. With LinkedIn, it’s crucial to put the literal definition of “connection” into practice and treat it less like a replacement for “follower”!
6. Send an invite to these folks. Bonus points if they are either a recruiter/talent acquisition specialist, hold a high title (Director, VP, etc), or have the same/similar job title to the one you are applying for. You can send a personalized message if you want, but, when you only have a few on the Free Plan, it isn’t entirely necessary here.
1. NOTE: Why these individuals?
1. Think of recruiters/talent acquisition specialists as the keeper of the keys. They are the first ones who see your application and move you on to a hiring manager. This would give them a face to a
name and an opportunity for you to make a good impression!
2. Directors, VPs, other “higher-ups” have influence. You make a meaningful connection with them, you might have someone to advocate for you in the recruitment process.
3. Folks with similar job titles are likely the ones who would work alongside the new hire. They want the hiring manager to pick someone they can get along with. Similar idea as above you want someone who will advocate for you. This would also be an enriching conversation for you, as they can give you a vivid picture of what the job actually entails!
3. When you have connected with these folks (sometimes you can actually message recruiters without connecting), you’re going to send them a nice message like this. Be sure to modify this script and make it your own to stand out!
1. Greeting + name + identifier (ex: recent MPH graduate in Epidemiology from XYZ University)
2. Reference commonality mentioned in Step 4 (ex: I was looking to expand my public health network and noticed you also know Dr. Smith! Small world!)
3. Mention your job hunt (ex: I also saw you work for DEF. I actually just applied for Position 123945 with them, as it matches my interest in JKL)
- LinkedIn cont'd on page 26
1. The Ask. NOTE: you are not asking about the position or asking for their help with getting the job you are demonstrating interest. (Ex: I’ve always been interested in the organization, and I would love to learn more about it as I pursue my options. I would particularly love to hear more about your experience with DEF and the company culture. Would you be willing to meet on Zoom or Teams for a brief informal chat [whenever]?
2. Be sure to say thank you!
2. Wait and follow through when possible!
1. NOTE: Acknowledge that some folks aren’t active on LinkedIn, some don’t have the capacity to help out, etc. Sometimes the strategy works and sometimes it doesn’t. If you do get a response and they are willing to chat with you, prepare! Write questions! Know what you want out of the chat and how to kindly ask for their help after learning more about the organization whether it be putting in a good word, sending other opportunities they know of, etc. Then, maintain the connection and follow up ask how they are, give updates, etc.
Someone once told me that most public health hiring processes come down to who knows who. For early-career professionals, it’s easy to think that this could put us at an inherent disadvantage, but maybe it doesn’t’ have to. We’re tech savvy and have tools, like LinkedIn, at our disposal to change that we just have to know how to use them to our greatest advantage!
So make those connections! Send messages! Schedule informational calls! Make LinkedIn work for you! Cold messaging can be daunting it’s scary to put yourself out there but who knows? It could lead to something good :)
Have another LinkedIn tip you think more people should know? Submit it here!
NOTE: This article was originally published by Public Health Hiring Help on Substack. To subscribe please click here: https://tinyurl.com/ms8tfnp5
Resources
UCLA Expands Its John Snow Website
Author: Ralph R. Frerichs, DVM, DrPH Professor Emeritus, UCLA (Epidemiology)
The new John Snow website has arrived, sponsored by the UCLA Fielding School of Public Health and the UCLA Department of Epidemiology. The site name remains the same as in the past, but has been completely transformed to a contemporary setting with historical maps and images, focusing on places and times of John Snow, bringing life to a remarkable legendary figure.
Every field benefits from a hero who captures its aspirations and successes. In epidemiology, that hero is British physician Dr. John Snow (1813 -1858). During 1999-2000, while active in the UCLA Department of Epidemiology as Professor and Chair, I created what turned out to be one of the first online extensive resources dedicated to John Snow's work. It provided a central access to historical London maps and other materials related to his cholera investigations, previously more difficult to locate, and introduced the field of epidemiology to a broader audience.
The site remained active for two decades until 2019 when the web adopted new safety standards, addressing risks of computer viruses and the like. By then I had been retired for some while and was engaged in different activities. Others, however, paid attention to the dangers, and were no longer willing to risk clicking on an “unsecured” website.
In late 2024, the Chair of Epidemiology urged me to consider upgrading the John Snow site, including finding new material (a joy), learning new programming skills (not so joyful), satisfying UCLA disability requirements, and making sure the material appears on phones, pads and desktops. It was a hard slog and a year later, the new site emerged in October 2025, on the web once more at: https:// episnow.ph.ucla.edu/.
What makes the new John Snow site special?
Rather than offering just snippets on Snow’s major accomplishments, the site with its many colorful maps and images is more comprehensive, presenting five streams of John Snow’s life, now deemed the “father of modern epidemiology.” The site’s intention is to remind epidemiologists of their glorious history, and to
- Snow cont'd on page 27
attract young people to the wonders of epidemiology, considering it as a possible career choice.
The opening three paragraphs of the website best capture what follows.
British physician John Snow (1813-1858) is considered by many as the "father of modern epidemiology" for his seminal investigations of cholera in London, long before the bacterial agent and its deadly toxin were widely known. During the mid-1800s, the prevailing notion of the cause of cholera was being overcome by "bad air” (the miasma theory). Snow's epidemiological investigations, however, pointed to the disease being transmitted through contaminated water, likely by a biological agent of some ill-defined form (the germ theory), a conclusion that was widely debated until well after Snow's death at age 45 in 1858. Unbeknownst to Snow, the Italian microbiologist Filippo Pacini (1812-1883) had already seen the causative agent of cholera in 1854 while Snow was conducting his famous field studies. The bacterium Vibrio cholerae was finally cultured and identified in January 1884 with great publicity by German physician and microbiologist Robert Koch who wrote widely of its distinctive comma shape, perhaps not aware of Pacini's earlier observations. While Koch hypothesized that the organism produced a toxin, another 75 years would pass before the cholera toxin and the exact method of pathogen transmission was clearly identified by Indian medical scientist Sambhu Nath De in 1959, a century after Snow's death.
One of Snow’s cholera investigations was in a neighborhood near his London home, termed the "Broad Street Pump outbreak," which led to authorities removing the handle from the pump, a lasting symbol of public health action to save lives in the face of uncertainty. Snow’s second major investigation was south of London’s River Thames, deemed the "Grand Experiment,” comparing cholera deaths in two sets of households, one receiving sewagecontaminated water from the nearby River Thames and the other receiving relatively clean water from an upriver location.
Innovative and personable, Snow was able with colleagues to support his epidemiological research, long before government funds or charitable organizations were there to assist. Instead he relied on: 1) data compiled from public listings provided by the Registrar General's Office, 2) amiable persuasion to assist with field work and 3) the earnings of his clinical practice as anesthesiologist. Snow's prominence as a master of anesthesia soared with his inventions, presentations and publications and when administering chloroform during the birth of two of Queen Victoria’s children. With his life of remarkable achievements in an era of biologic and anesthetic mystery, he remains a pioneering figure in the history of both epidemiology and anesthesiology.
- Snow cont'd on page 29
The website is organized into the five streams, or chapters if thinking of books, each with between 5 and 12 sub categories.
Stream 1 - Introduction
a. Encyclopedia Entry and “Greatest Doctor”
b. Images and Medal of Snow
c. Father of Modern Epidemiology
d. John Snow’s publications (126 between ages 25 and 45 [year of death])
e. Memoir of his friend Benjamin Ward Richardson
Stream 2 - Broad Street Pump Outbreak
a. Overview and Part 2 of Snow's 1855 Book, Map 1
b. Photo Tour of Snow's London Neighborhood (includes Snow’s 3 homes)
c. Photo Tour of Broad Street Pump Outbreak (includes Broad Street pub)
d. Investigation of Broad Street Pump Outbreak
e. Handle Removal, Index Case and Rev Whitehead
f. Map, Myth and Error Making in BS Pump Outbreak
Stream 3 - The "Grand Experiment”
a. Introduction and Part 3 Snow's Book, Map 2
b. Photo Tour of History of London's Water Supply (37 slides)*
*Water played a central role in John Snow's legacy, as he explained the spread of deadly cholera. Author and community lecturer Adrian Prockter (2007) presents the history of water acquisition in London, and sets the stage for the dramatic events of the mid-1800s that terrified this great city. Included is mention of John Snow's grand experiment in 1854.
c. Photo Tour of Tidal River Thames (36 slides)*
*The River Thames had much to do with the epidemic spread of cholera in nineteenth century London. When the water companies were told by Parliament in 1852 to move their intakes up river to above Teddington Lock, it served as a major step in improving the drinking water. One company (Lambeth) complied quickly, and the other (Southwark and Vauxhall) waited until the last minute, right before the August, 1855 deadline. When cholera reappeared in London during the mid-1800s, the delayed move of the Southwark and Vauxhall company provided the basis for Snow's grand experiment. Adrian Prockter offers a photo tour of these historical times.
d. “Grand Experiment” of 1854 (extensive details of the “Grand Experiment”)
e. Photo Tour of Southwark and Vauxhall Water Company (40 slides)*
- Snow
*The Southwark and Vauxhall Water Company (also known as the Southwark and Vauxhall Waterworks) was created in 1845 by merger of existing waterworks. The water intake from the River Thames of the merged company remained in the heart of London, supplying contaminated water which eventually included waste of cholera patients, as investigated by John Snow in his "Grand Experiment." Water contamination remained, until Southwark and Vauxhall Company moved its intake upriver in 1855 to Hampton. Author and community lecturer Adrian Prockter (2007) presents historic images and text of the formation of Southwark and Vauxhall Company, bringing visual life to an important event in the history of London.
f. Photo Tour of Lambeth Water Company pre-1852 (34 slides)*
*In his "Grand Experiment," John Snow demonstrated that persons drinking contaminated River Thames water were more likely to experience cholera than those drinking clean upriver water.
After 1852, the Lambeth Water Company became the source of clean water with its upriver move, leaving behind the Southwark and Vauxhall Water Company to provide contaminated water. Author and community lecturer Adrian Prockter (007) presents historic text and images of the formation and existence of the Lambeth Water Company (also known as Lambeth Waterworks) prior to the company moving upstream.
g. Photo Tour of Lambeth Water Company post-1852 (34 slides)*
*“ London was without cholera from the latter part of 1849 to August 1853. During this interval an important change had taken place in the water supply of several of the south districts of London. The Lambeth Company removed their water works, in 1852, from opposite Hungerford Market to up-riverThames Ditton; thus obtaining a supply of water quite free from the sewage of London.” - Snow, John. On the Mode of Communication of Cholera, 1855.
The photo journey of the history of Lambeth Water Company continues, following the 1852 upriver move, with text and slides provided by author and community lecturer Adrian Prockter (2007).
Stream 4 - John Snow’s Life
a. John Snow’s Early Years, Part 1
b. John Snow’s Early Years, Part 2
c. John Snow's Professional Years
d. Anesthesia for Queen Victoria
e. John Snow's Death
f. Remembrances and New The Lancet Obituary
- Snow cont'd on page 31
Stream 5 - Additional Items
a. Overview of Snow's Significance
b. Part 1 of Snow's 1855 Book
c. Part 4 of Snow's 1855 book
d. Other Cholera Outbreaks (1831-32, 184849, 1853-54)
e. Writings on Snow for Young People
f. Cholera Theories and Conflicts (includes miasma and germ theory)
g. First Discoverer of Vibrio Cholerae ( Italian microscopist Filippo Pacini)
h. William Farr - Campaigning Statistician (first a critic and then an ally)
i. Honoring John Snow in England and the USA (many sites and organizations)
j. Conversation with "The Ghost Map" Author (Frerichs and Seven Johnson)
k. The "Modern John Snow" - R. Piarroux, MD, PhD
l. Current Cholera Information and Implications of Snow
In summary, when viewing the John Snow site, the character and intelligence of the man should become readily apparent. This point was best made by Johns Hopkins Professor Wade Hampton Frost M.D., himself an impressive epidemiologist, when he wrote in 1936 in an introduction to a re-issuance of John Snow’s book, On the Mode of Communication of Cholera (1855): “Of Snow's character, the circumstances of his life, the range of his interests, and the position which he held in his profession, an illuminating account is given in the memoir by Richardson, his warm friend and admirer (Dr. Benjamin Ward Richardson, 18281896, presented in Stream 1e). It gives the picture of a man singularly endowed with the ability to think in straight lines and the courage to follow his own thought. In medicine these abilities placed him in the front ranks of his day; in epidemiology they carried him a generation beyond it” (and now even further). ■
Note that this month's Epi Word Search (on the next page) is dedicated to John Snow and his work.
John Snow - Historical Giant
The words in this month's puzzle comes to us from the article on the new John Snow website at UCLA. Good luck - don't let the easy words fool you!
For an interactive online version go to: https://tinyurl.com/2ky6u7z4
Words to find:
1. John Snow
2. Vibrio cholerae
3. Pump Handle
4. Shoe Leather
5. London
6. Broad Street
7. Queen Victoria
8. River Thames
9. Water
10. Grand Experiment
11. Sewage
12. Miasma Theory
13. Contamination
14. Deadly Toxin
15. Germ Theory
16. Filippo Pacini
17. Microbiologist
18. Pathogen
What We're Reading This Month
Editor's Note: All of us are confronted with more material than we can possibly hope to digest each month. However, that doesn't mean that we should miss some of the articles that appear in the public media on topics of interest to the epi community. The EpiMonitor curates a monthly list of some of the best articles we've encountered in the past month. See something you think others would like to read? Please send us a link at info@epimonitor.net and we'll include it in the next month
Washington DC Chaos
♦ CDC ‘Not Functional’ After Trump Administration Orders Mass Firings (Time)
https://tinyurl.com/4mp59ea5
♦ CDC rushes to hire back top scientists after they were sent layoff notices 'in error' (Daily Mail)
https://tinyurl.com/52fyydr4
In Honor of Halloween
♦ An epidemiologist explains how zombies are a metaphor for public health (PBS)
https://tinyurl.com/332vawxz
Public Health Topics
♦ Why a study claiming vaccines cause chronic illness is severely flawed – a biostatistician explains the biases and unsupported conclusions (The Conversation) https://tinyurl.com/ea96suu2
♦ How genetically modified mice could save a Massachusetts vacation town from a disease outbreak (The Independent)
https://tinyurl.com/233rwy85
♦ DNA Identifies 2 Bacterial Killers That Stalked Napoleon’s Army (NYT) https://tinyurl.com/4z4jy7ka
♦ How The Post found growing rates of young cancer in America's Corn Belt (WAPO via AppleNews)
https://tinyurl.com/5n7cbftj
- Reading cont'd on page 34
What We're Reading This Month
[Type a quote from the document or the summary of an interesting point. You can position the text box anywhere in the document. Use the Text Box Tools tab to change the formatting of the pull quote text box.]
- con't from page 33
Public Health Topics, cont.
♦ Scientists make concerning new discovery while studying dangerous mosquito-borne virus: 'Growing threat' (The Cool Down)
https://tinyurl.com/ycyuredr
♦ Bird flu confirmed in commercial N. Georgia chicken plant (11Alive)
https://tinyurl.com/2vsm2h46
♦ In Somalia, Diphtheria, a Once Vanquished Killer of Children, Is Resurgent (NYT)
https://tinyurl.com/3bduryy6
♦ Microbes trapped in permafrost AWAKEN after 40,000 years – as scientists warn they could spark the next pandemic (Daily Mail)
https://tinyurl.com/bdz6pmfy
♦ In Fight Against Malaria, an Unexpected and Snuggly Shield (NYT)
https://tinyurl.com/2bz9kwfc
♦ Oropouche in Panama: More than 600 cases confirmed; Health officials warn of spread in 7 regions (Outbreak News)
https://tinyurl.com/4msmmty2
♦ Epidemiology of 3 Vaccine-Preventable Infectious Diseases Within US Immigration Detention Centers (JAMA)
https://tinyurl.com/523jx886
Notes on People
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Named: The University of Pennsylvania has announced that Sunni Mumford, PhD, has accepted the position of Director of the Division of Epidemiology within the DBEI. Dr. Mumford has been serving as Deputy Director of the Division since 2023. She is a Professor of Epidemiology, Co-Director of the Women’s Health Clinical Research Center, Director of Enrichment for the Penn Center for Nutritional Science and Medicine, Chair of the Epidemiology Division Recruitment Committee, and Thematic Area Leader for the Center of Excellence in Environmental Toxicology.
Named: Brian Whitcomb, Professor of Epidemiology and Chair of the Department of Biostatistics and Epidemiology at the University of Massachusetts - Amherst, has been elected to the position of President-Elect of the Society for Epidemiologic Research (SER). He will serve a three-year term on the SER Executive Committee as President-Elect (2025-2026), President (20262027) and Past-President (2027-2028). He assumed the position on July 1, 2025.
Elected: George Mason University Reproductive and perinatal epidemiologist Michael Bloom was elected to the Leadership Committee of the Environment and Reproduction Special Interest Group in the American Society for Reproductive Medicine for a five-year term in leadership. He will serve in a different role each year, starting with vice chair, then chair-elect, chair, immediate past chair, and past chair.
Honored: Dr. Jason Salemi, professor and interim chair of the Department of Epidemiology at the USF College of Public Health (COPH), has been recognized with the Outstanding Mentorship Award from the American College of Epidemiology (ACE). The national award honors epidemiologists who demonstrate exceptional commitment to guiding and supporting the next generation of professionals in the field.
Notes on People, con’t
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Honored: The Department of Biostatistics at the School of Public Health at Boston University has named Revathi Ananthakrishnan (SPH ’17) the recipient of the 2025 Biostatistics Distinguished Alumni Award. Ananthakrishnan, a biostatistician at Bristol-Myers Squibb, accepted the award and gave a presentation on designing, analyzing, and interpreting immunooncology trials at SPH on October 3.
Honored: The University of Iowa College of Public Health has selected Bhramar Mukherjee, PhD, as the 2025 recipient of the Richard and Barbara Hansen Leadership Award. She is the Senior Associate Dean of Public Health Data Science and Data Equity, Anna M.R. Lauder Professor of Biostatistics, Professor of Epidemiology (Chronic Disease), and Professor of Statistics and Data Science (Secondary) at the Yale School of Public Health.
Named: The University of Iowa College of Dentistry has appointed Derek Smith as director of the Division of Biostatistics and Computational Biology within the Iowa Institute for Oral Health Research. Smith also joins the Department of Preventive and Community Dentistry as an associate professor. He began his appointment in August 2025.
Named: Fred Hutch Cancer Center has named Dr. Jingyi Jessica Li as the recipient of the Donald and Janet K. Guthrie Endowed Chair in Statistics. After earning her PhD in biostatistics at the University of California, Berkeley, she joined the faculty at the University of California, Los Angeles. Her research focused on improving statistical models to analyze “noisy” data (when there are so many data points that it’s unclear which are truly meaningful) to find patterns in how genes are turned on and off. She quickly became a leader in her field and has received numerous honors; most recently, the 2025 Mortimer Spiegelman Award for outstanding contributions to health statistics. -36-
Notes on People,
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Honored: Brown University Biostatistics Adjunct faculty member Joseph Cappelleri has received the 2025 Achievement (Industry) Award: Applied Public Health Statistics (APHS) Section of the American Public Health Association (APHA). Established in 1978, the APHS Achievement Award recognizes a distinguished career in statistical research and applications in public health, with a focus on academia, government, and industry. Cappelleri, a statistician from industry who has made outstanding contributions to public health statistics and data applications.
Retired: Douglas Heimburger, MD, MS, professor emeritus of Medicine in the Division of Epidemiology at Vanderbilt University, has retired. Heimburger joined the Vanderbilt University faculty in 2009 as a professor of Medicine in the Vanderbilt Institute for Global Health (VIGH), where he served as associate director for Education and Training until 2019. In that role, he oversaw training programs for Vanderbilt students and clinicians, helping create research training opportunities for doctoral and postdoctoral trainees at Vanderbilt as well as those from low- and middle-income countries.
Retired: Brown University has announced the retirement of Stephen McGarvey effective October 1st. He is Professor Emeritus of Epidemiology and Professor of Anthropology (Courtesy). He is also an elected Fellow of the American Association for the Advancement of Science, and on the editorial board of the American Journal of Human Biology. He was the recipient of the 2025 Franz Boas Distinguished Achievement Award from the Human Biology Association. McGarvey earned a Ph.D. in Anthropology from Pennsylvania State University in 1980, and an M.P.H. in Epidemiology from Yale University in 1984.
Retiring: Jonna Mazet, a world-renowned epidemiologist, wildlife veterinarian, and expert in emerging zoonotic disease surveillance and capacity strengthening, will retire at the end of 2025 after 30 years of exemplary service to UC Davis.
Mazet, the vice provost of Grand Challenges, came to UC Davis as an undergraduate to become a veterinarian. She earned four degrees over 10 years then joined the faculty in the UC Davis School of Veterinary Medicine, which she helped to elevate as a leader in global health.
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Retired: The Department of Epidemiology at UT Health Houston has announced the retirement of Professor Craig Hanis, PhD, after more than four decades of groundbreaking research, teaching, and mentorship. In recognition of his extraordinary contributions to public health, Hanis has been named Professor Emeritus, effective September 1st. His pioneering work in Starr County, Texas, laid the foundation for understanding the genetic and environmental factors contributing to chronic diseases such as type 2 diabetes in Mexican American populations. His leadership and commitment to community-based research have shaped national conversations around Hispanic health and continue to influence the field today.
Passed: Dr. Carrie Cottreau of Halifax, NS passed away on October 10, 2025, surrounded by family following a brief illness
Carrie grew up in a large, loving family in Yarmouth, NS, later moving to Halifax in pursuit of her scientific dreams. These eventually led her to Pittsburgh, Pennsylvania, where she remained until returning to Nova Scotia in 2020
Carrie dedicated her career as an epidemiologist to the study of cancers in women, especially ovarian cancer. She received her MSc in pathology from Dalhousie University and her PhD in epidemiology from the University of Pittsburgh, where she worked as a medical researcher and assistant professor of obstetrics and gynecology at the University of Pittsburgh Medical School. She authored a variety of scholarly papers in US medical and public health journals. Her work in women’s health led her to fellowships at the US National Institutes of Health and later at Harvard’s T.H. Chan School of Public Health. https://tinyurl.com/2cvbnmfj
Near Term Epidemiology Event Calendar
Every December The Epidemiology Monitor dedicates that issue to a calendar of events for the upcoming year. However that often means we don't have full information for events later in the upcoming year. Thus an online copy exists on our website that is updated regularly. To view the full year please go to: http://www.epimonitor.net/Events The events that we are aware of for the next month follow below.
November 2-5
Type: Conference
Title: APHA Annual Meeting & Expo
November 2025
Web: https://tinyurl.com/bdfkhrv3
Sponsor: American Public Health Association Location: Washington, DC
November 11-14
Type: Conference
Title: 18th European Public Health Conference
Sponsor: EPH Location: Helsinki, Finland
November 15-16
Type: Conference
Web: https://bit.ly/3jcNVcY
Web: https://tinyurl.com/2j6pbbfa
Title: Biostatistics in the New Era of Data-Driven Sciences
Sponsor: HTHealth Houston Location: Houston, TX
November 18-21
Type: Short Course
Web: https://tinyurl.com/7tcjta6b
Title: Leadership Development to Advance Equity in Healthcare
Sponsor: Havard University Location: Virtual
November 18-21
Type: Conference
Web: https://tinyurl.com/ukxk929m
Title: 17th International Conference on Molecular Epidemiology and Evolutionary Genetics of Infectious Diseases
Sponsor: Elsevier Location: Kolkata, India
November 24-25
Type: Conference Web: https://bit.ly/31SL1ln
Title: Infectious and Chronic Disease Conference
Sponsor: Pharmaweb Location: Dubai, UAE
Nov 30 – Dec 3
Type: Conference Web: http://bit.ly/2K5CCm0
Title: 10th Intl Conference on Infectious Disease Dynamics
Sponsor: Elsevier Location: San Diego, CA
December 2025
December 1-2
Type: Conference
Web: https://tinyurl.com/vbwk6s7z
Title: 14th Annual Conference on Tropical Medicine and Infectious Disease
Sponsor: Conference Series Location: Rome, Italy
Open Public Health Positions
What it means and why it matters
The list below has been compiled by Public Health Hiring Help the new Substack column that has been created to help individuals in the public health community find positions in the midst of the chaos that is now impacting governmental agencies and grant recipients. This list represents the most current positions PHHH has been able to identify. We thank PHHH for their permission to reprint these listings.
Child Health and Development Institute (Farmington, CT) Data Analyst
$62–78k + benefits | Master’s min | EPI, BIOS, BSHES
Assoc. of AAPI Community Health Orgs (Remote) Data Analyst
Weill Cornell Medicine — Biostatistics Intern Public Health Alignment: BIOS, EPI
What it means and why it matters
State of MA — Quality Improvement Intern Public Health Alignment: EPI, BSHES, HPM
Environmental Defense Fund Public Health Policy Intern Public Health Alignment: EH, HPM, GH
King County Health Outreach Worker (PT) Public Health Alignment: EPI, BSHES, GH
RAND Statistics Summer Research Associate Public Health Alignment: BIOS, EPI
PwC Healthcare Consulting Intern Public Health Alignment: HPM, BIOS, EPI
Moderna Biostatistics and Programming Intern Public Health Alignment: BIOS, EPI
Moderna Data Management and Clinical Data Standards Intern Public Health Alignment: EPI, BIOS, HPM
Moderna Infectious Disease Epidemiology Intern Public Health Alignment: EPI
Moderna Latent Virus Epidemiology Intern Public Health Alignment: EPI
NASA Lifelines Humanitarian Research Fellow Public Health Alignment: GH, EH, BSHES
Independence Blue Cross Population Health Intern Public Health Alignment: EPI, BIOS, HPM
LabCorp — Operations Intern Public Health Alignment: HPM, BIOS, EPI
Forvis Mazars US Healthcare Consulting Intern Public Health Alignment: HPM, BIOS, EPI
For Full Information on these jobs: http://www.epimonitor.net/JobBank
Your Ad Should Be Here
Do you have a job, course, conference, book or other resource of interest to the epidemiology community? Advertise with The Epidemiology Monitor and reach 35,000 epidemiologists, biostatisticians, and public health professionals monthly.
Advertising opportunities exist in this digital publication, on our website and social media pages, and in our Epi-Gram emails. For more information please contact: Michele Gibson / 770.309.7937 / michele@epimonitor.net
YLE can be found here: https://yourlocalepidemiologist.substack.com/
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, wife, and mom of two little girls. YLE reaches more than 305,000 people in over 132 countries with one goal: “Translate” the ever-evolving public health science so that people will be well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members.
To support the effort, subscribe or upgrade your existing subscription: https://yourlocalepidemiologist.substack.com/
The Epidemiology Monitor ISSN (2833-1710) is published monthly by Monitor Publishing & Communications, Inc.
All material in this publication is subject to copyright. For possible reprint permission please contact us at michele@epimonitor.net
Advertising options include but are not limited to:
Website only ads or website ads combined with digital print ads in this publication. Sponsorship for features in this newsletter or for the newsletter issue itself
Ads are accepted for open positions, events, programs, books, merchandise and other items of interest to our readers.
Subscriptions to this publication are free. Go to http://epimonitor.net/Subscribe.htm