This month the conversation turns to the devastation resulting from the funding cuts at NIH. The author lists proactive things you can do to make a difference and how to encourage others to do the same. We also have news about a group that is forming to save Epi Info™ which again represents an opportunity for your involvement. This month's Profile in Public Health highlights an epidemiology student from Uganda who is in the PhD program at the University of Georgia. Her story reminds us that, regardless of location, we are all facing similar issues.
Our look back at the beginning of Covid continues with a review of some of the proposed strategies from 2020 along with a reminder of the conflicts some epidemiologists were facing at the time.
As always, we continue to provide you with our popular monthly word game feature, Notes on People, an overview of what we are reading from the public media, and a listing of upcoming epidemiology events. Finally, don't miss the Job Bank offerings this month. We have some interesting opportunities.
Did you miss last month’s issue? Read it here: https://tinyurl.com/37uztj4y or here: https://tinyurl.com/yb8ctzym
In This Issue
NIH The quiet engine of science is being dismantled
Authors: Katelyn Jetelina, PhD, MPH Elizabeth Marnik, PhD
NOTE: This article was originally published on July 23, 2025 by Your Local Epidemiologist on Substack.
Years ago, when I was a professor, I studied how violence spreads through communities (much like infectious diseases) and how to interrupt the spread. My research was funded through federal grants from the National Institutes of Health (NIH) and the National Institute for Occupational Safety and Health (NIOSH). Several federal grants supported my research on the mental health of police officers people who routinely witness traumatic events that affect not just their wellbeing (think PTSD), but also how they engage with the communities they serve. Like many researchers, I became involved in this work because it held personal significance for me. My husband was a police officer.
The officers we worked with many of whom are MAGA supporters (and our dear friends!) weren’t passive subjects. They were collaborators. They opened their doors, welcomed us into their stations, shared coffee, and helped us ask and answer hard questions. Together, we eventually co-developed solutions that became policy across departments! The same grant that funded this work also supported the training of PhD students, many of whom continue this work today, grounded in relationships they built with officers years ago.
This is the power of public research. When
done well, it doesn’t just answer questions; it builds community, capacity, and long-term change for a healthier future.
I’ve been thinking about that project a lot lately. If it were up for funding this year, it would’ve been discontinued due to executive orders. Not one of those officers, regardless of political leaning, would have been okay with it because it was their project, too. However, those officers never really knew NIH/NIOSH was the invisible engine behind the magic.
In just six months, more than 5,500 research projects have been halted. That’s 5,500 unanswered questions. Thousands of communities left behind. Researchers stuck in limbo. And a generation of training lost.
All of this is happening quietly, strategically, and politically. But we in science and public institutions must also own our part: We haven’t done enough to make this work visible to the people it impacts. This invisibility has consequences. Because when people don’t see science working for them, it becomes easy to tear it down.
The good news is it’s not too late. There are real steps we can take now and in the future to change course.
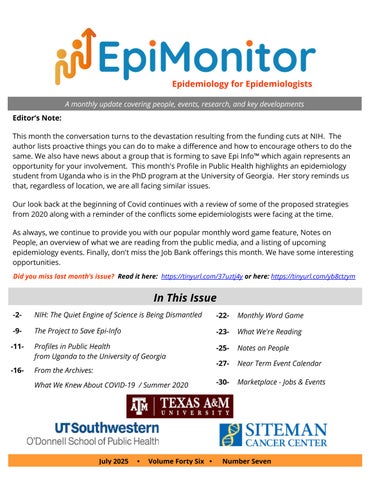
What is the NIH, anyway?
The National Institutes of Health (NIH) is the world’s largest public funder of research. It’s not one agency but a collection of 27 institutes and centers, each focused on specific areas like cancer (NCI), infectious diseases (NIAID), aging
- NIH cont'd on page 3
(NIA), and mental health (NIMH). NIH isn’t the only research engine in the United States (for example, there’s also the National Science
Foundation that funds NASA), but NIH is by far the biggest.
Getting a federal research grant is no small feat. Scientists spend months writing proposals, which are then reviewed rigorously by peers. Only the most promising, relevant, innovative, and well-designed research makes the cut, which is usually only the top 10-20% of applications. Securing a grant is a huge deal for your career. It is often the only way a scientist’s salary is paid, but it is also a guarantee that you’ll work on what you’re most passionate about for a few years.
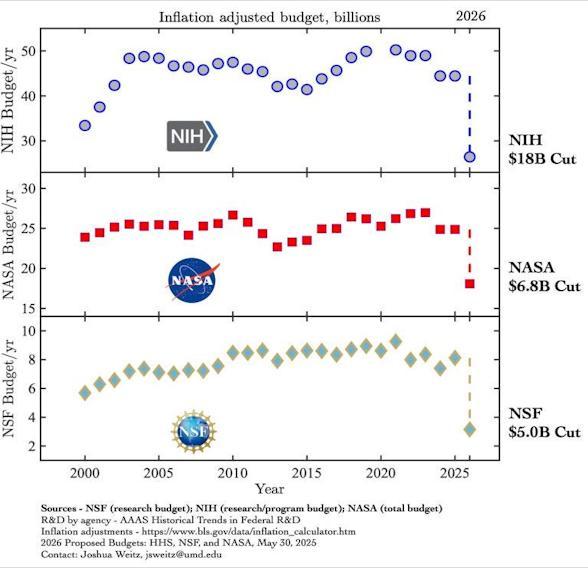
What's Being Cut and How
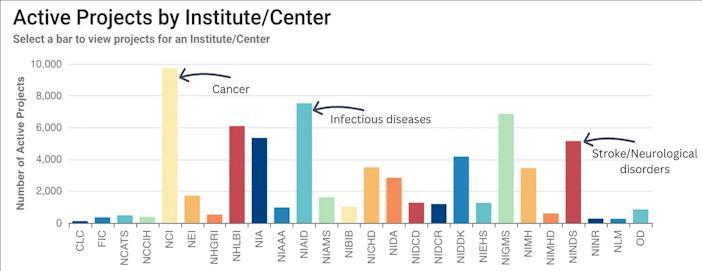
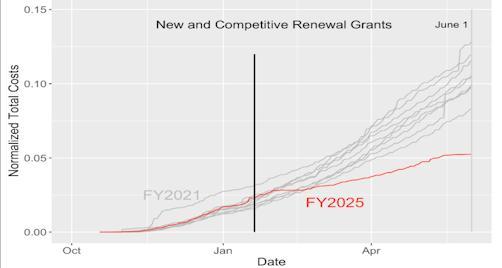
Research funding budgets rise and fall every fiscal year, depending on Congress's priorities, but this year is dramatically different. At the NIH alone, approximately 5,500 fewer research projects are being funded due to executive decisions, which is significantly lower than in any other year, as shown below.
Some of these projects support teaching and training the next generation of researchers, but funding has literally flatlined.
These cuts are currently being made through executive orders in three ways:
Cutting entire institutes, such as the Fogarty International Center, which supports global health research and pandemic preparedness.
Targeting research topics that don’t align with political agendas, like occupational health (my project), climate and health, LGBTQ+ health, gun violence prevention, healthy equity, misinformation, and vaccine confidence.
Targeting specific institutions that get awarded funds, like all grants to the Harvard School of Public Health that were cancelled last month.
And even where programs haven’t been cut outright, they’re in limbo. Peer review panels are stalled. People handling grants (called
program officers) are eerily reading from scripts when you call them. Researchers are waiting on funding decisions that should have arrived months ago.
Unfortunately, this is just the beginning. The Congressional budget has proposed an additional 40% cut to the NIH. NIH is the most significant cut in the Health and Human Services discretionary budget. To say that scientific discovery is being stripped to the bare bones is an understatement.
- NIH cont'd on page 5
Why does this matter?
Some politicians portray these cuts as trimming waste or targeting fringe projects that don’t apply to the average American. And, yes, some projects are very niche. But some projects are not. (Here is an ongoing database of cuts.)
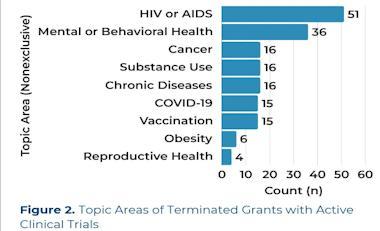
For example, more than 100 clinical trials have been cut, even for topics that MAHA supports, such as chronic disease, cancer, diabetes, and mental health.
- NIH cont'd on page
Here’s a sample of research that has been cut so far:
Research on long-term exposure to arsenic, and the co-occurrence of uranium, in public and private drinking water
Cancer in Your Community: Strategies to Reduce Cancer and Chronic Disease in the Arkansas Delta
Automated Digital Imaging for Cervical Cancer Screening
Racial Disparity in Diagnostic Evaluation of Uterine Cancer
Alzheimer’s Disease Research Center
HOPE in Action: A Clinical Trial of HIV-toHIV Liver Transplantation
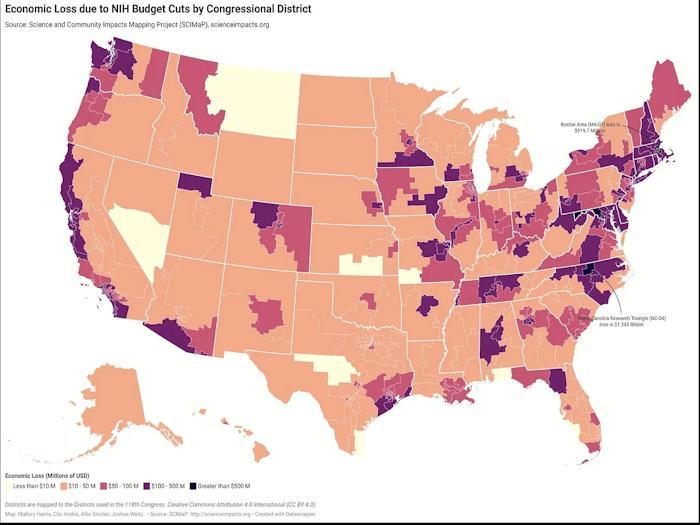
This also impacts local economies. If the NIH budget proposal moves forward, 200,000 jobs will be lost, resulting in $46 billion in economic losses. For each $1 invested in NIH, it returns $2.56 in local economies. For example, the University of Alabama, which receives significant support through the NIH, is the largest employer in the state.
Let’s be clear: NIH is not perfect. Ask any scientist, and you’ll hear it needs reform.
NIH has long been the invisible force powering vaccines, cancer therapies, diagnostics, and public health breakthroughs. However, that very invisibility science’s failure to communicate its impact on people’s lives in ways they can see and feel has made it vulnerable. For decades, much of science communication has lived behind paywalls, wrapped in jargon, distant from the communities it’s meant to serve, even though their tax dollars fund it.
Here are three starting points for reform:
1. Engage the public. NIH is publicly funded. The public deserves a better understanding of what’s being funded, why it matters, and how it’s improving lives. Grant requirements could include plain-language summaries and publicfacing updates.
2. Streamline applications. Scientists shouldn’t have to spend months writing proposals for a one-in-five shot. NIH should simplify the application process and improve transparency.
3. Balance funding across disciplines. Behavioral health, social determinants of
health (think housing, food insecurity),nutrition, and prevention strategies often get shortchanged despite their real-world relevance
There are many more ideas out there, too, like workforce improvements and exploring new funding models.
Good news! Silver linings and things you can do
The judicial system is responding. Last month, the U.S. District Court of Massachusetts ruled that the current administration’s decision to terminate NIH grants based on political objections to research topics was unlawful. The ruling only applies to the scientists and in the 16 states named in the lawsuit at this time. The administration could still appeal the decision or potentially ignore the ruling.
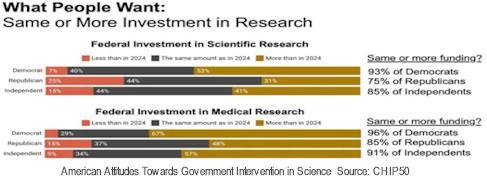
This topic is becoming increasingly bipartisan. We can see it in the polls (below). At the Senate HELP committee, Republicans, such as Senator Bill Cassidy, voiced concerns about research projects being cut. Senator Susan Collins, Republican, recently held a committee hearing on NIH achievements, the cuts, and how we can thoughtfully improve these systems.
Your voice matters.
The FY 2026 budget is still under negotiation and it’s not too late to stop these cuts. Staffers have informed me that it is particularly important to get people calling; a push from constituents before a vote can significantly influence senators’ decisions to vote yes or no. Republicans voters tend to push until the end; Democrats voters tend to peter out.
1. Contact your senators and representatives directly. Two senators in particular—Mike Rounds (SD) and John Kennedy (LA) are key votes on the budget committee and need encouragement.
And remember, the community is not merely a research target but an active partner. So if you’re a scientist or researcher, share stories:
Create an infographic based on your study after you have asked people to complete a survey.
Work with a patient organization.
Open your lab for community tours.
Host a community science storytelling event. Liz Marnik started this event because she knows that science belongs in community spaces, allowing people to see how it connects to their lives. Storytelling makes science personal, relatable and memorable. It helps people see themselves in the science, breaks down barriers, and builds trust in a way data alone can’t.
o HERE is a Taproom Tales guide, if you would like to host a similar event in your area!
Bottom Line
Federal research is the quiet engine behind the treatments, vaccines, and tools that keep us healthy. Americans are now getting at least 5,500 fewer research questions answered. This should serve as a wake-up call, not just for the public and policymakers, but also for scientists. Because if we want to protect this engine, we have to show people what it does.
Scientific discovery is one hell of a ride. And every American deserves a seat. Just like those police officers. They cared that someone showed up. That someone listened. That science worked for them.
And that’s what we have to fight to preserve.
■
This article was originally printed in Your Local Epidemiologist. To read more content from this source subscribe to Your Local Epidemiologist (YLE): https://tinyurl.com/47494ms4
Dr. Liz Marnik is an immunologist and Director of Science Education and Outreach at MDI Biological Laboratory. She is also a brilliant scientific communicator and a dear friend of YLE for years.
Author: Staff
The Project to Save Epi Info™
Last fall CDC announced that support, product development and technical assistance for Epi Info™ would cease effective September 30, 2025. After almost 40 years of use this announcement came as a surprise to many in the epidemiology community. CDC provided detailed information about the timeline for phasing the tool out and answers many common questions here:
https://tinyurl.com/4j6pfcky
Their hope was that by providing roughly a year's advance notice that users would be able to engineer a smooth transition. Their statement at the time read as follows:
This sunsetting decision is part of OPHDST's realignment of resources to focus on products that support our "One Public Health Approach" to data modernization…We recognize that Epi Info™ has been an integral part of users' public health work for nearly four decades. We appreciate the trust you have placed in Epi Info™ and CDC.”
Last November the EpiMonitor conducted a lengthy interview with Dr. Andrew Dean who was one of the original developers of Epi Info™ along with his wife and son: Drs. Consuelo Beck-Sagué and Jeffrey Dean. The elder Dean and Beck-Sagué were EIS officers at the time they created Epi Info™. Dr. Jeffrey Dean was a 16 year old high school student with a passion for computers, programming and science.
Epi Info started in 1985 at CDC as a free MS DOS program for epidemiologists to enter and analyze data. Over the last 40 years it has been updated to Windows and Web versions with a large number of added features for
epidemiology and public health purposes. Additional information on the history of Epi info can be found here:
https://www.cdc.gov/epiinfo/story.html.
Additional information on the history of Epi Info can also be found on Wikipedia:
https://en.wikipedia.org/wiki/Epi_Info
As described on the CDC website: “Epi Info™ is a public domain suite of interoperable software tools designed for the global community of public health practitioners and researchers. It provides easy data entry form and database construction, a customized data entry experience, and data analyses with epidemiologic statistics, maps, and graphs for public health professionals who may lack an information technology background. Epi Info™ is used for outbreak investigations; for developing small to mid-sized disease surveillance systems; as analysis, visualization, and reporting (AVR) components of larger systems; and in the continuing education in the science of epidemiology and public health analytic methods at schools of public health around the world.”
In response to the CDC decision to sunset Epi Info™, a group has started the “Save Epi Info” Project to ensure the continuity of this vital tool and exploring avenues for its preservation. The core team plans to identify individuals to explore possible options to continue the availability and support of Epi Info™. A critical challenge lies in securing funding for this
- Epi Info cont'd on page 6
ambitious project. Identifying potential sponsors and sustainable funding sources will be key to the project's success and longevity.
If you share our commitment to saving Epi Info, let's unite efforts and collaborate on a strategic plan. Interested individuals are encouraged to connect and contribute ideas by reaching out to Save.Epi.Info@gmail.com.
Information and progress on the effort will be made available at sites.google.com/view/saveepi-info
Together, we can work towards preserving and advancing the legacy of Epi Info for the benefit of public health initiatives worldwide.
SAVE EPI INFO!
Protect this valuable Public Health Tool from Being Unsupported
What is Epi Info?
A free software developed by the CDC Used by public health professionals worldwide Helps in outbreak investigations, data collection, analysis & visualization
Why It Matters:
✅ Supports rapid response during disease outbreaks
✅ Vital for training epidemiologists
✅ Trusted by global health institutions and NGOs
✅ Low-cost tool accessible to low-resource countries
Epi Info support by CDC is being discontinued. Without it, frontline health workers and researchers lose a critical resource.
Add your voice:
Join the Save Epi Info Project –email: Save.Epi.Info@gmail.com; website: sites.google.com/view/save-epi-info
Together, we can protect public health infrastructure. Don’t let this essential tool disappear.
Profiles in Public Health
From Uganda to the University of Georgia
Editor's note: The following interview was originally published by Words that Count and has been lightly edited for length. We look forward to presenting additional interviews that profile unique individuals in epidemiology, biostatistics and public health. To submit an article for consideration please send it to: info@epimonitor.net The original version of this interview can be found here: https://tinyurl.com/942h4emt
Meet Doreen, an emerging voice in the fields of Epidemiology and Biostatistics. She is contributing to critical public health research through data-driven approaches as part of her PhD research.
To kick us off, please give a brief introduction about yourself
My full name is Doreen Kibuule Kalemba, a Ugandan, based in the US. Currently, I am pursuing a PhD in Epidemiology and Biostatistics at the University of Georgia (UGA). I was born and raised in Jinja [Uganda], so that makes me a Musoga by tribe. I see myself as a career person, someone who enjoys learning about diseases. Lastly, I am a mother.
How did you join the world of Biostatistics and epidemiology?
Growing up, I was not a fan of Mathematics. I felt like it was either not fun or there was something wrong with the way it was taught. But then, my uncle constantly encouraged me to enjoy it. He always talked about how Mathematics should be done in school, and even took time off to teach me. It was not long before I realised that I would be finding Mathematics in everything else I enjoyed. At the age of 10, my love for the subject grew even more, and I started teaching the younger kids in our neighbourhood. It might have been a trauma response to the fact that I did not know a lot of Mathematics myself, or I just enjoyed teaching.
When I entered secondary school, I had a moment that significantly shaped my academic path. A classmate casually remarked that girls were not suited for mathematics, implying it was a subject meant for boys. Coming from primary school, where I had excelled in science and earned a distinction, this comment struck me deeply. It did not make sense. Why would someone’s gender determine their ability in a subject like mathematics? That moment stayed with me, not as a discouragement, but as a challenge. It planted a question in my mind: What happens when you go against expectations? Initially, my interest in mathematics was not about ambition. It was simply a decision to take a different path and test
- Uganda cont'd on page 11
Doreen K. Kalembe
the boundaries of what others assumed I could not do. And that decision marked the beginning of my journey into STEM.
By the time I reached Senior Four, the narrative around science subjects had become even more discouraging. Subjects like mathematics, physics, chemistry, and biology were labeled as difficult and were reserved only for the exceptionally gifted, usually boys. But having already chosen to challenge such assumptions, I was determined to excel in those very subjects. I focused on achieving strong grades, especially in chemistry, which I saw as deeply mathematical. The turning point came when I overheard students praising a girl for taking the PCB/Math combination, saying only brilliant students could manage it. That moment fueled my resolve to be counted among them. I wanted to prove to myself and others that academic ability was not incompatible with being a girl, or with being considered beautiful. If anything, I aimed to redefine what it meant to be both smart and seen.
After A’Level, my career options seemed limited to the familiar science-track expectations: become a doctor, or perhaps an engineer. But as I faced the reality of choosing a path, I discovered something important about myself. I was not comfortable with blood! Despite my interest in the medical field, I struggled during biology practicals. I came to terms with the fact that surgery or direct clinical work was not for me. Still, I did not want to give up on contributing to the health sector in some way.
Financial constraints further complicated my plans. Even with strong grades, my family could not afford medical school tuition, and I was not awarded a government scholarship for medicine. However, I did qualify for a government scholarship to study Education at Makerere University, specializing in Physics and Mathematics.
At first, it felt like a detour, but then it started to feel like a calling. Teaching had always been a part of me, even from childhood. I embraced the opportunity not just as a compromise, but as a platform.
During my undergraduate studies, I studied a course called Biomathematics in my second year. It was offered under the Mathematics Department, but to me, it felt like a new doorway into public health. It combined mathematical reasoning with medical relevance, and that intersection immediately resonated with me. As I progressed through the course, it felt like I had finally found my place. Biomathematics gave me the sense that I could still contribute to the medical field. From that point on, I knew this was the direction I wanted my career to take.
After completing my undergraduate degree, I applied for a scholarship at the African Institute for Mathematical Sciences (AIMS). This decision transformed my perspective in ways I had not anticipated. AIMS is often jokingly referred to as the African Institute for Missing Sleep because of the program’s intensity, but it truly lived up to its reputation as a place that stretches the limits of what you think is possible. Before AIMS, I saw mathematics and science as fields with clear boundaries, often tied to academic or technical work, mostly within computers or classrooms. But AIMS expanded that understanding. It introduced me to a world where math intersects with everything, from health and environment to technology and economics. Suddenly, the tools I had been learning could solve real-world problems in ways I had not imagined.
My interests widened rapidly. Beyond medicine, I became drawn to data science, artificial intelligence, and the many ways these tools could be applied
- Uganda cont'd on page 13
in healthcare, pharmaceuticals, education, and beyond. My thesis focused on infectious diseases, specifically a simulation of an SVEITR model for measles transmission in Uganda. That project deepened my understanding of disease dynamics, exposed me to public health modeling, and taught me how to interpret metrics like odds ratios and risk factors in real contexts. I continued learning more after AIMS, particularly in epidemiology and biostatistics. This sparked a clear sense of direction. I realized that public health was not just a fallback; it was a powerful, data-driven field where I could make a meaningful impact.
As I continued to explore the field, I began connecting the dots across mathematics, data, and health. Then, boom, COVID-19 happened. The pandemic was a turning point. It forced the world to pause, and for me, it created the space to reflect deeply on what I truly wanted to pursue within public health. It was during this time that everything came into sharper focus. I thought about how I wanted my career to evolve, how I could use the knowledge I had gained so far, and where I could make the greatest impact. That clarity led me to apply for a graduate program in public health, and I was accepted into the Department of Epidemiology and Biostatistics at UGA.
Moving into the next question, tell us about some of the challenging times you have faced as an African woman navigating the Epidemiology and Biostatistics world
One of the significant challenges I faced was navigating gender bias in professional spaces, particularly in leadership. I served as the Head of the Mathematics Department at Busoga College Mwiri, a role that came with both responsibility and resistance. I constantly felt the need to prove myself more than any of my male counterparts. Whenever I made decisions, called for meetings, or delegated tasks, I often encountered pushback,
not because the instructions were unclear or unreasonable, but because I was a woman in a leadership position. At the time, I was one of only two women in the department, and the other was still an intern. The rest of the team was entirely male, and that dynamic frequently made the work environment unnecessarily difficult.
Another challenge is with the double standard! If a man and I both applied for a leadership role, and he was selected, no one questioned his qualifications or whether he truly understood the work. But for me, despite holding the position, I was often second-guessed. That experience made me understand why many capable women shy away from leadership. There are additional, invisible barriers they must constantly push against just to be heard and respected.
Also, motherhood has been one of the most defining and challenging aspects of my career journey. Unlike many of my male counterparts, it is challenging for us to focus fully on our professional roles. I have had to navigate the intersecting responsibilities of being a wife, a mother, and a leader, all at once. At one point, I had to step back from active leadership for nearly two to three years to prioritize my family. It was not an easy decision, especially when I knew I could contribute more professionally, but I recognized that my presence was needed most at home during that time. Balancing these roles often felt overwhelming, but it also taught me resilience, patience, and the importance of pacing a career in a way that honors both personal and professional commitments.
How have you been able to navigate these challenges and still push forward? What’s your motivation?
What keeps me going is the responsibility I feel toward other girls and women who are watching, - Uganda cont'd on page 14
hoping, and drawing strength from my journey. I often remind myself why I started this, recalling the Senior Five student I once admired, who pursued a challenging science combination against the odds. Her courage inspired me, and I know that by continuing, I can offer that same spark to someone else. Giving up would not only be a disservice to myself but also to the many girls who need visible examples of what is possible.
Becoming a mother deepened this conviction. I want my daughter to grow up knowing that her life can be expansive. She should know that marriage, motherhood, and ambition can coexist, and that she is free to define success on her own terms.
I also carry the legacy of the women who fought hard to create the spaces we now occupy. The women who sacrificed greatly to shift the balance, even if only slightly, toward fairness. To step back entirely would feel like undoing part of their work. So I press on, not just for me, but for all the girls who deserve to see what resilience looks like.
Let us talk about the prestigious moments you have encountered on this journey of Epidemiology. We would like to celebrate those achievements with you One of my earliest and most memorable achievements came right after completing my bachelor’s degree. I applied for a grant and was selected to represent Makerere University’s Physics Department in a Materials Science project held in Dar es Salaam. It was a fully funded opportunity that significantly broadened my academic exposure and professional network.
Another major turning point was being awarded a scholarship to AIMS. Coming from a humble background, I was not sure how I would afford postgraduate studies, even though I was determined to continue. Winning that scholarship gave me access to world-class training and also
opened my mind to new possibilities in data science, AI, and public health.
Most recently, I was awarded a highly competitive, fully funded scholarship to pursue graduate studies in the United States, specifically in the Department of Epidemiology and Biostatistics in Georgia. This opportunity has been a profound affirmation of my journey and aspirations. Each of these achievements has shaped my path in meaningful ways, allowing me to grow, contribute, and dream even bigger.
Outside of all things Epidemiology and Biostatistics, who is Doreen?
With my PhD, free time is often scarce, but I make a conscious effort to care for my mental wellbeing. One of the ways I do this is by working out. I genuinely enjoy going to the gym and lifting weights; it clears my mind and brings me a sense of peace and balance. Swimming is another activity I find both relaxing and rejuvenating.
Beyond physical activity, I am deeply connected to my faith. I love going to church. It is an important part of who I am and how I stay grounded. I also enjoy spending time with friends whenever I can. Even if it is just an hour or two, catching up and having meaningful conversations helps me maintain strong relationships and reminds me of the world beyond academic life.
Do you have a favorite quote?
My all-time favorite comes from 2 Corinthians 5:7: “We walk by faith, not by sight.” I love this verse because it speaks directly to the unpredictable nature of life and career. In this journey, not everything unfolds the way we expect. There are times when you work hard on a project, only to see results that fall short. Other times, the effort pays off beyond what you imagined. This verse reminds
- Uganda cont'd on page 15
me that progress often requires trust that things will work out even when you can not see the full picture.
What is your word of encouragement for any African girl who is interested in Epidemiology and Biostatistics?
Do not hold yourself back from pursuing your goals just because certain things have not gone your way. Someone might hear my story and assume I had it easy, but the truth is, the journey has been far from easy. I have faced moments that nearly broke me, situations too personal and painful to even share. There were days I considered walking away from it all.
I have considered quietly retreating into a simpler life, maybe just focusing on motherhood or returning to my old primary school to teach and stay out of sight. But in those moments, I always came back to one question: Why did I begin this journey? That question reminded me not to limit -
myself. It stops me from defining my worth by whether I became a doctor, an engineer, a wife, or a mother.
Life does not end when one dream shifts or when circumstances change. Even if you have faced heartbreak, whether in your career, marriage, health, or personal life, you can still make a lasting impact. So please, do not let any single setback define your entire life. Stand up, dust yourself off, and keep going. It is not easy, I know, but it is necessary. The world keeps moving, and so must you. Keep reminding yourself of your purpose, and trust that things will work out in time. They always do. ■
Words that Count offers a free newsletter with more articles like this. To subscribe follow the link below and look for the subscription box near the bottom of the page. https://wordsthatcount.org/contact/
Your Ad Should Be Here
From Our Archives
What We Knew About COVID-19 in July 2020
What it means and why it matters
EDITOR'S NOTE: As we have now reached the 5th anniversary of the initial days of our awareness of COVID19, it seemed appropriate to begin looking back at what we knew, when we knew it and how our thoughts evolved over the early months of the pandemic. Accordingly, we will be reprinting our articles from that period over the next few months. We welcome your comments and suggestions about what you would like to see.
Deadly Failure To Control Transmission Of SARS-CoV-2 In The US Triggers Proposals For New Strategies Or Better Use Of Existing Countermeasures
The deadly failure of the US to achieve control of the current coronavirus pandemic has frustrated and angered many experts as well as everyday Americans. It has sent some infectious disease and policy experts back to the drawing boards to formulate alternative approaches or reinvigorate old ones that have the best chance of success at this relatively late phase in the pandemic in the United States.
Lessons Learned
A comprehensive review of the experiences of many US states as well as that of several other countries by the Center for American Progress entitled “A New Strategy to Control the Coronavirus” has identified several lessons learned. Based on these analyses and the success achieved by New York and other Northeast states in maintaining low incidence levels, the Center has proposed the following strategy to prevent future waves of cases in the coming year.
1. Close indoor dining and bars.
Experience has shown that these locations are foci of transmission and they should be kept closed or reclosed if reopened, particularly in hotspots. Support with good unemployment
insurance should be provided for workers as well as financial support to cover the fixed costs of businesses forced to close.
2. Monitor other potentially high-risk venues
Other potentially important sources of transmission such as gyms and places of worship could be closed or other measures used to lower risk such as requiring capacity limits, moving outdoors, or requiring masks. Nail and hair salons have not been linked to outbreaks but are inherently risky and should be monitored closely for breaches in compliance with face coverings. Public education about avoiding any indoor gatherings such as parties especially without masks is needed.
3. Mandate masks
This recommendation calls on governors and mayors to implement state and local mask mandates. Financial assistance to businesses should require mask mandates before the aid is provided.
4. Adopt cluster-based contact tracing. The goal of cluster -based tracing is to study
-
the patterns in chains of transmission to identify sources that can produce a large number of cases. These types of sources are super-spreading events and the focus should be on identifying and preventing them rather than tracing all chains of transmission. Bars are an example of such sources but contact tracing may identify others. According to the Center, the model for this approach is Japan which finds patterns in cluster-based contact tracing and uses the information to identify sources that could become major outbreaks.
Think Differently About Test Sensitivity
Another new strategic approach is being advocated by Michael Mina, professor of epidemiology at the Harvard School of Public Health. He was interviewed recently on the podcast This Week in Virology where he made the case for a different way of thinking about testing. Heretofore, the focus has been on having highly sensitive tests that are able to accurately determine if an individual is infected with SARS-CoV-2. This for the most part has meant relying on polymerase chain reaction or PCR tests to diagnose individuals. However, the PCR test is very sensitive and can even detect virus fragments that may not be capable of spreading and causing transmission to other persons. These tests are relatively expensive and are not easy and straightforward to carry out. Also there has been a long delay in reporting the test results which have made some contact tracing work ineffective because it is too late to halt transmission.
New Approach
A different approach argues Mina is to lower the bar for how sensitive tests need to be and to focus instead on other kinds of tests that are
cheap, easy to carry out, and provide results in minutes rather than days. The type of test Mina is calling for utilizes a thin paper strip that only requires a saliva sample and can deliver results in 15 minutes or less. This type of test will be less sensitive but may be considered sensitive enough to detect infectious persons. In this way of thinking, false negatives are of no concern because they are unlikely to be contagious and the test is good enough to be considered sensitive in picking up persons who are likely to transmit. Thus, if made widely available at low cost, these “contagiousness tests” could become ubiquitous and could serve to quickly determine if someone should be admitted to school or work or into any other environment where the risk of transmission exists. Positive persons would be kept away from others. And the test could be repeated daily if necessary to keep close monitoring of each situation.
Test, Test, Test
Mina’s idea was also explained recently in a feature article in the Atlantic. It described Mina’s idea this way. “Test negative, and you many enter the public space. Test positive, and you are sent home. In other words: Mina wants to test nearly everyone, nearly every day.”
Real Lockdown
Another idea has been put forward by Michael Osterholm at the Center for Infectious Disease Research and Prevention (CIDRAP) and Neel Kashkari, president of the Federal Reserve in Minneapolis. In an op-ed piece in the New York Times, Osterholm and Kashkari call for a second more rigid lockdown throughout the US. They believe the earlier lockdown was not carried out well enough and that the only way to get the
- Deadly cont'd on page 18
virus under control now is to get serious about keeping everyone at home for six weeks. The goal of the new lockdown would be to get reported cases to a level as low as 1 case per 100,000 because at that level public health control measures have a possibility of being effective. As rates stand now, the volume of cases is too large for effective testing and contact tracing, according to the authors.
New York Example
Failing such a rigorous intervention, Osterholm believes that another coronavirus “forest fire” will spread out of control in the US in future months. In one of the regular podcasts from CIDRAP, Osterholm said the US could look to the situation in New York State to envisage how the new lockdown could drive the seven day average numbers of cases and deaths lower.
New York had approximately 9800 cases and 921 deaths as of April 10. By June the cases had fallen to 662 and deaths to 39. By August 10, cases were at 651 and 8 deaths and the averages have been flat since June. According to Osterholm, New York has done what the rest of the country can and should now do.
Since we have to get through at least 6-8 months without a vaccine, according to Osterholm, the number of cases is going to get much worse. We should take our medicine now and get ready to manage the smaller caseload that will emerge after a rigorous lockdown, he said. It is a pay now or pay me later situation he believes. He is hopeful their proposed strategy can earn discussion and support.
NY Times Editorial Board
In perhaps a less surprising new strategy, the New York Times Editorial Board has proposed
making better use of the tools the US has to achieve a higher level of control that has eluded it. In its view, the US has never really had a true lockdown compared to other countries. It estimated that the US only closed down or “shuttered” half of the country rather than the 90% that was attained in other areas. Consequently the US never achieved the dampening effect that other countries were capable of producing.
The Board proposed a new strategy consisting of the following key steps:
1. Clear and consistent messaging. Because of the confusion that has been sown, it is now important to coordinate messaging at every level, especially from the top masks are essential, and social distancing is a civic responsibility.
2. Better Use of Data
Obtaining and sharing more information about how the pandemic is unfolding in various populations and places and how it is being managed could allow public health officials to provide better forecasts of what is coming so that people could adjust their plans accordingly.
3. Smarter shutdowns.
Alert levels could be created to warn people about what behaviors are permissible and which are not at different risk levels or at different levels of transmission in the community. Shutdowns would not need to be equally aggressive in all communities. Such color coded alert systems have been developed in Harris County Texas as an example.
- Deadly cont'd on page 19
4. Testing, Tracing, Isolation, and Quarantine
The US has failed at all of these. The Times calls for more effective and rapid diagnostics and the federal government should compel companies to make the needed tests available. Once testing is taking place at a high enough volume, then the other public health measures can be made effective to control the outbreak.
Epidemiologists and Public Health Officials Becoming Embroiled In Pandemic Control Conflicts
As uncontrolled community transmission of COVID-19 persists in the United States, epidemiologists and public health officials are involved in difficult situations. Media accounts of firings, resignations, harassment, and threats are proliferating. While there may be more than one reason for these conflicts, failure to use evidence as the primary basis for decision making is emerging as a common theme in several situations. So is the highly polarized social and political environment in the US.
Federal Level Preview
The challenges that are playing out at the state and local level are a reflection of similar challenges that have already produced headlines about similar conflicts at the federal level involving all of the major health agencies including the Centers for Disease Control and Prevention, the Food and Drug Administration, and the National Institutes of Health. Sometimes valid political and often serious economic considerations are bumping up against scientific facts or expertise.
List of Turnovers
A list maintained by Kaiser Health News (KHN) and the Associated Press reportedly contains almost 50 state and local officials who have resigned, retired, or been fired since April.
In an article in The Hill, NIH Director Francis
Collins stated: "To see this kind of really widespread resignations from critical roles at a time of great importance for our country ought to be a source for everyone to be concerned... I am very troubled to see that kind of turnover...The idea that you either have to pick to support the economy or pick public health measures is so upside down. The public health measures are going to get our economy going again. And yet somehow in many of these situations, these are pitted against each other in a way that causes a great deal of anger and resentment and political furor to kick in."
In a recent report, KHN quoted former CDC Director Tom Frieden “The overall tone toward public health in the U.S. is so hostile that it has kind of emboldened people to make these attacks.”
Bad Feelings
In the same report, KHN quoted former West Virginia public health commissioner Dr. Cathy Slemp, who was forced to resign by Republican Gov. Jim Justice in June. The past few months have been “frustrating and tiring and disheartening” for public health officials, said Slemp. “You care about community, and you’re committed to the work you do and societal role that you’re given. You feel a duty to serve, and yet it’s really hard in the current environment,” Slemp added.
Examples of these conflicts and challenges involving epidemiologists are described below.
Indiana Episode
The Indianapolis Star reports that Eileen White, the only epidemiologist working for the local city Fishers Health Department resigned earlier this month alleging too much interference by the city’s mayor, especially pushing hard to open classrooms too soon. In an account by the Indy Star, White says “This is a level of interference I had never seen before in a public health agency…I have never seen a health department set up as a business before… I have a feeling of failure that all of us in public health have right now…I had so much hope for what I could do. But we are continuing to see more pushback and politics in public health.” White previously worked for the Minnesota Health Department for three years. The mayor’s office and White’s supervisor pushed back hard in a written statement to the newspaper.
Official Response
"My administration, in concert with the Fishers Health Department, has had a constant focus on what is in the best interest and safety of our residents," the statement read. "That said, we continue to believe in, and follow the direction of, our public health department leadership, (Chief Medical Director) Dr. Indy Lane and (Public Health Director) Monica Heltz. Any assertion of anything other than that is categorically false."
Heltz said what White characterizes as interference she considers the full backing of the mayor.
"I have felt nothing but support from the city," she said. "The suggestion that it has been anything but supportive is disappointing."
Hawaii Episode
In Hawaii, the state epidemiologist Sarah Park has been sidelined for not having in place the required number of contact tracers needed to handle an upsurge of cases in the state. It apparently had a plan for controlling the virus that was not adequately implemented, according to the publication Civil Beat. Park reportedly had refused to accept outside help offered months before the upsurge because she believed the Department could bring on contact tracers quickly if needed. Only about 100 contact tracers are actively working when hundreds were called for three months previously. While continuing at the Department to focus on other aspects of the pandemic, Park will no longer oversee the contact tracing activities which have been transferred to a Department deputy director and the chief of the disease investigations branch.
Park Testimony
In her defense, Park gave testimony recently in front of a Senate Special Committee on COVID19. According to the Civil Beat article, “Park downplayed the importance of contact tracing, saying that some states no longer even do it. Park ultimately blamed the public for the surge in cases. She cited beach and house parties and other gatherings that people should have known not to engage in as causes for the surge in cases that quickly overwhelmed the system. She was quoted saying “What we could not have predicted, quite frankly, is how badly our community would behave.”
South Carolina Episode
In another situation in South Carolina, state epidemiologist Linda Bell has expressed regret in internal emails at not being more forceful
and speaking out in press briefings with the governor who has been reluctant to require mandates for mask use and other measures. According to the account published in The State, Bell said in emails to agency public relations specialists that Gov. Henry McMaster’s staff has been “somewhat manipulative” in meetings prior to news conferences about the coronavirus. Bell also said her not speaking out more from “a policy perspective is one of the reasons that South Carolina is now among the states with the worst outlook.”
After these emails became public, a group of organizations in the state issued an open letter of support for Bell.
In another development, South Carolina lawmakers have called for top health officials to speak out more frankly and forcefully about the pandemic.
Most people should be disturbed by the emails, SC House Minority Leader Todd Rutherford told The State.
He added, “We need to take steps to separate the governor from DHEC (state’s Department of Health and Environmental Control) and the governor from our chief epidemiologist so that we can get data that is unvarnished by someone’s political ideology.” ■
Your Ad Should Be Here
Epi
Famous Epidemiologists & Biostatisticians
We know summer is incredibly busy for our readers so this month, instead of a long crossword, we are bringing you a short word search. Good luck - don't let the easy words fool you!
For an interactive online version go to: https://tinyurl.com/3xsbpzv8
Names to find:
1. Daniela Witten
2. Katelyn Jetelina
3. Francis Galton
4. Larry Brilliant
5. Frank Harrel
6. Gertrude Cox
7. M Osterholm
8. Nancy Krieger
9. William Cochran
10. John Snow
11. J Battacharya
12. John Ioannidis
13. Paul Meier
14. Miguel Hernan
What We're Reading This Month
Editor's Note: All of us are confronted with more material than we can possibly hope to digest each month. However, that doesn't mean that we should miss some of the articles that appear in the public media on topics of interest to the epi community. The EpiMonitor curates a monthly list of some of the best articles we've encountered in the past month. See something you think others would like to read? Please send us a link at info@epimonitor.net and we'll include it in the next month
Washington DC Chaos
♦ I'm afraid of diseases I never thought I'd see (NYT)
https://tinyurl.com/ympd6sed
♦ The growing influence of vaccine skeptics inside HHS (STAT)
https://tinyurl.com/ys3r2z3z
♦ Secret changes to major U.S. health datasets raise alarms (PsyPost)
https://tinyurl.com/5bhnpdys
♦ Trump team withholds $140 million budgeted for fentanyl fight (NPR) https://tinyurl.com/y2ts8d56
♦ Columbia struck a deal to save research funding. How do its researchers feel about that? (Chronicle of Higher Education via AppleNews)
https://tinyurl.com/42rr582k
♦ White House agrees to exempt PEPFAR from cuts (The Hill) https://tinyurl.com/48dywvp9
♦ The conversations doctors are having about vaccination now (The Atlantic via AppleNews) https://tinyurl.com/yrj4vs2n
♦ States, cities face loss of vaccination programs and staff after ‘baffling’ cuts to federal funding (CNN)
https://tinyurl.com/y2evasww
♦ Trump EPA will propose repealing finding that climate change endangers public health (The Hill)
https://tinyurl.com/bdkupzc9
- Reading cont'd on page 24
What We're Reading This Month
[Type a quote from the document or the summary of an interesting point. You can position the text box anywhere in the document. Use the Text Box Tools tab to change the formatting of the pull quote text box.]
- con't from page 23
Public Health Topics, cont.
♦ A genetic tweak could prevent mosquitoes from transmitting malaria (NPR) https://tinyurl.com/yeyvb55t
♦ Arizona patient dies in emergency room from plague (NBC News) https://tinyurl.com/35w36rfm
♦ Doctors alarmed at rising meningitis cases in Gaza's children (Reuters) https://tinyurl.com/5dvjbbcc
♦ Doctors detected a mysterious antibody in a French woman. It signaled a new blood type. (Smithsonian Magazine via AppleNews) https://tinyurl.com/mwrj4nwk
♦ Meet the Oropouche virus. It may be visiting your city soon. (VOX via AppleNews) https://tinyurl.com/maafsnb2
♦ U.S. sees most measles cases in a single year since declaring disease eliminated in 2000 (STAT via AppleNews)
https://tinyurl.com/2s3tkf6w
♦ More than 14M children globally have not received a dose of any vaccine: WHO (ABC News)
https://tinyurl.com/3ecaw29y
♦ 'You Could Throw Out the Results of All These Papers' (The Atlantic via AppleNews) https://tinyurl.com/4s443saw
Notes on People
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Appointed: The University of Texas Medical Branch appointed Dr. Neil K. Mehta the inaugural Chair of the Department of Epidemiology in the School of Public and Population Health.
Mehta joined UTMB in 2020 as a faculty member in the Department of Preventive Medicine and Population Health. He joined the Department of Epidemiology when it was established as part of UTMB’s new School of Public and Population Health in 2022.
Elected: Brian Millen has been elected President of the American Statistical Association (ASA). Millen graduated from Ohio State University with a PhD in Statistics in 2001 and currently serves as vice president, global head of biostatistics, epidemiology, and real-world data analytics at Biogen. Prior to his current role, he served at Lilly in multiple senior leadership and technical roles across the clinical development lifecycle.
Named: UCF infection preventionist Dr. Cindy Prins has been named a fellow of the Association for Professionals in Infection Control and Epidemiology (APIC) – the highest honor for a scientist focused on better ways to prevent infectious diseases. Dr. Prins began her career as a virologist, before a passion for public health inspired her to transition to epidemiology, studying healthcare-associated infections, and how to prevent them from spreading.
Named: George Washington University has announced that Kelly A. Gebo will be the next Michael and Lori Milken Dean of the Milken Institute School of Public Health, effective Oct. 1. She will also be a professor of epidemiology. Gebo has spent over two decades at the Johns Hopkins University in various roles, working to improve the well-being and health outcomes of local, national and global populations. She is currently a professor of medicine at the Johns Hopkins University School of Medicine with a joint appointment at the Johns Hopkins Bloomberg School of Public Health in epidemiology.
Notes on People,
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Named: Ohio State University Biostatistics Professor Michael Pennell was named a 2025 fellow of the American Statistical Association (ASA), an honor that acknowledges his exceptional contributions to statistical sciences and his commitment to advancing the field.
The ASA selected Pennell for the prestigious fellowship for his notable methodological contributions to Bayesian non-parametrics, survival analysis, and risk assessment, along with extensive collaborative efforts. The association also noted Pennell’s exemplary mentoring, teaching and national service.
Passed: Dr. Thomas Mack passed away Sunday, June 22, after a long illness. Tom was a giant in the field of epidemiology and public health and made seminal contributions to smallpox epidemiology and transmission, and causes of cancer and chronic disease, first as a CDC Epidemiologic Intelligence Service officer, then as a faculty member at the Harvard School of Public Health and finally at the USC Keck School of Medicine, where he was a Professor in the Department of Population and Public Health Sciences for 47 years.
https://tinyurl.com/ju3a98nm
Passed: Dr. Frances J. Mather a former professor and administrator for 40+ years at her alma mater, Tulane University School of Public Health and Tropical Medicine, Biostat & Epi departments passed away on June 17th in Metarie, LA. In addition to her tenure as a faculty member, she also served as the Director of Academic Information Systems. She was one of the first women in Mining Engineering in the 50's, she marched for Women for Peace in the 60's (to her ex's chagrin), she bought a house (even as a divorcee, gasp!) in the 70's, which at the time was another milestone for women. The successive years were punctuated with teaching, grants, mentoring, and traveling.
https://tinyurl.com/3amff4p8
Near Term Epidemiology Event Calendar
Every December The Epidemiology Monitor dedicates that issue to a calendar of events for the upcoming year. However that often means we don't have full information for events later in the upcoming year. Thus an online copy exists on our website that is updated regularly. To view the full year please go to: http://www.epimonitor.net/Events The events that we are aware of for the next month follow below.
Do you have a job, course, conference, book or other resource of interest to the epidemiology community? Advertise with The Epidemiology Monitor and reach 35,000 epidemiologists, biostatisticians, and public health professionals monthly.
Advertising opportunities exist in this digital publication, on our website and social media pages, and in our Epi-Gram emails. For more information please contact:
Multiple Open-Rank Faculty - Epidemiology
The O’Donnell School of Public Health and the O’Donnell Brain Institute at UT Southwestern Medical CenterDallas, TX are seeking exceptional epidemiologist candidates for multiple tenured or tenure-track faculty positions preferably at the associate or full professor level. Both the School and the Brain Institute are undergoing significant expansions, and an outstanding startup package, along with opportunities for program development, will be provided.
We encourage applications from exceptional scholars with a national reputation in epidemiological and population research on Alzheimer’s disease and other dementias, stroke and cerebrovascular disorders, Parkinson’s disease, or other neurological disorders. Qualified candidates should hold a doctoral degree (Ph.D., D.Sc., Dr.PH., or equivalent) in Epidemiology or an MD with additional training in Epidemiology or Clinical Investigation (M.S., M.P.H., MSc., or Ph.D.). Candidates must demonstrate a successful, impactful research career with a strong record of securing external funding (e.g., NIH, CDC, AHRQ, PCORI, etc.). Experience in academic leadership, program development, teaching, and fostering multidisciplinary collaboration is highly desired.
OPEN RANK FACULTY - EPIDEMIOLOGY DEPARTMENT
Appointment rank will be commensurate with academic accomplishment and experience. Consideration may be given to applicants seeking less than a full-time schedule.
Candidate Requirements:
♦ Ph.D., M.D., Sc.D., DrPH, or equivalent doctoral degree in a relevant discipline
♦ Demonstrated ability to conduct scholarly research and capacity to obtain peer-reviewed funding
♦ Highly self-motivated individual, enthusiastic about scientific discovery and able to collaborate closely and effectively with other members of multidisciplinary research teams
♦ Desire to partner with healthcare systems, public health agencies, and/or community organizations to conduct research aimed at enhancing the health of the people of Texas and beyond
Apply Here: https://tinyurl.com/4yt4ytjd
OPEN RANK FACULTY - EPIDEMIOLOGY BRAIN HEALTH RESEARCH
Appointment rank will be commensurate with academic accomplishment and experience. Consideration may be given to applicants seeking less than a full-time schedule.
Candidate Requirements
♦ Ph.D., D.Sc., Dr.PH., or equivalent in Epidemiology or an MD with additional training in Epidemiology or Clinical Investigation (M.S., M.P.H., or Ph.D.)
♦ Candidates must demonstrate a successful, impactful research career with a strong record of securing external funding (e.g., NIH, CDC, AHRQ, PCORI, etc.).
♦ Experience in academic leadership, program development, teaching, and fostering multidisciplinary collaboration is highly desired.
Apply Here: https://tinyurl.com/3rdj676f
Postdoctoral Research Fellowships in Cancer Prevention and Control
Position Location: St. Louis, MO
Eligibility: PhD, DrPH, MD, or other doctoral degree in a public health related discipline, or a doctoral degree in another discipline with an interest in public health research. T32 applicants are limited to United States citizens, non-citizen nationals, or must be lawfully admitted for permanent residence and possess registration requirements.
Seeking postdoctoral fellowship applicants with an interest in cancer prevention and control to join diverse team of multidisciplinary researchers in the Division of Public Health Sciences and Siteman Cancer Center at Washington University in St. Louis. We welcome applicants from a variety of disciplines. Our multidisciplinary faculty conducts worldleading research on a wide range of health issues and leads community education and outreach to prevent cancer and other diseases, promote population health, and improve quality and access to health care in Missouri and beyond. Engaging community members, addressing key needs in our catchment area, and addressing cancer disparities are priorities in the work we do.
The Division has a diverse range of NIH funded projects and faculty mentors to see the full range, consult our website While we welcome applicants in any relevant research area, these are the highest priorities for the Training Program:
• Cancer Disparities and Access to Care
• Community-based and Community-engaged Research
• Cancer Epidemiology
• Intervention and Implementation Science
• Contextual Drivers of Health and Healthcare
Washington University School of Medicine is an equal opportunity employer. We particularly welcome applications from first generation college graduates and other backgrounds underrepresented in biomedical sciences.
Washington University offers excellent benefits. Support is available for tuition, books, software, conference travel, and research. Postdoctoral positions are partially funded by NCI grants (f32CA190194), with annual stipend starting at $61,428.00 for up to 2-3 years of training. Mentorship and career development are available to our vibrant cohorts of postdoctoral fellows. Our trainees have a strong track record of finding funding and faculty positions after completing their postdoctoral training. You’ll find ample opportunities to collaborate with investigators from a range of disciplines.
Send inquiries to: The T32 Program Coordinator at PHSpostdoc@wustl.edu. You can also contact Dr. Aimee James and Dr. Graham Colditz, Training Directors, at aimeejames@wustl.edu and colditzg@wustl.edu.
To apply: Fill out an application and submit your cover letter, curriculum vitae, and three professional references by visiting https://redcap.link/phs-postdoc.
You can also access the online application by scanning the QR code below.
Please email PHSpostdoc@wustl.edu with any questions. Applications are considered on a rolling basis.
Tenured: Professor & Department Head
The School of Public Health at Texas A&M University invites applications for consideration as Department Head and Professor (Tenured) for the Department of Epidemiology & Biostatistics. Located in College Station, TX on the flagship campus of the Texas A&M University System, the CEPH-accredited School of Public Health (SPH) has over 95 faculty across four distinct departments. Texas A&M University, a land-, sea-, and space-grant institution, was the state’s first public institution of higher learning, is a member of the prestigious Association of American Universities (AAU) and boasts world-class resources. The School of Public Health is currently ranked #1 in Texas and 27/219 by U.S. News & World Report and has the 5th largest student enrollment in the nation. The school has had record external funding growth over the past five years. This full-time, 9-month, hard-money-supported appointment would start Summer 2026, although this date is flexible.
The next department head will have the opportunity to build on the department’s strong foundation and craft a vision that will continue to foster scientific discovery and scholarly excellence. We seek a faculty-centered, student-supportive leader who will actively cultivate a dynamic environment in which all faculty, staff, and students will thrive.
The successful applicant will be an innovative thinker with a strategic vision for guiding the department to a higher level of excellence and who can communicate this vision to a constituency that includes academia, government, industry, and current and former students. The candidate must have notable accomplishments and experience in academic leadership, research, teaching, and scholarship.
Applicants can apply at https://apply.interfolio.com/167473 Please provide: (1) curriculum vitae, (2) cover letter outlining managerial and leadership philosophy, managerial and leadership experience, and managerial and leadership preparation to head a Department, (3) personal statement including philosophy and plans for research and teaching. Additionally, please provide a list of five (5) references; references will be contacted only if you are selected for an interview.
Questions regarding this academic leadership opportunity may be sent to Dr. Eric Wilson, Assistant Dean for Accountability and Strategic Initiatives, at eric.wilson@tamu.edu You may also contact the Search Chair, Dr. Adam E. Barry (aebarry@tamu.edu).
Equal Opportunity/Veterans/Disability Employer.
More Information: https://tinyurl.com/ye7jmm9c
YLE can be found here: https://yourlocalepidemiologist.substack.com/
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, wife, and mom of two little girls. YLE reaches more than 305,000 people in over 132 countries with one goal: “Translate” the ever-evolving public health science so that people will be well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members.
To support the effort, subscribe or upgrade your existing subscription: https://yourlocalepidemiologist.substack.com/
The Epidemiology Monitor ISSN (2833-1710) is published monthly
The Epidemiology Monitor
Editorial Contributors
Katelyn Jetelina, PhD, MPH Editor and Publisher
Operations
Christopher Jetelina Operations Manager
Advertising Sales
Michele Gibson sales@epimonitor.net
Advertising Rates
All
in a Digital Version is available FREE to subscribers
The Epidemiology Monitor is available exclusively online in the same familiar print format subscribers were accustomed to, and they can read through the publication on their electronic devices in the same manner they did with the print version. In addition, you can download and save copies of The Epidemiology Monitor for easy future access.