Special report
the training of
From myopia to online sales, balancing the evidence on key topics within optics
Practice team
In practice
importance of

and utilising data
www.optometry.co.uk Journal of the Association of Optometrists October/November 2022 Volume 62:05
Exploring
IP optometrists Page 34 CPD Recognising and managing keratoconus Page 80
The
collecting
Page 41
THE EVIDENCE EDITION
guide Supporting each other to achieve success







Welcome
During his recent bid to be Prime Minister, Rishi Sunak argued that government policy during the pandemic was too strongly influenced by scientists. That claim did not ring true to me. A few months earlier, the Institute for Government had published a report by Sense about Science director Tracey Brown on the UK’s response to COVID-19. The vast majority of those quoted in that report – me included – had testified that government had listened too little and responded too late to the scientific evidence.
Optometrists are, of course, scientists, and evidence is central to your day-to-day work. Among our members – and at Council and Board – there are incredibly knowledgeable academics who devote their professional lives to advancing the science of eye care. And, as this OT discusses, the sector has a commitment to expanding its knowledge base even further. This puts optometry on a strong platform to build from. But we need to go on assembling the evidence base to prove what we know to be true: that optometry is a key deliverer of healthcare benefit.
So the discussion of evidence is not just an academic one: it is one which is vital to our future. And the AOP need to play our part. That’s why we continue with our Voice of Optometry research surveys, which are invaluable for helping us raise the issues that matter within the profession with the media. And, later this year, we will be surveying you, our members, to find out your thoughts on the evolving profession and your career path. Plus, we are continuing to trawl through the information routinely collected in disparate parts of our sector to build the underlying evidence base behind our work.
Assembling the evidence is only half the battle; we need to bring it to life through effective communications. And that may mean packaging it up into easily saleable soundbites – something which is challenging and at times uncomfortable.
Evidence is an essential component in proper decision-making, but, as David Boyle argues in The TyrannyofNumbers, facts can mislead as much as they can inform. Asking the wrong question, measuring the wrong thing, tracking progress towards the wrong target – all are dangerous. So let us work to build our evidence base in optometry, but once we assemble it we have to use it right.
Adam Sampson, AOP chief executive
 Getty/Malte Mueller
Getty/Malte Mueller
“Assembling the evidence is only half the battle; we need to bring it to life through effective communications.”
OCTOBER/NOVEMBER 2022
October/November 2022 www.optometry.co.uk 3
Contents
07-23
SPOTLIGHT
The news in digest

Picture this
Man seeing grandchild for the first time following cataract surgery is captured
OT reports
The GOC answers key questions on its Education Training Requirements
The edit
Optics in 16 stories
Clinical round-up
A review of the latest clinical news and research papers

100% Optical
OTreports on the show’s latest updates
Industry profile
Raising the profile of the International Agency for the Prevention of Blindness, with Peter Holland

Supplier insight



Driving developments in OCT
AOP round up
Support for employers, a Whole life course project, and the HOAC 2022
Spotlight Member support
“We look to support members, not just as clinicians but as people, and this is reflected in our health and wellbeing programme”
Wendy Steele, AOP commercial director PAGE 22
25-30
HIT LIST

The trends, launches and looks
OT focuses on...
Seasonal eyewear styles

Me and my glasses
Street artist, Steve McCracken
Get the look // Anatomy of a frame
With Lizzy Yeowart
The shortlist
The October/November selection
Behind the brand
Cambridge Spectacle Co.
UPSKILLING
Fatima Nawaz,
Spring; Alberto Montresor; Chloe Farrant;

4 www.optometry.co.uk October/November 2022
16 41 Vision
Getty 28 34-38 IP: AN
WORKFORCE SPECIAL REPORT “There needs to be better connections with ophthalmologists”
IP optometrist
41-55
IN PRACTICE
Business insight and career development
The discussion
A deep dive into optical data wtih Specsavers and Leightons Opticians
Life as a locum
Bhargavi Zinzuwadia
How I got here
Optometrist, Siddhant Majithia
Eyes on wellbeing
Menopause in the workplace

How do I...
Incorporate new research into practice, advises Dr Ian Beasley
Pre-reg focus
Thaksha Sritharan, Holly Leitch and Caroline Mansfield
Key milestones
Switching to a private eye care model
PRACTICE
UNLOCKING POTENTIAL
Cover story The sweet spot
OTexplores the evidence on key topics within optics – from myopia and visual stress to racial bias and increasing happiness at work. Plus: the AOP’s experts, optometrists Dr Peter Hampson and Henry Leonard, share the Association’s perspective
PAGE 57-64
97-98
END NOTES
I could not live without...
”My WP10 pad,” says optometrist, Andy Britton
Last word
Matthew Stephenson’s secret life
OT and its wrapper are produced on paper from European mills, meeting the highest quality and environmental standards.
The journal and paper wrapper are fully recyclable.
CPD 65-90
Professional development for the eye care practitioner
65 CPD welcome
66 Adverse effects of periocular aesthetic treatments
73 How headsmart are you?
77 Communication in optometry
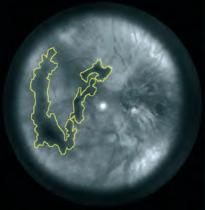
80 Keratoconus: considerations, recognition and magement with speciality contact lenses
86 Myopia management in clinical practice
88 Retinal cases of visual loss
90 CPD author Q+A: Lorcan Butler

ONLINE
OTvideo highlights
OT’s latest interactive CPD Video explores contact lens fitting

Watch the video on www.optometry.co.uk/CPD
Contact the OT team with your experiences, observations and lessons from practice today: newsdesk@optometry.co.uk

Follow us on Twitter

@OptometryToday
Like us on Facebook

OptometryTodayJournal
Follow us on Instagram
@optometry_today

October/November 2022 www.optometry.co.uk 5 CONTENTS
23 27 15
TEAM GUIDE
INSIDE









Spotlight
13 CLINICAL ROUND-UP
The impact of a sight loss diagnosis and low-cost 3D imaging
15 100% OPTICAL OT shares the latest news from the event, including plans for a new CPD timeline
16 INDUSTRY PROFILE Peter Holland from the IAPB on promoting eye care beyond World Sight Day

At first sight
A finalist in the International Agency for the Prevention of Blindness’ (IAPB) 2021 photography competition, photographer Ulrich Eigner captured the moment Mekonen Bezabeh, in Burkina Faso, saw his grandchild for the first time following successful cataract surgery.
The competition forms part of the annual World Sight Day campaign, and challenges amateur and professional photographers to illustrate what it means to
#LoveYourEyes. Simon Darvill, head of communications and campaigns at IAPB, said of the photographs: “They help us build awareness of eye health around the world, the positive impact it has on lives, and the losses that result when it is not easily accessible.”
Winners of the 2022 competition will be announced in November. Read more about the IAPB’s ambition to highlight the importance of eye health on page 16.
Ulrich Eigner for Light for the World, courtesy of IAPB
October/November 2022 www.optometry.co.uk 7
October/November 2022
Volume 62:05 Issn 0268-5485
ABC certificate of circulation

1 January 2021–31 December 2021
Editor: Emily McCormick emilymccormick@optometry.co.uk
Deputy editor: Lucy Miller lucymiller@optometry.co.uk
Features editor: Selina Powell selinapowell@optometry.co.uk
Senior reporter: Kimberley Young kimberleyyoung@optometry.co.uk
Web content and social media executive: Leah Boyle leahboyle@optometry.co.uk
Clinical editor: Dr Ian Beasley ianbeasley@optometry.co.uk

Clinical editor for multimedia: Ceri Smith-Jaynes cerismithjaynes@optometry.co.uk
Video production editor: Laurence Derbyshire laurencederbyshire@optometry.co.uk
CPD enquiries: 020 7549 2076 CPDhelp@optometry.co.uk
AOP membership and OT subscription team: subscriptions@aop.org.uk
EDUCATION TRAINING REQUIREMENTS: QUESTIONS ANSWERED ABOUT THE CHANGES TO OPTICAL UNDERGRADUATE EDUCATION
Last year, after an extensive four-year Education Strategic Review (ESR) process, the GOC signed off its plan for changes to its education and training requirements. Now moving to the implementation phase, the regulator’s head of education (development), Samara Morgan, answered students’ questions as universities prepare to begin the rollout of the new Education Training Requirements (ETR) from September 2023
1How is the GOC working with universities to implement the new ETR and when do you expect implementation to start? The GOC has already entered the implementation phase, Morgan confirmed, sharing that “all providers have been invited to start adapting to the new ETR.”
She explained the projected start date for implementing the new ETR is set by the education institution as the provider and “will be influenced by their own internal processes and development timescales.”
During the transition period, when courses will be produced to both the current and new standards, Morgan confirmed that the regulator will continue to quality assure all GOC-approved qualifications, until, eventually, all providers are offering programmes against only the new education and training requirements.
Asked how universities can involve students, staff and employers in the design and implementation of their new course structure, the GOC encouraged students to speak to their education providers.
Advertising: Matt Hall 020 3771 7257 matt.hall@thinkpublishing.co.uk
Advertising production: aop@ccmediagroup.co.uk
Senior designers: Grant Pearce, Juanita Adu
Client engagement director: Anna Vassallo
Executive director: Jackie Scully
Published bimonthly for the Association of Optometrists by Think Media Group
20 Mortimer Street, London, W1T 3JW
Printed by Acorn Web, Normanton Ind Estate, Loscoe Close, Normanton, West Yorkshire, WF6 1TW
All rights in and relating to this publication are expressly reserved. No part of this publication may be reproduced in any form or by any process without written permission from the AOP or the publisher.
The GOC is meeting with all providers in order to understand their needs and timescales “which will help us to ensure a smooth transition to the new requirements,” Morgan said. However, the GOC would anticipate that “most” will work towards enrolling students on courses that meet the new outcomes and standards from the 2023–24 or 2024–25 academic year. “Some providers may, in consultation with us, agree a later start date,” Morgan shared.
Morgan told OTthat within the new education and training requirements, the GOC expects “the design of the programme curriculum, and the delivery and assessment of the outcomes to be informed by feedback from a wide range of stakeholders, including patients, employers, students, placement providers, commissioners, members of the eye care team and other healthcare professionals.”
She added that “the new ETR is intentionally non-prescriptive,” allowing providers to use a range of methods to gather feedback depending on what works for them.
“We look forward to hearing about providers’ plans and the utilisation of innovative and creative solutions to drive forward good practice within the optical sector,” she said.
“All providers have been invited to start adapting to the new ETR”
8 www.optometry.co.uk October/November 2022
2How will the new requirements affect current and future optometry students?
There will be no disruption for students currently enrolled on any existing GOC-approved education or training programme, Morgan confirmed.
She explained to OT that during the transitional phase, which she referred to as the teach out or migration phase, the QualityAssuranceHandbooks foroptometry(2015)anddispensing opticians(2011),as well as the regulator’s policies on supervision and recognition of prior learning, will continue to apply to all existing GOCapproved and provisionally approved qualifications.
To current students who are concerned about the impact of the perceived standard of their degree in light of the new requirements, Morgan reassured: “Regardless of whether a student successfully completes their studies under the new or current requirements, they will be eligible to register with us,” adding that “all approved programmes will continue to be subject to the GOC’s robust quality assurance procedures.”
Discussing how the ETR would affect future optometry undergraduates, Morgan explained that a key change that will be introduced through the requirements is for education providers to fully integrate at least 48 weeks of clinical, patient facing experience into the course. “This will enhance the clinical capabilities of future optical professionals to increase their confidence to safely occupy current and future roles within service redesign,” she said.
“There is also a greater focus on key skills such as professional judgement, patient-centred communication, management of risk, and diagnostic consultation and clinical practice skills,” Morgan explained, adding: “Our new requirements will ensure that optometrists and dispensing opticians can meld critical thinking, clinical reasoning and decision-making; are well-
“There will be a greater focus on key skills such as profession judgement, patient-centred communication, management of risk, and diagnostic consultation and clinical practice skills”
prepared to take responsibility for decisions and actions; engage in research-informed clinical practice, and respond effectively to changing patent and service-user needs in each of the four nations.“
3What does the new ETR mean for the future of the pre-reg placement programme?
Under the new ETR, “optometry programmes will fully integrate practical and theoretical learning and experience, offering a single and direct route to registration with the GOC,” Morgan shared. As such, she expanded, “the preregistration period in its current form will cease to exist.”
Under the new requirements, courses must provide experience of
working with patients; interprofessional learning; and teamwork and preparation for entry into the workplace in a variety of settings. This includes in clinical practice, community, manufacturing, research, domiciliary and hospital. “This experience must increase in volume and complexity as a student progresses through a programme,” Morgan said.
Students must complete at least 1600 hours/48 weeks of patient-facing learning and experience for optometry and dispensing optics.
It is acknowledged that under the new ETR, with practical experience integrated into the course, students will no longer enter a paid prereg position. Some students have expressed concern for their future peers, questioning whether any grants or bursaries will be offered to students to offset the potential travel and placement costs.
Posing this to the GOC, the regulator said it has set up a Sector Strategic Implementation Steering Group (SSISG) in order to “discuss issues related to funding, supervision and workforce supply,” adding that within the SSISG a range of working groups have been meeting to discuss issues including tuition fees and funding.
SPOTLIGHT
October/November 2022 www.optometry.co.uk 9 Getty/ lemono
Jason Kirk, managing director for Kirk & Kirk, described his ambitions for the launch of a pop-up store in Shoreditch, hosted throughout September and designed to raise the profile of the brand. By cultivating a series of pop-up sites, the brand hopes to provide a unique experience of exciting eyewear to capture the attention of consumers.

Practice owner and optometrist, Valarie Jerome, shared the pressures facing businesses in her local community, as energy costs climbed this summer. Ahead of measures introduced by the newlyappointed Prime Minister, OT asked practices to share what the rising cost of business meant for them. Read more at: bit.ly/3Bg4xpP



Blind Veterans UK has launched a new campaign, sponsored by Specsavers, to encourage veterans to check if they could be eligible for support. The charity said that “there are many thousands more” veterans in need of support following sight loss.





A donation of €30,000 (approximately £26,000) from Andy Wolf Eyewear supported a summer school for children from Ukraine, in Styria, south east Austria. Run by Caritas Styria, the free holiday programme provided a mixture of learning and sports for children. Commenting on the donation, Andreas Pirkheim, CEO and founder of Andy Wolf Eyewear, said: “We wanted to help Ukrainian families to integrate and enable them to have an independent everyday life.”

Boots Opticians has introduced a new campaign, reflecting a repositioning of its brand identity. The campaign seeks to encourage the public to prioritise their eye health and “see what’s possible” with sharper vision. James Arrow, managing director for Boots Opticians, highlighted the “important role that each and every one of our colleagues and partners play by helping our customers have clear vision.”







Johnson & Johnson Vision Care has launched its Acuvue Oasys Max 1-Day contact lens in the UK and Ireland. The spherical and multifocal contact lens designs are designed to address increasing demands on the eye, with a study finding that two-thirds of people in Britain who wear vision correction felt the increased role of screens in modern life was have a negative effect on their eye comfort.





Julian Clarke, managing director of Caseco, described the supplier’s decision to relocate to The Eco Business Centre in Bicester, a carbon neutral site and the UK’s first non-residential Passivhaus Plus co-working space. Clarke said the move “satisfies our heartfelt desire to minimise our impact on the environment.”





 Kirk & Kirk
Caritas
Styria
Kirk & Kirk
Caritas
Styria
“For many people, the pandemic amplified an appreciation for our planet”
“We want everybody who comes through that door to really enjoy experimenting with eyewear”
“There is a lot of worry with local business owners”
INDUSTRY
10 www.optometry.co.uk October/November 2022
Full Catalogue & Prices Available Online 01438 740823 sales@bibonline.co.uk bibonline.co.uk For more information, please contact us on: Package deals New startRefits bibonline.co.uk
A study in The Lancet Global Health examining survival data in 4064 children with retinoblastoma from 149 countries found 40% of children die within three years of diagnosis in low income countries. This is compared to 1% of children who receive the diagnosis in high income countries, scientists found.

Dan Scarfe, chief executive of XRAI Glass, commented on the launch of a public preview of the company’s augmented reality glasses. XRAI Glass software converts audio into a subtitled conversation which appears on the wearer’s spectacle screen.
PROFESSIONAL SUPPORT
Scientists from the Yonsei University College of Medicine have highlighted a link between intermittent fasting and a reduced risk of developing age-related macular degeneration (AMD). Researchers examined records for 4500 patients aged 55 and older between 2015 and 2018. Assessing fundus photographs and corelating this data with information about meal frequency, signs of AMD were found in one in four participants.

The College of Optometrists has published updated guidance on myopia management. This covers the steps optometrists should take when introducing myopia management and the information that should be conveyed to parents and patients. The guidance assesses risks associated with management options and highlights the importance of obtaining informed consent. The advice suggests that optometrists should be able to explain what myopia is and the lifestyle factors that may affect its development. Read more at: bit.ly/3S3Pbvg

The General Optical Council has published a new guide to outline how it will approach quality assurance within the continuing professional development (CPD) scheme, with 10% of registrants set to have their CPD records reviewed over the three-year cycle. Those selected for review will be contacted by email. The guide outlines what reviewers will look for and potential outcomes. Read more about the guidance on OT: bit.ly/3REZR3p
IN PRACTICE
Speaking as part of OT’s Time to Speak series, optometrist Karan Vyas discussed how the optometry profession must tackle homophobia, sharing that: “If we don’t have a profession that is representative of the community around us, then we are not truly going to be able to serve the population.” Read the series on OT: ly/3ANAVje


Organisations across optics paid tribute to Queen Elizabeth II, who died on 8 September. The Queen was a patron of more than 600 charities in her lifetime, including a number of eye health organisations. AOP chairman, Dr Julie-Anne Little, shared: “During her 70-year reign, Her Majesty’s dignified service and unshakable integrity have been an inspiration for millions of people across the world. She leaves a profound mark and will be missed deeply.” Read more reflections on the life and work of Queen Elizabeth online: bit.ly/3BIXXtd
An ‘ambitious’ plan to reform eye care in Wales was given ministerial sign-off on 20 September. The new Welsh General Ophthalmic Services Contract, which will see ‘significant cultural change within the profession,’ will be rolled out over the next 18 months. The plans were announced by health and social care minister, Elenud Morgan. Details on financial packages that the profession can expect to see will be released soon. Read more on the refrom on OT: bit.ly/3SeFTgB
“We are so proud of the ability this innovative technology has to enrich the lives of people who are deaf and have hearing loss”
Getty/Tuan
Tran
Pixabay/skalekar1992
“It was like learning to understand myself”
Khalil Musani became an assistant store manager at Specsavers Leicester this year at the age of 21. He told OT how the diagnosis of multiple eye conditions as a child shaped his journey. Read more from Musani online: bit.ly/3RikUJj
SCIENCE & VISION
Getty/erdikocak THE EDIT 60 DAYS IN 16 STORIES SPOTLIGHT 40% 10%
October/November 2022 www.optometry.co.uk 11
























Clinical round-up
OT’s Selina Powell reviews the latest clinical news and research papers

SIGHT LOSS DIAGNOSIS “LIKE BEING HIT BY A BRICK”
Anglia Ruskin University scientists have examined the impact of a sightthreatening diagnosis on patients through a series of in-depth interviews.
The research, which was published in BMJ Open, examined the experiences of 18 patients diagnosed with eye disease in England.
A team of researchers led by Dr Jasleen Jolly highlighted that interactions with clinicians can have a lasting impact on how a diagnosis is experienced and how well the patient is able to come to terms with their visual impairment. Eye conditions patients were diagnosed with included retinitis pigmentosa, diabetic retinopathy, Stargardt disease and macular degeneration. A patient shared how the protracted wait for a diagnosis affected his work and relationships with people.
He waited 14 weeks for an initial consultation and then a further five months for the results of tests.
“Five or six months is a long time when you’re waking up every day worried, and you’re not sleeping well,” he said. Another common thread in the interviews with researchers was the
impact of the words clinicians chose. Speaking about the diagnosis, one patient recounted: “He looked at me, sort of shook his head and he said, ‘You poor, poor boy’ and… that has stayed with me my whole life… (it) really made me feel like it was something incredibly bad… it sort of tainted my view… of the condition.”
Another patient described her experience of being diagnosed as “like being hit by a brick.”
SCOTTISH RESEARCHERS DEVELOP LOW-COST 3D IMAGING DEVICE
University of Strathclyde researchers have developed prototype technology that could increase access to screening for eye conditions such as glaucoma.
The simple, inexpensive device can be added to a slit lamp, capturing 3D images of the retina and cornea.
Dr Mario Giardini, who was involved in the development of the device, highlighted that the technology enables patients to have images captured inexpensively, without the need for a specialist to be present.
“Our device reliably takes 3D images, and it is comfortable and fast, in less than a second,” he said.
Giardini added that the device has the potential to make eye diagnostics more accessible and reduce inequalities. “The technology has the potential to revolutionise the screening
and follow-up within the community of conditions such as glaucoma, as any optometrist, anywhere in the world, could afford it,” he said.
Consultant ophthalmologist, Dr Iain Livingstone, explained that the device uses visible light to recreate a highfidelity 3D representation of structures within the eye.
“It’s a crucial addition to the way we interpret information, harnessing digital to glean so much more from a slit lamp exam, with potential reach far beyond the hospital toward community optometry,” he emphasised.
While the price of the technology is commercially sensitive, Dr Giardini confirmed to OT that researchers were aiming for a cost to the end-user “in the order of the low-thousands.”
HEALTH
The impact of long COVID on the workforce
UK researchers have described the impact of long COVID on employment in the UK.
Writing in Applied Economics Letters, the authors highlighted that 1.4 million people aged between 17 and 69 suffered from persistent COVID-19 symptoms that lasted longer than four weeks after the initial infection.

Close to one million people within this age range experienced symptoms for longer than three months.
Research undertaken by the Office for National Statistics in 2020 found that optometrists ranked 17th out of 359 professions when it came to COVID-19 exposure risk.
Reuschke et al.
DOI: 10.1080/13504851.2022.2098239
GLAUCOMA
Racial disparities in vision loss
New research published in Translational Vision Science & Technology has examined racial disparities in the level of vision loss following a new diagnosis of primary open angle glaucoma.
Scientists from the New York Eye and Ear Infirmary of Mount Sinai applied an artificial intelligence algorithm to three prospective US population-based health professional cohorts who were free of glaucoma at the beginning of the study.
They found that black patients had a higher risk of early central and advanced visual field loss when compared to non-Hispanic white patients.
Kang et al. DOI: 10.1167/tvst.11.7.21
AMD
Elixer of youth? Key protein protects retina Scientists have investigated the role of a protein that protects retinal support cells in preventing agerelated eye disease.
In research published in the International Journal of Molecular Sciences, researchers highlighted that the loss of a protein called pigment epithelium-derived factor (PEDF) may drive diseases such as age-related macular degeneration.
Study author, Patricia Becerra, of the National Institute for Eye Health in the US, highlighted that PEDF is known as the “youth protein” because it is present at high levels in young retinas, but declines with ageing.
Rebustini et al.
DOI: 10.3390/ijms23147745
“He said, ‘You poor, poor boy...’ that has stayed with me my whole life”
October/November 2022 www.optometry.co.uk 13 SPOTLIGHT
Getty/ Witsarut Sakorn /EyeEm CLINICAL NEWS




























100% Optical

Opportunity abounds at 100% Optical 2023
The Studio is expected to grow in 2023
Registration has opened for 100% Optical 2023. Taking place on 25–27 February, it is set to be the “biggest show yet,” according to organisers.

The show has seen exciting developments in recent months as CooperVision committed to exhibit and deliver education at the 2023 event.
Encouraging delegates to register early, Nathan Garnett, show director, said of the event: “The strength and depth of the show is key for us. Having CooperVision at the show alongside Bausch + Lomb, Johnson & Johnson Vision and Safilens gives us a compelling contact lens offering to match up with what has always been a really strong eyewear offering.”
Organisers expect the Studio area of the show to be bigger than ever. To accommodate this, they are planning to introduce a bar to the area which will act as a networking hub where highend practices can meet with unique independent brands.
The release and booking of CPD has changed, with programme details to be released in phases from October, through November and December, before opening for bookings in January.
AOP members will have priority booking from 3 January, before the booking platform will open to all delegates the following week. Dr Ian Beasley, AOP head of education and OT clinical editor, shared: “By releasing the
“I’M LOOKING FOR… STAND-OUT EYEWEAR”

OT sought out long-loved and new eyewear brands to find out what to expect from the show
Modstyle: Modstyle will be launching its brands, Avanti Eclipse and Kaleyedoscope, to the UK. Managing director, Mark Wymond, shared: “Modstyle has been selling highquality affordable eyewear to the Australian market for 40 years.”
Maison Nathalie Blanc: Back for 2023, designer Nathalie Blanc said: “We want to continue the story we started last year with our British clients. We want to introduce the new collection and continue to increase awareness in the UK for Nathalie Blanc Paris, Monsieur Blanc, and Blanc.”
MAC Eyewear: The company will be presenting an update to its Prue Leith collection, along with the Priscilla collection from Ronit Furst and new styles across its brands. Mark Carpenter, managing director, added: “We might even have a few surprises up our sleeves as we are looking to bring in a new collection for 100% Optical 2023.”
Mokki Eyewear: New for 2023, Moshe Ohana, CEO and owner, said the Norwegian brand will be introducing its “innovative design of Mokki Click & Change eyewear for babies, toddlers and children” to the UK market.
programme in the new year, we hope people will have a better idea of when they want to attend.”
When the CPD programme opens in January, two thirds of seats will be available for booking, while one third will be retained for walk-in visitors on a first-come, first-served basis.
“We want people to book onto the sessions they intend to come to, and for those who decide to attend the event at short notice, to have the confidence that they will be able to consume educational content at the show,” Beasley added.
OT hears the latest updates from show organisers, from a new timeline for the CPD programme to the plans of independent eyewear brands
“We really enjoy catching up with optometrists from across the country and meeting other industry experts, and we can’t wait to see what the 2023 event has in store”
Greg Wharton, SpaMedica head of promotions
A WORD FROM A SPONSOR: SPAMEDICA
October/November 2022 www.optometry.co.uk 15 SPOTLIGHT
100% OPTICAL
PROFILE
Addressing a solvable global problem


We want to make World Sight Day a much more high-profile day – the day for people to recognise how important sight and, crucially, eye care, are. There are three things we want to achieve through World Sight Day, which takes place on 13 October this year. Firstly, getting everybody to recognise how important eye health is to them, then we’re encouraging people to draw the connection from their own eye health to the scale of the issue worldwide. Over one billion people worldwide have sight loss because they don’t have access to the eye care that they need. World Sight Day is an opportunity to make people aware of the magnitude of the problem.

We also want to communicate that this is a problem that is solvable. For the vast majority of people, it’s about access to glasses or a cataract
operation. These are some of the simplest and most cost-effective interventions in the whole of healthcare.
Running up to World Sight Day we want everybody to make a pledge to have their sight tested. We had a target of a million last year and got over three and a half million pledges. This year we have a target of five million. But we’re also bringing this home to decision makers, holding a series of sight screenings in parliaments and assemblies around the world, including at the UK Parliament.
Our Love Your Eyes global campaign launched this year. As a campaign it’s quite adaptable to different contexts. In the UK we think in the context of High Street opticians, but in many environments you don’t have that. Indeed, there is often quite a lot of stigma associated with simply wearing a pair of glasses. The feedback and experience we’ve had is that it provides
quite a helpful way of challenging some of those issues. Having a positive message about caring for your own eye health allows people to use it in contexts where it is less straightforward.

You need effective policy advocacy to influence decision makers. But ultimately, politicians listen to voters and their communities. If they are getting messages that people think this matters, then they are more likely to listen to us, and our members, about how important it is to invest in eye care. That is what is critical for the billion people who need investment in services.
We are within reach of eliminating trachoma as a public health issue across the world. A small country, Vanuatu, has just declared that it has managed to eliminate trachoma. But you have to keep investment in that. Like any of these public health problems, if you let up, even as you get very close, then the problem comes
Peter Holland, chief executive for the International Agency for the Prevention of Blindness, on raising the profile of eye health beyond World Sight Day
VisionSpring celebrating the launch of Love YourEyes
16 www.optometry.co.uk October/November 2022
INDUSTRY
VisionSpring
THE THREE STRANDS OF 2030 IN SIGHT
The IAPB has launched 2030In Sight, a sector strategy for the next decade, which aims to ensure that by 2030, no-one experiences unecessary or preventable sight loss. Holland explained the three strands at the heart of the strategy:
Elevate: raising the issue with decision makers, drawing out links to the wider impacts and making the case for proper investment in eye care, but also that there are crosscutting issues and relationships needed with schools and business
Integration: ensuring that eye care is properly integrated as part of mainstream health services
Activate: recognising that many people get much of their eye care through private providers, and so the market needs to work properly, encouraging demand.

back. It’s crucial that we keep going. Of course, it is that last mile that is always the most difficult.
We’ve introduced 2030 In Sight as a new strategy. The sector strategy has three elements to it: elevate, integrate and activate. A crucial message of the strategy is that this isn’t just a health issue, but a developmental, economic and social issue as well. Having good eye health means you can improve your education, stay in work, or just participate in daily life. In terms of work
and productivity, the Lancet Global Health Commission, published last year, estimated that globally the world loses US$411 billion (approximately £351 billion) a year in productivity due to vision impairment. They said that the figure was actually likely to be many multiples higher.
On the other side of the equation, the World Health Organization estimated that providing access would cost about US$25 billion (approximately £22 billion) a year. The return on investment is really significant. That was recognised at the United Nations (UN) last year when the General Assembly adopted a resolution on vision. This was the first time that the UN has had a resolution about vision.
To optometrists I would say: pledge your eye tests for World Sight Day. Write or speak to your local MPs and highlight the global, solvable problem.
October/November 2022 www.optometry.co.uk 17 SPOTLIGHT
Visit scotland and attend the UK’s largest one day cPd coUrse & exhibition * Preferential abdo & college of oPtometrists discoUnt aPPlies www.soc.scotScottish Optical Conference 3 Tracks Anterior Eye, Posterior Eye, Business/Marketing 50 Exhibitors Industry Experts 300 Attendees DOs, CLOs, OOs & IPs 20th Nov. 2022 Glasgow Radisson Blu £49 Fee* Best Value CPD in UK 45 CPD Points Interactive & Peer Discussion The IAPB’s campaign calls for goverment and industry leaders to support global eye health
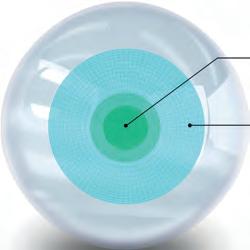
Early identifiers
One area in which discussions have been growing is OCT-A, a non-invasive imaging technique that captures the vascular structure, and that is more commonly used in ophthalmology.
Bennett shared: “I do find we are being asked more about the benefits of OCT-A in practice by optometrists and there is a definite intrigue to the value of being able to view these deeper structures and the flow within the retinal profile and how this can help aid clinical decision making alongside the many other factors of a patient’s eye examination.”
Driving developments in OCT
The development of optical coherence tomography (OCT) has “revolutionised clinics across both ophthalmology and the optometry sectors,” Nicola Bennett, Topcon clinical affairs manager for the UK and Ireland, told OT. “The driving force behind these developments I would believe to be the natural progression, development and revenue that can come from these technologies along with significant clinical prevalence and progression of eye disease.”
The benefit of safe monitoring, diagnosis, referrals and treatment of patients has had an impact, Bennett said, while the continued demand on eye services in the NHS also enhances the need for the technology to progress.
Claire Martin, business development manager, glaucoma and retina, for Zeiss, has also seen this demand. She said: “The high volume of elderly patients and NHS COVID-19 backlogs have driven a need for more community-based OCT and for patients to be seen more quickly and closer to home.”
Martin pointed to developments in additional modules, such as anterior segment OCT, widefield scans, OCTangiography (OCT-A) and ganglion cell analysis, as beneficial in diagnosing and managing glaucoma and other diseases.
Reflecting on the uptake of OCT and how this supports the scope of its
applications, she said: “As we see more practices embrace OCT and use the technology to its potential, we will see more patients being monitored and managed in community optometry, without the need for hospital review but with continuity of care thus giving optometry practices confidence in managing and referring patients.”
Optos recognised that there were benefits to incorporating OCT with its ultra-widefield retinal imaging, creating multi modalities on Optos devices.
“Our technology enables eye care professionals to discover, diagnose, document and treat ocular pathology that may first present in the periphery,” Gareth Steer, vice president of European sales at Optos, said. “Compared to traditional examination techniques, integrating the two imaging modes can aid quicker detection of disease or disorders in the retina, such as retinal detachments and tears, glaucoma, diabetic retinopathy and age-related macular degeneration.”
Considering whether this is something we will see more of within optometry in the community, she posed: “I can’t help but think there may be a potential of more services coming into the primary sector to help the NHS deal with the demand on eye care services, such as age-related macular degeneration or diabetic retinopathy, and this could be the opportunity that drives OCT-A into the optometry sector in the future.”
Zeiss’ Martin agreed that more optometrists are routinely enquiring about the platform, while one practice in Scotland is already actively using the Cirrus 6000A, an OCT-A device.

Discussing the technology, she told OT: “OCT-A further expands the optometrists’ knowledge in disease recognition, being able to identify early changes for diabetic retinopathy and
Above: Zeiss’ Cirrus-6000 provides high-speed OCT and OCT-A scans
Main image: Optos Daytona

OCT has become a must-have tool for many practices and still the technology continues to evolve. OT asked manufacturers about its development
SUPPLIER INSIGHT
“OCT has proven to be a valuable diagnostic tool, and there is strong evidence for widespread use in optometry”
Claire Martin, business development manager, glaucoma and retina, for Zeiss
18 www.optometry.co.uk October/November 2022
macular degeneration and allows for earlier referrals or monitoring patients already on the NHS pathway.”








Artificial intelligence
We are already seeing artificial intelligence (AI) used for certain features in optometry, including OCT.

Martin told OT that AI is embedded into its ultrawidefield (UWF) Clarus retinal camera. The camera uses deep learning to automatically find the optic nerve head, enabling clinicians to accurately derive the patient’s gaze, rather than relying on internal fixation. This can be particularly beneficial in cases where a patient has poor fixation.
“We will be having AI modules available for the Cirrus in the very near future,” Martin added.








Optos unveiled Optos AI, which has achieved CE marking in the UK and European Union, in spring 2022.

























Using optomap UWF images, the system provides automated evaluation of life-threatening diseases, including more-than-mild diabetic retinopathy and diabetic macular oedema.

Revealing the platform earlier this year, the company suggested that with the technology, healthcare practitioners “can improve access to diabetic retinopathy screening whilst quickly and efficiently determining whether diabetic patients should be referred for further evaluation and management.”
Detecting and monitoring
The companies identified the role of OCT developments in detecting disease.

Bennett said: “As OCT becomes more widely used within the optometry sector, the benefits that come from applying this enhanced technology to the patient’s eye examination are continuously growing.”
Faster, non-invasive and widefield scans enable efficient workflows, while detailed imaging allows clinicians prompt analysis and the potential for earlier diagnosis of eye disease. The enhancement of swept source OCT


enables clear visualisation of vitreous, retina and choroidal structures, Bennett added, supporting clinical interpretation.



As the benefits of OCT are more widely discussed, this helps patients to understand the importance of repeat scans as part of a regular eye check.
“This is becoming more of the norm,” Bennett said, adding that this means clinicians are able to safely monitor patients using enhanced progression and comparison tools.
Steer suggested that the ongoing development in OCT, UWF and retinal imaging enables clinicians to better detect and diagnose early stages of eye conditions and disease. Using optomap as an example, he shared that the technology enhances pathology detection, disease management and practice flow.
In recent years, Steer said, there has been a growing recognition of the importance of imaging the peripheral retina: “That’s why we are increasingly seeing our technology being adopted by hospital eye clinics, with many using our devices as a routine part of their patient consultation.”
Part of the clinical picture
“OCT has proven to be a valuable diagnostic tool, and there is strong evidence for widespread use in optometry,” Martin said, adding that it will “play an increasing role in the management of glaucoma and other ocular conditions within clinical practice.”
There are always considerations when introducing new developments, she acknowledged, emphasising that education on interpretation “will always be key” for its confident use.
Bennett highlighted the importance of the technology in caring for patients, but emphasised: “It is important to remember that this technology is part of a much bigger clinical picture with all aspects of the eye examination and patients medical and family history being paramount in the making of clinical decisions and patient management.”
“The benefits that come from applying this enhanced technology to the patient’s eye examination are continuously growing”
Nicola Bennett, Topcon clinical affairs manager for the UK and Ireland
October/November 2022 www.optometry.co.uk 19
CLM-1C Auto Lensmeter HDC-7000 Visual Acuity Software CDR-9000 Auto Phoropter CRK-1P Auto Refractor/ Keratometer 01438 740823 sales@bibonline.co.uk bibonline.co.uk























































Supporting practices and the individuals that make them
engagement in content delivered in partnership with Moorfields Private Eye Hospital.
Beyond education, employment and business tools, Steele said: “We look to support members, not just as clinicians but as people, and this is reflected in our health and wellbeing programme.”
Looking ahead, the AOP’s ambition to provide more tailored content will continue into 2023.
“Our programme will look to recognise where members work, and their changing roles and responsibilities in practice,” Steele said. “We know that the wider practice team are integral in the success of any optical business and our aim is to offer education and training that allows practices to be successful as a business as well as the individuals who work in them.”
With the output of educational content and resources from the AOP increasing, OT sought to review recent launches and find out what is next for members
The AOP has an ever-growing suite of content tailored to the different needs and goals of optometrists across modes of practice and career stages.

Reflecting on the output of content in recent years, Wendy Steele, AOP commercial director, shared how the AOP had worked to ensure members would have access to education during the pandemic, and with the launch of the continuing professional development (CPD) scheme in January 2022, she said: “We have continued to develop a programme of content that has supported our members’ transition to a CPD scheme.”
“Our online education offering has significantly increased, and this has allowed us to deliver a range of content tailored to members’ specific needs with a focus on their roles in practice through our long-running partnership with Johnson & Johnson Vision,” she continued.
series created to address the needs of the whole practice team, as well as the Locum Briefing, which covered practical advice, habits for safe practice and tips for managing the rising cost of living. Steele added: “We have increased the reach of content available to hospital optometrist members via our virtual events in 2020 and 2021, with more early career optometrists accessing the content.”
Myopia is set to continue to be an important clinical theme, with plans underway to ensure AOP members and OT readers have access to the most upto-date information on the topic.
“This will include a continuation of our education programme with CooperVision, through virtual and inperson events, and the return of the very successful MAYopia Day,” Steele added.
AOP TOOLS FOR MEMBERS
The renewal period for qualified AOP members begins from November. Make sure your communication preferences under MyAOP are correct to ensure you receive renewal emails.
In 2022, OT, in partnership with Johnson & Johnson Vision, released the Practice Team Guide – a two-part
Student and pre-reg optometrists have also been able to benefit from content delivered by the AOP: this included a range of freshers presentations delivered in person this autumn for the first time since 2019. Describing positive feedback on the content delivered so far this year, Steele said: “We work closely with our internal committees and industry partners to gather insight into member needs, and this informs the content we offer.” This combination resulted in more than 2300 attendees across the AOP's inaugural MAYopia Day event, as well as high levels of
Employer support: The online OT Jobs listing service was made free for members this year in order to support practice teams in filling vacancies. Find the service at: www.optometry.co.uk/jobs
Tailored content: Articles from the Practice Team Guide or Locum Briefing can be found on OT’s dedicated supplement page: www.optometry.co.uk/supplements
Locum support: The Locum Logbook, supported by Johnson & Johnson Vision, is available for all UK pre-reg and practising locum members: www.aop.org.uk/locumlogbook
Clinical knowledge: OT has more than 35 video skills guides available in its online Education Library: www.optometry.co.uk/educationlibrary
CPD and education: View the AOP’s range of tailored education or watch webinar recordings through the AOP’s Events page: www.aop.org.uk/events
AOP MEMBER SUPPORT Getty/Thomas Northcut
22 www.optometry.co.uk October/November 2022
The AOP introduces Whole Life Course
The AOP is encouraging members to share their experiences and patient stories to feed into the organisation’s lobbying and policy work.
The most recent call for contributions comes as the AOP begins work on the Whole Life Course, a project which will seek to demonstrate the contribution of optometry throughout people’s lives.
The AOP plans to produce campaigns that reflect the importance of eye health across an individual’s lifespan. Central to this work will be patient stories from members, providing accessible descriptions of key issues and examples of the contribution of optometrists.
Kathy Jones, policy adviser for the AOP, explained: “We want to show – to the public, to politicians and to the rest of the NHS – the important part that optometrists play at every point in a person’s life.”
Education
Vijay Anand, AOP Councillor for hospital optometrists

What are the aims of the Hospital Optometrists Annual Conference (HOAC)?
The aim is to bring together optometrists working in a hospital setting to learn and share ideas on working within both core optometry (paediatrics, medical contact lenses and low vision) and extended role clinics (glaucoma, medical retina, A&E/urgent care, adnexal and cornea clinics). Talks cover a wide variety of topics to give attendees the opportunity to keep their own knowledge up to date as well as expand their knowledge in areas of work they are not involved in.
What will the conference look like this year?
Due to the ongoing effects of COVID-19, this year will again be a virtual conference, held on Saturday 5 November 2022. We have four key lectures followed by two peer reviews, one for specialty optometrists (AS/SP/IP) and one for general optometrists. The conference is free to attend.
Are there any key focuses? We have lectures relating to medico-legal issues within ophthalmology, as well as a lecture on examining patients with learning difficulties and sensory needs. We also have a lecture relating to neuroophthalmology and a lecture related to glaucoma, but with a very different slant.
Who might want to attend? As this is a virtual conference, I would encourage all hospital optometrists to attend, whether they are working within an NHS settings or for an alternate healthcare provider. I would also encourage any community optometrists to attend the sessions, as they are relevant to all optometry colleagues. The event gives a good chance for community optometrists to gauge the kind of work that is undertaken within hospital settings. It may also encourage those attending for the first time to join the next conference, which we hope can return to being face-toface in 2023.
“Everything from the day-to-day miracle of giving a child the right pair of glasses, through to the extra work that optometrists do to support people who can’t access eye care easily, to the role of the optometrist in finding disease and securing or providing ongoing care for people with cataracts or macular degeneration,” she explained.
Members who would like to share their experiences, are encouraged to get in touch with the AOP by emailing communications@aop.org.uk
Communications: Serena Box, PR and media manager

What is the AOP’s 100% Respect campaign? We launched our 100% Respect campaign in March as part of an ongoing programme of work to unite optometry against discrimination. We believe in long term action that will support behavioural and cultural change through our guidance, employment services and campaigning.
How has the AOP been working to support equality, diversity and inclusion (EDI)? We’ve developed advice for both employers and employees including a suite of resources that promote inclusivity, from our expert legal and employment team. The AOP’s anti-racism and equality team (ARET), made up of AOP staff optometrists, also provides emotional and practical support where an individual is facing discrimination.
Experiences shared by members indicated that in 80%
of the incidents it was patients who were “the perpetrators of discrimination.” So we’ve created resources, such as practice posters, that highlight a zero tolerance approach alongside social media and digital assets to share online.
What is next for the AOP in this area?
Our EDI work is designed to help build inclusive workplaces where everybody can be accepted for who they are regardless of race, gender, sexuality, beliefs, age or disability.

We’re looking at how we can best support members to feel safe and protected. A large part of this work is not shying away from difficult conversations – making sure we’re there to engage, foster healthy debate and celebrate the milestones. But we’ve also launched a new template equal opportunities policy, and are producing CPD on the Equalities Act
Find the #100Respect campaign at: www.aop.org.uk/Respect and the new template policy at: www.aop.org.uk/templatepolicies
AOP EXPERT
Getty/Malte Mueller
The AOP is seeking member stories and experiences for a new project
AOP EXPERT
Communications
SPOTLIGHT
October/November 2022 www.optometry.co.uk 23








FOCUSES ON... SEASONAL STYLES
Hit list
The trends, launches and looks
Plant-based acetate
Neubau Eyewear has launched its first collection made from sustainable acetate. The eight frames in the Shapes of Motion range are made from a plantbased material composition of cotton and wood which uses only plant-based plasticizers and so is considered biodegradable. Styles include ‘Rupert’ (pictured) and are designed and handmade in a carbon-neutral production facility in Austria.
www.neubau-eyewear.com









Comfort in classics
Continental Eyewear has launched the new Puriti range of Japanese titanium frames. The new collection has been in development for more than three years and includes 26 models with two colourways each. The lightweight and hypoallergenic frames combine Japanese craftmanship with high-quality materials.

www.continental-eyewear.com
In the frame
International Eyewear has highlighted its episode collection, which aims to embody “femininity and fashion,” featuring inclusive sizing and eco-conscious packaging. A number of the frames, including ‘EP 294’ (pictured), are made from a bespoke material mix of three acetates, featuring handmade fronts and sides and OBE flex hinges, while a selection of combination styles have metal sides and an integrated hinge.



www.internationaleyewear.co.uk
Timeless titanium Charmant has released a new Titanium Perfection collection with three women’s models and four men’s frames. The frames are designed with pressure-mounted construction, featuring contrasting beta-titanium sides and transparent crystal end tips with inner colouring.
The women’s styles, including ‘CH16715’ (pictured), feature gradient patterns, demi colour rims or mono contrast on rim and sides.

www.charmant.com

October/November 2022 www.optometry.co.uk 25




















GET THE LOOK
Optometrist and lifestyle blogger, Lizzy Yeowart, on head-turning striped frames

Earn your sartorial stripes with eyewear in this season’s favourite pattern.
Head-turners
If head-turning eyewear is what you want, look no further than the Dutch brand Outspoken. Style ‘OA2124’ comes in five vibrant colourways, all guaranteed to attract compliments.
www.outspokenholland.com
Steve McCracken
The street artist, also known as NONE HERE, talks to OT about his classic style and collaboration with Bird Eyewear on a cleaning cloth


1Good vision is so important to me. I am a painter, so I am always looking at my pictures close-up and far away. I would be lost without my glasses. You have got to look after your eyes – you only get one pair. My favourite frame is a Bird Eyewear pair called ‘Blackcap.’ They are two-toned and made from wood.
2I’ve worn spectacles for about 25 years. When I was in primary school an optician came in and gave us all eye tests. I couldn’t read the letters. I can’t really remember my reaction but I don’t think I was too keen as glasses weren’t considered cool then. I love wearing glasses now, and they are definitely part of my identity.
3I am a street artist who paints birds. I paint and paste them all over the UK. My studio is in Exeter, like Bird Eyewear, and after seeing my bird paintings all over town they got in touch with me to propose a collaboration. I thought it was a cool idea. We had a chat and my piece suited the project perfectly.
Style accents
‘Tilde’ by Face a Face is named after the accent used in Spanish ( ~ ), which is illustrated in this frame by a cut-out colour accent along the sides. The sharp-edge polishing makes for futuristic styling.
www.faceaface-paris.com
4
It is a design I call ‘Pigeon Head Chaos.’ It is a repetition of my signature bird head with one coloured in. The single coloured-in bird represents the individual, whilst the others stand for the challenges we face day-today. At the same time, it expresses the idea that everyone has something special about them.
Seize the day
A regular exhibitor at 100% Optical, Ronit Fürst knows how to capture attention. Part of her Graffiti collection, ‘Model 5063’ is hand-painted and adorned with the famous idiom, Carpe Diem (‘Seize the day’).
www.maceyewear.co.uk




Chloe Farrant
HIT LIST Q&A ME & MY GLASSES
October/November 2022 www.optometry.co.uk 27
SHORTLIST THE LATEST PRODUCT LAUNCHES
Accessories
One bead at a time
Sunglasses
Catwalk trends
Marcolin has identified the key trends set to be driving eyewear design in the next season, suggesting the trend for reshaping styles in the spirit of the 70s will continue, while the linear shapes of European Bauhaus is a key inspiration and the digital urban movement will have an effect on emerging trends.
Amongst the new releases for the season, the brand highlighted the Moncler ‘ML0239,’ a unisex mask with a futuristic design. The bold shape and shaded lenses combine a sporty feel with seventies inspiration.
www.marcolin.com
Alberto Montresor
Chain and accessories brand, Coti Vision, has collaborated with the Nigerian company, Ilekeco, for its latest glasses chain which is made from recycled paper. Established by the designer, Anthony Uche Nsofor, Ilekeco transforms waste materials into wearable art.

Each bead in the glasses chain is hand rolled and painted, with approximately 384 strips of recycled paper used for a whole chain. The Ilekeco chain is available in four colours.
www.cotivision.com
Contact lenses
A lens for astigmatism
Alcon has launched Dailies Total1 for Astigmatism. The company described this as the “first and only” daily disposable toric lens to feature Alcon’s Water Gradient material, which features a gradual increase in water content approaching 100% water at the surface. The lens also integrates SmarTears Technology, a proprietary technology from Alcon, which releases an ingredient found naturally in tears that helps to stabilise the lipid layer of the tear film. The lens is designed to settle quickly to the proper on-eye position for stability.

www.alcon.com
Frames
Sophisticated style
Stepper Eyewear has introduced a new frame replicating the delicate patterns of lace. The ‘SI-30164’ frame has been made from a lightweight TX5 and titanium, making it both flexible and durable, as well as hypoallergenic. The lace-like pattern is embedded within a crystal front or available with solid colour fronts. The frame is available in four colours including grey/cerise, rose, dusky pink/grey, and blue-grey/bronze.
www.steppereyewear.com

28 www.optometry.co.uk October/November 2022
Digital marketing

Perfecting profiles
OptiCommerce has launched a new digital marketing product for independent practices to support with creating, updating and maintaining optical store profiles. The Online Listing Manager helps to ensure that online identities are correct and automatically syncs data to websites and social media platforms. The platform has been made to support an increase of in-practice traffic through the online profile, and also enables businesses to view how customers behave online.
www.opticommerce.co.uk


To feature in OT’s Hit list, contact kimberleyyoung@ optometry.co.uk

Frames
Make a statement
Mexx Eyes, an imprint of OWP Brillen, has released new styles for teenagers, providing stand-out pieces for younger wearers. The ‘5955’ (pictured) is a hexagonal shape in two-tone colour made from stainless steel. The components create a “delicate and stylish” frame for a “fashionable statement piece.”


www.mexx-eyes.com
Frames
Revisiting the classics Immagine98’s optical line designed for men, I-man, has launched a collection of “evergreen” styles made from acetate. The ‘Matthew’ (pictured) is a minimalist and contemporary optical navigator available in three colours: black, blue and stratified grey. All of the styles can support magnetic clip-on sun lenses.
www.immagine98.it
October/November 2022 www.optometry.co.uk 29
HIT LIST
Q&A BEHIND THE BRAND
Ahmed Ejaz, CEO, on the brand’s growth

Every frame takes inspiration from a location in Cambridge
The brand recently opened an operations HQ in Birmingham
Ejaz was invited to the Prime Minister’s office in 2022 to talk about the brand’s research aims.
What makes Cambridge Spectacle Co. unique?

We’re an optometrist-led great British eyewear brand. We have a passion for expertise and we put that into our brand and our frames, whilst also keeping a focus on design and style. We focus on building trust with patients at a fair price. Our brand has always been inspired by the city of Cambridge. Each frame has the name of a location or a road that we have taken inspiration from.

How has the company developed in just over a year?
I can only describe the journey so far as supercharged. We’re approaching this from the point of view of: ‘what would a fast-paced start-up do?’ We’re proud to announce that we have done a deal to supply Asda Opticians. When they looked at our brand they believed in our vision. They offer really great quality at really fair prices, so we fit in well with that part of their strategy. We’re going nationwide in quarter one next year.

What is next for the development of the brand?
Having worked as an optician for 10 years, and then being a CEO, I feel that there is a need for this brand out there, and we feel we can build a great community around it of people who are passionate about their vision, but believe in our social aims as well. We’re partnered with a research-based charity, St Paul’s Eye Research Foundation. A lot of customer feedback has been that they love what we’re doing in terms of giving back. We want our community to be part of that.
ANATOMY OF A FRAME
columnist Lizzy Yeowart
White matte stainless steel with a red signature on the left side
Clockwise from left: Finishing a pair of Cambridge Spectacle Co. frames; Ahmed Ejaz; the ‘Queens’ model
Visor-style aviator
Handcrafted in Italy Unpicking a standout frame, by OT
Ceramic nose pads Mirror and gradient sunglasses In a nutshell Manufacturer // Vysen Frame // ‘The Enzo EZ8’ Colour // White Web // www.vysen.com HIT LIST Cambridge Spectacle Co. 30 www.optometry.co.uk October/November 2022 CAMBRIDGE SPECTACLE CO. //
1 2 3
CAMBRIDGE SPECTACLE CO.

























































SPECIAL REPORT
IP: AN UPSKILLING WORKFORCE

A t�h n�umbe o� I� o�ptometrist g�rows OT �eviews �he obstacles to quali�cation, in the �rst of a new series of reports


The qualification process for independent prescribing (IP) has always had its challenges, as any qualification might, but some have only become harder following the pandemic. Meanwhile, we are seeing more discussion of extended services, a new NHS structure, and the General Optical Council’s (GOC) new requirements which will bring changes that could reshape the training of IP optometrists.
In the first of a new series that will explore the scope of IP optometry –present and future – OT sought to look into the training and qualification of the increasing numbers of IP optometrists.
The numbers
The number of registrants on the GOC’s independent prescribing specialty register has grown by 37% in the past five years, from 611 at the end of March 2018 to 1344 as of July 2022.
Meanwhile, interest in undertaking additional qualifications is growing.
The GOC’s Registrant Workforce and Perceptions Survey 2022 found that 40% of respondents planned to gain additional qualifications or skills when asked about their career plans over the next 12 to 24 months. Common reasons for this centred around delivering more services, helping more patients, and expanding their scope of practice.
Samara Morgan, head of education at the GOC, told OT: “It’s positive to see that so many optometrists are considering upskilling,” suggesting that this could be as professionals seek to gain a competitive edge in advanced multi-disciplinary environments, or to help ease pressure on secondary care with a wider range of optical health services delivered in local settings.
The College of Optometrists has also reported growing numbers of optometrists taking up IP – evident in the number of candidates taking its
Therapeutic Common Final Assessment
(TCFA) in IP, the final stage before receiving the qualification.
In 2021, 200 candidates sat the TCFA in IP, with 183 passing. This was a 32% increase in candidates compared to 2020, in which 152 people took the exam and 122 passed.
At the time of writing, 140 candidates have passed the exam so far in 2022.
34 www.optometry.co.uk October/November 2022 TRAINING AND FUNDING
Lizzy Ostler, director of education for the College of Optometrists, suggested the increase “may be due to the greater role the profession is fulfilling, particularly within new integrated eye care services and enhanced or supplementary care schemes.”
Universities across the UK also described high levels of interest in their IP optometry courses.
Ulster University has particularly seen a rise from clinicians wishing to expand their scope of practice, said Dr Julie McClelland, senior lecturer in optometry and course director for the Theory of Independent Prescribing for Optometrists, and Patrick Richardson, lecturer in optometry, optometry clinic manager and an IP optometrist.
The lecturers recognised the role of the pandemic in this, sharing: “Many practitioners made adaptations to their usual provision and worked closely with local GPs, pharmacists and
ophthalmologists to improve access to eye care and, as a consequence, they can see how gaining the IP qualification would help to facilitate this and ensure an ongoing enhanced level of eye care.”
With demand high during the pandemic, a number of universities received special permission from the GOC to create additional spaces.
For example, in June 2020, with many practitioners unable to complete full-time work, Glasgow Caledonian University provided additional theoretical IP training, enabled through extra funding provided by NHS Education for Scotland (NES) and the Scottish Government.
“During 2020–21, around 220 students completed our course, compared to approximately 100 in previous years,” Dr Mhairi Day, senior lecturer of the Department of Vision Sciences, said.
A question of funding
The approach to funding differs significantly: a mixture of self-funding, employer support, and regional funding models.
Colin Davidson, principal lecturer in optometry and programme lead for optometry independent prescribing and higher qualifications, explained that on the University of Hertfordshire’s IP course around half of the students are funded through their employer, hospital trusts or Health Education England, while the remaining half are self-funded.
“We’ve got nine students who are Health Education England sponsored to complete the course, and some hospital trusts funding,” Davidson said.
He noted that this is due to “a lot of work” by the university and Local Optical Committees.
The GOC’s Morgan recognised the varied pressures: “As nations design and deliver different models of care, underpinned by local government or commissioning approaches, this is likely to drive local education and employment strategies.”
The College also recognised that funding and placement availability “continue to represent potential
barriers to the future development of the profession.” Engaging in the GOC’s Sector Strategic Implementation Steering Group to support workforce planning, the College said it would continue to campaign for improved funding.
In Scotland, funded places on the IP course are available through NES, with both employed and locum optometrists able to apply annually.
IP optometrist Kevin Wallace, an AOP Councillor and clinical adviser, shared that he was part of a cohort in the first year this was offered by NES: “It’s a big advantage. You still had to take the time out of practice to do it, but you don’t have to think about paying for the course.”
“Optometrists in Scotland are the first port of call for all eye problems within the community,” explained Julie Mosgrove, chair of Optometry Scotland. Scotland currently has around 400 IP optometrists – making up about 30% of the profession in the nation.
He told OT: “I think, clinically, it is the right progression to be able to serve my patients and the community better.”
When the pandemic highlighted opportunities to be able to further support local communities, Sharma approached Hakim Group to discuss his interest in the qualification, and they sought to establish a special cohort through Ulster University. The university gained permission for a cohort of 120 places, made up of optometrists from Hakim Group as well as other independent practices.
Sharma suggested that the opportunity from Hakim Group and Ulster University made it easier for other optometrists to come on board. Describing it as ‘win-win,’ he said: “Firstly because there was financial support, and secondly because it presented an opportunity they wanted but hadn’t had the kick to do it.”
Specsavers has enshrined support for higher qualifications as part of its career pathways and has invested “hundreds of thousands of pounds” into helping fund optometrists’ courses, explained Paul Morris, director of professional advancement for the multiple.
“This care is managed by all optometrists as part of the GOS package. Optometrists with IP have NHS prescribing pads and all NHS prescriptions are free of charge to the patient,” Mosgrove explained, while acute ocular conditions are usually funded via a supplementary eye examination fee.
For Amit Sharma, an optometrist and director at a number of independent practices with Hakim Group, Pinder & Moore Opticians in Kingswinford and Davis Optometrists Group, the IP qualification was something he had always wanted to do.
“I think it’s wonderful that we’ve got the opportunity to do it. We have so many institutions that are able to make it accessible to people and I don’t think the costs are huge,” he added.
Describing the support provided to optometrists who want to complete the qualification, Morris said: “The people who want to go and do IP and other qualifications are so numerous, so keen, and it has a real practical use in most areas – we’ve been really happy to help fund some of that.”
Placement availability
Angela Whitaker, IP programme lead at Cardiff University, shared that funding and clinical placements can both be a concern for optometrists thinking of studying IP.

The GOC’s independent prescribing specialty register has grown 37% in five years
“Optometrists in Scotland are the first port of call for all ey problems within t community”
Julie Mosgrove, chair of Optometry Scotland
October/November 2022 www.optometry.co.uk 35
Getty/Marisvector
Asked about the impact of the pandemic, Whitaker said that placement availability was already an issue, but that “it became even more challenging and many found it impossible. The situation has improved slightly but remains very difficult.”
Sharma explained that since Hakim Group’s cohort of optometrists completed the IP course in February 2021, the challenge has been to secure clinical placements.
“Some have been lucky, being in localities where the hospital eye service is very pro-optometry. But some have been quite restricted, limiting the numbers of people in a consulting room,” he said.
During the pandemic, changes were made to support IP training, such as allowing part of the clinical placement to be virtual. While this was welcomed, Sharma reflected: “We thought that would open up a lot more opportunities, but it’s not changed the landscape too much from our perspective.”
The College acknowledged that, for many candidates, it is a challenge to find a placement with the capacity to offer experience. As a result, the College has agreed with the GOC to approve an extension to the timespan between the academic course and starting a placement, subject to the candidate undertaking and documenting suitable CPD. Ostler noted that candidates should contact the College if they think they may need an extension.
She added: “We will be seeking approval by the GOC to retain all these enhancements for as long as necessary to support optometrists training for the IP specialism.”
A case of connections
Optometrist Dr Keyur Patel, clinical director at Tompkins Knight & Son, an independent practice within the Hakim Group, completed his IP qualification after a period working in the US, which he said, “really opened my eyes to therapeutic optometry.”
200 candidates took the Therapeutic Common Final Assessment in IP in 2021
He explained that: “I was lucky to be working in a glaucoma clinic anyway, so I was under a consultant and got some of my sessions there. I know some private ophthalmologists who were kind enough to get me into local hospital services so I could get more of my sessions there.”
But reflecting on his experience, he added: “I’ve used the word ‘lucky’ and I think at the moment it still involves that. There is a lot of who-you-know involved in how fortunate you can be to get a place.”
Fatima Nawaz, AOP Councillor for independent prescribing optometrists and an ophthalmic director in an independent practice, was working in a multiple when she began her IP course and secured a placement in a private hospital. She said of the experience: “I was really blessed to have an amazing supervisor and consultants that didn’t mind me sitting in their clinics.”
“I’ve heard it’s really hard to get hospital placements,” she acknowledged, adding that she was grateful the private hospital gave her a supervisor as part of the placement.
“I don’t think I would have had the contacts at that point. If I had to do that on my own, I would have struggled to find an ophthalmologist to supervise me,” she said.
However, she also felt that changes could be made to improve access to placements, suggesting: “There
In 2021, Scope Eyecare launched its first Independent Prescriber Bursary Award. Sharing the reasons behind setting up the bursary, optometrist Mandy Davidson, medical and professional affairs manager for Scope Eyecare, told OT: “The pandemic really highlighted the important role that optometrists can play in enhanced services for patients. Scope is proud of the fact that optometrists really stepped up to the game, and saw and co-managed patients in really difficult situations.”
But the company recognised that barriers exist for some optometrists. Davidson explained: “One of the reasons for the bursary was to remove one of those obstacles.”
Over 70 applications were received for the bursary, with three optometrists selected for the reward of £1500 towards IP course fees.
The applications came from a wide range of backgrounds, Davidson said: “The appetite to upskill is across the board and that is really encouraging.”
SPECIAL REPORT: IP 36 www.optometry.co.uk October/November 2022
Number of registrants on the IP specialty register Year ending 3 �March Source: General Optical Council 2018 2020202220192021 AN APPETITE TO UPSKILL 611 940 749 1082 1260
needs to be better connections with ophthalmologists, maybe from the College’s side, and some incentive for supervisors.”
Expressing his concern around placement availability issues, Morris also told OT: “I think the profession as a whole needs to make more effort with ophthalmology and NHS stakeholders to make that work.”
Optometrists acknowledged the pressures faced by hospital departments. Morris commented: “We’re not quite in a post-COVID-19 world yet, we’re post restrictions, and it is difficult to have too many people in too small a place… But these are the things we have to face into. We have to show people the opportunity that it is going to make things easier for them in the future.”
A clinic approach
In many parts of Scotland, optometrists have access to NHS-funded Teach and Treat clinics, explained Mosgrove.
Overnight accommodation and travel is paid for those needing to travel a long distance for the training.
“The clinics are overseen by a consultant ophthalmologist within a hospital setting, giving optometrists experience of managing and treating a variety of ocular conditions,” she said.
“Naturally pressure for placements
has grown, with fewer IP placements being available during the pandemic,” Mosgrove said. Remote clinics were established in some health boards to help with the backlog and though faceto-face clinics have resumed, remote learning is still provided to those in rural settings.
Sharing his experience of a training clinic in Edinburgh, Wallace said: “It’s a brilliant facility with all the equipment we’d need – designed and funded to be a training clinic for optometrists.”
Asked if this is a model that could offer lessons for other parts of the UK, he commented: “I think it’s a really helpful model of having a dedicated training clinic. If you want optometrists to get the experience and see more of the pathology that has traditionally been seen in the hospital, that is the way to do it.”
Jill Campbell, chair of Optometry Northern Ireland, explained that services are regionalised in Northern Ireland with an IP placement scheme coordinated by the Belfast Trust.
The scheme was paused for a time during COVID-19, so there is likely to be a bottleneck, Campbell acknowledged.
“We’re very fortunate that the placements are free to the optometrist. They get a really good range of experience; they can observe glaucoma
clinics, eye casualty, corneal clinics and general ophthalmology so they get a good variety,” she explained, with a key benefit of the scheme being that optometrists have the opportunity to build connections with ophthalmology.
There is no specific pathway for utilising the skills of IP optometrists yet, though a pilot is in development.
Campbell explained: “The profession are aware that is being discussed and Optometry Northern Ireland are leading the discussions alongside a group of IP optometrists.”

Changing requirements
Earlier this year, the GOC published updated education and training requirements for approved qualifications in additional supply, supplementary prescribing and independent prescribing categories.
As part of the requirements, trainees will be required to have identified a designated prescribing practitioner (DPP) before or shortly after admission, who will supervise their approximately 90 hours of practice. The DPP can be an appropriately trained and qualified registered healthcare professional with independent prescribing rights, rather than an ophthalmologist.
While a positive change, Dr Peter Hampson, clinical and professional director for the AOP, pointed out that these may not be a straightforward solution to the challenges at hand.
Speaking to OT previously, the GOC had outlined that the DPP “must be an active prescriber competent in the clinical area(s) they will be supervising the trainee in, have the relevant core competencies and be trained and supported to carry out their role effectively.”
Hampson commented: “To fulfill the role of DPP, the practitioner would need to be able to fulfill the full range of patient types and be experienced in managing them themselves.”
“While there are some practices and practitioners with the correct case mix, unfortunately I don’t there there are that many,” Hampson noted. “While this is a positive step, it may not be the solution that some were hoping for.”
Under the requirements, trainees
“The situation has improved slightly bu r�emains very difficult
Angela Whitaker, IP programme lead at Cardiff University
October/November 2022 www.optometry.co.uk 37
Getty/Marisvector
will no longer be required to have been practising for two years before taking the qualification. Discussions around the future of IP also consider whether the theory could be integrated into new optometry courses.
Reflecting on this approach, optometrists pointed to similar training systems in primary care.
Chris Evans, optometrist director at Gwynns Opticians in Wales, said: “I don’t think IP is going to go back into the box. More people are going to do IP. Look at pharmacy. I think we’re more likely to see that model and people expanding their scope of practice.”
Patel pointed to approaches in the US, where students have three years of didactic training and slowly build up clinical experience, with a fourth year made up of clinical rotations in different settings. Of this, he said leaving university, graduates would have “the ability and foundations” to use IP.
Ulster University’s McClelland and Richardson told OT that, having delivered the IP qualification at a postgraduate level for six years, “we can see the value in optometrists having post-registration experience.”

The lecturers added, however: “The decision to incorporate IP into the undergraduate curriculum is also dependent on factors relating to funding, workforce issues and local commissioning, which vary across the UK. We look forward to working with commissioners to plan the training needs of the future members of the profession.”
The future workforce
Many optometrists felt that IP is a next step for the profession but noted that it may not be for everyone.
Wallace shared: “I’ve always seen it as the optometrist becomes the GP for eyes so that anybody with an eye problem knows that is where to go. Then we can deal with 90% of the conditions that come in with only a small number having to go on to hospital for specialist treatment.”
“It feels like it would be a gain for society. An efficient service, seeing patients closer to home, at a reasonable cost to the taxpayer,” he said, adding that an expanded workforce would provide the capacity needed for this.
Nawaz suggested it seems like “everyone is getting set up for the future,” but also highlighted the scope of practice that optometrists already have, emphasising that more could be done with existing schemes, such as Minor Eye Conditions Services.
“I do think it could be a lot better than it is at the moment. I just don’t feel like we’re having the right conversations,” she said. “I feel like until we get ophthalmology on side, the changes aren’t going to happen. Whether that is them understanding what we do, or the funding, but until they give us the work then I don’t think that everyone needs IP.”
Morris said he expects we will see a wider network of IP optometrists who would be able to see patients ordinarily seen in the hospital service.
However, he highlighted the important role that optometrists already play: “Do I think that IP is requisite for everyone? Probably not. But I do believe everyone should have the opportunity to do it in the fullness of time, depending on their requirements,” he said, continuing: “I believe IP has to be the direction of travel for a sizable cohort of colleagues over time.”
Recognising the opportunity that higher qualifications can provide, Campbell suggested that this could see more services provided in primary care, and “better experiences for our patients who want their care delivered in their community with someone they trust.”
OptometryTodaywill continue to explore this topic in future editions, including a focus on commissioning and the considerations of an IP workforce. Share your views at newsdesk@optometry.co.uk
PARTING WORDS ON IP

Nawaz: My ideal goal is to get into hospital. I will always promote IP because I do think it will help in the future, if things are done correctly.
Patel: If anyone is going to invest in any further qualifications, they should do IP. IP will change your life and it will change your patients’ lives. It is the qualification optometrists should be leaving university with.
Evans: The IP training has opened my eyes: what I’ve learned from it, and what I’m able to do, even down to the
way I look at an eye now. I think it’s probably the best thing you can do as an optometrist in the High Street.
Sharma: I think it’s really important that we continue to develop as a profession. We’ve got to be able to offer more than just the testing of sight, utilising the training we’ve done so that we can offer any forms of enhanced services.
Wallace: With an ageing population a lot of conditions will become more common and hospitals will get busier. It makes sense that we can deal with more of these things in the community and that will require more people with the skills to look after them.
Scotland has around 400 IP optometrists, about 30% of the profession in the nation
“I think it’s probably the best thing you can do as an optometrist in the High Street”
Chris Evans, optometrist director at Gwynns Opticians
SPECIAL REPORT: IP 38 www.optometry.co.uk October/November 2022









In practice
44 Life as a locum
Data in optometry: collecting, utilising, and informing the future
OT
Opticians
Data – how we gather, secure, and use it both in the short and longer term – is a subject that is liable to bring about a headache for businesses. Compulsory GDPR certification aside, where do we start? And
Business insight and career development
is data at scale even useful, especially to small companies?
These questions are likely even more pronounced with businesses that directly interact with the public, taking in large amounts
of potentially sensitive information that needs to be stored with the utmost care and security.

So, how can optometry practices ensure they are treading carefully in the data minefield? OT asked two of those with significant experience in this area –Andrew Bridges, director of professional services at Leightons Opticians and Hearing Care, and Paul Morris, director of professional development at Specsavers, for their insight.
Gathering and storing data
As with any type of healthcare data, guaranteeing the confidentiality of information held by optical practices is key. Patients trust practices implicitly with the data they share – whether it is personal, contact, financial, or special category health data. Bridges says, “We’ve got to maintain and safeguard that duty of care. We’ve got to hold all aspects of confidentiality at the highest order.”
patients? Are there practical solutions for its gathering and ongoing safe storage?
At Leightons, the process starts with training staff: data management protection, with compulsory modules that are revalidated on an annual basis. Staff understanding how to handle data is priority. Meanwhile, a paperless system means everything is stored securely, in the cloud.
The group is also working towards Cyber Essentials Certification, and enlisting external agencies to test the security of its systems. Seeking advice from professional advisers and an external data protection officer, Bridges said, ensures that all processes, policies, and procedures for meeting and exceeding regulatory requirements are in place. Morris emphasised the importance of following sector guidance, and ensuring that this is rolled out effectively at practice level.
DID YOU KNOW? Specsavers has 24 billion data points that have been taken directly from real patient examinations –the biggest repository of optometry data in the world
So, how do practices protect their data, once they have collected it from
At Specsavers, new patients are asked for their consent around data gathering and GDPR; if these questions are not answered or need to be renewed, a note will automatically be flagged within the system. If a
Former pre-reg contributor, Bhargavi Zinzuwadia, on lessons from one year of locuming
51 How do I... Incorporate new research into my practice? With AOP head of education, Dr Ian Beasley
55 Key milestones Practice owner, Dr Martin Smith, explains his journey into entirely private practice
47 Eyes on wellbeing The AOP offers resources and advice for handling menopause in the workplace
Getty/ Endai Huedl THE DISCUSSION October/November 2022 www.optometry.co.uk 41
takes a deep dive into the world of optical data with director of professional services at Leightons
and Hearing Care, Andrew Bridges, and director of professional development at Specsavers, Paul Morris
patient exercises their right to be forgotten, the request is handled centrally rather than falling on local partners.
An issue Morris raised is the use of mobile devices and the app-based versions of software, which can present “a real problem with having the good governance around what you’re viewing on practice premises and what you’re not.” Specsavers has a programme of mandated information governance security training, undertaken by “each and every one of our team members, both in the support office and in public facing roles,” on a yearly basis. This training “reminds you about the basics,” Morris explained, including “when to raise a concern, and what to do to safeguard yourself, especially if you’re travelling on public transport or using coffee shop-style public networks.”
He added: “It’s really important. We’ve all got an obligation to keep our patient data safe and secure, not just in the practice, but also in any way that it could be compromised.”
Decision making and the limits of data
Aside from security concerns, it is important to remember the value that data can have in guiding a business and the decisions that can be made within it. Can studying the demographics of patients
influence decisions about what services a practice offers, for example?
Bridges explained that, at Leightons, data provides insight on practice capacity, and, in certain areas, guides decisions on new services or products. Eight years ago, Leightons invested in optical coherence tomography, and “consideration was made in the investment, and the initial rollout in the right practices.”
Data is not the be all and end all, however. In fact, Bridges explained, “Sometimes, data is almost disregarded in order for us to meet our needs and desires to provide the highest quality of clinical care. That can override data.”
He added: “Last year, we reinstalled Optomap across each of our branch practices. That decision was made to ensure our optometrists have the latest clinical technology, so that we can provide rigorous care and clinical excellence. In that case, data wasn’t used – it was about quality of care.”

Bridges used the example of myopia awareness, which he explained should be spread as widely as possible.
“As eye care professionals, we’ve got a responsibility with the myopia pandemic,” he said. “We have to provide management advice, even if that’s limited to reducing screen use and close work and getting outside, through
“Data making a case for better and more consistent funding for what we do, particularly in England, where there is less congruity than you see in other devolved healthcare systems, is vital”
 Paul Morris
Paul Morris
to providing processes, be it a contact lens product or a spectacle lens product.”
He added: “I don’t think it should be limited to parents of a myopic child. It needs to be a widespread message, probably even more so with the grandparent power, where grandparents are often providing care for their grandchildren. They may be the ones that are providing funds to deliver that care, and if that’s ultimately ensuring the child retains quality of sight and life, it is important that that communication gets out there to everyone.”
Leightons provides myopia management information in all its communications, rather than only to particular patients. This includes a 16-page colour publication called Talking Points, which goes out to all patients and has recently included a feature on the condition.
Making sure messages reach as many people as possible is also key for Specsavers. Morris explained how collecting data led to an envelope redesign, which “increased uptake of recall, because people felt it looked important and that they should open and action it.”
He added: “That’s part of not only a business ideology, but a public health ideology. The more people respond practically to recall the better, because it means they’re engaging more readily in eye care.”
He also acknowledged the limits of data, however, and how easy it can be to rely too heavily on it.
“Data is only good provided you’re using it in a positive way,” Morris said. “It’s pointless collecting data for data’s sake. I often ask, ‘What are you going to use this for?’ You could get it X percent more accurate, or you could find X percent more or you could investigate this, but would it change what you’re looking to do?”
Specsavers has found it useful to collect data for forward booking. “Online availability of appointments is a huge driver in [to store],” Morris explained. “Practices that have good online availability have a better uptake of appointments than practices that don’t. It shows how frictionlessly the public want to access services. We can look at that data on an hourly basis if we wish to. That comes from investing in the right systems.”
Post-pandemic, Morris said, data analysis has allowed Specsavers to see which practices the previous patients of city centre stores, now largely working from home, are visiting. “They’re accessing care closer to home, rather than going during lunchtimes,” he explained.
“It’s interesting to be able to help those stores in their postCOVID-19 recovery, because some are still seeing 20% to 30% less volume.”
“We’ve got to maintain that duty of care and safeguard it. We’ve got to hold all aspects of confidentiality at the highest order” Andrew Bridges
42 www.optometry.co.uk October/November 2022
THE DISCUSSION
IN PRACTICE























“When you locum, it’s not just about yourself”
As she celebrates one year of locum life, OT’s former pre-reg contributor, Bhargavi Zinzuwadia, shares what she has learnt

When I started as a locum, I wish I had known…
How important it is to be as organised as possible. Get your diary set up. It’s about being prepared. It’s initially scary, so I think it’s important to ease yourself in. Everyone is really friendly when you start, so that’s quite nice. It’s been a really good experience, and a good learning curve. Every store is different, so you learn lots every day.
I realised this when…
I started booking days just before the locum work started for me, so not far in advance. But if you book in advance and get to know the team, you get to know more about the store. I realised the value of organisation early on, as soon as I started locuming, speaking to other locums and practice staff.
The people who helped me realise this…
Were my friends who locum as well, and also the store directors, all of whom
are very friendly. They understand that it’s different, moving from being a full time resident to a locum.
This level of organisation helps in my day-to-day practice because…
If you know what’s happening weeks in advance you can plan your days; you can plan your journey. You’re more at ease when you enter the clinics, because maybe you want to target certain stores, or you want to continue with a certain team.
It helps if you organise a few months ahead. Each store has a different database and different schemes, for example, diabetic clinics, or glaucoma clinics. Ask yourself, ‘what do I want to learn from this store?’ From an organisational point of view, you can plan your weeks to be able to learn a bit more. Locum work is vital in helping me expand my knowledge of optometry.
“Locum work isn’t restricted to multiples. There are independents, there are hospitals, there are universities. There are lots of things you can do”
My biggest challenge as a locum is…
I think the biggest challenges can be your follow-ups. I was a resident after qualifying and have worked with a lot of residents since. It’s a question of ‘Am I able to follow up that patient?’ In the stores that I have worked at, I have been fortunate enough that the senior optometrists have always let me know what happened to that patient. They have always got that communication going on. That’s nice for me and for my perspective, because I want to know what happened to that patient from a care point of view.
As a locum, I’ve adapted my days by…
Carrying forward all my learnings from residency onwards into locum work. Other than that, I haven’t really changed the way I practise at all. I am thoroughly grateful for all the learnings, from the moment I graduated.
Practices can make life easier for locums by…
I’ve been fortunate that most of my practices have gone through what their stores are like before I’ve started my work with them. I ask questions about how the team works before I actually do a day. I wouldn’t have asked for anything to have been done differently so far.
One change I’ve seen whilst working as a locum is… A lot of practices are really good at working as a team. The importance of being part of a team is reflected everywhere, from clinical assistants or optical assistants to clinical management.
My favourite thing about being a locum is…
The flexibility, but also the ability to learn a lot from different practices, different areas, and different clinicians. Locum work isn’t restricted to multiples. There are independents, there are hospitals, there are universities. There are lots of things you can do, and that variety is interesting for me at the moment. I’ve done a couple of hospital days. I do part-time at the university clinics and at multiples. It’s been a good experience. I’ve been lucky in that sense.
The highlight of my time as a hospital locum is…
Seeing a different side to my referrals. Asking, ‘Okay, maybe I could manage this in practice, but would I?’ It expands your knowledge. There are so many different ways to look at a patient or perspective, rather than just textbook, expanding from a practice scenario to what it would be from a hospital perspective. That’s been interesting for me: what I would think is urgent in practice might be routine in the hospital environment.
My last word after a year of locuming is…
When you locum, it’s not just about yourself. You’re entering a whole team. It’s nice to be flexible for that team, because everyone works differently. Understanding each store makes your life a lot easier. Teamship and friendliness, I would say, are key.
AOP support
If you are thinking about becoming a locum, and want to talk this through in more detail, contact regulation@aop.org.uk
LIFE AS A LOCUM
MY KITBAG ESSENTIAL IS... My retinoscope
44 www.optometry.co.uk October/November 2022











































“Continuous education keeps the job interesting”
From a young age, I was interested in healthcare.
I was amazed that a routine sight test can reveal anything from diabetes to brain tumours.
I studied optometry at the University of Bradford from 2014 to 2017. As a very practical course, it was excellent preparation for the pre-reg and my career.
I particularly enjoyed clinic rounds, where we were presented with patients with different conditions.
I was lucky to live with final year optometry students in my first year. I got a lot of advice on areas to focus on, as well as tips to living and studying away from home.
I joined Specsavers in 2015, during my summer holiday from university. I was looking for part-time work to help pay off my student loan.
I walked into Specsavers Leicester and was greeted by the lead optometrist, who introduced me to the practice director, and I was given an interview on the spot.
Beginning on the practice floor, I continued working during term-time by
commuting back every other weekend and went on to experience the various departments in a large practice. I started my pre-reg placement with the same practice in 2017.
By this point, the weekend work had allowed me to become a competent dispenser and pre-screener. The pre-reg was tough, with a lot of content to learn and
my OCT knowledge, gaining a distinction in my professional certificate in medical retina with University College London. Glaucoma is an area of interest for me, so I also did my professional certificate with the University of Bradford and passed with a distinction.
Early in the pandemic, I was the only optometrist working in my branch. This meant performing emergency and essential sight tests. I enjoyed working during this time. I was able to use my clinical expertise to make a difference during lockdown, when I saw the result of a lot of DIY accidents because many people did not have adequate ocular protection. I was able to help reduce the strain on the NHS. One patient had a fly stuck in his eye. The case went viral, and was published by the New York Post. This period was great for my development. It helps me as a director today.
“My Plan B?”
I would have pursued a healthcare profession that provides a similar career path, for example audiology, dentistry, or physiotherapy.
are the reasons I have progressed to this point. Continuous education keeps the job interesting. There is always time to learn and develop to be the best we can be, for both our patients and for our practice teams.
Working in primary care allows practitioners to work in many different areas of practice, including sight tests, contact lenses, ocular health, and paediatrics.
I have met clinicians from a range of backgrounds. Being able to see the benefit and impact of primary care at firsthand is invaluable.
As an optometrist, I am proud that we support the NHS by delivering these services. Working with Specsavers enables me to put primary eye care at the core of my practice, so I can make community eye care accessible for my patients.
put into practice. I was lucky to have a strong team around me. A highlight was when my colleagues created a mock objective structured clinical examination for me.
After qualifying, I completed my Wales Optometry Postgraduate Education Centre, Minor Eye Conditions Service and glaucoma accreditations. Optical coherence tomography (OCT) was then introduced into practice, and I took a lead clinical role as I strengthened
I started my Specsavers pathway programme – the route to directorship – in the summer of 2020, during the height of the pandemic. I completed it by the following summer and became director in Specsavers Towcester in November 2021.
Recently, I have started my independent prescriber qualification. I am currently working on my hospital placement and final assessment. Ongoing education and development
I supervised on a BTEC Level 3 Certificate for Ophthalmic Dispensing Assistants for an individual who is sight impaired. He progressed, and is working as an assistant store manager. This is the standout moment of my career. I hope to mentor others to develop future business partners and specialists for the industry.

Get in touch
Share your career journey with OT.Email lucymiller@ optometry.co.uk
Siddhant Majithia, optometry director at Specsavers Towcester, on going viral during the pandemic
HOW I GOT HERE
“I was able to use my clinical expertise to make a difference during lockdown... I was able to help reduce the strain on the NHS”
46 www.optometry.co.uk October/November 2022
M enopause Awareness Month gives a focused reason for women’s health to be at the forefront of public discussion – especially during conversations around workplace wellbeing.
In July, the first Women’s Health Strategy for England was published, aiming to ‘ensure women are better listened to’ and laying out key actions based on the concerns raised. The strategy promised to improve education on women’s health, after fewer than one in 10 respondents felt they had enough information on conditions in areas including the menopause.
Shadow Secretary of State for Health and Social Care, Wes Streeting, was quick to point out that not all concerns were accounted for, however. The shortage of Hormone Replacement Treatment, for example, has no specific focus in the strategy. Clearly, there is more work to do.
A survey by the Women’s Health and Equalities Committee, published in February, highlighted menopause stigma, as well as noting that one in three women have missed work because of symptoms, and that privacy concerns and fear of receiving an adverse reaction lead women not to seek out support. Most women, the report found, do not tell anyone at work that they are going through the menopause, despite most saying it affects their work.
AOP support
EYES ON WELLBEING
Menopause in the workplace
October is Menopause Awareness Month. OT looked into how the Government is tackling stigma, and what practical advice is available from the AOP
2022 has also seen the creation of the UK
Menopause Taskforce, which aims to address workplace stigma, alongside other issues, including better access to treatment. There are clear reasons for this need, aside from the general desire to improve women’s wellbeing.
Chair of the Women and Equalities Committee, Caroline Nokes MP, has highlighted the “legal, social and economic imperative” of supporting women “through a normal life transition, so we can hold on to role models for the next generation.”
So, what can women approaching or facing this period do to make things easier? The AOP has published guidance that addresses this question.
Handling the menopause: AOP guidance

The AOP advises those approaching the menopause consider their diet and
exercise regime. Because there is a high chance of osteoporosis during the menopause, keeping your bones strong in advance is a good idea. Strength training might help in this.
When it comes to the menopause affecting work, the AOP advises having an open and frank conversation with your employer. There are legal regulations in terms of how employers have to support women in the workplace who are experiencing the menopause, and especially symptoms
to accommodate your needs, whether that means allowing you to change what you wear to work if you’re experiencing hot flushes or altering your working hours to accommodate exhaustion.
If the menopause is causing declining mental health, time for appointments must be given as would be the case with any other health issue.
You should consider what you want to talk about ahead of time, and potentially go into the conversation with a list of things to address in case you do find yourself getting nervous or losing your pattern of thinking.
Arriving with solutions is helpful. Employers are often under-equipped to support women with menopause issues, so being able to help support them to support you is a good idea. Go in with ideas for what you would like to see changed, or what solutions you might want the business to put in place for you. This will put you in a more confident position, and help in exploring options.
It’s important to remember
“Go with ideas for what you would like to see changed, or what solutions you might want them to put in place for you”
that could affect the way they work. It is an employer’s duty to accommodate these.
The AOP has a suite of resources online that are aimed at making life easier for those dealing with the menopause. Advice includes how to support yourself during this period, how to handle stress, and how to navigate the menopause in the workplace. Find out more: www.aop.org.uk/menopause
It is understandable that you might feel more comfortable talking to a female colleague or line manager about the issue. If you have a male manager, though, you can still have the conversation – maybe take in a female colleague, if that makes you feel more comfortable. It’s the employer’s responsibility
that employers might not be aware of the challenges of the menopause, or what their responsibilities are towards staff. Giving them the link to the AOP’s menopause resources in advance, and allowing them to educate themselves, could be helpful.
Ultimately, your employer might need some guidance. After all, supporting you is going to benefit their business – so it pays to make it clear that you’re all in it together.
October/November 2022 www.optometry.co.uk 47 Getty/ SCIENCE PHOTO LIBRARY IN PRACTICE





















































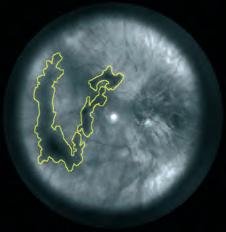
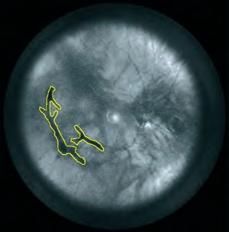




YOUR FUTURE IN FOCUS
PRACTICE TEAM GUIDE
UNLOCKING POTENTIAL

Supporting each other to achieve practice success

IN GOOD COMPANY
From boosting sustainability to fostering team wellbeing, OT explores how every staff member can contribute to practice success
The carbon footprint of an NHS sight test is 5.27 kgCO2e – roughly equivalent to washing and drying a load of laundry before tucking into a full English breakfast.
While it may not seem like much, with around 13 million NHS sight tests performed in optical practices each year, even incremental reductions in this number can have a large overall effect.
“It takes a healthy planet to have healthy people and communities,” Johnson & Johnson Vision’s Dr Rachel Hiscox shared with OT.
Alongside the question of how to tread a little lighter within the sector, optical staff working in different roles share insight on the qualities they value in colleagues. A common thread in successful practice teams
is that colleagues are always willing to learn from each other. This creates resilient workplaces that are ready to adapt when needed.
“Arguably the most crucial quality is communication,” optical assistant Irene Melville observed.
The influence of cost of living pressures is considered within optometrist Faye McDearmid’s advice on reducing contact lens drop out, while Neil Retallic and Peter Greedy share their thoughts on nurturing mentally healthy workplaces.
Within this guide, OT and the AOP have partnered with Johnson & Johnson Vision to recognise the value that cohesive teams bring to the optical profession.
Welcome to the Practice Team Guide – working together to protect the vision of our communities.
from
other
Optometrists share their tips for fostering mentally healthy workplaces
Optical staff share insight on the qualities they value in colleagues
on how to reduce the environmental impact of an optical business
The role of every team member in reducing contact lens drop out
“A common thread in successful practice teams is that colleagues are always willing to learn from each other”
PRACTICE TEAM GUIDE
2 www.optometry.co.uk Practice Team Guide 2022 3Managing team wellbeing
4View
the
side
6The sustainable optometry practice Tips
8Keeping in contact
CONTENTS
MANAGING TEAM WELLBEING
to improve wellbeing: nutrition, sleep, exercise, mindfulness, learning, service and creativity. Practice managers should reflect on how they can encourage healthy food choices at work – for example, by having suitable facilities to prepare food at work.
They could also provide the space for weary employees to have a recharging power nap. A lunchtime walk with a colleague can help to incorporate exercise into the working day – and walking with a peer provides accountability and motivation.
Greedy shared that mindfulness activities can easily be done in a quiet, dark room.
Many employers are now realising that a workplace which compromises employee happiness is not only detrimental in terms of individual wellbeing – but leads to a less productive workforce.

A study of call centre workers by University of Oxford researchers in 2019 found a strong link between happiness levels and sales performance.
The latest registrant survey by the General Optical Council published in August found that 62% of optometrists and dispensing opticians were satisfied in their role. The survey also revealed that there were significant variations in job satisfaction depending on the role, employer and region.
As well as reducing productivity, drains on employee wellbeing can lead to staff requiring extended breaks from work. Close to one in 10 optometrists and dispensing opticians had taken a leave of absence as a result of stress.
So how can you foster wellbeing within optical practices? OT asked optometrists Neil Retallic and Peter Greedy for their thoughts.
WORKPLACE CULTURE Retallic encouraged practices to adopt a positive mental health culture by encouraging open conversations.
“Individuals within the workplace can help shape a culture that encourages acceptance that mental health issues are not a failure or taboo subject and that actively talking about personal experiences and how they have overcome challenges is a strength,” he observed.
He noted that simple steps, such as setting personal daily targets to achieve a work-life balance, can be useful. This might include practising relaxation techniques or going for a walk during breaks. Reflecting on the key features of a happy workplace, Retallic described a team that is communicating with each other and feels free to outline changes that are required to support their personal and professional needs.
“Teams who take time to understand their colleagues’ personal interests, how to work best together and self-reflect will outperform those just focused on business operational activities,” he said.
SEVEN STEPS TO WELLBEING Optometrist, coach and leadership consultant, Greedy, highlighted seven areas that optometrists can focus on
“I focus on my breathing, note when my mind wanders and refocus on breathing,” he said.
Greedy encouraged practices to provide access to online learning for staff. He also highlighted that while optometry is a service profession, staff should consider how they frame the work they do.
“Do we approach it as an act of service or just go through the motions of the customer service playbook?” he asked.
Social media, frame selections, window displays and seasonal themes all provide opportunities for creativity within practice, Greedy highlighted.
PETER'S TIPS FOR A MINI-MINI BREAK
Five minutes: Do a breathing exercise. For example, box breathing is four seconds each of inhale, pause, exhale, pause, while visually tracing the sides of a rectangular object.
10 minutes: Consider a mindfulness exercise or micro nap. This could be a mindfulness exercise leading to a nap.
30 minutes: Go for a walk and listen to a podcast. If you use bone conducting headphones, you can also listen to the sounds of nature. In one activity you have three wellness benefits: exercise, learning, and connection with nature.
Optometrists Neil Retallic and Peter Greedy provide guidance on fostering mentally healthy workplaces
“Actively talking about personal experiences and how they have overcome challenges is a strength”
Practice Team Guide 2022 www.optometry.co.uk 3
NEIL RETALLIC Getty/simplehappyart
VIEW FROM THE OTHER SIDE
Optical staff share their words of wisdom on the qualities they value in colleagues working in other roles
Whether it is a colleague who remembers how everyone takes their tea or a team member who reliably helps new recruits, there are some staff who make the working day easier.
But how do you become that star worker within your team? And how can you ensure that you are providing the right kind of support for colleagues in every role within the optical practice?
OT approached an optometrist and two optical assistants for their views on the qualities they value in optical staff working in different roles.
AN OPTICAL ASSISTANT ON WHAT SHE VALUES IN A PRACTICE MANAGER

-
Name: Irene Melville
Role: Optical assistant
Practice: Bennett and Batty Opticians, and Crompton Opticians (Hakim Group practices)
As a practice manager, you need to interact well with patients and staff and so it’s really important to be professional but also very friendly. Organisation comes in super handy when you’re keeping an eye on frames, overheads and ensuring the practice really benefits from the hard work put in by being sensible about how it reinvests. As a practice manager, you should always be looking at the best ways to improve the practice.
Arguably the most crucial quality is communication. There needs to be interaction between the two roles at every opportunity; giving the optical assistant plenty of options, helping them with dispenses and giving them all the information they need to use machinery within the practice.
Every morning, my practice manager, Amelia, will sit down and run through the day ahead with the team, including the upcoming clinic and daily tasks, whether it’s figuring out what types of dispenses we can expect or just generally helping each other to tackle the day head on. There is a lot of
communication between the two of us and I always feel that her support is there if ever we need to back each other up. We are a team and we trust each other to follow up on anything, even if it’s outside of our work hours. I think it’s a really valuable way of going above and beyond. By forming that trust upon those key qualities, the result is a team that feels supported and confident and works much more efficiently.
“As a practice manager, you need to interact well with patients and staff”
IRENE MELVILLE
4 www.optometry.co.uk Practice Team Guide 2022
Getty/simplehappyart
ALWAYS LEARNING
The AOP has worked in partnership with Johnson & Johnson Vision to create a series of recorded webinars for the practice team: www.aop.org.uk/webinars
Name: Josie Evans

Role: Optometrist
Practice: Linklater & Warren Opticians
When handing a patient over for a dispense, I value when a dispensing optician makes eye contact with you when
-
Name: Gwen Eccles
Role: Optical assistant
Practice: Tyrrells and Embery Optometry (a Hakim group practice)
Since starting my job in 1978, optometry has advanced massively; we now do a lot of the pre-testing and visual field tests, and have more input upon improvements for our patients. Working with some very talented optometrists, I have learnt to value certain qualities. Along with a sense of humour, which anybody working with the general public needs, a key quality is patience: our patients range from young children to people over 100 years old, bringing a plethora of complex issues and requirements. Organisational skills are also a priority. It takes hard work to keep a clinic running to time when you’re in the test room and it’s vital to keep the whole practice running as it should.
Your optometrist needs to be able to identify the strengths and weaknesses of all practice staff. Regular training has helped our practice keep refreshed on topics and learn about new procedures and equipment as we offer a wide variety of services. This keeps our practice current and a place the patients feel safe and looked after. It also gives you confidence in answering patient questions that they’re a bit wary of discussing in the test room.
Our optometrist also encourages us to give a valued input in the choice of frames that we think will go well in the practice and fit the practice profile. That is the bit I really enjoy doing most of all. I absolutely love when people are thrilled with new glasses because it makes them feel good that they look good.


you’re walking towards them. This confirms they’re available to take the dispense and it also welcomes and acknowledges the patient, making it a smoother transition.
Time in the consulting room can be limited and dispensing opticians are the experts on different lens designs and frame choice. I really appreciate how our dispensing optician colleagues explore a patient’s lifestyle and working environment further outside of the consulting room, ensuring the patient has been recommended the best lens for their needs.
Likewise, if a patient is having difficulty with their glasses, a dispensing optician’s opinion
is invaluable. I find it useful to have notes of their assessment before a recheck is considered, for example –are the measurements correct? Have there been any changes in lens design compared to previous dispenses? What other solutions are available if the prescription is stable?
“A key quality is patience”
GWEN ECCLES
“If a patient is having difficulty with their glasses, a dispensing optician’s opinion is invaluable”
JOSIE EVANS
AN OPTOMETRIST ON THE TRAITS SHE APPRECIATES IN A DISPENSING OPTICIAN
AN OPTICAL ASSISTANT ON THE QUALITIES THAT MAKE A GOOD OPTOMETRIST
Practice Team Guide 2022 www.optometry.co.uk 5
THE SUSTAINABLE OPTOMETRY PRACTICE
Consumers are increasingly changing their behaviour in line with a more sustainable lifestyle as temperatures rise to record-breaking levels in the UK and the effects of climate change can be seen across the globe.
A survey in of 2000 adults in June this year by Deloitte found that 75% of UK residents recycled or composted household waste, while 64% of survey participants had limited their use of single-use plastic. More than half of respondents (59%) shared they had
limited new purchases, while 39% had reduced their intake of meat and animal products – up 9% and 20%, respectively, from the previous year. The focus on sustainability has extended from personal choices to the world of work. Within optometry, many optical practices are aiming to limit the impact that businesses have on the environment.
CALCULATING THE CARBON FOOTPRINT OF A SIGHT TEST
In February, the Centre for Sustainable Healthcare published a report calculating the annual carbon footprint
of NHS sight tests. Annual Carbon Footprint of NHS Sight Tests at Five Optometry Practices was produced in partnership with NHS England and NHS Improvement (Cheshire & Merseyside) and Cheshire Local Optical Committee. Across the five practices, 25,745 NHS sight tests were performed in 2020. The average carbon footprint per sight test equated to 5.27 kgCO2e.
The biggest contributor to the carbon footprint of the sight test was travel (69%) followed by energy (14%), procurement (11%) and waste (5%).
Taking these findings into account, the study authors recommended that
How can the optical sector reduce its environmental impact? OT explores the role of practice teams in creating a sustainable future
6 www.optometry.co.uk Practice Team Guide 2022
NHS England consider travel and accessibility when commissioning new optometry contracts – ideally offering services that can be reached by active or public transport. They also encourage the use of contact lens and spectacle lens recycling points, as well as collaboration between optometrist and industry to measure and reduce the carbon emissions of optical products and packaging.
ASKING THE RIGHT QUESTIONS
For Simon Berry, the sustainability of his optical practice has evolved over time.
In 2016, he developed an Ethical Supply Questionnaire to ensure that he could trace back the products that he stocks within his Durham practice.
“If I am selling something then I am endorsing it. I think that means I should make sure it is as sustainable as possible,” Berry explained to OT
A series of 10 questions assesses the company across a range of areas – from whether it has environmental policies to if it can trace the product back to raw materials.
Suppliers are quizzed on whether the product packaging is recyclable and if the company can calculate a carbon footprint for the product.
Berry is also involved in a research project with Durham University that is attempting to develop an algorithm that would estimate the carbon footprint of any frame taken off the rack.
Alongside individual practices, large optical companies have taken steps to assess and limit the environmental impact of providing products and
THE AOP AND SUSTAINABILITY
The AOP has established a steering group with the aim of meeting long-term sustainability goals within the membership organisation. The group will complete a sustainability assessment of the AOP, review procurement and move towards more sustainable member services and products.
services. Johnson & Johnson Vision (JJV) has prioritised energy efficiency, with 100% of electricity coming from renewable sources. The company recycles 89% of raw materials on location at its manufacturing sites.
As part of its Acuvue contact lens recycling programme, more than 8.8 million contact lenses, blister packs and foils in the UK have been recycled.
JJV has reduced the paper and singleuse plastics used in product packaging and guaranteed that all paper packaging comes from responsibly managed forests. The company has taken steps to reduce its annual carbon footprint by 48,000 tonnes.
Professional education and development manager for JJV, Dr Rachel Hiscox, highlighted that the company’s sustainability efforts are focused in three areas: climate change, waste reduction, and protecting natural resources.
“It takes a healthy planet to have healthy people and communities. That’s why we’re constantly innovating to find sustainable solutions to climate change, recognising its crucial role in helping to protect the planet,” Hiscox shared.
She noted that sustainability matters “more than ever” for the consumers and patients that optical practices serve. “We’re committed to finding sustainable solutions to existing challenges, as well as tackling key issues that affect us all. We’ll continue to demand more from ourselves too, as we work towards our sustainable vision and creating a healthier planet,” she shared with OT.
The Deloitte research found that around one in four consumers will consider whether a product is made from natural materials or a renewable resource when making a purchase.
Close to one in three (31%) would take into account whether a product uses minimal or recyclable packaging, while more than half of consumers would factor in whether the product was durable and long-lasting.
Find out more about how Johnson & Johnson Vision is helping the environment at: www.acuvue.co.uk/ sustainability
Practice Team Guide 2022 www.optometry.co.uk 7 69% STAFF AND PATIENT TRAVEL 14% ENERGY 11% PROCUREMENT 5% WASTE 1% WATER HOW DOES THE CARBON FOOTPRINT OF A SIGHT TEST COMPARE? 840 kgCO2e return flight, London to Tenerife 9 kgCO2e 30-mile car journey 5.27 kgCO2e sight test 3.7 kgCO2e full English breakfast 2.4 kgCO2e load of laundry (wash and tumble dry) 0.9 kgCO2e pint of beer 0.34 kgCO2e a large latte. Sources: The Centre for Sustainable Healthcare, Annual Carbon Footprint of NHS Sight Tests at Five Optometry Practices, TheGuardian, BBC, The Conversation, Carbon Footprint Calculator Dissecting the carbon footprint of a sight test Getty/simplehappyart
KEEPING IN CONTACT
Past AOP Awards Contact Lens Practitioner of the Year, Faye McDearmid, shares her tips on the role every team member has to play in reducing contact lens drop out


Changes in technology can be dramatic – the smartphone that brings entertainment, navigation and social connection to the palm of your hand is a distant cousin of its brick-like ancestors.
But less visible effects of innovation can have a profound impact on our daily lives. Within the field of contact lenses, developments in material technology have enhanced patient comfort and vision, as well as broadening the pool of potential wearers.
Optometrist, Faye McDearmid, highlighted to OT that just as it is unlikely for someone to own one mobile phone across their lifetime, it is also unlikely that they will wear one type of contact lens. “Let the patient know there is choice when it comes to lenses and it may be that something occasionally needs tweaking to make them happy again.”
As well as staying informed about developments in technology, optical professionals can offer patients choice in the context of the current financial climate. An OT poll of 65 optometrists in August found that 85% had seen a change in spending habits as a result of cost of living pressures. “The current worries about cost of living, inflation and the recession may have patients more concerned about costs, so know
the options you can offer,” McDearmid advised. For example, can ‘pay as you go’ customers be offered a monthly subscription at a lower rate? Or can those already on a subscription for 30 pairs be offered a subscription for 20 or 10 pairs? Common reasons for contact lens drop out relate to issues with comfort and vision, McDearmid highlighted.
comfort in lenses, it’s a shame for our patients to lose out on all the benefits and things they enjoyed about lens wear when it may be a simple fix.”
STARTING THE CONVERSATION
During the 17 years McDearmid has worked in the optical industry, she has observed that people will not hesitate to ask about new glasses after a change in vision. However, this same request does not come up in relation to contact lenses.
Her favourite questions to start a conversation about contact lenses include asking if a patient would like to reduce their reliance on glasses or enquiring about how they find wearing glasses during different sports and activities. For example, many runners and horse riders find it challenging to wear glasses. “They fog up, get rained on, slip and become more of a hindrance than help,” McDearmid shared.
She is then able to present contact lenses as alternative that can be tailored to their needs. For McDearmid, contact lens care does not end when the patient leaves the practice with their new lenses in hand.
“If you’re in the practice team and a patient comes to you with concerns about their lenses, is planning to reduce their wear frequency, or wishes to cancel their subscription – find out as much information as you can,” she advised.
This information can then be passed on to the clinician who may be able to address issues at a follow up appointment. “With improved materials and lens designs to support vision and

She emphasised the importance of keeping in touch between visits to ensure that the patient continues to receive optimal performance from their lenses.
“When people are fitted and don’t return, it’s often something simple that could easily be resolved if we knew about it,” McDearmid said.
She keeps in touch with any patients who are trialling contact lenses. “We make the emails personal, encouraging those who want the contact lenses for a specific activity to send in a photo, so that we can celebrate their success with them,” she shared.
OT supplement editor
Powell
editorial team
McCormick, Lucy Miller, Kimberley Young, Leah Boyle, Laurence Derbyshire
designer
Pearce
Client engagement director Anna Vassallo
by Think Printed by Acorn Web
All rights relating to this publication are expressly reserved. No part of this publication can be reproduced.
“When people are fitted and don’t return, it’s often something simple that could easily be resolved if we knew about it”
FAYE MCDEARMID
8 www.optometry.co.uk Practice Team Guide 2022
Selina
OT
Emily
Senior
Grant
Published
Getty/simplehappyart
Incorporate new research into my practice?
The AOP’s head of education, Dr Ian Beasley, explains how optometrists can approach new clinical research

More information
OT’s Education Library has over 500 CET and CPD articles, and Skills guides www.optometry.co.uk/ educationlibrary
A
s a busy practitioner, you may find it difficult to dedicate time to regularly trawl through peer-reviewed research papers alongside competing clinical commitments.
However, if you wish to explore a niche topic of interest, then using the advanced search function on PubMed can be a good place to start. The site provides abstracts of research papers along with some full articles available as open access.
While many articles require payment or a subscription to view the full content, if you are a member of the College of Optometrists you can request an ‘OpenAthens’ account, which will make certain publications accessible. Using the search function on Google Scholar offers an alternative to PubMed.
Utilising research
Reading short abstracts of full research papers may not always deliver the userfriendly experience you are looking for. Another option is regularly reading continuing professional development (CPD) content in professional journals, such as Optometry Today, which can offer a more easily digestible approach, providing you with a broad
understanding of the latest evidence base and, more importantly, relaying how these findings can translate into clinical practice.
How often you should consume new research depends on the specific clinical topic. There are some areas of practice that are evolving rapidly, for instance myopia management, whereas for others, such as binocular vision, the changes to the evidence base are more incremental.
You also need to consider your level of experience and current knowledge, and how this applies to your clinical role. This approach is at the heart of the General Optical Council’s new CPD scheme, where you should be tailoring your personal development plan (PDP) to consolidate and expand knowledge relative to your scope of practice, taking the opportunity to review this throughout the cycle and reflect periodically on the impact that changes to your role or to the clinical landscape have on your PDP.
Practical applications
As an optometrist, there are a lot of opportunities to stay up to date with evolving practice.
The AOP would advise taking time to read clinical articles, attending conferences and webinars, and networking with your peers. Subscribing to social media channels of interest on key clinical areas can be a relatively passive way to stay informed on updates and developments. Naturally, it is important to separate opinion from fact when consuming content via this route.
Of course, suppliers will be eager to update you on products that have translated from research to reach the market. It is worthwhile scratching beneath the surface of the glossy brochure and considering the weight of evidence that sits behind the product or products on offer. Are the headline claims underpinned by systematic reviews, randomised controlled trials, or case control studies?
Whether you want to take research forward and embed it into your own practise depends on the topic area and your level of prior knowledge and experience. If you read about developments in a particular clinical area, you
should ask whether this can be delivered safely within your current skillset, or whether specific training is required.
If the latter answer is true, there is a wealth of opportunity for you to expand your clinical skills with higher qualifications and accreditations from a range of optical institutions.
Patients will assume that decisions made about their care are based upon professional expertise. If there is a significant change to the way an ongoing condition should be managed, then it is reassuring to explain clearly the basis for that decision.
Useful resources
OT’s current CPD articles: www.optometry. co.uk/cpd
Past CPD articles in OT’s Education Library: www.optometry.co.uk/ educationlibrary PubMed: pubmed.ncbi.nlm. nih.gov
Google Scholar: scholar.google.com
Open Athens: www.openathens.net
Get in touch
Do you have a topic that you would like to see explored in OT? Email lucymiller@ optometry.co.uk
“It is important to separate opinion from fact when consuming content via this route”
October/November 2022 www.optometry.co.uk 51
HOW DO I...
IN PRACTICE
With the OSCEs in full swing, OT caught up with our 2022–2023 pre-reg focus cohort – Caroline Mansfield, Holly Leitch and Thaksha Sriatharan – to reflect on their feelings as qualification looms
What has been your standout moment during your pre-reg?
Caroline Mansfield (CM): The exhilaration that came with passing Stage 1 was my favourite moment so far. Work paying off is always what keeps me going. It also coincided with the week before my wedding, so that was a great week for me.
Holly Leitch (HL): A standout moment was with a patient who booked an appointment online the evening before, having had an eye exam the previous day elsewhere. When the patient attended, she was very upset. She felt she had been given bad news in the previous appointment, and was looking into health insurance and making a will. When I assessed her, the information given was incorrect, and there wasn’t anything to worry about – the issue just needed monitoring. This taught me the importance of clear communication and relationship building with patients, as well giving them time to ask questions to ensure they understand the outcome of their appointment.
Thaksha Sriatharan (TS): I came across a patient with advanced keratoconus, who could just about see the +1.30 logMAR binocularly in their glasses.
The patient came in for a contact lens fit assessment, and after spending time fitting rigid gas permeable lenses, I was able to bring their best corrected vision to +0.00 logMAR. The patient was very grateful, and it brought tears to their eyes. Helping that patient’s quality of life was a very humbling experience.
What was your scariest moment?
CM: The lead up to Visit 3. From the beginning of my pre-reg, I have been honing my routine and getting used to working through all the components that are required in a normal sight test, but being observed over a whole sight test with an assessor in person was daunting. I had not been under that kind of scrutiny since university.
Before that visit, my supervisor watched me and gave me pointers on what I did well and what I could work on. I found this very useful in the lead up. I thought I had ‘bigged-up’ that assessment in my head, but I felt all those same nerves for the Stage 2 visit. It’s silly, because I feel most confident in the practical elements and so these assessments should be the ones I feel good about.
HL: The scariest moment was when a young patient fell ill during the eye exam. I had to call an ambulance, wait with the family for it to arrive, and speak with the paramedics when they got to the practice.
This was two months into my pre-reg, and you aren’t expecting a situation like that to arise. I had to remain calm and help comfort the patient’s parent in the room, while dealing with the situation quietly so as not to alarm the rest of our patients.
TS: My scariest moment had to be when I was first starting out. The optometry department at the Manchester Royal Eye Hospital is big, and there were a lot of people to meet. Although everyone is friendly, it was intimidating to be working with worldclass leaders in the field.
How do you see your day-today changing now your prereg is over or almost over?
CM: I anticipate that my clinic times will be shorter, and my clinical decision-making process will have to become faster. However, there’ll be half the paperwork without all the pre-reg stuff, so it should be easier than I think.
I think it’ll be more stressful to begin with and the thought of not having a supervisor is daunting, but seeing more complex cases this year has prepared me well.
OT’s pre-reg focus contributors
Caroline Mansfield, pre-reg at Specsavers Haverfordwest, Wales
Holly Leitch, newlyqualified optometrist who completed her pre-reg at Urquhart Opticians, Kilmarnock Thaksha Sriatharan, pre-reg at Manchester Royal Eye Hospital.
HL: Over the past year I have worked closely alongside my supervisor in our Kilmarnock practice. Now that I am qualified, I can work between our different locations, and in smaller practices, where I will be testing on my own.
I’m looking forward to being independent in my clinical decision-making and working with different teams.
TS: I will be more independent in my decision making and patient management.
I also hope to learn more techniques, such as gonioscopy and advanced OCT interpretation, and I would like to be more active on social media in order to share my knowledge.
What are your plans for the coming year?
CM: To become fully registered, get Wales Eye Care Service accredited in
“Have some self belief: while it isn’t easy, it isn’t impossible”
“Work paying off is always what keeps me going”
Caroline Mansfield
PRE-REG FOCUS 52 www.optometry.co.uk October/November 2022
Education Library.
OT’s Education Library contains CPD and Skills guides on 31 topics www.optometry.co.uk/ educationlibrary
order to be able to continue to see the more challenging cases and become a more well-rounded optometrist, and then see what’s available in terms of further education.
HL: Urquhart Opticians has recently acquired new practices. I will be working in our Lanark store on testing days, managing a new team and building my patient base there. It will be great getting to know different clients in a different town. This is a fresh opportunity for me.

TS: I hope to be more confident in my clinical skills as I see patients unsupervised in the core clinics. I will have the chance to take on extended roles within the hospital, and also be involved in teaching and education.

Where do you see yourself in five years’ time?
CM: I hope to have a stable job and continue to do what I love, working alongside top professionals and learning more every day. I like the thought of creating a broad knowledge base in further education first, before specialising. At the moment, paediatric optometry has my name on it.
HL: In five years, I see myself continuing with Urquhart and being responsible for my own practice as a manager. By then I hope to have achieved my independent prescribing (IP) and have made further progress in my clinical ability.
TS: At this moment, I’m not sure where my career will take me. I see myself having completed further qualifications, such as IP. I love that as an optometrist the possibilities are endless, and there are many avenues that I can explore.

If you could say one thing to your early pre-reg self, what would it be?
CM: Don’t panic, take a breath, and remember everyone wants you to be competent and succeed.
HL: You can do it. And have some self-belief: while it isn’t easy, it isn’t impossible. When I was struggling, one of our directors, Peter, told me “If it was easy, everyone would do it” and that stuck with me throughout my pre-reg.
TS: Every patient is a new experience. Don’t be afraid to take on complex patients, because at the end of the day

“It will be great getting to know different clients in a different town. This is a fresh opportunity for me” Holly Leitch
they are who you learn the most from. Also, don’t be afraid to ask questions – it’s the best way to build your knowledge.
Can you tell us about your feelings ahead of your Objective Structured Clincal Examinations (OSCE)?
CM: I am nervous for the OSCEs, but I’m enjoying revision. I like revisiting university notes and reminding myself of the ways to remember different things. I will probably feel the nerves a lot more on the journey there on the day.
I’m not sure I have any tricks for dealing with my nerves: just reminding myself that I’m feeling them because I care about a good result and that, because I care, I’ve put the work and hours in to get it. In the moment I just need to remember to stay calm and actually answer what the question is asking.
TS: Ahead of sitting my OSCEs, I knew this was the last stretch of my pre-reg journey. I was one exam away from qualifying, and this was

something that made me both excited and nervous. OSCEs are intimidating. They are a unique style of exam. I’m sure everyone is capable of all the five-minute tasks that will be examined, but nerves can get the best of us. I tried to prepare by doing as many mock OSCE stations as I could. I attended the mock OSCE courses run by the Johnson & Johnson STEP programme and Out of the Box Optics. Manchester Royal Eye Hospital also ran a mock OSCE ring, which was helpful. I could identify my strengths and weakness through these sessions and tailor my practice accordingly. To aid my revision, I would practise stations with my supervisors whenever clinic allowed, and I used the Optotutor online portal and revision books to guide my studying.
What were your feelings after sitting the OSCEs?

HL: Relief that it was over. I had prepared well enough to take on the stations that came up, and only really panicked at one of them.
I felt positive to have made it to the end of my pre-reg. While waiting the three weeks for the results I started to feel nervous, but I’m delighted to have passed. I feel apprehensive moving forward without the support of my supervisor, but I’m very excited for the future.
“Don’t be afraid to take on complex patients, because at the end of the day they are who you learn the most from”
Thaksha Sriatharan
If you are newly-qualifed, upgrade your AOP membership by contacting membership @aop.org.uk or 0207 549 2010
IN PRACTICE October/November 2022 www.optometry.co.uk 53



“It’s more of an honest relationship”
Lincoln practice owner, Dr Martin Smith, explains what led his practice to switch to entirely private services in the summer of 2021

01 When I took over the practice 18 years ago, virtually every test was a General Ophthalmic Services (GOS) test. We bought our optical coherence tomography (OCT) machine 13 years ago, and that started us on the journey of shifting to paid clinical services.
It was a bit odd at first. The thing about that transition period is, you essentially start selling people clinical services, which I didn’t particularly like. People were coming in for a free test, and we were trying to sell them an extra service.
Now we’re private, they come for a sight test, it is a set fee, and we do everything we can in that time or book them for another appointment if needed. That’s a lot simpler than saying, ‘do you want an OCT for £35?’ We were quite early adopters of that, so we’ve made it through that slightly awkward period, and I feel we’ve come out the other side.
Because we’d been building up the clinical side of the business for a while, over the first COVID-19 lockdown we decided to implement a subscription scheme through Eyeplan. Patients on the scheme get lower prices on their spectacles, but obviously they’re paying more in clinical fees already. So, we’d already partially made the shift.
02
The decision to go entirely private was made in early spring 2021. I’d been thinking about it for ages. I had never liked the position that GOS puts us in as practitioners. I don’t like being essentially obliged to make up losses on sight tests by selling spectacles. It never sat well with me.
The thing that kicked me into going private, finally, was that two of the other practitioners in Lincoln also made the same decision.
I knew they were doing it, and we had discussed
“It’s not our duty as practitioners to make up for the fact that the Government doesn’t pay us adequately”
it previously. We all went private within a few months of each other.
03 I gave notice to NHS England in July last year, and then notified our patients and explained that we were going private. We then added £21 on to the current fee for our advanced sight test and stopped offering a basic NHS sight test, which I never thought we should be offering anyway. The vast majority of our patients didn’t have a free NHS sight test, so they were already used to paying us.
My profit margins are the same as they were preCOVID-19 – all we’ve done is shift some of the money from spectacle sales onto clinical services. Each pair of spectacles will make slightly less profit, but we’re putting that on clinical services, which is where it should have always been in the first place. I have nothing against selling spectacles: I love spectacles, I love nice lenses and frames, but I would rather people knew what they were paying for.
04
We lost very few patients and actually gained quite a few, some of whom have said that they specifically came to us because we are now private. There’s a degree of perception with some people that being private is more of a guarantee of quality. Or, maybe they realise that there isn’t so much pressure on us to sell them spectacles anymore. It’s more of an honest relationship.
There’s also a definite shift in the patient-practitioner relationship, which is noticeable. People look at the relationship slightly
differently than they did before, and I feel there’s more mutual respect. They’re choosing to pay and see a private practitioner because they value our services. There have been no negatives whatsoever.
05
The expectations of optometrists go up as the fees go down, and this probably wasn’t quite as clear to me until I stepped out of it and looked back at the GOS system from the outside. It’s a perspective that was there before, but has certainly increased since I swapped to an entirely private service.
You get people saying that not offering NHS services is unethical. But I feel it’s worse to offer people a service that you know you are making a loss on, and then have to recoup that loss somewhere – potentially from selling that patient spectacles.
It’s not our duty as practitioners to make up for the fact that the government doesn’t pay us adequately, in order that people who can’t afford the full fee have access to services. It’s not our moral duty to offer services that other people are paying for, because the Government won’t fund us.
There will be people who disagree and think that we should offer NHS services so that people who can’t afford the fee get access to services.
There is an argument there, but the argument is not that we should be making our other patients pay for them. It’s that the Government should be funding the service appropriately.
KEY MILESTONES
IN PRACTICE October/November 2022 www.optometry.co.uk 55








e are all guilty of it. You are busy describing how the scorch marks on your lacklustre brunch resemble Graham Norton when the waiter comes along to ask how your meal is.
The answer is, of course: fine, thanks.
But telling a white lie when your PeakyBlinders-obsessed boyfriend asks what you think of his new flat cap is a different matter entirely to sugar-coating the truth in the world of work. Optometrists have a
professional obligation to be honest and trustworthy. When a patient walks into an optometry practice, they are seeking insight not on what colour of curtains best suit their living room or the most appropriate outfit for a job interview – but on how to maximise and protect their vision.
It makes sense that when the service in question is the very way that patients perceive the world, providing clear, objective and considered advice is of the utmost importance.
This is not always easy. Conversion rates, limited testing times and the reality that optometry is an environment where healthcare and commerce combine can create challenges.
With the best of intentions, it is sometimes difficult to assess what guidance to give patients amid competing claims from industry, academia and professional bodies.


How should optometrists separate fleeting trends from a lasting
Balancing the evidence on key topics within optics – from myopia and visual stress to increasing happiness at work
Grant Pearce
Grant Pearce
October/November 2022 www.optometry.co.uk 57
IN A NUTSHELL: NUTRITION TIPS

Patients should be advised to eat dark, green leafy vegetables and fresh fruit daily, a serving of oily fish two to three times per week, a handful of nuts per week, choose low GI carbohydrates and limit the consumption of saturated fats and oils whenever possible.
Research by Downie et al. in 2017 found that two thirds of patients expected their optometrist to ask about their general health, while three in four patients indicated they would feel comfortable speaking about their diet with their optometrist.
development? How can pages of research be distilled into practical insight? In an effort to assist optometrists in taking an evidencebased approach to daily practice, OT approaches experts for their take on key issues within optics.
Nutrition
The idea that what a patient puts on their plate can help to protect their vision is an appealing one. But how much of this is based in evidence?
Associate professor Laura Downie, of the Melbourne Cochrane Eyes and Vision Centre for Evidence-Based Vision Care, highlighted that a person’s diet can influence their eye health.
“Extreme vitamin deficiencies can have severe, sometimes permanent, effects on eye health and vision,” she shared with OT.
A BMJ Case Report in March this year described how a Melbourne woman suffered corneal perforations after developing Vitamin A deficiency. Her “severely restricted” diet consisted of mostly bananas and yoghurt.

In another case published in 2021, a Singaporean woman suffered vision loss after developing severe iron deficiency as a result of a diet consisting of potato-based foods, and


biscuits. While not as extreme as these examples, the general UK population is also falling short when it comes to a nutritionally balanced diet.

intended to treat or prevent disease,” she added.

In 2018, only one in four UK adults were eating five or more portions of fruit and vegetables per day.
ZHUH�HDWLQJ�¿YH�RU�PRUH�SRUWLRQV�RI�
Downie highlighted that there is epidemiological evidence showing associations between specific dietary patterns and altered risk of eye disease – in particular age-related macular degeneration (AMD).
DVVRFLDWLRQV�EHWZHHQ�VSHFL¿F�GLHWDU\� DUH�WKH�PDLQ�PRGL¿DEOH�ULVN�IDFWRUV�



Cigarette smoking and nutrition are the main modifiable risk factors for AMD, which is the leading cause of irreversible vision impairment in developed nations.
“Given that diet is a modifiable risk factor for sight-threatening eye conditions such as AMD, optometrists have an opportunity to provide general advice about dietary patterns that can reduce the long-term risk of eye disease,” Downie shared.
Evidence supports the role of foods rich in antioxidants in limiting photoreceptor damage at the macula, while researchers have highlighted the anti-inflammatory and retinoprotective effects of omega-3 fatty acids.
Eating at least one portion of oily fish per week has been associated with a 50% reduction in the chance of developing wet AMD.
Turning to the use of nutritional supplements, Downie highlighted the importance of optometrists assessing the potential risks and benefits for each patient.

“Nutritional supplements are not intended to act as food substitutes as they cannot replicate the full spectrum of nutrients,” Downie said.
“Importantly, by definition, and unlike prescription medications, nutritional supplements are also not
She highlighted the value of wellconducted and up-to-date systematic reviews in considering the best current research on a topic.
Myopia management

There is an exciting question at the heart of myopia management. What if optometrists could bring the world of short-sighted children into focus, not solely through refractive correction, but through limiting the progression of myopia in the first place?
What if they could reduce the risk of generations of children developing eye disease in old age – at a time when ophthalmology departments across the globe will be grappling with the health burden of an ageing population?
A range of myopia management interventions are now gathering momentum, backed by multi-year trials and, in some cases, have gained regulatory approval.
However, without funding from the NHS, it is still up to patients to bear the cost of myopia management.
There are unanswered questions within the field. Not all children will respond to myopia management interventions and the research is still unclear on why that is.
Sharing her opinion when speaking with OT about MiSight 1 day contact lenses, Professor Nicola Logan highlighted that it makes sense to at least make people aware of an intervention that works in nine out of 10 patients.
“At a minimum, I think eye care practitioners should be speaking to children with myopia and their parents and saying there are interventions
“OPTOMETRISTS HAVE AN OPPORTUNITY TO PROVIDE GENERAL ADVICE ABOUT DIETARY PATTERNS THAT CAN REDUCE THE LONG-TERM RISK OF EYE DISEASE”
Dr Laura Downie
58 www.optometry.co.uk October/November 2022
THE EVIDENCE EDITION
available,” she said. “As a starting point, they can talk about behaviour and lifestyle changes that are likely to impact on myopia development and progression,” Logan shared with OT.
For example, research has found that an hour more of outdoor time each day can reduce a child’s chance of developing myopia by 45%.
In August, the College of Optometrists published updated guidance on myopia management.
The College states that optometrists can provide myopia management as long as it is within their scope of practice – meaning that the practitioner has the relevant knowledge and skills to provide this intervention acquired through training and experience.
The guidance summarises reasons for practitioners to consider myopia management – including the availability of effective management options and the link between myopia and developing eye conditions later in life. As with any form of therapeutic
intervention, optometrists should obtain informed consent in order to proceed with myopia management.
The importance of keeping upto-date with evidence about the effectiveness and safety of myopia management interventions is highlighted “as the evidence base is evolving at pace.”
Locum optometrist, AOP Councillor and Glasgow Caledonian University researcher and lecturer, Dr Stephanie Kearney, shared that the evidence shows that myopia management contact lenses and spectacle lenses can reduce myopia progression on average by approximately 50–60%. “However, some children will continue to progress, and it is unclear why some children respond better to treatment than others.”
Kearney noted that myopia management interventions are welltolerated and safe to use.
“In fact, there is better contact lens compliance in children than in adults resulting in lower rates of infection,” Kearney highlighted. Conundrums

Myopia management is an exciting area for the profession. Practitioners need to be mindful about the limits of the current evidence base, and be careful not to overstate the potential benefits. Some of the interventions which are currently available may involve a significant investment of time and money, with no guarantee that the intervention will work for the child. Therefore, it’s important that parents have enough information to make an informed decision about whether to proceed with treatment.
NUTRITION: COCHRANE SYSTEMATIC REVIEWS


Antioxidant supplements for slowing the progression of AMD: bit.ly/3dPhEpH

Omega-3 and omega-6 polyunsaturated fatty acids for treating dry eye disease: bit.ly/3AMcCDq
Vitamin A and fish oil for preventing the progression of retinitis pigmentosa: bit.ly/3PLOVPX
facing optometrists who have introduced myopia management in practice include when to stop treatment and what to do if progression continues.
Kearney believes that optometrists should be discussing the likelihood of myopia progression with patients and parents, increased disease risk and the available management options.
If a practice does not offer myopia management, in Kearney’s view optometrists should become familiar with practices that do so that
When discussing myopia management with patients and their parents or guardians, we recommend covering the following key points:
1 Myopia is becoming more prevalent and is associated with an increased risk of ocular complications in later life

THE AOP PERSPECTIVE


Head of clinical and regulatory, Henry Leonard, shares his thoughts on myopia management
When practitioners identify a child who is at high risk of myopia progression, they should be able to discuss the key points, and it’s good practice to record that this discussion has taken place. There is no obligation to offer myopia interventions, but where this is offered, practitioners should explain the current evidence base for intervention.

Spending time outdoors and reduced frequency of near work are known to be effective against the development of myopia
3 Specially designed spectacle and contact lenses have been shown to reduce axial length progression, but it’s not currently possible to: accurately predict which children will benefit from these interventions; or know how effective the intervention will be; or
conclude that reducing axial length will reduce the risk of ocular complications later in life.

4 Low dose atropine for myopia management is currently not licensed in the UK but may become a new treatment in the future.
 Dr Stephanie Kearney management
Dr Stephanie Kearney management
www.optometry.co.uk 59
DIGITAL DANGERS
1
Evidence shows patients are likely to present less frequently for aftercare visits, increasing the risk of undetected adverse ocular reactions
2Epidemiological studies demonstrate an increased risk of microbial keratitis

3
Internet vendors may substitute the prescribed lenses with brands that they have available and believe to be equivalent, despite the fact that true equivalence is rarely possible, often leading to compromised vision, comfort and ocular health

4

Patients may purchase lenses with incorrect specifications (for example, based on spectacle prescription uncorrected for vertex distance).


based
patients still have the option of receiving treatment. For practices that are offering myopia management, Kearney noted that subjective refraction can be variable and may not best suited for capturing the incremental effect of an intervention.
“There is a strong case that axial length should be measured. This noninvasive measurement is much more accurate and more directly correlates with disease risk,” she said.

Kearney shared that measuring axial length gives her confidence when deciding if a myopia management intervention is successful.
Turning to the future of myopia management, Kearney observed that in the near future low dose atropine may become available in the UK – offering hope to children who do not respond
paid for by parents until further UHVHDUFK�H[SORULQJ�WKH�FRVW�H╬HFWLYHQHVV�




to optical treatments. “For now, treatments will continue to be privately paid for by parents until further research exploring the cost effectiveness of treatment can be completed which can then be used to decide if public health funding could be considered,” she said.
refer to another local practice offering the service.
“As this is an evolving area of practice it is likely that guidance will change regularly and it is important practitioners stay up to date,” he concluded.
Visual stress and dyslexia
WKRVH�ZKR�FDQ�D╬RUG�WR�SD\�IRU�
Clinical and professional director at the AOP, Dr Peter Hampson, highlighted that currently only those who can afford to pay for treatment have the opportunity to see if myopia management will work for their children.
“If as a profession we are serious about reducing the potential future pathology risk, then we have to find a way to make it accessible to all who may benefit. To do that the evidence for how well it works has to be beyond challenge so that we can make the case that this should be NHS funded. It is therefore of the utmost importance that we proceed cautiously and continue to build the evidence base,” he said.
SDWKRORJ\�ULVN��WKHQ�ZH�KDYH�WR�¿QG� PD\�EHQH¿W��7R�GR�WKDW�WKH�HYLGHQFH�

Tasks that many complete without a second thought can present daily hurdles for those with dyslexia. From deciphering menus, to taking a telephone message and writing a shopping list, the written world can be challenging to navigate.
Professor Bruce Evans shared with OT that the evidence suggests around one in five people with dyslexia may also experience visual stress.

Visual stress is characterised by experiencing symptoms when viewing certain stimuli, particularly text.
Hampson added that while the College guidance recommends that optometrists should have the ability to explain myopia management options, the guidance does not go as far as placing an obligation on practitioners to discuss myopia management with potential candidates for treatment.
It also does not require practices that do not provide myopia management to
“The symptoms are often alleviated by individually prescribed coloured filters,” he shared.
There have been controversies within the field of visual stress. Evans highlighted that some people assume treating visual stress is capable of acting as a “cure” for dyslexia.
“Dyslexia is multi-factorial and only in some cases does visual stress seem to contribute to reading difficulties.”
EXAMPLES OF MISLEADING STATEMENTS
“Vision therapy treats dyslexia”
“We specialise in visual dyslexia”
“We treat dyslexia”
“Book a dyslexia test”
Source: Bruce Evans and Arnold Wilkins, Guidance for eye care professionals on publicity concerning dyslexia, visual stress, and related conditions
Professor James Wolffsohn assesses the evidence on risks associated with the online purchase of contact lenses
“Coloured filters are proven as a treatment for visual stress”
60 www.optometry.co.uk October/November 2022
1 Some people experience symptoms of visual perceptual distortions and eyestrain when viewing text, and this is often described as ‘visual stress’. Symptoms of visual stress include words appearing to move around or merge together
Alongside Professor Arnold Wilkins, Evans has authored the book, Vision, Reading Difficulties and Visual Stress, which provides an overview of the relevance of visual factors for those who struggle with reading.
A publicly available appendix (bit.ly/3CDE2Nn) provides guidance for eye care professionals on publicity. Evans shared that a 2017 study suggested diagnostic criteria for visual stress that may help to avoid overdiagnosing the condition.
Patients should have at least three of the following six typical symptoms: words move, words merge, patterns or shadows in the text, text seems to stand out in three dimensions above the page, words or letters fade or darken and discomfort with certain artificial lights.
As well as the above, the patient should meet two of the following three signs from investigations: the patient voluntarily uses an overlay for three months or more, the overlay improves performance on the Wilkins Rate of Reading Test and the patient has a Pattern Glare Test score of greater than three with mid-spatial frequency grating.
The online sale of contact lenses

As reliably as pumpkins are carved and the silhouettes of bats appear in windows, each October eye care

when reading, patterns or shadows appearing within a block of text and a strong aversion to striped patterns
THE AOP PERSPECTIVE
Head of clinical and regulatory, Henry Leonard, highlights the need for caution following practice complaints about dyslexia and visual stress advertising
The latest estimates are that visual stress is present in around 1 in 5 people with dyslexia, but although they may co-exist, visual stress and dyslexia are different conditions
3 Some people who suffer from visual stress find that their symptoms are alleviated by coloured filters, either in the form of coloured overlays or tinted lenses. Coloured filters are normally only considered once a sight test has been performed, and any other potential causes of visual difficulty have been addressed.

professionals urge caution when purchasing contact lenses online.
Aside from the potentially frightening consequences of a lastminute addition to a spooky costume, there are broader risks around the online sale of contact lenses.
Contact lenses purchased online may fall short of UK regulatory standards, while missing out on the guidance of an eye care professional can lead to risky contact lens behaviour.
The British Contact Lens Association’s Contact Lens Evidencebased Academic Report (CLEAR), published in 2021, notes that more than 19,000 peer reviewed academic papers on contact lenses have been published.
The report identified that the frequency of eye examinations is lower among individuals who purchase lenses exclusively online. Professor James Wolffsohn, of Aston University, highlighted that the evidence suggests among some demographics there are growing numbers of “self-taught” contact lens wearers, who may be at risk of non-compliance and poor practices. “Unregulated purchasing behaviour of contact lenses is associated with ocular complications such as a higher rate of infection and microbial keratitis,” he shared.
Wolffsohn highlighted that a contact lens fit cannot be predicted by lens parameters alone. “Assessment of a lens on eye by a registered eye care

professional before prescribing is essential,” he emphasised, adding that poor fitting lenses are associated with contact lens complications and dryness symptoms.
Professor Nathan Efron, of the Queensland University of Technology, shared that in his view contact lenses should never be purchased over the internet.
“Contact lenses should be prescribed, fitted and assessed by a qualified eye care practitioner in a clinic equipped with all the necessary instrumentation to undertake proper clinical oversight.”
However, Efron added that patients should be permitted to request contact lenses from their personal eye care provider either through the internet or by telephone. Efron conceded that there are both conceptual and technical challenges in regulating the online sale of contact lenses.
“The conceptual challenge is finding a balance between allowing the public to purchase contact lenses from the vendor of their choice, versus the imperative of protecting the ocular wellbeing of the public by ensuring that contact lenses can only be purchased with proper oversight by a registered ophthalmic practitioner,” he shared.
Technical challenges centre around implementing an effective, but not overly-onerous, mechanism of implementing the oversight of contact lens sales.
A number of optometry practices have recently received complaints regarding information they’ve published on their websites on the topic of visual stress and dyslexia. We recommend removing any references to diagnosing or treating specific learning difficulties such as dyslexia, but it would be reasonable to make the following points:
October/November 2022 www.optometry.co.uk 61 THE EVIDENCE EDITION
“This would mean only providing a new supply of contact lenses according to a prescription from a registered provider, but also providing a resupply of the same lens type with proper professional oversight,” Efron said.
“Then there are questions about exactly what needs to be specified in the prescription and designating appropriate expiry limits on the validity of the prescription,” he observed.
Happiness at work
We all want to start our working day with a spring in our step.
But what does the evidence say about how to achieve workplace satisfaction?
The latest Registrant Workforce and Perceptions Survey by the General Optical Council (GOC) found that 62% of optometrists and dispensing opticians were happy in their roles.
Professor Laurie Santos is a Yale University psychology professor and host of The Happiness Lab (bit.ly/3q08byA) where she examines the scientific evidence on happiness.
Santos shared with OT that the concept of job crafting, pioneered by Professor Amy Wrzesniewski, can help to boost job satisfaction.
In order to find out what factors contribute to meaningful work, Wrzesniewski carried out interviews with a group of janitorial staff at a US hospital. The cleaning staff who had the most satisfaction in their jobs expanded their job description beyond cleaning and saw themselves as playing an integral role in patient care.
For example, one cleaner would talk to patients who had not received visitors while another rearranged pictures in the rooms of comatose patients in the hope that it would have a positive effect.
“If you want to job craft as an optometrist, ask what you value, what strengths you have and consider the ways that you light up when you are doing certain things. Can you infuse that more into your work?” she shared.
Although it may be tempting to think that an increase in salary would boost job happiness, the evidence does not always support this assumption. Research carried out in 2009 found
SpaMedica patient coordinator, Julie Trowell, knits intricate squares to ease the worries of patients waiting for eye clinic appointments. She talks with OT about the motivating power of making a difference

Since November last year, Julie Trowell has created more than 20 knitted squares with intricate designs in her spare time.
The Romford-based SpaMedica patient coordinator started making the miniature works of art – which she has dubbed ‘twiddle squares’ – for anxious patients and those with dementia who come through the waiting room and may have restless hands.
Before she picks up her knitting needles, Trowell imagines a design that may bring a sense of familiarity and comfort to patients – often using vintage materials.
There are squares with rows of carrots and flowers for gardeners, a design with a ballgown for an 87-year-old patient who talks of her dancing days and a beach scene for a colleague whose grandmother

that once an individual is on a salary of $75,000 USD (£47,000 at the contemporary exchange rate), even if their salary is doubled or tripled there is not a significant improvement in positive emotions – or decrease in negative emotions.
“The connection between money and happiness is a complicated one. Money does equal happiness if you are not making very much money – if you are living below the poverty line or you are not making a decent middle-class income,” Santos shared.
can no longer remember her name but recalls family trips to the seaside. Each square takes a weekend to finish and is individually wrapped for patients to take home with them after their appointment.
“Every one of them is made with love, thought and care. Every time you are able to go the extra mile, your job satisfaction increases. I go home knowing I have made a difference to somebody’s day,” Trowell told OT.
Alongside the twiddle squares, Trowell has made more than 100 sets of worry beads which are available for any patient attending the clinic.

She noted that often patients will bring the worry beads back into the clinic when they have their second cataract operation.
“I would do anything for our patients. I would sit up until midnight making them because you can see what a difference it does make. You see them calm down. When they come out, they say, ‘It wasn’t as bad as I thought’,” Trowell shared.
“However, the evidence suggests that for many on middle class or upper middle class salaries, getting more money isn’t necessarily going to help you become happier,” she highlighted.
“My guess is that for many optometrists, increasing their salary isn’t necessarily going to bring happiness,” Santos added.
She shared that there is evidence to suggest that there are certain behaviours and mindsets that can help to boost happiness. “One of the biggest ones is social connection. Simply the act
“EVERY TIME YOU GO THE EXTRA MILE, YOUR JOB SATISFACTION INCREASES”
62 www.optometry.co.uk October/November 2022
AOP HEALTH AND WELLBEING RESOURCES
The AOP provides information to aid health and wellbeing in the optical profession, including access to support services that are available to members and the wider profession. Visit: www.aop.org. uk/wellbeing
of engaging with other people tends to make us happier over time,” she said.
“There’s also evidence that being nice to people can improve our happiness – either reframing the kinds of things that you are doing right now to help people, or to focus more on helping people generally can improve your happiness,” Santos observed.
Lastly, Santos emphasised the importance of gratitude. “A mindset of gratitude, being thankful for the things you have, can improve your happiness,” she said.
Turning to the issue of burnout, Santos noted that the term can be used flippantly in modern society.
¡LSSDQWO\�LQ�PRGHUQ�VRFLHW\��

DV�D�VSHFL¿F�FOLQLFDO�V\QGURPH�WKDW�

H╬HFWLYHQHVV��
Psychologists characterise burnout as a specific clinical syndrome that involves three features: emotional exhaustion, depersonalisation/ cynicism and a lack of personal effectiveness.

“Even after a good night’s sleep you still feel exhausted,” she shared.

“You feel like you are at your wit’s end all the time and you are constantly frustrated with the people around you,” Santos said.
The GOC survey revealed that close to one in ten optometrists and dispensing opticians (9%) had taken a leave of absence due to stress.
Santos emphasised that once someone is experiencing burnout “this is a time where simple hacks don’t help that much.”
“You really need to take a good hard look at your job and how you are interacting with your work to see if you can make some big changes. That can include taking time off, but
it can also include restructuring your relationship with your job – making sure that you prioritise other areas of your life in addition to your work,” she highlighted.
Racial bias within eye care



Ophthalmology registrar and research fellow at King’s College London, Dr Varo Kirthi, is passionate about the need for clinicians to recognise the impact of unconscious bias within healthcare.
“Optometrists will be seeing people walk in off the High Street from a variety of different backgrounds. The only way of reducing bias is to talk about it,” he emphasised.
“If you see people being treated differently, it is important to challenge that,” Kirthi highlighted.
Kirthi explored the impact of racial bias in a 2020 study of patients attending King’s College Hospital NHS Foundation Trust. Kirthi and colleagues described how black patients faced
TACKLING RACIAL BIAS IN PHARMACY AND MEDICINE
The General Medical Council and General Pharmaceutical Council are working to reduce disparities in professional conduct investigations
Racial bias within professional conduct proceedings is an issue that is not restricted to optometry, but evident across a range of healthcare professions.
Within the UK, BAME doctors are more than twice as likely to be referred to the General Medical Council (GMC) than white doctors.
GMC director of fitness to practise, Anthony Omo, shared that the regulator is committed to eliminating disproportionality related to ethnicity and place of qualification in fitness to practise referrals by 2026. The regulator also aims to eliminate differences in key measures of fairness in medical education and training by 2031.
“We’re working with employers and training bodies to make the health service a supportive and inclusive environment, which will be better equipped to train, attract and retain the doctors we already have, as the UK continues its postpandemic recovery,” Omo shared.
Asian and British Asian pharmacists account for 55% of concerns received by the General Pharmaceutical Council (GPhC), despite comprising
39% of registered professionals. In comparison, White pharmacists accounted for 26% of concerns received, while making up 40% of the register.
In meeting papers published in July 2022, the GPhC highlighted that there is a disproportionality in concerns received when compared to the profile of the register. “We want to understand the underlying issues and contributory factors that result in the disproportionate concerns we receive, and to identify what we can do about this and where we can work with others to make a difference.”
The GPhC has carried out anti-Semitism training and is planning to hold further sessions on Islamophobia for members of its statutory committees. From October 2022, information relating to a pharmacist’s ethnicity – including their name, place of birth, religion and university – will be redacted in the information presented to the investigating committee.
The project will be assessed on a monthly basis with a more comprehensive review after six months.
October/November 2022 www.optometry.co.uk 63
THE EVIDENCE EDITION
treatment delays for diabetic eye disease when compared with white counterparts.



Despite having a similar burden of disease at the point of referral, the time to treatment following a face-to-face consultation was significantly longer for black patients than white patients.
In his Eye article, Black eyes matter –do we treat Black patients differently in ophthalmology?, Kirthi highlighted that clinicians know how to identify bias when appraising research.
“Uncomfortable as it may be, current data suggest that we may also need to look for bias in our clinics. Addressing these difficult issues is the key to narrowing the inequity of care affecting those most in need of it,” he said.
Racial bias within healthcare is an issue that affects clinicians as well as patients.
Within fitness to practise proceedings specifically, non-White healthcare professionals across a range of disciplines face a higher rate of professional conduct investigations than their White peers.
In 2020, the GOC reported that nonWhite optometrists and dispensing opticians were 1.7 times more likely to be subject to a fitness to practise investigation than White registrants.
Despite comprising 41% of registrants, non-White optometrists and dispensing opticians accounted for more than half (52%) of fitness to practise investigations.
The most recent monitoring report in 2021 revealed that this level of disparity has narrowed – with non-White registrants accounting for 39% of fitness to practise proceedings, broadly in line with their registrant profile of 37%.
Once an optometrist or dispensing optician is subject to fitness to practise proceedings, there are also racial differences in whether the case progresses to committee stage. The 2021 monitoring report revealed that a higher rate (36.1%) of Asian and British Asian registrants are referred to
a fitness to practise committee when compared to cases involving White registrants (28.5%).


Conduct allegations are more frequently made against Asian or British Asian registrants, while clinical allegations are more frequently made against white registrants.
In 2021, 58% of allegations against white registrants were clinical and 31% related to conduct compared to 35% and 44% respectively for Asian and British Asian registrants.
A GOC spokesperson highlighted that the overall numbers involved in fitness to practise proceedings are very low. More than one in 10 registrants (14%) elected not to provide information on their ethnicity, meaning that the data may not reflect the actual split.
The regulator’s fitness to practise improvement programme for 2022 to 2025 contains a workstream to develop and implement guidance for decision-makers in recognising and addressing potential bias. The GOC also plans to commission research into the impact of its fitness to practise processes on different registrant groups.
Dry eye







For optometrist and dry eye specialist, Sarah Farrant, the publication of the Tear Film & Ocular Surface Society’s DEWS reports in 2007 and 2017 were milestone moments.

For the first time, an international panel of dry eye experts outlined definitions of dry eye disease. “Prior to that there was no universal definition of dry eye disease,” Farrant explained.


“That was a problem in academia because there was no standardised model to base the research on. You couldn’t easily compare data,” she said.
Farrant sees this definition as making progress towards debunking a common misconception about dry eye disease – that it is a minor inconvenience or an inevitable part
of ageing. “It’s not a normal state for the eye. We are now recognising that it is a genuine problem that we can’t ignore,” Farrant shared.
Alongside setting out the parameters of the condition, the DEWS II report (bit.ly/3R1Z3FG) can assist practitioners in taking an evidencebased approach to managing the condition in practice.
Experts assessed the available evidence on dry eye to inform a clear stage-based approach to treating the condition in practice.
TFOS is now finalising a new report, due to be published in 2023, that explores the wider context of how lifestyle factors are influencing key drivers of dry eye disease.
For example, air conditioned offices, reduced blink rates while working on screens and cosmetic use can all affect the development of dry eye disease.
“Our new TFOS report is called the ‘lifestyle epidemic’,” Farrant shared.
“There are many factors in our modern lifestyles that are either a direct or indirect cause of dry eye.”
BYE, BYE BABY (SHAMPOO)

Sarah Farrant shares her biggest gripe when it comes to the evidence-based management of dry eye disease
My biggest bugbear is the legacy of using baby shampoo for blepharitis. Some ophthalmologists, optometrists and GPs still recommend it. It is counter-productive. For years and years, we have known that commercial products are much better. Because baby shampoo is a surfactant, it breaks down the lipid layer of the tears. In applying soap to your eyelids, you get spill over into the ocular surface, which completely disrupts the quality of the tear film.
“THE ONLY WAY OF REDUCING BIAS IS TO TALK ABOUT IT”
Dr Varo Kirthi
64 www.optometry.co.uk October/November 2022
THE EVIDENCE EDITION
GH¿QLWLRQV�RI�GU\�H\H�GLVHDVH��¥3ULRU�WR�
CPD
IN THIS ISSUE
ADVERSE EFFECTS OF PERIOCULAR AESTHETIC TREATMENTS 66
C-102937
LEARNING OUTCOMES
Practitioners will be able to advise patients about adverse effects of periocular aesthetic treatments
Practitioners will be aware of the adverse effects and management of periocular aesthetic treatments.
HOW HEADSMART ARE YOU?
C-102919
LEARNING OUTCOMES
Practitioners will be able to elicit relevant detail from patients with brain tumours
Practitioners will be aware of the signs and symptoms of brain tumours in children.
REMEMBER TO UPLOAD YOUR CPD POINTS TO YOUR MYGOC
KERATOCONUS: CONSIDERATIONS, RECOGNITION AND MANAGEMENT WITH SPECIALTY CONTACT LENSES 80

C-103337
LEARNING OUTCOMES
Practitioners will be able to advise patients about contact lens options for keratoconus
Practitioners will be aware of the signs of keratoconus and be updated on contact lens management options.
COMMUNICATION IN OPTOMETRY 77
MYOPIA MANAGEMENT IN CLINICAL PRACTICE 86
C-102792
LEARNING OUTCOME
Practitioners will broaden their understanding of the implications and management of myopia.
C-102978
LEARNING OUTCOMES
Practitioners will learn strategies for communicating effectively with patients
Practitioners will learn strategies for communicating with colleagues to enable effective collaboration.
RETINAL CASES OF VISUAL LOSS 88
C-102771
LEARNING OUTCOME
Practitioners will be able to interpret a range of retinal images.
EXAM QUESTIONS, REFERENCES & DECLARING CPD POINTS
MCQs for OT’s CPD appear online at www. optometry.co.uk/CPD. Exams in this issue will be live from 8 October to 28 December, 2022. When taking an exam, the MCQs may require practitioners to apply knowledge that has not been covered in the related
CPD article. Visit www.optometry.co.uk/CPD, and click on ‘Related CPD article’ to view the article and accompanying references in full. In the new CPD cycle, registrants are responsible for declaring their CPD points viatheir MyGOC account (www.optical.org).
If you pass an exam with OT, you will receive a certificate to use as evidence when declaring your CPD points. Certificates will be available to download in your MyAOP.
ONLINE FROM 8 OCTOBER 2022
CPD
73
October/November 2022 www.optometry.co.uk 65
ADVERSE EFFECTS OF PERIOCULAR AESTHETIC TREATMENTS
IN BRIEF This article summarises the current literature on ophthalmic complications of the most common types of periocular aesthetic treatments.

INTRODUCTION
The popularity and variety of temporary and permanent periocular aesthetic treatments has increased over the past decade. The majority of these treatments are self-administered or performed in salons by aesthetic practitioners with no medical training. Patients may subsequently present to optometrists and ophthalmologists with the ophthalmic sequelae of these treatments. A careful history and examination are essential as many patients are embarrassed to disclose these treatments or do not feel they are relevant to their eye condition.
Early recognition of the ophthalmic sequelae of periocular cosmetics and aesthetic procedures will raise patient awareness, avoid long-term ocular discomfort and, in sight threatening cases, allow treatment to be initiated urgently. This review reports the ophthalmic complications of the most common periocular cosmetics and aesthetic treatments.
THE EFFECT OF COSMETICS ON THE OCULAR SURFACE AND THE NASOLACRIMAL SYSTEM
Cosmetics have been used since prehistoric times by people of all cultures to highlight eyes in order to enhance beauty and attractiveness. Kohl, an eyeliner commonly used in Asia and the Middle East, has been associated with heavy metal toxicity and migration of pigment to the conjunctiva and lacrimal system.1
Cosmetics more commonly used in the US and Europe, for example, eyeliner, mascara and eye shadow, are stringently regulated by the Food and Drug Administration (FDA) in the US and by European Union (EU) law. Despite this, these cosmetics may also adversely affect the ocular surface.
Migration of cosmetics from the periocular skin and eyelid margin onto the ocular surface is the main cause of cosmetic associated ocular surface disease. It causes blockage of meibomian glands and destabilisation of the tear film lipid layer, predisposing the user to evaporative dry eye disease. Migration is dependent on cosmetic viscosity and hydrophilicity, and blink
POINTS
frequency. Application of cosmetics to the posterior lid margin, concurrent topical eye drop use and eyelid rubbing may exacerbate the rate of migration.2-6
Ocular surface inflammation is a second mechanism that predisposes the individual to evaporative dry eye disease and generalised ocular discomfort. Accumulation of hydrophilic constituents of cosmetics within the aqueous and mucin layers of the tear film is thought to increase tear film osmolarity and mediate ocular surface inflammation.6 Use of cosmetics contaminated with microbes may also induce ocular surface inflammation.7,8 Inflammatory mediators within the tear film lead to conjunctival goblet cell loss and disruption to the mucin layer of the tear film, which can lead to ocular surface epithelial damage and drive further inflammation.
Allergy is a third mechanism that leads to cosmetic associated ocular surface disease. Periocular cosmetics and eye make-up removers contain a variety of chemicals, including fragrances, pigments and pearlescent additives. Any of these chemicals may induce allergic contact dermatitis and allergic conjunctivitis, leading to ocular inflammation and tear film instability.9 Preservatives in periocular cosmetics, including chlorhexidine, benzalkonium chloride and
Sonali Nagendran FRCOphth, Mohammad Javed Ali MD, PhD, FRCS, Murat Dogru MD, PhD and Raman Malhotra FRCOphth
Figure 1 Kohl deposits in the lacrimal sac of a long-term kohl user who developed nasolacrimal duct obstruction
66 www.optometry.co.uk October/November 2022
2 CPD
formaldehyde, have been demonstrated to have a toxic effect on corneal epithelial, conjunctival epithelial and meibomian gland cells. Benzalkonium chloride is known to destabilise the lipid layer of the tear film and has been associated with dry eye symptoms and a reduced tear break up time in vivo 10
Cosmetics have also been linked to nasolacrimal disorders. Mascara-laden casts within the canaliculus and lacrimal sac cause physical obstructions to the lacrimal drainage system.11-13 Other cosmetic pigments, particularly kohl, contain ingredients such as carbon, as well as heavy metals such as lead, silver and iron, which have been linked to inflammation and fibrosis within the nasolacrimal system, leading to stenosis and obstruction.14 Figure 1 demonstrates kohl deposits in the lacrimal sac of a long-term kohl user who developed nasolacrimal duct obstruction.
PROSTAGLANDIN SERUMS FOR EYELASH ENHANCEMENT
Hypertrichosis is a well reported side effect of topical prostaglandin analogues used in glaucoma treatment, with lashes becoming measurably longer, thicker and more pigmented. Occasionally this may lead to eyelash ptosis and growth of vellus hair on the eyelids. The mechanism of action is unclear, but one hypothesis is that prostaglandins may trigger the anagen phase (growth phase) in the telogen phase (resting state) in hair follicles or prolong the anagen phase.15-21
Long, thick, dark eyelashes are regarded as a beauty asset in many cultures and prostaglandin eyelash serums have become increasingly popular as a cosmetic aid. Currently there is only one FDAapproved prostaglandin eyelash serum, containing bimatoprost 0.03% (Latisse, Allergan). The majority of studies have documented the outcomes of bimatopost eyelash serum for chemotherapy-induced or idiopathic hypotrichosis. Reported side effects are similar to those reported for bimatopost glaucoma treatment, including conjunctival hyperaemia, punctate keratitis, eyelid erythema and pruritus, skin hyperpigmentation and hypertrichosis of vellus eyelid hairs. Eyelid hyperpigmentation and hypertrichosis of vellus eyelid hairs is related to the extent of skin contact with bimatoprost.22-24 Skin hyperpigmentation has been noted to develop at a faster rate with bimatoprost eyelash serum compared to bimatoprost glaucoma treatment, possibly due to greater contact with the eyelid skin.25
Others have documented the side effects of eyelash serum containing other prostaglandin analogues. Few side effects have been reported with the use of eyelash serum containing latanoprost, 15-keto fluprostenol isopropyl ester, 15-keto fluprostenol or dechloro-ethylcloprostenolamide.26-28 Skin hyperpigmentation has been noted with eyelash serum containing travoprost or isopropyl cloprostenate.29,30 Prostaglandin glaucoma drops are associated with periorbital volume loss. Prostaglandin eyelash serums containing a variety of different prostaglandins also demonstrated evidence of volume loss in one study which examined before and after photographs on company websites marketing these products.31
Following the success of bimatoprost eyelash serum, prostaglandin serum has also been trialled for eyebrow hypotrichosis, with no cases of skin hyperpigmentation or serious adverse effects reported so far.32,33
EYELASH AND EYEBROW DYE
Eyelash and eyebrow tints and dyes are a popular cosmetic treatment saving time and money on mascara and eyebrow pencil. Eyelash and eyebrow dye is not approved for use in the US but is approved in Europe, providing the dye is applied by professionals and appropriate counselling is offered. The main complication of eyelash and eyebrow dye is an allergy to one or more constituents; this commonly results in contact dermatitis, a type 4 hypersensitivity reaction that usually presents with eyelid swelling, eyelid oedema and allergic blepharoconjunctivitis. Contact dermatitis may develop many days after application, and as such, the link between eyelash or eyebrow dye and contact dermatitis may be overlooked.34-36
The most common allergen in eyelash dye is p-phenylenediamine (PPD), although toluene-2,5diamine and chloro-PPD have also been implicated. In addition, a wide range of different cleansers, lotions, and oils are used as part of the treatment, all of which may cause allergic reactions themselves.37,38 PPD sensitivity should not only be considered in cosmetic users, but also in hairdressers or beauticians who present with periocular contact dermatitis.39 Other reported complications of eyelash dye include loss of eyelashes and xanthelasma.40,41 Corneal argyria (silver deposition in Descemet’s membrane layer) may develop in patients self-applying eyelash dyes containing aqueous silver lactate.42
PATHOLOGY October/November 2022 www.optometry.co.uk 67
EYELASH EXTENSIONS
False eyelashes and eyelash extensions can give the appearance of longer, thicker eyelashes, saving time and money on mascara.
False lashes can be applied at home, glued just above the natural lash line. Eyelash extensions involve glueing a variable number of individual false lashes to each existing lash, a longer lasting, but more technically demanding technique that is usually performed in a salon.
The main reported complication of false eyelashes and eyelash extensions is an allergic reaction to the glue used for eyelash application.43-45

Contact dermatitis may only develop days later so the link between eyelash application and contact dermatitis may be overlooked. Components of glue that may be potential allergens include cyanoacrylate, formaldehyde, latex, ammonia and lead. Glue takes five to six hours to solidify, and migration of glue into the eye or release of vapours from the glue over this period may affect the ocular surface, resulting in allergic blepharoconjunctivitis and keratitis.
Eyelash extension removal gel also contains potential allergens, and results in the release of formaldehyde as the cyanoacrylate in the glue dissolves, in one case resulting in chemical conjunctivitis and diffuse lamellar keratitis.46
Other reported complications include accidental glueing eyelids shut, which may occur when applying false eyelashes, but has also occurred in children finding and playing with eyelash glue.47 There are also reports of bacterial keratitis arising from solidified eyelash glue at the lid margin scraping against the ocular surface, nylon fibres from eyelash extensions migrating subconjunctivally and eyelash extensions being set alight during a minor oculoplastic operation.48-50
COSMETIC TATTOOS
Eyeliner and eyebrow tattoos are a popular option for people who wish to save time and money on make-up and for those who have disabilities preventing makeup application. Permanent pigment is applied above the lash line to replicate the effects of eyeliner and, if correctly placed at the junction of the papillary and reticulated dermis, it sequesters within macrophages that have minimal migration, resulting in clinical stability of pigment deposition. Eyebrow tattoos traditionally involved injecting pigment into the dermis to produce a solid block shape. However, microblading, where tattoo pigment is deposited into the epidermis via cuts shaped to mimic eyebrow hair to give a more natural appearance, has gained in popularity. Complications of eyelid and eyebrow tattooing may be due to poor injection technique, allergy or disruption to adnexal structures and the ocular surface.
Poor injection technique may lead to pigment fanning beyond its intended location. Injection of pigment into deep dermis, orbicularis, tarsus or into macerated tissue is difficult to treat because of migration of pigment along deep tissue planes.51
Treatment of small areas of pigment fanning includes bleaching pigment via alcohol injections, tattooing a lighter pigment over the darker pigment, or using Q-switched Nd-YAG laser to break down pigment particles. Larger areas of pigment fanning may require surgical excision. Pigment fanning in eyebrow tattoos is more complex to treat than eyelid tattoos due to the combination of pigments used to mimic hair and skin colour and the need to preserve eyebrow hair.52-54
Injection of pigment into or too close to the mucocutaneous junction may lead to eyelash loss, eyelid margin necrosis and entropion. It may also result in continuous pigment shedding onto the ocular surface and loss of meibomian gland function, leading to tear film instability and ocular surface disease (see Figure 2).51,55,56
Full thickness penetration of the eyelid with the tattoo needle and accidental tattooing of the conjunctiva and cornea have been reported, fortunately without visual loss or globe rupture. These cases emphasise the need for the procedure to be performed using a protective corneal shield.57-59
Constituents of tattoo inks are classed as cosmetics and are not regulated by the FDA or EU. Inks may contain a variety of chemicals and heavy metals and allergy to these components may not be evident on patch testing, as deep dermal infiltration may be required to elicit a response.60 Allergy to tattoo ink in eyelid and eyebrow tattoos may present as delayed hypersensitivity reactions including contact dermatitis and cutaneous granulomas.60-64 There are several reports of cutaneous and systemic sarcoidosis
Figure 2 Illustrates a patient with severe meibomian gland dysfunction following cosmetic eyeliner tattoos
68 www.optometry.co.uk October/November 2022
presenting as granulomatous disease within eyelid and eyebrow tattoos, including one with associated intermediate uveitis. It is thought that chronic exposure of the immune system to the ink may precipitate the onset of sarcoidosis in genetically susceptible individuals.65-67 Hypopigmentation has also been reported as a delayed reaction to eyebrow and eyelid tattoos.68,69 There are also reports of localised cutaneous infections following eyebrow tattoos and, rarely, blood-borne infections.70
Cosmetic tattoo inks often contain heavy metals and there are a number of reports of magnetic resonance imaging (MRI) artifacts in the region of tattoos.71 Tattoos are not a contraindication to MRI scanning, but it is important to note that rarely, eyelid pain, swelling, erythema and first-degree burns have been reported in patients with eyelid tattoos undergoing MRI scans, even if the tattoo pigment does not contain iron.72
BOTULINUM TOXIN
Botulinum toxin, the exotoxin produced by the bacterium Clostridiumbotulinum, acts by inhibiting release of acetylcholine at the neuromuscular junction, resulting in temporary paralysis. Commonly used commercial preparations include onabotulinumtoxinA (Botox, Jeauveau), abobotulinumtoxinA (Dysport), incobotulinumtoxinA (Xeomin) and rimabotulinumtoxinB (Myobloc, Neurobloc). Studies have demonstrated similar efficacy among the different products.73 In an aesthetic setting, botulinum toxin is used to treat dynamic and static rhytids in the periocular region, primarily furrows arising from contraction of the frontalis, corrugator supercilii and glabellar muscles and lateral canthal ‘crow’s feet’. It has also been used to target brow depressors to reposition the brow and avoid the requirement for a surgical brow lift. Although the site and dose of botulinum toxin should be individualised, consensus recommendations have been published for its aesthetic use to reduce the risk of complications.74
There is little data in the literature specifically on the side effects of botulinum toxin administered for aesthetic purposes. Published data arises primarily from use in a medical setting, specifically to treat facial dystonia and periocular synkinesis secondary to facial nerve palsy. The most common side effects of botulinum toxin reported for essential blepharospasm are ptosis (13.4%), keratitis (4.1%), epiphora (3.5%), dry eyes (2.5%), facial weakness (0.9%) and lagophthalmos (3.0%).75
Spread of botulinum toxin beyond the target region is the main cause of side effects and complications, which can be avoided by injecting high concentration, low volume botulinum toxin into the target region.76 Botulinum toxin infiltrating through the orbital septum into the levator complex results in upper
eyelid ptosis. Botulinum toxin treatment for lateral canthal rhytids spreading inferiorly may result in partial lip ptosis.77

Botulinum toxin-induced orbicularis oculi chemodenervation, particularly in the lateral canthal region, may lead to incomplete blink, lagophthalmos, canthal laxity, lower eyelid retraction and even paralytic ectropion, with associated corneal exposure and evaporative dry eye disease.78-80 Spread of botulinum toxin from the lateral canthus and lateral brow region to the lacrimal gland disrupts parasympathetic innervation of the lacrimal gland and directly affects tear production, resulting in aqueous deficiency. Aesthetic use of botulinum toxin in the lateral canthal region is associated with clinical signs of aqueous deficiency such as reduced Schirmer measurements.78,81,82 However, botulinum toxin injections to the medial upper and lower eyelid have been shown to improve dry eye disease signs and symptoms. Paralysis of the medial orbicularis oculi muscle is thought to inhibit the function of the lacrimal pump, resulting in increased tear retention.83-85
Botulinum toxin has also been postulated to cause meibomian gland dysfunction and evaporative dry eye disease, although the evidence for this is limited. Chemodenervation of the pretarsal orbicularis oculi may impair secretion of the lipid layer component of tears from meibomian glands or disrupt the regulation of meibomian gland function via its effect on the parasympathetic nervous system.86
Figure 3 (Top) Patient with lower eyelid swelling secondary to hyaluronic filler; (middle) appearance immediately after dissolution with hyaluronidase; (bottom) appearance one-month after dissolution
PATHOLOGY October/November 2022 www.optometry.co.uk 69
TOPICAL ACETYL HEXAPEPTIDE
Acetyl hexapeptide (Argireline, Lipotec Group) is a synthetic peptide that acts as a competitive SNAP-25 inhibitor, inhibiting the release of acetylcholine at the neuromuscular junction and temporarily paralysing superficial facial muscles. It has been developed as a topical version of botulinum toxin, and compared to botulinum toxin A, the potency of Argireline with respect to inhibition of neurotransmitter release is lower but its acute toxicity is also less.87 A number of different formulations of Argireline are available, and as it is considered a cosmetic product rather than a drug, it is not regulated by the FDA.
Two studies compared the effect of topical Argireline to placebo over four weeks on periorbital rhytids in Chinese and American subjects. They used subjective measures (Daniell’s classification, Seeman’s standard) and objective measures (confocal microscopy of silicone replicas of periorbital skin before and after treatment). They demonstrated a greater improvement in subjective and objective measures of rhytids in the topical Argireline group (48.9% improvement compared to 10% improvement in the placebo).87-89
Another study demonstrated that, compared to placebo, topical Argireline applied to periorbital skin increased the time period between botulinum toxin injections in patients with blepharospasm compared to placebo (average 3.7 months compared to 3.0 months).90 No adverse effects have been reported, and although evidence is limited, Argireline may be considered a safer, if less effective, treatment option for periorbital rhytids.
PERIOCULAR FILLERS
Periocular fillers are increasingly used for facial rejuvenation in the periocular region to compensate for loss of periocular volume in the ageing face. In the US and Europe, fillers are regulated as medical devices. In many countries, including the UK, injections do not need to be performed by a medical practitioner if a prescription has been issued for the product.
Hyaluronic fillers are the most popular formulations used for the periocular region as they have a good safety profile and the advantage of being reversed using hyaluronidase if required. A variety of
hyaluronic filler formulations are available, based on source derivation, crosslinking, particle size and longevity. Other types of permanent and semipermanent fillers, for example, calcium hydroxyapatite and polyacrylamide, have greater longevity but they are not reversible, not suitable for the treatment of fine lines and may migrate over time.
Filler complications can be classified according to time of onset: immediate (within 24 hours); early onset (within four weeks); and delayed onset (more than four weeks). Complications may also be classified according to severity and whether they are ischaemic or non-ischaemic.91-96
Immediate and early-onset complications
Injectionsitereactions
Post-procedure erythema, swelling and bruising is common, usually transient and more evident in the periocular region due to thinner skin; this can be minimised by good injection technique, minimising the use of anticoagulant drugs and supplements, applying cold compresses before and after the procedure, and avoiding strenuous exercise post procedure.92
Earlyhypersensitivityreactions
Type 1 hypersensitivity reactions to fillers are rare and characterised by the development of localised or generalised facial oedema, erythema and itching within a few hours of the injection. Patients should be treated with antihistamines and monitored, as emergency anaphylaxis treatment is warranted if any signs of airway obstruction develop.92
Acuteinfection
Acute infections are typically due to common skin commensals and present with swelling, erythema and pustules. Infections can be prevented by stringent aseptic technique, minimising needle passes through skin and avoiding passes through inflamed skin and previous filler sites.97 In the periocular region, untreated preseptal cellulitis may progress to orbital cellulitis and visual loss. Antibiotic treatment should be initiated immediately and ophthalmology input sought if the periocular region is involved. Abscesses at the site of injection may require surgical drainage.
“HIGH QUALITY STUDIES EXAMINING THE COMPLICATIONS AND ADVERSE EFFECTS OF PERIOCULAR TREATMENTS ARE NEEDED”
70 www.optometry.co.uk October/November 2022
Contourirregularitiesandchangesinskincolour
Injection of too much filler or superficial filler placement may lead to contour irregularities and nodules. Superficial injection of filler has also been noted to result in a bluish tint to skin, previously attributed to the Tyndall effect, but now postulated to be from superficial vein colouration. If firm massage over the site does not improve the aesthetic outcome, filler may need to be dissolved or surgically removed.98
Vascularocclusionandskinnecrosis
The most feared complication following filler injection is vascular occlusion, usually due to injection of filler into arteries or veins. Prevention is helped by a detailed knowledge of facial anatomy and good injection technique. Early recognition of impending vascular occlusion, in particular pain, blanching or erythema of the skin in the distribution of the blood vessel, is key to prevent skin necrosis.
Treatment, based on expert opinion and consensus recommendations, is immediate cessation of filler injection and application of warm compresses and topical vasodilators, for example, 2% nitroglycerin paste while hyaluronidase is prepared. Hyaluronidase should be injected immediately at the original site of injection and over the whole area of ischaemia. Injections should be repeated hourly until there is clinical resolution and then daily to treat any residual ischaemia. Aspirin, low molecular weight heparin, and hyperbaric oxygen therapy have all been used as adjuvant treatment to prevent tissue necrosis. Tissue necrosis requires debridement and closure, with rotational flaps or skin grafts as necessary.99-101
Retinalarteryocclusion
Intravascular injection of dermal filler into branches of the facial artery may result in retrograde flow of filler emboli through the extensive network of anastomoses into branches of the ophthalmic artery. Patients with central retinal artery occlusion will present with loss of vision. Occlusion of other branches of the ophthalmic artery may result in periorbital pain, choroidal ischaemia, ischaemic optic neuropathy, ptosis and ophthalmoplegia.102-105 Retrograde flow of emboli into the ophthalmic artery has also been associated with cerebral infarction.106 The most common injection sites that have been reported to lead to retinal artery occlusion are the glabella (38.8%), nasal region (25.5%), nasolabial fold (13.3%) and forehead (12.2%).107
Early recognition of impending central retinal artery occlusion is key. Visual loss with or without pain often occurs within seconds of injection and may be associated with headache, nausea and vomiting along with neurological symptoms and signs. If suspected, practitioners should stop injecting immediately and arrange an urgent transfer to an emergency eye unit
for assessment, accompanying the patient. Treatment should be initiated within 60 minutes to prevent irreversible retinal ischaemia.
Treatment protocols, based on expert reviews and consensus recommendations, advise three main strategies:107-110
1 Lower the intraocular pressure: Lie the patient supine Administer intraocular pressure lowering agents, for example, topical timolol 0.5%, oral or intravenous acetazolamide
Perform anterior chamber paracentesis.
2 Dislodge the embolus to restore blood flow: Rebreathing into a paper bag to promote vessel dilatation
Ocular massage – digital or with a Goldmann lens.
3 Dissolve dermal filler emboli using hyaluronidase: Inject at the initial injection site and in the supratrochlear and supraorbital regions, massaging the area to aid hyaluronic acid breakdown
Peribulbar or retrobulbar injections may be attempted if experienced in the technique. Other measures attempted for this complication include subcutaneous, retrobulbar and intraarterial hyaluronidase, intra-arterial thrombolysis and hyperbaric oxygen treatment, with visual improvement noted in a few case reports.111-114 Adjuvant treatment given has also included anticoagulants and vasodilators. Unfortunately, the visual outcome for most patients with dermal fillerrelated central retinal artery occlusion remains poor. Ophthalmoplegia tends to recover spontaneously over time, but many patients go on to develop sensory strabismus.115
Late onset complications
Delayedhypersensitivityreactions
Type 4 hypersensitivity reactions to dermal fillers may present weeks or months after injection. Symptoms include oedema, granulomas, panniculitis, and rarely, systemic granulomatous and autoimmune disease. Non-antibody mediated oedema does not respond to antihistamines, requiring steroids and dissolution of filler with hyaluronidase to treat. Foreign body granulomas form as an immune reaction to filler material and present as papules, nodules, or plaques. Initial treatment is intralesional steroids and dissolution using hyaluronidase, but surgical excision may be required.116-118
Chronicinfection
Contamination of filler with skin commensals leads to biofilm formation adherent to filler deposits, causing chronic low-grade inflammation and the formation of inflammatory nodules. Repeat injections that disrupt existing biofilms may trigger abscess
PATHOLOGY October/November 2022 www.optometry.co.uk 71
formation or systemic infections. Initial treatment is with intralesional steroids and filler dissolution using hyaluronidase. Antibiotics should be prescribed if active infection is suspected.116-120
Skincolourchanges
Telangiectatic vessels may develop at injection sites days to weeks post-procedure from tissue expansion and trauma. These vessels usually fade spontaneously within 12 months, but persistent vessels may be treated with lasers or intense pulsed light (IPL). Postinflammatory hyperpigmentation may also develop at injection sites, particularly in patients with Fitzpatrick skin types IV-VI.121 First line treatment includes topical bleaching agents, for example, topical hydroquinone with tretinoin and sunscreen. Chemical peels, IPL and Nd:YAG laser treatment may also improve the appearance of hyperpigmented skin.91
Malaroedema
Malar oedema is a common complication of fillers, with a long-term incidence of 11%. Superficial placement of filler in the malar region is the most common cause, resulting in impairment of lymphatic flow superficial to the malar septum and persistent fluid accumulation. Dissolution of filler with hyaluronidase is often the only effective treatment.122,123 This appearance may be mistaken for lymphoedema and patients may be investigated for systemic conditions such as sarcoidosis and thyroid eye disease if the use of dermal fillers is not known.
Figure 3 illustrates a patient with lower eyelid swelling secondary to hyaluronic filler, before and immediately after dissolution with hyaluronic acid.
CONCLUSION
Periocular cosmetics and aesthetic treatments are widely used and highly regulated in Europe and the US. However, data on complications of these treatments is scarce, with most evidence from case reports and case series of patients attending emergency departments. High quality studies examining the complications and adverse effects of periocular treatments are needed to provide patients with sufficient information to make an informed choice on whether to use these products to enhance their appearance.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the staff at Queen Victoria Hospital NHS Trust library for their assistance in locating the references cited.
Sonali Nagendran is a consultant ophthalmic and oculoplastic surgeon at Hampshire Hospitals NHS Foundation Trust UK. Nagendran has a number of publications in the field of oculoplastics.

Mohammad Javed Ali is a consultant ophthalmic and oculoplastic surgeon at Govindram Seksaria Institute of Dacryology, L.V. Prasad Eye Institute, Hyderabad, India. Ali has published more than 500 papers and received 35 national and international awards.


Murat Dogru is a consultant ophthalmic surgeon at the Department of Ophthalmology, Keio University School of Medicine, Tokyo, Japan. Dogru is also a visiting senior fellow of UNSW, Brien Holden Eye Institute.
Raman Malhotra is a consultant ophthalmic and oculoplastic surgeon at Queen Victoria Hospital NHS Trust, East Grinstead. His specialist interests include oculoplastic surgery in ocular surface disease, facial palsy rehabilitation, reconstructive eyelid and orbital surgery, endonasal lacrimal surgery, facial dystonia and aesthetic eyelid rejuvenation.

72 www.optometry.co.uk October/November 2022
HOW HEADSMART ARE YOU?
POINT
INTRODUCTION
Optometrists are unique among healthcare professionals. We are often seen by the public as people who prescribe spectacles and contact lenses, but our real superpower is that we are trained to detect the signs and symptoms of ocular and systemic disease. This training enables optometrists to refer for timely treatment of sight- and life-threatening conditions.1
According to The Brain Tumour Charity, over 12,000 people in the UK receive the devastating news that they have a brain tumour every year.2 Over 500 of these people are children or teenagers. Sadly, a quarter of these children and teenagers don’t survive. Many of these young people are referred by their optometrist because of suspicious signs and symptoms.1,3 Indeed, Cancer Research UK states ‘Opticians have the skills, knowledge and equipment to identify warning signs of possible brain or CNS tumours’ and has indicated that optometrists are better placed than a general practitioner (GP) when it comes to assessing problems associated with eyes and vision.4 With this in mind, optometrists need to be aware of the presenting symptoms and signs so that patients can access secondary care for diagnosis and management as soon as possible.
Cancer is the leading cause of death in girls aged one to 19 years and in boys aged one to 14 years, and the third most common cause of death in boys in the 15 to 19 years age group (after self-harm and transport injuries).5
Childhood brain tumours are the leading cause of cancer death in children and teenagers. The five-year survival rate for childhood brain tumours is 70%. However, around two thirds of survivors are left with permanent mild or moderate disability; this has been attributed in part to the delay between onset of symptoms and the start of treatment.6 Very aggressive tumours (see Figure 1) tend to have a shorter time interval between symptom onset and treatment due to the rapid progression of symptoms. The converse is true for low grade tumours which have a slower rate of symptom onset and leads to a longer delay in diagnosis and treatment. During this
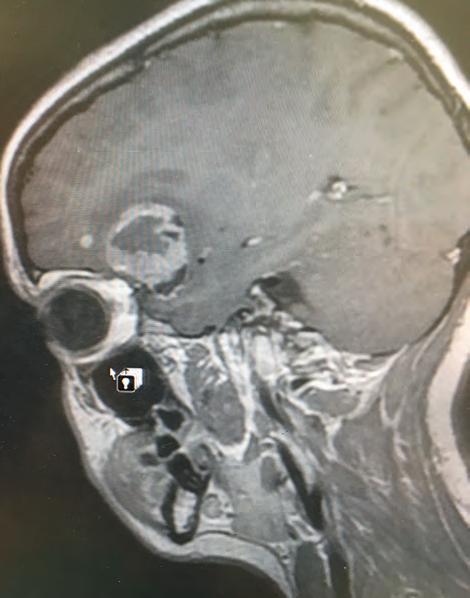
delay, the patient may acquire progressive permanent disabilities such as vision loss, mobility and cognitive difficulties.6-8
HeadSmart was introduced in 2011 in response to the concerns of healthcare professionals and families about the delay between onset of symptoms and diagnosis experienced by many patients.9 The expectation was that by improving awareness of the signs and symptoms of brain tumours for both healthcare professionals and the public, the time between symptom onset and diagnosis could be reduced, which would result in a decrease
Dr Deborah Armstrong PhD, MCOptom, DipTp (IP)
IN BRIEF This article is intended to raise awareness of the signs and symptoms of childhood brain tumours among optometric practitioners.
Figure 1 Stage 4 glioblastoma multiforme in an 18-yearold patient
NEUROLOGY, PATHOLOGY, VISUAL FIELDS
October/November 2022 www.optometry.co.uk 73
1 CPD
in the probability of both mortality and long-term disabilities.
In 2006, the median time between onset of symptoms and diagnosis in the UK was 14.4 weeks. As a result of the HeadSmart campaign, this reduced to 6.7 weeks by 2013.9 This article seeks to familiarise optometrists and other eyecare professionals with the HeadSmart guidelines to help in the fight against this dreadful illness.
HISTORY AND SYMPTOMS
Every eye examination should begin with an introduction and the practitioner should take the opportunity to observe the patient for signs of visual and mobility impairment while they progress towards the consulting room. Balance, co-ordination and walking problems are recognised signs and symptoms of a brain tumour in all three age groups described in the HeadSmart guidelines (see Figure 2). Abnormal head posture is included in possible signs of brain tumour for babies and children up to the age of 11 years. An abnormal head position may be adopted to overcome or reduce diplopia which has occurred as a result of muscle palsy. Abnormal head positions may include facial tilt, elevation or depression of the chin, or head tilt and these atypical positions can also occur concurrently. For example, in a superior oblique palsy, the face would be turned away from the affected eye, the chin would be depressed, and the head tilted away from the affected side. Differential diagnosis for proptosis in a child includes optic nerve, orbital or chiasm tumour10 and this needs to be investigated by ascertaining the onset and whether the proptosis is increasing. Past photographs of the child may be useful in deciding the latter.
Next, an accurate and detailed patient history should be taken with the practitioner asking pertinent questions depending upon their patient’s (and/or accompanying adult’s) descriptions. Undergraduates are often taught to ‘LOFTSEA’ our patients’ symptoms by asking questions about location, onset, frequency and duration, type/ severity, self-treatment, effect and associated factors.11
According to NHS and HeadSmart advice, common symptoms of brain tumours include headaches, seizures, nausea, vomiting, behavioural changes, paralysis and vision or speech problems.12 If alarm bells are ringing after hearing the chief complaint, it is important to ask in detail about family history of brain tumour since this is a risk factor for childhood disease along with family history of early onset breast cancer, leukaemia, sarcoma, neurofibromatosis and tuberous sclerosis.13
Headache is an important (but not exclusive) symptom of brain tumours, with studies reporting up to 64% of patients describing headaches on presentation.14-16 Often, headache is the first presenting symptom of a brain tumour..17 Tumour-associated headaches are frequently described as persistent (but unlike migraine) with the pain being worse on waking, coughing, exercise or with changes in posture. Headaches may be accompanied by vomiting or new neurological symptoms and are often unresponsive to pain medications that can be obtained from a pharmacy without prescription.18 It is important to remember that young children often don’t complain of headache, but their parents may notice other signs of headache such as the child holding their head in their hands, or that they appear generally unwell.
Seizures or fits can be experienced by patients with brain tumours. If a child experiences a tonic-clonic seizure (the type associated with epilepsy where
 Figure 2 The HeadSmart symptom card
Figure 2 The HeadSmart symptom card
74 www.optometry.co.uk October/November 2022
there is loss of consciousness and jerking body movements), they are highly unlikely to present first to the optometrist. However, other types of seizure may have symptoms that are noticed by parents and carers but are not recognised as seizures and it is these symptoms that might present to optometric practice.
Parents may have noticed that their child has had episodes when they seem ‘odd’ or ‘spaced out;’ they may appear to stare into space and be fixated on an invisible target. These episodes may in fact be ‘absent seizures’ and could be wrongly attributed to a vision problem. A ‘focal aware’ seizure may cause patients to complain of visual disturbances similar to those experienced by migraine sufferers, or of hallucinations – where the patient sees things that are not there19 – and these may trigger a visit to the optometrist.
PRELIMINARY INVESTIGATIONS
Research has shown that 70% of brain tumour patients have visual symptoms at diagnosis with 54% having cranial nerve palsies.20 Visual symptoms may include blurred vision, visual field defects, diplopia, photophobia, ptosis and nystagmus. Visual acuity should be investigated in the usual way with ageappropriate tests. Any reduction in visual acuity that cannot be attributed to an ocular cause should be regarded as suspicious.
Visual fields may be tricky to assess in infants, but studies have shown that children as young as five years may be successfully assessed using a SITA fast strategy21 and there are now game-based visual field tests available for use with children.22 Visual field defects that cannot be explained by an ocular cause should be referred for further investigation. Optometric practitioners should be aware of the characteristic visual field defects caused by lesions of the visual pathway. These include bitemporal and homonymous hemianopias and quadrantanopias with or without macular sparing (see Figure 3) Pupil reactions and ocular motor balance should always be performed as part of a routine eye examination.
A recent onset of a relative afferent pupillary defect (RAPD) should always ring alarm bells. Cranial nerve palsies secondary to raised intracranial pressure (ICP) may cause symptoms of diplopia due to the extra ocular muscles being affected. In addition, a patient may report photophobia (due to mydriasis) and express concern about recent onset ptosis. Any sudden onset strabismus and/or diplopia of unknown aetiology should be viewed as suspicious and referred for an ophthalmological opinion.
Colour vision may be defective in patients with a lesion of the visual pathway; this can manifest as poor discrimination of colours and a loss of colour saturation. The testing of colour vision in children is easily performed and should be carried out monocularly in these cases. Red desaturation should be investigated by presenting a red target to each eye in turn and asking the patient if they see any differences in colour or brightness between the eyes.
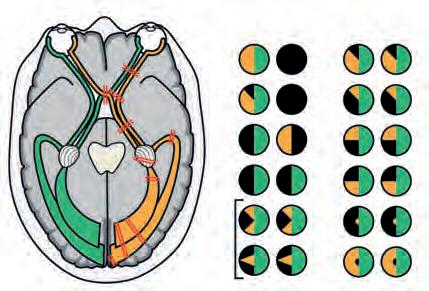
FUNDUS EXAMINATION
Brain tumours can lead to high ICP which causes swelling of the optic disc, that is to say, papilloedema (see Figure 4, page 76). In infants, the skull may expand as the tumour grows, so raised ICP may not occur.23 In some cases, papilloedema may be the first and only sign of raised ICP. If optic disc oedema is persistent, permanent damage to the vision can occur due to optic nerve atrophy.24 Early papilloedema is characterised by disc margin blurring (nasal margins are often the first to blur) and raised disc margins. Early papilloedema may be asymptomatic but it can also be accompanied by photophobia, nausea and headache. Severe papilloedema typically presents with obscured disc vessels (due to thickening of the nerve fibre layer) with flame-shaped haemorrhages at the optic disc alongside pallor, venous engorgement and the absence of the optic disc cup. The mechanical tension caused by the increase in ICP can cause the appearance of greyish lines which form concentric circles around the optic nerve head;
Location Defect
Decreased vision in the
Junctional scotoma
Bitemporal hemianopia
Left homonymous hemianopia
Left homonymous sectoranopias
Left homonymous superior hemianopic defect
Left homonymous inferior hemianopic defect
Left homonymous inferior quadrantopia
Left homonymous superior quadrantopia
Left homonymous macular-sparing hemianopia
Left homonymous scotomas
NEUROLOGY, PATHOLOGY, VISUAL FIELDS October/November 2022 www.optometry.co.uk 75
Figure 3 Visual pathway scotoma maps showing visual field defects resulting from various lesions of the visual pathway
1. Right optic nerve 2. Posterior right optic nerve 3. Chiasm 4. Right optic tract 5. Right lateral geniculate nucleus 6. Right temporal lope 7. Right parietal lobe 8. Right occipital lobe (upper bank) 9. Right occipital lobe (lower bank) 10. Right occipital lobe 11. Tip of the right occipital lobe Left eyeRight eye Right eye Right eye Left eye 11 2 4 3 6 5 7 8 9 10 11 6 2 7 5 10 11 4 9 3 8 Left eye
right eye
these are known as Paton’s lines.25 Severe papilloedema can be associated with transient loss of vision which may become apparent when the patient stands up from a seated position.
It is important to be aware that optic disc oedema can be imitated by a number of conditions and this is termed pseudopapilloedema. These conditions include tilted discs, small, congested hyperopic discs and optic disc drusen.
Changes to the optic nerve head appearance due to a brain tumour may, on rare occasions, mimic normal tension glaucoma26 with optic disc cupping and pallor being apparent. If an asymptomatic child or young person presents with these signs, the possibility of a brain tumour should be considered.
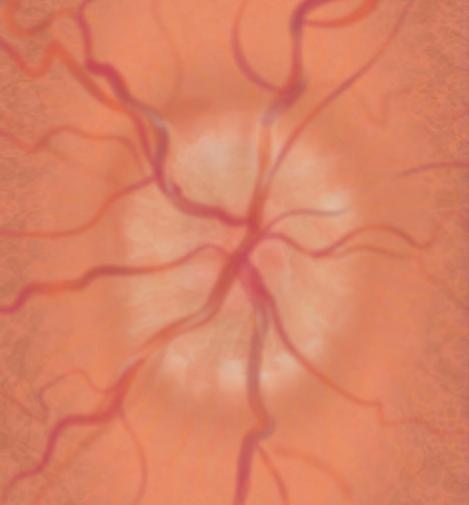
SUPPLEMENTARY TESTING
Optical coherence tomography (OCT) is an invaluable tool for differentiating between ocular conditions. Optic nerve head swelling is easily diagnosed using a retinal nerve fibre layer (RNFL) scan where the ‘TSNIT graph’ shows that the RNFL layer is thicker than those of agematched normals and indicates which areas of the RNFL
are affected most. Patients with pseudopapilloedema show no such swelling. Even very young children can be persuaded to position themselves at the OCT machine and since it is an objective test, it can prove very useful when examining these youngsters.
CONCLUSION
The HeadSmart awareness campaign aims to reach as many people as possible by displaying promotional material in places such as healthcare settings, schools and nurseries. The HeadSmart information and symptoms cards recommend that a patient who has one symptom should see their GP. With certain symptoms (persistent/recurrent headache, abnormal eye movements, abnormal head position, blurred or double vision and loss of vision) an examination by an optometrist is also advised. A patient who has two or more symptoms should be referred urgently for a specialist opinion. The HeadSmart website includes a decision support tool,27 which is aimed at healthcare professionals. This advises when to reassure or review and refer for each symptom and suggests appropriate investigations and assessments as well as highlighting potential diagnostic pitfalls. HeadSmart material and symptoms cards are available free of charge at www.headsmart.org.uk. The web page also has downloadable resources to use in practice. Optometrists who would like further information are welcome to call the support line on 0808 8000 004 where they will be directed to a suitable expert.
ACKNOWLEDGEMENTS
The author would like to thank the following people for their help in producing this article:

● Laura Nuttall for allowing an image of her brain scan to be used in Figure 1
● Piers Townley and HeadSmart for supplying research articles and Figure 2
● Dr Samantha Strong for allowing her artwork to be used in Figures 3 and 4.
Dr Deborah Armstrong graduated from Aston University. She worked as an optometrist in both a primary care setting and the hospital eye service before completing a PhD at the University of Bradford. Armstrong now combines work as a specialist optometrist in glaucoma for East Lancashire Teaching Hospitals NHS Trust with teaching at the University of Bradford.
Figure 4 Early papilloedema showing blurry disc margins and optic disc swelling
76 www.optometry.co.uk October/November 2022
COMMUNICATION
IN OPTOMETRY
Lorcan Butler BSc (Hons), MCOptom, FBDO, Prof Cert Paed Eye Care
This article discusses the importance of communication with patients, colleagues and other professionals, offering recommendations on best practice.
IN BRIEF
INTRODUCTION
Canadian physician, William Osler, famously stated: ‘A good physician treats the disease, while a great physician treats the patient who has the disease.’ The General Optical Council (GOC) recognises communication as being an integral part of the continuing professional development (CPD) scheme for registrants, specifically outlining the importance of being able to communicate effectively with the patient and any other appropriate person involved in their care.1
Communication within healthcare is considered effective when the receiver, either the patient or family member, understands clearly, the message being conveyed by the sender. For this to happen, the message has to be clear, concise, consistent and transparent, as well as being accessible and inclusive. Effective communication enables:
● The exchange of clear information and instructions on care needs
● The provision of direct (or indirect) emotional support to the patient (or family member)
● The development of positive relationships.
INTERNAL COMMUNICATION
Practitioners not only have to be good communicators with their patients, but also with other colleagues. The seamless transfer of care within a practice, especially when tasks are being delegated, is vital to ensure that patients receive the best care possible.
Communication errors were cited as the most commonly reported category in a pilot study looking at errors in an optometric practice.2 In the majority of cases, the errors related to poor communication between staff members, typically between professional and non-registered staff, highlighting the importance of staff training.
Practitioners should be reminded that if a task is delegated, they are entirely responsible for the test and its results. With this in mind, it is incumbent upon the professional to ensure that the staff member is competent, capable and trained to undertake the task safely; this includes having confidence that they are able to communicate effectively with patients and their carer, colleagues and others.
EXTERNAL COMMUNICATION
Working collaboratively with peers and other healthcare practitioners is evidently in the best interests of patients, so ensuring that communication is clear and effective is key. As collaboration between ophthalmology and optometry continues to grow with the rapidly changing landscape of co-managed care, it is essential that misinformation and miscommunication are minimised.
RESEARCH INSIGHT
A research project led by King’s College in conjunction with the College of Optometrists involved the video recording of over 60 optometric consultations, which were then subjected to scrutiny.3 Naturally, the findings from this work are highly relevant to practitioners in the sector. Workshops and seminars
COMMUNICATION
October/November 2022 www.optometry.co.uk 77
1 CPD POINT Getty/grivina
enabled optometrists to further their understanding of communication in the consultation and reflect on their own practices. The researchers discovered that asking the wrong question, using the wrong words or even facing the wrong way can all have a negative impact on communication success. Through this process they discovered how to ask the right questions, use the right words and the right direction with body position.
The right question
Open rather than closed questions can save time, make the patient feel more relaxed, invites them to lead the conversation, and most importantly, makes them feel listened to. It also offers insight into the communication style of the patient thereby allowing the practitioner to align their approach to meet individual preferences.
The right words
Patients can be reluctant to say ‘yes’ when asked if they are having any problems. They often feel it is the duty of the practitioner and the task of the eye examination to deduce whether any problems exist. Being able to talk in their own terms can help the patient to feel actively involved and important in the consultation, and therefore, enhance feelings of comfort, satisfaction and rapport with the clinician. Using softer words such as ‘burden,’ ‘worries’ or ‘concerns’ rather than ‘problem’ may elicit a better response from the patient.
The right direction
Facing the patient gets a better response with the individual likely to give more detail when there is eye contact. Record keeping is important but maintaining regular eye contact with the patient is also essential for good communication, especially at key times during the process. Loss of eye contact can lead to the patient repeating themselves and feeling that they are not being listened to properly.
THE IMPORTANCE OF NON-VERBAL COMMUNICATION
There is a positive correlation between nonverbal communication and patient satisfaction.4 Practitioners who employ appropriate nonverbal or behavioural attributes are seen to be more empathetic and connected to their patients.5 It is also important to be alert to unspoken signals which could indicate misunderstanding, discomfort or lack of consent.1
Active listening
Listening to patients and ensuring they are at the heart of the decisions made about their care is a primary expectation and practitioners should dedicate sufficient time to deal properly with their needs;1 this conveys respect for the patient and builds trust. Best practice guidelines, ample as they are, might not fully address a patient’s fears, grief over a diagnosis, or practical issues
of access to care. Overlooking these realities is perilous, both for the wellbeing of the patient and efficient delivery of care.6
Unfortunately, in a time sensitive clinical environment, despite best intentions, practitioners can spend too much time educating patients and steering them in a particular direction, that they can neglect to listen carefully enough. Through casual conversation, a patient can provide a lot of information about what they are thinking or where their priorities lie.
If the patient is unable to articulate why they have attended, and then cannot relate their care or management based upon that, then they will be left disappointed. A good practice to embed into the routine after history and symptoms are completed is to go back to the primary reason for the visit to paraphrase the patient’s key concerns. For example: ‘So Mr Smith, you have told me that your vision is fine, and your glasses seem to be adequate, it’s just that you are concerned about the redness in your right eye, is that correct?’
Eye contact
Eye contact displays to the patient that their needs are being taken seriously, and also if they have questions to ask, that they will be listened to. A second reason to maintain eye contact is that patients may be more likely to show lack of understanding or disagreement with facial expressions rather than verbally. Eye contact can be difficult in certain cultures, where a person may not want to do so as a mark of respect to the practitioner. Many cultures regard silence and indirectness as a sign of respect, whereas healthcare practitioners may interpret these silences as a failure to understand.7 Those on the autistic spectrum can also find it difficult to maintain eye contact and it is important to be sensitive to these nuanced behaviours.
TREATMENT COMPLIANCE
Good communication is essential when delivering either new treatment instructions or reiterating a preexisting regime which is not being adhered to correctly. For instance, medication usage for glaucoma, dry eye management regimes and contact lens wearing times. Many patients with glaucoma do not have symptoms, which can sometimes make it difficult to convince them that they have a sight-threatening condition. Effectively communicating with these patients and helping them to understand the disease can aid compliance. In 2019, a US glaucoma study revealed that 76% of patients were very or extremely concerned about losing their vision and how that would impact their independence.8 However, despite the concerns of this patient group, up to 50% of glaucoma patients in the UK are noncompliant with treatment.9 Given the consequences of treatment failure, it is vital to find out reasons for non-adherence and help each individual with measures
78 www.optometry.co.uk October/November 2022
of support to overcome these barriers. With this in mind, it is helpful to check that patients are managing to adhere to their treatment, reiterate the consequences of non-compliance and support them in doing so, for instance, by offering advice on instilling drops.
CONSEQUENCES OF MISCOMMUNICATION
The impact of miscommunication goes beyond the direct health implications of the patient’s condition and can affect their comprehension of the diagnosis, satisfaction with the practice and the practitioner, along with their level of hopefulness and psychological adjustment to the outcome of the consultation.
It is a sobering statistic that 40 to 80% of medical information provided by healthcare practitioners is forgotten immediately by the patient. Unsurprisingly, the greater the amount of information presented, the lower the proportion that can be recalled correctly.10 Almost 50% of information provided is remembered incorrectly.11
There is extensive data available on the impact of poor communication on legal cases against healthcare professionals. Within UK optometry, a poor history and symptoms is cited as one of the recurring themes in litigation cases.12 It is quite rare that a fitness to practice hearing does not involve some element of miscommunication.

It is essential to reinforce key verbal advice with other resources, such as patient information leaflets offered by the Association of Optometrists and the College of Optometrists, ensuring this is documented on the patient records; taking this step will support the practitioner in cases where it is alleged that proper communication did not occur. In cases where advice has been given over the phone then details of this communication should be detailed on the records.
Presenting information in an accessible way using non-clinical terminology is also very important. Language should be clear, honest and easy to understand, with an active tone. Avoid turns of phrase which patients themselves may not identify with, for example, ‘clinically extremely vulnerable’ or having ‘minor symptoms.’13
WHEN COMMUNICATION IS DIFFICULT
Practitioners often need to deal with scenarios where communication can be challenging in day-to-day practice.
Duty of candour
It can be difficult to take ownership and accountability of a problem where things have gone wrong. Being transparent and open is not the difficult part but looking into how the admission will affect the patient and their responses to the admission can sometimes be difficult for all clinicians, regardless of experience.
Breaking bad news
From explaining to a tearful child about the need for their first pair of glasses, to advising a patient they have a condition that is not amenable to treatment, are scenarios that practitioners frequently encounter; this is where the three main models of breaking bad news can be utilised:
● ABCDE: advance preparation, build relationship/ rapport, communicate well, deal with reactions, encourage/empathise
● SPIKES: setting up, perception, invitation, knowledge, empathy, summary/strategy
● BREAKS: background, rapport, explore, announce, kindle, summarise.
Unable to meet the driving requirements
Advising a patient that they no longer meet the driving standard can be one of the hardest pieces of news that a practitioner has to deliver. In these scenarios it is important to be very clear, concise and totally unambiguous with the communication. Using terms such as ‘close to,’ very near,’ or ‘close to the borderline’ of the legal driving requirements should be avoided. Practitioners should be familiar with the Assessing fitnesstodrive guidance published annually by the DVLA and use that as the rule book at all times.14 Clinical advisers from professional bodies can provide helpful support in dealing with difficult cases where required.
CONCLUSION
Communicating effectively with patients comes with experience and is a skill that requires careerlong learning. Building a good relationship with the patient and ‘speaking their language’ in a way they understand helps them to value the consultation journey.15 Practitioners should be mindful of body language, including eye contact, ask open questions and ensure that the patient’s primary reason for their visit is incorporated into diagnoses, management, and most importantly, the summary.
Lorcan Butler is the optical engagement manager for The Brain Tumour Charity and a qualified dispensing optician and optometrist. Butler has a keen passion for educating practitioners on the ocular manifestations of brain tumours and has delivered CPD on a range of topics including papilloedema and clinical decision making.
COMMUNICATION October/November 2022 www.optometry.co.uk 79
KERATOCONUS: CONSIDERATIONS, RECOGNITION AND MANAGEMENT WITH SPECIALTY CONTACT LENSES
INTRODUCTION
Keratoconus is the most common corneal irregularity and remains mysterious despite years of research. It is typically described as a progressive, asymmetric, bilateral and non-inflammatory corneal ectasia.1-3 The disease is characterised by central stromal thinning, scarring and protrusion, which generates high myopia and irregular astigmatism affecting visual quality.4 Typically, keratoconus starts to appear in adolescence,5-8 although it has been detected earlier8 and later,7 and is typically progressive until the third or fourth decade of life.9 This article will discuss the occurrence of keratoconus in a paediatric population, the diagnosis, psychological impact and its management with contact lenses.
PAEDIATRIC KERATOCONUS
Keratoconus can manifest in the first decade of life10 and the youngest documented case is age four.11 The early manifestation of keratoconus can have a significant impact on a patient’s social and educational development.10 It is known that keratoconus advances more rapidly in children compared to adults,10,12,13 which impacts clinical decision making after diagnosis. The Collaborative Longitudinal Evaluation of Keratoconus (CLEK) study found that over an eightyear time period, younger patients’ corneas progressed 1.80D more compared to older patients.14 Paediatric keratoconus appears to have both inheritance and environmental influences for its development and progression. It has been documented that 10% of diagnosed paediatric keratoconus patients have a family history of the condition.10,15,16-18 Paediatric keratoconus has been associated with coexisting conditions such as vernal keratoconjunctivitis, atopy, Down Syndrome, and Leber congenital amaurosis.19,20 Hormones, in particular androgens, may also play a role with paediatric keratoconus;10 this could explain the earlier onset and faster progression for boys compared to girls.10,18,21,22
Surgical management of paediatric keratoconus Corneal crosslinking (CXL), a treatment to increase
POINT
chemical bonding between collagen fibrils, should be considered at the initial diagnosis of keratoconus for a paediatric patient. The goal of CXL is to strengthen the cornea to halt or slow down the progression of topographical and refractive changes.12 However, it has been shown that the aggressive nature of paediatric keratoconus and persistent eye rubbing can result in progression years after treatment, potentiating the need for retreatment.12,23 Intracorneal ring segments (ICRS) are a select treatment strategy to flatten and stabilise the keratoconic cornea. However, ICRS is not a preferred strategy for children due to the potential of rapid progression, eye rubbing and non-compliance.12,24 Finally, penetrating keratoplasty is an option for the most advanced cases of paediatric keratoconus. Although penetrating keratoplasty is often successful in adults with advanced keratoconus, children typically do not fair as well as adults due to an increased risk of endothelial graft rejection12,25 and poor compliance. Deep anterior lamellar keratoplasty is an alternative surgical strategy to replace scarred stromal tissue while reducing the risk of endothelial cell loss and rejection.12,26
PSYCHOLOGICAL ASPECTS OF KERATOCONUS
Keratoconus is a disease of young patients who are often managing its ocular and visual effects during a key period of their education, career development and child-rearing years.27 It is important to note that keratoconus has been associated with depressive and anxiety disorders.28,29 The CLEK study found that visual acuity (VA) and corneal curvature were the measures that had the greatest association with visionrelated quality of life.30 Lower scores were seen in individuals who had binocular VA worse than 20/40 and >52D of corneal curvature.30 However, patients showed significant declines in vision-related quality of life even when they had binocular VA of 20/40 or better.27 A 10-letter decline in high-contrast binocular VA and 3D increase in corneal curvature were both associated with declines in scores.29 The visual function scores for keratoconus patients are similar to age-related macular degeneration patients, except for
Daddi Fadel DOptom, FSLS, FBCLA, FAAO, FIACLE and Dr Greg DeNaeyer OD, FAAO, FSLS
IN BRIEF This article outlines the clinical presentation of keratoconus and its management with a range of different contact lens options.
80 www.optometry.co.uk October/November 2022
1 CPD
health, where CLEK patients scored better, and ocular pain, where CLEK patients scored worse.30 Patients’ vision-related quality of life can also decline with worsening of keratoconus. Patients who have success with contact lenses may improve their vision related quality of life.31 In fact, in the CLEK study, contact lens wearers had higher visual function scores except for the category of ocular pain.30 The fact that patients’ mental status declines as keratoconus worsens further justifies the consideration of CXL during the early stages of the disease. CXL has been shown to reduce anxiety in keratoconus patients but not depression.28,32
DIAGNOSIS
Early diagnosis is important because this may rule out contraindicated refractive procedures and have maximum benefit from CXL.
Retinoscopy

Retinoscopy, although not high-tech, has been shown to be very useful as an initial screening technique for keratoconus diagnosis. The resultant retinal reflex of a keratoconus patient will give a scissoring appearance or Charleaux ‘oil droplet’ sign.33 AlMahrouqi etal screened 123 keratoconus suspects and keratoconus patients with retinoscopy and Pentacam (Scheimpflug) imaging.34 Results for retinoscopy were 97.7% sensitivity, 79.9% specificity, 70.8% positive predictive value and 98.4% negative predictive value.
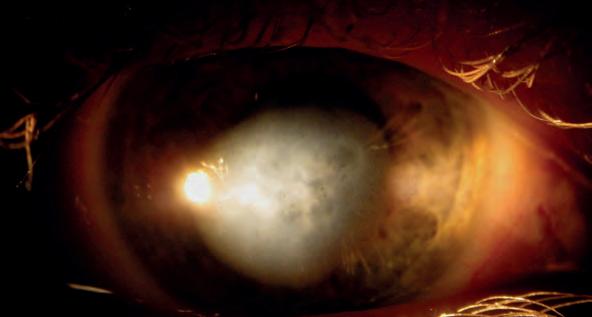
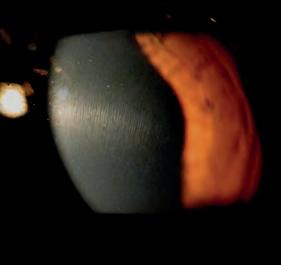


The authors concluded that retinoscopy is a reliable and sensitive technique for keratoconus screening. However, compared to imaging, keratoconus classification and match probability, retinoscopy underestimates keratoconus stages.35
Keratometry
Although used with decreasing frequency due to greater access to advanced technologies, measurement with a keratometer can still be useful for some clinicians when screening for keratoconus. Patients with keratoconus will have steep keratometry values, along with distorted and misaligned mires. Keratometers are of limited value because they are only able to measure the central 3mm area of the cornea resulting in relatively normal readings for more peripheral cases of keratoconus.
Slit lamp biomicroscopy
Examination with a slit lamp biomicroscope is critical for diagnosis and evaluation of keratoconus. Characteristic slit lamp findings for keratoconus include corneal protrusion, Vogt’s striae, Fleischer’s ring, Rizzuti’s sign and corneal scars.19,33 Nonspecific keratoconus findings include Munson’s sign, prominent corneal nerves and corneal thinning.33,35
Naderan etal evaluated slit lamp findings of 371 consecutive keratoconus patients revealing that more than 70% of patients had corneal protrusion, 55.5%
Figure 1 Clinical signs observed during biomicroscopy examination. (a) Munson’s sign in an eye with keratoglobus following penetrating keratoplasty. Munson’s sign may be also detected with the naked eye; (b) Fleischer’s ring; (c) Vogt’s striae; (d) Corneal thinning (e) Hydrops
CONTACT LENSES, CORNEA, PATHOLOGY October/November 2022 www.optometry.co.uk 81
A D E B C
had Fleischer’s ring and 47.7% had Vogt’s striae.33 The CLEK study reported that out of 1209 keratoconus patients, 86% had Fleischer’s ring, 65% had Vogt’s striae and 53% had corneal scarring.36 All clinical findings, including corneal thinning, prominent nerve fibres, Fleischer’s ring, Vogt’s striae, Munson’s sign, corneal scars, and Rizzuti’s sign, were found more frequently in severe keratoconus (see Figure 1) 33
Corneal topography

Topography has arguably had the biggest impact on diagnosis and monitoring changes of the keratoconus patient. Topography of the cornea allows the clinician to measure quantitative and qualitative morphological changes that are necessary for the diagnosis of keratoconus.37 The topographical maps are not only useful for diagnosis, but they can aid the clinician in distinguishing between nipple, oval and keratoglobus. These distinctions can be important for clinicians when determining contact lens selection.
Scheimpflug tomography
Another method of corneal analysis is using Scheimpflug tomography.37 The major advantage to this type of instrument is that it measures the front and back surface. Measuring the posterior cornea can be critical because posterior changes can be the first indication of keratoconus.38 A study by Ambrosio showed that posterior corneal changes were seen in 88% of contralateral eyes of patients previously diagnosed with unilateral keratoconus.39 Scheimpflug tomography can also generate corneal thickness maps, which is an important metric as thinning of the cornea has been shown to be diagnostic in keratoconus.40-43
Generally, topography and tomography systems not only aid in the diagnosis of keratoconus, but they are used to monitor for changes. Choi retrospectively analysed topographies of 84 keratoconus eyes and found that 25% of them progressed with a change in corneal topography from with-the-rule to oblique astigmatism.44
Optical coherence tomography (OCT)
OCT can also be used clinically for diagnosis and tracking changes or progression of keratoconus. Epithelial thickness maps generated from OCT measurement have been shown to detect forme fruste keratoconus. Temset etal evaluated OCT data of 145 eyes with early to severe keratoconus finding that epithelial maps can be used to detect early keratoconus.45 Pachymetry maps from OCT measurement can also be used for keratoconus diagnosis. Qin etal evaluated 163 eyes with keratoconus and normal eyes showing that when measuring pachymetry with OCT, 91.7% of keratoconus patients could be identified using a logistic regression formula.40
MANAGEMENT WITH CONTACT LENSES
In the early stages, spectacles may provide acceptable VA. However, despite the development of surgical treatments, the most common visual correction of keratoconus is achieved with contact lenses.46 The advancement in contact lens designs and materials has expanded the options to fit keratoconus patients, including soft and rigid gas permeable (RGP) designs.
Soft contact lenses
Patients with forme fruste keratoconus or mild keratoconus may be wearing soft contact lenses upon diagnosis. If the patient’s anterior segment sagittal height is approximately the same as a moulded lens design, a keratoconus patient may have success with spherical, toric and multifocal soft contact lenses. Soft lenses have been shown to offer similar improvements to quality of life as gas permeable lenses.47 These lenses become less successful with increasing sagittal height and irregularity secondary to advancing keratoconus.
Customised latheable soft contact lenses are available for mild to moderate keratoconus patients in hydrogel or silicone hydrogel materials. Latheable soft lens designs can have customised sagittal depths, diameters, power and centre thicknesses to optimise fit and vision. Purposefully increasing centre thickness can improve VA. Carracedo etalstudied four soft lens centre thicknesses (0.1, 0.2, 0.3, and 0.4mm) and found that keratoconus patients had significantly reduced higher order aberrations (HOA) and improved VA with lenses having 0.4mm centre thickness.48 The addition of wavefront optics can potentially correct for residual aberrations for keratoconus patients wearing soft lenses. Factors to be considered include pupil size and lens stability. Plus, it is unclear in deciding which corrected aberrations provide the maximum benefit and whether partial correction is the best strategy.49 Marsack etal reported on a case of a habitual soft lenswearing moderate keratoconus patient who was fitted with a wavefront-guided soft lens.50 The final lens improved the patient’s photopic high contrast vision by 1.5 lines and reduced HOA by 50%.
Figure 2 Corneal contact lens fit with three-point touch. The lens is slightly decentered inferiorly
82 www.optometry.co.uk October/November 2022
Rigid contact lenses
RGP contact lenses are the main refractive correction for early to advanced keratoconus.51,52 The firm nature of these lenses maintains the shape and creates a liquid reservoir between the lens and the corneal anterior surface that masks 89% of corneal anterior astigmatism,53 although will not necessarily correct HOAs.54 RGP lenses include corneal, scleral, piggyback and hybrid modalities.
Corneallenses
Corneal lenses have always been the gold standard in managing corneal irregularities. The rigid material provides the advantage of excellent visual performance when properly fitted on eyes with keratoconus. In early or mild keratoconus, corneal lenses may provide an optimal fit. However, in advanced stages, they may represent a challenge because of lens instability, apical touch, discomfort and suboptimal VA.55
There are three different types of lens fitting philosophies in keratoconus, which include apical clearance, three-point touch and apical touch.
Apical clearance is achieved when the back optic zone radius (BOZR) is steeper than the apical corneal curvature.56 The CLEK study developed a standard approach and suggests choosing the BOZR that exhibits definite apical clearance.57 This potentially reduces the risks of epithelial trauma and long-term corneal scars.57-59
Three-point touch is when the lens has a light touch on the apex and the majority of weight bearing in the mid-periphery (see Figure 2) 60 This approach is indicated in moderate and advanced keratoconus. When keratoconus is advanced, the lens will present a harsh bearing on the apex and less in the midperiphery.56
Apical touch is when the lens bears only on the apex of the cornea. The harsh bearing on the cornea may cause corneal erosions and potential scarring. It has been incorrectly assumed that an apical bearing fit may slow the progression of keratoconus since the lens provides a physical resistance to the disease. This has been demonstrated to be an apparent and transient flattening and does not retard the evolution of the corneal deformation.61 The CLEK study found that 32% of unscarred eyes at baseline fitted with apical touch developed corneal scarring by the eighth-year follow-up visit whereas only 14% of eyes fitted with apical clearance developed corneal scarring.57
Sclerallenses
According to the Scleral Lenses in Current Ophthalmic Practice Evaluation (SCOPE) study, the primary indication for fitting scleral lenses is for the management of keratoconus.62 Scleral lenses have the advantage over corneal lenses in vaulting the sensitive and irregular cornea with weight bearing on the bulbar
conjunctival tissue. Schornack etal successfully fitted 30 eyes of 19 keratoconus patients with scleral lenses that had failed with other nonsurgical visual correction options.63 The patients had an improvement of median best-corrected VA from 20/40 before scleral lens fitting to 20/20 after fitting. Scleral lenses may be a better option than corneal lenses for many keratoconus patients. There is evidence suggesting that a flat fitting corneal lens is associated with corneal scarring.57,64 Oxidative stress from the mechanical trauma of a flat fitting corneal lens is considered to be a mechanism for worsening keratoconus.65 Scleral lenses, by virtue of not contacting the corneal surface, reduces this potential complication (see Figure 3).
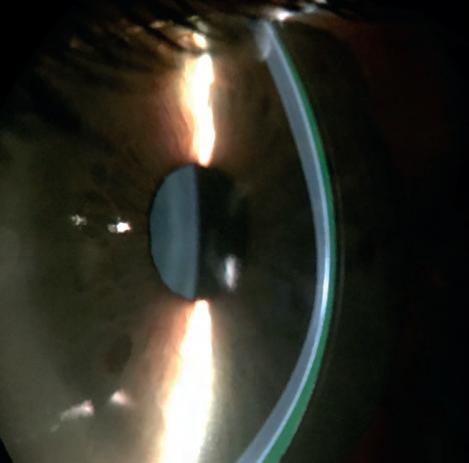
Front surface toricity and asphericity can be manufactured to improve visual function. Residual HOAs from the cornea and the crystalline lens can inhibit visual quality for keratoconus patients wearing scleral lenses. The relative rotational and translational stability of scleral lenses makes them an ideal platform for wavefront-guided optics.66 Patients may require neural adaptation before measuring significant visual improvement.66
Piggybacklenssystem
The piggyback contact lens system consists of wearing two contact lenses in one eye, with a corneal lens placed on top of a soft lens, usually a disposable silicone hydrogel lens (see Figure 4, see page 84). This system is indicated when a corneal lens is unstable on the eye, causes discomfort, three and nine o’clock staining or corneal scars.67,68 The use of a negative
Figure 3 Scleral lens fit in an eye with keratoconus. Corneal thinning may be observed. Excessive clearance at the peripheral cornea is created when fitting scleral lenses in advanced keratoconus
CONTACT LENSES, CORNEA, PATHOLOGY October/November 2022 www.optometry.co.uk 83
powered silicone hydrogel lens for piggybacking has been shown to be more appropriate in comparison to a positive powered contact lens.69 It has also been shown that only 21% of the effective power of a soft lens is transferred to the piggyback lens system.70 However, the final power of the rigid lens has been shown to be significantly more negative with positive lenses compared with negative lenses. This is explained by the modification of the mean central keratometry: a negative power of the soft lenses flattens the mean central keratometry and reduces the power of the corneal lens while a positive power steepens the mean central keratometry and increases the power of the corneal lens.69 The lighter weight of the rigid lens with less power will result in better centration on the eye. Furthermore, a negative powered soft lens might help to reduce spherical and coma aberrations, leading to an improvement in visual quality and allow better oxygen transmissibility at the centre of the piggyback.69
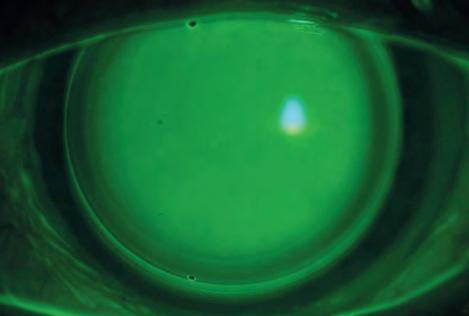
Hybridlenses
Hybrid lenses have a rigid component in the centre and a soft skirt in the periphery (see Figure 5). They are indicated when a corneal lens is unstable on the eye, in case of spontaneous lens ejection, discomfort and reduced wearing time.56 For these reasons, the
hybrid lens aims to combine a rigid contact lens visual performance and the characteristics of a soft contact lens in comfort and stability.70 A retrospective study of 44 patients reported successful fitting of SynergEyes hybrid lenses in 87% of patients after approximately eight months of follow-up. Fitting failures were due to lack of lens comfort.71 A comparative study has investigated the clinical and quality of life outcomes fitting SynergEyes ClearKone hybrid lenses and rigid lenses. Although VA was not significantly different between the two groups, higher overall satisfaction and vision-related quality of life were evident with hybrid lenses.72
CONCLUSION
Early recognition of keratoconus is crucial for the control of its progression, particularly given the impact on the patient as the disease worsens. Patients with keratoconus may report depressive, anxiety disorders and reduced quality of life. Specialty contact lenses are fundamental for its management and may improve the vision related quality of life. Scleral lenses in particularly have been shown to reduce the need for corneal transplants.52


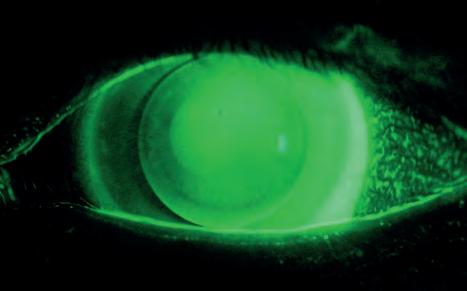 Figure 4 Piggyback system. The soft lens is fitted under the corneal lens to protect the cornea from mechanical stress of the corneal lens and to allow better centration
Figure 5 Hybrid lens fitted properly. Skirt curve is showing optimal fluorescein pattern and slight clearance in the inner landing zone. ImagecourtesyofSynergEyes, California,US
Dr Greg DeNaeyer practises at Arena Eye Surgeons with an emphasis on specialty contact lenses, is co-founder of the Scleral Lens Education Society and a fellow of the American Academy of Optometry. DeNaeyer is a contributing editor for ContactLensSpectrum and a contributor to ReviewofCorneaandContactLensesandOptometricManagement. He lectures internationally, and is a previous GPLI and Scleral Lens Education Society practitioner of the year.
Daddi Fadel is a contact lens designer, pioneer of modern lens designs and a specialist in contact lenses for the irregular cornea, scleral lenses, myopia control and orthokeratology. Fadel is author of the book ScleralLensIssues:TheirRecognition,Etiology,and Management, co-author of ClinicalGuideforScleralLensSuccessand editor-in-chief of the Journalof ContactLensResearch&Science
Figure 4 Piggyback system. The soft lens is fitted under the corneal lens to protect the cornea from mechanical stress of the corneal lens and to allow better centration
Figure 5 Hybrid lens fitted properly. Skirt curve is showing optimal fluorescein pattern and slight clearance in the inner landing zone. ImagecourtesyofSynergEyes, California,US
Dr Greg DeNaeyer practises at Arena Eye Surgeons with an emphasis on specialty contact lenses, is co-founder of the Scleral Lens Education Society and a fellow of the American Academy of Optometry. DeNaeyer is a contributing editor for ContactLensSpectrum and a contributor to ReviewofCorneaandContactLensesandOptometricManagement. He lectures internationally, and is a previous GPLI and Scleral Lens Education Society practitioner of the year.
Daddi Fadel is a contact lens designer, pioneer of modern lens designs and a specialist in contact lenses for the irregular cornea, scleral lenses, myopia control and orthokeratology. Fadel is author of the book ScleralLensIssues:TheirRecognition,Etiology,and Management, co-author of ClinicalGuideforScleralLensSuccessand editor-in-chief of the Journalof ContactLensResearch&Science
84 www.optometry.co.uk October/November 2022
MYOPIA MANAGEMENT IN CLINICAL PRACTICE
IN BRIEF This feature invites readers to consider the implications and management of myopia, accessing additional resources where required to answer the questions.
A 40-year-old male patient attends with visual acuity of 6/36 in his right eye and is otherwise asymptomatic. He was first prescribed spectacles at five years of age and had laser refractive surgery in his twenties.


01 Which of the following conditions is most likely shown in the image?
a) Myopic maculopathy
b) Toxoplasmosis scarring
c) Macular hole
d) Angioid streaks
02 Which of the following statements in relation to this presentation is true?
a) Other potential complications for this patient are retinal detachment and glaucoma
b) Axial length is likely to be greater than 26mm
c) The refractive error is probably greater than -6.00D
d) All of these options
03 Which of the following statements is false?
a) Undercorrection of myopia in childhood significantly slows myopia progression
b) There is a strong correlation between axial length elongation and myopia progression
c) OCT-based instruments can be used to measure axial length change
d) Early-onset myopia increases the likelihood of progressing to high levels of myopia
04 Which of the following statements regarding the treatment option shown is false?
a) A minimum Dk/t of 125 is required to avoid corneal oedema during sleep
b) This vision correction modality imposes relative peripheral hyperopic defocus
c) The lenses have a reverse geometry design
d) Studies show that these lenses offer a viable method of slowing myopia progression in children
05 Which of the following prescriptions is most suited to the lens type shown with the aim of slowing myopia progression?
a) -0.50DS
b) -3.25/-0.25 x 180
c) -8.00DS
d) -2.25/-2.50 x 90
06 Which of the following is an important consideration when offering this modality of wear to patients?
a) Time required for fitting and follow up appointments
b) Relatively high initial fee
c) Need for compliance with a strict hygiene regime
d) All of these options
IMAGE A IMAGE B
POINT
Prashant Shah MCOptom, PGDipOphth, DipClinOptom and Yashita Shah MCOptom, PGDipOphth
1 CPD
86 www.optometry.co.uk October/November 2022
07 The contact lens schematic illustrates a:
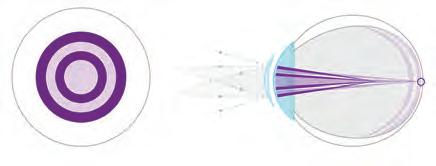
a) Dual-focus lens design
b) Centre-near bifocal
c) Orthokeratology design
d) None of these options
08 Which of the following prescriptions is suitable for the lens type shown?
a) R -1.75DS L -1.50DS
b) R -5.25/-0.50 x 40 L -5.00/-0.50 x 130
c) R -1.25/-0.75 x 180 L -2.75DS
d) All of these options
09 The lens design shown aims to slow myopia progression by:

a) Increasing accommodative lag
b) Imposing relative peripheral myopic defocus
c) Imposing relative peripheral hyperopic defocus
d) Increasing spherical aberration
Acknowledgements
Image B supplied courtesy of CooperVision Specialty EyeCare
Image C supplied courtesy of CooperVision
Image D supplied courtesy of Hoya.
10 Which of the following statements about the spectacle lens type shown is false?
a) The lens is based on a Defocus Incorporated Multiple Segments design
b) There is a lack of evidence to show that this spectacle lens type slows myopia progression
c) The array of +3.50D micro segments provide myopic defocus
d) The distance refractive error is corrected through the central optic zone
11 Which of the following statements regarding dispensing this lens type is false?
a) Pantoscopic tilt should be close to 00
b) Back vertex distance should be >12mm
c) The frame should have a B size of ≥25mm with at least 12mm above the pupil centre
d) The frame should have a face form angle of ≤50
12 The following prescriptions are suitable for the lens type shown except for:
a) R +0.50DS L -1.50DS
b) R -4.00/-3.25 x 90 L -3.50/-2.50 x 80
c) R -9.00DS L -8.00/-0.75 x 60
d) R -1.25DS 1.5∆ IN L -1.75/-1.75 x 180 1.5∆ IN
Prashant Shah completed his degree in optometry at City, University of London in 2004. He has postgraduate diplomas in ophthalmology and clinical optometry. Shah has worked in a variety of clinical settings including resident optometrist for a multiple, primary care ophthalmology alongside an ophthalmologist, supervising final year optometry students and a refractive surgery clinic. He currently works in private practice.

Yashita Shah completed her degree in optometry at City, University of London in 2004 and currently works in independent practice. Prior to this she worked in primary care ophthalmology alongside an ophthalmologist and supervised final year optometry students.
She holds a postgraduate diploma in ophthalmology and has a keen interest in myopia management and dry eye.

IMAGE C IMAGE D CONTACT LENSES, MYOPIA, PAEDIATRICS
IM A GE INTERP RE T A TION October/November 2022 www.optometry.co.uk 87
RETINAL CASES OF VISUAL LOSS
Himali Shah BSc (Hons), MCOptom, Prof Cert Med Ret
IN BRIEF Readers are invited to review the fundus images and consider the clinical features, using additional resources where necessary to answer the accompanying questions.
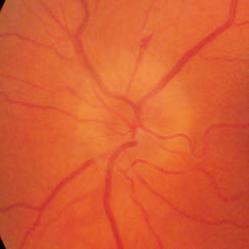

A 59-year-old female patient presents with sudden onset of a blurred patch in the central vision of her right eye.
01 Given the image and case history, what is the most likely diagnosis?
a) Nerve fibre myelination
b) Purtscher retinopathy
c) Branch retinal artery occlusion
d) Cilioretinal artery occlusion
02 Which of the following is leastlikely to be associated with the condition shown in the image?
a) Systemic hypertension
b) Hyperlipidaemia
c) Methotrexate
d) Pregnancy
03 The condition in the image can occur in:
a) Isolation
b) Patients with giant cell arteritis
c) Combination with central retinal vein occlusion
d) All of these options
A 61-year-old male patient presents after noticing obscured vision in the inferior nasal quadrant of his left eye. He has no other ocular or systemic symptoms.
04 Which of the following would be the most probable working diagnosis?
a) Retrobulbar neuritis
b) Papilloedema
c) Non-arteritic anterior ischaemic optic neuropathy
d) Neuroretinitis
05 Which of the following statements is false?
a) The right eye will demonstrate a relative afferent pupillary defect
b) Small crowded discs are at greater risk of developing this condition
c) Red desaturation is proportional to visual acuity loss
d) Disc oedema typically settles within four to six weeks and can be followed by neural retinal rim pallor
06 If the patient presented with eye pain, malaise, tender scalp and disc pallor, what would be the most probable working diagnosis?
a) Retrobulbar neuritis
b) Arteritic anterior ischaemic optic neuropathy
c) Non-arteritic anterior ischaemic optic neuropathy
d) Neuroretinitis
IMAGE A
IMAGE B
1 CPD POINT
88 www.optometry.co.uk October/November 2022
A 76-year-old female patient presents with progressive blurring of the vision in the right eye over the past few days.
07 What is the most likely diagnosis?
a) Ocular ischaemic syndrome
b) Hypertensive retinopathy
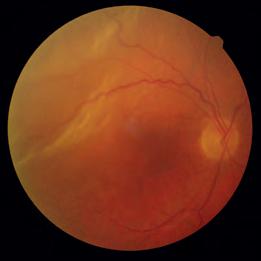

c) Central retinal vein occlusion
d) Background diabetic retinopathy
08 Which of the following is leastlikely to be associated with this condition?
a) Raised intraocular pressure
b) Iris neovascularisation

c) Vitreous haemorrhage
d) Disc oedema
09 Which of the following is a risk factor for this condition?
a) Hypertension
b) Diabetes
c) Raised intraocular pressure
d) All of these options
A 63-year-old female patient presents after noticing an increasing patch of misty vision in the inferior nasal quadrant of her right eye. She reports being in good health. A horseshoe tear is noted in the superior temporal quadrant.
10 What is the most likely diagnosis?
a) Rhegmatogenous retinal detachment
b) Tractional retinal detachment
c) Serous retinal detachment
d) Retinoschisis
11 Which of the following is a risk factor for this condition?
a) Posterior vitreous detachment
b) Myopia
c) Trauma
d) All of these options
12 In relation to treatment for this condition, which of the following is false?
a) Scleral buckling reduces vitreous traction and intraocular currents
b) Vitrectomy eliminates the effect of vitreous traction
c) Cryotherapy uses high temperatures to seal retinal breaks
d) Laser retinopexy can with used in combination with other treatment modalities
IM A
INTERP RE T
TION
Himali Shah graduated from Aston University in 2015 and currently works as an optometrist in primary care. Her interest in pathology led to the completion of a professional certificate in medical retina at City, University of London.
IMAGE C
IMAGE D
DIAGNOSTICS, PATHOLOGY, RETINA
GE
A
October/November 2022 www.optometry.co.uk 89
“I WANTED TO HELP PEOPLE”
Lorcan Butler
OPTOMETRIST
Tell us about what you do: I work to raise awareness of the link between brain tumours and eye exams. Early detection, early referral = a more favourable outcome.
Why did you become an optometrist? Because I wanted to help people in a health orientated profession.
If you could change one thing about optometry, what would it be and why?
To liaise and work better with other healthcare practitioners in the overall care of our patients. We tend to be siloed in our small, dark rooms too much.
Who inspires you?
Anybody who has overcome adversity and triumphed.
LORCAN’S 10-SECOND CHALLENGE
Face-to-face or Teams? Face-to-face Teaorcoffee?Tea Catsordogs?Dogs
Earlybirdornightowl?Earlybirdduring theweek,nightowlatweekends
Staycationorvacation?Vacation
Savouryorsweet?Sweet BakeofforMasterchef?Bakeoff.
What advice would you give newly-qualified optometrists?
It’s a long, tough year, but probably the most enjoyable one that you will have in your whole career. Enjoy it.
Tell OTabout one of your hobbies: I take part in pistol shooting.
Tell OTsomething unexpected about yourself: I was a hotel manager in a previous life.
What are you reading/watching at the moment? TheTerminalList
OT currently has a wide range of CPD available online covering all domains
n Microtropia: a practitioner-friendly guide
n Retinal detatchment: achieving the best outcome with posturing
n Practical tips for the identification of dry eye
n Bifocal lenses: are your standards up to standard?
The CPD articles are available at www.optometry.co.uk/CPD
n Retinal cases in secondary care
n All about the eyelids
n INTERACTIVE: Soft and RGP contact lens pearls.
CPDS COMING UP IN DECEMBER/JANUARY
n Strabismus: a simplified approach Professor Bruce Evans


n The detail is in the diagnosis: practical tips for diagnosing dry eye Megan Zabell
n The management of leukocoria Tavishi Kanwar, Guy Negretti, Sahar Parvizi and Mandeep Sagoo
n Inherited retinal diseases: preparing for emerging therapies Dr Alexis Ceecee Britten-Jones, Dr Jasleen Jolly
Dr Ian Beasley is the clinical editor for OTand head of education for the AOP. He began his career as an optical technician and later went on to train as a dispensing optician before qualifying as an optometrist in 1997. In 2013, Dr Beasley became the first person in the UK to graduate with a doctorate in optometry from Aston University. He is a visiting lecturer at Aston University, and recently completed a PhD which explored the effect of peripheral defocus on axial growth and modulation of refractive error in hyperopes.
Do you have an idea or request for a CPD article?
Email the clinical editor ianbeasley@optometry.co.uk
LIVE CPD Shutterstock 90 www.optometry.co.uk October/November 2022
CPD AUTHOR SPOTLIGHT














































Services and products for the practitioner Marketplace
MY WP10 PRESCRIPTION PAD
The Welsh Government recognises the potential for independent prescribers (IPs) and has made it very streamlined for us to get WP10 pads.
I’d been asking questions about how IPs could get access to pads before I was qualified. Our optometric adviser established a mechanism by which we could get access, and because of that the health board was very quick. It was only a couple of months between qualifying and having a WP10 pad. I’ve been using it since 2019.
I live in a remote, rural area, with low numbers of ophthalmologists and a very understaffed and geographically distant eye casualty. Some of my patients are travelling upwards of 50 miles to eye casualty, and there are challenges accessing that service, in terms of needing to speak to the triage nurse and then get through to the ophthalmologists on call. In the middle of a busy clinic, if you come across, for example, an iritis patient, making the diagnosis can be straightforward – but then you could spend half an hour on the phone, trying to arrange the appropriate care for the patient.
We pride ourselves in not sending patients with emergencies away, and 20% of my diary is held back for emergency and acute eye care type appointments, which can be complicated. If you’re waiting on the phone, that has an impact on your ability to deliver a service. You either can’t see as many patients, or the patient you should be seeing is being kept waiting, which is detrimental to your business. Obviously, patients
don’t enjoy waiting either. With a WP10 prescription pad, I can make the diagnosis, write up the prescription, and start treatment without the patient having to make a 100-mile round trip.
Patients who have recurrent eye problems know what the problem is. I know what the problem is. So, it’s about immediacy and appropriateness of care in a location closer to the patient, at a convenient time. It also reduces strain on hospitals, so secondary care is only having to deal with the problems only it can deal with.
I’m currently on the final phase of finishing my diploma in glaucoma,
which has meant that I can identify patients either having suboptimal responses or adverse reactions to glaucoma medications and communicate with ophthalmology to facilitate timely interventions.
Patients know that they can phone the practice and be seen the same day. They’re not trying to track down nurses or doctors. It improves my practice. I am a much more confident and competent optometrist by virtue of being able to do this, because you get to understand the nuances of treatment.
As an experienced IP optometrist, you’re delivering excellent clinical care, the patients like it, and if there’s a concern or a problem it’s very easy to review it. There’s a continuity of care.
There are two of us in my practice with WP10s. I’ve got a second colleague who obtained his a month ago, and another in training who is just waiting for a hospital placement. A fourth is just starting the IP course.
Within West Wales we have a scheme set up, where IP optometrists in the area should be the first port of call rather than the patient being sent to the hospital eye service. If a practice that doesn’t have access to an IP optometrist has a patient with a problem that could be dealt with by an IP optometrist, they should refer them to a practice that does. So, we have interprofessional referrals as well. I have phone calls from other practices, from other professionals in the area saying, ‘Look, Mrs Jones has got this problem. Can you see her please, Andy?’ It’s not just about looking after my patients, it’s about looking after the wider community.
Optometrist and director of Specsavers in Haverfordwest, Andy Britton, explains why access to a prescription pad is vital for patient care in his corner of rural Wales
I COULD NOT LIVE WITHOUT...
“As an experienced IP optometrist, you’re delivering excellent clinical care, the patients like it, and if there’s a concern or a problem it’s very easy to review it”
October/November 2022 www.optometry.co.uk 97
SpaMedica patient coordinator, Matthew Stephenson, on transforming into his drag queen alter ego, Emma Maezin – plus why his role is like an everlasting Christmas

MY SECRET LIFEAS...
M y role is patient coordinator for SpaMedica in Sheffield, which is a blend of administration and reception work. We help to improve people’s vision, providing NHS eye patient services, including cataract surgery. I can see a patient who has come for their assessment and has been apprehensive and nervous, I might be with them on their surgery day keeping them calm and then I get to see them thrilled when they have had their treatment. A lot of them write nice feedback or bring in chocolates. It’s like an everlasting Christmas.
I see drag as a way of dialling up my personality to 200. Everything I know as Matt helps Emma, and vice versa. There is that full circle. I remember how I felt watching RuPaul’sDragRace growing up and now I am probably that for other people. You can see the light in people’s eyes as they adore the performers living their authentic lives. I really love the peacock because it is the only species I can think of where the male is so much more vibrant, exotic and extravagant. I see my drag as a way of being a peacock. In my normal job I have my shirt and tie on – it is very formal. When I go into drag, I have my glitter, sparkles and rainbows.
The root of the name Emma Maezin (I’m Amazing) started with me not having that confidence in myself. I needed to find a name that would give
My secret life
Do you have a personal passion to share with readers?
Get in touch with selinapowell@ optometry.co.uk
me that switch in my brain –the name was like a shield of armour.
The very first time I did drag was at a competition called Drag Idol UK. I had my mum coming up on stage occasionally to pull down my dress. She has been there since day one and I can’t thank family and friends enough for their support.

At work, we celebrated Pride Month in June. One of our drivers, Nicky Taylor, is transitioning from male to female. It was the first time I had seen her come into work as female presenting, and I’m grateful to the business for giving people that opportunity to feel brave, supported and included. I had rainbows painted on my face and used a make-up tool to paint my colleagues too, to show our support to Nicky and Pride.
I get comments from people all the time asking why I don’t move somewhere bigger like Manchester, but I want to make the drag scene popular where I am in Sheffield. There is the realisation that if there are no opportunities, you have to make those opportunities.
I think it is really important to have safe spaces where people feel comfortable. What I am about in all aspects of my life is bringing people together and making sure they are having a nice time. I think that’s what life is.
“WhatIamaboutin allaspectsofmylifeis bringingpeopletogether andmakingsurethey arehavinganicetime. Ithinkthat’swhatlifeis”
98 www.optometry.co.uk October/November 2022
LAST WORD