








Practitioners



day
Health" - One-day lenses are the healthiest
to wear soft contact lenses. With silicone hydrogel material for high breathability and UV blocking·· for added protection.
Comfort - Optimised Comfort Edge'"and Wetloc"' Technology for all-day wearer comfort and hydration.
Adam Sampson

You need to feel that someone is on your side – and that someone is us, writes AOP CEO, Adam Sampson


Writing can be a horrible occupation. My father was a journalist, and some of my earliest memories are of emerging from my bed to be greeted by the sight of my dad, dishevelled and unshaven, sitting at his typewriter surrounded by coffee cups, with the floor covered in discarded drafts. You are reading this in the days of early spring. I am writing it in the dark, cold hours of early January. At a time when my contemporaries are starting to contemplate retirement, I find myself increasingly committed to work. Yes, on dank mornings like this, the temptation to pull the covers back and stay in bed is hard to resist, but I adore what I do.

At the AOP, spending time with my co-workers and the wider membership, I am part of a community – a family even. Yes –there are the formalities of the office, and the boundaries of our relationships are defined by the legalities of employment and membership duties. But within those boundaries, we act towards each other not as mere colleagues, but as members of a community. When people are having a difficult time, we offer help and support. Ring our legal team or talk to our clinical advisers, and you will get not just advice, but emotional understanding. Rules matter, but feelings matter too. This is one of the reasons why the AOP, both as an organisation and a membership body, has retained the loyalty of so many of our people. Over the three years I have been here, employee turnover has been amazingly low. Membership loyalty is incredible too: every year, over 97% of members renew, and the number who leave are more than made up for by the number who join. Among these are a small but significant number who leave temporarily (usually after graduation), later realising how vulnerable they are outside the AOP family.
As this edition of OTdiscusses, we understand how stressful it can be working in our sector and how important it is to have someone on your side. People tend to think the AOP is just about insurance (and OT). Yes of course, those things are important. But in truth, far more members need our help with the GOC, with disputes with their employer, with advice about clinical issues, and with access to CPD than ever face an insurance claim. The AOP is also there battling on your behalf with the Government to emphasise the importance of what optometrists (and DOs – we mustn’t forget those we have in our membership) can contribute to the nation’s health and wellbeing. On cold days like today (and in the equally cold days of February), you need to feel someone is on your side. That someone is us.
Adam Sampson, AOP chief executive


THE WIDEST MULTIFOCALRANGE FOR ASTIGMATISM NOW
AVAILABLEIN STOCKAND READYTO SHIP PARAMETERS







OT features a range of expert contributors who share their optometry expertise and insight. Here are some of those who helped us put this edition together

OTspeaks to Duncan & Todd about how the optical group has expanded it pre-reg recruitment programme, with students moving from Northern Ireland to Scotland In focusPAGE 40 -

February/March 2025
Volume 65:01 Issn 0268-5485
ABC certificate of circulation 1 January 2023–31 December 2023
Editor: Emily McCormick emilymccormick@optometry.co.uk
Deputy editor: Lucy Miller lucymiller@optometry.co.uk
Features editor: Selina Powell selinapowell@optometry.co.uk
Senior reporter: Kimberley Young kimberleyyoung@optometry.co.uk
Web content and social media manager: Leah Boyle leahboyle@optometry.co.uk
Clinical editor: Dr Ian Beasley ianbeasley@optometry.co.uk
Clinical editor for multimedia: Ceri Smith-Jaynes cerismithjaynes@optometry.co.uk
Video production editor: Laurence Derbyshire laurencederbyshire@optometry.co.uk
CPD enquiries: 020 7549 2076 CPDhelp@optometry.co.uk
AOP membership and OT subscription team: subscriptions@aop.org.uk
What is the most important tool in your toolkit for maintaining your workplace wellbeing and why?


“Spending long periods in front of screens, my Apple watch activity is a reminder to take a break. A sit-stand deck has also helped with my posture.”
Neil Retallic, optometrist
The cover story, page 10


“I have a photo of my two amazing daughters on my desk. Even during the most challenging days at work they always keep me smiling.”
Dr Grant Robinson, Cardiff University senior lecturer
How I got here, page 24

“My Outlook diary on my PC and phone supports meeting my commitments to a busy and varied schedule – giving peace of mind by planning.”
Sharon Beatty, Optometry Wales clinical adviser In focus, page 44
Advertising: Jamie Dawson 020 3771 7201 jamie.dawson@thinkpublishing.co.uk
Advertising production: aop@ccmediagroup.co.uk
Art director: Grant Pearce
Client engagement director: Kieran Paul Executive director: Jackie Scully
Published bimonthly for the Association of Optometrists by Think Media Group
65 Riding House Street, London, W1W 7EH
Printed by Acorn Web, Normanton Ind Estate, Loscoe Close, Normanton, West Yorkshire, WF6 1TW

All rights in and relating to this publication are expressly reserved. No part of this publication may be reproduced in any form or by any process without written permission from the AOP or the publisher. OT and its wrapper are produced on paper from European mills meeting the highest quality and environmental standards. The journal and paper wrapper are fully recyclable.






#EMILYMcCORMICK

Success and superheroes
What does success mean to you? was the theme of Hakim Group’s annual two-day retreat, which brought together over 2000 practice owners and their wider teams at the end of November. During a Comic Con-themed Saturday evening celebration, a number of practitioners from across the group were recognised, with special achievement awards given to Nick Rumney, Austin and Judith Roberts, Jonathan Foreman and Ivan Cammack.
0
Read our latest content, updated daily online: www.optometry.co.uk

OT’s latest skills guide series focuses on dry eye. Across the three videos, OT’s Ceri Smith-Jaynes and Laurence Derbyshire worked with Aston University’s Dr Sònia Travé Huarte to explore history and symptoms, the dry eye assessment and investigative techniques, and dry eye therapeutic management.

OT’s Emily McCormick travelled to Haverfordwest for the opening of Specsavers’ relocated practice, which boasts river-front views outside its 14 testing rooms following a £1.2million investment.


OT’s Laurence Derbyshire spoke to Professor David Thomson, optometrist and owner of Thomson Software Solutions, who volunteers at a community café every Thursday. The video interview is provided as an online exclusive to complement our I me edition cover story. Read more on page 10.
1 The impact of theft OT explores the rising levels of theft in optical workplaces

2
The Professor Bruce Evans episode
In the latest episode of The OT Podcast, we speak to Professor Bruce Evans
3
Not a dry eye in the practice
Optometrist Sarah Farrant on managing dry eye in practice and the importance of an armoury of options



Optical professionals share the activities that support their wellbeing in the wake of data that outlines challenging working conditions within the profession
WORDS: SELINA POWELL
PHOTOGRAPHY: ADRIAN JONES, LOUISE HAYWOOD-SCHIEFER




Some people have watches that remind them to take a break when they have been sitting for too long.
Optometrist Neil Retallic has a dachshund named Zeus. If Retallic has been sitting at his desk for too long, Zeus will roll a ball down the stairs before patiently descending the stairs to retrieve it and begin the cycle again.
His one-dog campaign for work-life balance has not gone unnoticed by Retallic. “Dogs know what is important,” he told OT “They always seem so happy to be part of your life and pleased about the small things,” Retallic shared.
Data from the General Optical Council (GOC) reveals that the optometry workforce is facing significant challenges when it comes to workplace satisfaction and wellbeing.
Published last July, the 2024 GOC Registrant Workforce and Perceptions Survey – which polled around 15% of registrant optometrists and dispensing opticians – found a noticeable increase in the proportion of respondents who were dissatisfied with their role.


One in four respondents said they were dissatisfied in their job, compared to one in five in 2023.
As part of Retallic’s own PhD research, he canvassed more than 1600 UK optometrists and pre-registration optometrists about their mental wellbeing through an online survey.
Retallic shared with OT that the survey found higher levels of mental wellbeing challenges among optometrists than the general population – in line with an earlier survey of Australian optometrists.
He added that around one in three optometrists surveyed were experiencing mental health challenges, with significantly higher levels among pre-registration optometrists.
Retallic reflected that pre-registration optometrists often lacked the time to build similar social networks to qualified optometrists, in part due to the additional demands of their professional training.
“They are a unique population because they are balancing study with a new job and clinical interactions, which isn’t easy,” he highlighted.
“It was also encouraging that they recognised the personal job satisfaction from supporting patients,” Retallic shared.
Common threads that arose from the survey were the importance of maintaining a good work-life balance, efficient clinic management, as well as the value of having support from colleagues.
Retallic highlighted that flexibility within roles – such as being given autonomy to take on additional qualifications or tailoring working hours to accommodate caring responsibilities – enhanced the wellbeing of optometrists. More than 1000 free text responses from optometrists included descriptions of how practitioners support their

Ò
Neil Retallic
own wellbeing, from therapy and mindfulness apps to taking a walk at lunch or meditating during a break.
“They’re not all massive changes. They’re little things that you can easily accommodate into your day,” Retallic highlighted.
One of the motivations for undertaking the study was to help inform the development of future support for the profession.
“We are already working on CPD sessions that will be delivered at 100% Optical and Specsavers events,” Retallic shared.
Adrian Jones
He emphasised the importance of addressing factors that can create challenges for wellbeing in the workplace. “It’s in everyone’s interest to take steps to create a happier
workforce,” Retallic said. “What we want to do is keep people in the profession for longer rather than losing them for avoidable reasons,” he added.
The 2024 GOC Registrant Workforce and Perceptions Survey found that 16% of respondents planned to leave the profession within the next two years.
Among this group, the most common reason cited for leaving the sector was ‘disillusionment with the profession’ (61%), followed by ‘to reduce stress/burnout/ fatigue’ (53%).


When it comes to his own wellbeing, Retallic pays tribute to his three dachshunds – Zeus, Dexter and Alexa.
He described to OT how they have added to his sense of purpose and routine. They have encouraged Retallic out of the house into nature and wreaked havoc on his household virtual assistant. “To be able to come back home to them has made such a difference,” he said. As well as being an advocate of pet ownership, Retallic supports his physical and mental wellbeing through regular gym sessions.
He shared that going to the gym gives him a sense of achievement and provides a break in the day when he is not looking at a screen or mobile.
“Our job is not as physically active as other occupations, so staying fit and healthy is important,” he said.
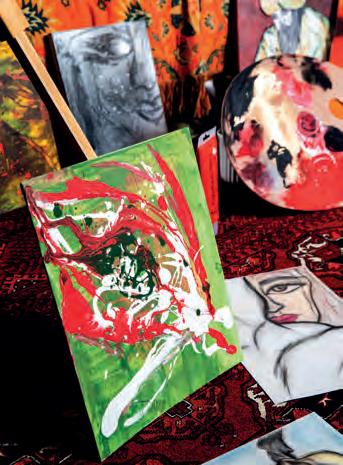
For dispensing optician and practice director, Shabnam Fazl, painting provides her with an anchor when dealing with everyday challenges.
“When things are not making sense – whether it is something personal or professional – the paint on the canvas

does,” she said. “After I paint, I have this incredible sense of calmness. I feel really grounded once I have put everything on the canvas,” Fazl shared.
After enjoying sketching as a child, Fazl began painting when her uncle made a canvas for her at the age of 16.
“From a young age, I watched him paint. He was my inspiration,” she said.
Fazl shared with OT that she has to be in a certain mood to paint. She keeps a blank canvas and brushes ready in case she feels the need to create an artwork.

She will sometimes wake up at midnight and begin painting in the office space she uses for her artwork.
Fazl observed that painting is similar to meditation. When she is working on a canvas, she has a sense of freedom.
“All stress, worries and anxieties seem to fade away as I get deeper and deeper into the paintings,” she said.
Fazl has infused her passion for creativity into her Broxbourne practice, E&G Opticians.
A range of artwork is displayed on the walls, including a series of pictures of eyes.
“A couple of patients have called our practice the eye gallery,” Fazl shared.
When KCM Community Café was on the verge of closing seven years ago, Professor David Thomson seemed an unlikely candidate to take over

the reins. “My main ventures into a kitchen are as a consumer, rather than someone with any culinary ability,” the founder of Thomson Software Solutions told OT.
However, faced with the prospect of losing a valuable community asset, Thomson decided to step out of his comfort zone and take over the management of the café.
“I thought, ‘Why not? I spend most of my life in front of a computer. Let’s do something completely different,” he said.
Although he originally envisioned making the café self-sustaining, then quietly withdrawing into the background, Thomson can be found each Thursday between 11am and 2pm chatting with regulars as they drink their tea and eat a baked potato.
“Much to my surprise, I absolutely loved it,” he said.
Thomson shared that the original idea behind establishing the café 18 years ago was to help people form connections over low-cost, nutritious meals.
“The idea was to provide a community hub where people could come and feel welcomed,” Thomson said.
Drawing on his software skills, Thomson wrote a bespoke café management system so that volunteers can take orders on tablets.
The café now has more than 100 regular attendees, from young parents to older customers who have forged new friendships through the café.
“The whole place has an amazing buzz about it, and the volunteers have formed a fairly close-knit group themselves,” Thomson said.
Thomson highlighted that his role at the café enhances his own wellbeing by giving him the sense that he is contributing to the community.
“You really come away feeling that you’ve done something worthwhile,” he said.
“There are a lot of lonely people out there, so in a very small way, in Potters Bar, hopefully we’re plugging that gap,” Thomson said.
He has on occasion made tea and coffee, but his culinary skills remain largely untested.
“They wouldn’t let me anywhere near preparing the food. I mainly go around, take the orders and chat,” Thomson shared.
“Despite my original intention to sneak out the back door after a year, here we are – seven years later. I love it. We will carry on for as long as we can, I think.”
After I paint, I have this incredible sense of calmness. I feel really grounded once I have put everything on the canvas
Shabnam Fazl
When he is not travelling to different areas of the UK and Ireland as Specsavers’ head of clinical performance, optometrist Russell Peake can be found at his 1960s Olivetti typewriter.
Since establishing the Spa Telegram service in 2021, Peake has typed close to 1000 telegrams.
The telegrams have marked a range of significant occasions, from births, marriages and exam results to a hand-delivered proposal and a transplant anniversary message between a mother who donated an organ to her son.
“I’m connecting people through the messages they send, and that’s a really lovely position to be in,” he shared with OT.
As someone who spends much of his working day in front of a computer screen, Peake enjoys the analogue nature of writing telegrams. The hobby also gets him outdoors as he delivers messages within the Leamington Spa and Warwick area by bike.
“This is genuinely something that supports my wellbeing, both mentally and physically,” he said.
Peake receives telegram requests through his website and Instagram page (@spatelegram), with £2 from each telegram ordered donated to LWS Night Shelter in Leamington. Messages have been sent as far afield as Australia, South Africa and Japan.
Reflecting on the pressures that exist within optometry, Peake shared that patients trust optometrists to look after their most important sense.



“It’s a job with responsibility and with that comes pressure,” he said.
Peake observed that optometrists may take their job home with them if they are worried about a management decision.
There is also potential for isolation in practices with a single optometrist. “It is important to have a peer network and the opportunity to be able to discuss any challenges,” Peake shared with OT.



As someone who visits a range of practices, Peake has observed factors that contribute to a positive workplace culture. These include having good systems in place for one-to-one meetings and personal development. Highly motivated and skilled support staff as well as strong teamwork is also key, Peake shared.
“There are no silos within the team. Everyone is working as one,” he said.

After a busy day, optometrist and practice owner, Zabir Ali, returns to his own small section of the Dorset countryside.
While he might hear the occasional honk of a peacock, when he is at home, Ali is largely insulated from the sounds of modern life.
“I wanted a place where I could go, close the gates and not hear any noise. There’s a real sense of relaxation,” Ali shared with OT.
On his acre and a half smallholding, Ali has four peacocks, four rescue alpacas, chickens and
ducks. He is close to both a beach and a forest. His surroundings are very different from his childhood in Birmingham, as one of five children growing up in a low-wage, single income household.
Ali has observed how the animals will change their behaviour as the temperatures drop.
“You learn so much from the natural world. We tend to be on this nine-to-five cycle every day of the year, which is not very natural,” Ali highlighted.
“This is the time of year where we’re meant to slow down, relax and get a bit more sleep,” he said.
Ali told OT that after the peacocks’ feathers fell out in autumn, he has noticed new growth in preparation for spring.
“You see that cycle year-in, yearout, and it gives you confidence that the world will be okay,” he shared. Alongside the wellbeing benefits of being immersed in nature, Ali enjoys a variety of exercise – from running and strength training to yoga and pilates.
He shared that the hardest part of exercising is often motivating himself to get out the door after a day at work.
However, Ali highlighted that the sense of achievement is worth the effort. “You could have been on the sofa eating crisps, but instead you have given something back to your body,” he said.
A health boost from hockey Hockey is a sport that has seen Jaclyn Payne represent Scotland and travel to France, Germany, Holland, Spain, Belgium and South Africa.
But aside from the opportunity to travel to far-flung locations, it is the daily boost to her physical and mental health that keeps the Specsavers Home Visits optometrist motivated to play – even when there are thunderclouds above or hail underfoot.
“Being out in the fresh air is wonderful. Exercise really does get the endorphins going to boost the mood,” Payne said.
Mehul Patel
As well as playing for the Huddersfield Dragons, Payne plays representative level hockey for two over 40s teams – Yorkshire and the North East, and Scotland.
She highlighted that hockey is a great sport for general fitness.
“There is a lot of sprinting, combined with pure endurance to last the game. You have to be strong to tackle but agile to change direction with your opponent,” Payne said.
The domiciliary optometrist emphasised the mental benefits of working towards a shared goal with a diverse range of people.
“We all have different things going on in our personal lives – ladies looking after elderly relatives, mums with kids driving them nuts, young women with relationship issues, teens going through exams. It’s such a great space to offload what has happened in your week if you choose to,” she said.
The employer perspective
Practice owner and AOP Councillor, Mehul Patel, feels a personal sense of duty towards his staff.
He knows their ambitions, their interests and their favourite hot drinks.
When he explains to his children the responsibilities of being a business owner, he tells them that he has 18 mouths to feed beyond their dining room table.
“I treat my team like a family,” he said. Team rewards have ranged from
weekends in Paris to a three-night Centre Parcs holiday for a longserving staff member. His practice manager, who turns 60 in March, has been gifted a five-night holiday in Malta.
Alongside these grand gestures, Patel believes that small acts of daily recognition are key – such as recognising exam results and celebrating birthdays.
“The personal touch is very important. We ensure that we value them, and something simple – like a birthday – is very important to recognise,” he said.
Patel believes that by investing in his staff, he will differentiate his practice as an employer.
He has observed in other workplaces how looking after staff can result in a more effective business.
“The restaurants where the waiters are happy are the ones that give you exemplary service,” he shared.
As a practice director at E&G Opticians, Fazl has focused on creating a positive work environment for her staff.
She encourages feedback from staff about any improvements that could be made to the business and is open to receiving any new ideas they may have. Fazl highlighted that investing in the team – and trusting them to make use of their skills – is a key priority. “Empowering individuals has always been my personal goal,” she said. “I don’t shy away from sharing work with them, allowing them to show their creativity and capability.”
0
Read the full article online, including the effect of high workloads on mental health: www.optometry.co.uk/the-cover-story

Selina Powell
OT features editor. Get in touch by email: selinapowell@optometry.co.uk
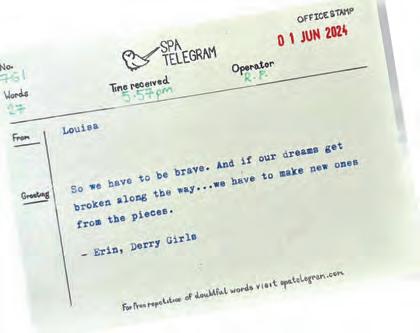
t'Excellent Vision' claim does not include ACUVUE® Soft Contact Lenses indicated for myopia management.
+Subjective Comfort Data has not been collected for the ACUVUE® drug-eluting [medication releasing] contact lenses.
1. JJV Data on File 2023: Survey among 150 eye care professionals in the United Kingdom between November and December 2023.
2. JJV Data on File 2022: Master Brand Claims on Clinical Performance and Overall Material Properties for ACUVUE® Brand Soft Contact Lenses.
Important Safety Information:
ACUVUE® Contact Lenses are indicated for vision correction. As with any contact lenses, eye problems, including corneal ulcers, can develop. Some wearers may experience mild irritation, itching or discomfort. Contact lenses should not be used in case of eye infections or any other eye conditions, or in case of a systemic disease that may affect the eye. For detailed product information, including contraindications, precautions and adverse reactions, please consult the Instructions for Use available on Johnson & Johnson website www.e-lFU.com or visit our Johnson & Johnson Vision website jnjvisionpro.co.uk
ACUVUE® is a registered trademark of Johnson & Johnson. © Johnson & Johnson and its affiliates 2025.

9
9

Canine companions and creative pursuits were centre stage in the I me cover story photoshoots

Artwork reminiscent of Dali and three dashing dogs featured in OT’s I me cover story photoshoots.
With a focus on wellbeing, OT explored the different hobbies that optical professionals pursue outside of practice to balance the stresses of working life.
Optometrist, Neil Retallic, was able to combine two activities close to his heart as part of his photoshoot – spending time with his three dogs, Zeus, Dexter and Alexa, and a rejuvenating gym workout. “I felt more at ease with the dogs featuring in most of the shots, and the time flew by, largely due to keeping the dogs on track,” he shared with OT
While Alexa was found to be the most flexible – she mastered balancing on top of a medicine ball – Zeus was the most athletic of the three, and Dexter focused on the simple joy of a good belly rub. Although they made a brief foray outdoors to take photos, the winter weather created challenges for these petite cameo stars.
“We popped to the park briefly, but it was clear the dogs were starting to feel the cold, so we headed home for a brew,” Retallic told OT.
Dispensing optician, Shabnam Fazl, was captured at home alongside her artwork – a pastime that helps to ground the director of Hakim Group independent, E&G Opticians.
She shared with OT that she was initially nervous but became calmer as the photoshoot progressed.
“Louise was an absolute delight. She made me feel so comfortable and at ease. Most importantly, we had a laugh and had a lot of fun,” she said.
Contributors Shabnam Fazl, Neil Retallic
Photographers Adrian Jones, Louise Haywood-Schiefer
You can watch our online exclusive video about volunteering at a community café with Professor David Thomson by following the QR code






a valuable prop on the
“It has been one of my favourite odysseys to become lost in a world of colour,” Shabnam told OT



describes painting as “a beautiful form of meditation”


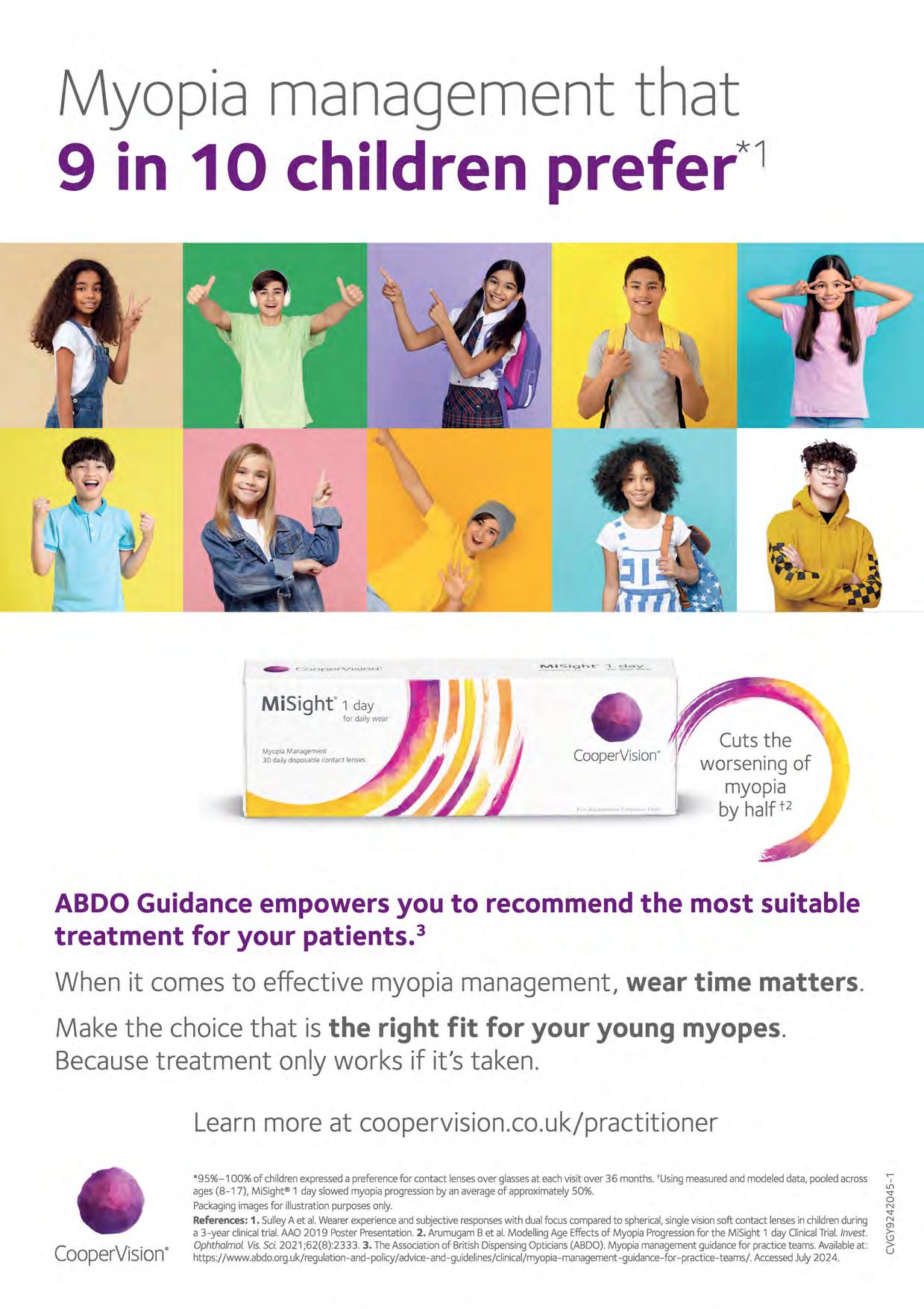
the worsening of
*95%-100% of childrenexpresseda preferencefor contact lensesover glassesat eachvisit over 36 months.'Using measuredand modeleddata, pooledacross ages(8-17), MiSight®1 day slowed myopia progressionby an averageof approximately50%. Packagingimagesfor illustrationpurposesonly.
References:1. SulleyA et al.Wearerexperienceand subjectiveresponseswith dualfocus comparedto spherical,singlevisionsoft contact lensesin childrenduring a 3-year clinicaltrial. AAO 2019 PosterPresentation.2. ArumugamBet al. ModellingAge Effectsof Myopia Progressionfor the MiSight 1 day ClinicalTrial.Invest. Ophtholmol.Vis.Sci.2021 ;62(8):2333. 3. TheAssociationof BritishDispensingOpticians(ABDO).Myopia managementguidancefor practiceteams.Availableat: https://www.abdo.org.uk/regulation-and-policy/advice-and-guidelines/clinical/myopia-management-guidance-for -practice-teams/. AccessedJuly 202 4.
Career paths and personal development
EDITED BY: LUCY MILLER

Working as a mental health champion in practice
DECODING DOMICILIARY
“It is one of the most rewarding roles in optometry”
24 30 35
Anish Mistry, optometry director at Specsavers Nottinghamshire 2 Domiciliary Home Visits, on the value of providing care for vulnerable patients
I became a domiciliary optometrist because... After several years working as a High Street optometrist, I felt ready for a new challenge. A medical camp in India gave me the confidence that I could be adaptable when delivering care for patients.
What I enjoy most about domiciliary optometry is... Each clinic offers a unique experience, requiring quick adaptation. Patients share fascinating life stories, and time flies by as you engage with their needs. It is one of the most rewarding roles in optometry.
The one thing I would change about domiciliary optometry is... Domiciliary patients face barriers in accessing care. NHS-commissioned visits in England require a pre-visit notification to the relevant NHS authority. This means that we can’t see any patients without giving 48 hours’ notice.
The most common misconception I hear about domiciliary optometry is... That domiciliary optometrists do a lot of travelling. As demand rises with an ageing population, clinics are becoming more clustered within single postcode
HOW I GOT HERE
Dr Grant Robinson on how teaching keeps him motivated
IP AND ME
Increasing discomfort in a dry eye disease patient
A DAY IN THE LIFE OF A BUSINESS OWNER
Sian Wilkie’s local ambitions

areas, reducing travel time. Flexible hours can support work-life balance, allowing clinics to start after and finish before school runs.
The one piece of advice I would give to those considering moving into domiciliary optometry is... Know that you are making a real difference to people’s lives.

Read about Anish’s experiences as a domiciliary optometrist in full on our website. 0

“THE
Cardiff University’s Dr Grant Robinson tells OT how postgraduate teaching keeps him motivated as a clinician
My interest in eyes goes back to childhood. My first school photograph shows me wearing glasses, and I remember having cycloplegic drops instilled regularly. Despite the momentary sting, I always enjoyed the experience as I got to wear my father’s sunglasses afterwards.
I gravitated towards science at school, and having skimmed through the stack of prospectuses in the library at the age of 18 I began to consider a career in healthcare. Having worn glasses every day for 13 years, I was most familiar with optometry compared to the other disciplines. I decided to explore the profession further via work experience with my family optometrist.
I decided I would give optometry a go, so off I went to study at Cardiff University. During my time as a student, I worked as an optical assistant and honed my communication skills as a barman at Ebbw Vale Rugby Club. One highlight occurred during my placement in eye casualty at the University Hospital of Wales, where I was able to assess a patient who had a penetrating, fishhook-related eye injury.
I enjoyed university so much that I stayed to do my pre-reg at the on-site clinic. I have since been informed I got the place over other candidates because I offered to get the staff a cup of tea and a biscuit when asked what I thought makes a successful team tick.
After I qualified, I moved to the North West of England and worked for various multiples. It was at this time I developed an urge to teach. It wasn’t entirely altruistic at first, as I would reinforce my own clinical knowledge by hosting weekly themed sessions for the optical assistants, one of whom is now a qualified optometrist himself.
I had always wanted to return to Cardiff, and when I saw a PhD advertised there in 2014, I thought: why not? I finished my role in Liverpool and headed back to Wales. My research involved conducting a randomised controlled trial to investigate the impact of light therapy on age-related macular degeneration. I was also lucky enough to work alongside some inspirational eye specialists at Bristol Eye Hospital’s clinical research unit.
During my PhD, I had the opportunity to teach first year optometry students. My experiences at that time have underpinned my career in academia. After my PhD finished, I worked
part-time as a locum optometrist and postgraduate teacher for the Wales Optometry Postgraduate Education Centre. I also had a short stint as co-founder of a cosmetic contact lens company for the television and film industry.
I“I have always valued retaining a day in clinic”
The balance between work in primary care and education slowly shifted to academia. However, I have always valued retaining a day in clinic, whether as a community optometrist or within a secondary care setting. As a firm believer of ‘practise what you preach,’ I have studied many postgraduate courses, including those in glaucoma, independent prescribing, medical retina, low vision and medical teaching.
Over the years I progressed to senior lecturer, and have also been the director of postgraduate taught programmes. Having oversight of the delivery and direction of postgraduate provision at the school gave me the opportunity to develop both as an educator and leader. The role was often challenging, but it was wonderfully rewarding too, and I got to lead an amazing team.
NAME: Dr Grant Robinson
ROLE: Senior lecturer, School of Optometry and Vision Sciences at Cardiff University
LOCATION: Cardiff
The students motivate me to ensure that the training we offer moves with developments in practice and technology. Even though education is only one piece of what happens in the optometry profession, I feel privileged to be involved with programmes that make a real difference to patient care, job satisfaction and career development.
I am proud to be an optometrist, and of all my optometry peers who I have seen successfully further their knowledge and skillset through postgraduate study.
0
Read more career insights online: www.optometry.co.uk/how-i-got-here
Any regrets?
I have never worked in my hometown of Brynmawr, in Blaenau Gwent, South Wales. I have also never performed an eye examination in the Welsh language, which I am still trying to learn. To give back to my local community and achieve these goals would give me an enormous sense of pride. Diolch am ddarllen.
"
NHS servicesnow available;*
• Cataract Surgery with Premium EDOF lens option
• YAG Laser Capsulotomy
• Glaucoma Management
• Minimally Invasive Glaucoma Surgery (MIGS)
• Medical Retina
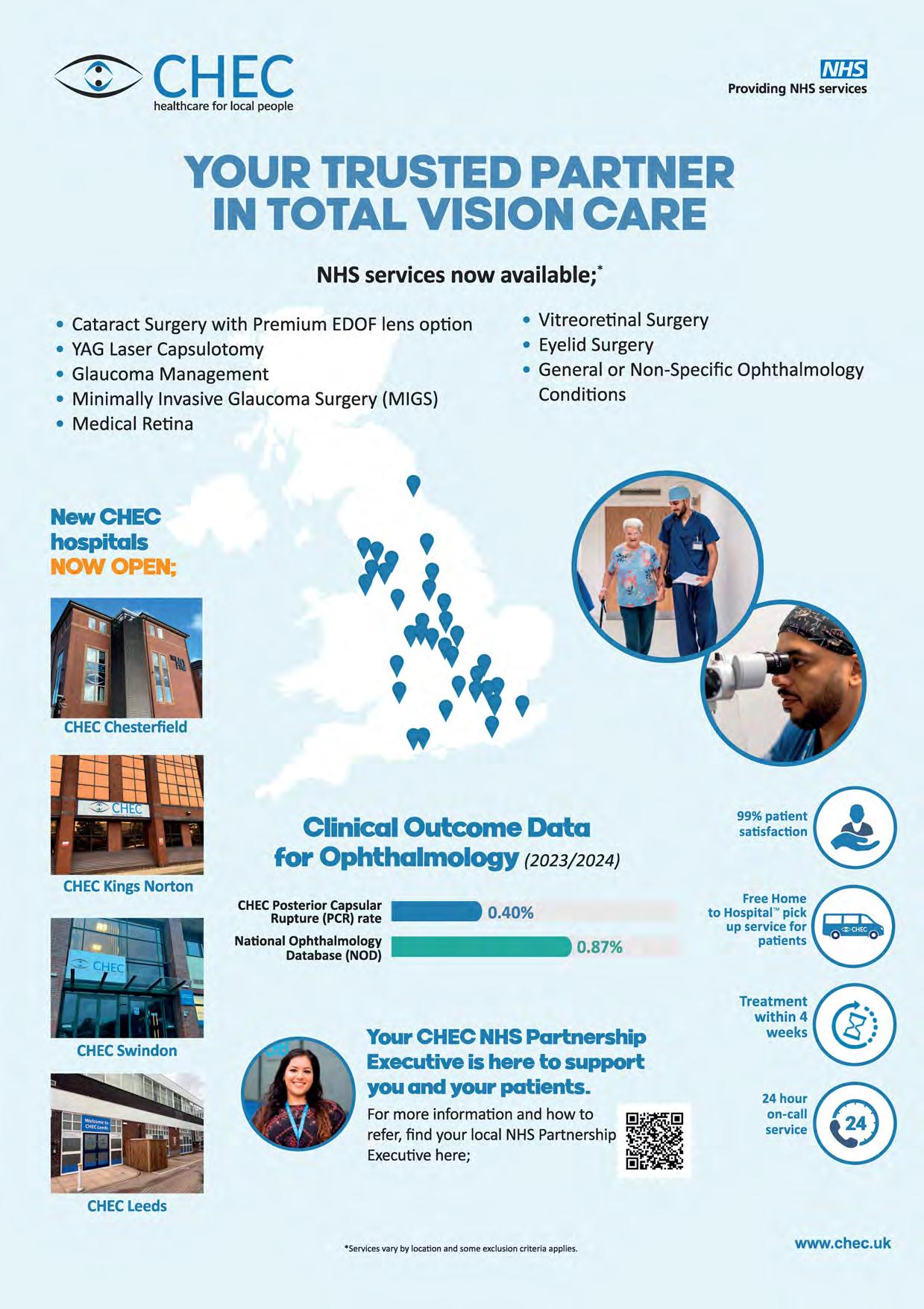
• Vitreoretinal Surgery
• Eyelid Surgery
• General or Non-Specific Ophthalmology Conditions
James Brawn tells OT how locuming has given him the opportunity to explore optometry from a variety of angles
Before I became a locum, I was working...
As a pre-reg at an independent, Parish and Green in Pencoed, just outside Bridgend. It was just me and my supervisor. I’ve never been a resident. As soon as I qualified, I was locuming.
When I started as a locum, I wish I had known… What the market rate was. Being selfemployed, you’ll say what your rate is for a day’s work. I had no idea. I found out six months later that I was being paid £100 less per day than the other locum. I was very much undercharging for the services I was providing.
The person who helped me as a locum was…
My pre-reg supervisor. The experience I had as a pre-reg meant I was prepared to make the jump to be a locum. I’d seen lots of pathology, and my supervisor had helped turn me into a competent and strong optometrist. I was able to make that leap from day one.
I made the decision to become a locum because of... Flexibility. I knew, once I qualified, that I wanted to go back and do a postgraduate degree at Cardiff. Being a resident would not have been compatible with pursuing that. Locuming has let me pursue different things without having to request time off. I’ve been in and out of study since I qualified. Currently, I’m retraining as a doctor, and I wouldn’t be able to do that without being able to locum to support myself.
My first day of locuming... Didn’t go well. There were four optometrists testing, including myself, and a lot of no-shows. They were doing a rolling
clinic, which meant that, as the residents were a bit quicker than I was, I ended up seeing about six patients on my first day. There were so many no-shows that there was no one left me to see. The director got quite upset with me, afterwards. It was quite a shock to the system. It made me realise that maybe not everyone at work would be as understanding as I’d found in my pre-reg.
One change I’ve seen whilst working as a locum is… The amount of clinical knowledge that you need has increased. In Wales, by virtue of the new contract, we all deliver some form of enhanced services, which means that we probably take on more complex patients than traditionally we might have done.
I“Locuming has let me pursue different things without having to request time off”
Practices can make life easier for locums by… Reaching out to ask if there is anything that, as locum, I need, or that I need to know. It could just be simple things such as passwords for computers, or whether there is a dispensing optician I can hand over to.
NAME: James Brawn
ROLE:
Locum optometrist
LOCATION: Bridgend

My favourite thing about being a locum is… Working in different places and meeting different people. One of my drivers towards locuming was that I didn’t like the idea of being in the same room, in the same practice, for the rest of my life. I liked the idea of having variety. I feel as though it has kept me fresh, especially when I was taking on more of a portfolio role. It has also allowed me to gain more experiences. It helps you become more of a rounded person and more of a rounded practitioner.
My advice for new locums is... To be organised in regard to your bookings, expenses, and invoicing. Number two would be to talk with other locums from your area, to understand things like the rates and what is acceptable practice.
Read more locum insights online: www.optometry.co.uk/life-as-a-locum

YOU HAD ME AT HOSPITAL
Krupa Mistry, advanced clinical hospital optometrist at St Thomas’ Hospital, on summoning the courage to leave the NHS trust that had been her home since qualification

When did you decide to become a hospital optometrist?
I was a pre-registration hospital optometrist at University Hospitals Coventry and Warwickshire. I was fortunate to end up doing my pre-registration year in a hospital. I’ve never really looked back – I’ve always stayed within the hospital eye service. I’ve been able to go into different roles, and that has allowed me to specialise in a specific niche, which I really enjoy.
How does working as a hospital optometrist support you as a High Street optometrist?
The experience that I’ve gained from hospital optometry – the specialist contact lens fitting that we do within the hospital service, such as fitting keratoconics and fitting complex contact lenses – is applicable in independent practice. The hospital work has allowed me to specialise in this in the community. If I didn’t work in a hospital setting, I don’t think I would be fitting those types of contact lenses on patients in the community.
How does working on the High Street benefit you in the hospital setting?
I don’t do any contact lens fitting anymore in the hospital eye service, so the High Street keeps me up to date with my contact lens knowledge, and aware of what new lenses are on the market.
Equally, because of the advanced clinical role that I now do within the hospital service, I don’t do any routine eye testing or refractions within the hospital anymore. It’s good to keep up my core skills as an optometrist in the community. If I completely specialised, I don’t think I would be keeping up with those skills.
What is hospital optometry’s biggest success in the past three years?
The Hospital and Specialty Optometrists Conference that the AOP held in September in Manchester. It was great because it wasn’t just for hospital optometrists – there were independent prescribing (IP) optometrists there as well. More optometrists are coming out with IP, and I think the conference is a great way to network. There are some really skilled


non-hospital optometrists out there, who really benefited from the lectures and talks over that weekend.
What is your biggest success in the past three years and why?
NAME: Krupa Mistry
ROLE: Advanced clinical hospital optometrist, St Thomas’ NHS Foundation Trust
LOCATION: London
Taking the leap of moving on from the trust where I did my pre-registration year. I was at Coventry and Warwickshire for eight years or so. It’s hard to make a jump when you feel comfortable with your work colleagues and the environment that you’re working in, especially when your colleagues have known you from being 22 and fresh out of university.
I really put myself out of my comfort zone, to even apply for a role that was not local to home. But I’m really proud, and I think it’s the best decision that I’ve made.
0
Read more hospital insights online: www.optometry.co.uk/you-had-me-at-hospital
One valuable moment
In January 2024, a team of us from my old job at Coventry and Warwickshire, along with a group of consultants, optometrists and nurses from across the UK, came together and volunteered in Cambodia. We provided cataract surgery for patients who didn’t have access to any healthcare. The skills of pre-assessment and postassessment that I learned from being a hospital optometrist allowed me to help carry out that voluntary work. That’s a time where I felt appreciated for the role that I do as an optometrist.

OT presents a clinical scenario to three of its resident IP optometrists. Here,
The scenario:
A 40-year-old woman who has previously been diagnosed with dry eye disease presents at your practice. The Hypromellose drops that she was previously prescribed have made her eyes more uncomfortable, and she is now struggling to work. How would you manage?
OT’s panel says...
Kevin Wallace: First of all, I would want to know more about the dry eye disease – so she needs a thorough examination of the external eye to see if there is anything else that needs to be done. I always explain to patients that it’s better to treat the problem rather than the symptoms, so if there is an element of, for example, lid margin disease, I’d want to treat that and then deal with what we have left.



Hypromellose is a basic drop, and is probably preserved, so that is a likely culprit for the discomfort. If I decide that lubrication is still required, I would switch to a preservative-free formulation of something more viscous. My usual regime is ‘qds and prn’ (four times a day, and as needed). I tell patients that it’s easier to keep an eye comfortable than it is to undry it once it gets dry. If they just use drops when they feel they have to, that isn’t as effective.









“In an ideal world, she would book a full dry eye work-up, which begins with a dry eye specific questionnaire”
Ceri Smith-Jaynes, OT clinical
multimedia editor
Ceri Smith-Jaynes: As Kevin said, the preservative in the drops, for example benzalkonium chloride (BAK), could be the culprit. Or is it just that the dry eye issue has been getting worse despite the use of an ocular lubricant?
In an ideal world, she would book a full dry eye work-up, which begins with a dry eye specific questionnaire, including questions about health and lifestyle. I’d like to know what her work involves. More people are working from home on multiple computer screens and, with online meetings and smartphones for socialising, screen time has increased. We know that blink rate reduces when people concentrate, allowing time for tears to evaporate between blinks and the osmolarity of the tears increases, causing inflammation.
After fully investigating, I’ll hopefully be able to diagnose evaporative dry eye, aqueous deficiency, or a mixture of both, and make some informed recommendations. This will be a conversation, followed by a written report, with lifestyle and dietary advice, homework to do (such as warm compresses, lid hygiene, use of drops), and in-clinic treatments if needed (such as lid debridement, meibomian gland expression, intense pulsed light, punctal plugs).
As an IP, dry eye and eyelid treatment may involve topical antibiotics or non-penetrating steroid drops. A recent study reported the use of topical ivermectin for improving Demodex-related blepharitis, but I have no personal experience of this so far (bit.ly/3WvfsHm).
I’d recommend referring to the TFOS DEWS II report to inform your dry eye practice. I’m looking forward to the DEWS III update, which I gather is in progress.
Ankur Trivedi: As already mentioned, my first thought is around this being an issue with preservative or an escalation of the underlying dryness issue.
As both Kevin and Ceri have outlined, a thorough examination, ideally focused on the external eye to identify the type of dry eye and ultimate causative factors at play, is required.
As well as the potential issues listed by Ceri, there could be hormonal changes that may be identified during the history and symptoms that can have a big impact on escalation of a pre-existing issue.
Also, mechanical issues with changes in time to the adnexa could have occurred, which may require referral to an ocuplastics specialist.
I agree that the use of topical antibiotics and topical steroids is very useful in getting patients with more marked dry eye issues to a much more manageable level, which then allows the self-management or home treatment to be more effective in controlling the symptoms.
In terms of warm compresses that I have found in the past 12 months, there has been a move toward electronic devices to produce the heat, with some that also have a vibrating or massage function.
The TFOS DEWS II report is a very useful tool to underpin establishing dry eye management in practice. I have found it allows a framework to manage dry eye patients. This work can be extremely rewarding and allows for great practice growth. I find that dry eye patients are often great advocates for a practice.
If you are unsure about how to manage a scenario in practice, contact the AOP’s regulation team: regulation@aop.org.uk










The UK’s first UKCA-approved VR eye testing platform with AI-optimized visual fields, supported by Swiss R&D and validated in clinical studies.







PRE-REG FOCUS
Habeeb Rahman tells OT about the importance of staying calm in stressful practice situations as he prepares for Stage 2
As I approach the end of Stage 1, I’m excited to have just a few competencies left to complete before moving on to Stage 2. My hybrid setup has made it easier to compile a wide variety of patient records for my visits, boosting my confidence and clinical decision-making skills. Overall, the journey has been enriching and fulfilling, and I feel well prepared to take on the challenges of Stage 2.
My pre-reg has reinforced my conviction that every patient is unique, and understanding their individual needs is at the heart of providing excellent care. Each day presents new challenges, and sometimes seeing conditions you haven’t come across before can be daunting. However, learning to adapt quickly and having the confidence to handle unexpected situations within a supervised environment allows me to refine my approach and develop my skills.
My day-to-day routine has been more varied than I had initially expected. I never imagined that during my pre-reg I would be removing a foreign body from a patient’s eye or assessing the anterior angle using a gonioscope lens. This felt like something I’d only observe, not perform so early on. These experiences have shown me just how hands-on and varied my role can be. Whether it’s dealing with unexpected emergency cases, attempting advanced techniques like gonioscopy, or handling patients with unique conditions, my pre-reg has kept me on my toes and constantly learning. Each day brings something new, and with it, opportunities to further my experience.
My supervisor has provided me with guidance and has pushed me to excel in my role. In addition to my primary supervisor at the independent practice, I’m fortunate to have multiple mentors at the hospital. This has allowed me to gain valuable perspectives in secondary care from a multidisciplinary team, enhancing the level of care I can provide.
The progress I’ve made since my first day as a pre-reg has been incredible. I’ve grown in confidence, from performing routine sight tests and contact lens appointments to managing more complex cases and playing a significant role in the delivery of our enhanced services. Beyond clinical skills, I’ve developed stronger communication and decision-making abilities, learning to put patients at ease. It’s exciting to see how much more independent and capable I’ve become.
NAME: Habeeb Rahman
ROLE: Pre-reg optometrist at James Bontoft Optometrist, the Royal Blackburn Hospital, and Burnley General Hospital
LOCATION: Barnoldswick
One stand-out moment was successfully removing a foreign body from a patient who was in severe pain. Despite their distress, I remained calm and focused, reassuring the patient while having my supervisor guide me. Having shadowed this procedure several times, I was well-prepared to handle the situation. Following the removal, the patient was overwhelmed with gratitude. This experience showed the immediate impact we can have on a patient’s quality of life and how much trust they place in us. It reinforced just how rewarding this profession can be.
Pre-reg is a unique opportunity to grow, learn, and develop. It’s also a rollercoaster journey where balancing full-time work with continuous assessments can feel overwhelming at times, but my advice is to try your best to enjoy it. Embrace the challenges as opportunities to improve, and don’t be afraid to ask questions or lean on your supervisors and peers for support. Every patient, every case, and every day will teach you something new.
Over the next few months, I plan to start preparing for Stage 2. This will involve tackling 100+ case scenarios and further refining my routine eye exam and contact lens techniques in preparation for the assessment.



Follow Zahrah, our Pre-reg focus video contributor, on OT’s Instagram page @optometry_today Zahrah Khan is a pre-reg optometrist at Moorfields Eyes Hospital. Watch her third video online now

Whateveryourlearningstyle, hangout with us.
At the CooperVisionLearningAcademy'"we believeeveryoneshouldlearn in a way that suits them best, whether that's fast or more laid back.That's why we offer everything from quick 30-minute 'espresso'sessionsto comprehensivelecturesand gamified learning-all accessible 24/7 on any device.Freefor every member of your practiceteam, from receptionto clinician. Ready to learn your way?
and
06:00
I get up when my little girl gets up, usually around 6am. The first thing I do is go through to her room, and get her ready for nursery. My husband then takes her to nursery, and I go to the gym for 7am.
08:00
I’m home from the gym at 8am, to walk the dogs and get ready to go into the practice.
09:15
I work from home for some of the week, but on the days I’m in, I will get into practice for quarter past nine.
Sian Wilkie, practice director at Wilkie’s Eyecare in Alexandria, on the balance of at home and in practice working, and the importance of the local High Street
I run the clinic on a Tuesday, so I am usually juggling between managing that alongside the diary for the day, and doing the business admin – bills, processing holiday requests, and marketing – and trying to get everything done in the time that I have.
14:00
The clinic lasts until lunchtime, so the practice is usually closed in the afternoon. Lunch doesn’t really exist for me. I’ll be working through, and then because I’m at home for the afternoon, I usually grab something on my way back. I come back at around two o’clock, and work from home for three hours.
15:00
Working from home is usually more admin: going through policies and statements, and processing the paperwork side of things, as well as looking at ways to grow the business. We write quite a lot of stories to
My fantasy practice...
NAME: Sian Wilkie
ROLE: Practice director, Wilkie’s Eyecare
LOCATION: Alexandria, West Dunbartonshire
If I had an unlimited practice budget, I would invest more in the service that we can provide for our customers, including having the best dry eye management. We already do visual stress and myopia control, but we would invest in the best equipment, so that we could diagnose in practice as quickly and efficiently as possible, and refer
promote who we are, and what we’re doing individually, as well as the practice. It’s also about improving the main street in Alexandria. Our recent Business Improvement District application was successful. For me, it’s about ensuring that the business survives and that the main street around it survives too. Our ethos is giving the best service to customers.
16:45 I close the laptop and finish work at around quarter to five. Taking time for myself is important. If I didn’t do that, the slump would kick in. Mentally, for me, it’s about physical exercise. That’s what gives me energy.
18:00
In the evening, we’ll watch anything that involves cooking. MasterChef – those sorts of programmes. Easy watching.

19:00
My go-to mid-week dinner, at this particular time of year, would be something really hearty –any sort of stew, anything with carbs, or a pasta dish.
My no.1 wellbeing tip is... Ensuring I carve out 45 minutes every day for myself
Read more business owner stories online: www.optometry.co.uk/ a-day-in-the-life
on to specialists where needed. Maybe in the pipeline, is opening our own private ophthalmic hospital. It would be a one-stop shop: patients coming into us, and us referring to Wilkie’s Eye Care Clinic, and we would do everything. The customer wants to be referred to somebody they trust, so that would be the goal: opening our all-singing, all-dancing clinic, to go along with our opticians. That would be invaluable.
A CONVERSATION ABOUT...
Optical assistants Chris Rosser and Kelly Cato, from Specsavers Haverfordwest, tell OT about the mental health support they are offering colleagues in practice
0
A point of contact for colleagues
Chris Rosser (CR): The first aspect of the role is as a point of contact for all our colleagues. If they’re struggling with their wellbeing, they’ve got someone to talk to. It’s a bit like being a physical first aider, where you’ve got an initial person to look after you and help you find the next stage of help if needed. They can come and talk to us in confidence, at any time, including if they want to talk outside of work. We can also approach people if we think they need a chat: put the time and the place in, and start the conversation.
NAME: Chris Rosser
ROLE: Optical assistant, Specsavers Haverfordwest
LOCATION: Haverfordwest
NAME: Kelly Cato
ROLE: Retail optical assistant, Specsavers Haverfordwest
LOCATION: Haverfordwest



The second stage is to encourage people to talk about their mental health. People find that hard, so we encourage them to talk about it, to try and reduce the stigma attached to poor mental health.
Kelly Cato (KC): I’ve got a good rapport with a lot of staff here. I get along with a lot of people, so they can come to me, and it’s the same with Chris. When it’s someone that they can get on with, they can approach us easily.
CR: I’ve been at the practice 17 years now, so I’ve worked with some people a long time. We’ve got some lifelong friends working here. Once they have talked to me, and I’ve made it clear it’s in confidence, colleagues are more comfortable coming back. I can check in regularly, keeping an eye on them.
Like a physical first aider, it’s essential to have one in every workplace. You cut yourself, you’re bleeding – what do you do? It’s understood by management that, if somebody is at crisis point, we will drop what we’re doing and look after them.
We created a list of contacts: phone helplines, websites, support groups. If people say they are struggling with anxiety, we can provide them with links. If they don’t feel like making a


“It’s a bit like being a physical first aider, where you’ve got an initial person to look after you”
Chris Rosser, optical assistant at Specsavers Haverfordwest
phone call themselves, we’ll sit with them or arrange appointments for them.
KC: We are both here most of the time. If someone is in crisis, we’re here to help them and point them in the right direction. It’s the first job I’ve had where we’ve had a mental health first aider in store. Where I worked in the past, that would have helped a lot.
CR: I’ve had patients ask me about it, and saying they’ve never heard of it before. When you explain the role, they’re interested. I think there are now one million mental health first aiders in the UK. It is becoming more widespread.
Finding balance
CR: We also have a wellbeing intranet page, which we update with contact information, and things to do monthly and every day. Management knows this is part of our role, so we make time for that. Like a first aid emergency, you drop everything, because that is more important.
The challenge is balancing it with everything else, and looking after your own wellbeing. If you’ve talked to a few different people, you do worry about them. You have to look after yourself too.
CR: Everybody is going through something that you know nothing about, often in their life outside of work. It can weigh on people. Stress is a huge thing. It makes people physically and mentally ill. Having somebody there, like a first aider, means someone to talk to and someone to share that load with, and it makes such a big difference. People think their problems are their own, and they can’t do anything about them. But actually, we can help them.
KC: I’ve had struggles, and I feel like, in helping my colleagues, I’m giving help back. It’s nice to return the help I received in the past.
0
Read more in this series online: www.optometry.co.uk/a-conversation-about

































OT heard from the event organisers in the final weeks before the show
Spring is rapidly approaching, a new continuing professional development cycle is underway, and 100% Optical 2025 is just around the corner.
Taking place from 1–3 March, the event will see the optical industry come together at ExCeL London.
More than 250 exhibitors will attend the show, highlighting the latest in design and technology in optics.
Exhibitors, new stands, and awards
Selin Pera, senior marketing executive at CloserStill Media, shared that, whether attending one day or all three: “It’s important to plan your time wisely, as there will be lots going on around the show.”
Delegates can find the exhibitor list on the 100% Optical website to take a look at the brands that will be represented at the show.
Pera recommended contacting exhibitors through the website, sharing: “This way, you’ll be able to book meetings with these brands pre-show.”
New exhibitors include Mykita, Hoffmann Natural Eyewear, Clayton Franklin Spectacles, Italart Occhiali, Wright & Bailey London, and Cerruti 1881. Dita Lancier will also take a space at 100% Optical for the first time this year to showcase its latest collection.
Pera explained that the brand is “one of the most requested exhibitors by delegates each year.”
The Love Eyewear Awards will return for 2025, with a celebration on the 100% Catwalk on the first day of the show.
A new category has been introduced to the awards this year for ‘Best Use of Social Media’ by a practice or optical retailer. A former winner of the ‘Eyewear Retailer of the Year’ award, dispensing optician, Nicos Antoniades, has also joined the judging panel this year.
Pera encouraged delegates to follow 100% Optical on social media for giveaways and competitions in the run-up to the show.
Ava Williams, events manager at the AOP, told OT: In addition to our education offering, the AOP Lounge is a hub for AOP members to network over a free cup of tea or coffee. Simply show your name badge, which will identify you as a member, at the AOP café to collect your hot drink. The AOP team will also be around during the show’s three days to answer questions about membership on our on-stand helpdesk.
Ramadan will coincide with 100% Optical, beginning from 28 February, and event organisers have highlighted that prayer rooms are available at ExCeL London.
The registration form for 100% Optical has been updated to allow visitors to add accessibility requests. Delegates who require a food voucher for Iftar are encouraged to contact 100% Optical organisers directly via marketing@100percentoptical.com with requests.
Those who have requested a food voucher for Iftar can collect it at the organiser’s office during the show. Pera said: “We can only accommodate those who contact us before to let us know that they will be observing Ramadan with special requests.”
Dr Ian Beasley, AOP head of education and OT clinical editor, commented: “With spring approaching and the fresh impetus of a new CPD cycle, 100% Optical 2025 marks an ideal opportunity to start ticking off those important boxes, such as your peer review requirement and meeting core domains.”
With more than 100 education sessions in the programme for 2025, there will be subjects to suit a variety of professional interests.
Beasley encouraged delegates to explore the whole education programme, available online.
He commented: “Why not look through the topics and themes covered in the education programme and use this as a springboard to inform the creation of your personal development plan for the new CPD cycle?”


“You could consider booking onto sessions covering topics that you notice you might want to consolidate your knowledge on, or new areas you are unfamiliar with,” he suggested.
Due to popular demand, additional capacity will be released across the education programme on 10 February, providing delegates with a further opportunity to book onto sessions of interest ahead of the show.
Beasley shared: “Space is also reserved in the programme for walk-ins, so delegates without bookings will still have the opportunity to join sessions on a first-come, first-served basis over the three days of the show.”
Event organisers encouraged delegates to arrive at their chosen seminars five to 10 minutes early for walk-in spaces.
In the weeks leading up to the show, OT will be exploring key topics identified in the education programme, with insight from AOP experts and 100% Optical speakers.
Delegates can discover what to expect from the programme in the areas of myopia, glaucoma, clinical imaging, clinical decision making, and patient communication.
Visit OT’s dedicated webpage to follow along with the series, and to keep up-to-date with the latest news from the show: www.optometry.co.uk/100-percent-optical 0




OT heard how Duncan & Todd has expanded its pre-registration recruitment programme
WORDS: KIMBERLEY YOUNG

The phrase ‘the world is your oyster’ is one often shared with those in their university years. An encouragement to make the most of new opportunities – to dream big – and perhaps sage advice from those who have experienced just how quickly the early years post-graduation can fly by.
While there is a great deal of truth to the saying, it is well-known that in some areas of the country,
finding opportunities can pose a challenge. Locations close to optometry schools can be in high demand, while practices further afield might struggle to recruit.
The General Optical Council’s (GOC) Business Registrant Survey 2024 found that respondents identified “substantial difficulties” in recruiting optical professionals, with the majority disagreeing or strongly disagreeing that they can easily recruit optometrists when needed (63%).
Around a quarter of registered businesses currently have arrangements with universities or the College of Optometrists to offer pre-registration placements to optical students, the survey found.
The GOC also found that the main perceived benefits to offering these placements are forward-looking, with the majority (70%) seeing a major benefit in “supporting the next generation of optical professionals” and providing a “future pipeline of newly-qualified optical professionals” (65%).
For Duncan & Todd, the optical and hearing group in Scotland, a key challenge is engaging student interest in rural locations.
Duncan & Todd has maintained a commitment to support pre-reg optometrists, primarily through partnerships with Scottish universities.
In 2022, Alix Buchanan, lead clinician optometrist, and Janna Swanson, HR adviser, made the decision to expand the group’s recruitment efforts.
Swanson explained: “We started visiting universities to engage directly with students, and during our visit to Ulster University, we received an overwhelmingly positive response from second-year students. Many expressed interest in relocating to Scotland for their pre-registration placements.”
Since that initial visit, the team has made a point of returning to Ulster University each year.
Swanson explained that visiting the students has highlighted that pre-reg placements in Northern Ireland can be quite limited, which often leads students to seek opportunities elsewhere in the UK.
“The Duncan & Todd Group offers a solution by providing students the chance to complete their pre-reg placements under Scottish regulations. Additionally, we guarantee a position with the company for those who successfully complete their pre-registration year with us, offering them a clear and secure path forward in their careers,” she added.
Ò
We encourage students to come and speak with us directly, and this opens up communication
Alix Buchanan, lead clinician optometrist, Duncan & Todd
application process easier. During our visit we encourage all students interested to apply and explain the process in detail, so students understand what to expect from the process.”
Applications are reviewed by the Duncan & Todd pre-reg programme team, and all students are invited to an initial interview to discuss their experience, skills, and current course.
“After each visit, we continue to stay connected with the successful candidates, helping facilitate their transition to Scotland to ensure they feel fully supported throughout their journey with us,” Swanson said.
Once location availability has been confirmed, the team provides as much detail as possible about the branch and location to the student and offers to facilitate a branch visit, “so the student is able to explore the area and feel comfortable in their decision.”
Students are encouraged to complete a summer placement with Duncan & Todd before starting their pre-reg placement. Buchanan explained that this enables the students to “get to know our staff and familiarise themselves with our systems and equipment, making for a smooth transition into their programme.”
Read more on how optometry is meeting the needs of remote communities in OT’s cover feature from The Future workforce edition 2024: www.optometry.co.uk/ everywhere
Duncan & Todd shared that it welcomed two students from Ulster University to its pre-reg programme in 2024.
The recruitment process begins with university presentations, in which the team speaks to students about the company, its locations, and the pre-reg programme offered.
Buchanan explained: “We encourage students to come and speak with us directly, and this opens up communication, making the
Feedback from previous and current students has been positive, the team told OT, particularly regarding the practice staff and supervisors who support students in onboarding, learning the role, and settling into the local community.
Swanson said: “Whilst our students may come onboard in varying locations across the
business, our goal is to provide them with all the support they require and make them feel part of a supported team.”
“Aside from the day-to-day support from our practice staff and managers, each student is provided with one-on-one supervision and has supported time with our lead clinician, Alix Buchanan, to explore any cases of interest,” Swanson added.
Asked to share what they have learned from expanding pre-reg recruitment in this way, Swanson said: “We believe that attending the university, speaking with the students directly, and keeping our points of contact consistent is key for building a trusting relationship with the university faculty and students.”
“Overall, our personal approach to pre-reg recruitment allows us to ensure a better candidate experience,” she added.
Given the success of the strategy, this is an approach that Duncan & Todd intends to continue in the future.
“ Our goal is to provide them with all the support they require and make them feel part of a supported team
Janna Swanson, HR adviser, Duncan & Todd
With the changes to the education of students and pre-registration optometrists going forwards, Buchanan explained: “We are continuing to review our recruitment process as we receive more information on the change to optometry education.”
She added: “We anticipate the continuation of welcoming newly-graduated students and supporting them with placements within the Duncan & Todd Group.”
Read more In focus : www.optometry.co.uk/in-focus
Workforce and recruitment challenges extend across professions in primary care. OT learnt about efforts to attract young professionals in dentistry
In 2024, NHS Dumfries and Galloway sought to address challenges in dental care by expanding the dental outreach programme for the region.
The NHS board worked with Glasgow University and NHS Education Scotland to increase the number of places for dentists in training to 12, making Dumfries the largest and busiest dental student outreach centre in Scotland.
The final year dental students training in Dumfries will provide single courses of dental care without charge to some members of the public who are not registered with an NHS dental practice in order to render them dentally fit. The students are supported and supervised by tutors and support staff.
Alison Milne, director of dentistry for NHS Dumfries and Galloway, told OT: “Having the extra students has allowed an opportunity for additional unregistered adult patients to attend clinics for a single course of treatment.”
It is hoped that the students will enjoy their experience in the region from both a clinical and social perspective.
Describing the workforce hurdles to OT, Milne said: “Recruitment of dentists and dental therapists to the Dumfries and Galloway area remains one of our main challenges.”
“Many General Dental Service practices are making huge efforts to recruit, and board officers continue to promote living and working in Dumfries and Galloway across a wide range of settings,” she added.
“This includes schools, universities, dental schools and other training programmes, where promotion of a career in rural dentistry in addition to a move to work in a beautiful but accessible new area are all promoted,” Milne added, continuing: “Highlighting living and working in Dumfries and Galloway is key, putting emphasis on our region and all that it has to offer.”

Mainline Instruments is excited to announce its participation in 100% Optical 2025, returning to exhibit at the show after another successful year.
Taking place from Saturday, 1 March to Monday, 3 March at London’s ExCeL, Mainline Instruments will showcase the latest advancements in optical technology through its market leading brands such as iCare, OCULUS, TowardPi,Tomey, Optomed, and more. Join us at our stand, E13, to explore groundbreaking innovations, interactive demonstrations, and insightful talks led by industry experts.
Expert-led talks: your gateway to advanced optical knowledge
Mainline Instruments is thrilled to be hosting three engaging talks during the show, each designed to empower practitioners with advanced knowledge and practical applications.
Talk one: Saturday, 1 March, 10:30am
Session:Freeform empirical contact lens fitting: corneal, limbal, scleral lens design
Speaker:Aneel Suri, principal optometrist at Moorfields Eye Hospital
Discover the future of contact lens fitting in this interactive session. Explore advanced corneal and corneoscleral topography, as well as CAD and CAM techniques that enable the design and manufacturing of highly customised lenses for patients with irregular corneas or surface disease. Keyhighlightsinclude:
•Basics of empirical lens fitting
•Customisation options for lens design
•Case studies demonstrating the benefits of freeform lenses
•Live lens design.
Accredited for one interactive CPD point.
Mainline Instruments will exhibit at 100% Optical, showcasing advanced technology and insights. Visit stand E13

Talk two: Sunday, 2 March, 10:30am
Session:Scanning confocal ophthalmoscopy: is a revolution on the horizon?
Speaker: Dr Adam Wylęgała, ophthalmologist at Wylegala Medical Center
Dive into the world of retinal imaging with this eye-opening presentation. Dr Wylęgała will discuss how scanning confocal ophthalmoscopy outperforms traditional fundus photography by delivering superior image quality and reliability, even in challenging cases such as cataracts. Keypointsinclude:
•Enhanced imaging for retinal diseases
•Cost and time efficiency in diabetic retinopathy screening
•Practical applications in routine and advanced care.
Accredited for one interactive CPD point.
Talk three: Monday, 3 March, 2:15pm
Session:Home monitoring of IOPs
Speaker: Ashish Chokshi, optometry lead for medical retina at Moorfields Eye Hospital
Learn how home monitoring of intraocular pressure (IOPs) is transforming patient care.This session covers everything from patient selection and clinical benefits to practical implementation in independent practice.

Topicsinclude:
•Identifying suitable patients for home IOP monitoring
•Understanding its importance in clinical pathways
•Integrating home monitoring into practice with robust, economically viable solutions.
Accredited for one interactive CPD point.
All sessions take place on the Mainline Instruments stand.
Innovation for every visual need
In addition to these must-attend talks, Mainline Instruments’ stand will feature hands-on demonstrations of the latest technologies in dry eye, optical coherence tomography, retinal imaging, and more. Attendees will have the opportunity to see how these advancements can elevate their practice and improve patient outcomes.
Join Mainline Instruments at 100% Optical to connect with industry leaders, explore advanced solutions, and gain practical insights for your practice. Don’t miss this opportunity to be part of the conversation shaping the future of optical care.
For further details, please contact Mainline Instruments directly.
Email: sales@main-line.co.uk Phone: +44 (0)121 458 6800


A quiet revolution in Wales has seen patients with urgent eye problems receive care in their own homes. OT talks to the optometrists creating parity between High Street and domiciliary care
WORDS: SELINA POWELL
Travelling between home and hospital can seem like a marathon effort when the distance between bed and sofa is an endeavor itself – only ventured a few times a day.
Before 2020, housebound patients in Wales who woke up with a sudden loss of vision or a red eye were faced with an unenviable choice. They could travel to receive care, or they could wait while their already small world diminished further.
Optometrist and clinical adviser, Sharon Beatty, told OT that a lack of equity between High Street and domiciliary NHS-funded urgent eye care prompted a series of reforms within Wales. “It was all about parity, safety and timely care,” she emphasised.
In 2020, the Domiciliary Emergency Eye Care Service was rolled out at pace in response to the pandemic. This was followed by overarching reforms to optometry in Wales in October 2023.
The overhaul saw the introduction of the WGOS2 domiciliary urgent eye care service and the removal of the pre-visit notification requirement in Wales for at least 48 hours’ notice before a domiciliary visit.
“The thought behind it was ‘How do we lose all the obstacles to providing safe and effective care for everybody?’,” Beatty explained.
Now, when a housebound patient has an eye health concern, they are no longer troubled by additional worries – such as the fear of being in an unfamiliar environment or burdening a relative with a request for a lift. The patient can see an

optometrist who they may already be acquainted with through routine domiciliary visits.
“You know your optometrist. They’ve been coming to your house for years,” Beatty said.
She added that, because there is a significant proportion of people living in rural areas in Wales, previously patients may have had to travel some distance to attend a hospital or GP surgery.
“The fact that we have a network of professionals who can bring that service to a patient’s own home means there is less travel involved,” Beatty shared with OT.
“It’s better for the patient, it’s better for the environment and it takes the pressure off our GP colleagues and secondary care,” she emphasised.

In addition to the benefits for patients, Beatty said that the WGOS2 national urgent eye care service has released thousands of appointments each month from GP practices and secondary care. “People can contact any optometry practice in Wales and receive free NHS-funded urgent eye care closer to home, or at home if meeting the eligibility requirements,” she highlighted.
Sharon Beatty
Care close to home
92% of urgent eye care patients are managed in primary care in Wales
29,000
domiciliary sight tests performed over the past year in Wales
243,445
annual number of WGOS2 urgent eye examinations in primary and domiciliary care.
Source: StatsWales
All practitioners in Wales on the NHS Performers List are signed up to deliver WGOS2 as a core NHS service, while some contact lens opticians have also undergone additional training to provide WGOS2 for anterior eye conditions. Beatty shared that there are benefits from a professional satisfaction point of view of providing the
Ò
Optometrists and dispensing opticians are working at the top of their licence
Sharon Beatty
service. “As part of optometry contract reform, optometrists and dispensing opticians are working at the top of their licence, which is wonderful to see,” she said.
Beatty hopes that the ability for patients to receive urgent eye care services, both on the High Street and in a domiciliary setting, will reinforce public understanding of optometrists as healthcare providers. “We need to ensure everyone knows to contact their optometry practice as the first port of call for any eye problems.”
Jason Scaife

Each year, the General Optical Council surveys around 2000 members of the UK public to find out where they would go if they woke up in the morning with an eye problem.
In Wales, 43% of respondents said they would go to their optometry practice in 2024, compared to 31% in England, 44% in Scotland and 41% in Northern Ireland.
Looking ahead, Beatty is hopeful that further advancements will be made in Wales supporting connectivity between primary and secondary care.
“I look forward to seeing further progress within the digital space so that the exchanging of images and patient data becomes a seamless process to support practice efficiencies,” she shared.
The optometrist perspective
Cardiff optometrist, Jason Scaife, provides domiciliary eye care services to patients from Caerphilly to Ceredigion through his role as optometry director of Specsavers Home Visits.
Scaife told OT that his team sees around 15 domiciliary patients each week through the WGOS2 domiciliary urgent eye care service.
Scaife highlighted the fulfilling nature of being able to provide urgent eye care to patients in their own homes. “These services enable us to provide urgent eye care to patients with serious, pressing, or sight-threatening conditions – patients we might not have been able to support in the
past,” he said. “Many of these individuals would otherwise face delays or significant challenges in accessing hospital-based care,” Scaife added.
This helps to prevent more serious complications that can arise due to treatment delays, he shared.
Scaife observed that being able to ease pressure on ambulatory services and secondary care adds to his sense of satisfaction with the service.
“It’s rewarding to know that our work is not just helping individuals but also contributing to a more efficient, sustainable and patient-focused healthcare system,” he said.
Scaife shared that being able to offer WGOS2 as a domiciliary business increases the volume of appointments and enhances the continuity of service provision.
The service also enables his business to reach a broader patient base. “Offering enhanced NHS services under WGOS2 allows most domiciliary eye care businesses to diversify their service offerings, contributing to long-term sustainability,” he said.
A year of urgent eye care in Wales
21,964
acute vision problems seen by High Street and domiciliary optometrists
39,070
red eye cases managed by optometrists through WGOS2
63,753 patients with eye pain or discomfort treated through WGOS2.
Source: StatsWales
“ It’s rewarding to know that our work is not just helping individuals but also contributing to a more efficient, sustainable and patient-focused healthcare system
Jason Scaife
Domiciliary optometrist, Lisa Evans, sees patients with a range of eye conditions in Cardiff, Vale of Glamorgan, and Rhondda Cynon Taff through WGOS2. “The eye conditions we detect from a WGOS2 examination are variable from very serious eye conditions such as iritis, angle closure glaucoma, sudden onset diplopia, retinal haemorrhages and retinal blood vessel occlusions to less sight-threatening eye conditions such as conjunctivitis and sub-conjunctival haemorrhages,” she said.
She added that the service means only patients who require treatment by the hospital eye service need to be transported to hospital.
“Patients really appreciate the service and the ability to be examined in their own home environment in a timely manner,” Evans highlighted.
Avoiding the need to travel to an optometry practice or hospital can reduce the physical exhaustion some patients experience – and in turn reduce their risk of a fall.
“Especially since the COVID-19 pandemic, patients value having a face-to-face examination in their own home,” Evans shared.
She added that the portability of domiciliary equipment minimises the amount that patients need to move in order to receive their eye care examination.
Evans highlighted that WGOS2 has reduced the strain on GP practices, with staff kept informed of the findings of examinations.
“This is appreciated by both patients and GP surgeries. With improved links within the NHS, WGOS2 is a great credit to all healthcare practitioners working collectively as a team for the best interest of the individual patient,” she said.
IP domiciliary services
A small number of domiciliary optometrists have completed their training in independent prescribing (IP).

Locum domiciliary optometrist, Hector Marcos, has been offering WGOS5 IP optometry services to patients in their own homes.
Marcos told OT that he decided to start studying IP during the pandemic. During the height of social distancing restrictions in Wales, primary eye care was predominantly provided by optometrists with IP qualifications. “I didn’t know of any optometrists who

“ Patients really appreciate the service and the ability to be examined in their own home environment in a timely manner
Lisa Evans
were offering IP in a home care setting. I thought I could upskill and use that qualification to help patients,” he said.
Since qualifying in 2023, Marcos has been able to manage and treat patients in their own homes with a range of conditions, including uveitis, marginal and bacterial keratitis, ocular hypertension and glaucoma.
He highlighted that patients are very grateful to be able to receive convenient care without the need to travel.
“Patients appreciate that you’ve gone the extra mile to help them, and you’ve seen them in the comfort of their own homes,” Marcos said.
He observed that previously patients could be nervous about leaving their own homes and reluctant to call an ambulance or request help from a relative.
“There is a sense of relief that they don’t have to burden someone else,” Marcos shared.
There are also benefits from a professional satisfaction point of view for the South Wales practitioner. “Even though it might be more difficult than a simple refraction, providing an IP appointment is very rewarding,” he said.
Read more In focus: www.optometry.co.uk/in-focus
30 minutesessions,packedwith stimulatingcontent.
by CooperVision/earningacademy
Havinga coffee break?Why not pop into the espressolearningzone and grab some insightfulCPD learningfrom the menu?Opento all,these half point sessionsare deliveredin a variety of ways to suit all learningstyles and cover a wide variety of contact lensrelatedsubjects.
If you haven'talready,pleaseregisteron the CooperVisionLearningAcademy™to accessespresso and muchmore.
Scan the QR code to find out more.
Sponsored by:








EXAMS CLOSE: 2 MAY 2025
Myth #1: Laser vision correction is relatively new, and the field is still developing so it is worth waiting
This article will address some of the myths surrounding refractive surgery, which still exist within parts of the optical sector and the public, allowing practitioners to provide evidence-based advice to patients.
Emma Brandon BSc(Hons) MSc MCOptom DipTp(IP)
Introduction
The demand for refractive surgery elevated following the COVID-19 pandemic; patients became frustrated with the repeated fogging of spectacles while wearing personal protective equipment (PPE), as well as the additional barrier created. Some patients also became increasingly concerned about hygiene and handling of contact lenses
during this time. There has also been heightened awareness surrounding the potential environmental impact of daily disposable contact lenses in recent years. Therefore, it seems appropriate to attempt to address some of the myths surrounding refractive surgery, which still exist among parts of the optical sector and the public. The article title states ‘Expert’ refractive surgery, and this is key. Refractive surgery performed to the highest standards by dedicated specialists using forefront techniques is critical to achieving safe and effective outcomes.
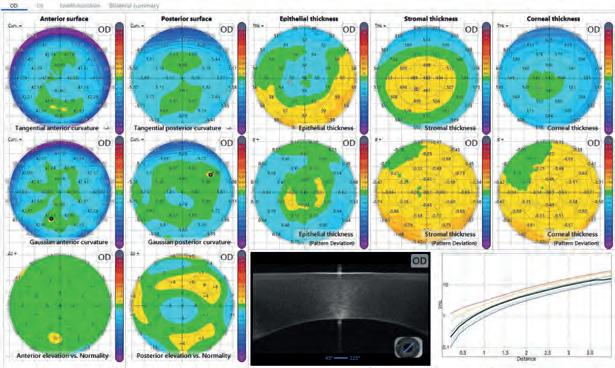
The foundation of modern laser refractive surgery can be traced back to the 1950s when Professor Jose Barraquer developed keratomileusis. The first sighted eyes were treated with photorefractive keratectomy (PRK) in 1988, and the incorporation of a microkeratome in 1990 led to laser in situ keratomileusis (LASIK), the basis of what we know today; this includes the development of small incision lenticule extraction (SMILE) in 2009, where a single femtosecond laser is used to create a small incision and a stromal disc of the required correction is removed through the incision.1-4 Laser refractive surgery is now one of the most well researched and developed specialties in medicine, with 50 million corneal refractive procedures performed globally by 2020. Long-term studies of at least 10 years demonstrate safe and effective outcomes, with modest post-treatment refractive shift largely being attributable to natural lenticular changes.5-7
Myth #2: Laser vision correction does not work well; you often still need glasses
The vast majority of patients are glasses free after the procedure. Today, in expert hands, more than 95% of patients achieve 6/6 vision or better, and 99% achieve 6/7.5, falling well within driving standards.2,5 For procedures such as laser blended vision (LBV), which will be considered later, low prescription balance glasses may be required for detailed tasks such as driving at night, but this is normally less than 5% of the time, and the benefit far outweighs the limitations with continuous use of reading spectacles. Very high prescriptions may also require top-up spectacle correction for fine detail, but again the relative freedom gained can be life changing.8
Using superior modern laser platforms, an expert refractive surgeon can successfully treat a range of hyperopia.2,9,10 As above, residual spectacle correction may be required for detailed vision in high hyperopes, but this is a fraction of the time, not to mention with more cosmetically acceptable spectacle lenses.
Myth
This is a common myth but in reality, astigmatic correction with a wellcentred treatment is excellent. Given the best laser platforms have the ability to remove as little as 0.25µm of tissue, it is no wonder the ablation can provide very accurate astigmatic correction. Corrections up to 6.00DC may be applied, where keratoconus has first been excluded. Enhancement may be indicated to ‘fine tune’ the outcome, where tissue safely allows.7,11
While there is yet no ‘cure’ for presbyopia, laser vision correction can provide an excellent option through LBV. LBV combines modified binocular vision with extended depth of field, achieved by aspheric laser ablation profiles.12–15 For hyperopes up to +5.75D, binocular vision of 6/6 has been achieved in 95% of patients, and near vision of N5 in 81% at 12 months.12 In myopia, up to 98% have achieved binocular uncorrected distance visual acuity (VA) of 6/6, and J5 in 99% at 12 months.14 Distance vision satisfaction rates following laser blended vision treatment are reported as 97% and 96% for myopia and hyperopia respectively, with near vison satisfaction ratings of 95% for myopes and 89% for hyperopes.15 It is also without the degraded optics frequently induced by multifocal intraocular lenses (IOLs), and simple balance spectacles can optimise vision for detailed tasks like night driving.
during laser vision
In expert hands, with application of premium technology and postoperative care, the combined risk of all potential complications causing a small amount of damage to the vision (up to two lines of corrected distance VA) is between 0.1% and <1%.5–7 The vast majority of complications can be managed to full resolution with expert care. This article does not have the scope to cover in-depth complication management. However, as an example, post-LASIK microfolds can be attended to by slit lamp smoothing immediately following surgery, or at day one postoperatively, to avoid them becoming embedded. While rare complications such as corneal ectasia do exist, high attention to detail and standardised procedures are key to avoidance, as well as their appropriate management, for example, with corneal collagen crosslinking. The incidence of contact lens related microbial keratitis is established at two to four per 10,000 wearers per year for daily soft lens wearers and 20 per 10,000 for overnight soft lens wearers.16 A large three-year longitudinal study found reported rates of infections and ulcers to be significantly less following LASIK compared to ongoing contact lens wear.17
Topical anaesthetic drops are administered (proxymetacaine and oxybuprocaine), as well as analgesics such as co-codamol perioperatively which help make the procedure as comfortable as possible, and certainly without pain. In modern refractive surgery, there may be a slight sensation of pressure during treatment, and a tightness as a speculum is applied to hold the lids. For example, the VISUMAX femtosecond laser (Carl Zeiss Meditec) uses a curved contact glass that requires very low suction to stabilise the eye during treatment, which enhances the
LEARNING OUTCOMES
Optometrists and dispensing opticians will identify when it is appropriate to direct patients to colleagues for expert guidance on refractive surgery options (s.10)
Optometrists and dispensing opticians will be able to provide evidence-based advice on refractive surgery options to patients (s.2).
patient experience. Postoperatively, the use of analgesics, steroid drops, and non-steroidal anti-inflammatory drugs (NSAIDs) where indicated, make the recovery relatively comfortable for the vast majority of LASIK and SMILE patients. The author’s personal experience of LASIK 15 years ago is that it was considerably more comfortable than many dental procedures. PRK can certainly be uncomfortable, but even here there are appropriate management strategies such as controlled short-term use of opioid pain relief, cold compress treatment and bandage contact lenses. In any case, PRK is reserved for a handful of cases such as those presenting with epithelial basement membrane dystrophy (EBMD) where it provides an appropriate treatment strategy.18
Myth #8: If you blink or move during the procedure it can go wrong
This is a myth with modern expertise and technology that surgeons have at their disposal. The eyes are held open by a speculum, so blinking is
virtually impossible. Topical anaesthetic makes this a relatively comfortable experience and further inhibits the blink reflex. There are fixation targets in place which help keep the eye aligned. If there is eye movement, an eye tracker allows for compensation, with some instruments tracking at 1050 frames per second. Therefore, eye movement is unlikely to result in complications.
Myth #9: Laser vision correction does not last very long and needs redoing
As previously described, there is now published long-term outcome data for corneal refractive surgery indicating stable results for at least 10 years, with changes being largely attributable to natural progression, and generally small relative to the refractive starting point.5-7 At the author’s clinic, long-term patient data shows the chance of needing an enhancement increases by ~1% per year, that is to say, 10 years after treatment, 10% of patients will have a second treatment.
Myth #10: The refraction needs to be stable before considering laser vision correction
While it is understandable why this myth poses concern, it is actually of less significance than commonly thought. Refractions change throughout our lives, most frequently due to lenticular thickening, or axial length changes. Of key importance is that an underlying cause for change is established, specifically to rule out keratoconus. Detailed tomography assessments of the
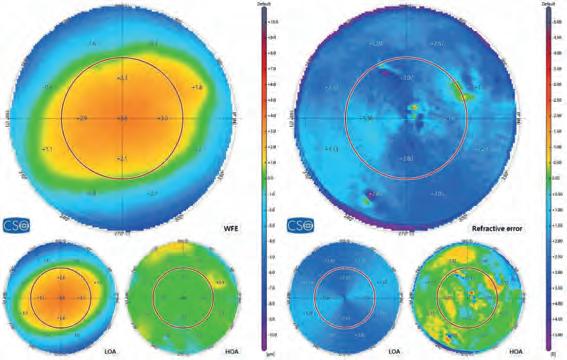
anterior and posterior corneal surface, as well as epithelial profiling and corneal pachymetry are key tools in establishing this preoperatively. It is also imperative to measure the thickness of the cornea in order to predict whether treatment can be conducted within comfortable safety margins. The patient also needs to be clearly counselled about future changes that naturally occur, and for the majority, enhancement may be safely carried out, tissue thickness allowing. Bear in mind that future changes are usually relative to the starting point, so the relative benefit of the treatment does remain in place.
Myth #11: If cataracts develop after laser vision correction, they cannot be treated
Cataracts can certainly be treated after laser vision correction, with excellent
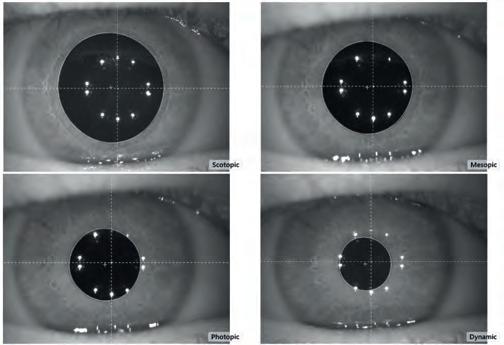
outcomes. Key information to retain and provide the patient with is their pre- and postoperative keratometry readings and prescription. These measurements allow for calculations of lens implant power to be made. However, with modern lens biometry it is possible to perform calculations even without this information. The American Society of Cataract and Refractive Surgery (ASCRS), Barrett True-K No History, or optical coherence tomography-based method are all examples of reliable formulae.19
Myth #12: Night vision is
This myth is really a hangover from the 1990s when small optical zone treatments were applied without transition zones. With older excimer lasers, significant glare could be induced by scotopic pupil dilation beyond the margins of the treated zone, creating a halo effect. Modern laser platforms with gaussian spot scanning profiles allow large optic zones, with further transition zones, meaning that there is no abrupt ‘cut off’ from the treated to untreated area. Furthermore, spherical aberration control is important as this further reduces induced night glare. SMILE is proving to be an excellent option as less spherical aberration is induced compared to traditional LASIK.20,21 Today, even patients with high prescriptions and large pupils experience little longterm induced night glare.22 Studies also demonstrate retained or improved
contrast sensitivity, and report patient satisfaction in quality of vision following refractive surgery interventions.23 In addition, previously degraded night vision can now be effectively ‘repaired’ through topography-guided treatments and zone expansion techniques.
Premium modern lasers allow for greater tissue conservation, and it is now possible to treat an impressive 98% of all prescriptions, with high myopia achieving excellent outcomes where tissue allows.7 Data for a range of high myopia from -8.00D to -14.25D showed that 83% of eyes were within 1.00D after primary correction, and 95% after enhancement, with 98% achieving 6/6 or better vision.8 SMILE treatment is an excellent option for high myopia as the stronger anterior stroma lamellae are preserved. which retains corneal integrity along with the anterior nerve plexus thus also reducing postoperative dry eye symptoms.23 This article has largely focused on corneal refractive treatment due to its less invasive nature; however, it is important to acknowledge the role of phakic lens implants in the form of implantable collamer lenses (ICL) for high myopia. There are cases where there is insufficient tissue to achieve a satisfactory result with corneal treatment, and ICLs are an effective solution. Careful patient selection is imperative, as risks such as cataract and intraocular pressure (IOP) changes are higher than with corneal treatments. However, safety can be optimised through appropriate anterior chamber depth selection and ultrasound sizing techniques.24,25
While a temporary increase in dry eye following corneal refractive surgery is common, the majority of symptoms subside within a few months and are easily managed using ocular lubricants.26 The principle mechanism of dry eye induction is due to temporary disruption to the anterior nerve plexus, thus reducing the lacrimal feedback mechanism; however, this does recover in most cases. Dry eye symptoms were not found to be significantly increased
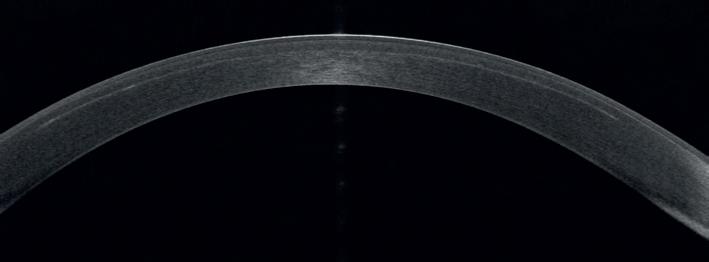
relative to preoperative levels at one year following LASIK among a large group (n = 819) of patients who wore contact lenses at baseline.17 Of the small percentage of long-term dry eye patients, this is most often secondary to underlying conditions such as blepharitis or inflammatory dry eye that should be managed preoperatively. Some of these higher risk patients should be excluded from treatment or counselled that the dry eye will remain afterwards. The advent of SMILE has further reduced postoperative dry eye, as the anterior plexus remains largely intact due to the absence of a flap. Evidence for reduced dry eye in SMILE is supported by studies on corneal nerve regeneration27 and recovery of corneal sensitivity.28
A frequently cited reason for preference to refractive lens exchange (RLE) is that there is refractive stability in the long term. However, refractions can also shift over time through corneal changes following lens replacement. The cornea does continue to evolve with age as anterior corneal astigmatism typically changes from with-the-rule to againstthe-rule, partly due to lid interaction, demonstrated in a large study of almost 4000 eyes in patients aged between 40 and 64 years.29 As previously indicated, it is imperative to bear in mind the increased surgical risk involved in lens exchange (~0.1% risk of significant vision loss) compared to corneal treatments (<0.1% risk of one to two lines of corrected distance VA for the majority of refractive errors), particularly where the patient has not developed visually significant cataract.
Patient satisfaction following corneal refractive surgery is extremely high. A recent study relating to LBV demonstrated that 98% of myopes and 97% of hyperopes were extremely satisfied with their vision quality for distance, 99% for both groups for intermediate vision, 96% of myopes for near vision, and 90% for hyperopes. Furthermore 95% of myopes and 92% of hyperopes experienced no symptoms of dysphotopsia.14 Another study of 1106 patients found high satisfaction levels with laser refractive surgery after three years, and more so for those who had originally worn contact lenses.17
In summary, modern refractive surgery provides a safe and effective option for vision correction, through expert surgical techniques and application of premium technology. It is important to emphasise the need for comprehensive preoperative evaluation and detailed postoperative care. Time invested preoperatively in thoroughly assessing patients, as well as clearly explaining the benefits, limitations and risks of treatment all pay forward towards excellent results and long-term patient satisfaction.
To read this article online, access the references and take the exam, visit: www.optometry.co.uk/cpd


Sponsored by:



This article outlines the importance of protection from ultraviolet radiation to enable practitioners to give appropriate advice to patients.
The risks of exposure to ultraviolet (UV) radiation are well known; however, the standards relating to UV protection can be confusing. This article seeks to present the facts around these issues and suggest ways practitioners can provide the highest level of care to their spectacle wearing patients.
The sun emits energy in the form of electromagnetic radiation resulting from the fusion of hydrogen nuclei within its core.1 This radiation is distributed in the form of electromagnetic waves and constitutes the electromagnetic spectrum. All elements of the electromagnetic spectrum exhibit wave-particle duality, that is to say, the ability to propagate as a wave, yet exchange energy like a particle.2 Therefore, the various elements of the spectrum are characterised by wavelength, frequency, and energy, where the relationship between these shows that the shorter the wavelength, the higher the energy contained.3,4
Cellular absorption of high energy radiation can lead to the breakage of bonds between atoms leading to the destruction of molecules; this is more likely with high energy photons and with an increase in intensity or irradiance which is influenced by various environmental factors.5
UV radiation is categorised according to wavelength into either UVA, UVB or UVC; of these, UVC has the highest energy. The stratospheric ozone layer effectively filters wavelengths up to 295nm which includes all UVC and a portion of UVB radiation.6
There are various standards relating to the UV spectrum. ISO 21348 is used by the aerospace industry, whereas ISO 13666 and ISO 4007 are used in the ophthalmic industry to provide consistency in the terminology used. As can be seen from Table 1, 7-9 there are inconsistencies in the standards with UVA, and indeed, the entire UV spectrum ending at 380nm according to ISO 13666 and ISO 4007. The US equivalent standard to ISO 13666 (ANSI Z80.3) also has a cut off of 380nm for UVA,10 while the Australian equivalent uses the enhanced cut-off of 400nm.11
UVB 280nm ≤ λ <315nm280nm to 315nm280nm to 315nm
UVC 100nm ≤ λ <280nm100nm to 280nm100nm to 280nm
TABLE 1 The constituent components of the UV spectrum according to different standards7-9
UVA radiation has lower levels of energy than UVB or UVC, but it is able to penetrate the atmosphere more effectively and is more abundant at the Earth’s surface. It is estimated that approximately 90% of the UV radiation we receive is contained within these wavelength ranges.12 UVA can penetrate deeply into the dermis where fibroblasts are found, compared to UVB which is mainly absorbed by epidermal layers, where keratinocytes are located.13
In terms of ocular penetration, wavelengths below 300nm (UVB) are mostly absorbed by the cornea with significant penetration of UVA to the lens (see Table 2, page 56).14 Wavelengths of 400nm have been shown to degrade cells in the retinal pigment epithelium, according to Dr Olaf Strauss, an expert researcher in this field:
“Theoutertissuesoftheeye,cornea andlensfullyabsorbUVlight.While UVBlightprimarilydamagesthe geneticmaterial,UVArayspenetrate deeper,causethermaldamageand magnifytheeffectsofUVBlight.The reasonswhytheWHOrecommends UV400protectionareclear.”15
Figure 1 illustrates the impact of the 20nm band (between 380–400nm) that does not form part of UK standards.16 The discrepancy in the various standards is due to difficulties in defining where UV radiation begins in the spectrum. UV radiation is defined as: ‘…optical radiation with wavelengths shorter than those for visible radiation.’17 It is, therefore, based on the limits of photodetection. As this varies by individual, the demarcation between
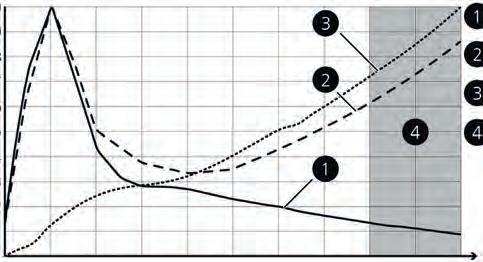

ICNIRP UVR hazard

Keratinocyte weighting

Fibroblast weighting

UVR hazard region not in ISO 8980-3
Optometrists and dispensing opticians will be able to advise patients about the importance of ultraviolet protection (s.2)
FIGURE 1 ICNIRP-UVR action spectrum weighted by the solar UVR spectrum in ISO 8980-3, keratinocyte effect and fibroblast effect. Image courtesy of Ivanov et al, UV-radiation oxidative stress affects eye health, 201816 (license link: https://creativecommons.org/ licenses/by/4.0/)
visible light and UV wavelengths is imprecise. The International Commission on Illumination (CIE) chose the mid-point of this range of wavelengths (360nm to 400nm) resulting in UVA ending at 380nm17 while the World Health Organization (WHO) and Standards Australia prefer to err on the side of caution by extending the range to 400nm.
Debate around reference to 400nm in the UK began in 198018 when the lens manufacturer Optical Radiation Corporation (ORC) began supplying lenses marked UV400, drawing the attention of the dermatological industry. Consequently, standards committees have convened to try and reach agreement on the definitions relating to the level of protection for products labelled in this way. To add confusion, the commonly used terms ‘blocking’ and ‘cut-off’ are ill-defined and may not adequately represent the ability of a lens or filter to limit transmission. The committees felt the adoption of the term alpha-blocking wavelength would be more appropriate as a descriptor of the performance of a lens. In 2009, the following definition was posited: “The highest wavelength, α, equal to or greater than 380nm for which the spectral transmittance is less than x% between 280nm and α nm.”18 In this definition the commonly seen UV400 marking would be re-phrased as 400-blocking, with the value for x being between 1% and 4%. However, the issue over labelling of products remains
unresolved, and the definition is yet to be formally adopted. Understanding of the hazards of high energy visible light (HEV) continues to evolve. In November 2023, the Vision Council published its Spectral Bands Task Force Technical Report19 setting out a new method for categorising wavelengths in the 380nm to 500nm range.
This report, signed by over 40 industry experts, communicated a new banding system for HEV, which was described as: “This provides comprehensive guidance for practitioners wishing to recommend enhanced protection using approved terminology that discards complicating language around ‘blue’ or ‘purple’ light hazards. The concept of the ‘blue light hazard’ is beyond the scope of this article, with research continuing in this field.”

Optometrists and dispensing opticians will recognise the risks of ultraviolet radiation and appropriate standards (s.5).
Returning to the 20nm gap in the standards, it is interesting to compare how clear lenses perform in their effectiveness in blocking this part of the spectrum. The transmittance properties for various ophthalmic plastic lenses are shown in Table 4.20 Untreated lenses are not able to provide protection up to 400nm and that these wavelengths can impact on ocular structures.
In 1995, the Global Solar Ultraviolet Index (UVI) was introduced to enable the public to understand the hazards of UV exposure on a given day. Revised in 2002 by the WHO, this is a globally recognised measure of the intensity of UV radiation (see Figure 2). The UVI is calculated using the International Commission on Illumination (CIE) reference action spectrum for UV induced erythema on the human skin (ISO 17166:1999/CIE S 007/E-1998).21,22 It has been reported as providing an adequate indication of the UV risk to ocular structures;23 however, considering that it is ‘... a measure of the UV radiation that is relevant to and defined for a horizontal
TABLE 2 Absorption of radiation by ocular structures and transmittance to the retina.
Note: figures in brackets denote absorption of incident radiation on the anterior surface of each structure14
surface,’21 this has limited relevance to ocular structures which are orientated vertically and are more influenced by ground reflection of UV radiation.24 It is entirely possible that the UV intensity may be deemed low risk regarding skin damage yet be of a high risk to the eyes.
There are further limitations when relying on the UVI due to the difficulty in accurately calculating a value. The amount of UV reaching the Earth’s surface is affected by:
1. Sun elevation – the higher the sun is in the sky, the greater the intensity
2. Latitude – higher intensity in equatorial regions
3. Cloud cover – clouds may transmit, reflect, and scatter UV depending on their shape and density. Nimbo form clouds will reduce this effect, but denser cloud cover may not always reduce UV intensity – cumulo clouds in particular can increase intensity as they tend be taller and have more surface area to reflect and scatter the radiation
4. Altitude – thinner atmosphere increases intensity
5. Ozone – variable concentrations throughout the day
6. Ground reflection – some surfaces reflect significant amounts of UV, increasing intensity.
To develop an accurate measure of UV intensity, it is necessary to make assumptions which can lead to over- or underestimation of the true index. For example, in its calculation of the UVI, the Meteorological (Met) office utilises a climatological value to represent the average value for ozone concentration based on the time of year,25 which reduces the accuracy of the index. Ozone plays a vital role in providing protection from UV radiation, blocking virtually all UVC and most (between 70–90%) UVB radiation.26 The UK experiences ‘low ozone events’ which are defined as a ‘departure of more than two standard deviations below the longterm monthly mean value for a site.’27 During such an event, the concentration of UVB increases leading to a higher risk of cellular damage (see Figure 3).26
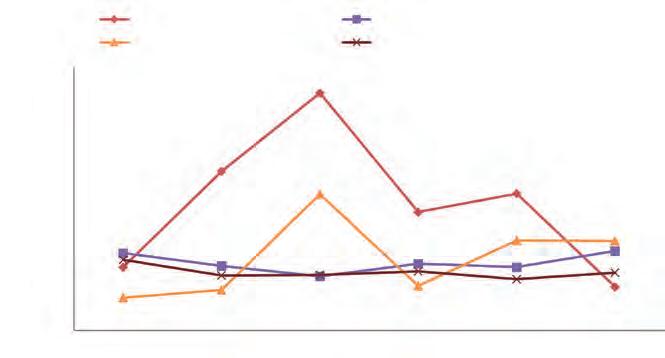
Computational models indicate that a reduction in ozone of 10% could lead to an additional 1.6–1.75 million cases of cataract worldwide.22
There have been attempts to create a measure of UV intensity which is more relevant to ocular structures. One method used mannequins to measure UV intensity at various times of the day,28 which provided a snapshot into why the current UVI is insufficient in providing information about ocular risk (see Figure 4).
Although UV has some positive health effects (enabling the natural synthesis of Vitamin D and endorphins in the skin), it is classified as a ‘complete carcinogen’ due to its ability to initiate and promote tumour growth;29 therefore, it is essential that adequate ocular protection is considered, taking into account the limitations of the UVI and the day-to-day variance in risk.
A spectral transmittance curve (see Figure 5, page 58) provides information on the wavelengths of light transmitted by a spectacle lens or a thin film coating. Although useful, it does not account for wavelengths which are indirectly transmitted to the eyes. There are various methods to increase UV absorption of a spectacle lens. A UV filter may form part of the substrate, be applied through a dye process (similar to dip tinting) or form part of the coating stack on the surface. However, consideration needs to be given to the effect of peripherally incident UV, which has been shown to increase the intensity of the light by a factor of around 20.14 This has been described as the Coroneo effect30 and is the result of the cornea refracting peripherally incident light onto the nasal corneal
Summer: 14/6/2012
Winter: 14/12/2011
FIGURE 4 UVI and Ocular UV Index (OUVI) levels at the eight-azimuth mean: (A) summer (June 14, 2012), and (B) winter (December 14, 2011). Figure courtesy of Hatsusaka et al. UV Index Does not Predict Ocular Ultraviolet Exposure (2021)27 License link: https://creativecommons.org/ licenses/by/4.0/legalcode.en
limbus and the nasal and inferonasal zones of the crystalline lens (coinciding with the most common location for cortical cataracts).31 In a study that investigated UV transmittance through various glass and plastic lenses, it was found that even when the lenses were covered with an opaque material, there was a small but significant quantity of UV radiation reaching the eye socket of a mannequin, both when the incident UV was in front and behind the head;32 this demonstrates the issues around rear surface reflection of UV.
Many anti-reflection (AR) coatings have been shown to increase reflectance of UV at the rear surface by around 25% (across all UV bands) compared to non-AR coated lenses and tinted lenses, which have a rear surface reflectance of around 4-6% for UVA and UVB, and less than 8% for UVC.32 It is therefore, imperative to ensure that AR treatments applied to lenses that will predominantly be used outdoors (clear or tinted) have an appropriate stack of layers on each surface, specifically designed to reduce UV reflectance.
The previous study31 also found that there was increased ocular exposure to UV for smaller, plastic lenses, with a reduction in radiation at the orbit as the surface area of the lens increased, highlighting the benefit of using larger eye sizes particularly for sunglasses. Finally, the study also investigated ocular exposure when the back vertex distance (BVD) was changed (0mm, 6mm and 12mm) and found that there is an increase in ocular exposure to UV as the BVD increases.31 Close fitting spectacles are vital to ensure patients have optimal protection, both in clear and tinted lenses.
To provide optimal protection from the harmful effects of UV radiation, ophthalmic lenses (whether clear or tinted), must satisfy a number of conditions, namely:
1. Contain a UV filter capable of absorbing wavelengths up to 400nm
2. Address the issue of back surface reflection of UV
3. Be large in size
4. Be fitted at a small BVD.
TABLE 3 The new bandings for HEV published by the Vision Council, November 202318
There are many UV filters available that have UV cut-offs of 400nm and beyond. It should be remembered that once a filter begins to block wavelengths in the blue region of the spectrum, the lens will feature a slight yellow tinge. While many patients do not find this an issue, those who are particularly sensitive – perhaps those with opacities and an already reduced contrast sensitivity – may find this effect problematic. Of course, the benefits outweigh this issue, and effective communication should be employed to set expectations.
Traditional AR coatings reduce reflections caused by visible light and allow more light to pass through the spectacle lens. To reduce rear surface UV reflectance, the coating needs to be adapted. This means the front and rear surface should have different coatings with respect to clear lenses, or those with a mirror finish. For tinted lenses, a front surface UV filter and UV specific rear surface AR is advisable.
The size of spectacles should be sufficient to provide adequate coverage of both the eye and the surrounding skin and to reduce the rear surface reflectance. For sunglasses, there are additional factors to consider from the relevant standards (ISO 123121:2013+A1:2015),33 which provide guidance on the appropriate size for sunglasses: “The sunglasses shall cover two ellipses with a

horizontal diameter of 40mm and a vertical diameter of 28mm, the centres of which are separated by 64mm and symmetrically placed on either side of the centre of the bridge of the frame, such as, its vertical symmetry axis.”
For children, the standards differ with a recommendation for the ellipses to have a horizontal diameter of 34mm and a vertical diameter of 24mm, with centres separated by 54mm.
The size, shape and fitting of sunglasses in particular (which are likely to be worn at times of the highest exposure) can affect the amount and intensity of radiation received by the ocular and surrounding structures. It has been shown that medium sized sunglasses (53mm x 57mm) result in increased levels of indirect UV
exposure compared to larger sizes and goggles.34 There is also a significant difference in exposure when wearing smaller sunglasses influenced by changing head position. This effect can be reduced with closer fitting, larger frames. Standards state for sunglasses tinted to the darkest category (Category 4), temple shields are required for spectacles with a pupillary distance greater than 54mm.33
GOC Standards of Practice state: “Only provide or recommend examinations, treatments, drugs or optical devices if these are clinically justified, and in the best interests of the patient.”35
The need for UV protection is an important consideration for all patients,
TABLE 4 Properties of different plastics materials measured in a study for the US military20
especially those at greater risk such as those with existing conditions known to be exacerbated by UV, such as cataract and pterygia, and those taking certain medications, for example, tetracyclines and oral contraceptives.36
As well as recommending the most appropriate eyewear, practitioners can extend advice to additional methods of protection, and give general lifestyle advice. It is also important to give relevant advice to those patients who do not require a prescription correction, particularly in the case of children to ensure they are protected in the most effective way. Ongoing discussions around HEV and the 400nm question will continue; so, it is important to keep up to date with communications from the standards authorities and provide the most current advice to patients.
To read this article online, access the references and take the exam, visit: www.optometry.co.uk/cpd


Sponsored by:
This article evaluates the influence of various lifestyle factors on myopia in comparison to genetic predisposition.
Dr
Sayantan Biswas PhD FHEA
Myopia is characterised by the disharmony between axial length (AL) elongation, and the eye’s optical power, whereby light entering the eye is focused in front of the retina.1 It leads to blurred images on the retina and the inability to see distant objects clearly.2 Myopia has become a global public health concern, with its prevalence escalating across the world.3 It is far beyond a mere inconvenience, and represents a highly prevalent, sight-threatening disease with implications for vision, health, education, social and quality of life (QoL). The World Health Organization (WHO) acknowledges myopia as an emerging problem in urban areas.4 By 2050, nearly half of the global population may suffer from some degree of myopia.5 Vision loss due to uncorrected myopia and pathological myopia-related complications are expected to rise with the growing prevalence of myopia.6 The International Myopia Institute (IMI) recognises the significant negative impact of myopia on health, QoL and the economy.7 The explosion in myopia prevalence is especially pronounced among school-aged children and young adults.8 While genetics plays a particular role in the development of myopia, lifestyle factors are increasingly recognised as crucial contributors to its onset and progression.3 Genes cannot fully account for the sudden increase in
myopia prevalence we are seeing in children today, and a child becoming myopic does not mean that the genetic factors were necessarily causative in each case. Single nucleotide polymorphisms (SNP) identified through genome-wide association studies can only explain about 18.4% of heritability of spherical equivalent.9 Also, these SNPs have small effect sizes (order of ±0.1D).10 Thus, parental myopia, that is to say, inheritance, does not necessarily mean genetics are causative of myopia. It may be linked to the shared lifestyle and parental factors that are myopiagenic. The rapid increase in the prevalence of myopia worldwide, without any significant change in the gene pool between generations, suggests the role of lifestyle and behavioural factors in myopia development.11
Numerous cross-sectional and longitudinal studies across countries have reported the association between increased time spent outdoors and reduced prevalence of myopia.3,12 Children spending more time on outdoor activities and longer daily outdoor light exposure have a lower prevalence of myopia. Daily outdoor
activity for 30 minutes for one year temporarily slowed myopic progression in children, albeit with a rebound effect on stopping the outdoor activity.13 Interventional randomised controlled trials in Chinese and Taiwanese school children observed the protective effect of recess time outdoors (40–80 minutes) against myopia incidence. This additional time outdoors (0, 40 and 80 minutes) has a small dose-response relationship with both myopia onset and progression.14 Moreover, engaging in outdoor activity for 120–150 minutes under a light intensity of 5000 lux per minute (cumulative exposure after two years: 600,000–750,000 lux) reduces myopia incidence by 15–24%.14 Thus, the protective effect is related to both the exposure duration and light intensity. The time spent outdoors is more protective in six-year-old children compared to 11- to 12-year-olds, probably because younger eyes are more sensitive to visual maturation.15 The protective effect of time spent outdoors has been reinforced by systematic reviews,16 meta-analyses,15,17 and overviews18,19 with evidence of 2–5% reduced odds of developing myopia and 24–46% relative risk reduction of incident myopia for every additional hour spent
“MYOPIA HAS BECOME A GLOBAL PUBLIC HEALTH CONCERN, WITH ITS PREVALENCE ESCALATING ACROSS THE WORLD. IT IS FAR BEYOND A MERE INCONVENIENCE, AND REPRESENTS A HIGHLY PREVALENT, SIGHT-THREATENING DISEASE”
every week outdoors. Conversely, decreased outdoor activity is shown to exacerbate myopia. The harmful effect of reduction in outdoor time on myopia was observed during COVID19-related home confinement and the related rise in myopia incidence and the rate of its progression.20,21
A review of the available evidence suggests that increased time outdoors might effectively prevent myopia onset in emmetropic eyes but does not slow progression in already myopic eyes. Nonetheless, interventional studies have shown mitigation of myopia progression by increasing outdoor time. A recent meta-analysis19 determined the reduction effect to be 0.13–0.17D spherical equivalent refraction (SER) or 0.03–0.08mm AL per year, which is sub-clinical (clinically significant change is 0.25D in SER or 0.11mm in AL annually).22
Despite the massive body of evidence supporting outdoor time with a reduced prevalence of myopia, some studies have found no association between the duration of time outdoors and myopia.3
Several studies have explored and reported the association of myopia with near work using parental surveys on activities such as school assignments, digital device use and watching television.3,23,24 In general, myopic children spend more time in near work (studying, writing and reading) compared to non-myopic children, with additional near work time among urban than rural children. More than 20.5 hours of engagement in near work every week heightens the risk of myopia among adolescents.25 Furthermore, near work intensity, duration of continuous reading (>30 minutes), close working distance (<30cm) and reading more than two books per week are associated with a higher risk of myopia.3,23 Myopic progression was found to be significantly associated with reading
scientific literature and practical near work among engineering students (young adults);26 this suggests that it is not just the number of hours doing near tasks but also the type and distance of near work undertaken related to myopia. Although in general, increased near work is associated with myopia, these findings should be cautiously interpreted due to the subjectivity of the questionnaires used. Objective measurements of near activity found myopic children engage in near work at close distances (<20cm) more often than non-myopic children.27 On the contrary, several studies failed to corroborate these findings. They found the number of books, increased near work, and the duration and distance of visual tasks did not significantly affect the refractive error or risk of myopia development in children.3 Systematic reviews and overviews provide substantial evidence recommending decreased reading time to reduce the risk of children developing myopia. For every additional dioptre-hour of near work per week, the odds of developing myopia increase by 2%.18,24
Paper-based reading and writing at close distances is traditionally considered near work. However, the last few decades has seen the adoption of digital devices and communication technologies into our daily lives.3 The advancement of screen resolution has further enhanced the use of devices such as smartphones, tablets and computers, which allows digital devices to be smaller and more handheld. The lightweight and smaller devices encourage prolonged screen time and a closer working distance.28 The use of electronic devices has become popular in children as young as three to four years old (average nine hours per week) in the UK, with average screen time rising to more than three hours per day (~21 hours per week) among eight to 12-year-olds.29 Furthermore, 97–98% of teenagers in
Optometrists and dispensing opticians will be able to outline modifiable myopia risk factors to patients and their parents (s.2)
Optometrists and dispensing opticians will recognise lifestyle factors that can elevate risk of myopia development and progression (s.5).
the UK30 and US31 have ownership or access to a smartphone. The ubiquity of digital devices in modern life is potentially a myopiagenic factor. Digital device use is hypothesised to induce accommodative stress and reduce blink rate, causing dry eye, and the emitted blue light may disrupt circadian rhythm and promote AL elongation.32 Spending 20 minutes or more on electronic devices without a break can lead to a higher risk of developing myopic refractive errors, especially for individuals with limited outdoor exposure.33 Even though the impact of digital screen time on myopic refraction is estimated to be 0.28–0.33D for every hour spent,34 recent meta-analyses35,36 found insufficient evidence of digital screen time on the risk of myopia. Screen time and viewing distance estimated using parental questionnaires are subjective and at risk of recall bias. 0 0
“SINCE CHANGING HABITS CAN BE DIFFICULT, IT IS IMPORTANT FOR CHILDREN AT RISK TO BE AWARE OF THEIR SUSCEPTIBILITY IN ORDER TO ADHERE TO LIFESTYLE RECOMMENDATIONS”
Longitudinal studies37,38 on the effect of high levels of time outdoors (>22.5–23 hours per week) in children performing high levels of near work (>19.5–25.5 hours per week) have reported a protective effect on myopia development. Spending less time outdoors has increased odds of myopia irrespective of the level of near work and low outdoor time (≤13.5–16 hours per week) combined with high near work results in an increased risk of myopia.
37
In several studies, physical activity (PA) is associated with a lower risk of incident myopia. Others report that PA is not associated with myopia development.3,18 However, moving away from subjective questionnaires to objective methods (accelerometers) of measuring PA, it was found that the reported PA mainly captured outdoor time information, that is to say, the influence of PA is confounded by outdoor time.16,18 Thus, the role of increased outdoor time is more crucial than PA. The use of the word ‘sports’ rather than ‘PA’ in questionnaires have mislabelled less physically demanding outdoor activities such as walking, cycling as leisure activity.3 Nevertheless, PA is most likely to occur outdoors, and it is important to note that promoting sports, benefits children by inspiring a healthier lifestyle.
39
Circadian rhythm is the internal physiological clock that follows a 24-hour cycle and is synchronised by
the central biological clock located in the suprachiasmatic nucleus (SCN). The dominant cue for entrainment of the SCN is the rhythmic variation in ambient illumination through the light/dark cycle.40 The absence of the Zeitgeber (constant light or constant darkness), which provides circadian time cues, can disrupt the circadian rhythm in the eye. This disruption in young, rapidly growing eyes often results in aberrant eye growth and failure to achieve emmetropisation.41 The SCN controls the rhythmicity of the pineal gland, which is responsible for melatonin secretion through both photic and non-photic inputs. The dim light melatonin onset (DLMO), a tool to assess melatonin secretion profile, can be a reliable biomarker of the circadian phase or entrainment.42 Even though DLMO has been linked with myopia, the findings are conflicting, with evidence of both difference and no difference in DLMO phase along with variable salivary and urinary melatonin amplitudes among refractive groups. Even though melatonin release and synthesis are light dependent, studies lack robust methodological design and definition of standard lighting conditions essential to investigate the relationship between melatonin dysregulation and myopia development. Since sleep is under circadian and homoeostatic control, it may have a role in controlling ocular growth and the resulting emmetropisation. Myopes have been reported to exhibit a significant DLMO phase delay, lower urinary melatonin levels, and delay in the onset of sleep and wake-up time, with diminished and lower-quality sleep compared
to emmetropes.43,44 Besides, lack of sleep or later bedtime could lead to additional near work and thus a higher risk of myopia. To date, the associations between different sleep disorders, such as insufficient duration, poor quality, irregular and late timing of sleep, and the incidence and progression of myopia remain unclear.43,44 Moreover, most studies have methodological differences in the definition of studied variables and participant demographics, lack of cycloplegic refraction resulting in overestimating myopia, insensitive outcome measures, and recall bias related to questionnaires estimating sleep characteristics.45 To summarise, there is insufficient evidence of an association between sleep, circadian rhythm and myopia.
The relationship between nutrition, diet and myopia is equivocal. On one hand, cholesterol intake and food like whole grains, saturated fat, and refined carbohydrates have been linked with increased axial growth and myopia.3 In contrast, some studies have found no link between myopia development and dietary factors such as protein, fat, carbohydrate, and vitamin A intake as determined by food frequency questionnaires.3 Earlier studies found lower vitamin D levels in myopes than in nonmyopes, whereas others did not find such evidence.46 The interrelation of vitamin D with myopia lacks biological plausibility. Furthermore, myopia is unrelated to rickets (vitamin D deficiency), implying that serum vitamin D level may indicate ultraviolet B exposure (time outdoors),
which exerts a protective effect.47 Systematic reviews of the evidence also suggest no significant association of myopia with nutritional factors and concluded that most studies are non-interventional with inconsistent evidence of an association.48,49
Studies have found higher socioeconomic status to be associated with myopia, while others failed to find any such relationship.3 The contradictory nature of the evidence may be rooted in differences in the definition and classification of socioeconomic status, which is generally determined by factors such as parental education, employment, income, type of school (private versus public) and housing.50 Additionally, immeasurable factors such as parental involvement, academic pressure, personal motivation and personality might also alter the education level. Higher socioeconomic status indicators (owning property, urban living, educational duration) are generally related to myopia. It has been hypothesised that economic development promotes further desire for wealth and improves social status, which increases educational pursuit and academic burden, reducing outdoor time and increasing near work, leading to myopia.50 Thus, the effect can be related to the increased near work time and less outdoor time. The level or years of education, higher intelligence quotient and better school performances have been observed as risk factors for myopia.51,52 Along with the child’s educational level, parental education can also affect ocular development and growth. However, this needs further research as this relationship is confounded by genetics (parental myopia), occupation, income and time spent outdoors.3 Besides, the child’s interest in academic
subjects, parental interest and time devoted to helping their children with schoolwork may also influence school performance.
Conflicting associations between smoking and myopia have been presented in earlier studies with confounders like education level, age, housing and socioeconomic status.3 While some studies have associated smoking with retinal and choroidal thinning, others have not supported the finding.3,32 The retinal nicotinic receptor-mediated causal pathway is also not robust. Nonetheless, large studies have associated second-
individuals to be outdoors less and do more near work. Frequent breaks are recommended for teenage smartphone users with one to two hours of daily outdoor activity.33 Physical activity is not an independent risk factor for myopia – other lifestyle factors like sleep, nutrition, socioeconomic status and smoking warrant further investigation. To successfully understand and address childhood myopia, the interaction between lifestyle and genes, and what enhances or triggers the effect of myopia genes must be considered.54 Studying this interaction can potentially be valuable in creating better prediction models for myopia, understanding individual
“IT IS CRUCIAL TO UNDERSTAND THE ROLE LIFESTYLE PLAYS IN THE DEVELOPMENT OF MYOPIA AND ITS SUBSTANTIAL IMPACT ON ITS PROGRESSION”
hand smoking exposure with myopia onset and progression in children.53 Although cross-sectional studies cannot prove a causal relationship, they have shown a dose-response effect of smoking on myopia and AL elongation.53 Although the relationship between smoking and childhood myopia is not definitively established, there is evidence suggesting a correlation.
It is crucial to understand the role lifestyle plays in the development of myopia and its substantial impact on its progression. The two most potent and opposing determinants of myopia are the protective effects of time spent outdoors and the exacerbation of risk with near work. The relationship between near work and myopia is not necessarily entirely causal, as myopia might force
susceptibility and further reducing the risk of myopia by developing bespoke therapies. The early onset of myopia in children increases the likelihood of developing high myopia. Engaging in outdoor activities can delay the onset of myopia, and in some cases, even prevent it. Since changing habits can be difficult, it is important for children at risk to be aware of their susceptibility in order to adhere to lifestyle recommendations.54
0
To read this article online, access the references and take the exam, visit: www.optometry.co.uk/cpd

Dr Sayantan Biswas is a lecturer in optometry at Aston University.


Sponsored by:








This article describes ocular biomarkers that have potential to enable early detection of ocular and systemic diseases.
Jason Higginbotham MCOptom
Prof Cert Glau Prof Cert Med Ret
Prof Cert LV FBDO MBCLA
A biological marker, or biomarker, is a measurable substance in an organism that indicates, or may indicate, the presence of a disease, a physiological abnormality, or psychological condition.
This article will consider the eyes and adnexa as ‘windows to the body,’ the modern terminology for which is oculomics and may be defined as a composite set of macroscopic, microscopic and molecular ophthalmic features associated with health and disease.1
Technological advances increasingly allow practitioners to view a range of physiological and psychometric characteristics, and some exogenous/ endogenous substances, which can be detected using a range of specialised eye tests.1,2
Biomarkers can be categorised as ‘visible’ or invisible.’ Visible biomarkers (see Table 1, page 66) refer to those that can be detected using conventional methods such as fundoscopy or
are evident through gross external examination (see Figures 1 and 2, page 67), whereas invisible indicators (see Table 2, page 68) require more specialised modalities such as optical coherence tomography (OCT).
This article will primarily focus on systemic conditions and their invisible ocular biomarkers where viable methods to detect these are available for practitioners to use in clinical practice. Biomarkers can also be categorised as:
• Anatomical – changes in the retinal morphology, vessel calibre and optic nerve head1
• Functional – classic physiological biomarkers such as visual fields and less common electrophysiological tests like electroretinograms (ERGs) and visually evoked potentials (VEPs)1
• Molecular – divided into proteomic (for example, cytokines in ocular surface disease)52 and metabolomic (for example, metabolic dysregulation in glaucoma or diabetic retinopathy)53
• Genetic – these are out of scope for this article but include genetic mutations to identify the risk or presence of ocular diseases like glaucoma and myopia54
• Imaging – detected with various high resolution multi-modal techniques

Optometrists and dispensing opticians will recognise the role biomarkers play with respect to ocular and systemic diseases (s.5).
such as OCT, confocal scanning laser ophthalmoscope (cSLO), and fluorescein angiography (FA), where subtle signs such as layer thickness changes and early oedema can be seen.
AGEs are a common form of toxic byproduct of metabolic processing of lipids, proteins and nucleic acids. They are generally endogenous, but can also be exogenous, either in highly processed foods or where food has been cooked at very high temperatures.
The production of AGEs is increased significantly where insulin uptake is impaired (resistance), glucose uptake is impaired, or as a result of oxidative stress, smoking, vascular endothelial cell damage, fatty food intake and other factors. They are, therefore, indicative of conditions like diabetes (and prediabetes) and cardiovascular
disease.24 A primary method of detecting AGEs is using autofluorescence (AF). It is possible to utilise the positioning of AGEs in the eye to capture a baseline status and then monitor the longterm metabolic status of a patient, for example, in diabetics, which may change how a person is treated or monitored.25,26 There is potential for an AGE reader in a range of medical and allied health settings, including optometry. It is estimated that globally, 7.5% of adults between 20 and 79 years of age have impaired glucose tolerance (IGT), essentially pre-clinical diabetes, which amounts to roughly 375 million people.25 These patients are at high risk of proceeding to clinical diabetes.
Impaired fasting glycaemia (IFG) is also referred to as pre-diabetes. There are roughly 300 million sufferers globally and these patients are at high risk of proceeding to clinical diabetes.55 Detecting IGT and IFG patients quickly and effectively can save health systems billions by avoiding the complications of undetected diabetes. Since prevention is better than cure, lifestyle changes can have a significant impact on these
Xanthelasma and arcus senilis3,4
Proptosis5,6
Scleritis/episcleritis7,8
Iritis/cyclitis9,10
Ptosis and binocular diplopia11,12
pre-diabetic individuals. By delaying or avoiding the onset of clinical diabetes, life expectancy and quality of life for many people will improve, while also generating substantial savings for economies worldwide.
In many cases, diabetics need to regularly monitor their blood glucose levels usually with an invasive process. Even the latest wearable devices use subcutaneous needles which then transmit information about the glucose status of the patient to smartphones.56 It is possible to take ultra-fine measurements of refractive index of the aqueous in the anterior chamber and monitor change over time. These measurements can be directly correlated with the glucose concentration in the blood stream, thus providing a completely non-invasive method of measuring and monitoring blood glucose levels; this has huge potential to improve the quality of life and ease of repeat measurements for diabetics.27
Measuring VEGF levels has potential to indicate the likelihood of a patient developing neovascular
diseases, particularly choroidal neovascularisation (CNV). It is theoretically possible to analyse the tear film to measure VEGF levels and establish the risk of CNV. A study in 2022 showed high sensitivity and specificity for identifying the stage of age-related macular degeneration (AMD) by measuring VEGF in the tears and also identified other risk factors such as hypertension.28
MMP-9 is one of a family of macromolecules involved in inflammatory processes29 and is a biomarker for corneal inflammatory disease (along with other parts of the adnexa). It is closely correlated with dry eye disease (DED), ocular surface disease and Sjögren’s syndrome.30 Commercially available devices permit measuring these levels in clinic.
TABLE 1 Visible ocular and systemic health biomarkers a a -
αSYN is a proteinaceous cytoplasmic inclusion, which when accumulated is known as a Lewy Body. It is one of the cerebral biomarkers of Parkinson’s disease (PD), along with loss of dopaminergic neurons in the substantia
Anterior eyeHypercholesterolaemia/dyslipidaemia
Anterior eyeHyperthyroidism/Graves’ disease
Anterior eyeRheumatoid, systemic lupus erythematosus and collagen vascular diseases
Anterior eyeAnkylosing spondylitis, psoriasis, and similar spondyloarthropathies
Anterior eyeMyasthenia gravis, medications, trauma, cancer, vascular disease/stroke, thyroid eye disease, infection or immunosuppression
Lens dislocation13 Anterior eyeMarfan’s syndrome
Lisch nodules and eyelid fibromas14 Anterior eyeNeurofibromatosis (type 1)
Retinopathy – dot, blot haemorrhages, microaneurysms, cotton wool spots15 Retina Diabetes
Arteriovenous nipping, vessel tortuosity, copper/silver wiring16 Retina Hypertension – atherosclerosis and arteriosclerosis
Cholesterol emboli17 Retina Hypercholesterolaemia/carotid artery stenosis
Roth spots18,19 Retina Bacterial endocarditis (80% of cases) or anaemia, leukaemia, hypertension, preeclampsia, diabetic retinopathy
Papilloedema20 Optic nerve headIntracranial hypertension, malignant hypertension, meningitis, cavernous sinus thrombosis, cerebral haemorrhage
Cytomegalovirus retinitis21 Posterior eyeHIV/AIDS primarily
Blood vessel calibre22 Optic nerve headCardiovascular disease risk
Enhanced posterior corneal elevation23 Anterior eyeEarly detection of ectatic diseases like keratoconus and pellucid marginal degeneration
nigrain the midbrain. PD can be notoriously hard to diagnose in its early stages.31,32 Lewy bodies can also be indicative of one of the more common forms of dementia, termed Lewy body dementia, often linked to later stage PD. It has been postulated that these accumulations can be detected in smaller concentrations, particularly in the retina. However, how these deposits can be detected and measured in a meaningful way is not yet understood. It is likely that ERGs, OCT, cSLO, fundus autofluorescence (FAF) and other diagnostic imaging methods could be used. Detection of apoptosing retinal cells (DARC) has shown considerable promise in this regard using a specialised form of imaging requiring the injection of Annexin V, a fluorescent locator for dying retinal ganglion cells (RGCs). DARC may also bind to Lewy Bodies, hence the potential to detect early PD.57
AD is the most common form of dementia and the leading cause of cognitive impairment in the elderly. It may be possible to detect accumulations of ß-amyloid, known as amyloid plaques, in the brain and potentially in the retina, using other methodologies, such as cSLO. Normally, this is achieved by blood samples and magnetic resonance imaging (MRI) scans.33
It has become evident that it may be possible to detect the effects of AD in the retina using OCT and OCT angiography (OCT-A).58 Even in mild cognitive impairment (MCI) and pre-clinical AD, signs are present within the retinal layers. One layer of most interest is the retinal nerve fibre layer (RNFL) and the
peripapillary RNFL measured at the optic disc.59 More recently, a paper has shown that reduced ß-amyloid peptide levels found in the tears correlates well with reduced retinal and choroidal thickness in patients with AD.60 It has also been shown that in-depth assessment of eye tracking can also help early detection of AD or a very early indication of increased risk in later life.45,46 With recent FDA approval of aducanumab for prevention of advancement to late-stage AD, early detection of AD and MCI is increasingly beneficial given the human and economic impact of this devastating condition.
As mentioned earlier regarding PD, there are certain proteins that bind to dying cells that can be detected or used to detect RGCs undergoing apoptosis. In glaucoma, there are several triggers for apoptosis of RGCs, including mechanical, vascular and inflammatory elements. Whatever the actual cause of this apoptosis, it is the RGC that dies in glaucoma. Using DARC to detect Annexin V, it is possible to detect these dying RGCs,35 which could serve as an early indicator of active glaucomatous loss.
In dry eye disease (DED), there are multiple inflammatory factors that are released, including cytokines, which can
potentially lead to damage to structures like conjunctival goblet cells, meibomian gland orifices and corneal epithelial cells. Ultimately, the greater the number of proteins, cells, and other material in the tear film, the higher the tear osmolarity. Thus, measuring osmolarity of the tears is a good indicator of the inflammatory status of the external ocular surfaces and the level of DED present;36 this is achievable in clinic using commercially available instrumentation.
LOX is one of a series of proteins that can be found in the tears involved in the regulation of collagen production in the cornea. In keratoconus, there appears to be dysregulation of LOX as well as MMP-9, levels of which can be detected in the tears.37 It is possible, in theory, to measure the levels of LOX to identify atrisk patients or detect the condition in its early stages. A recent paper has also shown that detection of LOX may help to identify heightened risk of glaucoma or diabetic retinopathy.38
DOPAC is a protein found in the vitreous, which appears to be directly related to dopamine release in ocular growth. In experiments with chicks, one group underwent continuous form
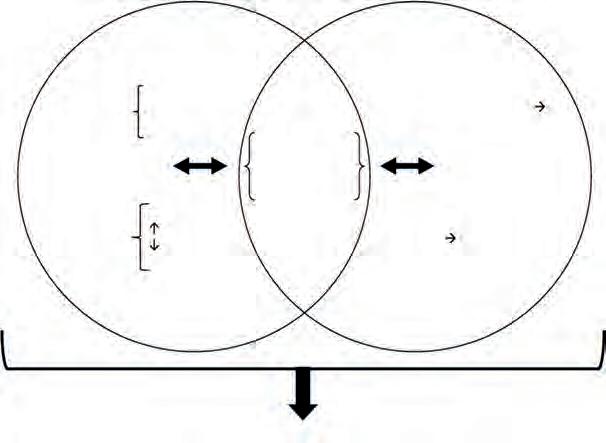
deprivation – a known driver for globe elongation and myopia development – and compared with a control group. Both groups of chicks were placed in conditions where they received 12 hours of bright daylight conditions, then 12 hours of dark conditions per day.39 The results of the study found that in the control group, DOPAC levels (and therefore dopamine levels) underwent expected diurnal variation, with release four times higher than in the darker conditions. However, in the deprived groups, even in the daytime levels, the DOPAC levels were only slightly raised compared to in dark levels; this suggests that light deprivation is linked to reduced dopamine levels, which in turn results in abnormal control of ocular growth. These levels were taken using chromatography, an invasive method that would not translate to the clinic. However, there is considerable potential for assessing and monitoring these levels invivo using developing modern imaging techniques, which could lead to improved understanding of a child’s risk of myopia development.
HSPs, along with an array of other proteomic biomarkers and the presence of autoantibodies, have been found to exist in glaucomatous eyes. These proteomic biomarkers have been shown to exist in eyes with intraocular pressure-independent neuropathy, thus normal and low-tension glaucoma40 and are included in newer models of glaucoma pathogenesis (see Figure 3). Reduction in levels of autoantibodies appears to reduce the protective autoimmune levels in the retina, increasing the risk of apoptosis in RGCs.40 Blood tests, and potentially, ocular imaging techniques, to measure HSPs and other proteomic biomarkers could help identify glaucoma at an early stage. More recent studies have shown that small HSPs can also identify cases of AMD, diabetic retinopathy as well as glaucoma.41 Another study specifically identified inhibiting production of HSP 90 can lower intraocular pressures in rabbits while having no effect on aqueous production.42 These outcomes show promise for future diagnostic therapies for many ocular conditions.
The subject of free radicals and dysregulation of oxidative stress is a complex topic and beyond the scope of this overview article. However, in brief, it is apparent that there are many degenerative ocular conditions linked to oxidative stress, which can affect numerous parts of the eye, including the cornea, retina, crystalline lens, anterior chamber and the optic nerve.43 The damage caused by processes linked to oxidative stress, and the presence of free radicals and reactive oxygen species (ROS), can lead to a range of conditions including AMD, glaucoma, keratoconus, cataracts and more.43 With the greater understanding of these processes, newer therapies, or existing options like antioxidant therapies, could lead to improved treatments for the myriad sight-threatening ocular conditions. Considering existing and developing diagnostic modalities and procedures, it is possible that invivotests that will detect and measure levels of free radicals and ROS could become available. Indeed, some rather esoteric imaging options already exist for
AGEs24-26 Crystalline lensRelative to HbA1c long-term levels. Auto-fluorescence detection. Can locate pre-diabetes and diabetes
AGEs 24-26 Retina, cornea, etc.A range of ocular and systemic conditions, for example cardiovascular disease, schizophrenia, and glaucoma
Refractive index27 Aqueous in anterior chamber It appears that the refractive index of the aqueous is well correlated with systemic glucose levels
VEGF28 Tears AMD, diabetic eye disease, ischaemic health issues
MMP-929,30 Tears Sjögren’s disease and DED (potentially cardiovascular disease)
α-synuclein31,32 Retina PD
ß-amyloid peptide33,34 Retina AD
Annexin V35 Retina Glaucoma
Osmolarity36 Tears DED
LOX37,38 Tears Keratoconus
DOPAC39 Vitreous Myopia risk
HSPs40-42 Anterior chamberGlaucoma
Free radicals and oxidative stress43,44 Whole eye Large range of conditions such as AMD, glaucoma, diabetes and many more
Eye tracking45,46 Visual systemAD
Bull’s eye autofluorescence47,48 Macula Hydroxychloroquine toxic retinopathy
Microvascular changes49-51 Posterior eye Diabetes and diabetic eye disease, cardiovascular disease
TABLE 2 Invisible ocular and systemic health biomarkers -
real-time detection of ROS in the retina, such as autofluorescence multispectral imaging.44
There is a growing body of evidence that dementia can have a detrimental effect on oculomotor control. Studies conducted in the past decade, including some in Glasgow, have shown that detailed assessment of gaze tracking and fine motor control tracking can indicate the likely risk of patients developing dementia in later life.61 There is evidence that a correlation exists between a lag in a patient’s ability to rapidly switch binocular gaze direction while following a target and the likelihood of them developing dementia.61 Unfortunately, with current treatment limitations, if a patient is identified as having such risks, which may not manifest for decades, there is little that can be done. However, it is likely that treatments and therapies are on the horizon and early identification of dementia risk could eventually lead to improved understanding of the condition and subsequently more effective therapies.45,46
FAF is a well-established technique used to identify an array of biomarkers in the retina and thus to screen for a range of ocular and systemic conditions.47 Recently, there has been an increased desire by NHS trusts to screen for the side effects of the long-term use of drugs like hydroxychloroquine used to treat rheumatoid arthritis and malaria. Long-term use of these drugs has been shown to lead to bull’s eye maculopathy, which affects the retinal pigment epithelium (RPE) in the central macular area. The damage occurs because these drugs bind strongly to the melanin in the RPE and can also cross the blood-retina barrier and are directly toxic to the RGCs. FAF can been used to screen for the early signs of the changes in the RPE found in bull’s eye maculopathy, which can guide when to alter treatment modalities. Research has shown that peripheral FAF imaging can
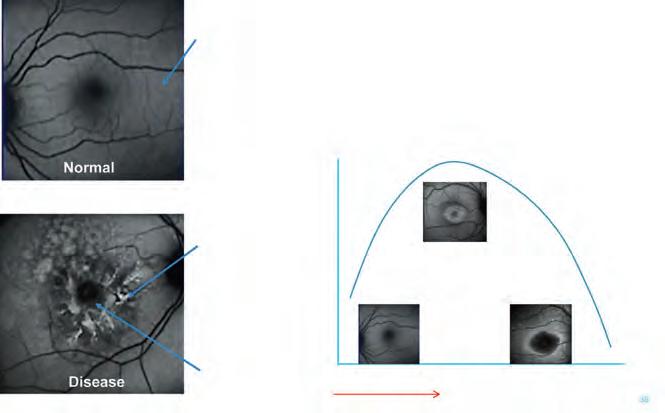
also locate earlier issues associated with hydroxychloroquine in an Asian population.48 Autofluorescence occurs when light of a specific wavelength incident on certain proteins and chemicals is absorbed and then re-emitted with lower energy and at a different specific wavelength. Such proteins and chemicals are known as fluorophores; many of these exist in the human body and are most easily excited in the skin and eyes. The benefit of FAF is that certain fluorophores are indicative of certain ocular and systemic diseases.62,63
The image in FAF appears monochrome as only one wavelength of light is used (including wavelengths outside of the visible spectrum). When the retina and RPE is healthy, the grey appearance is known as iso-fluorescence. Where there is a higher or lower than average degree of autofluorescence this is termed hyperor hypo-fluorescence, respectively (see Figure 4). Other modalities like FA, indocyanine green angiography (ICGA) and OCT-A can be used to assess the microvascular structure of the retina, choroid and optic nerve head in fine detail.49,50 These procedures then allow clinicians to detect a range of ocular and systemic conditions, including diabetic retinopathy, hypertensive retinopathy, wet AMD, glaucoma, vascular abnormalities, and others.
Hyperfluorescence (white region)
= RPE functional depression
= Abnormal lipofuscin accumulation
Hypofluorescence (black region)
= RPE functional loss
= Lipofuscin loss
There is evidence to show that early dry AMD can affect dark adaptation. Surprisingly, the rods appear to be affected sooner in dry AMD than the cones. Detecting changes in the adaptation curve in patients using new rapid dark adaptation tests can detect pre-clinical signs of dry AMD.64 Devices which can detect these changes in a rapid and easy way are becoming available.
Ocular biomarkers present a unique and accessible window into the body’s health, enabling early detection of a range of conditions. This trend towards early detection and personalised care has the potential to improve patient outcomes, allowing for preventive measures or early interventions that could mitigate the progression of serious systemic and ocular pathologies. A new field of oculomics has been established based around biomarkers and the eye, both for systemic and ocular health.65
To read this article online, access the references and take the exam, visit: www.optometry.co.uk/cpd


Your need to know industry insights
EDITED BY KIMBERLEY YOUNG
Jonathan Cohen, commercial manager for Seiko Optical UK, on lens production and a training academy

Emily
Steele, optical assistant
My role is: optical assistant at Edmonds & Slatter Opticians in Leicestershire. Time in the practice: Since December 2022.
What I love most about my practice is... The team I work with have all been so patient with me and really helped me, especially through my optical assistant course. They have always been willing to answer as many questions as I have. I also love how, as a company, we use the most up-todate technology we can, such as using the biometer to measure axial length for myopia management.
My role in the patient’s journey, in my view, is... I like to think of my role as being supportive – from booking initial sight tests, triaging patients and helping them to select their frames to arranging their collections, it’s important to ensure that they have someone as a point of contact if needs be.
One lesson I’ve learnt from a team member was... One of many valuable skills, aside from the optics knowledge, that I have been taught is to ensure constant communication, both within the team and with patients. Nothing gets sorted out if people don’t know what is happening, and the two
WHAT’S HAPPENING IN... Eyewear showcases at 100% Optical
ME AND MY GLASSES Marco Barp, CEO and designer at Tree Spectacles 75S 76
To feature in OT’s What’s happening section, contact: kimberleyyoung@optometry.co.uk

minutes it takes to pass on a message can save hours of frustration and confusion.
The practice supports colleague wellbeing by... We have lots of ongoing training and opportunities for personal development, along with lots of social events in order to maintain our strong team relationship.

For more from Emily on her practice team and her career goals, read the full profile on our website.

From devices for assessing visual fields, to highlights in eyewear, OT rounds up the latest from optics

EQUIPMENT
BIBOphthalmic
Instrumentshasbecome exclusiveUKdistribution partnerforPerivision’s virtualrealityeyetesting platform.TheVisionOneis UKCAapprovedandutilises analgorithmforvisualfield testingthatispoweredby artificialintelligence. bibonline.co.uk


FRAMES
JF Rey has expanded its Sledge Combi range, with new models featuring a monobloc titanium front with a refined acetate piece.The frames are equipped with the brand’s patented Combi Flex screwless hinge technology. jfrey.fr

1 Sun, sun, sun
FRAMES
Silhouette has released Sun Lite, an update on four classic styles, featuring subtle titanium accents and rich earthy colours in a range that draws inspiration from the West Coast of the US.The new models include a chic butterfly style, ‘Hermosa,’ named after Hermosa Beach. silhouette.com
EQUIPMENT
Grafton Optical has launched the Rexxam FieldNavigator, a headmounted perimeter using eye-tracking technology to assess visual fields.The FieldNavigator records all eye movements to allow for post-examination verification of results. graftonoptical.com

5 Fine steel
FRAMES
ItaliaIndependenthas introducedeightstylesin stainlesssteelfeaturing acetatetempletips. Acamotexturehasbeen re-introducedtotherange, inbluesandgreens,aswell asbrownsanddarkpurples. italiaindependent.com


Eyewear suppliers will showcase the latest in design

Bird Eyewear will showcase its largest range yet at 100% Optical, with highlights including its Pantix range of low-carbon acetate made with plant dyes, and the new WWF optical range, designed to celebrate and protect the Amazon rainforest. birdeyewear.co.uk


Morel will launch two new acetate models, ‘Jenny’ and ‘Noémie.’The ‘Jenny’ frame (pictured) gets creative with acetate and features an elegant arch.The ‘Noémie’ frame is a colourful design with bold contrasts. morel-france.com/en



Marcolin presents the latest collection from Max Mara, which features geometric shapes and refined lines, drawing inspiration from the architectural simplicity of designer, Eileen Gray.The acetate front of the ‘MM0117’ conceals its metal structure. marcolin.com

Kirk & Kirk will showcase the ‘Cat’ and ‘Falcon’ frames for the first time at a UK trade show. Made from the brand’s bespoke K-Lite material, each edge and angle is polished by hand.The frames are available in five colours including a new ‘Lagoon’ hue. kirkandkirk.com

FOR ALL Rebel Eyewear will make its second appearance at 100% Optical, bringing a refreshed offering for two of its brands: Kühl, the company’s most budget-friendly range, and Parker & Payne, described as “quintessentially English styles” with “Rebel flair.” rebeleyewear.com
Modstyle highlighted its latest launch, Avanti ‘Mode,’ inspired by the urban landscapes and contemporary street culture of Australia. The collection features statement styles with thicker, bolder acetates and rich colourways. modstyleeyewear.uk

The CEO and designer at Tree Spectacles on growing up surrounded by a passion for eyewear


The shapes I prefer are always very large and square. I almost exclusively wear acetate frames with significant thickness. It’s a type of frame with a bold and impactful design. As for colours, I have a very wide palette, but I always stick to shades that are never too bright or flashy.
My favourite model is the ‘Dite’ frame in crystal transparent. It’s quite large and thick. I love its very modern shape, which is not too extreme at the same time.The shiny gold metal detail adds a fashionable and luxury touch that makes the frame both elegant and trendy.
I come from a family of eyewear designers and manufacturers, so I’ve always been immersed in the world of eyewear. The main topic of conversation at home was eyewear.
Number of glasses owned: “Probably hundreds”
What does vision and eye health mean to you?
Being able to see well and take care of your vision is essential, in my opinion. Without proper vision correction, you experience a real deficit. It’s fundamental.
Growing up, I developed a deep passion for this field, especially thanks to my father and his contagious enthusiasm for glasses.
Wearing our glasses is the first thing we do every day. The face is what stands out the most when we meet someone, and it is through eyewear that we convey our personality and identity.There is nothing more significant we can wear to express who we are.
Inspiration can come from anything. I’m a big fan of design in general, from interior design, to ancient and contemporary art. I’m passionate about design books and photography. I live in Italy, the country of fashion, where beauty is everywhere. Of course, the eyewear world itself provides a lot of inspiration.Then, suddenly, an idea is born, and from there, the process of developing and making it credible begins.

Dispensing optician and AOP member, James Dawson, on: how should I approach dispensing frames for leisure and occupations?

Dispensingframesandlensesfor leisureandworkplaysavital roleinprovidingindividuals withthecorrectvisualaidsfor theirdailyactivities,soweshouldnever beconcernedaboutgivingadviceand multipleoptions–thisisourspecialty andwhyourclientscometous.
Understandingthepatient’sprimary activitiesiscrucial.Onlyafterhavinga meaningfulconversationwiththe client,explainingwhyyouareasking questionsandassessingtheir prescription,canyoureallybeginthe selectionandfittingofeyeweartailored totheclientandtheirspecificneeds. Findingoutabouttheclient’slifestyle andoccupationwillaidyouradvice andthepotentialformultiplepair dispensing.
Inleisureandworksettings,individuals oftenengagewithscreensforextended periods.Theprevalenceofdigitaleye strain,characterisedbysymptomssuch asdryeyes,blurredvision,and headaches,haspromptedaneedfor specialisedlensessuchasanti-fatigue andoccupationallensesthatmitigate theseeffects.Thus,understandingthe
nuancesofopticaldispensingis essential,notonlyforenhancingvisual comfortbutalsoforpromotinglongtermocularhealth.
Manyprofessionsrequireemployees toengageintasksthatoverworktheir eyes.Individualsmaybenefitfrom prescriptionlensesspecifictotheir workenvironments.Dispensingspecific opticalsolutionscanimprovework efficiencybyreducingvisualdiscomfort andenhancingfocusduringtasks.
Opticalleisureandoccupational dispensingrepresentacrucial intersectionbetweenthefieldsof optometry,ergonomics,andconsumer health.Associetybecomesincreasingly reliantondigitaldevicesforworkand recreation,thedemandforspecialised eyewearhassurged.Itisessentialto assessthespecificrequirementsof individualsbasedontheiractivities whileconsideringadvancementsinlens andframetechnology.
Forleisureactivities,suchassportsor outdoorpursuits,specificfeaturesin eyewearcanenhanceperformance. Forinstance,watersportsmaybenefit frompolarisedlensesthatreduceglare. Additionally,framesdesignedfor durabilityandasecurefitareessential

1
Open days and trunk shows are becoming a useful tool in promoting your business. It was great to see that people are still looking to find great eyewear, even at this difficult trading time in optics. We provided some amazing frames and lens combinations that help practitioners decide which models to stock going forward.
2
Therewasa weekoffinalising myCPDforthe lastcycle.Thepractice hostedapeerreviewwith Hoya.Itwasnicetointeractwith newconnectionsandtolearn fromtheirexperiences,aswellas sharemyinsight.Ifeltthiswasan essentialandvaluablepartofthe CPDrequirement–ithelpsyou findbestpracticeandshareideas.
3

I attended my first Hakim Group retreat – wow, what an event. With top class speakers, great business partners working with the stores to give them the tools to be successful, and an amazing Comic-Con themed party to celebrate success.
foractiveuserstominimisetheriskof losingordamagingtheireyewear duringvigorousmovements.Focusing onspecificsportswillalsogivegreater options,suchasswimminggogglesor divingandsnowmasks.

Jonathan Cohen, commercial manager for Seiko Optical UK, on a new

What is the latest from Seiko Optical UK?
The Seiko Vision Xperience Centre brings Seiko’s lens technologies to life in an interactive, immersive environment.This device allows patients to engage with the products first-hand, showcasing advanced lenses like Brilliance, polarised options, and Sensity lenses.The hands-on experience that not only demonstrates the performance and comfort of Seiko lenses, but also educates users about their benefits.
What did it mean for Seiko Optical UK to move manufacturing to the UK?
Our customers are in a highly competitive market, where they need to excel in both product and service to maintain their edge. One of the best ways we can support them is by building a strong, predictable, and reliable supply chain. If we deliver on time, they can deliver to their patients. While we already had a robust supply chain, this move allows us to support independent opticians even more. Being part


Seiko is all about staying close to customers, helping them shine and stand out by tapping into its unique brand, products, and services



of the larger Hoya Vision Care organisation enables us to tap into an incredibly reliable supply chain. From decision to the first UK-produced lens, it only took a few months.
Could you tell us about the intentions for the Seiko Training Academy?
While we continually train our customers nationwide through our business development managers and webinars, we realised that creating a dedicated facility to invite our customers would provide the ideal environment to play our role in continuously educating the market. Our simple belief is that the more we invest in our customers’ development, the more we will gain in return.This is a matter of mathematics. The second part of our strategy is to invite potential future customers. By showcasing our lab introducing them to the people behind the phone at our customer service office, and offering them a glimpse into Seiko’s culture, we hope to inspire them to see us as a strategic partner.
Three facts about Seiko Optical UK
Thecompanyisbasedin Wrexham,UK
InOctober2024,thefirst Seikolenswasmadein theUK
Thecompanyrecently hosteditsfirstSeiko VisionSpecialist conference.

OT spoke to three suppliers about giving guidance on vision correction for sports



Whether a career, a hobby, or even somewhere in between, for sporting enthusiasts it is all about performance. Fortunately, there are a number of solutions for patients looking to meet their vision correction needs, while unlocking their full potential.
Essential equipment
Ludwig Eberlein, international coordination, Vision Sensation at Silhouette Eyewear, highlighted the protective functions that sports eyewear can play, sharing: “90% of serious eye injuries could be prevented by wearing appropriate eyewear.”
Aside from protection, Eberlein suggested: “It is essential to offer the best contrast for every light circumstance, to ensure detailed vision and to avoid eye fatigue.”
In 2024, Silhouette brand evil eye introduced the ‘Peaklite’ goggle – a lightweight design with integrated optical inserts in the filter lens using an adapter system. This removes the requirement for additional clip-ins or a second lens.
Eberlein explained that there is a focus on prescription glazing throughout the frame development process, and athletes also test the products in real-world conditions.
“We are not just producing sports eyewear, we are producing sports eyewear as essential sports equipment,” he told OT When making a recommendation for sports eyewear to a patient, Eberlein shared: “Sports glasses are a classic second pair offer that must be offered proactively. Many patients simply do not know that sports eyewear with prescription lenses is available.”
Josie Barlow, head of customer support at Menicon UK, shared that in a conversation regarding a patient’s history and symptoms: “We think about people’s lifestyles, but we can sometimes be bit too focused on their job, rather than thinking about what they do outside of work which could influence what we are going to suggest.”
“We can get a holistic look at a whole person and that can give us some really good clues as to what contact lens would work for them,” she said.
For some patients engaged in sports, ortho-k can be a positive option.
Swimmers, rugby or football players and gymnasts, might all benefit from the freedom offered by ortho-k.
Barlow said: “While we talk about ortho-k for myopia progression, I think we don’t tend to talk about it quite so much with patients who would benefit from it – either from a lifestyle perspective or just being correctionfree throughout the day.”
In addition to a range of soft lenses, Menicon offers the Menicon Z Night ortho-k contact lens for non-progressing myopes, and the Menicon Bloom Night for children who require myopia control.
Sharing how she might discuss the option of ortho-k with a patient, Barlow gave the example of a patient who is a regular swimmer, suggesting she might ask: “Have you thought about this type of contact lens that you can sleep in overnight? In the morning when you wake up, you’re free of spectacles for the rest of the day.”
“I would explain that they could wear these contact lenses seven nights a week and they are not going to need any vision correction at all any other time of the day. They are going to be able to do everything with that one contact lens,” she said.
Sofia Fazal, professional services manager for Hoya, emphasised the importance of finding the right lenses for sports frames – particularly the wraparound frames that can be popular for patients involved in outdoor activities.

With these frames in particular, it is important to consider the peripheral visual system, Fazal shared: “It is critical for reaction time and how the individual wearer will perform.”
“This is where the challenge lies for us as lens manufacturers, because inevitably as you look off-axis to the periphery, you are going to perceive more distortion, more aberration, and induced prism where we don’t really want it,” she said.
To meet this need, Hoya has designed the Sportive range of lenses with both single vision and multifocal options, that uses a prism compensation technology to optimise the high-curved lenses for wrap frames.
The Sportive range supports wearer activities through power compensation and binocular vision design adaptation, with technology introduced to reduce perceived peripheral and prismatic distortion.
The lenses are also available in a number of tints and coatings to enhance contrast and reduce glare.

Advising that the practice team should be kept up-to-date on their knowledge of fitting and measurements, Fazal highlighted the need to ask enough questions of the patient.
Fazal commented: “Are you asking enough questions about working distances? Contrast, lighting, or colour perception requirements?”
She continued: “If they play a sport, what is the speed of objects as they move – are they static or moving? All these questions will help you to select the right sports lens.”

When Hasan and Hossain took their first steps, it should have been a moment of joy. Instead, their parents were filled with fear when they realised their sons couldn't see. Born with congenital cataracts, the twins faced a lifetime of blindness.
In the UK, a simple NHS surgery would restore their sight. But Hasan and Hossain are Rohingya Muslims living in the world's largest refugee camp in Bangladesh, and such treatment is out of reach.
Without intervention, the boys would remain blind. Just when it seemed all hope was lost, their
father Kholil visited an Orbis Vision Centre. Both boys underwent life-changing cataract surgery, restoring their sight.
Now Kholil can look forward to his boys' first day of school and a brighter future. Yet thousands more children like Hasan and Hossain still need urgent care to save their sight.
Your gift can help Orbis and our flying Eye Hospital continue our sight saving work and train more local eye care doctors to save sight in their local communities.
Will you help give children like Hasan and Hossain a brighter future?

For over 40 years, Orbis has helped to protect the sight of millions of people around the world.
We've provided screenings and treatment for millions of people who couldn't otherwise afford eye care. And because we train local eye care workers too, our supporters help create a lasting legacy of sharing skills and saving sight.
You can help our Flying Eye Hospital and teams on the ground reach children in Bangladesh and around the world, to save sight and give them a brighter future.
The Flying Eye Hospital, a state-of-the-art eye hospital on-board a converted plane, has visited 95 countries to date, training eye care teams to save sight for generations to come.
Help change a life by donating today
A gift of £25 could fund medicine to treat 25 patients' eye conditions.
A gift of £50 could train five community leaders to identify eye problems and learn where to send people for treatment.
A gift of £75 could go towards giving children with avoidable blindness the life-changing surgeries they need.


MI COULDN’T LIVE WITHOUT…
Laura Woolstenhulme, optometrist at Bainbridge Bespoke Opticians, on how a part-time working pattern reduces stress and optimises family time
yworkingpatternistwodaysperweek, andoneSaturdayeverymonth.Thatallows metospendmoretimewithmyson,whois 20monthsold.ItmeansthatI’mavailable ontheotherdaysintheweektodosimplethings, liketakinghimtotheGP,whichhappensquitealot. Itmakesthingsalotmoreflexible,inthatrespect.
Mypractice,BainbridgeBespokeOpticians,is reallyflexible.Withnursery,obviouslywecan’t changethedays.Ihadoriginallyrequestedtowork differentdays,andtheyhavebeenfinewiththat.
TheoneSaturdayamonth,wearrangeinadvance, soitsuitsboththepracticeandmyself.Thepractice managerdoestherota,andwewilldiscussit. If there’ssomethingthatIknowisgoingtopop up,likeaSaturdaywhereIknowthatIcan’twork, I’llsendheralistinadvance.Itwon’tjustbeaset Saturday.Wetryanddoitsothatitsuitsbothme andthebusiness.Itmeansmyhusbandisalways availabletolookafteroursonaswell.
If Ineedtodoashortdayforanyreason,they willalsoalwaysletmedoanotherdayinstead.That benefitsthem,becauseitmeansthatI’malways willingtogoaboveandbeyond.Iwanttohelpthem asmuchasIcantoo.
At the end of the day, if we haven’t got any patients, I’m often able to leave slightly early, which I appreciate. It means I can do nursery pick-up, and we can have more family time together. It makes me a happier person. It’s less stressful, which is the main thing. I know that, if I have to be slightly late or move something around, that the practice team is going to be fine about it. I’m much happier at work, because of that.
There is always a bit of give and take. In terms of the business, it means that if they need more cover or for me to do another day, if I’ve got enough notice, then I will help them out.
I used to work full-time. I was working five days a week, and then after my year of maternity leave, I came back part-time. We are looking at getting another optometrist to work part-time soon as well. That will work quite well, because it will offer balance and mean that somebody else can work the days that I am not working. The main thing is that family always comes first. That work-life balance is brilliant, for me.

Russell was diagnosed with AMO in 2011-one of over . • • 70,000 diagnosed each year. Thanks to innovative • .,,,, research, he can continue his sailing adventures. We -~ e ~·. at Sight Research UK fund research into eye disease • ·'/1;\ so people like Russell can live life to the fullest. • • SIGHT

Making connections for over 40 years
Join Us at 100% Optical -Stand ES!
Discover the latest in glazing equipment with Huvitz & MEI systems which deliver precision, efficiency, and quality to your lab.
With a huge range of practice consumables, expert advice, show offers and an exclusive product launch, take your practice to the next level.
Join us on Stand ES and explore just what is possible for your 2025!
The AOP’s employment law team is reminding employers of their duty to prevent sexual harassment in the workplace

A new statutory duty under the Equality Act 2010 came into effect on 26 October 2024, requiring employers to take ‘reasonable steps’ to prevent sexual harassment in the workplace.
The Equality Act provides legal protections against sexual harassment in the workplace, and this new duty creates an additional positive obligation on employers to work to prevent sexual harassment from happening, and if it has taken place, to prevent it from happening again.
As a result of the change, the Equality and Human Rights Commission is now able to take enforcement steps against employers who fail to take action.
It also means that employment tribunals will have the power, where a claim is successful, to increase compensation awarded to the claimant against the employer by up to 25%.
The AOP employment team has prepared guidance outlining the change and what it means for employers. This includes a link to guidance from the Equality and Human Rights Commission, along with guidance from the AOP on tackling workplace discrimination and harassment.
The AOP encourages a zero-tolerance policy towards any form of harassment or discrimination.
Templates are available from the AOP for an anti-harassment and bullying policy, diversity, equality and inclusion policy, and disciplinary and capability policy. This includes examples of gross misconduct – behaviour that could result in immediate dismissal without notice. These policies can be used as a tool by employers to send out a clear message around what behaviour is acceptable and what is not, the rules, and what will happen if those rules are breached.
There can be a misconception that sexual harassment in the workplace doesn’t really
NAME: Louise Wilkinson ROLE: Employment solicitor
These are significant penalties. It is a signal that employers can’t turn a blind eye to the possibility of sexual harassment happening in the workplace.

Resources and further reading
1
2
3
AOP update on tackling sexual harassment in the workplace: www.aop.org.uk/ sexualharassment
AOP template policies: www.aop.org.uk/ templatepolicies
OT’s Time to speak series profiles how discrimination in the workplace affects eye care professionals: www.optometry.co.uk/time-tospeak
4
The AOP Peer Support Line is available to members and non-members at any stage of their career to discuss problems with a trained, empathetic peer. Call: 0800 870 8401 or visit the AOP website: www.aop.org.uk/peersupportline.
happen anymore, but it is very common. Some employers may believe that having policies in place is enough to prevent sexual harassment, but that is unlikely to be the case.
The initial response for many on the receiving end of harassment can be to feel humiliated and ashamed. Employers need to not only be looking out for it, but creating a safe place for staff to bring it to their attention. That is where policies and procedures are important, because it sets the scene, but it needs to go further than that. Employers need to be at the forefront of bringing about cultural change.
Another myth that persists is that some people are just too sensitive – a common phrase used is that “it’s just banter.” If something humiliates, degrades, or offends another person, then that is harassment, regardless of the intention.
There are a number of steps that employers can take to prevent sexual harassment in the workplace, such as regular training for staff. If employers are concerned about the cost, there is a wealth of good material available online.
Employers have a duty to provide a safe place to work. Harassment needs to be talked about and tackled because the impact is devastating. Everybody needs to take action.
AOP members, whether an employee or employer, who have concerns about a member of staff can approach the legal team with any employment concerns. We can advise on how best to approach the situation and help to draft letters. Members will speak confidentially with an experienced employment lawyer or paralegal who will handle the conversation sensitively.
Find the AOP’s latest advice and guidance on employment law: www.aop.org.uk/advice-and-support/legal/employment
A review of AOP activity in the past two months



The AOP secured more than 400 items of coverage for its Don’t swerve a sight test campaign. Henry Leonard, head of clinical and regulatory, took to the BBC Breakfast sofa, CEO, Adam Sampson, appeared on ITV, and BBC Scotland interviewed clinical adviser, Kevin Wallace.
www.aop.org.uk/dontswerve

From business wins, to changing policy, to new qualifications, and community-work, OT asked contributors to share their standout moments from 2024. Experts also shared insight into key drivers in the eyewear market.
www.optometry.co.uk/ the-2024-viewpoint

For AOP members and OTsubscribers looking to get ahead in the new CPD cycle, OT has a variety of resources and education available on its website. Don’t forget to prepare a new PDP to structure the next cycle of your education.
www.optometry.co.uk/cpd
AOP Council applications February
Applications for some designated positions on the AOP Council will open in February. Find out more about the AOP Council and what is involved here: www.aop.org.uk/council
100% Optical 2025 1-3 March
Make the most of the education programme, see updates from suppliers, and network at the biggest optical industry event in the UK: www.100percentoptical.com
AOP events March
The AOP schedule of events for spring/summer will be published in March. Keep up-to-date with the latest events on the website: www.aop.org.uk/events
Josie Evans on how talking and chocolate supports her wellbeing and keeps her passionate about the profession
“ A problem shared is a problem
halved
1 You had me at hospital Krupa Mistry’s experiences as a hospital optometrist Page 29


As an optometrist the part of the role that I feel most stressed about is clinical decision making, and the possibility of missing something. This has always loomed over me, but became worse during lockdown when I was working as the sole optometrist in a practice – for the following year or two, I think my confidence had been shaken.
This feeling has receded as I’ve begun discussing more cases with colleagues, particularly cases that I’m unsure about, asking for a second opinion, and making sure I’ve thought of possible differential diagnoses. Two minds are always better than one, and addressing any uncertainty at the time means it’s less likely to travel home with me.
The more clinical experience I have, the more comfortable I feel with explaining to patients that I’m unsure of their diagnosis or management. This is usually followed by a plan to gain clarity, or an explanation of the differential diagnoses and what they should look out for. This transparency with patients has really helped ease my worry, and I think patients appreciate it too.
Over the years, when stresses begin to bubble to the surface, I have learnt to talk to someone, whether that be a friend, a family member or a colleague. Speaking to others helps to gain perspective, and often they’ve dealt with a similar stress before and can share their experiences. A problem shared is a problem halved.
I have also found it important to build in a routine to help me unwind at the end of the day. My partner would say that this sees me “eat a lot of chocolate.” Although this is somewhat true, it is usually preceded by a home cooked meal. Having a nourishing meal feels like a token to yourself after a day focusing on others. Generally, I find balance through the year by keeping most of my extra optometry-related activities to ‘term time’ and keep more availability in the summer and the festive period for friends and family. This variation helps; I appreciate the quieter periods and build energy for the busier ones.
In terms of staying motivated, I believe ‘the more you put in the more you get out.’ Although it tends to be a busier period, I am happier in my role when I am learning or when there is variety. Learning reignites my passion for optometry and it feels rewarding to apply something you’ve learnt in clinic. Variety is also key, whether it is having a mix of appointment types daily, or a mix of environments in the week, it prevents monotony and that auto-pilot feeling.
0
JOSIE’S TOP READS
2 IP and me
IP optometrists on a case of dry eye and an eye drop adverse reaction Page 30
3 In focus
A look at how urgent eye care is being delivered in peoples homes in Wales Page 44
Wear time matters for effective myopia
When you recommend a myopia management treatment, consider the lifestyle and preferences of your patients. Because wear time matters. 1• 2