










www.optometry.co.uk Journal of the Association of Optometrists freshthinking TO 100% OPTICAL 25-27th February 2023 ExCeL London | Stand: L300 BRING YOUR February/March 2023 Volume 63:01 Spotlight Growing opportunities in sports eyewear Page 16 CPD A guide to diagnosing optic neuritis in practice Page 76 In practice Looking after your financial wellbeing Page 55 The patient experience in optometry practices from London to Glasgow View from the chair In conversation Meeting the ocular demands of modern lifestyles Page 34 Optometry Today 1111 - - 0 Associatio~ of Optometrists , CooperVision·
LOOKING AT CONTACT LENS PRACTICE WITH
We’re thrilled to be an exhibitor and one of the AOP’s education partners at this year’s 100% Optical.
We’ve got some fresh ideas about contact lens practice, products and services that we’d love to share. We think you’ll have some pretty sharp ideas of your own too Come for a chat, bag some CPD points, definitely have fun, and help us create a fresh perspective.
fresh pairofeyes
a












freshthinking
As a global leader in contact lenses and myopia management, we’re bringing 14 hours of CPD to the event to support your fresh thinking.
ON STAND
CPD discussion workshops*
Saturday 25th, Sunday 26th, Monday 27th
freshthinking
We all know the practical and emotional benefits of contact lens wear for patients – but the journey to successful wear can sometimes be quite tricky.
Let’s face it, although contact lens technology has come a long way, the patient journey hasn’t changed much for decades.
WE’VE GOT SOME IDEAS. HAVE YOU?
• The art of prescribing for myopia.
• Myopia – putting the standard of care into practice.


• Presbyopia: myths and mishaps.
Further non-CPD discussion workshops for myopia management and specialty eye care available on the day.
AOP
LOUNGE
CPD discussion workshops*
Saturday 25th • Practice makes perfect.
• Presbyopia – myths and mishaps.


• Contact lens retention detention.
• Great expectations in myopia management.
MAIN STAGE CPD lecture*
Sunday 26th • Driving change to put the brakes on myopia.
For advanced bookings scan here:
We believe it’s time for some fresh thinking –and that’s where YOU can help.
INTERACTIVE SURVEY
Cast a fresh pair of eyes over current practice with our live survey and help create a vision of the future.
VIDEO BOOTH
How would you create a step-change in the contact lens patient journey? A chance to share your experience and fresh ideas.
BUZZ WIRE GAME
‘Bring your game on’ with a keen eye and steady hand as we present a literal ‘tortuous journey’ against the clock!
For more information scan here:


refreshyourbody,mind(andphone)
Phew! With all that fresh thinking you’re gonna need a boost. On stand you can grab a refreshing drink, relax while your phone is re-charged and let our stand staff blow your mind with the latest updates to our contact lens portfolio, technologies and services. On stand duty will be our CooperVision Business Development Managers, Myopia Management Specialists, Professional Affairs Consultants, and Specialty Eyecare Managers. We look forward to meeting you and hearing your fresh thinking!
25-27th February 2023 | ExCeL London | Stand: L300


CPD WORKSHOPS
ZONE
*3 CPD points for all interactive discussion workshops; 1 CPD point for main stage lecture.
, • - a I ,. CooperVision·
'
Welcome
Before Christmas, the GOC announced that, as part of its review of the Opticians Act, it was commissioning research to understand the public’s attitudes to the possibility of allowing dispensing opticians (DO) to refract. My immediate reaction was one of incredulity: in my experience, the public had little understanding of an eye exam, let alone what refraction involved or of the difference between a DO and an optometrist.
This sense of incredulity was strengthened when I read an article in TheGuardianby Adrian Chiles, who was complaining that his glasses kept slipping down his nose. “Opticians,” he said, “spend hours faffing around which line you can read, and which is clearer... And lately, they’ve started firing puffs of air at your eyeball to determine something or other.” But they had not cured the issue he had gone in with.

It was in this mood that I approached my latest eye appointment. The optometrist – an AOP Councillor – was someone I trusted. The experience was highly professional and reassuring. Sitting in the consulting room being asked to perform unfamiliar tasks may not be as stressful as, say, being in a dentist’s chair, but it is not without its tensions. One of my overwhelming takeaways is how much the soft, personal skills matter: each “well done” or “perfect” is vital in building confidence and rapport.
So, did I understand more at the end of that hour about the eye exam process? Yes – but largely because of the readiness of the optometrist to explain. There were parts of what was happening, which clearly spoke to refraction. But the purpose of many procedures was totally obscure to me. Had I not had such a fantastic optometrist, I would have left still unaware of the full purpose of what had just gone on. I had – thanks to Feb31st – already acquired frames. Yet, if the fitting process was relatively understandable, the discussion of the lenses took me into a mysterious, jargon-filled world. So I bowed to advice. For most of us, a visit to an optometrists is a mysterious process. What you do and why is obscure to us, and when we pay, we have a limited understanding of what we are purchasing. I paid £400 for my glasses. The GOC is set to pay much more for its public opinion research. I can now see more clearly. Will the GOC be able to say the same?
Adam

FEBRUARY/MARCH 2023 Getty/RobinOlimb
February/March 2023 www.optometry.co.uk 3
Sampson, AOP chief executive
0 OT
“Sitting in the consulting room being asked to perform unfamiliar tasks may not be as stressful as, say, being in a dentist’s chair, but it is nevertheless not without its tensions”
Contents
07-21
SPOTLIGHT
The news in digest
Picture this
A behind the scences look at our front cover shoot
OT reports
OTinvestigation reveals patients are losing their sight due to delays
The edit
Optics in 16 stories
Clinical round-up
A review of the latest clinical news and research papers
100% Optical
The latest updates before the show Supplier insight
Opportunities in sports eyewear Industry profile

Hakim Group founder, Imran Hakim, on business, values and community
AOP round-up
AOP Council appointments and the Association’s 2023 events programme
Spotlight AOP COUNCIL APPOINTMENTS
“You feel supported; you know your views and the views of the members you represent are being heard and valued”
Josie Evans, AOP Councillor PAGE 20
23-31
HIT LIST
The trends, launches and looks
OT focuses on...
OCT and imaging
Me and my glasses
Dispensing optician and personal stylist, Daniel Scott
Get the look // Anatomy of a frame With Lizzy Yeowart

The shortlist
The February/March selection Behind the brand Cubitts
34-36 IN CONVERSATION
With an increase in dry, tired eyes being reported, Johnson & Johnson Vision explains how its latest lens has been designed to meet the demands of modern lifestyles
“IMPROVED BIOCOMPATIBILITY HAS HELPED US MEET PATIENT NEEDS, AND IT IS EVEN MORE IMPORTANT TODAY WITH PATIENTS SPENDING MORE TIME LOOKING AT SCREENS”

Kamlesh Chauhan, director of professional affairs, UK, Ireland, Nordics and DACH

4 www.optometry.co.uk February/March 2023
16
28 48
0 0 0 0 0 0 0 0 0 0 0 0 0 0 OT
39-55 IN PRACTICE
Business insight and career development

The discussion
Balancing business and patient care with the cost of living crisis
How I got here
Optometrist, Scott Mackie
The workshop
Safeguarding in a domiciliary setting

IP and me
IP optometrists discuss how they would manage patients with swollen lids
Pre-reg focus
Akshay Shah and Isha Saghir
Key milestones
Specsavers’ TheBigIssuepartnership

What I have learned
The pre-reg and supervisor relationship
How do I...
Create a welcoming environment?
Eyes on wellbeing
Lloyd & Whyte on financial wellbeing
OT visits a range of optometry practices in different areas of Glasgow and London, including Munro Optometrists, Hynes Optometrists and Tom Davies Bespoke Opticians, for an on-theground view of life in practice PAGE 57-63


90-98

END NOTES
Career advice
Auerbach & Steele’s Gail Steele on why understanding the aims of the business is key I could not live without...
”My hospital equipment case,” says pre-reg optometrist and AOP Councillor, Laura Josephs
Last word
Jaclyn Payne’s secret life
OT and its wrapper are produced on paper from European mills meeting the highest quality and environmental standards. The journal and paper wrapper are fully recyclable.

CPD 65-89
Professional development for optometrists, DOs and CLOs
65 CPD welcome
66 Incomitance: tools and tips for everyday practice

71 Making the most of a management plan for dry eye
76 Clinical features of optic neuritis
81 Progressive additional lenses: are your standards up to standard?

86 Contact lens cases in practice
88 The iris and the angle
ONLINE
OTvideo highlights
OT’s latest skills guides
Watch the video on www.optometry.co.uk
Listen to The OT Podcast today
The Professor Nicola Logan episode and The Ian Cameron episode are available to listen to on all main podcast platforms
Contact the OT team with your experiences, observations and lessons from practice today: newsdesk@optometry.co.uk
Twitter

Facebook

Instagram

February/March 2023 www.optometry.co.uk 5
39 CONTENTS
98
Follow us on
@optometry_today Follow us on
@OptometryToday Like us on
OptometryTodayJournal
Cover story The view from the chair 25 Image: James
/ Art direction:
31
Tennessee Briandt
Eva Gaumé, Max Dreger,Getty
0 0 0 0 0 0 0 0 0 0 0 0 OT











Shining a light on daily practice
“Frank is a first-class optometrist,” he told OT. “When you go to get your eyes tested the whole process is very thorough. When I first visited he had just started out, so I have followed him all the way through.”
 14 100% OPTICAL OT showcases the latest developments from the trade show
16 SUPPLIER INSIGHT Opportunities in sports eyewear as the market experiences growth
18 INDUSTRY PROFILE Imran Hakim, CEO of Hakim Group, discusses the profession’s resilience
14 100% OPTICAL OT showcases the latest developments from the trade show
16 SUPPLIER INSIGHT Opportunities in sports eyewear as the market experiences growth
18 INDUSTRY PROFILE Imran Hakim, CEO of Hakim Group, discusses the profession’s resilience
Spotlight
Peter Sandground
Retired civil servant, Tony Watt, 73, was photographed at the Mount Florida branch of Munro Optometrists in Glasgow for OT's cover story. He has attended the practice for regular eye exam over the past 35 years (see P57-63).
February/March 2023 www.optometry.co.uk 7 0 OT
February/March 2023
Volume 63:01 Issn 0268-5485
ABC certificate of circulation

1 January 2021–31 December 2021
Editor: Emily McCormick emilymccormick@optometry.co.uk
Deputy editor: Lucy Miller lucymiller@optometry.co.uk
Features editor: Selina Powell selinapowell@optometry.co.uk
Senior reporter: Kimberley Young kimberleyyoung@optometry.co.uk
Web content and social media manager: Leah Boyle leahboyle@optometry.co.uk
Clinical editor: Dr Ian Beasley ianbeasley@optometry.co.uk

Clinical editor for multimedia: Ceri Smith-Jaynes cerismithjaynes@optometry.co.uk
Video production editor: Laurence Derbyshire laurencederbyshire@optometry.co.uk
CPD enquiries: 020 7549 2076 CPDhelp@optometry.co.uk
AOP membership and OT subscription team: subscriptions@aop.org.uk
NEW DATA SHOWS PATIENTS ARE LOSING SIGHT AS THEY WAIT FOR TREATMENT
Clinicians have reported more than 200 cases of patients losing sight as a result of delays to treatment since 2019, new data reveals.
In response to a FreedomofInformationActrequest by OT, NHS England revealed that there have been 551 reports to the National Reporting and Incident system that mention sight loss due to delayed outpatient appointments, or similar phrasing, since 2019.
Of those reports, 120 incidents involved moderate harm, 99 incidents involved severe harm, and one case in 2020 related to a patient who died. There were 144 cases where a low level of harm was reported, and 187 cases involving no harm.
One incident report described a patient with wet age-related macular degeneration (AMD) who lost useful vision in their left eye after their injection treatment was delayed. They were meant to have monthly injections but presented at clinic after three months had passed without receiving an appointment.
Another patient experienced a delay of a year from their appointment at eye casualty to being seen within the medical retina clinic. During this time their vision dropped from 6/4 to 6/24.
Advertising:
Matt Hall 020 3771 7257 matt.hall@thinkpublishing.co.uk
Advertising production: aop@ccmediagroup.co.uk
Art director: Grant Pearce
Senior designer: Juanita Adu
Associate director: Anna Vassallo
Executive director: Jackie Scully
Published bimonthly for the Association of Optometrists by Think Media Group 20 Mortimer Street, London, W1T 3JW
Printed by Acorn Web, Normanton Ind Estate, Loscoe Close, Normanton, West Yorkshire, WF6 1TW
All rights in and relating to this publication are expressly reserved. No part of this publication may be reproduced in any form or by any process without written permission from the AOP or the publisher.
In a third case, a clinician reported that after a four-month follow up appointment was recommended, a patient received their appointment one year and four months later. At this appointment a total retinal detachment was diagnosed. “It is very unlikely that the vision will be regained,” the reporting clinician noted, adding that this would affect the patient’s career as a paramedic.
“IT IS INCREDIBLY SAD TO SEE THESE CASES”
Cathy Yelf, Macular Society
In December, Macular Society chief executive, Yelf, shared that staff had received more than 25 calls in the past three months from people who were worried that they are going to lose vision because of delays.
“They are terrified at the prospect of losing vision. The ones who contact us are the ones who are actively trying to solve the problem. We have no idea how many people sit at home, quietly losing their vision and not making a fuss about it,” she shared. Yelf noted that there are good treatments available for wet AMD but at the moment many trusts do not have the capacity to deliver injections in a timely manner. “It is an absolute tragedy when delays in the system
means that people lose their sight when they didn’t need to,” she said, adding: “Losing sight is a devastating thing. To lose your sight when it didn’t need to happen is doubly devastating.”
President of the Royal College of Ophthalmologists, Professor Bernie Chang, shared that a lack of capacity is the underlying issue behind delays.
“There needs to be an expansion of the primary and secondary care workforce,” he said. 2
“THE STAFF SAY ‘SEE YOU IN SIX WEEKS’ BUT IT DOESN’T HAPPEN”
Val Robinson, 79
In Wales, founder of the Tenby Macular Support Group, Robinson, shared with OTthat she had waited 11 weeks for her last two appointments –
Shutterstock 8 www.optometry.co.uk February/March 2023
1
SPOTLIGHT
0 OT Optometry Today 0 Associationof Optometrists /J MIX Paper from responsible sources :!:.is FSC" C020533 OT
almost twice as long as the usual wait of six weeks between appointments.
“The deterioration is sad. I could read way down the eye chart before. Now I can only read four letters in my bad eye,” she said.
Robinson is quick to highlight her gratitude for the staff at Withybush Hospital, where she receives her treatment.
“The staff in the clinics are amazing, kind and brave. They worked throughout the pandemic and we were all so grateful for that,” she said.
But she now wonders what NHS founder Aneurin Bevan would think of the service that is being provided.
“Trusting, good people are being allowed to lose their sight,” she said.
While many were hesitant to receive their injections during the COVID-19 pandemic, Robinson continued to attend her appointments.
“A lot of people didn’t go during the pandemic because they were scared. I was more scared of losing my eyesight,” she said. Robinson shared that for the first two weeks following an injection the leakage in her eye dries up and she can see “substantially more.”
“That lasts for a while, then as you are coming up to six weeks, the leaks begin and your vision starts to go,” she said.
“What people don’t realise is that the thought of losing your eyesight can affect your mental health. That can’t be seen – people don’t know you’re suffering,” she said. The deterioration in her vision since Graham was diagnosed six years ago has meant that she has difficulties recognising people until she is close to them, and she has challenges with hand-eye coordination. She gave up her driving licence two years ago.
THE HEALTH BOARD RESPONDS
Andrew Carruthers, director of operations at Hywel Dda University Health Board
Christine Graham, 83 Fellow Tenby Macular Support Group member, Graham, has also seen the time between her injection appointments at Withybush Hospital close to double.
She told OT that the thought of losing her sight completely is “horrendous.” 4
“IT’S GOING TO CAUSE MORE TROUBLE IN THE LONG-RUN”
Joyce Cameron, 88 Tenby Macular Support Group member, Cameron, stopped receiving treatment for wet AMD during the pandemic. She did not experience delays in receiving injections when she was receiving treatment. “It wasn’t too bad then because we were still in the middle of COVID-19 and people weren’t going in to get their injections,” she said.
Cameron thinks that failing to address treatment delays will exacerbate issues within the NHS.
“It’s going to cause more trouble in the long-run because more people will have serious problems with their eyesight,” she said.
Workforce challenges within the NHS means that there are no easy solutions, Cameron added. “I think it’s awful, but what can they do about it if they don’t have the staff?” she said.
“I feel sorry for people who can’t get these injections and are so worried about it,” Cameron observed.
SIGHT LOSS DUE TO DELAYS SINCE 2019
551 REPORTS TO THE NATIONAL REPORTING AND INCIDENT SYSTEM
40% increase in reports of severe harm between 2019 and 2021
Source:FOIrequest –reportsinNational ReportingandIncident Systemthatmention “sightlossduetodelayed outpatientappointments” (orsimilarphrasing,for example:duetobacklog orwaitinglists)
“Within the health board’s wet AMD service, we have seen significant demand due to new referrals, the impact of the COVID-19 pandemic, the resulting disruption of services and recruitment challenges. This has all led to a backlog of demand and we are working with clinical experts and operational teams to try to reduce the backlog as soon as is practicably possible. Actions we are taking to improve the situation include providing people with the option to be seen elsewhere if it is quicker than in Withybush Hospital; providing additional weekend clinics in Withybush Hospital; recruiting to fill current vacancies; and using recently allocated funding to further enhance this service at Withybush Hospital.
“We wish to reassure people that we remain committed to continuing to develop this service within the health board which will enable us to treat our patients closer to home.”
5“IT IS ABSOLUTELY TRAGIC” Adam Sampson, AOP
Responding to the findings reported by OT, AOP chief executive, Sampson, said: “It is absolutely tragic that people should lose their sight due to a systemic issue and reasons that are completely preventable. There isn’t a silver bullet for many of the problems facing the NHS but with a national plan for eye care some of these challenges can be overcome to improve care and outcomes for patients.”
Emphasising the role optometrists could play in supporting the reduction of NHS wait lists, Sampson highlighted: “Part of the solution is working smart – optometrists are expertly trained, poised to help, but they’re underutilised in many parts of the country simply because of the way eye health care is commissioned and funded.”
3
“THE THOUGHT OF LOSING YOUR EYESIGHT CAN AFFECT YOUR MENTAL HEALTH”
February/March 2023 www.optometry.co.uk 9
of low or no
1 report involving the death of a patient 99 reports of severe harm 120 reports of moderate harm 331 reports
harm
Bryony Allen, professional services manager at Specsavers, told OT about the company’s three-pronged homelessness initiative, which includes partnerships with organisations Crisis and TheBigIssue, as well as local initiatives. Read the interview at bit.ly/3QcbIX3 or find out more about The Big Issue partnership on page 53.
Eyewear manufacturer, De Rigo, signed an agreement to acquire full ownership of Rodenstock Group’s eyewear division, in a transaction expected to be completed in the second quarter of 2023. The acquisition includes the brands Rodenstock Eyewear and Porsche Design Eyewear, which join De Rigo’s portfolio. Meanwhile, Rodenstock intends to focus on biometric ophthalmic lenses and growing as a med-tech company.














Julian Davies Opticians agreed a pre-pack administration deal for Bateman Opticians, which had been placed into administration and was facing closure. Through the agreement, four Bateman practices in Cardiff, Newport and Blackwood will stay open, with staff remaining in their roles.



Charities Fight

for Sight and Vision Foundation will merge and work as one organisation from 1 April. Together, they will become the only UK grant-maker that changes lives through funding both scientific research and innovative services, a joint release sharing the news stated. The boards of both charities voted unanimously to merge the organisations, which will be led by Fight for Sight CEO Keith Valentine. The move aims to expand reach and increase impact.

Scottish charities Sight Scotland, Oban and District Access Panel, and Disability Equality Scotland have launched a campaign calling for a statutory duty to be placed on businesses and retailers to provide braille labels on food products, detailing the name of the item, and the use by and sell by dates. Craig Spalding, chief executive of Sight Scotland and Sight Scotland Veterans, said: “Ensuring information is available in braille is vital for the inclusion of visually impaired people.”
Boots has re-opened its refurbished St Albans premises. The site is one of Boots’ first stores to feature a new open and stateof-the-art healthcare space, designed to make it easier for customers to access healthcare advice and products. It features Boots Opticians, Boots World of Hearing and the pharmacy. The immersive hearing care experience is the third to open in the UK, and the first inside of a Boots store.
Doug Bairner, country manager UK and Ireland at CooperVision, commented on a milestone in the contact lens manufacturer’s plastic neutrality partnership with the social enterprise, Plastic Bank, that saw the equivalent of more than 100 million plastic bottles prevented from entering the ocean.


INDUSTRY Boots
Pixabay/Igor
Ovsyannykov
“Small actions can make a massive difference when we all work together with a common purpose”
“The time really was right to step things up”
m idi ™ C M ibog ph Im gi g I c dib D pth-of-Fi d t io Im gi g & Vid o D t i d F u o c i L Fitti g Im gi g &Vid o Limbu to Limbu Topog ph - Now i Wid -Fi d Co ou S T t Optim : M t th n w Go d St nd d in o n Topog ph Th wm dmo t m idi ™ dv c d Topog ph & comp t D 01438 740823 sales@bibonline.co.uk www.bibonline.co.uk See us at: M160
10 www.optometry.co.uk February/March 2023 rn @)medmont 0 0 0 ,alyser. 0 ,............... . 0 0 0 BiB OPHTHALMIC INSTRUMENTS OT
Research published in Proceedings of the National Academy of Sciences, has offered insight on protecting dry eye patients from corneal injury. Scientists from the Washington University School of Medicine analysed the genes expressed by the cornea in mouse models of dry eye disease, as well as diabetes, ageing and homeostasis. They found that in mice with dry eye disease, the cornea activated expression of the SPARC gene. Higher levels of the SPARC protein were connected with improved corneal healing.
PROFESSIONAL SUPPORT
THE EDIT 60 DAYS IN 16 STORIES 5%
Eye health charities including the Macular Society have partnered with Diabetes UK to fund more research into diabetic eye disease. The partnership is investing in new research to improve understanding of who is at highest risk of eye damage and to provide more tailored treatment to prevent it. The charities have called for scientists to apply for the funding, with a deadline of 1 June 2023 for applications.
A study published in JAMA Network Open identified a link between lower visual acuity and depressive symptoms among middle-aged and older adults. Researchers examined data from 114,583 participants in the UK Biobank Study, finding that for every one-line decrease in visual acuity, there was a 5% higher risk of depression.
The Department of Health and Social Care has announced the extension of the provision of free personal protective equipment (PPE) for health and care staff in England for another year. PPE will remain free and accessible for primary care providers, NHS trusts, and adult social care providers until 31 March 2024, or when stock is depleted, whichever comes first. The scheme had been due to close on 31 March this year.

Janice Foster, CEO of the Local Optical Committee Support Unit (LOCSU), and Richard Knight, LOCSU head of policy, shared their vision for the year ahead, with a key priority being continuing to drive Optometry First forward. Read more about LOCSU’s expectations for the rest of the year: bit.ly/3Gh47lB
IN PRACTICE

Patient, Jean Bourne, shared her experience of the identification of a hard-to-spot retinal tear by optometrist, Alexandra Allen (pictured), from Walsh Opticians and Hearing Care, a Hakim Group independent practice.

CooperVision has named Muskaan Hussain from the University of Bradford as its 10th Future Ocular Research Creativity Event (FORCE) 2022 Student of the Year. University and college students from nine countries across Europe showcased contact lens or anterior eyerelated research projects as part of the annual competition. Hussain said: “Winning the 2022 FORCE final has been my best career experience so far.”

Myopia Profile has launched an upgrade of its public-facing My Kids Vision website, a free resource for parents. The website now holds more than 40 articles explaining myopia, treatment options and children’s vision. Printable graphics with QR codes linking to the website have also been created for practices. Co-founder of Myopia Profile, Dr Kate Gifford, said: “Communication is arguably the key ingredient in successful myopia management. We developed My Kids Vision as an information tool for eye care professionals to assist parents in understanding myopia and steps to help their children.”
Optometrist Elaine Styles told OT about her role with Vision Care for Homeless People. Read the interview at: bit.ly/3Zd0aXK
SCIENCE & VISION
“We see 2023 being a very big year for Optometry First”
Getty/Anna Ivonina
“The smile on people’s faces when they collect their glasses and see clearly for the first time in years is a fantastic reward”
“It could have so easily been overlooked”
February/March 2023 www.optometry.co.uk 11 SPOTLIGHT
0 0 0 0 0 0 0 0 OT
Pexels/Karolina Grabowska



















































































EXCEPTIONAL COMFORT 1 MEETS EXCEPTIONAL STABILITY 2 Astigmatic customers also deserve an exceptional wearing experience. They are even more likely to struggle with dryness and discomfort 3 Unique WATER GRADIENT MATERIAL with CELLIGENT™ TECHNOLOGY featured with PRECISION BALANCE 814™ DESIGN TM GRADIENT AVAILABLE NOW References: 1.Clinical Performance Evaluation of Two Frequent Replacement Silicone Hydrogel Torie. 2. In a clinical trial to evaluate on-eye performance of TOTAL30® for Astigmatism lenses where n=69; Alcon data on file. 3. Multi Sponsor Surveys Inc. The 2014 Gallup target market report on the market for toric contact lenses. *See instructions for use for wear, care, precautions, warnings, contraindications and adverse effects. 15130© 2022 Alcon Inc UKIE-T3A-2200024 Alcon
Clinical round-up
OT’s Selina Powell reviews the latest clinical news and research papers

‘SMART’ WALKING STICK ASSISTS VISUALLY IMPAIRED WITH DAILY CHORES

Engineers from University of Colorado Boulder (CU Boulder) have developed a ‘smart’ walking stick to help those with sight loss complete daily tasks.
Scientists at CU Boulder’s Collaborative Artificial Intelligence and Robotics Lab incorporated a camera and computer vision technology to a white and red cane.
The walking stick is capable of mapping and cataloguing its surroundings, as well as guiding the user with vibrations in the handle and spoken directions.
Trials were conducted to explore whether the assistive technology could help a user select a seat in a room with obstacles and other patrons.
“Imagine you’re in a café,” CU Boulder doctoral student, Shivendra Agrawal, shared. “You don’t want to sit just anywhere. You usually take a seat close to the walls to preserve your privacy, and you usually don’t like to sit face-to-face with a stranger,” he added.
During experiments, a sighted person wearing a blind fold used the ‘smart’ walking stick, which was connected to a laptop contained in the participants
backpack. The laptop used algorithms to identify different features within the room and calculate a route to the ideal seat.
In results reported at the International Conference on Intelligent Robots and Systems (23–27 October, Kyoto, Japan), researchers highlighted that study participants were able to find the correct seat in 10 out of the 12 trials.
Scientists are now exploring how the walking stick can help those with sight loss select items at a grocery store.
Users can scan the shelf with their walking stick in order to identify the correct product. The researchers plan further work to develop the technology – including making the system more compact so it can run off a smartphone attached to a cane.
EXPLORING THE RELATIONSHIP BETWEEN OBESITY AND AMD
Canadian researchers have gained new insight into the connection between obesity and a heightened risk of developing age-related macular degeneration (AMD).
Their research, which was published in Science, explored how stressors, such as obesity, can reprogramme immune system cells. The University of Montreal scientists found that transient obesity or a history of obesity leads to changes within the DNA of immune system cells that mean they are more susceptible to producing inflammatory molecules. These changes in innate immunity remain even following weight loss and normalisation of metabolism.
Study co-author, Masayuki Hata, explained: “Our findings provide important information about the
biology of the immune cells that cause AMD and will allow for the development of more tailored treatments in the future.”
University of Montreal ophthalmology professor, Przemyslaw Sapieha, highlighted: “Although considerable effort has been invested in understanding the genes responsible for AMD, variations and mutations in susceptibility genes only increase the risk of developing the disease, but do not cause it,” he said.
“This observation suggests that we must gain a better understanding of how other factors such as environment and lifestyle contribute to disease development,” Sapieha added.
Being overweight is the second riskiest non-genetic factor for the development of AMD, behind smoking.
MYOPIA Study examines genetics of myopia
Researchers from Cardiff University have described five genetic variants that increase the risk of myopia the longer a person stays in school.
The study, which was published in PLOS Genetics, analysed genetic and health data from 340,000 participants with European ancestry.
They identified genes that make a person more vulnerable to becoming myopic in combination with intensive schooling.
Clark et al.
DOI: 10.1371/journal.pgen.1010478
GENETICS
Stem cells used to grow ‘mini eyes’ Researchers from University College London have produced ‘mini eyes’ using stem cells generated from skin samples of patients with Usher syndrome.
The study, which is published in Stem Cell Reports, could help to provide greater understanding of the rare genetic disease.
Study author, Dr Yeh Chwan Leong, shared: “By using a small biopsy of skin, we now have the technology to reprogramme the cells into stem cells and then create lab-grown retina with the same DNA, and therefore the same genetic conditions, as our patients.”
Leong et al.
DOI: 10.1016/j.stemcr.2022.09.006
HEALTH
Rambling Rx: a five-minute walk every half hour
Colombia University researchers have examined the health effects of breaking up prolonged periods of sitting by taking short walks.
The study, which was published in Medicine & Science in Sports & Exercise, examined the effects of taking walking breaks at different intervals during an extended period of sitting down.
The research found that higher frequency, longer duration breaks were most effective in targeting both blood pressure and blood sugar levels, while lower doses of walking may be sufficient for targeting blood pressure. All variations that involved a break from sitting saw a significant decrease in blood pressure.
Duran et al.
DOI: 10.1249/MSS.000000000000310
SPOTLIGHT
Getty/Halfpoint Images CLINICAL NEWS February/March 2023 www.optometry.co.uk 13 0 OT
A buzzing trade show
OT
SPONSOR: CHARMANT
Taking place this year between 25–27 February at London ExCeL, 100% Optical is set to see 15% more exhibitors join the show than in 2022.


Nathan Garnett, 100% Optical show director, told OT: “In terms of exhibitors, we have the strongest line-up in all areas of the industry we have ever had, with the addition of new exhibitors like CooperVision for contact lenses; Inspecs in eyewear, bringing together Norville and Eschenbach to the show; Olleyes, the US tech company; Visionix in the equipment; Pampaloni in the
AOP LOUNGE
Plan your education and meetings for 100% Optical at: bit.ly/3ICyhT5
Not to be missed
Sharing updates from the show, Garnett noted: “100% Optical will feature a bigger focus on contact lenses than ever before.”

Major contact lens brands will be represented at the February show, with CooperVision joining the event, alongside Johnson & Johnson Vision, Bausch + Lomb, and Safilens, which are also confirmed.
The AOP Lounge will provide a space for networking and education at 100% Optical. Delegates will benefit from peer review sessions and presentations from the AOP’s legal, clinical and regulatory teams, as well as education hosted by Johnson & Johnson Vision and CooperVision.
The AOP Lounge will feature a clearly signposted helpdesk to guide members to where they can meet the AOP team to ask questions.
The stand will also offer a free cup of tea or coffee to members attending the show, providing a networking space to meet with other members and continue conversations following education sessions, explained AOP events manager, Ava Williams.
AOP LOUNGE: STAND W300
 Studio sponsored by Nikon, with its bespoke luxury eyewear; and last but not least, New Medical Systems and Staar Surgical for the strong ophthalmology offering.”
Studio sponsored by Nikon, with its bespoke luxury eyewear; and last but not least, New Medical Systems and Staar Surgical for the strong ophthalmology offering.”
gathered the latest updates on what to expect from the ninth 100% Optical event
100% OPTICAL
“Charmant will be supplying an ultimate guide to titanium and sustainability at 100% Optical and teaching front-of-house teams storytelling cues to inform and inspire your valued patients”
Nick Bandy, Charmant field sales manager
14 www.optometry.co.uk February/March 2023
A WORD FROM A
100% Optical/Media 10
-OT
Visitors to 100% Optical will also be able to gain insight into consumer trends as Euromonitor returns to the show. Eyewear expert and senior consultant, Natasha Cazin, will identify three factors from Euromonitor International’s Top 10 Global Consumer Trends that are expected to have the most impact on the eyewear industry in the near future. Following a short introduction, a panel of experts will discuss the themes of the presentation.
Meeting domains
Dr Ian Beasley, AOP head of education and OT clinical editor, explained that there will be over 140 continuing professional development (CPD) sessions over the three days.
“As we enter the second year of the CPD cycle, 100% Optical offers a unique opportunity to earn points and make sure you’re meeting the GOC’s requirements across all domains,” Beasley said, “there are a variety of peer reviews to engage in, and all points gained from the show are interactive.”
CPD sessions have approximately one third of capacity, which represents over 2500 seats, set aside to accept walkin delegates on a first-come-firstserved basis, ensuring more visitors can benefit from the programme. Beasley recommended: “It is a good idea to make notes during the session, or take pictures of the session slides for the purpose of writing reflective statements after the session, but also as a record of attendance for the future.”
Emails to confirm verification of attendance will be issued after 10 working days following the event, with visitors advised to check spam or junk folders.

As the optical trade show approaches, Garnett told OT: “The show has a great buzz about it, with live catwalk shows three times a day, main stage panel discussions and, of course, the CPD sessions. You won’t be short of things to do and see.”
“I’M LOOKING FOR… THE LATEST LENS DESIGNS”
OT heard what visitors can expect from lens manufacturers

Jai Kudo Lenses: The lens supplier will be showcasing its products and services, including its Glazed Package solution, offered in conjunction with Continental Eyewear, to provide frame, lenses and glazing “all under one roof,” explained Shaun Bace, key accounts, business development manager for Jai Kudo Lenses. The supplier’s Honeycomb lenses will be another focus, along with exclusive insights into current projects. The sculpture, ‘Heavy Light,’ created as a collaboration between Millmead Optical Group and designer, Yair Neuman, will also be on display.
Caledonian Optical: The manufacturing arm of Duncan and Todd Group will be highlighting its new £1.5 million laboratory at the show. Mark Robertson, head of manufacturing at Caledonian Optical, explained that the new lab in Dyce, Aberdeen, is more than double the company’s previous capacity and provides the company the opportunity for more sustainable practices.
The Caledonian Optical team will be joined on its stand by its lens design partner, IOT, to discuss the technology of the products.
Nikon Lenswear UK: The company will unveil its latest innovations, Jill McLellan, managing director of Nikon Lenswear UK, said, telling OT: “We’ll be sharing our cuttingedge products, as well as the tools and value we provide to independent practices above and beyond lenses.”
Headline sponsor of the Studio area, Nikon will also be hosting a networking bar where, McLellan said, “we will be sharing some of the details into how independents can complete the luxury experience in their practice.”

February/March 2023 www.optometry.co.uk 15 SPOTLIGHT
“We will be bringing a fully interactive environment and education space to the exhibition, asking eye care professionals what they see as the future of the contact lens patient journey”
Christina Olner, CooperVision head of professional affairs, UK and Ireland
“In a UK first, we are introducing Optos AI for Diabetic Retinopathy. Visitors can also experience our multi-modal imaging devices and learn how optomap improves practice efficiency and patient management”
A WORD FROM A SPONSOR: COOPERVISION A WORD FROM A SPONSOR: OPTOS
Rob Kennedy, CEO of Optos
0 OT
Visit OT’s page dedicated to the latest insights ahead of 100% Optical at: www.aop.org.uk/ot/100percent-optical-preshow-2023
Game on: opportunities in sports eyewear
Sports eyewear represents an opportunity for practitioners, suppliers suggest, both to enhance the sporting experience of their patients, and create an additional opportunity for revenue in practice.

Thomas Beier, director of vision sensation for Silhouette, which is behind the sports eyewear brand, Evil Eye, explained to OT: “According to our experience and our international markets, the segment of complete sports eyewear is developing really well.”
He suggested that, where traditional eyewear is returning to levels seen before the pandemic, sports eyewear is “steadily increasing double digits.”
Craig McNeil, UK sales manager for the sporting eyewear company, Bollé, described the changes seen in the market in recent years – with a rise in eyewear for cycling and running during the height of the pandemic, but a decrease in prescription eyewear as lockdowns restricted appointments in practice.
The company then saw an uplift in 2021 and a levelling in 2022, he said, with a strong market for skiing and ski goggles as the sporting seasons returned.
“Sports eyewear is a growth area without a shadow of a doubt,” McNeil explained. “Since I started 13 years ago, I would say we have seen continual growth year-on-year when it comes to prescription eyewear.”
Martijn van Eerde, senior director, marketing EMEA and APAC for eyewear manufacturer, Maui Jim, also described a
“tremendous opportunity, maybe almost an obligation” to raise awareness of eye protection for people playing sports.
He noted that while sportspeople will spend a significant amount of money on sports equipment, that doesn’t always translate to their approach to sunglasses.
“When we think about frame design, the lenses and the protection against impact and sun, I think it’s fair to say that in a lot of cases, it should be a premium product,” he said, “it’s an opportunity.”
Meeting needs
McNeil highlighted the role that eyewear can play as part of an individual’s sporting set-up, particularly for those requiring prescription lenses. He said: “You’ve got a performance-driven customer who is very into, say cycling, and so spends tens of thousands of pounds on a bike, but can’t read their Garmin and so wants to have a prescription pair.”
A key change McNeil has observed in this category has been an increasing percentage of customers from an older generation, who have a higher disposable income and are continuing to play sport later in life, even travelling abroad for sporting events.
“The optician who realises this, and has the option to be able to dispense those products, will get a multitude of different customers coming in,” McNeil added.
Beier noted that tints are a key part of the equation when choosing eyewear.
“It has to include a good filter to protect the eyes and, at the same time, reduce the bleed effect,” he said. In addition, anti-reflective coatings avoid the wearer seeing their own eye on the inside of the lens.
With safety a “must,” he added that the lens material itself should be “absolutely unbreakable.”
Prescription lenses in sports
Suppliers highlighted that customers are not always aware that prescription lenses are an option for sports eyewear.
McNeil said: “I think customers need guidance from the profession when it comes to sports eyewear. I find it amazing the number of customers we meet who weren’t aware they could get sports eyewear with prescriptions.”
While contact lenses will provide an option for many, this will not be the ideal solution for all and this is where prescription lenses can be beneficial, he said, adding that this could be a “cornerstone” for practices when it comes to sports eyewear.
Each of the suppliers benefit from laboratory facilities supporting the customisation of frames and lenses to the requirements shared by the practice.
Bringing sports in-house
Reflecting on how best to highlight sports eyewear solutions to patients, Beier suggested: “The most important advice we can give is to offer sports solutions to everybody who enters the practice.”
“It’s a win-win situation, because the wearer will discover greater comfort and better performance with sport glasses and lenses,” he said, adding that with the variety of designs, shapes, fits and lenses available, “practitioners can guide their patient towards a frame that enhances their experience of the sport.”
McNeil highlighted the role that practitioners play in understanding the patient’s lifestyle and making recommendations based on their requirements and prescription, suggesting: “I think the biggest driver is the optometrist in the consulting room.”
The sports eyewear market is a growth area and presents “tremendous” opportunities, suppliers suggest
SUPPLIER INSIGHT Evil Eye/Max Dreager
“Sports eyewear is a growth area without a shadow of a doubt”
16 www.optometry.co.uk February/March 2023 OT
Craig McNeil, UK sales manager, Bollé
What do you enjoy the most about sport eyewear and lenses?



McNeil: Being able to enhance sports with these products is exciting, and enabling people to enjoy the freedom of the outdoors and the best vision in the sport that they do.
Beier: The variety and possibilities available to support any type of sports – in plano as well as prescription.
Van Eerde: You could see an improvement in your game with premium sunglasses, and increase your enjoyment. You don’t realise how annoying light can be until you’ve worn something that lets through only what you need.
“Good optometrists, when testing, will discover what sports the patient is playing, and talk to them about what the dispensers can offer them in the practice when it comes to sports eyewear,” he said, adding that, outside of the consulting room, practices could utilise their digital presence or online shops to remind patients of the options available to them in sports eyewear at key times of the year.


McNeil acknowledged that stocking plano sports frames in order to show customers could feel like a hurdle for practices, but suggested: “We take an approach at Bollé, where practices don’t have to stock a lot of product.”
Practices can stock a core sports range to show customers and which could all be Rx-able, he said, and which “would be driven by training.”
Enquiring minds
Van Eerde emphasised the revenue opportunity that sports eyewear can present for practices, highlighting the importance of asking the “right” questions of patients.
“In our training, we talk about ‘selling the second pair first,’” he explained. “A lot of patients that come in for ophthalmic eyewear will be buying those anyway – they know they need correction. Before having them select
that, I think it’s important to ask the right questions in order to sell (Rx) sunwear and upsell with other options.”
This could mean asking, beyond work or driving: “What are the moments when your vision needs to be optimal?”
Beyond the aesthetics of eyewear, there are also questions that consumers should ask of the sports eyewear they try. He said: “I don’t think many people try on different lenses and consider: ‘Could I see the ball better, or estimate distances better, while wearing these?’”
These questions should be priorities when selecting eyewear for sports, van Eerde emphasised, and recommended educating consumers about the benefits of owning multiple pairs of frames, and the variety of choices in lenses.

Speaking to OT, he said: “We’re not selling them something they don’t need – on the contrary – it will enhance their lives, as well as being a boost to the revenue of the practice.”
An enhanced experience
At the heart of the category is a passion for enhancing patients’ vision to support their sporting endeavours.
The protection that sports eyewear provides cannot be understated. Beier emphasised: “Sports eyewear is a must if you want to optimise success and safety during sports.”
For McNeil, reflecting on the patients who might have “all the expensive gear” but struggle with fogged lenses, or when reading their fitness apps on-the-go, sports eyewear provides a solution: “We have a product for everybody that enables them to pursue their activities and feel stylish.”
Van Eerde agreed: “There is an opportunity to enhance people’s lives, and when it comes to sports, to enhance performance, enjoy the sport more and be better protected when practicing it.”
Maui
Jim
February/March 2023 www.optometry.co.uk 17 01438 740823 sales@bibonline.co.uk www.bibonline.co.uk See us at: M160 State Of The Art Tablet-Controlled Refraction with a 5-year warranty NEW PRODUCT LAUNCH OFFER Invest in: And you’ll receive: one FREE VX-36 Auto Lensmeter FREE £1995 Worth VX-36 Auto Lensmeter VX-65 Auto Phoropter, VX-22 Polarised Test Chart & VX-90 Auto Ref/Kera
\., v1s1on1x OPHTHALMIC INSTRUMENTS OT
Maui Jim’s ’World Cup’ in the colourway, Marlin
Remaining resilient through turbulence
Imran Hakim, CEO of Hakim Group, reflects on the current business environment, holding fast to practice values, and the benefit of community

to delivering eye care and eyewear in the community you serve, will be the yardstick by which businesses measure their success, as they look to emerge stronger through this period.


The last normal year that practices had was 2019. When COVID-19 hit, there was fear of the unknown, so frugality kicked in. Practices looked at controlling costs, maximising whatever opportunities arose for turnover, and used some of the Government’s support to ensure they finished 2020 in reasonably good shape.
This behaviour continued into 2021, but the demand and conversion rates were the highest we have seen in optometry. Patients wanted to spend money on themselves, because there were fewer places for them to spend it, and many patients had surplus money in the bank as a result of changes in consumer spending, predominantly COVID-19 related. Many practices had their best year of profitability in 2021.
Practices that had cash on the balance sheet by the end of 2021 then increased spending within the business, and simultaneously, in 2022, conversions dropped. While people have still been buying, the cost of doing business has been massively impacted by increased costs in supply chain, labour and double-digit inflation. The result being, most independent practices have
experienced a growth in turnover but a dip in profitability. This is similar to what many businesses have experienced in other industries, driven by the macroeconomic headwinds in the economy.
We are a fairly resilient industry. However, we are seeing an increasing number of demands on consumers’ pockets, and that means the resilience of the industry is being tested more than ever. Your positioning in the market as an independent practice has to be distinctive and compelling. If it isn’t, then you are at risk of becoming less relevant for a 21st century consumer who is more demanding, knowledgeable and sophisticated than at any time before.
The patients that come in have done their research. They know what they want, they have read reviews on the practice, and meeting their expectations is no mean feat. We have got to make sure we are a destination where consumers want to go to spend money in a recessionary environment.
When faced with the sort of turbulence we’re experiencing now, it’s all too easy to make short-term knee-jerk reactions. The ability to navigate a practice in light of the headwinds, whilst balancing the philosophy and ethos of your practice as well as your approach
The challenges we face will require business skills to be honed just as much as clinical skills. You almost need to be a mini-economist in the current climate, with the multitude of headwinds businesses are facing, and to be wellinformed but able to decipher the noise from what matters. This is where community and networks will be more important than ever. Everyone is facing the same kinds of challenges, and like we saw through COVID-19, we are stronger together and eminently capable of navigating exponential change together.
Independent practices are a valued part of the community they serve. Being aware of the challenges we face, and that are faced by our teams as well as our patients, whilst finding ways to support them in this time, is not easy. But the price is huge for getting it right. Eventually we’ll be in calmer waters, and people won’t forget how they were treated during the tough times.
It’s okay to feel overwhelmed, but don’t let this consume you. Be aware of the challenges, remove the noise and hype surrounding them, and focus all your energy on controlling the controllable. We will navigate this change together as a profession. But it requires business owners to stay educated on developments, connect with communities and networks, understand their businesses meticulously and not shy away from making difficult decisions. Remember: a smooth sea never made a skilled sailor.
18 www.optometry.co.uk February/March 2023
INDUSTRY PROFILE
SPOTLIGHT
0 OT
“Remember: a smooth sea never made a skilled sailor”









ultravisi Fromhyperopicto presbyopicandeveryonebetween... SEED1dayPureEDOFdailydisposablecontactlensescanbe usedat all stagesof yourpatient'svisualjourney. Onlyavailablethrough eyecareprofessionals Witha varyingpowerprofile,visualperformance is notdependenton pupilsizeor lenscentration. Proudto support independentpractices Freeproducttraining & ongoingsupport 32Ienses perpack Orderyourfreetrials,arrangetrainingorfindoutmore... SEED1da~ Pun~ ultravision.co.uk @) info@ultravision.co.uk (9 0800585115
Amplifying the voices of the profession
The newly-qualified and early career optometrists have a term of office of two years and can serve for three terms (a total of six years). All other designated positions have a three-year term from 2023.
In 2023, 14 designated posts on the AOP Council open for applications
The period for members to apply to join the AOP Council will open between 16 February and 15 March this year, as 14 designated posts open for applications. The designated positions open for application are:
Undergraduate student
Pre-registration optometrist
Newly-qualified optometrist
Additional hospital optometrist
Independent prescribing optometrist
Domiciliary care optometrist
Locum optometrist
Director of a multiple practice
Have you renewed your AOP membership for the year ahead? Members can contact the AOP with questions at membership @aop.org.uk
Employee of a multiple practice Director of an independent practice
Employee of an independent practice
Optometrist for Scotland
Optometrist for Wales
Optometrist for Northern Ireland. The undergraduate student and pre-registration optometrist positions have a term of office of one year.
WHAT THE AOP COUNCIL MEANS TO ME…
To mark their time representing members, several councillors reflected on what they most enjoyed about being part of the AOP Council
Looking back on their experience of AOP Council, a number of Councillors noted the benefits of meeting representatives from across the profession and the country.
Laura Josephs, AOP Councillor for undergraduate student optometrists, said: “Being on the AOP council has been an enlightening experience for me.” Josephs highlighted that Council presents opportunities to discuss topics “that are really important to optometrists today.”
Ali Yasen, AOP Councillor for newly-qualified and early career optometrists, also noted the opportunity to connect with others “on a national level and understand how the industry fits together and runs.”

“It’s lovely to be around like-minded people who are there to represent their cohorts, improve the quality of care for their patients and raise concerns in their areas where possible,” Yasen added.
Mehul Patel, AOP Councillor for directors of multiple practices, explained that he applied for council as a way
More information about the positions and eligibility criteria can be found on the AOP website. Applications can be made online, with appointments decided by the AOP Appointments Committee. Results will be announced in May.
The current AOP Council is made up of 34 members, with 14 elected to represent geographical areas across the UK, and 20 councillors with designated positions, representing the diversity of the AOP’s membership, from different types of work and workplaces, to differing career stages.
The AOP Council helps to ensure the views of members can be heard, representing members within their region or membership group at Council meetings held three times a year.
to give back to the profession: “I felt I wanted to give back to my colleagues and to the AOP, as they helped me a lot during the pandemic.”
Councillors also explained the ways that the AOP Council has enabled them to share and develop views on matters.
The AOP Councillor for Scotland, Dr Stephanie Kearney, shared that she enjoyed networking with practitioners across the UK, and having the opportunity to “be able to share and develop my views on important topics affecting our profession.”
AOP Councillor for employees of multiple practices, Karan Vyas, shared: “Council provides the opportunity to get things done, and amplify your voice and the voices of others around you.”
Josephine Evans, AOP Councillor for employees of independent practices, suggested that being part of the AOP Council provides an opportunity to “view our profession through a different perspective.”
Evans shared: “You feel supported; you know your views and the views of the members you represent are being heard and valued. As an individual, you are constantly learning and developing in this collaborative environment.”
Find out more about applying to be part of the AOP Council at www.aop.org.uk/council-appointments
AOP MEMBER SUPPORT
20 www.optometry.co.uk February/March 2023
0 0 0 0 0 0 OT 0 0 0 0 0 0
Education
Dr Ian Beasley, head of education and OT clinical editor

What can members expect from the AOP in 2023?
We will be building on the comprehensive programme we held in 2022, continuing with our programme of AOPled peer reviews for general optometrists, with a doubling of capacity relative to 2022 levels, as well as a suite of online peer reviews designed for specialty optometrists.
The AOP will continue to deliver content with our key strategic partners, including Moorfields Private Eye Hospital and CooperVision, and will collaborate with Johnson & Johnson Vision to deliver content aimed at independent practitioners, practice teams, and the wellbeing of members.
The year ahead will also see the exciting return of MAYopia Day, based on the success of the event in 2022, with a day of webinar education delivered online on 21 May.
The AOP will deliver two new events for locums, in partnership with Johnson & Johnson Vision as the headline sponsor. This includes a day of online education on 25 June, with content tailored to recognise the requirements of a locum audience, who will be able to consume the CPD content from their own homes.
In addition, the AOP will host a locum clinical skills conference in Birmingham on 27 November. This face-to-face event will present a mixture of clinical circuits and peer reviews, enabling locum members to consolidate and learn new skills across key areas of practice.
Any reminders for members?
The early months of 2023 are a good time to look at your personal development plans and ensure that it reflects your requirements, scope of practice, and current role.
AOP CAMPAIGN MAKES HEADLINES
The AOP’s cost of living campaign received coverage across regional, national and broadcast media
The AOP has reported a wide-reaching response to its cost of living campaign, which went live in late November.

The launch of the campaign followed the results of a public poll of over 1000 people, carried out in October, which found that two-thirds of respondents who wear glasses or contact lenses were “putting off” going to see an optometrist due to fear of the cost.
Adam Sampson, AOP chief executive, explained: “Our research shows that people are being forced to make decent vision an optional ‘extra’ – a truly concerning reality.”
The AOP warned of the effect of the cost of living crisis on eye health, and called for a 12.5% increase to
AOP membership survey launched
The second phase of the AOP’s research is live and invites members to participate in an online survey
The AOP has launched the second phase of its member research project, inviting practising and student members to share their views in an AOP survey.
Findings from the research will help the AOP understand how it can provide the right support at the right time across its membership, and will also underpin the delivery of its Five Year Strategy.
The AOP is working with the independent market research agency, Research by Design, on the project.
All members who are opted in to receive AOP surveys will have received a unique link to the online survey, that was sent by Research by Design after 25 January.
As a thanks to members that take part in the research, the AOP has said it will make a donation of £350 to the Optical Benevolent Fund. To thank participating student members, one respondent will be selected at random to receive the prize of a Volk Super Field Lens worth over £350, supplied with the support of Keeler. Three participating students will be awarded £50 each. The student research has been supported by Vision Express. A summary report will be published for members following analysis of the results.
Find out more about the research, and read the FAQs, on the AOP website: www.aop.org.uk/membersurvey2023
the NHS optical voucher, to help those struggling with rising costs to access eye care. Read more about the campaign on OT's website: bit.ly/3GlS2ve.
In the months since the launch, the campaign has made headlines across the UK. Media coverage included:
Nearly 40 broadcast hits across TV and radio. This included Channel 4’s Steph’s Packed Lunch as well as interviews with AOP spokespeople on BBC Northern Ireland and BBC South,
and 27 individual radio pieces on BBC Radio Scotland, BBC Asian Network, BBC Solent, UCB, and Radio Berkshire
12 national print and online pieces across The i, The Times, Sky News, Evening Standard, Daily Mail, Daily Star, Mirror, The Sun, and The Scottish Sun, as well as Yahoo!, MSN, and Money Saving Expert
More than 130 regional print articles in publications including: the Belfast Telegraph, The Northern Echo, South Wales Guardian, Glasgow Times, Bournemouth Daily Echo, Wandsworth Times, and Suffolk News
The campaign also received support from Labour MP for Battersea, Marsha de Cordova, who commented: “Proper eye care shouldn’t be a luxury and people shouldn’t have to choose between spending money on their sight or eating.”
The campaign uses the hashtag #EyeCareSupportNow. Read more at: www.aop.org.uk/costofliving
SPOTLIGHT Getty/ Endai Huedl February/March 2023 www.optometry.co.uk 21
The AOP’s spring/summer events programme will be published in early March. Keep up to date at: www.aop.org.uk/events
AOP EXPERT
0 0 0 0 OT





0 Associationof Optometrists The ROYAL COLLEGE of OPHTHALMOLOGISTS RN I B Seedifferently <D> MacularSociety Beating Macular Disease The Eyes Have It is a partnership between Rache, the Macular Society, RNIB, Fight for Sight, the Royal College of Ophthalmologists and the Association of Optometrists.
the activities of the partnership. ©2022 Roche Products Limited. All rights reserved. Roche Products Limited, Hexagon Place, 6 Falcon Way, Shire Park, Welwyn Garden City, AL71TW, United Kingdom. Date of preparation: February 2023. Material Number: M-GB-00010966.
Roche has funded
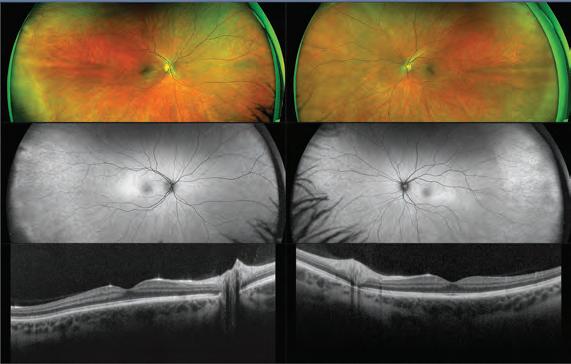
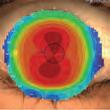
FOCUSES ON... OCT AND IMAGING




Enhanced practice workflow
Zeiss has updated the Cirrus 6000 HD-OCT device with seven new workflow pre-sets and new 21-point fixation targets, while the device also features an expanded field of view. A new wellness exam provides a wide-field OCT assessment of the optic nerve head and macular. The anterior segment premier module includes pachymetry maps with new epithelial thickness mapping, anterior segment analysis, and automatic detection of the anterior and posterior surface with the cornea caliper tool.

www.zeiss.ly/OCT-Devices
Hit list
The trends, launches and looks

Practice essentials
Haag-Streit UK has launched the Optovue Solix Essential from Visionix in the UK. The OCT provides images of the retinal structures using split-spectrum amplitudinal decorrelational angiography and motion correction technology, as well as 3D PAR 2.0 and vessel-to-vessel post processing alignment to minimise movement effects. The device also incorporates DualTrac and AI segmentation to support an advanced glaucoma system, and supports the anterior evaluation of pathologies with pachymetry, epithelial thickness mapping and 3D EnFace imaging.

hsuk.co/SolixEssential
High-speed scanning


BIB Ophthalmic Instruments has introduced the Optopol Revo FC130 all-in-one OCT and fundus camera. The device provides 130,000 A-scans per second with AccuTrack real time hardware eyetracking, as well as true colour fundus imaging, plus angio, topography, biometry and full visualisation of the anterior chamber. A new AI De-Noise allows for more detailed exams with a reduction in scanning time. www.bibonline.co.uk




Simultaneous capture
Grafton Optical has launched the Mocean 3000, a device configured with scanning laser ophthalmoscope (SLO) OCT imaging systems and an SLObased eye tracker. The SLO technology supports wide range real-time fundus imaging, to enable the user to locate the lesion area easily, while the eye tracker helps to reduce artefacts caused by movements.
www.graftonoptical.com
February/March 2023 www.optometry.co.uk 23
··•••• ---OT

























multi-award-winningRidseyewear BABY TO ADULT SIZES Fullyadjustable Ultralightweight Flexible Non-slip Comfortable Durable Headstrap Non-toxic www.tomatoglassesuk.com 01395 488188 info@tomatoglassesuk.com
GET THE LOOK
Optometrist and lifestyle blogger, Lizzy Yeowart, picks her top eyewear trends to watch out for in the year ahead

As we welcome the new sartorial season, we look at the three standout eyewear trends of 2023.
Daniel Scott
Design-wise
IHigh-tech processes combined with artistic craftsmanship. A pastel colour palette evokes harmony and calm. These are the yoga pants of the eyewear world. www.steppereyewear.com


100% Optical: www.100percent optical.com
The dispensing optician and trained personal stylist behind The Eyewear Stylist on his custom-made briefcase and creativity in eyewear

Soul space
1
If eyes are the window to the soul, then what is your shop window?
I keep my eyewear in a briefcase that was custom-made in Paris. I have about 15 pairs of frames. I pick my eyewear wardrobe very carefully. I hate the words ‘spare pair,’ in terms of something that lives in a drawer. I’ve always made sure that each pair is different from any other pair that I have, whether that is colour, shape or style. 2
Eyewear is so personal, because what can be more personal than your face. I think the best people embrace the fact that they are wearing glasses. You can completely change how you are perceived through that choice.
3
What I like about eyewear is that it is so multifaceted. You can think of eye health as just a need rather than a want, but I love the creative ways lens suppliers tackle it. Eyewear is not just the frames and the lenses, it is the combination of both, while also incorporating optical health. It is something to be embraced and to enjoy. 4
My favourite pair to wear currently is a Vinylize frame made from AC DC’s Back in Black album. With my background as a musician, anything I can tie back to music is brilliant and I love the story of the frames and knowing what the vinyl is.
A warm, bohemian palette influenced by nostalgia, romance, nature and comfort. This eyewear is akin to cosy cardigans and fluffy socks. www.maceyewear.co.uk

Full spectrum
Anything goes, from flamboyant Regency-inspired designs to upcycled “muck and brass” vibes – creating something beautiful from discarded materials. This epitomises joie de vivre.
www.wolfandbadger.com
HIT LIST
ME &
GLASSES
Q&A
MY
February/March 2023 www.optometry.co.uk 25
0
Catch Daniel's styling advice on the catwalk at
0
(bl
A SPOTLIGHT ON SAFILO

Emerging from what Safilo describes as a successful 2022, the Italian eyewear group enters 2023 with ambitions to continue building its licensed and core brands, while also “nurturing and supporting” its customers, both in independent opticians and selected partners/stores, despite the macro-economic challenges. OTspoke to Safilo country director, Oscar Cera, about the company and its aims for 2023 and beyond.
What impact did the pandemic have on business? And how did you respond?
We are pleased with the development of our business in 2022. Our strategic objective to build a Safilo with a strong and balanced portfolio of brands, geographies, products and channels is progressing well.
Throughout the pandemic, we accelerated our infrastructure-related efforts to improve our systems, completed our digital investments, enhanced our service quality and saw a strong resilience in the optical sector. After the pandemic, we had the opportunity to implement these efforts on the field. The positive feedback we received motivated us even more. We were lucky to be in an industry that could operate throughout the pandemic. The sun category was negatively affected due to the restrictions put in place on the global travel industry, which as a result slowed our business. The optical category, on the other hand, was resilient as consumers kept visiting their local optometrist when they needed a new prescription because health became a priority for all of us.
As a response, we closely partnered with our customers to find solutions to keep the business running despite the restrictions. The needs and expectations of customers are at the centre of our organisation and are always at the heart of what we do. We are committed to putting our customers first, and those who choose us are our trusted partners who value our choices and our way of doing business.
A CHANGING MARKET
WHAT TRENDS DOES SAFILO PREDICT IN 2023?

The pandemic had a real impact in consumer preferences and trends. The more relaxed workfrom-home pattern has increased demands for sporty, versatile styles as well as the tendency to shop more locally. The cost-of-living crisis has put a greater emphasis on value-for-money products as consumers are now more pricesensitive than ever before. With the restrictions relaxed, demand has increased for sporty styles as consumers are back to enjoying outdoor activities. This means that the market is looking for comfortable, versatile and stylish frames. In terms of consumer groups, we expect higher demands from the kids/teenager category requiring eyesight correcting solutions as a result of spending more time online.
As we move through the pandemic and into a cost of living crisis, how is Safilo managing the associated rising costs as a business?
We strongly believe that despite the resilience that our market has shown in the past, we must be more price sensitive and keep offering the best value for money solutions. Through licenses and acquisitions, we continuously aim at rebalancing our brand portfolio, with targeted additions that will allow us to gain a leading position in the various eyewear segments and reference markets.
How are you supporting customers in their businesses?
We are leveraging on our diverse brand portfolio to enable customers to be more competitive across different product segments. We are offering better flexibility, with trade terms enabling customers to effectively manage stock levels in line with macro-economic influences.
Our ambition is to become the privileged and strategic partner of opticians, which means that we will never try to replace them by entering retail with large acquisitions. The goal is to enable independent opticians to compete on the market through the digital and innovative tools that Safilo can provide.

“The needs and expectations of customers are at the centre of our organisation and are always at the heart of what we do”
Advertorial brought to you by OT Safilo Optometry Today SEETHEWORLOATITSBEST
SUSTAINABILITY MATTERS
Sustainability is of pivotal importance for Safilo. First and foremost it means, “protecting the environment and using renewable resources and materials, and greener production processes.” It can also be found in the company’s commitment to product design and production, as well as their impact on people.
What are Safilo’s short-term sustainabilty goals?
In line with our 2020–2024 plan, we started our sustainability journey and put in place a roadmap to guide our choices when it comes to planet, product and people. In 2022, Safilo Group joined The Fashion Pact, a global coalition of companies committed to key environmental goals in three areas: stopping global warming, restoring biodiversity and protecting the oceans. In the short term, Safilo Group is hoping to continue making positive changes when it comes to sourcing materials. We realise that sustainability is a journey, and we are committed to making it an important part of our business. Since 2021, we have been partners with Eastman and in 2022 we became the first player in the market to use all Eastman Renew materials for eyewear in its portfolio.
What are Safilo’s three sustainability pillars and how will they support the business through change?
In addition to the sustainable product choices we make, we wanted to build a holistic approach to sustainability by involving planet but also people. We added “people” not only because they are the heart of our business but because we also wanted to contribute to improving lives and supporting our ecosystems.
Since 2003, we have been proudly supporting Special Olympics, the international non-profit organisation dedicated to transforming the lives of people with intellectual disabilities.
DIGITAL TRANSFORMATION
Responding to change is key in business. How has Safilo responded to digital advancements?
Sustainability is a key pillar of our 2020–2024 plan. The other equally important pillar is digital transformation, enabling us to reshape our business 360 degrees. This encompasses developing B2B tools to enhance relationships with opticians and digitalising core business processes, including our B2B platform, You&Safilo, our WhatsApp channel, and our own new upgraded Sales Force Automation, which we are rolling out progressively.
Can you tell us about Safilo’s You&Safilo platform?
You & Safilo was established in 2020 as our one-stopshop solution designed to help independent opticians to browse our portfolio of brands, place orders, manage spare parts/warranties and interact with our customer service 24/7. Since its launch, we have been gathering insights from our network and introducing improvements to make You&Safilo an essential resource and help our opticians run their practices without the need for a physical interaction. We are proud to see that You&Safilo has already enabled us to improve our relationships with customers in remote areas, offering greater flexibility for both our sales representatives and our opticians.

SAFILO AT 100% OPTICAL
”We will showcase new collections for most of our brands, enabling our customers to purchase or just get a flavour of our latest designs and innovations. We plan to have two spaces dedicated to both sustainability and digital transformation with our B2B digital platform You&Safilo. We are looking forward to seeing everyone and welcoming all customers to our stand.”
SHORTLIST THE LATEST PRODUCT LAUNCHES
Children
ISecurity for the active
Exeter Eyewear has introduced a new collection of ultra-light TR-Lites and TR-Active frames, designed to fit securely for active young people. The straightsided models feature “super comfort” nose pads and a saw-tooth side channel design to enable a sliding ear lock to be attached. Eyewear can also be supplied with a free headband on request. Exeter Eyewear's TR-Lite and TR-Active ranges are available through Norville. www.exetereyewear.co.uk
Sunglasses
IMagnificent monograms
Emmanuelle Khanh launched its latest campaign, ‘Solstice,’ with a collection that signals a return to the design house’s jewellery monogram. The new monogram is crafted in Italy, plated in 18 carat gold and mounted by hand to Emmanuelle Khanh glasses in Oyannax. Artistic director, Eva Gaumé, said she wanted to revive the monogram seen in Emmanuelle Khanh’s vintage frames in a contemporary way. www.ek.fr/en


Cleanser
ISoothing formulation
The Body Doctor has launched the Eye Doctor Tea Tree Oil Lid Cleanser, as a result of the popularity of its lid wipes. The cleanser has been designed to remove dirt, debris and make-up from the eyelids and the base of the lashes, and is recommended for people with dry eye, meibomian gland dysfunction, blepharitis or demodex. The cleanser contains tea tree oil, as well as coconut oil, micellar water and argan oil. www.the-body-doctor.com

Frames
IContemporary colours

Part of Charmant Group, Ad Lib has shared a collection focusing on urban style and comfort. In the women’s line, Ad Lib has introduced the hexagonal ‘AB3290-BK’ frame (pictured) featuring contemporary colours, a gradient effect on the sides and 3D effects. The threetoned frames host contrasting matte and shiny finishes. www.charmant.com

28 www.optometry.co.uk February/March 2023
/ Art
Image: James Tennessee Briandt
direction: Eva Gaumé
-1-1 (ii:am . m.....,l m, 'vJ
(······
I
Image: James Tennessee Briandt
Art direction: Eva Gaume
To feature in OT’s Hit list, contact kimberleyyoung@ optometry.co.uk

Lenses
Light management
Transitions Optical has launched a new version of its Light Sensitivity Test, aiming to prompt patients to have conversations with eye care professionals about light management. The test can be accessed online or through a smartphone. Features include a light sensitivity score from 0–100, as well as a personal Transitions lens recommendation. Consumers can also use the Virtual Mirror tool to try out recommended lenses, and find a practice through the locator tool. www.transitionspro.com
Frames
Featherweight
Modo has debuted a range of seven new featherweight frames in its Air collection. A highlight in the collection is ‘4256,’ an optical frame featuring a titanium skeleton for durability, and contrasting colours between the inner and outer faces of the frame sides. All frames in the Air collection have a front made from memory plastic, a covered bridge and screwless hinge designs. www.modo.com



Precision design
Eyespace has launched four sunwear collections for 2023, adding over 60 styles to its portfolio of brand and house collections. Range Rover sees a selection of designer models with a focus on precision engineering. Selected from the new line, ‘RRS 306’ is a re-imagined round style with hexagonal upper eyerim. The Japanese raw edge finish of the outer rim contrasts with a highly polished front, while a metal trim extends from lug to the side of the frame. www.eyespace-eyewear.co.uk


February/March 2023 www.optometry.co.uk 29
HIT LIST
0OT
























THE LENS TO START IN AND STAY IN Contact your Alcon® representative to find out more. PRECISE VISION 1 LONG-LASTING COMFORT 1 EASE OF HANDLING 1 Reference: 1. Cummings S, Giedd B, Pearson C. Clinical performance of a new doily disposable spherical contact lens. Optom Vis Sci. 2019;96:E-obstroct 195375. See instructions for use for wear, care, precautions, warnings, contraindications and adverse effects. 15043 © 2022 Alcon Inc 08/22 UKIE-PRl-2200026 PRE-AND POST-FIT SUPPORT Alcon
Left and above:
CUBITTS //
The brand’s first customer was called Iris
In the early days of Cubitts, Tom hand delivered every pair of spectacles on his bicycle
Celebrity wearers include Steve Coogan, Helena Bonham Carter, and Alan Carr.
ANATOMY OF A FRAME
What is the latest campaign that Cubitts has released?
The Gloriously Awkward range embraces a variety of face shapes; Tom Broughton 1 2 3
At the start of this year, we released a new campaign that is all around individuality. The reason I got into the industry in the first place was that, to me, a pair of spectacles was a physical manifestation of the people who wore it. I was inspired by people like Morrissey from The Smiths and Jarvis Cocker from Pulp and other iconic spectacle wearers.

What went into Cubitts’ Gloriously Awkward collection and campaign?
The idea of Gloriously Awkward is to embrace outliers. When I first got into optics and spectacle design, one of the things that I found odd was the lack of sizing. Most of the industry is designed for the average, but the average served nobody, just that sliver of people in the middle. We built facial-scanning technology to build a true cephalometric database and scanned around 3300 faces and then tried to find patterns. That allowed us to identify a whole bunch of different people that were unserved. We matched that data to our existing frame collection to identify gaps and spent six to nine months developing collections specifically for those people.


What is Cubitts’ short-term and long-term goals?
Keep surviving. We’ll probably grow a little more, maybe open another couple of practices. We want to keep getting better – continue to improve the product, our lenses and service, and keep investing in the company as we go through what will be a difficult 12 months with the cost of living and recession – things that are out of our control.
Available in three types: wide, high, low
3D printed style from Polyamide so it is durable, stain-resistant, UV-resistant, skin-contact safe, and perspiration proof
HIT LIST
A play on bold, modern, and classic aesthetics Unpicking a standout frame, by OT columnist Lizzy Yeowart
in a choice of small, medium, large or custom sizes Made-to-measure frame In a nutshell Manufacturer // Reframd Frame // ‘Moni’ Colour // Black Web // www.reframd.com February/March 2023 www.optometry.co.uk 31
Available
Tom Broughton, founder
Q&A BEHIND THE BRAND CUBITTS
0 OT
Act early to helpslowthe
tUsing measuredandmodeleddata,pooledacrossages(8-17), MiSight" 1 dayslowedmyopiaprogressionby anaverageof approximately50%. f 12 monthspost-treatment.evidenceindicatesthat no accumulatedmyopiacontrolbenefitswerelostfollowing3 or 6-yearsof MiSight®1 daywear(onaverage,for childrenaged8-15 at start of wear).Instead,eyegrowth revertedto expected,age-normalrates.


1. Arumugam8 et al.ModellingAgeEffectsof MyopiaProgressionfor the MiSight1 dayClinicalTrial.Invest.OphthalmolVisSci.2021; 62(8): 2333. 2. ChamberlainPet al.A 3-year RandomizedOinicalTrialof MiSightLensesfor MyopiaControl.OptomVisSci.2019; 96(8): 556-567. 3. ChamberlainPet al.Long-termEffectof Dual-focusContactLenseson MyopiaProgression in Children:A 6-year MulticenterClinical Trial.OptomVisSci.2022; 99(3): 204-212. 4. ChamberlainPet al.Myopiaprogressionon cessationof Dual-Focuscontactlenswear:MiSight1 day7-year findings.OptomVisSci.2021; 98(E-abstract):210049.






5. ZadnikKet al.FactorsAssociatedw~h RapidMyopiaProgressionin School-agedChildren.Invest.Ophthalmol.Vis.Sci.2004; 45(13): 2306. 6. HammondD,A111mugamB,et al.MyopiaControlTreatmentGainsare RetainedafterTerminationof Dual-focusContactLensWearwith no Evidenceof a ReboundEffect.OptomV,sSci 2021; 98(E-abstract):215130.


© 2023 CooperVision.Cooperlosion®andMiSight®areregisteredtrademarksof TheCooperCompanies,Inc.andits subsidiaries.


MiSight"1 day Myopta Management Act1vContro1•Technology 30 dailydisposablecontactlenses CooperVision·
worseningof a child'smyopia (short-sightedness) 1 The world'sonly myopiamanagementcontact lens supportedby a 7 -year clinicaltrial2· 3 A
more at coopervision.co.uk/practitioner/myopia
Findout
CooperVision· CVGY323341-1 MiSight®1 day
Action Planfor the Future of Managing Myopia



00 Useyour existing skill set and build confidence
0 0

u.~l\ li'u/lf Raisethe subject early and involvethe whole family
Keepthe messagesimple,avoid scaremongeringand adopt a personalisedapproach
I •, I Reframe myopiaas a conditionthat needsmanagementas well as correction



I~ Manage parental concernsby sharingthe evidence
Adopt myopia managementas part of your plan to grow your business
pf~ Educateand activate the wider community
TIME TO SEE MANAGEMENT
Summary
CooperVision·
• [!] • DOWNLOAD NOW https:/ /www.coopervision.eo.uk/myopia-action
CREATING SOLUTIONS TO MEET DEMANDS ON THE EYES







With practices reporting seeing an increase in dry, tired eyes, Johnson & Johnson Vision explains how its ACUVUE® OASYS MAX 1-Day has been designed to meet the demands of modern lifestyles


What inspired the development of the ACUVUE® OASYS MAX 1-Day contact lens?












Jakob Sveen, managing director Northern Europe and General Manager UK and Ireland (JS): We recognise the last year has been particularly hard as we continue to navigate global challenges from the COVID-19 pandemic and the impact on supply chains. We remain committed to tackling these challenges while also continuing to drive innovation and category growth.
We are really proud to bring ACUVUE® OASYS MAX 1-Day contact lenses to the table as a solution




to feedback from eye care professionals (ECPs) that there has been a significant rise in dry, tired eyes at the end of the day, driven largely by changes in lifestyle. The shift to more hybrid working has increased our digital consumption; in fact, 81% of people in the UK who wear vision correction say they use at least five different digital screens per day.1
How have changing patient lifestyles altered what they need from their contact lenses?
JS: The biggest issues we have heard from ECPs is symptoms of dry eye as a result of longer days and





















increased use of digital devices. Increased screen time is creating widespread issues with symptoms of dry eye, with more than twothirds (67%) indicating the role of screens in modern life is detrimental to their eye comfort.1







These demands are even more troubling for ageing eyes. While digital screen use destabilises the tear film at all ages, the tear film breaks down 50% faster by age 50 and may exacerbate the feelings of dry eye and impact consistency of vision.2 Meanwhile, light scatter doubles by age 60, resulting in increased visual artefacts (starbursts, halos), affecting distance
Jakob







Sveen, managing director Northern Europe and general manager UK and Ireland



34 www.optometry.co.uk February/March 2023
“WE ARE REALLY PROUD TO BRING ACUVUE® OASYS MAX 1-DAY CONTACT LENSES TO THE TABLE”
e OT
The Digital Comfort Survey, commissioned by Johnson & Johnson Vision, found that, of people in the UK who wear vision correction:
81% use five different digital screens per day

2/3 indicated the role of screens is detrimental to their eye comfort
vision, and contributing to decreased ability to drive at night or read in dim light.3
How does the technology and material in these lenses address these new patient needs?
Kamlesh Chauhan, director of professional affairs, UK, Ireland, Nordics and DACH (KC): There are two unique new technologies we developed that make ACUVUE® OASYS MAX 1-Day contact lenses work harder for patients.

First, our TearStable™ technology optimises our existing wetting agent (PVP) for better distribution throughout the lens and surface.4 In other words, we’ve essentially made the contact lens more biocompatible with the eye tear film, both introducing more long-chain PVP, while also distributing it more evenly across the lens from edge-to-edge for improved comfort. Second, we have introduced the OptiBlue™ light filter, a technology that provides the highest-level blue-violet light filter at 60%,5,* to help reduce light scatter for increased visual clarity, day to night.6,7
When looking at a digital screen, we blink 60% less,
which can destabilise the tear film, affecting comfort and vision.8,9 Blue-violet light scatters from digital screens, florescent lights and the sun, which can impact visual clarity.10
So the two technologies work hand-in-hand to tackle these challenges, improving visual clarity and end-ofday comfort.
How does your approach to Eye-Inspired™ innovations help you better meet patient needs?

KC: The idea behind EyeInspired innovations is that our contact lenses are designed based on the eye’s natural physiology and anatomy, to make the most seamless wear experience possible.13 Improved biocompatibility has helped us to meet patient needs, and it is even more important today with patients spending more time looking at screens. By blinking less, our tear film disrupts faster. Using this as inspiration, we are continuing to innovate with the tear film front of mind.
For ACUVUE® OASYS MAX 1-Day we have incorporated both a tear like wetting agent and hydrated silicones into our stateof-the-art manufacturing process in a way that enhances tear-film stability and moisture retention between blinks. The goal is to have a lens that wearers barely think about.
How might this contact lens support retention, and support practices in their contact lens business?




JS: This is a great transitionary lens for presbyopes, as we can seamlessly transition wearers from sphere to multifocal with ACUVUE® OASYS MAX 1-Day Multifocal contact lenses. The multifocal contact lenses have the same benefit of sphere, so the hope is to see less drop-out and continuation of wear over time.
There is, of course, also the fact that the technology is new and will contribute towards providing exceptional end of day comfort and visual clarity in all lighting conditions. This will get many on board and retain patients who enjoy using them.
How do you recommend practitioners talk about the ACUVUE® OASYS MAX 1-Day with patients, in both its spherical and multifocal presentations?
KC: The key is to focus on patient needs by asking about their lifestyle and how that may impact the daily demands on their eyes. Ask how comfortable patients’ eyes are. Do they start to feel discomfort or eye dryness at the end of the day? Do patients prefer the way their eyes feel without lenses? For older patients who would prefer to stick to multifocal
glasses, practitioners can discuss the benefits and freedom that lenses will provide. Glasses can put a strain on patients’ necks when they constantly need to tilt their head to keep them positioned correctly. Some patients may be worried about price, but it may be the case that switching is a matter of 25p extra cost per day, less than a coffee per week. Putting the price into perspective, when vision and comfort is so critical and contributes towards their wellbeing, will be a clincher for some patients. There are options for everyone, and it’s worth discussing what is best for their needs.
IN CONVERSATION
“WE ARE CONTINUING TO INNOVATE WITH THE TEAR FILM FRONT OF MIND”
Kamlesh Chauhan, director of professional affairs, UK, Ireland, Nordics and DACH
February/March 2023 www.optometry.co.uk 35 VISION UV BLOCKING OASYS MAX 30~~~T;~; OT
GIVING PATIENTS THE OPPORTUNITY TO UPGRADE
Faye McDearmid, optometrist at Campbell & McDearmid Optometrists and professional affairs consultant for Johnson & Johnson Vision, on informing all patients about new technology

Between 25–40% of our patient base is contact lens wearers. When I see a patient, I am looking for a visual solution that fits with their lifestyle and work, helping them to be who they want to be.
I got my fitting kit for the ACUVUE® OASYS MAX 1-Day at the end of October 2022. I fitted one patient who, when I last saw him, was fitted with ACUVUE® OASYS 1-Day. He has a really demanding job but spoke about how much he was loving the contact lens. I told him that there is a new contact lens and his response was: ‘Great, can I try it? If I like it even better, can I have it?’
some time. Actually, we owe it to patients to tell them about these upgrades and let them experience the innovation.
FAYE’S TOP TIP FOR FITTING ACUVUE®
OASYS MAX 1-DAY


Even the patients who you think are happy: find out what they can improve on from their current contact lenses, and give them the opportunity to try it.
This was an eye-opener for me. He came in to tell me how great the lenses were that I had given him previously, but he still wanted to try the new technology.
If someone is happy in their contact lenses, it can be tempting in busy clinics to think: let’s keep them in that and catch up
MEETING VISUAL AND COMFORT NEEDS
Tuija Kankaanpaa, optometrist at TD Tom Davies, on digital device use and high expectations

I have never given out so many prisms as I have this year. People’s eyes are tired. Lots of my patients work with several monitors at different distances, which makes it tricky for their glasses, and a lot of patients like multifocal contact lenses because it gives them that depth of vision.
As our patients spend so much time in front of a screen, they expect really comfortable lenses.
The majority of our contact lens wearers are presbyopes. That is where we have seen the biggest growth continually for the last six or seven years. We are all doing more –wanting to be involved with family, or socially, or in leisure activities – and expectations for vision and comfort are still there. We know that as the eye has more birthdays, there is a correlation between that and a poor tear film. The people who I have upgraded to the new contact lens so far are all working-age presbyopes who are using screens or in offices, and they have really enjoyed the benefits.
The ACUVUE® OASYS MAX 1-Day has been really well received. The cost is higher, but my experience so far has been that it wasn’t as much as people thought it was going to be. With the cost of living on the news, practitioners can feel a bit hesitant

Dryness is a key issue now. The key challenges patients face are a 50-50 split between comfort and vision.

If we mention blue light filters, almost everybody we see who works with screens wants to have the filter. We are used to talking about and selling lenses with blue light filters with our glasses, so it is easy for me to say that we have a new contact lens with a blue lens filter. People are so aware of blue light nowadays that they ask about it. Having a contact lens with UV protection and a blue light filter is an excellent combination.*,†

As soon as I explain the benefits of the new contact lens, patients
Discussing lifestyle and contact lenses: “You wouldn’t play golf in high heels”


I will always ask people what they do and what a typical day or week looks like. I explain that I need to know this in order to be able to offer them the best vision care solutions – because they wouldn’t play golf in high heels or go to their best friend’s wedding in wellington boots. We can give them the best solution for what they are doing.
to show patients new contact lenses, but we can’t pass an opinion on what the person needs. If we can give them more comfortable vision and a sharper vision quality, then we owe it to them to let them decide.
want to try it. They don’t ask me about the price, and if it is a little more expensive, it hasn’t been an issue. The blue light filter does the magic – I think Johnson & Johnson Vision has nailed it.
Two of my multifocal patients used to have the 1-Day ACUVUE® Moist Multifocal. When one of them came to pick up their new ACUVUE® OASYS MAX 1-Day lenses, she told me: “I wish I had already been using them,” as she feels that she now sees much better.
References and further reading

* Filtering of HEV light by contact lenses has not been demonstrated to confer any systemic and/or ocular health benefit to the user. The eye care professional should be consulted for more information.
† All ACUVUE® contact lenses have Class 1 or Class 2 UV-blocking to help provide protection against transmission of harmful UV radiation to the cornea and into the eye. UV-absorbing contact lenses are NOT substitutes for protective UV-absorbing eyewear such as UVabsorbing goggles or sunglasses because they do not completely cover the eye and surrounding area.
ZHDU�WKHP�
I always test the lenses myself – I have dry eyes and challenges with my vision. I was a bit sceptical, but I love them. They are really comfortable and I wear them every day.
HYHU\�GD\��
References can be found online at www. aop.org.uk/ot/jjv-max
36 www.optometry.co.uk February/March 2023
IN CONVERSATION
~~VISION '' '' OT


In practice
the same varifocal that they had last time, removing the photochromic, or not having the second pair.”
“It’s anecdotal,” he explained. “If you look purely at sales, they haven’t dropped. But if you ask the staff what’s happening on the ground, they are hearing people say, ‘I want to keep costs down. I don’t want to have that this time. I’m not going to spend as much on my frame’.”

He added: “I’m having more conversations with patients who are concerned about their electric and gas. I’ll say to people, ‘you don’t need to upgrade this time.’ They say: ‘Good, because I was struggling to pay the gas bill’.”
Laura Whiting, practice manager at Valli Opticians in Hebden Bridge, West Yorkshire, explains that while certain patients are still choosing to pay upfront, “there’s definitely a middle ground where people are more cautious now.”
explained. “People have said, ‘I need to make sure I can pay my bills this winter.’ It’s awkward, because we’re a business. We want to retain our patients and not push them away when they’ve got other costs involved.”
Noticing behaviour changes in long-term patients, for example those who might once have spent a large amount no longer doing so, or requesting to set up a Direct Debit to make their purchase more affordable, is important when balancing business planning and communication with patients, Whiting believes. She added: “That would never have happened with certain patients once upon a time.”
As the cost of living crisis bites, optometry practices from Lancashire to Brighton are negotiating a tightrope of increasing business costs versus duty of care to patients – and especially to those who may already be vulnerable.
Neil Heyes, optometrist and


practice owner at Heyes Opticians, in Ormskirk, explained that top end sales at his practice are not being affected as patients cut back, but that he has noticed more caution “at the middle to bottom end of the range,” and that “people are downgrading: not having
Patient spending changes were more noticeable than usual in November and December, when Christmas hit “double barrel with the energy bill crisis,” she said.
“We have loyal patients who come time and time again, and you know their spend history,” Whiting
That patients with a high disposable income are not currently being affected but could be in the future is something that Jim Green, owner of Hakim Group independent practices Eyesite (Reading, Brighton, Weybridge and Winchester) and Walsh Opticians
Business
insight and career development
42 How I got here Scott Mackie on his varied career and embracing a better work-life balance
53 How do I... Peter Greedy on creating a welcoming environment for every patient
55 Eyes on wellbeing Wellbeing includes financial health, says Lloyd & Whyte’s Danny James
50 Pre-reg focus Moorfields Eye Hospital pre-reg, Akshay Shah, on his High Street placement
Getty/ We Are February/March 2023 www.optometry.co.uk 39
Four practices share how they are balancing business need with patient care during the cost of living crisis
“We want our reputation for having diverse patients to remain”
THE DISCUSSION
“We want to retain our patients and not push them away when they’ve got other costs involved”
OT
Laura Whiting
(Bogner Regis), is very aware of. With a patient base that values healthcare and is willing to prioritise spending accordingly, Green acknowledged that the resilience that his practices are seeing due could be affected by external factors at any time.
“There are patients who are currently less affected: they own their own home, they have savings, and the energy crisis is affecting them, but they can absorb that in their day-to-day life,” he said. But, “we still have to make sure we’re aware.”
Economic headwinds postBrexit had already led Green to consider how turbulent the situation might become.
“We’ve seen this coming for some time. It’s not something that is here one moment and gone the next,” he said.
Business response
So, how are businesses responding – both in terms of supporting patients, and in protecting revenue?
Green’s caution meant the Eyesite practices and Walsh Opticians had developed ‘tools in their armoury’ ahead of the current crisis, that they would be able to call upon when needed. These include a purchase plan, allowing patients to buy spectacles and pay for them off over a period of time. Green has ensured that the offering is more visible in recent months. It is, he said, “a way of being able to help patients spread the cost.”
At Valli, Whiting also offers an interest-free period on spectacle purchases.
“It’s something we are mentioning a lot more than we might previously have needed to,” she said.
Ryan Leighton, CEO of Leightons Opticians and Hearing Care, is looking to extend the group’s interestfree offering.

“We are encouraging our teams to provide interestfree payment plans to our patients to help spread the cost, and we are researching payment plans over longer time frames to ease the monthly cash burden on patients,” he said.
Leightons has also reduced the price of services including ear wax removal and has increased access to the services included in its MyLeightons Eye Plan, which has allowed it to keep eye examination fees stable.
At the same time, Heyes has found that certain clinical services that he might have previously offered out of goodwill can no longer be sustained.
“We have put private prices in place for certain things that we would have normally done as goodwill in the past,” he said. “We can’t do it anymore. We’ve got to make sure we charge for the chair time.”
He added: “You’ve got to look at it from three points of view: the patient point of view, and they’re struggling. The staff point of view: we don’t want them to struggle. And finally, making sure
the business is in a healthy position to provide support to both.”
The right dispensing experience
The practitioners are clear about the importance of listening to and interpreting customer need when it comes to budget, and how that can safeguard profits.
“Choosing the right dispensing experience means we see less vulnerability,” Green said. “We’re strategic with the brands we put in place.”
Heyes is also paying close attention to the frames his practice is supplying.
“We have been very conscious that this is coming, and we’ve made sure we’ve sourced frames, particularly from designer brands, that are a little bit lower in value,” he explained.
“We’ve made sure we’ve got a better offering at a slightly lower price point. We’ll say to patients, ‘Tell us what your budget is, and we will use it as wisely as we can, and make sure we don’t go over it.’ We’re protecting revenue by making sure patients don’t walk when they can’t afford what they had last time.”
Leighton agrees: “We take a forensic approach to

understanding our patients and their spending behaviours,” he told OT
Patient communication is vital in her practice’s small community, Whiting said – and it helps that her staff can talk openly to patients about their needs and requirements.
“We do get a diverse patient demographic,” Whiting said. “We get people who are on benefits who use a voucher towards their spectacles, and people who don’t bat an eyelid at spending £2000.

“It’s about managing what they want without them having buyer’s remorse. It’s a juggling act.”
She continued: “People are more vocal in saying that they’ve got a set budget now, which helps. You know straightaway where you need to start in terms of frames. My team members emphasise that frame prices start as little as X and go right the way up to X, rather than it being solely on the patient’s choice of style and then them being landed with a frame they can’t afford. It’s not just what you like that determines what you have to pay.”
“It’s quite a close-knit community,” Whiting added. “Everyone knows everyone, and we want our reputation for having diverse patients to remain. We’re not just for the higher spenders. We’ve got a screen in the front window, in this particular branch, that reminds everyone that NHS patients are welcome.”
40 www.optometry.co.uk February/March 2023
THE DISCUSSION
“We’re protecting revenue by making sure patients don’t walk when they can’t afford what they had last time”
Neil Heyes
“Choosing the right dispensing experience means we see less vulnerability. We’re strategic with the brands we put in place”
0
Jim Green
We look forward to seeingyou at 100%Optical!

When I left school, all I knew was that I wanted to work with people. In Glasgow, they used to say ‘Do you want to be a welder? Do you want to work in shipbuilding?’ because it was all heavy industry. I said, ‘I want to be an optician.’ They looked at me and said, ‘Nobody wants to be an optician, what are you talking about?’
I did not get into optometry, so I did two years of dispensing at Glasgow College of Technology and then a training year with Dollond & Aitchison in Clydebank, which was brilliant because it taught communication skills. I had to look at a person and not judge a book by its cover. There were people who were really poor, and would pay a pound a week for their contact lenses. It was a great learning experience.
Dollond & Aitchison made me a manager in East Kilbride, a town that was being built from scratch. I worked there for a year, then went back and did optometry for four years at university. In my final year, I decided people should be
continuing their education afterwards. This was before the General Optical Council (GOC) brought in CET. We set up a training course, and it was popular from day one. The minute I qualified, I set it up as a company.
For my pre-reg, I went to work in the hospital in Aberdeen. My supervisor, Professor John Forrester, was doing a PhD and was editor of the British Journal of Ophthalmology. He got me interested in research.
hospital is Glasgow, 35 miles away. People in these mining villages have never been to Glasgow, and they don’t want to. The first qualification I did after my PhD was in low vision. That was the start of a lot of postgraduate training. Since the minute I got the chance to do optometry, I’ve never looked back. That’s why I’ve been driven to have so many qualifications. I also did independent prescribing, as one of the first cohort.
My wife and I have done everything together. We met during our PhDs. We opened the practices together, we did the low vision certificate together, we did assessing and examining together. That led on to the GOC making CET compulsory, and we were some of the approvers.
I’ve been lucky that I’ve won a few awards. I stayed away from them for years, because it’s like tapping
“My Plan B?”
Reflecting now, I would’ve wanted to be an ophthalmologist.
we’re going to Cambodia. My friend, who is an ophthalmologist in the UK, has built a hospital there with funds from external stakeholders. Last week I sent 3000 pairs of glasses to them. We’re trying to recycle, and upskill people so they can do it themselves. I’ve got a lovely bunch of friends, and I just phone them and say, ‘let’s jump on a plane.’
During the pandemic we stayed open as an emergency eye care treatment centre, covering 26 practices. People were walking in who should’ve been in A&E. On the other end of the phone was a consultant, because all the juniors were on the COVID-19 wards. We were able to tell the NHS we needed access to hospital records and the medications people were on, and they gave them to us. It is amazing, the doors that open in a pandemic.
Afterwards, I was offered a PhD scholarship at what was by then Glasgow Caledonian University. I completed my PhD in 1996. It was on a very pragmatic topic: diabetes and how it affects eyesight.
We [Mackie and his wife, Roisin, also an optometrist] opened one practice, in Lesmahagow, in 1996, and another, in Bothwell, in 1997. We still have these practices today. The minute we started the practices, I could see what it was really like. Lesmahagow’s nearest

yourself on your back. But, it is great for marketing your practice. I’ve received the Macular Society Award, and the NHS Scotland Award for Optometrist of the Year. The icing on the cake was my fellowship from the College of Optometrists.
I wanted to give something back, so we started our own charity, Right to Sight. Opticians send us glasses, and we go into Barlinnie Prison in Glasgow. We’ve also done work in India, and this year (2023)
Now I’ve decided to step back from the committees, and just work in practice. I love the pace and interaction, and the communication. I’ve always loved working with patients. I plan to work in the practices, doing some innovative things, like myopia management, and just having a great time. All three kids are out of the house, so my wife and I can hopefully have a better work-life balance, which is a dream.
42 www.optometry.co.uk February/March 2023
Scott Mackie, of Mackie Eyecare, on his varied career and why he is ready to embrace a work-life balance
HOW
HERE
“I’ve always loved working with patients”
I GOT
“Since the minute I got the chance to do optometry, I’ve never looked back”


















100%0 ica ® LONDON THE UK'S LARGEST OPTICAL EVENT 25-27 FEBRUARY 2023 EXCELLONDON • Latest eyewear trends • Contact lenses, innovation and equipment • Fashion shows and networking www.lOOpercentoptical.com #1 00optical @100optical PRODUCT LAUNCHES I CPD POINTS I FASHION CATWALKS I 200+ EXHIBITORS OFFICIALUKPARTNER MEDIAPARTNER SPONSOR O =!~~~r I OT I SpaMedica ,,,.,,,,";) optos· GGt .. . ~+'"'""' v1s10• CHARMANT OLur.!:,~~-1• OptometryToday CooperV1s1on AMedia10event






'· UV-absorbing contact lenses are NOT substitutes for protect You should continue to use UV-absorbing eyewear as directed
Safeguarding in a domiciliary setting

The scenario
Jim, AOP member
“I’m starting a role as a domiciliary optometrist after working in High Street practice. As some of my new patients are likely to be vulnerable, can you advise me on explaining the associated costs of providing them with eye care, so I can ensure they fully understand what they will be paying for, along with any other specific things that I should be aware of?”
The advice
Paul ChapmanHatchett, AOP domiciliary Councillor and co-chair of the Domiciliary Eyecare Committee

Prior to your visit, ascertain whether the patient is eligible for an NHS sight test, explain this to them or their carer, and confirm that they are unable to attend a High Street practice unaided.
The next step is to explain how an eye test will work in the home, including in terms of space and lighting, duration, the equipment that will be used, our obligations as optometrists in completing an NHS test, and that you will issue a copy of the spectacle prescription and any recommendations. Also, explain that we can provide a dispensing service, and
access to lenses that they would see on the High Street. Select a mutually convenient day and time, and advise on who will be coming out to provide the service. If the person is not eligible for an NHS test, discuss the private sight test fee prior to the visit.
During the visit
There are seven main reasons why I would recommend new glasses to a patient in a domiciliary setting:
A change in prescription
The condition and fit of their current glasses is poor
The need for a lens upgrade, for example a move to tinted or photochromic lenses that they have not had before due to the patient now having cataracts
Change of lens design – for example, if a patient wears bifocals and is considered to be at risk of falls, changing to separate pairs
may be worth considering
Patient preference for a different frame or lens type
A dedicated pair for use when completing specific tasks, for example a pair of reading spectacles in addition to varifocals
The need for an additional pair/back-up glasses.
We can ascertain whether we can maximise the quality of life of our patients by discussing these points during history and symptoms.
You should provide the patient with information that explains the process, the frame and lenses differences, and their cost. This way we can ensure that all dispenses are clearly explained and how what we are recommending solves the problem the patient has explained to us.
Once all choices are made, make sure the patient and their carer are comfortable before proceeding, so we can avoid future problems. It is essential that discussions are clear, honest and open. It is important to listen to the patient, ensuring they don’t feel pressured in any way. Make sure you explain the expected delivery time, and that the patient has contact numbers for aftercare or further queries. As well as the full aftercare service we (at the OutsideClinic) offer the Care Plus package, which includes cover for maintenance and damage.
Remember that the patient also has the same rights as they would on the High Street in terms of taking their prescription elsewhere.
After the dispense
A lot of our patients have pathology and resulting sight loss, so having open
discussions about referral options and other support, such as sight loss charities and the appropriateness of a referral, are important. For example, an individual who drives may want referral for cataract surgery, but a housebound patient with the same level of cataract may feel a referral is not in their best interests. It is important to understand what local pathways are available, and to discuss the pros and cons of referring. Remember that if they decline a referral today it does not preclude them from changing their mind later, perhaps when they have discussed it with family.
As domiciliary optometrists, we need to make sure we get it right the first time, every time. That means an appropriate dispense of frames and lenses that meet patients’ expectations, requirements and budget, and the correct measurements. It is a privilege to be invited into someone’s home to offer a service. This must be the first and foremost consideration in everything we do. That trust must never be compromised. I use the ‘grandmother test’ – looking at the patient before you leave and asking yourself, ‘If this was my relative, would I be happy with the service I’ve provided?’ If you’re not 100% satisfied, go back, and fix it.
AOP support
Read the AOP’s guidance on safe practice in domiciliary eye care online: bit.ly/3FrubLj
46 www.optometry.co.uk February/March 2023
THE WORKSHOP
“It is a privilege to be invited into someone’s home to offer a service”
Will Amlot 0 0 0 0 0 0 0 0
Each edition, OT answers a question from an AOP member. This edition: safeguarding for domiciliary eye care patients
Want to Y1orkin a store you could end up 0Y1ning?
Diagnosing and managing swollen eyelids
OT presents a clinical scenario to three of its resident IP optometrists. This edition: advice on the management of patients with swollen eyelids
OT’s IP panel
Ceri Smith-Jaynes, OT clinical multimedia editor, IP-qualified: 2018
Farah Topia, AOP clinical adviser, IP-qualified: 2016 Kevin Wallace, AOP clinical adviser, IP-qualified: 2012.
The question: I’m looking for general advice on the management of patients with swollen eyelids. I’m unsure at which point to treat an internal hordeolum with antibiotics, and whether the antibiotics prescribed should be topical or systemic. What should I do if the condition is bordering on preseptal cellulitis?
OT’s panel says...
Ceri Smith-Jaynes (CSJ): There are many conditions that can cause the lid to swell, such as corneal abrasion, ocular rosacea, allergy, contact dermatitis, external or internal hordeolum, or preseptal or orbital cellulitis. You’ll have a good idea of what you are dealing with after a thorough history, but keep the differential diagnoses in mind until you’ve firmed up the diagnosis with the slit lamp. Is the redness and swelling unilateral or
bilateral, localised or spreadout? Don’t forget to check the visual acuity, check the cornea with fluorescein, and flip the lids over if you can. How is the patient feeling?
Farah Topia: A red and tender swelling of the eyelid is usually due to a bacterial infection. Internal hordeolum affect the meibomian glands and external hordeolum affect the glands around the eyelashes. Patients will complain of tenderness and redness, and there may be some discharge. A hot compress (five–10 mins several times a day) can help the lesion drain. In many cases, the condition can resolve spontaneously.
It is important to keep a close watch on things as there is a risk of the internal hordeolum recurring and developing into a chalazion, and of the infection spreading to other tissues and glands around the eye.
Topical antibiotics (chloramphenicol) may be prescribed in the first

instance if there is significant discharge. This can be in the form of either drops or ointment. I tend to recommend the ointment as it remains in the eye for longer, but some patients find the blurring effect annoying.
Kevin Wallace (KW): I agree that a warm compress is the most important treatment. Usually, I would only give antibiotic ointment if the lump is particularly red and angry. Most acute hordeola will resolve in a week or so and I find ointment applied to the eyelid quite effective. A chalazion can be frustrating for patients, but they can take months to resolve. Locally, our guidance is that curettage will only be considered after three months of moist heat, because the vast majority will resolve in that time.
CSJ: Patients can find a hordeolum distressing, but there’s often no quick fix. If it is external and just around one lash, it may help to epilate the lash. I encourage patience and persistence with the warm compress, gentle massage and lid cleaning (of both eyes, because it’s often due to neglected blepharitis). Blocked/infected meibomian glands are harder to get at and I generally find topical antibiotics aren’t effective because the infection is deep in the gland. Severe cases may require an oral antibiotic such as coamoxiclav. If it turns into a painless, hard lump, it’s a chalazion. If a chalazion is large, recurrent or inducing corneal astigmatism, it needs a referral to ophthalmology. In children, both preseptal cellulitis and orbital cellulitis are sight and life-threatening emergencies, requiring
immediate referral. Watch for fever and malaise, a warm, swollen lid that extends beyond just one gland, ptosis, pain, and restriction of eye movement. In adults, orbital cellulitis is an emergency, but if it is preseptal, I would still speak to the on-call ophthalmologist. In my area, they usually suggest that I start the patient on oral antibiotics, and then they will follow it up in their clinic. In simple cases, always advise the patient on what to expect, what to do if it gets worse, what symptoms to watch out for, and when to come back.
KW: The vast majority of lid infections need simple treatment, as we have already discussed. With practice, it gets easier to recognise those that may need something more intensive. The key is to seek advice when you’re unsure. Particularly in children, it’s important to have a low threshold for suspecting preseptal or orbital cellulitis.
For more information
If you are unsure about how to manage a scenario in practice, please contact regulation@aop.org.uk. If there is a scenario that you would like to hear our IP optometrists’ views to, please email: lucymiller@optometry.co.uk
Getty/KrizzDaPaul
IP AND ME
“It is important to keep a close watch on things as there is a risk of the internal hordeolum recurring and developing into a chalazion, and of the infection spreading”
Farah Topia, AOP clinical adviser
48 www.optometry.co.uk February/March 2023
0 0 0 OT 0
























































































































Moorfields Eye Hospital pre-reg, Akshay Shah, on the differences completing his High Street placement

Atypical week in the hospital includes a rotation of core clinics within the optometry department. These consist of refraction, contact lenses, dispensing, visual display unit tests, and paediatric clinics. The set schedule means I can become familiar with the specific clinics I work within, but also allows me to have a variety of sessions in a week.
At the end of November, I began my community practice experience, a fourweek placement in a High Street practice that is a requirement for hospital pre-reg optometrists as part of the Scheme for Registration. After being settled within the clinics at the hospital, a change in environment provided an exciting new experience, designed to show me another side to optometry. Similarly to the hospital, no day is the same, and I am seeing a range of patients. My day typically consists of performing routine eye examinations, which allows
me to detect and refer eye conditions into secondary care. I also get the opportunity to see a new variety of contact lens wear, ranging from soft contact lenses for presbyopic patients, to myopia control lenses for children.
Increasing in competence I definitely made the right decision with my choice of pre-reg, as I have been enjoying my time working within the hospital setting. I feel my experiences so

One of the greatest challenges of the pre-reg placement is being able to organise working fulltime with studying, and also finding moments to decompress. By planning ahead and using your time effectively you can find a balance between the two. One tip I have is using a cloud service to securely store my documents, as this allow me to access important files at any time, and from any location. I tend to use
Education Library. OT’s Education Library contains CPD and Skills guides on 31 topics www.optometry.co.uk/ cpd/education-library
service, in which patients are seen on a monthly basis for bandage contact lens replacements. These regular patients are seen by an ophthalmologist to monitor their prosthetic cornea, known as the k-pro, before seeing an optometrist to change their contact lens.
far have made me a more competent practitioner.
One skill that I believe I have developed particularly well is my retinoscopy technique. Learning from the range of patients and eye conditions I have seen has taught me how to make relevant adaptations to this part of the refraction.
My favourite part of the pre-reg is… working alongside knowledgeable individuals, who go the extra mile to ensure I am gaining as much experience as possible. I have also appreciated the patient interaction. Providing care and improving quality of life has given me great satisfaction.
My least favourite part of the pre-reg so far has been... breaking bad news to a patient,
the time spent commuting to and from work to ensure my logbook has been filled out daily, and to read through the elements of competence required when preparing for my next visit.
An interest in contact lenses
One of my favourite clinics is a specialist contact lens
as upon examination there was not much that could be done to improve their vision, due to their underlying pathology. This interaction put into perspective how much we rely on our vision, and how as practitioners we have to empathise whilst maintaining professionalism.
Before I started my pre-reg I wish I’d known… the level of organisation needed to progress.
The first time I saw a patient with these implants, I was amazed by what I had seen: a prosthetic cornea composed of titanium plates. Knowing that this specialist surgery is beneficial in maintaining even a small degree of vision, which can help to improve patients’ lives, is an incredible feeling. While many of these patients have extremely sensitive eyes, part of our role as optometrists within the hospital clinic typically involves the use of corneal anaesthetic for removal of existing lenses, iodine drops and a saline rinse for minimising risks of infections, and the replacement of new bandage lenses.
It only hit me two weeks before my Visit 1, so I was able to implement changes in time for this. By having a good work-life balance and being active in my learning I was able to achieve all the competencies required in both Visit 1 and Visit 2.
IshaSaghirisapre-reg optometristatBennettand BattyOpticians,aHakimGroup independentpracticeinLiverpool

50 www.optometry.co.uk February/March 2023
“I was amazed by what I had seen”
PRE-REG FOCUS
Isha says…
OT 0 OT
“After being settled within the clinics at the hospital, a change in environment is an exciting new experience”
KEY MILESTONES
01Specsavers was looking at how we could really embrace our sustainability credentials and look at all the things that we should be doing as the world changes post-pandemic. We have a long history of supporting the community and being a champion of the High Street. That’s part of our values, from the founders of the company. We’ve done work with the Royal National Institute of Blind People, Guide Dogs and Comic Relief, and overseas work in Zambia. This time, we wanted to help a group of people who weren’t getting the help they needed.
02 Most people can access health services via the NHS, but when we looked into it in more detail, we realised that there is a group of people, ie homeless people, who often struggled to access health services. That’s why we identified that particular group of people as really needing extra support: because often, through no fault of their own, they don’t have a permanent address – they’re living in temporary accommodation, or they could be refugees or migrant workers, or people coming out of the army. So, we knew that there was this group of people who really
needed additional support, and that’s when we decided that we were going to focus on putting some serious measures in place to support these people.
03 The Big Issue got in touch with us. It was really good timing, as we’d already decided to do this. We explained what we were trying to do, which was to improve accessibility and inclusivity for people with housing and accommodation issues. We talked more and then they said, “There might be an opportunity to help our vendors, because many of them have been homeless or are still homeless, and are trying to escape homelessness, not just by sponsoring their tabards to improve their visibility on the streets, but by giving them free eye care too.”
04 We spoke for months, working out the best way to get gift cards to vendors so they would feel comfortable. Any challenges have come from establishing our processes. We’ve sent all the vendors gift cards, which they can redeem in store as they would any regular gift card.
The Big Issue has said that its frontline workers will accompany anyone who feels uncomfortable coming into a busy retail environment. We’ve tried to make it as simple and as uncomplicated as possible.

05 Officially, we launched in October 2022. I did a photoshoot with the guys in the promotional pictures, Stephen (pictured above) and George. Everybody
we’ve spoken to has really welcomed it, and said what a good initiative it is. We need to see what we can do across the industry to help a group of people that have gone under the radar when it comes to accessing eye care.
06 The other part of the offering is free wax removal. Again, it’s about working out the process. We don’t have gift cards for wax removal, so we’ve had to work out another mechanism. It’s about how to make it as easy for the homeless person as possible to access services, so that there are no barriers in the way.
07 The partnership is ongoing. It’s going to take a while for all the vendors to get their tests, and there will be some people that have had a test recently and won’t need one.
The Big Issue has got around 1200 vendors, so it will take a while for all of them to come through. It’s too early to see the reaction, but that’s what we’ll be monitoring very closely.
Over the course of the next year or so, we hope that every single vendor will have an opportunity to come into our store and have an eye test. If they need them, they’ll get free glasses as well.
People who might be sleeping rough or leading quite chaotic lives are often more vulnerable when it comes to health issues and eye conditions, so we’re also including free optical coherence tomography in the service.
IN PRACTICE
Jo Delbridge, sustainability director at Specsavers,
talks
OT through the development of the optical group’s partnership with The Big Issue
“We have a long history of supporting the community”
February/March 2023 www.optometry.co.uk 51 0 OT
“We hope that every single vendor will have an opportunity to come into our store and have an eye test”
Newly-qualified optometrist, Chloe Fisk, and her pre-reg supervisor, Aashika Patel, reflect on what they have learnt from each other

Aashika Patel (AP), optometrist at Hakim Group practice, James Bryan Optometrists, in Chelmsford How long have you been a pre-reg supervisor?
AP: Chloe was my first prereg. I began her supervision when I joined the practice in April 2021. She had started her placement in the February.
How did you find coming into the relationship when Chloe had already started her pre-reg?
AP: Our director had set me up to know what to expect. Chloe had already settled into her placement, so there wasn’t much hand-holding at that stage. At the same time, I missed out on the beginning phase, which would have been nice to experience. I think I would have seen an even bigger growth, from the very beginning of her placement to what she has achieved now.
What level of growth did you see throughout your time supervising Chloe?
AP: I saw a massive level of growth. Chloe had always been very academic and book-smart, but being in a
practical situation pushes you out of your comfort zone. Chloe was quieter and more apprehensive when I first met her. Through receiving good feedback from her patients, as well as from us, she increased her confidence. I’ve seen a change in her personality, and that reflecting on her practical skills.
Has being a pre-reg supervisor helped your own clinical practice?
AP: Definitely. It’s nice to refresh my knowledge, and I think it helped for Chloe to have a fairly young supervisor, because I had recently gone through objective structured clinical examinations (OSCEs) and assessments myself. I could give her my insights, but even then, I realised how much I’d forgotten. It was a learning process for us both.
Any tips for those who want to become pre-reg supervisors?
AP: It’s easy to forget how it felt to be in that pre-reg year. Understand that they’re not going to be at that level you want them to be just yet: it’s going to take hard work, and perseverance. Be
understanding if they make mistakes or don’t know what you’re asking of them. Patience is important, as is having regular catch-ups and making sure your pre-reg feels comfortable with how things are going. Make sure they feel comfortable to ask questions. If you’re closed off, they might go to the wrong sources. That’s really important in your pre-reg and supervisory relationship.
Did you learn anything from Chloe while guiding her through the pre-reg?
AP: Chloe and I had different teaching backgrounds. She went to Cardiff University, whereas I went to City, University of London, so we realised there were quite a few differences in the teaching. It sometimes involved picking up research that she had found. It was very educational for me.
Chloe Fisk (CF), newlyqualified optometrist at Hakim Group practice, James Bryan Optometrists in Chelmsford How did your supervisor help in your patient interactions as a pre-reg?
CF: The first thing I did was sit in with Aashika for some of her clinics: sight tests, contact lenses, and some emergency appointments. That helped me gauge a specific kind of language spoken, as well as body language. I could choose language that came naturally for me, and then form my own routine.
Did you face any challenging moments with patients?
CF: Multifocal contact lenses were daunting. Aashika is a big contact lens advocate. She
made a document with all the steps, and we ran through it on some colleagues. If I had any fittings booked in my clinic, we discussed an action plan. That has led to a few nice multifocal fittings and some very happy patients.
What is the most important thing you learned from her?
CF: How much I can do for my patients. I’ve also realised all the options I have – for pressure recordings, for example, using a method like the iCare Tonometer. Also, realising where you can’t do much more for your patient: you might need a second opinion from the hospital. There’s only so much you can do within your expertise.
Do you have any advice for current or future pre-regs on building a good relationship with their supervisor?
CF: Honesty is key – being able to accept when you need a second opinion. Also, that if you’re confident with something you can say, “I’ve learned this and I’m happy with it,” and gain that self-approval. The other thing is the regular checkins. It’s important for your progress and to know how you’re getting along in the Scheme.
Share your story
Get in touch if you would like to share your experience with OT lucymiller@optometry.co.uk
52 www.optometry.co.uk February/March 2023
“It’s a learning process for both of us”
WHAT I HAVE LEARNED
“Chloe had always been very academic and very booksmart, but being in a practical situation pushes you out of your comfort zone”
0 OT
Aashika Patel
Create a welcoming environment for every patient?
Optometrist and coach, Peter Greedy, outlines the questions you should ask yourself in order to create a welcoming practice

Being a healthcare professional is such a privilege. We optimise people’s vision, ensure their eyes are healthy, and help them choose appropriate vision correction options. All of this is an important contribution to their lifestyle and wellbeing.
During my 30 years of performing eye examinations, people from almost every walk of life have sat in the ‘consulting chair’ – whether that’s been in a practice, in someone’s home, or in a makeshift tent clinic in Ghana.
Every person I’ve met has a story, and their stories are always interesting. How we see and interact with patients and clients is, in my opinion, the most important aspect of our job. It is an opportunity to connect and to make a contribution.
When we meet a patient for an appointment, what do we see? What thoughts go through our mind? How does what we see and hear (and sometimes smell) influence our thought process, and how we relate to and subsequently treat that person? Do we take an interest in the person sat in front of us, or do we plough through the appointment, conscious of the time, conversion rate, and other performance metrics?
How we welcome clients determines their first impression of us, and how we continue to communicate with them will determine the ongoing relationship we establish, which could last a lifetime.
Because of this, it is important to invest some thought and development into this aspect of our professional healthcare provider role. Here are some key considerations.
First impressions
Some of this did not come naturally to me. I have a highly-tuned sense of smell, and there have been times when I have felt nauseous from potent odours of stale nicotine, body odours, and worse. In the past these have generated biased stereotypes, which I would now be ashamed of.
The person in front of me is a human being just like me and, time and again, when I get curious and compassionate about their story, those biases and judgements disappear in tales of struggles, hardship, illness, suffering, and sometimes just a different
life story to mine. When you come across such a situation in practice, it is important to ask yourself: what story do I make up? What biases do I hold (remember that the biggest bias is, ‘I am not biased’)? What judgments do I make?
The assumption of positive intent

This is choosing to believe that people are doing their best, at that moment in time, in the circumstances in which they find themselves. Here’s a personal example. For years I had a poor attitude towards homeless people. I would avoid their gaze, and never stop to engage or give them money. This has changed dramatically as I have worked on my attitude and become more attuned to the privileges that I have.
It sounds silly to have to state this, but I’ve grown to understand that we are all equal, and my previous behaviour and attitude was dehumanising and unacceptable. What right do I have to judge someone else for addiction or mental health issues, or situations that I know nothing about? I could not imagine being in the position of being homeless, so who am I to judge what a homeless person might spend my
Read more articles from our extensive How do I... series on our website www.optometry.co.uk/ how-do-i
spare change on? Now, when I pass a person sleeping rough, I make a point of looking them in the eye and greeting them. I may give them money, or I may buy them a coffee and sandwich. But I always treat them as an equal, as that is what they are. It is vital that we take this attitude into our consultation rooms.
My personal ‘why’ statement is ‘to champion courageous, curious, compassionate conversations, so that people connect wholeheartedly.’ I am always pleasantly surprised when I do this during an eye examination. It is a safe space to engage with people, and almost everyone I get curious with has something interesting to tell me. We find common interests or connections, and this transforms the experience for both the patient and for me.
I encourage us all to take a moment to reflect on how we can better relate to those we are privileged to meet and serve in our work.
0
Peter Greedy is an optometrist, leadership consultant and coach. He can be contacted on 07906632378, or via his website: www.petergreedy.com
HOW DO I... Further reading
in touch
“Every person I’ve met has a story, and their stories are always interesting”
Get
February/March 2023 www.optometry.co.uk 53 IN PRACTICE - OT
OT
Associationof Optometrists
Make a difference to the future of optics
We're looking for members to join our Council
o Undergraduate student
o Pre-registration optometrist
o Newly qualified optometrist
o Additional hospital optometrist
o Independent prescribing optometrist
o Domiciliary care optometrist

o Locum optometrist
o Director of a multiple practice
o Employee of a multiple practice
o Director of an independent practice

o Employee of an independent practice
o Optometrist for Scotland
o Optometrist for Wales
o Optometrist for Northern Ireland
If you're passionate about the profession and representing your peers, we'd like to hear from you. No previous experience required.
Applications open 16 February. Find out more www.aop.org.uk/councilappointments
Financial wellbeing is about making sure your wealth and assets, however large or small, work for you. This includes keeping an eye on your future, as well as your present day-to-day income and expenditure.
Clearing debts
With high interest rates and the rising cost of living, clearing debts is a good place to start. If you have credit cards, store cards or overdrafts, consider paying them off or reducing them as much as possible.
If you have debts, ensure you always make at least the minimum payment each month and target the ones with the highest interest rate first. If it is going to take time to repay your debts, consider moving to an interest free credit card.
Your mortgage
Make sure you are on the best mortgage deal for your circumstances. Lloyd & Whyte’s mortgage advisers can help you with finding your future or reviewing your current mortgage. They are part of an independent financial adviser team, and are not tied into a specific provider, which means they can search a large panel of lenders and help find a mortgage to suit you.
Protecting income in the event of illness
You never know what is around the corner. Accidents and illness do happen, and we are not as invincible as we think we are.
Being unable to work due to an accident or illness is one of the largest risks you will probably face. Income protection can pay up to 65% of your salary until you
return to work. Compare this to the amount the state pays – £99.35 per week for up to 28 weeks – and you might want to consider taking out income protection as a ‘safety net.’
The benefits of income protection include:
Cover up to 65% of gross earnings paid tax free income after a waiting period
Benefits that can be paid up until retirement age Pay-out on incapacity, based on your income over the previous 12 months Payments until you return to work.
your ‘fixed expenditure.’
Remember to create an easily accessible cash ‘buffer’ for unexpected expenses or emergency costs. We suggest three to six months of your salary.
When you have a grasp on the ins and outs of your income and expenditure, you can work towards making your money work for you by starting to build up a nest egg for the important things in life. Our advisers can assist in making investment recommendations if you feel this would be of value. If investing seems to be
pension, the more peace of mind you could have.
Saving your money in the right places means your wealth works harder for you, rather than you work harder for your wealth.
Visualising your retirement
How do you want your retirement to look? If you haven’t considered planning for your retirement, now could be the time to start. Whether you intend to retire early, work part-time when you reach a certain age, or continue your career to later on in life, organising your savings, investments and pension(s) can make the difference between enjoying the longest holiday of your life to potentially struggling financially.
Practising ‘long-sighted’ planning around your financial wellbeing can be more beneficial than a short-sighted approach. Our independent financial advisers are experts in helping with investment strategies and pensions, helping you make the most of your hard-earned money.
Spending and saving
Are you a ‘spender’ or a ‘saver’? If you are already saving as part of your financial wellbeing – well done. If you err on the side of spending, Lloyd & Whyte can help.
To get you started, consider creating a budget. To do this, examine your ‘discretionary expenditure’ versus
a process which is not applicable to you, reconsider. You can start on a smaller scale and build up your portfolio over time.
Pensions
You often need to work for a long time until you can claim your State Pension, so the sooner you start thinking about organising your
Lloyd & Whyte practises a holistic strategy around clients’ financial wellbeing, which means every aspect of your finances, from paying off debts and managing income and expenditure to saving, investing and planning your pension, plays a part in your finances working for you.
Lloyd & Whyte is an AOP affinity partner. To talk to Lloyd & Whyte’s independent financial advisers, call 01823 250750.
February/March 2023 www.optometry.co.uk 55
“If you have debts, ensure you always make at least the minimum payment each month and target the ones with the highest interest rate first”
EYES ON WELLBEING
Looking after your wellbeing includes looking after your financial health. Lloyd & Whyte’s director of client services, Danny James, explains how
Getty/Ponomariova_Maria IN PRACTICE Learn more online For more on this subject, watch our financial wellbeing webinar on YouTube: bit.ly/3J393O2 0 0 0 0 OT 0
To look after yourself, first look after your finances



A TALE OF TWO CITIES
OT takes a seat at practices in Glasgow and London for an on-the-ground view of the issues facing optical professionals today
 SELINA POWELL
SELINA POWELL
February/March 2023 www.optometry.co.uk 57 OT
Peter Sandground
Frank Munro takes my coat and offers me a cup of tea inside the Mount Florida branch of Munro Optometrists. There is a Christmas tree nestled in the corner with blue baubles the same colour as the shopfront. Down the road, past posters that read ‘People make Glasgow,’ a notice in the window of J Lupton Family Butcher gently reminds pedestrians to order their turkey.
Munro tells me that during staff training he encourages new recruits to treat everyone who comes through the practice like a member of their family.
“Never walk past anyone – say hello to them,” Munro shares.
“Show some appreciation for the people who are in the building and you will never go far wrong,” he says.
Munro is one of the founding members of Optometry Scotland. Alongside Donald Cameron and Hal Rollason, Munro spearheaded the introduction of universal eye care in Scotland in April 2006.

On the afternoon I visit Munro in Glasgow, more than 400 miles away in London, Labour MP Marsha de Cordova is presenting the first reading of a bill that calls for a national eye health strategy in England.
If successful, the change would bring England in line with the other three nations of the UK, which already have a single plan overarching the eye care that is delivered in hospitals and optometry practices on a daily basis.
“We rely on our vision every day, yet we do not give much thought to our eye health until our vision changes,” de Cordova tells parliament.
This complacency about the value of sight is not limited to England, but a gradual shift in the public perception of eye health has occurred since the introduction of universal eye care in Scotland. Many patients view a visit
to the optometrist as an eye health check rather than simply a place to update a spectacle prescription.
Optometry Scotland chair, Julie Mosgrove, tells me over a video call that 2.2 million people have their eyes examined each year in Scotland, out of a total population of 5.5 million.
“They are coming for preventative reasons and overall health checks as well as with acute problems,” she says.
In England, there were 12 million NHS sight tests over the past year –meaning around 20% of people have an NHS-funded sight test each year, compared to 40% of people in Scotland.
Before the introduction of the new General Ophthalmic Services model in April 2006, Munro believes that cost was the biggest barrier that stopped people getting their eyes checked.
Alongside Cameron and Rollason,
Munro worked with the Scottish Government to redesign how eye care was offered in Scotland.
“The Scottish parliament was new, and wanted to make their mark by putting in free dental and eye checks for all. We made the most of that opportunity,” Munro explains.
“We had a blank sheet of paper –how did we see the service going? We were trying to anticipate what the challenges would be,” he shares.
As the plan for eye care was refined and revised, the trio of optometrists went back and forward between their practices and Holyrood for over a year. One day they went in and were told that they had secured the funding.
“That was a special day. Hal and I had a glass of wine and Donald had a cup of tea.”
Progress within Scottish eye care has continued since 2006. Alongside the primary eye examination, funding for supplementary and enhanced supplementary examinations enable optometrists to manage more complex levels of disease.
Munro shares that in England there has been a 70% increase in attendance at outpatient ophthalmology clinics since 2006, while in Scotland there has been a 3% rise over the same period.
Sandground
58 www.optometry.co.uk February/March 2023
“SHOW SOME APPRECIATION FOR THE PEOPLE WHO ARE IN THE BUILDING”
Frank Munro
Peter
OT
Optometrist and owner of Munro Optometrists, Frank Munro
“Scotland has more or less flatlined because the care has been retained in the community,” he says.
Around one in three optometrists in Scotland have an independent prescribing (IP) qualification.
Funded places are available for the course and every IP optometrist receives a prescription pad on qualification.
The majority of health boards in Scotland allow for direct electronic referral from optometry practices into secondary care.
Mosgrove explains: “Some practices are able to get feedback back from the hospital through the same system – the systems can talk to each other. Others may send in a referral and then they receive email feedback. On the whole, everyone is working towards electronic referral.”
Closing the gaps
While optometry has advanced in Scotland, as in other parts of the UK, there is room for improvement in reaching under-served communities.
“There is still a lot that we could be doing to promote healthcare – although the uptake is very good across all socioeconomic groups, it could be better,” Mosgrove shares.
“Practices are accessible – it is just making sure that people grasp that opportunity,” she adds.
Munro has six optometry practices within Glasgow. The Mount Florida branch I visit is a suburban practice located on Cathcart Road.
“We are a middle of the road practice,” he tells me.
“A mile down the road one way is very affluent. A mile and a half in the other direction is high deprivation,” Munro shares. South of Munro’s practice in King’s Park, around one in 10 people are experiencing
income deprivation according to data published by the Glasgow Indicators Project. To the north, in Govanhill, the figure is one in four. Munro has observed a higher proportion of people presenting with advanced pathology from lower income areas – and this has been exacerbated by the pandemic.
“After COVID-19, some of the things we have seen have been awful. People didn’t think we were open, but I was here every day,” he notes.
There are also challenges in letting migrant communities know that eye care is free to access when they are unfamiliar with the Scottish health system. “If people are not used to being in a healthcare system that is free to access, then they tend to present late with eye problems,” Munro shares.
The next generation
I arrive at Glasgow Caledonian University (GCU) as a free breakfast for staff and students is finishing up. Porridge, baked beans, scrambled eggs, fruit and a cup of tea or coffee are available Monday to Friday at the George Moore restaurant.
“It is hugely popular, there are long queues,” Professor Gunter Loffler tells me. “It is a recognition from the university that this is a tough time for
many students. This is a little way that the university can help,” he says.
We meet at the University’s Vision Centre – a modern, purpose-built facility where the next generation of Scottish optometrists, dispensing opticians and orthoptists hone their skills. Loffler initially trained as an optometrist in Germany before coming to the UK and completing a doctorate in visual perception.
He joined the GCU in 2001 and is currently the head of the university's vision sciences department, which provides training to undergraduate optometry, ophthalmic dispensing and orthoptic students.

Students can study towards their Master’s and PhD within the department, while an independent prescribing course is also offered.
GCU was the only provider of optometry training in Scotland until the University of Highlands and Islands (UHI) launched its course in September 2020, with the inaugural intake of UHI students yet to enter the workforce.
“The majority of optometrists in Scotland will have completed their training at GCU. It is not uncommon that I will be walking through a shopping centre and there will be someone who knows me and waves from an optometry practice. It is lovely,” Loffler shares. Dispensing optician and Vision Centre business manager, Michael Welsh, has shepherded generations of optical students through their training. “It gives me great pleasure when I
THE VIEW FROM THE CHAIR
“PRACTICES ARE ACCESSIBLE – IT IS JUST MAKING SURE THAT PEOPLE GRASP THAT OPPORTUNITY”Julie Mosgrove
“YOU NEED TO KNOW THE PATIENT. YOU GET PEOPLE BACK INTO PRACTICE BY HAVING POSITIVE RELATIONSHIPS WITH THEM”
Michael Welsh
receive a prescription where I see the signature at the bottom and think ‘Oh that is one of my former students’,” he tells OT.
Welsh started out as a glazing technician in 1980, crafting spectacle lenses on the second storey of a practice owned by two optometrists. He has since taught their granddaughter.
In Scotland, there are signs in hospitals, GPs and pharmacies telling patients to go to an optometry practice if they have a problem with their eyes –while some GP practices have the same message on their answering machines.

The fact that optometrists have become the first port of call for patients with any eye-related problem has informed the approach that the department takes to developing the next generation of optical professionals.
“We are acutely aware that there are challenges and opportunities awaiting our graduates. We need to provide the foundation for their future career,” Loffler shares.
He sees evidence-based practice as a key skill for the modern optometrist, orthoptist and dispensing optician.
“For that, you need to have an ethos that is underpinned by an understanding of research and the ability to evaluate publications and clinical evidence,” Loffler notes. He has observed the undergraduate education of optical professionals evolve to the point where the programmes offered by
GCU are now “almost unrecognisable” from the courses on offer when he first joined.
“Within optometry, there has been a remarkable shift from screening for disease towards the diagnosis and management of eye conditions,” Loffler says. In the future, Loffler believes it is conceivable that optometrists in the UK will take on further advanced practice roles.
career progression of dispensing opticians. The latest data from the General Optical Council reveals that while the number of optometrists in the UK is continuing to climb, dispensing optician numbers have remained relatively static since 2019. Over the same time period, student dispensing numbers have fallen by 25%.
Welsh believes that the value that dispensing opticians bring to practice is not confined to expertise in fitting spectacles.
“I have the family nickname of the ‘The Glasses Man’ – as my late motherin-law called me – but ophthalmic dispensing is much more than that,” Welsh observes.

“You need to know the patient. You get people back into practice by having positive relationships with them. They don’t just buy a pair of glasses – they buy into who you are and the experience they have,” he says.
Forging connections
Perhaps this is a not-too-distant future. When I speak with Munro, he has recently completed training in ocular plastics – learning to remove stitches, for example, when a patient has a tumour removed from an eyelid. Welsh would like to see employers raise the bar when it comes to the
I arrive at Specsavers The Forge as the sun is setting. It is four degrees outside – an illuminated ice cream van drives past silently like the ghost of summer. Clinical director and optometrist, Sufyaan Aslam, takes me through to a room where a ‘World’s Best Dad’ water bottle sits on the desk next to a half empty bottle of Irn Bru and stickers he gives to children after he puts drops in their eyes.
“The days I go home and I think, ‘That was a good day’ are not necessarily because it was a high sales day,” he tells me.
“It is because you had happy patients, a happy team, and everyone left with a smile,” Aslam shares.
Aslam started working on weekends at Specsavers The Forge in 2005, when he was in his third year of university. After completing his studies, he took on a pre-registration position before becoming a full-time optometrist, then supervisor and finally director.
Over the years he has learned the value of listening to patients and understanding where they are coming from. “If you listen to understand, rather than being on autopilot, then

60 www.optometry.co.uk February/March 2023
Peter Sandground
THE VIEW FROM THE CHAIR
“WE ARE ACUTELY AWARE THAT THERE ARE CHALLENGES AND OPPORTUNITIES AWAITING OUR GRADUATES” Professor Gunter Loffler
OT
Tony Watt receives a sight test at Munro Optometrists
very rarely will you be in a spot where you have missed something or you have an angry patient,” Aslam says.
The practice is Dementia Friends accredited, while practice staff speak a combined total of 15 languages, including Urdu, Mandarin, Arabic, Romanian, Greek and Polish.
Some patients will request to see someone who speaks a specific language, so they are booked in on a day when that team member is working.
“Patients love it. You can almost see their shoulders relax when they talk with someone who speaks their language,” Aslam says.
Data published by the Glasgow Indicators Project shows that four in 10 people in Parkhead are experiencing income deprivation, while half of children live in poverty. Life expectancy for men is 67.6 years and for women it is 75.8 years.
When headlines about the cost of living are in the news, he observes an effect on the shopping behaviour of people coming through The Forge.
“I have noticed this since the first credit crunch,” Aslam tells me.
“If in the headline it says ‘Universal Credit is getting scrapped,’ suddenly everyone is really concerned and the shopping centre gets quiet. Within a couple of weeks, things go back to normal,” he says.
Aslam sees higher levels of pathology among patients in Parkhead than he did when he worked days in the wealthier suburbs of West Glasgow. The health of the Parkhead population is affected by a combination of lifestyle and socioeconomic challenges.
He shares with me that the “heart is constantly warmed” at Specsavers The Forge. Aslam recalls a high myope in his 50s receiving his first pair of glasses. The man was deaf and struggled with his vision “but that is how he knew life to be.”
When the patient put on his new spectacles, for a moment he was stunned before he started jumping up and down, signing applause.
“His happiness was indescribable,” Aslam says. “Before, he would struggle
to see someone signing if they were too far away, but now he could see to the other side of the room,” he adds.
Around one in five patients who come through the practice are children. Dispensing optician, Sundas Afzal, explains that she always includes both the child and parent in the conversation when selecting spectacles.
“If the child feels like they are left out of the decision making, they might not want to wear their glasses or come back to the practice,” she says.
Positive feedback keeps her motivated in her job. She recently fitted a non-verbal adult patient with spectacles, who then immediately left her to go look around outside.
“He couldn’t say anything, but his eyes lit up,” she says.
Aslam, who is IP qualified, appreciates the variety of roles that are available to optometrists now compared to when he first qualified. He recently saw a patient with a several different conditions that required a battery of tests.
“About 20 minutes into the test he said, ‘Do you guys still measure for glasses?’ I said ‘Yes, we do, I promise I am coming to that.’ He was wondering if he was in the right place,” Aslam tells OT
Team work
Back in London on a rare snow day, I take the bus past fields blanketed in white and children making a snowman on a traffic island to Hynes Optometrists in Ealing.
Established as a house practice by optometrists Colin and Joy Hynes in 1982, Hynes Optometrists moved to its current High Street location in 1992. Over the decades, estate agents and
February/March 2023 www.optometry.co.uk 61
“IF THE CHILD FEELS LIKE THEY ARE LEFT OUT OF THE DECISION MAKING, THEY MIGHT NOT WANT TO WEAR THEIR GLASSES OR COME BACK TO THE PRACTICE” Sundas Afzal
“IF YOU LISTEN TO UNDERSTAND, RATHER THAN BEING ON AUTOPILOT, THEN VERY RARELY WILL YOU BE IN A SPOT WHERE YOU HAVE MISSED SOMETHING”
OT
Sufyaan Aslam
coffee shops have proliferated on the High Street while Northfield Avenue has said goodbye to independent butchers and the Owl and Pussycat children’s bookshop.
Hynes Optometrists has remained a constant, offering slices of home-baked orange polenta cake, Victoria sponge and tea at regular fundraising coffee mornings.
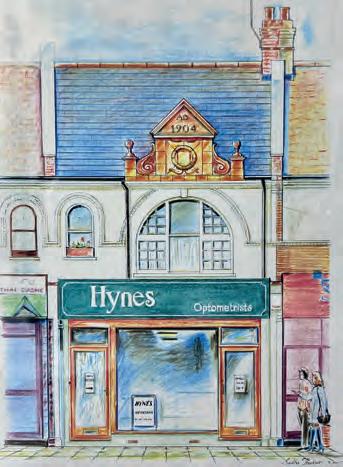
“Some of our patients live on their own and they look forward to these coffee mornings. Joy gets out her antique teacups,” practice manager and dispensing optician, Linda Menezes, tells me.

If it happens to be a patient’s birthday when they come through the practice, the staff will sing to them.
“We want to make them feel special for making the decision to come to us,” Menezes says.“It is about treating them as a special person, because that is exactly what they are,” Joy Hynes adds.
During the course of the interview, it becomes clear that Menezes and Hynes have the kind of friendship, formed over decades, that sees them finish each others’ sentences.
In the past, Menezes was a music teacher. Hynes had a vacancy for a dispensing optician and convinced her friend to study for the qualification by correspondence. Menezes believes that a stable staff base helps to build trust and loyalty with patients.
“When the patients come in, they see the same faces. They are very happy – there is that continuity of care,” she tells OT
Stories about Hynes father, who died when she was a young girl, have shaped her approach to working life. Hynes shares that his philosophy was to treat all his employees fairly, respectfully and with kindness in the knowledge that they would respond in kind.
“What is really important is that we work as a team. I am the boss, but we work with each other and for each other,” she says.
Bespoke service
Next to a thin strip of ice surrounded by a picket fence (‘This way to traditional Bavarian curling’), coins glint beneath the frozen surface of Sloane Square’s fountain. At Tom Davies Bespoke Opticians, beside
a black and white portrait of the eponymous designer, a video details the process of making bespoke frames. Store manager, Courtney Smith, shares that customers choose a template frame and colour before head, bridge and ear width is measured.
An eyewear design is then created using CAD software to translate the customer’s measurements into their own unique pair of frames, before the designs are sent for manufacture at Tom Davies’ West London factory.
Using i.scription technology (marketed by Zeiss as a “personal vision fingerprint”) the lenses within a Tom Davies frame can also be tailored to the individual.
With an hour set aside for each consultation, there is time to talk through the specific requirements of each customer.
“I always keep in my mind that this is a special moment for this person,” optometrist, Tuija Kankaanpaa, shares.
Many of the practice’s customers live in the local area, drawn to the practice on the recommendation of family members and friends.
There are also tourists who stop by on the way to visiting King’s Road and Harrods, and overseas residents with holiday apartments in London who time their appointments for when they are in the city.
Sloane Square sits within the Kensington and Chelsea borough, one of the wealthiest neighbourhoods in London. Life expectancy at birth is 83.9 years for men and 87 years for women.
On the store floor of Tom Davies, prices are absent from the rows of frames on display. Kankaanpaa notes that cost is far from the customer’s mind when they see the quality of the final product.
Sometimes customers are reluctant to part with their frames when their prescription changes, so the team will replace the lenses before taking care of the frame – polishing acetate and nourishing horn frames with cream.

62 www.optometry.co.uk February/March 2023
“I AM THE BOSS, BUT WE WORK WITH EACH OTHER AND FOR EACH OTHER”
Joy Hynes
Sudha Thakur
OT
LindaMenezes
Smith shares that a good pair of frames can have a transformative impact for the wearer.
“It can boost your confidence and change your life,” he says.
Smith adds that there is a family feel to the practice, with every customer given a warm welcome.

“I believe in treating customers in a way in which you would like to be treated. When I go somewhere I would like to be given good service from start to finish. I do the same with every customer who comes through the door,” he says.
Royal treatment
In August 2022, there were more than 800 royal warrant holders in the UK –covering goods and services from flags, church robes, candles and champagne, to asbestos removal and equine dental services.
Roger Pope Opticians in Marylebone holds two royal warrants for dispensing optician services to the royal household.
The practice was dispensing-only for a decade after opening in 1987. Optometrists were recruited to Roger Pope Opticians after the Harley Street consultants who had previously provided prescriptions stopped performing refractions.
With more than five decades of experience as a dispensing optician, Pope can look at someone who has walked into the store, mentally run through a catalogue of 800 frames and hopefully come up with a pair that are a good match.

“You can self-select, but on the whole people expect us to guide them through the whole process of choosing their spectacles,” Pope says.
Pope says that he is often working with customers who are at the top of their professions, and they demand the best from him in return. “You are not always looking at the cost aspect. If you say to someone, ‘I think this lens is the best lens for this prescription,’ they will often have the means to pay for that. It gives you a wider
scope,” he shares with OT. The range of lenses and coatings has expanded dramatically since Pope first qualified in 1971.
When he first started working, before varifocals and plastic lenses, Pope would select from a narrow range of glass bifocal NHS lenses.
“The world of lenses today is phenomenal. I think there are lenses out there to suit anybody, but you have got to listen to what their needs are,” he says.
The practice does small repairs for spectacle wearers – they do not need to be existing customers. Pope notes that people will often come back for frames after a good experience with a repair.
The practice will not sell poor quality frames, even if it is from a designer brand. “If it doesn’t meet certain criteria, we won’t stock
it. It’s no good to put a name on something if it doesn’t match the quality,” he says.

At the age of 76, Pope now comes into practice two days a week. But he is supported by a team that has decades of combined experience fitting spectacles for the varied community that lives in the West End.
“Everybody knows people by name when they come in,” Pope says.
He believes that dispensing opticians have an important role to play in translating what has been found in the consulting room into a well-fitting pair of spectacles with good quality lenses.
“I think dispensing optics does get pushed to the back. I think it is vital,” he says.
He will always shake the hand of new customers and walk them to the door when they leave.
“We would never let them wander off. I think that last impression can be as important as the first.”
February/March 2023 www.optometry.co.uk 63
“EVERYBODY KNOWS PEOPLE BY NAME WHEN THEY COME IN”
Tuija Kankaanpaa THE VIEW FROM THE CHAIR 0 OT
Roger Pope
The OT Podcast LISTENTODAY
The OT Podcast is hosted bimonthly by OT's clinical experts, Dr Ian Beasley and Ceri Smith-Jaynes



THE IAN CAMERON EPISODE: NEW Delve into the career of the Scottish IP optometrist and practice owner

THE PROFESSOR NICOLA LOGAN EPISODE: Take a deep dive into myopia management with the UK's Queen of myopia

The Optometry Today Podcast
A~pl~Podcasts 11 1 Listen on ••!I•Google Pod casts e Spotify Podcasts
CPD
INCOMITANCE: TOOLS AND TIPS FOR EVERYDAY PRACTICE
66
C-103858
LEARNING OUTCOME
Practitioners will understand how to investigate and manage cases of incomitance.
MAKING THE MOST OF A MANAGEMENT PLAN FOR DRY EYE
C-104001
LEARNING OUTCOMES
Practitioners will be able to outline anticipated treatment outcomes to dry eye patients Practitioners will be able to develop a management plan for patients with dry eye relative to their scope of practice.
PROGRESSIVE ADDITION LENSES: ARE YOUR STANDARDS UP TO STANDARD?
C-104217
LEARNING OUTCOMES
Practitioners will be able to verify progressive addition spectacle lenses to the relevant standards
Practitioners will be able to delegate the task of optical appliance verification to support staff in line with relevant standards.
C-104194
LEARNING OUTCOME
Practitioners will be able to manage a range of common contact lens-related presentations within their scope of practice.

CLINICAL FEATURES OF OPTIC NEURITIS
C-104147
LEARNING OUTCOMES
Practitioners will be aware of the presenting characteristics of optic neuritis that may be evident during history and symptoms
Practitioners will be familiar with the clinical characteristics of optic neuritis.
C-103750
LEARNING OUTCOME
Practitioners will be able to identify abnormalities of the iris and anterior chamber angle.
EXAM QUESTIONS, REFERENCES & DECLARING CPD POINTS CPD
MCQs for OT’s CPD appear online at www.optometry.co.uk/CPD. Exams in this issue will be live from 11 February to 5 May, 2023. When taking an exam, the MCQs may require practitioners to apply knowledge that has not
been covered in the article. Visit www.optometry.co.uk/CPD, and click on ‘Related CPD article’ to view the article and references in full. In the new CPD cycle, registrants are responsible for declaring their CPD
points viatheir MyGOC account. If you pass an exam with OT,you will receive a certificate to use as evidence when declaring your CPD points. Certificates will be available to download in your MyAOP.
ONLINE
UPLOAD
POINTS
MYGOC
FROM 11 FEBRUARY 2023 REMEMBER TO
YOUR CPD
TO YOUR
IN
ISSUE
THIS
CONTACT LENS CASES IN PRACTICE 86
IRIS
88 71 81 76
THE
AND THE ANGLE
February/March 2023 www.optometry.co.uk 65 0 0 0 -· _., 0 0 "·' - - ·-·: •••.•• ·: . 0 0 0 ,... - - ••. :.• 0 - : OT
INCOMITANCE: TOOLS AND TIPS FOR EVERYDAY PRACTICE
Professor Bruce JW Evans BSc, PhD, FCOptom, FAAO,
IN BRIEF This article provides a practical approach for the investigation and management of incomitancy
INTRODUCTION
In optometry, incomitance describes the abnormal situation when the two eyes do not move in a parallel, yoked, fashion. When looking at equidistant objects in various positions of gaze, the angle between the visual axes changes.1 Additionally, the angle of deviation differs according to which eye is fixating.1 This second part of the definition of incomitance is often forgotten, but is crucial to understanding the condition. This relates to primary and secondary angles of deviation, which will be discussed later.
A key distinction is between congenital and acquired incomitant deviations. Usually, the history will help with this classification. A new or changing incomitance requires referral as the aetiology may be pathological. This aspect is discussed further in the section on management.
The complete loss of action of a muscle is called a muscle paralysis. A partial loss is referred to as paresis The term palsyis used generically to include both paralysis and paresis. Incomitant deviations can be classified as:
• Neurogenic: a problem with the nervous supply (for example, third nerve palsy in diabetes)
• Myogenic: a problem with the muscle (for example, myasthenia gravis)
• Mechanical: where a muscle is mechanically restricted (for example, Duane syndrome, Brown syndrome).
ACTIONS OF THE CYCLOVERTICAL MUSCLES
Any consideration of incomitance must start with an understanding of the actions of the extraocular muscles; this is described in detail in the new edition of a standard textbook on binocular vision anomalies.1 A full description is beyond the scope of this article, but since the cyclovertical muscles are a common cause of confusion, their actions will be briefly summarised.
Just considering the action of the right superior rectus, Figure 1A shows the eye in its primary position (looking straight ahead). Here, if the muscle contracts
(along RA) the main action will be to elevate the eye. Because the insertion of the muscle is forward and slightly nasal to the centre of rotation of the eye (C), contraction in this position will have the secondary action of intorsion (rotating the top of the right eye nasally) and the tertiary action of adduction. The inferior rectus is approximately parallel to the superior rectus, but under the globe. So, in the primary position, the main (primary) action of the inferior rectus will be depression of the globe, with secondary actions of extorsion and adduction. The foregoing explanation of the actions of the superior and inferior recti in the primary position are useful when considering, for instance, the likely effects of underactions or overactions on cover test results when the patient looks straight ahead. A different scenario is motility testing, when we wish to consider the best way to elicit a muscle’s maximum action. In panel A, if we imagine how the situation would change if the right eye looks out (abducts) by approximately 23°, the sole action of the
1
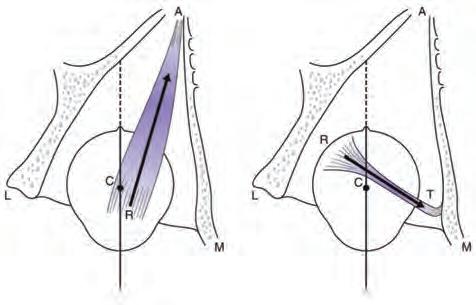
66 www.optometry.co.uk February/March 2023
FEAOO, FBCLA, DipCLP, DipOrth
CPD POINT
Figure 1 Schematic illustration of right orbit to highlight the action of the right superior rectus (A) and right superior oblique (B). See text for explanation. Reproducedwith permissionfromChapter17inEvansBJW(2021)Pickwell’s BinocularVisionAnomalies(sixthedition).Elsevier, Philadelphia
Abduction Adduction Abduction Adduction A B 0 OT
superior rectus will be to elevate the globe. Similarly, when the right eye abducts by a similar amount and looks down, we have isolated the action of the inferior rectus.
Considering the superior oblique (see Figure 1B), the muscle tendon runs through the trochlear pulley in the anterior medial aspect of the globe. The muscle is inserted into the globe posterior and lateral to the centre of rotation. Therefore, if it contracts in the primary position (as shown in Figure 1), its main action will be intorsion, secondary action depression, and tertiary action abduction. The power of the muscle to depress the eye will be maximal when the eye is adducted by approximately 45°.
The key point is that the actions of the extraocular muscles vary with the direction of gaze. The direction of gaze in which a muscle has maximum power to elevate or depress does not tell us about all of the muscle’s actions in the primary position.
PRIMARY AND SECONDARY DEVIATION
It was noted earlier that if an incomitancy is present, the angle of deviation will differ according to which eye is fixating. This occurs because of Hering's law of equal innervation and is explained by the example in Figure 2. The top panel shows normal binocular fixation. In this figure, ‘+’ signifies innervation to the lateral and medial recti muscles. In the second and third panels, the left lateral rectus has suffered a paresis. In the second panel, the non-paretic (right) eye fixates, as is most commonly the case. There will be approximately equal innervation to the right lateral and medial recti, and because the right eye is fixating, equal innervation to the left lateral and medial recti. Since the left lateral rectus is paretic, the left eye will be deviated inwards: the primarydeviation
In the bottom panel of Figure 2, the same left lateral rectus muscle is paretic but now the less common situation pertains, when the patient fixates with the paretic eye. Excessive innervation (+++) is required to the paretic left lateral rectus to maintain fixation in the primary position, and inhibition (---) to the left medial rectus. Hering's law means that the non-paretic right eye will receive similar innervation as the fixating left eye, and therefore, there will be much greater innervation to the right medial rectus than to the right lateral rectus. This will cause a secondarydeviation, which is significantly greater than the primary deviation that resulted when the non-paretic eye was fixating. The difference between primary and secondary deviations has several clinical manifestations. During the cover test in the primary position, the size of the deviation when each eye is covered can be compared, and if the deviation differs, this indicates the patient may have an incomitant deviation and can also indicate which eye has the underacting muscle. The difference between primary and secondary deviations also
explains why Hess and Lees screen plots are carried out twice, once with each eye fixating. If a patient has been habitually fixating with the unaffected eye and is then forced to fixate with the paretic eye (for example, if cataract is removed first in the paretic eye giving it better visual acuity), this can cause fixationswitchdiplopia. This typically causes symptoms and is one reason why, when a patient is referred for cataract surgery, the referral letter should include information about any incomitance or strabismus.
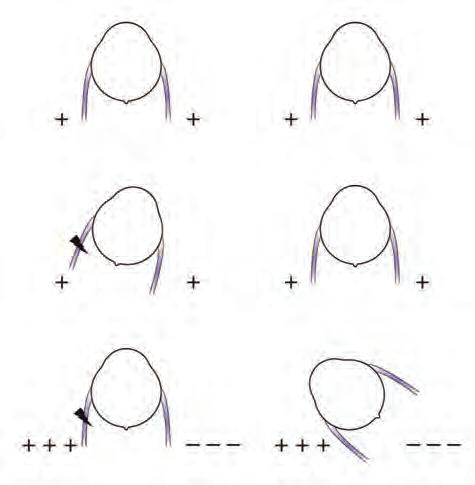
INVESTIGATION AND DIAGNOSIS
History and symptoms are essential in the investigation of incomitance, and anomalous head postures and facial asymmetry can help indicate longstanding cases.1
Motility test
It is recommended to carry out the motility test on children at every appointment, adults with suspicious symptoms (for example, diplopia) and new adult patients. Some practitioners would disagree with the author on the last point, but it can be useful to obtain a baseline result in case symptoms subsequently develop. This assumes that motility testing would detect a subtle longstanding underaction or overaction of which the patient may be unaware. Methods for improving the sensitivity of the motility test will now be discussed. There are really three different tests that can be carried out during the ocular motility test, and with incomitant patients the situation can be made simpler
BINOCULAR VISION
February/March 2023 www.optometry.co.uk 67
Figure 2 Illustration of primary and secondary deviations (see text for explanation). Reproducedwithpermission fromChapter17inEvansBJW(2021)Pickwell’sBinocular VisionAnomalies(sixthedition) Elsevier,Philadelphia1
Fixing Fixing Primary deviation Fixing Fixing Secondary deviation+Di+ +Di+ +IC)+ +Di+ +++~ ++~-OT
1 The best target is a point light source, which should be bright enough to allow the corneal reflexes to be clearly seen, but not so bright as to cause blepharospasm. For infants, any target that will catch their attention is recommended
2 The light should be held at about 50cm from the patient. It should be moved quite slowly, so that it takes about five seconds to move from extreme gaze on one side to extreme gaze on the other
3 The light should be moved in an arc, as if using an imaginary perimeter bowl
4 It is easier to observe the eye movements in extreme gaze if no spectacles are worn, but if there is an accommodative strabismus then spectacles should be worn, or the test repeated with and without spectacles
5 Various authors have preferences for different patterns of movement of the target. The star pattern is often used, but other patterns have been recommended and each has its own merits
6 The straight up and down (in the midline) positions are often also tested to look for an A or V syndrome
7 In young children, the head may need to be gently held. With infants, it is best not to hold the head but to move the target very far around the patient so that the eyes are forced to move when the head cannot turn any more
8 The motility test is performed while watching the reflection of the light in the corneae to detect any marked underactions or overactions
9 Any underactions or overactions can be graded from grade 1 (just detectable) to grade 5 (extremely noticeable)
10 Throughout the test, the corneal reflexes of the light are observed. If one disappears, either the light is misaligned or the patient’s view of the light has been obscured (for example, by the nose). This means that the light has been moved too far: the test should be carried out within the binocular field
11 In down gaze, patients often need to be asked to keep their eyes as wide open as possible. The lids should only be physically held open if this is the only way that the eyes can be seen
12 If any abnormality is observed on this binocular motility test, this can be investigated with a monocular motility test by occluding each eye in turn.
by performing the test three times to gather these three sets of data. The first of these three tests, the basic objective ocular motility test, is described in Table 1. Video clips of a variety of incomitant deviations obtained during motility testing are included as an online resource for a recently published book.1 If a marked deviation is present, then this may be revealed by the basic ocular motility test (see Table 1). However, this method relies on an observation of corneal reflexes,
which is an inaccurate method of assessing ocular alignment. The cover test is more accurate and can be carried out during ocular motility testing, as outlined in Table 2. Cover testing in peripheral gaze is an extremely useful test and, like the basic ocular motility test, provides objective data. It requires practice but is well worth the time that it takes to become skilled at this test. A more sensitive way of detecting incomitance is to use the patient’s own visual system to provide
1 A point light source is usually used, although in deviations with a significant accommodative element an accommodative target is better
2 An advantage of using a light is that binocular fixation can be monitored. It is pointless to carry out a cover test if one eye’s view of the target is already obscured by the nose
3 A cover/uncover and alternating cover test is carried out in each cardinal position of gaze. Usually, about four to six covers are required. Either the size of deviation can be estimated or measured with prisms1
Figure 3
The six cardinal positions of gaze, indicating the muscles with the maximum power to maintain the eyes in these directions. Reproducedwithpermissionfrom Chapter17inEvansBJW(2021)Pickwell’sBinocularVision Anomalies(sixthedition).Elsevier,Philadelphia1
4 Care must be taken to ensure that the occluder fully occludes – it will need to be angled as the target is moved into peripheral gaze.
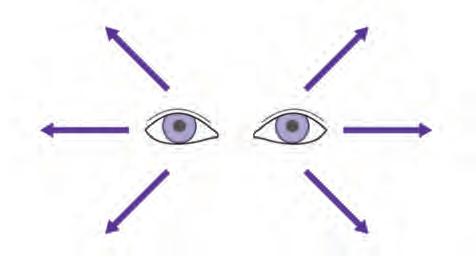
68 www.optometry.co.uk February/March 2023
Table 1 Procedure for carrying out the basic objective ocular motility test
RSR LIO RLR LMR R L RIR LSO RSO LIR RMR LLR RIO LSR OT
Table 2 Procedure for cover testing in peripheral gaze during the ocular motility test
feedback on ocular alignment through determining the subjective angle in different positions of gaze. This is made easier by using red and green goggles and this approach is described in Table 3. Although with some patients this can be extremely informative, with others it can be a source of considerable confusion. Patients can become dissociated as the test progresses, may be confused about diplopia, or may suppress in certain positions of gaze.
Neurogenic incomitancies often develop secondary sequelae, where other muscles become affected over time; this can complicate the appearance on motility testing. Ocular myasthenia gravis, a myogenic form of incomitance, can also have a confusing appearance owing to multiple muscles being affected and the clinical appearance can change over time.
Further diagnostic tools
If incomitance is suspected from ocular motility testing or symptoms, it is useful to carry out additional testing to investigate this further. One approach is to use clinical algorithms. Parks’ three-step method is well-known, but another approach, Lindblom’s method,2 is often easier in practice. These approaches are described in detail elsewhere.1 A permanent record of incomitance, which is ideal for monitoring over time, is to undertake a Hess plot. Thomson described a computerised system in 1990,3 and this software’s latest version (Binocular Vision Analyser) includes a variety of analytical tools.4
MANAGEMENT
In incomitant deviations of all kinds, treatment with spectacles or exercises is not likely to remedy the patient's deviation. Some patients with unchanging longstanding subtle incomitance can maintain binocular single vision in most directions of gaze. If such a case is struggling to maintain binocularity in the primary position, the prism indicated by the Mallett unit may alleviate symptoms.5
The over-riding priority is to recognise those cases which require urgent medical attention. For adults, new
1 For patients who do not experience diplopia, red and green goggles are required. Ideally, a bar light and goggles should be used since this allows torsional deviations to be assessed, but this equipment is no longer generally available
2 Patients who experience diplopia can do the test without red or green goggles. However, goggles still help in these cases to readily identify which image belongs to which eye
3 The patient is asked to indicate the relative positions of the two images in different positions of gaze. In its simplest form, this test consists of just drawing the relative positions of these images in the different boxes for different positions of gaze. This usually allows the position of gaze in which there is maximum diplopia to be clearly identified, which greatly assists in the diagnosis of an underacting muscle
4 Ideally, prisms can be used to bring the two images together and the deviation measured.
or changing incomitance is likely to be associated with symptoms; this is not always the case with children, although parents are likely to have noticed a turning eye or anomalous head position.
The main causes of acquired incomitant deviations are summarised in Table 4. Iatrogenic means secondary to treatment, and eye surgery can lead to incomitancies (for example, from an explant or plomb in retinal detachment surgery), as can some medications (see Table 5).6
Acquired neurogenic palsies can be a sign of lifethreatening pathology or of trauma. Nearly all myogenic palsies are acquired. Mechanical incomitancies can be congenital (eg, Duane syndrome) or acquired (eg, blowout fracture). Any new or changing incomitancy needs to be referred. The speed of onset of the incomitance is a good guide to the urgency of referral. For example, if
BINOCULAR VISION February/March 2023 www.optometry.co.uk 69
Vascular Neurological Other Diabetes Tumour Trauma Vascular hypertension Multiple sclerosis Thyroid eye disease Stroke Migraine Toxic Aneurysm (Myasthenia gravis) Iatrogenic Giant cell arteritis Idiopathic
Table 4 Main causes of acquired incomitant deviations. Myasthenia gravis is strictly speaking not of neurological aetiology, but myogenic ReproducedwithpermissionfromChapter17inEvansBJW(2021)Pickwell’sBinocularVisionAnomalies(sixth edition).Elsevier,Philadelphia1
OT
Table 3 Procedure for assessing the subjective angle of deviation in different positions of gaze
Table
Likelihood of diplopiaDrug
Very common (> one in 10)
Common (between one in 10 and one in 100)
Lacosamide
Zonisamide
Eslicarbazepine
Botulinum toxin
Rufinamide
Pregabalin
Perampanel
Temozolomide
Sildenafil (Viagra)
Gabapentin
Topiramate
Main uses of drug
Epilepsy, diabetic neuropathic pain
Epilepsy, Parkinson's disease
Epilepsy
Hemifacial spasm, cosmesis, EOM palsy
Epilepsy
Epilepsy, neuropathic pain
Epilepsy
Cancer
Erectile dysfunction, pulmonary artery hypertension
Epilepsy, neuropathic pain

Epilepsy, migraine
Uncommon (between one in 100 and one in 1000)
Zaleplon
Levetiracetam
Bortezomib
Amlodipine
Adalimumab
Pravastatin
Lamotrigine
Capecitabine
Insomnia
Epilepsy
Cancer
High blood pressure, coronary artery disease
Arthritis, spondylitis, Crohn's disease
Hypercholesterolaemia
Epilepsy
Cancer
Rare (between one in 1000 and one in 10,000)
Telithromycin
Voriconazole
Dextromethorphan/ Quinidine
Sertraline
Ciprofloxacin
a patient reports sudden onset diplopia for the first time that day and a new incomitant deviation is present, an emergency referral (within 24 hours)7 is required.
Occasionally, a longstanding incomitant deviation can decompensate causing symptoms; this can happen spontaneously or can be triggered by other factors, including poor general health. Decompensation can also occur if the patient is forced to look in the field of action of the affected muscle. For example, if a patient with a superior oblique underaction is forced to look down and in,
Bacterial pneumonia
Fungal infections
PBA (an emotional disturbance)
Depression, anxiety
Bacterial infections
this could cause symptoms; this could occur if a patient is prescribed multifocal spectacles for the first time.1
CONCLUSION
Most cases of incomitant deviations that optometrists encounter are likely to be longstanding and are easily identified as such by taking a history and by the absence of any change in symptoms. New or changing incomitancies should be referred, urgently or as an emergency, if of recent sudden onset. For other cases, the incomitance should be described in the clinical records so any change at subsequent appointments can be detected. 0
Professor Bruce Evans is director of research at the Institute of Optometry, and a visiting professor to City, University of London and London South Bank University. He is a fellow of the College of Optometrists and holds higher qualifications including, a Diploma in Contact Lens Practice and Diploma in Orthoptics. He has authored over 260 publications, has given over 250 invited lectures, and has authored eight editions of textbooks, including the third to sixth editions of Pickwell’sBinocularVisionAnomalies
70 www.optometry.co.uk February/March 2023
5 Drugs associated with diplopia. ReproducedwithpermissionfromChapter17inEvansBJW(2021) Pickwell’sBinocularVisionAnomalies(sixthedition).Elsevier,Philadelphia1 whomodifiedafterAlvesMetal,20156
0 OT
MAKING THE MOST OF A MANAGEMENT PLAN FOR DRY EYE
Megan Zabell BOptom, MClinOptom
IN BRIEF This article will discuss basic concepts that can be applied in order to simplify the process of forming a dry eye management plan.
INTRODUCTION
This feature follows two previous Optometry Today articles: Practical tips for the identification of dry eye; and Practical tips for diagnosing dry eye. It is important to not only ensure a patient meets all of the requirements for a diagnosis of dry eye, but to also confirm the major aetiology of their pathology, or subtype of dry eye, in order to help tailor an individual management plan. The Tear Film and Ocular Surface Society (TFOS) Dry Eye Workshop II (DEWS II) management and therapy report includes a suggested treatment algorithm consisting of four steps that can be worked through systematically or matched to the patient’s dry eye severity1 – there are certain elements of the earlier steps that should always be covered, even if the patient requires treatments suggested in the latter steps. Whether the patient has evaporative (EDE), aqueous deficient (ADDE) or mixed dry eye should also be taken into account.2 In order to remain concise, this article will focus on the first two steps in the TFOS DEWS II staged management algorithm, as these align well with the general scope of practice for optometrists in the UK.
STEP ONE ACCORDING TO TFOS DEWS II Education
Given the complicated nature of dry eye, the various risk factors, and the need for consistent, often longterm treatment to manage signs and symptoms,2 patient education is vital in ensuring compliance, as well as satisfaction with treatment.3
As it is common for patients to expect an immediate improvement in symptoms upon commencement of dry eye treatment, it is important to educate them on the need for longterm treatment, continuing after symptoms have reduced.2,3
Each treatment option recommended for the patient should be carefully explained. A brief description of the various treatments from steps one and two is provided below.
Environmental modification
The environment in which a patient lives and works can have an impact on their dry eye status, with lower humidity environments increasing rates of dry eye and higher humidity environments being considered healthier for dry eye.4,5 Education on avoiding environments that can induce dry eye symptoms is prudent, although it should be acknowledged that it is not always practical for patients to do so.
Using a desktop humidifier has been shown to increase tear breakup time and reduce dry eye symptoms.6 There have also been early indications that other lifestyle adjustments such as increased physical activity and dietary modifications have the potential to form part of a dry eye management programme, although further studies are required in this area.7
Essential fatty acid (EFA) supplementation
Oral essential fatty acid supplementation has been an area of focus for dry eye research for some time, commonly focusing on omega-3 (ω-3) and omega-6 (ω-6) and the effect this has on dry eye signs and symptoms.1 There has been a lot of attention paid to the recent DREAM study, as it was a large-scale, multi-centre, randomised, placebocontrolled study investigating the effects of ω-3 supplementation on dry eye.8 The study found that there was no significant difference between the patients receiving high-dose ω-3 supplementation and the placebo arm of the study. However, a more recent Cochrane review investigating the effects of ω-3 and ω-6 supplementation for dry eye found that long-chain ω-3 fatty acids could have a role in managing dry eye, although further research is needed due to uncertain and inconsistent evidence.9 As the literature tends to be in agreement about the possible role for oral ω-3 supplementation in dry eye, further guidelines need to be developed regarding the composition, dose and treatment duration recommended for such supplements.10
DRUGS, DRY EYE, THERAPEUTICS February/March 2023 www.optometry.co.uk 71
CPD POINT0 OT
Lid hygiene and warm compresses
Lid hygiene is widely prescribed, often as a firstline agent, to manage symptoms of a variety of lid conditions, such as blepharitis, that can cause or contribute to dry eye.1,11 Reducing the bioburden on the eyelid margin can improve the quality of the tear film lipid layer, thus reducing tear film evaporation.11 Using specialised products rather than diluted baby shampoo has been shown to elicit a bigger decrease in inflammatory markers on the ocular surface and they are also better-tolerated.1 Given that using baby shampoo has been associated with a decrease in mucin levels meaning that it may impair goblet cell function, TFOS DEWS II does not recommend its use for the purpose of lid hygiene, especially given the range of currently-available specialised products in the form of wipes, foams, sprays and more.1
Warm compresses are another first-line recommendation to help combat the symptoms of EDE by attempting to melt thickened meibum within the meibomian glands.1,12 There has also been suggestion that warm compresses may have an effect on Demodex infestations, given that Demodex mites have a preference for lower temperatures and may be harmed by temperatures that are considered therapeutic for the meibomian glands.12,13 While homemade warm compresses, generally consisting of a cloth soaked in warm or hot water, are still commonly used, it is unlikely that these are able to produce the level of heat required for the requisite amount of time to have a therapeutic effect on the meibomian glands (TFOS DEWS II recommends heating the palpebral conjunctiva and meibomian glands to ≥40°C; time periods of between two to five minutes have been investigated in various randomised clinical trials).1,14,15 Clinical management guidelines from the College of Optometrists recommend that warm compresses should be applied to the outer lid twice daily for not less than five minutes at 40°C.16
There are a number of devices available in order to perform warm compresses both at home and in a practice setting and these devices are available to suit a range of needs (portable, varying access to electricity, disposable or reusable).

Ocular lubricants
The TFOS DEWS II staged management algorithm recommends using ocular lubricants of various types in step one. Selection of an appropriate lubricant will be discussed later in this article.
STEP TWO ACCORDING TO TFOS DEWS II
Tea tree oil treatment for demodex
TFOS DEWS II recommends the use of tea tree oil in patients with Demodex blepharitis, which is supported by a more recent comprehensive literature review focussing on ocular Demodex 1,17 The active ingredient of tea tree oil that has been identified as most effective in eradicating Demodex is terpinene-4-ol. While tea tree oil has excellent antimicrobial, antifungal and anti-inflammatory properties, it should not be applied to the skin at 100% concentration due to the high likelihood of further skin irritation. Preparations with concentrations ranging from 3% to 50% tea tree oil content have been investigated.17 As tea tree oil can be toxic to the ocular surface, lower concentrations are recommended.16
Tear conservation
Step two includes the use of tear conservation approaches such as punctal occlusion or moisture chamber devices. Of these, punctal plugging is the most widely used method.1 It had been theorised that punctal occlusion may increase the inflammatory factors on the surface of the eye, given the inflammatory component to dry eye; however, this has not been demonstrated in studies with short periods of use.18 Punctal plugs are generally available as either permanent silicone plugs, or dissolvable (also referred to as absorbable) plugs which are often collagen-based.1 Punctal plugs are most commonly used to increase aqueous/ tear volume in ADDE, as their use in EDE is more controversial.1 Moisture chamber spectacles or glasses are another means of tear conservation, aiming to slow evaporation of the tear film by minimising air flow across the surface of the eyes and increasing the humidity at the surface.1 They have been shown to improve ocular comfort and tear film stability and are recommended as a dry eye treatment, which may be particularly useful to those working in adverse environments.19
Overnight treatments
TFOS DEWS II recommends overnight treatments to include moisture chamber goggles, as well as topical treatments like ointments. Higher viscosity lubricant formulations such as ointments are generally recommended as ancillary night-time treatments, or for more severe cases of dry eye,20 as the increased viscosity may cause blurry vision.
72 www.optometry.co.uk February/March 2023
OT
“GIVEN THE COMPLICATED NATURE OF DRY EYE, THE VARIOUS RISK FACTORS, AND THE NEED FOR CONSISTENT, OFTEN LONG-TERM TREATMENT TO MANAGE SIGNS AND SYMPTOMS, PATIENT EDUCATION IS VITAL”
In-practice heating and expression of meibomian glands
In-practice heating and expression of the meibomian glands can either be performed by the optometrist manually expressing the glands after heating, or by using a device that can heat and express the glands.1 Heating the glands would often be done as described in the warm compresses section earlier and is better done with a device designed specifically to warm the eyelids, rather than a facecloth soaked in warm water.1
The expression of the meibomian glands described for in-practice procedures is quite often called ‘forceful expression’, to differentiate from the diagnostic expression used to assess the quality and the ability to express ability a patient’s meibum. Repeated sessions of eyelid warming and forceful expression have been shown to increase the number of expressible glands, improve the quality of meibum excreted, and increase tear film lipid layer
thickness, to help reduce symptoms of dry eye.21 Another technique that can be performed prior to meibomian gland expression is lid debridement scaling, to remove the build-up of keratinised material that can occur with obstructive meibomian gland dysfunction (MGD). Lid debridement has been shown to improve meibomian gland function and decrease ocular staining and dry eye symptoms.22,23
In-practice intense pulsed light (IPL) therapy
IPL therapy was initially developed for the field of dermatology, using light of targeted wavelengths anywhere from 500nm to 1200nm to target various skin conditions.1 In 2002, it was discovered that patients undergoing facial IPL to address dermatological conditions such as acne and rosacea also had an improvement in their dry eye symptoms and the method of using IPL to treat dry eye (or more specifically MGD) was investigated.24
DRUGS, DRY EYE, THERAPEUTICS February/March 2023 www.optometry.co.uk 73
Getty/fizkesOT
While there are currently many ongoing investigations into the efficacy and long-term safety of IPL,25 the current literature suggests multiple mechanisms of action. When treating MGD, IPL is thought to remove superficial blood vessels from the eyelids to help reduce inflammation of the lid margins and eradicate Demodex to decrease the bioburden on lid tissues.26 It can also help to dissolve meibum and regulate the flow by heating the glands (making it a suitable treatment to use before forceful expression of the meibomian glands).26
Prescription drugs
For specialty optometrists with suitable experience, there are various prescription drugs recommended by TFOS DEWS II that may help to manage dry eye. Some of the more commonly used therapeutic agents are described below:
• Topical antibiotics: while practitioners are encouraged to avoid long-term use of topical antibiotics as a strategy for managing bacterial overload of the lids, it may be useful to employ a short course of antibiotic ointments or creams such as fusidic acid or ofloxacin in a case of blepharitis or obstructive MGD1
• Oral ivermectin: while current world events have rendered the anti-parasitic medicine ivermectin a controversial topic, its use has been shown to be an effective strategy to reduce Demodex on the lashes. It also has the benefit of being a single-dose treatment that is generally well-tolerated1
• Topical steroids have been shown to be effective in helping to break the inflammatory cycle of dry eye; however, serious ocular side effects such as raised intraocular pressure and cataract formation have been attributed to their long-term use. For this reason, patients should be considered for what is termed pulse-dose therapy, where the risk of these potential harmful side effects is minimised1
• Cyclosporine is an immune-modulating drug that is effective in relieving the signs and symptoms of certain types of dry eye with long-term use. The active ingredient has poor water solubility, although there are various drug delivery systems formulated in an effort to overcome this.1
• Oral antibiotics:
• Oral tetracyclines, a class of antibiotic drug, show anti-inflammatory properties and it is this combined antibiotic and anti-inflammatory
action that may be useful in the treatment of dry eye and associated ocular conditions such as MGD and blepharitis. In order to avoid contributing to the growing problem of antibiotic resistance, it has been shown that very low dose doxycycline (40mg/day) can treat rosacea without causing resistance. Further studies are needed to investigate the long-term side effects of oral tetracycline use, and its shortterm side effects are well documented, including gastrointestinal upset and photosensitivity1 • Oral macrolides, such as azithromycin, may decrease the clinical signs and symptoms of dry eye disease, possibly in combination with topical steroid therapy, although further studies are needed in this area.1
RECOMMENDATION OF LUBRICATING DROPS Drop ingredients
Although considered a mainstay of dry eye treatment, there is often confusion faced by both the patient and practitioner regarding the appropriate lubricating drops for various types of dry eye. Despite the biological plausibility, or common-sense view that a patient suffering from EDE requires a lubricating drop containing oils to support the tear film lipid layer, while a patient suffering from ADDE requires a drop with aqueous properties to support the tear film’s muco-aqueous phase, there had until recently been a gap in the literature comparing the efficacies of lipid and non-lipid lubricant drop formulations for different subtypes of dry eye.2 A six-month randomised controlled trial conducted by Craig et al in Australia, Canada, New Zealand and the UK, the results of which were published early in 2021, looked to provide data that clinicians could use to guide their selection of a lubricating drop based upon the presenting dry eye subtype classification and severity.2
The study used two lubricating drops with hydroxypropyl guar as a gelling agent in both types, but only one contained the addition of a lipid nanoemulsion. Participants in the study all had dry eye as classified by the TFOS DEWS II criteria and were randomised to being treated either with the lipid-containing or aqueous drop, regardless of dry eye subtype. Both lubricating drops investigated provided the dry eye patients with symptomatic relief and improvement of most signs; however, only the lipid-containing drop resulted in a significant
74 www.optometry.co.uk February/March 2023
OT
“IT IS IMPORTANT TO CONSIDER ALL OF THE WORK THAT HAS BEEN DONE IN CONFIRMING THE DRY EYE”
improvement to the tear film lipid layer grading, and these improvements were most significant for patients receiving the lipid-based drop that were suffering from EDE or a lipid deficiency.2 Therefore, the investigators concluded that patients suffering from EDE should be preferentially recommended a lipid-containing lubricating drop, which is in agreement with step one of the TFOS DEWS II staged management algorithm.1,2
Frequency and duration of drop use
As discussed earlier, it is important to set realistic expectations with dry eye patients, so they understand the likely duration of treatment required to improve their condition.
The Craig et al study demonstrated that for patients with mild to moderate dry eye, symptoms were improved (and that improvement sustained) after approximately one month of continuous lubricant eye drop use. However, the ocular signs of dry eye took several months of regular lubricating drop use to improve or resolve; this highlights the importance of encouraging regular drop use in dry eye patients, even after they feel that their symptoms have begun to resolve, to lead to the positive structural tear film changes. The frequency of dosage in this study was four times per day, although the severity of dry eye investigated were only mild-moderate cases.2
Preservatives
The TFOS DEWS II staged management algorithm recommends using non-preserved tear supplements from step two onwards, whereas in step one it is more important to focus on the inclusion of a lipid tear supplement in the case of EDE.1 While some practitioners prefer to forego preservatives entirely as a conservative approach, lubricating drops containing alternatives to benzalkonium chloride (BAK) offer a safe, cost-effective and well-tolerated option for many patients with mildmoderate dry eye disease.27 There is no official cut-
off regarding the frequency or duration of dosage which is considered unsafe to use a preserved eye drop for, although in the Craig et al study the patients were using various eye drops preserved with polyquaternium-1 four times per day for six months and the drops were well-tolerated by all participants.2
CONCLUSION
In forming a management plan for a dry eye patient, it is important to consider all of the work that has been done in confirming the dry eye and classifying the subtype and severity. TFOS DEWS II provides a fantastic staged management algorithm that can be worked through systematically to help guide treatment recommendations. Patient education is of vital importance to ensure compliance with treatment and satisfaction with their practitioner. While there is a myriad of proven adjunct therapies that can be used depending on the characteristics of the dry eye presented, one of the mainstays of dry eye treatment is still the use of lubricating eye drops. If used for a sufficient frequency and duration, eye drops can help to improve patient symptoms as well as the overall structure of the tear film. Lipid-containing supplements should be used if a patient has an evaporative component to their dry eye in order to improve the tear film lipid layer, although this change will most likely become more apparent with long-term use of the drops.
0
Megan Zabell graduated as a therapeutically endorsed optometrist from the University of Melbourne before beginning work in a private optometry practice alongside teaching pre-clinical optometry skills at her alma mater. Zabell joined Alcon’s professional affairs team in 2018 and recently completed her master’s degree in clinical optometry, again at the University of Melbourne.

DRUGS, DRY EYE, THERAPEUTICS February/March 2023 www.optometry.co.uk 75
-
0 OT -y.co.uk
CLINICAL FEATURES OF OPTIC NEURITIS
IN BRIEF This article outlines the characteristic signs and symptoms of optic neuritis to help guide differential diagnosis in practice.
INTRODUCTION
Optic neuritis is an acute, painful, symptomatic, inflammatory disorder of the optic nerve that may be idiopathic and localised to the optic nerve or associated with other systemic illnesses.
INCIDENCE AND RISK FACTORS
The incidence of optic neuritis in the UK, taken from a study of 11m NHS patient records, is 3.74 per 100,000,1 which is similar to cases cited in central Europe at five cases per 100,000.2 Mean onset is typically in the mid-thirties and is rare in those aged under 18 or over 50 years.3 More than 70% of cases are women,4 while Caucasian females are eight times more likely to be affected than Black females.5
CLASSIFICATION
Historically, cases of optic neuritis were classified as ‘multiple sclerosis (MS)’ or ‘non-MS.’ More recently, the approach has been extended to recognise specific conditions such as neuromyelitis optica (NMO), also known as Devic’s disease, along with myelin oligodendrocyte glycoprotein-associated disease (MOGAD) and other immune-mediated inflammatory disorders (IMIDs) which will be addressed later in the article.
Optic neuritis can also be classified by presentation:
• Typical or acute: accounts for 75% of cases and are usually retrobulbar in nature. Cases are usually idiopathic, self-resolving and may present as an isolated event or recurring episodes
• Atypical: accounts for 25% of cases and is characterised by neuroretinitis or papillitis.
CAUSES
Causes of optic neuritis can be categorised as demyelinating, inflammatory or infective. Demyelinating causes include MS and NMO. MS-related optic neuritis is thought to be immune-mediated, with systemic T-cells crossing the blood brain barrier leading to the release of cytokines and other inflammatory markers. This
CPD POINT
inflammatory response causes swelling of the myelinated nerve fibre sheath with a resultant breakdown and axonal loss. An initial swelling of nerve tissue, followed by myelin sheath breakdown, and a destruction of nerve fibres, results in the slowing of nerve conduction. Inflammatory causes include catscratch fever, syphilis, sinusitis, tuberculosis, sarcoidosis and Lyme disease. Infective cases of optic neuritis can arise from childhood infections such as chickenpox, rubella, mumps and measles.
SIGNS AND SYMPTOMS
Clinical diagnosis occurs in the consultation room. The classic presentation of optic neuritis includes loss of vision, peri-orbital eye pain, which often worsens on lateral eye movement, and optic nerve dysfunction. The patient can often specify a definite period of onset, whereas patients with papilloedema are unlikely to be able to do so. The vision loss usually worsens over several days to two weeks. It is rare that the patient would have maximum vision loss at onset, which would be more suggestive of an ischaemic event.
Monocular visual acuity (VA) is usually impaired, the extent of which can vary in each case. Patients often describe a blurry, loss of vision of fairly sudden onset. It may be acute, or subacute that has been progressively worsening since onset. They may confirm the presence of either Pulfrich or Uhthoff phenomenon when questioned. Pulfrich phenomenon is where an object swinging back and forth in the plane of vision is perceived as moving in a circle or tracing an elliptical pathway; this is due to a conduction delay in one optic nerve causing a slowing in neuronal transmission compared with the other optic nerve. Uhthoff phenomenon is where there is a worsening of visual symptoms with an increase in body temperature, such as running, or taking a hot shower or bath.
Peri-orbital pain is a common presentation and is usually worsened by lateral eye movements. In the optic neuritis treatment trial (ONTT), 92% of cases had pain on eye movement.6 The pain can precede or occur at the same time as the onset of blurred vision and is thought to be
76 www.optometry.co.uk February/March 2023
Lorcan Butler BSc (Hons), MCOptom, FBDO, Prof Cert Paed Eye Care
0 OT
due to the close proximity of the recti muscle insertions to the optic nerve sheath at the orbital apex. Contraction of these muscles pulls on the inflamed optic nerve resulting in pain.
Optic nerve dysfunction often results in colour vision impairment, which characteristically results in red desaturation and is disproportionate to VA, that is to say, colour vision may be profoundly affected whereas VA might remain relatively intact. Almost 90% of cases in the ONTT had an abnormal Ishihara test result.6 Contrast sensitivity can also be impaired which can affect driving, particularly in low contrast conditions. An ipsilateral relative afferent pupillary defect (RAPD) might be observed.
Visual field testing can reveal a variety of defects. In one large-scale study of 448 patients with acute optic neuritis, 48.2% of affected eyes had diffuse visual field loss, 20.1% had altitudinal or other nerve-fibre bundle defects and 8.3% had central or centrocaecal scotomas.7 In the ONTT, 56% of defects resolved by one year and 73% by 10 years.6
Differential diagnosis of optic neuritis type is detailed in Table 1. In cases of retrobulbar optic neuritis, the optic disc appears quite normal giving rise to the well-known statement: ‘The doctor sees nothing, and the patient sees nothing’.8 Since there are no ophthalmoscopic signs of note, initial diagnosis relies upon a good history from the patient, taking into account predispositions such as gender and age. MS is the most common association with retrobulbar optic neuritis in adults.
Cases of papillitis are associated with disc swelling and peripapillary flame-shaped haemorrhages.9 The optic nerve will be swollen in a third of cases.10 Neuroretinitis
is a term reserved for cases where inflammation spreads from the optic nerve to the retina and can result in a stellate macular star-like presentation of hard exudates. Retinal thickening and associated subretinal fluid may also be observed. As the macular star takes one to two weeks to manifest, only optic disc inflammation may be evident in its early presentation in association with visual symptoms. There are usually no disc haemorrhages. Differential diagnosis of other ocular conditions that can result in a macular star should include malignant hypertension and papilloedema; however, unlike the latter, neuroretinitis is usually monocular.
Optical coherence tomography (OCT) is becoming more standard in mainstream clinical practice to aid diagnosis and management. OCT is not very helpful in diagnosing acute optic neuritis; however, it is quite sensitive in detecting prior optic neuritis by observing changes to the retinal nerve fibre layer (RNFL) and the macular ganglion cell-inner plexiform layer.
Initial thickening of the optic nerve head occurs during the acute phase, followed by a thinning of the RNFL in its later stages. In one study, 74% of patients with acute optic neuritis demonstrated RNFL thinning within three months on OCT.11 In most patients, the RNFL thinning occurs by three to six months with stabilisation at around seven to 12 months. Interestingly, the unaffected eye can also show subclinical RNFL loss in OCT imaging.12 One study showed that RNFL thickness was reduced on average by 7.08μm in the unaffected eye of MS patients in comparison to 20.38μm in the eye affected by optic neuritis.13 As the total RNFL thickness is only ~100μm, to lose 20μm after one event is significant. RNFL changes
DIAGNOSTICS, OCT, PATHOLOGY February/March 2023 www.optometry.co.uk 77
Retrobulbar Papillitis Neuroretinitis Percentage of cases ~ 66% ~ 33% ~ 1% Disc swelling No Yes Yes Disc appearance Normal Swollen/hyperaemicSwollen Fundus features Majority – nonePeripapillary haemorrhages No haemorrhages Macular oedema
wool spots
star MRI characteristics HyperintensityNil Hyperintensity Aetiology MS Sinusitis (ethmoidal) Viral Syphilis Graves’ disease Tumour Lyme disease Cat-scratch fever
Cotton
Macular
OT
Table 1 Differential diagnosis of optic neuritis by type
can even occur in MS patients who have not had an episode of optic neuritis with an average decrease of 2μm per year which is 10 times more than those without MS.14 Macular ganglion cell-inner plexiform changes are seen as a more sensitive finding as it is not affected by the initial thickening and thinning that occurs in the RNFL. It is greatest during the first month, with the bulk of thinning occurring within three months following onset.15 Also, inter-eye differences in thickness have demonstrated higher sensitivity and specificity than inter-eye RNFL changes in detecting previous episodes of optic neuritis. An inter-eye difference in the macular ganglion cell-inner plexiform layer required to detect a previous unilateral subclinical episode of optic neuritis is 4μm.15
Although no further investigations are necessary for confirming the diagnosis, neuroimaging is needed to assess the risk of developing MS and to rule out any other disorders.
Optic neuritis can masquerade as other conditions, such as anterior ischaemic optic neuropathy (AION) and papilloedema, due to variable presentation, and
in particular, the range of vision loss that can occur. The characteristic features of optic neuritis, AION and papilloedema are detailed in Table 2. Other aspects of the clinical presentation that could point away from optic neuritis are male gender, age >50 years, bilateral presentation, and vision loss unaccompanied by eye pain.
OPTIC NEURITIS AND MULTIPLE
Optic neuritis is the presenting feature in 15-20% of MS cases and afflicts around half of these patients at some point during the course of the condition.16,17 With this in mind, optic neuritis can be the very first primary symptom in MS or an associated finding further along the disease course.
The risk of MS developing, after 15 years since optic neuritis, is 25% if there are no white matter lesions on magnetic resonance imaging (MRI) and 72% risk if there are white matter lesions on MRI at the time of initial presentation.17
date
a diagnosis
78 www.optometry.co.uk February/March 2023
SCLEROSIS
MRI can be used to stratify the risk of developing MS at
and
can
when Optic neuritis AION Papilloedema Age 20 to 45 years >50 years <35 years Gender Female > male Evidence is equivocal Female > male Eye pain on movement 92% of cases Uncommon Uncommon RAPD Present Present Present at late stage Onset Hours to days Subacute Sudden onset Associated with awakening Gradual Laterality 90% unilateral Unilateral Bilateral Disc swelling One third of patients Common Sectoral Bilateral Haemorrhage Retrobulbar – absent Papillitis – can be present Peripapillary On and off disc Visual field defect Variable Altitudinal Inferior nasal Enlarged blind spot Inferior Visual prognosis Most recover well within one month with continued slower recovery over one year Variable but often poor prognosis Variable
OT
some later
be made
Table
2 Differential diagnosis of optic neuritis, AION and papilloedema
the MRI in a patient with optic neuritis reveals two or more typical lesions of MS, where at least one of which is contrast enhancing. Optic neuritis with two or more noncontrast enhancing lesions typical of MS on MRI is called a ‘clinically isolated syndrome’ and is associated with a high risk of MS.
Uhthoff phenomenon tends to occur when the optic neuritis is receding, or when it takes a chronic course.18 While this phenomenon is MS-specific, it only arises in 50% of patients.19 Gender-related incidence of MS mirrors that of optic neuritis, that is to say, it is about three times more likely to occur in females.20
MANAGEMENT
The multicentre ONTT (1991 to 1998) was designed to evaluate the efficacy and safety of oral prednisolone versus intravenous methylprednisolone in comparison to a placebo. Prior to this trial, the management of optic neuritis in the US was typically oral prednisolone. The longitudinal data from the ONTT were a gamechanger in terms of guiding on best practice management for optic neuritis.21 However, this study is now over 30 years old and new approaches continue to evolve.22 A summary of the key outcomes from the ONTT are detailed as follows:
• Participants treated with the intravenous regimen recovered vision faster than the other two groups
• Treatment with oral steroids was associated with an approximately two-fold higher rate of recurrent optic neuritis during six to 24 months of follow-up (27%) than either the intravenous group (13%) or the placebo group (15%)
• The expected course, regardless of whether the patient is treated or untreated, is initial recovery within the first two weeks, with most recovery occurring within one month and further slow recovery over one year
• Intravenous steroids hasten recovery by approximately two weeks on average, but do not affect the overall visual outcome
• Steroids do not affect the long-term risk of MS development.
Visual prognosis is generally good with 69% of patients achieving a VA of 6/6 or better, while 92% recover to 6/12 or better. Nevertheless, 3% will be left with a profound impairment of 6/60 or worse. In addition to the visual recovery in the short-term, pain on eye movements tends to resolve within two weeks. Although optic neuritis resolves well either with or without treatment, it can
DIAGNOSTICS, OCT, PATHOLOGY February/March 2023 www.optometry.co.uk 79
“THE LONGITUDINAL DATA FROM THE ONTT WERE A GAMECHANGER IN TERMS OF GUIDING ON BEST PRACTICE MANAGEMENT FOR OPTIC NEURITIS”
Optic neuritisNMO Gender Female > maleFemale > male Ethnicity Caucasian > BlackBlack, Asian > Caucasian RAPD Present Maybe not Laterality 90% unilateralBilateral Dyschromatopsia Present Present Systemic features Weakness, shooting pains and burning sensation in arms and legs Blood test diagnosis No Yes, in 70% of cases MRI lesions Brain Spinal Residual vision 6/60 or worse 3% of cases 33% of cases
OT
Table 3 Key features of optic neuritis and NMO
cause visual disturbance and reduce the patient’s quality of life.23 Even though the patients VA may return to 6/6 in the affected eye, it is quite common to hear statements like ‘It’s not the same as it was before.’, or ‘I still feel it’s not right.’ Indeed, 50% of sufferers report problems such as poor vision when they are tired, difficulties with night vision, problems in bright sunlight, issues with colour perception, or finding it hard to focus on moving objects.6 Contrast sensitivity is likely to be impaired in a significant proportion of optic neuritis patients.24 In addition, 33% of cases have persistent deficits in low contrast visual settings even after 10 years, which correlates with poor night-time driving and poor vision in dim lighting conditions.25 It has been suggested that assessing vision at low contrast testing is a more sensitive indicator of impairment than at high contrast in patients with MS.26 Low contrast VA measures can also better detect asymptomatic or subclinical optic neuritis.26
ATYPICAL OPTIC NEURITIS
NMO/Devic’s disease
NMO is a condition with the potential for vision- and life-threatening consequences. It accounts for ~1-3% of optic neuritis cases.27 Patients with NMO can be affected by immunologically mediated vasculitis, which can result in central retinal artery occlusion and AION; therefore, ophthalmologists need to rule out NMO as being a cause in each case of optic neuritis to avoid irreversible sight loss. Females are affected more commonly than males and the average age of onset is 40 years. Incidence is around two to three times higher in those of Black or Asian ethnicity. Relapse rates during and directly after pregnancy are high. Within five years of NMO onset, more than 50% of patients are blind in one or both eyes; 60% of patients are legally blind after 15 years.27 Table 3 details the distinguishing features of optic neuritis to help aid differential diagnosis.
MOGAD
Myelin oligodendrocyte glycoprotein (MOG) is a transmembrane protein found on the surface of oligodendrocytes and myelin sheaths in the central nervous system. While its function is not fully understood, MOG is a target of the immune system in this disease. MOG antibodies found in the blood allow for diagnosis of the condition. In some cases, the MOG antibodies persist and relapses may occur. When a relapse occurs, the diagnosis of MOGAD is confirmed. Those with MOGAD may have previously been misdiagnosed with NMO, optic neuritis or MS. MOGAD-related optic neuritis has severe vision loss like NMO at onset but recovers much better. Optic neuritis is bilateral in 50% of presentations and recurs in half of cases. Disc oedema is present in 80% of patients.28
Non-MS IMIDs
Although each subtype on its own is rare, together, IMIDs outnumber MS-associated optic neuritis and typically require urgent management to preserve sight.1 Around 4m people in the UK are living with an autoimmune condition.29 Examples include sarcoidosis, psoriasis, Crohn’s disease, Sjögren’s syndrome, Behçet's disease, giant cell arteritis, polymyalgia rheumatica and Epstein Barr virus.
CONCLUSION
The landscape of optic neuritis will continue to evolve with the discovery of new antibodies and an everchanging spectrum of separate entities of optic neuritis that practitioners should be aware of. If left untreated, or poorly managed, atypical optic neuritis can lead to devastating visual outcomes. Although optic neuritis has been habitually associated with MS, practitioners should be mindful of other associations.
Lorcan Butler is the optical engagement manager for The Brain Tumour Charity and a qualified dispensing optician and optometrist. Butler has a keen passion for educating practitioners on the ocular manifestations of brain tumours and has delivered CPD on a range of topics including papilloedema and clinical decision making.

80 www.optometry.co.uk February/March 2023
0 0 OT
“THE LANDSCAPE OF OPTIC NEURITIS WILL CONTINUE TO EVOLVE WITH THE DISCOVERY OF NEW ANTIBODIES AND AN EVER-CHANGING SPECTRUM OF SEPARATE ENTITIES OF OPTIC NEURITIS”
PROGRESSIVE ADDITION LENSES: ARE YOUR STANDARDS UP TO STANDARD?
Jim Cox FBDO
IN BRIEF This article provides an overview of the standards that relate to progressive (and degressive) addition spectacle lenses.
INTRODUCTION
This feature follows two previous OptometryToday articles: Singlevisionlenses:areyourstandardsup to standard? and Bifocallenses:areyourstandards uptostandard? which looked at how to apply the BS EN ISO standards1 when checking edged and mounted single vision and bifocal lenses. In both of these, the relevant standard to refer to is BS EN ISO 21987:2017. Progressive (and degressive) addition lenses require reference to both BS EN ISO 21987:2017 and BS EN ISO 8980.2:2017 when verifying these types of optical appliances. While practitioners will be familiar with the terms progressive and degressive lenses, these lens types are referred to as powervariationlenses in the standards so the latter terminology will be used throughout this article.
LENS MARKINGS
Unlike single vision and bifocal lenses, power variation lenses do not have distinct and obvious optical centres to measure at. Due to the nature of the way the power variation occurs on the lens surface, the position of the measurement points varies by manufacturer. To allow practitioners to measure and validate a lens, there is an agreed standard for the layout of a power variation lens; this is set out in BS EN ISO 8980.2:2017 and comprises a series of permanent and non-permanent markings to guide the approach for verification (see Figure 1).
Permanent markings
The standard states that the following permanent markings should be present on a power variation lens:
1 An alignment reference comprised of two marks located 34mm apart, equidistant from a vertical
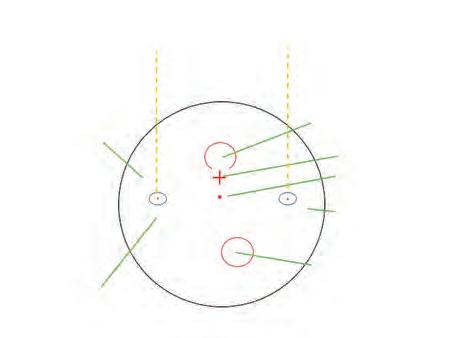
plane through the fitting point or prism reference point
2 For power variation lenses with two reference points, a mark indicating, in dioptres, the variation in power, that is to say, the addition or degression. If a power variation has only one reference point, they may be exempt from this requirement unless the lens is available with more than one variation power
3 An indication of the manufacturer or supplier or tradename or trademark.
Practitioners will be familiar with the experience of trying to find some of these markings on a lens and the difficulties that can arise.
Non-permanent markings
In addition to engraved, permanent markings, a lens should arrive from the lab with the following:
February/March 2023 www.optometry.co.uk 81
DISPENSING
CPD POINT
Manufacturer Alignment marks Distance reference circle Fitting point Prism reference point Design indicator Near reference circle Power variation MyLensCo 125 MyDesign0 6 OT
Figure 1 The layout of a power variation lens. Permanent markings are shown in blue while non-permanent markings are shown in red
1 The alignment reference marking. These should be ink or wax markings that are coincident with the permanent alignment reference marks. Always check this is the case
2 The indicator of the primary reference point - the distance reference circle
3 The indicator of the secondary reference pointthe near reference circle
4 The indicator of the fitting point - the fitting cross; this is what should be lined up with the pupil centre, not the distance reference circle
5 The indicator of the prism reference point; this is typically a single point mark, usually placed below the fitting cross midway between the two alignment markings and is the position that should be used when measuring any prism in a power variation lens.
VERIFICATION PROCESS
With knowledge of the principal points on the lens as outlined in Figure 1, practitioners should be able to ensure that the appliance received is within tolerance when compared to the order.
A useful starting point during the verification process is to check that the non-permanent alignment markings are coincident with the permanent markings; these are often applied in the lab by a machine that rotates and positions the lens, before a rubber stamp applies the ink. In cases where there is misalignment, the lens should be remarked using the manufacturer’s template to ensure all principal points are marked in the correct place prior to verification.
Once the position of the alignment markings has been confirmed, it is important to check they are in line horizontally. The alignment markings on a lens should deviate by no more than 2° from the horizontal. Figure 2 shows a method for checking the alignment of the permanent marking. Using a straight edge, such as a frame ruler, line up the lowest tangent of the lens, then using a line further up the ruler check that the markings on each lens are aligned. Note, each lens in a pair can have its
markings in a different vertical plane, for instance, in cases where unequal fitting heights are required. In the example shown in Figure 2, the left lens horizontal alignment is slightly off. Of course, it may be possible to rotate the lens in the frame and align the markings but this may impact the cylinder axis and base direction of any prism. This is why the author recommends ensuring that alignment is correct before attempting to measure the prescription elements.
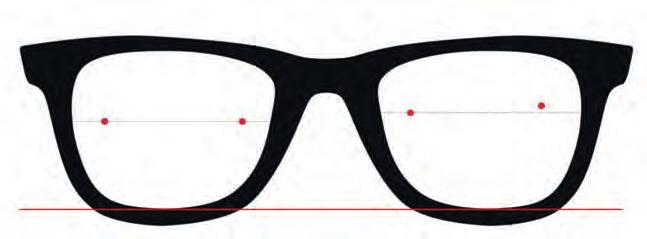
Distance power
The distance power of the lens should be measured on the back surface, that is to say, the back vertex power, as with any other lens type. The back surface of the lens should be placed on the focimeter or lensmeter with the aperture of the stop positioned centrally in the distance reference circle. The power measurement should then be read directly and the measured powers compared to the expected values. It is worth reinforcing at this point that if a bespoke or compensated lens design has been ordered then the expected powers will not be the same as those on the original order. When a compensated lens has been ordered, the lens manufacturer will provide the powers to be expected at the major reference points, which have taken into account parameters provided alongside the prescription such as wrap, pantoscopic tilt and vertex distance.
Table 1 shows the tolerances and power bands for power variation lenses. Practitioners will note that these have wider tolerances than the same powered lenses made in single vision or multifocal forms. This wider banding reflects the greater complexity of manufacturing power variation lenses.
Consider the following example prescription and the optical appliance received:
Ordered prescription
R +6.00/-0.75 x 36 Add 2.50
L +6.00/-1.50 x 45 Add 2.50
Measured prescription
R +6.12/-0.76 x 34 Add 2.61
L +6.06/-1.69 x 42 Add 2.63
82 www.optometry.co.uk February/March 2023
OT
Figure 2 Checking alignment of the permanent markings using a straight edge. Note the slight misalignment of the left lens
As with single vision and multifocal lenses, the validation process requires a three-point check to include measures of powers in both principal meridians and to determine the absolute cylinder power.
The first step should be to identify the principal meridians in each lens, which in this example are:
R +6.00, +5.25
L +6.00, +4.50
The tolerance for each principal meridian given in Table 1 for these principal powers is ±0.12D. For the measured prescription, the principal powers are:
R +6.12, +5.36
L +6.06, +4.37
This gives a difference from the ordered specification of:
R 0.12, 0.11
L 0.06, 0.13
In this example, three of four principal powers have a difference of less than 0.12D and pass the standard. The second principal power in the left lens is measuring at 4.37D against an expected value of 4.50 and so this gives a difference of 0.13D against a tolerance of 0.12 and, therefore, fails the standard.
Now consider the same example but for a compensated lens where the compensated powers provided by the lab are:
R +6.06/-0.79 x 33 Add 2.52
L +6.12/ -1.74 x 40 Add 2.49
Compensated principal meridian powers
R +6.06, +5.27
L +6.12,
Measured
DISPENSING February/March 2023 www.optometry.co.uk 83
+4.38
R +6.12, +5.36 L +6.06, +4.37 Power of principal meridians with higher absolute back vertex power (D) Tolerance on the back vertex power of each principal meridian (D) Tolerance on the absolute cylinder power (D) ≥0.00 and ≤0.75 >0.75 and ≤4.00 >4.00 and ≤6.00 >6.00 ≥0.00 and ≤6.00±0.12 ±0.12 ±0.18 ±0.18 ±0.25 >6.00 and ≤9.00±0.18 ±0.18 ±0.18 ±0.18 ±0.25 >9.00 and ≤12.00±0.18 ±0.18 ±0.18 ±0.25 ±0.25 >12.00 and ≤20.00±0.25 ±0.18 ±0.25 ±0.25 ±0.25 >20.00 ±0.37 ±0.25 ±0.25 ±0.37 ±0.37
principal meridian powers
Absolute cylindrical power (D) <0.12 ≥0.12 and ≤0.25 >0.25 and ≤0.50 >0.50 and ≤0.75 >0.75 and ≤1.50 >1.50 and ≤2.50 >2.50 Tolerance on the direction of the cylinder axis (°) No requirement ±16±9±6±4 ±3 ±2
Table 1 Tolerance of principal powers for power variation lenses
OT
Table 2 Tolerance of cylinder axis for power variation lenses
When checking against the compensated powers, all four meridians are within tolerance. It is also important to note that as the highest meridian power in each lens is now >6.00D, the tolerance is ±0.18D.
The validity of the cylinder powers now needs to be considered. From the difference between the principal powers for each lens, the absolute cylinder powers are:
R 6.12 – 5.36 = 0.76
L 6.06 – 4.37 = 1.69
The tolerance for both lenses is ±0.18D and both lenses clearly fall within this range.
Axis tolerance
The next step in the verification process is to check the axes against the tolerances in Table 2. Recall that the expected compensated axes in this example are R 33 L 40, against measured values of R34 L 42. As tolerances are 4° and 3° for the right and left lenses, respectively, the appliance passes this aspect of the standard.
Addition powers
For power variation lenses, the position of the near zone is clearly marked on the lens as shown in Figure 1, which is where the Add should be measured. As with multifocal lenses, the power should be measured on the surface on which the Add is located. For most lenses this will be the
back surface unless specified otherwise by the manufacturer.
The other important point to consider with modern power variation lenses is that the cylinder power and axis may differ at the near point from that found at the distance reference point and this is especially true of compensated lenses. The manufacturer will provide the expected Add power but when trying to confirm this without the original paperwork the practitioner should subtract the distance mean spherical equivalent from the near mean spherical equivalent.
In this case example, Add powers of 2.52D and 2.49D were expected and measures of 2.61D and 2.58D were found for the right and left lenses, respectively. Referring to tolerances in Table 3 shows that both lenses pass this aspect of the standards.
Prism and the prism reference point
(PRP)
For prism imbalance and power variation lenses BS EN ISO 21987:2017 directs the user to BS EN ISO 8980.2:2017. There is an issue with this, as this standard deals with individual lenses and individual prism values, not imbalance between lenses. With this in mind, practitioners should follow the process as set out in BS EN ISO 8980.1:2017 but use a common-sense approach to any resultant imbalance between the two lenses as follows. Practitioners can apply the tolerances for single vision lenses here which are detailed in
S – the highest principal meridian of the lens
Note: as stated, S is taken as the highest principal meridian in the pair
84 www.optometry.co.uk February/March 2023
Value of the addition power (D) ≤4.00 >4.00 Tolerance ±0.12 ±0.18
Highest ordered prism component Horizontal component Vertical component ≥0.00 and ≤2.00 ± [0.25 +(0.1 x S)]± [0.25 +(0.05 x S)] >2.00 and ≤10.00 ± [0.37 +(0.1 x S)]± [0.37 +(0.05 x S)] >10.00 ± [0.50 +(0.1 x S)]± [0.50 +(0.05x S)]
Table 3 Tolerances
for
the addition power
OT
Table 4 Tolerance of prism power for power variation lenses
a previous OptometryToday article: Singlevision lenses:areyourstandardsuptostandard? In short, it is reasonable to work on the basis that if an identically powered single vision lens is out of tolerance then so should a power variation lens be.
With power variation lenses, the prism should be checked at the PRP as shown in Figure 1. Due to the design of these lenses, practitioners should not expect to see the value of the ordered prism at the PRP; instead, the manufacturer will state the amount of prism that should be seen at this point.
Taking into account the design of power variation lenses, there are three important prism values to consider:
• Ordered prism – the amount of prism ordered by the practitioner
• Thinning prism – the amount of prism added to a lens to improve cosmesis
• Designed prism – the amount of prism that should be seen at the PRP, which is approximately equal to the combination of the ordered and thinning prisms.
Take the following example:
A prescription specifies prism of R 1.0Δ base in L 1.5Δ base in and the manufacturer then adds 1.5Δ base down in both eyes. The values provided by the manufacturer for these prisms are R 1.8Δ @304 and L 2.23Δ @315, which should be used for verification at the PRP. Unless the manufacturer states the resolved values, then these will need to be calculated; this can be done quickly using an online tool.2 In this example, the resolved values are R 1.01Δ in and 1.49Δ down L 1.58Δ in and 1.58Δ down.
Measuring the spectacles with the PRP over the lensmeter aperture, the values found are:
R 2.0Δ @300
L 2.1Δ @220
To determine if this meets the standards, the values need to be resolved into the component parts, which are as follows:
R 1.0Δ base in and 1.70Δ base down
L 1.6Δ base in and 1.34Δ base down
Table 4 sets out the tolerance for vertical and horizontal prism for each lens. If we take the

compensated sphero-cylindrical powers given in the earlier example, and note that the higher total prism component both horizontally and vertically is less than 2Δ, the tolerance values should be calculated as follows, where S is taken as the highest principal power:
Right lens
Horizontally
± [0.25 + (0.1 * S)]
± [0.25 + (0.1 * 6.06)] = 0.86Δ
Vertically
± [0.25 + (0.05 * S)]
± [0.25 + (0.05 * 6.06)] = 0.55Δ
Left lens
Horizontally ± [0.25 + (0.1 * S)]
± [0.25 + (0.1 * 6.12)] = 0.86Δ
Vertically ± [0.25 + (0.05 * S)]
± [0.25 + (0.05 * 6.12)] = 0.56Δ
All of the differences between the expected and measured values in this example are less than the tolerance values so again this pair of lenses pass the standard.
CONCLUSION
There is a lot more to consider when checking power variation lenses than other optical appliances and care should be taken to ensure that the correct reference points are identified before beginning the verification process. The checking of prism in power variation lenses requires calculation to work out the tolerance and are referenced in a different standard than the one used for everything else. As professionals, it is a key part of our role to ensure that any product we supply to the patient is fit for purpose and a rigorous checking process is integral to meeting these requirements.
0
Jim Cox is a dispensing optician and has worked in both multiple and independent practice as well as the manufacturing industry. During his career, he has been a store manager, area manager and business owner. Currently he works as vice president of operations for Eyoto Group Ltd.
DISPENSING February/March 2023 www.optometry.co.uk 85
-
0 OT
CONTACT LENS CASES IN PRACTICE
IN BRIEF This feature presents a series of contact lens-related cases. Readers are invited to review the images and use additional resources where necessary to answer the questions.
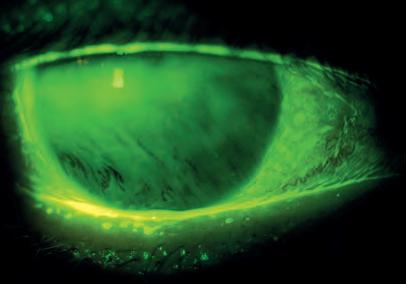
A 50-year-old female presents with the finding shown in the image.
01 What does the image show?
a) Non-invasive tear breakup
b) Invasive tear breakup
c) Corneal desiccation staining
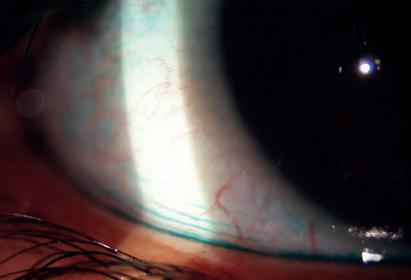
d) Corneal epithelial basement membrane dystrophy
02 Which of the following tests is not recommended for the diagnosis of dry eye disease in the TFOS DEWS II report?
a) Tear prism height evaluation
b) Non-invasive tear breakup time
c) Osmolarity
d) Ocular surface staining
03 Which of the following statements related to tear film changes in a presbyopic age group is true?
a) Tear breakup time reduces
b) Tear volume decreases
c) Tear film stability reduces
d) All of these options
A 34-year-old female patient has attended for a routine soft contact lens aftercare appointment.
04 What clinical sign is shown in the image?
a) Marx Line
b) Lid wiper epitheliopathy
c) Lid parallel conjunctival folds
d) Conjunctival chemosis
05 While the exact aetiology of the clinical sign in the image is unknown, which of the following theories has been proposed?
a) Increased friction between the ocular surface and lids during blinking
b) Reduced ocular surface lubrication
c) Decrease of conjunctival elastic fibres
d) All of these options
06 The clinical sign shown can be a predicator of contact lens discomfort. Which of the following lens properties is most likely to improve comfort?
a) High oxygen transmissibility
b) Low coefficient of friction
c) Increased thickness
d) Incorporating UV protection
IMAGE A
CPD POINT
IMAGE B
Monal Shah BSc (Hons)
86 www.optometry.co.uk February/March 2023 0 OT
A 24-year-old male contact lens wearer has attended for routine aftercare.
07 What does the image show?
a) Lid wiper epitheliopathy
b) Lid parallel conjunctival folds
c) Giant papillary conjunctivitis
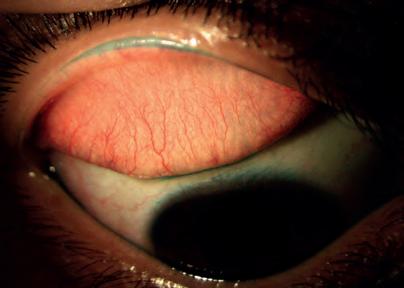
d) Staining of Marx Line only
08 Lissamine green can be used to observe the sign shown in the image. Which of the following statements about lissamine green is true?
a) It permeates the cytoplasm of living but damaged cells
b) It stains the cell membrane of dead or damaged cells
c) It is more uncomfortable than Rose Bengal
d) Observation of staining should be undertaken using a yellow Wratten (12) filter
09 Which of the following would not be an appropriate way to manage this patient?
a) Recommend ocular lubricants
b) Recommend a mast cell stabiliser
c) Refit with a contact lens that has a lower coefficient of friction
d) Manage any underlying tear quality issues

The image shows observation of the contact lens surface shortly after blink in a 34-year-old female patient.
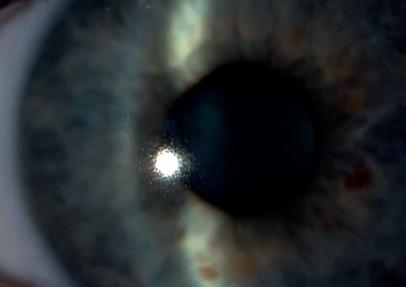
10 Which of the following symptoms is the patient leastlikely to report?
a) Dry eyes
b) Swollen eyes
c) Fluctuating vision
d) Tired eyes
11 Which of the following medications is not listed as a consistent risk factor for dry eye according to the TFOS DEWS II report?
a) Antihistamines
b) Hormone replacement therapy
c) Isotretinoin
d) Oral contraceptives
12 Which of the following is not listed as a consistent, non-modifiable risk factor for dry eye according to the TFOS DEWS II report?
a) Ageing
b) Female sex
c) Connective tissue diseases
d) Acne
IMAGE C IMAGE D CONTACT LENSES, DIAGNOSTICS
February/March 2023 www.optometry.co.uk 87 In partnership with VISION 0 OT liilii1 El m
Monal Shah qualified as an optometrist in 2008. She is a professional affairs consultant for Johnson & Johnson Vision, as well as a faculty member for the Johnson & Johnson Institute where she is involved in creating and delivering education.
THE IRIS AND THE ANGLE
Thurka Sivapalan MSc, BSc, MCOptom, BOptom, DipTp (IP), Dip Glauc, Prof Cert Med Ret
IN BRIEF This feature presents a series of anterior eye images. Readers are invited to review the images and access additional resources where necessary to answer the questions.
A 55-year-old myopic patient presents for a routine sight test with visual acuities of R 6/5 L 6/5 and intraocular pressures of R 15mmHg L 15mmHg.
01 What clinical sign is shown by the arrow in this image?
a) Corneal oedema
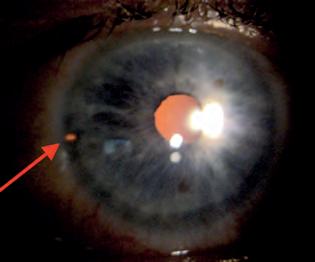
b) Epithelial microcysts
c) Keratic precipitates
d) Krukenberg’s spindle
02 Which of the following is leastlikely to cause this presentation?
a) Rubbing between the iris and lens zonules
b) Contact lens wear
c) Convection currents of the aqueous humour
d) Iris concavity
03 Which of the following conditions is associated with this clinical sign?
a) History of uveitis
b) History of trauma
c) Pigment dispersion syndrome
d) All of these options
A 49-year-old patient recently underwent the treatment evidenced in the image. Refraction R +5.00DS L +5.50/-0.50 x 180.
04 This procedure is usually indicated for:
a) Primary angle closure glaucoma
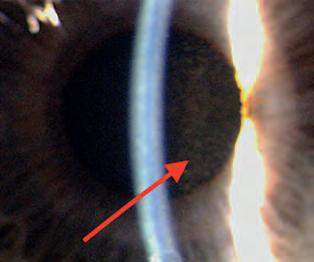
b) Primary open angle glaucoma
c) Ocular hypertension
d) Rubeotic glaucoma
05 Which randomised control trial considered the effectiveness of this treatment?
a) Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE)
b) Laser in glaucoma and ocular hypertension trial (LiGHT)
c) Ocular hypertension treatment study (OHTS)
d) Collaborative normal tension glaucoma study (CNTGS)
06 Which of the following risks is associated with this procedure?
a) Photopsia
b) Raised intraocular pressure
c) Hyphema
d) All of these options
CPD POINT
88 www.optometry.co.uk February/March 2023
IMAGE A
0 OT
IMAGE B
07 Which of the following statements bestdescribes the drainage angle in the image shown?
a) Open with pigmentation
b) Open with no pigmentation
c) Closed with pigmentation
d) Closed with pigmentation and neovascularisation
08 According to the NICE guidelines for glaucoma, updated in 2022, which anterior chamber test should be performed for the diagnosis of glaucoma-related conditions?
a) Van Herick technique
b) Gonioscopy
c) Anterior segment OCT
d) Smith’s method
09 Which of the following features can gonioscopy assess?
a) Anterior chamber angle
b) Level of pigmentation
c) Presence of blood vessels
d) All of these options
A 68-year-old pseudophakic patient attended for a routine sight test with cup to disc ratios of R 0.4 L 0.4.
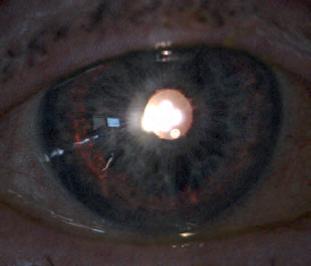
10 What slit lamp light illumination method is being used to identify this feature?

a) Retroillumination
b) Direct illumination
c) Optic section
d) Sclerotic scatter
11 Which of the following findings is leastlikely to be associated with this case?
a) Raised intraocular pressure
b) Normal intraocular pressure
c) Open angle
d) Narrow angle
12 What is the most likely cause of this finding?
a) Penetrating trauma
b) Pigment dispersion syndrome
c) Essential iris atrophy
d) Iris coloboma
Thurka Sivapalan graduated from Anglia Ruskin University in 2001 and became an independent prescriber in 2012. Over the past 10 years, she has gained specialist glaucoma skills and qualifications and works across two hospital trusts – Queen Victoria Hospital, East Grinstead and Sussex Eye Hospital, Brighton. Her main clinical responsibilities include the management of complex glaucoma cases, postoperative clinics, performing selective laser trabeculoplasty treatment and the supervision of glaucoma virtual clinics.

ANTERIOR SEGMENT, DIAGNOSTICS, PATHOLOGY
February/March 2023 www.optometry.co.uk 89
C IMAGE D 0 OT
IMAGE
Gail Steele, director at West London independent, Auerbach & Steele, explains why understanding the aims of the business is key for new recruits

What is the one piece of advice that you would give to someone who wanted to work for Auerbach & Steele?
We are very fortunate that we don’t have to advertise for staff very often, but we are always happy to talk to people interested in coming to join us. The most important thing is that they are on our wavelength and understand what we are trying to achieve as a high-end independent practice.
When you are shortlisting candidates, what’s the very first thing that you look for?
Enthusiasm, positive energy, and a natural understanding of good customer service.
How important is work experience?
Some experience in optical practice is highly desirable, but the right attitude is the most important quality.
How important is the cover letter in applications that you receive? The cover letter is important. I like to see enthusiasm. I know I sound like an old fogey, but I like to see that
applicants can write grammatically correct letters, and emails without spelling mistakes.
What is the biggest mistake that someone can make in an interview for Auerbach & Steele? Arrive late. If a candidate arrives late for interview without calling to let me know they have been delayed, or without apologising, then I won’t interview them.
What is the business ethos/most important values?
Our goal is, and has always been, to be the best. It is only possible to achieve that if you have a fantastic team of people working in harmony together. We offer top quality in everything we do, from the clinical services to the choice of goods. It is important to embrace change and always be happy to invest in the latest equipment and technology, and in the staff.
How do you go about ensuring fairness and equality in your hiring process? Do you have specific programmes in place to guarantee it?
We are very proud of our extremely diverse team, who have all been recruited on their ability and enthusiasm. Our hiring process would never discriminate because of ethnicity, gender, sexual orientation, age or religion. Everyone is treated fairly and
A new employee is preparing for their first week. What tip would you give them to be successful?
Don’t be afraid to ask questions, and flag up concerns early in your employment. We are a close, happy team, working together, who will be looking forward to welcoming new staff members. We are all here to help new employees settle in.
equally at Auerbach & Steele. We have professional advisers on employment law and health and safety, and would always refer to them if we have any doubts or need advice about our hiring process.
How important is employee wellbeing at Auerbach & Steele?
Employee wellbeing is absolutely paramount. I am always happy to support the staff in whatever way is necessary for them. We offer private medical insurance to all, a pension scheme, access to exercise classes, and lots of social activities. In independent practice the same people work together day-in, day-out. I probably spend more time with my workmates than I do with my husband. My team are like my family. I have always felt that it is my responsibility to look after their needs as far as I am able. Some have been with Auerbach & Steele for more than 25 years. A business can only be as good as the people in it.
Jobs www.optometry.co.uk/jobs
“My team are like my family. I have always felt that it is my responsibility to look after their needs as far as I am able to”
MY CAREER ADVICE
“I AM ALWAYS HAPPY TO SUPPORT STAFF IN WHATEVER WAY IS NECESSARY FOR THEM”
90 www.optometry.co.uk February/March 2023 • • OT 0



~~VISION
Association of Optometrists
It couldbe, if you'relookingfor a rolethat'sfocusedon clinicalcare and providinga high-quality serviceto NHS patients.Dueto our recentexpansion,we havevacanciesin multiplelocations, whereyou'llhavethe opportunityto workwith someof the UK'sleadingophthalmologists,nurses and HCTs.You'llbenefitfrom fantastictrainingand professionaldevelopmentopportunitiestoo.
WHO WEARE
We'repatient-focused,providingclinical expertiseand support for all our patientsthroughout everystep of their patientjourney.
We'rebusy-as the UK'slargest providerof NHS cataract surgery,we havethousandsof patients choosingour servicesand are proudto be ableto support them in improvingtheir sight and, ultimately, their quality of life.


Our patients reallyvaluethe servicewe deliver-we've received5-star reviewsfrom more than 10,000NHS patientsacross our 47 hospitals-you can readthese on NHSUK.
CONTACTUS TODAY:

This is a great opportunityto join one of the UK'sleading ophthalmologyserviceproviders.Pleasecall or email us today if you're interestedin joining our team.
WHAT WE'RE LOOKING FOR
You'll be GOCregistered,with at least 12 months' post-registration experience-we provide full training so previous hospital experienceisn't required.
You'll be someone that enjoys variety, is calm under pressure,great at problem solving and is willing to go the extra mile to providethe best service and advice for our patients.
Telephone:0330 058 4280 Email:careers@spamedica.co.uk www.spamedica.co.uk
Perth).
In a fast-growing, affluent area of Scotland. It benefits from spacious premises, modest rent, in an area of outstanding natural beauty. With excellent facilities, and Scottish GOS. It provides a comfortable living.

Please phone Des on 07961 637528 after 6pm or on the weekend.









Owen Aves is a long established, independent practice in Colchester, Essex. We are expanding our team and are looking for an optometrist with superb clinical skills, good business acumen, clinical enthusiasm and a personality to develop a strong patient following.

The practice offers a wide range of optometry services including contact lenses, MECS, Post-op cataract checks and Paediatrics.




You will find a happy team ready to support you in what will be a fulfilling role. No Sunday or bank holiday working.



salary
If you are interested in this great opportunity contact Andrew Chenery on andrew@owenaves.com or 01206 575693 Or Clive Roots on clive@owenaves.com

MARKETPLACE0 INSTRUMENTS OptopolREVOseries of OCT's & PTSVisual field perimeters ---Lead the way with the UK's most flexible, adaptable and affordable OCT & Visual field solutions. ll l PTS!J'1!1 OPHTHALMIC INSTRUMENTS 01438 740823 I sales@bibonline.co.uk I bibonline.co.uk Fordigital opportunitiescontact: MattHall matt.hall@thinkpublishing.co.uk
PRACTICE FOR SALE
for
or
due to
in
02037717257
Practice
sale
lease,
retirement,
Milnathort nr Kinross (between Edinburgh and
RECRUITMENT OWEN AVES OPTICIANS Enthusiastic and conun.itted Optometrist required
tune or full tune and possible partnership
Part
Competitive
February/March 2023 OT www.optometry.co.uk 93
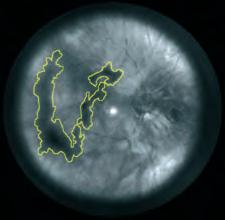
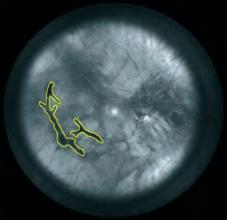





94 www.optometry.co.uk OT February/March 2023 4.5 4.0 3.5 3.0 2.5 2.0 Visualdisturbances







MARKETPLACE0 PRACTICE FITTING PRACTICE SOFTWARE integrate.automate.accelerate. free up yourtime & be moreoptician softwarefor opticians GOCARDLESS worksmartanytime,anywhere PC,Mac, iPad+ Tablet liveonlinebooking,directdebits & accountingsoftwarein1egrated fast, powerfulcloudsoftware with customclinicalrecords multipleusersand devices at no extracost upgrades,maintenance,support & backupFREEforeverMicrosoft Azure IntegratedSimplerDirectDebits IntegratedAutomatedAccounting Superfast,Secure& BackedUp CloudSoftwareSystem AutomaticReconciliation MakingTaxDigitalCompliant xeyex.co.uk/movetocloud call us on 01698 209609 February/March 2023 OT www.optometry.co.uk 95




Togetherwe providegreatoutcomes, ultimatelyimprovingour patients'qualityof life WORKING TOGETHER UK'slargest providerof NHScataract surgery,with 47 hospitalsacross the country NHSappointmentsavailablewithin four weeks of referral Freetransport for patients Patientsreturnto community optometrists for post-op assessment CONTACTUS TODAY: www.spamedica.co.uk SUPPORTING YOU & YOUR PATIENTS Regularcommunicationfrom SpaMedicaat everystage of the patient journey Specialistadviceto community optometrists to support you with your patients/referrals 24-houremergencyhotlinefor your patients Telephone:0330 058 4280 Email:contact@spamedica.co.uk
Services and products for the practitioner Marketplace
MY HOSPITAL EQUIPMENT CASE
Laura Josephs, AOP Councillor for undergraduate students, on how a humble make-up case has been invaluable during her placement at Manchester Royal Eye Hospital

F or my placement at Manchester Royal Eye Hospital, I use a carry case for all my equipment. Previously, when I was carrying everything, I kept dropping bits, and obviously the last thing you want to drop is your retinoscope. I thought, “I really need something that I can store my equipment in that’s also easy to carry.” So, I bought this case, and I love it. It’s not made for optometry equipment – it’s actually a make-up case. It’s got hard sides, removable compartments so that I can make certain bits bigger or smaller, and pockets for my occluder and other pieces of equipment.
Practicality on placement
On placements, I could have used my shoulder bag – but I wanted something nicer. Also, I’m short, and it has quite a long strap, so it was hitting the back of my knees when I was walking. I was struggling when I was carrying things, so it was easier to get another bag.
Buying the case evolved from an Amazon search. I originally thought I could get a pencil case – one with three compartments. They’re quite large,
“In the hospital setting it’s a confidence thing, because you don’t want to be worrying about what’s happening to your equipment when you leave it somewhere”
and they’ve got a middle bit and then two bits at the side. I thought all my retinoscope handles could go in there, and then my cross cyls in one side and other small pieces of equipment in the other. I wanted something hard, because I didn’t want to risk breaking
my retinoscope if I ever dropped it. So, I went down the rabbit hole on eBay and Amazon, and eventually found these makeup cases. I thought, ‘actually, this is better.’
If I hadn’t found this solution, I would be doing multiple trips to the place where I keep my equipment, which would be inefficient and annoying. Or, I’d be risking dropping something that is actually really difficult to replace. I really like it, because everyone knows it’s mine.
In the hospital setting it’s a confidence thing, because you don’t want to be worrying about what’s happening to your equipment when you leave it somewhere. I wouldn’t feel safe leaving it out – not because it might get stolen, but because we have trays, and other people put their things in the trays too. If someone put their bag on my retinoscope and didn’t realise that it was there, they might break it, whereas in this case I know it is padded and secure. I’m not worried about someone putting something on top of it, and I’m not worried about dropping it. I’m less worried, overall.
Laura explains why there is one person who she also could not live without…
I couldn’t possibly dream of living without my twin sister. Not only has she been a constant source of emotional and financial support throughout my degree (and a pandemic), she has also been my best friend, keeping me stocked up on tea and coffee, and having food on the table following long nights in the library. She’s sat through many a “practice scenario” for objective structured clinical examination prep, and never
once complained. She’s been there to commiserate when things have gone wrong, to share in my frustration when plans have gone awry, and has always been ready to celebrate even the smallest of my achievements.
I don’t know what I did in my past life, but I must have been a saint to have ended up with such an amazing sister. I definitely could not have made it through my optometry degree without her.
“SHE HAS BEEN A CONSTANT SOURCE OF EMOTIONAL AND FINANCIAL SUPPORT”
I COULD NOT LIVE WITHOUT...
February/March 2023 www.optometry.co.uk 97 0 OT
MY SECRET LIFEAS...
My hometown is Greenock, about half an hour from Glasgow. I started playing hockey when I was 10. I played for the school team, then for the district. At a district tournament I was selected to play for Scotland under-16s. I was asked at the age of 19 to step up and have a game for the seniors in Barcelona against Spain. I was quite nervous and young at the time. I remember as we were warming up for the match, one of the girls said ‘There’s a guy over there in a kilt. Who is that?’ I turned around and it was my dad. He knew it was my first senior cap for Scotland so he booked a flight over to surprise me.
Specsavers Home Visits
optometrist, Jaclyn Payne, on playing hockey for Scotland, the comradery of team sport, and the rewards of domiciliary care


I studied optometry at Glasgow Caledonian University. I would go to lectures in the morning, then go to the gym to do a weight session, then more lectures and at night I might have a club training. My parents ferried me about a lot until I could drive myself. Mum, bless her, would have meals ready, and she would do all the washing so I could just grab my hockey stuff and go.
With hockey I have travelled to many different places over the years. I’ve played in France, Germany, Holland, Spain, Belgium and South Africa.
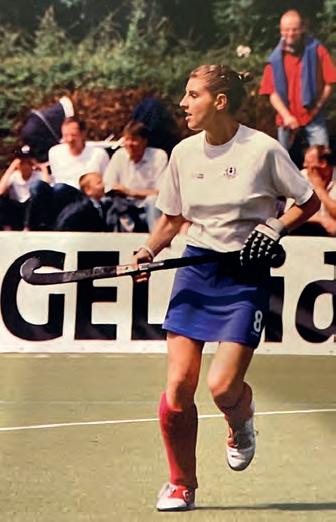
The best storm I ever saw was near Johannesburg. I was warming up and saw these black clouds in the distance rolling in, rumbling with thunder. We were standing
My secret life Do you have a personal passion to share with readers?

Get in touch with selinapowell@ optometry.co.uk
there, singing the national anthem and the rain started pummelling down. We all rushed back into the dugouts and within three or four minutes the pitch had flooded up to midshin height. In Glasgow, sometimes you couldn’t see the white lines because the pitch was covered in snow. I love the group effort of hockey. Moving down to West Yorkshire, my husband told me that I should seek out a hockey team because I needed that comradery and buzz that you get from the other girls. If you’ve had a rubbish week, you can talk about it with your teammates – a problem shared is a problem halved. You become a group of friends. You have to be quite disciplined in hockey and that is also the case for optometry. I have been doing domiciliary for nearly 10 years. I remember doing my first shadow day and thinking ‘This is fabulous –what a difference we can make for people.’
The older generation are just lovely. I saw a woman the other day who enjoyed doing jigsaws and crossword puzzles, but she was struggling to see them. We were able to correct her vision to the point where she could enjoy those activities again. To anybody who wanted to try domiciliary, I would say absolutely give it a go.
0

98 www.optometry.co.uk February/March 2023
LAST WORD
“Ifyou’vehada rubbishweek,you cantalkaboutitwith yourteammates–a problemsharedisa problemhalved”
OT
OT
THE COST OF CRISIS ££££££££ have seen a patient in the last three months who required vision correction but took no action because they couldn’t afford it* Download our resources and call on the Government to act now www.aop.org.uk/costofliving The NHS voucher should increase to reflect rising costs WE SAY: #EyeCareSupportNow Add your voice to our campaign 7in10 Optometrists *The Voice of Optometry panel, set up by the AOP in 2017, provides research from the optometry sector. 876 practising optometrists completed the online survey in September 2022. 0 Association of Optometrists LIVING















Look no further! J C p V g y™ CPD accredited for one interactivepoint u g u , g g g p WEBINARS Register now by scanning the QR code. On the look out for some great webinars? FREE TO ATTEND The science behind selection – contact lens recommendations. Wednesday 29th March 6:30pm-7:30pm. Sustainability for all. Wednesday 24th May 6:30pm-7:30pm. A lifetime of lens wear. Wednesday 26th July 6:30pm-7:30pm. Challenges with presbyopia. Wednesday 20th September 6:30pm-7:30pm. -·• CooperVision learningacademy™ HELPINGYOU GROW
