











The seeds of each edition of OT are sown many months before the hard copy arrives through your letterboxes. Ideas for topics are chewed over, rejected, improved and agreed upon. In the final weeks, news from across optics is compiled for our This month section.
The last two weeks has challenged all of OT's standard ways of working. As we send the April edition for press, the Chancellor of the Exchequer has announced a financial package that includes mortgage 'holidays' for those in financial difficulty, as well as £330bn in loans and £20bn in other aid to protect businesses facing losses as a result of the coronavirus outbreak. Unprecedented yes, and yet no one can say if it is going to be enough.
As your journal, OT is here to ask the questions that matter to you, and serve as a tool to support all AOP members in the optics community. Please use us. Tell us your stories, share your concerns and advice. The team may not be in the office but the work has not stopped. Keep up to date on the latest news online, including in-depth reports on the impact of the virus by visiting, www.optometry. i co.uk. It is a time when the Government <{ and communities have to find new ways " to come together. Businesses, careers and livelihoods are at stake.
John White, editor johnwhite@optometry.co.uk
Coronavirus (COVID-19)
The developing impact of the outbreak across optics -and where to find the latest advice and support
Pages07-17

of
practitioners in providing support Page67
Dr Deborah Armstrong considers questions that are commonly asked by patients when they are referred from primary care with suspect glaucoma Pagen

THIS MONTH
The news in digest
o Picture this
Eye-catching art installation represents Mexico-US border concerns
o OTreports
The latest updates on the Coronavirus (COVID-19) outbreak
o In brief
The month in 16 stories
o OT investigates
GOC reports 39% reduction in open FTP investigations
o 60 seconds with ...
Mitesh Gandhi of Clamp Optometrists on recieving a business award
o Clinical round-up
News and research papers
o AOP round-up
Supporting the GOC to tackle illegal online sales
The trends, launches and looks
o OT focuses on ...
Sunglasses
o Me and my glasses
Jeremy Hackett
o Get the look
Modem metallics
o The shortlist
The latest launches in April
Behind the brand
"Sustainability in optics is only going to become more important. Soon it will be the norm not the exception for businesses to show they understand the triple bottom linebusiness needs to be good for people and planet, as well as profit"
o Ed Bird, Bird Sunglasses PAGE 25
Voices from optics and beyond
o Perspectives
Henrietta Alderman, Poonam Patel
o Myvision
Dave Thomas, former professional footballer and guide dog owner
o Letters

''At a time when the opportunity for any individual to give a review that could reach many thousands has never been greater, keeping the customer close has never been more important"
o Henrietta Alderman, chief executive PAGE 27






Business insight and career development
o The challenge
The realities of creating a customer service culture
o Life as a locum
Craig McCoy
o Pre-reg focus
Daniel Chung and Samrina Awan
o The workshop
Handling complaints, the OCCS way
o How I got here
AOP award winner, Dipesh Chhatralia
o Key milestones
Sachin Nath on building his brand
0 Howdo I...?
Use communication to deliver patient loyalty
How a Moorfields Eye Hospital team has developed an award-winning telehealth initiative, utilising the expertise of community optometry to deliver outstanding patient care
PLUS: From driving to sightthreatening conditions, practitioners share their tips for tackling difficult conversations with patients
PAGE52-58
o Interview preparation
CV Writers' Michelle Hiseman
o I could not live without ...
Grafton's Optical LED slit lamp, says Alistair Duff
o Secret life
Jaime Patel's passion for painting
Education and training for the eye care practitioner
61 CET welcome
62 Ocular manifestations of child abuse
67 Seeing beyond the eyes
71 Referred for glaucoma -what happens next?
76 Clinical signs of ocular surface disease
79 CET interview: Deborah Armstrong
In this edition of OT, practitioners can test a range of competencies:
OPTOMETRISTS// 3
THERAPEUTIC OPTOMETRISTS// 2 DISPENSING OPTICIANS// 3 CONTACT LENS OPTICIANS// 1

OTvideo highlights
Tips and tricks from 100% Optical: introducing OCT into the practice
Watch the video on www.optometry.co.uk
Contact the OT team with your experiences, observations and lessons from practice today: newsdesk@optometry.co.uk



Followus on Twitter @OptometryToday
Likeus on Facebook OptometryTodayJournal
Followus on lnstagram @optometry_today


08 OT REPORTS
Coronavirus (COVID-19) outbreak puts pressure on practises and events
13 60 SECONDS WITH ... Clamp Optometrists' Mitesh Gandhi on winning a customer service award
17 AOP ROUNDUP
Rolling guidance on the novel coronavirus (COVID-19) outbreak for members


April 2020/Volume 60:04 lssn 0268-5485 a ABC certificate of circulation January 1 2019 -December 31 2019
Editor: John White johnwhite@optometry.co.uk
Deputy editor: Emily McCormick emilymccormick@optometry.co.uk
Assistant editor: Selina Powell selinapowell@optometry.co.uk
Senior reporter: Kimberley Young kimberleyyoung@optometry.co.uk
Web content and social media executive: Leah Boyle leahboyle@optometry.co.uk
Clinical editor: Dr Ian Beasley ianbeas/ey@optometry.co.uk
Clinical editor for multimedia: Ceri Smith-Jaynes cerismithjaynes@optometry.co.uk
Video production editor: Laurence Derbyshire laurencederbyshire@optometry.co.uk
CET enquiries: 020 7549 2076 CEThelp@optometry.co.uk
AOP membership and OT subscription team: AOP, 2 Woodbridge Street, London, EClR 0DG subscriptions@aop.org.uk
0Association of Optometrists
Advertising: Richard Ellacott 020 37717242 richard.e//acott@thinkpublishing.co.uk Kurran Jagpal 020 37717198 kurran.jagpal@thinkpublishing.co.uk
Advertising production: Simon Gould aop@ccmediagroup.co.uk
Senior designer: Juanita Adu
Executive Director: Jackie Scully
Published monthly for the Association of Optometrists by Think Capital House, 25 Chapel Street, London NWl 5DH
Printed by Acorn Web, Normanton Ind Estate, Loscoe Close, Normanton, West Yorkshire, WF61TW
All rights in and relating to this publication are expressly reserved. No part of this publication may be reproduced in any form or by any process without written permission from the AOP or the publisher.



PROFESSIONALSUPPORT CORONAVIRUS OUTBREAK PUTS PRESSURE ON PRACTICES AND INDUSTRY EVENTS
Characterised by the World Health Organization (WHO) as a "pandemic," the global outbreak of coronavirus (COVID-19) has led to an increased pressure on the optical sector.
In a statement released by the AOP, its policy director, Tony Stafford said: "It's increasingly clear that COVID-19 is likely to have a significant impact on optical practices, and on other primary healthcare providers and businesses."
Businesses have reported some impact in footfall and cancellations as patients follow the evolving guidance.
An online poll of OT readers in March reported that 40% of respondents had seen a drop in patient footfall over a period of seven days of 1-25%. Another 13% said footfall was down 26-50% while 6% said they had seen a drop of more than 50%.
AOP Board Member and owner of Thompson Opticians, Kevin Thompson, described to OT the measures in place at the practices to appropriately question patients making appointments and ensure personal and premises hygiene measures are adhered to.
However, Mr Thompson highlighted some barriers to following the guidance: "In trying to follow the most up-to-date guidance on cleaning and disinfection, despite optometry being a front-line health-related service, I am more than disappointed and frustrated at the apparent inability to be able to access very basic NHS supplies."


O The outbreak of COVID-19 was characterised as a pandemic by the World Health Organization at a media briefing on 11March
O Optrafair 2020 has been running for over 40 years and in 2019 the event expanded its reach to incorporate fashion, medicalisation and optics
O 2020 marks the 50th edition of the Italian trade show, Mido, which first opened its doors in 1970.
While he agreed there should be a prioritised list of healthcare professionals requiring materials for cleaning, disinfection and protection, optometry should be included.
Amidst public concerns, research scientists and associations have spoken out to "dispel myths and misinformation" and reassure consumers of the safety of wearing contact lenses.
The British Contact Lens Association confirmed there is no evidence to suggest a correlation between using contact lenses and the spread of the
"It'sincreasingly clear that COVID-19 is likely to have a significant impact on optical practices"
virus, and that "There is no evidence to date that contact lens wear should be avoided by healthy individuals."
Meanwhile, universities across the country have suspended face-to-face teaching, with many looking to establish on line alternatives.
The College of Optometrists announced the decision to stop all assessment activity on the Scheme for Registration from 18 March, cancelling all assessment visits at Stage 1 and 2 until further notice.
The College confirmed details would be provided regarding arrangements, adding: "We have not taken this decision lightly. It is to protect the safety of trainees, supervisors and assessors, as well as patients and the public."
Temporary measures included in the Government's 2020 Budget to support businesses through the outbreak have been welcomed, including business rate cuts, a temporary business interruption loan scheme and help with COVID-19related statutory sick pay (SSP).
SSP has been extended to those diagnosed with COVID-19 or selfisolating, while the Government advised self-employed individuals that employment support allowance for those affected by COVID-19 would be payable from the first day of sickness rather than the eighth.
Chancellor Rishi Sunak announced further support measures including giving retail businesses a business rates holiday for the next 12 months, increasing grants
to small businesses eligible for Small Business Rate Relief and providing further £25,000 grants to eligible businesses operating from smaller premises.
In light of the situation, industry events have been cancelled or postponed, with several now rescheduled for the autumn.
The eyewear tradeshow, Mido, was due to be held between 29 to 2 March. After postponing, the show was rescheduled for 5-7 July at the time of publication.
Vision Expo East, which was due to be held in March, is to be consolidated with its September event; Vision Expo West in Las Vegas. While Optrafair 20/20, due to have been held at NEC Birmingham in early April, has been postponed until 19-21 September.
Despite the challenges, organisers have been resilient, with Optrafair 20/20 organisers suggesting they would bring the "best ever" Optrafair later this year.
The situation surrounding the outbreak continues to evolve, please check ors website for the latest news and guidance.





















0 £138m
















Bath-based eyewear manufacturer, lnspecs, floated on London's AIM stock exchange in February. It was described as a landmark moment by lnspecs' chief executive and founder, Robin Totterman.








































o King's Lynn-based independent, Wigram and Ware Opticians, has marked its 100th anniversary. The practice celebrated the milestone with a 1920s-inspired tea party with fancy dress.
O Millmead Optical Group celebrates winning the AOP Awards 2020 Frame of the Year for Walter & Herbert by Optoplast Actman Eyewear.







o 11 Locums now represent a large proportion of eye care professionals in the UK11 Dr Rachel Hiscox, professional education and development manager Johnson 6. Johnson Vision, on providing new opportunities for locums to network and learn at 100% Optical 2020. Watch OT's video with Rachel online

0 8276
PEOPLEHAVE BEENSCREENED FOR GLAUCOMA IN INDIA BYTHE KEEPSIGHT INDIA INITIATIVE, ESTABLISHEDBYALLERGAN, SIGHTSAVERSAND THE INTERNATIONALAGENCY FOR THE PREVENTIONOF BLINDNESS, SINCE IT LAUNCHEDIN OCTOBER.







o Twenty-five per cent of Duncan and Todd's optometrist workforce are now qualified independent prescribers. The opticians, which has a portfolio of 41 practices across Scotland, confirmed that an additional four optometrists had gained their independent prescribing qualification in the last year.
o "It was a difficult decision, but ultimately The Vision Council's Board of Directors believes the safety and well-being of our members, exhibitors, attendees and staff must come first" Ashley Mills, CEO of The Vision Council, announces that Vision Expo East, due to be held in March in New York City, would be cancelled because of coronavirus concerns


Catch the news from OT on line -your daily digest of the latest stories in optics www.optometry.co.uk

o BMJ CaseReports authors have described their treatment of a 23-year-old patient who had two pieces of wood removed from her eye. The woman presented at hospital with a granuloma over the site of a facial laceration and visual acuity in her left eye of 6 / 60. After clinicians became suspicious of the presence of a foreign body they discovered and removed two pieces of wood measuring 33x6mm and 39x8mm using Blakesley forceps.
0 "Nockolds
has been instrumental in the success of the OCCS over the past five years and its understanding of the optical sector is second to none"
Director of casework and resolutions at the GOC, Dionne Spence, on the appointment of a new three-year contract funded by the regulator

retinal surgeon and medical retina specialist at Moorfields Eye Hospital, Professor Lyndon da Cruz, follows in the footsteps of Kylie Minogue, Professor Germaine Greer c and Clive James, having been named Australian of the Year in the UK 2020.
o Manchester Royal Eye Hospital consultant ophthalmologists and viteoreti na I surgeons, Felipe DhawahirScala and Niall Patton, performed viteoretinal procedures during the E-Learning Ocular Surgery conference held in Milan.
o A smart contact lens developed by Chinese researchers reacts to changes in pressure and moisture by changing colour. Describing the technology in Journal of Materials Chemistry B, the authors highlighted that contact lenses provide a suitable platform for point of care diagnosis of eye diseases. The smart contact lens is made from biocompatible hydrogel without the addition of chemical pigments.

O The Local Optical Committee Support Unit has launched a new online portal where practitioners can find and access the websites of local optical committees (LOCs) across England. The website, loc-online.co.uk, replacing loc-net.org.uk, includes a website design and hosting service to support LOCs in updating their online presence.

0 229,895
The number of women enrolling in a degree in science and technology subjects is rising, particularly in subjects aligned to medicine, according to analysis of Higher Education Statistics Agency figures. Figures revealed a 0.9% increase from the year 2017-18 when there were 227,725 female students enrolled, to 2018-19 when there were 229,895.
o The Royal National Institute of Blind People has worked with the Bank of England to produce a new £20 note with tactile markings that will make it easier for blind and partially sighted customers to distinguish between different bank notes.
o "OCT is really important to help you build your practice"
Optometrists and independent practice owners Alisdair Buchanan and Mark Holloway speak to OT at 100% Optical 2020. Watch the video on www. optometry.co.uk
Open fitness to practise investigations decreased by 39% in 2019,the General Optical Council (GOC) has highlighted.
A summary of the optical regulator's quarter three performance report was presented at the latest GOC meeting (26 February, London).
The document shows that the GOC's total fitness to practise caseload also reduced by 29% last year.
"This is a phenomenal outcome," the GOC's chief executive and registrar, Lesley Longstone highlighted.
The drop in open investigations follows the introduction of an enhanced triage process as pa rt of the GOC's fitness to
practise improvement programme. The time the GOC takes to resolve fitness to practise issues has been an Achilles heel in past annual performance reviews by the Professional Standards Authority.
Although the number of open fitness to practise cases has dropped, Ms Longstone highlighted that the average age of cases is a challenge. "If you
"If you reduce the number of open cases you are not going to have many short cases"

massively reduce the number of open cases you are not going to have many short cases," she said.
At the meeting, the GOC confirmed that Nockolds have retained the contract for the Optical Consumer Complaints service following a competitive tendering process, with a new contract to begin in April 2020.
"We look forward to continuing to work with them during the course of the next three-year contract," Ms Longstone highlighted.
The GOC has also announced plans to publish a gender pay gap analysis of staff within the organisation alongside its annual report.
As an employer with fewer than 250 staff, the optical regulator is not legally required to publish gender pay information because of the wide variations that can occur when percentages are based on small numbers.
However, the GOC has committed to making the analysis available in line with its commitment to transparency.
Plans to appoint a new GOC chair were also discussed at the meeting, with current chair Gareth Hadley to reach his maximum term in office on 21 February 2021.Mr Hadley has served in the role since his appointment in February 2013.



The clinical director and optometrist at Clamp Optometrists discusses the patient journey
The practice has won a Cambridgeshire Prestige Award. What does it mean to you? Winning the Eye Care Specialists of the Year award has strengthened our belief in the importance of the personal touch. In a world of efficient communication via the internet, our profession still relies on faceto-face contact.
How does the practice work to exceed patient expectations?
The journey begins from the point of booking an appointment. Those who use our on line system find it very easy to use and compliment us on it. Following that, we escort them to the waiting area which is tastefully decorated and relaxed; we have comfortable sofas and premium quality refreshments available. Before they are seen by me, they are pre-screened
using the latest equipment available; we have invested in the Heidelberg optical coherence tomographer, the Humphrey visual field analyser and the (non-puffer) I-care tonometer.
What makes the Clamp Optometrists customer journey effective?
A happy, motivated team makes all the difference between an average outcome and an excellent patient experience. We treat each of our patients like royalty and, generally speaking, in way that we would like to be treated. We have key words that resonate with our staff ethos displayed around the waiting room such as; professional, respect and honesty. This strengthens my sense of duty and purpose when interacting with staff and patients alike.
A pilot that is designed to provide patients with eye care "in the right place at the right time and closer to home" has been launched in five optometry practices across Wales by Cardiff and Vale University Health Board in March.
The project, which is being funded by Welsh Government, will see the five ophthalmic diagnostic treatment centres, provide enhanced patient pathways for glaucoma, macular degeneration, diabetic eye disease and

eye casualty services.
Patients will be referred to and receive the required tests and treatment in a High Street practice, with a hospital consultant able to virtually review images.
The latest Optical Goods Retailing report from research group Mintel has reported growth in the optical goods and services market, estimating consumer spend of more than £3.3bn in 2019.
The steady market growth has been particularly supported by an ageing population, while Mintel also suggests product innovation has bolstered the opportunities for opticians to upsell to consumers in order to gain added benefits from their eyewear.
Spectacles account for more than 60% of spend according to the survey and an eye exam was found to be a gateway to a purchase. Meanwhile, contact lenses formed 20% of consumer spend.
The market for contact lenses has been growing as people trade up for lenses replaced more frequently, or other valueadded products.
Mintel found that one in five of those surveyed shopped on line through a specialised seller for contact lenses, with the researchers predicting that shoppers for contact lenses may be more easily "tempted away" to internet retailers, particularly where there is a cost benefit.
Mintel suggests internet selling has a low share of spectacle shoppers. However, as technology to support shoppers to 'virtually' try on frames becomes simpler, Mintel expects internet sales will also grow.

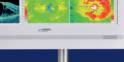
Observe and measure all the main structures and surfaces of the eye
• Posterior OCT
• Anterior OCT
• OCT-A Angio
• OCT-B Biometry
• OCT-T Topographic (due mid 2020)
• True colour fundus imaging
It's as simple as pressing the button




































Biotrue® ON Eday - The Lens with the Most Moisture 1
Maintains almost 100%*of moisture for a full 16 hours, so contact lens wearers can enjoy comfortablevisionfrom first thing in the morninguntillastthingat night2 , 3 A.5
PARAMETERS
Material
Now available for more of your patients
Biotrue® ON Eday
Spherical Contact Lens
More Moisture from Morning to Night 2

810 true
ONEdaylenses
Biotrue® ON Eday
NOW UPTO -12.00D For Astigmatism Contact Lens
Consistently clear and stable vision5 6

With Jan 2020 expanded range, excluding made-to-order lenses.
Lens material technology:
Water content:
Oxygen transmissibility:
Design:
Basecurve:
Diameter:
Centre thickness:
Spherical powers:
Visibility tint:
Modality:
42 Dk/t@ -3.00D93% OxygenFlux
Aspheric Optics
8.6mm
14.2mm
0.1mmat -3.00D
+6.00Dto -12.00D(0.25Dsteps;0.50D stepsover-6.50D)
light Blue
Daily Disposable
PackSizes: 30, 90
UVA/UVBtProtection: Blocksmorethan50% of harmfulUVAraysandmorethan90 %of UVBrays
PARAMETERS -2.75D Cyl will be available in Low Minus Powers across key axes mid 2020
Material: nesofilcon A
Technology: Surface Active TechnologyTM
WaterContent: 78 %
Oxygen Transmission:
Design:
Base Curve:
Centre Thickness:
Diameter:
2460
PARAMETERS
Powers:
Biotrue® ON Eday
More parameters than any other toric daily disposable lenst,9 For Presbyopia Contact Lens
With 3-Zone Progressive Design™

Precision Optics, SeamlessVision, Near, Far and ln-between 4 ·7. 8
Visibility Tint:
42 Dk/tat Centre-3.00D,93%OxygenFlux
EvolvedPeri-Ballast(PrismFree)
8.4mm
0.1mmfor -3.00D
14.5mm
PLto-6.00D (in 0.25D steps)
-6.50D to -9.00D (in 0.50D steps)
+0.25Dto +4.00D (in 0.25D steps)
LightBlue
-0.75,-1.25,-1.75 10°-180°(in10° steps)
-2.25 10°,20°, 10°, ao 0 90°, 100°,110°,160°,110°,100°
-0.75,-1.25,-1.75 10°,20°,60°,10°,00°,90°,100°,110°,120°,160°,110°,100°
-2.25 10°, 20°, 90°, 160°,170°, 180°
-0.75,-1.25,-1.75 10°,20°, 70°, 80°, 90°, 100°,110°,160°,170°,180°
-2.25 10°,20°, ao 0 90°, 100°,160°,170°,100°
Orientation Mark Orientation mark at 6 o'clock -Axis indicator varies with axis
Modality: DailyDisposable
PackSizes: 30
UVA/UVB' Protection: Blocksmorethan50 %of harmfulUVAraysandmorethan90 %of UVBrays
PARAMETERS
Material
Lens material technology:
Water content:
Oxygen transmissibility:
Design:
Base curve:
Diameter:
Centre thickness:
Spherical powers:
Spectacle Add power:
Visibility tint:
Modality:
Pack Sizes:
UVA/UVBtProtection:
nesofilcon A Surface Active Technology™ 78%
42 Dk/t@ -3.00D93% OxygenFlux
3-Zone Progressive Design TMwith Centre-Near Aspheric Optics
8.6mm
14.2mm
0.1mmat -3.00D
+6.00Dto -9.00D(0.25Dsteps)
Lowupto +1.50DHighfrom+1.75D light Blue Daily Disposable
30,90
Blocksmorethan50% of harmfulUVAraysandmorethan90 %of UVBrays
Rochester. 6. Bausch+ Lomb, 2016. Biotrue ONEdayfor Astigmatism (nesofilcon A Torie) Design Description. (#LDR165005A).Rochester. 7. Bausch+ Lomb, 2013. Perceptions of Bausch+ Lomb PureVision®2 for Presbyopia (#815) 8. Vogt, A.K.S., Hoving, K.R.Consistency of Multifocal Contact Lens Design. Poster Presentation. 9. Based on a comparison of manufacturer-provided

A new study by City, University of London scientists has investigated the potential of virtual and augmented reality to simulate the visual challenges faced by those with glaucoma.
The research, which was published in npj Digital Medicine, highlights that using head mounted displays to simulate sight loss could aid policymakers in better assessing the impact of visual impairment on patients.

The technology could also be used by architects to design more accessible buildings.
As part of the study, 22 participants without glaucoma wore head mounted displays while performing a variety of tasks in virtual or augmented reality.
Sensors within the head mounted displays tracked the position of each participant's eyes and generated a blurred area of vision that obstructed the same portion of their visual field wherever they looked.
Participants were slower to perform
tasks when a simulated visual impairment was present.
Dr Peter Jones, from City, University of London's Crabb Lab, highlighted that while it is impossible to exactly recreate what it is like to have glaucoma, digital simulators can allow people to experience some of the challenges that those living with the disease face.
"We are now working with architects to explore whether sight-loss simlulators can be used to design more accessible buildings and transport systems," he shared.
Researchers from University College London have developed a new screening method to identify jaundice in newborn babies using a smartphone app.
The study, which is published in PLOS One, involved taking smartphone pictures of the eyes of 37 infants.
The babies selected for the study had all been referred for tests to measure levels of bilirubin in
the blood; a substance which causes jaundice when it accumulates in .o thebody.
The images were then
It also identified cases that would not normally require treatment 60% of the time. This success rate is comparable to expensive hand-held devices recommended for use by midwives in the UK.
Felix Outlaw, from University College London's medical physics and biomedical engineering department,
"Being able to use smartphones for jaundice would have a significant impact"
.0 0 processed to remove 1distorting effects of background light and .sthe yellowness of the eye was quantified } to predict the level of bilirubin in -~the blood. The smartphone app ! successfully identified all cases of o jaundice that would usually be treated.
highlighted that the new screening method would only require a smartphone and is a tenth of the cost of commercial devices
commonly used within the United Kingdom.
"Given that smartphones are common even in poor and remote parts of the world, being able to use them to screen for jaundice would have a significant impact," Mr Outlaw emphasised.
Appointment attendance linked to acuity
New research published in JAMA Ophthalmology
•has highlighted that patients with age-related macular degeneration (AMD) who miss a single visit could be risking a drop in visual acuity.
Over a two-year period, researchers observed the attendance rates of 1178 AMD patients from 44 different clinical centres.
Patients were required to attend 26 visits over the period, or one appointment every 30 days.
The scientists found that patients who had the highest attendance levels also had the best visual outcomes.
Ramakrishnan, et al.
DOI: 10.1001/jamaophthalmol.2019.4577
New treatment for thyroid eye disease
A new study published in New England Journal of Medicine has explored the effectiveness of treating thyroid eye disease using teprotumumab. A total of 41 patients were given the drug while 42 received placebo.
After six weeks, 83% of patients who received teprotumumab had a measurable reduction in eye bulge compared to 10% in the placebo group. The response rate in the group receiving treatment was 78% compared to 7% in the control group.
Those receiving teprotumumab had better outcomes in terms of quality of life and diplopia.
Douglas et al.
DOI: 10.1056/NEJMoa1910434
Using gene therapy to rescue photoreceptors
Scientists have explored the effectiveness of replacing mutated genes in mice with congenital blindness.
Describing their findings in Nature Communications, researchers highlighted that replacing a mutated sequence in blind mice resulted in approximately 10% of photoreceptors being rescued.
Following the procedure, the light sensitivity and visual acuity of the mice improved. The new approach is an alternative strategy to gene supplementation, which has limitations when treating patients with defects in larger genes .
Nishiguchi et al.
DOI: 10.7038/s41467-019-14181-3















The General Optical Council (GOC) has sought to clarify its position on the use of lissamine green by registrants.
The GOC notes that lissamine green is available as a CE-marked product for use as a 'diagnostic agent when superficial corneal or conjunctiva! change is suspected.'
The optical regulator adds that the Medicines and Healthcare products Regulatory Agency considers lissamine green should be regulated as a medicine, but there is no marketing authorisation in place.
The position statement highlights that there will be circumstances where it is necessary for practitioners to use CE-marked lissamine green ophthalmic strips within the scope of their practice.
It also emphasises the need for optometrists and dispensing opticians to act in the best interests oftheir patients at all times.
"We hope the statement will give registrants clarity and reassurance"
The statement was developed through collaboration with a clinical consensus panel including representatives from the AOP, the Association of British Dispensing Opticians, the British Contact Lens Association, the College of Optometrists and the Federation of Ophthalmic and Dispensing Opticians.
GOC chief executive and registrar, Lesley Longstone, shared: "We hope [the statement] will give registrants clarity and reassurance about using CE-marked lissamine green ophthalmic strips within the scope of their clinical practice."
Clinical director at the AOP, Dr Peter Hampson, welcomed the GOC statement.
"We're pleased that they have now set out a position which clarifies use for practitioners," he said.
"This pragmatic approach will mean that optometrists and contact lens opticians, who deem lissamine green the most appropriate way to assesstheir patients eye health, can do so without being concerned that they may face regulatory action," Dr Hampson emphasised.
Novel coronavirus (COVID-19) advice
The AOP has issued a series of updates to members in response to the novel coronavirus (COVID-19), following the release of specific advice by NHS England for optical practices.
The AOP guidance covered basic hygiene measures, what to do if optometrists suspected that a patient may have coronavirus and what steps practitioners should take if they were concerned that they have contracted coronavirus. The guidance also included an OT skills guide video which showed the correct handwashing procedure to follow.
The AOP emphasised that it is highly unlikely that patients who present to an optical practice with cold or flu-like symptoms will have the coronavirus.
"If patients inform you that they have any cold or flu-like symptoms before they arrive for their appointment then it is acceptable to advise them to rebook their appointment for when they have fully recovered," the guidance stated.
"If the patient only advises you of any cold or flu-like symptoms when they present to the practice, given the prolonged duration of close contact during an appointment, it is acceptable to advise the patient that you are unable to see
OT'svideo guide to hand washing correctly
them, and they should rebook on another day when they have recovered," it added.
A series of four standard operating procedures for GPs, pharmacy, dentistry and primary care optical settings were published on the NHS England website. The guidance covered the national approach to responding to coronavirus, including the three guiding principles of identifying, isolating and containing potential cases of the virus.
For the latest updates and help finding further advice, visit www.aop.org.uk/advice-and-support
Off-payroll working Essilor/Luxottica and The AOP has published GrandVision guidance on changes
The AOP has updated to the way the off members on the payroll working rules Essilor/Luxottica and are applied. From GrandVision merger, in 6 April 2020 these light of the European changes will roll-out Commission's phase II for medium and large investigation. businesses.
Illegal sales Amazon UK has removed several listings of adjustable spectacles.
At the end of a Phase
The roll-out of these I investigation, the rules in April 2020, Commission concluded which are part of a that the merger might package of measures reduce competition known as IR35, shifts in both wholesale responsibility for and retail markets for making employment optical products, which status for tax could lead to higher determinations from prices for consumers. the person receiving Members have been payment to the encouraged to register practice paying for the their interest in being service. kept up to date on
The AOP is running a the AOP's community webinar on 23 April. For forum, or by contacting more information, visit the policy team directly www.aop.org.uk/events on policy@aop.org.uk

The GOC received 12complaints from the AOP relating to the illegal sale of adjustable spectacles on the multinational technology company's website.
After the GOC received complaints from the AOP. its legal team investigated and contacted Amazon asking the company to remove the sales Amazon marked the products as 'obsolete' to ensure that no further orders of the reported items can be taken through the Amazon catalogue.
To book on an AOP member event, visit www.aop.org.uk/events































The retro cool of Los Angeles (LA) in the 1970sis the inspiration behind the new Light Blue Capsule Collection from Komono. Said to take its visual cues from the sun-drenched teenage surfers who found their community in the wavelike empty swimming pools of suburban LA during the city's draught, the frames are smooth, rounded, and striking in sky blue. The campaign was shot at LA's legendary Pink Motel, an iconic symbol of this almostforgotten period of Americana. Frames include the rounded 'Ana' (pictured) and the widesided 'Avery.' www.komono.com

New from eyewear consultancy Vision of Tomorrow is Mita's Collezione 1 -an eyewear collection that "melds fashion and sustainability with the style of Miami and elegant Italian craftsmanship," the company said. Made from recycled water bottles and aluminium and biodegradable lenses, the range's ethical commitment is clear. www.vot-eyewear.com

The timeless elegance of the Parisian woman is the inspiration behind this new collection from longstanding fashion bible Elle and Charmant. The Sunwear 2020 collection is "all about modern urbanity and standing out from the crowd with a vibrant colour pop," the company explained. Six designs are available, ranging from square frames to bold rims set within a dark green frame (pictured). www.charmant.com

Sunglasses created for "urban free spirits," Serengeti's 'Hamel' model offers minimal design and maximum character. Ultra-light mineral lenses along with metal frames have a light, bright look ahead of the warmer months. Lenses are treated to ensure they are scratch-and impactresistance, and have an anti-reflective coating that aims to reduce glare. www.serengeti-eyewear.com





www.ucl.ac. uk/ioo/study


Founder of iconic tailors, Hackett London, tells OT why glasses are a fashion essential
1
1think you take on different personas when you wear different glasses. You behave differently. I would wear different glasses for different occasions. I'm not sure people used to think like that in the past. They just had this one pair of glasses that they wore forever.
2
Hackett's new Signature Collection through Mondottica was inspired by my cufflinks, which are my signature. We are using the best manufacturing to create the range, and I'm very happy with it. The glasses are made using Japanese acetate with a horn effect for a soft warm look. We are also using titanium, and lenses created by Zeiss. The gun metal plaque on the sides that bears my initials, }PH, adds panache to the design.
3
I have glasses going back years, if I haven't lost them of course. They are dotted around the house, in the car, in the office. I always forget them, or forget where I put them down. When I have good glasses, I tend to look after them. It's a bit like umbrellas: if you've got a cheap umbrella, you put it down; if you've got a good one, you go back and find it.
4
There are few things that men can wear without being overdressed.
I think glasses add a little bit of mystery and character to people, depending on what they choose. You can change your image from one pair of glasses to another. They can wear cufflinks, they can wear a nice watch, and they can wear glasses. O

Optometrist and lifestyle blogger, Lizzy Yeowart, takes a look at modem metallics

Coastal calling
This bronze, soft octagon frame from Prodesign ticks every trend box and combines functional, clean Danish design with colours and forms inspired by the Danish coast. Prodesign, '8127.'designeyeweargroup.com

Vintage chic
Bring retro styling right up to date with this luxury style by Vysen. The 'Arie' in rosegold stainless steel with rose-gold mirror lenses combines a vintage feeling with innovation and glamour. Vysen, 'Arie.' vysen.com

For the divas
This exclusive Chopard sunglass model with gradient lenses and precision-cast metal detail on the side is dedicated to the Red Carpet Collection. The mirrored palm leaf-effect provides diva-esque allure. Chopard, 'SCHD485,' www.derigo.com
Active folate
Ocufolin has launched an ocular dietary supplement, targeting AMD and diabetic retinopathy. The product, Ocufolin forte, contains L-Methylfolate calcium, the active, bioavailable form of folic acid. The company explained that the supplement "supplies the retina with active folate -the missing link in first-generation ocular supplements." The nutrient combination is said to reduce the disease-related increased homocysteine level in patients. The product is classed as a 'Food for Special Medical Purposes' by the British Specialist Nutritional Association. www.ocufolin.co.uk \;:..

Hit the slopes
For those seeking out the last of the season's powder, the new wraparound 'Florio' ski glasses from Finlay London are a carry-on must. The Zeiss lenses have full UVA/UVB protection, with scratchresistant coating. 'Florio' is best suited to heart, oval-shaped and round faces. Frames are available in matte pink and matte black, and lenses in gold, orange, purple or silver. Also available with prescription. www.finlayandco.com
70s inspired
Five new styles have been added to the Acetate Bold Series by Tree Spectacles. The frames are available in matt black, shiny gold and gun metal grey, and come in retro, 1970s-inspired shapes with a fresh and contemporary edge. Also new are the seven models in the Acetate Light Series (women's, men's and unisex), which offer a sleek aesthetic with 1.7mmframes in classic black. cappuccino and light blue. www.treespectacles.com




Sustainable eyewear brand Neubau has launched its first collection of100% bio-based frames, all of which are named after well-known environmental activists. Made in a 3D printer from entirely natural materials, 'Greta,' 'Bill,' 'Erin' and 'David' are designed to reinforce the company's commitment to creating sustainable products within an industry that has potential to create huge amounts of waste. www.neubau-eyewear.com
Sports, streetwear and fantasy make a heady combination that celebrates a decade of creative collaboration between Mykita and designer Bernhard Willhelm in this new sunglass collection. Sculptured silhouettes, hand-lacquering and airbrush gradients are utilised, bringing to mind the Venice Beach aesthetic of the early 2000s. The collection consists of four frames, each made up of two pairs: 'Super' and 'Lost,' and 'Total' and 'New.' www.mykita.com
To feature in OT's Hit list, contact kimberleyyoung@ optometry.co.uk
Luxury architecture
Fit, function and style are the key components behind the March 2020 collection from Evatik. Designed with minimalistic architecture in mind, the four styles that make up the collection are light and timeless, offering a choice between rectangular and round shapes, semi-rimmed and rounded, and an update on the classic navigator. Stainless steel is a key material, and a matte finish ties all of the frames in the collection together. www.evatik.com


Lens innovation
Avizor has launched Ever Clean Plus, which it promises to offer "the ultimate innovation in contact lens care." The 3% hydrogen peroxide solution is designed for deep elimination of the lipids that adhere themselves to contact lenses. With a four-step process that involves lipid cleaning, protein cleaning, disinfection and moisturising, the system is suitable for RGO (ortho-k), silicone hydrogel and soft contact lenses. The solution is preservative-free. www.avizor.es/





The AB Max™unique pulse mode gently cleans and massages the anterior eyelid margins, providing a more comfortable treatment experience and helping to reduce or alleviate symptoms of Anterior Blepharitis.
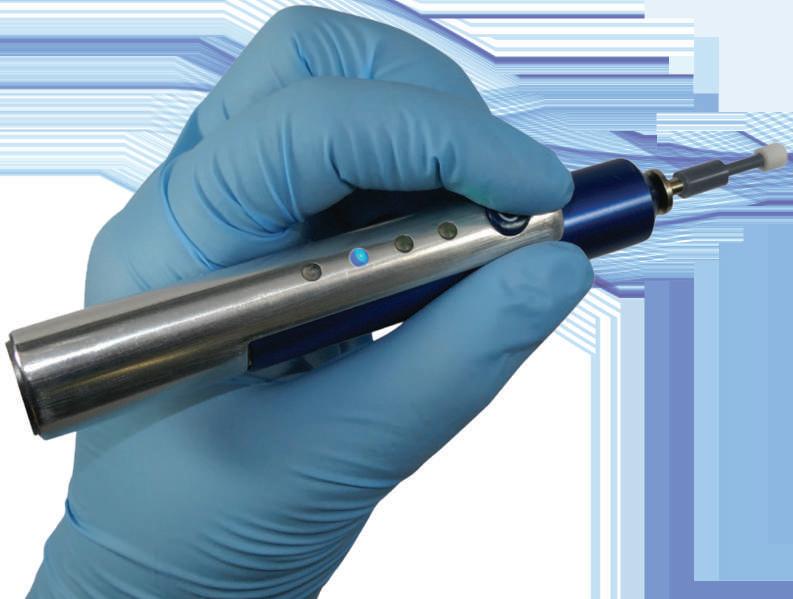

Contact us for information or buy online at graftonopti ca I .com/grafton-shop
For a quote or to arrange a demonstration please email sales@graftonoptical.com or call us on 01923 233980.





Co-founder of the eponymous brand, Ed Bird, talks to OT about his company's journey -and the increasing importance of doing good
1
Most of the frames are named after birds, and the designs and colours draw inspiration from birdlife
2 Bird products are available for purchase at Cornwall's Eden Project
3
Musicians love Bird frames: they've been on tour with Joss Stone and Rag 'n' Bone Man, and featured on US singer Kevin Max's album cover.



Clockwise from top left 'Strix' -cotton-based acetate tortoiseshell frame, with part wooden sides; 'Blackcap' -eight layers of real wood with two core layers of aluminium; 'Wren' -eight layers of real wood with two core layers of aluminium
Each month, OT columnist, Lizzy Yeowart, considers a classic dispensing scenario. This month we look at glasses for a 10-year-old high myope

Haseley and Co has an excellent selection of eyewear that is lightweight and durable. In a choice of colours, this grown-up shape will give kudos to every cool kid. Bondeye Optical, Haseley &.Co Kids Ophthalmics range, www.bondeyeoptical.co.uk
"It is true to say that finding a frame for a fashion-conscious 10-yearold isn't always an easy task. Give your 'tweenage' patients something to smile about with one of these stylish options."

Oversized
Tomato Glassesare highly adjustable and are made out ofTR90,which is safe, lightweight and flexible. Along with the adjustable sides, there are different nose pad sizeswhich can be adjusted into three different positions. Tomato Glasses, 'Junior A in camo' www.tomatoglasses.com
..,J,/















CKeeping the patient at the heart of everything we do and all the decisions we make are key
Henrietta Alderman
ustomer service is a vitally important part of any business, whether it's face-to-face or online. It is what binds a customer in, especially if there is a good relationship or they feel the business has worked especially hard for them to achieve a happy outcome. The reverse is also true of course. Poor customer service is the surest way of losing a customer. We all know that the cost and effort of gaining customers far outweighs the cost of retaining them.
The supplement in this month's OT celebrates the winners from our annual Awards, which took place at 100% Optical. Our award winners have demonstrated excellent
customer service in many ways and have exceeded the expectations of their patients. Success breeds success and the practice culture of going the extra mile to help patients brings rewards both personally and for the business. It is so good to see these individuals and practices being recognised.
We need your vote
problem. Sometimes it makes good business sense to accede to a customer's wishes, even if we know we are not in the wrong. In the optical sector we are fortunate to have the Optical Consumer Complaints Service, which does such a good job mediating and resolving issues at an early stage -many of which are related to retail and poor communication (read more on page 45 of this edition).
Protecting the good name of a business and brand matters, and at a time when the opportunity for any individual to give a review that could reach many thousands has never been greater, keeping the customer close has never been more important. Social media has changed the way we all make decisions. Reviews by users, for example about a holiday on TripAdvisor, play a part in our decision making.
The AOP is no different. Keeping you at the heart of everything we do and all the decisions we make enables us to deliver services and respond quickly when needed. For example, when you told us you would rather speak to a person when you call AOP rather than
"Success breeds success and the practice culture of going the extra mile to help patients brings rewards"
We all deal with difficult situations and customers during a career, and managing them so that everyone feels satisfied is part of good business. The maxim that the customer is always right may not work in every circumstance, but it offers a starting point. Fully understanding the problem before drawing conclusions is not easy, but it can save time in the long run. The time taken in dealing with complaints can be disproportionate to the
go through an automated system, we changed our system to enable you
to do this whenever possible.
And when you responded in your hundreds to a request for views on degree level apprenticeships, we were able to react quickly and represent your views appropriately. We need to know your views -either directly to the team here or through
your Council members. We want members to get involved in our work, which is why we encourage members to stand for election to our Council or to apply for one of the appointed positions. April will see voting for AOP Council seats across the UK. Voting closes on 23 April, so watch out for an email from Civica, which will contain your unique link to the online voting site.
0 Henrietta Alderman is chief executive oftheAOP
What is your view? Email OTwith your comments newsdesk@ optometry.co.uk

Iffl t!tffl I Voting for AOP Council opens on 1April www.aop.org.uk/ advice-and-support

CLet's help people to feel more in control of what is happening to them at the difficult stage of diagnosis
Poonam Patel
oming to terms with a diagnosis that has the potential to cause sight loss can be distressing. If patients are told in a manner that they find insensitive or in a way they can't completely understand, it can be even more traumatic. It's important for us as eye care professionals to remember that it is not just at the point of diagnosis that good communication is key, but that the need for further communication on this subject may be ongoing as a patient's eye condition or sight changes over time.
As an eye health information officer at the Royal National Institute of Blind People (RNIB), my role involves giving people information about eye health and eye conditions, taking the time to answer someone's eye health questions in clear and
"It's important that optometrists allow themselves time when discussing news of a diagnosis"
patients may often come to them for routine eye tests following a diagnosis at the eye clinic. Often when people hear bad news, they only take in a certain percentage of it, or don't even realise it is bad news. Optometrists are well placed within the community where patients can have a point of contact for further information or questions about what they have been told about their diagnosis. They can take time to explain and back up what they have understood about their eye condition and any future treatments.
It's important that optometrists allow themselves and the patient time when discussing news of a diagnosis that may cause or has caused sight loss. Allowing extra time to have this conversation is important so that the patient doesn't feel rushed, as well as giving them time to ask any questions. A lot of patients will often go home and, after reflecting, will have more questions. Inviting patients to come back and speak to you if they need to ask further questions can let them know that you are there for them.
SightlineDirecto
Services to help blind or partially sighted people
www.sightline directory.org.uk
simple language by phone or email.
The RNIB Eye Health Information team is part of a national telephone sight loss advice service. Most of our work is over the telephone, speaking to newly diagnosed people about their eye conditions. This may be anything from dry eye to age-related
macular degeneration to much rarer conditions. Our aim is to provide information that will hopefully enable people to feel more in control of what is happening to them at the difficult stage of diagnosis or when sight has been affected.
Optometrists are often the professionals who first spot something that may be a concern. When this is flagged to the patient, it may be the first time the patient is aware of a possible problem. Although the optometrist may not give a formal diagnosis, they do need to be able to explain that there is a potential concern that needs addressing. It can be a difficult balance between scaring the patient but also getting them to take it seriously. Communicating this in a calm way can help avoid panic, but it's also important not to downplay the seriousness of any action you wish for them to take, such as seeing their GP, attending eye casualty or complying with their glaucoma eye drops.
Although optometrists may not be the ones directly giving the diagnosis and prognosis,

It's also helpful for optometrists to be aware of local support available for someone facing sight loss. For example, having a list in the consulting room of local sight loss societies, local support groups as well as national organisations, such as RNIB, can mean you are able to signpost people to support early. The SightlineDirectoryis also a useful tool for searching for local sight loss support services.
0 Poonam Patel is an eye health information officer at RNIB and an optometrist



To find out more about Sensity 2, email: supportingyou@hoya.co.uk or visit our website www.hoyavision.co.uk

"Getting a guide dog was like winning the lottery. It is incredible"
Dave Thomas
After I left school at the age of 15, I did an apprenticeship at the Burnley Football Club. On your 17th birthday they call you in to say whether they are going to offer you a professional contract or not. I got the contract.
During my football career, I played for Burnley, Queen's Park Rangers, Everton and Wolverhampton. In the professional game, it is every player's dream to try and represent their country. I was lucky enough to do that eight times. I had a wonderful career. I value that so much. There is no better life than that of a professional footballer.
As a sportsman, there are lots of highs and lows. You are mentally prepared for certain things. Having a positive outlook on life has certainly helped me with the massive change in my life that has come through becoming a guide dog owner.

I had been approached in the past about an autobiography but I turned it down. The thing that convinced me this time around was that David Roberts, the publisher, has produced a commentary for blind and visually impaired Watford fans during every home game over the past 20 years. He doesn't get paid. I thought 'He is my type of guy.' Sometimes in life it is not about getting paid. It is about giving something back.
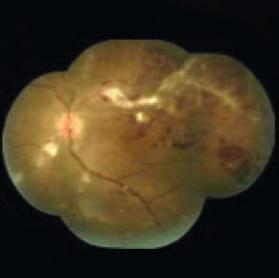
The diagnosis
I found out 20 years ago that I had glaucoma. When I did the medical for the football clubs, the one thing they never tested were my eyes. If I had my eyes tested all those years ago, I might not have been in the position that I am in now. I was 50 when I was diagnosed. It was
IzjfflffljttOttti
The AOP has produced a series of downloadable eye condition leaflets www.aop.org.uk/patients
the optometrist who picked it up. I felt like I needed glasses for reading so I went to the opticians. He told me I needed to see a specialist. I probably had the condition without knowing for years. Glaucoma is that sort of disease -it is a silent condition that comes in on you. When I lost my driving licence, that was a massive change in my life. A brown envelope came through the post one morning. It said, 'Dear Mr Thomas, I'm sorry to inform you that you have failed your fields of vision and you cannot drive again.' It was an absolute bombshell. You have two choices: you can either sink or swim. I was shocked but I got over it. The most awful thing before I had the dog was when there were loads of people around. When your peripheral vision goes, you feel as if you are going to walk into people. On the odd occasion we would go to people's houses where there was a crowd and I would just sit in the corner. It made me less social. I didn't want to talk to people.
Getting a guide dog was like winning the lottery. It is incredible how they match the dog to the owner. We are in the countryside. There are no footpaths or kerbs and we have one bus every hour in the village. We have horses, ducks, geese and chickens. You don't want a guide dog who is chasing after the chickens. They think of everything.
My dog Hannah is the most wonderful dog ever. She is a golden Labrador. Wherever I take her, I trust her so much that it gives me the confidence to go places where there are lots of people around. I can't tell you how much difference the dog has made. It is just absolutely fantastic. 0
Dave Thomas is a former professional footballer and guide dog owner. His autobiography, Guiding Me Home & Away, is published through Hornet Books.
Share your views. Send letters and tributes to OTvia email to johnwhite@optometry.co.uk
As the chair of Worcestershire LOC, I feel that several points that Nick Rumney raised need to be rectified in the article, The case for change (OT March 2020, page 56). Contrary to his belief that his neighbouring counties have 'zip' services compared to Herefordshire, we actually have four community services at present in the area, including MECS (which has been running for over 10 years in various guises), post-cataract assessment, IOP repeat readings and a children's pathway. We are also trialling a precataract assessment pathway. There are also services available in neighbouring Shropshire and Gloucestershire.
Perhaps Nick would like to talk with his neighbouring practices, especially those in Herefordshire who hold contracts to take part in our service. Please note that no practices in Worcestershire are able to hold a contract for Herefordshire -not for lack of trying, but as all contracts in Herefordshire are held singly and not by an overall Limited Company. Incidentally, any practice is welcome to apply for a Worcestershire contract via Optomanager.
I am sure it will give Nick much peace of mind that Herefordshire and Worcestershire are now one STP and the merger of our clinical commissioning groups from 1April 2020 will enable us all to provide a more uniform service in the future. We are all hopeful of and working towards more consistent commissioning of services in England, so that postcodes will no longer be a barrier for our patients, who we are all working hard for.
Mrs Harpreet Kular,optometrist and chair of WorcestershireLOC
points

After reading the four narratives in the article My strangest day in OT (January 2020, page 57), I was very encouraged by the care and actions of our dedicated optometrist colleagues. I think that many of us have gone through one of the 'strangest day' scenarios. I would even say that this might be a 'normal' day for many of us.
I have been working as a locum optometrist for many years. I have come across a number of emergencies such as urgent referrals or unwell patients. I wonder if a few multiples are moving more towards financial targets rather than patient care. I have been informed by one multiple that I had to do at least 20 eye examinations day otherwise my locum fee will be halved. I am sure one would need to spend at least 30 to 60 minutes on each challenging and interesting case.
As I've also worked as a junior doctor in a number of hospitals, I've been grilled extensively regarding patient safety and advocacy. I wonder who of us would like to work and be get paid half by advocating for patients and whether locum optometrists have been given enough support, especially new to the team.
Due to over capacity of eye care emergency, there is also pressure that has been put on optometrists to take on extra responsibility roles, such as MECS.
Dr T Nguyen, Robert Stanley Opticians, Oxford
"We are all hopeful of and working towards more consistent commissioning of services in England"



















With today's contact lens wearer being more health conscious than ever,2the case for silicone hydrogel material has never been stronger. CooperVision have over 50,000 power options in its silicone hydrogel range,1 so there's more opportunity to prescribe the benefits of silicone hydrogel to a wide range of patients according to prescription, modality choice, lifestyle and budget.3
Prescribeoxygen
Evidence supports the routine prescribing of silicone hydrogel contact lens materials in preference to conventional hydrogels to avoid hypoxic effects of soft contact lens wear.4
(Figure 1)
Oxygen map of lens at -3.00D5 5
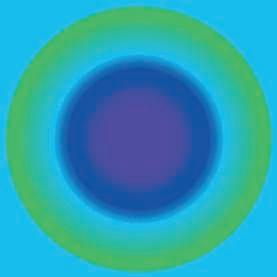
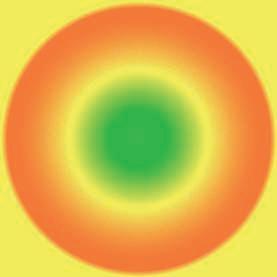

Oxygen maps allow a clearer understanding of the actual oxygen transmissibility across the entire profile of a contact lens. Typical lens profiles (Figure 1) of a silicone hydrogel and hydrogel lens illustrate the differing levels of oxygen transmissibility and how they perform relative to the established thresholds to avoid corneal swelling of 24Dk/t at the centre 9 and 33Dk/t at the periphery. 8
The CooperVisionsiliconehydrogel portfolio
Range - x5 more choice than any other large contact lens manufacturer. 1
Cost - A range of options to match lens performance and wearer needs; for new wearers, for those with busy lives, and those who demand high performance. 3
Comfort - Naturally wettable third-generation silicone hydrogel material technology, designed to resist dehydration. No need for surface treatments or coatings.
Health - Lenses designed to minimise or eliminate the effects of hypoxia; 10 a comprehensive daily disposable portfolio option, 11 with UV blocking. 12
Quality - Consistent, excellent quality of product with high precision, automated lens manufacture and constant quality innovation.
Benefitsof prescribingsiliconehydrogel
Good for patients - Most wearers would like to be more informed about the options available to them. 13
Good for you - Most wearers would have a positive opinion of their eye care professional if they were offered new products. 13
Good for business - Satisfied wearers are more likely to be loyal and recommend their eye care professional. 13

50,000 power parameters is a lot to choose from, so our FREEOptiExpert app makes lens selection easy.





Download the FREEOptiExpert'" app from the Apple and Play stores, designedto make lens selection easy and accurate.
1. At leastx5 more siliconehydrogelpower optionsthan other mainmanufacturers.CooperVisionDataon File.Basedon power options availableacrossall siliconehydrogelsoft lensesfrom four main manufacturersin UK May 2019. In stock, madeto order,sphere,toric & multifocal.Cosmeticand Photochromaticlensesnot included.Multiple basecurve variants not included. 2. Mintel. GlobalConsumerTrends2019. 3. Basedon CooperVisionrecommendedretail prices.Retailprice is solelyat the discretionof the retailerat all times, the above is not meant to influencethe price any retailercharges. 4. FonnD. and SweeneyD. TheBenefitsof SiliconeHydroge/DailyDisposableLenses.Contact LensSpectrum 2015. 5. PhaseFocus'"·HighresolutionDk/t profiles.The Dk/t scalehasbeen standardisedto enablecorrect like-for-like comparisonof Dk/t over the completelens.2016. 6. MyDay®dailydisposable.7. 1-DAYACUVUE®MOIST.ACUVUE®is a registeredtrademarkof JohnsonandJohnsonMedicalLimited. 8. Morgan,Brennanet al. Centralandperipheraloxygen transmissibilitythresholdsto avoidcornealswellingduringopeneye soft contactlenswear.J.AppliedBiomaterials.2010;92:361-5. 9. Holden,BA, Mertz, G.W.Criticaloxygenlevelsto ovoidcornealoedemafor daily andextendedwearcontactlenses.InvestOphthalmolVis Sci.25 (10):1161-1167. 19B4. 10. With higheroxygenpermeabilitythan hydrogelmaterials,siliconehydrogelcontact lensesminimiseor eliminatehypoxiarelatedsignsand symptomsduring lenswear. 11. Dailydisposablelensesare the healthiestway to wear soft contact lenses. 12. Warning:UV-absorbingcontact lensesare not substitutesfor protective UV-absorbing eyewear,such as UV-absorbinggogglesor sunglasses,becausethey do not completelycover the eye and surroundingarea.Patientsshouldcontinueto use UV-absorbingeyewearas directed. 13. CooperVisiondata on file. Consumerinsightstudy, July 2018. GBadultswho wear soft contact lenses.N~470 (DD~279, FRP~191). Appleandthe Applelogo aretrademarksof Apple Inc.,registeredin the U.S.and other countriesand regions.App Storeis a servicemarkof Apple Inc.GooglePlayandthe GooglePlaylogo aretrademarksof GoogleLLC. (c) CooperVision2020





















39 Life as a locum
Optometrist Craig McCoy discusses life locuming across Scotland and the Highlands
45 The workshop The OCCS' Richard Edwards explains how practices can deal with complaints
THE DISCUSSION
all
Optometrists-come-practice-owners Conor Heaney and Anthony Clarke on building their businesses
When it comes to exceeding patients' expectations in practice, for practice director Conor Heaney, it is all about an experience that starts for the customer before they
even walk through the practice door. Mr Heaney first entered practice ownership in 2005 when he jointly opened Seen Opticians in partnership with Tareq Moustafa.
47 How I got here
How do

It was during this venture that Mr Heaney realised that there was so much to business ownership that he did not know about and was not prepared for.
"[Owning a practice] is about much more than just what goes on in the testing room or when you dispense spectacles, and I very quickly realised that," he told OT.
A clinician by training, he set about building his business knowledge and know-how through a combination of reading, attending events and seminars, going to trade shows and "generally taking an interest in things outside of the realm of optometry," he explained.
Buildinga business
Today, Mr Heaney owns Jones and Co. Styling
Opticians, an independent based in Manchester. Mr Heaney' s aim was to build a high-end practice that offered something different to other opticians on the High Street. Its unique selling point would be its eyewear and dispensing experience. Today its average dispense ranges between £800-£900. The practice's philosophy is to be unique. "We are for people who want to look good and feel good in their glasses and we talk
"It was probably a chaotic process. There is a saying that success is cooked up in a messy kitchen and you have to try lots of stuff"
ConorHeaney
about this through our marketing," he highlighted.
Mr Heaney shared that when embarking on this journey, after investing in himself, he realised that it was equally as important to invest in his practice team. "Your team must understand and buy into the practice's mission too so they are able to deliver on the experience that you aim to provide. Trying to deliver on an experience is pointless if you are the only one who gets it," he said.
For Mr Heaney, developing a practice that meets and exceeds patient expectations does not happen overnight and change is constant and gradual. When asked about the changes he made that helped him towards his goal, Mr Heaney highlights taking frames off display as an eventual gamechanger.
"From a customer experience point of view, choosing glasses is difficult and most people hate the process because they don't know what fits or suits them. Recognising this and how it fits with our philosophy, we decided to take frames off display to eliminate this pain point and offer them a 45-minute styling consultation instead," he shared.
The consultation is designed to allow the dispenser to learn about the customer at a casual pace after which they handpick a selection of frames based on the customer's lifestyle, prescription and style.
Mr Heaney admits that the change was not an overnight success and

"We decided to take frames off display to eliminate a pain point and offered patients a 45-minute styling consultation instead"
Conor Heaney
people would question why there were no frames on display, but he persevered. When asked if there was a pivotal moment when he felt that things begun to change, Mr Heaney admits: "It was probably a chaotic process. There is a saying that success is cooked up in a messy kitchen and you have to try lots of stuff to see what works."
Happy to share his experiences with likeminded independents to help them succeed in practice too, Mr Heaney established the Optical Success Academy (OSA),
"The
practice is designed to be engaging and the time spent in practice is enjoyable - everything is done at a much slower pace"
Anthony Clarke
an organisation that provides coaching and training on all aspects of running an optical business.
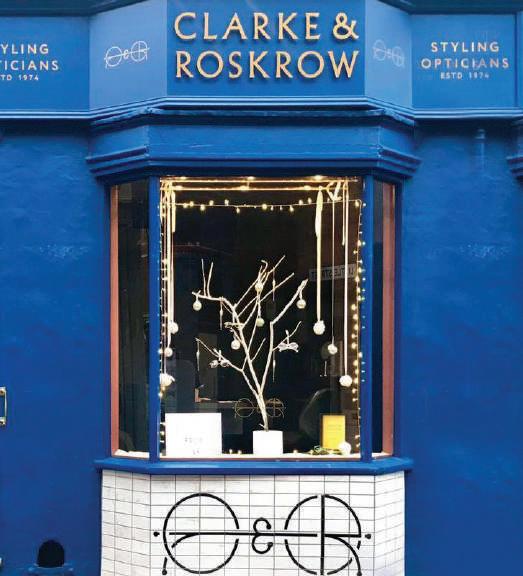
Supporting others Practice owner at Clarke & Roskrow Styling Opticians, Anthony Clarke, is a member of the OSA and advocates the support that it provides him and his business. Mr Clarke became a practice owner in May 2014 when he took over what was then K&G Roskrow Opticians.
Describing the practice that he purchased, Mr Clarke said: "It was a longestablished practice that had been in the town for 40 years. It was a secondgeneration practice; it was quite old school and was on a downward spiral."
Seeing the potential, Mr Clarke took the leap and because in his mind he knew the type of opticians that he wanted to create:
a mid-to high-end business that offered clients a unique eyewear experience that was different to what was available at other opticians in the area.
"We knew that there was a gap in the market for an optician in the town that could offer something unique and something special," he shared.
However, the optometrist realised that he did not know how to get there.
"I had a clear idea in my mind of what I wanted the final goal of the practice to be, but it quickly dawned on me that my clinical skills alone would not be enough and I didn't know how to get there," he said.
With support from the OSA, Mr Clarke was able to hone his ideas, build his business knowledge and in 2017 the practice embarked on a seven-month transformation.
"You wouldn't recognise us as an opticians," Mr Clarke shared.
"Differentiating ourselves and showing our clients that we are different was the goal," he added.
When discussing how the practice is exceeding patient expectations, he shared:
"It boils down to taking a genuine interest in the client who is sitting in front of us. The practice is designed to be engaging and the time spent in practice is enjoyableeverything is done at a much slower pace."
"We're engaging with our clients on a level that they have probably never experienced before and providing a personalised experience," he closed. 0














"Itry to keep up with referralsas I go"
Locum optometrist, Craig McCoy,discusses phasing out his full-time residency role to locum for independents across Scotland and the Highlands
Before the week be ins I try to keep myself bookedup a month or two in advance and at the start of each week I'll look at where I am going over the next seven days. If I am locuming in a practice where I haven't worked before, I always try to visit it in my own time before my first day. Being a locum, the worst thing in the world is having a patient in the testing room and not
ABOUT CRAIG
Qualified: 2014
Previous roles:
Full-time resident optometrist in a multiple
Based: Aberdeen.
being able to tum something on or flicking a switch and it doing something different from what you expect it to -visiting ahead of time eliminates this.
flii:iJ
In terms of travel, there isn't a typical journey. If I am locuming in Aberdeen, then I will walk to work. However, I will sometimes drive around an hour or so to the practice where I will be that day. In addition, sometimes I work in the Highlands and Islands for weekly periods and the practices will provide accommodation. On those occasions I wake up and I am already at work.
I always have a bag of equipment and my laptop
packed ready to go. The equipment that I tend to carry round is perhaps a bit more specialised than most because in Scotland there is a minimum amount of equipment that each practice has to have in order to comply with the General Ophthalmic Services contract.
(,Em I arrive 15--20minutes before my first patient so I have the time to get familiar with the testing room and make sure I can tum everything on. The first day in any practice can be a bit stop/ start, but after you have seen a few patients you know where you are moving to next.
l:fT:IiII I try to keep up with referrals as I go. Across most of Scotland we have access to electronic referrals. So I need to be assigned to a practice before I start a shift in order to be enabled to process referrals as I go. I try to keep up with referrals as I go so I don't have to stay late.
mmJ If I bring my own lunch, I go to the break room to eat. If I have referrals to do, I will try to get a couple done over lunch. In a new location, I always try to take a walk around the town too.
E':mJ At the end of the day I pack up my equipment and leave a note for the regular optometrist regarding anything that I feel they need to be made aware of, such as patients who have been booked in for a follow up. Before leaving I always take the time to do a doublecheck to make sure that I don't leave anything behindit has happened before. 0
When did you become a locum and why?
I first started locuming in June 2018.I had spent the months leading up to that considering my options away from being a full-time resident optometrist with a multiple. I had gone through a joint venture partnership pathway and decided that it wasn't for me. Based in Aberdeen, I was also aware that there was demand for locums in independent practice. Wanting to explore my options, I secured some pre-agreed locum work and slowly began to reduce the days I worked as a resident optometrist, moving from five to four days, and then to three, two and one before becoming a locum full-time.
What do you most like about locuming? What I most like is the freedom and flexibility that I have when it comes to weekend and holiday planning. Testing times are also more relaxed. I only work for independents now, as well as the odd sickness and annual leave cover for Duncan and Todd.
What is the one thing you know about locuming now that you wish you knew before you began? I took quite a long time considering the notion of locuming before taking the leap. The one thing I would say is to make sure that you have a few years' experience under your belt, especially if you are going into a practice where you will be the only optometrist present.


Designed to slow myopia progression in children -the system offers both orthokeratology and daily disposable contact lenses specifically CE-approved for myopia control. These are supported by a mobile app which enhances monitoring and communication between eye care professionals and patients.
Get in touch to find out how to become a certified Menicon Bloom™practitioner, by email at enquiries@menicon.co.uk or phone +44 (0)1604 646 216.
Pre-reg optometrist, Daniel Chung, on his one week hospital placement and preparing for Stage 2
Iam glad to report that I have now exceeded the number of patient episodes that are required of the pre-reg during the Scheme for Registration, with just the series of elements of competence for rigid gas permeable lenses to cover at my next visit. With this in mind, I have now shifted my focus to Stage 2 of the year.
One of the main reasons I am so passionate about optometry is the impact that you can have on people's lives by giving them spectacles or reassurance of their vision. However, testing many patients' sight during my pre-reg period, I have realised how patients underestimate just how much information an optometrist can identify about their health. One of the most common symptoms patients present with are headaches. Although many headaches do not have an ocular cause, those that do are likely refraction, binocular vision or idiopathic in origin. However, some can have a more serious presentation.


Last month, a patient presented complaining of headaches and thought they were simply because she had lost her spectacles. On thorough questioning, it became apparent that these were not your "average" refractive headaches. And after a comprehensive examination, it became clear that the patient had papilloedema, a condition I thought I'd never manage during my pre-reg training.
After being seen at Bristol Eye Hospital, the cause was not sinister, but further investigation was required. The patient came back into practice to thank me and reported: "I shall never neglect my two-year recalls." I shall hold this story closely to remind others why it is so important to get your eyes checked and never ignore symptoms, no matter how trivial.
Commonly, a difficulty faced in community practice is seeing sight-threatening
The biggest learning curve so far has been learning that during the pre-reg year it is okay to ask for help and make mistakes, and the more patients you see, the more opportunities you have to learn something new. Preparing for each visit has also been a learning curve in itself. For each visit I have
pathology such as uveitis because many of these patients will present to eye casualty.
As part of the pre-reg you must complete a minimum of one week in the hospital eye service. This is an enjoyable experience as you encounter conditions that are rarely seen in primary care and you can observe how the patients you refer into secondary care are managed. I completed my placement at Bristol Eye
"With all of these resources available to me, I definitely feel more prepared and at ease for the next part in my journey to become a proficient optometrist"
Hospital, which doubles as a teaching hospital for medical professionals. Primarily, you will observe specialist optometrists, consultants and nurses examining
been able to work on the feedback I received from the previous one, which has made revision a lot simpler.
When I am qualified I would like to broaden my skills and work in a variety of different settings, such as a busy multiple and hospital clinics. I would also be interested in
OTskills uides OT has developed a range of short video skills guides to aid students in their studies www.aop.org.uk/ otskillsguides
patients and carrying out surgical procedures, as well as obtaining witness testimonies for competencies you're unlikely to see in primary care. My advice to those who are yet to undertake their placement is to prepare as much as you can. This way you will get the best out of the sessions, and the discussions between the practitioners and patients will be easier to follow.
Preparingfor Stage 2 I will soon be working towards Stage 2. There are many courses out there to help pre-regs prepare for this, though one I would recommend is the J&JSTEP programme. Should you obtain a place on the course, at the end you are invited to mock Objective Structured Clinical Examinations which I have heard many good things about and look forward to.
Should all go to plan, I hope to share my experience of Stage 2 and provide some tips on how best to prepare shortly. 0
completing the independent prescribing course and achieving a diploma in glaucoma as it has been an ocular complication that I have seen consistently throughout my pre-reg year.
Samrina Awan is a pre-reg optometrist at Specsavers in Pinner.
OT spoke to optometrists about the positive impact the online GOS system has had for the practice and patients
For any business, making an important financial, regulatory or technical transition will involve time to prepare and adjust before making the leap.
One much-anticipated change for the optical profession last year was the launch of Primary Care Support England's (PCSE)electronic General Ophthalmic Services (eGOS) system. OT caught up with two optometrist practice owners to find out what their experience of using the system has been like, and why they are encouraging peers to make the switch.
Seeing the benefits in action
Optometrist Stewart Townsend explained that his practice, B Newbold, has had eGOS since September 2019 and was an original pilot site for the Optix eGOS system, which is one of a number of eGOS solutions created by practice management system (PMS) providers for their customers.

"Without question, eGOS has improved the running of the practice. It is easier to use, easier to administer and we get paid in a timely fashion and are able to reconcile that payment"
Stewart Townsend
He told OT: "From the beginning, it was clear Optix had really thought about how to implement this and make it seamless. The workflow of the eGOS system
specific, so needed to use PCSEOnline when he moved is straightforward and managed with a few clicks. It took about half a day for the whole practice team to be comfortable with all aspects of the system."
Optometrist and AOP Councillor, Stewart Mitchell, explained his practice uses a PMS that is not optometry-
to electronic payments. Representing the AOP and small businesses on the PCSECore User Group, the practice initially used the online service for GOSl and 3 forms. The success of the system now means that the practice submits all GOS forms using PCSEon line.
Following the rollout of online payments, a range of advantages have been identified that reflect the various
O To date, nearly 300 stores are already signed up to the electronic claims system. PCSE expect to see a marked increase throughout in the spring as pilots are ramped up into the full roll-out programmes
O PCSE processes in the region of 18 million GOS claim forms annually. Stacked on top of each other, that would equate to a paper tower that was higher than the Burj Khalifa in Dubai
O As of 4 March 2020, PCSE had over 60,000 on line claims submitted since launch, most of which have been made in the first two months of 2020
O Taking claims online can have a massive environmental benefit -an annual saving in CO2 emissions that's the equivalent to driving an average sized car non-stop for three years, running an optical store for nearly 50 years, or having one energy-saving lightbulb continuously lit for more than 500 years.
needs that different users have for the system. For Mr Townsend, the Optix integration means he is now fully aware of rejected claims "more or less instantly, and these are usually when the optometrists have not coded an early sight test."
He added: "The time and resources saved by not using and checking paper GOSl forms is significant. Not having to print, check and post is a great efficiency. The ability to batch-sign many forms at once is a bonus."
Mr Mitchell highlighted to OT that PCSEOnline works well for patients too. "In the past, when a patient who was GOS-eligible booked an appointment we had to prepare a paper form. Now, we add the patient's details and eligibility reasons on to the on line equivalent. The patient then simply signs an electronic declaration on a touchscreen in a way similar to signing for a parcel from a courier. Patients are impressed with the electronic forms -it shows we are moving with the times."
Mr Mitchell explained that a key advantage for practices of PCSEOnline is that it is not possible to submit a GOS that is not complete. "If you forget to tick a box and the patient signs, you
Advertorial
Stewart Townsend, B Newbold

O Single-site independent practice, nine days testing a week and performing around 250 GOS sight tests a month
O Running the online system since September 2019.
Stewart Mitchell (Eyecare)
O Single-site independent practice, with a mix of GOS and private, with around 50 GOS! a month
O Running the online system since August 2019.
He added: "The PCSE portal has been improved and so you can order supplies, make performer list changes and see your GOS payments all in one place. I find it easy to use and navigate. If you can use a PMS, you can you use this."
For Mr Townsend, the benefits of making the move to eGOS looked obvious in principle -but the system delivers on that promise.
"We were a very early adopter of eGOS in England and were very keen to use it. We had very few concerns going into the project because we could only see the upsides: less paper, less admin, lower costs. All of these considerations turned out to be true," he said.
Mr Townsend concludes: "Without can't progress to the next page of the online form. The errors need to be corrected prior to the patient re-signing the form. Once submitted it will be accepted for payment."
"Patients are impressed with the electronic forms - it shows we are moving with the times"
Stewart Mitchell
Staff not being taken off the shop floor to have to hand in signed-for post at the nearest post office is another benefit, he said. While highlighting that using the on line system may require the practice to invest in the purchase of a tablet, Mr Mitchell recommends shopping around. "We sourced two Acer Aspire Switch tablets online, which have 11-inch screens and run Windows 10.These have been a great buy."
Reflecting on the payment model, Mr Townsend explained eGOS is not only easier to use, but also helps with cashflow. "Every month we have had an email three to four days before our payment date informing us our statement is ready. We log into the improved PCSEportal and the statement is there telling you what you are going to be paid. You can export a detailed list and then reconcile it within Optix. This has improved our cash flow and accounting. You can also toggle whether you want to pay voluntary levies or not."
question, eGOS has improved the running of the practice. It is easier to run, easier to administer and we get paid in a timely fashion and are able
to reconcile that payment."
For those practices reluctant to use electronic claims, Mr Mitchell's assessment is straightforward. "It is essentially a GOS form but on line. The PCSEonline GOSl forms are great," he said.
Mr Townsend added that the Optix PMS environment is "easier, quicker and more efficient than the system it replaces. We have not found any negatives and wouldn't dream of going back."
www.pcse.england.nhs.uk/servives/ ophthalmic-payments
Whether you are a practice that plans to use PCSE Online or eGOS, you need to get registered and set up your new user administrators. These are needed to assign all the relevant roles in your organisation.
Go to www.pcse.england.nhs.uk/services/ ophthalmic-paymentsto find out more

Educating eye care professionals is very important to us at Thea. We are delighted to invite you to join our webinar programme for 2020, where some of the top speakers from the UK and beyond will provide enjoyable and thought-provoking talks. All webinars are free to attend and 1 CET point is available for each.














OT poses a monthly scenario from a practitioner. This month, we look at patient complaints
The scenario
Roopal, AOP member
"I am an optometrist who became a practice owner 18 months ago. We always strive to ensure that our customers have a pleasant experience and up until last month, I had not received a complaint. Recently a customer complained about the service, and it made me realise that the practice should be better prepared for complaints and how to deal with them. Can you share any advice on how to deal with a complaint effectively and resolve it at practice level?"

The advice
Richard Edwards, clinical consultant at the aces
As professionals, we do our utmost to ensure that the care we provide to patients is of the highest standard. However, on occasions, we disappoint a customer. Being prepared for those " situations and dealing with 1 them appropriately is key t to ensuring their swift and ] smooth resolution.
Complaints can be positive
While this sounds counterintuitive, complaints shouldn't be viewed as completely negative. A complaint gives the practice a chance to improve and get it right next time, as well as gain valuable insight into practice delivery as a whole. We can't get it 100% right every time, but we should view complaints and feedback as an opportunity to learn and improve. Viewing the complaint in this way is a positive and productive place to start.
Formalise the procedure
This is vital to reassure the patient that the complaint is being taken seriously and being dealt with efficiently. It is also reassuring for you when you spend much of the working day isolated in your consulting room. The procedure will vary from practice to practice but should always clearly outline the process for the patient and who will be dealing with it for them. It should also include a formal method of effectively recording and analysing the complaint and then agreeing a resolution. If there is no resolution, that's when engaging the OCCS should be considered. We can help with advice and mediation, if required, which is a service provided by experts at Nockolds Solicitors.
"If there is no resolution, that's when engaging the OCCS should be considered. We can help with advice"
Leave emotion at the door Complaints should never be taken personally. It's very rarely a personal slur or criticism of the optometrist's own level of care. The vast majority of issues we see at the OCCS are not clinical but relate to communication and expectation management.
Start by thanking the patient for bringing the issue to the practice's attention, and apologise for them having to do so. Then, try to avoid challenging the complaint. This is where the discussion can go downhill. In a health setting, there can often be an uncomfortable imbalance of knowledge between the patient and the health professional, and patients often tell us that they feel 'dismissed.' Using open questions to demonstrate an understanding of the full impact of the patient's complaint is a good tip. Try not to just focus on the technical aspect of a complaint, but also ask questions like 'how can I make this right for you?' I would always recommend mediation in any complaints that do not amount to allegations of serious professional misconduct. The most common issues raised during mediation relate to prescription or dispensing accuracy and manifest as a non-tolerance. The common denominator in these scenarios is the opportunity to learn and improve. If you're interested in learning more about mediation, visit Nockolds Solicitors' website, www.nockolds.co.uk. 0















I have worn glasses since the age of 12.so I have grown up going to the optometrist. I got my first job in optics as an optical assistant at the age of 17. It gave me an insight into the profession and helped me decide to pursue optics.
When I was looking for a pre-reg placement, it was really important to me to have a clinical placement where I could develop my skills. I did not want to just spend the year solely focused on passing the final professional assessments. I was lucky to get a hospital placement at the Oxford Eye Hospital -it was one of the best things that happened to me early on in my career. I was exposed to so many different areas of optometry, including specialist contact lens fittings, low vision and paediatric eye care, as well as ophthalmology clinics.
After completing my pre-reg year, I applied to do medicine and had an offer to go to Bristol. However, I deferred it for a year and in the end, after much thought, declined the offer. I decided to continue with optometry as I could see that there were lots of areas of the profession that I would enjoy, especially working with children, specialist contact lenses and running my own business.

"We listen to why they have come to see us"
Practice owner of Hammond & Parker Opticians, Dipesh Chhatralia, on business ownership and treating the patient the way he would like to be treated
After qualifying I split my time between Oxford Eye Hospital and primary care community practice. It was great to get an insight of how a practice is run. This experience made it apparent what I would do if I owned a practice in order to deliver the best standards of care I could.
I had always wanted my own practice from quite early on in my career. However, I wanted to develop my clinical skills and gain experience first so that I would have a good foundation to build a practice that delivered
I love IT and technology and try to incorpo r ate this into our business. So I would have ended up in that field.
outstanding clinical care. I met Sachin Patel, my business partner and fellow optometrist, in my pre-reg year when we were both doing evening clinics at the Institute of Optometry. We clicked because we were likeminded and would discuss owning a practice together to share the huge responsibility that this comes with.
In 2019 the Hammond &. Parker team won the AOP Awards Optical Team of the Year accolade. The whole team was happy and excited.
Having a team of staff that share our vision to be the best is first and foremost when it comes to meeting and exceeding patient expectations. We invest in staff training to ensure that
"It works well because we treat our patients in the same way we would like to be treated if we were on the other side"
we all continue to develop. At Parker & Hammond we have an ethos of putting the needs of the patients first and ensuring we deliver outstanding clinical care. We invest in technologies that we feel will make a positive difference to the care that we can deliver and try and remain at the forefront of new developments.
Throughout the customer journey at Parker&. Hammond we want our interaction with our patients to be as natural as possible and deliver the service that they want in a friendly, professional manner. We listen to why they have come to see us and address their problems. When appropriate, we offer our patients vision solutions that enhance their daily lives and discuss specific visual requirements. We ensure there is good communication when patients are handed over from one member of staff to another and service is centred around the patient's needs. It works well because we treat our patients in the same way we would like to be treated if we were on the other side. 0 Mli3i·l1t3P1
Share your career journey with OT. Email emilymccormick@ optometry.co.uk
Slowing myopia progression is more urgent than ever and can help to significantly reduce the risk of myopia-related complications, such as retinal detachment, myopic maculopathy and vision loss later in life. 2
Innovative MiSight® 1 day daily disposable contact lenses with ActivControl® Technology slow both axial length increase and myopia progression while correcting refractive error. 3A
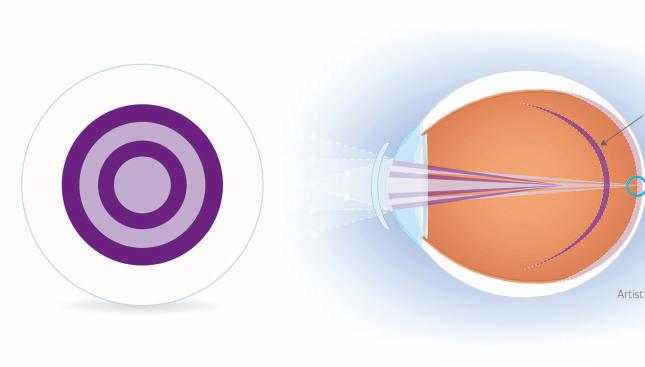

The MiSight® 1 day clinical study is the longest continuous soft contact lens study for myopia management and is setting a standard for myopia management clinical study designs. It adds to increasing evidence-based research supporting the practice of myopia management and part 1 of the study has been published in a peer-reviewed journal. 3 5




41 % of the MiSight® 1 day group showed no meaningful progression in refractive error• 3 t
MiSig~t® 1 day re~uced S g OL3 • myopia progression by 70
5 2 % reduction in axial elongation with MiSight® 1 day 3 *
Children from as young as 8 can be successfully flt with soft, daily disposable contact lenses3 §
MiSight" 1 day

of children strongly preferred, MiSight® 1 day contact lenses to glasses at year 5 4










''Reducing the incidence or prevalence of any disease by 40% is of huge public health significance. Slowingmyopiaby one dioptre may do just that for myopicmaculopathy. 7
Mark Bullimore, MCOptom, PhD, FAAO
Find out more about myopia management from CooperVision coopervision.co.uk/practitioner/clinical-resources/myopia-in-children
*Comparedwith a standardsingle-visionone-day lensover a three-year period.t No clinicallymeaningfulchangein refractive error -0.25D or lessfrom baselineafter 3 years comparedto 4% in the control group. :f:Childrennew to contact lenswear aged 8-12, n= 130@ 1 month after dispense.§ >95% of childrenw ere successfullyfit with MiSight®1 day or Proclear®1 day
I No slit-lamp observationsrecordedabovegrade 2 at any scheduledvisits apart from 1 observationof grade3 GPCattributed to a foreignbocy at the 1 month visit. ,r How much do you like wearingyour contact lenses?·87 /97 (90%) Topbox 'I likecontact lensesthe best' Subjectiveresponse@60M
References: 1. HoldenBA, FrickeTR, Wilson DA, et a/.Globalprevalenceof myopiaand high myopia and temporal trends from 2000 through 2050. Ophthalmology2016;123(5):10361042. 2. Flitcroft DI.The complex interactionsof retinal,optical and environmentalfactors in myopia aetiology. PragRetinEye Res. 2012;31 (6):622660 3. ChamberlainP,et al.A 3-year Randomizedclinicaltrial of MiSight®lensesfor myopia control. Optom V,sSci.2019;96:556-567. 4. CVI Data on File2019. 5. CONSORT2010 Explanationand Elaboration:
Updatedguidelinesfor reporting parallelgroup randomisedtrials BMJ. 2010;340:c869 doi: 10.1136/bmj.c869. 6. ChamberlainP,et al.Further comparisonof myopia progressionin new and establishedmyopiacontrol treatment (MiSight®1 day) groups.BCLApaper presentation2019. 7. BullimoreM, et al. Myopia Control:Why EachDiopter Matters. Optom VisSci 2019;96:463-46 © 2020 CooperVision.CooperVision®,ActivControl®,MiSight®and Proclear®are registeredtrademarksof The CooperCompanies,Inc.and its subsidiaries.


Optometrist Sachin Nath opened The Optical Co in Cobham earlier this year. He speaks to OT about the importance of creating the practice brand
01
We opened The Optical Co in Cobhamon 1 February this year.Prior to opening our doors, we spent seven months developing a practice with a unique and relaxed design and curated an eyewear offering that combines exclusive contemporary designer products and exquisitely manufactured vintage frames. Our brand and image have been specifically tailored to encapsulate this relaxed and less corporate ethos, from the logo through to the colour pallet we have chosen. Our aim was to create a mid-to high-end practice where it is not about patient volume.
I believe that the creation of a memorable brand starts with the development of a good logo, and this was one of the first things we did after finding a location for the business.
We knew that our logo had to tie in with the overall image that we wanted the brand to portray. Our brand resonates through everything we have done thereafte~ from the shop fit to the products
we sell and the services we provide -they all project this image.
Establishinga new practiceis not for the faint-hearted as it is sucha huge risk.Prior to practice ownership, I was a locum working in and around Cobham. I got to know the area and the potential patient demographic really well and identified a gap in the market for a mid-to high-end independent. We would say that we are Cobham' s only truly independent opticians. The first step was establishing the right location and this took a long time. Once we found a unit in the right location, myself and my wife Jeenal, who is co-director, went through all of the pros and cons of taking the leap into practice ownership to make sure it was the right move. Agreeing that it was,
the next step was to write a business plan so that we could secure funding. Finally, we needed to find another likeminded individual to work with us in the practice -someone who had the experience and ability to execute and deliver the same ethos and passion that we had to our customers.
03
Introducinga totally different conceptto people who are so usedto a corporateeye care vibe within an opticianshas really been the most challenging thing. The style and design of the practice, the layout and general welcome has a traditional feel. We offer standard eye tests that take 35 minutes and an advanced eye test with an optical coherence tomography scan that takes 45 minutes. The artisan and quirky frame ranges that we offe~ including
"I believe that the creation of a memorable brand starts with the creation of a good logo, and this was one of the first things we did after finding a location for the business"
Hublot, Maybach, Kirk & Kirk and Tom Davies, are an entirely different approach to delivering optics on the High Street today. We are a styling opticians and like to take the time with patients talking to them about their needs over a coffee, making them feel comfortable and guiding them in their frame choices.
04
A colleaguewho I have workedwith for a number of years,Simon,joined the team as practicemanager and dispenser- he really understandswhat we are trying to achievethrough the practice.The basics of creating our brand is in accepting that both the clinical and retailing aspects of the business go hand in hand. It's not just about the great clinical detail during the eye examination that I perform using the most cutting edge technology, but also having a great partner on the retail side who brings a wealth of experience and knowledge in retailing that helps build and develop The Optical Co's brand with our customers.
0 5 Over the many years I've workedwithin the optical industry,I've noted how a corporateimage, style and way of working hastaken over. I've always longed to re-introduce the passion and enjoyment that I get from my work back into a practice that has the patients at the heart of everything in a fashion that has almost been forgotten. Feedback from our customers has so far been really positive and business is going well. 0






























































































































































































































































































































































































Founder of Kirk & Kirk, Jason Kirk, shares advice on communicating effectively with your customers

communication with specialist medical approach? your customers starts You can decide, but you a long time before they must make it crystal-clear to enter your store, and the consumer and then get should never end. your message out there.
The public is sophisticated and has Be visible access to so much Your average high-spending information that they can customer is trawling walk through your practice through social media to find door knowing a lot about a retailer that suits them you. Therefore, you must before they talk to you, so communicate what you and make sure you are visible. your store stands for before You need an active you meet face-to-face. Instagram page in order to portray your story. You need "You need an active a Facebook page in order to gather your community. Instagram page in And you need a website to order to portray your share simple information. story. You need a
Maybe you need to Facebook page advertise in places where your potential client is in order to gather enjoying life - if you are your community" targeting the creative community, advertise in the local theatre, for example. Be crystal clear Whatever you do, talk You need to know what to your audience in their your practice stands for. environment in order to Sounds easy, right? build their confidence.
You need a clear and concise message that expresses your brand
Three steps purpose and convinces the to success customer to spend their hard-
O Bevisible earned money with you.
These days, practices that
0 Listen between the lines
0 Stay in contact. try to straddle different sections of the market generally struggle.
Is your practice about Once a client has made the high-end, independent decision to come to your designer frames? Is it practice, the way that you about your role in the communicate in-store leaves community? Or is it about a an irreversible impression.
No aspect of your communication can be neglected.
The manner in which you talk to your client needs to be correct, but there are so many other ways that you are communicating your values. These include through the store environment, the way that you are dressed, the products that you present and the way that you present them, and, let's not forget, the way that you listen to your client.
Listening between the lines shows your client that you care, and brings loyalty to the practice.
When the transaction is over, the relationship is just beginning. If your service has been great and the products offered exceptional, then you are halfway there.
If you sell a mass market product, the next time a client goes to purchase a frame, there is no reason for them to come to you. They will simply price-shop. If you offer a unique frame, they will want to find out what your next unique product will be.
Stay in contact. Follow up with a personal call a few weeks after to see how they are getting on

For more business management articles, visit the OTwebsite, which is updated seven days a week www.optometry.co.uk
with their new glasses. Ask them to sign up to your mailing list and keep your mailings concise and relevant.
"The way that you communicate in-store leaves an irreversible impression. No aspect of your communication can be neglected"
Stay in their world. They discovered you because your social media was visible, or your advertising was well-targeted.
Maintain those levels and they will continue to see your brand and the next purchase will automatically be yours.
You know when you are getting it right because they will come back to you for their next frame before they need a next frame.
Trust is everything in this relationship. Transactions in independent eyewear stores are usually north of £500, so you cannot cut any corners.
Give your customers an experience that they will remember, and they will communicate this experience for you to their network. 0
OT investigatesthe impact of an award-winning project that has halved referralsinto the hospitaleye service by using technology to connect ophthalmologistsand optometrists

When Dawn Sim joined Moorfields Eye Hospital, an acquaintance tried to convince her of the benefits of the private sector.
For some clinicians,working long hours within an overburdened NHS might have made this an inviting prospect. But this was not the case for Ms Sim.
"I remember saying, 'I can't. I have things to do.' I wanted to fix things that have been the bane of my life for a decade. Now I feel I am finally in a position where I can," she shared.
As a consultant ophthalmic surgeon and head of telemedicine at Moorfields, Ms Sim has led a remote referral project that has seen an increase in the number of cases managed by optometrists within the community rather than being referred to secondary care.
The remote referral system has been used in the management of around 300 patients across two Croydon and four Hampshire optical practices. The potential of the initiative was recognised
I"On the recipient end, to say that a referral is inappropriate is very arrogant. The focus needs to be on communication"
with the Telehealth Award at the 2019 Health Business Awards.
As part of the community optometry pilot, optometrists enter details into a system when they see a patient who they want to refer to secondary care. The technology prompts relevant follow-up questions after the initial information is entered.
"It is a decision tree. For example, if the patient has glaucoma in the family a few more questions will be asked," Ms Sim explained.
The optometrist then takes a scan of the patient's eye and the data is automatically uploaded to a platform for a Moorfields specialist to review.
Optometrists have the ability to ask questions within the system. "They might ask, 'I think this is X -do you agree?' It is a dynamic, two-way conversation," Ms Sim shared.
She highlighted that the enhanced ability for optometrists to collaborate with ophthalmologists opens up the potential of continual education throughout the working day.
Ms Sim shared with OT that she dislikes the phrase 'inappropriate referrals' because a referral is simply an indication that the referrer had a question. "On the recipient end, to say that a referral is inappropriate is very arrogant. I think the way in which referrals are made and handled
is inappropriate in our current digital age. The focus needs to be on communication and education," she said.
The pilot within community optometry has resulted in the number of cases that would be referred reducing by 50%. Within the hospital eye service, more than 2000 patients with stable eye disease have been seen using the same technology. A technician takes the history and scans before this information is passed on to a specialist clinician for review.
"In the beginning, 30% had to come back to a face-to-face clinic but now our technicians are able to gather information required and less than 10% are seen in clinic with 90% remaining in these stable diagnostic imaging clinics."
Ms Sim highlighted that the NHS is becoming increasingly open to technological solutions.
"What is exciting is that the appetite for change is finally reaching the decision makers within the NHS. Traditionally healthcare has been very riskadverse but times are moving on," she shared.
The NHS Long Termplan highlights that in ten years' time it is expected that models of care will look markedly different, with the NHS offering a 'digital first' option for most patients.
Taking this into account, Ms Sim believes that technology similar to the remote referral system will be integral to healthcare pathways looking ahead to the future. "The pathway's efficiency is obvious; not just in terms of cost efficiency but also access to care for those who require treatment. It is a no-brainer," she emphasised.
Head of optometry at Moorfields Eye Hospital, Sarah Canning, highlighted that teleophthalmology has "huge potential" to be embedded into most eye health patient pathways. She shared that the technology can be used to expand screening programmes as well as enhancing referrals and diagnostics and providing ongoing surveillance for those with chronic conditions.
"The benefits will be more timely diagnoses and subsequent interventions, which will improve patient care and ultimately reduce the risk of vision loss for many patients," she said. Ms Canning noted that teleophthalmology has the potential to build trust between primary care
I"As a profession we need to make sure that we're fully on board with telehealth"
optometrists and hospital teams by facilitating greater feedback. "As a profession we need to make sure that we're fully on board with telehealth. It brings fantastic opportunities to maximise the potential of optometrists as well as other eye care professionals, to ensure that patients have access to the best possible care."

Consultant paediatric ophthalmologist Peter Thomas is Moorfields' director of digital innovation. He highlighted that Moorfields has recently launched technology at the London hospital's accident and emergency department that allows clinicians to seek the advice of senior clinicians by attaching an adaptor to a smartphone during a patient examination.
"It is as if the doctor at home is looking down the slit lamp," Mr Thomas highlighted. "Already, in the first few days of the pilot, we have been able to get three patients with unusual conditions getting instant senior advice overnight," he said.
Moorfields is also completing early research into the potential for home-based monitoring of patients with conditions such as wet age-related macular degeneration; technology that Mr Thomas believes could become available within five years.
He highlighted that the ultimate goal is to provide the same quality of care that would traditionally be offered in hospital in a more responsive way closer to home, with less need to attend hospital for repeat visits. "I would hope that there are a lot of encounters where the patient has to go no further than their local optometrist with Moorfields then able to provide ophthalmology expertise without the patient needing to come in to hospital," Mr Thomas shared.
Like Ms Sim, Mr Thomas sees the creation of opportunities for enhanced efficiency through the use of telemedicine.
"There is a lot of cost involved with bringing a patient into hospital. If we can use telemedicine to let us manage conditions at home or in the community that frees up resources within the hospital," he observed.
As well as benefiting patients, this model of care has advantages for clinicians, Mr Thomas shared with OT.
"What everyone really wants to be doing is focusing on the patients who are most in need of our help. If we can use technology to create smoother pathways that are less intensive for the
"What everyone really wants to be doing is focusing on the patients who are most in need of our help"
patients who are well-controlled, then it will allow clinicians to practise at the top of their license," Mr Thomas said.
He observed that if less time is spent completing high-volume, repetitive tasks, clinicians will have more time for patients with complex needs. "This technology can help to free resources and space in brick and mortar locations to offer more services that patients will really benefit from. We will be able to offer all of the value-added services rather than spending so much time on the bread and butter services that could be delivered out of hospital," Mr Thomas concluded. 0


"WhatI like is having that extra bit of reassurance"
Optometrist David Barker on what remote referrals has meant for staff and patients at Rawlings Opticians
I met Dawn [Sim, Moorfields' head of telemedicine] around four years ago and she was talking about this platform that they were planning. It was still at an early stage at that point. We started using the technology in our two Croydon practices, and then expanded out to four of our practices in Hampshire. Hopefully two more will start using it in the near future.
What I like is having that extra bit of reassurance on those cases where you are not quite sure. Most optometrists were never trained in optical coherence tomography (OCT) -that is only just starting to happen. If you see something you are uncertain of, you can get an expert opinion without necessarily having to refer the patient. The other big plus is that you get feedback, which we traditionally haven't had.
The patient gets a report and we get a report. It is a partnership, with the optometrist able to add information to

the report. What we have found with our practices is that some of the new optometrists have used it quite a lot.
As they have become more experienced, they have only used it on the more unusual cases rather than the run-of-the-mill cases. Hopefully it will
I"It is a partnership, with the optometrist able to add information to the report"
reduce referrals. There is a concern that there will be a flood of referrals into secondary care with OCT devices in so many
practices. This technology would allow those borderline cases to be assessed within days by a consultant. 0
Navigating sensitive topics in practice can be a challenging task for optometrists. From driving to sight-threatening conditions, practitioners share their tips for tackling difficult conversations

Optometrist Holly Higgins shares her approach to communication working in a hospital diabetes clinic
I think that for situation or the someone they have anyone who has patients' emotions, proliferative diabetic a disease that offering support and retinopathy with mild might affect their a gentle empathetic parafoveal macular vision, honesty is tone where required. oedema means key. I don't think I think one of the nothing to a layperson. over-promising most important I think it's so or sugar-coating communication important to take your things is going to challenges with time to explain what be of benefit for the diabetic patients the condition actually patient. Clearly, it's is helping them means. This makes important to change to understand the the treatment easier your communication technicalities of to understand also. I for each patient, what is happening feel my patients leave reading the totheireyes. Telling the clinic happier
I"It is almost as important as the clinical assessment"
to proceed if the understanding of their condition has been covered.
Diabetic patients are,onthe whole, brilliant at communicating. On the flip side, the diabetic patients who are fed up with attending so regularly can be difficult to communicate with sometimes. In these instances, I think keeping communication open and creating a safe space for patients to tell you their take on things will really help. In a busy clinic, finding the time to do this is always a constant battle. However, it is almost as important


as the clinical assessment itself. In the past, taking this time with patients has revealed things such as patients who were coming to the hospital regularly as they were struggling with their diabetic control with very high blood sugars, due to the fact that they were struggling to see the dial on their insulin pen. Because I took this time to create an open environment for communication, I could resolve this issue with the help of our eye clinic liaison officer and diabetic nurse team.






Optometrist Marcello Leucci on how he approaches communication within the keratoconus service at Moorfields
As a hospital optometrist, I lead the keratoconus service at Moorfields Eye Hospital, while also working in the external disease and contact lens clinics. In general, many patients present with a lot of preconceptions having Googled either a diagnosis or symptoms in advance. This often leads to them reading about the worst-case scenario.
In the keratoconus clinic, I mainly deal with young patients who are otherwise fit and healthy. When their vision starts to deteriorate and they are referred to the hospital, a significant proportion of patients assume they are going blind. I feel that it is important to reassure patients at new appointments that this is not the case.
A clear and reassuring explanation of a diagnosis and treatment plan is very important since it fosters a patient's trust in you as a practitioner. When explaining a treatment or condition, I find it helpful to either show a patient their scans, or a model eye; even simply sketching what you're explaining can be helpful.
I have found that not all patients like it when things are explained exclusively in lay terms. Getting a feel for personalities, background and expertise can inform how things are explained. Keeping a patient engaged in their own care is very important. I think the best balance is to convey to the patient the need to attend and why they have to do so without worrying them.


IOptometry Wales chief executive Sali Davis on the benefits of good record keeping when it comes to talking with patients about driving and vision
The key with driving and vision, as always, is good record keeping. Document everything. I recommend taking some time to review the guidance from the College of Optometrists, notably its Clinical Management Guidelines.
We have always been a little timid as a profession to approach conversations that might keep a patient away from crossing our thresholds ever again. However, recent evidence from the Beaufort Research Study highlighted that patients actually expect to hear about health and wellbeing messaging from their optometrist.
Couching a conversation around general health and wellbeing and your own legal duties might soften a hard blow.
It's always best to seek the advice of your professional body if you feel anxious about how to deliver the news that someone should not drive again.
If you document what you did and what you said this will never be a bad thing to do.
As with all things, the more you have these difficult conversations, the easier they become. As a profession we need to get a little bit more comfortable with being uncomfortable. 0
"As a profession we need to get a little bit more comfortable with being uncomfortable"
,, It was a straightforward decision considering footprint, ability to upgrade in the future, thus keeping the equipment futureproof, and the fact that the system is already in the majority of UK hospitals. "
Douglas and Natalie Glass Glass & Glass Optometrists











































62/ Ocular manifestations of child abuse
Dr Sa bah Mehreen Janjua Raja MA, BM BCh (Oxon), MPH
Ms Tahmina Pearsall MBCHB, FRCOphth, FRCSEd, MRCOphth, MSc
67/ Seeing beyond the eyes
Daniel Williams
72/ Referred for glaucoma: what happens next?
Dr Deborah Armstrong PhD, MCOptom
76/ Clincal signs of ocular surface disease
Sonia Trave Hua rte BSc, MSc
Professor James Wolffsohn BSc, MBA, PhD, FCOptom
Course code: C-73846
Course code: C-74400
Course code: C-73896
Ocular manifestations of child abuse, page 62
Competency tracker
In this edition of OT, practitioners can test a range of competencies:
Course code: C-74029
"Eye specialists may be asked to perform a detailed eye exam by another clinician when child abuse is suspected or because of unexplained mental status changes, seizures or intracranial haemorrhage. Ocular manifestations of child abuse may also be picked up during a routine eye examination or as an emergency in eye casualty"
Sabah Mehreen Janjua Raja and Tahmina Pearsall
Referred for glaucoma: what happens next? page72
"It is every competent person's right to refuse referral to a medical practitioner. If a patient refuses referral, it should be an informed choice, therefore the optometrist should advise them of the possible consequences of refusing treatment, which for those with POAG would usually mean a slow progression of vision loss leading to restricted peripheral vision and eventually to blindness"
Deborah Armstrong
Dr Sabah Mehreen Janjua Raja MA, BMBCh (Oxon), MPH and Ms Tahmina Pearsall MBCHB, FRCOphth, FRCSEd, MRCOphth, MSc
This article will cover important considerations for the clinician in their assessment and management of children who may have suffered from non-accidental injury.
Optometrists
The National Society for the Prevention of Cruelty to Children has reported that 6.9% of young people aged 11-17 years have experienced abuse or neglect. 1 Around 40 children in the UK die per year due to maltreatment. 2
High profile cases of child abuse often highlight missed opportunities to intervene. One of the most horrific cases of child abuse is that of Victoria Climbie. Post-mortem examination found 128 separate injuries. A public inquiry ordered by the Secretary of State for Health found that on no fewer than 12 occasions did the relevant services have the opportunity to act. The inquiry laid forward numerous recommendations for child protection in England. Key failures of the system included poor communication and documentation, a lack of accountability, and poor training of frontline staff.
All clinicians involved in the care of children should have a good understanding of the red flags for child abuse and how to manage a suspected case. Preceding the diagnosis of non-accidental injury, a notable proportion of children have been seen with an ocular complaint and maltreatment missed. 3 Approximately 4-6% of abused children have ocular manifestations. 4
Eye specialists may be asked to perform a detailed eye examination by another clinician when child abuse is suspected or because of unexplained mental status changes, seizures or intracranial haemorrhage. Ocular manifestations of child abuse may also be picked up during a routine eye examination or as an emergency in eye casualty. In the UK, all clinicians have a duty of care to report suspected child abuse. In a case of sudden unexpected death of a child, an autopsy may require examination of the eye and orbital tissues, which may help to determine the cause of death.
Abuse may be classified into the following categories: physical, sexual, neglect, and emotional. This article
will primarily cover an approach to the management of physical abuse in the form of abusive head trauma. Sexual abuse, neglect, and Munchausen syndrome by proxy will also be briefly covered. For clinicians interested in further reading, there are a number of indepth articles available in the literature. 5-B
Abusive head trauma (AHT) includes all mechanisms of head injury, including shaking and blunt injury. Shaken baby syndrome (SBS)is a form of AHT characterised by repetitive acceleration-deceleration forces caused by violent shaking, with or without blunt trauma. The incidence of abusive head injury is highest in infancy and less frequently seen in children over three years of age. Mortality is more than 25%, and it is responsible for up to 50% of deaths from child abuse. 9
Following AHT, the child may present with irritability, lethargy and vomiting, which may be misdiagnosed as gastroenteritis or another infection, as the history of injury is withheld. The most common sign picked up on examination in AHT is retinal haemorrhages (RHs ).10 While the exact mechanism is controversial, there is now consensus that the forces required to cause RHs are unlikely to be inflicted accidentally, even through rough play or an attempt to rouse an unconscious child.11
This is usually a chronic form of abuse by a perpetrator, often well known to the child who uses a position of power to obtain sexual access.12 The child may present with conjunctivitis from a sexually transmitted organism, for example: chlamydia or gonorrhoea; a periocular infection, such as herpes simplex or pubic lice; or a systemic infection such as syphilis or human immunodeficiency virus (HN) with ocular manifestations. Several sexually transmitted diseases can be acquired in utero or during delivery. Nonsexual transmission of organisms such as herpes simplex and molluscum contagiosum is also common. This may also present as functional visual loss, as more than 50% of children with functional symptoms have psychosocial stressors. 13
____
Factors which contribute to a higher risk of abuse
Poverty
Maternal depression
Drug and alcohol abuse
Social stress
_____,Premature, disabled, or excessively crying babies
Siblings of abused children
Children subject to a child protection plan
Neglect should be suspected when scheduled visits are not attended, there is a delay in bringing the child in for serious problems, or there is non-compliance with treatment. Consideration should be given as to whether there are extenuating circumstances such as language barriers, an inability to afford care or transport to care, or absent family support. The child may be dirty, unkempt, and the caregiver may appear disinterested.
Munchausen syndrome by proxy
Munchausen syndrome by proxy is a rare diagnosis whereby the caregiver simulates illness in the child to seek medical attention. Ophthalmic manifestations include: recurrent conjunctivitis secondary to instillation of noxious substances; keratitis or corneal scarring; pupil and eye movement abnormalities due to topical or systemic medications; recurrent periorbital cellulitis due to injection of a foreign substance; and conjunctiva! haemorrhages secondary to covert suffocation. 12 Signs of medical child abuse include a disorder that does not respond to treatment and does not fit into any known diagnostic category with intermittent and unpredictable symptoms. The caregiver is overly involved in the care of the child and symptoms typically only occur in the presence of the caregiver. The caregiver is also unusually sociable and happy in the hospital environment.
When child abuse is suspected as part of a differential diagnosis, a carefully documented history is key. The time and mechanism of the injury should be recorded. Determine who was with the child at the time of injury. Details of the sequence of events before, during, and after the presenting complaint should be ascertained. The caregiver' s responses should be documented as these have a tendency to change over time in cases of abuse. It is useful to look for consistency in the history. This must be correlated with the clinical findings. The developmental stage of the child is key as it may provide
An inappropriate delay in presentation
Inconsistencies in the narrative with accounts changing over time
Injuries inconsistent with the mechanism described Injuries not in keeping with the developmental stage of the child, particularly injuries in a pre-mobile child
Multiple and unexplained injuries
An unusual lack of parental concern
clues as to how likely the child is to have obtained such injuries. 14 For example, a history of a one-month old baby sustaining a bruise by rolling and falling off a bed is not plausible as babies are not capable of rolling until after four months of age. Past medical history should also be sought, including any conditions that may predispose the child to bleeding, such as a history of haemophilia or leukaemia. The caregivers should be asked about any recent falls, motor vehicle accidents or other trauma. The history should be obtained in a neutral, nonthreatening manner and if the child is old enough, they should also be asked how they obtained their injuries. This may require creating a safe space to question the child in the absence of the caregiver. While obtaining a history, it is important to pay attention to the body language of the child and their guardian.
Examination of a child with suspected abuse should occur within 24 hours, and certainly within 72 hours, as findings such as RHs may be transient. Progressive increasing severity of RHs in AHT has not been reported. Both positive and negative findings should be carefully documented. Ideally, fundus photographs should be taken, which may be used in legal proceedings. General inspection is important to ascertain whether there are signs of neglect or other injuries. The child's interaction with their caregiver should be carefully observed. Both a detailed anterior segment and dilated indirect fundus exam should be performed. When pharmacologic pupillary dilation is contraindicated, as in children with severe central nervous system injury on close neurological observation, timely ophthalmologic assessment is still helpful. An attempt to view the retina and optic nerve using a direct ophthalmoscope, small pupil indirect ophthalrnoscopic techniques, sequential pharmacologic dilation, and/ or fast-acting mydriatics (for example, phenylephrine 2.5%) can yield important information. 15
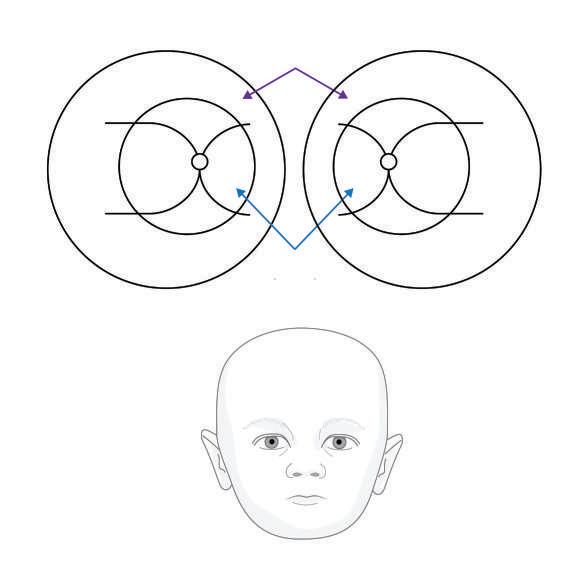
Figure 1 It is important to record the location and extent of any signs of potential AHT. /mage courtesy of the Dr Samantha Strong
The following approach is adapted from the Royal College of Ophthalmologists' guidance on appropriate documentation in cases of suspected child abuse: 16
O Patient details
O History
O Visual acuity
O Ocular motility
O Pupil size and pupillary reflexes
O Record of topical agent with which the pupils have been dilated
O Periocular bruising
O Subconjunctival haemorrhages
O Anterior segment findings
O Presence of RHs and features: -Number
O Few -one to 10
O Many-10 to 20
O Too numerous to count -Size
O Small < one-disc diameter
O Medium one to two-disc diameters
O Large > two-disc diameters -Location
O Preretinal
O Intraretinal
O Subretinal
O Multi-layered -Distribution
O Posterior pole/ periphery
O Few/ many/ too numerous to count for each
location -Morphology
O White centred
O Other
O Macular retinoschisis
O Peri-macular folds
O Optic disc
O Other findings
O Date and time
O Name and signature
O Method of fundus examination, for example, indirect ophthalmoscopy, fundus camera, optical coherence tomography (OCT).
Although several documentation and grading tools have been suggested, there is not yet a standard accepted tool. Acceptable terminology to describe the haemorrhages might include 'nonspecific' (with a differential diagnosis), 'suggestive,' or 'highly suggestive' of AHT.4 In the absence of a photograph, it is advisable to draw a diagram of findings (see Figure 1).
A summary of eye signs in ocular trauma is provided in Table 1(page 66). Other findings on clinical examination may include: old fractures; bruises of varying age on unexposed areas such as the ears, head, neck, buttocks, trunk and hands (bruising over extensor surfaces and bony prominences, particularly in the lower limb are typically accidental); burns; signs of neglect such as poor hygiene; and frozen watchfulness.
There are no pathognomonic fundus findings of child abuse. However, multi-layered, bilateral RHs involving the posterior pole and periphery associated with retinoschisis and retinal folds are highly suggestive of AHT, particularly in children under six months of age. Approximately 25% of victims of AHT have no RHs, and one-third of all cases have mild to moderate RHs.19 Frontal bone and orbital roof fractures are uncommon injuries in infants and young children and are even less common in those abused.
It is important to consider differential diagnoses in cases of suspect AHT:
O Accidental head or ocular trauma: around 2% of accidental paediatric head injuries result in RHs.20 In these cases, RHs are predominantly unilateral, few in number, pre-or intraretinal and confined to the posterior pole
O Normal birth: RHs are seen in more than one third of normal babies in the first 24 hours of life and are indistinguishable from those seen in AHT. However, these haemorrhages rarely involve the vitreous,
Multi-layered: preretinal, intraretinal and subretinal Too numerous to count and extend out to the retinal periphery, not just confined to the posterior pole
While a few intraretinal posterior pole haemorrhages may raise suspicion of AHT, such findings are non-
____,s~pec ifi c _________________ _
The more severe the haemorrhage, the higher the specificity for abuse
Greater concentration in a perivascular pattern and in the area of the ora serrata, often with sparing of the mid-periphery and posterior pole
RHs may be asymmetric or unilateral. RHs are reported to be bilateral in 83% of AHT cases compared with 8.3% in non-abusive head trauma•
Optic nerve sheath haemorrhages are common in AHT; however, these may also be seen in cases of accidental head injury
Dating cannot be ascertained precisely. The majority of birth-related RHs clear within two weeks though some intraretinal haemorrhages may persist up to 58 days•• Raised intracranial pressure, for example, from an intracranial tumour or meningitis, is associated with superficial RHs adjacent to the swollen optic nerve head, and does not cause RHs elsewhere
Seizures and excessive coughing do not cause RHs in children 27
The presence of macular retinoschisis, haemorrhagic macular cyst, or circumferential retinal folds are all highly specific for an abusive injury, unless there is a specific cause such as a high-speed motor vehicle accident
subhyaloid or subretinal space and typically resolve within four weeks in 95% of babies. 21 There have been no reports of retinoschisis or macular folds due to birth trauma
O Blood disorders: leukaemia, coagulopathy, anaemia, sickle cell retinopathy, haemorrhagic disease of the newborn, Henoch-Schonlein purpura, and thrombocytopaenic purpura. A bleeding diathesis should be excluded in all suspected cases of AHT with RHs
O Infection: sepsis, meningitis, cerebral malaria
O Genetic: familial exudative vitreoretinopathy, galactosaemia, tuberous sclerosis, X-linked retinoschisis, homocystinuria, glutaric aciduria, and osteogenesis imperfecta
O Inflammatory: vasculitis
O Active retinopathy of prematurity
O Purtscher retinopathy: associated with a contributing illness or event, (for example, long bone fracture, acute pancreatitis, renal failure) and Purtscher flecken and/ or superficial cotton wool spots.
Unlikely causes of RHs:
O Cardiopulmonary resuscitation: RHs are extremely rare, even if carried out by unskilled individuals. Haemorrhages would be few in number and posterior
O Intracranial bleed from a vascular anomaly (Terson syndrome): rare in young children and if haemorrhages occur, they tend to be concentrated around the optic disc
O RHs are rarely caused by seizures alone. If RHs are found in a child with convulsions, this finding should prompt a search for another cause
O RHs appear to be very rare as a result of the Valsalva manoeuvre in young children
O Acute life-threatening event (ALTE)has not been reported to be associated with RHs
O The association of RH and vaccinations has not been reported in children
o Short distance falls are unlikely to cause RHs if the injury is not severe
O Hypoxia resulting from apnoea or associated with choking or respiratory arrest during vomiting has not been shown to cause the clinical picture of AHT.17
A patient with suspect AHT is likely to undergo the following investigations:
O Fund us photographs: imaging of the retina in AHT supports detailed documentation of retinal findings and provides a permanent record of findings
O Computed tomography (CT) head and orbits: in cases of suspected fracture, cerebral haemorrhage or space-occupying lesion. Where possible, CT should be complemented by magnetic resonance imaging (MRI) two to three days later as this is better at delineating intraparenchymal damage. 22 Recently, diffusion weighted imaging has been used to identify cerebral ischaemia within minutes of onset and can distinguish between acute and chronic infarction faster than conventional CT or MRI. It is the most sensitive and specific means of identifying SBS20
O Blood tests: full blood count, platelet count, clotting screen including prothrombin time, partial thromboplastin time and bleeding time. Samples should ideally be couriered to the laboratory to ensure the sample is not tampered with en route
O OCT: this has been used to document the vitreoretinal interface and schisis cavities in AHT24
O Fluorescein angiography: may detect characteristic areas of peripheral retinal nonperfusion, especially in the months after the incident 25
O X-rays: a skeletal survey should be performed to rule out other injuries. If normal, this should be repeated at two weeks to evaluate for fractures not evident on the initial survey.
Periorbital trauma o Lid oedema
O Ecchymosis
O Subconjunctival haemorrhage (a possible 'sentinel injury' in child maltreatment, 14 as has previously been described for bruising or a torn labial frenum)
O Restricted eye movements
O Nystagmus on up gaze
O Crepitus and bony tenderness
O Altered sensation, particularly in the distribution of the infraorbital nerve
Anterior segment o Cornea: abrasion or laceration, acute corneal trauma oedema, tears in Descemet's membrane
O Hyphema
O Iris and pupil: radial sphincter tears, traumatic mydriasis, iris prolapse, iridodialysis
O Lens: Vossius ring, subluxation or dislocation of the lens, cataract
Posterior segment o Vitreous haemorrhage trauma
O Macular retinoschisis
O Macular hole
O Commotio retinae
O Retinal detachment
O RHs
O Choroidal rupture
O Traumatic optic neuropathy
O Optic nerve avulsion
Brain injury
O Nystagmus
O Cortical blindness
O Encephalopathy
O Cranial nerve palsies
O Subdural haemorrhage
O Subarachnoid haemorrhage
O Cerebral oedema
When abuse is considered as part of the differential diagnosis, there is a professional duty to report it. The case should be referred to the local safeguarding team to complete the assessment and order the necessary investigations. Communication between medical and non-medical teams is key. Child protection services are typically available 24 hours a day via the local hospital switchboard. You may be asked to testify as a fact witness or expert witness to provide unbiased, sciencebased testimony. Practitioners are encouraged to read the safeguarding guide for all optical staff and practices produced by the Optical Confederation in collaboration with the College of Optometrists and the Department of Health and Social Care. 26
Child abuse is common and may be picked up as part of a routine eye examination. All clinicians responsible for the care of children should be aware of red flags
Dr Sabah Raja is currently an ophthalmology specialty registrar in North London. She graduated with distinction from the University of Oxford and has recently completed a Master's in public health as a Frank Knox Fellow at Harvard University. Dr Raja has interests in health policy and global health. She has worked on school and community eye screening programmes in South Asia and Sub-Saharan Africa with Peek Vision.
Tahmina Pearsall is a consultant ophthalmic surgeon practising at Whipps Cross University Hospital. She is UK-trained in centres of excellence such as Moorfields Eye Hospital, St Thomas' Hospital and Addenbrooke's Hospital, which enables her to provide excellent medical and surgical care across all aspects of ophthalmology. Her research and surgical achievements have won many prizes both nationally and internationally and most recently she has been nominated for the Hospital Heroes award.
in the history and examination which lead them to suspect potential child abuse. When this is suspected, a thorough history and examination should be performed and carefully documented. The appropriate safeguarding team and child protection services should be informed. Communication between members of the multidisciplinary team is essential. O
Under the enhanced CETrules of the GOC, MCQs for this exam appear online at www.optometry.co.uk. Please complete online by midnight on 22 May 2020. You will be unable to submit exams after this date. Please note that when taking an exam, the MCQs may require practitioners to apply additional knowledge that has not been covered in the related CETarticle.
CETpoints will be uploaded to the GOC within 10 working days. You will then need to log into your CET portfolio by clicking on 'MyGOC' on the GOC website (www.optical.org) to confirm your points.
Visit www.optometry.co.uk, and click on the 'Related CETarticle' title to view the article and accompanying 'references' in full.
Course code: C-73846 Deadline: 22 May 2020
Learning objectives
Be able to identify signs of child abuse and respond accordingly to safeguard the patient (Group 2.11.1)
Be aware of signs of child abuse and be able to respond accordingly to safeguard the patient (Group 2.11.1)
Daniel Williams
This article charts the journey of patients with visual impairment, highlighting the role of practitioners in providing support in these cases.
Optometrists •
DispE:nsing • opt1c1ans
Introduction
A visit to the opticians is often the first port of call when patients experience visual deterioration. Optometrists play a key role in identifying the cause and deciding on the appropriate management. This article considers a series of cases, with a focus on the story of Katie, to highlight the hurdles faced by those with visual impairment, outlining the steps that can be taken by practitioners to improve the approach.
Case one: what more can be done for Katie?
Katie, an active woman in her fifties living in England, became worried when her vision started to deteriorate. After cutting her finger while preparing vegetables, falling when outside, scalding herself while making coffee and struggling to read print, she realised that she needed help.
She made an appointment with her local optometrist in the hope that her spectacle prescription needed updating. During the examination, the optometrist noted extensive dry macular changes and an optical coherence tomography (OCT) scan undertaken in practice identified an epiretinal membrane. During her sight test, she informed the optometrist that she'd had a number of falls, was struggling to recognise faces, was feeling lonely and low in her mood and didn't have any help at home. The optometrist referred her to an ophthalmologist. After waiting several weeks, Katie received a call from the hospital eye service (HES) saying she had missed her recent appointment. Katie explained that she has difficulty reading her mail and as a result didn't realise that she had received a letter offering an appointment. The HES rebooked her appointment while she was on the phone and one month later, she finally attended
for assessment. Under the Equality Act 2010, service providers have a duty to make reasonable adjustments to ensure a person with a disability isn't put at a severe disadvantage. 1 A reasonable adjustment in this situation would have been to provide the letter in large print or call the patient to inform them of their appointment.
At her appointment, the ophthalmologist diagnosed macular degeneration and she was asked to come back in three months' time for further monitoring. Katie was devastated by the news and broke down in tears saying that she felt so alone without any help or support at home.
Unfortunately, she didn't meet an eye clinic liaison officer (ECLO) who could have provided emotional and practical support, along with information and referral to services that can enable and empower people with sight loss. ECLOs are usually based within eye clinics; however, not every HES currently has coverage, and even if they do it doesn't necessarily mean that every patient is referred to one.
Katie went home following her appointment feeling devastated with her diagnosis and not knowing what to do next. She lives alone with no support network so continues to feel lonely, isolated and is struggling with everyday tasks such as cooking. When she is out and about, she regularly misjudges steps and kerbs causing her to fall.
Katie's retinal specialist explained that due to her sight loss, she would be eligible to be certified as sight impaired (SI).A certificate of vision impairment (CVI)-formerly BD8 -was completed and sent to Katie's local social services department. The specialist explained some of the benefits of being certified which are summarised in Table 1(page 68). 2
Katie waited two weeks to be called by the social services contact centre to assess her needs, at which point she was placed on a waiting list to receive support from a vision rehabilitation worker (VRW). During the call she was asked if she was happy to be registered on the local authority database of people with sight loss. After a further three months, a VRW
Table 1 Summary of concessions available to patients registered as severely sight impaired (SSI) or sight impaired (51)2
Benefit/concession
Blind person's tax allowance
Television licence fee reduction
Blue badge scheme -car parking
Free postage -'Articles for the blind'
Free NHS eye examination
Disabled person's railcard
Free or reduced bus travel fare
Free directory enquiries
Cinema pass for carer
Protection under the Equality Act
Assessment by social services
contacted Katie in order to carry out a home visit and assessment of her needs. Rehabilitation workers provide a home assessment looking at an individual's needs such as getting around, cooking safely in the home, white cane training, lighting in the home, and functional low vision therapy. They work with people to enable them to gain the confidence and skills to become independent following sight loss.
In total, Katie waited over six months before she got the support she needed and during this time her confidence plummeted. She barely left the house, and was afraid to cook. Katie's mental health dipped, and she began to suffer from anxiety.
The VRW helped her to regain confidence with getting out and about safely, trained her how to use a white cane and cross the road safely. They also gave her strategies and equipment for cooking and making hot drinks safely to avoid burning herself and referred her to social groups run by the local sight loss charity, where she could get peer support from other people with sight loss. She now participates with her local sight loss charity attending social groups, tandem cycling and walking clubs. Katie is beginning to feel less isolated and is facing the future with new-found confidence.
It is the eye care professional' s responsibility to have a working knowledge of pathways to support services and an awareness of what local charities, organisations, and groups can offer to patients with visual impairment. It is important for practitioners to find out what is available for patients locally.
With social services under pressure and underresourced, the role of the practitioner has become even more important for those with sight loss. However, the referring optometrist or dispensing optician must move away from the single-track referral pathway. If a low vision patient is struggling, an optometrist, dispensing optician, or optical assistant can direct patients to social services or local sight loss charities immediately. The patient doesn't have to be certified before these referrals are made.
The low vision leaflet (LVL)3enables a patient to contact social services directly. In England, the practitioner might wish to complete a referral of vision impairment (RVI),4 or another option might be to copy a referral letter to the local sight loss charity, eye clinical liaison officer (ECLO) or vision impairment team in social services. The other option would be to pick up the phone and give them call.
It is really important that the practitioner establishes links with sight loss professionals and local organisations as it is in everyone's interest, but most of all Katie's, to ensure there are as few barriers as possible to getting the support required. It should be apparent the quicker someone like Katie receives support the easier it is to rehabilitate them.
If Katie received support earlier in her sight loss journey, such as liquid level indicators, high contrast kitchenware, mobility training, smart phone apps, special lighting and magnifiers, this would have alleviated some of the problems she faced.
It is important to emphasise that referrals to outside agencies can be made prior to a CVI being issued. If a patient is struggling with day-to-day tasks and needs support, they should be referred to appropriate organisations regardless of their level of visual acuity. Every area has a social services department, and most have a local sight loss charity that can help. Patients can be referred to both local and national charities and organisations to get appropriate support.
The benefits of early intervention
Let's look again at the initial situation and see how earlier intervention could have really helped. Katie goes to her local optometrist because her eyesight is getting worse. She thinks there is a chance that she may lose considerable vision. The optometrist refers her to an ophthalmologist but this time, takes a proactive approach and meets their duty of care to the patient. To reiterate, confirmation of diagnosis is not required prior to referral to outside sight loss support services. With this in mind, the optometrist also does the following:

1. Refers Katie to social services for vision rehabilitation training
2. Gets in touch with a local sight loss charity who can offer practical advice and guidance ensuring Katie can access local services.
This time, with the essential signposting being done at the same time as the ophthalmology referral, Katie gets valuable support much sooner. This approach is far more proactive and allows her to enjoy a greater sense of independence. With technology moving so quickly, there is no need for patients to struggle for so long. With a little knowledge, simple advice about smart phone applications or affordable hardware can be given. To further illustrate the above points, three more case studies will now be considered.
A mother, with two small children, presents to her local optometrist with deteriorating vision due to a pre-existing ocular condition. The optometrist's initial thoughts take them towards a social services referral, for example, safeguarding. The patient feels very anxious about this, as she thinks her lack of eyesight will result E' in the ability to take care of her children being called into question. The optometrist therefore gives the patient
the details of Blind Mum's Connect and a small local charity that deals with the patient's specific eye condition. During this consultation, the optometrist has assessed the patient's visual status, discussed the condition and symptoms, and given the patient and partner the opportunity to access additional support and guidance. If the non-medical signposting to appropriate services had not been provided, it is possible that the patient would have become anxious, resulting in diminished mental health impacting upon the wider family.
A52-year-old man is diagnosed with a condition that is resulting in a gradual loss of eyesight. He has worked in a busy office environment for more than 20 years; as a result of the vision loss, he experiences anxiety and feels a mounting sense of hopelessness, with concern that he may not be able to do his job. The optometrist refers him to the RNIB for talking support, and to obtain assistance from the Access to Work programme. A few weeks later, the patient started a course of counselling, and Access to Work assessed his needs within the workplace and, along with his employer, has installed screen magnification and
screen reading software to allow him to continue his job. If these referrals had not have taken place, the patient may have suffered emotionally.
A patient presents with a marked visual impairment. A keen sportsman and former soldier, his mental health is suffering resulting in a sense of loss and demotivation. The optometrist refers him to a specialist who can better deal with his symptoms. However, this is only part of the story; the optometrist realises that sport and exercise promote a positive mental state, so he refers the patient to Blind Veterans UK, British Blind Sports, and the Thomas Pocklington Trust. These steps give the patient the opportunity to exercise and socialise, and along with clinical intervention, he soon begins to feel more positive. Six months down the line, he feels able to participate in mainstream sport and has an active social life.
These three snapshots give an idea of the power of referrals and the importance of slightly lateral thinking. Consultations naturally have time limitations and practices have limited resources and constraints; however, these factors should not get in the way of the moral and ethical duty of care to patients. It is, therefore, important to consider giving certain patients more consultation time in order to explore a full range of options. In some cases, delegation can help to meet the needs of the patient. The wider practice team can help to make sure that the patient has the information in a format they can access, and fully understand what support is available.
If a non-medical referral doesn't take place, a patient may be fortunate to be seen in a hospital setting where an ECLO is in place, helping to address their specific needs. However, there are many hospitals that do not employ an ECLO, and therefore the opportunity for support is very limited.
Sometimes eyesight cannot be saved. Some people may lose some, a lot, or all of their sight. While life will inevitably become more challenging, with appropriate action taken by the practitioner, the effects of vision loss can be minimised. For example, by ensuring the patient has the ability to read, is able to make a cup of tea safely, or to do the washing without fear of mixing colours. The chance to train again, to compete again, to act again, to feel like an important member of the family and society. Referrals can help these things happen. If everyone
does their job, referrals and signposting to non-medical services can truly change lives.
The author has developed a resource pack for professionals to make it quick and easy for optometrists and dispensing opticians to refer their patients for support which is available as a free download. 5 O
Under the enhanced CET rules of the GOC, MCQs for this exam appear on line at www.optometry.co.uk. Please complete online by midnight on 22 May 2020. You will be unable to submit exams after this date. Please note that when taking an exam, the MCQs may require practitioners to apply additional knowledge that has not been covered in the related CET article.
CET points will be uploaded to the GOC within 10 working days. You will then need to log into your CET portfolio by clicking on 'MyGOC' on the GOC website (www.optical.org) to confirm your points.
Visit www.optometry.co.uk, and click on the 'Related CETarticle' title to view the article and accompanying 'references' in full.
Daniel Williams is founder of Visualise Training and Consultancy and is a highly experienced trainer and qualified sight loss rehabilitation assistant. Being certified severely sight impaired due to retinitis pigmentosa, Daniel provides educational insights into sight loss to inspire dispensing opticians and optometrists to become more competent at understanding, supporting, and communicating with patients who live with low vision. Daniel is a supporter of the Prince"s Trust where he sits on business launch panels and considers business plans to enable young people to obtain support from the Trust to start their business. He is also an active member and volunteer for the Royal National Institute of Blind People.
Course code: C-74400 Deadline: 22 May 2020
Take relevent steps to ensure that patients with visual impairment receive appropriate support (Group 2.10.1)
Take relevant steps to ensure that patients with visual impairment receive appropriate support (Group 6.4.3)
Dr Deborah Armstrong PhD, MCOptom
This article provides answers to questions commonly asked by patients when they are referred from primary care with suspect glaucoma and subsequently managed within secondary care.
Optometrists g
Therapeutic optometrists ..,
Disp~nsing "' opt1c1ans
Introduction
Glaucoma is a group of progressive eye conditions that is characterised by structural changes in the optic nerve head and associated visual field loss. 1 Risk factors include increasing age, a positive family history, myopia, race, migraine, and raised intraocular pressure (IOP).2 When there is structural damage and visual field loss but the IOP remains within normal limits, this is termed 'normal tension' or 'normal pressure' glaucoma. 3 It has been reported that 30-40% of patients have normal tension glaucoma (NTG).4, 5 IOP remains the only modifiable risk factor for glaucoma.
If an optometrist detects signs and symptoms of primary open angle glaucoma (POAG) (with or without raised IOP), ocular hypertension (OHT), occludable angles or acute angle closure, this would result in referral
Figure 1

to the HES glaucoma clinic. Primary care practitioners are adept at detecting signs of glaucoma and referring patients to secondary care. Indeed, 95% of secondary care referrals for glaucoma are made by optometrists, 6 but how good are we at answering our patients' questions about what might happen when they attend their Hospital Eye Service (HES) appointment? Furthermore, if a patient who is being treated for glaucoma by the HES asks questions about what might happen next after being advised of signs of their glaucoma progressing -would you be able to give well-informed answers to reassure them?
This article aims to improve primary care optometrists' knowledge and understanding of glaucoma management by answering commonly asked questions so that practitioners can inform and reassure patients when they ask for advice.
referral to the glaucoma clinic
What will happen at the hospital appointment?
A patient arriving in the HES glaucoma clinic for the first time can expect a comprehensive eye examination. First, the HES practitioner will take a thorough history of eye and medical problems and any relevant family history. Next, baseline measurements are taken including visual acuity, central corneal thickness (CTI), IOPs, visual fields, and Van Herick assessment. Gonioscopy, a dilated (if safe) fundus examination, anterior segment assessment and optical coherence tomography (OCT) of the disc and retinal nerve fibre layer complete the battery of tests and examinations. Of course, it takes some time to perform all of these tests and given that they are often not all performed by the same practitioner, it would be advisable to tell your patient to expect the appointment to take up to two hours and that they should not drive to their first appointment.
What can the hospital do about narrow angles?
If the patient has narrow angles (Van Herick l:,,;0.25), they should be routinely referred to the HES glaucoma
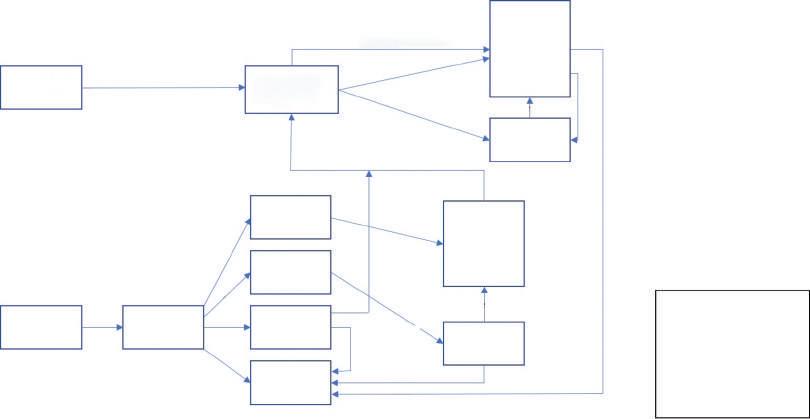
clinic for further investigation as a 'primary angle closure suspect' (PACS).When advising the patient, it is important to explain why occludable angles might be a problem. If the HES practitioner confirms occludable angles after gonioscopy, they might suggest performing a YAG peripheral iridotomy (see Figure 1)on each eye to improve drainage and reduce the chance of an acute angle closure episode.
What will the hospital do about the pressure? (when referred for POAG orOHT)
NICE Guidelines (2017) advise on protocols for the diagnosis and management of glaucoma and OHT.8 The guidelines state that on diagnosis of POAG or OHT with an IOP of ~4mmHg (where there is a risk of visual impairment within the patient's lifetime), that treatment in the form of a generic prostaglandin analogue should be offered to patients. Additional advice is given about further treatment should progression of visual
2 A flow diagram oftreatment options for primary open angle glaucoma based on the NICE guidelines (2017)8 loss occur, which is summarised in Figure 2. It is worth mentioning to the patient that even where the IOP remains within normal limits, treatment involves reducing the IOP.
Will the hospital perform laser treatment as a treatment option for glaucoma?
YAG peripheral iridotomy is used to treat narrow or closed angles and involves using a laser to create a small hole (located under the patient's upper lid) through which aqueous can drain. The main points for answering patients' questions about YAG peripheral iridotomy are found in Table 1.
Alternatively, phacoemulsification with intraocular lens implant would, in itself, likely result in improved drainage, and if the patient has cataracts, also provide improved visual acuity and less dependence upon spectacles; it has been suggested that this is a better method of IOP control in cases of PACS.7 A schematic diagram of the eye is a useful tool when explaining how the iris can be pushed forward into the angle (causing narrowing) by a lens that is increasing in thickness. When the lens is replaced by a thin implant, the iris moves away from the drainage apparatus, increasing aqueous outflow. This can be presented to the patient as 'killing two birds with one stone' in regard to cataract development.
Laser treatment is performed as a day-case procedure at a slit lamp biomicroscope using topical anaesthetic. The most common laser surgeries are selective laser trabeculoplasty (SLT)and YAG peripheral iridotomy. Written information about procedures are routinely given to patients who are listed for laser or surgery; however, if this has been misplaced or the patient finds it difficult to read, the optometrist might be their primary source of information.
SLT is an effective treatment for POAG with raised IOP and OHT.9 Short pulses of laser are used to target pigmented trabecular cells;10 it is thought that this stimulates the natural healing process to rebuild the cells which improves drainage. The procedure can be repeated if effectiveness reduces over time. The main points of information for answering patients' questions for SLT are summarised in Table 1.
A recent research study led by Gazzard received national news coverage when it suggested that SLT should be considered for first-line treatment in cases of POAG and OHT since it had been shown that it was more effective than drops for IOP control over three years. 2 It
Setting
Duration of procedure
Pain
Recovery time
YAG peripheral iridotomy
Slit lamp biomicroscope in clinic
Approximately five mins per eye
May be mild discomfort and/or photosensitivity for 24-72 hours
Minimal -advised not to drive for 24 hours
Aftercare IOP measured after procedure, then post-operative appointment for IOP measurement and gonioscopy in clinic
Possible complications
Vision after procedure
Effectiveness of procedure
Transient iris bleeding, cataract (rare), irregular pupil (rare)
May be slightly blurry for a few hours
Angle opens in around 84% of cases35
was successful in a population of patients with raised IOP who had not previously used topical anti-hypertensive drops, and where a skilled surgeon performed the procedure. Where patients are carefully selected, as in the study, SLT is an effective way of controlling IOP; however, it is not currently suggested as a first line treatment in the NICE guidelines (2017).8 Practitioners may need to advise patients that SLT is only effective for certain cases and if their IOP is within normal limits, they would not meet the criteria for a potentially successful procedure. In September 2019, NICE reviewed the evidence for glaucoma management in the wake of the Gazzard paper and concluded that the guidelines need to be changed. At the time of writing, new guidelines have not yet been published.
Why has the hospital not given any treatment for glaucoma?
Some patients may interpret a pre-referral explanation of 'I suspect you might have glaucoma' as 'You have glaucoma,' therefore, if they are discharged back to primary care without treatment, the optometrist may need to reiterate their explanation while telling them that it is great they don't have glaucoma. Referral to the HES for glaucoma does not always result in treatment or monitoring being given. Research has shown that even with referral refinement guidelines being followed, a false positive rate of around 15% might be expected 11 with the rate rising to around 36% when referral refinement guidelines are not implemented. 12 NICE guidelines (2017)recommend that patients with OHT who are not at risk of visual impairment within their lifetime are not offered treatment. 8 If the patient is very elderly or frail, the HES practitioner may decide that monitoring at suitable intervals is more appropriate than
Selective laser trabeculoplasty Slit lamp biomicroscope in clinic
Approximately five to 10 mins per eye
May be mild discomfort
Minimal -may have blurry vision for a few hours/days
IOP measured one hour after procedure, then post-operative appointment a few weeks later
Minimal, may have transient redness/blurry vision, bleeding (rare), very high IOP (very rare), macular oedema (very rare)
May be slightly blurry for a few hours/days
50-74% successful, 50% need repeating after five years'-36 37
instructing the patient to instil drops, which can be inconvenient, uncomfortable, and difficult for some.
What if the patient refuses referral for glaucoma?
It is every competent person's right to refuse referral to a medical practitioner.13 If a patient refuses referral, it should be an informed choice, therefore the optometrist should advise them of the possible consequences of refusing treatment, which for those with POAG would usually mean a slow progression of vision loss leading to restricted peripheral vision and eventually to blindness. The use of plain language is necessary in these situations so that the patient is in no doubt of the risks of declining treatment. An information leaflet such as those provided by the Association of Optometrists (AOP) or College of Optometrists can be given, and it should be made clear that the patient has the option to contact the practice to discuss the matter further or be referred if they change their mind. The patient's decision should be documented on their record card along with details about the information they have been given. In addition, it would normally be advisable to write to the patient by recorded delivery, setting out the findings and advice, and the possible consequences of not following this advice. A referral letter may also be included so that the patient can take this to their general practitioner (GP) (or accident and emergency department if the matter is urgent) if they change their mind. If the patient lacks capacity to make decisions about their own healthcare, the practitioner may need to take further steps, and seek advice on this from a professional body such as the AOP.
Table 2 The main points of information for XEN implant, Baerveldt tube and trabeculectomy
Setting
Duration of procedure XEN implant 15-30 minutes
Baerveldt implant Trabeculectomy
Operating theatre
Approximately 90 minutes 45-75 minutes
Pain Usually mild -controlled with simple painkillers, for example, paracetamol
Recovery time
Aftercare
Typically, two weeks off work. No swimming for four to six weeks
Antibiotic and steroid drops. Regular clinic follow-up
Possible Infection, bleeding, increased IOP. complications operation failure
Vision after Blurry vision for one to two weeks procedure
Effectiveness 80% controlling IOP without drops of procedure at 12 months••
What if the patient refusesreferralfor narrowangles?
The optometrist should explain to the patient what would happen if their narrow angles were to close and what might be the consequences in terms of vision loss so that the patient can make a fully informed decision. Research has shown that 22% of PACS patients go on to develop primary angle closure over five years, 14 and 38% of primary angle closure patients develop primary angle closure glaucoma (PACG) within five years. 15
Emergency referral for acute angle closure
When a patient presents with acute angle closure, they will have considerable pain and marked vision loss and will undoubtedly be very anxious. Often patients will want to know what is about to happen to them and
the optometrist can reassure them that the priority of the HES will be to reduce the IOP and pain quickly so as to preserve sight as far as possible. A patient with acute angle closure will be given oral and intravenous Diamox along with anti-hypertensive drops at regular intervals until the IOP has reached a satisfactory level (typically 10-12mmHg). At this point, the patient will be sent home with oral and topical medication and reviewed the next day when a YAG peripheral iridotomy would usually be performed to prevent a recurrence of the attack. The patient would then be reviewed in clinic approximately two months later to plan further management.
It has been shown that the ability of patients to recall medical information is variable, 16- 18 so it is not unreasonable to expect patients to need more information
Antibiotic and steroid drops. Regular clinic follow-up
Corneal damage, bleeding, cataract, infection, ptosis, irritation, tube blockage
Blurry vision for a few days to several weeks
83% controlling IOP without drops at 12 months 39
Antibiotic and steroid drops. Very regular clinic follow-up
Vitreous haemorrhage, anterior bleeding, hypotony, acute angle closure, sympathetic ophthalmia, cataract, infection, operation failure
Blurry vision for several weeks
83% still controlling IOP after five years••
about their treatment than they were able to recall after their HES appointment. Many patients will tum to the internet for information; however, some patients, especially the older generation, are less likely to turn to the web,19 20 and may prefer to ask their (more easily accessible) primary care optometrist for information.
Why have the drops been changed?
If glaucoma has progressed despite good adherence to drops then a different class of anti-hypertensive drop will be added to the treatment regime as appropriate. 8 It should be noted that an estimated 50% of patients are not entirely adherent to prescribed medicines,21 22 and that adherence to drops improves sharply in the week preceding an appointment before falling rapidly in the following weeks.23 A patient who is changed from a drop containing a single drug to a combination drop may perceive this as a change of drop rather than the addition of a drop.
Ocular surface disease (OSD) secondary to the use of preserved topical medication is a common occurrence among people who take drops for glaucoma and its prevalence increases with the number of topical treatments used. 24--27 OSD results in reduced adherence which can lead to loss of vision. 28 If left untreated, it can lead to corneal opacity and blindness. 29 When signs and symptoms of irritation and dryness occur, preservativefree drops are prescribed.
The pressureis still too high -what will be the next step in the treatment?
Patients who show raised IOP and/ or progression of glaucoma will move to the next stage in the treatment plan. Additional glaucoma drops, laser treatment or surgical treatment may be suggested if drops do not adequately control IOP.
The patient has been told they need drainage surgery - what does that involve?
A trabeculectomy or drainage implant may have been planned for the patient (see Table 2). The patient will have been given written information about the procedure; however, this may have been overlooked or misplaced when they ask their optometrist about the surgery. Drainage surgery is carried out as a day case procedure in an operating theatre and will involve the use of a general anaesthetic, local or topical anaesthesia depending upon the procedure.
A XEN gel implant is a 6mm stent made from porcine gel. It is inserted through the cornea with one end in the anterior chamber and the other in the subconjunctival space, thus aqueous humour is drained into the subconjunctival space. It is a type, amongst others, of a minimally invasive glaucoma surgery (MIGS) which is indicated for POAG where medical treatment has failed. 30
A Baerveldt implant is a silicone tube attached to a small plate which acts as a shunt to drain aqueous fluid into a subconjunctival bleb. 32 A patch of tissue from a donor eye is used to reinforce the conjunctiva in the region of the implant. The tube allows drainage of aqueous into a bleb under the conjunctiva.
Trabeculectomy surgery involves making a flap (often described to the patient as a 'trap door') in the sclera, underneath the upper lid to improve drainage. It is usually performed when maximum topical therapy is unable to control the IOP to a level where progression of visual loss is minimised.
Glaucoma surgery is often accompanied by the use of mitomycin C (MMC), which is an antimetabolite and is used to prevent scarring and healing. 33 The MMC is applied for a specified amount of time during surgery and then rinsed away. It has been shown to be both safe and effective when used during glaucoma surgery.34
The AOP and the College of Optometrists offer patient leaflets about glaucoma which are available free of charge to members. The International Glaucoma Association offers help and advice for glaucoma patients on their website in addition to free patient information leaflets and posters for the waiting room. In addition, the websites of the National Health Service, Moorfields Eye Hospital, and the Royal National Institute of Blind People also offer information for patients.
It is important for practitioners to understand the process patients are likely to follow when they are referred to secondary care with suspect glaucoma so that appropriate advice and reassurance can be given. O
Under the enhanced CET rules of the GOC, MCQs for this exam appear online at www.optometry.co.uk. Please complete online by midnight on 22 May 2020. You will be unable to submit exams after this date. Please note that when taking an exam, the MCQs may require practitioners to apply additional knowledge that has not been covered in the related CET article.
CET points will be uploaded to the GOC within 10 working days. You will then need to log into your CET portfolio by clicking on 'MyGOC' on the GOC website (www.optical.org) to confirm your points.
Visit www.optometry.co.uk, and click on the 'Related CETarticle' title to view the article and accompanying 'references' in full.
Dr Deborah Armstrong graduated from Aston University and worked in both independent and multiple practice and in the HES before completing the investigative ophthalmology and vision science glaucoma course at the University of Manchester and a PhD at the University of Bradford. She now combines work as a specialist optometrist in glaucoma for East Lancashire Teaching Hospitals NHS Trust with lecturing at the University of Central Lancashire.
Course code: C-73896 Deadline: 22 May 2020
Be able to explain to patients with suspect glaucoma about the implications of referral to secondary care (Group 1.2.4)
Be able to communicate effectively with patients to allow them to make an informed choice about referral for suspect glaucoma (Group 3.1.8)
Be able to explain to patients with suspect glaucoma about the implications of referral to secondary care (Group 1.2.4)
Sonia Trave Huarte BSc, MSc and Professor James Wolffsohn BSc, MBA, PhD, FCOptom
Readers are invited to review the images in this feature on ocular surface disease and use their clinical knowledge to answer the questions, accessing additional resources where required.
Optometrists
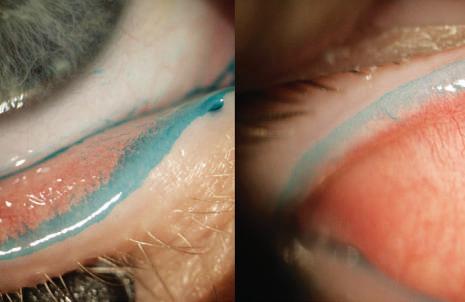
01 The staining in this image shows:
a) Marx line
b) Abnormal roughness of tarsal conjunctiva
c) Lid wiper epitheliopathy
d) Meibomian glands openings
02 Which of the following statements in relation to the sign displayed in the image is true?
a) It can be only found in patients with punctal plugs
b) It can be seen in patients where there is friction between the lid and the ocular surface
c) It is caused by an increase in tear meniscus height
d) It is caused by a thick lipid layer
03 In the first instance, patients with this type of presentation should:
a) Be referred to secondary care for further investigation
b) Be monitored with photography for future changes
c) Avoid screen time
d) Have artificial tears prescribed to lubricate the eye

04 What is the diagnosis?
a) Keratinisation of the lid margin
b) Obstruction of the meibomian gland orifices
c) Meibomian gland shortening or dropout
d) Increased lid roughness
05 When viewing this sign:
a) It will appear exactly the same under white or infrared light
b) It can only be seen under infrared light
c) It can only be seen under white light
d) The contrast of the glands will be seen better with white light than infrared light
06 Why does this image appear to have differently sized white grapevine-shaped structures?
a) Due to contrast of the image
b) Due to overexposure of the picture
c) Due to a shortening and loss of glands
d) Due to madarosis
Sonia Trave Huarte graduated in optics and optometry at the Faculty of Optics and Optometry in Terrassa FOOT (Barcelona). After completing her degree in 2016she completed a Master's in visual sciences with expertise in contact lenses in 2017.She is currently undertaking postgraduate research at Aston University on dry eye management and treatment.

07 Which of the following is not observable in the image?
a) Distorted Placido rings
b) Tear film debris
c) Colour fringe lipid layer
d) Corneal irregularity
08 If this patient was fitted with contact lenses what might we expect?
a) Lipid deposits on the lens
b) Complications because of the irregular lid margin
c) Lens discomfort because of blocked meibomian glands and telangiectasia
d) Excellent lens comfort due to the tear meniscus height
09 How thick might the lipid layer of this patient be?
a) Less than 13-lSnm
b) Between 13-lSnm
c) Between 90-140nm
d) More than 90-140nm
Under the enhanced CETrules of the GOC, MCQs for this exam appear on line at www.optometry.co.uk. Please complete on line by midnight on 22 May 2020. You will be unable to submit exams after this date.
Professor James Wolffsohn is deputy executive dean for life and health sciences at Aston University, teaching and researching in the field of anterior eye. He has been awarded fellowships from the International Association of Contact Lens Educators, the American Academy of Optometrists, the British Contact Lens Association, and the College of Optometrists.
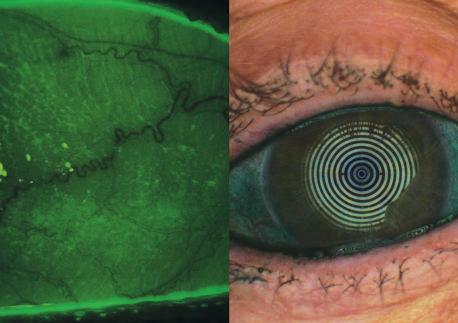
10 What do the images show?
a) Lid parallel conjunctiva! folds (LIPCOF)
b) Conjunctiva! abrasion
c) Punctate conjunctiva! staining
d) Lipid fluorescence
11Which subtype of dry eye disease does this indicate?
a) Aqueous deficient dry eye (ADDE)
b) Evaporative dry eye (EDE)
c) Mixed dry eye
d) More tests would be needed to make this decision
12 Which statement is incorrect? Corneal and conjunctiva! staining:
a) In severe dry eye is an informative marker related to the severity of the disease
b) Is a marker to diagnose dry eye
c) Correlates to the symptomatology of the patients
d) Occurs when there is a disruption of epithelial cell tight junctions
Course code: C-74029 Deadline: 22 May 2020
Be able to identify signs of ocular surface disease (Group 6.1.4)
Be able to assessthe ocular surface to identify abnormalities using appropriate techniques (Group 2.1.2)
Be able to identify ocular surface abnormalities in contact lens patients (Group 5.4.1)

Bespoke Trial Semi-ScieraI Contact Lenses
Optimum Extra (100Dk) Material, up to 16.50mm Diameter With full adjustability -
Apical Clearance -Limbal Clearance-Alignment Angle

Correct Your Vision While YouSleep
Bespoke Ortho-K
All off the above can be done using the Free Wave software v9.20 and above Current Compatible topographers Scout-Piccolo -Keratograph -Pentacam -Medmont

Tameside Business Park Windmill Lane,Denton, Manchester T 0161 336 9000 E contact@northern-lenses.co.uk
Call the above telephone number or email if this is of interest.

wDeborah Armstrong SPECIALIST OPTOMETRIST AND LECTURER
Deborah Armstrong works part-time at East Lancashire Teaching Hospitals NHS Trust, where she work as a specialist optometrist in glaucoma. She also works as a lecturer in optometry and ophthalmic dispensing at the University of Central Lancashire in Preston.
What is your current career goal?
I am currently working towards my independent prescribing qualification.
What are you most proud of?
I am very happy and proud of being an optometric researcher.
If you could switch career path, what would you choose todo?
I would love to be a (younger) female version of Sir David Attenborough.
What is the one thing you couldn't live without?
If it has to be a professional thing, it is my 78D lens. If not, it is my road bike.
How do you manage a work/life balance? Not very well. I seem to spend a lot of time doing work-things outside of work hours.
What do you do to unwind? I ride my bikes.
You have won the OT lottery. What are the first three things you would do with the £1mjackpot? First, I would buy a new road bike. Second, I would buy a new mountain bike. And third? Another bike. Seriously though, I'd like to do something that would help the climate crisis.
Do you have your next holiday booked? Where are you going?
I haven't booked any holidays yet this year, but I'd like to go back to Mallorca -for the road cycling obviously.

Cheese or chocolate? Chocolate Apple or Android? Android
Takeaway or fine dining? Takeaway Trainers or brogues? Trainers
Beach bum or culture vulture? Culturevulture
Strictly or X Factor? Never watched either of them so couldn't choose...
Clinical methods for slowing childhood myopia progression
Professor Carly SY Lam and Dr Wing Chun Tang
Myopia mysteries
Dr Kate Gifford
Orthokeratology for myopia control
Dr Paul Gifford
Anterior eye: keeping a lid on it
Nick Howard
OT has a range of articles available in the archive for therapeutic optometrists, including:
C-53202 / Does the solution to myopia progression come in a bottle?
C-42116 / Systemic associations and management ofuveitis
C-72205 / Anterior eye - cases in practice
C-72121/ Cases taken from community practice
C-62230 / Red eye and red flags.
The CET articles are available at www.optometry.eo.uk/cet

Dr Ian Beasley
is the clinical editor for OT and head of education for the AOP, with responsibility for delivering education in the journal and at face-to-face events. He began his career as an optical technician in 1989 and later went on to train as a dispensing optician ahead of qualifying as an optometrist in 1997.
In 2013,Dr Beasley became the first person in the UK to graduate with a doctorate in optometry from Aston University and received a research excellence award from the College of Optometrists in the same year for his published work investigating the susceptibility to pattern glare following stroke.
Dr Beasley maintains strong links with academia as a visiting lecturer at Aston, and is continuing his research by exploring the effect of peripheral defocus on axial growth and modulation of refractive error in hyperopes.
Email the clinical editor ianbeasley@optometry.co.uk

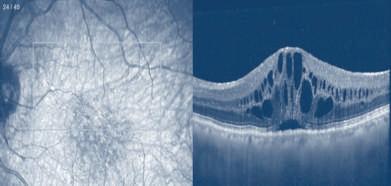


CV Writers Michelle Hiseman advises on studying the job description before an interview
job description is a key tool for preparing for the interview process. It will be used by the recruiter to draft their questions and set the interview strategy. Therefore, you need to do the same.
As soon as you decide to apply for a job, you should remember to download all of the available information about the role onto your computer because the web link could be taken down at any time.
Learning about the role
When applying for a role, avoid skipping past the section marked 'Introducing the role' because it often contains useful information about the culture of a company, where the role fits within the organisation and its corporate values.
But be aware that an NHS role will require a different interview preparation approach to one based in a private practice, as would working for a large retail chain versus a small independent.
'Tell me about yourself' is one of the most frequently asked questions in the interview process and you will need to tailor your answer to the specific role, culture and organisation that you are applying for. Look for the implied characteristics and core competencies related to the role that you are applying for and ask yourself 'how ] do I do this?' for every element listed.
j During this process, you should consider :, <5i the following:
0 Discussing vision-related matters with patients, offering advice and reassurance
0 Making the most of all sales opportunities whilst working towards achieving Key Performance Indicators (KPis).
"Face up to gaps in
your
CV, skill set and experience and prepare how you are going to answer questions on them"
For the first element above, consider customers who were particularly nervous which made the consultation more challenging, and answer how you used your communication skills to resolve the issue. For the second, find quantifiable information regarding your performance versus set KPis in your previous role.
Brainstorm the type of questions that you may be asked such as: 'Tell me about a time when you had to use your communication skills to reassure a nervous customer' and 'In the last 12 months how often have you achieved your targets?' Also, highlight areas where you might not match the criteria. Face up to gaps in your CV, skill set and experience and prepare how you are going to answer questions on them. Ignore these at your peril. 0


Workingfor Costcohasmany advantagesthat include:

• CompetitiveSalaryPackage(dependentonexperience)
• Privatemedical& dentalcover
• LifeInsurance
• 25 minuteeyeexams
• Nosalestargets
• GOCandIndemnityInsuranceRemuneration
• Excellentpensionplan
• Careerprogressionwithinthecompany



WearecurrentlyrecruitingQualifiedOptometrists at thefollowinglocations:
• CostcoBristol • CostcoMiltonKeynes
• CostcoChester • CostcoSheffield
• CostcoFarnborough • CostcoSouthampton
• CostcoLeeds • CostcoStevenage
• OCTinstalledin all practices
• CETtrainingto meetyourGOCrequirementsthroughouttheyear

Wearecurrentlyrecruiting a DispensingOpticianManager at thefollowinglocation: CostcoCardiff


'1wasunsurewhatto expectwhen I wasrecommended to workforCostco Opticianshoweversincejoiningin 2015I haveneverlookedback.Oneof Costco'sfoundingbeliefsisto takecareof ourmembersandI feelwetruly liveupto this.Thisis reflectedin thecontinuedinvestmentintothe latest technologysuchasthe implementation of OCTin all practices.Alongwith invaluabletrainingandsupport I feelI amableto providethebestclinicalcare to allourmembersandlookforwardtocontinuing11lisinthefuture."
AmritaSoorBSc(Hons)Mc0ptom- CostcoSunbury
Ifthis careerpath soundschallengingand exciting,we welcomeyou to apply. We want you to be part of our team! Applyby emailsmcclay@costco.co.uk or call : Ste McClay01923 830641




We are proudly independent, family-owned and family run group of 8 practices, in and around West and South Yorkshire, looking for a qualified Optometrist to join our friendly team.
Our Optometrists are an integral part of our team, providing our customers with excellent individual care with totally focused professional healthcare.
We focus more on care than targets.
This is an ideal position for a qualified Optometrist who's searching for a business who prioritise quality and customer satisfaction over quantity and sales targets.
Optometrists of all experience levels will be considered.
Please contact Steve Shaw email steve@ivisionopticians.com Tel 01226395015 or 07753837917
Ever dreamed of a job where patient centered care and clinical excellence are paramount?
Working alongside a strong and qualified team of Optometrists, Dispensing Opticians and support staff?
How about a guaranteed and secure income, with pension, private health insurance and encouragement for personal and professional growth?
Well, you might just be in luck, as Eye Academy is looking for you!
Eye Academy is an ever growing and expanding group of independent practices. Established in 2001, we may be a new name to some, but we have grown from strength to strength. We pride ourselves on good old traditional values of care, respect and service. We combine this with clinical excellence and attention to detail.
This is only possible by us recruiting and retaining a strong and dedicated team for each and every one of our practices.
We always welcome applications from talented individuals looking to combine clinical excellence and patient centred care.
Please get in touch if you are a GOC registered practitioner, whether FBDO, MCOptom or with higher certificates and IP.
For exceptional practice managers we make exceptions, but you must be open to working towards qualified status, which we will support.
• Clinical Optometrist -Full or Part-Time Rochester, Kent
• Clinical Optometrist -Part-Time Banbury, Oxfordshire
• Clinical Optometrist -Full or Part-Time Ferndown, Dorset
Base salary of up to £70,000 plus bonus
A real focus on your clinical development -including funded IP Training
45 minute testing with hospital grade equipment -including SPECTRALISOCT
The freedom to introduce work in areas of clinical specialism that interests you
No late nights and no Sunday's 5 weeks paid holiday plus bank holidays
Please send your CV and a note letting us know why you would love to join our team to Shaf at shaf.mohamed@eyeacademy.com
LOOKINGTO SELLYOUR PRACTICE?
For initial enquiries please contact romana.hashim@eyeacademy.com
Optometrist and director of Urquhart Opticians, Alistair Duff, discusses the importance of his LED camera slit lamp in the testing room
The slit lamp has always been a trusty piece of equipment for the optometrist and, in my opinion, having a slit lamp with a decent camera is a game changer in practice.
At Urquhart Opticians, we purchased our current slit lamp model that has an LED camera from Grafton Optical around 18 months ago as part of the business' ongoing investment in equipment, people and our group of four practices in general.
While the likes of our new optical coherence tomography (OCT) scanner can grab the headlines -and undeniably has significantly enhanced the service we provide -it is the new slit lamp camera that we purchased that I have found to be absolutely invaluable day in, day out.
The new arrival
Since it arrived, I have been furiously snapping away at any lump, bump or lesion that a patient presents with that looks remotely out of place.
Being a camera novice, I still have to play about with aperture and lighting, but it's pretty fool proof. The key is to take lots of photographs and save the best ones.
My artistic skills, like many optometrists, are zero, so these images play a really important part in referencing any issues with the external eye, meaning that subtle details can be noticed very quickly.
I tend to take a photograph of any unusual feature, as well as any external conditions. In fact, I take a picture of anything that I would like to chat to a patient about at the end of the examination. Cataracts, for example, are extremely common in the ageing

population, yet it can be difficult to explain what they are and the exact location. A photograph makes this extremely easy. I also use the video feature on the slit lamp just about as much as the camera. Dry eye is something we are dealing with on a daily basis and having the patient see how the tear film is evaporating under UV light with fluorescein is a powerful tool in getting the patient to fully understand the condition.
The images provide a fantastic resource for learning. At our practices we have two optometry students working with us who are both studying at Glasgow Caledonian University. Each week I collate the most interesting images that I have taken using the slit lamp and, with the patients' permission, share them with our students as we
discuss each case and any required treatment. This has proved to be invaluable for the students, who are making remarkable progress.
Arguably the most significant benefit is the slit lamp camera helps me to communicate with patients. Even with fairly minor issues such as blepharitis, an image brings the condition to life. I find that this also helps with the compliance of care instructions as the patient is eager for an improvement at their review appointment in the following weeks. I have even had a few people request a copy of their photo to show their family and friends.
Helping patients to better understand their eye conditions, and how and why the treatment offered is important, is fundamentally at the heart of what we do. So, in that respect, my slit lamp with its decent camera is one thing I could absolutely not live without. 0

WORKING TOGETHER I
• UK's largest provider of NHS cataract surgery
• NHS appointments available two weeks from referral -surgery within four weeks
• Free transport for patients
• Patients return to community optometrists for post-op assessment
SUPPORTING YOU &YOUR PATIENTS
• Regular communication from SpaMedica at every stage of the patient journey
• Specialist advice to community optometrists to support you with your patients/referrals
• 24-hour emergency hotline for your patients
Tel: 0330 058 4281 or Email: contact@spamedica.co.uk


Having served Optical professionals all over the country since its inception in 1993,


has built a wealth of knowledge and experience in dealing with taxation issues faced by Opticians. Our focus is on tax planning and compliance.
• Preparation of VAT returns and negotiations with HMRCon "full-cost apportionment" /Partial exemption or other special methods
• Advice surrounding incorporating your practice from sole proprietor or partnership to Limited Company
• Practice review/business planning including acquisitions and disposals
• Bookkeeping using cloud-based accounting software
• Ad hoc assistance with HMRC investigations and reviews
• Effective Tax planning
• Payroll services
• Quarterly management accounts and yearly practice accounts












MACHINERY




PRACTICE FITTINGS












• Fast, compact and future proof
• Multiple & single stimulus tests
• Customisable strategies
• Re-test individual locations
• Meets NHS requirements
• Now Windows 10 Compatible
















PRACTICE FITTINGS














Locum optometrist Jaime Patel tells OT how painting
has enriched her life
"Whenyou are creating art, you have to let go and see what happens"
My secret life Do you have a hobby to share with readers? Get in touch with selinapowell@ optometry.co.uk
a look around because she had grown up in the house. My dad let her in, she looked around the house, and when she got to the living room she asked about one of my paintings. My dad gave her my details and she called me within a couple of days and commissioned me. If someone is willing to spend their hardearned cash to buy something that you have produced, that is anhonour.
The journey has been very enjoyable and it has also been effortless. A lot of things in life are hard, but with this it seems to be something that always points me in the right direction. When you are creating art, you have to let go and see what happens. That is something that is bit alien to me because everyone always tells me that I tend to go for perfection. When I use alcohol ink in my work, often I have to go with what the ink wants to do because it has a mind of its own.

M yartwork started with a trip to Brighton with a friend around 15 years ago. He saw a piece of artwork that he liked. I don't know why I said this, because I had never painted anything in my life, but I looked at the artwork and thought 'I could do that.'
I have had a few commissions over the years. An older woman knocked on my dad's door when she was passing and wondered if she could have
I think there is something really beautiful about the iris. I look at them all the time in practice and I have a few ideas around experimenting with their shape and form. I can't put into words the feeling that creating artwork gives me.
If I go up into my studio, I can be up there for hours without realising. It is time to focus on what I am doing. You switch off, relax and go where the paint takes you. 0