TDA
Texas Dental Journal
October 2023
LEGISLATIVE LANDSCAPE Dr Matt Roberts
THE COUNCIL ON LEGISLATIVE, REGULATORY, AND GOVERNMENTAL AFFAIRS
POLITICAL PROCESS 101
MEET THE TDA LEGISLATIVE TEAM
HOW A BILL BECOMES A LAW IN TEXAS

PROTECTING THE PUBLIC: UNDERSTANDING THE TEXAS STATE BOARD OF DENTAL EXAMINERS’ ROLE IN REGULATING THE DENTAL PROFESSION
FOR DENTISTRY, I WILL
CHAMPIONING ACCESS TO CARE: TDA AS THE PREMIER MEDICAID & CHIP ADVOCATE
TDA’S INSURANCE LEGISLATION BENEFITS TEXAS DENTISTS AND DENTAL PATIENTS
DENTAL RECORD REQUESTS IN AN OIG INVESTIGATION
TDA LEGISLATIVE RESOURCE GUIDE

450 Texas Dental Journal | Vol 140 | No. 8 We’ll Take Care of Your Health Insurance. What’s the real difference between purchasing insurance through TDA Financial Services Insurance Program and somewhere else? You’ll always have attentive customer service from a team dedicated to TDA members and staff with TDA Financial Services Insurance Program. We work to make insurance easier for you and your staff. Go to our portal to review, compare, and buy your health insurance. Sign up through the portal. 2024 rates will be available on Nov. 1 . Portal at TDAmemberinsure.com For more information, call 800-677-8644 Enroll or learn more at tdamemberinsure.com Open Enrollment Begins Nov. 1 For coverage effective Jan. 1.
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner.
WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs: Principles of Pain Management
Fulfills rule 104.1 for all practitioners Use and Abuse of Prescription Medications and Provider Prescription Program
Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2

(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION RE PERMIT AVAILABLE!
(Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available):
American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs

NOTE: ACLS or PALS Renewal can be completed by itself at any combined program
Combined ACLS-PALS-BLS and Level 2, 3 and 4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home
Here are the distinct advantages of the webcast (contact us at 214 -384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the cou rse.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels. Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedat ion permits.
AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation

This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs.
Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
www.tda.org | October 2023 451
Live Programs
Approved PACE Program Provider FAGD/MAGD Credit. Approval does not imply acceptance by a state of provincial board of dentistry or AGD endorsement. 8/1/2018 to 7/31/2022 Provider ID# 217924
NOW Available: In -Office ACLS & PALS renewals; In -Office Emergency Program
Available Throughout Texas
Dr. Canfield
FEATURES
456 MEMBER HIGHLIGHT
Dr
502 DENTAL RECORD REQUESTS IN AN OIG INVESTIGATION
504 TDA LEGISLATIVE RESOURCE GUIDE
HIGHLIGHTS
462 In Memoriam
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
466
Dr
506 Oral and Maxillofacial Pathology: Case of the Month
509 Oral and Maxillofacial Pathology: Case of the Month Diagnosis and Management
512 Value for Your Profession: 2024 Open Enrollment and ACA Update
516 Classifieds
522 Index to Advertisers
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 140 | No. 8
Texas Dental Association
1946 S IH-35 Ste 400, Austin, TX 78704-3698
Phone: 512-443-3675 • FAX: 512-443-3031
Email: tda@tda.org • Website: www.tda.org
Texas Dental Journal (ISSN 0040-4284) is published monthly except January-February and August-September, which are combined issues, by the Texas Dental Association, 1946 S IH-35, Austin, TX, 78704-3698, 512-443-3675. PeriodicalsPostage Paid at Austin, Texas and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 1946 S IH 35 Ste 400, Austin, TX 78704. Copyright 2023 Texas Dental Association. All rights reserved.
Annual subscriptions: Texas Dental Association members $17. Instate ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax.
THE DENTAL PROFESSION
492 FOR DENTISTRY, I WILL
494 CHAMPIONING ACCESS TO CARE: TDA AS THE PREMIER MEDICAID & CHIP ADVOCATE
500 TDA’S INSURANCE LEGISLATION BENEFITS
TEXAS DENTISTS AND DENTAL PATIENTS
ERRATA: The Oral and Maxillofacial Pathology Case of the Month published in the July 2023 issue of the Texas Dental Journal was previously published in this publication and was inadvertently included. The editorial staff extends its apologies to the authors of this month’s case, which was originally scheduled for the July issue.
Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement included in the online September Annual Membership Directory or on the TDA website: tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
452 Texas Dental Journal | Vol 140 | No. 8 contents
LEGISLATIVE
Robert Henry Johnson 465 2023
LANDSCAPE
LEGISLATIVE LANDSCAPE
THE COUNCIL ON LEGISLATIVE, REGULATORY, AND GOVERNMENTAL AFFAIRS 476 POLITICAL PROCESS 101 478 MEET THE TDA LEGISLATIVE TEAM 480 HOW A BILL BECOMES A LAW IN TEXAS 486 PROTECTING THE PUBLIC: UNDERSTANDING THE TEXAS STATE BOARD OF DENTAL EXAMINERS’ ROLE IN REGULATING
Matt Roberts 474
Free Dental Practice Valuation Take the 1st step in selling your dental practice. Contact us to receive a free practice valuation. Terry Watson, D.D.S. Jeremy Brown, J.D. Frank Brown, J.D., LL.M. WBpracticesales.com 469-222-3200 *
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports

¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface
Professional, reliable service with hightechnology solutions so that you can better serve your patients. Call or email for free kits or consultation.
jkjpathology.com

281-292-7954 (T)
281-292-7372 (F)
johnkacher@jkjpathology.com
Protecting your patients, limiting your liability
Board of Directors Texas Dental Association
PRESIDENT Cody C. Graves, DDS 325-648-2251, drc@centex.net
PRESIDENT-ELECT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
PAST PRESIDENT Duc “Duke” M. Ho, DDS 281-395-2112, ducmho@sbcglobal.net
VICE PRESIDENT, SOUTHWEST Richard M. Potter, DDS 210-673-9051, rnpotter@att.net
VICE PRESIDENT, NORTHWEST Summer Ketron Roark, DDS 806-793-3556, summerketron@gmail.com
VICE PRESIDENT, NORTHEAST Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
VICE PRESIDENT, SOUTHEAST Shailee J. Gupta, DDS 512-879-6225, sgupta@stdavidsfoundation.org
SENIOR DIRECTOR, SOUTHWEST Krystelle Anaya, DDS 915-855-1000, krystelle.barrera@gmail.com
SENIOR DIRECTOR, NORTHWEST Stephen A. Sperry, DDS 806-794-8124, stephenasperry@gmail.com
SENIOR DIRECTOR, NORTHEAST Mark A. Camp, DDS 903-757-8890, macamp1970@yahoo.com
SENIOR DIRECTOR, SOUTHEAST Laji J. James, DDS 281-870-9270, lajijames@yahoo.com
DIRECTOR, SOUTHWEST Melissa Uriegas, DDS 956-369-9235, meluriegas@gmail.com
DIRECTOR, NORTHWEST
Adam S. Awtrey, DDS 314-503-4457, awtrey.adam@gmail.com
DIRECTOR, NORTHEAST
Drew M. Vanderbrook, DDS 214-821-5200, vanderbrookdds@gmail.com
DIRECTOR, SOUTHEAST
Matthew J. Heck, DDS 210-393-6606, matthewjheckdds@gmail.com
SECRETARY-TREASURER*
Carmen P. Smith, DDS 214-503-6776, drprincele@gmail.com
SPEAKER OF THE HOUSE*
John W. Baucum III, DDS 361-855-3900, jbaucum3@gmail.com
PARLIAMENTARIAN**
Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
EDITOR**
Jacqueline M. Plemons, DDS, MS 214-369-8585, drplemons@yahoo.com
LEGAL COUNSEL
Carl R. Galant
*Non-voting member
**Non-voting
454 Texas Dental Journal | Vol 140 | No. 8
PROTECT THE VALUE of Your Practice

Practice owners should always have an up-to-date Practice Valuation, meaning a professional appraisal that has been completed or updated in the past 12 months.
Besides helping you set a listing price when you are ready to sell your practice, ractice aluations are needed to:


• Evaluate what factors are affecting the value of your practice
• Write a Letter of Instruction (LOI)
• Apply for financing
• Form merger/partnership agreements
Henry chein Dental ractice chein Dental ractice ransitions valuation considers both tangible and intangible assets o and assets of the practice and can provide the many key factors that influence many factors that influence the practice’s value.
Practices For Sale
Since 1968
o get started on your practice valuation, give us a call at: 866-335-2947

or scan the Q code to schedule a complimentary consultation.

MULTI-MILLION DOLLAR OPPORTUNITY: Large GP located north of Houston with real estate is available. The office is in a stand-alone building with 8 ops and is in excellent condition, with digital x-rays, pano, and paperless charts. The office operates 45 hours per week with 3 clinicians. There is over 6,500+ active patients, 70% Medicaid & 30% PPO/ FFS, with an average of 96 new patients per month. Opportunity ID: TX-7894
REDUCED PRICE - WEST OF FORT WORTH: This thriving majority FFS practice with around 24% PPO, brought in impressive 2022 collections of $598,000+ on just 3 to 3.5 doctor and 3 hygiene days per week. Equipped with 6 ops, digital X-rays, and a 3D digital pano, this practice has it all! With almost 1,100 active patients and averaging 23+ new patients per month, the potential for growth is huge. Expand your hours and keep specialties in-house to take this practice to the next level. Opportunity ID: TX-7886
FORT WORTH ROOM FOR GROWTH/MERGER OPORTUNITY: GP located in the retail level of a live/work/play community. The office has 3 ops that are fully equipped with digital x-ray, Pan and paperless patient files. 2 additional ops are available. The office is in excellent condition with newer equipment. The practice currently operates on 4 doctor days and one hygiene day per week, leaving another area for growth. This practice has over 2,000 active patients that are a blend of 20% FFS, 65% PPO, & 15% Medicaid. Opportunity ID: TX-7883
$759K DALLAS OPPORTUNITY: GP in a retail center with 4 ops, all digital & paperless, and everything is in excellent condition, less than two years old. This practice operates 7 days a week, mainly evenings and weekends, with 1 FT & 1 PT associate currently in place. They have over 3,800 patients that are 100% FFS. The procedure mix is approximately 20% hygiene, 40% OS, 10% endo, 10% C&B, and 25% restorative. Opportunity ID: TX-7834


Go to our website or call to request information on other available practice opportunities!

www.tda.org | October 2023 455
© 2023 Henry chein, nc. o copying without permission. ot responsible for typographical errors. 23 2801 www henryscheinDPT com n C C n n B Y
800.232.3826 Practice Sales & Purchases Over $3.2 Billion www.AFTCO.net
We are pleased to announce...
Sarah B. Behmanesh, D.D.S. has acquired the practice of have acquired the practice of Houston, Texas
Bee Cave, Texas
We are pleased to have represented all parties in these transitions.
& David C. Sun, D.D.S.
Jini P. Kuruvilla, D.D.S.
Nehalben D. Patel, D.D.S.
Veronica Y. Chen, D.D.S.
Dr Robert Henry Johnson
One of America’s Oldest Practicing Dentists Has
a Secret to Staying Young
Dr Robert Johnson is 91, and he’s not quitting anytime soon.
It’s 1931. America is fraught with despair and instability—it’s in the midst of the Great Depression, Prohibition, and the Dust Bowl. That year of the Dirty Thirties saw the completion of the Empire State Building in New York City, gangster Al Capone sentenced to prison, and Herbert Hoover as president of the US.
Also that year on November 25, Robert Henry Johnson was born in Goldthwaite, Texas. Now, with an active dental license at 91 years old, Dr Johnson is one of the oldest practicing dentists in the United States. He goes into the office 5 days a week, taking off on Wednesday and Friday afternoons.
He grew up without running water or electricity, and the family used an outhouse and a smokehouse. His mother Virgie had a beauty shop, and the town waitresses were her best customers, Dr Johnson says. His father Bob ranched all his life. Two harder workers, you couldn’t find.

456 Texas Dental Journal | Vol 140 | No. 8
“We went to town on Saturday, got a dime and had 6 cents for a show and then 4 cents for candy. We’d stay until 3 PM, and then went home until the next Saturday,” he explains on an October 2022 YouTube video interview called “Dental Minute with Steven T. Cutbirth, DDS.”
He graduated from Baylor College of Dentistry in 1956, but getting there was no easy feat. He used the $20,000 he won from showing his grand champion steers at stock shows in Houston and Fort Worth to pay for tuition.


He credits 2 men with really giving his dental fate its teeth, Dr T. C Graves of Goldthwaite and Dr Eldon Knox of Dallas. He explains their influence on him in his youth, “There are 2 pretty good dentists! Looks pretty good to me! I’m going to be a dentist!”

Dr Graves attended his church and was his Eagle Scout leader. “He was an inspiration to me,” says Dr Johnson of the late Dr Graves, who is the grandfather of current TDA President Dr Cody Graves.
As a boy, he worked on the ranch for Dr Knox. “I already had a driver’s license at 12,” he says, explaining to Dr Cutbirth on the YouTube interview that he drove a truck to help his father and uncle. They made their 50-cent-anhour livings by commercially eradicating mesquite trees through a government program.
www.tda.org | October 2023 457
Dr Johnson (“PaPa”) treats one of his great grandsons.
Dr Johnson won Grand Champion Steer at the Houston and Fort Worth stock shows. He is pictured with his mother and father, Virgie and Bob, and he used that money to help pay for dental school.
Dr Knox “had this super huge 2-anda-half-story building, and in his living room, I couldn’t get the football to hit the ceiling, it was so tall,” he tells Dr Cutbirth. “And a 4-car garage! My eyes were pretty big for a little boy. I’d never seen anything like that.”
So, that small town young man with saucers for eyes took off to the big city of Waco to become a dentist, stopping first to buy slacks and blue suede shoes for $7.95. “I didn’t know nothing about nothing about city people. I was raised on a ranch. Jeans is all I knew, and boots, and all these people had slacks!”
He met his wife Pat at Baylor University, where she was the Homecoming queen and he’d caught her eye, regardless of his country look. She jumps in Dr Cutbirth’s YouTube interview here with a chuckle. “I tell you what I liked about him. He had on cowboy boots. I liked that!”
The couple remained friends through college and were married in May 1956. Dr Johnson then started his dental career at the Biggs Air Force Base in El Paso, now the Biggs Army Airfield. “That’s where, really and truthfully, you learn dentistry!”

They then moved to Big Spring, where he charged $5/filling, $5/extraction, and $30/crowns. “That’s hard to believe with inflation!”
Brownwood followed in 1970, and they raised their children, Bart and Robert, now 64 and 65, respectively. His practice prospered, and he prides himself on treating his patients like family, one of which was Dr Cutbirth whom he treated as a kid.

458 Texas Dental Journal | Vol 140 | No. 8
Dr Johnson began his dental career at the Biggs Air Force Base in El Paso, now the Biggs Army Airfield.
“His daddy called me, and he had 2 teeth in his hand, said he (Dr Cutbirth) tried to eat a baseball, but it ate him back,” Dr Johnson laughs in the YouTube video interview.
Dr Cutbirth remembers knocking out his bicuspid and lateral, but it wasn’t by a knockdown pitch or foul ball. He was trying to steal second base and ran into the shortstop’s knee. Dr Johnson performed a root canal and replanted the teeth, which lasted Dr Cutbirth until he was 55 years old.
Root canals, silver fillings, and extractions have given way to laminates, improvements to procedures, and more root canals and extractions. “I’m still doing all the same things. Really and truthfully, just upgraded from we used to do.”
He says that the innovations in equipment have been revolutionary to dentistry. “There is really no comparison. The fast equipment, it’s completely changed.”

Dr Johnson has treated generation after generation in Brownwood. “The patients are just part of my family.”
Really, it was always a family business of sorts. Pat helped him chairside over the years, and she laughs saying she was always on edge when the nuns in Big Spring made their way to his office. “I was so nervous because I thought, ‘Oh! I hope he doesn’t say a cuss word!’”
Dr Johnson’s secret to staying healthy while practicing for 66 years? “Sit down and work, and you’ll last 10 more years,” he says, adding it’s important to keep
Pat helped him chairside over the years, and she laughs saying she was always on edge when the nuns in Big Spring made their way to his office. “I was so nervous because I
current on CE courses and attend meetings.
He has another tip to eternal youth. “Heredity is the secret, but after that, we (he and Pat) have 2 drinks of vodka every night. That’s proven it’s good for you! Not 6, but 2!”
And, he golfs and keeps active but doesn’t follow a strict diet. “I was raised on fried food. It’s gotta be fried to be good!”
At 91 years old, he looks forward to a birthday in November, but he has no plans to retire anytime soon. “Money is not the answer. It’s the love of your patients you’ve had 50 years. They come in and say, ‘What am I going to do when you retire?’ And they mean it.”
www.tda.org | October 2023 459
Dr Johnson and his wife Pat treat their son Robert Jr in Big Spring.
thought, ‘Oh! I hope he doesn’t say a cuss word!’”

460 Texas Dental Journal | Vol 140 | No. 8
Fishing and golf are Dr Johnson’s favorite hobbies, and he won the TDA Smiles golf tournament in 1984 and 1986 in San Antonio.
He tells his patients he’ll retire when his hands shake, but until then, “We love each other! It’s like family!”
Near the end of the YouTube video, Dr Cutbirth says to Dr Johnson, “What an interesting life you’ve led.”
Indeed, Dr Johnson.
Watch Dr Cutbirth’s October 2022 YouTube interview with Dr Johnson and his wife Pat at https://bit.ly/ DentalMinute.
Dr Johnson has been a member of TDA since 1957, reaching Life membership status in 1998, 50-Year in 2007, and 60-Year in 2020.


www.tda.org | October 2023 461
Pictured quail hunting are grandson Bart Jr, Dr Johnson, son Bart, and grandson Blake.
Larry Steve Steinberger
Sugar Land

January 11, 1944–August 5, 2023
Good Fellow: 1996
Life: 2009
Fifty Year: 2018



Hubert Carl Askew Jr Houston
September 30, 1939– August 12, 2023
Good Fellow: 1992
Life: 2004
Fifty Year: 2017

Jack W Pool
San Antonio
May 7, 1946– August 16, 2023
Good Fellow: 2002
Life: 2011
Eugene H La Gesse Jr Austin
October 29, 1930– August 12, 2023




Good Fellow: 1986
Life: 1995
Fifty Year: 2011

Tommy Louis Thomson Austin
September 26, 1941– August 23, 2023
Good Fellow: 1994
Life: 2006
Fifty Year: 2019
Billy D Sturrock
Beaumont
April 3, 1953–July 19, 2023
Good Fellow: 2006
Life: 2018




462 Texas Dental Journal | Vol 140 | No. 8 in memoriam
1 0 k $ Sign on bonus up to careers.benevis.com/dentists APP-SOLUTELY RE-IMAGINED! Designed for dentists, with dentists, the new ADA Member App is here and ready to put the resources you need in the palm of your hand. • Chat 1:1 or with your network • Newsfeed customized to your interests • Digital wallet to store your important documents • Stream the new “Dental Sound Bites” podcast Tap into possibility at ADA.org/App
Those in the dental community who have recently passed
ORAL PATHOLOGY SERVICES
> Processing and interpretation of biopsy specimens

> Free biopsy kits
> Free mailing of specimens
> Access to oral pathologists for clinical/radiologic consultations
> One day turnaround after receipt of specimens
OUR BOARD-CERTIFIED ORAL PATHOLOGISTS
> Dr. Leticia Ferreira Cabido
> Dr. Madhu Shrestha
> Dr. Victoria Woo
> Dr. John M. Wright, Laboratory Director

Contact: 214 828 8111 oralpath@tamu.edu
https://dentistry.tamu.edu/departments/oral-pathology/
LAW OFFICES OF MARK J. HANNA
• Representation Before the Texas State Board of Dental Examiners
• Medicaid Audits and Administrative Hearings
• Employment Issues—Texas Workforce Commission Hearings
• Administrative (SOAH) Hearings and Counsel
• Professional Recovery Network (PRN) Compliance
• Employment/Associateship Contract Reviews
• Practice Acquisition and Sales
• Business Organizations,
•
www.tda.org | October 2023 463
PCs,
PLLCs
PAs,
and
Litigation 2414 Exposition Blvd., Suite A1 • Austin, Texas 78703 • Phone: 512-477-6200 • Fax: 512-477-1188 • Email: mhanna@markjhanna.com Not Board Certified by the Texas Board of Legal Specialization
Civil
Mark J. Hanna JD Former General Counsel, Texas Dental Association
EXPERIENCED LEGAL REPRESENTATION FOR TEXAS DENTISTS


www.tda.org | October 2023 465 466 474 476 478 480 486 492 494 500 502 504 Legislative Landscape Dr Matt Roberts The Council on Legislative, Regulatory, and Governmental Affairs Political Process 101 Meet the TDA Legislative Team How a Bill Becomes a Law in Texas Protecting the Public: Understanding the Texas State Board of Dental Examiners’ Role in Regulating the Dental Profession For Dentistry, I Will Championing Access to Care: TDA as the Premier Medicaid & CHIP Advocate TDA’s Insurance Legislation Benefits Texas Dentists and Dental Patients Dental Record Requests In an OIG Investigation TDA Legislative Resource Guide 2023 LEGISLATIVE Landscape Contents www.tda.org | October 2023 465
2023 Legislative Landscape
INTRODUCTION
Dr Matt Roberts, Chair
TDA Council on Legislative, Regulatory, and Governmental Affairs
The October issue of the Texas Dental Journal focuses on organized dentistry’s efforts in the legislative and regulatory arenas. Much of what dentists do every day in their practices is controlled by the Texas legislature, made up of 150 members of the Texas House of Representatives and 31 members of the Texas Senate. The Texas State Board of Dental Examiners (TSBDE), made up of 11 members including 6 dentists, 3 dental hygienists, and 2 members of the public, also plays a significant role in regulating dentistry in Texas. In addition, Texas statewide officials— including the governor, lieutenant governor, attorney general, and comptroller—have roles in the oversight and regulation of dentistry.

466 Texas Dental Journal | Vol 140 | No. 8
The practice and regulation of dentistry and dental hygiene are governed in state statute (law) by the Dental Practice Act (DPA) contained in the Texas Occupations Code. The DPA includes 16 chapters with over 200 sections pertaining to the practice and oversight of dentistry.
The TSBDE is charged with interpreting and enforcing the DPA and the other statutes/laws affecting dentistry, as well as promulgating and implementing rules to protect public health and safety.
Given the depth and complexity of the laws, regulations, and oversight of dentistry, it is imperative that the TDA commit adequate resources and personnel toward ensuring dentistry’s voice is not only present in Austin, but heard in all legislative and regulatory forums where dentistry is considered.
The TDA’s Council on Legislative, Regulatory, and Governmental Affairs (or CLRA) is made up of TDA member dentists from around the state who have experience and expertise in the legislative and regulatory fields. CLRA is charged with working with the legislature and the regulatory entities to represent the Association and implement its policies as set by the House of Delegates and Board of Directors.
The TDA legislative “team” (the TDA Department of Legislative and Regulatory Affairs staff and legislative consultants) work closely alongside CLRA members and the TDA leadership to assist with achieving organized dentistry’s goals.
The 88th Session of the Texas Legislature convened January 10, 2023, and concluded May 29. This session,
members of the Texas Senate and House focused most of their attention on the budget given there was a record surplus of tax dollars to work with— roughly $33 billion over the amount available in the previous session. The historic budget surplus had every stakeholder at the Capitol, including TDA, requesting funds for programs/ issues of importance to them. Time spent on budget-related issues left little time for all other issues.
Budget-related topics lawmakers deliberated include property tax cuts, public education funding and security, parental school choice/school vouchers, creating a new endowment for certain higher education university systems, mental health access, the state’s energy grid, higher education funding, and border security.
Other over-arching issues lawmakers spent precious time on include transgender health care, penalties for those associated with fentanyl distribution/poisoning, expanding broadband access to rural areas of Texas, preempting local regulations, and enhancing the state’s water infrastructure.
Also, the regular session concluded in atypical fashion with the House of Representatives voting to advance articles of impeachment against Attorney General Ken Paxton.
This session, TDA had its most aggressive legislative agenda ever including efforts to reform dental insurance law, increase funding to Medicaid dental and loan repayment, expand availability of health insurance options to TDA members through Multiple Employer Welfare Arrangements (MEWAs), and authorize
properly educated/trained dental hygienists to administer local anesthetic under certain conditions.
In addition to issues TDA pursued on “offense,” there were numerous issues on “defense” to work against including scope expansion efforts of non-dentists, unfavorable dental insurance proposals, and a DSO registration change attempt.
Each of these important oral health topics, and more, will be highlighted in this issue of the Journal.
On behalf of CLRA and the legislative team, thank you for being a member of the TDA and if your TDA legislative team can be of any assistance to you, please do not hesitate to contact me, Jess Calvert, Diane Rhodes, or Staci Rives in the legislative department.
www.tda.org | October 2023 467
TEXAS LEGISLATURE— OVERVIEW
The Texas Legislature is the chief policymaking branch of state government that the Texas Constitution vests with all legislative power in the state. It is a bicameral body composed of an upper chamber, the Texas Senate, and a lower chamber, the Texas House. The 181 members of the legislature are elected from districts throughout the state (31 senators, 150 representatives). The legislature enacts thousands of laws each session that govern behavior, allocate resources, and define the duties of government institutions. The only bill lawmakers are constitutionally required to pass every regular session, however, is the biennial state budget.
In addition to legislative powers, the legislature exercises other types of authority. Constituent powers include the ability to alter the state Constitution, and members have authority to exercise powers of attorney on behalf of their constituents. The legislature is also allowed by statute to create and regulate the state’s administrative system, which comprises boards, commissions and departments that oversee state agencies. The legislature establishes and funds the departments and agencies—such as the Texas State Board of Dental Examiners (TSBDE)—and defines their powers and functions.

468 Texas Dental Journal | Vol 140 | No. 8
TEXAS LEGISLATIVE SESSIONS
The Texas Constitution limits the regular legislative session to a maximum of 140 days every 2 years, but the governor has authority to call special sessions when necessary. Regular sessions begin on the second Tuesday of January in oddnumbered years. Special sessions are limited to 30 days each and are limited to a specific “call,” or subject matter, determined by the governor.
Governor Abbott called 2 special sessions of the 88th Legislature. The focus of both was primarily tax cuts/property tax reform. The Senate and House reached an agreement on property tax reform in the second called special session. Included in that agreement is an important change that could impact some TDA members. That change increases the franchise tax trigger point from $1 million to almost $2.5 million. Businesses, including dental practices, with less than $2.5 million in revenue will no longer pay the franchise tax. In addition, businesses that owe no franchise tax are no longer required to complete or file a report with the Texas Comptroller of Public Accounts.
It is anticipated that the governor will call a third special session later this year to focus primarily on public school vouchers and increasing public school teacher pay.
TERMS OF OFFICE— TEXAS HOUSE AND SENATE
House members serve 2-year terms. To qualify to run for the office, representatives must be at least 21 years old, have been Texas residents for at least 2 years and residents of the district they wish to represent for at least 1 year. There is no limit on the number of terms a member can be re-elected.
Senate members are elected to 4-year terms. To run for Texas Senate, candidates must be at least 26 years old, have been residents of Texas for 5 years preceding their election and residents of the district they are seeking for at least 1 year.
SENATE/HOUSE MEMBERSHIP—
88TH LEGISLATURE
Each election cycle brings change. Members of the Senate and House change each cycle—voluntarily, meaning some choose to leave, and involuntarily, meaning some are defeated.
In the last election, there was no significant change in terms of the overall party make-up of the chambers. Each chamber added 1 republican—19 republicans and 12 democrats in the Senate, 86 republicans and 64 democrats in the House. However, there was significant change in the members themselves—5 freshmen in the Senate, 27 in the House. Again, not much change in terms of overall party numbers but significant change in terms of members themselves.
In terms of leadership, Lt Governor Dan Patrick (R–Houston) was elected by Texas voters again as presiding officer of the Senate and Rep Dade Phelan (R–Beaumont) was elected by his House colleagues again as Speaker of the House of Representatives.
The TDA spends a majority of its time working with lawmakers on the Senate Health and Human Services Committee, House Public Health Committee, and House Insurance Committee. Chairs of these committees were the same this session as last with Senator Lois Kolkhorst (R–Brenham) chairing Health and Human Services, Stephanie Klick (R–Fort Worth) chairing Public Health, and Tom Oliverson (R–Cypress) chairing Insurance.
Of these 3 committees, Senate Health and Human saw the most significant membership change with 4 of the 9 members being new.
88TH LEGISLATIVE SESSION
As previously stated, the TDA had its most aggressive agenda ever this session. Your legislative team literally worked around the clock every day in support of the issues we had on offense, and against the issues we had on defense.
It is important to note and highlight that your TDA legislative team has been together for decades. That continuity and consistency benefits our efforts. Lawmakers and staff know your team well, and your team knows them well. Your team also knows dentistry.
Whether pursuing an issue on offense or defense, navigating the legislative process requires knowledge that only comes with experience, relationships with lawmakers and staff, instincts, strategy, communication, professionalism, camaraderie, and much more. Your team functions at a high level on your behalf, and they are respected at the Capitol.
www.tda.org | October 2023 469
TDA LEGISLATIVE AGENDA— ACTION SUMMARY
SECURED DENTAL INSURANCE REFORM— NEW SAFEGUARDS FOR DENTISTS
TDA secured passage of dental insurance reform for state-regulated insurance plans that brings relief to Texas dentists. HB 1527 is an example of TDA’s commitment to achieving a dental insurance landscape that promotes fairness and long-term success for patients and dentists.
HB 1527 addresses 3 dental insurance issues that Texas dentists commonly encounter:

1. Retroactive Denials—Dental insurers audit their claims payments after they are made to dentists to ensure accuracy and efficiency. When a carrier demands reimbursement of a paid claim after a significant amount of time has passed since the service was provided, the unexpected charges are distressing for patients who thought the claim was already paid by their insurance.
2. Disallowable Clauses—Health care decisions are personal, and treatment plans should be made between the patient and their dentist. However, many insurers have become not only the payor but also the arbiter of these personal clinical decisions through disallow clauses that both deny a dental benefit and prohibit the dentist from collecting fees from the patient for a service they provided.
3. Silent Network Leasing—In a “silent provider” network, the policy issuer
470 Texas Dental Journal | Vol 140 | No. 8
sells, leases, or rents its provider network to other insurance carriers or thirdparty payors of dental services without informing participating dentists. This lack of transparency erodes patient-dentist trust, which can lead to incorrect assumptions about treatment plans and unforeseen costs.
CSHB 1527 provides common sense solutions to address these issues in a fair and transparent manner by:
1. Creating reasonable procedures and a 180-day timeframe for insurance companies to engage in payment recovery efforts.
2. Preventing insurers from both denying a dental benefit and prohibiting the dentist from collecting fees associated with the services provided.
3. Creating transparency for dentists and patients by requiring insurers to follow fair and accurate network leasing laws that give dentists an opportunity to review contracts prior to the network being leased.
CSHB 1527 establishes fair and transparent procedures between dental insurers and dentists to protect the dentist-patient relationship.
TDA is grateful to Representative Tom Oliverson (R–Cypress) for authoring this legislation in the Texas House and to Senator Judith Zaffirini (D–Laredo) for sponsoring it in the Texas Senate. Both of these lawmakers and their staff worked extensively with the TDA legislative team to get this bill through the legislature and to Governor Abbott who signed it on June 18, 2023.
EXPANDED MULTIPLE EMPLOYER WELFARE ARRANGEMENTS (MEWA) AVAILABILITY
TDA-backed House Bill 290 which expands Multiple Employer Welfare Arrangements (MEWAs) eligibility to sole proprietors and professional organizations if those in the MEWA are in the same state.
MEWAs are arrangements under which a group of small employers join to obtain health care benefits that can be offered to their employees. MEWAs, by grouping together the purchasing power of several small employers, are often able to obtain access to health care coverage on more favorable terms than what would be available if those small employers were to each independently obtain health coverage on the commercial market. Through risk pooling of the participating small employers, MEWAs can offer comprehensive health coverage at rates that are similar to those that can be obtained by some larger employers.
There are limits to how helpful MEWAs can be to Texas employers because of certain limitations contained in Texas insurance law. Texas insurance law only allows employers to join a MEWA if they are in the same trade or industry. As such, if a MEWA offering benefits to law firms wanted to also offer benefits to dentist offices or accounting firms, for example, it would be prohibited from doing so. Additionally, Texas insurance law does not allow working owners of their own businesses to qualify as employers, meaning that MEWAs cannot offer benefits to sole proprietors.
www.tda.org | October 2023 471
TDA secured passage of dental insurance reform for stateregulated insurance plans that brings relief to Texas dentists. HB 1527 is an example of TDA’s commitment to achieving a dental insurance landscape that promotes fairness and longterm success for patients and dentists.
House Bill 290 amends Texas insurance law to allow the Texas Department of Insurance (TDI) to approve a MEWA that offers a comprehensive benefit plan to small employers within certain geographic areas, not limited by industry, as well as to sole proprietors.
House Bill 290 provides the ability for Texas small businesses and selfemployed individuals to join to obtain comprehensive health coverage at more affordable rates than what is available under current law. By expanding the coverage options of MEWAs, House Bill 290 increases the health care plans available to members of professional associations like the TDA.
TDA’s insurance vendor is currently researching potential MEWA health care options for TDA members, their families, and staff. This is an exciting opportunity for TDA to potentially offer better health insurance options for member dentists.
TDA thanks Rep Tom Oliverson (R–Cypress) for authoring House Bill 290 in the Texas House and Senator Kelly Hancock (R–North Richland Hills) for sponsoring it in the Senate. Both lawmakers spent significant time and effort to pass the bill and advance it to Governor Abbott who signed it on May 23, 2023.
ACHIEVED LEGISLATION AUTHORIZING HYGIENIST ADMINISTRATION OF LOCAL ANESTHETIC
In response to TDA member requests to authorize dental hygienists to administer local anesthetic and the TDA House of Delegates’ action changing TDA policy in May 2023, TDA successfully guided House Bill 3824 through the legislative process.
The historic legislation, resulting from extensive TDA-led negotiations with the Texas Dental Hygienists’ Association (TDHA), authorizes Texas dentists to delegate under direct continuous supervision to properly educated and trained Texas-licensed dental hygienists the administration of local infiltration anesthetic to a non-sedated or nitrous oxide/oxygen inhalation sedated patient who is 18 years of age or older in the context of delivering hygiene services.
TDA negotiations with TDHA on this issue include a signed agreement that there will be no additional scope of practice pursuits by TDHA for a term of ten years after House Bill 3824 becomes law. The effective date of House Bill 3824 is September 1, 2023, so the 10-year term does not expire until September 1, 2033.
As chair of the TDA Council on Legislative, Regulatory, Government Affairs, I have been involved with and seen TDA accomplish incredible things at the Capitol. I have never seen or been involved with an effort like this one. Work began more than a year before the session started to negotiate the terms of the agreement between TDA
and TDHA and to strategize potential pathways to successfully guide the legislation through both chambers at such a late stage of session.
The TDA HOD met in early May and changed TDA policy to permit hygienists to administer local anesthetic per the safeguards mentioned above. Session ended May 29 and deadlines in both chambers began as early as May 8. Despite the incredible odds against passing this bill with almost no time remaining at the Capitol, the TDA legislative team found a way to get it through the House and Senate in only 16 days.
Passing a bill in 140 days is almost impossible. Passing a bill in 16 days is unheard of and TDA’s legislative expertise and long-term relationships with key lawmakers made the difference.
The monumental actions and efforts by the TDA team and Senator Lois Kolkhorst (R–Brenham), Senator Bryan Hughes (R–Mineola), Representative Stephanie Klick (R–Fort Worth) and their staffs to get this done, cannot be overstated.
GUARDED DENTISTS FROM ONEROUS PATIENT BILLING REQUIREMENTS
TDA-amended Senate Bill 490 ensures that dentists are not held to tedious and burdensome itemized patient billing requirements. TDA’s advocacy resulted in dentists being removed from the bill so that the legislation focuses on its original intent of making hospitals provide itemized bills to patients upon request.
472 Texas Dental Journal | Vol 140 | No. 8
ENSURED ADDITIONAL STUDY FOR LICENSURE COMPACT
At TDA’s recommendation, the legislature agreed that more study is necessary to make an informed decision on whether Texas should participate in the Dentist and Dental Hygienist Interstate Licensure Compact.
The Compact would permit dentists and dental hygienists to practice in all states participating in it versus being licensed in those states independently. Considering the complexities and legal obligations involved for Texas to participate in the Compact, the legislative interim will give the time necessary to study dental workforce distribution in Texas and whether Compact participation is warranted.
ENHANCED TEXANS’ ACCESS TO DENTAL CARE
Senate Bill 1854 requires the Teacher Retirement System of Texas (TRS) to make available an optional insurance plan that provides coverage for dental care to all TRS retirees, dependents, and surviving spouses and surviving dependent children.
PROTECTED MEDICAID FUNDING
Although TDA tirelessly advocated for a Medicaid dental fee increase, the legislature declined to support the initiative that would have resulted in an ongoing increase to the state’s budget. However, TDA did protect Medicaid and CHIP dental funding from budget cuts.
TDA knows the vital role that Medicaid plays in Texas’ dental public health safety net. TDA will continue advocating for a fee increase that aligns with the program’s 2007 value when adjusted for inflation.
In addition to the issues highlighted above, TDA successfully worked against a number of efforts that would have negatively impacted Texas dentists, Texas dental patients, and/or the Association.

Your membership makes TDA’s advocacy efforts possible. The issues that dentistry faces at the Capitol are consistently becoming more complex, and there are more of them every session. Now more than ever, it is crucial for dentists to be strongly represented and properly positioned at the Capitol to protect the profession and the patients served.
Thank you for your membership and for being an advocate for your patients and your profession.
www.tda.org | October 2023 473
The Council ON Legislative, Regulatory, and Governmental Affairs
The Council on Legislative, Regulatory, and Governmental Affairs (CLRA) makes certain that the Texas Dental Association (TDA) has an effective voice in the legislative process and state government. CLRA works with the legislative and regulatory affairs staff and TDA contract legislative consultants to implement TDA’s legislative agenda and maintain positive working relationships with legislators, state officials, and allied professional groups. In conjunction with component societies, the council informs members about governmental actions and mobilizes the TDA’s grassroots organization. The council also works with regulatory agencies to help ensure a competitive marketplace for dentists and quality dental care for all Texans.
Dr Matthew B. Roberts, Chair
General dentist from Crockett, former TDA president, former member of the American Dental Association (ADA) Council on Government Affairs, former member of the ADA Council on Access, Prevention and Interprofessional Relations, and former member of the Commission on Dental Accreditation. Dr Roberts is serving his 20th year on CLRA.
Dr Jay C. Adkins, Member
General dentist from Lubbock, former TDA Board of Directors member, former member of the Texas State Board of Dental Examiners Dental Hygiene Advisory Committee, current TDA Smiles Foundation Board member (19th year), past regent for Texas in the International College of Dentists (ICD), and current chair of ICD 2023 Fellowship Orientation Program. Dr Adkins is serving his 12th year on CLRA.
Dr Paul A. Kennedy III, Member
Pediatric dentist from Corpus Christi, past president of the Nueces Valley District Dental Society, former adjunct professor in the department of pediatric dentistry at UT Health San Antonio. Dr Kennedy is serving his 6th year on CLRA.
Dr Debrah Worsham, Member
General dentist from Center, former TDA president, former DENPAC chair, former ADPAC vice-chair, former TDA Board of Directors member. Dr Worsham is serving her 21st year on CLRA.
Dr Georganne P. McCandless, President-Elect
Pediatric dentist from Tomball, current TDA president-elect, former member of Council on Dental Licensing, Standards, and Education, current LAC member 8th district. Dr McCandless is serving her 1st year on CLRA.
Dr Duc “Duke” M. Ho, Past President
General dentist from Katy, current TDA past president, current member of the ADA Council on Government Affairs, former chair of the ADA Council on Dental Practice, former chair of the TDA Strategic Affairs Committee, former president of the Greater Houston Dental Society, and has served on the ADA Fight Insurance Interference Strategic Task Force, the ADA Dental Practice Recovery (COVID) Task Force, and the ADA ERISA Special Committee. Dr Ho is serving his 5th year on CLRA.
Dr R. Shad Hattaway, New Dentist
General dentist from Carrollton, current member of the ADA ACE Panel, former roles in the Dallas County Dental Society include program chairman, SWDC New
Dentist CE Express chairman, membership committee, peer review committee, editor, and director. Dr Hattaway is serving his 1st year on CLRA.
Dr David A. Duncan, Consultant
General dentist from Amarillo, former TDA president, former TDA Board of Directors member, former Panhandle Dental Society president, former member of the ADA Council on Dental Practice, former member ADA’s political action committee (ADPAC). Dr Duncan is serving his 14th year on CLRA.
Dr Michael Najera, Consultant
Periodontist from El Paso, former president 16th District, current chair Legislative Action Committee 16th District, current DENPAC board member and chair of 16th District for past 17 years, past TDA and ADA delegate. Dr Najera is serving his 4th year on CLRA.
Dr Mark Peppard, Consultant
General dentist from Austin, served on the ADA’s political action committee (ADPAC), former TDA Board of Directors member, former TDA delegate, former ADA delegate, current DENPAC board member. Dr Peppard is serving his 18th year on CLRA.
Dr R. Lee Clitheroe, DENPAC
General dentist from Sugar Land, current DENPAC chair, former TDA vice president, former member of the Greater Houston Dental Society (GHDS) Foundation Board, former chair GHDS Legislative Action Committee, ICD and ACD fellow, and adjunct faculty at the University of Texas School of Dentistry at Houston. Dr Clitheroe is serving his 3rd year on CLRA.
Ms Janet Crow, Alliance
From Spicewood, current Alliance of the TDA (ATDA) treasurer, former ATDA president, former ATDA liaison to DENPAC and TDASF. Ms Crow is serving her 10th year on CLRA.
474 Texas Dental Journal | Vol 140 | No. 8
Row 1 (L-R)
Dr Matthew B. Roberts, Chair (Crockett)
Dr Jay C. Adkins (Lubbock)



Dr Paul A. Kennedy III (Corpus Christi)


Row 2 (L-R)
Dr Debrah Worsham (Center)
Dr Georganne P. McCandless (Tomball)



Dr Duc “Duke” M. Ho (Katy)
Row 3 (L-R)
Dr R. Shad Hattaway (Carrollton)

Dr David A. Duncan (Amarillo)
Dr Michael Najera (El Paso)
Row 4 (L-R)
Dr Mark Peppard (Austin)

Dr R. Lee Clitheroe (Sugar Land)
Ms Janet Crow (Spicewood)

www.tda.org | October 2023 475
POLITICAL

476 Texas Dental Journal | Vol 140 | No. 8
PROCESS 101
The Texas Dental Association takes pride in its legislative team and the participation in the political process by member dentists. Although mapping the legislative infrastructure may appear to be a daunting task, the processes can be navigated with the help of experts.
The Texas Senate and House of Representatives meets every 2 years on an odd-numbered year for no more than 140 days. At times, the business of the legislature may exceed the 140 days, and the governor may call a special session for up to 30 days. Although the legislative session is constrained by the time limitations, the truth is the legislators work in their districts all year long to meet with constituents, raise funds for campaigns, and learn which issues affect their areas.
During the 140 days that the legislature meets, the elected officials (31 members of the Senate and 150 members of the House of Representatives) review thousands of bills, listen to committee testimony, meet with visiting constituents and legislative staff, and become policy experts in many areas of law. While this may appear to be a lofty agenda for the elected official, the procedure for enacting a law is
particularly cumbersome involving numerous steps in both the House and Senate. At every point in the process, the bill’s survival is at risk. Also, at every point in the process, the public has the opportunity to make their opinions heard by meeting with their elected officials and attending committee hearings.
The lieutenant governor presides over the Texas Senate and is elected by a statewide popular vote to serve a 4-year term of office. However, the lieutenant governor is not a member of the Senate and only votes to break a tie. The lieutenant governor also appoints all chairs and members to all Senate committees and refers all of the bills to the committees as well. Lieutenant Governor Dan Patrick currently presides over the Texas Senate and the next election for the position is scheduled for 2024.
In the other chamber, the speaker of the house presides over the Texas House of Representatives. The presiding officer is elected by a majority of the House members and appoints all chairs and members to House committees. The speaker of the house also refers all of the bills to the House committees. Unlike the lieutenant governor, the
speaker of the house is a member of his/her chamber and has full voting rights as other House members. Speaker Dade Phelan currently presides over the House of Representatives.
While the legislative process is tedious and calculated, the democratic process relies heavily on civic participation and engagement. The process encourages constituents to meet with their legislators, understand the issues, and express their opinions to the offices of the officials. With today’s technology and the expertise of the TDA, member dentists have many valuable tools to help effectively voice their opinions.
From fundraisers for candidates and Legislative Day to letter writing campaigns and preparing for testimony before the House or Senate committees, the Texas Dental Association is ready and able to assist its members with political participation that supports the goals of organized dentistry and protect the future of the profession. With the influx of new senators and representatives into the Texas Legislature, the TDA hopes to encourage more member dentists to participate in the political process and be advocates for the profession.
www.tda.org | October 2023 477
TDA LEGISLATIVE
JESS CALVERT
is TDA’s director of public affairs. He serves as TDA’s in-house legislative consultant and oversees the day-to-day operations of the TDA Department of Legislative, Regulatory, and Governmental Affairs, including policy, DENPAC, and the contract legislative consultants. He began his career as an analyst at the Legislative Budget Board (LBB), where he was assigned to general government and natural resource agencies. After leaving the LBB, he served on the staff of the Texas House of Representatives Committee on Appropriations as an analyst assigned to education, criminal justice, and the judiciary. Prior to coming to work at the TDA, Jess was employed at General Motors Acceptance Corporation, where he managed several residential finance programs. A native of Austin, Jess earned a BA degree from Texas Tech University and a master of public administration from Texas State University.

NORA DEL BOSQUE
is a contract legislative consultant to TDA. Nora formerly worked as an associate to past TDA legislative consultant Dick Brown. Prior to that, she worked in public affairs and public relations for the Miller Brewing Company, serving as an industry lobbyist in Arizona, Colorado, New Mexico, and Texas. Before joining Miller Brewing Company, she worked in the Texas Legislature as chief clerk for the House Committee on Appropriations and as a legislative aide to the House Ways and Means Committee and for the late Representative James Hury (D-Galveston). A native of Abilene, Nora earned a BA degree from the University of Texas at Austin.

478 Texas Dental Journal | Vol 140 | No. 8
TEAM
SUSAN ROSS
is a contract legislative consultant to TDA and a former director of public affairs for the Association. Prior to representing TDA, she represented the nursing home industry for the Texas Health Care Association and worked as an aide to two influential legislative consultants, Bill Pewitt and Jack Gullahorn. Susan first came to the Capitol in 1993 as an aide to Senator Dan Shelley (R-Crosby). A native of Crosby, she earned a BS degree from Texas A&M University.
DIANE RHODES
is TDA’s senior policy manager. She works on legislative and regulatory issues and serves as staff liaison to the Texas State Board of Dental Examiners, the Council on Legislative, Regulatory, and Governmental Affairs (CLRA), the Council on Dental Licensing, Standards, and Education (CDLSE), and the Council on Public Health and Access to Care (CPHAC).
Prior to coming to TDA, Diane worked in the Division of State Grants in the governor’s office and as a legislative aide to Representative Tom Ramsay (D-Mount Pleasant). A native of Waco, Diane earned a BA degree from Baylor University.



STACI RIVES
is TDA’s PAC coordinator and policy analyst. She serves as staff liaison to DENPAC, the TDA Oral Health PAC (TOHPAC), the Council on Professions and Trends (CPT), and the Community Fluoride Committee (CFC). She worked 6 legislative sessions for various members of the Texas House of Representatives, most recently serving as chief of staff for Representative Ed Thompson (R-Pearland). She also spent time working as an insurance specialist for the Texas Department of Insurance. A native of Houston, Staci earned a BA degree from Southwestern University.
www.tda.org | October 2023 479
HOW A BILL BECOMES A LAW IN TEXAS
THE LEGISLATIVE BRANCH OF GOVERNMENT

480 Texas Dental Journal | Vol 140 | No. 8
The Texas Constitution divides state government into 3 separate but equal branches: the executive branch, headed by the governor; the judicial branch, which consists of the Texas Supreme Court and all state courts; and the legislative branch, headed by the Texas Legislature, which includes the 150 members of the House of Representatives and the 31 members of the state Senate.
Members of the House of Representatives are elected to 2-year terms and represent districts of about 200,000 people each. Senators serve 4-year terms and serve about 950,000 people each.
The legislature meets every odd-numbered year to write new laws and to find solutions to the problems facing the state. This meeting time, which begins on the second Tuesday in January and lasts 140 days, is called the regular session. The governor can direct the legislature to meet at other times also. These meetings, called special sessions, can last no more than 30 days and deal only with issues chosen by the governor.
On the first day of each regular session, the 150 members of the House of Representatives choose one of their members to be the speaker of the House. The speaker is the presiding officer of the House. He or she maintains order, recognizes members to speak during debate, and rules on procedural matters.
The speaker also appoints the chairs and vice chairs of the committees that study legislation and decides which other representatives will serve on those committees, subject to seniority rules. There are 31 committees, each of which deals with a different subject area, and 5 committees that deal with procedural or administrative matters for the House. Most members serve on 2 or 3 different committees.
In the Senate, the presiding officer is the lieutenant governor, who is not actually a member of the Senate. The lieutenant governor is the second-highest ranking officer of the executive branch of government and, like the governor, is chosen for a 4-year term by popular vote in a statewide election.
www.tda.org | October 2023 481
The Texas Constitution divides state government into 3 separate but equal branches: the executive branch, headed by the governor; the judicial branch, which consists of the Texas Supreme Court and all state courts; and the legislative branch, headed by the Texas Legislature, which includes the 150 members of the House of Representatives and the 31 members of the state Senate.
The first thing that the speaker of the House and the lieutenant governor ask their respective houses of the legislature to do is to decide on the rules that the legislators will follow during the session. Some legislative procedures are provided for in the state constitution, but additional rules can be adopted by a house of the legislature if approved by a majority vote of its members.
Once rules have been adopted, the legislature begins to consider bills.
INTRODUCING A BILL
A representative or senator gets an idea for a bill by listening to the people he or she represents and then working to solve their problem. A bill may also grow out of the recommendations of an interim committee study conducted when the legislature is not in session. The idea is researched to determine what state law needs to be changed or created to best solve that problem. A bill is then written by the legislator, often with legal assistance from the Texas Legislative Council, a legislative agency which provides bill drafting services, research assistance, computer support, and other services for legislators.
Once a bill has been written, it is introduced by a member of the House or Senate in the member’s own chamber. Sometimes, similar bills about a particular issue are introduced in both houses at the same time by a representative and senator working together. However, any bill increasing taxes or raising money for use by the state must start in the House of Representatives.
House members and senators can introduce bills on any subject during the first 60 calendar days of a regular session. After 60 days, the introduction of any bill other than a local bill or a bill related to an emergency declared by the governor requires the consent of at least four-fifths of the members present and voting in the House or four-fifths of the membership in the Senate.
After a bill has been introduced, a short description of the bill, called a caption, is read aloud while the chamber is in session so that all of the members are aware of the bill and its subject. This is called the first reading, and it is the point in the process where the presiding officer assigns the bill to a committee. This assignment is announced on the chamber floor during the first reading of the bill.
THE COMMITTEE PROCESS
The chair of each committee decides when the committee will meet and which bills will be considered. The House rules permit a House committee or subcommittee to meet: (1) in a public hearing where testimony is heard and where official action may be taken on bills, resolutions, or other matters; (2) in a formal meeting where the members may discuss and take official action without hearing public testimony; or (3) in a work session for discussion of matters before the committee without taking formal action. In the Senate, testimony may be heard and official action may be taken at any meeting of a Senate committee or subcommittee. Public testimony is almost always solicited on bills, allowing citizens the opportunity to present arguments on different sides of an issue.
A House committee or subcommittee holding a public hearing during a legislative session must post notice of the hearing at least 5 calendar days before the hearing during a regular session and at least 24 hours in advance during a special session. For a formal meeting or a work session, written notice must be posted and sent to each member of the committee 2 hours in advance of the meeting or an announcement must be filed with the journal clerk and read while the House is in session. A Senate committee or subcommittee must post notice of a meeting at least 24 hours before the meeting.
After considering a bill, a committee may choose to take no action or may issue a report on the bill. The committee report, expressing the committee’s recommendations regarding action on a bill, includes a record of the committee’s vote on the report, the text of the bill as reported by the committee, a detailed bill analysis, and a fiscal note or other impact statement, as necessary. The report is then printed, and a copy is distributed to every member of the House or Senate.
In the House, a copy of the committee report is sent to either the Committee on Calendars or the Committee on Local and Consent Calendars for placement on a calendar for consideration by the full House. In the Senate, local and noncontroversial bills are scheduled for Senate consideration by the Senate Administration Committee. All other bills in the Senate are placed on the regular order of business for consideration by the full Senate in the order in which the bills were reported from Senate committee. A bill on the regular order of business may not be brought up for floor consideration
482 Texas Dental Journal | Vol 140 | No. 8
The Legislative Process inTexas
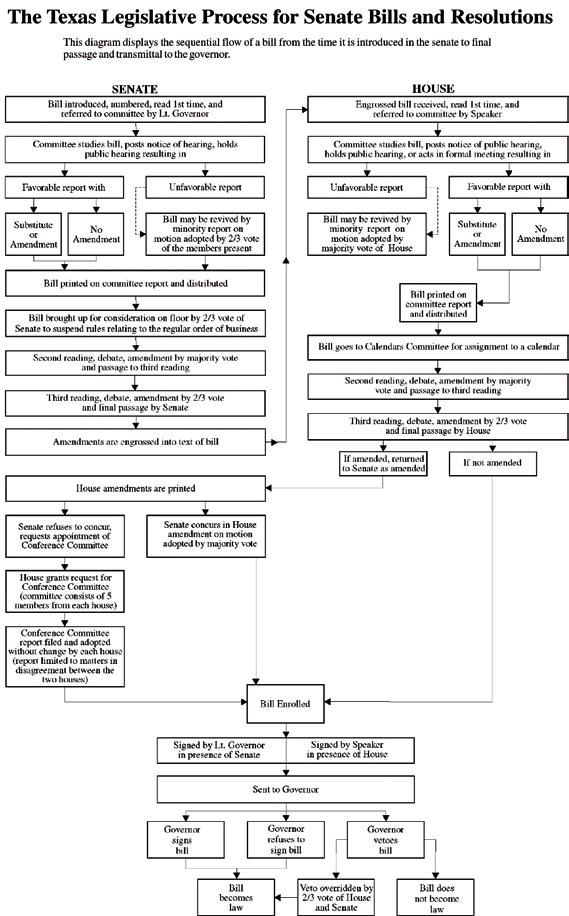
TheTexas Legislative Process for House Bills and Resolutions
Diagram of Legislative Process
Thisdiagramdisplaysthesequentialflowofabillfromthetimeitisintroducedinthehouseof representativestofinalpassageandtransmittaltothegovernor.
ThisdiagramdisplaysthesequentialflowofabillfromthetimeitisintroducedintheHouseofRepresentativestofinalpassageandtransmittal totheGovernor.AbillintroducedintheSenatewouldfollowthesameprocedureinreverse.
HOUSE SENATE
Bill introduced, numbered, read 1st time, and referred to committee by Speaker
Committee studies bill, posts notice of hearing, holds public hearing or acts in formal meeting resulting in
Favorable report with Unfavorable report
Substitute or Amendment
No Amendment
Bill may be revived by minority report on motion adopted by majority vote of House
Bill printed on committee report and distributed (1st printing)
Bill goes to Calendars Committee for assignment to a calendar
Second reading, debate, amendment by majority vote and passage to third reading
Third reading, debate, amendment by 2/3 vote and final passage by House
Amendments are engrossed into text of bill
House engrossed text with Senate amendments printed and distributed (2nd printing)
Houserefusestoconcur, requestsappointmentof ConferenceCommittee
Senategrantsrequestfor ConferenceCommittee (committeeconsistsof5 membersfromeachhouse)
ConferenceCommitteereport filedandadoptedwithout changebyeachhouse(report limitedtomattersin disagreementbetweenthe twohouses)
HouseconcursinSenate amendmentonmotion adoptedbymajorityvote
Engrossed bill received, read 1st time, and referred to committee by Lt. Governor
Committee studies bill, posts notice of public hearing, holds public hearing resulting in
Unfavorable report
Bill may be revived by minority report on motion adopted by majority vote of Senate
Favorable report with
Substitute or Amendment No Amendment
Bill printed and distributed
Bill brought up for consideration on floor by 2/3 vote of Senate to suspend rules
Second reading, debate, amendment by majority vote and passage to third reading
Third reading, amendment by 2/3 vote and final passage by Senate
If amended, returned to House as amended
If not amended
Bill Enrolled
Signed by Speaker in presence of House
Signed by Lt. Governor in presence of Senate
Sent to Governor Governor signs bill
Governor refuses to sign bill
Governor vetoes bill
Bill becomes law
Veto overridden by 2/3 vote of House and Senate
Bill does not become law
www.tda.org | October 2023 483
unless the Senate sponsor of the bill has filed a written notice of intent to suspend the regular order of business for consideration of the bill.
FLOOR ACTION
When a bill comes up for consideration by the full House or Senate, it receives its second reading. The bill is read, again by caption only, and then debated by the full membership of the chamber. Any member may offer an amendment, but it must be approved by a majority of the members present and voting to be adopted. The members then vote on whether to pass the bill. The bill is then considered by the full body again on third reading and final passage. A bill may be amended again on third reading, but amendments at this stage require a two-thirds majority for adoption. Although the Texas Constitution requires a bill to be read on three separate days in each house before it can have the force of law, this constitutional rule may be suspended by a four-fifths vote of the House in which the bill is pending. The Senate routinely suspends this constitutional provision in order to give a bill an immediate third reading after its second reading consideration. The House, however, rarely suspends this provision, and third reading of a bill in the House normally occurs on the day following its second reading consideration.
In either house, a bill may be passed on a voice vote or a record vote. In the House, record votes are tallied by an electronic vote board controlled by buttons on each member’s desk. In the Senate, record votes are taken by calling the roll of the members.
If a bill receives a majority vote on third reading, it is considered passed. When a bill is passed in the house where it originated, the bill is engrossed, and a new copy of the bill which incorporates all corrections and amendments is prepared and sent to the opposite chamber for consideration. In the second house, the bill follows basically the same steps it followed in the first house. When the bill is passed in the opposite house, it is returned to the originating chamber with any amendments that have been adopted simply attached to the bill.
ACTION ON THE OTHER HOUSE’S AMENDMENTS AND CONFERENCE COMMITTEES
If a bill is returned to the originating chamber with amendments, the originating chamber can either agree to the amendments or request a conference committee to work out differences between the House version and the Senate version. If the amendments are agreed to, the bill is put in final form, signed by the presiding officers, and sent to the governor.
Conference committees are composed of 5 members from each House appointed by the presiding officers. Once the conference committee reaches agreement, a conference committee report is prepared and must be approved by at least three of the 5 conferees from each house. Conference committee reports are voted on in each house and must be approved or rejected without amendment. If
approved by both houses, the bill is signed by the presiding officers and sent to the governor.
GOVERNOR’S ACTION
Upon receiving a bill, the governor has 10 days in which to sign the bill, veto it, or allow it to become law without a signature. If the governor vetoes the bill and the legislature is still in session, the bill is returned to the House in which it originated with an explanation of the governor’s objections. A two-thirds majority in each house is required to override the veto. If the governor neither vetoes nor signs the bill within 10 days, the bill becomes a law. If a bill is sent to the governor within 10 days of final adjournment, the governor has until 20 days after final adjournment to sign the bill, veto it, or allow it to become law without a signature.
CONSTITUTIONAL AMENDMENTS
Proposed amendments to the Texas Constitution are in the form of joint resolutions instead of bills and require a vote of two-thirds of the entire membership in each house for adoption. Joint resolutions are not sent to the governor for approval, but are filed directly with the secretary of state. A joint resolution proposing an amendment to the Texas Constitution does not become effective until it is approved by Texas voters in a general election.
484 Texas Dental Journal | Vol 140 | No. 8
www.tda.org | October 2023 485
PROTECTING THE PUBLIC:
UNDERSTANDING THE TEXAS STATE BOARD OF DENTAL EXAMINERS’ ROLE
IN REGULATING THE DENTAL PROFESSION
486 Texas Dental Journal | Vol 140 | No. 8
The Texas legislature convenes biennially for a 140-day session, evaluating thousands of bills, with only a select small number ultimately becoming laws. The enacted bills pertaining to dentistry are often codified within the Occupations Code section of the Texas statutes. The Texas Dental Practice Act is found in the Texas Occupations Code Chapters 251 through 267.
In accordance with the Texas Constitution, only the state legislature possesses the authority to enact laws like the Dental Practice Act (DPA). The DPA empowers the Texas State Board of Dental Examiners (TSBDE) to uphold state legislation and TSBDE regulations, conduct investigations of dental licensees and registrants, impose sanctions on offenders, and establish legally binding rules.
Unlike the Texas Legislature, which convenes every 2 years, the TSBDE’s rulemaking process is flexible. From December 2022 to August 2023, the dental board adopted 7 rule changes and 1 rule review.
Texas dentists must stay updated on evolving rules and their impact on dental practice in Texas. While this can be challenging, TDA membership offers a significant advantage with TDA’s advocacy efforts on behalf of member dentists both at the state capitol and the dental board. Furthermore, TDA keeps its members informed about TSBDE rule changes through written publications, emails, and podcasts, while also providing individual regulatory and compliance assistance for its members. Help with specific legislative and regulatory compliance questions or concerns is only a phone call or email away for TDA Members.
Individualized TSBDE Assistance
TDA provides individualized help for member dentists who need TSBDE assistance. Call or email Senior Policy Manager Diane Rhodes at drhodes@tda.org or 512-443-3675 ext 122.
TSBDE Rule Changes and review
Every 4 years the TSBDE is required to conduct a rule review to determine whether the rules under that review should be re-adopted, revised, or repealed. On March 10, 2023, the dental board published a rule review for Chapters 100 General Provisions, 101 Dental Licensure, and 102 Fees. At its May 5, 2023, meeting the dental board readopted the rule chapters in their entirety and in their current form. In addition to completing the rule review, the TSBDE also adopted the following 7 rule amendments.
TSBDE Rule Amendments
1. Permitted Dental Assistant Duties, effective March 16, 2023
This housekeeping amendment, making a non-substantive change to the rule, aligns the rule governing permitted dental assistant duties—22 Texas Administration Code §104.1— with the statutory language found in the Dental Practice Act §265.001 instead of under Dental Practice Act §265.005 that was repealed.
2. Dental Assistant General Qualifications for Registration, effective March 16, 2023
Another TSBDE housekeeping amendment that makes no substantive rule changes to 22 Texas Administrative Code §114.6, governing general qualification for dental assistant registration. The adopted amendment updates the rule language to comply with the applicable section of the Dental Practice Act—§265.001(d)—and not the previous section of the Dental Practice Act §265.005 that was repealed.
TDA provides individualized help for member dentists who need TSBDE assistance. Call or email Senior Policy Manager Diane Rhodes at drhodes@tda.org or 512-443-3675 ext 122.
www.tda.org | October 2023 487
TSBDE
Individualized
Assistance
3. Dental Assistant Registration Course and Examination, effective March 16, 2023
The adopted amendment to 22 Texas Administrative Code §114.21, Requirements for Dental Assistant Registration Course and Examination, removed language about the Dental Assistant Advisory Committee since the committee is no longer required in statute and the TSBDE has no need for the committee.
4. Permitted Duties Dental Hygienists, effective March 16, 2023
The adopted amendment updates the rule language found in 22 Texas Administrative Code §115.2, concerning the permitted duties of a dental hygienist, to reflect that the TSBDE no longer issues certificates to a dental hygienist to apply pit and fissure sealants or monitor nitrous oxide. However, dental hygienists must ensure that they meet all qualifications required by the Dental Practice Act or TSBDE rules before performing the permitted duty.
Delegating Nitrous Oxide Monitoring: Dental Hygienist
Before a dentist delegates monitoring nitrous oxide to a dental hygienist, the hygienist must have a specific N20 monitoring endorsement issued by the TSBDE.1
5. Continuing Education Providers, effective May 25, 2023
The TSBDE’s adopted amendment updates section 6 of the continuing education rule —22 Texas Administration Code §104.2, concerning continuing education providers. The amendment reflects the merger of the regional examining board
CDCA-WREB-CITA and adds the States Resources for Testing and Assessments (SRTA) examining board, and the American Association of Dental Boards— Accredited Continuing Education Program (AADB-ACE) as TSBDE-approved continuing education providers. The amendment also removes Dental Quality Assurance and Dentist Secure Labs as continuing education providers.
6. Fees, effective September 5, 2023
The dental board amended the fee rule to reflect the fees required to submit the following applications to the TSBDE: Registered Dental Assistant (RDA) Course Provider Application ($100) and Continuing Education Provider Application ($100).
7. Inspection of Sedation/Anesthesia Providers, effective September 5, 2023

The TSBDE’s amended a rule concerning the inspection of sedation/anesthesia providers—22 Texas Administrative Code §110.18—gives the TSBDE discretion on whether to pursue revoking a sedation/anesthesia permit holder’s dental license if an inactive status permit holder is found to have administered or delegated the administration of level 2, 3, or 4 sedation/anesthesia while in inactive status or in a non-exempt location.
Delegating Nitrous Oxide Monitoring:
Dental Hygienist
Before a dentist delegates monitoring nitrous oxide to a dental hygienist, the hygienist must have a specific N20 monitoring endorsement issued by the TSBDE.1
488 Texas Dental Journal | Vol 140 | No. 8
Delegating X-Rays
and N20 Monitoring: Dental Assistant
Dentists can only delegate taking patient X-rays to a dental assistant who has a TSBDE-issued Registered Dental Assistant (RDA) registration.3 For a dentist to delegate monitoring nitrous oxide to an RDA, the RDA must hold an N20 monitoring endorsement issued by the TSBDE.4
REMINDER: Check Your Team Members’ Licenses and Registrations
The dentist holds full responsibility for all tasks delegated to dental hygienists and dental assistants under their supervision. This includes verifying the dental hygienists and registered dental assistants have current licenses and registrations.2
Delegating X-Rays and N20 Monitoring: Dental Assistant

Dentists can only delegate taking patient X-rays to a dental assistant who has a TSBDE-issued Registered Dental Assistant (RDA) registration.3 For a dentist to delegate monitoring nitrous oxide to an RDA, the RDA must hold an N20 monitoring endorsement issued by the TSBDE.4
Dentists are also reminded that they cannot delegate coronal polishing or pit and fissure sealants to a dental assistant unless the dental assistant completes the required education and training prior to the delegation.5
Coronal Polishing and Pit and Fissure Sealants: Dental Assistants
The delegating dentist is responsible for verifying that the dental assistant has at least 2 years’ experience, current basic life support, and completed the required 8 hours of didactic and clinical education in coronal polishing and/or pit and fissure sealants prior to delegating those procedures.
TSBDE regulations mandate that training programs for coronal polish and pit and fissure sealants may only be offered by dental, dental hygiene, or dental assistant programs accredited by the Commission on Dental Accreditation (CODA) and approved by the TSBDE. Neither dental professional associations nor individual dentists may offer training courses unless they are offering a course taught by a CODA-accredited dental education program approved by the TSBDE.

www.tda.org | October 2023 489
Coronal Polishing and Pit and Fissure Sealants: Dental Assistants

The delegating dentist is responsible for verifying that the dental assistant has at least 2 years’ experience, current basic life support, and completed the required 8 hours of didactic and clinical education in coronal polishing and/or pit and fissure sealants prior to delegating those procedures.
Dentists must perform ongoing due diligence to ensure that all team members working in the dentist’s practice remain in compliance with the TSBDE’s license and registration requirements.
Delegating Infiltration Anesthetic to Dental Hygienists
Responding to TDA member requests for dental hygienists to administer local anesthetic, TDA played a pivotal role in guiding HB 3824 through the legislative process. The landmark legislation, achieved through extensive TDA-led negotiation with the Texas Dental Hygienists’ Association, gives Texas dentists the authority to delegate the administration of local infiltration anesthetic to properly educated and trained, Texas-licensed dental hygienists under direct continuous supervision. This delegation applies to non-sedated or nitrous oxide/oxygen inhalation sedated patients who are 18 years of age or older and is specifically limited within the context of the dental hygienist delivering hygiene services to the patient.
Remember that delegating local anesthetic to a dental hygienist is limited to:
• infiltration only;
• to non-sedated patients or patients only sedated with nitrous oxide/ oxygen inhalation;
• to patients 18 years of age or older, and;
• only when the hygienist is providing hygiene services within the dental hygiene scope of practice.
490 Texas Dental Journal | Vol 140 | No. 8
Although HB 3824 became law on September 1, 2023, the TSBDE has until January 1, 2024, to write rules establishing the minimum standard of care for dental hygienists administering local anesthetic by infiltration. These rules will also outline course requirements and the TSBDE approval process for CODA-accredited dental education institutions to offer a classroom course that trains dental hygienists to administer local anesthetic agents by infiltration. Details will be shared as the rule process continues under the “TSBDE Update” in the TDA Today publication.
Closing
Remember that TDA is here to serve you, the member, by helping advance dental positive legislation and regulations as well as keeping you up to date about state legislative and regulatory matters. TDA is vocal about the regulatory and legislative proposals affecting dentistry in Texas. TDA cannot and will not sit silently while decisions are made that impact your dental practice.
References
1. 22 Texas Administrative Code §115.2(a)(7), Permitted Duties
2. Texas Occupations Code §258.003, Responsibility of Delegating Dentist
3. 22 Texas Administrative Code §114.2, Registration of Dental Assistants
4. 22 Texas Administrative Code §114.4, Monitoring the Administration of Nitrous Oxide
5. 22 Texas Administrative Code §§114.3, Pit and Fissure Sealant; 114.5, Coronal Polishing
• Infiltration only;
• non-sedated patients or patients sedated only with nitrous oxide/oxygen inhalation;
• patients 18 years of age or older, and;
• only when the hygienist is providing hygiene services within the dental hygiene scope of practice.
www.tda.org | October 2023 491
Remember that delegating local anesthetic to a dental hygienist is limited to:
FOR DENTISTRY,
Dr R. Lee Clitheroe, Chair, DENPAC

You’ve put in a lot of work to get where you are today. Going to school. Studying for exams. Getting licensed. Keeping up with continuing education requirements. Maybe you pursued a specialty. Or opened your own practice. Regardless of the type of dentistry you practice, each day you’re working hard to provide quality oral health care for your patients. It takes time, effort, and sacrifice, but you’ve invested in yourself to be able to have a career that you love.
Have you thought about who is protecting that career? Organized dentistry is on the line every day. Legislative and regulatory actions can have a major impact on your day-today operations. But the Texas Dental
492 Texas Dental Journal | Vol 140 | No. 8
I WILL
Association has your back. TDA provides a powerful, united voice for organized dentistry through its political arm, DENPAC. DENPAC exists to protect your practice, your patients, and your profession. But we need your help.
Think about what dentistry means to you, and what you’re willing to do to protect it. While there are many possible answers to that question, let me share with you the simplest yet most effective solution: invest in DENPAC.
For dentistry, I will commit $10 a month.
For dentistry, I will ensure TDA has the resources they need to effectively advocate for me.
For dentistry, I will encourage my colleagues to donate.
For dentistry, I will ensure TDA has a constant presence at our state capitol.
For dentistry, I will make a $100 donation today.
We can’t afford to take TDA’s past legislative and regulatory successes for granted. Join me today in actively supporting DENPAC. Donating is easy:
• Scan the QR code with your phone’s camera.

• Visit denpac.org and click “Join Now.”
• Mail a check to DENPAC, 1946 S IH 35 Ste 400, Austin, TX 78704.
• Call 512-443-3675, ext. 123 to make a payment over the phone.
DENPAC uses voluntary donations from TDA members to contribute to election campaigns of state candidates who have demonstrated their concern for the preservation of dentistry as an independent profession, and for the dental health of the people of Texas. Every dollar donated to DENPAC goes directly to state candidates who are friends of dentistry, regardless of their political party. By contributing to these candidates, DENPAC facilitates relationships between the TDA legislative team, TDA member dentists, and key decisionmakers at the Capitol. These relationships are invaluable to TDA’s lobby efforts.
Thank you to all our current DENPAC members and anyone who has participated in previous advocacy efforts. We encourage everyone to become involved, regardless of your level of participation. Even if you can only contribute a few dollars today, your investment will make a difference, and your ongoing support is crucial to keeping our profession strong.
For more information, please visit denpac.org or contact our DENPAC Coordinator Staci Rives by email at srives@tda.org or by phone at 512-443-3675, ext. 123.
Disclaimer: Contributions or gifts to political action committees are not deductible as charitable contributions for federal tax purposes. Contributions to the Texas Dental Association Political Action Committee are voluntary and may be used to support state candidates and office holders. You may refuse to contribute without reprisal, and the Texas Dental Association and its local component societies will neither favor nor disadvantage anyone based on the amount or failure to make contributions. According to Texas state law, political action committees may only accept contributions from individuals, professional corporations, and professional associations. State law requires political action committees to request and make best efforts to report the name, mailing address, occupation, and employer for each individual whose contributions aggregate in excess of $100 in a calendar year.
DONATING IS EASY
Scan the QR code with your phone’s camera to donate now! You can also visit denpac.org, mail a check, or call 512-443-3675, ext. 123 to make a payment over the phone. If you practice dentistry in Texas, you can’t afford to not be politically engaged. Help DENPAC help you!
www.tda.org | October 2023 493
CHAMPIONING ACCESS TO CARE:
TDA AS THE PREMIER MEDICAID & CHIP ADVOCATE

494 Texas Dental Journal | Vol 140 | No. 8
The Texas Dental Association (TDA) represents a majority of dentists participating in Medicaid, the Children’s Health Insurance Program (CHIP), and other public health dental programs helping to make dental care accessible to all Texans. TDA prioritizes maintaining and strengthening Texas’ dental public health safety net by encouraging its member dentists to actively participate in Medicaid, CHIP, and other programs providing needed dental care to children, adults, and individuals with special health care needs.1
Ensuring oral health equity for lowincome Texans is vital. A dental safety net should be a source for comprehensive dental services and to promote oral health literacy. This will help Texans maintain overall well-being, as dental issues can impact general health and quality of life.2 Oral health can often be overlooked in the context of overall health and well-being.3
A dental safety net that preserves the dentist-patient relationship and enables the treating dentist to make clinical decisions tailored to an individual patient’s needs is crucial. Such a safety net helps prevent vulnerable Texans from facing urgent oral health issues. Often, dental diseases, which could have been prevented entirely or treated early, escalate to chronic infections, gum and bone loss, and tooth removal, straining Texas’ public health safety net.
A robust dental public health safety net deters policymakers and elected officials from promoting mid-level dental providers like dental therapists and advanced dental hygiene practitioners. Utilizing these less-trained and educated dental practitioners will result in a 2-tiered system of dental care in Texas, severing the dentist-to-patient relationship for some Texans.
TDA backs its member dentists delivering dental care within Texas’ dental public health safety net. TDA does this by consistently advocating for well-funded and streamlined public health dental programs. TDA’s advocacy extends to both legislative efforts and engagement with Texas Health and Human Services and other state health agencies to help ensure optimal dental programs for patients and dentists across Texas.
TDA Fought for Medicaid Dental Funding Increase: Protects Current Medicaid Dental Funding
For Texas’ Medicaid dental program to remain effective and cost-efficient, steps must be taken to ensure continued dentist participation. The most important step is a reimbursement rate adjustment so that dentists can continue program participation.
While TDA relentlessly championed a Medicaid dental fee increase during the recent legislative session, the legislature didn’t support the increase. Nonetheless, TDA succeeded in safeguarding Medicaid and CHIP dental funding from budget reductions.
Recognizing Medicaid’s crucial role in Texas’ dental public health safety net, TDA remains committed to seeking a funding increase during the 2025 legislative session. TDA will persist in advocating for a Medicaid dental fee increase that aligns with the program’s 2007 value when adjusted for inflation. Correcting Medicaid dental funding shortfalls is an essential part of setting Medicaid dental reimbursement rates
that help maintain a stable network of dentists.
Conclusion Rider 26 Workgroup
The workgroup, created by the Texas Health and Human Services Commission (HHSC) according to a budget rider from the 87th Regular Legislative Session, completed its report on Medicaid dental policy recommendations in November 2022. Rider 26 required HHSC to develop recommendations to improve the Texas Medicaid Provider Procedures Manual (TMPPM) in a manner that prevents fraud, waste, or abuse in Medicaid dental services, including changes related to the use of dental procedure codes by providers. Workgroup recommendations include: (1) Conduct a comprehensive review of the Texas Health Steps dental diagnostic services policy; (2) Complete the current comprehensive review of the Texas Health Steps dental preventive services policy; (3) Conduct a targeted review of certain Texas Health Steps dental therapeutic services policy; and (4) Implement a uniform Texas Health Steps orthodontic policy.
TDA Meets with HHSC Executive Commissioner
In late July, TDA Council on Public Health and Access to Care Chair (CPHAC) Dr Jason Zimmerman and TDA staff met with HHS Executive Commissioner Cecile Erwin Young and her dental leadership team. During the meeting, TDA advocated for Medicaid rate stability, improved operating room access for Medicaid-participating dentists, smoother Medicaid enrollment
www.tda.org | October 2023 495
and revalidation, and an appropriate fee for the new Medicaid dental facility code—G0330.
TDA Monitors Value-Based Payment Quality Improvement
TDA continues regular meetings with HHSC’s Health Quality Institute Director, and HHSC’s lead Value-Based Payment staffers to discuss the ongoing application of HHSC’s alternative payment models (APMs) to the dental maintenance organizations (DMOs).
At the time of this article, HHSC still has no plans to change the APM requirements or DMO data collection tools during 2023. However, in May 2023, HHSC began the APM adjustment process by analyzing results from the APM reports sent to the DMOs for their review. TDA will meet with HHSC in late 2023 to discuss the agency’s intentions for updating the DMO’s APMs. TDA will keep members informed about this process through periodic Medicaid updates in the TDA Today.
For more than a decade, HHSC has slowly transitioned its many Medicaid health programs away from fee-forservice payment models and into APMs within the value-based care (VBC) system. Since 2012, HHSC required that each DMO submit an annual report on its VBC activities with its dentists for HHSC information and planning purposes. As of 2021, HHSC requires that 50% of the DMO’s dentist provider payments be through an APM and not fee-for-service. Additionally, 10% of the DMO’s APMs must include financial risk for dentist providers.
TDA’s Role in APM Models
Throughout discussions over the past 11 years, TDA negotiated to achieve the best APM/VBP model for Texas dentists. TDA has met and will continue meeting, with both HHSC and the DMOs to help determine the best design for dentists. TDA identifies and advocates for APM/ VBP alternatives that allow the DMOs to meet the state’s APM/VBP requirement, without jeopardizing reimbursement to participating dentists.
TDA will keep promoting APM/ VBP efforts that positively reward participating dentists and not financially penalize participating dentists.
TDA Collaborates with HHSC on Medicaid Teledentistry Rule Development
TDA maintains ongoing communications with the HHSC associate commissioners responsible for rule development about the timeline for writing the teledentistry Medicaid rules. Currently, there is no date set, but HHSC will contact TDA when the process begins so that TDA can assist in writing the rules.
TDA Scores Win for Medicaid Dental
Responding to TDA’s advocacy, HHSC added D1354 (caries arresting medicament) as a new dental benefit for clients birth through 6 months
of age in the state’s Medicaid dental program, effective September 1, 2023. The agency also agreed to maintain coverage for dental procedure codes for space maintainers (D1520, D1527, D1556, D1557, and D1558).
According to an update published on the Texas Medicaid & Health Care Partnership (TMHP) website on July 14, 2023, silver diamine fluoride is the only material that may be used for D1354. The code is limited to 1 per lifetime per Tooth Identification (TID) Number (A-T and 3, 14, 19, and 30) by any provider for services rendered in the office setting. D1354 will be denied if billed on the same date of service for the same TID as procedure code D1351 and D1352 by any provider. D1354 will be denied if billed on the same date of service for the same TID as D1351 (sealant) or D1352 (preventive resin) by any provider. D9222 (deep sedation/ general anesthesia) and 00170 with modifier U3 will be denied if billed within 6 months of D1354 by any provider.
TDA Works to Improve Medicaid Operating Room Access
TDA has heard from members participating in the Medicaid dental program that there has been a significant decrease in operating room access for dental procedures. Patients are often waiting up to 6 months or more to access needed dental treatment under general anesthesia.
496 Texas Dental Journal | Vol 140 | No. 8
This is largely due to low Medicaid reimbursement rates for general anesthesia, and the facility fee that goes to the hospital or ambulatory surgical center (ASC). In early August 2023, TDA followed up its July meeting with HHSC officials by giving the agency details about the new Centers for Medicare and Medicaid Services (CMS) dental facility fee code to create a sustainable operating room billing mechanism for dental surgical services in both Medicare and Medicaid. Namely, designating a specific Medicare billing code—G0330— inclusive of fair reimbursement for dental services provided in a hospital operating room.
According to the American Dental Association (ADA), Medicare dental facility code G0330 does not apply to Ambulatory Surgical Centers (ASC), only hospitals. However, the ADA, the American Academy of Pediatric Dentistry, the American Association of Oral and Maxillofacial Surgeons, and other dental advocacy groups are strongly urging CMS to include the new code on the ASC Covered Procedures List (CPL) in the CY 2024.
Although G0330 is not on the Medicare ASC CPL, it is TDA’s understanding that state Medicaid programs, which historically provided ASC payment for CPT 41899 (miscellaneous dental procedures), can start coding Medicaid dental procedures requiring general anesthesia in a hospital or ASC setting under the Health Care Common Procedure Coding System (HCPCS) code G0330. CMS recommends a national average Medicare payment rate of $1722.43. TDA hopes that HHSC will designate the same reimbursement rate in Texas’ Medicaid dental program.
TDA remains committed to improving access to dental care for the segment of the Medicaid dental population that relies on receiving dental services under general anesthesia in operating room settings.
TDA Helps Dentists with Medicaid Enrollment and Revalidation Concerns
In response to TDA member complaints about Medicaid enrollment and revalidation, TDA hosted a virtual Medicaid enrollment and revalidation virtual town hall meeting with TMHP on June 23, 2023.
TMHP’s presentation addressed navigating the Medicaid enrollment process and timelines, common enrollment and revalidation mistakes, and tips and best practices for Medicaid enrollment and revalidation success. TMHP representatives were available during the town hall to answer questions.
TDA is working with TMHP and the DMOs on another town hall meeting in Fall 2023 that will address Medicaid enrollment, Medicaid revalidation, and credentialing with the Medicaid DMOs.
TDA’s Role in APM Models
Throughout discussions over the past 11 years, TDA negotiated to achieve the best APM/VBP model for Texas dentists. TDA has met and will continue meeting, with both HHSC and the DMOs to help determine the best design for dentists. TDA identifies and advocates for APM/VBP alternatives that allow the DMOs to meet the state’s APM/VBP requirement, without jeopardizing reimbursement to participating dentists.
TDA will keep promoting APM/VBP efforts that positively reward participating dentists and not financially penalize participating dentists.
www.tda.org | October 2023 497
TDA provides individualized help for member dentists with Medicaid and CHIP. For individual help, email Senior Policy Manager Diane Rhodes at drhodes@tda.org or call 512-443-3675 ext 122.
Texas Office of Inspector General Quarterly Reports
The Texas Office of Inspector (OIG) quarterly reports include information about Medicaid dental cases and recoveries. Cases include upcoding, billing for services not rendered, missing or inadequate documentation, medically unnecessary services, and failure to meet the professional standard of care.
OIG Quarterly Reports 2023
Quarterly Report, Quarter 1 FY 2023 bit.ly/OIGQ123
Quarterly Report, Quarter 2 FY 2023 bit.ly/OIGQ223
Quarterly Report, Quarter 3 FY 2023 bit.ly/OIGQ323
It is very important that dentists only bill for services provided, always bill the correct procedure codes, and maintain proper documentation in the patient’s dental record.
TDA Resumes Quarterly Meetings with HHSC Officials and Dental Managed Care Organizations
Starting in late Fall 2023, TDA will resume regular meetings with HHSC leaders and representatives from the DMOs to discuss program concerns and ways in which to improve the delivery of dental services for patients and dentists. These meetings are very productive and give TDA an opportunity to speak with all participating entities at the same time.
Closing
The state’s top legislative and agency decision-makers regularly seek TDA’s input about Medicaid, CHIP, and other public health programs. Every day, TDA represents its members helping protect patients and Medicaid- and CHIPparticipating dentists.
TDA provides individualized help for member dentists with Medicaid and CHIP. For individual help, email Senior Policy Manager Diane Rhodes at drhodes@tda.org or call 512-443-3675 ext 122.
All TDA’s advocacy efforts, both legislatively and within state agencies, result in program changes that improve Texas dentists’ experience with public health dental programs and lead to significant improvements in the delivery of dental care to Texans.
REFERENCES
1. Texas Dental Association. Policy 66-2010-H.
2. US Department of Health and Human Services, Oral Health in America: A Report of the Surgeon General (Rockville, MD: US Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2000), http://www.nidcr.nih.gov/ DataStatistics/SurgeonGeneral/ Documents/hck1ocv.@www. surgeon.fullrpt.pdf.
3. Ibid.
498 Texas Dental Journal | Vol 140 | No. 8
www.tda.org | October 2023 499 Quarter 1 Fiscal Year 2023 OIG Quarterly Report Texas Health and Human Services Inspector General OFFI C E OF I NSPECTOR GENERAL LAEH T H & HUMAN SERVICESCOMM I S NOIS TEXAS OIG Quarterly Report Fiscal Year 2023 OIG Quarterly Reports 2023 Quarterly Report, Quarter 1 FY 2023—bit.ly/OIGQ123 Quarterly Report, Quarter 2 FY 2023—bit.ly/OIGQ223 Quarterly Report, Quarter 3 FY 2023—bit.ly/OIGQ323
TDA’S INSURANCE LEGISLATION
BENEFITS TEXAS DENTISTS AND DENTAL PATIENTS
Texas Dental Association (TDA) members identify dental benefits and third-party payer issues as their top concerns. TDA has a proven track record of achieving insurance victories for its members. Working closely with the various insurance plans (including Medicaid managed-care plans), the Texas Department of Insurance (TDI), and the Texas Health and Human Services Commission (HHSC), TDA successfully addresses issues members are facing every day.

500 Texas Dental Journal | Vol 140 | No. 8
This year, TDA passed HB 1527, a landmark reform package targeting 3 major pain points: retroactive denials, disallowable clauses, and silent network leasing. Under the first provision in the bill, insurance companies will now be held to a 180-day timeframe to engage in payment recovery efforts, also known as retroactive denials. Retroactive denial allows insurance companies to require dentists to repay claims already paid to them when insurers discover they paid a claim mistakenly, even if the claim was processed years ago. This results in surprise billing at the expense of patients.
Now, state-regulated insurers will be prohibited from recovering an overpayment made to a dentist unless the carrier notifies the dentist in writing no later than 180 days after the dentist received the overpayment. The dentist will have 45 days after receiving the written notice of overpayment to agree or challenge the request. If the dentist disagrees with the recovery of funds request, the applicable plan or policy must provide the dentist with an opportunity to challenge or appeal the recovery attempt.
The second provision of the bill targets disallowable clauses, which can be found in most provider network agreements in place today. These clauses allow the insurer to both deny a dental benefit and prohibit the dentist from collecting fees for the dental services provided. This practice undermines the purpose of dental benefits, which exist to help patients with the cost of dental care, not to determine clinical decisions made by dentists and their patients. Disallowable clauses will now be prohibited by stateregulated insurers, ensuring that health care decisions remain transparent, fair,
and personal between the patient and their dentist.
The final provision addresses silent network leasing, a practice where insurance companies can pawn dentists off to different insurance networks without the provider’s knowledge or consent. When a network is leased without complete transparency, it can significantly impact the insurance benefits available to a dentist’s patients and result in an erosion of trust in the dentist-patient relationship. Stateregulated insurers will now be required to follow fair and accurate network leasing laws, allowing dentists to review contracts and decide whether to opt-out before an insurance network is leased.
In 2019, TDA secured passage of historic comprehensive reform for state-regulated insurance that brought much needed relief to dentists through HB 2486. The bill required stateregulated insurance plans to have a free website available for patients and dentists that includes information about the patient’s plan or policy. It also prohibited these plans from mandating payment methods to dentists. HB 2486 required state-regulated insurance plans to pay for dental treatment that has prior authorization. It also prevented the insurers from collecting an “overpayment” from a dentist who did not treat the patient where the overpayment occurred.
In 2015, TDA achieved coordination of benefits (COB) protection for dentists with the passage of HB 3024. That bill required state-regulated insurance plans to coordinate a patient’s primary and secondary insurance so that the secondary insurer also pays on a dental claim up to, but not exceeding, 100 percent of the total amount of
the claim. When both plans have COB provisions, the plan in which the patient is enrolled as an employee or the main policyholder is primary. The plan in which the patient is enrolled as a dependent would be secondary.
In 2011, TDA attained non-covered services protection for dentists through the passage of SB 554. State-regulated dental plans are prohibited from setting fees for dental services not covered by the plan. The only fees a dental plan may cap are fees for services the plan covers.
In 2003, TDA accomplished assignment of benefits protection for dentists, preventing state-regulated insurance plans from prohibiting or restricting a patient from making a written assignment of benefits to a dentist.
TDA will continue working with legislators and regulators to eliminate insurance issues plaguing dentists. Your involvement in advocacy and grassroots efforts is crucial to TDA’s success at the Texas Capitol, and with your help TDA will continue to make significant insurance improvements for Texas dentists.
www.tda.org | October 2023 501
DENTAL RECORD REQUESTS
IN AN OIG INVESTIGATION
A patient’s continuity of care relies on the dentist maintaining complete and accurate records. Documenting the patient’s history, images, diagnosis and treatment helps to ensure quality care and prevent errors. Records also demonstrate that work billed to Texas Medicaid was medically necessary and performed as billed.
When providers enroll with Texas Medicaid, they execute an agreement in which they agree to comply with various rules, regulations and requirements. One of the requirements relates to creating and maintaining records (see HHSC Medicaid Provider Procedures Manual section 1.7.3). The Texas Health and Human Services Office of Inspector General (OIG) performs investigations and provider record reviews to determine if these and other requirements have been met and to identify potential fraud, waste and abuse in Medicaid-supported services. Dentists are required by Texas statute and their Medicaid enrollment contract to promptly provide a patient’s clinical record if requested by the OIG.
What Medicaid and the OIG require
Providers must ensure that patient records are accurate, comprehensive, and complete. A clear narrative that ensures continuity of care for the patient also supports billing. Texas State Board of Dental Examiners rule 108.8 lists what documentation must be included when dental services are performed. During a medical record review, audit, inspection or investigation, the OIG relies on similar information, which includes but is not limited to:
• Patient’s medical history.
• Patient complaints and symptoms.
• Diagnostic quality x-rays.
• Treatment plans and progress notes, including prescriptions.
• Signed informed consent for treatment.
When dentists are notified of an OIG investigation or other fraud detection activity, they receive a records request that includes the documents listed above, as well as prior authorization, charting, referrals for specialty care, lab referrals, procedural notes, various business records, and type of software used for dental records and imaging. In addition to having a solid understanding of the requirements in their DMO contracts, providers are encouraged to stay abreast of any changes by regularly reviewing the provider bulletins posted to the Texas Medicaid & Health Care Partnership website and the Texas Medicaid Provider Procedures Manual

OIG investigations
The OIG investigates a dental provider typically after receiving a complaint from a patient or DMO. If a claims data review raises concerns or questions, an investigator requests records from the provider. The OIG dental team examines the patient
502 Texas Dental Journal | Vol 140 | No. 8
records to verify consent and that the dentist documented the exam or a procedure, any problems detected and how they were detected—along with supporting diagnostic radiographs and/ or intra-oral photographs—and whether the treatment was medically necessary. As part of the effort to ensure proper patient care and safety, the OIG checks for the proper permits if sedation is involved. Records requests and the associated records reviews are tailored specifically to the allegations at hand.
Potential outcomes
Following an OIG fraud detection activity, a case is closed without further action if patient records justify the billing and payments. However, if billing errors are found in the review—including billing Medicaid for services not delivered or lacking medical necessity— follow-up actions can include providing additional education, recouping erroneous payments, imposing administrative penalties, excluding the provider from future Medicaid program participation and referring the case to the Texas Office of the Attorney General for criminal investigation or the Texas State Board of Dental Examiners if there is a concern for patient harm. Providers are afforded the opportunity to appeal alleged billing or performance deviation determinations.
For example, the OIG settled a case in April with a dental provider who improperly billed Medicaid for a variety of dental services. Violations included billing and receiving reimbursement for services not rendered, up-coded services, and medically unnecessary services. Other violations involved missing or inadequate documentation to support billing and quality of care issues. The provider worked with the OIG by responding to the preliminary findings presented by the investigation. The provider later agreed to repay $24,000 in
overpayments over a 24-month period.
An OIG investigation led to another dentist’s five-year exclusion from Medicaid program participation. The investigation determined that over a five-year period the dentist allegedly billed for (or caused to be billed) restorations never performed, kept inadequate or incomplete records to document required services (including sedation), billed for services without required pre-operative x-rays or without diagnostic quality x-rays, and performed services using sedation without the required sedation permit for Medicaid services performed. The exclusion took effect in 2023.
Annual required review—Random sampling of all Medicaid claims
An additional circumstance where the OIG may request a dental or medical record from a provider comes from a statutory obligation set forth in Texas Government Code section 531.109, which requires the OIG to select a random, statistically valid sample of all Medicaid claims each year to review for potential fraud, waste or abuse. The OIG’s Data Operations team develops and applies a sampling methodology to all Medicaid claims to produce a sample of claims for review. Providers who submitted the randomly selected claims are notified via letter, which requests the records for a specific claim.
The letter requests an electronic copy of the entire original medical or dental record for the client(s) and claim(s) specified in the letter. The patient record must include all documentation to support that the services billed to Medicaid were medically necessary, provided in a quality manner and billed
appropriately. The medical record should include, as applicable:
• Dental or medical history.
• Consent for treatment.
• Treatment plans and progress notes, including prescriptions.
• Medicaid IDs.
• Referrals for specialty care.
• Prior authorizations, supporting requests and approvals.
• X-rays/images, maintained either as films or digital images.
• Any other record necessary to support that the services billed to Medicaid were medically necessary, provided in a quality manner and billed appropriately.
OIG teams compare the dental records with the selected claim to determine whether there is any indication of fraud, waste or abuse related to the specific claim.
Additional resources
The ADA and the American Academy of Pediatric Dentistry (AAPD) offer resources on documentation and record-keeping. Dentists will find more information in the Texas Medicaid Provider Procedures Manual and the Texas Administrative Code. (For specific requirements, see Texas Administrative Code §371.1667 (1)-(4).)
Everyone can play a role in protecting patient care and taxpayer dollars. If you suspect fraud, waste, or abuse in health care delivery, call the OIG Fraud Hotline at 800-436-6184 or use the fraud reporting form on the OIG website, ReportTexasFraud.com.
Connect with the Office of Inspector General:
Facebook: @TxOIG
Twitter: @TexasOIG
LinkedIn: Company/TxHHS-OIG
www.tda.org | October 2023 503
TDA Legislative Resource Guide
Resources
The staff at the Texas Dental Association stands ready to assist you. Please use this guide to identify staff members who are knowledgeable in areas of legislative and regulatory affairs. If you have questions or need assistance with any of these entities, or others not listed, please give us a call.
General Legislative & Regulatory Questions
1946 S IH35, Ste 400 Austin, TX 78704 512-443-3675, ext. 270
Director of Public Affairs
Jess Calvert
512-443-3675, ext. 132 jcalvert@tda.org
Senior Policy Manager
Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Policy Analyst/PAC Coordinator
Staci Rives
512-443-3675, ext. 123 srives@tda.org
DENPAC 1946 S IH35, Ste 400 Austin, TX 78704 512-443-3675, ext. 123
Texas State Board of Dental Examiners 1801 Congress Ave, Ste 8.600 Austin, TX 78701
P 512-463-6400
F 512-649-0797
www.tsbde.texas.gov
TDA Staff:
Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Office of Inspector General Chief Dental Officer
Dr Janice E. Reardon PO Box 85200 MC-1300
Austin, TX 78708
512-491-2060 janice.reardon@hhsc.state.tx.us
TDA Staff: Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Health and Human Services Commission
Texas Medicaid and CHIP Division 4601 W Guadalupe St Austin, TX 78711
512-424-6500
Emily Zalkovsky Chief Medicaid & CHIP Services Officer emily.zalkovsky@hhsc.state.tx.us
Dr Ensy Atarod Dental Director ensy.atarod@hhsc.state.tx.us
Texas Department of State Health Services
Oral Health Improvement Program Dr Rhonda Stokley State Public Health Dental Director MC 1938 PO Box 149347
Austin, TX 78714
1100 W 49th St Austin, TX 78756
512-776-2008 rhonda.stokley@dshs.texas.gov
www.dshs.texas.gov/dental-health
TDA Staff: Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Insurance
Texas Department of Insurance PO Box 12030
Austin, TX 78711
1601 Congress Ave
Austin, TX 78701
800-578-4677
www.tdi.texas.gov
Provider Resources
800-252-3439
www.tdi.texas.gov/hprovider/index.html
Consumer Protection
800-252-3439
www.tdi.texas.gov/consumer/complfrm. html
TDA Staff: Debbie Rogers
512-443-3675, ext. 152 drogers@tda.org
Medicaid and CHIP
Texas Medicaid & Health Care Partnership
General Inquiries Line: 800-925-9126
Provider Enrollment: 800-925-9126, option 3
www.tmhp.com
Texas Health Steps Dental
512-438-2366
www.hhs.texas.gov/doing-businesshhs/provider-portals/health-servicesproviders/texas-health-steps/dentalproviders
DentaQuest
800-896-2374
www.dentaquest.com/texas/providers
MCNA Dental
1-855-776-6262
www.mcnatx.net/dentists/#resources
TDA Staff: Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
504 Texas Dental Journal | Vol 140 | No. 8
Children’s Health Insurance Plan (CHIP)
Providers
Customer Service Department PO Box 1809
Alpharetta, GA 30023
866-521-2651
www1.deltadentalins.com/dentists.html
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Professional Recovery Network Statewide Toll-Free Help Line 800-727-5152 www.txprn.com
TDA Staff: Debbie Rogers 512-443-3675, ext. 152 drogers@tda.org
X-Ray Unit
Certification
Texas Department of State Health Services Radiation Control Program Attn: Registration 1100 W 49th St Austin, TX 78756 737-218-7110
xrayregistration@dshs.texas.gov www.dshs.texas.gov/radiation
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Prescriptions
DEA Diversion Control Program 800-882-9539 dea.registration.help@dea.gov www.deadiversion.usdoj.gov
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Texas Prescription Monitoring Program 333 Guadalupe, Ste 3-500 Austin, TX 78701 512-305-8050 texaspmp@pharmacy.texas.gov www.pharmacy.texas.gov/pmp
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Infection Control and OSHA Occupational Safety and Health Administration (OSHA) US Department of Labor Occupational Safety and Health Administration 200 Constitution Ave NW Room Number N3626
Washington, DC 20210 800-321-6742
www.osha.gov/dentistry
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Area OSHA Offices:
Austin: 512-374-0271
Corpus Christi: 361-888-3420
Dallas: 972-952-1330
El Paso: 915-534-6251
Fort Worth: 817-428-2470
Houston (North): 936-760-3800
Houston (South): 281-286-0583
Lubbock: 806-472-7681
San Antonio: 210-472-5040
Environmental Regulations
Texas Commission on Environmental Quality (TCEQ)
PO Box 13087
Austin, TX 78711
12100 Park 35 Circle
Austin, TX 78753 512-239-1000 www.tceq.texas.gov
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Tax Issues
Texas Comptroller of Public Accounts PO Box 13528, Capitol Station
Austin, TX 78711 111 E 17th St
Austin, TX 78774 888-334-4112
www.comptroller.texas.gov
TDA Staff: Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
www.tda.org | October 2023 505
ORAL
and maxillofacial pathology case of the month
Clinical History
A 73-year-old female presented for evaluation of a painful tongue mass she reported had progressively enlarged over the past year. The patient’s medical history was significant for arthritis, diabetes, hypertension, hypothyroidism, and arthritis, which were under pharmacologic control. She disclosed a history of breast cancer treated with a mastectomy in 1992. Extraoral examination revealed no facial asymmetry, swellings, neck masses, or lymphadenopathy. On intraoral examination, a 4.0 x 3.0 cm, fungating, exophytic mass with a papillary surface architecture was identified involving the right lateral tongue (Figure 1). The lesion extended

AUTHORS
Alberto Peraza
Labrador, BDS, MS
Oral and Maxillofacial Pathology Graduate Research Assistant, Texas A&M University School of Dentistry, Dallas, Texas
Jordan Chen, BS Student Dentist, Texas A&M University School of Dentistry, Dallas, Texas Bryan Ho, BS Student Dentist, Texas A&M University

School of Dentistry, Dallas, Texas Spencer D. Armuth, DMD, MD

Oral and Maxillofacial Surgeon, Private Practice, Las Vegas, Nevada

Victoria L. Woo, DDS Director of Pathology and Advanced Education Program, Clinical Professor, Texas A&M University School of Dentistry, Dallas, Texas

Disclosures: There are no financial, economic, or professional interest disclosures for this study.

506 Texas Dental Journal | Vol 140 | No. 8
Figure 1. Large fungating mass with a papillary surface involving the right lateral and dorsal tongue with posterior extension.
Figure 2. Panoramic radiograph showing generalized horizontal bone loss and multiple periapical radiolucencies associated with carious teeth. No overt evidence of right mandibular bone destruction was observed.

to the dorsal and ventral surfaces, causing mild restriction of tongue mobility. A panoramic radiograph showed generalized horizontal periodontal bone loss and periapical radiolucencies associated with multiple maxillary root tips; the right mandibular alveolar crest exhibited a smooth contour, and no overt evidence of bony destruction was appreciated (Figure 2).
An incisional biopsy was performed and submitted to an outside institution. The lesion was described as a polypoid proliferation of stratified squamous epithelium with reactive hyperplasia but no significant dysplasia. The diagnosis rendered was of an irritated squamous papilloma, and a comment was made that the lesion appeared benign and clinical follow-up should suffice. The oral surgeon remained concerned based on the reported pain and lesional growth as well as the patient’s prior oncologic history. After requesting a second opinion from an oral pathologist based on the clinical photo, he pursued an additional biopsy of the right posterior lateral tongue. The patient subsequently underwent a partial
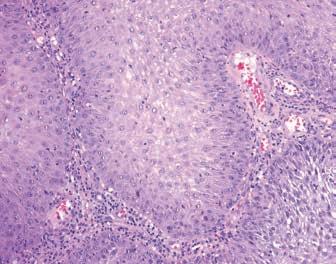
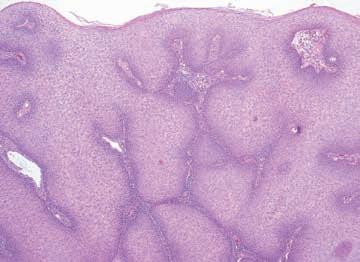
glossectomy with a modified radical right neck dissection and is currently under clinical surveillance every 3 months.
Pathologic Findings
Microscopic examination of the second lateral tongue biopsy revealed portions of mucosa surfaced by stratified squamous epithelium showing parakeratosis and a papillary architecture. Within the lamina propria were large islands of squamous cells with evidence of mild cellular pleomorphism and dyskeratosis; many of the neoplastic cells were terminally differentiated, and keratin pearls were occasionally seen (Figure 3A and B). No perineural, lymphovascular, or skeletal muscle invasion was identified. A comment was made that the submitted clinical photos were reviewed in conjunction with the submitted specimen.
What is the most likely diagnosis?
See page 509 for the answer and discussion.
www.tda.org | October 2023 507
3A
Figure 3. Photomicrographs of second biopsy. A. Medium-power view showing a neoplastic proliferation of squamous cells characterized by dyskeratosis and keratin pearl formation (hematoxylin-and-eosin stain, 4x); B. High-power view of neoplastic squamous cells exhibiting mild cellular pleomorphism and occasional mitotic figures (hematoxylin-and-eosin stain, 20x).
3B
508 Texas Dental Journal | Vol 140 | No. 8
ORAL
and maxillofacial pathology diagnosis and management—from page 506
Diagnosis: Oral Squamous Cell Carcinoma
Discussion
Oral cancer is the 16th most common cancer worldwide and accounts for approximately 2% of all cancers in the United States, excluding nonmelanoma skin cancers.1,2 The American Cancer Society estimates 54,540 new cases will be diagnosed, and 11,500 individuals will die of oral cancer in 2023.3 In the United States, a 2.5:1 male-to-female ratio has been reported, although this figure varies with age, race, and site of involvement.2 Squamous cell carcinoma (SCC) is the most common form of oral cancer and comprises more than 90% of malignancies affecting the oral mucosa proper.2 Oral SCC (OSCC) exhibits the highest incidence in White males over 65; however, there has been an observed increase in young adult and pediatric patients in recent years, especially among females without traditional SCC risk factors.4
The etiology of OSCC involves a multifactorial interplay of extrinsic factors, such as tobacco use and alcohol consumption, and intrinsic factors, such as immunocompromise and concomitant systemic diseases. Tobacco smoking remains a foremost risk factor for developing SCC of the oral mucosa, with more than a quarter of patients reported as current smokers at the time of diagnosis.5 Other risk factors of significance include alcohol consumption, use of smokeless tobacco and betel quid, iron and vitamin deficiencies, immunosuppression, and ultraviolet light exposure in lip cases.2 The activation of oncogenes and inactivation or mutation of tumor suppressor genes, such as epidermal growth factor receptor (EGFR) and p53, among others, also play important roles. The accumulation of these aberrant genetic and epigenetic events promotes genomic instability, which leads to tumor development and progression.6
OSCC can arise in any oral mucosal site but demonstrates a predilection for the lateral tongue, particularly the posterior-lateral tongue, and floor of mouth. OSCCs originating in these sites are associated with an increased tendency for invasion and metastasis, even in early-stage disease.7 The clinical presentation is variable, and lesions can range from subtle white plaques to fungating, ulcerative masses. Patients may complain of pain and paresthesia, although the early stages of development are generally associated with no or minimal pain. Most OSCCs are
preceded by a potentially premalignant oral lesion such as a leukoplakia or erythroleukoplakia or a potentially premalignant oral condition such as oral submucous fibrosis or proliferative verrucous leukoplakia. Irregular destruction of the underlying bone can occur, particularly in lesions located in close proximity to bone.
OSCC is characterized histologically by invasive islands of neoplastic squamous cells that show varying degrees of cellular pleomorphism, dyskeratosis, and mitotic activity. Keratin pearl formation is occasionally seen. Invasion of the neoplastic cells into skeletal muscle, around nerves (perineural invasion [PNI]), and into blood vessels (lymphovascular invasion [LVI]) can be found, which adversely affects prognosis. In addition to PNI and LVI, features such as host immunologic response, depth of invasion, and surgical margin involvement represent important elements of the pathology report that may impact treatment decisions, including the need for neoadjuvant (pre-treatment) or adjuvant (post-treatment) therapies.8 The presence of features such as PNI and LVI has significant prognostic implications as they are associated with a higher likelihood of recurrence and metastasis, respectively.6,9
The clinical stage of the tumor primarily determines the treatment of OSCC. One of the most commonly used staging systems for oral and oropharyngeal carcinomas is the American Joint Committee on Cancer (AJCC) cancer staging system, which utilizes the parameters of size (T), regional lymph node involvement (N), and distant metastasis (M) to classify tumors as Stage I through IV.10 Patients with early-stage OSCC (stages I and II) are
www.tda.org | October 2023 509
ORALand maxillofacial pathology continued
most often treated with surgical excision or radiation therapy if they are not surgical candidates. Patients with advanced-stage lesions typically require multimodal therapy consisting of surgery in conjunction with radiation therapy (RT) or combined RT and chemotherapy.11 Neck dissection can be performed in patients with confirmed cervical lymph node metastasis or who are at high risk for developing regional metastasis. The use of immunotherapeutic agents like cetuximab, pembrolizumab, and nivolumab for the treatment of head and neck SCC has expanded considerably in the past several years and holds tremendous promise as more targeted approaches to management.12
Clinical stage and tumor site remain the most important predictors of prognosis, with advanced stage, floor of mouth location, and continued smoking being among the factors that portend a poorer prognosis.2,13 The overall 5-year survival rate for oral and oropharyngeal carcinomas is 68.5%, with decreasing mortality rates over time due in part to the superior survival rates associated with human papillomavirus (HPV)-positive oropharyngeal SCC.14,15
Long-term follow-up and monitoring of the patients are mandatory as recurrences can develop over months to years. Moreover, patients with OSCC remain at risk for developing additional upper aerodigestive tract malignancies, particularly in those who continue to smoke or consume alcohol. According to Osazuwa-Peters et al., mortality is approximately twice as high in former smokers compared to non-smokers.2,16 Early diagnosis and treatment of OSCC are therefore of utmost importance. Metzger et al. reported the risk of death increases by 1.8% for each day of treatment delay.17 However, diagnostic delays are not uncommon and may be due to the subtle clinical presentation of early OSCCs.18
This case highlights the importance of clinical correlation and judgment in guiding the need to pursue additional diagnostic procedures. Furthermore, it underscores the value of requesting a second opinion when discrepant clinical and histopathologic diagnoses are encountered.
REFERENCES
1. Lingen M, Fujii S, Hille J, Hunter KD, Salo TA, et al. Oral squamous cell carcinoma. In: WHO Classification of Tumours Editorial Board. Head and neck tumours, 5th ed. [Internet; beta version ahead of print]. Lyon (France): International Agency for Research on Cancer; 2022.
2. Neville BW, Damm DD, Allen CM, and Chi AC. Epithelial pathology. In: Neville BW, Damm DD, Allen CM, and Chi AC, ed. Oral and Maxillofacial Pathology, 4th ed. Missouri: Elsevier; 2016: 374-389.
Long-term follow-up and monitoring of the patients are mandatory as recurrences can develop over months to years. Moreover, patients with OSCC remain at risk for developing additional upper aerodigestive tract malignancies, particularly in those who continue to smoke or consume alcohol.
510 Texas Dental Journal | Vol 140 | No. 8
3. Cancer Facts & Figures 2023. Accessed April 29, 2023. https:// www.cancer.org/research/cancerfacts-statistics/all-cancer-factsfigures/2023-cancer-facts-figures. html.
4. Mohideen K, Krithika C, Jeddy N, Bharathi R, Thayumanavan B, Sankari SL. Meta-analysis on risk factors of squamous cell carcinoma of the tongue in young adults. J Oral Maxillofac Pathol. 2019;23(3):450-457. doi: 10.4103/ jomfp.JOMFP_118_19. PMID: 31942130; PMCID: PMC6948024.
5. Duffy SA, Ronis DL, McLean S, Fowler KE, Gruber SB, Wolf GT, Terrell JE. Pretreatment health behaviors predict survival among patients with head and neck squamous cell carcinoma. J Clin Oncol. 2009;27(12):1969-75. doi: 10.1200/JCO.2008.18.2188. Epub 2009 Mar 16. PMID: 19289626; PMCID: PMC2669762.
6. Alberto PL, Kessler HP. Early Diagnosis and Treatment of Squamous Cell Carcinoma—A Case Comparison Highlighting its Importance. Biol Med (Aligarh). 2016;8:273. doi:10.4172/09748369.1000273).
7. Galli A, Bondi S, Canevari C, Tulli M, Giordano L, Di Santo D, Gianolli L, Bussi M. High-risk early-stage oral tongue squamous cell carcinoma, when free margins are not enough: Critical review. Head Neck. 2021;43(8):2510-2522. doi: 10.1002/hed.26718. Epub 2021 Apr 24. PMID: 33893752.
8. Dolens EDS, Dourado MR, Almangush A, Salo TA, Gurgel Rocha CA, da Silva SD, Brennan PA, Coletta RD. The Impact of Histopathological Features on the Prognosis of Oral Squamous Cell Carcinoma: A Comprehensive
Review and Meta-Analysis. Front Oncol. 2021;11:784924. doi: 10.3389/fonc.2021.784924. PMID: 34858861; PMCID: PMC8631280.
9. Li J, Liu S, Li Z, Han X, Que L. Prognostic Value of Perineural Invasion in Oral Tongue Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis. Front Oncol. 2021;11:683825. doi: 10.3389/fonc.2021.683825. PMID: 34322385; PMCID: PMC8311439.
10. Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR, Winchester DP. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93-99. doi: 10.3322/ caac.21388. Epub 2017 Jan 17. PMID: 28094848.
11. Gamez ME, Kraus R, Hinni ML, Moore EJ, Ma DJ, Ko SJ, Rwigema JCM, McGee LA, Halyard MY, Buras MR, Foote RL, Patel SH. Treatment outcomes of squamous cell carcinoma of the oral cavity in young adults. Oral Oncol. 2018;87:43-48. doi: 10.1016/j. oraloncology.2018.10.014. Epub 2018 Oct 22. PMID: 30527242.
12. Hartner L. Chemotherapy for Oral Cancer. Dent Clin North Am. 2018;62(1):87-97. doi: 10.1016/j. cden.2017.08.006. Epub 2017 Oct 12. PMID: 29126496.
13. Suresh GM, Koppad R, Prakash BV, Sabitha KS, Dhara PS. Prognostic Indicators of Oral Squamous Cell Carcinoma. Ann Maxillofac Surg. 2019;9(2):364-370. doi: 10.4103/ ams.ams_253_18. PMID: 31909017; PMCID: PMC6933976.
14. Cancer Stat Facts: Oral Cavity and Pharynx Cancer. Accessed April 29, 2023. https://seer.cancer.gov/ statfacts/html/oralcav.html.
15. Preissner SH, Nahles S, Preissner S, Heiland M, Koerdt S. Influence of sex on survival rates of HPVpositive oropharyngeal cancers. Front Oncol. 2022;12:917890. doi: 10.3389/fonc.2022.917890. PMID: 36119465; PMCID: PMC9472547.
16. Osazuwa-Peters N, Adjei Boakye
E, Chen BY, Tobo BB, Varvares
MA. Association Between Head and Neck Squamous Cell Carcinoma Survival, Smoking at Diagnosis, and Marital Status. JAMA Otolaryngol Head Neck Surg. 2018;144(1):43-50. doi: 10.1001/jamaoto.2017.1880. PMID: 29121146; PMCID: PMC5833596.
17. Metzger K, Moratin J, Horn D, Pilz M, Ristow O, Hoffmann J, Freier K, Engel M, Freudlsperger
C. Treatment delay in earlystage oral squamous cell carcinoma and its relation to survival. J Craniomaxillofac Surg. 2021;49(6):462-467. doi: 10.1016/j. jcms.2021.02.007. Epub 2021 Feb 12. PMID: 33648813.
18. Gómez I, Warnakulasuriya S, Varela-Centelles PI, López-Jornet P, Suárez-Cunqueiro M, Diz-Dios P, Seoane J. Is early diagnosis of oral cancer a feasible objective? Who is to blame for diagnostic delay? Oral Dis. 2010;16(4):333-42. doi: 10.1111/j.1601-0825.2009.01642.x. Epub 2010 Mar 9. PMID: 20233328.
www.tda.org | October 2023 511
2024 Open Enrollment and ACA Update
By Eric Tiedtke, CFP TDA Financial Services Insurance Program

What follows is TDA Financial Services Insurance Program’s annual update on health insurance for 2024. There has been a significant amount of new legislation passed and more changes ahead for individual and small group markets. Subsidies for the Affordable Care Act (ACA) individual plans have again been extended; and there are changes in the companies offering plans in Texas.
Market Changes:
Individual HMO rates increase or slightly decrease. Small Group rates increase.
If you have individual or small group coverage, there are changes coming. Filed rates are being reviewed to determine if proposed increases are based on reasonable cost assumptions and solid evidence. Final rates won’t be available until Nov. 1 when open enrollment starts, so you can’t really start comparing until then.
There are more individual companies offering plans but most other than Blue Cross are only available in limited areas of the state, not statewide. PLEASE NOTE: Rate increases are not the same for everyone. What part of Texas you live in and your age also impact your overall rate.
Individual Plans
Blue Cross will again be the only company offering individual plans statewide in Texas, and they will again be HMO only. Blue Cross filed for a .6% decrease on their most popular HMO. The other individual plans offered in Texas—United Health Care, Humana, Aetna, Community Health, Molina, and Friday Health Plan—filed for higher rate increases in the
512 Texas Dental Journal | Vol 140 | No. 8 Provided by: PERKS P R O G R A M value for your profession
range of 9% to 19%, so keep an eye out for your renewal.
There are no ACA-compliant individual PPO plans in Texas (at the time of this writing in mid-August). There are regional or local plans available in Texas—mostly HMOs—and in limited areas of the state where a hospital system has several facilities and offers a plan.
There are other companies offering individual plans in a few select major metropolitan areas; such as Community Health, Molina, Oscar, and Scott & White; and a few hospital-specific plans. Keep in mind the network being offered, as it could have limited or no coverage in parts of the state. Most of the plans incorporate tele-med, direct primary care, or concierge medicine as part of the coverage.
• Tele-med allows virtual visits with your physician that may or may not have a copay.
• Direct primary care and concierge arrangements typically provide certain services—such as an annual physical exam and specified treatment for a specific condition—and often don’t qualify as insurance, as you’re essentially pre-paying for a service.
• Virtual primary care sessions can include some prescriptions, durable medical equipment, lab tests, and diagnostic imaging.
Again, it’s very important to understand the scope of the networks, the coverage, and limitations—especially if you’re seeing specialists for an ongoing medical condition.
Don’t forget about subsidies or premium credits.
The ACA’s health insurance premium subsidies—also known as premium tax credits—normally adjust each year to
keep pace with premiums. And people with lower incomes are expected to pay a smaller-than-normal percentage of their income for the benchmark plan— as low as $0 for people with income that doesn’t exceed 150% of the poverty level.
The eligibility range was capped at household incomes of 400% of the federal poverty level (FPL). But that changed for 2021 and 2022. Pending legislation would eliminate the income cap for subsidy eligibility through 2025.
Small Group Plans
Small group plans continue to be the only option for getting true PPO plan options under the ACA. The group market has become smaller with Humana announcing they are leaving the market.
Rate increases filed for small group plans range from less than 5% to as high as 17% depending on the company. For 2024, it appears small group:
• PPO rates will again be slightly lower than individual HMO rates.
• HMO group rates will be 5% to 15% lower than individual plans (nonsubsidized).
Of the major companies, we anticipate Blue Cross will have the lowest rates (their filed rate increase for the PPO is 5.87% and HMO is around 1.31%) followed closely by United Health Care and Aetna. Several group plans have a smaller network or are linked only to a specific hospital system (Memorial Herman in Houston and Baylor Scott & White).
Coverage Options
Small group plans are less expensive than individual plans and have more options.
If you have a practice with at least one other full or part-time employee, you should consider a small group plan. Depending on how your practice is structured, the other employee could be your spouse. Contact TDA Financial Services Insurance Program at (800) 677-8644 for details.
Why go through the additional paperwork and effort for a small group?
• Small group plans will be less expensive than the individual plans, and you can still get a PPO.
• If you sign up during the special enrollment for new small groups (starting Nov. 1), the mandatory employer contribution towards employee premiums (as well as other requirements) will be waived. This is a good way to attract and retain high-quality employees while offering a lot of flexibility on plan designs.
• If you payroll deduct the employee premiums, it saves the practice and employees on taxes.
• You can offer more than one plan within your group—a base plan that’s less expensive for employees (perhaps an HMO with an Rx and office copay) and a PPO plan for you and your family.
We can start comparing rates for small group plans beginning October.
Here are the maximum out-of-pocket amounts for coverage in 2024:
In-network
• $9,450 for an individual
• $18,900 for a family
High-deductible plans intended to be HSA-compatible are subject to these out-of-pocket maximums:
• $8,050 for individual coverage
• $16,100 for family coverage
Out-of-network
If you have out-of-network expenses,
www.tda.org | October 2023 513
value for
your profession
the maximum can be double what’s listed above or more; or out-of-network expenses might not even be covered. The plans with the lowest premiums will have the highest out-of-pocket expenses.
This is Important.
It’s critical you check the network of the insurance company you select for 2024 and make sure your providers and hospitals are in-network. You need to know the company name and the network name. Some providers, for instance, might take a Blue Cross PPO, but not Blue Cross HMO.
What other options do I have for health insurance in 2024?
Level-Funded Plans
If your practice and its employees are generally healthy and not big users of health care, you might want to consider a level-funded plan. These are underwritten based on the health of the group and can be as much as 10% to 25% lower than regular ACA small group plans.
Keep in mind only 40% of groups will qualify based on underwriting, so this will not be a fit for all practices. Also, they typically don’t qualify for the special enrollment, so the practice must pay 50% of the employee premium and meet a participation requirement regarding the number of eligible employees that participate. Additionally,
there are other considerations, such as the different PPO networks, stop loss coverage, and just understanding how the plans work and what’s covered.
Faith-Based, Medi-Share and HealthShare Groups
These types of plans are not insurance and should not be considered a substitute. With these types of arrangements, you join a group and pay or contribute a monthly amount to the plan. After your deductible is met, you submit your medical bills and are reimbursed from the funds available or through others making additional contributions to cover your bill. Many have incorporated a PPO network, so you can get the discounted amount when you have treatment. However, remember you’re still responsible for the bill even if the health-share plan might reimburse you.
These arrangements also have stricter guidelines than traditional insurance companies on which procedures are eligible for reimbursement or cost sharing. As well, there’s normally a lifestyle guideline where a member agrees to live a certain way (abstain from illegal drug consumption, sex outside of marriage, tobacco use, and abuse of alcohol or prescription drugs). The payments of medical bills through these arrangements are not guaranteed in any way. Each member is always solely responsible for the payment of his or her own medical bills.
If you understand how the plans work and their limitations, these can be a less expensive option than ACA plans.
Short Term Medical
We don’t recommend you go without insurance; however short-term health insurance is an option if you’re without coverage because of a waiting period, you’re transitioning from one plan or coverage to another (e.g., in-between jobs), it’s outside the open enrollment period, or you’re close to being eligible for Medicare.
These plans are exempt from the definition of individual health insurance coverage under ACA provisions and usually don’t pay for pre-existing conditions. They’re designed to cover a new sickness or accident, with no treatment in the previous five years. They also have limitations on coverage (e.g., no maternity coverage) and don’t have all the same mandates, such as unlimited-benefits maximums. Currently these plans are available for up to 12 months of coverage and may be renewed for up to 36 months. PLEASE NOTE: There is pending executive action to limit the coverage on these plans to 3 months.
Limited Benefit Sickness-andAccident Plans
These plans are sometimes called “minimed plans” and are marketed as an ACA alternative with a PPO.
They may offer copays and Rx benefits, however, they don’t include the “essential minimum health benefits” required by the ACA.
These types of plans may include a PPO and provide a schedule of benefits that pay a certain amount per day or treatment and are limited to a maximum amount. A company selling these plans will often address this limitation by selling additional coverage for critical or specified illnesses.
514 Texas Dental Journal | Vol 140 | No. 8
Continued
These are underwritten based on good health and have some form of preexisting condition limitation, which means anything you’ve previously been treated for is not covered for a period—normally 12 months. If the plan is guaranteed issue with no pre-existing condition, make sure you’re not just buying a discount plan.
These plans can be an option, however you need to really understand the limitations and coverage, as you could be responsible for tens of thousands of dollars—even if you’re covered—if you have a major accident or illness.
Additional Options and Considerations
If you’re concerned about having a high deductible, limited, or no out-ofnetwork coverage, you might consider a supplemental product for accidents or hospital confinements. These types of plans pay you directly and in addition to your other coverage. They tend to be relatively less expensive and are a good option if you don’t want to self-insure high-deductible and out-of-pocket expenses.
HSA Plans
When picking a plan, keep the above numbers in mind, but also consider the following. Prescription-drug and office-visit copays are convenient plan features, but you need to know the combined cost of your total out-ofpocket exposure and your plan (the premium).
If you haven’t looked at HSA plans or didn’t think they made sense previously, you should look at them.
• HSA plans offer the lowest premium and can be a great way to build up a self-funding account for current and future medical expenses. This
can be especially important if you have to go out-of-network.
• Contributions are tax deductible (as much as $5,150 for an individual and $9,300 for a family).
• Earnings and interest accumulate tax-free.
• You own and control the funds.
• HSA plans are not a use-it or-lose-it vehicle.
ICHRA
Individual Coverage Health
Reimbursement Arrangement (ICHRA) presents an opportunity for employers to take more control over their benefits spend. An ICHRA allows them to set aside tax-advantaged dollars to reimburse their employees for individual health insurance plans; and is inflationresistant compared with group plan premiums. ICHRA brings more cost control and less risk for the employer and more purchasing power and choice for employees.
Keep in mind, however, that the individual health insurance plans offered are probably going to be HMO only; so no PPO. Additionally, the individual HMO plans are 10% to 15% higher than the group HMO plan, if unsubsidized. There’s also the ICHRA set up and additional administration for the practice, which isn’t particularly burdensome but should be taken into account.
HRA
Use of Health Reimbursement Accounts (HRAs) expanded because new regulations issued by the Departments of Labor, Treasury, and Health and Human Services, allow reimbursements for individual-market insurance premiums.
Before employers offer a benefit that includes individual HRAs, they should consider the implications related to the (ACA) employer shared-responsibility
mandate and the ability of their employees to obtain a premium tax credit (PTC) or subsidy on the ACA marketplace. Because of this indexing methodology, the maximum newcontribution amount for an excepted benefit HRA remained $2,150 for the 2024 plan year.
2024 Landscape Review
If you want or need full coverage, the small group market is still the best way to get coverage with more options available at lower cost than in the individual market. However, with proposed legislation, this could definitely change in 2024—so keep your ears open!
The alternative options discussed all have a place at the table, but you need to make sure you understand plan limitations and risks before making a change to something less expensive. Stay informed and get ready to review and compare your options and decide as soon as possible. You’ll be able to review individual plans and rates beginning Nov. 1 and small group plans and rates in early October.
Important Dates
The open enrollment period for health plans offered under ACA begins Nov. 1, 2023, with the effective date of Jan. 1, 2024. For individual plans, you’ll have until Dec. 15 to pick or change to a new plan with a Jan. 1 effective date; or until Dec. 31, if your plan terminates Dec. 31.
Please note: This article was submitted in mid-August, so some information may have changed by the time this article is published.
If you would like to receive more information or discuss available insurance options, please feel free to contact TDA Financial Services Insurance Program at 800-677-8644 or visit www.tdamemberinsure.com.
www.tda.org | October 2023 515
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members & $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/Member-Resources/TDAClassified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN-NORTH (ID #604): Legacy FFS practice with an impeccable reputation located in a budding community North of Austin. The office has relied solely on word-of-mouth referrals with very little marketing/advertising and refers out many specialty procedures leading to upside potential for an incoming buyer. The real estate is also available for purchase. HOUSTON-NORTHEAST, PEDO (ID #596): Pediatric dentistry practice in NE Houston suburb. High visibility retail center, 2,500+ sq ft office featuring 6 ops, computers throughout, digital radiography, intra-oral cameras, and paperless charts. It has a growing active patient base, sees approximately 80 new patients per month, and has an excellent online reputation. HOUSTON SUBURB (ID #610): GD practice plus real estate just 45 minutes from downtown Houston. Large PPO/FFS patient base, approx. 2,200 active patients, all perio, implants, and ortho is being referred out. The owner is retiring and open to a transition period. HOUSTON-SOUTHWEST (ID #614): State-of-the-art, modern GD practice in a rapidly growing suburb in southwest Houston.
516 Texas Dental Journal | Vol 140 | No. 8
Large FFS/PPO patient base, over 2,000 active patients, and a robust hygiene recall program (25%-30% of total annual production). Five operatories (4 fully equipped) with digital X-ray units, computers in operatories, intra-oral cameras, paperless charts, a digital scanner, and CBCT. Revenue of 7 figures over the past several years with consistent year-over-year growth. HOUSTON-NORTH (ID #615): Thriving, legacy, general dentistry practice approx. 60 miles north of downtown Houston with a multi-generational, primarily FFS, patient base. The large, free-standing building contains 9 fully equipped operatories with digital X-rays, a pano, Cerec w/milling unit, and intraoral cameras throughout. The real estate is also for purchase. HOUSTON-NORTH (ID #618): 100% FFS, legacy office located in a high traffic retail shopping center in a highly desirable suburb north of Houston. 4 fully equipped ops with digital sensors, intraoral cameras, computers in ops, and paperless charts. This is a rare opportunity to own an established, legacy practice in a sought-out community that is sure to move quickly! NORTHEAST TEXAS (ID #584): 100% FFS general dentistry practice in a desirable town in northeast Texas with 7 figures
in revenue and strong net income. The turn-key practice features 4 fully equipped operatories with digital radiography, intra oral cameras, paperless charts, CBCT, and a digital scanner.
TEXAS HILL COUNTRY, ORTHO (ID #616): Rare opportunity to purchase an orthodontic practice located in a serene, rapidly growing community in the Texas Hill Country (Austin, San Antonio, and the Texas wine country all available within a short drive). State-of-the-art facility with extensive, modern upgrades and top-of-the-line digital technology. The buyer will have the option of purchasing or leasing the real estate. The current owner will be retiring but is available to provide a transition period to the incoming buyer. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATES’ LISTINGS: Please register at www.dentaltransitions.com or contact us at 512-900-7989 or info@dentaltransitions. com.
AUSTIN: Fee-for-service private practice, 45 years same location with a 10-15 mile panoramic view over downtown Austin skyline. Associate to buy with a preferred long transition for the senior doctor. Nine years
www.tda.org | October 2023 517
classifieds
remaining current lease. Tremendous amount of residential growth immediately outside our huge windows. Ideally a GP interested in learning full scale orthodontics. Please email for information, info@austinskylinedental.com.
BEAUMONT: GENERAL (REFERENCE “BEAUMONT”). Small town practice near a main thoroughfare. 80 miles east of Houston. Collections in 7 figures. Country living, close enough to Houston for small commute.
Practice in a stand-alone building built in 1970. The office is 1,675 sq ft with 4 total operatories, 2 operatories for hygiene and 2 operatories for dentistry. Contains reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over 38 years. Practice sees patients about 16 days a month. Collection ratio of 100%. The practice is a fee-for-service practice. Building is owned by dentist and is available for sale. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com. HOUSTON
(SHARPSTOWN AREA): GENERAL (REFERENCE
“SHARPSTOWN GENERAL”). Motivated seller. Well-established general dentist with high-
6 figure gross production. Comprehensive general dentistry in the southwest Houston area focused on children (Medicaid). Very, very high profitability. 1,300 sq ft, 4 operatories in single building. 95% collection ratio. Over 1,200 active patients. 20% Medicaid, 45% PPO, and 35% fee-for-service. 30% of patients younger than 30. Office open 6 days a week and accepts Medicaid. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental. com. HOUSTON (BAYTOWN AREA): GENERAL (REFERENCE “BAYTOWN GENERAL”) MOTIVATED SELLER. Well-established general practice with mid-6 figure gross production. Comprehensive general dentistry in Baytown on the east side of Houston. Great opportunity for growth! 1,400 sq ft, 4 operatories in single story building. 100% collection ratio. 100% fee-for-service. Practice focuses on restorative, cosmetic and implant dental procedures. Office open 3.5 days a week. Practice area is owned by dentist and is available for sale. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental. com. WEST OF AUSTIN: ORTHODONTIC
(REFERENCE “HILL COUNTRY ORTHO”). Located in a rapidly growing small town, this practice is in the heart of the Texas Hill Country. This
518 Texas Dental Journal | Vol 140 | No. 8
practice serves the youth of the area. There are 4 operatories in the practice. The practice is 100% fee-for-service. Orthodontic care is the only service provided at this office. 1300 sq ft. Open 4 days per week. Digital X-rays and pano and Cloud9Ortho software. The practice has excellent visibility and is located near a hospital. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com.
HOUSTON, COLLEGE STATION, AND LUFKIN (DDR DENTAL Listings). (See also AUSTIN for other DDR Dental listings and visit www. DDRDental.com for full details. LUFKIN: GENERAL. Practice on a high visibility outer loop highway near mall, hospital and mature neighborhoods. Located within a beautiful single-story, free-standing building, built in 1996 and is ALSO available for purchase. Natural light from large windows within 2,300 sq ft with 4 operatories (2 hygiene and 2 dental). Includes a reception area, dentist office, a sterilization area, lab area, and break room. All operatories fully equipped. Does not have a pano but does have digital X-ray. Production is 50% FFS and 50% PPO (no Medicaid), with collection ratio above 95%. Providing general dental and
cosmetic procedures, producing mid six figure gross collections. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental. com and reference “Lufkin General or TX#540”.
HOUSTON: GENERAL (SHARPSTOWN). Well established general dentist with high-6 figure gross production. Comprehensive general dentistry in the southwest Houston area focused on children (Medicaid). Very, very high profitability. 1,300 sq ft, 4 operatories in single
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
www.tda.org | October 2023 519 www.dentaltransitions.com
DSO C S PRACTICE SALES Email: texas@dentaltransitions.com PRACTICE APPRAISALS Austin 512-900-7989 DFW 214-960-4451 Houston 281-362-1707 San Antonio 210-737-0100 South Texas 361-221-1990
classifieds
building. 95% collection ratio. Over 1,200 active patients. 20% Medicaid, 45% PPO, and 35% fee-for-service. 30% of patients younger than 30. Office open 6 days a week and accepts Medicaid. Contact Chrissy Dunn at 800-9308017 or chrissy@ddrdental.com and reference
“Sharpstown General or TX#548”. HOUSTON: GENERAL (PEARLAND AREA). General Located in southeast Houston near Beltway 8. It is in a freestanding building. Dentist has ownership in the building and would like to sell the ownership in the building with the practice. One office currently in use by seller. A 60 percent of patients age 31 to 80 and 20% 80 and above. Four operatories in use, plumbed for 5 operatories. Digital pano and digital X-ray. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com and reference
“Pearland General or TX#538”. HOUSTON:
PEDIATRIC (NORTH HOUSTON). This practice is located in a highly sought-after upscale neighborhood. It is on a major thoroughfare with high visibility in a strip shopping center. The practice has 3 operatories for hygiene and two for dentistry. Nitrous is plumbed for all operatories. The practice has digital X-rays and is fully computerized. The practice was
completely renovated in 2018. The practice is only open three and a half days per week. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com and reference “North Houston or TX#562”. WEST HOUSTON: MOTIVATED SELLER. Medicaid practice with production over $600,000. Three operatories in 1,200 sq ft in a strip shopping center. Equipment is within 10 years of age. Has a pano and digital X-ray. Great location. If interested contact chrissy@ddrdental.com.
Reference “West Houston General or TX#559”.
PORTLAND, TEXAS: Seeking full time associate in an established, fee-for-service, high quality dental practice. This is an exceptional opportunity to move into partnership after a successful initial employment phase. Must be committed to providing optimal patient care with exceptional technical skills, strong people skills and a passion for excellence. This practice has a dynamic, experienced team and a strong emphasis on CE and professional growth. Please send CV and a letter outlining your future objectives and goals to pam@ lifetransitions.com.
520 Texas Dental Journal | Vol 140 | No. 8
WATSON BROWN PRACTICES FOR SALE:
Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
FOR SALE
FOR SALE! Complete Dentsply Friadent motor, handpiece, Ankylos surgical and prosthetic kits, manuals and instruction discs. The total package, rarely used, $3,000. Will text pics, docjenk1@gmail.com.
FOR SALE! Complete Dentsply Friadent motor, handpiece, Ankylos surgical and prosthetic kits, manuals and instruction discs. The total package, rarely used, $3,000. Will text pics, docjenk1@gmail.com.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.
www.tda.org | October 2023 521

522 Texas Dental Journal | Vol 140 | No. 8 PRN Helpline (800) 727-5152 Visit us online www.txprn.com YOUR PATIENTS TRUST YOU. WHO CAN YOU TRUST? If you or a dental colleague are experiencing impairment due to substance use or mental illness, The Professional Recovery Network is here to provide support and an opportunity for confidential recovery. AFTCO ............................................................................ 455 Anesthesia Education & Safety Foundation, Inc.....451 Benevis Practice Services ...........................................462 Choice Transitions .............................. Inside Back Cover JKJ Pathology ................................................................. 454 Henry Schein Financial Services ................................ 455 Law Offices of Mark J. Hanna ..................................... 463 McLerran & Associates................................................ 519 Princess Dental Staffing ................................. Back Cover Professional Recovery Network ................................. 522 TDA Perks ............................................ Inside Front Cover Texas A&M School of Dentistry .................................. 463 Watson Brown .............................................................. 453 ADVERTISERS
Since 1996, our team of experts have provided successful transition services exclusively to dentists. Choice prides itself on its reputation for integrity, service and results.




C e. Considering selling to a DSO? Scan the QR code to watch a brief and informative video to help you decide. ) DSO-INF etr e walk oc t off ess str tia eceiv e f actice ver e o c ta es t g y fees! If y e c o a DSO y rec c ectly c s.
Questions Call us at 1-844-700-JOBS m psum








. Lorem psum
N