The Queen’s Medical Review is proud to present the first issue of our 18th edition—Legacy in Medicine. From medicine’s historical triumphs to devastating tragedies with disease, governance, and the human mind, this is our ode to the heroes of the past and challenge to the greats of our future. Extending beyond the humble Greek beginnings where tradition, medicine, and philosophy were intertwined, this edition harbors personal submissions of those who gave their life to the art of healing, and testimonies of those whose lives were changed by it forever.
We asked contributors to reflect on the legacies they feel are impactful to themselves or modern practice—whether personal, historical, or systemic. We encouraged perspectives that celebrate the achievements of medicine’s greatest practitioners and organizations, as well as challenges to existing structures set in place by our collegial ancestors. Finally, we sought hopeful consideration of the legacies we wish to leave with our patients, colleagues, and the broader community.
What resulted was a diverse and sincere amalgamation of our community’s collective perspectives. Within these pages you will find through various forms of art and written work, admiration for historical figures, reflections on personal legacies and the immediate impact of our actions, acknowledgment of institutional wrongdoing, introspective consideration of what it means to leave a legacy, and more.
We sincerely thank our contributors for their thoughtful and ongoing effort. We are also grateful for the opportunity to curate content that honours the past and embraces the future. As you explore this issue, we invite you to engage each piece with curiosity and to reflect on your personal legacies—both those that have shaped you and those you wish to leave behind.
Gratefully, Alex, Alice, Precious, Sarvesh, and Zier
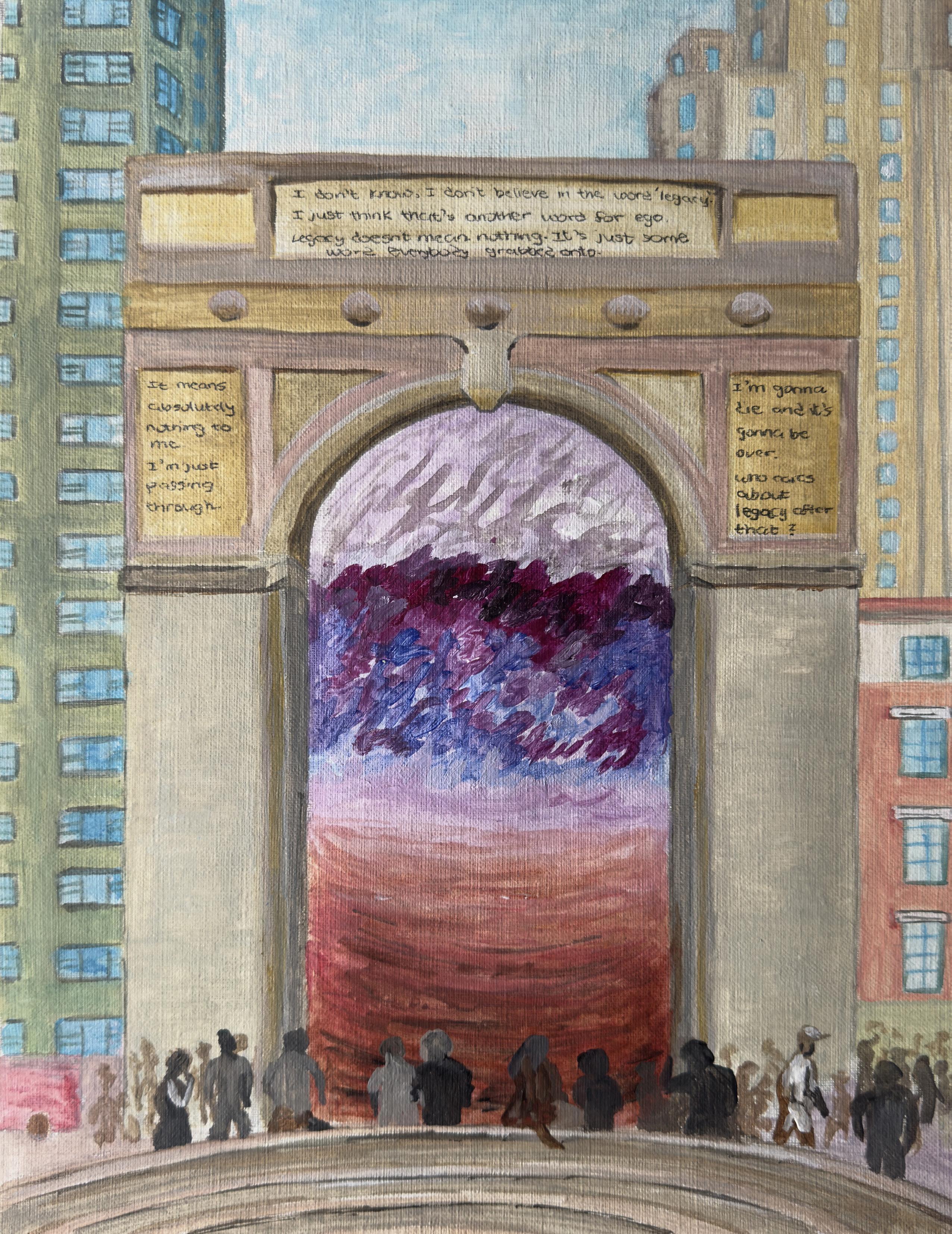
Wh o gets to h ave a legacy?
Written by: Alyssa Reddi, Class of 2028
“I don’t like the idea of legacy. It sounds elitist. It’s something that only white people get to have. It’s frivolous.”
These were my immediate thoughts when the Queen’s Medical Review asked us what comes to mind when we think of legacy.
My second set of thoughts: ...This is a weird reaction. Kind of dark. Am I being racist? Maybe I’m being racist. I should analyze that. So, I’m going to analyze it.
I am a second-generation Canadian. My dad came to Canada alone when he was 12 years old for boarding school, and my mom with her family in her early 20s, both from Guyana. The rest of their families either came before or later followed. Before that, my ancestors were brought to Guyana from India as indentured servants between 1838 and 1917 (UNESCO, 2011). I don’t know when, or exactly from where, or under what circumstances. My parents don’t know either and my grandparents aren’t available to ask due to a combination of early deaths, estrangement, and dementia.
Indentured servitude can be defined as “a contract committing one party to make a series of payments to or on behalf of the other... In exchange, the payee agrees to be completely at the disposal of the payor, or the payor’s assigns, for performance of work, for the term agreed” (Hoefte, 2017, p. 363). Today, indentured servitude is illegal in most countries.
The trauma of this form of slavery still endures. A small country in the warm and beautiful Caribbean, Guyana has the secondhighest suicide rate in the world (World Health Organization, 2021). Domestic violence, substance use disorders, other
mental health issues, and family estrangement are incredibly common, but often not acknowledged because of cultural stigma (Halley, 2023). Although these certainly aren’t facts of life for all Guyanese people, personally, I’ve seen or heard of all of these things happening throughout my extended family.
In contrast, my partner is white, of Irish and British descent. We visit his paternal grandparents, who were born in Belfast, a few times each year. They take great pride in their Irish heritage, and in being Canadian. They have fond memories of their home. The story we hear regularly is that on Sundays, when they were kids, everyone would go to church, followed by a gathering at their own grandparents’ house with dozens of siblings, cousins, aunts, and uncles for a big family meal. I have an ache deep in my soul when I picture this.
On a recent visit, his grandmother found out that I like antiques. Within minutes, she pulled out an entire set of English teacups and saucers from the early 1900s that she received from her mother, silver salt and pepper shakers that belonged to her own grandmother, and wanted to send them home with me (I was thrilled).
It occurred to me on our drive home that my family doesn’t have any “heirlooms.” I don’t know of anything that they brought with them from Guyana that they still have, besides their old passports. I rarely hear of fond memories. I don’t ask for details about childhoods anymore, because 1) I never knew my grandparents that well, and 2) eventually I was old enough to understand the puzzled looks I used to get in response meant they didn’t care to talk about it.
I know there is far more to family legacy than physical things. But it was the meaning behind the heirlooms—the memories attached to them, and the fact that these things were important and valuable enough for them to transport them all the way from Belfast to Canada, on a boat—that stuck out to me.
Still, I know that being white does not shield you from hardship and that having nice things doesn’t mean you have a good life. Few people escape the trauma of immigration, even those that leave their home by choice. My grandparents-in-law made the choice to leave Belfast during The Troubles, a violent conflict between Catholics and Protestants that spanned from the 1960s to the 1990s (Woodwell, 2005). I suppose it wasn’t truly a choice, if their decision to emigrate was based on their personal safety (or lack thereof).
In my partner’s extended family, there is also estrangement. There is substance use and there are mental health struggles,
and it seems that few families are untouched by this nowadays, regardless of race, class, or religion. Ireland, like many countries, did not escape the terror of British colonialism, as evidenced by The Troubles. There are Irish families whose ancestors came to Canada through indentured servitude as well, during the 1600s, though this wasn’t the case for my partner’s family (Suranyi, 2021). When I think about it like this, their story is not all that far off from my own family’s story. In fact, they sound almost identical. So why does it feel different?
I think there is privilege in knowing where you came from. Not in the factual sense, like what your country of origin is, but knowing the people that you come from. The stories that you hear of them. What they were like. What they did on Sundays. Maybe you can hear their laughter in the stories. Perhaps you can feel their warmth in the heirloom you hold in your hands.
My in-laws’ names can be found in the passenger lists of the Canadian archives. Their ancestry is documented in Northern Ireland. They have a family crest. Both sides of the family have a family Bible that has been passed down between generations, as evidenced by the names written in it. There is no denying that they have had their share of pain and suffering, and I cannot attribute my perceived privilege of their family legacy solely to them being white. But there are many things they have, or that are tied to them, that say, “We were here.” To me, that is the difference.
My family history was lost in the displacement from India to Guyana, and again during their tumultuous immigration experiences to Canada. My family did not get to build a legacy. Or maybe there is a legacy—but so far, from my experience, it’s been a legacy of pain, of trauma, of not being free. Although we are now free, in the physical sense of the term, those who are unable or unwilling to reconcile with the residue of these things experience a force opposing this relatively newfound freedom. The persisting pain and trauma actively and violently fight against one’s ability to build a good life. A physically and psychologically safe home. A family legacy.
But here I am. I am safe. I am healthy. I am the first in my family to go to medical school. My siblings and I are the first generation to not have to worry too much about money, thanks to how hard my parents worked, and how hard their parents before them worked to get them to Canada. I have the opportunity to build my own legacy for the family I will one day have with my partner. I’ve inherited a lot of pain and fear,
but each past generation inched forward enough that now, I am standing close to the light at the end of the tunnel. I can move forward if I choose to. It’s hard. It’s a decision I have to make over and over, every day.
With all this in mind, I’d like to alter my earlier opinion of what it means to have a legacy.
For me, a legacy is something that you have the time and privilege to build for yourself and, if you’re lucky, it’s something that endures as a positive memory for your family. It’s not necessarily an object, or a role in society, like “doctor,” or wealth. It doesn’t have to be grand or touch thousands of lives.
Last week, I looked back at an old journal entry I made 12 years ago. I talked about wanting to be a doctor. I had the privilege of having that dream, and I have the time and privilege to realize that dream now.
When I am long gone, I hope to be remembered in my family as someone who cared deeply for others, which is something that drove me to medicine. Ideally, I’ll share my life with at least a dozen more standard poodles (right now it’s just Leonard), like Queen Elizabeth II and her corgis. Maybe the antique teacups I now have will be handed down over generations as heirlooms. Maybe they’ll even have my old journals.
I cannot control how, or even if, I will be remembered. Nobody can. But now, I feel like I have the privilege of having the possibility that I will be remembered, at least in my family. The feeling is enough.
Maybe they will hear my laughter in the stories their parents tell. Perhaps they will feel my warmth in the heirloom they hold in their hands. I dream of my descendants feeling a sense of permanence, of being rooted, of belonging. Contributing to this is the legacy I hope to have.
I am not enough. And I will never believe that I can amount to anything. It doesn’t matter to me if I cure cancer. if I win a Nobel Prize.
The feeling persists.
This sense of success: Is meaningless. In the moment
But inadequacy and self-hate Glare at me in the bathroom mirror.
A façade of failures Instead of A senate of satisfaction.
“He
gets the job done” But think of all the people who said I was outdone.
Of course.
Am I even supposed to be here?
(Now read this poem line by line from the bottom to the top)
Written by: David Vaz, Class of 2026 (a poem in verse)
Neural Networks of Knowledge by
Mona Golmohammadzadeh, Class of 2028
Neural Networks of Knowledge
Figure
A Legacy of Courage: Dr. Gisella Perl
Written by: Lauren Breslin, Class of 2028
Could you practice medicine if your life was in danger? And if caring for patients put your life at greater risk? Would you risk your life and your livelihood to ensure the survival of your friends, your peers, complete strangers? These are questions that, luckily, most of us will never have to face. We live in Canada, where everyone has the right to healthcare and, in theory, the ability to access it. This is not necessarily the case around the world and has not always been the case in the past.
During the Holocaust, many Jewish, Polish, Roma, Sinti, and Soviet doctors were imprisoned, tortured, starved, and brutalized. Many were ultimately killed in concentration camps across German-occupied Europe. While doctors were considered valuable and noble professionals, this certainly did not save them from the Nazi regime and its mission to eliminate Jews and anyone that was not part of their Aryan race.
In this context, the story of one incredible Jewish female doctor, Gisella Perl, is particularly remarkable. Gisella was a gynecologist in Hungary, who after begging her father to become a doctor, became well known and successful. In 1944, she was deported to Auschwitz, a concentration and extermination camp in Poland where 1.3 million people were sent, 1.1 million of whom were ultimately killed, including 960,000 Jews. There, she was chosen by Joseph Mengele, ominously known as the Angel of Death, to work in the hospital, where she was ordered to inform the Nazis about the pregnant women in the camp and get them to come into the clinic with promises of better conditions and nutrition. Gisella soon realized that these women were being chosen for experimentation and almost certain death. She then dedicated her life and time in Auschwitz to saving as many of them as she could. She understood the power she held as a physician, even when stripped of all her rights and dignity, and nobly took it as her duty to save her people.
Rape of Jewish women in the camp was rampant, as was using sex in exchange for goods. As a result, many prisoners got pregnant, and when a pregnant woman came to Gisella, she would perform an abortion, so that the woman would not be subject to Mengele’s sadistic experiments. She performed these procedures with no medical equipment, no antiseptic, and no anesthesia. At the same time, she treated prisoners in the camp for the wounds they sustained from the torture of the Nazis. While she saved the lives of many women, the abortions also had a heavy cost—the lives of the babies. This weighed heavily on Gisella, even after being liberated. She suffered from depression, gave up the practice of medicine, and even attempted suicide after hearing of the deaths of both her husband and son. She was eventually convinced to go back into practice as a doctor, delivering around 3,000 babies into this world and fulfilling her true calling.
Gisella is an incredible example of the trailblazers in medicine who came before us. She overcame tremendous obstacles and pain in her lifetime, and instead of giving in to this pain, found the courage to help her patients and continue to bring life into the world. Gisella’s story is a reminder that taking care of patients and advocating for them can require courage and bravery. While I hope that we as a society are never faced with such peril and horror again, and that I, as a physician, am never faced with a situation that requires me to be as brave as Gisella, her example vividly illustrates that we can and must stand up for our patients, even when doing so is hard. Gisella’s story also makes me thankful each and every day for the privilege I will one day have of practicing medicine in an open, tolerant, and compassionate society like Canada. In the future, I hope to leave a legacy of deep compassion and caring for my patients, and to be inspired by the memory of the terrible circumstances under which some my predecessors operated.
Father Time by Sarvesh Ramlochun, Class of 2027
The Legacy of a Sausage Duel
Written by: Ethan Adler, Class of 2027
Leaving a legacy means leaving an impact, ideally positive, that is timelessly remembered. In the realm of healthcare, this would include advancements in our medical knowledge and practices of how we care for patients. However, generating a legacy is not, nor should be, our primary motivator. Rather, the drive should stem from the desire to address society’s larger problems, and in this unwavering pursuit of bettering our patients’ lives, a legacy is created.
Science and politics often conflict—addressing gaps in healthcare necessitates jumping into these clashes. In my view, doctors are inextricably tied to politics, whether they like it or not. Improving healthcare frequently requires challenging powerful forces, and I was eager to find a physician who exemplified this resolve.
I came across a notable figure in medicine: Dr. Rudolf Virchow. A prolific physician, he is often referred to as the founder of cellular pathology and the ‘father of modern pathology’. Though he made immense contributions in medicine, I would argue his greatest impact—his legacy—was not in the hospital but through his advocacy work for social and political reform.
His passion for social medicine arose in 1848 while he was investigating a typhoid outbreak in a Prussian province. In a scathing report, he concluded it “had only been possible under the wretched conditions of life that poverty… had created,” realizing, “medicine has imperceptibly led us into the social field…confronting directly the great problems of our time.” His goal? To help those “at the lowest level of moral and physical degradation.”
“Medicine is a social science, and politics is nothing more than medicine on a grand scale.”
In Virchow’s view, the only way to address this health disparity was through “education, liberty and prosperity.” He was one of the earliest physicians to recognize that tackling public health issues required a holistic approach to healthcare. Virchow’s work was revolutionary and ruffled many feathers among the ruling class.
Why was he so controversial? Virchow understood, “if medicine is to fulfill her great task, then she must enter the political and social life.” His life motto was that “physicians are the natural attorneys of the poor.” Linking poverty to disease, he argued the outbreak would have been less deadly “had [the people] been free, educated, and well-to-do.” In his mind, if medicine was to enter the social arena it “must be radical.” He became an ardent advocate for better housing, education, and ultimately democracy. His proposals for reform had four pillars: health is a social concern, it is affected by socioeconomic conditions, health promotion must have social and medical components, and statistics must provide objective measurements on progress.
Virchow faced immense pushback for his efforts to improve living conditions and combat poverty. He temporarily lost his hospital posting and was forced to stop the publication of his healthcare journal, Medical Reform. As a politician for a progressive party, he had frequent clashes with Prussian president Otto Von Bismarck. An anecdote recounts a confrontation between the two over military spending. An enraged Bismarck challenged Virchow to a duel. When offered to choose a weapon, Virchow held out two identical sausages. One was infected with a parasite. Given the option to choose first, Bismarck declined. Though a humorous (and likely exaggerated) tale, it underscores
the contentious nature of Virchow’s work and the repercussions he encountered.
The reason I’ve chosen to highlight Virchow is that despite the blowback, he was unwavering in his convictions supporting better living conditions for all. In taking a principled stand and fighting for his beliefs, Virchow created an immense legacy, as he is also known as the ‘founder of social medicine.’ His holistic approach remains a core principle of public health and his fortitude is an example to emulate.
Dr. Bennet Omalu is a contemporary physician who exemplifies this courage. Asked to perform an autopsy on former NFL player Mike Webster in 2002, Dr. Omalu was bothered by reports of his bizarre behavioural changes such as using super glue to adhere loose teeth. When results showed brain damage akin to an advanced Alzheimer’s patient, he published the results. Instead of concern, the NFL embarked on a malicious campaign attacking Dr. Omalu’s findings and credibility. Undeterred by immense pressure and attacks on his reputation, he continued researching. Vindication came in 2016 when the NFL finally acknowledged the connection between football and chronic traumatic encephalopathy (CTE).
What does this mean for those entering the medical field? Throughout our careers, we will inevitably find ourselves at a crossroad between politics and science. As physicians, it is vital to always act in the best interest of our patients and society, even if it questions the status quo. Being a selfless advocate, Virchow established a legacy. We would be wise to follow in his footsteps.
by Anonymous
rumi: on burnout
Rumi, a 13th-century Persian poet and Sufi mystic, famously wrote, “You are not a drop in the ocean, you are the ocean in a drop,” highlighting the boundless potential within each individual. This quote, a reflection on legacy, is interwoven throughout the poem to explore how, in medicine, even the smallest actions can carry a profound and lasting impact.
Written by: Zoë Mohan, Class of 2028
you are not a drop in the ocean yet you and i will be forgotten no matter whose lives we touch they too will be lost to time’s motion
you are the entire ocean in a drop merely a product of your strife full of life until you dry and leave all but a spot
you are not a drop in the ocean for every life you touch will take your words until the grave reduced beyond words to emotion
you are the entire ocean in a drop and you must bear the unbearable the lives of those before, the lives of those to come and ocean or not—you can never stop
you are not a drop in the ocean you may be able to leave your mark to show the world what only you can and evade the mind’s erosion
you are the entire ocean in a drop you leave behind more than yourself a ceaseless ocean of life after all, it’s just a drop.
rumi
Lending Strength:
A Reflective Piece on the Importance of Palliative Care
Written by: Helen Lin, Class of 2025
Tolstoy wrote in Anna Karenina:
“All happy families are alike; each unhappy family is unhappy in its own way.”
Similarly, in end-of-life care, suffering is wholly individual; no one person suffers the same way, and neither do their family members. Each family struggles differently when it comes to dealing with a terminal prognosis of their loved one. What can palliative care professionals do to ease that pain for patients and their families?
The most challenging aspect of this elective was witnessing families struggle with the imminent loss of their loved one. Grieving is complex in nature and individualized. In my first year of medical school, I wrote in our student-run newspaper about the complexities of grief and my own experience of losing my grandfather. I spoke about the dual process model of coping with bereavement by Stroebe and Henk; a model which I associated with my own grieving process. I likened myself to a ping-pong ball being bounced from a loss-oriented mindset to a restoration mindset until the ball slowed to a halt over time. However, anticipatory grief is a different beast. And that is where the palliative care physicians tread daily.
I’m reminded of Mr. B., whom I met on the first day of my palliative rotation. He was young, a travel nurse diagnosed with terminal gastric signet cell carcinoma, with a zest for photography and woodworking. He chose a career in nursing because he enjoyed helping others and wanted to
make a difference in their lives. His prognosis was clearly devastating to him and his family. I spoke in depth about this with my preceptor, after watching his family grasp at straws, desperate to give Mr. B every chance they got. They wanted him to cut down his opioid usage because it was making him too drowsy, even as he gasped for breath. They wanted to explore surgery, despite not even being able to speak more than a few words at a time without fatiguing. Understandable. How could it not be? From the palliative point of view, it was clear that Mr. B would die imminently. How could the family not see it? My preceptor shook his head and wrung his hands.
“The family is going to struggle after his death.”
If done right, palliative physicians can leave a lasting legacy that continues even after the death of the patient—and is one marked by healthy grieving, not complicated by guilt or doubts about whether the family’s loved one suffered unnecessarily. However, weaving through the intricacies of a conversation where the entire room is full of elephants seems incredibly daunting. No one wants to speak of death. How palliative physicians navigate the complex and volatile emotions of family members is like a tightrope walk—small steps at a time.
And so for Mr. B, we spoke with his family frequently, returning to his room time and time again. We opened space for the brother to talk about his guilt over their falling out. We
advocated for Mr. B’s comfort despite the sedating effects of opioids. We walked to his room again and again, and my preceptor would gauge the family’s understanding of Mr. B’s prognosis. I liken it to a good shepherd leading its flock back to its home. Mr. B’s family was lost, floundering in the complexities of a diagnosis that was allconsuming and devastating. They were grasping for any possibility for more time. However, in their desperation, they overlooked the suffering that Mr. B was experiencing.
Eric Cassell wrote in his pivotal piece, The Nature of Suffering and the Goals of Medicine, that “a person can suffer enormously at the distress of another, especially a loved one.” I watched Mr. B struggle with wanting to stay awake long enough to spend time with family, while at the same time, acknowledging his own pain and imminent death. He asked for more sedating medication frequently but changed his mind when his family was in the room. His family was also increasingly distressed by his impending death, but it had not “clicked” in their mind how he was in pain unnecessarily. The patient’s total pain was immense. Our preceptor spoke of total pain; the combination of physical, physiological, social, and spiritual pain that interact with one another, compounding the amount of suffering a patient experiences. The suffering was being transferred between patient and family in this situation, swelling over time like a tide.
My preceptor always redirected the conversation to how to have meaningful time while not sacrificing
his quality of life. It wasn’t until the last 2 days, and with copious counselling from my preceptor, that the family slowly understood and came to terms with Mr. B’s prognosis. I couldn’t hold back my tears watching Mr. B apologize to his brother, in between gasps for breath, for relenting to more sedating medication. As the patient drifted off to sleep with increased hydromorphone, his brother started to break down and voiced his guilt about keeping Mr. B from being comfortable. My preceptor and I remained by the brother’s side. We reassured him that Mr. B knew everything his brother did was out of love, and that feeling was reciprocated. We would do everything in our power now to make sure he was comfortable until the end.
Cassell reiterates that “[r]ecovery from suffering often involves help, as though people who have lost parts of themselves can be sustained by the personhood of others until their own recovers. This is one of the latent functions of physicians: to lend strength.” I have seen the impact that palliative physicians can have on patients and their families. They can provide guidance and comfort in the last days of someone’s life, and direct planning and supportive care in the months prior. They can ease suffering, whether physiological or spiritual. A good death, I believe, is just as important as a good life. Those two weeks on the service have informed my practice for years to come: the importance of treating not just symptoms but also ensuring a patient’s personhood remains intact through our treatments.
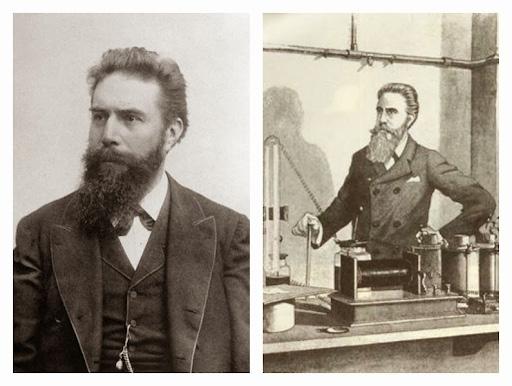
Written by: Alexandra MacMaster, Class of 2025
Cathode rays are the the flow of electrons emitted from a negatively charged electrode when voltage is applied in a vacuum environment (i.e. a vacuum tube). Numerous vacuum tube models, collectively known as cathode tubes, were created to evoke cathode rays, producing varying amounts of photoelectric effect that could be captured on a photoluminescent screen up to 8cm away from the cathode. He initially conducted his experiments using Lenard tubes, which allowed the cathode rays to exit through a small window in a thin sheet of aluminum foil, captured on a phosphor screen placed at the end of the tube. When Roentgen was initially experimenting, he held the phosphor screen very close to the window through the aluminum sheet, and the results were minimal. He decided instead that the Crookes-Hittorf tube, which utilizes thick glass at the area of focused cathode rays, would result in a higher magnitude and a more noticeable phosphorescent effect on the screen. He then attached a Ruhmkorff induction coil to maximize the electron velocity, releasing an electrostatic charge of up to 20,000 volts per pulse, yet the results were still minimal. He then covered the outside of the tube in cardboard cover in black paint, to stop cathode rays from escaping sideways, focusing all the electrons through the thick glass end of the tube, onto the phosphor screen—the results were still minimal. There was some luminescence, but nothing other scientists had yet prove.
Then, whether he was leaving from his usual Friday late night experiments, or purposely trying to limit the confounding visible light, he blew out all his candles. That’s when he noticed: another screen, on another lab bench, far away from the tube, a screen coated in barium platinocyanide, was glowing. Given the screen's distance compared to the tube, he knew these could not be the cathode rays. The black, non-conductive cardboard blocked visible light from leaving the sides of the tube and the lab was completely dark. Roentgen concluded the rays causing the fluorescence on the screen could not be from rays with wavelengths within the visible spectrum. The type of ray he just observed was unknown. Roentgen named these strange rays X-rays, X for “unknown.” Whether it was fate or a lucky break, on Friday, November 8th, 1895, Roentgen created the perfect formula of confounding variables that allowed him to notice and discover X-rays, changing his
With jittering excitement, Roentgen began attempting to stop the rays by placing various objects around his laboratory between the cathode tube and the screen: a book, different metals, and eventually his own hand. He saw shadows of his bones. He noted the varying penetration of the X-rays through materials. A few weeks after his initial discovery, he used his crude X-ray machine to photograph his wife Anna Bertha’s hand. “I have seen my death!” Anna exclaimed as she viewed the picture— the first radiograph (fig. 2). The famous image of Anna’s hand with the outline of her wedding ring has since been immortalized in medical history.
Professor Roentgen announced his discovery at the Würzburg Physico-Medical Society meeting in December 1895. His original paper was published on December 28th, 1895. Within the first few weeks following Roentgen’s announcement, X-ray photographs were used in Berlin to examine the results of recent surgical work, with before and after radiographs of the new fractures and then surgically repaired fractures. In Vienna, embedded bullets were being photographed with X-rays, instead of being surgically probed for, and subsequently removed with comparative ease. Radiography's life-saving capabilities then made international headlines with a story out of London. A sailor was brought to the hospital wounded and barely responsive from an unidentified injury. They discovered an object embedded in the spine using X-rays, which turned out to be a small fragment of a knife blade after it was successfully removed. The sailor lived thanks to the recently discovered X-ray machinery, and likely moreso thanks to the tetanus antiserum coincidentally discovered five years earlier.
By the turn of the century, more than 1,000 articles in X-rays were published worldwide. The first X-ray taken in North America was produced at Davidson College in North Carolina on January 12th, 1896. The first diagnostic X-ray photograph in North America was taken on February 3rd, 1896, at Dartmouth College in New Hampshire. Soon after, on February 17th, 1896, a radiograph was taken of Victorian singer Madame Emma Albani at the Royal Military College in Kingston, Ontario (fig. 3). Kingston General Hospital secured its place as one of the first in North America to obtain an X-ray machine for routine clinical work in the fall of 1896.
Roentgen refused to take out any patents on his discovery as he wanted society to benefit from the medical and practical applications of the newly discovered phenomenon. He received the Nobel Prize in Physics in 1901, much to the dismay of Philip Lenard, who claimed he was responsible for discovering X-rays since Roentgen used his tubes. However, the “glow” Lenard claimed to have previously discovered when he first made his vacuum tube model, was on a phosphorescent screen only a few inches away, whereas Roentgen documented X-rays as creating a photoluminescent effect on a fluorescent screen, at which point he was already experimenting with Crookes’ tubes. Lenard won his own Nobel Prize in Physics in 1905, which his antisemitic connections and views would later taint.
Roentgen’s legacy constitutes one of the most significant discoveries in the field of medicine that ignited exponential change in healthcare. From modest beginnings of incidental discoveries, radiology has become a cornerstone of modern medicine, blossoming into an integral role in the patient care continuum. From the radiograph exhibiting Anna Bertha’s wedding ring, to the clarity of today’s imaging technologies like MRI and CT, and the future of photon counting CT and virtual reality imaging assessments, Roentgen’s observation is celebrated as leaving a magnificent legacy in medicine and the overall advancement of humanity, biology, and physics.
Twice Daily After Meals
by Rahma Osman, Class of 2027
Interview with Art Historian Dr. Allison Morehead: On Munch and Medicine in the Modern Age
Written by: Zier Zhou, Class of 2027
Dr. Allison Morehead is a professor in the Department of Art History and Art Conservation at Queen’s University. One of her research areas is modern Scandinavian art and its intersections with the medical humanities. Currently, Dr. Morehead is curating the Lifeblood/Livsblod exhibition at the MUNCH Museum in Oslo, Norway, which is set to open from June 27 to September 21, 2025.
I reached out to Dr. Morehead because I was curious to hear more about her unique interests and perspectives. We met on Zoom and each sat on our own living room sofas, with some artworks of other places in the background. We talked about how Norwegian painter Munch and his Expressionist pieces are connected to medicine, her curatorial process for Lifeblood, and what she hopes people can gain from visiting this upcoming exhibition. Our conversation below has been condensed and edited for clarity.
Tell me about your background. What drew you to the medical humanities as a modern art historian?
While I was studying 20th-century art history in Europe, I was also working at a research institute and doing some editorial work. As I learned more about the history of medicine, I became interested in the interdisciplinary questions in the medical humanities. I’m drawn to studying [aesthetically pleasing] art that I like to spend time with and could live with, but not always.
Edvard Munch is a great example because he deliberately made “ugly” art and intended to provoke strong emotions. Sometimes, it’s about finding a work interesting and thinking that maybe it has something to tell us. Art can often help us understand things that maybe we haven’t yet been able to articulate, so it’s endlessly engaging.
How did you decide to focus on Edvard Munch's work? What makes his art compelling and connected to medicine?
Munch depicts universal themes of death, illness, love, consolation, loneliness, and jealousy. He’s an artist who tries to produce works that provoke empathy. One of my colleagues once referred to his paintings as “empathy machines.” At the same time, however, people can respond to an artwork in any number of ways. It’s very personal.
Since Munch’s father and his brother were medical doctors, he was quite familiar with the medical community growing up. Munch himself was quite sick when he was young, and his mother had died when he was young. Throughout his life, he formed close relationships with medical doctors. This gave him privileged access to medical care and significant lived medical experiences that were depicted in his art.
Critics have even accused his art of being pathological. Munch acknowledges depicting very difficult life experiences, such as illness, but argues it’s a healthy reaction that can help us deal with these challenges.
wax and cardboard in terrible condition. So, it’s the combination of subject matter and the media used that offended certain people.
Please describe your process for researching Munch's art and curating the upcoming Lifeblood exhibition at MUNCH.
Yes, I’m currently curating an exhibition for Munch called Lifeblood. It’s called Lifeblood because Munch referred to his art as his lifeblood. This idea of his art being fluid and circulating through the body is a very visceral metaphor, which speaks to these themes of health and medicine. One thing I wanted to do was combine Munch’s artworks with objects from the history of medicine. It’s not common for a modern art museum to combine artworks with non-artworks, so I’d say that’s one of my main creative contributions.
Of course, any curatorial project is deeply collaborative, so there’s also a whole team of people who bring their expertise to the table. I’m often writing for different audiences, including the museum, the museum director, and the public. We’re working with designers and architects who design the space and figure out how to hang the works on the walls. It’s an elaborate and creative process, but there are also practical considerations such as climate control, security concerns, and the transportation of works to Oslo from other European countries. A lot of care and attention goes into every single decision. It’s incredible.
There are many ways in which people can engage with art, so I’m totally open to those conversations. I don’t want to be too prescriptive—I guess that’s a good word to use in this context. However, each one of our lives has been impacted by medicine. While that can be great for our health, there are downsides, like the stigma associated with a diagnosis.
It’s easy for us to think of artists like Edvard Munch as abstractions and to forget that they were living people with real bodies. They struggled. In some ways that’s the stereotype, but not all the time—they were also funny and happy. Still, they had to deal with their bodies, which weren’t always healthy. By connecting people with these various life experiences, the art seems less out of reach.
Is there anything else that you hope audiences will take away after visiting Lifeblood?
I’m hoping Lifeblood is something that people can be inspired by. Instead of reading a paper, I’m hoping that this will encourage people to talk about what they’ve seen and say something like, “Oh, I knew the artist for The Scream, but I didn’t know that Munch also painted himself on an operating table, or all these pictures of nurses”. It’s hard to talk about the vulnerability of our bodies. If Lifeblood can encourage us to do so, then that would be my number one goal.
Shades of Grey by Alex Chen, Class of 2027
DOING HARM TO
The Darker Side of Medicine, Scientific Research, and Reflections Moving Forward
When called upon to reflect on medicine’s legacy, most will recount the innovation and landmark scientific progress that permeates into our practice today. From the development of the germ theory that transformed our understanding of disease and prevention, to the discovery of insulin that changed the landscape for people living with diabetes, there are countless innovations attesting to medicine’s ingenuity and resilience. It is evident that medicine is a field with an abundance of ideas and trailblazers that continue to push the boundaries of our current state of knowledge.
However, interwoven into the threads of medicine’s scientific legacy are its bleak origins that cannot be disentangled from the collective whole. Medical progress comes at the heavy cost of its insidious roots in racism, ableism, colonialism, and unethical human experimentation. Abuses of power and privilege permeate its advancement, but often remain hidden from the forefront of our considerations. As a public health researcher, medical student, and aspiring physician-scientist, there are a particular set of cases that I frequently and carefully reflect on.
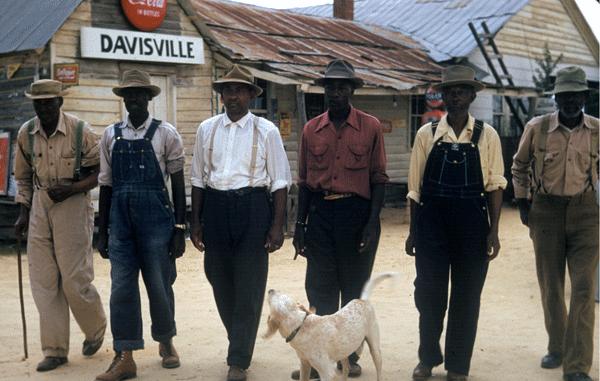
From 1932 to 1972, the United States Public Health Service recruited a group of 600 African American men for the Tuskegee study that aimed at “observing the natural history of untreated syphilis in Black populations.” Underscoring the motivations of this study were fundamentally flawed perceptions, scientific racism in the dominant culture, and the desire to reinforce racist social hierarchies. The recruited men were unaware of their syphilis diagnosis and were incentivized with free medical care they otherwise would not have received. During the 40 years, they were subjected to blood tests, x-rays, spinal taps, placebos,
and ineffective interventions. None of the infected men were treated despite penicillin becoming widely available in 1947 and being accepted as a safe and effective treatment for syphilis. At the end of the study in 1972, only 74 men were still alive, and most had died of syphilis or related complications. Beyond this, during the duration of the study, 40 of the men’s wives were also infected, and 19 children were born with congenital syphilis. The aftermath of this experiment was the tipping point that contributed to the creation of the Belmont Report, which identifies fundamental ethical principles and guidelines to uphold when conducting research with human subjects. Today, the effects of this unethical practice also permeate into continued distrust of the healthcare system and medical research in racialized populations, particularly for African American and Black communities.
Around the same period in the aftermath of World War II, the US military suffered a major jaundice outbreak that hospitalized ~50,000 people and affected ~300,000. This led to a scientific and medical interest in hepatitis, its transmission, strains, and immunization development to combat this viral infection. One of the most controversial and insidious studies occurred from the 1950s to 1970s in Staten Island at the Willowbrook State School, which at the time was the world’s
“DO NO HARM”
Written by Cindy Wen, Class of 2031
largest institution for children living with intellectual disabilities. A group of prominent researchers and physicians from New York University leveraged their power and privilege to lead several investigations that exploited the children and their families. To recruit subjects, they offered parents the ability to skip the waitlist to Willowbrook and placements in the newer and cleaner wards, on the condition that their children participated in the hepatitis experiments.
Broadly speaking, the researchers used ‘mild’ or ‘endemic’ hepatitis viruses and transmitted the pathogens to the children through ingesting material from the fecal matter of infected patients or injections with viral serum. The disturbing conduct of the research team eventually led to backlash from members of the medical community, broader public discourse, and community protests. Alongside this, the hidden inhumane conditions at Willowbrook were eventually exposed, and together, these factors led to the enactment of legislation such as the Developmental Disabilities Assistance and Bill of Rights Act and the Civil Rights of Institutionalized Persons Act, the first federal civil rights laws that protected people with disabilities. The Willowbrook study acts as a conflicting landmark of horrific violations of human rights and a pioneer in the
advancement of a vaccine for hepatitis B.
Moving closer to home, around the same period in the 1940s and 1950s, the Canadian government saw the pervasive malnutrition experienced by the Indigenous communities in Northern Manitoba and decided to exploit these disparities by conducting nutritional experiments. This series of unethical experiments eventually formed the initial basis of the well-known Canadian Food Guide. As shared by Historian Ian Mosby, at the core of these ‘investigations’ were racist beliefs and the “willful attempt to ignore the actual cause of the changes in Indigenous people’s diets”, which was rooted in elements of Canadian colonialism. The permeating effects of these actions, combined with other acts of colonialism and injustice still contribute to distrust, health inequities, and highlight the need for re-centering considerations for Indigeneity in our scientific research and medical practice.
Alongside these examples, there are other landmarks cases I encourage us all to reflect on: Henrietta Lacks and HeLa cells (her ‘immortal’ cells taken without her permission and now underpin much of the research in modern medicine), the Nuu-chah-nulth First Nation blood studies in British Columbia (blood samples collected originally for studying a disease impacting their community and was then taken to perform a number of other studies without informed consent), and many others around the world. Unfortunately, these cases are not unique or standalone—there remain countless disturbing examples of the exploitation of vulnerable and underserviced communities, unethical practice, biomedical elitism, and abuses of social or political power.
Today, these detrimental practices and experiments continue to shape how equity-deserving communities engage with providers in the pursuit of care and form the basis of medical distrust, collective peripheral trauma, and fear in navigating the healthcare system. As my responsibilities in scientific research and medicine become clearer, I often find myself a little disheartened. Science is rooted in generating and advancing knowledge. Medicine centres its practice on a commitment to humanity and to “do no harm.” What does it then mean to practice medicine, when it is rooted in evidence developed against its most fundamental value? What can we learn from our prior mistakes? Where do we go from here?
Unfortunately, I don’t think I’ll ever have the answer to these questions, but I can continue to reflect on the past, my own practice, and my hopes for the future. As I find my place in this ever-changing field, I know that I will continue to exist in this paradoxical state of being burdened by its history but inspired by it to craft a better future. Through reflecting on these historical cases, I see the emerging necessity of working towards community-based participatory research, where communities are empowered as partners in solving health-related problems that matter to them. The only way we can truly address the increasingly complex issues in medicine is through the inclusion of those we hope to service through our proposed innovations and advancements. As a discipline, we have undoubtedly seen progress and improvements in ethical practice, and commitment to communities, effectively ensuring that we “do no harm” while engaging in scientific inquiry. Not only have scientists and clinicians taken greater accountability, involvement of organizations, institutions, and governing bodies have catalyzed the commitments to ethical scientific conduct and ensuring the cycle of racism, colonialism, and ableism in medicine’s scientific history doesn’t repeat itself.
Reflecting on my own epidemiological and public health research, I have always committed to centering the principles of equity, humility, and reflexivity in my scientific conduct. This has been particularly essential in my previous qualitative health equity research
aimed at enhancing equitable access to living donor kidney transplantation for East Asian Canadians. Continuously challenging myself by reflecting on my power, privilege, and social positionality in my encounters with participants, patient partners, and community organizations has been transformative to my work and essential to producing good research. As I embark on my journey as a first-year MD/PhD student, I will continue to carry these values into all my research endeavours as I examine pressing contemporary public health issues facing Canadians today, particularly within high-risk and underserved communities. I hope I will be part of the group of physician-scientists that transform medicine’s scientific legacy into one of humility, self-awareness, and commitment to social justice in producing high-quality, robust, and ethical research that guides evidence-informed practice to enhance equitable care for all.
Beyond this, the foundational values I intend on upholding in my practice of medicine are rooted in the recognition of the accumulated trauma imposed by governing bodies, scientists, and physicians on equitydeserving communities. I am committed to acting as a champion of equity both inside and beyond the walls of the hospital and approaching all patient encounters with a sense of compassion and humility. Although sometimes the weight of medicine’s darker legacy is heavy, I feel hopeful in embodying these values and taking on the responsibility of unraveling past injustices while dismantling structures of social inequity, power, and oppression.
Moving forward, let our generation of physicians and researchers craft a new scientific legacy for medicine— one of compassion, equity, and ethical practice, where we uphold a commitment towards the communities and people that were previously harmed at the cost of medical innovation. I encourage us to reflect on our social positionalities, power, and privilege in all our encounters and place these lessons at the forefront of our minds so medicine can continue to grow as a discipline. I have a strong sense of optimism towards our collective capacity to ensure we “do no harm” in all that we pursue.
by Maggie Liu, Class of 2028
PRINCESS?
etrayal. My first memory. The nightmares always began with a suffocating heat that set my skin and breath ablaze. Wide-eyed aliens supplanted familiar faces. Feverish quarrels ordered an endless buffet of bitter leaves: kindling for the fire. Each breathless gasp stretched into an eternity, one second at a time, until the next came sputtering along.
Just as the agony seemed unbearable, a voice rose above the noise. Unlike the frantic shouts and panicked cries I’d grown used to, it was calm and soothing, like the tranquility of a silent ocean before barking dogs.
“It will only be a moment,” it said, accompanied by a soft embrace. Then something bitter, rancid, and revolting touched my tongue; all of my senses screamed. I cried, but more followed.
“Shhhhhhhhh,” the voice whispered. As it drew on, each competing noise faded away.
“Everything is going to be alright princess. Trust me.”
And there it was. How could I not?
. . .
The winter winds howled as the sun retreated beyond the mountains. Even in the confines of the fortress, the ever-present chill was a stark reminder of the inhospitable landscape. Such a place was hardly fit for a hardy shrub, let alone sustaining human life. It was the perfect place to hide for one who did not wish to be found; the kingdom rarely dedicated resources this far north, where fears of revolution or war were secondary to putting food on the table.
“Princess, the criminal is in the next room,” the young guard announced, puffing up his chest with pride. “Are you sure you want to see them?”
“Yes,” I said. “Lead the way.”
A flickering lantern was the first thing to catch my eye. Its dancing flame cast long shadows over a wizened crone, her emaciated body sprawled out on the stone floor—the sole occupant of the dreary prison. She was far too frail for the iron bangles that adorned her wrists, which threatened to slip off at any moment. The bars of the holding cell were not as merciful.
Despite my thick fur cloak, I felt a creeping chill crawl across my skin. Long-buried memories bubbled up, of heat, herbs, and a singular voice. I had so many questions. I closed my eyes and concentrated on calming my thumping heart. Slow, steady breaths. It had been a long journey, and an even longer hunt. But it was over now.
“Princess? Is everything alright?”
A flurry of stars swam through the air. Glistening constellations coalesced around a singular figure in the far distance, an arm’s stretch away. Features which were once handsome had rotted, a virile ooze leaking from every open orifice. Even still, he was immediately recognizable. His face was etched onto statues across the nation: the blessed founder; the first king. The royal
Written by: Alex Chen, Class of 2027
blade, sealed deep underground in the palace, was raised high. A guttural howl—
“You witch!” the guard cried, brandishing his spear. “What have you done to the princess?”
“Stand down,” I ordered, clasping my hands behind my back to nurse the freshly broken skin. To the young man’s credit, he spun into a salute and froze. “It was nothing more than a moment’s reprieve.”
He jerked awkwardly as he attempted to nod while maintaining the decorum of the salute. His face erupted into a pleasant shade of blood-red.
“Now tell me, what is this woman’s crime?” Witchcraft was no longer outlawed. I had made sure of that years ago.
“S-s-she’s a witch,” he stammered, “a-and we caught her babbling about you, so we rounded her up for treason against the crown. The Baron wants her executed.”
“That will not do,” I said. “Transfer her to the Royal Palace.”
“But the Baron—”
“I will speak to Donya,” I interrupted. “The witch will be kept under supervision and further questioned to uncover the root of any ill-conceived plot. Inform your superior officer immediately.”
He nodded, more confidently this time. “The rumours were true! We never thought about asking her anything. You really are wise beyond your y—”
“Immediately,” I repeated.
The young guard proudly marched out leaving thumping footsteps in his wake. Once the clattering of metal faded, I set the lantern down by the iron bars. The crone crawled towards the light’s warmth, revealing sagging skin and sunken cheeks framing hollow eyes ravaged by the cruelty of time. I knelt, reaching between the bars, and guided her into a more comfortable seated position. The filthy sodden gag was next to go.
“Thank you,” a raspy voice made out between hacking coughs. “Thank you, kind stranger. Thank you, thank you…”
“How are you feeling?” I asked, warming her freezing fingers with my own.
“I beg your pardon, for I am hard of hearing; this old body is not at its finest,” she said. “If you could only come a little closer, that I might be able to hear you, that I might be able to see you, it would mean the world to me.”
Had the head maid been here, she would have tutted endlessly about the state of my dress and the dangers of fraternizing with those of mundane birth. Fortunately, we were alone. The crone’s eyes widened as we came face to face.
“How beautiful! I never expected my saviour to be so lovely,” she cooed. “The founder was right to say that the body reflects the soul.” We shared a laugh in the cold cell.
“Now, if you could spare just one more thing,” she continued, “what is your name? I can hardly go on without knowing the name of my saviour.”
I smiled. “Anastasia Santon Livre Heidan Freesia.”
Her shrill scream shattered the lantern as she wrenched her hands free. A warm frothy fluid splattered across my cheek from parted lips left panting for breath. Her aged and decrepit features burned with inactionable fury, ignited by the spirit of a woman fifty years younger.
“You, you, you—”
“How have you been, princess?”
Ideas of Reference
As I reflect on the upcoming CaRMS process, the biggest piece of uncertainty has to be the reference letters. After all, who knows what my preceptors really thought of me? Sure, they say I’ll make a great internist, but is that enough? I couldn’t name the physical exam findings of severe aortic stenosis. I didn’t know the differences between complicated and uncomplicated UTIs. And I thought ‘emergent’ was less urgent than ‘urgent,’ confusing several consult teams coordinating my patient’s now-‘emergent’ eye clinic. Once the canvas that is my reference letter appears on their screens, how much will these mistakes obscure my final painting?
I truly wondered what it would feel like to be on that other side of the curtain, until it actually happened! I had a request from an undergraduate student I have worked with on a research project. He was a strong prospective medical student, and he loves everything healthcare-related while boasting a solid research background. I could see his drive, not unlike my own at the time. Unfortunately, the night before his OMSAS application was due, one of his referees still hadn’t replied. He pleaded with me to write him a strong reference, something I had actually offered in the past. And so appeared on my screen that same blank canvas.
My student has been truly exceptional. There was nothing on my mind but doing everything I could to help his application. Suddenly, my fears about my own reference letters came back, just with the roles reversed. Would I subconsciously be reminded of his mistakes and unintentionally hold back on positive language? Would I accidentally write negative feedback? Would the file reviewers consider my writing to be weak regardless?
But I just started writing. Sentences and paragraphs flowed from my mind, drawing from my experiences: his diligence in following through with his tasks, his communication and proactivity when faced with other commitments, his asking for help when needed, and his problem-solving skills, often researching his own questions online. These ideas all flew from my mind onto the canvas, illustrating to the admissions committees how suitable he would be for a career in medicine.
So, what about his mistakes? I asked after I finished. Sure, there were times he categorized papers incorrectly during abstract screening, but who hasn’t? Other times, he misinterpreted data in its clinical context, almost as if he had never gone to medical school. How much of that went into my comments? None! Mistakes are a normal part of his learning, and that doesn’t erode how exceptional he will be as a physician. I read over my answers again, and it was as glowing of a reference as I could make it. All positives. Flowery examples. All to showcase his greatness.
I hit submit, and when I told him, I could feel his anxiety melt away just through his texts. Then, I sat at my seat in reflection, something I do maybe too often. With the rapport I built with each of my attendings, I realized there really is no universe where my individual mistakes will trump my patient management, empathy, collaboration, and drive to learn. This extends to everyone in my class and everyone going through CaRMS right now. You don’t go through clerkship and stop improving.
I triggered my own reference letters a few weeks later, and soon my attendings began enthusiastically wishing me the best of luck this CaRMS season. If there was truly a red flag I didn’t know about, they would have politely declined, rather than tarnish my application. After all, how could their well wishes be accompanied by career-ending feedback?
In order to leave our legacy in this world, we first must climb this ladder of medical education. Anxiety while on these steps is inevitable, as they determine our future for the next half-decade and beyond. But as I came to experience, your attendings and supervisors, who have supported you from day one, want nothing more than for you to realize your own dreams. They see the big picture that is you, the you that always strives to work well with others and keep on learning. And when they sit down with your blank canvas, ready to paint, that will be the only picture of you on their mind.
Written by: Danny Ke, Class of 2025
by Ivan Quan & Zoë Mohan, Class of 2028
Baba #94 Varsity Estates Dr NW
Calgary, AB, T3B 3Y7
Dear Baba,
This letter is to let you know that dementia will not command your legacy. That I understand you, even when you can’t communicate everything you want to. And to say thank you, of course, for all that you have done for our family.
Years from now, when the dementia has finished its course and I think back to my Baba, my first thoughts will not be of the woman who can’t find the words, even though she has much to say. Instead, my first thoughts will be of ginger snap cookies and rhubarb crisps—the best that anyone has ever tasted. One day my sister and I will make these desserts for our children, and though I’m sure we’ll never get them to taste quite like yours did, I can promise that we’ll think of you each time that we try.
I will think of the woman who raised my dad and aunt. Who had the patience to deal with my father’s mischief and the grace to quell an unrelenting current of intersibling squabbles, all while ensuring the house was kept and that there was always food in the fridge.
I will think of cribbage games, snakes and ladders, plastic army men in the basement, and reading my favourite childhood book in the guest bedroom made up specially for me. My mind will surely go to memories of being pushed on the swing set for hours until it gets dark, and to innumerable walks along the ridge. How many thousands of miles have you and Grandpa put on that ridge and the quiet pathway by the river below?
I will remember a persistent and determined woman, stubborn in her own way, amongst a family of iron-willed people. I will think of countless family gatherings centered around happy hour on the porch, and 12-dish Christmas Eve dinners with huge servings of trout and pierogies before exchanging gifts in the living room. When my children hear of their great-grandmother, I will tell them about the woman who made all of this possible.
I’ll remember you sitting beside Grandpa in the stands, watching whatever sport I was exploring at the time. I’ll remember talking with you after the game, and I’ll pull up photos of us standing next to each other, with you looking happy and with me usually sporting a newly earned bruise or fresh coat of mud over my uniform, and with both of us smiling in the same way.
Written by: Anonymous
Of course, I’ll recall that you grew up on the farm, were educated in Edmonton, and worked as a nurse. Though I didn’t get to observe this aspect of you directly, I will know that you took your work seriously and gave your best to all those who fell under your care, as I hope to do. When dad got sick, I remember sitting with you in the gray waiting room of the intensive care unit at that hospital in London. A heartbroken stranger walked in and settled into a chair next to you. She was quiet for a few moments, then suddenly burst into the type of sob that is known only to the waiting room outside the ICU. I saw you reach to her with a form of grace that is uniquely yours, put your hand on her back, and provide a comfort to her that no other person could in that moment.
Over the past decade, I have moved away to pursue my own educational and career goals. Selfishly, I have taken my own direction, and greedily have I pursued opportunities to learn and to develop into the man I hope to become. And it all has come at the cost of time spent next to you and Grandpa, I know. With this comes a guilt that I can only abate with a solemn promise to you both—that I give my best to all that I pursue.
I hope all who I meet will come to know your care through me; I will be led forever by your example of compassion and love for others. Perhaps one day, by my actions, you will comfort another sobbing woman in the waiting room outside of the ICU.
All this to say, Baba, that I love you and am grateful to call you my grandmother. I see that your disease traps you in your own body and hides the words that you would speak. I understand that you have so much more you want to tell me, and I hope you know that there is so much more I want to hear from you. I know that you want to converse and bond with my partner, who is entering our family, and that you want to participate in family discussions as you did in the past. You have an isolating and nasty disease, but I also know that it has not changed who you are. Behind your dementia is the same person who has anchored our family for so many years. Your eyes give it away! In them I see the same love that I have known since birth, and when I speak to you and watch them carefully, I hear all that you would tell me.
So don’t fret, Baba, and know that you are understood even when you cannot speak. Though there is still much life to be lived, I hope we can both look to our history with joy. For in the past, nothing is irretrievably lost, but everything irrevocably stored and treasured. I will cherish the time we have already spent together, as I will cherish the time we have yet to spend together. Though the course of your disease and the future more broadly is uncertain, I want you to know now that I will always look upon you and see the Baba that I have always known.
With love, Your Grandson
Women in Wartime: Rebellion in Healthcare
Written by: Chen Chen, Class of 2027
“Why did you choose a career in healthcare?”
It’s a question we are used to hearing— in interviews, at orientations, when meeting someone new. Our answers can vary from wanting to care for others to pursuing biomedical innovation to emulating role models from our childhood. We seek to keep learning about the fascinating intricacies of the human body. We want improvement for our patients. Very few of us come into healthcare to disrupt or to dissent.
Yet, if we dare imagine ‘better,’ we must resist and refuse to accept inequality within the structures in which healthcare has existed.
There are a plethora of examples rebuffing the status quo within medicine. Here is a microcosm—three women immersed in the extraordinarily terrible challenges of the Second World War, and these are their legacies.
Dr. Margaret Chung
Dr. Margaret Chung was born in California in 1889 amidst the tensions caused by the Chinese Exclusion Act which made it illegal to grant citizenship to Chinese immigrants. Her father eventually passed away from occupational injuries after being denied care from US hospitals. In 1916, she was the first Chinese American woman to complete medical school. However, she was continually denied residency and fellowship opportunities due to her race and sex.
Dr. Chung opened a practice in San Francisco, one of the only clinics that provided Western medical care to Chinese patients, and became head of the OBGYN department at the newly opened San Francisco Chinese Hospital which she helped establish in 1925 for the local Chinese community.
Dr. Chung began treating Navy pilots in the 1930s, and provided them with food and Christmas gifts. Her generosity was extended throughout the Navy, with those she cared for naming themselves ‘Mom Chung’s Fair-Haired Bastard Sons.’ Through a recruitment role in the government and her ‘sons,’ Dr. Chung built connections to establish the first US Women Accepted for Volunteer Emergency Service (WAVES) Naval Reserve Branch in 1942 amidst widespread opposition. However, she was still barred from joining this branch due to her ethnicity and suspected homosexuality.
“Women of every nation, every country, should learn medicine, so that they can teach the women of their countries and their races how to care for themselves and their children—how to improve the coming generation.” – Dr. Margaret Chung, Los Angeles Herald, 1914
Dr. Chung’s ‘sons’ famously included several mayors and senators, as well as former President Ronald Reagan and esteemed pilot Amelia Earhart. The WAVES branch that Dr. Chung helped form eventually served 900 stations and consisted of almost 87,000 women recruits. She paved the way for Chinese women and Chinese patients in the American healthcare system.
Dean Vera Nieh
Following WWI and the ‘Spanish Flu’ pandemic, attention shone upon health deficits among the general population of numerous countries. Public health departments had to be developed, of which nurses were the front lines of primary care, preventative health, and education.
Vera Nieh was born in 1905 in Hebei, China. She earned her diploma from Peking Union Medical College, the only university offering nursing education in China, before completing fellowships at the University of Toronto, University of Michigan, and other US universities. In 1940, Nieh was the first Chinese person and woman to serve as Dean of PUMC School of Nursing.
In the face of the brutal WWII invasion of China, Nieh famously negotiated and refused to allow entry to Japanese troops occupying PUMC the day following Pearl Harbor so as not to disturb nursing students while they completed their National Nursing examinations. While the Japanese military ultimately imposed the closure of PUMC by the beginning of 1943, Nieh ensured students’ safe returns home or continuation of education elsewhere according to their wishes.
“I asked the [nursing service] to type up [for] each student what more theory they need[ed], and how many hours, and what kind of [nursing] service they need[ed] to practice before they can graduate.” – Vera Nieh, 1942
Dean Nieh then made a two-month 1800-km-journey to Chengdu, China, in order to reopen PUMC there for the rest of the war. Several of her colleagues were injured or died enroute, including her brother, and she persisted through numerous active war zones to reach Chengdu. As a result of these efforts, PUMC staff and students were able to critically support a waning nursing service in wartime China. Despite her advocacy and organizational strengths, Dean Nieh was perceived by male superiors as a ‘difficult personality’ or a ‘psychiatric instability.’
However, post-war, she was credited with keeping the nursing school functioning during the war and developing a baccalaureate degree in nursing at West China Union University. Nieh was unafraid to challenge traditional medical norms and established a new order of nursing leadership that fostered the development of muchneeded advanced education pathways for nurses, especially in the realm of public health.
Nurse Tsen Shui Fang
Nurse Tsen Shui Fang was born in 1875 in Wuhan, China, beginning her career at the local Wuchang Nursing School. In 1924, Tsen moved to Nanjing and became a director at Ginling Women’s College alongside Minnie Vautrin.
In 1937, Japanese troops began a vicious massacre of at over 100,000 soldiers and civilians, infamously known as the ‘Rape of Nanjing.’ Tsen Shui Fang, then aged sixty-two, remained in the city despite most staff having escaped. She and Vautrin converted Ginling College, built to house 2,750 students and staff, into a refugee camp that eventually served over 10,000 women and children. She bought food for the refugees housed at Ginling and personally guarded the gates. As the only nurse in Ginling College, Tsen provided medical aid to the refugees, including tending to pregnant women and delivering babies. She would also brave regions outside the Nanjing Safety Zone to provide care to wounded soldiers. Tsen and Vautrin kept Ginling running for several years, almost every day directly driving Japanese troops away from raping refugees.
Tsen kept a careful daily diary of the suffering and atrocities she witnessed in Nanjing at the hands of the Japanese Army, and went to great lengths to keep the diary secret from the Japanese military. Her diary was translated by the Second Historical Archives of China
and is still the only account preserved of someone Chinese experiencing the Nanjing Massacre. It was used as evidence during the International Military Tribunal for the Far East where Japanese generals and politicians were tried for their crimes against humanity. Her diary has become crucial in the fight for justice against continued historical denialism surrounding the atrocities of the Nanjing massacre.
“Each night, outside, every place is burning… I do not want to write anymore. When thinking about the Chinese people, I cannot help but feel heartbroken.” – Diary of Nurse Tsen Shui Fang
“Japanese soldiers would enter the grounds on the pretext of looking for soldiers but were in fact looking for our girls… In spite of all that she and I and the rest of us could do on the night of December 17, 1937, the soldiers entered the grounds and carried off eleven girls… We never heard any more of the other two girls.” – Nurse Tsen Shui Fang, Statement to International Military Tribunal for the Far East
LITTLE OLD LADY IN
NO APPARENT DISTRESS
Written by: Hassait Hilawe, Class of 2027
Legacy is often seen through the lens of history as widespread recognition. In reality, the concept is a derivative of impact that is focused on its source.
At lunch, the physician mentioned that one of today’s patients, Avery, was a little crazy and dramatic, and would best be seen at the end of the day. A few hours later, it was time to review Avery’s X-rays at 5 weeks post-operation. What it showed was unequivocally mangled: the bone was still broken and the fixating screw had slipped out of position, now gnawing at the surrounding bone. As if this image wasn’t alarming enough, at the bottom of the screen sinisterly lingered a single set of X-rays from 1-week post-operation. With a single click, the existing images inflated and immediately bore a nauseating hole through the chest of all who viewed it: the two X-ray sets were almost identical. Hopelessly scrolling through 5 weeks of charting demonstrated follow-up visits and radiology notes without any concerns regarding complications—as well as 5 weeks of persistent concerns regarding “severe, immobilizing pain.” Ultimately, this unsuspecting patient had been attempting to rebuild her life on a crucially broken bone, with the damage growing with each passing day. The physician swore silently before resolving to embark on what was to be an undoubtedly excruciating visit for all.
Avery was a little old lady, and as any reasonable person might expect, she was in very apparent distress. She pleaded to be listened to in her entirety as she tried to explain her agonizing pain through her tears. It was clear this was not a privilege she had been afforded throughout the last 5 weeks—not from the healthcare providers overseeing her transition to physiotherapy, nor the physiotherapist who extended her weightbearing and movement goals despite Avery’s objections. Now, with the monstrous anatomy seen on imaging, she had gained the currency of credibility at the cost of excruciating pain in every waking hour of her life for the past 35 days. So how could it come as any surprise that she no longer wanted to live? Seated, she slowly clasped her hands together, looked up with sunken eyes, and began to beg for a referral to initiate the process of MAiD.
In her state, she was unable to entertain a discussion about yet another surgery to revise the damage. She lifted the sleeve of her sweater to reveal a small silver bracelet with 6 charms, and began to explain how each charm represented an interaction with medicine that was marred with suffering and met with dismissal. As if on cue, the physician, exasperated with the task of convincing this woman to ever go near an operating table again, interrupted Avery. She begrudgingly pressed her to tuck the bracelet away, denied any relation between this and past experiences, and began to discuss when a revision surgery could be scheduled. Somewhere in the bitter storm of grievances on both the patient’s and physician’s parts, compassion was violently ripped away from that room, alongside humility. The explanation Avery and her husband received that afternoon did not at all include the honest and truly unfortunate mistakes that shrouded the last month of her life in agony.
Little Old Lady in No Apparent Distress (LOL in NAD)
by Hassait Hilawe, Class of 2027
“What you leave as a legacy is not what is etched in stone monuments, but what is woven into the lives of others.”
- Author Unknown
Legacy is a derivative of impact, focused on its source. Impact itself is centered on those who receive the consequences of action, and how those consequences are woven into their lives. In medicine, those who are impacted are patients and their loved ones whether directly affected by the immediate actions of their physician, or indirectly affected through receiving care at standards formed by research and advocacy. For Avery, the impact of medicine has been forged through repeated misery and rejection. That, like the impact of medicine on most patients, will not receive widespread recognition, or even be recorded, at least not beyond that of a small silver bracelet. In considering legacy in medicine, a critical aspect insurmountable by sheer volume, yet relatively unrecognized ultimately lies in the perspective of the patient.
by Isha Gill, Class of 2027
ON THE LEGACY OF RELIGION IN CANADA’S HEALTHCARE
Did you know that hospitals can refuse patient care due to the belief systems they are founded upon? I certainly didn’t, and that’s why I was so surprised to learn that in Kingston, out of our three hospitals, two of them limit the provision of gynecological care related to contraception, gender affirming care, and medical assistance in dying (MAiD). They are Hotel Dieu Hospital (HDH) and Providence Care Hospital (PCH), and both of them, at one point in their history, were affiliated with the Catholic Church.
I think my reaction is a common sentiment shared among Kingstonians. Albeit far from classified, the influence of the Church on where you can receive the aforementioned care seems far from public knowledge. I imagine for some patients, it may be unrealistic to be referred to Kingston General Hospital (KGH) to receive comprehensive care, nor is it logistically effective amidst our strained healthcare resources. When I first learned about this issue at a seminar hosted by our upper year classmates and residents, I was quite surprised. But as my surprise morphed into frustration with our institutions, I decided to dive into the rabbit hole and learn more about the role of religious faith in our hospitals. With the theme of this issue of the Queen’s Medical Review being ‘Legacy’, this piece reflects what I learned from my brief readings and peer anecdotes about the legacy of the Catholic Church on our healthcare systems, the beginnings and extent of their influence, and what that means for our patients in Kingston.
The idea of the Hotel Dieu comes from the 10th century in French speaking countries. The literal meaning, House of God, represents a place where the poor and
Written by: Henry Li, Class of 2028
needy can receive healthcare free of charge run by the Catholic Church. At the time, this attracted doctors to the Hotel Dieu for the sake of practicing their skills, and the Hotel Dieu became some of the oldest known hospitals. As this idea was transitioned to Canada before the Canada Health Act in the 1980s, the construction and operation of many hospitals were graciously funded by the Catholic Church to serve their communities. In fact, much of the land which our hospitals today are built on is or was owned by the Catholic Church, including PCH in Kingston.
Although this is not inherently an issue, as most patients go through HDH and PCH without discovering any barriers of access to the care they need, the funding and operations of our hospitals nowadays are mostly by our provincial and federal governments. This means that despite the funding of our healthcare being secularized, our access to care at HDH and PCH is still held to the standards of Catholic ethics. In a sense, we are funding our own barriers to access of abortion care, genderaffirming care, and MAiD at these facilities in Kingston. Once again, this does not necessarily pose a problem, as non-religious hospitals do exist and patients should be able to choose where they receive their care. But in contrast to other institutions funded by the church, such as Catholic schools, patients often end up at a hospital simply because it was the one closest to them during an emergency, regardless of if they are owned by a religious institution. In fact, most patients do not know that contraceptive care is not provided at HDH until they are denied it, which makes this also an issue of transparency.
My first reaction to learning this was:
Is this even legal in 2024?
To me, I believe if our modern public healthcare system is funding the operation of both Catholic and secular hospitals the same way, we should be providing care equally in either contexts. But the truth is, the legacy left by religious institutions on Canada’s healthcare system is evident in the law itself. Catholic and secular hospitals are both governed by the same provincial legislation, which provisions employment, reporting, et cetera, but these laws also permit hospitals to refuse services for religious reasons. Much like how physicians are not required to provide care that goes against their faith, religious hospitals can do the same at an institutional level. In Ontario’s Public Health Acts of 1990, our government is unable to order a Catholic hospital to provide care against their religion’s ethics, as “A directive [by the Minister] shall not unjustifiably … require the board of a hospital that is associated with a religious organization to provide a service that is contrary to the religion related to the organization.”
So what types of care are limited by Catholic ethics in Kingston? From my knowledge, HDH limits provision of tubal ligations for contraceptive purposes, as well as laparoscopic hysterectomies and bilateral salpingectomies for gender-affirming purposes. Unfortunately, as Dr. Chris Vicenza, an obstetrics and gynecology resident at KHSC, mentioned in an interview with the Queen’s University Journal, there are close to six times more gynecological operating room spaces offered at HDH compared to KGH. Since KGH is a secular hospital with no limits on what type of gynecological care is provided, it does not make logistical sense for it to receive a lower capacity for gynecological care than HDH when both hospitals are located in such close proximity. In a similar vein, Kingston’s major long-term care hospital PCH, due to its Catholic affiliation, does not provide MAiD. As many
patients at PCH tend to have more complex disease progressions, palliative and end-of-life care makes up a large portion of care provided at PCH, which makes it all the more contradicting when MAiD is not offered to this patient population.
Looking back, there has been a lot of discourse on this topic over the past few years. In 2023, Dr. Danielle Kain’s appointment as Interim Clinical Director of Palliative Care at PCH provoked concern over the future of Catholic affiliation in Kingston’s hospitals due to her being a proponent and practitioner of MAiD. Most recently last year, an open letter organized by residents and medical students addressed to Queen’s School of Medicine regarding contraceptive and gender-affirming care has again sparked interest, a spark that inspired me to look more into the legacy of Catholic healthcare.
When I began writing this piece for QMR, my intentions were never to bash the Catholic affiliations in Kingston’s hospitals. In fact, I acknowledge that most of our healthcare infrastructure in Kingston would never have existed without the generosity of the Catholic Church, an appreciation for which has only grown as I researched this topic more. With the announcement of ‘Legacy’ as the theme of this QMR issue, I did not initially plan to write about a topic so entrenched in religion. As someone who is not religious, I wondered if it was appropriate for me to criticize the ethics of an organization I have little affiliation with. But as I dove into discussions with peers, I began to realize this instead became a question of accessibility, and the almost clandestine legacy in which accessibility in healthcare has not been prioritized due to religion.
My hope is that while we move forward in this discourse, we keep in mind the legacy we are criticizing as we try to make medicine accessible for all.
When the lights shut off and it’s my turn to settle down, my main concern.
by Sarvesh Ramlochun, Class of 2027
Medical Legacies Through Nature’s Lens
by Jaskarn Dhaliwal, Class of 2027
Similar to nature, legacies in medicine are prevailing. Just as sprouts emerge from the soil, new medical professionals learn, adapt, and grow—creating roots that will influence their careers. Over time, they will create legacies of their own. At the same time, the experiences of today’s medical professionals are influenced by those who came before. Like nature’s cycles of change and renewal, each new generation of physicians builds on those that came before them. However, there is always room for change and growth in response to new societal needs. This piece, created using items found in nature and a watercolor painting, embodies my perception of legacies in medicine.
QMR VOICES ESTABLISHING A LEGACY IN MEDICINE
Written by: Tim Song, Class of 2028
To look upon your legacy, one requires a precedent; for many individuals with no prior connection to medicine, this means that they are the first to step forward into new territory. This is an extremely daunting process to navigate on top of the everyday stressors of learning medicine. From disparities in knowledge to network, students first in their family to pursue medicine—or post-secondary education at large—face additional challenges during their journey in medicine. Firstgeneration medical students carry not only their own ambitions but also the hopes and dreams of those who came before them. Through determination and the legacies they aim to create, they redefine what it means to leave a mark on the field of healthcare.
Understanding the experiences of first-generation medical students informs the support needed to help them successfully progress through medical school to residency. A qualitative interview-based study of firstgeneration American medical students (Havemann et al., 2023) on the challenges they faced led to the emergence of four prominent themes: isolation and exclusion related to the ‘hidden curriculum’ (the discrepancy between what is taught in the classroom vs. the informal flow of professional practice); resource insecurity for educational and basic resources (i.e., food, rent, transportation); lack of faculty or institutional support; and a constant sense of needing to rely on grit and resilience to survive.
So what do these experiences look like within Queen’s Medicine? We asked first-generation students
within our community four to five different questions about what their journey to medicine looks like. In this context, we defined first-generation as students first in their family to attend medical school, whereas the term has historically been used for students who are first in their family to pursue post-secondary education overall. Given Queens’ smaller student body, we opted to use this alternate definition to receive more student responses but understand the limitations that this may place in understanding first-generation student experiences.
1. What do your parents/family members do? How has your family background shaped your drive to pursue medicine?
“My mom always spoke of wishing to pursue the sciences, but never did as higher education was discouraged in her family.”
Family backgrounds play a pivotal role in shaping the drive to pursue medicine. For many, their families instilled values of hard work, resilience, and community service. One student reflected on their parents’ sacrifices: “My parents worked really hard and took large risks just for me to have an education. This motivated me to work hard.” Others found inspiration from family members’ unfulfilled dreams, such as grandparents who aspired to become physicians but were unable to due to sociopolitical barriers. Students were also often instilled with
values of community service, which brought forward medicine as a viable career path for them despite unfamiliarity of the career in the family. For some, personal experiences with the healthcare system ignited their passion for medicine. Whether through navigating complex medical histories of family members or witnessing disparities in access to care, these experiences cultivated a desire to make a difference. As one student shared, “I knew from a young age that I wanted to pursue medicine, driven by curiosity and the desire to assist my family in navigating the healthcare system.”
Student Responses:
My mom influenced my path by always being adamant that I should love what I do, and that I should keep as many doors open as I could. She is also the most altruistic person that I have ever encountered, and the work that she does as a high school principal at a specialized school for at-risk youth has inspired me. On the other hand, my dad always advocated that I find myself in a stable profession where the skills that I obtained in my education would be useful—to him it did not matter whether that was a trade, dentistry, or engineering, but it was important that what I chose would be highly employable.
I was raised on values of community service. Living in the GTA, I found that there weren’t many spaces where true community building and community service existed, where you know the people in your community and feel a part of something greater. Medicine could give me that no matter where I ended up geographically.
I grew up in a blue collar family with my dad working as meat cutter and my mom as a stay at home. My parents worked really hard, sacrificed a ton, and took large risks just for me to be able to have an education. This motivated me to work hard. My childhood was pretty rough. My family was going through difficult times financially and it was a very hostile environment. I experienced physical abuse throughout my childhood, which in a weird way motivated me to pursue medicine. Firstly, I wanted to get out of this hostile environment and be self-sufficient. I also wanted to prove to myself
that I didn’t need my parents. But also I saw first-hand how difficult times can really tear a family apart, and a large part of being a doctor for me was to be able to try and mitigate that for other families.
My grandparents were all manual labourers in communist China. Two of them actually had dreams of becoming physicians in their youth but could not pursue higher education during the Cultural Revolution and the subsequent years of quote-onquote "education reforms". Although they could not pursue post-secondary education themselves, or even finish secondary education, they never de-prioritized education in their lives and for my parents. My grandparents were all exceptional life-long learners, even without the accessibility of formal training. Growing up, I could always see their passion for learning and their continued curiosity. My grandpa has often told me how much of a privilege it is to be able to attend school because it requires so much luck to live in a peaceful time without war, to be physically healthy enough to attend school, and to be financially secure enough to afford it (monetarily and the time investment it takes before earning an income).
Medicine was something I knew I wanted for myself—it wasn’t tied to their professional paths but rather my own passion and curiosity. However, their dedication and sacrifices have undoubtedly shaped the foundation that allowed me to dream big and follow this path. Growing up, they made countless sacrifices for my siblings and me, ensuring we had the opportunities and support to pursue whatever we were passionate about. Even now, as an adult, their encouragement hasn’t wavered. Their belief in me inspires me to keep pushing forward, not just for myself but for the values they instilled in me.
2. What are your family's thoughts on your pursuit of medicine?
“Their unwavering support reminds me of the strength of family and inspires me to keep pushing forward, not just for myself but for them as well.”
Despite lacking firsthand knowledge of the medical field, families of first-generation students have often been unwavering in their support. Students expressed profound gratitude for this emotional encouragement, which has been critical in their journeys. One shared, “Their belief in me inspires me to keep pushing forward, not just for myself but for the values they instilled in me.”
For some, the pursuit of medicine has fulfilled longheld family aspirations. Another student recounted an emotional conversation with their grandparents: “It signified the fulfillment of three generations of dreams in my family.”
Student Responses:
At times I felt like they would try really hard to help but just couldn't because they didn't know the ins and outs of the process. That being said their emotional support was unmatched and is definitely the reason I am in medical school today.
They are very happy for me. throughout the process, they did not think I could get in to medical school due to how competitive it is.
Both of my parents are very proud that I have chosen a path that is meaningful and provides me with stability. They both recognize that this career will work for me and represents the values that they have instilled in me. However, they would have been proud no matter what I chose to pursue so long as I was true to who I am in selecting a life-path.
I've always known that my grandma wanted to pursue medicine as a young adult and was not afforded the opportunity to do so, but it was only after I received my acceptance that I learned from my other grandpa that he too had dreams of pursuing medicine when he was younger. He has never shared that with us before because he always considered it unhelpful to share his burdens and lost dreams from decades ago, but it was this story that made me realize the weight and meaning of my medical degree to my family. While this acceptance was tremendously happy news for myself, it
also signified the fulfillment of 3 generations of dreams in my family. I could hear my grandparents' voices crack with emotion and excitement when I called to share the news and they are able to see their own buried dreams, from what feels like a lifetime ago, fulfilled in their grandchild. That emotional conversation was profoundly impactful for me. My grandpa's words from long ago rang in my ears and it helped me appreciate all the more what a privilege it is to live in a country where higher education is relatively accessible and in a time when we have the luxury of studying in peace.
I come from a family with three siblings, all in very different fields, and I’m the only one to pursue postsecondary education. Despite the differences in our paths, my parents and siblings are equally proud of all of us, celebrating our unique journeys and achievements.
3. What challenges have you faced as the first in your family to pursue medicine?
First-generation medical students frequently navigate unfamiliar academic and professional pathways with little guidance. A recurring theme was the challenge of learning the “unspoken rules” of the field—from securing research opportunities to preparing for the MCAT (Medical College Admission Test) and medical school applications.
Students highlighted the importance of self-advocacy and seeking mentorship. One described the need to “forge my own connections and figure out everything myself,” while another emphasized the value of mentorship, saying, “I had to seek my own mentors at every phase of my life.” Despite these challenges, many expressed pride in their resilience and the lessons learned along the way.
Student Responses: Definitely a lack of knowledge on the unspoken “It felt like I was going against the tide.”
rules and requirements. These are things that I found were known among people who had family members in the field, but I had to learn from trial and error.
You have to forge your own connections and figure out everything yourself. Things as simple as applying to university, paperwork, general advice and guidance were things I didn’t have.
In high school, I had no idea how to best set myself up to get into medical school. I found myself asking university fair reps about the medical school application process and what kind of traits and experiences the admission committees look for. This sometimes yielded helpful information and other times didn't. I was distressed thinking about which program I should enter as I debated between following more of a broad health or life sciences route vs. following something more niche and 'what I truly loved'. When it came to studying for the MCAT, I had absolutely no idea where to begin and this led me to putting it off for quite some time. I spent a lot of time and stress trying to figure out the best strategy for studying and managing working, volunteering and other commitments. I know this is a common story for most medical students regardless of if they are a first-generation medical student or not, but I think these challenges and stressors are augmented when you don't know the testing and application system at all and you're truly going into the whole thing blind. At a younger age trying to create opportunities was extremely daunting, and the imposter syndrome of not knowing what research really entailed, or not knowing if I was qualified enough for certain jobs definitely delayed the process of getting critical lifeexperiences that prepared me for medical school.
While I am the first in my family to pursue medicine, I do not think that I am disadvantaged by that in any way. I do, however, strongly believe that the socioeconomic status of my parents (being in the same tax bracket as physicians) does contribute to my perception.
medicine, I know that I carry the weight of many people's dreams on my shoulders. While there is great hope alive and resilience represented by my presence in a medical school, there is also great pressure. Pressure to not let anyone down. Pressure to be a doctor my family and the society expects/respects. And pressure to honour all those who've gone before me.
Without a family background in healthcare, I had to navigate complex academic and professional pathways largely on my own, learning through trial and error, without a built-in roadmap or family members who could share firsthand insights into the process. It was often frustrating not having anyone fully understand what I was experiencing—whether it was the rigor of my studies or the complexities of processes like the MCAT or application process. At the same time, this unfamiliarity came with a silver lining: my family’s unwavering belief in my abilities. They genuinely think I can do anything I set my mind to because they don’t know the challenges of the field, and their confidence in me has been a constant source of encouragement. It’s both humbling and heartwarming to be surrounded by people who not only support me but also see me as the bee’s knees. I know their praise and involvement come from a place of love, and it fuels my determination to make them proud. Balancing these dynamics has taught me resilience and gratitude. It’s helped me appreciate the importance of building my own network of mentors while cherishing the unconditional support of my family. Their belief in me reminds me why I embarked on this journey—to inspire others and show that with dedication, even the most challenging paths are worth pursuing. Despite the challenges, it’s been empowering to carve out my own path and lean into my resilience and determination.
4. What legacy would you like to leave as a future healthcare professional, and the first in your family to pursue medicine?
“I aspire to leave a legacy rooted in compassion, resilience, and advocacy.”
As the first in my extended family to pursue
When envisioning their legacies, first-generation medical students aspire to inspire future generations, foster equity, and bring compassionate care to their communities. One student articulated a desire to “leave a legacy of someone who is an inclusive leader and who advocates for equity and social change.” Another hopes to “bring a compassionate perspective toward newcomers and the unique challenges they face.” For some, the idea of legacy extends beyond their professional achievements to embody hope and resilience. As one student shared, “I want my legacy to be one of conveying hope to patients and future generations, showing that no matter how dark the present may seem, there is always hope.”
Student Responses:
Honestly, speaking to classmates that have family members who are physicians, it’s beautiful to see the way that they have positively influenced and inspired them to go into medicine. I hope that I can do the same for the future generations in my family!
I hope to inspire others to never give up on their dreams (applied a few times before getting in), to not be afraid if you're the first to do it, and to approach each obstacle as exactly that—just something in the way that you can, and will, overcome.
I hope to bring a compassionate perspective toward newcomers and the unique challenges they face, especially navigating cultural and linguistic barriers. My family had no background in healthcare, and added on with being new to Canada, our family couldn't access or wasn't aware of many services available. We were lucky our family physician was very caring and provided guidance on many facets of our journey, and I hope to continue a similar caring approach to my community.
I don't think that I am very interested in leaving a legacy, necessarily. I would like to add to the general goodness of the universe by doing the right thing and making the right choices day-to-day, and to lead by example in making those choices. I would like for my name to die with those who loved me.
I would like to leave a legacy of hope. While my grandparents were not able to pursue their dreams, there was resilience and hope nonetheless. There was hope as they raised another generation, and that generation raised another. As future physicians, we will hold a lot of life in our palms and my wish is that we can convey this message of hope to all of our patients and people we interact with. No matter how dark the present may seem, there is always hope, and with that hope comes resilience. There are always more stories left to be written and I'm excited for what the future holds for us and how we will impact the world around us. Let us run the race set before us with hope, grace, strength, and endurance and not lose heart.
My journey is not only about becoming a skilled healthcare professional but also about honoring my heritage and addressing the unique health challenges faced by Indigenous communities. I want to inspire future generations—both within my family and my community—to dream boldly, overcome barriers, and believe in the power of education and determination. I hope to be remembered for combining clinical expertise with cultural humility and empathy, ensuring my patients feel seen and respected. Moreover, I aim to contribute to health equity by advocating for culturally sensitive healthcare and addressing disparities that disproportionately affect Indigenous populations. My legacy will be one of paving the way for others, fostering understanding between cultures, and demonstrating that our traditions and modern medicine can coexist to create a healthier future for all.
5. Is there anything else you would like to share about your experience as the first in your family to pursue medicine? What is some advice you would give to other students with no familial background pursuing medicine?
“Try your best, be kind to yourself, and understand uncertainty is part of the process.”
Queen’s Medicine students encourage the following: to seek mentorship, stay informed, ask for help, and be
vigilant. They emphasize the importance of networking and staying connected; word of mouth is a powerful source of information. This rings true in the medical application process, but also beyond.
Student Responses:
Seek out experiences and perspectives. Knowledge is power! and seeking out as much information and mentorship as possible, as early as possible makes a huge difference.
If you have a dream, work like hell if you want to achieve it. But don’t forget to take some time to be present and live life.
My advice would be to talk to as many people as you can (I literally would talk to walk-in doctors, other healthcare professionals and family friends) about the process and be cautious not to weigh one person's opinion or experiences too heavily as what worked for one person may not be the strategy or lifecourse that works best for you. I would also encourage first-generation medical students to obtain as much information as possible on the application process in undergrad. The earlier you can have a grasp on the road to medical school as well as what traits and skills are required of you once you get there, the better choices you can make regarding your own unique path to becoming a physician.
Seek out mentors, peers, and advisors who understand the journey and can provide guidance. Also, don’t be afraid to ask questions or seek help—no one expects you to have all the answers, especially when you’re blazing a new trail. I also learned very quickly that people who have gone through this process are eager to answer questions and want to see you succeed, so don't be afraid to reach out to current med students or residents! Stay focused on your ‘why.’ Remember what drives you, whether it’s a passion for helping others, a desire to make an impact, or personal experiences that inspired you to enter the field. Also, celebrate your victories, no matter how small. Every step forward is an achievement, and it’s worth acknowledging how far you’ve come. Finally, be kind to yourself. This journey
is tough, but it’s also incredibly fulfilling, and you’re proving that it’s possible to break barriers and achieve your dreams.
Conclusion
This interview series of Queen’s Medicine found that our community faced challenges like limited mentorship, financial barriers, and imposter syndrome, but drew strength from family support and personal resilience, aspiring to inspire others, address health inequities, and mentor future generations. However, the earlier study on first-generation American medical students (Havemann et al., 2023) found that a constant need to rely on grit and resilience to survive correlates with increased levels of stress, physical and emotional fatigue, lower perceived social support, and lower likelihood to practice self-care. While grit and resilience are important individual qualities for navigating medical school, systemic interventions and peer support groups are thus required to address the disproportionate challenges first-generation medical students encounter navigating medical school (Alves-Bradford, 2023). It is thus important to achieve educational equity by creating a network of academic, identity, and financial resources to support medical students.
Queen’s Medicine fosters supportive learning environments in many ways, it is important for us as students to continue to uphold high standards for ourselves to support learners and ultimately the patients that we will serve. We call for increased diversity within medical school classes—as a core value, not just a target quota (Shin et al., 2023), as research has shown that medical student and physician diversity is correlated with improved educational experiences (Gurin et al., 2002) and health care (Snyder et al., 2023). Encouraging and supporting students who may not have initially considered a career as a physician to enter medical school is a meaningful way to diversify the physician workforce, ensure a robust learning environment for all, and improve patient outcomes.
We would like to thank the eight participants who shared their experiences with the Queen’s Medical Review team.
“The truth is people who are sick, people who have suffered have something beautiful to give to the world.”
- Claire Wineland
Claire Wineland by Annie Liu, Class of 2028
Shaping Tomorrow’s Wings
by Ivan Quan, Class of 2028
WE MUST STOP REACHING
An unconventional review of When Breath Becomes Air by Dr. Paul Kalanithi, 2016
“My journey from medical student to professor of neurosurgery was almost complete: after ten years of relentless training… I had earned the respect of my seniors, won prestigious national awards, and was fielding job offers from several major universities. My program director at Stanford had recently sat me down and said, “Paul, I think you’ll be the number one candidate for any job you apply for. Just as an FYI: we’ll be starting a faculty search for someone like you here…” At age thirty-six, I had reached the mountaintop; I could see the Promised Land, from Gilead to Jericho to the Mediterranean Sea… I could see myself finally becoming the husband I’d promised to be.”
— Dr. Paul Kalanithi, When Breath Becomes Air, 2016
My first time reading this autobiography was the summer before starting medical school, in July of 2023. I was in the beautiful, lush countryside of Midi-Pyrénées, at a musician’s retreat in Chateau d’Aix, a 1400s castle in the south of France. Paul Roberts was my teacher for the week—a wise, gentle man who had published books extensively on Debussy and Liszt—and I was there to live and breathe music one last time before I embarked on a new chapter in medicine. I figured it was a rite of passage for every aspiring medical student to read Dr. Kalanithi’s autobiography, so it was my book of choice between the masterclasses and concerts.
My initial thoughts of the book were odd. The foreword was written not by a family member or a dear colleague, but by the clerkship director at Stanford University medical school, Dr. Abraham Verghese, who introduces himself as someone who “got to know Paul only after his death.” Verghese sings praises—without personal connection—about Paul being the image of courage and bravery…only for the reader to be let down.
Let me explain.
The first half of the book felt like Dr. Kalanithi was not only convincing the reader, but also himself, that he had the most ethical reasons for becoming a doctor. He writes that he had not seriously considered medicine until the eighteen months before he had applied, out of motivation to continue finding the deeper answers on suffering and death. Kalanithi credits his realization to the voice of Augustine (yes, the literal philosopher’s), instructing him to “set aside the books and practice medicine” (p. 29). I still remember rolling my eyes as I read that passage, as I found it incredibly unconvincing that he claims he had not previously considered a career in medicine despite both his parents being physicians. As someone with first hand experience in the challenges, sheer resources, and detailed planning needed to even apply to medical school, I did not appreciate that the first half of his book—a book that he wanted to leave behind as his legacy— was a lengthy expansion of a particularly pretentious premed statement on why he had the purest, holier-than-thou motivations for becoming a doctor.
Here was a man claiming that he wanted to observe the humanity in medicine, but he himself came off as less than humane. If this pursuit of knowledge was his only motivation, would he not be already living his dream as a medical student or neurosurgery resident? Why is his ‘mountaintop’ likened to a professorship at Stanford?
What of his wife, Lucy? His friends? His family? Dr. Kalanithi spoke only in an active voice concerning his academic pursuits, and frequently used passive voice at the mention of his wife and family. It felt almost obligatory, like he believed he needed to include them in his autobiography, but they were always an afterthought. If you read carefully, one will notice that Lucy was only mentioned in detail in the context of conflicts they have had, or being there to support him in his medical appointments, but never in light of her own goals or accomplishments. Heck, he even talked about his first girlfriend, Abigail, with arguably more passion as a key inspiration for pursuing biology and neuroscience
FOR THE “PROMISED LAND”
Written by: Alice Li, Class of 2027
as his undergraduate degree—perhaps she was the one who got away? Lucy is not a real-time relationship, but an afterthought that he is looking forward to reacquainting with, after he reaches his “Promised Land” of prestigious tenure-track professorship.
One passage revealed the condescending nature which Dr. Kalanithi regarded other medical specialties in comparison to his selection of neurosurgery: “In the fourth year of medical school, I watched as, one by one, many of my classmates elected to specialize in less demanding areas (radiology or dermatology, for example) and applied for their residencies… The idealism of their med school application essays tempered or lost” (p. 40). This, combined with him bringing up the Stanford job he was a ‘shoe-in’ for no less than four times throughout the book, paints a picture of how Dr. Kalanithi viewed the world— that neurosurgery, or climbing the ladder to the top, was the best and most admirable way to live.
Now I understand that I may sound overly critical of Dr. Kalanithi’s autobiography, but I do respect Dr. Kalanithi for his pursuit towards a noble career in neurosurgery. As a medical student, I find his operating room stories and the sacrifices he made towards his career quite commendable. Furthermore, writing a book as the final project of his life is very brave because it requires introspection and vulnerability. However, I maintain that Dr. Kalanithi’s legacy is not one as admirable as he would lead the reader to believe—because the apparent motivator for writing his book was to let the world know that he had so much potential he did not fulfill, and for his accomplishments to be remembered (did you know, he would’ve been a professor in neurosurgery at Stanford had he not been ill?). All at the cost of what? A man consumed by climbing, and achieving, and decorating himself, obsessed with his legacy so much that he wrote a book, finished with sincerity by his wife (whom they had almost separated due to not prioritizing their relationship before his cancer diagnosis), with a foreword written by someone who did not know him before death.
And yes, I have considered that it is unfair to judge Dr. Kalanithi so harshly as I was not a personal friend, and he never finished his autobiography due to cancer (his wife, Lucy, finished the last pages with refreshing candor). However, like the phenomenon of seeing our “life flash before our eyes” in the final moments before death, the stories that he chose to inscribe in his last months likely carried the most significance in his life. And, like any work of published literature, these stories are open to interpretation and judgement.
Now that same summer, I read Paul Robert’s book—the pedagogue I was fortunate to study with at the music retreat—Reading Franz Liszt. In this book, Mr. Roberts talks about Goethe’s Faust and the towering mountain ranges in Switzerland that inspired catalogues of Liszt’s most monumental piano works. Here, Mr. Roberts writes with pure curiosity for his art, generous with his knowledge and revelations, showing that legacy should not be something one sets out to conquer out of desperation, but the parting kiss after immersing oneself fully in the beauty and depth of their pursuit.
In the end, I wish to find myself in the Swiss Alps where Liszt stood, content at its base in admiration—the same mountains that Paul Roberts writes about with spirited wonder and excitement for the journey it took to reach the top. I prefer this over a race to the peak of Mount Academia, where we forget to live and love, and climbing becomes an ultimate end in itself. So Dr. Kalanithi’s autobiography, though applauded by many, reads to me as a warning that life is preciously finite and our breaths will inevitably become air.
Jericho is not the gateway to the Promised Land, the Promised Land is here.
GEHNA
by Priya Thethi, Class of 2027
As a medical student of Indian ethnicity, I am fond of the ‘Bani Thani’ style of paintings, which originate from my family’s hometown. Traditionally, these paintings displayed Indian women admiring objects that were considered to be "feminine". In my paintings, the women are adorned with intricate jewelry, yet their eyes speak of something far deeper—a yearning for healing and selfeducation. One gazes tenderly at animals, one feeds them with affection, and another holds a bouquet of flowers absentmindedly, her attention captivated by a book. These women reflect how I imagine I might have been,
had I lived in their time—carrying a blend of compassion and intellectual curiosity.
Many women of the past carried within them the passion and ambition to pursue careers, perhaps even in medicine, but were denied the opportunities to do so. Despite these barriers, their legacy endures. They have passed down values of compassion, resilience, a thirst for knowledge, and a profound desire to heal. I am deeply grateful for the traits that previous generations have instilled in me, enabling me to seize the opportunities they never had and to honor their legacy in my own journey.
Gehna
REFERENCES: WHOGETSTOHAVEALEGACY?(PAGE4)
1. UNESCO. (2011). Records of the Indian Indentured Labourers.
2. Hoefte, R. (2017). 4.4. Indentured labour. Handbook The Global History of Work, 363.
3. World Health Organization. (2021). Suicide worldwide in 2019: Global health estimates.
4. Halley, C., & Cowden, S. (2023). Reconciling a broken heritage: Developing mental health social work in Guyana. International Journal of Environmental Research and Public Health, 20(20), 6931.
5. Woodwell, D. (2005). The “Troubles” of Northern Ireland. Understanding civil war: Evidence and analysis, 161.
6. Suranyi, A. (2021). Indentured servitude: Unfree labour and citizenship in the British colonies (Vol. 4). McGill-Queen’s University Press.
REFERENCES: LASTFRIDAYNIGHT(PAGE16)
1. Linton, O. (2012). History of radiology. Academic Radiology, 19(10), 1304.
2. Bell, D., & Goel, A. (2013). Wilhelm Roentgen. Radiopaedia.org.
3. Cadogan, M. (2024, November 7). November 8, 1895. Life in the Fast Lane.
4. Blattenberger, K. (2021). After class: X-rays, October 1960 Popular Electronics. RF Cafe.
5. Schwarcz, J. (2023, March 3). The right chemistry: Discovery of X-ray changed medicine forever. Montreal Gazette.
6. The Nobel Prize in Physics 1901. (2024). NobelPrize.org.
REFERENCES: DOINGHARMTO‘DONOHARM’(PAGE24)
1. Alsan, M., Wanamaker, M., & Hardeman, R. R. (2020). The Tuskegee study of untreated syphilis: A case study in peripheral trauma with implications for health professionals. Journal of general internal medicine, 35(1), 322–325.
2. McVean, A. (2019, January 25). 40 years of human experimentation in America: The Tuskegee Study. McGill Office for Science and Society.
3. Muscente, K. K. (2020, August 3). Ethics and the IRB: The history of the Belmont Report.Teachers College Columbia University.
4. Halpern, S. (2021). Dangerous medicine: The story behind human experiments with hepatitis. Yale University Press.
5. Rosenbaum, L. (2020, June 15). The hideous truths of testing vaccines on humans. Forbes.
6. Disability Rights TN. (2023, January 6). Willowbrook 51 years later: A look at history and modern advocacy. Disability Rights Tennessee.
7. Tennant, Z. (2021, April 19). The dark history of Canada’s Food Guide: How experiments on Indigenous children shaped nutrition policy. CBC Radio.
8. Mosby, I. (2013). Administering colonial science: Nutrition research and human biomedical experimentation in Aboriginal communities and residential schools, 1942–1952. Histoire Sociale / Social History, 46(1), 145–172.
9. Nature. (2020). Henrietta Lacks: science must right a historical wrong. Nature, 585(7823), 7.
10. Dalton R. (2002). Tribe blasts ‘exploitation’ of blood samples. Nature, 420(6912), 111.
REFERENCES: QMRVOICES(PAGE45)
1. Alves-Bradford, J. M. (2023). Supporting first-generation medical students—Improving learning environments for all. JAMA Network Open, 6(12), e2347475.
2. Havemann, C., Mason, H. R. C., Russell, R. G., Casillas, A., Nguyen, M., Boatright, D., Webber, A., Parrilla, J. A., Gallegos, A., & Wyatt, T. R. (2023). Challenges facing first-generation college graduates in medical school: A qualitative analysis. JAMA Network Open, 6(12), e2347528.
3. Romero, R., Miotto, K., Casillas, A., & Sanford, J. (2020). Understanding the experiences of first-generation medical students: Implications for a diverse physician workforce. Academic Psychiatry, 44(4), 467–470.
4. Shin, Y. B., Stojcevski, A., Dupuis-Miller, T., & Kirpalani, A. (2023). Racial and ethnic diversity in medical school admissions in Canada. JAMA Network Open, 6(7), e2324194.
IMAGE CREDITS: ALEGACYOFASAUSAGEDUEL(PAGE10)
Rudolf Virchow [Photograph]. Encyclopædia Britannica. Retrieved March 22, 2025, from https://www.britannica.com/biography/ Rudolf-Virchow#/media/1/629797/15084
IMAGE CREDITS: LASTFRIDAYNIGHT(PAGE16)
Fig. 1—Willhelm Conrad Roentgen portrait photograph published in 1900; on the right is an illustration of Roentgen next to his crude X-ray machine with the Crookes cathode tube model. Photo taken from: https://thex-rayellica.blogspot.com/p/the-history. html
Fig. 2—Anna Bertha’s hand radiograph, with the famous outline of her gold wedding ring, taken on December 22nd, 1895. Photo taken from: Kirkman, M. A. (2014). The role of imaging in the development of neurosurgery. Journal of Clinical Neuroscience, 22(1), 55–61. https://doi.org/10.1016/j.jocn.2014.05.024
Fig. 3—Hand radiograph of Victorian singer Madame Emma Albani taken at the Royal Military College in Kingston, Ontario, on February 17th, 1896, courtesy of the Museum of Health Care in Kingston – item accession number 997029001 a-b, under ‘Archival Radiology’. https://mhc.andornot.net/en/permalink/artifact1019
IMAGE CREDITS: DOINGHARMTO“DONOHARM”(PAGE24)
Participants in the Tuskegee Syphilis Study - National Archives and Records Administration. https://catalog.archives.gov/id/824600 Children’s beds at Willowbrook State School - Willowbrook State School, Staten Island, New York City. IC-05: Eric C. L. Aerts Photographs, IC-05. CSI Archives & Special Collections.
IMAGE CREDITS: WOMENINWARTIME(PAGE36)
Vera Nieh - Barnes, N.E. (2009). The Rockefeller Foundation’s China Medical Board and Medical Philanthropy in Wartime China, 1938-1945. ISSUELAB. Retrieved March 22, 2025, from https://www.issuelab.org/resources/27979/27979.pdf
Margaret Chung - Wikipedia contributors. (2025, March 22). Margaret Chung. Wikipedia. Retrieved March 22, 2025, from https:// en.wikipedia.org/wiki/Margaret_Chung
Nurse Tsen - Hu, H., & Lian-Hong, Z. (2010). The Undaunted Women of Nanking: The Wartime Diaries of Minnie Vautrin and Tsen Shui-Fang. https://muse.jhu.edu/chapter/322740/pdf