How can mindfulness be used to promote movement in spinal cord injury rehabilitation?
Debate
Should our health care provision model move towards a two-tiered public and private system?
Rainbow roads
A piece on the importance of accompaniment with our LGBTQ+ patients through a personal narrative
Experience how love is both moving and halting across two reflective poems rise and fall
Movements
In This Issue
Managing Team
Sigi Maho
Mahshid Hosseini
Staff Contributors
Sarenna Lalani
Jessica Nguyen
Helen Lin
Jehan Irfan
Anna Tran
Devyani Premkumar
Meghan Jenkins
Imran Syed
Mili Milivojevic
Colin Faulkner
Amelia Boughn
Annie Kang
Kaitlyn Rourke
Kassandra McFarlane
Design
Jessica Nguyen
Fiona Raymond
Tanya Narang
Colin Faulkner
Molly Cowls
Kaitlyn Rourke
Suffia Malik
Joshua Lowe
Andrew Lloyd—Kuzik
Jehan Irfan
Sarah Sloss
Helen Lin
Kiera Liblik
Editors
Amelia Boughn
Sarenna Lalani
Helen Lin
Haya Abuzuluf
Anna Tran
Annie Kang
Meghan Jenkins
Mili Milivojevic
Colin Faulkner
Cover Art
Kendra Zheng
Letter From the Editors
We are proud to introduce Queen’s Medical Review Volume 15.2: Movements in Medicine!
As an active, highly engaged student body, we are always in motion. From one class to the next, from one DIL to the next, or from one wellness run to the next, we are seldom rooted in place. People talk about the importance of ‘seizing the moment’ but time is so transient that remaining stagnant is seldom a desired option, let alone a possibility. On a larger scale, we are subject to movements in society and shifts in political ideologies. We are constantly on a pendulum of change. The truth is movements are multidimensional and we are constantly subject to shifts in time, body, and space.
What moves us and what roots us in place are delicately intertwined, and in this issue we have collected narratives, commentaries, and art that capture this delicate balance. Our contributors wrote about physical movements. Meagan Wiederman connects movement between mind and body, writing a compelling piece on the use of mindfulness in promoting movement in spinal cord injury rehabilitation. Amelia Boughn highlights the importance of keeping moving and provides a breakdown of all of the running trails around Kingston for all of your activity needs. Our writers also described social movements in time. Sarenna Lalani and Laura Wells debate the future of our health care provision model, and whether we should move towards a two-tiered public and private system. Imran Syed highlights the idea of anti-intellectualism and relates it to the current Freedom Convoy movement. Our contributors also moved us, by writing compelling pieces that discussed notions of moving on and moving forward. Helen Lin discusses grief and bereavement from both a personal and academic perspective. Joseph Sanfillipo writes a moving piece on the importance of accompaniment with our LGBTQ+ patients through a personal narrative. From poetry and art to reading lists to thoughtful reflective pieces like the ones above, Movements in Medicine is an issue packed with thoughtprovoking discussions, deeply moving reflections, and insightful conversations that attempt to move the dialogue on important social issues forward.
As always, we have many thank yous. First, a huge thank you to the incredible contributors that have truly moved us this issue. The writing was raw, honest, and deeply personal. We feel an immense sense of privilege that you would share your stories with us and our readers. We are forever grateful to you. Second, we would like to take the opportunity to thank our incredible production team. Every single member of QMR is so incredibly invested in making this publication everything it is and more. From attention to detail to imaginative creation, our QMR team truly breathes life into each word, each illustration, and each design. We are so thankful for all of you and cannot tell you enough how much your time and effort is appreciated. And last, but most certainly not least, a sincere thank you to our readers. Your unrelenting support and encouragement is the reason we are so motivated to make QMR the best it can be. Without you, there would be no QMR - so thank you for keeping us inspired.
And with that, we invite you to move to the first page of ‘Movements’ - an issue that is all about putting your thoughts and feelings into motion.
healthcare in Canada should move to a two-tiered system both public and private provision of services
Artwork by Kiera
Liblik, Meds ‘23
A long overdue wake up call
Prior to the COVID-19 pandemic, I feel that Canadians were conditioned to believe that we live in some sort of healthcare utopia. The healthcare system exudes the image of poised perfection — with it’s sparkly “universal” title, high quantity of hospitals in major cities, and the stateof-the-art cancer centres, the system seems idyllic. That is, until you have to use it. A 2015 Ipsos poll found that three in four Canadians believed that we lived in the best healthcare system in the world. A December 2021 poll, however, showed that 71% of Canadians feel our system to be too bureaucratic, with 58% believing we need to allow private entrepreneurs in.1 Sure, I will be the first to admit that we are fortunate to live in a (mostly) developed nation, with some level of universal healthcare. However, I think that anyone who claims our healthcare system to be infallible need only look at the crippling burdens placed upon it today to put that claim to rest. COVID-19 has highlighted some serious shortcomings in the Canadian healthcare system; nursing and bed shortages, resource scarcity and exorbitant delays are only a few of the issues the pandemic has brought to light. More frightening, however, is that the demands that will be placed upon our healthcare system as we compensate for missed care opportunities will assuredly amplify the paucities we are already
seeing. The ugly truth is that the Canadian healthcare system has been crumbling for a very long time, and the pandemic only shook things up so that we could see just how unsteady our system was. I think it’s about time that we move to resurrect, and reinvent, it.
If only we could put the quality in equality
Before I get into why I think a twotiered system would improve both functionality and efficiency of our healthcare system, I want to address a common misconception about hybrid healthcare. There is a belief that those who contend for a two-tiered system fundamentally oppose the concept of fair and equal access to healthcare. To this, I say two things:
First, to believe a hybrid healthcare system will destroy equal access to healthcare, one must inherently believe that the status quo is an equal system. I simply do not buy that this is true. The social determinants of health already create unequal access to healthcare systems and services; factors like location, age, education, employment, language, and culture are already impacting the ability of Canadian residents to access healthcare services. Our “universal” system is hardly universal at all — the challenges that would face an Indigenous person living in Moose Factory requiring an emergent procedure or a rural Labrodorite seeking abortion care are a testament to this. If you believe our current healthcare system to be fair
system with
and equal, I would urge you to take another look.
Second, and more importantly, I am not sure that I believe equality should be the endpoint of our healthcare system. Equality does not equal quality. An equally miserable healthcare system is still just that — a miserable healthcare system — only everyone is suffering from it. I think aiming for an improvement in healthcare quality is a far more important goal; we ought to decrease wait times, improve access, and promote primary care and if it takes adding in a paid system to do that, I think the ends will most certainly justify the means.
Pay to play, and get out of the way
A common belief is that a hybrid system will create two radically different healthcare systems, one of tremendously superior quality than the other. Our current facilities would likely constitute the public portion of the new system, so it is unlikely that care would drastically worsen within the public queue. If anything, I would argue that the vast majority of healthcare would be similar to what we are seeing now, with a few added benefits of course. The first of these is a decreased burden on wait times. Canadians are more than used to waiting their turn when it comes to receiving healthcare. The newest report from the Fraser Institute shows that we wait a whopping 26 weeks, on average, between seeing our GPs and receiving treatment for our medical issues.2 We also wait for imaging, appointments with our GPs, and to see specialists. The queues, unfortunately, are something we have come to accept as part and parcel of our healthcare system. However, maybe we don’t
have to. In a hybrid system, private payers would be able to expedite their care in a lower burdened and less bureaucratic system. Not only does this hasten their care, but it also removes them from the public waitlists, thus shortening wait times there too. Not only will they free up spots for imaging or specialists, but there will also be a decreased load in the public system, thus equating to a greater dollar amount per healthcare user. This would hopefully mean that our taxpayer dollars would reach further, since less bodies would have to be covered by the system. If shortened wait times mean a private payer gets to undergo an MRI in a twinkling glass building while public users must face the painted brick of hospital walls, I would argue that it’s a small price to pay for quicker healthcare overall.
Hardly working to working hard
So, you may be wondering how we will staff this brand new system and continue to cover the ongoing burden in the public sector. Remember that change isn’t going to happen overnight. Some physicians will inevitably move from the public to private sector, but so will some patients. Over time the existence of two systems will widen the job market for healthcare workers. As future physicians, this would bode really well for our job prospects! A new market might mean that the ortho gunners need not complete two fellowships after a gruelling five year residency to be considered employable. It also means that there will be increased capacity for training, both at student and resident levels, and an overall increase in the number of providers able to care for patients. Perhaps accompanying this will be an increased robustness of primary care, along with greater availability of specialists in both systems. Some may argue that all practitioners will shift to the private sector, I mean, who would say no to better pay and shinier equipment, right? To this I would say a few things. First, if this was a real fear, I think we would already see a gross disappearance of our physicians to our southern neighbours. The “brain drain”
not currently a pressing issue, and has actually been on the decline since the mid-90s.3 Second, doctors in the public sector are pretty well paid as it is, and they are often the first to admit it. I don’t buy that a few thousand dollars will suddenly motivate everyone to switch over to the private sector. That additional income comes with a headache of its own — lofty overhead clinic fees and fancy (and pricey!) equipment are inherent to working in the private sector. If people are going to pay, they are going to expect firstclass treatment, and the physicians within the private sector will have no choice but to accommodate. Lastly, the basic rules of supply and demand will keep people in check. If there is an overabundance of supply and a low demand in the private sector, doctors there may actually make less than their public counterparts. Over time, a natural balance will be struck between the two systems.
It is time to move on
It is high time that we stop pretending that our healthcare system is perfect and paradisiacal and start actually providing accessible care to our population. The fear of our system turning into an American one is both unrealistic and unfounded, with a different model that includes universal care at baseline, we are bound to see different results. There may be uncertainties and adjustments that lie ahead, however, what is certain is that our system is cracking, and throwing more money at it is not going to change that. We need to move away from a system that is not serving Canadians (at any socioeconomic status) well, and move towards increased efficiency and functionality. It is about time we add a second tier to the Canadian healthcare system.
References: 1. Canadians Largely Satisfied with Healthcare System, But Eager for Increased Access | Ipsos. Accessed January 31, 2022. https://www.ipsos. com/en-ca/news-polls/canadians-largely-satisfied-healthcare-systemeager-increased-access
2. Waiting Your Turn: Wait Times for Health Care in Canada, 2021 Report | Fraser Institute. Accessed January 31, 2022. https://www.fraserinstitute. org/studies/waiting-your-turn-wait-times-for-health-care-in-canada-2021
3. Freeman TR, Petterson S, Finnegan S, Bazemore A. Shifting tides in the emigration patterns of Canadian physicians to the United States: A crosssectional secondary data analysis. BMC Health Serv Res. 2016;16(1):1-8. doi:10.1186/S12913-016-1908-2/TABLES/1
4. Chris Selley: Canadians feel smug about their health-care system right up until they need it | National Post. Accessed January 31, 2022. https:// nationalpost.com/opinion/chris-selley-canadians-feel-smug-about-theirhealth-care-system-right-up-until-they-need-it
NAY
Laura Wells, Meds’23
The COVID-19 pandemic has placed an enormous amount of pressure on Canada’s public healthcare system. The rising case numbers with the Omicron variant led to a large demand for COVID-19 tests in early December – a demand which could not be met by the public system at the time. As a result, Ontario started seeing pop-up, for purchase PCR tests being made available individuals who could afford it. The introduction of such services and strain from the COVID-19 pandemic suggests the need to re-evaluate the age-old debate of the pros and cons of a two-tiered system with private and public delivery of healthcare in Canada. A brief discussion of the potential shortcomings of a two-tiered system makes it clear why it should not be considered.
There will be fundamental, inequitable differences between the care provided in the public versus private systems. People who can afford it will be able to walk up and pay for the healthcare service they want with no delay. Conversely, people who cannot afford the luxuries of the private system, most notably members
of equity-deserving groups who have been traditionally disadvantaged in society, will be forced to wait in the public system for access to necessary healthcare. Furthermore, the creation of a two-tiered system will change the quality of care provided in the public system. Healthcare providers may choose to work more frequently in the private system as it provides the opportunity to make more income without the limitations of the public system. Over time, more healthcare professionals could choose to provide care in the private system, resulting in shortages of providers in the public system. This could lead to a reduction in access to high quality healthcare professionals in the public system, and consequently poorer healthcare for those who need it the most. Canada is a country that prides itself on its universal, accessible, portable, publicly administered, and comprehensive healthcare (yes, I did just quote the Canada Health Act, as flawed as it may be), and a two-tiered healthcare system directly contradicts Canadian values.
The potential for reduced wait-times in the public system with the introduction of private healthcare is often one of the biggest allures of a two-tiered system. However, this theory hasn’t been shown to hold-up in practice. For example, in the UK and Australia, areas with larger private sectors have longer wait times in public systems compared to regions with less private sectors in the same country. To put things in a Canadian context, in Manitoba there are several private clinics performing cataract surgeries. The private clinics continue to have very short wait times, and members of the public system waiting for surgery are often redirected to the private system if they can afford it to get their surgery sooner. However, for the same surgery in the public system, there continues to
be long wait times. In fact, due to the COVID-19 pandemic, Manitoba has experienced the largest percentage decrease in cataract surgeries than any other province. Private healthcare services may result in faster access to care for many people who are willing to pay for it, but those who can’t afford to skip the line will get left behind.2
In summary, a two-tiered system should not be considered for healthcare delivery in Canada as it introduces inequitable access to care based
services, redirection of funds to improving access to care, and thinking of alternative funding models for healthcare and healthcare providers in Canada to improve care for all (but those are topics for a future issue). No matter what the future of our healthcare system, there is one thing we can all agree on: something has got to change. ⚚
Mindfulness in Promoting Movement in Spinal Cord Injury Rehabilitation
Written by Meagan Wiederman, Meds ‘23
Artwork by Kaitlyn Rourke, Meds ‘23
Movement in the Physical Medicine & Rehabilitation Wards
On the Dr. Marc L. Smith Memorial Summer Studentship in Physical Medicine & Rehabilitation (PMR), I had the opportunity to see patients with spinal cord injury (SCI). An essential part of the studentship was observing and learning about the role of interdisciplinary healthcare providers in caring for PMR patients.
I specifically followed one patient who had an SCI at the level of C7 after a tumor grew and was resected, making him paralyzed from the waist downwards with limited control of bowel and bladder. He had some control of the arms, including shoulder movement, but his elbow naturally contracted and his fingers were in a tight ball without botulinum injections. I had a memorable learning experience where I attended the physiotherapy session with this patient, once during their first week on the unit and again two weeks later. I could see how much working with the physiotherapist was improving this patient’s functional abilities: between these weeks, he went from having difficulties with transferring with assistance to grasping the handrails well enough to support their weight and transfer mostly independently. The patient sometimes missed their other appointments because of their pain levels but would never skip psychotherapy because they felt it was directly supportive of their pain management and recovery.
Importance of early movement in SCI
SCI is the fracture, dislocation, or compression of a vertebra, disk, or ligament of the spinal column or impingement of spinal cord nerves due to a car crash, fall, infection, or lack of blood supply. In 2010, 85,556 Canadians had SCI (Noonan et al., 2012). As I learned on my experience in PMR, physiotherapy is a mainstay of the treatment of SCI. Physical rehabilitation has been shown to improve functional independence (activities of daily living [ADLs]): ability to transfer, mobilize, eat, toilet, bathe, and dress one’s self) and the American Spinal Injury Association (ASIA) motor score (Sumida et al., 2001).
The current care guidelines outlined by the American Association of Neurological Surgeons/Congress of Neurological Surgeons recommendation that early treatment is the most controllable important factor in treating SCI (Ahuja
et al., 2017). Early treatment can include early detectiona and diagnosis by imaging, priority transfer to specialized centre, fast decompressive surgery, blood pressure management, and prescription of methylprednisolone. The long-term outcomes associated with early treatment include improvement in the American Spinal Injury Association Impairment Scale rating (Hachem et al., 2017; Sharif & Jazaib Ali, 2020). This concept has been coined “time is spine”. This concept also appears to apply to physical rehabilitation as subgroups that begin rehabilitation earlier have better functional and motor outcomes for their ADLs at 6 months post-treatment (Sumida et al., 2001).
How to get to early movement after SCI
There are many ways to achieve early movement therapy in SCI patients. For example, one randomized clinical trial identified significantly superior improvement in the Walking Index for SCI-II and Functional Independence Measure (FIM) scores when participants received roboticassisted gait training compared to standard physiotherapy (Yıldırım et al., 2019). However, implementing these supports isn’t practical at every rehabilitation program due to the financial cost.
In interacting with the patients on the PMR wards, they anecdotally reported that their most significant barriers to early movement were pain and anxiety. The literature supports these anecdotes. SCI is debilitating as it can compromise a patients’ independence due to muscle paralysis, loss of bladder/bowel control, recurrent urinary tract infection, pressure injury, autonomic dysregulation, among others. The severe disability associated with SCI can result in loss of employment (Nas et al., 2015). This lack of independence, functional limitation, chronic pain, and psychosocial/financial burden contributes to a higher rate of mental health problems (48.5%) and clinical stress (25%) in SCI
patients (Migliorini et al., 2008). Stress negatively impacts recovery from SCI (Maldonado Bouchard & Hook, 2014) and interferes with functional gains and quality of life.
Given that the stress of pain and anxiety are barriers to accessing movement, decreasing them should improve access to physiotherapy and, in turn, improve outcomes. Additionally, while physical rehabilitation is essential to address functional deficits after a traumatic injury like SCI, psychological factors also affect recovery in and of themselves (Vincent et al., 2015). SCI patients who learn coping skills from occupational therapists (Pillastrini et al., 2008) have better rehabilitation outcomes (Krupa et al., 2009). Other stress-reduction therapies, like mindfulness meditation (MM), may improve rehabilitation by reducing pain to enable patients to do rehabilitation/movement earlier.
Support for mindfulness as a tool to get moving after SCI
MM is a meditation practice focused on acknowledging the present (Brown & Ryan, 2003). MM has been used as an adjuvant treatment in many populations such as patients with fibromyalgia (Goldenberg et al., 1994; Kaplan et al., 1993), cancer (Carlson et al., 2001; Lengacher et al., 2009; Speca et al., 2000), and addiction (Goldberg et al., 2018). MM is an effective treatment, on par with cognitive behavioural therapy (CBT) and better than pharmacologic treatment, for reducing stress (Irving et al., 2009) and improving anxiety and depression (Khoury et al., 2013). MM was shown to reduce the rating of thermal pain experience in a dosedependent manner (Zgierska et al., 2016) and increase pain tolerance of sports injuries (Mohammed et al., 2018). Preliminary research proposed that MM works mechanistically to improve physical health by training stress-resilience neural pathways (Creswell et al., 2019) and decreasing pain rumination (Gu et al., 2015).
The literature supports that MM can reduce pain and improve therapeutic outcomes in a patient model similar to SCI: chronic lower back pain (CLBP). For CLBP patients, MM increased pain acceptance (Esmer et al., 2010; Morone et al., 2008; Randolph et al., 1999) and decreased pain perception and functional disability for up to 1 year compared to a wait-list control (Morone et al., 2009) and on par with CBT (Cherkin et al., 2016). Yet, on the contrary, other research shows no short or long-term benefits of therapeutic use of MM to CLBP or back-related disability (Esmer et al., 2010; Morone et al., 2008). In another population distinct from SCI, but with some shared qualities is orthopedic trauma patients. Research on orthopedic trauma suggests that early treatment of stress after injury with holistic approaches, pastoral care, coping skills, peer visitation, educational resources, and mindfulness improves short-term patient outcomes (Vincent et al., 2015). I am researching whether MM can reduce pain and stress and improve
QOL and mental health in SCI patients. Further research may investigate whether the use of MM in an inpatient setting improves early access to physiotherapy and physical function to increase movement after SCI. ⚚
References
Ahuja, C. S., Schroeder, G. D., et al. (2017). Spinal Cord Injury-What Are the Controversies? Journal of Orthopaedic Trauma, 31 Suppl 4, S7–S13.
Bamber, M. D., & Kraenzle Schneider, J. (2016). Mindfulness-based meditation to decrease stress and anxiety in college students: A narrative synthesis of the research. Educational Research Review, 18, 1–32. Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848.
Carlson, L. E., Ursuliak, Z., et al. (2001). The effects of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients: 6-month follow-up. Supportive Care in Cancer: Official Journal of the Multinational Association of Supportive Care in Cancer, 9(2), 112–123. Carmody, J., & Baer, R. A. (2008). Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31(1), 23–33.
Cherkin, D. C., Sherman, K. J., et al. (2016). Effect of Mindfulness-Based Stress Reduction vs Cognitive Behavioral Therapy or Usual Care on Back Pain and Functional Limitations in Adults With Chronic Low Back Pain: A Randomized Clinical Trial. JAMA, 315(12), 1240–1249.
Cramer, H., Haller, H., et al. (2012). Mindfulness-based stress reduction for low back pain. A systematic review. BMC Complementary and Alternative Medicine, 12, 162.
Creswell, J. D., Lindsay, E. K., et al. (2019). Mindfulness Training and Physical Health: Mechanisms and Outcomes. Psychosomatic Medicine, 81(3), 224–232.
Eberth, J., & Sedlmeier, P. (2012). The effects of mindfulness meditation: A meta-analysis. Mindfulness, 3(3), 174–189.
Esmer, G., Blum, J., et al. (2010). Mindfulness-based stress reduction for failed back surgery syndrome: A randomized controlled trial. The Journal of the American Osteopathic Association, 110(11), 646–652. Goldberg, S. B., Tucker, et al. (2018). Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clinical Psychology Review, 59, 52–60.
Goldenberg, D. L., Kaplan, et al. (1994). A controlled study of a stress-reduction, cognitive-behavioral treatment program in fibromyalgia. Journal of Musculoskeletal Pain, 2(2), 53–66.
Gu, J., Strauss, C., et al. (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37, 1–12.
Hachem, L. D., Ahuja, C. S., et al. (2017). Assessment and management of acute spinal cord injury: From point of injury to rehabilitation. The Journal of Spinal Cord Medicine, 40(6), 665–675.
Irving, J. A., Dobkin, P. L., et al. (2009). Cultivating mindfulness in health care professionals: A review of empirical studies of mindfulness-based stress reduction (MBSR). Complementary Therapies in Clinical Practice, 15(2), 61–66.
Kaplan, K. H., Goldenberg, D. L., et al.(1993). The impact of a meditation-based stress reduction program on fibromyalgia. General Hospital Psychiatry, 15(5), 284–289.
Keng, S.-L., Smoski, M. J., et al. (2011). Effects of Mindfulness on Psychological Health: A Review of Empirical Studies. Clinical Psychology Review, 31(6), 1041–1056.
Khoury, B., Lecomte, T., et al. (2013). Mindfulness-based therapy: A comprehensive meta-analysis. Clinical Psychology Review, 33(6), 763–771.
Krupa, T., Fossey, E., et al. (2009). Doing daily life: How occupational therapy can inform psychiatric rehabilitation practice. Psychiatric Rehabilitation Journal, 32(3), 155–161.
Lengacher, C. A., Johnson‐Mallard, V., et al. (2009). Randomized controlled trial of mindfulness-based stress reduction (MBSR) for survivors of breast cancer. Psycho-Oncology, 18(12), 1261–1272.
Maldonado Bouchard, S., & Hook, M. A. (2014). Psychological Stress as a Modulator of Functional Recovery Following Spinal Cord Injury. Frontiers in Neurology, 5.
Migliorini, C., Tonge, B., et al. (2008). Spinal cord injury and mental health. The Australian and New Zealand Journal of Psychiatry, 42(4), 309–314.
Mohammed, W. A., Pappous, A., et al. (2018). Effect of Mindfulness Based Stress Reduction (MBSR) in Increasing Pain Tolerance and Improving the Mental Health of Injured Athletes. Frontiers in Psychology, 9, 722.
Morone, N. E., Greco, C. M., et al. (2008). Mindfulness meditation for the treatment of chronic low back pain in older adults: A randomized controlled pilot study. Pain, 134(3), 310–319.
Morone, N. E., Rollman, B. L., et al. (2009). A mind-body program for older adults with chronic low back pain: Results of a pilot study. Pain Medicine (Malden, Mass.), 10(8), 1395–1407.
Nas, K., Yazmalar, L., et al. (2015). Rehabilitation of spinal cord injuries. World Journal of Orthopedics, 6(1), 8–16.
Noonan, V. K., Fingas, et al. (2012). Incidence and Prevalence of Spinal Cord Injury in Canada: A National Perspective. Neuroepidemiology, 38(4), 219–226.
Pillastrini, P., Mugnai, R., et al. (2008). Evaluation of an occupational therapy program for patients with spinal cord injury. Spinal Cord, 46(1), 78–81.
Randolph, P., Tacone, T., & et al. (1999). The long-term combined effects of medical treatment and a mindfulness-based behavioral program for the multidisciplinary management of chronic pain in West Texas. 9, 103–112.
Schellekens, Melanie. P. J., et al. (2017). Mindfulness-Based Cancer Recovery (MBCR) versus Supportive Expressive Group Therapy (SET) for distressed breast cancer survivors: Evaluating mindfulness and social support as mediators. Journal of Behavioral Medicine, 40(3), 414–422.
Sharif, S., & Jazaib Ali, M. Y. (2020). Outcome Prediction in Spinal Cord Injury: Myth or Reality. World Neurosurgery, 140, 574–590.
Slocum, C., Shea, C., et al. (2020). Early Trauma Indicators and Rehabilitation Outcomes in Traumatic Spinal Cord Injury. Topics in Spinal Cord Injury Rehabilitation, 26(4), 253–260.
Speca, M., Carlson, L. E., et al. (2000). A randomized, wait-list controlled clinical trial: The effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosomatic Medicine, 62(5), 613–622.
Sumida, M., Fujimoto, M., et al. (2001). Early rehabilitation effect for traumatic spinal cord injury. Archives of Physical Medicine and Rehabilitation, 82(3), 391–395.
Vincent, H. K., Horodyski, M., et al. (2015). Psychological Distress After Orthopedic Trauma: Prevalence in Patients and Implications for Rehabilitation. PM & R: The Journal of Injury, Function, and Rehabilitation, 7(9), 978–989.
Yıldırım, M. A., Öne‐, K., et al. (2019). Early term effects of robotic assisted gait training on ambulation and functional capacity in patients with spinal cord injury. Turkish Journal of Medical Sciences, 49(3), 838–843. Zgierska, A. E., Burzinski, C. A., et al. (2016). Mindfulness Meditation and Cognitive Behavioral Therapy Intervention Reduces Pain Severity and Sensitivity in Opioid-Treated Chronic Low Back Pain: Pilot Findings from a Randomized Controlled Trial. Pain Medicine (Malden, Mass.), 17(10), 1865–1881.
Anti-Intellectualism in Medicine
Written by Imran Syed, Meds ‘25
Passing through Ottawa on a weekend in late January, 2022, I was overwhelmed by the loudness of horns that could be heard all the way down the Rideau Canal where we were skating. As it turns out, the so-called “Freedom Convoy” had attracted a larger than expected turnout, spanning multiple days. This convoy, which initially aimed to reverse a single federal policy, had eventually cascaded into a large demonstration of people with a list of policy demands, including the reversal of any COVID-19 regulations and removal of the Prime Minister. For Canadians, I worry of the long-term social repercussions, not just of this convoy, but of the influencing trends.
“So how will you deal with anti-intellectualism in your career?” I was taken back when someone asked me this past summer, as I awaited the start of medical school. While it may not be a movement inherent within medicine, antiintellectualism presents a growing barrier and challenge for healthcare workers, physicians included, in providing patient care. How then should our community navigate changing landscapes in patient care with this new variable?
What is anti-intellectualism?
Anti-intellectualism can be defined as “the generalized distrust of experts and intellectuals” and can explain how the public engages the advice it receives from physicians and other scientists.1 It is important to understand this concept, as trust in these institutions can be particularly important during public health crises, such as the current COVID-19 pandemic.
How extensive is this issue?
The trucker’s convoy is but one of among many overt examples of this trend. This convoy followed many Ontariobased demonstrations for “anti-vax”, “anti-masking”, and “anti-mandate” aimed at Queen’s Park throughout 2020 and 2021.2 Similarly, there was the famous disobedience by Adamson Barbecue, a small Etobicoke based restaurant that refused to close indoor dining when public health warranted so in early 2021.3 Many of the above have garnered growing support, throughout the pandemic; for example, the trucker’s convoy raised over $10 million dollars in financial support on Gofundme, before the parent site shut down their campaign.4
Even within medicine, anti-intellectualism can be problematic. Famously, was the episode where President Donald Trump cited a fringe scientist, Dr. Stella Immanuel, instead of the majority of the scientists at the time, with regards to use of hydrochloroquine to treat COVID-195, which was determined to be unproven in effectiveness and potentially dangerous, leading to increased mortality.6 This public relations incident was soon followed by multiple accidental deaths by those opting to self-treat using the drug.7
But beyond overt examples, anti-intellectualism and its sub-trends can be problematic for common pro-health habits that affect the lives of physicians and their patients. For example, anti-intellectualism was found to be associated with poor adherence to mask usage and social distancing among Canadians, in addition to altered perceptions of COVID-19 related news, according to one study published in Nature.8
Unsurprisingly, there is a lack of physician practice guidelines for dealing with anti-masking, vaccine hesitancy or any other trends that result from anti-intellectualism, but perhaps there should be. Chou and Benudenz (2020) for example, recommend that physicians attenuate to patient fears and anxieties, disarm the the emotional manipulations poised by anti-vaccine disinformation efforts, and inspiring positive affirmations, such as hope and altruism to bolster vaccine education endeavours.9
Similarly, writers for the American Medical Association recommend education, monitoring social media for disinformation, and emphasizing ethical responsibility in an effort to encourage vaccination among healthcare workers and offer similar advice for vaccine hesitant patients.10,11
Anti-intellectualism is indeed a modern-day social movement: one that many of us in the medical community will hold in peril for the foreseeable future. While there are many unfortunate social effects of the pandemic, I believe that continuous politicization of our profession is probably one of the more regrettable ones that many medical students and physicians would rather not have to deal with. Regrettably, like anti-intellectualism, this is just another trend we may have to deal with for years to come. ⚚
References
1. Merkley, E., & Loewen, P. J. (2021). Anti-intellectualism and the mass public’s response to the COVID-19 pandemic. Nature Human Behaviour, 5(6), 706-715.
6. Axfors, C., Schmitt, A. M., Janiaud, P., van’t Hooft, J., Abd-Elsalam, S., Abdo, E. F., ... & Hemkens, L. G. (2021). Mortality outcomes with hydroxychloroquine and chloroquine in COVID-19 from an international collaborative metaanalysis of randomized trials. Nature communications, 12(1), 1-13.
8. Merkley, E., & Loewen, P. J. (2021). Anti-intellectualism and the mass public’s response to the COVID-19 pandemic. Nature Human Behaviour, 5(6), 706-715.
9. Chou, W. Y. S., & Budenz, A. (2020). Considering emotion in COVID-19 vaccine communication: addressing vaccine hesitancy and fostering vaccine confidence. Health communication, 35(14), 1718-1722.
This commitment to honoring racial diversity is not exceptionally illustrated in medical school, faculties, and government ministries.
Written by Meghan Jenkins, Meds ‘25
Canada’s diversity is often celebrated as a global success story because its citizens come from many countries of origin and cultural backgrounds. Justin Trudeau commented that “[Canada’s] commitment to diversity and inclusion isn’t about Canadians being nice and polite—though, of course, we are. In fact, that commitment is a powerful and ambitious approach to making Canada, and the world, a better, and safer, place.”
According to the 2016 Census, 37.5% of the total population of Canadian children were born outside of Canada or had at least one parent born outside Canada. This population will likely grow to between 39.3% and 49.1% of the entire population of children aged 15 and under in 2036. In 2011, 47% of individuals in Toronto identified as a visible minority. The diversity of Canada’s population is both beautiful and promises, as Trudeau pointed out, “a better, and safer, place.”
Despite Trudeau’s proud words and these details, this commitment to honoring racial diversity is not exceptionally illustrated in medical schools, faculties, and government ministries. Division heads and faculty members at Canadian medical schools are primarily Caucasian and predominantly male, and presented material is typically demonstrated on Caucasian patient examples. Despite this systemic example of racism, a group of racially aware Queen’s medical students noticed the problem and set to find how deep it ran. Iku Nwosu (Meds’ 22), Aquila Akingbade (Meds’ 22), Shakira Brathwaite (Meds’ 21), and Eric Zhang (Meds’ 23) reviewed pre-clerkship learning materials and found 90% of lectures discussing skin conditions to use only images of white skin. Bringing this information to the Queen’s Medical faculty’s attention, professors found that the lack of skin tone variety was due to inaccessibility to diverse media.
As a solution, Nwosu, Akingbade, and Zhang spearheaded an initiative that mobilized resources acquired through VisualDX with the help of Michelle Gibson, Queen’s Medicine’s Assistant Dean. This promising commitment opened the conversation of decreased skin cancer identification in patients of racial minorities, and the higher proportion of Black people who are likely to die from the disease due to diagnosis at a much more lethal stage, according to Akingbade. Recognizing this, promoting resources such as the ‘Mind the Gap’ handbook—a highlighting series of clinical dermatological signs in ethnic minorities—and VisualDX should be further emphasized in preclerkship education at Queen’s and beyond.
With a better representation of Canada’s diversity in provided medical teachings, the care of our diverse population will indeed encourage Canada’s progression towards “a better and safer place.” ⚚
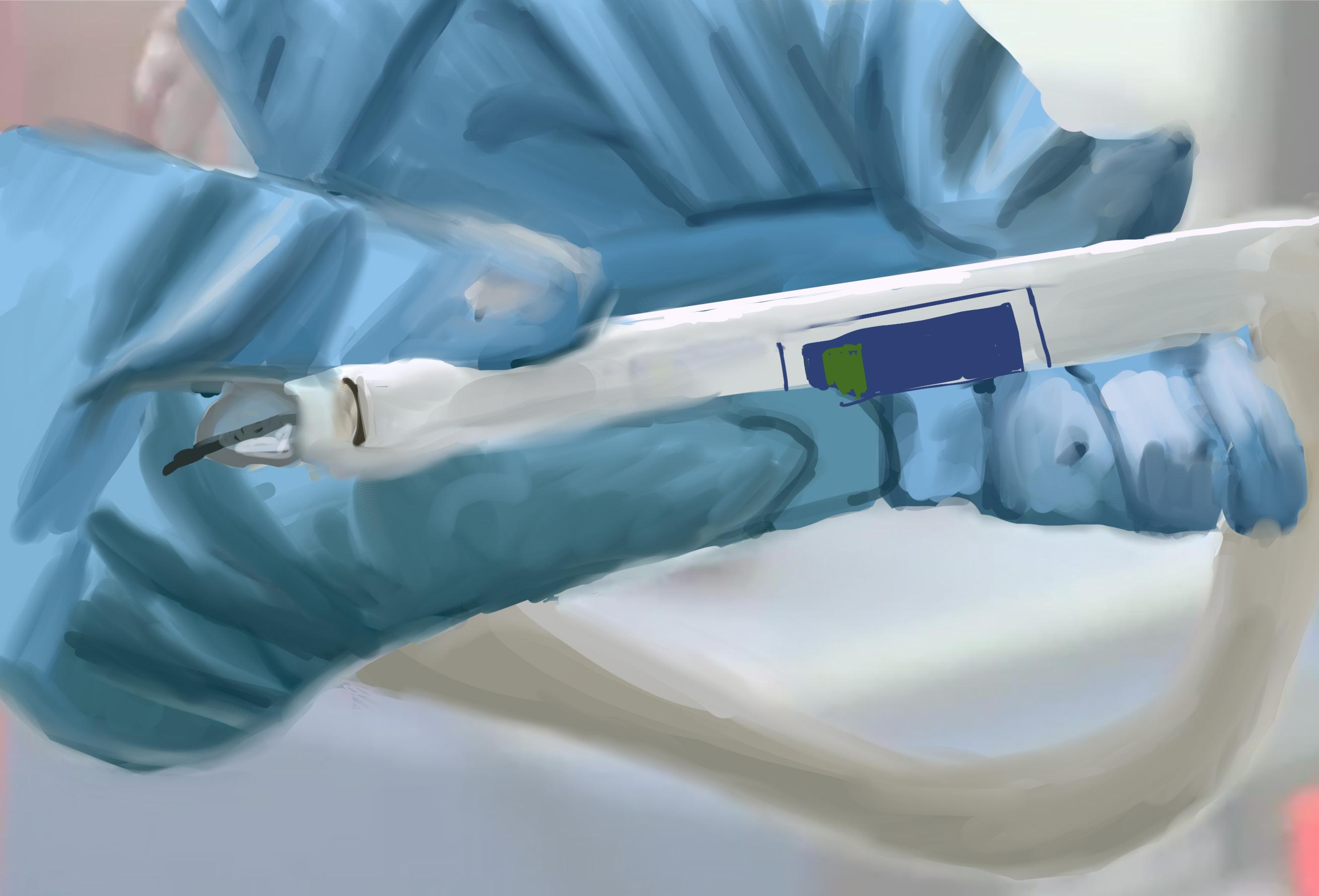
The Cutting-edge of Cancer Introducing the iKnife
Written by Kaitlyn Rourke, Meds ‘23
Artwork by Kailtyn Rourke, Meds ‘23
Surgery to remove cancer from healthy tissue is extremely challenging. It is necessary to remove all the cancer — even a small amount left can cause recurrence. However, it is difficult for the surgeon to distinguish cancer from healthy tissue. The iKnife is a cutting-edge (pun intended) solution to the issue: it analyzes the tissue as it cuts, informing the surgeon as to whether there is any cancer left. The device was invented in 2010 by Zoltan Takats, and has been used in cervical, ovarian, breast and colon cancer. It was Dr. Zoltan who brought the iKnife to Kingston, where its potential was immediately realized. The iKnife is currently being researched by the Department of Surgery in Kingston, led by surgical oncologist Dr. Jay Engel. The iKnife is a product of technology and innovation, with a real and significant potential to improve patient outcomes
The iKnife exploits the principle that cancer tissues express different molecules than healthy tissue. The handle of the iKnife contains a mass spectrometer. A mass spectrometer is a molecular analysis that creates unique ‘fingerprint’ readouts for every molecule. Due to the unique molecular composition of cancer, the mass spectrometer creates a different fingerprint for cancer cells than healthy tissue. However, mass spectrometry requires vaporized and ionized substrates, creating a challenge when analyzing human tissue, which is electrically neutral and solid.
The iKnife ingeniously solves this issue. The “knife” component of the tool is a form of electrocautery. Electrocauterization is a method of cutting tissue that uses heat, produced by an electric current, to simultaneously coagulate the small vessels, minimizing operative blood loss. Electrocautery accomplishes two tasks that aid the iKnife. First, the heat transforms some of the tissue to gas (which can normally be smelt by everyone in the OR), and
second, the electricity ionizes the tissue. Thus, the perfect substrate for mass spectrometry is created. The ionized vapor enters the tube of the knife, where it is analyzed in less than a tenth of a second.
The final step of the iKnife is analysis by the built-in software. This software contains the molecular readouts of numerous types of tissue (breast, cervical, skin, fat), as well as numerous types of cancer. The software matches the sample tissue to one in the database. Within 10 seconds, it can present the result to the surgeon, with an identification accuracy of higher than 92%. Moreover, this accuracy is consistent with identifying ovarian cancer, breast tumor and colorectal cancer from the healthy counterpart.
The iKnife is a game-changer for surgical oncologists. Using the iKnife reduces the chance of leaving cancer behind, which would previously require a new operation. “
The iKnife is a game-changer for surgical oncologists. Using the iKnife reduces the chance of leaving cancer behind, which would previously require a new operation. For patients, this is heartbreaking news. Dr. Engel explains, “[the surgeons] were all motivated by years of frustration of sitting down with the patient and saying, well we didn’t get it all.” Along with reducing the need for a second operation, the iKnife cuts out the need for a pathologist to analyze the tissue, reducing the length of time the operation takes. In the current Canadian healthcare climate, this is especially important as OR time is limited to reduce COVID-19 transmission. ⚚
Cancer Research:
rise and fall
Written by Ivneet Garcha, Meds ‘24
Artwork by Sigi Maho, Meds ‘24
These pieces were inspired by the theme ‘Movements’. Love is both moving and halting. It can bring us forward or hold us back.
This two poem ‘couplet’ describes the rise and fall of a budding relationship that never reaches full bloom. The prose is meant to entangle the reader in juxtaposition; the rise of the relationship encapsulated by the consuming feeling of falling in love, and the fall of the relationship captured by the slow rise to self-realization.
The transitions from union to separation to selfawareness are also visualized through contrasting imagery, shifts in tone, and the physical structures of
Falling
the poems. As the narrator moves through each phase, so too the landscapes move with them. You can see this shift most strikingly at the end of ‘Falling’ and beginning of ‘Rising’, as the narrator climbs to new heights, only to ultimately come down to a new grounded sense of self.
Where the spacing in Falling is written to emulate the visceral cascade into a state of love, it also structurally imitates the visual appearance of a fresh rain fall. Similarly, Rising is structured to show the highs and lows the narrator navigates before finding their path to a new sense of self. But most importantly, in finding their compass, they find direction and bring you on this journey with them. ⚚
Like still waters to raging monsoons, Like waterfalls rising from calming lagoons, When the rainfall falls, I fall too.
Free fall, free falling. Keep falling for you. And,
It’s rhythmic raindrops like irregular heartbeats, Precipitate pitter patter on concrete set streets. Drizzling downpour in soaking wet sheets, Send shivers down spines, stories that fleet.
Like the weathering weather, we’ve weathered before. Like settling ships, returning from unsettling wars.
Like the rumbling thunder of great lion’s roar, I am a swimming brown ocean, reaching your shores.
Like fiery first suns from longing last moons, Like melodious midnights to whimsy warm noons, When sunbeams beam, I beam too.
Beaming, still beaming Beaming for you.
Sometimes,
Even brimming beams don’t reach hilltops, The sun rises to summits, but at summits it drops. Like the far cry of a raven, distance echoes in speech. Silent heights grow to cliff faces, but cliff faces birth new peaks.
And I know now,
Moving you, Is like moving mountains.
From roaring river mouths to stoic stone faces, Rocks and boulders, sprouting between hard places. When a tall tree falls, birds fly to new spaces. Even suns die, and a new son replaces.
Kicking up settled dust to make up lost ground.
A mother moves roots to where richer soils are found. Even seedless seeds sown, where once drowned. Can find new terrain, budding flowers abound.
Soaring self-ascension, in dissent I rise. Finding new life growing, where an old life left to die. Finding vision in new viewpoints, like the eagle, hawk’s eye. For you, I would have parted a thousand ocean tides.
The ebb of bodies flow in and out
While the door pulses its own beat
Amongst hands that beat its handle
flow
One after another the machines speak Hoping to cause a scandal
There’s movement within a room, without a room
Emotion flowing in between
The crying, the laughing, the gagging, the silent The crunch and swish of the garbage and broom
An ever-moving scene
And I stood within it
Trying to understand
The dance that seemed ages old
The dance I was learning
The dance I am learning
Written by Grace Lin, Meds ‘23
Artwork by Suffia Malik, Meds ‘24
moving mountains
Written by Devyani Premkumar, Meds ‘25
Artwork by
Sigi Maho, Meds ‘24
we move mountains for the ones we love ignore the burning in our legs the sweat building on our back
we stop the storms from creating floods push and pull of the rain no more rope giving us slack
stillness and silence, you try to avoid keep your world spinning you don’t give yourself a choice
for others, you try to do your best but who, is lifting the mountain weighing heavy on your chest?
As learners, there is a monumental expectation, partly one we put on ourselves, to move mountains. There can be a great deal of emotions we associate with this, ones not always so pleasant. To anyone who has graciously taken the time to read these words, I hope you know that it is ok to breathe. To pause on your trek and understand that not every mountain was made to be moved. There are some people who you may never please. There are some goals that may feel out of reach. This is not me telling you to give up. Some journeys are worth it. But you can only complete them if you cut yourself some slack, ask for the right help, and enjoy your climb along the way.
*cue
“It’s the Climb” by Miley Cyrus* ⚚
Moving Forward and
Nyssa Sharp, 2015
and Moving Onwards: A Study of Grief
Written by Helen Lin, Meds ‘25
Thesaurus dot com shows 72 associated words for grief that range from bereavement and despair to melancholy and misery. Yet there is no one word for the concept of moving on from grief. Grief is not a physical symptom in the literal sense, it’s an emotion. But how is it that we can feel such powerful physical symptoms of grief that parallel the butterflies we feel when we’re in love?
When I was younger, the concept of grief and death were obscure and intangible. As a child I had no reason to consider death and all its implications, until one day, a teacher in the second grade asked us to write a brief reflection on our summer. A girl in our class, Rachel, who was incredibly gifted and intelligent for her age, volunteered to read to the class what she had written. It was a moving tale about the loss of her uncle over the summer, and how challenging it was for her to process and understand what was taking place. Most people would consider children to be oblivious to grief, unable to truly grasp the finiteness of death. But for Rachel to express, and so eloquently, her inner struggle at the age of eight made a lasting impression on me to this day. Not only was it very impressive but also extremely courageous to share such vulnerability at her age. It begs the questions of whether we are truly able to process grief better as adults and how exactly we’re able to do so, physically and emotionally.
How is it that we can feel grief so viscerally? Can these visceral reactions become physical symptoms that affect our health? Early research has shown that grief, especially traumatic grief, can be associated with a variety of poor outcomes.1 Inflammatory markers have been shown to distinguish between higher and lower grief severity in bereaved spouses, indicating that inflammation is an important marker for elevated levels of depression.2 Bereaved survivors have also been shown through research to have higher mortality rates than control participants from cardiovascular disease and infectious disease.3 In what is termed Normative Grief, non-pathological grief is characterized by a mixture of physical, cognitive, psychological, and spiritual symptoms that can intensify suffering.3 Common physical symptoms to the loss
of a loved one can include shortness of breath, tightness in the throat, feeling of emptiness and heaviness, physical numbness, feeling outside one’s body, muscle tension, body aches, headaches, dizziness, nausea, gastrointestinal problems and heart palpitations.3 Normative grief can also cause perceptual disturbances such as visual and auditory hallucinations, impaired memory, slowed disorganized thinking and constant worry.3
We cannot ignore the psychological toll that grief can play on our mental wellbeing. Guilt and depression are symptoms commonly experienced while processing grief, although it is important to note that psychologists have distinguished Major Depressive Disorder from the newly recognized disorder of Complicated
Photograph by K. Mitch Hodge on Unsplash
Grief. In many with complicated grief, where bereaved individuals continue to experience maladaptive reactions and psychiatric symptoms that don’t improve with time, these feelings of loss are debilitating.3 In a study by Li et al., guilt was found to be significantly associated with depression and complicated grief in Chinese populations.4 They also found that responsibility guilt, indebtedness guilt, and degree of guilt feeling were more prominent aspects of guilt in complicated grief than in depression.4 Other symptoms related to depression from grief include feeling sad or low, withdrawing from friends and family, an
inability to focus or make decisions, and even thoughts of suicide.3
But how do we move on from these feelings? From loss? This is where most people would agree that the process of recovering from loss is highly individual and doesn’t follow a predictable course. Factors that influence grief and bereavement have to do with the nature and circumstances of the loss, the relationship with the deceased, and the characteristics of the bereaved.3 We’re all familiar with the five stages of grief or the KublerRoss model, whether it be in a comical
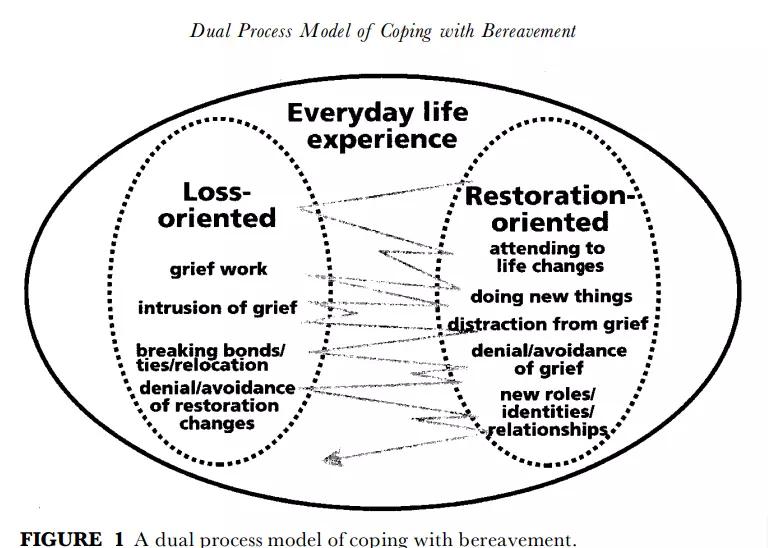
sense or the literal sense. This model is considered outdated and inaccurate. However, Margaret Stroebe & Henk Schut developed a theory in 1995 called the Dual Process Model of Coping with Bereavement that challenges the more common stages (Figure 1). This model identifies two types of stressors, loss- and restoration-oriented, and describes a dynamic, regulatory coping process of oscillation whereby the grieving individual at times confronts, at other times avoids, the different tasks of grieving.5 The model proposes that adaptive coping is composed of confrontation– avoidance of loss and
but we move forward with loss
Figure 1. A dual process model of coping with bereavement.
restoration stressors.5 It also argues that the need for dosage of grieving, that is, the need to take respite from dealing with either of these stressors, as an integral part of adaptive coping.5 Stroebe & Henk agree that the reality of loss needs to be confronted, but not relentlessly.5
Stroebe & Henk refer to the Loss-Oriented portion of their model as the grief work that focuses on the relationship with the deceased person which involves rumination, yearning, crying. They describe the emotions as coming and going, sometimes unwilled and unexpected. In the early days, negative affect predominates, but as time goes on, positive affect plays a larger role in the recovery process. Stroebe & Henk do not propose a sequence of stages, but rather a waxing and waning, an ongoing flexibility, over time. The Restoration-Orientation portion focuses on how the loss is dealt with whether it be dealing with new arrangements without the loved one or taking on a new role from “spouse” to widower”. These new experiences will inevitably cause stress and anxiety but can also come with a myriad of emotional reactions from relief and pride over the new skills learnt. In short, the central component of the model is the oscillation between the two portions. Stroebe and Henk suggest that at times the bereaved will be confronted by their loss and other times they will avoid memories and be distracted or seek relief from other things. Over time, habituation will have taken place, and the bereaved will have weakened reactions to the loss.
When I think of grief, I inadvertently associate it with the death of my maternal grandfather. Undoubtedly it was the first experience of intense grief I’ve had which made it so much more impactful and long-lasting in my mind. I certainly experienced many of the symptoms I’ve mentioned previously, most of which was guilt. I felt guilt over the lack of time I had to spend with him. I felt guilt over the many questions I never got to ask him. I felt guilt over the way he would sit outside my kindergarten in the snow for hours on end to reassure four-year-old me, poking my head out the window, that I was not alone when we first moved to Ottawa. These memories often bring on a nostalgic wave of grief. I find myself agreeing with Stroebe & Henk, that grieving is a dosing process. I imagine it like a spoonful of medicine being gulped down periodically when something triggers a memory in you. It brings about the heart palpitations and the tightness in the throat. Mary Poppins once said: a spoonful of sugar makes the medicine go down. My memories do taste bittersweet in the moment, and sometimes I do find myself oscillating between pain and joy. But like droplets of paint swirling down a sink, they tend to blur after a while.
Confronting loss is challenging. Maybe that’s why we don’t move on from loss, but we move forward with loss. However, it doesn’t always have to be painful; it can be bittersweet. Interestingly, thesaurus dot com only has four synonyms for bittersweet. ⚚
1. Prigerson HG, Bierhals AJ, Kasl SV, Reynolds CF, Shear MK, Day N, Beery LC, Newsom JT, Jacobs S. Traumatic grief as a risk factor for mental and physical morbidity. American journal of psychiatry. 1997 May 1;154:61623.
2. Fagundes CP, Brown RL, Chen MA, Murdock KW, Saucedo L, LeRoy A, Wu EL, Garcini LM, Shahane AD, Baameur F, Heijnen C. Grief, depressive symptoms, and inflammation in the spousally bereaved. Psychoneuroendocrinology. 2019 Feb 1;100:190-7.
3. Strada EA. Grief, demoralization, and depression: Diagnostic challenges and treatment modalities. Primary psychiatry. 2009 May 1;16(5):49.
4. Li J, Tendeiro JN, Stroebe M. Guilt in bereavement: Its relationship with complicated grief and depression. International Journal of Psychology. 2019 Aug;54(4):454-61.
5. Schut MS. The dual process model of coping with bereavement: Rationale and description. Death studies. 1999 Mar 1;23(3):197-224.
a waxing and waning, an ongoing flexibility, over
loss
Rainbow Roads
On the importance of accompaniment with our LGBTQ+ patients
Written by Joseph Sanfilippo, Meds ‘22
Artwork by Fiona Raymond, Meds ‘23
Some 15 years ago, in the mid2000s, I went to an intake appointment with my new family physician. I was a typical teenager in many ways. I slouched in my chair and probably stared at the floor for much of the visit. My new doc asked me the standard new-patient questions, and we started by walking through medical history, family history, medications, and allergies. After a few minutes, we arrived at social history, and he asked
a question that to him probably felt like a perfectly innocuous question to ask a teenage boy: “Do you have a girlfriend yet?”. I looked up and felt a twinge of panic. The question was a fork in the road, and I suspected we were about to go down separate paths.
“No,” I answered.
It was the truth, but it wasn’t the whole truth. In that moment, my mind was
flooded with the kinds of questions that descend on any closeted person whose truth is at risk of being known: Am I safe? If he’s asking about a girlfriend, does that mean he thinks having a boyfriend is unacceptable? Would he treat me differently? Failing to come up with satisfying answers to my mind’s racing questions in this split second, I repeated myself: “No”. I left it at that, and we moved on to diet and exercise.
Ultimately, the conclusion I arrived at was that my physician might not be amenable to an answer that strayed outside the bounds of his question’s underlying assumption. It’s not difficult to imagine the ways in which quality of care could be compromised by this sort of glib gloss-over of a significant aspect of a patient’s life. Indeed, I was this physician’s patient until I moved out of the country several years later, and I never mustered the audacity to revisit his original question.
So, my physician and I walked on separate roads, as it were, throughout our time together.
Part of my motivation to pursue medical school, years later after I had finally stepped out of my closet, was to become the kind of doctor who could and would provide a safe space for
care to those who felt that aspects of their identities made them vulnerable.
If there’s one thing I’ve learned in medical school, it’s that a listening mind is one of the most valuable universal tools we have to offer our patients.
A physical exam may or may not localize a lesion, labs may or may not nail a diagnosis, and medications may or may not confer a benefit, but there is always therapeutic value in accompanying patients and bearing witness to their story. We do them a disservice if we don’t give them every opportunity to be heard and understood.
My final elective rotation of clerkship this winter was at a community pediatrics clinic in rural Ontario with a wonderful pediatrician. What I didn’t know until my first day of the elective is that this pediatrician is known throughout the region for her gender-affirming approach and for providing comprehensive transgender care to youth. As a result, a significant proportion of her patients are transgender adolescents. I couldn’t have asked for a more profound clinical experience to cap off my medical school training, and it was a motivating reminder of the leaps and bounds medicine has made in its approach to LGBTQ+ patients even in the last 15 years.
Given that these patients typically return to the clinic every one to three months for hormone therapy, there are frequent opportunities to check-in with them on how they are doing overall. Many of these patients have reticent family members, and advocacy often begins at the level of the family: modeling appropriate terminology and attending to correct
pronouns, providing education and resources to parents, facilitating constructive means of communication, and reminding patients that they are not responsible for other people’s feelings about their identities. Most of these are remarkably easy things to do, and the frequent opportunities for allyship clearly make a difference in these patients’ lives.
Over the course of my rotation I encountered many of these patients, and I recognized some familiar patterns.
When I first walked into the rooms and introduced myself, I was often met with floor-staring and a familiar skepticism.
I was, after all, an unknown presence. I would ask how school was going. I would ask if things were okay at home. I would ask if they were having any medication side-effects. “Fine,” “yeah,” and “no” – all-too-familiar one-word answers – were the most common responses I received, at first. One particularly reserved transgender teen eventually mentioned to me that
he was unhappy at the fact that he was only 5’6” and might not grow any taller. “I can definitely understand how you might feel disappointed by that,” I told him, “but you know, most of the men in my family are shorter than 5’6”, and I think they would actually be envious of you!”. He looked up and met my eyes for the first time. Seemingly satisfied that I was sincerely on his team, his eyes curved into half-moons, and I was quite certain that there was a relieved smile behind his mask.
Everybody deserves the opportunity to be heard, understood, acknowledged, and accepted for who they are.
As I graduate and move on from Qmed this year, I am grateful to you all for being a part of the movement in medicine that allows a transgender teen to smile in a medical office in rural Ontario, and I hope we will all carry a spirit of compassion, sensitivity, openness, and unreserved kindness with all our patients as we walk the paths of this privileged profession. ⚚
Running a pandemic love story
Written by Amelia Boughn, Meds ‘25
Artwork
by Kiera Liblik, Meds ‘23
Like many runners (28% of them, according to Running Magazine), I am a pandemic convert.
A lifetime ago, in March 2020, just as my competitive hockey career ended, COVID made its entrance into our lives. I was used to spending 4-5 hours a day at the rink, skating, working out, and hanging out with teammates. Then somehow, after almost two decades of playing the game, hockey as I’d always known it was over. Predictably, I had a lot of pent-up energy and no clue what to do with it. So, once the weather warmed and the restrictions eased up, I turned to running. I had run cross-country in high school, but since then hadn’t given the sport much thought. Running, in my mind and the minds of most of my hockey teammates, was something we had to do during the summer to pass fitness testing in the fall. I equated running with the beep test. I didn’t see it as an activity one would engage in voluntarily, and balked at the thought of doing it for fun. But, slowly, somehow, I began to enjoy it. It started with a couple of short runs
a week. Then, working from home last year, I became a morning runner. I began to look forward to every morning before work when, the city still sleeping, I’d lace up my shoes and pace my familiar routes. While the routes were predictable, the sky never was. Each morning brought a new sunrise – cotton candy pinks, brilliant reds, and warm, glowing oranges – to entertain and amaze me; a splash of the unexpected in days otherwise filled with predictably stressful news and a whole lot of Zoom.
I was hooked.
I’d heard from friends that Kingston was a running city, and it didn’t take me long to realize that they were right. I’ve even found some Kingston pals to run with. So, here are my three favourite short to mid-length Kingston routes (starting from Brock and Bagot), for running, walking, cycling, rolling, wheeling, or whatever your favourite form of movement is.
Enjoy!
1. The RMC Loop (6.1 km)
Head down Brock, past city hall, to Ontario Street. Once you get to Ontario, take a left and follow the road as it turns right towards the Causeway. Head across the Causeway (a great spot to watch the sunrise) and then take your first left towards the RMC Memorial Arch. Head through one of the smaller gates on the side of the Arch and continue straight on Valour Drive until you reach a right on Point Frederick Drive. This road will take you on a beautiful stretch along the water, with views of downtown. Eventually, this road will curve left and uphill. Follow it until you reach Precision Drive, then take a right towards the gate that leads back to Highway 2. For an extra couple of kilometers, turn right here and head up the hill to Fort Henry. Once back onto Highway 2, head left towards the Causeway and over the bridge towards downtown.
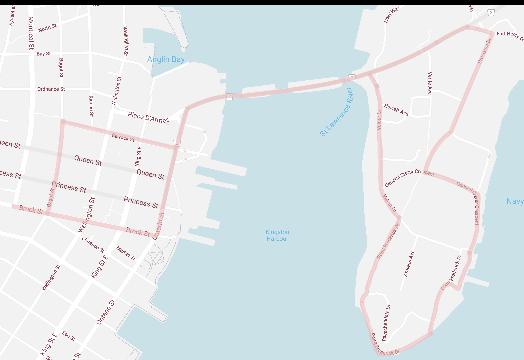
3. The K and P Loop (5.07 km)
Head towards the water on Brock and turn left onto Wellington. Wellington will take you out of downtown and past the Marina to a small park by the water. You’ll see the K and P trail pick up here. Get on the trail and enjoy the beautiful views of the water to your right. There’s also a pretty neat street art exhibit to your left. The trail will take you past the old Woolen Mill, built in 1882. Past the Kingston Rowing Club, the trail turns left onto River Street, then about 100 m later takes a right before it reaches Rideau Street (Note: this path is not accessible for wheels in the winter. For an alternative route take Rideau until it meets Montreal). Travelling parallel to Rideau, the trail pops out again where Rideau meets Montreal. Take a sharp left onto Montreal and follow Montreal back downtown (for a longer run, take a right where the trail heads toward the road and head through the golf course towards Belle Island. I’d recommend doing this with a buddy, as it’s easy to take a wrong turn). ⚚
2. The Waterfront Tour (6.4 km)
Head down Brock towards the water, and hop onto the Waterfront Path in Confederation Park just South of the Delta Hotel. Follow the signs for the path as it takes you out onto Delta’s Walkway, through Battery Park, past the Marine Museum of the Great Lakes, up to King along the edge of City Park, then finally back down to the water by Murney Tower, KGH, and Gord Downie Pier (Note: parts of this path are not accessible for wheels in the winter. As an alternative route, stay on King). At the Peer, turn right up Beverly Street. Follow Beverley (which becomes Victoria), until Brock, then turn left on Brock and head back downtown (which is, thankfully, all downhill).
Rising stars Rising stars
Written by Ivneet Garcha, Meds ‘24
Welcome to another edition of Rising Stars! QMR’s Issue 15.2 is all about Movements. Astrology is all about movements too – the movements of planets, moons, and stars. Having recently survived a Venus AND Mercury retrograde, I am sure we were all propelled into some serious self-reflection about what we
Aries: Aries, you’re so playful. You love to tease and jest, all at the cost of your love interest. Much like the kindergartener who pulls their crush’s hair in a desperate attempt to get their attention, you have yet to master, let alone understand, the not-so-subtle difference between roasting and flirting. You’re genuinely surprised that when you hit your crush from FSGL with “I hate you”, they think you actually do? Shocked and confused. Eventually your simmering passionate side will win them over, but please for once, choose love not violence.
Taurus: You’re steady and romantic, and you take love seriously. Despite being the bull, you’re not one to be charging after red flags. Your ‘grab love by the horns’ mentality actually means that you are purposeful in your choice of partners. You move slow, but once you’ve chosen, that person has you 100%. The problem, Taurus, is you expect that person to be in the bullpen with you 100% too. But for your crush, that bullpen quickly turns into a bull prison as they try and understand why exchanging a few Facebook messages means you’re QMed exclusive. Taurus, if you want to herd your crush towards a commitment, coax them in with your good taste and loyalty. Be a bull, not a bully.
want, or more interestingly who we want. Celestial bodies have a way of making stars align, but how does your sun sign make their love story align?
Read below to see how you’re making your move on that cutie in your interest group exec or how that classmate is making a move on you ;)
Gemini: You’re witty and charming, and always know exactly what to say, how to say it, and to whom. In fact, you wear so many faces, you can seduce just about anyone you want. And honestly, you often do and often succeed. Yesterday, you sent that upper year hottie a Zoom private chat, thinking nothing of it, and a series of messages later, you find yourself exchanging numbers. What a thrill! But things take a dark turn quick. Later that week, you’re aghast when they follow up and ask you to grab coffee? Well, well, well. Look at you, having to deal with the consequences of your own actions. Just because you can make anyone fall in love with you, doesn’t mean you should… unless?
Cancer: When you make a move, it is anything but low stakes. People flirt to flirt; you flirt to marry. You are intuitive, sentimental, and can create a safe home for anyone. But the problem, Cancer, is that when you see a stray, it’s coming back to that home whether it should be there or not. You’ll gladly take the string of red flags your crush is displaying, sew them into a cape, toss it over them, and claim that as your own personal hero. Your desperate attempt to save a relationship that will definitely end, only ends up in your friends having to save you. So do us all a favour, choose right and swipe left on that upper year you know isn’t looking for anything serious.
Leo: You love love. You are passionate and demonstrative. And so you need your QMed love interests to reciprocate that energy. When it comes to love languages, you love physical touch, but really your favourite kind of strokes, are strokes of your own ego. Your first impression is less about the person, and more about how much you can talk up the INCREDIBLE, PASSIONATE, STUNNING person that you are. In fact, you know that the partner that compliments you, is literally the partner that compliments you. And if they’re not going to do it, you can bet you’re going to do it yourself.
Capricorn: You might be the GOAT, but your crush has you feeling like a silly billy. Not that they would ever know. Even though you are a stable, direct, and loyal lover, you’re not one to readily express how you feel. When you ask out that impressive classmate who’s gunning for that competitive speciality, you know you’ve found your match. Your career is your first love, but you’ve finally found someone who makes you want to put love first (some of the time). Have to start calling you CapriCORNY.
Scorpio: *STARES AT CRUSH* Is the intent seduction or murder? Your crush will never know, Scorpio. Dark, dangerous, mysterious. Your crush is scared. I’m scared. Honestly, all of QMed is scared. And that’s exactly how you want it to be.
Sagittarius: Sagittarius, everyone knows you as the archer. But really you’re more your own personal Cupid. You’re firing that arrow, shooting that shot, and 16 times out of 10, you’re hitting the target of your affections with a direct and playful energy that leaves them… wounded. You’re confused why they can’t just keep it chill. You didn’t ask them to pour their heart out to you. They have a crush on you?? You’re embarrassed for them. You thought it was abundantly clear that you were just having fun. You’re WAY too young to be that serious. People should realize Cupid is a literal baby after all.
Virgo: *stares at crush* Virgo, you’re so in love. You’re so devoted. You are nurturing and kind and genuinely have all the makings for the perfect partner, but sadly none of the makings for making a move. Your game is just not playing games at all (read: non-existent). The rest of us just don’t know how to get you out of your head and into your crush’s pants. I know when you brushed some snow off of that classmate’s hair and they smiled back, it sent you in a three-day analysis of whether they like you. Honestly Virgo, they probably do, but they definitely don’t know that you feel the same. So speak up, lest you be left as the zodiac Virgin forever.
Rising Stars
Libra: If flirting was a sport, you would definitely be a 10x gold medalist. The romantic aerobatics you do have your lovers spinning. But you’re also a sign that strongly believes in fairness. And to be fair, you flirt with everybody. In your eyes, true equality can only be achieved when everyone feels loved… loved by you that is. It’s pretty jarring for you when your multiple QMed ‘friends’ don’t understand that there is more than enough of you to go around. When it comes to your love life, it is definitely a “Justice for All” kind of approach, especially justice for you when you’re caught sending the same “you up?” text to multiple people in the same friend group.
Aquarius: As the water bearer Aquarius, you are constantly filling up everyone’s cups. You love your friends, but you love that one friend just a little extra more, don’t you? They’re pouring out all of their philosophical thoughts and intellectual hot takes, like a tall drink of water. Relax Aquarius, you’re looking a little thirsty. Your approach is engaging them in deep existential discussions, but still having a go with the flow energy. Still waters run deep for you Aquarius, but try not to drown them with questions like “which branch of the aorta are you and why?” The only anatomy they’re trying to study is yours.
Pisces: You’re romantic and dreamy, spending more time in your head than with your crush… sorry, love of your life. You’re confused why they haven’t realized that you reacting with a ‐‐ and not ‐to their Facebook message in your FSGL group chat was a clear expression of interest. Like what more do they need? In a last-ditch effort to make it exceedingly clear that you have every intention of living out the romantic novel that you’ve written in your head, you send them THE song that perfectly captures your love story. If they don’t get it now, then they are obviously not worth your time…. until the next time they ask you if you finished your case of the month question. *Deep sigh* ⚚
QMR Reading List
1. East of Eden – John Steinbeck
2. These Truths – Jill Lepore
3. In the Realm of Hungry Ghosts – Gabor Maté
4. The Lord of the Rings – J. R. R. Tolkien
5. Lullabies for Little Criminals – Heather O’Neill
6. A Carnival of Snackery – David Sedaris
7. Educated – Tara Westover
8. Do No Harm – Henry Marsh
9. The Body Keeps The Score: Brain, Mind and Body in the Healing of Trauma – Bessel van der Kolk, MD
10. The Invisible Life of Addie LaRue – V. E. Schwab
11. Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic Future – Ashlee Vance
12. Harry Potter and the Goblet of Fire – J.K. Rowling
13. Know My Name – Chanel Miller
14. Normal People – Sally Rooney
15. The Heart Principal – Helen Haong
16. Les Misérables – Victor Hugo
17. Klara and the sun – Kazuo Ishiguro
18. The Beauty of Discomfort – Amanda Lang
19. Superior: The return of race science – Angela Saini