Trends in financialisation of outpatient care across OECD countries by Valerie Paris
Trends in financialisation of outpatient care across OECD countries and challenges for competition authorities
Half of 20 OECD countries report that financialisation in outpatient care is a high or moderate trend in their countries
Financialisation = entry of for-profit financial firms and nonfinancial entities whose main business lies outside healthcare
Outpatient services is a new target after hospitals and nursing homes
Private equity and insurance companies reportedly involved
Most affected specialties (survey responses)
Note: Nb of countries reporting each specialty in the top 3 affected (N=14)
Financialisation of outpatient healthcare services
High growth in market shares of Dental Services Organisations between 2015 and 2018 (x2 in Denmark, Spain, USA and UK to reach 10% in Spain and 20% in the UK. Old data!
Radiology and radiotherapy seems to be a recent target for financial investors, owning 5% of practices in USA to 15% of pratices in France
Ophtalmologie: significant surge in private equity investment over the past decade. Development of networks of centers.
In laboratories, consolidation occurred before financialisation in the US (1980’s), mainly between public institutions in the UK (2010’s), but with financialisation in France since the 2010’s.
Primary care: not a priority but present in Sweden (1/8 PC centres), Finland (3 groups own 70¨of PC centres)
Drivers of financialisation in healthcare
Financial incentives
Rising demand for health care largely publicly financed
Budget constraints creating business opportunities
Healthcare organisation and professionnals
Potential for consolidation and productivity gains
Professionals preferences and constraints
Across OECD countries, the share of the population aged 65+ projected to increase from 18.5% in 2023 to 26.4% by 2050
Public spending accounts for 72% of Health spending on average in 2024
Shrinking budgets may impact public coverage and public provision of health care services Creating opportunities for private supply & insurance
Especially in capital-intensive sectors
Young professionals unable to compete with offers of financial investors to purchase practices of retiring physicians
New preferences of professionals for salaried practices
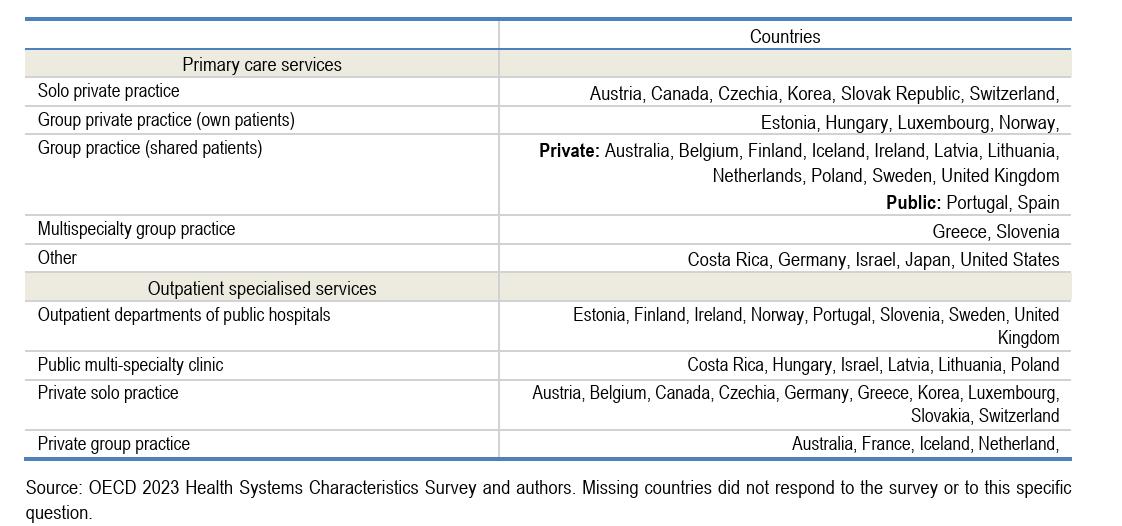
Predominant mode of service delivery for outpatient care
Health systems characteristics define opportunities for financialisation of services
Services not included in the benefit package
Healthcare services with poor public coverage
Low or underfunded public coverage of health care
Under-provision of services + population ability to pay
Service with high cost-sharing requirements
Long waiting times, possibility to pay to jump the queue or go privately for quicker access to health care
Ability for private insurance to cover private services
Often imposes thresholds for non-health professionals’ participation to ownership – partly circumvented +
Regulation of ownership of private practices
Varies across countries, across regions within countries, and across sectors of care
Potential and measured impact on access, quality and prices?
Empirical evidence?
Pros Cons
Infusion of capital for investments in health technologies
Operational efficiency through management expertise
Market consolidation of fragmented activities
Economies of scale and negotiating power
Short term focus on financial gains over long term quality
Increased costs due to leveraged buyouts
Access issues due to cherry picking of patients or activities
Price increase due to monopoly position
Survey - 9/10 countries have NO evaluation of impact of financialisation of outpatient care services
Most empirical literature is for US markets (hospitals, nursing homes)
Existing evaluations for outpatient services show:
- Increase in prices and cost per patient after PE acquisition with varying magnitude across specialties, due to change in service mix and/or coding practices
- Finland - increased prices in acquired clinics and dental services
- NB- Prices can only increase where they are not regulated
- Mixed impact on access
- Limited evidence on impact of quality – although private investment in technology may improve standards of care (eg Biology in France)
Specific challenges for competition authorities
Monitoring capacities
Mergers & acquisitions and risks of anti-competitive behaviours cannot be systematically monitored in large healthcare markets – eg US FTC works on cases brought to its attention
Data availability
In many countries, data are not organised in a way enabling the analysis of impact of ownership of healthcare practices on access, price and quality
Quality indicators
Quality indicators in the outpatient sector are under-developed by comparison to other sectors of care