Kryuchka Yaroslav


“As an organisation, it is our duty to advocate for critical access to affordable and essential health services and basic human rights, and to ensure that there's highest achievable quality health outcomes in the country.” – Dr Mzulungile Nodikida (SAMA CEO).
S NATIONAL HEALTH INSURANCE (NHI) once again dominated headlines after the President signed the Bill into law just before the elections, the South African Medical Association (SAMA) is gearing up for legal action. “SAMA continues to express its profound concern and opposition against the NHI in its current form,” said Dr Mvuyisi Mzukwa (SAMA chair). “As it stands, it fails to adequately address the critical social, economic imbalances and inequalities of the past that continue to plague our health system.” Dr Mzukwa was speaking during a webinar hosted by SAMA addressing critical legal updates now that the NHI Act has been passed.
“While the intention of the bill to transform our healthcare system is commendable, the implementation strategy lacks the necessary depth and practicality required to achieve meaningful and sustainable change,” he said. “For one, the funding mechanism is
flawed in its heavy reliance on general tax revenue, the payroll tax, and surcharges on personal income, not to mention systems and structural challenges such as ethical governance and leadership.
“It’s clear that the NHI is not a viable solution to realise universal health coverage for the South African population. We had hoped and remained optimistic that the President was going to refer the Bill back to Parliament for further stakeholder engagement, to assist with insights and expertise, with the aim to resolve the challenges the Bill will pose and to bring all parties and the country closer to realising universal healthcare in our lifetime. Sadly, these calls for a better healthcare system were ignored. As the South African Medical Association, we believe that it is our duty to advocate for equitable access to affordable essential healthcare services, and it is a cause that we are ready to fight for. In protecting our health care services, SAMA’s legal team is preparing to launch this challenge in relevant courts in this country.”
SAMA PREPARING FOR COURT
Assuring SAMA members, “We’ve been
preparing for this for months, if not years,”
Dr William Oosthuizen (head of SAMA Legal Affairs Department) introduced Elsabe Klinck, who specialises in health law, policy, and ethics, a key member of the legal team who will be challenging the Bill for SAMA. Warning that although we may all be pulled back into the legal aspects during the next phase of the NHI Act, Klinck said it was important not to lose sight of the narratives around the Act too as these were important.
“What affects SAMA membership tremendously is the fact that the Act is structured around three buckets for contracting,” namely primary care contracting, specialist and hospital services, and emergency services. Klinck explained that while it makes sense for specialist and hospital services to be rolled into one in the public sector, the same isn’t true in the private sector, “because the private hospital and the practitioners are in different legal entities. It’s also for entities to whom SAMA’s members may be referring, or entities that they use
such as blood services.” However, the Act isn’t clear how that would work or where they would fit in. Using the example of orthotics and prosthetics Klinck said they could fall into all three buckets. “So, an OMP (occupational medicine practitioner) that contracts, the question is how would they contract and how would their income be calculated? Because the remuneration for primary care would be on a capitated basis. For specialists and hospital services it will be an all-inclusive fee, so presumably the private hospital would get a fee and would then need to divide that. This in turn raises issues in terms of practitioners who are not hospital based or who see a whole range of their patients outside of the hospital setting, and then emergency services on a case basis.”
This brings us to accreditation. Klinck explained that one would not be able to contract into the NHI without the necessary accreditation. “That means being registered at the relevant body – nurses at nursing council, doctors at HPCSA, etc – then being accredited by the Office of Health Standards Compliance (OHSC). This is one of the things that will legally put brakes
on the NHI because we know that the OHSC at this stage is accrediting private and public hospitals, and public sector clinics, but it's not accrediting private medical practices, for example, or physiotherapy practices.”
While Klinck believed the standards for GPs were further advanced, she wasn’t clear how far the standards for other practitioners, like occupational therapy for example, were.
Next the Act calls for practices to submit a budget impact analysis. “It's not clear what that is and what will happen to that, because if all practices in the country make a submission – there are tens of thousands of practices that could potentially be contracted in – who will evaluate all the budget impact assessments?” Klinck asked.
The Act specifies that one would need to provide the services as prescribed by the Minister of Health (MoH): “You will need to have the right number and mix of professionals in a hospital and practice [as required by the MoH] to be contracted in. Certain specialists, and supportive professionals like occupational therapists for example.” But as that's not clear yet, Klinck explained that we needed to wait for regulations as to what those services could be. “Then one would have to adhere to treatment protocols and guidelines, and one would be obligated to prescribe and procure goods from the NHI funds list.” Stressing how strict this is, Klinck explained that “the Act talks about being kicked off the system if you don’t adhere to this.”
Furthermore, one would have to adhere to referral pathways, submit information to the National Health Information Service (NHIS), and adhere to the pricing regimen. “This pricing regimen implies a price regulatory, price fixing type of system.”
It’s not as simple as you can just clock in at either a public or private facility as some politicians have been saying, Klinck warned. “That facility you’ve clocked into would need to be both accredited and contracted to the NHI Fund. For that to be possible the NHI Fund would need to be in existence which is probably going to take another three years.”
1. We already have NHI under the existing National Health Act – free at point of care
"The only people who are not benefiting from that are medical scheme members and people who are receiving compensation for compensable occupational diseases. The only difference under the NHI Act is we’ll be bringing those people into the system too. The important question is if we already have this for primary care, why isn’t it working?” Klinck asked.
2. The private sector only services 15% of the population (ie only medical scheme members)
SAMA’s own research shows that private practices see far more than just medical scheme patients. “To say that the private sector is an elitist self-serving entity that only serves rich people is not correct,” said Klinck.
3. You don’t know how much we will pay you, doctor, but you will be better off due to increased volumes
“What we do know is that taxes cannot be raised now,” said Klinck. Currently the public sector spends R5 000 per patient per year, while the public sector spends R25 000 per patient per year. “If we want to create an average of R9 000 per patient per year we will need to start taxing, which isn’t yet possible. Furthermore, saying we’ll pay you less, but you can see more patients is problematic for doctors already at capacity who cannot see more patients,” Klinck said stressing that the idea of having to focus on volume but not necessarily ensuring quality of care is understandably very uncomfortable for practitioners.
4. Taxes will not be raised at present, but functions (and its associated monies) will shift
In the public sector, hospitals and facilities that were provincially driven will now be controlled at a national level. We currently have nine provinces controlling 52 districts and hospitals, a total of 3 741 facilities, that will be replaced by one overarching oversight entity under the MoH. “They will all become national government components," said Klinck. “This is significant for SAMA members working in the public sector because it implies a change in the employer and who controls how healthcare is rendered in that entity. “With provinces no longer in control human resources in terms of healthcare professionals would move to national government.”
SAMA’S LEGAL CHALLENGE
Looking ahead at the legal battles set to unfold in court and the possibility of SAMA joining forces with other stakeholders in their legal challenge, Dr Oosthuizen said: “With many similar arguments raised, we foresee many of these cases will be consolidated into one and as such there will possibly be some cooperation between various legal teams. However, our case looks very different to Discovery’s for example or any of the other funders. SAMA is concerned about our members, the profession, the health system, and I suppose most importantly – and this probably goes against the narrative out there – our patients. We’re really concerned about them and what NHI means for them, so it’s critically important for us to consider all those facts.”
Explaining that SAMA’s challenge will be a constitutional one, Klinck said, “These cases are complex, this is not a theoretical thing.” While there are lots of issues to be fought around the Act, Klinck said SAMA’s legal team will be focusing on what’s important to the associations’ members and their patients.
Stressing that SAMA was not opposing universal health coverage (UHC), just the NHI Act in its current form, Dr Mzulungile Nodikida (SAMA CEO) said, “As an organisation, it is our duty to advocate for critical access to affordable and essential health services and basic human rights, and to ensure that there's highest achievable quality health outcomes in the country. We remain firm in our commitment of championing health and the well-being of all South Africans, and we are still resolute in our endeavours to actively participate in the realisation of UHC.”

EAR DEVOTED READERS,

Our cover story addresses the growing controversy surrounding the National Health Insurance (NHI). The South African Medical Association (SAMA) is gearing up for a legal challenge against the NHI, emphasising the need for accessible and high-quality health services.
In terms of global health, we explore strategies to reduce out-of-pocket expenses for noncommunicable diseases (NCDs). Adrian van den Hoven, chair of the International Generic and Biosimilar Medicines Association, highlights how promoting generic competition can significantly lower medicine prices.
Case studies from India and Colombia illustrate how generic competition has made essential NCD medications more affordable, offering a viable
solution to a pressing global issue.
This issue also includes an analysis of the cardiovascular safety of testosterone use in ageing men. Two landmark studies provide valuable insights into the relationship between sex hormones and cardiovascular outcomes, contributing to the ongoing debate and informing clinical decisions.
Look out for the webinar announcements, as we have some exciting topics coming up, presented by experts in their respective fields. Additionally, this issue features a Continuing Professional Development (CPD) article focused on winter ailments, to see us through the cold months.
Thank you for your dedication and contribution to the medical field.
Happy reading

The rise of antimicrobial resistance (AMR) is a growing threat, posing a significant danger to global health. The World Health Organization (WHO) estimates AMR is responsible for 1.2 million deaths annually, with projections suggesting this number could reach 10 million by 2050.
By Nicky Belseck, medical journalist
AMR IS A looming global health crisis that has been identified by the WHO as one of the most pressing threats facing humanity. Responsible for approximately 1.2 million deaths annually, and associated with around five million deaths, the toll of AMR is significant and escalating. Without intervention, the future could see up to 10 million deaths per year by 2050, along with severe disruptions to medical interventions, a rise in extreme poverty by 24 million people, and a substantial global economic impact, potentially reducing the annual GDP by up to 3.8% by 2050.
CURRENT STATE OF THE ANTIBIOTIC
The antibiotic pipeline today is insufficient to counter the growing threat of AMR. A recent report by the International Federation of Pharmaceutical Manufacturers & Associations (IFPMA) highlights this troubling reality. Despite the urgency, there have only been 10 new antibiotics or combinations approved by stringent regulatory authorities between 2017 and 2023, with just two classified as innovative by the WHO. Disturbingly, none of these represent a new class of antibiotics. The situation is even more critical for pathogens deemed a critical priority by WHO, with only one antibiotic candidate currently in Phase III clinical trials.
The primary challenge in antibiotic research and development (R&D) is the economic disincentive. Antibiotics, by design, should be used sparingly to avoid resistance, leading to limited sales and returns on investment. This economic paradox has led to an exodus of expertise and investment from the field. To reverse this trend and rebuild a robust pipeline, new economic incentives are imperative. These incentives must attract private investment by ensuring sufficient returns on successful developments.
New modelling the IFPMA conducted with predictive health intelligence experts
from Airfinity outlines two potential future scenarios:
• Scenario one: no new incentives
Without new incentives, the antibiotic pipeline is projected to decline. Current funding for late-stage (Phase II and III) studies is expected to dwindle from 2026 onwards. While eight new approvals might be expected over the next decade, the number of candidates in Phase III trials would drop to just three by 2033. The overall pipeline would stagnate, failing to keep pace with rising resistance.
• Scenario two: effective incentives introduced in 2025
Introducing effective incentives in 2025 would stimulate significant private investment. The model predicts 19 new approvals by 2033, compared to just eight without these incentives. The pipeline would see 72 treatments in clinical trials, with 41 in late stages. This scenario boosts the number of approved antibiotics and enhances the pipeline's robustness and resilience.
A more robust antibiotic pipeline could dramatically improve public health outcomes. Modelling the burden of disability-adjusted life years (DALYs) from four WHO critical priority pathogens underlines the potential benefits. According to the report, without new antibiotics, the DALY burden in high-income countries (HICs) is expected to rise by 35% over the next decade. However, with new antibiotics helped by effective incentives, this burden could be reduced by more than 50%. Although this model focuses on HICs, similar benefits would likely be seen globally.
While the global community acknowledges the critical need to strengthen the antibiotic pipeline, the IFPMA cautioned that action remains limited. High-profile international forums, including the UN General Assembly and the G7 and G20 summits, are prioritising AMR. However, concrete steps are needed to incentivise R&D. Current efforts, such as the
UK's novel subscription model and Japan's antibiotic revenue guarantee pilot, are promising but insufficient alone. Legislative actions in the US and EU must also advance to provide the necessary economic framework.
The future of the antibiotic pipeline hinges on our ability to implement effective pull incentives that attract and sustain investment in antibiotic R&D, the IFPMA reported. By shifting from resistance to
resilience, we can ensure the development of new, innovative antibiotics that are essential for global health security. Governments must act decisively to establish a sustainable economic model for antibiotic R&D, ensuring a resilient pipeline capable of meeting the challenges of AMR. The stakes are high, but with the right incentives, IFPMA believes we can safeguard the future of medical treatments and protect public health worldwide.




The high cost of non-communicable diseases: challenges and solutions.
NON-COMMUNICABLE DISEASES
(NCDs) like heart disease, diabetes, and cancer are the leading cause of death worldwide. They place a heavy financial burden on individuals, healthcare systems, and entire economies, particularly in low- and middle-income countries (LMICs).A significant portion of NCD treatment costs falls on patients themselves through out-of-pocket (OOP)
expenditure. This can be devastating, forcing individuals to forego treatment, deplete savings, and even borrow money. High OOP expenditure also hinders progress towards Universal Health Coverage (UHC), which aims to provide everyone with access to affordable, quality healthcare.
The WHO Department for NCDs, Rehabilitation, and Disability recently held a talk looking at how to reduce out-of-pocket
EPCLUSA® is indicated for the treatment of chronic hepatitis C infection irrespective of genotype in treatment naïve or treatment experienced patients aged 12 years and older and weighing at least 30 kg:
- without cirrhosis or with compensated cirrhosis
- with decompensated cirrhosis in combination with ribavirin 1
(OOP) expenditure in NCD medicines.
THE PROBLEM WITH HIGH OOP EXPENDITURE
People suffer financial hardship in health when their OOP health spending threatens their living standards or compromises access to essential goods such as food, shelter, clothing, or education. Matthew Jowett (WHO head of a.i. Health Financing

Footnotes: aDespite unknowns in baseline characteristics of some patients, such as: HCV genotype, fibrosis stage, former/current IV drug use, PPI use at baseline and treatment history.3 bA large-cohort international real-world study showed that patients with unknown genotype (n = 42), unknown fibrosis score (n = 82) and unknown treatment history (n = 33) were cured with EPCLUSA® for 12 weeks. Cure is defined as SVR i.e., undetectable HCV RNA after treatment completion.3,4 cCases of HBV reactivation, some of them fatal, have been reported during or after treatment with direct acting antiviral agents including EPCLUSA®. HBV screening should be performed in all patients before initiation of treatment. Treatment with EPCLUSA® should not be initiated in patients who screened positive for hepatitis B virus infection. HBV/HCV coinfected patients are at risk of HBV reactivation, and should therefore be monitored and managed according to current clinical guidelines.1 dPatients with decompensated cirrhosis use EPCLUSA® + ribavirin for 12 weeks.
References: 1. Epclusa Professional Information approved by the medicine’s regulatory authority. 10 March 2022. 2. Lawitz E, Bourliere M, Han L, McNally J, Stamm LM, Brainard DM, et al. Treatment with SOF/VEL or SOF/VEL/VOX is well tolerated and results in high SVR12 in genotype 1-6 HCV-infected patients with minimal fibrosis: a retrospective analysis of the ASTRAL and POLARIS clinical studies. Poster THU-273 presented at the International Liver Congress 2017, April 19–21, Amsterdam, The Netherlands. Available at: https://www.natap.org/2017/EASL/EASL_07.htm [Accessed 24 March 2022]. 3. Mangia A, Milligan S, Khalili M, Fagiuoli S, Shafran SD, Carrat F, et al. Global real-world evidence of sofosbuvir/velpatasvir as simple, effective HCV treatment: Analysis of 5552 patients from 12 cohorts. Liver Int 2020;40:1841–1852. 4. National Guidelines for the Management of Viral Hepatitis. Department of Health Republic of South Africa Available at: https://sahivsoc.org/Files/SA%20 NDOH_Viral%20Hepatitis%20guideilnes%20final_.pdf [Accessed 10 March 2022]. For full prescribing information refer to the professional information approved by the Medicines Regulatory Authority. S4 EPCLUSA® 400 mg/100 mg
and 100 mg velpatasvir.
gilead.com or drugsafetysouthafrica@gilead.com | EPCLUSA® the EPCLUSA® Logo, GILEAD and the GILEAD
By Nicky Belseck, medical journalist
Unit, Department of Health, Financing, and Economics) expressed concern around at the number of people around the world that are facing catastrophic OOP spending and the fact that these numbers continue to increase (9.6% of the world population in 2000, 13.5% in 2019).
Research reveals significant disparities in NCD treatment costs. Public and private healthcare facilities have different cost structures, and socioeconomic factors like wealth and insurance coverage significantly impact what patients pay. Mental health and neurological disorders add substantially to household healthcare expenditure.
The cost of medicines is a major driver of OOP expenditure. Adrian van den Hoven (chair, International Generic and Biosimilar Medicines Association) argued that promoting generic competition can dramatically reduce medicine prices, citing examples from India and Colombia where generic competition led to significant price drops for essential NCD medicines.
“Even in Europe we see catastrophic spend, but in some countries, there can be up to 20% of households facing catastrophic OOP expenditure,” James Anderson (executive director, Global Health, the International Federation of Pharmaceutical Manufacturers and Associations) said emphasising the importance of UHC in addressing catastrophic OOP expenditure. Expanding health insurance coverage, particularly in LMICs, is crucial. However, achieving UHC requires better data collection on OOP expenditure to inform policy decisions, he explained.
FOR REDUCING OOP EXPENDITURE
Several strategies were raised to reduce OOP expenditure beyond just medicine prices. These included:
• Public-private partnerships to create insurance mechanisms for the uninsured
• Technology-based solutions to improve access to healthcare financing
• Tiered pricing approaches for NCD medicines, with lower prices for LMICs
• Regulations to control markups in the medicine distribution system
• Shifting from percentage markups to fixed markups to better align prices with patient needs.
Speakers agreed that achieving progress requires a collaborative effort from governments, the pharmaceutical industry, healthcare providers, and other stakeholders. By working together, we can implement effective strategies to ensure equitable access to affordable NCD care for all.






Strengthening decision-making for essential medicines and beyond: the future of health technology assessment in the NHI era.
ASSESSMENT (HTA) has become a crucial component in the South African public sector's selection of essential medicines. The Essential Medicines List (EML), a key tool in this process, guides the procurement of vital medicines in the public sector, while the Prescribed Minimum Benefits (PMBs) outline entitlements in the private sector. HTA ensures a transparent,
evidence-based link between emerging technologies and the foundational values guiding their integration into healthcare. This approach streamlines decision-making, avoids redundancy, and allows for dynamic feedback on real-world effectiveness, enabling corrective actions when necessary.
In SA, various players including private
sector funders, hospital groups, nonprofits, academia, and public sector guideline developers are involved in HTA processes. However, coordination among these entities has been imperfect, often resulting in duplicated efforts and a lack of transparency. Over the past two decades, the public sector has increasingly utilised HTA in selecting essential medicines through the National Essential Medicines List Committee (NEMLC), appointed by the Ministry of Health.
HTA has moved public sector medicine

2 May 2024





By Nicky Belseck, medical journalist
gap between public and private healthcare sectors through the NHI fund, which will purchase services from both sectors to provide equitable access to quality healthcare.
With the NHI Bill signed into law by the president earlier this month, HTA is poised to play a vital role in maximising the impact of NHI spending, supporting equitable and transparent decision-making.







The Benefits Advisory Committee (BAC) will advise the Minister on priority-setting for the NHI fund, developing cost-effective treatment guidelines. The Ministerial Advisory Committee on HTA will serve as a precursor to a formal HTA agency, using evidence on cost-effectiveness and efficiency to review health interventions. In the short term, the Ministerial Advisory Committee on HTA will establish policies, engage stakeholders, and pilot HTA methodologies. In the medium term, national HTA resources will be utilised more extensively, with ongoing capacity building. In the long term, HTA processes will become entrenched in decision-making, potentially evolving into an independent national agency. SA's fragmented HTA processes have not yielded outcomes proportional to healthcare spending. The establishment of NHI offers an opportunity to formalise HTA, ensuring its integration into decision-making for all health interventions. As the NHI Bill progresses, stakeholder consultation and buy-in will be crucial for implementing a robust HTA framework. Transparent decision-making, strong governance, and political will are essential for the successful adoption of a formalised HTA process, ultimately improving healthcare outcomes across
Jugathpal, J., Parrish, A., Jamaloodien, K., Blecher, M., & Daven, J. (2023). Institutionalizing Health Technology Assessment in South Africa—An Opportunity in National Health Insurance. Health Systems &

Microsoft Surface for Business presents a diverse range of devices tailored to provide the ultimate experience for Windows 11 and Microsoft 365, empowering healthcare providers to deliver superior patient care.
IN THE EVER-CHANGING realm of healthcare, technology serves as a cornerstone in elevating patient care standards, streamlining operational processes, and fostering seamless collaboration among healthcare professionals. As the healthcare sector continues its digital transformation journey, selecting the right devices becomes increasingly critical to ensure optimal efficiency and effectiveness. Amidst the multitude of options available, the Microsoft Surface Pro 9 and Laptop 5 emerge as the top contenders for healthcare organizations seeking devices that offer reliability, adaptability, and cutting-edge innovation.
MICROSOFT SURFACE PRO 9: REDEFINING MOBILITY AND FLEXIBILITY
At the forefront of healthcare technology, the Microsoft Surface Pro 9 embodies the perfect synergy of power and portability. Designed to meet the demanding requirements of healthcare professionals, this versatile device seamlessly transitions between tablet and laptop modes, providing unparalleled flexibility in various clinical settings.
With its lightweight and compact design, the Surface Pro 9 is the ideal companion for on-the-go healthcare professionals. Whether conducting patient rounds, attending telehealth appointments, or collaborating with colleagues, its portability ensures uninterrupted productivity and seamless workflow integration. Equipped with the latest Intel processors and ample RAM, the Surface Pro
9 delivers exceptional performance, enabling healthcare professionals to multitask effortlessly and access critical patient information with ease.
The Surface Pro 9's innovative features, such as the Surface Pen and touchscreen functionality, facilitate intuitive input and interaction, allowing clinicians to annotate medical images, complete electronic health records (EHRs), and capture signatures with precision and accuracy. Combined with advanced security features, such as Windows Hello facial recognition and BitLocker encryption, the Surface Pro 9 ensures robust data protection and compliance with stringent healthcare regulations, safeguarding patient confidentiality and privacy.
MICROSOFT
The Surface Laptop 5 grants healthcare workers access to premium Microsoft features, facilitating efficient patient interactions with its highly portable design, extended battery life, and reliable Wi-Fi 6 connectivity. Healthcare professionals can seamlessly transition between keyboard, pen, or dictation for digital notetaking during appointments. They can also multitask between critical business applications, imaging software, and communication tools while on the move. Exceptional visual and auditory experiences during Microsoft Teams calls are ensured through top-quality cameras, finely tuned microphones, and integrated Omnisonic speakers. For healthcare providers valuing
both performance and style, the Microsoft Surface Laptop 5 embodies elegance and efficiency. Its sleek and lightweight design seamlessly blends desktop power with laptop portability, catering to clinical and administrative needs alike.
With a vibrant PixelSense display and responsive keyboard, the Surface Laptop 5 offers an immersive computing experience, enabling clear and precise review of medical images, diagnostic reports, and collaborative patient care planning. Powered by the latest Intel processors and integrated graphics, it facilitates seamless multitasking and smooth performance for tackling complex tasks with ease.
Furthermore, the Surface Laptop 5's extended battery life ensures sustained productivity throughout busy shifts, while robust security features such as Windows Defender Antivirus and built-in malware protection provide comprehensive defence against cyber threats, safeguarding sensitive patient data and ensuring compliance with regulatory standards.
In clinical environments, the Surface Pro 9's versatility allows seamless transitions between tablet and laptop modes, catering to the dynamic needs of healthcare professionals.
Its lightweight design and robust performance make it an ideal companion for clinicians conducting rounds, attending telehealth appointments, or collaborating on care plans. Intuitive features such as the Surface Pen enhance clinical productivity and facilitate seamless interaction with electronic health records (EHRs) and diagnostic imaging.
Similarly, the Surface Laptop 5 enhances productivity and performance for healthcare professionals in administrative roles. Its sleek design, vibrant display, and extended battery life ensure uninterrupted productivity, while advanced security features provide comprehensive protection against cyber threats. From managing administrative tasks to collaborating on care plans, the Surface Laptop 5 empowers healthcare professionals to work efficiently, driving operational excellence and enhancing the quality of care delivery.
Investing in the Surface Pro 9 and Laptop 5 is a strategic decision that positions healthcare organizations at the forefront of innovation and excellence. These devices empower organizations to achieve new levels of efficiency, productivity, and patient satisfaction. By harnessing the power of these cutting-edge devices, healthcare organizations can navigate the complexities of modern healthcare delivery confidently, driving transformative change and shaping the future of healthcare for generations to come.
Elevate your practice to new heights with the cutting-edge Surface devices available through Altron HealthTech and Tarsus Distribution.
Experience the transformative power of Surface technology firsthand by visiting Altronhealthtech.com/surface/ today. Alternatively, connect with our dedicated team at healthtech.sales@altron.com to discover how we can empower your practice with the innovation it deserves. Don't settle for ordinary – embrace the future of healthcare with Surface.
In the dynamic landscape of modern healthcare, primary care practitioners are tasked with a delicate balance: delivering personalised patient care while navigating the complexities of administrative demands.
AMIDST THESE CHALLENGES,
Engage Mx emerges as a beacon of efficiency and effectiveness, poised to redefine patient care management for optimal outcomes and streamlined practice operations.
Engage Mx stands out as a tailored solution, simplifying patient care management by facilitating timely reminders for individuals to consult their healthcare professionals. This is achieved through a comprehensive understanding of each patient's unique health profile, condition, and risk assessment. Let us delve into how Engage Mx addresses a critical challenge for healthcare providers, offering dual benefits for both patients and practitioners.
Engage Mx transformspatient care management byconsolidating information andautomating reminders and follow-ups
Primary healthcare providers often grapple with the formidable task of ensuring every patient receives timely follow-ups and screenings. This challenge frequently results in gaps in care, missed intervention opportunities, and compromised patient well-being. Through the experiences of practitioners, it becomes evident that a solution transcending sole reliance on patient responsibility is imperative.
rates and reducing healthcare costs associated with advanced disease stages.
More than just software, Engage Mx serves as a catalyst for positive change in primary healthcare delivery. By streamlining patient care management, fostering
compliance, and enabling proactive screening, Engage Mx drives improved patient outcomes and ensures the resilience of primary healthcare practices.
Discover the transformative potential of Engage Mx and elevate your practice to
unprecedented levels of efficiency and effectiveness. Experience seamless patient care management and proactive health interventions with Engage Mx today, and embrace the future of healthcare delivery.

Engage Mx transforms patient care management by consolidating information and automating reminders and follow-ups. Renowned for its capacity to monitor and coordinate all facets of patient care within a unified platform, this software streamlines practice operations while fostering personalised care plans and enhancing health outcomes.
The management of chronic conditions demands meticulous adherence to treatment plans and follow-up appointments. Engage Mx assumes a pivotal role in identifying and recalling non-compliant patients, thus contributing to improved condition management and operational efficiency within healthcare practices.
Furthermore, Engage Mx transcends conventional medical condition screening by proactively recalling patients based on their health profiles. This feature underscores its significance in early detection and intervention, ultimately mitigating mortality

Medical coding and billing is a topic not for the faint of heart! This article will introduce you to the new online ethical CPD-accredited course (3 CEU), Introduction to Medical Coding & Billing.
ARE often uncertain about the rates they may charge for their services. How medical practices are managed and, specifically, how rates and codes are applied during the billing process has become increasingly complex over time.
GoodX Courses created an introductory course to
1. Bring those working in the industry up to date on best practices about coding and billing
2. Make practical suggestions on how to manage and maintain successful coding and billing.
The course follows the flow of the Intro to Medical Coding & Billing diagram.
1. Survey
The course starts by surveying the history of coding and billing, the differences between coding and billing, the role-players involved and the role of tariff masters in the industry.
Good news for those who need an introduction to the world of medical coding&billing
2. Billing Structures
The course then delves deeper into billing structures. It explains the different types of billing structures in a practice and the different medical industry categories and disciplines. The differences between practice rates and scheme rates are discussed, and what to look out for in implementing the different rates in the healthcare practice.
3. Practice Billing Policy
Of great benefit to any practice is to write a practice billing policy. The what's and why of the policy are described, and how each section of the policy will provide clarity to all staff involved in coding and billing. It will also provide a strategy for implementing the policy and navigating the legal landscape.
4. Billing Rules and Guidelines
The next section of the course will explain
the billing rules every practice needs to be considered by billing experts.
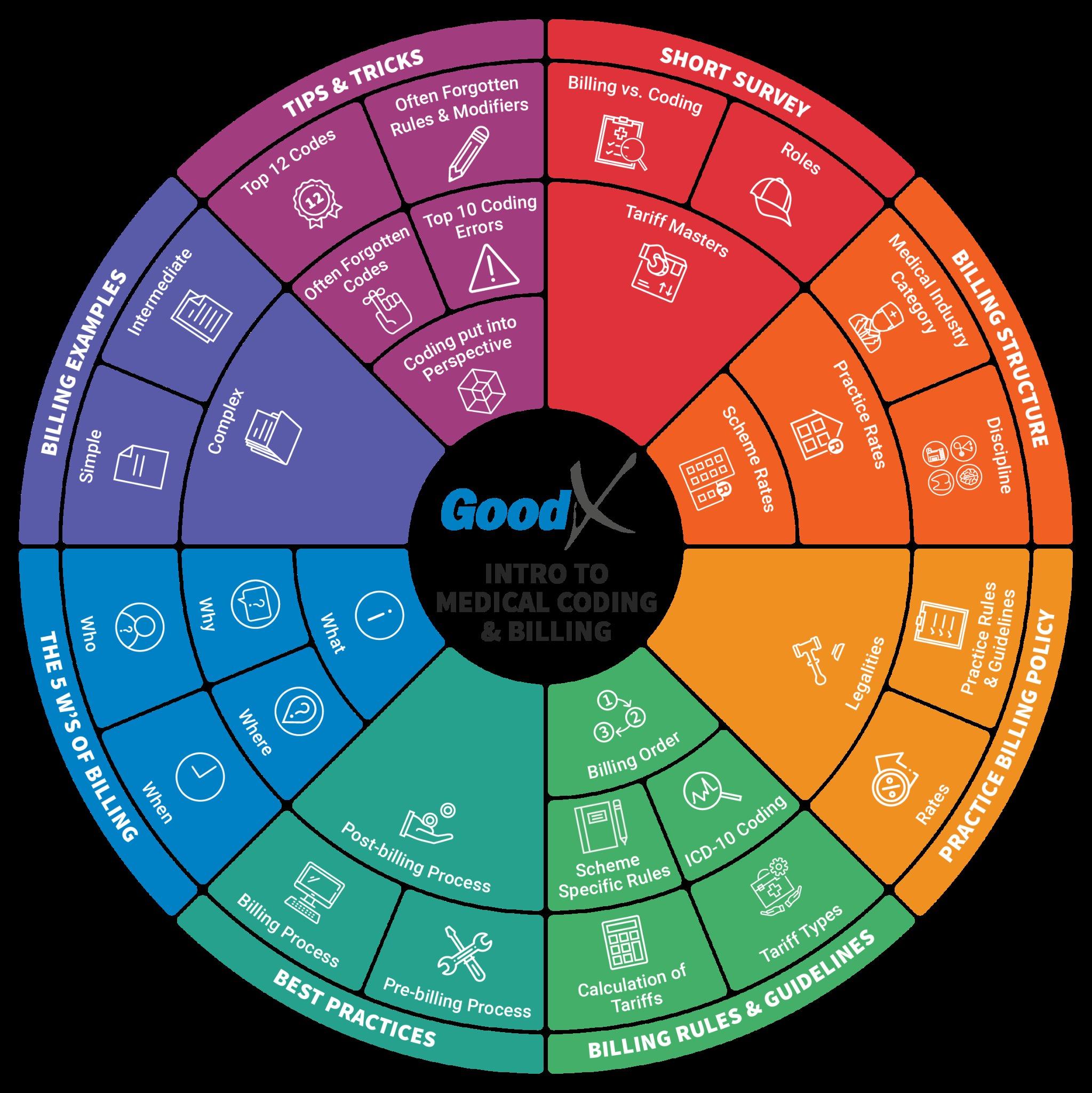
5. Billing Best Practices
After learning the theory of coding and billing, the course focuses on the practicalities of invoicing. The basics when gathering the information to optimise billing are explained to ensure your claims go through without rejection or resubmission.
6. The 5 W’s of Billing
The coding process is simplified using the 5 W’s of coding. This helps the billing expert to follow due process to optimise the outcome.
7. Billing Examples
The course provides billing examples and explanations so that learners can understand how to apply the theoretical concepts practically.
8. Tips and Tricks
The course ends with providing useful tips and tricks to help maximise your effectiveness as a billing expert.
Any person involved in a healthcare practice will find that the course provides a solid foundation to become well-versed in the language and skills of medical coding and billing. To enroll for the course, please visit courses.goodx.co.za. It is a selfservice platform where you can register as a user, pay, and enroll by clicking on the Introduction to Medical Coding and Billing course listed on the homepage.

1 2 Features Voice to typing/Dictation
Billing
Stylus compatible for those who think when writing
Turn your phone into a clinical camera (Capture App)
Facial recognition

The sore throat is one of the most common conditions encountered in a general practice. Pharyngitis is inflammation of the mucous membranes that line the back of the throat, or pharynx. This inflammation can cause discomfort, dryness and difficulty swallowing.

common conditions encountered in a general practice. Pharyngitis is inflammation of the mucous of the throat, or pharynx. This inflammation can cause discomfort, dryness and difficulty swallowing.
IA sore throat is one of the most common conditions encountered in a general practice. Pharyngitis is inflammation of the mucous membranes that line the back of the throat, or pharynx. This inflammation can cause discomfort, dryness and difficulty swallowing.
NFLAMMATION OF THE throat is a common medical issue, and it can result from a variety of causes, including:
• Laryngitis
symptoms may appear depending on the type of infection, such as cold or flu symptoms.
I• Tonsillitis
• Throat ulcers.
NFLAMMATION OF THE throat is a common medical issue, and it can result from a variety of causes, including:
• Laryngitis
• Tonsillitis
• Throat ulcers.
symptoms may appear depending on the type of infection, such as cold or flu symptoms.
Acute pharyngitis is characterised by the rapid onset of sore throat and pharyngeal inflammation (with or without exudate). Absence of cough, nasal congestion and nasal discharge suggests a bacterial, rather than viral aetiology. Acute pharyngitis
The main symptom of pharyngitis is a sore, dry, or itchy throat. Additional
The main symptom of pharyngitis is a sore, dry, or itchy throat. Additional symptoms may appear depending on the type of infection, such as cold or flu symptoms.
Acute pharyngitis is characterised by the rapid onset of sore throat and pharyngeal inflammation (with or without exudate). Absence of cough, nasal congestion and nasal discharge suggests a bacterial, rather than viral aetiology. Acute pharyngitis can be caused by a variety of viral and bacterial pathogens, including group A Streptococcus (GAS), as well as fungal pathogens (Candida). Bacterial pharyngitis is more common in winter (or early spring), while enteroviral infection is more common
Acute pharyngitis is characterised by the rapid onset of sore throat and pharyngeal inflammation (with or without exudate). Absence of cough, nasal congestion and nasal discharge suggests a bacterial, rather than viral aetiology. Acute pharyngitis

in the summer and fall. Acute pharyngitis is generally a self-limited condition with resolution within two weeks.
can be caused by a variety of viral and bacterial pathogens, including group A Streptococcus (GAS), as well as fungal pathogens (Candida). Bacterial pharyngitis is more common in winter (or early spring), while enteroviral infection are more common in the summer and fall. Acute pharyngitis is generally a self-limited condition with resolution within two weeks.
conditions in the mouth and throat. Its unique chemical nature and mechanism of action makes benzydamine unique.

Quality of life in patients with acute pharyngitis or tonsillitis is significantly lower than in healthy persons, and it should be taken into account when efficacy of new therapeutic options is investigated.
Benzydamine hydrochloride is a nonsteroidal anti-inflammatory molecule with local anaesthetic and analgesic activity, that delivers targeted relief from inflammatory
can be caused by a variety of viral and bacterial pathogens, including group A Streptococcus (GAS), as well as fungal pathogens (Candida). Bacterial pharyngitis is more common in winter (or early spring), while enteroviral infection are more common in the summer and fall. Acute pharyngitis is generally a self-limited condition with resolution within two weeks.
Quality of life in patients with acute pharyngitis or tonsillitis is significantly than in healthy persons, and it should be taken into account when efficacy of new therapeutic options are investigated.
CHEMICAL NATURE OF BENZYDAMINE vs OTHER NSAIDS
Quality of life in patients with acute pharyngitis or tonsillitis is significantly lower than in healthy persons, and it should be taken into account when efficacy of new therapeutic options are investigated.
Benzydamine hydrochloride is a nonsteroidal anti-inflammatory molecule with local anaesthetic and analgesic activity, that delivers targeted relief from inflammatory
Unlike other NSAIDs, which are aspirin-like and therefore acidic chemical molecules, benzydamine is a base. This explains its tendency to preferentially concentrate in inflamed tissues. Once at the site of inflammation, benzydamine acts on a
Benzydamine hydrochloride is a nonsteroidal anti-inflammatory molecule with local anaesthetic and analgesic activity, delivers targeted relief from inflammatory


number of inflammatory mechanisms to relieve pain, redness and swelling.
BENZYDAMINE’S MECHANISMS OF ACTION
Cytokines are cell-signalling proteins that have a specific effect on the interactions and communications between cells and immune responses, and stimulate the movement of cells towards sites of inflammation. Benzydamine’s main anti-inflammatory activity results from its inhibition of the production of proinflammatory cytokines, mainly tumour necrosis factor alpha (TNF- α) and
Interleukin-1 beta (IL-1β), a major driver of inflammation, and monocyte chemotactic protein-1 (MCP1). These are common proinflammatory cytokines. So although it is classified as a NSAID, it works as a CSAID (cytokine-suppressive anti-inflammatory drug). Benzydamine acts as a modulator of cytokines, ensuring it does not inhibit antiinflammatory cytokines: Interleukin-10 (IL10) Interleukin-1ra (IL-1ra).
Benzydamine also elicits supportive anti-inflammatory activity, through cell membrane stabilisation, reducing both capillary vasodilation and the release of proinflammatory substances. Benzydamine’s
local anaesthetic effect may be related to its capability for inhibiting the release of inflammatory mediators such as substance P, which causes the release of histamine from mast cells. The prevention of substance P release further contributes to an anti-inflammatory effect.
BENZYDAMINE’S SAFETY PROFILE
Benzydamine’s chemical structure makes it highly lipid soluble, with low plasma protein binding capacity. This promotes its absorption and selective binding into inflamed tissues, where it accumulates, reducing the possibility of systemic side
effects. Benzydamine’s targeted activity makes it ideal for topical application and it has no known drug interactions. Benzydamine is only a weak inhibitor of prostaglandin synthesis, even following oral application, meaning it is an efficacious, more gastro-friendly anti-inflammatory choice. It is a well-established molecule with over 50 years of clinical experience. Its unique triple action provides antiinflammatory, analgesic and local anaesthetic relief for your patients with inflammatory conditions of the mouth and throat.
OF CHLORHEXIDINE/ BENZYDAMINE MOUTH SPRAY ON PAIN AND QUALITY OF LIFE IN ACUTE VIRAL PHARYNGITIS
Cingi et al conducted a prospective, randomised, double-blind, placebocontrolled, multicentre study to assess the efficacy of chlorhexidine gluconate/ benzydamine hydrochloride mouth spray for reducing pain and improving quality of life in patients with acute viral pharyngitis.
Benzydamine’s chemical structure makesithighly lipidsoluble,with lowplasmaprotein bindingcapacity. Thispromotesits absorptionand selectivebindinginto inflamedtissues, whereitaccumulates, reducingthe possibilityof systemicside effects
Chlorhexidine belongs to the antimicrobial class of drugs. It works by decreasing the amount of bacteria in the mouth, providing a broad spectrum antiseptic activity, killing or inhibiting the growth of bacteria, viruses and fungi. Prior to treatment, patients rated the intensity of their pain on a visual analogue scale and evaluated their quality of life on the 36-Item, Short-Form Health Survey. Patients were then randomised to receive either paracetamol plus chlorhexidine/ benzydamine or paracetamol plus placebo for seven days. On days three and seven of treatment, the participants again rated the intensity of their pain, and on day seven, they again rated their quality of life.
A total of 164 patients were evaluable at study's end-80 in the chlorhexidine/ benzydamine group and 84 in the control group. A comparison of self-evaluations revealed that the active treatment group reported less pain on both day three (p <0.001) and day seven (p = 0.002). Likewise, the chlorhexidine/benzydamine group reported a significantly better quality of life on day seven (p < 0.001).
Chlorhexidinegluconateand benzydaminehydrochloride combinationmouthspray, added to standard antibiotic treatment,significantly alleviatetheintensityof clinicalsignsinpatientswith streptococcalpharyngitis

Chlorhexidine/benzydamine was well tolerated, and no serious adverse events were observed.
The same study author assessed the effect of chlorhexidine gluconate and benzydamine hydrochloride mouth spray, used in conjunction with antibiotic treatment, on the intensity of clinical signs and quality of life of patients with group A streptococcal tonsillopharyngitis. Methods: Patients (n = 147) with streptococcal tonsillopharyngitis were recruited and randomly allocated to either the treatment group (penicillin plus chlorhexidine and benzydamine; n = 72) or control group (penicillin plus placebo; n = 75). Blinded assessments were conducted before and after 10 days' treatment, using an intensity rating scale for clinical sign severity, a visual analogue scale for subjective health state, the Short Form 36 Health Questionnaire for quality of life, and a customised questionnaire for side effects.
Results: The treatment group showed a statistically significant reduction in the intensity of clinical signs, compared with the control group. On treatment day seven, there was no significant difference in quality of life between the treatment and control groups. The treatment drugs were well tolerated, and no serious adverse events
were observed.
Conclusion: Chlorhexidine gluconate and benzydamine hydrochloride combination mouth spray, added to standard antibiotic treatment, significantly alleviate the intensity of clinical signs in patients with streptococcal pharyngitis.
Chlorhexidine belongstothe antimicrobial classofdrugs. Itworksby decreasingthe amount of bacteria inthemouth, providing abroadspectrum antisepticactivity
In cases of persistent sore throat, it is important to reconsider the initial diagnosis. Consider an alternative diagnosis or further investigation if the individual has not responded to a course of antibiotics. Consider a neoplasm if the sore throat is
persistent, especially if there is a neck mass. Indications for urgent referral include:
• An unexplained persistent sore or painful throat −‘persistent’ refers to a time frame of three-four weeks
• Red, or red and white patches, or ulceration or swelling of the oral/ pharyngeal mucosa for more than three weeks
• Odynophagia or dysphagia for more than three weeks
• Unexplained hoarseness accompanied by persistent sore throat.
Consider non-infectious causes of sore throat (eg gastro-oesophageal reflux disease, chronic irritation from cigarette smoke, alcohol or hay fever).
CONCLUSION
Clinical studies show that benzydamine/ chlorhexidine sprays significantly reduce the pain of a viral sore throat without causing any serious side effects, while in Strep throat the combination has shown to alleviate the intensity of clinical signs when used alongside a standard antibiotic treatment.
REFERENCES
Claassen J. The sore throat. Continuing Medical
Education, [S.l.], v. 30, n. 9, p. 306-313, sep. 2012. ISSN 2078-5143. Available at: <http://www.cmej.org. za/index.php/cmej/article/view/2447/2535>. Date accessed: 26 May. 2021.
Cingi C, Songu M, Ural A, Erdogmus N et al. Effect of chlorhexidine gluconate and benzydamine hydrochloride mouth spray on clinical signs and quality of life of patients with streptococcal tonsillopharyngitis: multicentre, prospective, randomised, double-blinded, placebo-controlled study. J Laryngol Otol. 2011 Jun;125(6):620-5. doi: 10.1017/S0022215111000065. Epub 2011 Feb 11. PMID: 21310101.
Cingi C, Songu M, Ural A et al. Effects of chlorhexidine/benzydamine mouth spray on pain and quality of life in acute viral pharyngitis: a prospective, randomized, double-blind, placebocontrolled, multicentre study. Ear Nose Throat J. 2010 Nov;89(11):546-9. PMID: 21086279. IMS Total Private Market Value MAT. December 2020. Impact Rx, December 2020.
Almazan NA. Benzydamine HCl 0.15% for Oropharyngeal Diseases and Surgeries: A Review of Clinical Trials. Philippine Scientific J 2009; 42(1):38-42.
Andolex®-C Oral Rinse approved package insert. February 2017.
Turnbull RS. Benzydamine Hydrochloride (Tantum) In the Management Of Oral Inflammatory Conditions. J Can Den Assoc 1995;61(2):127-134.
Sironi M, Massimiliano L, Transidico P, et al. Differential effect of benzydamine on pro- versus antiinflammatory cytokine production: lack of inhibition on interleukin-10 and interleukin-1 receptor antagonist. Int J Clin Lab Res 2000;30:17-19.
Mathivanan S, De La Torre Martinez R, Wolf C, et al. effect of econazole and benzydamine on sensory neurons in culture. J Phys and Pharm 2016;67(6)851-858. Benzydamine. Available from: https://www.drugbank.ca. Accessed date: 26 May 2021.
Allergic rhinitis stands as the most prevalent allergic condition globally, affecting approximately 18% to 40% of the general population.
WHILE ANTI-ALLERGIC medications, including certain antihistamines, offer relief, they often come with adverse effects such as drowsiness, further compromising quality of life.
Addressing allergic rhinitis (AR) remains a formidable task in global healthcare, with existing treatments offering limited relief from its burdensome symptoms. Despite decades of available options, patients still struggle with compromised quality of life due to persistent symptoms.
AR stems from exposure to allergens like pollen, mites, and animal dander, triggering a cascade of immune responses in susceptible individuals. This includes the activation of specific immunoglobulin E (IgE) receptors on mast cells and basophils, leading to early and late-phase reactions characterized by various inflammatory processes. The resulting nasal and ocular symptoms significantly impair daily functioning and quality of life.
PRESENT PHARMACOLOGICAL LANDSCAPE
Current pharmacological management relies on symptomatic relief through antihistamines, corticosteroids, nasal decongestants, and leukotriene receptor antagonists. Traditional antihistamines have fallen out of favour due to side effects, paving the way for newer-generation options like desloratadine and levocetirizine, which offer improved safety profiles. Intranasal formulations provide targeted relief, while corticosteroids serve as primary therapy by suppressing immune responses. Combination therapies, such as intranasal antihistamines with corticosteroids, have shown superior efficacy.
Montelukast, a leukotriene receptor antagonist, stands out for its efficacy in reducing night-time symptoms, particularly when combined with H1 antihistamines. While nasal decongestants alleviate congestion, their overuse can lead to rebound symptoms.
Innovative Combination Therapy Recent studies explore the efficacy of combining montelukast and levocetirizine, offering a promising approach to AR management. Panchal et al (2021) conducted a Phase III trial, demonstrating the superior efficacy of this combination over monotherapy in seasonal allergic rhinitis (SAR) patients. The fixed-dose combination (FDC) significantly improved daytime nasal symptoms, nighttime symptoms, and overall quality of life, with favourable safety profiles.
Mahatme et al (2016) compared montelukast-levocetirizine with montelukast-fexofenadine combinations,
highlighting the former's cost-effectiveness alongside significant symptom reduction.
BILAYER TECHNOLOGY
Similarly, Rathod et al found that combining montelukast with levocetirizine presents notable advantages over individual drug administration, particularly for patients experiencing persistent allergic rhinitisrelated impairment.
Montelukast sodium, being alkaline and stable, and levocetirizine dihydrochloride, possessing acid stability, present a formulation challenge when combined in a matrix tablet. Their interaction may render the formulation unstable over its shelf life. Thus, a bilayer tablet is recommended to enhance stability. This bilayer configuration ensures prolonged stability of both drugs in combination, surpassing the performance of matrix tablets in stability studies.
Ciebiada et al conducted a study to evaluate the impact of treating persistent allergic rhinitis using montelukast, desloratadine, and levocetirizine either individually or in combination on quality of life.
Methodology: The study, spanning 32 weeks, employed a randomised, doubleblind, placebo-controlled crossover design with two arms. In one arm, 20 patients received montelukast 10 mg/d and/or desloratadine 5 mg/d or placebo, while in the other arm, 20 patients received montelukast 10 mg/d and/or levocetirizine 5 mg/d or placebo. Treatment periods were separated by two-week washout intervals, and quality of life was assessed before initiating treatment and at the end of each treatment period using the Rhinoconjunctivitis Quality of Life Questionnaire. Sleep issues were also evaluated.
Findings: In the arm receiving desloratadine plus montelukast, the qualityof-life score mean (SEM) prior to treatment was 3.1 (0.41). After placebo, it decreased to 2.16 (0.43), further decreased to 1.79 (0.38) after desloratadine, to 1.48 (0.37) after montelukast, and to 1.59 (0.37) after the combination of montelukast and desloratadine. In the arm receiving montelukast plus levocetirizine, the pretreatment quality of life score mean was 2.58 (0.49), dropping to 1.78 (0.46) after placebo, and further decreasing to 1.38 (0.42) after levocetirizine, to 1.36 (0.37) after montelukast, and to 1.26 (0.39) after the combination of montelukast and levocetirizine.
Conclusion: Placebo, montelukast, desloratadine, and levocetirizine all led

to significant improvements in quality of life. Combining montelukast with either levocetirizine or desloratadine provided additional benefits compared to individual agents and could be considered for patients experiencing impaired quality of life due to persistent allergic rhinitis.
In another study by Ciebiada et al, the authors evaluated the treatment outcomes of patients with persistent AR receiving montelukast, levocetirizine, desloratadine alone, or in combination with montelukast.
Results revealed that montelukast alone, levocetirizine alone, desloratadine alone, and the montelukast/antihistamine combinations significantly alleviated nasal symptoms within the initial 24 hours. This improvement continued to escalate over the six-week treatment period, particularly among patients receiving montelukast alone or in combination with antihistamines in both arms. Notably, patients treated with the combination of montelukast and levocetirizine exhibited significantly greater improvement on day 42 compared to day one of therapy. These findings underscore the gradual and sustained improvement in nasal symptoms achieved with montelukast alone or in combination with antihistamines over a six-week treatment duration in patients with persistent AR.
Combining montelukast and levocetirizine represents a significant advancement in AR treatment, offering enhanced symptomatic relief and improved quality of life compared to monotherapy. Moreover, its costeffectiveness makes it a practical option for patients with affordability concerns. Healthcare providers should consider both clinical efficacy and economic
feasibility when selecting treatment options for AR. The synergistic combination of montelukast and levocetirizine presents a balanced solution, enriching the arsenal of therapies available for AR management.
Rathod RT, Misra D. FDC of montelukast with levocetirizine: focus on bilayer technology. J Indian Med Assoc. 2009 Aug;107(8):562-4. Erratum in: J Indian Med Assoc. 2009 Oct;107(10):734. PMID: 20112841. Bjermer L, Westman M, Holmström M, Wickman MC. The complex pathophysiology of allergic rhinitis: scientific rationale for the development of an alternative treatment option. Allergy Asthma Clin Immunol, 2019:16;15:24. Doi: 10.1186/s13223-018-0314-1. PMID: 31015846; PMCID: PMC6469109. Mahatme MS, Dakhale GN, Tadke K, Hiware SK, Dudhgaonkar SD, Wankhede S. Comparison of efficacy, safety, and cost-effectiveness of montelukastlevocetirizine and montelukast-fexofenadine in patients of allergic rhinitis: A randomized, double-blind clinical trial. Indian J Pharmacol, 2016;48:649-53. Pawankar R, Mori S, Ozu C, Kimura S. Overview on the pathomechanisms of allergic rhinitis. Asia Pac Allergy, 2011;1:157-67. Doi: 10.5415/apallergy.2011.1.3.157. Epub 2011 Oct 11. PMID: 22053313; PMCID: PMC3206239.
Nur Husna SM, Tan HTT, Shukri N, Mohd Ashari NS and Wong KK. Allergic Rhinitis: A Clinical and Pathophysiological Overview. Front Med, 2022. Doi: 10.3389/fmed.2022.874114
Panchal S, Patil S, Barkate H. Evaluation of efficacy and safety of montelukast and levocetirizine FDC tablet compared to montelukast and levocetirizine tablet in patients with seasonal allergic rhinitis: a randomized, double blind, multicentre, phase III trial. Int J Otorhinolaryngol Head Neck Surg, 2021;7:83-90. Ciebiada M, Ciebiada MG, Kmiecik T, DuBuske LM, Gorski P. Quality of life in patients with persistent allergic rhinitis treated with montelukast alone or in combination with levocetirizine or desloratadine. J Investig Allergol Clin Immunol. 2008;18(5):343-9. PMID: 18973097.
Ciebiada, Maciej & Gorska-Ciebiada, Malgorzata & Barylski, Marcin & Kmiecik, Tomasz & Gorski, Pawel. Use of Montelukast Alone or in Combination with Desloratadine or Levocetirizine in Patients with Persistent Allergic Rhinitis. American journal of rhinology & allergy. 2011:25. e1-6. 10.2500/ ajra.2011.25.3540.

www.glenmarkpharma.co.za.
Levocetirizine dihydrochloride 5
Levocetirizine (second-generation antihistamine) and montelukast (leukotriene receptor antagonist)1
Levocetirizine & montelukast combat both early and late-phase seasonal allergic rhinitis. 2,3
Montelukast targets the underlying inflammation, while levocetirizine provides symptom relief by blocking histamine. 1,2
The cardiovascular safety of testosterone use in ageing men has been a subject of extensive debate and research. Two landmark studies offer valuable insights into the associations between sex hormones and cardiovascular (CV) outcomes.
EAP et al's STUDY investigates how circulating sex hormones affect mortality and cardiovascular disease (CVD) risk in ageing men. This study aims to clarify the relationships between testosterone, sex hormone-binding globulin (SHBG), luteinizing hormone (LH), dihydrotestosterone (DHT), and oestradiol
incident CVD events. The study accounted for various covariates, such as age, BMI, marital status, alcohol consumption, smoking, physical activity, hypertension, diabetes, creatinine concentration, cholesterol ratios, and lipid medication use.
From nine studies with data encompassing 255 830 participant-years
Androgel Targeted AD (MC).pdf 1 2024/05/28 12:48
including 24 109 participants, key findings emerged. Men with testosterone levels below 7.4 nmol/L had higher all-cause mortality, and those with levels below 5.3 nmol/L had higher CVD mortality. Higher all-cause mortality was associated with LH levels above 10IU/L and was linked to oestradiol levels below 5.1pmol/L. Lower


all-cause and CVD mortality. In terms of DHT, there was a nonlinear association with mortality, where both low and very high levels increased all-cause and CVD mortality risks. Very low DHT also increased the risk of incident CVD events.
• Testosterone: Low levels are consistently associated with higher all-cause and CVD mortality, suggesting a direct impact regardless of the underlying cause.
• SHBG: Higher SHBG concentrations correlate with increased all-cause mortality, likely due to its role in modulating the bioavailability of sex hormones.
• DHT: Exhibits a U-shaped relationship with mortality, indicating that both low and high levels are detrimental.
• LH and oestradiol: High LH and very low oestradiol levels are linked to higher allcause mortality but not specifically to CVD mortality.
SEX HORMONES AND CVD
Lincoff et al's TRAVERSE study addresses uncertainties about the cardiovascular safety of testosterone-replacement therapy in middle-aged and older men with hypogonadism. It specifically examines whether this therapy increases the risk of CV events in men with pre-existing CVD or multiple risk factors. The FDA initiated a review of testosterone products in 2010 after a small trial indicated increased cardiovascular events. Subsequent metaanalyses showed inconsistent results. This trial, larger than all previous ones combined, provided a more definitive assessment. The consistency of results across analyses confirmed the noninferiority of testosterone therapy. In a randomised, placebo-controlled trial involving 5198 men over a mean followup of 22 months, testosterone therapy was noninferior to placebo concerning major adverse cardiac events (MACE), with a hazard ratio of 0.96 (95% CI, 0.78 to 1.17). The findings support the cardiovascular safety of testosterone-replacement therapy in middle-aged and older men with hypogonadism, even among those with cardiovascular disease or multiple risk factors. Previous trials have shown additional benefits such as improved sexual function, bone mineral density, correction of unexplained anaemia, and reduced depressive symptoms.
SUMMARY
While low testosterone is associated with higher all-cause and CVD mortality, testosterone-replacement therapy is noninferior to placebo regarding major adverse cardiac events, offering reassurance to clinicians and patients considering this treatment.
References available on request.
Erectile dysfunction (ED) is a prevalent condition characterised by the inability to achieve or maintain an erection sufficient for sexual intercourse.
THIS CONDITION CAN significantly impact quality of life and often indicates underlying health issues. Understanding the multifactorial nature of ED is crucial for effective diagnosis and management.
DEFINITION AND PREVALENCE
ED is a penile disorder affecting erection by preventing adequate blood flow to the erectile tissue. It can result from physical, psychological, or combined factors. It is the most reported sex-related condition among men aged 40 to 70, with prevalence increasing with age and comorbid health conditions.
Vascular: The most common type, vascular ED, involves blood vessel issues in the penis and is often linked to cardiovascular diseases, atherosclerosis, hypertension, and hyperlipidaemia.
Neurogenic: Neurogenic ED results from nerve damage preventing signal transmission from the brain to the penis due to pelvic trauma, spinal cord injuries, neurological diseases, or pelvic surgeries.
Hormonal: Hormonal imbalances, particularly testosterone deficiency, can lead to ED. Thyroid disorders also fall under this category. Psychogenic: Psychogenic ED arises from psychological factors such as stress, anxiety, depression, or relationship issues, often requiring psychological counseling or therapy.
SYMPTOMS AND DIAGNOSIS
Symptoms include difficulty achieving or maintaining an erection, reduced rigidity, and needing extensive stimulation. Diagnosis involves medical and sexual history, physical examination, and targeted laboratory tests, including:
• Blood tests (CBC, lipid panel, liver and kidney function, thyroid function, testosterone levels)
• Urinalysis
• Penile Doppler ultrasound
• Penile biothesiometry
• Vasoactive injection tests
• Magnetic resonance angiography.
MANAGEMENT AND TREATMENT
Lifestyle changes like more exercise, quitting smoking, managing weight, and healthy eating are first-line interventions. Oral medications such as phosphodiesterase type 5 inhibitors (sildenafil, vardenafil, tadalafil, avanafil) are commonly prescribed. Intracavernosal injections with alprostadil or combination therapies provide alternatives.
Device-based therapies like penile low-intensity focused shockwave therapy (LiSWT) and vacuum erection devices enhance penile blood flow.
Penile implants offer a surgical solution
for severe cases. Testosterone replacement therapy is beneficial for documented testosterone deficiency. Psychogenic ED often requires therapy, counseling, and psychiatric medication. Partner communication and support are critical.
CONCLUSION
Erectile dysfunction requires a comprehensive approach to diagnosis and treatment. Early identification and management improve outcomes and quality of life. Clinicians should suspect underlying health issues in ED patients

and adopt a holistic treatment approach, including lifestyle changes, medication, devices, hormonal treatment, and psychological support.
References available on request.











Pain science has long been mired in historical biases and misconceptions that reinforce systemic inequities.
medicine have reinforced harmful beliefs. Nobles and colleagues, in their Nature editorial, ‘Science must overcome its racist legacy’, highlight how scientific practices have endorsed racism through colonisation, apartheid, imperialism, and eugenics. Similarly, the exclusion of women from scientific professions and clinical trials has perpetuated gender disparities in pain research and treatment.
Bourke's exploration of pain sensitivity from 1800-1965 reveals how misconceptions about pain based on race, sex, and religion reinforced social hierarchies. These historical biases persist today, influencing pain assessment and management. For example, gender stereotypes often lead to the underestimation of pain in women due to beliefs that women are more emotive and men more stoic. Similarly,
racial misconceptions, such as the belief that black individuals have higher pain tolerance, continue to affect pain treatment recommendations.
Disparities in pain management are profound and persistent. Racial minority groups have been historically undertreated for pain, a problem recognised three decades


ago but still prevalent today. Biases and misconceptions influence pain care based on sociodemographic characteristics, including race, ethnicity, age, sex, gender identity, socioeconomic status, and sexual minority status. The very groups that bear the highest burden of pain are often underrepresented in pain research, exacerbating disparities.
To address these issues, editors of major pain journals endorse four principles to guide inclusive pain research and publication practices:
1. Promote inclusive and representative scholarship and fair, unbiased reviews.
• Authors should ensure diverse citations and consciously avoid omitting work based on sex, gender, race, ethnicity, or institution reputation
• Reviewers and editors must embrace diversity to foster broader perspectives and more generalisable science.
2. Use language that is inclusive and minimises bias
• Authors should use respectful and neutral language, avoiding stigmatising terminology
• Inclusive language guidelines from APA and AMA provide best practices for describing demographic characteristics respectfully.
3. Include representative populations in pain research and comprehensively report data
• Inclusion of diverse groups by sex, gender, age, race, and ethnicity is crucial for addressing pain inequities
• Authors should report demographic data comprehensively, reflecting on limitations when representative samples are not included.
4. Report demographic variables and use social frameworks for interpretations
• Authors should analyse and report data by demographic variables, considering social and cultural experiences in interpretations
• Misinterpretations of racial and ethnic differences as biological rather than social constructs must be avoided to prevent reinforcing stereotypes.
Addressing these principles is not merely about avoiding offense but is fundamental to improving the quality of pain science. By fostering inclusion, diversity, and equity, the scientific community can develop treatments that better serve all individuals experiencing pain. The commitment to these principles across pain journals aims to yield more valid research and a broader impact on the field, marking a significant step towards eliminating disparities in pain science.
REFERENCE
Palermo TM, Davis KD, Bouhassira D, et al. Promoting Inclusion, Diversity, and Equity in Pain Science. Pain Med. 2023 Feb 1;24(2):105-109. doi: 10.1093/pm/pnac204. PMID: 36622210; PMCID: PMC9890303.


Dr Tshegofatso
Date: 18 July 2024
Time: 7:00pm
Topic: The benefits of the FDC of Levocetirizine/Montelukast vs Oral antihistamines
Speakers: Dr Tshegofatso Mabelane
CLICK TO REGISTER https://bit.ly/GlenmarkWebinar18Jul24
Dr Tshegofatso Mabelane is the first HPCSA certified Family Physician Allergist in South Africa. She obtained her subspecialist qualification in Allergology through the University of Cape Town and College of Medicine South Africa. She also did the allergy exam with the European Academy of Allergy and Clinical Immunology under the European Union of Medical Specialists.


Dr Mabelane is the director of About Allergy, involved in clinical trials for asthma and clinical immunology. She serves as an executive committee member of the Allergy Society of South Africa, Chairperson of the Diploma in Allergy for the College of Medicine South Africa. Her research in allergy led to the diagnosis of the 4th largest cohort in the world with red meat allergy.

Montelukast 10 mg
Levocetirizine dihydrochloride 5 mg
Montelukast (leukotriene receptor antagonist) and levocetirizine (second-generation antihistamine)1
Montelukast targets the underlying inflammation, while levocetirizine provides symptom relief by blocking histamine. 1,2
Montelukast and levocetirizine combat both early and late-phase seasonal allergic rhinitis. 2,3
scientific rationale for the development of an alternative treatment option. Allergy Asthma Clin Immunol. 2019;15:24. 3. Panchal S, et al. Evaluation of efficacy and safety of montelukast and levocetirizine FDC tablet compared to montelukast and levocetirizine tablet in patients with seasonal allergic rhinitis: a randomized, double blind, multicentre, phase III trial. Int J Otorhinolaryngol Head Neck Surg. 2021;7(1):83-90. For full prescribing information,
Rupatadine is a novel second-generation antihistamine that combines potent H1 receptor antagonism with platelet-activating factor (PAF) inhibition, offering a unique approach in managing allergic diseases.
RUPATADINE IS INDICATED for the treatment of allergic rhinitis and urticaria in those over 12 years of age.
PHARMACOLOGY AND KINETICS
Rupatadine, a selective long-acting H1 antagonist, shows high affinity for peripheral H1 receptors. Its metabolism is primarily facilitated by cytochrome P450
CYP3A4, with a half-life of 5.9 hours and high plasma protein binding (98%-99%). Food intake delays the time to peak plasma concentration by about one hour but does not alter the maximum concentration.
ANTI-INFLAMMATORY AND ANTIHISTAMINERGIC EFFECTS
Rupatadine shows significant efficacy in
animal and human models, outperforming loratadine and fexofenadine in suppressing histamine reactions. It inhibits histamineinduced skin reactions dose-dependently, with greater efficacy at higher doses (10-40 mg).
PAF ANTAGONIST ACTIVITY
PAF plays a crucial role in inflammatory




from the same mould.1





responses associated with allergic conditions. Rupatadine exhibits competitive PAF antagonism, reducing PAF-induced inflammatory responses more effectively than other antihistamines.
CLINICAL EFFICACY
Allergic rhinitis: Clinical studies confirm rupatadine's efficacy in reducing symptoms of seasonal (SAR), perennial (PAR), and persistent allergic rhinitis (PER). Rupatadine consistently showed fast onset of action and was more effective than placebo and comparable or superior to other antihistamines like cetirizine, loratadine, and ebastine. Chronic urticaria: Rupatadine significantly reduces pruritus and wheal formation in chronic urticaria patients, with a rapid onset of action. Studies show it is superior to placebo and as effective as levocetirizine, with notable quality of life improvements.
TOLERABILITY AND SAFETY
Rupatadine is well tolerated, with headache, drowsiness, and dry mouth as common side effects. No significant ECG changes occur, even at high doses. It has minimal CNS effects and does not impair psychomotor performance or driving ability at therapeutic doses.
DRUG INTERACTIONS
Rupatadine's exposure increases when co-administered with CYP3A4 inhibitors like ketoconazole and erythromycin, but without QT interval prolongation or increased side effects. Grapefruit juice increases rupatadine exposure and should be avoided.
GLOBAL SAFETY EVALUATION IN ALLERGIC RHINITIS AND URTICARIA González-Núñez et al (2016) showed rupatadine is:
• Highly selective for histamine H1receptors
• Exhibits additional PAF antagonism in in vitro and in vivo studies
• Does not cross the blood-brain barrier
• Has similar adverse events comparable with other second-generation antihistamines
• Is safe and well tolerated, with no central nervous system or cardiovascular effects and can be taken with or without foods.
Rupatadine, with its dual action as an H1 antihistamine and PAF antagonist, provides effective relief from allergic rhinitis and chronic urticaria with a good safety profile. Its rapid onset of action, minimal central nervous system effects, and favourable safety data make it a valuable option for managing these allergic conditions. Coadministration with certain drugs and grapefruit should be avoided.


LEAN is a set of operating philosophies that help create maximum value for patients by reducing waste. It emphasises consideration of customers' needs, employee involvement, continuous improvement, and harm reduction.
THIS CONCEPT AIMS to fundamentally change the organisations thinking and value, which should lead to the transformation of organisation behaviour and culture over time. Originally there were ‘7 Wastes of LEAN’ which were categorised by Taiichi Ohno, one of the fathers of the Toyota Production system. He separated the waste he saw, into seven categories, which made them easier to identify and eliminate.
Over time the LEAN philosophy changed to accommodate new situations and learnings. As such, an eight waste was recognised and added in the early 2000’s. The 'Waste of human potential' or the 'Waste of talent'.
Based on the Toyota model, it focuses on how new efficient resources are being used and asks what is being added for the customer in every process. Recently the healthcare industry has shown success in applying these principles in the United States, United Kingdom, Australia and now Canada. The principle of LEAN was proposed as a solution to the unsustainable increases of healthcare costs. The principle and aim were to rein in costs and add value to patients.
Essentially LEAN in healthcare aims to continuously improve by minimising waste in every process, procedure, and task. “Using the LEAN principle, all members of the organisation from clinicians to operations and administration staff, continuously strive to identify areas of waste and eliminate anything that does not add value to the patients.” [NEJM Catalyst: April 27, 2018]
One of the areas of focus is increasing 'customer’s' (patients and payer) satisfaction. The Foundational Principle of LEAN Philosophy is to end waste at every level of the organisation and 'LEAN thinking' requires buy in from every team member for it to be successful. This embeds into the organisation’s culture and promotes innovations at every level.
By adopting LEAN healthcare strategies, organisations are also improving patient satisfaction, as decisions and processes become more and more patient focused. The healthcare Industry adopted LEAN as a positive solution to this rising demand for improved healthcare quality while managing costs. To be successful both
the healthcare providers and managers in the microlevel, as well as healthcare policy makers in the macrolevel, strive to figure out how to improve healthcare outcomes for all stakeholders. LEAN principles have shown to be one of the most future promising means to achieve this aim. Despite indications that LEAN benefits healthcare, many researchers regard its implementation to be pragmatic, patchy, and fragmented. The application of LEAN management in healthcare can also be holistic such as transformation of an overall business strategy. With the lack of knowledge and misunderstanding of the preconditions of LEAN implementations in the healthcare Industry, practitioners have adopted tools in several processes which have resulted in the anticipated outcomes, though it is limited at this stage. Gomez et al (2010) pointed out that by optimising only one process in the entire value chain, sub optimising components would be at risk and eventually affect the entire value chain.”
Implementing LEAN in an isolated process would undermine the overall LEAN efforts in the healthcare organisation. Errors and mistakes in healthcare can be all parties since human life is at risk. As reported by Kohn et al (2000) nearly 90 000 patients admitted to hospitals lost their lives because of preventative medical errors and nosocomial infections.
Wagner (2004) identifies in hospital errors, as one of the leading causes of death in the United States. This stresses the need for healthcare organisations to incorporate LEAN management principles and integrate operations management to improve overall performance and minimise or eliminate harm during delivery of healthcare.
LEAN in healthcare goes beyond efficiency, it’s about creating a culture of continuous improvement and patient centric care.[Lisa Chang]
John Roberts a LEAN consultant for hospitals adds, “The key is to view the healthcare system from the patient’s perspective and continuously ask how we can deliver more value.”
Adopting LEAN in healthcare comes with the challenges - of which one is the complexity of healthcare systems, and the
variability of patients’ needs. To address this, many of the organisations have employed cross functional teams to map out patients journeys and show efficiencies. A major challenge is resistance to change, which can be overcome through effective communication and involving staff at all levels in LEAN initiatives.
Implementing LEAN principles has significantly improved patient care by reducing wait times and enhancing the accuracy of diagnoses and treatment through streamlined processes. Scientifically structured care pathways reduce harm and mitigate risks and adverse events, decreasing morbidity and mortality in facility-based interventions. In the rural environment, better supply chain management meant that patients always had access to the necessary medical supplies, improving overall care quality and safety.
Cut out the 'eight waste' Implementing LEAN in healthcare can reduce waiting and idle times by addressing the eight wastes.
Patients sitting in waiting rooms, meetings stalled for late comers, appointment waiting lists and idle hightech equipment are all areas that are opportunities for healthcare organisations to tap the creativity and imaginations of their teams to reduce waste. Minimal inventory represents tied up capital and storage costs, surplus supplies and medications superfluous equipment, extraneous data or stockpiles of preprinted forms, all translate to inventory waste. Employees can be trained to recognise excessive inventory and find novel ways to reduce it.
Eradicate defects to improve quality and increase reimbursement process or system failures, medical mistakes and misdiagnoses are examples of defect waste in healthcare. Other examples of defect waste include healthcare acquired conditions such as blood clots and infections, medications or surgical errors, avoidable readmissions, preventable allergic reactions, and incomplete erroneous medical records. LEAN principles advocate to mobilise
every employee to eradicate defect waste and improve quality to positively impact the bottom line and most importantly avoid mistakes.
Decrease the movement of patients, supplies, and equipment to improve patient flow. LEAN thinking can be used to analyse patient and caregiver movement through hospital facility to save time, reduce injury and improve patient flow.
PREVENT INJURIES AND SAVE TIME BY REDUCING MOTION
Waste in motion occurs whenever hospital workers perform movement within their workplace that does not add value for patients. This can include increased walking due to poor building design or nonergonomic patient transfers between beds, wheelchairs or operating tables are potential instances of motion waste. Duplication of tests and extending hospital stays beyond medical necessity are all issues that healthcare organisations can address by applying LEAN principles.
REMOVE WASTE FROM OVERPROCESSING
Over-processing occurs when unnecessary work goes into treating patients. By viewing all processes through the lens of LEAN healthcare, staff can help identify repetitive, redundant, or less than valuable processes to save time and money. Understand how healthcare waste leads to untapped Human Potential - THE PINNACLE OF WASTE IN HEALTHCARE.
When workers time is consumed by any of the above, they are unable to use it to leverage their creativity and talents for work that promotes patient care and optimised operation. Adopting a LEAN culture not only leads to improvements in care quality and decreased costs, but it also leads to improved employee morale and commitment. “As healthcare continues to evolve the adoption of lean principles offers promising pathways to meet the challenges of an increased complex healthcare landscape, ultimately leading to better patient outcomes and more sustainable healthcare systems.” Clive Hays, LEAN agile leadership expert.


Prof Natalie Schellack
Registered pharmacist
Date: 27 June 2024
Time: 18h00 - 19h00
Topic: The elemental Journey: Navigating the path to wellness
Speaker: Prof Natalie Schellack
CLICK TO REGISTER
https://bit.ly/P_GHealthWebinar27Jun24
Natalie Schellack is a registered pharmacist, Professor and currently the head of the Department of Pharmacology, University of Pretoria. She holds three degrees, two bachelor degrees (nursing and pharmacy) and a PhD in Pharmacy. Outside the University, she serves on the Gauteng Provincial Pharmacy and Therapeutics committee and nationally she serves as a member of the Tertiary and Quaternary Expert Review Committee for the National Department of Health. Her research interests are centred on the broad area of clinical pharmacy as related to paediatrics, ototoxicity and infectious diseases (eg TB and HIV). More specifically interested in quantifying antimicrobial utilisation data, pharmacokinetic and dynamic levels of antibiotics in blood levels. More recently her research area has been more focused on finding innovative ways of measuring antimicrobial utilisation using health technology. Research gate score is 32.68 and the information can be obtained at https://www.researchgate.net/profile/Natalie_Schellack?ev=prf_highl Twitter handle: @NSchellack


Publications: Google Scholar https://scholar.google.co.za/citations?hl=en&user=TC_ vFwcAAAAJ&view_op=list_works&gmla=AJsN-F5OL67Zbd0GlNYxeQ1O4qqEUt7lLKQP2In bk-s71hWV-klRnx1uSa4En5aEU2hkR8XrSxJgPRifSkCo0TKtqP735nq8RsG2P9Na6Qz2IUbI7 OA6nxg
She is a co-founder of the South African Society of Clinical Pharmacy (SASOCP). She has also been awarded the following, Best Established Researcher in the School of Health Care Sciences, Best Overall Female Researcher, Best Overall Researcher in the University and the Chancellor’s Distinguished Teaching and Learning Excellence Award. In 2018 she has also been nominated as the woman of the year – health care category for “woman of stature” in South Africa. She has been elected as a member of the South African Pharmacy Council. She is also a rated researcher (C2) as awarded by the National Research Foundation (NRF), furthermore she is the fourth elected member of the South African Antimicrobial Stewardship Programme (SAASP).
Social anxiety disorder (SAD) is often overlooked and misunderstood, frequently mistaken for mere shyness or an introverted disposition.
NLIKE THESE TEMPERAMENTAL traits, SAD leads to significant and enduring social impairment. Globally, it ranks as the third most common mental health condition after depressive and addictive disorders. Diagnosing SAD can be challenging due to cultural, gender, and situational factors, such as work and school environments, which influence social interactions. Social anxiety involves the fear of scrutiny in social situations, ranging from meeting new people to performing tasks as mundane as eating in front of others. While some anxiety is situationally appropriate, such as before a major presentation, SAD is characterised by persistent negative thoughts about being judged or ridiculed. This disorder can severely impact various aspects of life and doesn't necessarily stem from traumatic social experiences. According to the DSM-5, a diagnosis of SAD requires symptoms to persist for at least six months. In children, SAD may manifest as school refusal, potentially being mistaken for separation anxiety. For teenagers and young adults, it can hinder social interactions like making new friends or asking someone out. In individuals with visible medical conditions or disfigurements, diagnosing SAD requires distinguishing between general anxiety and excessive or unrelated fears. The disorder also includes specific phobias such as paruresis, the fear of urinating in public restrooms. In the US, SAD affects approximately 7% of the population, with higher rates in women. Globally, prevalence ranges from 5% to 10%, with a lifetime prevalence of 8.4% to 15%. Research indicates a slow increase in cases from the 1960s to the early 2000s, predominantly among married and educated individuals. The relationship between SAD and problematic internet use is not fully understood, but studies suggest a link between anxiety and excessive internet usage. Common coping mechanisms for SAD include using alcohol or other substances and blushing, a hallmark physiological response. The DSM-5 identifies a subtype of SAD known as performance-only anxiety, where fear is confined to public speaking or performing. This can be particularly debilitating in educational or professional settings. Avoiding feared situations often leads to missed opportunities and significant personal and professional costs. Milder symptoms include anxiety, over-preparation, or needing a companion for events. Diagnosing SAD involves screening for comorbid conditions such as other anxiety disorders, substance use, and mood disorders like depression. Tools like the Social Phobia Inventory and the Liebowitz Social Anxiety Scale aid in diagnosis.
primary treatment for SAD in both adults and younger individuals. Mindfulness and acceptance-based therapies, such as acceptance and commitment therapy (ACT) and mindfulness-based stress reduction (MBSR), also show promise. CBT typically involves 15 to 20 sessions focused on gradual exposure to feared social situations, cognitive restructuring, and altering core beliefs to improve quality of life and prevent
DE
relapse. For young patients, parental education and involvement are crucial.
PHARMACOLOGICAL INTERVENTIONS
First-line pharmacotherapies include selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors These medications require 4–6 weeks for noticeable benefits. While monoamine oxidase inhibitors like show high response
rates, their adverse effects limit their use as first-line treatments. Emerging evidence supports combining CBT with paroxetine for enhanced outcomes. Additionally, new treatments like nasal anti-anxiolytics show potential for short-acting, as-needed relief before anxiety-provoking situations.
Source: Psychiatric Times, 2023.

PSYCHOTHERAPEUTIC INTERVENTIONS
Cognitive-behavioural therapy (CBT) is the

Dr Dion Craig Opperman
Date: 31 July 2024
Time: 7:00pm
Topic: Managing the complications/symptoms of MS
Speaker: Dr Dion Craig Opperman

CLICK TO REGISTER: https://bit.ly/ActivoHealthWebinar31Jul24
Fellow of the College of Neurologists of South Africa (FC Neurol) by peer review since 2008.
Research: MMed dissertation on Myotonic Dystrophy
Clinical Trials: We took part in various clinical trials including: Alnitidan, Aricept, SP511, Lamictin, Elitriptan, Zomitriptan, Topiramate (for migraine prophylaxis), Epilepsy, 3 Migraine trials, Devco D.
Specific Fields of Interest
• Multiple Sclerosis
• Parkinson’s Disease

• Dystonia (I run a Botox clinic for dystonia)
• Headache
• Epilepsy
• Peripheral Neurology (Nerve Conductions and EMG)
Publications
Co-author: Giampaolo, D, Bhigjee, A, Retief, C, Isaacs, M, Britz, M, Opperman, D, Govender, R, & van Rensburg, M (2013). Guideline for the diagnosis and management of multiple sclerosis: A Southern African perspective. South African Medical Journal, 103(9), 670-691.

Isotretinoin is an oral prescription medication primarily used to treat severe acne by affecting sebaceous glands.
PPROVED BY THE US Food and Drug Administration (FDA) in 1982, it is particularly effective for severe, nodular acne that does not respond to conventional treatments, including systemic antibiotics. Isotretinoin is effective for severe acne and has several non-FDAapproved uses, including moderate acne, cutaneous T-cell lymphomas, neuroblastoma, and preventing squamous cell carcinoma in high-risk patients. It is also used to treat rosacea, folliculitis, and pyoderma faciale.
MECHANISM OF ACTION
As a systemic retinoid taken orally, isotretinoin inhibits sebaceous gland function and keratinisation, reducing gland size and sebum production. Though its exact mechanism is unknown, it effectively treats acne at doses of 0.5 to 1mg/kg per day. For neuroblastoma, it decreases cell proliferation and induces differentiation.
ADMINISTRATION
Isotretinoin is available in capsule form and is highly lipophilic. To maximise absorption, it should be taken with a meal and a full glass of water to prevent oesophageal irritation. The typical dosing starts at 0.5mg/kg per day, gradually increasing to 1mg/kg per day, with a treatment course lasting 15 to 20 weeks for sustained remission.
ADVERSE EFFECTS
Common dose-dependent side effects: cheilitis (dry lips), dry skin, dry mouth, dry nose, and sun sensitivity. Patients should use sun protection, moisturisers, and avoid skin procedures during and six months after treatment. Frequent laboratory monitoring is necessary for hypertriglyceridemia and increased erythrocyte sedimentation rate. Other potential adverse effects include pruritis, irritation, hair thinning, dry eyes, skin infections, rashes, bone or joint pain, and muscle aches. Paediatric patients often report back and joint pain.
LABORATORY ABNORMALITIES
Common laboratory abnormalities include decreased HDL, increased liver function tests, increased creatinine phosphokinase, decreased haemoglobin and haematocrit, decreased erythrocyte and leukocyte counts, and increased platelet counts. Isotretinoin should be discontinued if neutropenia or agranulocytosis occurs.
SERIOUS REACTIONS AND PRECAUTIONS
Recent studies do not significantly correlate controversial associations with inflammatory bowel disease or depression. Serious skin reactions like Stevens-Johnson syndrome and toxic epidermal necrolysis warrant discontinuation. Acute pancreatitis has also been reported, necessitating cessation if symptoms appear.
Patients should avoid blood donation during and for one month after treatment due to the risk of embryo-foetal toxicity. Screening for depression and other psychological conditions is recommended, and isotretinoin should not be combined with tetracyclines due to the risk of pseudotumor cerebri.
CONTRAINDICATIONS AND MONITORING
Sotretinoin is contraindicated in pregnant women due to severe birth defects. The FDA's iPLEDGE program ensures compliance with pregnancy prevention measures, requiring negative pregnancy tests and the use of two forms of birth control.
Monitoring: Females of child-bearing potential must have two negative pregnancy tests before starting isotretinoin and monthly tests thereafter. All patients
should have baseline liver function tests, lipid profiles, blood glucose, creatinine phosphokinase, and complete blood counts. Biweekly monitoring is necessary during the initial treatment phase.
REFERENCE
Pile HD, Sadiq NM. Isotretinoin. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK525949/


For the first time since its publication, the World Happiness Report (WHR) provides a comprehensive analysis of happiness trends across generations, giving separate rankings by age group.
EN Z’ REFERS TO anyone born from 1997 onward. This group’s wellbeing is down in the Anglosphere, Western Europe, and South Asia but up in Central and Eastern Europe. Notably, the USA has fallen out of the top 20 ‘happiest countries’ for the first time, driven by a significant drop in the wellbeing of Americans under 30: it now ranks 62nd in the world for the young! The UK ranks 20th, but its youth ranks 32nd – why are young adults in the west so unhappy?
Social media has been publicised as the cause of the decline in Gen Z’s mental health and happiness, but it can’t be the only reason. For Mental Health Awareness Week, we looked into this drop – and find it’s a mystery.
Dr Michael Plant, research director at the Happier Lives Institute and Fellow at the Wellbeing Research Centre, Oxford University, points out the problem without laying all the blame on social media:
“Over the past 20 years, we have seen young people become less happy in North America and Western Europe. But, over the same period, youth wellbeing in Central and Eastern Europe has gone up. Social media is everywhere. I expect it’s one cause of reduced wellbeing, but it’s hard to see how it could be the only culprit.”
What does explain the drop in Western countries? Researchers aren’t sure. “There is no consensus among academics regarding the role of social media, at least from a global perspective. Interestingly, regions like Central and Eastern Europe, with similar levels of social media use, exhibit divergent wellbeing trends. In general, it is not clear yet what is driving negative and positive trends in different parts of the world, and
this is partly due to limited data availability in non-Western countries,” says Dr Jose Marquez, a WHR chapter author on youth wellbeing.
Prof Lara Aknin, co-editor of the WHR, emphasises the multifaceted nature of the issue. “Pinpointing a single cause proves challenging. Yet, the data suggests that today’s North American youth face increased stress and anxiety, lower satisfaction with their living situation, diminished social support, and declining trust in governmental institutions,” she explains.
There are many possible explanations on the table, but researchers haven’t yet analysed these factors to identify their importance. Some options include:
• The pervasive influence of social media1
• The culture of comparison, amplified by digital platforms2
• Media portrayal, both traditional and social, contributing to negative perceptions3
• Societal polarisation and widening inequality4
• Diminishing prospects and quality of life5
• The rise of wealth disparity and resource monopolisation6
• Lingering anxieties about the future, fuelled by climate concerns and economic uncertainties7
• A sense of disconnection and over work culture8
• Declining religious affiliations affecting communal bonds9
• A prevailing sense of disillusionment with politics and societal structures.10
Mental distress: Some respondents reported experiencing mental distress, including thoughts or attempts of suicide and the use of antidepressants. Those with absent fathers were particularly prone to these issues. Female influence: There was a notable strong female influence, both in upbringing and in role models.
Collectivist society: Interviewees often come from large, multigenerational households, highlighting a collectivist society that supports the elderly, unemployed adult dependents, and differently-abled individuals, in contrast to the individualistic mindset prevalent in the West.
Delayed adulthood: Many young adults are delaying traditional markers of adulthood; they often live with their parents, remain unmarried, and do not own cars or property.
Workplace identity: This fracturing of identity extends to the workplace, where young people maintain strictly professional personas and are cautious about revealing personal details to colleagues and employers
Education and employment disconnect: Many unemployed interviewees are highly educated, revealing a gap between their education and the skills needed by industry. Often, their career aspirations differ significantly from their current or past studies.
Perceptions of racism: About half of the sample have experienced racism, yet the same proportion believes that racism is an issue primarily for older generations.
As we navigate through plausible speculations and empirical realities, one thing is clear – the decline in Western wellbeing defies a simple explanation.
“Frankly, I don’t know why youth wellbeing has dropped so fast in Western Countries – but not elsewhere. I’m not sure anyone does. While I want to see schools trial things like whole-day phone bans, given the terrifying, unexplained scale of the drop in Western youth wellbeing, researchers need to investigate the global picture, identify the causes, and work out what we need to do to restore happiness to Gen Z and those that come after,” says Dr Plant.
Closer to home, Flux Trends and Student Village have published the 30/30/30 Project Report, which includes interviews with 30 young South Africans under the age of 30, 30 years into the country's democracy.
To learn more about the Happier Lives
Institute and Dr Michael Plant’s work, go to: www.happierlivesinstitute.org.
REFERENCES
1. https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC10476631/ 2. https://www.nature.com/articles/s44159-02300244-2 3. https://www.protectingourstudents.org/ understanding-medias-influence-on-school-shootingsgun-control-and-youth-perceptions/
4. https://www.brookings.edu/articles/risinginequality-a-major-issue-of-our-time/
5. https://www.usnews.com/news/best-countries/ articles/2020-09-11/a-global-anomaly-the-usdeclines-in-annual-quality-of-life-report 6. https://www.nber.org/papers/w27922
7. https://www.nature.com/articles/d41586-02400998-6
8. https://hbr.org/2023/08/why-we-glorify-overworkand-refuse-to-rest
9. https://www.nature.com/articles/s41599-02100797-8 10. https://academic.oup.com/pa/ article/69/4/876/2468902?login=false#41827133


Dr HV Pitamber
Dermatologist in private practice in Johannesburg, South Africa
MBBCh (WITS) FCDERM (SA)
IMPORTANT ACHIEVEMENTS:
Date: 17th July 2024
Time: 19h00
Topic: The do’s and don’ts of prescribing isotretinoin for GPs
Speaker: Dr HV Pitamber
Publications: CLIN EXP DERMATOL 2003; 28: 17-21.
Pitamber HV, Grayson W.
Five cases of Cutaneous Rosai-Dorfman Disease
CLINICS IN DERMATOLOGY (2005); 23, 258-266
Hetesh V Pitamber, E Joy Schulz.
Dermatoses in Life- threatening Metabolic and Endocrine Disorders
Professional Affiliations and Involvement:
Member of the Dermatological Society of South Africa
Member of the Dermatological Surgical Society of South Africa.


Ex Member of the South African Melanoma Advisory Board (SAMAB) (involved actively in the prevention of skin cancer and melanoma campaigns viz with the Springbok Rugby Team in November 2010).
Ex member of the Africaderm Network.
Key opinion leader for various dermatological companies.
Regular attendance of the Congress of the European Academy of Dermatology and Venereology (EADV) and American Academy of Dermatology Congresses.
Other: Guest speaker on national television: Bonita House Call, SABC NEWS International, Health Issues guest speaker for local radio stations: Radio Islam, Channel Islam, 702 Talk Radio and Eastwave Radio on current dermatological issues contributor to various magazines on dermatological topics: Cosmopolitan, Oprah, Femina and Netcare and Skin Deep magazines.



The WELLTH Fund has had a powerful impact in encouraging people to complete their annual Health Checks and reinforced the value of preventive care in increasing the lifespan and health span of members of Discovery Health Medical Scheme. pays out more than R600 million since January 2023
SINCE THE INTRODUCTION of the WELLTH Fund in January 2023, more than 500 000 beneficiaries of Discovery Health Medical Scheme (DHMS) have activated and claimed from the benefit. The once-off benefit will be available until 31 December 2024.
To-date, over R600 million has been paid out to providers and members from the WELLTH Fund. Members have predominantly used their WELLTH Fund to access dentists, GPs, physiotherapists, optometrists, obstetricians, and gynaecologists. DHMS claims data shows that during January to December 2020, the first year of the Covid-19 pandemic, annual Health Checks carried out by members dropped by 52%, compared to the same period in 2019.
With the introduction of the WELLTH Fund in January 2023, we are pleased to note that the health checks rate has
not only returned to pre-Covid levels but exceeded expectations. In 2023, we saw more than double the number of Health Checks compared to 2021. In comparison to 2022, there was a 47% increase in health checks in 2023.
HOW DOES THE WELLTH FUND WORK?
The WELLTH Fund is activated once all beneficiaries on a DHMS plan have completed their Health Checks. For adults, this is the annual Health Check (funded from the existing DHMS Screening and Prevention Benefit), and for children (two years and older), the annual online Kids Health Review.
- The Health Check available to DHMS adult members involves tests for blood pressure, blood glucose, cholesterol, and waistadjusted Body Mass Index (BMI). The assessment also includes a voluntary non-
smoker’s declaration and HIV screening.
- Health Checks can be completed inperson at a Discovery Store, an accredited pharmacy, a GP’s rooms in the Discovery Health Wellness Network or at an employer’s Wellness Day.
Once the WELLTH Fund is activated, each adult beneficiary is allocated R2 500 and children between the ages of two and 18 years of age are allocated R1 250 each –up to a limit of R10 000 per family. Children under the age of two have full access to the fund once a primary member has activated the benefit, without first having to complete any health check.
The WELLTH Fund gives members access to six broad categories of preventative health services. These include:
• General health screenings including screenings for visual, hearing, dental and skin conditions.
• Physical health screening at a dietician, chiropractor, biokineticist and/or physiotherapist.
• Mental health wellness check-ups.
• Women and men’s specific health screening such as gynaecological, prostate and/or heart consultations with a doctor and bone density checks.
• Children’s specific health screening in the form of a child wellness visit which includes growth and developmental milestone assessments with an occupational therapist, speech therapist and/or physiotherapist.
• Medical monitoring devices for personal monitoring of key health metrics including blood pressure, cholesterol, blood sugar management and respiratory.
A groundbreaking HIV vaccine candidate developed by the Duke Human Vaccine Institute has demonstrated the ability to stimulate low levels of a crucial type of broadly neutralising HIV antibodies in participants of a 2019 clinical trial.
published on May 17 in the journal Cell, not only validates the vaccine's capacity to induce these antibodies, which are pivotal in combating diverse strains of HIV, but also highlights its ability to initiate this process within a matter of weeks, thus initiating a vital immune response.
The vaccine candidate targets a specific area on the HIV-1 outer envelope known as the membrane proximal external region (MPER), which stays relatively stable despite the virus's mutations. Antibodies directed against this region of the virus's outer coat have the potential to block infection by numerous circulating strains of HIV. According to senior author Barton F Haynes, MD, director of the Duke Human Vaccine Institute, this breakthrough represents a significant advancement in HIV vaccine research. He emphasises that while the induction of neutralising antibodies against the most challenging strains of HIV is promising, the ultimate goal is to elicit even more potent neutralising antibodies against other vulnerable sites on the virus to prevent viral escape.
Theultimategoal is to elicit even more potent neutralising antibodiesagainst other vulnerable sites on the virus topreventviral escape
The study, which analysed data from a phase 1 clinical trial, involved twenty healthy, HIV-negative participants. After just two immunisations with the investigational vaccine, a remarkable 95% serum response rate and a 100% blood CD4+ T-cell response rate was observed, indicating robust immune activation. Importantly, the vaccine induced broadly neutralising antibodies after just two doses, a feat that typically takes several years post-infection to achieve. Despite the trial being halted due to a participant experiencing a non-life-threatening allergic reaction, the researchers remain optimistic about the vaccine’s potential.
Lead author, Dr Wilton Williams, underscores the challenge of recreating the complex series of events necessary to induce broadly neutralising antibodies within a shorter timeframe using a vaccine. However, he notes the excitement of witnessing the emergence of neutralising antibodies within weeks of vaccination, thanks to this vaccine molecule. The
researchers acknowledge that further work is needed to enhance the vaccine’s effectiveness and target additional regions of the virus envelope. They envision a successful HIV vaccine consisting of multiple components aimed at vulnerable sites on the virus envelope to prevent viral escape.
CONCLUSION
This study demonstrates the feasibility of inducing broadly neutralising antibodies in humans through vaccination. With this knowledge, researchers are poised to replicate and build upon these findings, paving the way for the development of a highly effective HIV vaccine that could
transform the landscape of HIV prevention and treatment.
REFERENCE
Williams WB, Alam SM, Ofek G, et al. Vaccine induction of heterologous HIV-1-neutralizing antibody B cell lineages in humans. Cell, 2024; DOI: 10.1016/j. cell.2024.04.033.




Prof Claudia Gray, a paediatrician with specialised accreditation in allergology and paediatric pharmacology, part-time consultant at the Allergy and Asthma clinic at Red Cross Children’s Hospital, and an Associate Professor in Paediatrics at the University of Cape Town, recently presented a webinar on the interplay between allergic rhinitis (AR) and asthma. The webinar was sponsored by Inova in the interest of education, awareness, and support.
AR, OFTEN KNOWN as hay fever, extends beyond being a mere seasonal inconvenience. It manifests when the immune system reacts excessively to harmless substances, resulting in symptoms like itching, sneezing, congestion, and eye irritation.
Despite sometimes being trivialised, AR can significantly impact both physical and emotional well-being, causing discomfort and reducing functionality in daily life.
Understanding the immune response involved in AR reveals the formation of specific immunoglobulin E antibodies upon initial allergen exposure. Upon subsequent encounters, these antibodies trigger mast cells to release various mediators, leading to symptoms like itching, sneezing, and congestion. Additionally, cytokines released during this process can perpetuate inflammation, worsening symptoms over time. Traditional classification focused on seasonal versus perennial AR, but newer guidelines prioritise symptom duration and severity. The Allergic Rhinitis and its Impact on Asthma guidelines categorise AR into intermittent and persistent forms,
with further subdivisions based on impact on quality of life (QoL). AR, especially when moderate to severe, disrupts sleep, hinders work or school performance, and interferes with leisure activities. It is vital to recognise AR's substantial impact beyond inconvenience and address it comprehensively to improve patients' QoL, stressed Prof Gray. Early testing for environmental allergies in children is feasible and beneficial, helping differentiate between infections and allergies for appropriate treatment.
MYTHS AND MISCONCEPTIONS
Correcting misconceptions about AR is crucial for accurate diagnosis and treatment. Differentiating between allergies and infections can be challenging due to overlapping symptoms, but allergy testing is instrumental in proper classification.
A prevalent myth is that allergy medications should only be taken when symptoms are present. In reality, proactive medication use can be more effective as allergic inflammation can occur before symptoms emerge, noted Prof Gray.
Furthermore, the belief that using only one brand of allergy medication leads to tolerance build-up lacks evidence. Dispelling these myths can lead to better-informed treatment decisions and improved patient outcomes, she stressed.
It
MANAGING ALLERGIC RHINITIS
Managing AR involves minimising allergen exposure and utilising pharmacological interventions tailored to individual
needs. Intranasal corticosteroids and antihistamines are mainstays in treatment, with newer formulations offering improved efficacy and reduced side effects.
According to Prof Gray, antihistamines capable of inhibiting both histamine and platelet-activating factor hold a theoretical advantage for alleviating allergic AR symptoms, particularly nasal congestion - a benefit that many antihistamines lack. Furthermore, combination nasal sprays containing intranasal antihistamine corticosteroids offer an advantage by providing multiple benefits in a single device.
Recognising the interconnectedness of AR and asthma and adopting a proactive approach to treatment is essential for optimal disease control, she concluded.
Comprehensive management of AR requires understanding its pathogenesis, tailoring treatment, and considering the latest advancements in pharmacotherapy. Addressing both symptom relief and underlying inflammation is key to enhancing outcomes and improving patients' QoL



DUAL-ACTION RUPANASE® BLOCKS HISTAMINE FOR RELIEF OF DAYTIME SNEEZING, RUNNY, ITCHY & BLOCKED SYMPTOMS, AND PAF* FOR RELIEF OF NASAL CONGESTION AT NIGHT2-6
Once-daily 24 hour relief2,7,8 Starts to work from the first dose9
*platelet activating factor
§Allergic Rhinitis
†based on once a day dosing
Non-drowsy8
Relieves chronic urticaria symptoms from the first week10

Based on 2,5 ml daily dose
Syringe included
References: 1. South African Medicine Price Registry. Database of Medicine Prices, 01 November 22 [online]. [cited 2022 Nov 17]; Available from URL: http://www.mpr.gov.za/. 2. Marmouz F, Giralt J, Izquierdo I, et al. Morning and evening efficacy evaluation of rupatadine (10 and 20 mg), compared with cetirizine 10 mg in perennial allergic rhinitis: a randomized, double-blind, placebo-controlled trial. J Asthma Allergy 2011;4:27–35. 3. Picado C. Rupatadine: pharmacological profile and its use in the treatment of allergic disorders. Exp Opin Pharmacother. 2006;7(14):1989-2001. 4. Ridolo E, et al. Rupatadine for the treatment of allergic rhinitis and urticaria: a look at the clinical data. Clin Invest 2014;4(5):453-461. 5. Smolensky MH, Lemmer B, Reinberg AE. Chronobiology and chronotherapy of allergic rhinitis and bronchial asthma. Adv Drug Deliv Rev 2007;59:852–882. 6. Alfaro V. Role of histamine and platelet-activating factor in allergic rhinitis. J Physiol Biochem 2004;60(2):101-112. 7. Valle M, et al. PD39 - Application of population pharmacokinetic modeling and simulation in the design of the optimal dose regime of rupatadine in children 2-5 year old children. Clin Transl Allergy 2014;4(Suppl 1):P39. 8. RUPANASE Junior approved professional information, June 2020. 9. Potter P, et al. Rupatadine oral solution in children with persistent allergic rhinitis: A randomized, double-blind, placebo-controlled study. Pediatr Allergy Immunol. 2013;24(2):144-150. 10. Potter P, et al. Rupatadine is effective in the treatment of chronic spontaneous urticaria in children aged 2–11 years. Pediatr Allergy Immunol. 2016;27(1):55-61.
Scheduling status: S2 Proprietary name (and dosage form): RUPANASE 10 Tablets. Composition: Each tablet contains 12.80 mg rupatadine fumarate equivalent to Rupatadine 10 mg base. Contains sugar: lactose monohydrate 61.1 mg per tablet. Registration number: 46/5.7.1/0119. Name and business address of applicant: iNova Pharmaceuticals (Pty) Ltd, Co. Reg. No. 1952/001640/07, 15e Riley Road, Bedfordview. Tel. No. 011 087 0000. www.inovapharma.co.za. For full prescribing information, refer to the professional information as approved by the SAHPRA (South African Health Products Regulatory Authority) available at www.inovapharma.co.za. Further information is available on request from iNova Pharmaceuticals. 21828L. IN4808/23
S THE PREVALENCE OF autism diagnoses increases, Dr Nerica Ramsundhar, a neurodevelopmental paediatrician at Netcare St Augustine’s Hospital in Durban, highlights the signs and symptoms parents should watch for. “In the past five or six years, the number of autism diagnoses has risen from one in 56 to one in 36 children, according to the 2023 US Center for Disease Control (CDC) guidelines. Autism affects more males than females,” she notes.
Autism is characterized by neurodevelopmental differences affecting socialization, communication, and behavior. “People with autism often have unique ways of socializing and communicating, accompanied by repetitive behaviours and fixated interests. Sensory processing can also be affected,” says Dr Ramsundhar. Children on the autism spectrum may communicate differently. “This impacts expressive language (ability to talk), receptive language (ability to understand), and non-verbal communication (facial expressions, eye contact, gestures, and
body language). Their use of expressive language varies greatly. Some may have fluent speech but struggle with conversational skills, making undirected, non-purposeful, delayed, or scripted utterances. Others might create their own words or speak in a singsong manner.”
Autistic children might also have affinities for languages other than their home language, and they may respond inconsistently to their names or exhibit auditory processing differences. “Reduced eye contact and the absence of common gestures like pointing are typical. Facial expressions may appear flattened or muted,” explains Dr Ramsundhar. Repetitive behaviours such as hand flapping, jumping, body twirling, and object spinning are also common.
Understanding restrictive behaviours in autistic children is crucial. “These children thrive on routine and familiarity, often becoming upset by changes. They may insist on specific orders of things and have difficulty with applied knowledge. Fixated interests, such as an intense focus on a
particular hobby or topic, can impede their ability to connect with others.”
Social interaction can be altered as well. Some autistic children may avoid social interaction, while others might be overly friendly. “Challenges in taking turns, sharing, and engaging in functional play with toys are often observed,” she adds. Early clues to autism can include difficulties with breastfeeding, fragmented sleep patterns, being hard to soothe, and a lack of response to their name or decreased eye contact.
As they grow, children might show delayed expressive language and reduced use of gestures. “They might not clap, blow kisses, or wave goodbye. Play behaviours can also indicate autism; they may show a late interest in toys, prefer to play alone or engage in parallel play, and exhibit repetitive play patterns. Difficulty in regulating emotions, particularly when faced with changes, is another sign to investigate,” advises Dr Ramsundhar.
Neurodevelopmental paediatrics, a subspecialty focused on conditions affecting a child’s development and behavior, plays
a key role in diagnosing autism. “The diagnostic process includes a parental interview covering pregnancy, birth, developmental, and medical history, and a review of three generations of the family. This interview, which should be conducted away from the child, explores the family’s observations on play, sociability, repetitive behaviours, and processing differences,” she explains.
Following the interview, an interaction and observation session with the child is conducted. “We assess how the child interacts, their interest in parents, their requests to others in the room, and the coordination of expressive language with gestures. A clinical examination checks for neurological factors that might explain the symptoms, such as epilepsy, cerebral palsy, traumatic brain injury, or genetic causes,” says Dr Ramsundhar.
She emphasizes the importance of community support for children with autism and their families. “Support from the community through simple gestures, caring, and kindness is crucial,” she concludes.



Date: 1 August 2024
Time: 6pm
Topic: The Dry Eye Wheel
Speaker: Dr Marsha Oberholzer CLICK TO
Dr Marsha Oberholzer is a proud South African that has earned three academic degrees from the University of Johannesburg in South Africa. After completing her B.Optom degree, she pursued her Master’s degree in Optometry and thereafter, her PhD in Visual Science which she completed in 2015. After her undergraduate studies, she embarked on a career starting out as an Independent Optometrist, practicing in Johannesburg, South Africa after which she spent four years assisting an Ophthalmologist and Refractive Surgeon in his practice. Dr Oberholzer joined the Optometry School of the University of the Free State in South Africa in 2008 as a senior lecturer, lecturing and training undergraduate and postgraduate students in especially the niche fields of Ocular Pathology and Neuro-Optometry. Her teaching background includes the management of the undergraduate Optometry programme at this university and involvement in the Professional Board (HPCSA) accreditation and re-curriculation of the undergraduate Optometry programme. During this time, she travelled across the world lecturing and training clinicians in a variety of optometric fields, mostly in the field of Higher Order Aberrations, which was the focus of her PhD Studies. She also served as a key opinion leader for Alcon Laboratories during this time, after which she then permanently joined Alcon as the South African Professional Education


















and Development manager in 2019. Her journey with Alcon has given her the opportunity to not only train within the field of contact lenses locally and export markets, but also the opportunity to travel globally, being involved in the extensive training to GEM (Growth and Emerging markets) associates, distributors and Eye Care Professionals. Since September 2023, Marsha has been appointed as the Vision Care Professional Education and Product Training HEAD for GEM at Alcon.
Dr Oberholzer has won multiple awards during her career, under which the most valued are the winner of the 'Excellence in teaching and learning' award in the category Junior Lecturer at the UFS in 2011, Alcon AAA and GEM awards as well as the SA Alcon Hero award in 2022.
Currently Dr Oberholzer is expanding her horizons with more extensive trainings globally at Alcon. She is also still an affiliated postgraduate lecturer at the University of the Free State where she continues to actively lead Masters and PhD Optometry students in their postgraduate studies. Even though her first love may be 'eyes', she is also a musician, actively playing the violin and viola in professional Orchestras in South Africa. She is a wife, and mother of three (one daughter and two sons) which keeps her on her toes and humble. GSA-VC-2400004





There is a growing preference among both consumers and healthcare professionals to use natural medications and cough syrups before resorting to conventional chemical treatments.
as thyme, ivy, and marshmallow root have been employed for over a millennium to alleviate coughs, demonstrating clinical efficacy and safety. Healthcare practitioners have observed better compliance and potentially fewer side effects with natural products compared to their chemical counterparts.
According to Dr Peter Voitl, a specialist paediatrician and paediatric expert for the European Medicines Commission for Paediatrics with special focus on phytotherapy, one could make the argument that demulcents like Althaea officinalis, more commonly known as marshmallow root extract, could be used as a first-line treatment for cough.
Althaea officinalis, commonly known as marshmallow root extract, is an herbal demulcent traditionally used to treat oral or pharyngeal irritation and associated dry cough. This extract, recognised in European Medicines Agency (EMA) and World Health Organization (WHO) monographs, is also used as an emollient for wounds and dry skin. Marshmallow root extract is rich in carbohydrate mucilage, which coats the cough receptors in the throat, forming a protective barrier that relieves irritation and soothes inflamed tissues. This coating effect reduces the sensitivity of cough receptors, thereby diminishing the urge to cough. Research by Al-Snafi (2013) attributes these demulcent effects to the high content of polysaccharide hydrocolloids in marshmallow root, which soothe local irritation and inflammation, significantly reducing the frequency and intensity of cough episodes.
Marshmallow root extract consists of long-stranded polysaccharides that are not systemically absorbed, allowing it to be safely used with expectorants. Combining an expectorant with a demulcent can be particularly beneficial during colds, as it facilitates mucus expulsion while locally reducing the urge to cough.
Honey is another effective demulcent, particularly recommended for children over the age of one by the WHO. Honey rapidly coats the throat, reducing both the frequency and severity of cough while protecting the pharyngeal mucosa against irritants. This makes honey especially valuable for nighttime use, ensuring a peaceful rest. Dr Voitl highlights that demulcents are crucial for alleviating cough in children, who often experience painful

throat irritation. Studies, such as those cited by Goldman (2014), support the use of a single dose of honey to reduce mucus secretion and cough in children. However, honey should not be used in infants under one year due to the risk of botulism.
For secretolytic action, Dr Voitl prefers thyme as an expectorant. According to the EMA monograph, thyme extract has been traditionally used to treat various respiratory conditions, including coughs, bronchitis, and laryngitis. Thyme's essential oils stimulate the serous glandular cells and ciliated epithelium, improving mucociliary clearance and reducing mucous gland activity. Studies suggest that thyme (Thymus vulgaris) offers expectorant, mucolytic, and antispasmodic effects, along with potential antibacterial,
antifungal, and antiviral activities.
CONCLUSION
Dr Voitl concludes that marshmallow root extract, honey, and thyme are safe and effective first-line therapies for cough. He emphasises the underestimated value of demulcents in treating coughs and highlights the importance of taste in paediatric treatments. For children, a palatable, safe, and effective product is essential for ensuring compliance and therapeutic success.
REFERENCES
WHO monographs on selected medicinal plants (Volume 1). World Health Organization, Geneva. 1999. Al-Snafi A. (2013). The Pharmaceutical importance of Althaea officinalis and Althaea rosea: A review. International Journal of PharmTech Research. 5. 1378-1385.
Ciuman RR. Phytotherapeutic and naturopathic
adjuvant therapies in otorhinolaryngology. Eur Arch Otorhinolaryngol. 2012 Feb;269(2):389-97. doi: 10.1007/s00405-011-1755-z. Epub 2011 Sep 16. PMID: 21922427; PMCID: PMC3259400. Paul IM, Beiler J, McMonagle A, et al. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Arch Pediatr Adolesc Med 2007; 161:1140-6. doi: 10.1001/archpedi.161.12.1140. PMID: 18056558. Oduwole O, Udoh EE, Oyo-Ita A, Meremikwu MM. Honey for acute cough in children. Cochrane Database of Systematic Reviews 2018, Issue 4. Art. No.: CD007094. DOI: 10.1002/14651858.CD007094. pub5.
Goldman RD. Honey for treatment of cough in children. Can Fam Physician. 2014;60(12):1107-1110.
Assessment report on Althaea officinalis L., radix. 2016. European Medicines Agency.
Sultana, S., Khan, A., Safhi, M.M., & Alhazmi, H. (2016). Cough Suppressant Herbal Drugs: A Review. Capasso F., Gaginella T.S., Grandolini G., Izzo A.A. (2003) Plants and the Respiratory System. In: Phytotherapy. Springer, Berlin, Heidelberg. https://doi. org/10.1007/978-3-642-55528-2_18
Assessment report on Thymus vulgaris L., vulgaris zygis L., herba. 2013. European Medicines Agency.













Dual action; working locally and systemically
Forms a protective coating on the pharynx
Reduces sensitivity of the cough receptors
Relieves local irritation
Reduces the urge to cough
Reduces severity of cough
Thins mucus and helps open airways
Forms a protective barrier against irritants
e.g. post-nasal drip
Reduces the urge to cough at night
Diaphoretic effect helps relieve mild fever
Mildly sedative to promote sleep
Not known to be habit-forming
Not known to cause respiratory depression
Citingrabiesasaclassic exampleoftheveryclose connection between human and animalhealth,ProfTambyah said control of this disease in animal hosts was critical
As Africa faces burgeoning infectious disease outbreaks, including Mpox in the Democratic Republic of the Congo and cholera in multiple countries this year alone, the International Society for Infectious Diseases (ISID) has urged the continent to accelerate multidisciplinary One Health solutions to curb the threat.
THE INTERSECTION OF infectious diseases in humans, animals, and the environment is a global concern, with limited-resource countries worst impacted, warned ISID president, Prof Paul Tambyah. “Understanding this integration is critical if we are to address the complex health challenges we face and save lives.” Prof Tambyah was speaking ahead of the 20th International Congress on Infectious Diseases, being held in Cape Town, South Africa, this December. More than 3 000 infectious disease experts from more than 100 countries are expected to attend, with One Health-related health threats a priority agenda item. The largest congress of its kind globally, will showcase an accredited programme focused on clinical infectious disease knowledge and practice, novel translational science, infection prevention protocols, and the epidemic intelligence of Infectious Diseases.
While health, food, water, energy, and the environment are all wider topics with sector-specific concerns, collaboration across sectors has been shown to address health challenges more effectively such as the emergence of infectious diseases, antimicrobial resistance, and food and
water safety.
Citing rabies as a classic example of the very close connection between human and animal health, Prof Tambyah said control of this disease in animal hosts was critical, given that rabies kills more than 50 000 people every year, mostly children in Africa.
“The most effective way of reducing human rabies is to control the animal reservoirs through vaccination of dogs and other animal hosts, which has worked extremely well in high-, middle- and lowincome settings alike which have launched combined veterinary and public health programmes to control the disease,” he explained.
The One Health concept is not entirely new to Africa, research shows, although serious implementation gaps remain. Between 2007 and 2009, the approach was successfully used to control an outbreak of Rift Valley fever in Kenya, in part due to coordination between the Kenya Ministry of Health and the Ministry of Agriculture, Livestock and Fisheries. In 2006 in Nigeria, the One Health approach enabled a successful multi-sectoral emergency action plan that led to the elimination of the highly pathogenic avian
influenza virus H5N1 in Nigeria.
More recently, said Prof Tambyah, effective vaccination of commercial poultry, which has been used in many parts of Asia for more than a decade, has virtually eliminated human disease in those settings.
Cholera, meanwhile, is a clear example of the link between environmental factors and human health. Between January 2023 and March 2024, more than 270 000 cases and nearly 6 000 deaths were reported in 18 African countries, driven by persistent gaps in access to safe water and sanitation.
“Provision of clean water and safe sanitation has probably saved more lives from infectious diseases than any other intervention, long before the advent of antibiotics and chlorination of municipal water,” said Prof Tambyah.
At the upcoming Congress, he added, a special ICID Ubuntu Community Village, built within the programme, would enable activists and patient groups to interact with researchers, clinicians, and public health professionals – and give a voice to those impacted by infectious diseases from all walks of life, both globally and locally. A policy forum would allow policymakers to hear directly from people living and working
with infectious diseases and share their plans for public health interventions.
“If we are to scale up the One Health approach sufficiently to make a real difference among worst-affected populations, it is important to hear from those whose ground-up initiatives are taking the lead, to turn the tide on this evergrowing threat in Africa and worldwide,” Prof Tambyah said. For more information about ICID 2024, visit https://isidcongress.org/
In December, Cape Town will welcome over 3 000 delegates from first-time attendees to key thought leaders to the Cape Town International Convention Centre (CTICC) for the 20th International Congress on Infectious Diseases (ICID 2024).The ISID is dedicated to developing partnerships and finding solutions to the problems of Infectious Diseases across the globe and encourages collaborative efforts of human, veterinary, and environmental health communities working locally, nationally, and globally for the best control and management of infectious diseases.
Prof Richard van Zyl-Smit recently shared insights and strategies for navigating this diagnostic puzzle during a webinar for Medical Chronicle, sponsored by Cipla.
THE HUMAN LUNG, often likened to a complex sponge, plays a pivotal role in facilitating the exchange of oxygen and carbon dioxide in our bloodstream. However, when patients present with symptoms that don't neatly fit into the categories of asthma or chronic obstructive pulmonary disease (COPD), medical professionals are challenged to unravel the mysteries of interstitial lung diseases (ILDs).
DECONSTRUCTING THE LUNG
Central to understanding ILDs is a grasp of the lung's fundamental function: oxygenation and carbon dioxide removal. Dyspnoea, or shortness of breath, often heralds an ILD diagnosis. Van Zyl-Smit emphasised the importance of meticulous inquiry into the patient's symptoms, such as onset, exacerbating factors, and associated sensations like chest pain or dizziness.
Recognising the subtleties of ILDs requires a keen clinical eye. Certain clues may raise suspicion: a gradual onset of symptoms, typically in older patients, accompanied by a persistent cough and crackling sounds upon chest examination. Finger clubbing, a physical sign often overlooked, can be a crucial indicator of an underlying lung pathology. Van Zyl-Smit cautions against the pitfalls of 'anchoring' – the tendency to fixate on a presumed diagnosis –urging physicians to maintain a broad differential approach.
The hallmark of ILDs is shortness of breath during exertion, prompting a comprehensive evaluation. Beyond the traditional asthma or COPD assessment, thorough auscultation of the chest and cardiac examination are warranted.
Diagnostic imaging, including chest X-rays, serves as an initial step in the diagnostic journey, but the importance of revisiting the patient for a detailed history cannot be overstated.
Navigating the labyrinth of ILD terminology requires familiarity with the jargon. ILD encompasses a spectrum of conditions, from the ominous idiopathic pulmonary fibrosis (IPF) to less severe forms like nonspecific interstitial pneumonia (NSIP). Understanding these classifications, such as usual interstitial pneumonia (UIP) patterns on imaging, is pivotal in guiding further management.
KEY TAKEAWAYS: THINK SPONGE...
Prof Van Zyl-Smit captured the essence of ILD diagnosis in a mnemonic: “Think sponge.” This mantra emphasises key

clinical features: shortness of breath and crackles on auscultation, suggesting a need for further evaluation. Patients with ILDs may possess unique characteristics, such as the ability to lie flat without exacerbation, challenging the conventional wisdom of heart failure as the primary aetiology. Prof van Zyl-Smit underscored the importance of clinical judgment, cautioning against overreliance on radiology reports and advocating for a multidisciplinary approach involving lung function tests, high-resolution CT scans, and collaboration with specialists. In conclusion, navigating the landscape of interstitial lung diseases requires a blend of clinical acumen, diagnostic precision, and a holistic approach to patient care. By embracing a comprehensive evaluation strategy and remaining vigilant for subtle clues, medical professionals can unravel the complexities of ILDs and deliver optimal outcomes for their patients.

Dr Eleonora Cinelli (dermatologist with a rich academic background) and Kim Louw, National Commercial Manager at Cosmetiques de France, The French Skincare Specialists, recently presented a webinar on Avène's acne range. The following article is based on their presentations.
ACNE IS A prevalent skin condition characterised by the development of non-inflammatory lesions like comedones and inflammatory lesions such as papules, pustules, and nodules, which may leave behind scars or pigmented macules.
Recent data from a global study involving over 50 000 individuals aged 16 and above from 20 countries revealed an overall acne prevalence of 20.5%. The highest prevalence was observed in the age group of 16 to 24, reaching 28.3%. Additionally, there has been a noted increase in adult acne, with approximately one in five individuals between 25 and 39 years old being diagnosed with acne.
The impact of acne extends beyond physical effects to encompass psychological effects and a diminished quality of life. Hence, effective management strategies are crucial, with dermocosmetics playing a significant role. Understanding the pathophysiology of acne-prone skin has
highlighted the potential of skincare products in maintaining homeostasis and preventing microcomedone formation, a pivotal aspect of long-term acne therapy.
Avène offers a comprehensive range of products tailored to address the diverse needs of acne-prone skin. These products include cleansers like Cleanance cleansing gel and micellar water, which effectively remove impurities and excess sebum while respecting the skin's sensitivity. Additionally,
the Cleanance comedomed Anti-blemishes concentrate targets an early stage of comedogenesis, reducing lesions and preventing their recurrence.
The range also features exfoliating serums and mattifying emulsions that regulate sebum production and refine skin texture. Ingredients such as Comedoclastin™ and Avène Thermal Spring Water work synergistically to control hyperseborrhea and provide soothing
and anti-irritant effects. Furthermore, the soothing cream is ideal for alleviating irritation and restoring the skin barrier in acne-affected skin undergoing treatment.
A recent 12-month international real-life cohort study demonstrated the efficacy and safety of Avène products in acne management. Participants experienced a significant reduction in clinical lesion counts, with a sustained improvement observed over time. The products were well-tolerated, with minimal withdrawals due to intolerance.
In conclusion, Avène's range of dermocosmetic products offers comprehensive support for acne management, targeting not only visible lesions but also underlying infra-clinical abnormalities. By maintaining homeostasis in acne-prone skin, these products play a vital role in long-term therapy, empowering patients of all ages to achieve clearer, healthier skin.

The field of allergy diagnosis has seen significant advancements. In a CPD-accredited webinar sponsored by Thermo Fisher Scientific, Dr Magnus Borres, a leading specialist in paediatric allergology and immunology, presented on diagnosing IgE-mediated food allergies. This article summarises key points from Dr Borres’ presentation, highlighting the new EAACI guidelines and the clinical utility of allergen component testing.

EVOLUTION OF ALLERGY DIAGNOSIS
Dr Borres began by tracing the history of allergy diagnosis, emphasising the shift from traditional methods to more precise diagnostic tests. A central theme of his presentation was the use of allergen components in diagnosis. Unlike whole allergen extracts, specific IgE (sIgE) testing to allergen components offers higher specificity, which is particularly beneficial for foods like peanuts, hazelnuts, cashew nuts, and sesame.
KEY ALLERGEN COMPONENTS AND THEIR CLINICAL UTILITY
Understanding the role of specific allergen components is critical for accurate diagnosis. Dr Borres highlighted several components with significant clinical utility:
• Ara h 2 (Peanut)
• Cor a 14 (Hazelnut)
• Ana o 3 (Cashew)
• Omega-5 gliadin (Wheat)
• Ovomucoid (Egg)
• Casein (Milk)
• Jug r 1 (Walnut)
• Ses i 1 (Sesame).
These components are instrumental in distinguishing true food allergies from cross-reactivities, particularly in pollensensitised patients, where false positives can occur. For instance, Ara h 2 is highly
specific for peanut allergy, while other peanut proteins may indicate crossreactivity to pollen.
THE ROLE OF 2S ALBUMINS
A significant portion of the webinar focused on 2S albumins, described by Dr Borres as ‘the bad guy’ in food allergies. IgE antibodies to 2S albumins are strongly associated with IgE-mediated food allergies. These albumins are also pivotal in understanding allergic reactions to sesame seeds and storage proteins in peanuts and nuts, which are linked to higher inflammatory markers in asthma.
DIAGNOSTIC TESTS: COMPONENT TESTING
Component testing stands out as a secondline diagnostic tool, providing more specific results than traditional methods. Dr Borres explained that sIgE to allergen components like Ara h 2, Cor a 14, and Ana o 3, combined with a confirmed history and positive extract testing, ensures a more accurate diagnosis of food allergies. This method is particularly useful for patients with pollen sensitivities, where cross-reactive allergens can lead to false-positive results.
ECONOMIC ASPECTS AND RETESTING
Dr Borres also touched on the health economic benefits of using allergen
components in clinical settings. Component testing can reduce the need for oral food challenges (OFCs), which are both costly and time-consuming. He advocated for retesting food-allergic children to monitor the development of tolerance, an essential step in managing and potentially overcoming food allergies.
INCREASING PREVALENCE OF NUT ALLERGIES
The webinar also addressed the rising prevalence of nut allergies globally. In the US, nut allergy prevalence increased by a massive 373% from 2005 to 2014. Similar trends were observed in Canada and Sweden. Dr Borres discussed the accuracy of diagnostic testing for tree nut allergies, emphasising that testing for storage proteins like Cor a 14, Cor a 9, Jug r 1, and Ana o 3 enhances diagnostic specificity for hazelnut, walnut, and cashew allergies.
Identifying individuals at risk for tree nut allergies is crucial. The HealthNut Study in Australia revealed that children with egg and peanut allergies often have IgE to tree nuts, with cashew being the most common. Dr Borres highlighted the importance of monitoring these patients over time, as many develop tree nut allergies by the age of six.
The BSACI and UK guidelines for managing nut allergies recommend a cautious approach. While complete avoidance is the safest strategy, it is often impractical and can lead to significant dietary restrictions. Patients are advised to continue consuming nuts they are not allergic to, while being aware of cross-contamination risks, especially in restaurant settings.
Dr Borres concluded by discussing milk and egg allergies, where self-diagnosis and over-diagnosis are common. He stressed the importance of introducing small amounts of these foods to allergic children to help develop tolerance. Component testing can aid in determining whether tolerance has been achieved, facilitating the return to a normal diet.
Dr Borres’ presentation provided a comprehensive overview of the latest advancements in allergy diagnosis, particularly the use of allergen component testing. These insights are invaluable for healthcare professionals aiming to enhance diagnostic accuracy, improve patient outcomes, and manage the rising prevalence of food allergies effectively.

Sexual dysfunction, particularly erectile dysfunction (ED), is a prevalent and distressing complication of diabetes, affecting the quality of life for many patients. Renowned sexual health expert Dr Jireh Serfontein recently addressed this issue in a CPD-accredited webinar, sponsored by Accord Healthcare.
THE WEBINAR PROVIDED a comprehensive overview of the impact of diabetes on sexual health, strategies for management, and the importance of addressing these concerns in clinical practice.
THE SCOPE OF THE PROBLEM
Globally, diabetes affects 366 million people, with South Africa home to 3.5 million diabetics, comprising 6% of the population. An additional five million South Africans are pre-diabetic, with Type 2 diabetes being the most common and preventable form. The link between diabetes and sexual dysfunction is significant, with 85% of diabetic men and 84% of diabetic women experiencing some form of sexual dysfunction. Men with diabetes are three times more likely to suffer from ED.
The Multinational Survey of Ageing Males (MSAM) highlighted the importance of sexual health, with 83% of men aged 40-70 affirming that sexual desire and interests are crucial aspects of life.
Sexual health is essential for overall well-being, influencing personal identity, mental health, and social relationships.
The World Health Organization defines sexual health as a state of physical, mental, and social well-being in relation to sexuality, needing a positive and respectful approach to sexual relationships.
UNDERSTANDING SEXUAL DYSFUNCTION
Sexual dysfunction in diabetes can arise from various factors:
1. Psychological factors: Chronic illness and associated stress.
2. Hyperglycaemia: Leading to macrovascular and microvascular complications, including neuropathies.
3. Hypogonadism: Often due to low Sex Hormone-Binding Globulin (SHBG) from insulin resistance and increased aromatisation in visceral fat, converting testosterone to oestradiol.
Other contributing factors include hypertension, dyslipidaemia, obesity, depression, and medication side effects.
HYPOGONADISM AND ITS CONSEQUENCES
Low testosterone levels, or hypogonadism, can result from diabetes. This condition leads to various health issues such as loss of libido, sexual problems, cardiovascular risks, and obesity. Testosterone replacement therapy can mitigate these effects by improving body composition, insulin resistance,erectile function, and bone health. However, monitoring is essential, particularly for prostate-specific antigen (PSA) and haematocrit (HCT) levels.
ERECTILE DYSFUNCTION IN DIABETES
Erectile dysfunction in diabetic men is notably severe, occurring 10-15 years
earlier than in non-diabetics and being less responsive to treatment. The causes are multifactorial, involving both psychological and organic factors such as vasculopathy, neuropathy, visceral adiposity, and hypogonadism. Risk factors include age, depression, alcohol abuse, smoking, hypertension, and cardiovascular disease.
TREATMENT STRATEGIES FOR ERECTILE DYSFUNCTION
Management of ED includes:
1. Lifestyle modifications: Can reduce ED risk by 70%.
2. Mechanical devices: Rings and vacuum erection devices.
3. Pharmacological treatments: PDE5 inhibitors like sildenafil, tadalafil, and vardenafil, which require sexual stimulation to be effective. Intra-cavernous injections (eg, Caverject) provide an alternative when nerve function is impaired.
4. Surgical interventions: Considered in severe cases.
FEMALE SEXUAL DYSFUNCTION
In diabetic women, sexual dysfunction can stem from hyperglycaemia, infections, vascular and neurological damage, and hormonal disorders. Management includes counselling, lifestyle changes, lubricants, devices, hormonal treatments (testosterone, DHEA, oestrogens), and pharmacological options like bupropion.
ADDRESSING SEXUAL HEALTH IN

CLINICAL PRACTICE
A significant barrier to effective management is the reluctance of patients to discuss sexual health issues with their doctors, fearing embarrassment or dismissal. The PLISSIT model offers a structured approach to address these concerns:
1. Permission: Encouraging open discussion about sexual concerns.
2. Limited information: Providing information to dispel myths.
3. Specific suggestions: Offering tailored advice for specific issues.
4. Intensive treatment: For more complex cases requiring specialised therapy.
TOOLS FOR ASSESSMENT
Using standardised tools such as the Female Sexual Function Index (FSFI), the International Index of Erectile Function (IIEF-5), and the Ageing Male Score (AMS) can aid in the assessment and management of sexual dysfunction in diabetic patients.
Dr Serfontein's webinar underscores the importance of recognising and addressing sexual dysfunction in diabetic patients. With a comprehensive approach that includes psychological support, lifestyle changes, and medical treatments, healthcare providers can significantly improve the quality of life for their diabetic patients.
Dr Johan Grobbelaar recently presented an enlightening webinar exploring advanced sinus solutions. This webinar was sponsored by Austell Pharmaceuticals.
DR GROBBELAAR DIVED into the intricacies of sinusitis; a condition marked by inflammation of the sinuses. Sinusitis can be classified into acute, chronic, and recurrent forms, each with distinct characteristics and diagnostic criteria.
DIAGNOSTIC TOOLS FOR SINUSITIS
1. VAS Score: A simple visual analogue scale to rate the severity of symptoms.
2. SNOT-22: A self-reported questionnaire with 22 questions scored from 0 to 5, totalling 110 points.
3. Lund MacKay Score: A CT score assessing sinus opacification on a scale from 0 (clear) to 2 (completely opacified), with a maximum of 24 points.
INTERNATIONAL DEFINITION OF SINUSITIS
To diagnose sinusitis, two or more of the following symptoms must be present, with at least one being nasal blockage or discharge:
• Blockage/obstruction/congestion
• Anterior/posterior nasal discharge
• Facial pain/pressure
• Loss/reduction of smell
Additionally, diagnostic confirmation requires endoscopic signs or CT changes. TYPES AND SPECTRUM OF SINUSITIS
1. Acute rhinosinusitis (ARS): Lasts less than 12 weeks.
2. Chronic rhinosinusitis (CRS): Persists for more than 12 weeks.
3. Recurrent acute rhinosinusitis (RARS): Four or more episodes per year.
4. Acute exacerbation of chronic rhinosinusitis (AECRS): Worsening of CRS symptoms.
ACUTE RHINOSINUSITIS (ARS)
ARS can be viral or bacterial, with the majority being viral. Common viruses include rhinovirus, influenza, and coronavirus.
Bacterial ARS often involves Streptococcus pneumoniae and Haemophilus influenzae.
Predisposing factors for ARS
• Smoking (active and passive)
• Odontogenic problems
• Anatomical variations
• Ciliary dysfunction
• Immunodeficiency
• Mechanical issues (eg, deviated septum, nasal polyps).
BACTERIAL vs VIRAL SINUSITIS
Determining when antibiotics are necessary is crucial. Indicators for bacterial sinusitis include discoloured discharge, severe unilateral pain, high fever, and elevated CRP/ESR levels. Overuse of antibiotics can lead to resistance and adverse effects
without significantly improving outcomes for viral infections.
Treatment of ARS
Viral ARS (common cold)
• Education on the condition
• Decongestants (less than 10 days)
• NSAIDs/Paracetamol
• Zinc and Vitamin C
• Nasal rinses
• Herbal medicine (eg. BNO1016, cineole).
BACTERIAL ARS
• Similar initial treatments as viral ARS
• Antibiotics after 7-10 days if symptoms persist or worsen.
CHRONIC RHINOSINUSITIS (CRS)
CRS is divided into CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP). The former is often associated with allergies and treated with steroids, while the latter may follow untreated acute bacterial rhinosinusitis and requires antibiotics.
FACTORS CONTRIBUTING TO CRS
• Genetic predisposition
• Environmental factors (eg, pollution, smoking)
• Microbial dysbiosis

• Host factors (eg, immune deficiencies, anatomical variations).
Treatment approaches for CRS
• Topical and systemic steroids
• Nasal rinses
• Surgery (eg, Functional Endoscopic Sinus Surgery – FESS) for refractory cases.
INNOVATIONS IN TREATMENT
Dr Grobbelaar highlighted the role of biofilms in CRS, which are resistant bacterial communities. Treatments include surgical removal, aggressive irrigation, and use of topical antibiotics like mupirocin.
COMPLICATIONS OF SINUSITIS
Severe complications can arise, particularly from bacterial infections, including:
• Orbital cellulitis
• Intracranial abscesses
• Meningitis.
PREVENTION STRATEGIES
Preventive measures include the use of probiotics, regular exercise, and Vitamin D supplementation. Annual flu vaccines are also recommended to reduce the incidence of viral infections leading to sinusitis
Dr Grobbelaar’s webinar emphasised the importance of accurate diagnosis, appropriate use of antibiotics, and innovative treatments for managing sinusitis effectively
Medical Chronicle recently hosted a product webinar on the launch of Tavirant, highlighting it as a crucial alternative when necessary. Dr Kay Mahomed, the keynote speaker, provided an in-depth analysis of Tavirant, a product developed by Cipla, emphasising its role as a first-line antiretroviral therapy (ART) option.
R MAHOMED DISCUSSED several factors that underline the importance of alternative ART options like Tavirant, particularly in the context of an ageing HIVpositive population and those with various comorbidities. Key issues include:
• Ageing population: Increased incidence of comorbidities such as hypertension and diabetes mellitus
• Renal issues: Both inherent renal complications and those arising from HIV-associated nephropathy and certain medications
• Chemotherapy: For patients undergoing cancer treatment
• Medications: Interactions with drugs like Purbac, acyclovir, amphotericin B, kanamycin, and NSAIDs
• Acute and opportunistic infections: Such as osteoporosis and a history of fractures, especially in elderly and postmenopausal women.
Given these factors, Dr Mahomed
stressed the importance of having alternative ART options that are safe, have minimal side effects or toxicity, and are suitable for various populations including children and adolescents.
TDF vs TAF: UNDERSTANDING THE DIFFERENCES
Dr Mahomed highlighted the differences between tenofovir disoproxil fumarate (TDF) and tenofovir alafenamide (TAF), both of which are key components in ART regimens.
• Virological efficacy: Both TDF and TAF exhibit similar virological efficacy
• TDF: Dosage of 300mg, known for reduced dyslipidaemia
• TAF: Dosage of 25mg, a prodrug with 90% lower plasma concentration. It achieves four times higher levels in lymphocytes and hepatocytes, reducing proximal tubular toxicity and the risk of bone mineral density loss.
CLINICAL APPLICATIONS OF TDF, ABC, AND TAF
Dr Mahomed provided guidance on the use of TDF, abacavir (ABC), and TAF based on patients’ glomerular filtration rate (GFR):
• GFR >60: TDF is recommended
• GFR <60 and >30: TAF is preferred as an alternative to ABC, with the benefits of not requiring Hepatitis B surface antigen testing or human leukocyte antigen typing
• GFR <30: ABC is recommendedOsteoporosis: Patients with osteoporosis in the lumbar spine or femoral neck should consider TAF
• Adolescents and paediatrics: Considerations around pill size for ease of administration
• Cost: A factor in the selection of the appropriate regimen.
PERSONAL OBSERVATIONS
Drawing from personal experience,

Dr Mahomed shared insights on the successful use of Tavirant:
1. Usage abroad: Tavirant has been employed as a first-line option with positive outcomes
2. Liver function: Patients with abnormal liver function tests switched from TEE (a combination of TDF, emtricitabine, and efavirenz) to TER (TAF, emtricitabine, and rilpivirine) without virological failure (VF) or significant side effects
3. Neurological side effects: Shift workers experiencing neurological side effects on TEE switched to TER, with no VF or side effects observed.
4. Long-term switch: All patients initially on TEE were switched to TER a decade ago, with sustained success and no VF or side effects.
5. Proactive switching: Emphasis on the importance of not waiting for renal issues to arise before switching to more suitable alternatives like TER.
Over 80 million people suffer from moderate-to-severe chronic obstructive pulmonary disease (COPD).
To view the webinar recording and still earn a CPD point, visit: https://event.webinarjam.com/replay/770/w8948cog4brpguo41f76rk
MEDICAL CHRONICLE HOSTED a CPD-accredited webinar on improving COPD outcomes, sponsored by Cipla and presented by Prof Guy Richards. This article summarises highlights from his talk. Asthma, a heterogeneous disease characterised by chronic airway inflammation, presents with respiratory symptoms like wheezing, shortness of breath, chest tightness, and cough, along with variable expiratory airflow limitation (GINA, 2017). COPD, a common, preventable, and treatable disease, is marked by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities, typically from significant exposure to harmful particles or gases (GOLD 2017).
Asthma-COPD overlap (ACO), characterised by persistent airflow limitation with features of both asthma and COPD, is identified clinically by its shared features. This is not a strict definition but a clinical description, encompassing various phenotypes and mechanisms.
COPD MORTALITY
Over 80 million people have moderate-to-severe COPD, with half dying within ten years of diagnosis. In 2012, COPD claimed three million lives.
GOLD: GOALS OF THERAPY
Reduce symptoms:
• Relieve symptoms
• Improve exercise tolerance
• Improve health status.
Reduce risk:
• Prevent disease progression
• Prevent and treat exacerbations
• Reduce mortality.
Bronchodilator therapy deflates the lungs, improving airflow. Forced expiratory volume (FEV1) measures how much air one can force out in one second.
Bronchodilator therapy improves volumes like forced vital capacity (FVC) and inspiratory capacity (IC).
Bronchodilators are central to managing stable COPD symptoms. Short-acting beta agonists (SABAs) and short-acting muscarinic antagonists (SAMAs) provide symptom relief.
COMBINATION THERAPIES
• Long-acting bronchodilator combinations (LABAs) and long-acting muscarinic antagonists (LAMAs) significantly improve pulmonary function tests (PFT), shortness of breath (SOB), quality of life (QOL), and reduce acute exacerbations (AE)

• LAMAs decrease AE and hospitalisations compared to LABAsCombination LAMA/ LABAs increase FEV1 and reduce symptoms and AEs compared to monotherapy Tiotropium enhances exercise performance during rehabilitation.
LABA/LAMA COMBINATIONS
For COPD not controlled on one bronchodilator, combining two with different mechanisms may lower doses, reduce adverse effects, simplify regimens, and improve compliance. LABA/ LAMA combinations offer greater bronchodilation and better patient-reported outcomes:
• Superior to LABA, LAMA, or LABA and inhaled corticosteroids (ICS) in reducing hyperinflation
• Long-acting β2-agonist indacaterol/longacting muscarinic antagonist glycopyrronium (IND/GLY) is superior to IND alone in increasing IC
• IND and the LAMA tiotropium (TIO) surpass TIO alone in improving IC
• LABAs formoterol (FORM) and TIO significantly reduce end-expiratory lung volume (EELV) versus FORM.
SINGLE INHALER TRIPLE THERAPY
An observational study on single-inhaler triple therapy vs dual bronchodilators in real-world clinical practice (UK’s Clinical Practice Research Datalink) showed:
• Patients starting single-inhaler triple therapy (n=4106), or single-inhaler dual bronchodilator (n=29,702) were followed for one year; hazard ratio (HR) of first moderate or severe AE on triple vs dual was 1.08 (1.00–1.16)
• AE risk was lower with triple therapy in patients with ≥2 prior exacerbations, a prior asthma diagnosis, and blood eosinophil count >300 cells/µL
• Severe pneumonia (HR 1.50, 95% CI 1.29–1.75) increased with triple therapy.
TREATMENT ESSENTIALS
Smoking cessation (including cannabis) is crucial. Pharmacotherapy reduces symptoms, frequency, severity of AEs, and improves health-related quality of life. Individualised pharmacotherapy, considering the ABE classification system, cost, response, preference, and device, is important. Regularly assess inhaler technique. Influenza and PCV13 vaccines lower respiratory tract infection rates. Physical rehabilitation improves symptoms and health-related quality of life.





Southern African


Congress will be held from 16 - 18 August 2024, and we invite all health care practitioners, case managers, medical aid advisors, nurses, pharmacists, primary care providers, researchers, and students from both private and public sectors. The CPD-accredited event features a scientific program with updates on guidelines, clinical lectures, debates, practical advice, ethical discussions, and the latest research. The theme for this year is "Controlling Hypertension in Southern Africa: The New Frontier," focusing on cardiac and kidney disease, stroke, obesity, and genetics. The congress offers multidisciplinary learning, interaction, and networking opportunities with international experts such as Prof Gianfranco Parati, Prof Dike Ojji, Prof Albertino Damasceno, Prof Alta Schutte, and local opinion leaders in hypertension



To Register Scan with Smart Phone Camera or visit

www.hypertension.org.za









particularly diabetic neuropathy, casts a pervasive shadow over the lives of those it affects. “Imagine waking up to brew your morning coffee only to feel as though you're treading on hot coals,” Dr Coetzee said. This sort of continuous discomfort can also result in sleeplessness, which is often the reason patients seek medical advice.
“Diabetic peripheral neuropathy accounts for more hospitalisations than all other diabetic complications combined,” Dr Coetzee pointed out. “And we know that, specifically in type 1 diabetes, early intervention is extremely important for managing glucose levels. Multiple studies have proven that early can delay the microvascular complications significantly.”
“And we also know about the legacy effect from a cardiovascular perspective in people with type two diabetes, where again, early intervention gives you significant bang for your buck. However, the problem in people with type 2 diabetes is that many of these individuals have a significant
history of prediabetes,” Dr Coetzee said. Additionally, these patients often have other risk factors such as obesity and hyperlipidaemia. A significant proportion of patients do not actually experience pain during the course of their peripheral neuropathy. “But around one out of two patients, even if they are not symptomatic at the start, will become symptomatic in future,” Dr Coetzee said. “Patients usually explain the sensation as a tingling sensation or a feeling of numbness.”
“If you've got a foot peripheral neuropathy, 90 per cent of the time it will turn out to be a symmetrical polyneuropathy in the setting of diabetes,” Dr Coetzee explained. However, she urged clinicians to be aware that peripheral neuropathy seldom starts in the hands. “You need significant progression before you see peripheral neuropathy symptoms manifesting in the hands,” she said.
“This is important because there are many mimics of diabetic peripheral sensory neuropathy. And many other conditions
such as chronic inflammatory demyelinating polyneuropathy, for instance, can co-occur in high frequency in people with diabetes.”
VITAMIN B12 DEFICIENCY
Vitamin B12 deficiency is one of the most prevalent common denominators in diabetes patients. “In someone with type 1 diabetes, we need to be vigilant that they might present with autoimmune gastritis with a concomitant vitamin B12 deficiency,” Dr Coetzee said.
“In people with type 2 diabetes, this deficiency is even more prevalent, since T2DM patients use a lot of medications that can cause vitamin B12 deficiency by various mechanisms,” Dr Coetzee said, pointing out that two of the biggest culprits are metformin and PPIs. A decline in vitamin B12 levels can occur as early as four months after starting treatment. This deficiency can also be compounded by vegetarian lifestyle. “Current guidelines are not very succinct in guiding us as to when to test for B12 deficiency,” Dr Coetzee said. “I test
any patient with a new onset peripheral neuropathy that has been on metformin –even if they've only been on it for a year.”
Dr Coetzee noted that she also tests for vitamin B12 deficiency in the following scenario: "If a patient has peripheral neuropathy that’s been stable for a while, but suffers a sudden deterioration, and they've been on metformin, I always check for B12 levels.”
But how does long term metformin use lead to vitamin B12 deficiency? “Well, firstly, it interferes with intrinsic factors so that there’s a reduced B12 absorption,” Dr Coetzee said. “It's very similar to an iron block that we get with inflammation and chronic disease where you have iron that can’t be utilised by the systemics or the system.” When should one refer a patient who presents with peripheral neuropathy? How does one perform a sensory assessment for this condition via telemedicine? How many podiatrists work in the public sector in the Western Cape (spoilers: it’s one).

Medical Chronicle recently hosted a webinar on the rational use of medications for insomnia, presented by Dr Alison Bentley. This webinar was sponsored by Pharma Dynamics.

THE SESSION PROVIDED a comprehensive overview of effective treatment strategies for this prevalent sleep disorder, offering valuable insights for both healthcare providers and patients..
Insomnia affects a significant portion of the population, with up to 10% experiencing insomnia disorder and around 25% reporting insomnia symptoms. Despite its prevalence, only 37% of those suffering from insomnia seek medical advice. Reasons for this include reluctance to use medications, scepticism about the effectiveness of medical consultations, and a preference for consulting pharmacists for nonprescription alternatives.
FACTORS INFLUENCING HYPNOTIC USE
Patients typically turn to hypnotics based on the frequency and severity of their symptoms, particularly difficulties in falling asleep. Insomnia severity increases with age, and patients with multiple comorbidities are more likely to use hypnotics. For example, in GP practices, 16% of patients take hypnotics, although the prevalence of insomnia is 55%.
CONSEQUENCES OF UNTREATED INSOMNIA
Untreated insomnia can lead to a range of negative outcomes, including:
• Poor daytime functioning, attention deficits, memory issues, and fatigue
• Increased body mass index due to decreased exercise and increased calorie intake
• Elevated risks of depression (up to 40 times higher for chronic insomnia), diabetes, cardiovascular disease (40% increased risk of myocardial infarction), and dementia.
TYPES AND CAUSES OF INSOMNIA
Insomnia is not a single disorder but can be categorized into acute and secondary types:
• Acute insomnia: Often related to psychological stress, acute medical problems, postoperative conditions, pain disorders, and asthma attacks
• Secondary insomnia: Associated with psychiatric disorders (depression and anxiety), long-term medical issues (arthritis), restless legs syndrome, obstructive sleep apnoea, and circadian rhythm disorders.
NEUROLOGICAL SYSTEMS AND SLEEP
Two major systems regulate sleep
and wakefulness:
• Wake-promoting system: Involves neuropeptides like orexin and neurotransmitters like histamine that activate arousal regions and inhibit sleeppromoting areas
• Sleep-promoting system: Involves neurotransmitters like GABA and melatonin, which promote sleep by inhibiting wakepromoting regions.
Dr Bentley emphasised the importance of tailored treatment strategies, highlighting the benefits of both pharmacological and nonpharmacological approaches:
• Cognitive behavioural therapy for insomnia (CBT-I): Recommended as the first-line treatment for chronic insomnia by various sleep societies. CBT-I has shown better longterm efficacy compared to hypnotics and can significantly reduce hypnotic use.
• Medications:
- Benzodiazepines and Z-drugs: Effective for increasing total sleep time and improving sleep quality but can alter sleep architecture.
Melatonin: Particularly useful for circadian rhythm disorders and conditions like jet lag, shift work, and neurodevelopmental disorders. Longterm therapy may be needed for conditions with reduced or irregular melatonin secretion
- Other medications: Tricyclic antidepressants and antipsychotics like quetiapine may be used, although their efficacy for primary insomnia is limited and associated with significant side effects.
- Appropriate use of medications.
Dr Bentley advised careful consideration when prescribing hypnotics, including:
• Ensuring there are no underlying biological reasons for insomnia
• Combining hypnotics with CBT-I to enhance treatment outcomes
• Using minimal effective doses and considering intermittent rather than nightly dosing to reduce the risk of dependence and adverse effects.
Accurate diagnosis and a balanced approach to treatment are crucial for managing insomnia effectively. While hypnotics are appropriate for acute and secondary insomnia, CBT-I remains the preferred treatment for chronic insomnia. The goal should be to improve daytime functioning and overall quality of life, rather than merely increasing sleep duration.

Date: 22nd - 25th August 2024
Venue: Sandton Convention Centre, Johannesburg












Patient safety is a subset of healthcare and is defined as the avoidance, prevention and amelioration of adverse outcomes or injuries stemming from the processes of healthcare.
ATIENT SAFETY ALWAYS comes first for healthcare providers. It is difficult to keep all patients safe.
Medical error is the third leading cause of death in the United States, leading to over 250 000 deaths each year. Sentinel events associated with medical errors are preventable through technology.
The challenge isn’t in creating best practices for patient safety, but rather in implementing with consistency.
Technology consistently certifies a reduction in errors, a decrease in miscommunications, and an assurance in provider compliance.
In 1999, the Institute of Medicine [IOM] report To err is human called for developing and testing new technologies to reduce medical errors and in 2001 the report Crossing the Quality Chasm called for information use.
The 1999 IOM report dramatically increased public awareness of medical error. It is estimated that each year 44 000 to 98 000 people die of an iatrogenic injury, either as a main or a contributing cause, and that 1.3 million are injured by medical treatment.
The mortality estimates were extrapolated primarily from two large studies, one in New York State (The Harvard Medical Practice Study) and the other in Colorado and Utah.
Even though some controversy surrounds the accuracy of these mortality estimates, all agree that the number of deaths attributed to iatrogenic injury is too high. In 1984 Harvard Medical Practice Study showed an overall adverse event rate of 3.7 per 100 admissions for inpatients, and 0.6 and 2.1 per 100 admissions for newborns and children aged 15 years or younger, respectively.
Most common adverse events in this study were complications of medicine use (19.4%), followed by wound infections, operative complications, and diagnostic mishaps. Of these adverse events, 71% resulted in a disability that lasted less than six months, 3% caused permanent disability and 14% led to death.
Technology as a key first step in transforming the healthcare environment to achieve better and safer care. In the past several decades, technology advances have opened new possibilities for improving patient safety. Using technology to digitise healthcare processes has the potential to increase standardisation and efficiency of clinical workflows and to reduce errors and cost across all healthcare settings.
However, technology approaches and applications must be used appropriately, following standardised evidence-based guidelines and domains. The adoption of Generative AI and technology in healthcare ecosystems has just begun.
Providers rightfully are still cautious about use of AI, yet generative AI is a transformative technology that cannot be ignored. Generative AI / Technology support can improve patient care, safety, and better outcomes. If implemented appropriately :
- Digital solutions will become common in all aspects of healthcareImprove patient care and safety
- Improve certain experiences of care
- Make interactions quicker
- Quicker completion of pre-authorisation processes with digital scribe
- Improve record keeping
- Bridging the gap between provider and patients.
The benefits and use in hospitals and facilities also show enormous benefits and promote safety. AI is used to help optimise hospital workflows, inventory control, ensure proper staffing, due to application of data and use of scientific algorithms.
Clinical Decision Support [CDS]
CDS provides clinicians, patients, and other individuals with relevant data (patient specific information), purposefully filtered, and delivered through a variety of formats and channels to improve and enhance care.
One of the main applications of CDS is Computerised Patient Order Entry (CPOE) is a process used by clinicians to enter and send treatment instructions via a computer application. The change from paper to electronic order entry itself can reduce errors (due to unclear handwriting or manual copy errors), research conducted in 2022 showed that there is still room for improvement in order entry systems, as well as some novel approaches. Two studies looked at the frequency of and reasons for medication errors in the absence of CDS and CPOE and showed that:
- Medication errors occurred during the ordering or prescribing stage
- Most common prescribing errors was incorrect dose.
Further research, such as the AHRQ Medication Safety Measure Development project aims to develop and validate measure specifications for wrong-patient, wrong dose, wrong medication, wrong route, and wrong frequency medication orders within EHR systems, to better understand and capture health IT safety events.
Errors of this type can be avoided or at least reduced using effective CPOE and CDS systems. However, with optimal application of CDS and CPOE tools, errors can still occur and even be caused by the systems themselves.
One study reviewed duplicate medication orders and found that 20% of duplicate orders resulted from technological issues, including alerts being overridden, alerts not firing and automation issues ( prefilled fields). Studies have shown that a fully implemented CPOE systems significantly reduced specific serious and commonly occurring prescribing and procedural errors.
In 2022, a particular CPOE feature showed significant improvement: automatically discontinuing medication orders and relaying pertinent information to pharmacies. Deprescribing is a planned and supervised process of dose reduction or stopping of a medication that is no longer beneficial or could be causing harm. The study showed an immediate and sustained 78% increase in successful discontinuation after implementation of the software.
A second study on the same functionality found that currently only one third to one half of medications are e-prescribed, and the study proposed that e-prescribing should be expanded to increase the impact of the deprescribing software.
In the last decade, much of Health Information Technology started with adoption of EHR by medical facilities. These records provide a central repository of the patient medical history, allowing for the sharing of information, including physician notes, test results and information on prescription of drugs and clinical decisions. EHR considers the impact of Human factors in healthcare, improving communication and providing 'one source of truth' on the patient’s health and treatment for better coordination of the patient
care process. The impact of information technology has expanded beyond just information visibility and sharing to utilising information for data informed patient care.
Health Information Technology has emerged as the most cost-efficient, costeffective, and safe alternative to traditional methods in improvement of patient safety and quality of care.
Errors can occur with diagnostic testing, such as lab work or imaging, especially with manual processes. It is easy to mislabel an Xray. Digitised diagnostic tools and communication systems enhance patient care and safety.
These assessments ensure patients are matched to the correct tests and providers have instant access to results.
One of the largest areas of burgeoning technologies in healthcare has been AI.
AI and machine learning use algorithms that absorb large amounts of historical data, predict outcomes, recommend treatments, and are being integrated into EHR and CDS systems. Using machine learning to improve and filter CDS alerts can reduce alert volumes by 54% while maintaining high precision, potentially alleviating alert fatigue and habitual overriding. Another topic explored in a scoping review was the use of AI to reduce Adverse Drug Events.
Data from devices, scans, and prior patient encounters can be incorporated into Electronic Medical Records.
Efforts are underway to anonymize or tokenize data for sharing across hospitals. Predictions suggest this will enhance operational tasks and support clinical decisions with AI.
This technology is used in operating and procedure rooms to count, locate, and detect swabs and sponges, with accuracy validated by research in AORN practice guidelines. It is crucial for preventing Retained Surgical Items (RSI).
AI and technology play an important role in improving population health and safety, enabling informed decision-making. The key dimensions of technology in healthcare focus on enhancing patient safety and the quality of care.

AMIE ROSSOUW, 36, is a self-confessed workaholic.
He started his appliance store when he was just 18, and as he had a small team to begin with, he had to do a lot of the heavy lifting himself. Although he was very fit, participating in cross-fit training, boxing, and running, the backbreaking work eventually took its toll. “I sell household appliances, and back then, I was lifting between 200 and 300 appliances each day. These included stoves, fridges, washing machines, and tumble driers.” When Rossouw started to experience lower back pain, he began a journey that would eventually lead him to consult a South African orthopaedic spine surgeon who is doing groundbreaking work, for a lasting solution to his debilitating problem. After consulting other medical practitioners without success, in desperation Rossouw began to do his own research. “I thought, surely, there was another way to treat this and discovered that there was an endoscopic procedure being done in the USA. I was even exploring the possibility of going to see a surgeon there. But then, on Google, I found that Dr Shawn Venter, who works from the Spine Centre at Netcare Kuils River Hospital, is charting the way forward for biportal endoscopic spinal surgery in South Africa.”
Rossouw unluckily contracted hepatitis and had to postpone both his honeymoon and the interventional pain treatment. After he recovered from the hepatitis, he had the discectomy done to alleviate his leg and back pain in September 2023. Unfortunately, his leg pain returned a few weeks after surgery and Dr Venter diagnosed a re-prolapse.
“This fairly rare occurrence happens in only about five to ten per cent of people after a discectomy,” explains Dr Venter. “Again, all efforts to treat his pain conservatively to acceptable levels failed.” Rossouw decided that despite his young age, the endoscopic spinal fusion would provide lasting relief. Also, considering the demands of his work, he needed to be able to do all the heavy lifting without any concerns about his back.” The biportal endoscopic spinal fusion was agreed upon as the next step. Dr Venter explains that although the literature quotes longer theatre times for endoscopic fusions, he has been able to reduce his surgical time to less than that of open surgery, with a single level spinal TLIF (transforaminal lumber interbody fusion) taking less than two hours. This procedure means there is much less surgical trauma to the patient’s back muscles, which means fewer risks and less post-operative pain compared to traditional open surgery.
“Blood loss is reduced and there is a lower infection risk as the wound is constantly irrigated during the procedure. There is also no delay in mobilising a patient post-operatively,
and Rossouw returned home three days after his spine fusion fully functional, able to sit, stand and lie down with no restrictions. He was able to resume driving after 10 days.”
“Worldwide there are less than 100 surgeons currently performing this endoscopic fusion surgery, however this number is growing exponentially as the benefits of this type of surgery become more evident,” says Dr Venter.
He explains that a spinal fusion is made up of small procedures put together. “First, we do a decompression to open up the space for the nerves, then a discectomy to take out all of the diseased disc. The void is filled with a spacer and bonegraft harvested locally, and lastly, screws keep everything in place while the bone grows into the vertebra.”
Dr Venter says that the minimally invasive approach provides hope for patients previously deemed unfit for spinal surgery. “I’m now able to offer surgical relief to a wider range of patient demographics compared to the past. These include patients with extreme BMIs who wouldn’t even be considered for open surgery, elderly patients, as well as those requiring simple and multilevel fusions. Probably the most beneficial component is that frequently a more targeted type of endoscopic surgery can be performed, rather than altogether avoiding spinal fusion.”
He cautions that an open or endoscopic fusion is always the last resort surgery, but it’s a very good choice when the indications are right. “We try and find a solution for everyone. If a patient is not a candidate for endoscopic surgery, my partner, Dr Reggie King, has an amazing skill set for salvage and deformity correction surgery.”
Dr Venter says he chooses to operate at Netcare Kuils River Hospital because the theatre he works in is specially modified and automated, with larger space to allow for the specialised equipment he uses. “It includes a navigation system, which is a powerful 3D reconstruction of the spine that I can scan in theatre as well as the best endoscopic tools and cameras. The unit has also been set up to allow optimal training of other surgeons.” A much-relieved Rossouw said his recovery had been “absolutely amazing”. “Instead of going to the stepdown clinic after my hospital stay, Dr Venter let me go straight home. I had two weeks of rest and did some walking, and then I was back to work using my back brace. It made things a whole lot easier,” he says. “I’ve worked extensively with a personal trainer and done the necessary core exercises. I go for needling and physiotherapy to make sure the muscles there are not too tight. At 16 weeks post-surgery, I’ve even started running slowly. I’m feeling great, and I’m over the moon with the way things have worked out.”
Copyright Medical Chronicle 2024
EDITORIAL
EDITOR: Claire Rush McMillan
Claire.Rush@newmedia.co.za
NEWS WRITER: Nicky Belseck
Nicky.Belseck@newmedia.co.za
SUB-EDITOR: Gill Abrahams
EDITORIAL CONTRIBUTORS
Conrad Strydom, Prof Morgan Chetty, Rene Bosman.
LAYOUT & DESIGN: Naresh Budraj
ADVERTISING
ADVERTISING EXECUTIVES
Anel du Plooy - Tel: 082 786 9517
Anel.duPlooy@newmedia.co.za
Cindy Riederer - Tel: 082 492 0229
Cindy.Riederer@newmedia.co.za
DISTRIBUTION & SUBSCRIPTIONS
Felicity Garbers
Email: felicity.garbers@newmedia.co.za
Update your details here: www.medicalacademic.co.za
PUBLISHING TEAM
GENERAL MANAGER: Dev Naidoo
GROUP ACCOUNT DIRECTOR: B2B: Johann Gerber
Email: Johann.Gerber@newmedia.co.za
DIGITAL MANAGER: Varushka Padayachi
PRODUCTION MANAGER: Angela Silver
ART DIRECTOR: David Kyslinger
CONTACT
Johannesburg Office:
New Media, Ground Floor
272 Pretoria Avenue, Randburg 2194
COVER PRICE
Medical Chronicle per issue R60.00 VAT Incl.
Published by New Media, a division of Media24 (Pty) Ltd
Printed and bound by Novus Print - Montague Gardens, Cape Town
MANAGEMENT TEAM
CEO : Aileen Lamb
COMMERCIAL DIRECTOR: Maria Tiganis
STRATEGY DIRECTOR: Andrew Nunneley
CHIEF FINANCIAL OFFICER: Venette Malone
CEO: MEDIA24: Ishmet Davidson
HEAD OFFICE
New Media, a division of Media24 (Pty) Ltd 8th floor, Media24 Centre, 40 Heerengracht Cape Town, 8001 www.newmedia.co.za
Unless previously agreed in writing, Medical Chronicle owns all rights to all contributions, whether image or text.
SOURCES: Shutterstock, supplied images, editorial staff. While precautions have been taken to ensure the accuracy of its contents and information given to readers, neither the editor, publisher, or its agents can accept responsibility for damages or injury which arise therefrom. All rights reserved. © Medical Chronicle. No part of this publication be reproduced, stored in a retrieval system or transmitted in any form or by any means, photocopying, electronic, mechanical or otherwise without the prior written permission of the copyright owners. Attention African readers: Please note that some products might not be available in your region and product names could vary. Please contact your local distributors, agents or pharmaceutical companies concerned for any discrepancies.