HLTPAT005 - Collect specimens for drugs of abuse testing
Learner Guide
In completing this course you will learn how to collect specimens for drug and alcohol abuse testing.
HLTPAT005 Learner Guide v1.7 - 9/09/2021
Outline
HLTPAT005 - Collect specimens for drugs of abuse testing
This unit describes the skills and knowledge required to confirm collection requirements, prepare client and equipment and collect specimens via urine and/or oral and breath testing following the special procedures that apply for drugs of abuse testing.
This unit applies to individuals working in collection centres, in hospitals, in other health care environments and workplaces where drugs of abuse testing takes place.
Drug use in Australia and the Workplace
Prevalence and Patterns of Alcohol and Other Drug Use in Australia
Alcohol and drug use is a fact of Australian culture. For many people, use of alcohol, or recreational drugs, is an occasional event, which does not impact their lives. However, there is no denying that alcohol and other drug use is a major cause of preventable disease, illness and death in Australia. There is also a major impact on the Australian work force, because the majority of Australians who use alcohol or other drugs are also employed. It should be no surprise then, that patterns of harmful use are evident in the workforce as well.
The majority of Australians drink alcohol regularly and a substantial proportion have tried cannabis. However, few Australians are regular users of other illicit drugs.
The below table refers to people aged 14 years and over.
Source: NDSHS 2019
The majority of Australians who use alcohol or other drugs are also employed. It should be no surprise then, that patterns of harmful use are evident in the workforce as well.
Harmful alcohol and other drug use can be found at all levels across a broad range of organisations. Some industries and occupations have higher levels of harmful use than others as indicated by the 2016 and 2019 NDSHS.
For example, in the transport industry some drivers use amphetamines to ‘stay awake’ and in some areas of the manufacturing industry there are higher levels of cannabis use compared to other industries.
Similarly, nurses, doctors and others employed in the health industry may be more likely to misuse pharmaceuticals compared to others.
Heavy Drinking Occupations/Industries:
CEOs, general managers, legislators are now the number one occupation for high alcohol consumption.
Work Sectors and Why they Screen for Drugs and Alcohol
There is significant legislation around work health and safety and occupational safety. One aspect of creating a safe workplace would be ensuring that the people in that workplace are fit for work. In addition, testing does occur in social and community programs.
In light of all this, workplace drug and alcohol screening is now conducted in a variety of different work sectors such as the following.
Work Sector
Workplaces
Social Services
Prisons
Testing Reason
Test to assess fitness for work.
Test to assess if drug use is occurring within rehab programs.
Test to track and confirm drug use among both prison population and staff.
Medical Facilities Perform pre-employment medicals which include drug screens.
Hospitals May perform post accident screen.
Legal Testing as part of court orders or in determining custody of children.
Potential Negative Consequences of Alcohol & Other Drug Use For The Workplace
While alcohol and other drug use in the workplace can reflect use in the general community, harmful use in the workplace is often indicated by increased injuries, absenteeism, lost production, workers compensation and rehabilitation.
Studies show lost production from harmful alcohol and other drug use costs Australian industry in excess of $6 billion per year. Australian workers admitted to taking almost 11.5 million sick days as a result of their alcohol and/or drug use which costs the economy an estimated $500m.
In addition, research indicates that up to 15% of all Australian workplace accidents may be associated with alcohol use and that at least 5% of all Australian workplace deaths are associated with alcohol use (4).
The alcohol and other drug consumption patterns of the workforce can have a variety of negative consequences for the workplace and employees, including the following:
Accidents
• Accidents resulting in injury or death
• Lost employee work time
• Damage to tools and equipment
• Increased insurance costs/workcover levy
• Possible bad publicity and even prosecution
Consequences for other employees
• Unsafe work environment with risk of accidents
• Covering for poor work performance
• Disputes
• Reduced morale
• Embarrassment if forced to ‘dob in a mate’ for their own good
Lower productivity
• Lower quantity & quality of work
• Loss of business
• Loss of skill when employee terminated/ injured/ill
• Co-workers covering for affected employees
Staff turnover
• Costs of dismissal or premature retirement
• Replacement of employees
• Training of new employees
• Loss of skills and experience
• Loss of investment in employees
Consequences for individual employee
• Possible injury to self & others
• Demotion, discipline or dismissal
• Problems with family, friends & workmates
• Loss of self-esteem
• Loss of wages
• Cost of medical expenses
Absenteeism
• Lost production
• Disruption of operations
• Covering for lost employee time
Types Of Drugs, Their Effects & Potential Consequences For The Workplace
People may use alcohol or other drugs for a variety of reasons and not all uses have harmful outcomes. Alcohol use can be an enjoyable and pleasurable experience for many people and there is some evidence to suggest that low levels of alcohol consumption may have positive health benefits for older people. However, excessive use of alcohol is also associated with substantial health and social problems.
Australians are among the heaviest drinkers in the world. Drinking alcohol is often socially expected and many people do not view alcohol as a drug. However, alcohol is a drug and in large quantities can have a toxic effect on the human body.
Alcohol is a depressant and excessive consumption or consumption in combination with other depressant drugs can cause death.
Reasons People give for Using Alcohol or other Drugs:
• to relieve physical or emotional pain
• to relax or relieve stress
• bored
• enjoyment
• peer pressure
• to socialise
Drug Effects, Use and Abuse
Many people have heard about the dangerous effects of drugs that are used recreationally.
That makes it very hard to understand the reasoning behind any use of recreational drugs at all. Good drug education should acknowledge that some drugs, used in safe dosages, result in pleasant effects on the user. Acknowledgment of that fact is not to advocate recreational drug use, because there are serious risks associated with use, and the worst of these is the “unknown” factor.
Recreational drugs are usually not drugs that are manufactured under strict controls. While some people use pharmaceutical drugs as recreational drugs (not in prescribed therapeutic doses), the majority of illegal drug use is substances such as cannabis, (in all its varied forms from hashish and hash oil, smokable leaves, edible items and concentrates) psychedelics, (LSD, mushrooms, peyote) empathogens, (MDMA, also called X, Pingas, ecstasy, PMA, Mephedrone, also called Meow or Plantfood, and Ethylone, also called Bath Salts) and stimulants (including meth and ice, cocaine and crack). Any drug that is not regulated is essentially a game of Russian Roulette. What you see may not be what you get. So, let’s look at the promises and the realities of recreational drug use.
Stimulants
Common stimulants include methamphetamine (ice), amphetamines, cocaine or crack, nicotine and caffeine.
Stimulants accelerate messages between the brain and the body. They can make a person feel more awake, alert, confident or energetic. In higher doses, or with overuse, they can also cause a person to feel anxious, aggressive or paranoid. Use of stimulants can result in loss of appetite, sleep difficulties, as well as increased heart rate and blood pressure. Long term, these effects are seriously damaging to the body.
Consistent use of stimulants may result in a user feeling they need more to get the same effect, particularly if they are becoming sleep deprived. Higher levels lead to greater side effects, and increased likelihood of dependence. Some users will mix stimulants for greater effect. When different stimulants are taken at the same time, such as cocaine and ice, the likelihood of cardiovascular damage increases.
How stimulants work
Stimulants like cocaine and methamphetamines (ice) both increase the production of, and inhibit the absorption of the neurotransmitters serotonin and dopamine. This increase in serotonin and dopamine levels makes a person feel the “high” associated with this drug. This flood in serotonin may lead to a person experiencing serotonin syndrome (ref ADF.org.au: effects of polydrug use), which includes symptoms like diarrhea, and muscle spasms, and when severe, can cause muscle rigidity, high fever, and seizures. Combining stimulants also increases the risk of psychosis, anxiety, or panic attacks. Other side effects of stimulants are weakened ability to curb impulsive behaviour, and depression and fatigue when the drug wears off. Recovery from this “come-down” can take days, even weeks depending on the amount used. Dependence on stimulants can be both psychological and physical, and withdrawal symptoms can include fatigue, insomnia or hypersomnia, psychomotor agitation or retardation, vivid unpleasant dreams, increased appetite. Milder
symptoms can include irritability, body aches, depressed mood, and impaired social functioning. Studies show that these symptoms persisted for between five days and three weeks.
Overdose of stimulants can result in death. Even caffeine has been implicated in overdose deaths. Mixing of stimulants with depressants confuses the central nervous system and can result in seizures or death (polydrug syndrome).
Depressants
How Depressants Work
Depressants do not make a person feel “depressed”. Depressant substances affect the central nervous system by increasing activity of gamma-aminobutyric acid (GABA), a chemical that inhibits brain activity. This slows down the messages between the brain and the body. This can result in a person feeling calm, mellow and relaxed. Common depressant drugs are alcohol, benzodiazepines, opiates and opioids, and sleeping tablets. Cannabis can also have depressant effects.
Opiates (and opioids) are also used to treat pain. They affect the opioid receptors in the brain and are usually derived from the opium poppy. Like other depressants, opioids slow the central nervous system and messages between the brain and the rest of the body. Common opiates are morphine, codeine, heroin, oxycodone, fentanyl, methadone and tramadol.
Depressants reduce concentration, inhibitions, and coordination. They are sometimes used to help with insomnia or to reduce feelings of anxiety, particularly social anxiety. Higher doses can result in serious loss of coordination, greatly reduced reaction time, and extreme sleepiness. In an overdose, depressants slow heart rate, reduce respiratory rate, and can result in loss of consciousness, coma or death.
Mixing depressants and stimulants places the body under enormous stress as it tries to deal with the competing effects. This can result in heart problems, respiratory difficulties, including infections and bronchitis, dehydration, over- heating, kidney failure, seizures and death. (ref ADF.org.au: effects of polydrug use).
Empathogens
How Empathogens Work
Empathogens include substances that cause the brain to release dopamine and serotonin. This is essentially the same effect that stimulants have. Therefore, when discussing the medical impact of these drugs, they are considered stimulants. They can increase feelings of connection and empathy, pleasure and energy levels. Users may experience visual and auditory hallucinations or floating sensations. The most common empathogen is MDMA, or “Ecstasy” or it’s synthetic version PMA and PMMA.
The effect of these drugs can vary according to a number of factors including:
• size, weight and health of user
• whether the person is used to taking it
• whether other drugs are taken around the same time
• the amount taken
• the strength of the drug (varies from batch to batch).
One of the most serious risks of these “party” drugs comes from the inability to differentiate between MDMA and its imitations, without an actual test.
Drugs sold as MDMA (ecstasy) may not contain any methylenedioxymethamphetamine (MDMA); they can be a mix of amphetamine, paramethoxyamphetamine (PMA), ketamine, NBOMe, synthetic cathinones or other substances.
There is a much greater risk of overdose with PMA and PMMA because the side effects are more severe, but the euphoric effects are lower and can take longer to “come on”. This results in users thinking they got a dud MDMA pill and double dosing. PMA and PMMA also result in a rapid increase in blood pressure and body temperature.
Other side effects of MDMA and other empathogens may include.
• Unpleasant hallucinations
• Dilated pupils
• Jaw clenching, teeth grinding
• Overheating, excessive sweating, heat stroke
• Risk of dehydration/overhydration (can cause death)
• Anxiety, paranoia, irrationality
• Racing heart
• Seizures and death
Long term or regular use of MDMA can reduce immune response, create memory or concentration problems, dependency, depression, and liver problems.
Empathogens and other drugs
Using empathogens with other drugs can be dangerous, in particular with other drugs that increase the amount of serotonin in the brain, including antidepressants, SSRIs, L-Tryptophan and other empathogens. High levels of serotonin can lead to serotonin toxicity or serotonin syndrome. This is a serious condition with symptoms such as confusion, agitation, sweating, increased heart rate and muscle spasms, and can be fatal. So don’t mix and match!
Psychedelics
How psychedelics work
Psychedelics are also known as hallucinogens. They can cause hallucinations, or change a person’s thoughts, mood, sense of time or perception of their environment or themselves. There are many different kinds of psychedelics. Some occur naturally, in trees, vines, seeds, fungi and leaves. Others are made in laboratories. Common psychedelics are LSD, peyote and psilocybin. These drugs alter the sensory input part of the brain, causing a user to see, feel, hear, smell and taste things that are not there.
Generally, people who use psychedelics don’t take them on a regular basis, but on occasions that may be weeks or months apart. (ref: ADF.org.au/drug facts)
Like MDMA, psychedelics affect everyone differently, based on:
• size, weight and health of user
• whether the person is used to taking it
• whether other drugs are taken around the same time
• the amount taken
• the strength of the drug (varies from batch to batch).
The effects of psychedelics can last several hours and vary considerably, depending on the specific type of psychedelic. Users may experience hallucinations, feelings of euphoria, relaxation and well-being.
Less pleasant effects can be unpleasant hallucinations, confusion, dizziness, loss of balance and blurred vision.
Breathing rate may increase, heart rate can be fast or irregular. Sweating, chills and vomiting may occur.
Regular use of psychedelics will not result in a physical dependency but may result in psychological addiction. There are no withdrawal symptoms with cessation of use.
Psychedelics are also associated with reported “flash backs”, which is a re-experience of the drug and can occur days, weeks or even years later. Flash backs can range from being pleasant to causing severe anxiety. They are usually visual and only last for a minute or two.
The greatest risk with psychedelic use occurs when combining psychedelics with other drugs, or when using psychedelics in risky situations, (outdoor activities, sports, using vehicles or machinery).
Marijuana and THC
Cannabis and Cannabinoids
The word cannabis refers to all products derived from the plant Cannabis Sativa. Marijuana refers to parts or products of the plant that contain tetrahydrocannabinol (THC). THC is the substance that’s primarily responsible for the effects of marijuana on a person’s mental state. It is used in a variety of forms from smokable dried leaves and flowers, to hashish, the dried plant resin, and concentrates used in food preparation, (edibles) and for vaping.
Cannabinoids are a group of substances found in the cannabis plant. The main cannabinoids are THC and cannabidiol (CBD). Besides THC and CBD, more than 100 other cannabinoids have been identified. These substances have a variety of medical applications.
The effects of THC will vary widely from person to person, however common effects are feelings of relaxation and euphoria, a sense of well being, spontaneous laughter, and increased appetite. Side effects may be intense anxiety, increased mental health symptoms (for people with existing mental health issues), dry mouth, memory impairment, and slowed reflexes.
The long term risks of smoking include reduced immune response, greater susceptibility to asthma and upper respiratory illnesses. While cannabis is not associated with cancer, users who smoke marijuana with tobacco have increased emphysema and cancer risks.
Long term risks of vaping are unknown at this time, however vaping has been associated with severe lung injury and in the US alone, 68 deaths due to vaping occurred in 2020. (ref CDC.gov)
Long term marijuana use can result in development of tolerance, and dependency. Withdrawal from marijuana can be challenging with symptoms ranging from anxiety, irritability, upset stomach and loss of appetite to sweating, chills and tremors, insomnia, and restless sleep. (ref adf.org.au/drug-facts) There are no significant complications of withdrawal that would necessitate inpatient treatment.
Dealing With Alcohol & Other Drug-Related Harm in The Workplace
Many traditional workplace responses have taken the problem orientated approach (Figure 1) which focuses resources on identification and treatment of individual problem users through DISCIPLINE, DISMISSAL or REHABILITATION.
Occasional and/or low-risk users
Moderate and/or risky users
Tertiary Treatment
High Risk and/or dependent users
Traditional focus of attention
This approach places the emphasis on dealing with problems after they occur which is a tertiary treatment approach rather than a prevention approach.
Research indicates that most of the cost borne by alcohol and other drug problems comes not from the relatively few dependent users, but from the much larger numbers of infrequent or moderate users whose occasional consumption patterns can become problematic.
This suggests that responses need to focus on all workers in the workplace and resources need to target moderate and occasional users as well as the heavy or dependent users (Figure 2).
Primary prevention includes education and information dissemination strategies regarding alcohol and other drug health and safety risks and includes the identification of risk factors in the workplace that could contribute to alcohol and other drug-related harm.
Secondary prevention strategies identify and deal with workers whose alcohol or drug use is problematic and allows workers to seek assistance. Secondary prevention strategies provide the framework for the identification and removal or reduction of risk factors in the workplace and includes the training of supervisors and other staff who often play a crucial role in determining the success of any strategy.
Occasional
Moderate and/or risky users
New focus of attention Tertiary
High Risk and/or
Figure 1
Figure 2
The Law
Work Health and Safety Legislation
All workers have a duty to take reasonable care for their own health and safety and ensure they don’t adversely affect that of others. This means they must be fit and well enough to do their job, not be under the influence of alcohol or drugs, or use alcohol or illegal drugs while at work.
In some jobs such as road and rail transport, maritime and mining occupations, the law sets down a legal blood alcohol level and may prohibit a worker from being affected by any drugs—legal or illegal.
In many instances organisations have explicit policies to test their workers for alcohol and illicit substances. This is particularly important if a worker could kill or seriously injure themselves, another worker or a member of the public. (Safework Australia, 2021)
The Work Health and Safety Act does not require drug testing for managing risk in the workplace, however, testing is an option to be considered.
There are legislative provisions currently in place for specific occupational groups in relation to alcohol consumption in the workplace. For example, there is legislation to protect public safety in transport (covering commercial road transport, the railways, civil aviation, and marine transport) through restrictions on the use of alcohol and drugs and the development of drug and alcohol management (including testing) plans. (PN10875 - Framework for alcohol and drug management in the workplace 2012, Worksafe Queensland)
Laws Relevant To Alcohol And Other Drug Issues In The Workplace
Road Traffic Legislation
Under the National Australian Road Rules (1999) and various state Acts and Regulations, it is illegal to drive (or attempt to drive) a motor vehicle under the influence of alcohol or any drug to the extent of being incapable of exercising effective control of the vehicle. Depending on the legislative jurisdiction, this may extend to prescription and over-the-counter medications.
Currently, in all Australian jurisdictions the prescribed limit for being under the influence of alcohol is 0.05g/100ml blood alcohol concentrate.
For certain categories of vehicles and drivers the limit will be 0.000g/100ml such as:
• Heavy vehicles;
• Vehicles carrying dangerous goods;
• Buses and other vehicles primarily used for transporting passengers;
• Provisional license or ‘P’ plate drivers.
It is also generally accepted that an individual’s ignorance of the effect of a drug is not an excuse.
Depending on the legislative jurisdiction, an individual who is caught driving under the influence of alcohol or other drugs may be charged with a criminal offence. An individual driving under the influence of alcohol or other drugs who kills another person while driving may be charged with an additional criminal offence. Furthermore, insurance companies are likely to disallow claims when the driver is under the influence.
Common Law / Vicarious Liability
Under common law provisions, an employer may be held legally and financially responsible for the actions of employees who are under the influence of alcohol or other drugs.
Criminal Legislation Concerning Illicit Drugs
Under various federal and state criminal legislation, employers may be held accountable for any activities involving illegal drugs that occur at work. For example, according to the Controlled Substances Act 1984 (South Australia) a person is considered to be taking part in the manufacture, sale, supply, or administration of an illicit drug if they provide the premises in which this takes place, or if they let any step in the process take place in the premises of which they are the owner or manager.
Indicative Australian Case Law
A number of cases addressing the development and application of drug and alcohol policies have been brought before the various Industrial Relations Commissions in Australia.
BHP Iron Ore Pty Ltd V. Construction, Forestry, Mining & Energy Union Western Australian Branch
Random drug testing policies were first tested in Australia when BHP Iron Ore Pty Ltd presented its program for drug testing to the Western Australian Industrial Relations Commission for approval in 1998.
BHP had developed the program with the assistance of employees and unions with the exception of the Construction, Forestry, Mining and Energy Union (CFMEU), who opposed the program.
The program that was developed, stipulated that employees would be required to submit a urine sample if they were randomly selected to undertake the test. If they tested positive they would be sent home on leave with pay. If they recorded a second positive result within two years, they would be sent home on leave without pay. If they had a third positive result within the same period, their employment with the company would be up for review.
BHP advised that a counselling service would be available for anyone, not just the people that have tested positive, and that any records would be kept in strict confidence for two years, and destroyed thereafter. BHP also set levels for cannabinoid metabolites at twice the Australian standard (DR06557: Procedures for specimen collection, detection and quantitation of drugs of abuse in urine) in an attempt to account for occasional or social use. It also argued that although the tests were not impairment tests, the higher levels allowed would be an indicator of potential impairment if an employee tested positive.
BHP argued that the program was needed to satisfy its obligation under the Mining Safety and Inspection Act (1994) WA (this act prohibits a person being in a mine whilst under the influence of alcohol or drugs) and the OHS duty to maintain a safe workplace.
The Full Bench of the Commission ruled that the program was reasonable. They gave the following reasons for their ruling:
1) That the program was accepted by the majority of unions and employees;
2) That safeguards against wrongful use of the test results were in place, and;
3) The company had agreed to review the policy if new technology or research found a less intrusive test.
Australian Railway Union of Workers, West Australian Branch & Ores V. West Australian Government Railways Commission
Mr Worden was dismissed when he returned to work after an off-duty period, due to a positive drug test result which was obtained after the conclusion of his previous work period.
The Commissioner observed that:
1) There was no evidence to suggest that the company had ever conducted any random testing (in spite of the company’s stated policy);
2) The company had hired people who had shown a positive drug result in their preemployment testing;
3) Their drug and alcohol policy was rarely enforced, and;
4) The policy did not mention that the consequences of a positive result could lead to dismissal.
The Commissioner also commented that the company’s expert witness was not able to confirm whether the marijuana that Mr Worden had consumed was whilst on duty or not. As such, the Commissioner ruled the dismissal as unfair and awarded Mr Worden compensation for lost wages.
Pioneer Construction Materials Pty Ltd V. Transport Workers’ Union of Australia, Western Australia Branch
Pioneer Construction Materials Pty Ltd introduced a policy for fitness for duty which required that employees undergo random urine testing for illicit drugs and alcohol.
The employees undertook industrial action when two employees were stood down for refusing to take the test. The company delayed the introduction of the policy while the Western Australian Industrial Relations Commission dealt with three issues relating to the policy which included:
1) The company’s right to conduct urine testing (as opposed to saliva testing sought by the union);
2) The requirement that employee’s declare and provide an appropriate doctor’s certificate in respect of any over-the-counter medication which could lead to a positive test; and
3) The stipulation that where a health assessment is required by the respondent and an employee chooses not to attend for assessment with one of the company recommended medical practitioners, that an employee’s attendance at his/her own medical practitioner is at his/her expense.
The Commission found that the proposal to conduct urine testing was reasonable, particularly as there is no standard in Australia that covers detecting the presence of illicit drugs in saliva but there is for the detection of illicit drugs in urine. The company stated it would consider saliva testing once a standard was endorsed. The Commission also found that it was reasonable that employees provide an appropriate doctor’s certificate in respect of any over- the-counter medication which could lead to a positive test, as long as the company paid the employees’ reasonable medical costs.
The Commission endorsed the employees’ right to attend their own medical practitioners, and found that company’s subsequent decision to pay an employee’s reasonable medical costs of obtaining a health assessment from their own doctor was also reasonable.
Summary of Legal Findings
1) A policy should be clear, easy to understand, written in plain English and applicable to the entire workforce from executive/owners to apprentices/trainees;
2) A policy should be communicated to all employees who should indicate their understanding of the consequences of the policy, preferably in writing;
3) A policy should be brought to the attention of the employees regularly.
Developing a Drug and Alcohol Policy
The central component of any response to alcohol and other drug-related issues in the workplace is the development and implementation of an alcohol and other drug policy.
What is a Drug & Alcohol Policy
A drug and alcohol policy is a set of guidelines and strategies for dealing with all aspects of alcohol and other drug issues in the workplace.
The main aim of the policy should be to create a work culture that does not mix alcohol and other drugs with work and that prevents hazardous and harmful alcohol and other drug use.
The objectives of the policy should be to detail procedures for prevention, recognition and early action concerning harmful alcohol and other drug use.
Why Have a Policy?
Under occupational health and safety legislation, an employer has a responsibility to provide a safe working environment. Every employer must prepare policies on health and safety issues in the workplace.
Occupational health and safety policies demonstrate that there is a commitment to ensuring the health and safety for all employees.
A drug and alcohol policy should be a part of the health and safety policy. Employers may risk prosecution and penalties if any employee is injured by the actions of another employee who was intoxicated at the time.
The effectiveness of any drug and alcohol policy is dependent on the inclusion of key components during the policy development and implementation stages:
1) Consultation
2) Universal application
3) Organisation specific
4) Comprehensive
5) Instructions and procedures
6) Drug testing considerations
7) Gradual and informed change
8) Publicity
9) Information dissemination, education and training
Evaluation
Evaluation of the Policy Serves Three Purposes:
1) Evaluation assesses how well the policy meets its objectives;
2) It ensures accountability at the managerial and organisational level and;
3) It provides important information for predicting future policy success or failure.
Potential Issues for Consideration in Evaluation of a Drug and Alcohol Policy
Include:
• The extent to which policy implementation applies to all employees;
• The achievement of anticipated outcomes;
• The identification of impaired employees;
• The effectiveness of treatment and counselling interventions;
• The effectiveness of the policy implementation process.
The Process of Developing and Implementing a Policy
Agreement within the organisation (management/union)
Appointment of steering committee and coordinator
Feasibility study and risk assessment
Reduction/removal of risk factors
Development and production of policy document
3. Phases involved in developing, implementing and managing an alcohol and other drug policy.
The Design Phase
The success of any response to alcohol and other drug issues in the workplace directly relates to the quality of planning and preparation. The design phase in particular plays a crucial role in determining the credibility and uptake of the policy. The design phase begins with an ‘in principle’ agreement within the organisation that a policy is necessary.
The Implementation Phase
The development and production of a policy document. The removal or reduction of risk factors. Awareness and information campaign/education and training. All components of the implementation stage are also components of the ongoing management phase of the policy.
Figure
The Management Phase
Awareness campaigns, education and training are continuing processes in effective policies. Apart from the need to reinforce the policy at regular intervals during employment, the employment of new staff require that education and training are ongoing.
Evaluation
Evaluation is essential in order to determine how well the policy meets its objectives. This ensures accountability at the organisational level and provides important information for predicting future policy success or failure.
The process of evaluation should result in continual improvements in the policy, and allow for ongoing identification of risk factors.
Managing Alcohol & Other Drugs in the Workplace
A guide for Managers and Supervisors
• The procedure for dealing with alcohol or other drug use in the workplace should be the same regardless of what drugs may be involved.
• Managers, supervisors and other staff are usually not qualified to make clinical diagnoses of dependency, nor are they qualified to provide treatment or counselling for alcohol or other drug problems.
• Work performance and safety rather than what employees do outside of work should be the the central focus in dealing with alcohol and other drugs issues in the workplace.
• It needs to be made clear to everyone in the workplace that the use of alcohol or illicit drugs will not be tolerated for both legal and safety reasons.
Intoxication at Work
• If an employer believes a person is not capable of performing work in a safe manner (e.g., due to suspected intoxication) they must ensure that the person is not at any risk personally, nor in a position to create a risk to others.
• An individual should not be allowed to work until they are considered able to safely and productively perform their job.
• If an employee is suspected of being intoxicated and is asked to leave the workplace for this reason, they must comply. If an employee is too intoxicated to legally drive, the employer should ensure safe transport for the employee.
Poor Work Performance
Criteria for evaluating poor work performance:
1) Lost time (not including sick leave)
2) Quality of work
3) Quantity of work
4) Safety
5) Effects on work team
6) Effects on clients or customers
Informal Approach
Below is a an example of how a policy may be implemented. Each business will have to define the consequences of a breach within its own policy. Consequences may also change on a case by case basis, as the risk of potential harm may be far greater in some circumstances. Some companies may choose to implement a “one strike” policy, where others may choose a more informal approach. Policies may also differ for casual employees vs permanent full time employees.
• Initial discussions with the employee regarding work performance can be on an informal basis. This needs to outline the concerns and make it clear that improvement is necessary.
• If an informal approach does not result in any improvement in work performance then a formal ‘constructive confrontation’ procedure is the next stage.
Constructive Confrontation Approach
The ‘constructive confrontation’ approach motivates behaviour change primarily using the threat of disciplinary action and encourages workers to improve and perform at their best. It fulfils all legal requirements in the event of dismissal.
The three stages of the ‘constructive confrontation’ approach are:
1) Advise; 2) Caution; 3) Confront.
Poor work performance
Written details recorded
Informal discussion of work performance problems
Work performance continues to be unacceptable
FORMAL APROACH
INTERVIEW 1
Advise person of problem
Monitor performance
Assess whether work performance has improved
Work performance continues to be unacceptable
INTERVIEW 2
Caution about the effects of continued poor performance
Continue monitoring performance
Assess whether work performance has improved
Work performance continues to be unacceptable
FINAL INTERVIEW
Confront with consequences, including dismissal
Continue monitoring performance
Assess whether work performance has improved
Work performance continues to be unacceptable
DISMISSAL
Satisfactory work performance Resume normal supervision
1. Advise
After sufficient written evidence of unsatisfactory or deteriorating job performance has been collected, an initial interview needs to be arranged with the person concerned. The objective of the first interview is to advise the person of the work performance problem, supported by examples.
2. Caution
If the first interview has been unsuccessful and work performance has not improved, a second interview needs to be arranged.
The aim of the second interview is to caution the employee, to provide specific evidence of how the employee’s work performance has remained unsatisfactory and to provide recommendations on seeking help or advice.
The employee needs to be further cautioned that dismissal or other disciplinary action will result if work performance does not improve. Details of the interview must be documented, agreed upon and signed by both parties.
Following the second interview, the employee’s performance needs to be continually monitored and documented. If the second interview does not achieve any significant improvements in performance a third interview must be arranged to confront the employee.
3. Confront
The third interview gives the employee a clear option to improve their work performance or face disciplinary consequences, including dismissal. The option to seek help is no longer voluntary and a mandatory assessment is required.
The employee should be given the opportunity to have a witness or representative present at this third interview stage.
Details of the third interview must be documented, agreed upon and signed by both parties. The costs of dismissing an employee and of training a replacement far exceed the costs of helping them.
Understand your relevant industrial relations legislation and unfair dismissal, unlawful dismissal and antidiscrimination legislation for all employees.
Extra Tips
• Offer help and discuss possible disciplinary action
• Keep a written record
• Do not try to diagnose the problem
• Sick leave may need to be offered if the employee’s diagnosed dependence on alcohol or drugs is considered a medical issue
• Maintain confidentiality throughout the process
• Continue monitoring through the designated period, documenting performance and details of any improvements
The Supervisor’s Role
Supervisors play a key role in the constructive confrontation process. The goal of the supervisor is to identify performance decrements, not to diagnose the cause of the decrement.
The supervisor’s focus in the constructive confrontation process must be on the performance issue, not determining the impact of an employee’s personal problems on performance. Supervisors may remind employees that if personal problems are affecting work performance they should seek access to appropriate services to rectify the problem.
The alcohol and other drug policy should clearly emphasise that performance should return to acceptable levels within an agreed time frame. Supervisors and employers should not specify what route employees should take to meet the goal of performance improvement, however, they can advise of the availability of counselling or treatment services.
Workplace Considerations
Unions
In workplaces where there are union members the employee needs to be advised that a union representative can be present at each interview if requested.
The union movement has placed much emphasis on occupational health and safety in recent years. By reducing alcohol and other drug problems, workers themselves stand to gain both better personal health and safer work conditions.
Workplace Factors
Consideration of the individual is important. However, consideration also needs to be given to factors in a workplace that may have an influence on drinking or drug use:
• Physical work environment;
• Availability and access to alcohol and other drugs;
• Stress;
• Job characteristics;
• Management style.
Workplace Compensation
Workers compensation agencies may not compensate for any injuries that occur if alcohol or other drugs are a factor.
Complimentary Health & Safety Practices
Responding to alcohol and other drug-related problems in the workplace complements other activities aimed at ensuring a safe and healthy work environment.
Therefore, alcohol and other drug responses and policy needs to be part of wider occupational health and safety practices and policies.
The suitability of these strategies for individual workplaces, and the availability of resources to support these strategies, will largely be determined by the feasability study and risk assessment conducted during the design stage of the policy.
Employee Assistance Programs (EAP’s)
An EAP is a workplace intervention designed to detect and resolve any workplace or personal problem that negatively impacts on work performance.
EAPs are not restricted to workplace alcohol and other drug issues. EAPs provide support tools to assist with family problems, relationship problems, financial problems, emotional problems, health problems and alcohol or other drug problems.
The main purpose of an EAP is to provide assessment and short-term counselling to employees who have voluntarily accessed the EAP services and to employees referred to the EAP by a supervisor.
Employees who have severe alcohol or other drug problems are identified and referred on to specialist treatment.
The services provided by any EAP depend on the needs and resources of individual workplaces. Services can range from minimal assessment and referral to fully integrated programs.
Fully integrated services usually include:
• Employee awareness and education;
• Supervisor training;
• Assessment and referral;
• Diagnosis and treatment;
• Monitoring and follow-up.
Brief Interventions
Most individuals do not require long and relatively expensive interventions to reduce alcohol and other drug-related harm and may only require brief interventions which are efficient and cost effective. Brief interventions include a range of strategies that can assist employees to modify their alcohol or other drug use. Brief interventions may consist of assessments and provide feedback or relevant information.
What
Are The Key Components of a
Best Practice Workplace Drug and Alcohol Testing Program?
The Main Considerations Under Australian Standards are:
• Collector/technician must be properly trained;
• Training should be accredited;
• Initial positive on-site test must be subjected to confirmatory testing at an accredited laboratory;
• Cut off levels for on-site and lab tests must not be less than levels prescribed in the Standards;
• Testing to be conducted only after informed consent is given by the employee;
• The Standard’s chain of custody must be followed;
• Provision made for a referee sample to be collected.
Establish a Need for Testing
• More likely to be accepted by workforce;
• More likely to be accepted by potential job applicants;
• Provides some protection from unfair dismissal claims.
Engage with Employees
• Consult with the workforce prior to introducing any testing program;
• Allow for mutually acceptable goals and procedures to be developed;
• Increases acceptance and credibility of program;
• Allow time for employees to consider the proposed testing program;
• Ensure adequate question and answer sessions;
• Place focus on rehabilitation/treatment with dismissal as a last resort.
Ensure Adequate Education & Training
• Must be early and on-going;
• Before testing is introduced and after implementation;
• Ensures acceptance and compliance;
• Provides a process for workers to come to understand the policy;
• Content must include more than just the testing procedures and process. Include information and skills on alcohol and drug use in the workplace, risks, and strategies to minimise harm.
A Drug Testing Program Should be Based on Formal Written Policy & Procedures
• Policy should be simple and easy to understand;
• Employees should be required to indicate acknowledgement and understanding of the policy;
• Employees should be reminded of the policy in a timely and regular manner;
• The policy should be applied consistently and without discrimination.
Australian Standards Relevant to Workplace Testing
• AS/NZS 4760:2019 Procedure for specimen collection and the detection and quantification of drugs in oral fluid
• AS3547:2019 Breath alcohol testing devices for personal use
• AS/NZS 4308:2008 Procedures for the collection, detection and quantification of drugs of abuse in urine
Testing
What Occurs in a Drug and Alcohol Test?
Workplace drug testing is a method of identifying drug use that may affect workplace safety. It is a two-stage process that involves a point of collection test (POCT) and a laboratory analysis.
POCT on-site screening, (immunoassay test)
Advantages
• Usually less expensive than laboratory testing
• Relatively easy to administer, little training required
• Test result is generally available within minutes of screen being conducted
Disadvantages
• Less accurate and reliable than laboratory analysis;
• The range of drugs that can be detected by a single test device is limited;
• Test result cannot distinguish between prescription/over-the-counter and illicit drugs;
• Test device does not allow for results to be kept for medical or legal reasons;
• Visual display markers vary widely and are subject to misinterpretation;
• Risk that poorly trained staff may be exposed to health and safety hazards, inappropriately conduct the test, or misinterpret results.
Laboratory Analysis (GC-MS, or LC-MS spectrometry tests)
Advantages
• More reliable and accurate than onsite POCT screens;
• Can detect a wider range of drugs than POCT devices;
• Better able to distinguish between prescription/over-the counter and illicit drugs than POCT devices;
• Can detect the adulteration or dilution of specimen samples;
• Results can be stored for future medical or legal access;
• Lab staff have higher levels of expertise/ training in conduct and interpretation of tests.
Disadvantages
• Generally more expensive than POCT;
• Slower turnaround time for test results.
Types of POCT On-site Screening
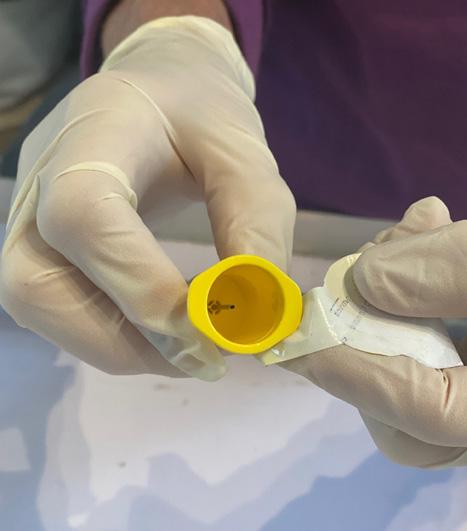
Urinalysis
involves the employee producing a urine sample into a sterile tamper proof container
Advantages
• Inexpensive;
• Fully developed methodology;
• More reliable for detecting past use;
Saliva Testing
Disadvantages
• Intrusive;
• Wide window of detection for cannabis (days/weeks);
• May not detect very recent use of some drugs;
• Requires appropriate collection facilities;
• Donor may not be able to readily provide a specimen;
• Dilution, adulteration, or substitution of urine easier compared to other methods.
involves collection of a sample of saliva from inside the mouth using a swab or pipette
Advantages
• Relatively non-intrusive;
• Swab wipe only;
• Narrow window of detection;
• Can detect current/recent use;
• Specimen available immediately;
• Less opportunity for substitution, dilution, or adulteration.
Breath Analysis
Disadvantages
• Can be difficult to collect sufficient quantities for confirmatory analysis;
• Oral contamination can adulterate or dilute the sample;
• Donors need to be supervised for up to 30 mins prior to sample collection to minimise oral contamination;
• Ability to reliably detect cannabis use questioned.
involves the employee exhaling into a usually hand held breathalyser
Advantages
• Onsite test that can indicate alcohol intoxication/impairment;
• Un-intrusive, breath sample only;
• Window of detection is narrow and produces a result similar to blood.
Disadvantages
• Only detects alcohol use;
• Testing equipment relatively expensive, requires ongoing maintenance and Calibration;
• Can not store sample for confirmation.
What Types of Workplace Testing Programs are Used?
Pre-Employment Screening
Positives
• Considered most acceptable to employees and unions.
Random Testing
Positives
• Considered to be procedurally fair.
For-cause Testing
Positives
• Generally supported by employees and unions.
• More cost effective than other forms of testing.
Post-accident Testing
Positives
• Generally supported by employees and unions.
• More cost effective than other forms of testing.
Negatives
• Easily evaded - only likely to detect uninformed or severely addicted applicants.
Negatives
• Most contentious testing program, places the onus on employee to prove they are not a drug user.
• May result in legal challenges if nonsafety sensitive work roles are tested at the same rate as those in safety sensitive roles.
Negatives
• Potential for false accusations, employee bullying
Negatives
• Can result in under-reporting of minor accidents and near misses.
What Are The Possible Readings?
An ideal test accurately measures what it is supposed to measure.
That is, an ideal test indicates drug use when drugs have been taken (a true positive) and shows no use of drugs when drugs have not been taken (a true negative).
POCT on-site screens are likely to produce a higher rate of false positives and false negatives than laboratory analysis.
The risk of false positive on-site POCTs is reduced by subsequent confirmatory laboratory analysis, but false negatives are likely to go undetected.
What is a non-negative?
This is where the initial test result was at or above the specified cutoff levels and requires confirmation testing to determine the cause of the result.
Is a Drug Present?
Is a Drug Detected?
1) A true positive (a drug is detected and is present);
2) A false positive (a drug is detected, but no drug is present);
3) A false negative (no drug is detected, but a drug is present);
4) A true negative (no drug is detected and no drug is present);
The Collection Procedure
Duty of care and work role boundaries
Businesses, workers, and collectors are all responsible for safe testing. There is a duty of care that applies to each party in drug and alcohol testing.
The business has a responsibility to provide a safe environment for testing, appropriate procedures and proper equipment, including PPE.
The donor has a responsibility to follow the procedural directions and use care to not place themselves or others at risk for biohazard contamination.
The collector has a responsibility to conduct the testing in a safe manner, use proper PPE and protect themselves and the donor from biohazard contamination. Additionally, collectors should avoid confrontation with donors.
There is an additional duty of care issue which may arise in the course of testing. If a donor makes a statement to the collector about harming themselves, or harming others, this then falls under Mandatory Reporting obligations. A collector would have an obligation to report that statement to appropriate authorities.
Collectors, and by extension, businesses, must be aware of the work role boundaries that apply when doing drug or alcohol testing. It is not appropriate to use information gathered or otherwise obtained during a drug or alcohol screen to initiate discussion about personal health matters. A collector with a medical background may feel a urine test has indicated that a donor has a medical condition, however, their job is not to diagnose medical conditions in this role.
Safety considerations in drug and alcohol testing
There are several considerations to take into account when conducting drug and alcohol testing. It is important to ensure that your testing procedures are designed to ensure the safety of the collector and the donor.
If you are the collector, you must bear in mind, some donors will be uncooperative, unwilling, or even potentially aggressive during the testing process. The consequences of a non-negative result could be very serious, and some participants may become very difficult if they know or are concerned that their results may cost them their income or employment. How should you handle uncooperative or aggressive participants?
When commencing the drug or alcohol screening, the collector will gain consent, first verbally, then in writing. A good practice is to start with asking the donor, “are you familiar with the company’s drug and alcohol policy” and if they confirm, then ask “do you consent to participate in this test?” If the participant says, “no” or indicates they were unaware of the policy, or suggests that they are not consenting willingly, this is the time to stop. Ask the company representative to take the participant to HR to discuss this. Your job as a collector is not to argue with a participant about what they know or do not know. It is only to ensure that they are clear on the policy, and they are consenting to be tested.
When setting up your testing area, it is advisable to keep communication equipment (mobile phone) with you, work in teams where possible, and maintain clear access to exit doors in the testing room. If a participant becomes agitated with a result, do not conflict with them. State that the test is a screen, and nothing is confirmed until it has been sent to a lab. If a participant becomes aggressive, remain calm, attempt to de-escalate the situation. If you feel unable to de-escalate the situation, exit the testing area
immediately. Your role is not to force anything, or threaten any disciplinary actions, but only to conduct a test. If the participant is unwilling, your job is done. Remember, key points to safe collecting:
• Always confirm the donor understands the policy.
• Always confirm informed consent.
• Do not argue or engage in conflict with the donor, refer them back to HR if needed.
• De-escalate if donor becomes agitated or aggressive.
• Exit the room if unable to de-escalate.
Infection Control
Many infectious agents are present in biological secretions or excretions.
There are six major types of infectious agents:
1) Bacteria
2) Viruses
3) Fungi
4) Protozoa
5) Helminths
6) Prions
The main mode of transmission of infectious agents is direct contact, airborne or droplet.
Successful infection prevention and control involves implementing work practices that prevent or minimise the transmission of infectious agents.
When testing for drugs and alcohol, using potentially infectious agents, it is essential for testers to know the following:
• Risk created by the exposure
• Precautions to be taken to protect themselves and others
• Proper use of PPE and clothing
• Correct infection control procedures to follow
Recommended Precautions
The Australian and New Zealand standards AS/NZS 4308:2008 Procedures for specimen collection and the detection and quantitation of drugs of abuse in urine contains an Appendix D titled “Recommended precautions for handling biological specimens”.
This document has been developed to reflect appropriate precautions in a laboratory environment but could also be appropriate for workplace testing.
Disinfecting
The recommended precautions state that a disinfectant such as freshly prepared 1:10 dilution of bleach in water should be used to clean surfaces, spills and equipment. This can be unrealistic in a workplace testing environment as it could be potentially dangerous transporting the chemical to various worksites and could pose a challenge in preparing a fresh solution multiple times throughout the day.
Infection control procedures for workplace testing should include the following:
• Only performing tests where plastic backed absorbent pads are used on flat surfaces where testing equipment and consumables are to be placed
• Wearing PPE as appropriate
• Isolating the area
• Soaking up any spill immediately with disposable towels or absorbent material
• Washing the affected area with hot water and detergent
• Drying the area
• Disposing of any waste materials appropriately
• Washing your hands
• Do not use alcohol-based or antibacterial wipes on breathalyser equipment while testing.
PPE
Medical gloves should be used when conducting any workplace drug and/or alcohol testing. A fresh pair of gloves should be applied for each new sample being collected.
The recommended precautions state that the handling of biological samples should not be performed by persons with cuts and abrasions. However, according to the majority of workplace policies/guidelines it is sufficient to cover any affected areas with a water resistant occlusive dressing which is changed as necessary and is further reinforced by double gloving.
Planning and Preparation
Workplace testing may occur across many worksites or remote locations. It is important that planning and preparation for a testing session includes the following:
• Requesting authority: this is the person or entity who is requiring the test. Usually this will be the employer.
• Day and time for testing
• Location of testing facility
• Nominated company representative contact details
• Any special instructions particular to the site
• The nature and scope of sample collection
• Expected number of donors
• Required testing equipment
• Waste hazard bags and waste sharps container
• Reason for conducting test (random/post-incident/pre-employment/reasonable grounds)
The above information should be established from reviewing the instruction/job sheet which will be largely determined by legislative requirements, industry standards or organisation specific policies.
Testers/collectors may be employees of the organisation that is requesting the testing. When this is the case, it is recommended that an additional company representative is provided to assist.
Ensure an appropriately private screening area is available. Provide sufficient quantities of PPE, paperwork and testing consumables. Allow for extra screening devices and lab packs to accommodate the potential need for retests due to adulterated samples or non-valid devices. Ensure any electronic equipment is within calibration date and any consumables are within their expiry dates.
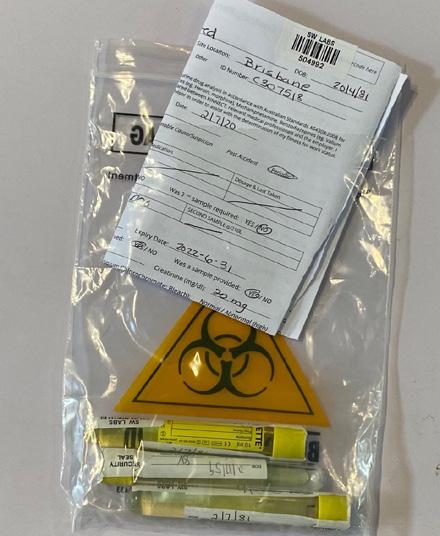
Storage and Transport
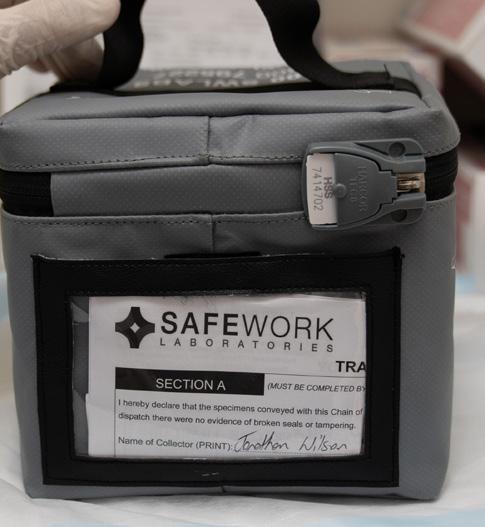
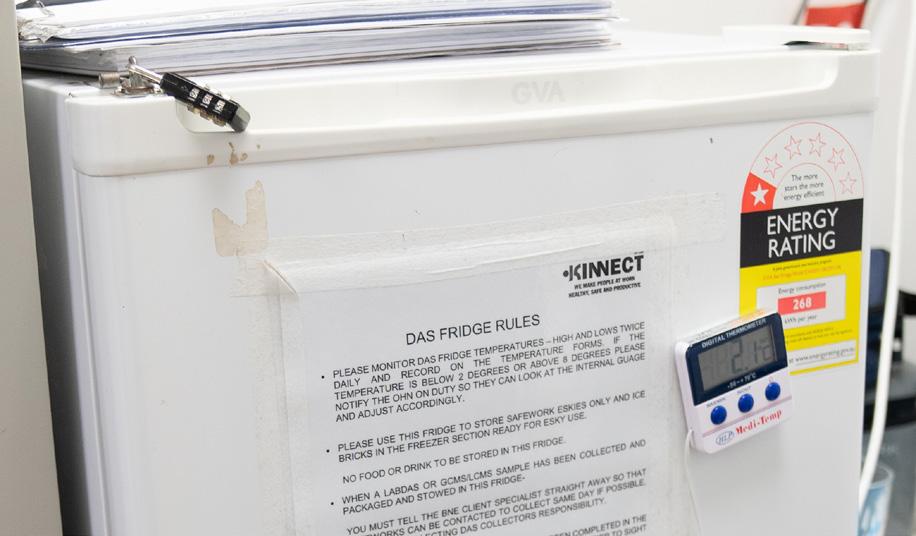
When transporting equipment and consumables to the worksite, place in a cool controlled container/ pack and not in direct sunlight (check manufacturers instructions) as this may compromise their effectiveness.
Ensure you have a coldpack/icepack, fridge, esky or insulated cooler to store any potential samples that must be sent to a lab for analysis. Do not freeze collected samples.
Communication and Documentation
Communication to the Donor
The collector should confirm the donor understands why the test is being conducted (i.e. random, post incident).
It is the responsibility of the Nominated Company Representative (NCR) to communicate to the donor/s any information regarding their policies and procedures.
It is normally outside the scope of the collector/tester to explain these issues in depth and where any misunderstanding or dispute arises the donor should be referred back to the nominated company representative. However, the collector/tester should confirm with the donor that they have been made aware of their rights and obligations and that they have an obligation to provide accurate information and a true sample. The donor must sign a consent prior to a sample being collected.
Documentation
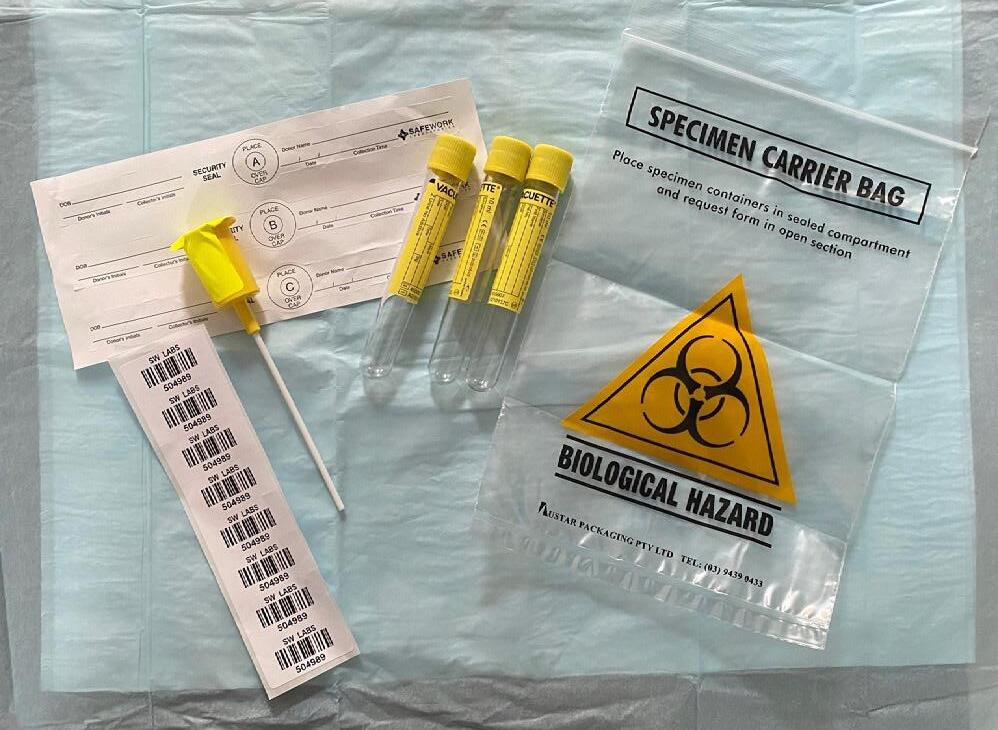
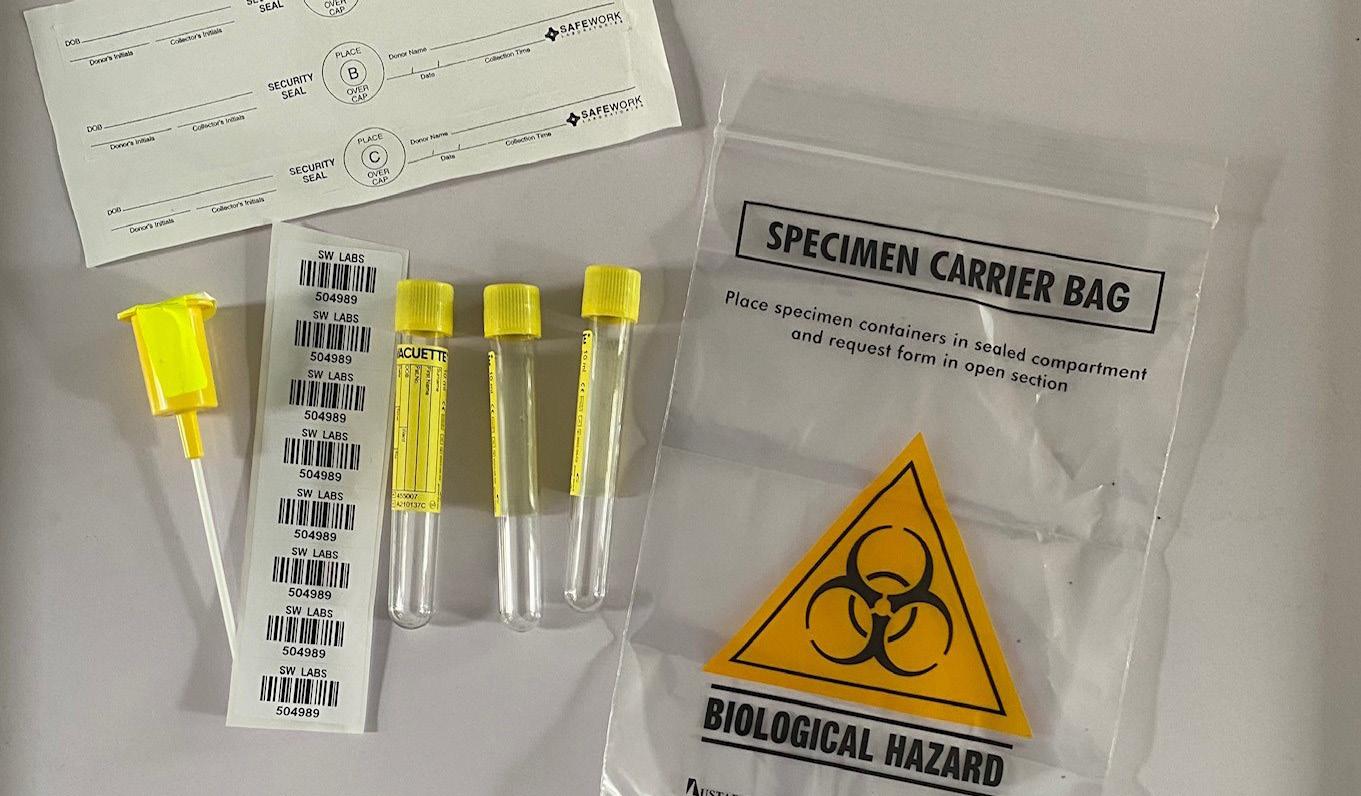
When performing any drug and alcohol testing procedures, certain documentation is required. This can vary according to company policies. At a minimum, there will be two types of documents which are required.
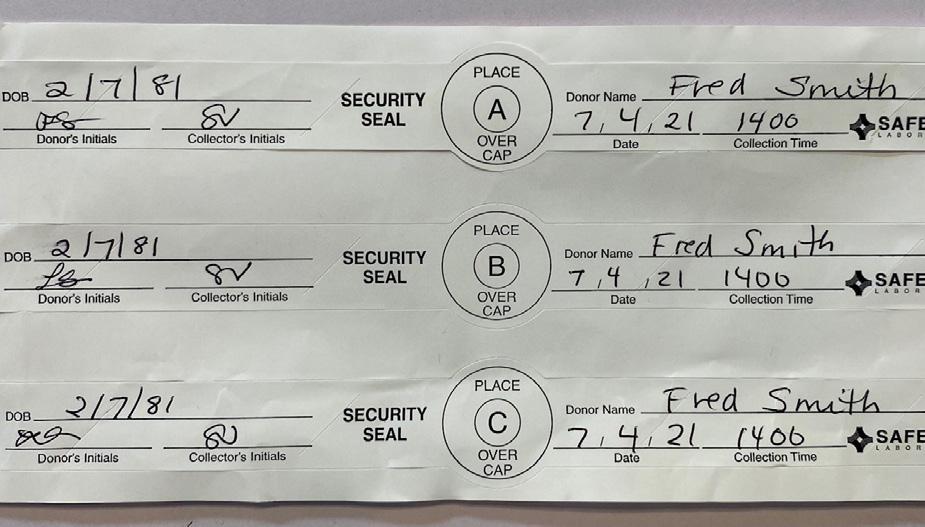
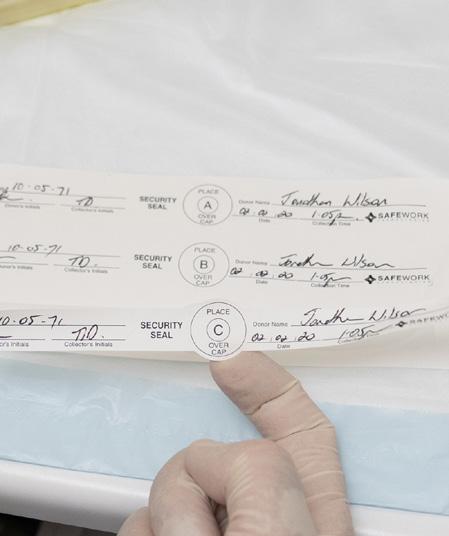
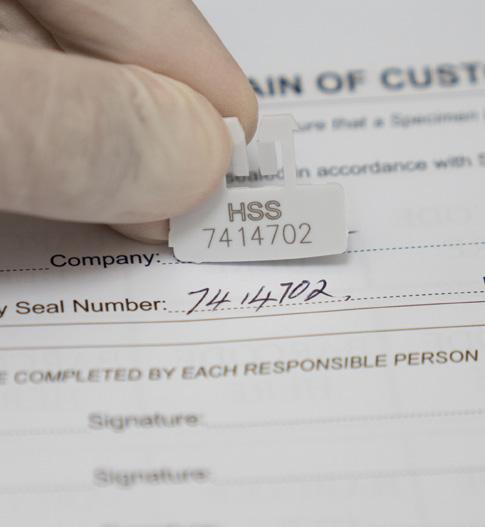
1) Chain of custody form (usually in triplicate)
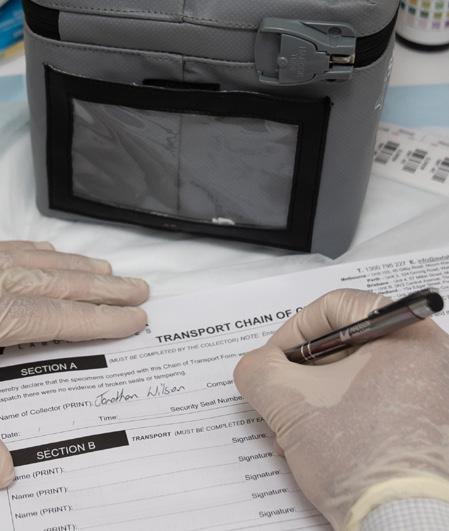
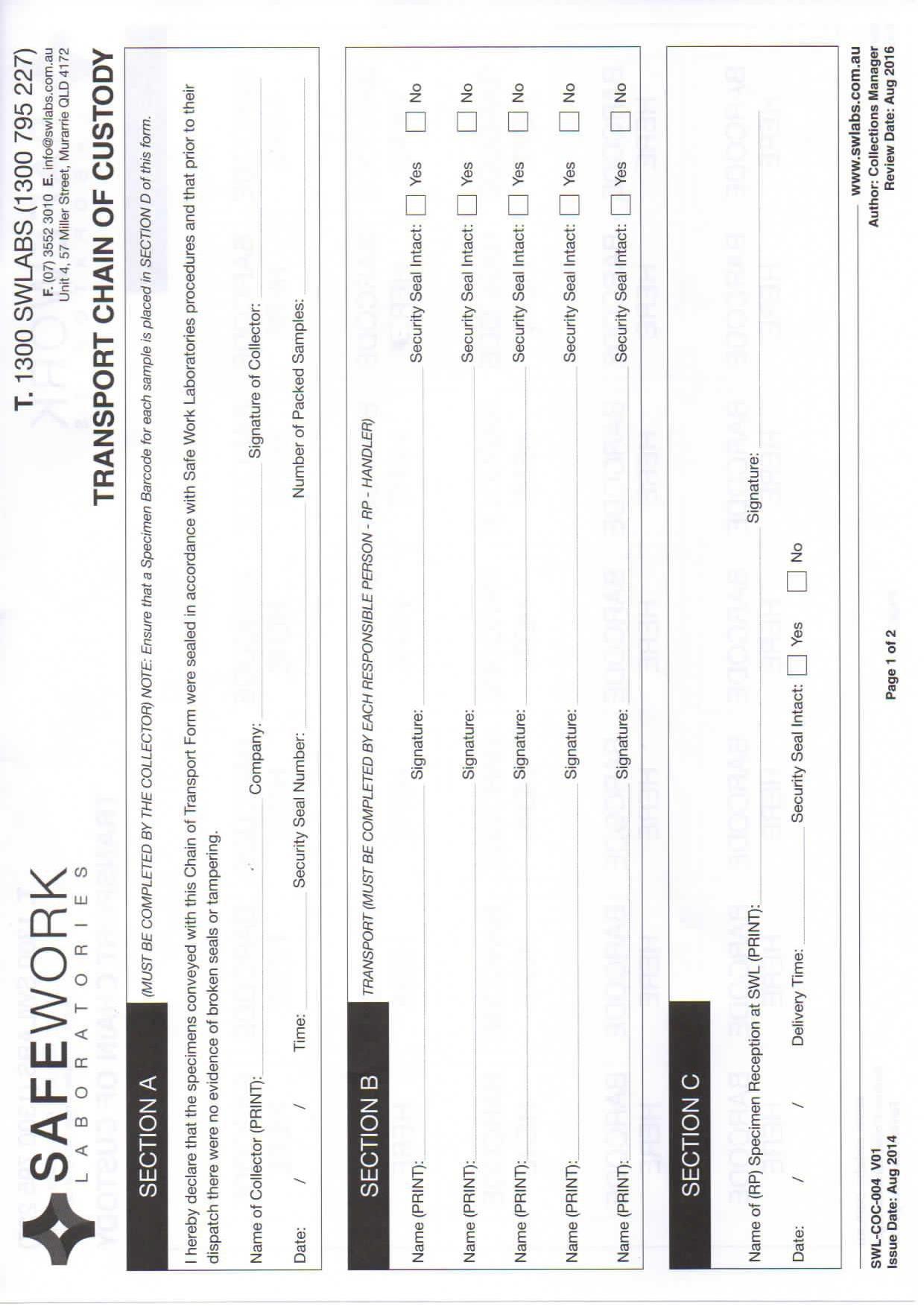
2) Transport chain of custody form
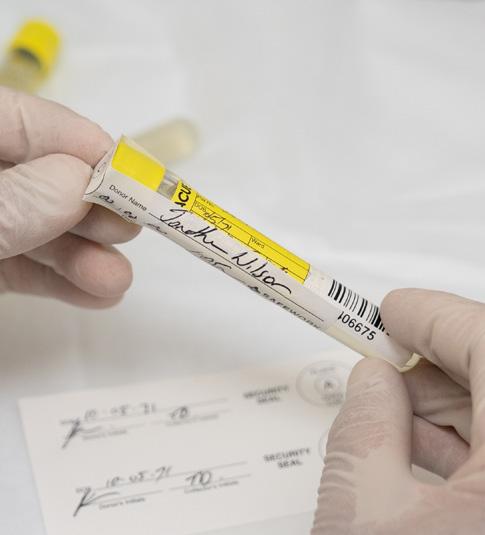
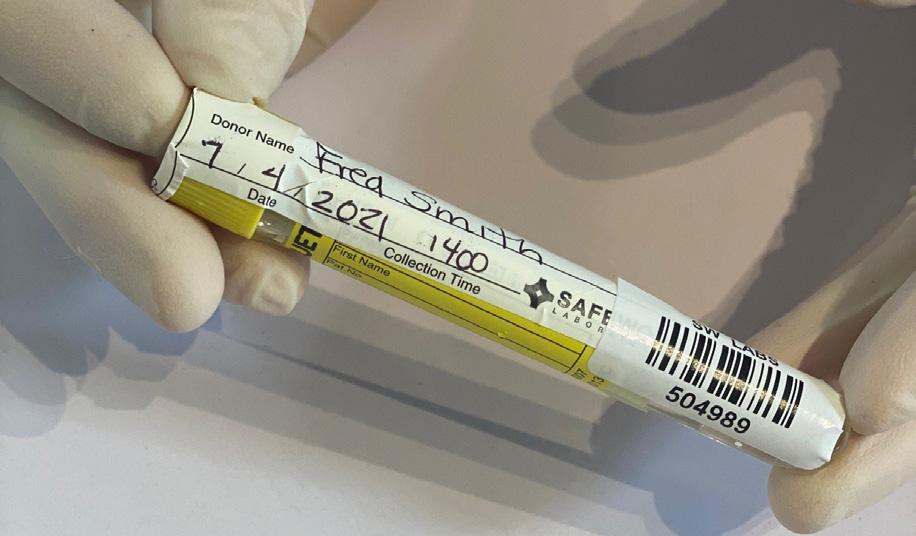
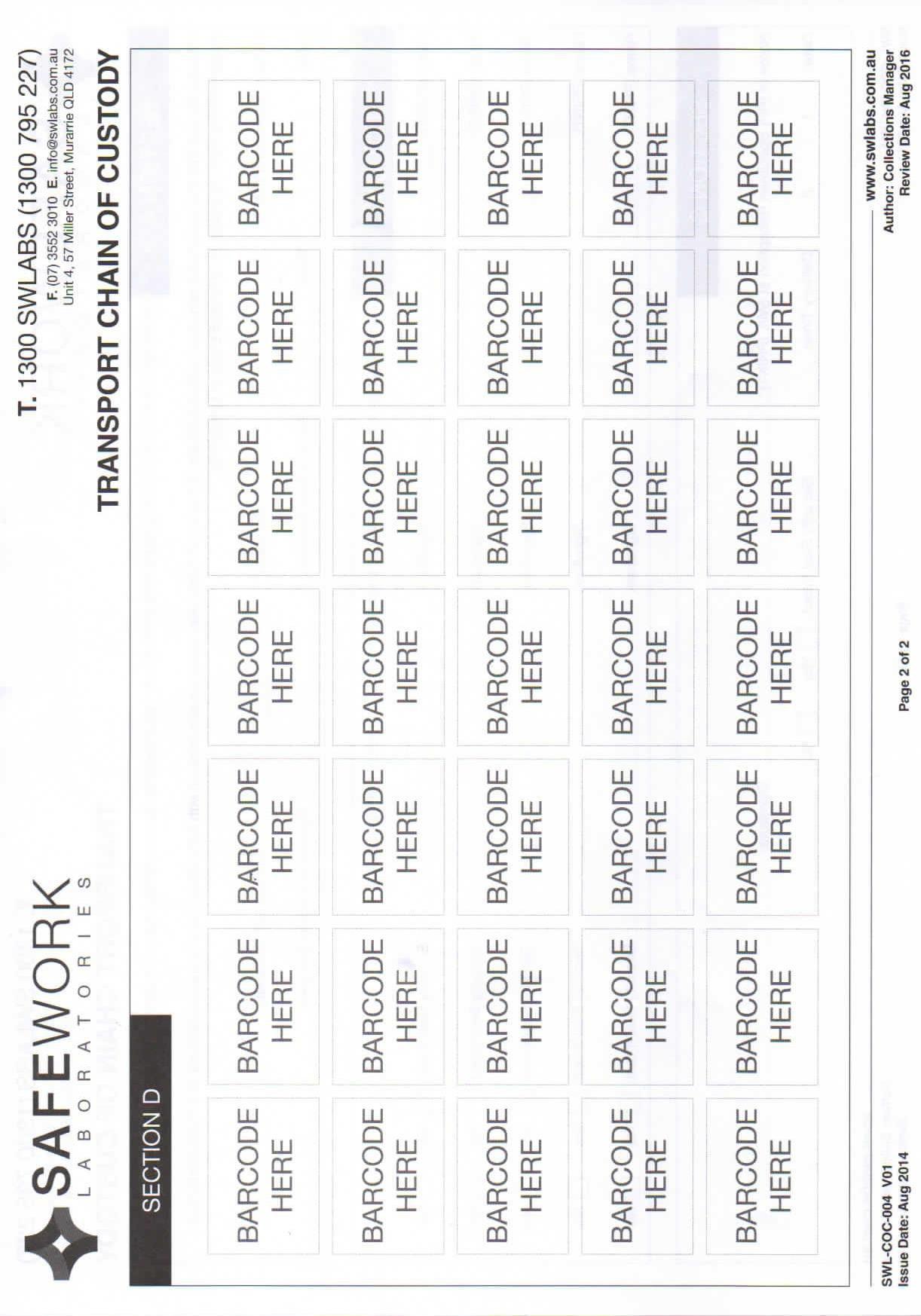
The chain of custody form is the initial documentation for any test. It will have donor’s identifying information, medication declarations, and consents. It will also state who the requesting authority is, types of tests being conducted, and reasons for tests.
These documents must be filled out in blue or black ink. Errors must be corrected with single line strikethrough. All corrections must be initialled by both collector and donor. No spaces should be left blank, write nil or N/A or strike through any spaces that have no information.
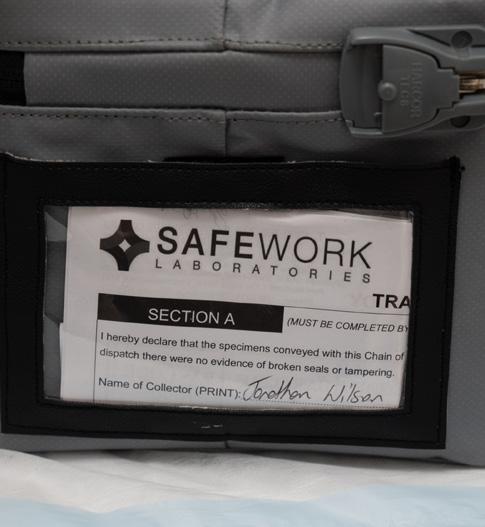
The transport chain of custody is a document that identifies the number of samples, the barcode identifiers of the samples, the collector’s name, the names of the couriers who carry the sample, and the name of the lab personnel who receive the sample. This document goes to the lab with the sample and is evidence of an intact chain of custody.
Testing Consent & Chain of Custody Form:
Urine Screening /Breath Alcohol Screening
Donor Details
Participant consent: I do hereby consent to undergo a breath and/or urine analysis, in accordance with AS3547:2019 and AS 4308:2008 for the following substances: alcohol, THC, cocaine metabolites, opiates/opioids, methamphetamine, amphetamines, and benzodiazepines. I understand that the information from this assessment will be shared between the authorised collector, relevant medical professionals and the employer requesting the screen. I understand that I may be asked to discuss my medical history with a medical advisor to assist with the determination of my fitness for work status. I understand that I may request an independent witness during this screening.
Date
Medication taken in the past 30 days
I certify that the donor’s identification has been verified and that the specimen identified on the form has been provided to me by the donor certified above.
Donor Declaration: I
certify that the specimen accompanying this form is my own and was provided by me to the authorised collector. I also certify that the specimen containers were sealed with tamper evident seals in my presence and that the information provided on this form and on the labels is correct. I consent to the analysis of the specimen for the following drugs and their metabolites; amphetamine type substances, benzodiazepines, cannabis metabolites, cocaine metabolites, opiates/opioids. I consent to the release of the results of these tests to the authority that requested the screening, i.e. employer, medical professional, or their authorised representatives.
Collector Declaration: I certify that I witnessed the donor signature above and that the specimen identified on the form was provided to me by the donor whose certification appears above, and that it has been collected, tested, divided, labelled, and sealed in accordance with the instructions provided in the Standard AS/NZS 4308:2008. Reason for test
Laboratory Use Only
Breath Alcohol Test
Drug Screen
Collector Certification
Breath Alcohol Testing
A breath alcohol assessment is the measure of the concentration of alcohol vapour in the subjects expired breath, a measured amount of which is drawn from the mouthpiece into the device.
The use of alcohol breathalyser units in the workplace has become a popular method of testing for alcohol intoxication. Many organisations now routinely use personal hand held devices as a fast and simple way to check employee sobriety as they enter the workplace for random testing or following an incident.
The effects of alcohol and the rate it is metabolized into the bloodstream may vary between individuals. Many factors can play a role in the rate at which the body absorbs alcohol.
AS 3547-2019 is the Australian Standard for breath alcohol testing .
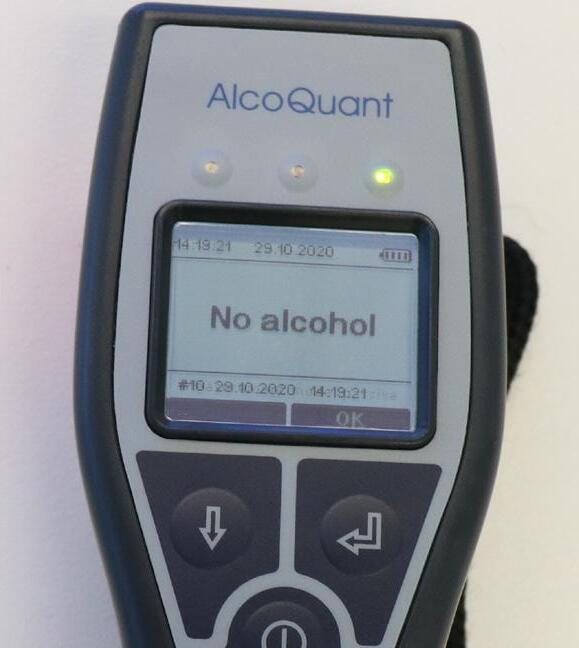
Passive Mode Collection
When conducting an breath alcohol test, a variety of methods can be used. Many industries including mining and construction have introduced a 100% testing format when arriving at the workplace and use the procedure known as passive mode collection .
This method involves the donor talking into the device whilst held close to their mouth, it may include speaking their name or counting numbers e.g. 1 to 15. Once the breathalyser has completed analysing it will indicate a result of Alcohol or No Alcohol. If the breathalyser does not detect any alcohol then the donor can continue to work. If the breathalyser detects alcohol, then the donor will be required to repeat the test in the active mode collection immediately.
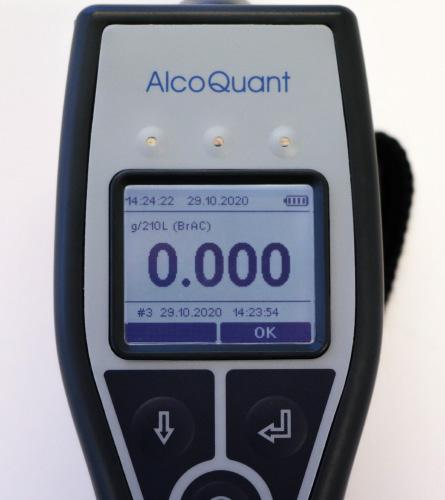
Active Mode Collection
This method involves the collector switching the breathalyser to the active test mode , which requires attaching a mouthpiece/straw to the device.
The collector should carefully pull the plastic strip cover back and insert the straw into the device, leaving about an inch of wrapper over the end of the straw that the donor will remove prior to placing their mouth over the straw. This will provide confidence that the straw is hygienic and not contaminated.
Testing in active mode will indicate a Breath Alcohol Concentration (BrAC) percentage reading e.g. 0.045% - this would mean the donor has some alcohol in their system, but is under the legal driving limit (in Australia) of 0.050%. If the reading is 0.000% then the donor has no alcohol in their breath.
Breath Testing Procedure
Prepare for Testing
1) Prepare a private testing environment including equipment, consumables, paperwork and PPE.
2) Ensure device is in calibration.
Conducting the test
1) Introduce themselves.
2) Ask donor if they are familiar with the company drug and alcohol policy, and if they consent to be tested.
3) Ask if the donor has had anything to eat or drink in the last 20 minutes or had a smoke in the last 5 minutes.
4) Confirm the donor’s identity with an id card or a supervisor’s confirmation.
5) Read consent to the donor and then have donor sign consent to perform the test.
6) Turn on the device and check the current calibration date. Show the calibration date to the donor.
7) Record the serial number, and calibration date of breathalyser.
8) Ask the donor to blow continuously into the mouthpiece until you ask them to stop. (If the testing device indicates “blow failure” then the collector will reset and ask donor to try again).
9) Once the testing device has analysed the result it will be shown as a 4 decimal % reading (0.000%). Show the result to the donor.
Results
1) If the result is 0.000 the collector records it on the chain of custody form as First Sample, including time of test.
2) If the reading is anything apart from 0.000, record the result and inform the donor they will be required to repeat the test in 20 minutes. During this time they should be supervised by a company NCR. They must remain nil by mouth the entire time.
3) After 20 minutes, re-test the donor using a fresh mouthpiece.
4) Once the testing device has analysed the result, the collector is to show the donor and record in the second sample section of the form.
5) If re-test result is 0.000 then the breath test is completed and donor may return to work.
6) If secondary test result is above 0.000, collector to complete documentation and advise NCR. They will manage the donor according to company procedure.
Tips
• Do not store or use the breathalyser unit near or with ethanol wipes, gels or sprays
• Do not clean the breathalyser unit with disinfectant wipes
• Collector to remain in control of the device at all times
• Do not conduct a test if the donor has smoked in the previous 5 minutes
• Never allow anyone to blow liquid through the mouthpiece
• Don’t block the breathalyser exhaust port with a finger
• Always show the donor the screen result
• Always ask donor to take a deep breath
• Always keep device in manufacture’s case during transportation
• Always use hygienic methods when handling mouthpieces
Testing Consent for Breath Alcohol Screening
Donor Details Signature
Surname: Given Name: DOB:
Job Title: Site Location:
ID # Driver’s Licence: Passport: 18+ Card: Other:
Reason for test Pre-employment Random For Cause Post-Incident Periodic Other Date:
Requesting Authority:
Participant consent: I hereby acknowledge that I am required to undergo tests to determine the existence of alcohol which may affect my performance; I consent to the analysis of a specimen of my breath for alcohol; I declare that the information provided in this form is true and correct; I consent to the release of the test results to the requesting authority.
I certify that the donor’s identification has been verified and that the specimen identified on the form has been provided to me by the donor certified above.
Serial
Urine Drug Testing
Urine drug testing is one of the most common testing methods used.
Urine drug tests screen the urine for the presence of a drug or its metabolites (a drug metabolite is a byproduct of the body breaking down, or “metabolizing,” a drug into a different substance). Immunoassay tests cannot predict when a drug was taken or how much the person used, it only indicates the presence of the drug, or it’s metabolites.
Urine drug testing is an immunoassay based on the principle of competitive binding. Drugs which may be present in the urine specimen compete against their respective drug conjugate for binding sites on their specific antibody. During testing, a urine specimen migrates upward by capillary action. A drug, if present in the urine specimen below its cut-off concentration, will not saturate the binding sites of its specific antibody. The antibody will then react with the drug-protein conjugate and a visible colored line will show up in the test line region of the specific drug strip.
AS/NZS 4308:2008 is the Australian Standard for urine testing.
This standard sets out procedures for specimen collection, screening, confirmation, quantitation and reporting of drugs in human urine as well as integrity testing of the specimen.
The procedure tests for all the following drug classes:
• Amphetamine type substances (includes Methamphetamine)
• Benzodiazepines
• Cannabis metabolites
• Cocaine metabolites
• Opiates
On-site drug testing is a more cost efficient method for effectively detecting drug abuse amongst employees. Urine testing is more reliable for detecting past use and in some cases can detect cannabis use for days/weeks.
Drug Test Detection Times
Drug detection times can vary, based on individual metabolism, amount used and frequency of use. Detection times listed by individual products also vary, but will remain within an average.
Urinalysis Oral Fluid
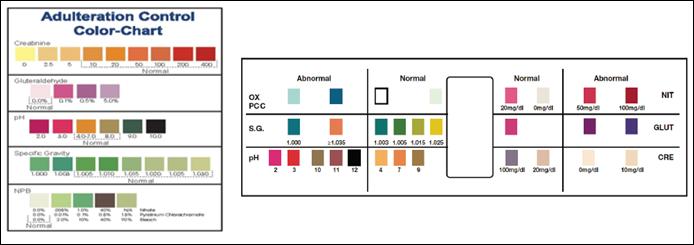
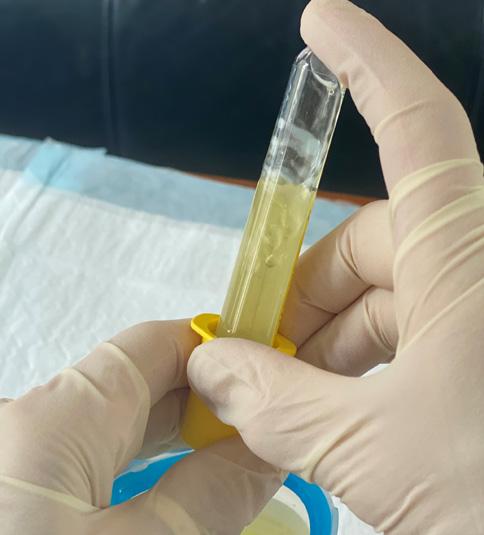
Integrity Testing
Integrity testing of the donor sample is the first step to make sure it is a valid sample and to detect if the sample has been adulterated.
Adulterants
An adulterant is a pejorative term for a substance found within other substances.
There are two categories of adulterants:
1) The first kind is urine substitute or fake urine . Urine substitute contains normal urine substances, such as pH buffer, sodium chloride, creatinine, protein, bilirubin, etc.
2) The second category of adulterants include chemicals intended to disable or lower the sensitivity of drug tests . Commonly used adulterants include nitrites, peroxides, bleach (Hypochlorite), and cross-linking agents (glutaraldehyde), etc. These chemicals affect drug test by altering the reaction environment or the active ingredients, enzymes, antibodies, or drugs of interest.
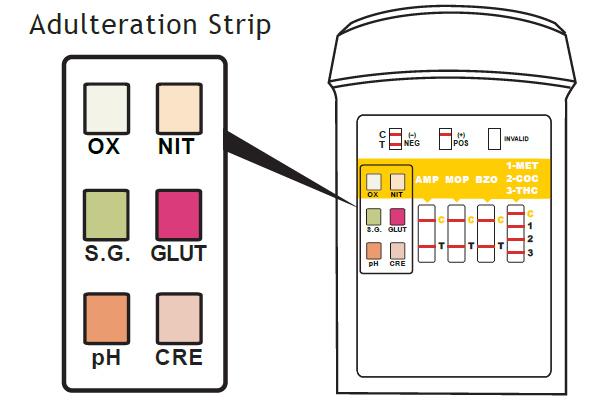
Creatinine (CRE)
Specific Gravity (S.G.)
Creatinine is a waste product of creatine, an amino acid contained in muscle tissue and found in urine.
This test is a way to check for dilution of the sample and to ensure the sample is consistent with human urine.
If there is no creatinine reading on a sample, then this is an indication the sample is not human, low levels off creatinine could indicate potentially dilution, a result of water loading to dilute drug levels below cut of levels.
Tests for sample dilution, this is the least reliable indicator and if abnormal in isolation of all other adulterants, it should be ignored.
Tests for the alkalinity or acidity of the sample.
PH (pH)
Nitrite (NIT)
Oxidants (OX)
Glutaraldehyde (GLUT)
If the PH level is recorded as high (greater then 9) or low (below 4) this may indicate that the sample has been adulterated with a chemical such as cleaning agent or an acid may have been added to the sample.
Nitrite tests for commonly used commercial adulteranats such as Klear or Whizzies. They work by oxidising the major cannabinoid metabolite THCC00H.3. Normal urine should contain no significant trace of nitrite. Positive results could also be found due to urinary tract infections or bacteria contamination.
This tests for the presence of oxidising agents e.g. bleach, hydrogen peroxide, persulfate and pyridinium chlorochromate.
Normal human urine should not contain any trace of oxidants and if recorded is an indication of adulteration.
Tests for the presence of aldehyde, a chemical used for sterilization making it difficult to detect any illicit drugs in urine.
It is not a normal component of human urine and should not be present in normal urine and if recorded is an indication of adulteration.
Adulterant Test
What it detects
Integrity Test Failure Process
If the integrity of a donor sample cannot be verified by temperature or the listed adulterants, do not record the results. Retain the first sample and request the donor to provide a further sample. For this second sample, start a new chain of custody form. If the second test does not pass integrity checks, both samples will be sent to the lab for screening. If the second test passes integrity checks, and the result is negative, you may discard both samples. If the second test passes integrity checks and the result is nonnegative, both samples should be sent to the lab for screening and confirmation.
Do not read or record the results of a drug screen for a sample which does not pass integrity checks.
If samples are to be sent to lab, follow the laboratory confirmation procedure and mark the chain of custody form that the sample validity could not be established.
Notify the nominated company representative of the result and inform them that only a laboratory can provide a confirmed positive result.
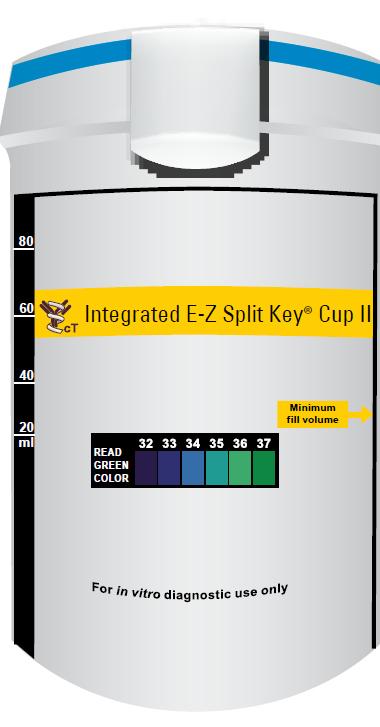
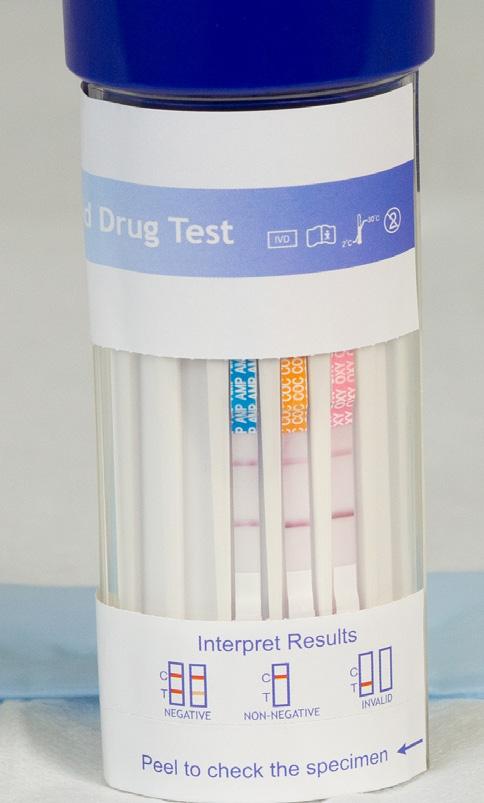
Reading a Urinalysis Cup
Before conducting a drug test, you should become familiar with the device you are testing with. Most devices offer a similar method in how they display results, as most devices display a control and test line. The urine cups generally have a key printed on them that shows you how to interpret the results. To demonstrate how to read and interpret results, we will use the Integrated E-Z Split Key Cup, which is AS/NZS4308:2008 compliant and can test up to 6 drugs.
Looking at the E-Z split cup you can see each drug class has a corresponding testing segment. These segments display 3 possible testing results which includes: Negative, Non-Negative, and Invalid.
Negative (drug not detected)
This is when there is a coloured line in the control region (C) and a coloured line in the test region (T). The shade of the line in the test region (T) may vary, however it should be considered a negative whenever there is faint coloured line.
Non-Negative (drug detected)
This is when there is a coloured line in the control region (C) but no line in the test region (T) for the drug it indicates.
Invalid (failed test)
This is when the control line (C) fails to appear. The most common reason for this is an insufficient amount of specimen or procedural failure. Repeat the test with a new test cup if this happens.
Urine Testing Procedure
Prepare for Testing
1) Prepare a private testing environment including equipment, consumables, paperwork and PPE.
2) Prepare a designated stall: close taps, seal cistern, add blue dye to bowl. Stall should not be accessible to the public or other workers during the testing period. Remove any items from the stall such as bowl cleaners, brushes, bins or deodorants.
3) Place an absorbent, disposable pad (blue hospital pad) on the testing table.
Conducting the Test
1) Collector to introduce themselves.
2) Ask donor if they are familiar with the company drug policy, and if they consent to be tested.
3) Confirm donor identity, with an id card, or a supervisor’s confirmation, and record information on Chain of Custody, (COC) form.
4) Read consent to the donor and then have donor sign consent to perform the test.
5) Collector to sign form stating their name and role as collecting technician.
6) Ask donor to provide information to complete medication declaration.
7) Ask donor to select a sealed test cup, and then record the lot number and expiry date on the COC form.
8) Ask donor to remove bulky clothing, empty pockets and leave all belongings in the screening area.
9) Take donor to the toilet and allow donor to wash hands with water only.
10) Advise the donor the preferred volume required on the testing cup (preferred minimum is 30ml).
11) The donor is asked to place the closed sample on the cistern and instructed NOT to flush the toilet.
12) Donor may now be provided with soap to wash hands.
13) Check the toilet for any foreign objects.
14) Return to screening area with donor, place sample on absorbent pad.
Results
1) Record the temperature reading and visually check the colour for any abnormalities.
2) Read the adulterant strips and record results on the COC form, (if integrity issues are present, the donor will be required to provide a second sample).
3) If no integrity issues the collector should now read the drug test panel.
4) Record the result on the COC form as either negative or non-negative.
5) If result is negative, complete paperwork and give the donor a copy and the test is concluded. Go to Results step 12
6) If result is non-negative, inform the donor of results and the next required steps of the process.
7) Package sample into supplied sealed vials for transport to laboratory. Seal and sign each vial with the donor.
8) Put a barcode on the COC document, on the Transport COC document, and one on each vial.
9) Donor to sign declaration confirming sample is their own and permitting lab assessment of same.
10) Sample is placed in chilled, locked container prior to transport to lab.
11) Privately advise the nominated company representative of the result, the NCR will then manage the donor as per the company’s procedure during this time.
12) Dispose of sample into toilet, flush, and prepare toilet for next donor.
13) Place gloves, pipette, used cup and any other refuse in waste bag. Prepare area for next test.
Testing Consent & Chain of Custody Form:
Urine Screening /Breath Alcohol Screening
Donor Details
Participant consent: I do hereby consent to undergo a breath and/or urine analysis, in accordance with AS3547:2019 and AS 4308:2008 for the following substances: alcohol, THC, cocaine metabolites, opiates/opioids, methamphetamine, amphetamines, and benzodiazepines. I understand that the information from this assessment will be shared between the authorised collector, relevant medical professionals and the employer requesting the screen. I understand that I may be asked to discuss my medical history with a medical advisor to assist with the determination of my fitness for work status. I understand that I may request an independent witness during this screening.
Date
Medication taken in the past 30 days
I certify that the donor’s identification has been verified and that the specimen identified on the form has been provided to me by the donor certified above.
Donor Declaration: I
certify that the specimen accompanying this form is my own and was provided by me to the authorised collector. I also certify that the specimen containers were sealed with tamper evident seals in my presence and that the information provided on this form and on the labels is correct. I consent to the analysis of the specimen for the following drugs and their metabolites; amphetamine type substances, benzodiazepines, cannabis metabolites, cocaine metabolites, opiates/opioids. I consent to the release of the results of these tests to the authority that requested the screening, i.e. employer, medical professional, or their authorised representatives.
Collector Declaration: I certify that I witnessed the donor signature above and that the specimen identified on the form was provided to me by the donor whose certification appears above, and that it has been collected, tested, divided, labelled, and sealed in accordance with the instructions provided in the Standard AS/NZS 4308:2008. Reason for test
Laboratory Use Only
Breath Alcohol Test
Drug Screen
Collector Certification
Tips
• Be aware of your own safety, and use proper PPE
• As the collector always remain with the donor until test procedure is finalised
• Do not conduct a test if the donor has not consented
• Use a privacy sign on toilet doors
• Do not conflict with donors. If faced with an aggressive response, de-escalate or leave the room.
Protocol for Non-Negative Results
Once a non-negative result has been recorded, advise the donor that the screening result can only be confirmed by an accredited laboratory. Explain the next steps which include the packaging of the urine sample.
Different laboratory companies will have their own procedure and equipment and you will need to confirm which company you are to use and their protocol and procedures.
Safework Laboratories Protocol and Procedure
Obtain a laboratory split kit confirmation pack and place all pieces on the blue absorbent mat.
The kit will contain the following:
• 3 x specimen tubes
• 3 x security seals
• 1 x specimen transport bag
• 1 x set of barcodes
• 1 x vacuum straw
1. Select a Vacutainer Spike Kit
2. Fill in the security labels
3. Place a barcode on the Chain of Custody document and on the Transport Chain of Custody Section D
4. Remove the seal and place the straw into the cup. Use care as the pipette contains a spike
5. Insert the vacuette onto the spike and press in to suck up the sample
*Do this for all 3 vacuettes
6. Attach the security seal stickers to all 3 samples
7. Affix a barcode to all 3 samples
*Make sure the barcodes are stuck parallel to the label so the lab can scan them properly
8. Place the vacuettes and paperwork into the sample bag and place sample in locked fridge or transport cooler with ice bricks
9. Fill out Section A of the Transport Chain of Custody form
*Select a safeworks bag seal and write the seal number in this section
10. Slip the full Transport Chain of Custody form into the Esky pouch
*Fold up pages 1 and 2 together
11. Seal the Esky by pressing in the security tag into the seal
12. Place the Esky into a locked fridge until pickup to preserve the sample
Preparing samples for transport to lab
1) When you have completed your screening, you will then need to send the samples you have collected to the laboratory for confirmatory testing.
2) Complete the Transport Chain of Custody (COC) document, section A, with your details.
3) Count the number of samples. Record number of samples on Transport COC
4) Confirm that barcodes on packed samples match barcodes on back of Transport COC document
5) Place all samples in transport cooler bag or satchel.
6) Lock bag with a security tab key
7) Record number of security tab key onto Transport COC document.
8) Place Transport COC document in sleeve window of Cooler Bag or with Satchel for transportation.
9) Ensure that courier fills out section B of Transport COC document upon pickup.
Oral Fluid Drug Testing
Oral fluid screening involves the collection of saliva from the mouth. Saliva is secreted by the parotid, submandibular and sublingual glands via ducts that empty near the teeth, tongue and the floor of the mouth. There are also many smaller glands in the lips, inner cheek and in the lining of the mouth and throat that all contribute to saliva production.
The role of saliva is to moisten the mouth, initiate digestion and offer protection to teeth against decay. Oral fluid production is mediated by several physiological factors such as age, gender, food intake and some drugs that may affect its production.
Oral fluid testing is becoming more popular in the workplace as it is considered to be more time and cost effective, less invasive and more easily conducted. It also gives an indication of most substance usage within the past 24 hours. This is because saliva identifies the parent ingredient of an illegal drug, not the metabolite, which is in contrast to urine screening. However, indication times may differ if the donor is a very heavy user or is using a long-acting BZO to manage epilepsy. Further, according to Clonal (a manufacturer), some compounds may show up as long as 2-3 days.
For this reason an oral fluid specimen may be used to establish recent drug use at a workplace. The relationship between blood or plasma concentration of drug and oral fluid concentration allows an inference to be made of relatively recent use of drugs to be made (within hours) compared to urine concentrations only being able to establish past use of a drug (days to weeks).
A variety of on-site oral fluid testing devices are available, including devices that provide a instant screen result on the device via the saliva running across the test strips off the device, and some devices provide an electronic screen result.
Testing devices can also vary in pricing, test result times and varied saliva collection procedures. Most devices will require the donor to place a swab pad in to mouth, actively swabbing inside including cheeks, gums and tongue until sufficient saliva is collected. This could take a number of minutes depending upon donor’s ability to produce saliva.
Once enough saliva has been collected a coloured strip will indicate that the test is ready to screen for drug use. If a test line is not present then you must activate devise according to the manufacturer’s instructions and specified timeframes.
Once a device has indicated control lines, and test lines the result can be read. If this first device produces a non-negative result, a second sample must be taken with a Quantisal device which preserves the sample for laboratory confimation testing. The initial test device cannot be use for lab testing.
The Quantisal package has two vials so that you may collect a test sample and a referee sample. These are sealed and signed in much the same way a urine sample is. These samples should also be stored in a chilled, locked container prior to transport to the lab.
All POCT tests that provide a non-negative result will require laboratory confirmation.
Drug Test Detection Times
Drug detection times can vary, based on individual metabolism, amount used and frequency of use. Detection times listed by individual products also vary, but will remain within an average.
Urinalysis
Oral Fluid
Reading an Oral Fluid Device
Before conducting a drug test, you should become familiar with the device you are testing with. The saliva drug testing devices display results much like the urinalysis cups with a control line and test line to indicate whether a drug is present or not. Saliva drug testing devices also have a key printed on the device to help you interpret the result. To demonstrate how to read and interpret results, we will use the Clonal 6 Panel Oral Fluid Drug Testing Device, which is AS/NZS 4760:2019 compliant and can test up to 6 drugs.
Looking at the Oral Fluid device, you can see each drug class has a corresponding testing segment. These segments display 3 possible testing results which includes: Negative, Non-Negative, and Invalid.
Negative (drug not detected)
This is when there is a coloured line in the control region (C) and a coloured line in the test region (T). The shade of the line in the test region (T) may vary, however it should be considered a negative whenever there is faint coloured line.
Non-Negative (drug detected)
This is when there is a coloured line in the control region (C) but no line in the test region (T) for the drug it indicates.
Invalid (failed test)
This is when the control line (C) fails to appear. The most common reason for this is an insufficient amount of specimen or procedural failure. Repeat the test with a new test cup if this happens.
Oral Testing Procedure
Prepare for Testing
1) Prepare a private testing environment including equipment, consumables, paperwork, and PPE.
2) Place an absorbent, disposable pad (blue hospital pad) on the testing table.
Conducting the test
1) Collector to introduce themselves.
2) Ask donor if they are familiar with the company drug policy, and if they consent to be tested.
3) Ask the donor if they have had anything to eat or drink in the last 20 minutes. (donor must be nil by mouth for 20 minutes prior to collection).
4) Confirm donor identity, with an id card, or a supervisor’s confirmation, and record information on Chain of Custody, (COC) form.
5) Read consent to the donor and then have donor sign consent to perform the test.
6) Collector to sign form stating their name and role as collecting technician.
7) Ask donor to provide information to complete medication declaration.
8) Ask donor to select a testing device and then record the lot number and expiry date on the COC form.
9) Advise donor of the procedure for collecting oral fluid, ( i.e., lean forward, do not chew on sponge, keep sponge in mouth while collecting, advise collector when sponge is very soft).
10) Check the colour indicator if using a device that has one to show adequate collection amount.
11) Place collection wand into testing devise and compress to close.
12) Remove label and wait for control lines to appear before reading test results.
13) Keep device upright at all times.
Results
1) Confirm control lines are visible
2) Read the results of the screen.
3) Record the result on the COC form as either negative or non-negative.
4) If result is negative, complete paperwork and give the donor a copy and the test is concluded. Go to Results step 12.
5) If result is non-negative, inform the donor of results and the next required steps of the process.
6) Explain that donor must provide a second oral fluid collection onto absorbent paddles for preservation in Quantisal vials.
7) Seal and sign each vial with the donor.
8) Put a barcode on the COC document, on the Transport COC document, and one on each vial.
9) Donor to sign declaration confirming sample is their own and permitting lab assessment of same.
10) Sample is placed in chilled, locked container prior to transport to lab.
11) Privately advise the nominated company representative of the result, the NCR will then manage the donor as per the company’s procedure during this time.
12) Dispose of original sample and any other refuse in waste bag. Prepare area for next test.
I
Testing Consent & Chain of Custody Form:
Oral Fluid Screening / Breath Alcohol Screening
Donor Details
Participant consent: I
do hereby consent to undergo a breath and/or oral fluid analysis, in accordance with AS 3547/2019 and AS/NZS 4760:2019 for the following substances: alcohol, cannabis, amphetamine-type stimulants, opiates, benzodiazepines, cocaine and metabolites, or other identified drugs. I understand that the information from this assessment will be shared between the authorised collector, relevant medical professionals and the employer requesting the screen. I understand that I may be asked to discuss my medical history with a medical advisor to assist with the determination of my fitness for work status. I understand that I may request an independent witness during this screening.
Medication taken in the past 30 days
Results (Circle negative or further testing)
(OPI, MOP)
(OXY)
(BZO)
Confirmation Testing Required No (end form) Yes (complete the next section)
Confirmation Testing
Donor Declaration: I certify that the specimen accompanying this form is my own and was provided by me to the authorised collector. I also certify that the specimen containers were sealed with tamper evident seals in my presence and that the information provided on this form and on the labels is correct. I consent to the analysis of the specimen for the following drugs and their metabolites; amphetamine type substances, benzodiazepines, cannabis metabolites, cocaine metabolites, opiates/opioids. I consent to the release of the results of these tests to the authority that requested the screening, i.e. employer, medical professional, or their authorised representatives.
Collector Declaration: I certify that I witnessed the donor signature above and that the specimen identified on the form was provided to me by the donor whose certification appears above, and that it has been collected, tested, divided, labelled, and sealed in accordance with the instructions provided in the Standard AS/NZS 4308:2008.
Tips
• Be aware of your own safety and PPE
• The collector must remain with donor until test procedure is finalised
• Do not conduct a test if the donor has not consented
2-4 days; cutoff level: 300 ng/ml Dilates pupils, increased heart rate and Bp; anesthesia, euphoria, sensitive to sound; and touch, less need for food, cardiotoxic
1 day
up to 14 days; up to 30 days with chronic users; cutoff level: 25 ng/ml
users feel euphoric, then sleepy; used as a date rape drug; slows breathing and heart rate
1-2 joints: 2-3 days; oral ingestion: 1-5 days; moderate smoker: 5 days; heavy smoker(daily): 10 days; chronic smoker-5 joints per day: 14-18 days or as long as a month; cutoff level: 50 ng/ml
analgesia, amnesia, hallucinations, foul-tasting drip from nasal passages; users feel they are outside of their body, vomiting, seizures, dissociation
hydromorphone (Dilaudid), codeine, Tylenol with codeine, morphine ( avinza, Kadian, mS contin, oramorph Sr, hydrocodone (Vocodin): pos. at 300 cutoff
oxycontin, percodan, percocet, roxicodone, Tylox, oxycontin is a time-released form of oxycodone
days;
level: 2000 ng/ml or 300 ng/ml
as amphetamines; may grind teeth and clench jaw, sweating and increase in body temp.
Same as amphetamines; hallucinations, increase in body temp.; tachycardia, agitation, very talkative
pupils constricted, pulse and Bp lowered, body temp. lowered, euphoria initially and then drowsy, respiratory depression, convulsions, constipation, coma
Dissociative anesthetia-analgesia and amnesia, dissociated from environment but not asleep, pulse and Bp elevated, coma
Same as opiates
elevated body temperature, elevated pulse and Bp, pupils dilated, agitation, delirium, seizures, constipation, dry/ flush skin
Useful Resources and Contacts
Alcohol & Other Drugs Council of Australia (ADCA):
The ADCA website provides links to help-lines and information and fact sheets on specific drugs and alcohol and strategies to minimise harm, an online searchable DRUG database and links to other Internet resources pertaining to alcohol and other drugs.
Community Alcohol Action Network (CAAN):
The CAAN website provides a list of links to information and treatment services, telephone counselling available in each Australian jurisdiction, support groups, research and education.
Australian Drug Foundation (ADF):
The ADF website provides links to resources such as videos, posters, pamphlets, booklets, educational kits and manuals and free downloadable fact sheets. The ADF supports the Community Action on Alcohol Network and the Drug Info Clearinghouse and the ADF website contains links to both resources.
Drug Info Clearinghouse:
The DrugInfo Clearinghouse provides information about alcohol and other drugs pertaining to various people, drug-related fact sheets and statistics, laws relating to drugs and information relating to drugs and driving. Toolkits for workforce development and drug education are provided along with links to other alcohol and other drug related organisations and/or services. Drug information in languages other than English is also provided.
Australian Drug Information Network (ADIN)
ADIN is funded under the National Illicit Drug Strategy and is managed by the Australian Drug Foundation (ADF). The ADIN website provides links to a variety of websites and information on alcohol and other drugs. Organisations and individuals can use the search function on the ADIN website to locate relevant information on a range of drugs and drug issues.
Australian National Council on Drugs (ANaCD)
The ANCD website provides publications on alcohol and other drugs, links to websites of alcohol and other drug-related organisations and Australian drug-use information.
National Centre for Education & Training on Addiction (NCETA)
NCETA provides a variety of publications and resources concerning alcohol and other drug related issues in the context of the workplace. Particular emphasis is placed on the role of workplace culture, and its impact on behaviours such as risky drinking, and strategies to manage alcohol- and other drug-related harm in the workplace.
Interlock Employee Assistance Program
Interlock is a not-for-profit organisation under the auspice of the Alcohol and Drug Foundation Queensland (ADFQ) that was established to introduce and maintain Employee Assistance Programs (EAPs) within organisations in Australia. The Interlock website provides information on EAPs, such as what an EAP is, the components and principles of an effective EAP and a link to National Guidelines for Employee Assistance Programs:
http://www.interlock.org/guide.html
Unionsafe
The UnionSafe website provides links to online resources relating to workplace safety, an A to Z list of hazards information in which tobacco smoking and passive smoking appear with the health effects of the hazard, useful references in the subject area and a comprehensive series of drug and alcohol fact sheets covering issues that pertain to the use of alcohol and other drugs at work (the effects and impairment, performance and counselling, the law, possible factors, employee assistance services, costs and testing for misuse).
National Drug & Alcohol Research Council (NDARC)
The NDARC website provides a list of alcohol and drug information services and other key agencies across Australia as well as links to alcohol and other drugs information, services and treatment. A series of fact sheets on a range of drugs are also available.
The Australian Drug Foundation Alcohol & Work Website
Alcohol and Work website is provided by the Australian Drug Foundation (ADF). The ADF Alcohol and Work website provides information and advice to prevent alcohol-related problems at work in ways that are fair, effective and ethical. The aim of the website is to use the workplace as an environment to raise awareness about alcohol issues and to help reduce alcohol-related harm in the community.
National Drug Research Institute (NDRI)
The main aim of NDRI is to conduct and disseminate high quality research that contributes to the primary prevention of harmful drug use and the reduction of drug related harm in Australia. The NDRI website provides information on the National Alcohol Indicators Project (NAIP), which monitors and evaluates the effectiveness of state and national alcohol policies, and the School Health and Alcohol Harm Reduction Project (SHAHRP) which aims to reduce alcohol related harm among secondary school students. Links to other useful Australian and international websites are also available.
Comparison of Urine and Oral Fluid for Workplace Drug Testing
Casolin, A. (2016). Comparison of Urine and Oral Fluid for Workplace Drug Testing. J Anal Toxicol, 40(7), 479–485. doi: 10.1093/jat/bkw055
Aim
The aim of the study was to compare relative detection rates of urine versus oral fluid testing in a safety sensitive (i.e. high-risk) industry as well as the correlation between diagnosed substance use disorders and the possible impairment at work.
Method
The study involved 1,500 paired urine and oral fluid tests in accordance with Australian Standard/ New Zealand Standard (AS/NZS) 4308:2008 and AS 4760:2006. Workers who returned a positive test were screened for substance use disorders, as defined by DSM-5, and for possible impairment at work following that particular episode of substance use.
Results
Substances were detected in 3.7% (n = 56) of urine samples and 0.5% (n = 8) of oral fluid samples (p < 0.0001). One worker (0.07%) had a substance detected on oral fluid alone versus 49 workers (3.3%) who had substances detected on urine alone. Twelve workers returned a positive result, defined as being consistent with the use of an illicit drug or a controlled substance without a clinical indication and prescription. Nine workers tested positive on urine alone, one on oral fluid alone and two on both (p = 0.0114). Of note, 6/11 workers who tested positive on urine had possible impairment at work and 2/11 had a substance use disorder versus 2/3 and 0/3, respectively, who tested positive on oral fluid.
Conclusion
This study has shown that urine drug testing performed in accordance with AS/NZS 4308:2008 is more likely to detect overall substance use and illicit drug use than oral fluid testing conducted in accordance with AS 4760:2006. The results of this study also suggest that urine testing performed in accordance with AS/NZS 4308:2008 may be more likely to detect workers with possible impairment at work and substance use disorders than oral fluid testing performed in accordance with AS 4760:2006. Urine, therefore, is recommended as being the testing matrix of choice for routine random drug testing in safety sensitive industries in Australia. This study has also confirmed that urine drug testing may miss very recent use of cannabis by a previously abstinent person and thus the use of both urine and oral fluid would provide a greater level of assurance and could be indicated in selected circumstances, such as for targeted or post-incident testing, in a similar way to that considered and endorsed by Commissioner Cambridge (8). Further study of the paired results of such a program would provide greater evidence concerning the risks described in this study and further study is also required to determine whether the findings in relation to possible impairment and substance use disorders are replicated and reach significance in a larger cohort.
HLTPAT005 Learner Guide v1.7 - 9/09/2021
Workplace Drug and Alcohol Testing Course
HLTPAT005 - Collect specimens for drugs of abuse testing