Journal of The Association of PAs in Cardiothoracic and Vascular Surgery
Figure 1: TEE image showing all four cusps.
Figure 2: TEE image showing Mild AR of the Aortic Valve. with vena contracta of 0.297cm2
Official Journal of The Association of Physician Assistants in Cardiothoracic and Vascular Surgery
JAPACVS
Journal of the Association of PAs in Cardiothoracic and Vascular Surgery
Editor-in-Chief
Aaron R. Morton, DMSc, MMSc, PA-C, ATC, FAPACVS Emory University, Atlanta, GA
Associate Editor—International Vicky Vink PA Switzerland
Associate Editor Writer Development
Edward A. Ranzenbach, PA-C, MPAS, CAQ-CVTS, FAPACVS, DFAAPA Misenheimer, NC
Editorial Board
Cardiac Section Editor
Michael Lalonde, MHA, PA-C Branford, CT
Thoracic Section Editor
Matthew Vercauteren MPAS, PA-C, FAPACVS Pittsburgh, PA
Vascular Section Editor
Daniel Geersen MPAP, PA-C Morrisville, NC
Editorial Member at Large
Hantz B. Fontaine PA-C New York, NY
Publisher
David E. Lizotte, Jr. MPAS, PA-C, FAPACVS
Executive Director APACVS Festus, MO
EDITORIAL MISSION:
The JAPACVS is the official clinical journal of the Association of PAs in Cardiothoracic and Vascular Surgery. The mission of the JAPACVS is to improve Cardiac, Vascular and Thoracic Surgical and CVT Critical Care patient care by publishing the most innovative, timely, practice-proven educational information available for the physician assistant profession.
PUBLISHED CONTENT IN THE JAPACVS: Statements and opinions expressed in the articles and communications herein are those of the authors and not necessarily those of the Publisher or the Association of PAS in Cardiothoracic and Vascular Surgery (APACVS). The Publisher and the APACVS disclaim any responsibility or liability for such material, including but not limited to any losses or other damage incurred by readers in reliance on such content. Neither Publisher nor APACVS verify any claims or other information appearing in any of the advertisements contained in the publication and cannot take responsibility for any losses or other damage incurred by readers in reliance on thereon. Neither Publisher nor APACVS guarantees, warrants, or endorses any product or service advertised in this publication, nor do they guaranty any claim made by the manufacturer of such product or service.
SALES OFFICE
APACVS 1208 Victoria Crossing Festus, MO 63028 Phone (502) 321-6155 admin@apacvs.org
JAPACVS/Journal of the Association of PAs in Cardiothoracic and Vascular Surgery is published quarterly (4 issues per volume, one volume per year) by APACVS 1208 Victoria Crossing, Festus, MO 63028. Volume 6, Number 4, spring 2025. One year subscription rates: $40 in the United States and Possessions. Single copies (prepaid only): $20 in the United States
7 QUADRICUSPID AORTIC VALVE: A CASE OF A 46-YEAR-OLD SYMPTOMATIC FEMALE
Tanmay Acharia, DMSc, MBA, PA-C
Kayapanda Muthuna Mandana, MBBS, MS, MCh
Ashima Bhelotkar, MBBS, MS, DNB
Saikat Badyopadhyay, MBBS, MD
Loknath Tiwary, BSc, PGDFT
Dhanik Lal Mandal, PA-C
Peer Reviewed Content
15 Understanding Paraganglioma: An In-Depth Look
Michael E. Champion, DHSc, PA-C, RN, MBA
San Antonio, TX
APACVS is the only association representing Cardiac, Thoracic and Vascular Surgery and CTV Critical Care PAs. By PAs, For PAs!
Aaron R. Morton, DMSc, MMSc, PA-C, ATC, FAPACVS Editor-in-Chief
From the Editor's Desk
As the new year begins, it's common for people to reflect on their lives, consider changes they'd like to make, and set New Year’s resolutions. What follows are often determined efforts to maintain those resolutions. While I find this practice both interesting and, in some cases, admirable, I personally don't subscribe to it. Instead, I focus on reflecting upon the successes of the past year and expressing gratitude for those who contributed to the wins and supported me through the challenges.
This year was no different. As I envisioned the future of JAPACVS, I found myself thinking about the many individuals whose efforts have been vital to its growth and success.
While it would be impossible to list every contributor, certain key figures stand out as foundational to the development of this journal. One early champion, thought leader, and current Associate Editor for Writer Development, Edward Razenbach, played a critical role in shaping the journal’s concept. His energy, passion, and prior experience in publication, combined with the support of senior board leaders and past presidents Mr. Steve Gottesfeld and Mr. Scott
Balderson, laid the groundwork for JAPACVS.
Their support helped establish a space for PA publications and fostered a community dedicated to showcasing peer research. Both Mr. Gottesfeld and Mr. Balderson faced the challenge of advocating for PA publications in surgical journals that are often dominated by Physicians and less welcoming of PA contributions.
These early efforts were carried forward by Mr. David Bunnell, a former Editor-in-Chief who oversaw the publication of the journal's inaugural issues. Many of you may know Mr. Bunnell for his numerous roles supporting and advocating for our community nationally, or perhaps from his thoughtful "coffee consultations" on social media. His unwavering commitment to the PA profession, from education to advocacy, has had a profound impact.
Our progress would not have been possible without the expertise and dedication of our talented publisher, Mr. David Lizotte. As a long-standing member, past APACVS President, and current Executive Director of APACVS, Mr. Lizotte has worked tirelessly to ensure the journal’s professional presentation and success. Digital publication requires immense time, effort, and talent, and Mr. Lizotte's contributions have resulted in a journal we can all be proud of.
Reflecting on these contributions fills me with gratitude for the intellect, talent, and selflessness that have built a strong foundation for JAPACVS. The continued success of the journal depends on the engagement and support of our community. I urge each reader to honor the vision of these pioneers by contributing manuscripts, electronic media, or letters to the editor. Together, we can ensure the journal's ongoing growth and success.
Join Getinge for the Virtual North American EVH Summit
Join leading EVH experts and your peers for an engaging virtual experience at the Getinge North American EVH Summit — discover advanced techniques, share challenges, and gain insights for your endoscopic vessel harvesting practice. Register today!
Wednesday, April 16, 2025
6:00 PM EST (3:00 PM PST)
William Johnson, PA-C (Atlanta, GA)
ERAH: Procedural Optimization, and Utilizing Tourniquet vs. Non-Tourniquet for Endoscopic Radial Harvesting
Chelsey Martin, CRNFA (Nashville, TN)
Vein Harvesting: Solutions for Vein Prep and Optimizing Leg Positioning Techniques in Greater Saphenous Vein Harvesting
Register now for April 16!
www.getinge.com
Thursday, April 17, 2025
6:00 PM EST (3:00 PM PST)
Gary Cook, DMSc, PA-C (Camden, NJ) Historical Perspective and Perioperative Evaluation for Conduit Harvesters
John Skinner, PA-C (Charlotte, NC)
EVH 1-on-1’s: A Conversation with John Skinner, PA-C - Pioneering Radial Artery Harvesting
Register now for April 17!
QUADRICUSPID AORTIC VALVE: A CASE OF A 46-YEAR-OLD SYMPTOMATIC FEMALE
Authors: Tanmay Acharia, DMSc, MBA, PA-C
Physician Assistant & Team Leader, Fortis Hospital, Anandapur, Kolkata, India.
Kayapanda Muthuna Mandana, MBBS, MS, MCh (CTVS).
Director, Cardio-Thoracic and Vascular Surgery, Fortis Hospitals, Anandapur, Kol kata, India
Ashima Bhelotkar, MBBS, MS, DNB (CTVS).
Senior Consultant, Cardio-Thoracic and Vascular Surgery, Fortis Hospitals, Anandapur, Kolkata, India.
Saikat Badyopadhyay, MBBS, MD (Anaesthesia)
Senior Consultant Anaesthesiologist, Cardio-Thoracic and Vascular Surgery, Fortis Hospital, Anandapur, Kolkata, India.
Loknath Tiwary, BSc, PGDFT
Head of the Department of Perfusion Technology, Fortis Hospitals, Anandapur, Kolkata, India.
Dhanik Lal Mandal, PA-C
Physician Assistant (CTVS), Fortis Hospitals, Anandapur, Kolkata, India
INTRODUCTION
A Quadricuspid aortic valve (QAV) is a rare congenital heart defect characterized by four leaflets in the aortic valve instead of the normal three.1-4 QAV has an incidence which is less than 0.05%.2 Several cardiac anomalies are associated with QAV,3 with a higher prevalence of aortic regurgitation (AR) than aortic stenosis (AS).2,4 QAV is typically diagnosed using transthoracic echocardiography, but transesophageal echocardiography (TEE) can provide a more detailed and accurate visualization of the valve.2,3 Other imaging modalities such as computed tomography (CT) and cardiac magnetic resonance imaging (MRI) can be used if the quality of the images obtained through echocardiography is not conclusive.1,2,5 Patients with QAV can remain asymptomatic, and QAV can be an incidental finding in such patients.2,6 Surgical intervention is required for QAV patients due to AR and the hemodynamic consequences it causes, although AS is also
included.1,3 Surgical management of QAV can involve valve replacement using a mechanical or bioprosthetic valve, Bentall's procedure, Ross procedure, or bi- or tricuspidization of the valve without root replacement.3
CASE PRESENTATION
A 46-year-old woman presented with worsening symptoms, including dyspnea on exertion, palpitations, fatigue, dizziness, and occasional chest pain over the three months. She had a history of laparoscopic cholecystectomy in 2018 and no history of syncope. Echocardiography done in 2018 revealed QAV with mild AR. Upon examination, the patient was afebrile with a blood pressure of 130/80. Laboratory tests, including complete blood count, electrolytes, and kidney function, were all normal. An electrocardiogram showed normal sinus rhythm, and auscultation revealed an early diastolic murmur best heard at the left lower sternal border.
The patient was recommended to undergo echocardiography due to her progressively worsening shortness of breath during increased physical activity and palpitations, as well as her previous diagnosis of having QAV with mild AR six years ago. The echocardiogram revealed that she had QAV with severe AR, mild concentric left ventricular (LV) hypertrophy, and a normalsized LV cavity. Her LV ejection fraction was measured at 61%. The right ventricle was normal size and function, while the left atrial pressure was slightly elevated. Both the mitral and tricuspid valves appeared normal in structure and function. The aortic valve was noted to have normal cusp separation, an aortic root diameter of 2.8cm, and a sino-tubular junction diameter of 2.4cm.
The patient was advised to undergo cardiac catheterization before Aortic Valve Replacement (AVR), which showed normal coronary arteries. An intraoperative TEE was performed to assess the valve more clearly. The TEE initially showed QAV (Fig 1) with mild AR, with a vena contracta of 0.297 cm2 (Fig 2) at a blood pressure of 100/60 mmHg and a heart rate of 50 – 55 beats per minute.
Figure 1: TEE image showing all four cusps.
Figure 2: TEE image showing Mild AR of the Aortic Valve. with vena contracta of 0.297cm2
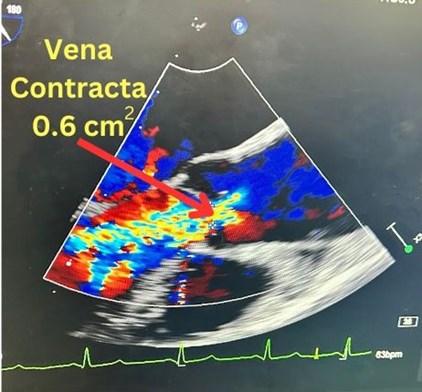
It was then decided to simulate the experience of a patient climbing a flight of stairs by increasing the blood pressure to 150-170 and raising the heart rate to the 90s. This was accomplished by subjecting the patients’heart to dobutamine-induced stress. Afollow-up TEE showed severeAR with a vena contracta of 0.6 cm 2 (Fig 3).
Figure 3: Repeat TEE showing severe AR with a vena contracta width of 0.6 cm2 .
The patient underwent AVR with a 19mm Cardiamed Mechanoprosthesis and her post-operative recovery was uneventful.
DISCUSSION
In 2018, the patient was diagnosed with QAV with mild AR during a laparoscopic cholecystectomy. The patient remained mostly symptom-free and did not require treatment for the next six years. There were no other associated anomalies besides the QAV. This case study aims to demonstrate how patients with QAV remain symptom-free and how echocardiography shows mild AR when the heart rate and systolic blood pressure are within normal limits. It also aims to highlight that an increase in systolic blood pressure and heart rate induced by inotropes can worsen the severity of AR. Therefore, patients with QAV need to undergo regular cardiac screening, and TEE is the gold standard for assessing the severity of AR in patients with QAV and determining if surgical intervention is necessary.
QAV is a rare congenital heart valve anomaly.4 A study conducted at Mayo Clinic screened over 60,000 patients from 1982 to 1988 and identified only 8 cases of QAV, highlighting its rarity.4 Due to its uncommon occurrence and limited research, the outcomes of patients with QAV are not well-defined.7 The exact cause of QAV development is still unknown.2 Still, it is speculated that inflammatory events during early heart development may play a role in the abnormal septation leading to QAV formation.2
Hurwitz and Roberts classified QAV into 7 subtypes (labelled A to G) based on the relative size of the four cusps.8 Subtype B, with three equal-sized larger cusps and one smaller cusp,8 has the highest prevalence at 41%.3 They were followed by subtype A, with all four equal cusps, having a prevalence of 32%. Subtypes E and F, with one larger cusp and three equal-sized smaller cusps, and two equal-sized larger cusps and two unequal-sized smaller cusps, respectively, have the lowest prevalence at 2% each.3,8 Vali et al. added subtype H to this classification in 2010, which features one large cusp, one intermediate-sized cusp, and two small cusps of equal size.3,9 Nakamura has classified QAV into 4 subtypes, numbered I to IV. His classification is based on the position of the supernumerary cusp relative to the left, right, and non-coronary cusps.3,10 However, Hurwitz and Roberts system of classification is most followed.3
Patients with QAV may exhibit symptoms as late as their 40s to 60s.2,3 Typically, QAV patients experience symptoms of AR such as shortness of breath when active, chest pain, widened pulse pressure, and a murmur during the resting phase of the heartbeat.1,3
Echocardiography is considered the most reliable method for diagnosing patients with QAV.1-3 In 1984, two-dimensional transthoracic echocardiography was first used to diagnose QAV.3 Two-dimensional echocardiography is useful for evaluating valvular morphology, function, aortic root size, and left ventricular function and diameter.11 Recently, TEE has become more important in diagnosing QAV. TEE provides a clear view of all four cusps of the aortic valve and helps assess AR and the displacement of coronary ostia.11 Additionally, computed tomography can be utilized to evaluate leaflet coaptation and degree of AR in patients with QAV.11
Surgical intervention is often necessary due to the worsening severity of AR and malfunction of the QAV in association with other issues.2,3 However, aortic stenosis rarely requires surgery.3 These patients can undergo surgery using various methods including mechanical or bioprosthetic valve implantation, the Bentall procedure, the Ross procedure, and bi- and tricuspidization of the valve.3 Transcatheter aortic valve replacement is an option for older patients.3,12
Most patients with QAV will need surgery before left ventricular dysfunction or heart failure develops.1,13 Therefore, it is essential to regularly screen these patients for any increase in AR severity or enlargement of the LV, as these could indicate impending LV failure.2 TEE should be used to diagnose AR in patients with a QAV, as it is considered the gold standard due to its superior imaging quality and its ability to better evaluate the mechanism of AR.1,13
CONCLUSION
QAV is a rare congenital heart defect. Most patients with QAV start showing symptoms in their 50s or 60s. It is crucial to regularly screen these patients to assess the severity of AR under normal conditions and when the heart is working harder. TEE is the preferred method for diagnosing QAV because it provides superior image quality and better evaluation of valvular
REFERENCES
1. Douglas A, Patel A, Batsides G, Safi L. Quadricuspid Aortic Valve: A Rare Cause of Aortic Regurgitation. CASE (Phila). 2020;4(4):244-247. Published 2020 May 15. doi: https:// doi.org/10.1016%2Fj.case.2020.04.002
2. Al-Qaysi A, Sayeh N, Al-Qaysi Z, Al Ghoul Y, Elhouni E. Quadricuspid Aortic Valve: A Case Report of an Asymptomatic Middle-Aged Man. Cureus. 2023;15(9):e45262. Published 2023 Sep 14. doi: https://doi.org/10.7759%2Fcureus.45262
3. Saith S, Saith S, Murthy A. Quadricuspid Aortic Valve: An Introduction for Clinicians. Cardiol Res. 2022;13(1):2-10. doi: https://doi.org/10.14740%2Fcr1308
5. Alomari M, El-Sayed Ahmed MM, Ali M, Wadiwala IJ, Pham SM, Sareyyupoglu B. Quadricuspid Aortic Valve: Imaging, Diagnosis, and Prognosis. Tex Heart Inst J. 2024; 51 (1): e238256. doi: https://doi.org/10.14503/THIJ-23-8256
6. Khatun N, Kaliounji A, Alkoutami SS, Francois J, John S. Quadricuspid Aortic Valve: An Incidental Finding in an Elderly Man. Cureus. 2023;15(5):e39536. Published 2023 May 26. doi: https://doi.org/10.7759%2Fcureus.39536
7. Liu Y, Zhai M, Mao Y, et al. Transcatheter aortic valve replacement in patients with quadricuspid aortic valve in a single center. Front Cardiovasc Med. 2022;9:1011466. doi: https:// doi.org/10.3389%2Ffcvm.2022.1011466
8. Yang E, Balkhy HH, Patel B, et al. Cardiovascular computed tomography for the detection of quadricuspid aortic valve: A case report. Radiol Case Rep. 2023;18(10):3544-3548. doi: 10.1016/ j.radcr.2023.06.056
9. Vali Y, Rajendra R, Nishtar S. A previously undescribed type of quadricuspid aortic valve: type H. J Heart Valve Dis. 2010;19(6):792-793. Accessed September 10, 2024. https:// pubmed.ncbi.nlm.nih.gov/21214107/
10. Nakamura Y, Taniguchi I, Saiki M, Morimoto K, Yamaga. Quadricuspid aortic valve associated with aortic stenosis and regurgitation. Jpn J Thorac Cardiovasc Surg. 2001; 49: 714–716.
11. Yuan SM. Quadricuspid Aortic Valve: A Comprehensive Review. Braz J Cardiovasc Surg. 2016;31(6):454-460. doi: https://doi.org/10.5935%2F1678-9741.20160090
12. Liu Y, Zhai M, Mao Y, et al. Transcatheter aortic valve replacement in patients with quadricuspid aortic valve in a single center. Front Cardiovasc Med. 2022;9:1011466. Published 2022 Sep 28. doi: https://doi.org/10.3389%2Ffcvm.2022.1011466
13. Vasudev R, Shah P, Bikkina M, Shamoon F. Quadricuspid Aortic Valve: A Rare Congenital Cause of Aortic Insufficiency. J Clin Imaging Sci. 2016;6:10. Published 2016 Mar 30. doi: https://doi.org/10.4103%2F2156-7514.179417
Understanding Paraganglioma: An In-Depth Look
Author: Michael E. Champion, DHSc, PA-C, RN, MBA
San Antonio, TX 78261
Abstract
Paragangliomas are rare neuroendocrine tumors originating from the paraganglia, presenting significant diagnostic and therapeutic challenges. Recent advances in imaging, particularly Cardiac Magnetic Resonance (CMR) and 131I-MIBG scintigraphy, have improved diagnostic accuracy, as discussed by Paolisso et al. (2024) and Hou et al. (2022). Intraoperative hypertensive crises, a notable risk in surgical management, are highlighted by Araujo-Castro et al. (2024). Case reports by Xu et al. (2023) and Zaresharifi et al. (2023) provide valuable insights into the management of complex cases. Innovative therapies, including high-specific-activity iodine 131 metaiodobenzylguanidine, show promise for treating metastatic paragangliomas, as detailed by Jimenez et al. (2020). Pathological and radiological insights are critical for understanding and managing these tumors, as explored by Wang et al. (2018) and Diehn and Krecke (2021). This article provides a comprehensive overview of the current state of knowledge on paragangliomas, emphasizing the importance of a multidisciplinary approach in their management.
Introduction
Paragangliomas are rare tumors originating from neuroendocrine cells called paraganglia, which are distributed throughout the body. These tumors can develop in various locations, including the head, neck, thorax, abdomen, and pelvis. Paragangliomas can be benign or malignant, and their management poses significant clinical challenges due to their diverse
presentations and potential complications. This article aims to provide an in-depth overview of the current state of knowledge on paragangliomas, focusing on diagnosis, risk factors, surgical challenges, therapeutic approaches, and case studies.
Advances in Imaging for Diagnosis
Cardiac Magnetic Resonance (CMR)
Accurate diagnosis of paragangliomas often relies on advanced imaging techniques.
Paolisso et al. (2024) highlighted the role of Cardiac Magnetic Resonance (CMR) in predicting the malignancy of cardiac masses. The study introduced the CMR Mass Score, which helps distinguish malignant from benign cardiac masses. This scoring system can be particularly useful when paragangliomas involve the heart, aiding in early and accurate diagnosis.
131I-MIBG Imaging and 99mTc-HYNIC-TOC Scintigraphy
Hou et al. (2022) conducted a comparative study on the efficacy of 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy in detecting nonmetastatic extra-adrenal paragangliomas. Their findings indicated that the site-based performance of these imaging modalities significantly impacts diagnostic accuracy. By improving detection rates, these imaging techniques facilitate better clinical management and treatment planning.
Risk Factors and Surgical Management
Intraoperative Hypertensive Crisis
Intraoperative hypertensive crises are a significant risk during surgeries for pheochromocytomas and sympathetic paragangliomas. Araujo-Castro et al. (2024) identified specific risk factors that increase the likelihood of such crises, including tumor size, location, and catecholamine secretion levels. Their research emphasizes the need for meticulous preoperative planning and intraoperative management to mitigate these risks and improve surgical outcomes.
Surgical Challenges
Surgical treatment of paragangliomas, especially those located in challenging anatomical regions,
requires a nuanced approach. Lu et al. (2018) presented a case report detailing the difficulties encountered in the surgical treatment of undiagnosed functional paragangliomas. Their report underscores the importance of comprehensive preoperative assessment and the potential for unexpected complications during surgery. Understanding these challenges is crucial for developing effective surgical strategies and improving patient outcomes.
Case Reports and Literature Reviews
Case reports provide valuable insights into the management of rare and complex cases of paragangliomas. Xu et al. (2023) described a case of a middle mediastinal paraganglioma, providing a thorough review of the literature and highlighting the unique challenges associated with this rare tumor location. Similarly, Zaresharifi et al. (2023) discussed the successful management of a giant retroperitoneal ancient schwannoma, which mimicked malignant tumors. These case reports contribute to the growing body of knowledge on paraganglioma management and can serve as reference points for clinicians faced with similar cases.
Therapeutic advancements have also been made in the treatment of metastatic pheochromocytoma and paraganglioma. Jimenez et al. (2020) explored the use of high-specific-activity iodine 131 metaiodobenzylguanidine (131I-MIBG) for treating these conditions. Their research highlighted the potential of this novel therapy to improve outcomes for patients with metastatic disease, offering hope for a condition that is often difficult to treat.
Individualized Treatment Plans. Yen and Lodish (2021) reviewed current trends in the management of pheochromocytomas and paragangliomas, providing a comprehensive overview of therapeutic options. Their work emphasized the importance of individualized treatment plans, considering the diverse presentations and progression patterns of these tumors. By tailoring treatment to each patient's unique clinical profile, clinicians can optimize therapeutic outcomes and minimize adverse effects.
Pathological and Radiological Insights
Understanding the pathological features of paragangliomas is crucial for accurate diagnosis and effective treatment. Wang et al. (2018) provided a detailed case report on the pathological features of paraganglioma in the lumbar spinal canal. Their findings highlight the importance of recognizing the distinct pathological characteristics of paragangliomas, which can vary significantly depending on their location. These insights are essential for pathologists and clinicians in developing accurate diagnostic and therapeutic strategies.
Radiological Imaging
Radiological imaging plays a pivotal role in the diagnosis and management of paragangliomas. Diehn and Krecke (2021) discussed neuroimaging techniques for spinal cord and cauda equina disorders, including paragangliomas. Their work underscores the advancements in imaging technology that have improved the detection and characterization of these tumors, facilitating better clinical management. The use of advanced imaging modalities helps clinicians accurately localize tumors, assess their extent, and plan appropriate interventions.
Cardiac Complications. Paragangliomas can also lead to severe cardiac complications, particularly when they involve the cardiac region. Batisse-Lignier et al. (2015) conducted a systematic analytical review of acute and chronic pheochromocytoma-induced cardiomyopathies, providing insights into the prognoses of these conditions. Their review highlighted the variability in outcomes, emphasizing the need for timely diagnosis and tailored therapeutic approaches. Understanding the cardiac implications of paragangliomas is crucial for cardiologists and oncologists in managing these patients effectively.
Conclusion
The management of paragangliomas requires a multidisciplinary approach, integrating advancements in imaging, surgical techniques, and therapeutic interventions. The recent literature underscores the importance of accurate diagnosis, careful surgical planning, and innovative treatment options in improving patient outcomes. As research continues to evolve, a
deeper understanding of the biological behavior and clinical management of paragangliomas will undoubtedly enhance our ability to treat this complex and diverse group of tumors effectively.
References
Paolisso, P., Bergamaschi, L., et al. (2024). Cardiac Magnetic Resonance to Predict Cardiac Mass Malignancy: The CMR Mass Score. Circulation: Cardiovascular Imaging, 17(3), e016115. doi:10.1161/ CIRCIMAGING.123.016115.
Araujo-Castro, M., Garcia Sanz, I., Minguez Ojeda, C., et al. (2024). Risk factors for intraoperative hypertensive crisis in patients with pheochromocytomas and sympathetic paragangliomas. J Hypertens, 42 (2), 252-259. doi:10.1097/HJH.0000000000003596.
Zaresharifi, N., Karimzadhagh, S., Ebrahimian, R., et al. (2023). Successful management of a giant retroperitoneal ancient schwannoma mimicking malignant tumors: A case report and literature review. Ann Med Surg (Lond), 85(12), 6279-6284. doi:10.1097/MS9.0000000000001445.
Xu, S., Hu, G., Du, J., Ma, L., Zou, L., Li, Q. (2023). Middle mediastinal paraganglioma: A case report and review of the literature. Medicine (Baltimore), 102(47), e36327. doi:10.1097/MD.0000000000036327.
Hou, G., Jiang, Y., Li, F., Zhu, Z., Jing, H. (2022). Site-based performance of 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy in the detection of nonmetastatic extra-adrenal paraganglioma. Nucl Med Commun, 43(1), 32-41. doi:10.1097/MNM.0000000000001490.
Sachani, H., Tripathi, M., et al. (2021). Thoracic Extradural Paraganglioma Localized on 68GaDOTANOC PET/CT. Clin Nucl Med, 46(9), e471-e472. doi:10.1097/RLU.0000000000003643.
Yen, K., Lodish, M. (2021). Pheochromocytomas and paragangliomas. Curr Opin Pediatr, 33(4), 430-435. doi:10.1097/MOP.0000000000001029.
Diehn, F., Krecke, K. (2021). Neuroimaging of Spinal Cord and Cauda Equina Disorders. Continuum, 27 (1), 225-263. doi:10.1212/CON.0000000000000926.
Jimenez, C., Nunez, R., Wendt, R. (2020). High-specific-activity iodine 131 metaiodobenzylguanidine for the treatment of metastatic pheochromocytoma or paraganglioma: a novel therapy for an orphan disease. Curr Opin Endocrinol Diabetes Obes, 27(3), 162-169. doi:10.1097/MED.0000000000000544.
Liu, S., Zhou, X., Song, A., et al. (2019). Surgical treatment of malignant paraganglioma with spinal invasion in a juvenile patient: A case report. Medicine (Baltimore), 98(39), e17145. doi:10.1097/ MD.0000000000017145.
Wang, Z.-H., Wang, Y.-T., Cheng, F., Hu, Y. (2018). Pathological features of paraganglioma in the lumbar spinal canal: A case report. Medicine (Baltimore), 97(41), e12586. doi:10.1097/ MD.0000000000012586.
Lu, L., Yang, Z., Zhang, G., An, B., Lin, Y., Zheng, X. (2018). Challenges in the surgical treatment of undiagnosed functional paragangliomas: A case report. Medicine (Baltimore), 97(38), e12478. doi:10.1097/ MD.0000000000012478.
Lichtenberger, J., Franco, D., Kim, J., Carter, B. (2018). MR Imaging of Thoracic Aortic Disease. Top Magn Reson Imaging, 27(2), 95-102. doi:10.1097/RMR.0000000000000165.
Batisse-Lignier, M., Pereira, B., Motreff, P., et al. (2015). Acute and Chronic Pheochromocytoma-Induced Cardiomyopathies: Different Prognoses?: A Systematic Analytical Review. Medicine (Baltimore), 94(50), e2198. doi:10.1097/MD.0000000000002198.
Richardson, B., Wandtke, J., Hobbs, S. (2015). Imaging of the Superior Mediastinum. Contemp Diagn Radiol, 38(12), 1-5. doi:10.1097/01.CDR.0000466213.63286.58.