Jane Webster PhD Researcher Illustrated Reader February- July 2024

CONTENTS:
Page 1.....Tutorial from the pre- IMR upgrade practice run through.
Pages 2-3.....Presentation slides from the IMR upgrade presentation.
Pages 4-5.....Content and feedback of the IMR upgrade presentation.
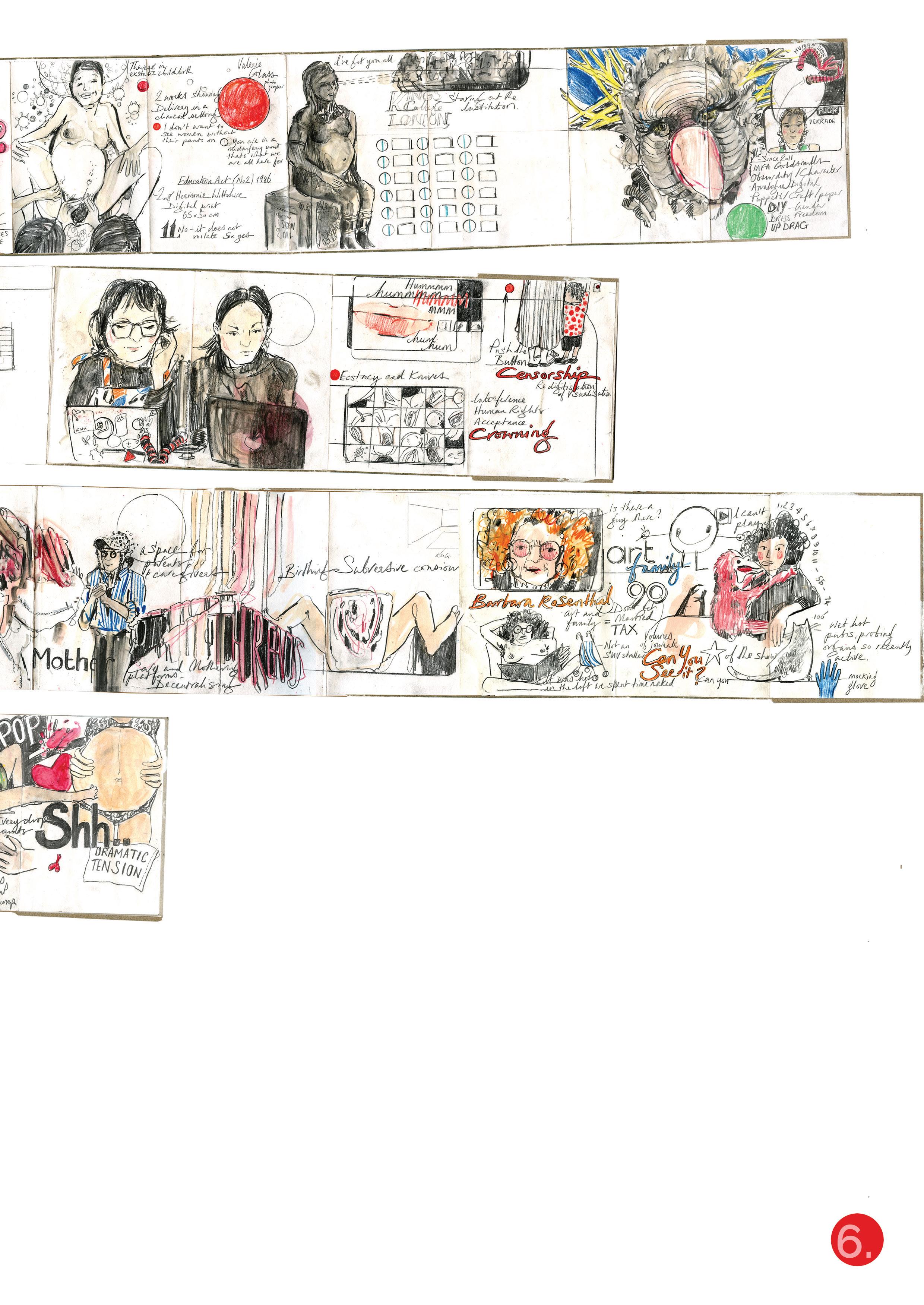
Page 6-11.....Notes and drawings from the Birth Rites Collective Summer School.
Page 12......BRC Presenter Biographies.
Page 13......Film created in response to the collection
Page 14-15......Ethics notes- Consideration and consent form.
Page 16-17.....Ethics notes- What am I asking of the participants?
Pages 18-19.....Ethics - Kingston University direction and guidance.
Pages 20-21.....What’s in the news? Media coverage of birth issues & NHS cover-ups.
Pages 22-23......Description of articles.
Pages 24-25......Panorama Maternity Scandal: Fighting for the Truth.
Page 26......Mental Canvas Potential.
Page 27......Gestational Diabetes Screening brief.
Pages 28-29......Illustration Animation experimentation: Blastocyte Implantation.
Pages 30-31......Listening with Alannah and Georgina.
Pages 32-33......Listening continued. Reflections from Reader 6.
Anke teaches sustainable design. Still, in terms of research, the main aspects of work I know of her is designing sensory environments for people with dementia. So she’s got a well-established interest in art, design, and healthcare, although —she’s not an illustrator.
There’s the internal stakeholder of an illustrator, an illustration practitioner, or an illustration educator. There’s a whole world there regarding how this, you know, illustration practice research projects. But then there are the external stakeholders, the ones who are going to benefit the people you are targeting and the professionals within those other realms
The panel will want to know where it is headed. Do you know your diagram with the two halves at the end of the board? When you presented that, this was the start of the presentation .................
For example, you mentioned ethics clearance, which is because it involves working with the NHS. That could take time. I’m getting through Kingston’s processes one thing, but you will have to get NHS ethics clearance as well, which will complicate things. But it immediately begs the question, what do you need ethics clearance for? Who are you working with, people preparing to give birth and going through midwifery consultations and such? Well, what would you want to do with them?
That’s identified from my own experience, but especially in what Sheila Kitzner writes about birth crisis and about the fact that you know, we’re introduced to what most hospitals are run in a very kind of patriarchal way as well. If your body doesn’t give birth, it takes a long time in preparation for your body, which is why I want to explore the importance of oxytocin and how we don’t acknowledge that as being important in having some level of control.
It’s really good to say that, to highlight the learning that you are undertaking. ................
Everyone comes to something with existing knowledge, whether that existing knowledge is real or not. And it’s imperative to some people to come up with existing knowledge that may have gone down generations of women, which is different from how you present it. Are you going to, you know, delineate? There’s faux knowledge, and there’s a kind of professional knowledge. The premise of the project is as follows: What’s important?
The presentation is a perfect device for locating your focus.
Okay, so this demonstrates what we’ve got at the moment now is it’s not working, and it’s leaving lots of women with a sense of failure, having to live with a feeling that they weren’t in control of something, they weren’t allowed the choices that they wanted. You are so vulnerable now but are part of this time line if you are accessing free NHS healthcare
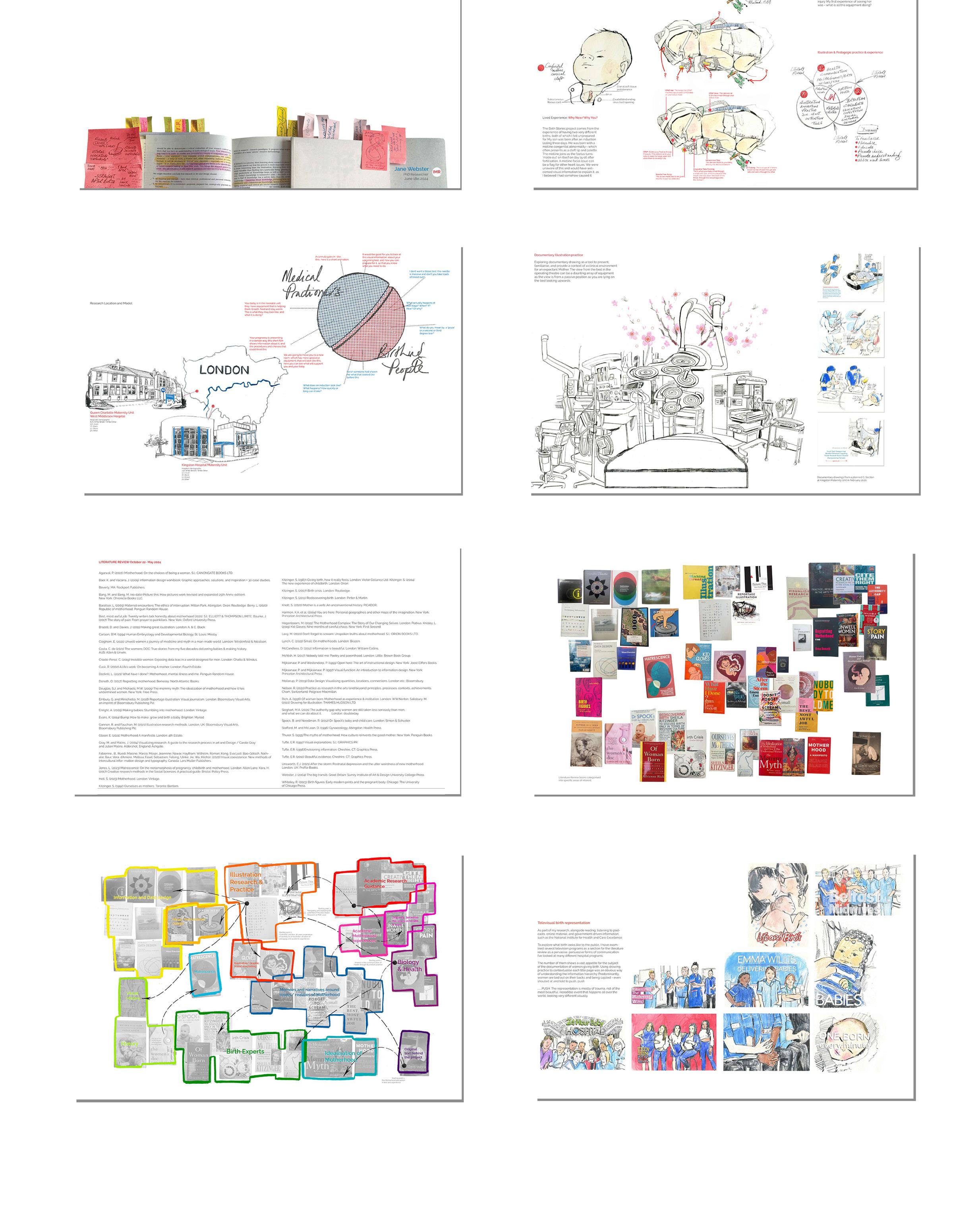
My name is Jane Webster. My project is centred around birth stories and advocacy around birth for women; I’m just going to start with the premise of ‘why now and why you’. My experience comes from my experience as a senior lecturer and an academic, as well as the two experiences of birth, which turned out to be quite different from the narratives I thought they might be.
The first one was with my son after a long three-day induction. I did not know that he had a congenital midline cervical cleft, which often presents itself as a cleft palate. Then my daughter, who was born quite early, at thirty-three weeks, after a full placental of abruption.
In both instances, we were very grateful to the NHS. When I saw my daughter for the first time, she looked like this first image in the middle, and I didn’t know what all these things were. I would have liked to have known these things at this time,
For the first two years of this project, I’ve established working with Kingston Maternity Unit and now with Queen Charlotte Maternity Unit, which is West Middlesex Hospital. Both hospitals are situated in South West London but have different demographics. Kingston is slightly more white and middle class, but other social housing groups surround it. Middlesex has a more extensive Asian and non-English speaking stakeholder base, with over 87 languages spoken.
From my research, I’ve realised that to do this project on two sides of the ball, from a medical practitioner’s point of view and through birthing mothers, asking these different questions.
These are just examples on this slide. What does induction look like? What happens? How quickly or how long does it take? From the medical practitioners’ point of view, your baby is in a neonatal unit. They have lots of equipment helping them, which is what it’s doing for them.
All women giving birth will be given a cannula, but they may need to know how it works. This is what will be inside your hand, and there is a short film to show this. Another example is - a blood test -’ I have heard the needle’s massive/ I don’t know what that is going to be like.’ Here’s information about what perennial tears look like.
I am an illustrator. I’ve 25 years of experience with documentary illustrations and a lot of experience with documentary illustrations, so this is an example of a documentary illustration produced in a clinical environment, which is what the theatre looks like. My daughter was born in this operating theatre, and I remember it being huge, but it’s not very big. When I showed this back to the staff I was having all these initial conversations with at Kingston, they were, ‘Oh, that’s really, really complicated. They then invited me to draw some births. So, this is the birth of a woman who had low placenta previa. It was a fantastic opportunity. It was entirely balletic to see how people work and also understand the amazing job that the NHS do.
For the last few years, I’ve been exploring a literature review which looks like this. I’m very visual, so this is how I have categorised these books; I’ve arranged them into sections to determine what I’m looking at and why.
The first book is down at the bottom right. It’s by Rachel Cusk, and I read this when I was first pregnant 19 years ago and thought, how could you write a book like that? That’s shocking because she wrote about the reality of birth, parenthood and pregnancy and how difficult and miserable it can be lonely.
I’ve got these different starting points, so looking at illustration research practice, the idealisation of motherhood, birth experts, visual history, history, and how information and data design works maps and instructional work. So the two books in the middle here are Kid Gloves and Bump. I’m doing a presentation at Graphic Medicine about these two books and how these two different narratives articulate the different aspects of birth.
The other thing I’ve been looking at is one of the most pervasive mediums we have in television. What does birth look like in terms of how different programs present it? From the anxious midwife to the kind of carefree teen mom who looks like they are in a bar, to, like, we’re all waiting for your baby to come out. This example - Your baby looks like a science experiment to one born every minute, your caucasian baby is calm and is asleep. So this is very timely at the moment because the House of Commons birth trauma debate came out on the 13th of May-
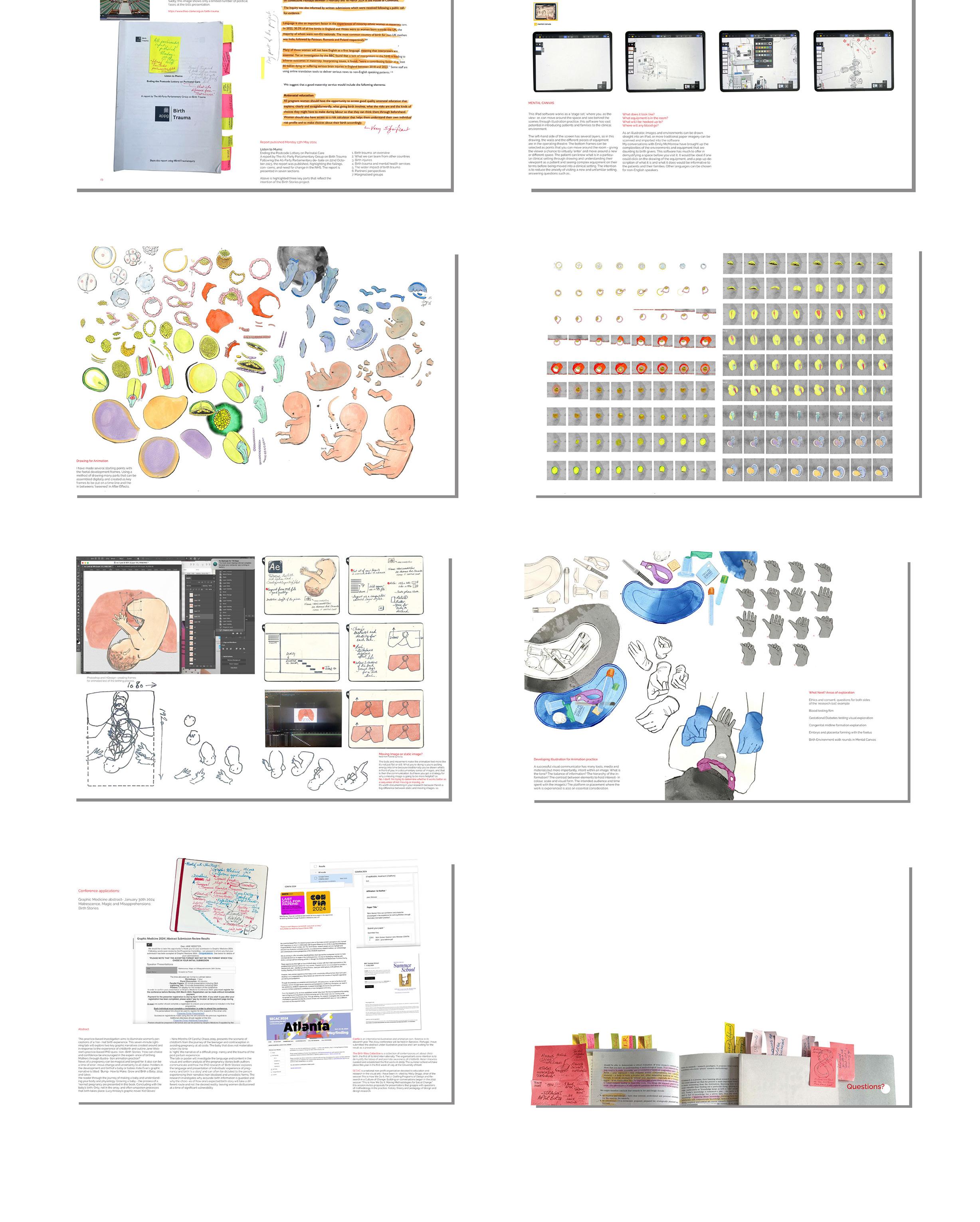
Following Theo Clark’s October presentation, it is wonderful that these conversations are happening. This is the published all-party paper; there are three very significant things which are about language being essential for the experience for minority groups and people that don’t speak English, but many women do not get the perceived experience that they think they’re going to have due to lots of different reasons which have increased since my experience with giving birth, primarily through social media, but also that all pregnant women should have the opportunity to access good quality and natural education that explains clearly and straightforwardly what give birth involves, what the risks are and the kind of choices they might have during the labour so that they can think about them beforehand. Women should have access to a risk calculator that helps them understand their individual risk profile and make choices about their birth accordingly.
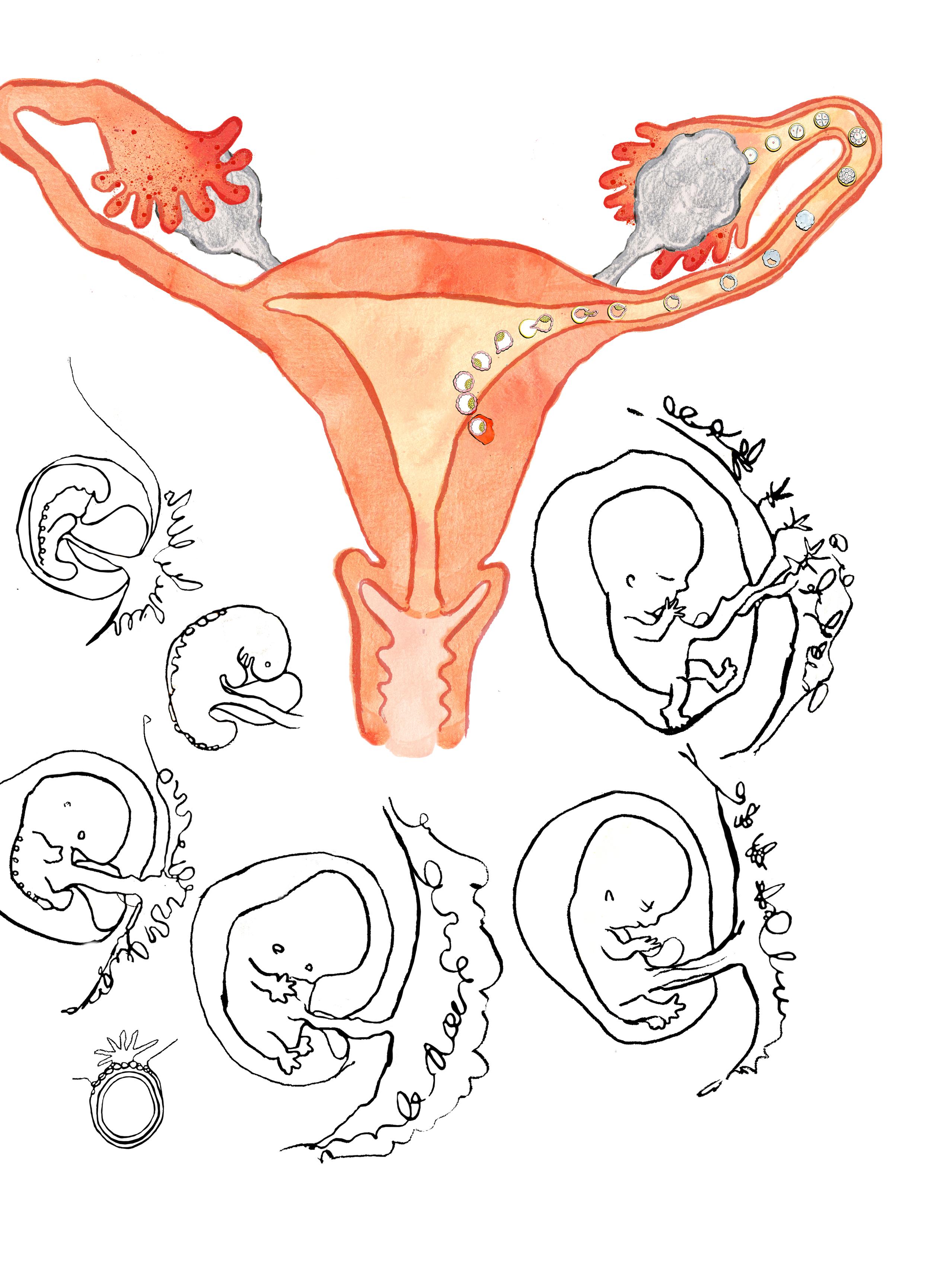
That’s great; it’s in words, but consider how this could look in visuals. We’re looking at this programme at Mental Canvas, with the premise that you might give birth. So you can be shown this: you will be taken to a different room, which will look like this. Ideally, this equipment will look like this. This is based on the drawing on the third slide. And then, through this project in the last two years, I’ve been exploring my illustration animation practice. So, what are these things that need to be looked at? So, how is the baby formed?
There’s no information about how a blastocyte goes into the uterine lining and then comes back out as a formed yolk sac that the baby shows development in the womb. So that is what I’m exploring. I’ve also been looking at how I’m not an animator. Still, I’m learning about animation, so there’s an after-effect of how you have different layers that make this experience look alive.
I am developing illustrations for animation practice, so the areas of exploration I’m looking at in the next part of my PhD are ethics and consent, as well as questions for both sides of this research ball I showed you in the first slide.
So, what do these two different groups need to know from each other? Looking at an animation test for what a blood test looks like, gestational diabetes testing and the visual exploration, so if English isn’t your first language, look at what a congenital midlife formation explanation looks like because I would have loved to have seen that at the time so I wouldn’t have felt what did I do wrong, looking at embryo and placental forming within the foetus so people can understand how that works and the fact that most people fertilisation happens in the fallopian tube. Birth environments walk rounds and mental canvas. I will establish that through conversations with people from both services, health professionals, and women giving birth. I’m presenting at these little conferences, so this is graphic medicine; I’m going to Atlanta in October to present the second part of this project to This is How We Do It, and then I’m attending summer school in Kent.
Do you have any questions?
Dr. Beatrice Jarvis
Dr. Anke Jacob
Dr. John Miers
This is an impressive body of work clearly demonstrating the potential of this doctoral research going forward.
The viva voce examination was highly successful, showcasing Jane’s profound and incredibly thorough professional research practice. Jane demonstrated a comprehensive understanding of her research area, articulated her methodology effectively, and engaged critically with the committee’s questions.
Going forward, we would recommend considering aspects listed below to benefit the research. This include applying generally a more systematic approach in the research process as well as clearer articulation of the aspects listed below.
- Key insights and key research methods
- Main learnings from secondary research and how did the gained knowledge inform your practice - overall methodological approach: research methods applied for data collection ensuring rigor; recruitment of participants - Research Question(s) and Aims of the PhD.
These should include:
1. Contextual research (secondary research / literature review etc.) – insights gained; conclusions drawn from synthesizing information; critical-reflective summary informing primary research (2.)
2. Practical research - based on / informed by 1., methods employed for data gathering (e.g. user engagement/research, illustration practice)
3. Proposed intervention (based on / informed by 2.)
- envisaged contribution to knowledge in the field of, e.g., illustration research and practice, art and design for health and well being (therapeutic methods, humanizing medical care by providing better access to information) etc.
- potential limitation and challenges of the research and research process might pose
Jane has undertaken a substantial amount of work, demonstrating an extensive and nuanced understanding of her research topic. She exhibits a sophisticated and unique grasp of the relevant literature and theoretical frameworks. Her ability to synthesize interdisciplinary perspectives into her research is particularly commendable and could be highlighted even more in her final submission. Jane’s methodological approach is both innovative and well-structured, indicating a high level of competence in research design and execution.
Refinement of Research Questions:
The committee strongly recommends a detailed review and refinement of the research questions. This process should involve narrowing the scope to focus on specific, well-defined aspects of the topic. By doing so, Jane will be able to provide a more precise and coherent analysis in her final thesis. Example: Instead of broadly investigating the
impact of health literacy on patient outcomes, the research could focus specifically on the influence of health literacy on medication adherence in a particular demographic.
Refinement of Research Questions:
The committee strongly recommends a detailed review and refinement of the research questions. This process should involve narrowing the scope to focus on specific, well-defined aspects of the topic. By doing so, Jane will be able to provide a more precise and coherent analysis in her final thesis. Example: Instead of broadly investigating the impact of health literacy on patient outcomes, the research could focus specifically on the influence of health literacy on medication adherence in a particular demographic.
Ethical Considerations:
Jane must ensure that all ethical considerations are thoroughly addressed. This includes obtaining informed consent, ensuring confidentiality, and being mindful of the potential impacts of the research on participants.
A detailed ethics section should be included in the methodology chapter, outlining how these ethical principles will be upheld throughout the research process. This should include plans for informed consent, data protection, and participant well-being. Developing a participant information sheet and consent form that clearly explains the research objectives, procedures, and participant rights will be essential. Jane should prepare and submit a detailed ethics application that addresses all potential ethical issues. This application should include plans for informed consent, data protection, and participant well-being.
Consideration of Practical Applications:
Jane’s project demonstrates significant potential value to the NHS and reflects her desire to create a socially meaningful project. However, it is essential to consider whether certain aspects, such as the televisual documentation and the reflections on the impact of social media, might sideline the main research enquiry. These aspects could lead to another detailed enquiry, such as exploring the impact of televisual documentation and social media on birth narratives.
To ensure timely and impactful research, it might be beneficial for Jane to refine three very precise research questions. This will help her hone in on timely, relevant, and impactful research areas. It might be ideal within a supervisory meeting to discuss what the final PhD will look like and how it will culminate.
The committee noted that the current suite of portfolio supporting monthly progress of the research process is incredibly professional and a pleasure to review. However, it is crucial to consider how these elements will culminate to generate a final research output and how they will weave together to avoid overcomplicating or diluting the general research narrative.
While Jane’s desire for a specific notion of a final output is admirable, it is worth considering whether this needs to happen as part of the PhD or could be generated post-PhD as a practical application. The timeline for getting the research into the NHS, evaluating, and demonstrating impact may be more extended than the PhD timeframe allows.
The viva voce examination for Jane was a success, highlighting the candidate’s significant potential for doctoral research. The recommendations provided aim to refine and focus the research, ensuring a clear and rigorous PhD thesis. The committee commends Jane for her dedication and professionalism and looks forward to her continued
FIRST SUPERVISOR’S REPORT
Progress that the candidate has made so far
As demonstrated by both the format and content of her IMR submission, Jane’s doctoral work continues to draw very successfully on her extensive experience as an illustrator and educator. Reflective creative practise is embedded throughout her process both as a means of testing potential communicative outcomes and responding to a wide variety of research activities and sources. Although she is rightly confident in her existing abilities as a visual communicator, she has maintained an openness to new ideas and approaches and a consistent willingness to challenge herself throughout the project, as reflected throughout the submission in responses to discussions with supervisors and colleagues, and her reflections on the value of compiling and summarising her work for the upgrade process. She remains engaged with professional scholarship, with upcoming contributions to significant conferences, and her undiminished passion for this project is strongly evident in every interaction.
Action Plan for the forthcoming year (including training needs identified)
The detailed and purposeful action plan reflects the thorough and active engagement with all aspects of the project as mentioned above, and there is an appropriate focus on ethics clearance necessary for the next stages of the project
SECOND SUPERVISOR’S REPORT
Progress that the candidate has made so far
I fully concur with the supervisory colleagues evaluation. The work is developing well through stages that step address the complexities of the subject matter without losing focus on its main objective of changing the understanding of the maternity journey through visual communication. The action plan demonstrates a clear structure around the core questions and looks well considered to deliver tangible outcomes. The conference presentations test the core research questions and add valuable insight to meet objectives.
Day 1. Start
Day 2. Start
Day 3. Start

02/07/24 Tuesday
Performing the collection introduction by Leni Dotham
Developing group work
Presentation of group works.
Artist Talk: Puck Verkade
Artist Talk: Barbara Rosenthal
Questions and end of day round up.

01/07/24 Monday
Welcome:
Introduction to the BRC Summer School. Participants introduce themselves.
Tour of the collection and the history of censorship, the rights and law in artworks in public spaces.
Visit to the Medical school and Law school Jury Role-play workshop.
Form a jury and consider if showing the image of ‘Terese’ or ‘Kinderwunsch’ constituting harassment in the workplace? Jury decision.
Film screening
Puck Verkade
Barbara Rosenthal
1. End
2. End
03/07/24 Wednesday
Leni Dotham debriefing following contention from the previous days performance piece.
Developing independent practice
Independent practice tutorials
Artist Talk: Dyana Gravina
Artist Talk: Ana Casas Broda
Questions and end of day round up.
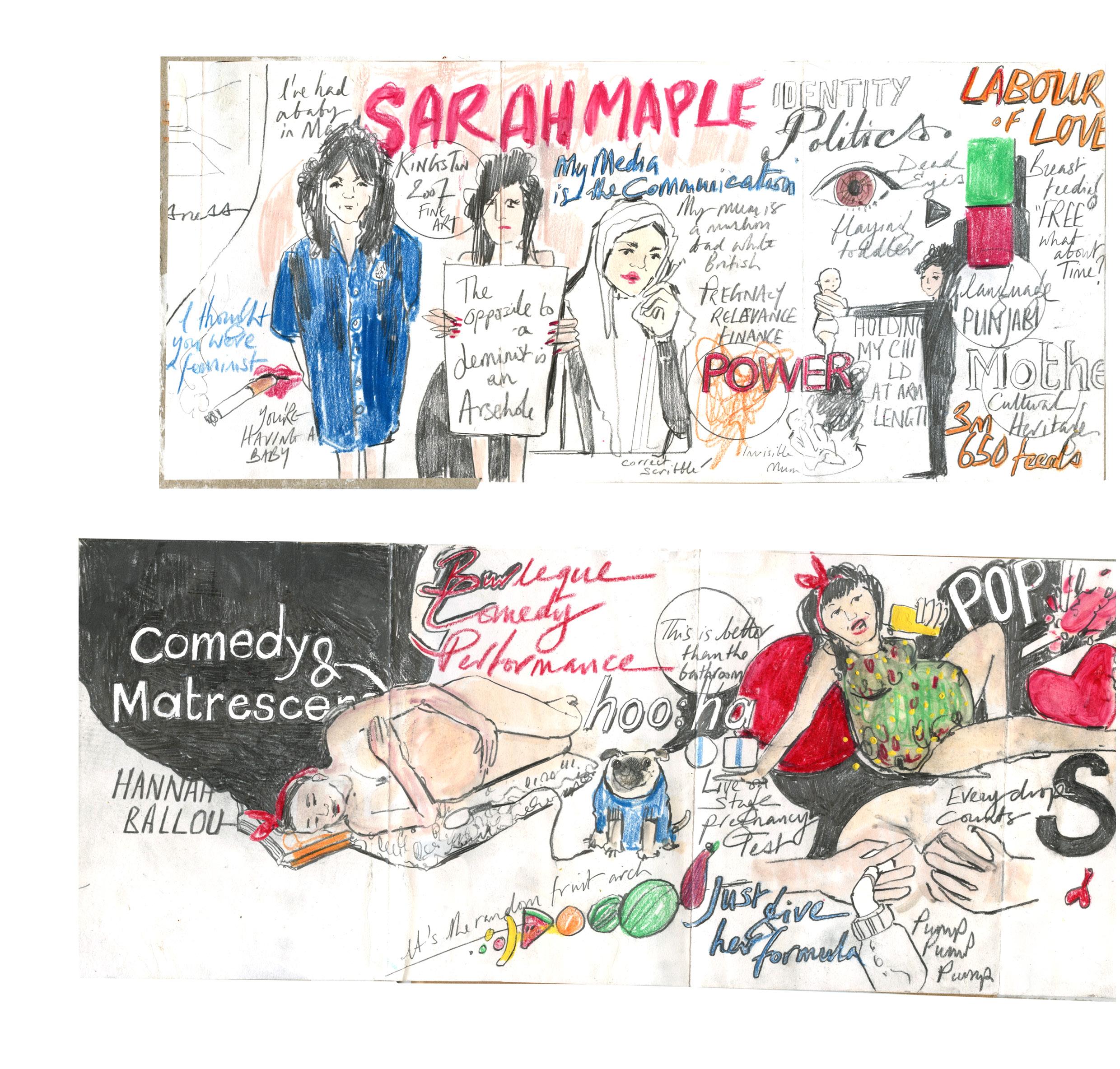
The final day hosted the best talks from Sarah Maple and Hannah Ballou. The inclusion of humour and irony was welcome after such a range of heavy and a rather bat-shit presentation from New York veteran artist Barbara Rosenthal, where she presented a range of films of her children burping the alphabet and her naked presentation with a monkey puppet in the late 70’s. Day 4. End
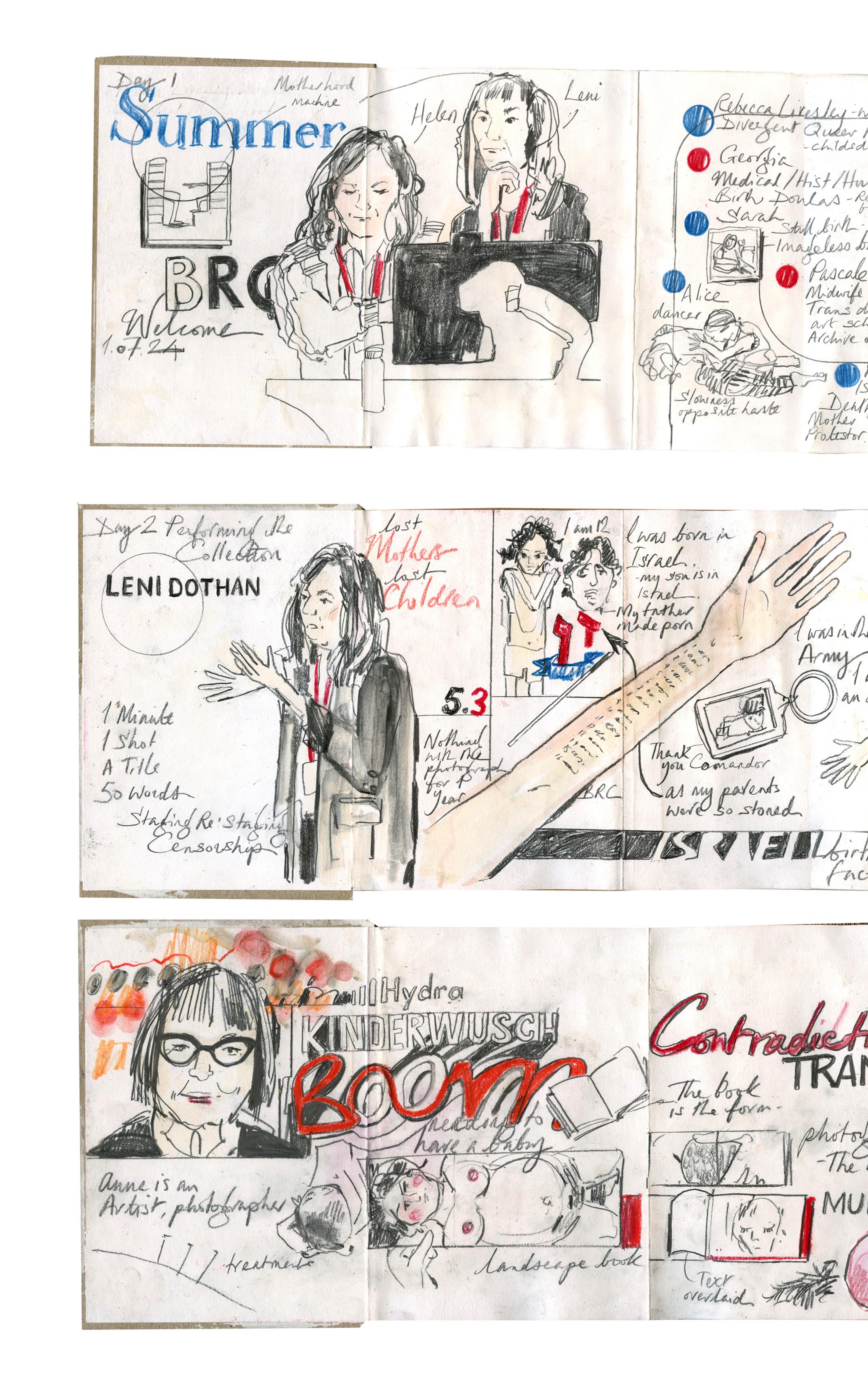
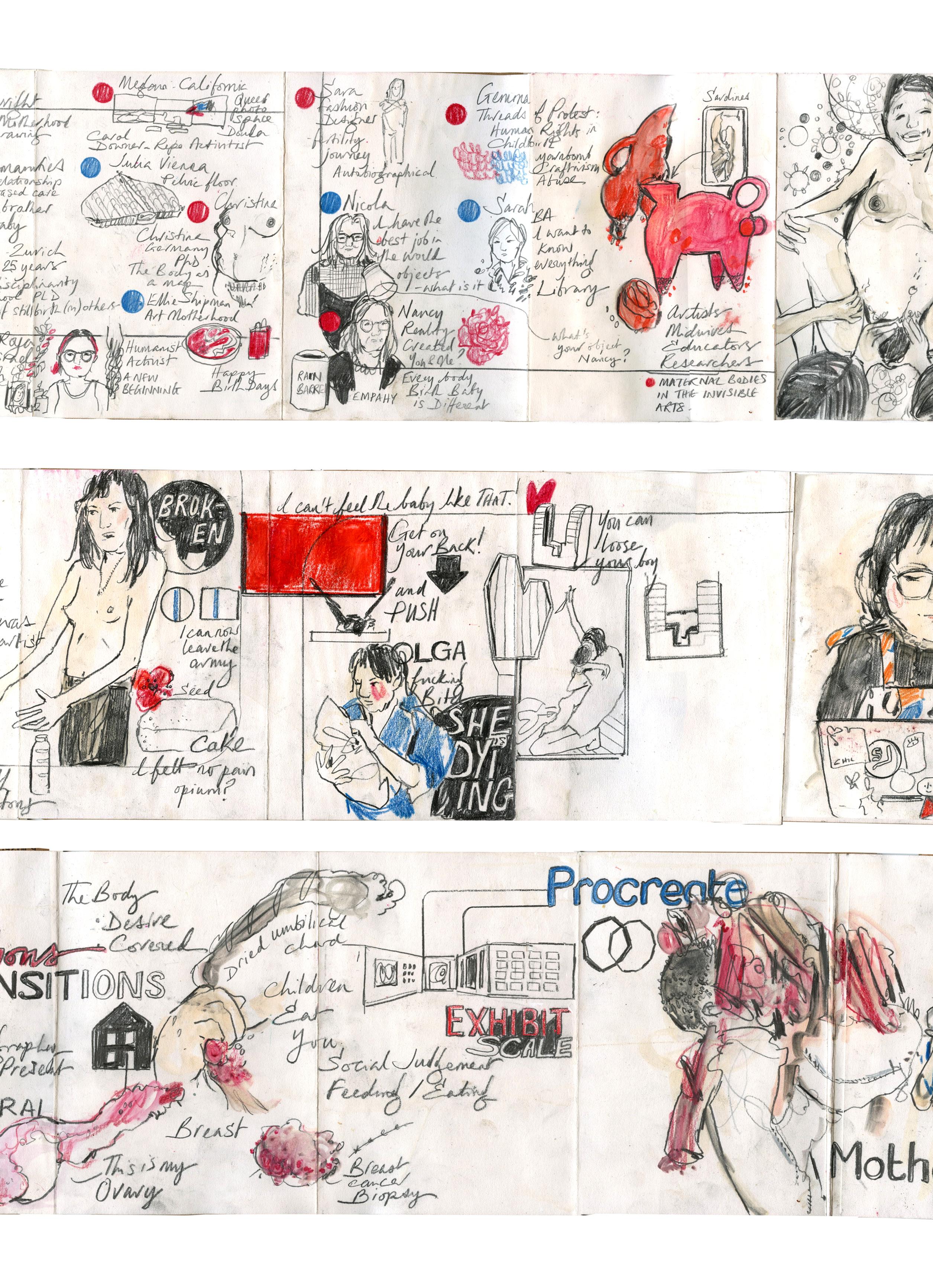
Kent University at Canterbury hosted the BRC Summer School from the 1st- 4th July 2024. It was an intense experience, with workshops and talks responding to the collection. Birth Rites Collection was founded by curator Helen Knowles in 2009. This was following a touring exhibition curated by Knowles, working alongside Phoebe Mortimer on public programmes. Birth Rites is a collection of contemporary art on childbirth- the first in the world. The collection aims to facilitate the production of new works by artists who might not typically address the subject because of its taboo status within contemporary art practice, to support the work of artists whose work already engages with issues on this subject, and to acquire relevant existing works to expand the collection. BRC encourages debate and increases awareness around childbirth practice. The project highlights issues like the shift towards medical intervention in birth and explores the impact of technological biomedical advances. The curator aims to examine whether society’s focus on propelling women onto an equal footing with men in the workplace erodes their importance as mothers and investigates how free women are to give birth in the way they want.
The ‘students’ who had signed up for the course- including myself- had diverse backgrounds, ranging from childbirth, academics, doulas, and midwives to artists. This diversity was a testament to the interdisciplinary nature of the course.
ranging from childbirth, academics, doulas, and midwives to artists. This diversity was a testament to the interdisciplinary nature of the course. Notably, not all attendees had experienced pregnancy and birth, further enriching the range of perspectives. Most of the attendees were in person, with a handful joining remotely. Everyone’s experience of holding events partially online with TEAMS will know that this practice is fraught with frustration with films not running and audio issues. The talks included visiting the artworks, creating a group response and a personal final ‘piece.’ Some talks were very contentious; the focus leaned towards a ‘performative’ approach -which I found rather painful. Discussions about whether you should share any negative experiences of childbirth with your child were divisive. On the second day, co-presenter Leni Doham gave a talk after removing her top about her traumatic birth narrative and the subsequent loss of her son to her partner in Israel. Many attendees found this method of delivery somewhat triggering, and the mood was a strange sense of trauma competition. The summer school was quite gruelling in the content of the talks. A sense of being so immersed in the subject made me both question how valid and valuable my PhD enquiry is and, on the other side of the same coin, the need for women to have spaces to talk about and decompress their experiences and expectations and understanding of their rites in this life-changing event. On reflection, I am glad I attended this event, although it took a few weeks to realise this. The BRC has asked me to donate the documentary drawings from the c-section I drew in 2020.
04/07/24 Thursday
Between staging and documenting, fiction and the real.
Introduction to the day.
Artist Talk: Sarah Maple
Artist Talk: Hannah Ballou
Final presentation of individual works.
Questions and end of day round up.
Barbara Rosenthal
Avant-garde Barbara Rosenthal (b.1948) artist, writer, performer, photographer, diarist, print and artists book maker, videographer, and experimenter with new media, electronic media, installation, surrealism, existentialism, philosophy, conceptual art. Almost all of her works are produced in editions that combine camera, text, and performative aspects. During her frustrating haphazard presentation dominated by Teams issues, she discussed her projects she created with her children in the 70’s and 80’s which constituted a lot of nudity as the New York loft in the Bronx was very hot.
Helen Knowles
Helen Knowles (b. 1975) is an artist and curator of the Birth Rites Collection. She has a BA Hons from Glasgow School of Art and an MFA Fine Art from Goldsmiths Universityformer British Council, Young Creative Entrepreneur.
Dr Leni Dothan
Leni Dothan (b.1981) is an Israeli-born artist, architect and researcher based in London who blends her skills and knowledge in dealing with the overlooked representations of women and especially mothers in art history and contemporary culture, as well as eco-political urgent subjects. As a mother to a boy living away from her birth home, she creates sculptures, photographs, videos and installations that suggest new narratives other than the perfect, ideal vision of a mother-and-child relationship. Dothan aims to touch on the less discussed and underrepresented aspects of the mother and child relationship and help the public to question their own bodies, social norms and political structures.
Terese in Ecstatic Childbirth, 2008
Ina May Gaskin
Hermione Wiltshire spent time observing the preparation of expectant parents at birth workshops given by the President of the National Childbirth Trust, Gail Werkmeister. Here Hermione witnessed the anxieties and hopes of parents-to-be. She became very aware of the prevalence of negative images of birth. She says, “My work often reflects my interest in images that are politically charged. I am particularly interested in the cultural anxiety around images of crowning. [This] moment … is seen as shocking, stimulating the same response as a pornographic image.”
Ana Casas Broda
Ana Casas Broda (b.1965) A Mexican photographer ‘Kinderwunsch’ is a book and an exhibition in which texts and photos construct a narrative that approaches maternity as a setting of complex interactions, where her children’s identity is created and my profound transformations as a mother are explored. Motherhood as an identity is one that is not fixed and is grounded in daily acts and sensations. The body and the home are fundamental axes of this project. This work elaborated during several years and was exhibited during the month of October 2013 in The Photographers’ Gallery in London.
Puck Verkade
Puck Verkade (b.1987) work is held in private and public collections internationally such as Fondazione Sandretto Re Rebaudengo in Turin, Servais Family Collection in Brussels, EKARD Collection in Wassenaar, amongst others. Unborn addresses the sensitivity of reproductive choice in an absurd but openly vulnerable manner. The lead character of the film, embodied by Verkade dressed as a human-sized pigeon, grapples with possible parenthood and reproductive rights issues informed by both societal expectations and biological determinism.
Sarah Maple
Sarah Maple (b.1985) is an award winning multidisciplinary artist known for bold artworks that challenge notions of identity. Her work spans a variety of media such as performance, painting, installation, collage and photography. Much of Maple’s inspiration originates from her mixed religious and cultural upbringing. She often using herself as a conduit to challenge stereotypes and normative behaviour, she is adept at confronting complex issues that we are all thinking about with wit and irony.
Dr Hannah Ballou (B.198_?) She has a PhD in Feminist comedy and a fear of balloons which she bravely faces live on stage in her part 2 of Goo:ga performance. She is a comedian, performance artist, researcher, writer, and Senior Lecturer who feels at home (on stage) working live with children and complicated props where she announced her pregnancy test result.
On the facing page is stills from the 40 second film I made in response to the talks and collection. The written comments are from a conversation I had with a consultant in KMU, in response to him asking about my second birth. The voice over is dialogue with myself and daughter. The image is the small scale of her wrist band to frame the conversation.
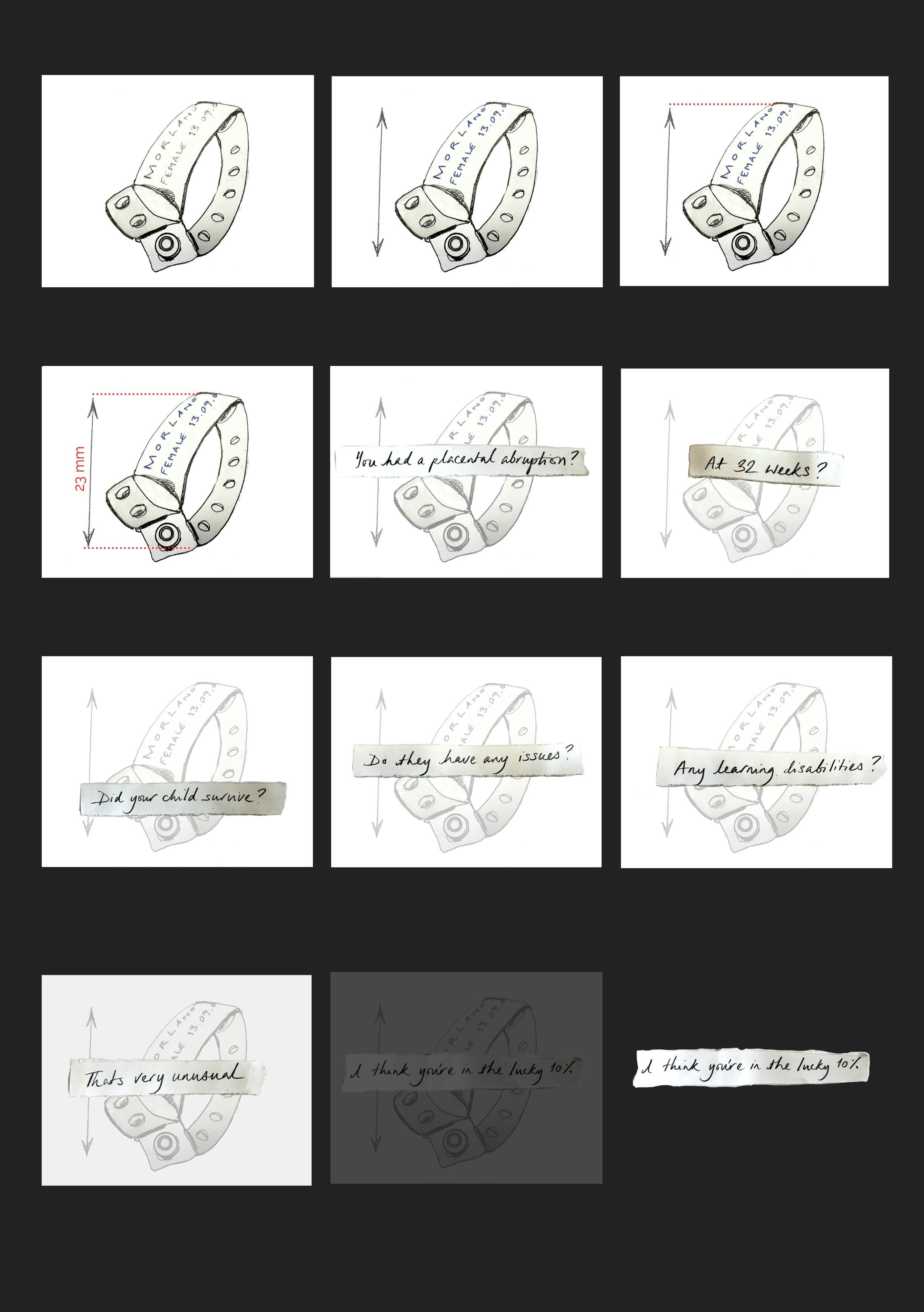
And basically it meant that it was quite a dangerous birth and you had to have a C-section.
It meant that after I was born, because of what happened throughout my birth, you couldn’t have any kids afterwards.
But I also know that I was expected to have some learning deficiencies, I don’t know what it was,
The Birth Stories research project centres around creating advocacy around birth for women through clear visual communication in the form of illustration and animation regarding the choices and narratives in pregnancy and childbirth. Through the collection of stories and experiences of birth stories, from those experiencing pregnancy and birth and those working with pregnant women.
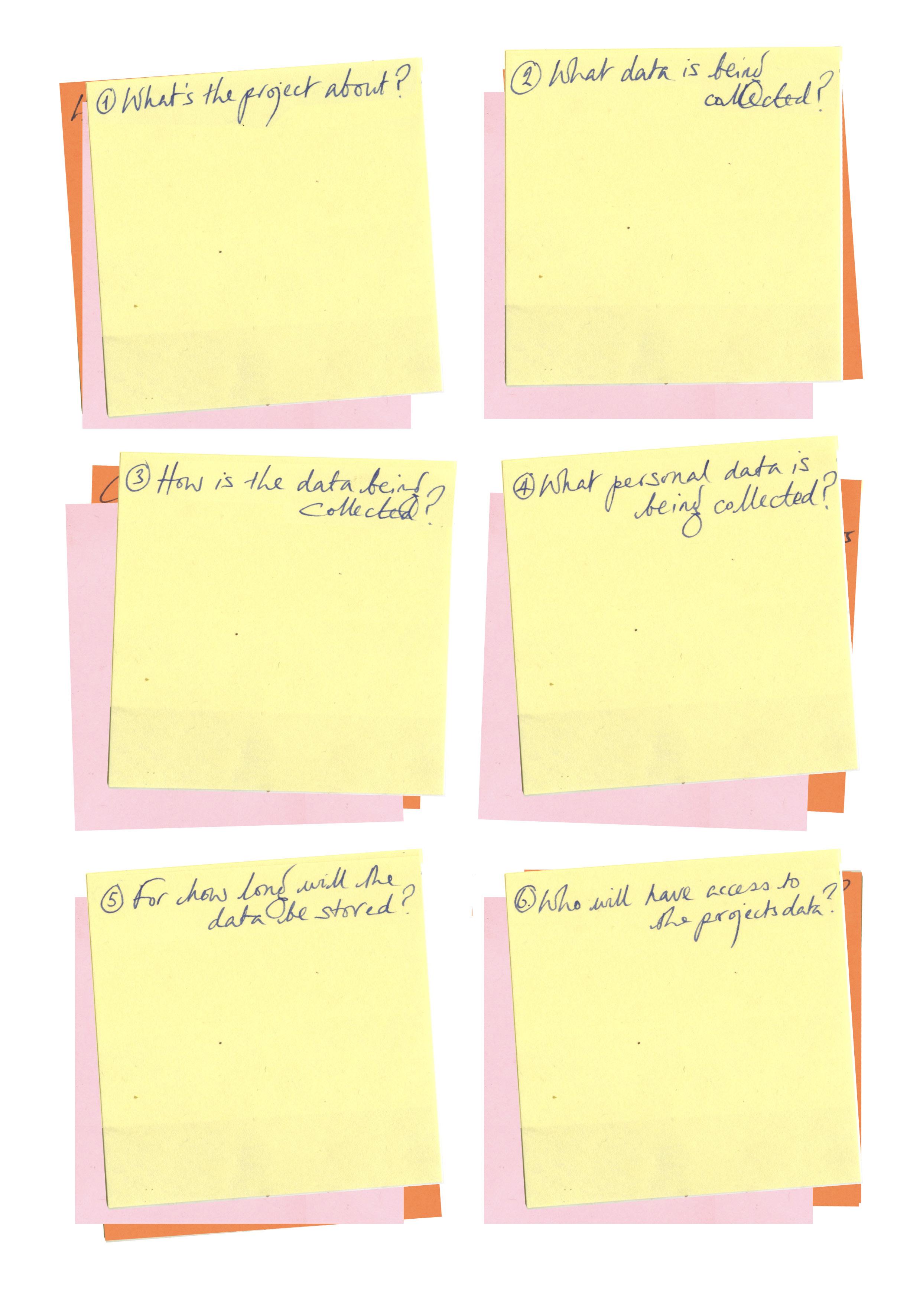
Data will be collected from participants via a variety of methods. Interviews, illustrations, diagrams, annotations drawn by the participants, focus groups and photo/object elicitation interviews. Data generated through conversations (Interview/focus group data) will be audio recorded with the consent of the participant, and then transcribed interviews and focus groups will be recorded on mobile phones, after which they will be transcribed into Cockatoo and Grammarly.
Interview data will be audio recorded and then transcribed, after which the audio recordings will be deleted. Illustrations or diagrams will be recorded on paper and kept as part of the project; drawings will be anonymised.
Participation might also participate in activities such as drawing illustrations or diagrams, talking about experiences, or talking about their thoughts from their births.
Primary Data: Singular & Small group Interviews, imagery in the form of documentary drawing Primary data will be accessed by the volunteering participants.
The qualitative data collected for the project will be stored for the duration of the PhD research. (approximately 4 years.)
Findings from the research will be disseminated via academic publications and or conference papers. Outputs from the project will be disseminated to wider public audiences via platforms established within the research. These will be digital to avoid costs of print material.
Considerations of what am I asking of the contributors and participants.
You have been invited to participate in the project as a pregnant woman, a person who has recently given birth, or a person who works with women as their pregnancy and birth stories develop.
The benefits are that you will contribute to developing illustration animation research to encourage the choice, understanding, and communication of experiences encountered during pregnancy and birth.
There is always a risk that participants might become upset by the process of recalling a negative or emotional birth experience.
You will have the opportunity to review what you have said and redact anything that has been stated which might compromise you or another person.
Your inclusion in the project will involve talking about your pregnancy and birth experiences. Questions will centre around your birth story, how your experience aligns with your expectations and the communication you encountered from your experience.
No, it is your choice whether to participate or not to. Participation in these activities is at the participant’s discretion. In some instances, participants might tell their stories in small groups; this is also at the participant’s discretion.
You will have full control over whether you wish to remain anonymous and to remove any identifying or sensitive material. Personal information, such as contact details, will be collected only to liaise with participants. Contact details are not part of the data set and will be stored separately from the project data. You will have the opportunity to decide if and how your identity is disclosed.
This study will have been reviewed and approved by the University’s Research Ethics Committee. Interview data and photographed sketch maps, map annotations, illustrations or diagrams will be stored on the University’s password encrypted server. Hard copies will be stored in locked filing cabinets

All participants will have the option to withdraw from the project at any time up to the point at which the data or outputs from the data are made available in the public domain. I will direct you to support services that can help you with any negative or emotive issues you might experience.
Participants have the right to lodge complaints (In accordance with Article 77 of the General Data Protection Regulation Considerations) about this research. If you do have concerns of complains please contact the Faculty Dean, Professor Amir Alani at m.alani@kingston.ac.uk
To withdraw from the project, you will need to contact me. If you have chosen to be anonymous in the project, you will need your participant information number. This is a number that you will receive at the start of the project which will be attached to your contribution. Without this number it will not be possible to identify your stories from the data set and therefore not be possible to remove your contribution to the project as the data set will be anonymous (except for those who have consented to be identified). Only you and I will know this number.
Data will be analysed using qualitative/thematic coding. The research’s findings will be disseminated through academic publications and/or conference papers. Creative outputs- illustrations and animations developed from the project will be disseminated to wider public audiences via appropriate platforms.
Research Ethics (sharepoint.com)
via RBI > Research and Impact > Ethics.
If your answer to the first question (below) and to any of the other questions is YES, then a research ethics application must be submitted to KUREOS (Kingston University Research Ethics Online System) and a favourable ethical opinion received before the research project is conducted
Is your work a research project? -YES
Will your research involve living human participants? -YES
Will your research involve data on humans? -YES
Will your research involve human biological material? -NO
For further information regarding which studies require ethical review please refer to Section 6 of the Ethics Guidance and Procedures for Undertaking Research involving human participants.
Depending on the nature of your research ethics application it may take up to 20 working days for you to receive an initial response. As a researcher it is your responsibility as the applicant to submit your research ethics application in good time so that any data collection can start as planned and only after a favourable ethical opinion (FEO) has been awarded.
At this point you may be asked to carry out a number of amendments and thus it will take a number of weeks before you receive a Favourable Ethical Opinion (FEO) and are able to commence your research project.
You must allow plenty of time for your research ethics application to be reviewed and possibly amended before you commence your research. Until you have received a favourable ethical opinion from Kingston University you cannot start collecting your data. You will be asked to confirm that you have read the University’s Guide to Good Research Practice.
You will be required to complete and upload the combined Epigeum programme certificate Ethical Research. (This comprises the two research ethics courses ‘Becoming and Ethical Researcher’ and ‘Research Ethics in Practice’).
You will be required to complete and upload the GDPR training for researchers. If your study involves recruitment of patients or staff through the NHS; the use of NHS data or be conducted on NHS premises, you will need to apply to the Health Research Authority (HRA) for review If you have received a favourable ethical opinion (FEO) from another institution or organisation you need to upload your FEO documentation and application onto KUREOS
If you are considering undertaking research that involves the use of human tissue, you must first contact the University’s ‘Human Tissue Act Designated Individual’ and prefix any KUREOS applications with HTA.
You will need to provide supporting documentation when completing your KUREOS application, such as (but not limited to): Recruitment / advertising material (letters, emails, advertisements, posters)
Data management plan - see guidance here Participant information sheet(s) Informed consent form template(s) All survey tools to be used, such as published standardised tools; questionnaires with weblinks to the platform.
Agreement correspondence / letters from organisations / departments that have agreed for you to access their data
Debrief sheet(s)
All research has certain ethical implications to be considered. This process is integral within any research project. It is the researcher’s responsibility to ensure that they conduct their studies in a responsible manner, treating others with integrity, respect and empathy. An indicator of good ethical practice is to question whether you are treating others, be they participants, audiences, colleagues or collaborators, in a way you would be happy to be treated
Positioning
When acting as a researcher, positioning refers to the relationship and dynamic between yourself, your project and the subject/s of your investigation. Power relations can be shaped through public discourses, media and institutions as well as human, social and cultural factors such as gender, race, religion, sexuality and different abilities. The illustrator researcher may approach their subject from a range of positions. These might be informed by subjective interpretation such as personal interests, their own areas of creative expertise, their own personal experiences. The position the researcher adopts can inflect on the viewpoint, narrative and / or opinion described in the research project.
Ethnocentricity
This can be mitigated against by being self-aware of the factors informing your own knowledge, experiences and viewpoints. This reflection will allow you to recognise and confront your own prejudices and assumptions. A good practice is to simply be mindful that everyone is prejudiced and to consider how these might be informing the wider research project.
Who benefits?
A responsible practitioner considers who benefits from a research project and any outcomes. For example, how does a documentary project impact on the community being described; do they gain experiences, recognition or some other value from the project? Funding bodies, institutions and stakeholders might also benefit through their support or association with a project. What are the benefits to the illustrator conducting the project?
Consider what will be achieved through conducting the project. Motivation is likely lead by a number of factors: to raise awareness of a cared for cause; to obtain a higher academic achievement, to further employment opportunities. One rationale is not necessarily more worthy than another, but it is important to acknowledge the full spectrum of motives and potential impacts behind any work.
Legacy
Illustrators should be aware of the responsibilities they carry when making work about real people and lived experiences, be they living in the contemporary moment or distant past. Even the stories of the dead may have impact in the here and now; relations may be living or affected by events long past. How we document knowledge of ourselves and others carries the potential to leave a legacy. The information, messages and narratives, even the most seemingly mundane content conveyed in illustrative works can be used to provide insight of the here and now to future societies.
Informed consent
First ascertain who the participants within your project are. A participant may be the subject of research: those being documented or interviewed; a test audience for an illustrative work etc. Participants should normally be given a choice as to whether or not they take part in your research, and informed consent should be sought, usually in written form. Institutions (whether academic or otherwise) may be able to provide ethics forms and pro forma consent letters, which can be adapted for specific use. Being on familiar terms with participants (a family member or friendship group for example) doesn’t preclude them from ethical considerations, and informed consent should still be sought. Gaining informed consent ensures individuals have a clear understanding that they are participants in a project. Clear and plain language should be used in all records and correspondence to ensure clarity. Participants should be provided with copies of consent forms. Consent forms vary according to the nature of the research activity but should specify:
The name of the illustrator /researcher and brief project details including any working title.
An invitation to participate and a brief description of the research activity, i.e., an interview, a workshop, a drawing exercise etc.
Permission to name participants (if necessary).
Details of how the research activity will be recorded or documented.
Details of how the information gained might be used, for example, will drawings be exhibited publically or published?
Details of how this documentation will be stored and for how long.
Contacts details should participants need to correspond after the research activity has taken place.
The explicit right to withdraw their consent to take part after the research activity has taken place
If working with at risk groups such as children, vulnerable adults etc. it may be necessary to gain additional consent from a parent or guardian. Working with an institute or organisation may require an application for ethical approval through their internal ethical committee. There are circumstances in which ethical clearance cannot be obtained, particularly when working covertly or in busy public environments. Consent may not be needed if there is no way an individual can be identified in the research outcomes.
Research Ethics Reading List
https://kingston.alma.exlibrisgroup. com/leganto/public/44KU_INST/ lists/7067481690001931?auth=SAML
Research Ethics Canvas page
https://canvas.kingston.ac.uk/courses/498/ pages/ethics-for-pgrs
My Kingston (linked to from Canvas page)
https://kingstonuniversity.sharepoint.com/ sites/mykingston/myuni/research-governance/
Data Management Plan
https://dmponline.dcc.ac.uk/ Very useful tool, log in with KU credentials and you will see Data Management Plans shared by colleagues
KU Research Data Repository
https://researchdata.kingston.ac.uk/ Useful to review entries in order to better understand what full data sets and metadata are, and what is appropriate for particular types of research
Researching with KU students as participants Data protection privacy notice for enrolled students
https://www.kingston.ac.uk/aboutkingstonuniversity/howtheuniversityworks/policiesandregulations/privacy-notices/2021-22/ enrolled-students/
See “how we use your information, To manage the academic experience” research (for example, academic research, evaluation research, student surveys and market research)
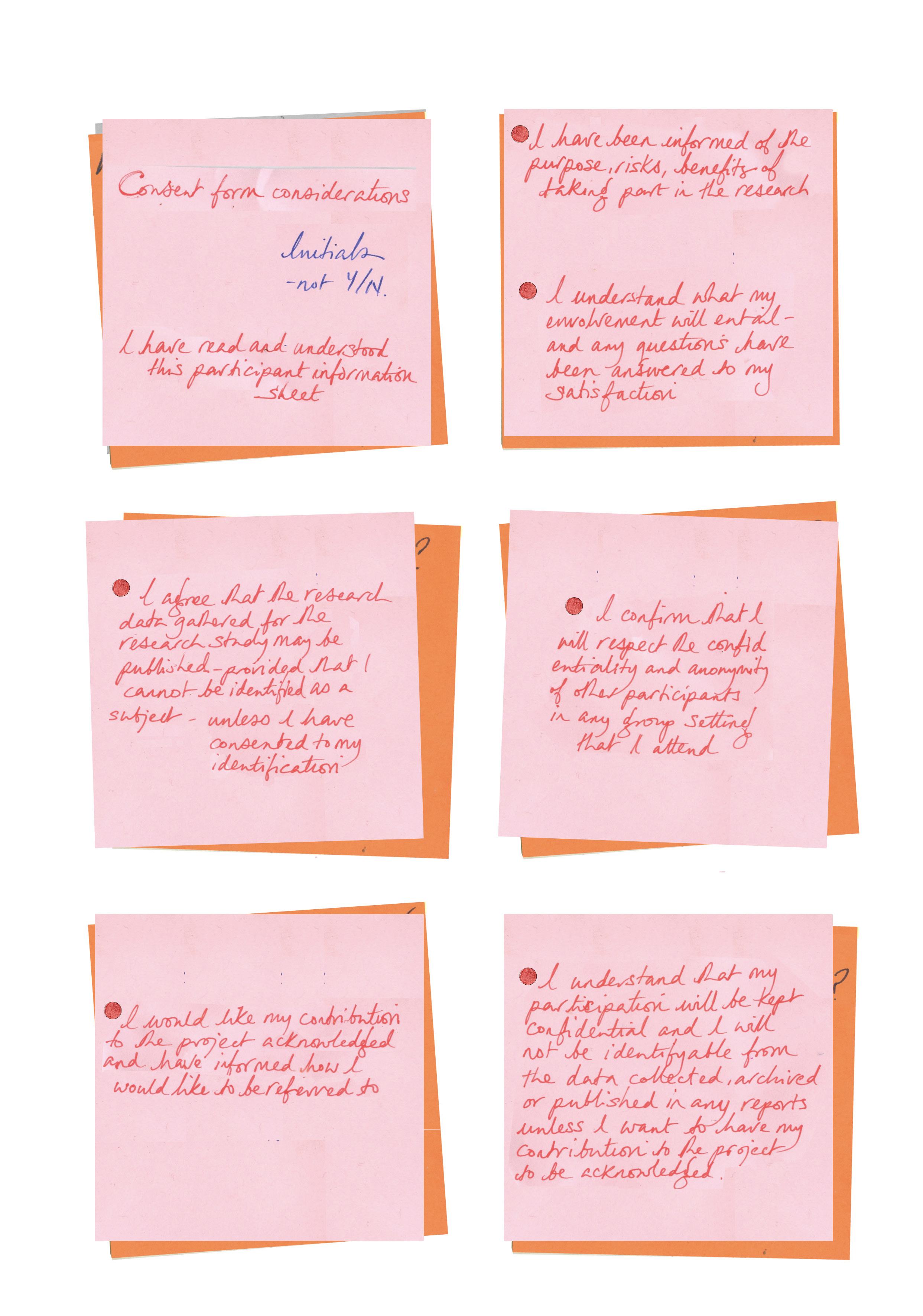
Research Consent
Participants will be given a participant information sheet which will inform them about the project. After reading the information sheet they will have the opportunity to ask questions. Informed consent will then be sought by asking participants to sign a consent form where they will also indicate if they want to remain anonymous or to be identifiable in the project. If participants want to be identifiable then they will let the research team know how they would like to be referred to.







What am I doing any why?
Summer of 2024- Following a monumental bout of imposter syndrome after my IMR Upgrade. I have been completing the project’s relevance and whether there is anything original in the world anymore. I have been re-reading some of the many articles I haven’t looked for but have come across in the paper as I flick through daily. Here are ten from the end of January, exploring a range of opinions and critical issues regarding how the UK treats pregnant women and giving birth. Here, I have outlined the content of each piece, many of which overlap with the issues and problems presented.



The All Party Parliamentary report published in May, ‘Listen to Mums: Ending the Postcode Lottery on Perinatal Care,’ also highlights the need for change for the support and consideration of mothers. One aspect focussed on is poor communication, especially in terms of women’s understanding and content of tearing and consent when giving birth.
I have spent some time in hospital environments this Summer following my Dad having a stroke. From this experience, I have been reassured that there is a need for clear, concise visual information to explain complex information when people need it.

At St George’s Hospital, during a vascular appointment, the consultant tried to explain the extent of the blockage to the carotid arteries. These are the major blood vessels that provide the brain’s blood supply. You have two carotid arteries, one on either side of your neck. Carotid artery disease causes up to a third of all strokes. A stroke occurs when one on either side of your neck. Carotid artery disease causes up to a third of all strokes. A stroke occurs when something blocks the blood flow to the brain, causing brain injury.
The consultant described this with a diagram he had drawn with a biro; he was colouring a

percentage of blockage in an environment of the central vascular ward, machines beeping, trolleys crashing, and patients groaning. He was explaining a complex issue to a man who had recently had a stroke and is also quite deaf but refuses to admit it. My point here is that my enormous conflict of confidence and sense of impostorism may need to take a back seat as correct, precise and clear visual information in a time-critical setting or moment about health is relevant and empowering when you are at your most confused and vulnerable.
07/07/24. The Times Culture Magazine
Books‘Why are we addicted to motherhood horror stories?’
Martina Kemp
‘Bringing up a baby is no fun,’ according to what started as a trickle and is now a flood of books and TV shows in a diverse scope and style. These books unite in ‘their political charge and the unvarnished portrait they paint’ about the loss of self. ‘To live in your body before [birth]is one thing,’ the protagonist of Elisa Albert’s novel After Birth says. ‘To live in your body after is another.’
15/07/24. The Times- News
‘Birthing mothers ‘dehumanised by lack off respect from NHS.’
Eleanor Hayward
Hayward’s article discusses the issues around consent and how thousands of women are having intrusive ‘normalised’ procedures during childbirth. The most common is an episiotomy- a surgical incision between the vagina and the perineum. It is usually performed during the second stage of labour to quickly enlarge the aperture, allowing the baby to pass through. The incision can be done from the posterior midline of the vulva straight toward the anus or at an angle to the right or left. Waters broken and unwelcome cervical sweeps are commonplace—a lack of communication and a fundamental lack of dignity due to time pressures in hospital environments.
05/02/24. The Times Health Commission
‘A report into the state of health and social care in Britain Today’
Lead Commissioner: Rachel Sylverster
This comprehensive report covers a ten-point plan for health- the scale of the problem, waiting lists, primary care, workforce and culture, social care, technology, mental health, health inequalities, obesity and public health. Maternity issues fall under Patient safetythe devastating consequences of medical negligence and the culture of blame, making legal battles lengthy and preventing crucial lessons from being learned. The dismissal as mothers being ‘overly anxious’ when raising concerns about their own physical health or that of their babies.
25/05/24. The Times Saturday Magazine
Paloma Faith Bad Sex, Men, Miscarriage, Birth Trauma- What no one told me about being a woman.
Paloma Faith is candid in her rare interview about her struggles to conceive and the birth trauma she experienced with both her children. Long labours are not communicated with in advance, and they do not feel prepared for the shock of episiotomy and the subsequent pain when trying to manage the experience of postpartum feeding and the expectation of just ‘getting on with it.’
13/05/24. The Times News
‘Birth trauma report calls for tsar to end postcode maternity lottery.’
Geraldine Scott
‘A national plan to improve maternity care will be introduced after Britain’s first parliamentary inquiry into birth trauma found ‘negligent care’ was putting mothers and babies at risk of injury and death. This article is in response to the All-Party Parliamentary report ‘Listen to Mums: Ending the Postcode Lottery on Perinatal Care led by Theo Clarke and Rosie Duffield.
18/01/24. The Times News
‘I felt frightened giving birth on NHS ward, says health secretary.’ Eleanor Hayward
As a woman living with type 1 diabetes, where the process of birth can be very medicalised, Victoria Atkins, the then health secretary. At the beginning of this year, she spoke about her ‘frightening’ experience of having an emergency birth in a hospital. She was promoting £25 million in funding for ‘one-stop health shops’ for women’s health. All women should be given a health check on mental and physical check-up within eight weeks of giving birth.
03/ 02/ 24. The Times - Weekend Essay
‘The NHS is stuck in a cover-up culture- there is a better way.’
Rachel Sylvester
Families bereaved after avoidable deaths in hospital face further trauma when they are pitted against the health service in legal battles- what can we learn from our mistakes? The article focuses on blame-shifting after things go wrong in the NHS. Every year, there are 11,000 avoidable deaths in the UK, and thousands more patients are harmed. This publication claims that maternity negligence costs during 2023 cost 60% of the total payout budget at £8.2 billion. This number is disputed online by ‘fullfact’ as being inaccurate, and the total is £2.6 billion in 2022/23, up from £2.4 billion in 2021/22still, maternity payouts cover a third of all medical payouts across all medical negligence claims.
https://fullfact.org/health/maternity-nhs-compensation-clinical-negligence/
23/06/24. Sunday Times Magazine
‘Cutting the cord- With trust in NHS maternity services at a low, women are turning to private midwives and doulas, some with extreme views on childbirth. What happens when that dream home both goes wrong?’
Rosie Kinchen
This article explores what happens when there is a growing distrust of health care services. These stories come from a wide range of forums and pieces in the public eye—such as these I am including in my research. The term BBA is new to me. (It is born beyond arrival.) It is a term applied when a baby arrives before the midwives do. It is a choice made by the mother and family to intentionally keep the health professionals away to have an uninterrupted birth. Kinchen’s article highlights the nervousness and the turning away from medicalised birth to using doulas and more radical ‘birthkeepers,’ some of whom advocate no medical intervention. We have a national shortage of midwives, midwives, and training, and experienced midwives are leaving the profession. There are 700 doulas registered with Doula UK - the representing body. The word translates from the Greek for ‘female slave.’ The natural birth movement in the 1970s saw the first doulas becoming a newly valuable source of support in the birthing environment. Doulas are usually not medically trained and do not carry out the clinical midwifery duties. Their skills are utilised in working through and processing birth preparation and fears and nerves, as well as providing techniques to support through labour and to manage the birth and the crucial postpartum stage. Having experienced help in breastfeeding support, help around the house, and help with other children must be an absolute middle-class dream.
12/04/24. The Sunday Times Magazine
‘Blood was pouring out of me like a hose- I begged for a c-section from the start. But it was too late. Giving birth to my son ruined my health - for life.’
Louise Carpenter
Another media personality is talking openly about their experience. Louise Thompson is an example of someone with a reality star and influencer ‘perfect life.’ She had a c-section which went wrong; she lost vast quantities of blood, she was discharged too soon, and eight days later, another haemorrhage occurred. Her son was in ICU, so she felt no bond, and as she gave birth at the height of the pandemic, she suffered from a lack of support mentally and emotionally. Thomson recently had part of her damaged bowel removed and now has a stoma. ‘Who is taking accountability for the fact I can’t carry another baby now?’ She appreciates that her experience was an unlucky catalogue of errors and that none of this matters, as she has been given another chance.
23/02/24. The Times News
‘Instagram and Facebook ban posts on women’s health as pornographic.’ Rosie Taylor & Eleanor Hayward.
The depressing title and article content surrounding the perception of practical health visuals as inappropriate are outside the research project. Women’s health campaigners such as Clio Wood, founder of CensHERship, quote, ‘It is especially galling, as everyday uncensored and hypersexualised pictures are ignored in their thousands. Women’s health campaigners must resort to the use of numbers or symbols to avoid censorship.
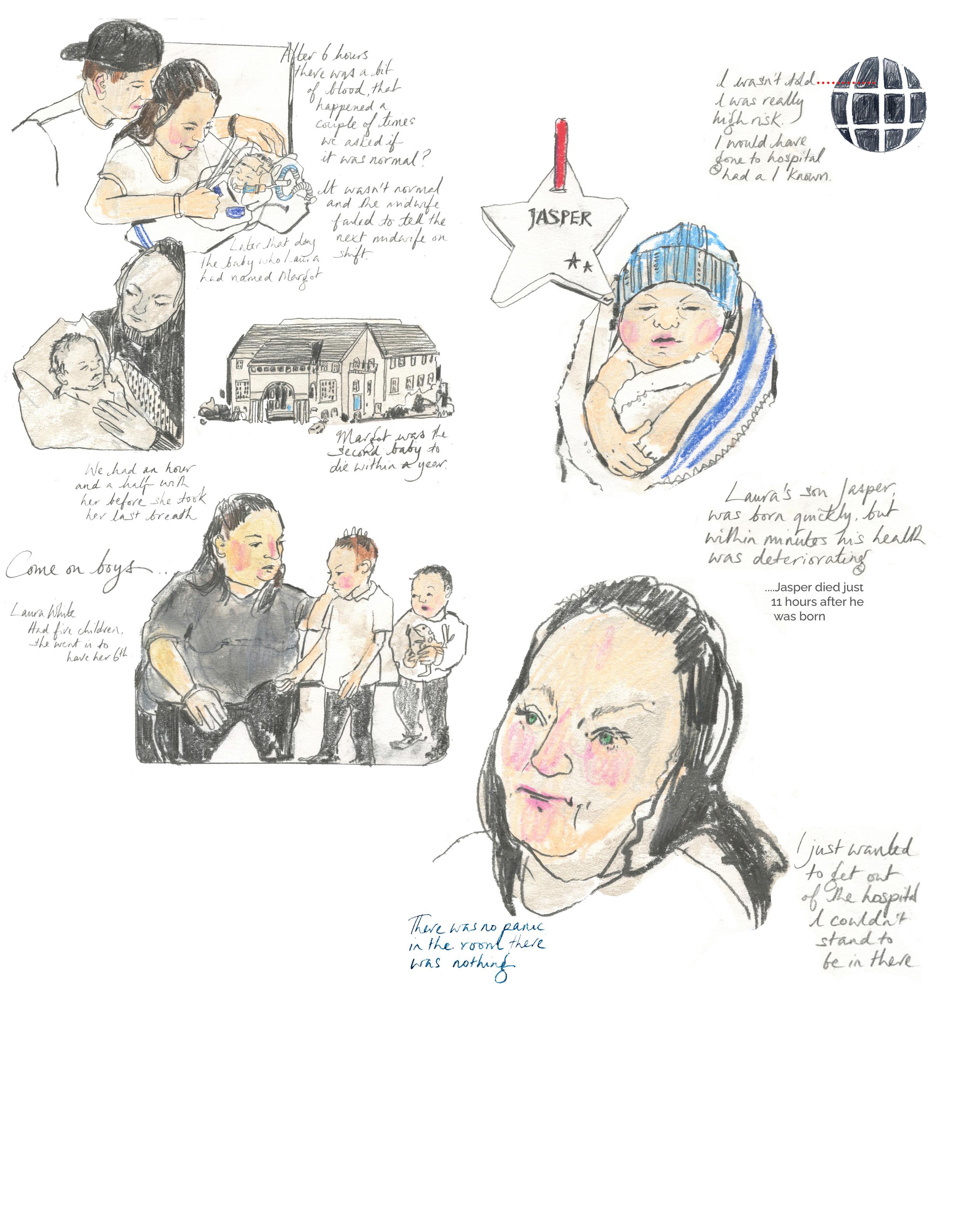
Maternity Scandal: Fighting for the Truth
Panorama: Season 33, Episode 8
Air date: 23 February 2022
Director: Alys Cummings
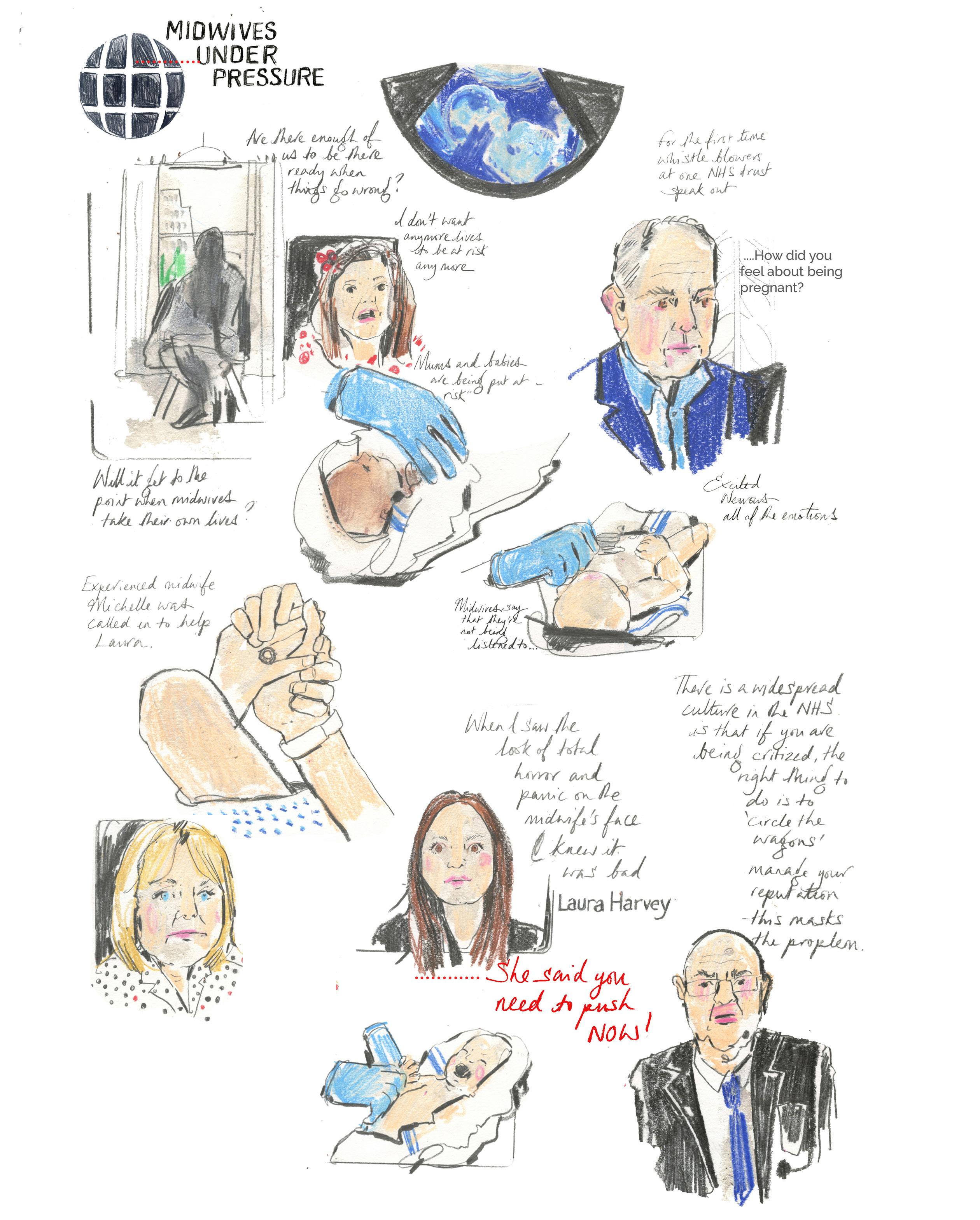
Panorama is an investigative journalism programme with a seventy history of unpacking relevant and critical subjects since 1953.
In this shocking programme, Panorama investigates the crisis in maternity care that is putting women and babies at risk. Whistle blowers at a trust in Gloucestershire tell reporter Michael Buchanan about the deaths of mothers and babies, the dangers of the under staffing and a culture that they say has failed to learn from mistakes, and subsequent mistakes being covered up as a toxic culture of misleading and hidden information.
The regulator, the Care Quality Commission, has said that the trust’s maternity services are inadequate, and Panorama has calculated that maternal deaths there are almost double the national average. The trust says that it is deeply sorry for failings in its care and has improved its maternity services.
This programme follows on from an aired show covering one of the biggest scandals in the history of the NHS, where many babies died whilst others were left with life-changing injuries following repeated failures in maternity care at hospitals in Shropshire. Michael Buchanan, who first investigated the extent of this hidden tragedy, meets families who have never spoken out before and former insiders who describe a dysfunctional culture that contributed to the truth being buried.
This software has much to offer in demystifying a space before you visit it. It would be ideal if one could click on the drawing of the drawing of the equipment, and a pop-up description of what it is and what it does would be informative to the patients and their families. Other languages can be chosen for non- English speakers.
As an illustrator, images and environments can be drawn straight into an iPad, or more traditional paper imagery can be scanned and imported into the software. My conversations with Emily McMorrow have brought up the complexities of the environments and equipment that are daunting to birth givers.
As a ‘stage set,’ where you, as the viewer, can move around the space and see behind the scenes through illustration practice, this software has vast potential in introducing patients and families to the clinical environment.
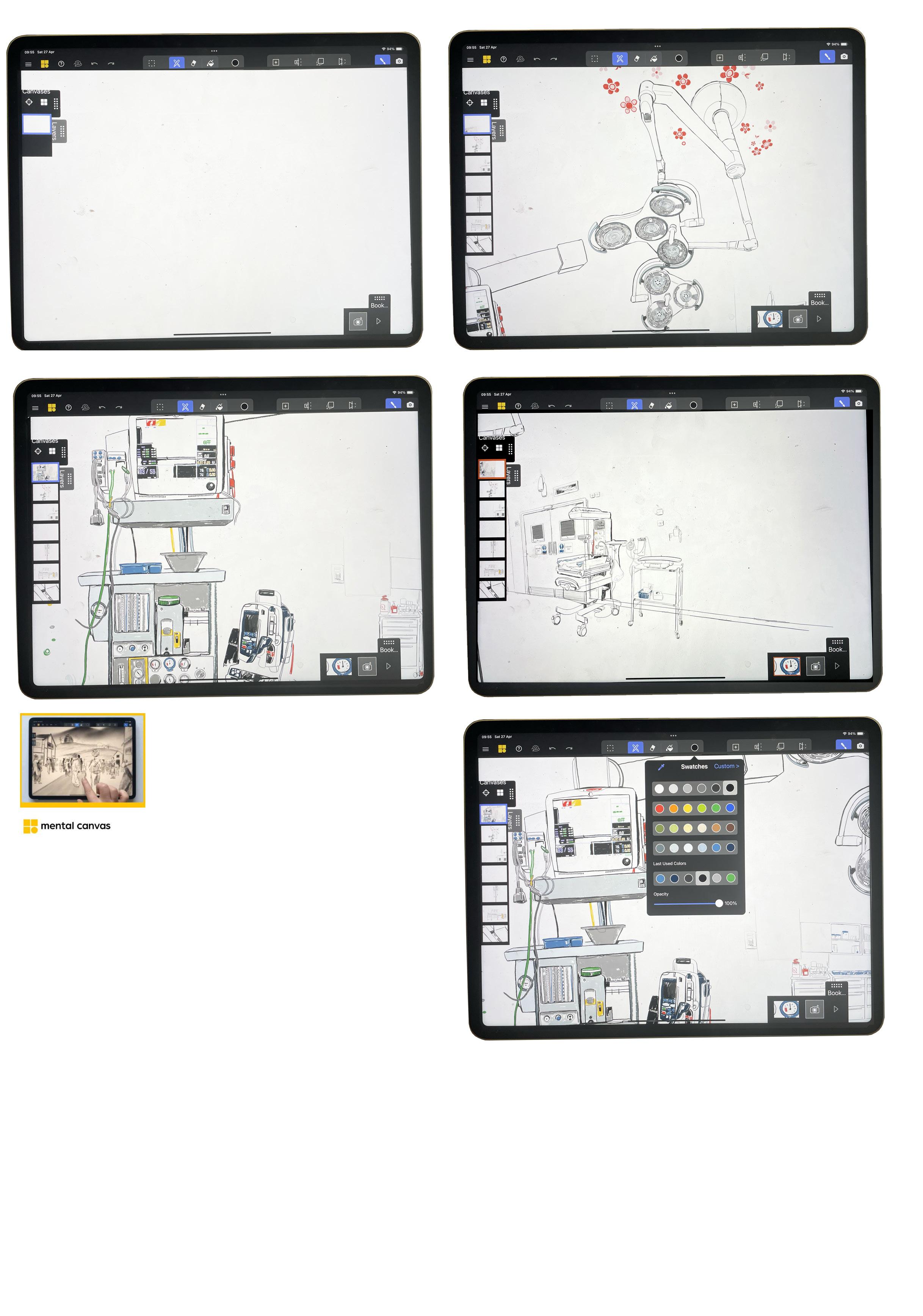
The left-hand side of the screen has several layers, so in this drawing, the walls and the different pieces of equipment are in the operating theatre. The bottom frames can be selected as points that you can move around the room - giving the viewer a chance to virtually ‘enter’ and move around a new or different space. The patient can know what is in a particular clinical setting through drawing and understanding their viewpoint as a patient and seeing complex equipment on their terms before being moved into a clinical setting.
The intention is to reduce the anxiety of visiting a new and unfamiliar setting, answering questions such as..
What does it look like?
What equipment is in the room? What will I be hooked up to?
Where will any blood go?
Talking with Emily McMorrow Midwifery Worker Kingston Maternity Unit
I want to find out about your gestational diabetes. Your health provider suggested that you look at this part of the process.
As I said, I explained the book in the notes. The first page you open lists almost everything that can go wrong, the most immediate things that can go wrong. That can feel confrontational and alarming. Whereas if you have been told, okay now, you’ve been diagnosed with gestational diabetes, I need to find out about that, let me have a look at that, I wonder if there’s any information about that, oh, absolutely yes there is.
I remember what you told me: before you go for your routine urine test, don’t eat Cocoa Pops or drink orange juice for breakfast, or you’ll be in trouble. Only eat something sugary after you do have completed your urine test.
It costs the NHS money.
Only eat chewing gum after you do it.
Yes, absolutely. Oh my gosh, that’s such a good point at the moment; well, it will because, for example, we’ve gone from giving people letters with a printout about the glucoside test to not consistently attaching a written guide.
Now, women are coming to me for a glucose tolerance test after having eaten, rendering the test undoable. The premise and procedure must be transparent to the patient—this is how the test works. Women say,
I Googled it, and it said don’t eat from midnight.’
Every hospital carries out the test differently. It’s Kingston Hospital’s policy—we say you have to fast for 12 hours, so I can’t do the test now. And they’re very upset.
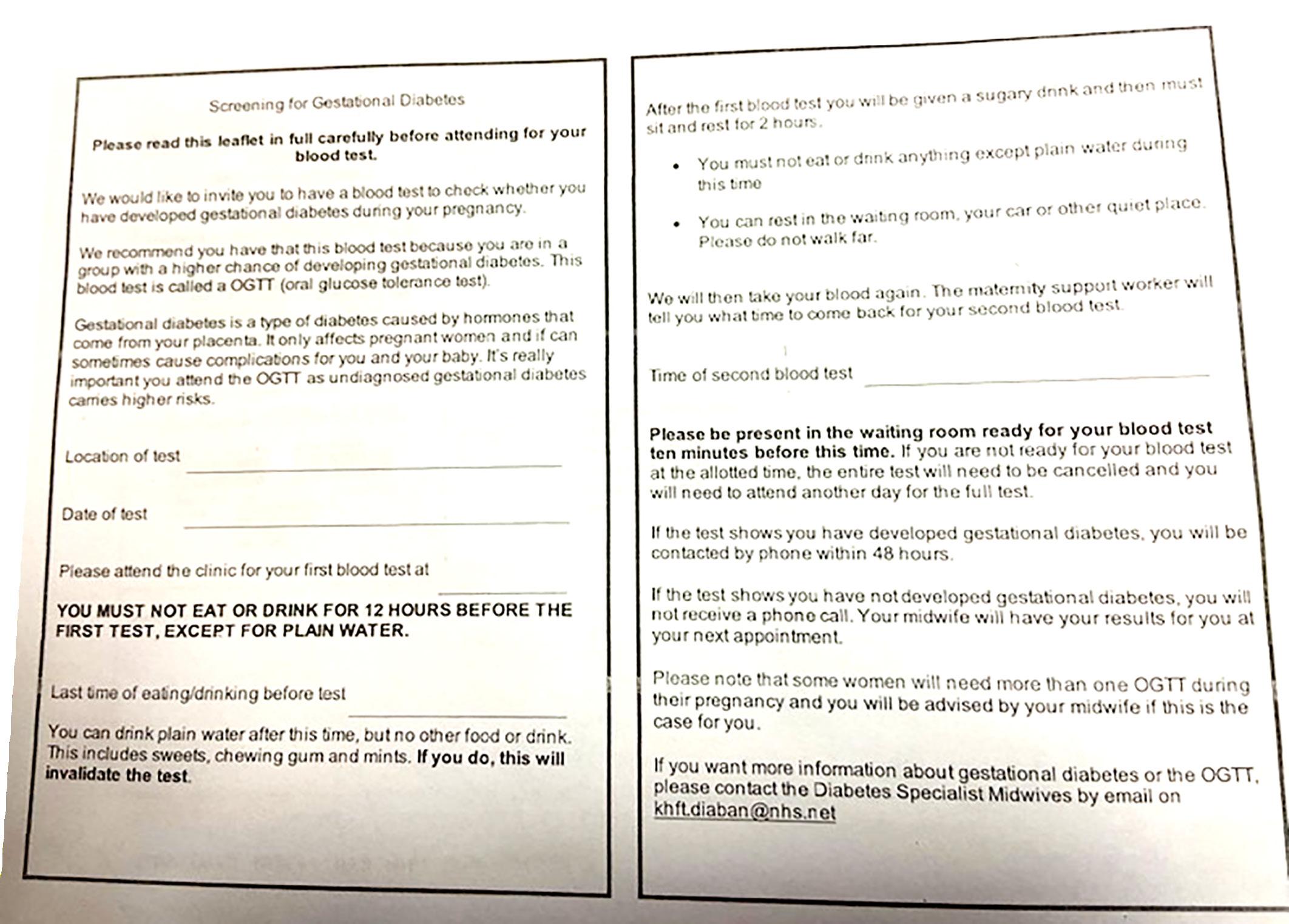
Could I design a visual version of the written PDF?
Oh my god, that would be a brilliant idea. Jane, it would save the NHS, hospital trust, and patients time, money, and energy— also, approach John Grellier, the head of improvement.
I know him, so I will.
Again, then the language barrier could be addressed, or it could be designed with the top 5 KMU patient languages. I will text you a copy of this leaflet that should be sent out to patients having that.
Please do.
A digital attachment would be so helpful as women often have booked a day off work. Also, it’s our time as practitioners, the appointment time, and the fact that women have fasted. They may have had to put other children into childcare. Also, remember that it’s a two-hour test, so they have to sit in the hospital for that time. So if they have to rebook it, that is a lot of wasted resources.
That’s a lot of NHS time. Thanks Emily, I’ll send it tomorrow.
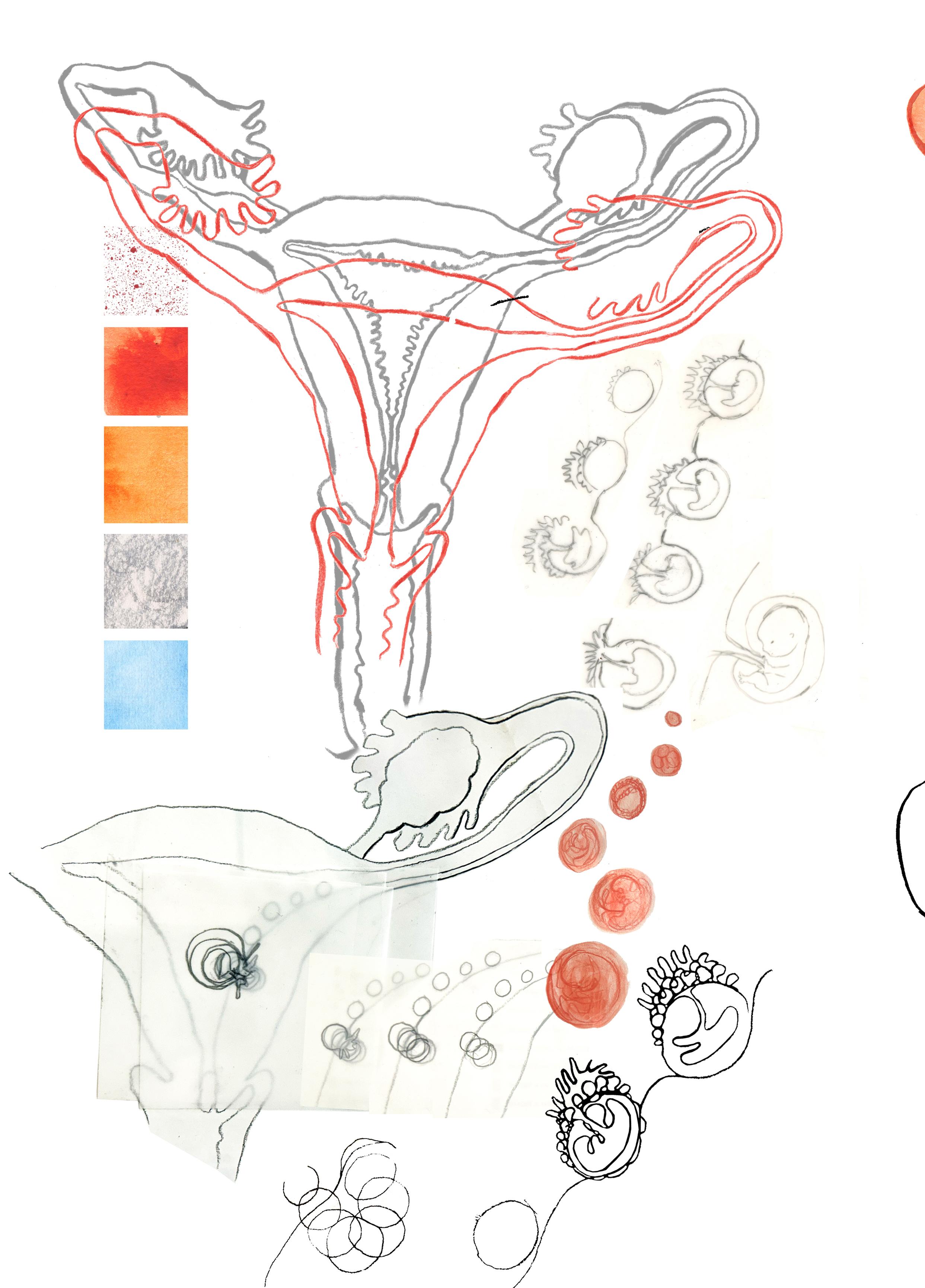
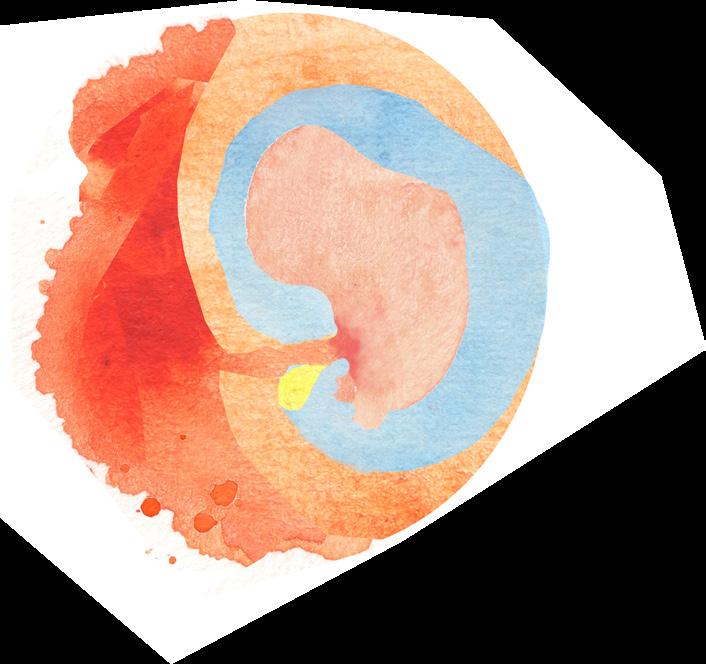
The visual information that exists of a blastocyte embedding into the uterine wall and then developing into an embryo, the imagery always jumps to the next frame as being inside the embryonic sac. Here, I am visualising the process of the embryo returning to the womb cavity as it develops into a foetus.
The drawings on this page are working out how I can visualise this. I am much happier with the visual of this womb than the imagery in Reader No. 3, as the colour and the key line feel more organic, and the splatter crackle has an energy to it.
Listening with Alannah Smith and Georgina Moore.
Friday 5th June 2024
JW- Black text
AS Red text
GM Blue text
I am here with Alana and Georgina, and Alana and Gee are going to talk and I’m going to listen i an informal way about their thoughts about being pregnant and giving birth. Do you want to say hello?
Hello I am Alannah and, I am Gee,
So let’s go, I you both have just completed your degrees and about to go out into the world- I want to ask; what are your thoughts about being pregnant?
So like, obviously we’ve been to school when you got to see that horrendous video at the end of Year 6.
Yes. Oh yeah, with the weird songs.
I actually... I don’t particularly know all that much, I haven’t learned any things recently, more so than in my school education, but I don’t know anyone close to me that’s pregnant. It sounds awful, but I don’t really know, like, technical things. All I know is we spend a lot of consideration and effort on not getting pregnant.
How old are you both?
I’m 23.
Yep, I’m also 23, so we could be pregnant. We could be mothers.
Yes, some 23 year olds are and if you go back 40 years- most probably you would have been by 23
We could have been mothers NOW!.
People in my year group that have, from school, they have children. Whole actual human beings.
I like the idea of being a mum, but I think the idea of birth actually does put me off.
Like you get really extreme fluctuations of temperature in your body. Don’t you? Is that the thing that puts you off?
No the pain puts me off! and not being able to control things. And I think like if you do have to like, if I only just found out that you have to second birth your like sack that keeps the baby alive, so that comes after the baby and that blew my mind a bit. Is that?
No, keep going.
I can’t think what it is called
The placenta
Yeah, but like, I don’t know, it’s just a world away, but it could happen. And also like pregnancy, like so many pregnancy scares, but then I’ve never really thought about what like that is leading up to something that I’m frightened of, that like pregnancy.
Do you think, that’s a really interesting thing to say, I think as young women we spend a lot of time investing on not being pregnant.
Yeah, yes we do, and money. And it’s not about the child at all. And it’s our job.
I’ve always bought the condoms because like, it’s going in me. Yeah, it’s really bizarre to me when they don’t care about that, when they’re really chill about that. And it’s like, you don’t understand the implications of what that would mean for me, not you, if something were to happen.
Yeah.
So what do you know about pregnancy in terms of, I don’t know, t or what to expect?
So for me? I know words in there, like trimesters,
Yeah.
I’ve heard someone refer to a fourth trimester,
Like post partum? Okay. I heard about that. Like a more mental... In that you’re still going through the process of being pregnant because your body has to heal and do all these other things after the baby’s actually come out. Yeah, because they always say like, bounce back, she’s bounced back after pregnancy and then they’ve magically become sexy again and that’s really strange. You still have to like, you’re still like, proceeding. Yeah, you’ve still got all of this excess, even skin. So much, yeah. Excess skin.
I’ve heard so many horror stories.
Like what?
Well, one of them, well, okay. One of my friends, her sister, gave birth, she went in and she had a caesarean. And she went into the hospital room afterwards and she said it smelled like a butcher shop. Because it’s raw meat. I was like, that’s horrible. Wonder if that being able to smell your own meat. Because it would smell. You never really think about the smells of pregnancy. It’s horrible. And then there’s all the things about epidurals and then if you’re too far gone they don’t give you the drugs and then it really hurts.
Yeah. My mum’s had three cesareans. Three cesareans? Yeah. I don’t know why, I think it was like a fad. Everyone had cesareans at one point.
What year were you born? 2000?
1999
Me -2000.
Yes, that’s interesting.
I wonder? Was there like a section of time where everyone I don’t I don’t know actually and it’d be really interesting to look at that but then do you think that’s presented as an easy solution it probably was because at the emergency solution yeah but why did my Mum had three like- you have had two - you might as well have another. And this was the thing as well, we were asking someone recently, when you have a C-section scarring, do they do the same line?
No, they do different ones.
I thought it was the same one, like a little- oh there’s already a line, we’ll go back in there. Like a zip.
No, you have to have a different, I asked my mum, I was like, no, she’s got three scars.
From the research I have looked at - if you used the same scar it would be in danger of rupturing in the latter stages of the next pregnancy. If you have a c-section scar and you are having subsequent operations, like a hysterectomy they then go through the same scar.
Oh,
Makes sense.
What do you think, when you just said the word a natural birth, what is that?
I don’t know. But I think it seems like it was that because a natural birth doesn’t really have to be with any interactions form anyone else. If a baby is breach in the end you have to have one- a c-section, then it’s not natural. What is it called? Assisted or instrumental?
I think a natural birth is like you’re just kind of there in the stirrups and then like it comes out head first and you’re just pushing on every time they count down and breathe with you. That’s what I would imagine is a natural birth. Probably you would have drugs.
So would the drugs be a natural birth or not?
And why would you be in stirrups?
Because that’s what they do, isn’t it?
Where have you seen that- or where would you see a birthing woman in stirrups?
It was a historical thing?
I knew about this because they there were women like that on Casualty and, and what’s it called? One Born.....
One born every minute.
Yes, yes!
Interesting -Because it’s not the ideal position to be in.
Is it not?
No, not in all cases.
Are you meant to be crouched?
Gravity wise- it can be a good idea. You’re meant to be in the pool, in the birthing pool.
I’m not sure about the birthing pool.
I want to have a birthing pool. Because that sounds great, the baby just floating out.
But then you have to swim in it. Swim in all the liquids But I think, I thought stirrups are... No, but also, think -when you go to the toilet, it’s better to have your knees up and push down.
Wouldn’t the baby come out on the ground?
I think midwives avoid that happening!
I know that when I was born. Well they need to keep me alive in it’s little box with all the other babies.
Have you seen pictures of yourself being in a nursery of other babies?
Yes
Oh, that’s really interesting
I was a home birth, in my bedroom that is my old one now.
Wow. Was that your mum’s choice? Did she have to fight for that?
Yeah, I don’t know if she had to fight for it, that was her plan I think. But you should see... She’s had two births already, and I think, at least one of them was at hospital, I’m not sure if my other brother was at home or not because that was in the plan. But I think she’s had C-sections before that.
Do you know where your Mums were born?
My mum was born in Bath Hospital.
My mum was born at home in Bristol.
I remember in your Chelsea and Westminster presentation you mentioned that your mum had a really long time in hospital before you were born.
Yeah, well... So she went in in... early June, and I obviously came out in September.
3 months! So she was in there for a long time.
And she’d had two c-sections before, with my older brothers. And she’d had... I don’t think she’d mind me saying this, but she’d had a couple of miscarriages just before Michael, who’s the eldest, and then two after him. So she doesn’t really have a smooth ride of birthing. And, yes, so she’s in there because it was... It was a... a placenta previa that happened. I’m not quite sure what that is. But, yeah, it just meant that she was in there for three months and she got really, like, used to and started just like living life in there which was kind of a crazy sort of I don’t know like living your normal life in a hospital which is always like working on such a schedule I think would be really interesting to follow. I’m sure she’d talk about it but um yeah I thought I’ve chatted to her about it pretty recently because I’ve been interested in it but I was just gonna come out very, very early probably not survive so they just kept like I don’t know what they did but they just like but they would have wanted your lungs to develop yeah I wasn’t I wasn’t at all you know do you know how what gestation you were born out how many weeks but I can find out but I think I was very small still no I was okay I was like there was nothing wrong. It started with like she’d leaked waters, so they took her in - I think they put some sort of stitch in. I was six or so weeks early, even with the three months in hospital.
It’s interesting to hear to talk of her being so institutionalised so quickly. My daughter was in hospital for a month, I was only there for two weeks as I had a three year old to get
home to. And also there was Swine Flu- so only the parents could visit. Which meant he couldn’t come and see his sister. Yeah. She was there for a month, but I was just like, I’ve got to go home at some point.
Because that was like, my mum talked really like, emotionally about the visiting, because obviously she needed to see her family. And that was almost a deal that she’d go home. She had two older boys. Yeah, Charlie was three, Michael was six. And I remember my mum telling me that Michael came and was like, when are you coming home, mummy? Like anything like that, and it just would push her because like she’s clearly feeling so emotional about missing her two other boys growing and like Michael had his birthday coming up as well and she was gonna miss that and it was all just she was just stuck in this place that all of these women were she was seeing having babies and being happy for them and things going wrong and being so emotionally like in touch with these women that were just next door to her but knowing that it wasn’t gonna be her for a very long time. It would be quite like emotionally like yeah very tiring on her definitely.
You touched on something about the whole thing about being like having to be like amazing after your baby.
Yeah
Yes,
What are your thoughts about that?
Well they always do it don’t they? Whenever like a person in the public eye is having a baby.
So like, on the front cover of a magazine, or even like health people, like people that go to the gym a lot, are like, they’re like, I’m already exercising, I’m already doing this, and I exercise throughout the pregnancy. And they’re always like bouncing back, their tummies are like, it’s hard again, and it’s as if they haven’t been making a whole life in their tummy. But yeah, of course your body’s going to change and adapt. Yeah, and it’s always going to change. It’s going to be different afterwards, forever, right? And then it’s like, yeah. But they talk about it as if it should be like, sexy again, like immediately. And it’s like, I don’t know, that’s a mad expectation and a mad judgment and it’s quite like, I don’t know, that’s kind of...
It’s very cruel. Yeah.
To have this thing where there’s a huge expectation of women to have children, and then it’s like, you’re not allowed to actually exist. You have to be sexy when you’ve had them. It’s like, it doesn’t mean anything. Yeah, it’s really...
It’s like a before and after shaming thing.
I was really interested, I was watching a programme from about 2005, which was Jamie Redknapp’s wife, who had kids the same age as me, and she was in a girl band, I can’t remember what they’re called now. She was the white girl. But anyway, she had this underwear shoot planned for post her second child, which seemed really nuts. But the programme was from 2005, which was basically about people keeping themselves very, very
thin during pregnancy and obviously the dangers of that are your baby could die. But obviously you’re in a different situation like when I had my children there wasn’t Instagram. Yeah it’s like the constant because you’re always viewed and viewable and then keeping up appearances.
I think maybe the Kardashians are really bad for that as well. They’re always pumping out babies. And they’re not actually. They’re always so, like their skin never has any stretch marks.
Nothing. They’re all like so airbrushed and beautiful. I hate saying that that’s beautiful, but it’s so false and it’s so weirdly clinical and not correctly real.
It feels as though they also hide it away when they are pregnant or having children.
Yeah.
Like hide it away and then pretend that they were just... It’s just happened. I’m like, oh, now I look like this. And then I obviously had surgery. My mum does get very annoyed at, like, seeing celebrities after, like, birth or, like, ageing. And she’s like, oh, they’ve had this, this, this done. And I’m just like, why does that annoy you? But it works, because it’s like... Yeah.
It’s not real.
It’s not real, yeah, but she’ll always pick up on it. And I’m just like, oh, it’s just noise like it’s just I think like maybe our generation.
What do you think about your careers and the thought of having children?
Careers in that is in fitting it in with the career? Yeah because paternity things, paternity leave is like kind of more of a thing than it was, but maternity leave is still, yeah but there’s still sort of difficulty with women being hired over men because they have the expectation that they will be off having children. So not as desired in job roles. Because they’ll be gone. But it’s like, what’s the alternative? And then what was it, how does that work if you’re freelancing?
Yeah, because we will probably be freelancing. Exactly. So it’s like, how would that work? I’ve not given it a huge amount of thought because No I have had much. I mean children is always like a... I definitely want children. But like I’m not in a rush. Isn’t that popular anymore? Like a lot of people when you ask they’re like no never.
I’ve never really... I mean like I think at some point I’ll want them but like I’m not like in a rush. No. My life would have to come first.
What’s your priority?
I think money and the state of the house first. I don’t want to have children and not give them what I think they deserve.
I’d like to be, I’d like to be that happy, like, I’d like to know that I’d be a good influence
Yes.
Because what’s the point?
I want to have children that I can give them a good life. Yeah, I’d like to be wise.
When I become wise I’ll have something. And I don’t think I’d be against being like an older parent.
I know. I want to have a good life before I have them.
Yeah, because then you will say like, you have your life, and then they have their lives. Yeah. I think that would be nice. And then once you have them, they’re there, and their is no going back.
They are the whole thing, they’re your whole world.
For like quite a long time!
What would be your ideal age to be a parent?
To have a baby, I’ve had much thought about this. So like when I was younger I’d say like 27, and now I’m 23, I’m like, I don’t really like anyone that much. And then you need to like them for a long time. So I would say like, I’d want to be below 35 I think. So like, 33? Let’s say 33.
What about you, Gee?
I think I am the same, thinking that I would want to have children in my late 20’s, but they seem to be flying by and I am totally not ready in way emotionally, financially or in terms of housing. So I would certainly now say my 30s, but it’s not like I’d have a.... It depends on who I met as well. If there was someone I really wanted to have a baby with, then I would eventually do that.
Oh, that’s both of you for talking so candidly and providing such inciteful answers! Right, that’s great. Thanks both.

Reflections
This reader feels it has been forever in the making, following the Summer School, a birth baptism of fire. Following that, the Summer revolved around family, and here we are back in September. The first version of the ethics considerations has been slow in realising what that can look like; breaking it into post-it notes and their non-committal nature has been helpful, having everything in a moveable form. Feedback from my supervisory team will be beneficial, and seeing other examples of ethics clearance questions would also be welcome. I need to look at other PhD researchers’ theses as I don’t have a picture of what this could look like. I aim for the project to feel like I am drilling down and focussing this year. The last two years have been about establishing the territory, but it has felt like I have been flitting around and making a range of starting points but not having the time to invest in committing to seeing anything through.
I spoke to other researchers this week who have had issues with their supervisory team, such as not getting their project or seeing the practice base elements as an add-on to the academic content. One researcher looking at a comparable health-related enquiry at the same journey stage, post-IMR, seemed utterly lost and disillusioned by the process. I am grateful that the supervisory team understands my practice and intentions. Seeing Hannah present at the BRC Summer School was great, and seeing the respect for her work and the refreshing hilarity of her talk gave me a real sense of pride- She’s supervising my project! I am extremely grateful for the quality of the supervision, in it is supportive whilst not spelling out what to do. The feedback form the IMR panel was also very constructive and considered.
The Listening experience with the students post-graduation was inciteful in how patchy their understanding of pregnancy and birth was. The conversation could have gone on and on as the setting was informal and chatty, the questions were not preset in advance, and the premise was they asked to have the discussion when we were on a bus to the West Middlesex Hospital for the CW+ residency ‘take-over’ day. Quite rightly, the main concerns on their radar have been centred around avoiding pregnancy at all costs. The birth rate at the moment in the UK, as with many first-world countries, is at an all-time low. The birth rate for the UK in 2023 was 11.267 births per 1000 people, a 0.49% decline from 2022. The birth rate for the UK in 2022 was 11.322 births per 1000 people, a 0.48% decline from 2021. The birth rate for the UK in 2021 was 11.377 births per 1000 people, a 0.49% decline from 2020. In 1955, the birth rate was 18,000 to every 1,000 people; now, it is at 11,100 to 1,000 people.
A steady decline, hearing the pressure felt by Alannah and Georgina in not having the perfect set-up before considering having a child in finding the right job, person, house, and everything, let alone the fear of the pain and the representation of a woman pinned down in stirrups. I aim to listen to a much wider group of young women to hear how pregnancy and birth are represented to them and to see if this is the case for many. These young women are in a place of privilege in their education and class; it would be interesting to hear the thoughts of other women of a similar age who have not just invested fifty or sixty thousand pounds in their education and may not see such a range of options in front of them.
https://www.macrotrends.net/global-metrics/countries/GBR/united-kingdom/birth-rate#:~:text=The%20birth%20rate%20for%20U.K.,a%20 0.49%25%20decline%20from%202020.