

CONTENTS:
Pages 1-2.....10x10 Interview with PhD researcher Hannah Rollings.

Pages 3-8.....Visceral Bodies Symposium Kingston University.
Page 9.....Interview with Suzanne Achillios Senior Lecturer and Midwife.
Pages 10-11...Tutorial 2: Supervisors John Miers, Hannah Ballou and Geoff Grandfield.

Pages 12-15.....National Maternity and Perinatal Audit Kingston Hospital KMU.
Pages 16-17.....Social Media- @Badassmotherbirther - What does birth look like? Part 1.
Pages 18-19.....Interview with Angie Phillips 33 weeks plus 2 days.
Page 20....Reflections
Page 21.....Time line and Methodology Diagram.
Pages 22-23.....Selection of illustrated material generated academic year 2022-23.
Pages 24-25.....Annual Monitoring Report content.
Pages 26-27.....KSA Post Graduate Research Festival Presentation‘The Illustrated Reader.’
Pages 28-29.....Tutorial 3: Supervisors John Miers, Hannah Ballou and Geoff Grandfield.
Pages 30-31.....Interview with Katharine Gale BSc RN Hons MSc- Director of FluxState
Page 32.....Conclusion of KG interview.
Page 32..... Bibliography Year 1. 2022-23.
Jane Webster and Hannah Rollings. 22.4.23
Hello, I’m having a conversation with Hannah Rollins. We are doing the 10x 10 activity for Geoff for the dialogues Illustration Animation Department PhD Researcher submission.
So, hi Hannah, how are you?
Hi Jane, good thank you.
I’m going to ask you the first question which is, how do you define illustration within your project and within your research practice?
It’s based on my practice-based experience, a sort of expanded autoethnographic practice which is basically recording through the lens of being a mother, small holder, and witnessing my family’s connections to nature. And through my illustration practice, I aim to encourage woodland stewards of the future. So, it’s been a sort of very reflective process, a diaristic, I suppose, practice, which it didn’t really start out as, but having children through my practice PhD, it’s all centred really around that and it’s opened my experience and my viewpoint of illustration to encourage this connection with nature for children.
So has your practice-based PhD changed your illustration practice in terms of, obviously it’s changed within your focus, within the depth of inquiry, but I think from having a conversation with you before, you were talking about how previously your illustration practice was far more commercial?
Yeah, so much more commercial and trying to gain commissions. So I started out by interviewing publishers, looking for sort of gaps in the market, and the environmental picture book at that time, when it started, I was interviewing publishers and a lot of them were saying it was still very niche, that there were only a few sort of breakout titles. They sort of mentioned ‘The Promise’ by Nicola Davies and Laura Carlin as being one. So I was, I think, quite on the precipice of non-fiction, resurgence of the nonfiction picture book and especially environmental issues. And I think since Covid, that whole experience I think has made people a lot more connected to the environment and to nature and the well-being possibilities of that. And I suppose my practice has become a bit more participatory through my workshops and through working with my children.
You’re at the latter end of your PhD journey. So, I can imagine that the landscape or the amount or choice, has that changed in that kind of seven years, in terms of what is available, or is that still a niche market?
No, it’s definitely massive now. It’s a huge business, I think, the environmental issues within publishing. So, it’s really opened up. But, I’ve sort of moved away from working with publishers and I’m more interested interested in the experience of being, from a personal position really, experience of being in nature and recording that. So I suppose my whole practice has changed and I’ve just recently, past this week, I was working with some children in a school outside painting trees and the landscape, so that was really lovely. And just to see them kind of excited, a bit more connected, you know, rather than looking at pictures or rather looking at screen or, you know, they’re actually having to deal with the physical and the senses.
I think we’re both interested in the position in relation to both our practices. I think there’s crossovers isn’t there? You just talked about how your experience of being a mother, bringing two people into the world has completely changed the way of seeing the world and I think that’s hugely important, I believe for both of our practices, and everything that we bring to it. My work is about advocacy in birth and childbirth. The one thing that everyone in the whole world has got in common, that we were all born and not manufactured in a, in a lab.
Absolutely, absolutely! How do you define your work in terms of is, it documentary?
My work has always been about trying to explain things, whether it’s how a Pontefract cake gets manufactured, how a location works, the story of a business model or how to get from A to B, so that hasn’t changed. My practice has always been about it being explanatory, thinking about the language of it and how that language communicates. So I think the ‘joining up’ of the subject matter is the essence. The way that I draw and make work, has been commented on quite a lot in the fact that it feels quite feminine, it doesn’t feel aggressive in any way. It’s quite layered, and it’s a from of ‘peeling back’ information. I’m at the beginning of my journey and then some of the things that I’ve been looking at, so I went back to the Wellcome Trust to look at all the different models that they had about pregnancy and birth. One of the ones that they had, it was the first thing I drew that went from being on my B.A. here.
So I think that’s really interesting that those things that are kind of in you and that have resonated in you for all those years. Keep coming back.
My position in relation to the PhD practice is having two very different experiences, and both experiences having left those with a sense of, well, failure and disillusionment, but also massive gratitude to the NHS. So I think my position is that I really want to do something that’s useful
that is actually going to help people understand what’s meant to be the most natural process in the world, but actually every process of giving birth is a completely different story, and so you can’t prepare for all those eventualities. But I think it’s really important that women, because they tend to give birth more, have a space to ask questions, to digest complex information in a time-based activity where there’s two patients and things are changing literally week by week. You know, from week 8 where someone says to you, where do you want to have your baby, most women are thinking, well, I’d quite like to get to week 12, when I can actually tell people I’m having one. So it’s this massive change, and from this project, I’m beginning to explore timebased work.
I’m just thoroughly enjoying the process of studying and learning and reading and reflecting and thinking and putting things together. It’s really interesting, isn’t it? You suddenly see your project absolutely everywhere in everything.
Yes! it’s quite astonishing. The time-based element is going to be really interesting, isn’t it?
There are 40 weeks, leading up to it and beyond. I’ve had two different experiences, one of a 42-week pregnancy and one of a 32 and a half week pregnancy so both very different.
So in your research obviously you’re much further down the line than I am, what is it you want to achieve with the project that you’ve been so involved with?
I suppose it’s a hard one isn’t it? Because you come out, you have, when you start things you think of these huge kind of issues and actually you might make, which is maybe a bit depressing, but you might make a really small contribution. You know, it’s because you focus down and you can only, maybe you can only affect a smaller number of people or maybe it’s kind of that affects something and it kind of leads to something. But it’s been changing for my practice, you know, I’ve completely sort of opened up my practice and moving away from a commercial position as I said.
But I think for others I suppose, I did a trail with the Forestry Commission which was really great to connect with people and talk about the outdoors and how they felt about being in trees and the well-being associated with that. So that was really good. I suppose it’s just to continue having small effects. Because I think if it was with a publisher, if it was with a commercial, because I did, I did, was talking with a publisher, but then they wanted to change things quite a lot and it didn’t really resolve itself. And I suppose they’re always, you know, it’s the next thing, what’s the next story or what’s the next issue. And I think, I think it’s about slowing things down,
actually, for me, and being a bit slower, and being a bit slower about my practice, and not worrying about, obviously, you need to make a living.
But I suppose it’s, yeah, being a bit more honest with my own practice and my own self, and trying to create images that reflect that, so I don’t think there’s any great big goals or outcomes. But it’s interesting you say, you know, that whole thing you start a project and your intentions are this is going to change the world, but I guess, you know, you become the expert in that quite specific pool of things that you’ve just surrounded yourself with and, you know, it’s like anything, you start whatever activity you’re doing with a breadth of knowledge and then it’s kind of, you know, you go further and further into the depth of it. So I think that’s really interesting. I guess as a researcher you actually become the more, the niche, the specialist in that area. Yeah. And it’s, you have to work, you know, where to take it. Yeah, I don’t know where it will take, where things will go. I mean, it was really nice to meet with these children and work outside with them and, you know, think about images of trees.
I think the UK,, we aren’t great at being outside. In Norway there’s a phrase that says, ‘There’s no such thing as bad weather, there’s just bad clothes.’ They have their very tiny kids outside all the time. They learn outside. It’s interesting, we’ve got a forest school in the school behind us here and they have lots of kids who can’t learn in a classroom, but they can learn outside. So, I wonder, you know, if you’re... Have you thought about working with forest schools?
Yeah, I think that would be another thing to do, another next step. Because that’s kind of, yeah, where my research has been into sort of forest schools and, you know, children spending too much time in front of screens, sitting at desks, not involved in that sort of free play outdoors.
I find it astonishing when you see people pushing kids around in pushchairs and they’re on a screen! Wow, how can your child not be experiencing the world in a first-hand way and you’ve basically given them a digital dummy to shut them up.
I think it’s where we’re going with screens and all of these sort of things and being so disconnected. And it goes through everything, doesn’t it? Through food and just everything connected. So yeah, I’d love to do more.
My project’s opposite in making people look at the screen in the fact that everyone has a phone and that’s, I’m assuming, going to be the portal where this research is going to be experienced. Because if you look at, I’ve just got a pregnancy pack here. I mean, it’s pretty dreadful as you have material that’s printed, reprinted, reprinted, reprinted.
You give it to someone and you struggle to read it, if English isn’t your second language, then you really can’t read or access it. But no, it’s interesting, isn’t it? Your research is that way and my research is the other opposite, which constitutes, please look at your screen so you understand this information.
But there’s a place for it obviously. Are you thinking about participatory activities?
Yes, I had a really interesting conversation with an academic but who is an SL on the midwifery course here at university and they were talking about the pressures on the NHS where and also the fact that so few people want to be midwives anymore because of pay being no incentive. So in lots of places they’re encouraging midwifery assistants to take on a much bigger role. She was saying this would be an ideal place for where this information lives. So potentially if the information has been agreed by the Royal College of Midwifery, potentially it could be delivered by someone who’s a level 4, a grade 4 healthcare professional, not perhaps a grade 5. Grade 5&6 HCP’s time are taken up with other things. So the midwifery assistant has more time and has a different connection in the fact that they’re not maybe seen as someone that’s so seniorly clinically trained.
So that’s really exciting, where would this research actually really matter?
So you’ve got 20 different tests at the beginning of a pregnancy, or about week 20, and some of the information on that is quite complex. My intention and what I want to achieve is for women to ask questions and to hopefully save the NHS time and cost, you know, in terms of wasted appointments, you know, and I think for anyone who’s had a medical experience where the consultant draws you a biro diagram of your insides, and from the conversations I’ve had with healthcare professionals, is- please don’t Google it if it’s anything medical.
So, I think the similarities in the research is like let’s try and make this world slightly better are completely on the same intentions aren’t they? Let’s get yeah better and healthier.
That’s so important. I feel so privileged to be given the opportunity to study as a grown-up. I think you should only be allowed to study when you’re over 35! I know from both our experience of teaching, where you work with students and think what do you do with your time? It’s so precious. So, I’m really looking forward to seeing you complete as you are at the latter stages of your PhD.
Thanks, I think, you know, the whole importance of why is illustration practice important in the fact that it does allow conversations, it does encourage people to understand the spaces that they’re in.
think it’s more democratic, isn’t it? And it has a... there’s an accessibility about illustration that maybe the other disciplines don’t quite have. It’s sort of a bit of a... a bit of a nomad, isn’t it? It’s a bit lost sometimes. And actually, that’s its sort of strength, in a way.
I think, like, shapeshifter, isn’t it? Illustration is an amazing sort of shapeshifter, you know, and especially in the way that it’s changed so much in the last, you know, 20, 15, 10, five years in terms of, you know, the potential of what these different practices are and different methods of how you reach the audiences that you’re intending to reach.
So, we’ve gone 20 minutes, Hannah. Lovely! we’ve waffled on for 20 minutes about illustration practice. There’s something in there that might be up to it
Exactly. I hope it’s then record button worked!
Visceral Bodies Symposium 27-28th April 2023

This two-day, transdisciplinary symposium will explore how renewed attention to the human (and specifically female) body in philosophy, politics, literature and psychosocial studies has paved the way for a rethinking of motherhood, reproductive loss, disability and death beyond biological categories. How does this reflection contribute to naming, elaborating, and making visible concrete aspects of human life in their connection to gender, race, sexuality?
“Pregnant women should not be so obviously deprived of their full capacity just because they enter the maternity ward.” Professor Stella Villarmea’s research brings together philosophers, lawyers and health workers and looks at how all are influenced by ageold stereotypes about childbirth, allowing violence in the labour ward to be considered normal.
“Unnecessary episiotomies or caesareans, vaginal examinations conducted without a woman’s consent – all are examples of routine violence in countries considered to have some of the best health systems in the world,” Her paper presented how women are not allowed the space and time to Trust their own bodies, in western medicine we are encouraged to use the opposite gravitational potential and to lie down to birth, being hurried along and scalded for ‘not progressing’ in the appropriate allotted timed birthing slot.’ Her work focusses on “Philosophy, which Plato called the ‘medicine of the soul’, can it use its scalpel to open up the theories and practices which still oppress and denigrate women’s bodies?”
Obviously, as my supervisor, I wanted Hannah’s presentation to be absolutely brilliant and it delivered everything I hoped for. Bold, funny poignant and breath holding. As she presented Goo:ga ll her second pregnancy overshadowed with the heart defect of her unborn baby. ‘Your baby’s heart is a water balloon and it’s gonna blow.’ I experienced Hannah’s presentation knowing her baby was fine, I was interested if any of the audience would ask if the baby was ok? and how the presentation is experienced if you weren’t are of a good outcome. The concept of ‘one body and two people- the doubling of the pregnant subject and split body.’ How we are in a temporal state whist carrying a child, a version of your past and a vessel for your future. A fantastic talk.
Anna Argirò, Between Private and Public: Reframing Maternity with Hannah Arendt
Argirò’s very quiet presentation presented her PhD inquiry which is focussed on the German born American historian and political philosopher Hannah Arendt. Maternity - the private and public sphere. How matrional labour sits within the unseen private sector of bodies, reproduction and ‘bodily necessities.’ This paper in the verbal presentation of it was quite difficult to follow. The importance of looking up and engaging with the audience is essential to keep them with you.
 Hannah Ballou
Hannah Ballou
Paul
In his 20 minute presentation Paul takes us on a very visceral journey of gay sexual hook up experiences, using shock frank language of fluids and the landscape of the bodies orifices, he certainly had everyone’s attention. He uses humour and frankness of vulnerability and expectation in delivery of one a poem written from experiences of gay male hook-up culture. They centre sex as a setting and practice to think about things like touch, clumsy translation, the pleasures and perils of inviting someone into your home, and hosting of the body. Certainly an educational presentation, my thoughts in response are, ‘it doesn’t sound very loving.’
Anna McFarlane, A Fantastic Voyage: Abortion, Child Loss and Science Fiction
McFarlane first talks about being stalked, a horrible experience which must completely derail you in trusting society. The hiding and shit made her body need to to protect itself so she became pregnant. A routine scan reveals that the baby will not be viable outside the womb. A 45 hour abortion ending in an emergence surgery to remove the placenta. A horrendous experience that she compares with the scene from Alien. The opposite is the saccharine imagery of muted coloured tops on pregnant women’s bulging bellies as they are cradled in the expectant mothers’ hands.
 Paschal, Poetry reading “Love to all lovers”
Paschal, Poetry reading “Love to all lovers”
Emma Mitchell, Let the Body Tell Her Tales: Fiction and Her story through Embodied and Experiential Writing Practice
Emma Mitchell vocalised the struggles she has accumulated along her life’s journey. She navigates her story around the lunar and menstrual cycle, and how she has ‘journey home’ to body after an extensive list of trauma and events which affect many women in their parallel lives. Mitchell presents a very colourful array of physical symptoms, post traumatic stress disorder, perimenopause, childhood trauma, separation and bodily presence. She talks candidly about her writing struggle in a global post pandemic environment. There is a lot of content in a twenty minute presentation.
Charlotte Warne Thomas, Tainted Love
Charlotte Warne Thomas screened a short video titled Tainted Love (2023), which followed edited shots of the production of gold shot on location at Baird & Co, the UK’s largest gold refinery. The film is juxtaposed with the text offering different definitions of love. It is ambiguous whether these shots are a sofa or a soft body that has housed a baby as a vessel. The film explores love’s value, the worth of gold and the worth of the work of domesticity and caring. The role that many women to undertake domestic care and parenting. Her presentation as part of her practice based PhD in Fine Art, which explores invisible labour, with a particular focus on the ‘motherload.’

Hannah Voegele, Your Body Belongs to You? Self-Ownership’s Troubles in Reproductive Struggles.
Hannah Voegele’s presentation examined the question of your body and its ownership. She begins with the rights of trans teens and the policing of age being able to transition from eighteen, to twenty one to twenty six- seemingly ridiculous. She continued to address how the medical care of the trans child is sexualised. How consent and the capability to make decisions is threatened if you are someone who is not considered to be ‘being at the improvement of the race.’ Lots to think about.
Kingston University’s catering for the event was very generous. Considering the price of a sandwich in the refectory, I think at least £1500 of pastries, sandwiches and refreshments went in this symposium.
The process of note-taking through drawing is integral to my practice as an illustrator. The illustrated notes are a visual prompt of the talks content, and the essence of it can be recounted and retained.
Visceral Bodies Conference.
Apart from six cups of tea, two tiny custard pastries, an odd beetroot wrap, and a decent feta salad, what did I learn from the conference?
“[T]he body in extremis – the body experiencing itself acutely as a body – is a human reality to which mothers cannot help but have access, although once again they are expected to put a lid on it, to make everything sweet and nice. They can, they must, love, hold, coddle their babies, but on condition of warding off the danger of any spillages – blood, guts, misery and lust. Their task is to prevent such intensities from going too far, to clean out the drains, on behalf of everyone. […] So how to tell the tales of love of and for mothers? Or, how to listen to the tales that mothers choose to tell?”
Jacqueline Rose, Mothers
Rose, J (2023) Visceral Bodies
https://visceralbodies.squarespace.com/ 12/5/23
This quote is the first page of the website for the conference. It is descriptive and accurate from my experience as a mother. It has the intention of what my project seeks to do. To articulate these experiences to others, to open a space where the conversation about the joyous, the dull, the crappy, and the overrated bits can be put out there without judgement. To be not afraid of being judged as you are ‘So lucky to have him/her/them.’ The talks were as on the tin all ‘Visceral.’ I have never been partial to a monologue regarding the practicalities and the experience of gay hook-up sex. As Paul Paschal quoted, the Clattern Lecture theatre was a space to hear, ‘What does it mean to relax when large instruments are being inserted into your anus?’ I’m guessing it’s probably quite difficult to relax in that scenario.
Where are the spaces where we hear other people’s lived experiences and stories? We feel safe and not judged in the places we work, socialise, and study. All speakers in this conference setting used their platforms to articulate their experiences. The themes that resonated with my area of research were the truths around the amount of free work women provide in the motherhood and domestic setting and how this country is particularly bad at not allowing mothers and fathers to have adequate paid time off to look after and enjoy their children. Hannah Ballou’s new project, ‘Shhh’, shows her taking her child to work as she performs to a live audience while trying to settle, soothe and keep a toddler asleep.
Shhh
1. Be an artist
2. Make it much harder by having a child
3. Turn all money you make gigging over to babysitters


4. Bitch about this ceaselessly
5. Commit to a date for the debut of a new performance
6. Do not book a babysitter for this date
7. Do not ask a partner, friend, or relative to look after your child
8. Bring your child to the theatre
9. Get them to go to sleep on their buggy between 30 and 5 minutes before you’re due on stage
10. Do this in a broom cupboard, conference room, or other unsuitable space
11. House lights down
12. Stage lights up
13. Roll your (hopefully) sleeping child on stage
14. Wait an uncomfortably long amount of time
15. Enter
16. Entertain
17. Don’t wake the baby
Ballou, H (2023) ‘Shhh’ 28/4/23
This performance has fantastic humour and a depressing reality, where the existence of juggling a child and a career more often falls to the mother. Charlotte Ware Thomas’ ‘Tainted Love’ presentation also focussed on the production of one of the most valued materials in the world and the production of creating and bringing a child into the world and raising them as a well-rounded human being- without having too much guilt.
“Combined with text offering different definitions of love, the video reflects upon love’s value, and hints at its role in persuading women to undertake domestic care and parenting. This will be linked to the wider context of her practice-based PhD in Fine Art, which explores invisible labour, with a particular focus on the ‘motherload’ – loosely defined as the additional emotional labour undertaken, principally by women, in managing a household and maintaining harmonious familial relationships. More broadly, the research seeks to establish a link between women’s’ unpaid domestic care work and the additional invisible labour undertaken by female artists in a male-dominated / market-oriented art world.”
Warne Thomas, C (2023)https://www.instagram.com/charlottewarnethomas/?hl=en
On the 15th of April, 2023, I had a Teams conversation with a Senior Lecturer of Midwifery at Kingston University. Suzanne Achillieos discussed the need to question how women feel able to ask questions about their choices in their labour and birth. She wants to promote dialogue with the women they work with. ‘Have you asked questions about why this is important at this stage?’ This conference also focussed on the need to ask questions about why decisions are made for and with us- especially in a time of vulnerability and transition.
Anna McFarlane, in her presentation, talked about the ‘truth’ of her abortion experience. She found the imagery associated with birth is all sugar-coated, pastel colours and not the reality of a visceral experience related to trauma and shame. She recommended reading the book ‘Phenomenology of Pregnancy.’ An academic text published by Sodertorn University Sweden.
Jonna Bornemark 2012 9789187843389
The conference had a keynote speaker Stella Villarmea, based in Madrid, Spain. Her areas of specialisation: Epistemology and Feminist Philosophy
Field of interest: Philosophy of Birth
Stella Villarmea is a Professor of Philosophy at the Complutense University of Madrid. She is currently researching the Philosophy of Birth, i.e., how our notions of childbirth reflect our view of the human being. She has worked in epistemology, philosophy of feminism, and metaphilosophy. She is interested in conceptual innovation, our beliefs’ moral and political justification, and the relationship between knowledge and emancipatory action. Until I saw Professor Villarmea talk, the philosophy of birth had completely been off my radar and is certainly an area that I want to explore within this project.
Complutense University of Madrid
e-mail: svillarm[at]ucm.es -https://ucm.academia.edu/StellaVillarmea

PhD meeting 2.
 John Miers and Geoff Grandfield in attendance. Bullet points of the meeting and what to take forward.
John Miers and Geoff Grandfield in attendance. Bullet points of the meeting and what to take forward.
*Looking at KMU’s Birth statistics as a foundation.
*Looking at what a doe a modern day ‘Godsip’ or female birth role model look like?
*Looking backward to plan what form this research take in the next academic year
As above- what is meaningful? To which groups of people using KMU’s services?

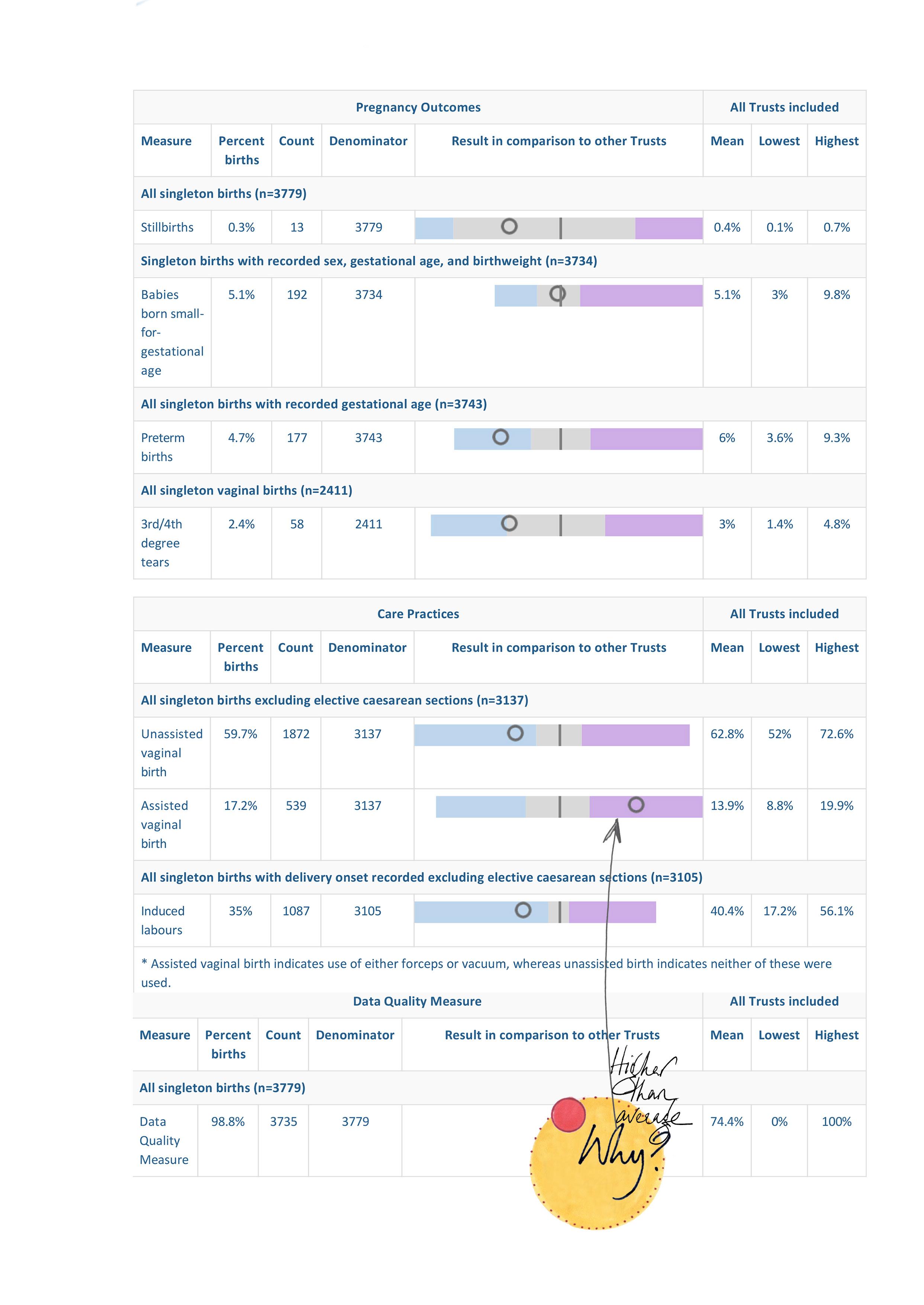
National Maternity and Perinatal Audit Rapid Quarterly Reporting: NHS hospital results

On the following page is the results for a Kingston Hospitals NHS Foundation NHS Hospital (Trust.) These can be compared to the national average and to other hospitals. You can select the hospital and the period you would like to see results for (either the most recent 12 months data are available for or the 12 months prior to that). If a result for your hospital is missing, this is because it did not pass our data quality checks.
The percentages of each measure are presented with the numerator (the number of patients who had the indicator) and the denominator (the number who could have had it). The national average (mean), highest, and lowest percentages are also presented for reference. Each result is also shown on a spine chart. This shows the result for the hospital compared to the national average and the expected range of results around that average. A percentage outside the expected range means there is statistical evidence (p<0.05) that the hospital’s result is different to the national average. This could be due to different clinical practices or differences in the patient case mix.
The site provides information on care practices to help interpretation of the maternity outcomes reported. For example, the percentage of third or fourth degree tears (an outcome) will be influenced by a hospital’s selection of patients for interventions such as assisted delivery (a care practice). However, it is important to note that there are no ‘correct’ values for care practices to take: a higher or lower than expected result does not indicate a hospital is better or worse than average.
I have an appointment with the Head of Improvement - Jon Grellier in the next few weeks to discuss how to better understand these results and to fully establish the demographic that Kingston Hospital serves. This will be helpful in establishing the specific communicative issues KMC have in ensuring that their families can get the best experience from this research project.
https://maternityaudit.org.uk/Audit/Charting/
NHS Maternity Survey 2021
- Benchmark Report
https://nhssurveys.org/wp-content/surveys/04-maternity/05-benchmarks-reports/2021/Kingston%20Hospital%20 NHS%20Foundation%20Trust.pdf
Births by parents’ country of birth, England and Wales: 2021
https://www.ons.gov.uk/peoplepopulationandcommunity/ birthsdeathsandmarriages/livebirths/bulletins/parentscountryofbirthenglandandwales/2021
Births by parents’ country of birth, England and Wales: 2021
Annual statistics on live births including, countries of birth for nonUK-born mothers and fathers.
* There were 624,828 live births in England and Wales in 2021, an increase of 1.8% from 613,936 in 2020, but still below the 2019 figure (640,370); 2021 remains in line with the long-term trend of decreasing live births seen before the coronavirus (COVID-19) pandemic.
* The total fertility rate (TFR) increased to 1.61 children per woman in 2021 from 1.58 in 2020; the first time TFR has risen since 2012.
* Fertility rates increased overall; however, younger age groups saw declining fertility rates while older age groups saw fertility rates increase.
* There were 2,597 stillbirths in 2021, an increase of 226 from 2020; this is similar to the 2,522 stillbirths in 2019.
* The stillbirth rate in 2021 increased to 4.1 stillbirths per 1,000 total births.
* In 2021, 28.8% of live births were to non-UK-born women; this is a decrease from 29.3% in 2020.
* The total fertility rate (TFR) increased for UK-born women to 1.54 children per woman; the TFR for non-UK-born women remained at 2.03 children per woman.
Live births and fertility rates
For the first time since 2015, the number of live births in England and Wales increased annually. In 2021, there were 624,828 live births, an increase of 1.8% compared with 2020 (613,936). However, the number of live births in 2021 is lower than the number of pre-coronavirus (COVID-19) births in 2019 and is in line with the long-term trend of decreasing live births.
The TFR for England and Wales in 2021 rose to 1.61 children per woman.
This is the first annual increase since 2012. The TFR is 1.9% higher than in 2020 (1.58), but 2.4% lower than in 2019.
The total fertility rate (TFR) is the average number of live children that a group of women would bear if they experienced the age-specific fertility rates of the calendar year throughout their childbearing lifespan. The rate provides a timely measure of fertility levels and can be affected by changes in the timing of childbirth, completed family size and the population structure.
Age-specific fertility rate (ASFR)
The number of live births to mothers of a particular age per 1,000 women of that age in the population. Useful for comparing fertility of women at different ages or women of the same age in different populations. The rates for women under 20 years and 40 years and over are based on the female population aged 15 to 19 years and 40 to 44 years respectively. Age-specific fertility rates for 1981 are based on a 10% sample because of the late submission of some birth registrations caused by a registrars’ strike. The population estimates used to calculate fertility rates from 1938 to 1980 are rounded to the nearest hundred and are therefore of a slightly lower level of accuracy than the fertility rates for 1981 onwards.
Stillbirths
There were 2,597 stillbirths in England and Wales in 2021. This is a 9.5% increase compared with 2020 and similar to the 2,522 stillbirths seen pre (COVID-19) in 2019. The stillbirth rate increased to 4.1 stillbirths per 1,000 total births in 2021, from 3.8 in 2020. This is higher than the pre-Covid (3.9 stillbirths per 1,000 total births) in 2019
*Stillbirth
A stillbirth is a baby born after 24 or more weeks completed gestation and which did not, at any time, breathe or show signs of life. On 1 October 1992 the Still- Birth (Definition) Act 1992. came into force, altering the definition of a stillbirth to 24 or more weeks completed gestation, The stillbirth rate is defined as the number of stillbirths per 1,000 live births and stillbirths.
Live births and fertility rates
For the first time since 2015, the number of live births in England and Wales increased annually. In 2021, there were 624,828 live births, an increase of 1.8% compared with 2020 (613,936). However, the number of live births in 2021 is lower than the number of pre-coronavirus (COVID-19) births in 2019 and is in line with the long-term trend of decreasing live births.
*Live birth
A baby showing signs of life at birth.


*BADASSMOTHERBIRTHER
Flor Cruz is an advocate for the normalisation of birth. She’s an American woman who works as a doula and runs birthing classes, a website full of information. Cruz hosts an enormously successful Instagram presence of 820 thousand followers. After her first disappointing birth experience of her child, a breech baby and a c-section, which she felt bullied into. She’s committed to spreading awareness and the normalisation of the birthing process. Within her online presence, she shares uncensored and raw images of birth: some photos and many videos from around the world. Cruz aims to advocate and allow women to understand that they have a choice in how they’re treated along the pregnancy journey and in the delivery setting.
Her website https://badassmotherbirther. com/ has a visual language akin to a tattoo parlour. She introduces herself as

‘DOULA+INFLUENCER+ADVOCATE’. Set out are the stories of her three very different experiences. In the disappointing C-section, the hospital VBAC and her home birth. In the third experience, she chose to have no interventions and no cervical checking for dilation. This birth story isn’t saccharin, and the baby has a shoulder dystopia- where a shoulder becomes stuck in the birth canal. Knowledgeable midwifery deals with this scenario, and her baby son is fine. She has no tearing and records the experience. ‘I want you to see and hear my story of my home birth, my 2nd VBAC, and how competent midwifery care can be. That emergency can be handled at home. That my team would have indeed called an ambulance and transferred me to a hospital if I or my son needed it. But we didn’t, and I’m beyond amazed by the expertise of my team.’ Her experiences have led to
her career working with midwifery professionals to host birthing classes on Zoom - so they can be attended anywhere in the world. She publishes images and stories of women showing empowering birth positions, which feel right and natural. Not feeling that you have to ask and have permission on positioning and choices in birth. America has the most significant baby mortality rate in the developed world and the highest ceasarean rates. Badassmotherbirther provides a space for women to compare stories, seek solace and feel advocated in seeing and normalising the seeing of women’s births. Interestingly, 60 per cent of the stories on her Instagram page are behind a censored ‘watch at your own peril’ warning. The one and only thing we all have in common is that we have all been born. Why does it remain such a taboo and uncomfortable subject? We simply don’t see births.

Interview with Angie Phillips
Hello Angie.
I’m having a conversation with Angie who I believe is 33 weeks?
Yes correct, and 2 days!
Oh - what a guess!
So you’re coming to the end of your pregnancy. I’m going to ask you the same questions, the first being. So how are you feeling?
Yeah, at the moment I’m feeling really positive and prepared. It’s definitely not a linear journey! There’s a sense of like, like the several hurdles of anxiety overcome and the fact that you can really see you’re growing day by day, baby movements are really strong now so there’s like that, I think where my main anxiety before was I felt baby movements quite late, I would say. Well, they say 16 to 24 weeks. And mine was definitely more like 24 weeks. Even though I knew on the 20-week scan that everything was fine it was just that that kind of and I don’t know if it’s me just being busy and I wasn’t feeling that connected to the baby I think I had this sort of protective mental state of having a bit of distance but then now everything seems really real and I got to know the baby’s movements and I feel like it’s happening. So it feels more real, so I feel like much more relaxed.
Yeah, and I guess this is all about, the stage I’m at now is all about just preparing physically like for my body, mind and the stuff and the house and making space for the baby in your life kind of thing.
How do you feel about the kind of care that you’ve had in terms of being looked after in whichever hospital you’re at?
I had a choice of St. Michael’s or Southmead where I’m located and I went with Southmead because they have a birth centre which is midwife led that currently It’s like a four-star hotel, very holistic care. That would have been a dream, but they aren’t open due to staff shortages.
In Bristol, Southmead, they have a midwife-led centre called Mendip Centre, which is lots of birthing pools, and then if I need to be transferred to, I’m just next next to a proper hospital. The transition is five minutes. That’s the reason I chose there.
In terms of my care, I’m really happy with it. I think I’ve had a consistent midwife up until maybe 30 weeks and then recently I’ve had some different ones but they’re all lovely. There’s something about a lovely midwife that just makes you feel calm and reassured. I’ve also been visited by a health visitor two weeks ago so I’ve been introduced to this person who’s going to come and see me after the baby’s born.
But yeah, so I’m happy with my care. There’s a few private things I’ve gone ahead and done. Cause I guess I’ve got the privilege of being able to and maybe I can’t afford it, but I can afford to spend the money on self care.
I am aware that a lot of people obviously wouldn’t. So, it’s less like in the second trimester, my pelvic girdle pain came on really quickly and I could have, instead of sort of raising it with my midwife, I decided to go see a private physio because I wanted to sort it off my own back and then just having a kind of reassurance and some exercises to do it was fine. The other kind of things I’m invested in is antenatal classes. I chose a more independent one than NCT and NHS one it’s called New Line and it’s really well put together midwife led. Great. And then the other thing is just like constant pregnancy yoga which has helped just educated me in terms of how as your body changes, labouring positions. And I think that’s helped me really accept my body changing and not, you know, there’s things you can’t do.
You have to change the way you move. The way you sleep.
Exactly, yeah. So, stuff like that, really. So yeah, I recognise that those things are a bit of a privilege that not a lot of everyone would be able to afford on top of life. So I think that needs to be taken into account. Like if I was just had the NHS, there’d be a bit of lack of understanding and maybe acceptance of the changes but I have to say yes I have been looked after really well.
That’s great. Do you feel pressured in any way like leading up to the birth in you know having to do it naturally or your perceptions of you know what potentially is meant to be a good birth experience?
I feel like there’s a lot of information out there now on social media. What are you looking at on social media? So, the Positive Birth Company, I guess it’s hypno-birthing course. I feel quite educated in terms of what will happen and how to sort of be open minded about labour but also expect to be prepared with a preference plan but be also prepared that anything could happen. I think that’s probably a really best way to approach that. Yeah it’s like I kind of see it like training for a marathon but you just don’t know what will happen on the day and all you can do and the only thing you can control. So try and stay relaxed but again, it’s like you don’t know, I don’t know how I’ll feel.
It’s a really interesting analogy, a marathon, because they say when you get to mile 20 you think, oh my god, I can’t do this and I’m going to give up.
I’ve had quite a lot of conversations with a gynae consultant, she said the marathon comparison is apt -the thing about getting you past that point so that then your body takes over.
Are you up for that 20 mile mark and are you welcoming interventions? Are you happy to have pain relief?
Yeah I think so. I think this is, I’ve changed my mind a bit. I think I was set out to be really like, I don’t want, I want it to be as natural as possible. But now I think I’ve got to a point where at the end of the day it’s not about So whatever happens-happens for the right reasons. And I think the hypno-birthing course sort of prepares you to the acronym ‘brain.’
So what does it stand for?
Benefits, risks, instinct, alternative and then nothing. So it’s like preparing yourself so you understand the risk and the benefit but being open to like what are the stats and what like are people panicking around me or is it the right thing for me and the baby? But yeah so I guess I’m really open-minded to what would happen and I think I could still have a really positive ceasarean and I could still have a really positive experience of epidural. Whereas I think a few months ago, I was more like, no, I really want to stay away from those things because they seem medicalised. Whereas now I’m just, yeah, I guess it’s like, it’s just so unknown and you don’t know what the position the baby’s gonna be in.
Do you feel like you’ve had loads of people just throwing advice at you all the time?
Yeah, I think I over the years I’ve definitely heard a lot of people’s birth stories and for me I actually think it’s only ever helped me understanding that more. Like for instance my friend just had- what she would describe as a really positive birth, but she had every intervention thrown at her, and that just because the longevity of the labour, every stage is very long, and but her her end experience is like I met my baby and the baby’s healthy. So that’s what I took away from that. Whereas other people, you know, they just want to share their trauma. But yeah, I’ve kind of seen it as a way of learning. But in the way like a athlete prepares Like kind of have to this is where I see it like I have to I have to just ignore everyone else’s experiences And just think mine is going to be my own yeah experience,
I believe every experience is different everyone. There’s no normal experience
It’s like you say you know if everyone ran a race There’s like you know are you
prepared for that.
Have you found that whole business about people touching you? Have you found that or do people not do that anymore?
Yeah I mean people I think people definitely are touching my belly but they’re like people close to me yeah and people do ask and I think because I’m just a sort of person that welcomes it in a way that’s like - I am quite proud of my belly. Yeah quite Like if someone asked me if no one’s asked me where I didn’t want it to happen basically that’s good Whereas it’s some people close to me have said can I touch your belly and I said yes, of course!
So I haven’t been in a position where I’ve had to feel uncomfortable.
I’m really proud of my body. It’s like, I actually feel more comfortable in my pregnant body than I do in my normal body.
That’s brilliant. Absolutely brilliant to hear. Because it’s such a thing, like, purposeful about having a belly. Yeah. And I like it. mean, it’s such an amazing thing, isn’t it?
That you’re one person, but you’re actually two people at the same time.
I loved being pregnant. I felt really empowered and felt really like, you know, I am Mother Earth,and this is probably the most important thing I’m ever going to do.
I think my struggles come later on when I’m tired. So, I think I’m just embracing it. Yeah, and be kind to your body,
Don’t try and like you know push it back into shape too quickly. I did that stupid thing of basically going on a diet which then meant that my milk dried up which was just stupid.
What’s your baby up to this weekend, do you know?
Oh, the apps?, yeah. At first I was really obsessed. Yeah. And then, now I haven’t been looking, but I have a look now.
Is your baby doing a crossword?
Ha ha, I don’t know. I know baby’s pushed down and into the pelvis and the kind of movement feels like a big bum moving across the tummy.
That’s quite weird isn’t it? It’s like alien. Yeah. Amazing.
Will you be open for a chat after you’ve had the baby or literally just before you go in?
Of course.
It’s such a privilege to be able to ask someone about their pregnancy as you’re living it.
Yeah of course, so on the app, the lanugo, yeah, is a hair isn’t it? By this time most of this lanugo body hair is gone.
The baby ingests that fine hair which is what the meconium black poo is when they come out.
Oh really? Yeah. That’s interesting.
They do this really weird tar-like poo, and that’s because they’ve ingested all of that hair.
Ah. And it can be ranging or black or brown. The immune system, your baby’s immune system is no longer relying on the antibodies from the placenta and the digestive system is fully working by itself your baby is peeing up to a pint of urine a day into the amniotic fluid.
Wow.
The app tells me it’s quite a hidden process, they help you visualise it, but now I’m kind of obviously pregnant, I think I’m relying on it less, like looking at it less.
So yeah, they are good though.
So you’re 33 weeks now. So would your baby’s due date be like July?
The 29th of June is my due date. But I think it’ll be early July. Yeah. If not before.
Well, feel free when I do ask you just to say no, if you’re too tired. But it would be lovely to speak to you just before and then maybe afterwards when you feel the way.
Oh, I got some really brilliant advice from a mid, from a doula. She said put every job in the house that you want done into a jar. Yeah, so walk the dog, clean the oven, fridge, make me a cup of tea, da da da. So that when you have the baby and people come round and they go, what can I do? And you won’t really want them to be picking up your baby and like putting germs all over it. And then you can give them a little job out of the jar.
Yeah. Without feeling guilty. People just want to hold the baby, but really, just like, could you do my washing up, please?
Yeah. Yeah. I mean, the whole reason I moved back to Bristol is to be near my mum.
That’s brilliant it sounds like your mum’s really hands-on.
Yeah, well she was a midwife, sorry, not a midwife, she was a health visitor. A nurse, health visitor. She’s been busy helping my sister with her three kids for ten years.
Now it’s your turn!
Yeah, she’s nagged, but she’s really good. Oh, that’s brilliant.
Well done for having a mum that’s on it. That’s great. And you’re... are you still working? Yeah, going to work into mid-June.
OK. Oh, thank you, Angie. We’re actually animating some films for Tommy’s charity
You’re living it!
So, yeah, they’re very understanding, we get it. That’s good.
Oh, thank you, Angie Have a lovely day. Thank you very much, it was nice to speak to you. And I’ll speak to you soon.
Take care. Bye then, bye.
Birth Stories
Reflection 14th May 2023
How can choice and confidence be promoted in the experience of birthing Mothers through Illustration Animation practice?
Visual narrative based on observational drawings will drive the research of one of humanity’s most critical time-based activities: giving birth.
“There is no such thing as a normal birth Natural birth is a myth, as all births likely have a different narrative.”
Emily McMorrowThe research aims to create a universal communication tool based on observational drawings. A tool that can be accessed on a phone that is free and accessible for everyone—supporting the use of translation with emphasis on images rather than words to avoid misunderstandings driven by fear, shyness and intimidation.
The birth experience is a highly personal, mostly private and, in most cases, physically painful experience. Based on conversations with people working at Kingston Hospital maternity unit, there is a great need for up-todate, clinically correct, visually engaging accessible Information for patients and their families. To develop visual tools to encourage Mothers to feel listened to on a journey that relies heavily on understanding key procedures to create dialogue and a bond of trust in one of life’s critical stages of being human.
Why now?
To generate visual information which creates awareness, engagement, interest and trust in the supporting medical team and patients.
To support, encourage and enhance dialogue between the medical team and patients.
In preparation to ease fear elements in individuals and pressure on NHS. There should be an emphasis on general knowledge transfer to create a more expansive knowledge pool to work against stigmatising or generalising that evolves around one of life’s most powerful times of being under physical and mental pressure. There is a need to be exposed to the truth of facts and shared experiences, personal stories make it less clinical, more approachable, more personal. To debunk that mystery of misconception of trendy interventions. Moreover, the fear of failure when it does not go ‘to plan.’
Why this?
Dry and outdated produced and re-produced data with limited visual references versus energetic, moving, empathetic, inclusive, visually culturally inclusive material visual-driven society, Instagram and TikTok generation. (When words do not do it.)
Why you?
Experienced illustrator animator, teaching practitioner working and researching at the pulse of time of testing and incorporating visual, technical and consumer development programmes and experimentations in a teaching environment.
Why a practice-based PHD?
One of the outstanding factors within this research lies in the processes of NHS medical support accessing more than one patient as it concerns mother & child or children in multiple births. There is a lot of ‘Information on the market, primarily written, often fragmented and not joined up.
There are no up-to-date enough, relevant, engaging and encouraging resources available that allow communication in preparation for a pregnancy journey when it runs ‘normal’ when the NHS is under enormous pressure. Building on NHS, ‘the Birth Plan’, with the staff at KMU, we are working with what is already available and exploring how to expand on the visual levels of essential information needed.
This journey will allow unique on-location in real-time research to be collated through observational drawings. Illustration animation practice will provide a space to create a helpful resource so stakeholders leave appointments feeling listened to and understand what lies ahead.
Considered and communicative illustration animation practice saves time to improve people’s understanding and prepare them for what might lie ahead. The themed can include general and specific health, exercise, eating and weight gain— the potential of the range of birth stories.
Considered and communicative illustration animation practice saves time to improve people’s understanding and prepare them for what might lie ahead.
The themed can include general and specific health, exercise, eating and weight gain—the potential of the range -of birth stories.
I have been looking at the normalisation of understanding, as generally, we do not see birth in everyday life—for example, @badassmotherbirther.
The research aims for the patients to process information away from the medical environment. Instead of googling keyword information, this project aims to support what is the most current and up-to-date visual Information at that point for mothers giving birth. The unique hand signature in the artist’s observational drawings will provide visual insights translating an approach that photographic documentary recording does not. Through observational drawing, the artist can edit, select, and focus on the importance and hierarchy of the content, narrative, or information.
Points to consider
*NHS ethics clearing needs to be approved and granted
*Sound recordings on location
*Developing animation practice and experience
*Adhering to midwiferies ‘gold standard of information’
- Royal College of Midwives
Timeline- I am on track with the schedule of six years part-time, achieving the proposal in June. The co-design element will be further down the line, with ethics clearance. The first year - or six months, in reality, it has been an experience of scoping, conversations and establishing the requirement for the research.

Selection of drawings from year one, Collections, previous visits to KMU, Birth Rites, and Baby Life Line Talks.


1.a-
My first year of practice-based research has led me to establish and examine the first year of my ‘outlined plan’ or methodology diagram. I have conducted various interviews with staff at KMU regarding their questions and concerns in communicating information about pregnancy. These have highlighted the need for visual resources:’ There is no such thing as a normal birth; every Birth is a story.’ I have attended the ‘Big Room,’ where recent birth experience cases are presented and discussed with the intention of continual improvement. My interviews with acquaintances currently experiencing pregnancy have been inciteful in the perception and anticipation of new mothers before the experience of birthing a baby. I will continue these conversations very near their due dates and postnatally. During this first year part-time, much of my focus has been on the literary review. (See attached bibliography.)
The media has provided many case studies, from treating mothers of colour and the statistics of injury and death: maternity payouts and the cumulative cost of obstetric litigation to the NHS—several maternity scandals across the UK and the Ockenden Report.
Within my illustration practice (IP), I have reviewed the retrospective work and interests that have resided in my practice for the last thirty years within the Birth Stories realm. I have explored the development of still imagery and drawn shapes in animating. I have been developing imagery from documentary experience into drawn animating.
I Presented the intention of my PhD to the SECAC 2022 Watershed Conference in Baltimore, USA. 28/10/22
The conference sought to foster intersections between art, art history, education, and social and environmental justice. Others received the presentation- mostly American Academics and visual practitioners- as informative and original, using illustration practice to convey the intention and content.
I have attended and visually documented the ‘Visceral Bodies’ conference. The speakers provided an inciteful view into other PhD students’ experiences and journeys. The specialist keynote speakers have provided a wider international pool of researchers in this specialist field.
The year has formed and focussed the research into the following questions.
*How can Illustration animation practice facilitate communication about the pregnancy and birth process so that those giving birth have a sense of preparation and empowerment- not vulnerable and scared?
*How can observation illustration create a less intimidating space than live-action filming or photography?
To support, encourage and enhance dialogue between the medical team and patients. In preparation to ease fear elements in individuals and pressure on NHS
1.b.-
As a .8 member of fractional staff and a year leader to a cohort of 90 plus Level 6 undergraduate students and an external illustration freelance practice, this year has left me feeling time-poor and frustrated. I am an organised facilitator of ‘getting things done’- however, the lack of depth of time I have to engage with my project feels enviable.
As a member of staff who uses Canvas to communicate, disseminate information and assess submitted work, I question why OSIS is the best way to submit in a smooth form. I have issues with uploading information - to have my supervisor check that I have done so as it is missing. This has been time-consuming at the pinch point of the academic year of assessment.
Highlights:
The support from my supervisory team has guided and shaped my focus, especially in terms of not over-promising what the scale of a project this size in this time frame can realistically achieve.
Presenting the proposal for the practice-based PhD at an international conference made me focus on the intention and question whether the purpose could be appropriate in other countries.
Research methods _Qualitative:
As a visual practitioner, I have kept abreast of my practice-based research in the form of ‘Illustrated Readers’ These take a publication form of 36 pages. The book form holds a visual representation of the creative and research journey. Interviews, diagrams, documentary references, articles, tutorials, drawings, and animation developments document and guide the reader through the journey.
Information seeking:
I have attended the PGR planned activities and sessions.
GR Induction: Faculty Welcome to new PGR students.
What Does a Thesis Look Like?
Research Tools: Search Engines and Archives
Publishing Workshop
Giving Conference Papers and Presentations Questions and Argument
Writing for Research (1): Abstracts and Audience Profiles and Career Planning
2.1. aKnowledge and intellectual abilities As a Senior Lecturer and Year leader, my extensive teaching experience demonstrates links between my research and real-world affairs. Students are encouraged and supervised to develop their Extended Practice Research projects around social issues and activism and to use their creative skills to bring to the fore challenging content that can be synthesised through illustration and animation processes. I educate and guide others in selecting and using research design, information and data collection management in their analysis of how they adopt appropriate creative methods and technical processes. I mentor new staff as our course grows and develops, both in educational approaches and subject expertise.
My intellectual insight, innovation and risk with my personal development this year as a PhD researcher, Senior Lecturer and Year Leader, enthusiasm, resilience, integrity, and self-confidence are necessary for managing a workload, people, curriculum development and initiating and maintaining subject relevance. I have high expectations of myself, the staff I work with and the cohort I lead.
Successful Illustration as a discipline requires analytical thinking and problem-solving. The context of where the work ‘lives’ is critical to those approaches; illustrators as designers have a heightened awareness of the audience, and a successful practice relies on whether the work communicates and clarifies the content. This year I have learned to take on board supervisor experience and commentary - if you are stating a project’s intent - you need to travel to that destiny and provide the evidence of the journey. Many illustrators are often ‘people pleasers,’ intending to use a project to ‘solve everything’ within the subject area.
2.1.b-
Personal Effectiveness
I position my investment in the subject through my experience as a mother, educator, illustrator animator practitioner. I am self-aware and self-critical, having a heightened awareness of my strengths and weaknesses. With all of my UG colleagues- we strive to make helpful illustration projects poignant and, most importantly -communicative. My L6 experience enables students to establish their research projects at the UG level. It allows articulating the ‘how and why’ that specific enquiry needs exploring and to which audiences. My PhD research is a continuation of my professional development as a domain within my appraisal process.
2.1.c-
Research governance and interpretation
Supervising the UG Level 6 final projects provides the opportunity to introduce students to the importance of ethics and the impact of their practice. I clearly understand the expectations and ensure
ethical principles are adhered to within my research environment. I implicate students and less experienced staff in the importance of IP and for them to challenge others who do not. I use a range of project management strategies to manage the strands of my employment and creative practice. Prioritising, planning, understanding and delivering expectations are critical for stability so that success can be achieved and built upon.
2.1.dEngagement, Influence and impact
I promote fairness and collegiality, regardless of status, the dialogue ideas and intentions of students are as relevant as staff and practitioners with numerous year of experience. We live in a society which proves changing and challenging. I have developed teaching practices which provide students with a voice for themselves and their peers, challenging the traditional form of ‘the crit.’ Develops skills as a mentor and uses own mentorship effectively. Encourages peers and less experienced researchers to present at conferences, I have published and written papers about my teaching and research. I have also with my CHS colleague promoting the relationship between students academic and studio practice.
2.2.
Are there any specific areas where you need development for skills
Ethics management and further academic writing were two sessions that I missed due to clashes with my academic timetable and the PGR sessions. I need to continue to work on the citing of sources using Zotero and Cite them right.
3.
Plan for next academic year
Schedule of Studies Part Time
Academic Year 2023-24
June 2023
Presenting ‘The Illustrated Reader’: a research documentation process
Session 4
at KSA PGR Festival of Research Symposium 2023
*Re- Interviewing
P. Halstead
A. Phillips
M. Tsakiri-Scanatovits
All one month to go
Completion reader Three
*Application for Ethics Clearance
July - Summer Break
August
*Re- Interviewing
P. Halstead
A. Phillips
M. Tsakiri-Scanatovits
All 4-6 weeks postnatal
SEPTEMBER 2023
Birth Rites Collective Summer School
Themes include:
How the collection informs and unpacks different perspectives in midwifery, medicine and education, and its potential to improve practice and policy.
Artistic and midwifery practices that address reproduction in the digital age including AI, simulation, VR, blockchain and NFT tech and, new reproductive technologies.
Changing perspectives on the non-binary and notions of kinship.
The Collection’s impact on feminist art practices and the rehabilitation of visual discourses of birth into art history.
Censorship of artworks on birth, institutional responses, ethics and the law.
October 2023
*Re- Interviewing
P. Halstead
A. Phillips
M. Tsakiri-Scanatovits 3 months postnatal
Design and production of Reader Four
October 2023- May2024
Continuation of Reading List/ Literary Review- focussing on academic titles including:
Chadwick, Rachelle (2018). Bodies That Birth Vitalizing Bith Politics Routledge ISBN 9781138123342
Dahlen, Hannah/ Kumar-Hazard, Bashi/ Schmied, Virginia (2020). Birthing Outside the System: The Canary in the Coal Mine Routledge ISBN 9780367506605
Kitzinger, Sheila (2006). Birth Crisis Routledge ISBN 0-415-37266-6
Penn Handwerker, W (2021). Births and Power: Social Change and the Politics of Reproduction Routledge ISBN 9780367163129
Marland, Hilary (1994). The Art of Midwifery: Early Modern Midwives in Europe Routledge ISBN 9780415116756
Mander, Rosemary/ Fleming, Valerie (2002). Failure to Progress, The Contraction of the Midwifery Profession Routledge ISBN 9780415235587
January2024
Design and production of Reader Four
March 2024
Sharing visual tests with Kingston MU and Royal Free MU
Feedback loop
April 2024
Writing up the narrative and findings of this year.
Production of Reader six
May 2024
IMR.
November 2023
Development of questionnaires for pregnant participants for NCT Group
November 2023 February 2024
Drawing for Animation Completion of animated tests Blood test animation Pregnancy animation
The ‘Illustrated Reader’: a research documentation process.

Abstract:
How do you organise and present your research in a way that might be accessible and useful to another researcher by establishing and collating the content that best compliments and summarises the findings? As an illustrator and creative practitioner, putting together the research’s influences, discoveries, and stories in a way that feels intuitive and visually led has enabled the content to be shared and accessed in an immediate and user-friendly form.
As a PhD researcher, choosing a method of organising using editing, design and art direction has made the narrative of the year clear to me as the researcher, alongside as a tool to communicate with other stakeholders in the project. The publications have been a tool to communicate to other stakeholders in the project. It has been a space to test illustration and animation research methods and to keep abreast of PGR training, interviews, reflection, tutorials and events unfolding in the media.
This methodology has been developed from my teaching practice in Level 6 where students are encouraged to visualise the content of their academic practice - their dissertation. How can their creative abilities allow parties, peers, staff and the wider public access to their written research and findings.
The readers allow me to organise, structure and make links to the strands of the enquiry. The form is informal in 32 page ‘bite-sized’ magazines. The printed and published form has enabled me to move on to the next phase and most importantly to be able to look back, to make the subsequent progression. I hope that this form will be particularly helpful at the writing up and dissertation latter stages of the project.


Hello Geoff, so you and John be used to these forms.
I’ve seen them since 2015, you know.
Great- that will be very helpful
They don’t have to be particularly lengthy.
I’ve populated most of it, but I’ve just got it in one form. So what would be fantastic is to just clarify what that bit is, what that bit is, what that bit is, and then I can go back through it and edit it back again.
John is joining us in a moment- what you do in 1A is bring up several that could be considered aims or particular phrases. If I were you, I’d be careful about how many you introduce at this stage or the ones who do get in there.
You say these are the ones you’re focused on now because of you. Hence, you talk about a visual narrative based on observational drawing now that in itself as a research topic is enormous because you’ve got, you know, the twin disciplines of what is a visual narrative and what is observational drawing. So those two territories are immense in their own right.
Then you do a universal communication tool. Well, that is, it’s a nice phrase, isn’t it, but it’s again it’s a bloody massive subject. What is universal? A lot of visual communication is culturally specific, and it’s being coded by culture, so that must be handled carefully.
You talk about the misunderstanding, fear, shyness, and intimidation that come in; those are all amazing but also complex emotional elements, aren’t they? So, do you want me to go on as you go?
Yes, please.
Is it useful? So you then talk about a phone base. Now that, as you know, we know it’s like there’s loads of complexity in that in terms of how big an image can be if you’re going to view it through your phone, how much detail, so the scaling of the imagery becomes a research question, what is going to work if someone’s holding a phone.
Then you talk about visually engaging, well again, as a phrase, it’s compelling, but what does it mean? Do you know what it is? I think this is one of the critical things that you’re going to be examining is this is the is like the spaces between what is visually informative and what is visually engaging, because there is this kind of thing that if it’s just diagrammatic, then it’s not emotional, it doesn’t have a sort of a load into it does it, and you refer to the thing about how your practice is about making something that appeals to the eye you know it’s like something that people engage with?
There’s a question there, and as I say, you don’t have to do all this. I mean, this is just like, but every time you include a particular topic at this stage of your inquiry, you’ve got to be absolutely careful you don’t include topics and then don’t demonstrate that you’ve, you know, looked at that so you might want to take some of that stuff out. So in your experience, as you know, you’ve seen several projects through what it sounds. The last one you just talked about is about visual information that engages through it, not feeling cold.
Is this the thing that I need to focus on?
Absolutely. Is there an emotionally reassuring because you are identifying particular characteristics that you want to bring to this?
Still, one is clarity, but one is like demystification; one is saving time, and one is joining up the current fragmented nature of the existing visual forms that might be encountered.
You’ve got to be careful about using the universal because it’s too massive to think you’re going to. I think you want to bring it down to NHS and current materials because even that is probably a pretty massive thing to evaluate what is currently out there, take a look at what does work, what doesn’t work, and why doesn’t it work and do questionnaires or something for people to try, because you comment on it and say it’s dry and outdated, but what’s the evidence for that? Another person could say what you call dry is very clear, so it’s like halves to an outdated again. What does that mean it’s like this thing about up-to-date is that because we now have more sophisticated imaging devices for what goes on inside the body or can the more sophisticated scanning, CAT scan, all that stuff, be able to generate so much information, it becomes less clear about what you’re looking at. This is precisely where, as you described, like the hand of an artist, it’s like somebody who can select and prioritise the information rather than throw everything at somebody.
Absolutely, and that is entirely the intention of the project and the research.
So, Hello John- Geoff’s been helpful in just talking about some of the aims that I’ve been talking about are enormous and bringing those down into what is tangible and manageable in a six-year project at illustration language and how it’s perceived through diagrammatic processes but also the hand of the artist and how we understand an image or a moving image where it’s not. Did you see in the third reader, I was lookng at the work of that lady called, uh, ‘@badassmotherbirther’? So, looking at her- content’s terrific. She’s got an enormous following and calling to get to her classes. I was drawing her content. So on Instagram, you’ve got provocative content,-explicit content, in some instances
deemed as ‘pornographic’ context. It shows how, and I think what was interesting from looking at all the work and several different people is that we’re not used to seeing anyone give birth. If someone’s got a dog that has puppies in the house, that’s very exciting, but still, it’s a bit ‘ewww’ and surprising. We grow up in a culture where we don’t ever see that.
Well, that might well be a contributing factor. I mean, you talk about the kind of shyness or the fear and things like that,
In 1a, which is the progress that made section, and then a couple of other bits, but basically, Jane-as yet has not tackled two yet 2.1, which is the four domains knowledge and intellectual ability personal effectiveness research governance and organisation and engagement interest impact. So what all I was doing was advising that the scope and range in 1a as it can you access it in essence.
If monitoring reports Committee date on the 5th of July. This is what I need to be looking at. So you’ve got until the 31st of May. Right. But for you, for John, for you to review this. Yeah. And then open it for others, for Hannah and then for me, and it goes in that kind of linear thing. This is not good or bad, but this is how they do it here. So the progress you made during the year is that you put a lot of speculative things in here which are essential for you and what you’re doing, but they’re about something other than the progress. The progress all it needs to be is like. What did you do in the last year?
Really OK, well the progress, I assume the progress is all in the readers that I’ve done that shows what I’ve been doing. I can put that into words.
I wouldn’t elaborate any more than you need to. It can be shorter than what you’ve done. It is just describing what you’ve done this year. OK, what is one ‘B’? Is as if you know any difficulty one ‘C’ has any positive features? If I were you, I’d be put the development of the readers in there or something to say that that’s your strategy of dealing with this thing as a practice-based researcher rather than an academic researcher. You’ve got your conference in there. 1E, any ethical issues have arisen. You have had discussions with the ethics people. So it’s a good idea to give a little commentary on, if you like, you can call it the tension or the friction or whatever because you’ve had some people ask....
The head of ethics at Kingston said why do you want to scare these women?
I wouldn’t go journalistic on it, but you just described what’s been happening. When we get to two, you start discussing the knowledge, like what you’ve learned. In B, how well have you? Now I might get this wrong, so John, please correct me, but
personal effectiveness is how well you have managed to negotiate and handle the research you’ve conducted and how you’ve negotiated that. Research governance and organisation is very much about how you’ve taken what you’ve discovered and started to organise it in a form you will use as a basis for the next stage of the plan.
As far as I understand, the engagement, influence and impact are whether you have actually shared, so in that case, it would be the conference, and you wouldn’t need to put the description in there because you’ve already described it. I would suggest the response or the discussions you had when you were at the conference that would be a good place for that, and then yes, specific areas and particular skills again if you say, well, you know I’ve never done this before, so that’s the place to sound kind of well actually it’d be constructive for me to have something in that particular field.
Gosh, no, that sounded right to me, Geoff. It is one thing. Can you go if we can go back to? I mean overall, you know, overall this is about documenting what you’ve done and, you know, I take, I tell you’re correct to say that yes you have covered that in the reader, but of course, you know, we’re dealing with a formal university process here. So, as we are familiar with, it’s got to be put into the particular set of boxes they want it put into.
So, yeah, we’ve covered that. So that information does need to be extracted from the reader. But it was worth saying that, so we’re looking at this page at the top; it’s researcher development, not just research development. So it does; it frames it in terms of research skills training.
So how you’ve developed your research skills during the past year, and what training you’ve undertaken? So in each of these domains, let’s say in engagement, influence and impact. I mean engagement with relevant scholarly communities you had through your experience of presenting in Baltimore. Still, also you know if you’ve been to any search training.
I have, reporting as a postgraduate researcher.
This needs to go as a standard format to a panel looking at around 150 of these across two or three days.
Okay, thanks so much both of you. Tha’ts very inciteful. I know Hannah is going to add some thoughts as she isn’t here.
JW- blue
GG -black
JM- red
Tutorial date 4pm Tuesday 23/5/23
Feedback from Hannah 24/5/23
1. I may only take on illustration PhD students after the luxurious reading experience you’re giving me, Jane!
2. Joking aside, it is so interesting to see how you collate and understand and ultimately manifest some form of embodied knowledge about the ‘practice-review’ by drawing all the the votive figures and models etc. This raises a methodological question for me; does drawing these models (as opposed to simply looking at them) inform your own designs? Why (and how?) or why not? To give an example from a different discipline while I amass an enormous practitioner-framework in my own research (i.e. watching performances) very rarely would I re-perform the work, though of course it influences my own practice. Is this a standard method in illustration practice research?
3. I laughed when you noted that the maternity unit in Surrey bought your Soft Pregnancy (1997) as a piece of hospital art instead of their intended use as communicative tools. Then I realised that depending on where they are displayed, they might be doing their job after all; we do spend A LOT of time in those waiting rooms. Perhaps blurring lines between aesthetics and functionality.
4. When you and Phoebe are discussing the birth plan as a design challenge, that made me wonder (and forgive me if we’ve already discussed this) whether an illustration tool for articulating the plan (or ‘preferences’ as we all know them to be) is something that would be one of the outcomes? Using the same visual language that you use for communicating the clinical information? Unbelievably some hospitals still make pregnant women haul around an enormous folder of notes to each appointment, and if I recall correctly, the ‘preferences’ are just notes jotted down by a rushed midwife. Last time we talked I remember discussing the enormous scope of the gestation and birth experience and you note the necessity of narrowing down the ‘key stages’ and ‘specialist stages’ that will be the focus of the practice. Has the birth plan/preferences fallen within that? Again, apologies if I’m behind on this.
5. How did you go about designing your questions for your interview with Phoebe, and is there anything that you would have added or changed upon reflection?
6. That ‘cost of harm’ graph is incredibly grim.
7. I was struck by the inclusion of the pregnancy dolls in the misemono popular entertainment in 19th century Japan. Women’s reproductive physiology seems to reside in a ‘need to know’ category in contemporary Western culture.
Hello Kate, It is lovely to see you after so much time. Can we start with what is your experience of women’s health care? You’ve got tons of experience, so let’s start there.
So, I am Katherine Gale, a nurse for 30 years, I have always worked in women’s health, and passionate about helping women to understand their bodies, know what’s going on in regards to how they can advocate for their health and make an informed choice about what’s right for them has been something that’s always been a priority for me. And so I’ve worked in different specialities. I’ve worked on the gynae ward, so that would be operations, hysterectomies, let’s say, and the decision whether to have a hysterectomy. Then I worked in early pregnancy, and again, it was decisions around care For example, if it was a miscarriage, whether they wanted to have different treatment options, so whether it was to have a general anaesthetic or whether to have medication or to have what we call conservative management - which is no treatment at all, we watch and wait and support them as best we can. And then into abnormal bleeding, so quite a lot to do with postmenopausal bleeding ladies and interpreting the ultrasound scan and talking to them about whether they want to have their marina coiled or changing their HR. So it’s always been about my value of radical simplicity. It’s taking complex things and helping them to understand it. Because I might have all the knowledge, but I don’t know what’s best for them. So we always start from a place of trying to get them to understand what’s ‘normal,’ what’s not, what the options are, what the advantages and disadvantages are, and then respect their decision. That’s the background.
Fantastic - do you use much visual material in your field? There’s a lot of traditional; for example, you go into a consultant’s room, and there’s a kind of medical illustration on the wall, or there might be a model of a pelvis or something like that. What kind of visual material do you use, if any?
So there was a picture book that I always found quite helpful. And things have yet to move on from there, so it was diagrams, all in a book; all the different procedures were in there. Its a medical text, so quite dry - called Patient Pictures: Gynaecology
Illustrated by Dee McLean.
ISBN: 1899541101. When I started working with adolescents, I had many adolescents or young women coming in and talking about their abnormal vulva. And so I started using some picture illustrations, all the different types of what’s a normal vulva
because it usually’s always ‘normal.’ We used to get mums to come in and say my daughter’s vulva Is abnormal. And it might be different to hers, but it didn’t mean it was abnormal. And so we often used pictures to show how we’re all different. And that’s probably the only time I’ve ever used any illustrations or anything like that.
Where do you think kind of illustration animation could be helpful or could sit in that kind of gap between, as you said, you’ve got a lot of highly complex knowledge that you’re trying to put in a manageable format, which is probably I’m assuming your appointments always very time Based you know where you work in a larger organisation - which I assume is all time-based. We’re dealing with pregnancy menstrual cycles, even in terms of you as a woman. It’s all time-based.
You’re absolutely right, and the other thing is we’ve got to consider giving people a tremendous amount of information in a short time while there’s emotion to how much we have spoken. We then give them loads of leaflets that rely on their above-average reading age and use scientific words we often need to define or explain. So I know that in our organisation, particularly for obstetrics, they’ve been putting information on an app, so women have that. But again, it relies on above-average reading aid and comprehending what’s there and then interpreting it from your point of view.
What would you like to see? What would be useful?
Women’s voices are compelling, so I would love to have people’s stories before people’s decisions. People relate to it more than they do with a leaflet. So I’d like to see us reusing more visuals before they come in to decide if we possibly can because I think then the emotions flow, they might be able to have access to that in their own time, they might be able to browse through something, it might then be I’ve come in and asked questions, or I didn’t understand what was said about this. Whereas we put it the other way round, we often give people information and send them away.
That’s fascinating, Kate, because this project came from me asking to draw after drawing an elective C-section for a lady who had placenta previa; I then said about not drawing a normal birth, and the midwife laughed and said there’s no such thing as a ‘normal’ birth Jane, every birth is a story and that’s where the premise for the whole project.
I’ve been reading a lot about how, within a Western culture in the medicalisation of female health, we rely less on other women historically. So the women that would be around your delivery were called. Initially, they were named ‘godsips,’ where the word ‘gossips’ comes from, because they chat about the weather and the lady down the road what you are up to.
So they’d be there to cajole and to take the woman’s mind off the pain. When we talk to other women about experiences- on the whole, we try not to catastrophise an experience. You feel like there’s no way you could say that to someone who hasn’t gone through that experience, the reality of it.
Today- a lovely friend of mine sent me a picture of her week-old baby. She went entirely off-grid for two weeks but had a six-day early labour and then a C-section. I’ve just been reading her birth intentions in a previous interview before she had her baby. I would never in a million years say her experience may not align with that. I’m so relieved that she’s OK; the baby’s gorgeous. She just said it was just a complete roller coaster. Her pre-birth intention was to have a hypno-birthing experience in a pool. How do we put these narrative parts together so that they don’t...
What was the term you said about the catastrophising?
Yes, we don’t want to catastrophise, and we don’t want to instil fear. There’s so much fear in how women are presented and understand their bodies. You’ll have some people who will always think about the worst-case scenario. And then you will always have other people who think it will all be a-okay. And there’s a whole range in between where you are. And so it’s, that’s the important thing.
So it’s a spectrum, isn’t it?
We talk about risk a lot, such as early labour or needing a caesarean section. Struggle with the concept of risk because it depends where their mindset and actually for them to interpret; one person might say, oh my goodness, that’s such a high risk; I definitely would like to have a cesarean section because I wouldn’t want to have an emergency cesarean section, whereas the other person would automatically think they will not need an emergency section. Do you know what I mean? It’s a number, but our interpretation can be wholly different.
It depends on our mindset and how we view information. For example, a map is designed to help you get from A to B, but is a map more helpful if you have a shit sense of direction? Or if you are confident in where you are going? It’s how you interpret that language, whether it be auditory, whether it be narratives or visual.
I definitely, in my menopause work, we quite often use, ‘one in ten people have endometriosis, for example, or, you know, 27 out of a thousand women will get breast cancer.’ It’s a diagram of people, like the boxes, don’t you, a hundred people. But even that, people have different reactions to it. It’s essential that we provide information in lots of different ways. It takes a long time for things to sink in as well. That’s where the power of a picture can say a thousand words, can’t they?
That is the correct term. And I’m hoping to do this project because I had a Norwegian friend who gave birth at Kingston, and because English wasn’t her, she speaks better English than I do. And because English wasn’t her first language, she was poorly treated - not listened to because she was deemed a non-native speaker. And yes, so if you can’t speak excellent English and English isn’t your second language, again, you’re talking about this additional layer of medicalised language that, you know, you work with, if you were explaining to me what you have just been looking at with bloods, that would be complex to me- but in your clinical knowledge it would be like you talking about going down the road and buying a, I don’t know, a Mars bar. It’s entirely different for someone who doesn’t understand that language.
You’re right; when people speak a different language, they convert it in their brains. There are often no words or equivalent words in their language, making it even more difficult.
That’s an excellent point because very few, well, no languages translate directly. They’re all a variant of, aren’t they? And also when you’re talking to people who, you know, you’re perceived with, they’ve kind of, you know, they’ve got that expertise, often your brain does something where you miss that, don’t you? Because you’re so busy trying to understand it, we always encourage people to make notes and decide their intention for this appointment when you leave. But yes, it’s that. And you are then having a selective memory of that experience as well.
I think there’s also, you know, the impact of trauma as well, and previous trauma would change how you interact probably with somebody who you might empower or, you know, saying no to a procedure. So it’s important you take all that into account as well. I think that’s where my personal stories come in because it’s like we think it’s black and white, but how somebody can interpret it through their own lens on what they’ve experienced in the past, what maybe you know siblings or friends have been through. And we sugarcoat many things because we’re afraid of frightening somebody else. And it’s not to scare anyone, but we also have a responsibility, to be honest.
Have you seen there’s an Instagram called Badass Mother Birther? The content comes with a warning as if you’re about to see someone horrific. She shows many different births from around the world and, with the whole thing, that the more you see something, the more normal it is. We live in a clinical world where we don’t see people giving birth. So then it’s not normal to see. I would like to see your thoughts on her account.
Fascinating; you’re right. There’s desensitisation, isn’t there? The more we see something, the more normalised it is if
think about it. There are still people who will be triggered by it, for examplebreastfeeding in public; thankfully, we see more of that now. It will still trigger some people, though. If you see lots of births, some will trigger some people and not others, and It’ll be helpful to see more births. So I, one born every minute, watched that quite a lot before having my child, and once I had my own birth experience, I wasn’t interested.
It’s interesting. I’ve been watching all those back, and so many programs exist. There are just loads and loads and loads from the Yorkshire Home Birth Team to Teen Mom UK! There is an appetite out there because they won’t make those programs if they do not sell them to different franchises, are they? The Merino Coil sponsored Teen Mom show.
So it was all sponsored by the pharma, which is just mindblowing. At the end of the season, they would be asked how they managed not to get pregnant. The reply was, ‘I’m on the merino coil.’ And then, yeah, and then the credits were like, this is sponsored by whatever big pharma brand makes it. Before my hysterectomy, I had this female consultant who insisted that I had to have it, and I was adamant that I did not want it. I’ve been sterilised-I don’t want any more hormones. The lovely nurses look at me like, look, love, and you won’t go without it. And she did it, and I was outraged that she didn’t listen and cornered me into it. Then, nine days later, it came out, and I woke up in a pool of blood. I’m relatively outspoken, and I’m not a complete fool. How can I have not been allowed to say no when this woman’s got her hand inside my uterus?
I think that that’s right. I think we diminish women’s opinions about things, you know, that’s happened for many years. That’s sort of like, ‘oh well, it’s normal to have pain when you have your period,’ but it’s not normal to faint. It depends on that person’s experience; we seem to diminish pain without explaining why. For example, you can’t have an epidural because you’re already 10 centimetres dilated, but what could have happened beforehand? You know, leading up to that point, if she was struggling with pain, now you’re saying no. So I think there’s something around our judgment of other people’s pain, the amount they’re bleeding, or the impact on their quality of life. It will be different for everybody.
You’ve got a brilliant network of people, haven’t you, that you would have worked with and around for years; the more I become invested in this project. I need to get this ethics clearance sorted, but are there people you know who are clinical/ medical practitioners but have invested in seeing the value of image-making as a toolkit to bridge communication gaps through visual materials? Who would be the relevant people/ teams/organisations to talk to?
I don’t expect you to answer that now, but if you have a little think, that’d be great.
Yes, and I feel so passionate about it. It’s about ethics and maternity; is that what you’re thinking?
Yeah, it’s very much about, because otherwise, it would be too massive, but yeah, especially about, you know, so whether it’s about when are the timings good for that, is it when you’re trying to explain to someone about different behaviours, is it about you’re about the different methods, even the different stages of birth and labour? Or is it a kind of, almost like, a podcast of different women talking that’s got, you know, or, you know, so, yeah, is it something that’s animated to other people’s voices? Yeah, or is it much more of a kind of your healthcare provider goes, you’re going to have this, look at this little film, and that will explain exactly what you need to do before that procedure. So don’t chew gum before a gestational diabetes appointment; don’t have coca pops and sugar before you have a general pee stick test. So just those behaviours or, and I was talking to a friend of mine who’s a midwife, and she said quite often, you know, babies will have like, you know, hernias and stuff like that, and it’s like, OK, this is what it is, and this is what we’re going to do.
Yes, and quite often, they’re found out quite early on either between, usually around 20 or 20 weeks back. Yeah, there’s a lot of time there’s a whole 20 weeks before birth, and what can we do to help? And also that whole thing about so people don’t Google.
You know, so I think what I, I intend that the information is entirely supported by health professionals but put in a way where it can go across language, it can be kind of, actually if you look at this, this will kind of, reiterate what we’re talking about. Yeah. Or show this is how we’re going to move a baby around. And this is how a baby has to go over that bit, which is the painful bit, the transitional bit, and then you’re on the other side.
I love that. OK, yeah, I’ll reach out.
I’m also so invested in your project on how HRT is the most fantastic invention ever. But think about what I could do for you with a skill set that I’ve got to help you with, and I don’t know, whether it’s something to do with a campaign or something that, you know, yeah.
Yeah, because I’m currently doing this campaign, which is the hashtag is menopause countdown. One is going to be focused on the 18th of October is Menopause Day. I can count down to that. I’m going to use the campaign afterwards. I want that we are all on a countdown to menopause at some point. If we can get ahead of that, educating so that it’s not a shock, it’s not a surprise.
And it’s not an embarrassment, either. And you’re treated like suddenly you’ve just gone off. You’re like some old stale egg that’s just gone off. There’s something around that, but also I know the big lifetime decisions people make around this time.
You’ve often got teenagers where you go. It’s OK for a teenager to behave in a kind of bonkers way because it’s all about their hormones. And then you’ve got these two people having a hormone crisis, quite often in the same house, under the same roof.
One’s tolerated, one’s not. One’s seen to be some miserable, you know, yes, again, Miserable or moaning, and you know the whole unpleasantness of like your skin itching and all those different things. Yes, so having a GP that is is kind. I’ve got many friends who have been back and forwards because their GPs may not have as far as they have gone on that course or aren’t female. There are not many photos or imaging of menopause. It’s all like, if you type it in when I’m looking for marketing pictures, it’s all going to be grey hair, lots of wrinkles, probably, you know, put a bit of weight on.
Yeah, and also what I’ve achieved in my life so far, and also the fact that I’ve got an established skill set that could be useful for da-da-da-da-da, the same with everyone. There are many things, but yeah, even women’s bodies, if we look in the diagrams in textbooks and the shape of a woman, you know and then the anatomy. But there are no black bodies, you know and also the fact that there are not enough black bodies. So that’s what I want you to look at, that badass mother-birther. I’m going to start thinking about imagery that’s positive for menopause. Yes, that would be good. We think menopause is midlife, and actually, there are a whole lot of younger women, 20 under 30 and older. I’m happy if you want to send me some questions about the readers. Or do you want me to talk about what I think about them in audio? Would that be good? I will see you soon. Thanks Kate
See you soon Jane
Year One Bibliography: 2022-23
Kata, Helen (2015). Creative Research Methods In the social sciencesA practical guide Policy Press ISBN 978-1-44731-627-5
Agarwal, Pragya (2021). (M) otherhood
On the choice of being a woman
Cannon Gate ISBN 978-1-83885-321-1
Baraitser, Lisa (2009). Maternal Encounters. The Ethics of Interruption
Routledge ISBN 978-0-415-45501-5
Cleghorn, Elinor (2020). Unwell Women A Journey through Medicine and Myth in a Man-Made World Orion ISBN 978-1-4746-1687-4
Criado Perez, Caroline (2019). Invisible Women
Exposing Data Bias in a World Designed for Men
Penguin, RH ISBN 978-1- 784-70628-9
Cusk, Rachel (2001). A Life’s Work, on becoming a mother.
ISBN 1- 84115-487-3
Dockrill, Laura (2020). What Have I Done? Motherhood Mental Illness and Me
Penguin, Random House ISBN 978-15291125-42
Donath, Orna (2017). Regretting Motherhood: A Study. North Atlantic Books
ISBN 978-1-62317-137-7
Douglas, Susan J. (2004). The Mommy Myth
The Idealization of Motherhood and How it has Undermined Women
Free Press ISBN 0-7432-5999-8
Enright, Anne (2004). Making Babies Stumbling into Motherhood
Vintage
ISBN 978-0-099--43762-8
Embury, Gary Minichiello, Mario (2019). Reportage Illustration
Visual Journalism
Bloomsbury ISBN 978-1-4742-2459-8
Evans, Kate (2014). Bump How to make, grow and birth a baby
Myriad Editions ISBN 978-1-908434-35-7
Gannon, Rachel Fauchon, Mireille (2021). Illustration research Methods
Bloomsbury ISBN 978-1-350-05143-0
Glasner, Eliane (2021).
Motherhood: A Manifesto
4th Estate ISBN 978-0-00-831188-9
Gray, Carole Mallis, Julian (2004) Visualizing Research
A guide to the research process in Art and Design
Ashgate ISBN 0-7546-3577-5
Hogenboom, Melissa (2021). The Motherhood Complex
The Story of our changing selves
ISBN 978-0-349-42657-0
Kitzinger, Sheila (2006). Birth Crisis Routledge ISBN 0-415-37266-6
Kitzinger, Sheila (2000). Rediscovering Birth. Pinter & Martin ISBN 978-1-905177-38-7
Kitzinger, Sheila (2004). The New Experience of Childbirth. Orion ISBN 0-75286-137-9
Kitzinger, Sheila (1989). Giving Birth, How it Really Feels. Victor Gollancz ISBN 0-575-04110
Kitzinger, Sheila (1992). Ourselves as Mothers. Bantam Books ISBN 0-553-40549-7
Knisley, Lucy (2019). Kid Gloves Nine-Months of careful chaos :01 First Second ISBN 978-1-62672-808-0
Levy, Marianne (2022). Don’t Forget To Scream Unspoken Truths about Motherhood Phoenix ISBN 978-1-4746-2365-0
Lynch, Claire (2021). Small on Motherhood brazen ISBN 978-1-914240-05-8
Nelson, Robin (2013). Practice as Research in the Arts: Principles, Protocols, Pedagogies, Resistances.
Palgrave Macmillan ISBN 978-1137282903
McNish, Hollie (2017). Nobody Told Me: Poetry and Parenthood. Blackfriars ISBN 978-0-349-13451-2
May, Katherine (2020). The Best, Most Awful Job Twenty writers talk honestly about Motherhood.
Elliott & Thompson ISBN 978-1-78396594-6
Rich, Adrienne (1976). Motherhood
As Experience and Institution
Norton ISBN 978-0-393-31284-3
Smellie, W (1752). A Treatise on the Theory and Practice of midwifery Baillière Tindall ISBN 0-7020-0522-3
Thurer, Shari L. (1994). The Myths of Motherhood How Culture Reinvents the Good Mother Houghton Mifflin Company ISBN 0-39558415-9
Unsworth, Emma Jane (2021). After the Storm Postnatal Depression & the Utter Weirdness of Motherhood Profile Books ISBN 9781788166549
