





















Page 11
Allergies
Page 13
Age-Related
Macular
Degeneration
Page 15
Blepharitis



Page 19 Clearing
Congestion in Children Page 21 Cough Page 23 Decongestants



Page 25
Dental Health in Children Page 27
Dry Eye Syndrome Page 29 Hair Loss







Page 31 Haemorrhoids
Page 33 Heartburn
Page 35
Irritable Bowel Syndrome
Page 37 Incontinence



















Is your brand the one that is recommended?
With the BMA recommending that GPs no longer prescribe for minor ailments, pharmacies now play a key role in administering advice and recommending products.
This Educational Training Guide offers a quick and easy way for the pharmacy staff to learn and to re-cap their knowledge in a specific area.
Alongside each learning module will feature an advertisement for your associated therapy medicine.
There is only one brand associated per therapeutic area - offering exclusive category ownership.
PAUK offers
7 out of 8 pharmacy visitors interact with counter assistants, and 1 in 5 are seeking advice.
Immediate impact of category knowledge
Raise Brand awareness
Encouraging product recommendation
Boost product stocking
Pharmacy Assist UK (PAUK) is an Educational and Training Directory designed with counter assistants in mind, identifying, managing and treating minor ailments and health complaints across 40 topics.
Using the popular WWHAM acronym.
W - Who is the patient?
W - What are the symptoms?
H - How long have the symptoms been present?
A - Action already taken?
M - Medication?
PHARMACY ASSIST UK 2025

Training on when to refer to the pharmacist, self-care and advice and patient support lines is included. Circulation:
14,000 targeting every independent pharmacy and chain in the UK - Distributed by the Royal Mail.
United Kingdom 14,000 England 11,500 Scotland 1,400 Wales 650 Northern Ireland 450
Cover Pack Shot Image
Module Sponsorship Spread
Front Cover Advert
Planner Sponsorship
Page Spread Advert
Page Advert
Listing in Directory
Back Cover Advert
Cover Advert

As a member of the pharmacy team, counter and pharmacy assistants will deal with many different situations which call for effective communication. These will always include responding to OTC requests for information, and counselling patients on their medications.
WWHAM is one of the many mnemonics that allow you to do that effectively and it is included in every article within this booklet. It is the most basic method of questioning used by Pharmacy teams, but it is direct, and asks most of the necessary questions.
It is used as follows:
WWHAM
• Who is the presenting complaint about? (patient or other)
• What are the symptoms present?
• How long have the symptoms been present?
• Action already taken?
• Medication being taken?
In order for WWHAM to work effectively, the pharmacy team do need to work on the communication process between health professionals and patients.
An effective relationship forms the base that allows a patient to meet professional responsibilities in patient care.
In addition to creating an atmosphere of trust, it further facilitates the exchange of information necessary to assess the patient’s health condition, implement treatment of medical problems and evaluate the effects of treatment on a patient’s quality of life.
Effective communication allows for WWHAM to work in that it is also involves a number of basic processes which include:
• Initiating a conversation: In many situations patients can be uneasy, concerned or embarrassed when they come to speak to the pharmacy team. When beginning the conversation it is important to focus on the patient in front of you, greet the customer and introduce yourself and be conscious of how the patient may be feeling. Similarly, establish immediately who the patient is: are they there for themselves or for someone else?
• Obtaining information: Obtaining information is a complex process including the acts of listening, questioning, checking your understanding and reading non-verbal signals. Stop talking and allow the patient to explain why they are here. Look at the other person to help you concentrate and show the other person that you are indeed listening. Similarly, react to ideas, not to the person.
• Action already taken: Any action taken by the patient should be established, including the use of any medication to treat the symptoms. About 50% of patients will have tried at least one remedy before seeking a pharmacist’s advice. Treatment may have consisted of OTC medicines bought from a pharmacy or elsewhere, other medicines prescribed by a doctor on this or a previous occasion, or medicines ‘borrowed’ from a friend or neighbour or ‘found’ in the medicine cabinet. Homoeopathic or herbal remedies may have been used. The cultural traditions of people from different ethnic backgrounds include the use of various remedies that may not be considered as ‘medicines’.
• The identity of any medicines taken regularly by the patient is important for two reasons: possible interactions and potential adverse reactions. Such medicines will usually be those prescribed by the doctor, but may also include OTC products. Pharmacies have an increasingly important role in detecting adverse drug reactions and consideration should be given to the possibility that the patient’s symptoms might be an adverse effect caused by medication. Where you suspect an adverse drug reaction to a prescribed medicine, you should discuss with the doctor what action should be taken.
Notes to the counter assistant: The views and opinions expressed within this Pharmacy Assist directory are those of the authors and it is provided to you only as guidance. All of the information is published in good faith and for general information purposes only. Please share with your supervising pharmacist for his/her review in order to tailor it to the specific needs and practices of your individual pharmacy. It can be shared with counter staff at your discretion for training purposes.
All rights reserved by IPN Communication Ltd. All material published in Pharmacy Assist is copyright and no part of this document may be reproduced, stored in a retrieval system or transmitted in any form without prior written permission. IPN Communications Ltd have taken every care in compiling Pharmacy Assist to ensure that it is correct at the time of going to print, however the publishers assume no responsibility for any effects from omissions or errors.
No two pharmacies are the same. Whether you are working within a pharmacy chain or in a smaller, independent pharmacy; staff, opening hours, protocols and allied healthcare professionals will differ. It is important therefore that you are knowledgeable as to your pharmacy's business and services provided. In addition, you should be educated in knowing the roles and remits of your colleagues.
Pharmacy name: .................................................................................................................................................................
Pharmacy address: .............................................................................................................................................................
Pharmacy telephone number: ..........................................................................................................................................
Pharmacy fax number: ......................................................................................................................................................
Pharmacy website: ..............................................
Pharmacy Social Media Streams
Pharmacy email address: .....................................................................

Leading Stockist of Ostomy & Urology
Care products with a dedicated support team.
•Continuously expanding our range with over 3,000 products from all leading suppliers.
•Complimentary bag cutting service, cutting in excess of 8,000 bags per week.
•Five dedicated team members with over 50 years combined experience.
•Over 25,000 calls annually taken and the team upskills their knowledge every 6 weeks.
•In collaboration with Convatec we provide complimentary wipes and bags for you to offer your customers.
•Exclusive Ostomy Excellence Programme: Pharmacy staff training & in store clinics run by nurses for your patients in collaboration with Coloplast.

Tel: 01 4632347www.udw.ie


Cetrine Allergy 10mg Film-Coated Tablets available in packs of 7s and 30s. Always read the leaflet.
ABBREVIATED PRESCRIBING INFORMATION
Product Name: Cetrine Allergy 10mg lm-coated tablets & 1 mg/ml oral solution.
Composition(s): Each tablet contains 10 mg cetirizine dihydrochloride. One ml of the oral solution contains 1 mg cetirizine dihydrochloride. Description(s): White, oblong lm-coated tablets, scored on one side. Can be divided into equal halves. Clear, colourless liquid with banana avour.
Indication(s): Tablets: Adults and paediatric patients 6 years and above. Oral solution: Adults and children 2 years and above. Relief of nasal and ocular symptoms of seasonal and perennial allergic rhinitis (hay fever); relief of symptoms of chronic idiopathic urticaria.

Dosage: Tablets: Adults, elderly and children aged 12 years and over: 10 mg once daily. Children from 6 years to 12 years: 5 mg (half a tablet) twice daily. Moderate renal insu ciency (creatinine clearance CrCl 30-49 ml/min): 5 mg once daily. Severe renal insu ciency (creatinine clearance ≤30 ml/min): 5 mg once every 2 days. Children under 6 years: Not recommended. Oral solution: Children aged from 2 to 6 years: 2.5 mg twice daily (2.5 ml oral solution twice daily (half a measuring spoon twice daily)). Children aged from 6 to 12 years: 5 mg twice daily (5 ml oral solution (a full measuring spoon twice daily)). Adults and adolescents over 12 years of age: 10 mg once daily (10 ml oral solution (2 full measuring spoons)). Not recommended in children aged less than 2 years. Moderate renal insu ciency (creatinine clearance CrCl 30-49 ml/min): 5 mg once daily. Severe renal insu ciency (creatinine clearance ≤30 ml/min): 5 mg once every 2 days. In paediatric patients su ering from renal impairment: Adjust dose on an individual basis taking into account the renal clearance of the patient, his age and his body weight. Contraindications: History of hypersensitivity to the active substance, to any of the excipients, piperazine derivatives or hydroxyzine. Severe renal impairment < 10 ml/min creatinine clearance.
Warnings and Precautions for Use: Cetirizine may increase risk of urinary retention, therefore caution in patients with predisposition factors of urinary retention (e.g. spinal cord lesion, prostatic hyperplasia). Caution in epileptic patients and patients at risk of convulsions. Discontinue use of cetirizine three days before allergy testing. Pruritis and/or urticaria may occur when cetirizine is stopped, even if the symptoms were not present before treatment initiation. In some cases, the symptoms may be intense and may require treatment to be restarted. The symptoms should resolve when the treatment is restarted. Tablets contain lactose. Oral solution contains sorbitol, propylene glycol, sodium (essentially ‘sodium free’), methyl - & propyl-parahydroxybenzoate.
Interactions: Caution is advised when taken concomitantly with alcohol or other CNS depressants. Cetirizine does not potentiate the e ect of alcohol (0.5 g/l blood levels). The extent of absorption of cetirizine is not reduced with food, although the rate of absorption is decreased.
Pregnancy and Lactation: Caution during pregnancy and breast-feeding.
Ability to Drive and Use Machinery: Usually non-sedative, patients should take their response to the product into account. In sensitive patients, concurrent use with alcohol or other CNS depressants may cause additional reductions in alertness and impairment of performance.
Undesirable E ects: Cetirizine at the recommended dosage has minor adverse e ects on the CNS, including somnolence, fatigue, dizziness and headache. In some cases, paradoxical CNS stimulation has been reported. Although cetirizine is a selective antagonist of peripheral H1-receptors and is relatively free of anticholinergic activity, isolated cases of micturition di culty, eye accommodation disorders and dry mouth have been reported. Instances of abnormal hepatic function with elevated hepatic enzymes accompanied by elevated bilirubin have been reported which resolves on discontinuation of the drug. Uncommon: Agitation, diarrhoea, pruritus, rash, asthenia, malaise, paraesthesia. See SPC for all adverse reactions. Marketing Authorisation Holder: Rowex Ltd, Bantry, Co. Cork.
Marketing Authorisation Number: PA0711/075/002-003. Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417 E-mail: rowex@rowa-pharma.ie
Legal Category: Not subject to medical prescription.
Date of Preparation: March 2021

Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing Rowex pv@rowa-pharma.ie
An allergy is a reaction the body has to a particular food or substance. Allergies are very common. They’re thought to affect more than one in four people at some point in their lives. They are particularly common in children. Some allergies go away as a child gets older, although many are life-long. Adults can develop allergies to things they weren’t previously allergic to.
Having an allergy can be a nuisance and affect your everyday activities, but most allergic reactions are mild and can be largely kept under control. Severe reactions can occasionally occur, but these are uncommon.
House dust - although many allergens in the environment can trigger allergic symptoms, house dust is the main culprit in indoor allergies. House dust is an airborne mixture that might contain fine particles of soil and plant material from indoors or outdoors, particles of human and animal skin dander and hair, fabric fibres, mould spores, dust mites, fragments of insects that have died and their waste, food particles, and other debris. Some dust is present in every home, regardless of how often or how thoroughly the house is cleaned.
Dust mites - often, when people believe they are sensitive to dust, they are in fact sensitive to the dust mites and their waste particles that are found in household dust. Dust mites can be found in most homes, usually in beds and bed covers, upholstered furniture and fabrics. Preventative measures include: using a dehumidifier or air conditioner, washing bedding on a hot cycle (non-washable bedding can be frozen overnight to kill dust mites), replacing wool or feathered bedding with synthetic materials or allergen-proof bedding, using a vacuum cleaner with a HEPA filter and avoiding the vacuumed area for 20 minutes to allow any dust and allergens to settle.
Pet dander - the allergic reaction to an animal is not caused by the animal’s hair. It is caused by substances in the animal’s saliva, urine, and especially dander (dead skin flakes that become loosened from the animal’s skin). The allergens become crusted on the animal’s fur and skin from urination or the animal licking or scratching itself; once dry, the allergens are released into the air, where they join the other components of house dust. Cats and dogs are most likely to cause allergic reactions.
Moulds - moulds generally live outdoors but can normally be found in almost any indoor environment. They easily pass through open doors and windows and settle indoors, especially where there is excess heat and humidity. They grow and produce mildew which thrives in places like shower cubicles. Non-visible moulds can grow in unseen areas of the house, such as under flooring materials and behind walls. To grow, mould requires water; for example, from a leaking pipe or
roof, or condensation. As it grows, mould releases more spores, many of which become part of house dust. While moulds can trigger allergic symptoms, like any other allergen, they rarely cause serious health problems, except in people who are seriously immunecompromised or on chemotherapy.
•Itchy, congested nose
•Clear nasal discharge
•Itchy, watery, swollen or red eyes
•Sneezing
•Tickly, swollen throat
•Coughing or wheezing
•Tightness in the chest
•Reactions to animal allergens may be very mild or quite severe. Symptoms may occur immediately after exposure to the allergen, or they may build gradually for 8-12 hours after exposure or become persistent.
First generation antihistamines are more likely to cause drowsiness. Depending on the product, the duration of action is often shorter than newer antihistamines and may necessitate taking the drug three to four times each day.
Second generation antihistamines can be taken over the long term with minimal side effects and are unlikely to cause sleepiness. The nonsedating antihistamines are convenient to take since they are taken once or twice daily. Saline nasal rinses reduce the symptoms of nasal allergies and can offer relief in conjunction with conventional treatment.
Maintaining clear and nasal passages is important - the tiny hairs (cilia) inside the nasal passage work to carry dust, pollution and allergens to the back of the throat where they are swallowed and destroyed, before they can multiply and cause harm. If the nasal passages are dry or blocked, they become less efficient.
Who is the patient? Sensitivity to indoor allergens is very common and occurs at every age.
What are the Symptoms? Itchy, congested nose, clear nasal discharge, irritated eyes, sneezing, tickly throat, coughing or wheezing.
How long have the symptoms been present? Indoor allergies tend to be at their worst in the late summer, when dust mites are at most prevalent.
Action already taken? Patients may have tried antihistamines but not be aware of the benefits of nasal hygiene.
Medication? Saline nasal rinses and sprays are drug free and do not contain preservatives, so will not interact with other medication.

MacuShield Original + and MacuShield Original chewable contain B2 and MacuShield Gold contains zinc, both help to maintain normal vision

Pharmacists cannot stop the progressive loss in central vision that comes with age-related macular degeneration, but they can help patients understand the treatment options.
Age-related macular degeneration (AMD) is a chronic disease leading to progressive central vision loss. The symptom of central vision loss is due to the fact that the damaged macula is in the centre of the retina. Patients with AMD may be unable to recognise faces, read, or drive a vehicle.
AMD is the most common cause of sight loss in people over the age of 50 in Ireland and it’s estimated that 7% of Irish people over 50 years of age are living with AMD. On account of our ageing population, the number of people in Ireland affected by this condition is expected to increase.
Symptoms of AMD include decreased central vision, central scotoma, and metamorphopsia. Scotoma is an area of partially diminished vision surrounded by a field of normal or well-preserved vision. Metamorphopsia is a visual defect that causes people to see objects in a distorted manner; straight objects appear wavy or curvy. Patients will complain of distorted vision, lack of bright colours, or blurred vision.
There are 2 types of macular degeneration: dry and wet. Dry macular degeneration, also known as the nonexudative form, is more common and found in approximately 90% of AMD patients. The onset of dry AMD is subacute. Management of dry AMD includes attempts to prevent progression to and frequent monitoring for the development of wet macular degeneration.
Wet (also known as exudative or neovascular) macular degeneration occurs in about 10% of AMD patients. It is the more acute form and more likely to cause vision loss.
Wet age-related macular degeneration develops when abnormal blood vessels grow into the macula. These leak blood or fluid which leads to scarring of the macula and rapid loss of central vision. Wet AMD can develop very suddenly but it can now be treated if caught quickly.
• Gaps or dark spots (like a smudge on glasses) may appear in their vision, especially first thing in the morning. Objects in front of them might change shape, size or colour or seem to move or disappear.
• Colours can fade.
• Sufferers may find bright light glaring and uncomfortable or find it difficult to adapt when moving from dark to light environments.
• Words might disappear when they are reading.

• Straight lines such as door frames and lampposts may appear distorted or bent.
The exact cause of AMD is unknown. However, extensive research efforts over the last decade are playing an important role in uncovering some of the clues as to what may be causing the disease.
Researchers know that certain genes can cause AMD, but they don’t know what triggers the gene. While AMD can be inherited, many lifestyle choices can make progression of the disease worse.
Some risk factors that are believed to increase the chances of developing AMD include being over the age of 50 and having a family history of AMD. Having high blood pressure, a poor diet or being overweight are also thought to be risk factors for this condition.
Because the exact causes of AMD are not yet known, some people may develop AMD even in the absence of these risk factors.
Age-Related Studies (AREDS1 and AREDS2) have shown that a combination of vitamins
and antioxidants may help reduce the risk of progression of Early AMD to late-stage AMD. The recommendations include supplements containing vitamins C and E, zinc, copper, lutein and zeaxanthin.
Treatment for Wet AMD is most often through a series of injections into the eye using a drug called anti-VEGF (anti-vascular endothelial growth factor). This treatment works by reducing the growth of new blood vessels. Response to this treatment is usually better in the early stages of Wet AMD, although even later stages can be stabilised. In some cases, individuals may notice improvements in their vision.
It is important to remind patients at risk for AMD to have regular eye exams, even when they are symptom-free. Patients complaining of a recent or chronic loss or change of vision should be urged to see an ophthalmologist immediately. A healthy lifestyle may help prevent AMD. This includes not smoking, eating a healthy diet, and being physically active. Following the recommended guidelines and the use of appropriate pharmacologic agents may help patients with AMD slow vision loss progression, increase visual acuity, and experience a greater quality of life.
Who? Dry eye is usually older people; red eye, anyone.
What are the symptoms? Dry, gritty eye for dry eye; grit and stick eye for conjunctivitis.
How long have they had the symptoms? If this persists for longer than a few weeks or is a particularly severe case, refer to GP.
Action already taken? Customers may have already tried eye drops.
Medication? Check the medication of patients with dry eye as it may be causing it, check if patients are contact lens wearers and what lubricants they use.



Blepharitis is a common and usually mild condition where the edges of the eyelids become inflamed, red and swollen.
Blepharitis is usually a long-term condition. Most people experience repeated episodes, separated by periods without symptoms.
There are three main types of blepharitis:
• Anterior blepharitis - where the inflammation affects the skin around the base of the eyelashes
• Posterior blepharitis - where the inflammation affects the Meibomian glands, found along the eyelid margins behind the base of the eyelashes
• Mixed blepharitis - a combination of both anterior and posterior blepharitis
• Anterior blepharitis can be caused by either a reaction to Staphylococcus bacteria - these usually live harmlessly on the skin of many people, but for unknown reasons they can cause the eyelids to become inflamed.
Seborrhoeic dermatitis, a skin condition that causes skin to become oily or flaky and sometimes can irritate the eyelids, causing the Meibomian glands to become blocked.
Posterior blepharitis is caused by a problem with the Meibomian glands, where the glands do not function properly and can get blocked by either debris, skin flakes or inflammation.
Sometimes blockages in the Meibomian glands are associated with rosacea. If too much oily substance is being produced, this may be caused by seborrhoeic dermatitis.
Mixed blepharitis, which is the most common, is caused by a combination of both anterior and posterior blepharitis.
Blepharitis isn’t usually serious, although it can lead to a number of further problems.
For example, many people with blepharitis also develop dry eye syndrome. Serious, sight-threatening problems are rare, particularly if any complications that develop are identified and treated quickly.
Patients with blepharitis may present with eyelash changes, watering, crusting and mattering around the lashes and canthus, photophobia, pain, and vision changes. The symptoms are usually worse in the morning, after a night of closed eyes has kept eyelids in contact with the ocular surface.
Patients’ visual function may decline pursuant to corneal damage and inflammation, scar formation, loss of surface smoothness, and clouded corneas. If severe inflammation develops, corneal perforation can occur. The normal progression may include eyelid damage to the lids with trichiasis, or entropion

and ectropion (respectively, inward or outward turning lids that cannot close properly).
Ophthalmologists and opticians encourage blepharitis sufferers to establish a systematic, long-term commitment to eyelid hygiene, because management will require lifelong vigilance. The exact process varies. Antibiotic drops or ointments, or low-dose antibiotic courses should be considered if hygiene changes are ineffective.
Pharmacy staff should keep certain tips in mind when helping patients who have blepharitis. First, pharmaceutical preparations like ointments and gels will stay in contact with the lid margin longer than solutions. These are usually preferred for blepharitis, but drops are preferred for corneal disease because they spread evenly.
There is one key message which should be given to patients at every visit: when applying any ointment to lid margins, using a clean application device, such as a cotton swab or a clean fingertip, is critical, as is gentle eyelid handling.
A warmed wet towel or eyelid-warming mask can help to improve gland function. This is
usually recommended for 10 minutes twice daily, but manufacturers’ instructions for eyelid-warming masks may vary.
• For 5 minutes once or twice daily, apply a wet washcloth, soaked gauze pads, or flax-filled mask, that has been warmed. This step softens gland secretions and promotes evacuation and cleansing of secretory passages.
• Gently wash the eyelid margins while avoiding the lids or eye surface to remove adherent scurf (dead epidermal cells), collarettes (rims of thickened epidermis), and crusting. This also cleanses glandular orifices. Although many clinicians recommend washing with water, some suggest adding a few drops of baby shampoo.
• Apply an antibiotic ointment like erythromycin or sulfacetamide, but only for short courses of treatment (chronic use is contraindicated). Generally, ointments are applied at bedtime so blurry vision is not a problem.
Who? Can occur in any age group but more common in young children and people over 50.
What are the symptoms? Eyelash changes, watering, crusting, pain and vision changes.
How long have they had the symptoms? If this persists for longer than a few weeks or is a particularly severe case, refer to GP.
Action already taken? Customers may have already tried eye drops.
Medication? check the medication of patients with dry eye as it may be causing it, check if patients are contact lens wearers and what lubricants they use.



Nasal congestion happens when blood vessels and tissue in the nasal cavity fill up with too much fluid. It can make it hard to sleep and lead to problems like a sinus infection (sinusitis). A baby may also have trouble feeding if he or she is congested. There are some tell-tale signs that can help you tell the difference between viral and bacterial infections.
For example, if a child has a runny nose, the colour of the discharge is an important clue. Clear and watery discharge at first usually come from a virus, though the mucus may turn white, green, or yellow for a few days before it turns clear again.
Blocked noses can be caused by a mild infection, like the cold or flu, but it’s worth checking if a child has accidentally blocked a nostril themselves.
A gentle option is to wash away the mucus that’s causing the blockage, so the child can breathe more easily. A natural treatment like a nasal spray of saline drops can help to do this.
Some of the causes of nasal congestion include:
• Infections: the common cold and other respiratory tract infections, including influenza (flu) and sinusitis.
• Allergies, including hay fever
• Persistent rhinitis.
When temperatures start turning colder and kids are inside and interacting with each other in greater numbers, cold and flu season inevitably follows.
Children under the age of 6, and particularly under age 2, are at an especially high risk during cold and flu season. Advise on keeping the child hydrated to help reduce cold and flu symptoms and make them feel better. Fevers can result in dehydration. Children suffering with the cold or flu may not feel as thirsty as they normally would, and they may be uncomfortable when drinking, so it’s important to encourage them to drink plenty of fluids.
Medicated nasal sprays aren’t recommended for young children. Fortunately, there are several easy ways to clear up a stuffy nose without medication.
Use a cool-mist humidifier in the child’s room. This will help break up mucus. Another option is using a saline nasal spray or drops, which makes thin mucus easier to blow out or remove with a bulb syringe. This is especially helpful before feeding and bedtime.
• Get the timing right. It’s hard to use a nasal spray when a baby’s feeling wriggly, so try dosing them when they are nice and relaxed, like after a bath or a feed.

If a child’s under 2:
1. Lay the child down and turn their head to one side.
2. It’s sometimes helpful to lay them on a pillow, so you can tilt their head back slightly.
3. Put the nozzle into a nostril and press the spray head once.
4. Then repeat in the other nostril.
If they’re over 2:
1. Put the nozzle into one nostril, holding the bottle vertically.
2. Press the other nostril closed.
3. Press the spray head once and spray deeply, asking your child to breathe in at the same time.
4. Then repeat in the other nostril.
• Don’t worry about misfires If a little spray gets in their eye, don’t panic. It may surprise them a little but saline solution is very gentle and shouldn’t cause any harm.
• If it is tricky to use a nasal spray with a young baby, try using nasal drops instead, as some people find these easier.
Moisture and warmth can help too. Try advising a parent to take the child into the bathroom while they run a steamy shower or bath.
Advise the parent to make sure their little one gets plenty of restful sleep – this will really help give them the strength they need to recover.
If the child is older than one, advise the parent to prop up the child’s pillow. It can help the child breathe more easily while they sleep.
A range of plug-in products which release vaporised oils into the child’s room or vapour rubs are also available for young children.
Who? All children are prone to congestion and colds.
What are the symptoms? Stuffy nose, irritability.
How long have they had the symptoms? An infant will have difficulty communicating their symptoms.
Action already taken? Steam, moisture and warmth can help to alleviate symptoms.
Medication? Decongestants for adults or older children should not be used on young children.

Available in 800g powder
Supplier code: 12458581
New SMA® Comfort is a nutritionally complete, easy to digest formula1, suitable from birth to 12 months and offers a unique combination of ingredients proven to help manage symptoms of colic and constipation1-7 This product should be used under medical supervision.
SIGNIFICANT IMPROVEMENT IN STOOL CONSISTENCY
Associated with increased magnesium levels*2-4
REDUCED CRYING TIME IN INFANTS WITH COLIC
Associated with lower lactose levels**5†
AN INCREASE IN BENEFICIAL BACTERIA IN THE INFANT GUT MICROBIOME
Due to the presence of GOS/FOS6
Contains 100% whey, partially hydrolysed protein which is easier to digest than intact protein1
REFERENCES:
1. Billeaud C et al. Gastric emptying in infants with or without gastro-oesophageal reflux according to the type of milk. Eur J Clin Nutr 1990; 44: 577–583. 2. Chao et al. Therapeutic effect of NovalacIT in infants with constipation. Nutrition 2007;23:469–473. 3. Infante et al. Modification of stool’s water content in constipated infants: management with an adapted infant formula. Nutrition Journal 2011; 10:55-8. 4. Benninga MA; MENA Infant Constipation Study Group, Vandenplas Y. The Magnesium-Rich Formula for Functional Constipation in Infants: a Randomized Comparator-Controlled Study. Pediatric Gastroenterology Hepatology and Nutrition 2019 May;22(3):270-281. 5. Kanabar D et al. Improvement of symptoms in infant colic following reduction of lactose load with lactase. J Hum Nutr Dietet 2001; 14: 359-363. 6. Moro G, et al. Dosage-related bifidogenic effects of galacto- and fructooligosaccharides in formula-fed term infants. J Pediatr Gastroenterol Nutr. 2002 Mar;34(3):291-5.
IMPORTANT NOTICE:
The World Health Organisation (WHO) has recommended that pregnant women and new mothers be informed on the benefits and superiority of breastfeeding – in particular the fact that it provides the best nutrition and protection from illness for babies. Mothers should be given guidance on the preparation for, and maintenance of, lactation, with special emphasis on the importance of a well-balanced diet both during pregnancy and after delivery. Unnecessary introduction of partial bottle-feeding or other foods and drinks should be discouraged since it will have a negative effect on breastfeeding. Similarly, mothers should be warned of the difficulty of reversing a decision not to breastfeed. Before advising a mother to use an infant formula, she should be advised of the social and financial implications of her decision: for example, if a baby is exclusively bottle-fed, more than one can (400 g) per week will be needed, so the family circumstances and costs should be kept in mind. Mothers should be reminded that breast milk is not only the best, but also the most economical food for babies. If a decision to use a formula is taken, it is important to give instructions on correct preparation methods, emphasising that unboiled water, unsterilised bottles or incorrect dilution can all lead to illness. This product must be used under medical supervision. SMA® Comfort is a special formula intended for the dietary management of bottle-fed babies with colic and constipation. It is suitable as the sole source of nutrition up to 6 months of age, and in conjunction with solid food up to 12 months of age.
For any questions contact SMA Careline® UK 0800 081 81 80 www.smahcp.ie
The only Comfort formula in the UK & I to have increased magnesium levels (still within regulatory limits of infant FSMP Delegated Regulation (EU) 2016/128 for food for special medical purposes). Magnesium content of new SMA Comfort is 8.1mg/100ml compared to SMA PRO First Infant Milk which contains a magnesium level of 5.7mg/100ml
**Where lactose intolerance is a cause of the colic
Since the 1950’s, colic has been described as unexplained paroxysmal crying for longer than three hours per day, for three days per week, for at least three weeks. More recently the Rome IV diagnostic criteria include infants who are less than five months when symptoms start and stop, who have recurrent and prolonged periods of infant crying, fussing or irritability with no obvious cause, that cannot be prevented or resolved by caregivers, with no evidence of failure to thrive, fever or illness. The condition is most frequent within the first six weeks of life and effects up to a quarter of infants. It is equally common in breastfeeding and formula feeding babies. Excessive infant crying is a frequent reason for parents to support from healthcare professionals and is a risk factor for non-accidental injury.
Some would argue that the term colic is outdated, and that infant crying is part of normal newborn behaviour. It would be expected that a newborn infant would cry or be unsettled for 2-3 hours a day, with peak incidence of crying occurring at about six weeks of age. Parents often perceive a baby’s cry as pain, however this is only means they have to communicate any discomfort to their caregiver. Infant crying can lead to parental distress and parents should be encouraged to seek support and also be aware of the risk of postnatal depression.
If parents are concerned about their baby’s crying, they should be encouraged to speak to a healthcare professional and have a clinical exam and weight measurement. Reassurance can be beneficial. Fever (>38°C), bilious vomiting, projectile vomiting, poor weight gain, blood in the stool or any signs of injury are all reasons to seek medical attention. Typically, the ‘colicky’ baby gains weight well and is keen to feed. They frequently appear quite happy and content when they visit the doctor.
The aetiology of colic is undefined and is likely multifactorial – behavioural and biological components, gut microflora and dysmotility factors are the focus of research. Lactose intolerance and presence of allergens in formula or breast milk have been investigated as causes. The intestinal microbiome has been found to be different in infants with and without colic. Immature gut motility has also been investigated.
Once no red flags are present, the mainstay of treatment is support and parental reassurance. Babies are unable to self-soothe. Responding to them quickly reduces the crying time. Parents should be reassured that they will not ‘spoil’ their baby by holding them.
The most recent Cochrane Review on Dietary Modifications for Infantile Colic was published in 2018. 15 studies of 1121 infants were included. Modification of the maternal diet to reduce intake of potential allergens was not found to be beneficial. If the breastfeeding

mother decides to exclude allergens from her diet, baby’s symptoms should be monitored with reintroduction of normal eating as soon as possible if there is no effect. Longer term dietary modification should be supported by a dietitian in order to support a healthy balanced diet for the mother.
Use of hydrolysed formula has not been shown to reduce crying times in any meaningful way. Similarly reduced lactase intake or use of lactase drops showed no difference in crying times. There is no evidence to say that changing formula type will influence colic or crying times. The different types of formula have been discussed above.
Probiotics have been studied for use in infantile colic (Cochrane 2019). 6 studies of 1886 infants compared probiotics with placebo. There was no evidence to suggest that probiotic use prevented colic.
A meta-analysis of three studies showed a
Who? Newborn babies and infants.
reduction in crying time of approximately 30 minutes per day with use of probiotic when compared with placebo, the most studied agent was Lactobacillus reuteri. A metaanalysis (Paediatrics 2018) of probiotics concluded that there was insufficient data to recommend use in formula fed infants.
Simethicone is an anti-flatulent medication, however it is no better than placebo at treating colic. Gripe water typically contains sodium hydrogen carbonate and some other agents such as fennel which are thought to reduce wind. Gripe water has not been shown to reduce infant colic.
For crying infants, once red flag signs and symptoms have been out ruled, no treatments have been found to reduce infant crying by any clinically meaningful amount. Parents need support and reassurance. It should be acknowledged that caring for a crying baby is frustrating and tiring and they should be encouraged to ask for help.
What are the symptoms? Persistent crying, fussing or irritability with no obvious cause.
How long have they had the symptoms? If a child cries for more than three hours in a row on three or more days of the week they may be considered colicky.
Action already taken? Parents may have already considered a number of home actions to soothe symptoms.
Medication? Mainstay of treatment is support and parental reassurance.

1,2

1 Associated with Common Cold, Bronchostop Junior is a MD. 2 Based on Traditional use, Bronchostop Adult is a THR. * Based on combined IQVIA Data - June 2022. Buttercup Bronchostop Cough Syrup contains thyme herb extract and marshmallow root extract. A traditional herbal medicinal product for the relief of coughs, such as chesty coughs and dry, tickly, irritating coughs and catarrh, exclusively based upon long-standing use as a traditional remedy. Adults and children over 12 years: 15ml every 4 hours, 4 times per day. Max 6 doses (90ml) per day. Max dose should not be exceeded. To be taken 30 to 60 minutes before or after intake of other medicines. Not recommended for children under 12 years. To be administered undiluted or diluted in water or warm tea. Seek medical advice if symptoms persist after 7 days or if dyspnoea, fever or purulent sputum occurs. Contraindications: Hypersensitivity to marshmallow root, thyme, to other members of the Lamiaceae family or to any of the excipients. Warnings and precautions: Asthmatics and atopic patients should consult a doctor before using the medicine. Contains E218 and E216 that may cause allergic reactions (possibly delayed). Patients with HFI, glucose-galactose malabsorption or sucrase-isomaltase insufficiency should not take themedicine. The additive effect of concomitantly administered products containing fructose (or sorbitol) and dietary intake of fructose (or sorbitol) should be considered. Pregnancy and lactation: Not recommended. Side effects: pruritus, rash, urticaria, angioedema, anaphylactic reaction, oral mucosal blistering, abdominal pain, diarrhoea, nausea, vomiting, dyspnoea, exacerbation of asthma. Legal classification: GSL. TR 2006/001/001.TR Holder: Kwizda Pharma GmbH, Effingergasse 21, A-1160 Vienna, Austria. RRP (ex VAT): €4.99 Date of preparation: 05/2022. SPC: http://www.medicines.ie/medicine/16380/SPC/Buttercup+Bronchostop+Cough+Syrup/ Bronchostop Junior is a medical device according to Directive 93/42/EEC, used to relieve any cough (dry & chesty) associated with a cold for children from 1 year. Children under 3 years of age should consult with a doctor to exclude more serious diseases being present. Use in children under 1 year of age is not recommended. Children aged 1 year and above: 5ml up to 3 times daily. Children 2 to 3 years: 5ml up to 4 times daily. Children 4 to 5 years: 7.5ml up to 4 times daily. Children 6 to 11 years: 15 ml up to 4 times daily. Always read the Instructions for Use. Date of preparation: 05/2022.
Date of preparation: August 2022. IRE/BRO/2022/37
Cold and flu season is the time of the year when pharmacists are more likely to see patients scanning the pharmacy shelves in search of the perfect remedy to manage a cough. Patients may be overwhelmed by the numerous OTC cough products, but pharmacists are in an ideal position to evaluate and aid patients in selecting a cough product for self-treatment, as well as to encourage patients to seek further medical care when warranted.
During winter, most coughs are caused by viruses such as colds and flu and can be safely managed at home using OTC remedies. Coughs are classified as “acute” or “chronic”. An acute cough is most common and lasts up to three weeks. It’s usually caused by a cold or flu virus and most improve after one to two weeks.
Chronic cough lasts for eight or more weeks. The most common causes include acid reflux, asthma, TB, COPD, bronchitis and smoker’s cough. Red-flag signs include:
• Coughing up blood
• Unexplained weight loss
• Night sweats
• Cough worsening after three weeks
• Shortness of breath
• Voice changes
• Lumps/swellings in neck
• Chest pain
A dry cough is caused by inflamed airways due to a viral infection such as a cold or flu. A chesty cough produces phlegm. This is caused by the lungs producing extra fluid due to an infection.
It is important to get a detailed overview of the patient’s symptoms. Is their cough productive? How long have they had the cough and what action has been taken? Pharmacists should ask if a patient has any medical conditions that may affect any treatment or product you recommend.
The role of cough medicine is to ease symptoms while the body heals. There are many brands of OTC cough medicines. But there are only three basic types:
Expectorants help thin mucus, making it easier to cough up. The ingredient is guaifenesin.
Suppressants help cut the number of times someone coughs. The active ingredient listed is usually dextromethorphan (DM). Other cough suppressants include camphor, eucalyptus oil, and menthol.

Combination cough products have more than one active ingredient. They have both guaifenesin and dextromethorphan. Cough medicines may also contain ingredients to help coat and soothe the throat.
Combination products may have medicines to ease other symptoms, that may include decongestants for stuffy nose, antihistamines for allergies or a runny nose, or painkillers.
Cough drops can also help relieve a cough and may ease a sore throat.
When temperatures start turning colder and kids are inside and interacting with each other in greater numbers, cold and flu season inevitably follows.
Children under the age of 6, and particularly under age 2, are at an especially high risk during cold and flu season. Whilst it is known that antibiotics won’t help when it comes
Who? Anyone can be affected.
to clearing up an infection, there are steps pharmacists can advise parents to take to help their child feel better while their immune system battles the virus.
Advise on keeping the child hydrated to help reduce cold and flu symptoms and make them feel better. Fevers can result in dehydration. Children suffering with the cold or flu may not feel as thirsty as they normally would, and they may be uncomfortable when drinking, so it’s important to encourage them to drink plenty of fluids.
Medicated nasal sprays aren’t recommended for young children. Fortunately, there are several easy ways to clear up a stuffy nose without medication.
Use a cool-mist humidifier in the child’s room. This will help break up mucus. Another option is using a saline nasal spray or drops, which makes thin mucus easier to blow out or remove with a bulb syringe. This is especially helpful before feeding and bedtime.
What are the symptoms? Depend on type of cough to suggest if it is allergic or viral.
How long have they had the symptoms? Coughs should clear after 3 weeks, is it short or persistent?
Action already taken? Customers may already have purchased cough medicines.
Medication? Some of the ingredients in cough medicines should not be given to children such as opioids. Antacids may interfere with other medicines.








We recommend using Stérimar Isotonic and Stérimar Baby two to six times a day (or more) in each nostril for as long as you need it or as long as and as often as your doctor recommends.
Stérimar Hypertonic is recommended for a short period. Use two to four times a day in each nostril for light congestion and up to six times a day for severe congestion.
Can Stérimar be used with other medication?
Yes. Stérimar is drug-free and doesn’t contain preservatives so there is no known risk of interaction with any other medication. However, in all cases it is best to check with your doctor.
Am I likely to experience any irritation from using Stérimar?
Stérimar Isotonic and Stérimar Baby are purified sea water solutions with the same concentration of salts as the cells in the human body. As such, irritation is highly unlikely. Stérimar Hypertonic has a higher salt content than Stérimar Isotonic but the solution is still less salty than sea water. A sensation of dryness may occur and should disappear within a few days.
Always follow instructions and/or doctor’s recommendations.
Can I use Stérimar if I am pregnant, diabetic or suffer from high blood pressure?
Yes, Stérimar is completely safe to use with these conditions, but it is always a good idea to check with your doctor.
Can I use Stérimar for my three year old?
Yes, Stérimar Isotonic is suitable for the whole of the family, even babies from 3 months old. Stérimar Hypertonic is suitable for all adults and children over three years of age and Stérimar Baby can be used with babies from birth to 3 years old.
Is the nozzle safe to use?
Yes. The Stérimar nozzle has been specifically designed to fit any shape and size of nostrils.
Stérimar Baby has a specific nozzle with a protective flange. The nozzle cannot be pushed too far into the nose to avoid any risks of injury.
How long will Stérimar keep?
Stérimar products can be kept for a maximum of three years after manufacture or until all solution has been used. The expiry date can be found at the bottom of the can and carton. Each
dose of Stérimar delivered is aseptic. The valve on top of the can prevents air from entering. Also, because the solution is kept in a sterilised pouch it never comes into contact with either the aluminium can or the non-flammable nitrogen gas within.
Why is it important to clean the nozzle after each use?
You must clean the nozzle in soapy water to remove any microorganisms left after use to help avoid any cross-contamination.
What does micro-diffusion mean?
The unique Stérimar micro-diffusion system produces a fine spray of sea water. As the droplets produced by Stérimar are microfine, they remain in contact with the walls of the nasal passages for longer, making Stérimar even more effective.
Why are the copper and manganese in Stérimar Hypertonic important?
Copper and manganese are found in very small amounts in the human body. They stimulate the body’s self defense mechanisms and help keep it healthy.

Please
Decongestants can help relieve a congested (stuffy) nose caused by a cold virus or by the flu, sinusitis, or allergies. Most decongestants come in pill or liquid form.
They work by helping to shrink swollen tissues in the nose, sinuses, throat, and the space behind the eardrum (middle ear). This may relieve pressure, pain, and stuffiness (congestion).
Decongestants are available as:
• nasal sprays
• drops
• tablets or capsules
• liquids or syrups
• flavoured powders to dissolve in hot water
Most people who also have allergies are familiar with nasal congestion. This can include a stuffy nose, clogged sinuses, and mounting pressure in the head. Nasal congestion is not only uncomfortable. It can also affect sleep, productivity, and quality of life.
Antihistamines may help prevent allergy symptoms. But sometimes sufferers may need to take additional medications. This is especially the case if they need to relieve sinus pressure and a congested nose. Decongestants help break this cycle of congestion and pressure.
Nasal sprays feature a decongestant that is delivered directly into the nasal cavities. It is generally recommended that patients don’t use spray decongestants for longer than three days at a time as the body may grow dependent on them, and then the products will no longer be effective in alleviating congestion.
Nasal spray decongestants may provide temporary relief from congestion. However, they’re especially prone to inducing tolerance for the drug.
Both oral and topical nasal decongestants are contraindicated for patients with heart disease (they increase the workload of the heart), hypertension (they raise blood pressure), thyroid disease (they increase the risk of adverse reactions), diabetes, or, in men, difficulty in urination caused by an enlarged prostate.
Clearing congestion in a small child can be a challenge. For starters, it’s not always obvious what’s causing a stuffy nose. Infants and toddlers often catch colds because they are just starting to build up their immunity to common viruses. But there are many other potential causes of congestion.
If a child has a stuffy nose, breathing in steam with added essential oils, such as eucalyptus or rosemary, may help to relieve

it. For babies, placing a few drops of saline (salt water) just inside their nose, before they feed, will help to relieve a blocked nose. Saline drops are available.
Cold medicines for relief of older children and adults are not recommended for infants and toddlers. Fortunately, there are plenty of safe and effective treatments.
One of the safest and most effective ways to help clear a baby’s congestion is with a saline (salt water) spray or natural nose drops. These products are available without a prescription and are preservative free.
The drops or spray work to maintain daily nasal hygiene by gently cleansing “nasally” nostrils and preserving the natural balance of the nasal mucosa of the infant/child. They can improve the evacuation of mucus, which ultimately prevents colds and limits the occurrence of allergic symptoms like hay fever. By clearing the child’s nose and allowing them to breathe more freely, this also results in improved sleeping and feeding.
If advising the use of drops, tell the parent to place two drops in each nostril to loosen the
mucus inside. A suction bulb can be used to withdraw the saline and mucus.
• It is unlawful to supply a product or combination of products which contain more than 720mg of pseudoephedrine OR 180mg of ephedrine in a single transaction, without a prescription
• It is unlawful to sell or supply any pseudoephedrine product together with an ephedrine product without a prescription
• Sale or supplies should either be made personally by the pharmacist or by pharmacy staff who have been trained on pseudoephedrine and ephedrine issues, knowing when to refer to the pharmacist where necessary
• Even when a request is made for a lawful quantity, the sale or supply can be refused where there are reasonable grounds for suspecting misuse
• Be vigilant for signs of misuse.
WWHAM
Who? All who are prone to congestion and colds.
What are the symptoms? Stuffy nose, irritability.
How long have they had the symptoms? An infant will have difficulty communicating their symptoms.
Action already taken? Steam, moisture and warmth can help to alleviate symptoms.
Medication? Decongestants for adults or older children should not be used on young children.



Children have different needs as they grow older. Step by Step is a unique kids range that follows the children's development and offers tailored design with different features to make brushing easy and effective at every age. The handle, head size, bristles and design are all tailor made to help you establish good dental care habits from the first tooth. Choose the one that fits your child.


Teething is the natural process by which the primary (baby) teeth are triggered to move into mouth through the gums. As the teeth move to the surface in a protective sac, enzymes break down the gingiva allowing the teeth to pass through - there is no damage to the flesh or ‘cutting’ it is a begin process beginning at approximately 6-8 months.
A baby’s lower front teeth will usually erupt first, followed by the upper front teeth, in pairs. By approximately 3 years old children will have 20 primary teeth – 10 on the maxilla & 10 on the lower. Dentists tend to be more concerned about teeth that erupt out of sequence, or are missing their partner, than teeth that are slow to come through.
Children display symptoms to varying degrees, with some being completely unaffected and teeth appearing to the surprise of caregivers, while others seem to feel every tooth. It is thought that a dull teething pain can be present approximately 4 days prior to the tooth emerging from the gum – then resolving over the next 2-3 days – a 7-8 day teething window.
Generally topical agents are lidocaine-based preparations, with cetylpyridinium chloride as an antibacterial to reduce infection as teeth part the gingiva. Lidocaine hydrochloride is rapidly absorbed through mucous membranes, giving rapid, but temporary, pain relief.
Systemic analgesics can also be used. Sugar-free paracetamol liquid is the systemic medication of choice for teething infants, given its action in reducing pain and pyrexia.
The primary teeth that start erupting as a very small baby play a massive role in smiling, appearance, eating, & speech. Children start losing primary teeth at age 6-7 years but many people don’t realise is that many of those primary teeth that we get as infants are not lost until age 11 or 12 years. It is important to keep the primary teeth until they exfoliate naturally as they guide the permanent teeth into position by holding the space. If primary teeth are lost early due to decay there is a high risk of malocclusion & crowding in the adult teeth.
Dental decay is a preventable disease. Unfortunately 50% of Irish 5 year olds have visible cavities in their teeth. Decayed teeth affect every aspect of childrens’ lives –eating sleeping, anxiety, behaviour, school performance & growth. Many children experience social issues due to the poor appearance of decayed teeth.

The primary teeth should be cleaned the minute they erupt. A damp muslin or face cloth is effective. There are also special baby brushes & finger brushes which are soothing to chew on.
It is important to discourage night feeding. Water is the only safe drink at night time, children should be ‘fed & put to bed not put to bed then fed’. If teeth are bathed in milk for long periods during the night they are at increased risk of decay. Water & milk are the only tooth safe day time drinks – fruit juices should be avoided.
Orthodontic soothers are recommended by some paediatricians until 6-12months. If soothers are used long term they can severely affect tooth growth & alignment. Soothers should NEVER be dipped in sweetened substances e.g. honey.
From the age of 2 a smear of fluoridated toothpaste can be used. It is not recommended to use fluoride toothpaste before 2 years in Ireland. It is best not to rinse toothpaste out after brushing to maximise the beneficial effects.
Caregivers should be encouraged to bring babies to their local family dentist before their 1st birthday. This is to get good preventive advise from the outset & also to familiarise children to the dental setting. Many children experience unnecessary dental anxiety because their first dental experience is when they are in pain or in need of treatment –we can avoid this: First Dental Visit by first Birthday.
Please prescribe sugar free medications wherever possible.
WWHAM
Who? Teething from 6 months.
What are the symptoms? Dull pain and itch.
How long have they had the symptoms? 4 days prior to tooth emerging; 7-8 day teething window.
Action already taken? Cool soothers; Orthodontic soothers.
Medication? Topical agents such as lidocaine-based preparations and systemic analgesics.

An estimated 10% to 30% of the population older than 40 years suffers from some degree of dry eye disease (DED). The condition tends to affect people above 60, and it is more common in women than men.
Around one in 13 people who are in their fifties experience dry eye syndrome, and the condition becomes more common with age. Up to a third of people age 65 or older may have dry eye syndrome.
DED, which is also sometimes referred to as dry eye syndrome or keratoconjunctivitis sicca, is considered the most prevalent ophthalmic disorder that affects the anterior eye and is most often associated with the aging process, especially in postmenopausal women.
DED is a multifactorial disease of the tears and ocular surface that results in discomfort, tear film instability, and visual disturbance, with potential for damage to the ocular surface. DED can be classified as chronic or temporary. DED can be also attributed to Bell palsy, collagen disorders such as rheumatoid arthritis, corneal or eye lid defects, Sjögren syndrome, and thyroid-related eye disease.
Other medical conditions associated with DED include diabetes, lupus, and scleroderma.
Dry eyes can be caused by ordinary things that increase tear evaporation, such as looking at a computer screen too long; being outside in windy, dry conditions; or just being tired. Cigarette smoke may also cause dry eyes. Other common causes of dry eye include:
• Aging. Tear production tends to decline with age. Dry eyes are common in individuals older than 50 years.
• Gender. A deficiency of tears is more common in women, especially with hormonal changes caused by pregnancy, the use of birth control pills, or menopause.
• The use of cold or allergy medicines, antidepressants, and drugs for high blood pressure; acne; birth control; and Parkinson’s disease.
• Wearing contact lenses.
• An eye injury or other problem with your eyes or eyelids.
• Diabetes.
• Thyroid disorders.
• Vitamin A deficiency.
SYMPTOM CHECKER
The symptoms of dry eye syndrome usually affect both eyes and may include:
• feelings of dryness, grittiness or soreness, which get worse throughout the day

• redness of the eyes
• watering eyes, particularly when exposed to wind
• eyelids that stick together when waking up
These symptoms may get worse in smoky or hot environments.
When a patient presents with symptoms of a dry eye condition, such as irritation, grittiness, burning, soreness, watery eyes and visual disturbances generally affecting both eyes, a detailed history should be recorded by the pharmacist because it may elicit information about contributing factors.
Briefly, this should include details of the signs and symptoms, duration of symptoms and exacerbating factors, such as the environment, changes in humidity or computer use.
It should also record details of topical and systemic medicines taken by the patient, whether the patient wears contact lenses and if the patient has any dermatological, inflammatory or other systemic diseases.
A differential diagnosis for other eye conditions (such as conjunctivitis, allergy and acute red eye) should be established because initial presentation may be similar.
Once dry eye syndrome develops, some people have recurring episodes for the rest of their lives. There is no cure for dry eye syndrome, but a range of treatments can control the symptoms. In rare cases, more severe cases of dry eye syndrome may require surgery.
The ultimate goal of dry eye treatment focuses on symptomatic relief, usually using tear
WWHAM
supplements. Despite this, the underlying mechanism of symptomatic improvement with tear supplementation is still poorly understood. It is thought that increased tear volume, improved tear stabilisation, reduced tear osmolarity or a dilution of inflammatory biomarkers or a combination of these factors play a vital role.
Topical ocular lubricants are the mainstay of dry eye treatment, with the choice of tear substitute depending on the severity of the condition. Pharmacological interventions in all forms of dry eye conditions range in formulation, such as drops, sprays, gels and ointments.
For occasional or mild dry eye symptoms, OTC eyedrops (artificial tears) used regularly may provide relief. Preservative-free artificial tears are preferred, as they cause less irritation. Wearing glasses or sunglasses that fit close to the face (wraparound shades) or that have side shields can help slow tear evaporation from the eye surfaces. An indoor air cleaner to filter dust and other particles can help prevent dry eyes, as can a humidifier by adding moisture to the air, avoiding dry conditions, and allowing the eyes to rest when performing activities that require someone to use their eyes for long periods of time.
Pharmacologic agents that have anticholinergic properties—including antihistamines, decongestants, and antihypertensives such as antidepressants, beta-blockers, and diuretics—are common causes of DED.
Additionally, DED may be caused or exacerbated by allergens and environmental conditions such as dry climates, failure to blink regularly when staring for long periods at electronic devices, smoke, and wind. Laser eye surgery may also cause temporary dry eye.
Who? Can affect all but mainly women and those over age 60.
What are the symptoms? Feelings of dryness, grittiness, soreness, redness, watering of the eyes.
How long has the patient had the symptoms? Symptoms can be recurring.
Action already taken? The patient may already be using eye drops, reducing computer screen time and avoiding exacerbating factors.
Medication? Topical ocular lubricants, OTC eye drops, glasses and wraparound sunglasses can help.
Our supplements feed the root from within 25 years of research in the science of hair

Supported by 10 clinical trials
Hair-loss, for both men and women, can be distressing, and is a subject which needs careful and sensitive handling by pharmacists and pharmacy staff. It is important you are educated in the types of hair-loss, what causes it and that you understand which treatments are available.
A hair growth cycle consists of three phases. During the anagen phase, hair grows actively. This phase may last for years. During the catagen phase, hair stops growing and separates from its follicle, which is the structure beneath the skin that holds the hair in place. The catagen phase lasts about 10 days. During the telogen phase, the follicle rests for two or three months, and then the hair falls out. The next anagen phase begins as a new hair grows in the same follicle. Most people lose 50 to 100 hairs per day as part of this natural cycle.
If this cycle is disrupted, or if a hair follicle is damaged, hair may begin to fall out more quickly than it is regenerated, leading to symptoms such as a receding hairline, hair falling out in patches, or overall thinning.
Hair-loss is mainly genetical but can be caused by some other factors like sedentary lifestyle, unhealthy diets, ageing and hormonal imbalance and increasing chronic disease like arthritis, cancer, hypertension and depression.
Androgenetic alopecia is the most common form of hair loss for both men and women. It can be caused by either hormonal or hereditary factors.
Androgenetic alopecia is an androgendependent hereditary disorder in which dihydrotestosterone is a significant contributing factor. The condition affects Caucasian men more than men of other ethnicities. It can start at any age, but approximately 30% of men will experience some hair loss by the age of 30 years, 50% by the age of 50 years, and 80% by the age of 70 years.
In men, hair loss can begin any time after puberty and progress over the course of years or decades. It starts above the temples and continues around the perimeter and the top of the head, often leaving a ring of hair along the bottom of the scalp. Many men with male pattern hair loss eventually become bald.
In women, hair slowly thins all over the scalp, but the hairline usually doesn’t recede. Many women experience this type of hair loss as a natural part of aging, although hair loss may begin any time after puberty. Female pattern hair loss can cause hair to thin dramatically, but only rarely does it lead to baldness.
Telogen effluvium, a type of hair loss, occurs when large numbers of follicles on the scalp enter the resting phase of the hair growth cycle, called telogen, but the next growth phase doesn’t begin. This causes hair to fall out all over the scalp without new hair growth.
Telogen effluvium does not generally lead to complete baldness, although some may lose 300 to 500 hairs per day, and hair may appear thin, especially at the crown and temples. A medical event or condition, such as a thyroid imbalance, childbirth, surgery, or a fever, typically triggers this type of hair loss. Telogen effluvium may also occur as a result of a vitamin or mineral deficiency—iron deficiency is a common cause of hair loss in women—or the use of certain medications, such as isotretinoin, prescribed for acne, or warfarin, a blood thinner. Starting or stopping oral contraceptives (birth control pills) may also cause this type of hair loss.
Anagen effluvium is rapid hair loss resulting from medical treatment, such as chemotherapy. These potent and fast-acting medications kill cancer cells, but they may also shut down hair follicle production in the scalp and other parts of the body. After chemotherapy ends, hair usually grows back on its own.
Alopecia areata is an autoimmune condition, which means the body’s immune system attacks healthy tissues, including the hair follicles. This causes hair to fall out and prevents new hair from growing.
This condition can affect adults and children, and hair loss can begin suddenly and without warning. Hair from the scalp typically falls out in small patches and is not painful. Hair in other parts of the body, including the eyebrows and eyelashes, may also fall out.
Tinea capitis, also called scalp ringworm, is a fungal infection of the scalp that’s a common cause of hair loss in children. This condition causes hair to fall out in patches, sometimes circular, leading to bald spots that may get bigger over time.
The affected areas often look red or scaly, and the scalp may be itchy. Sores or blisters that ooze pus can also develop on the scalp.
There are ranges available from pharmacy that encompass a full system for consumers to use that includes supplements, fibres and densifying shampoo, conditioner and elixir. The haircare products help to ensure the scalp

is healthy and nourished, while helping the hair to look thicker and fuller.
Minoxidil reinvigorates shrunken hair follicles – they increase in size and re-grow thicker hair over time. Minoxidil works by helping the blood flow to the hair follicles and increasing follicular size and hair shaft diameter, stimulating and prolonging hair growth.
Minoxidil increases blood flow which stimulates hair follicles, promoting hair regrowth in 4 ways:
• Reverses miniaturisation of follicles
• Increases blood flow around follicles
• Stimulates follicle movement from resting to hair growth phase
• Extends each follicle’s growth phase
Alpecin Shampoo is caffeine based treatment, with additional zinc, vitamin A and niacin. There are several small research papers showing some effectiveness of Alpecin in improving hair strength and increasing activity in hair roots after a few months of regular use.
Tinea capitis needs to be treated with oral antifungal medication and a medicated antifungal shampoo to reduce spread of the fungus to other people.
Who? Both men and women can be affected by thinning hair due to a number of factors. Androgenetic alopecia will affect 30% of men will by the age of 30 years, 50% by the age of 50 years, and 80% by the age of 70 years. In addition, up to 13% of premenopausal women experience some degree of androgenetic alopecia.
What are the symptoms? Most people will lose some hair every day. Patients with androgenetic alopecia experience hair loss with no signs of inflammation or scarring.
How long has the patient had the symptoms? If a patient develops sudden hair loss they should be referred to a GP.
Action already taken? Eating a balanced diet can aid hair health.
Medications? Minoxidil reinvigorates shrunken hair follicles; Alpecin Shampoo; Anti-fungal medications/shampoos.



















Anusol™ Cream (GSL): Each 100g contains Bismuth oxide 2.14g, Balsam Peru 1.8g, Zinc oxide 10.75g. Anusol™ Suppositories (GSL): Each suppository contains: Bismuth subgallate 59mg, Bismuth oxide 24mg, Balsam Peru 49mg, Zinc oxide 296mg. Anusol™ Plus-HC Ointment (P): Each 100g contains: Hydrocortisone acetate 0.25g, Benzyl benzoate 1.25g, Bismuth subgallate 2.25g, Bismuth oxide 0.875g, Balsam Peru 1.875g, Zinc oxide 10.75g. Indication. For the symptomatic treatment of internal and external (ointment only) haemorrhoids and pruritus ani. MA holder. Church & Dwight UK Ltd., Premier House, Shearway Business Park, Pent Road, Folkestone, Kent, CT19 4RJ. Information about this product, including adverse reactions, precautions, contra-indications, and method of use can be found at: Anusol cream: https://www.medicines.org.uk/emc/product/1486/smpc; Anusol Suppositories: https://www.medicines.org.uk/emc/product/1488/smpc; Anusol Plus-HC Ointment: https://www.medicines.org.uk/emc/product/1470/smpc. Latest revision of SmPCs: April 2018.
Haemorrhoids are one of the most common ano-rectal ailments. More than half of people will develop haemorrhoids, usually after the age of 30. A HTA on referral thresholds for haemorrhoid procedures has shown that half the Irish population “experience symptomatic haemorrhoid disease at some point in their lives, with the peak incidence of symptomatic disease between the ages of 45 and 65 years.”
Also known as piles, these are swellings that contain enlarged blood vessels that are found inside or around the bottom (the rectum and anus).
Most haemorrhoids are mild and sometimes don’t even cause symptoms. When there are symptoms, these usually include:
• bleeding after passing a stool (the blood will be bright red)
• itchy bottom
• a lump hanging down outside of the anus, which may need to be pushed back in after passing a stool
Symptoms may include rectal bleeding resulting from irritation of internal haemorrhoids, with bleeding usually occurring immediately after defecation. Other symptoms may include itching, perianal discomfort, and soiling.
Constipation, pregnancy, heavy lifting, or strenuous exercise may exacerbate these symptoms. Prolonged sitting, obesity, and low-fibre diets are other possible contributing factors.
The exact cause of haemorrhoids is unclear, but they’re associated with increased pressure in the blood vessels in and around the anus. This pressure can cause the blood vessels in the back passage to become swollen and inflamed.
Many cases are thought to be caused by too much straining on the toilet, due to prolonged constipation – this is often due to a lack of fibre in a person’s diet. Chronic (long-term) diarrhoea can also make sufferers more vulnerable to getting haemorrhoids.
Other factors that might increase the risk of developing haemorrhoids include:
• being overweight or obese
• age – as a person gets older, the body’s supporting tissues get weaker, increasing the risk of haemorrhoids
• being pregnant – which can place increased pressure on your pelvic blood vessels, causing them to enlarge
• having a family history of haemorrhoids
• regularly lifting heavy objects
• a persistent cough or repeated vomiting
• sitting down for long periods of time
Supportive care strategies may include

lifestyle changes, such as adopting a highfibre diet, increasing fluid intake, avoiding straining during defecation, and using topical products for symptom relief.
As haemorrhoidal tissues are inflamed, topical vasoconstrictors are commonly used to shrink blood vessels in the anorectal area and temporarily relieve swelling. Topical analgesics may also be used to relieve pain, itch, and irritation.
OTC treatments - various creams, ointments and suppositories are available from pharmacies without a prescription. They can be used to relieve any swelling and discomfort. These medicines should only be used for five to seven days at a time. They may irritate the sensitive skin around your anus if you use them longer than this.
Any medication should be combined with the diet and self-care advice discussed above. Pharmacists can advise about which product is most suitable.
Corticosteroid cream - a GP may prescribe corticosteroid cream, which contains steroids, if there is severe inflammation in and around the back passage.
Painkillers - common painkilling medication, such as paracetamol, can help relieve the pain of haemorrhoids. But if a sufferer has
excessive bleeding, they should avoid using non-steroid anti-inflammatory drugs (NSAIDs), such as ibuprofen, as they can make rectal bleeding worse. They should also avoid using codeine painkillers as they can cause constipation.
Banding - carried out as a day procedure, this involves placing a very tight elastic band around the base of the haemorrhoids to cut off their blood supply. The haemorrhoids should then fall off within about a week of having the treatment. Banding is usually a day procedure that doesn’t need an anaesthetic, and most people can get back to their normal activities the next day.
Sclerotherapy - may be used as an alternative to banding. During sclerotherapy, a chemical solution is injected into the blood vessels in the back passage. This relieves pain by numbing the nerve endings at the site of the injection. It also hardens the tissue of the haemorrhoid so a scar is formed. After about four to six weeks, the haemorrhoid should decrease in size or shrivel up.
Surgery - although most haemorrhoids can be treated using the methods described above, around one in every 10 people will eventually need surgery. Surgery is particularly useful for haemorrhoids that have developed below the dentate line – unlike non-surgical treatments, anaesthetic is used to ensure sufferers don’t feel any pain.
Who? The risk of haemorrhoids increases as a person gets older.
What are the symptoms? Pain or discomfort, especially when sitting, pain during bowel movements, itching or irritation around the anal region, bright red blood on stools, swelling around the anus.
How long have they had the symptoms? If OTC products have not helped the symptoms within a week the sufferer should be referred to a doctor.
Action already taken? Sufferer can be advised of a number of lifestyle changes which can lessen the symptoms or reduce the risk of haemorrhoids returning.
Medication? A number of OTC treatments are available. Sufferers should avoid ibuprofen and codeine.
Famotidine, Magnesium Hydroxide, C alcium C arbonate.
Neutralises existing acid Reduces acid production Effective relief in just one dose
Lasts all day or night

Calcium Carbonate and magnesium hydroxide neutralises the exisiting acid in the stomach.
Famotidine actively reduces the amount of acid produced.

active substances or to any of the excipients. Severe renal failure. Cross sensitivity in H2-receptor antagnonists has been observed. Famotidine/antacid combination should not be administered to patients with a history of hypersensitivity to other H2-receptor antagonists. Special warnings and precautions for use. Warnings: Patients with renal or hepatic impairment should consult a physician before using Pepcid Duo Chewable Tablets. In case of rena failure, monitoring of serum magnesium and calcium should be undertaken. Pepcid Duo is contraindicated in patients with severe renal failure. As some serious underlying conditions can have symptoms in common with simple indigestion, it is recommended patients seek medical advice in case of: indigestion symptoms accompanied by unintentional weight loss, dif culty swallowing, persistent abdominal discomfort, heartburn occurring for the rst time or if these symptoms have recently changed. Patients with pre-existing known hypercalcaemia, hypermagnesaemia, hypophosphataemia, hypercalcuria, a history of renal calculi or nephrocalcinosis should consult a physician before using famotidine/antacid combination. As this product contains lactose, glucose and benzyl alcohol: Patients with rare hereditary problems of galactose intolerance, total lactase de ciency or glucose-galactose malabsorption should not take this medicine. Patients with rare glucose-galactose malabsorption should not take this medicine. This medicine contains 0.000238 mg benzyl alcohol in each tablet which is equivalent to 0.000129 mg/g. Benzyl alcohol may cause allergic reactions. High volumes of benzyl alcoho should be used with caution and only if necessary, especially in subjects pregnant or breastfeeding, or with liver or kidney impairment because of the risk of accumulation and toxicity (metabolic acidosis). With long term use, especially during concomitant treatment with other calcium products and/or Vitamin D products, there is a risk of hypercalcaemia with subsequent kidney function impairment. Patients should stop use and consult a physician if new symptoms
Heartburn typically presents as a burning sensation in the chest, just behind the breastbone known to appear directly after or while eating, after exercise at night time or when lying down. It is caused by stomach acid travelling up the oesophagus towards the back of the mouth primarily due to dysmobility of the lower oesophageal sphincter, which is supposed to prevent the regurgitation of gastric content and/or gastric acid.
For anyone experiencing the discomfort associated with heartburn and dyspepsia, finding rapid relief is a top priority. Heartburn and dyspepsia are common gastrointestinal (GI) complaints that, if left unresolved, may negatively affect an individual’s overall quality of life and restrict or limit activities or ingestion of certain foods.
Because many patients elect to self-treat mild to moderate cases of heartburn and dyspepsia, pharmacists are likely to encounter patients seeking advice on the various non-prescription products available for the prevention and treatment of both conditions. Pharmacists also are instrumental in identifying patients at increased risk for developing heartburn and dyspepsia because of certain medications, medical conditions, or lifestyle habits.
Heartburn, or pyrosis, is characterised as a burning sensation arising from the substernal area and moving toward the neck or throat. There are 2 main types: postprandial heartburn occurs within 2 hours after a meal, when bending over, or when lying down, and nocturnal heartburn occurs during sleep and often is responsible for interrupting it.
The groups at risk include those in poor health, particularly the over 55s who are more likely to be overweight and/or have other medical conditions, and people exposed to stress.
Most patients know what causes their heartburn. Citrus juices, bread, coffee, cucumber, and rich and spicy meals are common triggers. Overindulgence in food and alcohol (especially right before bed), smoking, excess weight, and stress are other common causes.
If someone has heartburn incidences more than three times a week they may have a more serious underlying problem such as gastro oesophagael reflux disease (GORD). This condition results in the contents of the stomach to back up, or reflux, into the oesophagus.
Pharmacy staff should ask open-ended questions about concurrent medications and supplements, such as NSAIDs, aspirin, glucosamine, and others, that may list heartburn among their side effects.
Sometimes pointed questions about lifestyle can help patients select appropriate lifestyle modifications. Pharmacists should remember that for gastrointestinal reflux, certain symptoms should raise an alarm. If patients

report any symptom indicative of one of these, referral to a physician is warranted.
• Am I/my team familiar with the differences between heartburn, GORD, indigestion and other GI disorders to make an educated diagnosis?
• Am I/my team aware of the symptoms of heartburn?
• Am I/my team aware of contributing causes of heartburn in order to advise sufferers of lifestyle changes?
• Do I know what to recommend if a customer returns saying the treatment has not worked?
• Am I aware of the drug interactions for OTC heartburn medicines?
Who? 73% of people can experience indigestion and heartburn interchangeably. As many as eight out of 10 women experience indigestion at some point during their pregnancy.
What are the symptoms? Pain in the lower chest, abdomen or top of the stomach, feeling bloated, needing to burp or pass wind, nausea or vomiting and loss of appetite.
How long have they had the symptoms? The symptoms are usually experienced after eating or drinking, but there can sometimes be a delay between eating a meal and developing indigestion. Women may experience indigestion at any point during their pregnancy. Symptoms may be more frequent and severe during the third trimester.
Action already taken? People may have taken antacids but not be aware how to eliminate triggers until they start to keep a food diary
Medication? Antacids can be taken safely during pregnancy to treat indigestion.


Pharmacy teams can play an essential role for patients with Irritable Bowel Syndrome (IBS) by helping them identify symptoms, discussing possible treatment options, and educating them about the disease.
Counter assistants and staff can help to recognize patients who likely have IBS and either attempt to self-medicate with various OTC products such as herbal supplements or have prescriptions for antidiarrheals or laxatives.
Proactive questioning of the patient will allow pharmacy staff to assess the appropriateness of the medications or identify a need for referral to other health care professionals for further evaluation. Finally, it is also important to reassure the patient that IBS remains a manageable illness for the most part.
Irritable bowel syndrome (IBS) is quite common with as many as 1 in 5 people affected. It is twice as common in women as men and happens most often to people in their 20s and 30s.
IBS is a disorder of the gut whereby the function of the gut is disturbed. However there are no physical or structural abnormalities. It causes a variety of symptoms, which are discussed in further detail below. It usually first appears in teenagers and young adults.
Symptoms of IBS include loose, frequent stools, constipation, bloating, and abdominal pain and cramps. Patients may notice symptoms following the intake of specific foods or that symptoms, such as stool consistency or pain location, change over time. Patients may also present with headache, lethargy, nausea, bladder symptoms or faecal incontinence.
Pain and discomfort may occur in different parts of the abdomen. Pain usually comes and goes. The length, severity and timing of each bout of pain can also vary greatly. The pain often eases when passing stools (motions or faeces) or wind. Many people with IBS describe the pain as a spasm or colic.
Bloating and swelling of the abdomen may develop from time to time. Sufferers may pass more wind than usual. Other symptoms can sometimes occur and include: nausea (feeling sick), headache, belching, poor appetite, tiredness, backache, muscle pains, feeling quickly full after eating, heartburn, and bladder symptoms (an associated irritable bladder).
Some people have occasional mild symptoms. Others have unpleasant symptoms for long periods. Many people fall somewhere in between, with flare-ups of symptoms from time to time.

Most IBS sufferers believe that certain foods cause or exacerbate their symptoms and thus exclude these foods from their diet. Insufficient evidence exists, however, to support exclusion diets or food allergy testing once lactose intolerance and celiac sprue are excluded.
Alternatively, some may find it helpful to keep a food diary to determine if gas-producing foods (eg, beans, cabbage, onions, broccoli), carbonated drinks, sorbital, lactose, or wheat aggravate their symptoms and then avoid or limit them to determine if symptoms improve.
Many IBS patients who seek medical care suffer from anxiety or depression and benefit from psychological therapies, including
cognitive-behavioural therapy, hypnotherapy, and dynamic psychotherapy.
Pharmacologic treatment is aimed at relieving the predominant GI symptom, but the goal should be to improve the overall or global symptoms, including altered stool frequency and consistency, abdominal pain and discomfort, bloating, and quality of life.
Antispasmodics may provide short-term relief of abdominal pain and discomfort in IBS, but support for long-term efficacy is not available. Antispasmodics are associated with adverse effects (eg, dry mouth, blurred vision, dizziness, urinary retention), which may limit their use and should be avoided in IBS-C or IBS-M, as they may worsen constipation.
Who? As many as 1 in 5; twice as common in women as in men; more frequently occurs in those aged in their 20’s and 30’s.
What are the symptoms? Loose, frequent stools; constipation; bloating; cramps.
How long have they had the symptoms? Pain usually comes and goes; bloating and swelling may occur from time to time.
Action already taken? May have altered diet and/or kept a food diary to determine flare-ups and causes.
Medication? Antispasmodics may provide short-term relief of pain and discomfort.



Result of product demonstration consisting of pouring 4x 10 ml liquid to 1 Always Unnoticeable Protection for Incontinence Normal & 1 Al ways Ultra Long pad. 20 minutes from finishing last pour, plotting paper pressed on both pads, resulting in measuring the level of dryness.

Incontinence is a condition that most people are too embarrassed to talk about, yet one that affects one in three women and one in nine men, and costs the HSE ¤100 million every year.
Urinary Incontinence (UI) can have a hugely negative impact on a person’s quality of life, mood and confidence with some sufferers becoming virtual prisoners in their own homes.
Urinary incontinence is loss of control of the bladder. It can affect anyone, regardless of age. It is a condition which ranges from mild to uncontrollable and embarrassing wetting. Incontinence can often be caused by an illness, such as a urinary tract infection, and often when the infection gets better the incontinence improves.
Bladder control problems have a significant effect on the quality of life of sufferers on a physical, emotional and social level. Continence is a necessity for comfortable social adjustment and conversely, urinary incontinence frequently causes profound psychological and social consequences and restricts social activities.
Stress incontinence - happens when a person wets themself during exercise, coughing, sneezing, laughing or other movements that put pressure on the bladder. It is the most common type of incontinence and usually affects women, however, men can also develop stress incontinence after a prostate operation.
Urgency/urge incontinence - occurs when a person cannot hold on long enough to reach a toilet. This may be caused by an over-active bladder, infection, medication or poor mobility. In men, it may be sign of an enlarged prostate.
Overflow incontinence - happens when the bladder does not empty completely. Urine builds up and then may overflow, often as frequent dribbling. This type of incontinence is more common in men and may be due to an enlarged prostate gland, but constipation may also be a cause.
Reflex incontinence - is where the bladder empties when it is full and the person is usually unaware of this. The cause is a break in the signals between the brain and bladder, which may be caused by a stroke or spinal injury.
While incontinence products aren’t a treatment for urinary incontinence, they are useful for managing the condition while a person is waiting to be assessed or for treatment to take effect.
• Absorbent products, such as incontinence pants or pads. Liners, pads, disposable underwear, and reusable underwear absorb moisture. Products made for incontinence control catch the leaks and pull moisture away from the skin. That allows sufferers to go longer between changes.Many disposable pads, liners, and undergarments have a waterproof backing. This helps prevent overflow from reaching clothes. The waterproof systems
use a “breathable” plastic film that helps reduce skin irritation.There’s also a range of disposable undergarments with built-in protection - not just in the crotch, but throughout the entire garment. Styles range from pull-ons with elasticised legs and waists resembling a traditional cloth underwear to underwear that slips on with Velcro or adhesive tabs for a customised fit. There are also open-sided “thong style” pants held together by straps in the front and back that rest on top of the hip bone. Incontinence bed sheets are also available.
• Handheld urinals
• A catheter, a thin tube that is inserted into the bladder to drain urine
• Devices that are placed into the vagina or urethra to prevent urine leakage – for example, during exercise
The treatment a medical professional will recommend for urinary incontinence will depend on the type of incontinence a patient has and the severity of their symptoms. If the incontinence is caused by an underlying condition, they may receive treatment for this alongside incontinence treatment.
Conservative treatments, which don’t involve medication or surgery, can be recommended first. These include:
Lifestyle changes
• reducing caffeine intake – caffeine is found in tea, coffee and cola, and can increase the amount of urine the body produces
• altering how much fluid is drunk a day –drinking too much or too little can make incontinence worse
• losing weight
Pelvic floor muscle training (Kegel exercises)
The pelvic floor muscles are the muscles used to control the flow of urine as the body urinates. They surround the bladder and urethra, the tube that carries urine from the bladder outside the body. Weak or damaged pelvic floor muscles can cause urinary incontinence, so exercising these muscles is

often recommended. A GP may refer a patient to a specialist to start a programme of pelvic floor muscle training.
The specialist will assess whether the person is able to squeeze (contract) their pelvic floor muscles and by how much. If they can contract their pelvic floor muscles, they’ll be given an individual exercise programme based on their assessment.
When diagnosed with urge incontinence, one of the first treatments offered is bladder training. Bladder training may also be combined with pelvic floor muscle training if a person is suffering from mixed urinary incontinence. It involves learning techniques to increase the length of time between feeling the need to urinate and passing urine. The course will usually last for at least six weeks.
Mid-urethral slings are minimally invasive procedures developed in Europe in the 1990s to treat female stress urinary incontinence. These slings are narrow, polypropylene (a commonly used suture material) tapes that are surgically placed beneath the middle part of the urethra (water pipe) to provide dynamic support to stop leakage from the bladder. They have been shown to be as effective as more invasive traditional surgery with major advantages of shorter operating and admission times, and a quicker return to normal activities together with lower rates of complications.
Who? Anyone, regardless of age. Women are more prone to stress incontinence than men.
What are the symptoms? Depends on the type of incontinence, but generally wetting oneself or dribbling.
How long have they had the symptoms? Medical advice should be sought when symptoms present.
Action already taken? Lifestyle changes or pelvic exercises may help.
Medication?A range of products to manage the condition are available.







To request more information on Active Iron, please contact your Pharmed Ireland representative or email info@activeiron.com
For more information, please visit www.activeiron.com/activeiron/healthcare-professionals/

Iron deficiency anaemia occurs when there is a reduced number of red blood cells because the body does not have enough iron to produce them. The main symptoms are tiredness and lethargy (lack of energy).
An estimated 20% of all women, 50% of pregnant women, and 3% of men do not have a sufficient amount of iron in their bodies.
Research suggests that women living with inadequate iron levels is a global problem affecting approximately 1 in 4 women. Certain groups are more at risk, including:
• Pregnant & post partum women
• Endurance exercisers
• Restricted diets e.g vegetarians
Iron is an essential mineral because it is an integral component of haemoglobin (Hb), which enables oxygen to be bound, stored and carried around the body in the blood. Reduced iron in the body therefore results in less oxygen being delivered to tissues and organs.
This lack of iron can be caused by either reduced iron intake or an increased loss of iron from the body. Non-anaemic iron deficiency or latent iron deficiency is a condition in which there is iron deficiency but Hb levels are normal and symptoms often include fatigue, hair loss, lack of concentration and irritability.
Iron is found in meat, dried fruit and some vegetables. It is used by the body to make haemoglobin, which helps store and carry oxygen in red blood cells. Haemoglobin transports oxygen from the lungs to the rest of the body. If there is a lack of iron in the blood, the organs and tissues will not get as much oxygen as they usually do.
Iron deficiency anaemia affects up to one in 20 men and one in 20 post-menopausal women (after a woman’s menstrual periods have stopped). Iron deficiency anaemia is more common in women who are still menstruating (having periods). This is because menstruation and pregnancy can cause iron deficiency.
The oral iron market is dominated by poorly absorbed and poorly tolerated products. Treatment for iron deficiency anaemia involves increasing dietary iron intake or taking iron supplements to replace the missing iron in the body. This is usually very effective and the condition rarely causes any serious complications.
Due to poor absorption, oral iron can cause inflammation and oxidation in the gastrointestinal system, resulting in side effects.
• A majority of patients report GI side effects from traditional iron including stomach upset, nausea, constipation and diarrhoea.
• Around half of them have stop taking them due to these side effects, resulting in treatment failure.
• Some patients will progress to anaemia and need medical intervention with injectable iron.
• Others continue on the cycle – take, side effect, stop, repeat

Patients with iron deficiency anaemia may need to be monitored to check that the treatment is working and that their iron levels have returned to normal.
For those customers who decide to take an iron supplement, it’s important pharmacy staff assist them in selecting one that is kind on their stomach and strong on absorption.
Gastrointestinal blood loss
Bleeding in the stomach and intestines is the most common cause of iron deficiency anaemia in men and in women who have been through the menopause (when a woman’s monthly periods stop).
In women who are still menstruating (having monthly periods), the most common causes of iron deficiency anaemia are:
• menstruation (monthly periods)
• pregnancy
Menstruation
Usually, only women with particularly heavy periods develop iron deficiency anaemia. If you have heavy bleeding over several consecutive menstrual cycles, it is known as menorrhagia.
It is very common for women to develop iron deficiency during pregnancy. This is because their body needs extra iron so that your baby has a sufficient blood supply and receives all of the necessary oxygen and nutrients. Many
pregnant women require an iron supplement, particularly from the 20th week of pregnancy.
Other conditions or situations that cause blood loss and may lead to iron deficiency anaemia include:
• inflammatory bowel disease: a condition that causes inflammation (redness and swelling) in the digestive system, such as Crohn’s disease and ulcerative colitis
• oesophagitis: inflammation of the gullet (oesophagus) that is caused by stomach acid leaking up it
• schistosomiasis: an infection that is caused by parasites and is mainly found in subSaharan Africa
• blood donation: donating a large amount of blood may lead to anaemia
• trauma: a serious accident, such as a car accident, may cause you to lose a lot of blood
• nosebleeds: if you have a lot of nosebleeds, this may lead to anaemia, although it is rare
• haematuria (blood in your urine): this is also rare and may be the symptom of another condition
Unless a customer is pregnant, it is very rare for iron deficiency anaemia to be caused solely by a lack of iron in their diet.
Pregnant women may have to increase the amount of iron-rich food that they consume during their pregnancy to help avoid iron deficiency anaemia.
Who? Anyone, but women, and particularly pregnant women are more likely to suffer.
What are the symptoms? The main symptoms are tiredness and lack of energy.
How long have they had the symptoms? Best controlled as soon as the symptoms are diagnosed.
Action already taken? Treatment for iron deficiency anaemia involves increasing dietary iron intake or taking iron supplements to replace the missing iron in the body.
Medication? Prescribed medication may lead some people to get side effects such as constipation or diarrhoea, tummy pain or a feeling of sickness.


analgesic

References: 1. Merry A, et al. AFT-MX-1, a prospective parallel group, double-blind comparison of the analgesic effect of a combination of paracetamol and ibuprofen, paracetamol alone, or ibuprofen alone in patients with post-operative pain. Department of Anaesthesiology, University of Auckland, New Zealand 2008. *compared with the same daily dose of standard paracetamol or ibuprofen alone.

Easolief DUO 500 mg/150 mg film-coated tablets Each tablet contains paracetamol 500 mg and ibuprofen 150 mg. Presentation: White, capsule shaped tablet with breakline on one side and plain on the other side. Indications: Shortterm symptomatic treatment of mild to moderate pain. Dosage: Adults/elderly: The usual dosage is one to two tablets taken every six hours up to a maximum of six tablets in 24 hours. Children: Easolief DUO is contraindicated in children under 18 years. Contraindications: Severe heart failure, known hypersensitivity to paracetamol, ibuprofen, other NSAIDs or to any of the excipients, active alcoholism, asthma, urticaria, or allergic-type reactions after taking acetylsalicylic acid or other NSAIDs, history of gastrointestinal bleeding or perforation related to previous NSAID therapy, active or history of recurrent peptic ulceration/haemorrhage, severe hepatic failure or severe renal failure, cerebrovascular or other active bleeding, blood-formation disturbances, during the third trimester of pregnancy. Warnings and precautions: This medicine is for short term use and is not recommended for use beyond 3 days. Clinical studies suggest that use of ibuprofen, particularly at a high dose may be associated with a small increased risk of arterial thrombotic events. Patients with uncontrolled hypertension, congestive heart failure, established ischaemic heart disease, peripheral arterial disease and/or cerebrovascular disease should only be treated with ibuprofen after careful consideration and high doses should be avoided. Careful consideration should be exercised before initiating long-term treatment of patients with risk factors for cardiovascular events. The use of paracetamol at higher than recommended doses can lead to hepatotoxicity, hepatic failure and death. Patients with impaired liver function or a history of liver disease or who are on long term ibuprofen or paracetamol therapy should have hepatic function monitored at regular intervals. Severe hepatic reactions, including jaundice and cases of fatal hepatitis, though rare, have been reported with ibuprofen. Paracetamol can be used in patients with chronic renal disease without dosage adjustment. There is minimal risk of paracetamol toxicity in patients with moderate to severe renal failure. Caution should be used when initiating treatment with ibuprofen in patients with dehydration. The use of an ACE inhibiting drug, an anti-inflammatory drug and thiazide diuretic at the same time increases
the risk of renal impairment. Blood dyscrasias have been rarely reported. Patients on long-term therapy with ibuprofen should have regular haematological monitoring. Like other NSAIDs, ibuprofen can inhibit platelet aggregation. GI bleeding, ulceration or perforation, which can be fatal, has been reported with all NSAIDs at anytime during treatment. Combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) should be considered. Use with concomitant NSAIDs including cyclooxygenase-2 selective inhibitors should be avoided. NSAIDs may lead to onset of new hypertension or worsening of pre-existing hypertension and patients taking antihypertensive medicines with NSAIDs may have an impaired anti-hypertensive response. Fluid retention and oedema have been observed in some patients taking NSAIDs. NSAIDs may very rarely cause serious cutaneous adverse events such as exfoliative dermatitis, toxic epidermal necrolysis and Stevens-Johnson syndrome. Acute generalised exanthematous pustulosis (AGEP) has been reported in relation to ibuprofencontaining products. Products containing ibuprofen should not be administered to patients with acetylsalicylic acid sensitive asthma and should be used with caution in patients with pre-existing asthma. Adverse ophthalmological effects have been observed with NSAIDs. For products containing ibuprofen aseptic meningitis has been reported only rarely. NSAIDs may mask symptoms of infection and fever. In order to avoid exacerbation of disease or adrenal insufficiency, patients who have been on prolonged corticosteroid therapy should have their therapy tapered slowly rather than discontinued abruptly when products containing ibuprofen are added to the treatment program. Interactions: Warfarin, medicines to treat epilepsy, chloramphenicol, probenecid, zidovudine, medicines used to treat tuberculosis such as isoniazid, acetylsalicylic acid, other NSAIDs, medicines to treat high blood pressure or other heart conditions, diuretics, lithium, methotrexate, corticosteroids. Fertility, pregnancy and lactation: Easolief DUO is contraindicated during the third trimester of pregnancy. Driving and operation of machinery: Dizziness, drowsiness, fatigue and visual disturbances are possible after taking NSAIDs. If affected patients should not drive or operate machinery. Undesirable effects: Dizziness, headache, nervousness, tinnitus, oedema, fluid retention, abdominal pain, diarrhoea, dyspepsia, nausea, stomach discomfort, vomiting, flatulence, constipation, slight gastrointestinal blood loss, rash, pruritus, alanine aminotransferase increased, gamma-glutamyltransferase increased, abnormal liver function tests, blood creatinine increased and blood urea increased. Refer to Summary of Product Characteristics for other adverse effects. Adverse reactions should be reported via HPRA Pharmacovigilance, website: www.hpra.ie. Pack size: 24 tablets. Marketing authorisation holder: Clonmel Healthcare Ltd. Marketing authorisation number: PA0126/294/1. Supply through pharmacies only. Date last revised: June 2022. Date of preparation: July 2022. 2022/ADV/EAS/197H.
Painful conditions are among the most commonly presenting minor ailments in general practice, and the scope for pharmacy input into self-care for painful minor ailments is evident. It is imperative that pharmacists and pharmacy support staff have relevant and evidence-based knowledge to inform their practice.
Pain is one of the most common symptoms presented to pharmacists and its presence is almost ubiquitous in all diseases and injuries. Pain can be mild, moderate or severe. It can be treated using different strengths of painkiller, depending on the level of pain. A pharmacist can assess a patient’s pain before prescribing the best painkillers to help control it.
Effective assessment is the keystone of pain management and it is important to focus on the patient’s experiences and circumstances.
Acute pain is short-term and usually follows an injury, such as an operation, fracture or infection. Acute pain is usually self-limiting, resolves once the underlying problem is treated or heals – which generally takes days or weeks – and typically responds well to analgesics, including those available OTC from pharmacies.
Acute pain is often treated with non-opioid drugs and anti-inflammatory drugs. Sometimes opioids are used to treat mild pain. A patient’s description of pain should be considered the most reliable indicator of suffering.
On the whole, pains encountered in community pharmacies will be mild to moderate and self-limiting (less than one week), and will generally respond to any one of the wide range of over-the-counter analgesic products available.Typical conditions presented include toothache, headache, dysmenorrhoea and musculoskeletal injuries.
Mild pain is often successfully treated with painkillers such as paracetamol and antiinflammatory drugs.
Paracetamol can be used for most types of mild pain. It can be bought it from a pharmacy or supermarket. It has few side effects, but it is very important not to take more than the recommended dose. Higher doses can damage the liver. Paracetamol does not reduce inflammation.
Anti-inflammatory drugs such as ibuprofen help reduce inflammation and swelling. They are good for treating pain in the skin, muscle or bone. These can be bought from a pharmacy or supermarket. Other antiinflammatory medicines need to be prescribed by a doctor.
Advice should be given by a medical professional before these types of medicines are taken. They do not always work for everyone and may not mix well with other medicines you’re taking.
Anti-inflammatory drugs can cause indigestion and may irritate the lining of the stomach, so it’s important to take them after a meal or snack. A doctor may prescribe another medicine to help protect the stomach. If a patient has had problems with stomach ulcers before, a doctor may suggest they don’t take anti-inflammatory drugs at all. Or they may
suggest they use an anti-inflammatory gel, which you can rub onto the skin.
When taking these drugs, always check the recommended dose on the packet and never take a higher dose.
Other medicines or tablets that are sold from a pharmacy or supermarket, such as cold and flu remedies, may also contain paracetamol or anti-inflammatory drugs. If a person is taking painkillers, they should be careful which other medicines they take, so that they don’t take more than the recommended doses. A pharmacist can give advice about over-thecounter medicines.
Compound analgesics are made from a combination of two different drugs. New combination painkillers combining full strength paracetamol and ibuprofen are available and suitable for the treatment of mild to moderate pain.
Compound analgesics containing low doses of codeine are available over the counter from pharmacists, but stronger ones are only available on prescription. They can be used for moderate pain.
A number of other methods can be recommended for managing pain
• Applying heat to the skin can help some types of pain. Use compresses or products such as sprays, creams, ointments, gels and patches to help swelling and inflammation.
• Support from bandages or compression hosiery can help with sprains and strains.
• Acupuncture or Transcutaneous Electrical Nerve
• Stimulation (TENS) are alternatives to medication for pain control
• Rest
• Exercise (if the patient is able to)
• Headache, migraine
• Toothache
• Period pain
• Minor injuries, strains and sprains
• Backache, muscle aches, joint pains
Topical OTC treatments broadly divide into those with active ingredients and those that are drug-free.
Formats available include gels, creams, ointments, sprays, patches and wraps. Patients will often use
OTC topical analgesics for the treatment and management of musculoskeletal injuries and disorders.
These products may have local analgesic, anesthetic, antipruritic, and/or counterirritant effects.
Topical analgesics for musculoskeletal pain can be used alone or in conjunction with oral analgesics when appropriate and warranted. External analgesic products may contain one or more of the following ingredients: methyl salicylate, camphor, menthol, methyl nicotinate, capsicum, and trolamine salicylate.
Who? Anyone suffering mild to moderate pain. What are the symptoms? Persistent and nagging pain.
How long have they had the symptoms? If the symptoms persist after taking OTC medication further advice should be offered.
Action already taken? Rest and exercise can help with managing mild to moderate pain.
Medication? A number of painkillers are available OTC. Stronger painkillers are available with prescription.





Nappy rash is one of the most common skin conditions in babies and it is also the most common skin problem in early childhood. Most children aged 0-3 years old develop nappy rash in some way and it is usually presents in babies from 6-8 months.
Nappy rash can be caused by a number of factors including a combination of excess moisture, warmth, urine, faeces and friction in a baby’s nappy. It is a difficult environment for baby skin.
The nappy rash creates an enclosed area around the bottom and this increases warmth, moisture and encourages the growth of micro-organisms that can cause infection. Chafing, due either to skin rubbing against the nappy, or from skin folds, can damage and irritate the skin and ongoing contact of the skin with urine, faeces or both, can lead to a formation of ammonia which can irritate a baby’s skin.
There is also a common link made between nappy rash and teething, as well as the transition to solid foods.
Pharmacists can ease a worried parent by telling them that most nappy rashes are mild and can be treated with a simple skin care routine. Most babies will not feel any pain or discomfort and it is very rare that a baby will contact a severe form of nappy rash where infection is involved.
There are various causes of a nappy rash. Examine the rash and explain what type it is, and how to treat it most effectively.
Nappy rash can occur a baby soils or wets itself and the nappy is left on for a longer time than usual, the urine and faeces can encourage the production of the chemical ammonia, which can irritate the baby’s skin, causing it to become sore and inflamed.
Where there has been close contact with the nappy, the baby’s skin will look red and inflamed. Most affected will be the genitals, the outer skin on the folds of thighs, and the bottom. The affected areas can appear either dry or moist, and look shiny or pimply.
The best way to treat this is to keep the bottom as clean and dry as possible and change nappies often. It’s also a good idea to apply a barrier ointment/cream or medicated powder after every change.
Fungal nappy rash is often a complication of initial nappy rashand looks different. If the baby’s skin is warm and damp for long periods of time, it can cause the fungus ‘candida’, to grow. Like ammonia, candida can irritate the baby’s skin. The area of skin will be inflamed, with spots around the edges. The infection will be bright red and also present in the folds of the skin.

If a patient’s baby has severe or reoccurring nappy rash, they should be advised to visit their GP as it will usually require prescribed medication. Nappy rash should clear up within a few days of over the counter treatment.
There are a number of treatments for severe nappy rash.
• Corticosteroids help to reduce the inflammation of the skin and relieve any itching and redness.
• Hydrocortisone cream, which should only be applied once a day should not be used for more than seven days
• An anticandidal medicine helps to treat any fungal infection that may cause a rash. Some commonly prescribed anticandidal medicines include: Clotrimazole, econazole, ketoconazole, miconazole and nystatin.
Who? Predominantly newborn babies up to one year of age.
What are the symptoms? Nappy rash can affect the genitals, the outer skin on the folds of the thighs and the buttocks. The affected areas can appear either dry or moist and may sometimes look shiny or pimply.
How long has the patient had the symptoms? Severe nappy rash or recurring nappy rash should be referred.
Action already taken? Parents may already be following self-care tips such as leaving baby’snappy off and changing regularly.
Medication? If baby’s rash is caused by thrush, don’t use a barrier cream or ointment, as this can make the rash worse.

Fish oils are sometimes called the beauty and brains supplement. The DHA ingredient in fish oils is known to be a building block for brain and nerve formation.
It is added to baby formulas to support brain and nerve development. Fish oil’s popularity has soared in recent years, propelled by research that suggests consuming omega-3 fatty acids can ward off heart disease. Community pharmacists play an important role in helping patients make informed decisions about fish oil and omega-3 supplementation.
But with hundreds of OTC options available (and labels claiming that the supplements treat everything from bipolar disorder to menstrual cramps) how can pharmacists distinguish between them to help patients
Fish oils are a type of polyunsaturated fatty acids (PUFAs). They are the omega-3 and omega-6 fatty acids. Regarding heart health, the active ingredients in fish oils are DHA and EPA. The hypothesis is that omega3s offer protection from cardiovascular disease by reducing the heart’s susceptibility to arrhythmias, decreasing platelet aggregation and lowering blood pressure and

Sold by pharmacists since the early years of the 20th century, cod liver oil is one of the oldest and most well-known food supplements. The oil first gained its reputation as an effective preventative against rickets because of its high vitamin D content and it was taken by generations of children, decreasing in popularity only when, in the 1960s, the British government decided to phase it out as a welfare food.
Fish oils are most commonly used in supplements for conditions related to the heart and blood system. They may also be used for many kidney-related problems.
There is little doubt that n-3 fatty acids have an important role in nutrition. They are significant structural components of the phospholipid membranes of tissues throughout the body, particularly in the brain and retina. Because of their role in cell membranes, n-3 fatty acids are essential for the formation of new tissue and are therefore important for development and growth (eg, during foetal and infant development).
For optimal foetal health, women can be advised to take a DHA dominant Omega-3 oil from the start of their pregnancy.
Long chain n-3 fatty acids (and other fatty acids) are present in breast milk and European Union regulations now allow their addition to infant formulas.
Pharmacy team should be aware of, and understand, the following key points:
• Those who could benefit from an increased intake of n-3 fatty acids. The typical Irish diet contains relatively low amounts of these.
• Fish oil appears to reduce the risk of CHD. It may help to reduce the risk of thrombosis (by increasing bleeding tendency), reduce blood levels of triacylglycerols, prevent atherosclerosis and arrhythmias and reduce blood pressure.
• Fish oil may have a role in various mental disorders, such as depression, schizophrenia and Alzheimer’s disease, but research in this area is in its infancy.
• Fish oil supplements appear, in general, to be safe. However, patients on anticoagulants or with blood clotting disorders should be monitored.
• Fish oil could have beneficial effects in inflammatory conditions such as rheumatoid arthritis, Crohn’s disease and ulcerative colitis, but evidence of any benefit in asthma and psoriasis is poor.
Who? Certain vitamins are recommended for specific patient groups. Keep educated on their target populations.
What are the symptoms? Take a full symptom and medical history in order to direct the customer to the most appropriate vitamin/ supplement.
How long have they had the symptoms? N/A
Action already taken? Some customers may have already commenced a more balanced and healthy approach to diet and lifestyle, recommend continuation of this to include exercise.
Medication: A full medication history is essential to ensure the right product is selected for the right customer as many vitamins and supplements can cause side effects if used inappropriately.



paracetamol/caffeine
DUAL ACTIVE FORMULA PROVIDES 30% MORE POWERFUL PAIN RELIEF THAN STANDARD PARACETAMOL1
GENTLE ON THE STOMACH AND NON-DROWSY**
SOLUBLE RELIEF FOR TOUGH PAIN, INCLUDING HEADACHES, PERIOD PAIN AND DENTAL PAIN
*compared to standard paracetamol. **when used as directed/always read the label before use.
Reference: 1. Laska EM et al. JAMA 1984; 251(13): 1711-1718.
Product Information: Please consult the summary of product characteristics for full product information. Panadol Extra 500mg/65mg Soluble Effervescent Tablets, paracetamol 500mg, caffeine 65mg. Indications: Relief of mild to moderate pain including rheumatism, neuralgia, musculoskeletal disorders, headache, symptoms of colds and flu, fever, toothache and menstrual pain. Dosage: Adults and children 16 years and over: 2 tablets up to 4 times a day. Do not exceed 8 tablets in 24 hours. You may need a lower dose if you are underweight (<50kg), malnourished, dehydrated or if you have alcohol problems. Children aged 12-15 years: 1 tablet up to 4 times a day. Do not exceed 4 tablets in 24 hours. Do not give to children under 12 years. Minimum dosing interval: 4 hours. Contraindications: Hypersensitivity to paracetamol, caffeine or any ingredients. Precautions: Avoid concurrent use with other paracetamol-containing products. Diagnosed liver of kidney impairment. Patients on concomitant treatment with drugs that induce hepatic enzymes. Patients with depleted glutathione levels or chronic alcoholism or sepsis. Avoid excessive caffeine intake. Caution in those with hereditary sugar intolerance or on a low sodium diet. Should not be used in pregnancy or lactation without medical advice. Caution, due to paracetamol, if administered with flucloxacillin due to increased risk of high anion gap metabolic acidosis. Do not exceed the stated dose. Prolonged use except under medical supervision may be harmful. If high fever, or signs of secondary infection occur or if symptoms persist for longer than 3 days, consult your doctor. Side effects: See SPC for full details. All very rare: Thrombocytopenia, hypersensitivity reactions including anaphylaxis and skin rash, angioedema, Stevens-Johnson syndrome, Toxic Epidermal Necrolysis, bronchospasm, hepatic dysfunction. Frequency unknown: Nervousness, dizziness. When combined with dietary caffeine intake, higher doses of caffeine may increase potential for caffeine related adverse events such as insomnia, restlessness, anxiety, irritability, headaches, GI disturbances and palpitations. Overdose: Immediate medical advice should be sought in the event of an overdose, even if symptoms of overdose are not present. Legal Category: Supply through pharmacy only. MA Number: PA 678/39/10. MA Holder: GlaxoSmithKline Consumer Healthcare (Ireland) Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24. Additional information is available upon request. Text prepared: September 2022. Contains paracetamol. Always read the label/leaflet. Trade marks are owned by or licensed to the Haleon group of companies. PM-IE-PAN-21-00017.
Oral analgesics are used commonly for relieving pain such as headache, menstrual pain, toothache, back pain and arthritis. Some analgesics work on the body’s peripheral and central nervous systems to block or decrease sensitivity to pain. Others act by inhibiting the formation of certain chemicals in the body that mediate pain. They are available in various oral forms such as tablets, capsules, syrups, suspensions and powders. The analgesics market has experienced its fair share of ups and downs in recent years but is still growing and is likely to continue doing so.
There are two kinds of analgesics:
Non-opioid: Non-opioid analgesics include paracetamol and nonsteroid anti-inflammatory drugs (NSAIDs) such as Aspirin and Ibuprofen. Non-opioid analgesics are the first choice analgesics for treating mild to moderate pain and are also used in moderate to severe pain to potentiate the effects of opioids.
Opioid: Opioid analgesics block or decrease sensitivity to pain in the body’s peripheral and central nervous systems. Most of the opioid analgesics are prescriptiononly medicines and are suitable for moderate to severe pain, particularly of visceral origin. They can be further classified into two categories: mild and potent opioids. Mild opioid analgesics include codeine and tramadol. Strong opioid analgesics examples are morphine and methadone.
• Always follow the dosage instructions on the packaging or as instructed by your doctor or pharmacist. Do not take more than the recommended dose as this will increase the risk of serious side effects.
• Painkillers should not be shared with anyone else, as different people may experience pain with different cause and severity.
• Avoid drinking alcohol if you are taking analgesics as it may increase the risk and severity of side effects of the medicines
WARNINGS FOR ORAL ANALGESICS
Paracetamol: Taking excessive amounts can cause Liver damage and less frequently kidney damage following over doses. It should be used with caution for patients with impaired kidney or liver function, alcohol dependence, chronic malnutrition or dehydration
NSAIDS: These should always be taken with food or milk. The medication should be stopped immediately and the patient referred to a GP if the patient has abnormal or black stools. Those taking NSAIDS should avoid smoking and drinking large amounts of alcohol as these activities can increase the risk of developing a stomach ulcer Oral Pain
ORAL PAIN IS A BIG MARKET FOR ANALGESICS
Many common conditions cause oral pain or discomfort. Examples of these conditions include cold sores (see separate entry), toothaches; tooth sensitivity; teething; minor oral mucosal injury or irritation; oral mucosal disorders, such as recurrent aphthous stomatitis ([RAS]; and xerostomia (dry mouth). There are OTC products available for the selftreatment of each of these sources of oral pain and discomfort, including topical analgesics/ anaesthetics, toothpastes formulated for sensitive teeth, artificial saliva products for dry mouth, and oral mucosal protectants, as well as products that provide treatment of and relief from pain due to cold sores.
In general, the goals involved in the treatment of minor oral pain are to provide immediate symptomatic relief from discomfort and irritation and to promote healing. Patients should be assessed for the appropriateness of therapy and educated on the proper use of these
products. Pharmacy teams should advise patients to seek medical care if their conditions worsen or show signs of infection.
In an effort to self-medicate, some patients may try using analgesics to ward off pain caused by more serious health conditions and pharmacy staff are in an ideal position to monitor such situations without being too intrusive.
Toothache is pain in and around the teeth and jaws that is most often caused by tooth decay. The pain usually starts suddenly and it can vary from mild discomfort to a severe throbbing, which is often worse at night. The area of the jaw close to the infected tooth may also be sore and tender to the touch.
Toothache can either come and go or be constant. Eating or drinking can make the pain worse, particularly if the food or drink is hot or cold. Painkillers such as paracetamol and ibuprofen may help reduce pain and discomfort whilst sufferers are waiting for an appointment.
Who? Those suffering from pain such as dental pain.
What are the symptoms? Pain anywhere in the body.
How long has the patient had the symptoms? Symptoms will usually clear up within 7 days of treatment.
Action already taken? Sufferers may already have tried analgesics. If the pain persists longer than 2 weeks, the patient should be referred to a GP.
Medication? Check for underlying conditions before suggesting a specific pain relief.
*To verify contact verify@perrigo.com
Solpa-Extra 500mg/65mg Soluble Tablets contains paracetamol and caffeine. For the treatment of mild to moderate pain. Adults and children over 16 years: 1-2 tablets dissolved in water every 4-6 hours. Max 8 tablets a day. Children 12-15 years: 1 tablet dissolved in water every 4-6 hours. Max 4 tablets a day. Not suitable for children under 12 years. Contraindications: Hypersensitivity to the ingredients. Precautions: Particular caution needed under certain circumstances and medical advice sought for renal or hepatic impairment, Gilbert’s Syndrome, chronic alcoholism, glucose-6-phosphatedehydrogenase deficiency, haemolytic anaemia, glutathione deficiency, malnutrition or dehydration, the elderly, patients weighing less than 50kg. Precautions needed in asthmatic patients sensitive to acetylsalicylic acid, patients on a controlled sodium diet and with rare hereditary problems of fructose intolerance. Patients should be advised not to take other paracetamol containing products concurrently. Immediate medical advice should be sought in the event of overdose even if the patient feels well because the risk of irreversible liver damage. Excessive intake of caffeine should be avoided while taking this product. Interactions: warfarin and other coumarin, other medicines following the same metabolic pathway, cholestyramine, probenecid, chloramphenicol, metoclopramide, domperidone, sedatives, tranquilizers and some decongestants. Pregnancy and lactation: Not recommended during pregnancy and breastfeeding. Side effects: Rare: allergies. Very rare: thrombocytopenia, anaphylaxis, bronchospasm, hepatic dysfunction, cutaneous hypersensitivity reactions, very serious skin reactions, TEN, drug-induced dermatitis, SJS, AGEP, sterile pyuria. Unknown: nervousness, dizziness, neutropenia, leukopenia. Further information is available in the SmPC. Legal classification: P. PA 1186/017/001. MAH: Chefaro Ireland DAC, The Sharp Building, Hogan Place,Dublin 2, Ireland. Date of preparation: 04/2022. RRP (ex. VAT): €5.07. SPC: https://www.medicines.ie/medicines/solpa-extra-soluble-tablets-33783/smpc
When patients experience muscle and joint pain, pharmacists can recommend topical analgesics (rubs, creams and sprays) to help provide relief for their symptoms. Helping customers choose the right topical analgesic for their individual needs is key if they are to gain optimum benefit.
Musculoskeletal pain is likely to affect a significant percentage of the population and encompasses a huge range of conditions.
Low back pain, for example, is acknowledged to be the leading cause of disability worldwide and osteoarthritis is purported to affect 60% of 60-year-olds.
While musculoskeletal conditions and the pain, stiffness and immobility that go with them can compromise the lives of sufferers in many obvious physical ways, mental health and wellbeing is also affected.
Patients will often use OTC topical analgesics for the treatment and management of musculoskeletal injuries and disorders. These products may have local analgesic, anaesthetic, antipruritic, and/or counterirritant effects. Topical analgesics for musculoskeletal pain can be used alone or in conjunction with oral analgesics when appropriate and warranted. External analgesic products may contain one or more of the following ingredients: methyl salicylate, camphor, menthol, methyl nicotinate, capsicum, and trolamine salicylate.
Patient confusion regarding the wide array of topical products and formats available can also hinder usage. Consumers want help and reassurance when it comes to self-treating. They do not understand the difference between various types of topical – hot, cold and non-steroidal anti-inflammatory drugs – or how to use them. Following the introduction of the codeine regulations, pharmacists now encourage the use of acetaminophen as first in line choice of pain relief, followed by ibuprofen, before codeine-based analgesics.
In addition, patients must be made aware of how to use the medication properly and must be informed by pharmacists of the possible side effects that can occur when a product is used after the recommended period of three days. Products may have local analgesic, anaesthetic, antipruritic, and/ or counterirritant effects.
Topical pain killers, or analgesics, are sprayed on or rubbed into the skin over painful muscles or joints. Although all are designed to relieve pain, different products are made up different ingredients. Counterirritants are approved for the topical treatment of minor aches and pains of muscles and joints.

They are often employed for the treatment of acute musculoskeletal injuries and as an adjunct therapy in the treatment of chronic musculoskeletal disorders.
Counterirritants differ from other external analgesics in that pain relief results more from nerve stimulation than depression. Topical analgesics for musculoskeletal pain can be used alone or in conjunction with oral analgesics when appropriate and warranted.
External analgesic products may contain or more of the following ingredients: methyl salicylate, camphor, menthol, methyl nicotinate, capsicum, and trolamine salicylate.
Salicylates: These same ingredients that give aspirin its pain-relieving quality are found in some creams. When absorbed into the skin, they may help with pain, particularly in joints close to the skin, such as the fingers, knees, and elbows.
Capsaicin: The main ingredient of hot chilli peppers, capsaicin is also one of the most
effective ingredients for topical pain relief. When first applied, capsaicin creams cause a warm tingling or burning sensation. This gets better over time. Users may need to apply these creams for a few days up to a couple of weeks before they will notice relief from pain.
Topical analgesic products are available in a variety of formulations, including gels, ointments, creams, lotions, and patches in single-entity or combination formulations. Topical heat therapy patches are also available in various sizes for treating joint and muscle pain and provide eight to 12 hours of continual, portable heat therapy.
OTC topical analgesics are intended to be used for mild to-moderate pain for no longer than seven days. The factors that a pharmacist may consider when recommending a topical analgesic include dosage form, cost, ease of use of product, as well as the patient’s medical history, including possible allergies.
Who? Anyone suffering from pain, musculoskeletal problems or fever.
What are the symptoms? Dependent on the condition suffered.
How long has the patient had the symptoms? Dependent on the condition suffered.
Action already taken? Pain relief.
Medication? Apply topical products only to intact skin. Areas treated with counterirritants should not be covered with tight bandages or occlusive dressings. Patients on anticoagulation therapy should be advised not to use topical products that contain salicylates, because concomitant use has been associated with prolonged prothrombin time.

ABBREVIATED PRESCRIBING INFORMATION
ABBREVIATED PRESCRIBING INFORMATION
Product Name: Brupro for Children 100mg/5ml Oral Suspension & Brupro for Children Six Plus 200mg/5ml oral suspension.
Composition: Each 5 ml of oral suspension contains 100 mg or 200 mg ibuprofen respectively.
Product Name: Brupro for Children 100mg/5ml Oral Suspension & Brupro for Children Six Plus 200mg/5ml oral suspension.
Description: White or almost white suspension, homogeneous after agitation
Composition: Each 5 ml of oral suspension contains 100 mg or 200 mg ibuprofen respectively.
Description: White or almost white suspension, homogeneous after agitation




Indication(s): 100 mg/5 ml: Reduction of fever and relief of mild to moderate pain, such as cold and flu symptoms, teething pain, headache, sprains and strains and to ease the pain of sore throats and earache. For short term use only. 200 mg/5 ml: For the short-term symptomatic treatment of mild to moderate pain. For the short-term symptomatic treatment of fever.
Indication(s): 100 mg/5 ml: Reduction of fever and relief of mild to moderate pain, such as cold and flu symptoms, teething pain, headache, sprains and strains and to ease the pain of sore throats and earache. For short term use only. 200 mg/5 ml: For the short-term symptomatic treatment of mild to moderate pain. For the short-term symptomatic treatment of fever.
Dosage: Infants aged 3-6 months who weigh more than 5kg. Do not dose more frequently than at 6 hourly intervals and do not exceed the recommended dose. For infants aged 3-5 months medical advice should be sought if symptoms worsen or not later than 24 hours if symptoms persist and no later than 3 days in children aged from 6 months and in adolescents. Recommended time interval is 3 times in 24 hours: 100 mg/5 ml: 3-12 months (5-9 kg bodyweight): 2.5 ml; 1 to 3 years (10-16 kg): 5 ml; 4 to 6 years (17-20 kg): 7.5 ml; 7 to 9 years (21-30 kg): 10 ml (two 5ml spoonfuls); 10 to 12 years (31-40 kg): 15 ml (three 5ml spoonfuls). 200 mg/5 ml: Not for use in children under 6 years of age or under 20 kg body weight. 6-9 years (20-29 kg): 5ml (200 mg); 10-12 years (30-40 kg): 7.5ml (300 mg).
Renal insufficiency: No dose reduction in mild to moderate impairment. Hepatic insufficiency: No dose reduction in mild to moderate impairment.
Contraindications: Hypersensitivity to the active substance or to any of the excipients. In patients: - who have previously shown hypersensitivity (e.g. bronchospasm, asthma, rhinitis, angioedema or urticaria) associated with acetylsalicylic acid, ibuprofen or other non-steroidal anti-inflammatory (NSAID) medicinal products; - with a history of gastrointestinal bleeding or perforation, related to previous NSAID therapy; - with active, or a history of recurrent peptic ulcer/haemorrhage (two or more distinct episodes of proven ulceration or bleeding); - with cerebrovascular or other active bleeding; - with severe hepatic failure or severe renal failure; - with severe heart failure; -with unclarified blood-formation disturbances; -with severe dehydration (caused by vomiting, diarrhoea or insufficient fluid intake). During the last trimester of pregnancy. Warnings and Precautions for Use: Refer to the SPC for detailed warnings. Undesirable effects may be minimized by using the lowest effective dose for the shortest duration necessary to control symptoms and patients should report any unusual symptoms especially any GI bleeding. Elderly: Have an increased frequency of adverse reactions to NSAIDs especially gastrointestinal bleeding and perforation which may be fatal. Are at increased risk of the consequences of adverse reactions. Caution in: Systemic lupus erythematosus as well as those with mixed connective tissue disease, due to increased risk of aseptic meningitis; Congenital disorder of porphyrin metabolism (e.g. acute intermittent porphyria); Gastrointestinal disorders and chronic inflammatory intestinal disease (ulcerative colitis, Crohn’s disease). Consider combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) and also for patients requiring concomitant low dose acetylsalicylic acid, or other drugs likely to increase gastrointestinal risk; A history of hypertension and/or heart failure as fluid retention and oedema have been reported in association with NSAID therapy; Renal impairment as renal function may further deteriorate; Hepatic dysfunction; Dehydration; Directly after major surgery; Hayfever, nasal polyps or chronic obstructive respiratory disorders as an increased risk for them of allergic reactions occurring. These may be present as asthma attacks (so-called analgesic asthma), Quincke’s oedema or urticaria; In patients who have already reacted allergically to other substances, as an increased risk of hypersensitivity reactions occurring also exists for them on use of this product; Bronchospasm may be precipitated in patients suffering from, or with a history of, bronchial asthma or allergic disease. Dermatological effects: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome and toxic epidermal necrolysis, have been reported very rarely in association with the use of NSAIDs. Patients appear to be at highest risk of these reactions early in the course of therapy, the onset of the reaction occurring in the majority of cases within the first month of treatment. Acute generalized exanthematous pustulosis (AGEP) has been reported. Discontinue Brupro for Children at the first appearance of signs and symptoms of severe skin reactions, such as skin rash, mucosal lesions, or any other sign of hypersensitivity. Symptoms of underlying infections and fever can be masked which may lead to delayed initiation of appropriate treatment and thereby worsening the outcome of the infection. This has been observed in bacterial community acquired pneumonia and bacterial complications to varicella. Monitoring of infection is advised. In nonhospital settings, the patient should consult a doctor if symptoms persist or worsen. Exceptionally, varicella can be at the origin of serious cutaneous and soft tissues infectious complications. It is advisable to avoid use of ibuprofen in case of varicella. Cardiovascular and cerebrovascular effects: Ibuprofen, particularly at a high dose (2400 mg/day) may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke). Low dose ibuprofen (e.g. ≤ 1200 mg/day) is suggested not to be associated with a small increased risk of arterial thrombotic events. Patients with uncontrolled hypertension, congestive heart failure (NYHA II-III), established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease should only be treated with ibuprofen after careful consideration and high doses (2400 mg/day) should be avoided and consider carefully if long term treatment is needed. Other notes: Severe acute hypersensitivity reactions (for example anaphylactic shock) are observed very rarely. Discontinue treatment immediately and seek medical attention. Ibuprofen may temporarily inhibit the blood-platelet function (thrombocyte aggregation). Monitor patients with coagulation disturbances carefully. Check liver values, kidney function and blood count in prolonged treatment. Be aware of diagnosis of medication overuse headache (MOH), suspected in patients who have frequent or daily headaches despite (or because of) the regular use of headache medications. Alcohol may increase adverse effects that concern the gastrointestinal tract or the central nervous system. Renal: Habitual use of analgesics, especially the combination of different analgesic drug substances, can lead to lasting renal lesions with the risk of renal failure (analgesic nephropathy). There is a risk of renal impairment in dehydrated children. Contains sorbitol and propylene glycol. Interactions: Refer to the SPC for detailed information on the interactions. Avoid in combination with: Other NSAIDs including cyclooxygenase-2 selective inhibitors; Acetylsalicylic acid; Antihypertensives, (ACE inhibitors, beta-receptor blocking medicines and angiotensin-II antagonists) and diuretics; Cardiac glycosides: e.g. digoxin; Lithium; Potassium sparing diuretics; Phenytoin; Methotrexate; Tacrolimus; Ciclosporin; Corticosteroids; Anti-coagulants; Anti-platelet agents and selective serotonin reuptake inhibitors (SSRIs); Mifepristone; Sulphonylureas; Zidovudine; Probenecid and sulfinpyrazone; Baclofen; Ritonavir; Aminoglycosides; Quinolone antibiotics; Cholestyramine; Captopril; CYP2C9 inhibitors: e.g. voriconazole and fluconazole.
Dosage: Infants aged 3-6 months who weigh more than 5kg. Do not dose more frequently than at 6 hourly intervals and do not exceed the recommended dose. For infants aged 3-5 months medical advice should be sought if symptoms worsen or not later than 24 hours if symptoms persist and no later than 3 days in children aged from 6 months and in adolescents. Recommended time interval is 3 times in 24 hours: 100 mg/5 ml: 3-12 months (5-9 kg bodyweight): 2.5 ml; 1 to 3 years (10-16 kg): 5 ml; 4 to 6 years (17-20 kg): 7.5 ml; 7 to 9 years (21-30 kg): 10 ml (two 5ml spoonfuls); 10 to 12 years (31-40 kg): 15 ml (three 5ml spoonfuls). 200 mg/5 ml: Not for use in children under 6 years of age or under 20 kg body weight. 6-9 years (20-29 kg): 5ml (200 mg); 10-12 years (30-40 kg): 7.5ml (300 mg). Renal insufficiency: No dose reduction in mild to moderate impairment. Hepatic insufficiency: No dose reduction in mild to moderate impairment. Contraindications: Hypersensitivity to the active substance or to any of the excipients. In patients: - who have previously shown hypersensitivity (e.g. bronchospasm, asthma, rhinitis, angioedema or urticaria) associated with acetylsalicylic acid, ibuprofen or other non-steroidal anti-inflammatory (NSAID) medicinal products; - with a history of gastrointestinal bleeding or perforation, related to previous NSAID therapy; - with active, or a history of recurrent peptic ulcer/haemorrhage (two or more distinct episodes of proven ulceration or bleeding); - with cerebrovascular or other active bleeding; - with severe hepatic failure or severe renal failure; - with severe heart failure; -with unclarified blood-formation disturbances; -with severe dehydration (caused by vomiting, diarrhoea or insufficient fluid intake). During the last trimester of pregnancy. Warnings and Precautions for Use: Refer to the SPC for detailed warnings. Undesirable effects may be minimized by using the lowest effective dose for the shortest duration necessary to control symptoms and patients should report any unusual symptoms especially any GI bleeding. Elderly: Have an increased frequency of adverse reactions to NSAIDs especially gastrointestinal bleeding and perforation which may be fatal. Are at increased risk of the consequences of adverse reactions. Caution in: Systemic lupus erythematosus as well as those with mixed connective tissue disease, due to increased risk of aseptic meningitis; Congenital disorder of porphyrin metabolism (e.g. acute intermittent porphyria); Gastrointestinal disorders and chronic inflammatory intestinal disease (ulcerative colitis, Crohn’s disease). Consider combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) and also for patients requiring concomitant low dose acetylsalicylic acid, or other drugs likely to increase gastrointestinal risk; A history of hypertension and/or heart failure as fluid retention and oedema have been reported in association with NSAID therapy; Renal impairment as renal function may further deteriorate; Hepatic dysfunction; Dehydration; Directly after major surgery; Hayfever, nasal polyps or chronic obstructive respiratory disorders as an increased risk for them of allergic reactions occurring. These may be present as asthma attacks (so-called analgesic asthma), Quincke’s oedema or urticaria; In patients who have already reacted allergically to other substances, as an increased risk of hypersensitivity reactions occurring also exists for them on use of this product; Bronchospasm may be precipitated in patients suffering from, or with a history of, bronchial asthma or allergic disease. Dermatological effects: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome and toxic epidermal necrolysis, have been reported very rarely in association with the use of NSAIDs. Patients appear to be at highest risk of these reactions early in the course of therapy, the onset of the reaction occurring in the majority of cases within the first month of treatment. Acute generalized exanthematous pustulosis (AGEP) has been reported. Discontinue Brupro for Children at the first appearance of signs and symptoms of severe skin reactions, such as skin rash, mucosal lesions, or any other sign of hypersensitivity. Symptoms of underlying infections and fever can be masked which may lead to delayed initiation of appropriate treatment and thereby worsening the outcome of the infection. This has been observed in bacterial community acquired pneumonia and bacterial complications to varicella. Monitoring of infection is advised. In nonhospital settings, the patient should consult a doctor if symptoms persist or worsen. Exceptionally, varicella can be at the origin of serious cutaneous and soft tissues infectious complications. It is advisable to avoid use of ibuprofen in case of varicella. Cardiovascular and cerebrovascular effects: Ibuprofen, particularly at a high dose (2400 mg/day) may be associated with a small increased risk of arterial thrombotic events (for example myocardial infarction or stroke). Low dose ibuprofen (e.g. ≤ 1200 mg/day) is suggested not to be associated with a small increased risk of arterial thrombotic events. Patients with uncontrolled hypertension, congestive heart failure (NYHA II-III), established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease should only be treated with ibuprofen after careful consideration and high doses (2400 mg/day) should be avoided and consider carefully if long term treatment is needed. Other notes: Severe acute hypersensitivity reactions (for example anaphylactic shock) are observed very rarely. Discontinue treatment immediately and seek medical attention. Ibuprofen may temporarily inhibit the blood-platelet function (thrombocyte aggregation). Monitor patients with coagulation disturbances carefully. Check liver values, kidney function and blood count in prolonged treatment. Be aware of diagnosis of medication overuse headache (MOH), suspected in patients who have frequent or daily headaches despite (or because of) the regular use of headache medications. Alcohol may increase adverse effects that concern the gastrointestinal tract or the central nervous system. Renal: Habitual use of analgesics, especially the combination of different analgesic drug substances, can lead to lasting renal lesions with the risk of renal failure (analgesic nephropathy). There is a risk of renal impairment in dehydrated children. Contains sorbitol and propylene glycol. Interactions: Refer to the SPC for detailed information on the interactions. Avoid in combination with: Other NSAIDs including cyclooxygenase-2 selective inhibitors; Acetylsalicylic acid; Antihypertensives, (ACE inhibitors, beta-receptor blocking medicines and angiotensin-II antagonists) and diuretics; Cardiac glycosides: e.g. digoxin; Lithium; Potassium sparing diuretics; Phenytoin; Methotrexate; Tacrolimus; Ciclosporin; Corticosteroids; Anti-coagulants; Anti-platelet agents and selective serotonin reuptake inhibitors (SSRIs); Mifepristone; Sulphonylureas; Zidovudine; Probenecid and sulfinpyrazone; Baclofen; Ritonavir; Aminoglycosides; Quinolone antibiotics; Cholestyramine; Captopril; CYP2C9 inhibitors: e.g. voriconazole and fluconazole.
Pregnancy and Lactation: Pregnancy: During the first and second trimester of pregnancy, ibuprofen should not be given unless clearly necessary. If ibuprofen is used by a woman attempting to conceive, or during the first and second trimester of pregnancy, the dose should be kept as low and duration of treatment as short as possible. Contraindicated during the third trimester of pregnancy. Breast-feeding: Ibuprofen and its metabolites can pass in low concentrations into the breast milk. No harmful effects to infants are known to date, so for short-term treatment with the recommended dose for pain and fever interruption of breast feeding would not generally be necessary. Fertility: There is some evidence that substances which inhibit cyclo-oxygenase/ prostaglandin synthesis may cause impairment of female fertility by an effect on ovulation. This is reversible upon withdrawal of treatment. Ability to Drive and Use Machinery: For short-term use this medicinal product, has no or negligible influence on the ability to drive and use machines. Undesirable Effects: Gastro-intestinal: abdominal pain, nausea and dyspepsia, diarrhoea, flatulence, constipation, heartburn, vomiting and slight gastrointestinal blood losses that may cause anaemia in exceptional cases. Refer to the SPC for other undesirable effects. Marketing Authorisation Holder: Rowa Pharmaceuticals Ltd., Bantry, Co. Cork. Marketing Authorisation Number: PA0074/067/004-005 Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417 E-mail: rowex@rowa-pharma.ie. Legal Category: Not subject to medical prescription. Date of Preparation: March 2021
Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing Rowex pv@rowa-pharma.ie
Pregnancy and Lactation: Pregnancy: During the first and second trimester of pregnancy, ibuprofen should not be given unless clearly necessary. If ibuprofen is used by a woman attempting to conceive, or during the first and second trimester of pregnancy, the dose should be kept as low and duration of treatment as short as possible. Contraindicated during the third trimester of pregnancy. Breast-feeding: Ibuprofen and its metabolites can pass in low concentrations into the breast milk. No harmful effects to infants are known to date, so for short-term treatment with the recommended dose for pain and fever interruption of breast feeding would not generally be necessary. Fertility: There is some evidence that substances which inhibit cyclo-oxygenase/ prostaglandin synthesis may cause impairment of female fertility by an effect on ovulation. This is reversible upon withdrawal of treatment. Ability to Drive and Use Machinery: For short-term use this medicinal product, has no or negligible influence on the ability to drive and use machines. Undesirable Effects: Gastro-intestinal: abdominal pain, nausea and dyspepsia, diarrhoea, flatulence, constipation, heartburn, vomiting and slight gastrointestinal blood losses that may cause anaemia in exceptional cases. Refer to the SPC for other undesirable effects. Marketing Authorisation Holder: Rowa Pharmaceuticals Ltd., Bantry, Co. Cork. Marketing Authorisation Number: PA0074/067/004-005 Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417 E-mail: rowex@rowa-pharma.ie. Legal Category: Not subject to medical prescription. Date of Preparation: March 2021 Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing Rowex pv@rowa-pharma.ie
It can be a challenge to recognize the symptoms of pain in children. Are they really hurting, or are is the parent overreacting? Pain is a highly individual and complex experience. Here we take a look at reading the symptoms of pain in children.
Unlike with older children, crying isn’t always a reliable pain indicator in babies. That’s because crying is a baby’s way of expressing a whole host of needs. Here are signs that a baby may be in pain.
Changes in crying patterns. A baby’s distressed cry sometimes, but not always, sounds different from ordinary crying. Changes in a baby’s behavior can also be a tip-off. For example, crying that can’t be soothed with a bottle, diaper change, or cuddling could signal pain. Also, a calm baby who becomes unusually fussy could be in pain.
Crying while nursing. The baby who cries while nursing could very well have a painful ear infection.
Prolonged, intense crying, often at the same time each day. This behavior is common with colic. It often starts at the age of 2 weeks, peaks at 6 weeks, and then gradually declines.
Crying and drawing the legs up to the abdomen. The baby could have colic or a serious medical condition.
Withdrawing. Chronic pain can sap a baby’s energy, causing him or her to become still, quiet, and to avoid eye contact.
SYMPTOMS
Fortunately, at this age, children in pain can talk. They will often also clutch the part that hurts. Pulling or rubbing the ear is common in toddlers and although it can sometimes indicate ear pain, it may be habit. Suspect an ear infection if the child has had cold symptoms or a fever and begins to tug at the ear suddenly.
SYMPTOMS
Chronic or recurrent pain is common in children and adolescents. Research has shown that as many as 30% to 40% complain of pain at least once a week.
Acute abdominal pain. Pain that comes on suddenly can be caused by viral infections or by something more serious like appendicitis. If a child’s pain seems to be localised to the right of the belly button and is accompanied by nausea, vomiting, and desire to stay very still, they should be evaluated for appendicitis.
Recurrent stomach aches and headaches. A stomach ache that goes away after a bowel movement could signal a problem with

constipation or, less often, inflammatory bowel disease. Daily abdominal pain without nausea, vomiting, or diarrhea could be a special form of migraine, or could fall under the category of chronic recurrent abdominal pain, a common but frustrating complaint in children.
Communicating with and involving children in taking their medications will have a significant impact on their adherence. Children take responsibility for their medications at different ages. Children are often not present when their parents collect their medications from the pharmacy and, therefore, this prevents them from receiving support and advice from community pharmacists so ensure parents are well educated on the symptoms, medications and side effects.
• Check parents understand what the medication is for and supplement knowledge if needed;
• Ensure parents are aware of the most common adverse effects and what to do if these occur;
• Explain what to do if their child misses a dose;
• Explain anything relevant to the particular medication (e.g. to take phenoxymethylpenicillin on an empty stomach);
• Check parents understand how to administer the medication to their child;
Discomfort during a febrile illness is often due to associated pain; e.g. myalgia, sore throat, headache. Ibuprofen and paracetamol may be considered to improve comfort (with
accompanying improvements in feeding activity and irritability), because they may also provide relief from pain and may reduce the risk of dehydration. They should be used to make the child more comfortable and not used routinely with the sole aim of reducing the temperature. The use of antipyretic medication and attention to the fever must not detract from monitoring the child’s activity and level of consciousness (as an indicator of worsening illness) and paying attention to adequate hydration.
Both paracetamol and ibuprofen are safe and effective for short-term use in children. The practices of combining or alternating paracetamol and ibuprofen have limited value and are not recommended. Dose of antipyretic medication in children should be accurately based on body weight and should not merely be estimated. For accurate dosing, liquid medicines should be administered with a syringe. The use of NSAIDs has been associated with an elevated risk of severe skin and soft-tissue infections in patients with varicella zoster virus infection. Therefore, paracetamol is recommended as the antipyretic of choice in children with chicken pox. Medicines containing combinations of NSAID(s), paracetamol, codeine and/or antihistamines should not be used in children.
Nonpharmacological measures can be used as an adjunct therapy in the management of pain in both adults and children. Nonpharmacological strategies such as physical and psychological comfort measures are useful in conjunction with pharmacological options to help lower levels of anxiety, distress and pain. Some physical comfort measures include the use of massage or heat and/or cold compresses, applying pressure or vibration and repositioning. Psychological comfort measures include use of imagery, distraction and relaxation techniques.
Who? Babies, toddlers and children under 9.
What are the symptoms? Changes in crying patterns, lacking energy, high temperature, discomfort when feeding, touching where they hurt.
How long have they had the symptoms? Colic can start at 2 weeks and peak at 6 weeks, symptoms of other pain can be acute and/or recurrent.
Action already taken? Changing feeds, administering pain relief such as paracetamol and/or ibuprofen, keeping child cool and hydrated.
Medication? Paracetamol and ibuprofen.

LEADING For over 100 years baby nutrition research

SMA® Anti-Reflux For the dietary management of reflux and regurgitation
Discover our full range at www.smahcp.ie

SMA LF® Lactose Free For babies with lactose intolerance
Did you know that feeding issues, such as colic, constipation, reflux & regurgitation occur in up to 55% of all infants in the first 6 months of life?1

SMA® Comfort For the dietary management of colic and constipation
REFERENCES: 1. Iacono G. et al. Gastrointestinal symptoms in infancy: a population-based prospective study. Dig Liv Dis 2005;37(6):432–438.
SMA High Energy® For medically identified high-energy needs
IMPORTANT NOTICE: The World Health Organisation (WHO) has recommended that pregnant women and new mothers be informed on the benefits and superiority of breastfeeding – in particular the fact that it provides the best nutrition and protection from illness for babies. Mothers should be given guidance on the preparation for, and maintenance of, lactation, with special emphasis on the importance of a well-balanced diet both during pregnancy and after delivery. Unnecessary introduction of partial bottle-feeding or other foods and drinks should be discouraged since it will have a negative effect on breastfeeding. Similarly, mothers should be warned of the difficulty of reversing a decision not to breastfeed. Before advising a mother to use an infant formula, she should be advised of the social and financial implications of her decision: for example, if a baby is exclusively bottle-fed, more than one can (400 g) per week will be needed, so the family circumstances and costs should be kept in mind. Mothers should be reminded that breast milk is not only the best, but also the most economical food for babies. If a decision to use an infant formula is taken, it is important to give instructions on correct preparation methods, emphasising that unboiled water, unsterilised bottles or incorrect dilution can all lead to illness. •SMA LF® is a lactose-free milk based formula for babies and young children who are intolerant to lactose or sucrose, or who are experiencing symptoms such as diarrhoea, tummy ache or wind caused by temporary lactose intolerance. It is suitable as the sole source of nutrition up to 6 months of age, and in conjunction with solid food up to 18 months of age. The following products must be used under medical supervision •SMA® Anti-Reflux is a special formula intended for the dietary management of bottle-fed babies when significant reflux (regurgitation) is a problem. It is suitable as the sole source of nutrition up to 6 months of age, and in conjunction with solid food up to 12 months of age. If the baby’s reflux does not improve within 2 weeks of starting SMA® Anti-Reflux, or if the baby fails to thrive, the family doctor should be consulted. •SMA High Energy® is a milk based formula for the dietary management of babies and young children with medically determined high energy requirements as identified by a healthcare professional. It is suitable as the sole source of nutrition up to 6 months of age, and in conjunction with solid food up to 18 months of age. SMA High Energy® is not intended for use with preterm babies, for whom fortified breast milk or a low birthweight formula such as SMA Gold Prem® 1 is more appropriate. •SMA Comfort is a
Infant reflux occurs when food backs up (refluxes) from a baby’s stomach, causing the baby to spit up. Sometimes called gastroesophageal reflux (GER), the condition is rarely serious and becomes less common as a baby gets older. It’s unusual for infant reflux to continue after age 18 months.
Reflux occurs in healthy infants multiple times a day. As long as the baby is healthy, content and growing well, reflux is not a cause for concern.
The muscle at the bottom of the food pipe acts as a kind of door into the stomach – so when food or milk travels down, the muscle opens allowing the food into the stomach. However, while this muscle is still developing in the first year, it can open when it shouldn’t (usually when a baby’s tummy is full) allowing some food and stomach acid to travel back up again. Acid in the stomach is normal and a necessary part of the digestion process – it helps break down food.
In most babies, reflux is nothing to worry about (as long as they are healthy and gaining weight as expected). However, in some cases (though very few) reflux can cause a lot of pain when strong acid travels up into the food pipe. When reflux becomes painful and it happens frequently, this is known as ‘gastro-oesophageal reflux disease’ (GORD).
Baby reflux symptoms include:
• constant or sudden crying when feeding

Reflux medications aren’t recommended for children with uncomplicated reflux. These medications can prevent absorption of calcium and iron, and increase the risk of certain intestinal and respiratory infections.
However, a short-term trial of an acid-blocking medication — such as cimetidine (Tagamet HB) or famotidine (Pepcid AC) for infants ages 1 month to 1 year or omeprazole magnesium (Prilosec) for children ages 1 year or older — might be recommended if a baby:
• Has poor weight gain and moreconservative treatments haven’t worked
• Refuses to feed
• Has evidence of an inflamed esophagus
Did you know that feeding issues, such as colic, constipation, reflux & regurgitation occur in up to 55% of all infants in the first 6 months of life?
• bringing up milk during or after feeds (regularly)
• frequent ear infections
• lots of hiccups or coughing
• refusing, gagging or choking during feeds
• poor weight gain
• frequent waking at night
Infant reflux usually clears up by itself. In the meantime, you can recommend the following to worried mums:
• Giving the baby smaller, more-frequent feedings.
• Interrupting feedings to burp baby.
• Holding baby upright for 20 to 30 minutes after feedings.
• Eliminating dairy products, beef or eggs from mum’s diet if they are breast-feeding, to test if baby has an allergy.
• Switching the type of formula.
• Using a different size of nipple on baby bottles. A nipple that is too large or too small can cause a baby to swallow air.
• Thickening formula or expressed breast milk slightly and in gradual increments with rice cereal. Although recognized as a reasonable strategy, thickening adds potentially unnecessary calories to a baby’s diet.
• Has chronic asthma and reflux
It is important that all parents know that night time sleeping problems are very common in refluxing infants. Research shows that 13% of infants over 3 months of age wake their parents three or more times a night, however a study completed on infants with Gastro-Oesophageal Reflux Disease (GORD) found that 50 to 60% of infants over 3 months of age suffering from GORD woke their parents frequently at night.
Sleep issues that can be due to reflux include:
• waking in the middle of the night with a burst of crying;
Who? Newborn babies.
• waking frequently overnight, a child may initially sleep for three or four hours, but then will wake every one or two hours for the rest of the night and be difficult to resettle;
• infants and children may be more comfortable in a fully upright position and may object or cry when put to lie down;
• day time sleeping tends to be for short periods and usually are cat naps for 10 to 40 minutes with the child waking distressed;
• older children with reflux can be restless during sleep and may cry, moan or swallow even when asleep
If the baby:
• Isn’t gaining weight
• Consistently spits up forcefully, causing stomach contents to shoot out of his or her mouth (projectile vomiting)
• Spits up green or yellow fluid
• Spits up blood or a material that looks like coffee grounds
• Refuses food
• Has blood in his or her stool
• Has difficulty breathing or a chronic cough
• Begins spitting up at age 6 months or older
• Is unusually irritable after eating
What are the symptoms? Hiccups, coughing, sudden crying, bringing up milk, poor weight gain.
How long has the patient had the symptoms? Can occur up to age 18 months. Action already taken? Mums may already have tried switching feeds, feeding times, holding baby upright .
Medication: Short-term trial of an acid-blocking medication for infants ages 1 month to 1 year may be recommended in some instances.


There are many causes of scarring, both avoidable such as acne scarring and unavoidable including post trauma, surgery, lipoatrophy and inflammatory skin diseases. There are also a variety of different types of scars and the treatment to remodel and improve them is dictated by the individual morphology.
Scars form as part of the body’s healing process. The body builds tissue to repair damaged skin and close gaps due to an injury. Scars come in all shapes and sizes. They can result from accidents, burns, surgery, acne and illness. Over time, most scars fade away. Several treatments can make scars less noticeable.
Nearly everyone develops some type of scar, whether from an accident, a surgical procedure, acne or an illness like chickenpox. Scars affect people of all ages and genders.
When a scar first develops on lighter skin, it’s usually pink or red. Over time, the pinkish colour fades, and the scar becomes slightly darker or lighter than the colour of the skin. In people with dark skin, scars often appear as dark spots. Sometimes scars itch, and they may be painful or tender.
A scar’s appearance depends on several factors, including:
• Injury or event that caused the scar, such as surgery, a burn or severe acne.
• Size, severity and location of the wound.
• Treatment you received for the wound, such as stitches or bandages.
• Age, genes, ethnicity and overall health.
A minor wound like a cut will usually heal to leave a red, raised line, which will gradually get paler and flatter over time. This process can take up to two years. The scar won’t disappear completely and the customer will be left with a visible mark or line.
Fine line scars are common following a wound or after surgery. They aren’t usually painful, but they may be itchy for a few months.
On darker skin types, the scar tissue may fade to leave a brown or white mark. A pale scar may be more obvious on tanned skin because scar tissue doesn’t tan.
A keloid scar is an overgrowth of tissue that occurs when too much collagen is produced at the site of the wound. The scar keeps growing, even after the wound has healed.
Keloid scars are raised above the skin and are red or purple when newly formed, before gradually becoming paler. They’re often itchy or painful, and can restrict movement if they’re tight and near a joint.
Like keloid scars, hypertrophic scars are the result of excess collagen being produced at the site of a wound. But not as much collagen is produced in hypertrophic scars compared with keloid scars.
Also, unlike keloid scars, hypertrophic scars don’t extend beyond the boundary of the original wound, but they may continue to thicken for up to six months. Hypertrophic scars are red and raised to start with, before becoming flatter and paler over the course of several years.
Some scars caused by skin conditions, such as acne and chickenpox, can have a sunken or pitted appearance. Pitted scars, also known as atrophic or “ice-pick” scars, can also occur as a result of an injury that causes a loss of underlying fat.
If a wound takes 10 or more days to heal, this increases the risk of scarring. Once the wound is completely healed, lots of massage will help to break down scar tissue.
Customers can use a hand massager and an evidence-based silicone product as soon as possible. Some of these products are rubbed on the skin, normally twice a day. The sheets need to be applied to the skin for seven to 12 hours a day.
Silicone gels are the first line treatment for scars by healthcare professionals including plastic surgeons. This treatment forms an occlusive layer over the scar tissue to help create an optimal healing environment for scars to normalise collagen production and help improve the appearance of scars. It has a patented formulation which helps to soften and flatten raised scars as well as reducing discolouration and redness. It also relieves itching, discomfort and pain associated with scars.
Who: Anyone can suffer from scarring.
Be sure to ask a patient what aspect of their scar or stretch marks is troubling them so you can advise them accordingly.
Like any sensitive topic, asking questions can be a good way to initiate a positive discussion. Scars and stretch marks are extremely common – so reassure customers that it is something the pharmacy team is used to advising on. Ask a customer if they would prefer to talk in private and, if so, move the conversation to a consultation room.
• Considering the aspects of wound and skincare that they need to address, and keeping up-to-date with product developments and launches.
• Stocking a range of products including dressings, surgical tape, antiseptic wipes, wound cleaners, spray skin, swabs, plasters, adhesive removers, bandages, massage oil (for aftercare), and antiseptic creams and ointments.
• Featuring the best sellers and sizes in each brand and focusing on a specific skin concern.
• Avoiding overstocking the category by focusing on the top two or three brands, including ones that pharmacy teams particularly advocate and use.
• Engaging with customers to research what they are looking for in a skincare range and whether anything is missing from a pharmacy’s skincare category.
• Setting up a campaign to support wound care, promoting good practice to customers.
What are the symptoms? Fine line scars, keloid scars, pitted or sunken scars, hypertrophic scars are some of the most common types of scarring. How long have they had symptoms? Dependent on size and severity of the wound.
Action already taken? Sufferers may have tried camouflaging, moisturizing and scar appearance reduction oils.
Medication: OTC creams, ointments and gels, surgical removal, laser treatment, steroid injections.

Despite increased awareness on the importance of sleep, many people with sleep disorders do not seek help from a physician for the diagnosis or management of the disorder and many even choose to selfmedicate. This results in many sleep disorders remaining undiagnosed and untreated.
Historically there have been three major classification systems for sleep disorders. These are (1) International Classification of Sleep Disorders (ICSD), (2) Diagnostic and Statistical Manual of Mental Disorders (DMS) and (3) American Psychiatric Association and the International Classification of Diseases (ICD). In total there are over 80 sleep disorders with insomnia being the most common.
Acute (short term/transient) insomnia is a common complaint, and a stressor can usually be identified. The insomnia complaint usually subsides once the stressor is eliminated. Prevalence of acute insomnia is generally between 30-50 % of the population (pre COVID-19).
Chronic Insomnia, according to the ‘European guidelines for the diagnosis and treatment of Insomnia,’ is defined as one or more of the following: (1) Difficulty initiating sleep (2) Difficulty maintaining sleep (3) Early awakenings (4) Resistance to going to bed. The reported sleep/wake complaints occur despite adequate opportunity for sleep. The sleep disturbance and daytime consequences must occur at least 3 times per week and must have been present for at least 3 months. The sleep/wake difficulty is not explained by another sleep disorder.
Women are twice as likely to suffer from insomnia, individuals with a history of shift work, older adults, post-menopausal women, those with a medical or psychiatric condition and even those from a lower socio-economic background are at greater risk. In recent times, employment stresses are playing an increased role in the development of an insomnia disorder. Bereavement, relationship issues, or any kind of life changes have the potential to cause an insomnia disorder. Since the start of COVID-19 pandemic, worries and anxiety around health have played a huge role in the increase of insomnia.
Management of insomnia can differ depending on the disorder being acute or chronic. The pharmacist can play a vital role in the management of acute insomnia and when to advise the patient to see a GP as the disorder becomes chronic or if short-term treatments are unsuccessful.
Insomnia disorder has a prevalence of between 6% and 20%. This increases to between 30% and 48% of the general population at a symptom level. Being older,
female, or being from a socioeconomic background are independent risk factors for the development of insomnia. Having a previous episode of insomnia also increases the risk of a future episode.
Pharmacological treatment for insomnia should be limited to short term use only, if CBT-I is unavailable or if a patient does not respond to CBT-I. Available substances that are commonly used include benzodiazepines (BZ), benzodiazepine receptor agonists (BZRA), antidepressants, anti-psychotics, antihistamines, phytotherapeutic substances and melatonin. A variety of side-effects of hypnotics have been reported, including hangover, nocturnal confusion, falls, rebound insomnia, tolerance and dependency.
Restless legs syndrome (RLS) is a neurological sleep disorder. It is also called Willis-Elbom disease (WED). Prevalence of RLS ranges from 0.6% to 15% of the population. This increases to 27% in pregnant females. The disorder is defined by the classic clinical symptoms of an overwhelming urge to move the legs while resting in the evening and night. This is accompanied by an uncomfortable/
unpleasant sensation in the legs with patients often describing it as a crawling sensation. Symptoms are partially or totally relieved by walking or stretching the legs. Symptoms may return as soon as the movement stops, particularly in severe cases.
Nonpharmacological: Good sleep hygiene is advised and alcohol should be avoided in the evening as it can aggravate symptoms.
Pharmacological: Moderate to severe RLS treatment generally involves four categories of medications; dopaminergic agents, alpha-2-delta ligands, opioids and benzodiazepines. All pharmacological treatments are palliative and occasional drug holidays should be considered to assess the need for continuing treatment.
A sleep diary is an easy achieved assessment tool that provides a daily record of a patient’s perception of their sleep. (They can also be used to monitor progress after intervention). They are inexpensive and easy to complete. They consist of blocks of time slept over cycles of 24 hours. They gather subjective data on sleep timing, routines, quality of sleep etc.
Who? Insomnia impacts 30-50% of the population; women are twice as likely to suffer as men.
What are the symptoms? Finding it hard to go to sleep; waking up several times during the night; feeling tired after waking up; finding it hard to nap during the day.
How long have they had the symptoms? Some sufferers may have symptoms at least three times per week for at least 3 months.
Action already taken? A sleep diary may already have been started. Medication? Pharmacological treatments should be limited to short-term use; good sleep hygiene is advised and alcohol should be avoided.


Nicorette QuickMist 1 mg/spray, oromucosal spray, solution. One spray delivers 1 mg nicotine in 0.07 ml solution. 1 ml solution contains 13.6 mg nicotine. Excipient with known effect: Ethanol (less than 100 mg of ethanol/spray). Propylene glycol, Butylated hydroxytoluene. Pharmaceutical form: Oromucosal spray, solution. A clear to weakly opalescent, colourless to yellow solution. Indications: For the treatment of tobacco dependence in adults by relief of nicotine withdrawal symptoms, including cravings, during a quit attempt (or to cut down smoking before stopping completely. Permanent cessation of tobacco use is the eventual objective. Nicorette QuickMist should preferably be used in conjunction with a behavioral support program. Dosage: Subjects should stop smoking completely during the course of treatment with Nicorette QuickMist. Adults and Elderly: The following chart lists the recommended usage schedule for the oromucosal spray during full treatment (Step I) and during tapering (Step II and Step III). Up to 4 sprays per hour may be used. Do not exceed 2 sprays per dosing episode and do not exceed 64 sprays (4 sprays per hour, over 16 hours) in any 24-hour period. Step I: Weeks 1-6: Use 1 or 2 sprays when cigarettes normally would have been smoked or if cravings emerge. If after a single spray cravings are not controlled within a few minutes, a second spray should be used. If 2 sprays are required, future doses may be delivered as 2 consecutive sprays. Most smokers will require 1-2 sprays every 30 minutes to 1 hour. Step II: Weeks 7-9: Start reducing the number of sprays per day. By the end of week 9 subjects should be using HALF the average number of sprays per day that was used in Step I. Step III: Weeks 10-12: Continue reducing the number of sprays per day so that subjects are not using more than 4 sprays per day during week 12. When subjects have reduced to 2-4 sprays per day, oromucosal spray use should be discontinued. To help stay smoke free after Step III, subjects may continue to use the oromucosal spray in situations when they are strongly tempted to smoke. One spray may be used in situations where there is an urge to smoke, with a second spray if one spray does not help within a few minutes. No more than four sprays per day should be used during this period. Regular use of the oromucosal spray beyond 6 months is generally not recommended. Some ex-smokers may need treatment with the oromucosal spray longer to avoid returning to smoking. Any remaining oromucosal spray should be retained to be used in the event of sudden cravings. Gradual cessation through progressive reduction in smoking: For smokers who are not willing or ready to quit abruptly. The oromucosal spray is used between periods of smoking in order to prolong the smoke-free intervals and with the intention to reduce smoking as much as possible. The patient should be aware that an incorrect use of the spray may enhance adverse effects. A cigarette is replaced with one dose (1-2 sprays) and a quit attempt should be made as soon as the smoker feels ready and no later than 12 weeks after start of treatment. If a reduction in cigarette consumption has not been achieved after 6 weeks of treatment, a healthcare professional should be consulted. After quitting smoking, gradually reduce the number of sprays per day. When subjects have reduced to 2-4 sprays per day, oromucosal spray should be discontinued. Regular use of the oromucosal spray beyond 6 months is not recommended. Some ex-smokers may need treatment with the oromucosal spray longer to avoid returning to smoking. Any remaining oromucosal spray should be retained to be used in the event of sudden cravings. Paediatric population: Do not administer this medicine to persons under 18 years of age. There is no experience of treating adolescents under the age of 18 with this medicine. Method of administration: After priming, point the spray nozzle as close to the open mouth as possible. Press firmly the top of the dispenser and release one spray into the mouth, avoiding the lips. Subjects should not inhale while spraying to avoid getting spray into the respiratory tract. For best results, do not swallow for a few seconds after spraying. Subjects should not eat or drink when administering the oromucosal spray. Behavioural therapy advice and support will normally improve the success rate. Contraindications: Hypersensitivity to nicotine or to any of the excipients. Children under the age of 18 years. Those who have never smoked. Special warnings and precautions for use: This medicine should not be used by non-smokers. The benefits of quitting smoking outweigh any risks associated with correctly administered nicotine replacement therapy (NRT). A risk-benefit assessment should be made by an appropriate healthcare professional for patients with the following conditions: Cardiovascular disease: Dependent smokers with a recent myocardial infarction, unstable or worsening angina including Prinzmetal’s angina, severe cardiac arrhythmias, recent cerebrovascular accident and/or who suffer with uncontrolled hypertension should be encouraged to stop smoking with non-pharmacological interventions (such as counselling). If this fails, the oromucosal spray may be considered but as data on safety in this patient group are limited, initiation should only be under close medical supervision. Diabetes Mellitus. Patients with diabetes mellitus should be advised to monitor their blood sugar levels more closely than usual when smoking is stopped and NRT is initiated as reduction in nicotine induced catecholamine release can affect carbohydrate metabolism. Allergic reactions: Susceptibility to angioedema and urticaria. Renal and hepatic impairment: Use with caution in patients with moderate to severe hepatic impairment and/or severe renal impairment as the clearance of nicotine or its metabolites may be decreased with the potential for increased adverse effects. Phaeochromocytoma and uncontrolled hyperthyroidism: Use with caution in patients with uncontrolled hyperthyroidism or phaeochromocytoma as nicotine causes release of catecholamines. Gastrointestinal Disease: Nicotine may exacerbate symptoms in patients suffering from oesophagitis, gastric or peptic ulcers and NRT preparations should be used with caution in these conditions. Paediatric population: Danger in children: Doses of nicotine tolerated by smokers can produce severe toxicity in children that may be fatal. Products containing nicotine should not be left where they may be handled or ingested by children. Transferred dependence: Transferred dependence can occur but is both less harmful and easier to break than smoking dependence. Stopping smoking: Polycyclic aromatic hydrocarbons in tobacco smoke induce the metabolism of drugs metabolised by CYP 1A2 (and possibly by CYP 1A1). When a smoker stops smoking, this may result in slower metabolism and a consequent rise in blood levels of such drugs. This is of potential clinical importance for products with a narrow therapeutic window, e.g. theophylline, tacrine, clozapine and ropinirole. The plasma concentration of other medicinal products metabolised in part by CYP1A2 e.g. imipramine, olanzapine, clomipramine and fluvoxamine may also increase on cessation of smoking, although data to support this are lacking and the possible clinical significance of this effect for these drugs is unknown. Limited data indicate that the metabolism of flecainide and pentazocine may also be induced by smoking. Excipients: This medicine contains about 7 mg of alcohol (ethanol) in each spray which is equivalent to 97 mg/ml. The amount in one spray of this medicine is equivalent to less than 2 ml beer or 1 ml wine. The small amount of alcohol in this medicine will not have any noticeable effects. This medicinal product contains less than 1 mmol sodium (23 mg) per spray, i.e. essentially ‘sodium- free’. This medicine contains 12 mg propylene glycol in each spray which is equivalent to 157 mg/mL. Due to the presence of butylated hydroxytoluene, Nicorette QuickMist may cause local skin reactions (e.g. contact dermatitis), or irritation to the eyes and mucous membranes. Care should be taken not to spray the eyes whilst administering the oromucosal spray. Undesirable effects: Effects of smoking cessation: Regardless of the means used, a variety of symptoms are known to be associated with quitting habitual tobacco use. These include emotional or cognitive effects such as dysphoria or depressed mood; insomnia; irritability, frustration or anger; anxiety; difficulty concentrating, and restlessness or impatience. There may also be physical effects such as decreased heart rate; increased appetite or weight gain, dizziness or presyncopal symptoms, cough, constipation, gingival bleeding or apthous ulceration, or nasopharyngitis. In addition, and of clinical significance, nicotine cravings may result in profound urges to smoke. This medicine may cause adverse reactions similar to those associated with nicotine given by other means and these are mainly dose-dependent. Allergic reactions such as angioedema, urticaria or anaphylaxis may occur in susceptible individuals. Local adverse effects of administration are similar to those seen with other orally delivered forms. During the first few days of treatment irritation in the mouth and throat may be experienced, and hiccups are particularly common. Tolerance is normal with continued use. Daily collection of data from trial subjects demonstrated that very commonly occurring adverse events were reported with onset in the first 2-3 weeks of use of the oromucosal spray, and declined thereafter. Adverse reactions with oromucosal nicotine formulations identified from clinical trials and during post-marketing experience are presented below.
has been estimated
Pharmacies are ideally placed to advise people on how to stop smoking and to provide information on the supply of medication. Many will also be able to provide treatment for smokers who want to stop. The contribution pharmacists can make to improving the health of the population has been widely recognised.
Pharmacy staff are at the front line to encourage customers to take a look at the reasons why they smoke and consider giving up. Combining behavioural advice with pharmacotherapy for smokers who visit the pharmacy with an ailment or long standing condition could increase their chances of stopping.
The suggestion that giving up smoking will improve a smoker’s overall health, speed up the healing process and help prevent against disease could help build their motivation to quit. With an appropriately trained pharmacy team pharmacies can offer services such as carbon monoxide testing and one-on-one advice on an ongoing basis, all year round.
Many who have attempted to kick the smoking habit would probably agree that it is often easier said than done, and that it can be both overwhelming and challenging.
Pharmacists are in a pivotal position to help patients find the most effective methods to successfully quit smoking and choose from the many OTC smoking cessation products currently on the market.
The key elements of brief smoking cessation advice are:
1. Ask the patient if they smoke;
2. Advise them to quit;
3. If they would like to quit smoking, provide assistance by referring them to the NHS stop-smoking service, or if they do not want to attend the service, provide an alternative.
In addition, there are numerous over-the-counter aids.
This treatment reduces or removes withdrawals associated with giving up smoking. Patches suit the moderately addicted smoker. They can be used for 16 hour or 24 hour periods. There is no difference in the effectiveness of 16 hour and 24 hour patches. They work by giving a steady dose of nicotine into the blood through the skin. The 24 hour patch keeps the nicotine levels constant and is for people who smoke as soon as they wake up and people who smoke during the night.
Customers should be advised to put the patch on a different part of the body each day so it won’t irritate the skin. Some people may have high skin sensitivity or react badly to the adhesive or latex in the patches. If this happens, advise a switch to a different form of NRT.
Nicotine gum relieves withdrawal symptoms and gives ‘something to do with the mouth’ in place of smoking. This can help change a habit of smoking.
The gum is available in various strengths depending on how the level of addiction to nicotine.

The inhaler (sometimes called an inhalator) is made up of a mouth piece and cartridges which contain nicotine. When it’s inhaled, the nicotine and menthol vapour is sucked into the body. This is absorbed into the blood through the lining of the mouth and throat.
The lozenge comes in various strengths depending on the level of addiction. Some people prefer the taste of lozenges over other oral forms of NRT. Lozenges may irritate the mouth and stomach and cause hiccups as the nicotine is swallowed.
Because tobacco smoke interacts with various pharmacologic agents through pharmacokinetic or pharmacodynamic mechanisms that may result in decreased therapeutic efficacy or, less commonly, increased toxicity, pharmacists are key in identifying possible drug interactions and contraindications associated with tobacco use.
Examples of drug interactions with tobacco smoke include hormonal contraceptives, betablockers, theophylline, and benzodiazepines
There are a number of tips and techniques that can assist pharmacists in their quest to help smokers kick the habit.
Advise a quit date. Deciding upon a specific date allows for adequate preparation including coming to terms with it mentally, which can have a huge impact on the outcome.
• Relevance: patients should be encouraged to think about the reasons why quitting is important
• Risks: patients should be asked to identify the negative health consequences of smoking
• Rewards: patients should be asked to identify any potential benefits they anticipate from cessation
• Roadblocks: help the patient identify barriers to quitting and assist in overcoming these. E.g. stressful periods, trigger factors such as always having one with a cup of tea, boredom, negative side effects of quitting
• Repetition: repeat the message when possible
Always acknowledge and congratulate a patient’s efforts, this can promote a positive mental attitude. Remind patients that slip-ups are normal and that they shouldn’t punish themselves. Promoting patients to take their cessation journey one day at a time, often allows for more reasonable goals.
In addition, for cravings, promoting “The 4 Ds” is a good way to overcome them:
• Distract
• Delay (until the urge passes, usually within 3-5 minutes)
• Deep breathe (about 20 times)
• Drink (patients find water extremely beneficial)
How long have they had the symptoms? The length of time they have smoked and the volume is essential to determining what NRT to recommend. Action already taken? Sufferers may already be trying to cut down or stop smoking all together.
Medication: No more than 15 of the higher strength NRT lozenges should be used per day. Inhalators should be used in caution with patients with COPD or chronic throat disease.
Can be used to treat a chesty cough (productive cough)*
Contains thyme liquid extract
180ml pack size
Sugar free Suitable for vegans
For relief of painful, irritated sore throats
30ml pack size
Gluten free
Local Anaesthetic effect
Medithyme Cough Syrup contains liquid extract from Thymus vulgaris L., herba (Thyme herb). Contains: ethanol, maltitol (E965) and benzoate salt (E211). For oral short-term use only. Contraindications: Hypersensitivity to thyme or to other members of the Lamiaceae (mint) family, or to any of the excipients. For supply through general sale. TR 126/319/001. *Medithyme Cough Syrup is a traditional herbal medicinal product, for use in case of productive cough associated with cold, exclusively based on longstanding use. Medispray is indicated for the symptomatic relief of painful, irritated sore throats. Additional therapy is required in the event of bacterial infection accompanied by fever. Adults, adolescents and children over 12 years. The dose is 3 to 5 sprays (0.3 - 0.5 ml). This can be repeated 6 to 10 times per day. The lowest effective dose should be used for the shortest duration necessary to relieve symptoms. Repeat the dose every hour as needed up to a maximum of ten times in 24 hours. Supply through pharmacy only. PA 126/300/001
A copy of the summary of product characteristics for both products is available on request or alternatively please go to www.clonmel-health.ie PA/TR Holder: Clonmel Healthcare Ltd., Clonmel, Co. Tipperary. Date prepared: June 2022. 2022/ADV/MED/164H

Sore throat (also called pharyngitis) is typically caused by a viral or bacterial infection. An estimated 200 to 300 different strains of virus cause colds and sore throat.
In up to 90% of cases, sore throat is caused by viruses linked to the common cold or flu. The other 10% of cases result from bacterial infections or some other medical condition. The bacteria that most commonly cause sore throat are streptococci. Infection with streptococcal bacteria is commonly called strep throat.
The following are some of the most common sore throat causes:
• Strep throat: The bacteria group A Streptococcus is the most common cause of strep throat.
• Sore throat (viral pharyngitis): Viruses are the most common cause of sore throat, including rhinoviruses or a respiratory syncytial virus. These viruses can cause other symptoms, such as:
o a cold
o earache
o bronchitis
o sinus infection
The majority of sore throats do not require referral to the GP and antibiotics do not significantly improve the outcomes. Therefore, pharmacists have an important role in managing sore throat. Explanation, reassurance, and symptomatic treatment is frequently all that is necessary when a person presents with a sore throat. However, there is still an important role in checking the need for referral when certain warning signs or symptoms are present.
The degree of throat discomfort can range from itch to severe pain. Sore throats are often associated with other symptoms such as fever and headache. Cough, rhinorrhoea and hoarseness are uncommon with bacterial infection and may be suggestive of a viral cause.
Some of the signs of strep throat will be visible. They may include
• white patches on the tonsils or throat,
• dark red splotches or spots on the roof of the mouth, and
• a skin rash.
Those white spots are pus pockets. In addition, some patients may exhibit swollen, tender lymph nodes in the neck and some with fever above about 101-102 F. The signs and symptoms are the same for both children and adults.
Although these signs may indicate strep, a visit to their GP is necessary to make a full determination. A full diagnosed is impossible by visual signs alone.

Adults are less likely to have this disease than children. For school-age children, their odds of a sore throat being strep are about 20% to 30%. For adults, the odds are more like 5% to 15%.
Sore throats are often caused by viruses, making them difficult to cure. They can also be caused by
• dry air,
• irritants like pollution,
• smoke, including cigarette smoke, and
• allergies.
Unlike strep throat, everyday sore throats usually go away on their own without any antibiotic treatment. In fact, antibiotics are useless against viral infections like colds and the flu, the most common causes of the diseases that cause sore throat.
Beyond the throat itself, a few more symptoms include
• runny nose,
• watery eyes,
• cough,
• sneezing,
• post-nasal drip, and
• a low fever (below 101 F).
Swollen lymph nodes under the chin and the front of the neck could indicate any kind of infection. They could accompany an ear infection or sinus infection, for example.
Ibuprofen and paracetamol can be used as an antipyretic and/or analgesic. Some
patients may wish to try medicated lozenges containing either a local anaesthetic, a nonsteroidal anti-inflammatory drug (NSAID) or an antiseptic for symptomatic relief.
People with a sore throat caused by streptococcal bacteria are more likely to benefit from antibiotics. FeverPAIN criteria is a clinical scoring tool that can help identify people in whom this is more likely. People who are most likely to benefit from an antibiotic have a FeverPAIN score of 4 or 5.
Complications include otitis media and parapharyngeal abscess.
The patient should be admitted immediately to hospital if they have stridor, breathing difficulty, or dehydration.
The person should be advised to seek follow up if:
• symptoms have not improved after 3 or 4 days of antibiotic therapy
• pain does not improve after 3 days, and/or there is fever over 38.3°C
• it becomes difficult to swallow saliva or liquids, if any difficulty in breathing develops, or if there is any one-sided neck or throat swelling
• if the person is taking a diseasemodifying anti-rheumatic drug (DMARD), carbimazole, is on chemotherapy, has known or suspected leukaemia, asplenia, aplastic anaemia or HIV/AIDS or is taking an immunosuppressive drug following a transplant.
Who? Although anyone can get a sore throat, some factors make you more susceptible, including: Age. Children and teens are most likely to develop sore throats.
What are the symptoms? Painful scratchy throat, especially when swallowing; redness at the back of the mouth; white patches on the tonsils or throat; skin rash.
How long have they had the symptoms? Symptoms usually occur for 3-7 days.
Action already taken? May have already tried gargling with warm salty water; eating cold foods; sucking ice cubes or ice lollies.
Medication? Paracetamol and ibuprofen; medicated lozenges; anaesthetic spray.
LiftPlus 360 Citrus: a fresh citrus scent for added discretion
AbsorbaGel: solidifying agent to minimise odour*
DeoGel: enzyme action helps to reduce pouch odour*
Check the fit is snug around the stoma to help prevent skin issues1
Lift Plus Wipes and LiftPlus 360: help to reduce the pain associated with the removal of stoma pouch adhesives
Lift Plus: can be used to help remove any sticky residues left on the skin around a stoma
Skinsafe: an effective barrier film that helps protect the skin and prevents skin stripping
AbsorbaGel: fast acting discharge solidifying agent, which solidifies stoma output into a gel and reduces pouch related noise and leaks*
Skinsafe: a highly effective barrier to help protect the peristomal skin
DeoGel: lubricates the pouch walls and helps prevent static problems such as pancaking, with the nozzle allowing for simple application to the inside of the pouch
LiftPlus 360 (50ml spray): order code 5506
LiftPlus 360 Citrus (50ml spray): order code 5507
LiftPlus sachets (30 per pack): order code 5502
LiftPlus spray (50ml): order code 5503








Skinsafe (50 wipes per pack): order code 6600
AbsorbaGel (150 sachets per pack): order code 9900
DeoGel bottle (200gsm): order code 2010
If problems persist, consult your Stoma Care Nurse or GP
For further information or samples, please contact: Sheila Sweeney RGN/ RSCN SCN (Stoma Care Nurse) sheila@opus-healthcare.ie 0667181636
* Not intended for urostomy patients
Reference: 1. Stoma Complications https://www.bladderandbowel.org/bowel/stoma/stoma-complications/ Last accessed Oct 2021. Code: JB-001240 Date of Preparation: Oct 2021
The word stoma comes from the Greek word meaning mouth or opening. There are many kinds of stoma but the main ones are colostomy, ileostomy and urostomy (ileal conduit). A stoma is a surgically created abdominal opening to which part of the bowel is attached.
It is estimated that over 13,500 people in the UK and Ireland have stoma surgery each year. The most common conditions resulting in stoma surgery are colorectal cancer, bladder cancer, ulcerative colitis, Crohn’s disease and accidental Injury.
A stoma normally looks like a small button, deep pink in colour, (similar to the colour of the gums) and although it appears to look sore it has no nerve endings hence no feeling and pain free.
As many pharmacists know, waste matter comes out of the stoma and is collected in a stoma bag. The type of bag used depends on the type of stoma.
Stoma patients around Ireland can take some time to adjust to having a stoma but with the help of pharmacy teams their stress can be eased.
Pharmacy staff are in an ideal position to advise patients on how to maintain a normal life while living with a stoma.
Always make patients aware that it can take a while to get used to living with a stoma. However once patients are assured that life can continue on, albeit a little differently, and the quicker they learn to manage their stoma, the less effect it will have on their day to day life. Always advise patients that with time, things like going to work or socialising with friends and family will get easier.
It is normal for patients to feel worried about how they will look, and how others may react to them and they will experience practical worries about the bag being noticeable, or smelling. When patients query about the bag this is the pharmacist’s opportunity to remind them that the stoma bags are very well designed, they should not smell and they cannot be seen through their clothes.
When a patient presents in Pharmacy with a stoma it is always important to remember that the stoma has no nerve supply so should not be painful.
Each person’s stoma is different and will probably be swollen immediately after surgery, though this will shrink over the next few weeks. It is normally red in colour,

and can bleed easily, especially if handled roughly. This type of bleeding is normal but if it continues the pharmacist should advise the patient to contact their stoma care nurse or doctor.
One of the most important things to remember is to advise the patient to take good care of the skin around the stoma. In practice, a stoma requires the same hygiene as an ordinary toilet visit. If the bag is applied and managed correctly there should be no odour or leakage.
How often a patient changes their stoma bag will depend upon the type of stoma and bag the patient uses.
Always advise the patient that as with any surgery, they will need time to recover which can take up to a few months. Having a stoma involves adjustment and learning new habits and although this can seem unpleasant and difficult in the beginning, it can, with time, become a natural part of the patient’s daily routine.
When recommending appropriate medications for those with an intestinal stoma, there are some additional considerations. Ostomists are more prone
to gastrointestinal side-effects of medicines, such as constipation or discolouration of the stools, and need to be counselled appropriately regarding suitable management.
They are also more likely to experience significant fluid and electrolyte losses associated with the use of diuretic medications, so these should be carefully titrated and monitored.
Patients with an intestinal stoma may also experience issues with the absorption of some orally administered medications due to their reduced intestinal length and associated pathophysiological changes. The use of enteric-coated and modified release preparations should be avoided, and those patients with rapid transit times and associated high stoma output may not sufficiently absorb some standard release formulations.
If patients experience recurrence of symptoms or poor disease control despite optimal medical management, particularly if accompanied by the appearance of apparently intact tablets or capsules in their stoma bag, then absorption problems should be suspected and alternative formulations or medications may be required.
Who? Common reasons include bowel cancer, bladder cancer, inflammatory bowel disease (Crohn’s Disease or Ulcerative Colitis), diverticulitis or an obstruction to the bladder or bowel.
What are the symptoms? Stomas can cause bloating, skin irritation, bowel obstruction and leakage. Stoma blockage can cause bloating and swelling in the tummy, cramps, a swollen stoma, nausea and/or vomiting.
How long have they had the symptoms? Typically patients may notice swelling not decreasing post surgery, sudden onset of discharge and pain.
Action already taken? Taking care of skin around the stoma and maintaining appropriate hygiene measures.
Medication? N/A




Suppositories may not be the most pleasant product anyone will ever use but they can make it easier to take medicine that some people are unable to swallow or that their stomach or intestines wouldn’t absorb well.
Analgesic suppositories can be used in similar circumstances to oral formulations, although there are some considerations unique to this mode of administration. The rectum needs to be empty, if possible, when a suppository is administered.
Ideally, the patient should evacuate the bowel prior to administration or administration should be delayed until a bowel movement has occurred. Where the lower rectum is loaded with faeces, the administration of a suppository can trigger reflex bowel emptying which extrudes the suppository before it is fully absorbed, thus reducing it’s efficacy.
Most patients find it difficult to empty the bowel on demand. In children this can be impossible. Postponing administration until after a natural bowel movement is not practical for treatment of an acute condition. Where patients have diarrhoea, frequent bowel movements may also reduce the usefulness of the rectal route.
In recent years, analgesic suppositories have become more widely used for symptomatic treatment of conditions associated with pain and fever in infants and children.
Suppositories have a base made from substances like gelatin or cocoa butter that surrounds the drug. As the warmth of the body melts the outside, the drug slowly releases.
Different types of suppositories go into the rectum, vagina, or the urethra.
Suppositories which are correctly formulated are absorbed in to the bloodstream in a comparable way to oral formulations in terms of both rate and extent of absorption. Thus, suppositories work as quickly as oral formulations and their effect lasts a similar length of time.
Two of the most commonly used analgesic suppositories are paracetamol and ibuprofen, both of which are available without prescription.
Just as with paracetamol tablets and liquids, the dose of paracetamol suppositories should be carefully selected based on the weight of the patient.
This is particularly important in children. Parents are often unaware of the weight of their child and standard mechanical weighing scales are not accurate enough for this purpose. Thus, suppositories are often administered according to the age of the child. With the increase in childhood obesity, underdosing can be a problem.
On the other hand, anorexic or dehydrated children are at risk of overdose and

consequent serious liver damage. Pharmacists may have a role in advising parents on the correct dose even to the extent of weighing the child using accurate, calibrated electronic weighing scales.
Analgesic suppositories are effective for symptomatic treatment of mild to moderate pain and fever in children and are likely to become more popular as the range of suppositories expands in Ireland. Paracetamol suppositories are now available in strengths suitable for all ages from infants and children to adults. Ibuprofen suppositories are also available for use in infants and children and though a more recent arrival on the market, are likely to become just as popular as parents realise that they now have another option for treatment of mild conditions.
Suppositories are usually safe. Yet there can be some problems when a patient takes medicine this way:
• Some of the medicine might leak back out.
• Sometimes the body doesn’t absorb the drug as well as if taken by mouth.
• The medicine can irritate the spot where it was put it in.
Those who have:
• An irregular heartbeat
• Have had recent surgery on the rectum
• Males who have had prostate surgery recently
• Females who have had surgery or radiation treatment to the vaginal area
Who: Adults and Children aged 6 plus.
What are the symptoms? Mild to moderate pain (from headaches, menstrual periods, toothaches, backaches, osteoarthritis, or cold/flu aches and pains) and to reduce fever.
How long have they had symptoms? N/A
Action already taken? Some patients may have already tried oral medications but are unable to swallow.
Medication: 3 types of suppositories; rectal, vaginal and urethral.




Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Please refer to the Summary of Product Characteristics (SmPC) for full details of Prescribing Information.
Motusol Max (diclofenac sodium) 2% w/w gel Abbreviated Prescribing Information. Presentation: White to almost white, homogeneous gel. 1g of gel contains diclofenac as 23.2mg diclofenac diethylamine corresponding to 20mg of diclofenac sodium. Indications: Local symptomatic treatment of pain in acute strains, sprains or contusions following blunt trauma. For short term treatment only. Dosage and administration: For cutaneous use. Apply to affected parts of the body thinly and gently rub into skin. Wash hands after application unless area to be treated. Allow gel to dry on skin before applying bandages. Adults and adolescents aged 14 years and over: depending on the size of the affected site, apply a cherry to walnut size quantity 2 times a day (preferably morning and evening). Should not be used for longer than 1 week without medical advice. Children: no data in children and adolescents under 14 years of age. Elderly: no dosage adjustment required. Monitor patient carefully. Renal and hepatic impairment: no dosage adjustment required. Contraindications: Hypersensitivity to active substances or excipients; patients with a history of hypersensitivity reactions such as asthma, bronchospasmus, urticaria, acute rhinitis in response to acetylsalicylic acid or non- steroidal anti-inflammatory drugs (NSAIDs); open injuries, inflammations or infections of the skin as well as on eczema or mucous membranes; in the last trimester of pregnancy; in children and adolescents under 14 years of age. Precautions and warnings: Systemic undesirable effects cannot be excluded if applied on larger areas of skin over a prolonged period of time. Must only be applied to intact, not diseased or injured skin. Must not come into contact with eyes and oral mucous membranes. Must not be taken orally. May be used with non-occlusive bandages, but not with airtight occlusive dressing. Consult doctor if symptoms worsen or do not improve after 3-5 days. Patients suffering from asthma, hay fever, swelling of nasal mucous membranes (so called nasal polyps) ) or chronic obstructive pulmonary disease, chronic
respiratory infections (particularly associated with hay fever-like symptoms), and patients with hypersensitivity to painkillers and anti-rheumatic medicinal products of all kinds are rather at risk to asthma attacks (so called analgesic intolerance / analgesic asthma), to local skin or mucous membrane swelling (so-called quincke edema) or to urticaria than other patients when treated with Motusol Max. In these patients, Motusol Max may only be used under certain precautions (emergency preparedness) and direct medical supervision. The same applies for patients who are also allergic to other substances e.g. with skin reactions, itching or urticaria. Discontinue treatment if skin rash occurs. Photosensitivity can occur with the appearance of skin reactions after exposition to sunlight. Avoid children coming into contact to the skin areas where the gel has been applied. Contains butylhydroxytoluene which may cause local skin reactions or irritation to the eyes and mucous membranes. Contains fragrance with benzyl alcohol (0.15mg/g), citral, citronellol, coumarin, eugenol, farnesol, geraniol, d-limonene and linalool which may cause allergic reactions. In addition, benzyl alcohol may cause mild local irritation. Interactions: None known. Pregnancy and lactation: Should not be used during first and second trimester unless clearly necessary. Contraindicated during third trimester. Should only be used during breast-feeding under advice from a healthcare professional and should not be applied on the breasts, nor elsewhere on large areas of skin for a prolonged period of time. Effects on ability to drive and use machines: No or negligible influence. Adverse reactions: Hypersensitivity, angioedema, dermatitis bullous, Common: dermatitis (including contact dermatitis), skin rash, erythema, eczema, pruritus. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: Wash skin with water where applied. If ingested, apply general therapeutic measures normally adopted to treat poisoning with non-steroidal anti-inflammatory medicinal products. Gastric lavage and use of activated charcoal should be considered. Legal category: Pharmacy. Marketing Authorisation Number: PA1986/093/002. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00036. Date of Preparation: June 2021
Job Code: Dic-IE-00009. Date of Preparation: November 2022
When patients experience muscle and joint pain, pharmacists can recommend topical analgesics (rubs, creams and sprays) to help provide relief for their symptoms.
Helping customers choose the right topical analgesic for their individual needs is key if they are to gain optimum benefit.
Musculoskeletal pain is likely to affect a significant percentage of the population and encompasses a huge range of conditions. Low back pain, for example, is acknowledged to be the leading cause of disability worldwide and osteoarthritis is purported to affect 60% of 60-year-olds.
While musculoskeletal conditions and the pain, stiffness and immobility that go with them can compromise the lives of sufferers in many obvious physical ways, mental health and wellbeing is also affected.
Patients will often use OTC topical analgesics for the treatment and management of musculoskeletal injuries and disorders. These products may have local analgesic, anaesthetic, antipruritic, and/or counterirritant effects.
Topical analgesics for musculoskeletal pain can be used alone or in conjunction with oral analgesics when appropriate and warranted. External analgesic products may contain one or more of the following ingredients: methyl salicylate, camphor, menthol, methyl nicotinate, capsicum, and trolamine salicylate.
Patient confusion regarding the wide array of topical products and formats available can also hinder usage. Consumers want help and reassurance when it comes to self-treating. They do not understand the difference between various types of topical – hot, cold and non-steroidal anti-inflammatory drugs – or how to use them.
Following the introduction of the codeine regulations, pharmacists now encourage the use of acetaminophen as first in line choice of pain relief, followed by ibuprofen, before codeine-based analgesics.
In addition, patients must be made aware of how to use the medication properly and must be informed by pharmacists of the possible side effects that can occur when a product is used after the recommended period of three days.
Products may have local analgesic, anaesthetic, antipruritic, and/or counterirritant effects. Topical pain killers, or analgesics, are sprayed on or rubbed into the skin over painful muscles or joints. Although all are designed to relieve pain, different products are made up different ingredients.
Counterirritants are approved for the topical treatment of minor aches and pains of muscles and joints. They are often employed for the treatment of acute musculoskeletal injuries and as an adjunct therapy in the treatment of chronic musculoskeletal disorders.

Counterirritants differ from other external analgesics in that pain relief results more from nerve stimulation than depression. Topical analgesics for musculoskeletal pain can be used alone or in conjunction with oral analgesics when appropriate and warranted. External analgesic products may contain or more of the following ingredients: methyl salicylate, camphor, menthol, methyl nicotinate, capsicum, and trolamine salicylate.
Salicylates: These same ingredients that give aspirin its pain-relieving quality are found in some creams. When absorbed into the skin, they may help with pain, particularly in joints close to the skin, such as the fingers, knees, and elbows.
Capsaicin: The main ingredient of hot chilli peppers, capsaicin is also one of the most effective ingredients for topical pain relief. When first applied, capsaicin creams cause a
warm tingling or burning sensation. This gets better over time. Users may need to apply these creams for a few days up to a couple of weeks before they will notice relief from pain.
Topical analgesic products are available in a variety of formulations, including gels, ointments, creams, lotions, and patches in single-entity or combination formulations. Topical heat therapy patches are also available in various sizes for treating joint and muscle pain and provide eight to 12 hours of continual, portable heat therapy.
OTC topical analgesics are intended to be used for mild to-moderate pain for no longer than seven days. The factors that a pharmacist may consider when recommending a topical analgesic include dosage form, cost, ease of use of product, as well as the patient’s medical history, including possible allergies.
Who? Anyone suffering from pain, musculoskeletal problems or fever.
What are the symptoms? Dependent on the condition suffered.
How long has the patient had the symptoms? Dependent on thHere you goe condition suffered.
Action already taken? Pain relief.
Medication? Apply topical products only to intact skin. Areas treated with counterirritants should not be covered with tight bandages or occlusive dressings. Patients on anticoagulation therapy should be advised not to use topical products that contain salicylates, because concomitant use has been associated with prolonged prothrombin time.
9/10 patients did not require antibiotics with Utipro® Plus*
Urinary tract infections (UTIs) are among the most common infections affecting adult women. One-half of all women will experience at least one UTI in their lifetime. Recurrence of UTIs is common, with a reported rate of 25% within 6 months of the first occurrence.
Urinary tract infection (UTI) is the collective term used to describe infections involving any part of the urinary tract, which includes the kidneys, ureters, bladder and urethra. Infections of the bladder (cystitis) and urethra (urethritis) are known as lower UTIs and infections of the kidneys (pyelonephritis) or ureters are classed as upper UTIs.
Diagnosis of UTI is based primarily on signs and symptoms.
The incidence of UTIs in adult males under age 50 years is low. Up to 40% of women develop a UTI at some point in their life, compared to 12% in men. In men, cystitis is often associated with infection and inflammation of the prostate gland (prostatitis). Anatomically, the female urethra is shorter and located closer to the anus than in males, which makes it easier for bacteria to reach the female urethra and bladder.
Adult women are 30 times more likely than men to develop a UTI, with almost half of them experiencing at least one episode during their lifetime and one-in-three women experiencing their first episode by the age of 24 years. UTIs are most commonly seen in sexually-active young women.
UTIs can be classified as ‘uncomplicated’ (sometimes referred to as a ‘simple’ UTI) or ‘complicated.’ Uncomplicated infections present most frequently in women without any structural or functional abnormality of the urinary tract, any history of renal disease, or other comorbidity (e.g. immunocompromised patients or those with diabetes), which may contribute to more serious outcomes. Complicated UTIs are associated with a condition or underlying disease that interferes with the patient’s immune mechanisms and increases the risk of acquiring infection.
Recurrent UTIs, defined as at least two UTIs in 6 months or three UTIs in 1 year, are a significant burden for the patient and result in high costs to the health system. The most commonly prescribed regimens are trimethoprim-sulfamethoxazole (or trimethoprim alone), nitrofurantoin, cephalexin and the fluoroquinolones at a quarter of the usual daily dose for 6 months.
Symptoms may include:
• Pain or a burning sensation when passing urine
• Needing to urinate more often during the night
• Urine that looks cloudy
• Needing to urinate more urgently than usual
• Blood in the urine
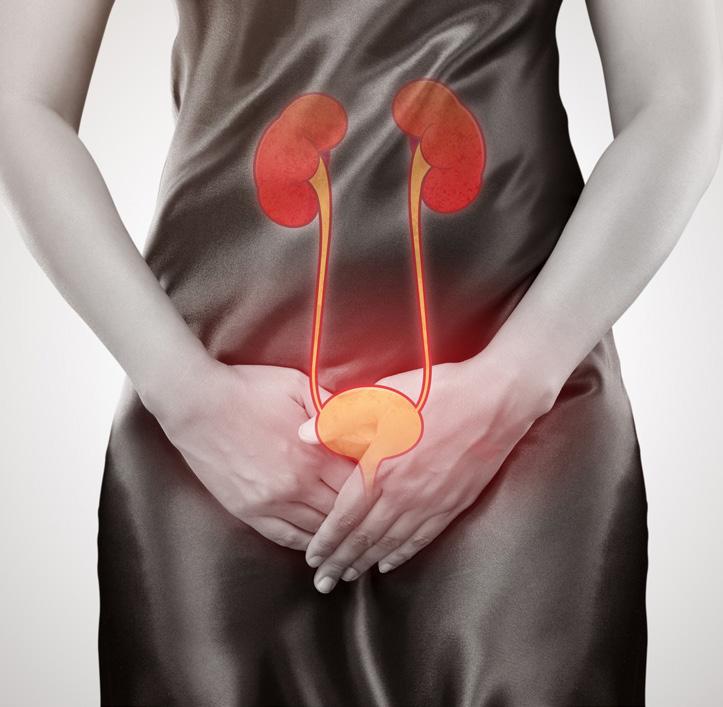
Children with UTIs may also:
• Have a high temperature
• Appear generally unwell
• Wet the bed or themselves
• Be sick
When to Refer:
• Someone who has symptoms of a UTI for the first time
• A child has symptoms of a UTI
• A man with symptoms of a UTI
• Pregnant women with symptoms of a UTI
• Symptoms of a UTI after surgery
• Symptoms get worse or do not improve within 2 days
Those suffering with UTIs can be advised to take paracetamol up to four times a day to help reduce pain and a temperature. Children can take liquid paracetamol. They should also be advised to rest and drink fluids so that they can pass urine more regularly during the day.
Who? Adults, mainly women.
It may also help for sufferers to avoid sexual intercourse until symptoms have passed.
Drinking cranberry juice may help to prevent UTIs. For those with recurring UTIs, higher strength cranberry capsules are recommended.
However, advise customers that they should not consume cranberry juice or cranberry capsules if they are taking warfarin.
Constipation (where it is difficult to pass stools) can increase the chances of developing a UTI.
Recommended treatments for constipation include:
• increasing the amount of fibre in the diet (20g to 30g of fibre a day)
• using a mild laxative on a short-term basis
• drinking plenty of fluids
What are the symptoms? Pain when urinating, urinating more frequently, high temperature, frequent urinating at night.
How long has the patient had the symptoms? Recurrent UTIs can be as frequent as 2 in six months.
Actions already taken? Cranberry juice and drinking water regularly may help. Avoiding constipation can be a deterrent.
Medication: Antibiotics.
THE UK’S NO.1 GP RECOMMENDED BRAND FOR VAGINAL DRYNESS.* If you’re su ering from vaginal dryness and irritation, Replens is the perfect solution for you. Unlike lubricants, Replens is a specially made vaginal moisturiser that helps replenish your natural moisture. This 2 in 1 gel soothes and treats symptoms to give you up to 3 days of long-lasting relief. So, you can wave bye-bye to vaginal dryness and say hello to happier days to come, whether that be rekindling your love life or simply feeling like you again.



Normally, the walls of the vagina stay lubricated with a thin layer of clear fluid. The hormone estrogen helps maintain that fluid and keeps the lining of your vagina healthy, thick, and elastic. A drop in estrogen levels reduces the amount of moisture available and can lead to vaginal dryness.
It is a common but treatable problem that many women experience at some point in their lives. It can be a problem at any age, but is a particular issue for women who are going through or have experienced the menopause. Sufferers will often feel embarrassed about seeking help but can be advised that there are a number of treatments that can help.
Some women only have symptoms of vaginal dryness at certain times, such as during sex, while others have them all the time. Problems associated with having a dry vagina include:
• vaginal irritation, discomfort, itchiness or a burning sensation
• discomfort during sex
• a reduced sex drive
• difficulty getting aroused and reaching orgasm
• the surface of the vagina looks pale and thin
• narrowing or shortening of the vagina
• needing to pass urine more often than usual
• repeated urinary tract infections (UTIs)
Causes of a dry vagina include:
• the menopause - decreased levels of the hormone oestrogen during the menopause can cause persistent vaginal dryness (also known as vaginal atrophy or atrophic vaginitis)
• breastfeeding or childbirth - oestrogen levels can temporarily decrease after giving birth and make the vagina feel drier than usual
• not being aroused before sex - if a woman doesn’t feel aroused before having sex, her vagina may not produce natural lubricant and sex may be uncomfortable
• some types of contraceptionthe combined contraceptive pill and contraceptive injection can occasionally cause vaginal dryness, although this is uncommon
• cancer treatment - radiotherapy to the pelvic area, hormonal cancer treatments, and sometimes chemotherapy can cause vaginal dryness
Vaginal dryness is also sometimes caused by an underlying condition such as diabetes or Sjögren’s syndrome, where the immune attacks the glands in the body that produce fluid.
Sufferers of vaginal dryness can be advised that it’s worth trying self-help options first. It can help to:
• try using a lubricant or vaginal moisturiserthese can be bought without a prescription
• give yourself enough time to become aroused before having sex - read more about female arousal and get good sex tips
The most common treatment for vaginal dryness due to low estrogen levels is topical estrogen therapy. These replace some of the hormone the body is no longer making. That helps relieve vaginal symptoms, but it doesn’t put as much estrogen in the bloodstream as the hormone therapy in pills.
Lubricants - liquids or gels that are applied to the vulva, vagina or the partner’s penis just before having sex to keep the vagina moist. They offer immediate but short-term relief from vaginal dryness. Several different brands of lubricant are available to buy from pharmacies without a prescription.
Vaginal moisturisers - creams that are applied inside the vagina to keep it moist. They may be better than lubricants if the
dryness isn’t just causing problems during sex, as they tend to have a longer-lasting effect. They usually need to be applied every few days.
Vaginal oestrogen - a GP may prescribe vaginal oestrogen if the dryness is caused by the menopause. This works by increasing the level of oestrogen that declines during and after the menopause.
Vaginal oestrogen is available as pills that are placed in the vagina (pessaries), vaginal creams and vaginal rings. Oestrogen treatment can be more effective than lubricants and moisturisers for menopausal women, and it generally causes few side effects.
However, it can take a few weeks to start working, so the patient may want to use a lubricant or moisturiser as well to begin with. Treatment usually needs to be continued indefinitely, as the dryness tends to return if treatment stops.
Hormone replacement therapy - HRT is a treatment that involves taking medication to replace the hormones that start to decline during the menopause.
It’s available on prescription from a GP either as tablets, a skin patch, an implant under the skin, or a gel that’s applied to the skin.
HRT has a wider effect on the body than vaginal oestrogen, so may be best if the person has other menopause symptoms, such as hot flushes. However, it also has more side effects.
Who? All women, but more prevalent during the menopause.
What are the symptoms? Vaginal irritation, discomfort, itchiness or a burning sensation, discomfort during sex, a reduced sex drive, difficulty getting aroused and reaching orgasm, the surface of the vagina looks pale and thin, narrowing or shortening of the vagina, needing to pass urine more often than usual, repeated urinary tract infections (UTIs).
How long has the patient had the symptoms? Many women will delay seeking medical advise because they may be embarrassed about the symptoms.
Action already taken? A number of self-care treatments may already have been used by the sufferer.
Medication? Topical estrogen therapies replace some of the hormone the body is no longer making.

Contributes to:


• maintenance of normal bones
• normal function of the immune system
• maintenance of normal muscle function
Food supplements do not replace a varied, balanced diet and a healthy lifestyle. Always read the label carefully.
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product.
Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system HPRA Pharmacovigilance, Website: www.hpra.ie
Adverse reactions/events should also be reported to the marketing authorisation holder at email address: pv.ireland@viatris.com or phone 0044 (0) 800 1218267.
Viatris, Newenham Court, Northern Cross, Malahide Road, Dublin 17, Dublin, Ireland. www.viatris.ie
Job code: COL-2022-0005
| DOP: August 2022
Vitamin D is often called the “sunshine vitamin” because it’s produced in the skin in response to sunlight. It is a fat-soluble vitamin in a family of compounds that includes vitamins D-2, and D-3.
Vitamin D is unique because it can be made in the skin from exposure to sunlight. It can also be sourced through certain foods and supplements to ensure adequate levels of the vitamin in the blood.
Vitamin D deficiency is generally classified as serum 25-hydroxyvitamin D [25(OH)D] concentrations of less than 30 ng/m. There is limited available evidence regarding the optimal level of vitamin D, but some studies suggest about 50 ng/ml.
Groups at risk of vitamin D deficiency include the following: breastfed infants; older adults; individuals with limited sun exposure; patients with dark skin; individuals with inflammatory bowel disease and other conditions causing fat malabsorption; and patients who are obese or have undergone gastric bypass surgery.
Vitamin D has several important functions. Perhaps the most vital are:
1. REGULATING THE ABSORPTION OF CALCIUM AND PHOSPHORUS, AND FACILITATING NORMAL IMMUNE SYSTEM FUNCTION
• Getting a sufficient amount of vitamin D is important for normal growth and development of bones and teeth, as well as improved resistance against certain diseases.
2. SUPPORTING THE PARATHYROID
• These work minute to minute to balance the calcium in the blood by communicating with the kidneys, gut and skeleton. When there is sufficient calcium in the diet and sufficient active Vitamin D, dietary calcium is absorbed and put to good use throughout the body. If calcium intake is insufficient, or vitamin D is low, the parathyroid glands will ‘borrow’ calcium from the skeleton in order to keep the blood calcium in the normal range.
• Vitamin D insufficiency affects almost 50% of the population worldwide. In childhood/ adolescence, there are periods of intensive bone growth, with Vitamin D deficiency causing improper bone mineralisation, causing rickets. This leads to a severely bowlegged appearance due to the softening of the bones. Evidence suggests that rickets prevalence is increasing globally, with levels in the UK the highest seen in 5 decades. A recent study by Trinity College Dublin, also found that low vitamin D is highly prevalent (51%) in Ireland, with girls, those over 12 years and those assessed in winter most at risk.
• Similarly, in adults, vitamin D deficiency manifests as osteomalacia, or softening of the bones. Osteomalacia results in poor bone density and muscular weakness. Osteoporosis (fragile bones) can also result, which can lead to increased fractures & falls particularly in the elderly.
• Vitamin D interacts with receptors on macrophages, B lymphocytes & T lympocytes to help activate & regulate immune responses. Within the respiratory tract, it also stimulates our production of natural anti-microbial factors such as the anti-biotic like proteins known as defensins. Studies involving over 19,000 adults show that having low levels of vitamin D increases the likelihood of developing common cold symptoms by 36% compared to people with high levels. Deficiency is especially harmful for people with lung diseases - lack of vitamin D increases the risk of respiratory infection in those with asthma & COPD.
• Vitamin D deficiency has links to high blood pressure in children. A 2018 study found a possible connection between low vitamin D levels and stiffness in the arterial walls of children.
• The American Academy of Allergy Asthma and Immunology (AAAAI) suggest that evidence points to a connection between low vitamin D exposure and an increased risk of allergic sensitization. An example of this is children who live closer to the equator and have lower rates of admission to hospital for allergies plus fewer prescriptions of epinephrine autoinjectors. They are also less likely to have a peanut allergy.
• Furthermore, vitamin D may enhance the anti-inflammatory effects of glucocorticoids. This benefit makes it potentially useful as a supportive therapy for people with steroid resistant asthma.
Who? Anyone – the young and elderly are more susceptible to winter illness.
What are the symptoms? Cold, congestion, sore throat and cough.
How long have they had the symptoms? Symptoms of a cold generally only last a few days, flu symptoms can make people feel very unwell often leaving them unable to leave the house or go to work.
Action already taken? People may have tried pain relief – but may not be aware of combination products, for example ones containing combinations of antihistamine, analgesic and stimulant.
Medication? Pseudoephedrine is contraindicated in patients with diabetes mellitus, cardiovascular disease, severe or uncontrolled hypertension, severe coronary artery disease, prostatic hypertrophy, hyperthyroidism, closed angle glaucoma, and pregnant women.


The Vitamins, Minerals and Supplements (VMS) has always been an important category in pharmacy in Ireland. There has been an upsurge in the past few years as people have become more aware of nutrition and what they can take to help aid their bodies to operate to their full capacity. People have begun to learn and understand that VMS are important at any stage of life from birth right up to the elderly.
Over the past year with the incidence of the Covid-19 pandemic there has been a significant increase in the incidence and demand for the VMS category when compared to previous years. Initially with the outbreak of the pandemic, there was a surge in demand for Vitamin C and Zinc and other products that could aid and strengthen the immune system to help fight off any possible infection. As the year progressed and more information and research about the Coronavirus emerged, there was a significant increase in the requests for Vitamin D.
Current guidelines state that all women thinking of having a baby should have a folic acid supplement, as should any pregnant woman up to week 12 of her pregnancy. Folic acid can help to prevent neural tube defects, such as spina bifida.
Pregnant and breastfeeding women are also at risk of vitamin D deficiency and should take a daily supplement containing 10 micrograms – a point pharmacy teams could raise with expectant mothers.
Fish oil supplements should be pregnancyspecific to avoid high doses of vitamin A and breastfeeding women should continue with vitamin D and fish oil supplementation.
Statistics have shown that a large number of the over-50s are falling short of the nutritional goals needed to maintain optimal health. The take-home message is clear - Supplements, such as a daily multivitamin, can provide an effective strategy for maintaining health, supporting nutrient intakes, plugging dietary gaps and helping to address the nutritional challenges associated with ageing.
Vitamin C (ascorbic acid) is a nutrient your body needs to form blood vessels, cartilage, muscle and collagen in bones. Vitamin C is also vital to your body’s healing process.
Vitamin C can be obtained from a healthy diet as it is present in citrus fruits, berries and spinach.
Severe vitamin C deficiency can lead to a disease called scurvy, which causes anemia, bleeding gums, bruising and poor wound healing.

The recommended daily amount of vitamin C is 90 milligrams for adult men and 75 milligrams for adult women.
Vitamin C is available in many formulations ranging from chewable tablets, oral tablets and effervescent tablets. It is common to see Vitamin C products also containing zinc to help the immune system and there definitely is an increase in requests for such products coming into the winter months.
Zinc is essential for the body’s growth and development and wound healing. It also helps regulate immune function, exhibits antioxidant activity, and helps support a balanced inflammatory response in the body.
Your immune system needs zinc to function properly. A zinc deficiency reduces your ability to eliminate pathogens, mount a response against threats, and produce antibodies. It has been shown that if zinc is taken soon after cold symptoms appear, it may also shorten the length of a cold.
The recommended daily amount of zinc is 8 milligrams (mg) for women and 11 mg for adult men.
Zinc is available on its own mainly in tablet form but is quite popular in a chewable form combined with Vitamin C. The combination products appear to be more popular amongst customers due to ease of taking a single tablet.
Magnesium keeps the immune system strong, helps strengthen muscles and bones, and supports many body functions from cardiac functions to brain functions.
The amount of magnesium recommended is: 300mg a day for men (19 to 64 years) and 270mg a day for women (19 to 64 years)
Care should be taken as high doses (more than 400mg) for a short time has been shown to cause diarrhoea. Having 400mg or less a day of magnesium from supplements is unlikely to cause any harm.
Magnesium is available in tablet form at varying strengths and also in sachet form as a soluble powder for consumption.
The most important thing we take into consideration when merchandising this area in the pharmacy to achieve optimum footfall would be to rotate our displays to reflect the current situation. For example, all the Vitamin D products are always at eye level and then when schools began to reopen, all the multi vitamin and mineral products were made more visible. Special offers were highlighted in store, e.g. if an item was at a special price or included a free item with purchase these were very eye catching for consumers.
Who? Certain vitamins are recommended for specific patient groups. Keep educated on their target populations.
What are the symptoms? Take a full symptom and medical history in order to direct the customer to the most appropriate vitamin/supplement.
How long have they had the symptoms? N/A
Action already taken? Some customers may have already commenced a more balanced and healthy approach to diet and lifestyle, recommend continuation of this to include exercise.
Medication: A full medication history is essential to ensure the right product is selected for the right customer as many vitamins and supplements can cause side effects if used inappropriately.
The Safety, Health and Welfare at Work Act 2005, which repealed and replaced the Safety, Health and Welfare at Work Act 1989 was brought in to make further provision for the safety, health and welfare of persons at work. This Act clarifies and enhances the responsibilities of employer‘s, the selfemployed, employees and various other parties in relation to safety and health at work. The Act also details the role and functions of the Health and Safety Authority, provides for a range of enforcement measures that may be applied and specifies penalties that may be applied for breach of occupational safety and health.
The 2005 Act came into force on 1st September 2005 WHO DOES THE ACT APPLY TO?
The Act applies to all employers, selfemployed and employees in all places of work. It also places duties on designers, suppliers, manufacturers and others concerned with work activities.
Employers have extensive duties under the Act. The different requirements are split up into the following headings:

General duties of the employer include:
• To ensure the safety, health and welfare at work of his or her employees
• To manage and conduct work activities in such a way as to ensure the safety, health and welfare at work of all employees
• To manage and conduct work activities in such a way as to prevent any improper conduct or behaviour likely to endanger employees
• As regards the place of work concerned, the employer must ensure the design, provision and maintenance of:
- a safe, risk-free place of work,
- safe means access to and egress from it
- plant and machinery that are safe and without risk to health
• To ensure safety and the prevention of risk arising from the use of articles or substances or the exposure to noise, vibration, radiation or any other ionizing agent
• To provide systems of work that are planned, organised, performed, maintained and revised as appropriate so as to be safe and risk free
• To provide and maintain facilities and arrangements for the welfare of employees at work
• To provide information, instruction, training and supervision, where necessary
• To implement the safety, health and welfare measures necessary for protection of employees, as identified through risk assessments and ensuring that these measures take account of changing circumstances and the general principles of prevention specified in Schedule 3.
• To provide protective clothing and equipment where risks cannot be eliminated or adequately controlled
• To prepare and revise emergency plans and procedures
• To report accidents and dangerous occurrences to the relevant authority (prescribed under section 33)
• To obtain where necessary the services of a competent person for the purpose of ensuring safety and health at work
• To ensure that all safety measures take into account both fixed term and temporary workers and that that any measures taken do not involve financial cost to his or her employees
When giving information to employees, employers must:
- Ensure that it is given in such appropriate form, manner and language that it is likely to be understood by the employees concerned
- Ensure that the information includes the workplace hazards and risks identified, the protective and preventive measures taken and the names of the safety representative and all other persons named in evacuation procedures etc.
• Where persons from other employment are engaged in work activities in an employer‘s undertaking, the employer must ensure that the person‘s employer receives the above information
• The employer must ensure that the safety representative (section 25) and designated competent persons (section 18) have access to:
- The Risk Assessment
- Information relating to reportable incidents and accidents
- Information arising from protective or preventative measures
• The employer must provide information relating to the following before a fixed term or temporary employee commences work:
- Any potential risks
- Health surveillance
In response to stress, the body’s nervous system is activated due to the sudden release of hormones.
This is known as the fight or f light response, which evolved as a survival mechanism, enabling people and other mammals to react quickly to life-threatening situations as your body becomes ‘ready’ and in a ‘state of alert.’The released hormones increases heartbeat and respiration rate in order to provide the energy and oxygen to the body that will be needed to fuel a rapid response rate. This can have a positive effect on your performance as it can help you to prepare and focus, however if this state of alert becomes prolonged or permanent, your performance abilities become restricted.
The viscious circle
Modern life can be stressful and demanding, as we struggle to find a balance between the needs of the family, pressures from work and our own health and well-being. Neuro Balance may help you to find your inner balance.
The lack of a regular balance between tension and relaxation may have effects on your cardiovascular system, immune system and digestion. Your nervous system suffers from prolonged stress too, and constant stimuli can lead to nervous restlessness. The roundabout of thoughts just doesn’t stop and it can become difficult to relax at night which results in beginning the next day already exhausted.
Simple tips to help yourself
Taking a daily timeout may release the present state of stress. Taking a relaxing bath without access to your phone and social media can help you switch off and unwind.
Take exercise - whatever type you choose, be it swimming, cycling or walking, it’s a perfect outlet in order to release the stress caused by accumulated energy.
Being out in the fresh air can have many benefits, both physically and mentally. If you cannot get out, even sitting by the window can help.
Try relaxation techniques such as Yoga, Tai Chi, Qigong, meditation and special breathing techniques, which can help you to relax and restore balance.
A bedtime routine can help the body and mind to wind down and prepare you for sleep. Writing a diary may enable you to leave your thoughts of the day behind.
Floradix Neuro Balance, with its contained ashwagandha root and herbal extracts of passion flower, lavender, lemon balm and rosemary, may help you to find your inner balance.
What is Ashwagandha?
Ashwagandha is an evergreen shrub, also known as Indian ginseng or winter cherry, that is found in India and parts of Africa. The plant, particularly its root powder has been used for hundreds of years for medicinal purposes and to help improve the body’s resistance to stress.

- Any special occupational qualifications or skills required
- Any increased specific risks which the work may involve
An employee, while at work must:
• comply with all relevant statutory provisions
• take reasonable care to protect the safety of themselves and others who might be affected by their acts and omissions
• ensure they are not under the influence of an intoxicant or in such a state that they might be a danger to themselves or others.
• submit to reasonable, appropriate testing, if reasonably required by the employer .The Act gives scope for Regulations to be made that provide for employees to be required to undergo tests for intoxicants to be carried out by or under the supervision of a registered medical practitioner. Such Regulations are yet to be developed and until they are made, an employer may not require such testing although local agreements may apply. The employer may, however, prevent an employee from working if it is apparent that he or she would be a danger to themselves or others.
• co-operate with his or her employer so far as is necessary to enable compliance with the relevant statutory provisions
• not engage in any improper conduct or dangerous behaviour
• attend training and undergo such assessment as may be necessary
• make correct use of any article or substance provided for use or for the protection of the employee, including protective clothing and equipment
• report to his or her employer as soon as practicable:
- any work being carried out which might endanger themselves or others
- any defects in the place of work, the system of work, any article or substance which might endanger themselves or others
- any contravention of the relevant statutory provisions of which he/she is aware
• Notify the employer or the employer‘s nominated registered practitioner if they become aware that they are suffering from any disease or physical or mental impairment which affects their performance of work activities that could give rise to risks to the safety, health and welfare of persons at work. The duty is on the employee to protect themselves and others.
An employee may not:
• misrepresent himself or herself to an employer with regard to their level of training
• interfere, misuse or damage anything provided for the safety, health and welfare or employees
• place at risk the safety, health and welfare of persons in connection with work activities
In order to prevent bullying, horseplay, harassment or any other behaviour that has a potential to endanger employee’s safety, health and welfare at work, appropriates procedures must be put in place.
Bullying and Harassment Prevention procedures and disciplinary procedures need to be put in place. Ensuring that competent staff are in place and that appropriate Codes of Conduct are applied will help in complying with these legal requirements.
Download further Information and guidance on Bullying and the Prevention of Violence in the workplace.
ARE THERE ANY REGULATIONS ON TESTING FOR INTOXICANTS IN THE WORKPLACE?
There are no regulations on testing for intoxicants other than in Railway Safety Act 2005. Many companies already have policies on intoxicants and testing may be one element of this policy.
There is already a requirement on employees under Section 13(1)(b) of the 2005 Act not to be under the influence of an intoxicant to such an extent as to endanger themselves or others.
Section 13(1)(c) makes provision for testing as may be prescribed by the Minister.
WHEN MAY AN EMPLOYEE
The 2005 Act gives scope for Regulations to be made that may allow for employees to be required to undergo tests for intoxicants carried out by or under the supervision of a registered medical practitioner.
Regulations are yet to be developed and until they are made, an employer may not require such testing unless a local agreement applies within the contract of employment. The employer may, however, prevent an employee from working if it is apparent that he or she would be a danger to themselves or others.
The duty of the employee not to be under the influence of an intoxicant is effective immediately.
For further information see the Intoxicants at Work Information Sheet.
The Act requires an assessment of the medical fitness to work of employees involved in certain work activities or occupations. Theses activities and occupations are to be detailed in Regulations. Registered medical practitioners nominated by the employer will carry out the assessments.
If the medical practitioner is of the opinion that the employee is unfit to perform work activities, he or she must notify both the employer and the employee as soon as possible giving the reason for the opinion and the likelihood of early resumption of work for rehabilitation purposes. The amount of information that can be passed on to the employer is limited by Doctor/ Patient confidentiality.
When an employee is informed by their General Practitioner or other medical practitioner that they are unfit to carry out an occupation or activity specified in the regulations they must inform either the employer or the employer‘s registered medical practitioner.
When an employer is notified of the unfitness of the employee they must immediately take appropriate action to comply with the general duties of employers to ensure the safety, health and welfare of all employees at work.
These are both defined in Section 2 of the 2005 Act.
An article is:
any plant, machine, machinery, appliance, apparatus, tool or any other work equipment for use or operation at work any article designed for use as a component in, part of or to control any of the foregoing or any work equipment any other product used by persons at work.
A substance is any natural or artificial substance, preparation, or agent in solid or liquid form or in the form of a gas, vapour or microorganism.
In addition to the requirements for articles, referred to above, the substance supplier or manufacturer must supply information with regard to the identification of the substance, any risk arising from its inherent properties, any relevant test results and any conditions necessary to ensure its safe use, handling, processing, storing, transportation or disposal.

Clinically tested in 'Memory Investigation with Nutrition for Dementia' Trial at Nutrition Research Centre Ireland, SETU, Waterford
Unique, patented food supplement with carotenoids, omega-3 fatty acids and vitamin E
Helps to support normal brain function*
All natural ingredients, no side-effects
Diabetic friendly and gluten free
Approved by Supplement Certified *DHA
order from



WHAT ARE THE DUTIES OF DESIGNERS, MANUFACTURERS, IMPORTERS AND SUPPLIERS OF ARTICLES AND SUBSTANCES UNDER THE 2005 ACT?
Manufacturers, importers and suppliers of equipment, machinery, articles, or substances used at work have the duty of ensuring safety and health concerning the use of the materials that they produce or supply. Manufacturers, importers and suppliers must provide information on the correct use of the materials to ensure safety and health at work.
Users must be provided with information about the safe use of the article and updated information must be supplied if it becomes known to the supplier or manufacturer that there is any risk to health, safety and welfare. Information provided must relate to the use for which the article has been designed, manufactured or tested and must include information on its safe installation, use, maintenance, cleaning, dismantling or disposal without risk to safety or health.
Designers, manufacturers, importers and suppliers of articles who retain a responsibility under a rental, leasing or other agreement,
In 2009 slips trips and falls (on the level) were the second highest reported accident trigger in the Healthcare Sector.
30% of reported incidents resulted in the person involved being absent from the workplace for over one month.
Consider the following contributing factors when managing the risk from slips, trips and falls.
• Floor surface - it must be suitable for the work activity and kept in good condition.
• Floor contamination and obstaclesprevent contamination (wet floors, greasy floors, paper wrappings etc) and improve housekeeping and you will reduce if not eliminate the risk.
• Floor cleaning - stop pedestrian access to wet floors, spot clean where possible.
• Environmental aspects - ensure adequate lighting for walkways and level changes, good entrance design (e.g. canopies) can help.
• People - their behaviour and physical attributes can be influencing factors. A positive attitude to health and safety by all in the workplace will create a safer working


must maintain the article in a safe condition and in compliance with health and safety laws. Designers and manufacturers must carry out research to discover if the article gives rise to risks with a view to reducing these risks. Persons who erect, assemble or install an article for use at the place of work must ensure that it is done so safely and without future risk.
environment. Taking account of physical disabilities such as poor vision, limited mobility etc in planning and design will help reduce the risk.
• Footwear - wearing suitable footwear for the environment and work activities will help reduce the risk.
• Have a system in place to manage health and safety
• Risk assess and identify high risk areas
• Consult with and involve staff
• Get the flooring right from the start, it must be suitable for the work activities
• Have a system in place to deal with spills without delay
• Encourage good housekeeping
• Encourage a ‘see it sort it’ mentality
• Clearly mark slopes and changes in level
• Review your cleaning procedures to ensure they do not contribute to slips and trips
• Provide slip resistant footwear where other controls are not adequate, trial footwear in the workplace to ensure it is effective.
• Co-operate with your employer to reduce the risk from slips and trips
• Report any health and safety risks to your employer/manager
• Deal with spills straight away
• Adopt and encourage good housekeeping practices
• Report any accidents or near misses
• Wear and take proper care of any safety footwear provided.
Is your brand the one that is recommended?
With the BMA recommending that GPs no longer prescribe for minor ailments, pharmacies now play a key role in administering advice and recommending products.
This Educational Training Guide offers a quick and easy way for the pharmacy staff to learn and to re-cap their knowledge in a specific area.
Alongside each learning module will feature an advertisement for your associated therapy medicine.
There is only one brand associated per therapeutic area - offering exclusive category ownership.
PAUK offers
7 out of 8 pharmacy visitors interact with counter assistants, and 1 in 5 are seeking advice.
Immediate impact of category knowledge
Raise Brand awareness
Encouraging product recommendation
Boost product stocking
Pharmacy Assist UK (PAUK) is an Educational and Training Directory designed with counter assistants in mind, identifying, managing and treating minor ailments and health complaints across 40 topics.
Using the popular WWHAM acronym.
W - Who is the patient?
W - What are the symptoms?
H - How long have the symptoms been present?
A - Action already taken?
M - Medication?
Training on when to refer to the pharmacist, self-care and advice and patient support lines is included.
PHARMACY ASSIST UK 2025
Circulation:
14,000 targeting every independent pharmacy and chain in the UK - Distributed by the Royal Mail.
United Kingdom 14,000 England 11,500 Scotland 1,400 Wales 650 Northern Ireland 450

Health Research Charities Ireland has approx. 40 member charities. Together, they represent well over 1 million people across Ireland. Our members range from large research funding charities to small, voluntary-run patient organisations. They span many areas of health, including rare diseases, childhood illnesses, dementia, mental health, and many forms of chronic illness and disability. All have a strong focus on health or social care research.
The members of HRCI invested more than ¤15 million in research in 2019 (for context, that is one third of the annual HRB budget) and every extended family in Ireland is connected to at least one of these organisations. Beyond financial investment, they ensure the relevance of research to the communities they represent, communicate its findings and insist that it has impact for people. Together these charities provide a beautiful example of what research means to people and families and how the impact of research reaches every village in Ireland.
Note: while we frequently use the terms patients, due to our strong focus on health research, some of our members represent older adults, carers and other groups in society.

The 22q11 Ireland Support Group was set up to provide help, support and accurate information to Irish families. 22q11 Deletion syndrome is a complex variable condition with over 180 different symptoms caused by a micro-deletion on the 22nd chromosome. No two persons with 22qDS will have exactly the same symptoms and some individuals will develop newer ones over time.
https://www.22q11ireland.org/

The Adelaide Health Foundation is a voluntary charitable organisation which has as its principal object the advancement of healthcare. We deliver this through investment in nursing and medical education and health policy research. We also support patients and patient care in Tallaght University Hospital and in the local community.
http://www.adelaide.ie/

A collaborative of hospices, health & social care organisations & universities which advances education.
http://aiihpc.org/

The Alpha One Foundation was established in 2001 to promote research into Alpha-1 Antitrypsin Deficiency (Alpha-1) and to improve the diagnosis, treatment, life expectancy and quality of life of people with this inherited condition.
www.alpha1.ie
The Alzheimer Society of Ireland is the leading dementia specific service provider in Ireland. It is a national voluntary organisation that aims to provide people with all forms of dementia, their families and carers with the necessary support to maximise their quality of life.
www.alzheimer.ie

Arthritis Ireland is the only national charity dedicated to improving the quality of life for people of all ages with arthritis.
www.arthritisireland.ie

Breakthrough Cancer Research funds the efficient and effective development of new treatments for cancer. We work to significantly impact the number of people who can survive this disease.
www.breakthroughcancerresearch.ie

Breast Cancer Ireland is a charity registered in Ireland, triple locked for governance and transparency to raise funding to support pioneering research and provide education and awareness on the importance of good breast health to women of all ages in Ireland.
www.breastcancerireland.com
CRY (Ireland) is an all-island charity, dedicated to supporting families bereaved through the loss of a young person from sudden cardiac death (SCD). It was established in 2002. CRY Ireland provides access to free cardiac screening and assessment at its Centre at Tallaght University Hospital, Dublin for families who have lost a young person or who are affected by or at risk from inherited conditions that cause SCD and emotional support services in an empathetic environment and supporting research into the prevention of sudden cardiac death in collaboration with other likeminded bodies.

CARD rheumatology at St Vincent’s University Hospital is a EULAR Centre of Excellence for research and education. Our main focus is on patients with early, inflammatory arthritis eg. rheumatoid / psoriatic and vasculitis eg. Giant Cell Arteritis. We aim to provide patients with state-of-the-art treatment and information about their conditions. Our key scientific focus is on understanding mechanisms of inflammation in rheumatic diseases, with a view to providing the most relevant treatment to individual patients
https://arthritissvuh.com/

Working together to make a positive difference to the lives of people with disabilities, their families, and carers.
https://www.crc.ie/

The Conor Foley Neuroblastoma Cancer Research Foundation was set up after we lost our son Conor to this disease. Conor did a lot for research in the latter years of his life by participating in new drug trials and allowing his tumour samples to be collected and used for research. As very little developments in new agents or survival rates had changed in the 10 years that Conor was cancer free, we decided to continue Conor’s legacy in research to hopefully one day be a part of a team that finds a cure for this horrible childhood cancer.
http://foleye5.wixsite.com/conor-foley

Cystic Fibrosis Ireland was set up in 1963 to increase knowledge and awareness of CF and to give advice and support to people with Cystic Fibrosis and their families.
http://www.cfireland.ie/

The CFRI is a registry organisation which records, stores and analyses relevant data about the health and medical treatment of people with cystic fibrosis (CF) in the Republic of Ireland. By collecting and analysing information on all people with CF in Ireland, we can better understand their health and wellbeing, and the treatments they receive.
www.cfri.ie

Cystinosis Foundation Ireland is an all volunteer, non-profit organisation dedicated to providing services and suppport for those in affected by Cystinosis. The Foundation also funds research into the causes and improved treatments of Cystinosis. www.cystinosis.ie

DEBRA Ireland is the national charity established in1988 to provide patient support services and to drive research into treatments and cures for those living with the genetic skin condition, epidermolysis bullosa (EB).
http://www.debraireland.org/

Diabetes Ireland Research Alliance is a subsidiary of the Diabetes Federation of Ireland. It was set up to promote Ireland as a knowledge base for global diabetes research and increase the level of diabetes research being undertaken in Ireland.
https://www.diabetes.ie/research/what-is-research/dira/

The aims of Dystonia Ireland are to promote and encourage scientific research into the causes and treatments of dystonia, raise the level of awareness amongst the general public and the medical profession, offer support and information to all people with dystonia and their families nationwide.
As the national support group for dystonia, we also represent the interests of our members with international support agencies and dystonia networks.
http://www.dystonia.ie/

The Emer Casey Foundation was established after Emer’s death of uterine/ovarian cancer when she was only 28 years old. The Foundation aims to promote research into uterine/ ovarian cancer, to raise standards of care for patients and to raise awareness of the disease. http://www.emercaseyfoundation.com/

Epilepsy Ireland is committed to improving the lives of people with epilepsy in Ireland. Brainwave provides a wide range of services aimed at people with epilepsy, their parents, families and friends as well as raising epilepsy awareness and funding epilepsy research.
http://www.epilepsy.ie/

FCI is a national membership charity for carers, working to improve supports, services, and recognition for anyone living with the challenges of caring for a family member or friend who is ill, frail, disabled, or has mental health difficulties. Through out network of 22 resource centres and 66 support groups we engage with approximately 20,000 family carers throughout the year.
https://familycarers.ie/

Fighting Blindness is an Irish patient-led charity funding & enabling world-leading research into treatments & cures for blindness. Through education and advocacy Fighting Blindness works to empower everyone in Ireland living with severe vision impairment. For more information, visit www.FightingBlindness.ie

Friends of the Coombe is a charity organisation established in 1982 to raise funds to assist the development of the Coombe Women & Infants University Hospital. We are one of the largest and most comprehensive providers of Women & Infant healthcare in Europe. www.friendsofthecoombe.ie/

The Irish Cancer Society aims to improve the lives of those affected by cancer, by providing up to date information and a range of services, by influencing change and raising awareness of cancer issues.
www.cancer.ie

The Irish Heart Foundation is a national charity whose mission is to lead in improving the cardiovascular health of people living in Ireland so they do not experience disability or die from preventable heart, stroke and other blood vessel diseases.
www.irishheart.ie
The Irish Kidney Association is a national charitable voluntary organisation founded in 1978. It is a charity for patients led by patients. We are dedicated to meeting the needs of people living with and affected by end-stage kidney disease. These needs are spread across all aspects of life – medical, social, and psychological. The profile of the kidney patient ranges from infanthood to the elderly who are undergoing various methods of treatment: haemodialysis, peritoneal dialysis, and kidney transplantation.
www.ika.ie

The Irish Nephrology Society is comprised of doctors and scientists working in the care of patients with kidney disease, either at a clinical or research level. The mission of the Irish Nephrology Society is to ensure a high quality care for patients with kidney disease by promoting the highest standard of medical practice.
www.nephrology.ie

The Irish Thoracic Society is the official society for the broad spectrum of healthcare professionals involved in the care of people with chronic or acute respiratory disease in Ireland www.irishthoracicsociety.com

MSD Action Foundation and SavingDylan.com were established in 2015. To promote and support research advancements that will lead to improvements in clinical outcomes, life expectancy and quality of life for patients suffering from Multiple Sulfatase Deficiency. www.savingdylan.com/

MS Ireland exists to enable and empower people affected by Multiple Sclerosis to live the life of their choice to their fullest potential. www.ms-society.ie

Muscular Dystrophy Ireland aims to provide information, advice and support to people with neuromuscular conditions and their families through a range of support services. http://www.mdi.ie/

Our goal is to facilitate research into the diagnosis, treatment and prevention of childhood diseases, through the award of research grants funded by the Children’s Medical Research Foundation(CMRF) www.nationalchildrensresearchcentre.ie

The National Institute for Prevention and Cardiovascular Health (NIPC) is an independent, not-for-profit organisation, established in 2014. It has a strategic partnership with the National University of Ireland, Galway and Croí, the West of Ireland Cardiac & Stroke Foundation. It is based at the Croí Heart and Stroke Centre, Moyola Lane, Newcastle, Galway, Ireland. https://nipc.ie/

Research Motor Neurone (RMN) was founded in 2007, for the purpose of promoting and facilitating research into the causes and treatments of motor neurone disease (MND), also known as ALS. RMN also strives to increase awareness of this incurable disease at both a national and international level.Ongoing research is needed to discover the cause, treatment and methods of improving quality of life for MND sufferers and their families.
http://mnd.ie

The Rett Syndrome Association of Ireland is an association of parents and families of people affected with Rett Syndrome and other related disorders.
http://www.rettsyndrome.ie/

The main function of the Research Foundation is to provide equipment and financial support to staff members at the Royal Victoria Eye and Ear Hospital. It also carries out Research Projects throughout the country for subsequent publication in the literature and presentation at Medical Conferences.
http://www.rveeh.ie/rveeh/departments/Research_Foundation.html


The development of Sage Advocacy has been influenced by the scandals of Leas Cross in 2005, and Áras Attracta and Portlaoise Hospital in 2014. First established in June 2014 as a support and advocacy service for older people by the HSE, The Atlantic Philanthropies and Third Age, it was in 2016 asked to explore how it might address some of the more systemic issues relating to people with intellectual disabilities in the South-East. Sage Advocacy clg was established in September 2017 and on March 1st 2018 it assumed full responsibility for the governance and future development of the service. In July 2018 the patient advocacy services, previously provided by Patient Focus, moved to Sage Advocacy which is now a support and advocacy service for vulnerable adults, older people and healthcare patients.
https://www.sageadvocacy.ie/
Sickle Cell and Thalassaemia Ireland advocates for and supports Sickle Cell patients and their families. Since its foundation in 2012 SCTI projects include: educational programmes on Sickle Cell; training for physicians; supporting young people in disease management; provision of basics for children attending hospital; advocating for national screening programme.
http://sicklecellireland.ie/

St John of God Research Foundation
The Saint John of God Research works to promote and support the development of research strategies in the areas of Intellectual Disability, Adult Mental Health and Child and Adolescent Mental Health, in line with the Order’s research mission and national / international developments.
http://www.sjog.ie/

St Patrick’s Mental Health Services
St Patrick’s Mental Health Services is Ireland’s largest independent, not-for-profit mental health service. The hospital, in conjunction with the TCD School of Psychiatry and St. James’ Hospital have developed a vigorous and broad-based programme of clinical research over the past thirty years.
www.stpatricks.ie

St Vincent’s Anaesthesia Foundation
St. Vincent’s Anaesthesia Foundation is a Charity Trust , set up to support and promote the advancement of education & research in relation to Anaesthesia, Intensive Care & Pain Medicine.
http://www.sedda.ie/

Childrens Health Foundation
Children’s Health Foundation raises money to enable the Temple Street Children’s University Hospital to provide world class care and to pioneer new treatments and cures for childhood illnesses.
http://www.templestreet.ie/

The Rotunda Foundation
The Rotunda Foundation (formerly known as the Friends of the Rotunda) is committed in its support of the Rotunda Hospital to strongly embrace the concept of conducting high quality research and new procedures that lead to better patient care.
https://rotunda.ie/rotunda-foundation/

Abbott House, Vanwall Business Park, Vanwall Road, Maidenhead SL6 4XE
Website: freestylediabetes.ie/health-care-professionals | Help Line: 1800 77 66 33
Products: The FreeStyle Libre system
At Abbott, we believe people with diabetes should have the freedom to enjoy a full, active life. That’s why we’re focused on making breakthrough technology accessible and approachable for all. Our groundbreaking sensing technology is revolutionising how people monitor their glucose and providing healthcare teams with more data to drive better informed treatment decisions.

United Drug House,Magna Business Park,City West Road, Dublin 24, Ireland
Type of company: Healthcare group including prescription medicines, devices, OTC brands, cosmetics and herbal remedies.
Website:www.alliancepharmaceuticals.com
Alliance Pharma PLC, Registered Office, Chippenham, Registered in England, Company Number 04241478
Please use the contacts on our global website.
Help Line Number: Phone +44 [0]1249 466966 | Local Contacts: Adrian Curley Mobile +353 (0)87 298 8226
Company Information: From its origins in the UK 20 years ago, Alliance has grown to become a significant international healthcare group, marketing over 90 products in over 100 countries world-wide and employing over 200 people.
Recent years have seen a broadening in the scope of Alliance’s product portfolio. In addition to the established niche prescription products which formed the original focus of the company’s activities, our portfolio now includes medical devices and consumer products, covering a wide range of therapy areas.
In addition to its UK presence, the Group now has eight further offices across Europe, the Far East and the US. This geographic presence is enhanced by a broad network of international distributors, covering more than 100 countries worldwide. An acquisitive company by nature, we have completed more than 35 acquisition or in-licensing deals over the last 20 years, fuelling both our portfolio development and international expansion.
Local Brands in Ireland include: NuSeals®, MacuShield®, Kelo-Cote®, Vamousse®, Opus® Stoma Accessories, Anbesol®, Gelclair®, Hydromol®, Aloclair®, Naseptin® andAmetopl®

Ballytramon Business Park, Ardcavan, Castlebridge, Co. Wexford Y35 Y19A
Tel: (053) 917 9007 | Fax: (053) 915 9494 | Order Line: (053) 917 9007 | Email: info@brandshapers.ie | Website: www.brandshapers.ie
Type of company: Sales, Marketing, Wholesale and Distribution
Brands: Baby - Ella’s Kitchen, Bear, InfaCare, Kandoo, Kendamil Beauty - Sculpted by Aimee, Benefit, Real Techniques, IsaDora, EcoTools, Remesca, Profusion Personal Care - iWhite, Bulldog, Blistex, Breathe Right, Sugar Coated, Vagisil, Kidsner, Moxi Loves, Banana Boat, Human + Kind VMS - Chewy Vites, VOOST, MyVitamins, Ulla Vitamins Supplements - MyProtein Functional Drinks - Parachute, LoBros
Contacts: Simon Byrne – Field Sales Manager (Pharmacy) Simon.Byrne@brandshapers.ie | Mob: +353 86 2259208 Sharon Cahill – Key Account Manager Sharon.Cahill@brandshapers.ie | Mob: +353 87 405 5364
Customer Service: customerservice@brandshapers.ie

Unit 20A, Second Floor, Beckett Way, Park West Business Park, Nangor Road, Dublin 12 Website: www.clonmelhealthcare.ie
Services: Distributors of Medicines and OTC Products direct to Pharmacies, Hospitals and via Wholesalers
Ethical: 4SURE Blood Glucose Monitoring; Amidex; Amitriptyline; Amlodipine; Amoxicillin Clonmel, Amlodipine/Valsartan; Amlodipine/Valsartan/HCT; Anxicalm; APO-Go; Aripiprazole; Aspirin; Atenomel; Atorvastatin Clonmel, Axid; Azacitidine; Azithromycin Clonmel; Binosto; Bisoprolol; Bortezomib; Calvepen; Candist; Candist Plus; Casomide; Caspofungin; Cimeldine; Cinacalet; Ciprotan; Clavamel; Clavamel Forte; Clonactil; Clonocid; Clopidogrel TAD; Co-Tipol Max Suppositories; Cozatan; Cozatan Comp; Crystapen; Darunavir; Dasatinib; Denzapine; Donesyn; Doxatan; Doxatan XL; Duloxetine; Emtricitabine/Tenofovir Disproxil; Distaclor; Distaclor LA; Distaclor LA Forte; Etalopro; Ezetimibe/Simvastatin; Famotidine; Flucloxacillin; Febuxostat; Fesoterodine; Folic Acid; Fungasil; Furosemide; Ibandronic Acid; Irbesartan Clonmel; Isomel SR; Itami; Keflex; Lecigon Intestinal Gel; Lenalidomide; Lercanidipine Clonmel; Letrozole; Levetiracetam Clonmel; Linezolide; Losamel; Maxilief; Melfen; Memantine; Memantine Drops; Minimed MIO Advance Infusion Set; Miramel; Montelair; Movymia; Mycophenolatemofetil Clonmel; Nebimel; Nepramel; Nizoral Shampoo; Nytamel; Olanzapine; Olanzapine ODT; Olmesartan/Amlodipine HCT; Olmesartan; Olmesartan HCT; Osteomel; Oyavas; Pantium; Paracetamol; Pemetrexed; Perdamel; Phenobarbital; Pipercin; Posaconazole; Pravamel; Prednisolone; Pregabalin; Profloxin; Prosentio; Prozamel; Ramitace; Rasagaline Clonmel; Rabeprazole; Rinozal; Risontel; Rosuvastatin; Sametec Airmaster; Serimel; Seropia, Seropia XR; Sildenafil Clonmel; Simtan; Solifenacin; Tamnic; Tamnexyl XL; Tadalafil; Telmisartan; Telmisartan HCT; Temozolomide; Tipuric; Toltertan SR; Valtan; Valtan Comp; Venex XL; Xymel; Xymel SR; Xymel Comp; Zestan; Zomel; Zopitan. OTC: Acriflex; Anti-Hist Allergy; Caldease; Caldesene; Caldesene Adult; CaldeSpray; CaldeBaby Teething Gel; Cerumol; Cerumol Olive Oil; Clonfolic; Desenex; Easofen for children strawberry oral suspension; Easofen; Easofen Max; Easolief DUO; Eye Drops from the makers of Anti-Hist Allergy; Electrosal; Eucryl; Eurax; Flexitol Rescue Heel Balm, Flexitol Nourishing Foot Cream; Flexitol Rapid Relief Hand Balm; Galfer Caps, Galfer Syrup; Gloup Zero Swallowing Gel; Hedrin Treat and Go, Hedrin Protect and Go Spray, Hedrin Dual Pack, Hedrin ONCE; Just a Drop; Maxilief, Medispray, Medithyme Cough Syrup, Nicochew 2mg Gum, Nicochew 4mg Gum; Nizoral Dandruff Shampoo; Nizoral Care Scalp Tonic; Oilatum Bar Soap; Oilatum Emollient; Oilatum Junior Liquid Bath; Paralief 500mg Tablets; Paralief Effervescent Tablets; Paralief Extra; Paralief Hot Lemon Drink; Paralief Night; Paralief Sinus; Ridonex; Savlon Antiseptic Cream; Savlon Advanced Healing Gel; Thermacare; Tefin Suppositories; Tipol Suppositories; Viralief 2g cream; ViraSoothe Gel, ViraSoothe Spray

Unit 3/4, Ballymount Business Park, Ballymount Drive, Ballymount Industrial Estate, Walkinstown, Dublin 12, D12 F884 Website: www.eurosalesinternational.ie | Tel: 00 353 1 450 7771 | Order Line: 00 353 405 0900
Products: 1000 Hour, 7th Heaven, Bathefex, Beverly Hills, Biovene, Broadway, Cuticura, e.l.f. Cosmetics, Egypt Wonder, I LOVE Cosmetics, Inecto, Jordan, Kennedy & Co., KISS, King of Shaves, Lip Smacker, MAM, NOTE Cosmetique, P20, Palmers, Perspirex, Profinish, Provoke, Q+A, Soft & Gentle, Softsole, Sunkissed, Tangle Teezer, True Beauty by Aideen Kate, Vegan Tan, wet n wild Sales Team: Shane Halpin (Monaghan, Cavan, West Meath, Meath, Louth & North Dublin) Phone: 086 234 4408 Email: shane@eurosalesinternational.ie
Jenny Vernal (South Dublin, Wicklow, Wexford & Carlow) Phone: 0872563544 Email: jenny@eurosalesinternational.ie
Helen Fallon (Kildare, Laois & Kilkenny) Phone: 087 432 5891 Email: helen@eurosalesinternational.ie
Suzanne Cooney (Waterford, Cork, Kerry & Tipperary) Phone: 087 210 5126 Email: suzanne@eurosalesinternational.ie
Catherine Flanagan (Limerick, Clare, Galway, Mayo, Roscommon, Leitrim, Longford, Offaly, Sligo) Phone: 087 763 6914 Email: catherine@eurosalesinternational.ie
Allyson White (Belfast, Mid and East Antrim, North Down, Antrim, Newtownabbey, Kilrea, Coleraine, North Coast) Phone: 0044 7407 709109 Email: allyson@eurosalesinternational.ie
Clodagh Birney(Donegal, Fermanagh, Tyrone, L/Derry, Armagh) Phone: 0044 7748 113044 Email: clodagh@eurosalesinternational.ie
Telesales: Aimee Roche / Sandra Cheung - orders@eurosalesinternational.ie
Aimee: Phone: 087 258 0384 l Email: aimee@eurosalesinternational.ie
Sandra: Phone: 01 405 0900 l Email: sandra@eurosalesinternational.ie
Order Online: https://b2b.eurosalesinternational.ie/customer/account/login/ Or register here: https://www.eurosalesinternational.ie/register/
Haleon, 12 Riverwalk, Citywest, Dublin 24, Ireland
Type of company: Consumer Health
Website: www.haleon.com Tel: 01 495 5000 Help Line: customer.relations@@haleon.com
Brands: Pain Relief: Panadol, Voltarol, Excedrin & Anadin. Oral Health: Sensodyne, Sensodyne Pronamel, Corsodyl, Aquafresh, Poligrip & Biotene. Wellness: Nexium, Centrum, Emergen-C, Nicotinell, Caltrate, Andrews, Driclor, Imedeen & Preparation H. Respiratory: Piriton, Flixonase, Otrivine, Night & Day Nurse, Beechams, Panadol Cold & Flu, Robitussin & Advil Cold & Flu. Skin: Zovirax, Lamisil, Duofilm & Chapstick.
Local Contacts: North Leinster, Brian Kelleher Email: brian.x.kelleher@haleon.com Mobile: 087 775 5657 - South Leinster, Stuart Keegan Email: stuart.x.keegan@haleon.com Mobile: 087 986 8819 - West, David FitzPatrick Email: david.x.fitzpatrick@haleon.com Mobile: 087 188 1353South, Paul Hayes Email: paul.x.hayes@haleon.com Mobile: 087 647 4877
Airton Road, Tallaght, Dublin 24 D24 WR89
Type of company: Consumer Health
Website: www.jnj.com Tel: 01 466 5200 Help Line Number: 1800 22 00 44
Products: Nicorette®, Calpol®, Benylin®, Imodium®, Motilium®, Regaine®, Sudafed®, Sinutab®, Actifed®, Johnson’s®, Aveeno®, Neutrogena®, OGX®, Listerine®

Unit H, 1st Floor, Citywest Shopping Centre, Saggart, Co.Dublin D24 TYT9
Type of company: Pharmaceutical Supplier of Generic Ethical Medication
Website: www.krka.ie | Tel: 01 413 3710 | Help Line: 01 413 3710 | Order Line: 01 413 3710
Local Contacts: Ciaran Brennan Sales & Marketing Manager 01 413 3710

Minami, Nestlé Ireland,3030 Lake Drive, Citywest Business Campus, Dublin 24.
Type of company: Nutrition
Website: www.minamihealth.co.uk | Tel: 00800 6378 5385 | Help Line: 00800 6378 5385
Products: MorEPA Platinum Elite + 1000IU Vitamin D, MorEPA Original, MorDHA Prenatal, PluShinz0-3, VeganDHA, MorEPA Move, MorDHA KIDS 3+, MorEPA KIDS 6+, MorEPA Mind, DHA+EPA Liquid Kids + Vitamin D
Local Contacts: Jason McGarry +353852374764
Any other info: At Minami, we create omega-3 products tailored to different lifestyles and life stages. Our unique, advanced production process ensures our products are highly concentrated and highly sustainable, for a purity you can feel and trust.

Suites 3&4, Marine Point, Belview, Waterford
Type of company: Financial Advisers
Website: www.mwm.ie | Tel: 086-8603953 | Help Line: 051 -832 839
Products: Pensions, Investments, Life Cover, Serious Illness, Income Protection
Any other info: As Certified Financial Planners™ and recommended providers of Financial Advice to IPU member you can have the confidence of knowing your financial advice is at the highest accredited standard worldwide.

PrecisionBiotics Ltd, Building 4400, Airport Business Park, Kinsale Road Cork T12N84F
Website: www.precisionbiotics.com | Tel: (021) 206 6012 | Email: Ask@precisionbiotics.com
Type of company: Food Supplements
Any other info: POver 20 years ago, our scientists began researching thousands of bacterial cultures, together with experts from one of the world’s leading centers of microbiome research, the APC Microbiome Institute in UCC, Ireland. Since then, they’ve discovered hundreds of different bacterial cultures and they’ve put each one through rigorous scientific tests. Amongst these hundreds are a handful of special bacteria that stand out because of the precise and significant impact they make to human gut health. When these unique cultures pass all our tests, which include clinical trials in the UK and Europe, the PrecisionBiotics® team are proud to produce them in a high quality and convenient form for consumers and clinicians. Our leading product Alflorex, containing the bacterial culture 35624©, which has won numerous awards including Best Digestive Product at the IPN Awards in 2022 for the 6 time.
Our innovative team has developed 1714© in partnership with leading clinicians which is the culture in Zenflore© aimed at reducing fatigue. We also launched Alflorex Immune in 2019.
For information on any of our products contact our sales partner Pamex Limited, Moneen Business Park, Castlebar, Co. Mayo (info@pamex.ie – 094 902400)

14 Moneen Business Park, Castlebar, Co. Mayo
Type of company: Pharma Distribution
Website: www.pamex.com | Tel: 094 9024000 | Email: admin@pamex.ie
Products include: Alflorex, Zenflore, Utipro Plus AF, KIN Dental, Arthelio Joint Support, Dermatonics, Mycosan, Marimer, Sorefix, Carmex, De Facto Shaving Oil, BioXtra, Nubit, Balance Activ.
Any other info: Pamex distribute and promote over the counter pharmaceuticals, dental & personal healthcare products to pharmacies nationwide.

Sharp Building 10-12 Hogan Place, DO2TY74, Dublin 2
Key Contact: Fiona Clancy, Senior Brand Manager, 00353872212475 | Website: www.perrigo.com

Greenogue Business Park, Rathcoole, Co Dublin
Type of company: Sales & Distribution
Website: www.prl.ie
Tel: +353 1 257 4650
Help Line: +353 1 257 4650
Order: pgsales@prl.ie
Products: Gillette, King C Gillette, Old Spice, Venus, OralB, Fixodent, Seven Sea’s, Ilvico, Vicks, Clearblue, Always, Always Discreet, Tampax, Head & Shoulders, Pantene, Herbal Essence, Aussie, Olay

Liosban Industrial Estate, Unit 6A, Tuam Road, Galway, H91 A580
Type of company: Food Supplement Company
Website: www.reviveactive.com
Tel: IE: 1800 910 000 UK: 0800 901 2152
Help Line Number: IE: 1800 910 000 UK: 0800 901 2152
Order Line: IE: 1800 910 000 UK: 0800 901 2152
Products: Revive Active, Zest Active, Junior Revive, Teen Revive, Joint Complex, Beauty Complex, Meno Active, Mastermind, Ubiquinol Coenzyme Q10
Local Contacts:
Kevin Barry, National Sales Manager - kevin@reviveactive.com Tel: +353 91 769803
Stephen Kean, Area Sales Manager, South Dublin & South Leinster - skean@reviveactive.com Tel: +353 86 1437727
Andra Rooney, Area Sales Manager, North Dublin & North Leinster - andra@reviveactive.com Tel: +353 85 8776110
John Lalor, Area Sales Manager, Connacht & Donegal - John@reviveactive.com Tel: +353 87 2594399
Rhys Phillips, Area Sales Manager, Munster - rphillips@reviveactive.com Tel: +353 86 7925757
Georgina McKeown, Area Sales Manager, Northern Ireland - georgina@reviveactive.com Tel: +44 7769 224494

Newtown, Bantry, Co. Cork, Ireland
Tel: +353 27 50077
Fax: +353 27 50417
Email: PV@rowa-pharma.ie
Any other info: Rowex Ltd. was established in 1993 as the Irish marketing division of Rowa Pharmaceuticals Ltd. It is now one of Ireland’s leading providers of generic pharmaceuticals, supplying the Irish market with high-quality, branded generic pharmaceuticals. We exercise a strong commitment to the local community, sponsoring projects such as the Bantry Hospice project and the Matt Kingston Third level Scholarship. Rowex is committed to providing high quality products which are available to all your patients.

3030 Lake Dr, Citywest Business Campus, Dublin 24
Type of company: Infant Nutrition
Website: www.smababy.ie and www.smahcp.ie | Tel: 1800 931832
We are a specialised maternal and baby nutrition company who have been caring for babies for over 100 years. During that time, we have used our industry leading research to bring ever better products to families. SMA® Nutrition is part of the largest food and nutrition research network in the world, with around 40 research and development sites, including one in the UK and one in Ireland.

Hoffmann Park, Little Island, Cork,T45 YX04 Tel: +353 (021) 4510220 | Email: info@solvotrin.com
Products: Active Iron, Active Folic and Active Immune
Product Information: www.activeiron.com / info@activeiron.com
Distribution: Pharmed Ireland, Mullingar Email: customerservice@pharmed.ie | Tel: +353 (0)44 939 6188

Digital Office Centre Swords, Suite 101 – 103, Balheary Demense, Balheary Road, Swords, Co. Dublin, K67E5AO
Type of company: Global pharmaceutical company | Website: www.Teva.ie | Tel: 00353 1 9127700 | Help Line: 1800 201 700 Products: Bisodol, Buplex, Cetriz, Cymex, Exorex, Infacol, Sudocrem, Orovite, Motusol
Local Contacts: Paul Neill, Director Generic Products Ireland
Any other info: We offer high quality generic, specialty and OTC medicines to patients across a wide range of therapeutic areas. And, we are continually expanding our range of products and services to better meet the needs of Irish patients and healthcare professionals. Teva employs around 800 people in Ireland and has two sites in the Republic of Ireland.
Commercial Division: Teva’s commercial activities span the sales and support services for Teva’s large portfolio of medicines, both generics and branded innovative medicines, along with over-the-counter consumer health products.
We supply medicines to treat a wide range of diseases and conditions – from multiple sclerosis, asthma, cancer and Chronic Obstructive Pulmonary Disease, to pain relief, cholesterol reducers and antibiotics. Dosage forms include extended and immediate release tablets and capsules, injectables, creams, ointments, solutions, suspensions and inhalers. Whether they’re used in hospitals or by GPs, nurses, or independent pharmacists, our medicines are supported by comprehensive advice and information from our Medical teams.
In additional to the field-based sales teams covering both primary and secondary care in Ireland; Teva’s commercial teams and support functions are based in Swords, near Dublin.

Golden Mile Industrial Park, Breaffy Rd. Castlebar, Co. Mayo, Ireland F23 D299
Type of company: Ophthalmology – Eye Care | Website: www.theapharma.ie | Tel: +353 94 925 0290
Any other info: Théa Pharma Ireland is the Irish subsidiary of Laboratoires Théa, Europe’s leading, pioneering and innovative Eye Health group founded in 1994 by Henri Chibret. The Chibret family has been dedicated to Ophthalmology for more than 150 years.
Théa was the pioneer and remains the world leader in 100% preservative-free eye care products. Thanks to Théa, ophthalmology has entered into the preservative-free era, allowing patients to benefit from a whole range of eye care treatments which respect their visual potential.
Théa Pharma was introduced in 2018 in Ireland and within only a year managed to earn the trust of Ophthalmologists, Pharmacists and consumers all around the country and become their #1 choice for Eye Care. Our strength lies within our people: a team of dedicated, highly motivated and driven professionals ready to satisfy with the most efficient and effective way the increasing needs and wants of our Customers and Consumers for Eye Health.
We are uncompromising in our approach to developing the best eye care solutions that won’t damage or irritate eyes. That’s why we are committed to being 100% preservative-free!

United Drug, Magna Drive, Magna Business Park, Citywest Road, Dublin 24, D24 XKE5
Type of company: Pharmaceutical distribution of products & services
Email: Reception.UDW@united-drug.com
Consumer Email: Consumer@united-drug.com
Distribution Email: Distribution@united-drug.com
Wholesale Email: Wholesale@united-drug.com
Website: www.united-drug.com
Tel: +353 1 463 2300 | Fax: +353 1 463 2333
United Drug Wholesale (Ballina)Crossmolina Road, Ballina, Mayo, F26 W6R6, Ireland. Tel: +353 096 72555 | Fax: +353 096 72400
United Drug Wholesale (Limerick) Johnsgate House, Old Clare Street, Limerick, V94 E3F1, Ireland. Tel: +353 061 315411 | Fax: +353 061 315012

Newenham Court, Northern Cross, Malahide Road, Dublin, Ireland.
Type of company: Pharmaceuticals, generics, brand products and OTC medicines
Website: www.viatris.com
Tel: +353 1 8711600





Extra Strength 2% w/w Gel (diclofenac diethylammonium) easy-to-open cap*
Powerful Anti-Inflammatory Provides All-Day Joint & Muscle Pain Relief**
Making life easier for your patients with pain in their hands
Contains a unique permeation enhancer – up to 3x increased skin permeation of diclofenac†1
Clinically proven to demonstrate deep penetration into tissue 2
Reduces pain on movement – to help patients get moving again
Patient convenience – twice daily application for clinically proven 12 hour-pain relief

*100g pack only. **with twice daily application. †compared with Voltarol Emulgel 1% in vitro study. 1. Quartarone & Hasler-Nguyen 2014; GSK data on file 2. Seefried et al. Ther Adv Musculoskel Dis (2020) Vol. 12: 1-13. Product Information: Please consult the Summary of Product Characteristics for full product information. Voltarol Emulgel 1% w/w Gel (diclofenac) and Voltarol Emulgel Extra Strength 2% w/w Gel (diclofenac). Indications: For the local symptomatic relief of pain and inflammation in trauma of tendons, ligaments, muscles and joints, localised forms of soft tissue rheumatism. Dosage: Adults and adolescents 14 years and over: Voltarol Emulgel 1% w/w Gel: 2g to 4g of gel, applied topically 3-4 times daily. Maximum treatment duration is 7 days. Voltarol Emulgel Extra Strength 2% w/w Gel: 2g to 4g of gel, applied topically 2 times daily – morning and evening. Maximum treatment duration is 14 days. All gels: Patients should consult their doctor if the condition does not improve within 7 days, or worsens. Contraindications: Patients with or without chronic asthma in whom asthma, angioedema, urticaria or acute rhinitis are precipitated by aspirin or other non-steroidal anti-inflammatory agents. Hypersensitivity to diclofenac, acetylsalicylic acid or other non-steroidal anti-inflammatory drugs. Hypersensitivity to any other ingredient of the gel. Use in third trimester of pregnancy. Use in children and adolescents aged less than 14 years. Warnings and precautions: Apply only to intact, non-diseased skin and not to skin wounds or open injuries. It should not be used with occlusion. Do not smoke and avoid naked flames. It should not be allowed to come into contact with the eyes or mucous membranes and should never be taken by mouth. Application over extensive areas for prolonged periods or application in excess of recommended dosage may give rise to systemic effects. These include gastrointestinal disturbances and bleeding, irritability, fluid retention, rash, hepatitis, renal dysfunction, anaphylaxis and rarely blood dyscrasias, bronchospasm and erythema multiforme. Discontinue if rash develops. Use with caution in patients with a history of peptic ulcers, gastrointestinal bleeding, hepatic or renal insufficiency, or bleeding diathesis, or intestinal inflammation. Side effects: Very rare: rash pustular, hypersensitivity (including urticaria), angioedema, asthma, photosensitivity reaction. Rare: Dermatitis bullous. Common: Dermatitis (including contact dermatitis), rash, erythema, eczema, pruritus. MA Holder: GlaxoSmithKline Consumer Healthcare (Ireland) Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24, Ireland. MA Number: Voltarol 1% w/w Gel: PA 678/140/2. Voltarol 2% w/w Gel: PA 678/140/3. Legal Category: 1%: GSL, 2%: Pharmacy only. Text revised: March 2022. Further information available on request. Contains diclofenac diethylammonium. Always read the label/leaflet Haleon, formerly part of GSK. Trade marks are owned by or licensed to the Haleon group of companies. PM-IE-VOLT-21-00011. Find out more at our