































October 2022 Volume 14 Issue 10 THE INDEPENDENT VOICE OF PHARMACY In this issue: NEWS: Budget 2023 must address pharmacy underfunding Page 6 PROFILE: Keane’s CarePlus showcase their Digital Journey Page 14 FEATURE: Menopause and Dry Eye Disease Page 22 CPD: Management of Acute Pain Page 41 AWARDS: The Secret Sauce for McCabes Pharmacy Page 46 CORPORATE: Keeping ‘Eyes’ on Future Growth Page 68 EDUCATION: 5-Minute Module on Cough Page 72 PHARMACYNEWSIRELAND.COM This Publication is for Healthcare Professionals Only Introducing... Haleon, formerly part of GSK MGK9299 Haleon Trade Ads.pdf 1 10/08/2022 14:58
Explore the Kelkin Vitamin Immunity Range





 Stephen Moloney
Julie Webster
Julie.webster@valeofoods.ie
Stephen Moloney
Julie Webster
Julie.webster@valeofoods.ie
087 699 9344 stephen.moloney@valeofoods.ie
086 462 1723
David Keane 087 279 2860 david.keane@valeofoods.ie Fintan Byrne 087 647 0764 fintan.byrne@valeofoods.ie Eamonn Connolly 087 238 5648 eamonn.connolly@valeofoods.ie
For more information on promotions and POS, contact Valeo Healthcare Account Manager or Sales Rep
Page 5: School of Pharmacy HRB funding success
Page 8: Sharon Foley takes up Pharmacy position

Page 10: Illegal prescription medicines posing a threat
Page 12: New antimicrobial network launched for pharmacists
Page 14: John Keane talks about moving into the digital era

Page 26: Menopause and Urinary Incontinence
Page 32: Local Pharmacy Group launches fertility service

Page 66: Vaccination Guidance issued for pharmacists
Page 87: Learning from international models in Pharmacist Prescribing
IPN Communications Ireland Ltd.
Clifton House, Fitzwilliam Street Lower, Dublin 2 00353 (01) 6690562
MANAGING DIRECTOR
Natalie Maginnis n-maginnis@btconnect.com
EDITOR


Kelly Jo Eastwood: 00353 (87)737 6308 kelly-jo@ipn.ie
ADVERTISING EXECUTIVE
Amy Evans: amy@ipn.ie
EDITORIAL/ EVENTS & MARKETING EXECUTIVE
Aoife Jackson: aoife@ipn.ie
CONTRIBUTORS
Donna Cosgrove | Kieran Moore
Adam Esa | Deirdre Garvin
Dr Deirdre Lundy
Dr Genevieve Ferraris
Dr Claire McCarthy
Dr Catherine Riordan
Loretta Dignam
Dr Louise O’Toole
Theresa Lowry-Lehnen
Mary-Claire Kenedy
DESIGN DIRECTOR
Ian Stoddart Design
Foreword
As Irish Pharmacy News was going to press with this October issue, the HSE launched a new service to provide free prescription and emergency contraception for 17 to 25 year old women and people. The news has been broadly welcomed, as this service will significantly reduce costs barriers which prevent people using contraception effectively.
However, the IPU has said that barriers to accessibility remain, and recommend that the service should be expanded to provide the option of accessing oral contraception, directly from their local pharmacy, through consultation with a pharmacist and be aligned to the model of care and access provided for in the emergency hormonal contraception service.
Community pharmacist and Chair of the IPU’s Pharmacy Contractors’ Committee, Kathy Maher said, “This is a very welcome and positive development for the healthcare of young women in Ireland. The ambition of this plan is to ensure that women can access the contraception they need, and it successfully removes cost as a barrier of doing so for younger women. We must now focus on ensuring that access is not a barrier either.
“This new service quite rightly gives women the choice over what form of contraception they wish to use. However, they are not being provided with a choice on where to access this contraception. Young women who wish to use oral contraception (the pill) should be able to access it directly from pharmacies without first having to get a prescription from a GP.” Turn to page 54 for more details on this and we will have full coverage in the next issue.
In other news, pharmacists have said the upcoming budget must take steps to address the underfunding of the pharmacy sector here. An impossible trend has set in, according to the IPU, where pharmacists are having to provide more services to the state and dispense more medicines to patients than ever before, but the payments received from the HSE continue to decline. You can read more about this on page 6.
This issue also has an extensive special Women’s Health section with clinically contributed articles such as Loretta Dignam on Menopause in the Workplace, Dr Catherine Riordan on Menopause and Urinary Incontinence and Dr Claire McCarthy on Considerations for Medication use in Pregnancy.
Meanwhile the search has been ongoing for The People’s Pharmacist 2022. The offices at IPN have been inundated with nominations telling stories of phenomenal inspiration, dedication and commitment. Make sure you catch the November issue for the details of all our Finalists.
Regulars
independent, multiple Pharmacists and academics in Ireland.
All rights reserved by Irish Pharmacy News. All material published in Irish Pharmacy News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission.

IPN Communications Ltd. has taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
FEATURE:
CHRONIC OBSTRUCTIVE PULMONARY DISEASE P34
FEATURE: OSTEOPOROSIS P62
CPD: PAIN P41
FEATURE: ORAL CARE P80
TEAM TRAINING: VACCINATIONS P84
CLINICAL PR: P96
3 PHARMACYNEWSIRELAND.COM 8
NEWS 5 10 PUBLISHER:
PHARMACYNEWSIRELAND.COM @Irish_PharmNews IrishPharmacyNews Contents 14
Uniphar in talks for McCauley Group
Uniphar is in talks to buy the Sam McCauley Health & Beauty Pharmacy chain, Irish Pharmacy News has learned.

Osteoporosis Screening
University of Galway clinicians, computer scientists and engineers are using enhanced x-ray technology used to measure bone density in people across Galway, Leitrim and Sligo to develop new osteoporosis screening and testing strategies for early identification of the condition in patients.
Funded by the Health Research Board, the Dual-energy X-ray Absorptiometry Management Application Project (DXA MAP), uses state of the art machines to develop a personalised, patientcentred tool for osteoporosis screening and fracture prediction.
Investment fund Carlyle Cardinal Ireland (CCI) owns a majority stake in the pharmacy group. She acquired the stake in 2017 in a deal valued at over ¤50 million.
The McCauley Pharmacy chain has watched its revenues slide over recent years amid reports that Uniphar may be in line to buy the company.
Sam McCauley has warned that state intervention is needed to avoid the closure of chemists around Ireland, as new figures showed it has cut more than 230 jobs over the last four years.
The company, which owns and runs 37 pharmacies around Ireland, employed 441 staff in its 2021 financial year, down from 674 in 2018, accounts filed with the Companies Registration Office (CRO) show.
In a note attached to its most recent accounts, James Tolan, the chairman of McCauley Pharmacies, said the chemist retail

sector was facing “very significant inflationary challenges as well as a growing shortage of pharmacists.
“If the state continues to pursue a non-strategic approach to its relationship with the pharmacy retail sector then over time there will be less pharmacies and there will be reduced opening hours,” he said.
Meanwhile, Irish-listed healthcare group Uniphar, who have it’s Irish headquarters in Citywest, has said it traded in line with expectations during the first six months of the year, while it achieved organic gross profit growth of about five per cent.
The company, which accounts for more than a fifth of the retail pharmacy market in the Republic, is an international business that services the requirements
Future of pharmacIE Event
The Future of pharmacIE, hosted by APPEL, will return on October 20th, 2022. This event is an online careers event for pharmacy students and professionals. Panel discussions will take place with pharmacy professionals which will showcase the varied and exciting career paths for pharmacists.

Those who attend will get inspiration for their future in pharmacy and the chance to meet future colleagues.
Exhibition booths will allow APPEL placement providers to promote their business or practice area to the pharmacists of the future and build their talent pipeline.
This is a unique networking event with many opportunities for pharmacy students and professionals alike.
Visit www.appel.ie to register your interest in attending.
of more than 200 multinational pharmaceutical and medical technology manufacturers.
It recently announced details of an unaudited trading update for the six months ended June 30.
The business performed “in line with the group’s expectations” in terms of both gross profit and earnings before interest, taxes, depreciation and amortisation level (Ebitda), while it also delivered normalised free cash flow conversion “in line with mediumterm guidance”.
The company described the performance as “strong” and “demonstrating resilience” in the face of continued macroeconomic uncertainty and inflationary pressures. It continues to maintain “a strong liquidity position”.
Professor of Medicine at University of Galway and Clinical Lead for DXA, Osteoporosis and Metabolic Bone Disorders, at Galway University Hospitals, John Carey said, “The cross disciplinary expertise enables the development of a smart screening methodology to reduce health costs, maximise healthcare efficiencies, reduce waiting times and improve patient care and quality of life.”
The DXA MAP tool will be underpinned by artificial intelligence, recommended diagnostic criteria, reference standards and visualisation approaches to support osteoporosis and fracture risk prediction, clinical interpretation and clinical-patient communication. The DXA MAP project also aims to support clinician interpretation through more automated processes and could predict Covid-19 and multi-morbidity risk using DXA secondary-data.
The project will be carried out by the University’s College of Science and Engineering and the College of Medicine, Nursing and Health Science, and led by Dr Attracta Brennan, Professor John Carey and Associate Professor Mary Dempsey.
It is estimated that up to 300,000 people in Ireland have osteoporosis. Although more common in females who have gone through the menopause, it can also affect men and children.
Osteoporosis is a condition that affects the inside of bones. It causes bones to become fragile, so they break easily.
It is called the silent disease because there are no signs or symptoms prior to a person breaking (fracturing) bones.
Sam McCauley of McCauley Health & Beauty Pharmacy
PHARMACYNEWSIRELAND.COM 4 News
Medicine Shortages
The Health Products
Regulatory Authority has been notified of a shortage of the following products:
• Artelac 3.2 mg/ml Eye Drops, Solution - PA23259/004/001
• Ceftazidime 2g Powder for Solution for Injection or Infusion - PA0281/224/002
• Concerta XL 18mg Prolonged-Release TabletsPA22612/002/001
• DuoPlavin 75mg/75mg Film-Coated TabletsEU/1/10/619/002
• Dynastat 40mg Powder for Solution for InjectionEU/1/02/209/005
• Gamanil 70mg Film-Coated Tablets - PA1701/004/001
• Macrolief 13.8g sachet, Powder for Oral olutionPA0711/224/001
• Minocin SA 100mg Modified Release CapsulesPA2010/060/001
• Nebilet Plus 5mg/25mg Film-Coated TabletsPA0865/015/002
• Noxafil 40mg/ml Oral Suspension - EU/1/05/320/001
• Palladone SR 2mg Prolonged Release CapsulesPA1688/007/007
• Provera 10mg TabletsPA0822/134/003
• Taxotere 20mg/1ml Concentrate for Solution for Infusion - EU/1/95/002/003
• Toviaz 4mg Prolonged Release Tablet - EU/1/07/386/003
• Vidisic Preservative Free Single Dose Unit - PA23259/008/002
• Xymel 50mg CapsulesPA0126/099/001
The following shortages have been resolved and supply has resumed to the Irish market:
• Acerycal 10mg/10mg TabletsAcerycal 10mg/10mg tablets
• Calvepen 333mg TabletsPA0126/137/001
• Cozaar Comp 100mg/25mg Film Coated TabletsPA23198/001/003
• Deslor 0.5mg/ml Oral SolutionPA0711/202/002
• Doxatan XL 4mg Prolonged Release TabletsPA0126/202/004
• Fentanyl 50mcg/ml Solution for Injection (2ml presentation only) - PA2165/011/001
• Fucidin 20mg/g CreamPA0046/004/012
• Loniten 5mg TabletsPA0822/130/001
• MST Continus 5mg Prolonged Release TabletsPA1688/004/001
• Palladone SR 8mg Prolonged Release CapsulesPA1688/007/009
Pharmacy Success in HRB Funding
The CEO of Six RCSI researchers have been awarded funding totalling more than €2.2 million by the Health Research Board (HRB) under the Investigator-Led Projects (ILP) 2022 scheme announced.
The funding is part of an overall investment of ¤10m by the HRB divided across 33 new projects to support high-quality research in patient-oriented research, population health research, and health service research.
The successful RCSI lead applicants were:
• Professor Annette Byrne, Department of Physiology and Medical Physics, for the project ‘Interrogation of novel Glioblastoma Subtypes towards an improved Precision Medicine Approach for Brain Tumour Patients’
• Professor Mary Cannon, Department of Psychiatry, for the project ‘Exploring the risk factors and consequences of cannabis use in adolescence using population-based data: the CANNARISK study’
• Professor David Cotter, Department of Psychiatry, for the project ‘Investigating the relationship between the Complement Pathway and outcomes in Psychosis; from Clinical High Risk to First Episode Psychosis’
Dr Roger Preston, School of Pharmacy, RCSI
• Professor Dermot Cox, School of Pharmacy and Biomolecular Sciences, for the project ‘Study of the role of platelets In Sepsis (SEPSIS)’

• Dr Sudipto Das, School of Pharmacy and Biomolecular Sciences, for the project ‘Examining the diagnostic and functional role of a novel DNA methylation signature in predicting Colorectal Cancer Metastasis – INTERACT’
• Dr Roger Preston, School of Pharmacy and Biomolecular Sciences, for the project ‘Increased Thrombotic Risk in Patients with Myeloproliferative Neoplasms: Linking Inflammation, Metabolism and Hypercoagulability - the CLIMB study’
The 33 successful investigatorled projects were selected by an international panel of experts
following a rigorous application process. As a matter of course, a public review was undertaken alongside the scientific peer review to assess whether the research is in the best interests of the patient or the general health of the population. Successful projects were selected based on their scientific quality and innovation, impact, and feasibility. Each project will be funded for a maximum of four years.
LloydsPharmacy Winter Health Index 2022 Shows Concern
The 2022 Winter Health Index from LloydsPharmacy has shown a lack of concern from the Irish public towards the flu ahead of the ‘twindemic’ COVID-19 and winter flu season. The concern follows the latest trends seen in Australia where the winter flu, combined with COVID-19 led to a difficult winter for the health service.
It is often observed that winter flu difficulties experienced in Australia are replicated across Europe in the months that follow. This year, Australia saw the flu virus affecting all age groups, and not just the elderly or vulnerable. Research commissioned by LloydsPharmacy shows 71% of Irish adults aged 35-44 intend to either not go for flu vaccination or are still unsure, despite the evidence of the flu vaccination playing a vital role in keeping people well and healthy during the tough winter months.
LloydsPharmacy believe in encouraging patients to proactively manage their health, providing advice and support to help prevent sickness and boost immunity during winter months.
Research showed amongst those that currently take daily vitamins or supplements, just over half (56%) claim they take them for general health, with 48% claiming they take them to boost immunity and just over a third (36%) to boost energy. Vitamin D once again continues to be the most popular vitamin (58%) taken by respondents who take a daily vitamin, followed by a multivitamin (44%). To help support their local communities this winter, LloydsPharmacy are running a Buy One Get One Half Price offer throughout September where you can mix and match on selected vitamins and supplements. LloydsPharmacy colleagues are available to advise customers on how to help keep their family
healthy this winter, whether it is the best medication for cough and colds or what vitamins and supplements can support their immune system.
Denis O’Driscoll, LloydsPharmacy Superintendent Pharmacist said “We have seen worrying trends coming from Australia as Ireland prepares for the combination of COVID-19 and flu season together. LloydsPharmacy are on a mission to ensure our communities are fully protected this winter, offering our customers their flu vaccination and COVID-19 booster. Our highly trained colleagues are always on hand to offer tailored advice and support for the health and wellbeing of families in our communities.”
PHARMACYNEWSIRELAND.COM 5
News
Budget 2023 Must Address Underfunding of Pharmacy Sector
The upcoming budget must take steps to address the underfunding of Ireland’s community pharmacy sector, the Irish Pharmacy Union (IPU) has said. An impossible trend has set in, according to the IPU, where pharmacists are having to provide more services to the state and dispense more medicines to patients than ever before, but the payments received from the HSE continue to decline. The situation is now close to a breaking point with the risk of pharmacy services being severely curtailed, which will significantly impact on patient services.
Derek Reilly, IPU Head of Contract
ministers for health. Now, more than two years into the lifetime of this government, we have seen no actions towards a new contract.
Enhanced Community Care Conference 2022
Outlining the importance of supporting community pharmacies, IPU Head of Contract Derek Reilly said, “Pharmacies are part of the fabric of the local communities they serve. Over half the population lives within one km of a pharmacy, with 85% living within five km. As a result, with 1.5 million visits to pharmacies each week, they are the most accessed part of our health service. As we demonstrated during the pandemic this is an invaluable resource and one that must be protected.”
Pharmacies are coming under increasing financial pressure according to Mr Reilly. “Nine out of every ten pharmacies are family-owned businesses. They operate on tight margins and share the struggles of any other small business. However, unique to our sector is the importance of state-run schemes to our viability. Pharmacies are paid by the HSE to dispense medicines to medical card patients, and this essential service simply could not exist without the cooperation of pharmacies. However, the payments we receive for providing this service have been declining and are now at an unsustainable rate.
“Since 2009 the number of medicines pharmacies dispense annually, through this PCRS scheme, has dramatically increased. In 2021 there were almost 82m prescription items, an
increase of 19.5% in twelve years. However successive cuts in the fees pharmacists can charge, from an average of ¤6 in 2009 to just ¤4.74 last year, put pharmacies in a precarious position. Over that time, we have seen average revenues in pharmacies decrease by 6%, but costs are soaring, powered by an 18.5% increase in staff costs in the last decade.
“We are calling on the government to commit to a new flat dispensing fee of ¤6.50 per item in Budget 2023. This modest increase, just a 7% increase on the rate paid 12 years ago, would go a long way towards securing the financial future of many pharmacies across the country.
A growing shortage of pharmacists is also having an impact on the sector Mr Reilly stated, who called for government support.

“The length of time it is taking to fill pharmacist vacancies in pharmacies is becoming an increasing concern for the sector. We need the government to support greater levels of training at home by funding more third level places for pharmacy students. In the short term the pharmacy regulator the PSI should be adequately resourced to ensure it can rapidly facilitate the registration of non-EU pharmacists to avoid any delays.”
The IPU has also called for negotiations to start on the introduction of a new Community Pharmacy Contract. “The contract which governs the work conducted by pharmacies on behalf of the state is hopelessly out of date. More than a quarter of a century old it no longer reflects the nature of a modern pharmacy.
Reform of this contract has been a commitment of successive governments and successive
Another key demand is for the recruitment of a Chief Pharmaceutical Officer (CPO) as a matter of priority. The appointment of a CPO would ensure a strategic vision for the future of communitybased pharmacy care within the Department of Health.
The absence of an Irish CPO makes us an outlier in modern healthcare systems. Those jurisdictions that have created such a position have demonstrated the value it represents. For example, pharmacists in Scotland operate according to a clear national pharmacy strategy which is integrated into the wider health service. Through this simple but effective structure, pharmacists’ specialist knowledge in medicines is utilised to best affect for people’s health and well-being.
The IPU has also recommended a range of new clinical services which it says could be introduced by pharmacies to support the national health service. These include a call for Irish women to be provided with convenient access to contraception without prescription from a pharmacy as is available to women in the UK, USA, Canada, New Zealand, and other similar countries as well as the development and roll-out of a national Community Pharmacybased Triage Programme including a Minor Ailment Scheme, use of Emergency Medicines, and Minor Injuries.
Derek Reilly, Head of Contract in the IPU concluded “The government must embrace the tremendous potential of the pharmacy sector. That must include adequate funding and resources to maximise our potential in every conceivable way. Failing to do so, ignoring the challenges and maintaining the status quo, will increase pressures on an already stretched sector. Pharmacies cannot continue to do much more with much less – we need support.”
The HSE and the Department of Health recently hosted the Enhanced Community Care Conference 2022. This event is designed to bring together our community teams from all over the country to mark progress on implementing the Enhanced Community Care Programme and support ongoing change as our teams invest in community services and improve patient experience.
Attendees heard from senior colleagues in the HSE, expert speakers working in integrated care, including the keynote speaker Professor Sir Chris Ham, former CEO of the Kings Fund UK, and also representatives from our HSE teams around the country about the programme’s latest developments, and the first hand experiences of people benefitting from this programme.
Paul Reid, HSE CEO, underlines the importance of bringing services closer to home and acknowledges staff for their dedication and commitment in rolling out the new programme adding, “The HSE’s Enhanced Community Care programme is improving the experience of our patients and aims to reduce our reliance on hospitals. The fast pace of this implementation would not be possible without the hard work and dedication of the committed staff working around the country. So far over 2,200 staff have been recruited or at an advanced stage of employment and we have an additional recruitment of 1,400 staff planned for 2022. 87 Community Healthcare Networks have been set up and we have established 21 Community Specialist Teams for Older People and 14 Community Specialist Teams for Chronic Disease so far.
“Today’s conference will bring together the full range of stakeholders in health and social care services to learn, network and share their knowledge and experience. I am delighted to celebrate the progress made in implementing the programme and welcome attendees for an exciting and thought-provoking day.”
PHARMACYNEWSIRELAND.COM 6 News
utipro®Plus

AF
for the Control and Prevention of






Improves the symptoms of acute uncomplicated cystitis*
Reduces the use of antibiotics
*Garcia-Larossa A, Alexe O.Efficacy and safety of a medical device versus placebo in the early treatment of patients with symptoms of a urinary tract infection: a randomised controlled trial . Clin. Microbiol. 5,1 (2016).
in Pharmacies or
at
9/10 patients did not require antibiotics with Utipro® Plus*
Significantly reduces recurring UTIs
www.utipro.ie Available
online
www.utipro.ie
Sharon Takes up Pharmacy Position
Sharon Foley has taken up the position of Secretary General of the Irish Pharmacy Union (IPU). Ms Foley from Ballylinan Co. Laois, whose appointment was announced in May, had previously served as Chief Executive Officer of the Irish Hospice Foundation since 2011.

Speaking at the outset of her tenure Ms Foley said, “I am excited to be taking up the position of Secretary General of the Irish Pharmacy Union. The role pharmacists have been playing at the front line of healthcare in our communities, has never been more important. As was seen through the COVID vaccine campaign the pharmacy sector can play a continually active role in supporting the national health service.
“My priority as Secretary General will be to maximise the potential of pharmacies, while ensuring that they are adequately supported by all stakeholders. It is clear that the growing shortage of pharmacists is causing significant pressure and securing government action to address this will be a key concern of mine.”
IPU President Dermot Twomey wished Ms Foley every success in the role saying, “We are excited to be welcoming Sharon to the IPU today as our new
New Pharmacy App Launched
LloydsPharmacy, Ireland’s leading pharmacy chain has today launched a new app for customers.
This reflects the ongoing investment and focus on digital transformation, and the goal to further enhance the omni channel shopping experience for customers. The LloydsPharmacy app mainly focuses on a new appointment booking service, as well as a prescription upload service known as DigiScript, both of which are available in all LloydsPharmacy’s nationwide.

The LloydsPharmacy app will streamline the appointment booking experience, allowing app users to book appointments with their local pharmacy. The new functionality means it is now even easier for customers to schedule appointments for services including LloydsPharmacy’s new Travel Vaccinations, HPV Vaccination and Shingles Vaccination services, as well as booking COVID booster and Flu vaccinations in the coming weeks when available.
LloydsPharmacy is innovating how they connect and serve their
customers with the addition of this new app to its product offering. The new app will give customers an even greater sense of ease as they will be able to conveniently manage their prescription ordering services from their android or iPhone. The new DigiScript service allows users to upload an image of their prescription through the website or app and send it to their LloydsPharmacy of choice. The pharmacy will contact the customer once their prescription is ready for collection. This new service offers LloydsPharmacy customers a more convenient and efficient way to pick up their medication.
App users will also be able to browse and shop LloydsPharmacy’s online store, avail of the free click and collect service and stay up-to-date with the latest health advice. All orders over ¤40 placed through the App or Lloydspharmacy.ie website are eligible for free home delivery within Republic of Ireland.
Secretary General. She brings exemplary experience to this role as demonstrated by her highly successful tenure as CEO of both the Irish Hospice Foundation and the Crisis Pregnancy Agency.
“Ireland’s pharmacy sector is the most accessible and accessed component of our health service. There is huge ambition amongst the profession to expand our role, all for the benefit of patients. This will require action and support from Government, but with Sharon’s experience and dedication I am sure much progress will be made. On behalf of the IPU and indeed Ireland’s wider pharmacy profession I wish her every success in the role.
Ms Foley holds a Master’s Degree in Research from Trinity College Dublin, a MA in Health Promotion from NUI Galway and a BSc in Nutrition & Dietetics from TCD/TUD as well as other qualifications in leadership and change management.
World Alzheimer’s Month
Marking World Alzheimer’s month last month, the HSE Dementia: Understand Together campaign has urged people across the country who may be recently diagnosed, awaiting diagnosis, concerned about their memory or having difficulty with mental tasks to seek support within the community.
There are approximately 64,000 people living with dementia in Ireland at this time. With this number expected to more than double to 150,131 by 2045, many more of us are going to be living with dementia, or supporting a loved one with the condition.
Every September, people come together from all around the world to raise awareness and to challenge the stigma that persists around dementia. This year’s theme, Know Dementia, Know Alzheimer’s is focused on diagnosis, the warning signs of dementia, the continued effect of COVID-19 on the global dementia community and more.
Professor Sean Kennelly, Consultant Geriatrician and Director of the Institute of Memory and Cognition, Tallaght University Hospital said, “The diagnosis experience can understandably be challenging, and for some people, being told they have dementia can feel completely devastating at first. An integral part of a dementia diagnosis disclosure is to empower people with a sense of hope that they can continue to “live well” with dementia, and that the diagnosis doesn’t define them. There has been significant investment into care and support services nationwide in recent years meaning that vital support can be accessed more easily than before.
“While the aim of the month is to continue to raise awareness and understanding of dementia, we’re also encouraging communities to take actions that will help to include and support those affected by the condition.
To mark the new app launching, LloydsPharmacy is offering 25% off first-time orders through the app for a limited time using the code LLOYDS25%APP. To download, search LloydsPharmacy Ireland in your App or Google Play store.
“A full list of these support groups are also available on understandtogether.ie.”
Sharon Foley
PHARMACYNEWSIRELAND.COM 8
News
PNEUMOCOCCAL VACCINATION

PNEUMOCOCCAL
PNEUMONIAVS
Help prevent pneumococcal pneumonia with the proven protection of Prevenar 131,2 Proven to reduce the risk of community-acquired pneumonia: Results from the Community-Acquired Pneumonia Immunisation Trial in Adults (CAPiTA) – one of the largest vaccine efficacy trials ever conducted in older adults.2,3

ABBREVIATED PRESCRIBING INFORMATION
Prevenar 13* Suspension for Injection
Pneumococcal polysaccharide conjugate vaccine (13-valent, adsorbed)
Presentation: Each 0.5ml dose of Prevenar 13 contains 2.2 micrograms of each of the following pneumococcal polysaccharide serotypes: 1, 3, 4, 5, 6A, 7F, 9V, 14, 18C, 19A, 19F, 23F and 4.4 micrograms of pneumococcal polysaccharide serotype 6B. Each pneumococcal polysaccharide is conjugated to CRM197 carrier protein and adsorbed on aluminium phosphate. 1 dose (0.5 ml) contains approximately 32 µg CRM197carrier protein and 0.125 mg aluminium. Indications: Active immunisation for the prevention of invasive disease, pneumonia and acute otitis media caused by Streptococcus pneumoniae in infants, children and adolescents from 6 weeks to 17 years of age. Active immunisation for the prevention of invasive disease and pneumonia caused by Streptococcus pneumoniae in adults ≥18 years of age and the elderly. Dosage and Administration: The immunisation schedules for Prevenar 13 should be based on official recommendations. It is recommended that infants who receive a first dose of Prevenar 13 complete the vaccination course with Prevenar 13. For intramuscular injection. Infants aged 6 weeks-6 months: Three dose primary series: The recommended immunisation series consists of four doses, each of 0.5ml. The primary infant series consists of three doses, with the first dose usually given at 2 months of age and with an interval of at least 1 month between doses. The first dose may be given as early as six weeks of age. The fourth (booster) dose is recommended between 11 and 15 months of age. Two dose primary series: Alternatively, when Prevenar 13 is given as part of a routine infant immunisation programme, a series consisting of three doses, each of 0.5ml, may be given. The first dose may be administered from the age of 2 months, with a second dose 2 months later. The third (booster) dose is recommended between 11 and 15 months of age. Preterm infants (< 37 weeks gestation): In preterm infants, the recommended immunisation series consists of four doses, each of 0.5 ml. The primary infant series consists of three doses, with the first dose given at 2 months of age and with an interval of at least 1 month between doses. The first dose may be given as early as six weeks of age. The fourth (booster) dose is recommended between 11 and 15 months of age. Unvaccinated infants and children ≥ 7 months of age: Infants 7-11 months: Two doses, each of 0.5 ml, with at least a 1 month interval between doses. A third dose is recommended in the second year of life. Children aged 12-23 months: Two doses, each of 0.5 ml, with at least a 2 month interval between doses. Children and adolescents aged 2-17 years: one single dose of 0.5 ml. Prevenar 13 vaccine schedule for infants and children previously vaccinated with Prevenar (7-valent) (Streptococcus pneumoniae serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F): Infants and children who have begun immunisation with Prevenar may switch to Prevenar 13 at any point in the schedule. Children aged 12-59 months: Children who are considered completely immunised with Prevenar (7-valent) should receive one dose of 0.5 ml of Prevenar 13 to elicit immune responses to the 6 additional serotypes. This dose of Prevenar 13 should be administered at least 8 weeks after the final dose of Prevenar (7-valent). Children and adolescents aged 5-17 years: One single dose of Prevenar 13 if they have been previously vaccinated with one or more doses of Prevenar. This dose of Prevenar 13 should be administered at least 8 weeks after the final dose of Prevenar (7-valent). Adults ≥18 years of age and the elderly: One single dose. The need for revaccination with a subsequent dose of Prevenar 13 has not been established. Regardless of prior pneumococcal vaccination status, if the use of 23 valent polysaccharide vaccine is considered appropriate, Prevenar 13 should be given first. Special Populations: Individuals who have underlying conditions predisposing them to invasive pneumococcal disease (such as sickle cell disease or HIV infection) including those previously vaccinated with one or more doses of 23-valent pneumococcal polysaccharide vaccine may receive at least one dose of Prevenar 13. In individuals with an haematopoietic stem cell transplant (HSCT), the recommended immunisation series consists of four doses of Prevenar 13, each of 0.5 ml. The primary series consists of three doses, with the first dose given at 3 to 6 months after HSCT and with an interval of at least 1 month
between doses. A fourth (booster) dose is recommended 6 months after the third dose. Contra-indications: Hypersensitivity to any component of the vaccine or to diphtheria toxoid. As with other vaccines, the administration of Prevenar 13 should be postponed in subjects suffering from acute, severe febrile illness. However, the presence of a minor infection, such as a cold, should not result in the deferral of vaccination. Warnings and Precautions: Do not administer intravascularly. Appropriate medical treatment and supervision must be readily available in case of a rare anaphylactic event. This vaccine should not be given as an intramuscular injection to individuals with thrombocytopenia or any coagulation disorder that would contraindicate intramuscular injection, but may be given subcutaneously if the potential benefit clearly outweighs the risks of administration. Prevenar 13 will only protect against Streptococcus pneumoniae serotypes included in the vaccine, and will not protect against other microorganisms that cause invasive disease, pneumonia, or otitis media. As with any vaccine, Prevenar 13 may not protect all individuals receiving the vaccine from pneumococcal disease. Individuals with impaired immune responsiveness, whether due to the use of immuno-suppressive therapy, a genetic defect, human immunodeficiency virus (HIV) infection, or other causes, may have reduced antibody response to active immunization. Safety and immunogenicity data are available for a limited number of individuals with sickle cell disease, HIV infection, or with an HSCT. Safety and immunogenicity data for Prevenar 13 are not available for individuals in other specific immuno-compromised groups (e.g., malignancy or nephrotic syndrome) and vaccination should be considered on an individual basis. Infants and children aged 6 weeks to 5 years: Prevenar 13 does not replace the use of 23-valent pneumococcal polysaccharide vaccine in at risk children ≥ 24 months of age. Children ≥ 24 months of age at high risk, previously immunised with Prevenar 13 should receive 23-valent pneumococcal polysaccharide vaccine whenever recommended. The potential risk of apnoea and the need for respiratory monitoring for 48-72 hours should be considered when administering the primary immunisation series to very premature infants (born ≥ 28 weeks of gestation) and particularly for those with a previous history of respiratory immaturity. When Prevenar 13 is administered concomitantly with Infanrix hexa (DTPa-HBV-IPV/Hib), the rates of febrile reactions are similar to those seen with concomitant administration of Prevenar (7-valent) and Infanrix hexa. Increased reporting rates of convulsions (with or without fever) and hypotonic hyporesponsive episode (HHE) were observed with concomitant administration of Prevenar 13 and Infanrixhexa. Antipyretic treatment should be initiated according to local guidelines for children with seizure disorders or with a history of febrile seizures and for all children receiving Prevenar 13 simultaneously with vaccines containing whole cell pertussis. Adults aged 50 years and older: When Prevenar 13 was given concomitantly with trivalent inactivated influenza vaccine (TIV), the immune responses to Prevenar 13 were lower compared to when Prevenar 13 was given alone, however, there was no long-term impact on circulating antibody levels. The immune responses to Prevenar 13 were noninferior when Prevenar 13 was given concomitantly with quadrivalent inactivated influenza vaccine (QIV) compared to when Prevenar 13 was given alone. As with concomitant administration with trivalent vaccines, immune responses to some pneumococcal serotypes were lower when both vaccines were given concomitantly. Fertility, Pregnancy & Lactation: There are no data from the use of pneumococcal 13-valent conjugate in pregnant women. It is unknown whether pneumococcal 13-valent conjugate is excreted in human milk. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity.
Side Effects: Analysis of postmarketing reporting rates suggests a potential increased risk ofconvulsions, with or without fever, and HHE when comparing groups which reported use of Prevenar 13 with Infanrix hexa to those which reported use of Prevenar 13 alone. Adverse reactions reported in clinical studies or from the post-marketing experience for all age groups are listed in this section per system organ class,in decreasing order of frequency and seriousness. The frequency is defined as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (≤ 1/10,000), not
known (cannot be estimated from available data). Infants and children aged 6 weeks to 5 years: Very common (≥ 1/10): Decreased appetite, fever, pyrexia, irritability, any vaccination-site erythema, induration/swelling or pain/tenderness, somnolence, poor quality sleep. Vaccination-site erythema or induration/swelling 2.5cm – 7.0 cm (after the booster dose and in older children [age 2-5 years]. Common (≥ 1/100 to < 1/10): Vomiting, diarrhoea, rash, pyrexia >39 °C, vaccination-site movement impairment (due to pain), vaccination-site erythema or induration/swelling 2.5cm – 7.0cm (after infant series). Uncommon (≥ 1/1,000 to < 1/100): Convulsions (including febrile convulsions), urticaria or urticaria-like rash, vaccination-site erythema, induration/swelling >7.0cm, crying. Rare: Hypersensitivity reaction including face oedema, dyspnoea, bronchospasm, hypotonic-hyporesponsive episode. Not known: Lymphadenopathy (localised to the region of the vaccination site), anaphylactic/anaphylactoid reaction including shock, angioedema, erythema multiforme, vaccination site urticaria, vaccination-site dermatitis, vaccination-site pruritus, flushing. In clinical studies infants vaccinated at 2, 3 and 4 months of age, fever ≥ 38°C was reported at higher rates among infants who received Prevenar (7-valent) concomitantly with Infanrix hexa than in infants receiving Infanrix hexa alone. After a booster dose at 12 and 15 months of age, the rate of fever ≥ 38°C was greater in infants who received Prevenar (7 valent) and Infanrix hexa at the same time compared to infants receiving Infanrix hexa alone. These reactions were mostly moderate (less than or equal to 39°C) and transient. Additional information in special populations: Apnoea in very premature infants (≤ 28 weeks of gestation). Children and adolescents aged 6 to 17 years of age: Very common (≥ 1/10): Decreased appetite, irritability, any vaccination-site erythema, induration/swelling or pain/ tenderness, somnolence, poor quality sleep, vaccination-site tenderness (including impaired movement). Common (≥ 1/100 to < 1/10): Headaches, vomiting, diarrhoea, rash, urticaria or urticaria-like rash, pyrexia. Additional information in special populations: Children and adolescents with sickle cell disease, HIV infection or an HSCT transplant have similar frequencies of adverse reactions, except that headaches, vomiting, diarrhoea, pyrexia, fatigue, arthralgia, and myalgia were very common. Adults ≥18 years of age, and the elderly: Very common (≥ 1/10): Decreased appetite, headaches, diarrhoea, vomiting,(in adults aged 18 to 49 years), rash, chills; fatigue; vaccination-site erythema; vaccination-site induration/swelling; vaccination-site pain/tenderness (severe vaccination-site pain/ tenderness very common in adults aged 18 to 39 years); limitation of arm movement (severe limitation of arm movements very common in adults aged 18 to 39 years), arthralgia; myalgia. Common (≥ 1/100 to < 1/10): Vomiting (in adults aged 50 years and over), pyrexia(very common in adults aged 18 to 29 years). Uncommon (≥ 1/1,000 to < 1/100): Nausea, hypersensitivity reaction including face oedema, dyspnoea, bronchospasm, lymphadenopathy localized to the region of the vaccination site. Additional information in special populations: Adults with HIV infection have similar frequencies of adverse reactions, except that pyrexia and vomiting were very common and nausea common. Adults with an HSCT have similar frequencies of adverse reactions, except that pyrexia and vomiting were very common. For full prescribing information see the Summary of Product Characteristics. Legal Category: S1A. Package Quantities: Pack of 1 single-dose prefilled syringe (with separate needle) or pack of 10 single- dose pre-filled syringes. Marketing
Authorisation Numbers: Single-dose pre-filled syringe (with separate needle) pack of 1: EU/1/09/590/002, single-dose pre-filled syringe pack of 10: EU/1/09/590/003. Marketing
Authorisation Holder: Pfizer Europe MA EEIG, Boulevard de la Plaine 17, 1050 Bruxelles, Belgium. For further information on this medicine please contact: Pfizer Medical Information on 1800 633 363 or at EUMEDINFO@pfizer.com. For queries regarding product availability please contact: Pfizer Healthcare Ireland, Pfizer Building 9, Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24 + 353 1 4676500.
Date of preparation: 11/2018.
*Trade mark.
Ref: PN 11_0 IE.
of Preparation: February 2021 | PP-PNA-IRL-0005
The persons depicted are models used for illustrative purposes only.
References: 1. Prevenar 13 Suspension for Injection Summary of Products Characteristics. 2. Bonten M.J.M., Huijts S.M, Bolkenbaas M, et al. Polysaccharide Conjugate Vaccine Against Pneumococcal Pneumonia in Adults. The New England Journal of Medicine. 2015;372:1114-25. 3. Pfizer Inc. Press Release Mar 18, 2015. INDICATED FOR THE PREVENTION OF PNEUMOCOCCAL PNEUMONIA IN ADULTS1
Date
Increased Awareness Calls on Prescription Medicines
The Health Products Regulatory Authority (HPRA) has stated that whilst the volume of detained illegal medicines in the first half of 2022 has fallen significantly compared to the same period in 2021, a substantial amount of product is still being sourced online which poses risks to people’s health. The HPRA enforcement section detained nearly half a million (486,088) dosage units of falsified and other illegal medicines between January and June 2022 (895,591 for the first half of 2021). Announcing its mid-year update of detention figures, the HPRA reminded the public of the health risks associated with prescription medicines purchased online from unauthorised sources.
Grainne Power, Director of Compliance, Health Products Regulatory Authority
risks through online channels and, where possible, to influence the decision of the buyer prior to purchase. We hope our campaign will make people stop and think before they seek to purchase prescription medicines online and ultimately persuade them not to use this route.”
As part of its regulatory activities in this area, the HPRA routinely monitors websites, social media sites and e-commerce listings selling prescription medicines into Ireland and will take action to remove or amend content when necessary.
In the first six months of 2022, the main categories of illegal products detained included sedatives (28%), anabolic steroids (12%), erectile dysfunction medicines (9%) and analgesics (7%). The breakdown is:
• Sedative medicines – 137,587 units detained (434,157 units detained Jan – June 2021).
• Anabolic steroids – 59,764 units detained (59,750 units detained Jan – June 2021).
• Erectile dysfunction - 41,635 units were detained (56,878 units detained Jan – June 2021).
• Analgesic medicines – 33,542 units detained (105,769 units detained Jan – June 2021).
• 43,707 units of Covid-19 medicines detained (23,172 units detained Jan – June 2021).
• 287 websites, e-commerce listings and/or social media pages amended or shutdown (167 Jan – June 2021).
According to Grainne Power, Director of Compliance with the HPRA, the reduction of detentions in the first half of 2022 cannot be linked to any one factor alone.

“Although the volume of detentions has decreased, we are still
observing significant levels of potent, prescription medicines that are being illegally supplied into Ireland. These levels remain very concerning with so many people prepared to take a chance in ordering prescription medicines online. When you acquire medicines from unregulated sources, you simply have no idea what you are getting. This isn’t merely about people wasting money on falsified or counterfeit products, it is also about the very real dangers of significant side effects, of using a product without supervision where there is no guarantee of what it contains and of experiencing interactions with other medicines being taken. All of these risks have the potential to make your condition worse or cause serious harm to health,” Ms Power says.
To highlight the health risks of sourcing prescription medicines online, the HPRA today announced the launch of a new multi-platform digital information campaign to warn the public of the issue. Incorporating both social media and display advertising, the campaign will target members of the general public and highlight to them the very real dangers presented when buying prescription medicines online.
Ms Power outlined the role HPRA’s digital campaign can play in increasing public awareness and understanding of the safe supply routes for medicines and the associated dangers of buying prescription medicines online.
“Given the fact that so many transactions take place online, it is particularly important and appropriate to highlight those
The HPRA works in close cooperation with colleagues from An Garda Síochána and Revenue’s Customs Service with whom there is significant inter-agency collaboration to combat the illegal supply of health products into and within Ireland. It also co-operates and shares intelligence with other regulatory and law enforcement agencies worldwide to prevent the illegal manufacture, importation and distribution of medicines, medical devices, and cosmetics.
The HPRA is responsible for prosecuting cases where it considers that there is a significant risk to public health or where there are persistent non-compliances. The HPRA also supports prosecutions brought by the Director of Public Prosecutions in relation to the illegal supply of medicines.

“Although the volume of detentions has decreased, we are still observing significant levels of potent, prescription medicines that are being illegally supplied into Ireland. These levels remain very concerning”
PHARMACYNEWSIRELAND.COM 10
News
An Unbeatable Way of Quitting Smoking
*Provides significant improvement in quit rate vs patch alone. To verify contact: verify@perrigo.com
Lindson N et al. 2019 Different doses, durations and modes of delivery of nicotine replacement therapy for smoking cessation. Cochrane Library. IRE NIQ 2022 27 NiQuitin CLEAR 24 hrs transdermal patches contain nicotine and are indicated for the relief of nicotine withdrawal symptoms including cravings as an aid to smoking cessation. Indicated in adults and adolescentsaged 12 years and over. NiQuitin patches should be applied once a day, at the same time each day and preferably soon after waking and worn continuously for 24 hours. Apply a patch to non-hairy clean dry skinsurface, a new skin site should be used every day. Therapy should usually begin with NiQuitin 21 mg/24 hrs and reduced according to the following dosing schedule: Step 1: NiQuitin Clear 21 mg/24 hrs transdermalpatches first 6 weeks. Step 2: NiQuitin Clear 14 mg/24 hrs transdermal patches next 2 weeks. Step 3: NiQuitin Clear 7 mg/24 hrs transdermal patches last 2 weeks Light smokers (less than 10 cigarettes per day)are recommended to start at Step 2 (14 mg) for 6 weeks and decrease the dose to NiQuitin 7 mg/24 hrs for the final 2 weeks. In some instances (e.g. heavy smokers, those who have relapsed after NRT, or whenone NRT product is not enough to control cravings), NiQuitin patches may be used in combination with a nicotine oral format (refer to the package leaflet for dosing guidance). Contraindications: Non-smokers, hypersensitivity, children under 12 years and occasional smokers. Precaution: Supervise use if hospitalised for MI, severe dysrhythmia or CVA, if haemodynamically unstable. Use with caution in patients withactive oesophagitis, oral and pharyngeal inflammation, gastritis, peptic ulcers, GI disturbances, susceptible to angioedema,

https://www.medicines.ie/medicines/niquitin-clear-21-mg-24-hours-transdermal-patch-33084/spc
Mini 2mg/4mg Mint Lozenges contain nicotine and are used for the treatment of tobacco dependence by relief of nicotine withdrawal symptoms and cravings. Indicated in adults and adolescentsaged 12 years and over NiQuitin Mini 2 mg are suitable for those who smoke 20 cigarettes or less a day. NiQuitin Mini 4 mg are suitable for smokers who smoke more than 20 cigarettes a day. Place a lozengein the mouth whenever there is an urge to smoke, allow to dissolve completely. Do not chew or swallow whole. In heavy smokers, those who have relapsed after NRT, or when one NRT is not enough to controlcravings, NiQuitin Minis may be used in combination with NiQuitin patches (refer to the package leaflet for dosing guidance). Abrupt cessation: Use a lozenge whenever there is an urge to smoke, maximum of15 lozenges a day. Continue for up to 6 weeks, then gradually reduce lozenge use. Gradual cessation Use lozenges whenever there is an urge to smoke in order to reduce the number of cigarettes smoked for upto 6 weeks, followed by abrupt cessation. Adolescents (12-17 years): Only with advice from a healthcare professional. Should not quit with a combination NRT regimen. Contraindications: Hypersensitivityto nicotine or any of the excipients, children under the age of 12 years and non-smokers. Precaution: Supervised use in dependent smokers with a recent myocardial infarction, unstable or worsening anginapectoris including Prinzmetal’s angina, severe cardiac arrhythmias, uncontrolled hypertensions or recent cerebrovascular accident. Use with caution in those with; stable cardiovascular diseases, diabetesmellitus, susceptibility to angioedema & urticaria, renal/hepatic impairment, phaeochromocytoma & uncontrolled hyperthyroidism, GI disease & seizures. Side effects: Nausea, mouth/throat and tongueirritation, irritability, anxiety, insomnia, sleep disorders, dizziness, headaches, cough, sore throat, vomiting, diarrhoea, upper abdominal pain, GI and oral discomfort, flatulence, hiccups, heartburn, dyspepsia,dry mouth,

*
urticaria, renal/hepatic impairment, hyperthyroidism, diabetes, phaeochromocytoma,seizures & epilepsy. Discontinue if severe persistent skin rash. Pregnancy and lactation: Oral formats preferable to patches unless nauseous. Remove patches at bedtime. Side effects: Sleep disorders, abnormaldreams, insomnia, headache, dizziness, nausea, vomiting, application site reactions, nervousness, palpitations, dyspnoea, pharyngitis, cough, dyspepsia, upper abdominal pain, diarrhoea, constipation, drymouth, sweating, localised pain, urticaria, hypersensitivity, tremor, nervousness, palpitations, tachycardia, contact & allergic dermatitis, photosensitivity, arthralgia, myalgia, asthenia, malaise, influenza-typeillness, fatigue, chest or limb pain, pain, seizures and anaphylaxis. Legal classification: GSL: PA 1186/018/004, PA 1186/018/005 & PA 1186/018/006. MAH: Chefaro Ireland DAC, The Sharp Building, HoganPlace, Dublin 2, Ireland. Date of preparation: 04/2022. RRP (ex. VAT) 7 pack €19.83, 14 pack €35.73. SPC: https://www.medicines.ie/medicines/niquitin-clear-7-mg-24-hours-transdermal-patch-33085/spc https://www.medicines.ie/medicines/niquitin-clear-14-mg-24-hours-transdermal-patch-33083/spc
NiQuitin
constipation, ulcerative stomatitis, pharyngitis, pharyngolaryngeal pain, nervousness, depression, palpitations, heart rate increased, dyspnoea, rash, angioedema, pruritus, erythema, hyperhidrosis,urticaria, fatigue, malaise, asthenia, chest pain, anaphylactic reactions, hypersensitivity, tremor, dysgeusia, paresthesia mouth, seizures & epilepsy, dysphagia, eructation, salivary hypersecretion, influenza likeillness. Legal classification: GSL: PA 1186/018/017 & PA 1186/018/012 MAH: Chefaro Ireland DAC, The Sharp Building, Hogan Place, Dublin 2, Ireland. Date of preparation: 07/2022. RRP (ex. VAT) 20 pack €7.55, 60 pack €21.05, 100 pack €28.00. SPC: https://www.medicines.ie/medicines/niquitin-mini-2mg-mint-lozenges-35237/spc https://www.medicines.ie/medicines/niquitin-mini-4mg-mint-lozenges-33091/spc Nicotine “Since I quit, I enjoy a smoke-free life with my family” Paul
New Network Launched for Pharmacists
We need to curb, and hopefully reverse, the growing trend of antimicrobial resistance in order to have effective antimicrobials to enable us to deliver an optimal level of healthcare. We need, as healthcare workers, to feel empowered to play our part by learning how to incorporate antimicrobial stewardship in our day to day practice. To assist all pharmacists in doing this a new network has been established the Pharmacist Antimicrobial Stewardship Network (PAMS-net).
Join the network
The PAMS-net webpage is hosted on the IIOP website. It provides a discussion forum and resources section. Members receive updates through the network and network events are organised regularly.
3 reasons to join the PAMS-net
knowledge and learning in the area of antimicrobial stewardship.
net is a more joined up approach to AMS across the pharmacy profession. Pharmacists across all settings have guided the development of this vision through participation in focus groups, feedback sessions and membership of the PAMS net working group.
1. Networking & support through our online discussion forum and educational network events
All pharmacists with an interest in responsible antimicrobial use are welcome to join this network. The network aims to bring together pharmacists from a diverse range of settings including community, hospital, education, researchers, other HSE and national bodies. The network welcomes pharmacists from all professional backgrounds, those who are considered experienced antimicrobial pharmacists and those who wish to further their knowledge.
antimicrobials are kept effective for future generations.
The functions of the network are:
PAMS-net vision
As healthcare workers we all have a role to play as antimicrobial stewards, as detailed in the recently published HSE antimicrobial stewardship (AMS) guidance for all healthcare settings. We need to curb, and hopefully reverse, the growing trend of antimicrobial resistance in order to have effective antimicrobials to enable us to deliver an optimal level of healthcare. We need, as healthcare workers, to feel empowered to play our part by learning how to incorporate antimicrobial stewardship in our day-to-day practice. To assist all pharmacists in doing this a new network has been established the Pharmacist Antimicrobial Stewardship Network (PAMS-net)
The PAMS-net launched on the 15th August 2022. It is a collaboration between the HSE Antimicrobial Resistance and Infection Control (AMRIC) team and the Irish Institute of Pharmacy (IIOP) and is open to all registered pharmacists.
• To share knowledge, information, learning and experience in AMS, both across and within sectors
2. CPD through our resources and educational network events
• To provide a discussion forum for members
• To share AMS work and foster creativity and innovation in AMS
• To assist in the provision of CPD for pharmacists with an interest in AMS
Join the network
The vision of the PAMS-net is a more joined up approach to AMS across the pharmacy profession. Pharmacists across all settings have guided the development of this vision through participation in focus groups, feedback sessions and membership of the PAMS-net working group.
3. Protect antimicrobials for future generations! Optimising antimicrobial use in all patients reduces patient harms and it limits the development of antimicrobial resistance so that antimicrobials are kept effective for future generations.
Antimicrobial stewardship
The PAMS net webpage is hosted on the IIOP website. It provides a discussion forum and resources section. Members receive updates through the network and network events are organised regularly.
The functions of the network are:

• To share knowledge, information, learning and experience in AMS, both across and within sectors
3 reasons to join the PAMS net
1. Networking & support through our online discussion forum and educational network events
To become a member of the network go to the “Courses and Events” page on the IIOP website and click the “Forum” tab (see below).

The network is a fantastic opportunity for pharmacists across all settings to collaborate in education, promotion and implementation of best practice so we can achieve our shared goal of enabling responsible use of antimicrobials in all patients and limiting the emergence of antimicrobial resistance (AMR). Through the PAMS net discussion forum and member events pharmacists can come together to provide support and advice to one another. Pharmacists across different settings can share knowledge and learning in the area of antimicrobial stewardship.
The PAMS-net launched on the 15th August 2022. It is a collaboration between the HSE Antimicrobial Resistance and Infection Control (AMRIC) team and the Irish Institute of Pharmacy (IIOP) and is open to all registered pharmacists.
2. CPD through our resources and educational network events
• To provide a discussion forum for members
• To share AMS work and foster creativity and innovation in AMS
3. Protect antimicrobials for future generations! Optimising antimicrobial use in all patients reduces patient harms and it limits the development of antimicrobial resistance so that antimicrobials are kept effective for future generations.
To learn more about antimicrobial stewardship and view national antibiotic prescribing guidelines and resources visit antibioticprescribing.ie.
The network is a fantastic opportunity for pharmacists across all settings to collaborate in education, promotion and implementation of best practice so we can achieve our shared goal of enabling responsible use of antimicrobials in all patients and limiting the emergence of antimicrobial resistance (AMR). Through the PAMS-net discussion forum and member events pharmacists can come together to provide support and advice to one another. Pharmacists across different settings can share
Antimicrobial stewardship (AMS) can encompass any action that promotes responsible use of antimicrobials. Some examples of AMS in pharmacy practice include: checking if antibiotic prescriptions align with antibiotic prescribing guidelines; recognising when an antibiotic agent, dose or duration is not in line with guidelines and highlighting this to the prescriber; providing advice when a patient presents with a self-limiting or viral infection.
Antimicrobial stewardship
Overuse and misuse of antimicrobials causes increasing AMR as well as other patient harms. Over the last 20 to 30 years we have seen many antimicrobials become less effective or even not effective at all for treatment of some infections due to AMR. AMS is vital in limiting and potentially reversing the development of AMR so that
• To assist in the provision of CPD for pharmacists with an interest in AMS
Keeping antibiotics effective for future generations -it’s everyone’s responsibility
All pharmacists with an interest in responsible antimicrobial use are welcome to join this network. The network aims to bring together pharmacists from a diverse range of settings including community, hospital, education, researchers, other HSE and national bodies. The network welcomes pharmacists from all professional backgrounds, those who are considered experienced antimicrobial pharmacists and those who wish to further their knowledge.

To become a member of the network go to the “Courses and Events” page on the IIOP website and click the “Forum” tab.
Antimicrobial stewardship (AMS) can encompass any action that promotes responsible use of antimicrobials. Some examples of AMS in pharmacy practice include: checking if antibiotic prescriptions align with antibiotic prescribing guidelines; recognising when an antibiotic agent, dose or duration is not in line with guidelines and highlighting this to the prescriber; providing advice when a patient presents with a self limiting or viral infection.
Women in Leadership Event
The Pharmaceutical Manufacturers’ Institute (PMI) are hosted a Women in Leadership lunch which takes place on Thursday, October 13th in Kingswood House Hotel, Kingswood. Following on from the previous Women in Leadership event in May where Eimear Caslin was guest MC; for this event the team are joined by Melissa Fisher, General Manager with Viatris.
Overuse and misuse of antimicrobials causes increasing AMR as well as other patient harms. Over the last 20 to 30 years we have seen many antimicrobials become less effective or even not effective at all for treatment of some infections due to AMR. AMS is vital in limiting and potentially reversing the development of AMR so that antimicrobials are kept effective for future generations.
PAMS-net vision
Guest speaker is Lisa Clancy, Vice President of the Paralympics Olympics Ireland and Owner of Clansult – a consultancy agency. She has been to the fore in leadership across Irish sport for a number of years and in a number of different roles, and is currently creating a pathway for leaders of the future through the Women in Sport Leadership Programme. A passionate advocate for mentorship and driving women in leadership, Lisa works with companies, athletes & senior executives to help them reach their full potential and make a strategic impact.
A new network for pharmacists just launched - Pharmacist Antimicrobial Stewardship Network (PAMS-net)
PHARMACYNEWSIRELAND.COM 12 News
Pain relief for lit tle ones
Pain relief for lit tle ones
And a sigh of relief for grown-ups
And a sigh of relief for grown-ups
ACTS FAST ON PAIN & FEVER
For Children

ABBREVIATED PRESCRIBING INFORMATION
ABBREVIATED PRESCRIBING INFORMATION
Product Name: Brupro for Children 100mg/5ml Oral Suspension & Brupro for Children Six Plus 200mg/5ml oral suspension.
Product Name: Brupro for Children 100mg/5ml Oral Suspension & Brupro for Children Six Plus 200mg/5ml oral suspension.


Composition: Each 5 ml of oral suspension contains 100 mg or 200 mg ibuprofen respectively.
Composition: Each 5 ml of oral suspension contains 100 mg or 200 mg ibuprofen respectively.
Description: White or almost white suspension, homogeneous after agitationIndication(s): 100 mg/5 ml: Reduction of fever and relief of mild to moderate pain, such as cold and flu symptoms, teething pain, headache, sprains and strains and to ease the pain of sore throats andearache. For short term use only. 200 mg/5 ml: For the short-term symptomatic treatment of mild to moderate pain. For the short-term symptomatic treatment of fever.
Dosage: Infants aged 3-6 months who weigh more than 5kg. Do not dose more frequently than at 6 hourly intervals and do not exceed the recommended dose. For infants aged 3-5 months medical adviceshould be sought if symptoms worsen or not later than 24 hours if symptoms persist and no later than 3 days in children aged from 6 months and in adolescents. Recommended time interval is 3 times in 24hours: 100 mg/5 ml: 3-12 months (5-9 kg bodyweight): 2.5 ml; 1 to 3 years (10-16 kg): 5 ml; 4 to 6 years (17-20 kg): 7.5 ml; 7 to 9 years (21-30 kg): 10 ml (two 5ml spoonfuls); 10 to 12 years (31-40kg): 15 ml (three 5ml spoonfuls). 200 mg/5 ml: Not for use in children under 6 years of age or under 20 kg body weight. 6-9 years (20-29 kg): 5ml (200 mg); 10-12 years (30-40 kg): 7.5ml (300 mg).
Renal insufficiency: No dose reduction in mild to moderate impairment. Hepatic insufficiency: No dose reduction in mild to moderate impairment.Contraindications: Hypersensitivity to the active substance or to any of the excipients. In patients: - who have previously shown hypersensitivity (e.g. bronchospasm, asthma, rhinitis, angioedema or urticaria)associated with acetylsalicylic acid, ibuprofen or other non-steroidal anti-inflammatory (NSAID) medicinal products; - with a history of gastrointestinal bleeding or perforation, related to previous NSAIDtherapy; - with active, or a history of recurrent peptic ulcer/haemorrhage (two or more distinct episodes of proven ulceration or bleeding); - with cerebrovascular or other active bleeding; - with severe hepaticfailure or severe renal failure; - with severe heart failure; -with unclarified blood-formation disturbances; -with severe dehydration (caused by vomiting, diarrhoea or insufficient fluid intake). During the lasttrimester of pregnancy. Warnings and Precautions for Use: Refer to the SPC for detailed warnings. Undesirable effects may be minimized by using the lowest effective dose for the shortest durationnecessary to control symptoms and patients should report any unusual symptoms especially any GI bleeding. Elderly: Have an increased frequency of adverse reactions to NSAIDs especially gastrointestinalbleeding and perforation which may be fatal. Are at increased risk of the consequences of adverse reactions. Caution in: Systemic lupus erythematosus as well as those with mixed connective tissue disease,due to increased risk of aseptic meningitis; Congenital disorder of porphyrin metabolism (e.g. acute intermittent porphyria); Gastrointestinal disorders and chronic inflammatory intestinal disease (ulcerativecolitis, Crohn’s disease). Consider combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) and also for patients requiring concomitant low dose acetylsalicylic acid, or otherdrugs likely to increase gastrointestinal risk; A history of hypertension and/or heart failure as fluid retention and oedema have been reported in association with NSAID therapy; Renal impairment as renalfunction may further deteriorate; Hepatic dysfunction; Dehydration; Directly after major surgery; Hayfever, nasal polyps or chronic obstructive respiratory disorders as an increased risk for them of allergicreactions occurring. These may be present as asthma attacks (so-called analgesic asthma), Quincke’s oedema or urticaria; In patients who have already reacted allergically to other substances, as anincreased risk of hypersensitivity reactions occurring also exists for them on use of this product; Bronchospasm may be precipitated in patients suffering from, or with a history of, bronchial asthma or allergicdisease. Dermatological effects: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome and toxic epidermal necrolysis, have been reported very rarely inassociation with the use of NSAIDs. Patients appear to be at highest risk of these reactions early in the course of therapy, the onset of the reaction occurring in the majority of cases within the first month oftreatment. Acute generalized exanthematous pustulosis (AGEP) has been reported. Discontinue Brupro for Children at the first appearance of signs and symptoms of severe skin reactions, such as skin rash,mucosal lesions, or any other sign of hypersensitivity. Symptoms of underlying infections and fever can be masked which may lead to delayed initiation of appropriate treatment and thereby worsening theoutcome of the infection. This has been observed in bacterial community acquired pneumonia and bacterial complications to varicella. Monitoring of infection is advised. In nonhospital settings, the patientshould consult a doctor if symptoms persist or worsen. Exceptionally, varicella can be at the origin of serious cutaneous and soft tissues infectious complications. It is advisable to avoid use of ibuprofen in caseof varicella. Cardiovascular and cerebrovascular effects: Ibuprofen, particularly at a high dose (2400 mg/day) may be associated with a small increased risk of arterial thrombotic events (for examplemyocardial infarction or stroke). Low dose ibuprofen (e.g. ≤ 1200 mg/day) is suggested not to be associated with a small increased risk of arterial thrombotic events. Patients with uncontrolled hypertension,congestive heart failure (NYHA II-III), established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease should only be treated with ibuprofen after careful consideration andhigh doses (2400 mg/day) should be avoided and consider carefully if long term treatment is needed. Other notes: Severe acute hypersensitivity reactions (for example anaphylactic shock) are observedvery rarely. Discontinue treatment immediately and seek medical attention. Ibuprofen may temporarily inhibit the blood-platelet function (thrombocyte aggregation). Monitor patients with coagulationdisturbances carefully. Check liver values, kidney function and blood count in prolonged treatment. Be aware of diagnosis of medication overuse headache (MOH), suspected in patients who have frequent ordaily headaches despite (or because of) the regular use of headache medications. Alcohol may increase adverse effects that concern the gastrointestinal tract or the central nervous system. Renal: Habitualuse of analgesics, especially the combination of different analgesic drug substances, can lead to lasting renal lesions with the risk of renal failure (analgesic nephropathy). There is a risk of renal impairment indehydrated children. Contains sorbitol and propylene glycol. Interactions: Refer to the SPC for detailed information on the interactions. Avoid in combination with: Other NSAIDs including cyclooxygenase-2selective inhibitors; Acetylsalicylic acid; Antihypertensives, (ACE inhibitors, beta-receptor blocking medicines and angiotensin-II antagonists) and diuretics; Cardiac glycosides: e.g. digoxin; Lithium; Potassiumsparing diuretics; Phenytoin; Methotrexate; Tacrolimus; Ciclosporin; Corticosteroids; Anti-coagulants; Anti-platelet agents and selective serotonin reuptake inhibitors (SSRIs); Mifepristone; Sulphonylureas;Zidovudine; Probenecid and sulfinpyrazone; Baclofen; Ritonavir; Aminoglycosides; Quinolone antibiotics; Cholestyramine; Captopril; CYP2C9 inhibitors: e.g. voriconazole and fluconazole.
Description: White or almost white suspension, homogeneous after agitationIndication(s): 100 mg/5 ml: Reduction of fever and relief of mild to moderate pain, such as cold and flu symptoms, teething pain, headache, sprains and strains and to ease the pain of sore throats andearache. For short term use only. 200 mg/5 ml: For the short-term symptomatic treatment of mild to moderate pain. For the short-term symptomatic treatment of fever. Dosage: Infants aged 3-6 months who weigh more than 5kg. Do not dose more frequently than at 6 hourly intervals and do not exceed the recommended dose. For infants aged 3-5 months medical adviceshould be sought if symptoms worsen or not later than 24 hours if symptoms persist and no later than 3 days in children aged from 6 months and in adolescents. Recommended time interval is 3 times in 24hours: 100 mg/5 ml: 3-12 months (5-9 kg bodyweight): 2.5 ml; 1 to 3 years (10-16 kg): 5 ml; 4 to 6 years (17-20 kg): 7.5 ml; 7 to 9 years (21-30 kg): 10 ml (two 5ml spoonfuls); 10 to 12 years (31-40kg): 15 ml (three 5ml spoonfuls). 200 mg/5 ml: Not for use in children under 6 years of age or under 20 kg body weight. 6-9 years (20-29 kg): 5ml (200 mg); 10-12 years (30-40 kg): 7.5ml (300 mg).Renal insufficiency: No dose reduction in mild to moderate impairment. Hepatic insufficiency: No dose reduction in mild to moderate impairment.Contraindications: Hypersensitivity to the active substance or to any of the excipients. In patients: - who have previously shown hypersensitivity (e.g. bronchospasm, asthma, rhinitis, angioedema or urticaria)associated with acetylsalicylic acid, ibuprofen or other non-steroidal anti-inflammatory (NSAID) medicinal products; - with a history of gastrointestinal bleeding or perforation, related to previous NSAIDtherapy; - with active, or a history of recurrent peptic ulcer/haemorrhage (two or more distinct episodes of proven ulceration or bleeding); - with cerebrovascular or other active bleeding; - with severe hepaticfailure or severe renal failure; - with severe heart failure; -with unclarified blood-formation disturbances; -with severe dehydration (caused by vomiting, diarrhoea or insufficient fluid intake). During the lasttrimester of pregnancy. Warnings and Precautions for Use: Refer to the SPC for detailed warnings. Undesirable effects may be minimized by using the lowest effective dose for the shortest durationnecessary to control symptoms and patients should report any unusual symptoms especially any GI bleeding. Elderly: Have an increased frequency of adverse reactions to NSAIDs especially gastrointestinalbleeding and perforation which may be fatal. Are at increased risk of the consequences of adverse reactions. Caution in: Systemic lupus erythematosus as well as those with mixed connective tissue disease,due to increased risk of aseptic meningitis; Congenital disorder of porphyrin metabolism (e.g. acute intermittent porphyria); Gastrointestinal disorders and chronic inflammatory intestinal disease (ulcerativecolitis, Crohn’s disease). Consider combination therapy with protective agents (e.g. misoprostol or proton pump inhibitors) and also for patients requiring concomitant low dose acetylsalicylic acid, or otherdrugs likely to increase gastrointestinal risk; A history of hypertension and/or heart failure as fluid retention and oedema have been reported in association with NSAID therapy; Renal impairment as renalfunction may further deteriorate; Hepatic dysfunction; Dehydration; Directly after major surgery; Hayfever, nasal polyps or chronic obstructive respiratory disorders as an increased risk for them of allergicreactions occurring. These may be present as asthma attacks (so-called analgesic asthma), Quincke’s oedema or urticaria; In patients who have already reacted allergically to other substances, as anincreased risk of hypersensitivity reactions occurring also exists for them on use of this product; Bronchospasm may be precipitated in patients suffering from, or with a history of, bronchial asthma or allergicdisease. Dermatological effects: Serious skin reactions, some of them fatal, including exfoliative dermatitis, Stevens-Johnson syndrome and toxic epidermal necrolysis, have been reported very rarely inassociation with the use of NSAIDs. Patients appear to be at highest risk of these reactions early in the course of therapy, the onset of the reaction occurring in the majority of cases within the first month oftreatment. Acute generalized exanthematous pustulosis (AGEP) has been reported. Discontinue Brupro for Children at the first appearance of signs and symptoms of severe skin reactions, such as skin rash,mucosal lesions, or any other sign of hypersensitivity. Symptoms of underlying infections and fever can be masked which may lead to delayed initiation of appropriate treatment and thereby worsening theoutcome of the infection. This has been observed in bacterial community acquired pneumonia and bacterial complications to varicella. Monitoring of infection is advised. In nonhospital settings, the patientshould consult a doctor if symptoms persist or worsen. Exceptionally, varicella can be at the origin of serious cutaneous and soft tissues infectious complications. It is advisable to avoid use of ibuprofen in caseof varicella. Cardiovascular and cerebrovascular effects: Ibuprofen, particularly at a high dose (2400 mg/day) may be associated with a small increased risk of arterial thrombotic events (for examplemyocardial infarction or stroke). Low dose ibuprofen (e.g. ≤ 1200 mg/day) is suggested not to be associated with a small increased risk of arterial thrombotic events. Patients with uncontrolled hypertension,congestive heart failure (NYHA II-III), established ischaemic heart disease, peripheral arterial disease, and/or cerebrovascular disease should only be treated with ibuprofen after careful consideration andhigh doses (2400 mg/day) should be avoided and consider carefully if long term treatment is needed. Other notes: Severe acute hypersensitivity reactions (for example anaphylactic shock) are observedvery rarely. Discontinue treatment immediately and seek medical attention. Ibuprofen may temporarily inhibit the blood-platelet function (thrombocyte aggregation). Monitor patients with coagulationdisturbances carefully. Check liver values, kidney function and blood count in prolonged treatment. Be aware of diagnosis of medication overuse headache (MOH), suspected in patients who have frequent ordaily headaches despite (or because of) the regular use of headache medications. Alcohol may increase adverse effects that concern the gastrointestinal tract or the central nervous system. Renal: Habitualuse of analgesics, especially the combination of different analgesic drug substances, can lead to lasting renal lesions with the risk of renal failure (analgesic nephropathy). There is a risk of renal impairment indehydrated children. Contains sorbitol and propylene glycol. Interactions: Refer to the SPC for detailed information on the interactions. Avoid in combination with: Other NSAIDs including cyclooxygenase-2selective inhibitors; Acetylsalicylic acid; Antihypertensives, (ACE inhibitors, beta-receptor blocking medicines and angiotensin-II antagonists) and diuretics; Cardiac glycosides: e.g. digoxin; Lithium; Potassiumsparing diuretics; Phenytoin; Methotrexate; Tacrolimus; Ciclosporin; Corticosteroids; Anti-coagulants; Anti-platelet agents and selective serotonin reuptake inhibitors (SSRIs); Mifepristone; Sulphonylureas;Zidovudine; Probenecid and sulfinpyrazone; Baclofen; Ritonavir; Aminoglycosides; Quinolone antibiotics; Cholestyramine; Captopril; CYP2C9 inhibitors: e.g. voriconazole and fluconazole.
Pregnancy and Lactation: Pregnancy: During the first and second trimester of pregnancy, ibuprofen should not be given unless clearly necessary. If ibuprofen is used by a woman attempting to conceive, orduring the first and second trimester of pregnancy, the dose should be kept as low and duration of treatment as short as possible. Contraindicated during the third trimester of pregnancy. Breast-feeding:Ibuprofen and its metabolites can pass in low concentrations into the breast milk. No harmful effects to infants are known to date, so for short-term treatment with the recommended dose for pain and feverinterruption of breast feeding would not generally be necessary. Fertility: There is some evidence that substances which inhibit cyclo-oxygenase/ prostaglandin synthesis may cause impairment of femalefertility by an effect on ovulation. This is reversible upon withdrawal of treatment.
Pregnancy and Lactation: Pregnancy: During the first and second trimester of pregnancy, ibuprofen should not be given unless clearly necessary. If ibuprofen is used by a woman attempting to conceive, orduring the first and second trimester of pregnancy, the dose should be kept as low and duration of treatment as short as possible. Contraindicated during the third trimester of pregnancy. Breast-feeding:Ibuprofen and its metabolites can pass in low concentrations into the breast milk. No harmful effects to infants are known to date, so for short-term treatment with the recommended dose for pain and feverinterruption of breast feeding would not generally be necessary. Fertility: There is some evidence that substances which inhibit cyclo-oxygenase/ prostaglandin synthesis may cause impairment of femalefertility by an effect on ovulation. This is reversible upon withdrawal of treatment.
Ability to Drive and Use Machinery: For short-term use this medicinal product, has no or negligible influence on the ability to drive and use machines.
Ability to Drive and Use Machinery: For short-term use this medicinal product, has no or negligible influence on the ability to drive and use machines.
Undesirable Effects: Gastro-intestinal: abdominal pain, nausea and dyspepsia, diarrhoea, flatulence, constipation, heartburn, vomiting and slight gastrointestinal blood losses that may cause anaemia inexceptional cases. Refer to the SPC for other undesirable effects. Marketing Authorisation Holder: Rowa Pharmaceuticals Ltd., Bantry, Co. Cork.
Undesirable Effects: Gastro-intestinal: abdominal pain, nausea and dyspepsia, diarrhoea, flatulence, constipation, heartburn, vomiting and slight gastrointestinal blood losses that may cause anaemia inexceptional cases. Refer to the SPC for other undesirable effects. Marketing Authorisation Holder: Rowa Pharmaceuticals Ltd., Bantry, Co. Cork.
Marketing Authorisation Number: PA0074/067/004-005 Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417
Marketing Authorisation Number: PA0074/067/004-005 Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417
E-mail: rowex@rowa-pharma.ie. Legal Category: Not subject to medical prescription. Date of Preparation: March 2021
E-mail: rowex@rowa-pharma.ie. Legal Category: Not subject to medical prescription. Date of Preparation: March 2021


Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing Rowex pv@rowa-pharma.ie
Adverse events should be reported. Reporting forms and information can be found on the HPRA website (www.hpra.ie) or by emailing Rowex pv@rowa-pharma.ie
Supply status: Supply through pharmacies only
Supply status: Supply through pharmacies only
of Preparation
of Preparation
Date
: 07-22 CCF 25112
Date
: 07-22 CCF 25112
CarePlus and Keane’s bring Digital Pharmacy to Dublin
Having opened their doors in June of this year, the team at Keane’s CarePlus Pharmacy in Drumcondra is looking forward to the return of university students this month, promising another boost to their growing customer base in the community.
tasks during the day. That means their time can be spent getting to know customers, building up those all-important relationships when it comes to offering real understanding and care.”
The journey towards a digital pharmacy offering began in May 2019, when CarePlus Pharmacy’s in-house team began working on innovations to create a new concept for the sector.
The aim was to put technology to work to tackle some perennial problems like errors, operational inefficiencies, date rotation, theft, live stock counts and a feeling that pharmacists could be ’trapped’ and under-utilised when they were standing behind the counter, as well as move the sector towards the digital age.
Two and a half years since the first digital operation was rolled out in County Meath, the concept has proven highly successful for CarePlus Pharmacy. Its latest version uses a software system from Irish tech company, ScreenVend, which offers multiple omni-channel opportunities. The screens and dispensing system are linked to a large Gollmann robot, which brings chosen products to the point of sale via a specially designed chute system. The robot can store up to 20,000 individual items, all of which are accessible through a click on the screen or via the dispensary system.
John Keane says the digital experience has aligned closely with what customers were using in other areas of their day-to-day lives: “Customers were already familiar with online retail and this in-store experience mirrors that, while supporting easy product selection and promoting sales opportunities. The system is designed to recreate an “online” experience in store - and I think it does a great job”.
Proprietor and pharmacist, John Keane, says it’s been an excellent start for his first outlet in the capital, “We’ve had a fantastic summer and we are very lucky to have such a great team and support from the community. Our staff has grown since opening and we now employ five people in this store, which will hopefully expand further in the future.”
The CarePlus Pharmacy outlet, located within a building that also houses Drumcondra’s new Lidl store, is a significant arrival for another reason, too. It’s the first hybrid CarePlus Pharmacy in Dublin, offering customers a digital and traditional experience, and the fifth of its kind in Ireland.

John has plenty of experience with the two formats, given this is his seventh CarePlus Pharmacy outlet. He says the feedback from
staff and customers to the hybrid store has been very positive: “I think people are intrigued when they visit for the first time and see a lovely, airy shop with the shelves on one side and these bright, inviting screens across the floor. They’ve embraced the technology and convenience of the digital option. The staff are happy too - the system saves them plenty of time and labour on numerous repetitive
The overarching belief was that cutting edge technology could be designed to fulfil certain tasks, freeing up staff to do what machines couldn’t, i.e., build relationships with customers and become trusted advisers within their communities.
Whichever type of service customers at the Drumcondra store choose, John and his team are determined to establish a valuable presence in the community: “Being on one of the busiest thoroughfares in Dublin and adjacent to a university (Dublin City University) brings a really interesting opportunity to build loyalty among a younger market. As a group of people, third level students aren’t often very unwell, but they may have
The hybrid store in Drumcondra combines CarePlus Pharmacy’s state-of-the-art digital screens with a bespoke robotics system, allowing customers to easily browse and select items for purchase, with instant delivery to point of sale.
 John Keane, pictured at another CarePlus Pharmacy he operates in Mullingar, Co Westmeath. Keane’s CarePlus Pharmacy in Drumcondra is John’s seventh store in the network. Photo: Shane O’Neill
Photo: Alan Rowlette
John Keane, pictured at another CarePlus Pharmacy he operates in Mullingar, Co Westmeath. Keane’s CarePlus Pharmacy in Drumcondra is John’s seventh store in the network. Photo: Shane O’Neill
Photo: Alan Rowlette
PHARMACYNEWSIRELAND.COM 14 Profile
*Ryaltris™ is indicated in adults and adolescents 12 years of age and older for the treatment of moderate to severe nasal symptoms associated with allergic rhinitis1





Ryaltris™ 25 mcg/actuation + 600 mcg/actuation nasal spray, suspension. Prescribing information


Please consult the Summary of Product Characteristics (SmPC) for full prescribing information.


Presentation: One delivered dose contains mometasone furoate monohydrate equivalent to 25 mcg mometasone furoate and olopatadine hydrochloride equivalent to 600 mcg olopatadine. White, homogeneous suspension.
Uses: In adults and adolescents 12 years of age and older for the treatment of moderate to severe nasal symptoms associated with allergic rhinitis.
Dosage: For nasal use only. Adults and adolescents (12 years of age and over) two actuations in each nostril twice daily (morning and evening). Elderly: no dose adjustment required. Children under 12 years: not recommended. Renal and hepatic impairment: no dose adjustment expected.


Contraindications: Hypersensitivity to the active substance or to any of the excipients. Presence of untreated localised infection involving the nasal mucosa, such as herpes simplex. Recent nasal surgery or trauma until wound healing has occurred.


Warnings and Precautions: Instances of nasal ulceration and nasal septal perforation have been reported. Not recommended in case of nasal septum perforation. Patients using Ryaltris™ over several months or longer should be examined periodically for possible changes in the nasal mucosa and for evidence of Candida infection. Instances of epistaxis have been reported. Visual disturbance may be reported with systemic and topical corticosteroid use. Consider referral to ophthalmologist with symptoms such as blurred vision or other visual disturbances as cataract, glaucoma or rare diseases such as central serous chorioretinopathy have been reported after use of systemic and topical corticosteroids. Hypersensitivity reactions, including wheezing, may occur - discontinue. Immunosuppression: use with caution, if at all, in patients with active or quiescent tuberculous infections of the respiratory tract, untreated local or systemic fungal or bacterial infections, systemic viral or parasitic infections, or ocular herpes simplex. Potential systemic effects of corticosteroids include Cushing’s syndrome, Cushingoid features, adrenal suppression, growth retardation in children and adolescents, cataract, glaucoma and more rarely, a range of psychological or behavioural effects including psychomotor hyperactivity, sleep disorders, anxiety, depression or aggression (particularly in children). Hypercorticism and adrenal suppression may appear at higher than recommended dosages or in susceptible individuals at recommended dosages - discontinue slowly. Increased risk of signs or symptoms of hypercorticism and/or suppression of the HPA axis possible with concomitant use with other inhaled corticosteroids. Careful monitoring needed for acute adrenal insufficiency in response to stress in patients previously treated for prolonged periods with systemic corticosteroids and transferred to topical corticosteroids. In patients with asthma or other conditions requiring long term systemic corticosteroid treatment, too rapid a decrease in systemic corticosteroids may cause a severe exacerbation of symptoms. Somnolence has been reported following administration of Ryaltris™ in clinical studies. Caution in patients operating machinery or driving a motor vehicle. Avoid concurrent use with alcohol or other central nervous system (CNS) depressants. Increased risk of antihistamine adverse effects with concomitant use of olopatadine or other antihistaminic drugs administered via nasal, ocular or oral route. Paediatric population: It is recommended that the height of children receiving prolonged treatment with nasal corticosteroids is regularly monitored. Contains 0.02 mg benzalkonium chloride in each actuation. Benzalkonium chloride may cause irritation or
swelling inside the nose, especially if used for a long time. Interactions: No interaction studies have been performed with Ryaltris™. Any interactions from the combination of olopatadine and mometasone furoate are expected to reflect those of the components taken individually, no pharmacokinetic interaction between olopatadine and mometasone furoate was observed when administered in combination. Olopatadine: No interactions with other drugs expected. Mometasone Furoate: Cotreatment with CYP3A inhibitors should be avoided unless the benefit outweighs the increased risk of systemic corticosteroid side-effects and patients should be monitored. Pregnancy and Lactation: Avoid use during pregnancy unless potential benefit to mother justifies potential risk to mother, foetus or infant. Assess before prescribing in lactating mothers.
Side Effects: Common: dysgeusia, epistaxis, nasal discomfort. Uncommon: dizziness, headaches, somnolence, nasal dryness, dry mouth, abdominal pain, nausea, fatigue. Rare: bacterial vaginosis, anxiety, depression, insomnia, lethargy, migraine, blurred vision, dry eye, eye discomfort, ear pain, nasal inflammation, nasal mucosal disorder, oropharyngeal pain, sneezing, throat irritation, constipation, sore tongue, laceration. Frequency not known: pharyngitis, upper respiratory tract infection, hypersensitivity (including anaphylactic reactions, angioedema, bronchospasm, dyspnoea), cataracts, glaucoma, increased intraocular pressure and nasal septum perforation.

Pack Sizes: One bottle containing 30ml suspension (240 actuations).
Legal Category: POM.
Product Authorisation Numbers: PA 1543/002/001


Product Authorisation Holder: Glenmark Pharmaceuticals s.r.o., Hvezdova 1716/2b, 140 78 Prague 4, Czech Republic.
Marketed by: A. Menarini

Pharmaceuticals Ireland Ltd.

Further information is available on request from A. Menarini Pharmaceuticals Ireland Ltd., 2nd Floor, Castlecourt, Monkstown Farm, Monkstown, Glenageary, Co. Dublin A96 T924 or may be found in the SmPC.
Date of Preparation: June 2022.
IR-RYL-11-2022 May 2022
Two

1. Ryaltris™ Summary of Product Characteristics July 2021
sprays per nostril twice daily 1
needs around medication which helps build the business with them. For many, this is the first time they will be engaging with a pharmacist independently as they enter a new phase of their lives. So, we’ll be tailoring our offering to the health needs that go along with being a third level student, as well as providing advice around health issues if they need it. For example, the government recently announced a free contraception scheme for women aged 17 to 25, so we’ll be on hand to support our customers with that if needed.”
The CarePlus Pharmacy network is also known for providing a wide range of screening around concerns like COVID-19, blood pressure, asthmatic and diabetic care etc., which is useful for a range of demographics. As autumn arrives, John is preparing for a busy vaccination season: “A growing number of people avail of the flu vaccine every year, which is a really positive trend, and we’ll be offering it to eligible cohorts. We will also be keeping up to date with COVID boosters as they’re made available for more people”.

John has been spending time working the pharmacist shift in the Drumcondra store recently, which gave him the chance to really get to know the area, his team and the customers. He’s planning a great event to mark the official opening this month.

“We’ve had a few months to bed everything down here in Drumcondra, the team has got to know each other, and the customers are getting to know us too. We’re pulling out all the stops for our big opening weekend, with plenty of hampers, weekend discounts and special offers, face painting and giveaways. I might even cut a ribbon outside to mark the occasion. We want to make a splash and let the locals know we’re a friendly bunch that wants to look after them, and hopefully we’ll be here for a long time to come.”
 Keane’s CarePlus Pharmacy in Drumcondra also features interactive screens behind the counter, where staff can help patients with their choices. Pictured are (l-r) Pharmacy Assistant Jessica Wilson and Pharmacy Manager Hazel Kelly. Photo: Alan Rowlette
(l-r) Pharmacy Assistant Jessica Wilson, Pharmacist Manager Hazel Kelly and Store Supervisor Geraldine Cooper are looking forward to Keane’s CarePlus Pharmacy’s official Drumcondra opening event in October. Photo: Alan Rowlette
(l-r) CarePlus Pharmacy Assistant Jessica Wilson and Pharmacist Manager Hazel Kelly demonstrate the digital screen technology. Photo: Alan Rowlette
Keane’s CarePlus Pharmacy in Drumcondra also features interactive screens behind the counter, where staff can help patients with their choices. Pictured are (l-r) Pharmacy Assistant Jessica Wilson and Pharmacy Manager Hazel Kelly. Photo: Alan Rowlette
(l-r) Pharmacy Assistant Jessica Wilson, Pharmacist Manager Hazel Kelly and Store Supervisor Geraldine Cooper are looking forward to Keane’s CarePlus Pharmacy’s official Drumcondra opening event in October. Photo: Alan Rowlette
(l-r) CarePlus Pharmacy Assistant Jessica Wilson and Pharmacist Manager Hazel Kelly demonstrate the digital screen technology. Photo: Alan Rowlette
PHARMACYNEWSIRELAND.COM 16 Profile


Call: 091 769803 | Email: customerservice@reviveactive.com | Web: reviveactive.com BEAUTY Offer available while stocks last. Food supplements should not be used as a substitute for a varied diet & healthy lifestyle WELLBEING ESSENTIALS STARTER KIT The Per fect Gift RRP € 49.95 PROMO PRICE € 39.95 INCLUDES Three 7-Day Super Supplement Trial Packs Energy Immune System Heart Brain Function Cognitive Function Mental Performance
Navigating Menopause in Thrombosis Patients
Levels of female reproductive hormone will start to become less predictable and then drop; sometimes gradually with age, sometimes abruptly as a result of disease or medical treatments.
 Written by Dr Deirdre Lundy, Clinical Lead, Complex Menopause Service, NMH, Holles St Picture: Gerry Mooney
Written by Dr Deirdre Lundy, Clinical Lead, Complex Menopause Service, NMH, Holles St Picture: Gerry Mooney

The transition typically kicks off naturally from about the mid- 40’s and the symptoms resulting from hormone derangement or loss are commonly referred to as “The Menopause” by patients and HC (even though we know that the word ‘menopause’ actually means “end of the monthly”). So while menopause officially is defined as the last ever natural menses and most commonly occurs in the early 50’s, the symptomatic phase of the lead into sex hormone changes - more accurately referred to as ‘perimenopause’, often precede the final menstrual period by many months or even years. We use those terms interchangeably. This transitional time (‘Perimenopause’) puts some patients in the unenviable position of having to juggle midlife hormonal symptoms as well as contraceptive concernsfertility may decline in your 40’s & 50’s but it’s not gone!
Some but thankfully not all patients struggle with perimenopausal symptoms and seek our advice in primary care. The amount of issues that may be uncovered in a first menopause visit are legion.
The classic physical symptoms are easily recognized: night sweats, hot flushes, heavy and/ or irregular periods, loss of vaginal elasticity and lubrication, decrease in metabolism (+/- weight gain), hair and skin changes, joint complaints, bladder complaints, et al.
The psychological symptoms are just as prevalent and possibly more likely to be misinterpreted. They include; depression, mood swings, anxiety, irritability/ rage, tiredness, memory loss, poor concentration, loss of libido, PMStype symptoms, et al.
The first thing to do is confirm the diagnosis. Easier said than done as hormone blood tests are often within normal ranges for perimenopausal patients and so are not recommended as having any part in the diagnostic process. In addition, not everything a patient experience in their middle life is related to perimenopause hormones changes. It can be challenging to identify whose mood symptoms are arising directly from the perimenopause vs. pre-existing mood issues being
exacerbated by the approach of menopause. A thorough history - maybe even expedited by pre consult symptom self-assessment questionnaires- may be of use. The most effective treatment for menopause related symptoms is HRT but it is not a ‘miracle cure’ and some people won’t need it, won’t want it or have been advised to avoid it. Clinicians are reminded that menopause care should be individualised- using a comprehensive approach that pays attention to advice on exercise, optimising weight, stopping smoking, and reducing alcohol consumption as well as management options such as HRT.
Talking about Thrombosis
One of the more important aspects of the history taking (apart from a kind ear which is of immeasurable benefit) is the need to exclude comorbidities that might affect the range of treatment options available to that patient. Some people will be keen to consider menopause hormone balancing or replacement therapy for their menopause symptoms (MHT or HRT). MHT involves providing small dose of estrogen in all cases and usually some low dose progestagen for the patient with a uterus. Occasionally, in cases of hypoactive sexual desire or arousal, some testosterone may also be offered. Each of these
individual hormones come with their own lists of contraindications and special precautions. Some contraindications are absolute but some special situations mainly require a conversation with either a menopause specialist or the consultant team that manages the patient’s medical condition; this is according to the British Menopause Society. One such situation is in the case of patients with a personal past history of thrombosis. If a perimenopausal patient who has had a VTE has considered and/ or explored nonhormonal options for managing their symptoms and now is keen to consider HRT, they can but we need to be much more cautious when prescribing for them. Our first job is to make sure as much is being done to optimise any modifiable risks that they carry. We know venous thrombosis particularly can be liked to modifiable issues such as:
- Immobilization
Smoking
Long plane or car trips of more than 4 hours &
Certain contraceptives – any high-dose, strong estrogen – like the ones in all the combined pills, rings and patches – can increase thrombosis risk; similar to the elevated risk linked to being pregnant. Some progestagens have been linked to increased VTE risk too, but not at the typical doses we see in progestagenonly contraceptives.
So keeping active and reducing or stopping smoking, keeping hydrated and avoiding the avoidable triggers is an important part of a menopausal chat for someone with a past history of VTE.
PHARMACYNEWSIRELAND.COM 18 Menopause

Exclusive to Pharmacies & Health Stores
Menopause
Now traditionally the estrogen in HRT was considered contraindicated for people with a past history of VTE as we expected the estrogen in HRT to have a similar effect on clotting mechanisms to the estrogens in contraceptives. High levels of estrogen (and certain progestagens) in the blood can be ‘Pro- thrombotic’. Oral oestrogen goes straight from the GI tract to the liver, where it is metabolized. During this first run through the liver is where the impact on clotting molecules occurs. But even non oral estrogens can impact clotting risk if the doses are high or the estrogen molecule is particularly potent - so the contraceptive patch and vaginal ring are just as likely to promote VTE as oral contraceptive pills. Risk is maximally elevated at initiationwhen a patient is commencing an estrogen containing contraceptive - and wanes with time, so using estrogen based contraceptives for a short time is not safer than staying on them for months or
years. In addition, every time a patient switches brands or comes off for a few weeks or months ‘to see if everything is still working in there’, they increase their clot risk when they restart.
So, knowing all this it was only logical that we assume HRT - type estrogen would also be risky for women with elevated VTE risk?
Well, apparently this is not the case.
While it is true that the estrogens in ORAL HRT can increase clot risk, there is an abundance of research to confirm that lowdose, ovarian - similar HRT oestrogen does not affect clot risk when used transdermally. This is supported by all the menopause guideline groups as well as by the gynaecology and haematology guidance groups. The go-to data to support this is the nested case-control study by Yana Vinogradova, et al that looked at women diagnosed with VTE between 1998 and 2017. Ref 2 With regard to progestagens,
this study did not actually review micronized progesterone for some reason, but it did look at dydrogesterone and found it also to be a safer option when there is concern about blood clots.
So we tell patients this: while people who are smoking, overweight or who have had a blood clot in the past should not use estrogen contraceptives nor should they use oral estrogen in HRT, they can safely try transdermal estrogen HRT products, in modest doses after discussion with their haematologist or menopause specialist.
According to the UK’s National Institute for Health and Care Excellence: ‘The risk of venous thromboembolism (VTE) is increased by use of an oral oestrogen-containing HRT product compared with baseline population risk, but the risk associated with transdermal HRT given at standard therapeutic doses is no greater than baseline population risk.’
Be warned though; the information leaflets that come with transdermal HRT estrogen products (and even with local vaginal oestrogen, which has never been suspected of increasing DVT risk) say: May cause blood clots or Do not use if you are at risk of blood clots. So patient counselling is key.
If someone is already on an anticoagulant, they may also consider low dose transdermal HRT oestrogen.
1. National Institute for Health and Care Excellence. Menopause: diagnosis and Management. NICE, 2015
2. Vinogradova Y, et al. Use of hormone replacement therapy and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ. 2019 Jan 9;364:k4810. doi: 10.1136/ bmj.k4810. Erratum in: BMJ. 2019 Jan 15;364:l162. PMID: 30626577; PMCID: PMC6326068.
NewsHeart Disease and Stroke in Menopausal Women
1 in 4 women in Ireland die from heart disease and stroke with women six times more likely to die from cardiovascular disease than breast cancer, these are the stark messages from a new campaign ‘Her Heart Matters’ by the Irish Heart Foundation which aims to raise awareness of heart disease and stroke in women.
Medical Director of the Irish Heart Foundation and consultant cardiologist, Dr Angie Brown

their lifestyles and make vital, sustainable changes to improve their heart health.
CSO data shows that in 2021, a total of 4,145 women died from cardiovascular disease which accounts for 26 per cent of all female deaths. The 2021 data also revealed that 686 women died from breast cancer in the same year, which means that women in Ireland are six times more likely to die from cardiovascular disease than breast cancer.
This comes as a surprise to most. According to a poll conducted by Ipsos on behalf of the Irish Heart Foundation, more than half of women (58%) surveyed said this was higher than they thought.
From about the age of 40, a woman’s risk of heart disease and stroke increases as she moves into menopause. And yet the Ipsos poll revealed that almost onethird (30%) of women do not have enough time each day to focus on their health.
As a result, the Irish Heart Foundation has launched the ‘Her Heart Matters’ campaign which aims to encourage women in their 40s, 50s and beyond to review
Speaking about the launch of the ‘Her Heart Matters’ campaign, Medical Director of the Irish Heart Foundation and consultant cardiologist, Dr Angie Brown, explained why cardiovascular disease was something women need to take seriously.
“Cardiovascular disease in women remains understudied, underrecognised, underdiagnosed, and undertreated. Early detection and management of cardiovascular risk factors are essential if we are to improve women’s heart health and reduce early deaths in women.”
Women’s risk of cardiovascular disease increases as they move into their 40s and 50s and experience menopause.
“Menopause causes a drop in the levels of the hormone oestrogen and blood vessels need oestrogen to stay healthy and flexible. Lower
oestrogen due to menopause leads to higher LDL, or bad cholesterol. This can increase plaque buildup, stiffening the arteries and leading to high blood pressure. Therefore, it’s important that women in their 40s and 50s really take stock of their health and make efforts to live healthily,” Dr Brown explained.
Despite the risk of heart issues increasing as women enter their 40s and 50s, the Ipsos poll revealed that just 13 per cent of women associate experiencing menopause with an increased risk of cardiovascular disease and the situation is even worse for stroke – just 4 per cent associate the menopause with an increased risk of the condition.
The link between menopause and heart disease should be more widely discussed but more than two-thirds of women aged 35+ (68%) surveyed said that even the topic of menopause itself was never brought up by a healthcare professional during a consultation.
PHARMACYNEWSIRELAND.COM 20
A new way of comfortable expressing.
Breast milk is the best nourishment a baby can receive and breastfeeding encourages that special bond between mother and baby. But for those moments when expressing milk is desirable, the new MAM Breast Pump is the best solution. The ergonomic shape and the easy handling and cleaning makes it ideal at home, work or on the go. A soft funnel and quiet pumping guarantee a hassle-free use anytime and everywhere. Plus the milk is expressed straight into the bottle for immediate use or safe and hygienic storage. To find out more about our unique easy-to-use Breast Pump, visit mambaby.com
free



Teamwork with medical experts for maximum safety. Only after approval by medical experts is a MAM innovation ready for baby life.



°BPA/BPS free: All MAM products are made from materials free of BPA and BPS.






























 DEVELOPED WITH MEDICAL EXPERTS
DEVELOPED WITH MEDICAL EXPERTS
Breast PadsNipple Shields Discover our additional breast feeding range from MAM: Easy Start™ 0+
BPA BPS
Easy & efficient pumping! Storage Solution
Menopause and Dry Eye Disease

Menopause is currently a hot topic (pun intended!). Many people are familiar with the typical symptoms of the menopause transition – vasomotor symptoms (hot flushes), mood changes, insomnia and genitourinary symptoms. However there are over 40 recognised symptoms of menopause, and this article aims to explore one of the lesser known symptoms; dry eyes.
Written by Dr Genevieve Ferraris MBBCh, The Menopause Hub
providers who treat patients in perimenopause and menopause. These practitioners should ask about and assess for symptoms of dry eye disease and provide education to help women manage their eye health.4

Patients should be encouraged to add an appropriate omega 3 supplement to their diet.
Dry eye disease is a multifactorial disease of the ocular surface, occurring due to a loss of homeostasis of the tear film.1
Patients present with symptoms of eye irritation, including redness, excessive tearing, a sensation of grittiness or burning, blurry vision and light sensitivity.2 Dry eye disease is not a unique symptom specific to menopause, and may also occur in patients with diabetes, Sjogren’s syndrome and as a side effect of various medications. However as it may point to an underlying hormonal issue if it occurs in a woman of menopausal age, it should prompt the healthcare provider to ask about other symptoms of menopause.
There are various risk factors for the development of dry eye disease, but of relevance here is advanced age, female sex, and hormonal changes associated with pregnancy, oral contraceptive use, and menopause. The underlying hormonal change is a decrease in androgens, either from reduced ovarian function or increased levels of sex hormone binding globulin.1 Androgen and estrogen receptors are located in the lacrimal and Meibomian glands, and a reduction in circulating sex hormones seems to affect both the functional and secretory aspect of the lacrimal gland as well as the loss of the lipid layer in Meibomian gland secretions.1 There is also hormonal dysregulation of secretory glands in general in menopause, putting menopausal women at a higher risk of dry eye disease.3
The pathophysiology of dry eye disease is multifactorial. A healthy eye tear film relies on the interaction of lacrimal glands, eyelids and the ocular surface. Dysfunction of any of these components can lead to dry eye disease.2 There are two major types of dry eye disease – aqueous deficient dry eye and evaporative dry eye. Evaporative dry eye results from tear film lipid deficiency as a result of Meibomian gland dysfunction. Aqueous dry eye, as a result of reduced tear production from the lacrimal glands, can also exacerbate Meibomian gland dysfunction.3 It is now believed that in most cases of dry eye disease both mechanisms are present.2
Dry eye disease may have significant impact on activities of daily living, workplace productivity and social functioning.2 When it appears in the menopause transition it is likely to be accompanied by other distressing symptoms, which may further affect work, life and socialising. Patients are also likely to incur medical costs through visits to various healthcare professionals as well as pharmacological and non-pharmacological therapies.2 Often when patients come to see me for the management of their menopause they report previous visits to the optometrist, GP and even the emergency department to seek relief of their dry eye symptoms.
Diagnosis is based on characteristic patient symptoms, and supportive findings on examination include conjunctival injection, excessive tearing, blepharitis and breakdown of ocular surface.2 When taking a history from female patients it would be prudent to ask about any menstrual irregularities, whether or not she is on contraception or HRT and if she is experiencing any other menopausal symptoms. Her presentation for dry eye may be her first presentation at a healthcare provider for a menopause-related symptom. One should also consider the screening opportunity for healthcare
First line treatment of dry eye disease involves1
• patient education around the condition, management and prognosis
• reviewing current medication and modifying if possible (if contributing to symptoms)
• modification of the patient’s environment
• tear supplementation (artificial tears)
The aims of tear supplementation are increased tear production, reduced tear evaporation and resorption and less ocular surface inflammation.2 Artificial tears generally contain cellulose to maintain viscosity and a spreading agent like polyethylene glycol to prevent evaporation. They come in liquid, gel and ointment forms – choice of formulation would be down to patient preference although a gel or ointment may temporarily affect vision and would be preferable to use at night.1
Oral omega 3 supplementation has been found to be protective against Meibomian gland dysfunction4 and has anti-inflammatory properties which aid in the production of tears and improve ocular surface function.1
Although HRT has been consistently shown to improve menopausal symptoms when compared with placebo and remains the most effective treatment for menopausal symptoms for most women,5 evidence is lacking as to whether it will specifically improve dry eye disease in menopause. A systematic review and metaanalysis published in the Canadian Journal of Ophthalmology in 2020 showed no significant reduction in dry eye symptoms with HRT over a 6 month period, however they noted that ‘more goodquality randomized control trials are needed to make accurate conclusions’.6
In summary, women going through the menopause transition may experience dry eyes as a symptom. They should be offered treatment specifically to manage this symptom, but healthcare providers should also be aware of the link between menopause and dry eye disease and be open to discussing this with the patient. HRT should not be offered specifically to treat dry eye but it may still be appropriate for a patient with other menopausal symptoms in addition to her ophthalmological complaints.
www.themenopausehub.ieIreland’s only dedicated multidisciplinary menopause clinic. References available on request
PHARMACYNEWSIRELAND.COM 22 Menopause/Dry Eye
every step of the
For
information on this
please visit www.pregnacare.com/mostrecommended.


Journal of the American College of Nutrition, Vol.18, No.5, 487-489 (1999).
A beneficial effect can be obtained from a maternal daily intake of 200mg DHA in addition to the recommended daily intake of 250mg DHA / EPA for adults - Annex of Commission Regulations (EU) No. 440/2011.




more
research,
2.
3.
With you
way Wellbaby For your new arrival Most trusted by mums1 Most recommended by midwives1 Pregnacare® Breast-feeding With 21 nutrients including 10µg vitamin D & 300mg DHA2 which contributes to normal brain and eye development in breast-fed infants.3 Pregnacare® New Mum With iron which contributes to a reduction of tiredness and fatigue, plus biotin to help maintain normal skin & hair. Contact Valeo Healthcare sales reps to place your order for our ‘award-winning’ products Julie Webster 086 462 1723 Julie.webster@valeofoods.ie Fintan Byrne 087 647 0764 fintan.byrne@valeofoods.ie Eamonn Connolly 087 238 5648 eamonn.connolly@valeofoods.ie
Considerations for Medication use in Pregnancy and Lactation
initiation rates in Ireland in comparison to other developed countries, with 62.3% of women initiating breastfeeding in 2020.4
The HSE Breastfeeding Action Plan notes the importance of healthcare provider education in the support of breastfeeding. Community pharmacists consistently top polls as the most trusted group of healthcare professionals,5 and are often the first port of call for healthcare advice, as well as dispensing of medications. The importance of pharmacist involvement in this is noted in the Competence Framework for Breastfeeding Support, which outlines the minimum level of knowledge that various healthcare providers should aspire to have.6
Written by Dr Claire McCarthy, Consultant Obstetrician/ Gynaecologist, Rotunda Hospital, Dublin

It is clear that there are challenges with respect to gathering evidence on medicines in pregnancy, with the majority of information being obtained through studies examining accidental or planned use in pregnancy, or extrapolated from animal studies. As such, the evidence continues to evolve with respect to the use of medications in pregnancy and lactation and it is important to continually evaluate the evidence available and update our knowledge.
provide information on specific medication with respect to medication use in pregnancy and lactation.
Further afield, the LactMed database contains information on drugs that mothers may be exposed to and presents an evidence based review to allow counselling of patients.10 The UK Teratology information Service provides an online resource in “Bumps” (Best use of medicines in pregnancy) with information leaflets for patients and healthcare providers to guide counselling and choice of therapy.11 UKTIS, who run the Bumps website, is part of a wider European Network (ENTIS) that provide position statements and publications on a number of different medications in pregnancy.12 Finally, Hale’s Medication and Mothers’ Milk is one of a number of textbook resources that can be referred to for medication use in lactation.13 Some of these are available as mobile and desktop applications to allow frequent access.
Dr Claire McCarthy is a Consultant Obstetrician/Gynaecologist with a special interest in managing medical conditions in pregnancy. Dr McCarthy is also involved with the Irish Medicines in Pregnancy Service (IMPS), a multidisciplinary service based at the Rotunda Hospital, which provides information and expertise to support safe and effective use of medicines before, during and after pregnancy and in lactation.
The use of medication in pregnancy and breastfeeding is exceedingly common, with the majority of women taking either over-the-counter or prescribed medication at some point during the antenatal or peripartum period.1 While some women enter pregnancy with a pre-existing health condition, others develop one in pregnancy or during the postnatal period. It is essential that women and their support networks receive clear, coherent and accurate counselling to support their treatment during pregnancy and in the postnatal period. We know that a well-controlled medical condition in pregnancy is preferable to deterioration of a condition that could lead to maternal and fetal/infant complications.2
From a breastfeeding perspective, the Health Service Executive (HSE) implores that the promotion, support and protection of breastfeeding are a priority, with additional funding granted to increase lactation consultant numbers in 2021.3 This is important given lower breastfeeding
When considering medication use in the pregnant or breastfeeding woman, we need to give consideration to maternal, fetal and neonatal physiology. Pregnancy can alter the pharmacokinetics and pharmacodynamics of medications, due to and separate to maternal physiological changes.7 From an infant perspective, the relative infant dosage (RID) provides an indication of how much of the maternal dose an infant is receiving.8 This is dependent on factors such as infant age, gestational age at delivery and other maternal factors, but generally an RID of less than 10% is acceptable.
Any discussion on medication use in pregnancy or lactation should be balanced on the risks and benefits, with the risks communicated in a way (i.e. language/ visual/numerical) that is acceptable to the patient, taking into account the clinical perspectives unique to their situation.
There are a wide range of resources available to us when assessing suitability and risk/ benefits of medications in pregnancy. Nationally, the National Medicines Information Centre (NMIC) based at St James’ Hospital in Dublin provides regular NMIC Bulletins and publications (Therapeutics Today) and evidence-based information on medication use in pregnancy and lactation.9 The IMPS at the Rotunda Hospital provides information for patients attending the Rotunda Hospital for antenatal care, in conjunction with the maternal medicine service. Other hospitals also have medicines information pharmacists who can
Pharmacists, obstetricians and neonatologists in maternity units can provide information or evidence on the use of medications in pregnancy and lactation. There are also regular conferences (both physical, online and hybrid) that discuss this topic, such as the Royal College of Physicians of Ireland conference which has a “Medications in Pregnancy and Lactation” Study Day running annually in March.
It is important to acknowledge that the use of medications extends to vaccination in pregnancy and lactation, as we have seen during the COVID pandemic as well as annual influenza seasons, with many women accessing pharmacy services for advice and vaccination. It is essential that pharmacists and staff within the pharmacy can present balanced information to women and their families on this topic, advocating for protection from disease through vaccination. COVID vaccination information and decision aids can be accessed through resources such as the Royal College of Physicians of Ireland.14
As healthcare providers, it is essential that we empower our patients by educating ourselves and advocating for them and their healthcare needs. This will allow us to continue to offer contemporaneous advice and support in order to manage their acute and chronic healthcare conditions in pregnancy, as well as obtain their breastfeeding goals.
References available on request
24 | PHARMACYNEWSIRELAND.COM



IMMUNE New With Extra Strength Vitamin D For Immune Support* Contains the unique PB-VIR™ culture, a PrecisionBiotics strain *Vitamin D contributes to the normal function of the Immune System More information available at www.precisionbiotics.com Available Now Distributed by Scienti callyStudied PB-VIR 14 Moneen Business Park, Castlebar, Co. Mayo, Ireland. Tel: +353 94 9024000 Fax: +353 94 9022824 Email: info@pamex.ie Your Sales Partner in Ireland
Menopause and Urinary Incontinence
Almost every tissue in the body has estrogen receptors, which suggests that estrogen has a role to play in their function. This is true of the genitourinary system, which includes the external genitalia, vagina, bladder and urethra. The loss of estrogen which comes with menopause has several effects on these tissues which, used to come under terms such as atrophic vaginitis, vulvovaginal atrophy, and various urinary conditions including urinary incontinence. More recently, the term Genitourinary Syndrome of Menopause (GSM) is used to refer to these issues as a group.
Written by Dr Catherine Riordan, The Menopause Hub
Dr Riordan is a Fellow of the Royal College of Surgeons, England. She spent several years as a fertility specialist at both Sims and ReproMed IVF clinics. She is a member of the Urology team at St Michael’s Hospital, Dun Laoghaire and a Surgeon Prosector in the anatomy department of the RCSI.

“Genitourinary syndrome of menopause (GSM) is a more accurate and inclusive term that describes the multiple changes occurring in the external genitalia, pelvic floor tissues, bladder and urethra, and the sexual sequelae of loss of sexual function and libido, caused by hypoestrogenism during the menopause transition and post menopause. These genitourinary changes primarily occur in response to reduced estrogen levels and aging, and do not settle with time”. (Kim et.al, 2015)
There are two main types of incontinence; stress urinary incontinence (SUI) and urge urinary incontinence (UUI). Aging is a large factor in the development of urinary incontinence, but menopause can have an added impact. By the age of 70, 1 in 2 women has a degree of urinary incontinence and it has an enormous impact on quality of life.
SUI is leakage of urine when the pressure on the bladder is increased from within the abdomen, as happens when the abdominal muscles are tightened during coughing, laughing, sneezing or lifting something heavy. It can also happen when there is extra pressure applied to the pelvic floor while running, or classically, jumping on a trampoline - a major no-no for many mothers! Having a baby increases the chance of having SUI from 1 in 10 to 1 in 3.
UUI is leakage which happens when you have the sudden urge to pee and can’t quite hold on until you get to the toilet. It is less common than SUI, affecting approx 1 in 30 women, but becomes more common with age and with the onset of menopause. It is caused by overactivity of the muscle of the bladder wall, also known as overactive bladder syndrome (OAB) and is associated with reduced bladder capacity, urinary frequency, urgency and the need to get up multiple times at night to pass urine. You may have OAB without leakage.
The bony pelvis is like a bowl without a bottom, into the top of which rest the abdominal contents. The pelvis itself contains the bladder, uterus and rectum, all of which would fall out through the bottom of the bowl were it not for a muscular sheet or diaphragm stretched across it. This group of muscles is collectively referred to as the pelvic floor. It contains condensations of muscle fibres around the bladder neck and a sling around the lower rectum which act as sphincters to prevent unwanted escape of their contents. When you are about to cough or sneeze etc, there is a reflex tightening of the pelvic floor muscles a split second beforehand, so that when the cough occurs, everything is sealed tight and no urine or faeces are squeezed out. If the pelvic floor is weak, this may not happen strongly or quickly enough and leakage occurs. If the pelvic floor is significantly weak, over time the pelvic organs, ie the bladder, uterus and rectum, may slip downwards and bulge through it in the form of a prolapse. If the bladder bulges through the pelvic floor, this is known as a cystocele.

There are many factors that can weaken the pelvic floor, such as a chronic cough or excess intra
abdominal fat. Women are at higher risk than men because of their childbearing potential. Firstly, the birth canal passes through the pelvic floor which necessitates a third opening and thus a further potential weakness. Secondly, the pelvic floor is subjected to stretching during pregnancy and childbirth. Even carrying a baby for 9 months puts pressure on the pelvic floor and will stretch it. Pushing a baby through it during vaginal delivery, particularly if the passage is rapid or if instruments are required, stretches it even more dramatically. Indeed, the muscles can tear. Not only are the muscle fibres stretched, but the elastic and collagen fibres are also stretched or broken. The result is a loss of muscle tone and strength of the pelvic floor as a whole. Pelvic floor exercises are extremely important in the post delivery phase, to restore as much muscle tone as possible, but the pelvic floor will never be as taught as before pregnancy. Awareness and exercise of the pelvic floor before pregnancy is very beneficial in terms of minimising any damage during pregnancy and childbirth.
As we get older, our muscle tone in general will tend to reduce. A sedentary lifestyle or reduced participation in exercise contributes to this loss of muscle tone. With menopause, when estrogen levels fall, this reduction accelerates because low estrogen leads to loss of muscle tone and strength, including that of the pelvic floor muscles. A fall in estrogen results in a loss of collagen of up to 30% in the first 5 years of menopause. On top of that, with aging, our metabolism slows and lower estrogen levels make women prone to gaining weight and to store any extra fat around their abdomen.
This additional abdominal fat adds to the pressure on their pelvic floor. As a result, women who previously had things under control, may find that leakage now becomes a problem.
Another factor is the atrophy of the vaginal and urethral epithelium, which comes with a decline in estrogen. From a continence point
PHARMACYNEWSIRELAND.COM 26 Menopause
of view, if the urethral lining is less puffy, it is less able to hold in any urine which may try to escape. The cells of the urethra and the trigone of the bladder may become more sensitive, leading to increased irritability, urinary frequency and discomfort. Finally, the loss of glycogen-rich vaginal secretions leads to a decline in the Lactibacillus population in the vagina. This causes an increase in vaginal pH, a disruption of the previously healthy and stable vaginal microbiome, and an increased propensity to population with pathogenic bacteria such as E.Coli. With menopause, may women find themselves prone to recurrent urinary tract infections (UTI). Anyone with even slight SUI or UUI, may find it worsened in the presence of a UTI.
Treatment
The first thing to bear in mind is that most women are reluctant to bring up incontinence with their doctor, either because they think it is a normal part of aging and something to be put up with, or because they are embarrassed. Without direct questioning, the problem may not be revealed. Secondly, an accurate diagnosis is important. It can be very clear which type of incontinence someone has, but quite commonly, women have a combination of both SUI and UUI, known as Mixed Urinary Incontinence. It can sometimes be difficult to determine how much each contributes to the problem and, therefore, which is the best treatment option. In this case, a urodynamic study may be helpful.
SUI
Pelvic floor exercises (PFE) can achieve significant improvement in up to 75% of women with SUI and may well avoid the need for any further treatments. However, 1 in 2 women have difficulty identifying and contracting their pelvic floor as the contractions are internal and the effect unseen.
Assessment by a specialist pelvic floor physiotherapist can be invaluable, both to identify an individual’s particular muscle weakness and ensure the most appropriate exercises are done, using the correct technique. Some improvement may be seen within weeks, but maximal benefit may not be seen for up to 6 months. As with all muscle exercise, continued exercise is necessary to maintain the effect, of course. Physiotherapists may use tools such as biofeedback and electrostimulation for women who have difficulty in contracting their pelvic floor.
The avoidance of constipation is important, as any loading of the rectum will increase pressure on the bladder and straining to open the bowel further increases pressure on the pelvic floor. Stool softening agents and plenty of fluid intake is helpful. The use of a footstool to raise the knees above hip height relaxes the abdomen and pelvic floor and helps with defaecation. Weight loss is essential for those with increased abdominal fat. Many exercises such as those which are part of a pilates or yoga programme, can help to restore muscle tone. Vaginal pessaries may be useful for support of the bladder neck.
When conservative measures have failed, surgical options may be required. These procedures are generally only provided by urogynaecologists or urologists with a special interest in this field and referral to a general urologist may delay accessing the appropriate treatment. Procedures include the injection of bulking agents around the bladder neck, mid-urethral slings to elevate and support the bladder neck or colposuspension. It is important to rule out UUI as surgery for SUI may unmask or make UUI worse, so a urodynamic study may be required pre-operatively.
UUI
Vaginal estrogen reverses the atrophy of the vaginal and urethral epithelium, making them thicker,

less sensitive and reducing the incidence of UTI. It may also reduce the sensitivity of the bladder itself, thus reducing overactivity of the muscle. There is minimal systemic absorption of vaginal estrogen, with an initial peak, then almost no further absorption. Hence, it is perfectly safe for the vast majority of women to use and, indeed, is now to become available over the counter in the UK.
Pelvic floor physiotherapy is useful for both rehabilitation of the pelvic floor and retraining of the bladder to hold larger amounts of urine. As with SUI, weight loss and avoidance of constipation is beneficial.
Bladder irritants such as fizzy drinks, caffeine and alcohol are best avoided. Although most people with OAB tend to instinctively restrict their fluid intake, this can be counter productive as concentrated urine is an irritant to the bladder and increases the risk of UTI.
Good diabetic control is vital as glucosuria is a bladder irritant and increases the risk of UTI. Over time, high blood glucose may also lead to neuropathy and a neurogenic bladder.
The addition of an anticholinergic or beta-3 adrenergic agonist may be required. If conservative treatment has failed, other options again require referral to a urogynaecologist or a urologist with a special interest. Treatments include intravesical Botulinum toxin (Botox) injections, percutaneous tibial nerve stimulation or sacral nerve stimulator implants.
It is important to bear in mind that rapid onset of symptoms of bladder irritation, particularly in older women or those with a history of smoking and also the presence of haematuria, may signify a bladder neoplasm and such symptoms should be carefully monitored. Lack of response to conservative management, should trigger referral to a urologist for possible cystoscopy.
Although SUI and UUI are the main types of urinary incontinence, one can also have overflow incontinence. This can be caused by obstruction which prevents the bladder emptying adequately, such as happens in men with enlarged prostates. Symptoms may begin with issues similar to OAB but develop to include weak urinary flow or a dribble, small amounts of urine passed, a feeling of incomplete emptying, having to get up multiple times at night to pass urine, incontinence and recurrent UTIs. In women, a significant cystocele may result in kinking of the urethra, thereby causing an obstruction. Many women find that they can initiate a second void by shifting position on the toilet and it is important that they do try to empty completely, if possible. Another cause of overflow incontinence is a neurogenic bladder, as can happen with certain neurological conditions such as Parkinson’s or MS. Neuropathy can also be the result of poorly controlled diabetes. Treatment of overflow incontinence depends on the cause and may entail surgery to elevate the bladder neck, learning how to self-catheterise or using an indwelling urinary catheter.
Finally, functional incontinence occurs when an issue such as poor mobility means you can’t make it to the toilet in time or arthritis means you cannot undo your clothes quickly enough. This increases with age and is not a direct result of menopause. In this situation, products such as pads and absorbent underwear may be the best option. For some, an indwelling urinary catheter can be useful.
With all aspects of GSM, it is important for healthcare professionals to bring the subject up. Awareness among the general public is increasing, but women still tend to be reluctant to do it themselves. Once out in the open, treatment can be simple, rapid and life-changing.
Types of pelvic organ prolapse
PHARMACYNEWSIRELAND.COM 27
in Work
Menopause in the Workplace
Menopause for far too long has been a taboo and stigmatised topic both in society and in the workplace. For a condition that affects 50% of the population and may impact the other 50%, menopause has been almost secret and has been spoken about in hushed tones This is finally changing. Women no longer have to suffer in silence. We are experiencing a menopause revolution! And it is long overdue!
Written by Loretta Dignam, CEO & Founder, The Menopause Hub
39% took time off work due to menopause and 22% took 3 or more days
2. Employers need and want to optimise employee performance
3. In this tight talent market retention is paramount and talent attraction vital.

1. Fatigue 40%
2. Hot flushes 35%
3. Focus & concentration 34%
4. Anxiety & worry 32%
86% said they did not tell their employer / manager the real reason for time taking time off The data, where it exists, in other countries is similarly shocking.
4. Employers are at legal risk on the grounds of gender, age and disability discrimination. There are increasing numbers of employment tribunals taking place in the UK & Ireland with decisions being made in favour of the menopausal woman.


5. Insomnia 30%
By 2030 there will be 1.1bn menopausal women on the planet, or 12.5% of the global population. That equates to 1 in every 8 people on the planet will be a menopausal woman! And every year 47 million menopausal women will enter that cohort.
Menopause is an important societal issue, an important workplace issue, an important healthcare issue and an important economic issue. The average age of perimenopause is 45 and menopause is 51. Therefore, menopause is clearly not an older woman’s condition! In the workplace in Ireland there are 350,000 menopausal women, in the UK 4.4m, in Australia 2m and in the US 27m.
The vast majority of these women will go through the menopause transition during their working lives. And, given the myriad of menopause symptoms (there are 40+) women at work can be impacted by psychological/ emotional/mental, physical and genitourinary symptoms at work.
Research* conducted by The Menopause Hub in Ireland 2021 among 1150 menopausal women highlighted the following startling statistics:
80% of women said that their menopause symptoms impacted their performance at work (50% said a little, 30% said a lot)
12% of women gave up work due to menopause
There is clearly a strong business case for supporting women experiencing menopause at work. These women are often at the peak of their skills, experience, and careers. Negative impact on self-confidence means that women are reluctant to seek promotion or forgo promotional opportunities. This is counter to all of the gender equality and diversity and inclusion work that has enabled women to progress at work in recent years.
From an organisation’s perspective there are 4 clear reasons why employers need to take note and engage in the menopause conversation.
1. Legally employers have a duty of care to their employees through the Health & Safety at Work Act
Why hasn’t it been addressed before?
There is still a real taboo when it comes to the menopause at work. While some menopausal women receive help and understanding from colleagues and managers, many are too embarrassed to discuss the issue or think their manager would be embarrassed. 70% of menopausal women in our survey said they would not be comfortable discussing menopause with their line managers. And 60% said they would be uncomfortable discussing menopause with colleagues.
The top 5 symptoms that women said that affected them most at work were as follows:
Often a few small practical adjustments at work could make a world of difference to those experiencing the oftenuncomfortable symptoms of menopause. However, having conversations with those affected, being empathetic and supportive, non-judgemental or prescriptive can uncover what the most effective reasonable accommodations will be. Unfortunately, few managers or HR professional are educated about menopause or confident in having an informed discussion. This needs to change and quickly.
Menopause is seen by many as a taboo topic in the workplace. What can employers do to help overcome this?
In our survey we asked menopausal women what they wanted to see employers do to better support them. The response was overwhelming, 92% wanted awareness training for colleagues, 96% wanted education & training
40% considered leaving work or cutting back their hours
PHARMACYNEWSIRELAND.COM 28 Menopause
Anxiety Overwhelmed Weeping/Crying Grumpy Bursts of Anger Panic Attacks Flat Mood Loss of Confidence Hot Flushes Insomnia No Energy / Fatigue Dry, Papery, Itchy or Crawling Skin Hair Loss PMS like Bloating Sore/Swollen Breasts Increased Chin Hair Pimples/Acne Deepening Voice Migraine / Headaches Weight Gain S Heart Palpitations tiffness/Aches and Pains Loss of Libido Painful Sex Vaginal Dryness Vaginal Discharge M e n t a l / E m o t i o n a l S y m p t o m s P h y s i c a l S y m p t o m s none mild moderate severe Bladder Issues (UTIs / Incontinence) Receding Gums Dry Eyes Brain Fog Burning Tongue/Mouth Digestive Problems Tingling Extremities Brittle Nails Irregular Periods Muscle tension Allergies G e n i t o u r i n a r y S y m p t o m s Memory Loss Mood Swings Depression none mild moderate severe Symptom Checker none mild moderate severe












AGE ABSOLU SKIN IS REDENSIFIED, PLUMPER, AND LOOKS YOUNGER. NEW AGE LIFT FOR ALL SKIN TYPES ANTI-AGEING INNOVATION ACTS ON SIGNS OF AGEING AND DAILY AGGRESSIONS WHICH DAMAGE THE SKIN. FOR 30yrs +FOR 50yrs + & MENOPAUSAL SKIN GRAHAM ANTHONY DISTRIBUTION BECOME A STOCKIST: +35318222711 EMAIL: sales@gadistribution.ie
Menopause in Work
•
Performance
a little
• 30% said performance was affected a lot
EMPLOYEE SURVEY
1152
Missing work due to symptoms
• 39% said they missed work because of their symptoms
• 22% said that they missed 3 or more days
• 86% were not comfortable telling their line manager the real reason
What employees are asking for from their employers
• 92% Would like awareness training and education for staff
Giving up work
• 40% Said that they considered giving up their work
• 12% gave up work
About Ibec
Ibec is Ireland’s
About The Menopause Hub
• 96% said they would like menopause awareness training for managers & HR
• 93% said they would like to see a menopause in the workplace policy introduced at work.
EMPLOYER SURVEY
272 HR managers, Sep-Oct 2 by IBEC
79% of respondents to this survey stated that menopause is relevant to their organisation.
25% of respondents said that it was ‘very likely’ that they would introduce menopause specific supports in the next 1 – 2 years.
Of the supports provided to menopausal women in the workplace, the availability of supports through the company EAP service was the most common (70%), with flexibilities such as ability to schedule annual leave around appointments (47%), and option to avail of flexible working if needed (39%) also being popular. (46%) stated that their employees can avail of paid sick leave where needed.
companies,
for managers and 93% wanted their employer to introduce a menopause policy.
It is clear that the only way to overcome the taboo and help to normalise the conversation around menopause is to start talking and educating people about the topic. Menopause is not unlike where mental health in the workplace was 10-15 years ago. And many of the programmes and structures that organisations have put in place can be adapted for menopause.
The Menopause Hub encourages employers to adopt best practice in supporting their colleagues. We offer awareness education for staff, managers, HR professionals and Menopause Champions (not unlike mental health First Aiders) who will signpost and offer support groups and buddies for those experiencing menopause at work. Through this training we want everyone to engage, as menopause is not just a woman’s issue. Having male allies is critical for progress as is senior leadership sponsorship. Many of our clients have also developed an organisational framework which encompasses training for line managers on
sensitive conversations and reasonable adjustments. Many have also developed menopause workplace policies.
Interestingly the research The Menopause Hub conducted with IBEC amongst employers highlighted that
70% offered menopause support through their EAP services
most popular supports
future
47% offered flexibility for staff to schedule annual leave around appointments
accredited e-learning programme, in multi-media format, interactive with expert interviews, case studies from menopausal women, animation and quizzes. Each module is accompanied by downloadable handbooks, toolkits and guides for four key audiences: colleagues, managers. HR professionals and Menopause Champions.
46% said employees could avail of paid sick leave when needed
39% said they offered flexible working arrangements if needed
This may be the case, but clearly employees and staff are unaware that this applies to menopause and/ or are not comfortable mentioning menopause in this context. Either way, employers need to work on opening up the conversation to include menopause.
Tell us more about the support material
We have just launched our CPD
All modules include practical guidance aimed at helping to normalise the conversation around menopause at work. Also included are developing frameworks of support and education, helping to create diverse and inclusive cultures. We are already working with a number of organisations who are pioneering menopause at work. Lild Ireland and NI have partnered with us and have launched their menopause policy. They are rolling out training and offer paid for consultations for their staff at our clinic. We are working with ESB, Accenture, Comreg, DCU, UCD, Irish Aviation Authority, INMO (Irish Nurses and Midwives Organisation), Queally Group, Avvio, HSE, Bar Council of Ireland, VHI, Axa, Cappagh Orthopaedic Hospital and many, many, more. We hope that more organisations
KEY FINDINGS:
will use our practical guidance to affect change and tailor to their individual organisation’s contexts and cultures.
If you could tell employers just one thing about menopause at work, what would it be?
Don’t assume that all women will experience menopause in the same way. Some might experience very few symptoms, while others might experience severe physical and psychological symptoms that can last for 10 years or more. The average length of menopause is 7.4. years and there are over 40 symptoms. One of the most important things you can do as an employer is to train line managers to be confident to have sensitive conversations that consider individual needs and offer adjustments that help with the specific symptoms that are being experienced.
*Research conducted online by The Menopause Hub in Sept / Oct 2021 among 1150 menopausal women

** IBEC Employer Survey, conducted among 272 HR Managers in Sept / Oct 2021

The
Maeve
PHARMACYNEWSIRELAND.COM 30
Menopause Hub and Ibec present the first “Menopause in the Workplace” survey results. ‘This is the first data in Ireland to provide insight into how women feel as they transition through menopause in the workplace, and demonstrates how employers are and should be supporting their staff.’ Loretta Dignam, Founder & CEO of The Menopause Hub’
McElwee, Director of Employer Relations at IBEC says’ ‘It is really positive to see that 79% of respondents to this survey stated that menopause is relevant to their organisation. of which 350,000 are in paid employment (CSO 2016) There are 570,000 women in the menopausal cohort in Ireland (CSO 2016)
women, ROI, Sept / October 21 by The Menopause Hub
and ability to do the job
52% said performance was affected
Of these
the
planned for the
were • Education and training for management/HR (74%) • Communications/events to increase employee awareness (70%) • A specific company policy on menopause (62%) • Menopause champions/ambassadors or similar (48%) • Supports available through the EAP service (46%)
largest lobby and business representative group. With over 250 employees, Ibec engages with key stakeholders in Ireland and internationally.
The Menopause Hub is Ireland’s first and only dedicated multidisciplinary menopause clinic, offering a range of services to optimise the health and wellbeing of menopausal women. For further information please contact: Loretta Dignam, The Menopause Hub T: 086 8146603 E: loretta.dignam@themenopausehub
Floradix
Chapped lips, brittle hair, constant fatigue and palpitations are not on a prospective mum’s wish list. They are, however, some of the tell-tale signs of iron deficiency, which is common amongst pregnant women. Iron is needed to make haemoglobin, the chemical that transports oxygen in the blood. A range of stressful symptoms can indicate a deficiency, but severe cases can lead to anemia, total exhaustion and a weakened immune system. Throughout pregnancy, eating for two also means that your body requires twice the amount of iron to stay healthy.
Keeping levels healthy
A healthy, balanced diet with ironrich foods will provide most of the iron you need during pregnancy. This should include lean meats; pulses such as peas, beans and lentils; fruit such as prunes, apricots and raisins; and dark green leafy vegetables such as spinach.
However, it can be difficult to absorb enough iron from a balanced diet alone for you and your growing baby, particularly if you have a deficiency as you need to eat a lot of iron-rich foods to correct it. This is where Floradix can really help. This high quality liquid supplement contains organic iron gluconate, and its easy absorption into the body is enhanced by vitamins C and B complex, herbal extracts and fruit juice concentrates. This special blend of ingredients mean that it’s easy to digest and the unpleasant side effects of many iron preparations, such as stomach cramps and constipation, are avoided. So it’s no wonder Floradix is recommended by numerous midwives and health care professionals. What’s more, it’s completely free of chemical preservatives, colourings or flavourings, and is also available in a gluten-free form called Floravital.

Helping Absorption
Vitamin C, animo acids, fructose and glucose all help your body absorb more iron from foods and supplements. Other elements of our diet will decrease absorption, such as calcium, milk proteins, black tea, coffee, fibre, vitamin E and phosphates (found in soft drinks). So to maximise the amount of iron you are getting, take an iron supplement before eating.
Warning signs of iron deficiency
• pale skin under eyes and nails
• brittle hair
• cracked skin around mouth
• breathlessness when exercising
• heart palpitations
• rapid pulse
• difficulty concentrating
• cold hands and feet
• increased frequency of infection
Addressing the Fertility Service Gap
Local Pharmacy Group
Launches new Fertility Service
According to the HSE, one in six couple will experience fertility issues here in Ireland. That means approximately eight in 10 couples will successfully conceive within a year. This leaves those struggling to conceive often searching for assistance. Leading fertility consultants within Ireland estimate that between 8,000 and 10,000 people seek medical treatment or assisted conception per year; with almost half of them leaving Ireland specifically for IVF treatment. This includes heterosexual couples and also single women looking to get pregnant. Ireland is the only state in the European Union to not offer publicly funded IVF as well as being ranked 40th out 43 nations for access to fertility treatment.
methods of business research and so applied the same method for developing this service. This involved taking a qualitative approach which included identifying a problem statement. Through this, we could then identify a solution.
which could confidently explain the protocol and educate patients on supplementary support would go a long way in making their journey seamless and stress free. This also includes offering lifestyle support such as smoking cessation and supplement recommendation.
Unfortunately couples and in particular women often feel stigmatised for not having children by a certain age. Further, the lack of conversation and accessibility can further enflame fertility as a taboo subject as well.
The good news is that Pharmacy is facing a dynamic shift from being a simple one-stop shop for health, beauty and dispensing to being recognised as wellness clinics for all things health. Pharmacists are empowered more so with being experts in medication and clinical matters. Therefore, with pharmacy being an integral part of any community, the doors to discuss sensitive issues should now be accessible at all times.
With the advance of technology, this elevates healthcare accessibility and makes it easy to connect patients with healthcare professionals. Digital technology can also serve as a powerful tool for increasing organisational efficiency and so improve health outcomes within communities.
Our pharmacy group is on a mission to cultivate community wellness by innovating with services. This includes tackling community problems such as taboo topics - one of which is fertility.
The challenges we face as pharmacists however is finding the time so that we are able to provide a high level of quality services.
We are all over burdened with administrative tasks which often consumes any free time we have.
As a superintendent pharmacist, part of my role is to look at processes within our organisation and make them efficient and lean, all whilst complying with legislation. For that reason, I have been developing a new software which essentially free’s our pharmacists up with time. In addition, we innovate our services within the software, which allows for service optimisation and hence, a greater quality of care.
With that being said, How did we develop the new fertility service? And how does that tie in with digital technology.
We used a unique approach to identifying a need for the new fertility service. We acknowledged there was a gap in fertility knowledge by health care professionals and so we sought to explore this further.
Having completed my MBA back in 2019, I learnt about different

We held in depth discussions with cohorts of patients undergoing fertility treatment. Topics discussed included: Their fertility journey, choice of pharmacy, failings within pharmacy, pharmacy service solution and additional pharmacy support. These discussions were held in a non-structured way which allowed for patients to truly express themselves. From a research perspective, this also allowed for us to identify common themes in an unbiased way. We further held discussions with various other stakeholders such as fertility clinics, GPs, pharmacists and nurses. Once we had gathered all data, we then began to identify reoccurring phrases, words, sentences and topics. This then allowed for us to establish key themes.
Amongst the key themes identified, the most common one was: Pharmacist knowledge.
Patients wanted to go to pharmacies whose staff were confident in empowering and supporting them along their journey. For patients undergoing fertility treatment, the process can often be overwhelming and stressful. Often fertility protocols can be lengthy, with medications needing to be administered at certain stages of the cycle. Injections can further complicate things, with patients being unaware of the additional equipment required for administration. Patients also lacked confidence in being able to apply the correct technique for administering injections.
As pharmacy would be the final step before commencing the fertility protocol, patients felt they would benefit in receiving added reassurance from their pharmacies. The best way of doing so is through knowledge. Having a pharmacy
Lifestyle support further extended to those starting their fertility journey with patients also wanting their pharmacists to provide advice on weight loss and diet.
Having taken into consideration all the key themes, we developed a service based around empowerment. We upskilled all of our pharmacists in being able to describe the entire fertility journey and everything in between. From counselling patients to providing accurate and up to date fertility advice. We integrated that into our in-house developed software, which allows for us to carry out a review in a coordinated, professional and cohesive manner. Once completed, our software exports the discussion points into a document which can then be printed and provided to the patient. This can then be given to the patient for record keeping purposes and so that they can provide this to other interdisciplinary teams.
The result… Fantastic!
What is the future of our new fertility service? We really believe in the power of technology for advancing healthcare. We’re currently exploring the option of integrating artificial intelligence as part of our software. AI systems operate through absorbing large amounts of data, analysing for data patterns, and then using these to predict future outcomes. Therefore, over a period of a time, our software will adopt machine learning which can then be used to better enhance our services for patients to come.
We’re looking to roll out our technology to as many pharmacies as possible. We’re currently running through our beta phase and will be soon to launch officially.
“Having a pharmacy which could confidently explain the protocol and educate patients on supplementary support would go a long way in making their journey seamless and stress free. This also includes offering lifestyle support such as smoking cessation and supplement recommendation”
Written by Adam Esa, Superintendent Pharmacist, Local Pharmacy Group
PHARMACYNEWSIRELAND.COM 32 Fertility
Healthy Skin From Within*
95% of women would recommend Cleanmarine® For Women for healthy skin†

Clinical Prize for Dr Porter at Irish Melanoma Forum
Dr Emma Porter, dermatology registrar at University Hospital Limerick (UHL), was awarded the poster Clinical Research Prize at the 10th Annual Scientific Meeting of the Irish Melanoma Forum held in University College Dublin, in May 2022.
Dr Sinead Field, Ms Evelyn Power and Dr Emma Porter, Dermatology Dept. University Hospital Limerick
The poster presented preliminary findings from a collaborative research initiative examining the impact of a visual sun protection campaign on sun-related attitudes and behaviours of healthcare workers.
During summer 2021, the Irish Skin Foundation, Ms Evelyn Power, Clinical Nurse Specialist in skin cancer and Dr Sinead Field, Consultant Dermatologist, UHL, in association with the Health Service Executive’s National Cancer Control Programme, University of Limerick Hospital Group (ULHG), and the Healthy Ireland SunSmart campaign, launched a series of five video animations, to encourage people to build SunSmart behaviours into their everyday routine, especially from April – September when the intensity of sunburn producing ultraviolet radiation is greatest.
The videos played on visual display units throughout ULHG hospitals and hospital social media channels throughout the summer, as part of a research initiative to evaluate the effectiveness of these assets in raising awareness of sun protective behaviours amongst staff.

cancer, and 65% said it influenced them to discuss sun protection with others.
Available in Pharmacies & Health Stores
Dr Sinead Field says of the launch of the video animation series, “Traditional health promotion campaigns have had to be reimagined in light of COVID-19 public health restrictions. Our aim in developing these animations was to bring the SunSmart messaging to life by creating a novel skin cancer awareness campaign in response to these changed circumstances and explore how digital health promotion initiatives can support all of us in adopting healthy sun protective behaviours.”
Preliminary findings
Skin cancer is the most common cancer in Ireland with around 13,000 cases diagnosed annually. This figure represents a steep increase compared to just 10 years ago and is projected to more than double again by 2045. However, the majority of skin cancers could be prevented; ultraviolet radiation exposure (emitted naturally in sunlight or from artificial sources e.g. sunbeds) is the main risk factor.
Cancer prevention offers the most cost effective, long term approach to cancer control and remains a cornerstone of the National Cancer Strategy 20172026. Consequently, public health efforts including Ireland’s first National Skin Cancer Prevention Plan 2019-2022, are directed towards encouraging those at risk to adopt sun-safe practices.
*Vitamin B2 contributes to the maintenance of normal skin. Vitamin B1 contributes to normal energy yielding metabolism. † Source: Cleanmarine Skincare Survey, December 2020, with 120 Cleanmarine For Women customers
The study was open to all staff of ULHG. Preliminary findings revealed that 64% of participants reported the campaign improved how they protect their skin. 79% reported raised awareness of skin
In terms of promoting the SunSmart message, particularly given the increased skin cancer incidence projections for Ireland to 2045, these study findings lend support for the potential to leverage digital health promotion initiatives into the future.
PHARMACYNEWSIRELAND.COM 33
News
Disease Management of COPD

COPD Support Ireland & The Chronic Disease Management Programme
Healthy Ireland policy which seeks to improve health through preventive strategies and supporting people to live healthier lives, which in turn reduces demand for hospital care.2,4,7
Written by Deirdre Garvin, Respiratory CNS, Mayo University Hospital/Board Member, COPD Support Ireland

The health and life expectancy of the Irish population has improved, and with this comes a greater need for healthcare in chronic disease in Ireland.
The Slaintecare report (2017) of the Oireachtas Committee on the Future of Healthcare set out the vision for health service reform to improve the health of the nation.7 The aim is to provide a universal healthcare system and to move care delivery from the acute health care setting, which is unsustainable, to care closer to home which includes promoting health and wellbeing and meets the patients’ needs in a fair and equitable way.4,5,7
The integrated model of care for the prevention and management of chronic disease (IMPCD) is the essence of the national framework for integrated prevention and management of chronic disease in Ireland 2020-2025 and details how end to end care will be available in Ireland.4,5
Integrated care is the process of providing this Slaintecare vision for patients and integrated care has been shown to improve care by meeting population health need.4,5 Research shows patients with chronic diseases, including respiratory, when managed and cared for in primary care with good governance and clinical leadership have improved care and outcomes than if provided in acute services.7
Integrated care for chronic disease is care provided at the lowest level of complexity, close to home with services to support and empower individuals to optimise their health and minimise risk factors for developing or progression of their chronic disease.
Health promotion and education by preventing illness in the first place and preventing progression is in line with
The framework is the mechanism of delivering care, which is person centred, holistic to the person and preventative.19 The various models of care and national clinical care programmes including the COPD model of care, have all adapted an integrated approach and are developing care around the framework which is line with policy.3,4,5,7
the hospital setting which will support access to diagnostic, specialists’ services and specialists’ opinions. Health care will primarily be delivered in the community with supports available to allow this by providing specialist care when needed within the community in chronic disease including COPD and this care will then be delivered closer to home.4,5,7
The treatment, burden and management of chronic illnesses account for a large share of health resources, including 80% of all general practitioner (GP) visits, 40% of acute admissions, 75% of hospital bed days and accounts for poorer quality of life.3,6,7,8,9
The Integrated Model of Care for the Prevention and Management of Chronic Disease
Slaintecare and the integrated framework detail the health reform including the development of 6 Regional Health Areas (RHA,). These are then further broken down into 96 Community Healthcare Networks (CHNs).4,5
The ‘Integrated Model of Care for the Prevention and Management of Chronic Disease’ is at the heart of the ‘National Framework for the Integrated Prevention and Management of Chronic Disease’ and demonstrates how “end-to-end” care can be provided within the Irish health services.
The Model of Care (Figure2) describes the five levels of service, and examples of each service, that need to be provided for a population in order to deliver integrated end-to-end care for chronic disease. These are the five levels of service that local areas need to strengthen and provide in an equitable manner to their population.
CHN’s are geographical based units which serves a population of approximately 50,000 and three CHN’s will be served by a specialist ambulatory care hub for chronic disease serving a population of approximately 150,000. An ambulatory care hub will be a clinical site away from
In the area of respiratory the true prevalence of respiratory conditions such as COPD in Ireland is unknown. It is estimated that 500,000 have COPD, however only approx. 200000 are diagnosed and many are unaware of their condition.1,8,9 COPD is a major health burden and causes morbidity and mortality in Ireland with over 1500 deaths and 15,000 patients admitted to hospital annually.3,8,9 Ireland has the highest rate of hospital admission with COPD of any country in the OECD.8,11
Figure 2. Model of care for the Integrated Prevention and Management of Chronic Disease
Implementation GuideDisease
34
Levels ofCare Examples ofService 0.Livingwellwith chronicdisease DiabetesPrevention MakingEveryContactCount Telehealth/RemoteMonitoring Self-managementSupport AssessDeterioratingPatient ScheduledReview VirtualCarePlanClinics TelephoneTriage1.GeneralPractice Cardiac/PulmonaryRehab SpecialistTeams(CNS,Physio, StructuredDietitians,Podiatrists)DiagnosticsPatientEducation2.Community AmbulatorySpecialistCare 3.Acute AmbulatorySpecialistCare AlternativeOPD Pathways Respiratory Outreach 4. Specialist Hospital Care ED/ AMAU, ComplexCare, InpatientCareHospital Care Specialist Ambulatory Hub Care in the Community


















There was considerable variability in COPD care with variation in length of hospital stay, access to diagnosis, access to Pulmonary Rehabilitation and COPD Outreach.3
The national framework for Integrated prevention and management of Chronic diseases which includes COPD is a whole system approach to integration that incorporated population health, wellbeing, preventative, acute, non-acute and community-based services.4,5
The framework is person centred, holistic proactive and preventative in endeavours to make care accessible and equitable for all. It will improve care for our COPD patients by providing access to diagnostic, specialist expertise, pulmonary rehabilitation, and COPD outreach across the country.3,4,5,10
The national framework for the integrated prevention and management of Chronic Disease in Ireland along with the accompanying 10 step guide document details how care will be delivered and details the 5 levels of care as seen in below diagrams.4,5
The MOC for COPD takes a holistic, person centred and life course approach to the provision of services.3,10 It reflects the principles of integrated care which in essence is to provide patients with the right care at the right time by the right team in the right place and to reduce inequalities and describes what services will be provided at each level of care.3
It is anticipated that patients through their journey will move through the levels of care, however primarily care will be provided in the community and a greater emphasis now is on primary prevention, health promotion and population health.3,10
Through early identification of risk factors through professionals using, Making every Contact Count (MECC) this will allow early detection and diagnosis, therefore appropriate management and in turn prevent or delay the onset of COPD.3,5,10
This will improve care for all patients across the levels of care as appropriate, allowing for specialist inpatient, specialist ambulatory care, specialist support to General Practice and chronic disease prevention and management in primary care, all supported by patient self-management with the aims of saving lives of people with COPD and in turn the reduction of hospitalisations and morbidity of COPD patients.3,4,5,10
The model of care details the 4 levels of service and level 0 care is included in the resource document on COPD integrated Service model.
In general terms level 0 care is about keeping communities healthy and to keep those with chronic disease living well.3,4,10 The integrated framework describes how services are being developed to support and empower individuals living in our communities to prevent and manage their chronic diseases.4,5 Services include education, support to manage their diseases and each RHA and CHN is tasked with
mapping all services available including HSE funded, voluntary and community.
This allows development of services that are lacking but also making best use of services that are in fact available. However, it is of paramount importance that all health care professionals (HCP’s) are aware of available services and can sign post patients and their families to these services The making every contact count (MECC) as a health promotion ensures health promotion is a focus of each HCP and patient encounter and should be a focus for us all.
This includes each patient encounter albeit in the GP’s surgery during an acute illness, during a structured chronic disease review, or a pharmacy visit. This requires staff to be aware of what’s available to support patients in their communities.
Level 0 care available and appropriate for COPD patients
• Living Well with chronic disease programme
• Self-Management programme
• Stress management Programme
• COPD Support Ireland Website
• Social Prescribing,
• Flourish programme
• Sing strong programme
• Making every Contact count
• Tele-Health, remote monitoring
• COPD support Groups
• COPD support Ireland nurses phone line
• Smoking Cessation services
COPD Support Ireland (COPDSI) was established in 2013 as Irelands National COPD Support and Advocacy organisation and has established over 35 communitybased COPD exercise and peer support groups across the country.
It supports patients and their families living with COPD throughout Ireland through various channels. The work of COPD Ireland supplements the work of the integrated framework for chronic disease and the model of care and can support patients and their families across all the 5 levels of care.
Patients can access information and services throughout their disease trajectory from diagnosis onwards. COPDSI work complements the work of the integrated care programme and model of care for chronic disease as much of its work focuses on providing services that supports those to live well and education on self-management.
Equally it is a great source of knowledge for those who are undiagnosed and may want to learn a bit more about the disease and then seek help. Those who seek advice and are supported through various channels often are better equipped to manage their condition and COPDSI can support this.
It is important that those of us working in healthcare are aware of supports available
to our patients and can sign post patients and their families to the resources available. COPDSI has recently sent correspondence to Respiratory physicians of the valuable services it provides to help support their patients and this in turn can support the health service.
Services provided by COPDSI include:
COPD Adviceline 1800 83 21 46 is a HSE funded freephone service, delivered with the Asthma Society of Ireland; for people who want to discuss or learn more about their COPD and its Self-Management from a specialist respiratory nurse or physiotherapist. It is a valuable resource for patients and their families to learn more about COPD.
COPD & Me Exercise Programme
COPDSI developed a community-based COPD exercise programme delivered by fitness professionals. Classes take place weekly, either virtually, or in person at a local support group location. Participation in these classes has been shown to increase exercise capacity & gait speed and to reduce anxiety. You can refer patients to the COPD & Me exercise programme through the HCP referral link on www.copd.ie
COPD & Me Book
Is a comprehensive patient information and Self-Management education Book. Designed in collaboration with the Respiratory National Clinical Programme and supported by the Chronic Disease Management Programme, this book is now available to HSE COPD services nationally during 2022. To order copies, email info@copd.ie.
Sing Strong – Singing for better Lung Health
In COPD Self-Management, airway clearance and breathing control are taught to help control dyspnoea. Sing Strong is a novel, fun and popular way to learn and implement these techniques through singing. Created by vocal coach Ms. Ciara Meade and lecturer of cardiovascular and respiratory physiotherapy, Dr. Roisin Cahalan, SingStrong is delivered virtually or in person, over 10-weeks through COPDSI.
In conclusion the rolling out of the national framework for integrated prevention and management of Chronic Disease and Model of care for COPD is a welcome development for those suffering and or at risk of developing COPD. Care and services which meets population health needs will be accessible and available and not a post code lottery service of services available in certain locations. COPDSI is a valuable resource to both HCP’s and patients and its work needs to be communicated to those who may benefit from its services.
References on request
36 | PHARMACYNEWSIRELAND.COM



























































Visit us at macushield.com SUITABLE FOR VEGANS * Vitamin B2 helps maintain normal vision. JB-000871. Mar21 NEW A NEW WAY TO TAKE MACUSHIELD • ONE-A-DAY • EASY TO TAKE • CHEWABLE TABLET • ™ NUTRIENT BLEND • BILBERRY FLAVOUR • VEGAN FRIENDLY NOW AVAILABLE MACUSHIELD CHEWABLE
Management of Macular Oedema
Written by Dr Louise O’Toole, Consultant Medical Ophthalmologist, Bon Secours Hospital Glasnevin, DublinMater Private Network, Dublin
Macular oedema is the end common pathway for many prevalent ophthalmic conditions. It is one of the leading causes of central visual loss.
The condition is characterized by the accumulation of fluid in the outer plexiform layer and the inner nuclear layer of the retina; it occurs secondary to the breakdown of the blood-retinal barrier. This causes an abnormal passage of proteins into retinal tissues resulting in osmotic water retention and consequent swelling.
When macular oedema occurs, patients may be aware of a fall in their central vision, they may also experience distortion and reduced colour vision.
Macular oedema can be diagnosed at the slit-lamp using high magnification; however Ocular Coherence Tomography (OCT) imaging facilitates both detection and quantification of the oedema. In recent times, the availability of OCT imaging has increased, allowing patients to access this investigation through both optometric as well as ophthalmic practitioners. Depending on the aetiology of the macular oedema, it has a different nomenclature.
A common cause of macular oedema is retinal vein occlusion (RVO). This may be secondary to a central, branch or hemiretinal vein occlusion. The prevalence of RVO increases with age. The most common association with RVO is undiagnosed hypertension. It is to be recommended that when patients are diagnosed with macular oedema secondary to RVO that they undergo 24-hour blood pressure monitoring. Open-angle glaucoma, diabetes mellitus, and hyperlipidemia have all been implicated as other primary risk factors for RVO. A hypercoagulable state also predisposes to the development of RVO. Conditions such as polycythemia, multiple myeloma, cryoglobulinemia, and Waldenstrom macroglobulinemia place patients at a higher risk of developing RVO. In a young patient who presents with a RVO a full systemic workup is mandated to detect such potential underlying causes.
The primary treatment of macular oedema secondary to RVO is to address the underlying cause. Macular oedema secondary to advanced hypertension can resolve following adequate hypertensive control. Otherwise, patients are treated with a course of intravitreal therapy. The agents used may either be steroids or more commonly an anti-Vascular endothelial growth factor (VEGF) agent. Such agents include ranibizumab (Lucentis), aflibercept (Eylea), and bevacizumab (Avastin). Intravitreal steroids have a longer duration of action but are associated with an increased risk of cataract formation and can cause raised intraocular pressure. When the macular oedema resolves, the patient’s visual acuity generally improves unless there is associated non perfusion of the macula. Patients may require ongoing treatment for several months to years to preserve their vision.
Patients with either Type 1 or Type 2 Diabetes Mellitus can develop diabetic macular oedema (DME). If the macular oedema does not involve the fovea, it can be treated by laser

photocoagulation. However, laser scars can enlarge with time and encroach on the fovea leading to visual loss, so intravitreal therapy with either anti-VEGF agents or steroids is preferred by some for treating cases of DME with and without foveal involvement. Improving glycaemic control, regularising hypertension and treating hyperlipidaemia are known interventions to treat diabetic maculopathy. If DME has been present for some time, secondary structural changes can occur in the retina. These changes are termed disorganisation of retinal inner layers (DRIL). When these changes are seen, the visual prognosis for the patient is guarded.
Neovascular age related macular degeneration (nAMD) is associated with swelling of the central macula. Choroidal neovascularisation leads to both subretinal and intraretinal leakage of fluid as well as haemorrhage. The presence of chronic intraretinal fluid is associated with a poorer visual outcome. Treatment of nAMD is with sustained intravitreal anti-VEGF therapy to dry up the intraretinal fluid and prevent the development of fibrosis. Patients are monitored with serial OCT imaging and their intravitreal treatment frequency adjusted accordingly.
Cataract surgery is a recognised cause of macular oedema. When this occurs, it is termed pseudophakic cystoid macular oedema (CMO). The cataract surgery may have been either a complicated or an uncomplicated procedure. The patient may initially have good vision post cataract surgery which then falls in the following month, or else the vision may fail to improve vision at all post operatively. Many patients have subclinical CMO that is only detectable on OCT imaging and is self-limiting in nature. CMO is believed to be secondary to intraocular inflammation. The majority of patients with CMO will undergo resolution of their macular oedema following a course of combined topical NSAIDs and steroids. Sometimes intensive hourly treatment is required ab initio. A small subset of patients will require either a periocular or an intravitreal injection of steroid to settle this inflammatory condition.
If cataract surgery is planned for their fellow eye, prophylactic anti-inflammatories are prescribed by many surgeons.
Macular oedema may also occur as a complication of other intraocular procedures. These procedures include panretinal photocoagulation and YAG laser. Cryotherapy is another procedure which is known to cause macular oedema.
Uveitis, no matter where it is located within the eye -anterior, intermediate, or posterior can result in macular oedema and consequently reduced vision. The treatment of macular oedema secondary to uveitis is to treat the inflammatory cause with immunosuppressive agents. Chronic inflammatory changes at the macula can result in the development of choroidal neovascularisation.
Another cause of macular oedema is drug related. Fingolimid associated macular oedema (FAME) is well described. Fingolimid is an oral disease-modifying therapy indicated for the treatment of multiple sclerosis. The risk of FAME is dose dependent. A baseline OCT is required before commencing Fingolimid and the patients should undergo regular monitoring while on treatment. Latanoprost is a topical therapy commonly used to treat primary open angle glaucoma and CMO is a recognised side effect. CMO has been reported following nicotinic acid and niacin supplementation with doses of greater than 1.5g/day.
Patients with retinitis pigmentosa have a reduced peripheral visual field. They may also develop CMO which will then further reduce their remaining central visual function. CMO in retinitis pigmentosa responds well to treatment with oral acetazolamide, topical dorzolamide or brinzolamide drops.
Macular oedema has a disparate range of causes and accordingly treatments. It can cause mild to profound visual loss, if left untreated as in the case of nAMD the visual loss can be irreversible. OCT imaging facilitates the early detection of macular oedema and with early intervention, patients’ sight can be preserved.
OCT image of left macular oedema
38 | PHARMACYNEWSIRELAND.COM
TILDA publishes research on Brain Blood Oxygen
The group has previously studied the blood pressure response to standing, but in this study - published in the journal Experimental Gerontology - cerebral oxygenation was examined.
The study used data from 2,764 community-dwelling participants. The size of the study enabled researchers to account for a range of confounding factors.
Key Findings:
• Women experienced a smaller drop in cerebral oxygenation compared to men.
• Women took longer to return to their normal level.
• Older age groups had a larger initial drop in cerebral oxygenation and impaired stabilisation.
• Those taking blood pressure lowering medications took longer to recover.
• Blood pressure levels also only partly explained some of the differences that we found.
Louise Newman is the lead author of the study and Research Assistant
in Medical Gerontology at Trinity.
She said, “We know that age affects how quickly blood pressure recovers when a person stands up, but we didn’t know if it was the same for cerebral oxygenation.
"We used novel equipment, nearinfrared spectroscopy, to measure the change in blood oxygen in the brain during a standing task. We found that women experienced a smaller drop in cerebral oxygenation compared to men, but women took longer to return to their normal level. We also found that those taking antihypertensive medications took longer to recover.
“However, there were no differences in the cerebral oxygenation response in those who told us they felt dizzy, light-headed or unsteady when standing up. Blood pressure levels also only partly explained some of the differences that we found.”
She explained, “The study highlights the need for standing cerebral blood measures to be assessed in older patients, regardless of symptoms.”
Professor Rose Anne Kenny, TILDA’s Principal Investigator, added, “Brain cells survive and function according to how much oxygen they receive and how quickly the cells and circulation can clear toxins from the brain cells. We stand up 30-50 times per day and each time our bodies must react quickly to ensure that the flow of blood and therefore oxygen is kept constant. For the first time in such a large adult study we have measured such brain blood flow when TILDA participants stood up and demonstrated that the ability to react quickly and maintain flow is impaired year on year over 50 years.
“Furthermore, men and women react differently. Muscle strengthening exercises and other interventions can change in a beneficial way these responses, so early recognition of problems, using this novel technology, should trigger treatments and lifestyle behaviour changes. As a
Exciting Developments at Uniphar
result of this research, we have started to use the new technology in clinical settings to improve patient management.”
The study, Age and sex related differences in orthostatic cerebral oxygenation: Findings from 2764 older adults in the Irish Longitudinal Study on Ageing, is published in the journal Experimental Gerontology and is freely available to all online.
Uniphar are very excited to welcome Martin Slattery to the Uniphar Supply Chain & Retail division. Martin joins Uniphar as Wholesale Commercial Director having spent the last 15 years in senior leadership roles across both the retail and FMCG wholesale sectors so brings with him a wealth of experience in driving good business and the importance of customer partnerships.
He spent the last 8 years at the head of Musgrave MarketPlace overseeing a period of significant sales growth having led a complete brand transformation and customer offer across their nationwide sites.
Prior to this Martin was part of Lidl Ireland’s early success across a period of 7 years working in various key roles and divisions finishing as Sales Director.

He also spent 2 years working in marketing in the Financial sector. He holds a Masters in Marketing from NUI Galway.
Uniphar have also confirmed the appointment of Louise Martin as the new Retail Director for Uniphar Supply Chain & Retail.


Louise joined Uniphar 2 years ago as Consumer Business Unit Manager. Prior to Uniphar, Louise held several senior commercial positions in McKesson UK, Lloyds Pharmacy Ireland and Tan Organic. During her time as Head of Category Management for McKesson UK, Louise built a strong team, grew retail sales in what was a challenging retail environment at the same time as managing an aggressive store refit programme.
Over the last two years during Louise’s management the Consumer business has doubled its turnover and profit. Louise has brought an energy and passion for pharmacy retail, customer focus, brilliant basics and cross functional collaboration to the Consumer business. She has
fostered a positive work culture within Consumer, focused on building a commercially focused and highly motivated team.
Louise leaves the Consumer team in an excellent place for success as they are embarking on a new phase of growth and opportunity.
Professor Rose Anne Kenny, TILDA
New research from The Irish Longitudinal Study on Ageing (TILDA) examined how blood oxygen levels in the brain (“cerebral oxygenation”) are affected when a person stands up. Blood flow to the brain provides oxygen and nutrients for normal function. A reduced supply has been associated with adverse events such as falls, depression and cognitive decline.
Louise Martin, Retail Director, Uniphar Supply Chain & Retail
Martin Slattery, Wholesale Commercial Director, Uniphar Supply Chain & Retail
PHARMACYNEWSIRELAND.COM 39News
Fighting Blindness to Host Leading International Eye Researchers

Retina, the annual gathering of international eye experts organised by Fighting Blindness, returns to Dublin this November for the first time since 2019.
‘Back in the Room’
For Dr Ellen Moran, Research Manager with Fighting Blindness, Retina 2022 provides an opportunity for the international eye research community to come together, share ideas and develop partnerships:
challenges before us and how these can best be overcome. Retina is unique in providing earlystage researchers and established experts a joint platform to share their insights and develop personal connections and collaborations.”
Unlocking Retinal Cells
The scientific stream of the conference takes place from November 3-4 and brings together leading clinicians and scientists at the vanguard of ophthalmology research.
Now in its 14th year, Retina aims to enable participants share the advances they are making with their peers, to offer a springboard for ideas, and to provide an opportunity for collaboration in the collective human effort to find treatments and cures for vision impairment and blindness.
With latest figures showing that there are approximately 272,000 people in Ireland living with blindness or vision impairment, this event will be of interest to all those working in eye healthcare, from researchers working at the bench, to clinicians working at the bedside.
Registration for the conference, which is taking place in the Radisson Blu Royal Hotel, Golden Lane, Dublin 2, will open on October 1 at www.retina.ie
Day 1 – StarT Symposium
The first day of the conference, Thursday November 3, features a StarT symposium, organised by StarT, a European Training Network, established to advance diagnosis, understanding and treatment of Stargardt disease.
Among the speakers will be Professor Mariya Moosajee, Francis Crick Institute London, whose work ranges from developing new therapies for inherited retinal diseases (IRDs) to developing patient understanding with the creation of the Gene Vision online resource on rare genetic eye disorders.
Day 2 – Scientific Conference
The second day of the conference, Friday November 4, features a wide range of speakers who will offer perspectives on topics such as the use of adaptive optics in Age-Related Macular Degeneration (AMD), developments in gene editing for inherited retinal diseases, and the use of artificial intelligence in offering precision diagnosis for eye disease.
Speakers include:
• Professor Catherine Bowes Rickman, Duke University, USA, one of the world’s leading experts on AMD who will speak on the pathobiology of AMD and her work to find a cure
• Professor Austin John Roorda, University of California, Berkeley, USA, inventor of the Adaptive Optics (AO) Scanning Laser Ophthalmoscope, who will address the use of AO in studying AMD and evaluating treatments to slow its progression
• Dr Alessandra Recchia, Associate Professor in Molecular Biology, University of Modena and Reggio Emilia, Italy, who will update on gene editing in inherited retinal diseases and her application of the CRISPR/Cas gene therapy tool in retinitis pigmentosa


• Professor Rando Allikmets, Columbia University, New York, who discovered the first gene associated with AMD, among other discoveries, will speak on precision ophthalmology and using state-of-the-art genetic testing for personalised treatment of Stargardt/ABCA4 disease
“We are delighted to welcome some of the world’s foremost thinkers in ophthalmology research to Dublin for what promises to be the most inspiring Retina conference yet. It was 2019 when the eye research community last had an opportunity to gather in-person for Retina and the intervening period has been particularly challenging for the IRD community, with several potential therapies not making it through clinical trials. Many in the community feel some of these therapies have indeed shown promise, but that success is perhaps only being judged in improving, as opposed to maintaining vision, and that keeping current levels of sight should also be deemed a win. The unfortunate reality is that while mutations have now been identified in over 300 genes for IRDs, therapies continue to elude us. We owe it to the approximately 5,000 people in Ireland with an IRD to put our shoulders to the wheel in driving forward innovation in this area.
“That’s why Retina 2022 provides such a valuable opportunity to allow people to get ‘back in the room’, to meet face-to-face, and to showcase the positive scientific research advances being made, as well as to address some of the
One of the conference speakers, Dr Abigail Fahim, Assistant Professor, Kellogg Eye Centre, Michigan, USA, adds:
“Retinal pigment epithelial cells, or RPE cells, form a supportive layer adjacent to the light-sensing cells of the retina. RPE cells are critical for the health of the retina and the health of the underlying blood vessels, called the choroid. In certain inherited retinal dystrophies, such as choroideremia, dysfunction of RPE cells can disrupt this support system and can lead to damage of the adjacent retina and choroidal vasculature, causing irreversible vision loss. My lab examines abnormalities of protein transport and release from RPE cells in choroideremia, and how these released proteins may be damaging neighboring tissues. We hope to establish a platform for testing new treatments in choroideremia and other diseases with RPE dysfunction. This is the next step to give these patients hope.”
Retina 2022 is supported by AbbVie, Novartis, Roche and Specsavers. For more information on the conference proceedings and to register, visit www.retina. ie, or follow on Twitter @fight_ blindness #RetinaDublin
Dr Ellen Moran, Research Manager, Fighting Blindness
Dr Abigail Fahim, Assistant Professor, Kellogg Eye Centre, Michigan, USA
PHARMACYNEWSIRELAND.COM 40
Ophthalmology News
Continuing Professional Development
CPD
60 Second Summary
The International Association for the Study of Pain (IASP) defines pain as an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.
The reason we experience pain is to notify the body of a stimulus in order to avoid further tissue damage. It is usually proportional to the severity of the injury, and resolves when the tissue heals fully.
In pain perception, three main stages generally occur, firstly pain sensitivity, then pain transmission from the periphery to the DH, and finally, transmission of these signals to the higher brain, e.g cortex, through nerves in the central nervous system (CNS).
Pain is strongly associated with self-care management and acute pain is responsible for consumption of large quantities of over the counter (OTC) non-steroidal anti-inflammatory drugs (NSAIDS). Pharmacist-led management of pain, including the identification of the cause and knowledge of the treatments available, helps optimise outcomes in selfmedicating people.
Ibuprofen is the first line treatment recommendation for a range of aches and pains including lower back pain, period pain and toothaches. Although aspirin can also be used for many aches and pains, other NSAIDs like ibuprofen tend to be better tolerated, so are the preferred option.
There are no specific clinical guidelines that provide information on how to manage acute pain with OTC analgesics, but there are a few available that are still relevant such as the NICE management of acute postoperative pain, and several indication specific guidelines for e.g headache, back pain, dysmenorrhoea, and sprains and strains.
AUTHOR: Donna Cosgrove PhD MPSI

Donna graduated with a BSc in Pharmacy from the Royal College of Surgeons in Ireland. She then returned to university to complete a MSc in Neuropharmacology. This led to a PhD investigating the genetics of schizophrenia, followed by a postdoctoral research position in the same area. Currently Donna works as a pharmacist in Galway, and as a clinical writer.
1. REFLECT Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN If I have identified a

knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings.
Published by IPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author. SOLPA-EXTRA has no editorial oversight of the CPD programmes included in these modules.

Management of Acute Pain in Pharmacy
Introduction
Pain is a distressing sensation, as well as an emotional experience.1
The International Association for the Study of Pain (IASP) defines pain as an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage. IASP expand further with these points to put the definition in context:2
Pain is always a personal experience that is influenced to varying degrees by biological, psychological, and social factors.
to the severity of the injury, and resolves when the tissue heals fully. Acute pain lasts for less than 3 months and is most commonly caused by musculoskeletal conditions. Chronic pain persists beyond the tissue healing time, or beyond three months.3 Prolonged pain which lasts for longer than the expected period of healing can be caused by an inappropriate increase of afferent input into the dorsal horn (DH), leading to central sensitisation.1
Types and Causes of Pain
Pain and nociception are different phenomena: pain cannot be inferred solely from activity in sensory neurons.
Through their life experiences, individuals learn the concept of pain.
A person’s report of an experience of pain should be respected.
Although pain usually serves an adaptive role, it may have adverse effects on function and social and psychological well-being.
The experience of pain occurs through the activation of receptors in the primary afferent fibres: the unmyelinated C-fibre and myelinated Aδ fibre. These receptors are only activated in the presence of noxious stimulus and are normally quiet. Three types of neurons that exist in our body are sensory neurons (afferent neurons), interneurons (which relay the signals between afferent and efferent neurons) and motor neurons (efferent neurons). (See figure 1 on page 42)
Transduction occurs initially. The painful stimulus is converted to chemical tissue events, then chemical tissue and synaptic cleft events are converted into electrical events in the neurons, and finally electrical events in neurons are transduced as chemical events in the synapses.
Transmission then occurs, i.e. the propagation of electrical events along the neuronal pathways and across synapses.
Modulation then takes place at all levels of nociceptive pathways through the primary afferent neuron, DH and higher brain centres, up or downregulating the sensation.
There are multiple types of nerve fibres in the body that have different roles. Based on the velocity of a conducted impulse, axon’s diameter, and function of an axon, the sensory (afferent) neurons are classified into three main groups—Group A, B and C.
Verbal description is only one of several behaviours to express pain; inability to communicate does not negate the possibility that a human or a nonhuman animal experiences pain.
The reason we experience pain is to notify the body of a stimulus in order to avoid further tissue
In pain perception, three main stages generally occur, firstly pain sensitivity, then pain transmission from the periphery to the DH, and finally, transmission of these signals to the higher brain, e.g cortex, through nerves in the central nervous system (CNS). This pathway carrying the signal to the brain is the ascending pathway, and the nerves that connect the brain to e.g. muscles involved in reflex are
Aα nerve fibres are the thermal and mechanical nociceptors. They are also the smallest myelinated nerves, with a relatively fast conduction velocity.
Aδ fibres are responsive towards short-lasting and pricking pain.
Group B nerve fibres are mainly nociceptive in function with moderate conduction velocities, and include those of the autonomic nervous system (ANS) and general visceral
41CPD: Acute Pain CPD
2x FASTER Solpa-Extra 500mg/65mg Soluble Tablets. For the treatment of mild to moderate pain. Always read the leaflet. To verify contact: verify@perrigo.com IRE SOL1 2022 20* Based on absorption data. GETS TO WORK * THAN JUST PARACETAMOL FIND OUT MORE
Hyperalgesia is the natural occurrence of enhanced pain perception at the site of injury due to the lowered pain threshold to thermal/mechanical pain stimuli. PGs are the main culprits for receptor sensitisation. Some inflammatory mediators activate receptors outside the trauma site, covering a larger area than is actually injured.
Allodynia describes central sensitisation that leads to a pain response from a stimulus that normally does not provoke pain, such as a light touch. Both hyperalgesia and allodynia occur due to the increase of prostaglandin E2 (PGE2) in the inflamed tissue after activation of the COX pathway in the DH of the spinal cord.
tumour necrosis factor α (TNFα), strong proinflammatory molecules that promote hyperalgesia, are also present.
Prostaglandins are produced from the action of cyclooxygenase (COX) on arachidonic acid (AA). PGE2 (from COX 2, binds to prostaglandin E2 receptors 1-4) and PGI2 (from COX1, binds to prostaglandin receptor IP) are two major PGs that lead to afferent sensitisation.
Leukotriene B4 is produced within the leukocytes, and is responsible for recruiting neutrophils to the site of tissue damage, as well as promoting cytokine production.
Adenosine triphosphate (ATP) is an intracellular messenger released locally by damaged tissues and directly stimulates its receptors.
In pain perception, three main stages generally occur, firstly pain sensitivity, then pain transmission from the periphery to the DH, and finally, transmission of these signals to the higher brain, e.g cortex, through nerves in the central nervous system (CNS). This pathway carrying the signal to the brain is the ascending pathway, and the nerves that connect the brain to e.g. muscles involved in reflex are the descending pathway (1).
Group C nerve fibres are unmyelinated and have a relatively slow conduction velocity. They are polymodal, activated by thermal, mechanical and chemical stimuli. The activation of C-fibres gives rise to poorly localised sensations, such as burning sensation of the skin.
These are located in the viscera and are usually insensitive to mechanical stimuli, but can be sensitised by the chemical mediators produced during inflammatory reactions.
There are a range of endogenous compounds responsible for the generation of pain:1
Nerve Growth Factor is a neuropeptide released at the site of injury causing rapid onset of hyperalgesia after activation of the NGF receptor, widely expressed in primary afferent neurons. It also causes further mast cell degranulation.
● Transduction occurs initially. The painful stimulus is converted to chemical tissue events, then chemical tissue and synaptic cleft events are converted into electrical events in the neurons, and finally electrical events in neurons are transduced as chemical events in the synapses.
Motor (efferent) neurons carry the impulses of motor signals out from the spine to the peripheral effector organs, the skeletal muscle and smooth muscles.

● Transmission then occurs, i.e. the propagation of electrical events along the neuronal pathways and across synapses.
Once the nociceptive signal from the ascending pathway reaches the somatosensory cortex, the descending pain modulation pathway is triggered. Descending pain control pathways can be facilitatory as well as inhibitory: facilitatory pathways enhance pain perception whereas inhibitory pathways suppress pain perception.4
Pain can be grouped into three different classifications: nociceptive, neuropathic, and inflammatory:
Nociceptive: Aδ and C-fibres are mostly found in superficial organs, such as the skin, whereas deeper structures such as muscles and joints are mainly supplied with C-fibres. There is an additional nociceptor type called silent nociceptors.
Neuropathic: this type of pain generally serves no purpose. It is commonly described as nerve injury or impairment and is associated with allodynia (central pain sensitisation). Nerve neurochemistry can be damaged after compression, stretching, or hyperexcitability propagated from other peripheral nerves.
Inflammatory: This is a normal biological response to harmful stimuli that is required to start tissue repair. Neutrophils are usually the first cells to gather at the site of injury. Redness and swelling at the site of injury is due to the increased blood flow and increased vascular permeability, which can also induce pain. Chemical inflammatory mediators including 5-HT, kinins, histamine, nerve growth factors (NGF), adenosine triphosphate (ATP), prostaglandins (PGs), glutamate, leukotrienes and nitric oxide (NO) are produced from the necrotic tissues during inflammation, and interact to activate nociceptors within the inflamed area.
Tachykinins (substance P, neurokinins A and B) are neuropeptides produced in the periphery that bind to neurokinin type receptors, NK1, 2 and 3, to elicit excitation.
Calcitonin Gene-Related Peptide (CGRP) is a peptide in both the CNS and PNS. CGRP receptors (calcitonin receptor-like receptors) are found in the nucleus accumbens, meaning that CRGP mediated pain transmission is controlled centrally.
Bradykinin, produced locally at the site of inflamed tissue, binds to the bradykinin receptors (B1 or B2). It initiates production of other inflammatory mediators, as well as being responsible for nociceptor sensitisation to heat stimuli.
Glutamate is the most common excitatory neurotransmitter, and is released by the sensory afferents to modulate nociception.
The following mediators act to mitigate the sensation of pain:
GABA is the most widely distributed inhibitory neurotransmitter. It can inhibit the sensation of pain.
Opioid peptides (enkephalin and dynorphin) bind to mu, delta and kappa opioid receptors, widely distributed throughout the body. These inhibit the release of excitatory neurotransmitters, reducing pain sensation.
Cytokines are released following degradation of e.g. mast cells during inflammation. Platelet activating factor (PAF) causes 5-HT production, which leads to plasma extravasation and pain. Histamine is also produced after mast cell granulation, adding to inflammation. Cytokines like interleukin 1β (IL-1β) and
Cannabinoids (most notably tetrahydrocannabinol, THC) bind to CB1 (brain and spinal cord) and CB2 receptors (predominantly in the immune system). They result in a reduction of neuronal excitation and mast cell degranulation.
Pharmacy Role in Acute Pain Management
Pain is strongly associated with self-care management and acute pain is responsible for consumption of large quantities of over the counter (OTC) non-steroidal antiinflammatory drugs (NSAIDS).
Figure 1. Joints most often affected by OA4
to
Figure 1. Signal pathways for nociception summary (4).
42 CPD: Acute Pain
IPN: How
Support Patients with Acute Pain in Community Pharmacy Donna Cosgrove PhD MPSI 2
2x FASTER Solpa-Extra 500mg/65mg Soluble Tablets. For the treatment of mild to moderate pain. Always read the leaflet. To verify contact: verify@perrigo.com IRE SOL1 2022 20* Based on absorption data. GETS TO WORK * THAN JUST PARACETAMOL FIND OUT MORE
Pharmacist-led management of pain, including the identification of the cause and knowledge of the treatments available, helps optimise outcomes in selfmedicating people.5 It is important to initiate conversations with patients about what they have taken before and how in order to help improve efficacy and safety. The underlying cause of pain should be treated where possible, and the full therapeutic dose tried before switching to an alternative analgesic. For this reason, combination analgesics should not be used as the first line in some cases to allow independent titration of single constituent medicines and assessment of efficacy.
The aims of pain management should be discussed with each individual, but may include some or all of the following:3
Reducing the intensity of pain

Enhancing physical functioning
Improving psychological functioning
Promoting return to work or school and/or role within family and society
Improving health-related quality of life
Ibuprofen is the most frequently used OTC analgesic in Europe.5
A Cochrane review investigating the effects of analgesics/analgesic combinations (given as single doses postoperatively) concluded that there is evidence supporting the efficacy of these OTC drugs that are available without prescription, with ADRs generally not different from placebo.6
There are risks associated with OTC NSAID intake in certain groups such as pregnant women, older people, and people taking additional medications although data suggests overall that the risk of severe ADRs from OTC analgesics remains low. Improving safety relies on increasing consumer awareness of risks, which is done by pharmacists, pharmacy technicians and OTC staff on a daily basis.5
Over-the-Counter Analgesia and Evidence
A review of the comparative effectiveness of opioid, nonopioid pharmacologic, and non pharmacologic therapy in acute pain conditions was conducted. Opioid therapy was associated with decreased or similar effectiveness as an NSAID
for some acute pain conditions, but with increased risk of shortterm adverse events.7 Evidence on nonpharmacological therapies was limited, but heat therapy, spinal manipulation, massage, acupuncture, acupressure, a cervical collar, and exercise were effective for specific acute pain conditions. Authors of a separate Cochrane review on the efficacy of OTC analgesics in acute pain made the following observations.6
There was evidence to show that simple, inexpensive, readily available analgesics give good pain relief to many patients with acute pain, such as toothache, sprains and strains.
Of particular note was an absence of evidence to support efficacy of low-dose codeine preparations in acute pain.
pain intensity reduction. Diclofenac plasters (except fhr the brand Flector) also had a low NNT of 3.2.
The authors also question the standard advice supplied with ibuprofen and other NSAIDs to take them with food: the absorption of these drugs is faster on having an empty stomach which increases efficacy. Some ibuprofen product PILs have in fact been changed to reflect this advice
In a Cochrane review specifically looking at the efficacy of topical NSAIDs for musculoskeletal conditions, authors found that.8
The most effective OTC drugs used were ibuprofen/ paracetamol combinations in 400mg/1,000mg and 200mg/500mg doses; respectively, providing relief to 70% of people, and with a NNT of less than 2.
Topical NSAIDs provided good levels of pain relief in acute conditions such as sprains, strains and overuse injuries, probably similar to that provided by oral NSAIDs.
Ketoprofen gel had an NNT of 2.5 (but less well defined outcomes).
Ibuprofen gel had an NNT of 3.9 as measured by outcomes of marked improvement or complete remission.
Data was insufficient to make comparisons between individual topical NSAIDs or against the same oral NSAID.
Local skin reactions were generally mild and transient, and did not differ from placebo, and very few systemic adverse events.
Notably, etofenamate topical preparations were not included in this review.
Fast acting ibuprofen formulations were effective in over 50% of patients, with a NNT of 2 to 3.
Formulations of topical diclofenac, ibuprofen, and ketoprofen in particular demonstrated significantly higher rates of clinical success (more participants with at least 50% pain relief) than matching topical placebo.
Paracetamol alone helped about 40% of patients and had a NNT of between 3 and 5, which was dose dependent.
For diclofenac, the Emulgel formulation had the lowest NNT of 1.8 for at least 50%
In terms of specific nonpharmacological approaches, review authors7 found that heat therapy was probably associated with moderate decrease in pain compared to usual care or placebo, particularly for lower back pain. Further evidence for the use of non-pharmacological measures in this review were not robust enough to make recommendations, however.
43
2x FASTER Solpa-Extra 500mg/65mg Soluble Tablets. For the treatment of mild to moderate pain. Always read the leaflet. To verify contact: verify@perrigo.com IRE SOL1 2022 20* Based on absorption data. GETS TO WORK * THAN JUST PARACETAMOL FIND OUT MORE
Pain
Non-Steroidal Anti-inflammatories
Ibuprofen is the first line treatment recommendation for a range of aches and pains including lower back pain, period pain and toothaches. Although aspirin can also be used for many aches and pains, other NSAIDs like ibuprofen tend to be better tolerated, so are the preferred option.3
Non-steroidal anti-inflammatory drugs work through mediation of prostaglandin and thromboxane A2 production through reversible inhibition of the enzyme cyclooxygenase (COX). Prostaglandins mediate many physiological functions including inflammatory and nociceptive processes; also maintaining the gastric mucosal barrier, regulating renal blood flow and endothelial tone.6 These medicines should not be taken in people with active gastrointestinal bleeding/ulcers, previous hypersensitivity to NSAIDs, severe heart failure, or severe liver or kidney impairment.3
Paracetamol
This is a great first line choice for mild to moderate pain. It has no known GI, renal or cardiac adverse effects at the usual OTC and prescribed doses; however, the patient should be reminded of the maximum daily dose over 24 hours to reduce the risk of accidentally exceeding this. Paracetamol appears to inhibit COX 1 and COX 2, although it does not inhibit COX in peripheral tissues. It is for this reason that paracetamol has no peripheral anti-inflammatory effects like traditional NSAIDs.9
Codeine
Codeine and paracetamol combination products should only be offered for e.g. managing acute lower back pain if an NSAID is not suitable or has been ineffective.3 Opioids are not suitable to recommend for acute treatment of tension type headaches or migraines. Tolerance and dependence can occur with use of weak opioids, so caution should be used. The codeine and paracetamol OTC products are not suitable in acute ulcerative colitis, or conditions that may include abdominal distension or inhibition of peristalsis as a symptom. Peripheral receptor binding can cause nausea, vomiting and constipation.6
Caffeine
Caffeine does not have any pain
relieving effect itself, but rather is added as an adjuvant to ibuprofen, aspirin and/or paracetamol products to enhance their analgesic effects. It is a competitive antagonist of adenosine A1 and A2 receptors, so it is possibly the disruption of normal adenosine signalling responsible for any enhanced analgesia.10
Pain Management Guidelines
There are no specific clinical guidelines that provide information on how to manage acute pain with OTC analgesics, but there are a few available that are still relevant such as the NICE management of acute postoperative pain, and several indication specific guidelines for e.g headache, back pain, dysmenorrhoea, and sprains and strains.3 These guidelines should be considered along with the ever changing evidence base, particularly important if there is a few years since the guidelines were updated.
The WHO analgesic ladder, published in 1986, provided guidance on how to provide adequate pain relief in cancer. It has gone through several modifications since its initial appearance, and is now used for the treatment of pain in additional types of conditions like degenerative disorders, musculoskeletal diseases, neuropathic pain, and other types of chronic pain.11 The original version was unidirectional, starting with NSAIDs or paracetamol as step 1, and heading up to weak (step 2) and strong (step 3) opioids, with or without adjuvants, depending on the patient’s level of pain. It has been suggested that step 2, which recommends the use of weak opioids, be eliminated, as there is little evidence that these offer much for pain control. Instead, reduced doses of strong opioids may be more useful. However, opioids aside, one main limitation of the original pain ladder was lack of inclusion of non-pharmacological approaches into the pain treatment path. Subsequently, a fourth step has been added to the pain ladder. This integrates non-pharmacological evidence based interventions like epidural anaesthesia, intrathecal administration of analgesia, neurosurgical procedures, neuromodulation strategies, nerve blocks, and ablative procedures (the removal or destruction of a body part or tissue or its function),
among others. There is more of a focus on quality of life with the updated WHO pain ladder, with a bidirectionality that offers de-escalation if pain improves as well as stepwise escalation for worsening pain. Some of the main elements are:
Oral dosing of drugs whenever possible
Around-the-clock administration for pain control rather than on-demand
announces Revised Definition of Pain. Available https://www. iasp-pain.org/publications/iaspnews/iasp-announces-reviseddefinition-of-pain/
3. Youssef, S. (2019). Clinical guidelines and evidence base for acute pain management. Pharm J, 303(7929), 44-48.
4. (Physiopedia. (n.d.) Pain Facilitation and Inhibition. Available https://www.physiopedia.com/Pain_Facilitation_ and_Inhibition)
Analgesics must be prescribed according to pain intensity as evaluated by a scale of pain severity. For this purpose, a clinical examination must combine with an adequate assessment of the pain.
Individualised therapy (including dosing) addresses the concerns of the patient. This method presupposes that there is no standard dosage in the treatment of pain, maybe the biggest challenge in pain management, as the dose must be continuously adapted to the patient, balancing analgesic effects with potential side effects.
5. Perrot, S., Cittée, J., Louis, P., Quentin, B., Robert, C., Milon, J. Y., ... & Baumelou, A. (2019). Self-medication in pain management: The state of the art of pharmacists’ role for optimal Over-The-Counter analgesic use. European Journal of Pain, 23(10), 1747-1762.
6. Moore, R. A., Wiffen, P. J., Derry, S., Maguire, T., Roy, Y. M., & Tyrrell, L. (2015). Non-prescription (OTC) oral analgesics for acute pain, an overview of Cochrane reviews. Cochrane Database of Systematic Reviews, (11).
Proper adherence to pain medications, as alteration in the dosing can lead to a recurrence of pain.
With evidence that pharmacistled management of pain helps to optimise outcomes in selfmedicating people, pharmacy teams have a very important role in the acute management of pain. Using up to date research evidence and guidelines can help pharmacy teams with the provision of the most effective treatment strategies. Advice on appropriate OTC analgesia tailored to each patient, considering age, medical conditions and other medications can be offered, as well as advice about topical vs. oral administration. Appropriate referral to a GP for stronger medication can be made if necessary.
References
1. Yam, M. F., Loh, Y. C., Tan, C. S., Khadijah Adam, S., Abdul Manan, N., & Basir, R. (2018). General pathways of pain sensation and the major neurotransmitters involved in pain regulation. International journal of molecular sciences, 19(8), 2164.
2. International Association for the Study of Pain. (2021). IASP
7. Chou, R., Wagner, J., Ahmed, A. Y., Blazina, I., Brodt, E., Buckley, D. I., ... & Skelly, A. C. (2021). Treatments for acute pain: a systematic review. Available https://europepmc.org/article/ nbk/nbk566506
8. Derry S., Moore R.A., Gaskell H., McIntyre M., Wiffen P.J. Topical NSAIDs for acute musculoskeletal pain in adults. Cochrane Database of Systematic Reviews 2015, Issue 6. Art. No.: CD007402. DOI: 10.1002/14651858.CD007402. pub3.
9. Wishart DS, Knox C, Guo AC, Shrivastava S, Hassanali M, Stothard P, Chang Z, Woolsey J. Drugbank: a comprehensive resource for in silico drug discovery and exploration. Available: https://www. drugbank.ca/drugs/DB00316.
10. Derry, C. J., Derry, S., & Moore, R. A. (2014). Caffeine as an analgesic adjuvant for acute pain in adults. Cochrane Database of Systematic Reviews, (12). Available https:// www.ncbi.nlm.nih.gov/pmc/ articles/PMC6485702/
11. Anekar, A. A., & Cascella, M. (2021). WHO analgesic ladder. In StatPearls [Internet]. StatPearls Publishing.
44 CPD: Acute
2x FASTER Solpa-Extra 500mg/65mg Soluble Tablets. For the treatment of mild to moderate pain. Always read the leaflet. To verify contact: verify@perrigo.com IRE SOL1 2022 20* Based on absorption data. GETS TO WORK * THAN JUST PARACETAMOL FIND OUT MORE
Supported by an unrestricted educational grant from
FREE COPD WEBINAR FOR PHARMACISTS
Pharmacy supporting COPD patients this winter
Live | 8pm – 9pm, Tuesday 22nd November 2022

DR DEREK FORDE
Chairman of Primary Care Respiratory Society Ireland, Former Clinical Lead, Respiratory Disease Ireland, Primary Care

DR BREDA CUSHEN MB BCh BAO PhD MRCPI, Consultant Respiratory Physician, Beaumont Hospital

Following significant interest generated by our Diabetes Technology webinar on 12th October, Uniphar is excited to announce a second educational webinar, covering COPD management. The webinar, open to pharmacists and pharmacy technicians, will provide current, evidence-based, best practice guidelines for supporting your COPD patients.

The webinar will feature Dr Derek Forde and Dr Breda Cushen, two of Ireland’s leading experts on the management of COPD. We will discuss COPD pathophysiology and risk factors, GOLD COPD Strategy 2022 updates and the key role that pharmacists can play in optimising both clinical and quality of life outcomes for COPD patients.
Scan QR code to register your attendance

webinars
New Developments a Winning Formula for McCabes Pharmacy
McCabes Pharmacy Group – Winners of the Uniphar Category Development Award 2022

Through analysis of external market trends, alongside internal data analysis, McCabes Pharmacy were inspired to further invest in the vitamins category across the business and enhance consumer experience. Operating our innovative strategy allows McCabes to continually thrive and stay ahead of the market curve as well as competitors.
The Irish Pharmacy
McCabes Pharmacy is 100% Irish owned and run, established by Roy and Margaret McCabe in 1981. McCabes customers are at the heart of the company. With 28 pharmacies across the country, McCabes employ over 350 employees who are constantly striving to provide the best service and care for customers.

Developing the Category
The global vitamin supplements market was expected to expand at a CAGR of 6.2% from 2021 to 2028, with the western European region forecasted to grow annually by 3.66% (CAGR 2022-2025) (Statista).
Teresa Mullen, Group Buying Manager with McCabes Pharmacy
Blanchardstown Store Manager Lynsey with Sales Assistant Brenda
explains, “Through analysis of external market trends, alongside internal data analysis, McCabes were inspired to invest in the vitamins category, through successful implementation of this initiative, McCabes have enhanced consumer experience as well as increasing category sales.
“Though the pandemic expedited the development of the vitamins category online, this was previously identified as a key area for development, due to gaps in this category being serviced by
the Irish market. Since the launch – development of the vitamins category has been key to driving traffic and conversion rates of the website.
“Further investment was made to improve the in-store customer experience at the beginning of 2022; a roadmap was put in place to improve the navigation and flow of the category through the rollout of the below, creating superior customer experience in store, resulting in increase in store category sales.”
“Through analysis of external market trends, alongside internal data analysis, McCabes were inspired to invest in the vitamins category, through successful implementation of this initiative, McCabes have enhanced consumer experience as well as increasing category sales”
PHARMACYNEWSIRELAND.COM 46 Awards
Awards2022
Staff training was going to be key for the Group in enhancing their category development. Teresa adds, “We noticed that our staff members were not completely comfortable with regards to their vitamin and supplements knowledge, and therefore implemented new training strategies for all staff members.
With investment in online infrastructure, McCabes were able to react quickly and ensure smooth, safe and speedy supply of a wide range of vitamins online in uncertain times. Choosing to develop the vitamins category online has been key to driving traffic to the website, ensuring a wide range of products was available, and offering a bestin-class service has allowed McCabes to become market leaders particularly in terms of range width in relation to other Irish online retailers.
Teresa notes that the measurable benefits of their initiative have been six-fold:
• This initiative ensures McCabes are operating at best practice levels and has led to improvements in operational efficiency.


• This initiative has allowed McCabes to create a more streamlined collaborative approach encouraging open innovation between management and staff overall improving company culture, with more visibility in the business
• This has resulted in increased sales
• This has resulted in strong visual presence in stores, improving customer experience

• This initiative has contributed to the McCabes sustainability policy, – reducing paper consumption, and wastage, investing in online technology reducing the need to print in stores
• This project has greatly assisted staff, making the section easier to merchandise and quicker timeframe


Informing Customer Purchases
“To ensure the customer has all information needed to make an informed purchase each staff member is trained on each product in the vast offer of vitamins with over 700 options on offer in top tier stores, ensuring there is something to appeal to all
McCabes customers. Through specific training programmes, every endeavor has been made to ensure there is a best-in-class service level in terms of expert advice. With such a high level of advice on offer from McCabes staff the customer journey has been improved which can be seen in our reviews.
“The accessibility through the digitalization of this category has cut out the need for numerous communication emails, and reduced time on this task. Instant online access to the category plan at any place or time has made a task that was previously very time consuming, much more efficient and enjoyable for staff, allowing staff more time to spend with customers and other areas or improvement in store.
“Not only have the results been seen financially, but the visual impact created in stores through the application of this initiative has significantly improved the
consumer experience, while also contributing to operational efficiencies at McCabes.”
Teresa told us after winning the award, “Everyone at McCabes Pharmacy works tremendously hard, either in the dispensary, on the shop floor or behind the scene. We have made extra efforts to ensure we are experts in our field, offering our customers the best in choice and the best in advice. This recognition from the Irish Pharmacy Awards and Uniphar cements our position as leaders within category development and we are extremely proud of everyone that has helped to make this happen.”
Louise Martin, Consumer Business Unit Manager with Uniphar commented, “Uniphar are delighted to welcome all of our finalists to this year’s Irish Pharmacy Awards. Congratulations to all of them who have put in so much work and especially to McCabes Pharmacy.

“I would like to say on behalf of the Uniphar team, Thank You to Irish pharmacies and your teams’ for your dedication and commitment to the local community and for always putting the patient first.
Uniphar is proud to be Irish owned, set up by a small group of Irish community pharmacists more than 50 years ago to ensure a reliable supply of medicines for our patients. We remain steadfast in our commitment to putting the patient first in everything we do. This award demonstrates Irish Pharmacy at it’s best.”




 Louise Martin, Consumer Business Unit Manager, Uniphar with Sarah Fitzgerald and Teresa Mullen, McCabes Pharmacy Group
McCabes Pharmacy Group’s winning Category Development
Louise Martin, Consumer Business Unit Manager, Uniphar with Sarah Fitzgerald and Teresa Mullen, McCabes Pharmacy Group
McCabes Pharmacy Group’s winning Category Development
PHARMACYNEWSIRELAND.COM 47
A Rising Star in Pharmacy

The Irish Pharmacy
His Superintendent Pharmacist comments, “Damien has a great ability to share and explain his medical knowledge with staff, meaning all our colleagues can actively improve the health and wellbeing of our customers and provide correct and safe information.”
During the COVID19 pandemic Damien was responsible for the coordination and administration of almost all vaccines. This was an immensely stressful time but due to Damien’s high level of communication and organisation the pharmacy staff were able to adapt to the increased pressure. He
made sure all staff were informed of any new updates regarding vaccine rollout so they could answer queries appropriately. He went above and beyond to make sure all his patients had access to these vaccines if they wished and contacted those of the highest priority.
He also offered other seasonal vaccines such as the flu vaccines.
He has often visited the homes of those who are housebound in order to administer these.
Damien played an active role in organising clinics for those people/children with additional needs, if they wanted to, they could come in during a quieter
time to make the process as comfortable as possible. He offered a range of other health services such as blood pressure monitoring, emergency hormonal contraception, BMI and antigen testing.
Damien’s ability to work well under pressure and make crucial decisions while maintaining a calm demeanour was pivotal in saving a patient’s life. A man presented to the pharmacy with wheeziness and shortness of breath, he then collapsed the ground. Damien immediately came to assistance, he assessed the scene and instructed one staff member to get
the defibrillator and another to ring an ambulance. Damien performed CPR until the ambulance arrived. Thankfully the patient survivedDamien was a true hero!
“Damien is a much-loved member of the Baldoyle community,” his Superintendent continues. “He has a very close relationship with all our customers and most will come to him first for advice and support before going to other healthcare professionals. Damien greets every patient with a smile and seizes every opportunity to positively impact their health.
“Engaging with the local community is very important to
“Damien has had a very positive impact on our pharmacy and community since working in Baldoyle. His love for the profession and management has given our pharmacy the tools to excel in the services we provide”
Jason Bradshaw, Partner, JPA Brenson Lawlor with Damien O’Brien, Pharmacist, Adrian Dunne Pharmacy Baldoyle
Damien has been the driving force in the promotion of public health services in his community. His commitment to his customers and wealth of knowledge has allowed Adrian Dunne Pharmacy in Baldoyle to flourish and become the main point of contact for health advice in Baldoyle.
Damien O’Brien, Adrian Dunne Pharmacy Baldoyle winner of the JPA Brenson Lawlor Young Community Pharmacist of the Year Award 2022
PHARMACYNEWSIRELAND.COM 48 Awards
Awards2022
Damien and he is very passionate about educating people on important health issues. He has organised talks with groups in the community which cover important topics such as Men’s Health.
“Damien has been actively involved in charity events held by our pharmacy. These events have been a great way to bring the community together and put a smile on the faces of those who need it most. For example; He was involved in organising a sponsored walk for a 13-year-old patient of ours who was diagnosed cancer undergoing treatment in England.”
Damien also has a great working relationship with the local doctors, they trust and respect him and turn to him for any queries they might have.
Damien completed his preregistration year in Baldoyle 2017/18, he continued to work for Adrian Dunne for 2 and a half years before coming back to Baldoyle as a Support and then Supervising Pharmacist in 2021. His journey really reflects how hard-working and dedicated Damien is to the profession and how he has excelled as a pharmacist in such a short period of time. Damien took over as Supervising Pharmacist during the most stressful time in pharmacy history. The pandemic led to increased prescriptions, vaccine rollouts, staff shortages and legislation changes. Damien’s calm and reassuring approach guided us through these unprecedented times.

“Damien has had a very positive impact on our pharmacy and community since working in Baldoyle. His love for the profession and management has given our pharmacy the tools to excel in the services we provide. He keeps all staff members up to date with the latest pharmacy news and changes in legislation which was very important during the COVID pandemic so our staff could give the appropriate information to customers.
“He gives all OTC staff and pharmacy technicians over the counter and is always on hand for advice, ensuring our patients receive the safest and most effective care.
“He is actively involved in the development and confidence of our technicians especially during their Level 3 diploma. He loves sharing his own knowledge of the field to better the understanding of others and is always happy to help and answer any questions a member of staff or customer has.
“Since Damien has become the manager of Baldoyle it
has become a very enjoyable place to work. His high levels of organisation, communication and leadership has created a great working environment where we all have the potential to increase our skills, learn from one another and excel in our careers. This has led to an increased job fulfilment throughout the team.
“His dedication to putting the patient first, paired with his strong leadership skills has created a team who can confidently provide reliable and safe information and services to the public.”
Damien truly cares for the health and well being of others and does his best to positively impact their lives. They continue, “He plays a pivotal part in the Baldoyle community who we all turn to for advice and support. He works tirelessly even beyond the working day to come up with ways he can improve the services we provide and grow the business.
“His medical knowledge is second to none and his dedication to continual professional development means he can only keep growing as a great pharmacist. His communication, organisation and leadership skills make him the great Supervising Pharmacist he is. His friendly and caring personality make him very approachable for staff and customers, he definitely is a reason our patients always come back. Damien’s ability to work under pressure, making crucial decisions and meet deadlines all while maintaining a calm demeanour and ‘can-do’ attitude helps to create a great work environment. His commitment to educating others and furthering
their understanding of medicines not only increases our job satisfaction but makes our jobs that bit easier. His love for his job really shines through in his work and its evident in all decisions he makes to benefit his patients.
“Damien’s ability to administer 1200 vaccinations, manage a large pharmacy whilst still carrying out his duties as a pharmacist and his performance of CPR to a patient in need that resulted in saving the man’s life is outstanding.”
Damien said on the night, “I am very grateful to accept the JPA Brenson Lawlor Young Pharmacist of the Year Award. I am privileged to be chosen for this Award by the judging panel as these awards have showcased the enormous talent present in community pharmacy in this country.
“These Awards are particularly important as they emphasise the vital role that community pharmacy plays in the healthcare system. This has been particularly evident over the last couple of years, where pharmacies have kept their doors open and continued to provide an outstanding service to their patients.
“Although this may be classified as an individual award, I would view it as a team award. It gives recognition for all the hard work
that all my team members have contributed throughout the last number of years. I would also like to thank all the sponsors, particularly JPA Brenson Lawlor, for contributing to a great night and for all their support throughout the year.”
Partner with JPA Brenson Lawlor, Jason Bradshaw told us, “I would like to congratulate all the finalists of the Irish Pharmacy Awards 2022 and especially offer our congratulations to Damien, a very worthy recipient of this Award.
“The past two years have been incredibly difficult, but we have all seen how pharmacists are working hard to meet the needs of their patients. Young pharmacists have an ever-growing role and I have been able to meet many of them while providing business lectures to the pharmacy students at Royal College of Surgeons in Ireland (RCSI). I have also had the pleasure of providing 1:1 meetings with interested first time buyer pharmacists in order to assist them with acquiring their first pharmacy.”
Damien O’Brien, Pharmacist, Adrian Dunne Pharmacy Baldoyle
PHARMACYNEWSIRELAND.COM 49
Awards
Putting the ‘Super’ in Superintendent

Elaine has been Superintendent Pharmacist for Meaghers Pharmacy Group since August 2019 and in her time as Superintendent she has championed a number of public health initiatives. Described as someone who has a great passion for the role of the pharmacist in preventative healthcare, she truly believes that the position of the pharmacist can be utilised to help patients live healthier lives and to not only care for patients when they are ill but help them remain well.
Elaine Lillis began her career as an Intern Pharmacist in Meaghers in 2011, throughout the years she has grown and progressed as a pharmacist, a leader, a patient advocate and as a business leader. Throughout her time in Meaghers Elaine has worked as an Intern, a support pharmacist, a supervising pharmacist, the support to the superintendent pharmacist and now as a superintendent she brings with her all the interpersonal, patient care and business skills to the role.
For the past few years, Elaine has been the driving force behind the Meaghers group flu vaccine campaign. Since taking on the role of superintendent, the number of flu vaccines delivered in Meaghers has increased dramatically year on year. Elaine has also organised, co-ordinated and delivered Flu vaccine clinics off site, delivering easy access to vaccinations to corporate customers to improve health and wellness in workplaces and in nursing homes and assisted living facilities helping to protect the most vulnerable patients in our communities.
Despite the significant challenges posed during the pandemic Elaine’s hard work and tenacity has helped countless people.
Elaine’s work with the Meaghers’ covid vaccine clinics has allowed her team to be part of the recovery of society and communities by delivering thousands of doses of covid vaccines so far.
Oonagh O’Hagan, Managing Director of Meaghers Pharmacy Group comments, “When the pharmacy vaccination program was announced Elaine was determined that we would play our part in Meaghers to bring our country and out communities out of the isolation and desperation caused by the pandemic, Elaine successfully rallied our

pharmacists to organise the swiftest and most efficient system of vaccination within the stores and her efforts certainly were successful. We will continue to deliver booster doses and run vaccine clinics within the Meaghers group.”
Elaine has a great passion for the role of the pharmacist in preventative healthcare, she truly believes that the position of the
“Elaine’s passion for serving the communities in which she serves has proven to be a rallying call for the entire Meaghers team, Elaine leads from the front and has been instrumental in formulating strategies to allow the Meaghers business better serve patients and communities”
Paul Hatton, National Field Sales Controller, Perrigo with Elaine Lillis, Superintendent Pharmacist, Meaghers Pharmacy Group
The Irish Pharmacy
Elaine Lillis: Winner of the Perrigo Superintendent Pharmacist of the Year Award 2022
PHARMACYNEWSIRELAND.COM 50
Awards2022
pharmacist can be utilised to help our patients live healthier lives and that pharmacies can not only care for patients when they are ill but can help them remain well.
There is a silent epidemic of Non-Alcoholic Fatty Liver Disease (NAFLD) in Ireland and patients with type 2 diabetes, obesity, and high cholesterol are at greater risk of developing this disease which, if undiagnosed and left untreated, may lead to cirrhosis of the liver.
Elaine teamed up with leading Consultant Hepatologist and Gastroenterologist Professor Suzanne Norris, to run several successful liver scans clinics in a number of Meaghers pharmacies, the country’s only pharmacy-led Diabetes Liver Screen Initiative.
Oonagh continues, “As part of this initiative, our type 2 diabetic patients were invited into our pharmacies for a free liver fibroscan with the aim of identifying those with liver fibrosis. The highly ambitious programme is the first trial of its type in Europe and from our patient cohort an astonishing 67% had abnormal scans. Results of scans were sent to patients GPs and those with a high liver stiffness measurement were fast-tracked to a specialist hepatology clinic for treatment. If caught early, NAFLD can be reversed through healthy eating, exercise and weight loss and Elaine has plans to continue to educate and empower those at risk. Elaine hopes to run future Liver clinics in our pharmacies in 2022 targeting additional patient cohorts including those with high BMI and high cholesterol.”
Elaine’s passion for serving the communities in which she serves has proven to be a rallying call for the entire Meaghers team, Elaine leads from the front and has been instrumental in formulating strategies to allow the Meaghers business better serve patients and communities.

Meaghers recently launched a Travel Antigen Testing Service to enable local communities to travel safely and limit the spread of infection.
Elaine says, “In March 2022 we partnered with a qualified physiotherapist to supply online pelvic training exercises to our customers and next month we will be running in store pop-up clinics where our patients can come into the pharmacy to speak to our Expert Physiotherapist.
“Also, in process at the moment is the setting up Meaghers Pain Clinics. This will be the first type of pain clinic run in pharmacies in Ireland. The free appointment
Elaine Lillis, Superintendent Pharmacist, Meaghers Pharmacy Group
will allow patients to review their current pain medication with a specifically trained pharmacist and then allow them to use Bio-electric devices to assist in managing their pain. These devices are showing to have a huge benefit in managing chronic pain, musculoskeletal pain and injury and also helping to reduce recovery time from acute injury or surgery. This novel initiative could bring huge benefit to many of our patients allowing them to reduce the amount of pain medication taken daily and to live a happier and more active lifestyle.”
Oonagh adds, “We are lucky to have Elaine at the helm, leading our team but the Pharmacy profession is also lucky to have such a passionate, innovative and proactive pharmacist working in the community sector. Elaine is incredibly passionate about the future of Irish Pharmacy and works with TCD educating and developing future pharmacists.”
In her role as an Adjunct Assistant Professor in TCD she designs and delivers communication and conflict workshops to secondand third-year undergraduate pharmacy students as part of their Practice of Pharmacy Module and works as an assessor in Trinity End of term OSCEs. She has also acted as an assessor in the Pharmacy Professional Registration Exam (PRE) in both Trinity & RCSI, the final exam pharmacy students must sit before becoming a fully qualified pharmacist.
Elaine is a champion of continued personal development and is instrumental in leading the training and upskilling of the entire Meaghers team. She works with the individual team member to ascertain what training and development would benefit them and their patients most and works tirelessly to lift them up, support them and encourage them to be the best they can be.
“Elaine also works to help our pharmacists develop and upskill in their profession, organising pain management workshops, gut health workshops and many more.
“Elaine manages the special relationship between Meaghers and the Nursing homes and assisted living facilities that we supply medicines to, she has worked with the teams there in designing courses for education
and training of nurses in managing patients’ medicines, increasing patient safety and has introduced new platforms, software and systems to Meaghers to ensure a better and more efficient integration between the pharmacy and the care facility. Most recently she made a change to the medication packs we supply to our nursing home, to a type which ensure medication rounds are carried out more efficiently and the risk of administrative errors are greatly reduced.
“Having held the role for a short number of months before the first lockdown hit Elaine had a baptism of fire in her role as superintendent, she never once faltered, she remained professional, kept her focus on patient care, team and patient safety and despite all challenges that came her way thrived and pushed the Meaghers Business forward. We are extremely proud of our superintendent and blessed to have her lead our team.
She said after receiving her Award, “This Award really is a shout out to my team. Having been nominated by my peers, it is rewarding to get that recognition from them; to then be announced as the winner is really the highlight for me. I am honoured to lead the team that I do and it has been a particular honour to lead
them during the last two years, during a time that has probably been the most challenging for the profession as a whole. They too have been an amazing support network for me.”
Paul Hatton, National Field Sales Controller with Perrigo added, “It is super to be involved with the Irish Pharmacy Awards. Within Perrigo, the core nature of our business is built around self-care and recognising excellence in community pharmacy is a great alignment for our business.
“With our healthcare landscape facing unprecedented change, our consumers are increasingly looking for self-care products that will improve their health and wellbeing. We would not be where we are today without the help of our local pharmacies and pharmacists. Congratulations to all the finalists and especially to Elaine on winning the Perrigo Superintendent Pharmacist of the Year Award.”
PHARMACYNEWSIRELAND.COM 51
Boots Ireland – Leading from the Front
This was the first year of the Roche Point of Care Testing Award, won on the night by Boots Ireland. Boots Ireland responded to the Covid-19 pandemic by rapidly implementing testing services, the foundation of the country’s fight to manage and mitigate the disease. They were the first pharmacy in Ireland to offer PCR testing in December 2020 and again the first to offer professionally administered antigen testing to facilitate travel under the EU Digital Covid Certificate scheme in July 2021.
Boots Ireland, winner of the Roche Diagnostics Points of Care Testing Pharmacy of the Year Award. Pictured is Noor Bajalan, Boots Ireland, Len Marshall, Head of Healthcare Development, Roche Diagnostics and Susan O’Dwyer, Pharmacy Strategy and Development Manager, Boots Ireland

Susan O’Dwyer, Pharmacy Strategy and Development Manager with Boots Ireland says, “The arrival of the COVID-19 pandemic set the world on a path never seen before in our lifetimes.
“As COVID cases swept the country, work from home and shelter in place orders were enforced and the healthcare sector worked tirelessly to continue to provide vital services and treat this new, unknown, disease. In the initial phases of the pandemic Government taskforces worked to implement regimes of testing to manage case numbers and to protect people from the harshest symptoms of the disease.
“Recognising that there was no testing provision under the National Testing Strategy for patients that were not experiencing symptoms and conscious of the allowances being made to facilitate international travel over the Christmas 2020 period Boots Ireland worked quickly to design, develop and implement the first private pharmacy delivered Covid-19 PCR testing service in the country.
Designed for asymptomatic individuals who required PCR testing for international travel or as a re-assurance when interacting with family over the Christmas period Boots were able to provide
a convenient and accessible solution to support the national programme by increasing access to testing.”
Susan continues, “Significant innovation was required to design, develop, implement and re-define this service over time in response to the ever-changing nature of the pandemic as follows:
• We developed a patent journey for the service that adhered to public health guidance, kept our colleagues, customers and patients safe and responded rapidly to changing guidance over time
• We sought out and evaluated potential laboratory partners to ensure we were providing access to high quality, appropriately accredited PCR testing that was cost competitive and subject to efficient turnaround times.

“Recognising the need for minimal patient contact we have an almost entirely digital journey, the majority of which is completed by the patient outside of the pharmacy setting to minimise dwell time in the pharmacy”
Irish Pharmacy
Boots Ireland: Winners of the Roche Diagnostics Point of Care Testing Award 2022
PHARMACYNEWSIRELAND.COM 52 Awards
Awards2022The
• We implemented an internal training programme, based on HSE training for community swabbers in HSE run testing centres, initially for pharmacists and later for a newly created role of Covid-19 Testing Service Advisor, that provided colleagues with the skills to accurately, safely and confidently collect swab samples, maintain proper infection control, accurately label and package test samples, interpret results and provide relevant public health advice to service users. A corresponding system of colleague and premises authorisation to provide the service was implemented.
• We developed an online journey that incorporated the use of online appointment booking, digital consultation record forms, remote payment, sample registration and laboratory integration to facilitate minimal patient contact, no duplication of data entry, tracking of samples from collection, to receipt at the laboratory, to result generation and communication with the patient through their online portal.
• We worked with national bodies such as the HSE Public Health Departments and the Department of Health to ensure timely notification of positive cases and to gain access to the national EU Digital Covid Certificate service
Where Boots lead others follows as evidenced by the number of pharmacy providers of Covid-19 testing services in the pharmacy market. This supports scope of practice development and expansion across the sector and increases access to pharmacy led services nationwide, something that is of benefit to the sector and to the patients and communities.
“Whilst the need for Covid-19 testing services may be diminishing the lessons learned in service implementation can be used to re-introduce the service at pace into the future should that be required and/or to introduce similar services with a different disease target.
“The Covid-19 pandemic fundamentally changed the lives of people around the globe in an unprecedented way. The national public health emergency had, and continues to have, a significant impact on the way public and private healthcare services are delivered across the country.
Community pharmacy has been at the forefront of the pandemic response, remaining open and accessible at all times through the crisis whilst simultaneously battling
Boots Ireland, winner of the Roche Diagnostics Points of Care Testing Pharmacy of the Year Award. Pictured is Susan O’Dwyer, Superintendent Pharmacist, Boots Ireland, Noor Bajalan, Boots Ireland and Len Marshall, Head of Healthcare Development, Roche Diagnostics

its own workplace challenges in times of fear, pressure and workforce constraints.
The National Testing Strategy saw the implementation of community testing for symptomatic individuals as a means of identifying cases and contacts and thus limiting spread of the disease.
As society started to re-open and international travel started to reopen Boots recognised that more private services, for asymptomatic individuals wishing to determine their Covid-19 status and travel freely on foot of a negative result, were required. We worked relentlessly over a very short time period in late 2020 to implement the first private PCR testing service in community pharmacy in Ireland.
“Front and centre in our minds when developing the service was the need to protect colleagues who would deliver the service as well as other colleagues within the pharmacy. Detailed analysis of infection prevention and control measures, sourcing of high-quality PPE as utilised in the hospital setting (FFP2 masks, gowns, visors, gloves) and consideration for ventilation in the testing areas formed the very initial stages of the assessment of suitability of the pharmacy as a location for delivery of this much needed service. Risk assessments were carried out and risk mitigation measures implemented.
“We created a bespoke training programme to support out teams to deliver the service to the highest standards. Alongside this we implemented a robust system of accreditation for colleagues to ensure only those who successfully complete the programme and pass a series of competence assessments are authorised to deliver the service. Governance and professional standard requirements are outlined in a
series of SOPs and detailed result interpretation and communication guides are also provided to teams.
Recognising the need for minimal patient contact we have an almost entirely digital journey, the majority of which is completed by the patient outside of the pharmacy setting to minimise dwell time in the pharmacy. Working with a thirdparty provider, and in collaboration with the laboratory and the antigen test kit provider, we have a unique digital portal that allows scanning of a barcoded sample that is assigned to an individual patient to ensure accuracy of result reporting. Results and associated Certificates (including EU Digital Covid Certificates) are issued through this digital portal thus ensuring accuracy of reporting and efficiency in terms of result communication and Certification generation.
“It was imperative that our messaging was responsibly handled to ensure that only those eligible to attend store did so to prevent the spread of infection to other customers and Boots Ireland colleagues working in the store. This included criteria such as not having any symptoms when attending store for testing. It was also important that people understood that a negative antigen test did not mean that they could ignore the Government’s guidelines at the time. Therefore, time was spent to develop robust messaging and Q&A documents to guide communications ensuring that the eligibility to attend the store to access testing was adhered to.
“We feel that the innovative use of technology and digital solutions to facilitate more accessible care, the focus on designing and delivering a high quality, professional service,
underpinned by strong infection prevention and control measures and adherence to public health guidance, the execution of a very strong engagement plan at both national and regional levels and the long term engagement of our colleagues and customers is very deserving of the BOI Payment Acceptance (BOIPA) Innovation & Service Development (Chain) Award 2022.
The Award was given out on the night by Len Marshall, Head of Healthcare Development with Roche Diagnostics. He said, “Over the past number of years the profession has shown great innovation and agility in expanding the services that are offered. This includes services that support prevention, early detection, and management of chronic diseases such as diabetes.
“During the pandemic pharmacies remained open and, building on the experience with the Flu vaccination programme, became centres for Covid-19 vaccination. This award category recognises the pioneering pharmacy teams that have embraced this opportunity. Well done to all the finalists and most importantly, Boots Ireland on their fantastic win.”
PHARMACYNEWSIRELAND.COM 53
New Lithium Therapy Patient Booklet
Saint John of God Hospital Pharmacy, the HSE National Medication Safety Programme, and the Irish Pharmacy Union have joined forces in a novel new initiative to launch a new patient Information Booklet on Lithium Therapy.
Jonathon Morrisey, Chair, IPU Community Pharmacy Committee

contains important safety and clinical information as well as providing a handy means of recording essential information on lithium levels and blood test results.
Additional information is also provided on different lithium products on the market, blood testing and frequency, monitoring, side-effects, and how to recognise signs of Lithium toxicity.
The Patient Information Booklet on Lithium Therapy is being distributed throughout September by the HSE directly to Hospital Pharmacies and to Community Pharmacies via the Irish Pharmacy Union.
GPs can direct patients towards Community Pharmacists to avail of the booklet and an electronic template is available online.
The joint initiative aims to promote safer lithium therapy and empower patients to engage more with their Healthcare Professional on all aspects of lithium therapy including monitoring and potential side-effects.
Lithium is a mood stabiliser that is prescribed to treat mood disorders. It is specifically used as a treatment and prophylaxis in Bipolar Disorder and in more severe depression. It is thought that at least 10,000 people are prescribed Lithium every year in Ireland.
The new Lithium Therapy patient information booklet has been produced by Audrey Purcell, Pharmacy Dispensary Services Manager, Saint John of God Hospital, in conjunction with Professor Dolores Keating, Head of Pharmacy, Saint John of God Hospital, and the Saint John of God Hospital Drug and Therapeutics Committee.
Published in Plain English format, the easy-access booklet is intended for patients and healthcare professionals and
Welcoming the publication Dr Orla Healy, National Clinical Director Quality and Patient Safety with the HSE said, “The HSE National Quality and Patient Safety Directorate are delighted to support this initiative and to share the excellent practice from our colleagues in Saint John of God Hospital with people who are prescribed lithium and healthcare professionals engaging with them throughout the country. Lithium is a highly effective therapy which needs to be monitored
Free Emergency Contraception
and managed carefully, and the booklet is a high quality resource to contribute to safe, effective and informed use.”
Marking the publication Emma Balmaine, Chief Executive, Saint John of God Hospital said, “This is a timely publication on an important public health issue –lithium is a highly effective therapy in treatment of more severe depression and Bipolar Disorder but requires ongoing close medical supervision and ongoing monitoring and patient education.
Saint John of God Hospital, as a leading independent provider of mental health services, plays an active role in promoting best practice guidance around use of medications and managed care. This initiative will have real and practical benefits for those who need Lithium therapy.
Jonathon Morrissey, Chair of the IPU’s Community Pharmacy Committee said, “We are delighted to see the launch of the Lithium Therapy Patient Information Booklet, which will be an important information source for patients. Community pharmacists will find the content of the booklet invaluable as a tool to support and educate patients on the safe use of lithium and the Irish Pharmacy Union is committed to playing its part in helping keep the public informed on this important health issue.”
The free contraception service will cover the full cost of prescription contraception, including the cost of:
GP or doctor’s appointments - to talk about contraception options and for repeat prescriptions when needed
any prescriptions given by your doctor - these will be given free of charge at participating pharmacies
your choice of contraceptionfrom a wide range of short-term and long-term contraceptives
such as the patch, pill, ring, implant, injection and IUDs
fittings and removals of implants and IUDs or IUSs (coils)
any check-ups or other follow up care needed, relating to your implant or coil
emergency contraception (morning after pill).
Maeve O'Brien, Interim Programme Lead for the HSE Sexual Health and Crisis Pregnancy Programme commented, “This new service is a welcome development. As part of the service, the HSE is
launching a campaign to promote the free contraception service and the range of contraceptive options available over the coming weeks. As a first step, we are encouraging those who may be eligible to visit SexualWellbeing. ie to learn more about the service, the contraception options available and how they work. This information will help to support discussions with your GP.”
Dr Ciara McCarthy, ICGP/HSE GP Clinical Lead in Women's Health added, “Finding a suitable method of contraception will depend on your needs, your medical history
and your own preferences. I would encourage anyone thinking about contraception for the first time, or thinking about changing their contraception, to speak to their GP about the options available.
GPs are in a good position to discuss the options and advise about side effects or the method that will suit your needs best. The free GP consultations covered under the new service will give anyone considering availing of free contraception the chance to discuss these questions in full before making an informed decision.”
PHARMACYNEWSIRELAND.COM 54
News
The HSE has launched a new service to provide free prescription and emergency contraception for 17 to 25 year old women and people.
Future of pharmacIE
The future of pharmacy is in your hands – where will you take it?
Join APPEL on the 20th of October for the return of our virtual careers event!
What to expect at Future of pharmacIE?
An online careers event for pharmacy students and professionals.
Panel discussions with pharmacy professionals will showcase the varied and exciting career paths for pharmacists. Get inspiration
for your future in pharmacy and get the chance to meet your future colleagues!
Our online Exhibition Hall is a chance for organisations to promote themselves to attendees and for attendees to see what opportunities are available for them. Exhibitors from community pharmacy, hospital pharmacy, the pharma industry, regulation, education, and more will be there to tell you more about their work.
Unique networking opportunities for pharmacy students and professionals alike make this an unmissable event! You will have the ability to set up your own networking rooms to connect with groups of people or have one-to-one video chats with your new connections.
Find out more about the Future of pharmacIE on the APPEL website or by contacting us at ops@appel.ie.

United Drug raise 50k for their official Charity Partner, Aware
Following a two-year partnership with Aware as their official Charity Partner, McKesson Ireland have expressed a massive thank you for all the fundraising efforts from their employees across the four businesses of United Drug, Lloyds Pharmacy, TCP Homecare and Median Healthcare.

Over the two years, they have completed many fantastic initiatives to raise these muchneeded funds for Aware, from Hiking, Running and Walking to Cycling the entire length of Ireland to name just a few.



Collectively the teams raised ¤50,000 through their fundraising initiatives, had lots of fun along the way, and maybe a few of them even got a bit fitter!
The team at Aware are delighted with the donation. Stephen Butterly, Head of Fundraising at Aware:
“On behalf of the whole team in Aware, I would like to take this opportunity to thank the McKesson Ireland team for their significant sum of ¤50,000. Fundraising of this nature goes a long way towards supporting the provision of support and education services by Aware to almost 50,000 people impacted by depression and bipolar disorder each year.”
Paul Reilly, CEO of McKesson Ireland commented, “As a
company, we want to make a positive difference in Ireland.
The Charity Programme gives our colleagues the chance to
support a cause that is close to their hearts and benefits the local communities where we work and live. I am immensely proud of
Irish Osteoporosis Society Annual Conference
The Irish Osteoporosis Society Annual medical conference will be held virtually on Saturday 22nd October 2022.

The event, which is CPD applied for, features a wide ranging programme with the opening address being delivered by President of the Society, Professor Moira O’Brien.
the efforts and commitments our teams have shown to support such a worthy cause.”
Other keynote speakers include; Dr Kevin McCarroll, Consultant Physician & Geriatrician at the Bone Health Unit in St James Hospital talking about ‘Hyperparathyroidism’ – Ms Aoife Ni Eochaidh, Chartered Physiotherapist, Clinical Specialist Physiotherapist at Bon Secour Consultant’s Clinic speaking about ‘Women’s Health’ and Dr Derek Bennett, President of the Irish American Orthopaedic Society and Member of the European Board of Orthopaedic & Trauma Surgeons who will be looking at ‘License to Kill – The Double O’s of Bone Health.’
Furthermore there will be oral abstracts and question and answer chaired sessions. You can find out more by visiting www.irishosteoporosis.ie
PHARMACYNEWSIRELAND.COM 55News
Together We Raised €50,000
The Best Shots this Autumn: Influenza and COVID-19 vaccination
Written by Dr Tom Barrett, Senior Medical Officer, National Immunisation Office

has exceeded the 5 year average. During this influenza season in Australia, the groups with the highest rates of disease are among children aged 5-9 years, followed by children aged under 5 years, and adolescents.
Influenza in children
4750 children aged 0-14 years have required hospitalisation as a result of influenza.
Influenza vaccination for children in Ireland
Influenza
Influenza is a very common acute viral respiratory illness which affects all age groups. The virus is seen all year round but peaks every winter. The degree of influenza infection is unpredictable, however, each year in Ireland influenza is responsible for between 200 and 500 deaths and as many as 1,000 during a particularly severe season (2008/2009).
As we head into autumn the 2022/2023 influenza season presents a significant challenge to the delivery of healthcare services both in primary care and in hospitals, especially as there may also be a resurgence of cases of COVID-19.
During the 2020-2021 flu season, the first flu season of the pandemic, influenza cases were not reported in Ireland because the public health measures recommended to prevent COVID-19 infection were very successful in preventing influenza virus transmission.
In the 2021-2022 flu season, though influenza cases numbers increased, they remained far below pre-pandemic levels because of ongoing COVID-19 preventative measures. However, throughout the 2022/2023 influenza season there is likely to be a limited recent community natural immunity to influenza, especially for children born since 2020.
In this year’s southern hemisphere flu season, Australia reported influenza–like-illness notifications that peaked at the beginning of the influenza season and the weekly number of notifications
Children are among the most susceptible to influenza infection. It is estimated that 20-30% of children develop influenza during each influenza season compared to 5 to 10% of adults. Children, because they have limited preexisting immunity, are primary vectors of influenza transmission in the community and shed the virus at higher viral titres. Children transmit the influenza virus for a longer period than adults; they can transmit the influenza virus for 10 or more days, compared to 6 days in adults, therefore increasing spread of the disease and contributing significantly to influenza outbreaks.
Influenza vaccination of young children can not only protect against severe illness in children but may also assist in reducing influenza transmission to other vulnerable populations, such as those aged 65 years or older who due to immunosenescence develop less immunity after vaccination.
Approximately 10% of children under 15 attend their GP with influenza in an average influenza season. Influenza is an important cause of pneumonia, bronchitis, otitis media, croup and bronchiolitis in children. Incidence rates are highest in the younger age groups leading to high rates of excess GP and outpatient visits, hospital admissions and medicines prescriptions, increasing pressure on the healthcare system.
In Ireland during the 2018/2019 influenza season, 1245 children were hospitalised with influenza. Children aged less than 5 years had the second highest hospitalisation rates for influenza after those aged 65 years and older.
Between the 2009/2010 and 2018/2019 influenza seasons:
For the 2022/2023 influenza season the Department of Health, will continue to provide funding to the HSE to offer Quadrivalent Live Attenuated Influenza (LAIV) vaccine free to all children aged 2 to 17 years inclusive. This vaccine was introduced during the 2020/2021 influenza season, however uptake of the LAIV vaccine remains very low. For 2021/2022 Flu season vaccine uptake in children aged 2 to 17 was 16.6%. Therefore it is important to encourage up take of the LAIV vaccine.
The aim of the childhood influenza programme is to reduce:
morbidity and mortality from influenza in children
transmission of influenza to the elderly and persons in risk groups
the number of hospital admissions
transmission to health care workers in families with children
absenteeism of children from school and their parents from work
Influenza vaccination for children in other countries
Nine European countries, US, Canada and Australia recommend influenza vaccine for children. The UK offer LAIV to children. Finland, US and Canada offer LAIV or QIV to children.
In the US, LAIV has been recommended since 2004. LAIV has been authorised for use in Canada since 2011.
In 2013, the UK introduced trivalent LAIV for 2 and 3 year olds with pilot programmes for primary school children. Quadrivalent LAIV was introduced during the 2014/2015 influenza season. The programme has extended year on year to include all children from 2 up to 11 years.
In Finland, annual inactivated influenza vaccine was recommended for children aged 6–35 months in 2007. LAIV was introduced in 2015 to enhance
vaccine uptake. Since then, all 2 and 3 year old children have been eligible for vaccination with either LAIV or inactivated influenza vaccine. The programme is now extended to include all children to 6 years of age.
Live Attenuated Influenza vaccine (LAIV) for 2022/2023 influenza season
Quadrivalent Live Attenuated Influenza vaccine (LAIV) Fluenz Tetra is manufactured by Astra Zeneca. It is administered intra-nasally.
The vaccine contains the following four vaccine virus strains as recommended by the World Health Organization (WHO):
Egg-based influenza vaccines
• an A/Victoria/2570/2019 (H1N1) pdm09-like virus;
• an A/Darwin/9/2021 (H3N2)-like virus;
• a B/Austria/1359417/2021 (B/ Victoria lineage)-like virus; and
• a B/Phuket/3073/2013 (B/ Yamagata lineage)-like virus.
LAIV may contain residues of egg proteins (ovalbumin), with a maximum amount of less than 0.024 micrograms and gentamicin. LAIV does not contain any adjuvants, or preservatives.
LAIV effectiveness
Since LAIV contains live attenuated viruses, it mimics natural infection with wild-type viruses, with the development of both mucosal and systemic immunity. Local mucosal antibodies protect the upper respiratory tract and may be more important for protection than serum antibodies, inducing more durable immune memory and so providing better longterm protection to children than inactivated influenza vaccines such as QIV.
In some studies, LAIV has been shown to be more effective in children compared with inactivated influenza vaccines. In addition, LAIV may offer some protection against strains not contained in the vaccine, as well as virus strains that have undergone antigenic drift.
PHARMACYNEWSIRELAND.COM 56
Immunisations
and role models for their peers, colleagues and the rising stars of tomorrow
The Dynamic 100 is a network of the most influential professional in the Irish pharmacy industry who act as ambassadors
within Community Pharmacy. How to enter: Please submit 250-800 words, describing how you/they have achieved something special, gone above and beyond or behaved dynamically. We also require a high-resolution photograph of the entrant for print publication. Each entry must be within the pharmacy industry. Pharmacists have continued to provide a first-class service in the face of adversity, with each pharmacy team displaying the highest levels of resilience, determination, and courage. And now the time has come to reward that resilience. That determination. That courage… Nominations are sought from across the pharmacy profession in Ireland. DYNAMIC 100 NOMINATE TODAY Email nomination(s) to aoife@ipn.ie or Kelly-jo@ipn.ie DEADLINE MONDAY 3rd OCTOBER Dynamic
Dose
One
•
A recent meta-analysis of LAIV suggested an efficacy against confirmed disease of 83% (95% confidence interval 69-91%).
•
The UK pilot primary school programme introducing LAIV was evaluated in 2014/2015 and showed:
94% reduction in primary school age children GP influenza-like consultations
In Ireland the National Immunisation Advisory Committee (NIAC) has recommended healthy children require one dose of LAIV. However children in a medically at risk group aged 2 to 8 years inclusive are recommended 2 doses of LAIV if they have never had any influenza vaccine before. (Table 1). The two doses should given 4 weeks apart.
• Influenza antiviral medication within the previous 48 hours
• Those with severe neutropoenia (absolute neutrophil count <0.5 × 109/L) to avoid an acute vaccine related febrile episode
marketing surveillance, overall rates of fever were similar to the rates following other childhood vaccines and were generally mild and of short duration.
Very rare (less than 1 in 10,000): Immediate allergic reactions.
• Those on combination checkpoint inhibitors (e.g. ipilumumab plus nivolumab) because of a potential association with immune related adverse reactions.
Contraindications
The following are NOT contraindications
• Asymptomatic HIV infection
•
74% reduction primary school age Emergency Department attendances with respiratory complaints
93% reduction in primary school age confirmed influenza hospitalisations
•
59% reduction in adults GP influenza-like illness consultations.
LAIV dose and administration
Each LAIV vaccine comes as a prefilled nasal applicator and each applicator contains 0.2ml nasal suspension. The vaccine is administered by the nasal route. One dose of LAIV is 0.2ml administered in divided doses into each nostril i.e. 0.1ml in each nostril.
If the child’s nose drips after vaccination, the vaccine dose does not need to be repeated. The vaccine is immediately absorbed after administration. For the same reason, the vaccine does not need to be repeated if the child sneezes or blows their nose after vaccination.
LAIV can be given together with or at any time before or after the administration of any other live attenuated (e.g. MMR) or inactivated vaccines including COVID-19 vaccines.
• Children receiving topical or inhaled corticosteroids
low dose systemic corticosteroids
replacement therapy corticosteroids (e.g. adrenal insufficiency).
Contraindications to LAIV:
• Anaphylaxis following a previous dose of influenza vaccine or any of its constituents1 (other than ovalbumin – see Precautions)
• Asthma
• Acute exacerbation of symptoms increased wheezing and/or additional bronchodilator treatment in the last 72 hours
• Seek specialist advice if on regular oral steroids or previous ICU admission
• Significant immunosuppression due to disease or treatment
• Children who live with severely immunosuppressed persons (i.e. post haematopoietic stem cell transplant)
• Concomitant use of aspirin/ salicylates
Precautions
Defer until recovered from an acute severe febrile illness.
As LAIV has an ovalbumin content <0.1 micrograms per dose, it can be given to children with confirmed egg anaphylaxis or egg allergy in a primary care setting except children who have required ICU admission to hospital for a previous severe anaphylaxis to egg who should be given LAIV in hospital.
Aspirin/salicylates should not be be used for 4 weeks after vaccination unless medically indicated, as Reye’s syndrome has been reported following the use of salicylates during wild-type influenza infection.
Avoid influenza antiviral medication for 2 weeks post vaccination.
Children aged 2 to 17 years for whom LAIV is contraindicated should be offered QIV vaccine (provided there are no contraindications to QIV).
LAIV side effects
Very common or common (More than 1 in 10 to 1 in 100): Nasal congestion/rhinorrhoea, decreased appetite, malaise, fever, headache, and myalgia. In post
Very rare cases of Guillain-Barré syndrome (GBS) have been observed in the post-marketing setting following influenza vaccination. The risk of GBS following influenza infection is significantly greater than that following influenza vaccination.
Can LAIV vaccine cause virus shedding?
The attenuated vaccine viruses in LAIV are cold adapted. They can replicate at the lower temperatures found in the nose but cannot replicate efficiently at body temperature elsewhere in the body.
Vaccinated children can shed the attenuated virus for a few days after vaccination but the virus that is shed cannot cause infection. Peak incidence of shedding occurred 2-3 days post-vaccination in Fluenz clinical studies. Therefore the weakened viruses do not cause flu infection in others, or in the person vaccinated.
Increasing uptake of influenza vaccine
Influenza remains a major public health issue and never more than after more than two years of the COVID-19 pandemic. Influenza vaccination is the best intervention available to prevent influenza.
Extending the influenza vaccination programme to all children aged 2-17 years aims to protect children and reduce transmission to others, thereby reducing the burden on our health services at this crucial time.
PHARMACYNEWSIRELAND.COM 58 Immunisations
Table 1. Doses of LAIV required for children aged 2-17 years vaccine before. (Table 1). The two doses should be given 4 weeks apart. Table 1. Doses of LAIV required for children aged 2-17 years Group Age Previous vaccination
Medically at risk 2 to 8 years Have never had any influenza vaccine Two doses 4 weeks apart Have had any influenza vaccine before One dose 9 to 17 years Not relevant
dose Healthy 2 to 17 years Not relevant One dose The following are NOT contraindications
Asymptomatic HIV infection
Children receiving o topical or inhaled corticosteroids o low dose systemic corticosteroids o replacement therapy corticosteroids (e.g. adrenal insufficiency).
to LAIV:
Anaphylaxis following a previous dose of influenza vaccine or any of its constituents 1 (other than ovalbumin see Precautions)
Asthma • Acute exacerbation of symptoms increased wheezing and/or additional bronchodilator treatment in the last 72 hours • Seek specialist advice if on regular oral steroids or previous ICU admission • Significant immunosuppression due to disease or treatment • Children who live with severely immunosuppressed persons (i.e. post haematopoietic stem cell transplant) • Concomitant use of aspirin/salicylates salicylates
and Support
The Ostomy & Urology Care team at United Drug strive for the best advice, service and support, enabling you to give your Ostomy & Urology Customers confidence and peace of mind that they are receiving the best possible care through your pharmacy.
Education
We do this through our three-tiered approach:
United Drug helps facilitate in-store
training to pharmacy staff, online
Striving for Best in Class Advice, Service and Support
training, and one-to-one Quality of Life consultations with patients.
EducationCustomer Care
The Ostomy & Urology Care team at United Drug strive for the best advice, service and support, enabling you to give your Ostomy & Urology Customers confidence and peace of mind that they are receiving the best possible care through your pharmacy.
Speak to our team of 5 dedicated Ostomy Care specialists. Call us on 01 4632347
Extensive Product Range
We do this through our three-tiered approach:
with 35 leading manufactures, we have over 3000 Ostomy and Urology products.
United Drug helps facilitate in-store training to pharmacy staff, online training, and one-to-one Quality of Life consultations with patients.
EducationCustomer Care
Speak to our team of 5 dedicated Ostomy Care specialists. Call us on 01 4632347

Extensive Product Range
with 35 leading manufactures, we have over 3000 Ostomy and Urology products.
Get in touch!
Customer Care Team 01 4632347 udwmarketing@united-drug.com
United Drug helps facilitate in-store training to pharmacy staff, online training, and one-to-one Quality of Life consultations with patients.
Order online www.udw.ie | Contact our dedicated Customer Care Team 01 4632347
Get in touch!
Contact Marketing to recap on any of our online webinars : udwmarketing@united-drug.com
Order online www.udw.ie | Contact our dedicated Customer Care Team 01 4632347
Contact Marketing to recap on any of our online webinars : udwmarketing@united-drug.com
Immunisations
Research, both in Ireland and elsewhere, has consistently shown that doctors and other healthcare professionals are the most trusted sources of information on vaccination. A recommendation by a trusted healthcare professional for their patients who are at an increased risk of influenza-related complications to attend their GP or pharmacist for vaccination has been shown to increase vaccine uptake.
Medical conditions that are associated with an increased risk of influenza-related complications:
• Those with chronic illness, e.g. chronic heart disease (including acute coronary syndrome), chronic liver disease, chronic neurological disease (where the neurological condition compromises clearance of respiratory secretions), chronic renal failure, chronic respiratory disease (including chronic obstructive pulmonary disease, cystic fibrosis, moderate or severe asthma, and bronchopulmonary dysplasia), diabetes mellitus, or haemoglobinopathies
• Those with immunosuppression due to disease or treatment, including
asplenia or hyposplenism, and all cancer patients
• Those with any condition that can compromise respiratory function (e.g. spinal cord injury, seizure disorder, or other neuromuscular disorder,) especially those attending special schools/ day centres
• Children and adults with Down syndrome
• Children with moderate to severe neurodevelopmental disorders such as cerebral palsy and intellectual disability
• Children on long-term aspirin therapy (because of the risk of Reye syndrome)
• Those with morbid obesity (Body mass index >40)
• Residents of nursing homes, old people’s homes, and other long stay facilities where rapid spread is likely to follow introduction of infection
COVID-19 vaccinations: National Immunisation Advisory Committee (NIAC) new COVID-19 vaccines recommendations (July 2022)
NIAC strongly recommends those who to date are unvaccinated or are incompletely vaccinated should
for COVID-19 vaccines
complete a primary COVID-19 vaccination course and booster vaccination to protect themselves against COVID-19 infection.
Using currently available mRNA COVID-19 vaccines, NIAC advise the following groups are recommended COVID-19 booster vaccination 4 months after their last COVID-19 vaccination (a 3 months interval may be used in exceptional circumstances):
1. A third mRNA COVID-19 booster vaccine is recommended for
• those aged 65 years and older (5th COVID-19 vaccine)
• those aged 12–64 years with immunocompromise associated with a sub optimal response to vaccines at the time of their primary or booster vaccination (6th COVID-19 vaccine).
When practicable, these booster doses of COVID-19 vaccine and influenza vaccine can be given at one visit.
• those aged 12–49 years who have underlying medical conditions associated with a higher risk of severe COVID-19 e.g. DM (4th COVID-19 vaccine)
• those aged 12–49 years who have underlying medical conditions who are residents of long term care facilities (4th COVID-19 vaccine).
3. A second mRNA COVID-19 booster vaccine is recommended for
• healthcare workers, and when practicable, should be given at the same time as seasonal influenza vaccine (4th COVID-19 vaccine).
4. To enhance maternal protection and provide optimal benefit to the infant, an additional mRNA COVID-19 booster vaccine is recommended in pregnancy at 16 weeks gestation or later for those who have not received a booster vaccine in the current pregnancy (4th COVID-19 vaccine). This timing is to enhance protection to the mother and the infant.
Chapter 5a COVID-19
Chapter 5a COVID-19
2. A second mRNA COVID-19 booster vaccine is now recommended for
• those aged 50-64 years (4th COVID-19 vaccine).
and
COVID-19 vaccines by age and immune status July 2022
Group
years
years
years and older
years
term
compromise associated with a sub optimal response to vaccines
dose primary course (one dose if JCOVDEN/COVID-19 vaccine Janssen)
16 weeks gestation or later
not already boosted in this pregnancy
New recommendations for children aged 5 to 11 years with immunocompromise
5. A first mRNA COVID-19 booster vaccine is now recommended for those aged 5–11 years with immunocompromise associated with a sub optimal response to vaccines at the time of their primary or additional vaccination (3rd COVID-19 vaccine).
See Table left
https://www.hse.ie/eng/health/ immunisation/hcpinfo/guidelines/ covid19.pdf
mRNA booster vaccines should be given as follows:
• aged 30 years and older: Comirnaty® (0.3ml/30 mcg) or Spikevax® (0.25ml/50 mcg)
• aged 12-29 years: Comirnaty® (0.3ml/30 mcg)
• aged 5-11 years: Comirnaty® (0.2ml/10mcg)
Nuvaxovid® Novavax vaccine is recommended if there is a contraindication to an mRNA vaccine. Jcovden® Jansen vaccine is recommended only if there is a contraindication to both Novavax and the mRNA vaccines.
Implementation of these new NIAC COVID-19 vaccine recommendations has now commenced.
References
from National Immunisation Office
PHARMACYNEWSIRELAND.COM 60
available
Table 5a.1 Recommendations for COVID-19 vaccines by age and immune - status July 2022 Chapter 5a COVID-19 COVID-1929 July 2022 Click here to return to contents Table 5a.1 Recommendations for COVID-19 vaccines by age and immune status July 2022 Group Primary course* Additional dose 1st booster 2nd booster 3rd booster 65 years and older √√ √ √ √ 50-64 years √√ √ √ 12-49 years Underlying medical condi tions √√ √ √ Residents of long term care facilities √√ √ √ Healthcare workers √√ √ √ Others √√ √ Pregnancy √√ √ √** 5-11 years √√ 12 years and older Immuno compromise associated with a sub optimal response to vaccines √√ √ √ √ √ 5-11 years √√ √ √ *two dose primary course (one dose if JCOVDEN/COVID-19 vaccine Janssen) **at 16 weeks gestation or later if not already boosted in this pregnancy
COVID-1929 July 2022 Click here to return to contents Table 5a.1 Recommendations for
Primary course* Additional dose 1st booster 2nd booster 3rd booster 65
and older √√ √ √ √ 50-64 years √√ √ √ 12-49 years Underlying medical condi tions √√ √ √ Residents of long
care facilities √√ √ √ Healthcare workers √√ √ √ Others √√ √ Pregnancy √√ √ √** 5-11
√√ 12
Immuno
√√ √ √ √ √ 5-11
√√ √ √ *two
**at
if
COVID-1929 July 2022 Click here to return to contents Table 5a.1 Recommendations
by age
immune status July 2022 Group Primary course* Additional dose 1st booster 2nd booster 3rd booster 65 years and older √√ √ √ √ 50-64 years √√ √ √ 12-49 years Underlying medical condi tions √√ √ √ Residents of long term care facilities √√ √ √ Healthcare workers √√ √ √ Others √√ √ Pregnancy √√ √ √** 5-11 years √√ 12 years and older Immuno compromise associated with a sub optimal response to vaccines √√ √ √ √ √ 5-11 years √√ √ √ *two dose primary course (one dose if JCOVDEN/COVID-19 vaccine Janssen) **at 16 weeks gestation or later if not already boosted in this pregnancy
The People’s Pharmacist for 2022 –The Wait is Almost Over
Members of the public all across Ireland have spent weeks nominating their local pharmacist for the coveted title of The People’s Pharmacist 2022.


The offices at IPN have been inundated with stories of true dedication, commitment and outstanding customer service; going well above and beyond the phenomenal role already played by our community pharmacists across the country.

The difficult task of shortlisting the Finalists now begins. Make sure you catch the November issue of IPN for details of all the Finalists and their inspiring stories.
In association with
Osteoporosis: The Silent Disease
 Interview with Theresa Lowry Lehnen (GPN, RNP, PhD) Clinical Nurse Specialist and Associate Lecturer South East Technological University (SETU)
Interview with Theresa Lowry Lehnen (GPN, RNP, PhD) Clinical Nurse Specialist and Associate Lecturer South East Technological University (SETU)

It is estimated that up to 300,000 people in Ireland have osteoporosis. Although more common in females who have gone through the menopause, it can also affect men and even children.
It is commonly known as the “Silent Disease”, and is characterised by low bone mass and structural deterioration of bone tissue, leading to bone fragility and an increased risk of fractures.
Osteoporosis is the most common metabolic bone disease in Ireland and increases the risk of ‘fragility fractures’. These fractures occur mainly at the hip, vertebrae, and distal forearm and are associated with significant morbidity, mortality, and reduced quality of life, attributed not only to the fracture itself but also to the high prevalence of comorbidities in this patient population.
According to the Irish Osteoporosis Society (IOS), 20% of people aged 60 and above who sustain a hip fracture will die within 6 to 12 months, due to secondary complications and 50% of people over the age of 60 who sustain a fractured hip will lose their independence. Only 15% of people in Ireland are diagnosed with bone loss, leaving an estimated 280,000 people undiagnosed.
Causes of Osteoporosis
According to Theresa Lowry Lehnen, Clinical Nurse Specialist and Associate Lecturer South East Technological University, osteoporosis is multifactorial in origin. “It occurs when there is an imbalance between new bone formation and old bone resorption,” she explains.
Modifiable and Non modifiable Risk Factors for Osteoporosis
Modifiable and Non-modifiable Risk Factors for Osteoporosis
Modifiable Risk Factors
Sex hormones: The reduction of oestrogen levels in women at menopause is a strong risk factors for developing osteoporosis. Men have a gradual reduction in testosterone levels as they age. Treatments for prostate cancer that reduce testosterone levels in men and treatments for breast cancer that reduce oestrogen levels in women accelerate bone loss.
Endocrine: Too much thyroid hormone can cause bone loss. This can occur in hyperthyroidism or if too much thyroid hormone medication is used to treat an underactive thyroid. Osteoporosis has also been associated with overactive parathyroid and adrenal glands and hypogonadism
Medication use: Long term use of certain medications, such as glucocorticoids and some anticonvulsants can lead to loss of bone density and fractures. Depo Provera contraceptive has been proven to cause bone loss, particularly high risk if given during adolescence when bone is being laid down.
Non modifiable Risk Factors
Sex: Women are much more likely to develop osteoporosis than men. Women have less bone tissue and lose bone faster than men because of the changes that occur with menopause
Age: The risk of developing osteoporosis as bones become thinner and weaker increases with age.
Body size: People who have small body frames tend to have a higher risk of developing osteoporosis because they have less bone mass to draw from as they age
Ethnicity: White and Asian women are at highest risk. African American and Hispanic women have a lower but significant risk. Poor diet increases the risk for osteoporosis. Low calcium and Vitamin D intake contributes to diminished bone density, early bone loss and an increased risk of fractures.
Lifestyle factors: An inactive lifestyle can lead to weakened bones and increased risk of osteoporosis. Cigarette smoking and excessive consumption of alcohol increases the risk of bone loss and fractures
Eating disorders, severely restricting food intake, low BMI and being underweight weakens bone in both men and women.
Diagnosis
Osteoporosis can be diagnosed by:
1. The presence of a fragility fracture
Genetic: A family history of osteoporosis is a very strong risk factor People whose parents have a history of fractures also seem to have reduced bone mass and may be at greater risk for fractures.
62 | PHARMACYNEWSIRELAND.COM
“Bone turnover is regulated by the interaction between osteoblasts and osteoclasts. Osteoblasts form new bone and osteoclasts are responsible for bone resorption. Both types of cell are under hormonal regulation. Up to 90 percent of peak bone mass is acquired by age 18 in females and age 20 in males. The amount of bone mass in the skeleton can keep increasing until a person reaches their late 20’s, at which point, bones have reached their maximum strength and density, known as peak bone mass. As people age the rate of bone resorption by osteoclast cells exceeds the rate of bone formation, so bone weakens.”
Theresa adds that the greatest cause of osteoporosis is oestrogen deficiency which results in increased bone turnover in which resorption exceeds formation. “Corticosteroids can also induce osteoporosis in which trabecular bone is particularly affected from suppression of osteoblastic activity,” she says.
Diagnosis
Osteoporosis can be diagnosed by:
1. The presence of a fragility fracture
2. Measurement of bone mineral density (BMD)
3. Bone biopsy: Bone biopsy is a diagnostic procedure restricted to untypical, unclear and complicated cases in evidence-based guidelines on diagnosis and treatment of osteoporosis. Bone Biopsy is not routinely used and should never be undertaken without consultation with a specialist in osteoporosis and metabolic bone disease.
Theresa continues, “Most fractures occurring after 50 years of age are osteoporotic. All persons presenting with a fragility fracture after 50 years of age or menopause should be considered as possibly osteoporotic. A detailed history of the fracture occurrence, physical examination and evaluation for other fractures is carried out while noting any presence of back pain, kyphosis, and height loss. Baseline laboratory tests include: Full blood count: Serum chemistry levels: Liver function tests: Thyroid-stimulating hormone level: 25-Hydroxyvitamin D level: Serum protein electrophoresis: 24-hour urine calcium/creatinine: Testosterone (total and/or free) and luteinizing hormone/ follicle-stimulating hormone.
“Additional testing should include measurement of bone mineral density (BMD) and if there is height loss and/ or back pain, imaging of the spine. On average BMD is lower in women than in men, because women have smaller bones and smaller trabeculae. Women, as they also go through the menopause lose more bone in their lifetime than men; 50% in females Vs 35-40% in males.”
Osteopenia is the early stage of osteoporosis and places a person at risk of developing osteoporosis. The Irish Osteoporosis Society divides osteopenia into three categories:
1. Mild Osteopenia is a T-score of -1 to -1.49 and usually requires lifestyle changes; however, causes should be investigated and addressed.
2. Moderate Osteopenia is a T-score of -1.5 to -1.9 which usually requires lifestyle changes. Causes should be found and addressed and the person may require medication, depending on the cause, or if they have had a fragility fracture.
3. Marked Osteopenia is a T-score of -2 to -2.49 which requires lifestyle changes. Causes should be found and addressed and the person may require medication, depending on the cause, or if they have had a fragility fracture.
Treatment
Osteoporosis is treatable and fractures are preventable. “The primary goal of osteoporosis therapy is to reduce the risk of fracture,” she says. “A comprehensive osteoporosis treatment program includes a focus on proper nutrition, exercise, and safety issues to prevent falls that may result in fractures. In addition, medication to slow or stop bone loss, increase bone density, and reduce fracture risk may be prescribed.
“The treatment selected for each individual is based on their risk of fracture or re-fracture, causes of osteoporosis, age, DXA scan results and medical history. Assessment of bone markers before and at three and six months after the commencement of treatment will give an earlier indication of the response to treatment.”
Calcium and Vitamin D supplements
Calcium and vitamin D are essential for the prevention and treatment of osteoporosis. “Bone is a major store of calcium and phosphate. Every cell in the body requires calcium. Vitamin D helps to regulate cell growth and the immune system and is essential for the absorption of calcium. It increases the body’s ability to absorb calcium by 30-80%. Vitamin D is the only vitamin required by the body that does not have to be consumed through food or supplements as it is manufactured through the skin, when exposed to sunlight,” adds Theresa. “Supplements are generally only recommended when the daily amounts of calcium and Vitamin D from dietary sources are not being met.
HRT – Hormone Replacement Therapy
Oestrogen replacement for women going through the menopause can help to maintain bone density and reduce fracture rates while they are on the treatment. “There is a direct relationship between the lack of oestrogen after menopause and the development of osteoporosis. Early menopause before age 45 and any long phases in which the woman has low hormone levels and no or infrequent menstrual periods can cause loss of bone mass. Oestrogen therapy and oestrogen with progesterone hormone therapy are approved for the prevention of osteoporosis in postmenopausal women provided there are no contraindications. HRT is not suitable for people who have a history of breast cancer in their family, particularly in early menopausal patients or patients who have had a history of deep vein thrombosis,” she says.
Hormone Replacement Therapy
PHARMACYNEWSIRELAND.COM | 63
Recommended Daily Allowances of Calcium and Vitamin D Age (years) Calcium (mg/day) Vitamin D (µg/day) Babies 0 1 N/A 5 (as supplement) Children 1 3 800 10 4 6 800 0 10 7 10 800 0 10 Males & Females 11 14 1200 0 15 15 18 1200 0 15 Males & Females 19 64 800 0 10 65+ 800 10 Pregnancy 1200 10 Lactation 1200 10 Reference: Irish Nutrition + Dietetic Institute (INDI, 2013) HRT
Oestrogen replacement for women going through the menopause can help to maintain bone density and reduce fracture rates while they are on the treatment. “ There is a direct relationship Reference: Irish Nutrition + Dietetic Institute (INDI, 2013
Selective Estrogen Receptor Modulators (SERMs)
Theresa continues, “SERMs, brand name Evista® work in a similar manner to oestrogen on bone, by preventing bone loss in postmenopausal women who do not have hot flushes and provided there are no other contraindications. It is used for the prevention and treatment of osteoporosis in postmenopausal women and to reduce risk of invasive breast cancer in postmenopausal women at high risk or with osteoporosis. Evista helps to maintain bone density and reduce fracture rates, specifically at the spine. It is administered as a 60mg tablet once daily. Evista can be taken with or without food or drink and at the same time as calcium and vitamin D supplements. Appropriate weight bearing exercise is also necessary.”
Monoclonal Antibody
Denosumab, brand name Prolia, is a monoclonal antibody which binds to RANK Ligand, inhibiting the maturation of osteoclasts, therefore protecting the bone from degradation. “Prolia is indicated for the treatment of osteoporosis in postmenopausal women and in men at increased risk of fractures. In postmenopausal women Prolia reduces the risk of vertebral, non-vertebral and hip fractures. Prolia is also indicated for the treatment of bone loss associated with hormone ablation in men with prostate cancer at increased risk of fractures. It is the first choice of drug for those at high risk of hip fracture or who have had a hip fracture over the age of 75 with T scores < −2.5 at femoral neck or with a humeral fracture. The
recommended dose of Prolia is 60 mg administered as a single subcutaneous injection once every 6 months into the thigh, abdomen or upper arm. Patients must be adequately supplemented with calcium and vitamin D.”
Bisphosphonates
“Parathyroid Hormone – (PTH) brand name preotac is a bone forming agent that stimulates the formation of new bone administered as a daily 100mcg dose, subcutaneous injection in the thigh or abdomen for 24 months. It can only be prescribed by a Consultant, as it is a ‘high tech’ drug for severe osteoporosis. It is contraindicated in patients with cancer. Patients need to have follow up tests done at 1, 3 and 6 months, for elevated serum or urinary calcium. The patient should then have a repeat DXA scan and a new treatment plan should be implemented at the end of the course of treatment.
“Parathyroid hormone - (PTH) teriparatide, brand name Forsteo is a recombinant human parathyroid hormone 1-34 and a bone forming agent that stimulates the formation of new bone. Foresto is a ‘high tech’ medication that can only be prescribed by a Consultant. It is given as a daily 20mcg, subcutaneous injection in the thigh or abdomen for 24 months. The patient should then have a repeat DXA scan and a new treatment plan should be implemented at the end of the course of treatment. PTH is usually recommended for those with severe osteoporosis or fractures and those who cannot tolerate other medications. Forsteo can help with the pain of vertebral
fractures and the reduction of vertebral and non-vertebral fractures in women.”
Theresa reflects that other treatments for osteoporosis can include Kyphoplasty and Vertebroplasty:
“Kyphoplasty is a surgical treatment involving a balloon being placed into the fractured vertebrae, followed by “bone cement” being injected into the balloon.
Vertebroplasty is a non-surgical treatment involving a needle with “bone cement” inserted into the fractured body of the vertebrae under imaging guidance. The decision to perform these techniques is made by a multi-disciplinary team to ensure that this is the correct approach to managing the collapse.
“Many of the consequences of osteoporosis, particularly vertebral fractures, are associated with severe pain. Patients with established osteoporosis should be treated for pain relief and physiotherapy offered for the secondary effects of osteoporosis. Pharmaceutical and non- pharmaceutical measures can be used to alleviate pain. Patients should be advised of all the options, and encouraged to try different approaches until they find what works best for them.
“Prevention of osteoporosis should ideally start in utero. Childhood and teenage years, are critical periods for developing a strong healthy bone, especially before puberty, between the ages of 8 and 12 years. If good peak bone strength is achieved in early childhood, the risk of osteoporosis in later life is reduced.”
References available on request
¤3.2m for Degenerative Retinal Diseases
The project (EYE-D) will target diseases that can result in severe loss of vision and are estimated to affect 224,000 people in Ireland, and 40 million people worldwide.
underlying causes of degenerative eye diseases.
The funding for EYE-D was announced by Simon Harris, Minister for Further and Higher Education, Research, Innovation and Science. Science Foundation
Ireland will provide ¤1.6 million funding to EYE-D, matched by project partners.

The proposed partnership involves separate collaborations with three companies: Roche, Disarm/Eli Lilly, private ophthalmology clinic, Progressive Vision Research, and the charity Fighting Blindness Ireland.
Cumulatively, these groups will fund ¤1.6 million to advance various research programmes focused on identifying the
Professor Matthew Campbell said, “We are excited about the potential developments that will emerge from this grant. Spearheading a project with a cumulative budget of ¤3.2 million will allow us to make a major impact on the international stage of vision research. In addition, our research endeavours put us in a perfect position to identify the cause of some of the most common forms of blindness.”
Co-PI, Professor Sarah Doyle, added, “This funding will allow us to build on the major successes our group has had in understanding degenerative eye diseases. Added to this, we can now recruit the most talented group of scientists internationally
and place Ireland at the forefront of vision research.”
Professor Philip Nolan, Science Foundation Ireland, said, “We are looking forward to working with the researchers and collaborators of EYE-D research project as they work to find solutions to vision loss caused by retinal diseases. The project highlights the impact that the Strategic Partnership Programme can deliver. I welcome the broad partnership involved in supporting this research which includes industry, charities and higher education institutes.”
TheEYE-D research project seeks to identify new therapeutic treatments for Age Related Macular Degeneration (AMD), glaucoma, and other inherited diseases that cause vision loss.
Professors Matthew Campbell and Sarah Doyle, Trinity College Dublin
64 | PHARMACYNEWSIRELAND.COM
News
MICROLITERS SOLUTION FOR INJECTION

Each
(corresponding to
Presentation: Glass cartridge. Indications: Movymia is indicated in adults. Treatment of osteoporosis in postmenopausal women and men at increased risk of fracture. In postmenopausal women, a significant reduction in the incidence of vertebral and non-vertebral fractures but not hip fractures has been demonstrated. Treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk for fracture. Dosage: The recommended dose is 20 micrograms administered once daily. Patients should receive calcium and vitamin D supplements if dietary intake is inadequate. The maximum total duration of treatment is 24 months. The 24 month course should not be repeated over a patient’s lifetime. Following cessation of teriparatide therapy, patients may be continued on other osteoporosis therapies. Teriparatide must not be used in severe renal impairment. Use with caution in moderate renal impairment and impaired hepatic function. Teriparatide should not be used in paediatric patients (less than 18 years), or young adults with open epiphyses. Method of administration: Movymia should be administered once daily by subcutaneous injection in the thigh or abdomen. It should be administered exclusively with the Movymia Pen reusable, multidose medicine delivery system and the injection needles which are listed as compatible in the instructions provided with the pen. The pen and injection needles are not included with Movymia. However, for treatment initiation a cartridge and pen pack should be used. Movymia must not be used with any other pen. Patients must be trained to use the proper injection techniques. Contraindications: Hypersensitivity to the active substance or excipients. Pregnancy and Breast-feeding Pre-existing hypercalcaemia, severe renal impairment, metabolic bone diseases other than primary osteoporosis or glucocorticoid-induced osteoporosis, unexplained elevations of alkaline phosphatase, prior external beam or implant radiation therapy to the skeleton, patients with skeletal malignancies or bone metastases. Warnings and precautions: In normocalcaemic patients, slight and transient elevations of serum calcium concentrations have been observed following teriparatide injection. Serum calcium concentrations reach a maximum between 4 and 6 hours and return to baseline by 16 to 24 hours after each dose of teriparatide. Therefore, if blood samples for serum calcium measurements are taken, this should be done at least 16 hours after the most recent teriparatide injection. Routine calcium monitoring during therapy is not required. Teripa ratide may cause small increases in urinary calcium excretion, but the incidence of hypercalciuria did not differ from that in the placebo-treated patients in clinical trials. Teriparatide should be used with caution in patients with active or recent urolithiasis because of the potential to exacerbate this condition. In short-term clinical studies with teriparatide, isolated episodes of transient orthostatic hypotension were observed. Typically, an event began within 4 hours of dosing and spontaneously resolved within a few minutes to a few hours. When transient orthostatic hypotension occurred, it happened within the first several doses, was relieved by placing subjects in a reclining position, and did not preclude continued treatment. Caution should be exercised in patients with moderate renal impairment. Experience in the younger adult population, including premenopausal women, is limited. Treatment should only be initiated if the benefit clearly outweighs risks in this population. Women of childbearing potential should use effective methods of contraception during use of teriparatide. If pregnancy occurs, teriparatide should be discontinued. The recommended treatment time of 24 months should not be exceeded. Contains sodium. Interactions: Digoxin, digitalis. Fertility, pregnancy and lactation: Women of child bearing potential should use effective methods of contraception during use of teriparatide. If pregnancy occurs, Movymia should be discontinued. Movymia is contraindicated for use during pregnancy and breast-feeding. The effect of teriparatide on human foetal development has not been studied. The potential risk for humans is unknown. Driving and operation of machinery: Teriparatide has no or negligible influence on the ability to drive and use machines. Transient, orthostatic hypotension or dizziness was observed in some patients. These patients should refrain from driving or the use of machines until symptoms have subsided. Undesirable effects: Nausea, pain in limb, headache, dizziness. Refer to Summary of Product Characteristics for other adverse effects. Pack size: 1. Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2; Tel: +353 1 6764971; Fax: +353 1 6762517. Website: www.hpra.ie; E-mail: medsafety@hpra.ie. Marketing authorisation holder: STADA Arzneimittel AG, Stadastrasse 2-18, 61118 Bad Vilbel, German. Marketing authorisation number: EU/1/16/1161/001-003. Medicinal product subject to medical prescription. Date last revised: July 2019.

Janjigian YY
Oncol. 201814(23):2403–2414.*
DON’T WAIT UNTIL OSTEOPOROSIS STRIKES AGAIN MOVYMIA®: THE NEW TERIPARATIDE BIOSIMILAR FROM CLONMEL HEALTHCARE Rebuild bone before it breaks again—with Movymia®1 RELIABLE: Movymia®’s quality, safety and efficacy is highly similar to its reference product1,2,* EFFECTIVE: Anabolic MoA effectively rebuilds bone through the stimulation of osteoblasts1,3 AFFORDABLE: Allows more eligible patients to benefit due to its cost advantage4,5 RE-USABLE: One high quality reuseable pen for the entire treatment period1 MOVYMIA 20 MICROGRAMS/80
dose of 80 microliters contains 20 micrograms of teriparatide. One cartridge of 2.4 ml of solution contains 600 micrograms of teriparatide
250 micrograms per ml).
1. Movymia® SmPC. 2. Movymia® EPAR – public assessment report, available at: https://www.ema.europa.eu/documents/assessment-report/movymia-epar-public-assessment-report_en.pdf 3. Brixen KT et al. Basic Clin Pharmacol Toxicol. 200494(6):260–70. 4. Lyman GH et al. N Engl J Med. 2018378(21):2036–2044. 5.
et al. Future
Forsteo® October 2019. 2019/ADV/TER/122H
News
Coadministration of Vaccines – Guidance for Pharmacy
The International Pharmaceutical Federation (FIP) has released the new guidance “Optimising vaccination through coadministration of influenza and COVID-19 vaccines: Guidance for pharmacists”.
Vaccination is a key strategy in the prevention of COVID-19 and influenza, improving quality of life. Administering vaccines against COVID-19 and influenza at the same time is safe and increases uptake of each vaccine and increases protection against both diseases, according to new guidance “Optimising vaccination through coadministration of influenza and COVID-19 vaccines: Guidance for pharmacists” published by FIP.
The guidance includes focus on opportunities for coadministration of the two vaccines and how pharmacists can contribute to global health by supporting this. It explains that while there is a need for more data on safety and effectiveness of different combinations of vaccines, the currently available evidence supports coadministration, as highlighted by guidelines issued by the World Health Organization.
Gonçalo Sousa Pinto, FIP lead for practice development and transformation, and coauthor of the guidance, said: “Many countries still do not have pharmacy-based vaccine administration services. FIP encourages pharmacists around the world to advocate pharmacy vaccines administration programmes and to seek legislative approaches to facilitate their implementation. Where such regulations are already in place, advocating pharmacybased coadministration of flu and COVID-19 vaccines will contribute to improving vaccination coverage against both diseases”.
Says the report, “Vaccination is key to preventing disease and improving quality of life for people of all ages. In the past couple of years, vaccination has become an important topic on the agendas of policy makers, healthcare professionals and society overall. The recent pandemic highlighted the central role that immunisation
plays as a pillar of primary health care and universal health coverage.
“While vaccination against seasonal influenza has been well established for decades and is recommended in many countries on a yearly basis, particularly for older adults and other vulnerable population groups, flu vaccination coverage rates remain below the World Health Organization (WHO) recommended target of 75% of adults above 65 years of age except in a handful of nations. As COVID-19 evolves into a post-pandemic phase, with multiple variants of the virus that, albeit less lethal, are highly transmissible, it will continue to affect millions around the world and to be a significant threat — just as flu is — to the health and lives of the most vulnerable members of our communities. Having access to the vaccine is therefore an important step to prevent disease and alleviate pressure on health systems.
“Coadministration of COVID-19 and influenza vaccines can provide a critical opportunity to increase protection of patients and the community against the dual impacts of the respiratory illness caused by these viruses, as highlighted by this publication.
This publication explores how vaccination strategies for two important respiratory conditions — COVID-19 and influenza — can and should be considered together, combined in an effective way to improve uptake rates for both vaccines.
“Pharmacists can highlight the importance of vaccination to highrisk groups, as those are frequently visiting community pharmacies to access medicines and services. Pharmacies were used in several countries as places to deliver COVID-19 vaccines and to provide another extensive access point to these vaccines. Many countries
Key messages
also provide influenza vaccination in pharmacies. However, as many countries still do not have pharmacy-based vaccine administration, it is important to reflect on the main aspects that can facilitate its implementation in the future. Coadministration of vaccines can have a big impact on the increase in vaccination coverage rates, as it can be convenient, save patients’ time and increase the probability that people will be fully vaccinated, as they might not return for a second vaccine in situations where they are given separately.”
• Scientific evidence and WHO guidelines support that coadministration of influenza and COVID-19 vaccines with inactivated vaccines is acceptable in terms of safety and reactogenicity, as well as efficacy and immunogenicity.
• The WHO considers that “coadministration of an inactivated seasonal influenza vaccine and any dose of a COVID-19 vaccine is acceptable, given that the known risk of serious illness for adults infected with influenza virus or SARS-CoV-2 is substantial”.
• Coadministration is convenient, saves time, avoids missed opportunities and provides a safe and effective win-win for people and healthcare professionals.
• Each time a person walks into a pharmacy is an opportunity to engage in conversations about vaccination.
• Leveraging the accessibility, convenience and professionalism of community pharmacies to build confidence in vaccines, raise awareness of the importance of vaccination — especially among vulnerable groups — and ultimately to administer vaccines is an effective and powerful way of increasing vaccine uptake.

• Actively promoting the coadministration of the influenza and COVID-19 vaccines in the same visit further enhances convenience, which is a central pillar of any person-centred approach to vaccination.
• Pharmacists can highlight the importance of vaccination to high-risk groups, as these frequently visit community pharmacies to access medicines and services.
• High-risk groups for flu and COVID-19 vaccination include older adults and people with comorbidities, among other groups that pharmacists may target — in addition to getting vaccinated themselves.
PHARMACYNEWSIRELAND.COM 66
The complete range of pain relief
Paralief Range Pain Relief - Full prescribing information is available on request. For sale through pharmacies only. THE STATED DOSE SHOULD NOT BE EXCEEDED. Please refer to the individual product Summary of Product Characteristics.





Paralief Sinus Tablets contains paracetamol and pseudoephedrine hydrochloride PA 126/339/1
Paralief Night Film-coated Tablets Contains paracetamol and diphenhydramine HCl PA 126/338/1






Paralief Extra Film-coated Tablets Contains paracetamol and caffeine PA 126/337/1




Paralief 500mg soft capsules – contains paracetamol PA 126/020/007
Paralief 500mg Tablets Contains paracetamol PA 126/20/1 (24 pack size)





Paralief Hot Lemon 600mg Powder for Oral Solution in Sachet Contains paracetamol PA 126/20/6


Paralief 500mg Effervescent Tablets Contains paracetamol PA 126/20/4
PA Holder: Clonmel Healthcare Ltd., Clonmel, County Tipperary







































For more information go to www.clonmel-health.ie


Date prepared: January 2022

2022/ADV/PAR/006H
Keeping Their Eyes on the Future
This year has marked milestones for many businesses, not just across Ireland but across Europe. As the waves of the Covid-19 pandemic continue to ebb away, new opportunities and those which had previously been put on the backburner are arising.
We spoke with Country Manager Diarmuid Gavin to learn more about the exciting developments in the pipeline for this industry leader.
Driving Innovation
This is especially true for Théa Pharma, who are embracing the potential of the future.
Théa Pharma is renowned as being the Number 1 ophthalmology brand in Ireland; an innovative company solely dedicated to developing high-quality products that support ophthalmic care and eye health across Ireland.
2022 has already been a special year for the company. “In many ways, it is the year we have all been waiting for,” Diarmuid tells us.
“Driving Innovation, Education and Professionalism in improving Eye Health has been our motto from day one. This year Théa Pharma Ireland has become a reality

moving from a joint venture to a full subsidiary of Théa global, allowing us to offer our customers and patients the full Théa experience.
“Our brand-new, state of the art offices located in Castlebar, Co Mayo offer us the opportunity to invest further in Ireland while staying closer to the increasing wants and needs of customers and patients for improved eye care and a better quality of life.”
By developing treatments, providing information and sharing knowledge with specialists around
Diarmuid Gavin, Country Manager Théa Pharma Ireland
“The key to Théa’s growth is a combination of scientific, technical, regulatory and commercial expertise, unique in the world of Ophthalmology”
PHARMACYNEWSIRELAND.COM 68 Corporate Profile
the world, Théa Pharma enable everyone to keep their eyes wide open. Théa specialise in preservative-free treatment.
What led the company to their leading ranking? Diarmuid explains, “Théa possesses 150 years of knowledge and expertise in ophthalmology. We are 100% dedicated to eye health and world leaders in 100% preservative free eye care solutions.
“The key to Théa’s growth is a combination of scientific, technical, regulatory and commercial expertise, unique in the world of Ophthalmology. The Chibret family own and run Théa, they pride themselves on reinvesting in discovering future innovations.
Road Mapping for Pharmacists
“Over the last few years we have placed a strong emphasis on OTC. We provide Pharmacies with a full scope of trade and digital marketing offerings, merchandising and emerchandising, a clear roadmap for Pharmacists to increase profitability while enjoying high margins, as well as working together to provide expert Eye Care advise and raising awareness on the importance of Eye Health.
“And I want to thank wholeheartedly all Pharmacists throughout Ireland for helping us raise awareness on the importance of eye care. The Eyes are the windows to our soul and body. Let’s take good care of them!”
Much like the rest of the industry, the team behind Théa were not without their challenges when it comes to the pandemic, presenting the company with one of their largest hurdles to date. But as Diarmuid points out, ensuring their team and their customers are kept at the heart of everything has driven morale and resilience.
So what sets Théa apart from their competitors?
Diarmuid says the answer to this is four-fold. “Firstly, our products are 100% preservative free which means they wont damage or irritate the eyes. Secondly, our products are clinically tested and proven to treat various symptoms of eye care conditions. For example for Dry Eyes, which is a rapidly growing market, we offer Thealoz Duo eye drops which are Europe’s number one dry eye drop, 100% preservative free and clinically proven to treat symptoms of dry, stingy, tired eyes. In Blepharitis we have Ireland’s No 1
daily eyelid cleanser Blephaclean which is 100% preservative free and clinically proven to treat symptoms of eyelid inflammation.
“Furthermore, each product offering allows the Pharmacist to enjoy high levels of margin and profitability, and lastly, because we are 100% dedicated to eye health, our product portfolio is extensive and covers all eye care needs including Dry Eyes, Glaucoma, Eyelid inflammation, Blepharitis, Eye nutrition, Infection and Allergy.”
Overcoming Challenges
“Dealing with the Covid-19 pandemic has been, above all, about people,” he reflects. “From all the people working in the healthcare sector, who have willingly put themselves in harm’s way, to the people who have kept essential services running, we owe them all a tremendous thanks – today more than ever. The Covid-19 pandemic has gone through phases, each of which is characterised by a different set of needs and requirements that have impacted all businesses.
“What it did for us, was to force us to respond to, cope with, and look beyond the crisis. People are
the first line of resilience for the workforce during a crisis. From the very first moment we stayed close to our people ensuring they have all they needed, strengthening the ‘work from home’ experience with much needed fun that kept morale at a high level.
“We provided guidance on alternative ways of working while protecting productivity, performance, and safety for each work location. We adopted our work environment to be more agile, flexible, and clear open communication gave our team reassurance and short-term direction.”
It can be true to say that the pandemic also forced the hand of many businesses into the digital era.
Diarmuid adds, “Furthermore, we accelerated the digitalisation of our internal, customer and supply chain interactions and their internal operations by three or four years. Once ‘nice to have,’ digital capabilities are now a ‘must have’ to build resilience for a sustainable future ahead.
“While we can put 2021 under the theme ‘new normal’ we are now in a transition phase toward

“I want to thank wholeheartedly all Pharmacists throughout Ireland for helping us raise awareness on the importance of eye care. The Eyes are the windows to our soul and body. Let’s take good care of them!”
Diarmuid Gavin, Country Manager Théa Pharma Ireland
PHARMACYNEWSIRELAND.COM 69
the “next normal.” We learn as we go and can build on this experience to be prepared for future disruptions. Perhaps most important is long-term adaptability and resilience. We will undoubtedly face new challenges caused by geopolitical events, climate change, health crises, energy crisis and the like. Companies must be able to actively manage continuous change and adapt to new circumstances.”
The Ophthalmology Market Value
The ophthalmology market and its value to pharmacy has been steadily increasing over the last number of years but more recently it has visibly accelerated.
Diarmuid adds, “The pandemic accelerated rapidly the growth that was already occurring the previous years. In 2019, 1 out of 5 adults suffered from dry eyes. Within just 3 years we saw a
Diarmuid Gavin, Country Manager Théa Pharma Ireland
“The market is growing rapidly and Pharmacists need to be aware of the increasing needs for eye health that more and more people and families around Ireland have. Education is the key. Preservative free products are the present and future in ophthalmology. As the number 1 Group in Eye Care in Europe and world leader in 100% preservative free products, Théa Pharma continues to stay ahead and complete its range of eye care solutions to satisfy the full needs of all Ophthalmologists, Optometrists, Pharmacists and Patients.
“Already in 2022 we have launched 4 new pioneering and innovative eye health products that cover a wide range of eye care needs from eyelid warming and cleansing to evaporative dry eye solutions and leading products for dry eyes caused by allergies.”
The eye care market continues to show significant growth, how can community pharmacists make the most of this segment in reaching customers? Diarmuid concludes by stating,
“I would urge all pharmacy teams to consider this. How much space and time have you dedicated to eyecare?”
“Community pharmacists play a crucial and significant role in promoting the right eye care solutions for their patients. We brush our teeth morning and evening and yet we rarely take care of our eyes unless we have a problem; You can replace a tooth but not an eye.
dramatic increase and as of 2022 dry eye sufferers account for 1 out of 2 of the general population which means almost half of the population are suffering from dry, tired, itchy, stingy eyes.
“Eight out of 10 dry eye sufferers experience symptoms of blepharitis. Google search for eye health keywords increased by a staggering +1,078% during the pandemic. The increase in screen time use, the Mask Associated Dry Eye symptoms (MADE), our environment, air conditioning, menopause, poor tear quality and ageing are some of the contributing factors for this new, harsh reality.”
According to IQVIA’s Ireland General Manager, Gwynne Morley, the OTC market is recovering faster than expected following the impact of Covid-19. Is this sentiment true for eye care we asked Diarmuid.
“It is. The eye care market is increasing significantly and will continue to do so in the years to come. Based on IQVIA data over the last 5 years the Dry eye market has increased by +37%. Between 2016-2021 the eyelid market increased by +62%.
1 out of 5 people is allergic and more than 60% of them have eye related allergy symptoms. Studies show that younger people are also affected more and more by dry eyes.”
Opportunities for Pharmacy
Diarmuid is keen to highlight the upcoming opportunities and potential within ophthalmology for community pharmacists here, and explains more about how he and his team will be supporting the profession in embracing these.

“Eyecare is the second most valuable and important product category based on total value within the Irish Pharmacy, just behind skincare,” he notes.
“Quality plays a huge role when proposing an eye care product. Is the solution 100% preservative free? Is it clinically proven and tested?
“Our products are indicated to battle and treat various serious eye symptoms such as dry eyes and blepharitis. Most importantly, we ensure high margins and profitability as well as full online and offline marketing support including merchandising to ensure the right shelf space for the eye care category. We have a full Pharmacy team that regularly visit Pharmacies around Ireland as well as dedicated Medical, Surgical and GP teams for dedicated visits to Ophthalmologists, GPs and Hospitals. Education is the key and we offer numerous webinars and training. We are fully dedicated to eye care therefore we guarantee high quality products with high margins and an expert team to help and train Pharmacy teams around Ireland to deliver the best advice and care for patients.”
“I would urge all pharmacy teams to consider this. How much space and time have you dedicated to eyecare?”
PHARMACYNEWSIRELAND.COM 70 Corporate Profile





TIRED, RED OR STINGY EYES? www.theapharma.ie Abak® System The most widely used preservative-free bottle in the world BEST EYE CARE PRODUCT 2021 IPN ThealozDuo OTC & Retail cy Produc Awards IRISH PHARMACY 2021Fixed combination of Trehalose and Hyaluronic acid for synergistic action Hydrates – Lubricates – Protects – Repairs Clinically proven to treat symptoms of Dry Eyes 100% preservative FREE Suitable for ALL dry eye sufferers including contact lens wearers
5
Minute Module:

Management and Treatment of – Cough
Following
Learning Objectives
After
After completing this module, you should recognise the varying types of cough that may present to the pharmacy and the OTC treatments available for each. Where pharmacy management is appropriate you will be able to explain to patients the nature of their type of cough and suggest possible solutions. You will be able to give advice on current recommendations symptom management and know how to signpost to relevant resources. Where a patient wishes to purchase OTC treatments, you should be able to support that person to make appropriate choices.

Cough is a common symptom and complaint, particularly during the winter months, and is associated with a wide variety of aetiologies and clinical conditions. A cough is one of the most common medical complaints, and is the most common symptom for which people seek advice at their community pharmacy.
Coughs are classified as acute, subacute or chronic. A cough is considered ‘acute’ if it is present for less than 3 weeks. A ‘subacute’ cough, is one lasting 3 to 8 weeks, most often due to a recent
respiratory infection. A cough of greater than 8-week duration is considered a ‘chronic’ cough.
Most coughs are self-limiting and will usually self-resolve within 3 weeks, however, it is important for the person to see or be referred to the GP, if the cough lasts more than 3 weeks, or if the person is coughing up blood (haemoptysis).
Smoking is a leading risk factor for coughs, and additional common causes of an acute cough include acute rhinosinusitis, pertussis, acute exacerbations of COPD, allergic rhinitis, asthma, congestive heart failure, pneumonia, aspiration syndromes, and pulmonary embolism. An acute cough is also a main symptom of SARS-CoV-2 (Covid-19) infection, and this must always be considered when a patient presents with a cough, and investigated and treated appropriately.
Those presenting to the pharmacy with a cough should be referred to their GP if they:
• Are finding it difficult to breathe
• Are short of breath or have a wheeze
• Are coughing up blood (Haemoptysis)
• Have a hacking cough or cannot stop coughing and it is getting worse
• Have a recurrent nocturnal cough
Coughs and colds in children are frequent and usually self-limiting, and there is no clear evidence to support the use of these products in children under six. Children under six years should not be given OTC cough and cold medicine containing;
• brompheniramine, chlorphenamine maleate, diphenhydramine, doxylamine, promethazine or triprolidine (antihistamines)
• dextromethorphan or pholcodeine (cough suppressants)
• guaifenesin or ipecacuanha (expectorants)
• phenylephrine hydrochloride, pseudoephedrine hydrochloride, ephedrine hydrochloride, oxymetazoline, or xylometazoline hydrochloride (decongestants)
Certain cough remedies however, made with mainly natural ingredients including traditional herbal medicinal products (THRs) are licenced for sale in Ireland, available in pharmacies nationwide, and suitable to use for children over 12 months old. A range of products are specifically formulated for children from 1 year of age, and can be used to treat dry or chesty coughs.
Opioid derivatives are commonly sold as cough suppressants / antitussives to suppress the cough reflux from the medulla in the brain stem to provide relief from frequent coughing. Common drugs include dextromethorphan, pholcodine, dihydrocodeine, and codeine. Preparations may be sold as syrups, medicated lozenges, tablets or capsules.
Medication licensed for the management of productive coughs fall into two categories: expectorants (protussives) and mucolytics. Like antitussives, these drugs come as syrups, medicated lozengers, tablets or capsules.
Herbal medicines are popular in the treatment of minor medical conditions, including coughs. Herbal medicines are those with active ingredients made from plant extracts such as leaves, roots and flowers. Like conventional medicines, herbal medicines have an effect on the body, and can be potentially harmful if not used correctly. While traditional herbal remedies are safe to use for most people, some herbal medicines may not be suitable for certain individuals including; those taking other medicines; people with serious health conditions, such as kidney or liver disease; people who are undergoing surgery; pregnant or breastfeeding women; some older people and children.
There are a wide variety of herbal remedies available for coughs in pharmacies. Consumers should check for a traditional herbal registration (THR) marking on the product packaging, which means the medicine complies with quality standards relating to safety and manufacturing, and provides information about how and when to use it.
Now I should:
Update my knowledge of the signs, symptoms, causes and treatment of cough
Reassess my and my staffs’ ability to do a risk assessment
Train my pharmacy counter assistants to ensure they can meet the points in the training checklist
72 | PHARMACYNEWSIRELAND.COM
on from the September issue Continuing Professional Development on the Management of Cough, this 5-Minute Learning Module is designed to enhance the community pharmacy team understanding and ask further questions as to how you can support and advise patients.
studying this module, pharmacy teams will: Understand that cough is a common symptom and complaint, and is associated with a wide variety of aetiologies and clinical conditions. Be aware of the different types of presenting cough (acute, subacute or chronic) and identify the correct pharmacy treatments Identify red flags and/ or danger symptoms, and know when a patient needs to be referred to the GP or seek urgent medical attention. Be aware of any potential drug-drug interactions or contraindications, considerations and questions to ask the patient before supplying OTC or prescribed cough medication
IRELANDS No.1 COUGH BRAND*

1

Associated with Common Cold, Bronchostop Junior is a MD. 2 Based on Traditional use, Bronchostop Adult is a THR. * Based on combined IQVIA Data - June 2022. Buttercup Bronchostop Cough Syrup contains thyme herb extract and marshmallow root extract. A traditional herbal medicinal product for the relief of coughs, such as chesty coughs and dry, tickly, irritating coughs and catarrh, exclusively based upon long-standing use as a traditional remedy. Adults and children over 12 years: 15ml every 4 hours, 4 times per day. Max 6 doses (90ml) per day. Max dose should not be exceeded. To be taken 30 to 60 minutes before or after intake of other medicines. Not recommended for children under 12 years. To be administered undiluted or diluted in water or warm tea. Seek medical advice if symptoms persist after 7 days or if dyspnoea, fever or purulent sputum occurs. Contraindications: Hypersensitivity to marshmallow root, thyme, to other members of the Lamiaceae family or to any of the excipients. Warnings and precautions: Asthmatics and atopic patients should consult a doctor before using the medicine. Contains E218 and E216 that may cause allergic reactions (possibly delayed). Patients with HFI, glucose-galactose malabsorption or sucrase-isomaltase insufficiency should not take themedicine. The additive effect of concomitantly administered products containing fructose (or sorbitol) and dietary intake of fructose (or sorbitol) should be considered. Pregnancy and lactation: Not recommended. Side effects: pruritus, rash, urticaria, angioedema, anaphylactic reaction, oral mucosal blistering, abdominal pain, diarrhoea, nausea, vomiting, dyspnoea, exacerbation of asthma.

Legal classification: GSL. TR 2006/001/001.TR Holder: Kwizda Pharma GmbH, Effingergasse 21, A-1160 Vienna, Austria. RRP (ex VAT): €4.99 Date of preparation: 05/2022. SPC: http://www.medicines.ie/medicine/16380/SPC/Buttercup+Bronchostop+Cough+Syrup/ Bronchostop Junior is a medical device according to Directive 93/42/EEC, used to relieve any cough (dry & chesty) associated with a cold for children from 1 year. Children under 3 years of age should consult with a doctor to exclude more serious diseases being present. Use in children under 1 year of age is not recommended. Children aged 1 year and above: 5ml up to 3 times daily. Children 2 to 3 years: 5ml up to 4 times daily. Children 4 to 5 years: 7.5ml up to 4 times daily. Children 6 to 11 years: 15 ml up to 4 times daily. Always read the Instructions for Use. Date of preparation: 05/2022.
Date of preparation: August 2022. IRE/BRO/2022/37

TO RELIEVE ANY COUGH1,2









Funding for New Health Projects






The Health Research Board has announced its support for three University College Cork-led projects that will tackle health inequality, prevent childhood obesity, and explore how our gut can affect our memory, concentration, and social interactions.
The Health Research Board (HRB) announced that it was funding nine new projects under Emerging Investigator Awards for Health (EIA) 2022, three of which are led by researchers at University College Cork (UCC).

Based in UCC’s Institute for Social Science in the 21st Century (ISS21), Dr Monica O’Mullane has been funded to develop a Health Impact Assessment Implementation Model (HIA-IM) - a tool aimed at tackling health inequalities.
“Public health research has shown that our health and wellbeing are affected by the circumstances into which we are born, grow, live, work and age,” Dr Mullane explained.

“HIA-IM is now needed more than ever to ‘health-proof’ public policies as we cope with challenges such as the global climate emergency. HIA-IM will help reduce the risk of policies that impact adversely on health and wellbeing, with particular reference





to Ireland’s marginalised groups,” she said.




A lecturer in UCC’s School of Public Health, Dr Karen Matvienko-Sikar has been awarded funding to develop a standardised approach to measuring infant feeding outcomes to prevent childhood obesity.
“Approximately one in five children experience obesity worldwide, making it a major public health challenge. What, how and when children are fed in the first year of life contributes to childhood obesity risk,” Dr Matvienko-Sikar said.
“This research aims to provide researchers, practitioners, and policymakers with a toolkit of measurement instruments, such as questionnaires and clinical assessments, to better evaluate infant-feeding interventions and prevent childhood obesity.
“This will enhance the evaluation of interventions to prevent




















childhood obesity, with potential for significant impact on, and meaningful improvements for, population health,” she said.
Dr Linda Katona is a neuroscientist based at UCC’s Department of Anatomy and Neuroscience and the APC Microbiome Ireland SFI Research Centre has also been awarded by the HRB’s Emerging Investigator Awards for Health. Her research seeks to identify the gut microbiome-responsive brain biomarkers of cognitive impairments relevant to schizophrenia.
“Ireland has among the highest rates of mental illness in Europe, and schizophrenia is one of the leading psychiatric diagnoses nationally and the one carrying the biggest economic cost. Schizophrenia patients have problems remembering their past, are unable for social interactions and cannot retain information long enough to use it. Gut microbes
affect our mood and motivation and interfere with our mental abilities,” Dr Katona said.

“Recent research shows that information from our gut gets transferred to our brain through the vagus nerve, and that disruptions in the communication between gut microbes, vagus and brain often accompany the core symptoms of schizophrenia. This project will examine this and attempt to answer questions such as how our gut microbiome, through the vagus nerve, interferes with our memory, how it influences our social interactions, and how it can affect our concentration.
“By exploiting these gut-brainbehaviour relationships for novel, better-targeted therapeutic interventions, this study could revolutionise how schizophrenia and similar brain disorders are treated, significantly improving the lives of millions of people globally,” she said.
PHARMACYNEWSIRELAND.COM 75
News *suitable for children from 6 months & pregnant women If symptoms persist beyond the recommended usage timeframe, the causes of constipation should be investigated by a doctor. Always read the label. Distributed in Ireland by Clonmel Healthcare Ltd. *consultation with a doctor is advised. Pharmacy only brand To place an order, contact your Clonmel Healthcare Area Representative or call our freephone order line on 1800 262626 WORKS WITHIN 24 to 72hrs WORKS WITHIN 24 to 72hrs GENTLE RELIEF GLUTEN LACTOSE & SUGAR FREE WORKS WITHIN 24 to 72hrs GENTLE RELIEF GLUTEN LACTOSE & SUGAR FREE 2022/ADV/DUL/237H ORAL SOLUTION Gentle & effective relief of constipation and irregularity 250ml DOUBLE ACTION POWDER FOR ORAL SOLUTION Gentle relief of constipation and bloating 200g
Peak Trading 2022: A Pharmacy Guide to Success
The holiday and therefore peak trading period is just around the corner. Following several years of lockdowns, reduced social contact and uncertainty consumers are ready to return to their pre pandemic festive traditions and for many that includes shopping.
 Written by Orla Cooney, Chief Operating Officer, Magico
Written by Orla Cooney, Chief Operating Officer, Magico

products, this is a fantastic way to encourage your customers to increase their basket value. Examples of these products include offering a tanning mitt with a tanning cream or make up brushes with makeup
• Employ Out of Stock email alerts so you never miss an opportunity to convert a sale when you restock
Providing excellent customer service can also help you stand out from the competition during peak trading periods. Superior customer service will also bring customers back to your online store long after the peak trading period. Everything from their first interaction with you, to transparent and fair delivery and returns policies are crucial in developing long lasting relationships with your customers. Surprise your customers, add free samples with orders, allow your customers to add gift messages, go above and beyond with customer service, or offer a discount on next purchase.
help those shoppers who have run out of ideas.
In the peak shopping frenzy, customers are likely to browse numerous online stores and place multiple items in their shopping carts. Often the customer gets distracted by another product or promotion and these carts become abandoned. Use email to entice these customers back, remind them of their potential purchases and consider offering a promotional incentive to encourage conversion.
This year however consumers are facing unfamiliar pressures to their disposable income resulting from increases to cost of living and spiralling energy costs and retailers continue to face relentless supply chain issues. It is clear that in a highly competitive market online pharmacists will need to work harder than ever to ensure a successful peak trading period.
Where to begin? With Planning
September & October is all about planning. Consider your stock, resourcing, promotions, and digital marketing strategies, by October you want to ensure that you have all the plans in place to maximise the peak trading opportunity. Do you know what product ranges you want to push, have you sufficient stock, what discounts to offer, what campaigns to run, what channels to use and do you have the assets and resources in place to make the magic happen.
Also consider the customers user experience when they visit your website. Optimise your online store ahead of the shopping rush to keep your customers converting.
• Advanced site search will offer your customers search as you type functionality and ensure that the most relevant products appear first, increasing your conversion chances.
• Personalisation services will customise their online shopping experience and make recommendations based on individual browsing histories.
• Take every opportunity to upsell and feature complimentary
• For high ticket items like hair dryers, styling tools etc, why not offer the option for the customer to pay in instalments. Great way to entice and convert the organised early shopper particularly when customers are more considered about spending this year
• For multi outlet retailers allow customers to view instore stock availability across your store network from the product detail page. Offer them the control to select home delivery or the option to collect from their local store.
• Optimising your checkout to provide a painless checkout process boosts your conversion rate and gives customers more reason to return to your online store.
At the heart of your planning should be your omnichannel strategy, successful Retailers don’t think of online retail and physical retail as separate functions, it is all Retail. Your customer could see a product on your Instagram page, order it online via your website but return it in-store OR see a product in-store and go home and buy it later online so make sure that your various marketing channels are synced and do not function independently
November is the time to capitalise on the organised shopper, those who know what they want and are price sensitive. Marketing should be focussed on showcasing your best offers and ensuring you stand out from the competition. Email & SMS marketing are excellent means of staying connected with customers during this time, promote your offers in advance, create a buzz with pre-sale exclusive offers and reward loyalty with access to this years “must haves” before stock runs out.
Customers are also more green conscious then ever and are using their buying power with a renewed desire to buy from brands that demonstrate a genuine commitment to sustainable business practices. Sourcing ecofriendly materials, the consolidation of shipments, reducing the distance packages travel and minimising paper and packaging used for shipments and returns are ways that Retailers can contribute to a more sustainable future.
December is the time to target the last minute shopper.
Time is of the essence with Christmas approaching so take the stress out of your customers shopping experience and focus on your delivery and customer service terms. Reassure your customers that their purchases will arrive on time and that you will deal with any issues that might arise without delay. Building this trust will not only convert Christmas shoppers but will have those shoppers returning post-festivities. For the reluctant shopper make it easy with gift guides like Gifts for Mum and Gifts for Teenagers etc, Gift Hampers and Gift Cards will also
Post-Christmas will see the return of the deal hunter, it is important that you have your promotions in place, and you are ready to again stand out from the competition. Depending on what stock you have left over you also need to be prepared to pivot your plans and react to the opportunities that may present themselves.
To succeed this peak trading period you need to consider the organised shopper, the deal hunter and the last minute frenzied shopper and create a shopping experience that exceeds all your customers’ expectations.
Orla Cooney, Chief Operating Officer, Magico with over 20 years’ experience. Orla’s strength is in her ability to focus on the practical application of ecommerce strategies for her clients, she works with clients to identify the best strategy for them and how to deliver it.
Magico (www.magico.com) is a client-first, innovative eCommerce Agency based in Ennis, Co. Clare, that has been delivering websites for Irish retailers since 1999 and specialises in getting pharmacies online & helping them to grow fast.
PHARMACYNEWSIRELAND.COM 76 Pharmacy Retail

Functionality tailored to pharmacy industry Existing integrations with top pharmacy software Supporting Ireland’s leading pharmacy retailers Bring your pharmacy online & grow fast ocooney@magico.com | www.magico.com IRELAND ' S PHARMACY ECOMMERCE SPECIALISTS CONTACT
Children’s Health and Wellness in Ireland
Paediatric healthcare in Ireland is currently undergoing a revolution
Children’s Health Foundation is working to support sick children and their families in Children’s Health Ireland (CHI) hospitals, Crumlin and Temple Street, and urgent care centres Tallaght and Connolly. We raise vital funds to support sick children and their families in CHI hospitals and urgent care centres.
standards of care, world-class facilities, and benefit from the most up-to date research that will change young lives for the better.
Children’s Health Ireland was formed January 1st, 2019, following the enactment of the Children’s Health Act 2018 in November 2018. This provided for a dedicated board, appointed by the Minister for Health, to take over responsibility for services currently provided by Dublin’s three children’s hospitals, Our Lady’s Children’s Hospital, Crumlin, Temple Street Children’s University Hospital, and the National Children’s Hospital, Tallaght. Latterly an urgent care centre in Connolly Hospital, Blanchardstown joined under Children’s Health Ireland’s governance, this is in operation today and will serve as one of two urgent care centres supporting the new children’s hospital, along with Tallaght hospital. Children’s Health Ireland (CHI) governs and operates acute paediatric services for the greater Dublin area and all national paediatric services, some of which are on an all-island basis.
In addition to this, a new state-of the art paediatric hospital is being built in Dublin city at the St James
site. This hospital will form the centre of a hub-and-spoke model which will provide care for every single child all over Ireland. The new children’s hospital is the central cog of the National Model of Care for child healthcare in Ireland.
Childhood illness in all its forms is persistent, indiscriminate, and often devastating. As many of the children who pass through the doors of CHI sites every day have rare and complex conditions that are life-limiting or life-threatening, Children’s Health Foundation know all too well that the burden of disease can have a significant impact on a child and their family.
Children’s Health Foundation is the largest fundraising charity in Ireland supporting sick children. From the funding of cutting-edge equipment and technologies to the refurbishment of critical hospital facilities, Children’s Health Foundation is committed to supporting the provision of world class care for children in need.
Ensuring that patients continue to have access to the very highest
This can only be achieved through supporters’ funding, bringing real long-term impact for sick children and their families. From understanding disease progression in children with cystic fibrosis, to providing tailored treatment options for children who have been diagnosed with cancer, these funds will allow Children’s Health Foundation to invest in the innovative research programmes that will make each day easier for those children battling chronic illness, enable us to provide state-of- the-art equipment and treatment programmes, and allow us to offer supports to children and their families.
Sona has partnered with the Children’s Health Foundation



since 2019 as one of their charity partners. This October, Sona will launch a Golden Ticket campaign in aid of Children’s Health Foundation to support the life-saving work of CHI hospitals and urgent care centres. A golden ticket will be hidden inside a product from the Sona Children’s range.
During this October and November, Sona will launch a Golden Ticket campaign in aid of Children’s Health Foundation to support the life-saving work of CHI hospitals and urgent care centres. A golden ticket will be hidden in the packaging of one Sona’s products. Whoever finds the golden ticket will win ¤1,000 in cash, and will also trigger a ¤30,000 donation from Sona to Children’s Health Foundation. For more information, visit www.childrenshealth.ie/sonagolden-ticket and or visit www. Sona.ie
PHARMACYNEWSIRELAND.COM 78 Children’s Health





FIND THE PLUS Sona will donate €30,000 to Children’s Health Foundation in support of Children’s Health Ireland at Crumlin, Temple Street, Tallaght, and Connolly. Hidden inside a product from the Sona children’s range & WIN €1000 The lucky winner of the Sona Golden Ticket will get to present the cheque to Children’s Health Foundation on behalf of Sona Nutrition. The Sona Golden Ticket competition will run Oct / Nov 2022 GOLDEN TICKET Congratulations, you are the lucky winner of the €1000 cash prize Sona proudly Support S RCN: 20042462 CHY: 13534 Ir ISH v I tam I n S
Promoting good Oral Health in the Pharmacy
Oral health plays a key role in general health and wellbeing and is important at all stages of life. The available evidence shows that oral diseases share important common risk factors with the four leading chronic disease – cardiovascular diseases, cancer, chronic respiratory diseases and diabetes. Oral diseases such as tooth decay, periodontal (gum) disease and mouth head and neck cancer can be detected with the help of the pharmacy community delivering oral health promotion messages and information. Evidence has also shown that pharmacist-led continuity of care, can and does improve patient outcomes.
For some people, a visit to the dentist can be put on hold, as something non urgent, for a variety of reasons, and indeed, may only attend if they require treatment. However, people frequently visit their local pharmacy and will listen to advice from the Pharmacist who is well equipped to help. For example, currently it is possible to purchase a temporary filling material repair kit from a pharmacy if a loose filling/crown needs to be repaired (temporarily) before visiting the dentist. A pharmacist may be asked about denture repair kits for broken dentures, or to recommend appropriate over the counter pain medication in the case of a toothache (rinsing the mouth with warm salt water may also help), until the person visits a dentist.
Tooth Decay and Oral Hygiene
Tooth decay is the most widespread noncommunicable disease according to the World Health Organization and can be traumatic for both child and adult, and may result in pain, lead to infection and result in hospitalisation and extraction of teeth under general anaesthetic. Good oral health is also essential for healthy ageing, a healthy mouth will improve general well-being and quality of life. Tooth loss and ill-fitting dentures in older people affects their ability to eat, speak or socialise properly. It also puts them at a higher risk for malnutrition, cardiovascular disease and infectious respiratory diseases such as pneumonia.
Poor oral hygiene and frequent consumption of sugary foods and drinks (cakes, biscuits, chocolate, sweets, fizzy drinks) are the main causes of tooth decay. Acidic foods and drinks like fruit juice and smoothies can also
cause dental erosion. Tooth decay is largely preventable, and the pharmacist can play a key role in reinforcing messages about healthy eating and good oral hygiene. General advice for both children and adults is as follows:

• When a baby is born, the first set of teeth is already under the gums so a clean damp cloth should be used to wipe the gums after a feed. As soon as the first tooth appears brush twice a day (at night-time and one other time with a soft toothbrush and water, do not use toothpaste for under 2’s unless advised by a dentist).
• Parents/carers should supervise teeth brushing until the age of seven years old and use a pea-sized amount of fluoride toothpaste (at least 1000ppm) for 2–7-yearolds, twice a day.
• Spit out toothpaste but don’t rinse after brushing (as this will wash the fluoride off the teeth
• Adults, brush twice daily with fluoride toothpaste (at least 1000ppm) at night and one other time, spit out toothpaste and don’t rinse. Floss daily.
• Make healthy food choices by eating more fruit and veg and avoid sugary snacks and drinks between meals.
• Unflavoured milk and water are the best drinks.
• Read food labels for sugar content, less than 5g per 100g is considered a low sugar.
It is not only the physical removal of plaque that is important in oral hygiene practices, but also noting that fluoride in toothpaste gives the tooth enamel the potential to heal. The pharmacist can recommend oral health products such as toothbrushes (these should be changed when the bristles are worn, about every 3 months), fluoride toothpaste, interdental brushes, floss etc. However, it is also important that the patient is encouraged to seek oral health advice and a professional opinion from a dentist.
Gum Disease
Gum disease is caused by a build-up of plaque on the teeth and around the gums, causing red swollen gums which bleed when brushing. If left untreated, gum disease (or gingivitis) will progress to periodontal disease which causes bad breath, receding gums, wobbly teeth and, ultimately, loss of teeth. Smoking also increases the risk of periodontal disease, smokers are more likely to get periodontal disease and prematurely lose their teeth than non-smokers.
Poorly controlled diabetes increases the risk of periodontal disease development, which in turn can make it more difficult to control diabetes. People with diabetes should be encouraged to have a good oral hygiene routine and regular visits to their dentist.
It’s also worth noting that hormonal changes during pregnancy can make women’s gums more vulnerable to pregnancy gingivitis. Advice to pregnant women about their oral health during pregnancy is important to both the mother and baby. Studies suggest a link between poor oral health and women delivering pre-term, low birth rate babies. Making healthy choices can positively affect their baby’s development including their teeth.
80 | PHARMACYNEWSIRELAND.COM






THE ANTIBACTERIAL PROPERTIES OF ESSENTIAL OILS HELPS LEAVE THE WHOLE MOUTH CLEAN AND FRESH 96% natural origin & biodegradable formula Helps maintain healthy gums For stronger teeth* * Enamel Protect only Alcohol & dyes 100% recyclable bottle* Made from 50% recycled plastic *Safety seal excluded. DISCOVER NATURALS KILLS UP TO 99% OF GERMS LEFT AFTER BRUSHING IE-LI-2200039
Mouth Head and Neck Cancer
Mouth Head and Neck Cancer is the sixth most common cancer in the world. Smoking and drinking alcohol are the most important risk factors, alcohol plays a role in up to half of all cancers of the mouth, head and neck in men in Ireland. It is useful to able to be signpost to alcohol and smoking cessation support services such as https://www2.hse.ie/ alcohol/ and www.quit.ie
Early detection saves lives so if a concerned customer has any of the following symptoms for more than 3 weeks refer them to their dentist or doctor:
A sore or ulcer in the mouth that does not heal, white or red patches inside the mouth, a lump in the mouth or neck. thickening or hardening of the cheek or tongue, difficulty chewing, swallowing or moving the tongue, numbness of the tongue or face, a persistent sore throat and hoarseness persistent nosebleeds and a stuffy nose or unexplained loose teeth.
A lesser-known fact is that the human papillomavirus (HPV) is also a risk factor for Mouth Head and Neck Cancer. Students in their first year of secondary school are offered the HPV vaccine as part of the school vaccination programme. For more information about mouth head and neck cancer, please see www.mouthcancer.ie
Medication
Some liquid medicines have a high sugar content. The Dental Health Foundation recommends sugar-free alternatives if they are available, especially where medicines are given frequently or are long term.
Dry mouth is a side effect of some medication. This is particularly uncomfortable and often gives rise to difficulty in speaking and eating and impacts negatively on quality of life. Furthermore, reduced saliva flow can give rise to an increased incidence of tooth decay, gum disease and also an increase in oral infection, such as candida albicans.
Saliva substitutes are generally available in pharmacies and useful if used just before eating, at night if you wake up because of dry mouth, or first thing in the morning. Sucking sweets regularly e.g., mints, boiled sweets or consuming sugary drinks can give temporary relief but will cause severe tooth decay in the absence of saliva. Chewing sugar-free gum may offer relief. We advise to limit the frequent consumption of drinks sweetened with sugar e.g., soft drinks, sugary tea, and also sugar-free drinks, because sugar/acid content may cause tooth decay and erosion. Sipping water frequently, and with your meal is best (fluoridated tap water will help to prevent tooth decay).
Some people require nutritional supplements or fortified drinks to maintain their calorie input, and these can have a high free sugar
content, putting them at further risk of dental caries, so recommend a sugar free option if suitable.
Visit the Dentist
It is highly recommended that everyone visits a dentist at least once a year, (even if they have no teeth of their own or wear dentures). The dentist will ensure that teeth and gums stay healthy and will also carry out a mouth cancer examination
Support and Resources
The Dental Health Foundation is at the heart of oral health promotion for over 40 years and supports all health professionals, including Pharmacists, by providing evidence based best practice resources to increase awareness amongst the public, empowering them to make healthier oral and general health lifestyle choices. Having the right information on tooth tips, diet and general health will help keep teeth healthy for a lifetime. Good oral health is of vital importance to the general health of everyone in Ireland.
Health Promotion is about empowering people to take control of their own lives so make every contact count. For further information about the Dental Health Foundation and to download our free resources please see www.dentalhealth.ie or link in with us on Twitter, Facebook, LinkedIn. Be aware of the factors that affect oral health and know where to go to get the best help and advice: www.dentalhealth.ie www.dentist.ie
For information about dental entitlements see www.citizensinformation.ie
International Symposium on Dental Hygiene
TePe were delighted to be key sponsors at International Symposium on Dental Hygiene 2022 this week and were on hand to showcase their full dental range of sustainable products and solutions.

The event is took place in the Convention Centre in Dublin for three days and the theme of the event was “The Future in Our Hands”. The symposium featured three days of presentations from a handpicked selection of global speakers, a full poster exhibition, sponsored sessions, and a packed exhibition hall.
The Association of Dental Educators in Europe (ADEE) has confirmed that ISDH 2022 is a peer reviewed event and attendance equates to 16 hours CPD or ECEC(d).
From left to right, Judy Caesley TePe UK, Amanda Sheehan TePe UK, Lina Gassner Kanters TePe Sweden and Edel Quinn Ocean Healthcare TePe Ireland
82 | PHARMACYNEWSIRELAND.COM
Promoting good oral health since 1965








Developed in collaboration with dental experts, TePe is the UK’s No. 1 selling Interdental Brush (IDB) and most recommended by dental hygienists.* IDB’s are highly effective in removing dental plaque between teeth and TePe offers a wide range in multiple sizes and handle lengths to suit everybody.



















We’re using a range of initiatives from raw materials to energy supply that reduces our IDBs carbon footprint by 80% – without compromising on product quality, efficiency or design.

Get the det ail s at tepe.com

* S ource: A sur vey of 20 1 dent al hygienist s in t he UK , Ip s o s ( 20 19) 2 Made in Sweden 80% l e s s CO
Topic Team TrainingShingles
In this series of articles, we provide pharmacists with information to develop and implement OTC team training sessions, aimed at ensuring safe and suitable recommendations, and appropriate pharmacist referral. Thanks to the team at totalhealth and Haven Pharmacies for this month’s topic: Shingles.

What is Shingles?
Shingles (Herpes Zoster) is a painful rash the occurs when a nerve underneath the skin becomes infected by the varicellazoster virus, the same virus that causes chicken pox. Unlike chicken pox, shingles is usually confined to one area of the body, although it may spread around the body depending on where the infected nerve lies and travels. Most people become infected with chicken pox during childhood; shingles is a reactivation of that virus.
Signs and Symptoms
The first sign of shingles is usually a tingling sensation or pain in one area of the skin. It may be accompanied by a headache or feeling generally unwell. The rash usually appears a few days later. Shingles rash is usually characterised by red blotches that quickly develop into fluid-filled blisters. Blisters may continue to develop for up to a week. Swelling under the rash and pain may also be experienced. Blisters slowly dry up and transform to scabs. Scarring can often occur. Pain is usually localised to the location of the rash but can be very severe.
Treatment
Anyone suspected of being infected must be referred to their GP immediately for treatment. Prescription treatments may include:
• Pain Killers
• Antiviral Medicines
• Steroids.
Consider:
Reflect on the following in assessing your own knowledge and your team’s training:
Is your knowledge up to date on shingles symptoms?
Are you familiar with shingles treatments, both Rx and OTC?
Is your knowledge up to date on shingles risk factors, including transmission risks?
Is your team aware of what patients must be referred to the pharmacist?

Self-Care
Patients diagnosed with shingles may benefit from OTC pain relief (provided it is safe with any prescription medication – always refer to the pharmacist). The following advice may also help relieve discomfort:
• Keep the rash clean and dry to reduce risk of further infection
• Wear loose-fitting clothing
• Apply a cool compress on the rash site several times a day.
It is not recommended to use antibiotic or antibacterial creams on a shingles rash, or to let dressing or plasters stick to a raw rash. Simple emollients or calamine lotion can be used to ease itching, and nonadhesive plasters can be used to cover weeping blisters.
Transmission
As already mentioned, shingles is the result of the reactivation of varicellazoster virus in those who have previously been infected with chicken pox. You cannot catch shingles from somebody with shingles. Reactivation of that virus is usually due to a lowered immune system, because of illness, immune-suppression, stress, or age. People who have NOT had chicken pox may be at risk of developing chicken pox when encountering someone who has shingles. The infection is spread through direct contact with a ‘live’ rash, i.e., skin-to-skin contact with a shingles rash before it has scabbed over.
Key Points:
Ensure your team understands and is confident explaining the following:
The OTC treatment options for patients experiencing shingles
Those people that should particularly be avoided by someone infected with shingles
The patients who should be referred to the pharmacist and why
How shingles is spread and how to avoid transmission.
Risks and Complications
There are potentially severe consequences associated with shingles infection, as well as with the transmission of chicken pox by those with shingles infection. In some cases, shingles can lead to complications, such as postherpetic neuralgia, where pain lasts for several months after the rash has gone. This is usually experienced by older people or those with a weakened immune system. There is also a risk of post-viral fatigue syndrome following a shingles infection.
Those infected with shingles should especially avoid:
• Pregnant people who have not had chickenpox before
• People with a weakened immune system – e.g., someone having chemotherapy
• Babies less than 1 month old.
Vaccination
There are two shingles vaccines licenced for administration by pharmacists in Ireland. Neither is part of the National Immunisation Plan and therefore must be paid for by recipients.
Those who may benefit from shingles vaccination include:
• Those aged over 50
• Anyone aged 18 and over with a compromised immune system
• Those who have not had chicken pox before.
Actions:
Your action plan for Shingles should include the following:
Your team has been trained on shingles symptoms and treatments
You have the appropriate range of products available
The risk factors and transmission dangers associated with shingles
WWHAM Protocol forms the basis of all interactions at the OTC counter
Update your CPD record.
84 | PHARMACYNEWSIRELAND.COM
powder and suspension for injection in vials (Please refer to SmPC before prescribing)
Composition: After reconstitution, one dose (0.5 mL) contains: Varicella Zoster Virus glycoprotein E antigen1,2 50 micrograms. (1 adjuvanted with AS01B containing: plant extract Quillaja saponaria Molina, fraction 21 (QS-21) 50 micrograms, 3-O-desacyl-4’-monophosphoryl lipid A (MPL) from Salmonella minnesota 50 micrograms, 2 glycoprotein E (gE) produced in Chinese Hamster Ovary (CHO) cells by recombinant DNA technology). Therapeutic indications: Prevention of herpes zoster (HZ) and post-herpetic neuralgia (PHN) in adults 50 years of age or older and in adults 18 years of age or older at increased risk of HZ. The use of this vaccine should be in accordance with official recommendations. Posology and method of administration: For intramuscular injection only, preferably in the deltoid muscle. Primary Vaccination: Initial dose of 0.5 ml followed by a second 0.5 ml dose 2 months later. For flexibility the 2nd dose can be administered between 2 and 6 months after the first dose. For subjects who are or might become immunodeficient or immunosuppressed and whom would benefit from a shorter vaccination schedule, the 2nd dose can be given 1 to 2 months after the initial dose. Booster doses: need not established. Contraindications: Hypersensitivity to the active substances or any of the excipients. Special warnings and precautions for use: The name and the batch number of the administered product should be clearly recorded. Appropriate medical treatment and supervision should be readily available in case of an anaphylactic event. Administration of Shingrix should be postponed in subjects suffering from an acute severe febrile illness. However, the presence of a minor infection, such as cold, should not result in deferral. A protective immune response may not be elicited in all vaccinees. Never administer intravascularly or intradermally; subcutaneous administration not recommended as it may lead to an increase in transient local reactions. Caution in individuals with thrombocytopenia or any coagulation disorder since bleeding may occur following intramuscular administration. Syncope can occur following, or before any vaccination as a psychogenic response. This can be accompanied by several neurological signs such as transient visual disturbance, paraesthesia and tonic-clonic limb movements during recovery. It is important that procedures are in place to avoid injury from faints. There are no data to support replacing a dose of Shingrix with another HZ vaccine. There are limited data to support the use of Shingrix in individuals with a history of HZ and in frail individuals including those with multiple comorbidities. The benefits and risks of HZ vaccination should be weighed on an individual basis. Interactions: Shingrix can be given concomitantly with unadjuvanted inactivated seasonal influenza vaccine, 23-valent pneumococcal polysaccharide vaccine (PPV23) or reduced antigen diphtheriatetanusacellular pertussis vaccine (dTpa). The vaccines should be administered at different injection sites. Fertility, pregnancy and lactation: There were no effects on male or female fertility in animal studies. It is preferable to avoid the use of Shingrix during pregnancy. The effect on breast-fed infants of administration of Shingrix to their mothers has not been studied. It is unknown whether Shingrix is excreted in human milk. Effects on ability to drive and use machines: Shingrix may have a minor influence on the ability to drive and use machines in the 2-3 days following vaccination.
to
site
(
Headache, GIT symptoms, myalgia, injection site reactions, fatigue, chills, fever. Common (

lymphadenopathy, arthralgia. Rare (
1/1000 to
Hypersensitivity reactions. Legal Category: POM
Date

YOUR PATIENTS AGED 50 YEARS OF AGE OR OLDER ARE AT INCREASED RISK OF DEVELOPING SHINGLES.1 YOU CAN PREVENT IT.2,3 SHINGRIX demonstrated >90% efficacy against shingles in all age groups aged 50 years of age or older, based on pooled data from two large, phase 3 randomised control trials.2,3 SHINGRIX IS NOW AVAILABLE PM-IE-SGX-JRNA-220001 | Date of Preparation: March 2022 Trade marks are owned by or licensed to the GSK group of companies ©2022 GSK group of companies or its licensor. For more information on SHINGRIX, please scan the QR code. References : 1. Gauthier et al. Epidemiology and costs of herpes zoster and postherpetic neuralgia in the United Kingdom. Epidemiol infecti. 2009 137 38-47. 2. Lal H et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med. 2015; 372(22):2087-96. 3. Cunningham AL et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. 2016; 375(11):1019-32. This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. Shingrix
Undesirable effects: Very common
≥1/10):
≥1/100
<1/10): injection
pruritus, malaise. Uncommon (≥1/1000 to <1/100):
≥
<1/100):
A. Marketing Authorisation Number: EU/1/18/1272/001. Marketing Authorisation Holder: GlaxoSmithKline Biologicals S.A., Rue de l’institut 89, B-1330 Rixensart, Belgium. Further information is available from GlaxoSmithKline (Ireland) Ltd. 12 Riverwalk, Citywest Business Campus, Dublin 24. Telephone: 01-4955000. Code: PI-7757.
of preparation: March 2021. Adverse events should be reported directly to the Health Products Regulatory Authority (HPRA) on their website: www.hpra.ie. Adverse events should also be reported to GlaxoSmithKline on 1800 244 255.






















































































Prescribing
Pharmacist Prescribing: Learning from international models and opportunities for pharmacists in Ireland
Independent and supplementary/collaborative prescribing, also known as non-medical prescribing, has been introduced in many countries in recent decades. Since 2007, nurses and midwives in the Republic of Ireland have been able to become registered prescribers with An Bord Altranais, upon completion of a programme of study1. The contribution of independent prescribers to the quality and safety of patient care has been studied and discussed within published literature.
Pharmacist prescribers can make a meaningful impact on patient care, enhancing timely access to care which is delivered in a safe and effective manner. Focusing on a specialty or specific clinical area helps pharmacists to become established and integrated as prescribers in a multidisciplinary team. Within secondary care pharmacist prescribers have been demonstrated to make a positive contribution to the management of acute conditions in addition to the ongoing management of chronic conditions through outpatient clinics2,3. There are also studies currently being conducted to understand the contribution of pharmacist prescribers to care home or nursing home settings4
A Cochrane review examining prescribing by medical and nonmedical prescribers for chronic disease management in primary and secondary care concluded that specific outcomes such as the extent of diabetes control, adverse events and patient adherence were comparable when care was overseen by a medical practitioner or independent prescriber5. Furthermore, a study examining prescribing errors has demonstrated that independent pharmacist prescribers make fewer errors than their medical counterparts6. It is reasonable to say that pharmacist prescribers make a meaningful and highquality contribution to patient care.
I have been Programme Lead for Independent and Supplementary Prescribing at the University of Leeds since 2016 so I have first-hand experience of the education of trainee prescribers who are pharmacists, nurses, midwives, physiotherapists, paramedics and podiatrists. Since I joined the University, more than 500 healthcare professionals working in many different practice settings across Yorkshire and the Humber, including small and large hospitals, GP surgeries, community pharmacies, prison and custody settings, nursing homes and palliative care have completed the prescribing programme at Leeds. Having arrived as a novice Lecturer in Pharmacy Practice to the University in 2015, scarcely aware
of the existence of prescribing pharmacists, it has been a source of pride (and sometimes bemusement) that I could play such an instrumental role in the progression of the profession in the UK, while longing to see similar advancements in Ireland.
The UK could be considered to have the most advanced model of independent and supplementary prescribing, which has evolved over time, having existed in some form since 1992. It was introduced following the publication of the Cumberlege Report (1986) and the Crown Report (1989), these reports suggested that patient care would be enhanced by permitting nurses to prescribe medications, although limited these items to the Nurse Prescriber Formulary7
From 2003, pharmacists were permitted to become supplementary prescribers, and in 2006 could become independent prescribers. Independent prescribing powers enable pharmacists to prescribe licensed and unlicensed medications, and controlled drugs, although there are some exceptions (i.e. drugs prescribed to treat addiction)8
Supplementary prescribing is defined as a partnership between an independent prescriber and supplementary prescriber to implement an agreed patient specific clinical management plan (CMP) with the patient’s agreement, particularly but not only in relation to prescribing for a specific non-acute medical condition or health need affecting the patient. For example, if managing a patient with hypertension, the supplementary prescriber might be able to implement dose adjustments or introduce new medications to the management plan, provided this has been set out in the CMP and has been agreed with an independent prescriber.
At present in the UK, becoming an independent or supplementary prescriber requires that the pharmacist undertakes an accredited training programme with a Higher Education Institution (HEI) and completes a specified period of training in practice. There is an established model of funding
Written by Mary-Claire Kennedy PhD SFHEA MRPharmS, Programme Lead for Independent and Supplementary Prescribing, University of Leeds

of prescribing programmes and accreditation of these programmes by professional regulators. Health Education England (HEE), an executive non-departmental public body of the Department of Health and Social Care, which commissions places on prescribing training programmes in HEIs. Usually commissioned places can only be offered to healthcare professionals working within the geographical proximity of the HEI and providing care to patients through the NHS. Those who wish to attend an HEI outside of their geographical area or those caring for patients outside of the NHS, can opt to pay privately for a place on an accredited course. A large part of the success of the prescribing pharmacist role within the UK is the development of roles such as advanced clinical pharmacists in secondary care or GP based pharmacists where prescribing is a fundamental part of effective care, and also the allocation of specific funding for training of these pharmacists. There are currently around 9000 pharmacists registered as prescribers in the UK, representing approximately 15% of the total number of registered pharmacists 9. However, this number will increase considerably in the coming years, as from this academic year onwards, prescribing training will be integrated into the MPharm curriculum, such that pharmacists will be automatically permitted to prescribe upon initial registration with the General Pharmaceutical Council (GPhC) or Pharmaceutical Society of Northern Ireland (PSNI)10
Until now only pharmacists who were more than two years qualified could apply to complete a prescribing programme offered by one of the more than forty
accredited HEIs within the UK. These courses focus primarily on developing pharmacists’ clinical evaluation, communication, diagnostic and decision-making skills. Courses usually combine a number of face-to-face study days as well as online learning materials. All teaching, learning and assessment materials are mapped to the thirty-two learning outcomes defined by the GPhC11
The Royal Pharmaceutical Society’s Core Competency Framework for All Prescribers, which details the skills, knowledge and behaviours that all prescribers should demonstrate, also informs teaching and assessment for many courses. The RPS Framework can also assist with planning learning and undertaking reflection when working as prescriber12
During the period of learning with the HEI, pharmacists are also required to complete 90 hours in practice under the supervision of a Designated Prescribing Practitioner (DPP). DPPs can be a medic, pharmacist, nurse or allied health professional with more than 3 years’ prescribing experience and who have sufficient training or experience of clinical supervision in the workplace. During this period of supervised practice, pharmacists have an opportunity to develop the knowledge and skills specifically relevant to their specialist area so that they can become a competent prescriber. It is therefore essential that a trainee pharmacist prescriber has the
PHARMACYNEWSIRELAND.COM 87
Prescribing
full support of their employer and the clinical team they work with, as they will need to work closely with these individuals to gain a sufficient depth and breadth of experience in practice.
Other International Models
Many other countries have a version of independent and supplementary/collaborative prescribing for pharmacists, although the latter is most common. I will mention a few different models here to give you a sense of the various approaches that are adopted by different countries. Prescribing rights for pharmacists in Canada differ between provinces. Pharmacist practising within the province of Alberta are permitted to prescribe all Schedule 1 drugs (those requiring a prescription) and blood products. There are no lists of drugs; instead, all pharmacists are expected to limit their prescribing to situations where they have an adequate understanding of the patient, the condition being treated, and the drug being prescribed. Pharmacists may not prescribe drugs regulated by the Controlled Drugs and Substances Act such as narcotics, benzodiazepines and anabolic steroids. Prescribing pharmacists can order laboratory tests, access laboratory test results and authorise the administration of medications and blood products. Pharmacists are reimbursed for their prescribing in a deal brokered between the advocacy body, Pharmacists Association of Alberta and Alberta Health13
One of the key drivers for independent prescribing in New Zealand was the number of GPs due to retire within the next
decade, this mirrors issues with the number of GPs in Ireland that have been widely discussed within the media. Prescribing powers were therefore broadened to other groups of healthcare professionals in New Zealand to enable equitable access to healthcare and timely access to medications.
Pharmacist prescribers must work collaboratively with a medical prescriber whereas nurse prescribers can work independently 14. Recently a further 200 medications were added to the list of medications that be prescribed by pharmacists. However, the number of registered pharmacist prescribers remains relatively low with only 37 currently registered as such in New Zealand. These pharmacists generally work as part of a multidisciplinary team15
There are four broad models of prescribing in place in the USA, patient specific collaboration of prescribing through collaborative prescribing agreements (CPAs), population specific prescribing, state-wide protocols and class specific prescribing16. CPAs create a formal practice relationship between pharmacists and other health care professionals, whereby the pharmacist assumes responsibility for specific patient care functions that are otherwise beyond their typical “scope of practice,” but aligned with their education and training. Services can include initiation and modification of drug therapy. The extent of the services authorised under the collaborative agreement depends on the state’s statutory and regulatory provisions, and the specific agreement between the pharmacist and other health care professionals. There are acknowledged to be a number
of opportunities for further development of pharmacist prescribing in the USA including standardisation of prescriptive authority and giving pharmacists greater access to electronic medical records16
Prescribing Pharmacists in Ireland: The opportunities and challenges

The role of pharmacist prescribers differs considerably among countries, this is likely to be a product of many different factors such as health service systems and structure, the legislative context and the perceived need for pharmacist prescribers by key stakeholders. A common feature amongst many countries is the evolution of prescribing powers over time, initially restricted to a limited formulary or collaborative/ supplementary prescribing and moving to independent or autonomous prescribing over time, with fewer restrictions on what can be prescribed. Additionally, the introduction of independent and supplementary prescribing rights is rarely implemented in isolation, they are combined with advanced practice skills such as diagnostic and clinical decision-making skills, which further enable the pharmacist to work autonomously and effectively in a range of settings.
The Future of Pharmacy Practice report identified opportunities for pharmacist prescribing in Ireland17. Indeed, there are pockets of innovative practice within some of our hospitals, striving to upskill pharmacists as prospective prescribers, supported by medical staff. However, there are undoubtedly several major changes required before such an advancement can be widely
introduced in Ireland. Firstly, there is the legislative change which would rely upon the support and leadership of key stakeholders. Training and education programmes would need to be established and models of funding for such programmes considered. Support of medical and nursing colleagues will be essential for training of pharmacist prescribers in practice. There is also the challenge of placing pharmacists within roles and practice settings where their contribution as a prescriber is routinely incorporated into the delivery of care to patients, such as outpatient clinics or GP-based consultations. Consideration also needs to be given to pay and reimbursement for an enhanced role and responsibility. Perhaps of greatest consequence is the acceptability of pharmacist prescribers to other groups of healthcare professionals, to patients and to the pharmacy profession itself. It must be acknowledged that gaining annotation as a prescriber without then utilising the skill will not benefit the healthcare system nor will introduction of the qualification with relatively few pharmacists seeking to become annotated as prescribers. In other words, there must be a determination and willingness for the profession to embed prescribing as part of our professional practice. Gaining acceptability and support is likely to be incremental. Perhaps starting with supplementary/collaborative prescribing could provide evidence of the value of pharmacist prescribers. Over time, as has been the case in many countries, this can evolve into a greater breadth of prescribing powers.
References available on request.
PHARMACYNEWSIRELAND.COM 88
ABBREVIATED PRESCRIBING INFORMATION
Prevenar 13* Suspension for Injection
Pneumococcal polysaccharide conjugate vaccine (13-valent, adsorbed)
Presentation: Each 0.5ml dose of Prevenar 13 contains 2.2 micrograms of each of the following pneumococcal polysaccharide serotypes: 1, 3, 4, 5, 6A, 7F, 9V, 14, 18C, 19A, 19F, 23F and 4.4 micrograms of pneumococcal polysaccharide serotype 6B. Each pneumococcal polysaccharide is conjugated to CRM197 carrier protein and adsorbed on aluminium phosphate. 1 dose (0.5 ml) contains approximately 32 µg CRM197carrier protein and 0.125 mg aluminium. Indications: Active immunisation for the prevention of invasive disease, pneumonia and acute otitis media caused by Streptococcus pneumoniae in infants, children and adolescents from 6 weeks to 17 years of age. Active immunisation for the prevention of invasive disease and pneumonia caused by Streptococcus pneumoniae in adults ≥18 years of age and the elderly. Dosage and Administration: The immunisation schedules for Prevenar 13 should be based on official recommendations. It is recommended that infants who receive a first dose of Prevenar 13 complete the vaccination course with Prevenar 13. For intramuscular injection. Infants aged 6 weeks-6 months: Three dose primary series: The recommended immunisation series consists of four doses, each of 0.5ml. The primary infant series consists of three doses, with the first dose usually given at 2 months of age and with an interval of at least 1 month between doses. The first dose may be given as early as six weeks of age. The fourth (booster) dose is recommended between 11 and 15 months of age. Two dose primary series: Alternatively, when Prevenar 13 is given as part of a routine infant immunisation programme, a series consisting of three doses, each of 0.5ml, may be given. The first dose may be administered from the age of 2 months, with a second dose 2 months later. The third (booster) dose is recommended between 11 and 15 months of age. Preterm infants (< 37 weeks gestation): In preterm infants, the recommended immunisation series consists of four doses, each of 0.5 ml. The primary infant series consists of three doses, with the first dose given at 2 months of age and with an interval of at least 1 month between doses. The first dose may be given as early as six weeks of age. The fourth (booster) dose is recommended between 11 and 15 months of age. Unvaccinated infants and children ≥ 7 months of age: Infants 7-11 months: Two doses, each of 0.5 ml, with at least a 1 month interval between doses. A third dose is recommended in the second year of life. Children aged 12-23 months: Two doses, each of 0.5 ml, with at least a 2 month interval between doses. Children and adolescents aged 2-17 years: one single dose of 0.5 ml. Prevenar 13 vaccine schedule for infants and children previously vaccinated with Prevenar (7-valent) (Streptococcus pneumoniae serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F): Infants and children who have begun immunisation with Prevenar may switch to Prevenar 13 at any point in the schedule. Children aged 12-59 months: Children who are considered completely immunised with Prevenar (7-valent) should receive one dose of 0.5 ml of Prevenar 13 to elicit immune responses to the 6 additional serotypes. This dose of Prevenar 13 should be administered at least 8 weeks after the final dose of Prevenar (7-valent). Children and adolescents aged 5-17 years: One single dose of Prevenar 13 if they have been previously vaccinated with one or more doses of Prevenar. This dose of Prevenar 13 should be administered at least 8 weeks after the final dose of Prevenar (7-valent). Adults ≥18 years of age and the elderly: One single dose. The need for revaccination with a subsequent dose of Prevenar 13 has not been established. Regardless of prior pneumococcal vaccination status, if the use of 23 valent polysaccharide vaccine is considered appropriate, Prevenar 13 should be given first. Special Populations: Individuals who have underlying conditions predisposing them to invasive pneumococcal disease (such as sickle cell disease or HIV infection) including those previously vaccinated with one or more doses of 23-valent pneumococcal polysaccharide vaccine may receive at least one dose of Prevenar 13. In individuals with an haematopoietic stem cell transplant (HSCT), the recommended immunisation series consists of four doses of Prevenar 13, each of 0.5 ml. The primary series consists of three doses, with the first dose given at 3 to 6 months after HSCT and with an interval of at least 1 month
between doses. A fourth (booster) dose is recommended 6 months after the third dose. Contra-indications: Hypersensitivity to any component of the vaccine or to diphtheria toxoid. As with other vaccines, the administration of Prevenar 13 should be postponed in subjects suffering from acute, severe febrile illness. However, the presence of a minor infection, such as a cold, should not result in the deferral of vaccination. Warnings and Precautions: Do not administer intravascularly. Appropriate medical treatment and supervision must be readily available in case of a rare anaphylactic event. This vaccine should not be given as an intramuscular injection to individuals with thrombocytopenia or any coagulation disorder that would contraindicate intramuscular injection, but may be given subcutaneously if the potential benefit clearly outweighs the risks of administration. Prevenar 13 will only protect against Streptococcus pneumoniae serotypes included in the vaccine, and will not protect against other microorganisms that cause invasive disease, pneumonia, or otitis media. As with any vaccine, Prevenar 13 may not protect all individuals receiving the vaccine from pneumococcal disease. Individuals with impaired immune responsiveness, whether due to the use of immuno-suppressive therapy, a genetic defect, human immunodeficiency virus (HIV) infection, or other causes, may have reduced antibody response to active immunization. Safety and immunogenicity data are available for a limited number of individuals with sickle cell disease, HIV infection, or with an HSCT. Safety and immunogenicity data for Prevenar 13 are not available for individuals in other specific immuno-compromised groups (e.g., malignancy or nephrotic syndrome) and vaccination should be considered on an individual basis. Infants and children aged 6 weeks to 5 years: Prevenar 13 does not replace the use of 23-valent pneumococcal polysaccharide vaccine in at risk children ≥ 24 months of age. Children ≥ 24 months of age at high risk, previously immunised with Prevenar 13 should receive 23-valent pneumococcal polysaccharide vaccine whenever recommended. The potential risk of apnoea and the need for respiratory monitoring for 48-72 hours should be considered when administering the primary immunisation series to very premature infants (born ≥ 28 weeks of gestation) and particularly for those with a previous history of respiratory immaturity. When Prevenar 13 is administered concomitantly with Infanrix hexa (DTPa-HBV-IPV/Hib), the rates of febrile reactions are similar to those seen with concomitant administration of Prevenar (7-valent) and Infanrix hexa. Increased reporting rates of convulsions (with or without fever) and hypotonic hyporesponsive episode (HHE) were observed with concomitant administration of Prevenar 13 and Infanrixhexa. Antipyretic treatment should be initiated according to local guidelines for children with seizure disorders or with a history of febrile seizures and for all children receiving Prevenar 13 simultaneously with vaccines containing whole cell pertussis. Adults aged 50 years and older: When Prevenar 13 was given concomitantly with trivalent inactivated influenza vaccine (TIV), the immune responses to Prevenar 13 were lower compared to when Prevenar 13 was given alone, however, there was no long-term impact on circulating antibody levels. The immune responses to Prevenar 13 were noninferior when Prevenar 13 was given concomitantly with quadrivalent inactivated influenza vaccine (QIV) compared to when Prevenar 13 was given alone. As with concomitant administration with trivalent vaccines, immune responses to some pneumococcal serotypes were lower when both vaccines were given concomitantly. Fertility, Pregnancy & Lactation: There are no data from the use of pneumococcal 13-valent conjugate in pregnant women. It is unknown whether pneumococcal 13-valent conjugate is excreted in human milk. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. Side Effects: Analysis of postmarketing reporting rates suggests a potential increased risk ofconvulsions, with or without fever, and HHE when comparing groups which reported use of Prevenar 13 with Infanrix hexa to those which reported use of Prevenar 13 alone. Adverse reactions reported in clinical studies or from the post-marketing experience for all age groups are listed in this section per system organ class,in decreasing order of frequency and seriousness. The frequency is defined as follows: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (≤ 1/10,000), not
known (cannot be estimated from available data). Infants and children aged 6 weeks to 5 years: Very common (≥ 1/10): Decreased appetite, fever, pyrexia, irritability, any vaccination-site erythema, induration/swelling or pain/tenderness, somnolence, poor quality sleep. Vaccination-site erythema or induration/swelling 2.5cm – 7.0 cm (after the booster dose and in older children [age 2-5 years]. Common (≥ 1/100 to < 1/10): Vomiting, diarrhoea, rash, pyrexia >39 °C, vaccination-site movement impairment (due to pain), vaccination-site erythema or induration/swelling 2.5cm – 7.0cm (after infant series). Uncommon (≥ 1/1,000 to < 1/100): Convulsions (including febrile convulsions), urticaria or urticaria-like rash, vaccination-site erythema, induration/swelling >7.0cm, crying. Rare: Hypersensitivity reaction including face oedema, dyspnoea, bronchospasm, hypotonic-hyporesponsive episode. Not known: Lymphadenopathy (localised to the region of the vaccination site), anaphylactic/anaphylactoid reaction including shock, angioedema, erythema multiforme, vaccination site urticaria, vaccination-site dermatitis, vaccination-site pruritus, flushing. In clinical studies infants vaccinated at 2, 3 and 4 months of age, fever ≥ 38°C was reported at higher rates among infants who received Prevenar (7-valent) concomitantly with Infanrix hexa than in infants receiving Infanrix hexa alone. After a booster dose at 12 and 15 months of age, the rate of fever ≥ 38°C was greater in infants who received Prevenar (7 valent) and Infanrix hexa at the same time compared to infants receiving Infanrix hexa alone. These reactions were mostly moderate (less than or equal to 39°C) and transient. Additional information in special populations: Apnoea in very premature infants (≤ 28 weeks of gestation). Children and adolescents aged 6 to 17 years of age: Very common (≥ 1/10): Decreased appetite, irritability, any vaccination-site erythema, induration/swelling or pain/ tenderness, somnolence, poor quality sleep, vaccination-site tenderness (including impaired movement). Common (≥ 1/100 to < 1/10): Headaches, vomiting, diarrhoea, rash, urticaria or urticaria-like rash, pyrexia. Additional information in special populations: Children and adolescents with sickle cell disease, HIV infection or an HSCT transplant have similar frequencies of adverse reactions, except that headaches, vomiting, diarrhoea, pyrexia, fatigue, arthralgia, and myalgia were very common. Adults ≥18 years of age, and the elderly: Very common (≥ 1/10): Decreased appetite, headaches, diarrhoea, vomiting,(in adults aged 18 to 49 years), rash, chills; fatigue; vaccination-site erythema; vaccination-site induration/swelling; vaccination-site pain/tenderness (severe vaccination-site pain/ tenderness very common in adults aged 18 to 39 years); limitation of arm movement (severe limitation of arm movements very common in adults aged 18 to 39 years), arthralgia; myalgia. Common (≥ 1/100 to < 1/10): Vomiting (in adults aged 50 years and over), pyrexia(very common in adults aged 18 to 29 years). Uncommon (≥ 1/1,000 to < 1/100): Nausea, hypersensitivity reaction including face oedema, dyspnoea, bronchospasm, lymphadenopathy localized to the region of the vaccination site. Additional information in special populations: Adults with HIV infection have similar frequencies of adverse reactions, except that pyrexia and vomiting were very common and nausea common. Adults with an HSCT have similar frequencies of adverse reactions, except that pyrexia and vomiting were very common. For full prescribing information see the Summary of Product Characteristics. Legal Category: S1A. Package Quantities: Pack of 1 single-dose prefilled syringe (with separate needle) or pack of 10 single- dose pre-filled syringes. Marketing

Authorisation Numbers: Single-dose pre-filled syringe (with separate needle) pack of 1: EU/1/09/590/002, single-dose pre-filled syringe pack of 10: EU/1/09/590/003. Marketing
Authorisation Holder: Pfizer Europe MA EEIG, Boulevard de la Plaine 17, 1050 Bruxelles, Belgium. For further information on this medicine please contact: Pfizer Medical Information on 1800 633 363 or at EUMEDINFO@pfizer.com. For queries regarding product availability please contact: Pfizer Healthcare Ireland, Pfizer Building 9, Riverwalk, National Digital Park, Citywest Business Campus, Dublin 24 + 353 1 4676500.
Date of preparation: 11/2018.
*Trade mark.
Ref: PN 11_0
IE. References: 1. Prevenar 13 Suspension for Injection. Summary of Product Characteristics. 2. Shea K, Edelsberg J, Weycker D, et al. Rates of Pneumococcal Disease in Adults with Chronic Medical Conditions. Open Forum Infectious Disease. 2014;1-9. 3. Bonten M.J.M., Huijts S.M, Bolkenbaas M, et al. Polysaccharide Conjugate Vaccine Against Pneumococcal Pneumonia in Adults. The New England Journal of Medicine. 2015;372:1114-25. 4. Pfizer Inc. Press Release Mar 18, 2015. INDICATED FOR THE PREVENTION OF PNEUMOCOCCAL PNEUMONIA IN ADULTS1 IN ADULTS AGED ≥ 65 YEARS With each additional comorbid condition, the risk for pneumococcal pneumonia multiplies compared to healthy adults of the same age2 Proven to reduce the risk of community-acquired pneumonia: Results from the Community-Acquired Pneumonia Immunisation Trial in Adults (CAPiTA) – one of the largest vaccine efficacy trials ever conducted in older adults.3,4 Alcoholism Asthma Chronic cardivascular disease Chronic liver disease Chronic pulmonary disease Current smokers Diabetes These underlying conditions included2: Date of Preparation: February 2021 | PP-PNA-IRL-0006 Help prevent pneumococcal pneumonia with the proven protection of Prevenar 131,3 4.2x increased risk 2 underlying conditions 2.1x increased risk 1 underlying condition 9.2x increased risk >3 underlying conditions
To AVC or not to AVC, that is the question
Making Additional Voluntary Contributions (AVC’s) to your existing employer-funded pension scheme is perhaps the most underutilised tax break currently available. Why is this?
Written by Kieran Moore QFA, SIA, Director,Moore Wealth Management Ltd

Moore Wealth Management has been advising the Irish Pharmacy Community for over 20 years with extensive knowledge of the sector. They can be contacted at 086-3801868, kieran@mwm.ie or www.mwm.ie
• Back service credits for additional employer pension contributions will also be created going back ten years, these would be approximately ¤150,000 for John and ¤90,000 for Mary. In total in year one approximately ¤272,000 of additional funds could be extracted from the company to the pensions free of all income tax. With an additional ¤32,000 every year thereafter.
• The company can claim the pension contributions against its profits and therefore reduce its corporation tax liability.
AVC’s are permissible by the revenue on the following agerelated scale as a percentage of salary to a maximum allowable salary of ¤115,000
Age Percentage Limit
Under 30 15 %
30-39 20 %
40-49 25 % 50-54 30 % 55-59 35 % 60 or over 40 %
We all remember the popularity of the government SSIA savings accounts Introduced in the Finance Act 2001. This was primarily because both the message and benefits were clear. The SSIA was structured so that the Government contributed one euro for every four invested by the account holder. The maximum contribution was ¤254 per month. A great deal for all concerned, the government topped up your investment by 25% effectively giving you a return of at least 25% before any other investment returns were considered.
So how does this compare to the benefits currently offered by AVC’s?
Let’s look at a case study to see. John aged 50 owns a Pharmacy for the last 10 years and currently pays himself ¤80,000 and his spouse Mary also aged 50 has a salary of ¤30,000. The revenue commissioners at their respective ages will permit employer pensions contributions of circa 80% of both salaries. With this in mind, they currently have annualised employer contributions to two company paid pensions of ¤64,000 and ¤24,000 respectively. They also have ¤50,000 surplus cash sitting on deposit earning nothing and are looking to invest these funds for the longer term.
If john increases his salary to ¤100,000 and makes an AVC contribution of ¤30,000 (using his full 30% allowance) into the existing employer pension before the tax deadline this year
his taxable salary will reduce to ¤70,000. If Mary’s salary is increased to ¤40,000 with another AVC for her of ¤12,000 reducing her taxable salary to ¤28,000.
The following benefits will accrue to them
• The combined taxable income has decreased from ¤110,000 to ¤98,000 with an estimated saving on tax, PRSI and levies of ¤5,700
• The ¤42,000 invested in the AVC’s only cost them ¤25,200 thanks to the government tax break. In other words, the immediate return on the ¤25,200 was 67%.
So, the benefits of an AVC are almost 3 times better than the offer the government made under the terms of the very popular SSIA scheme.
But the benefits do not stop there, here is some of the other benefits that John and Mary can now enjoy.
• All investment returns on the funds invested in AVC’s will be free of tax for the duration of the contract (unlike SSIA investment returns which were taxable). This gross roll-up of returns will add significantly to the final overall pension pot.
• Because employer contributions are linked to salary and service, the increased salaries will now trigger two additional sets of increases. Annual contributions for John can increase to ¤80,000 per annum and for Mary she can increase to ¤32,000.
Over ten years even with no investment growth the pensions would be boosted by the following John AVC’s ¤300,000
Lump sum employer contributions ¤150,000
Additional employer annual contribution ¤160,000
Additional pension contributions ¤610,000 Mary AVC’s ¤120,000
Lump sum employer contributions ¤90,000
Additional employer annual contribution ¤80,000
Additional pension contributions ¤290,000
So, by increasing John and Mary’s salaries and using an AVC to offset the tax on these increases we could achieve the following benefits
• Reduce income tax
• Boost their pensions
• Reduce corporation tax
There is no doubt that AVC’s should play a larger role in your financial planning, especially for those of you who have both personal and corporate cash deposits. As we have explained in a previous article the erosion of the purchasing power of funds left on deposit in the medium to longer term is dramatic. Using these funds toward increased employer contributions or introducing AVC’s would be an excellent starting point in tax efficiently growing your wealth.
In other significant pension news
You may have heard in recent changes that there have been significant changes to the regulation of the type of pension that most of you as business owners are operating at the moment that you need to be aware of.
The Technical Piece
Institutions for Occupational Retirement Provision(IORP II) a European Directive was transposed into Irish law in April 2021. Ireland, like other EU Member States, had the option to exempt pension schemes with under 100 members from certain onerous and costly requirements but decided not to. While 100-member schemes would be significant to remove from the regulations, the fact that onemember pension arrangements like yours were not exempted came as a major shock. Ireland has a high number of these that operate under a trust system that falls under IORP II unlike other countries where there isn’t a requirement for a trust meaning the level of compliance and regulation on your schemes is already very high.
Under threat of penalty from the pensions authority for the pension holder, the trustee and the life office, all the major providers of pensions in Ireland withdrew from the market and in the process cut off the only viable pension funding option for business owners at a time when we are continually told about the looming pensions timebomb. In a nutshell, the pensions authority has put the same requirements that govern large schemes (500+ members) onto schemes with one member.
PHARMACYNEWSIRELAND.COM 90 Finance
The idea of schemes for one member under a trust arrangement recognized the nature of starting and running your own business where due to cashflow you may not be in a position to fund your pension in the early years. It recognized the peaks and troughs and rewarded entrepreneurship for building a business. The structure allowed for a backdated contribution to your pension for past service where you had not been in a position to save for your future.
Take a scenario where a 50-yearold business owner with ten years of service to date on a salary of ¤75,000 had not been able to fund a pension. Under revenue maximum funding calculations the option to extract ¤580,000 from the business tax-free was
available. Under the only option now available with these changes which is a PRSA the same person could fund their pension to the amount of ¤22,500, a near 96% decrease.
PRSAs were typically not recommended for business owners for the following reasons
• Lower Allocations – that means 100% of your contribution may not reach your fund and be swallowed up in life company charges

• Higher fees
• Limited fund choices
• Benefit in Kind on employer contributions which did not apply to one member schemes
• No ability to contribute for back service as a tax-efficient means of extracting company cash.
• More limited monthly contribution levels
Industry Response
Due to the threat of fines and sanctions from the pensions authority the providers were left with no option but to stop the set up of any new schemes. Despite intensive talks and lobbying the authority have refused to change their stance and currently the market is looking at various options that satisfy IORPS II. These include potentially a retail master trust arrangement but there is no estimate on when this will be available. This is a very fluid matter and we will have further updates as they arise.
Possible changes in Pipeline for Finance Bill 2022?
• Similar tax relief structures for pension contributions to PRSAs as one member schemes – This will involve the removal of BIK on employer contributions above current limits
• Proposal to provide in scheme drawdown as opposed to ARF
• PRSA – An individual pension for life
• No new Personal Retirement Bond or Personal Pension contracts
What do you do if you already have a one-member scheme
• There is a 5-year derogation for existing schemes which means
Pre-Budget Submission on Diabetes
that apart from investment restrictions on unregulated investments such as direct property which came into place in April 2021 your scheme does not change.
• What you have you hold – the rules are not retrospective but future investment decisions must adhere to the new rules.
• The governance, policy, and procedures changes, while not required until 2026 will in general be applied by trustees as best practice in advance of this date
• Trustee Annual Report optional before 2026
Opportunity
What this has shown to current pension holders is that you hold a supremely tax-efficient vehicle for accumulating retirement wealth and extracting funds from your business and are in an enviable position. As per the examples shown if you have accumulated cash in your business and want to contribute for backdated service now would be a good time to have a consultation to determine if this is an option for you.
Before you finalise your income tax return this year, seek advice on how to integrate the tax, investment and retirement planning to its greatest effect. The example earlier illustrates that if you are utilising all the tax breaks and revenue allowances for pensions permissible it can greatly enhance your ability to create wealth. Perhaps it starts with a simple AVC.
Diabetes Ireland presented its Pre-budget Submission 2023 to the Minister for Health Stephen Donnelly TD recently and called on him and the Government to take a number of immediate actions to improve diabetes healthcare services for people with diabetes nationwide.
Diabetes is a serious global public health issue which has been described by the World Health Organisation as one of the top ten most challenging health problems in the 21st century with a high individual, social and economic burden. According to the International Diabetes Federation Diabetes Atlas 2021 Ireland is ranked 7th in the world for diabetes related health expenditure per person and in the Euro Diabetes Index 2014, Ireland was placed 20th out of 30 countries in the rank for the
access to and quality of care and its outcomes One of the reasons for this low score was the lack of a diabetes registry, which helps to monitor the outcomes and supports health-services planning. Since 2014 nothing has changed in this matter and Ireland is still one of the very few countries in Europe which does not have a registry or routinely undertaken annual national audits of diabetes clinical services and diabetes outcomes. Both these issues need to be addressed as a priority in the coming budget.
Dr Kate Gajewska, Research and Advocacy Manager, Diabetes Ireland said, “If the HSE wants to aspire to deliver high-quality diabetes care, they need to know how many people live with diabetes in Ireland and where those people live. They also need to regularly monitor the standard of clinical care being provided along with diabetes outcomes. Only then can they begin to effectively plan staffing resources, determine the cost of providing care and improve health outcomes for our community.”
There is no accurate figure available
for the number of people living with diabetes in Ireland, but based on the Scottish prevalence data and the newest census, we estimate there are now approximately 300,000 people living with diabetes in Ireland. Furthermore, recent research has identified diabetes as the most prevalent chronic condition in people between 45 to 74 years of age in Ireland further implies the necessity of having access to appropriate data and health information so better decision making and planning can be undertaken.
PHARMACYNEWSIRELAND.COM 91
News





































We’ve got your future Confidential Pension Second Opinion Service We give you the peace of mind that comes with knowing the advice you received was in your best interest A Certified Financial Planner ™ will provide you with that reassurance and clarity so your retirement is what you want it to be www.mwm.ie What are we looking for ? 1 Fees – Why pay more than you need to? You don’t do it for stock in your business so why do it for your pension 2 Performance – How does your pension compare to best in class 3 Risk – Are you over exposed to risk. 4 Was there actually financial advice? - Did you just get sold products or do you have a comprehensive personalized financial plan with full cashflow modelling? Moore Wealth Management Limited trading as Moore Wealth Management is Regulated by the Central Bank of Ireland Reg number 55195 colm@mwm.ie 086 860 39 53 | kieran@mwm.ie 086 380 18 68
Conjunctivitis: Infectious and Non-Infectious
Conjunctivitis, also known as red or pink eye, is an eye conditions caused by infection or allergies. We recently spoke to Theresa Lowry Lehnen (PhD), Clinical Nurse Specialist and Associate Lecturer South East Technological University for a further insight into the infectious and non-infectious diagnosis of this very common and prevalent condition.
Conjunctivitis, also known as red or pink eye, is an eye conditions caused by infection or allergies. We recently spoke to Theresa Lowry Lehnen (PhD), Clinical Nurse Specialist and Associate Lecturer South East Technological University for a further insight into the infectious and non-infectious diagnosis of this very common and prevalent condition.
Conjunctivitis can be acute or chronic and infectious or noninfectious. Viruses and bacteria are the most common infectious causes. Theresa explains, “Non-infectious conjunctivitis includes allergic, toxic, and cicatricial conjunctivitis, as well as inflammation secondary to immune-mediated diseases and neoplastic processes.2 Prevalence of conjunctivitis varies according to the underlying cause, which may be influenced by the patient’s age, as well as the season of the year.”
Viral conjunctivitis is the most common cause of infectious conjunctivitis both overall and in the adult population and is more prevalent in summer. Theresa points out that the signs and symptoms of viral conjunctivitis at presentation are variable - it usually does not require treatment, she says.
“Bacterial conjunctivitis is the second most common cause of infectious conjunctivitis, with most uncomplicated cases resolving in 1 to 2 weeks. Bacterial conjunctivitis is responsible for the majority of cases in children and occurs more frequently in winter. The majority of bacterial conjunctivitis cases are self-limiting and no treatment is necessary in uncomplicated cases. However, conjunctivitis caused by chlamydia or gonorrhoea and conjunctivitis in contact lens wearers should be treated with antibiotics. Allergic conjunctivitis occurs most often in spring and summer. Treatment with antihistamines and mast cell stabilisers usually alleviates the symptoms.”1 Treatment with antihistamines and mast cell stabilizers alleviates the symptoms of allergic conjunctivitis.
Symptoms
The classic symptoms of the three most common types of conjunctivitis are:2
Viral: symptoms of itching and tearing, history of recent upper respiratory tract infection, watery discharge, inferior palpebral conjunctival follicles, tender pre-auricular lymphadenopathy.
Bacterial: symptoms of redness and foreign body sensation, morning matting of the eyes, white-yellow purulent or mucopurulent discharge, conjunctival papillae, infrequently pre-auricular lymphadenopathy.

Allergic: symptoms of itching or burning, history of allergies/atopy, watery discharge, oedematous eyelids, conjunctival papillae, no pre-auricular lymphadenopathy.
Diagnosis
“A focused history and ocular examination are important for making a diagnosis and appropriate decisions about the treatment and management of conjunctivitis,” says Theresa. Labs and cultures are rarely indicated to confirm the diagnosis of conjunctivitis. Cultures and cytology are usually reserved for cases of recurrent conjunctivitis, those resistant to treatment, suspected gonococcal or chlamydial infection, suspected infectious neonatal conjunctivitis, and adults presenting with severe purulent discharge.1, 2
“Ocular history includes timing of onset, prodromal symptoms, unilateral or bilateral eye involvement, associated symptoms, previous treatment and response, past episodes, type of discharge, and presence of pain, itching, eyelid characteristics, periorbital involvement, vision changes, photophobia, and corneal opacity.2 The ocular exam should focus on visual acuity, extraocular motility, visual fields, discharge type, shape, size and response of pupil, the presence of proptosis, corneal opacity, foreign body assessment, tonometry, and eyelid swelling.2
“Eye discharge type and ocular symptoms can help determine the cause. A purulent or mucopurulent discharge is often due to bacterial conjunctivitis, a watery discharge is more characteristic of viral conjunctivitis and itching is associated with allergic conjunctivitis. However,
An interview with Theresa LowryLehnen (PhD), CNS, GPN, RNP, South East Technological University

clinical presentation is often nonspecific and relying on the type of discharge and patient symptoms does not always lead to an accurate diagnosis.1
“Similar to redness and discharge, other common signs and symptoms of conjunctivitis are nonspecific and can make determining the underlying cause more difficult.” For example, she told us, itching is historically correlated with allergic conjunctivitis and while in the context of watery discharge and a history of atopy this is likely the case, one study found that 58% of patients with culture-positive bacterial conjunctivitis also reported itchy eyes.2
Papillae, a nonspecific finding in conjunctivitis can be present in both infectious and noninfectious conjunctivitis. Theresa adds, “Papillae, small elevations usually under the superior tarsal conjunctival, with central vessels are often present in bacterial conjunctivitis, allergic conjunctivitis, and contact lens intolerance. Papillae in chronic allergic conjunctivitis can lead to a cobblestone appearance of the conjunctiva.2 While also non-specific, the presence of follicles, in conjunction with other findings, can help differentiate the aetiology of conjunctivitis. Follicles are small elevated yellow-white lesions found at the junction of the palpebral and bulbar conjunctiva and are a lymphocytic response often present in chlamydial and adenoviral conjunctivitis.2
“Differential diagnosis can include glaucoma; iritis; keratitis; episcleritis; scleritis; pterygium; corneal ulcer; corneal abrasion; corneal foreign body; sub-
conjunctival haemorrhage; blepharitis; hordeolum; chalazion; contact lens over use and dry eye. Other signs and symptoms that can point to diagnosis other than conjunctivitis include localised redness, redness not including the entire conjunctiva, ciliary flush, elevated intraocular pressure, vision loss, moderate to severe pain, hypopyon, hyphema, pupil asymmetry, decreased pupil response, and trouble opening the eye or keeping it open.2
It is important to differentiate conjunctivitis from other causes of “red eye” associated with severe sight- or life-threatening consequences.” Theresa also notes that while presentations can often overlap, a systematic approach including a thorough history and ocular exam should safely out rule acute sightthreatening diagnoses and identify the likely cause of conjunctivitis.7
keeping it open.2 It is important to differentiate associated with severe sight- or life threatening presentations can often overlap, a systematic should safely out rule acute sight threatening 7
Viral Conjunctivitis
Viral Conjunctivitis
Image: creative commons. https:// creativecommons.org/
Image: creative commons. https://creativecommons.org/
Viruses are responsible for up to 80%
Viruses are responsible for up to 80% of all cases of acute conjunctivitis. She continues, “Clinical accuracy in diagnosing viral conjunctivitis is less than 50% compared with laboratory confirmation and many cases
“Clinical accuracy in diagnosing viral conjunctivitis confirmation and many cases are misdiagnosed 90% of cases of viral conjunctivitis are caused conjunctival fever and epidemic keratoconjunctivitis, associated with viral conjunctivitis.
“Pharyngo conjunctival fever (PCF) caused by the presence of fever, pharyngitis, conjunctivitis. Additional ocular surface
PHARMACYNEWSIRELAND.COM 93Conjunctivitis
Incubation and communicability are estimated to be 5 to 12 days and 10 to 14 days, respectively.1
Conjunctivitis
are misdiagnosed as bacterial conjunctivitis. Between 65% and 90% of cases of viral conjunctivitis are caused by adenoviruses, which can produce pharyngoconjunctival fever and epidemic keratoconjunctivitis, two of the common clinical entities associated with viral conjunctivitis.
“Conjunctivitis caused by the herpes simplex virus is usually unilateral. The discharge is thin and watery, and accompanying vesicular eyelid lesions may occur. Topical and oral antivirals are recommended, however, topical corticosteroids should be avoided because they potentiate the virus and may cause harm.1
Incubation and communicability are estimated to be 5 to 12 days and 10 to 14 days, respectively.1
“Pharyngo-conjunctival fever (PCF) caused by HAdV types 3, 4 and 7 is usually characterised by the presence of fever, pharyngitis, periauricular lymphadenopathy, and acute follicular conjunctivitis. Additional ocular surface findings include oedema, hyperaemia, and petechial haemorrhages of the conjunctiva as a result of interaction between proinflammatory cytokines and conjunctival vasculature.
“Conjunctivitis caused by the herpes simplex virus is usually unilateral. The discharge is thin and watery, and accompanying vesicular eyelid lesions may occur. Topical and oral antivirals are recommended, however, topical corticosteroids should be avoided because they potentiate the virus and may cause harm.1
for hyperacute conjunctivitis secondary to N gonorrhoea is intramuscular ceftriaxone, and concurrent chlamydial infection should be managed accordingly. Conjunctival hyperemia, mucopurulent discharge, and lymphoid follicle formation are hallmarks of chlamydial conjunctivitis. Discharge is often purulent or mucopurulent, however, patients often present with mild symptoms for weeks to months.
inflammatory response of the conjunctiva to allergens such as pollen, animal fur and other environmental antigens. Redness and itching are the most consistent symptoms.2

“Herpes zoster virus, responsible for shingles, can involve ocular tissue, especially if the first and second branches of the trigeminal nerve are involved. Eyelids are the most common site of ocular involvement, followed by the conjunctiva. Corneal complication and uveitis may occur. Patients with suspected eyelid or eye involvement or those presenting with Hutchinson sign (vesicles at the tip of the nose, which has high correlations with corneal involvement) should be referred for a thorough ophthalmic evaluation. Treatment usually consists of a combination of oral antivirals and topical steroids.”1
“Herpes zoster virus, responsible for shingles, can involve ocular tissue, especially if the first and second branches of the trigeminal nerve are involved. Eyelids are the most common site of ocular involvement, followed by the conjunctiva. Corneal complication and uveitis may occur. Patients with suspected eyelid or eye involvement or those presenting with Hutchinson sign (vesicles at the tip of the nose, which has high correlations with corneal involvement) should be referred for a thorough ophthalmic evaluation. Treatment usually consists of a combination of oral antivirals and topical steroids.”1
Bacterial Conjunctivitis
Bacterial Conjunctivitis
“Herpes zoster virus, responsible for shingles, can involve ocular tissue, especially if the first and second branches of the trigeminal nerve are involved. Eyelids are the most common site of ocular involvement, followed by the conjunctiva. Corneal complication and uveitis may occur. Patients with suspected eyelid or eye involvement or those presenting with Hutchinson sign (vesicles at the tip of the nose, which has high correlations with corneal involvement) should be referred for a thorough ophthalmic evaluation. Treatment usually consists of a combination of oral antivirals and topical steroids.”1
Bacterial Conjunctivitis
“This condition is self-limited, often resolving spontaneously in two–three weeks without any treatment.6 The most severe ocular manifestation of adenoviral infection is epidemic keratoconjunctivitis (EKC) which affects both the conjunctiva and cornea, leaving behind long-lasting and permanent ocular surface changes and visual disturbances. Serotypes,8, 19, 37 and less frequently serotype 4 were believed to be associated with EKC, but more recently, HAdV-D53 and HAdV-D54 have been identified in several outbreaks and thought to be responsible for the majority of EKC cases.6 Ocular manifestations of EKC include conjunctival discharge, follicular conjunctivitis, corneal sub epithelial infiltrates (SEI), corneal scarring, development of conjunctival membranes and pseudo membranes and symblepharon formation.6
https://creativecommons.org/
“Chlamydial conjunctivitis is often acquired via oculogenital spread or other intimate contact with infected individuals and in new-borns the eyes can be infected after vaginal delivery by infected mothers. Treatment with should be investigated.”
“Ocular allergic conditions can be classified into three main categories: IgE-mediated reactions, including seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC); combined IgE and non-IgEmediated reactions, including VKC and AKC; and non-IgE-mediated reactions, including giant papillary conjunctivitis (GPC) and contact dermatoconjunctivitis (CDC).6
“Treatment involves avoidance of the offending antigen and the use of saline solution or artificial tears to dilute and remove the allergens. Topical decongestants, antihistamines, mast cell stabilisers, nonsteroidal anti-inflammatory drugs and corticosteroids may be indicated. Steroids must be used judiciously and only when indicated.”1, 7
chlamydial infection should be managed accordingly. Conjunctival hyperemia, discharge, and lymphoid follicle formation are hallmarks of chlamydial Discharge is often purulent or mucopurulent, however, patients often present symptoms for weeks to months.

Treatment and Management
Bacterial conjunctivitis can be contracted from infected individuals or result from abnormal proliferation of the conjunctival flora.
Images: creative commons. https://creativecommons.org/
Images: creative commons. https://creativecommons.org/
Chronic bacterial conjunctivitis is used to describe any conjunctivitis lasting more than 4 weeks. Staphylococcus aureus, Moraxellalacunata, and enteric bacteria are the most common causes. Ophthalmologic consultation should be sought for management.
Bacterial conjunctivitis can be contracted from infected individuals or result from abnormal proliferation of the conjunctival flora.
“Lymphadenopathy occurs in up to 50% of viral conjunctivitis cases and is more prevalent in viral conjunctivitis compared with bacterial conjunctivitis. Treatment with antihistamines and mast cell stabilizers alleviates the symptoms of allergic conjunctivitis.
Viral conjunctivitis secondary to adenoviruses is highly contagious and spreads through direct contact example via contaminated fingers, medical instruments, swimming pool water, or personal items.” Incubation and communicability are estimated to be 5 to 12 days and 10 to 14 days, respectively.1
Bacterial conjunctivitis can be contracted from infected individuals or result from abnormal proliferation of the conjunctival flora.
“Chlamydial conjunctivitis is often acquired via oculogenital spread or other intimate with infected individuals and in new borns the eyes can be infected after vaginal infected mothers. Treatment with systemic antibiotics such as oral azithromycin doxycycline is efficacious. Patients and their sexual partners must be treated and with gonorrhoea should be investigated.” 1, 2, 6
Signs and symptoms include red eye, purulent or mucopurulent discharge, and chemosis.
“Contaminated fingers, oculogenital spread, and contaminated fomites are common routes of transmission. Certain conditions such as compromised tear production, disruption of the natural epithelial barrier, abnormality of adnexal structures, trauma, and immunosuppressed status can predispose to bacterial conjunctivitis. Bacterial conjunctivitis is much more common in children than adults, and the pathogens responsible vary depending on the age group. The most common pathogens responsible for bacterial conjunctivitis in adults are staphylococcal species, followed by Streptococcus pneumoniae and Haemophilus influenzae In children, the condition is often caused by H influenzae, S pneumoniae, and Moraxella catarrhalis. The infection usually lasts 7 to 10 days. 1, 2
Theresa concludes by adding that effective management of conjunctivitis includes timely diagnosis, appropriate differentiation of the various aetiologies, and appropriate treatment.
“Contaminated fingers, oculogenital spread, and contaminated fomites are common routes of transmission. Certain conditions such as compromised tear production, disruption of the natural epithelial barrier, abnormality of adnexal structures, trauma, and immunosuppressed status can predispose to bacterial conjunctivitis. Bacterial conjunctivitis is much more common in children than adults, and the pathogens responsible vary depending on the age group. The most common pathogens responsible for bacterial conjunctivitis in adults are staphylococcal species, followed by Streptococcus pneumoniae and Haemophilus influenzae In children, the condition is often caused by H influenzae, S pneumoniae, and Moraxella catarrhalis The infection usually lasts 7 to 10 days. 1, 2
“Conjunctivitis caused by the herpes simplex virus is usually unilateral. The discharge is thin and watery, and accompanying vesicular eyelid lesions may occur. Topical and oral antivirals are recommended, however, topical corticosteroids should be avoided because they potentiate the virus and may cause harm.1

Contaminated fingers, oculogenital spread, and contaminated fomites are common routes of transmission. Certain conditions such as compromised tear production, disruption of the natural epithelial barrier, abnormality of adnexal structures, trauma, and immunosuppressed status can predispose to bacterial conjunctivitis. Bacterial conjunctivitis is much more common in children than adults, and the pathogens responsible vary depending on the age group. The most common pathogens responsible for bacterial conjunctivitis in adults are staphylococcal species, followed by Streptococcus pneumoniae and Haemophilus influenzae In children, the condition is often caused by H influenzae, S pneumoniae, and Moraxella catarrhalis The infection usually lasts 7 to 10 days.1, 2
Theresa adds that incubation and communicability are estimated to be 1 to 7 days and 2 to 7 days, respectively.
Chronic bacterial conjunctivitis is used to describe any conjunctivitis lasting weeks. Staphylococcus aureus, Moraxellalacunata, and enteric bacteria common causes. Ophthalmologic consultation should be sought for management.
Signs and symptoms include red eye, purulent or mucopurulent discharge, and
“Hyperacute bacterial conjunctivitis presents with decreased vision and a severe copious purulent discharge. There is often accompanying eyelid swelling, eye pain on palpation, and preauricular adenopathy. It is often caused by Neisseria gonorrhoeae and carries a high risk for corneal involvement and subsequent corneal perforation. Treatment for hyperacute conjunctivitis secondary to N gonorrhoea is intramuscular ceftriaxone, and concurrent
“Hyperacute bacterial conjunctivitis presents with decreased vision and a severe copious purulent discharge. There is often accompanying eyelid swelling, eye pain on palpation, and preauricular adenopathy. It is often caused by Neisseria gonorrhoeae and carries a high risk for corneal involvement and subsequent corneal perforation. Treatment for hyperacute conjunctivitis secondary to N gonorrhoea is intramuscular ceftriaxone, and concurrent
“Hyperacute bacterial conjunctivitis presents with decreased vision and a severe copious purulent discharge. There is often accompanying eyelid swelling, eye pain on palpation, and preauricular adenopathy. It is often caused by Neisseria gonorrhoeae and carries a high risk for corneal involvement and subsequent corneal perforation. Treatment
Bilateral mattering and adherence of the eyelids, lack of itching, and no history of conjunctivitis are strong positive predictors of bacterial conjunctivitis,” she says. “Severe purulent discharge should always be cultured and gonococcal conjunctivitis should be considered. Conjunctivitis not responding to standard antibiotic therapy in sexually active patients warrants a chlamydial evaluation. The possibility of bacterial keratitis is high in contact lens wearers, who should be treated with topical antibiotics and referred to an ophthalmologist. A patient wearing contact lenses should be asked to remove them.”1, 6
“Most acute bacterial conjunctivitis infections are self-limiting and do not require topical antibiotics. Acute bacterial conjunctivitis is usually unilateral with yellow-white mucopurulent discharge and symptoms usually resolve within 5-7 days without treatment. If topical antibiotics are considered necessary a delayed prescription for 3 days should be considered to see if symptoms resolve with self-care and without antibiotic eye drops.7
Theresa adds that incubation and communicability are estimated to be 1 to 7 days, respectively.
“Bilateral mattering and adherence of the eyelids, lack of itching, and conjunctivitis are strong positive predictors of bacterial conjunctivitis,” she purulent discharge should always be cultured and gonococcal conjunctivitis considered. Conjunctivitis not responding to standard antibiotic therapy in patients warrants a chlamydial evaluation. The possibility of bacterial keratitis contact lens wearers, who should be treated with topical antibiotics and ophthalmologist. A patient wearing contact lenses should be asked to remove Allergic conjunctivitis
Allergic conjunctivitis
“Antibiotic ointments last longer than drops, however they tend to interfere with vision. Chloramphenicol is not recommended in pregnancy or breastfeeding. In 2021 the Summary of Product Characteristics for Chloromycetin® 0.5% Redi-Drops was updated to contra-indicate use of the drops in children under 2 years. This is due to a risk of toxicity from boron. This excipient is not present in the ointment formulation and the contra-indication applies to the drops only.”7
Image: creative commons. https:// creativecommons.org/
Allergic conjunctivitis is the
“Antibiotic drops are indicated for complicated bacterial conjunctivitis, in conjunctivitis caused by gonorrhoea or chlamydia, and in bacterial conjunctivitis in contact lens wearers.5 The recommended treatment for gonococcal
Allergic conjunctivitis is the inflammatory response of the conjunctiva to allergen pollen, animal fur and other environmental antigens Redness and itching consistent symptoms. 2
“Ocular allergic conditions can be classified into three main categories:
 Image: creative commons. https://creativecommons.org/
Image: creative commons. https://creativecommons.org/
PHARMACYNEWSIRELAND.COM 94
except for herpes zoster, as they can prolong the condition or potentiate the infection, resulting in complications including corneal damage and blindness.1, 2

“Treatment for allergic conjunctivitis consists of allergen avoidance, artificial tears, cold compresses, and a wide range of topical agents. Topical agents include topical antihistamines alone or in combination with vasoconstrictors, topical mast cell inhibitors and topical glucocorticoids for refractory symptoms. Oral antihistamines can also be used in moderate to severe cases of allergic conjunctivitis.1, 2
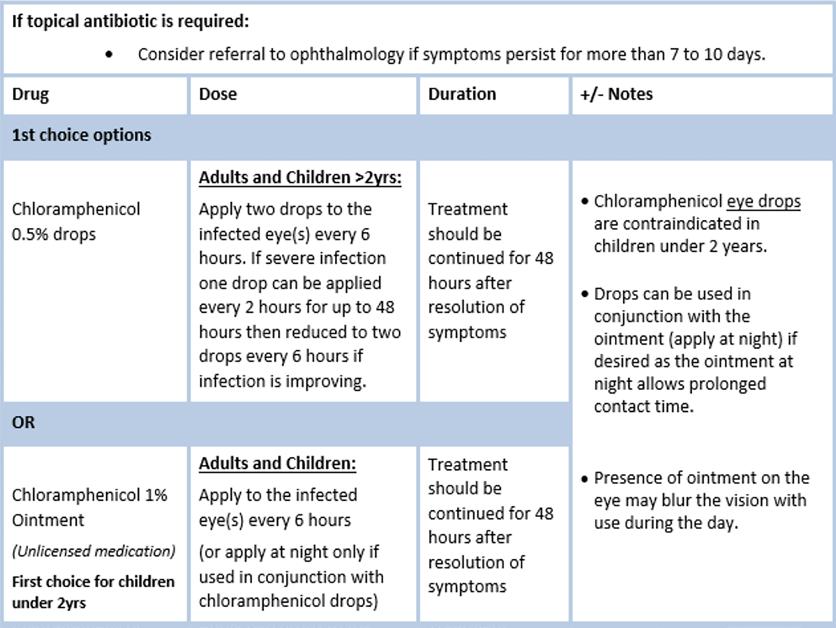
“Any patient with moderate to severe pain, vision loss, corneal involvement, severe purulent discharge, conjunctival scarring, recurrent episodes, lack of response to therapy, or herpes simplex keratitis should receive a prompt referral to an ophthalmologist. In addition, patients requiring steroids, contact lens wearers, and those with photophobia should also be referred to an ophthalmologist. 2
“Viral and bacterial conjunctivitis can spread by direct contact and have high transmission rates. Patient education is important to prevent transmission and the importance of hand hygiene should be highlighted.
Caution with steroids/ antibioticsteroid combination drops
HSE (2021).
https://www.hse.ie/eng/services/
conjunctivitis is ceftriaxone 1gm IM, and it is also recommended to treat for concurrent chlamydial infection with 1gm azithromycin orally. The neonatal dosing for gonococcal conjunctivitis is 25 to 50mg/kg ceftriaxone IV/IM with a max dose of 125mg, with 20mg/ kg azithromycin PO once daily for three days.2
“Viral conjunctivitis due to adenoviruses is usually self-
limiting, and treatment should target symptomatic relief including cold compresses and saline solution or artificial tears.2

“Herpes simplex keratitis requires antiviral therapy such as aciclovir or ganciclovir and the patient should be reviewed by an ophthalmologists to monitor for complications.2 Treatment of herpes zoster conjunctivitis includes a combination of oral antivirals and
topical steroids, however, steroids should only be part of therapy in consultation with ophthalmology. Antiviral doses differ from those used for herpes simplex and consist of oral acyclovir 800mg five times a day, oral famciclovir 500mg TDS, or oral valacyclovir 1g TDS for 7 to 10 days.”3, 4
Topical corticosteroids are not recommended for cases of bacterial or viral conjunctivitis,
“Steroids should be used with caution. Steroid drops or combination drops containing steroids should not be used routinely. Topical steroids are associated with cataract formation and can cause an increase in eye pressure, leading to glaucoma. 1 if an undiagnosed corneal ulcer secondary to herpes, bacteria, or fungus is present, steroids can also worsen the condition, leading to corneal erosion and blindness.1
Complications
“Complications of acute conjunctivitis are rare. However, patients who fail to show improvement should be referred to an ophthalmologist for further evaluation. Patients with HZV conjunctivitis are at the highest risk of complications including corneal complications and uveitis, and should always see an ophthalmologist for close re-evaluation. Patients with N. gonorrhoea are also at high risk for corneal involvement and secondary corneal perforation and should be treated appropriately,” 2 she concludes.
References available on request
PHARMACYNEWSIRELAND.COM 95
Conjunctivitis: Antibiotic Prescribing. Available at:
list/2/gp/antibiotic-prescribing/conditions-and-treatments/skin-soft-tissue/conjuncitivitis/ conjuncitivitis-ophthalmology.html
Clinical Profiles
BOOTS IRELAND ANNOUNCES PARTNERSHIP WITH THE HYGIENE BANK IRELAND
Boots Ireland has announced a new partnership with The Hygiene Bank Ireland, providing drop off points in ten stores where people can donate hygiene products which are provided to those in need. People are invited to donate a range of unopened and unused products such as dental products, deodorants, body wash, nappies, baby wipes, razors and shaving foam, period products, hairbrushes, shampoo and conditioner.
This new partnership was announced ahead of National Hygiene Week, from 12 – 18th September 2022, which aims to raise awareness about hygiene poverty and its impact on those who are affected.
Hygiene poverty is not being able to afford many of the everyday hygiene and personal grooming products most of us take for granted. The reality of low income is that it restricts people’s options, leaving people caught between being able to heat homes, pay rent, eat or be clean. The Hygiene Bank Ireland is a grassroots organisation, which tackles hygiene poverty by delivering donated hygiene and household cleaning products to community partners who work with vulnerable and marginalised communities.
Initially Boots Ireland will be operating ten drop-off points around the country, and everyone is invited to donate products if they are able to do so. The stores in the initial phase include five locations in Dublin – Dundrum, Carrickmines, Swords, Liffey Valley and Blanchardstown, Letterkenny Retail Park, Letterkenny, two locations in Cork – Blackpool and
Boots Hygiene Bank Letterkenny, Martha Ryan, Vic Riley, Margaret McFadden, Carla Harkin

Half Moon Street – as well as Shop Street, Galway and Abbey St., Wicklow Town.
Speaking at the launch of the new partnership, Ciára Dalton, Head of Marketing, The Hygiene Bank Ireland said, “Everyone has the right to an adequate standard of living, yet with 640,000 people at risk of poverty and the cost of living on the rise, hygiene products can often be at the bottom of the shopping list for people who are struggling to make ends meet. The impact of this can be immense.
As the national charity for hygiene poverty, The Hygiene Bank Ireland is dedicated to working towards eradicating this problem whilst supporting those most at-risk of hygiene poverty with the products they need.”
CALLS TO SCRAP VAT ON DEFIBRILLATORS
The VAT on defibrillators is a “tax on saving lives” and must be scrapped, the Irish Heart Foundation insisted in its preBudget submission recently.

The charity claims the average cost of an automated external defibrillator (AED) - ¤1,500 including ¤345 VAT - makes them unaffordable for many community organisations.
It wants Minister for Finance, Paschal Donohoe, to remove the 23% tax burden levied on the portable, computerised devices in next month’s Budget.
The Foundation’s Resuscitation Manager, Brigid Sinnott, said sporting and voluntary groups are also being hit with an estimated extra ¤100 in VAT when they replace pads and batteries –required regularly to keep the AEDs in working order.
“The VAT on defibrillators is a tax on saving lives and it’s time it was removed,” said Ms Sinnott, who is also a community first responder trained to administer defibrillation before paramedics arrive.
“The more AEDs there are available in local communities and accessible to the public, the more lives can be saved.”
In some cardiac arrests, AEDs deliver a shock to the heart to resume its normal rhythm.
More than 8,400 people so far have signed an online petition launched by the charity as part of its drive to have the VAT on AEDs scrapped.
“We hope the Minister will have listened to the thousands of individuals who have supported our petition by the time he delivers his Budget,” Ms Sinnott added.
Volunteer group Community First Responders Ireland (CFR Ireland) is also backing the call.
To sign the AED petition, visit: https://my.uplift.ie/petitions/ scrap-vat-on-aeds-it-s-a-tax-onsaving-lives.
CHRONIC PAIN IRELAND MARKS 30TH ANNIVERSARY WITH EVENTS TO PROVIDE ADVICE AND RESPITE

Chronic Pain Ireland (CPI), an organisation dedicated to supporting people living with
chronic pain and their families, is to mark the 30th anniversary of its foundation by hosting a series of events for Pain Awareness Month, which starts today (September 1st).
The World Health Assembly (WHA) – a subsection of the World Health Organization (WHO) – has declared September Pain Awareness Month. The event is designed to bring patients and advocacy groups from around the world together to highlight the condition of chronic pain.
CPI, in conjunction with the HSE, is supporting its members throughout Pain Awareness Month via its Living Well with Chronic Pain selfmanagement programmes. These seven-week online programmes are available for free and are designed
Resuscitation Manager with the Irish Heart Foundation Brigid Sinnott with Community First Responders Ireland chairperson John Fitzgerald
Chair of Chronic Pain Ireland Martha Phelan
PHARMACYNEWSIRELAND.COM 96
to support those living with chronic pain conditions to self-manage by providing them with tools, techniques and coping strategies.
CPI and the HSE are also working together to offer specific programmes for those aged 18-30. Top university researchers who engage with CPI through its patient and public involvement (PPI) partnerships will also be on hand to provide insights on their studies into chronic pain.
Also part of CPI’s 30-year milestone celebrations is the launch of the Hidden Disabilities Sunflower initiative to highlight the plight of those living with chronic pain and non-visible disabilities. Sunflower lanyards are being gifted to all CPI members from today and can be worn in public to discreetly indicate to others that the wearer has a hidden disability and may require additional support.
Chronic pain is classified as pain that persists beyond the time of healing, typically around three months. While many people suffer chronic pain due to injury or illness, others can experience pain in the absence of any obvious cause.
According to figures released by Irish Pain Society, Ireland has just 27 dedicated pain consultants operating across the public system, meaning that 41% of patients are currently waiting more than 12 months for their first appointment with a chronic pain specialist, while 18% are waiting the same length of time for their first treatment.
The Irish Pain Society’s figures estimate that chronic pain costs the Irish economy around ¤4.7billion per year, more than 2.5% of GDP. Among those with chronic pain, 29% cannot work because of their condition, while 42% said they think others doubt the existence of their pain. Some 21% said their pain was so intense that they wanted to die.
OVER-50S URGED TO ‘UNDERSTAND SHINGLES’
Broadcaster Teresa Mannion has called on the over-50s in Ireland to speak with their doctor, practice nurse or pharmacist about the risk factors for shingles and shingles prevention. New research conducted on behalf of GSK shows that almost one-fifth of respondents (19%) over-50 reported that they had experienced shingles and over half (55%) of those surveyed said they knew someone who was affected by it.
The GSK ‘Understanding Shingles’ research1 looked at awareness levels, knowledge and perceptions
of shingles among the over-50s in Ireland. Ms Mannion made the appeal because despite over half of respondents (56%) perceiving shingles to be a serious disease, a considerable number of respondents - 43% - said they felt it was unlikely that they would develop shingles over the next year.
Ms Mannion also urged the over50s to find out about the risk factors as one-in-three people who have had chickenpox are at risk of developing shingles in their lifetime.2, 3 While most people make a full recovery, shingles can potentially lead to serious and long-lasting complications. Post-herpetic neuralgia (PHN) is the most common complication, a prolonged nerve pain in the area affected by shingles that can last for months or even longer.4 PHN occurs in around 20% of all shingles cases, with the over-50s particularly at risk.5
The survey shows that 57% of respondents said they were extremely or somewhat knowledgeable about shingles and reveals good awareness of many of the main symptoms - including a red rash (76%), pain, burning, numbness or tingling in one part of the body (71%) and itching (55%). It also demonstrates that some of the main risk factors associated with shingles are well understood, with recognition of a weakened immune system (62%), being under stress (48%) and agerelated declining immunity (47%).
Additionally, 42% felt that shingles had an ‘extremely negative’ impact on quality of life.
Commenting on the research findings, Ms Mannion said: “I can speak from personal experience as I developed shingles and it really stopped me in my tracks. It can be a severely painful, debilitating condition, and it impacted my personal and professional life, so it is not to be taken lightly. I’m heartened to see that over half of the respondents believe shingles is a serious condition, but I’m also concerned that many of the over 50s don’t feel that they are at risk.
As shingles has a broad range of risk factors, I’d advise anyone in that age group to contact their doctor, practice nurse or pharmacist to discuss options.”
Chair of Chronic Pain Ireland, Martina Phelan, added: “Shingles can be very painful. This pain is described as burning, shooting, stabbing or even constant unbearable itching. It does not happen to everyone, and it may only last for a few weeks, but some people can experience postherpetic neuralgia (PHN), a chronic condition that is difficult
to treat and may cause pain for months, or longer. People don’t know as much as we’d like about shingles and there are many misconceptions. We are pleased to be part of the Understanding Shingles campaign as we find shingles is not always taken as seriously as it should be.”
Visit www.understandingshingles.ie to learn more about shingles.
RHYTHM PHARMACEUTICALS ANNOUNCES IMCIVREE® (SETMELANOTIDE) GRANTED MARKETING AUTHORIZATION BY EUROPEAN COMMISSION FOR TREATMENT OF OBESITY AND CONTROL OF HUNGER IN BARDET-BIEDL SYNDROME
Rhythm Pharmaceuticals, Inc. (Nasdaq: RYTM), a commercialstage biopharmaceutical company focused on transforming the lives of patients and their families living with hyperphagia and severe obesity caused by rare melanocortin-4 receptor (MC4R) pathway diseases, has announced that the European Commission (EC) has expanded the marketing authorization for IMCIVREE® (setmelanotide) to include the treatment of obesity and control of hunger associated with genetically confirmed Bardet-Biedl syndrome (BBS) in adult and pediatric patients 6 years of age and older.
“Patients and families have long endured a significant need for a therapy to address the burdens of hyperphagia and severe obesity often associated with BBS,” said Philip Beales, M.D., University College London, UCL Great Ormond Street Institute of Child Health. “Having new treatment options available can help address the physical and emotional aspects of this devastating disease, offering patients and their families relief and improved quality of life.”
BBS is a rare genetic disease that affects approximately 2,500 people in the European Union (EU) and United Kingdom (UK). People living with BBS may experience insatiable hunger, also known as hyperphagia, and severe obesity beginning early in life. Approximately 1,500 patients have been diagnosed with BBS and are now being cared for at academic settings in the EU and UK.
Under the terms of the Revenue Interest Financing Agreement with HealthCare Royalty Partners announced on June 16, 2022, Rhythm is now eligible to receive an additional investment of $37.5 million following EC marketing authorization for setmelanotide for BBS. Rhythm had received an initial investment amount of $37.5 million from HealthCare Royalty
as a result of the approval of setmelanotide by the U.S. Food and Drug Administration (FDA), and the Company remains eligible for an additional investment amount of $25 million, which would be payable upon the achievement of certain agreed sales milestones in 2023.
Priority Review Status Granted for New Drug Submission for Setmelanotide in Canada
Rhythm also announced today that Health Canada has granted Priority Review for Rhythm’s New Drug Submission for setmelanotide, indicated in adult and pediatric patients 6 years of age and older with impairments in the MC4R pathway due to genetic diseases, for the treatment of obesity and control of hunger in BBS or biallelic pro-opiomelanocortin (POMC), proprotein convertase subtilisin/ kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency.
Priority Review shortens Health Canada’s submission review performance target to 180 days, in comparison to 300 days for non-priority review. Priority Review may be granted for drug submissions in Canada for a serious, life-threatening or severely debilitating disease or condition for which there is substantial evidence of clinical effectiveness that the drug provides effective treatment, prevention or diagnosis of a disease or condition for which no drug is presently marketed in Canada or a significant increase in efficacy and/or significant decrease in risk such that the overall benefit/risk profile is improved over existing therapies, preventatives or diagnostic agents for a disease or condition that is not adequately managed by a drug marketed in Canada.
“These two important regulatory milestones underscore the global unmet need to treat the hyperphagia and severe obesity associated with these rare MC4R pathway diseases,” said David Meeker, M.D., Chairman, President and Chief Executive Officer of Rhythm. “We are working closely with Health Technology Assessment bodies and payers throughout the EU on a country-by-country basis to achieve market access and reimbursement in order to make IMCIVREE available to eligible patients as rapidly as possible. Taken together with the recent FDA approval for BBS in June, we are making significant advances in our mission of delivering the first precision medicine for MC4R pathway diseases to patients across the world.”
PHARMACYNEWSIRELAND.COM 97
Profiles
ACCORD HEALTHCARE LAUNCH ABIRATERONE ACCORD 250MG FILM-COATED TABLETS
Accord Healthcare Launch Abiraterone Accord 500mg FilmCoated Tablets
Accord Healthcare is delighted to announce the launch of another medicine to their already extensive high-tech portfolio: Abiraterone Accord 500 mg filmcoated tablets which comes in a pack of 56 tablets.
Abiraterone Accord is indicated with prednisone or prednisolone for:
• the treatment of newly diagnosed high risk metastatic hormone sensitive prostate cancer (mHSPC) in adult men in combination with androgen deprivation therapy (ADT).
• the treatment of metastatic castration resistant prostate cancer (mCRPC) in adult men who are asymptomatic or mildly symptomatic after failure of androgen deprivation therapy in whom chemotherapy is not yet clinically indicated.
• the treatment of mCRPC in adult men whose disease has progressed on or after a docetaxel-based chemotherapy regimen.
Please refer to the Summary of Product Characteristics (SPC) for further information. The SPC will be available from the launch date at www.hpra.ie and for Healthcare Professionals at www.accordhealthcare.ie.
Abiraterone Accord 250 mg filmcoated tablets will be available from both full line wholesalers from launch. For further information please contact Accord in Cork on 021 461 9040 or visit www.accord-healthcare.ie
Think High-Techs, Think Accord ASTELLAS’ EVRENZO
(ROXADUSTAT) TO BE REIMBURSED UNDER THE HIGH TECH DRUGS SCHEME IN IRELAND FOR ADULTS WITH SYMPTOMATIC ANAEMIA ASSOCIATED WITH CHRONIC KIDNEY DISEASE (CKD)
Astellas Pharma Company Ltd. (part of the Astellas Pharma Inc group TSE: 4503, President and CEO: Kenji Yasukawa, Ph.D., “Astellas”) is pleased to announce that EVRENZO™ (roxadustat) has been granted reimbursement, in line with its marketing authorisation under the High Tech Drugs Scheme in Ireland from 1st September, 2022, as an option for treating adult patients with symptomatic anaemia associated with CKD.
Roxadustat is the first and only HIF-PH inhibitor licensed and reimbursed for use in Ireland. The licence was based on results from a comprehensive pivotal Phase 3 programme comprising of eight multicentre and randomised studies, which involved 9,600 patients worldwide.6-11 The results of this programme support roxadustat as efficacious in achieving and maintaining target haemoglobin (Hb) levels (10–12 g/ dL) in patients with symptomatic anaemia of CKD regardless of dialysis status and irrespective of prior erythropoiesis-stimulating agent (ESA) treatment.6-10
The safety profile observed in the roxadustat development programme is reflective of the CKD populations studied and comparable to ESAs.6-11
‘This is an excellent demonstration of how a ground-breaking, Nobel Prize winning, scientific discovery can inform and pave the way for innovative medicines that can benefit patients.’ said Dr. Timir Patel, Medical Director, Astellas UK and Ireland. ‘Through its novel mechanism of action, roxadustat offers physicians an orally administered option to tackle anaemia of CKD, a complex and multi-faceted disease that can be hugely debilitating.’
Roxadustat activates the body’s natural response to reduced oxygen levels in the blood via inhibition of the HIF-PH pathway. The response involves the regulation of multiple, coordinated processes that improve iron absorption and mobilisation, and increase red cell production, and can therefore assist in the management of anaemia of CKD.
According to The WHO, around 20% of people living with diagnosed CKD suffer from anaemia.3,4 Anaemia of CKD symptoms include dizziness, fatigue and headaches, and can be associated with significant impairment in quality of life.12-15
Additionally, patients with CKD that also suffer from anaemia have impaired health-related quality of life compared to patients without the added complication of anaemia.5
‘Chronic kidney disease patients suffer frequently from anaemia and this complication of CKD has greater impact as CKD worsens. Anaemia significantly impacts patient’s quality of life and vitality’, said Prof. Donal Reddan, Consultant Nephrologist, Galway University Hospital.
‘This licence enhances patient care by providing a novel alternative option for managing anaemia and improving patient’s quality of life’.
PATIENT GROUP CALLS FOR EXPANDED ACCESS TO MEDICAL CANNABIS ON ‘NATIONAL DAY OF ACTION’
A leading patient advocacy group has called for a major overhaul of Ireland’s cannabis laws on the day that campaigners rally outside the Department of Health.
The Patients For Safe Access (PFSA) group said little progress has been made since the Medical Cannabis Access Programme (MCAP) was introduced here, and they insisted that more action is needed immediately.
PFSA organised a large-scale event outside the Department of Health’s offices in Dublin where speakers called for changes to be made to expand access to medical cannabis.
Speakers at the event included Martin O’Brien and Alicia Maher of PFSA, Deputy Gino Kenny, Peter Reynolds of the Cannabis Industry Council and the activist Martin Condon.
Martin O’Brien, the PFSA director, said that until major changes are made to Ireland’s drugs, barriers to access would continue to inflict real suffering on patients, some of whom are emigrating to escape needless constraints.
“Many patients and those who care about this issue hoped that the limited MCAP reforms would represent a new dawn. Unfortunately, three years on, it has become abundantly clear that the existing law is not fit for purpose.
“People with a range of serious medical conditions are not able to access cannabis legally. In spite of the evidence showing the benefits of cannabis in treating the chronic pain which so many people suffer from, the Government has slammed the door shut.
“Under MCAP, patients have to exhaust several other medical avenues before being allowed onto it, but we firmly believe that the Programme should be open to any patient with a condition that can be treated with medical cannabis,” O’Brien said.
Another leading voice within PFSA is Alicia Maher, a PhD candidate in the University of Limerick who left Ireland in 2019 to move to Spain, where she can legally access cannabis to cope with chronic pain.
“Nobody should have to struggle to get the medicine they need, but for the many Irish people who require medical cannabis, that is the reality. And for more than a few people, that entails travelling back and forth between countries, bringing sick relatives on journeys they should not have to make, or in
my case, having to leave my family just to be able to get by. This has to end,” Maher said.
LATE-BREAKING DUPIXENT® (DUPILUMAB) DATA AT ERS 2022 SHOW CONSISTENT EFFICACY AND SAFETY PROFILE FOR UP TO TWO YEARS IN CHILDREN AGED 6 TO 11 YEARS WITH MODERATE-TO-SEVERE ASTHMA
Results from a Phase 3 openlabel extension trial demonstrated the efficacy and safety profile of Dupixent® (dupilumab) as a maintenance therapy when added to other asthma medications was consistent for up to two years in children aged 6 to 11 years with uncontrolled moderate-to-severe asthma with evidence of type 2 inflammation. These results were presented today in a late-breaking session at the 2022 European Respiratory Society (ERS) International Congress, which coincides with the milestone that more than 500,000 people around the world have been treated with Dupixent in its approved indications.
Professor of Pediatrics, Director of the Center for Pediatric Asthma Research, Monroe Carell Jr. Children’s Hospital, Vanderbilt University Medical Center
“Children with uncontrolled moderate-to-severe asthma may experience long-term persistent coughing, difficulty breathing, unpredictable asthma attacks and impaired lung function, which can lead to complications later in life as they grow and develop. An established safety profile balanced with efficacy is always a priority when treating children with a chronic disease, such as those with uncontrolled moderate-to-severe asthma with an eosinophilic phenotype or oral corticosteroid dependent asthma. These new data further support the consistent safety profile of longterm Dupixent - which is indicated for the treatment of uncontrolled moderate to severe asthma with an eosinophilic phenotype or oral corticosteroid dependent asthma - and its ability to provide sustained improvements in lung function and reductions in asthma exacerbations in children as young as 6 years old.”
The results are from data in children who entered the extension trial after finishing active treatment or placebo in the Phase 3 trial (pivotal trial). Children in the extension trial were treated for up to an additional year with Dupixent, providing up to two years of data
PHARMACYNEWSIRELAND.COM 98 Clinical
™
in total. Children treated with Dupixent in the extension trial experienced a:
• Low rate of severe asthma attacks with an average of 0.118-0.124 events per year, compared to 2.16-2.56 events per year at baseline in the pivotal trial.
• Sustained improvement in lung function at 52 weeks of 9.43-12.6 percentage points from baseline in the pivotal trial, measured by percent predicted FEV1 (FEV1pp). FEV1pp seeks to evaluate a patient’s change in lung function compared to their predicted lung function based on age, height, sex and ethnicity to account for children’s growing lung capacity at different stages of development.
o Children who switched from placebo in the pivotal trial to Dupixent in the extension trial demonstrated improvement of 8.71 percentage points in lung function at two weeks.
The safety results of the trial were generally consistent with the known safety profile of Dupixent in its approved respiratory indications. Over the 52-week treatment period, the overall rates of adverse events (AEs) were 61-68%. The most common AEs (≥5%) were nasopharyngitis (9-10%), pharyngitis (6-10%), upper respiratory tract infection (4-8%), influenza (5-6%), eosinophilia (3-6%), allergic rhinitis (3-7%), diarrhea (4-6%) and injection site reactions (3-7%).
IRELAND’S LEADING FITNESS AND WELLNESS EXPERT, KARL HENRY TO BRING AN EXTRA BOOST TO PHARMATON WITH NEW PARTNERSHIP
The newest face of Pharmaton is leading fitness and wellness
expert, and Podcast host Karl Henry. From tv screen stardom to bestselling author, no personal trainer in Ireland has a larger wheelhouse than Karl Henry. For the past decade he has led the charge in changing the wellbeing and lifestyle of the Irish public through his columns, guides, and television cameos. Karl will be involved in promoting Pharmaton’s latest immunity supplement, Immuno10; built to boost immunity and help you get back to living better faster.
Karl Henry’s voice and image will be taking over the health and fitness market as the face of Pharmaton with the campaign running from September 1st for two months across outdoor, radio, online and national print with an investment in excess of ¤250,000. The campaign itself will include in-store support in the form of window materials, floor stands and counter display units.
Pharmaton is a leading multivitamin pharmacy-only brand that has been available in the Irish market for the last 20 years. Widely recommended by pharmacists, the range is high in vitamins and minerals designed to support energy, vitality and immunity.

Personal Trainer and fitness expert Karl Henry was recently announced as brand ambassador.
Olivia Reilly, Marketing Manager Consumer Healthcare (Sanofi) said: “We are thrilled to have Karl on board to increase awareness around the importance of multivitamins in increasing health and wellbeing. There has been a great response from pharmacies excited to have Pharmaton on their shelves after months spent inside without any exposure to sickness, immune systems have let their guard down. Immuno10 was created to tackle this problem and bring our immunity back to and beyond its previous performance level. This product is made for the fast-paced modern life, boosting both our mental and physical endurance so we can get back to living faster and better.”
• Immune System: High in Vitamins A, C and B Complex (B6, B9, B12) plus minerals Iron, Zinc, Copper and Selenium, that each contribute to the normal function of the immune system –ideal as we approach the Cold / Flu season.
• Vitality: Iron and magnesium are known to reduce fatigue and tiredness whilst Vitamin B complex (B1, B2, B3, B6) and Biotin all contribute to energy
yielding metabolism which we need for all functions and activities of the body including exercise.
• Mental Performance: Vitamin B5 contributes to normal mental performance – the tricky balancing act of hectic daily schedules needs all the support it can get!
Pharmaton is available over the counter from almost all pharmacies nationwide (RRP: ¤17.95). The recommended daily dose is one film-coated tablet per day in the morning with a glass of water, preferably at breakfast. Immuno10 is suitable for adults 18 years +. Food supplements should not replace a balanced diet or healthy lifestyle. Always read the label.
BOOTS IRELAND LAUNCHES
THIS YEAR’S BOOTS NIGHT WALK IN AID OF THE IRISH CANCER SOCIETY
Boots Ireland has partnered with TV presenter and broadcaster Darren Kennedy, to launch this year’s Boots Night Walk in aid of the Irish Cancer Society Night Nursing service which provides end-of-life care for people living with cancer in Ireland. The Irish Cancer Society Night Nursing service provides up to 10 nights of care, free to people who avail of it, and it is funded almost entirely by donations. Boots Ireland has partnered with the Irish Cancer Society since 2012 and through the support of their Team Members, patients and customers have raised ¤2.5 million for the service so far, helping to provide 7,200 nights of care.
This year, the Boots Night Walk is back in person and hopes to be the biggest one yet, with Boots Ireland calling upon the public to sign up and walk 5km together

this autumn in support of the Irish Cancer Society Night Nurses.
Alongside the walk, Honour Tags are now on sale in Boots stores nationwide for ¤2. Customers can purchase a tag in honour of someone who has survived or passed away from cancer. The front of the tag allows for the name of the individual with space on the back for a personal message. One metre will be walked in honour of that person by members of the Boots Ireland team.
All funds raised from the Boots Night Walk will go towards the Irish Cancer Society Night Nursing service which provides end-of-life care for cancer patients, allowing them to spend their final days at home surrounded by family and loved ones, as well as giving much needed respite for the family caring for them.
Managing Director at Boots Ireland, Stephen Watkins, said, “This year the Boots Night Walk is back in person and hopes to be the biggest one yet The Boots Night Walk helps to raise funds and awareness of the incredible work these Night Nurses undertake. Over the past 10 years an incredible ¤2.5 million has been raised for this service so we want to say a big thank you from Boots Ireland to the public as this cannot be done without your fundraising and support.”
Boots Night Walks Campaign ambassador TV Presenter and Broadcaster Darren Kennedy, launches the Boots Night Walks in aid of the Irish Cancer Society Night Nursing service
PHARMACYNEWSIRELAND.COM 99




= than sanitary pads 4x drier Result of product demonstration consisting of pouring 4x 10 ml liquid to 1 Always Unnoticeable Protection for Incontinence Normal & 1 Al ways Ultra Long pad. 20 minutes from finishing last pour, plotting paper pressed on both pads, resulting in measuring the level of dryness. for SENSITIVE BLADDER www.prl.ie pgsales@prl.ie +353 1 257 4650 PRL SALES ULC, Greenogue Business Park, Rathcoole, Co. Dublin Logistics Solutions In-Market Solutions Integrated Services
