Ireland’s Dedicated Hospital Professional Publication
KISQALI® is now reimbursed to treat HR+/HER2- Early Breast Cancer (eBC) patients in Ireland
KISQALI® is indicated in: Scan here to access the KISQALI® SmPC on www.medicines.ie
KISQALI® in combination with an aromatase inhibitor is indicated for the adjuvant treatment of patients with hormone receptor positive (HR+), human epidermal growth factor receptor 2 negative (HER2-) early breast cancer at high risk of recurrence. In pre- or perimenopausal women, or in men, the aromatase inhibitor should be combined with a luteinising hormone releasing hormone (LHRH) agonist.* 1
KISQALI® is also indicated and available in Ireland for the treatment of HR+/HER2- advanced breast cancer. Please see the SmPC for a full list of prescribing information.1
*KISQALI® is not recommended for use in combination with tamoxifen.1
1. KISQALI (ribociclib). Summary of Product Characteristics. www.medicines.ie. Legal categories: POM. MAH: Novartis Europharm Limited, Vista Building, Elm Park, Merrion Road, Dublin 4. Full prescribing information is available upon request from Novartis Ireland Ltd. Vista Building, Elm Park Business Park, Merrion Road, Dublin 4, D04 A9N6, or at www.medicines.ie See inside for further details.
Novartis Ireland Ltd, Vista Building, Elm Park Green, Merrion Road, Ballsbridge, Dublin 4, D04 A9N6
THIS ISSUE: NEWS: Pharmacy Aseptic Unit opens at Tallaght University Hospital Page 4 BUDGET: Record Budget Marks a Turning Point Page 6 REPORT: Women’s Health and Hospital Pharmacy Page 9 CONFERENCE: Precision Oncology Ireland Page 12
WOMEN'S HEALTH: Polycystic Ovary Syndrome Page 43
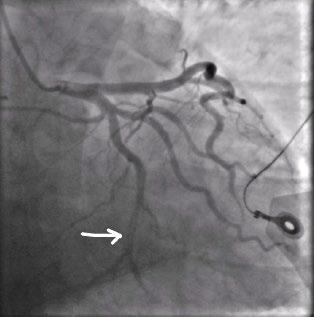
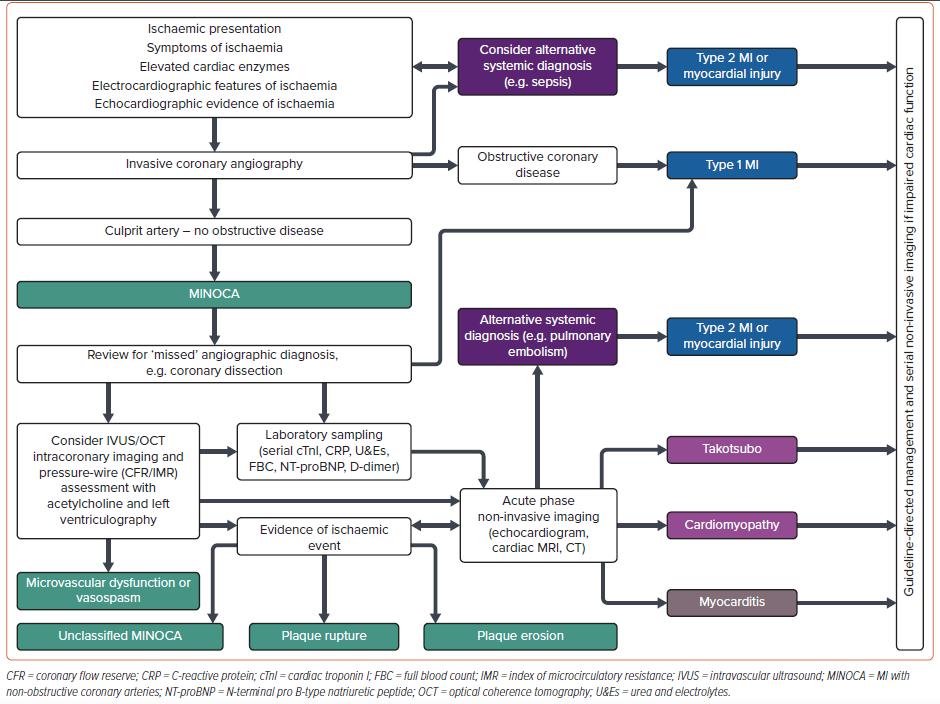
FEATURE: Myocardial Infarction Page 54
STUDY: Confronting Stigma in Pain Page 57 October 2025 | IE11536023
Call for papers: make your contribution to Hospital Professional News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
Contents Foreword
Pharmacy Aseptic Unit Opens at Tallaght University Hospital P4
Fellowship for Professor Kelly P5
Government’s Budget 2026 has set a new record for health spending P6
Women’s Health and Hospital Pharmacy in Ireland: The Changing Landscape P9
¤28M Programme to Deliver Next Generation Cancer Care P12
Women’s Health: Bladder Cancer P22
New Study identifies potential new treatment of Breast Cancer P36
REGULARS
Women’s Health: Cervical Cancer P42
Editor
October arrives with both anticipation and reflection as Ireland’s 2026 Budget announcement takes centre stage across the healthcare landscape. This month’s issue explores what the measures mean for our sector — from the perspectives of those shaping and delivering care every day.
The Irish Medical Organisation (IMO) and the Irish Pharmaceutical Healthcare Association (IPHA) have offered early and candid reactions, highlighting the potential impacts on frontline services, medicine access, and workforce sustainability. Meanwhile, insights from the Department of Health provide important context on how the new funding commitments will translate into practical delivery across community and hospital settings.
Feature: Cholesterol Metabolism P50
Feature:
Myocardial Infarction P54
Study: Chronic Pain Stigma P57
Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only.
All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission.
IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
As always, we aim to move beyond the headlines to examine how policy decisions resonate at the level of patients, practitioners, and pharmacy teams. The conversation around Budget 2026 underscores the delicate balance between fiscal responsibility and the urgent need to invest in primary care, digital infrastructure, and prevention — areas that directly influence the daily work of healthcare professionals across Ireland.
Fittingly, our October special focus on Women’s Health shines a spotlight on several key therapeutic and clinical areas that continue to demand attention and understanding. We feature a series of expert, evidence-based articles written by clinicians and specialists, addressing conditions such as cervical cancer, polycystic ovary (PCO) syndrome, and breast cancer. These features not only highlight current best practice in diagnosis and management but also emphasise the vital role of early detection, patient education, and community engagement.
October is also Breast Cancer Awareness Month — a timely reminder of the importance of screening and of ensuring that women feel empowered to discuss their health openly and without stigma.
We hope this issue offers readers a clear, balanced view of the evolving healthcare environment while providing practical, clinically grounded content that supports continued professional learning and patient care.
I hope you enjoy the issue.
Pharmacy Aseptic Unit Opens Doors
A new pharmacy Aseptic Unit has opened in Tallaght University Hospital (TUH) following a ¤8.8 million capital investment from the HSE. This new, purpose-built Aseptic Unit, is a cutting-edge facility designed to deliver the highest standards in sterile medicine preparation.
The new facility has been constructed to meet Good Manufacturing Practice standards, ensuring the safe preparation of sterile products, including cancer treatments, clinical trials and other high-risk injectable medications. With the latest cleanroom technology, validated processes,
and strict environmental controls, the Aseptic Unit will support both inpatient and outpatient services with reliable, high-quality, ready-to-administer medications.
The new facility is 200 square metres and four times the size of the original Aseptic Unit. It is located beside the main pharmacy. The unit features multiple cleanrooms with varying grades of sterility and is equipped with four isolators. A number of efficiencies have been introduced such as an Environmental Monitoring System and CCTV which means important checks to ensure the environment is sterile can be monitored
Members of the team from left to right are: Yvonne Keogh, Senior Pharmaceutical Technician; Louise Byrne, Aseptic Unit Manager; Deirdre Mooney, Senior Pharmaceutical Technician-Team Leader; Iarlaith Doherty, Senior Pharmacist; Katie Brophy, Senior Pharmaceutical Technician; Aisling McGowan, Senior Pharmacist; Nicola Ward, Pharmaceutical Technician. Pharmacy Technicians absent from the image are Laura Ryan, Senior Pharmaceutical Technician; Niamh Cullen, Senior Pharmaceutical Technician, and Hannah Berman, Pharmaceutical Technician
electronically. This will ensure all of the drugs are produced to the very highest of standards.
Commenting on the opening of the new Aseptic Unit, TUH CEO, Barbara Keogh Dunne said, “This new facility is a major step forward for our Hospital. Trained Specialist Pharmaceutical Technicians and Pharmacists will manage production, quality assurance, and validation to ensure full compliance with standards and product integrity. This new cutting-edge facility which contains the latest technology has the potential to treat more patients and has been future-proofed for the introductions of robotics at a later stage.”
New Masters of Pharmacy Programme
A new Master’s of Pharmacy (MPharm) Degree Programme at South East Technological University (SETU) has been accredited by the PSI – the Pharmacy Regulator. SETU intends to offer the MPharm Programme from next September 2026 at its Waterford campus.
This is the third new pharmacy programme accredited this year by the PSI. It brings to six the number of MPharm courses that will be available from 2026 to people wishing to study pharmacy in Ireland.
This new pharmacy programme is established following the Government commitment to funding for expanded healthcare places, including the creation of three new MPharm Programmes. The MPharm provides the qualification necessary for registration to practise as a pharmacist and is a five-year
integrated programme that incorporates clinical and other experiential learning placements.
Speaking about the accreditation of the new programme, PSI Registrar and Chief Officer, Joanne Kissane, said: “Congratulations to all those involved in establishing the new programme at South East Technological University. The PSI has been pleased to support the expansion of pharmacy programmes through our accreditation role since first proposed by Government through the Higher Education Authority (HEA) in 2023. Approval of this new MPharm Programme is positive for SETU, the southeast region, and for students wishing to study pharmacy within Ireland.”
“The availability of a greater number of student places is significant for those interested in this field of study, for the future provision of patient care,
and for our evolving healthcare services. Today’s announcement is another positive milestone for our ongoing work with the Department of Health and many other stakeholders in relation to workforce planning for pharmacy and for the range of healthcare services and industries where pharmacists can contribute their expertise.”
“Our role as the Pharmacy Regulator is to maintain and support patient safety and public trust in pharmacy. This includes accrediting and approving educational programmes for pharmacy and for setting the accreditation standards that must be met on an ongoing basis by the approved pharmacy programme providers. Our aim is to ensure that future pharmacists are equipped to meet their professional and clinical obligations, the needs of patients and the health system.”
One of the key drivers of this exciting new project is Chief 2 Pharmacist & Aseptic Services Manager at TUH Louise Byrne. “This new Aseptic Unit represents our ongoing commitment to excellence in patient care and medication safety. It enables us to meet rising clinical demands, support complex therapies, and improve turnaround times, all the while following the highest sterility and quality standards. With this investment, we are future-proofing our pharmacy services and creating a more resilient and responsive infrastructure to meet the evolving needs of our patients.”
Other staff who have helped support the development of this important project at TUH include Deirdre Mooney, Aseptic Unit Team Leader and Niamh Cullen, Senior QA Pharmaceutical Technician. The Hospital’s Head of Pharmacy, John O‘Byrne and his predecessor, Tim Delaney. Other key players were the Deputy CEO, John Kelly; Head of Project Management in our Facilities Department, Seamus Foran, Brendan Redington HSE Estates Manager Quality & Standards, Chief Operations Officer (former), Shane Russell, Operations Project Manager, Sean Humphreys along with the entire team in the Aseptic Unit itself.
Dr Claire Lennon, Head of the Department of Pharmacy at SETU, commented “Our multidisciplinary cross-campus MPharm development team at SETU is very proud to have received Pharmaceutical Society of Ireland accreditation. The team has worked extremely hard to develop an innovative and impactful, future-focused MPharm programme. Pivotal to programme development has also been the collaborative input and support of our pharmacy professional advisory committee, and stakeholders from community, hospital, and industry pharmacy settings across the southeast. This will ensure graduates meet the requirements of modern pharmacy practice and the skills needs of the sector, all the while maintaining a patient-centred focus. We look forward to welcoming our first group of 40 students to the programme in 2026.”
Talks to Commence on Supply and Pricing of Medicines
The Minister for Health Jennifer Carroll MacNeill has announced the commencement of discussions between the State and Irish Pharmaceutical Healthcare Association (IPHA) on the Framework Agreements on the Supply and Pricing of Medicines.
These discussions will aid the development of a new Multiannual Agreement which supports the financial sustainability of medicines and improves access to innovative new medicines for patients.
The commencement of formal talks follows extensive preliminary engagement between the Department of Health, Department of Public Expenditure, Infrastructure, Public Service Reform and Digitalisation, the
Health Service Executive (HSE) and IPHA.
Minister Carroll MacNeill said, “I am pleased that these formal talks have commenced. This longstanding relationship has been an important one, particularly for patients in Ireland, contributing towards a sustainable supply of innovative medicines.
"We remain committed to supporting timely access to new and innovative medicines. This is underpinned by the continued collaboration between the State and the pharmaceutical industry on our shared objectives of reaching decisions on applications within the context of existing legislation for the benefit of patients.
“I look forward to continuing to work in partnership with the pharmaceutical industry to realise our shared ambition for enhanced access and affordability of medicines in Ireland.”
IPHA has welcomed the confirmation. The commencement of the talks was enabled by assurances to IPHA by the Minister that “in the context of a new Agreement and the engagements to support the development of same, the State is committed to working with you [IPHA], productively, with the explicit aim of achieving the timelines set out in legislation.” Those timelines, which have been highlighted by IPHA, refer to the HSE making a decision on an application for
Fellowship for Professor Kelly
Professor Cathal Kelly, Vice Chancellor, Chief Executive Officer and Registrar of RCSI, has been awarded an Honorary Fellowship of the American College of Surgeons (ACS), one of the most prestigious distinctions in international surgery.
The award was conferred during the Convocation Ceremony at the ACS Clinical Congress in Chicago on 4 October 2025.
In conferring this honour, the ACS acknowledges Professor Kelly’s contribution as an international leader who has transformed surgical education and care quality in Ireland and beyond.
A graduate and Fellow of RCSI, Professor Kelly served as Dean of the Faculty of Medicine and Health Sciences (2006-2009) before his appointment as Chief Executive and Registrar in 2009. Prior to taking up these leadership roles, he was a consultant general and vascular surgeon with a special interest in endovascular surgery in Beaumont Hospital. He combined his career in surgical practice with chairmanship of the surgical division and an academic position in RCSI as Vice-Dean for curriculum change.
He completed his basic and higher surgical training in Dublin and went on to undertake a research fellowship at the University of Pennsylvania in Philadelphia, USA.
Professor Cathal Kelly, Vice Chancellor, Chief Executive Officer and Registrar of RCSI
Professor Kelly completed an MBA at the Institut de Empresa (IE), the Stanford Executive programme and is a Chartered Director.
Professor Kelly has published 75 research papers and given 102 invited lectures and presentations, largely focused on development of surgical practice, advancement of education and research in healthcare, and healthcare quality improvement and assurance. He also is a recipient of the Moynihan Intercollegiate Medal and an honorary fellowship of the Royal
reimbursement of a new medicine within 180 days (excluding clock stops), as set out in the Health Act 2013. We believe this is the first time a Minister for Health has confirmed a policy to achieve the timelines in the 2013 legislation.
IPHA stated, “We believe that this is a significant confirmation from the Minister for Health that can deliver faster access to new medicines for patients in Ireland. We fully agree with the Minister’s position that to achieve this target of 180 days “requires a shared understanding of the role played by all actors in achieving this and where necessary appropriately targeted interventions, including evidencebased capacity investments.”
College of Physician and Surgeons of Glasgow.
Under Professor Kelly’s leadership, RCSI has experienced a period of remarkable growth and transformation, with the achievement of full university status in 2019 marking a major milestone in its evolution.
During this time, the institution has broadened its academic offering through the establishment of new schools and programmes, including Schools of Pharmacy and Biomolecular Sciences, Population Health and Dentistry.
It has also introduced innovative undergraduate and postgraduate programmes aimed at meeting the evolving needs of modern healthcare systems, alongside a significant transformation of RCSI’s medical curriculum.
Professor Kelly has also overseen major campus development projects in support of this growth, most notably the opening of the award-winning 26 York Street building in 2017 and the ¤95 million development at 118 St Stephen’s Green.
Record Budget Marks a Turning Point — or Another Test of Delivery
The Government’s Budget 2026 has set a new record for health spending — a ¤27.4 billion allocation, representing a ¤1.5 billion (6.2%) increase on 2025. Ministers have described the package as a “performance-led investment” designed to improve access, reduce waiting times, and modernise how Ireland delivers care.
But while the figures are historic, reactions across the healthcare sector have been mixed. Industry voices have welcomed new funding for medicines and workforce expansion, while frontline doctors warn that hospitals remain dangerously overburdened and under-bedded.
“We cannot continue to spend more without spending smarter.”
— Minister for Health, Jennifer Carroll MacNeill TD
A Performance-Led Model for a Regionalised Health System
Minister for Health Jennifer Carroll MacNeill TD has made clear that Budget 2026 signals a shift away from pure expenditure growth towards measurable performance. Under the new framework, all six Health Regions will have greater autonomy to direct funds according to local needs, with accountability tied to outcomes and access improvements.
“The State must spend smarter, not just spend more,” the Minister said. “We’re striving for increased productivity in all regions, and driving innovation as we develop faster, smarter and safer ways of delivering healthcare.”
The Department of Health describes the new approach as part of the evolution of Sláintecare — aiming to integrate care closer to home while ensuring national consistency in standards. Hospital and community services will be expected to collaborate under shared performance goals, supported by digital and AI-enabled systems to track outcomes.
Focus on Access, Waiting Times and Workforce
The 2026 allocation targets four broad pillars: equity of access, safety and prevention, capacity and reform, and productivity and value for money.
Budget Figures at a Glance
A major emphasis will be on reducing waiting times, extending operating theatre hours, and shifting more hospital activity to community and virtual settings.
The budget also funds an additional 3,300 whole-time equivalent (WTE) staff for the Health Service Executive (HSE), alongside targeted initiatives such as the expansion of GP out-of-hours services, more home support hours, and investment in digital transformation.
3,300 new HSE staff planned
— 10% of them dedicated to mental health
However, the implementation of seven-day service delivery and regional resource autonomy raises practical challenges. Hospital managers will need to adapt to new performance metrics while continuing to contend with recruitment difficulties, rostering constraints, and space limitations. Hospitals: Capacity Constraints Dominate
For hospital professionals, the single most pressing issue remains bed capacity. Despite the record spend, only 220 new acute hospital beds are planned for 2026.
The Irish Medical Organisation (IMO) has been sharply critical, warning that this number is “simply not credible” given the scale of overcrowding and the ageing population.
Minister for Health Jennifer Carroll
“Talking of record health budgets is nothing more than a smokescreen masking the real problems around capacity and workforce deficits.”
— Dr Anne Dee, President, IMO
The IMO highlighted that although 215 new beds were promised in 2025, just one had been delivered by the end of August. Even with new capacity coming online in Limerick later this year, the gap remains vast.
Clinicians across the system report that chronic Emergency Department overcrowding, delayed discharges, and theatre cancellations continue to undermine patient safety and morale. While the budget’s emphasis on productivity and extended hours could ease bottlenecks, many professionals view these as partial fixes rather than systemic solutions.
Mental Health: Expansion and Reform
Mental health services see one of the most detailed expansions within Budget 2026. The allocation allows for the recruitment of 300 additional WTE staff, including new
Advanced Nurse Practitioner (ANP) and Clinical Nurse Specialist (CNS) posts in Emergency Departments.
Minister for Mental Health Mary Butler TD said the investment will “fundamentally change how we respond to the needs of people in distress,” with out-of-hours coverage and new crisis cafés in Donegal, Kerry and the Midlands.
There will also be:
• 21 new CAMHS inpatient beds
• 10 new Intensive Care Rehabilitation Unit beds at the National Forensic Mental Health Service
• 12 new Suicide Crisis Assessment Nurses working in community GP settings
The reforms aim to provide alternatives to Emergency Departments for people in crisis and to strengthen the bridge between hospital-based and community care.
For hospital professionals, this expansion could relieve some acute pressure, particularly in Emergency Departments where mental health presentations have surged post-pandemic. However, staffing and training capacity remain limiting factors.
Older Persons and Community Care: Building Capacity at Home
Ireland’s rapidly ageing population has prompted a substantial ¤215 million increase for older persons services — a 7.1% uplift on 2025.
Minister for Older People Kieran O’Donnell TD said the funding will deliver 26.7 million home support hours next year, along with an additional ¤92 million for the Fair Deal scheme and ¤2 million for Meals on Wheels — a 30% increase on 2025.
A further ¤2.3 million will enhance dementia diagnostics, memory assessment, and day care expansion, bringing the total number of dementia advisers to 36 nationwide.
O’Donnell said the measures would help more people “live well in their own homes and communities,” aligning with Sláintecare’s goal to shift care out of hospitals.
For hospitals, stronger community and home support provision could help reduce delayed discharges and unnecessary admissions — provided the new hours and staffing materialise in practice.
Public Health and Inclusion Health: Prevention as Investment
Public health spending will rise by ¤11 million, with a renewed focus on prevention and inclusion.
Minister Jennifer Murnane O’Connor TD said the aim is to “lay the foundations for a healthier future,” including campaigns on youth vaping, sexual health, obesity, and child wellbeing.
The budget also provides for expanded drug and inclusion health services across all Health Regions,
new resources for Traveller health programmes, and additional Environmental Health Officers to support school meals inspections.
While modest compared to acute care spending, these investments reflect a growing recognition that prevention reduces long-term pressure on hospitals — an argument that resonates strongly with clinicians who see preventable illness driving demand.
Medicines and Innovation: Industry Welcomes Commitment
The Irish Pharmaceutical Healthcare Association (IPHA), representing Ireland’s researchbased biopharma sector, has welcomed the ¤30 million allocation for new medicines within the ¤217 million PCRS medicines budget.
IPHA Chief Executive Oliver O’Connor said the funding should enable reimbursement for up to 32 innovative medicines in 2026, potentially benefitting 6,000 patients across cancer, cardiovascular disease, diabetes, and rare conditions such as Friedreich’s ataxia.
Crucially, O’Connor highlighted the Minister’s commitment to implementing the statutory 180day reimbursement timeline under the Health Act 2013. “This is the first time a Minister for Health has confirmed a policy to achieve the timelines set out in legislation,” he said.
“Budget 2026 funding for new medicines, along with the State’s commitment to legislative timelines, represents a significant step forward for patient care.”
— Oliver O’Connor, CEO, IPHA
Dr Anne Dee, President, IMO
Budget2026
IPHA also welcomed the increase in the R&D Tax Credit from 30% to 35%, describing it as an important signal of Ireland’s competitiveness amid global market uncertainty.
For hospitals, faster access to reimbursed medicines could shorten treatment pathways, particularly in oncology and metabolic diseases — but success will depend on efficient HSE decision-making and supply chain readiness.
The Frontline Reaction: Divided Views
While industry sees opportunity, frontline clinicians remain sceptical.
The Irish Medical Organisation (IMO) contends that the budget “has failed to plan for a future health service capable of meeting population needs.” Dr Anne Dee, IMO President, said the Government “should be honest with the public that services will not improve” under current capacity constraints.
The IMO’s key criticisms include:
• Insufficient hospital bed expansion
• Lack of targeted investment in General Practice
• Overreliance on “productivity” rhetoric instead of structural solutions
The Organisation argues that structured, funded chronic disease management in primary care could reduce hospital pressures far more effectively than efficiency measures alone.
Despite these critiques, hospital leaders have cautiously welcomed commitments to expand diagnostics, virtual care, and community services, which could ease acute demand over time.
What It Means for Hospital Professionals
For those working within the hospital system, Budget 2026 represents both promise and pressure.
Opportunities:
• More staff (particularly in nursing, mental health, and community care)
• Extended theatre and diagnostic hours
• Potential relief through improved home support and mental health pathways
• Faster access to reimbursed medicines
Challenges:
• Limited acute bed expansion relative to demand
• Workforce fatigue and recruitment challenges
• Complex implementation of seven-day services
• Balancing productivity metrics with clinical quality
The transition to a performanceled model will require robust data infrastructure, clear accountability, and cultural change. Many hospital managers are calling for realistic timelines and adequate local flexibility to deliver measurable improvements.
Looking Ahead to 2027
As the health system prepares to absorb and implement this record allocation, the coming year will test whether Ireland can turn financial inputs into tangible outcomes.
Key issues to watch:
• Delivery of promised hospital and community beds
• Recruitment and retention of the planned 3,300 new staff
• Real progress on regionalisation under Sláintecare
• Achievement of reimbursement timelines for new medicines
• Integration between hospitals and community care
If the system succeeds in these areas, Budget 2026 could mark the start of a more responsive, sustainable health service. If not, hospital professionals may once again find themselves facing rising demand without matching capacity — despite another record spend.
As Minister Carroll MacNeill put it, “We must measure our performance not just by health outcomes, but on how our patients are met when they turn up to our health services.” The next 12 months will determine whether Ireland’s record health budget delivers that vision — or simply repeats familiar patterns of ambition outpacing delivery.
Oliver O'Connor, CEO, IPHA
Women’s Health and Hospital Pharmacy in Ireland: The Changing Landscape
By Chantal Alexander
In the acute hospital settings of Ireland, the pharmacy team is moving into sharper focus when it comes to women’s health. While gynaecology, obstetrics and midwifery remain front of mind, the contribution of hospital pharmacists is increasingly vital for women whose healthcare journeys cross multiple specialties, multiple transitions, and often multiple medicines.
Women’s health in Ireland has climbed the policy agenda. The 2024–2025 national Women’s Health Action Plan reflects a real shift, tracking a more than ¤140 million investment in women’s health since 2020. This places a spotlight on conditions such as endometriosis, menopause and cardiovascular disease, all historically under-researched and under-prioritised in the Irish system. In this evolving environment, hospital pharmacists are not simply dispensers of medicines but core members of multidisciplinary teams. They ensure that women
admitted for care receive medicines that align not only with their presenting condition but also with their gender-specific physiology, life stage and transition points. The role may not always make headlines, but its potential impact on women's outcomes is significant.
Take for example a woman aged 53 admitted for unstable angina, who is peri-menopausal, hypertensive, diabetic and on statin and ACE-inhibitor therapies. A hospital pharmacist reviewing her medicine chart can identify the interface between menopausal hormone therapy (HRT) and cardiovascular risk, check bone health in light of osteopaenia, optimise her discharge medicines and ensure the community pharmacy follow-up is aligned with her gender-specific needs. That kind of medicines-integrated, gender-informed approach is exactly what hospital pharmacy can offer.
Recent Irish research supports this. A study from an Irish teaching
hospital found that among over 1 200 patients reviewed, 55.8 per cent were female and pharmacistled interventions were significantly associated with the female gender. The implication is clear: women frequently derive real additional benefit from pharmacist input in hospital settings.
Yet the pathway is not without challenges. Staffing pressure within hospital pharmacy services remains a key barrier. Meanwhile, women still face difficulties in speaking about medicines associated with female health – for example, vaginal health products – even in structured care settings, signalling a cultural gap that persists.
What gives this moment extra momentum is the timely arrival of new policy and investment in 2025. In April, the Minister for Health announced that the national state-funded HRT scheme would commence from 1 June 2025, covering both medication and dispensing fees
at participating pharmacies. This shift means eligible women will access HRT at no charge in community settings. The implications for hospital pharmacy lie in the hospital-to-community interface and ensuring female patients discharged on HRT continue seamlessly in the community setting with the correct medicines and information in place.
Research into cardiovascular health among women has also gained traction. In April, three Women’s Health Fund projects launched with approximately ¤570, 000 in funding, based at University College Dublin in collaboration with the heart failure unit at St Michael’s Hospital in Dun Laoghaire and St Vincent’s University Hospital in Dublin. These projects focus on postpartum cardiovascular risk after hypertensive disorders, on the social determinants of women’s self-care, and on early diagnostic strategies for heart failure in women. The implication
“The treatment is now seen as an entirely standard part of managing menopause and perimenopause. Given the importance of HRT within women’s healthcare, eliminating all costs would be of significant benefit.”
— Kathy Maher, Chair, Pharmacy Contractors Committee, Irish Pharmacy Union
for hospital pharmacy is clear: pharmacists must bring genderspecific medicines review into areas like cardiology and heartfailure care, where female patients may present differently and receive different risk-modifying therapies.
In the hospital pharmacy context, the gender lens is especially pertinent in several key areas: menopause and HRT management; female cardiovascular risk and medicines optimisation; obstetrics, gynaecology and oncology intersections; polypharmacy in older women; and transitions of care from hospital to community pharmacy.
Menopause care is a paradigmatic example. Women entering peri- or post-menopause who are admitted for other reasons may have HRT, bone health, cardiovascular risk and multiple medicines in play. Hospital pharmacists can review all those domains, intervening on HRT appropriateness in the context of comorbidities, advising
on bone-density monitoring, liaising with gynaecology or endocrinology teams, and ensuring discharge medicines consider both acute and long-term female health. In cardiology wards, women are still under-represented in clinical research despite cardiovascular disease being a leading cause of female mortality. Hospital pharmacists can drive genderaware medicines review, ensure women receive guidelinerecommended therapies and actively participate in the team discussion about how female physiology and presentation differ from male equivalents.
When it comes to gynaecology, oncology and obstetrics, the hospital pharmacist’s medicines expertise is often underutilised. These are areas where pharmacokinetic changes, fertility or menopausal transitions, polypharmacy and complex discharge planning all intersect. Embedding a pharmacist in those multidisciplinary teams
“There’s a huge gap in education about women’s bodies. Women don’t have the language to talk about them or the knowledge to look after them.”
— Laura Dowling, Pharmacist and Women’s Health Educator
elevates care, ensures medicines are managed appropriately and supports safe discharge. Transitions of care are particularly important for women. Women live longer, often accumulate more comorbidities and medicines, and frequently serve as caregivers. Hospital pharmacists, in partnership with community pharmacy, can ensure the medication journey continues smoothly from admission to discharge to the community –especially for women’s health medicines such as hormone therapy, osteoporosis treatments, contraceptives and other femalespecific prescriptions.
Yet there remains a data gap. Few hospital pharmacy departments in Ireland currently capture sex-disaggregated metrics on pharmacist interventions or women-specific medicine outcomes. Moving forward, departments should collect data on interventions in female patients, outcomes, costavoidance and patient-reported experiences specifically within women’s health domains.
Training is another frontier. While hospital pharmacists receive broad clinical mentorship, specialist modules in women’s health (menopause, HRT, female cardiovascular medicine, bone health, fertility pharmacology) are not yet standard. For pharmacists to deliver on the genderresponsive promise, continued professional development must include these domains.
From a hospital policy and service-design angle, there are clear recommendations. Hospital pharmacy departments should introduce a “Women’s Health Medicines Review” protocol for in-patients aged 45 and above or for women with multiple comorbidities. Integration of hospital pharmacy teams with gynaecology and menopause clinics will ensure that the pharmacist voice is heard early. Publication of female-specific metrics will help demonstrate value and secure investment. Community-hospital discharge pathways for women’s medicines must be strengthened, and training offered for hospital pharmacy staff on female-specific pharmacotherapy.
The new Irish policy initiatives of 2025 create a powerful backdrop for hospital pharmacy. The rollout of free HRT from June, the cardiovascular research projects targeting women, and the broader investment in women’s health services mean hospital pharmacists are positioned to proactively shape
how medicines-optimised care for women is delivered.
In the Irish hospital environment, the pharmacy team stands at the nexus of medicines optimisation, multidisciplinary care and continuity of treatment. For women’s health, this is a moment of opportunity. With policy momentum, expanding roles, evolving training and robust hospital pharmacy infrastructure, Irish hospital pharmacists can become central to delivering gender-responsive medicines care. Their contribution may be subtle but is far from minor –from reviewing HRT for a woman with cardiovascular disease, to reconciling complex medicines for a breast-cancer patient, to supporting a perimenopausal admission in a cardiology ward.
Ultimately, when hospital pharmacy services recognise and embrace the unique needs of women – in the ward, at discharge and beyond – women’s health in Ireland will not just improve, it will thrive. And hospital pharmacists will be part of that transformation.
Fact Box: Women’s Health & Hospital Pharmacy in Ireland
• Women’s health remains under-researched in Ireland. Cardiovascular disease accounts for about one quarter of all female deaths.
• Pharmacists in Ireland now comprise approximately 64 per cent female registrants.
• A Cork-based study found that 55.8 per cent of patients reviewed by a clinical pharmacist were female and gender was significantly associated with intervention frequency.
• Demand for HRT in Ireland has doubled over the past two years.
• Hospital pharmacy teams number more than 1 800 professionals across Irish hospitals and are increasingly involved in direct multidisciplinary care.
Atorvastatin Teva Pharma is indicated as an adjunct to diet for reduction of elevated total cholesterol (total-C), LDLcholesterol (LDL-C), apolipoprotein B, and triglycerides in adults, adolescents and children aged 10 years or older with primary hypercholesterolaemia including familial hypercholesterolaemia (heterozygous variant) or combined (mixed) hyperlipidaemia (corresponding to Types IIa and IIb of the Fredrickson classification) when response to diet and other non-pharmacological measures is inadequate.
Atorvastatin Teva Pharma is also indicated to reduce total-C and LDL-C in adults with homozygous familial hypercholesterolaemia as an adjunct to other lipid-lowering treatments (e.g. LDL apheresis) or if such treatments are unavailable.
Prevention of cardiovascular disease
Prevention of cardiovascular events in adult patients estimated to have a high risk for a first cardiovascular event, as an adjunct to correction of other risk factors.
Atorvastatin Teva Pharma Film-Coated Tablets Abbreviated Prescribing Information. Presentation: Each film-coated tablet contains 10mg, 20mg, 40mg and 80mg atorvastatin (as atorvastatin calcium). Indications: Hypercholesterolaemia: Atorvastatin Teva Pharma is indicated as an adjunct to diet for reduction of elevated total cholesterol (total-C), LDL-cholesterol (LDL-C), apolipoprotein B, and triglycerides in adults, adolescents and children aged 10 years or older with primary hypercholesterolaemia including familial hypercholesterolaemia (heterozygous variant) or combined (mixed) hyperlipidaemia when response to diet and other nonpharmacological measures is inadequate. Atorvastatin Teva Pharma is also indicated to reduce total-C and LDL-C in adults with homozygous familial hypercholesterolaemia as an adjunct to other lipid-lowering treatments (e.g. LDL apheresis) or if such treatments are unavailable. Prevention of cardiovascular disease: Prevention of cardiovascular events in adult patients estimated to have a high risk for a first cardiovascular event, as an adjunct to correction of other risk factors. Dosage and administration: For oral administration. Adults: Usual starting dose is 10mg once a day, with adjustment of dose made at intervals of 4 weeks or more. Maximum dose is 80mg once a day. Primary hypercholesterolaemia and combined (mixed) hyperlipidaemia: Majority of patients are controlled with Atorvastatin Teva Pharma 10mg once a day. A therapeutic response is evident within 2 weeks, and the maximum therapeutic response is usually achieved within 4 weeks. Heterozygous familial hypercholesterolaemia: Patients should be started with Atorvastatin Teva Pharma 10mg daily. Doses should be individualised and adjusted every 4 weeks to 40mg daily. Thereafter, either the dose may be increased to a maximum of 80mg daily or a bile acid sequestrant may be combined with 40 mg atorvastatin once daily. Homozygous familial hypercholesterolaemia: Limited data available. The dose of atorvastatin in patients with homozygous familial hypercholesterolemia is 10 to 80mg daily. Atorvastatin should be used as an adjunct to other lipid-lowering treatments (e.g. LDL apheresis) in these patients or if such treatments are unavailable. Prevention of cardiovascular disease: In the primary prevention trials the dose was 10mg/day. Higher doses may be necessary in order to attain (LDL-) cholesterol levels according to current guidelines. Children aged 10 years and above for Heterozygous Familial Hypercholesterolemia: Recommended starting dose is 10mg per day which may be increased to 80mg daily, according to the response and tolerability. Elderly: Efficacy and safety in patients older than 70 using recommended doses are similar to those seen in the general population. Renal impairment: No dose adjustment required. Hepatic impairment: Atorvastatin Teva Pharma should be used with caution in patients with hepatic impairment. Atorvastatin Teva Pharma is contraindicated in patients with active liver disease Contraindications: Atorvastatin Teva Pharma is contraindicated in patients with: hypersensitivity to the active substance or to any of the excipients; active liver disease or unexplained persistent elevations of serum transaminases exceeding 3 times the upper limit of normal; during pregnancy, while breast-feeding and in patients of child-bearing potential not using appropriate contraceptive measures; treated with the hepatitis C antivirals glecaprevir/pibrentasvir. Precautions and warnings: Liver function tests should be performed before the initiation of treatment and periodically thereafter. Patients who develop any signs or symptoms suggestive of liver injury should have liver function tests performed. Atorvastatin Teva Pharma should be used with caution in
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland.
Freephone: 1800 - 201 700 | Email: info@teva.ie
Prescription Only Medicine.
patients who consume substantial quantities of alcohol and/or have a history of liver disease. For patients with prior haemorrhagic stroke or lacunar infarct, the balance of risks and benefits of atorvastatin 80mg is uncertain, and the potential risk of haemorrhagic stroke should be carefully considered before initiating treatment. Atorvastatin may in rare occasions affect the skeletal muscle and cause myalgia, myositis, and myopathy that may progress to rhabdomyolysis, a potentially life-threatening condition characterised by markedly elevated creatine kinase (CK) levels (> 10 times ULN), myoglobinaemia and myoglobinuria which may lead to renal failure. There have been very rare reports of an immune-mediated necrotizing myopathy (IMNM) during or after treatment with some statins. IMNM is clinically characterised by persistent proximal muscle weakness and elevated serum creatine kinase, which persist despite discontinuation of statin treatment, positive anti-HMG CoA reductase antibody and improvement with immunosuppressive agents. In few cases, statins have been reported to induce de novo or aggravate pre-existing myasthenia gravis or ocular myasthenia. This medicinal product should be discontinued in case of aggravation of symptoms. Atorvastatin should be prescribed with caution in patients with pre-disposing factors for rhabdomyolysis. A CK level should be measured before starting statin treatment. The risk of treatment should be considered in relation to possible benefit, and clinical monitoring is recommended. If CK levels are significantly elevated (> 5 times ULN) at baseline, treatment should not be started. Exceptional cases of interstitial lung disease have been reported with some statins, especially with longterm therapy. Presenting features can include dyspnoea, non-productive cough and deterioration in general health (fatigue, weight loss and fever). If it is suspected a patient has developed interstitial lung disease, statin therapy should be discontinued. Some evidence suggests that statins as a class raise blood glucose and in some patients, at high risk of future diabetes, may produce a level of hyperglycaemia where formal diabetes care is appropriate. Patients at risk (fasting glucose 5.6 to 6.9mmol/L, BMI>30kg/ m2, raised triglycerides, hypertension) should be monitored both clinically and biochemically according to national guidelines. Interactions: Please refer to the SmPC for a comprehensive list of drug interactions (including the effect of medicinal products on atorvastatin, and the effect of atorvastatin on other co-administered medicinal products). Risk of rhabdomyolysis is increased when atorvastatin is administered concomitantly with potent inhibitors of CYP3A4 or transport proteins (e.g. ciclosporin, telithromycin, clarithromycin, delavirdine, stiripentol, ketoconazole, voriconazole, itraconazole, posaconazole, letermovir and HIV protease inhibitors including ritonavir, lopinavir, atazanavir, indinavir, darunavir, tipranavir/ritonavir, etc). The risk of myopathy may also be increased with the concomitant use of gemfibrozil and other fibric acid derivates, antivirals for the treatment of hepatitis C (HCV) (e.g. boceprevir, telaprevir, elbasvir/grazoprevir, ledipasvir/ sofosbuvir), erythromycin, niacin, or ezetimibe. If possible, alternative (noninteracting) therapies should be considered instead of these medicinal products. In cases where co-administration of these medicinal products with atorvastatin is necessary, the benefit and the risk of concurrent treatment should be carefully considered. When patients are receiving medicinal products that increase the plasma concentration of atorvastatin, a lower maximum dose of atorvastatin is recommended. In addition, in the case of potent CYP3A4 inhibitors, a lower starting dose of atorvastatin should be
considered, and appropriate clinical monitoring of these patients is recommended. The risk of myopathy and/or rhabdomyolysis may be increased by concomitant administration of HMG-CoA reductase inhibitors (e.g. atorvastatin) and daptomycin. Consideration should be given to temporarily suspend Atorvastatin Teva Pharma in patients taking daptomycin unless the benefits of concomitant administration outweigh the risk. If co-administration cannot be avoided, CK levels should be measured 2-3 times per week and patients should be closely monitored for any signs or symptoms that might represent myopathy. Atorvastatin must not be coadministered with systemic formulations of fusidic acid or within 7 days of stopping fusidic acid treatment. In patients where the use of systemic fusidic acid is considered essential, statin treatment should be discontinued throughout the duration of fusidic acid treatment. There have been reports of rhabdomyolysis (including some fatalities) in patients receiving fusidic acid and statins in combination. The patient should be advised to seek medical advice immediately if they experience any symptoms of muscle weakness, pain or tenderness. Statin therapy may be re-introduced seven days after the last dose of fusidic acid. In exceptional circumstances, where prolonged systemic fusidic acid is needed, e.g. for the treatment of severe infections, the need for co-administration of Atorvastatin Teva Pharma and fusidic acid should only be considered on a case-by-case basis and under close medical supervision. Pregnancy and lactation: Patients of childbearing potential should use appropriate contraceptive measures during treatment. Atorvastatin Teva Pharma is contraindicated during pregnancy. Atorvastatin Teva Pharma should not be used in patients who are pregnant, trying to become pregnant or suspect they are pregnant. Treatment with Atorvastatin Teva Pharma should be suspended for the duration of pregnancy or until it has been determined that the patient is not pregnant. Patients taking Atorvastatin Teva Pharma should not breast-feed their infants. Atorvastatin is contraindicated during breast-feeding. Effects on ability to drive and use machines: Atorvastatin Teva Pharma has negligible influence on the ability to drive and use machines. Adverse reactions: Thrombocytopenia, anaphylaxis, peripheral neuropathy, myasthenia gravis, hearing loss, pancreatitis, hepatitis, hepatic failure, cholestasis, angioneurotic oedema, dermatitis bullous including erythema multiforme, StevensJohnson syndrome and toxic epidermal necrolysis, myopathy, myositis, rhabdomyolysis, muscle rupture, lupus-like syndrome, immune-mediated necrotizing myopathy, gynaecomastia, peripheral oedema. Common: Nasopharyngitis, allergic reactions, hyperglycaemia, headache, pharyngolaryngeal pain, epistaxis, constipation, flatulence, dyspepsia, nausea, diarrhoea, myalgia, arthralgia, pain in extremity, muscle spasms, joint swelling, back pain. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: Specific treatment is not available for atorvastatin overdose. Should an overdose occur, the patient should be treated symptomatically and supportive measures instituted, as required. Liver function tests should be performed and serum CK levels should be monitored. Due to extensive atorvastatin binding to plasma proteins, haemodialysis is not expected to significantly enhance atorvastatin clearance. Legal category: POM. Marketing Authorisation Number: PA1986/125/001-004. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00099. Date of Preparation: July 2025
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie.
Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Further information is available on request or in the SmPC. Product Information also available on the HPRA website. Date of Preparation: August 2025 | Job Code: GEN-IE-00149
¤28M Programme to Deliver Next Generation Cancer Care
Siobhan Gaynor, Advanced Cancer Patient Council member and patient researcher; Prof Donal Brenan, UCD Professor of Gynae-Oncology, Consultant Gynaecological Oncologist at the Mater Hospital, and DeputyDirector of POI; Prof Walter Kolch, Director of Precision Oncology Ireland and Systems Biology Ireland (based at UCD); Dr Siobhan Roche, Director of Science for the Economy, Taighde Éireann–Research Ireland; Prof Kate Robson Brown, UCD Vice-President for Research, Innovation and Impact.
Photo credit: Angela Halpin, photographer
Minister for Further and Higher Education, Research, Innovation and Science, James Lawless TD, launched Phase 2 of Ireland’s leading and largest ever cancer research programme, Precision Oncology Ireland (POI).
POI is a cancer research consortium dedicated to advancing personalised cancer research and care. Its mission is to develop tailored diagnostic and therapeutic solutions using cutting-edge technologies and data, ensuring every patient receives the right treatment at the right time.
The programme is an ambitious and unique strategic partnership model, co-funded through Research Ireland, industry and the not-for-profit sector, coordinated by the Systems Biology Ireland centre based at University College Dublin (UCD), which is led by Professor Walter Kolch.
Minister Lawless said:
“Breakthroughs in cancer research are most likely when clinicians, scientists, industry leaders, patients, charities and other stakeholders come together with a shared purpose. The first phase of Precision Oncology Ireland
stands as proof that strong, sustained collaboration can unlock innovation and accelerate transformative solutions. I congratulate the team on the advances made to date and wish them every success as they embark on this next phase of funded research.”
Professor Walter Kolch said, “Research is the engine behind new medicines. POI-2 is all about linking top notch cancer research to clinical translation. This includes the development of advanced computer simulations of the disease, so that we can design the best diagnostic and treatment approaches for each individual patient.”
UCD Professor of GynaeOncology, Consultant Gynaecological Oncologist at the Mater Hospital, and DeputyDirector of POI, Professor Donal Brennan said: “The first phase of this programme delivered
significant achievements. We now aim to strengthen collaboration with clinical partners and move towards embedding research within standard cancer care, so that patients and society across Ireland – and beyond – can benefit from improved outcomes, enhanced healthcare innovation, and more sustainable delivery of cancer services.”
The first phase of POI established a pioneering cross-sector collaborative model, bringing together academics, industry partners, charities, and patients.
Dr Diarmuid O’Brien, CEO, Research Ireland, said: “The highlyimpactful Precision Oncology Ireland strategic partnership is enabling breakthroughs in cancer biology, supporting the development of new treatments, training the next generation of researchers, nurturing biotech start-ups, and strengthening critical research infrastructure.
“The challenge has moved to focus on qualityof-life needs as well as the need for more real-world data to be gathered to better inform service delivery and hopefully improve our care. In addition, we are hoping to better educate the public and the health service about the realities of living with an advanced cancer diagnosis.”
“This programme has built a unified community that is creating a lasting impact on how we approach cancer research in Ireland. Phase 2, now, represents a substantial increase in investment, scale and ambition, as we work to deliver the next generation of cancer care.”
Patient advocate and researcher Siobhan Gaynor supports the launch of POI-2. Siobhan lives with advanced breast cancer which is a life-limiting disease. She volunteers on several cancer research committees and conducted a survey via Cancer Trials Ireland in 2023 to capture never before-seen input from stage IV cancer patients. Her research was awarded the Irish Cancer Society Public and Patient Involvement (PPI) project of the year in 2025.
Following the survey, Siobhan was also behind the creation
of an Advanced Cancer Patients Council, which ensures dissemination of the survey results and campaigns for changes in Irish advanced cancer care by patients and for patients.
Speaking at the launch, Siobhan said: “Most Stage IV cancers are incurable, although thanks to science and research, we are now living longer. The challenge has moved to focus on qualityof-life needs as well as the need for more real-world data to be gathered to better inform service delivery and hopefully improve our care. In addition, we are hoping to better educate the public and the health service about the realities of living with an advanced cancer diagnosis.”
POI-2 will build on the success of Phase 1 by deepening interdisciplinarity through stronger clinical engagement, broadening scientific scope and
Professor Walter Kolch, Director of Precision Oncology Ireland and Systems Biology Ireland (based at UCD)
infrastructure, enhancing patient and public involvement, expanding training opportunities, and fostering collaboration across the cancer research and healthcare communities from the outset.
UCD Vice-President for Research, Innovation and Impact, Professor Kate Robson Brown said: “The launch of POI-2 marks a pivotal step in realising our collective strategic vision to advance precision medicine, accelerate interdisciplinary collaboration, and harness the transformative power of AI and digital technologies. Most importantly, it reflects our unwavering commitment to translating groundbreaking research into tangible improvements in patient care and outcomes. This programme exemplifies the future of healthcare research and innovation and we are proud to be at the forefront.”
New report highlights only three of 28 targets met in National Cancer Strategy
The Irish Cancer Society has launched new figures that highlight only three of 28 defined targets have been met in the National Cancer Strategy. With Ireland’s cancer mortality rate the third highest in Western Europe, the Society has warned that things will get worse unless increased investment is provided in budget 2026.
The Irish Cancer Society’s NCS Scorecard highlights performance against the 28 defined targets in the National Cancer Strategy in 2024 and 2025.
Of these targets only three have been met. 14 have not been met; seven have no data available; 1 is considered unlikely to meet its 2026 target given its current trajectory, and three have a 2026 deadline which cannot yet be assessed.
CEO, Averil Power said, “One in two of us will get cancer in our lifetime. When we do, we deserve to be given the best possible chance of surviving the disease. But as the National Cancer Strategy Scorecard highlights, target waiting times for vital cancer tests and treatment are not being met. As a result, our cancer death rate is the third highest in Western Europe.
“The National Cancer Strategy was launched in 2017 and will expire in 2026. As we head into the final year of the Strategy, it's clear most targets are not being met. That will only change if Government provides additional investment in the National Cancer Strategy in next week’s budget.”
Professor John Kennedy, Chair of the last National Cancer Strategy, said, “We are deeply concerned about the impact lack of investment in the National Cancer Strategy is having on people with cancer in Ireland. The fact of the matter is that patients are being let down.
“Without Government investment in cancer services, staff, and infrastructure, it is cancer patients who continue to pay a too high price. Budget 2026 must prioritise the National Cancer Strategy, with ringfenced new recurrent development funding for the National Cancer Control Programme of at least ¤20 million each year. The huge challenges posed by the combination of a growing and increasingly aged population along with ever more complex, expensive and effective therapy, can only be addressed by coherent planning for, and multiannual funding of, the next National Cancer Strategy over its lifetime.”
The Irish Cancer Society is calling for increased investment in Budget 2026 towards cancer staff, buildings, and equipment to ensure target waiting times are met. Specifically:
• Provide sufficient investment in staff, buildings, and equipment to enable targets of the current National Cancer Strategy to be met.
• Plan and resource the next National Cancer Strategy.
• Improve the availability of data to support transparency and decision-making.
TIME IS IN YOUR HANDS
ERBITUX® + FOLFIRI or FOLFOX:
Combining strength of clinical data with a manageable tolerability profile
• ERBITUX® combined with FOLFIRI or FOLFOX shows improved mOS in RAS wild-type mCRC patients compared with chemotherapy alone2,3*†
• ERBITUX® has a manageable adverse event profile1,5
ERBITUX® is indicated for the treatment of patients with EGFRexpressing RAS wild-type mCRC in combination with irinotecan-based chemotherapy, in first-line in combination with FOLFOX, or as a single agent in patients who have failed oxaliplatin- and irinotecan-based therapy and who are intolerant to irinotecan.1
Legal category: POM.
Prescribing information and adverse event reporting information for ERBITUX® is available on the next page. GET UPDATES
Scan this QR code with your smartphone to receive updates by email and/or SMS from Merck Serono Limited.
PRESCRIBING INFORMATION - Ireland
Please refer to the Summary of Product Characteristics for further information
Erbitux 5 mg/ml solution for infusion cetuximab.
Presentation:
Glass vial containing 20 ml or 100 ml of Erbitux solution for infusion at a concentration of 5 mg/ml. Total: 100 mg or 500 mg Erbitux per vial.
Indications:
Treatment of Epidermal Growth Factor Receptor-expressing, RAS wild-type metastatic colorectal cancer (mCRC) in combination with irinotecan-based chemotherapy; in first-line in combination with FOLFOX (oxaliplatin, 5-FU and folinic acid) or as a single agent in patients who have failed oxaliplatin- and irinotecan-based therapy and who are intolerant to irinotecan. Treatment of squamous cell cancer of the head and neck (SCCHN) in combination with radiation therapy for locally advanced disease or in combination with platinumbased chemotherapy for recurrent and/or metastatic disease.
Dosage and administration:
Erbitux may be administered in a weekly or every other week dose regimen for all indications, with the exception of locally advanced squamous cell carcinoma of the head and neck (SCCHN) in combination with radiation therapy, where it is administered only on a weekly basis.
Weekly dose regimen: Erbitux is administered once a week. The initial dose is 400 mg cetuximab per m2 body surface area (BSA). All subsequent weekly doses are 250 mg/m2 each.
Biweekly dose regimen: Erbitux is administered once every other week. Each dose is 500 mg cetuximab per m2 body surface area.
Children: safety and efficacy have not been established.
Administration must be supervised by a physician experienced in antineoplastic medicinal products. Administer intravenously with infusion pump, gravity drip or syringe pump using a separate infusion line. The initial dose should be given slowly to minimize risk of infusion related reactions. The recommended infusion period is 120 minutes. For subsequent administration the infusion rate must not exceed 10 mg/min. If initial infusion is well tolerated the recommended infusion period for weekly dose regimen of 250 mg/m2 is 60 minutes and recommended infusion period for biweekly dose regimen of 500 mg/m2 is 120 minutes.
Premedicate first infusion at least one hour before with an antihistamine and a corticosteroid. Premedication recommended for all subsequent infusions.
Flush line with sterile 0.9% NaCl at end of infusion. Closely monitor patient throughout infusion and for at least 1 hour afterwards. Resuscitation equipment must be available. mCRC: Evidence of wild-type RAS status is required before initiating treatment. Mutational status should be determined by an experienced laboratory using validated test methods for detection of KRAS and NRAS (exons 2, 3 and 4). Refer to product information for concomitantly used chemotherapeutic agents for dosage. Administer Erbitux first and do not administer concomitantly used chemotherapeutic agents earlier than 1 hour after end of Erbitux infusion. Continue treatment until disease progression. Locally advanced SCCHN: start Erbitux one week before radiation therapy and continue treatment until the end of the radiation therapy period. Recurrent/ metastatic SCCHN: use in combination with platinum-based chemotherapy followed by Erbitux as maintenance therapy until disease progression. Do not administer chemotherapy earlier than 1 hour after the end of Erbitux infusion.
Contraindications:
Severe (grade 3 or 4) hypersensitivity to Erbitux. In combination with oxaliplatin-containing chemotherapy in patients with mutant RAS mCRC or for whom RAS mCRC status is unknown. Consider contraindications to concomitantly used chemotherapeutic agents or radiation therapy.
Precautions:
Discontinue infusion immediately and permanently in the event of severe infusion-related reactions (symptoms may include: bronchospasm; urticaria; increase or decrease in blood pressure; loss of consciousness or shock; rarely: angina pectoris; myocardial infarction or cardiac arrest) – emergency treatment may be required. Some of these reactions may be anaphylactic or anaphylactoid in nature or represent a cytokine release syndrome (CRS). Anaphylatic reactions may occur as early as within a few minutes of the first infusion. The risk is increased in patients with a history of allergy to red meat, tick bites of positive results of tests for IgE antibodies against cetuximab. A CRS typically occurs within one hour after infusion and is less commonly associated with bronchospasm and urticaria. It is normally most severe in relation to the first infusion. Monitor all vital signs closely for at least two hours for the first dose. If an infusion-related reaction occurs during the first 15 minutes, stop the infusion. Perform careful benefit/risk assessment including whether patient may have pre-formed IgE antibodies, before giving a subsequent infusion. If an infusion-related reaction develops later during the infusion or at a subsequent infusion, further management depends on its severity – see SPC. Warn patients of possible delayed-onset severe infusionrelated reactions. Decrease infusion rate if mild or moderate infusion-related reaction occurs (symptoms may include: fever; chills; dizziness; dyspnoea)
and use lower rate in all subsequent infusions. Closely monitor patients, particularly during the first administration and those with reduced performance status and pre-existing cardiopulmonary disease.
Cases of interstitial lung disease (ILD), including fatal cases, have been reported, with most patients being from the Japanese population. Factors such as concomitant chemotherapy known to be associated with ILD or pre-existing pulmonary diseases were frequent in fatal cases. Monitor such patients closely. In the event of symptoms or radiographic findings suggestive of ILD, prompt diagnostic investigation should occur. Discontinue Erbitux if ILD is diagnosed. Skin reactions are very common. Consider prophylaxis with oral tetracyclines (6-8 weeks) and topical 1% hydrocortisone cream with moisturiser. Skin reactions may become severe, especially in combination with chemotherapy. The risk of secondary infections is increased and cases of staphylococcal scalded skin syndrome, necrotising fasciitis and sepsis, in some cases with fatal outcome, have been reported. Interrupt treatment if patient experiences an intolerable or severe skin reaction (≥ grade 3 CTCAE). Only resume if reaction resolves to grade 2. With second or third instances of severe skin reactions, resume at lower dose (200 mg/m2 BSA in the weekly dosing regimen, 400 mg/m2 BSA in the biweekly dosing regimen) after the second occurrence and with a dose reduction of 40% (150 mg/m² BSA in the weekly dosing regimen, 300 mg/m² BSA in the biweekly dosing regimen) after the third occurrence. A fourth occurrence of severe skin reaction, or failure to resolve to grade 2 during interruption, necessitates permanent discontinuation of Erbitux. Determine serum electrolyte levels (e.g. magnesium, potassium, calcium) prior to, and periodically during Erbitux treatment and replete as appropriate. In combination with platinum-based chemotherapy, severe leukopenia or neutropenia may occur, leading to infectious complications such as febrile neutropenia, pneumonia and sepsis. Careful monitoring is recommended in such patients, particularly in those who experience skin lesions, mucositis or diarrhoea. An increased frequency of severe and sometimes fatal cardiovascular events and treatment emergent deaths has been observed in non-small cell lung cancer, SCCHN and colorectal carcinoma patients. In some studies (non-small cell lung cancer) association of these with age ≥ 65 years has been observed. When prescribing, take into account the cardiovascular and performance status of the patient and concomitant administration of cardiotoxic compounds such as fluoropyrimidines. Do not use Erbitux in colorectal cancer patients whose tumours have RAS mutations or for whom RAS tumour status is unknown.
Promptly refer patients with symptoms of keratitis to an ophthalmology specialist. If ulcerative keratitis is confirmed, interrupt or discontinue Erbitux. Consider the benefits/risks of continuing treatment if keratitis is diagnosed. Use Erbitux with caution in patients with a history of keratitis, ulcerative keratitis or severe dry eye. Contact lens use is a risk factor for keratitis and ulceration. Only use in pregnancy if potential benefit justifies potential risk to foetus. Breast feeding is not recommended during Erbitux treatment or for up to 2 months after last infusion.
Side effects: Very common: skin reactions (acne-like rash; pruritus; dry skin; desquamation; hypertrichosis; nail disorders); hypomagnesaemia; increase in liver enzyme levels; mild or moderate infusion-related reactions; mucositis, in some cases severe, which may lead to epistaxis. Common: headache; diarrhoea; nausea; vomiting; severe infusion-related reactions, in some cases fatal; conjunctivitis; fatigue; dehydration normally secondary to diarrhoea or mucositis; hypocalcaemia; anorexia which may lead to weight decrease. Uncommon: blepharitis; keratitis; pulmonary embolism; DVT, interstitial lung disease which may be fatal. Very rare: Stevens-Johnson syndrome/toxic epidermal necrolysis. Unknown frequency: superinfection of skin lesions; aseptic meningitis. Refer to product information of concomitantly used chemotherapeutic agents for side effects. In combination with fluoropyrimidines, the frequency of cardiac ischaemia and hand-foot syndrome was increased compared to that with fluoropyrimidines. In combination with capecitabine and oxaliplatin (XELOX) the frequency of severe diarrhoea may be increased.
In combination with platinum-based chemotherapy, the frequency of severe leukopenia or neutropenia may be increased, leading to a higher rate of infectious complications such as febrile neutropenia, pneumonia and sepsis compared with platinum-based chemotherapy alone.
Prescribers should consult the summary of product characteristics in relation to other side-effects.
Legal category: POM.
Marketing Authorisation Holder:
Merck Europe B.V., Gustav Mahlerplein 102, 1082 MA Amsterdam, The Netherlands
For further information, including price queries, contact: Merck Serono, 4045 Kingswood Road, Citywest Business Campus, Dublin 24. Tel: 01 4687590.
Date of preparation: December 2024 Job Bag No: IE-ERB-00008
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Merck Serono Limited. Tel: 1 800 719 881 or email: medinfo.uk@merckgroup.com
EGFR, epidermal growth factor receptor; FOLFIRI, fluorouracil, leucovorin and irinotecan; FOLFOX, fluorouracil, leucovorin and oxaliplatin; mCRC, metastatic colorectal cancer; mOS, median overall survival; PFS, progression-free survival.
References
1. Erbitux® Summary of Product Characteristics. Available at: https://www.medicines.ie/medicines/erbitux-5mg-mlsolution-for-infusion-32054/spc (Last accessed June 2025).
2. Van Cutsem E et al. J Clin Oncol. 2015;33:692–700.
3. Qin S et al. J Clin Oncol. 2018;36:3031–3039.
4. García-Foncillas J et al. Front Oncol. 2019;9:849.
5. Petrelli F et al. Oncology. 2018;94:191–199.
Recent Patterns and Trends in Global Prostate Cancer Incidence and Mortality: An Update
Written by Elizabeth J. Schafera, Mathieu Laversanneb, Hyuna Sunga, Isabelle Soerjomataramb, Alberto Brigantic,d, William Dahute, Freddie Brayb and Ahmedin Jemala
aSurveillance and Health Equity Science, American Cancer Society, Atlanta, GA, USA
bCancer Surveillance Branch, International Agency for Research on Cancer, Lyon, France
cDivision of Experimental Oncology/Unit of Urology, Urological Research Institute, IRCCS Ospedale San Raffaele, Milan, Italy
dVita-Salute San Raffaele University, Milan, Italy
eOffice of the Chief Scientific Officer, American Cancer Society, Atlanta, GA, USA
Prostate cancer (PC) is the second most commonly diagnosed cancer and the fifth leading cause of cancer death among men worldwide, with more than 1 460 000 estimated cases and 396 000 deaths in 2022.1 It is predicted that by 2040, the PC burden will have increased to approximately 2.4 million cases and 712 000 deaths solely because of the aging and growing global population.2 This increase in mortality translates to approximately 7.5 million life-years lost, with Africa, Asia, and Latin America/Caribbean experiencing the steepest increase in predicted life-years lost.3
Previous studies of trends in international PC incidence and mortality rates4, 5 are based on data up to 2016. There have been recent changes in early detection recommendations in many countries,6, 7 as well as improvements in treatment8 and an increase in the number of countries covered by highquality population-based cancer registries.9 Here we examine global patterns and time trends for PC incidence and mortality using incidence data from populationbased cancer registries worldwide up to 2021, and national mortality data from vital registration systems up to 2022.
Materials and methods
Data sources
The International Agency for Research on Cancer (IARC) GLOBOCAN 2022 estimates were obtained from the Global Cancer Observatory (https://gco.iarc.who. int/today/en) and used to describe PC incidence and mortality (International Classification of Disease-10 code C61) estimated for 185 countries or territories, covering approximately 98% of the global population. The countryspecific methods for estimation depend on the coverage, timeliness, and accuracy of the incidence and mortality data recorded in each country.10
PC incidence data for 50 countries/territories with at least 10 yr of data available between 1980 and 2021 were obtained from the IARC Cancer Incidence in Five Continents Plus (CI5plus) database, a quinquennial series of high-quality population-based cancer registry data at the national or subnational level that covers approximately 5% of the global population.9, 11 Inclusion in CI5 volumes is based on the data quality of each registry over time, which is assessed in terms of the comparability, completeness, and validity of the data submitted. Incidence data for the USA were supplemented with more recent data from the Surveillance, Epidemiology and End Results 8 (SEER-8) registry database, representing approximately 8% of the US population, to examine incidence rates for Black and White men separately because of known racial disparities.12 Cancer mortality data between 1980 and 2022 for 59 countries/ territories were obtained from the World Health Organisation (WHO) mortality database as compiled by IARC, representing approximately 22% of the global population. The quality of these data, which is measured according to coverage and completeness, varies across countries.13
Long-term PC incidence trends are presented for 50 countries/ territories, and long-term PC mortality trends for 59 countries/ territories. However, the recorded rates include White and Black men in the USA, yielding 52 populations for incidence and 61 populations for mortality.
Statistical analysis
All incidence and mortality rates were age-standardised to the 1966 Segi-Doll world standard population using the direct method.14, 15 Secular trends in age-standardised rates were visualised and quantified using Joinpoint regression by estimating
the annual percentage change (APC), allowing a maximum of four joinpoints. A weighted average of the APC (AAPC) was also calculated for the most recent 5-yr period, with weights based on the length of each APC interval. Trends were described as increasing or decreasing when the APC or AAPC was statistically significant according to a two-sided p value <0.05, or otherwise as stable. Analyses were performed with R v4.3.3, Rcan v1.3.82, and Joinpoint v3.53.
Results
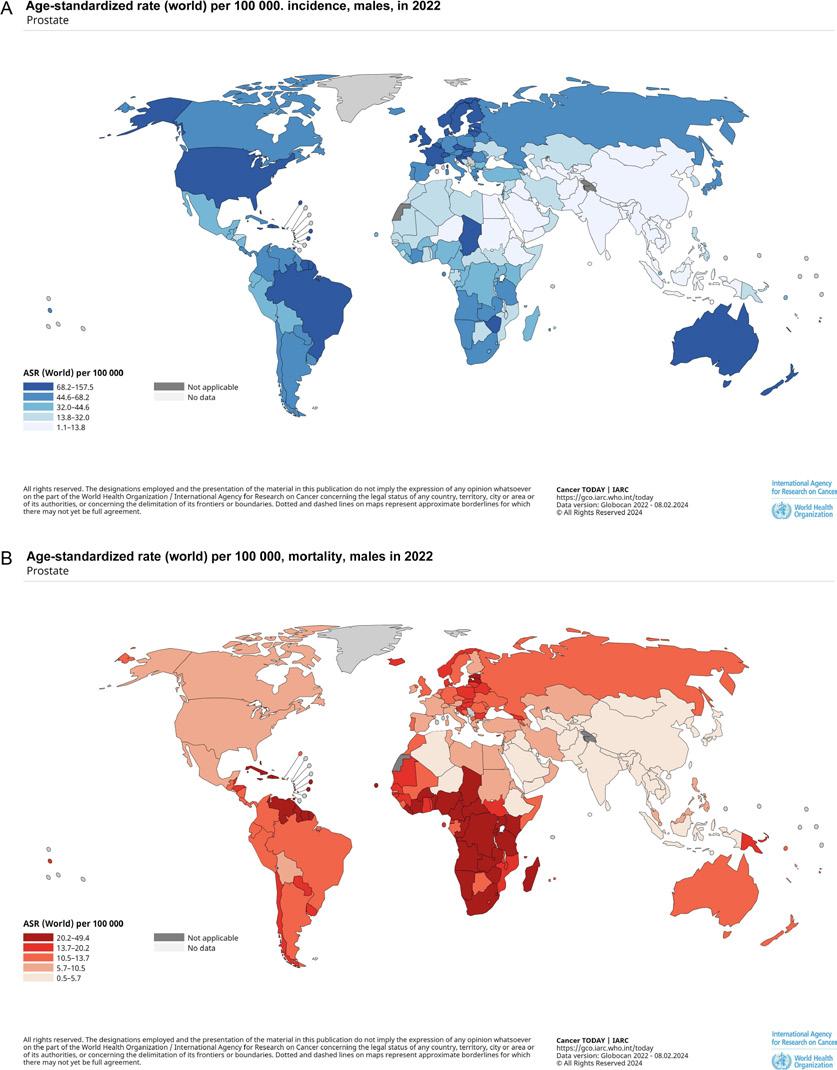
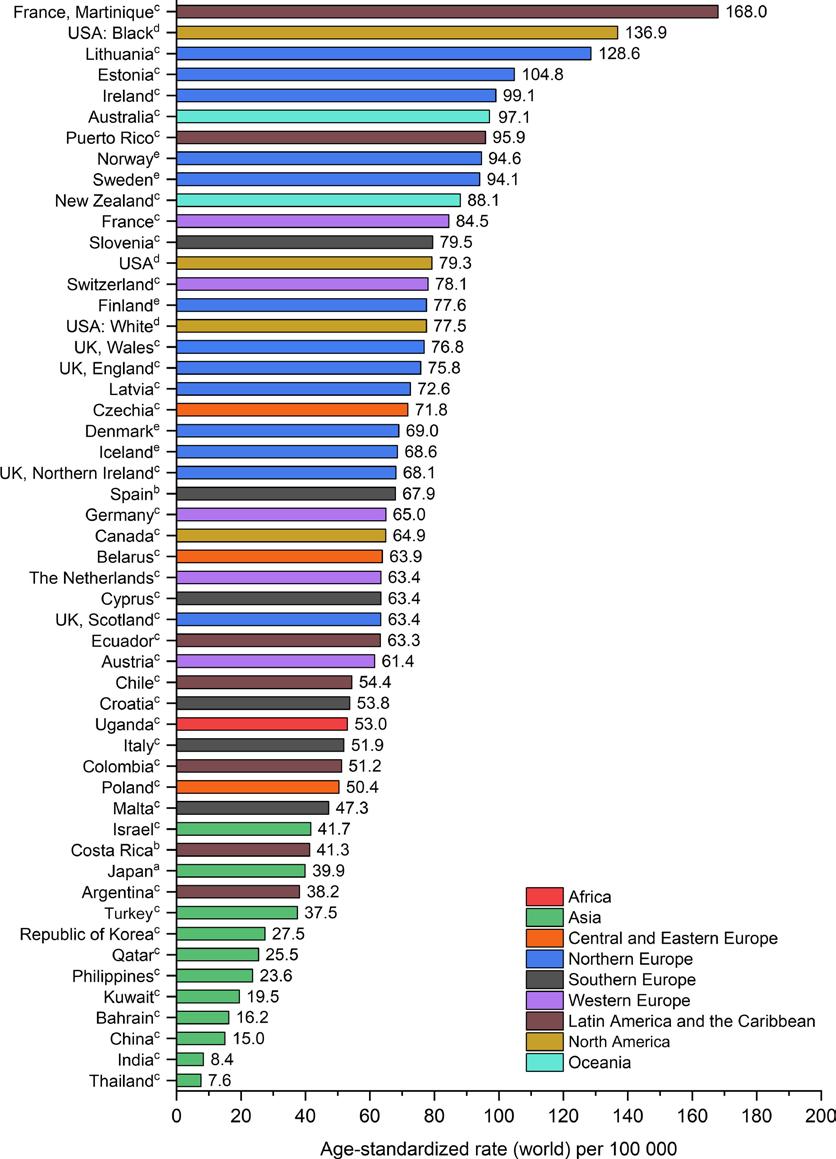
Estimated PC incidence and mortality rates for 2022 across 21 world regions and 185 countries
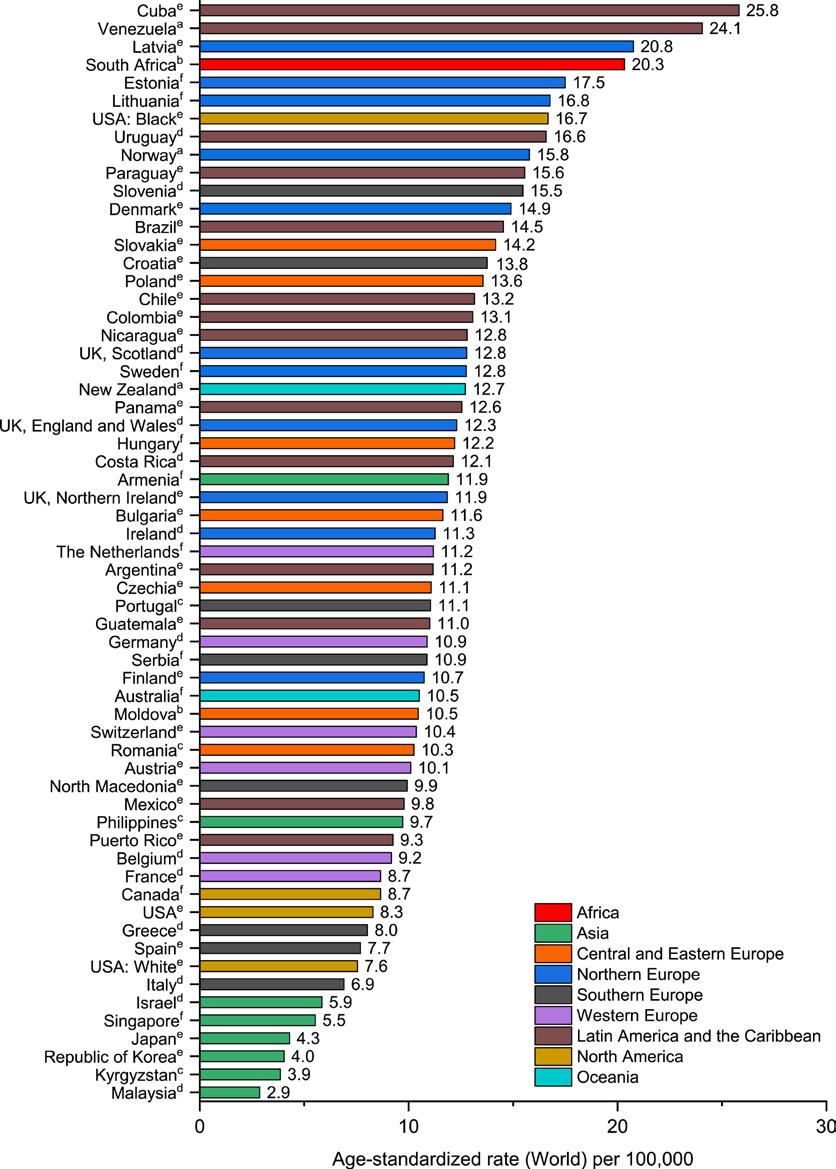
In 2022, PC incidence and mortality rates varied approximately 13-fold and 9.5fold, respectively, across world areas. Northern Europe had the highest estimated incidence rate (82.8 per 100 000 men) and Southern Africa had the highest mortality rate (29.7 per 100 000 men). South-Central Asia had the lowest rates for both incidence (6.4 per 100 000 men) and mortality (3.1 per 100 000 men). At the country level, the highest incidence rates were found in Australia, New Zealand, the USA, Brazil, and several countries in the Caribbean and Northern Europe (Fig. 1). By contrast, mortality rates were highest in many sub-Saharan African and Caribbean countries, such as Barbados, Jamaica, and Chad, and were lowest across Asia (Fig. 1).
Patterns in recorded incidence and mortality rates for the last 5 yr of available data
Fig. 2, Fig. 3 illustrate PC incidence and mortality rates recorded during the most recent 5-yr period with data available from 52 and 61 populations, respectively. Incidence rates per 100 000 men varied approximately 22-fold across countries, from 7.6 in Thailand to 168.0 in Martinique. Mortality rates per 100 000 men
varied approximately ninefold, ranging from 2.9 in Malaysia to more than 24.0 in Cuba and Venezuela. In general, countries in Asia had the lowest incidence and mortality rates, while countries with a higher proportion of men of African ancestry (sub-Saharan Africa and the Caribbean) and some Eastern European countries (eg, Lithuania and Estonia) had the highest incidence and mortality rates.
Africa
The incidence rate in Uganda was 53.0 per 100 000 men, and rates have been increasing by 2.3% per year since 1993 (Fig. 2). South Africa had the fourth highest mortality rate among all countries included in the study at 20.3 per 100 000 men, and rates have been increasing by 1.6% per year since 1996 (Fig. 3).
Asia
Countries throughout Asia had some of the lowest incidence (7.6 to 41.7 per 100 000) and mortality (2.9 to 11.9 per 100 000) rates during the most recent 5-yr period (Fig. 2, Fig. 3). Incidence rates during the latest 5-yr period continued to increase by approximately 4.0–5.0% per year in China, India, and Thailand, decreased by 2.2–6.2% per year in Turkey and Israel, and remained stable in Bahrain, Philippines, Republic of Korea, and Qatar. However, incidence rates recently stabilised in Japan and Kuwait after increasing up to the early 2010s. By contrast, mortality rates during the most recent 5-yr period increased by 0.5% per year in the Philippines, decreased by 1.5–5.2% per year in Japan, the Republic of Korea, and Armenia, and were stable in the remaining countries.
Central and Eastern Europe
Incidence rates in Central and Eastern Europe ranged from 50.4 to 71.8 per 100 000 men (Fig. 2), while mortality rates ranged from
Fig. 1. Estimated age-standardised (A) prostate cancer incidence and (B) prostate cancer mortality rates in 2022.
ASR = age-standardized rate; IARC = International Agency for Research on Cancer.
Source: GLOBOCAN 2022.
10.3 to 14.2 per 100 000 (Fig. 3). During the most recent 5-yr period, incidence rates increased in Belarus (4.4% per year) and Poland (10.0% per year) and remained stable in Czechia (Fig. 4). By contrast, mortality rates decreased by approximately 1.0–3.0% per year in Hungary, Czechia, and Slovakia, increased by approximately 1.0–5.0% per year in Romania, Bulgaria, and Moldova, and were stable in Poland.
Northern Europe
In Northern Europe, incidence
rates varied twofold across the 13 countries included in the study, from 63.4 per 100 000 men in Scotland to 128.6 in Lithuania, the third highest rate among all countries (Fig. 2). Similarly, mortality rates varied approximately twofold across the 11 countries, with the highest rate in Latvia at 20.8 per 100 000 men, the third highest rate among all populations (Fig. 3). Incidence rates during the most recent 5-yr period continued to increase by 4.0% annually in Latvia and by 0.7% per year in Scotland,
in Slovenia, while mortality rates per 100 000 men ranged from 6.9 in Italy to 15.5 in Slovenia (Fig. 2, Fig. 3). During the most recent 5-yr period, incidence rates increased by 9.2% per year in Croatia, decreased by 3.1% per year in Spain, and remained stable in Cyprus, Italy, Malta, and Slovenia. By contrast, mortality rates decreased by approximately 1.0–2.0% per year in all countries except North Macedonia, where the rate remained stable.
Western Europe
decreased by approximately 1.0–2.0% per year in five countries (Denmark, Finland, Ireland, Norway, and Sweden), and were stable in the remaining countries. By contrast, mortality rates during the most recent 5-yr period decreased by approximately 1.0–8.0% per year for all 11 Northern European countries except for Latvia, where the rate remained stable.
Southern Europe
Across Southern Europe, incidence rates per 100 000 men ranged from 47.3 in Malta to 79.5
Incidence rates per 100 000 men ranged from 61.4 in Austria to 84.5 in France, while mortality rates per 100 000 men ranged from 8.7 in France to 11.2 in the Netherlands (Fig. 2, Fig. 3). During the most recent 5-yr period, incidence rates decreased by approximately 2.0% per year in Germany and the Netherlands and remained stable in Switzerland. However, incidence rates increased by 3.6% per year in Austria and stabilised in France, a change from the previously declining trends. Mortality rates continued to decrease by approximately 1.0–3.0% per year in Belgium, Germany, Switzerland, and France, and stabilised in Austria and the Netherlands (Fig. 3). Latin America and the Caribbean Incidence rates per 100 000 men varied more than fourfold across the seven countries located in Latin America and the Caribbean, ranging from 38.2 in Argentina to 168.0 in Martinique (Fig. 2). Mortality rates per 100 000 men ranged from 9.3 in Puerto Rico to 25.8 in Cuba (Fig. 3). The region encompasses four of the top ten populations with the highest mortality rates in the study (Cuba, Venezuela, Uruguay, and Paraguay). During the most recent 5-yr period, incidence rates continued to decrease by approximately 1.0% per year in Argentina, Colombia, and Puerto Rico, and were stable in the four remaining countries. Mortality rates during the most recent 5-yr period decreased by approximately 1.0–4.0% per year in eight of the 14 countries examined, increased by approximately 1.0–8.0% per year in Venezuela, Paraguay, Cuba, and Guatemala, and were stable in Mexico and Nicaragua.
North America
Incidence rates per 100 000 men were 79.3 in the USA and 64.9 in Canada. Mortality rates were relatively similar between Canada and the USA, at 8.7 and 8.3 per 100 000 men, respectively. Black men in the USA had the second highest incidence rate among all men included in the study at 136.9 per 100 000 men and had a 77% higher incidence rate and a 120% higher mortality rate in
BPH
Fig. 2. Prostate cancer incidence rates in selected countries. a Rates are from 2011–2015. b Rates are from 2012–2016. c Rates are from 2013–2017. d Rates are from 2015–2019. e Rates are from 2017–2021.
Source: Cancer Incidence in Five Continents; Surveillance, Epidemiology and End Results (SEER) program.
comparison to White men (Fig. 2, Fig. 3). During the most recent 5-yr period, the incidence rate increased by 4.2% per year in the USA and stabilised in Canada after rapidly declining in the previous decade. By contrast, the mortality rate during the most recent 5-yr period continued to decline in Canada, albeit at a slower pace, and stabilised in the USA following two decades of steady decline.
Australia and New Zealand had the sixth (97.1 per 100 000 men) and tenth (88.1 per 100 000 men) highest incidence rates, respectively, among all men included in the study. The incidence rate decreased by 3.8% per year in Australia since 2008 and by 0.7% per year in New Zealand since 1995 (Fig. 2).
reflecting higher uptake of prostate-specific antigen (PSA)-based testing in these countries.8, 16 By contrast, mortality rates were highest in many parts of sub-Saharan Africa and Latin America/Caribbean, largely because of the higher proportion of individuals of African ancestry, who are genetically more susceptible to developing PC, and the limited availability of early detection and treatment services.17 During the most recent 5-yr period, incidence rates increased in 11 countries and mortality rates increased in nine, largely confined to countries within Africa, parts of Asia, Latin America/Caribbean, and Europe. In most countries, however, incidence and mortality rates decreased or stabilised.
In general, trends in PC incidence in many high-income countries follow trends in PSA-based screening, with the incidence rate rising when PSA-based screening uptake increases and falling when it decreases.18, 19 For example, the decline in the PC incidence rate since 2008 in Australia coincided with the fall in PSA-based screening prevalence beginning in the same year among men aged 45–84 yr.18 In addition to declines in PSA-based screening uptake, increased use of multiparametric magnetic resonance imaging (mpMRI) to reduce overdiagnosis20 may have contributed to the recent decrease in incidence rate in some countries. For example, in Sweden, where incidence rates are decreasing, the STHLM3-MRI trial found that incorporation of mpMRI in the diagnostic pathway reduced diagnosis of clinically insignificant tumors by 64% and benign findings on biopsy by 74% among men biopsied after a positive MRI test in comparison to men who underwent transrectal ultrasonography-guided prostate biopsy for elevated PSA.21 Over the past few years, many national or regional organisations, including the European Association of Urology22 and the American Urological Association,23, 24 updated their guidelines on early PC diagnosis to recommend mpMRI before prostate biopsy to decrease the number of clinically insignificant PC diagnoses at biopsy.
Similarly, the mortality rate has decreased by 1.0% per year in Australia since 2014 and by 2.7% per year in New Zealand since 1997(Fig. 3).
Discussion
The estimated PC incidence rates in 2022 were highest in North America, Australia, New Zealand, Brazil, and in many Northern European countries, probably
Incidence rates increased in 11 of the 50 countries examined, including Uganda, the USA, and several countries in Asia and Europe. Such trends may in part reflect increases in incidental detection of tumors via transurethral resection of the prostate (TURP) for lower urinary tract syndrome and benign prostatic hyperplasia,25, 26, 27 greater awareness of the disease,8, 28 and opportunistic PSA testing.29, 30 A 2022 meta-analysis revealed that the prevalence of incidental
Oceania
Fig. 3. Prostate cancer mortality rates in selected countries. a Rates are from 2012–2016. b Rates are from 2014–2018. c Rates are from 2015–2019. d Rates are from 2016–2020. e Rates are from 2017–2021. f Rates are from 2018–2022.
Source: World Health Organisation mortality database.
PC following TURP was higher in Africa (22.0%) and Asia (9.0%) than in North America (1.0%).31 The rising prevalence of potential risk factors such as obesity, which is associated with advanced-stage disease,32 and a Western diet32,33
may have also contributed to the rising incidence of PC. The increase in PC incidence rate since the mid-2010s in the USA, largely driven by advanced-stage disease, was not preceded by a marked increase in PSA-based screening practices.34 Further studies are needed to elucidate reasons underlying this rising trend.
The declining trend for mortality rates in many countries throughout Europe, North America, Oceania, and Latin America/Caribbean
are probably the result of improvements in early detection of advanced-stage cancer8, 35 and in treatments.8, 36 Previous modelbased studies estimated that PSA-based screening accounted for 45–70% of the decline in the PC mortality rate in the USA,37 and improvements in treatments for 22–33% of the decline by 2005.36 A 2021 study in Lithuania, where a nationwide PSA-based PC screening program in 2006, found that among individuals diagnosed with PC, the PCspecific standardised mortality risk ratio was higher for who did not participate in the national screening program (20.95, 95% CI 20.00–21.94) than for those who did (8.99, 95% CI 8.63–9.37).38
In contrast to the declining or stabilising mortality trends in the majority of the 59 countries included in the study, rates increased in nine countries, including South Africa, the Philippines, Cuba, Moldova, Bulgaria, and Guatemala. These increasing mortality trends may reflect increasing incidence as well as limited availability of high-quality early detection and treatment services.39 For example, according to WHO, there are fewer than three radiotherapy machines per million population in South Africa and Cuba, compared to more than 10 machines per million population in the USA, Germany, and Sweden.40, 41, 42 Only 28% of PC patients survive for 5 yr in South Africa, compared to more than 90% in high-income countries such as the USA (97.0%),41 France (93.1%),43 and Australia (94.5%),44 where early detection and treatment services are more accessible.
Conclusions
Our analysis of high-quality population-based data across the five continents revealed that PC incidence and mortality rates decreased or were stable in the majority of countries examined. However, increasing trends were found in a few countries located in Africa, Asia, Latin America/ Caribbean, and Central and Eastern Europe, possibly because of an increase in detection (incidence) and limited access to and the availability of treatments (mortality only). These findings reinforce the need for improvements in access to early detection and treatment services to mitigate the undue high burden of the disease in these countries. Furthermore, improvements in data availability and quality, particularly in lowand middle- income countries in Asia and Africa, will enhance our understanding of current disparities and prioritisation of early detection and treatment approaches.
References available on request
Masters of Pharmacy Programme
A new Master’s of Pharmacy (MPharm) Degree Programme at South East Technological University (SETU) has been accredited by the PSI – the Pharmacy Regulator. SETU intends to offer the MPharm Programme from next September 2026 at its Waterford campus.
This is the third new pharmacy programme accredited this year by the PSI. It brings to six the number of MPharm courses that will be available from 2026 to people wishing to study pharmacy in Ireland.
Having been engaged with universities towards accreditation over the past two years, the Council of the PSI, the pharmacy regulator’s governing board, was pleased to accredit the SETU programme at its meeting on 2 October*.
This new pharmacy programme is established following the Government commitment to funding for expanded healthcare places, including the creation of three new MPharm Programmes. The MPharm provides the qualification necessary for registration to practise as a pharmacist and is a five-year integrated programme that incorporates clinical and other experiential learning placements.
Speaking about the accreditation of the new programme, PSI
Registrar and Chief Officer, Joanne Kissane, said, “Congratulations to all those involved in establishing the new programme at South East Technological University.
The PSI has been pleased to support the expansion of pharmacy programmes through our accreditation role since first proposed by Government through the Higher Education Authority (HEA) in 2023. Approval of this new MPharm Programme is positive for SETU, the southeast region, and for students wishing to study pharmacy within Ireland.”
“The availability of a greater number of student places is significant for those interested in this field of study, for the future provision of patient care, and for our evolving healthcare services."
"Today’s announcement is another positive milestone for our ongoing work with the Department of Health and many other stakeholders in relation to workforce planning for pharmacy and for the range of healthcare services and industries where pharmacists can contribute their expertise.
“Our role as the pharmacy regulator is to maintain and support patient safety and public trust in pharmacy. This includes accrediting and approving educational programmes for pharmacy and for setting the accreditation standards that must
be met on an ongoing basis by the approved pharmacy programme providers. Our aim is to ensure that future pharmacists are equipped to meet their professional and clinical obligations, the needs of patients and the health system.”
The President of SETU, Professor Veronica Campbell, added, “Accreditation of our MPharm programme represents a major step for SETU in expanding healthcare education and training in Ireland. Our provision of the programme will ensure that students across the southeast can pursue their studies regionally. More broadly, it allows our university to have a direct impact on the development of pharmacy in healthcare, community, and industry settings. The programme supports the need for expansion of the national pharmacy workforce, and the establishment of our new Department of Pharmacy directly responds to these national, regional, and university imperatives. It also builds on SETU’s existing strengths in pharmaceutical science, bioscience, nursing and healthcare, teaching and research. I would like to acknowledge and thank the HEA and the Department of Further and Higher Education, Research, Innovation, and Science (DHERIS) for their support in bringing the MPharm programme to fruition."
Dr Aisling Croke (MPSI), Lecturer in Pharmacy; Dr Claire Lennon, Head of Department of Pharmacy; Sarah Brown (MPSI); and Dearbhla Walsh (MPSI), both Lecturers in Pharmacy
Dr Claire Lennon, Head of the Department of Pharmacy at SETU, commented, “Our multidisciplinary cross-campus MPharm development team at SETU is very proud to have received Pharmaceutical Society of Ireland accreditation. The team has worked extremely hard to develop an innovative and impactful, future-focused MPharm programme. Pivotal to programme development has also been the collaborative input and support of our pharmacy professional advisory committee, and stakeholders from community, hospital, and industry pharmacy settings across the southeast. This will ensure graduates meet the requirements of modern pharmacy practice and the skills needs of the sector, all the while maintaining a patient-centred focus. We look forward to welcoming our first group of 40 students to the programme in 2026.”
Commending the availability of the new pharmacy programme, the Minister for Health, Jennifer Carroll McNeill, said, “I extend my sincere congratulations to South East Technological University on the successful accreditation of its Masters in Pharmacy programme. This innovative programme will provide students in the South East with the opportunity to pursue a career in pharmacy closer to home and reflects the Government’s strategic investment in regional education and our commitment to expanding access to high-quality healthcare training across all regions of the country.
"I look forward to seeing the first group of students begin their journey in pharmacy education in Waterford from September 2026 and to the lasting impact they will have on patient care and public health across Ireland.”
Prospective students for the new MPharm Programme are encouraged to communicate with the relevant universities directly.
IHCA Annual Conference 2025: Leading from the Frontline
Clinician-led leadership is the key to a fairer, safer, and more sustainable health service, the President of the Irish Hospital Consultants Association (IHCA), Professor Gabrielle Colleran, stated ahead of the Association’s Annual Conference in Kilkenny.
The IHCA hosted its Annual Conference 2025 as HPN was going to press, on Saturday, 18 October at Mount Juliet Estate, Kilkenny, under the theme ‘Leading from the Frontline: Medical Negligence & Clinical Leadership’.
The event brought up to 200 consultants and healthcare leaders from across Ireland to examine two of the most pressing issues facing the health system today: medical negligence and clinical leadership A Focus on Compassion, Leadership, and Reform
The morning session, MedicoLegal Matters: Law Meets Humanity, exploreed how Ireland can achieve fairer, faster, and more compassionate resolution for patients and clinicians caught in protracted medical negligence processes. This discussion built on the IHCA’s constructive engagement with the Department of Justice, the State Claims Agency, and the Expert Witness Site to advance pre-action protocols and strengthen the role of Irish-based expert witnesses.
The afternoon session, Leading from the Frontline: Clinical Leadership, examined how
IHCA President Professor Gabrielle Colleran
clinical leadership can drive cultural change and improve patient outcomes, and the role of Clinical Director in meeting those objectives. Speakers included Robert Watt (Secretary General, Department of Health), Dr Colm Henry (Chief Clinical Officer, HSE), and Professor Deborah McNamara (President, RCSI), alongside clinical leaders such as Dr Ike Okafor (Children’s Health Ireland), Dr Amanda Burke (HSE Child and Youth Mental Health) and Professor Nóirín Russell (CervicalCheck).
Dr Burke told the conference that Clinical Directors and Executive Clinical Directors must be strategic leaders in the health service, not just operational managers.
A Constructive Voice for Consultants
IHCA President Professor Gabrielle Colleran said the event reflects the Association’s renewed focus on being a constructive, credible, and courageous advocate for consultants and patients alike:
“As hospital consultants, we carry not just the responsibility of care, but the right to share, to share our thoughts, our insights, our hopes, and our dreams for a better, fairer, and more functional health service for every patient in the country.”
“Our discussions this year move beyond criticism to collaboration. We want to light a candle, not curse the darkness, to show that clinician-led leadership is the key to a fairer, safer, and more sustainable health service.”
Driving a New Era of ClinicianLed Reform
IHCA CEO Jim Daly said the Annual Conference comes at a pivotal moment for healthcare reform in Ireland, “The IHCA is entering a new chapter, one that puts consultants at the heart of shaping reform, driving quality improvement, and strengthening trust in our health system.
“This year’s Conference reflects that shift. It’s not just about identifying problems, but offering solutions rooted in the daily
realities of clinical care. Our members are leading teams, managing complexity, and caring for patients under immense pressure, and their experience must guide the next phase of national reform.”
Celebrating
Excellence
The day concluded with the presentation of the President’s Awards, honouring consultants who have made exceptional contributions to patient care, education, and leadership.
Full coverage in next month’s issue.
Dr Amanda Burke, National Clinical Lead for HSE Child and Youth Mental Health
Professor Rhona Mahony, Consultant Obstetrician, National Maternity Hospital
Improving Diagnosis and Management of Epilepsy
A new clinical trial co-led by researchers at FutureNeuro and RCSI University of Medicine and Health Sciences is investigating how advanced brain monitoring could improve the diagnosis and management of epilepsy.
Led in Ireland by consultant neurologists Professor Norman Delanty of RCSI and Beaumont Hospital and Dr Daniel Costello of Cork University Hospital (CUH) – two of the country’s busiest neurology departments – the trial involves multiple sites across Europe, with Irish patients making up more than half of those enrolled.
Traditional diagnostic methods for epilepsy face significant limitations. Short-term EEGs (typically around 30 minutes) and seizure diaries can be unreliable, especially when seizures are infrequent or hard to classify. While inpatient video-EEG in epilepsy monitoring units (EMUs) remains the gold standard, it is resourceintensive and difficult to access. Ireland has just six dedicated EMU beds, and patients often require hospital stays of up to eight days.
The trial in collaboration with Danish medical technology company UNEEG Medical A/S, focuses on the use of UNEEG EpiSight, a subcutaneous EEG (sqEEG) system that enables
remote monitoring of brain activity for up to 36 months in people with epilepsy. Designed as a complementary tool within epilepsy services, the UNEEG EpiSight records continuously, including during sleep, and transmits data wirelessly to support clinical decision-making. Implantation is performed through a brief outpatient procedure, carried out by Consultant Neurosurgeons Mr Kieron Sweeney at Beaumont and Beacon Hospitals, and Mr Wail Mohammad at Cork University Hospital, along with their expert teams.
The innovation builds on promising findings from a previous study led by Professor Delanty, Consultant Neurologist at Beaumont Hospital, Opens in new windowFutureNeuro investigator and Honorary Clinical Professor at RCSI, recently published in Epilepsia, which showed that an earlier version of the technology reliably detected all recorded seizures and 90% of significant brain abnormalities in patients with drug-resistant epilepsy. Until now, this level of detailed monitoring has only been possible through admissions to EMUs.
This trial will assess whether longterm, outpatient sqEEG monitoring can address these challenges.
By capturing brain activity in real-world settings over extended periods, the system could help clinicians detect seizure patterns that might otherwise go unnoticed, particularly those that happen at night, support earlier diagnosis, and reduce the need for repeated hospital visits.
Professor Delanty said: "FutureNeuro's involvement reflects our commitment to embracing the huge progress in the safe use of technology in clinical practice. This trial will help us better understand the clinical impact of long-term brain monitoring, with the potential for significant downstream benefits – such as reducing inpatient admissions, shortening time to diagnosis, and avoiding unnecessary treatments. By improving diagnostic accuracy and efficiency, this type of technology could ease pressure on epilepsy services, support better resource allocation, and ultimately lead to more personalised and costeffective care for patients."
Dr Daniel Costello added: "This diagnostic tool holds significant potential for clinical care. It could help detect seizures that go unrecognised, provide a clearer picture of seizure frequency, and reveal the cumulative impact on brain function. Just as importantly,
it may offer reassurance when seizures are well-controlled and help distinguish between epileptic seizures and other events. The potential to monitor brain activity long-term, outside of hospital, is an important step forward."
Peter Murphy, Epilepsy Ireland CEO commented: "We are excited by the potential of this trial and delighted that so many Irish patients are involved, highlighting the world-class epilepsy research taking place here. Epilepsy is highly individual, and finding the right treatment often requires trial and error. The more accurate information clinicians have, the better the chances of identifying the right treatment sooner. This innovative technology could provide that insight without long hospital stays or lengthy waiting lists, improving quality of life for people with epilepsy while easing pressures on hospital services. We will follow this important trial closely and look forward to its findings."
This trial represents a fundamental shift toward precision medicine in epilepsy care, where treatment decisions can be based on comprehensive, objective data rather than limited traditional monitoring methods. The strong Irish participation in this international study reflects FutureNeuro's established position in translating brain research discoveries into clinical practice, demonstrating how Irish research centres are driving innovation in global epilepsy care.
Professor Norman Delanty, RCSI & Beaumont Hospital
¤28M to enhance the Diagnosis and Treatment of Cancer Patients News
Researchers at University College Cork (UCC) will partner with a consortium of Irish Universities, charities and international companies in a unique strategic partnership aiming to deliver next generation cancer care in Ireland.
Minister for Further and Higher Education, Research, Innovation and Science, James Lawless TD, recently launched Phase 2 of Ireland’s leading and largest ever cancer research programme, Precision Oncology Ireland (POI-2).
POI-2 has received a total of ¤28M over a five-year period under the Research Ireland Strategic Partnership Programme. The programme is dedicated to advancing personalised cancer research and care. Its mission is to develop tailored diagnostic and therapeutic solutions using cutting-edge technologies and data, ensuring every patient receives the right treatment at the right time.
Coordinated by University College Dublin, POI-2 builds on the success of Precision Oncology Ireland (POI), an initiative first launched in 2019 that was the first of its kind in Ireland in terms of combining expertise from third level institutions, charities and industry to co-develop precision medicine for cancer patients.
Minister Lawless said: "Breakthroughs in cancer research are most likely when clinicians,
Photo (L-R): Professor Mark Tangney, POI-2 Grant Holder at Cancer Research @UCC, Deirdre Stuart, Secretary of Cork University Foundation, Professor Roisin Connolly, Director of Cancer Research @UCC.
Image credit: UCCTV
scientists, industry leaders, patients, charities, and other stakeholders come together with a shared purpose. The first phase of Precision Oncology Ireland stands as proof that strong, sustained collaboration can unlock innovation and accelerate transformative solutions. I congratulate the team on the advances made to date and wish them every success as they embark on this next phase of funded research."
Professor Mark Tangney of Cancer Research@UCC will lead on the OncoBioMaps Ireland work package, focusing on the identification of the cancer microbiome. OncoBioMaps will build a platform for biological mapping of cancer patients across Ireland,
2025 Ronnie Fehily Medalo
underpinned by the microbiome as a common biomarker.
"The funding allocated to UCC under this strategic partnership will enable us to develop a standardised national platform to collect and analyse multiple sample types from cancer patients across Ireland. With Cancer Research@UCC at its centre, this uniquely positions Ireland in having multiple laboratories studying the same patients in different ways, to develop 'biological maps' of patients", said Professor Tangney.
Professor Roisin Connolly, Director of Cancer Research@UCC said:
"We are delighted to support this exciting POI-2 initiative which bridges state of the art microbiome research with our patients at regional and national cancer
centres. Collaboration across academia and healthcare is critical to move the needle for improving cancer outcomes and we are excited to see tangible patient benefit in the coming years under Professor Tangney’s leadership."
Professor John F. Cryan, UCC Vice President for Research and Innovation said: "Congratulations to Professor Mark Tangney and his team in Cancer Research@UCC on the key role they will continue to play in Precision Oncology Ireland, a major national strategic programme aiming to develop new diagnostics and therapeutics for personalised cancer treatment in Ireland. Their work in developing biological maps of patients using the microbiome as a biomarker will play a major role in cancer treatment for patients."
Dr Jane Pears, consultant paediatric oncologist (right), is presented with the 2025 Ronnie Fehily Medal by Naomi Roche, daughter of Ronnie Fehily.
Dr Pears and Professor Michael Capra were jointly awarded the medal by Brain Tumour Ireland for their outstanding dedication and exceptional service to children with brain tumours in Ireland for more than 20 years.
Ronnie Fehily, who sadly died of a brain tumour in 2012, was the inspiration behind the establishment of Brain Tumour Ireland—the Ronnie Fehily Foundation.
The presentation took place during National Brain Tumour Awareness Week as part of the National PPI Festival at the Royal College of Surgeons in Ireland. For more information on the research activities undertaken by Brain Tumour Ireland, visit www.braintumourireland.com
Naomi Roche with Professor Michael Capra
Women’s Health: News
Landmark Study in Women’s Health Launched
UCC launches a study on women’s experiences seeking diagnosis for chronic health conditions
A new study seeks to understand the experiences of women in Ireland navigating a diagnosis for chronic health conditions.
Researchers at University College Cork (UCC) want to hear from women experiencing chronic health conditions such as endometriosis, migraine, postural orthostatic tachycardia syndrome (POTS), premenstrual dysphoric disorder (PMDD), and mast cell activation syndrome (MCAS).
Launched recently, the research will explore issues including diagnostic delays, patient–doctor interactions, ranging from symptom dismissal to supportive engagement, and how women use symptom-tracking apps to document and share their experiences with healthcare professionals, and responses to that data.
Diagnostic delays and medical gaslighting
Delays in diagnosis are welldocumented across women’s health. Internationally, endometriosis takes an average of nine years to diagnose, while POTS can take five. Conditions such as PMDD, MCAS, and less common migraine subtypes remain under-recognised despite their disabling impact. These conditions often overlap with one another, as well as with neurodivergence and connective tissue disorders like Ehlers-Danlos Syndromes, and may emerge or worsen after COVID-19 infection, creating complex healthcare needs that are poorly understood and managed in current clinical practice.
Many patients report feeling disbelieved or having their symptoms minimised, a
Supporting Thrombosis Patients
phenomenon often described as “medical gaslighting.” This contributes to years-long diagnostic delays. The study will examine both negative and positive healthcare experiences, including moments of validation and support.
Irish women’s experiences of diagnosis
“Too often, we hear patients speak about delays in diagnosis, and the barriers that contribute to them, such as symptom dismissal, minimisation, or normalisation. We want to hear about these experiences, as well as good patient–doctor interactions, so that we can learn from both and improve women’s healthcare,” Jenny Cooney-Quane, lead researcher on the project and Research Associate in UCC School of Applied Psychology, said.
The study will also investigate how patients use symptom-tracking apps to record symptoms and identify patterns, and how doctors respond to this patient-generated data in relation to diagnosis, treatment, and communication.
“Digital health transformation in Ireland has the potential to respond meaningfully to historic and contemporary issues in women's health, particularly more accurate diagnosis. However, it is imperative that this innovation is informed by the experiences of women and doesn't take away from existing healthcare provision,” Dr Sarah Foley, Principal Investigator and Lecturer in UCC School of Applied Psychology, said.
“These conditions are deeply under-researched, underdiagnosed, and under-funded. So many of us were told our debilitating, life ruining symptoms were normal. Nothing to be concerned about, just anxiety. You can spend a decade trying to get someone to take you seriously and then spend 3 years on a waiting list to be seen by someone else and still be dismissed. This study is so important and so validating,” a member of the PPI Panel Member said.
The study acknowledges that non-binary individuals and trans men may also be affected by these health conditions, often facing additional diagnostic challenges. The survey is designed to ensure their experiences are represented. In doing so, the research aims to deliver findings that are relevant and meaningful to all groups affected.
The Irish Heart Foundation announced the expansion of the cardiac conditions supported by the organisation, with the addition of thrombosis. The move comes as Thrombosis Ireland, a charity aiming to increase awareness of the condition and advocate for those affected, is wound down.
Thrombosis occurs when blood clots form in the blood vessels (arteries or veins), stopping the blood from flowing normally. The blood clot can then travel to the heart, brain, lungs, or other organs. It is a serious condition and can be life-threatening.
As of July 1st, 2025, the Irish Heart Foundation will include thrombosis in the cardiac conditions it covers, to offer information, including about the signs and symptoms, and support to those affected by the condition. As the national stroke and heart charity, adding the new condition further supports the charity’s mission to eliminate preventable death and disability from heart disease and stroke, and to support and care for those living with these life-changing conditions.
Venous thrombosis, including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common condition, affecting approximately 1 to 2 people per 1,000 annually in Western populations. About two-thirds of these cases are DVT, and one-third are PE. It is the third most common cardiovascular disease after myocardial infarction and stroke. Around 4,000 people die of thrombosis related deaths – venous thromboembolism or blood clots in the veins each year.
Pictured are Dr Sarah Foley and Jenny Cooney-Quane, UCC School of Applied Psychology
Women’s Health: Ovarian Cancer
From Fallopian Tube to Ovarian Cancer: Understanding the Evaluation and Management of Serous Tubal Intraepithelial Carcinoma Lesions
Opinion Piece: Division of Gynecologic Oncology, Department of Surgery, City of Hope National Medical Center, Duarte, CA, USA - Vinita Popat & Ernest Han - Contributions: V.P. - wrote the main manuscript text, reviewed the manuscript. E.H. - Reviewed the manuscript.
Ovarian cancer remains one of the most formidable challenges in gynecologic oncology, characterised by significant morbidity and mortality. It has long stood as a leading cause of death among cancers arising from the female reproductive tract.1,2 Within this disease spectrum, high-grade serous carcinoma (HGSC) represents the most common histological subtype, demonstrating particularly aggressive behavior and poor survival outcomes.3 Survival rates beyond the ten-year mark have remained disappointingly low at around 30%, likely due to diagnosis at advanced stages.4 This highlights the need for enhanced approaches in both prevention and early detection. Although screening tools for ovarian cancer have been explored extensively, widespread screening is generally not recommended due to inadequate specificity and sensitivity, as well as the lack of demonstrable mortality benefit.5, 6
Given these challenges, a critical focus has been placed on identifying individuals at increased genetic risk, as targeted prevention strategies may offer the best opportunity to reduce ovarian cancer incidence. In recent years, there has been increasing recognition of genetic risk factors that predispose certain individuals to ovarian cancer. Individuals harboring germline mutations, such as BRCA1 and BRCA2, face a substantially increased lifetime risk of ovarian cancer as compared to the general population.7 Consequently, many carriers of these pathogenic variants are counseled regarding the option of prophylactic surgery, typically in the form of risk-reducing salpingooophorectomy (RRSO), to diminish the likelihood of future malignancy.8 This preventive measure has proven effective in lowering the incidence of HGSC and thus remains central to the management strategy in high-risk cohorts.
Understanding the pathogenesis of HGSC is essential for uncovering the mechanisms that drive cancer development and identifying key targets for early detection and prevention. Alongside advances
in genetics, greater appreciation of the pathogenesis of HGSC has emerged. A wealth of evidence indicates that a notable proportion of these carcinomas originate in the fallopian tube, particularly at the tubal-peritoneal junction [9]. This area is believed to undergo significant epithelial transformation and, in many patients, is the apparent source of tumor precursor lesions that eventually seed the ovary or peritoneum.10,11 A spectrum of tumor precursor lesions has been identified along the tubal-peritoneal junction, including p53 signatures, serous tubal intraepithelial lesions (STILs), and serous tubal intraepithelial carcinomas (STICs), each representing a progressive step toward malignant transformation. STICs are associated with as many as 60% of all HGSCs.12, 13 With molecular evidence strongly supporting their role in the early stages of carcinogenesis, STICs have been suspected to be a direct precursor to HGSC. Given their potential role in the development of ovarian cancer, the detection and management of STICs may provide a crucial opportunity for cancer prevention.
The recognition that STIC lesions can be significantly present, sometimes even in patients without hereditary risk, has generated interest in opportunistic salpingectomy for women who have completed childbearing. This proactive approach has the potential to reduce the incidence of ovarian and primary peritoneal malignancies later in life. Though considerable progress has been made, many questions remain unanswered regarding STICs. In particular, if STIC represents a direct precursor to HGSC, a critical concern is determining the appropriate clinical course when these lesions are identified. Should the detection of STIC prompt immediate intervention, or is conservative management a viable option? Current data suggest that occult invasive carcinoma or peritoneal disease is detected in up to 30–60% of cases where STIC is found, raising concerns that some patients
may already harbor microscopic cancer at the time of diagnosis.13 This parallels the established progression model of endometrial intraepithelial neoplasia (EIN) as a precursor to endometrial carcinoma, where the presence of EIN often warrants definitive treatment with hysterectomy, due to its strong association with invasive disease.14 However, unlike EIN, the natural history of STIC remains less well characterised, making management decisions more complex. Some clinicians advocate for routine surgical management and even chemotherapy in select high-risk scenarios, whereas others lean toward enhanced surveillance, highlighting the ambiguity stemming from the limited body of evidence.15 ** Achieving a uniform and standardised characterisation of STIC—both morphologically and molecularly—is essential to ensure consistent diagnosis across pathology and clinical settings, reducing variability in interpretation and guiding more precise management strategies.
With continued research, the hope is that more personalised risk stratification and treatment algorithms will emerge, optimising outcomes for patients diagnosed with these precursor lesions. This literature review will focus on the current understanding of STIC, its relationship with ovarian cancer and its management.
STIC and Association with Ovarian Cancer
STIC is considered a rare entity in the general population, though growing awareness and the adoption of meticulous pathology protocols has likely increased its detection rate. Among patients diagnosed with HGSC, investigators have identified STICs more than half of the time during pathological review of the resected adnexa and in patients with STICs, concurrent HGSC is present 10.7% of the time.16, 17 Patients with STICs identified on pathology may ultimately develop HGSC up to 29% of the time later in their life.18 Historically, the incidence of STIC among those undergoing salpingectomy for benign indications has been
reported to be under 1%.19 However, in high-risk populations, specifically those with BRCA germline mutations who undergo risk-reducing salpingooophorectomy, STIC lesions have been noted in a substantially higher percentage of cases. Reports suggest that anywhere from 2 to 10% of BRCA-positive individuals receiving RRSO might harbor STIC.16, 20 Moreover, the presence of p53 signatures— an even earlier precancerous marker—can be found in as many as one-quarter of these patients, further corroborating the notion that tubal involvement precedes ovarian involvement in the malignant process.20 Risk-reducing surgery offers a significant benefit in these high-risk individuals, but even so, there remains a 0.4–0.9% residual chance of peritoneal carcinomatosis.18, 21 This is possibly due to either undetected STICs, exfoliation of malignant tubal epithelium into the peritoneal cavity, or an alternative, non-tubal pathway of carcinogenesis. While the tubal hypothesis provides a compelling framework for understanding the origins of highgrade serous carcinoma, it may not fully account for all cases of ovarian and peritoneal malignancies.13 Further research is needed to investigate non-tubal sources of carcinogenesis, which may contribute to the observed rates of subsequent peritoneal disease even after complete removal of the fallopian tubes and ovaries.
Besides genetic factors, there are other demographic and clinical variables that influence the incidence of STIC, further shaping individual risk profiles and guiding prevention strategies. Several demographic and clinical variables influence the incidence of STIC including age and germline pathogenic variant status. Notably, the likelihood of detecting STIC at the time of RRSO appears to increase with advancing age.18 Another factor that has consistently emerged is the presence of multiple STIC lesions. In patients with high-risk pathogenic variants undergoing RRSO, more than 50% of patients with STICs had evidence of multiple tubal precursor lesions,
Women’s Health: Ovarian Cancer
suggesting that a higher number of precursor lesions may portend an increased risk of developing HGSC.18 Overall, recognising the interplay of these risk factors and identifying precursor lesions when present is a critical component of improving patient outcomes.
How a STIC leads to Ovarian Cancer
Epithelial ovarian cancers have historically been described as malignancies arising from the surface epithelium of the ovary. Over time, however, this notion has shifted toward understanding the fallopian tube as the primary site of origin for many of these tumors, particularly the high-grade serous subtype.11 The molecular events underlying malignant transformation in the adnexa involve an interplay between genomic instability and chronic exposure to oxidative stress, as well as other mediators of inflammation.22
Early molecular alterations are believed to manifest in the form of p53 mutations in otherwise normal-appearing fallopian tube epithelium.11 Such changes can persist for years, possibly decades, before evolving into more advanced lesions.23 Some of these early lesions are designated as “p53 signatures,” which can be present in normal tubal epithelia without overt histologic atypia.11 Over the span of several decades, these p53 alterations may lead to greater genetic aberrations, culminating in STIC lesions. STICs, in turn, seem to have the capacity to progress in a relatively condensed timeline of 5–7 years into a frank HGSC (Fig. 1).23
While the tubal hypothesis provides a compelling explanation for the pathogenesis of many high-grade serous carcinomas (HGSCs), it does not appear to account for all cases of ovarian or peritoneal malignancies. Notably, not all ovarian or peritoneal cancers exhibit the classic p53 mutationdriven pathway, suggesting that alternative mechanisms of carcinogenesis must be present.11 Similarly, not all STICs are associated with subsequent cancer development, and conversely, not all HGSCs have an identifiable STIC precursor. These observations raise important questions about the existence of non-tubal origins of ovarian cancer, which warrant further investigation.
One proposed alternative mechanism is the direct malignant transformation of residual Müllerian epithelial tissue, which includes the endometrium, cervix, and peritoneal inclusion cysts, as well as the potential contribution of endometriosis-associated
Figure 1
malignancies.13 Additionally, primary ovarian carcinogenesis remains a possibility, particularly in cases where precursor lesions are absent in the fallopian tube. While serous ovarian tumors are believed to frequently arise from tubal epithelium that has implanted on the ovarian surface, intrinsic ovarian epithelial transformation cannot be ruled out as a rare but distinct pathway.13
The mechanical and environmental factors within the pelvic cavity also likely contribute to the pathogenesis of ovarian cancer. Repeated ovulatory events bathe the tubal fimbriae and adjacent peritoneum in follicular fluid, which contains elevated levels of reactive oxygen species, proteolytic enzymes, and other bioactive molecules.22 These components can damage cellular DNA in the fallopian tube epithelium, especially at the fimbriated end. It is postulated that this microenvironment fosters the malignant transformation of the tubal mucosa, which eventually enables the spread of neoplastic cells to the ovary, omentum, and
other peritoneal surfaces. There is a notion of “early metastasis”, that STICs can detach from the fallopian tube surface and migrate into the pelvis to implant on surrounding peritoneal tissue, ultimately manifesting as primary ovarian or peritoneal HGSC.23 This provides a sound explanation for the occurrence of primary peritoneal HGSC in individuals who have previously undergone prophylactic removal of both ovaries, as undetected STICs may have already been seeded the peritoneal cavity before surgery. However, the persistence of peritoneal carcinomatosis in some individuals post-RRSO also suggests that alternative carcinogenic pathways may be at play, reinforcing the need for continued investigation into the full spectrum of ovarian and peritoneal cancer origins.
Diagnosing STIC
The diagnosis of STIC largely depends on meticulous pathological examination of the fallopian tubes. There is currently no reliable imaging modality to
detect these lesions preoperatively. In fact, STICs are often microscopic and asymptomatic, remaining elusive on standard ultrasound or cross-sectional imaging. Accordingly, diagnosis frequently arises as an incidental finding when surgical specimens from salpingectomy are subjected to detailed pathological review. Morphologically, STIC is characterised by marked epithelial atypia, including cellular crowding, enlarged pleomorphic nuclei, and a loss of normal polarity.24 Immunohistochemical analysis typically shows strong p53 overexpression (or complete absence in the case of a truncating mutation) and a high Ki-67 proliferative index.25 This molecular profile helps to distinguish STIC from lower-risk lesions such as STILs (serous tubal intraepithelial lesions), which may share some morphological changes but have a lower proliferation rate.24 Pathologists now widely employ the Sectioning and Extensively Examining the FIMbriated end (SEE-FIM) protocol, a method
that entails serial sectioning of the fimbrial portion of the fallopian tube at short intervals, thereby maximising the likelihood of identifying subtle precursor lesions.26 This approach is considered the gold standard in patients deemed high risk, particularly those carrying BRCA mutations or those undergoing RRSO for other hereditary syndromes.27 Despite the recognised utility of SEE-FIM, it has not yet been universally implemented among average-risk patients in all clinical practices. Nevertheless, incidental STIC detection in low-risk salpingectomies underscores the potential value of standardised protocols for pathologic evaluation. However, while universal adoption of SEE-FIM for all patients may enhance early detection, it presents a significant strain on resources, requiring considerable pathologist time, labor, and financial cost for identifying a relatively rare histologic entity— one that, even in high-risk cases, is still a precursor lesion rather than an overt malignancy.
While STICs most frequently arise in the tubal fimbriae, it is also important to recognise that they may appear elsewhere along the tubal lumen. Although rarer, involvement of the proximal tube has been documented, raising the possibility that any region of the salpinx harboring sufficiently damaged epithelium may become an incipient site of malignancy [28]. This highlights the importance of complete resection of the entire fallopian tube at time of resection and thorough pathologic examination to identify even small foci of neoplastic change. It is important to note that the diagnosis of STIC can be subject to interobserver variability among pathologists, owing to the sometimes ambiguous histological distinction between early neoplastic changes and reactive epithelial atypia.29 In a study conducted by Carlson et al., interobserver concordance in the diagnosis of STIC lesions was found to be at best fair to good, even among experienced gynecologic pathologists [29]. Notably, a proportion of STICs could not be consistently identified, highlighting the inherent subjectivity in pathologic interpretation. Given these challenges, corroboration of STIC diagnoses with a second observer may be warranted to enhance diagnostic accuracy and reduce variability.30
Efforts are ongoing to improve diagnostic reproducibility through more precise criteria, standardised immunohistochemical (IHC) thresholds, and consensus
guidelines.25 In this context, Vang et al. have proposed an algorithmic approach to more uniformly identify STICs, stratifying cases into three morphologic categories: unequivocal STIC, suspicious for STIC, and not suspicious for STIC.24, 25 To further refine classification, each category is then subcategorised using p53 and Ki-67 IHC staining, as STIC lesions are often p53-positive and demonstrate high Ki-67 proliferative indices. This method has been shown to increase diagnostic confidence and concordance among pathologists, but it has yet to be validated in larger studies. Nevertheless, the routine use of p53 and Ki-67 IHC on lesions suspicious for STIC may serve as an adjunctive tool to confirm diagnosis and enhance diagnostic uniformity.30
Lastly, significant morphologic and molecular heterogeneity exists within lesions diagnosed as STICs, which may explain why some instances of STIC progress to malignancy, while others do not.31 As further molecular characterisation is undertaken, it is hoped that distinct subsets of STICs can be identified— those that are highly associated with progression to HGSC and predictive of poor outcomes, versus those that may remain indolent. This level of stratification could provide critical insights into which patients may benefit from more aggressive intervention versus conservative management, ultimately refining the clinical approach to STIC diagnosis and treatment.
Management of STIC and Prevention of Ovarian Cancer
Opportunistic Salpingectomy in the General Population
One of the most pivotal developments in ovarian cancer prevention in recent years has been the adoption of opportunistic salpingectomy in women who have completed childbearing. By removing the fallopian tubes during procedures such as hysterectomy or even at the time of cesarean section, it is believed that a significant proportion of future HGSCs could be prevented with an ovarian cancer risk reduction of approximately 80%.32,33 A landmark populationbased retrospective cohort study in Canada further substantiated this association, revealing a significantly decreased incidence of ovarian cancer among patients who underwent opportunistic salpingectomy compared to those who did not.34 This intervention has been shown to reduce up to 14.5% of ovarian cancer related deaths and decrease healthcare costs by million dollars annually.35 Given the relative feasibility and
safety of salpingectomy, major professional societies, including the American College of Obstetricians and Gynecologists (ACOG) and the Society of Gynecologic Oncology (SGO), now advocate for opportunistic salpingectomy as a routine prophylactic measure in average-risk women who have completed childbearing and do not desire future fertility36,37,38
Nonetheless, this strategy is not without caveats. A critical consideration is the possibility of preexisting, subclinical STIC lesions, which may have already disseminated into the peritoneal cavity by the time of surgery. In such cases, meticulous surgical technique—minimizing manipulation of the fallopian tubes and ensuring containment of the specimen—may reduce the risk of iatrogenic exfoliation of malignant or premalignant cells.15 While these precautions are theoretically sound, the empirical evidence supporting their efficacy remains limited and warrants further investigation. Moreover, while opportunistic salpingectomy is generally safe— with no significant increases in postoperative complications, hospital readmissions, transfusion rates, or length of stay — clinical judgment must guide its application.39 Specifically, the surgical approach should not be altered solely to facilitate salpingectomy, as the marginal benefit of the procedure does not justify additional morbidity associated with more invasive techniques.37 As such, the implementation of opportunistic salpingectomy must be contextualised within broader surgical planning, patient characteristics, and ongoing research into optimal timing, technique, and long-term outcomes.
Management in BRCA-Positive Patients
For carriers of BRCA1 or BRCA2 mutations, prophylactic removal of the ovaries and fallopian tubes is the standard-of-care recommendation, especially after childbearing is complete. RRSO is recommended in patients with BRCA 1 at age 35–40 years and at 40–45 years for women with BRCA2, conferring a marked decrease in the risk of developing ovarian cancer and is associated with improved survival outcomes.5
As demonstrated in the US Nurse’s study, premenopausal oophorectomy has been associated with significant detrimental impact on allcause mortality.40 Many women have delayed RRSO due to concerns for cognitive decline, increased risk for cardiovascular disease, osteopenia, and sexual dysfunction, symptoms associated
with surgical menopause from oophorectomy.41, 42 A metaanalysis found that 30–70% of high-risk women postpone RRSO, highlighting the need for alternative risk-reduction strategies and improved postsurgical management.42 Bilateral salpingectomy alone may demonstrate a benefit for ovarian cancer risk reduction which is currently being studied in clinical trials.11 An emerging concept known as “radical fimbriectomy” has been introduced in France as an alternative strategy for those who are reluctant to undergo oophorectomy at a younger age.43 By removing the entire fallopian tube, including its fimbrial extremity and any adjoining ovarian tissue at the tubal–ovarian junction, this procedure aims to mitigate cancer risk while preserving ovarian endocrine function until natural menopause. Early results have been encouraging, with some studies reporting zero incidence of HGSC over years of followup.43 Nevertheless, ongoing trials, such as the SoROCk trial, comparing salpingectomy alone to the established gold standard of bilateral salpingo-oophorectomy, will be instrumental in determining whether delaying oophorectomy is safe and effective in high-risk populations [44]. We caution that although salpingectomy alone might reduce risk, it has not yet been proven to match the effectiveness of removing both tubes and ovaries.
Given the recognised association between STIC and hereditary predisposition, any patient diagnosed with an incidental STIC and unknown mutation status should be offered thorough genetic counseling and testing.27,45 In certain studies, up to 12% of previously untested individuals discovered to have STIC on a surgical specimen were subsequently found to carry a BRCA pathogenic variant or an unclassified variant.46
Additionally, the role of routine peritoneal biopsies in the setting of RRSO has been a subject of debate. While some clinicians may seek to identify occult disease, others point out that random peritoneal biopsies sample only an infinitesimal fraction of the peritoneal cavity and rarely alter clinical management.47, 48 Moreover, such sampling may add operative time, cost, and potential morbidity. Similarly, the role of pelvic washings is also often controversial with mixed practice patterns based on provider and institution, as some providers routinely obtain pelvic washings and some never obtain washings. This is likely due to the relatively rare incidence of positive pelvic
Continuing Professional Development
CPD
CPD
60 Second Summary
Hypertension is a significant global health problem and an important cause of morbidity and mortality worldwide, serving as an important risk factor for cardiovascular disease (CVD), chronic kidney disease (CKD), stroke, and dementia.
The prevalence of hypertension increases with age in both sexes, particularly after 40 years of age. In women, the prevalence is slightly lower than in men between the ages of 40 to 59 years (59.4% in men vs 49.9% in women). However, by 60 years of age, women have nearly caught up with men, with hypertension prevalence of 75.2% in men and 73.9% in women.
Epidemiological studies have shown associations between clinical BP or diagnosed hypertension in youth with atherosclerotic CVD and premature mortality. The menstrual cycle affects arterial compliance and may change systolic and diastolic BP; however, these variations in normotensive women appear to be modest and larger studies are needed.
Specific antihypertensive therapy is required for: (1) chronic treatment to gradually lower BP to maintain goal range, or (2) acute lowering of severe-range BP. The timing and setting of intervention along with the selection of antihypertensive agents will differ between these scenarios.
Changes in BP after menopause seem to be related to alterations in estrogen and progesterone levels along with other factors including genetic predisposition, obesity, type 2 DM, endothelial dysfunction, salt sensitivity, and arterial stiffness.
Increased BMI greater than 25 kg/m2 is associated with greater risk of hypertension and mortality, whereas weight loss can reduce risk of hypertension. Data support up to a 20-mm Hg drop in BP with 10 kg of weight loss.
Written by Niloofar Nobakht MD a, Yalda Afshar MD, PhD e, Marmar Vaseghi MD, PhD b, Zhaoping Li MD, PhD c, Ines Donangelo MD, PhD d, Helen Lavretsky MD, MS f, Thalia Mok MD e, Christina S. Han MD e, Susanne B. Nicholas MD, MPH, PhD a
a Division of Nephrology, Department of Medicine, at the David Geffen School of Medicine at University of California, Los Angeles, CA, USA
b Division of Cardiology, Department of Medicine, at the David Geffen School of Medicine at University of California, Los Angeles, CA, USA
c Division of Clinical Nutrition, Department of Medicine, at the David Geffen School of Medicine at University of California, Los Angeles, CA, USA
d Division of Endocrinology, Department of Medicine, at the David Geffen School of Medicine at University of California, Los Angeles, CA, USA
e Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, at the David Geffen School of Medicine at University of California, Los Angeles, CA, USA
f Department of Psychiatry at the David Geffen School of Medicine at University of California, Los Angeles, CA, USA
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings.
Published by HPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author.
Hypertension Management in Women With a Multidisciplinary Approach
Hypertension is a significant global health problem and an important cause of morbidity and mortality worldwide, serving as an important risk factor for cardiovascular disease (CVD), chronic kidney disease (CKD), stroke, and dementia. The prevalence of hypertension was estimated to be 1.27 billion globally, with ∼626 million women living with hypertension, worldwide.1 Nearly 1 of 2 adults in the United States has hypertension (116 million), with more than 50% reported to be women (44.9 million women and 40.8 million men).2 Optimal management of hypertension can improve both cardiovascular outcomes and mortality. It has become evident that, although hypertension is more prevalent in men,3 the risk factors for developing hypertension and the blood pressure thresholds for its diagnosis may differ by sex. However, the current guideline does not provide different blood pressure values for men and women.4 Specific risk factors related to lifecycle changes are present in women that affect both development and management of hypertension. A multidisciplinary approach may lead to better blood pressure (BP) control in hypertensive females. This review, which was conducted using PubMed, OVID, EMBASE,
and Cochrane library databases between 1995 and 2023, provides a comprehensive summary of the presentation and treatment of hypertension as it relates to women across the lifespan and includes reference to specific racial and ethnic minority groups. It describes relevant clinical studies and ongoing challenges and outlines unanswered questions pertinent to the optimal management of hypertension in women.
The 2017 American College of Cardiology/American Heart Association Clinical Practice hypertension guideline recognises the importance of risk calculators to determine when to initiate antihypertensive therapy. It also includes major changes in BP values, lowering the treatment target from less than 140/90 mm Hg to less than 130/80 mm Hg,5 and supporting improved cardiovascular outcomes with treatment aimed at lower targets. These changes were derived from evidence of increased CVD risk associated with BP 130-139/80-89 mm Hg, along with data supporting better associated cardiovascular outcomes.3 According to the new guideline, BP is “normal” if it is less than 120/80 mm Hg. The guideline also categorises hypertension by stages: patients with systolic BP between 130 and 139 mm Hg
or diastolic BP between 80 and 89 mm Hg have stage 1 hypertension, whereas those with a systolic BP greater than or equal to 140 mm Hg or diastolic BP greater than or equal to 90 mm Hg have stage 2 hypertension.5 6 The guideline remains consistent for both men and women, targeting BP less than 130/80 mm Hg for patients with coexisting coronary artery disease (CAD), diabetes mellitus (DM), CKD, peripheral vascular disease, and cerebral vascular accident (CVA) events without consideration for patient sex or physiological state at different life cycles.5 6 In this review, several sex-specific strategies to achieve optimal management of hypertension in women using a multidisciplinary approach are discussed. Importantly, socioeconomic conditions and transitions across different life stages from premenopause to menopause are also considered.
Risk of Hypertension Across the Woman’s Lifespan
The prevalence of hypertension increases with age in both sexes, particularly after 40 years of age.7 In women, the prevalence is slightly lower than in men between the ages of 40 to 59 years (59.4% in men vs 49.9% in women). However, by 60 years of age, women have nearly caught up with men, with
30 CPD 120: HYPERTENSION
hypertension prevalence of 75.2% in men and 73.9% in women.7
The current guideline does not provide specific recommendations related to the management of hypertension by sex. According to all major society guidelines, accurate measurements, diagnosis of hypertension with repeat visits, ambulatory blood pressure monitoring (ABPM), or home BP monitoring via commercial devices are important in the diagnosis of hypertension for both women and men. Home and ABPM measurements are less likely to be confounded by white coat or masked hypertension Although nearly all major clinical trials use clinic BP readings, ABPM can supplement these readings because data indicate that ABPM is a stronger predictor of clinical outcomes compared with clinic measurements8, 9, 10 and allows for measurement of nocturnal pressures.11, 12, 13
A 10% to 20% decrease in nighttime BP compared with daytime is expected,5 6 and patients who are nighttime “nondippers” or “reverse dippers” have higher risk for stroke, cardiac hypertrophy, and silent CVA events.8,11,14,15 Reverse and nondipping BP, for women more than men, increase the risk of cardiovascular events with age. Middle-aged and postmenopausal women who are nondippers are at highest risk for cardiovascular events, particularly if they present with comorbid conditions.16 Nondipping is associated with a higher left ventricular mass in both sexes, although this is the case to a greater extent in women.17
Ambulatory BP monitoring has also allowed for assessment of important changes in BP over the lifetime of males vs females. Using ABPM data in 15,913 women and 14,600 men, diastolic BP was noted to fall at a very early age (22.3 years) in women, whereas in men, diastolic BP begins to fall at age 46.5 years.18 Finally, there is a greater prevalence of masked hypertension in men than women, as detected by ABPM.19, 20, 21
Hypertension During Reproductive Age
Epidemiological studies have shown associations between clinical BP or diagnosed hypertension in youth with atherosclerotic CVD and premature mortality 22 The menstrual cycle affects arterial compliance and may change systolic and diastolic BP; however, these variations in normotensive women appear to be modest and larger studies are needed.
Although most patients have primary (essential) hypertension, the proportion of individuals affected by secondary hypertension is higher in women of reproductive age, despite a lower prevalence of primary hypertension in this age group. The diagnosis of secondary causes requires a high index of suspicion, and appropriate testing based on clinical presentation. Early detection of secondary hypertension is pivotal because timely diagnosis and management of underlying condition allow for prevention of hypertension-mediated organ damage (HMOD).
Several recognised endocrine causes of secondary hypertension include primary aldosteronism (PA), pheochromocytoma, Cushing syndrome, thyroid disease, acromegaly, and hyperparathyroidism 23 Primary aldosteronism is the most common cause of secondary hypertension, with a prevalence of 5% among patients with hypertension, and up to 20% in individuals with resistant hypertension 24 25 The most common cause of PA is bilateral adrenal hyperplasia, followed by aldosterone-producing adrenal adenoma, representing in 60% and 30% of cases, respectively.26 Unilateral PA is more common in men, whereas bilateral adrenal hyperplasia is more common in women.27 Observed differences in incidence are further modified by age, where women diagnosed with unilateral adrenal hyperplasia are more likely to be younger than men. The inverse of this is true for bilateral adrenal hyperplasia, as male patients with this diagnosis tend to be younger than female patients.27 The prevalence of PA is similar in men and women, but estrogen can affect plasma renin concentration (PRC), and may interfere with laboratory investigation of PA. Although there is good correlation between plasma renin activity (PRA) and PRC, estrogen use or pre-ovulatory (luteal phase) estrogen surge in women is associated with false positive case detection testing when using PRC but not PRA. Plasma renin activity may be more suitable for PA case detection in premenopausal women or in those taking oral estrogen.26,28
Salt-sensitive BP characterised by an increase in BP following salt loading or a drop in BP following salt depletion is reported in up to 50% of hypertensive patients.29 This is more common in women than men and increases with age.30,31 The mineralocorticoid pathway may be implicated in the mechanism for salt-sensitive hypertension in younger women. Premenopausal women may have heightened aldosterone production to stimuli and expression of endothelial mineralocorticoid receptor (MR) mediated by sex hormones that lead to endothelial dysfunction and hypertension. Therefore, MR antagonism may be preferred in the treatment of salt-sensitive hypertension in premenopausal
women.32 The role of MR activation and augmented aldosterone production diminishes after menopause. In postmenopausal women, as in men, dysfunctional renal physiology leading to impaired natriuresis is the main contributor to salt-sensitive hypertension.16,32
Renovascular hypertension is among the most common causes of secondary hypertension, primarily from atherosclerotic lesions (60%-90%) followed by fibromuscular dysplasia (10%-30%).33 Fibromuscular dysplasia has a female/male ratio of 84%/16% in the United States and is predominantly diagnosed in middle-aged subjects.33 It is a noninflammatory disease of medium-size arteries which may lead to stenosis, occlusion, and or dissection.34 Approximately 90% of these patients have hypertension, and a significant proportion of them may present with major vascular events such as CAD, cerebrovascular and renal events including ischemia, infarction, and renal failure. Earlier diagnosis and vascular interventional treatment with angioplasty will improve outcome and adverse events 33,34
Preconception Care
Optimising the care of the pregnant person with hypertension, even before pregnancy, is the ideal. As such, a preconception consultation with a multidisciplinary care team, including maternal-fetal medicine, is recommended in reproductive-age people who desire pregnancy.43 The goal of preconception care is to affirm pregnancy intention, mitigate potential harm, and recognise modifiable risk factors related to pregnancy while stratifying pregnancies on a continuum of low to high risk.43 Although most patients with wellcontrolled hypertension will have uncomplicated pregnancies, patients with hypertension should have a clear understanding of the possible complications in pregnancy, potential effects of pregnancy on BP, and the need for heightened increased maternal and fetal surveillance. Patients with modifiable risk factors such as obesity, smoking, and poorly controlled diabetes may benefit from a discussion on lifestyle modifications. These include weight loss, diet, exercise, and smoking cessation to improve BP control and decrease rates
of hypertension disorders of pregnancy (HDP) and associated adverse maternal and fetal outcomes.44 45 All patients in need of renin-angiotensin-aldosterone (RAAS) blockade agents should have a discussion of effective contraceptive options along with negative pregnancy test before.
Selection of Antihypertensive Agents in Pregnancy
Specific antihypertensive therapy is required for: (1) chronic treatment to gradually lower BP to maintain goal range, or (2) acute lowering of severe-range BP. The timing and setting of intervention along with the selection of antihypertensive agents will differ between these scenarios. Labetalol or nifedipine extended release are preferred for the long-term treatment of hypertension in pregnancy 55 Methyldopa, previously considered first-line, has shown lower efficacy with greater adverse effects 77 Diuretics can be considered second- or third- line HDP treatment, and their use during pregnancy and breastfeeding is generally tolerated but should be closely monitored.78 Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers are avoided due to potential teratogenic risks and associations with fetal growth restriction and neonatal kidney failure.79 There is evidence demonstrating the risk of beta-blockers, primarily atenolol, and its association with small for gestational age infants 79
For severe hypertension (systolic ≥160 mm Hg or diastolic ≥110 mm Hg) and if it is persistent (>15 minutes) requires prompt pharmacologic treatment. Therapy should be initiated within 30 minutes of diagnosis to decrease maternal risks. Medications used include intravenous labetalol, hydralazine, or oral immediaterelease nifedipine 80 Hypertension disorders of pregnancy require timely treatment because CVA and hypertensive encephalopathy occur at lower BPs compared to outside of pregnancy. Pregnancies complicated by HDP should undergo increased antenatal surveillance for maternal health and risks to the neonate, including fetal growth restriction. Delivery timing depends on the underlying HDP diagnosis and the control of the disease process. The delivery
mode (ie, vaginal vs cesarean birth) is not dictated by HDPs and is based solely on routine obstetrical indications.52
Hypertension and Menopause
Changes in BP after menopause seem to be related to alterations in estrogen and progesterone levels along with other factors including genetic predisposition, obesity, type 2 DM, endothelial dysfunction, salt sensitivity, and arterial stiffness 83
Estrogen plays a significant role in the observed sex differences in hypertension and CVD.16 84 The mechanism for its vascular protective role is complex, and many pathways remain to be clarified. Estrogen contributes to vascular homeostasis by upregulation of endothelial nitric oxide pathway, augmenting prostacyclin release, reducing oxidative stress and fibrosis, and stimulating angiogenesis. Decline in estrogen has been associated with augmentation of ACE and angiotensin II pathways and lower MR expression.32 85 Estradiol deficiency results in RAAS system dysregulation with switch to proinflammatory pathways that contributes to impaired immune response and CVD.86 Estrogen modulates sympathetic tone by attenuating α-adrenergic receptor-mediated vasoconstriction, while enhancingβ-adrenergic receptor effect. This may be a cause of age-related increase in hypertension among women that is at least in part caused by falling estrogen levels during menopause.16,84
Although observational studies in humans and experimental studies in animals provide evidence that estrogen replacement protects post-menopausal women against CVD, randomised control trials did not support this concept.87 The reason for the disparity remains unclear; yet, it is hypothesised that several factors, including the type of estrogen used, interaction with progesterone, women’s age, and timing of the treatment, contribute to these results.88,89 There is evidence that estrogen therapy may be cardioprotective if started around menopause transition and may be harmful if started >10 years after menopause.
90 Replacement with endogenous 17 β-estradiol shows superior cardiovascular benefit compared to replacement with oral conjugated equine
estrogen, which is associated with a greater risk of hypertension development.91 92 Data on possible benefits of hormone replacement therapy on CVD are controversial.
93, 94, 95
International medical societies, including the American Association of Clinical Endocrinologists, Endocrine Society, American College of Obstetricians and Gynecologists, and North American Menopause Society recommend against menopausal hormone therapy for primary or secondary prevention of CVD, especially for those older than 60 years or more than 10 years after menopause.96 Estrogen is a safe option for treatment of menopausal symptoms when initiated in healthy women younger than 60 years of age or within 10 years of menopause onset when it is used at the lowest effective dose and for the shortest total duration based on risk benefit analysis (typically <5-10 years).97
However, estrogen may have a plaque-destabilising effect in the setting of advanced atherosclerosis, favoring thrombosis. Therefore, it is contraindicated in women with atherosclerotic CVD, BP greater than 180/110 mm Hg, venous thrombosis or pulmonary embolism, cerebrovascular disease, and congenital heart disease 98 Selected younger (<60 years of age) women with one or more cardiovascular risk factor including obesity, controlled hypertension, diabetes, and dyslipidemia may use menopausal hormone therapy; however, the transdermal route of estrogen is preferred and there should be an emphasis on optimising primary prevention efforts. Additionally, cardiovascular risk must be regularly reassessed.93, 94, 95 Additional studies are needed to better understand the consequences of menopause on CVD and to determine the value, timing, and dosing of hormone replacement therapy on BP.
Lifestyle Modifications and Hypertension Management in Women
Lifestyle modification plays a pivotal role in preventing and managing hypertension. In fact, 24.3 million (21%) adults with hypertension can be treated with lifestyle modifications alone, without the need for
antihypertensive medications.110
Nutrition and Hypertension Management in Women
The Dietary Approaches to Stop Hypertension (DASH) diet has emerged as a balanced dietary strategy for preventing and treating hypertension.111 This diet emphasises fruits, vegetables, and low-fat dairy products and recommends reduced amounts of saturated fat, total fat, and cholesterol and is rich in potassium, magnesium, calcium, and fiber. Importantly, the DASH diet lowers BP beyond the level achievable by simply reducing sodium intake. It has been demonstrated that it not only results in the expected lower BP, but can benefit cardiometabolic health, decreasing body mass index (BMI), body fat content, fasting glucose, insulin, and leptin concentrations.112 113
The consensus from studies on sex differences in dietary patterns and hypertension outcomes remain unclear. One study on sex differences in those between 40 and 69 years of age found that diets higher in the consumption of vegetables, potatoes, fruits, beans, and seaweeds were related to lower BP.114 Another study concluded a diet rich in whole grains and legumes was inversely associated with the risk of hypertension in women, suggesting sex differences in association with diet and hypertension.115 Additional studies are needed to evaluate diet-based recommendations for women in the various stages of life cycle relative to hormonal alterations, aging, sodium retention after menopause and by race and ethnicity.
Weight and Body Mass and Hypertension in Women
Increased BMI greater than 25 kg/m2 is associated with greater risk of hypertension and mortality, whereas weight loss can reduce risk of hypertension.121,122 Data support up to a 20-mm Hg drop in BP with 10 kg of weight loss.123 Combined use of DASH diet and weight loss can further lower BP.5 Results from a study on women who had a BMI greater than 25 kg/m2 at the age of 18 years showed a relative risk of 2.2 for developing hypertension.121 Recent data indicate that indices of central adiposity including waist circumference (WC), and waistto-height ratio (WHtR), may have
32 CPD 120: HYPERTENSION
Figure 1. Lifestyle modifications have potential positive impacts that measurably reduce blood pressure. Data from the American College of Obstetricians and Gynecologists.5 DASH, Dietary Approaches to Stop Hypertension.
better predictive value for the risk of hypertension in women.124 The WC and waist to hip ratio and WHrR may increase with parity and is consistently associated with an increase in WC and a reduction in hip circumference in women 18 to 30 years of age.125
Impact of Physical Activity on Hypertension in Women
Approximately 80% of US adults are insufficiently active. Regular, mild-to-moderate aerobic activity can independently decrease BP by 5 to 8 mm Hg in women, regardless of weight loss.126 127 Few studies have assessed the combined impact of body weight and physical activity in relation to hypertension among women. A report studying a large cohort of French women concluded that higher physical activity was associated with a lower risk of hypertension, but only within a BMI range of 22.5 to 25.0 kg/ m2 128 Further studies are needed to provide guidance on the
duration and intensity of physical activity on BP reduction and HMOD in women.
Impact of Sleep on Hypertension in Women
Sleep disturbances are associated with increased risk of morbidity and mortality.129 Key sleep disorders that can impact BP are obstructive sleep apnea (OSA), short sleep duration, and poor sleep quality.130 131 132 One study of 277 perimenopausal women with a mean age of 56 years and a mean BMI of 28 kg/m2 showed that women with moderate to severe OSA were more likely to be hypertensive, use more medications to reduce BP, and have higher awake and nocturnal BP and increased arterial stiffness.133 Results from the Nurses’ Health Study supported the need for sufficient sleep to reduce hypertension incidence and prevalence.131 The prevalence of hypertension was significantly higher among women who slept 5 hours or less per night. Studies suggest that night shift work, short sleep duration,
or poor sleep with circadian disruption might increase the risk of hypertension because acute sleep restriction has been shown to increase BP and sympathetic nervous system activity.131,134 Figure 1 summarises the effects of lifestyle modifications on BP with the largest impacts being from the DASH diet and weight loss.5
Pharmacotherapy Treatment for Women with Hypertension
Antihypertensive therapy choices vary among women across different phases of life. Therapy choices are limited during the reproductive age including the preconception phase and during pregnancy given the risk of teratogenicity and the side effects on the fetus. This limits access to RAAS blockade agents for patients with diabetes, CKD, or cardiac disease 55 79 Therapy choices during perimenopause and post menopause are more similar to those with men in relation to comorbidities; there is greater attention to MR antagonists as
a preferential treatment for premenopausal women who have been diagnosed with salt-sensitive hypertension with recent evidence that aldosterone production is sex-specifically heightened in salt-sensitive hypertensive women.5,32 Adverse effects of antihypertensive therapy can be higher in women than men with some class of medications such as ACE inhibitor–induced cough or edema with calcium antagonists
Conclusion
There is a significant clinical need for the diagnosis and optimal management of hypertension in women across the lifespan. With the continued growth of hypertension in women and the anticipated increase in prevalence of HDPs due to the obesity epidemic, increasing maternal age, and the rising prevalence of metabolic syndrome, additional strategies in a multidisciplinary fashion are needed to address unmet needs. References available on request
Women’s Health: Menopause
Menopause, Gut Microbiota, and Mental Health
Menopause marks a natural biological transition in a woman’s life, signalling the end of reproductive capability and the cessation of menstrual cycles due to declining ovarian function. While menopause typically occurs between the ages of 45 and 55, the perimenopausal period—the years leading up to menopause— is often when the most disruptive symptoms begin to emerge. These hormonal fluctuations profoundly influence multiple physiological systems, particularly the brain and gut, with growing evidence linking the gut microbiota to mood, cognition, and overall mental wellbeing during this phase.1
In Ireland, it is estimated that over 400,000 women are currently peri- or post-menopausal, and this number will continue to rise as life expectancy increases.2 Globally, over 25 million women enter menopause each year, and by 2030, more than 1.2 billion women worldwide will be post-menopausal. As women in developed countries now spend up to one-third of their lives in menopause, this transition is not only a natural biological stage but also an important public health issue.3
The prevalence and impact of menopausal symptoms are significant and multifaceted. Studies indicate that approximately 85% of women experience symptoms during perimenopause and menopause, with 25% reporting them as severe. The FemmeBiome™ Perimenopause and Menopause Symptom Survey, conducted in collaboration with Health Innovation Hub Ireland and University College Cork, found that the most severe and prevalent symptoms were brain-related.4
Three out of four respondents reported sleep disturbances, over 60% experienced anxiety and brain fog, and half struggled with concentration difficulties. Furthermore, 40% reported mood changes directly attributable to perimenopause. These findings echo global data demonstrating that cognitive and mood-related symptoms significantly affect quality of life and occupational functioning.4
Irish data from The Menopause Hub highlight similar trends: 61% of women said menopause negatively affected their relationships, and 84% reported an adverse impact on work performance. Alarmingly, one in three women considered leaving the workforce because of unmanaged symptoms. Such
figures underscore the need for systemic improvements in awareness, diagnosis, and support. Beyond quality-of-life metrics, the healthcare burden of menopause is substantial. Increased risks of cardiovascular disease, osteoporosis, metabolic dysfunction, and depression during the post-menopausal years add long-term strain to healthcare systems.5
Menopause is marked by a progressive decline in oestrogen production, particularly oestradiol, which exerts regulatory effects across multiple organ systems. Oestrogen receptors are widely distributed throughout the body— including the central nervous system, gastrointestinal tract, cardiovascular system, and skeletal tissue—reflecting the hormone’s systemic influence. Consequently, oestrogen depletion initiates broad physiological and neuropsychological alterations that characterise the menopausal transition.6
Oestrogen exerts neuroprotective effects by modulating synaptic plasticity, neurogenesis, mitochondrial function, and neuroinflammation. It also regulates key neurotransmitters such as serotonin, dopamine, and GABA, all central to mood and cognition. When oestrogen levels fluctuate, neurochemical stability is disrupted, leading to symptoms such as mood swings, anxiety, irritability, memory lapses, and cognitive difficulties like memory lapses and reduced attention often referred to as "brain fog".7
Hot flushes and night sweats— caused by dysregulation of the hypothalamic thermoregulatory centre—are often accompanied by sleep disturbances. Poor sleep, in turn, exacerbates stress, fatigue, and cognitive dysfunction, perpetuating a self-reinforcing cycle of psychological distress.8
The gut microbiota is well known to synthesise neuroactive compounds such as serotonin, dopamine, and short-chain fatty acids (SCFAs) that modulate brain function. Conversely, psychological stress and emotional states influence microbial composition via the bidirectional gut–brain axis.9 Declines in oestrogen can alter gut microbial composition, leading to inflammation and impaired neurotransmitter synthesis. In turn, stress and depression can further disrupt gut microbiota, forming a vicious cycle of neuroendocrine imbalance.10
Written by Mariarosario Cuozzo, Postdoctoral Fellow, Eimear Gleeson, Senior Postdoctoral Fellow and Professor Siobhain M. O’Mahony PhD - Principal Investigator, Department of Anatomy and Neuroscience, APC Microbiome Ireland
Emerging research suggests that gut dysbiosis—an imbalance in the gut microbiota—can exacerbate menopausal symptoms. The estrobolome, a subset of gut bacteria capable of metabolising and regulating circulating oestrogens, plays a crucial role in maintaining hormonal balance. When microbial diversity declines, oestrogen metabolism becomes dysregulated, potentially intensifying symptoms like mood instability, cognitive decline, and metabolic dysfunction. This bi-directional relationship—the oestrogen–gut–microbiota axis—is now recognised as a key player in the pathophysiology of perimenopausal depression, anxiety, and cognitive decline.11
Menopausal symptom severity varies among women and is influenced by a multifactorial interplay of genetic, hormonal, lifestyle, and environmental determinants. Modifiable risk factors—including smoking, obesity, physical inactivity, poor diet, and chronic stress— are strongly associated with increased vasomotor, cognitive, and psychological symptoms. Accordingly, preventive and therapeutic strategies should integrate both endocrine and microbial health.12 Lifestyle-based interventions remain central to symptom management and long-term well-being. Regular physical activity, adequate sleep, and stress-reduction approaches such as mindfulness and cognitive behavioural therapy (CBT) have been shown to enhance mood stability, cognitive function, and resilience.13 Nutritional strategies supporting the gut microbiome—such as prebiotic fibres, fermented foods, and plantbased phytoestrogens (e.g., soy isoflavones, flaxseed lignans)— can modulate both gut and brain function and promote hormonal balance.14 Emerging evidence
underscores the therapeutic potential of microbiome-targeted interventions. Probiotic and synbiotic supplementation with Lactobacillus and Bifidobacterium species has demonstrated promise in enhancing microbial diversity, reducing inflammation and improving mood, anxiety, metabolic regulation, and overall quality of life during menopause.15 Recent findings from large-scale studies, such as the Zoe Predict project, have identified specific bacterial taxa linked to menopausal symptom severity and dietary patterns, suggesting that nutritional modulation of the microbiome may influence endocrine and neurochemical pathways.16
In Ireland, the Irish Menopause Guidelines (HSE, 2023) have introduced a more standardised national approach to menopause care, emphasising shared decision-making, and the inclusion of lifestyle and psychosocial interventions as first-line support.17 Concurrently, the FemmeBiome™ initiative is advancing translational research into the microbiome–hormone–brain axis, using data from over 100 women to develop targeted interventions for perimenopausal mental health.4
Integrating microbiome science into menopause care represents a promising advancement in women’s health. The interplay between nutrition and the microbiome is essential for developing personalised interventions, tailoring dietary and probiotic strategies to each individual’s microbial profile. In particular, understanding the role of the estrobolome—the collection of gut bacteria involved in oestrogen metabolism—and supporting it through psychobiotic supplementation may help women maintain hormonal balance and overall well-being.
References available on request
Women’s Health: Bladder Cancer
Bladder Cancer – Risk factors, warning signs and the positive outcomes of early detection
Each year in Ireland, 500 men and women are diagnosed with bladder cancer. Sadly, around 236 people die from the disease each year. But this does not have to be the case. When detected early, bladder cancer is very treatable.
Bladder cancer begins when cells in the bladder start to grow uncontrollably. As more cancer cells develop, they can form a tumour which can spread to other areas of the body. It usually takes a long time to develop, so it is most common in older people.
3 in 4 people (over 75%) who get bladder cancer in Ireland are 65 years or older. Although less common in people under 50, it is very worthwhile staying vigilant. More men than women get bladder cancer. This may be because more men than women have smoked or been exposed to chemicals/dyes at work in recent decades.
We don’t know exactly what causes most bladder cancers but there are some factors that may increase your risk.
Smoking cigarettes increases your risk of bladder cancer. Over a third of all bladder cancers are caused by smoking. Your risk of getting bladder cancer if you smoke is up to 4 times that of someone who has never smoked.
People with the highest risk are those who:
• smoke heavily
• started smoking at an early age
Written
by Helen Forristal, Director of Nursing, Marie Keating Foundation
Blood in the urine is the most common symptom of bladder cancer. 4 out of 5 people with bladder cancer (80%) have some blood in their urine.
• have smoked for a long time
• Cigar and pipe smoking can also increase your risk.
Certain industrial chemicals have been linked with bladder cancer. Workers in other industries that use certain organic chemicals also may have a higher risk of bladder cancer. It is always worth checking with your Health and Safety officer, regarding your safety when using
certain chemicals. Thankfully there is far more regulation around the use and exposure to chemicals than there was many years ago.
If you have been diagnosed with bladder cancer, it is worth finding out if you have ever been exposed to a chemical mentioned here. If you have, talk to your urologist or cancer doctor.
• Arylamines
• Polycyclic aromatic hydrocarbons
• Chlorine and trihalomethanes
• Chlorine
There are also risk factors that are beyond your control
Race and ethnicity– Caucasians are about twice as likely to develop bladder cancer as Black and Hispanic people. Asian Americans and Native Americans have slightly lower rates of bladder cancer. The reasons for these differences are not well understood.
Age – Bladder cancer usually takes a long time to develop, so it is most common in older people. 3 in 4 people (over 75%) who get bladder cancer in Ireland are 65 years or older. It is rarer in people under 50.
Gender – Bladder cancer is much more common in men than in women.
Chronic bladder irritation and infections – Urinary infections, kidney and bladder stones, bladder catheters left in place for a long time, and other causes of chronic bladder irritation have been linked with bladder cancer (especially squamous cell carcinoma of the bladder), but it’s not clear if they cause bladder cancer.
Personal history of bladder or other urothelial cancers such as kidney.
Genetics and family history –People who have family members with bladder cancer have a higher risk of getting it themselves.
Prior chemotherapy or radiation therapy.
Signs and symptoms
These are the possible symptoms of bladder cancer. Your symptoms
are unlikely to be cancer, but it’s important to get them checked by a doctor.
Blood in the urine
Blood in the urine is the most common symptom of bladder cancer. 4 out of 5 people with bladder cancer (80%) have some blood in their urine. Doctors call blood in the urine haematuria (pronounced heem-at-you-ree-ah). It is important to remember that blood in urine can sometimes be caused by stones in the urinary tract, a Urinary Tract Infection or even Prostatitis.
Sometimes the blood is there in such small amounts that you can’t see it. (called microscopic haematuria) But a urine test will still show if blood is present and if it is further tests will be carried out.
The bleeding is not usually painful but tell your doctor whether you had any pain when you peed (passed urine) with blood in it as it will help them to make their diagnosis.
It can also help your doctor if you tell them whether:
• There is blood only when you start to pee
• The blood is mixed with all the urine you pass
Problems with passing urine may be a symptom of other conditions but a bladder cancer should be ruled out.
You should see your doctor if you:
• Notice blood in your urine
• Need to pass urine very often
• Need to pass urine very suddenly
• Have pain when passing urine
Please go to your doctor if you have any concerns, it is better to have these signs and/or symptoms checked out early and remember that early detection saves lives. Many cancers can be treated and potentially cured if caught early.
For more information and support around bladder cancer or any of the most common cancers please go to www.mariekeating.ie or reach out to info@mariekeating.ie with any questions.
Women’s Health: Endometriosis
Living with Pain: The Hidden Burden of Endometriosis in Ireland
Endometriosis affects around one in ten women in Ireland yet remains one of the most commonly overlooked conditions in women’s health. Despite its prevalence, the average time to diagnosis still ranges between seven and nine years. Many women are misdiagnosed multiple times before receiving appropriate care. The delay is not due to rarity, but because pain in women continues to be minimised, normalised, or misunderstood.
Endometriosis occurs when tissue similar to the endometrium, the lining of the uterus, grows outside it, commonly on the ovaries, fallopian tubes, bladder, or bowel. The result is inflammation, scarring, and often excruciating pain. It can cause infertility, chronic fatigue, digestive problems, and psychological distress. Globally, it affects an estimated 190 million women and girls yet remains one of the least prioritised reproductive disorders in terms of research and funding.
Dr Hugh O’Connor, Consultant Gynaecologist at the Coombe Women and Infants University Hospital, says the condition is still too often dismissed as “bad periods.” “We are dealing with a systemic under-recognition of women’s pain. Endometriosis is not just a menstrual disorder. It is a chronic inflammatory disease that requires a multidisciplinary approach and long-term support.”
Several studies indicate that women frequently see up to five healthcare professionals before receiving a diagnosis. Irish research conducted by Trinity College Dublin in 2024 found that nearly 60 per cent of women with endometriosis had initially been treated for unrelated conditions such as irritable bowel syndrome or urinary tract infections. The emotional impact of being dismissed or misdiagnosed repeatedly is profound. Many women report frustration, self-doubt, and exhaustion from years of unrelenting pain without answers. The complexity of endometriosis makes diagnosis difficult. Symptoms vary, imaging can be inconclusive, and definitive diagnosis still requires laparoscopic surgery. However, awareness among general practitioners, hospital teams,
and pharmacists is improving. Pharmacists, in particular, have become crucial advocates. They identify patterns of repeated pain medication use, assist with hormonal therapies, and counsel patients on side effects associated with gonadotropin-releasing hormone (GnRH) analogues, progestins, and oral contraceptives used in management.
In hospital settings, pharmacists also contribute to peri-operative care, reviewing analgesics and ensuring post-surgical pain relief aligns with patient-specific regimens. As more advanced hormonal therapies and novel treatments emerge, pharmacists play an increasing role in monitoring for bone density loss, mood changes, and metabolic effects. Their continuity of care bridges the gap between acute treatment and long-term management.
“Endometriosis is not just a menstrual disorder. It is a chronic inflammatory
disease that requires a multidisciplinary approach and long-term support.”
The scale of the problem in Ireland is sobering. According to the HSE, more than 34,000 women and girls are currently waiting for outpatient gynaecology appointments, including more than 500 teenagers. Nearly 750 women remain on waiting lists for endometriosis surgery, with
over 170 of them waiting between three and six months. The Health Service Executive has pledged to perform more than 100 additional surgeries under the new National Framework for Endometriosis Care launched in October 2025.
That framework marks a major step forward. It introduces a tiered model of care, with specialist centres at Tallaght University Hospital and Cork University Maternity Hospital leading diagnostic and surgical excellence. A further three regional hubs are planned to reduce waiting times and ensure equitable access nationwide. It also emphasises integrating physiotherapy, mental health, and pharmacy into coordinated care pathways, recognising that pain management and emotional wellbeing are inseparable. Pharmacological research continues to evolve globally. New oral GnRH antagonists such as elagolix and relugolix have demonstrated effectiveness in managing moderate to severe symptoms while reducing side effects associated with older injectable formulations. Studies exploring immune and genetic mechanisms behind endometriosis are paving the way for earlier, less invasive diagnostic tools. Irish clinicians are already collaborating in international trials examining biomarkers and the role of immune modulation.
Public health education remains a crucial frontier. Surveys from the Irish Family Planning Association reveal that nearly half of Irish women under 30 cannot correctly
By Chantal Alexander
identify endometriosis symptoms. Campaigns now target schools, workplaces, and healthcare training institutions to normalise discussion of menstrual and pelvic pain as potential warning signs, not inconveniences to endure.
For hospital pharmacists, the opportunity to influence outcomes lies in patient education, early recognition, and interdisciplinary collaboration. Through careful medication management, empathetic counselling, and coordination with consultants and pain specialists, they play a central role in improving both quality of life and long-term outcomes.
Endometriosis is not rare, invisible, or inevitable. It is a condition that deserves the same urgency and resources afforded to any chronic disease. Changing that reality begins with recognising that the pain is real, the delays are unacceptable, and that women’s voices must finally be believed.
“We still see women who have been living with pain for a decade before getting a formal diagnosis. Early intervention changes everything.”
— Dr Hugh O’Connor, Consultant Gynaecologist, Coombe Women and Infants University Hospital
References available on request
Dr
Hugh O’Connor, Consultant Gynaecologist at the Coombe Women and Infants University Hospital
Women's Health - News
Potential New Target in Breast Cancer
A new study from RCSI, conducted through the pioneering Precision Oncology Research Initiative for Metastatic Breast Cancer (PRISM) research programme, has identified a potential new way to slow the growth and spread of advanced hormone-positive breast cancer.
The research is the first to show that a gene regulator known as CDK12 directly teams up with a hormone receptor and a key co-factor protein to drive cancer progression in difficult-to-treat breast cancers. The findings point to CDK12 as a promising new target for future therapies designed to stop breast cancer from spreading and becoming resistant to treatment.
This study is among the first to be published from the PRISM programme, a four-year initiative led by the Beaumont RCSI Cancer Centre to study the mechanisms that drive breast cancer’s spread. The programme is funded by Breast Cancer Ireland, the Research Ireland Strategic Partnership Programme, and Carrick Therapeutics, whose collaboration is central to translating PRISM’s scientific discoveries into future clinical applications.
“This discovery highlights a completely new pathway that we could potentially target to slow the progression of advanced ER+ breast cancer,” said Professor Leonie Young, RCSI Department of Surgery and joint senior author of the study.
“These findings are especially encouraging because they emerge from PRISM – a programme designed to unite leading academic researchers, clinicians and industry partners like Carrick Therapeutics to accelerate progress in cancer treatment and improve outcomes for patients.”
Towards better treatments
The researchers focused on breast cancers that are hormone receptor-positive, the most common subtype of the disease. Often, these cancers become resistant to treatment and spread to other parts of the body, including the brain.
By studying tumour samples from patients as well as laboratory models of advanced disease, the team discovered that the gene regulator CDK12 plays a critical role in driving aggressive growth in these cancers. When CDK12 was blocked using a new drug developed by Carrick Therapeutics, and now being investigated through the PRISMCarrick collaboration, cancer cells were less able to grow and spread. This discovery is especially timely, as Carrick Therapeutics has recently advanced this drug into a first-in-human Phase 1 trial.
The study also found that high levels of CDK12 were associated with poorer survival, particularly in patients with hard-to-treat types of breast cancer.
“We’ve shown that CDK12 acts like a control switch, turning on genes that help breast cancer
Dr Damir Vare�lija and Professor Leonie Young
grow and spread,” said Dr Damir Vare�lija, joint senior author.
“While more research is needed before these findings can be translated into clinical treatments, the study opens the door to new possibilities for tackling advanced breast cancer – particularly in patients who currently have limited treatment options” he added.
Aisling Hurley, CEO of Breast Cancer Ireland, said: “We are immensely proud to support research of this calibre through the
Abstract
Background
PRISM initiative. Discoveries like this bring us one step closer to understanding and overcoming the mechanisms that drive treatment resistance in advanced breast cancer. It’s an excellent example of how collaboration between academia, clinicians, industry and patient-focused organisations can deliver real hope for patients and their families.”
The study led by Dr Daniela Ottaviani, Dr Damir Vare�lija and Professor Leonie Young was published in the Journal of National Cancer Institute (JNCI). It was funded by Breast Cancer Ireland and Research Ireland with additional support from Enterprise Ireland, Breast Cancer Now and EU Interreg, and Carrick Therapeutics as a key collaborative industry partner driving translational impact within the PRISM programme.
Cyclin-dependent kinase 12 (CDK12) regulates general gene transcription elongation, and plays multiple roles in RNA splicing, DNA damage-response, cell cycle and genomic stability. However, transcriptional partners that guide CDK12-specific gene programs have not been identified. Genomic alterations in CDK12 have been observed in multiple cancers, exhibiting both pro-tumorigenic and tumor-suppressive functions, suggesting a context-dependent mechanism of action.
Methods
CDK12 copy number alterations and gene expression levels were analyzed in matched primary and brain metastatic patient tumors. Clinical significance was assessed by immunohistochemistry in a large cohort of primary breast cancer patient tumors. RNA-sequencing, ChIP-sequencing and molecular studies were conducted to explore CDK12’s mechanism of action, and pharmacological studies were performed both in vitro and in vivo using models of advanced (endocrine-resistant and metastatic) estrogen receptor positive (ER+) disease.
Results
CDK12 amplifications and gene overexpression were observed in brain metastatic tumors. In ER+ primary patient tumors, high CDK12 protein expression significantly associated with poor overall survival, particularly within the ER+/HER2-negative group. In ER+ endocrine resistant models, CDK12 regulated estrogen signaling pathways, with ER/MED1 identified as the master transcriptional complex directing CDK12-specific pro-tumorigenic gene programs. Pharmacological inhibition of CDK12 significantly reduced viability in endocrine resistant and metastatic cell and organoid models in vitro, and decreased metastatic spread in vivo.
Conclusion
This work describes a novel mechanism for CDK12, suggesting a potential vulnerability in ER+ breast cancer. These findings provide a basis for further investigation into the role of CDK12 inhibition as a therapeutic approach, particularly in advanced disease settings.
KISQALI® is the only CDK4/6i approved for the broadest range of HR+/ HER2- patients including those with high-risk N0 or N+ disease 2,15,16
KISQALI® demonstrated a predictable, manageable and reversible safety profile. Most AEs are asymptomatic and QoL was maintained compared to baseline. The most common grade 3/4 AEs were neutropenia, abnormal liver function tests and leukopenia2,8-11 NATALEE1 iDFS ACHIEVED
KISQALI® reduced the relative risk of invasive disease recurrence by 28.4% vs NSAI alone1
Fictional healthcare professional and patient.
AEs, adverse events; aBC, advanced breast cancer; CDK4/6i, cyclin-dependent kinase 4 and 6 inhibitor.
ABBREVIATED PRESCRIBING INFORMATION
Please refer to Summary of Product Characteristics (SmPC) before prescribing. Kisqali (ribociclib) 200 mg film-coated tablets
Presentation: Film coated tablets (FCT) containing 200 mg of ribociclib and 0.344 mg soya lecithin. Indications: Early breast cancer - Kisqali in combination with an aromatase inhibitor is indicated for the adjuvant treatment of patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative early breast cancer at high risk of recurrence (see section 5.1 for selection criteria). In pre- or perimenopausal women, or in men, the aromatase inhibitor should be combined with a luteinising hormone-releasing hormone (LHRH) agonist. Advanced or metastatic breast cancer - Kisqali is indicated for the treatment of women with HR-positive, HER2-negative locally advanced or metastatic breast cancer in combination with an aromatase inhibitor or fulvestrant as initial endocrine-based therapy, or in women who have received prior endocrine therapy. In pre- or perimenopausal women, the endocrine therapy should be combined with a LHRH agonist. Dosage and administration: Patient selection for treatment with Kisqali based on the tumour expression of HR and HER2 should be assessed by a CE-marked in vitro diagnostic (IVD) medical device with the corresponding intended purpose. If the CE-marked IVD is not available, an alternative validated test should be used. Adults: Early breast cancer - The recommended dose is 400 mg (two 200 mg FCT) taken orally, once daily for 21 consecutive days followed by 7 days off treatment, resulting in a complete cycle of 28 days. In patients with early breast cancer, Kisqali should be taken until completion of 3 years of treatment or until disease recurrence or unacceptable toxicity occur. When Kisqali is used in combination with an aromatase inhibitor (AI), the AI should be taken orally once daily continuously throughout the 28-day cycle. Please refer to the Summary of Product Characteristics (SmPC) of the AI for additional details. In pre- or perimenopausal women, or in men, the aromatase inhibitor should be combined with a LHRH agonist. Advanced or metastatic breast cancer - The recommended dose is 600 mg (3 x 200 mg FCT) taken orally, once daily for 21 consecutive days followed by 7 days off treatment, resulting in a complete cycle of 28 days. When Kisqali is used in combination with an AI, the AI should be taken orally once daily continuously throughout the 28 day cycle. Please refer to the Summary of Product Characteristics (SmPC) of the AI for additional details. When Kisqali is used in combination with fulvestrant, fulvestrant is administered intramuscularly on days 1, 15 and 29, and once monthly thereafter. Please refer to the SmPC of fulvestrant for additional details. Treatment of pre and perimenopausal women with the approved Kisqali combinations should also include an LHRH agonist in accordance with local clinical practice. Management of severe or intolerable adverse reactions (ARs) may require temporary dose interruption, reduction or discontinuation of Kisqali. Please see section 4.2 of SmPC for recommended dose modification guidelines. Kisqali can be taken with or without food (see section 4.5 of SmPC). The tablets should be swallowed whole and should not be chewed, crushed or split prior to swallowing. Special populations: ♦Renal impairment: Mild or moderate: No dose adjustment is necessary. Severe: A starting dose of 200 mg is recommended in patients with severe renal impairment. Kisqali has not been studied in breast cancer patients with severe renal impairment. Caution should be used in patients with severe renal impairment with close monitoring for signs of toxicity. ♦Hepatic impairment: No dose adjustment is necessary in patients with early breast cancer with hepatic impairment (see section SmPC 5.2). In patients with advanced or metastatic breast cancer, no dose adjustment is necessary in patients with mild hepatic impairmentModerate or severe: Dose adjustment is required, and the starting dose of 400 mg once daily is recommended. ♦Elderly (>65 years): No dose adjustment is required. ♦Pediatrics(<18 years): Safety and efficacy have not been established. Contraindications: Hypersensitivity to the active substance or to peanut, soya or any of the excipients. Warnings/Precautions: ♦Neutropenia was most frequently reported AR. A complete blood count (CBC) should be performed before initiating treatment. CBC should be monitored every 2 weeks for the first 2 cycles, at the beginning of each of the subsequent 4 cycles, then as clinically indicated. Febrile neutropenia was reported in 1.7% of patients exposed to Kisqali in the phase III clinical studies. Patients should be instructed to report any fever promptly. Based on the severity of the neutropenia, Kisqali may require dose interruption, reduction, or discontinuation as described in Table 2 (see section 4.2 of SmPC). ♦Hepatobiliary toxicity increases in transaminases have been reported. Liver function tests (LFTs) should be performed before initiating treatment. LFTs should be monitored every 2 weeks for the first 2 cycles, at the beginning of each of the subsequent 4 cycles, then as clinically indicated. If grade ≥2 abnormalities are noted, more frequent monitoring is recommended. Recommendations for patients who have elevated AST/ALT grade ≥ 3 at baseline have not been established. Based on the severity of transaminase elevations, Kisqali may require dose interruption, reduction, or discontinuation as described in Table 3 (see section 4.2). ♦QT interval prolongation has been reported with Kisqali. The use of Kisqali should be avoided in patients who have already or who are at significant risk of developing QTc prolongation. This includes patients with long QT syndrome, with uncontrolled or significant cardiac disease, including recent myocardial infarction, congestive heart failure, unstable angina and bradyarrhythmias and patients with electrolyte abnormalities. The use of Kisqali with medicinal products known to prolong QTc interval and/or strong CYP3A4 inhibitors should be avoided as this may lead to clinically meaningful prolongation of the QTcF interval (see SmPC sections 4.2, 4.5 and 5.1). If co-administration of Kisqali with a strong CYP3A4 inhibitor cannot be avoided, the Kisqali dose should be changed as described in SmPC section 4.2. QT interval prolongation in early breast cancer –study O12301C (NATALEE), a QTcF interval increase >60 msec from baseline was observed in 19 (0.8%) patients receiving Kisqali plus AI. The ECG should be assessed prior to initiation of treatment. Treatment with Kisqali should be initiated only in patients with QTcF values <450 msec. The ECG should be repeated at approximately Day 14 of the first cycle then as clinically indicated. In case of QTcF prolongation during treatment, more frequent ECG monitoring is recommended. Appropriate monitoring of serum electrolytes (including potassium, calcium, phosphorous, and magnesium) should be performed prior to initiation of treatment, at the beginning of the first 6 cycles, and then as clinically
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the
indicated. Any abnormality should be corrected before the start of Kisqali treatment. Based on the observed QT prolongation during treatment, Kisqali may require dose interruption, reduction, or discontinuation as described in Table 4 (see section 4.2 of SmPC). Based on the E2301 study QTcF interval data, Kisqali is not recommended for use in combination with tamoxifen. ♦Critical visceral disease. The efficacy and safety of ribociclib have not been studied in patients with critical visceral disease. ♦Severe cutaneous reactions Toxic epidermal necrolysis (TEN) has been reported with Kisqali treatment. If signs and symptoms suggestive of severe cutaneous reactions (e.g. progressive widespread skin rash often with blisters or mucosal lesions) appear, Kisqali should be discontinued immediately. ♦Interstitial lung disease/pneumonitis ILD/pneumonitis has been reported with CDK4/6 inhibitors including Kisqali. Patients should be monitored for pulmonary symptoms indicative of ILD/pneumonitis which may include hypoxia, cough and dyspnoea and dose modifications should be managed in accordance with Table 5 (see section 4.2 of SmPC) Based on the severity of the ILD/pneumonitis, which may be fatal, Kisqali may require dose interruption, reduction or discontinuation as described in Table 5 (see section 4.2 of SmPC). ♦Blood creatinine increase ribociclib may cause blood creatinine increase – if this occurs it is recommended that further assessment of the renal function be performed to exclude renal impairment. ♦CYP3A4 substrates ribociclib may interact with medicinal products which are metabolised via CYP3A4, which may lead to increased serum concentrations of CYP3A4 substrates (see section 4.5 of SmPC). Caution is recommended in case of concomitant use with sensitive CYP3A4 substrates with a narrow therapeutic index and the SmPC of the other product should be consulted for the recommendations regarding co administration with CYP3A4 inhibitors. Pregnancy, Fertility and Lacation ♦Pregnancy: Pregnancy status should be verified prior to starting treatment as Kisqali can cause foetal harm when administered to a pregnant woman. Kisqali is not recommended during pregnancy and in women of childbearing potential not using contraception. ♦Women of childbearing potential who are receiving Kisqali should use effective contraception (e.g. double-barrier contraception) during therapy and for at least 21 days after stopping treatment with Kisqali. ♦Breast‑feeding: Patients receiving Kisqali should not breast feed for at least 21 days after the last dose. ♦Fertility: There are no clinical data available regarding effects of ribociclib on fertility. Based on animal studies, ribociclib may impair fertility in males of reproductive potential. ♦Effects on ability to drive and use machines Patients should be advised to be cautious when driving or using machines in case they experience fatigue, dizziness or vertigo during treatment with Kisqali. Interactions: ♦Concomitant use of strong CYP3A4 inhibitors should be avoided, including, but not limited to, clarithromycin, indinavir, itraconazole, ketoconazole, lopinavir, ritonavir, nefazodone, nelfinavir, posaconazole, saquinavir, telaprevir, telithromycin, verapamil, and voriconazole. Alternative concomitant medicinal products with less potential to inhibit CYP3A4 should be considered. Patients should be monitored for ARs. If concomitant use of a strong CYP3A4 inhibitor cannot be avoided, the dose of Kisqali should be reduced (see section 4.2 of SmPC). ♦Grapefruit or grapefruit juice should be avoided. ♦Concomitant use of strong CYP3A4 inducers should be avoided, including, but not limited to, phenytoin, rifampicin, carbamazepine and St John’s Wort (Hypericum perforatum). An alternative medicinal product with no or minimal potential to induce CYP3A4 should be considered. ♦Caution is recommended when Kisqali is administered with sensitive CYP3A4 substrates with narrow therapeutic index (including, but not limited to, alfentanil, ciclosporin, everolimus, fentanyl, sirolimus, and tacrolimus), and their dose may need to be reduced. ♦Concomitant administration of Kisqali with the following CYP3A4 substrates should be avoided: alfuzosin, amiodarone, cisapride, pimozide, quinidine, ergotamine, dihydroergotamine, quetiapine, lovastatin, simvastatin, sildenafil, midazolam, triazolam. ♦Caution and monitoring for toxicity are advised during concomitant treatment with sensitive substrates of drug transporters P-gp, BCRP, OATP1B1/1B3, OCT1, OCT2, MATE1 and BSEP which exhibit a narrow therapeutic index, including but not limited to digoxin, pitavastatin, pravastatin, rosuvastatin and metformin. ♦Co-administration of Kisqali with medicinal products with known potential to prolong the QT interval should be avoided such as anti-arrhythmic medicinal products (including, but not limited to, amiodarone, disopyramide, procainamide, quinidine and sotalol) and other medicinal products known to prolong the QT interval including, but not limited to, chloroquine, halofantrine, clarithromycin, ciprofloxacin, levofloxacin, azithromycin, haloperidol, methadone, moxifloxacin, bepridil, pimozide and intravenous ondansetron. Kisqali is not recommended for use in combination with tamoxifen. Adverse reactions – advanced or metastatic breast cancer: ♦Very common: Infections, neutropenia, leukopenia, anaemia, lymphopenia, decreased appetite, headache, dizziness, dyspnoea, cough, nausea, diarrhoea, vomiting, constipation, stomatitis, abdominal pain, dyspepsia, alopecia, rash, pruritus, back pain, fatigue, peripheral oedema, asthenia, pyrexia, abnormal liver function tests. ♦Common: thrombocytopenia, febrile neutropenia, hypocalcaemia, hypokalaemia, hypophosphataemia, vertigo, lacrimation increased, dry eye, syncope, dysgeusia, hepatotoxicity, erythema, dry skin, vitiligo, dry mouth, oropharyngeal pain, blood creatinine increased, electrocardiogram QT prolonged, interstitial lung disease (ILD)/pneumonitis. ♦Rare: Erythema multiforme ♦Not known: Toxic epidermal necrolysis (TEN) ♦ Please refer to SmPC for a full list of adverse reactions. Adverse reactions - early breast cancer: ♦Very common: Infections, neutropenia, leukopenia, headache, Cough, Nausea, diarrhoea, constipation, abdominal pain, alopecia, fatigue, asthenia, pyrexia, abnormal liver function tests ♦Common: Anaemia, thrombocytopenia, lymphopenia, hypocalcaemia, hypokalaemia, appetite decreased, dizziness, dyspnoea, interstitial lung disease (ILD) / pneumonitis, vomiting, stomatitis, hepatotoxicity, rash, pruritus, peripheral oedema, oropharyngeal pain, blood creatinine increased, electrocardiogram QT prolonged ♦Uncommon: Febrile neutropenia ♦ Please refer to SmPC for a full list of adverse reactions. Legal Category: POM. Pack sizes: Unit packs containing 21, 42 or 63 FCTs. Not all pack sizes may be marketed. Marketing Authorisation Holder: Novartis Europharm Limited Vista Building
Adverse events can also be reported to Novartis preferably at www.novartis.com/report, by emailing
References 1. Crown JP, et al. Presented at the European Society For Medical Oncology Congress 2025, 17–21 October, Berlin, Germany. 2. KISQALI (ribociclib). Summary of Product Characteristics. 3. Hortobagyi GN, et al. Ann Oncol. 2024:S09237534(24)04064-X. 4. Hortobagyi GN, et al. N Engl J Med. 2022;386(10):942–950. 5. Neven P, et al. Breast Cancer Res. 2023;25:103. 6. Im S-A, et al. N Eng J Med. 2019;381:307–316. 7. Yardley DA, et al. Ann Oncol. 2022; 33(S7):S629. 8. Verma S, et al. Br Cancer Res Treat. 2018;170:535–545. 9. Beck JT, et al. Cancer Res. 2019;79 (4_Supplement):P6-18-14. 10. Fasching PA, et al. Breast. 2020;54:148–154. 11. Harbeck N, et al. Ther Adv Med Oncol. 2020;12:1–8. 12. Fasching PA et al., Annals of Oncology, Volume 34, Issue 10, 2023, Pages 951-953. 13. Lu et al., JCO 42, 2812-2821(2024). 14. Burris et al.Br J Cancer. 2021 Aug;125(5):679-686. 15. Slamon DJ, et al. Ther Adv Med Oncol. 2023;15:1–16. 16. Slamon D, et al. N Engl J Med. 2024; 390:1080-1091. 17. Fasching PA, et al. Oral LBA13. Presented at the European Society for Medical Oncology Congress 2024, 13–17 September, Barcelona, Spain. October 2025 | IE11536045 Novartis Ireland Ltd, Vista Building, Elm Park Green, Merrion Road, Ballsbridge, Dublin 4, D04 A9N6
Women's Health
Managing Women’s Heart health
Cardiovascular disease (CVD), including heart disease, stroke, and blood vessel disease, is the leading cause of death among women worldwide. In Ireland, CVD claims the lives of around 4,500 women each year—over a quarter of all female deaths. Women are six times more likely to die from CVD than from breast cancer, and approximately 30,000 women are discharged from public hospitals annually with a cardiovascular condition.
Despite this CVD in women is under-researched, underdiagnosed, and under-treated. This represents a large amount of preventable disease, disability, and death, and contributes unnecessarily to pressures on frontline health services. Women’s heart health has also been underrepresented in clinical guidelines, and medical education.
Historically it’s been believed that heart disease and stroke affect men more than women. Indeed 70% of women believe they are more likely to die from breast cancer than heart disease and stroke whereas they are
6 times more likely to die of a cardiovascular disease than breast cancer.
Worryingly 50% of women are unsure of the signs and symptoms of a heart attack. Women may downplay their symptoms which may be vaguer and though chest pain remains the commonest presenting symptom, there may be a heaviness in the chest, radiating to the arms particularly the left arm, the neck or back. There may be breathlessness, diaphoresis, dizziness and nausea is more common in women. The only way to diagnose a heart attack (STEMI and NSTEMI) is to have an ECG and troponin so it’s crucial that anyone who thinks they are having a heart attack dials 999 or 112 for an ambulance and go to the ED.
The quicker a person who is experiencing heart attack symptoms calls for help, the more likely they are to receive timely treatment, thereby reducing infarct damage. In the last Irish Heart attack audit only 47% of patients arrived directly by ambulance within 60 minutes of the onset of symptoms. Less women (36%)
Written by Dr Angie Brown MD Medical Director Irish Heart Foundation Consultant Cardiologist
called an ambulance within 60minutes of symptom onset than men (52%).
Furthermore for women with heart failure, receiving an official diagnosis takes on average five weeks compared with three weeks for men. Women are twice as likely to only be diagnosed after attending the emergency department, when the disease has already advanced, highlighting a failure of early recognition. They are also less likely to understand their prognosis (43% versus 35% of men), and the impact of late diagnosis is more likely to strain personal relationships (39% compared with 25%).
This misconception may be due to the fact that there are differences in the aetiology and presentation of heart disease in women. Clinicians frequently underestimate women’s risk of CVD, particularly in those under 54, leading to a failure to prescribe preventative therapies, timey treatment and sometimes leading to a misdiagnosis. For instance, younger women are more likely to have heart attacks in the absence of obstructive
coronary artery disease (MI with non obstructive coronary arteries MINOCA / ischaemia with non obstructive coronary arteries INOCA), from spontaneous coronary dissection (SCAD) or due to Takotsubo cardiomyopathy.
INOCA is a chronic coronary syndrome condition that is increasingly being recognised as a substantial contributor to adverse cardiovascular mortality and outcomes, including myocardial infarction and heart failure with preserved ejection fraction (HFpEF). It is thought to be due to microvascular ischaemia or coronary spasm, it is commoner in women and often underdiagnosed, it is associated with poorer outcomes if not addressed.
The true prevalence of SCAD is unknown as it is significantly under diagnosed but it is likely to be between 1.7 – 4%. The prevalence is much higher in women (women account for 90-95% of the population with SCAD) and in particular young women (less than 55 years of age) presenting with ACS. It is a life threatening condition but the diagnosis can be challenging. Though the commonest presenting symptoms is chest pain, arm, neck pain, dyspnoea, diaphoresis, and back pain can occur with time from symptoms to hospital presentation 1.10 days with further misdiagnosis and delays in hospital prior to investigation and treatment. Accurate diagnosis is important as the management differs from atherosclerotic CAD. Though coronary angiography is widely available it has limitations dedicated Intravascular imaging (intravascular ultrasound /OCT) can improve the diagnostic accuracy, but it is not widely available and is associated with additional risks and costs. Angiography therefore remains important in diagnosis so it’s important there is an awareness of this as a potential differential diagnosis as well as the angiographic variants seen in SCAD. Increased awareness includes understanding the risk factors of SCAD. It can be associated with pregnancy, hormonal influences, fibromuscular dysplasia, some connective tissue diseases, severe hypertension and drug use such as cocaine or other illegal drugs as well as intense emotional or physical stress.
Stress induced Cardiomyopathy or Takotsubo cardiomyopathy accounts for 1-2% of ACS and can also occur in situations of
Women’s Health: Breast Cancer
An Overview of Breast Cancer in Ireland
Breast cancer is the second most common cancer in women in Ireland. On average 1 in 11 Irish women, up to the age of 75, will develop breast cancer in their life time. Most common cancer in women in Ireland (excluding NonMelanoma Skin Cancer, NMSC).
The incidence of breast cancer in females is rising significantly since 2014.
• 1:11 Irish women will develop breast cancer (to the age of 75) and 1:7 in their life time
• 3.587 female cases diagnosed each year
• 753 women die from breast cancer annually
However, more women are surviving breast cancer. Latest statistics from the national cancer registry in Ireland (NCRI) indicate that the 5 year survival for women with breast cancer is now 88%. Early detection of breast cancer leads to better outcome so the earlier it is detected the better.1
Breast cancer is rare in men
• About 30 men are diagnosed each year in the Ireland with breast cancer
• Average of 8 men die yearly from breast cancer in Ireland
• Invasive ductal carcinoma is the most common type of breast cancer in both women and men
• Men can also develop rarer types of breast cancer, such as inflammatory breast cancer
• More common in men over 60, but can occur in younger men
• Men, as well as women, can inherit faulty genes that increase their risk of breast cancer (BRCA1 and BRCA2)1, 2, 3
RISK FACTORS - Modifiable risk factors:
• Overweight or obesity particularly after the menopause
• Being inactive
• Alcohol intake - one standard alcoholic drink per day is associated with a 9% increased risk
• Alcohol is now responsible for 1:8 breast cancers in Ireland with new research from Breakthrough Cancer Research: https:// breakthroughcancerresearch.ie/ cut-down-on-alcohol/
• Smoking – Small increased risk in women who smoke compared to those who have never smoked
• Oral contraceptives – returns to normal 10 years after you stop taking it
• HRT – risk is low but highest for those using combined HRT
Non-modifiable risk factors:
• Getting older; 8 out of 10 cases occur in women over 50
• A family history and inherited genes (BRCA 1 & BRCA 2)
• Early menarche (before age 12) or late natural menopause (after age 55)
• Dense breast - Risk of breast cancer is higher in women with the densest breasts compared to those with less dense breasts
• Having no children or late age pregnancy
• Benign breast disease4, 5, 6 What is BRCA?
Everyone has BRCA 1 and BRCA 2 genes. They are important genes that stop the cells in our body from growing and dividing out of control. By doing this, the genes help to protect us from getting cancer. They are often referred to as tumour suppressor genes. Everyone has two copies of each of the BRCA 1 and BRCA 2 genes—one copy inherited from each parent.
Both men and women can inherit a faulty BRCA1 or BRCA2 gene from their father or their mother.
People who inherit a faulty BRCA1 or BRCA2 gene have an increased risk of developing different types of cancers including female breast cancer, ovarian cancer, prostate cancer and to a lesser degree male breast cancer and pancreatic cancer. They also tend to develop cancer at younger ages than people who do not have a faulty BRCA1 or BRCA2 gene.8, 9
Breast changes to look and feel for include the following:
• Skin changes such as puckering, dimpling, a rash or redness of the skin
• Orange peel appearance
• Prominent veins
• Nipple changes - inverted, change in direction or shape, flattened, discharge, rash, flaky or crusted skin
• Change in size, shape or feel of the breast
• Breast lump, swelling or thickening
• Armpit lump
Written by Bernie Carter, Assistant Director of Nursing, Marie Keating Foundation
Know what is normal for you and what changes to check for:
One of the most important things that you can do for your health is to get to know your breasts. Know what is normal for you and know what changes to look out for. The best time to check your breast is several days after your menstrual period as the breast can be tender and lumpy at the time of the menstrual period. It is important to check at the same time every month. If you have gone through menopause, do your exam on the same day every month. We would suggest in the Marie Keating Foundation choosing your birthday date.
Visit your doctor if you notice any of the above changes or anything new for you. Don’t panic, remember 9 out of 10 breast lumps (90%) are normal. This means they are not cancer. 5, 7
Please visit the Marie Keating foundation website, mariekeating.ie to view a short video on how to check your breasts for changes.
What to do if you find something not normal for you:
• See your GP if you notice any new changes in your breasts, including nipple changes or new lumps or swellings in either of your armpits
• Most breast lumps (90%) aren't cancerous, but it's always best to have them checked by your doctor
• If necessary, your GP will refer you to a specialist breast centre for further tests & investigations
• The earlier it's picked up the higher the chance of successful treatment
Treatment for breast cancer
Depends on the stage and grade of your cancer. Treatment may include one or combination of the following:
• Surgery -
Breast conserving surgery (Lumpectomy or wide local excision )
Mastectomy-removal of breast
• Chemotherapy
• Radiotherapy
• Hormone treatment (Also called - Endocrine therapy)
• Targeted therapies
• Breast reconstruction surgery
A Multi-Disciplinary Team (MDT), which is a team of doctors and other health professionals with expertise in a specific cancer, come together and discuss the best treatment plan for a specific patient.
Staging and Grading of Breast Cancer
Doctors use the Stage and Grade of a cancer to help decide on the best treatment.
• Staging means the Size of the cancer and whether it has Spread
• Grading describes what a cancer cell looks like under the microscope and whether they are similar or very different to normal cells
Breast cancer is not something you have to go through alone.
The Marie Keating Foundation is here to support you. We have lots of valuable information on our website mariekeating.ie. We offer a free ‘Ask The Nurse service’ that allows you to ask questions to a qualified senior oncology cancer nurse about any cancer related health issues you may have. We have many services for those with a BRCA alteration so please do visit our website to find more information.
Our mission in the Marie Keating Foundation is to make cancer less frightening by enlightening and to achieve a world free from the fear of cancer.
References available on request
Women's Health
overwhelming grief or stress. It is also more common in women (88%). Again, this can be misdiagnosed due to the lack of traditional risk factors and an atypical presentation.
Various hypotheses have been postulated and include elevated levels of circulating plasma catecholamines and their circulating metabolites due to underlying stress, microvascular dysfunction or microcirculatory disorder, inflammation, Oestrogen deficiency, spasm of the epicardial coronary vessels, and aborted myocardial infarction. This leads to symptoms that can mimic a heart attack. The catecholamine hypothesis is the most widely accepted pathophysiologic mechanism, and elevated levels of plasma catecholamines and neuropeptides (norepinephrine, epinephrine, and dopamine) have been observed in patients with TC. Catecholamines can cause microvascular spasms, dysfunction, myocardial stunning, or direct myocardial injury. Oestrogen exerts protective effects on the cardiovascular system, including vasodilation, protection against atherosclerosis, and endothelial dysfunction. Therefore, post-menopausal women exhibit exaggerated vasoconstriction, altered endothelium-dependent
vasodilatation, and sympathetic activation in response to psychosocial stress. Unlike myocardial infarction caused by a partial or complete occlusion of a coronary artery the arteries in stress induced cardiomyopathy have a transient interruption in the blood supply to the heart but the arteries aren’t blocked. In most people this resolves completely after supportive medical care though in some people it can lead to permanent heart damage or very occasionally death. Sometimes it is recurrent.
ST elevation MI is more common in males (77%), with females presenting at an older age (69, versus 62 in males) and with a higher burden of co-morbidities. Women tend to present with atherosclerosis about 10 years later than men as they are protected by their hormones until they reach the menopause. After this the protective effects of Oestrogen are lost and women’s risk catches up to that of men.
Though some risk factors are the same for women and men such as high blood pressure, high cholesterol, obesity and sedentary lifestyles, women are more sensitive to the effects of smoking and have a higher risk of developing vascular disease if they
smoke than men, smokers tend to present with an STEMI 10 years earlier than non smokers. Similarly, women with diabetes have an even higher risk of developing cardiovascular disease then men and may be less likely to develop chest pain if they are having a heart attack. Women are also more at risk from the adverse effects of alcohol which increases the heart rate and blood pressure as well as the risk of arrhythmias.
In addition, there are sex specific risk factors that are often not considered. A premature menopause /premature ovarian insufficiency- POI (before age 40), preeclampsia or gestational diabetes (high blood pressure and diabetes in pregnancy) and some autoimmune diseases like Lupus are associated with an increased risk. POI is being recognised as a growing public health issue the prevalence is likely to be over 3.7%. Lack of oestrogen leads to endothelial dysfunction, a reduction in nitric oxide levels, increasing oxidative stress and altering lipid profiles. This leads to impaired vasodilatation reduced blood flow increased arterial stiffness and increased risk of CVD. Menopause and POI are associated with higher LDL and Tg levels. There is a change in fat distribution with the accumulation of central and
visceral adiposity. Hypertension is more prevalent in women with POI. These changes all increase the risk of premature CVD.
Other under recognised factors are unemployment, socioeconomic status, cultural disparities, race, and poverty are linked to higher CVD risk.
Psychological factors are also important to consider. Depression and stress are more prevalent in women and are linked to increased CVD risk.
Mental health and mental health conditions interact with CV health and CVD in a multidirectional way. Positive features of mental health at an individual and societal level are associated with better CV health, while people with mental health conditions are more likely to be at greater risk of CVD.
Acute CV events or chronic CVD impacts on mental health, worsening pre-existing mental conditions or triggering new conditions and poor mental health can worsen CVD prognosis.
People with mental health conditions are often the most disadvantaged, experiencing social and economic hardship as well as dealing with stigma, stereotypes, and prejudice.
People with mental health disorders are more vulnerable and are less likely to receive the same diagnostic and treatment efforts as persons without mental health conditions. This group of patients therefore particularly need targeted risk assessment and treatment.
Constant chronic stress can also affect heart health. Everyone has stressful moments, at times stress can be useful helping performance in meetings or for major deadlines etc. Chronic stress however can affect wellbeing. Stress releases adrenaline /epinephrine which can increase the heart rate and causes vasoconstriction, increasing blood pressure. Stress also releases Cortisol this sustains the effect of adrenaline and increases blood sugar levels, affects lipid levels, also increases the blood pressure. Long term these effects can damage the blood vessels and cardiac myocytes. High blood pressure causes left ventricular hypertrophy and causes endothelial damage increasing the susceptibility to the development of atherosclerotic plaque.
The long-term activation of the stress response system with too much exposure to cortisol and other stress hormones can disrupt almost all the body's processes and exacerbate underlying conditions such as hypertension and diabetes increase the risk of developing cardiovascular disease.
Stress can lead to a poor diet and comfort eating, people also often tend to drink more alcohol and if they smoke, smoke more.
Anxiety, irritability and depression can occur and can lead to poor sleep patterns. Stress may make it harder to maintain a regular exercise regimen.
Furthermore, people respond to stress in different ways. Genetics can have a role. The genes that control the stress response may vary, Genes involved in the sympathetic system or in the hypothalamic-pituitaryadrenocortical axis are associated with altered stress responses. Most people are in a fairly steady emotional level, only sometimes does stress prime the body for fight or flight. More active or less active stress responses may stem from slight differences in the genetic profile
Women can also experience more profound effects of stress due to hormonal fluctuations during menstruation, pregnancy, menopause as well as differences in stress responses and increased susceptibility to microvascular dysfunction
A study presented at the ACC showed the expected lower absolute risk in young women (<50 years) but noted a higher level of risk of developing CVD in women with depression and anxiety. This increased risk is related to higher rates of hypertension, diabetes and higher cholesterol levels in these individuals. The study showed larger increases in stress related neural activity.
As 80% of premature cardiovascular disease is
preventable its crucial that there is an awareness of all of these risk factors. The last Irish Heart Attack audit showed that 46% of patients presenting with an STEMI had hypertension, 42% Hypercholesterolaemia 35% were smokers and b2 % Diabetics. A substantial proportion of patients had multiple (>3) potentially modifiable cardiovascular risk factors on presentation. Identifying these individuals with multiple risk factors at an earlier stage in primary care, chronic disease management programmes and the ‘making every contact count’ programme and, most importantly, adequately addressing those modifiable risk factors provides an opportunity to help reduce the incidence of cardiovascular events.
To try and counter the effects of stress it’s important to eat a healthy diet and get regular exercise and try to get plenty of sleep. Relaxation exercises such as yoga, deep breathing, massage or meditation can help. Time for hobbies, such as favourite sporting activities, reading or listening to music and fostering healthy friendships, regularly talking with friends and family is important. Organise what you need to get done at home and work and remove tasks that aren't needed. If levels of stress are out of control seek professional counselling. A counsellor can help with specific coping skills to manage stress.
Cardiovascular disease in women has been under recognised under diagnosed and under treated in the past, this is only now starting
to change but there is still a wide variation in female representation in cardiovascular trials by disease states, intervention, region and sponsor type. The lack of women’s involvement in clinical trials has limited our knowledge of the efficacy, safety, and correct dose of many therapies in women compared to men which has led to the underutilisation of preventative treatments and interventions for CVD in women. Its therefore important to remove barriers for women entering clinical trials and encourage their participation so we can better understand their specific risk factors and response to treatment.
In conclusion women in Ireland are disadvantaged at every stage of the cardiovascular journey, from delayed and missed diagnoses to underrepresentation in research.
Addressing these challenges requires coordinated action including comprehensive education on sex-specific risk factors for both healthcare professionals and the public, robust research that includes women and analyses results by sex, and a cardiology workforce that is inclusive, flexible, and representative.
The Irish Heart Foundations campaign Her Heart Matters is important in raising awareness of the prevalence of heart disease and stroke, the risk factors including sex specific risks and the symptoms of a heart attack in women.
For more information see herheartmatters.ie
Women’s Health: Cervical Cancer
What is Cervical Cancer?
Cervical cancer is cancer that starts in the cells of the cervix. The cervix is the lower part of the womb (uterus), also called the neck of the womb. Cervical cancer usually develops slowly over time.1 What causes cervical cancer?
Most cases of cervical cancer (at least 9 in 10) are caused by the human papillomavirus (HPV). HPV can cause cells in the cervix to become abnormal. These abnormal cells can develop into cervical cancer over time. It usually takes 15 to 20 years for abnormal cells to become cancer but rarely it can develop quicker.
The following can increase your risk of getting cervical cancer:
• smoking - if you smoke you are twice as likely to develop cervical cancer
• having a weakened immune system
• being sexually active in your early teens
• if your birth mother took the hormonal drug diethylstilbesterol (DES) while pregnant with you2 What is HPV?
HPV is very common. At least 80% of people will get a HPV infection in their life. There are at least 100 different types of HPV and around 14 types are considered high risk for cervical cancer. You can get HPV by having vaginal, anal, or oral sex with someone who has the virus. It is also spread through close skin to skin contact, usually during sexual activity. Most HPV infections cause no symptoms and resolve spontaneously.3
What are the symptoms of cervical cancer?
Not everyone diagnosed with cervical cancer will have symptoms. That's why it's important to attend for regular
Written by Bernie Carter, Assistant Director of Nursing, Marie Keating Foundation
People with a cervix age 30 to 65 are screened every 5 years from age 30 to 65.
If you have never had a cervical screening test, you can ask any registered GP or clinic for a free cervical screening test up to age 65.
Is 5 years a big gap between screening?
It is safe to wait for 5 years between screening tests if you do not have a HPV infection.
This is because:
cervical screening. The most common symptoms include:
• unusual vaginal bleeding
• pain or discomfort during sex
• vaginal discharge
• pain in the area between the hip bones (pelvis)
If you have any of these symptoms, see your GP. Don't panic as many of those symptoms can be caused by other conditions which are not cancer.4
What is HPV cervical screening?
HPV cervical screening is a new way of cervical screening which was introduced in Ireland in 2020. It has replaced the previous screening test known as ‘The Smear.’ This type of screening has already been introduced in Australia, England, and Wales.
HPV cervical screening:
• is a better way of cervical screening
• prevents more cancers
• taken in the same way as the smear
• if your sample tests positive for HPV, this same sample will then be checked for abnormal cells (pre-cancerous)
• It is important to note that precancerous cells are not cancer
Screening age
All eligible women and people with a cervix will now be screened up to the age of 65 instead of age 60. The number of years between your screening tests changes depending on your age.
People with a cervix age 25 to 29 are screened every 3 years. You are screened more often than people over 30 because you are more likely to have HPV.
• your risk of developing cell changes is very low
• a test showing that you do not have a HPV infection is more reliable than a test finding normal cells
In most cases, it takes 15 to 20 years for a HPV infection to develop into cervical cancer.7
HPV Cervical Screening Results
You'll usually get your results by letter within 4 weeks of your screening test.
There are 14 high-risk types of HPV that can cause cervical cancer. Cervical screening looks to see if you have any of these. It does not tell us which HPV type, or how many types, were found.
Your results may say:
• HPV not found
o Next Cervical Screening in 3 or 5 years depending on your age
• HPV found and no abnormal cell changes found
o Repeat test in 12 months
o No HPV present then return to screening every 3 or 5 years
o HPV found in repeat test then a Colposcopy will be scheduled
• HPV found and abnormal cell changes found
o Scheduled for a Colposcopy
• Inadequate or unsatisfactory sample
o Issue with the sample, repeat test in around 3 month
o If 3 inadequate results in a row you will be referred for a colposcopy8
Please speak to your GP for further explanations on the results of your cervical screening.
Irelands plan to eliminate cervical cancer
Ireland is on target to eliminate cervical cancer by 2040. A global initiative led by the World Health Organization (WHO). Elimination does not mean eradication of cervical cancer. Elimination is defined as less than 4 cases of cervical cancer per 100,000.5
Cervical cancer is highly preventable and highly curable if caught early. Nearly all cervical cancers could be prevented by HPV vaccination, routine HPV cervical screening, and effective treatment of high grade abnormal cervical disease.6
To achieve elimination Ireland must meet the following targets:
• 90% of girls vaccinated against HPV by age 15
• 70% of women screened by age 35 and again by age 45
• 90% of people identified with cervical disease treated
The HSE’s Cervical Cancer Elimination Strategy Group are working closely together to help make this a reality. We can do this through HPV vaccination, HPV cervical screening and effective treatment of high grade abnormal cervical disease.
Visit the Marie Keating Foundation at www.mariekeating.ie for more information about cervical cancer, other types of gynaecological cancer, specific cancer types, cancer prevention, and our support services.
References
1. Cervical cancer | Cancer Research UK
2. Causes of cervical cancerHSE.ie
3. About Genital HPV Infection | STI | CDC
4. Cervical Cancer Symptoms | Cancer Research UK
5. HSE launches Cervical Cancer Elimination action plan as latest figures show Ireland is on track to reach historic goal by 2040
6. Cervical Cancer Causes, Risk Factors, and Prevention - NCI
International Evidence-Based Recommendations for Polycystic Ovary Syndrome in Adolescents
Written by Alexia S Peña1, Selma Feldman Witchel2, Jacky Boivin3, Tania S. Burgert4, Carolyn Ee5, Kathleen M Hoeger6, Marla E. Lujan7, Aya Mousa8, Sharon Oberfield9, Chau Thien Tay10 and Helena Teede11
1. Discipline of Paediatrics and Endocrine Department, The University of Adelaide Robinson Research Institute and Women’s and Children’s Hospital, 72 King William Road, North Adelaide, SA, 5006, Australia - Alexia S Peña
2. Division of Pediatric Endocrinology, UPMC Children’s Hospital of Pittsburgh, University of Pittsburgh, 4401 Penn Avenue, Pittsburgh, PA, 15224, USASelma Feldman Witchel
3. School of Psychology, Cardiff University, 70 Park Place, Cardiff, Wales, CF10 3AT, UK - Jacky Boivi
4. University of Missouri Kansas City, 3101 Broadway, Kansas City, MO, 64111, USA - Tania S. Burgert
5. NICM Health Research Institute, Western Sydney University, Locked Bag 1797, Penrith, Australia - Carolyn Ee
6. University of Rochester, 500 Red Creek Drive, Suite 220, Rochester, NY, 14623, USA - Kathleen M Hoeger
7. Division of Nutritional Sciences, Cornell University, Ithaca, NY, 14850, USA - Marla E. Lujan
8. Cornell Nutrition, 244 Garden AvenueRoom 216, Savage HallIthaca, NY, 14853, USA - Marla E. Lujan
9. Monash Centre for Health Research & Implementation, School of Public Health and Preventive Medicine. Faculty of Medicine Nursing and Health Sciences, Monash University, Melbourne, VIC, 3168, Australia - Aya Mousa
10. Division of Pediatric Endocrinology, Columbia University Irving Medical Center, CUIMC/Presbyterian Hospital, 622 West 168 Street, Suite 307 West, New York, NY, 10032, USA - Sharon Oberfield
11. Monash Centre for Health Research and Implementation, Monash University, Clayton, VIC, 3168, Australia - Chau Thien Tay
12. Monash Centre for Health Research and Implementation, School of Clinical Sciences, Monash University, Clayton, VIC, 3168, Australia - Helena Teede
Polycystic ovary syndrome (PCOS) is a common endocrine condition affecting 8% of adolescents.1 The adolescent PCOS diagnostic criteria have been controversial due to the overlap of the pubertal changes with adult PCOS diagnostic criteria. These pubertal changes including menstrual irregularities, acne, and polycystic ovarian morphology (PCOM) are well recognised.2, 3 Given the prevalence of menstrual irregularities during the early postmenarcheal years, mild acne or PCOM, these PCOS diagnostic criteria during adolescence can result in overdiagnosis. Conversely, disregarding diagnostic features can result in delayed or underdiagnosis with adverse long-term consequences.2,4,5,6 Delayed diagnosis has been reported by individuals who described symptoms starting in adolescence.7 Hence, nuanced diagnostic criteria are key to accurate and timely diagnosis.
The original consensus-based Rotterdam criteria for PCOS diagnosis were upgraded to evidence-based criteria in the 2018 and 2023 International Evidence-based PCOS Guideline. The 2023 Guideline recommends adult diagnosis on the basis of the identification of at least two of these recognised features: (1) menstrual irregularities/ ovulatory dysfunction, (2) clinical/ biochemical hyperandrogenism, and (3) PCOM on ultrasound or elevated anti-Müllerian hormone (AMH) levels;4, 8, 9 however, neither PCOM nor AMH levels
are suitable for diagnosing PCOS during adolescence.2, 4, 9
In the 2023 update of the PCOS International Evidence-based Guideline (“The Guideline”), we aimed to develop and provide comprehensive evidencebased recommendations for diagnosis, assessment, and treatment to improve the lives of those with PCOS worldwide from adolescence to adulthood.8, 9 This manuscript highlights the adolescentspecific recommendations from the 2023 Guideline with supporting evidence. The term “adolescent” refers to individuals between 10 and 19 years of age according to the World Health Organisation definition and women within 8 years postmenarche (gynecological age of 8 years or less) have also been identified for specific recommendations.
Methods
Methods used to develop, update, and expand this Guideline align with international best practices and comply with the Appraisal of Guidelines for Research and Evaluation (AGREE II) process. Databases (OVID MEDLINE, All EBM, PsycInfo, EMBASE, CINAHL) were searched until August 2022. Evidence synthesis procedures included integrity assessments using the Research Integrity in Guideline Development framework, which incorporates tools such as the Research Integrity Assessment and the Trustworthiness in Randomised
Women’s Health: PCO
Controlled Trials checklist.1, 10, 11
Full details of the methodology are included in the publicly available Guideline and Technical report (https://www.monash.edu/ medicine/mchri/pcos/guideline).1, 8
An international advisory board, project board and five guideline development groups (GDGs) with 80 members representing 39 organisations across six continents (71 countries) were engaged over 12 months. The GDGs included individuals with PCOS and multidisciplinary experts in PCOS including pediatricians, endocrinologists, gynecologists, reproductive endocrinologists, psychologists, allied health professionals, researchers, and others, who were involved at all stages of guideline development. The guideline addressed 55 questions via 52 systematic reviews and three narrative reviews conducted and/or overseen by an evidence team. The quality of the evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach. Judging each outcome for risk of bias, inconsistency, indirectness, imprecision, and other considerations, evidence quality was ranked from very low to high, reflecting certainty in the effect estimate from evidence synthesis (Tables 1 and 2).12
The Guideline recommendation categories were then formulated by applying the GRADE evidence-to-decision framework (Table 3).13 GDGs members drafted recommendations that
From: International evidence-based recommendations for polycystic ovary syndrome in adolescents
From: International evidence-based recommendations for polycystic ovary syndrome in adolescents
were international peer reviewed by partnering societies and the general public. Evidence was required to support recommendation modifications. Peer review results are available online: https://www.monash. edu/medicine/mchri/pcos/ guideline, and the final Guideline was approved by the Australian National Health and Medical Research Council and endorsed by participating societies.
Results
The full 2023 Guideline update provides recommendations in five areas: screening, diagnosis, and risk assessment; psychological features; lifestyle; management of nonfertility features; and infertility.8, 9 This paper summarises 63 adolescent recommendations and does not cover infertility.
Screening, diagnostic, and risk assessment
The criteria required to diagnose adolescent PCOS include menstrual irregularities and hyperandrogenism, following the exclusion of conditions that mimic PCOS.
1. 1)
Diagnostic criteria required
o 1a) Menstrual irregularities
o The updated search using the clinical question “In adolescents, at what time point after onset of menarche do irregular cycles indicate ongoing menstrual dysfunction?” revealed no studies that met the selection criteria.1 Based on the natural history of menstrual cycles/ ovulation in healthy adolescents, there was no change in the previous definition of irregular menstrual cycles according to years postmenarche.1,2,4,9 Menstrual irregularities can occur during the physiological maturation of the hypothalamicpituitary-ovarian axis over several years.14, 15 The timing at which menstrual irregularities may indicate PCOS remains unclear as the cycle’s length can vary considerably in the first postmenarcheal years. However, by the third postmenarcheal year, 95% of cycles had an average adult length of 28 days (range 24–35 days).14,16 Therefore, well defined menstrual irregularities are one of the two criteria required for adolescent PCOS diagnosis.
o 1b) Hyperandrogenism: biochemical and/or clinical
o The updated search using the clinical question “In women with suspected PCOS, what is the most effective measure to diagnose PCOSrelated hyperandrogenism (biochemical)?” revealed 17 studies (two studies including 249 adolescents).1, 17, 18 Most studies (n = 11) have evaluated total testosterone and calculated the free androgen index (FAI). Four evidencebased recommendations (EBRs) were generated and supported by a meta-analysis showing that compared with other androgens, the calculated free testosterone level and FAI had the best sensitivity (80.3% and 80.2%) and specificity (93.3% and 86.4%) for the diagnosis of hyperandrogenism. Total testosterone, androstenedione, and dehydroepiandrosterone had sensitivity of approximately 70% and specificity of approximately 75–85% and are not routinely recommended for diagnosis.1
o The updated search using the clinical question “In women with suspected PCOS, what
From: International evidence-based recommendations for polycystic ovary syndrome in adolescents
From: International evidence-based recommendations for polycystic ovary syndrome in adolescents
Table 3
is the most effective measure to clinically diagnose PCOSrelated hyperandrogenism?” identified seven studies (none in adolescents) with significant heterogeneity.1 Only consensus recommendations (CRs) were made for adolescents. These findings were based on the fact that mild acne is common in adolescents, but severe acne during perimenarcheal years is uncommon and is more likely to indicate hyperandrogenism.1,2 Modified Ferriman-Gallwey score cut-offs were based on adult studies.1, 2
1. 2)
Investigations not recommended for adolescent PCOS diagnosis
Pelvic ultrasound for PCOM evaluation and AMH levels are not recommended for the PCOS diagnosis until 8 years postmenarche, when the hypothalamic-pituitary-ovarian axis is deemed mature and evidencebased criteria for the diagnosis of PCOM are available. Normative data on ultrasonographic and serum markers of ovarian morphology show a rapid increase in ovarian size and follicle populations during adolescence, peaking in early adulthood (20 years).19, 20 The elevated and dynamic nature of ovarian morphology during adolescence renders adult definitions for PCOM inappropriate for use during this developmental stage.1,17, 18,21,22 While pooled evidence suggests that ovarian volume and AMH have some diagnostic value in adolescents, these data are limited by small sample sizes, a focus on older adolescents, the use of multiple imaging modalities or assays, and variable criteria to define adolescent PCOS cases.1, 8, 17, 18, 21, 23,24,25
1. 3)
Adolescents “at risk” of PCOS
Adolescents who have only one of the two features required for adolescent PCOS diagnosis (menstrual irregularities/ovulatory dysfunction or hyperandrogenism) should be considered “at risk” for PCOS and require longitudinal evaluation.
Evidence-based recommendations (EBR) Evidence-based recommendations are made where evidence is sufficient to inform a recommendation made by the guideline development group
Consensus recommendations (CR)
Practice points (PP)
Consensus recommendations have been made by the guideline development group in the absence of adequate evidence on PCOS and informed by evidence from the general population
Practice points have been made by the guideline development group where important issues arose from discussion of evidence-based or consensus recommendations and where evidence was not sought
From: International evidence-based recommendations for polycystic ovary syndrome in adolescents
1. 4)
Other risks associated with PCOS
While PCOS in adults is associated with increased cardiovascular disease, impaired glucose tolerance/type 2 diabetes, obstructive sleep apnea, endometrial hyperplasia, and cancer, PCOS in adolescents is associated with increased risk for impaired glucose tolerance/ type 2 diabetes. While there were studies evaluating the performance of tests for dysglycemia in adult women with PCOS, there were none in adolescents with PCOS. These studies showed that the 75 oral glucose tolerance test was the most accurate test to assess dysglycemia in women with PCOS regardless of body mass index (BMI). Recommendation in adult women also highlighted that if an oral glucose tolerance test cannot be performed, fasting plasma glucose and/or glycated hemoglobin could be considered noting reduced accuracy. In the absence of evidence, the Guidelines did not recommend any specific test to assess dysglycemia in adolescents.1 An increased risk of diabetes also occurs in first degree relatives of those with PCOS.1, 8
Psychological features
Four EBRs were formulated for psychological features. The first recommends screening for depression on the basis of a meta-analysis of 47 studies (six studies including1098 adolescents) showing up to a four-fold higher prevalence of depression in adolescents with PCOS than those without PCOS.1, 26,27,28,29,30,31 Generic online screening resources are available1, 32 and should be used for screening and rescreening according to clinical
judgment, life changes, and risk factors. A qualitative evidence synthesis reported challenges for adolescents in interactions with healthcare professionals. These challenges were attributed to their impression that their symptoms were normalised, dismissed, or not taken seriously, that doctors failed to discuss all available options with them, that follow-up plans were inappropriate because they focused primarily on future fertility, and that the immediate concerns of young people were overlooked.1,7 Healthcare professionals should become more knowledgeable of shared decisionmaking and methods for sharing medical news and supporting patient activation in adolescents.
Other EBRs underscore awareness regarding other psychological comorbidities in adults with PCOS. EBRs were based on a meta-analysis of 27 studies (3 studies including 455 adolescents) showing that adults with PCOS had a greater prevalence of anxiety that did those without PCOS; however, this was not reflected in the small number of adolescents. 1, 27, 29, 30 Similarly, few studies on negative body image and eating disorders have not shown a higher prevalence in adolescents with PCOS compared to controls.1,27,33 However, healthcare providers should note the limited studies to date, the associations in adulthood and the fact that negative body image and eating disorders are commonly observed in adolescents without PCOS.
Lifestyle
Excess weight and weight gain risks are prevalent in the general population and are exacerbated in adolescents and adults with PCOS, due to our obesogenic
environment.34 Obesity and excessive weight gain adversely affect reproductive, metabolic, and psychological health and are particularly challenging in adolescents when their self-image is developing.35 The risk associated with excess weight should be discussed with sensitivity to avoid weight bias and stigma. Similarly, health care professionals should consider asking permission prior to obtaining weight.36
Lifestyle interventions have been shown to have beneficial effects on adolescents, but randomized intervention trials to inform best practice are limited.1,37,38 On the basis of population data, it is recommended that all adolescents, including those who are not currently overweight, pursue healthy lifestyles, and prevent excess weight gain. If the adolescent’s goal is to achieve weight loss, a tailored energy deficit could be prescribed, considering individual energy requirements, weight, and physical activity levels.
EBRs highlight that no specific diet or exercise over another is recommended. Rather evidencebased general population strategies should focus on healthy individual preferences that are sustainable, recognising the role of broader family engagement. The CR in relation to the duration of exercise was also based on population guidelines.1, 39
Management of nonfertility features
Regardless of whether an adolescent is diagnosed with PCOS or is “at risk” for PCOS, specific individual concerns should guide interventions. The first management step involves a decision-making discussion with the adolescent and parents/
Women’s Health: PCO
guardians to identify specific treatment goals. The topics that merit discussion include the following: (1) lifestyle changes, (2) the use of combined oral contraceptive pills (COCP) and metformin for PCOS is evidencebased, (3) both COCP and metformin are generally “off-label” for PCOS, and (4) considerations of other interventions.
COCP could be considered for the management of hirsutism and/or menstrual irregularities in adolescents with or “at risk” of PCOS according to 10 studies (420 adolescents).1, 40, 41 Metformin alone could be considered in adolescents with or “at risk” of PCOS for cycle regulation, acknowledging limited evidence (six studies [185 adolescents]).1,42 Metformin could be used over COCP for metabolic features and COCP could be used over metformin for hirsutism and/or menstrual irregularities based on four studies (142 adolescents).1,43 The combination of COCPs and metformin in those with a body mass index < 30 kg/m2 has minimal additional benefit in women with no data in adolescents. The role of antiandrogens is limited according to 26 studies (two studies in adolescents that used antiandrogens combined with two insulin sensitizers).1, 44
No specific adolescent recommendations were made for anti-obesity medications and cosmetic therapies due to lack of data in this population. However, anti-obesity medications have beneficial effects in individuals with obesity and there is some evidence in PCOS. Additionally, laser and light therapy are effective treatments for hirsutism and related psychological features according to eight studies in adults with PCOS. Inositol preparations cannot currently be recommended in adolescents as no data exist in this population and only biochemical efficacy has been demonstrated in adults with PCOS.1, 45
Models of care and transition
Limited data are available regarding models of care in women and adolescents with PCOS.1, 35, 46, 47
Only one qualitative study evaluated the transition to adult care.48 Adolescents with PCOS and those “at risk” of PCOS should have longitudinal followup; hence, appropriate transition to adult care is important.2 Some
adolescents have failed to connect with healthcare professionals for several years. During these years, obesity, dysglycemia, dyslipidemia, depression, and subfertility often progress. Consequently, reliable accurate information sources, including the free AskPCOS app, are important. Prior to transition, healthcare professionals and adolescents should discuss comorbidities and develop lifelong plans.48 Shared decisionmaking discussions to educate adolescents regarding their health care needs are designed to improve their ability to assume responsibility for self-care during and beyond transition. Transition should be a planned process with the ultimate goals of continued, high-quality health care and increased patient responsibility for self-care.
Discussion
This manuscript summarizes specific adolescent recommendations from the 2023 International Evidence-based PCOS Guideline.8, 9 The Guideline was a result of extensive international engagement and robust methodological evidencebased processes and was independently reviewed. This manuscript provides healthcare professionals, adolescents, and their families with the most recent evidence-based recommendations to improve health outcomes. There are fewer recommendations for adolescents than for adult women highlighting the limited number of adolescent PCOS studies and emphasising the need for further research.
Adolescent PCOS diagnosis has always been challenging as normal physiological changes overlap with adult PCOS diagnostic criteria resulting in delayed and underdiagnosis as well as potential overdiagnosis.2, 3 While evidence supports the use of PCOM and AMH levels for the diagnosis of PCOS in adults,1, 8, 9 PCOM or AMH should not be used for diagnosis in adolescents to minimise the risk of overdiagnosis.2, 4,5,6, 9 PCOM or AMH can be used at approximately 8 years postmenarche when the hypothalamic-pituitary-ovarian axis is mature and evidence-based criteria for PCOM are available.8, 9
For adolescent PCOS diagnosis, the Guideline recommends the combination of menstrual irregularities defined according to the time postmenarche and clinical/biochemical hyperandrogenism following the
exclusion of other disorders.8,9 The use of these well-defined criteria for PCOS diagnosis during adolescence will promote accurate and timely diagnosis during this life stage. This approach will allow the detection of adolescents at considerable risk of weight gain and diabetes by establishing early screening with the management of long-term metabolic risks and enabling the optimisation of long-term fertility outcomes.1,6,34 As delayed diagnosis has been reported in adolescents,7 adolescents with either menstrual irregularities or clinical/ biochemical hyperandrogenism can be considered “at risk” for PCOS. This tactic addresses concerns of inappropriately labeling an adolescent with a PCOS diagnosis while avoiding delayed diagnosis when appropriate follow-up is in place.
Adolescents “at risk” of PCOS require ongoing follow-up and management according to symptoms.2, 8, 9 Timing of follow-up and re-evaluation of the diagnosis should be discussed and emphasized with adolescents and their families to avoid disruption in care which frequently occurs during transition. Adolescents “at risk” of PCOS can be diagnosed with PCOS during follow-up if they present with a combination of both menstrual irregularities and hyperandrogenism, even before 8 years postmenarche. Thus, reevaluations before and following transition are essential to ascertain outcomes. Additionally, recent data suggest that adolescents “at risk” for PCOS have abnormal metabolic profiles.49 Prospective longitudinal studies evaluating adolescents “at risk” of PCOS and healthy adolescents are needed to provide evidence-based data to better advise on the timing of follow-up and the future risk of developing PCOS.
The Guideline provides increasing evidence of psychological features and highlights the need for routine screening and management of depression in adolescents with PCOS due to the high prevalence of this condition.1, 8, 26,27,28,29,30,31
Adolescents with PCOS reported suboptimal emotional wellbeing management and dissatisfaction in relation to the education and emotional support offered.7 More research is required on other psychological features and on strategies to optimise emotional wellbeing management and evaluate anxiety, quality of life, body image, and eating disorders in adolescents with PCOS.
A lifelong health plan, including age-appropriate education, healthy lifestyles, timely screening for long-term metabolic risks, reproductive life plans, and the transition to adult care, is recommended. Management should be guided by shared decision-making addressing adolescent-specific concerns.8,9,48 The Guideline recommends that adolescents with PCOS or “at risk” of PCOS be treated with COCP for menstrual irregularity and hyperandrogenism. COCP with lowest effective estrogen dose are recommended but specific types or doses of progestins, estrogens, or combinations of COCP cannot currently be recommended. Although relatively safe, COCP have absolute and relative contraindications that need consideration, and this should be guided by general recommendations from the World Health Organisation Medical Eligibility Criteria. When prescribing COCP to adolescents “at risk” of PCOS, adolescents and parents should be counseled about the potential need of at least 3-month withdrawal of COCP for re-evaluation of diagnosis especially if there is lack of hyperandrogenism and there is a possibility of hypogonadism. Metformin is recommended for metabolic features and cycle regulation in adolescents with PCOS or “at risk” of PCOS. Of note, assessment of insulin resistance can be challenging and while most common in those with a higher BMI adolescents with normal BMI can have insulin resistance and metformin therapy have been beneficial in this population. More studies are needed to evaluate other treatments in adolescents with PCOS, including patient preferences for contraception, hair reduction therapies, antiandrogens, and antiobesity medications. The latter addresses one of the most important adolescent concerns: weight management.7, 48
The strengths of the Guideline include the following: extensive international engagement including consumers and a range of multidisciplinary healthcare professionals, rigorous methods aligned with international best practices and complying with AGREE-II, and detailed evidence synthesis processes including integrity assessments.1, 10,11,12 Additionally, the Guideline was independently evaluated as being of high quality and has a comprehensive and multifaceted translation program aiming for consistent worldwide
implementation of evidence-based care.47, 50 Limitations include that priorities were determined mostly from women with PCOS, not adolescents. However, data are accumulating in adolescents highlighting similar priorities except for infertility.7, 48 Despite an increased number of studies involving adolescents with PCOS, studies including “only adolescents” or those defining the postmenarcheal period or applying current Guideline diagnostic criteria are limited
in number and quality.1, 2 This highlights that research, using well defined cohorts of adolescents with PCOS, on the natural history of PCOS, emotional wellbeing, optimal treatments, strategies to improve weight, models of care, and transition, is a priority. Additionally, where there are no adolescent studies, some adult recommendations are likely to have applicability, but they need to be considered in the context of adolescence.
Conclusions
Adolescent-specific recommendations from the 2023 International Evidencebased PCOS Guideline enable accurate and timely diagnosis with well-defined Guideline criteria for PCOS diagnosis during adolescence that differ from adult diagnostic criteria. Additionally, recommendations highlight the importance of identifying and managing adolescents “at risk” of PCOS, screening for depression
and glucose abnormalities in adolescents with PCOS and establishing management strategies guided by adolescents’ concerns including a lifelong health plan. The overall evidence is limited and of low to moderate quality, highlighting the critical need for further research on PCOS during adolescence and in the longer term.
Anticoagulation therapy in the context of women’s health
References available on request
Women’s Health: Thrombosis
Anticoagulation therapy in the context of women’s health
Written by Dr Katie Liston Haematology Specialist Registrar in Haematology and Dr Maeve Crowley Consultant Haematologist, Cork University Hospital
Background: Anticoagulants are frequently prescribed medications. In Ireland, direct oral anticoagulants are the anticoagulants of choice in most cases but vitamin K antagonists still have a vital role to play, especially in the management of patients with metallic heart valves and antiphospholipid syndrome. Anticoagulants remain high risk medications (https://ipu.ie/wpcontent/uploads/2022/03/highrisk-medicines.pdf). Women face specific and evolving bleeding and thrombotic challenges throughout their lives (Figure 1.)
Women and Iron deficiency:
The WHO estimate that ~half a billion women worldwide aged 15-49 are anaemic. In 2019 30% of non-pregnant women and 37%of pregnant women in this age group were anaemic and the most common cause of this anaemia was iron deficiency (www. who.int/news-room/fact-sheets/ detail/anaemia). During this period, women have an increased requirement for iron in the form of menstruation and pregnancy. Iron supplementation outside of dietary sources is not always easy to tolerate so once you become iron deficient, it can be difficult to resolve. This is important in the context of anticoagulation as if you know menstruating women are commonly anaemic at baseline, putting on a treatment that leads to increased and prolonged bleeding is only likely to make things worse. Heavy menstural bleeding (HMB): HMB is common and can be caused by structural issues (e.g. polyps, leiomyomas, malignancy or adenomyosis)
Background: Anticoagulants are frequently prescribed medications. In Ireland, direct oral anticoagulants are the anticoagulants of choice in most cases but vitamin K antagonists still have a vital role to play, especially in the management of patients with metallic heart valves and antiphospholipid syndrome. Anticoagulants remain high risk medications (https://ipu.ie/wpcontent/uploads/2022/03/high-risk-medicines.pdf). Women face specific and evolving bleeding and thrombotic challenges throughout their lives (Figure 1.)
Figure 1. Bleeding and Thrombotic Challenges Faced by Women. HRT=Hormone Replacement Therapy. days and a median blood loss of 57ml/cycle. HMB is a loss of > 80mls/cycle or excessive menstrual blood loss that interferes with a woman’s physical, social, emotional, or material quality of life. It is important to identify if a woman has an underlying menstral disorder prior to starting them on anticoagulation as we know that anticoagulation is likely to make things worse. About 2/3 of women on anticoagulation experience heavy menstural bleeding and almost ¾ of women on rivaroxaban (De Crem N et al. Thromb Res. 2015 Oct).
Figure 1. Bleeding and Thrombotic Challenges Faced by Women. HRT=Hormone Replacement Therapy.
Women and Iron deficiency: The WHO estimate that ~half a billion women worldwide aged 15-49 are anaemic. In 2019 30% of non-pregnant women and 37%of pregnant women in this age group were anaemic and the most common cause of this anaemia was iron deficiency (www.who.int/newsroom/fact-sheets/detail/anaemia). During this period, women have an increased requirement for iron in the form of menstruation and pregnancy. Iron supplementation outside of dietary sources is not always easy to tolerate so once you become iron deficient, it can be difficult to resolve. This is important in the context of anticoagulation as if you know menstruating women are commonly anaemic at baseline, putting on a treatment that leads to increased and prolonged bleeding is only likely to make things worse.
Table 1. Clinical Features of Heavy Menstral Bleeding
Changing sanitary products more than every 2 hours or requiring double protection
Leaking or soaking through clothing or needing to change sanitary products overnight
Periods lasting >7 days
Passing clots >2.8cm (1.1 inch)
or non-structural issues (e.g. anovulatory cycles, medications, coagulopathy); (Samuelson Bannow B et al. Res Pract Thromb Haemost. 2021 Aug).
Consequences of HMB include iron deficiency +/- anaemia, impaired quality of life, missing school/work, missed doses of anticoagulation due to fear of HMB and missing out on social activities and sport.
A 2015 European survey (Fraser IS et al. Int J Gynaecol Obstet. 2015 Mar) found that ~27% of the women surveyed had experienced
2 or more HMB symptoms in the previous year; 46% of these women had never consulted a physician about it. 7% of the respondents completed an extended survey –63% of these women had been diagnosed with iron deficiency or iron deficiency anaemia but only 46% had been prescribed supplementation. To identify menstrual problems, it’s important to know what is normal. A normal cycle length is 21-35 days with each cycle lasting 2-7 days and a median blood loss of 57ml/cycle.
When trying to assess if a women has an underlying menstrual disorder, Table 1 contains some things to ask women about.
HMB is a loss of > 80mls/cycle or excessive menstrual blood loss that interferes with a woman’s physical, social, emotional, or material quality of life. It is important to identify if a woman has an underlying menstral disorder prior to starting them on anticoagulation as we know that anticoagulation is likely to make things worse. About 2/3 of women on anticoagulation experience heavy menstural bleeding and almost ¾ of women on rivaroxaban (De Crem N et al. Thromb Res. 2015 Oct).
Heavy menstural bleeding (HMB): HMB is common and can be caused by structural issues (e.g. polyps, leiomyomas, malignancy or adenomyosis) or non-structural issues (e.g. anovulatory cycles, medications, coagulopathy); (Samuelson Bannow B et al. Res Pract Thromb Haemost. 2021 Aug) Consequences of HMB include iron deficiency +/- anaemia, impaired quality of life, missing school/work, missed doses of anticoagulation due to fear of HMB and missing out on social activities and sport. A 2015 European survey (Fraser IS et al. Int J Gynaecol Obstet. 2015 Mar) found that ~27% of the women surveyed had experienced 2 or more HMB symptoms in the previous year; 46% of these women had never consulted a physician about it. 7% of the respondents completed an extended survey – 63% of these women had been diagnosed with iron deficiency or iron deficiency anaemia but only 46% had been prescribed supplementation. To identify menstrual problems, it’s important to know what is normal. A normal cycle length is 21-35 days with each cycle lasting 2-7
Starting a menstruating women on anticoagulation: It is good practice to try to address 4 issues when starting a menstruating women on anticoagulation. (Figure 2.)
Written by Dr Katie Liston Haematology Specialist Registrar in Haematology and Dr Maeve Crowley Consultant Haematologist, Cork University Hospital
When trying to assess if a women has an underlying menstrual disorder, Table 1 contains some things to ask women about.
Women’s Health: Thrombosis
Starting a menstruating women on anticoagulation: It is good practice to try to address 4 issues when starting a menstruating women on anticoagulation. (Figure 2.)
Figure 2. Issues to address when starting a menstruating women on anticoagulation. HMB = Heavy Menstrual Bleeding.
Exploring these factors allows clinicians to counsel women about the most appropriate modality for them.
Inhibitors (SSRIs) are commonly prescribed antidepressant medications. Many of the haemostatic functions of platelets are mediated through serotonin so SSRIs potentially can make the haemostatic function of platelets less effective and increase the bleeding risk (Ann Med. 2022 Dec). Over the counter medications such as non-steroidal anti-inflammatory drugs (NSAIDs) are also important to ask about as they also have an antiplatelet effect. It may not be possible to stop these medications but at least you can flag that the patient may be at a higher risk for bleeding and counsel them regarding this.
Figure 2. Issues to address when starting a menstruating women on anticoagulation. HMB = Heavy Menstrual Bleeding.
When trying to assess if a women has an underlying menstrual disorder, Table 1 contains some things to ask women about.
ensure they have some reserve. In general, a multifaceted approach works best.
This is particularly important if a patient is going to be on indefinite anticoagulation. If a women has underlying menstrual disorders, they may need further investigations such as imaging or a review by a gynaecologist or haematologist. Different anticoagulants have different risk of menorrhagia so agent choice is important. If a women has always had HMB and sinister causes have been out-ruled, it is better to consider measures early to ameliorate the issue rather than risk the woman
Starting a menstruating woman on anticoagulation: It is good practice to try to address 4 issues when starting a menstruating women on anticoagulation. (Figure 2.)
This is particularly important if a patient is going to be on indefinite anticoagulation. If a women has underlying menstrual disorders, they may need further investigations such as imaging or a review by a gynaecologist or haematologist. Different anticoagulants have different risk of menorrhagia so agent choice is important. If a woman has always had HMB and sinister causes have been out-ruled, it is better to consider measures early to ameliorate the issue rather than risk the woman experiencing significant bleeding. Ensuring that women are iron replete is vital as you are lowering their bleeding threshold so you want to
Anticoagulant choice: Rivaroxaban appears to be associated with the highest rates of menorrhagia, when compared with apixaban, dabigatran or warfarin (Samuelson Bannow B et al. Res Pract Thromb Haemost. 2021) – see Table 2. Quality of life is also differently impacted (Patel JP et al. Res Pract Thromb Haemost. 2023). The ongoing randomized MEDEA (Hamulyák EN et al. Res Pract Thromb Haemost. 2020 Dec) study will hopefully provide further evidence to guide agent choice in the future.
Concurrent medications: It is important to review a patients regular medications to look for drug-drug interactions as well as those that may increase the bleeding risk. Co-prescription of antiplatelet agents increases the risk of bleeding. The prescription of an anticoagulant may negate the need for an antiplatelet agent. Selective Serotonin Reuptake
experiencing significant bleeding. Ensuring that women are iron replete is vital as you are lowering their bleeding threshold so you want to ensure they have some reserve. In general, a multifaceted approach works best.
Anticoagulant choice: Rivaroxaban appears to be associated with the highest rates of menorrhagia, when compared with apixaban, dabigatran or warfarin (Samuelson Bannow B et al. Res Pract Thromb Haemost. 2021) – see Table 2. Quality of life is also differently impacted (Patel JP et al. Res Pract Thromb Haemost. 2023). The ongoing randomized MEDEA (Hamulyák EN et al. Res Pract Thromb Haemost. 2020 Dec) study will hopefully provide further evidence to guide agent choice in the future.
Hormonal therapy: The combined oral contraceptive pill (COCP) is associated with an increased risk of venous thrombosis. Women are prescribed it for many reasons, including contraception, HMB, acne, endometriosis, polycystic ovarian syndrome, dysmenorrhoea, cycle regulation. It is important to find out what the indication for the COCP was when you are considering if it should continue or be changed to an alternative. Whatever their indication, it is reassuring the note that if a women is on therapeutic anticoagulation, then their risk of recurrent VTE appears similar if they are on oestrogen containing therapies or no hormonal therapy (Martinelli I et al. Blood. 2016 Mar). Therefore, if a woman is remaining on anticoagulation, they can stay on the COCP but if they are stopping anticoagulation, an alternative needs to be found. Different modalities have different levels of efficacy in terms of contraception thrombosis risk and amenorrhoea rates (DeLoughery E et al. Hematology Am Soc Hematol Educ Program. 2022 Dec).
Table 2. Relative risk of Heavy Menstrual Bleeding by choice of Anticoagulant.
uterine
*statistically significant , P<0.01. CRNMB= Clinically Relevant Non-Major Bleeding. MB=Major Bleeding. Adapted from ‘Management of heavy menstrual bleeding on anticoagulation’ Samuelson Bannow B. Hematology Am Soc Hematol Educ Program. 2020 Dec
*statistically significant , P<0.01. CRNMB= Clinically Relevant Non-Major Bleeding. MB=Major Bleeding. Adapted from ‘Management of heavy menstrual bleeding on anticoagulation’ Samuelson Bannow B. Hematology Am Soc Hematol Educ Program. 2020 Dec
Concurrent medications: It is important to review a patients regular medications to look for drugdrug interactions as well as those that may increase the bleeding risk. Co-prescription of antiplatelet agents increases the risk of bleeding. The prescription of an anticoagulant may negate the need for an
agent.
Tranexamic acid (TXA): TXA is an antifibrinolytic agent which stops the breakdown of clots. A Danish historical prospective cohort study attempted to estimate the risk of thrombosis in women aged 15-49, not on anticoagulation with a standard risk of thrombosis. They looked at data on 2 million women followed for 13.8 million person years. The incidence of venous thrombosis appeared to be increased but the number of women who needed to get a 5 day course of TXA to cause harm was >78,000 (Meaidi A et al. EClinicalMedicine. 2021). There was no increased risk of thrombosis in the high risk patients recruited to the CRASH2 and WOMAN studies which is reassuring. It is frequently used in the prevention and management of bleeding in patients with bleeding disorders. It is not well studied in patients with thrombosis or on anticoagulation. A survey of clinicians’ prescribing habits showed that there is often a reluctance to use it in the acute setting, with 1/3 of those surveyed never prescribing it in the first 3 months and 46% very concerned with the risk of progression or recurrence. (Abdulrehman J et al. Thromb Res. 2024 Jan).
Conclusion: It’s important to be both frank and open when starting a woman on anticoagulation. Heavy Menstrual Bleeding is common, especially in woman on anticoagulation. Women are often reluctant to talk about it without prompting. Discussing where they are at present in terms of menstruation and their past experiences will help you predict how they will be on anticaogulation. If they are anaemic or iron deficient, this is a good time to address it.
Anticoagulation stewardship is an emerging movement focusing on the appropriate use of anticoagulants, which persist in being high risk medications despite the availability of newer agents. Choosing the correct agent, following consideration of patient and disease factors, at the correct dose, for an appropriate duration should ensure maximum efficacy with the minimal amount of harm.
Educational resource: The team in Kings College hospital have developed a short educational video for patients entitled ‘anticoagulants and your periods’ which is freely available on youtube https://youtu.be/ kAIirzFVFKc?si= IrSfQUGvygKQcZDS
Hidden in Plain Sight: Addressing the Rise of Uterine Cancer in Ireland Women’s Health: Uterine Cancer
By Chantal Alexander
Uterine cancer, most commonly endometrial carcinoma, is now one of the fastest-growing cancers among women in Ireland. Once considered relatively uncommon, its incidence has risen steadily over the past two decades, largely driven by lifestyle factors, hormonal influences, and an ageing population. According to the National Cancer Registry Ireland (NCRI), more than 530 Irish women are diagnosed each year, with most cases detected after menopause. The encouraging news is that, when found early, uterine cancer is highly treatable. The challenge lies in ensuring women recognise the warning signs and that the healthcare system, from general practice to hospital pharmacy, responds swiftly and cohesively.
The most common symptom is abnormal uterine bleeding — any post-menopausal bleeding should prompt investigation. Yet too often, women delay seeking help, assuming that spotting or changes in bleeding patterns are part of ageing. Consultant Gynaecological Oncologist Dr Fionnuala McAuliffe from the Mater Misericordiae University Hospital notes, “We still see women who wait months to present. Awareness is our strongest tool, because early diagnosis leads to excellent survival rates.”
Hospital pharmacists are closely tied to the care continuum for uterine cancer. They play a vital role in managing chemotherapy, hormonal therapy, and newer immunotherapy protocols. Adjuvant treatments such as carboplatin-paclitaxel combinations remain standard
“We still see women who wait months to present. Awareness is our strongest tool, because early diagnosis leads to excellent survival rates.” — Dr Fionnuala McAuliffe, Consultant Gynaecological Oncologist, Mater Misericordiae
University
Hospital
Case Vignette: Listening Beyond the Prescription
Anne, a 69-year-old woman, was referred to a Dublin hospital after several months of postmenopausal bleeding. Initially hesitant to seek help, she finally mentioned her symptoms during a medication review at her local pharmacy. The pharmacist encouraged her to consult her GP immediately. A biopsy confirmed early-stage endometrial carcinoma. Surgery followed swiftly, and Anne’s prognosis was excellent. “I only went because my pharmacist said not to ignore it,” she recalls. “Otherwise, I might still be putting it off.”
This everyday interaction underscores how pharmacists, both in the community and hospital, can influence early detection through patient engagement. Hospital pharmacists also assist in postoperative care, reviewing analgesic and anticoagulant use and monitoring for potential drug interactions, particularly in older patients managing comorbidities such as diabetes or hypertension.
microsatellite instability (MSI) and mismatch repair deficiency (dMMR) guides the use of immunotherapy. Pharmacists are at the forefront of implementing these personalised approaches, ensuring testing results are integrated into prescribing systems and that patients understand the purpose behind new treatment pathways.
In advanced or recurrent uterine cancer, pharmacists support combination regimens and help mitigate toxicities such as fatigue, hypertension, and diarrhoea. They also monitor for hormonal side effects in patients using progestin therapy and ensure consistent access to medications across hospital and outpatient settings. “Continuity is everything,” says an oncology pharmacist at Cork University Hospital. “When a patient leaves our care, they must still have clarity about their treatment plan and when to seek advice.”
for advanced disease, but novel agents like pembrolizumab and lenvatinib are being introduced for recurrent or metastatic cases. Pharmacists ensure these complex regimens are safely dispensed, counsel patients on managing side effects, and coordinate supportive therapies that protect quality of life.
Endometrial cancer is strongly associated with oestrogen exposure unopposed by progesterone. Risk increases with obesity, polycystic ovary syndrome, and tamoxifen therapy. Ireland’s rising obesity rates have contributed significantly to the growing incidence. Public health campaigns now emphasise maintaining a healthy weight and managing metabolic risk as part of cancer prevention.
Molecular profiling has transformed treatment. Identifying
Psychological support is increasingly recognised as part of holistic uterine cancer care. Pharmacists and nurses, often closest to patients during treatment, provide reassurance and practical guidance. Fear of recurrence, body-image concerns, and menopause-related symptoms are common. Ensuring open dialogue reduces anxiety and strengthens adherence.
Nationally, initiatives by the HSE’s National Cancer Control Programme (NCCP) are expanding multidisciplinary care for gynaecological cancers, including uterine malignancies. Hospitals such as St James’s, Cork University Hospital, and the Mater are leading collaborative models where oncologists, surgeons, pathologists, and pharmacists review every case collectively. These meetings refine treatment plans and ensure consistency across Ireland’s cancer network.
Dr Fionnuala McAuliffe, Consultant Gynaecological Oncologist, Mater Misericordiae University Hospital
Uterine cancer may not attract the same public attention as breast or cervical cancer, but its rising prevalence demands focus. For hospital pharmacists, every interaction is an opportunity to contribute to earlier detection, safer therapy, and improved survivorship. The disease may begin quietly, but through vigilance, communication, and compassion, its outcomes need not remain so.
References available on request
Cholesterol
The impact of sex and the cheese matrix on cholesterol metabolism in middle-aged adults
Written by Martina Rooneya b, Aileen O'Connora b, Simone Dunnea b, Emma L. Feeneya b and Eileen R. Gibneya b
aFood for Health Ireland, University College Dublin, 4, Dublin,
Ireland
bInstitute of Food and Health, School of Agriculture and Food Sciences, University College Dublin, 4, Dublin, Ireland
Cardiovascular disease (CVD) is a leading cause of mortality globally, accounting for 20.5 million deaths in 2021, approximately a third of all deaths worldwide.1 Encompassing disorders of the heart and blood such as coronary heart disease and cerebrovascular disease, CVD is traditionally more prevalent in men compared to women, with ischaemic heart disease responsible for 159.59 deaths per 100.000 males, and 146.27 deaths per 100,000 women in Western Europe in 2019.2 In recent years, sex-related perceptions of CVD risk are evolving, as there is recognition of higher mortality rates and poorer prognosis following acute cardiovascular (CV) event in women3 in addition to different presentation of CV events between men and women4,5 and disparities in management of acute coronary syndromes.6 Women have smaller arteries than males, and are more likely to present with ischaemia with non-obstructive coronary arteries (INOCA), whereas obstructive coronary artery disease is more typical in men.4,7,8 Femalespecific risk factors for CVD include age of menarche and menopause, polycystic ovarian syndrome, parity, pregnancy loss, and adverse pregnancy outcomes.9
Interest into the effect of sexual dimorphism in nutrition has grown, as men and women often respond differently to dietary intervention.10, 11 A comprehensive analysis of the biochemical profiles of 853 men and 903 women identified sex differences in one-third of the serum metabolites examined, including fatty acids and lipids.12 Causes of such variation are relatively unknown, but such sexual dimorphism in lipid metabolism may be a result of hormone action13 or genotypic variation.14 In post-menopausal women a less-favourable lipid profile and increased CVD risk occur in response to a decline in oestrogen levels8 while genomewide association studies (GWAS) have identified single nucleotide polymorphisms (SNP's) associated
with cholesterol and triglyceride metabolism.14,15 Coupled with guidelines which are established from clinical trial data where men are over-represented,16 there is a need to understand the interaction between sex and CVD in order to provide effective treatment to both sexes. Elevated cholesterol concentrations have long been linked with increased CVD risk, with sex differences evident throughout the lifecycle. Men have higher LDL cholesterol until the fifth decade, while LDL, and therefore total, cholesterol concentrations increase in women in response to decreased oestrogen levels in the postmenopausal state, although women exhibit higher HDL cholesterol concentrations than men at all ages.17 Furthermore, women have a lower likelihood of achieving target LDL cholesterol concentrations than men.18
Dairy products, such as milk and cheese, provide a range of nutrients such as protein, calcium, iodine, vitamin D and vitamin B12 and as such, play an important role in health.19 However, dairy products are also a source of saturated fat, which is implicated in elevated cholesterol concentrations, and those at risk of CVD may limit intake of these nutritious foods.20 In the past decade the view on dairy products and CVD risk appears to be changing as meta-analyses of randomised controlled trials (RCT) and prospective cohort studies demonstrate dairy products to have neutral or beneficial effects on CVD event or mortality21, 22, 23 and cholesterol concentrations.24, 25, 26, 27 Moreover, evidence suggests markers of dairy intake are associated with lower CVD risk.28 It is thought the dairy matrix, the complex structure of protein, fat and nutritional components may be responsible for the cardioprotective effects of cheese compared to butter observed in the published literature,29,30 and compelling evidence from recent RCT's investigating the cheese matrix and cholesterol concentrations support this.
Feeney et al., explored the effect of fat consumed in different dairy matrices to differentially effect cholesterol concentrations in a cohort of middle-aged, overweight adults.31 They found that fat consumed within the cheese matrix, as cheddar cheese, reduced cholesterol concentrations to a greater extent compared to a reduced fat cheddar cheese and butter group or a macronutrient matched butter and protein powder group.31 However, the study by Feeney et al.,31 and others in the area32, 33, 34, 35, 36 did not stratify results by sex, thus the interaction of sex and dairy intervention on lipid metabolism remains unknown. It must be noted that these RCT's considered small sample sizes and may have been underpowered to detect such effects. Further understanding of the interaction of sex and dairy intervention will help tailor nutritional advice and precision nutrition for those at risk of CVD, however the evidence base for sex-specific recommendations must first be established.10
The aim of the present study is to investigate if men and women respond differently to intervention with dairy fat in different matrices by combining data from two RCT's investigating the effect of long-term cheese and butter consumption on markers of cardiometabolic health.
Materials and methods
Participants
In the original studies, volunteers were recruited from Dublin, Ireland, and the surrounding areas.31,36 The inclusion criteria for both studies were for participants to be healthy, aged ≥50 years and with a BMI ≥25 kg/m2. Exclusion criteria included being prescribed medication for cholesterol or blood pressure lowering, following a prescribed diet or actively trying to lose weight. Written, informed consent was obtained from all participants prior to commencement. Both studies were approved by the Human
Research Ethics Committee at University College Dublin (LS-1544-Feeney-Gibney and LS-1978-Gibney) and study protocols conform to the ethical guidelines of the 1975 Declaration of Helsinki. The trials are registered as ISRCTN86731958 and ISRCTN11913510. Full details are available elsewhere.31,36
Study design
The present study is secondary analysis of two previously conducted studies which share a similar study design; the Cheese Matrix Study31 and the Cheese Melting Study.36 In brief, both studies were four-arm randomised controlled trials, testing the effect of fat eaten in different dairy matrices. Both studies had intervention arms investigating 120g Irish cheddar cheese and a ‘deconstructed cheese’ group comprising 49g butter, 30g calcium caseinate powder, and a calcium supplement (CaCO3).31,36 The groups were matched for macronutrients and calcium, each providing 475 kcal, 40g fat, 29g protein, and 820 mg calcium per day. Tirlán provided cheese and Kerry Group supplied butter for the interventions. Protein powder was purchased from Bacarel and Company Ltd and calcium supplements were purchased from Holland and Barratt. All intervention diets provided between 38 and 41g/day of dairy fat in different dairy matrices over a 6-week period, and were matched for total energy, macronutrients and calcium.31 Data from the cheese and deconstructed cheese groups from each trial were combined for the present analysis (Fig. 1).
Appointments were conducted at the Institute of Food and Health, University College Dublin. Anthropometric measurements were collected before and after intervention. Fasting body weight was measured using a Tanita scale, Model BC-420ma, and height was measured with a free-standing SECA stadiometer.
Fig. 1. Study flow chart. Participants from two previously conducted RCT's31,36, who were assigned to the cheese or deconstructed cheese group were included in the present exploratory analysis (Completer approach, n 197; Per Protocol approach, n 164). Reasons for dropouts are found in the original publications.31,36 Both trials were of six weeks duration, recruited free-living subjects aged ≥50 years with a BMI ≥25 kg/m2, and followed similar protocols.31,36 The cheese used in both RCT's was grass-fed, full-fat mature Irish cheddar cheese. The butter group in each trial was matched to the cheese intervention for energy, macronutrients and calcium by including protein powder (calcium caseinate) and a calcium supplement (CaCO3).
Seated blood pressure was measured using an Omron digital monitor (Model M6 HEM-7360-E).
Serum and plasma fasting blood samples were collected at baseline and post-intervention. In one study, blood lipids were analysed on a Pentra 400 clinical analyser (Randox, Antrim, Northern Ireland) at University College Dublin.31 In the second study blood lipids were analysed by LabCorp Inc (Morrisville, North Carolina, USA) using nuclear magnetic resonance (NMR) spectroscopy using the Vantera NMR Clinical Analyser using the LipoProfile-4 algorithm.36 Strong correlations between clinical chemistry analysis and NMR analysis were found for triglycerides (r = 0.907, p < 0.001) and HDL cholesterol (r = 0.898, p < 0.001; data not shown). LDL cholesterol was calculated using the Friedewald equation in each study.37 Fasting insulin was analysed in serum samples at University College Dublin using Mercodia Insulin ELISA kits (Uppsala, Sweden). Dietary intakes were also assessed at both timepoints using a 3-day food diary or
the validated EPIC-Norfolk Food Frequency Questionnaire (FFQ). For a more detailed description of the study design, see Feeney et al.,31 and O'Connor et al.36
Results
Data from a total of 164 subjects from the two previously conducted RCT's were included in this analysis, 69 (42.1 %) men and 95 (57.9 %) women. The mean ± SD for age was 59.5 ± 6.5 years, 80.2 ± 13.8 kg for weight and 28.0 ± 3.6 kg/m2 for BMI. There were no significant differences in anthropometry between the groups before or after dairy intervention.
With respect to biomarker data, no sex × treatment interaction was observed for glycaemic control or blood pressure, although sex was shown to have an effect on total (p = 0.008) and HDL cholesterol (p = 0.031) concentrations and treatment was seen to have an effect on LDL cholesterol. Upon stratification by sex, some significant differences in response were observed, as shown in Fig. 2. For total
cholesterol concentrations, there was no significant difference in response in males between cheese and deconstructed cheese ( 0.24 ± 0.57 mmol/L vs 0.11 ± 0.61 mmol/L, p = 0.189), while within females total cholesterol concentrations decreased by 0.19 ± 0.77 mmol/L in response to the cheese diet and increased by 0.10 ± 0.73 mmol/L in response to the deconstructed cheese diet (p = 0.004). A similar trend was observed for LDL cholesterol, with no difference between the groups within men ( 0.19 ± 0.47 mmol/L vs 0.10 ± 0.54 mmol/L, p = 0.386) but LDL cholesterol concentrations were seen to decrease by 0.18 ± 0.62 mmol/L in response to the cheese diet and remain stable in response to the deconstructed cheese diet (0.03 ± 0.58 mmol/L, p < 0.001) within women. No sex differences were observed in response to cheese or deconstructed cheese for HDL cholesterol, triglyceride, glucose or insulin concentrations (all p > 0.05). Sex was shown to have an effect on both systolic (p = 0.045) and diastolic (p = 0.034) blood pressure.
Pre-intervention intakes of fat (37.5 ± 6.8 %TE vs 40.0 ± 7.1 %TE, p = 0.028) and SFA (14.8 ± 4.1 %TE vs 16.1 ± 3.9 %TE, p = 0.045) were lower in the group who consumed cheese compared to those who consumed deconstructed cheese. There was a greater reduction in energy intake in the group who consumed cheese ( 200 ± 671 kcal) compared to an increase in those who consumed deconstructed cheese (131 ± 683, p = 0.001). Protein intakes increased by 2.1 ± 3.9 %TE in response to the cheese diet but decreased by 0.4 ± 4.5 %TE in response to the deconstructed cheese diet (p < 0.001). Dietary intake stratified by study is presented in Supplemental Table 4. Using the Keys et al. prediction equation38 an increase in total cholesterol was predicted in response to both interventions, based on dietary changes across the intervention period. An overview of the present analysis is presented in Fig. 3.
Discussion
Meta-analyses of RCT's have demonstrated the cholesterollowering effects of cheese, compared to butter24,25 however, the key RCT's included in these meta-analyses did not consider the role of sex in this interaction.31, 32, 33, 34, 35, 36 In line with the published evidence, cheese
Cholesterol
was found to lower total and LDL cholesterol concentrations, compared to a deconstructed cheese diet comprised of butter, calcium caseinate and a calcium supplement, in this group of middle-aged overweight adults, with no effect on other markers of metabolic health observed. Although no sex × treatment interaction was demonstrated, within sex differences were detected as total and LDL cholesterol were shown to respond differently to intervention with dairy fat in females, but not in males. These results indicate sex may contribute to inter-individual cholesterol response to dairy fat and that the dairy matrix effect may be stronger in women.
In the present study, women responded differently to intervention with dairy fat, an effect which is largely in agreement with the published literature,41, 42, 43 while the findings within the male group is in line with some44 but not all published studies considering males.45,46 A small study by
Fig. 2. Changes in total, HDL, and LDL cholesterol and triglyceride concentrations (mmol/L) for delta visit 2 – visit 1. Panel A, all subjects (n 164); Panel B, men only (n 69); Panel C, women only (n 95). Shaded boxes represent the cheese group, hatched boxes represent the deconstructed cheese group. Values are mean differences ± SEMs. *p < 0.05.
Thorning et al.,43 found total, LDL and HDL cholesterol concentrations decreased in response to cheese in an acute and chronic investigation of 14 postmenopausal women, who had similar baseline cholesterol concentrations to the women in the present study, while Lacroix et al., found butter to increase total, LDL and HDL cholesterol concentrations in 61 young, normocholesterolaemic women.41 Females have been shown to respond differentially to varying sources of dietary fat42,47,48 which may explain the response observed here and further support the role of the cheese matrix in lipid metabolism. Brassard et al., investigated the differential effects of dietary fatty acid type on cholesterol response, and while they did not stratify their results by sex,48 secondary analysis identified a potential sexual dimorphism in the cholesterol efflux capacity (CEC) response to dietary fat32 which may offer some insight into the variation observed between men and women in response to the deconstructed cheese diet in
the present study. In the Brassard et al., secondary analysis, an increase in HDL-mediated CEC after butter compared with cheese was found in men, but not women, whereas in women, an increase in HDL-mediated CEC after a MUFA-rich olive oil diet compared to cheese was observed.32 These sex-dependent differences in cholesterol response to saturated and unsaturated fats have been reported in other studies49,50 and genetic factors, such as DNA methylation, may explain this variance,51,52 although, it has been noted that many studies into cardiovascular epigenetics lack stratification of data by sex, despite the established sex differences in CVD.53 Although not considered in this present study, it is important to consider the influence of genetic variation in response to dietary intervention. Nonetheless, in the present study women responded more favourably to cheese compared to deconstructed cheese, thus the dairy matrix effect may be stronger in women.
The present study considers traditional markers of metabolic health, such as cholesterol concentrations, however novel, more sensitive markers, such as lipoprotein particle number and size, may offer further insight into the cholesterol lowering effects of cheese compared to butter, and any sex differences that may exist in this relationship. In observational analysis of 1574 males and 1692 females from the Framingham Offspring Study, women were shown to have higher concentrations of larger LDL and HDL particles, and therefore a less atherogenic profile, compared to men.54 Looking more closely at the effect of cheese on lipid particle size response, in a 12-week crossover RCT Raziani et al., found neither full-fat nor reduced-fat cheese to differentially effect cholesterol concentrations, compared to a carbohydrate control, in either the group as a whole, or when stratified by sex in intention-totreat primary analysis.35 However, in sub-set analysis investigating particle size, within men fullfat cheese led to a reduction in LDL cholesterol concentrations whereas reduced-fat cheese increased LDL cholesterol, an effect which was driven by decreased concentrations of cholesterol in the medium- and small-sized LDL particles in the regular compared to reducedfat cheese groups.55 Within females, HDL concentrations in the full-fat dairy group increased significantly compared to the carbohydrate control group, an effect driven by an increase in cholesterol in the smaller HDL particles.55 It must be noted only blood samples for 85 of the 139 subjects who completed the study were available for this secondary analysis, and only 23 (27 %) of these participants were male, thus limiting the power of this subgroup analysis. Nonetheless, the findings by Raziani and colleagues indicate middle-aged men may have a more favourable lipoprotein response to regular-fat than reduced-fat cheese, compared to middle-aged/postmenopausal women,55 and thus support the findings from the present analysis. These results also highlight the importance of considering the dairy matrix effect and fat content when examining changes in blood lipids. Similarly, men and women were found to have different postprandial lipoprotein subclass responses after intake of comparable meals containing 45g dairy fat, although an opposing trend was demonstrated, perhaps owing to the younger participants with a healthy BMI.56 In the study by Hansson et al., women were found to have a greater decrease
Fig. 3. Graphical abstract of the present analysis. Abbreviations: *, P < 0.05; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; Total-C, total cholesterol.
in LDL-particles and a greater increase in extra-large- and largeHDL particles, therefore a shift to a more protective profile, compared to men.56 In a separate study of middle-aged, overweight subjects, it was reported that reductions in LDL cholesterol observed after chronic dairy fat consumption were driven by reductions in small LDL particles and a shift towards larger LDL particles overall, however this study did not investigate the effect of sex on this interaction.57 Given the shift in particle size patterns observed in response to dairy foods and between sexes, further studies in larger samples are warranted to investigate the mechanism behind the cholesterollowering effects of cheese compared to butter, and any sex difference that may exist.
This study is unique in that it combines data from two RCT's which followed similar protocols and has a greater sample size than other studies in the area. Despite this, the Per-Protocol analysis is limited by the male sub-analysis being under-powered based on power calculations employed in the initial studies, although findings from the Completer Approach are in line with the Per Protocol analyses, and are available in Supplemental Tables 1-3. Furthermore, the authors recognise that a crossover
design would have been optimal, however this analysis combines two different datasets with a parallel-arm design to answer the research question and ‘study’ was used as a covariate in the statistical analysis. Moreover, the original studies were conducted by the same researchers with consistent methods across the studies. A limitation of the original trials is the lack of a run-in phase, which may give rise to random findings due to differences at baseline and regression to the mean. Furthermore, a Per-Protocol approach was applied to the analysis, although it is recognised that this may also introduce bias into the comparison between groups.39 The Completer analysis followed similar trends as the Per-Protocol approach and is available in Supplemental Table 2. In the present study, the observed findings deviate from the response predicted by equations based on dietary changes. This study was in free-living individuals, and therefore we cannot completely rule out the risk of bias as being a potential explanation, although several independent studies support the findings observed here.24,25 While sex hormones, such as oestrogen, regulate cholesterol metabolism,58 this is not likely to have an effect in the present study as participants were aged ≥50 years and as such, are likely
to be postmenopausal, although information on this and use of hormone replacement therapy was not collected. Furthermore, one RCT was conducted during the COVID-19 pandemic, which may have impacted the findings, for example there was a higher level of attrition in this trial with n 37 (25.3 %) dropouts36 compared to n 24 (21.4 %) in the earlier trial.
31 Some significant differences in nutrient intake between the groups cannot be overlooked. While the analysis is adjusted for change in energy intake, there is a small possibility some of the observed effects may also be mediated by differences in nutritional intake such as energy, protein or fat. The present study only considers traditional markers of cardiometabolic health, i.e., cholesterol concentrations and as explored earlier, investigation of lipoprotein particle size may provide more sensitive insight into the sex differences observed here. Given the limited number of studies investigating the role of sex in the cholesterol-lowering effects of cheese compared to butter, further investigations in larger sample sizes are warranted.
Understanding sex differences in metabolism is critical to optimise prevention, diagnosis and therapeutic intervention for both males and females. Clinical guidelines for many conditions exist for normal and diseased populations, for example National Institute for Health and Care Excellence (NICE) guidelines for cardiovascular disease outline
recommendations for healthy individuals and those with type 2 diabetes mellitus, but sex is overlooked.59 A review of such guidelines to incorporate sex differences may be warranted given the emerging evidence on the sex differences in progression, presentation and treatment of CVD.4,5,8 Furthermore, increased understanding of sex differences in response to dietary intervention, such as dairy fat, add to the evidence base to provide more tailored, personalised nutrition to those at risk of CVD, and therefore improve treatment and management of CV health through lifestyle modifications. This is especially pertinent as there have been recent calls for early, personalised treatment of dyslipidaemia in women.8
In conclusion, no sex × treatment interaction was observed for any markers of metabolic health in the present analysis, however when stratified by sex, men and women were shown to respond differently to dairy fat contained within or outside the cheese matrix, with the dairy matrix effect appearing to be stronger in women compared to men. Overall, cheese was found to improve lipid profiles in middleaged adults at increased risk of metabolic disease. Further work investigating sex differences to dairy intervention are warranted to optimise prevention and treatment for cardiometabolic health in both men and women.
References available on request
Cardiotoxicity (e.g., chemotherapy)
Coronary MINOCA
Myocardial Infarction
Myocardial Infarction with Non-Obstructive Coronary Artery Disease: review of diagnosis and management approach
most frequent category, involving mechanisms where the coronary arteries myocardial ischaemia despite the absence of flow-limiting atherosclerotic
Common aetiologies include:
Dr Ross O’Grady
Written by Dr. Muslim Madhag (Cardiology Registrar), Dr Ross O’Grady (Cardiology SPR) Dr. Samer Arnous (Consultant Cardiologist)
Dr Muslim Madhag
Plaque rupture or erosion (most common)
Coronary artery spasm
Dr S Arnous
• Coronary artery spasm
Spontaneous coronary artery dissection (SCAD) — further classified into three by angiographic morphology: (8)
• Spontaneous coronary artery dissection (SCAD) — further classified into three types by angiographic morphology:8
Type 1: Classic appearance of longitudinal radiolucent flap with contrast staining.
Coronary embolism
Coronary thrombosis
Myocardial bridging
Dr Ross O’Grady
Introduction
Cardiovascular disease remains the leading cause of mortality among both men and women worldwide. In Ireland, acute coronary syndrome (ACS) accounts for approximately 6,000 hospital admissions annually.1
Between 5% and 15% of patients diagnosed with myocardial infarction (MI) have nonobstructive coronary arteries on invasive angiography—typically defined as <50% diameter stenosis in a major epicardial vessel. This clinical entity is termed myocardial infarction with nonobstructive coronary arteries (MINOCA) and remains common yet often underrecognised.2,3
o Type 1: Classic appearance of longitudinal radiolucent flap with contrast staining.
Type 2: Long, diffuse, smooth tubular narrowing with abrupt calibre change.
Type 3: Focal, tubular stenoses mimicking atherosclerosis.
Dr S Arnous
magnetic resonance (CMR), and provide aetiologyspecific management principles with key evidence where available. We also highlight prognosis and followup considerations, including rehabilitation and psychosocial support.
Classification of MINOCA
MINOCA encompasses a heterogeneous group of conditions and can be broadly classified into two categories based on whether the underlying mechanism is coronary or noncoronary in origin.3
1. NonCoronary MINOCA
(a) NonCardiac causes
• Cardiac trauma
• Cardiotoxicity (e.g., chemotherapy)
2. Coronary MINOCA
This is the most frequent category, involving mechanisms where the coronary arteries contribute to myocardial ischaemia despite the absence of flowlimiting atherosclerotic stenosis. Common aetiologies include:
• Plaque rupture or erosion (most common)
o Type 2: Long, diffuse, smooth tubular narrowing with abrupt calibre change.
o Type 3: Focal, tubular stenoses mimicking atherosclerosis.
• Coronary embolism
• Coronary thrombosis
• Myocardial bridging
1. Invasive coronary angiogram showing SCAD of the mid left circumflex artery with an intimal flap
Dr S Arnous
MINOCA is a working diagnosis made in patients who present with clinical features of ACS and a rise/fall in cardiac troponin consistent with acute myocardial injury, in whom coronary angiography does not demonstrate obstructive coronary artery disease (CAD). Compared with MI due to obstructive CAD (MICAD), patients with MINOCA are more often women and tend to have fewer traditional cardiovascular risk factors.2,3 Scope of this review. We summarise the contemporary classification of MINOCA (coronary and noncoronary causes), outline a practical diagnostic pathway integrating invasive angiography, intracoronary imaging and physiology, and cardiac
These conditions cause myocardial injury via supply–demand imbalance rather than direct coronary pathology, sometimes labelled Type 2 MI. Common examples include:
Invasive coronary angiogram showing SCAD left circumflex artery with an intimal flap.
• Sepsis
• Pulmonary embolism (PE)
• Severe anaemia
• Acute respiratory failure
(b) Cardiac, noncoronary causes
These conditions directly injure the myocardium without obstructive CAD, leading to troponin elevation. Key examples:
• Myocarditis
• Cardiomyopathies
• Takotsubo (stressinduced) cardiomyopathy
Figure
Dr. Muslim Madhag
Dr Ross O’Grady
Dr. Samer Arnous
Diagnostic Approach
Clinical Assessment
Diagnosis begins with a thorough history and examination. Certain features may point toward specific aetiologies—for example, ACS after exertion in young women may suggest SCAD; a history of illicit drug use raises suspicion of coronary vasospasm; and chest pain following intense emotional or physical stress may indicate Takotsubo cardiomyopathy.
Initial Investigations
The cornerstone investigation in diagnosing patients with MINOCA is invasive coronary angiography. Prior to angiography, baseline laboratory and bedside tests should be performed to guide differential diagnosis.
• Transthoracic echocardiography to assess left ventricular systolic function and wallmotion abnormalities
Invasive Coronary Angiography
Invasive coronary angiography remains central to the evaluation of suspected MINOCA. A meticulous, framebyframe review of angiographic images is essential, as subtle findings such as plaque rupture, small thrombus, or SCAD may otherwise be missed.
When the angiographic appearance is uncertain or atypical:
• Intracoronary imaging with optical coherence tomography (OCT) or intravascular ultrasound (IVUS) can clarify the presence of plaque disruption
or SCAD. Given the procedural risks, these modalities should be reserved for situations where angiography alone is inconclusive.
• Intracoronary pharmacological testing: Administration of intraarterial glyceryl trinitrate can relieve vasospasm, aiding diagnostic accuracy.
• Coronary physiology: In patients where microvascular dysfunction is suspected, physiological indices may be measured. Abnormal values are defined as coronary flow reserve (CFR) <2.0 and/or index of microvascular resistance (IMR) ≥25.
• Left ventriculography: Injection of contrast into the left ventricular cavity can reveal characteristic wallmotion abnormalities consistent with Takotsubo syndrome, such as apical ballooning.
Cardiac Magnetic Resonance (CMR)
CMR offers detailed myocardial tissue characterisation, enabling differentiation between myocarditis, Takotsubo syndrome, infarction, and other cardiomyopathies. It can demonstrate oedema, inflammation, fibrosis, and scar, while also providing accurate functional assessment. CMR is therefore recommended in all patients with a working diagnosis of MINOCA, ideally within two weeks of presentation to maximise diagnostic yield.4 Delays in access may significantly reduce sensitivity, particularly for detecting transient conditions such as myocarditis or Takotsubo cardiomyopathy.
Figure 2 Diagnostic algorithm for Patients with working diagnosis of MINOCA. By Sykes R, Doherty D, Mangion K, Morrow A, Berry C. What an Interventionalist Needs to Know About MI with Non-obstructive Coronary Arteries. Interventional Cardiology Review 2021;16:e10. https://doi. org/10.15420/icr.2021.10
Figure 1 Diagnostic algorithm for Patients with working diagnosis of MINOCA. By Sykes R, Doherty D, Mangion K, Morrow A, Berry C. What an Interventionalist Needs to Know About MI with Non- obstructive Coronary Arteries. Interventional Cardiology Review 2021;16:e10. https://doi.org/10.15420/icr.2021.10
Figure 2: Diagnostic algorithm for patients with MINOCA4
Myocardial Infarction
Integrated Imaging Strategy
A multimodality approach— incorporating invasive angiography, intracoronary imaging, coronary physiology, and CMR—can identify a specific aetiology in up to 85% of patients initially labelled with MINOCA.2,4 The choice and sequence of tests should be individualised according to clinical presentation and haemodynamic stability, balancing diagnostic benefit against the risk of iatrogenic complications. A rigid, onesizefitsall pathway is not appropriate; investigations should be tailored to the patient’s clinical context.
Management
General Principles
Management of MINOCA should be guided by the underlying aetiology whenever identified. In the absence of large-scale randomised controlled trials, current recommendations rely primarily on observational data and expert consensus.4,5
Secondary prevention strategies, modelled on those used in obstructive MI, are often considered beneficial—especially when plaque rupture or erosion is suspected. These typically include highintensity statins, ACE inhibitors or ARBs, betablockers, and appropriate antiplatelet therapy.
AetiologySpecific Management
• Plaque rupture or erosion: Treat as for atherosclerotic ACS, with dual antiplatelet therapy (DAPT) for 12 months followed by lifelong single antiplatelet therapy, highdose statins, betablockers, and ACE inhibitors/ARBs.4
• Spontaneous coronary artery dissection (SCAD): Conservative management is preferred, as >70% of lesions heal spontaneously within weeks to months (7). Revascularisation with PCI or CABG should be considered only in highrisk scenarios such as left main stem involvement, persistent ischaemia, malignant arrhythmia,
or haemodynamic compromise. Medical therapy generally includes betablockers and aspirin; statins and ACE inhibitors may be added, and a second antiplatelet agent can be considered in selected patients.7,9
• Coronary vasospasm: Calcium channel blockers are firstline therapy, often in combination with nitrates if tolerated. Avoid precipitants such as cocaine and sympathomimetic drugs.
• Microvascular dysfunction: Antianginal therapy (betablockers, calcium channel blockers, nitrates, ranolazine) is the mainstay, with lifestyle modification and riskfactor control.
• Takotsubo cardiomyopathy: Supportive therapy is indicated, often with betablockers and ACE inhibitors. Management should follow ESC heart failure guidance if LV dysfunction is significant.
• Myocarditis or cardiomyopathies: Treatment should follow diseasespecific guidelines, with supportive heart failure therapy where appropriate.
Heart Failure and Secondary Prevention
Patients who develop LV dysfunction should be managed according to ESC heart failure guidelines, with optimisation of guidelinedirected therapy and followup in a specialist heart failure service. All MINOCA patients should be referred to a structured cardiac rehabilitation programme.
Prognosis
Compared with MI due to obstructive CAD (MICAD), patients with MINOCA generally have a more favourable prognosis. Nevertheless, their risk of major adverse cardiovascular events (MACE) remains significantly higher than that of the general population. (2) Prognosis varies according to underlying aetiology—for example, SCAD typically carries a good
PMI Annual Charity Lunch
mediumterm outlook with vessel healing, whereas myocarditis or microvascular dysfunction may be associated with recurrent symptoms. Importantly, MINOCA patients remain at risk of recurrent MI, heart failure, and arrhythmia, underscoring the need for close followup and secondary prevention.
Psychological sequelae— including anxiety, depression, and posttraumatic stress disorder—are not uncommon after MINOCA. Timely referral for screening, counselling, and rehabilitation services should therefore be integrated into holistic care.8
Conclusion
MINOCA represents a heterogeneous clinical syndrome encompassing a wide range of coronary and noncoronary pathologies. It should be regarded as a provisional working diagnosis, prompting thorough investigation to establish the precise mechanism of myocardial injury. A multimodality diagnostic pathway—combining angiography, intracoronary imaging and physiology, and CMR—can clarify the underlying cause in most cases.
Management must be tailored to the identified aetiology, with secondary prevention applied judiciously. While outcomes are generally better than for MICAD, MINOCA still confers a substantial risk of adverse events compared to the general population. Ongoing research and clinical trials are needed to refine treatment strategies and improve prognosis.
References
1. Shannon J. Heart attack audit shows need for new cardiovascular strategy. Irish Heart Foundation. Available at: https://irishheart. ie/news/heart-attack-audit-shows-need-for-new-cardiovascular-strategy (Accessed March 2025).
2. Bakhshi H, Gibson CM. MINOCA: Myocardial infarction with nonobstructive coronary artery disease. Am Heart J Plus Cardiol
The PMI Annual Charity Lunch takes place this year on December 11th from 12-4pm in the Dublin Royal Convention Centre, Dublin.
This much-loved annual event is a perennial highlight of the PMI events calendar; bringing members, colleagues and guests together for an afternoon of good food, great company and the opportunity to support an amazing charity.
This year the PMI are proud to support Make-A-Wish Ireland, an incredible organisation that grants life-changing wishes to children living with life-threatening illnesses. Make-A-Wish has granted over 3,350 unique wishes to date. More than just experiences, each wish creates treasured memories and gives children and their families hope, joy and precious moments together.
Don’t miss this opportunity to connect and celebrate all while supporting an incredible cause. Tables of 10 and 12 are available and sell out quickly each year – secure yours today by contacting the PMI office or visiting www.thepmi.com
Res Pract. 2023;33:100312. doi:10.1016/j.ahjo.2023.100312.
3. Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44:3720–3826. doi:10.1093/eurheartj/ehad191.
4. Sykes R, Doherty D, Mangion K, Morrow A, Berry C. What an interventionalist needs to know about MI with nonobstructive coronary arteries. Interv Cardiol Rev. 2021;16:e10. doi:10.15420/ icr.2021.10.
5. Montone RA, Caffè A, Yasumura K, Kini A. Routine diagnosis of ANOCA/INOCA: pros and cons. EuroIntervention. 2025;21:e293–e295. doi:10.4244/EIJ-E-24-00072.
6. Lindahl B, Baron T, Erlinge D, Hadziosmanovic N, Nordenskjöld A, Gard A, Jernberg T. Medical therapy for secondary prevention and longterm outcome in patients with myocardial infarction with nonobstructive coronary artery disease. Circulation. 2017;135:1481–1489. doi:10.1161/CIRCULATIONAHA.116.026336.
7. Khiatah B, Jazayeri S, Yamamoto N, Burt T, Frugoli A, Brooke DL. Cardiovascular disease in women: A review of spontaneous coronary artery dissection. Medicine (Baltimore). 2022;101(38):e30433. doi:10.1097/ MD.0000000000030433.
8. Krittanawong C, Gulati R, Eitzman D, Jneid H. Revascularisation in patients with spontaneous coronary artery dissection: Where are we now? J Am Heart Assoc. 2021;10(13):e018551. doi:10.1161/JAHA.120.018551.
9. Tweet MS, Kok SN, Hayes SN. Spontaneous coronary artery dissection in women: What is known and what is yet to be understood. Clin Cardiol. 2018;41:203–210. doi:10.1002/clc.22909.
Chronic Pain
Changing the Narrative: Confronting Stigma in Chronic Pain
1. Introduction
Up to one in three people in Ireland live with chronic pain, and one in five report pain lasting more than ten years. It is now widely accepted that chronic pain is both a sensory and emotional experience, dynamically shaped by biological, psychological and social factors.
While chronic pain itself is complex and frequently misunderstood, stigma adds a further, often invisible, layer of suffering.
Listening to patients—or even a cursory scan of the literature— reveals the near-ubiquitous presence of stigma in the lives of those living with pain.
“I think the stigma that goes with back injuries is fairly nasty… I don’t tell people I have a back injury. I’d rather tell them I was dying of something.” - Slade et al. (2009), Pain Medicine
“I was labelled ‘drug-seeking.’ I felt like I had to prove I was really in pain.” - Bean et al. (2022), Pain Reports
“I wasn’t listened to or believed. I felt violated.” - Wallace et al. (2021), International Journal for Equity in Health
These accounts echo what we hear from patients in Irish pain clinics. They are often loaded with the emotional weight of life-altering pain, compounded by accumulated wounds inflicted by stigma—intentional or otherwise.
Stigma is not always explicit, or obvious. It can manifest as subtle disbelief, avoidance, or the quiet omission of timely referrals. Understanding how stigma operates is not only a matter of empathy—it is a clinical and systemic necessity.
2. Stigma is a Clinical Risk Factor: What the Evidence Tells Us
A 2024 meta-analysis in Pain found that higher levels of stigma are significantly associated with worse pain intensity, disability, and depression (Hickling et al., 2024). Stigma is particularly potent in conditions where the pathology is invisible or contested, such as fibromyalgia. People with both fibromyalgia and rheumatoid arthritis reported significantly more stigma and poorer wellbeing than those with rheumatoid arthritis alone (Van Alboom et al., 2021).
Stigma can be enacted (e.g. being labelled "drug-seeking," having symptoms dismissed), or internalised, when individuals begin to believe negative assumptions others hold. These processes can erode confidence, suppress help-seeking, and amplify pain.
Krishnan and Mathur (2025) describe stigma operating at three levels:
Krishnan and Mathur (2025) describe stigma operating at three levels:
Structural
System-level barriers to equitable pain care
Underfunded services, long waitlists, inadequate staff training
Public Societal attitudes that minimise or invalidate pain “It’s all in your head”; disbelief from family or professionals
Internalised Self-directed stigma shaped by external judgements
Shame, social withdrawal, reduced helpseeking
These layers often intersect with social determinants of health such as gender, race, or socioeconomic status. Crucially, research shows stigma may amplify pain through overlapping neural pathways between physical pain and social exclusion (e.g., via the anterior cingulate cortex and insula).
In Ireland, a national audit revealed that patients often wait more than 18 months to access public chronic pain services, which remain critically under-resourced (Purcell et al., 2022). Sheridan et al. (2025) identified four common experiences in Irish pain services: the dominance of biomedical care, fragmentation of support, the desire for more holistic care, and barriers to self-management like short appointments and long waits.
3. Drivers of Stigma
Chronic pain challenges the biomedical model, especially when it doesn’t neatly correspond to test results or visible injury. While neuroscience and psychology have made strides in understanding central sensitisation and pain processing, these insights have not fully permeated public or clinical consciousness.
Further contributors include:
• Out-group bias: pain expressed by people from marginalised groups is more likely to be discounted
• Perceived blame: when pain is viewed as self-inflicted, empathy decreases
Written by Dr Rosemary Keane, Principal Specialist Clinical Psychologist, Pain Team at the Mater Misericordiae University Hospital; Secretary, Pain Psychologists Ireland (PPI)
Chronic Pain
While neuroscience and psychology have made strides in understanding central sensitisation and pain processing, these insights have not fully permeated public or clinical consciousness.
These layers often intersect with social determinants of health such as gender, race, or socioeconomic status. Crucially, research shows stigma may amplify pain through overlapping neural pathways between physical pain and social exclusion (e.g., via the anterior cingulate cortex and insula).
In Ireland, a national audit revealed that patients often wait more than 18 months to access public chronic pain services, which remain critically under-resourced (Purcell et al., 2022). Sheridan et al. (2025) identified four common experiences in Irish pain services: the dominance of biomedical care, fragmentation of support, the desire for more holistic care, and barriers to self-management like short appointments and long waits.
3. Drivers of Stigma
Chronic pain challenges the biomedical model, especially when it doesn’t neatly correspond to test results or visible injury. While neuroscience and psychology have made strides in understanding central sensitisation and pain processing, these insights have not fully permeated public or clinical consciousness.
Further contributors include:
• Out-group bias: pain expressed by people from marginalised groups is more likely to be discounted
• Perceived blame: when pain is viewed as self-inflicted, empathy decreases
• Clinical discomfort: professionals may struggle with uncertainty, especially without training
(De Ruddere & Craig, 2016)
4. A Vicious Cycle: Masking, Disconnection, and Identity Loss
Pain is not just felt—it’s communicated and interpreted. But when expressions of pain are
ignored or misread, people often respond by masking symptoms. This coping mechanism, though understandable, reduces opportunities for validation and increases isolation. Over time, it contributes to a shrinking sense of identity and unmet emotional needs.
5. Breaking the Cycle: Validation
In Abraham Verghese’s Cutting for Stone, a surgeon asks: “Tell us, please, what treatment in an emergency is administered by ear?” The answer—“words of comfort”—reminds us that compassionate presence is a powerful intervention.
These statements reflect not only emotional relief but also potential clinical benefit. As Vowles and Thompson (2011) emphasise, emotionally safe, group-based interventions can reduce shame, increase connection, and promote psychological flexibility—a key mechanism in recovery.
Such services rebuild trust and provide a model of stigma-resilient care. Unfortunately, these are the exception rather than the rule across Ireland.
7. Breaking the Cycle: Education and Awareness
Chronic Pain Ireland’s 2025 Pain Awareness Month focuses on stigma across healthcare, work, and life. Tuning into lived experience is essential. Listening is not passive—it is an active form of care. More at chronicpain.ie
8. Conclusion: What Can We Do Today?
Stigma manifests in subtle and overt ways—from offhand comments to system-level neglect. Yet small shifts in how we speak, listen, and relate can have outsized effects. Begin with a question. Offer space. Choose words with care. Every staff member in the hospital system has the capacity to change the narrative of chronic pain and help to reduce the invisible burden carried by so many.
between stigma and health outcomes in people with chronic pain: A meta-analysis. Pain. Advance online publication. https://doi.org/10.1097/j. pain.0000000000003077
Scott, W., Buchman, D.Z., Vasiliou, V.S. (2025). The multi-dimensional stigma of chronic pain: A narrative review, Current Opinion in Psychology (62):101980
https://doi.org/10.1016/j. copsyc.2024.101980.
Purcell, A., Channappa, K., Moore, D. et al. A national survey of publicly funded chronic pain management services in Ireland. Ir J Med Sci 191, 1315–1323 (2022). https://doi. org/10.1007/s11845-021-02673-5 Sheridan, R., Coote, S., et al. (2025). The lived experience of pain services: A comparison of service users and service providers in the Irish health services. Pain Research and Management, Article ID 4608906. https://doi.org/10.1155/2025/4608906
Slade, S. C., Molloy, E., & Keating, J. L. (2009). Stigma experienced by people with nonspecific chronic low back pain: A qualitative study. Pain Medicine, 10(1), 143–154.1 https://doi.org/10.1111/j.15264637.2008.00540.x
Van Alboom, M., De Ruddere, L., Kindt, S., Loeys, T., Van Ryckeghem, D., Bracke, P., Mittinty, M., Goubert, L. (2021) Well-being and Perceived Stigma in Individuals With Rheumatoid Arthritis and Fibromyalgia: A Daily Diary Study. The Clinical Journal of Pain 37(5):p 349-358 https://doi.org/10.1097/ AJP.0000000000000929
though understandable, reduces opportunities for validation and increases isolation. Over time, it contributes to a shrinking sense of identity and unmet emotional needs.
When pain is invisible, language and empathy matter. The strategies below can enhance clinical validation:
6. Breaking the Cycle: Interdisciplinary Pain Care
5. Breaking the Cycle:
References
Validation
Bean, D. J., Johnson, M. H., Kydd, R. R., & Dean, S. (2022). The determinants and effects of chronic pain stigma: A review and conceptual model. Pain Reports, 7(1), e967. https://doi.org/10.1097/ PR9.0000000000000967
Verghese, A. (2009). “Cutting for Stone”. Knopf.
Vowles, K. E., & Thompson, M. (2011). The patient-provider relationship in chronic pain. Current Pain and Headache Reports, 15(2), 133–138. https://doi.org/10.1007/s11916-0100170-3
The Mater Hospital’s eightweek interdisciplinary programme involves psychology, physiotherapy, and nursing. Patients describe the impact of this stating; “I especially felt listened to,”, “Helping us to understand pain and move on,”, “Everyone had a voice.”
De Ruddere, L., & Craig, K. D. (2016). Understanding stigma and chronic pain: A state-of-the-art review. Pain, 157(8), 1607–1610. https://doi. org/10.1097/j.pain.0000000000000512
Hickling, L. M., Allani, M., Cella, M., & Scott, W. (2024). The relationship
Wallace, C., et al. (2021). "I wasn’t listened to or believed": A qualitative analysis of experiences of chronic pain stigma in healthcare. International Journal for Equity in Health, 20, Article 72. https://doi.org/10.1186/s12939021-01416-y
In Abraham Verghese’s Cutting for Stone, a surgeon asks: “Tell us, please, what treatment in an emergency is administered by ear?” The answer “words of comfort” reminds us that compassionate presence is a powerful intervention.
When pain is invisible, language and empathy matter. The following strategies can enhance clinical validation:
Strategy Application
Acknowledge the reality of pain
Listen without rushing to fix
Validate emotional responses
Choose language carefully
Recognise coping effort
Offer hope through partnership
Accept pain as described by the patient. Trust their account.
Prioritise understanding before advising.
Normalise fear, frustration, shame, or anger.
Avoid stigmatising phrases like “medically unexplained” or “non-compliant.” Clinical notes shape future care.
Acknowledge the unseen work patients do to function day to day.
Encourage autonomy and shared decision-making.
6. Breaking the Cycle: Interdisciplinary Pain Care
NEW BREAST HEALTH PROGRAMME FOR FÓRSA MEMBERS LAUNCHES NATIONWIDE
Cornmarket Group Financial Services Ltd., in partnership with Fórsa and Breast Cancer Ireland, this week officially launched a twoyear breast health awareness and education programme at Fórsa HQ, Nerney’s Court, Dublin.
The programme, which began on a trial basis in July 2025, will now be rolled out to Fórsa workplaces nationwide in a phased regional approach. Delivered by Breast Cancer Ireland’s Outreach Coordinator and breast cancer survivor, Juliette O’Connell, the initiative will provide 88,000 Fórsa members with complimentary practical, engaging presentations on breast health, and the importance of early detection, along with information on the 8 signs and symptoms of breast cancer to be aware of.
Juliette, herself a breast cancer survivor, with lived experience of the disease, will travel to Fórsa workplaces across Ireland in a distinctive pink Breast Cancer Ireland branded car to deliver these education and awareness sessions in person, whilst Fórsa members can also access presentations online. Sessions can be arranged at any time during the working day, making the programme as accessible, as possible, to all programme participants.
This initiative is being delivered to Fórsa members in partnership with Cornmarket Group Financial Services Ltd., and their longstanding partner Breast Cancer Ireland, making vital health education available directly to union members.
Clodagh Ruddy, Cornmarket Group Financial Services Ltd, Aisling Hurley, CEO of Breast Cancer Ireland and Julie Flood, Fórsa Senior Vice President
Clodagh Ruddy, speaking on behalf of Cornmarket Group Financial Services Ltd., said at the launch “Early detection of breast cancer can save lives and the programme’s main focus is about driving awareness. The effect of this programme in the short and longer term will be hugely significant and has the potential to really make a difference to the lives of Fórsa members and their colleagues. Cornmarket is proud to partner with Breast Cancer Ireland and Forsa on this important new initiative, and to build on our existing relationship with Ireland’s leading breast cancer charity”
Aisling Hurley, CEO of Breast Cancer Ireland, added:
“We’re delighted to partner with Cornmarket Group Financial Services and Fórsa to extend the reach of our breast health awareness programme nationwide. We are ever so grateful for this support of the work that we do. Juliette’s personal experience and expertise help bring the importance of early detection to life, empowering people with the knowledge to take action. Together, we can improve survival rates and support research that changes outcomes for future generations – and indeed become the generation that ends breast cancer once and for all”
Julie Flood, Fórsa Senior Vice President added “We at Fórsa are delighted and proud to launch our breast cancer awareness campaign in conjunction with Breast Cancer Ireland and Cornmarket. Raising awareness in workplaces is an extremely important step in assisting early detection and in turn, saving lives. Our campaign will educate our members about risk factors and symptoms, encourage selfexamination, promote regular screenings and help to dispel myths about breast cancer. Breast cancer is the second most common factor affecting women.
Statistics show one in seven women in Ireland will be diagnosed with breast cancer in their lifetime.” Fórsa members who wish to arrange a presentation in their workplace can do so by emailing forsa@bciresearch.ie
HIQA PUBLISHES REVIEW ON THE DESIGN AND DELIVERY OF URGENT AND EMERGENCY HEALTHCARE SERVICES IN HSE MID WEST
The Health Information and Quality Authority (HIQA) has published its independent Review to inform decision-making on the design and delivery of urgent and emergency healthcare services in HSE Mid West.
Commenting on the publication of the Review, HIQA’s Director of Healthcare Regulation, Sean Egan, said: “This Review was prompted by significant concerns for patient safety in HSE Mid West, which have remained the utmost priority informing the advice provided to the Minister for Health. This Review was delivered with the support of a number of organisations and individuals, including patients and their families, whom HIQA wishes to thank for their contributions.”
Dr Máirín Ryan, Director of Health Technology Assessment and Deputy CEO at HIQA said: “HIQA also wishes to acknowledge the significant work undertaken by the Economic and Social Research Institute (ESRI) at the request of the Department of Health in relation to future bed requirements for the Mid West, which informed HIQA’s advice.”
Dr Ryan continued: “HIQA found that the core issue impacting urgent and emergency healthcare delivery in HSE Mid West is the significant inpatient bed capacity deficit relative to demand from patients presenting with more serious or complex care needs. This is intensified by an evergrowing demand for services, which will continue into the future as highlighted by the ESRI projections for the period up to 2040. The current situation caused by the demand-capacity gap at University Hospital Limerick (UHL) and across HSE Mid West, presents a risk to patient safety.”
HIQA’s advice highlighted an immediate need for action and investment to address current risks to patient safety in the shortest timeframe and safest way possible. The solution must also have regard for the ESRI projected capacity requirements to 2040.
HIQA has presented the Minister for Health with three options for how this might be achieved. These include the expansion of capacity at UHL on the Dooradoyle site
(Option A); the extension of the UHL hospital campus to include a second site in close proximity under a shared governance and resourcing model (Option B); and the development of a Model 3 hospital in HSE Mid West, providing a second emergency department (ED) for the region (Option C).
HIQA is of the view that Options A or B will likely yield the required inpatient capacity in the Mid West within a shorter timeframe, thereby addressing the immediate risk to patient safety. Option C may have the potential to meet longer-term bed requirements, but would be least capable of addressing immediate capacity deficits, while being associated with the longest lead times. Given that the ESRI projections span a wide range in terms of additional beds required, it will be important to ensure that decisions made around the future design and delivery of urgent and emergency healthcare services enable flexibility in how services are planned and developed. It is essential that there is ongoing monitoring of actual demand for services relative to the ESRI capacity projections, to support timely decision-making.
HIQA’s Director of Healthcare Regulation, Sean Egan, continued: “In working to progress any of these options, HIQA recommends the development of a comprehensive strategic plan. This should remain focused on addressing the safety concerns which prompted this Review, while having regard to the future demographic and policy considerations. Ongoing communication and engagement with the people of the Mid West will also be crucial to its delivery.”
HIV IRELAND CALLS ON GOVERNMENT TO PUBLISH A NATIONAL ACTION PLAN TO END NEW TRANSMISSIONS OF HIV BY 2030
HIV Ireland is urging the Government to honour its Programme for Government pledge to publish a National HIV Action Plan, warning that without clear timelines and accountability, Ireland risks falling short of its goal to end new HIV transmissions by 2030. The call comes ahead of the HIV Ireland and Fast Track Cities UK & Ireland National HIV Conference, Towards a National Action Plan for HIV in Ireland, which takes place today at the Aisling Hotel in Dublin.
HIV Ireland Executive Director Stephen O’Hare said “We have the knowledge and tools to end new HIV transmissions. What we need now is political will and leadership. A National HIV Action Plan, informed by both clinical and community expertise, with
Clinical R&D
specific targets and oversight, is the only way Ireland can meet its UNAIDS commitment to end new transmissions by 2030.”
The landmark conference brings together leading experts from Ireland and the UK including UCD’s Centre for Experimental Pathogen and Host Research led by Infectious disease specialist Prof Patrick Mallon, Sussexbased Irish Clinical Professor and Consultant in HIV Medicine & Sexual Health Prof Yvonne Gilleece and UK Government advisor on HIV and chair of the HIV Action Plan Implementation Group for England Prof Kevin Fenton as well as people living with HIV and advocates. The conference aims to share best practice and effective initiatives on prevention, testing, and combatting HIV related stigma to focus on turning the government’s promise into action.
In June, Ireland published an updated National Sexual Health Strategy 2025-2035. The Strategy commits to developing a HIV Action plan and HIV Model of Care. A similar plan is in place in England, which was published in 2021. Speaking of the success of the National HIV Plans in England, Scotland and Wales Prof Yvonne Gilleece said “The experience across the UK demonstrates how a structured, evidence-based plan can lead to measurable improvements in HIV prevention and treatment outcomes. Developing a similar framework in Ireland is critical if the stated goal of ending new transmissions by 2030 is to be realised.”
Prof Patrick Mallon said “In recent decades, advances in testing, treatment and prevention have substantially changed the trajectory of HIV in Ireland. Of the new cases identified this year, fewer than 200 will constitute new transmissions. Ending new transmissions by 2030 is not insurmountable, but only if we redouble our efforts now.”
Rebecca Tallon de Havilland is an advocate living with HIV. Speaking on the Government’s commitment to better support people living with HIV, she said “When I was first diagnosed, I thought my life would be defined by HIV. Over time, with treatment and the right support, I’ve learned that it doesn’t have to be that way. Living well with HIV is possible and it’s important that the right supports are in place.”
The conference is supported by Gilead Sciences and Viiv (GSK) and represents a milestone moment for HIV advocacy in Ireland and a critical opportunity to ensure the Government fulfils its promise to end new HIV transmissions by 2030.
MICROSOFT DRAGON COPILOT HAS LAUNCHED IN IRELAND
Dragon Copilot brings together the trusted natural language voice dictation capabilities of Dragon Medical One (DMO) with the ambient listening capabilities of Dragon Ambient eXperience (DAX) Copilot, fine-tuned generative AI and healthcare-adapted safeguards. Part of Microsoft for Healthcare, Dragon Copilot is built on a secure modern architecture that enables organisations to deliver enhanced experiences and outcomes across care settings for clinicians and patients alike.
More than 200 clinicians with a wide range of medical disciplines across seven healthcare organisations, in the UK and Ireland, tested Dragon Copilot as part of a private preview programme that involved over 10,000 consultations.
In September, The Department of Finance published a long-term demographic outlook projecting sustained ageing trends over the next four decades. Meanwhile, the HSE’s "Medical Workforce Analysis Report 2024-2025" outlines workforce retention challenges. These national challenges mirror broader European trends; according to the OECD’s “Health at a Glance: Europe 2024 – State of Health in the EU Cycle” the EU faces a health workforce deficit that stems from an ageing population, impacting both patients and the health workforce, as well as difficult working conditions that are contributing to staff burnout and retention challenges. The report notes that technologies, such as AI, will be essential to augment the health workforce’s productivity and ability to focus more on patient care.
Recognising the pressing challenges facing Ireland’s healthcare—including an ageing population, workforce shortages, and persistent waiting lists— “Dragon Copilot is helping to reshape how clinicians manage time-consuming administrative tasks, such as documentation, referrals, and after-visit summaries, freeing up valuable time for patient care,” said Ciara Perciavalle, Head of Health at Microsoft Ireland. “By streamlining workflows and integrating seamlessly with electronic patient records (EPR), Dragon Copilot not only enhances operational efficiency, but also supports clinician well-being, retention, and patient experiences. As Ireland continues to address growing demand and resource constraints, solutions like Dragon Copilot are vital in building more resilient and compassionate healthcare for the future.”
In a recent Microsoft commissioned report, 40 percent of patients surveyed reported having a consultation where they felt the clinician was too focused on the screen to provide their full attention. With the clinician-patient experience serving as the heart of high-quality care, AI solutions like Dragon Copilot offer practitioners a solution that helps improve human connection by reducing administrative tasks and facilitating more personalised care with enhanced data-driven insights.
Dr Peter-Marc Fortune, Paediatric Intensive Care Physician and Chief Medical Information Officer at the Manchester University NHS Foundation Trust, agrees that clinical AI assistants like Dragon Copilot “should reduce the burden of ensuring that [clinicians are] capturing everything, so they can actually focus on the interaction with the patient. [Consultations now feel more] face-to-face… like would have happened in the GP surgery 20 years ago, before everybody had PCs on their desk. The most important thing is to develop a relationship with a patient.”
STRIKING PORTRAIT BASED ON EXTENSIVE IRISH RESEARCH, REVEALS THE LIVED EXPERIENCE OF CHRONIC SPONTANEOUS URTICARIA
A unique piece of art, developed through a partnership with an Irish researcher and artist, was created to increase awareness and understanding of Chronic Spontaneous Urticaria (CSU), a debilitating chronic autoimmune condition. The portrait, "A Shared Canvas: The Untold Stories of Urticaria", will be on display at the Royal College of Physicians today. CSU, characterised by spontaneous hives, uncontrolled
itching and unpredictable episodes of disfiguring swelling of the skin can significantly impact the quality of life of those affected, causing physical discomfort and emotional distress.1 It is estimated that 1 in 100 people in Ireland suffer from chronic spontaneous urticaria.2,3 For the majority of these, they can be treated with over-the-counter antihistamines if diagnosed correctly. However, even with antihistamine treatment, the literature indicates that up to 9000 patients in Ireland could have uncontrolled symptoms.4
At the heart of the event in the RCPI is the unveiling of a striking portrait by artist Valentina Vittorio. This isn't just any painting; it is a co-designed artwork, deeply informed by extensive Irish patient research conducted by PhD student Jennifer Donnelly from the RCSI. The research, based on in-depth patient interviews, uncovered the often-invisible psychosocial and emotional burdens of living with uncontrolled flares of hives, including profound loneliness, isolation, a devastating loss of identity, burning sensations and relentless sleep deprivation.
"Chronic Spontaneous Urticaria is a condition under recognised in public discourse. Our research over the past few years has highlighted the raw, often hidden, emotional toll including the loneliness, the isolation, the burning sensation that goes beyond the skin" said Jennifer Donnelly, PhD student, RCSI. "I had so many text documents of quotes and interviews, but it was Artist Valentina Vittorio who took on the task of translating these perspectives into her artwork.”
“Turning the different experiences of individuals living with CSU into a visual form was really moving and challenging " Artist Valentina Vittorio explained. "The feedback from the patients was that I should focus on the themes of loneliness, isolation and that intense burning sensation. These were challenging to put into art, but it helped to have this input and direction. I aimed to create one portrait to represent all the different emotions and experiences. I hope it helps others better understand the unseen side of this condition."
Speaking about the symptoms, Professor Niall Conlon, Consultant Clinical Immunologist, St James’s Hospital and Senior Clinical Lecturer, Trinity College Dublin, said: "The uncontrolled itch from CSU substantially impacts quality of life, disrupting sleep and interrupting daily activities. This condition disrupts relationships, sleep, work, school and mental wellbeing. Around the world, patients often feel unable to
Ciara Perciavalle, Head of Health at Microsoft Ireland
participate fully in society due to the unpredictability and discomfort of urticaria. It is not only a medical issue but a significant barrier to living a full and confident life. The global burden of this disease must be recognised and addressed with urgency.”
Agron Hasani, Country Head of Medical Affairs and Chief Medical Officer at Novartis Ireland said: "At Novartis, our purpose is to reimagine medicine to improve and extend people's lives. Raising awareness of this research ‘A Shared Canvas: The Untold Stories of Urticaria' underscores our commitment to the CSU community. It is important to work alongside health care practitioners and patient advocates to address the unmet needs and ultimately improve the lives of those affected by this challenging condition."
Ireland is home to a designated UCARE Centre at St James’s Hospital in Dublin, focused on improving management and research for urticaria patients.
#ChronicSpontaneousUrticaria
#UDAYYourJourney
#UnmetNeedInHives #UDAY2025
#CSU
CHANELLE PHARMA ANNOUNCES THREE STRATEGIC APPOINTMENTS TO BOARD OF DIRECTORS
Chanelle Pharma (“Chanelle”), Ireland’s largest indigenous pharmaceutical company and a leading manufacturer of generic pharmaceuticals for human and animal health, today announced the appointment of Steven Mahoney, Rafik Amrane, and Jean Hoffman to its Board of Directors, effective immediately.
Steven, Rafik, and Jean will bring decades of global leadership experience across healthcare, manufacturing, and entrepreneurship, further strengthening Chanelle’s governance framework and supporting the company’s ambitious growth in both veterinary and human health markets.
Carsten Hellmann, Chair of the Board at Chanelle Pharma, said: “Steven, Rafik, and Jean each bring unique perspectives and decades of global leadership, especially in the Animal Health space. Their broad international experience will deepen the Board’s strategic insight and strengthen
A unique piece of art, developed through a partnership with an Irish researcher and artist, was created to increase awareness and understanding of Chronic Spontaneous Urticaria (CSU), a debilitating chronic autoimmune condition. The portrait, "A Shared Canvas: The Untold Stories of Urticaria", will be on display at the Royal College of Physicians today. Pictured were Susanne O'Reilly Head Communications & Patient Advocacy , researcher Jennifer Donnelly, PhD Scholar at the RCSI with artist Valentina Vittorio, Lisa Bashorum, Senior Patient Advocacy Manager and Prof Niall Conlon, Consultant immunologist St James's Hospital. Picture Jason Clarke
our ability to building a strong Chanelle platform.”
Angelo Gatto, CEO and Board Member of Chanelle Pharma, added: “The addition of these distinguished professionals brings to Chanelle world-class expertise that will help us scale faster, innovate smarter, and deepen our impact across global markets. Their vast knowledge and experience will be instrumental as we continue our growth journey.”
Steven Mahoney is a seasoned healthcare executive with 35 years’ experience. He spent most of his career at Merial where he held key leadership roles across Asia Pacific, the U.S. and Latin
America focusing on regional strategy, commercial operations, and integration. His expertise in managing complex global teams and driving growth in regulated markets aligns directly with Chanelle’s international ambitions.
Rafik Amrane currently leads Global Operations at Opella, a 5 Billion Euro turnover HealthCare company, overseeing Manufacturing, Supply Chain and Quality across 13 manufacturing sites, 140 CMOs and more than 5,000 professionals worldwide. His background includes transformational leadership roles at Toyota, Merial and Sanofi, bringing deep operational insight and a strong track record in driving manufacturing excellence and supply chain innovation. Rafik has also led large scale performance transformation in various industries at McKinsey & Co.
Jean Hoffman is an accomplished entrepreneur and board director who has successfully built and exited two healthcare companies, including Putney Inc., a leading U.S. generic veterinary pharmaceutical firm acquired for $200 million. Jean’s expertise spans portfolio strategy, commercial growth and governance, providing Chanelle with valuable experience in scaling high-growth businesses.
ST PATRICK’S MENTAL HEALTH SERVICES MARKS 20 YEARS OF SERVICE USER ADVOCACY THIS WORLD MENTAL HEALTH DAY
This World Mental Health Day, St Patrick’s Mental Health Services is celebrating 20 years of structured service user engagement via its Service Users and Supporters (SUAS) Council, with a campaign focused on one clear message:
Steven Mahoney, Rafik Amrane, and Jean Hoffman
Clinical R&D
Lived experiences must be central to the design and delivery of mental healthcare services.
Established in 2005 as the Patient and Carers Council, today’s Service User and Supporters Council has always been led by the voices of people with lived experience. Its members, all experts by experience, advocate on behalf of service users to shape and improve the care provided at St Patrick’s Mental Health Services. SUAS now stands as a cornerstone of the organisation’s commitment to involving service users in the planning, management and evaluation of their treatment and support.
With over 30 members contributing their time and expertise over the last 20 years, SUAS Council members have:
• Provided invaluable insights into clinical care and evidence-based research
• Championed the voices of fellow service users
• Helped raise awareness about mental health at a national level.
Speaking about the crucial role of service user engagement, Paul Gilligan, CEO, St Patrick’s Mental Health Services said: “This year, as we celebrate 20 years of structured service user involvement at St Patrick’s Mental Health Services, we recognise and commend the invaluable role that SUAS has in shaping and improving services. The commitment and insight of our Council members has not only influenced how we deliver care here in St Patrick’s, but has also helped to challenge stigma, inform national policy and drive meaningful change.
The work of SUAS is a powerful reminder of the importance of lived experience in building services that are effective and grounded in human rights. As we look ahead, we do so with renewed determination to deepen this impact and ensure the voices of service users continues to guide everything we do.”
At an event to celebrate the 20th anniversary of SUAS, and in the lead up to World Mental Health Day 2025, current and former Council members, staff, supporters and partners of St Patrick’s Mental Health Services came together to reflect on 20 years of SUAS’ impact and its key achievements, such as:
• Improving care experiences:
- From playing a key role in redesigning the inpatient admission process to introducing peer-led hospital tours and talks, SUAS has consistently worked
to ensure service users feel supported from the very first point of contact.
• Shaping staff learning and support:
- Initiatives such as the Caring with Respect eLearning module and the Carers and Supporters Information Guide have helped staff and families better understand and respond to service users’ perspectives and needs.
• Driving innovation in digital health and service development:
- SUAS play a central role in consultations on new digital initiatives at St Patrick’s, including the launch of the eSwift electronic health record and Ireland’s first online service user portal, Your Portal.
• Influencing policy and challenging stigma nationally
- The Council has contributed to policy reform, including collaborating with Amnesty International on capacity legislation; providing input to St Patrick’s advocacy submissions process; engaging in national campaigns and media interviews; and earning recognition from the Mental Health Commission for its impact on service quality.
Speaking at the 20th anniversary event, Chris Miley, Chair of the Service User and Supporters Council at St Patrick’s Mental Health Services, said: “Involving those with lived experiences in the development and delivery of mental health services is key to providing care and treatment that is effective, responsive and person-centred.
As experts by experience, our perspectives and insights are crucial to informing approaches to care that truly respond to the needs and rights of service users. I have been proud to work alongside my peers on SUAS over the last several years to advance meaningful participation, and I look forward to what the future will bring as we continue to champion the service user voice and advocate for positive change across the mental healthcare system.”
Since SUAS was launched 20 years ago, St Patrick’s has continued to expand opportunities for service user involvement. Today, service users contribute through the Service User Advisory Network, which now has more than 100 members getting involved in a range of service improvement initiatives and strategic projects; the Family Carers and Supporters Network; the Remote Care Advisory Forum, which shapes
digital health initiatives and improves remote access to care; and the Academic Institute Steering Committee, where service users guide research priorities.
HPRA HEALTH WARNING
An ongoing investigation by the Health Products Regulatory Authority (HPRA) and Revenue’s Customs Service has identified a small consignment of counterfeit tirzepatide injection pens that have been found to contain insulin and could pose a serious health risk for consumers. The HPRA is advising members of the public to only source prescription medicines from a registered pharmacy using a valid prescription to ensure they are accessing legitimate authorised medicinal products. The consignment detained, which included falsified pens, was sourced online and originated from outside Europe. Laboratory tests confirm that two of the pens contain insulin instead of tirzepatide, posing a serious risk to unsuspecting users due to the possible onset of severe hypoglycaemia upon administration.
Tirzepatide is a manufactured peptide designed to help manage type 2 diabetes and support weight loss. The counterfeit products appear similar to the authorised form of tirzepatide, branded as Mounjaro®
Hypoglycaemia occurs when blood sugar levels, also called blood glucose levels, drop too low. It must be treated quickly to stop it getting worse. Symptoms of low blood sugar can include feeling hungry, feeling dizzy, sweating, shaking, heart palpitations, changes in vision and feeling confused. More severe symptoms include extreme drowsiness, seizures and loss of consciousness. If left untreated, severe low blood sugar can be life-threatening.
The HPRA advises anyone who suspects they may have used any falsified tirzepatide or other GLP-1 type product, and who are experiencing symptoms of hypoglycaemia, to seek medical attention immediately.
The HPRA confirms that, to date, no reports of harm have been received in connection with this issue, nor is there evidence that these particular counterfeit products have reached end users. It continues to work closely with Revenue’s Customs Service, whose decisive action in this case successfully intercepted the falsified pens and prevented their entry into the country via the postal system.
As recently as September, the HPRA confirmed that it detained almost 400,000 units of illegal medicines in first half of 2025. It reminds the public that purchasing prescription medicines from unregulated sources means you can't be sure what you're getting. These products may be unsafe, ineffective, or fake – and could seriously harm your health.
ST JOHN OF GOD RESEARCH FOUNDATION OPENS
DEDICATED PSYCHOSIS RESEARCH CENTRE
The St John of God Research Foundation (SJOG Research) announces the opening this week of a new Centre dedicated specifically to Psychosis Research. The newly established St John of God Psychosis Research Centre builds on the organisation’s respected heritage of supporting those with mental ill health.
With up to 45,000 people affected by psychosis at any one time in Ireland, the SJOG Psychosis Research Centre will aim to harness research activity and coordinate efforts across all of St John of God (SJOG) group and to offer the opportunity to strengthen collaborations nationally with other leading specialists in the area. The research outputs will inform the delivery of psychosis treatment across all relevant SJOG services and support its policies and advocacy programmes to develop improved mental health services.
A key initiative of the SJOG Psychosis Research Centre will be Patient and Public Involvement (PPI) meaning people with lived experience will be actively involved in the planning, conducting, and sharing of research findings. Conor Gavin, who has been recruited as the Psychosis Research Centre Co-Ordinator has himself lived experience in this area and is looking forward to bringing it to bear in the development of the Centre.
“As a person with my own lived experience of psychosis, I am thrilled to be a part of this new initiative in St John of God. It’s inspiring to see the work that has been done over the last number of decades to strive for better outcomes in this area of mental health. My motivation always stems from my own personal experience, and I often ask: ‘What would have worked for me?’ when I approach research questions. I am hugely excited to work with St John of God Research Foundation, researchers and clinicians alongside others with lived experience to help bring this project to fruition.”
SJOG has provided services in Ireland for those with mental
has informed international services and policies.
Professor Mary Clarke, Consultant Psychiatrist , St John of God DETECT Service said:
ill-health for nearly 150 years and research began over 40 years ago. The SJOG Research was incorporated in 2011 to solidify SJOG commitment to research.
Dr Lesley O’Hara, CEO SJOG Research said,
We are incredibly proud to support the establishment of the St John of God Psychosis Research Centre. Our organisation has a long-standing reputation as leaders in this field of research, and we welcome the opportunity to extend our expertise to include research across the life span, and with disability and minority groups. A central focus of the new Centre is the person with psychosis, and their family. They will have the opportunity to shape the strategy, ensuring the research conducted is truly reflective of what is important to the people we support.
Collaboration has always been a key part of SJOG with many international researchers in psychosis spending time training in St John of God in Ireland.
The SJOG Early Intervention in Psychosis (EIP) Service known as ‘DETECT’ was founded in 2005 and was the first of its kind in Ireland. It has continued to provide opportunities for building alliances across the globe and it
The St John of God Psychosis Research Centre builds on a strong legacy of clinical research in psychosis, grounded in the collaboration of clinicians, researchers, and the lived experience of individuals with psychosis and their families. We are excited by the opportunity to bring diverse areas of expertise together and to learn from one another, fostering a culture of shared purpose, curiosity and respect, in pursuit of better outcomes for individuals with psychosis. We are committed to translating research into better care, from early detection and intervention to long-term recovery.
The research evidencing and acting on early intervention programmes and initiatives is a step in better care for people.
In addition, the SJOG Psychosis Research Centre will provide research training, with a focus on supporting people to be leaders in this field. It goes further to support the full health service development and improvement cycle for psychosis, from research to policy and from implementation to evaluation.
Uniquely, the SJOG group of companies delivers services but also funds and carries out research on mental ill-health, implements its research findings into policy and practice, and builds clinical services based on the evidence.
impression made by their team further solidified our confidence in this partnership. It seems we are a natural fit in both values and working style.”
For over 30 years, OxygenCare has been transforming digital healthcare through clinical systems and working with innovative products and solutions throughout Ireland. The Medanets integrated nursing app supports point-of-care documentation and immediate access to key patient data, making it a natural fit with OxygenCare’s digital portfolio.
Combining OxygenCare’s connectivity solutions with Medanets' mobile solutions can provide significant added value both to organisations already using an electronic health record (EHR) and to hospitals beginning their digital journey.
OXYGENCARE EXPANDS DIGITAL HEALTHCARE OFFERING WITH MEDANETS
OxygenCare is delighted to announce the introduction of the Medanets integrated Point of Care Nursing app to its ever-expanding Digital Healthcare solutions portfolio. The collaboration brings together two companies with a shared vision for improving patient care through innovative digital healthcare solutions.
Stephen Nicholson, Digital Health Manager, OxygenCare, explains: “Medanets simplifies nursing routines, supports decision making, complements and integrates with EHR systems, and releases time to care for patients.’
The CE and MDR certified app was developed in collaboration with healthcare professionals.
OxygenCare is a multi-awardwinning, family-owned business with over 50 years supporting healthcare throughout the island of Ireland.
“Their dedicated digital health team and prior experience in delivering complex ICU and anaesthesia systems make them an ideal partner for us,” says Medanets CEO Juha-Matti Ranta. “On top of that, their deep market knowledge and the
“We can offer healthcare providers a fast-track way to modernise operations, even in settings where an EHR is not yet in place. For instance, Medanets supports "lightweight IT" approaches such as sending PDFs directly to a document archive—a direct impactful step forward in digital empowerment,” Ranta explains. Maurice Moran, Managing Director of OxygenCare, adds: “This Medanets offering complements our portfolio, and we see strong market potential. Together, we are currently conducting exploratory efforts in the market to identify opportunities and tailor our approach to local needs. Through this new partnership, all care phases can be managed digitally through a single provider. This partnership marks a promising step toward improving healthcare outcomes in Ireland and underscores the strength of collaboration in driving innovation forward."
Conor Gavin, Psychosis Research Centre Co-Ordinator, Professor Mary Clarke, Consultant Psychiatrist, SJOG DETECT,Lesley O’Hara, CEO SJOG Research Foundation.
Photo: Aidan Oliver
Pictured left to right: Stephen Nicholson, Digital Health Manager, OxygenCare; and Maurice Moran, Managing Director, OxygenCare