Ticagrelor Teva co-administered with acetylsalicylic acid (ASA), is indicated for the prevention of atherothrombotic events in adult patients with acute coronary syndromes (ACS) or a history of myocardial infarction (MI) and a high risk of developing an atherothrombotic event
unless specifically contraindicated. Adults: ACS: Should be initiated with a single 180mg loading dose (two tablets of 90mg) and then continued at 90mg twice daily. Treatment with Ticagrelor Teva 90mg twice daily is recommended for 12 months in ACS patients unless discontinuation is clinically indicated. Adults: History of MI: 60mg twice daily is the recommended dose when an extended treatment is required for patients with a history of MI of at least one year and a high risk of an atherothrombotic event. Treatment may be started without interruption as continuation therapy after the initial one-year treatment with Ticagrelor Teva 90mg or other adenosine diphosphate (ADP) receptor inhibitor therapy in ACS patients with a high risk of an atherothrombotic event. Treatment can also be initiated up to 2 years from the MI, or within one year after stopping previous ADP receptor inhibitor treatment. Children: Not suitable for use in patients under 18 years of age. Elderly: No dose adjustment is required. Renal impairment: No dose adjustment is necessary. In patients with ACS, it is recommended that renal function is also checked one month after initiating the treatment with ticagrelor, paying special attention to patients ≥75 years, patients with moderate/severe renal impairment and those receiving concomitant treatment with an angiotensin receptor blocker (ARB). Hepatic impairment: No dose adjustment is necessary for patients with mild hepatic impairment. No dose adjustment is not recommended for moderate hepatic impairment, but ticagrelor should be used with caution. Ticagrelor has not been studied in patients with severe hepatic impairment and its use in these patients is contraindicated. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Active pathological bleeding. History of intracranial haemorrhage. Severe hepatic impairment. Co-administration of ticagrelor with strong CYP3A4 inhibitors (e.g. ketoconazole, clarithromycin, nefazodone, ritonavir and atazanavir), as co-administration may lead to a substantial increase in exposure to ticagrelor. Precautions and warnings: The use of ticagrelor in patients at known increased risk for bleeding should be balanced against the benefit in terms of prevention of atherothrombotic events. Ticagrelor should be used with caution in the following patient groups: Patients with a propensity to bleed (e.g. due to recent trauma, recent surgery, coagulation disorders, active or recent gastrointestinal bleeding) or who are at increased risk of trauma. Patients with concomitant administration of medicinal products that may increase the risk of bleeding (e.g. non-steroidal anti-inflammatory drugs (NSAIDs), oral anticoagulants and/or fibrinolytics) within 24 hours of ticagrelor dosing. Patients should be advised to inform physicians and dentists that they are taking ticagrelor before any surgery is scheduled and before any new medicinal product is taken. If a patient is to undergo elective surgery and antiplatelet effect is not desired, ticagrelor should be discontinued 5 days prior to surgery. ACS patients with prior ischaemic stroke can be treated with ticagrelor for up to 12 months. Patients with an increased risk of bradycardic events (e.g. patients without a pacemaker who have sick sinus syndrome, 2nd or 3rd degree AV block or bradycardic-related syncope) have been excluded from the main studies evaluating the safety and efficacy of ticagrelor. Therefore, due to the limited clinical experience, ticagrelor should be used with caution in these patients. Caution should be exercised when administering ticagrelor concomitantly with medicinal products known to induce bradycardia. Bradyarrhythmic events and AV blocks have been reported in the post-marketing setting in patients taking ticagrelor, primarily in patients with ACS, where cardiac ischemia and concomitant drugs reducing the heart rate or affecting cardiac conduction are potential confounders. Dyspnoea was reported in patients treated with ticagrelor. Dyspnoea is usually mild to moderate in intensity and often resolves without need for treatment discontinuation. Central sleep apnoea including Cheyne-Stokes respiration has been reported in the post-marketing setting in patients taking ticagrelor. If central sleep apnoea is suspected, further clinical assessment should be considered. Hyperuricaemia may occur during treatment with ticagrelor. Caution is advised in patients with history of hyperuricaemia or gouty arthritis. As a precautionary measure, the use of ticagrelor in patients with uric acid nephropathy is discouraged. Thrombotic Thrombocytopenic Purpura (TTP) has been reported very rarely with the use of ticagrelor. It is characterised by thrombocytopenia and microangiopathic haemolytic anaemia associated with either neurological findings, renal dysfunction or fever. TTP is a potentially fatal condition requiring prompt treatment including plasmapheresis. Co-administration of ticagrelor and high maintenance dose ASA (>300mg) is not recommended. Premature discontinuation of treatment should be avoided, as this could
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland. Freephone: 1800 - 201 700 | Email: info@teva.ie
result in an increased risk of cardiovascular (CV) death MI or stroke due to the patient’s underlying disease. Interactions: Strong CYP3A4 inhibitors (e.g. ketoconazole, clarithromycin, nefazodone, ritonavir and atazanavir) are known to reduce the Cmax and AUC of the active metabolite of ticagrelor, therefore, their concomitant use is contraindicated. Moderate CYP3A4 inhibitors (e.g. amprenavir, aprepitant, erythromycin and fluconazole) can be co-administered with ticagrelor. A 2-fold increase of ticagrelor exposure was observed after daily consumption of large quantities of grapefruit juice. CYP3A inducers (e.g. phenytoin, carbamazepine and phenobarbital) would be expected to decrease the exposure to ticagrelor. Coadministration of ticagrelor with potent CYP3A inducers may decrease exposure and efficacy of ticagrelor, therefore, their concomitant use with ticagrelor is discouraged. Co-administration of cyclosporine with ticagrelor increased ticagrelor Cmax and AUC. No data are available on concomitant use of ticagrelor with other active substances that also are potent P-gp inhibitors and moderate CYP3A4 inhibitors (e.g. verapamil, quinidine) that also may increase ticagrelor exposure. If the association cannot be avoided, their concomitant use should be made with caution. Co-administration of ticagrelor with heparin, enoxaparin and ASA or desmopressin did not have any effect on the pharmacokinetics of ticagrelor or the active metabolite or on ADP-induced platelet aggregation compared with ticagrelor alone. Co-administration of ticagrelor with simvastatin increased simvastatin C and AUC. Ticagrelor may have similar effect on lovastatin, therefore, the concomitant use of ticagrelor with doses of simvastatin or lovastatin greater than 40mg is not recommended. Co-administration of ticagrelor with atorvastatin increased atorvastatin Cmax and AUC, but these increases are not considered clinically significant. Ticagrelor is a mild CYP3A4 inhibitor. Co-administration of ticagrelor and CYP3A4 substrates with narrow therapeutic indices (i.e. cisapride or ergot alkaloids) is not recommended, as ticagrelor may increase the exposure to these medicinal products. Appropriate clinical and/or laboratory monitoring is recommended when giving narrow therapeutic index P-gp dependent medicinal products like digoxin concomitantly with ticagrelor. Co-administration of ticagrelor with tolbutamide resulted in no change in the plasma levels of either medicinal product, which suggests that ticagrelor is not a CYP2C9 inhibitor and unlikely to alter the CYP2C9 mediated metabolism of medicinal products like warfarin and tolbutamide. Ticagrelor may affect renal excretion of rosuvastatin, increasing the risk for rosuvastatin accumulation. Co-administration of ticagrelor and levonorgestrel and ethinyl oestradiol increased ethinyl oestradiol exposure approximately 20% but did not alter the pharmacokinetics of levonorgestrel. No clinically relevant effect on oral contraceptive efficacy is expected when levonorgestrel and ethinyl oestradiol are co-administered with ticagrelor. Due to observations of mostly asymptomatic ventricular pauses and bradycardia, caution should be exercised when administering ticagrelor concomitantly with medicinal products known to induce bradycardia. Due to reports of cutaneous bleeding abnormalities with SSRIs (e.g. paroxetine, sertraline and citalopram), caution is advised when administering SSRIs with ticagrelor as this may increase the risk of bleeding. Pregnancy and lactation: Patients of childbearing potential should use appropriate contraceptive measures to avoid pregnancy during ticagrelor therapy. Ticagrelor is not recommended during pregnancy. Regarding lactation, a risk to newborns/infants cannot be excluded. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from ticagrelor therapy taking into account the benefit of breastfeeding for the child and the benefit of therapy for the patient. Effects on ability to drive and use machines: Ticagrelor has no or negligible influence on the ability to drive and use machines. Dizziness and confusion have been reported with treatment, therefore, patients who experience these symptoms should be cautious while driving or using machines. Adverse reactions: Thrombotic thrombocytopenic purpura, hypersensitivity including angioedema, syncope, and haemorrhage (including intracranial, ear, eye, gastrointestinal, retroperitoneal). Very Common: Blood disorder bleedings, hyperuricaemia, and dyspnoea. Common: Gout/gouty arthritis, dizziness, headache, vertigo, hypotension, respiratory system bleedings, diarrhoea, nausea, dyspepsia, constipation, subcutaneous or dermal bleeding, rash, pruritus, urinary tract bleeding, blood creatinine increased, post procedural haemorrhage, and traumatic bleedings. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: In the event of an overdose, any of the above listed adverse reactions could occur, as well as prolonged duration of bleeding risk associated with platelet inhibition. ECG monitoring should be considered. There is currently no known antidote to reverse the effects of ticagrelor, and ticagrelor is not dialysable. Treatment of overdose should follow local standard medical practice. If bleeding occurs other appropriate supportive measures should be taken. Platelet transfusion is unlikely to be of clinical benefit in patients with bleeding. Legal category: POM. Marketing Authorisation Number: PA1986/123/001. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00092. Date of Preparation: May 2025
Product subject to prescription which may be renewed (B) Further information is available on request or in the SmPC. Product Information also available on the HPRA website. Date of Preparation: May 2025 | Job Code: GEN-IE-00139 Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Call for papers: make your contribution to Hospital Professional News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
Contents Foreword
Mutual Stewardship of medicines.ie P4
World Conference on Tobacco Control P6
Major EU Funding for XR Cancer Survivorship Project P7
The Role of the Dairy Matrix in Cholesterol Management P20
¤34m Research Ireland ARC Hub P23
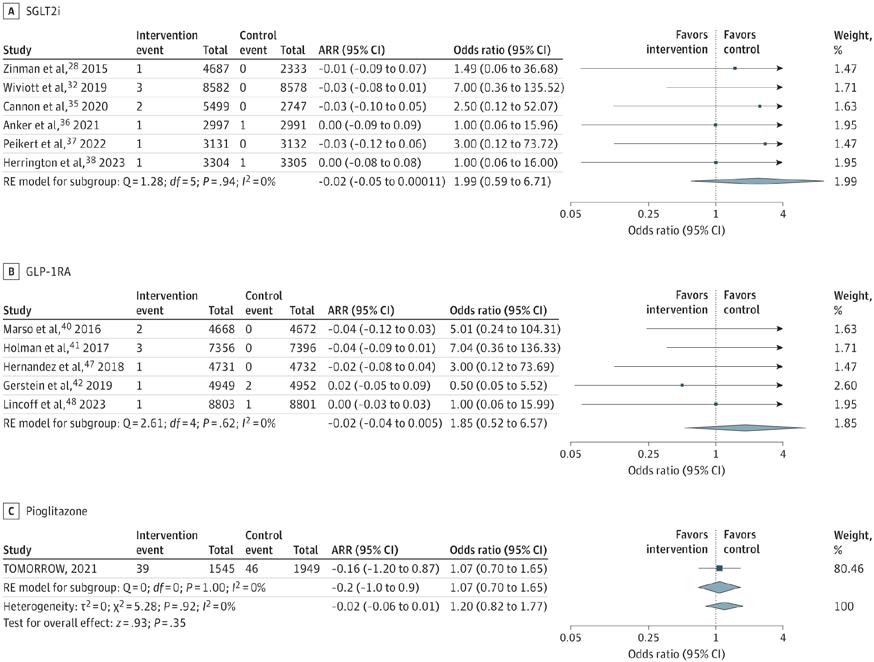
Knowledge is Central: Presentations from ASCO 2025 P34
REGULARS
Feature: Advancements in Diabetes Technology P16
Feature: Cardioprotective Glucose-Lowering Agents and Dementia Risk P24
CPD: Breast Cancer P29
Study: Osteoporosis P40
Clinical PR: P79
Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only.
Editor
In one of our lead news stories this month, the Irish Hospital Consultants Association (IHCA) has said that the slowdown in the growth in the number of approved Consultant post needs to be addressed if the increasing demand for specialist hospital and community care is to be adequately met.
Commenting on the publication of two new reports from the HSE National Doctors Training and Planning (NDTP) unit, the IHCA said that the growth rate in the number of consultant posts was just 4% in 2024, compared with and averaged 8% per annum over the 2020 to 2024 period and 6% per annum since 2015.
Last year saw a considerable drop in the number of new and replacement Consultant posts approved by the HSE’s Consultants Applications Advisory Committee (CAAC) –from 393 posts in 2023 to 287 posts last year, or a decrease of 27%.
Read more about this on page 5.
On page 9, Darren Walsh and Ita Fitzgerald give an overview of the recent Hospital Pharmacists Association of Ireland annual conference. This year’s Hospital Pharmacist Association of Ireland (HPAI) conference was a resounding success from a research perspective. The conference saw over 100 abstract submissions, a range of high quality oral presentations and held the inaugural conference meeting of the Education and Research Specialist Interest Group (SIG).
All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission.
IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
The National Maternity Experience Survey returns for its second cycle this year, providing a vital opportunity to assess the quality of maternity care in Ireland. This nationwide initiative enables women who have recently given birth to share their experiences, ensuring that the voices of mothers are at the heart of future service improvements. A more indepth look at this is provided by Director of the National Care Experience Programme Rachel Flynn on page 19.
Meanwhile, our ‘Ask The Expert’ series contains some thought-provoking articles from healthcare leaders such as Professor Eoin Feeney, Consultant in Infectious Diseases, St. Vincent's University Hospital and Tara Ramsbottom, ID SpR, who highlight advances and challenges in HIV care (page 66); Áine Toher, Deputy Pharmacist Executive Manager at the National Maternity Hospital on Pharmacy Views on VTE (page 68) and Aideen Stack, Health Psychologist who discusses Rheumatoid Arthritis (page 71).
I hope you enjoy the issue.
Mutual Stewardship of medicines.ie
The Irish Pharmaceutical Healthcare Association (IPHA) and cormeo, the newly established German based Pharma Tech holding company under Bertelsmann, announces its Venture in the mutual operation of medicines.ie, Ireland’s trusted information provider of accurate and reliable medicines information. This joint effort is exemplary in combining the knowledge and voice of the pharmaceutical industry, with cormeo’s innovative capabilities, enabling better care for patients in Europe.
medicines.ie, established by IPHA, has earned its reputation as
the reliable source for healthcare professionals and patients by providing comprehensive, upto-date and regulatory-approved information on medicines in Ireland. The platform offers detailed product descriptions, patient information leaflets (PILs), and summaries of product characteristics (SmPCs), serving as an essential tool for informed healthcare decision-making across Ireland.
By partnering with cormeo, medicines.ie strengthens its commitment to delivering trusted, up-to-date medicinal product information to healthcare
Oliver O'Connor, Chief Executive, IPHA
professionals and patients in Ireland. Leveraging cormeo’s proven expertise—demonstrated through platforms like Germany’s Rote Liste—this collaboration enhances the visibility and accessibility of medicines information while preserving the high standards that medicines.ie is known for.
“We are looking forward to working together with the cormeo team”, says Oliver O’Connor, Chief Executive of IPHA. “The partnership will allow us to broaden the medicines.ie offering to pharmaceutical companies and continue the great work we have built to support healthcare professionals in their decision making, ultimately benefiting patients across Ireland”.
“With medicines.ie, we are thrilled to welcome another trusted and
Hospital Pharmacy Educational Event
The European Association of Hospital Pharmacists (EAHP) BOOST event, a two-day educational event will take place in the beautiful city of Prague on 14-15 November 2025.
The event will focus on tackling the global challenge of medicines and medical device shortages, exploring strategies to strengthen supply chains and ensuring continuous patient care.
Shortages not only pose risks to patient care but also have significant economic consequences, including increased healthcare costs, strain on national healthcare budgets, and disruptions to the broader economy, as healthcare providers must adjust their service delivery strategies to manage limited financial and human resources. For more than a decade, EAHP has been working on increasing the awareness of shortages and
the importance of their timely mitigation in order to protect the wellbeing of patients. The first EAHP Survey on shortages was launched back in 2013, initiating similar efforts by other healthcare professional associations and stakeholders. In order to bring everyone together with the single purpose of combating shortages, EAHP presents its 2nd BOOST edition around
this major public health issue, affecting our healthcare systems across Europe. BOOST will bring together experts, regulators, and industry leaders to discuss effective solutions to address the emerging challenge of shortages.
A key feature of this event will be the interactive workshops. These hands-on sessions are designed to engage participants directly in addressing real-world challenges
well-established platform for medicinal product information for healthcare professionals and patients to the cormeo family”, says Peter Koop, CEO of cormeo. “By this investment we underscore our commitment to optimizing the accessibility of compliant and up-to-date medicines information across countries.”
The dedicated team at medicines. ie will continue to drive operations and maintain service excellence, ensuring continuity and stability while driving the expansion of its portfolio. Aligned in purpose, IPHA and cormeo, as partners in that venture will jointly steward the future of medicines.ie as members of the board, offering valuable expertise and insights to guide the company’s strategic direction, while also contributing to various initiatives, driving the company’s innovation and growth.
As part of the cormeo portfolio, medicines.ie is set to play an even greater role in advancing the digital transformation of the life sciences sector in Ireland. This collaboration enhances our ability to support healthcare professionals with accurate, accessible information— empowering better decisionmaking and contributing to improved patient outcomes across Europe.
related to shortages. Participants will work with colleagues and facilitators to simulate the implementation of strategies, explore innovative solutions, and discuss the practical steps you can take to improve shortages management in your own healthcare settings.
Visit www.eahp.eu for further details.
Welcome for Latest Capacity Report
The Irish Hospital Consultants Association (IHCA) has welcomed the publication of the new report from the Economic and Social Research Institute (ESRI), which highlights the pressing need to expand Ireland’s acute public hospital capacity, and said its findings align with the Association’s long-standing concerns regarding the critical shortage of hospital beds.
The IHCA, which said this latest evidence-based analysis reinforces the need for sustained investment in hospital infrastructure, has urged the Government to expedite the implementation of its Acute Hospital Inpatient Bed Capacity Expansion Plan, published in May 2024, which aims to open 3,378 new beds by 2031.
The IHCA has also urged the six HSE Health Regions to publish in-depth regional projections of their acute hospital bed capacity requirements up to 2040, in order to identify where to locate up to 6,800 additional inpatient beds needed to meet future demand for care.
Consultants have also suggested that this regional analysis should identify where this additional hospital capacity can be accommodated on existing hospital campuses, and where new hospital builds may be needed.
While both the Government plan and ESRI report are positive steps in the right direction, Consultants emphasised that timely delivery is crucial, with any delays in expanding bed capacity having
direct consequences on patient care, leading to longer waiting times and increased pressure on our health service.
The IHCA also welcomed today’s ICU Audit Report by the National Office of Clinical Audit, which found that despite a reported ICU bed occupancy rate of 96% being well above the recommended average of 85%, the health system is delivering high quality outcomes for patients.
The Association again called for ICU bed numbers to be increased from the current 330 to the minimum 579, as recommended a decade ago, and to over 900 critical care beds to reach the OECD average on a population basis.
The Association also reiterated its call to expedite the delivery of the
Government urged to Invest in Dementia
The Alzheimer Society of Ireland (The ASI) is calling on the Government to invest ¤9million in dementia supports and services to address major inequity of access across the country.
The ASI is calling on Government to improve equity of access for people living with dementia and family carers through investment in community day care services, dementia-specific home care, counselling for people with dementia and family carers and dementia research.
The recommendations are contained in The ASI’s Pre-Budget Submission 2026; Building on the Potential of the Programme for Government: A stepping stone to a more dementia-inclusive Ireland in Budget 2026 which was launched today at Buswell's Hotel in Dublin. There are 64,000 people with dementia in Ireland, and this is forecast to more than double to 150,000 by 2050. There are 11,000 new cases of dementia in Ireland each year and anyone can get dementia – including people in their 30s/40s/50s.
The ASI’s CEO Andy Heffernan said, “Our Pre-Budget Submission 2026 looks to address the growing need for dementia supports and services. There was a 55% increase in day care at home hours
Action is required to address the workforce challenges in homecare including training, career pathways, recruitment, retention and the structural barriers to reimbursement of travel expenses particularly in rural areas.
from 2023 to 2024 and a 24% increase in Day Care attendances. Our services also recorded a 20% increase in social supports attendances in 2024. Demand continues to outpace this growth, and many core ASI services have growing waiting lists.
promised six surgical hubs, for a positive decision to be made on a seventh surgical hub proposed for the North West in Sligo, and for the four new elective hospitals to progress at speed, in order to meet their target of receiving their first patients in 2027.
Workforce issues must also be addressed in tandem with the delivery of infrastructure, to ensure that new beds translate into improved patient care.
The IHCA supports this evidencebased approach to healthcare planning and urges policymakers to act swiftly on the ERSI report’s findings to ensure Ireland’s hospital system is equipped to meet both current and future patient demand.
“A key service is home care for people living with dementia. Action is required to address the workforce challenges in homecare including training, career pathways, recruitment, retention and the structural barriers to reimbursement of travel expenses particularly in rural areas.
“Investing in dementia-specific day care, both in day centres and at home, will help alleviate pressure on residential care services. These services provide care in the community and can help a significant portion of people who need care, and in a dementiaspecific manner.”
Alzheimer Society of Ireland CEO Andy Heffernan
World Conference on Tobacco Control
As Ireland welcomes the international public health community to the World Conference on Tobacco Control 2025, the Royal College of Physicians of Ireland (RCPI) calls on political leaders to urgently recommit to the nation’s Tobacco Free Ireland goals.
Despite being a pioneer in global tobacco control, Ireland is falling short of its 2025 target to reduce smoking prevalence to below 5%. Today, smoking still claims nearly 100 lives and causes over 1,000 hospitalisations every week across the country.
Dr Paul Kavanagh, Chair of the RCPI Clinical Advisory Group on Smoking and E-Cigarettes, warns that Ireland remains in the grip of a smoking-related health crisis:
“Ireland has led the way with bold tobacco control measures, but we are still deep in an epidemic of harm. The toll of smoking is visible every day in our hospitals and communities. Through our Clinical Advisory Group, doctors are using their voice to provide leadership toward a Tobacco Free Ireland.”
The RCPI Clinical Advisory Group provides expert clinical
Dr Paul Kavanagh, Chair of the RCPI Clinical Advisory Group on Smoking and E-Cigarettes,
guidance to reduce smokingrelated harm and has played a critical role in shaping recent public health policies, including the ban on e-cigarette sales to children and young people and the upcoming Tobacco 21 legislation.
Despite this progress Ireland’s smoking prevalence of 17% falls short of the 5% target, and historic declines in smoking have stalled in the last five years.
As global experts gather in Dublin, Dr Kavanagh sees a critical opportunity. “We welcome the dialogue with international leaders
at this pivotal conference. It’s an important moment for Ireland to show renewed leadership and deliver a new roadmap to achieve a Tobacco Free Ireland for the next generation.”
Dr John Gannon, a member of the RCPI Clinical Advisory Group on Smoking and E-Cigarettes, will present the findings of his recently published study at the World Conference.
Published in the European Journal of Public Health, the global study reveals a growing consensus among young people in support of a tobacco-free society, highlighting a generational momentum toward a tobacco-free future.
“The survey found that young people in Ireland and internationally are strongly supportive of tobacco end-game measures,” Dr Gannon says.
“Measures with strong support among respondents include T21 legislation, restricting tobacco sales to a limited number of licensed shops, reducing nicotine content in cigarettes and accountability for tobacco companies footing the bill for health costs from smoking.”
The Royal College of Physicians of Ireland is committed to working with Government to reduce tobacco-related health dangers and calls on political leaders to reaffirm commitment to deliver a new plan for a Tobacco Free Ireland.
‘Dumbing Down’ of Psychiatric Services having Adverse Effect
The Chair of the Consultants’ Committee of the Irish Medical Organisation (IMO) has warned that the “dumbing down” of psychiatric services is having an adverse effect on patients through increased waiting lists, and poor governance and oversight of services.
Professor Matthew Sadlier, who is also a consultant old age psychiatrist, was speaking at a panel discussion entitled ‘Confronting the Care Deficit for Patients with Severe and Enduring Mental Illness’ at the IMO AGM in Killarney recently.
Professor Sadlier said that the move of psychiatric services from hospital to community settings has resulted in patients not being
able to have adequate monitoring of medications and diagnostic investigations, leading to potentially negative outcomes.
He added that the distributed model of service delivery has led to a significant postcode lottery for access across the country. This model leads to difficulty in governance, with non-consultant hospital doctors (NCHDs) and supervisors working in separate locations, and unnecessary travel leading to significant wastage of time and subsequent productivity.
He said, “Psychiatry is a complex medical specialty, but the HSE treats it as it is a form of applied social care. The move to community psychiatric services
is a logistical mess, with several key stakeholders regularly working in different locations and the availability of accessible services increasingly determined by a patient’s Eircode.”
Professor Sadlier added that there had been a consistent downgrading of the expertise of psychiatry. He said that the Assisted Decision-Making Capacity Act and proposed Mental Health Act attempted to make a false equivalence between different professions.
He added that practitioners from eight different specialties can determine if a patient lacks capacity and subsequently hand
over control of their affairs to another person. These specialties include occupational therapists, registered midwives, registered nurses, social workers and speech and language therapists. He said that many practitioners from these specialties would have neither the requisite training nor expertise to make a decision on a patient’s capacity.
“Neurocognitive assessment is a complex task that requires specialisation to complete adequately. Given that this function can lead to the loss of personal liberty guaranteed by the constitution, not making this a specialist function is mind-boggling.”
Major EU Funding for XR Cancer Survivorship Project
Announced during International Men’s Health Week (June 9th15th), University College Cork has received funding to lead a major new ¤6 million European project that will revolutionise how adolescents and young adults (AYAs) across Europe understand and manage the long-term effects of testicular cancer.
Testicular cancer is the most common cancer in people assigned male at birth aged 15 to 39 years, with incidence rates in Europe doubling over the past 40 years. While survival rates exceed 95%, survivors can face a lifetime of complications - physical, psychological, and social.
TRANSCEND-XR, a 5.5-year project funded by Horizon Europe, will ethically co-create and evaluate a cutting-edge eXtended Reality (XR) experience aimed at improving the quality of life of AYA testicular cancer survivors.
This project marks a radical shift from traditional strategies to an engaging, interactive medium tailored to young people’s digital fluency. Virtual Reality, Augmented Reality & Digital Reality will be considered in this innovative cancer survivorship research project. The TRANSCEND-XR intervention will be tested in a randomised controlled trial involving 230 testicular cancer survivors across Europe, using a digital platform co-designed with survivors, their loved ones, and healthcare professionals.
The initiative brings together 15 partners from 12 countries and 15 disciplines, including clinicians, epidemiologists, XR developers, 3D artists and, crucially, testicular cancer survivors themselves.
A Crisis in Young Men’s Health
"Announcing TRANSCENDXR during Men’s Health Week
underlines our commitment to tackling an overlooked yet deeply impactful men’s health issue," said Dr Mohamad Saab, Senior Lecturer at UCC’s School of Nursing & Midwifery and TRANSCEND-XR Project Coordinator.
"We know that young survivors of testicular cancer often face a heavy burden of late effectsfrom cardiovascular disease to mental health challenges - yet few resources speak directly to their lived experience. TRANSCEND-XR will change that."
TRANSCEND-XR aims to:
• Explore the unmet needs of testicular cancer survivors, their families and healthcare teams;
• Co-create a fully immersive, evidence-based XR educational intervention;
• Evaluate the effectiveness, costefficiency and acceptability of the intervention;
• Translate research into real-world care, policy and education.
Innovation in Cancer Recovery Support
"This project will serve as proof of concept for developing and implementing ethical, immersive educational tools that support cancer survivorship," added Dr Saab.
Governance, patient involvement and long-term sustainability are core to the project’s success, with pathways in place to scale the intervention across health systems.
TRANSCEND-XR builds on Dr Saab’s research at UCC and his prior success using virtual reality to improve awareness of testicular diseases among young men. A prior UCC study found that virtual reality gaming may be effective
Stakeholder Briefing – HSE Update
Dr Mohamad Saab, Senior Lecturer at UCC’s School of Nursing & Midwifery and TRANSCEND-XR Project Coordinator. Image credit Rubén Tapia (UCCTV)
in promoting men’s awareness of testicular diseases and increasing testicular self-examination. Now this UCC-led research project, will take the next step: empowering survivors to reclaim health, knowledge, and agency after cancer.
Professor John F. Cryan, Vice President for Research and Innovation at UCC said: "Congratulations to Dr Mohamad Saab and his UCC project partners on securing this funding that will tackle a critical healthcare challenge in young men. Building
on the success of the HRB-funded E-MAT trial, TRANSCEND-XR exemplifies how interdisciplinary research can drive innovation, and can tackle complex healthcare challenges that will improve the lives of people affected by cancer."
This Horizon Europe funded project will be conducted in 12 European countries over a 5.5-year period, commencing June 2025.
UCC partners in the TRANSCEND-XR team: L-R: Dr Maria O’Malley (School of Nursing & Midwifery), Mr David Murphy (School of Computer Science and IT), Professor Josephine Hegarty (School of Nursing & Midwifery), Dr Mohamad Saab (School of Nursing & Midwifery), Dr Aileen Murphy (Department of Economics), Dr Ann Kirby (Department of Economics), Dr Sheena McHugh (School of Public Health), Professor Jack Gleeson (CUMH and Cancer Research), Professor Francis Shiely (School of Public Health and Clinical Research Facility)
The Pharmaceutical Managers’ Institute September stakeholder breakfast will host Damien McCallion, Chief Technology and Transformation Officer and Deputy CEO of the HSE. Damien will give an update on the HSE’s ongoing transformation which will include the following topics:
o The rollout and development of the new health regions and appointment of the REOs
o Rollout of the new patient app and the plans to extend it’s functionality
o Patient waiting times & how this is being addressed
o Short to medium plans for HSE
There will also be an opportunity to pose questions. This breakfast provides an excellent opportunity to meet with one of the most senior stakeholders in the industry in an informal setting and hear first-hand the current situation and future plans for the health service as well as meeting with industry colleagues. The briefing takes place on September 24th, 2025 from 7.30-9.30am in the Clayton Hotel, Liffey Valley, Dublin.
Improving Lung Cancer Survival
Results from a phase 3 clinical trial published in the New England Journal of Medicine, have show that patients with lung cancer who received an immunotherapy drug, nivolumab, along with standard chemotherapy before surgery had improved long term survival compared to those who received chemotherapy alone, at 5 years after completing treatment.
Professor Patrick Forde of the Trinity St. James’s Cancer Institute (TSJCI), Trinity College Dublin School of Medicine presented the findings at the American Society of Clinical Oncology Annual Meeting in Chicago recently.
Professor Forde led the CheckMate 816 trial which enrolled 358 patients globally who were diagnosed with the most common type of lung cancer, non-small cell lung cancer (NSCLC), at a stage where it could be removed by surgery. However, despite undergoing surgery >50% of patients with stage 2 or 3 lung cancer will eventually have relapse of their cancer. Immunotherapy drugs known as immune
checkpoint inhibitors, in particular those that block a receptor called PD-1, have led to improved survival for patients with advanced cancers by unmasking the tumour to the patient’s immune system.
However, up until now, no study had shown long-term benefit to this treatment in helping to cure earlier stage lung cancer.
Earlier in his career as an oncologist at Johns Hopkins in the United States Professor Forde led the first clinical trial of immunotherapy prior to surgery (neoadjuvant therapy) for lung cancer which was published in the New England Journal of Medicine in 2018. That study showed that among 20 patients who underwent surgery after 2 doses of immunotherapy almost half had little or no remaining cancer at the time of their operation.
In an earlier report of the CheckMate 816 trial, patients with lung cancer who received immunotherapy along with chemotherapy prior to surgery were more likely to have had their
Date for your Diary: Return of the Great Debate
The Pharmaceutical Manufacturers’ Institute (PMI) is bringing back one of their most anticipated events – The Great Debate. This year, they tackle one of the pressing questions for healthcare’s future: Healthcare 2030: The Price of Progress – Can Innovation and Affordability Coexist?
Join the team for an evening of sharp insights, bold arguments, and expert perspectives as their panel of thought leaders go head-tohead, moderated by MC, Ivan Yates. After the debate, stay with for refreshments and the chance to connect with colleagues and industry leaders.
The event takes place on Thursday, 16th October at 6.30pm for a 7.30pm start at the RCSI, Dublin. Visit www.thepmi.com for more details.
cancer eliminated completely by the time of surgery and also had lower rates of cancer relapse. Side effects were not increased with the addition of immunotherapy and in general surgeries went well. These findings led to the approval of the neoadjuvant nivolumab plus chemotherapy in several countries globally, including as a standard treatment for eligible patients in Ireland.
In the latest update from the trial patients who received immunotherapy plus chemotherapy before surgery were approximately 10% more likely to be alive at 5 years than those who just received chemotherapy. Among the 24% of patients treated with immunotherapy plus chemotherapy who had no cancer remaining at the time of surgery, known as a pathologic complete response, no patient had died from lung cancer by 5 years.
Professor Forde is also co-leading an international clinical trial open in Ireland at TSJCI, Beaumont, Galway and Mater Hospitals that is aimed at further improving outcomes for patients undergoing surgery. Results from part of this study were also published recently in the prestigious Nature Medicine
journal. In the NeoCOAST-2 trial, patients who received standard chemo-immunotherapy plus a new treatment called an antibody drug conjugate (ADC) before surgery were more likely to have no viable cancer remaining at the time of surgery, suggesting that this additional treatment could improve outcomes further.
Professor Forde said, “Immunotherapy has helped many patients with stage 4 lung cancer live longer with good quality of life. Until recently we have not had new treatments available that can increase the chances of cure after lung cancer surgery. The use of immunotherapy with chemotherapy before lung cancer surgery has now been shown to reduce the risk of cancer coming back and improve long term survival. Cancer clinical trials are key to improving outcomes for patients with cancer and offer the potential for early access to the latest cutting edge cancer treatments. I am delighted to be able to help expand clinical trial options for patients in Ireland.”
In 2024, Professor Forde joined the Trinity St. James’s Cancer Institute (TSJCI) as the Patrick Prendergast Professor of Clinical Immuno-Oncology. This position was established by a philanthropic gift from Dr. Stanley Quek, Trinity alumnus and former Pro-Chancellor of the University.
In collaboration with colleagues across Ireland Professor Forde’s goal is to improve access for patients to this cutting edge cancer clinical trial.
You can find further coverage of the 2025 American Society of Clinical Oncology Annual Meeting in Chicago on page 33 of this issue.
Professor Patrick Forde
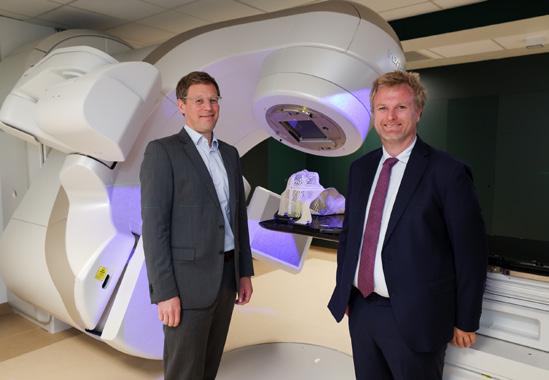
¤5.6m Investment in Innovative Cancer Care Technology
New radiotherapy technology, TrueBeam LINAC with HyperSight imaging, offers faster, more precise treatment, improving patient outcomes and experience
Mater Private Network has announced a ¤5.6 million investment in Ireland’s first TrueBeam LINACs with HyperSight– an advanced radiotherapy system that uses high-quality imaging to deliver faster, more precise cancer treatment. The new system, now available at its Dublin hospital and soon to be available in its Limerick Radiation Oncology Centre, enables clinicians to target tumours with greater accuracy, improving outcomes, reducing side effects and reducing treatment times for patients.
The recent announcement builds on a series of strategic investments by Mater Private Network, which has invested ¤20 million over the last five years to enhance cancer services across its network. This latest upgrade reflects its ongoing commitment to innovation, clinical excellence, and faster access to care.
Hugh Healy, Director of Cancer, Mater Private Network, said, “Today marks a major milestone for cancer care in Ireland and builds on our ongoing investment in oncology services. This is the first time this technology is available in the country. The TrueBeam LINAC with HyperSight is capable of producing high quality scans in just six seconds, enhancing the precision of tumour targeting while making treatment times quicker for patients. Within our network, we will be able to offer best-in-class stereotacticcapable machines incorporating
The launch was officially marked with a ribbon-cutting ceremony earlier today at Mater Private Network’s hospital in Dublin
Varian HyperSight and Brainlab Exactrac Dynamic in both the east and west of the country, as part of the newest fleet of LINAC machines and planning CTs. We’re proud to be the first healthcare network in Ireland to introduce this treatment technology, reaffirming our commitment to ensuring that patients have access to the most advanced treatments available.”
Radiation oncology at Mater Private Network is led by a team of seven sub-specialty radiation oncologists, dedicated to delivering personalised, patient-centred care. Working closely with the Medical Oncology Department, and the multidisciplinary team at The Mater Hospitals and UCD Cancer Centre and University Hospital Limerick, the team works to optimise individualised treatment pathways and patient outcomes.
Radiation oncology at Mater Private Network is led by a team of seven sub-specialty radiation oncologists, dedicated to delivering personalised, patient-centred care
Thanks to improved workflows and more efficient technology, patients referred to Mater Private Network for radiotherapy, including for prostate, brain, lung, and other site-specific cancers, can typically be seen within one week and begin treatment within one month of referral, ensuring expedited access to potentially life-saving care.
Professor Daniel Cagney, Clinical Director of Radiation Oncology,
Professor Daniel Cagney, Clinical Director of Radiation Oncology, Mater Private Network and Hugh Healy, Director of Cancer, Mater Private Network
Mater Private Network said, “These new capabilities, including the TrueBeam LINAC with HyperSight and Brainlab Exactrac Dynamic, are transforming how we deliver radiotherapy. With clearer imaging and faster scans, we can ensure more precise treatment and personalised care. As the first and only healthcare network currently offering this technology, we’re ensuring more people have access to world-class treatment close to home. Ultimately, it’s about better outcomes and giving patients confidence and peace of mind during a very difficult time.”
The launch was officially marked with a ribbon-cutting ceremony earlier today at Mater Private Network’s hospital in Dublin.
An Overview of Head and Neck Cancer
Introduction:
In Ireland we see on average 800 new cases of head and neck cancer diagnosed every year. Men are at a higher risk of the disease,1 with men being more than twice as likely to develop it (4.6%) compared to women (1.8%).1
The risk of head and neck cancers increase as we get older with the majority occurring over the age of 50 years, however they can also develop in people younger.2
Types of Head and Neck Cancers:
Head and neck cancer can be used as an umbrella term to describe a number of different cancers that can develop in the soft tissues of the head and neck. They can include cancers such as:
- Laryngeal Cancer – cancer of the larynx or voice box.
- Nasopharyngeal Cancer –cancer in the area where the nose and back of the throat meet.
- Mouth and Oropharyngeal Cancer – area of the mouth including the lips, gums and sides of the mouth and the oropharyngeal area (area of the throat just behind the mouth).
- Nasal and Paranasal Sinus Cancer – space behind the nose or within the bones close to the nasal cavity.
- Oesophageal Cancer – cancer of the oesophagus an area where food is transported from the mouth to the stomach, also known as the gullet or food pipe.
Written by Áine Finn, Community and Online Information Nurse, Marie Keating Foundation
“The most common type of head and neck cancer is squamous cell carcinoma. About 9 out of 10 head and neck cancers (90%) start in squamous cells.4 Treatment will vary depending on the location of the cancer”
- Salivary Gland Cancer – there are three main salivary glands in the mouth along with 100s of smaller ones in the mouth and throat.
- Throat Cancer – cancer developing in any part of the throat.
- Tongue Cancer – cancer at the front or back of the tongue
- Tonsillar Cancer- cancer occurring in the tonsils of the mouth.
- Ear Cancer – cancer developing in any of the three areas of the ear, the inner, middle or outer sections.3
The most common type of head and neck cancer is squamous cell carcinoma. About 9 out of 10 head and neck cancers (90%) start in squamous cells.4 Treatment will vary depending on the location of the cancer.
Risk Factors and Causes:
We do not know the cause of most head and neck cancers however there are certain factors that can increase our risk.5 The three main
causes of head and neck cancers are tobacco and alcohol and the human papillomavirus (HPV).
Tobacco
This includes cigarettes, cigars and pipes as well as smokeless or chewable forms of tobacco.
Alcohol
No alcohol is best however when consuming alcohol the recommendation is to try not to exceed the weekly recommended guidance.6 The risk of alcohol consumption can be further increased when alcohol and tobacco are used together. This is due to an increased absorption of harmful chemicals from both tobacco and alcohol into the cells in our body when combined.
HPV (Human Papillomavirus)
The human papillomavirus is a very common virus which most people will be exposed to at some point in their life. It is spread through close skin to skin contact, usually during sexual activity such as sexual intercourse, anal sex or oral sex. There are over 100 different strains of HPV and they can be classified as low-risk strains and high-risk strains. Our own immune system can play a role in clearing this virus, with the majority of people able to clear it within two years. However, with high-risk strains of this virus, if we are unable to effectively clear the virus ourselves, it can increase the risk of developing some mouth and oropharyngeal cancers.5, 7
Other risk factors:
Age:
As previously mentioned, the risk of head and neck cancers increases with age with the majority of people diagnosed over 50 years of age.2
Sex:
Men are more than twice as likely to develop head and neck cancers compared to women. Head and neck cancers are the fifth most common cancer in men excluding non-melanoma skin cancer.1
Weakened immune system:
When our immune system is weakened, we are at an increased risk for being unable to clear HPV. People who are on immunosuppressant drugs or those with a weakened immune system can be at an increased risk of developing some head and neck cancers.7
UV Exposure:
Exposure to harmful ultraviolet (UV) rays from the sun or from sunbeds can increase the risk of cancer of the mouth in particular of the lips. Therefore, it is important to apply sunscreen to protect our lips from harmful UV rays and to avoid sunbed use.2, 7
Signs and symptoms
- Hoarseness
- Persistent sore throat
- Pain to the ear, head or neck
- Difficulty swallowing or food getting caught or stuck
- A lump to the mouth, throat or head
- Numbness or issues with moving the tongue
- New changes to your gums, cheeks or tongue such as red or white patches,
- Mouth ulcers or blisters that don’t heal
- Loose tooth that is unexplained
- Droop in the side of your face
- Gums that don’t fully heal -after dental work.2, 8
Head and neck cancers can be treated successfully if caught in time. Therefore, it is important that if a person has any one or combination of the above symptoms, especially if they persist for more than three weeks, that they seek medical advice. People can also help to reduce their risk by regular dental checkups and by self-checks at home on a regular basis.2
Treatment:
Treatment is dependent upon a number of factors including the stage and grade of the cancer, the type and location as well as the general health of the person. The main treatment options for head and neck cancers are:
- Surgery
- Chemotherapy
- Radiotherapy
- Combination of chemotherapy and radiotherapy
- Targeted therapies
- Immunotherapies9, 10, 11, 12
References available on request
Ticagrelor Teva
90 mg Film-coated Tablets
ticagrelor
56 tablet pack
Indications
Ticagrelor Teva co-administered with acetylsalicylic acid (ASA), is indicated for the prevention of atherothrombotic events in adult patients with acute coronary syndromes (ACS) or a history of myocardial infarction (MI) and a high risk of developing an atherothrombotic event
Ticagrelor Teva Film Coated Tablets Abbreviated Prescribing Information.
Presentation: Each film-coated tablet contains 90mg ticagrelor. Indications: Ticagrelor Teva coadministered with acetylsalicylic acid (ASA), is indicated for the prevention of atherothrombotic events in adult patients with acute coronary syndromes (ACS), or a history of myocardial infarction (MI) and a high risk of developing an atherothrombotic event. Dosage and administration: For oral use. Patients taking Ticagrelor Teva should also take a daily low maintenance dose of ASA 75-150mg, unless specifically contraindicated. Adults: ACS: Should be initiated with a single 180mg loading dose (two tablets of 90mg) and then continued at 90mg twice daily. Treatment with Ticagrelor Teva 90mg twice daily is recommended for 12 months in ACS patients unless discontinuation is clinically indicated. Adults: History of MI: 60mg twice daily is the recommended dose when an extended treatment is required for patients with a history of MI of at least one year and a high risk of an atherothrombotic event. Treatment may be started without interruption as continuation therapy after the initial one-year treatment with Ticagrelor Teva 90mg or other adenosine diphosphate (ADP) receptor inhibitor therapy in ACS patients with a high risk of an atherothrombotic event. Treatment can also be initiated up to 2 years from the MI, or within one year after stopping previous ADP receptor inhibitor treatment. Children: Not suitable for use in patients under 18 years of age. Elderly: No dose adjustment is required. Renal impairment: No dose adjustment is necessary. In patients with ACS, it is recommended that renal function is also checked one month after initiating the treatment with ticagrelor, paying special attention to patients ≥75 years, patients with moderate/severe renal impairment and those receiving concomitant treatment with an angiotensin receptor blocker (ARB). Hepatic impairment: No dose adjustment is necessary for patients with mild hepatic impairment. No dose adjustment is not recommended for moderate hepatic impairment, but ticagrelor should be used with caution. Ticagrelor has not been studied in patients with severe hepatic impairment and its use in these patients is contraindicated. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Active pathological bleeding. History of intracranial haemorrhage. Severe hepatic impairment. Co-administration of ticagrelor with strong CYP3A4 inhibitors (e.g. ketoconazole, clarithromycin, nefazodone, ritonavir and atazanavir), as co-administration may lead to a substantial increase in exposure to ticagrelor. Precautions and warnings: The use of ticagrelor in patients at known increased risk for bleeding should be balanced against the benefit in terms of prevention of atherothrombotic events. Ticagrelor should be used with caution in the following patient groups: Patients with a propensity to bleed (e.g. due to recent trauma, recent surgery, coagulation disorders, active or recent gastrointestinal bleeding) or who are at increased risk of trauma. Patients with concomitant administration of medicinal products that may increase the risk of bleeding (e.g. non-steroidal anti-inflammatory drugs (NSAIDs), oral anticoagulants and/or fibrinolytics) within 24 hours of ticagrelor dosing. Patients should be advised to inform physicians and dentists that they are taking ticagrelor before any surgery is scheduled and before any new medicinal product is taken. If a patient is to undergo elective surgery and antiplatelet effect is not desired, ticagrelor should be discontinued 5 days prior to surgery. ACS patients with prior ischaemic stroke can be treated with ticagrelor for up to 12 months. Patients with an increased risk of bradycardic events (e.g. patients without a pacemaker who have sick sinus syndrome, 2nd or 3rd degree AV block or bradycardic-related syncope) have been excluded from the main studies evaluating the safety and efficacy of ticagrelor. Therefore, due to the limited clinical experience, ticagrelor should be used with caution in these patients. Caution should be exercised when administering ticagrelor concomitantly with medicinal products known to induce bradycardia. Bradyarrhythmic events and AV blocks have been reported in the post-marketing setting in patients taking ticagrelor, primarily in patients with ACS, where cardiac ischemia and concomitant drugs reducing the heart rate or affecting cardiac conduction are potential confounders. Dyspnoea was reported in patients treated with ticagrelor. Dyspnoea is usually mild to moderate in intensity and often resolves without need for treatment discontinuation. Central sleep apnoea including Cheyne-Stokes respiration has been reported in the post-marketing setting in patients taking ticagrelor. If central sleep apnoea is suspected, further clinical assessment should be considered. Hyperuricaemia may occur during treatment with ticagrelor. Caution is advised in patients with history of hyperuricaemia or gouty arthritis. As a precautionary measure, the use of ticagrelor in patients with uric acid nephropathy is discouraged. Thrombotic Thrombocytopenic Purpura (TTP) has been reported very rarely with the use of ticagrelor. It is characterised by thrombocytopenia and microangiopathic haemolytic anaemia associated with either neurological findings, renal dysfunction or fever. TTP is a potentially fatal condition requiring prompt treatment including plasmapheresis. Co-administration of ticagrelor and high maintenance dose ASA (>300mg) is not recommended. Premature discontinuation of treatment should be avoided, as this could
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland.
Freephone: 1800 - 201 700 | Email: info@teva.ie
Product subject to prescription which may be renewed (B)
result in an increased risk of cardiovascular (CV) death MI or stroke due to the patient’s underlying disease. Interactions: Strong CYP3A4 inhibitors (e.g. ketoconazole, clarithromycin, nefazodone, ritonavir and atazanavir) are known to reduce the Cmax and AUC of the active metabolite of ticagrelor, therefore, their concomitant use is contraindicated. Moderate CYP3A4 inhibitors (e.g. amprenavir, aprepitant, erythromycin and fluconazole) can be co-administered with ticagrelor. A 2-fold increase of ticagrelor exposure was observed after daily consumption of large quantities of grapefruit juice. CYP3A inducers (e.g. phenytoin, carbamazepine and phenobarbital) would be expected to decrease the exposure to ticagrelor. Coadministration of ticagrelor with potent CYP3A inducers may decrease exposure and efficacy of ticagrelor, therefore, their concomitant use with ticagrelor is discouraged. Co-administration of cyclosporine with ticagrelor increased ticagrelor Cmax and AUC. No data are available on concomitant use of ticagrelor with other active substances that also are potent P-gp inhibitors and moderate CYP3A4 inhibitors (e.g. verapamil, quinidine) that also may increase ticagrelor exposure. If the association cannot be avoided, their concomitant use should be made with caution. Co-administration of ticagrelor with heparin, enoxaparin and ASA or desmopressin did not have any effect on the pharmacokinetics of ticagrelor or the active metabolite or on ADP-induced platelet aggregation compared with ticagrelor alone. Co-administration of ticagrelor with simvastatin increased simvastatin Cmax and AUC. Ticagrelor may have similar effect on lovastatin, therefore, the concomitant use of ticagrelor with doses of simvastatin or lovastatin greater than 40mg is not recommended. Co-administration of ticagrelor with atorvastatin increased atorvastatin Cmax and AUC, but these increases are not considered clinically significant. Ticagrelor is a mild CYP3A4 inhibitor. Co-administration of ticagrelor and CYP3A4 substrates with narrow therapeutic indices (i.e. cisapride or ergot alkaloids) is not recommended, as ticagrelor may increase the exposure to these medicinal products. Appropriate clinical and/or laboratory monitoring is recommended when giving narrow therapeutic index P-gp dependent medicinal products like digoxin concomitantly with ticagrelor. Co-administration of ticagrelor with tolbutamide resulted in no change in the plasma levels of either medicinal product, which suggests that ticagrelor is not a CYP2C9 inhibitor and unlikely to alter the CYP2C9 mediated metabolism of medicinal products like warfarin and tolbutamide. Ticagrelor may affect renal excretion of rosuvastatin, increasing the risk for rosuvastatin accumulation. Co-administration of ticagrelor and levonorgestrel and ethinyl oestradiol increased ethinyl oestradiol exposure approximately 20% but did not alter the pharmacokinetics of levonorgestrel. No clinically relevant effect on oral contraceptive efficacy is expected when levonorgestrel and ethinyl oestradiol are co-administered with ticagrelor. Due to observations of mostly asymptomatic ventricular pauses and bradycardia, caution should be exercised when administering ticagrelor concomitantly with medicinal products known to induce bradycardia. Due to reports of cutaneous bleeding abnormalities with SSRIs (e.g. paroxetine, sertraline and citalopram), caution is advised when administering SSRIs with ticagrelor as this may increase the risk of bleeding. Pregnancy and lactation: Patients of childbearing potential should use appropriate contraceptive measures to avoid pregnancy during ticagrelor therapy. Ticagrelor is not recommended during pregnancy. Regarding lactation, a risk to newborns/infants cannot be excluded. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from ticagrelor therapy taking into account the benefit of breastfeeding for the child and the benefit of therapy for the patient. Effects on ability to drive and use machines: Ticagrelor has no or negligible influence on the ability to drive and use machines. Dizziness and confusion have been reported with treatment, therefore, patients who experience these symptoms should be cautious while driving or using machines. Adverse reactions: Thrombotic thrombocytopenic purpura, hypersensitivity including angioedema, syncope, and haemorrhage (including intracranial, ear, eye, gastrointestinal, retroperitoneal). Very Common: Blood disorder bleedings, hyperuricaemia, and dyspnoea. Common: Gout/gouty arthritis, dizziness, headache, vertigo, hypotension, respiratory system bleedings, diarrhoea, nausea, dyspepsia, constipation, subcutaneous or dermal bleeding, rash, pruritus, urinary tract bleeding, blood creatinine increased, post procedural haemorrhage, and traumatic bleedings. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: In the event of an overdose, any of the above listed adverse reactions could occur, as well as prolonged duration of bleeding risk associated with platelet inhibition. ECG monitoring should be considered. There is currently no known antidote to reverse the effects of ticagrelor, and ticagrelor is not dialysable. Treatment of overdose should follow local standard medical practice. If bleeding occurs other appropriate supportive measures should be taken. Platelet transfusion is unlikely to be of clinical benefit in patients with bleeding. Legal category: POM. Marketing Authorisation Number: PA1986/123/001. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00092. Date of Preparation: May 2025
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie.
Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Date of Preparation: May 2025 | Job Code: GEN-IE-00139
Further information is available on request or in the SmPC. Product Information also available on the HPRA website.
Insulin
Insulin Prescribing, Administration, and Glucose Monitoring Trends in a Hospital Setting
Written by Diana Hogan-Murphy1, Lisa Reddington2, Michael Conall Dennedy2,3,
Laurence Egan3,4, Julie Okiro2, John Given1, Sinead Donnellan1 and Ridhwaan Salehmohamed2
1. Department of Pharmacy, Galway University Hospitals, Galway, Ireland
2. Department of Endocrinology, Diabetes and Metabolism, Galway University Hospitals, Galway, Ireland
3. Department of Pharmacology and Therapeutics, School of Medicine, National University of Ireland, Galway, Ireland
4. Department of Gastroenterology, Galway University Hospitals, Galway, Ireland
Abstract
Aims
Insulin is a high-alert medication which can cause significant patient harm when used inappropriately. The aim of this study was to conduct a prospective audit on insulin prescribing, administration, and glucose monitoring trends in Galway University Hospitals. Methods
This audit was conducted over one day in March 2022. The audit was approved by the local Clinical Audit Committee, piloted on two inpatients, and communicated to all data collectors prior to commencement. Generated data were anonymous and securely stored. Independent analysis was conducted by three researchers to confirm reliability of results.
Results
Four hundred and fifty-four inpatients were reviewed of which 17% [75] had diabetes and 9% [41] were prescribed insulin. The overall insulin error rate with one or more errors comprising prescribing and/ or administration per inpatient drug record was 90% [37]. In total, 95% [235] insulin brand names and 89% [220] dose units were clearly prescribed, 84% [208] administration times were clearly specified by a prescriber, 87% [214] orders were signed, 58% [25] prescribers clearly documented their registration number/bleep/name at least once for contact purposes, 35% [30] meal time supplements were documented clearly by a nurse, 70% [202] administrations were double checked by a second person, 53% [142] administration times were documented by a nurse, and 26% [10] of inpatients were administered insulin by a nurse when not prescribed.
Conclusion
Results will assist in developing quality improvement initiatives to optimise patient care.
Introduction
Diabetes mellitus (DM) is a heterogeneous complex metabolic condition characterised by hyperglycaemia with a degenerative potential resulting from changes in the production, secretion and/or inability of insulin to adequately exercise its effects1. The most common classifications include Type 1 DM and Type 2 DM, the latter accounting for more than 90% of all cases2. Type 2 DM is characterised by insulin resistance and a relative deficiency of insulin secretion which progressively worsens over time3,4 Type 1 DM results in an absolute deficiency in beta-cell function with autoimmune destruction of beta-cells a common origin5 Current estimates suggest more than half a billion adults live with DM worldwide, a rise of 16% since previous estimates in 20196. This is predicted to escalate to almost 800 million by 20456. In Ireland, in the absence of a national DM registry, the current approximate projection is 5.6%7
DM is a leading cause of death globally8 and described as the most challenging health problem in the 21st century9,10 driven primarily by rising levels of obesity and an ageing population9,11. A systematic review and meta-analysis on the epidemiology of DM and its complications amongst adults in Ireland found variables from 7–25% for retinopathy; 3–32% for neuropathy; and 3-5% for nephropathy12. The economic burden also plays heavily with Ireland ranked 7th in the world for DM related health expenditure per person7, and as high as ¤1.4 billion annually with costs mostly associated with hospitalisations and treatment of complications6 Insulin is a critical high-alert medicine used in the treatment
of DM which bears a heightened risk of causing significant patient harm. With limited Irish data availability and few local incidents reported, anecdotal evidence suggests insulin accounts for a substantial number of medication errors13,14. A review by the States Claims Agency of over 20,000 medication incidents reported by Irish acute hospitals in 2017 and 2018 found insulin was the fourth most commonly implicated therapeutic subgroup15, many comprising omissions leading to hyperglycaemia and inaccurate dosing leading to hyperglycaemia and hypoglycaemia16
Insulin has been identified as a significant medication safety concern in Galway University Hospitals (GUH). The aim of this study was to conduct a prospective audit on insulin prescribing, administration, and glucose monitoring trends in GUH in order to identify and develop agreed quality improvement initiatives to enhance patient care.
Methods
A prospective audit on insulin prescribing, administration, and glucose monitoring was conducted over one day in March 2022 on 24 wards in GUH. GUH comprises University Hospital Galway (UHG), a Model 4 public hospital, and Merlin Park University Hospital (MPUH), a Model 2 public hospital, and provides a comprehensive range of services to emergency and elective patients within the Saolta University Healthcare Group in the West of Ireland.
Inclusion criteria comprised inpatients prescribed/administered insulin in UHG and MPUH for the previous 72 hours until 9am on the morning of audit. Exclusion criteria comprised non-admitted patients, Day Wards, Emergency Department, Acute Medical Unit, Short Stay Unit, Emergency Surgical Unit, Critical Care including Post Anaesthetic Care
Diana Hogan-Murphy
Unit, Maternity Department, and Psychiatry Department. Content of the audit protocol and tool was informed by the research objective, local practices, and existing evidence-based international and national literature. The audit tool was piloted on a medical ward in UHG with two random inpatients prescribed and administered insulin. Minor amendments were made to its content and the pilot was excluded from data analysis.
The audit was led by two lead researchers and conducted by 29 data collectors comprising endocrine consultant and nonconsultant hospital doctors, diabetic nurse specialists, and pharmacists. The audit tool was guided by the protocol which was communicated to all data collectors prior to the audit via video conferencing and face-to-face meetings and emails. This audit was conducted in accordance with the HSE Code of Governance (2021) and HSE Healthcare Audit Quality Assurance and Verification Standards (2019) and was approved by the GUH Clinical Audit Committee prior to commencement. All audit forms were anonymous and securely stored in a locked cabinet and all generated data were securely stored on an encrypted password protected work computer. Any audit records will be destroyed after full dissemination of audit findings. Independent analysis was conducted by the two primary researchers and a specialist registrar in endocrinology to confirm reliability of results. This process
Figure 1: DM/Insulin prevalence
Overall insulin error rate per inpatient drug record
The overall insulin error rate with one or more errors comprising prescribing and/or administration per inpatient drug record was 90% [n=41] as presented in Table 1.
Table 1: Overall insulin error rate per inpatient drug record
Insulin name not clearly prescribed
Insulin dose units not clearly prescribed 11%
Insulin administration times not clearly specified by the prescriber 16%
Insulin orders not signed by the prescriber 13%
Prescriber MCRN/bleep/name unclear for contact purposes 42%
Meal time supplement documented incorrectly 65%
Insulin administration times not documented 47%
Insulin administration not double checked by a 2nd person 30% Administration error 89%
Insulin administered when not prescribed 26%
Insulin prescribing patterns
Table 1: Overall insulin error rate per inpatient drug record
Nineteen inpatients [n=37; 51%] were prescribed the same insulin as pre-admission, four inpatients [n=37; 11%] were not prescribed the same insulin as pre-admission, and 14 inpatients [n=37; 38%] were not on insulin pre-admission and were either prescribed a meal time supplement [10 inpatients; n=37; 27%] or were newly prescribed insulin on admission [4 inpatients; n=37; 11%].
involved independently inputting content of paper audit forms into excel, analysing data, and comparing results. No significant discrepancies were identified.
Results
specialty comprised medical [27, 66%], surgical [12, 29%], and paediatric [2, 5%].
Overall insulin error rate per inpatient drug record
and were either prescribed a meal time supplement [10 inpatients; n=37; 27%] or were newly prescribed insulin on admission [4 inpatients; n=37; 11%].
A total of 247 insulin doses were prescribed of which 235 orders [95%] had the insulin name clearly documented Two hundred and twenty [89%] insulin dose units were clearly prescribed, 208 [84%] administration times were clearly specified by a prescriber, and 214 [87%] orders were signed by a prescriber (Figure 2).
General participation and prevalence
In total, 454 inpatients were reviewed of which 41 [9%] were prescribed insulin and included in the audit. The number of inpatients using an Insulin and Glucose Monitoring Record was 117 [26%] of which 75 inpatients [17%] had a documented history of DM (Figure 1). This equates to 55% of all inpatients with DM were treated with insulin. Patient
The overall insulin error rate with one or more errors comprising prescribing and/or administration per inpatient drug record was 90% [n=41] as presented in Table 1.
Insulin prescribing patterns
Nineteen inpatients [n=37; 51%] were prescribed the same insulin as pre-admission, four inpatients [n=37; 11%] were not prescribed the same insulin as pre-admission, and 14 inpatients [n=37; 38%] were not on insulin pre-admission
DM/Insulin Prevalence GUH
Number of inpatients documented with DM
Number of inpatients on Insulin
Number of inpatients using an Insulin and Glucose Monitoring Record
Number
A total of 247 insulin doses were prescribed of which 235 orders [95%] had the insulin name clearly documented. Two hundred and twenty [89%] insulin dose units were clearly prescribed, 208 [84%] administration times were clearly specified by a prescriber, and 214 [87%] orders were signed by a prescriber (Figure 2).
Twenty-five prescribers [n=43; 58%] clearly documented their medical council registration number (MCRN)/bleep/name on the insulin drug record at least once for contact purposes and 25 inpatients [61%] had the meal time supplement signed by a prescriber. The meal time supplement was documented clearly 30 times out of a total of 86 entries [35%].
Insulin administration patterns
Two hundred and eighty-seven doses were administered of which 202 [70%] were double checked by an independent second person. Administration times were documented for 142 doses [n=270; 53%] as illustrated in Figure 3. Ten inpatients [n=39; 26%] were administered insulin by a nurse when not prescribed.
Glucose management
The GUH DM team reviewed/was contacted to review 21 inpatients insulin drug record [55%, n=38]. Twenty-five inpatients [61%; n=41] had changes to their insulin regimen made during their inpatient stay. This included changes to a brand name of insulin [4; n=37; 11%], the initiation of insulin and/or a meal time supplement [14; n=37; 38%], and/or a dose change [9; n=32;
Insulin
Insulin Prescribing Patterns
What number of insulin orders have been signed by the prescriber?
What number of insulin administration times are clearly specified by the prescriber?
Insulin Prescribing Patterns
What number of insulin dose units are clearly prescribed?
What number of insulin orders have been signed by the prescriber?
What number of insulin orders have the name clearly prescribed?
What number of insulin administration times are clearly specified by the prescriber?
What number of insulin doses have been prescribed?
What number of insulin dose units are clearly prescribed?
What number of insulin orders have the name clearly prescribed?
had the insulin name, dose, and administration times clearly documented and signed by the prescriber which are positive findings. However, less than three out of five prescribers clearly documented their MCRN/ bleep/name on the insulin drug record at least once for contact purposes leading to possible time delays and patient care issues if communication is required.
Twenty-five prescribers [n=43; 58%] clearly documented their medical council registration number (MCRN)/bleep/name on the insulin drug record at least once for contact purposes and 25 inpatients [61%] had the meal time supplement signed by a prescriber. The meal time supplement was documented clearly 30 times out of a total of 86 entries [35%]
28%; median 3; range 1-6]. Three inpatients had their insulin omitted after an episode of hypoglycaemia (blood glucose <4 mmol/L).
What number of insulin doses have been prescribed?
inpatients in 206 NHS hospitals were insulin dependent and 36% of inpatients with DM were treated with insulin18
inpatient drug record was 90%.
This is significantly higher than the NaDIA 2019 report which found 18% of inpatient drug records had one or more insulin errors17
Discussion
Insulin administration patterns
Figure 2: Insulin prescribing patterns
Insulin Administration Patterns
Insulin administration patterns
This study identified 17% of inpatients had DM on audit day of the audit in GUH of which 9% were insulin dependent and 55% of all inpatients with DM were treated with insulin. This is similar to the most recently published National Health Service (NHS) National Diabetes Inpatient Audit (NaDIA) England 2019 report which found 18% of all inpatients in 188 NHS hospitals had documented DM17. The NaDIA England and Wales 2015 report identified a lower prevalence of 6% of all
What number of doses with administration times are documented?
The majority of inpatients in this audit were medical and prescribed the same insulin as pre-admission. All inpatients not prescribed the same insulin as pre-admission were altered by the DM team during admission and were therefore appropriately changed. The remaining inpatients were not on insulin pre-admission and were either prescribed a meal time supplement or were newly prescribed insulin on admission. The overall insulin error rate comprising both prescribing [80%] and administration [89%] per
Whilst the majority of inpatients were prescribed a meal time supplement, it was only documented clearly by nurses for approximately one in every three inpatients potentiating administration errors and significant patient harm. Almost one in three insulin doses were also not double checked by an independent second person and almost half administration times were not documented. Insulin is a high-alert medication which requires a two-person check of both dose preparation and administration at the bedside as well as precise administration timing to minimise hypoglycaemia, hyperglycaemia, wide glycaemic excursions, and diabetic ketoacidosis.
Two hundred and eighty-seven doses were administered of which 202 [70%] were double checked by an independent second person. Administration times were documented for 142 doses [n=270; 53%] as illustrated in Figure 3. Ten inpatients [n=39; 26%] were administered insulin by a nurse when not prescribed.
This figure is also higher than findings from an analysis of the National Reporting and Learning System database of patient safety incidents concerning insulin reported from NHS providers in England and Wales over a six year period which found 61% of incidents occurred at the administration stage and 17% at the prescribing stage19 The most common medication error types were wrong dose, strength, or frequency followed by omitted or delayed insulin19 Most prescriptions in this audit
More than one in four inpatients were administered insulin by a nurse when not prescribed. A nurse may only administer a non-prescribed medication in a situation that requires immediate intervention in lifethreatening situations and there is no immediate access to an appropriate prescriber. All insulin doses should be prescribed prior to nurse administration.
Twenty-five prescribers [n=43; 58%] clearly documented their medical council registration number (MCRN)/bleep/name on the insulin drug record at least once for contact purposes and 25 inpatients [61%] had the meal time supplement signed by a prescriber. The meal time supplement was documented clearly 30 times out of a total of 86 entries [35%]
Two hundred and eighty-seven doses were administered of which 202 [70%] were double checked by an independent second person. Administration times were documented for 142 doses [n=270; 53%] as illustrated in Figure 3. Ten inpatients [n=39; 26%] were administered insulin by a nurse when not prescribed.
What number of doses are double checked by an independent second person?
Insulin Administration Patterns
What number of doses have been administered?
What number of doses with administration times are documented?
Glucose management
What number of doses are double checked by an independent second person?
The GUH DM team reviewed/was contacted to review 21 inpatients insulin drug record [55%, n=38]. Twentyfive inpatients [61%; n=41] had changes to their insulin regimen made during their inpatient stay. This included changes to a brand name of insulin [4; n=37; 11%], the initiation of insulin and/or a meal time supplement [14; n=37; 38%], and/or a dose change [9; n=32; 28%; median 3; range 1-6]. Three inpatients had their insulin omitted after an episode of hypoglycaemia (blood glucose <4 mmol/L).
What number of doses have been administered?
Figure 3: Insulin administration patterns
The GUH DM team reviewed or was contacted to review more than half of the inpatients prescribed insulin. More than three out of five inpatients had changes to their insulin regimen made during their inpatient stay including brand of insulin, the initiation of insulin, and dose changes. Three inpatients had their insulin omitted after an episode of hypoglycaemia. This is lower than a study evaluating insulin information on discharge summaries in a United Kingdom (UK) hospital which found 33 out of 42 patients [79%] had changes made including the initiation and/or discontinuation of insulin therapy, insulin dose changes, and insulin preparation/brand20
As per best practice some of the current interventions implemented in GUH specific to insulin include an updated inpatient Glucose and Monitoring Drug Record; updated/newly approved policies, procedures, protocols and guidelines; piloting of a self-administration policy; development of a collaborative practice agreement for nurse prescribing; continuous education
Figure 2: Insulin prescribing patterns
Figure 3: Insulin administration patterns
Figure 2: Insulin prescribing patterns
Figure 3: Insulin administration patterns
and training to patients as well as medical, nursing, and pharmacy undergraduate students and employees in GUH; expansion of a medication safety portal inclusive of educational videos; use of hospital screens and social media to disseminate prudent information; and promotion of error reporting.
Based on results of this audit as well as evidence from local insulin error reporting, local practices, and best practice, future quality improvement interventions for consideration to optimise patient
care include implementing a dedicated insulin safety team that comprises a broad membership to facilitate sustainability and spread of interventions to improve insulin prescribing practice; recruiting a clinical pharmacist with a special interest in DM; mandatory e-learning for nurses and doctors on insulin prescribing and administration incorporating individual reflection and assessment; electronic prescribing as a part of the ongoing implementation of a new pharmacy
system; widespread roll out of the self-administration insulin policy; an insulin inpatient and discharge checklist; promotion of an annual national audit on insulin prescribing, administration, and glucose monitoring trends similar to the UK; and further promotion of insulin error reporting. Once interventions are in situ it is hoped and anticipated that results of a re-audit on insulin prescribing, administration, and glucose monitoring trends in GUH will be favourable.
Declaration of Conflicts of Interest
The authors report no conflict of interest.
Corresponding Author: Dr Diana Hogan-Murphy, Department of Pharmacy, University Hospital Galway, Galway
E-Mail: diana.hogan-murphy@hse.ie
References available on request
Latest Pharmacy Appointments
The Minister for Health, Jennifer Carroll MacNeill T.D., has appointed six members to the PSI Council with four new appointments and two reappointments. Their appointments commenced on 21 June for a four-year term on the PSI’s governing board.
The new appointees are pharmacists Margaret Donnelly, Leon O'Hagan, Áine Mac Grory and Nigel Moloney. A fifth pharmacist, Adj. Professor John Given, has been reappointed to serve a second term, along with the Health Products Regulatory Authority (HPRA) nominee, Grainne Power. All members of the PSI Council are appointed by the Minister for Health to act in the public interest in overseeing the regulatory responsibilities of the PSI as the pharmacy regulator.
At a recent meeting, the PSI Council also elected Dr Denis O’Driscoll as PSI President (chair) and Professor Laura Sahm as Vice-President. The President and Vice-President are elected from amongst the Council for a oneyear term and may hold office for up to two years.
Dr Denis O’Driscoll was appointed to the PSI Council in 2023 and has served as the PSI VicePresident. He is a pharmacist with many years of experience working across a variety of pharmacy practice settings, notably as Chief Pharmacist with the HSE’s Addiction Services for over twenty years. Since 2018, he has been the Superintendent Pharmacist for the McCabe’s Pharmacy group (formerly Lloyds Pharmacy). He is also the voluntary independent chair of the Naloxone Advisory Group for the HSE
Dr Denis O’Driscoll, PSI President
Strategy on Overdose Prevention and lectures on pharmacy and public health programmes at Trinity College Dublin.
Professor Laura Sahm was also appointed to the PSI Council in 2023. She is the current representative on the Council for the Schools of Pharmacy in Ireland. Laura is the Vice Dean of the School of Pharmacy and Head of Clinical Pharmacy Practice at University College Cork (UCC). She has worked previously as a pharmacist in a range of community, hospital and research positions in Europe and Ireland.
Together with the Council, the President and Vice-President will continue to support the work of the PSI and ensure its good
governance. This includes its statutory regulatory responsibilities and initiatives set under the Council’s recently launched Corporate Strategy 2025-2028, including a significant role in implementing national policy actions envisaged for pharmacy in the short and medium term.
The PSI – the Pharmacy Regulator is governed by a 21-member
Council, with a non-pharmacist majority. Council members are appointed by the Minister for Health in accordance with the Pharmacy Act 2007. The Council meets at least six times each year and is responsible for setting the strategy for the PSI, and overseeing the functions of the PSI, in the public interest. The full list of Council members is on the PSI website.
Diabetic Technology
Advancements in Diabetes Technology: Optimising Care with CGMs and Insulin Pumps
A guide for hospital clinicians on the use of modern diabetes technology within the Irish healthcare system
Written
by Professor Derek O’Keeffe, Consultant Physician/ Professor of Medical Device Technology, University Hospital Galway, Ireland/Digital Health Principal Investigator, LERO, University of Limerick, Ireland, National Clinical Lead Diabetes, HSE and Dr Lyle McVicker, University Hospital Galway
Diabetes technology has undergone a revolutionary transformation in recent years, fundamentally changing how we monitor and manage both Type 1 and Type 2 diabetes. With increasing proportions of people living with diabetes now using these technologies, clinicians of all disciplines are more likely to encounter them in their daily work. Having a familiarity with the commonly used diabetes technologies and how they work is critical to ensuring safe patient care in an increasingly complex hospital system. This article provides practical guidance on continuous glucose monitors (CGMs) and insulin pump therapy, with specific reference to access pathways and implementation within the Irish healthcare system.
Glossary of Diabetes Technology Terms
rtCGM (Real-time Continuous Glucose Monitoring): A system that automatically displays glucose readings every few minutes and provides alarms for high or low glucose levels. Users can view their glucose levels at any time without scanning.
isCGM (Intermittently Scanned Continuous Glucose Monitoring): Also known as "flash" monitoring, this requires manual scanning
of the sensor with a reader or smartphone to obtain glucose readings and trends.
HCL (Hybrid Closed-Loop): An automated insulin delivery system that links an insulin pump to a CGM with software algorithms that automatically adjust insulin delivery. Sometimes called an "artificial pancreas," though it still requires user input for meals.
Open Loop Therapy: A traditional insulin pump that delivers programmed insulin doses but doesn't automatically adjust based on glucose readings. All adjustments must be made manually by the user.
Artificial Pancreas: A fully automated insulin delivery system that would require no user intervention. Current systems are "hybrid" as they still require meal announcements and other user inputs.
Basal Rates: The continuous background insulin delivery programmed into an insulin pump, typically varying throughout the day to match the body's natural insulin requirements.
Insulin-to-Carbohydrate Ratio (ICR): The amount of carbohydrate (in grams) that one unit of insulin will cover. For example, a ratio
of 1:10 means one unit of insulin covers 10 grams of carbohydrate.
Correction Factor/Insulin
Sensitivity Factor (ISF): The amount (in mmol/L) that one unit of insulin will lower blood glucose. For example, an ISF of 3.0 means one unit reduces glucose by 3.0 mmol/L.
TIR (Time in Range): The percentage of time glucose levels remain within the target range (typically 3.9-10.0 mmol/L). The goal is >70% for most adults.
TAR (Time Above Range): The percentage of time glucose levels are above target range (>10.0 mmol/L).
TBR (Time Below Range): The percentage of time glucose levels are below target range (<3.9 mmol/L). The goal is <4% overall and <1% below 3.0 mmol/L.
Understanding Continuous Glucose Monitoring
Continuous glucose monitors represent a paradigm shift from traditional fingerstick glucose monitoring. These devices measure glucose levels in interstitial fluid every few minutes, providing real-time data that enables more precise diabetes management. The technology comprises a small sensor attached to the arm or abdomen, paired with either a dedicated reader or smartphone application.
The clinical evidence supporting CGM use is compelling across multiple domains:
Glycaemic Control
Improvements: The DIAMOND randomised controlled trial demonstrated a 0.6% reduction in HbA1c among adults with Type 1 diabetes using CGM compared to usual care, with participants spending significantly more time in target glucose range and experiencing fewer episodes of hyperglycaemia and hypoglycaemia.
Hypoglycaemia Reduction: Perhaps more striking is the HypoDE study, which showed CGM use resulted in a 72%
reduction in hypoglycaemic events among people with Type 1 diabetes and impaired awareness of hypoglycaemia. This technology proved particularly beneficial for nocturnal hypoglycaemia, with over 50% reduction in night-time episodes—a finding with profound implications for patient safety and quality of life.
Early Intervention Benefits: Recently published research demonstrated that initiating CGM within the first year of Type 1 diabetes diagnosis in children and adolescents leads to improved glycaemic control in multi-year follow-up studies compared to those who begin CGM use at later stages, suggesting that early adoption of this technology provides lasting benefits.
Current Guidelines and Recommendations
The evidence has influenced international guidelines significantly. The 2025 American Diabetes Association (ADA) Standards of Care guidelines now recommend CGM for all people living with Type 1 diabetes, regardless of their current level of glycaemic control. This represents a major shift from previous recommendations that limited CGM to those with problematic hypoglycaemia or suboptimal control.
The 2024 Irish National Clinical Guideline for management of Type 1 Diabetes aligns with this approach, recommending that adults should be offered a choice between real-time CGM or intermittently scanned CGM based on individual preferences, needs, and device functionality. The emphasis on shared decisionmaking reflects the recognition that patient engagement and preference significantly influence successful technology adoption.
HSE Coverage and Access Pathways
Access to CGMs has improved significantly through The HSE Medicines Management Programme (MMP). The programme currently recommends
Professor Derek O'Keeffe
Dr Lyle McVicker
two preferred CGM systems for people with diabetes who are not insulin pump users: the FreeStyle Libre 2 and Dexcom One+. They make this distinction because not every CGM allows insulin pump integration.
Both systems offer high and low glucose alerts and integrate with smartphone applications that enable family members or carers to monitor glucose levels remotely—a
feature particularly valuable for parents of children with diabetes. The FreeStyle Libre 2 uses a 14day sensor suitable for ages four and above, worn on the back of the arm. The Dexcom One+ features a 10-day sensor approved from age two, with placement options varying by age group.
For patients with Type 1 diabetes, these CGM systems are available free of charge where clinically indicated. The diabetes team makes the application on the patient's behalf, with ongoing supplies provided through community pharmacy under the Long-Term Illness scheme.
Insulin Pump Therapy and Hybrid Closed-Loop Systems
Insulin pump therapy represents another significant advance, particularly when integrated with CGM technology. Modern insulin pumps are small electronic devices worn 24 hours daily, delivering insulin continuously through a tiny subcutaneous tube. The insulin used within the pump is generally rapid acting such as Novorapid or Humalog with a continuous background infusion acting as a basal rate with accompanying boluses delivered via the pump to cover meals or to correct for rising blood glucose levels. Most contemporary pumps integrate with CGM systems, automatically adjusting insulin delivery based on glucose readings via sophisticated algorithms—a technology known as hybrid closed-loop (HCL) systems. The benefits of pump therapy are substantial. Patients gain greater flexibility with meal timing and insulin dosing, often achieving more stable blood glucose levels. The integration with CGM technology reduces the burden of diabetes management while improving outcomes, with Time in Range (TIR) serving as the primary metric for success. Research demonstrates that each 10% increase in TIR correlates with a 40% reduced risk of microalbuminuria and 64% reduced risk of retinopathy.
Insulin Pump Therapy Evidence
Image 4: mylife Ypsomed Pump from Ypsomed
Efficacy Data: A 2008 metaanalysis reported that severe hypoglycaemia was reduced by a ratio of 2.89 in randomised controlled trials and 4.34 for before/after studies when using continuous subcutaneous insulin infusion (CSII). The reduction was greatest in those with initial high rates of hypoglycaemia. The mean HbA1c reduction was 0.21% (2.3 mmol/mol) in RCTs and 0.72% (7.9 mmol/mol) in before/after studies.
Quality of Life: CSII can reduce glycaemic variability and improve aspects of quality of life, particularly in relation to diet and physical activity flexibility.
HCL Benefits: Evidence suggests average HbA1c improvements of approximately 0.5% (5.5 mmol/ mol) can be achieved with the addition of CGM to CSII when the CGM component is in use at least 60-70% of the time. HCL systems that stop insulin delivery when hypoglycaemia occurs or is predicted have been shown to significantly reduce the frequency and severity of hypoglycaemia.
Available Systems in Ireland
Within the HSE system, several insulin pump options are available, including the Tandem t:slim X2,
Image 1: Dexcom One+ from DexCom, Inc.
Image 2: Freestyle Libre 2 from Abbott Laboratories
Image 2: Freestyle Libre 2 from Abbott Laboratories
Image 3: Medtronic MiniMed 780G from Medtronic Diabetes
Image 4: mylife Ypsomed Pump from Ypsomed
Image 3: Medtronic MiniMed 780G from Medtronic Diabetes
Image 4: mylife Ypsomed Pump from Ypsomed
Diabetic Technology
fibrosis-related diabetes, and hospital settings (including ICU and surgical environments) show promise. CGM devices continue to get smaller and last longer without need for replacement –improving acceptability to patients. Non-invasive glucose monitoring techniques using optical methods remain under development, potentially eliminating the need for subcutaneous sensors entirely.
2. If no improvement in 2 hours: give correction with insulin pen and check ketones
3. Consider pump/infusion set failure—ask patient to perform infusion set change if possible
4. Transition to alternate form of insulin delivery following infusion set change if no improvement and seek specialist advice
Never stop or suspend pump therapy without ensuring backup insulin is provided
Key Safety Points
• Pump users have no long-acting insulin depot—interruptions in insulin delivery are dangerous
• Most pump complications relate to infusion set problems (kinking, blockage)
Medtronic MiniMed 780G, and Ypsomed YpsoPump. Each system integrates with specific CGM devices: the Medtronic system uses Guardian 4 or Simplera sensors, while the Tandem and Ypsomed pumps work with Dexcom sensors (G6 currently, with G7 integration expanding).
While Ireland does not have specific guidelines surrounding the use of insulin pump therapy, the Diabetes Technology Network Ireland (DTN-IRL) recommends that teams use the Best Practice Guide for Insulin Pumps, which is based on the NICE Technology appraisal guidance (2022). This states that pumps therapy should be offered to those with T1DM who struggle with debilitating hypoglycaemia or those who fail to reach glucose targets despite optimal multiple daily injectable therapies. In reality, many practitioners are more aggressive about getting their patients onto pump therapy such are the possible benefits.
Each pump has specific advantages and disadvantages and the choice of pump should be guided by individual patient characteristics and preferences. For instance, the Ypsomed system offers unique advantages for certain populations. It's the only pump currently approved for use during pregnancy, with target ranges that can be set sufficiently low to meet pregnancy requirements. The pump is controlled via smartphone, allowing screen magnification for visually impaired users, though this population faces particular challenges with diabetes technology that the field continues to address.
While Ireland does not have specific guidelines surrounding the use of insulin pump therapy, the Diabetes Technology Network Ireland (DTN-IRL) recommends that teams use the Best Practice Guide for Insulin Pumps, which is based on the NICE Technology appraisal guidance (2022). This states that pumps therapy should be offered to those with T1DM who struggle with debilitating hypoglycaemia or those who fail to reach glucose targets despite optimal multiple daily injectable therapies. In reality, many practitioners are more aggressive about getting their patients onto pump therapy such are the possible benefits.
Illness scheme. The main barrier of access to pump therapy is the limited availability of skilled clinical staff to provide the necessary training for onboarding new pump users and support their continued care. Waiting lists for pump therapy can be long in some institutions and not every service operates a dedicated pump service as of yet. However, there is a widespread appreciation that the demand and clinical need for diabetes technology services will increase massively in future years and significant efforts are being made to train diabetes staff around the country to provide pump services. Examples of these efforts include running national diabetes technology training days around the country and the establishment of a DTN-IRL.
Connected insulin smartpens such as the NovoPen represent an intermediate technology gaining traction and can be effective for patients not using a pump. These devices capture insulin delivery data including timing and dosing, integrating with CGM platforms to provide comprehensive diabetes management insights. In simple terms, while before you could see only a 24-hour glucose tracing and rely on the patient’s recollection to inform when insulin was taken, a smartpen allows you to see exactly when insulin was given, at what dose and how glucose levels reacted in response to this. While not currently reimbursed through the HSE, they show promise for improving medication adherence and achieving modest improvements in TIR.
Fortunately, each pump is funded through the HSE at no cost to the patient and consumables required to utilise the pump are available under the Long-Term Illness scheme. The main barrier of access to pump therapy is the limited availability of skilled clinical staff to provide the necessary training for onboarding new pump users and support their continued care. Waiting lists for pump therapy can be long in some institutions and not every service operates a dedicated pump service as of yet. However, there is a widespread appreciation that the demand and clinical need for diabetes technology services will increase massively in future
Future Directions and Emerging Technologies
Each pump has specific advantages and disadvantages and the choice of pump should be guided by individual patient characteristics and preferences. For instance, the Ypsomed system offers unique advantages for certain populations. It's the only pump currently approved for use during pregnancy, with target ranges that can be set sufficiently low to meet pregnancy requirements. The pump is controlled via smartphone, allowing screen magnification for visually impaired users, though this population faces particular challenges with diabetes technology that the field continues to address.
Fortunately, each pump is funded through the HSE at no cost to the patient and consumables required to utilise the pump are available under the Long-Term
The field continues to evolve rapidly with pumps becoming more sophisticated and easier to use by patients with each iteration. Patch pumps such as the Omnipod, which eliminate tubing and offer more discrete insulin delivery, are available in many countries though not yet on offer to the Irish market. The advent of HCL systems has led to significant improvements in patients’ abilities to achieve TIRs >70% however many still struggle to achieve good control and oftentimes this can be related to issues surrounding meal time boluses, when the user has to interact with their pump more directly. The concept of an artificial pancreas—fully automated insulin delivery systems which require less user input—moves closer to reality with each technological iteration and represents a major frontier in diabetes technology.
For CGM technology, expansion beyond Type 1 diabetes appears inevitable. Applications in Type 2 diabetes on insulin, cystic
Essential Hospital Management of Diabetes Technology
Immediate Safety Assessment
For Insulin Pump Users:
• Ensure backup rapid-acting insulin pens are available— pump failure can cause diabetic ketoacidosis within hours
• Check if pump is functioning (no alarms, infusion set connected)
• Verify patient can operate their device safely – caution in acute confusional states
For CGM Users:
• Remember CGM readings lag blood glucose by several minutes
• Use fingerstick glucose for rapid changes, hypoglycaemia treatment, or when CGM readings don't match clinical picture
• Communicate plan for how blood glucose will be monitored and recorded with patient and nursing staff
Managing Pump Problems
Unexplained hyperglycaemia (>13 mmol/L):
1. Patient takes correction bolus via pump
• Patients should perform infusion set changes every 2-3 days, ideally early in the day
• Both pump and CGM users should have traditional backup supplies available
Discharge Planning
• Ensure diabetes technology is functioning before discharge
• Verify backup insulin supplies are available – these should be prescribed on discharge prescription
• Arrange appropriate diabetes team follow-up for any technology issues
• If technology has failed, ensure interim management plan until specialist review
When in Doubt
Default to traditional glucose monitoring and insulin delivery methods while seeking diabetes specialist input—patient safety takes priority over technology convenience.
Understanding these principles enables clinicians to safely manage patients using diabetes technology while maximising the benefits these innovations provide.
Additional Reading and Resources:
• HSE National Clinical Guideline No. 17 Adult Type 1 Diabetes Mellitus v2
• Diabetes Technology Network UK (DTN-UK): https://abcd. care/current/abcd-diabetestechnology-network
• YpsoPump Explorer app and t:simulator app available to download from Google Play/Apple store for device familiarisation
• HSE Medicines Management Programme guidelines for CGM reimbursement applications
Image 5: Tandem t:slim X2 from Tandem Diabetes
Image 5: Tandem t:slim X2 from Tandem Diabetes
Inequalities in Diabetes Prevalence
New research from RCSI University of Medicine and Health Sciences highlights significant inequalities in diabetes prevalence across Ireland, linked to differences in socio-economic status, age and education levels.
The research, led by the RCSI School of Population Health, analysed data from the Healthy Ireland survey spanning 2015 to 2023. The team found that those from disadvantaged areas, as well as those with lower levels of education are more likely to have, or develop, diabetes.
Among disadvantaged communities, 6% of individuals reported having diabetes – almost three times higher than the 2.2% recorded among those in more affluent areas. Similarly, research reveals that diabetes rates are three times as high among those who have not progressed beyond primary school education when compared to those with postgraduate degrees.
While these findings underscore stark inequalities in diabetes prevalence, the study suggests that targeting existing diabetes prevention programmes at these groups could improve diabetes prevalence among the Irish population over time.
Dr Gintare Valentelyte, Lead Author of the study
An Individualised Approach
Professor Edward Gregg, co-investigator on the study and Head of RCSI’s School of Population Health, said: “The research shows that, while our overall diabetes rates are stable, the high prevalence in lower socio-economic areas remains. In order for diabetes prevention strategies to be effective, we must account for, and accommodate, the specific challenges faced by various marginalised groups across the country.”
Lead author of the study, Dr Gintare Valentelyte, added, “The need for targeted and accessible support among all social demographics is evident from our research findings. I hope this research highlights the existing gap in services and education and that it inspires a more individualised approach to diabetes prevention.”
Strong Partnerships
The study provides critical insights to guide more equitable public
Date for your Diary 2026
The calendar recently marked a one-year countdown to the International Social Pharmacy Workshop 2026, taking place in Cork, Ireland from 28th June - 2nd July!
ISPW 2026 Co-chairs Laura and Michelle in statement said, “It’s difficult to believe that it’s been nearly a whole year since the wonderful time we spent in Banff, Canada for ISPW 2024.
“It has been a busy but exciting period of planning. The international committee have met frequently, and with their guidance, we have been putting some very exciting arrangements in place. A wonderful venue, programme and social calendar across the five days is being finalised, complementing the theme for this gathering, “Pharmacy First, People Foremost.”
“The sponsorship prospectus will be released shortly, but we’re absolutely delighted to confirm that ISPW will
health interventions aimed at reducing diabetes prevalence across Ireland.
This publication has emanated from research conducted with the support of Science Foundation Ireland, as well as a Research Ireland Research Professorship Programme for Professor Edward Gregg.
The research was carried out in partnership with Imperial
be sponsored once again in 2026 by Research in Social and Administrative Pharmacy (RSAP) and Exploratory Research in Clinical and Social Pharmacy (ERCSP), with published abstracts for accepted submissions!
Huge thanks to Dr Shane Desselle and colleagues for their continued championing of pharmacy research, and for supporting this bi-annual meeting of colleagues and friends.
“You’ll be hearing lots more from us over the coming months. Stay tuned for important updates on additional sponsorship opportunities, registration opening, calls for abstracts, keynote speaker reveals, and all the extra information that you’ll need to make your trip to the Emerald Isle and the banks of Cork’s River Lee something really special.
“We cannot wait to welcome you, so get those dates in the diary, (if they aren’t there already!) and please help us to spread the word on socials and via your networks.”
College London, Department of Epidemiology and Biostatistics; School of Health, University of the Sunshine Coast; Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne; and the School of Medicine, Western Sydney University. You can also find more information on the causes, risks and symptoms of diabetes in the HSE publication, Diabetes Prevention: A Guide to Healthy Living.
Cholesterol
The Role of the Dairy Matrix in Cholesterol Management
Written by Dr Martina Rooney, Prof Eileen R Gibney and Dr Emma L Feeney.
Food for Health Ireland, Institute for Food and Health, UCD.
Milk, cheese and yogurt are rich sources of nutrients important for health, including protein, fat, calcium, iodine, phosphorus, vitamin D, vitamin B12, riboflavin and other nutritive and bioactive compounds. These nutrients are essential for biological function including bone growth and development, bone health, energy and nutrient metabolism, nervous and immune system function and many others. Dairy products are an important contributor to the intake of these nutrients, on average in the Irish population, dairy provides 39% of calcium, 34.5% of vitamin B12 and 10.5% of magnesium intakes (1). However, these findings are from 2010 when 99% of the sampled population consumed some form of dairy. The most recent analysis from 2024 indicates 84% of those sampled consumed milk, while 62% ate cheese, with an average population intake of ~1 glass and a cheese portion daily (2). Delving into these figures further, cheese alone provides 9.1% of calcium, 12.6% of retinol, 3.7% of protein, 3.4% of vitamin B12 and 3.2% of riboflavin intakes (1). The critical role of dairy in nutrition and health is further emphasised by recent global analysis highlighting widespread deficiency several nutrients of concern, particularly B vitamins, iodine and calcium (3). Globally, the triple burden of malnutrition has recently been highlighted with 820 million chronically undernourished people, and greater than 2 billion people suffering from ‘hidden hunger’, i.e. insufficient
micronutrient intake despite consuming enough calories (4). Given the rich nutritional profile of dairy foods, particularly in ‘nutrients of concern’, such as calcium, iodine and riboflavin, dairy foods can play an important
role in assisting populations to achieve optimal nutritional intakes and health outcomes.
However, dairy also contains saturated fat, high intakes of which are linked with elevated
LDL-cholesterol concentrations, which in turn is associated with increased cardiovascular disease (CVD) risk (5). Globally, nutrientbased dietary guidelines have a blanket recommendation for saturated fat intake, of 10% of total energy intake or less (6-8). Consequently, those with elevated cholesterol concentrations are often advised to limit dairy intake, particularly cheese, thus this population may be missing out on important nutrients, such as calcium and protein (9). Experts in the field of dairy and health have made recent global calls to challenge these guidelines, given the compelling evidence that the dairy matrix can influence the physiological and health effects of nutrients, including saturated fat (10). The dairy matrix refers to the nutrients and interactions of the proteins, fats and other nutritive and bioactive compounds within the dairy food. Different dairy structures and common processing methods may enhance interactions between nutrients in
Full-fat cheese
Reduced-fat cheese and butter
Deconstructed cheese ingredients
Cholesterol response to full-fat cheese (teal), reduced-fat cheese (green) and ‘deconstructed’ cheese ingredients (blue) in the RCT by Feeney et al., published in the American Journal of Clinical Nutrition (2018). Full-fat cheese, where all dairy fat was contained within the dairy matrix, significantly lowered total and LDL cholesterol concentrations compared to both reduced fat cheese and butter (where some fat was within the dairy matrix, and some outside), and deconstructed cheese ingredients, where all dairy fat was outside the dairy matrix.
* indicates significant difference in response between groups.
Dr Martina Rooney, Research Scientist/Research Progamme and Grants Manager, UCD
Prof Eileen Gibney, Full Professor of Nutrition, UCD Nutrition, UCD
Figure 1: Effect of dairy fat in different matrices
Unmelted cheese
Melted Cheese
Deconstructed cheese ingredients
Cholesterol response to unmelted cheese (teal), melted cheese (purple) and ‘deconstructed’ cheese ingredients (blue) in the RCT by O’Connor et al., published in Food & Function (2024). Here, the dairy matrix was disrupted by applying heat, i.e., melting. Consumption of melted cheese was shown to significantly increase total cholesterol and triglyceride (not shown) concentrations, compared to butter, in middle-aged adults with overweight and obesity.
* indicates significant difference in response between groups.
the dairy matrix, which may modify the metabolic effects of dairy consumption (11).
Approximately 60% of the fat in dairy is saturated fat, however, the nature of the dairy matrix can mitigate the effects of saturated fat on health. Specifically, when the same amount of fat is eaten in the form of cheese vs in the form of butter, we see that cheese raises cholesterol significantly less than butter. This has been shown independently in a number of trials and summarised in meta-analyses, an approach which combines the results of multiple studies which address the same research question in order to provide a more comprehensive overview. The most recent meta-analysis (12) considered the effect of cheese vs butter on 264 participants from seven randomised controlled trials (RCTs), with findings indicating that consumption of 135g/day (~4 servings) of cheese for at least two weeks decreased total cholesterol by 0.24 mmol/L and LDL cholesterol by 0.19 mmol/L, compared to 52g butter (~three pats of butter). These findings, from independent research groups in Denmark, Australia, Ireland and America, indicate the beneficial effects of cheese, compared to butter, on cardiometabolic health. But what are the mechanisms underpinning this relationship? Several potential pathways have been proposed, each rendering saturated fat less available
for cholesterol synthesis and in turn, lowering cholesterol concentrations. Cheese is a rich source of calcium, which can bind with fat and form calcium soaps, making the fat less digestible and subsequently increasing faecal fat excretion (13, 14). Therefore, when contained within the cheese matrix, it may be that not all of the fat is digested. Within the dairy food category, the foods themselves have different matrices with milk having a liquid matrix, yogurt has a gel matrix and cheese a semi-solid matrix. The disintegration of the matrix is a key factor influencing nutrient release during digestion, with in-vitro studies demonstrating a much slower release of fat from cheese, compared to milk or yogurt, owing to the matrix structure (15). Furthermore, disrupting the physical structure of the matrix by applying heat, i.e., melting, has been shown to increase total cholesterol and triglyceride concentrations in middle-aged adults (16).
Research at Food for Health Ireland (FHI), a dairy technology centre based at University College Dublin, has been investigating this over the past decade and researchers have gained further insight into the dairy matrix effect. In order to investigate the effect of the cheese matrix on cardiometabolic health, the team at FHI disrupted the cheese matrix by deconstructing the ingredients
(17) and the structure, i.e., through melting (16) in a series of human intervention studies. The first study investigated how dairy fat contained within or outside the cheese matrix affected health, in 127 people (17). The test diets comprised of either a full-fat cheddar cheese, a reduced fat cheese and butter intervention or ‘deconstructed’ cheese ingredients (butter, powdered calcium caseinate, and a calcium supplement to match the overall macro and micronutrient profile of cheese). Each of the test diets provided ~40g dairy fat in different matrices and were matched for energy (calories), fat, protein and calcium. This was important so that any effect observed could be attributed to the matrices (structures) and not any nutritional differences between the test diets. The authors also note the high ‘dose’ of 120g of cheese eaten daily in this study, which was above recommended guidelines of 3 portions of dairy per day. However, it was important to provide enough of the cheese to demonstrate a difference in cheese vs butter in the relatively short 6-week study time period. Participants recruited for these studies were healthy adults with overweight or obesity, of middle age, and who were not prescribed any medications for cholesterol or blood pressure management or therapeutic diets. Evidence suggests any benefits from cheese
consumption would be greatest in a slightly older, heavier cohort. When full-fat cheddar cheese was consumed, i.e., all dairy fat was contained within the cheese matrix, total and LDL cholesterol concentrations decreased by 0.52 mmol/L and 0.45 mmol/L, respectively, after 6-weeks. In response to the reduced-fat cheddar cheese and butter group, i.e., when some dairy fat was within the cheese matrix and some was outside the matrix, reductions of 0.37 mmol/L and 0.27 mmol/L in total and LDL cholesterol concentrations were observed. Finally, when all the dairy fat was outside the cheese matrix, i.e. the ‘deconstructed’ cheese ingredients, total cholesterol lowered by 0.10 mmol/L and LDL cholesterol by 0.07 mmol/L. As can be seen from the results, a step-wise reduction in cholesterol concentrations was observed, with the greater improvements when more fat was contained within the dairy matrix. This seminal RCT was the first to confirm the role of the dairy matrix in cardiometabolic health, by the investigating the presence of dairy fat within or outside the cheese matrix. While other studies had previously compared cheese to butter, none had nutrient-matched the interventions in this way to test the effect of the matrix structure.
The next step was to test the role of the dairy matrix form, or structure, on cardiometabolic health The second RCT disrupted the dairy matrix by deconstructing the physical structure, by applying heat, i.e., melting (16). Here, two of the test diets were identical to the original study, i.e., full-fat cheddar cheese (participants were advised to eat cheese unmelted, in its natural form) and deconstructed cheese ingredients; however, the novel test arm was a full-fat cheddar cheese that was melted by grilling or micro-waving before consumption. Otherwise, the protocols were identical across both RCTs. Again, on this occasion the dairy matrix effect was demonstrated, as when the matrix was disrupted through melting significant differences in cholesterol response were observed between the melted and unmelted cheese groups (16). There was no change in lipid parameters after consumption of unmelted cheese, however total cholesterol and triglyceride concentrations increased in response to melted cheese. This can be explained by the physical breakdown of the cheese structure when melted, where the fat escapes from the protein structure, and can pool on the surface, known as ‘oiling-off’. It must be noted that in the original study reductions in cholesterol
Figure 2: Effect of cheese form (structure)
Cholesterol
Full-fat, unmelted cheese
Deconstructed cheese ingredients
When data from both RCTs was pooled and split by sex, there was no difference in cholesterol response between cheese and butter within males
concentrations in response to cheese vs butter were observed (17) whereas in the second RCT maintenance or an increase in these markers were observed, despite identical recruitment criteria and study protocols between the studies. However, sampling for the second RCT
started in March 2020, just as Ireland entered a Covid-19 related lockdown, which altered diet and lifestyle factors for many people.
CVD is traditionally considered to affect males more than females, with ischaemic heart disease responsible for 159.59 deaths per
100,000 males, and 146.27 deaths per 100,000 females in Western Europe in 2019 (18). In recent years, there has been growing realisation of the difference in presentation and treatment of CVD in males compared to females, with calls for action for sex-specific CVD guidelines (19).
Female-specific CVD risk factors include age of menarche and menopause, polycystic ovarian syndrome, parity, pregnancy loss, and adverse pregnancy outcomes (20). Furthermore, interest into the effect of sexual dimorphism in nutrition has grown, as males and females often respond differently to dietary intervention (21, 22). Thus, pooling of data from the abovementioned RCT, allowed further insight into sex differences in the cholesterol lowering effect of cheese compared to butter (23). When data from all those who consumed (a) unmelted, full-fat cheddar cheese or (b) the deconstructed cheese ingredients were combined, LDL cholesterol was shown to be significantly lowered following 6 weeks cheese consumption, compared to butter. When stratified by sex, there was there was no difference in cholesterol response between cheese and butter within males. However the ‘dairy matrix effect’ appeared to be particularly strong in females, with a decrease of 0.19 ± 0.77 mmol/L in total cholesterol in response to the cheese diet and an increase of 0.10 ± 0.73 mmol/L in response to the deconstructed cheese diet (23). These findings are particularly relevant for personalised nutrition, as heavier, middle-aged females are often advised to limit cheese intake for dietary management of cholesterol concentrations, however this group may actually benefit most from cheese, for both lipid management and nutrient intake and health. The rationale behind these observed sex-related differences are unknown, although HDL-mediated cholesterol efflux capacity response to dietary fat has been shown to vary between males and females (24). Whilst, genetic factors were not considered as part of this analysis, the influence of genes cannot be ruled out. Furthermore, carryover effects from pregnancy-related outcomes and subsequent impact on health may be implicated.
The dairy matrix effect may be stronger in females.When data from both RCTs was pooled and split by sex, there was a significant difference in response to total and LDL cholesterol after consumption of cheese and butter, within middle-aged females with overweight and obesity. * indicates significant difference in response between groups.
Patients, and medical practitioners, are familiar with the traditional lipid markers of total, LDL and HDL cholesterol concentrations. More recently, however, the field has advanced to develop novel and more sensitive markers of cardiovascular health such as lipoprotein particle concentration and size. Total, LDL and HDL cholesterol biomarkers consider the amount of cholesterol circulating around the body, whereas lipoprotein particle markers reflect the number and size of the particles carrying the cholesterol (25). In order to understand this marker and health, smaller, more denser LDL particles are more atherogenic than larger,
more buoyant LDL particles. In follow-up analysis of the cheese matrix study for more sensitive biomarkers, an increase in LDL particle size and reduction in LDL particle density was observed after consumption of full-fat cheese, compared to the other test diets. These findings indicate when cheese is consumed within its whole or intact food matrix it may lead to improvements in atherogenic lipid profile, compared to the formulated diets where the fat was eaten as butter (26). Preliminary analysis suggests sex may also play a role in this relationship, with more favourable effects of cheese on lipoprotein particle profiles observed in females compared to males.
Whilst this article has focused mainly on cholesterol concentrations, other markers of cardiometabolic health, such as
anthropometry, glycaemic control and blood pressure, cannot be ignored. In our cheese matrix studies despite providing an additional energy intake, no net change in body weight or body fat percentage was observed. This is in line with other studies, although displacement of other foods in the background diet cannot be ignored. However, it is also worth noting that in an observational analysis of a representative Irish population, higher dairy intake was associated with lower body mass index, percentage body fat, waist circumference and waist-to-hip ratio (27). While the cohorts in the cheese matrix studies were normotensive at baseline, no effect on blood pressure was observed in response to cheese. Again this is in line with other studies considering cheese and blood pressure, while evidence
suggests that mixed dairy intakes, i.e., including milk, cheese and yogurt in the daily diet (28) may have the greatest blood pressure lowering effects in populations with overweight or obesity (29). These findings highlight the neutral effects of cheese consumption on cardiometabolic health, and thus how cheese, and dairy, can play an important role in nutrition and health.
The evidence for the role of dairy in nutrition and health is compelling. Milk, cheese and yogurt are a key source of essential nutrients that billions of people worldwide are lacking. On the other hand, evidence suggests cheese has neutral or beneficial effects on cardiometabolic health, despite containing saturated fat. But what does this mean for health professionals and their practice?
Considering the evidence provided
¤34m Research Ireland ARC Hub
Significant Research Ireland funding has been announced today for the ARC Hub for HealthTech which is led by Professor Garry Duffy, Head of Department of Anatomy and Regenerative Medicine at RCSI and Professor of Health Technology Innovation at University of Galway.
The ARC Hub for HealthTech aims to boost translational research in chronic disease management, focusing specifically on aspects such as decision support and intervention planning, smart implants, advanced wearables, novel sensors, and algorithms and artificial intelligence/machine learning models.
Funded by Research Ireland, along with the European Regional Development Fund (ERDF) and the Government of Ireland, ARC Hub for HealthTech will be implemented across Northern and Western Regions of Ireland. The innovation-led programme will fast track research projects, boosting healthcare access across regional parts of Ireland.
Minister for Further and Higher Education, Research and Innovation James Lawless added: “Enhancing the existing academic-enterprise healthcare and technology ecosystems, the ARC Hub will deliver a suite of impactful, on-the-ground supports, benefitting everyone in the process – researchers, engineers,
Pictured (l-r): Director of the ARC Hub for HealthTech Professor Garry Duffy, Head of Department of Anatomy and Regenerative Medicine at RCSI and Professor of Health Technology Innovation at University of Galway; ARC Hub for HealthTech Co-lead Professor Richard Costello, Professor of Respiratory Medicine, RCSI; Dr Aoife Gallagher, Head of Innovation, RCSI; Research Ireland’s Interim CEO, Celine Fitzgerald; and Dr Seamus Browne, Head of Strategic Research Initiatives and Industry Partnerships, RCSI.
technologists, manufacturers, clinicians, physicians and, critically, patients. The ARC Hub for HealthTech will play an instrumental role in accelerating the commercialisation of research and getting health solutions to those that need them, faster.”
Professor Fergal O’Brien, Deputy Vice Chancellor for Academic Affairs at RCSI, commented on RCSI’s involvement, saying: “Supported by RCSI’s Office of Research and Innovation, we are delighted to be play a key role in such an important initiative for translational research. RCSI is dedicated to boosting development and commercialisation in medtech, digital health, and biomaterials and we look forward to advancing our efforts in these areas through our ongoing collaboration with ARC Hub for HealthTech”.
here when offering patientcentred care is a positive next step. If a patient is lacking intake of essential nutrients, it is worth encouraging milk, cheese and yogurt as a digestible, accessible, affordable source of protein and a range of micronutrients. When offering lifestyle and dietary management of elevated cholesterol concentrations, reassuring cheese-lovers that consuming cheese can be neutral or even beneficial for their cardiometabolic health, particularly if they are middleaged, with overweight/obesity or female, can make dietary advice more acceptable and varied, and therefore effective. Personalised nutrition and positive messaging around dairy and health is a winwin for both the practitioner and the patient.
References available on request
The five RCSI projects funded under the new ARC Hub for HealthTech programme are:
• Developing novel biosensor technology to improve heart failure management – Dr Aamir Hameed, Tissue Engineering Research Group, RCSI.
• Developing a novel medical device to improve the accuracy of diagnosis of lung conditions, overcoming current spirometer limitations – Professor Richard Costello, Department of Medicine, RCSI.
• Developing an algorithm for early-stage breast cancer prediction and treatment
guidance – Professor Darran O’Connor, School of Postgraduate Studies, RCSI.
• Creating a decision support and intervention planning digital obesity treatment platform for adolescents –Dr Grace O’Malley, School of Physiotherapy, RCSI.
• Developing a novel device to overcome the major challenges associated with current brain stimulation devices used for deep brain stimulation in epilepsy – Dr Ian Woods and Professor Fergal O’Brien, Tissue Engineering Research Group, RCSI.
Diabetes & Dementia
Cardioprotective Glucose-Lowering Agents and Dementia Risk: A Systematic Review and Meta-Analysis
Written by Allie Seminer, MSc1; Alfredi Mulihano1; Clare O’Brien, MD2; et al
1HRB Clinical Research Facility, University of Galway, Galway, Ireland
Dementia is a leading cause of disability globally, and is projected to affect approximately 75 million people by 2030.1 2 Diabetes is a risk factor for dementia, estimated to account for approximately 5% of the populationattributable fraction of all dementia.3 4 Diabetes is also a risk factor for ischemic stroke,5 which may mediate an association with vascular dementia. Identification of population-level interventions, such as tailored management of common risk factors (eg, diabetes), may reduce the global burden of dementia. However, there is a lack of robust evidence to support the efficacy of glucose-lowering therapies in reducing the risk of dementia, which may relate to variations in cardioprotective efficacy among glucose-lowering therapies.
In patients with type 2 diabetes and cardiovascular disease or risk factors, guidelines recommend use of sodium-glucose cotransporter-2 inhibitor (SGLT2i) and glucagonlike peptide-1 receptor agonist (GLP-1RA) drug classes as first-line treatments, based on findings from phase III randomised clinical trials reporting a significant reduction in cardiovascular events, and metformin and pioglitazone are recommended as secondline treatments.6 7 Observational evidence suggests that certain glucose-lowering drug classes, such as SGLT2is and GLP-1RAs, may have a neuroprotective effect.8 9 However, to date, the association of cardioprotective classes of glucose-lowering therapies with risk of dementia has been inconsistent, prompting the need for an updated meta-analysis of randomised clinical trials.10 11
The aim of this meta-analysis was to determine whether cardioprotective glucose-lowering therapy, compared with controls, was associated with a reduction in risk of dementia or cognitive impairment, and among primary dementia subtypes.
Methods
We performed a systematic review and meta-analysis, adhering
to the Cochrane Collaboration guidelines, and reported our findings according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.12,13 The meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42024557562). The data that support the findings of this study are available from the corresponding author upon reasonable request.
Data Sources and Search Strategy
We systematically searched the PubMed and Embase databases for articles published from inception of the database to June 11, 2024. The included search terms are detailed in the eMethods in Supplement 1. The reference list of studies selected for inclusion and published systematic reviews of glucose-lowering therapy were also screened for studies that met our inclusion criteria. Two reviewers (A.S. and A.M.) independently screened titles and abstracts. Full texts were sourced for relevant articles. To ascertain if cognitive outcomes were reported, the full text, supplementary appendix, and ClinicalTrials. gov record were reviewed for each study that met inclusion criteria related to the population, intervention, and comparator. Inclusion criteria were assessed independently and inconsistencies were resolved by consensus.
Eligibility Criteria
Studies were considered eligible if they (1) were randomised clinical trials; (2) included adults older than 18 years; (3) evaluated cardioprotective glucose-lowering therapy based on guideline recommendations and findings from phase III randomised clinical trials compared with controls; (4) reported dementia, cognitive impairment, and/or change in cognitive score; and (5) had a 6-month minimum follow-up duration. Eligible glucose-lowering interventions included the following drug classes and agents: SGLT2is, GLP-1RAs, metformin, and
pioglitazone. These drug classes are recommended as glucoselowering therapy for individuals with cardiovascular disease or risk factors6 7 on the basis of randomised clinical trial evidence demonstrating a reduction in cardiovascular events (SGLT2is and GLP-1RAs)14-16 or suggesting cardiovascular benefit (metformin and pioglitazone).17 18 The following drug classes were excluded due to lack of current evidence of efficacy in cardiovascular outcome trials: dipeptidyl peptidase-4 inhibitors,19 sulfonylureas,20 and insulin.21 22 Controls were defined as placebo, usual care, or no glucoselowering therapy. Trials evaluating the effect of glucose-lowering therapy in a population with a prior diagnosis of cognitive impairment or dementia were excluded.
Data Extraction
Data were abstracted independently by 2 authors (A.S. and A.M.) using a standardised data collection form. For each study, we abstracted the title, year of publication, glucose-lowering drug (class, drug name, and dose), control, design (open label or placebo controlled), intervention and control numbers, definition of dementia used, all-cause dementia, dementia subtypes, and change in cognitive score. We reported outcomes from the point of longest available follow-up. Data were compared for inconsistencies and merged into a prefinal dataset, which was checked independently by a third reviewer (C.R.).
Outcomes
The primary outcome of this meta-analysis was dementia or cognitive impairment on follow-up. We used a hierarchical approach in which we included trials that reported incident dementia, or a composite of dementia or cognitive impairment (if dementia alone was not reported), on follow-up.23 Secondary outcomes included dementia subtypes, including vascular dementia and Alzheimer dementia, and change in cognitive score.
Risk-of-Bias Assessment
The methodological quality of eligible trials was assessed using the Cochrane Risk of Bias 2 tool.24 Two independent reviewers (A.M. and C.O.) performed risk-of-bias assessments, and disagreements were resolved by a third reviewer (C.R.). If 1 of the domains was rated as high risk, the study was considered at a high risk of bias.
Data Synthesis and Analysis
We calculated the odds ratio (OR) and 95% CIs for each outcome of interest from individual studies. Weighted pooled treatment effects were calculated overall and individually for individual drug classes, using restricted maximum likelihood (REML) estimation to fit a random-effects meta-analysis model. REML estimation was chosen because it has been shown to be less biased than the DerSimonianLaird estimator.50 51 Absolute risk reductions (ARRs) and 95% CIs were calculated for each study; the Mantel-Haenszel method was used to obtain a pooled estimate of the risk difference. The variability across studies due to heterogeneity was investigated using forest plots and I2 statistics. Differences in cognitive scores were not meta-analyzed due to lack of data and heterogeneity of score used. Publication bias was assessed using a funnel plot.
We tested for heterogeneity between drug classes (GLP1RAs vs SGLT2is) by dividing the difference in log relative risk by its standard error.52 A priori subgroup sensitivity analyses that assessed pooled estimates for trials that reported follow-up above and below the median number of months of follow-up, and including only trials with low risk of bias, was performed. P values were 2-sided with a significance threshold of <.05.
Results
The systematic search of articles published before June 11, 2024, identified 3831 articles. After
TOUJ0O® From the start,1 there to help your patients on their basal insulin journey 1 insulin glargine 3D0U/mL
• Help your patients find balance between HbA le reduction and hypoglycaemic risk1 -7
Toujeo® DoubleStar ™ prefilled pen is recommended for patients requiring at least 20 units per day.1
t Toujeo® is available in easy-to-use pens, .s.9 to be administered once daily at any time of the day, preferably at the same time every day.1 When needed, patients can administer Toujeo� up to 3 hours before or after their usual time of administration. Flexible dosing time was evaluated in two randomised, open-label clinical studies, in patients with T2DM.1
prescribing Information: Toujeo®(insulin qlargine 300 uni ts/ml) Please refer to Summary of Product Characteristics (SmPC) before prescribing. Presentation: Toujeo SoloStar and DoubleStar pre-filled pens. Each ml contains 300 units of insulin glargine. SoloStar pen contains 1.5ml (450 units) of solution for injection. DoubleStar pen contains 3ml (900 units) of solution for injection. Indication: Treatment of diabetes mellitus in adults, adolescents and children from the age of 6 years. Dosage and Administration: Toujeo is administered subcutaneously, by injection into the abdominal wall, the deltoid or the thigh, once daily, at any time of the day preferably at the same time every day. Injection sites must be rotated within a given injection area from one injection to the next in order to reduce the risk of lipodystrophy and cutaneous amyloidosis. The dose regimen (dose and timing) should be adjusted according to individual response. Do not administer intravenously. In type 1 diabetes mellitus, Toujeo must be combined with short-/rapidacting insulin to cover mealtime insulin requirements. In patients with type 2 diabetes mellitus, recommended daily starting dose is 0.2 units/kg followed by individual dose adjustments. Toujeo can also be given together with other anti-hyperglycaemic medicinal products. Switch between insulin glarqine 100 units/ml and Tou;eo: Insulin glargine 100 units/ml and Toujeo are not bioequivalent and are not directly interchangeable. When switching from insulin glargine 100 units/ml to Toujeo, this can be done on a unit-to-unit basis, but a higher Toujeo dose (approximately 10-18%) may be needed to achieve target ranges for plasma glucose levels. When switching from Toujeo to insulin glargine 100 units/ml, the dose should be reduced (approximately by 20%). Switching from other basal insulins � A change of dose and/or timing of the basal insulin and concomitant anti-hyperglycaemic treatment may be required. Dose adjustments may also be required if the patient's weight or lifestyle changes, the timing of insulin dose is changed, or other circumstances arise that increase susceptibility to hypo- or hyperglycaemia. Toujeo must not be mixed or diluted with any other insulin or other medicinal products. Close metabolic monitoring is recommended during a switch and in the initial weeks thereafter. SoloStar 1-80 units per single injection in steps of 1 unit and DoubleStar 2-160 units in steps of 2 units. When changing from Toujeo SoloStar to Toujeo DoubleStar, if the patient's previous dose was an odd number then the dose must be increased or decreased by 1 unit. Toujeo DoubleStar prefilled pen is recommended for patients requiring at least 20 units per day. Special Populations: Insulin requirements may be diminished in the elderly or patients with renal or hepatic impairment. Paediatdc: When switching basal insulin to Toujeo, dose reduction of basal and bolus insulin needs to be considered on an individual basis, in order to minimise the risk of hypoglycaemia. The safety and efficacy of Toujeo in children and adolescents below 6 years of age have not been established. Contraindications: Hypersensitivity to insulin glargine or any excipients. Precautions and Warnings: Traceability: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Toujeo is not the insulin of choice for treatment of diabetic ketoacidosis. Patients must be instructed to perform continuous rotation of the injection site to reduce the risk of developing lipodystrophy and cutaneous amyloidosis. There is a potential risk of delayed insulin absorption and worsened glycaemic control following insulin injections at sites with these reactions. A sudden change in the injection site to an unaffected area has been reported to result in hypoglycaemia. Blood
Intended for Healthcare Professionals in the Republic of Ireland only.
glucose monitoring is recommended after the change in the injection site, and dose adjustment of antidiabetic medications may be considered. Hypoglycaemia: In case of insufficient glucose control or a tendency to hyper/hypoglycaemic episodes, the patient's adherence to the prescribed treatment regimen, injection sites and proper injection technique and all other relevant factors must be reviewed before dose adjustment is considered. Particular caution should be exercised, and intensified blood glucose monitoring is advisable for patients in whom hypoglycaemic episodes might be of clinical relevance and in those where dose adjustments may be required. Warning signs of hypoglycaemia may be changed, less pronounced or absent in certain risk groups, potentially resulting in severe hypoglycaemia and loss of consciousness. Risk groups include patients in whom glycaemic control is markedly improved, hypoglycaemia develops gradually, an autonomic neuropathy is present, or who are elderly. The prolonged effect of subcutaneous insulin glargine may delay recovery from hypoglycaemia. lntercurrent illness: Requires intensified metabolic monitoring and often it is necessary to adjust the insulin dose. Insulin antibodies: administration may cause insulin antibodies to form. Use with pioglitazone: Cases of cardiac failure have been reported when pioglitazone was used in combination with insulin, especially in patients with risk factors for development of cardiac heart failure. If the combination is used, patients should be observed for signs and symptoms of heart failure, weight gain and oedema. Pioglitazone should be discontinued if any deterioration in cardiac symptoms occurs. Medication errors: Insulin labels must always be checked before each injection to avoid errors between Toujeo and other insulins. Patients must be instructed to never use a syringe to remove Toujeo from the SoloStar or DoubleStar prefilled pen, A new sterile needle must be attached before each injection. Needles must not be re-used. Pregnancy and lactation: There are no data from exposed pregnancies in controlled clinical trials. However there is a large amount of data on use of insulin glargine 100 units/ml in pregnant women indicating no specific adverse effects on pregnancy and no specific malformative nor feta/neonatal toxicity. The use of Toujeo may be considered during pregnancy, if clinically needed. Careful monitoring of glucose control is essential. It is unknown if insulin glargine is excreted in breast milk. Interactions: Substances that affect glucose metabolism may require adjustment of insulin glargine. Adverse Reactions: Very common· Hypoglycaemia. Prolonged or severe hypoglycaemia may be life-threatening.� Lipohypertrophy injection site reactions, including redness, pain, itching, hives, swelling, or inflammation. Prescribers should consult the SmPC in relation to other adverse reactions. Legal Category: POM. Marketing Authorisation Number: SoloStar 5 pen pack: EU/1/00/133/035; Double5tar 5 pen pack: EU/1/00/133/038. Marketing Authorisation Holder: Sanofi Aventis Deutschland GmbH, D-65926 Frankfurt am Main, Germany. Further information is available from: Medical Information, Sanofi, 18 Riverwalk, Citywest Business Campus, Dublin 24 or contact IEmedinfo@sanofi.com. Date of preparation: July 2022
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie; email: medsafety@hpra.ie Adverse events should also be reported to Sanofi Ireland Ltd. Tel: 01 403 5600. Alternatively, send via email to IEPharmacovigilance@sanofi.com
Abbreviations: HbAlc, Hemoglobin A1c; PD Pharmacodynamics; PK Pharmacokinetics; TlDM. Type 1 Diabetes Mellitus; T2DM, Type 2 Diabetes Mellitus.
References: 1. Toujeo', Summary of Product Characteristics 2. Home PD, et al Diabetes Care 2015;38(12):2217-2225. 3. Matsuhisa M, et al Diabetes Obes Metab 2016;18(4):375-383. 4 Danne T. et al. Diabetes Care 2020: 43(7):1512-1519, 5. Riddle MC, et al. Diabetes Care 2014;37:2755-2762. 6. Yki-Jarvinen H, et al Diabetes Care 2014;37:3235-3243. 7. Bolli GB et al. Diabetes Obes Metab 2015;17:386-394. 8 Singh R, et al. Eur Endocrinol 2018;14:47-51. 9 Pohlmeier H, et al. J Diabetes Sci Technol 2017;11;263-269.
MA T IE-2500032 (v2 .OJ I April 2025
Diabetes & Dementia
From: Cardioprotective Glucose-Lowering Agents and Dementia Risk: A Systematic Review and Meta-Analysis
Association of Glucose-Lowering Therapy With Vascular DementiaSquares and bars represent the mean values and 95% CIs of the effect sizes, while the size of the squares reflects the weight of the study. Arrows indicate that the values are outside the range of the x-axis. Diamonds represent the combined effects and the vertical dotted lines, the lines of no effect. ARR indicates absolute risk reduction; RE, random effects
title and abstract screening, 505 articles were considered potentially relevant. Following full-text and ClinicalTrials.gov review, 26 trials were included. Twenty-three studies reported the incidence of a composite of dementia or cognitive impairment on follow-up and were included in the primary meta-analysis. Three studies were included for the secondary outcome of change in cognitive score only.
Study Characteristics
Overall, 164 531 participants were included from 26 trials, with a mean (SD) age of 64.4 (3.5) years and 34.9% were women. The mean duration of followup was 31.4 (range, 10.1-73.2) months. The publication years ranged from 2015 to 2024; 24 trials were conducted in international sites25 -36 38-45 48 and 2 were conducted in North America.46 ,47 All included trials were placebo controlled.
Risk of Bias
Risk of bias was assessed for all included trials. The overall risk of
bias was categorised as low for all trials. The measurement of the outcome domain was deemed to be low risk for all studies. While there was limited information regarding method of outcome ascertainment, participants and investigators of all included trials were blinded to the intervention allocated. There was no evidence of publication bias for the primary outcome.
Association of Cardioprotective Glucose-Lowering Therapy With Cognitive Impairment or Dementia
Twenty-three trials reported dementia or cognitive impairment on follow-up (160 191 participants), 12 trials evaluated SGLT2is, 10 trials evaluated GLP-1RAs, and 1 trial evaluated pioglitazone (no trials of metformin were identified).25 -39 41-45 Dementia or cognitive impairment was diagnosed in 93 participants in the intervention group and 119 participants in the control group on follow-up. Glucose-lowering therapy was not significantly associated with a reduction in
cognitive impairment or dementia (0.12% vs 0.14% over a mean follow-up of 31.8 months; OR, 0.83 [95% CI, 0.60-1.14]; ARR, 0.02% [95% CI, 1.00% to 0.09%]; I2 = 6.6%). Glucoselowering therapy with GLP-1RAs (OR, 0.55 [95% CI, 0.35-0.86]), but not SGLT2is (OR, 1.20 [95% CI, 0.67-2.17]), was statistically significantly associated with a reduction in cognitive impairment or dementia. Meta-regression analysis showed no significant association of the proportion of women enrolled with all-cause dementia (P = .08).
Association of GlucoseLowering Therapy With Dementia Subtypes
Dementia subtypes included vascular dementia, Alzheimer dementia, Lewy body dementia, and frontotemporal dementia. Ten trials reported rates of vascular dementia on follow-up (94 648 participants).28 ,29,3133 38 39 41 42 45 Vascular dementia was diagnosed in 6 participants in the intervention group and 16 participants in the control group
on follow-up. Glucose-lowering therapy was not significantly associated with a reduction in vascular dementia (0.01% vs 0.03% over a mean follow-up of 35.7 months; OR, 0.45 [95% CI, 0.19-1.07]; I2 = 0.0%). This was consistent across drug classes (SGLT2i OR, 0.35 [95% CI, 0.09-1.36]; GLP-1RA OR, 0.38 [95% CI, 0.18-1.61]; P value for heterogeneity = .93; Figure 2). Twelve trials reported rates of Alzheimer dementia (115 840 participants).25 ,29,32-35,3841,45,49 Alzheimer dementia was diagnosed in 56 participants in the intervention group and 51 participants in the control group on follow-up. Glucose-lowering therapy was not associated with a significant reduction in Alzheimer dementia (0.09% vs 0.09% over a mean follow-up of 37.1 months; OR, 1.20 [95% CI, 0.82-1.77]; I2 = 0.0%). This was consistent across drug classes (SGLT2i OR, 1.99 [95% CI, 0.596.71]; GLP-1RA OR, 1.85 [95% CI, 0.52-6.57]; pioglitazone OR, 1.07 [95% CI, 0.70-1.65]; Figure 3). Four trials reported rates of
From: Cardioprotective Glucose-Lowering Agents and Dementia Risk: A Systematic Review and Meta-Analysis
Association of Glucose-Lowering Therapy With Alzheimer DementiaSquares and bars represent the mean values and 95% CIs of the effect sizes, while the size of the squares reflects the weight of the study. Arrows indicate that the values are outside the range of the x-axis. Diamonds represent the combined effects and the vertical dotted lines, the lines of no effect. ARR indicates absolute risk reduction; RE, random effects.
Lewy body dementia (47 287 participants).29 38 42 45 Lewy body dementia was diagnosed in 1 participant in the intervention group and 3 participants in the control group on follow-up. Glucose-lowering therapy was not associated with a significant reduction in Lewy body dementia (0.004% vs 0.01% over a mean follow-up of 37.9 months; OR, 0.58 [95% CI, 0.12-2.86]; I2 = 0.0%). There were insufficient data to report a meta-analytic estimate for the frontotemporal dementia subtype (1 trial).39
Association of GlucoseLowering Therapy With Change in Cognitive Score
Three trials reported on change in cognitive score.46-48 McGarry et al reported no significant difference in cognition, measured by Scales for Outcomes in Parkinson’s Disease Cognition, between exenatide and placebo over a mean follow-up
of 36 months.46 The Pioglitazone in Early Parkinson’s Disease trial reported no difference in cognition, measured by Mattis Dementia Rating Scale scores, between the pioglitazone and placebo groups over a mean follow-up of 10.1 months.47 The Insulin Resistance Intervention After Stroke trial reported no significant difference in cognition, measured by Modified Mini-Mental State Examination, associated with pioglitazone compared with placebo over a mean follow-up of 57.6 months.48
A priori subgroup sensitivity analyses for the primary outcome assessing pooled estimates for trials that reported years of follow-up above and below the median follow-up duration did not materially alter findings.
Discussion
This meta-analysis, which included 23 trials with 160 191 participants for the primary outcome analysis,
did not report a significant reduction in dementia or cognitive impairment when all drug classes were considered. However, glucose-lowering therapy with GLP-1RAs, but not SGLT2is or pioglitazone, was associated with a significantly lower risk of dementia or cognitive impairment, compared with controls. Glucose-lowering therapy was not associated with a significant reduction in vascular or Alzheimer dementia. Vascular dementia event rates were numerically lower (not statistically significant) in the glucose-lowering group compared with controls. In contrast, Alzheimer dementia event rates were numerically higher (not statistically significant) in the glucose-lowering group compared with controls.
These findings add new information to existing literature. A 2023 meta-analysis of randomised clinical trials did not report a
significant reduction in dementia, and included 21 randomised clinical trials, including DPP4 inhibitors, GLP1-RAs, and SGLT2is.8 This meta-analysis differed in that the analysis was confined to glucoselowering therapy with proven effectiveness in reducing the risk of cardiovascular disease, and included additional trials for GLP1-RA and SGLT2i classes. A selected pooled analysis of 3 randomised clinical trials and a nationwide Danish registry-based cohort reported that GLP-1RA exposure was associated with reduced risk of dementia.10 These findings extend the findings of this study by including additional trials evaluating GLP-1RAs identified through a systematic search, and also including other drug classes that have demonstrated cardiovascular benefit, which allowed treatment effects to be determined among drug classes.
Diabetes & Dementia
Diabetes is associated with an increased risk of dementia, expected to be primarily mediated through vascular injury, but may also increase brain atrophy through other mechanisms.53 The study hypothesis was that glucoselowering medications associated with significant reductions in cardiovascular events would also reduce the risk of dementia, acknowledging that, in general, the magnitude of association of common vascular risk factors with dementia is lower than risk reported for cardiovascular events. For example, antihypertensive therapy is associated with a 27% relative risk reduction in stroke,54 but a 7% relative risk reduction in dementia.23 As a result, large sample sizes with extended periods of follow-up are
Navigator Tool
required to detect a significant reduction in dementia risk. Animal studies suggest that GLP-1RAs may reduce dementia risk through a number of potential mechanisms, in addition to neuroprotection mediated through reduced cardiovascular risk (eg, through anti-inflammatory effects on neuronal structures, antioxidative effects, and reduction in neuronal apoptosis).55 Similarly, SGLT2is have demonstrated neuroinflammatory and antioxidative effects in addition to cardiovascular prevention.56
In this meta-analysis, a larger risk reduction in dementia was associated with randomisation to receive GLP-1RAs than SGLT2i classes. This may be partly explained by differences
in populations enrolled, with a higher all-cause dementia event rate noted among the control group of GLP-1RA trials compared with SGLT2i trials (0.14% vs 0.05%), with a resultant increase in statistical power to detect associations. Indirect comparison also suggests that GLP-1RAs may have a larger magnitude of effect on cardiovascular risk than SGLT2is.16 57 While none of the eligible clinical trials included a specific population with cognitive impairment, findings may have implications for choice of glucose-lowering therapy in patients with diabetes and higher risk of dementia. However, large randomised clinical trials should be conducted that are dedicated to addressing optimal glucoselowering therapy in patients with
cognitive impairment. It is plausible that the efficacy of glucoselowering therapies for dementia outcomes may differ by sex and APOE4 status due to differences in glucose metabolism.58 59 Future studies reporting dementia outcomes by APOE4 status and sex are required to evaluate this.
A limitation of this meta-analysis is that the majority of clinical trials did not systematically evaluate participants for dementia, resulting in a low event rate. Other possible reasons for the low event rate include mean age of trial participants and relatively short duration of follow-up. However, as all clinical trials were placebo controlled, the relative risk estimates are expected to be unbiased. The incidence of all-cause dementia and vascular dementia among adults with diabetes in prospective cohort studies was estimated to be 14.2 to 16.8 per 1000 patient-years and 1.8 to 3.2 per 1000 patientyears, respectively, more than double the rate reported in this study.60 61 Therefore, the absolute risk reduction reported is most likely an underestimate, and the real-world absolute risk reduction of cardioprotective glucoselowering therapy is likely to be greater by approximately 0.5% to 0.6%.
A number of randomised clinical trials evaluating the neuroprotective effects of GLP1-RAs and SGLT2is are in progress. Studies are ongoing among populations with early Alzheimer disease or mild cognitive impairment, such as EVOKE (NCT04777396)62 and LIGHT-MCI (NCT05313529), and healthy volunteers with vascular risk factors, such as OxSENSE (NCT06363487).
Minister for Mental Health Mary Butler has launched ‘Navigator’ a signposting tool designed to support the mental health and wellbeing of young people aged 14 to 34 across Ireland.
Navigator was launched in collaboration with spunout, the Department of Health and the Health Service Executive (HSE). The signposting tool, a Programme for Government commitment, was developed by spunout in response to the challenges young people face in accessing mental health support, including stigma, low mental health literacy, and fragmented access to services. This innovative web-based and mobile-first tool offers anonymous, immediate, and personalised access to mental health information, resources, and services, addressing the gap in the availability of a single, national repository for tailored youth mental health support.
Minister for Mental Health Mary Butler today emphasised the importance of this tool, “spunout’s Navigator is a national digital gateway that empowers young people to take the first step toward support in a way that is simple, private, and tailored to their needs. By answering just three short questions, users of the tool will receive clear, trustworthy, and relevant results, helping them find the right support, right now.
“The launch and promotion of this important tool was included in the Programme for Government which was agreed at the beginning of this year, and I’m delighted to see this commitment being delivered on so early in the lifetime of this government.”
The digital tool includes a wide range of mental health resources, including factual information, lived experience articles and videos, expert-approved mental health apps, books, and podcast recommendations, as well as guided activities like grounding exercises and safety planning. The tool also provides direct service connection to 24/7 support through spunout’s ‘Text About It’ service for immediate support and signposts to specific and relevant local and national services for ongoing support.
Continuing Professional Development
CPD
CPD
60 Second Summary
Breast cancer screening programmes can lead to better disease outcomes, but women from deprived backgrounds are less likely to participate and more likely to present with late-stage cancer. This study aimed to explore associations between deprivation and breast cancer screening outcomes in Ireland during 2009–2018.
Data on all female breast cancer cases diagnosed in Ireland during 2009–2018 were extracted from the National Cancer Registry Ireland. Associations between area-level deprivation, using the Pobal Haase-Pratschke deprivation index, and detection of breast cancer through BreastCheck, Ireland’s breast screening programme, and stage of screen-detected breast cancer were explored. Unadjusted risk ratios (RRs) and 95% confidence intervals (CIs) were calculated.
Among screening eligible women in Ireland in 2009–2018, there was no difference in risk of breast cancer detection through BreastCheck across deprivation quintiles (RR for most compared to least deprived group: 1.01, 95% CI: 0.96–1.06). In women with screen-detected breast cancer, the risk of late-stage cancer detection increased with deprivation in 2009–2013 (RR for most compared to least deprived group: 1.45, 95% CI: 1.10–1.93), but no association was observed between deprivation and cancer stage in 2014–2018.
Notwithstanding its limitations, including the risk of confounding by uncontrolled variables, this study suggests screening eligible women in Ireland have had similar outcomes from breast cancer screening, regardless of deprivation level, since the national roll-out of BreastCheck.
Associations between deprivation and screening outcomes should continue to be monitored to ensure Ireland’s breast cancer screening programme is helping to reduce health inequities.
Written
by Philippa White1,*, Aline Brennan2, Joe McDevitt2, Deirdre Murray2, Caroline Mason Mohan1, Patricia Fitzpatrick3, Therese Mooney3, Alan Smith1, Maeve Mullooly 4 and Niamh Bambury2
1Public Health Department, National Screening Service, Dublin, Ireland
2National Cancer Registry Ireland, Cork, Ireland
3Programme Evaluation Unit, National Screening Service, Dublin, Ireland
4School of Population Health, Royal College of Surgeons in Ireland, Dublin, Ireland
*Corresponding author. Public Health Department, National Screening Service, King’s Inns House, Parnell Street, Dublin 1, Ireland. E-mail: philippa.white2@hse.ie.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings. Published by HPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author.
Screen-detected breast cancer and cancer stage by area-level deprivation: a descriptive analysis using data from the National Cancer Registry Ireland
Introduction
Breast cancer is the leading cause of cancer mortality in women worldwide1 and accounts for approximately 12% of the cancer burden globally.2 Excluding nonmelanoma skin cancer, breast cancer is the most common cancer in women in Ireland,3 with approximately one in every seven women receiving a diagnosis during their lifetime.4 In Europe, Ireland has the eighth highest incidence and fourth highest mortality rate.5 Socioeconomic disparities in breast cancer outcomes in Ireland are also stark. Women from the most deprived backgrounds have a 41% higher age-adjusted risk of dying from breast cancer within five years of diagnosis than women from the least deprived backgrounds and a 24% higher risk of being diagnosed with late-stage disease. Moreover, many of these disparities have remained unchanged over the last two decades.6
Similar to the international setting, in Ireland affluent women typically have a higher incidence of breast cancer than more deprived women.6, 7 This may be due to reproductive factors such as lower parity, older age at first full-term pregnancy, and lower age at menarche, as well as other factors such as higher
use of hormone replacement therapy and higher participation in screening being more prevalent in more affluent women.8 Despite this higher incidence of breast cancer in more affluent women, deprived women tend to have worse disease outcomes.9 This may be due to a number of factors. Firstly, participation in breast cancer screening is considerably lower among women from deprived backgrounds than women from less deprived backgrounds.10 In Europe, women from low income households are up to 45% less likely to participate in mammography screening than women from high income households.10 Low levels of education, immigrant status, and lack of home ownership have also been shown to be associated with a significantly lower attendance at breast cancer screening.11
Additionally, women from more deprived backgrounds are more likely to experience delays to diagnosis after an abnormal mammogram.12 Further, there are important socioeconomic differences in breast cancer stage at diagnosis, with more deprived women being more likely to present with late-stage disease.13
Organised breast cancer screening programmes aim to detect breast cancer at its earliest
stages, when treatment can lead to better disease outcomes.14
Mammography-based screening is effective and has been shown to reduce breast cancer mortality and the incidence of late-stage disease.15 The population benefits conferred by screening are not always evenly distributed, however, and as previously described, health inequities in breast cancer persist.12
BreastCheck—The National Breast Screening Programme, is Ireland’s population-based breast cancer screening programme and is delivered by the National Screening Service (NSS). Since 1998, BreastCheck has provided free biennial mammography screening to eligible women.16 In the first phase of the programme roll-out starting in 2000, BreastCheck was available in the east of the country, providing services to 14 of the 26 counties in the Republic of Ireland. Starting in late 2007, the second phase saw the national expansion across the country.17 Initially, the eligible age range for participation was 50–64years and in 2015 this was extended upwards on a phased basis with those aged 50–69years being eligible to participate from 2020.16
The relationship between deprivation and screening outcomes in Ireland remains
Sensitivity analysis
30 CPD 119: BREAST CANCER
In women with screen-detected breast cancer, those in the more deprived quintiles had a higher risk of being diagnosed with latestage disease over the entire study period (Table 3). There was a clear gradient between increasing deprivation and increasing risk of late-stage screen-detected breast cancer in 2009–2013, with the risk diagnoses were observed (Supplementary Table S3).
Table 1. Characteristics of all female breast cancers (all ages) diagnosed in Ireland between 2009 and 2018 (n ¼ 30 560)
a: This included breast cancers detected through symptomatic presentation, autopsy, opportunistic screening, incidental findings, and unknown methods of detection.
unclear. This study aimed to assess the associations between area deprivation and both risk of breast cancer being detected by organised, population-based screening and risk of later stage screen-detected breast cancer. It also aimed to assess these associations over time, between 2009 and 2018, as the BreastCheck programme was rolled out to the entire country.
Methods
Sources of data
Data on breast cancer cases (i.e. cancers categorised under code C50 of the tenth revision of the International Classification of Diseases, [ICD-10]) are collected by the National Cancer Registry Ireland (NCRI). Since 1994, the NCRI has collected data on all cancer cases from all areas in the Republic of Ireland. Under secondary legislation, the NCRI collects data on all cancer cases from different sources and covers all public and private hospitals nationally.18 The registry obtains the majority of its data through electronic sources including pathology laboratories, medical records, and death certificates. Its case ascertainment of invasive
cancers in Ireland, excluding nonmelanoma skin cancer, is very high and estimated to be 97%. Data collected by the NCRI includes sex, age, area of residence, year of cancer diagnosis, tumour site and type, and method by which the individual presented with cancer. Cases’ data are validated manually by Cancer Data Registrars, who are assigned to hospitals around Ireland and access various data sources. Population data were obtained from the Central Statistics Office (CSO), Ireland’s national statistical office, which organises five-yearly censuses.19 Data from the population censuses of 2006, 2011, and 2016 were used to provide denominator data for these years. Mid-year estimates were used for intercensal years in 2004–2015, and population estimates calculated by the NCRI were used for 2017 and 2018, as no mid-year population estimates for 2017 and 2018 were available from the CSO at the time the analysis was performed.
Study population
Registration data on all female cases of primary breast cancer (n=30560) diagnosed between 2009 and 2018 in Ireland were
Excluding women with an unknown cancer stage from the analyses of the associations between deprivation and cancer stage at in the east of Ireland had no impact on the direction and magnitude of the associations seen in the primary analyses (Supplementary Table S4). In other words, no statistically significant association between deprivation and cancer stage for women with screen-detected breast cancer was observed.
Discussion
Summary of findings
extracted from the NCRI. Conforming with international reporting guidelines for cancer registries, the NCRI defines primary breast cancer as breast cancer in which the breast is the primary tumour site, and not a site of cancer recurrence, metastasis, or extension.20 Where a case has breast tumours from more than one broad morphological group (e.g. adenocarcinoma and sarcoma), however, multiple cancers are captured by the NCRI and were included in these data. As previously described, the age range for eligibility for BreastCheck expanded during the study period: until 2015, women aged 50–64years were eligible to attend screening, but in late 2015 the upper screening age was extended from 65 to 69years on a phased basis. As this extension was not completed until 2020, for the purpose of this study screening eligible women denotes women aged 50–64years only. As the national roll-out of BreastCheck did not occur until late 2007,17 our primary analysis includes national data from 2009, the first year for which comprehensive national data on female breast cancer cases in Ireland are available, to 2018, the most recent year for which comprehensive national data on female breast cancer cases are available. A subgroup analysis of female breast cancer cases confined to 14 counties in the east of Ireland, where breast cancer screening was available before BreastCheck’s national roll-out in 2007, was performed to assess associations between deprivation and breast cancer screening over a longer period of time (between 2004 and 2018).
an unknown electoral division being categorised as having an ‘unknown’ deprivation quintile.
Outcome variables
We found little evidence to suggest breast cancer screening outcomes vary significantly according to deprivation. In our primary analysis, there was no association between deprivation and having breast cancer diagnosed through screening, as opposed to other diagnostic pathways, in the screening eligible population nationally in 2009–2018. This was supported by a subgroup analysis of the screening eligible women in the east of Ireland in 2004–2018, which also found no association. Secondly, we observed a deprivation gradient in the risk of screen-detected breast cancer being detected at a late-stage in our primary analysis, with the risk being higher in deprived women in 2009–2013. There was, however, improvement with time and in 2014–2018 no associations were observed between deprivation and cancer stage in women with screen-detected breast cancer. The reason for the disappearance of this deprivation gradient over time may be due to a higher burden of prevalent, more advanced cancers being detected in more deprived women after the initial roll-out of BreastCheck. In the general population, deprived women have a higher risk of presenting with more advanced breast
The outcomes of interest were method of cancer detection and breast cancer stage at diagnosis. Method of breast cancer detection was categorised as a binary variable—detected through organised breast cancer screening versus detected through other methods. The latter category included breast cancers detected through symptomatic presentation, autopsy, opportunistic screening, incidental findings, and unknown methods of detection. The NSS informs the NCRI of all breast cancer cases detected by BreastCheck and the NCRI liaises with NSS on an ongoing basis to cross-check its data. Therefore, it is unlikely that there would be a meaningful amount of misclassification of this outcome variable. Cancer stage at diagnosis was also categorised as a binary variable—diagnosed at a late stage (i.e. stage III or IV according to the American Joint Committee on Cancer TNM system24) versus diagnosed at all other stages. The latter category included breast cancers with an unknown stage at diagnosis.
Statistical analysis
Exposure variable
The exposure variable was arealevel deprivation, measured using the Pobal Haase-Pratschke (Pobal HP) deprivation index, an arealevel index of deprivation.21 Using the Pobal HP deprivation index, the NCRI assigns the deprivation quintile to the electoral division in which each cancer case resided at the time of cancer diagnosis.6 The index measures area deprivation using a combination of census-based indicators of relative affluence and deprivation. Quintile 1 corresponds to the most affluent areas and quintile 5 to the most deprived areas.22 The missing indicator method, as previously described,23 was used for missing exposure variable data, with women residing in
Descriptive statistics were used to describe breast cancer characteristics among women diagnosed in Ireland in 2009–2018. For the primary analysis, unadjusted risk ratios (RRs) and 95% confidence intervals (95% CIs) were calculated to compare the risk of breast cancer being detected through populationbased screening in screening eligible women with high compared to low deprivation levels in 2009–2018. Unadjusted RRs and 95% CIs were also calculated to compare risk of late-stage screen-detected breast cancer by deprivation level in 2009–2018. Similar analyses were used for the subgroup analysis of breast cancer cases in the east of Ireland over the longer 2004–2018 period.
Sensitivity analyses were conducted to investigate whether the direction and magnitude of the effect estimates changed when women with an unknown stage of cancer were excluded from the primary and subgroup analyses. This sensitivity analysis was performed because it is possible
Table 2. Breast cancer cases by deprivation quintile and cancer detection method in screening eligible women (age 50–64 years), Ireland, 2009–2018 (n ¼ 12 301)
Abbreviations: CI ¼ confidence interval; RR ¼ risk ratio.
Table 3. Breast cancer cases by deprivation quintile and cancer stage at diagnosis in screening eligible women (age 50–64 years) with screen-detected breast cancer, Ireland, 2009–2018 (n ¼ 7027)
that women classified as having an ‘unknown’ cancer stage had late-stage breast cancer, thus leading to misclassification of the outcome variable.
All P-values reported are twosided and P<.05 was considered statistically significant. Statistical analyses were performed in Microsoft Excel and P-values for RRs were calculated as described.
Ethical considerations
cancer in Ireland in 2009–2018 (Table 1). Among the breast cancers diagnosed, 40.3% were within the target age range for breast screening (i.e. age 50–64years) and 24.6% (n=7525) were screen-detected. Women from the most affluent quintile (Quintile 1) represented the highest proportion of breast cancers (n=6278; 20.5%). In total, 74.2% (n=22688) of breast cancers were diagnosed at an early stage (stages 0, I, or II).
Cancer stage in women with screen-detected breast cancer (2009–2018)
Deprivation and cancer stage
The NCRI has the authority to collect and classify information on all cancer cases which occur in Ireland under the National Cancer Registry Board (Establishment) Order, 1991, and has a confidentiality protocol covering the collection, processing, and release of data.25 All analyses were performed by the NCRI as part of routine service evaluation procedures. Additionally, aggregate data, containing no personal data, were collated and analysed for this study. Therefore, ethical approval was not required.
Method of breast cancer detection in screening eligible women (2009–2018)
Epidemiology of female breast cancer cases (2009–2018)
In total, 30560 women were diagnosed with primary breast
Among screening eligible women, there were no differences between deprivation quintiles and method of breast cancer detection over the entire study period (i.e. 2009–2018) and in 2014–2018 (Table 2). However, women with an unknown deprivation quintile had a significantly higher risk of having breast cancer detected through screening than women in all deprivation quintiles in 2009–2013 (RR 1.12, 95% CI: 1.01–1.24) and over the entire study period (RR 1.10, 95% CI: 1.03–1.17).
In women with screen-detected breast cancer, those in the more deprived quintiles had a higher risk of being diagnosed with late- stage disease over the entire study period. There was a clear gradient between increasing deprivation and increasing risk of late-stage screen-detected breast cancer in 2009–2013, with the risk ncreasing almost monotonically as area deprivation rose. Women in Quintiles 3 (RR 1.67, 95% CI: 1.12–2.51), 4 (RR 1.67, 95% CI: 1.11–2.51), and 5 (i.e. the most deprived group, RR 1.74, 95% CI: 1.17–2.60) had a significantly higher risk of their screen-detected breast cancer being diagnosed at a late stage compared with those in Quintile 1, while the risk in women in Quintile 2 was higher, but not significantly so. In 2014–2018, no associations were observed between deprivation and cancer stage in women with screen- detected breast cancer.
Sensitivity analysis
stage at diagnosis were excluded. No difference in the direction or magnitude of the associations seen in the primary analyses were observed. Therefore, in women with screen-detected breast cancer with a known cancer stage at diagnosis, the risk of late-stage disease increased with higher levels of deprivation in 2009–2013 and during the entire study period, but no significant associations were found in 2014–2018.
Subgroup analysis of women in the east of Ireland (2004–2018)
Deprivation and method of breast cancer detection
There was no association between deprivation and method of breast cancer detection in screening eligible women in the east of the country in 2004–2008, 2009–2013, and 2014–2018 or during the entire 2004–2018 period).
Deprivation and cancer stage in the east subgroup analysis (2004–2018)
In women with screen-detected breast cancer in the east of the country, no associations between deprivation and late-stage diagnoses were observed. cancers [6, 26]. Screening, however, reduces the burden of late-stage disease for the entire screened population [15] and can lead to reductions in socioeconomic inequities in stage at diagnosis [13, 27] and overall survival [28]. Therefore, it is possible that once BreastCheck became well-established nationally and the prevalent, more advanced cases were detected, women from all deprivation quintiles benefitted from early disease detection afforded by BreastCheck and we thus saw no between-group differences in cancer stage.
It is imperative that these associations continue to be monitored into the future, as the BreastCheck programme matures further. While eliminating inequities in screening participation and breast cancer stage at diagnosis is important to help reduce inequities in breast cancer outcomes, inequities in survival and mortality may nonetheless exist due to other factors, such as differences in access
to healthcare, treatment, and comorbidity burden between deprivation groups [13, 29]. Therefore, survival and mortality rates according to deprivation quintiles in women with screen-detected breast cancer should be regularly assessed to ensure BreastCheck is truly reducing inequities in breast cancer outcomes in Ireland.
In a sensitivity analysis, women who had an unknown cancer
Comparison with the literature
Our study’s finding of no association between deprivation and risk of breast cancer detection through population-based screening is both encouraging and surprising. In contrast to our study, a study examining differences in breast cancer case characteristics between socioeconomic groups in Wales over an 11-year period found there are proportionally fewer women being diagnosed with breast cancer through the NHS breast cancer screening programme in more
32 CPD 119: BREAST CANCER
Sensitivity analysis
Excluding women with an unknown cancer stage from the analyses of the associations between deprivation and cancer stage at in the east of Ireland had no impact on the direction and magnitude of the associations seen in the primary analyses. In other words, no statistically significant association between deprivation and cancer stage for women with screen-detected breast cancer was observed.
Discussion
Summary of findings
We found little evidence to suggest breast cancer screening outcomes vary significantly according to deprivation. In our primary analysis, there was no association between deprivation and having breast cancer diagnosed through screening, as opposed to other diagnostic pathways, in the screening eligible population nationally in 2009–2018. This was supported by a subgroup analysis of the screening eligible women in the east of Ireland in 2004–2018, which also found no association. Secondly, we observed a deprivation gradient in the risk of screen-detected breast cancer being detected at a late-stage in our primary analysis, with the risk being higher in deprived women in 2009–2013. There was, however, improvement with time and in 2014–2018 no associations were observed between deprivation and cancer stage in women with screendetected breast cancer. The reason for the disappearance of
this deprivation gradient over time may be due to a higher burden of prevalent, more advanced cancers being detected in more deprived women after the initial roll-out of BreastCheck. In the general population, deprived women have a higher risk of presenting with more advanced breast cancers.6, 26 Screening, however, reduces the burden of late-stage disease for the entire screened population15 and can lead to reductions in socioeconomic inequities in stage at diagnosis13, 27 and overall survival.28 Therefore, it is possible that once BreastCheck became well-established nationally and the prevalent, more advanced cases were detected, women from all deprivation quintiles benefitted from early disease detection afforded by BreastCheck and we thus saw no between-group differences in cancer stage.
It is imperative that these associations continue to be monitored into the future, as the BreastCheck programme matures further. While eliminating inequities in screening participation and breast cancer stage at diagnosis is important to help reduce inequities in breast cancer outcomes, inequities in survival and mortality may nonetheless exist due to other factors, such as differences in access to healthcare, treatment, and comorbidity burden between deprivation groups.13, 29 Therefore, survival and mortality rates according to deprivation quintiles in women with screen-detected breast cancer should be regularly assessed to ensure BreastCheck is truly reducing inequities in breast cancer outcomes in Ireland.
Comparison
with the literature
Our study’s finding of no association between deprivation and risk of breast cancer detection through population-based screening is both encouraging and surprising. In contrast to our study, a study examining differences in breast cancer case characteristics between socioeconomic groups in Wales over an 11-year period found there are proportionally fewer women being diagnosed with breast cancer through the NHS breast cancer screening programme in more socially deprived areas.30 Previous Irish31, 32 and international studies33, 34 have demonstrated that deprivation, low income, and low levels of education are associated with lower uptake of screening. As our study explored the association between deprivation and risk of having breast cancer diagnosed through BreastCheck, making direct comparisons between it and studies that explore the association between deprivation and breast cancer screening uptake is difficult. Our findings are nonetheless surprising, as if screening uptake was lower in more deprived areas, it might be expected that affluent women have a higher risk of having breast cancer detected through screening than deprived women. It is possible that our findings are explained by deprived women in Ireland having a higher burden of breast cancer and a lower screening uptake, but the fact that the incidence of breast cancer in Ireland is significantly higher in affluent women compared to deprived women refutes this hypothesis.6
Our finding of a positive association between deprivation and cancer stage in women with screen-detected breast cancer in the early years of BreastCheck, with an elimination of the deprivation gradient in more recent years can be interpreted in the context of the limited, mixed evidence on the effect of breast cancer screening programmes on socioeconomic inequities in cancer stage at diagnosis. Two separate studies from New Zealand and the United States (US) found that racial disparities in breast cancer stage at diagnosis were removed in screened populations.27, 35 Another study in the Netherlands using cancer registry data showed that differences in survival between socioeconomic groups with screen-detected breast
cancer were due to differences in comorbidity, rather than disease stage at diagnosis, whereas for women with non-screen-detected breast cancers cancer stage was the main driver of inequities, indicating that screening may have significantly reduced inequities in cancer stage.13 On the other hand, a matched case-control study in France found women with low socioeconomic status had double the risk of having latestage breast cancer diagnosed than high socioeconomic status women, even when their breast cancer was detected through population-based screening.36 misclassification of exposure has occurred in our study. Second, this study did not control for factors such as ethnicity, education, comorbidities, or marital status, that may confound the associations between deprivation and the outcome measures in this study, as these variables are not collected by the NCRI. Nonmarried women,37 women from ethnic minority backgrounds,38 and women with lower educational attainment39 and comorbidities40 are more likely to be diagnosed with advanced breast cancer. Therefore, these factors may have positively confounded the associations we observed between deprivation and cancer stage in women with screen-detected breast cancer, potentially reducing the validity of our findings. Third, the NCRI uses an area-level index to measure deprivation, thus it may not accurately reflect the individual level of deprivation of each breast cancer case in this study, leading to misclassification of exposure.
Conclusion
Overall, our findings suggest that the benefits of organised population-based breast cancer screening have largely been distributed equally across deprivation quintiles in Ireland as the BreastCheck programme has been fully rolled out nationwide. The associations between deprivation and breast cancer screening outcomes should continue to be monitored, as well as survival and mortality rates for screen-detected breast cancer according to deprivation quintile, to ensure BreastCheck is having a sustained effect on reducing disparities in breast cancer screening outcomes in the Irish population.
References available on request
Global First in Surgical Training: SURGhub
Marking a major milestone in the fight to close the global surgical education gap - which leaves 93% of people in sub-Saharan Africa and millions more worldwide without access to safe surgical care when needed - a groundbreaking e-learning platform has brought the classroom directly to the homes and clinics of more than 19,000 healthcare workers across 190 countries in just two years.
The majority of the world’s population lacks access to safe, affordable surgical care, a crisis driven in part by a severe shortage of trained surgeons, anaesthetists, obstetricians, and nurses. This shortage is compounded by a chronic lack of accessible, affordable, and contextappropriate training resources - an educational gap that the United Nations Global Surgery Learning Hub (SURGhub) was specifically created to address.
In a new report published recently, it was revealed that the remote learning system, launched in June 2023, is not just transforming but revolutionising how surgical, anaesthetic, obstetric, and surgical care professionals in low-resource and conflict-affected regions access high-quality training. This pioneering platform addresses
a long-standing crisis that has crippled health systems for decades - bridging a gap that has long left millions without the surgical care they need. By prioritising low-bandwidth delivery, free access, and culturally relevant content, SURGhub is dismantling longstanding barriers of cost, geography, internet access, and language, demonstrating how digital tools can democratise education even in the most challenging environments.
SURGhub is a product of the global surgery community, powered by over 200 volunteers. It is an initiative of the Global Surgery Foundation (GSF) and the United Nations Institute for Training and Research (UNITAR) supported by RCSI University of Medicine and Health Sciences in association with the Johnson and Johnson Foundation.
The platform now hosts over 100 educational courses, contributed by 27 international organisations, with content quality maintained by more than 200 volunteer experts. The impact is particularly visible in countries where surgical education is often out of reach.
At least 1,700 learners are based in conflict-affected regions, including the Democratic Republic
of Congo, Sudan, Ukraine, Yemen, and Palestine, with thousands more in low- and lower-middleincome countries.
For learners navigating immense challenges, the platform’s accessibility is transformative.
“Where was this platform when I was a resident? When I was struggling? There was nothing to guide me then… I didn’t know where to find readings and references,” said one user, capturing the frustration of years spent searching for reliable training that simply wasn’t there.
“This is what equitable scalability in global health looks like", said Eric O’Flynn, lead author of the report, and Programme Director of Education, Training and Advocacy in the Institute of Global Surgery, RCSI University of Medicine and Health Sciences, Dublin.
“SURGhub proves that with the right partnerships and the right technology, we can break down barriers that have held back surgical education for generations. Now the task is to take this further -so lifesaving teams, regardless of where they are based, have the tools they need to deliver safe surgical care.”
Dr Phumzile Mlambo-Ngcuka is a member of the GSF Foundation Board. She said, "With SURGhub now reaching more than 19,000 healthcare professionals in over 190 countries, we’re demonstrating how innovative, collaborative approaches can meet the critical needs in surgical education. By expanding access to high-quality training— particularly in low-resource and crisis-affected settings—we’re not only strengthening health systems but also advancing better outcomes for women, families, and communities worldwide. This is the type of scalable, impact-driven solution that global health needs more of."
Expanding content in languages beyond English is also a top priority, as is strengthening the ability to measure how training translates into real-world improvements in clinical practice and patient outcomes. But the challenge, and the opportunity, extends far beyond the platform itself. Continued investment, collaboration, and global partnerships will be critical to achieving SURGhub’s mission of transforming surgical education at scale.
Inaugural European Meeting on PFA Education and Innovation
On June 27th, Professor Gábor Széplaki and the Cardiac Electrophysiology Team at Mater Private Network hosted the inaugural meeting of Europe’s leading cardiology experts in the field of pulsed field ablation (PFA). The session was in partnership with Boston Scientific and focused on sharing clinical experiences and shaping the future of PFA education.
Key topics included workflow integration with FARAVIEW™ software, advancing clinical strategy, and building training programmes to drive the next wave of cardiac ablation technology.
Mater Private Network is proud to play a leading role in the safe and effective adoption of PFA as a FARAPULSE Academy Centre of Excellence through structured proctorship and peerto-peer learning. Recognised for expert patient care, extensive
experience, and with a strong focus on education, Mater Private Network was selected as part of the international network of centres dedicated to advancing best practices in cardiac ablation. The meeting provided a vital platform for collaboration, enabling clinicians to shape the next phase of educational programming in this rapidly advancing field.
Speaking on the meeting, Professor Gábor Széplaki, Head of Cardiac Electrophysiology at the Mater Private Hospital, Dublin said, “It’s a great honour to host today’s summit at Mater Private Network with our partners Boston Scientific, bringing together the pioneers of pulsed field ablation. Events like this ensure our patients receive not only the best cardiac care but have access to international best practice and cutting-edge innovation, ensuring faster recovery and better outcomes.”
Mater Private Network remains committed to advancing clinical excellence and fostering international collaboration in the
education and implementation of next-generation cardiac ablation technologies.
Prof. Gábor Széplaki and the Cardiac Electrophysiology Team at Mater Private Network
Knowledge is Central: Presentations from ASCO 2025
From 30 May-2 June 2025, the world’s cancer researchers were in Chicago for the year’s biggest cancer conference: the American Society of Clinical Oncology (ASCO) annual meeting.
The conference was opened by President Dr Robin Zon who addressed delegates stating, “Throughout ASCO’s existence, knowledge has been central to its mission. But we know that knowledge alone doesn’t conquer cancer; it must be applied. Knowledge applied universally will help us ask the right questions, solve problems, make the best decisions for patients, and save more lives. Yet, despite years of increasing scientific knowledge, we’re ironically facing more and more barriers to delivering care.
“Our environment is becoming more uncertain, more volatile, and more challenging with each passing year. All of which makes the three words under my theme so critical right now: technology, advocacy, and community. These are the drivers that propel knowledge to action and empower us to achieve our goal of quality patient care for all.”
Dr Zon discussed the importance of technology in healthcare and its future direction adding, “Technology can mean a lot of things, but today I want to talk about artificial intelligence (AI)—a powerful tool for driving knowledge to action.
“Just as we can no longer imagine our world without cell phones and the internet, it will soon be impossible to imagine living without AI. We are now at the crossroads of long-imagined possibilities and actionable solutions.
“AI tools are scheduling appointments and managing patient records. They are helping us more accurately and rapidly dictate notes, access patient information, and record patient conversations. Now, we can actually look at our patients during a visit instead of our computers!
“AI is providing translation tools to bridge the gap between providers and patients who speak different languages. Remote monitoring devices are alerting providers to health concerns of patients in rural and other underserved areas.
“AI-enhanced radiology and pathology services are revolutionizing care. In fact, a recent study demonstrated that AI-supported mammography can detect cancer faster and more accurately than two radiologists while reducing their workload by almost half.
“Perhaps most important, AI is improving our ability to acquire, assimilate, and organise knowledge. Did you know there is at least one new medical article published every 26 seconds? You would have to read 5,000 articles a day to keep up! It’s not surprising that simply trying to stay current is one of the causes of burnout, but AI is helping dramatically.
“This is why I am so excited to share that ASCO and Google are working together on a new tool designed to help us provide cutting edge care to every patient, every day, everywhere. It’s called the ASCO Guidelines Assistant. In response to your specific queries, the Guidelines Assistant will deliver the latest published information from ASCO’s guidelines, developed and kept current by ASCO experts.”
She concluded, “We must also remember that knowledge, no matter how evidence-based, doesn’t drive itself to action. That’s also up to us. Research shows that if we consistently apply what we already know,
we can greatly improve patient outcomes. For instance, following breast cancer treatment guidelines was associated with more than a 30% reduction in the risk of death and improved disease-free survival. Adherence to lung cancer guidelines, including biomarker testing, reduces mortality up to 20%; those with stage IV cancer experienced the highest benefit.
“But, as we’ve heard more than once from the Institute of Medicine, evidence-based medicine is not consistently delivered. That’s where our growing domestic and international program, ASCO Certified, can help.
“Years ago, a patient inspired me to walk in beauty and strength. This is our call: a call to live with authenticity, harmony, and resilience. We must and will forge ahead with unwavering determination, harness technology, and advocate tirelessly to ensure every patient across the globe benefits from the latest innovations in cancer care.
“Let’s nurture our community, which begins here at ASCO. My hope is that you feel enlightened and empowered by the knowledge that we are stronger than cancer. Together, we are defining cancer care for generations to come with hope fueled by the many successes we achieve together at ASCO, with hope from the
Asco President Dr Robin Zon
enduring commitment, courage, and passion from our volunteers and members, and with hope from the communities we have built along the way. Rest assured, we are transforming the future at its most intimate level—in the room with our patients, who look to you as their beacon of hope.”
Below we take a look at some of the key studies that were presented.
GLP-1 Receptor Agonists May Modestly Reduce Risk of Fourteen Obesity-Related Cancers for People with Diabetes
A large observational study of more than 170,000 patients with diabetes and obesity in the United States has found that GLP-1 receptor agonists may modestly reduce the risk of fourteen obesity-related cancers, especially colorectal cancer, when compared to DDP-4 inhibitors.
About the Study
“Although obesity is now recognised as an increasingly important cause of cancer in the United States and worldwide, no medications have been proven to lower the cancer risk associated
with obesity. Our study begins to fill that gap by evaluating GLP-1 receptor agonists, a relatively new but widely prescribed medication that treats diabetes, obesity, and related conditions. Our results suggest they may modestly cut the chance of developing certain cancers—especially cancers of the colon and rectum—and reduce rates of death due to all causes. These data are reassuring, but more studies are required to prove causation,” said lead study author, Lucas A. Mavromatis, ScB, a medical student at the NYU Grossman School of Medicine in New York, New York.
This large observational study included 170,030 adults from 43 health systems in the United States. The patients had a BMI of 30 kg/m2 or higher and a diagnosis of diabetes. Between 2013 and 2023, based on examining health systems data, half (85,015) had started treatment with a GLP-1 receptor agonist and half with a DPP-4 inhibitor. DPP-4 inhibitors work by blocking the action of the enzyme DPP-4 but unlike GLP-1RAs, they have not been shown to help lower weight. The average age of the participants was 56.8 years. About half of the participants were women, more than 70% were White, and more than 14% were Black. The average BMI was 38.5 kg/m2
This was a target trial emulation study, which is an observational study using large groups of patients who have already received the two treatment types instead of randomly assigning a treatment. It used propensity score matching to ensure the two groups had similar characteristics thereby creating more comparable groups and reducing bias.
Key Findings
• Patients who took GLP-1 receptor agonists had a 7% lower risk of developing an obesity-related cancer and an 8% lower risk of death from any cause compared to those who took a DDP-4 inhibitor.
• In the GLP-1 receptor agonist group, there were 2,501 newly diagnosed cases of obesityrelated cancer out of 85,015. In the DDP-4 inhibitor group, there were 2,671 cases of obesityrelated cancer out of 85,015.
• Researchers looked at the difference between the risk of obesity-related cancer in men and women:
o For men, there was not
a statistically significant difference between the two treatment groups for either obesity-related cancers or all causes of death.
o Women treated with GLP-1 receptor agonists had an 8% lower risk of obesity-related cancer and a 20% lower risk of all causes of death compared to women treated with DDP-4 inhibitors.
• Taking a GLP-1 receptor agonist was also protective against two related types of cancer: colon and rectal cancer:
o There were 16% fewer colon cancer cases and 28% fewer rectal cancer cases in the group prescribed GLP-1 receptor agonists.
o This group also did not have an elevated risk of any of the 14 obesity-related cancers.
Next Steps
The investigators hope to follow patients taking GLP-1 receptor agonists longer than four years to continue to study risk and look at cancer risk for people taking GLP1 receptor agonists who do not have diabetes.
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health.
"This trial raises an intriguing hypothesis: that the increasingly popular GLP-1 medications used to treat diabetes and obesity might offer some benefit in reducing the risk of developing cancer. I see many patients with obesity,
and given the clear link between cancer and obesity, defining the clinical role of GLP-1 medications in cancer prevention is important. Though this trial does not establish causation, it hints that these drugs might have a preventative effect. Future research is needed to validate these findings, including in patients who do not have diabetes,” said Dr Robin Zon, MD, FACP, FASCO, ASCO President.
Molecular Assay May Help Identify People With NonSmall Cell Lung Cancer Who Could Benefit From Adjuvant Chemotherapy
Results from an international clinical trial show that a 14-gene molecular assay can help identify patients with early-stage non-squamous non-small cell lung cancer (NSCLC) who could benefit from adjuvant chemotherapy after surgery.
About the Study
“This is the first large prospective randomised trial to demonstrate that a 14-gene molecular assay can identify who could benefit from adjuvant chemotherapy among a high-risk group of patients with stage IA-IIA non-squamous non-small cell lung cancer who otherwise may not typically receive such therapy,” said lead study author David Spigel, MD, FASCO, Sarah Cannon Research Institute in Nashville, Tennessee.
This study enrolled 421 patients with stage IA-IIA non-squamous NSCLC who had surgery to remove their tumor(s). Those tumors were tested and categorised as low, intermediate, or high risk via a 14-gene assay
called the RiskReveal assay. At the time of this interim analysis, there were 194 intermediate- and high-risk patients who could be evaluated. Patients who were categorised as intermediate or high risk were randomised to four cycles of platinum-based adjuvant chemotherapy (87 patients) or to observation (107 patients). Researchers then compared the time to disease recurrence in each group. About 55% of each group had IA NSCLC, and demographics between the two groups were similar.
Key Findings
After 24 months, patients who received adjuvant chemotherapy had a 78% lower risk of cancer recurrence compared to the observation group.
In the adjuvant chemotherapy group, 96% of patients did not have a cancer recurrence. In the observation group, 79% of patients did not have a cancer recurrence. The trial’s median disease-free survival endpoint was not reached in either group, meaning more than half of patients would not have experienced disease recurrence in either group.
At the time of the interim analysis, the Data Safety Monitoring Board recommended that the clinical trial stop enrolling new patients because of how successful the assay was at determining which of these patients could benefit from
David Spigel, MD, FASCO, Sarah Cannon Research Institute in Nashville, Tennessee
36 Conference
adjuvant chemotherapy. Follow-up continues with those who were already enrolled.
Next Steps
Researchers will continue to follow the patients already enrolled in this study and will look at how advances in targeted therapy and immunotherapy could be applied to earlier stages of NSCLC.
Combination of Encorafenib and Cetuximab With Chemotherapy Helps Some Patients With Advanced Colorectal Cancer Live Longer
Results from an international phase 3 study show that the targeted therapy combination of encorafenib and cetuximab with mFOLFOX6 chemotherapy helps patients with BRAF V600E-mutant metastatic colorectal cancer (mCRC) live longer. After early results from the BREAKWATER trial showed a significant benefit, the U.S. Food and Drug Administration (FDA) granted accelerated approval of encorafenib/cetuximab with mFOLFOX6 chemotherapy as a first-line treatment for patients with BRAF V600E-mutant mCRC.
About the Study
“BRAF V600E-mutant metastatic colorectal cancer is characterized by its aggressive nature, and the
standard therapeutic options have limited efficacy. Despite the high unmet need in this subtype, prior to the accelerated FDA approval based on initial overall response rates from the BREAKWATER study, there were no approved biomarker-driven therapies specifically indicated for people with previously untreated BRAF V600E-mutant metastatic colorectal cancer,” said lead study author Elena Elez, MD, PhD, Vall d’Hebron Institute of Oncology, Barcelona, Spain.
The BREAKWATER randomised clinical trial was designed to test the targeted therapy drugs encorafenib and cetuximab, with or without mFOLFOX6, for BRAF V600E-mutant mCRC. Encorafenib is a BRAF inhibitor. Cetuximab is an EGFR inhibitor. The mFOLFOX6 chemotherapy regimen combines multiple drugs to treat colorectal cancer, including folinic acid, fluorouracil, and oxaliplatin. The encorafenib/cetuximab combination with and without mFOLFOX6 was compared to the current standard of care treatment of chemotherapy with or without bevacizumab.
The BREAKWATER study included 637 participants. The median age of the participants was approximately 60 years and about half were women.
Key Findings
• The study originally included three treatment arms: encorafenib/cetuximab alone (158 patients), encorafenib/ cetuximab with mFOLFOX6 (236 patients), and the control arm of chemotherapy with or without bevacizumab (243 patients).
o When early results showed that the encorafenib/ cetuximab with mFOLFOX6 arm had a statistically significant improvement in objective response rates (ORR), enrollment in the encorafenib/cetuximab alone arm was closed in a protocol amendment.
• Overall survival was 30.3 months in the encorafenib/ cetuximab with mFOLFOX6 arm, 19.5 months in the encorafenib/ cetuximab alone arm, and 15.1 months in the control arm.
• Patients treated with encorafenib/cetuximab with mFOLFOX6 had a 51% lower risk of dying than patients treated with the standard of care chemotherapy with or without bevacizumab.
• Progression-free survival was 12.8 months in the encorafenib/ cetuximab plus mFOLFOX6 arm, 6.8 months in the encorafenib/ cetuximab alone arm, and 7.1 months in the control arm.
• Patients treated with encorafenib/cetuximab with mFOLFOX6 had a 47% lower risk of cancer progression than patients treated with the standard of care chemotherapy with or without bevacizumab.
• ORR, which is the percentage of people who have a partial or complete response to the treatment, was 65.7% in the encorafenib/cetuximab plus mFOLFOX6 arm, 45.6% in the encorafenib/cetuximab alone arm, and 37.4% in the control arm.
Most of the side effects for these treatments were manageable. Serious side effects caused by the treatments occurred in 30% of patients in the encorafenib/ cetuximab alone arm, 46% of
Elena Elez, MD, PhD, Vall d’Hebron Institute of Oncology, Barcelona, Spain.
the encorafenib/cetuximab with mFOLFOX6 arm, and 39% of the control arm. The most common side effects for the encorafenib/ cetuximab with mFOLFOX6 treatment were nausea, anemia, and diarrhea.
Next Steps
Researchers will continue to study the encorafenib/cetuximab combination with another chemotherapy regimen called FOLFIRI, which combines the common chemotherapy drugs folinic acid, fluorouracil and irinotecan.
Movement Is Medicine: Structured Exercise Program
May Lower Risk of Cancer
Recurrence and Death for Some Colon Cancer Survivors
New study results show that a structured exercise program following surgery and adjuvant chemotherapy reduced the risk of recurrent or new cancer and increased survival for patients with stage III and high-risk stage II colon cancer.
About the Study
“After completing surgery and chemotherapy, about 30% of patients with high-risk stage II and stage III colon cancer will eventually experience recurrence of their disease. As oncologists, one of the most common questions we get asked by patients is ‘what else can I do to improve my outcome?’ These results now provide us with a clear answer: an exercise program that includes a personal trainer will reduce the risk of recurrent or new cancer, make you feel better, and help you live longer,” said lead study author Christopher Booth, MD, FRCPC, Queen’s University in Kingston, Canada.
Between 2009 and 2023, the international CHALLENGE clinical trial enrolled 889 participants from six countries, with most participants enrolling from Canada and Australia. The median age of the participants was 61 years and 51% were female. Most of the patients (90%) had stage III colon cancer. The remaining 10% had high-risk stage II colon cancer. All patients had previously received intent-to-cure surgery and adjuvant chemotherapy. The patients were randomly assigned to participate in a structured exercise program (445 patients) or to receive health education materials promoting physical activity and healthy nutrition (444 patients).
All participants also received standard cancer surveillance and follow-up care. Patients in the structured exercise program worked with a physical activity consultant twice a month for coaching sessions and supervised exercise sessions. The consultants gave each patient an “exercise prescription.” After 6 months, patients met with their physical activity consultant once a month, with additional sessions available for extra support if needed.
Key Findings
• Patients in both groups improved their physical function and sustained it, but it was significantly higher for patients in the structured exercise program. They had improvements that were maintained over all three years, in recreational physical activity, predicted VO2 max, and distance they could walk in six minutes.
• After a median follow-up of 7.9 years, 93 patients in the structured exercise program had their cancer recur, compared to 131 patients in the health education materials group. At five years, the disease-free survival rate was 80% in the structured exercise program and 74% in the health education materials group. Patients in the structured exercise program had a 28% lower risk of recurrent
or new cancers developing than patients who only received health education materials.
• There were 41 people in the structured exercise program and 66 people in the health education materials group who died. After 8 years, overall survival was 90% in the structured exercise program and 83% in the health education materials group. Patients had a 37% lower risk of death if they participated in the structured exercise program.
Patients in the structured exercise program reported more musculoskeletal adverse events, such as muscle strains or bone fractures (19%), compared to the health education group (12%). Ten percent of these adverse events in the structured exercise program were related to their participation in the program.
Next Steps
Researchers will explore how exercise reduces cancer recurrence by studying blood samples of the patients who participated in CHALLENGE.
Treatment Combination With Inavolisib Extends Survival, Delays Chemotherapy for Some Patients With Advanced Breast Cancer
New findings from the phase 3 INAVO120 trial show that adding inavolisib to palbociclib and fulvestrant can help extend survival and delay the time until treatment with chemotherapy in patients with previously treated PIK3CAmutated, HR-positive, HER2negative advanced breast cancer.
About the Study
“The INAVO120 study was designed to address a need for more potent and tolerable therapies for PIK3CA-mutated, hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the first-line setting. The INAVO120 trial findings support an inavolisib-based regimen as an emerging new standard of care that helps people live longer, as well as substantially improving how long treatment works,” said lead study author Nicholas C. Turner, MD, PhD, Royal Marsden Hospital, London, United Kingdom.
Inavolisib (Itovebi™) is a type of targeted therapy drug called a PI3K inhibitor. It works by targeting the PIK3CA mutation, which can stop cancer cells from dividing and spreading. In 2024, the U.S. Food and Drug Administration approved inavolisib in combination with palbociclib (Ibrance®) and fulvestrant (Faslodex®) to treat people with HR-positive, HER2negative advanced breast cancer with a PIK3CA mutation that has grown following treatment with hormone therapy. Palbociclib is a targeted therapy drug that inhibits the activity of CDK4/6 enzymes, and fulvestrant is a hormone therapy drug.
This approval was based on previous results from this phase 3 INAVO120 clinical trial, which found that progressionfree survival (PFS) significantly improved in patients who received inavolisib in combination with palbociclib and fulvestrant. In this INAVO120 update, researchers analysed the final overall survival (OS) data.
Christopher Booth, MD, FRCPC, Queen’s University in Kingston, Canada
38 Conference
Key Findings
INAVO120 included 325 patients with PIK3CA-mutated, HR-positive, HER2-negative locally advanced or metastatic breast cancer that had grown during or following treatment with hormone therapy. The patients were randomly assigned to receive either inavolisib in combination with palbociclib and fulvestrant (161 patients) or a placebo with palbociclib and fulvestrant (164 patients).
After a median follow-up of just under 3 years (34.2 months), researchers found that:
• The median OS was 34 months for patients in the inavolisib group vs. 27 months for those in the placebo group.
• Overall, the inavolisib combination reduced the risk of death by 33% for participants.
• For those who received inavolisib, the probability that they would still be alive after treatment was:
o 96.8% at 6 months after treatment (vs. 90.1% in the placebo group)
o 87% at 1 year after treatment (vs. 76.7%)
o 74.3% at 1.5 years after treatment (vs. 67.2%)
o 65.8% at 2 years after treatment (vs. 56.3%)
o 56.5% at 2.5 years after treatment (vs. 46.3%).
• The objective response rate – the percentage of patients whose tumors shrank by more than 30% in response to treatment – was 62.7% for patients in the inavolisib group vs. 28% in the placebo group.
• The median time until patients needed to start chemotherapy was 35.6 months in the inavolisib group vs. 12.6 months in the placebo group.
• With the final results now in hand, the median PFS was recalculated from 15 months in the inavolisib group to 17.2 months while the median PFS remained 7.3 months in the placebo group.
Serious side effects occurred in most patients in both groups:
• 90.7% of patients in the inavolisib group experienced a grade 3 or 4 adverse event compared to 84.7% of those in the placebo group.
• Hyperglycemia, or high blood sugar, of any grade was particularly common in the inavolisib group (63.4% of patients vs. 13.5% in the placebo group).
• 6.8% of patients in the inavolisib group discontinued treatment due to side effects vs. 0.6% in the placebo group, though discontinuation rates were generally low.
Next Steps
Beyond INAVO120, inavolisib is currently being investigated in three other phase 3 studies: INAVO121, INAVO122, and INAVO123. All 3 studies are in PIK3CA-mutated locally advanced or metastatic breast cancer using various treatment combinations.
Vepdegestrant Could Extend Progression-Free Survival for Some People With ESR1-Mutated Advanced Breast Cancer
Results from VERITAC-2, the first global phase 3 clinical trial of a PROTAC, a targeted therapy that breaks down the estrogen receptors found on cancer cells, showed that the PROTAC vepdegestrant could extend progression-free survival for people with previously treated estrogen receptor (ER)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer with an ESR1 mutation.
About the Study
“Patients with estrogen receptorpositive, human epidermal growth
factor receptor 2 -negative advanced breast cancer whose tumors harbor ESR1 mutations have limited treatment options if the disease progresses and becomes resistant to available endocrine therapies. Newer therapies with differentiated mechanisms of action, longer clinical benefit, and tolerable safety profiles that can improve outcomes are now emerging. The findings from the VERITAC-2 study provide support for vepdegestrant as a potential oral treatment option,” said lead study author Erika P. Hamilton, MD, Sarah Cannon Research Institute, Nashville, Tennessee.
Vepdegestrant is a type of investigational drug called a proteolysis-targeting chimera, or PROTAC. It works by targeting and breaking down the estrogen receptors found on cancer cells, which can shrink or stop ER-positive breast cancers from growing. Previous phase 1/2 research has shown that vepdegestrant might help improve outcomes in people with advanced breast cancer who have received other treatments, but VERITAC-2 is the first global phase 3 clinical trial to study the safety and efficacy of vepdegestrant in these patients.
VERITAC-2 enrolled 624 patients with ER-positive, HER2-negative advanced breast cancer. The patients, 99.5% of whom were women, ranged in age from 26 to 89 years old, with a median age of 60. The patients in the study had already received treatment with hormone therapy and a CDK4/6 inhibitor. One additional line of hormone therapy was also allowed. Patients who previously received chemotherapy for advanced disease or who had already received fulvestrant were not eligible to enroll in the study. Fulvestrant is a type of hormone therapy called a selective estrogen receptor degrader (SERD) that indirectly leads to estrogen receptor degradation. In contrast, vepdegestrant directly degrades the estrogen receptor because of its binding properties.
Key Findings
The patients were randomly assigned to receive treatment with either vepdegestrant (313 patients) or fulvestrant (311 patients). Vepdegestrant was taken orally each day, while fulvestrant was given intramuscularly on days 1 and 15 of the first cycle of treatment and day 1 of each subsequent treatment cycle. A total of 43.3% of patients had
ESR1 mutations (136 patients in the vepdegestrant group and 134 in the fulvestrant group).
The researchers found that:
• For patients with ESR1 mutations, the median PFS for those who received vepdegestrant was 5 months vs. 2.1 months for those who received fulvestrant. However, the same PFS benefit was not seen when looking at vepdegestrant vs. fulvestrant in all patients regardless of ESR1 mutational status.
• The clinical benefit rate was 42.1% in the vepdegestrant group vs. 20.2% in the fulvestrant group.
• The overall response rate was 18.6% in the vepdegestrant group vs. 4% in the fulvestrant group.
Most of the side effects in the vepdegestrant group were mild or moderate, but severe side effects were slightly more common in this group. In these patients, 23.4% experienced a grade 3 or higher adverse event vs. 17.6% of those in the fulvestrant group. Finally, few patients from either group discontinued treatment due to side effects, but more patients in the vepdegestrant group stopped treatment because of side effects (2.9% of patients vs. 0.7% in the fulvestrant group).
Next Steps
Researchers will share the data from VERITAC-2 with global regulatory authorities to potentially support filings for drug approval.
Large National Cancer Institute-Funded Trial Shows Atezolizumab Combined With Chemotherapy Leads to Improved Survival in Deficient Mismatch Repair Colon Cancer
The results of an international phase 3 clinical trial sponsored by the National Cancer Institute show that patients with deficient mismatch repair (dMMR) colon cancer that are treated with the chemoimmunotherapy combination of FOLFOX and atezolizumab had a 50% reduction in disease recurrence and death compared to those treated with chemotherapy alone.
About the Study
“Colon cancers with deficient mismatch repair have shown relative resistance to chemotherapy. However, these tumors show a high burden of
mutations which are immunogenic and can lead to stronger antitumor immune responses when treated with immunotherapy. These findings apply to patients with Lynch syndrome, the most common hereditary colon cancer syndrome, and the more common deficient mismatch repair colon cancers that are sporadic in that they can’t be traced to a known hereditary cause or family history,” said lead study author Frank A. Sinicrope, MD, Mayo Clinic, Rochester, Minnesota.
The ATOMIC randomised study tested whether adding the immunotherapy drug atezolizumab to FOLFOX chemotherapy improved outcomes for patients with stage III dMMR colon cancer, as compared to FOLFOX chemotherapy alone. The study enrolled 712 patients. The median age was 64 years old and about half (55.1%) were female. There were 355 patients randomly assigned to receive atezolizumab plus FOLFOX and 357 patients randomly assigned to receive FOLFOX alone.
Key Findings
After a median follow-up of 37.2 months:
• Out of 712 patients, 124 patients in the trial had a disease-free survival (DFS) event of cancer recurrence or death.
• In the atezolizumab plus FOLFOX group, 86.4% of patients did not have any evidence of cancer after 3 years. In the FOLOFX alone group, 76.6% of patients had not experienced any evidence of cancer recurrence or death.
• Patients treated with atezolizumab plus FOLFOX had a 50% lower risk of recurrence and death compared to patients treated with FOLFOX alone. The atezolizumab plus FOLFOX treatment was effective across all subgroups, including patients older than age 70, low-risk patients and high-risk patients.
Severe side effects (grade 3 and higher) were experienced in both treatment groups but were manageable and consistent with the known toxicities of the drugs.
Next Steps
The ATOMIC clinical trial is ongoing, and the study investigators will continue to follow these patients. They will also study biospecimens from the trial and try to identify biomarkers that can predict which patients treated with
chemoimmunotherapy are more likely to receive benefit as well as who might be at a higher risk of cancer recurrence.
Pro-Inflammatory Diets Associated With Worse Outcomes for Patients with Stage III Colon Cancer
Results from a large, prospective cohort study show that eating a less inflammatory diet may reduce the risk of death for patients with stage III colon cancer.
About the Study
"One of the most common questions that patients ask is what diet they should be following to maximally reduce their risk of cancer recurrence and improve survival. While there have been many studies examining dietary factors and the risk of developing colorectal cancer, there is significantly less known about how diet impacts colon cancer outcomes after diagnosis. This study sheds light on the relationship between dietary patterns and survival in patients with stage III colon cancer,” said lead study author Sara K. Char, MD, Dana-Farber Cancer Institute in Boston, Massachusetts.
To assess the effects of diet on the risk of colon cancer recurrence, the diet habits of a subset of patients enrolled in the phase 3 CALGB/SWOG 80702 clinical trial were analysed in a prospective cohort study. The CALGB/SWOG 80702 clinical trial tested 3 months vs. 6 months of adjuvant chemotherapy, with or without celecoxib, an anti-inflammatory medication. A prospective cohort study follows patients with similar characteristics who differ in a key factor over time to see if that factor impacts outcomes.
Of the approximately 2,500 patients enrolled in CALGB/SWOG 80702, there were 1,625 patients followed as part of this study. The patients all had stage III colon cancer that had been removed with surgery. The average age of the participants was 60.9 years. The patients reported their diet and exercise habits at six weeks after being randomly assigned to a treatment group in the CALGB/ SWOG 80702 study and again 14 to 16 months after random assignment. Their diets were scored using the empirical dietary inflammatory pattern (EDIP) tool.
The EDIP tool is a weighted sum of 18 food groups: 9 pro-inflammatory and 9 antiinflammatory. Examples of pro-inflammatory foods include
red meat, processed meats, refined grains and sugary drinks. Examples of anti-inflammatory foods include coffee, tea, dark yellow vegetables and leafy green vegetables. A high EDIP score indicates a pro-inflammatory diet. A low EDIP score represents a less inflammatory diet.
Key Findings
• Patients who consumed the most pro-inflammatory diets and had the highest EDIP scores were:
o More likely to be younger (average age 58.7 vs. 61.3)
o More likely to be female (64% vs. 48.9%)
o Have an ECOG score of 1 or 2, indicating a lesser ability to perform daily activities (35.7% vs. 19.4%)
o Less likely to be White (76.6% vs. 92.0%)
o More likely to be Black (15.4% vs. 3.7%)
• Pro-inflammatory diets were associated with worse outcomes. Patients with the highest EDIP scores and very pro-inflammatory diets had an 87% higher risk of death than those who ate highly antiinflammatory diets.
• Exercise habits, another modifiable factor associated with systemic inflammation, also impacted overall survival. Patients who consumed less inflammatory diets and exercised more often (9 or more metabolic equivalent [MET] hours per week) had the best overall survival, with 63% lower risk of death compared to patients who ate pro-inflammatory diets and exercised less (less than 9 MET hours pers week).
• There was no significant difference in disease-free survival between the patients who ate a pro-inflammatory diet and those who ate an antiinflammatory diet.
• Low-dose aspirin use and which treatment regimen the patients received as part of the CALGB/ SWOG 80702 trial were not significantly different between the groups.
Next Steps
Researchers will continue to study how diet and inflammation, as well as exercise, affect outcomes for patients with colorectal cancer.
Osteoporosis
Utilisation and expenditure on medicines for the management of osteoporosis in Ireland: A repeated cross-sectional study
Written by Amelia Smith1,2, Lisa Kelly1,2, Claire Gorry1,2,Bernard Duggan1,2 and Michael Barry1,2
1Department of Pharmacology & Therapeutics,Trinity College Dublin, Trinity Centre for Health Sciences, St James's Hospital, Dublin, Ireland
2Medicines Management Programme, Health Services Executive, Trinity Centre for Health Sciences, St James's Hospital, Dublin, Ireland
The reimbursement price of certain medicines for the management of osteoporosis in Ireland has seen a reduction due to patent expiry and the introduction of generic medicinal products, and subsequent implementation of automatic substitution and reference pricing as legislated for in the Health (Pricing and Supply of Medical Goods) Act 2013.12 In 2015 reference pricing was introduced for risedronate and alendronate, with a further reference price reduction for alendronate in 2022.13–15 Medicinal products containing a combination of alendronate and colecalciferol underwent a price reduction in 2016 as a result of reference pricing.16 Similarly, the addition of biosimilar medicines and hybrid medicinal products for teriparatide to the reimbursement list in 2019 triggered a price reduction in the originator brand in line with the provisions set out in the Framework Agreements between industry representative bodies and the health service.17,18
Osteoporosis is a systemic skeletal disease that is characterised by low bone mass, micro-architectural deterioration of bone tissue and compromised bone strength. This results in bone fragility and increased susceptibility to fracture.1 Osteoporosis is the most common bone disease worldwide and is associated with high morbidity and mortality, as well as socio-economic costs.2 Although the prevalence of osteoporosis currently is highest in North America and Europe, it will increase in developing countries as population life expectancy in these countries continues to increase.3 Medicines commonly used in the management, ie, treatment and prevention, of osteoporosis may reduce the rate of bone turnover (antiresorptive therapies) or stimulate bone formation (anabolic therapies). Antiresorptive therapies include bisphosphonates, denosumab, hormone replacement therapy and selective oestrogen receptor modulators (SERMs), while teriparatide has an anabolic or bone-forming action. A number of medicines for the management of osteoporosis are available for reimbursement in Ireland. In Ireland in 2005, over 87 000 patients received bisphosphonates, calcitriol, calcitonin, strontium, raloxifene or tibolone, with an associated expenditure of ¤22.12 million.4 In the same year, there were 606 prescription claims for teriparatide, with an associated expenditure of ¤1.99 million.4
Since 2005, the range of medicines reimbursed in Ireland for the management of osteoporosis has expanded to include the human monoclonal IgG2 antibody denosumab (2010) and the SERM bazedoxifene (2012).5,6 Internationally, osteoporosis treatment guidelines recommend using bisphosphonates first line in the management of osteoporosis.7–11 Some guidelines also support the use of denosumab as an alternative first-line treatment.10,11 Others recommend denosumab
The aim of this study was to determine the utilisation and expenditure associated with medicines for the management of osteoporosis on the community drug schemes (CDS) and High Tech (HT) arrangement in Ireland. The demographic characteristics (age and gender) of people in receipt of these medicines are described and the duration of use of certain medicines used in the management of osteoporosis was determined.
osteoporosis on the CDS from 2011 to 2023 and the associated total annual expenditure. The number of individual patients with claims for these medicines has increased slightly over the 13-year period, from 109 235 patients in 2011 to 127 887 in 2023. Total annual expenditure fell from ¤28.7 million in 2011 to just over ¤24.8 million in 2015, likely due to a decrease in eligible patient numbers over this time period, in combination with the introduction of reference pricing. Total annual expenditure increased from 2018 onwards, reaching ¤33.8 million in 2023.
3.1 Utilisation and expenditure on osteoporosis medications
There has been a significant change in the utilisation patterns of medicines used for the treatment of osteoporosis in Ireland. Figure 1 illustrates the number of individual patients in receipt of medicines licensed for the management of
Figure 2 outlines the utilisation of the individual medicines from 2011 to 2023. The number of patients in receipt of denosumab has substantially increased, from just under 3000 patients in 2011 to over 75 000 patients in 2023. The number of patients in receipt of bisphosphonate treatment has declined over the same period, from 95 579 patients in 2011 to 52 755 patients in 2023. Of these, 41 000 received alendronate in 2011, reducing to 23 161 people in 2020 and increasing again to 32 053 in
2023. A similar reduction was seen in the number of people receiving medicinal products containing alendronate in combination with colecalciferol (vitamin D3): 19 694 patients in 2011 and 9043 in 2023. Similar patterns can also be seen for the other bisphosphonates. As strontium ranelate has been withdrawn from the Irish market, there is a significant reduction in the utilisation of this medicine on the CDS. In 2011, there were 11 438 people in receipt of strontium ranelate on the CDS, fewer than 10 patients in 2022 and no patients in 2023. There has been an increase in the number of patients in receipt of teriparatide in Ireland; in 2011 there were just over 1600 patients in receipt of teriparatide and in 2023, just over 2600 patients. In 2023, the majority of patients in receipt of medicines for the treatment of osteoporosis were female: 90.9% for denosumab, 80.8% for bisphosphonates, 98.9% for selective oestrogen receptor modulators (SERMs), 99% for tibolone and 86.8% for teriparatide. In 2023, the majority of patients in receipt of denosumab, bisphosphonates,
should be noted that this analysis considers GMS claims only.
4 DISCUSSION
To our knowledge, this is the first Irish study of the utilisation and expenditure on medicines for the management of osteoporosis using national-level dispensed claims data between 2011 and 2023. There has been a significant change in the utilisation of medicines for the management of osteoporosis over the timeframe, with an increase in the utilisation and expenditure associated with the monoclonal IgG2 antibody, denosumab.
FIGURE 1 Total number of individual patients in receipt of medicines for the management of osteoporosis on the community drug schemes from 2011 to 2023 and associated total annual expenditure.
SERMs or teriparatide were aged over 70 years (Figure 3). The majority of patients in receipt of tibolone were aged 64 years and under.
Figure 4 shows the total annual expenditure on medicines for the management of osteoporosis on the CDS from 2011 to 2023. The total expenditure was ¤28.6 million in 2011 and ¤33.8 million in 2023. While the total annual expenditure has not changed significantly over this 13-year period, the distribution has changed significantly. For example, expenditure on denosumab accounted for ¤0.97 million in 2011 (less than 5% of the annual total), but had increased substantially to ¤26.4 million in 2023 (almost 80% of the annual total).
Figure 5 highlights the breakdown of expenditure on the individual bisphosphonates within the drug class. The total expenditure associated with bisphosphonates has decreased significantly over the study timeframe, as shown in Figure 4. In 2011, the total expenditure reached almost ¤18 million, in contrast to a total expenditure of just over ¤3 million in 2023. Alendronic acid, alendronic acid and colecalciferol combinations, and ibandronic acid comprised the majority of expenditure on bisphosphonates over the study timeframe.
3.2 Prescribing rate of osteoporosis medication per 1000 GMS eligible patients
The prescribing rate per 1000 GMS eligible patients in shown in Table 1. There has been a large decrease in the prescribing rate of bisphosphonates from over 426.4 per 1000 GMS eligible in 2011 to 220.1 per 1000 GMS eligible in 2023. There has been
an increase in the prescribing rate of denosumab over the study period, from 1.7 per 1000 GMS eligible in 2011 to 49.1 per 1000 GMS eligible in 2023. As the prescribing rate per 1000 GMS eligible is based on the number of claims per 1000 population with GMS eligibility, the apparently low prescribing rate of denosumab is reflective of the low number of claims dispensed per patient per year due to a dosing schedule of once every 6 months.
3.3 Adherence to osteoporosis medication:bisphosphonates, denosumab and teriparatide
In 2019, there were 9952 new users of denosumab. The proportion of patients considered adherent to denosumab treatment 1-year post treatment initiation was high, at 73%. However, the proportion of patients adherent 2 years post treatment initiation was much lower, at 44%. Similar patterns of adherence were seen for bisphosphonates FIGURE 4 Total expenditure on medicines licensed for the management of osteoporosis on community drug schemes from 2011 to 2023. SERMs, selective oestrogen receptor modulators. FIGURE 3 Age category breakdown of patients in receipt of medicines for the management of osteoporosis in 2023. SERMs, selective oestrogen receptor modulators. and teriparatide. In 2019, there were 7588 new users of bisphosphonates; 1 year post treatment initiation the proportion of patients considered adherent was 60%. The proportion of patients considered adherent to bisphosphonates 2 years post treatment initiation was 49%. In 2019, there were 944 new users of teriparatide; the proportion of patients considered adherent 1
year post treatment initiation was 65%, decreasing to 43% at 2 years post treatment initiation. The results of this analysis are shown in Table 2.
Due to potential disruptions to medicines utilisation during the COVID-19 pandemic, we repeated this adherence analysis using data from new users of osteoporosis medicines in 2017. In 2017, there were 8951 new users of denosumab; the proportion of patients considered adherent to denosumab treatment 1 year post treatment initiation was high at 75%, with the proportion of patients' adherent 2 years post treatment initiation at 47%. In 2017, there were 7607 new-users of bisphosphonates; 1 year post treatment initiation the proportion of patients considered adherent was 56%. The proportion of patients considered adherent to bisphosphonates 2 years post treatment initiation was 42%. In 2017, there were 783 new users of teriparatide; the proportion of patients considered adherent 1 year post treatment initiation was 67%, decreasing to 41% at 2 years post treatment initiation. The results of this analysis are shown in Table 3.
3.4 First-line use of denosumab for the treatment of osteoporosis
In 2017, there were 8951 new users of denosumab. Of these, 2401 (26.8%) patients had a claim for a bisphosphonate in the 6 months prior to denosumab initiation and 2773 (31%) patients had a claim for a bisphosphonate in the 12 months prior to denosumab initiation. This suggests that up to 70% of patients are being treated with denosumab first line. However, it
While there has been an overall decrease in the number of patients in receipt of bisphosphonates, there has been an increase in patient numbers since 2021; this is most likely due to a reduction in the payment threshold for the DP scheme. In November 2020, the DP scheme payment threshold was reduced from ¤124 to ¤114 per month. The threshold was further reduced to ¤100 and subsequently ¤80 in January 2022 and March 2022, respectively. This results in more patients meeting the payment threshold and thus being captured in the dispensed claims database. The lack of increase in the prescribing rate of bisphosphonates on the GMS scheme also suggests that the increase in patient numbers may be due to an increased number of individuals meeting the threshold for reimbursement support under the DP scheme.
The patient demographics seen in this study are similar to those observed in other Irish studies of osteoporosis treatments.4,20 A recent document by the International Osteoporosis Foundationestimated that 209 000 people in Ireland have osteoporosis, 77.5% of whom are female.21 This document also highlights that the Irish population aged 50 years or more is projected to increase by 38% between 2019 and 2034, which is higher than the EU average of 11.4%. The increases in the numbers of men and women aged 75 years or more are even more marked: 78.9% for men and 69.0% for women.21 As such, the number and burden of fragility fractures are likely to increase, and utilisation of agents for the management of osteoporosis is likely to continue to increase.21 The Irish Central Statistics Office highlights that Ireland has had an aging population over the last 10 years, with the proportion of people aged 45 or over increasing from 35.4% in 2013 to 40.6% in 2023.22
In 2011, the average annual cost per patient on bisphosphonates was approximately ¤188, which
Osteoporosis
is in contrast to 2023, which had an annual cost per patient of approximately ¤60. This is likely driven by patent expiries, the introduction of generic medicinal products and reference pricing, which was introduced for risedronate in January 2015 and alendronate in May 2015, and for medicinal products containing a combination of alendronate and colecalciferol in August 2016.13,14,16 The reference price for alendronate was revised in February 2022.15 In Ireland, The Health (Pricing and Supply of Medical Goods) Act 2013 provides for the introduction of reference pricing, which involves the setting of a common reimbursement price, or “reference price”, for a group of medicines that are deemed interchangeable by the Health Products Regulatory Authority (HPRA).12 In addition, under the Health Act 2013, medicines on the interchangeable list may be substituted for each other to create financial efficiencies for the health service. The publication of an interchangeable list by the HPRA facilitates automatic substitution by allowing pharmacists to safely dispense a lower-cost alternative to a medicine where a specific brand has been prescribed.
The savings generated from the introduction of reference pricing for bisphosphonates appear to have been negated by the increased utilisation and expenditure associated with the uptake of denosumab, as demonstrated in Figure 5. The number of patients in receipt of denosumab has increased from 2800 patients in 2011 to over 75 000 patients in 2023, reaching a total expenditure of almost ¤26.4 million in 2023. In 2023, almost 60% of patients in receipt of medicines for the management of osteoporosis were treated with denosumab. The annual cost per patient on denosumab, based on ingredient cost alone and a twice-yearly dosing schedule, is approximately ¤400 per year. A study from the United States has reported the utilisation of denosumab as having increased since its launch in 2010, accounting for approximately 20% of almost 950 000 patients treated for osteoporosis in March 2020.23 In Australia, the data show a greater uptake in its utilisation, with denosumab comprising 76.1% of patients dispensed any osteoporosis medicine in 2018 on the Pharmaceutical Benefits Scheme.24
Financial efficiencies were also created through a best-value medicine (BVM) initiative. Where a biosimilar medicine and/ or hybrid medicinal product become available for a biological medicine, such as teriparatide,
the Medicines Management Programme may evaluate the biological medicine in question and issue a recommendation as to the BVM.18 Since 1 March 2023, it has been HSE policy that all adult patients who are commencing treatment with teriparatide should be prescribed one of the recommended BVMs for teriparatide.25
In February 2024, the HSE agreed to approve reimbursement of romosozumab (Evenity®) for postmenopausal women with severe osteoporosis who have had a major osteoporotic fracture (within the previous year and who are at imminent risk of another fragility fracture).26 The health technology assessment (HTA) summary for romosozumab in the Irish setting estimates a 5-year cumulative gross and net drug budget impact (including VAT) of ¤15.2 million and ¤3.2 million, respectively.27 In the HTA, the Marketing Authorisation Holder also included cost offsets, which assumed a reduction in healthcare resource use secondary to reduced incidence of fragility fractures. Accounting for these cost offsets, the 5-year cumulative net healthcare budget impact for romosozumab (including VAT) was estimated to be ¤3.8 million.27 Reimbursement is subject to a managed access protocol that imposes specific eligibility criteria for reimbursement, specifically restricting reimbursement to a subpopulation of the product licence.28 Managed access protocols are used by the HSE to actively manage the utilisation of medicinal products, with the aim of providing a measure of cost containment and cost certainty regarding reimbursement decisions for new medicines.29
Adherence to medications has been defined as the process by which patients take their medications and has three components: initiation, implementation and discontinuation. This study focused on the first two components of medication adherence, initiation and implementation for up to 2 years.30 Persistence with osteoporosis medications both in Ireland and internationally has been shown to be suboptimal, with a range of studies demonstrating 2-year persistence rates in the region of 50% or below.20,31–34 In an Irish study using prescribing data from GP practices, 2-year persistence was found to be 49.4% for oral bisphosphonates and 53.8% for denosumab.20 In a systematic review investigating the persistence and adherence with parenteral osteoporosis treatments, the adherence rates for teriparatide were examined
in 29 studies and were 21-89% at 1 year and 37-68% at 2 years. Denosumab was investigated in 19 studies, with 1- and 2-year dosepersistence rates of 61-100% and 36-99%, respectively.35 A study investigating the economic burden of poor adherence with osteoporosis medications found that poor adherence results in a 50% reduction in the potential benefits observed in clinical trials and a doubling of the cost per quality adjusted life year (QALY) gained.34 When denosumab was evaluated for cost-effectiveness compared with bisphosphonates in the Irish setting by the National Centre for Pharmacoeconomics, denosumab had a high probability of costeffectiveness and reimbursement was recommended.5 It is unknown what assumptions were made regarding treatment adherence in that analysis. There are some limitations of the PDC method when assessing medication adherence. For example, as the PDC method considers the proportion of time a patient has medication available, based on prescription claim reimbursement data, it may overestimate adherence by masking non-persistence. This can occur when a patient stops taking the medication for a period (considered non-persistence) and then resumes refilling prescriptions later. In addition, in this study, the PDC method measures whether the medication claim is reimbursed but not whether it is taken as prescribed. Patients might receive dispensed medications but not take them as prescribed, which again may overestimate the adherence value.36
In this study, up to 70% of patients were initiated on denosumab as first-line treatment in the management of osteoporosis. A recent study of Irish GPs cited the vast majority of GP participants (90%) had prescribed denosumab in the last year, with 43% using it as a first-line therapy. Reasons for use of denosumab as first-line therapy included gastrointestinal upset, poor compliance with oral therapy, convenience, severe osteoporosis and renal impairment.37
A global questionnaire study was conducted by the International Osteoporosis Foundation and National Osteoporosis Foundation to ascertain the impact the COVID-19 pandemic had on osteoporosis management from the perspective of healthcare workers. Healthcare workers reported an increase in telemedicine consultations, delays in dual-energy X-ray absorptiometry (DXA) scanning, interrupted supply of medications and reductions in the use of
parenteral medications.38 Furthermore, in addition to the effects of COVID-19 on osteoporosis management, measures used to prevent the spread of COVID-19 may have contributed to bone loss. For example, a decrease in physical activity during quarantine and stay-at-home guidance may have contributed to decreased bone mineral density and increased frailty and fall risk, particularly in older adults.39
Our study was based on claims data for medicines dispensed under the CDS; this excludes medicines administered in the hospital setting. Zolendronic acid is an intravenous bisphosphonate, licensed at a dose of 5 mg once yearly for the treatment of osteoporosis and Paget's disease of the bone in adults.40 While individual patient level claims data for medicines administered in the hospital setting are not available, unpublished HSE data suggest that approximately 550 units of zolendronic acid 5 mg/100 mL were dispensed through acute hospital pharmacy departments in 2023. This suggests that there is not widespread use of intravenous bisphosphonates for the treatment of osteoporosis in the hospital setting, and provides assurance that the absence of individual patient-level claims data from this setting is unlikely to bias the outcomes of our study.
Our study was conducted using a large, robust national pharmacy claims database. However, it is important to note some limitations. The PCRS database does not include indication for treatment, and we assumed that those in receipt of medicines for the management of osteoporosis had had an osteoporosis diagnosis. As the data included in this study are based on reimbursement claims, there are negligible missing data, however, we could not ascertain if patients had taken medicines as prescribed. It should also be noted that the expenditure data included in this study are representative of ingredient cost alone and exclude patient care fees and VAT. Therefore, the actual state expenditure associated with medicines for the management and treatment of osteoporosis is higher than quoted here. In Ireland, non-oral medicines (such as denosumab and teriparatide) are liable to VAT at the standard rate, currently 23%. Confidential commercial arrangements with marketing authorisation holders, which further reduce the cost of medicines, are excluded from our analyses.
References available on request
IPHA Respond to Transparent Payments Bill
The Irish Pharmaceutical Healthcare Association (IPHA), representing the research-based biopharmaceutical industry in Ireland, have noted Sinn Féin’s proposed Healthcare (Transparent Payments) Bill 2022 due for Second Stage Debate in the Dáil towards the end of last month (June).
The bill, sponsored by Darren O’Rourke TD, David Cullinane TD and Seán Crowe TD, seeks to make it mandatory for pharmaceutical companies and medical equipment suppliers to declare payments, gifts, donations and all other transfers of value made by them to healthcare professionals and organisations.
Teachta O’Rourke said, “We know payments to healthcare professionals and organisations can create a conflict of interest. Evidence shows that receipt of payments from the pharmaceutical industry is, for example, associated with higher prescribing rates, higher prescribing costs, increased use of specific drug classes, including opioids, and lower prescribing quality.
“The popular show ‘Dopesick’ highlighted this to great effect in the context of the opioid epidemic in the United States.
“In Ireland, tens of millions of euros are paid to healthcare professionals and organisations each year by the pharmaceutical industry.
“While a voluntary register of these payments is currently in place and maintained by the Irish Pharmaceutical Healthcare
Teachta Darren O’Rourke
Association, research conducted at the Royal College of Surgeons in Ireland found that the identity of many recipients is anonymous, while other payments may not be reported at all.
“The current voluntary system is inadequate. The Healthcare (Transparent Payments) Bill 2022 is needed to bring Ireland in line with international best practice, and is a measure in the interest of industry, professionals, organisations and the general public.”
Issuing a statement, IPHA said, “Ahead of this debate, we would like to reaffirm IPHA’s unwavering commitment to integrity and transparency in all interactions between our member companies and healthcare professionals (HCPs) and healthcare organisations (HCOs).
“The shared ambition of our member companies is to bring innovative treatments to Irish patients under the guidance of qualified HCPs. We place great value on our longstanding, ethical relationships with doctors, nurses, dentists, and pharmacists, whose experience and insight are essential to advancing the development and appropriate use of new medicines.
“Our industry has already taken significant steps to ensure accountability and transparency in all such engagements with the healthcare community. Since July 2016, in line with the IPHA Code
of Practice for the Pharmaceutical Industry, companies have disclosed financial transfers of value—whether direct or indirect, in cash or in kind—made to HCPs and HCOs. IPHA members are required to disclose, and these disclosures are publicly accessible on www.transferofvalue.ie which is open to all pharmaceutical companies to use, not just IPHA members. Currently, of the 50 companies who publish their data through the platform, 11 are non IPHA members.
“For 2023 data, we achieved 100% named disclosure for HCOs and 96% for HCPs. We expect the 2024 data, due for publication on June 30th, 2025, will maintain or exceed these strong levels of transparency.
“Our aim is to reach 100% named disclosure for HCPs, and we will
continue to support our member companies in using legitimate interest as a legal basis for making these disclosures under data protection law.”
IPHA believes that any legislative proposals in this area must be informed by the progress that has already been made by the industry. “We are very willing to work with Government to ensure more companies, and indeed other sectors such as medical devices, use this already established and effective website to disclose their payments to HCPs and HCOs. “Constructive engagement with stakeholders, including Oireachtas members, remains a priority as we continue to uphold the highest standards of conduct in support of patient care and public confidence,” they add.
Teva Launches Ticagrelor Teva 90mg Film Coated Tablets
Teva Pharmaceuticals is pleased to announce the launch of Ticagrelor Teva 90 mg Film-coated Tablets.
Ticagrelor Teva co-administered with acetylsalicylic acid (ASA), is indicated for the prevention of atherothrombotic events in adult patients with acute coronary syndromes (ACS) or a history of myocardial infarction (MI) and a high risk of developing an atherothrombotic event.
For any queries or further information, please contact your local Teva representative or contact Teva on 1800 201 700.
Further product information is available upon request or from the SmPC available at hpra.ie.
Adverse events should be reported. Reporting forms and information can be found at hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com.
Date of preparation: May 2025
Job code: GEN-IE-NP-00146
TIME IS IN YOUR HANDS
ERBITUX® + FOLFIRI or FOLFOX:
Combining strength of clinical data with a manageable tolerability profile
• ERBITUX® combined with FOLFIRI or FOLFOX shows improved mOS in RAS wild-type mCRC patients compared with chemotherapy alone2,3*†
• ERBITUX® has a manageable adverse event profile1,5
ERBITUX® is indicated for the treatment of patients with EGFRexpressing RAS wild-type mCRC in combination with irinotecan-based chemotherapy, in first-line in combination with FOLFOX, or as a single agent in patients who have failed oxaliplatin- and irinotecan-based therapy and who are intolerant to irinotecan.1
Legal category: POM.
Prescribing information and adverse event reporting information for ERBITUX® is available on the next page. GET UPDATES
Scan this QR code with your smartphone to receive updates by email and/or SMS from Merck Serono Limited.
PRESCRIBING INFORMATION - Ireland
Please refer to the Summary of Product Characteristics for further information
Erbitux 5 mg/ml solution for infusion cetuximab.
Presentation:
Glass vial containing 20 ml or 100 ml of Erbitux solution for infusion at a concentration of 5 mg/ml. Total: 100 mg or 500 mg Erbitux per vial.
Indications:
Treatment of Epidermal Growth Factor Receptor-expressing, RAS wild-type metastatic colorectal cancer (mCRC) in combination with irinotecan-based chemotherapy; in first-line in combination with FOLFOX (oxaliplatin, 5-FU and folinic acid) or as a single agent in patients who have failed oxaliplatin- and irinotecan-based therapy and who are intolerant to irinotecan. Treatment of squamous cell cancer of the head and neck (SCCHN) in combination with radiation therapy for locally advanced disease or in combination with platinumbased chemotherapy for recurrent and/or metastatic disease.
Dosage and administration:
Erbitux may be administered in a weekly or every other week dose regimen for all indications, with the exception of locally advanced squamous cell carcinoma of the head and neck (SCCHN) in combination with radiation therapy, where it is administered only on a weekly basis.
Weekly dose regimen: Erbitux is administered once a week. The initial dose is 400 mg cetuximab per m2 body surface area (BSA). All subsequent weekly doses are 250 mg/m2 each.
Biweekly dose regimen: Erbitux is administered once every other week. Each dose is 500 mg cetuximab per m2 body surface area.
Children: safety and efficacy have not been established.
Administration must be supervised by a physician experienced in antineoplastic medicinal products. Administer intravenously with infusion pump, gravity drip or syringe pump using a separate infusion line. The initial dose should be given slowly to minimize risk of infusion related reactions. The recommended infusion period is 120 minutes. For subsequent administration the infusion rate must not exceed 10 mg/min. If initial infusion is well tolerated the recommended infusion period for weekly dose regimen of 250 mg/m2 is 60 minutes and recommended infusion period for biweekly dose regimen of 500 mg/m2 is 120 minutes.
Premedicate first infusion at least one hour before with an antihistamine and a corticosteroid. Premedication recommended for all subsequent infusions.
Flush line with sterile 0.9% NaCl at end of infusion. Closely monitor patient throughout infusion and for at least 1 hour afterwards. Resuscitation equipment must be available. mCRC: Evidence of wild-type RAS status is required before initiating treatment. Mutational status should be determined by an experienced laboratory using validated test methods for detection of KRAS and NRAS (exons 2, 3 and 4). Refer to product information for concomitantly used chemotherapeutic agents for dosage. Administer Erbitux first and do not administer concomitantly used chemotherapeutic agents earlier than 1 hour after end of Erbitux infusion. Continue treatment until disease progression. Locally advanced SCCHN: start Erbitux one week before radiation therapy and continue treatment until the end of the radiation therapy period. Recurrent/ metastatic SCCHN: use in combination with platinum-based chemotherapy followed by Erbitux as maintenance therapy until disease progression. Do not administer chemotherapy earlier than 1 hour after the end of Erbitux infusion.
Contraindications:
Severe (grade 3 or 4) hypersensitivity to Erbitux. In combination with oxaliplatin-containing chemotherapy in patients with mutant RAS mCRC or for whom RAS mCRC status is unknown. Consider contraindications to concomitantly used chemotherapeutic agents or radiation therapy.
Precautions:
Discontinue infusion immediately and permanently in the event of severe infusion-related reactions (symptoms may include: bronchospasm; urticaria; increase or decrease in blood pressure; loss of consciousness or shock; rarely: angina pectoris; myocardial infarction or cardiac arrest) – emergency treatment may be required. Some of these reactions may be anaphylactic or anaphylactoid in nature or represent a cytokine release syndrome (CRS). Anaphylatic reactions may occur as early as within a few minutes of the first infusion. The risk is increased in patients with a history of allergy to red meat, tick bites of positive results of tests for IgE antibodies against cetuximab. A CRS typically occurs within one hour after infusion and is less commonly associated with bronchospasm and urticaria. It is normally most severe in relation to the first infusion. Monitor all vital signs closely for at least two hours for the first dose. If an infusion-related reaction occurs during the first 15 minutes, stop the infusion. Perform careful benefit/risk assessment including whether patient may have pre-formed IgE antibodies, before giving a subsequent infusion. If an infusion-related reaction develops later during the infusion or at a subsequent infusion, further management depends on its severity – see SPC. Warn patients of possible delayed-onset severe infusionrelated reactions. Decrease infusion rate if mild or moderate infusion-related reaction occurs (symptoms may include: fever; chills; dizziness; dyspnoea)
and use lower rate in all subsequent infusions. Closely monitor patients, particularly during the first administration and those with reduced performance status and pre-existing cardiopulmonary disease.
Cases of interstitial lung disease (ILD), including fatal cases, have been reported, with most patients being from the Japanese population. Factors such as concomitant chemotherapy known to be associated with ILD or pre-existing pulmonary diseases were frequent in fatal cases. Monitor such patients closely. In the event of symptoms or radiographic findings suggestive of ILD, prompt diagnostic investigation should occur. Discontinue Erbitux if ILD is diagnosed. Skin reactions are very common. Consider prophylaxis with oral tetracyclines (6-8 weeks) and topical 1% hydrocortisone cream with moisturiser. Skin reactions may become severe, especially in combination with chemotherapy. The risk of secondary infections is increased and cases of staphylococcal scalded skin syndrome, necrotising fasciitis and sepsis, in some cases with fatal outcome, have been reported. Interrupt treatment if patient experiences an intolerable or severe skin reaction (≥ grade 3 CTCAE). Only resume if reaction resolves to grade 2. With second or third instances of severe skin reactions, resume at lower dose (200 mg/m2 BSA in the weekly dosing regimen, 400 mg/m2 BSA in the biweekly dosing regimen) after the second occurrence and with a dose reduction of 40% (150 mg/m² BSA in the weekly dosing regimen, 300 mg/m² BSA in the biweekly dosing regimen) after the third occurrence. A fourth occurrence of severe skin reaction, or failure to resolve to grade 2 during interruption, necessitates permanent discontinuation of Erbitux. Determine serum electrolyte levels (e.g. magnesium, potassium, calcium) prior to, and periodically during Erbitux treatment and replete as appropriate. In combination with platinum-based chemotherapy, severe leukopenia or neutropenia may occur, leading to infectious complications such as febrile neutropenia, pneumonia and sepsis. Careful monitoring is recommended in such patients, particularly in those who experience skin lesions, mucositis or diarrhoea. An increased frequency of severe and sometimes fatal cardiovascular events and treatment emergent deaths has been observed in non-small cell lung cancer, SCCHN and colorectal carcinoma patients. In some studies (non-small cell lung cancer) association of these with age ≥ 65 years has been observed. When prescribing, take into account the cardiovascular and performance status of the patient and concomitant administration of cardiotoxic compounds such as fluoropyrimidines. Do not use Erbitux in colorectal cancer patients whose tumours have RAS mutations or for whom RAS tumour status is unknown.
Promptly refer patients with symptoms of keratitis to an ophthalmology specialist. If ulcerative keratitis is confirmed, interrupt or discontinue Erbitux. Consider the benefits/risks of continuing treatment if keratitis is diagnosed. Use Erbitux with caution in patients with a history of keratitis, ulcerative keratitis or severe dry eye. Contact lens use is a risk factor for keratitis and ulceration. Only use in pregnancy if potential benefit justifies potential risk to foetus. Breast feeding is not recommended during Erbitux treatment or for up to 2 months after last infusion.
Side effects: Very common: skin reactions (acne-like rash; pruritus; dry skin; desquamation; hypertrichosis; nail disorders); hypomagnesaemia; increase in liver enzyme levels; mild or moderate infusion-related reactions; mucositis, in some cases severe, which may lead to epistaxis. Common: headache; diarrhoea; nausea; vomiting; severe infusion-related reactions, in some cases fatal; conjunctivitis; fatigue; dehydration normally secondary to diarrhoea or mucositis; hypocalcaemia; anorexia which may lead to weight decrease. Uncommon: blepharitis; keratitis; pulmonary embolism; DVT, interstitial lung disease which may be fatal. Very rare: Stevens-Johnson syndrome/toxic epidermal necrolysis. Unknown frequency: superinfection of skin lesions; aseptic meningitis. Refer to product information of concomitantly used chemotherapeutic agents for side effects. In combination with fluoropyrimidines, the frequency of cardiac ischaemia and hand-foot syndrome was increased compared to that with fluoropyrimidines. In combination with capecitabine and oxaliplatin (XELOX) the frequency of severe diarrhoea may be increased.
In combination with platinum-based chemotherapy, the frequency of severe leukopenia or neutropenia may be increased, leading to a higher rate of infectious complications such as febrile neutropenia, pneumonia and sepsis compared with platinum-based chemotherapy alone.
Prescribers should consult the summary of product characteristics in relation to other side-effects.
Legal category: POM.
Marketing Authorisation Holder:
Merck Europe B.V., Gustav Mahlerplein 102, 1082 MA Amsterdam, The Netherlands
For further information, including price queries, contact: Merck Serono, 4045 Kingswood Road, Citywest Business Campus, Dublin 24. Tel: 01 4687590.
Date of preparation: December 2024 Job Bag No: IE-ERB-00008
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Merck Serono Limited. Tel: 1 800 719 881 or email: medinfo.uk@merckgroup.com
EGFR, epidermal growth factor receptor; FOLFIRI, fluorouracil, leucovorin and irinotecan; FOLFOX, fluorouracil, leucovorin and oxaliplatin; mCRC, metastatic colorectal cancer; mOS, median overall survival; PFS, progression-free survival.
References
1. Erbitux® Summary of Product Characteristics. Available at: https://www.medicines.ie/medicines/erbitux-5mg-mlsolution-for-infusion-32054/spc (Last accessed June 2025).
2. Van Cutsem E et al. J Clin Oncol. 2015;33:692–700.
3. Qin S et al. J Clin Oncol. 2018;36:3031–3039.
4. García-Foncillas J et al. Front Oncol. 2019;9:849.
5. Petrelli F et al. Oncology. 2018;94:191–199.
Prostate Cancer
Focal Therapy for Prostate Cancer - High Intensity Focused Ultrasound
High intensity focused ultrasound (HIFU) ablation for localised prostate cancer involves delivery of ultrasound energy to a focal area of the prostate via a transrectal ultrasound probe. Ultrasound energy pulses are delivered in an area of 9x3mm with a rapid rise in temperature (>80 degrees Celsius) in the region of interest. This leads to melting of cell membrane lipids and denaturation of protein and thus cell death (coagulative necrosis, cavitations and cell death). HIFU ablation is repeated over multiple zones with a good surgical margin. The surrounding tissues and areas remain unaffected, limiting damage to surrounding nerves, vessels, external urinary sphincter, rectum and bladder neck.
Prostate cancer is the second most common cause of invasive cancer death in Ireland and most common cancer in men in Ireland with 4000 cases diagnosed on a yearly basis. A recent study on patients with a new diagnosis of prostate cancer in a tertiary center in Dublin showed that nearly 30% of patients were ideal candidates
and 50% were suitable candidates for focal HIFU. The first focal HIFU case in the Republic of Ireland was performed at Beacon Hospital in November 2024 using the Sonablate HIFU machine.
International guidelines (European association of Urology, National institute for health and care excellence) and local guideline (National cancer control programme) have incorporated focal therapy into their up-todate guidelines. Focal therapy should only be offered as part of a clinical trial or a prospective registry. In appropriately selected patients, focal therapy offers better functional outcomes. Patients should be informed of the lack of long-term oncological outcome. Current standard of care for localized prostate cancer treatment includes surgery (Robotic assisted laparoscopic prostatectomy) or radiotherapy (External beam radiotherapy or Brachytherapy), where the whole prostate gland is treated, regardless of the location or volume of disease. Radical treatments are associated
Written by Mr Mohammud Shakeel Inder, Consultant Urological Surgeon at Beacon Hospital
with a significant risk of rectal complications, incontinence and impotence. Focal therapy in which only areas of known cancer are targeted may improve the therapeutic ratio. Multiple studies have shown that preservation of genitourinary function can be high following focal therapy and cancer control in the short to medium term is good. Over two thousand cases treated with focal therapy in the United Kingdom over the last 10 years, with an average follow-up of 7 years and maximum follow-up of 10 years. Urinary incontinence after focal therapy is < 2% and erectile dysfunction occurs in 5-15% of men. From an oncological viewpoint, there is a 20% risk of infield recurrence, 5% risk of out of field recurrence and a 5-10% salvage rate. Both surgery and radiotherapy are feasible after focal therapy. Cancer specific survival is > 99%. Comparative data using a propensity matched analysis has shown that compared to radical prostatectomy and radiotherapy, focal HIFU have similar survival, metastases free survival and transition to salvage therapy.
Alternative ablation techniques include cryotherapy and nanoknife irreversible electroporation (IRE). Both needle therapies treat only the affected areas of the prostate gland. The use of different ablation techniques is based on multiple factors, including location of clinically significant cancer and prostate volume.
The consensus amongst focal therapy experts regarding eligibility for focal HIFU are as follows:
1) PSA ≤ 20
2) MRI Staging ≤ T3a
3) Visible lesion on MRI (PIRADS 3 or 4 or 5)
4) Intermediate risk prostate cancer
- Unilateral disease: Any cancer length and MRI lesion PIRADS 3 or 4 or 5
- Bilateral disease: MRI lesion PIRADS 3 or 4 or 5 with confirmed Gleason 7 disease on one side and contralateral Gleason 6 disease with maximum cancer length (MCL) ≤ 6mm)
5) Low-risk disease (MCL of ≥ 6mm and MRI lesion PIRADS 3 or 4 or 5)
HIFU focal therapy for prostate cancer is performed under general anesthesia, as a day case procedure or an overnight stay. All cases are discussed at a multidisciplinary meeting and recorded as part of a prospective registry. The Sonablate system is used to define the ablation zones with adequate overlapping. HIFU energy is delivered with real time monitoring of specific changes (near field heat absorption and dissipation, prostate swelling and quality of ablation). A urinary catheter is placed at the end of ablation. Urinary catheter remains in situ post operatively for 7-14 days. Patients are discharged home on analgesia and antiinflammatory medications, laxatives, alpha blocker, antibiotics and beta 3 agonist as required.
Focal therapy is a good alternative treatment option in appropriately selected patients, with a better functional outcome compared to current standard of care.
¤6.5m Horizon Europe Bone Regeneration Project
Dr Ciara Murphy, Senior Lecturer from the RCSI Department of Anatomy and Regenerative Medicine, the Research Ireland Centre for Advanced Materials and BioEngineering Research (AMBER) and RCSI Tissue Engineering Research Group, has been named a partner on a prestigious ¤6.5 million Horizon Europe grant.
The funding will support HYDROHEAL, an ambitious research initiative aimed at developing smart, sustainable biomaterials to transform the treatment of bone loss and fractures.
As part of the international HYDROHEAL consortium, Dr Murphy will advance the development of injectable hydrogels made from natural, renewable sources. These hydrogels are designed not only to support bone healing – particularly in the spine and jaw – but also to deliver therapeutics precisely when and where they are needed, activated by external signals.
“What sets HYDROHEAL apart is the integration of intelligent biomaterials with advanced
Dr Ciara Murphy, Senior Lecturer, RCSI
drug delivery systems,” said Dr Murphy. “Our goal is to create eco-friendly, scalable solutions that don’t just support healing – they actively enhance it, improving outcomes for patients with serious skeletal injuries.”
The project addresses a significant clinical need. Fractures caused by injury, infection, osteoporosis or cancer remain a major global health challenge, and current treatments such as bone grafts and bone cement have limitations in effectiveness and safety. HYDROHEAL’s bioengineered hydrogels will incorporate features to support healing, fight bacterial infection, and enable real-time treatment monitoring. They will also be enhanced through machine learning and digital design tools, helping ensure sustainable, cost-effective production at clinical scale.
In addition to scientific innovation, HYDROHEAL will be informed by
public and patient involvement (PPI). Patient groups affected by spinal and jawbone injuries will be directly engaged through focus groups, surveys, and consultation activities. The project aims to collaborate with at least five patient associations, ensuring that patient needs and priorities guide the research.
Professor Fergal O’Brien, Deputy Vice Chancellor for Research and
Diabetes Ireland DICE Event
Almost 450 healthcare professionals and researchers attended the Diabetes Ireland Conference and Exhibition (DICE) in Croke Park on 22nd of May 2025, where they heard from a top line-up of international and national speakers presenting on the day.
From a paediatric diabetes care perspective, excellent presentations were delivered by international and national experts covering diabetes education, sports performance and type 1 diabetes, managing different types of diabetes in children and learning from the National Childhood Diabetes Register. Highly renowned, Professor Klemen Dovc from Slovenia discussed the benefits of technology in paediatric diabetes, and UK Psychologists, Drs Corah Lewis and Mary Owen, outlined the challenges associated with living with type 1 diabetes and neurodiversity.
In the pregnancy stream, complex and complicated cases were explored, alongside presentations on resources to support women
with diabetes. The importance of nutrition in gestational diabetes was discussed, as well as strategies for preparing for pregnancy with pre-existing diabetes, presented by Ms Cathy Jones (UK) and the significance of mental health during pregnancy was also highlighted.
In the acute stream, the importance of integrating psychology services into diabetes clinics was emphasised by Dr Rose Stewart and Dr Steve Stanaway from Wales, who explained both the rationale and practical steps for implementation. Expertise was also shared on managing Type 1 diabetes in individuals who follow alternative diets, and a presentation outlined the key concerns and priorities of people living with Type 1 diabetes. In the community stream, Ms Una O’Neill highlighted the need for awareness around Latent Autoimmune Diabetes in Adults (LADA) in primary care. Hormonal influences on diabetes, particularly in relation to menopause, were explored, and the role of dietitians
in supporting people with diabetes within the Chronic Disease Model of Care was also highlighted.
Dr PJ Boyle shared his expertise on engaging effectively with minority groups. Dr. Amar Puttanna (UK) discussed diabetes complications, screening, and the often-overlooked link with oral health. Finally, Dr. Mark Davies (Belfast NHS Trust) addressed the critical issue of burnout among professionals working in diabetes care, offering insights on prevention and support
The Keynote Lecture was delivered by a real diabetes trailblazer and one of the most recognised researchers in the field of diabetes, the president of the European Association for the Study of Diabetes (EASD), Professor Chantal Mathieu. Professor Mathieu’s talk on the ‘New Face of Diabetes’ outlined where we are and where we are going with managing and living with diabetes and its prevention. This excellent talk gave hope to many that the health and well-being of people living with diabetes or at risk of diabetes are continuously
Innovation at RCSI, welcomed the award, “This Horizon Europe funding reflects the outstanding calibre of Dr Murphy’s work and the strategic impact of RCSI’s regenerative medicine research. HYDROHEAL is an excellent example of how scientific innovation, when grounded in clinical need and sustainability, can drive meaningful change in healthcare.”
improving, and the research work is ongoing, bringing us closer to finding the cure for diabetes.
Following the keynote lecture, the youngest-ever DICE presenter, Ms. Hazel O’Grady, who along with her group were highly commended at the BT Young Scientist and Technology Exhibition this year for their project “Plastic not so fantastic: Sustainability in diabetes management”, was joined by Professor Michael O’Grady to explore the oftenoverlooked topic of diabetes and the environment. Their discussion served as a powerful reminder of the importance of environmental sustainability in healthcare and encouraged all attendees to take steps toward going green.
The event concluded with a series of short national updates, including: an overview of Diabetes Ireland activities, progress on the Language Matters initiative, insights from the National Paediatric Diabetes Audit (presented on behalf of the National Office for Clinical Audits), and an update on the National Diabetes Registry by its national lead.
Prostate Cancer
Lived Experience of Men with Prostate Cancer in Ireland: A Qualitative Descriptive Study
Written by Seidu Mumuni,Claire O’Donnell and Owen Doody School of Nursing
and
Midwifery,
University of Limerick, V94 T9PX Limerick, Ireland
Introduction
Prostate cancer, the second most prevalent malignancy among men globally, remains a significant health concern with complex implications for those affected.1,2 With a staggering 1,467,854 new cases and over 397,430 deaths in 2022 alone,3 this disease is a profound public health issue. According to the Irish Cancer Society (ICS) over 4000 men are diagnosed with prostate cancer annually in Ireland, meaning approximately one in six men will be diagnosed in their lifetime.4 The disease predominantly originates in the peripheral zone of the prostate (70% of cases), with central and transition zone cancers comprising 10% and 20%, respectively.4 Although adenocarcinoma accounts for 95% of prostate cancers, rarer forms including primary carcinoid, sarcoma, and primary small-cell carcinomas, highlighting the need for targeted screening and early detection strategies.5
Prostate cancer incidence varies significantly across regions, with rates in Oceania and North America being over six times higher than in Asia, suggesting an interplay of genetic, environmental, and lifestyle factors.2,6,7 Age is a major risk factor, with incidence rising from 1 in 350 men under 50 years to 1 in 52 by ages 50–59, and further escalating in those over 65, who account for 55% of prostate cancer deaths.1,8 Despite high survival rates, advanced prostate cancer frequently metastasizes to the bone, lymph nodes, lungs, and liver, leading to severe complications that affect both quality of life and survival outcomes.9 These challenges highlight the need for comprehensive screening programs, such as prostatespecific antigen (PSA) testing, despite ongoing debates about its potential for overdiagnosis.10
Focusing on Ireland is particularly important, as prostate cancer remains one of the most diagnosed malignancies among Irish men. While advancements in early detection and treatment have improved outcomes, the Irish healthcare system faces
challenges related to screening accessibility, specialist availability, and psychosocial support. Issues such as long waiting lists, limited access to urologists, and inconsistencies in screening recommendations contribute to diagnostic delays, which can negatively impact survival and quality of life. Furthermore, cultural and societal factors may influence men’s health-seeking behaviours, awareness levels, and willingness to undergo screening. Addressing these gaps in knowledge is crucial to understanding the barriers men face and informing policy decisions aimed at improving prostate cancer care in Ireland.
Current evidence suggests that modifiable lifestyle factors, including diet, smoking, and alcohol consumption, contribute to prostate cancer risk alongside non-modifiable factors such as age, race, and family history.11,12 African American and Caribbean men face up to three times the risk compared to Caucasian men, while individuals with a family history of prostate cancer are at significantly increased risk, with the likelihood escalating based on the number of affected relatives.12,13,14 As a result, many health organisations, including the US Preventive Services Task Force,15 recommend PSA testing for men aged 55–69, though there remains ongoing debate regarding mass screening.16
The European Association of Urology opposes universal screening, instead advocating for early detection among highrisk men.16 Given this complex landscape, research into men’s experiences with prostate cancer screening and diagnosis is essential, not only to address clinical challenges but also to explore how these factors impact men’s lives. In Ireland, where many cases are diagnosed incidentally or at later stages due to insufficient proactive screening, understanding patient experiences can bridge gaps in early detection and intervention strategies. Beyond survival, prostate cancer presents men with substantial physical and psychological challenges. Urinary difficulties, including weak flow, bladder fullness, painful
urination, and incontinence, are common, alongside back pain and nocturia.17,18,19,20 The indolent nature of prostate cancer means symptoms often develop silently, leading to potentially curable cases going undetected.1,11
This reinforces the importance of understanding Irish men’s perspectives on screening, treatment decisions, and posttreatment support. Given Ireland’s healthcare infrastructure and cultural dynamics, a deeper examination of patient experiences can help identify gaps in support services and improve prostate cancer care.6,21
Psychologically, a prostate cancer diagnosis often elicits significant distress, manifesting as anxiety, depression, and diminished selfesteem.6,22 Many men experience concerns over treatment-related side effects, particularly those affecting masculinity, sexuality, and bodily functions, which contribute to emotional and psychological burdens.23,24 Erectile dysfunction and urinary incontinence, for instance, can undermine selfworth and strain relationships with partners and families.25,26 These concerns highlight the importance of research exploring Irish men’s specific experiences, including their emotional responses to diagnosis, decision-making processes, and available support structures. Insights from this research could inform healthcare policies that prioritize not only medical treatment, but also psychosocial interventions tailored to men’s unique needs.
Prostate cancer disproportionately affects racial and sexual minority groups, who may experience stigma, healthcare disparities, and lower screening uptake rates. African American men, for example, often report negative healthcare experiences, deterring them from timely screening.27 Similarly, LGBTQ+ individuals face barriers to screening, though some studies suggest that gay and bisexual men may be more proactive in seeking screening options.28,29 These disparities underscore the need for culturally sensitive, inclusive research to fully understand the diverse experiences of men with prostate cancer.
Addressing these challenges requires interventions that improve communication, accessibility, and reduce societal stigma. Given the complexity of men’s experiences with prostate cancer, further research is needed to examine factors influencing both diagnosis and treatment. By focusing on Ireland, this study aims to generate insights that will enhance screening initiatives, improve healthcare delivery, and inform policies that recognise the diverse ways prostate cancer impacts men’s lives. Ultimately, understanding these experiences will contribute to better health outcomes, increased awareness, and a more patient-centred approach to prostate cancer care in Ireland.
METHODOLOGY
Study Design and Settings
The study employed a qualitative descriptive design to explore the lived experiences of men with prostate cancer in Ireland. This design was chosen as it allows for an in-depth exploration of participants’ experiences, enhancing the depth and authenticity of the study.30 To facilitate participant recruitment, the research team obtained ethical approval and permission to engage with the Irish Cancer Society and other relevant prostate cancer and men’s health organizations, such as Men’s Sheds. These organisations provide crucial support networks, offering Irish men a space to address various health and social concerns impacting both their communities and individual well-being.
Study Population and Eligibility Criteria
The study included men living with prostate cancer in Ireland, recruiting participants through various men’s health and prostate cancer organisations. To capture a diverse range of experiences, the study included men who were recently diagnosed, undergoing treatment, or in post-treatment stages. However, individuals who were critically ill or had cognitive impairments were excluded.
Sample Size and Sampling Procedure
The study employed purposive sampling to recruit participants. Information about the study, including an invitation letter, email, and participant information leaflet, was disseminated through relevant organisations. Additionally, study promotion was conducted via leaflet distribution and radio announcements. A total of 11 men participated, with the sample size determined based on the saturation principles (theoretical, data, code/theme and meaning) outlined by Rahimi.31
Data Collection Tool
This study utilised a semistructured interview guide, developed based on a review of existing literature and adapted to align with the study’s objectives. In-depth data on the lived experiences of men with prostate cancer were collected through face-to-face, Microsoft Teams, or phone interviews. Pretesting was conducted to ensure the relevance and effectiveness of the interview questions in the data collection process.
Data Collection Procedure
The interviews were conducted by the lead investigators (SM, OD, and CO’D) between March 2024
and February 2025. Depending on participant preference, interviews were held face-to-face, virtually via Microsoft Teams, or by telephone. Probing questions were used to explore responses in greater depth and clarify participants’ perspectives. Field notes were taken to capture non-verbal cues and contextual details that could not be recorded by the audio device. The in-depth interviews lasted between 30 and 40 min.
Data Analysis
All interviews were audio-recorded and transcribed verbatim. The transcribed data were uploaded to NVivo 12.0 software(QSR International, Melbourn, Australia) for data organization and text coding. The principal investigators independently conducted iterative readings of the transcripts with an open, exploratory approach to gain a comprehensive understanding of each participant’s narrative. Coding was employed to identify patterns within the text, aligning with the predetermined categories outlined in the research objectives. After multiple transcript reviews,32 thematic analysis framework (see Table 1) was applied to facilitate theme development and deeper interpretation. Categories were constructed based on key phrases within text segments, and subthemes were identified within each category by the lead investigators.
RESULTS
Participants Characteristics
A total of 11 participants took part in the study, with 2 being black Irish and 9 being white Irish. The youngest participant was 62 years old, while the oldest was 81 years old, with a mean age of 72.8 years. The marital status of the participants was as follows: single (n = 3), divorced (n = 2), married (n = 6). Regarding their stage of diagnosis: three were early stage, five were intermediate stage, and three advanced or recurrent stage. Some of the participants (n = 5) were from urban cities, while the remaining (n = 6) were from rural areas. During the study four participants were working, two on the verge of retirement, and five were fully retired and not working.
Themes Identified
The experience of Irish men with prostate cancer revealed five major themes: (1) systemic obstacle in timely cancer detection; (2) the role of efficient system in cancer care; (3) emotional resilience in cancer recovery; (4) redefining normalcy post-treatment; (5) harnessing specialised support network in coping strategies.
Theme 1: Systemic Obstacle in Timely Cancer Detection
hospital) and tell them to hurry up? …. and they said, oh we cannot …… it is between me and (named the other hospital)”.
(p5)
Other concerns raised included a lack of awareness of alternative diagnostic centres and poor communication between healthcare providers.
“Nine months to get a biopsy ……. they should have noticed something sooner... they could have told me the biopsy can be done in a private place for a few hundred euros”.
(p5)
Delays heightened stress and may cause poorer outcomes.
“The waiting list was so long; … it felt like forever before I got a diagnosis” (p6)
“I had symptoms for months, but getting a referral took ages” (p5)
Theme 2: The Role of the Efficient System in Cancer Care
Table 1. Braune and Clarke 2021 reflective thematic analysis framework
To ensure credibility and alignment with the study’s objectives, the authors examined emerging meanings from the analytic outputs, categories, and themes (see Figure 1).
Table 1. Braune and Clarke 2021 reflective thematic analysis framework
Phase Description
Phase One: data familiarization
Phase Two: Code generation
Phase Three: Searching of theme
Phase Four: Reviewing of themes generated
Phase Five: Naming and Defining themes
Phase Six: Report production
During the interviews, participants frequently expressed frustration over delays in diagnosis caused by systemic inefficiencies. Many reported long waiting times for biopsies, diagnostic imaging, and cancer referrals.
“I rang (named hospital), and I said, would you ever ring (named other
This stage is reading and rereading transcript to dote down initial impression
At this stage, one systematically looks for meaningful features or patterns across all data inductively and reflectively.
Codes are grouped together to make meaningful subthemes or themes.
Generated themes reviewed in relation coded data ensuring correlation, cohesion and accuracy.
Finally theme clearly defined, named and described.
Writing a narrative about the generated themes with supporting evidence.
Application to Study
Many participants expressed satisfaction and gratitude for the treatment they received once inside the healthcare system. However, they also highlighted gaps in guidance on long-term management, side effects, and post-cancer care.
“The doctors and nurses were excellent …. but I had to figure out post treatment care on my own”.
(p3)
Researchers went through all 11 interviews and noted down the need information e.g., Emotional needs, unmet needs.
Researchers generated codes like shock, fear, anxiety with the help of a qualitative analysis software.
Generated codes were used by researchers to form subthemes like psychological adaptation and coping mechanisms.
Sub-themes reviewed again in relation to the codes to help ensure correlation and distinctions.
Researchers ensure identified theme final theme is distinct and has never been used or identified in other literatures.
Developed themes were used by the researchers to write a cohesive narration to make a meaningful statement.
Prostate Cancer
Participants emphasised the need for multidisciplinary treatment and advocated for early involvement of specialists such as radiotherapists, oncologists, and other support services.
“There needs to be more multidisciplinary involvement (urologists, oncologists, radiologists, pathologists, specialist nurses, psychologists, physiotherapists, primary care physician) from the start” (p4)
This theme highlights the importance of structured follow-up procedures and patient education to improve long-term outcomes.
Theme 3: Emotional Resilience in Cancer Recovery
Upon receiving their diagnoses, many participants described experiencing a rollercoaster of emotions, including shock, disbelief, and fear, particularly among those with limited prior knowledge of prostate cancer.
“I did not expect it at all……. there is a lot of fear that hits all at once” (p6)
Concerns about recurrence and uncertainty also emerged, especially among those diagnosed with intermediate or advancedstage prostate cancer.
“How long will I live”.
(p2)
However, some participants demonstrated emotional adaptability, finding ways to accept their diagnosis and focus on recovery.
“Eventually I found acceptance by focusing on the present and what I can control”
(p5)
Theme 4: Redefining Normalcy Post Treatment
The study revealed that the physical toll of prostate cancer treatment, including surgery, chemotherapy, radiotherapy, and hormonal therapy presented significant challenges such as fatigue, incontinence and erectile dysfunction.
“My body just did not feel like my own for a long time”
(p6)
Participants described undergoing major adjustments that altered their activity levels, expectations, and overall sense of normalcy.
“I have adjusted to a slower pace……things are just different now”
(p5)
As a result, many participants emphasised the need to redefine their sense of normalcy and adapt to new physical and emotional realities post-treatment.
Discussion
This qualitative descriptive study provides a comprehensive exploration of the lived experiences of men with prostate cancer in Irish society, uncovering five key themes that encapsulate the emotional, systemic, and social dimensions of their journey and survivorship. These themes highlight the interplay between the healthcare system, personal resilience, and support networks, offering valuable insights into areas that require increased awareness and intervention. The findings revealed systemic obstacles in timely cancer detection, the role of an efficient healthcare system in cancer care, emotional resilience in cancer recovery, redefining normalcy post-treatment, and harnessing specialised support networks in coping strategies. These themes align with the Biopsychosocial Model,35 which recognises prostate cancer survivorship as shaped
by physical health challenges, emotional resilience, and social support structures.
Participants consistently reported delays in diagnosis as a significant challenge, citing prolonged waiting times for biopsies, diagnostic imaging, and hospital referrals. Early cancer detection is crucial for improving prognosis and survival rates, yet these findings align with recent studies showing that men with prostate cancer often experience longer diagnostic and treatment waiting times compared to other cancers, leading to psychological distress and potentially worse outcomes. Diagnostic delays and lack of support networks negatively impact the clinical trajectory and psychosocial wellbeing of men.36 Fragmented communication between care services and lack of support networks contribute to cancer progression and reduced survival. These results are consistent with with studies by Mottet et al. and the American Cancer society which underscore the critical importance of early detection in improving prostate cancer outcomes globally.36,37 However, systemic barriers such as limited healthcare access and cultural stigma often hinder early detection efforts. Additionally, delayed diagnosis increases
Figure 1.
psychological distress, with many patients experiencing uncertainty and anxiety about the disease’s progression.38 To address these diagnostic delays and improve survival rates, streamlined referral processes, improved public awareness, and enhanced primary care provider training are necessary.39 The Biopsychosocial Model further emphasizes the importance of integrating social health determinants into cancer detection strategies, advocating for community-based screening programs, patient navigation services, and culturally competent healthcare delivery. Delayed diagnosis in hospitals requires policy commitment, workflow redesign, patientcentred approaches, and technology integration for timely prostate cancer diagnosis, enhancing clinical efficiency and humanised care.38,39
While 9 out of 11 of the participants expressed satisfaction and gratitude for the care they received after diagnosis, gaps in post-treatment guidance and follow-up care were evident. Effective cancer care systems require seamless coordination across diagnosis, treatment, and survivorship. However, fragmented healthcare services often result in delays, miscommunication, and suboptimal treatment outcomes.40 These findings align with research by Garcia-Baquero et al. and Shore et al. which indicate that a well-planned, comprehensive multidisciplinary approach significantly improves treatment outcomes and patient experiences.41,42 Participants advocated for earlier involvement of oncologists, radiotherapists, and mental health professionals, reinforcing the importance of integrated care pathways. Studies by Kord et al., Østergaard et al. and de Resende Izidoro et al. emphasize the benefits of personalized survivorship programs that address psychological, physical, and sexual health post-treatment.43,44,45 Additionally, patient navigation initiatives which guide patients through the treatment process, have been shown to improve treatment adherence and reduce healthcare disparities.46 The Biopsychosocial Model underscores the necessity of a patient-centred approach, integrating biological, psychological, and social factors through a multidisciplinary team. Recent studies highlight the value of biopsychosocial screening initiatives in oncology, as they help identify distress, unmet psychological needs, and barriers to treatment at early stages.47 Moreover, ref.48 suggests that AI-driven decision support
systems and electronic medical records can enhance coordination among multidisciplinary teams and improve continuity of care. Participants described experiencing a range of emotions upon diagnosis, including shock, fear, anxiety, and eventual acceptance. Cancer diagnosis and treatment place significant psychological burdens on patients, affecting their mental well-being and resilience. This finding aligns with studies emphasizing the role of adaptive coping strategies in managing the psychological impact of prostate cancer.49 Emotional resilience is a crucial factor in successful recovery, requiring support systems, time, and coping mechanisms. Activities such as exercise, outdoor engagement, meditation, and creative outlets help manage stress and emotional challenges.50,51 The Psychological Model of Coping supports these findings, highlighting adaptive coping strategies as essential in managing chronic disease stressors.52 Professional counselling and peer support have been identified as effective in reducing depression and anxiety.53,54 However, stigma and societal expectations often discourage men from expressing psychological distress, necessitating gender-sensitive interventions to improve mental health engagement.55 Interventions such as cognitive-behavioural therapy (CBT) and mindfulnessbased stress reduction (MBSR) have proven effective in reducing anxiety, depression, and fear of recurrence, leading to improved quality of life and treatment adherence.51,56 The Biopsychosocial Model suggests that incorporating self-efficacy strategies, goal setting, and meaning-making interventions into cancer care can further support resilience-building.
A total of 10 out of 11 participants faced significant physical and emotional challenges of posttreatment, including fatigue, urinary incontinence, and erectile dysfunction, which often disrupted their sense of identity and masculinity. Studies by Chung et al. and Talvitie et al. corroborate these findings, demonstrating that prostate cancer treatment frequently impacts masculinity and selfperception.57,58 To navigate these changes, participants recalibrated their expectations, developed new routines, and adopted coping mechanisms. Research suggests that sexual health awareness programs, physical rehabilitation, and fatigue management initiatives significantly improve post-treatment quality of life.59 The Biopsychosocial Model
emphasises the importance of personalised survivorship care plans to manage long-term effects of cancer.60
While peer support groups, mental health organisations, and advocacy groups emerged as valuable resources, 7 out of 11 participants expressed reluctance to seek help. Studies by Wilkerson et al. indicate that older men often avoid disclosing struggles due to societal norms equating vulnerability with weakness, leading to increased depression, anxiety, and social isolation.61 The Biopsychosocial Model highlights the need for comprehensive support networks beyond clinical settings. Ref.62 found that online support communities, peer-led groups, and men’s advocacy organizations help cancer patients express emotions, share experiences, and build community connections. Expanding access to support networks in rural and underserved areas is essential to addressing disparities in prostate cancer care. Refs.63,64 emphasise that patient-centred support groups foster resilience, motivation, and improved quality of life.
The high prevalence of prostate cancer in Ireland is multifactorial, influenced by demographic trends, genetic predisposition, lifestyle factors, and robust cancer surveillance systems. In Ireland the primary risk factor for prostate cancer like many other countries is the aging population. Prostate cancer is the most diagnosed cancer in Irish men, with most cases occurring in those over 60 years of age.65 Genetic and familial risk factors play a significant role and men with a family history of prostate cancer are at higher risk, and certain inherited gene mutations (e.g., BRCA1 and BRCA2) can increase susceptibility and Irish men have a relatively high burden of hereditary cancer risk, which may contribute to incidence.66 Lifestyle and dietary factors may also influence prevalence. Diets high in animal fats and red meat, which are common in Western countries, including Ireland, have been associated with increased risk, although evidence remains inconclusive. Another important factor is increased awareness and widespread PSA testing, especially in past decades, which has led to higher detection rates. While PSA screening has been debated for its risks of overdiagnosis, it has undoubtedly contributed to identifying more cases, including those that may have remained undetected otherwise. Lastly, population-based cancer registration in Ireland is relatively comprehensive, contributing to more accurate and complete
incidence reporting compared to some other countries.
Improving delayed diagnosis in hospitals, particularly for conditions like prostate cancer, requires a multifaceted approach focused on system-level changes, better clinical practices, and increased patient engagement. Adopting structured diagnostic pathways can significantly reduce the time to diagnosis. For instance, the Rapid Assessment for Prostate Imaging and Diagnosis (RAPID) pathway demonstrated a reduction in median diagnostic time from 32.1 days to 15.9 days.67 The integration of mpMRI into the diagnostic process has improved the accuracy of prostate cancer detection as mpMRI allows for better visualisation of prostate lesions, facilitating targeted biopsies and reducing the detection of indolent tumors.68 The formation of dedicated prostate cancer units comprising urologists, radiologists, oncologists, pathologists, and other specialists ensures comprehensive patient evaluation with regular multidisciplinary meetings to facilitate coordinated care, leading to reduced diagnostic delays and improved patient outcomes. The use of clinical decision support systems within electronic health records can prompt clinicians to follow evidence-based guidelines, ensuring timely follow-ups on abnormal findings, reduce diagnostic errors and enhance the efficiency of the diagnostic process. Implementing national guidelines, such as the NHS England’s timed diagnostic pathway, sets standards for achieving diagnosis within 28 days of referral providing a framework for consistent and timely prostate cancer diagnosis across healthcare settings69
Conclusions
This study contributes to the existing literature on prostate cancer by highlighting the multifaceted physical, psychological, emotional, and social factors that shape patients’ experiences. Addressing systemic disparities, enhancing peer and social support networks, and promoting multidisciplinary care are crucial steps toward fostering a more patient-centered approach in prostate cancer management. Implementing comprehensive, evidence-based survivorship care frameworks can significantly improve the quality of life for prostate cancer survivors. Future research should explore the long-term effects of integrated care models and develop targeted strategies to optimise survivorship outcomes and enhance patient well-being.
References available on request
Hepatitis B
Community prevalence of blood-borne viruses (hepatitis B and HIV) in Ireland
Written by P. Aiden McCormick1, Marie O’Grady2, Paul Holder3, Cillian F. De Gascun3, John S. Lambert4, Orla Crosbie5, Susan McKiernan6, Maeve Skelly7, Garry Courtney8, Brian Hennessy9, Kevin Walsh10, Roisin Twohig3, Kate Browne3, Tessa O’Gorman11, Vivion Crowley6, Seán J. Costelloe5, Roz O’Byrne7, Orla Gildea9 and Noreen Montgomery10
1 National Hepatitis C Treatment Program HSE, Liver Unit, St Vincent’s University Hospital and UCD, Elm Park, Donnybrook, Dublin 4 DO4 T6F4, Ireland
2 National Hepatitis C Treatment Program, HSE, Dublin, Ireland 3 National Virus Reference Laboratory, UCD, Dublin, Ireland
4 Mater and Rotunda Hospitals and UCD, Dublin, Ireland 5 Cork University Hospital and UCC , Cork, Ireland
6 St James’s University Hospital, Dublin, Ireland 7 University Hospital Limerick, Limerick, Ireland 8 St Luke’s Hospital, Kilkenny, Ireland
9 University Hospital Waterford, Waterford, Ireland 10 Sligo University Hospital, Sligo, Ireland 11 Mater Misericordiae University Hospital, Dublin, Ireland
Abstract
Background: Chronic infection with hepatitis B virus and HIV causes significant morbidity and mortality. Effective antiviral treatment is available for both. Ireland has historically been considered a low prevalence country. However, with increasing inward migration and diversity, this may be changing.
Aims: The aim of this study was to measure the community prevalence of hepatitis B virus and HIV infections in Irish resi-dents born between the years 1965 and 1985.
Methods: Anonymised residual serum samples from blood tests ordered by community general practitioners and tested in eight general hospital laboratories, spread across Ireland, were analysed for the presence of Hepatitis B surface antigen and antibodies to HIV.
Results: A total of 6080 samples were analysed for hepatitis B surface antigen including 2993 males, 2807 females and 280 samples for which gender was not recorded. HBsAg was detected in 28/6067 samples giving an estimated prevalence of 0.46% (95% CI 0.32–0.67%). Antibodies to HIV were identified in 18/6064 giving an estimated prevalence of 0.33% (95% CI 0.19–0.47%). The prevalence of both hepatitis B and HIV was significantly higher in Cork (Southwest Ireland) than other centres: hepatitis B (12/1050 vs 16/5017, p = 0.014) and HIV (11/1049 vs 7/5015, p < 0.001).
Conclusions: The prevalence of hepatitis B virus and HIV infections in this cohort appear to be higher than previously esti-mated. In addition, their prevalence in the Cork area appears particularly high. Whether this represents a true prevalence or a chance finding will require confirmatory studies.
Keywords: Cirrhosis · Hepatitis B · Human immunodeficiency virus · Migration
Introduction
Blood-borne viruses hepatitis B (HBV), hepatitis C and human immunodeficiency virus (HIV) cause serious illness and significant morbidity and mortality. Effective treatment is now widely available for all three viruses. Hepatitis C virus can be eliminated with a short course of oral anti-viral medication. Conversely, while neither chronic hepatitis B nor HIV can be cured, they can be controlled with long-term oral antiviral therapy, thus preventing further end-organ damage. It is also important to diagnose and treat individuals with these viral infections, from a public health perspective, to prevent onward transmission. Accurate information on community prevalence and transmission patterns is essential for designing appropriate screening and treatment strategies. The epidemiology of these infections is likely to change as a result of migration patterns and other social and cultural trends.
We previously reported that the community prevalence of hepatitis C in Ireland was much lower than previously reported, approximately 0.1% compared to previous estimates of about 1%.1 This study was performed on anonymised routine biochemistry blood samples sent by general practitioners to general hospital laboratories. Individuals born between 1965 and 1985 were included as public health notification data suggested 70% of those infected were in this age cohort. The population prevalence of both hepatitis B and HIV is believed to be low in Ireland at between 0.1 and 0.2%.2, 3 We now report results for hepatitis B and HIV in the same birth cohort previously studied for hepatitis C.
Methods
This study looked at residual serum samples from general practitioner-requested blood tests from eight general hospitals, three of which were in Dublin.
These hospitals included St Vincent’s University Hospital, Mater Misericordiae University Hospital, St James’s Hospital, Cork University Hospital, University Hospital Limerick, University Hospital Waterford, St Luke’s Hospital Kilkenny and Sligo University Hospital (Fig. 1). All patients were in the birth cohort (born in years 1965–1985) and the study included equivalent numbers of males and females.
Residual samples were anonymised, batched, and sent to the National Virus Reference Laboratory in UCD for analysis. The only information retained on the samples was the sex of the patient. These samples were initially tested for the presence of hepatitis C virus antibody. If positive, the samples were checked for the presence of hepatitis C antigen. Ethical permission was then obtained to test residual samples for HBV and HIV from the research ethics committees in St Vincent’s
University Hospital, Mater Misericordiae University Hospital, St James’s Hospital, University Hospital Limerick, Cork University Hospital and University Hospital Waterford. Sligo University Hospital and St Luke’s Hospital Kilkenny accepted the ethics approval from St Vincent’s University Hospital.
Laboratory methods
HIV status was determined using the Abbott Architect HIV Combo Ag/Ab assay (Abbott Diagnostics, Wiesbaden, Germany). Specimens exceeding the manufacturer’s signal to cut-off (S/Co) ratio of 1.0 were tested using the Biomeriéux HIV DUO Ultra assay (MarcyL’Etoile, France). Persistently reactive samples were further investigated using the Fujirebio INNO-LIA HIV I/II Score assay (Fujirebio Europe N.V., Ghent, Belgium) to determine the true anti-HIV status of the sample and determine the HIV type.
Fig. 1 Geographic distribution and number of samples from eight general hospitals participating in the epidemiological study
p < 0.01) and HIV antibody in 11/1050 (prevalence 1.05%, CI 0.53–1.87%, p < 0.01). None of the samples in any of the hospitals was positive for both HBsAg and HIV antibody. One patient had hepatitis C antibodies and HBsAg (male) and one had hepatitis C antibodies and was anti-HIV positive (female). Both patients were in the Cork cohort. The proportion of females with hepatitis C antibodies was higher in Cork than in the other centres (6 female/3 male vs 3 female/16 male, p < 0.05).
Discussion
HBV status was determined initially using the Abbott Architect HBsAg Qualitative II assay (Abbott Diagnostics, Wiesbaden, Germany). Specimens generating a S/Co ≥ 15 were directly investigated for HBV markers using the following assays, Abbott Architect HBeAg (Abbott Diagnostics, Wiesbaden, Germany), Abbott Architect Anti-HBe (Abbott Diagnostics, Wiesbaden, Germany), Abbott Architect anti- HBc IgM (Abbott Diagnostics, Wiesbaden, Germany) and Abbott Architect anti-HBc II (Abbott Diagnostics, Wiesbaden, Germany). Weakly reactive HBsAg samples using the Architect assay (generating HBsAg result above the manufacturer’s S/Co of 1.0 but less than 15.0) or HBeAg and anti-HBe Ab negative samples were further investigated using the Murex HBsAg Confirmatory
Version 3 assay (DiaSorin Italia
S.p.A UK Branch, Dartford, UK) to determine the true HBsAg status of the sample.
1. There was insufficient volume HBsAg and 16 samples for HIV antisummarised in Table 1. HBsAg was identified in 28/6067 samples (18 male, 10 female) giving an estimated prevalence of 0.46% (95% CI 0.32–0.67%). HIV antibody was identified in 18/6064 samples (11 male,
Statistical analysis
Differences between groups were evaluated using the chisquare (and Fisher’s exact) test using the Prism 10 statistical program (GraphPad Software Inc., California, USA). Confidence intervals (95%) for the estimated prevalence in each sample were calculated using the Clopper-Pearson method [ref1] implemented in the R package epitools.4
Results
A total of 6080 samples were available for analysis, including 2993 males, 2807 females and 280 samples for which gender was not recorded. The geographical distribution of samples is shown
in Fig. 1. There was insufficient volume to test 13 samples for HBsAg and 16 samples for HIV antibody. The results are summarised in Table 1. HBsAg was identified in 28/6067 samples (18 male, 10 female) giving an estimated prevalence of 0.46% (95% CI 0.32–0.67%). HIV antibody was identified in 18/6064 samples (11 male, 7 female) giving an estimated prevalence of 0.3% (95% CI 0.19–0.47%). Hepatitis C antibodies were detected in 28/6080 (19 male and 9 female), but of these, hepatitis C antigen was detected in only 2/28 (7%) (1 male, 1 female). The geographical distribution of positive samples was nonrandom. The prevalence of both virus infections was significantly higher in Cork. HBsAg was present in 12/1050 samples (prevalence 1.14%, CI 0.59–2.0%,
In this study, we found the prevalence of hepatitis B surface antigen was 0.46% and the prevalence of HIV antibodies was 0.3% in this community-based cohort of individuals born between 1965 and 1985. These figures appear higher than previously published estimates. As would be expected, approximately twothirds of those infected were male. A surprise finding was that the prevalence rates of both hepatitis B and HIV were significantly higher in Cork than the other centres combined. We are not aware of a reason for this and it may represent a chance finding. Nevertheless, further investigation is warranted to confirm or refute this finding.
There are limited data on the epidemiology of hepatitis B and HIV in the community in Ireland. A recent publication from the European Centre for Disease Control (ECDC) and Bristol University suggested a population prevalence of 0.21% for HBsAg and a prevalence of 0.26% among prisoners.5 All pregnant females in Ireland are offered screening for hepatitis B and HIV. The Coombe maternity Hospital in Dublin reported 6974 babies born in 2023. All expectant mothers are checked for hepatitis B, HIV and hepatitis C. Seven were HBsAg positive (0.1%), 18 had HIV (0.26%), 10 had antibodies to hepatitis C but
Hepatitis B
*p < 0.05. **p < 0.01; Cork prevalence vs other centres combined
Table 1 Results of testing for hepatitis B surface antigen (HBsAg), HIV antibodies, hepatitis C antibodies and hepatitis C antigen (HCV Ag) in 6080 community sourced birth cohort samples (born 1965–1985)
none was PCR positive.6 The Rotunda Hospital delivered 8442 babies in 2023. Thirtytwo had HBsAg (0.38%) and 25 (0.3%) had antibodies to HIV.7 The prevalence of HBsAg in first time blood donors in Ireland (1999–2022) was very low at 0.009% (monthly donation testing report, UK Health Security Agency). These figures are for donors born in Ireland or the UK, but would constitute a special population as individuals with risk factors are discouraged from donating.
International protection applicants in Ireland are offered blood-borne virus screening as many are from high prevalence countries. Uptake is variable but the national reception centre for international protection applicants, in Balseskin, Dublin, reported that of those tested in 2023, 2.2% were HBsAg positive, 4.3% were HIV positive and 0.3% had chronic hepatitis C infection.8 The UNAIDS program estimates the prevalence of HIV infection in the general adult population in Ireland in 2023 was 0.3%.9 All pregnant females are offered antenatal testing for HIV. The national prevalence for 2023 was 0.2%.10 Only 14% of these were new diagnoses suggesting high rates of previous diagnosis, awareness and treatment in this cohort.
The strengths of this study are that it was community based, with a wide geographical spread and was not targeted at
higher risk groups. The major limitation is that the samples were anonymised so we have no clinical information about the infected individuals. It is possible that chance over-representation from higher risk groups may have skewed the results, particularly with regard to Cork, in the southwest of the country.
This study suggests that the epidemiology of hepatitis B and HIV infections is changing in Ireland and that the community prevalence of both is higher than previously estimated. This has implications for screening and service provision. It highlights the importance of up-todate epidemiological studies, particularly in societies affected by large-scale migration and social changes.
Acknowledgements We would like to thank Dr David McConnell, Senior Statistician, National Center for Pharmacoeconomics (NCPE), for providing statistical assistance.
Funding Open Access funding provided by the IReL Consortium Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creativecommons.org/licenses/ by/4.0/.
References
1. McCormick PA, O’Grady M, De Gascun CF and others (2024) Hepatitis C community prevalence is over-estimated: a prospective, birth cohort study. Ir J Med Sci 193:1257–1260
2. Nardone A, Anastassopoulou CG, Theeten H and others (2009) A comparison of hepatitis B seroepidemiology in ten European countries. Epidemiol Infect 137:961–969
3. Tuite H, Horgan M, Mallon PW and others (2015) Patients accessing ambulatory care for HIV-infection: epidemiology and prevalence assessment. Ir Med J 108:199–202
4. Aragon T (2020) Epitoole: epidemiology tools. R package version 0.5–10.1. http:// CRAN.R- proje ct. org/ packa ge= epito ols
5. Trickey A, Bivegete S, Duffell E and others (2023) Estimating hepatitis B virus prevalence among key population groups for European Union and European Economic Area countries and the United Kingdom: a modelling study. BMC Infect Dis 23:457
6. The Coombe Hospital. Annual Report 2023. Available at: https:// www. coombe. ie/ annual- report. (Accessed 31/12/2024)
8. (2023) Health Screening, National Reception Centre, Balseskin. Annual Report. Health Service Executive
9. UNAIDS HIV and AIDS estimates for Ireland 2023. Available at https:// www. unaids. org/ en/ regio nscou ntries/ count ries/ irela nd. (Accessed 31/12/2024)
10. Antenatal HIV testing in Ireland. Health Protection Surveillance Centre. Available at https:// www. hpsc. ie/a- z/ hivan daids/ anten atalh ivtes ting/. (Accessed 24/12/2024)
Publisher's Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Atorvastatin Teva Pharma is indicated as an adjunct to diet for reduction of elevated total cholesterol (total-C), LDLcholesterol (LDL-C), apolipoprotein B, and triglycerides in adults, adolescents and children aged 10 years or older with primary hypercholesterolaemia including familial hypercholesterolaemia (heterozygous variant) or combined (mixed) hyperlipidaemia (corresponding to Types IIa and IIb of the Fredrickson classification) when response to diet and other non-pharmacological measures is inadequate.
Atorvastatin Teva Pharma is also indicated to reduce total-C and LDL-C in adults with homozygous familial hypercholesterolaemia as an adjunct to other lipid-lowering treatments (e.g. LDL apheresis) or if such treatments are unavailable.
Prevention of cardiovascular disease
Prevention of cardiovascular events in adult patients estimated to have a high risk for a first cardiovascular event, as an adjunct to correction of other risk factors.
Atorvastatin Teva Pharma Film-Coated Tablets Abbreviated Prescribing Information. Presentation: Each film-coated tablet contains 10mg, 20mg, 40mg and 80mg atorvastatin (as atorvastatin calcium). Indications: Hypercholesterolaemia: Atorvastatin Teva Pharma is indicated as an adjunct to diet for reduction of elevated total cholesterol (total-C), LDL-cholesterol (LDL-C), apolipoprotein B, and triglycerides in adults, adolescents and children aged 10 years or older with primary hypercholesterolaemia including familial hypercholesterolaemia (heterozygous variant) or combined (mixed) hyperlipidaemia when response to diet and other nonpharmacological measures is inadequate. Atorvastatin Teva Pharma is also indicated to reduce total-C and LDL-C in adults with homozygous familial hypercholesterolaemia as an adjunct to other lipid-lowering treatments (e.g. LDL apheresis) or if such treatments are unavailable. Prevention of cardiovascular disease: Prevention of cardiovascular events in adult patients estimated to have a high risk for a first cardiovascular event, as an adjunct to correction of other risk factors. Dosage and administration: For oral administration. Adults: Usual starting dose is 10mg once a day, with adjustment of dose made at intervals of 4 weeks or more. Maximum dose is 80mg once a day. Primary hypercholesterolaemia and combined (mixed) hyperlipidaemia: Majority of patients are controlled with Atorvastatin Teva Pharma 10mg once a day. A therapeutic response is evident within 2 weeks, and the maximum therapeutic response is usually achieved within 4 weeks. Heterozygous familial hypercholesterolaemia: Patients should be started with Atorvastatin Teva Pharma 10mg daily. Doses should be individualised and adjusted every 4 weeks to 40mg daily. Thereafter, either the dose may be increased to a maximum of 80mg daily or a bile acid sequestrant may be combined with 40 mg atorvastatin once daily. Homozygous familial hypercholesterolaemia: Limited data available. The dose of atorvastatin in patients with homozygous familial hypercholesterolemia is 10 to 80mg daily. Atorvastatin should be used as an adjunct to other lipid-lowering treatments (e.g. LDL apheresis) in these patients or if such treatments are unavailable. Prevention of cardiovascular disease: In the primary prevention trials the dose was 10mg/day. Higher doses may be necessary in order to attain (LDL-) cholesterol levels according to current guidelines. Children aged 10 years and above for Heterozygous Familial Hypercholesterolemia: Recommended starting dose is 10mg per day which may be increased to 80mg daily, according to the response and tolerability. Elderly: Efficacy and safety in patients older than 70 using recommended doses are similar to those seen in the general population. Renal impairment: No dose adjustment required. Hepatic impairment: Atorvastatin Teva Pharma should be used with caution in patients with hepatic impairment. Atorvastatin Teva Pharma is contraindicated in patients with active liver disease Contraindications: Atorvastatin Teva Pharma is contraindicated in patients with: hypersensitivity to the active substance or to any of the excipients; active liver disease or unexplained persistent elevations of serum transaminases exceeding 3 times the upper limit of normal; during pregnancy, while breast-feeding and in patients of child-bearing potential not using appropriate contraceptive measures; treated with the hepatitis C antivirals glecaprevir/pibrentasvir. Precautions and warnings: Liver function tests should be performed before the initiation of treatment and periodically thereafter. Patients who develop any signs or symptoms suggestive of liver injury should have liver function tests performed. Atorvastatin Teva Pharma should be used with caution in
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland.
Freephone: 1800 - 201 700 | Email: info@teva.ie
Prescription Only Medicine.
patients who consume substantial quantities of alcohol and/or have a history of liver disease. For patients with prior haemorrhagic stroke or lacunar infarct, the balance of risks and benefits of atorvastatin 80mg is uncertain, and the potential risk of haemorrhagic stroke should be carefully considered before initiating treatment. Atorvastatin may in rare occasions affect the skeletal muscle and cause myalgia, myositis, and myopathy that may progress to rhabdomyolysis, a potentially life-threatening condition characterised by markedly elevated creatine kinase (CK) levels (> 10 times ULN), myoglobinaemia and myoglobinuria which may lead to renal failure. There have been very rare reports of an immune-mediated necrotizing myopathy (IMNM) during or after treatment with some statins. IMNM is clinically characterised by persistent proximal muscle weakness and elevated serum creatine kinase, which persist despite discontinuation of statin treatment, positive anti-HMG CoA reductase antibody and improvement with immunosuppressive agents. In few cases, statins have been reported to induce de novo or aggravate pre-existing myasthenia gravis or ocular myasthenia. This medicinal product should be discontinued in case of aggravation of symptoms. Atorvastatin should be prescribed with caution in patients with pre-disposing factors for rhabdomyolysis. A CK level should be measured before starting statin treatment. The risk of treatment should be considered in relation to possible benefit, and clinical monitoring is recommended. If CK levels are significantly elevated (> 5 times ULN) at baseline, treatment should not be started. Exceptional cases of interstitial lung disease have been reported with some statins, especially with longterm therapy. Presenting features can include dyspnoea, non-productive cough and deterioration in general health (fatigue, weight loss and fever). If it is suspected a patient has developed interstitial lung disease, statin therapy should be discontinued. Some evidence suggests that statins as a class raise blood glucose and in some patients, at high risk of future diabetes, may produce a level of hyperglycaemia where formal diabetes care is appropriate. Patients at risk (fasting glucose 5.6 to 6.9mmol/L, BMI>30kg/ m2, raised triglycerides, hypertension) should be monitored both clinically and biochemically according to national guidelines. Interactions: Please refer to the SmPC for a comprehensive list of drug interactions (including the effect of medicinal products on atorvastatin, and the effect of atorvastatin on other co-administered medicinal products). Risk of rhabdomyolysis is increased when atorvastatin is administered concomitantly with potent inhibitors of CYP3A4 or transport proteins (e.g. ciclosporin, telithromycin, clarithromycin, delavirdine, stiripentol, ketoconazole, voriconazole, itraconazole, posaconazole, letermovir and HIV protease inhibitors including ritonavir, lopinavir, atazanavir, indinavir, darunavir, tipranavir/ritonavir, etc). The risk of myopathy may also be increased with the concomitant use of gemfibrozil and other fibric acid derivates, antivirals for the treatment of hepatitis C (HCV) (e.g. boceprevir, telaprevir, elbasvir/grazoprevir, ledipasvir/ sofosbuvir), erythromycin, niacin, or ezetimibe. If possible, alternative (noninteracting) therapies should be considered instead of these medicinal products. In cases where co-administration of these medicinal products with atorvastatin is necessary, the benefit and the risk of concurrent treatment should be carefully considered. When patients are receiving medicinal products that increase the plasma concentration of atorvastatin, a lower maximum dose of atorvastatin is recommended. In addition, in the case of potent CYP3A4 inhibitors, a lower starting dose of atorvastatin should be
considered, and appropriate clinical monitoring of these patients is recommended. The risk of myopathy and/or rhabdomyolysis may be increased by concomitant administration of HMG-CoA reductase inhibitors (e.g. atorvastatin) and daptomycin. Consideration should be given to temporarily suspend Atorvastatin Teva Pharma in patients taking daptomycin unless the benefits of concomitant administration outweigh the risk. If co-administration cannot be avoided, CK levels should be measured 2-3 times per week and patients should be closely monitored for any signs or symptoms that might represent myopathy. Atorvastatin must not be coadministered with systemic formulations of fusidic acid or within 7 days of stopping fusidic acid treatment. In patients where the use of systemic fusidic acid is considered essential, statin treatment should be discontinued throughout the duration of fusidic acid treatment. There have been reports of rhabdomyolysis (including some fatalities) in patients receiving fusidic acid and statins in combination. The patient should be advised to seek medical advice immediately if they experience any symptoms of muscle weakness, pain or tenderness. Statin therapy may be re-introduced seven days after the last dose of fusidic acid. In exceptional circumstances, where prolonged systemic fusidic acid is needed, e.g. for the treatment of severe infections, the need for co-administration of Atorvastatin Teva Pharma and fusidic acid should only be considered on a case-by-case basis and under close medical supervision. Pregnancy and lactation: Patients of childbearing potential should use appropriate contraceptive measures during treatment. Atorvastatin Teva Pharma is contraindicated during pregnancy. Atorvastatin Teva Pharma should not be used in patients who are pregnant, trying to become pregnant or suspect they are pregnant. Treatment with Atorvastatin Teva Pharma should be suspended for the duration of pregnancy or until it has been determined that the patient is not pregnant. Patients taking Atorvastatin Teva Pharma should not breast-feed their infants. Atorvastatin is contraindicated during breast-feeding. Effects on ability to drive and use machines: Atorvastatin Teva Pharma has negligible influence on the ability to drive and use machines. Adverse reactions: Thrombocytopenia, anaphylaxis, peripheral neuropathy, myasthenia gravis, hearing loss, pancreatitis, hepatitis, hepatic failure, cholestasis, angioneurotic oedema, dermatitis bullous including erythema multiforme, StevensJohnson syndrome and toxic epidermal necrolysis, myopathy, myositis, rhabdomyolysis, muscle rupture, lupus-like syndrome, immune-mediated necrotizing myopathy, gynaecomastia, peripheral oedema. Common: Nasopharyngitis, allergic reactions, hyperglycaemia, headache, pharyngolaryngeal pain, epistaxis, constipation, flatulence, dyspepsia, nausea, diarrhoea, myalgia, arthralgia, pain in extremity, muscle spasms, joint swelling, back pain. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: Specific treatment is not available for atorvastatin overdose. Should an overdose occur, the patient should be treated symptomatically and supportive measures instituted, as required. Liver function tests should be performed and serum CK levels should be monitored. Due to extensive atorvastatin binding to plasma proteins, haemodialysis is not expected to significantly enhance atorvastatin clearance. Legal category: POM. Marketing Authorisation Number: PA1986/125/001-004. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00099. Date of Preparation: July 2025
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie.
Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Further information is available on request or in the SmPC. Product Information also available on the HPRA website. Date of Preparation: August 2025 | Job Code: GEN-IE-00149
Ask the Expert: Migraine
More than a Headache
Migraine is one of the most common neurological disorders worldwide, affecting up to 12% of the population, yet it remains underdiagnosed, undertreated, and often misunderstood. For many patients it is far more than “just a headache” — it is a debilitating condition that disrupts daily life, work, and wellbeing. Over the past three decades, major advances such as triptans, CGRP-targeted therapies, and neuromodulation devices have transformed the treatment landscape, but access to care and persistent misconceptions continue to challenge both patients and clinicians.
We sat down with Dr. Edward O’Sullivan, Director of the Headache & Migraine Clinic at Cork University Hospital, to discuss the evolution of migraine management in Ireland, the pressures facing specialist services, and where the next opportunities for improvement lie.
Could you tell us about your background and how you came to lead the Cork Headache & Migraine Clinic?
I was appointed Director of the Headache/Migraine Clinic within the Department of Neurology, Cork University Hospital, in September 2000. The clinic runs two outpatient sessions each week, on Tuesdays and Fridays, and is fully supported by registrars, SHOs, a clinical nurse specialist and clerical staff. We also have ready access to diagnostic services, particularly radiology and laboratory testing.
My own interest in headache began in my junior hospital doctor days during a neurology rotation. Even after moving into general practice I maintained that interest. Towards the end of the 1990s, as triptan therapies began to emerge, awareness of migraine as a serious and debilitating disorder grew. Around the same time the Migraine Association of Ireland was founded by Audrey Craven, who has been a tireless advocate for patients for decades. I became medical advisor to the Association and increasingly
involved in the evolving landscape of migraine management.
The Association lobbied for the establishment of dedicated migraine clinics in hospitals. The first was set up in Beaumont Hospital, followed soon afterwards by the Cork clinic which I now direct.
How do you approach diagnosis in the clinic?
Migraine is a recurrent clinical disorder, and accurate diagnosis depends first and foremost on a comprehensive history and examination. The International Headache Society has helped bring uniformity with internationally adopted diagnostic guidelines.
One crucial element is recognising “red flag” symptoms that suggest possible secondary causes of headache. In those cases we order appropriate neuroimaging or laboratory investigations. For follow-up, we ask patients to keep headache diaries, which provide invaluable information and help us to refine management.
Dr. Edward O’Sullivan
The management of migraine has become increasingly complex. There is now a wide variety of acute and preventative therapies available, and patients being considered for newer treatments such as CGRP antagonists must meet specific clinical criteria. The most challenging group are those with chronic migraine—defined as more than 15 headache days per month. These patients now represent the largest proportion attending our clinic.
How common is migraine, and what does that mean for clinics like yours?
Migraine affects around 10–12% of the population, but those who attend specialist headache or neurology clinics represent only the tip of the iceberg. The majority of people with migraine remain undiagnosed in the community, or assume that little can be done.
At the clinic our challenge is triage: identifying those with the highest levels of disability and poorest quality of life. Even with triage, our waiting lists are long. This reflects the sheer prevalence of
migraine, and the rising demand for specialist input.
What misconceptions about migraine still affect patient care?
The biggest misconception is that migraine is “just a headache.” When patients present to emergency departments or are admitted to hospital, once a secondary cause has been ruled out, concern for the patient often diminishes. This can lead to suboptimal care.
All too often patients are prescribed compound analgesics such as paracetamol with codeine, or even narcotics, despite guidelines recommending triptans as the first-line treatment for acute attacks. Many of these patients should also be considered for a preventative therapy.
These barriers have been difficult to break down. Greater education—both for healthcare professionals and for patients— remains essential.
How did triptans change the management of migraine?
The first targeted specific acute migraine therapies, the triptans, 5HT1B/1D receptor agonists have been available since the late 1990’s and are listed in fig 1.
Fig: 1
Triptans: 5HT1B/1D Receptor Agonists
1. Sumatriptan 50mg, 100mg, Nasal: 10mg, 20mg.
2. Zomitriptan 2.5mg
3. Frovatriptan 2.5mg
4. Eletriptan 40mg
5. Naratriptan 2.5mg
6. Almotriptan 12.5mg
The arrival of triptans (5HT1B/1D receptor agonists) in the late 1990s represented a milestone in migraine therapy and our understanding of pathophysiology. Today we have six oral triptans available (sumatriptan, zolmitriptan, frovatriptan, eletriptan, naratriptan and almotriptan), as well as intranasal formulations.
Despite proven efficacy in numerous clinical trials, triptans remain under-prescribed. A recent meta-analysis published in the BMJ (September 2024) showed that only 20–25% of migraine patients in Western societies have ever been prescribed a triptan. The authors concluded that triptans should be first-line for acute migraine, ahead of simple or compound analgesics and NSAIDs.
Can you explain the role of CGRP and the development of targeted therapies?
Pivotal research in the late 1980s by Goadsby and Edvinsson demonstrated that calcitonin gene-related peptide (CGRP) was elevated in jugular venous blood during migraine attacks. CGRP is concentrated in the trigeminal system, and its release activates the trigeminovascular pathway.
This scientific breakthrough lead to investment in drug development which specifically targeted C.G.R.P. and ultimately lead to the approval of C.G.R.P. monoclonal antibody antagonists and small molecule ‘’gepants’’. Fig 2. These advances have brought us to a new era in migraine management with recommended guidelines and best practice changing and evolving all the time.
GALCANEZUMAB 200MG LOADING AND 100MG S.C MONTHLY INJECTION
EPTINEZUMAB 100MG IV INFUSION EVERY 3 MONTHS
2. SMALL MOLECULE GEPANTS:
RIMEGEPANT 75MG BOTH AS ACUTE AND PREVENTATIVE THERAPY ALTERNATE DAYS
ATOGEPANT 30MG AND 60MG DAILY AS PREVENTATIVE THERAPY
“The management of migraine has become increasingly complex. There is now a wide variety of acute and preventative therapies available, and patients being considered for newer treatments such as CGRP antagonists must meet specific clinical criteria”
Today we have two categories:
• CGRP monoclonal antibodies (erenumab, fremanezumab, galcanezumab, eptinezumab) used as preventatives, administered by injection or infusion.
• Small molecule “gepants” (rimegepant and atogepant) which can be used both acutely and preventatively.
These advances mark a new era in migraine care, with clinical guidelines evolving rapidly.
What are the eligibility requirements for these therapies in Ireland?
In Ireland, CGRP antagonists are available only through neurology departments under the HSE’s Medicines Management Programme. Patients must meet strict criteria:
• For monoclonal antibodies: diagnosis of chronic migraine (>15 headache days/month, including 8 migraine days) and documented failure of at least three conventional preventatives (such as propranolol, amitriptyline, topiramate, candesartan, venlafaxine, pizotifen, or botulinum toxin). Supporting documentation from the patient’s dispensing pharmacist is required.
• For gepants: approved in episodic migraine (>4 migraine days/month) as well as chronic migraine, but patients must also have failed three preventatives. These hurdles take time, create delays, and add pressure to already stretched neurology services.
Are devices also part of modern management?
Yes. Neuromodulation devices such as trigeminal nerve
stimulators (Cefaly), external vagal nerve stimulation (gammaCore), and transcranial magnetic stimulation are available. These can be used both acutely and preventatively, particularly for patients who fail to respond to drug therapies.
However, they are not reimbursed by the HSE. Patients must pay out-of-pocket, which limits access
How are these new therapies impacting services?
The arrival of CGRP antagonists has led to a surge in referrals. GPs and patients are aware of the real-world data showing these therapies are superior to conventional preventives. However, because prescribing is restricted to neurology, the pressure on Headache/Migraine Clinics has increased dramatically.
With current resources, clinics cannot meet demand. This leaves many eligible patients unable to access therapies that could transform their quality of life.
Beyond medications, how important are multidisciplinary approaches?
Migraine is the second leading cause of disability worldwide, and management is rarely just about tablets. Multidisciplinary input is vital: physiotherapy, cognitive behavioural therapy, stress management, and lifestyle interventions all play a role.
Clinical nurse specialists are an essential part of this team. In some centres they manage follow-up patients, increasing clinic capacity, and act as a vital contact point between appointments. They explain medications, side-effects, trigger management, and provide reassurance. Their role significantly enhances patient care and should be expanded.
Are the current restrictions on prescribing CGRP antagonists fit for purpose?
In my view, no. The restrictions imposed by the Medicines Management Programme are at odds with best clinical practice. International evidence consistently demonstrates the safety and effectiveness of CGRP therapies.
Meanwhile, many of the conventional preventives have significant drawbacks. Sodium valproate and topiramate are teratogenic and require contraception in women of childbearing age. Beta-blockers and candesartan may cause hypotension and dizziness. In many cases, patients are forced to try medications with more risk and less efficacy before being allowed access to targeted therapies.
What changes would improve services for patients?
The appointment of more clinical nurse specialists with expertise in migraine would make an immediate difference, increasing capacity, supporting patients between appointments, and helping reduce waiting times.
Longer term, we need to revisit prescribing restrictions. Broader access to CGRP antagonists— supported by evidence and patient outcomes—would align policy with best practice and ease the pressure on neurology clinics.
Looking back, how do you see the progress in migraine care?
From the early days of triptans to the new generation of CGRP therapies, progress has been remarkable. Patients who once had few options now have access to highly effective, targeted treatments.
The challenge is no longer a lack of therapies, but ensuring equitable access, adequate resourcing, and education—both for clinicians and for the public—to overcome the misconceptions that still surround migraine.
In summary: migraine remains one of the most common and disabling neurological disorders. But with targeted treatments, better service structures, and multidisciplinary care, outcomes for patients in Ireland can continue to improve. As Dr. O’Sullivan stresses, the science has brought us far—the next step is ensuring patients can benefit.
Ask the Expert: Diabetes
Rethinking Diabetes as a System Disease
Diabetes is often thought of as a blood sugar problem, but it is far more complex: a systemic disease driving cardiovascular, renal, and metabolic complications. In recent years, new approaches — particularly the treatment of obesity — have shifted how clinicians view type 2 diabetes, making remission a realistic goal for some patients. We spoke with Professor Carel Le Roux, Head of Pathology at St Vincent’s University Hospital and University College Dublin, about misconceptions in diabetes care, the rise of cardio-renal-metabolic medicine, and the practical steps hospitals can take now to improve outcomes.
Can you share your current role and what drew you into diabetes care?
I am a chemical pathologist at St Vincent’s Healthcare Group. My interest in diabetes stems from my wider focus on metabolic medicine — diabetes is central to understanding how deranged metabolism drives cardiovascular, renal, and other complications that increase morbidity and mortality.
What inspired your focus on diabetes within hospital practice?
What excites me most is that we can now disrupt diseases like type 2 diabetes by effectively treating obesity. Not only can this dramatically improve glycaemia, but it can also enhance patients’ functionality and even put many diabetes-related complications into remission. It’s very rewarding to see patients’ lives transformed in this way.
What are the biggest challenges hospitals face in managing Type 1 versus Type 2 diabetes?
The growing incidence of both type 1 and type 2 diabetes places significant pressure on hospital services. Managing such large patient numbers effectively — while also addressing their complications — is an ongoing challenge.
How do these challenges impact patients in day-to-day hospital care?
For type 2 diabetes in particular, delays in providing optimal care for patients with established cardio-renal-metabolic complications remain a concern. At the same time, preventing those complications in patients who are earlier in the disease course is equally challenging. Both sides of this spectrum need attention if we are to reduce morbidity and mortality.
What misconceptions about diabetes management do you frequently encounter?
Some misconceptions still persist. A few patients and even healthcare professionals continue to think diabetes is caused by “eating too much sugar,” or that the sole aim of treatment is to reduce blood glucose.
Fortunately, understanding is shifting. More and more clinicians now see diabetes as a system disease — one that requires us to address its underlying pathophysiology. By doing so, we can control the disease and, in some cases, achieve remission.
What promising developments do you see in diabetes research or therapy?
The fact that we can now prevent type 2 diabetes and even create glycaemic remission by effectively treating obesity has been a true game-changer. These advances not only improve long-term outcomes but also quality of life, which means patients are actively seeking care in ways they might not have before.
What role do multidisciplinary teams play in improving diabetes outcomes?
Multidisciplinary teams are critical. But one member has stood out as especially important: the primary care physician. Their central role in coordinating care, identifying risks early, and supporting patients day to day
has transformed outcomes for many people living with diabetes.
What systemic changes are needed in Ireland to strengthen diabetes care?
To reduce hospitalisations and mortality, we need a sharper focus on patients with cardiorenal-metabolic complications. The tools now exist to help these patients live longer and better lives — but we need to make sure they are implemented consistently and effectively.
Three practical things hospitals can do this year to improve care for people with diabetes?
1. Identify the highestrisk cohort: patients with established cardiovascular disease, a urine albumincreatinine ratio >30, and BMI >27 kg/m2. Escalating care in this relatively small group could prevent a great deal of morbidity and mortality in the next year.
2. Deliver guideline-directed therapy: ensuring that evidence-based, optimal care is consistently applied for patients with cardio-renal-metabolic complications.
3. Strengthen collaboration between primary and secondary care: building on the strong foundation we already have, so that patients benefit from a more integrated and seamless system of care.
In summary: Diabetes is not simply about high blood sugar — it is a systemic condition with far-reaching consequences.
As Professor Carel Le Roux stresses, the most powerful advances in recent years have come from treating obesity and focusing on cardio-renalmetabolic complications. With multidisciplinary teamwork and sharper prioritisation of high-risk patients, hospitals in Ireland can deliver more effective, life-changing care.
Professor Carel Le Roux
PREVENT
THE DISRUPTION OF MIGRAINE1
The only oral once-daily calcitonin gene-related peptide (CGRP) receptor antagonist for both episodic and chronic migraine patients1,2
Tablet not actual size.
Typical characteristics of migraine are headache of unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity and association with nausea and/or photophobia and phonophobia.3
ABBREVIATED PRESCRIBING INFORMATION. AQUIPTA® (atogepant) 10 mg tablets; 60 mg tablets. Please refer to the Summary of Product Characteristics (SmPC) before prescribing. PRESENTATION: Each tablet contains: 10 mg atogepant in 10 mg tablet, 60 mg atogepant in 60 mg tablet. INDICATION: Prophylaxis of migraine in adults who have at least 4 migraine days per month. DOSAGE AND ADMINISTRATION: The recommended dose is 60 mg taken orally once daily with or without meals; swallowed whole and not split, crushed or chewed. Missed dose to be taken as soon as it isremembered. If forgotten for an entire day, missed dose to be skipped and next dose taken as scheduled. Dose Modification: The recommended dosage of atogepant with concomitant use of strong CYP3A4 inhibitors or strong OATP inhibitors is 10 mg once daily. Special Populations: Elderly: No dose adjustment needed. Renal impairment: In patients with severe renal impairment (creatinine clearance [CLcr] 15-29 mL/min), and in patients with end-stage renal disease (ESRD) (CLcr <15 mL/min), the recommended dose is 10 mg once daily. For patients with ESRD undergoing intermittent dialysis, atogepant should preferably be taken after dialysis. No dose adjustment is recommended for patients with mild or moderate renal impairment. Hepatic impairment: Avoid use of atogepant in patients with severe hepatic impairment. No dose adjustment is recommended for patients with mild or moderate hepatic impairment. Paediatric Population: The safety and efficacy of atogepant in children (< 18 years of age) have not yet been established. CONTRAINDICATIONS: Hypersensitivity to active substance or any of the excipients. SPECIAL WARNINGS AND PRECAUTIONS: Serious hypersensitivity reactions reported, including anaphylaxis, dyspnoea, rash, pruritus, urticaria and facial oedema. Most serious reactions have occurred within 24 hours of first use, however, some hypersensitivity reactions can occur days after administration. Patients should be warned about symptoms of hypersensitivity. If a reaction occurs, discontinue atogepant and institute appropriate therapy. AQUIPTA 60 mg tablets contain 31.5 mg sodium per tablet; this is equivalent to 1.6% of the WHO recommended maximum daily intake of 2 g sodium for an adult. AQUIPTA 10 mg tablets contain less than 1 mmol sodium (23 mg) per dose, that is to say essentially ‘sodium-free’. Atogepant has no or negligible influence on the ability to drive and use machines. However, if affected by somnolence, patients should exercise caution
before driving or using machinery. FERTILITY, PREGNANCY AND LACTATION: Pregnancy: Atogepant is not recommended during pregnancy and in women of childbearing potential not using contraception. Breast-feeding: It is unknown whether atogepant is excreted in human milk. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from therapy taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman. Fertility: No human data on the effect of atogepant on fertility are available. Animal studies showed no impact on female and male fertility with atogepant treatment. UNDESIRABLE EFFECTS: Common (≥ 1/100 to < 1/10): Decreased appetite, nausea, constipation, fatigue/somnolence, weight decreased. Refer to Section 4.8 of the SmPC for details of other side effects, and for further information.
This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance; website: www.hpra.ie.
LEGAL CATEGORY: POM (S1B). MARKETING AUTHORISATION NUMBERS: EU/1/23/1750/001 AQUIPTA 10 mg tablets in blisters, in cartons of 28 tablets; EU/1/23/1750/003 AQUIPTA 60 mg tablets in blisters, in cartons of 28 tablets. MARKETING AUTHORISATION HOLDER: AbbVie Deutschland GmbH & Co. KG, Knollstrasse, 67061, Ludwigshafen, Germany. Further information is available on request from: AbbVie Limited, 14 Riverwalk, Citywest Business Campus, Dublin 24. DATE OF REVISION: November 2024. PI/1750/002.
References: 1. AQUIPTA® Summary of Product Characteristics, available at www.medicines.ie. 2. Morena-Ajona D, et al. J Clin Med. 2022;11(6):1656. 3. Ferrari MD, et al. Nat Rev Dis Primers. 2022;8(1):2.
Ask the Expert: Medicine Shortages
Tackling Medicine Shortages in Hospital Pharmacy
Medicine shortages are no longer rare, short-term issues — they have become a persistent challenge for hospitals, pharmacies, and patients alike. From routine generic switches to critical shortages of lifesaving drugs such as insulin, the impact is felt across every level of healthcare.
For this edition of Ask the Expert, we speak with Barry O’Sullivan, Senior Manager of Outpatient Pharmacy across four Diabetes and Endocrine Centres in the UAE about the global and local drivers of shortages, how they affect patient care and hospital workflows, and what practical steps hospitals in Ireland can take to build resilience into their supply chains.
The pharmacist’s perspective
Every pharmacist and pharmacy technician working directly with patients has some level of involvement in managing medicine shortages. For Barry, the first taste came during summer work in a busy community pharmacy in Cork.
“One brand of a generic ACE inhibitor might be unavailable, but we could easily switch to another. For high-volume generic medicines, this is straightforward — and that’s reflected in the HPRA’s interchangeable medication list, first published in 2013.”
The picture becomes more complicated when medicines are novel or delivery methods unique — such as pen devices or insulins. “In those cases, shortages are not so easily navigated, and the impact on patients is much greater.”
Today, as Senior Manager of Outpatient Pharmacy across four Diabetes and Endocrine Centres in the UAE, supply chain management is a daily focus for Barry and his team.
“We’re a high-volume network, dispensing over 100,000 items per month. My role is to make sure patients can access the right medications, sensors, needles, and consumables to support their care plans. Even though I’m not directly in procurement, shortages affect my team of 80 staff across four sites every day.”
Why shortages happen
The causes of shortages are multiple and interconnected. “It’s a mixed bag of geopolitics, economics, regulatory hurdles, and fragile supply chains,” Barry explains.
Drug discovery and manufacturing are expensive, and global markets drive allocation. “Often, more profitable or larger markets are supplied first. Ireland, as a small market with relatively low reimbursement rates, can end up further down the list for replenishment. Regulatory requirements here can also delay the launch of medicines compared to other countries.”
This vulnerability has been highlighted repeatedly in recent years.
• Insulin shortages in 2024: “When all the major manufacturers encountered supply issues, it created a major challenge across diabetes services. Managing this required in-depth case-by-case discussions between physicians, patients, and families, with clear documentation and communication.”
• GLP-1 shortages in 2024: Demand for GLP-1 drugs surged due to off-label use for weight loss in countries like the USA, UAE, and Qatar. “Manufacturing couldn’t scale quickly enough, creating lags in supply.”
• Valsartan recall (2018–2020): Detection of potential carcinogens in the active pharmaceutical ingredient from one factory in Asia led to widespread shortages, forcing patients onto alternative ARBs such as telmisartan and losartan. “The clinical management of switching was time-consuming, complex, and anxiety-inducing for patients.”
Barry adds, “These events show how fragile supply can be. When a high-alert, life-saving
medicine becomes unavailable, the burden on healthcare teams for counselling, education, and safe switching is immense. And in Ireland, where reimbursement for such services is limited, the resource strain is even greater.”
The impact on patients and hospitals
For patients, shortages are deeply unsettling. “There’s often genuine concern that they’re on a suboptimal therapy, or that they may take a medication incorrectly because their usual brand or device has changed. Adherence risks rise during shortages,” he notes.
For hospitals, the consequences are operational as well as clinical. “Shortages disrupt workflows, consume staff time, and force repeated communication with clinical teams and families. Even when managed well, they create anxiety and inefficiency.”
Clearing up misconceptions
One common misconception is that shortages are the fault of pharmacy teams. “Of course, occasional errors in ordering or
“Pharmacy sits at the intersection of procurement, logistics, and patient care — and often becomes the focal point for frustration when shortages hit.”
Barry O'Sullivan
delivery happen, but the reality is far broader. Pharmacy is the intersection point of procurement, logistics, clinical teams, and payers. We are face-to-face with patients, so frustrations often land with us. But the causes are usually systemic and global.”
The broader societal risks of supply breakdown are stark.
“The recent Netflix series The Hostage illustrated how civil unrest was fuelled in part by a broken medicines supply chain, delaying access to chemotherapy and asthma drugs. It’s a reminder that medicine shortages are not just clinical inconveniences — they can destabilise communities.”
Strategies and technologies
Hospitals and health systems are adopting new strategies to anticipate and mitigate shortages. Predictive analytics and AI tools are becoming especially important. “Demand-planning systems can ensure purchase orders and contracts are aligned to likely need. They can’t prevent global shortages, but they can reduce frequency and severity for local services.”
Other practical strategies include:
• Medication governance committees to approve core drug lists and clinically appropriate alternatives.
• Par levels with higher reserves for 20–30 key medicines.
• Cluster purchasing between hospitals to increase buying power and reduce waste.
• Alternative equivalents built into clinical software to allow rapid switching when shortages hit.
The policy dimension
Barry emphasises the importance of national and international collaboration. “Sometimes it feels like the pharmacy voice isn’t truly heard by policymakers. But policy support is essential to strengthening supply resilience.”
He points to the UK as a recent example. “In August 2025, the Department of Health and Social Care, with NHS England, released a paper called Managing a Robust and Resilient Supply of Medicines. It acknowledged the global nature of supply chains and set out measures to strengthen resilience across the system. That’s the kind of framework other countries, including Ireland, should adopt.”
Long-term solutions for Ireland
For Ireland, Barry suggests several steps to strengthen supply chain resilience:
• Peer-to-peer transfer of stock between hospitals and pharmacies.
• A national dashboard of key medicines, similar to the High-Tech Medicines initiative, to track availability and share resources efficiently.
• Adopting WHO guidance: “The WHO’s biannual essential medicines list, most recently updated in September 2025, gives clear direction on which drugs should be prioritised for resilience planning.”
Collaboration is key
Ultimately, medicine shortages cannot be solved by pharmacy alone. “Collaboration between pharmacists, clinicians, and policymakers is vital. Hospitals must balance cash flow and perishability, but clustering, bulk purchase, and shared risk all strengthen resilience.”
And while procurement strategies are critical, so too are communication and education. “Clear communication with clinicians and patients, and good documentation, are the difference between a safe switch and a dangerous one.”
Three actions hospitals can take this year
To build resilience now, Barry recommends three practical steps:
1. Stock more of the essentials: Identify 20–30 core items,
increase stockholding, and align par levels with higher reserves.
2. Create approved alternative lists: Through governance committees, agree clinically appropriate substitutes in advance, and activate them when core stock drops.
3. Cluster and bulk purchase: Partner with other facilities to increase purchasing power, reduce cost, and share risk of expiry.
Conclusion
Medicine shortages are a fact of modern healthcare, driven by global markets, fragile supply chains, and complex regulatory environments. While pharmacists are often the visible face of the problem, solutions lie in systemic collaboration, smarter demand planning, and robust national policies.
As Barry concludes, “Pharmacy sits at the intersection of procurement, logistics, and patient care. We may not control all the levers, but with the right strategies and stronger collaboration across the system, we can make shortages less disruptive and ensure patients continue to access safe, effective treatment when they need it most.”
Ask the Expert: Diabetes Diabetes Safety in the Hospital Setting
Diabetes is one of the most common chronic conditions encountered in hospitals, yet its management is anything but routine. With complex medication regimens, rapidly changing insulin needs, and an expanding array of devices and therapies, safe diabetes care requires constant vigilance. Errors can have serious consequences — but with the right systems, teamwork, and education, they are preventable. We spoke with Diana Hogan Murphy, Chief II Pharmacist for Medication Safety at Galway University Hospitals and Adjunct Professor at the University of Galway, about the evolving challenges and opportunities in hospital diabetes care.
Can you share your current role and what drew you into diabetes care?
I am Chief II Pharmacist for Medication Safety at Galway University Hospitals, and Adjunct Professor at the College of Medicine, Nursing and Health Sciences, University of Galway.
What drew me into diabetes care was seeing first-hand how easily things can go wrong with diabetes medicines, especially insulin. It’s a high-alert drug
that can cause significant harm if used incorrectly, and in my role I encountered incidents that highlighted the critical importance of safe prescribing, administration, and monitoring.
I also teach safe prescribing to final-year medical students, which keeps me motivated to stay current in diabetes care. My goal is to ensure future doctors are equipped with the skills and awareness to prevent medication errors. The pace of change in diabetes treatments — with new
drugs, new delivery systems, and digital tools — adds another layer of complexity, but also opportunity.
What inspired your focus on diabetes within hospital practice?
Diabetes is one of the most common chronic conditions we see in hospitals. Because it affects such a large proportion of patients, improving medication safety here can make a big difference to outcomes overall.
Insulin management is especially complex: it requires precise dosing, timing, and monitoring, and errors can lead to severe hypoglycaemia, diabetic ketoacidosis (DKA), or hyperosmolar hyperglycaemic state (HHS).
Working as part of a multidisciplinary team — doctors, nurses, and pharmacists together — means we can embed safety into policies, protocols, and education. For example, since 2022 we’ve run annual insulin audits at Galway University Hospitals led by an interprofessional team. These have already resulted in tangible improvements in quality and safety.
What are the biggest challenges hospitals face in managing Type 1 versus Type 2 diabetes?
Type 1 diabetes is uniquely challenging because patients rely entirely on insulin, which is unforgiving if mismanaged. Doses and timing must be exact, yet requirements often change rapidly in hospital due to illness, stress, nutrition, or reduced activity. At home, patients usually self-manage, but in hospital our policy is that insulin is stored and administered by nursing staff. This means nurses must quickly get to grips with each patient’s highly individual regimen.
Poor glycaemic control in hospital is not just an inconvenience — it’s linked to longer length of stay, hospital acquired infections, and higher morbidity. On the patient side, it’s also stressful.
Diana Hogan Murphy
Type 2 diabetes patients often take multiple oral agents, sometimes combined with insulin, and frequently have cardiovascular or renal comorbidities that complicate treatment. Certain drugs, such as SGLT2 inhibitors, may be inappropriate during acute illness. Knowing when to stop, switch, or restart medicines is essential.
For both groups, the biggest risks come from miscommunication — within teams, between teams, or with patients. Managing blood glucose fluctuations around surgery, fasting, or acute illness is another challenge. Robust protocols and ongoing staff training are essential safeguards.
How do these challenges impact patients day to day in hospital?
Poor glycaemic control in hospital is not just an inconvenience — it’s linked to longer length of stay, hospitalacquired infections, and higher morbidity. On the patient side, it’s also stressful. Hospitalisation disrupts people’s normal routines and self-management. Patients may feel anxious, frustrated, or excluded from decisions about their own care.
From a safety perspective, insulin doses need constant adjustment for meals, stress, or acute illness. If that’s not managed correctly, patients can tip into DKA or HHS within hours.
What misconceptions about diabetes management do you frequently encounter?
Some of the most common examples we see include:
• Holding long-acting insulin after a hypo — which risks ketones and DKA within hours. Long-acting insulin should never be stopped.
• Checking glucose too soon after corrective insulin — leading to “insulin stacking” because the first dose hasn’t had time to work.
• Skipping mealtime insulin if glucose is high — which risks worsening hyperglycaemia. Insulin is needed with each meal, regardless of prior levels.
• Confusion between CGM and fingerstick readings — CGM measures interstitial glucose, with a lag of about 15 minutes, so they won’t always match.
• Continuing oral agents during acute illness — metformin and SGLT2 inhibitors should be held when risks like lactic acidosis, renal impairment, or euglycaemic DKA are present.
• Sound-alike/look-alike drug errors — e.g. NovoRapid vs NovoMix, Humalog vs Humalog Mix, which can cause dangerous mix-ups.
Education and vigilance are key to preventing these errors.
How are CGMs, pumps, and digital tools changing the landscape of diabetes care?
The impact has been transformative.
• Continuous glucose monitors (CGMs): These now provide 288 readings per day and can send alerts in real time. Parents of children with Type 1 diabetes, for example, no longer have to wake up multiple times at night to check glucose — the CGM does it for them. In Ireland, CGMs are now free for all patients with Type 1 diabetes, which has been a game-changer for safety and quality of life.
• Insulin pumps: Particularly common in children and young adults, pumps simplify dosing by calculating insulin requirements based on carbohydrate counting. The newer hybrid closed-loop systems automatically adjust insulin delivery using CGM data, keeping glucose in range much more effectively.
• Digital tools: Integration with smartphones, cloud platforms, and AI-driven analytics has empowered patients and clinicians to identify patterns and make informed decisions. Telemedicine has also expanded access, particularly for those who live far from specialist clinics.
The key principle in hospital is to let capable patients continue to manage their devices. Overriding patient autonomy can cause harm if staff are less familiar with the device than the patient is.
What promising developments do you see in research or therapy?
There is a lot of excitement around:
• Stem cell and beta-cell regeneration therapies, which could one day restore natural insulin production.
• Immunotherapy, aiming to halt or slow the autoimmune process in Type 1 diabetes.
• Fully closed-loop insulin delivery systems, though these are limited by the relatively slow absorption of subcutaneous insulin.
While these remain largely experimental, they represent real hope for the future.
What role do multidisciplinary teams play in improving outcomes?
They are absolutely central. Diabetes impacts almost every system in the body — macrovascular and microvascular complications, mental health, nutritional needs, physical activity, and more. No single profession can address it all.
Endocrinologists, diabetes nurses, pharmacists, dietitians, physiotherapists, psychologists, occupational therapists, and social workers all bring different expertise. Together, they can create care plans tailored to individual patients, improving adherence and outcomes. Education is another cornerstone — empowering patients to take ownership of their condition is just as important as prescribing the right drug.
What systemic changes are needed in Ireland?
We need a National Diabetes Strategy to drive policy and resource allocation. A national diabetes registry would help us track outcomes, plan services, and benchmark progress. Expanding access to diabetes technologies
like CGMs and pumps is vital, as is better integration between primary and secondary care.
Three practical steps hospitals could take this year to improve care?
1. Annual insulin audits: Just as we’ve done in Galway University Hospitals since 2022, every hospital should implement a standardised audit to benchmark and improve practice.
2. Promote reusable and smart pens: These are more sustainable, cost-effective long term, and provide features like dose memory, reminders, and data sharing.
3. Intensify training for staff and patients: Focus on safe insulin use, the importance of never withholding long-acting insulin, and involving patients in shared decision-making from the start.
In summary: Diabetes care in hospitals is complex, fastmoving, and high-stakes. With the right systems, multidisciplinary teamwork, and ongoing education, hospitals can significantly reduce errors and improve outcomes. As Diana Hogan Murphy emphasises, the science and technology are advancing rapidly — the challenge is embedding safety and patient partnership into every step of care.
Ask the Expert: Sepsis
Sepsis Care in Ireland
Sepsis remains one of the greatest challenges in modern healthcare, claiming millions of lives globally each year and leaving many survivors with lasting complications. In Ireland, it is a condition that stretches across all specialties and patient groups, demanding rapid recognition, coordinated treatment, and long-term support.
For this edition of Ask the Expert, we spoke with Dr Michael O’Dwyer, Clinical Lead for the HSE’s National Clinical Programme for Sepsis and Consultant in Intensive Care Medicine and Anaesthesiology at St Vincent’s Healthcare Group, about why sepsis is so complex, the challenges facing Irish hospitals, and how clinicians can improve outcomes now and into the future.
A career shaped by sepsis
For Dr Michael O’Dwyer, sepsis has been a central thread running through his clinical and academic career. Today he serves as the Clinical Lead for the HSE’s National Clinical Programme for Sepsis and practices as a consultant in Intensive Care Medicine and Anaesthesiology at St Vincent’s Healthcare Group, as well as in private practice. But his path into this area was set early on.
“As a junior doctor I enrolled in a PhD programme at Trinity College Dublin,” he recalls. “My supervisor, Dr Tom Ryan, was an ICU consultant with a keen interest in sepsis and the immune pathways that become dysregulated as a consequence. My PhD explored genetic predispositions to sepsis, and the differences between patients who developed sepsis and those who had bloodstream infections but did not progress.”
This early work left him fascinated by the complexity of immune responses in infection. After completing an ICU fellowship in Australia, his first consultant post was at Barts Health NHS Trust in London, where he also served as a senior lecturer at Queen Mary,
Dr Michael O’Dwyer
University of London. There he led a large translational research group examining immune responses to sepsis, trauma, and major surgery.
“That experience really deepened my appreciation of just how much we don’t know about sepsis. Even with sophisticated techniques, understanding which immune responses are protective and which are harmful is enormously challenging.”
Why sepsis became a lifelong focus
While ICU practice meant frequent encounters with sepsis, Dr O’Dwyer says it was his academic immersion that revealed the global
scale of the problem. “Sepsis is not a rare, specialist condition. It’s one of the world’s leading causes of death, responsible for millions of cases every year. From an academic point of view, it’s fascinating. From a clinical point of view, it’s devastating.”
He points out one of sepsis’s most puzzling features: variability. “Two patients of similar ages, with similar infections, can have completely different outcomes. One might have a mild illness, the
A genome-wide gene expression array demonstrating the profound genomic changes during the early time course of sepsis
other could progress to multiorgan failure. That unpredictability is part of what makes sepsis so dangerous, and part of why I remain fascinated by it.”
The diagnostic dilemma
Despite decades of research, sepsis remains notoriously hard to diagnose. “Our so-called ‘gold standard’ — blood cultures — is not good enough,” Dr O’Dwyer says. “In about half of confirmed sepsis cases, blood cultures remain negative. When they are positive, results take 24 to 48 hours, which is far too slow in a condition where minutes matter.”
Molecular techniques, capable of detecting microbes without the need for culture, show promise but have limitations. “They can detect organisms with much greater sensitivity, but they also pick up microbes in healthy people. For example, brushing your teeth releases bacteria into the bloodstream, which can be detected using these methods, but that doesn’t mean you’re septic. The false-positive rate is too high for routine clinical use.”
As a result, clinicians still rely on a combination of patient history, physiological signs, and rapid blood tests to risk-stratify patients. “This is imperfect,” he admits. “Experienced clinicians may pick up subtle cues, but for juniors it can be very difficult. And because sepsis can occur in anyone, from any infection, it means cases will inevitably be missed every year.”
The treatment balancing act
When it comes to treatment, speed is critical — but so is caution. “There’s an understandable impulse to lower the threshold for giving antibiotics, because delays can be fatal. But overtreatment carries its own risks: antimicrobial resistance, allergic reactions, disruption of the microbiome, even associations with conditions such as inflammatory bowel disease,” Dr O’Dwyer explains.
ICU capacity has been one of the biggest determinants of improved survival in sepsis over recent decades. “The ability to support failing organs with ventilators, dialysis, or circulatory support has transformed outcomes. But our ICU bed capacity in Ireland is far below international norms. Too often, critically ill patients are managed on general wards because there simply isn’t space in ICU. In Germany or Australia, those patients would almost certainly be in intensive care.”
The COVID-19 pandemic exposed these gaps starkly. “COVID was essentially a pandemic of viral sepsis. The pressure it placed on ICU services revealed just how
vulnerable we are with our limited bed stock.”
The long shadow of sepsis
Even when patients survive, the story doesn’t end at hospital discharge. “Sepsis survivors often develop long-term complications — what we call post-sepsis syndrome,” Dr O’Dwyer explains. “This overlaps with post-ICU syndrome and includes fatigue, weakness, cognitive impairment, anxiety, and depression. It can profoundly affect quality of life.”
Awareness of this syndrome remains limited, both among clinicians and the public. “Globally, post-sepsis syndrome doesn’t get the attention it deserves. Patients are left struggling, with little structured support. That’s why in our Sepsis Strategy 2026–2031, we’re advocating for formal screening and rehabilitation pathways for survivors.”
Misconceptions and training gaps
Ireland benefits from strong governance structures and a high standard of training, but misconceptions persist. “Senior staff often feel they don’t need sepsis support tools, because they are confident in their clinical judgment. And while that’s often true, it creates a culture where junior staff mimic that behaviour. Subtle cases can be missed.”
The HSE’s sepsis support forms, which guide diagnosis and treatment, are designed to be accessible across experience levels. A newly redesigned form, now rolling out nationally, has addressed usability concerns.
“If senior staff visibly use the forms, it normalises best practice and ensures standardised care across the board,” Dr O’Dwyer emphasises.
What could change the game?
Asked which developments could transform sepsis care, Dr O’Dwyer highlights two: real-time diagnostics and immune-based therapies.
“A device that could accurately detect true pathogens in the bloodstream, distinguish them from harmless microbes, and do so within hours rather than days — that would be revolutionary,” he says.
Equally transformative would be the ability to profile immune responses in real time. “If we could identify whether a patient’s inflammation is sterile or infective, or whether they’re responding to a virus versus a bacterium, we could tailor treatment far more precisely.”
In terms of therapies, he points to oncology as an inspiration. “Cancer
care has been transformed by immunotherapies, which harness the patient’s own immune system. I believe the next seismic advance in sepsis care will come from something similar. Right now, our improvements are incremental, driven by better systems and processes. The next leap will come when we can safely modulate the immune system itself.”
The next five years in Ireland
Realistically, Dr O’Dwyer doesn’t foresee a step-change in diagnostics or therapies in the immediate future. Instead, he sees incremental but important gains.
“Increasing ICU bed stock will make the biggest difference, allowing us to care for more critically ill patients in the right environment. Expanding our audit process will give us richer national data, which will help us target interventions. Closer collaboration with AMRIC will strengthen antimicrobial stewardship.”
He also stresses the importance of embedding sepsis protocols beyond hospitals. “As Sláintecare reforms push more care into the community, sepsis recognition and management must follow. And if we continue to invest in public awareness campaigns, I hope people will present earlier — and be met by a healthcare system better equipped to respond.”
Teamwork saves lives
Sepsis can affect anyone, at any time, so vigilance must be system-wide. “We advocate for every healthcare worker in patient-facing roles to have basic sepsis training,” Dr O’Dwyer says. Simulation training, designed to strengthen both technical and nontechnical skills, is a future priority for the programme.
Later in the patient journey, recovery is heavily dependent on a multidisciplinary approach. “Sepsis survivors may be profoundly weak and deconditioned. Rehabilitation requires physiotherapists, occupational therapists, speech and language therapists, psychologists, and social workers. This holistic input can make the difference between returning to independent life or living with longterm disability.”
The same applies to postsepsis syndrome. “Managing fatigue, cognitive issues, and psychological sequelae requires a team approach. In our strategy, we are strongly advocating for this multidisciplinary follow-up.”
Systemic changes to strengthen sepsis care
What would improve outcomes
nationally? Dr O’Dwyer is clear: ICU capacity, data, and technology.
“Ireland has fewer ICU beds per capita than many comparable countries. Increasing bed numbers and associated staffing would allow us to manage more patients in critical care rather than general wards.”
He also calls for a national sepsis audit. “Annual, granular data would let us understand where deficiencies lie and how best to target interventions.”
Longer term, he sees technology as a powerful tool. “I believe hospitals will eventually admit patients with wearable monitoring devices, overseen by AI systems capable of detecting deterioration earlier than current tools like INEWS. That kind of system-level revamp could transform sepsis outcomes.”
Practical steps hospitals can take now
Despite the complexity of sepsis, Dr O’Dwyer identifies three straightforward actions every hospital can take this year:
1. Training: Ensure all staff complete the HSEland module on sepsis recognition and management.
2. Standardisation: Champion the sepsis support tool and forms, using them consistently to improve care and strengthen national data.
3. Audit: Conduct local audits to identify deficiencies and implement targeted improvements, with support from regional sepsis ADONs. Looking ahead
For Dr O’Dwyer, the future of sepsis care in Ireland will be defined by steady improvements in training, systems, and capacity, alongside anticipation of the next scientific breakthrough. “Antibiotics were the first great leap, and the development of ICU was the second. The third leap, I believe, will come from immunotherapies. Until then, our focus must be on doing the basics well, standardising care, and ensuring that every patient suspected of sepsis gets timely, appropriate treatment.”
In summary: Sepsis remains one of the most complex challenges in modern medicine. Its diagnosis is imperfect, its treatment a balancing act, and its recovery a long journey. Yet with coordinated national strategy, multidisciplinary teamwork, and continued investment in both systems and science, Ireland has the tools to steadily improve outcomes.
Ask the Expert Advances and Challenges in the Care of HIV and Viral Hepatitis in Ireland
The landscape of care for people living with HIV and viral hepatitis has changed dramatically in recent decades. Yet despite scientific breakthroughs, challenges remain in diagnosis, access, and stigma. We spoke Professor Eoin Feeney, Consultant in Infectious Diseases, St. Vincent's University Hospital and Tara Ramsbottom, ID SpR, about where Ireland stands today—and what the future may hold.
Professor Eoin Feeney
“Timely diagnosis remains a real issue. In 2023, almost 40% of new HIV diagnoses in Ireland were late, with a CD4 count under 350. Many clinicians still don’t think of HIV when faced with indicator conditions like recurrent shingles, unexplained weight loss, or bacterial pneumonia”
How would you describe the current state of care for people living with viral hepatitis and HIV in Ireland?
Prof. Feeney: In many respects, Ireland has made excellent progress. If a patient receives a diagnosis of HIV or viral hepatitis today, they can usually be seen in a specialist clinic very quickly. Antiviral therapy for HIV and hepatitis C is provided free of charge, which is hugely important. In the case of hepatitis C, short oral courses of direct-acting antivirals (DAAs) achieve cure rates above 95%. That’s an
extraordinary change from the era of interferon, when treatment lasted a year, caused significant side effects, and cured less than half of patients.
Dr. Ramsbottom: Communitybased care is also developing. Some patients with hepatitis C can now be treated outside hospitals, which improves access. Inclusion health initiatives have made a real difference too— supporting patients experiencing homelessness or those in international protection who often face the greatest barriers to care.
But challenges remain. Specialist centres are concentrated in large urban hospitals, which means many patients face long journeys to appointments. Even once they attend, access to allied health services—physiotherapy, occupational therapy, clinical psychology—is limited. That’s a particular concern for our ageing HIV population, many of whom are living with multiple comorbidities and the impact of stigma or past trauma. Care is still largely hospitalbased rather than being integrated into community services.
What recent advances have had the most impact?
Prof. Feeney: For HIV, the concept of undetectable equals untransmissible (U=U) has been transformative. The knowledge that people with a suppressed viral load cannot transmit HIV to their partners is empowering and destigmatising.
Dr. Ramsbottom: Treatment itself has also changed. We now have two-drug regimens instead of traditional triple therapy, which means fewer side effects for many patients. Long-acting injectable therapies—currently given every two months—are available in Ireland, though still resourceintensive. They can be lifechanging for people who struggle with daily tablets, whether due to adherence issues, pill burden, or difficulties storing medication in shared accommodation.
For hepatitis C, DAAs have completely altered the landscape. What was once a debilitating and often unsuccessful treatment journey is now short, simple, and curative for almost all patients. That’s reduced not just prevalence, but also the downstream complications we used to see regularly—cirrhosis, hepatocellular carcinoma, and liver transplantation.
And for hepatitis B, new guidelines from the European Association for the Study of the Liver and WHO recommend treating patients earlier, at the first
signs of fibrosis or inflammation. While HBV is rarely curable, suppressive oral therapy can prevent long-term complications.
Where are the biggest gaps when it comes to early diagnosis?
Prof. Feeney: Timely diagnosis remains a real issue. In 2023, almost 40% of new HIV diagnoses in Ireland were late, with a CD4 count under 350. Many clinicians still don’t think of HIV when faced with indicator conditions like recurrent shingles, unexplained weight loss, or bacterial pneumonia.
Dr. Ramsbottom: There have been positive steps. The SH24 online programme allows people to order postal test kits for HIV, hepatitis B and C, which has improved access. Antenatal screening now routinely includes hepatitis C as well as HIV and HBV. But gaps remain. Optout screening isn’t consistently offered in busy emergency departments, prisons, drug treatment centres, or international protection accommodation.
Socioeconomic factors are also crucial. People who inject drugs or who come from endemic countries are among those least likely to seek asymptomatic screening, even if they have risk factors or symptoms. So, while the tools exist, reaching those most at risk remains challenging.
How well is Ireland doing in terms of equitable access to treatment?
Prof. Feeney: Broadly speaking, Ireland is performing well. A 2023 audit by the Health Protection Surveillance Centre showed that 90% of people living with HIV know their status, 99% of those are on treatment, and 99% of treated patients are virally suppressed. That puts us in a strong position internationally.
Dr. Ramsbottom: But we mustn’t overlook inequities. Patients outside major cities face difficulties
travelling to tertiary centres, particularly if they’re working, have limited English, or are financially constrained. And while HIV and hepatitis C therapies are free, patients with hepatitis B must pay for their medications, which are often lifelong. That inconsistency creates avoidable barriers.
Stigma continues to be raised as an issue. What is the situation today?
Dr. Ramsbottom: Stigma is still a daily reality for many patients. HIV and hepatitis disproportionately affect groups who already experience social exclusion— gay and bisexual men, people who inject drugs, migrants from endemic areas. Misconceptions about transmission remain common, and not everyone knows that U=U or that treated patients can live full, healthy lives.
Prof. Feeney: Unfortunately, stigma isn’t limited to the general public. A survey from the RCSI found that 75% of healthcare workers had witnessed stigmatising remarks about patients with infectious diseases. That’s concerning. In our hospital we make a point of marking World AIDS Day and Sexual Health Awareness Day with education campaigns, stands, and social media posts to challenge stigma within healthcare. Campaigns like You, Me and HIV are also helping shift the narrative by sharing real patient stories.
How are treatment strategies evolving?
Prof. Feeney: For hepatitis C, the next challenge is eradication. DAAs have given us the means, but
success will depend on expanding testing and decentralising treatment. Other countries have shown that community pharmacies and outreach services can deliver effective test-and-treat models, and that’s something we need to look at more seriously.
Dr. Ramsbottom: For HIV, injectables are the biggest innovation right now. Cabotegravir and rilpivirine are already in use in Ireland as two-monthly injections. While they bring challenges—site reactions, more frequent clinic visits, and increased resource needs—they offer a valuable alternative. Longer-acting agents, such as lenacapavir, which could reduce dosing to just twice a year, are particularly exciting.
How do you approach coinfections in practice?
Prof. Feeney: Integrated care makes all the difference. In St. Vincent’s, we run combined infectious diseases and hepatology clinics, which allow us to streamline visits, manage complex drug-drug interactions, and reduce pill burden. For example, tenofovircontaining regimens can treat both HIV and hepatitis B effectively.
Dr. Ramsbottom: Supportive care is also key. We try to address the risk factors that led to infection in the first place—providing opiate substitution therapy, needle exchange programmes, vaccinations, condoms, and routine sexual health screening. Co-infected patients often face a double layer of stigma, so referral for psychological support is sometimes just as important as the prescriptions we write.
Are we on track for the WHO hepatitis C elimination targets?
Prof. Feeney: Encouragingly, yes. Notification rates for hepatitis C have halved since 2012, down to 9 per 100,000 in 2024. The WHO elimination goal is fewer than 5 per 100,000 by 2030, so we’re within touching distance.
Dr. Ramsbottom: The WHO also targets ≥90% of patients diagnosed and ≥80% treated. Around 70% of people with chronic HCV in Ireland have already been treated. To reach the remainder, we’ll need to broaden testing strategies—optout screening in EDs, targeted programmes in prisons and drug services, and outreach in international protection centres. Reinfection risk in high-risk groups also needs ongoing attention, with harm reduction and repeat testing.
Looking ahead, what innovations are you most hopeful about?
Prof. Feeney: Long-acting HIV therapies are particularly exciting. At CROI 2025, phase II data showed six-monthly lenacapavir plus broadly neutralising antibodies maintained suppression in 96% of patients. If longer-acting agents become standard, they’ll significantly ease treatment burden.
Dr. Ramsbottom: Cure research is ongoing for both HIV and hepatitis B, though we’re not there yet. The few HIV “cures” so far have only been possible with stem cell transplants for malignancy—too risky for widespread use. But progress is being made with novel antivirals and immunotherapies.
In the shorter term, what gives us the most hope is scaling up testing, breaking down barriers to access, and addressing stigma. Those steps will have the biggest impact in the next decade.
Finally, what lessons have you learned from your own practice that you’d like colleagues to bear in mind?
Prof. Feeney: Adherence challenges are rarely about patients being careless. More often, they reflect underlying problems—unstable housing, addiction, stigma, or mental health issues. Recognising those challenges, and offering support rather than judgement, can make all the difference.
Dr. Ramsbottom: Compassion and patient-centred care are as important as the drugs we prescribe. When patients feel heard, respected, and supported, adherence improves, outcomes improve, and stigma is reduced.
At a time when treatment options have never been stronger, the challenge is ensuring every patient—regardless of background—has equal access to care, and that stigma is replaced by understanding. As Professors Feeney and Ramsbottom emphasise, science may provide the tools, but it is compassion and inclusivity that will drive real progress.
References:
1. HSE-Health Protection Surveillance Centre. HIV Slideset 2023. Dublin: HPSC; November 2024
2. British HIV Association/British Association for Sexual Health and HIV/British Infection Association Adult HIV Testing Guidelines 2020
3. HIV Treatment Audit 2023 and progress towards UNAIDS 95-95-95 targets, Ireland. HSE. November 2024. Dublin.
4. HSE-Health Protection Surveillance Centre. Epidemiology of hepatitis C in Ireland; Trends from 2004 to 2024.
5. A Study of Teropavimab and Zinlirvimab in Combination With Capsid Inhibitor Lenacapavir in Virologically Suppressed Adults With HIV-1 Infection
ClinicalTrials.gov ID NCT05729568
Ask the Expert: VTE Pharmacy Views on VTE
Venous thromboembolism (VTE) remains one of the leading causes of maternal mortality worldwide, despite being largely preventable with timely risk assessment and prophylaxis. In Ireland, national initiatives such as the recently launched Eve Protocol are driving standardisation and raising awareness of VTE prevention across hospital and community settings.
At the National Maternity Hospital, Áine Toher, Deputy Pharmacist Executive Manager, has combined her expertise in clinical pharmacy, informatics, and education with a personal passion shaped by family experience to champion safer prescribing, electronic risk assessment, and multidisciplinary collaboration in women’s health. We spoke with Áine about her role, her motivations, and the continuing challenges in preventing VTE.
Can you share your role and how you came to specialise in thrombosis/VTE?
I am the Deputy Pharmacist Executive Manager in The National Maternity Hospital (NMH), with a special interest in venous thromboembolism (VTE) prevention, especially in the context of women's* health. I am passionate about raising awareness of VTE risk factors among patients, the public and healthcare staff as well as the potential for standardisation of measures to aid VTE prevention for all patients.
I am also a member of the Dublin South East VTE Service Review Group and part of the Clinical Advisory Group to the National Clinical Programme for VTE (NCPVTE)
There has been a long established haematology service, VTE prevention programme and maternal medicines clinic in the NMH. I work alongside the haematologist and haematology specialist midwife to review the VTE risk assessments, optimise low molecular weight heparin (LMWH) prescribing and providing patient and staff education.
With the introduction to the NMH of the National Maternal and Newborn Clinical Management System (MN-CMS) Electronic Health Record (EHR), as part of my role in informatics, I worked with the MN-CMS National Meds Team to develop and introduce NMH specific packages (care plans) which promote safe LMWH prescribing for our obstetric and gynecology patients.
I also collaborated with the haematology and MNCMS teams to introduce to the EHR - NMH specific electronic VTE risk
assessment forms to replace the paper versions.
In conjunction with the Dublin South East VTE Service Review Group, I coordinate the ongoing collection, analysis and presentation of NMH data to the hospital and DSE hospital group on VTE risk assessment and prophylaxis using an electronic VTE audit application.
What inspired your interest in clotting disorders and hospital care?
I have a professional and personal interest in the prevention, diagnosis and management of VTE as well as the follow-up care provided to patients.
My family has a history of thromboembolic disease. My father experienced and was treated for an unprovoked DVT in his 20s. There was very little follow-up at the time and he subsequently developed what is now known as post-thrombotic syndrome, it didn’t hold him back and managed symptoms with exercise and tubigrib when his leg was swollen. I also have had first-hand experience attending a haematology service, sourcing and self-administrating a LMWH during the postnatal period and the value of aftercare follow-up as well as discussion regarding contraceptive choices.
All of this has influenced my clinical awareness and the importance of the patient perspective and voice when designing models of care.
Early in my career, when I first qualified, there was a case that deeply impacted me. A young mother with three small children, was in the rehabilitation ward after suffering a postpartum stroke
secondary to a thrombotic event and was unable to hold her new baby due to the neurological deficits. Witnessing the emotional and physical toll on the young woman and her family was heartbreaking. It reinforced the importance of recognising and managing VTE risk, especially in pregnancy and the postpartum period.
What are the biggest challenges hospitals face in diagnosing and managing VTE that can impact on patient care?
I am aware that working in a specialised maternity hospital with a long established haematology, VTE prevention service and access to an electronic healthcare record is a position of privilege. Therefore, VTE is likely to be considered in those who present with symptoms and/or risk factors. We are linked with St Vincent’s University Hospital and all patients with suspected VTE
are transferred without delay for screening and diagnosis.
However, it is important to note that VTE remains one of the leading causes of maternal mortality worldwide. Thrombosis and thromboembolism was reported to be the leading cause of maternal death in the 2025 MBRRACE-UK report which looks at the care of 643 women who died during or up to one year after pregnancy in the UK and Ireland (2021-2023).
VTE prevention is key but it is also a challenge as there are different risk assessment tools available. This can contribute to inconsistent or incomplete use across specialities.
Patients can have overlapping risk factors which makes assessment difficult e.g. surgery, cancer, immobility, age, family history, pregnancy, weight changes. For younger patients, VTE risk
assessment may be overlooked despite risk factors such as oral contraceptives or smoking etc.
If an initial assessment is not carried out, it can be difficult to reassess risk if there is a change in clinical status.
Prophylaxis guidelines usually include mechanical and/or pharmacological options. If risk assessments are missed or incomplete or bleeding risks present concerns, this can result in inappropriate prophylaxis choices, incorrect doses as well as gaps or delays in prophylaxis.
Diagnostic challenges may be present in all patient groups as VTE symptoms can overlap with other conditions and pregnancy symptoms e.g. breathlessness, fatigue, leg pain and swelling.
Diagnostic tests and tools may have limitations depending on the patient cohort, availability of out of hours diagnostic imaging, balancing the radiation and contrast risks for pregnant patients and for those with renal failure.
Management
Compression stocking sizes may not be available for those at extremes of body weight and intermittent pneumatic compression devices may not be available or suitable.
Pharmacological anticoagulation choices may vary and considerations must be made depending on the treatment group. Other factors to consider are, for example, renal function, cancer, drug interactions, contraindications, dose adjustment, treatment durations, bleeding risk and monitoring.
Therapeutic choices remain limited in pregnancy as warfarin is teratogenic and DOACs have limited evidence of safety, therefore they are not recommended in pregnancy or breastfeeding. This leaves LMWH as the main option with unfractionated heparin (UFH) reserved for emergency use or in high-risk cases during labour and delivery. Education and planning for staff and patients regarding timing of doses around labour, delivery and anaesthesia is important to prevent bleeding or thrombosis.
Transitions of care
Risk can occur if there is no clear documentation in patient notes
and/or if communication is not effective between teams and patients; especially when patients move between settings and on discharge. As a result, missed doses, incorrect continuation/ stopping of anticoagulants, risk of VTE recurrence or bleeding can increase, poor adherence, and patients may not be followed-up.
Adherence to prophylaxis, especially on discharge, can be difficult to assess if follow-up is not scheduled.
Daily subcutaneous injections can be painful and intimidating for patients and this can impact compliance, particularly if LMWH is the only choice e.g. in pregnancy and postpartum.
Staffing and resources
Adequate staffing, resources, creation and maintenance of posts including succession planning, especially in specialised areas like haematology and VTE stewardship are essential components for safe provision and continuity of care. Not all Irish hospitals have a multidisciplinary VTE team to provide ownership or accountability for VTE-related services. This could potentially lead to delayed implementation and compliance with guidelines and national recommendations and therefore pose a risk for patient safety.
Staff shortages, loss of expertise if posts are not replaced and gaps in staff training and education can lead to missed assessments, delays in prophylaxis, incorrect dosing, contraindications and inappropriate treatment decisions. Challenges can also arise if there is limited time and staff experience with providing patient information, especially before discharge. Other challenges to consider are language, literacy and health literacy barriers.
Adequate pharmacy staffing is important as pharmacists play a critical role in optimising safe and effective anticoagulant use. They collaborate on guideline development, provide staff and patients with education, support accurate risk assessment and optimise prescribing and dosing (especially in high-risk groups).
At discharge, pharmacists help to ensure continuity of care through medication review, prevention of error and communication with community pharmacies and GPs. Their involvement in quality improvements, informatics and
audits further strengthens VTE safety protocols and reduces preventable harm.
Are there common misconceptions about VTE among staff or patients?
Although staff awareness of VTE in the NMH is good, misconceptions regarding VTE can still exist and can impact care.
Common ones are:
Those requiring surgery or having a C-section are at risk while young people are low-risk,
Anticoagulation must be avoided if there is a bleeding risk and in pregnancy/breastfeeding,
If the patient is mobile or once they are mobile post-surgery, they don’t need prophylaxis and
Risk stops at discharge.
Patients often link blood clots to long flights and older people, but may not be aware of other risk factors. Commonly patients are familiar with leg swelling and pain as symptoms but can attribute signs and symptoms like fatigue, swelling and breathlessness to pregnancy or other health conditions. Concerns regarding harm to the baby if taking medication are common.
VTE prevention and management is collaboration across a wide variety best outcomes. Doctors, nurses, midwives, diagnostic imaging teams, physiotherapists informatics, quality and safety teams play. Multidisciplinary teamwork with guidelines, reduces errors an improves be considered as part of the team and (‘Making Every Contact Count), leading adherence to treatment.
reduces errors an improves safety. Patients and their families should always be considered as part of the team and included in any decisions related to their care (‘Making Every Contact Count), leading to increased trust, understanding and adherence to treatment.
New prevention protocols and systemic changes most needed in Ireland to reduce VTE-related harm?
New prevention protocols and systemic changes related harm?
The National Clinical Programme for VTE (NCP-VTE) provides governance for the prevention, diagnosis, management and long term care of VTE in hospitals and community settings.
The National Clinical Programme for VTE (NCP diagnosis, management and long term care
In reality, clear guidelines with optimisation of education for staff and patients is important as VTE risk is multifactorial and clots can present silently or with mild symptoms. Due to the complexities of individual VTE risk and in order to balance clot risk and bleeding risk, assessment, prophylaxis and treatment should be individualised. Individualisation of care can also help maximise understanding and adherence especially at transitions of care.
The recent launch of the National Clinical Guideline Eve Protocol, named in memory of Eve Cleary framework for best practice in prevention, patient education
The recent launch of the National Clinical Guideline on Venous Thromboembolism (NCG-VTE) Eve Protocol, named in memory of Eve Cleary who tragically died due to VTE, provides a framework for best practice in prevention, assessment, diagnosis, treatment, recovery and patient education
Contributing to this guideline as part of the family representatives was a rewarding experience.
Contributing to this guideline as part of the multidisciplinary team, including patient and family representatives was a rewarding experience.
What role do multidisciplinary teams play in preventing and managing VTE?
VTE prevention and management is complex and requires clear communication and collaboration across a wide variety of disciplines and teams to ensure best practice and best outcomes. Doctors, nurses, midwives, haematologists, pharmacists, radiologists, diagnostic imaging teams, physiotherapists, occupational therapists, administration, informatics, quality and safety teams as well as, patients and families, all have roles to play. Multidisciplinary teamwork with shared responsibility improves compliance with guidelines,
National Clinical Guideline on Venous Thromboembolism (NCG-VTE) Eve Protocol
https://www2.healthservice.hse.ie/ files/534/
Ask the Expert: VTE
Systemic changes are needed to ensure the Eve’s Protocol is implemented nationwide to improve care and reduce VTE-related harm. Changes needed include:
Mandating the establishment of thromboprophylaxis policy and use of standardised VTE risk assessment tools at key time points in hospitals e.g. admission, post-surgery, postpartum and if the patient condition changes.
Investing in VTE stewardship roles (pharmacists, nurses/ midwives) and VTE multidisciplinary teams, including IT, in hospitals. Implementing change takes time. Therefore, investing in local champions and teams with protected time, resources and responsibility for oversight and compliance is essential for sustainability of service.
Launching National education and awareness campaigns for healthcare workers and staff.
Raise awareness of the signs and symptoms of clots, risk factors, prophylaxis and treatment options.
Provide plain language and consistent education, patient information leaflets and training materials to patients. Translations into other languages is hugely beneficial (e.g. the blood clot alert cards).
Provide education modules on VTE in all healthcare undergraduate courses
Strengthen standardised surveillance and audit locally and nationally.
Robust reporting identifies trends over time and allows targeted intervention
Without consistent data it is hard to identify areas of concern or track improvements.
Digitalising VTE risk assessments and tools. Provide resources to allow EHR integration of VTE risk assessments. Develop digital clinical decision support packages for safe prescribing and administration.
Progression of the Health Digital for Care Framework 2030 to improve care and
safety across services through introduction of the:
National Shared Care record and
Electronic Health Record availability and functionality in all hospital settings
Balancing our digital health footprint with the provision of safe healthcare while minimising climate impact.
The Dublin South East hospital group are at the forefront of implementation with many of the recommendations are already being acted upon in the hospitals within the group.
It has an established and active multidisciplinary VTE service review group with patient representation to highlight and discuss key priorities for patients.
Audit and feedback relating to VTE risk assessment and prophylaxis using an electronic VTE audit application is promoted and used to track and monitor trends in;
percentage of admitted patients with documented VTE risk assessment;
percentage of adherence to guidelines;
percentage of patients receiving appropriate prophylaxis.
The numbers of hospital acquired thromboses are also collated.
The introduction of the National Maternal and Newborn Clinical Management System (MNCMS), enhanced collaboration, standardization and safety in obstetric and neonatal care across the 5 sites that are currently live. The National meds team of informatics pharmacists in conjunction with clinical
pharmacists working in the live sites have helped to digitalise local VTE risk assessments. Clinical decision support tools and packages have been developed to enhance safe monitoring and prescribing of anticoagulation.
Three practical actions hospital teams can take right now to improve VTE care.
a. Prioritise VTE risk assessment completion (on paper or as part of an EHR) at all key time points e.g. admission, post-surgery, postpartum and if the patient condition changes
b. Establish clear links between VTE risk assessment and mechanical and/ or pharmacological prophylaxis. Include guidance for dose recommendations and treatment duration on the paper drug kardex or embedded with decision support and alerts/ triggers in the EHR for safety. Facilitate pharmacists and nurses/midwives in the regular review of VTE risk assessment completion and appropriate prescribing of prophylaxis.
c. Design and implement staff and patient education and awareness programs using patient information leaflets from the National Clinical Programme for VTE, the Irish Heart Foundation and World Thrombosis Day resources. Provide plain language and consistent education and training materials to patients at discharge relating to VTE risks, management and administration of medication at home. ‘Make Every Contact Count’ for better health, safety and chronic disease prevention.
Footnote: *including those who identify as women and all those who may not identify as female but share female biology and experience*
National clinical guideline on vte (ncg-vte): Supplementary appendix
Ask the Expert: Rheumatoid Arthritis
Living with Rheumatoid Arthritis in Ireland: A Health Psychologist’s Perspective
for Doctors and Nurses
Rheumatoid arthritis (RA) is often thought of as a disease of the joints, but for patients it is far more complex: a lifelong condition that touches every aspect of identity, work, relationships, and wellbeing. Alongside the physical burden of inflammation and pain, people in Ireland living with RA face the psychological weight of uncertainty, stigma, and navigating a stretched health system.
In this article, expert Aideen Stack, Health Psychologist (B.A.P., M.Sc., Pg.Dip.), explores how RA shapes lives beyond the clinic, the barriers created by the Irish healthcare context, and the practical steps clinicians and multidisciplinary teams can take to support patients’ mental health, adherence, and quality of life.
Aideen’s professional website is Whole Health Psychology and can be found at: wholehealthpsychology.ie
Rheumatoid arthritis (RA) is far more than just a disease of the joints. It is a chronic, systemic autoimmune condition that can reach into every aspect of a person’s life—family, friends, work, identity, and mental wellbeing. For clinicians, particularly doctors and nurses, it is important to recognise that alongside the biological processes of inflammation and damage, patients in Ireland maybe managing the psychological challenges of an RA diagnosis. Psychological challenges may include a grief process following a life changing diagnosis, uncertainty, fatigue, stigma, and the daily demands of navigating a complex health system. As a health psychologist, I want to explore how RA shapes people’s lives, how the Irish healthcare system can create unique challenges for patients, the issues and importance around adherence to medication, and what practical steps multidisciplinary teams can take to support RA patients’ shortand long-term quality of life.
The Psychological Impact of RA
The diagnosis of RA is often experienced as a major life event. Some patients feel an initial sense of relief at finally putting a name to their persistent pain and stiffness, but this relief can soon be overshadowed by a sense of confusion, loss and uncertainty. RA can feel like the beginning of a “before and after” narrative, where the previous identity—independent worker, parent, student, or caregiver—no longer seems manageable. Many patients describe mourning the loss of an identity and the shift to seeing themselves as a person with a chronic condition can
be challenging. For clinicians, recognising this grief as a normal response rather than pathology is essential; it can help validate the patient’s experience and foster the doctor – patient relationship.
The uncertainty of living with RA can also be difficult to come to terms with for patients. The unpredictable flare pattern means that patients may not reliably plan social events, holidays, or even day-to-day tasks. Cancelling on friends and family commitments may lead to guilt, frustration, and feelings of being a burden. This uncertainty can create a sense of anxiety worrying about when the next flare may be, and patients may become hypervigilant to bodily sensations, wondering whether each twinge signals the beginning of another flare. In this context, clear communication about early signs of a flare, and what to do should a flare happen, can help a person feel more confident in their ability to manage their condition. When patients are
involved in shared decision-making and provided with concrete flaremanagement plans, they may feel a sense of control in their life.
Pain and fatigue of living with RA can have a particularly detrimental effect on a person’s mental health. Persistent pain is not only physically taxing but also mentally draining, amplifying perceptions of threat in the body, hypervigilance to body changes and can lead to lower resilience in coping with life. Fatigue— often underestimated by those around the patient—is frequently described as the most debilitating aspect of RA. Fatigue can impact concentration, memory, and mood. These cognitive difficulties may effect relationships, the person’s ability to enjoy hobbies, run a household, or go to work or education. Furthermore, pain and fatigue can contribute to cycles of withdrawal, inactivity, and depression. Integrating psychological strategies—such as pacing activities, encouraging
good sleep hygiene, and connecting with a psychologist or therapist - into rheumatology care may be significantly beneficial to a patient.
Finally, the invisibility of RA as a condition poses its own challenges for a person. Patients often encounter scepticism from employers, colleagues, or even family members who assume that if someone looks “fine,” they cannot truly be in pain or struggling. This disbelief can push patients into social withdrawal and silence, or even avoid acknowledging their condition to themselves, throwing themselves into activities trying to appear “normal” yet further contributing to the likelihood of a flare or pain. For clinicians, simply acknowledging the “invisible load” of living with RA—the effort of planning around fatigue, enduring pain in silence, and negotiating stigma—can profoundly reduce patients’ sense of isolation.
Aideen Stack
Ask the Expert: Rheumatoid Arthritis
RA and the Irish Healthcare System
The Irish healthcare system may present specific structural challenges for people living with RA. Access to rheumatology services remains uneven across the country. According to the Irish Society for Rheumatology, consultant rheumatologists per capita in Ireland (one consultant rheumatologist per 125,000–200,000 population) is lower than in many other European countries (one per 80,000), and waiting lists for initial appointments can stretch into months, sometimes over a year. This delay means that patients may spend long periods in pain and uncertainty before receiving definitive diagnosis and treatment, which in turn heightens distress and risk of mental health difficulties.
Once under specialist care, patients typically engage with hospital-based rheumatology clinics, day wards for infusions, general practice for shared care, and community pharmacies for dispensing. Navigating this system can be tricky for some patients, and awareness of this aspect of care may be important for clinicians. Access to Biologic medication is free of charge but requires registration, approval, and coordination between hospital consultants and community pharmacies. While this scheme ensures financial protection for patients, the administrative complexity can be daunting, particularly for those already struggling with fatigue or cognitive difficulties.
Geography and location of the patient can also play role in treatment access and adherence. Patients living in rural areas may have to travel long distances to tertiary hospitals for infusions or specialist reviews, incurring travel costs and time off work. For those reliant on public transport, attending appointments can be a day-long ordeal. Weather events, such as heavy rain or snow, further disrupt access for rural patients. The unequal distribution of services means that a person’s postcode continues to shape their healthcare experience, and can add to the burden of stress for these patients.
Workforce shortages compound these issues. The number of clinical nurse specialists in rheumatology has grown in recent years according to Irish Society for Rheumatology, but the demand remains high. Access to allied health professionals such as
physiotherapists, occupational therapists, podiatrists, and psychologists can be limited or varied depending on the hospital. Many patients report being discharged from hospital clinics back to general practice with little access to community-based rheumatology supports.
Furthermore, employment matters can contribute to stress and uncertainty. Deciding whether to disclose RA to an employer involves weighing the potential benefits of accommodations against the risk of stigma or reduced career opportunities. Flexible hours, ergonomic adaptations, and phased return after flare can make an enormous difference, yet many patients lack guidance in navigating these conversations. Clinicians can provide vital advocacy by offering medical letters that describe functional limitations clearly and by signposting patients to resources such as Arthritis Ireland, which offers practical advice and peer support.
Quality of Life: Short- and Long-Term
In the short term, particularly in the first two years after diagnosis, patients often experience disruption of daily routines, anxiety about treatment regimens, and significant emotional adjustment. Initiating disease-modifying drugs, including biologics, introduces unfamiliar medical language and new tasks, such as managing injections or coordinating infusions. Fear of side effects, coupled with needle anxiety or difficulties with drug storage, can undermine confidence. At the same time, role renegotiation within families can create guilt or conflict, as patients struggle with asking for help or stepping back from responsibilities.
Over the long term, even with good disease control, the cumulative impact of RA on life trajectory is profound. The cycle of flares and remissions, the threat of disability, and the constant need to manage treatment routines can gradually erode career opportunities and social participation. Comorbidities, particularly cardiovascular disease and osteoporosis, further threaten health and independence. Life transitions such as pregnancy, parenting, menopause, and retirement are all influenced by the presence of RA and its treatments. Yet many patients also demonstrate resilience, reframing their identities around advocacy, peer support, or expertise in selfmanagement, particularly when
healthcare teams validate and support this growth.
The Importance of Adherence
Adherence to medication for a patient is less about willpower and much more related to beliefs, history of medication and context. Patients weigh perceived necessity against concerns: “Do I really need this drug?” versus “What might it do to me?” Social influences matter as well—stories from peers, social media, or family members often shape behaviours. If a patient sees RA as simply a problem of “bad joints,” the rationale for immune-modulating treatment such a biologics is weak. Some patients may dread injections or find it difficult to arrange travel for hospital infusions. Others struggle with storing cold-chain medicines safely in crowded homes. Patients who experience a flare while on treatment may interpret this as failure and discontinue their regimen prematurely. Here, reframing is crucial: flares are not evidence of futility but data points that guide treatment refinement.
The importance of clinicians explaining the underlying immune processes driving inflammation and clear communication about treatment works and the consequences of poor adherence, is paramount to ensuring adherence.
Practical Support for RA
Simple and practical strategies for embedding support into routine Irish rheumatology care can go a long way in helping RA patients. Validating the patient’s lived experience and seeing life from their perspective helps build compassionate care. When patients feel believed and understood, they are more open to education about the condition and information about treatment.
Building adherence can be through encouraging small, concrete changes, whilst understanding the patient’s lived experience and barriers they may be facing that impact adherence. Encouraging patients to link medication to existing routines, to use reminders, or to prepare injection kits reduces the cognitive burden of treatment. Needle anxiety can be addressed through gradual exposure, paced breathing, or numbing techniques. Motivational interviewing—asking about both the benefits and the fears of treatment—helps patients articulate their own reasons for adherence.
Addressing fatigue and sleep disturbance is also vital. Teaching pacing, emphasising good sleep hygiene practices, and energy management helps patients avoid the boom-and-bust cycle that can exacerbate symptoms.. Psychological interventions, whether through brief CBT, acceptance and commitment therapy, or mindfulness approaches, can support emotional wellbeing and resilience in patients.
In Ireland, access to dedicated psychological services for people with RA remains limited, and patients who are struggling may have to rely on overstretched community mental health services. Expanding psychology provision within rheumatology clinics would be a cost-effective way of improving adherence, reducing healthcare utilisation, and enhancing quality of life. In the meantime, doctors and nurses can integrate basic psychological strategies—validation, motivational interviewing, practical problemsolving—into routine consultations.
Conclusion
Rheumatoid arthritis is never only about joints. It is about disrupted identities, moving through grief of diagnosis, and the struggle for agency in the face of an unpredictable illness. In Ireland, systemic challenges—long waiting lists, geographical inequities, workforce shortages, and administrative burdens—intensify the psychological load of the disease. Yet there is also promise: biologic therapies transform outcomes, and organisations such as Arthritis Ireland provide vital peer support.
For clinicians, the task is to see the whole person, not just the swollen joints. This means validating grief and uncertainty, supporting adherence through practical and psychological strategies, and smoothing the patient’s journey through the healthcare system. It means integrating brief psychological tools into everyday practice and advocating for greater access to dedicated psychology within rheumatology services.
When care is psychologically informed and systemically supportive, adherence improves not because patients are pressured but because treatment fits their lives. The aim should be to ensure that patients with RA do not merely cope but live fully and meaningfully, on their own terms, with the support of a compassionate, coordinated healthcare system.
Ask the Expert: Diabetes Diabetes in Pregnancy
We spoke with Ciara Coveney, Advanced Midwife Practitioner in Diabetes in Pregnancy, about the realities of hospital care, common misconceptions, and the opportunities ahead for Irish maternity services.
Ciara Coveney works as an Advanced Midwife Practitioner specialising in Diabetes in Pregnancy. Her decision to enter this field stemmed from seeing first-hand how tailored, expert-led care can transform outcomes for both women and their babies.
“Pregnancy is already a huge journey,” she explains. “When diabetes is added, it brings extra challenges that can feel overwhelming. What drew me in was the opportunity to combine advanced clinical decision-making with the heart of midwifery — supporting women, giving them clear information, and helping them feel more confident. That blend of specialist expertise and personalised support can truly change outcomes.”
Different challenges in Type 1 and Type 2 diabetes
In hospital practice, the challenges of supporting women with Type 1 and Type 2 diabetes diverge significantly.
For Type 1 diabetes, the complexity lies in the constant adjustments required. “Insulin sensitivity shifts dynamically during pregnancy,” Ciara says, “so frequent dose changes are essential. Technology such as hybrid closed-loop pumps and continuous glucose monitors (CGMs) help enormously, but they still require extensive expertise to interpret and manage safely.”
Women with Type 1 diabetes may also present with advanced comorbidities such as renal or retinal disease, hypertension, or vascular complications, requiring close collaboration across specialties. Some will also need input from maternal–fetal medicine experts, something Ciara feels fortunate to have access through the specialist obstetricians on the diabetes in pregnancy team.
For Type 2 diabetes, the picture is often different. Many women enter pregnancy with limited prior engagement with specialist teams or pre-conception care. “They may be on multiple agents not suitable for pregnancy, requiring a rapid transition to safer alternatives. Add to this the high burden of comorbidities such as obesity and hypertension, and it can feel overwhelming for women early on in pregnancy,” Ciara notes. Encouragingly, she highlights the role of chronic disease hubs in creating better pathways and earlier specialist input for these women.
Day-to-day realities for women
Regardless of type, diabetes in pregnancy means frequent monitoring, multiple hospital visits, and ongoing adjustments to care. “For women who are used to independently managing their diabetes, the intensity of hospital-based care can feel disempowering,” Ciara says.
Technology plays a role in alleviating some of this burden, particularly CGMs and pumps that reduce the need for constant finger-pricking or manual dose adjustments. “We hope that in the near future, technology will be made more widely available to women with Type 2 diabetes too,” she adds.
The team works hard to streamline care and ensure women feel listened to and involved in decisions. “Pregnancy changes the landscape of diabetes care,” Ciara reflects. “Our job is not just to monitor closely, but to make sure women still feel empowered and supported.”
Misconceptions that persist Ciara regularly encounters myths that can undermine care.
• That all types of diabetes are essentially the same. “In reality, Type 1, Type 2, and gestational diabetes require very different approaches,” she stresses.
• That technology alone is the answer. “Insulin pumps and CGMs are fantastic tools, but they don’t solve everything — they still need education, expertise, and active engagement from women and staff alike.”
• That poor control is simply a matter of lifestyle. “There’s stigma attached to diabetes, and assumptions about personal choices. But in pregnancy, hormonal changes make management uniquely complex. Women are often working incredibly hard, and part of my role is to challenge those misconceptions and make sure women feel supported, not judged.”
“CGMs provide real-time feedback, reducing the burden of fingerpricks and giving us a much clearer picture of glucose patterns,” she explains. “Insulin pumps and hybrid closed-loop systems allow for more precise insulin delivery and adapt to the rapid changes that happen in pregnancy. They play a vital role
Ciara
Coveney
in maintaining the tight glycaemic control needed for fetal growth and development.”
Digital platforms that share data remotely are also changing how maternity teams work. “Women can upload glucose readings from home, and we can adjust treatment without needing an in-person visit. That’s a huge step forward in reducing the burden of frequent hospital appointments.”
This shift towards proactive, rather than reactive, care means complications can be avoided, interventions made earlier, and women feel more confident day to day.
The most exciting advances, Ciara says, are in technology. Hybrid closed-loop systems are showing strong evidence for safe use in pregnancy, helping to achieve tighter glucose control while reducing hypoglycaemia risk.
Another important area is screening and prevention of complications. Retinal screening has been strengthened, with a pregnancyspecific pathway launched by Ireland’s Diabetic RetinaScreen programme. “The ability to detect and intervene earlier in diabetic retinopathy is a huge step forward in protecting women’s long-term health,” she notes.
“What excites me most,” Ciara adds, “is that these advances aren’t just about hitting glucose targets — they’re about supporting women to feel safer, more confident, and less burdened during such a critical time.”
The power of the multidisciplinary team Ciara emphasises that diabetes in pregnancy is never just about glucose control. “It impacts midwifery, obstetrics, fetal growth, mental health, and long-term maternal wellbeing,” she explains.
“The strength of the multidisciplinary approach is that it reduces silos, gives women confidence through joined-up thinking, and improves both maternal and neonatal outcomes.”
Building a stronger system in Ireland
For Ciara, the priorities are clear: workforce, technology, and integration.
• Workforce: “We need more specialist staff across all disciplines, not just in tertiary centres, so every woman has equitable access to expertise.”
• Technology: Expanding CGMs, pumps, and digital platforms to become standard in pregnancy care.
• Integration: Stronger pathways between maternity hospitals, GPs, and community teams. She is currently contributing to the update of the national guideline for diabetes in pregnancy, being written with multidisciplinary stakeholders. A key aim is to align with the Diabetes in Pregnancy: A Model of Care for Ireland launched in February 2024.
Three steps hospitals can take now
Ciara identifies three immediate actions maternity hospitals can take to improve care for women with diabetes in pregnancy:
1. Strengthen multidisciplinary teams with adequate specialist midwifery, obstetric, endocrinology, and dietetic support.
2. Embed technology into routine care, making CGMs and datasharing platforms standard for women with pre-existing diabetes.
3. Improve integration with GPs and community teams to prevent women from falling through the cracks.
“These are achievable steps,” Ciara says. “While we work towards national implementation of guidelines and models of care, hospitals can act now to make a difference.”
Fresenius Kabi is introducing Azacitidine
Kabi
25 mg/ml powder for suspension for injection (azacitidine)
Fresenius Kabi
Azacitidine Kabi is indicated for the treatment of adult patients who are not eligible for haematopoietic stem cell transplantation (HSCT) with: 1
• Intermediate-2 and high-risk myelodysplastic syndromes (MDS) according to the International Prognostic Scoring System (IPSS),
• Chronic myelomonocytic leukemia (CMML) with 10-29% marrow blasts without myeloproliferative disorder
• Acute myeloid leukemia (AML) with 20-30% blasts and multi-lineage dysplasia, according to World Health Organization (WHO) classification,• AML with > 30% marrow blasts according to the WHO classification.
* Please refer to the abbreviated prescribing information overleaf forfull details on the indications
Azacitidine Kabi
Abbreviated prescribing information
PRESCRIBING INFORMATION – Azacitidine Kabi 25 mg/mL powder for suspension for injection. Consult the Summary of Product Characteristics (SmPC) for full information. Additional information is available on request. Active ingredients: Each vial contains 100 mg azacitidine. After reconstitution, each mL of suspension contains 25 mg azacitidine Indications: Treatment of adult patients who are not eligible for haematopoietic stem cell transplantation (HSCT) with: Intermediate-2 and high-risk myelodysplastic syndromes (MDS) according to the international prognostic scoring system (IPSS), chronic myelomonocytic leukaemia (CMML) with 10-29% marrow blasts without myeloproliferative disorder, acute myeloid leukaemia (AML) with 20-30% blasts and multi-lineage dysplasia, according to World Health Organisation (WHO) classification, AML with > 30% marrow blasts according to the WHO classification. Dosage and administration: Initiate and monitor under supervision of a physician experienced in the use of chemotherapeutic agents. Patients should be premedicated with anti-emetics for nausea and vomiting. Recommended starting dose for the first treatment cycle, for all patients regardless of baseline haematology laboratory values, is 75 mg/m2 of body surface area, injected subcutaneously, daily for 7 days, followed by rest period of 21 days (28-day treatment cycle). Recommended that patients be treated for a minimum of 6 cycles. Treatment should be continued for as long as the patient continues to benefit or until disease progression. Monitor for haematologic response/toxicity and renal toxicities (see section 4.4 of SmPC for further guidance) a delay in starting next cycle or dose reduction may be necessary. Should not be used interchangeably with oral azacitidine. Dose and schedule recommendations for oral azacitidine differ to injectable azacitidine – verify medicinal product name, dose and administration route. Determine liver function tests, serum creatinine and serum bicarbonate prior to therapy initiation and each treatment cycle. Perform complete blood counts prior to therapy initiation and as needed to monitor response and toxicity, but at a minimum, prior to each treatment cycle. Elderly patients - No specific dose adjustments recommended. May be useful to monitor renal function. Renal impairment - Can be administered to patients with renal impairment without initial dose adjustment. If unexplained reductions in serum bicarbonate levels to <20 mmol/L, reduce dose by 50% on next cycle. If unexplained elevations in serum creatinine or blood urea nitrogen (BUN) to ≥ 2-fold above baseline values and above upper limit of normal (ULN) occur, delay next cycle until values return to normal or baseline and reduce dose by 50% on next treatment cycle. Hepatic impairment - No formal studies conducted in patients with hepatic impairment. Carefully monitor patients with severe hepatic organ impairment for adverse events. No specific modification to starting dose recommended for patients with hepatic impairment prior to starting treatment; subsequent dose modifications should be based on haematology laboratory values. Contraindicated in patients with advanced malignant hepatic tumours. Paediatric population - Safety and efficacy in children aged 0-17 years not yet been established. Currently available data described in sections 4.8, 5.1 and 5.2 of SmPC but no recommendation on posology. Method of administration - Inject reconstituted Azacitidine Kabi subcutaneously into upper arm, thigh or abdomen. Rotate injection sites. Give new injections at least 2.5cm from previous site and never into areas where site is tender, bruised, red, or hardened. Suspension should not be filtered after reconstitution. For instructions on reconstitution of the medicinal product before administration, see section 6.6 of SmPC Contraindications: Hypersensitivity to active substance or to any of the excipients, advanced malignant hepatic tumours, breast-feeding. Special warnings and precautions for use: Haematological toxicity Azacitidine treatment is associated with anaemia, neutropenia and thrombocytopenia, particularly during first 2 cycles. Perform complete blood counts as needed to monitor response and toxicity, but at least prior to each treatment cycle After administration of recommended dose for first cycle, reduce dose for subsequent cycles or delay administration based on nadir counts and haematological response. Advise patients to promptly report febrile episodes. Hepatic Impairment Patients and physicians also advised to be observant for signs and symptoms of bleeding. Patients with extensive tumour burden due to metastatic disease reported to experience progressive hepatic coma and death during azacitidine treatment, especially where baseline serum albumin <30g/L. Azacitidine is contraindicated in patients with advanced malignant hepatic tumours Renal impairment Renal abnormalities ranging from elevated serum creatinine to renal failure and death reported in patients treated with intravenous azacitidine in combination with other chemotherapeutic agents. Renal tubular acidosis, defined
as a fall in serum bicarbonate to <20 mmol/L in association with an alkaline urine and hypokalaemia (serum potassium < 3 mmol/L) developed in 5 subjects with chronic myelogenous leukaemia (CML) treated with azacitidine and etoposide. If unexplained reductions in serum bicarbonate (< 20 mmol/L) or elevations of serum creatinine or BUN occur, dose should be reduced or administration delayed. Advise patients to report oliguria and anuria to the health care provider immediately. Closely monitor patients with renal impairment for toxicity since azacitidine and/ or its metabolites are primarily excreted by the kidney. Laboratory tests Determine liver function tests, serum creatinine and serum bicarbonate, prior to therapy initiation and each treatment cycle. Perform complete blood counts prior to therapy initiation and as needed to monitor response and toxicity, but at a minimum, prior to each treatment cycle Cardiac and pulmonary disease Safety and efficacy of azacitidine in patients with history of severe congestive heart failure, clinically unstable cardiac disease or pulmonary disease has not been established. Recent data from a clinical study in patients with a known history of cardiovascular or pulmonary disease showed a significantly increased incidence of cardiac events with azacitidine; exercise caution when prescribing azacitidine to these patients. Consider cardiopulmonary assessment before and during treatment. Necrotising fasciitis, including fatal cases, reported in azacitidine treated patients. Therapy should be discontinued if necrotising fasciitis develops and appropriate treatment promptly initiated. Patients with high tumour burden prior to treatment are at risk of tumour lysis syndrome; monitor closely and take appropriate precautions. Cases of differentiation syndrome (also known as retinoic acid syndrome) reported in patients receiving injectable azacitidine. Consider treatment with high-dose IV corticosteroids and haemodynamic monitoring at first onset of symptoms or signs suggestive of differentiation syndrome. Differentiation syndrome may be fatal. Please see SmPC for further details. Consider temporary discontinuation of injectable azacitidine until resolution of symptoms and if resumed, caution advised. Caution recommended when driving or operating machines. Fertility, pregnancy and lactation: Women of childbearing potential have to use effective contraception during and for at least 6 months after treatment. Men should be advised not to father a child while receiving treatment and must use effective contraception during and for at least 3 months after treatment. Due to the potential serious adverse reactions in the nursing child, breast-feeding is contraindicated. Undesirable effects: Very common (≥1/10) – Pneumonia (bacterial, viral, fungal), nasopharyngitis, febrile neutropenia, neutropenia, leukopenia, thrombocytopenia, anaemia, anorexia, decreased appetite, hypokalemia, insomnia, dizziness, headache, dyspnoea, epistaxis, diarrhoea, vomiting, constipation, nausea, abdominal pain, petechiae, pruritus, rash, ecchymosis, arthralgia, musculoskeletal pain, pyrexia, fatigue, asthenia, chest pain, injection site erythema, injection site pain, injection site reaction. Common (≥ 1/100 to < 1/10) – Sepsis, neutropenic sepsis, respiratory tract infection, urinary tract infection, cellulitis, diverticulitis, oral fungal infection, sinusitis, pharyngitis, rhinitis, herpes simplex, skin infection, pancytopenia, bone marrow failure, dehydration, confusional state, anxiety, intracranial haemorrhage, syncope, somnolence, lethargy, eye haemorrhage, conjunctival haemorrhage, pericardial effusion, hypotension, hypertension, orthostatic hypotension, haematoma, pleural effusion, dyspnoea exertional, pharyngolaryngeal pain, gastrointestinal haemorrhage, haemorrhoidal haemorrhage, stomatitis, gingival bleeding, dyspepsia, purpura, alopecia, urticaria, erythema, rash macular, muscle spasms, myalgia, renal failure, haematuria, elevated serum creatinine, bruising, haematoma, induration, rash, pruritus, inflammation, discoloration, nodule and haemorrhage at injection site, malaise, chills, catheter site haemorrhage. Uncommon (≥1/1,000 to <1/100) – Hypersensitivity reactions, pericarditis, hepatic failure, progressive hepatic coma, acute febrile neutrophilic dermatosis, pyoderma gangrenosum, renal tubular acidosis. Rare (≥1/10,000 to <1/1,000) – Tumour- lysis syndrome, interstitial lung disease, injection site necrosis. Frequency not known – Necrotising fasciitis, differentiation syndrome, cutaneous vasculitis. Legal category: POM Marketing authorisation number: EU/1/23/1777/001 Marketing Authorisation Holder: Fresenius Kabi Deutschland GmbH, Else-Kroener-Straβe-1, Bad Homburg 61352, Germany. Further information: Available from Fresenius Kabi Limited, Cestrian Court, Eastgate Way, Manor Park, Runcorn, Cheshire, WA7 1NT. Tel +44 (0)1928 533 533. Date of preparation: July 2025 IE--2500022
Adverse events should be reported. Reporting forms and information can be found at: https://www.hpra.ie/report-an-issue
Adverse events should also be reported to Fresenius Kabi Limited, Cestrian Court, Eastgate Way, Manor Park, Runcorn, Cheshire, WA7 1NT Tel +44 (0)1928 533 533.
Fresenius Kabi Limited
Fresenius Kabi Ireland
Unit 3B Fingal Bay, Balbriggan, Co. Dublin, Ireland
Website: www.fresenius-kabi.com/ie/
Email: FK-enquiries.ireland@fresenius-kabi.com
Phone: +353 (0)1 841 3030
Job Code::IE--2500025
Date of Preparation: August 2025
Ask the Expert: Blood Cancer
Genomics, Myeloma, and the Future of Blood Cancer Care in Ireland
Blood cancers such as leukaemia, lymphoma, and multiple myeloma remain some of the most challenging diseases in modern medicine. Advances in genetics and immunotherapy are transforming how these conditions are understood and treated — yet Ireland still faces significant gaps in diagnostics, access, and awareness.
In this edition of Ask the Expert, we speak with Dr Róisín McAvera, Clinical Scientist at the Royal College of Surgeons in Ireland (RCSI) and Beaumont Hospital, Dublin. Her work focuses on bringing genomic testing into routine care for blood cancers, with a particular emphasis on multiple myeloma.
A scientist at the crossroads of research and clinical care
Dr McAvera’s current role sits at the intersection of laboratory science and clinical practice. Working with the multiple myeloma research group led by Professor Siobhan Glavey, she implements new genomic tests for blood cancers, particularly myeloma.
“Day to day, I receive samples from myeloma patients across Ireland and carry out genomic tests to determine whether their disease is high-risk or standardrisk. This distinction is critical because it can influence treatment decisions,” she explains.
Much of her work focuses on transitioning assays developed in research settings into routine clinical practice. That means rigorous validation of both the testing process and the reporting of results to meet clinical standards. “It’s about ensuring that cutting-edge science translates
into safe, reliable tools that can be used in everyday patient care.”
A calling sparked in Belfast
Her path into haematology began during her Biomedical Science degree at Queen’s University Belfast. “I quickly discovered how much I enjoyed haematology,” she recalls. That passion deepened during her PhD at Queen’s, where she focused on multiple myeloma but was also exposed to research across a wide range of blood cancers.
Working with the charity Leukaemia & Lymphoma Northern Ireland gave her perspective beyond the lab bench. “Meeting patients and families affected by blood cancers was hugely inspiring. Their experiences motivated me to continue in this field.”
After completing her doctorate, Dr McAvera moved to Dublin to focus on multiple myeloma research, a path that has shaped her clinical and scientific career ever since
Dr Róisín McAvera
Filling the gaps in Ireland’s genomic landscape
One of the key contributions of McAvera’s role is helping to build a clearer picture of the genetic landscape of multiple myeloma in Ireland.
“Genomic testing for myeloma is not as widely available here as it is in other countries. That means patients with high-risk disease aren’t always identified early, and they may not receive the more intensive treatments they need,” she explains.
By expanding access to these tests, the goal is to ensure patients are managed more precisely and effectively. “In the longer term, the data we gather will also help researchers identify new therapeutic targets and inform the next generation of treatments.”
Encouragingly, she notes, change is underway. “We’re seeing genomic testing expand across Irish hospitals for most blood cancers, with significant progress already at Beaumont Hospital and St James’s Hospital in Dublin.”
Challenges in haematology today
From her perspective as a scientist, one of the biggest challenges in Irish haematology is the limited routine use of genomic profiling. “Compared with other countries, far fewer genetic tests are carried out here. Many still have to be sent abroad, which creates long turnaround times. Patients often begin treatment before we fully understand their disease at the molecular level.”
This lag can have major consequences. High-risk patients might not be identified in time, and opportunities for more targeted treatment are missed. However, Dr McAvera remains optimistic. “The trajectory is positive. Genomic testing is expanding, and there’s a clear recognition of its importance.”
“By introducing genomic tests, we can identify high-risk myeloma patients earlier and tailor treatment to improve their outcomes.”
“Multidisciplinary teams ensure blood cancer care is never just about one test or one doctor — it’s about combining expertise for the best possible outcome.”
Different diseases, different treatments
Although grouped together as “blood cancers,” leukaemia, lymphoma, and myeloma are biologically distinct, and their treatments reflect those differences.
• Leukaemia affects blood and bone marrow. Treatments may include chemotherapy, targeted drugs such as tyrosine kinase inhibitors, immunotherapies including CAR-T, and stem cell transplantation in high-risk or relapsed cases.
• Lymphoma arises in the lymphatic system and is typically treated with combinations of chemotherapy, immunotherapy (monoclonal antibodies), radiotherapy, or in resistant cases, stem cell transplant or CAR-T therapy.
• Multiple myeloma primarily affects the bone marrow. While considered incurable, it can be controlled with a combination of proteasome inhibitors, immunomodulatory drugs, and monoclonal antibodies. Many patients also undergo high-dose chemotherapy with autologous stem cell transplant, alongside supportive care for bone, kidney, and immune complications.
“Each blood cancer type progresses differently and responds differently to therapy,” Dr McAvera notes. “Understanding those nuances is essential.”
Misconceptions about blood cancers
Misunderstandings persist — both among patients and even some healthcare professionals outside haematology.
“One common misconception is that ‘blood cancer’ is a single
disease. Most people know about leukaemia and lymphoma, but few have heard of multiple myeloma,” she says.
In reality, the picture is far more complex:
• Four main types of leukaemia (with further rarer forms).
• More than 70–90 subtypes of lymphoma, under Hodgkin and non-Hodgkin categories.
• Myeloma, distinct from “melanoma” (a skin cancer), which is often confused by name alone.
“Because of this, we’re working hard to improve awareness of multiple myeloma in Ireland. Our research group has produced a patient information leaflet, and the newly formed Irish Multiple Myeloma Society is advocating for patients nationally.”
Advances shaping personalised treatment
Among the many innovations in blood cancer care, Dr McAvera is particularly enthusiastic about minimal residual disease (MRD) testing.
“MRD refers to very low levels of cancer cells that remain even after treatment appears successful. Its presence strongly predicts relapse risk. What’s exciting is that MRD testing is now used more routinely to gauge treatment depth and guide intensity. It’s helping us tailor therapies more precisely to each patient.”
For myeloma especially, the growing emphasis on achieving MRD negativity marks a shift toward more personalised care, where treatments are refined based on each patient’s molecular response.
CAR-T, targeted drugs, and the next frontier
Few developments have generated as much excitement as CAR-T cell therapy. Ireland’s first CAR-T treatment centre opened at St James’s Hospital in 2021, offering hope to patients with otherwise untreatable lymphomas and leukaemias.
“CAR-T therapy has shown remarkable success in relapsed or refractory disease. For patients who had no options left, it offers the possibility of long-lasting remission. Availability for multiple myeloma is anticipated in 2026, which will be transformative.”
Alongside CAR-T, targeted drugs are reshaping therapy. “The move towards tailoring treatment based on a cancer’s genetic features means we can design far more personalised strategies. Together, CAR-T and targeted drugs represent a new era of blood cancer care.”
What’s next in blood cancer research?
Looking ahead, Dr McAvera sees cell-based immunotherapies as the most exciting frontier.
“CAR-T has already changed the landscape, but it’s just the beginning. The challenge now is to expand its use, improve safety, and make it more widely accessible.”
One particularly promising area is NK (natural killer) cell therapy. Unlike CAR-T, NK therapies can be developed as “off-the-shelf” products, sourced from donors or stem cells. “That means they could be delivered more quickly and at lower cost. Early trials suggest they may be effective with fewer side effects. In the next five years, NK and other cell-based therapies could significantly change how we treat blood cancers.”
Genomic profiling will underpin these advances. “As we learn more about the molecular landscape of each cancer, we’ll be able to match patients to therapies more precisely — improving both outcomes and quality of life.”
The importance of multidisciplinary teamwork
Blood cancers are complex, and no single discipline can manage them alone. For Dr McAvera, multidisciplinary teamwork is essential.
“The lab provides key insights — genetic and molecular results — but these only make sense when combined with clinical findings, imaging, and the patient’s overall circumstances. Multidisciplinary meetings bring haematologists, oncologists, nurses, pharmacists, and scientists like myself together to make evidence-based, individualised treatment plans. That collaboration is vital for ensuring patients get the best possible outcome.”
Conclusion
From genomic testing to cuttingedge immunotherapies, blood cancer care is entering a new era. Yet challenges remain: limited genomic profiling, long turnaround times, and gaps in awareness mean Ireland still has progress to make.
For Dr Róisín McAvera, the task ahead is clear. “By embedding genomic testing into routine practice, expanding access to advanced therapies, and strengthening multidisciplinary collaboration, we can ensure patients with blood cancers in Ireland are not only treated but treated with precision, compassion, and hope.”
Almost 400,000 Units of Illegal Medicines
The Health Products Regulatory Authority (HPRA) has reported that 382,395 dosage units* of falsified and other illegal medicines were detained between January and June 2025. Recent detentions include sedatives, anabolic steroids, erectile dysfunction medicines, and more than 10,000 unauthorised GLP-1 patches claiming to contain semaglutide or tirzepatide. The HPRA is reminding the public today that purchasing prescription medicines from unregulated sources means you can't be sure what you're getting. These products may be unsafe, ineffective, or fake—and could seriously harm your health.
• Sedative medicines – 114,916 units detained (65,913 units in H2 2024)
• Anabolic Steroids – 62,751 units detained (42,981 units in H2 2024)
• Erectile dysfunction medicines – 60,184 units detained (46,658 units detained in H2 2024)
• GLP-1 products – 11,350 units detained (716 units detained in H2 2024)
• Analgesics – 17,454 units detained (17,074 units detained in H2 2024)
A total of 11,350 GLP-1 type medicines were detained including products promoted as containing semaglutide, liraglutide or tirzepatide. Authorised GLP-1
In the first six months of 2025, the most significant categories of illegal products detained included sedatives (30%), anabolic steroids (16%), erectile dysfunction medicines (16%), GLP-1 products, (6%), and analgesics (5%). The breakdown, with comparisons to the previous six-month period (Jul-Dec 2024), is as follows:
prescription-only medicines are intended for specific medical purposes such as diabetes or weight management under certain conditions. While 533 of the detained products included unauthorised tablets, pens and vials containing powder or clear liquid, the HPRA also detained a further 10,817 transdermal delivery microneedle patches. It is claimed these patches contain semaglutide or tirzepatide. The online promotion of these unauthorised products, an emerging trend identified in early 2025, make claims as to HPRA approval as well as endorsement from national charities, hospitals and individual healthcare professionals.
As part of its enforcement remit, the HPRA continues to monitor and disrupt online activity promoting unapproved medicines, medical devices, and cosmetics.
Gráinne Power, Director of Compliance at the HPRA,
Landmark New Hospital begins Opening
Bon Secours Health System welcomed its first patients on Monday 15th September, as its new ¤213 million stateof-the-art private hospital in Ballysimon, Limerick officially opened its doors. This landmark development, the first new acute hospital built in Ireland in nearly two decades, is set to transform healthcare in the region.
The new hospital represents one of the largest healthcare investments ever made in the region. When fully operational, it will significantly boost healthcare capacity while also providing a major economic and employment lift for the region and local communities.
The phased opening begins with the relocation of the first set of services, including the hospital’s
new cardiac catheterisation laboratory, which is the first such private cath lab in Limerick and the wider Mid-West. In coming weeks, the hospital will expand further, relocating additional services including surgery and related specialties.
In the months ahead, the hospital will also broaden access to a wide range of specialties including
highlighted the ongoing detentions of illegal and unauthorised medicines and emphasised the serious risks they pose to the public.
Ms Power stressed that “prescription medicines obtained online or from unregulated sources may be counterfeit, falsified or contaminated. These factors pose a serious threat to the health of anyone who uses them. The HPRA strongly advises the public to safeguard their health by only using prescription medicines under the guidance of a qualified healthcare professional and by sourcing products authorised for the Irish market from a registered pharmacy. We urge anyone who has purchased prescription medicines from unauthorised sources to stop using them immediately and seek advice from a healthcare professional if they have any concerns.”
cardiology, respiratory medicine, neurology, ophthalmology, dermatology and advanced diagnostic imaging.
Alan Sharp, Group Chief Executive Officer of Bon Secours Health System, said, “The opening of the Bon Secours Hospital Limerick marks yet another proud milestone for our organisation and for healthcare in Ireland. This ¤213 million investment reflects our long-term commitment to expand access to high-quality care, supporting medical innovation and creating meaningful employment opportunities in the Mid-West. This new hospital embodies our mission to bring world-class, compassionate healthcare to the communities we serve.”
Jason Kenny, CEO of Bon Secours Hospital Limerick, added, “This is a historic day for Limerick and the Mid-West as we welcome our very first patients to this world-class facility. Our investment represents a major commitment to both patients and the community. From day one, patients will benefit from access to cutting-edge technology and expert care. This hospital will not only help transform healthcare delivery, but it will also create strong and sustainable career opportunities for hundreds of healthcare professionals in the region.’
EUROPEAN COMMISSION AUTHORISES TWICE-YEARLY LENACAPAVIR FOR HIV PREVENTION
Gilead Sciences, Inc. (Nasdaq: GILD) has announced that the European Commission (EC) has granted marketing authorisation for lenacapavir for PrEP (under the brand name Yeytuo®)—the company’s twice-yearly injectable HIV-1 capsid inhibitor—for use in combination with safer sex practices for pre-exposure prophylaxis (PrEP) to reduce the risk of sexually acquired HIV-1 in adults and adolescents with increased HIV-1 acquisition risk, who weigh at least 35kg. Initiation of lenacapavir requires 2 days of oral tablets at the time of the first injection. Lenacapavir for PrEP is licensed for use in the European Union’s 27 member states, as well as Norway, Iceland and Liechtenstein.
The marketing authorisation application (MAA) was reviewed under an accelerated timeline based on the assessment by the European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) that twice-yearly lenacapavir for PrEP is a product of major interest for public health. In July, the CHMP adopted a positive opinion recommending lenacapavir for PrEP for EC authorisation.
The EC authorisation follows authorisation by the U.S. Food and Drug Administration (FDA) in June, as well as the issuance of guidelines by the World Health Organisation (WHO) in July that recommended twice-yearly lenacapavir as an additional PrEP option for HIV prevention.
EC authorisation of lenacapavir for PrEP is supported by efficacy and safety data from two Phase 3 trials
The EC authorisation of lenacapavir for PrEP was supported by data from the Phase 3 PURPOSE 1 and PURPOSE 2 trials conducted by Gilead. In the PURPOSE 1 trial (NCT04994509), data at the primary analysis showed that administration of twice-yearly subcutaneous lenacapavir led to zero HIV infections among 2,134 participants, 100% reduction in HIV infections and superiority of prevention of HIV infections when compared with once-daily oral emtricitabine 200mg and tenofovir disoproxil fumarate 300mg(F/TDF) in cisgender women in sub-Saharan Africa. In the PURPOSE 2 trial (NCT04925752), at the primary analysis there were two HIV infections among
2,179 participants in the twiceyearly subcutaneous lenacapavir group, demonstrating 99.9% of participants did not acquire HIV infection and superiority of prevention of HIV infections when compared with once-daily oral F/TDF among a broad and geographically diverse range of cisgender men and gender-diverse people. In both trials, lenacapavir demonstrated superiority of prevention of HIV infections when compared with background HIV incidence and was generally well-tolerated, with the most common adverse reactions in PURPOSE 1 and PURPOSE 2 being injection site reactions (71% and 85% respectively), almost all of which were mild or moderate in intensity. Data from both trials were published in The New England Journal of Medicine.
HSE APPROVES
MIRIKIZUMAB FOR THE TREATMENT OF ELIGIBLE ADULTS WITH MODERATELY TO SEVERELY ACTIVE ULCERATIVE COLITIS
Eli Lilly and Company have announced that the HSE has approved mirikizumab for the treatment of adult patients who have had moderately to severely active Ulcerative Colitis (UC) who had inadequate response with, lost response to, or were intolerant to either conventional therapy or a biologic treatment. Reimbursement is restricted to use as a subsequent line of therapy following treatment with a lowercost biologic therapy.
“This decision means mirikizumab will now be made available in Ireland for the treatment of adults with moderate to severe Ulcerative Colitis. Ulcerative Colitis is a chronic, relapsing inflammatory disorder affecting the large intestine. It is characterised by symptoms of diarrhoea, bleeding and urgency, and often has negative effects on patients’ personal, psychological, professional and social well-being,” said Professor Glen Doherty, Consultant Gastroenterologist at The Centre for Colorectal Disease at St Vincent’s Hospital, Dublin. “I am delighted that an additional treatment option will now be available through Ireland’s healthcare system for eligible patients diagnosed with Ulcerative Colitis.”
Victoria Spillane, Chief Operating Officer of Crohn’s & Colitis Ireland, welcomes the news: “Over 40,000 people in Ireland are living with Crohn’s Disease and Ulcerative
Colitis. They are lifelong conditions for which there is no known cure, and the symptoms are painful and debilitating. Existing medications may not work for some people or indeed stop working for others. Expanding the treatment options for eligible people living with Colitis is a promising step forward and we welcome the HSE’s decision to recommend mirikizumab.”
This approval for reimbursement was based on results from the LUCENT program, which included two randomised, double-blind, placebo-controlled Phase 3 clinical trials, consisting of one 12-week induction study (LUCENT-1) and one 40-week maintenance study (LUCENT-2) for 52 weeks of continuous treatment.
INIZIO APPOINTS RYAN QUIGLEY AS ITS NEW CHIEF EXECUTIVE OFFICER
The board of Inizio, a leading commercialization partner to health and life sciences companies globally, has announced the appointment of Ryan Quigley as Chief Executive Officer, effective 9 September 2025. Ryan succeeds Paul Taaffe, who will continue to work with Ryan to support the transition until the end of the year. Ryan has served as Inizio’s Chief Operating Officer since 2021, driving the company’s commercial strategy, innovation agenda, and investment roadmap, as well as playing a pivotal role in developing Inizio into the leading commercialisation partner to health and life sciences companies globally.
With $1.6bn in revenue and more than 10,500 employees across five connected business units, Medical, Advisory, Evoke, Engage and Biotech, Inizio partners at scale with more than 700 large pharma and biotech clients globally to support their clinical development and commercialisation journeys, improving patient access and experience. Inizio brings a fully connected suite of technologyenabled capabilities, combined with specialised scientific expertise across all therapeutic areas, to support clients through every pivotal moment of their asset’s lifecycle, maximizing asset potential and impact, and enhancing treatment outcomes.
Prior to being appointed to his current role, Ryan’s 25-year career spanned some of the world’s largest healthcare and pharmaceutical companies. Most notably, he held senior leadership roles at Abbott and AbbVie, where he was responsible for
launching blockbuster brands across major markets.
Ryan said: "This is an exciting time to lead Inizio as we continue to grow and help biopharma clients with integrated solutions to bring highly complex new drugs to market. At Inizio, it’s the combination of our people and our expertise that makes the difference: we connect talent from across the organization to create innovative solutions that make a meaningful difference for our clients and patients. Together, we will continue to unlock new opportunities, reimagine how healthcare engages with patients, professionals and society, and build on the momentum we have achieved over the last few years."
Liam FitzGerald, Chairman of the Board, said: "Ryan has an exceptional track record as a leader who combines strategic vision with deep operational expertise. He embodies the values of Inizio and has the energy, ambition and client focus to lead the business into its next chapter of growth and success.”
“I would like to thank Paul personally and on behalf of the Board of Directors for his contribution to the successful development of Inizio as its CEO. He oversaw the creation of the company and built a market leader well positioned for sustained growth. Paul will remain closely involved with Inizio as a board member going forward.”
New Chief Executive Officer, Inzio, Ryan Quigley
Clinical R&D
ALL-ISLAND PRIVATE HEALTHCARE EXCELLENCE AWARDS
Mark Regan, CEO of Kingsbridge Healthcare Group, has been recognised for his outstanding contribution to the healthcare sector across the island of Ireland.
Mr Regan accepted the award at the inaugural All Island Private Healthcare Excellence Awards which took place recently in Belfast, and also recognised the exceptional clinics, practitioners, service providers and private hospitals providing outstanding care throughout Northern Ireland and the Republic.
Mark joined Kingsbridge, which now operates four private hospitals with two in Belfast, and others in Derry/Londonderry and Sligo, in 2005 after several years as a radiographer with the NHS and in medical innovation with Phillips. He was part of the team that sold the first CT Scanner to 3fivetwo Healthcare, which later became the Kingsbridge Healthcare Group.
The highly esteemed independent judging panel, headed up by Dr Tom Black FRCGP, were keen to recognise Mark’s continued drive and mission for the private sector to supplement the NHS as it continues to face daily challenges.
The Private Healthcare Excellence Awards were founded by one of Northern Ireland’s leading NHS GPs and owner of two private health clinics, Dr Carla Devlin and Sarah Weir, Managing Director of Weir Events, with expert guidance from clinical advisor Dr Jenny Addley.
Outstanding Contribution to the Industry - Mark Regan, CEO, Kingsbridge Healthcare Group
Dr Devlin commented; “We set up the Awards to facilitate collaborative, cross border shared learning opportunities, and help shine a light on practices and individuals who are delivering outstanding care and sharing improved medical knowledge North and South of Ireland. Everyone in the room on Saturday night, and beyond, will know of Mark Regan’s passion and commitment towards access to healthcare across Ireland.
“Mark has been a pioneer in revolutionising not only private healthcare services through Kingsbridge, but also the provision and access of such services, communicating how those needing non-urgent care can advocate for themselves and access it efficiently. He is an advocate for both the NHS and private services, and has demonstrated a respect and learning for both that we can all aspire towards.”
Kingsbridge Healthcare Group recently signed a new agreement with Vhi, Ireland’s largest health insurer, that will enable its 1.2 million members to access Kingsbridge’s services in Belfast, a move that brings the accessibility of cross border care to so many more.
Vhi was also a winner on the night, picking up the awards for Excellence in Patient Care, one of the most hotly contested categories, for its Hospital at Home services in Dublin, and Mental Health Initiative of the Year for their Paediatric Mental Health Occupational Therapy Services in Dublin.
Alanna Denny, Paediatric Clinical Nurse Education Facilitator at Vhi Health & Wellbeing also won the Nursing & Midwifery Project of the Year for the Essentials in Paediatrics project.
Marble Arch Health picked up the Excellence in Cross Border Collaboration award for its Project Healthcare Without Borders operation in Enniskillen, providing all-island expert care and support for women dealing with complex health issues.
Other winners on the night included Dr Patrick Campbell for Excellence in Female Healthcare and Gentle Dental & Implant Clinic in Newry, which took home both the Excellence in Patient Care (Cosmetic Medicine/Dental) and Dental Practice of the Year awards. Anna Gunning of Cosmed Medical Aesthetics Training Academy in Dublin was recognised with the Excellence in Leadership award, and Dr Steven Kinnear of Dundonald Consulting Rooms in East Belfast won Excellence in Patient Care (General Practice).
Newry Private Clinic won Medical Clinic of the Year while Loughview Health, Lurgan won Private General Practice of the Year and St. Vincent’s Private Hospital, Dublin won Private Hospital Innovation of the Year. (See full list of winners and highly commended in notes to editors.)
DUPIXENT APPROVED IN THE US AS THE ONLY TARGETED MEDICINE TO TREAT PATIENTS WITH BULLOUS PEMPHIGOID
The US Food and Drug Administration (FDA) has approved Dupixent (dupilumab) for the treatment of adult patients with bullous pemphigoid (BP).
BP primarily affects elderly patients, and is characterized by intense itch, painful blisters, and lesions, as well as reddening of the skin. It can be chronic and relapsing with underlying type 2 inflammation. The blisters and rash can form over much of the body and cause the skin to bleed and break down, resulting in patients being more prone to infection and affecting their daily functioning. Available treatment options are limited and can add to overall disease burden by suppressing a patient’s immune system.
The FDA approval is based on data from the pivotal ADEPT phase 2/3 study that evaluated the efficacy and safety of Dupixent compared to placebo in adults with moderateto-severe BP. Patients were randomised to receive Dupixent 300 mg (n=53) or placebo (n=53) added to standard-of-care oral corticosteroids (OCS). During treatment, all patients underwent a protocol-defined OCS tapering regimen if control of disease activity was maintained. During
the FDA review, the analyses were updated; the FDA-approved results at 36 weeks in the label for Dupixent compared to placebo are:
• 18.3% of patients experienced sustained disease remission compared to 6.1% (12.2% difference; 95% confidence interval: -0.8% to 26.1%), the primary endpoint
• 38.3% of patients achieved clinically meaningful itch reduction compared to 10.5%
• Median cumulative OCS dose was 2.8 grams compared to 4.1 grams
In this elderly population, the most common adverse events (≥2%) more frequently observed in patients on Dupixent compared to placebo were arthralgia, conjunctivitis, blurred vision, herpes viral infections, and keratitis. Additionally, one case of acute generalized exanthematous pustulosis was reported in one patient treated with Dupixent and zero patients treated with placebo.
George D. Yancopoulos, MD, PhD Board co-Chair, President, and Chief Scientific Officer at Regeneron said, “This approval extends the remarkable ability of Dupixent to transform treatment paradigms for people living with a variety of diseases with underlying type 2 inflammation, from common conditions like asthma and atopic dermatitis, to rarer ones such as eosinophilic esophagitis and prurigo nodularis, and now including bullous pemphigoid. Dupixent has shown the potential to improve the most challenging effects of bullous pemphigoid, while helping some patients achieve sustained disease remission and decreased oral corticosteroid use. Additionally, this approval further reinforces the demonstrated safety profile of Dupixent in a broad age range of patients, from infants to elderly people, and across dermatological, respiratory, and gastrointestinal diseases.”
The FDA evaluated Dupixent under priority review, which is reserved for medicines that represent potentially significant improvements in efficacy or safety in treating serious conditions. Dupixent was previously granted orphan drug designation by the FDA for BP, which applies to investigational medicines intended for the treatment of rare diseases that affect fewer than 200,000 people in the US. Additional regulatory applications are also under review around the world, including in the EU, Japan, and China.
PROCEIVE SUPPORTS FÉILEACÁIN IN THE VHI WOMEN’S MINI MARATHON
On Sunday 2nd June, members of the Proceive team proudly took part in the Vhi Women’s Mini Marathon in support of Féileacáin, a not-for-profit organisation that provides support to anyone affected by the death of a baby during or after pregnancy.
Féileacáin offers vital services such as counselling, memory boxes, and nationwide support groups, providing comfort and care to families during an unimaginably difficult time.
As a brand dedicated to supporting individuals and couples on their fertility and pregnancy journeys, Proceive recognises that while this path can be full of hope, it can also involve heartbreak. Supporting Féileacáin reflects the brand’s deep commitment to families at every stage of this journey.
This cause holds both professional and personal significance for the team at Proceive. A team member has experienced Féileacáin’s support first-hand, making the brand’s involvement in the initiative especially meaningful.
Participating in the Mini Marathon was a way to honour those affected by baby loss and to raise awareness of the essential work Féileacáin does across Ireland.
The Proceive team has raised over ¤2,500 for the charity. To learn more or make a donation, visit www.feileacain.ie.
VHI 360 HEALTH CENTRE OFFICIALLY OPENS IN GALWAY EXPANDING AVAILABILITY OF VHI SERVICES IN THE WEST OF IRELAND
Vhi has officially opened its new 360 Health Centre in Galway today, marking a major milestone in its nationwide healthcare network. The opening of the redeveloped and enhanced Health Centre introduces Vhi’s 360 model of care to the West of Ireland, aiming to provide an integrated approach to patient health and wellbeing to ultimately improve health outcomes.
To celebrate the opening, Síle Seoige, Galway native and ambassador for the Vhi 360 Health Centre in Galway, toured the facility, learning more about the range of services now available to Vhi members in the region.
patients quickly and discharge them within 90 minutes. Follow-up care with orthopaedic consultants or wound care nurses is also available on-site.
by cancer, who are experiencing a treatment-induced menopause.
Menopause, Diet & Cancer is designed to offer practical, evidence-based guidance on how dietary and lifestyle choices can alleviate menopausal symptoms and enhance overall well-being.
Developed by CORU-registered dietitians Dr. Samantha Cushen and Ms Katie Johnston from School of Food and Nutritional Sciences and Cancer Research @ UCC, University College Cork, in partnership with the Irish Cancer Society, the book emerged from the Women’s Health Initiative
“Linking You with Support and Advice” (LYSA) Trial.
Situated on the Headford Road, Vhi 360 Health Centre offers access to Vhi’s integrated clinical services including:
• Urgent Care for minor injuries and illnesses, available 365 days a year without appointment
• X-ray and diagnostics
• Medical Screening by appointment
The Vhi 360 Health Centre in Galway also serves as a hub for Vhi’s Hospital@Home, a referralonly service where expert nurses and doctors deliver care directly to members in their homes, with the team already supporting patients in the region. In addition, members can access specialist services such as paediatrics and women’s health care as part of Vhi’s suite of integrated services.
Speaking about her visit to the Vhi 360 Health Centre in Galway, Síle Seoige said: “As a Galway native, living in the area with my young family, I’m thrilled to see Vhi’s 360 Health Centre open in Galway. This new facility will allow people to access expert care, support and information in one welcoming space close to home. Having faced my own health challenges in the past, I am passionate about proactive health and wellness, and I believe that the availability of services through Vhi’s 360 Health Centre will make a real difference to people in Galway.”
For the first time in the West of Ireland, Vhi members will have walk-in access to a Vhi Urgent Care Clinic. The six-bay Urgent Care Clinic aims to assess
The facility is open seven days a week, 10am to 7pm, and joins existing Vhi 360 Health Centres in Dublin, Cork, and Limerick.
At the opening of Vhi’s 360 Health Centre in Galway, Anne O’Connor, Managing Director of Vhi Health and Wellbeing, said: “Today marks an important milestone for Vhi and our members in the West of Ireland as we open our new Vhi 360 Health Centre. This facility brings our connected model of healthcare to the region, offering access to a multidisciplinary team and integrated clinical services. With services including urgent care for minor illnesses and injuries, as well as medical screenings that support early detection, our members will benefit from timely, expert care focused on achieving the best possible health outcomes. This opening reflects our ongoing commitment to helping our members live longer, stronger, and healthier lives.”
Vhi’s 360 Health Centre in Galway is now open and can be found by searching Eircode: H91 E2R8. Urgent care is available to Vhi members seven days a week, 365 days a year from 10am to 7pm. For more information on services available at Vhi 360 Health Centre in Galway, please visit www.vhi.ie/360.
NEW VITAL RESOURCE LAUNCHED FOR WOMEN NAVIGATING MENOPAUSE AND DIET AFTER CANCER
Recently, on International Day of Action for Women’s Health, a new vital and innovative resource has been launched for women affected
Cancer treatments can sometimes trigger a sudden, intense menopause, often leading to more severe symptoms than those of natural menopause. For some, these symptoms are manageable, while others may find them overwhelming. They can impact quality of life and compound the physical and emotional burdens many women face during and after their cancer journey.
The resource integrates lived experiences, sound scientific evidence, and the invaluable perspectives of patients themselves, making it a trusted companion for women embarking on this complex journey.
Samantha Cushen, Lecturer in Human Nutrition and Dietetics & co-author of Menopause, Diet & Cancer said: “Navigating menopause after cancer is hard enough—finding clear nutrition advice shouldn’t be. For too long, women have been left to piece together guidance from too many, often conflicting, sources. In a world full of nutrition misinformation, this book brings it all together—offering clarity, compassion, and credible answers in one evidence-based guide designed to support, inform, and reassure.”
Katie Johnston, Oncology Research Dietitian & co-author of Menopause, Diet & Cancer said: “There is a serious lack of dedicated dietetic support for women managing the longterm, often debilitating, effects of cancer and treatment-induced menopause. All too frequently, my colleagues and I found ourselves in clinic, reaching for a resource that simply did not exist—one our patients clearly needed. Shaped by the voices of 16 women who helped design what they needed most – Menopause, Diet and Cancer is not a clinical manual; it’s
Members of the Proceive team proudly took part in the Vhi Women’s Mini Marathon in support of Féileacáin
Clinical R&D
a book designed to be part of your everyday life—and your kitchen.”
Jointly, the authors state: “The launch of Menopause, Diet and Cancer marks a crucial breakthrough in Ireland, where dietetic support for cancer survivors is virtually non-existent. This resource takes an important step toward making trusted dietetic advice a standard part of care for women after cancer—but much more needs to be done to ensure every woman has access, and we are determined to make that a reality.”
“This is the first Irish publication that has truly made me feel seen—not just in terms of my diagnosis, but in the full complexity of what I’m dealing with. Beyond understanding, this book offers clear, science-based nutritional advice and practical strategies I hadn’t been able to find elsewhere.”
HUMAN TISSUE ACT 2024
The HSE has welcomed the Human Tissue Act 2024 Part 2 which now provides a national legislative framework for organ donation and transplant services in Ireland for the first time.
The donation of an organ is an incredible gift that is life changing for the recipient and their families. Consent is the cornerstone of this new legislation. Under this new legislation, all adults in Ireland will be considered to have agreed to be an organ donor when they die, unless they have recorded a decision not to donate on the National Organ Donation Opt-Out Register or are in one of the excluded groups. This is commonly referred to as a soft opt-out organ donation system.
organs donated go to people most in need of a transplant. Consent is at the heart of this change.
When someone dies, their family must agree to donate their organs. It is important to inform your family and friends about your decision regarding organ donation, as they will always be consulted and your wishes should be central to any decision.
The Act sets out who is considered a “designated family member” and this is usually the family member who has been the main point of contact for clinicians in their treatment of the deceased. This is the person who has to provide consent to the organ donation. If no consent is received or no designated family member is found then the donation will not proceed.’’
Both Noel and Michael O’Brien had experienced symptoms commonly associated with aortic valve disease, a condition where the valve narrows or leaks, forcing the heart to work harder to pump blood. If untreated, the condition can lead to heart failure and other serious complications. Patients with aortic valve disease, either stenosis (blocked) or regurgitant (leaky), often require valve replacement
The Avalus Ultra valve is a next-generation aortic valve replacement that offers improved durability, enhanced surgical handling, and easier placement. Its introduction places UHG at the forefront of cardiac surgical innovation in Ireland.
Family members will always be consulted before any action is taken and if they do not agree, then the donation will not proceed. Those who do not wish to donate their organs, for whatever reason, and have recorded their objection on the new National Organ Donation Opt-Out Register will have their wishes respected, and their family will not be approached on the issue of organ donation.
The Act also provides a framework for living donation and will, for the first time, provide a way for people who wish to donate a kidney to someone they don’t personally know, the opportunity to do so.
This is known as non-directed altruistic donation. They are donating an organ for someone on a waiting list who needs it.
Speaking on the register, Dr Colm Henry, CCO, HSE said, “The opt-out organ donation system will bring us in line with international best practice. Organ transplantation is one of the great advances in modern medicine. It offers a second chance at life to people with life-threatening illnesses or injuries to their vital organs. Every year, more than 200 people in Ireland have their lives improved or saved by the gift of organ donation. At any given time, approximately 600 people in Ireland are on waiting lists for organ transplants. I encourage you to have a conversation with your family or next of kin and let them know your wishes around organ donation.”
Dr Brian O'Brien, National Director, HSE Organ Donation Transplant Ireland added: "Not everyone who dies is a potential organ donor. A donor needs to be in hospital and on a life support machine. All
The HSE is running an information campaign to inform the public of the changes around organ donation and how to access the opt-out register.
THE HEART OF THE MATTER – SIBLINGS UNDERGO SAME LIFE-SAVING HEART PROCEDURE
University Hospital Galway (UHG) achieved a significant milestone in cardiac care last October by becoming the first hospital in Ireland and the UK to implant the Avalus Ultra biological aortic valve, a major advancement in the field of valvular heart surgery.
The ground-breaking procedure was first performed on Noel O’Brien from County Galway, marking the hospital’s inaugural use of the innovative valve. In a remarkable turn of events, Noel’s brother, Michael, underwent the same life-changing procedure, becoming the eighth patient to receive the implant last month. Both surgeries were successfully carried out by Professor Alan Soo and his team at UHG.
Professor Alan Soo, Consultant Cardiothoracic Surgeon praised the development, stating, “The introduction of the Avalus Ultra valve represents a new chapter in heart valve surgery. We are proud to lead the way in offering our patients the very latest in cardiac technology, ensuring better outcomes and improved quality of life.”
The successful adoption of this advanced valve system underscores UHG’s commitment to pioneering treatments and delivering world-class cardiac care to patients across Ireland.
CÚRAM AND B. BRAUN COLLABORATE ON SIMULATED VASCULAR ACCESS RESEARCH
A research collaboration is to deploy cutting-edge simulation technologies to redefine best practices training and innovation
Noel and Michael O’Brien from Tynagh in County Galway with Professor Alan Soo, Consultant Cardiothoracic Surgeon, University Hospital Galway
Katie Johnston & Samantha Cushen
for vascular access – the process of inserting a small tube or catheter into a vein to administer medication, fluids or take blood.
The project involves CÚRAMthe Research Ireland Centre for Medical Devices at University of Galway - and B. Braun, a global leader in medical technology. It leverages B. Braun’s expertise in medical device development and University of Galway’s leadership in clinical simulation research to deliver evidence-based advancements in vascular access training. Known as the SIMETRIC project (Simulation and Imaging Methods for Eye Tracking and Recording Intravenous Catheter Insertion), it is harnessing cuttingedge simulation technologies to enhance clinical protocols, ensuring safer and more effective patient care. The initiative integrates eye-tracking systems, high-resolution video, wearable devices and motion analysis tools to assess and refine clinician performance in real-time.
This level of precision training is expected to significantly enhance competency, safety, and patient care standards.
The study, led by Dr Peter Carr, CÚRAM Funded Investigator and Associate Professor at the School of Nursing and Midwifery, University of Galway, will evaluate how simulation-based training can enhance clinician performance in ultrasound-guided long peripheral catheters.
The project will assess clinicians using three types of ultrasoundguided long peripheral catheters, including an innovative device from B. Braun´s long peripheral catheter (Deep Access) range. Dr Carr said: “Strong partnerships drive real change in healthcare. By combining clinical expertise, cutting-edge technology and industry collaboration, we are shaping the future of vascular access training and device innovation.” The SIMETRIC project highlights the importance of interdisciplinary collaboration, bringing together nurses, vascular access specialists, biomedical engineers and researchers.
B. Braun said: “At B. Braun, we firmly believe that industryacademic-clinical collaboration is essential for advancing healthcare innovation and improving patient outcomes. By fostering strong partnerships between these sectors, we can leverage diverse expertise, drive groundbreaking research and develop cutting-edge medical solutions. Guided by our vision to protect and improve the health of people around the world,
Dr Orlaith Hernon, Assistant Professor, School of Nursing and Midwifery; Dr Peter Carr, Associate Professor, School of Nursing and Midwifery; Dr Jing Wang, Post Doctoral Researcher, School of Nursing and Midwifery; Ms Jiaxin Deng, PhD Scholar, School of Nursing and Midwifery; and Dr Brian Deegan, Lecturer in Electrical and Electronic Engineering. Photo: Andrew Downes
we are committed to collaborative efforts that enhance the quality of care and ensure a healthier future for all.” This partnership aligns with B. Braun’s commitment to advancing healthcare through innovation, creating new opportunities to collaborate with frontline clinicians and academic experts to develop smarter training solutions and cuttingedge medical devices.
Dr Carr said: “This project will aim to ensure that the new device is underpinned by robust evidence before it can be adopted in a clinical setting. We also want to demonstrate how technology can be leveraged by clinical academics to provide training simulation that leads to improved clinical and patient care. Nurses and vascular access specialists play a pivotal role in this study and their clinical expertise is invaluable in the development and evaluation of new technologies.”
Vascular access is considered a routine yet high-risk procedure in healthcare. Problems can arise from improper catheter insertion and ensuring healthcare workers have the highest level of skill, precision, and real-time feedback is critical for improving patient outcomes.
In response to growing demand from clinical partners, University of Galway is launching three new micro-credential modules based on the project’s findings. These courses will focus on ultrasoundguided cannulation and advanced vascular access techniques, supporting the increasing adoption of ultrasound-guided long peripheral catheters across a wider range of patient groups. The outcomes of SIMETRIC will contribute to academic training, real-world clinical applications, and the future of vascular access education. By investing
in collaborative research and professional development, the University of Galway and B. Braun are setting new benchmarks for innovation in medical training and patient care.
ABBOTT INTRODUCES MIXED REALITY EXPERIENCES TO DRIVE BLOOD DONATIONS IN IRELAND
Abbott, the global healthcare company, today unveils two new mixed reality experiences to support the need for more blood, platelet and plasma donations in Ireland. The experiences aim to reduce fear in donors and encourage more younger people to donate.
Only 3% of people eligible in Ireland donate blood, yet 3,000 blood donors are needed every week and one in four people in Ireland will require donated blood at some point in their lifetime. Just one donation can save up to three lives. Critically, there is no substitute for human blood[1].
A study with two blood centers in the US found that the use of mixed reality decreased anxiety in 68% of donors and 89% of donors reported they were very or extremely likely to donate again 2.
Participants wear lightweight headsets with a translucent visor, so the eyes of donors are always visible to clinical staff, ensuring constant monitoring and evaluation. Intergalactica is a new experience designed using gaming engagement principles in which donors build a team of robots to explore planets, solve puzzles, and defeat enemies – and Irish donors will be the first in the world to experience it. In another mixed reality experience called Zen Garden, donors listen to soothing music while planting seeds. Both experiences will be piloted in
partnership with the Irish Blood Transfusion Service for a limited time, between May and June.
Joana Araujo, Global Marketing Director, Transfusion Medicine, Abbott said: "As a global leader in health technology, Abbott is always exploring new ways in which innovations can help improve the donor experience. These headsets balance complex computing with a simple insight –many people fear donating blood and mixed reality technology makes it easier to donate blood by giving the donors something else to focus on while they give blood. We hope that the improved experience leads to more people wanting to donate blood in Ireland."
Paul McKinney, Director of Donor Services and Logistics, IBTS said: "This innovative technology introduces a gaming-like experience which evidence and feedback suggests makes blood, platelet and plasma donation less intimidating and more fun for the donor. We also hope it will encourage many people, of all ages, who want to donate but have been nervous about doing so in the past."
The pilot initiative will run between May and June in a number of IBTS donation centres in Dublin and Cork.
NEW PATIENT ADVICE AND LIAISON SERVICE COORDINATOR
Sligo University Hospital (SUH) is delighted to announce the appointment of Lorraine Cooney to the role of Patient Advice and Liaison Service (PALS) Coordinator. Lorraine, a native of County Roscommon, has over 15 years clinical experience as a Radiation Therapist, and for the past two years, she worked as the PALS Coordinator at Mayo University Hospital, prior to her recent appointment.
The Patient Advice and Liaison Service Coordinator acts as the main contact between patients, their families, carers and the hospital. They ensure that the patient voice is heard either through the patient directly or through a nominated representative.
If a patient wants to provide feedback or make a comment about the hospital and the care they received, the PALS Coordinator will assist them in doing so, or refer them to the appropriate person who will be able to assist them further.