Page 10: Budget marks a Turning Point or Another Test
Page 12: What Europe’s vision means for Irish pharmacists
Page 14: PHX Ireland Recognising People
Page 16: Steady deals and shifting dynamics in Pharmacy
Page 19: Masters of Pharmacy Programme gains accreditation
PUBLISHER:
IPN Communications
Ireland Ltd.
Clifton House, Fitzwilliam Street
Lower, Dublin 2 00353 (01) 6690562
MANAGING DIRECTOR
Natalie Maginnis
natalie@ipn.ie
EDITOR
Kelly Jo Eastwood: 0044 787654 8989
kelly-jo@ipn.ie
SALES DIRECTOR
Debbie Graham
debbie@ipn.ie +353 8727 99317
CONTRIBUTORS
Adam Esa | Frank Olden
Bernie Carter | Helen Forristal
Chantal Alexander
Patrick J McGee
Eamonn Brady
Dr Emer Guinan
Dr Marie Tierney
Dr Muslim Madhag
Dr Ross O’Grady
Dr Samer Arnous
DESIGN DIRECTOR
Ian Stoddart Design
Foreword
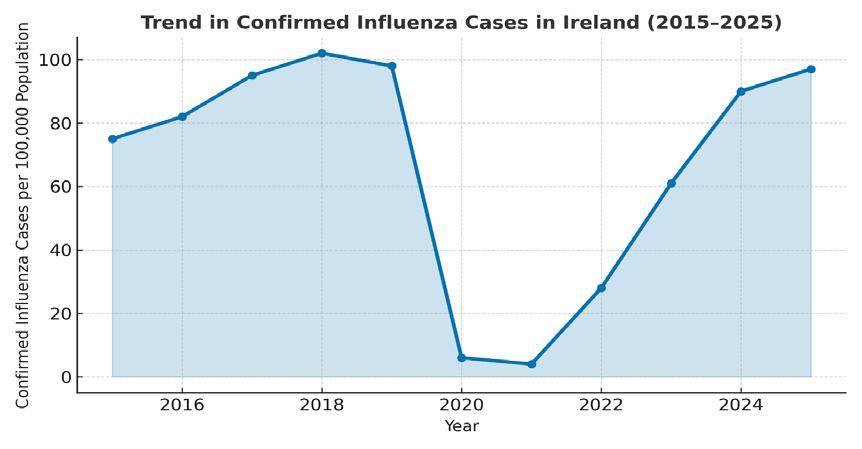
As Ireland’s pharmacists take stock of another year of change, one message stands out clearly across every new report and headline — pharmacy is moving from a place of endurance to one of evolution.
Page 24: Men’s Hormonal Health Conversations Contents 12
The Government’s record ¤27.4 billion health budget promises a “performance-led” future, aiming to deliver care closer to home through regional autonomy and smarter spending. For community pharmacy, that ambition offers both opportunity and accountability. The profession is being asked not simply to dispense more, but to demonstrate more — more value, more integration, more measurable impact on patient outcomes.
4 19
Two recent analyses remind us just how wide that horizon is. The Fitzgerald Power M&A Review reveals a market that has matured without losing its vitality. Pharmacy ownership is consolidating around capability, professionalism, and confidence. Deal activity may be steady rather than spectacular, but stability itself is now a sign of strength — proof that community pharmacy remains one of Ireland’s most resilient health assets.
6 Irish Pharmacy News is circulated to all independent, multiple Pharmacists and academics in Ireland. All rights reserved by Irish Pharmacy News. All material published in Irish Pharmacy News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd. has taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
Across Europe, the PGEU Report on Pharmacy Services points to where that strength can go next. Pharmacies are delivering vaccinations, chronic-disease management, and prevention programmes as integral parts of national health systems. It’s a vision of pharmacy not as a distribution network, but as a clinical service platform — precisely the direction the Irish sector must embrace as the new Community Pharmacy Agreement begins to take shape.
Taken together, these developments signal a sector on the cusp of transformation. The investment is there, the evidence is there, and the public trust is already yours. What remains is to ensure that policy, funding, and professional leadership move at the same pace.
This issue explores that transition — from financial confidence to clinical capability — and the shared responsibility that comes with it. Because the real test of progress in 2026 won’t be how much you spend, but how much difference pharmacy makes.
I hope you enjoy the issue.
All-Ireland Recognition for Pharmacy Plus Birr
Pharmacy Plus Birr has been officially recognised as the Business All-Star Community Pharmacy of the Year 2025 by the All-Ireland Business Foundation.
Founded by David O’Meara in 2006, Pharmacy Plus Birr has grown to become a cornerstone of the local community. In addition to its comprehensive pharmacy services, the business includes Vision Plus Opticians, offering professional eye care and a wide range of eyewear solutions under one roof. Conveniently located in the heart of Birr, the store combines friendly, personal service with innovative healthcare offerings.
David O’Meara is the Founder and Superintendent Pharmacist of Pharmacy Plus Birr and Vision Plus Opticians. A proud Offaly native, David has spent nearly two decades building a healthcare business that is as much about people as it is about prescriptions.
After qualifying as a pharmacist, David set out to create something different – an independent pharmacy where patients could count on expert advice, friendly faces, and a genuine connection. In 2006, he opened Pharmacy Plus Birr in the heart of the town, combining professional care with a neighbourly touch that quickly won the loyalty of the local community.
Kieran Ring, Deputy Chair, Adjudication Board said, “Pharmacy Plus Birr represents the
very best of community healthcare, delivering excellence in service while making a tangible difference to people’s lives. In reviewing their accreditation application, it was clear that this is a business built on trust, compassion, and a deep understanding of its community’s needs.
“David O’Meara and his team have gone beyond the traditional role of a pharmacy, offering not only exceptional healthcare and optical services, but also serving as a reliable source of advice, support, and reassurance for local residents. It is businesses like Pharmacy Plus Birr that remind us of the vital role independent, community-focused enterprises play in the fabric of Irish life.”
Transparency of Medicines
Speaking after accepting the accolade, David O’Meara, Founder of the Pharmacy added, “This accolade is deeply meaningful for our team. Our mission has always been to combine professional expertise with a warm, personal approach, so that every customer feels valued and cared for. We’re proud to serve this community and grateful for the trust people place in us every day!
Hypertension Pharmacy Toolkit
A version of the International Pharmaceutical Federation (FIP) Hypertension Toolkit focusing on uncontrolled hypertension, one of the leading risk factors for cardiovascular disease, has been shared with the profession.
The toolkit empowers community pharmacists and their teams to identify and manage patients with uncontrolled hypertension through motivational counselling, timely interventions, and ongoing support. It provides practical tools, such as an educational guide, assessment tool, patient leaflet, and referral letter to help integrate blood pressure management into pharmacy practice and strengthen collaboration with other healthcare professionals.
Supporting patients with uncontrolled hypertension: A toolkit for pharmacists has been developed to support community pharmacists and pharmacy support teams in identifying and managing patients with uncontrolled hypertension. It aims to enhance pharmacists’ role in providing motivational counselling and empowering individuals to achieve and maintain optimal blood pressure control through timely interventions and ongoing support.
The Minister for Health Jennifer Carroll MacNeill TD has welcomed the publication of new guidance supporting the transparency of medicine pricing and fees for pharmacy services.
This guidance has been developed by the Pharmaceutical Society of Ireland (PSI) – the pharmacy regulator – to assist pharmacists in providing clear and accessible pricing information to the public.
Minister Carroll MacNeill said, “Community pharmacies are at the heart of our healthcare system; they are among the most trusted and accessible healthcare professionals. This guidance will strengthen that trust even further, with access to information about the cost of services pharmacists deliver being made available to the public for the first time
“I am grateful to the PSI for developing this guidance as I believe patients need visibility of the fees they are paying for dispensing services when purchasing their prescription medicines.
"We are growing the role pharmacists play in our community with the recent Community Pharmacy Agreement and this guidance on pricing transparency, beginning from 1 December, will help people better understand exactly what they’re paying for their medication and associated services.”
• From 1 December 2025:
Pharmacies will be required to display information about the cost of all professional services on a clear notice in a conspicuous location, visible to patients.
• From 2026:
Patients will receive a detailed, a receipt for any transaction outlining the costs of the medicine dispensing fee (where applicable) the cost of any other professional service.
PSI Registrar, Joanne Kissane added, “The PSI is committed to assuring safe, high-quality pharmacy services are available to patients and the public. As part of this, we believe that access to pricing information is essential to empower individuals to make informed healthcare decisions. While we do not determine the prices charged by pharmacies, patients have a right to transparent and accurate information on the price of the medicines and health services they access.
“Transparency of fees and pricing maintains and enhances public confidence in pharmacists and enables patients to make informed decisions about their health and treatment. The new guidance will provide patients with an improved understanding of the fees they pay for the products and services they use in pharmacies.”
This resource is designed to motivate and enable pharmacy teams to establish or strengthen community-based services focused on the management of uncontrolled hypertension. It promotes a standardised approach to care, integrates blood pressure monitoring and management into the pharmacy workflow, and fosters collaboration with prescribers to optimise treatment outcomes.
The toolkit is structured around four core elements: an educational guide, an assessment tool, a patient information leaflet, and a primary care referral letter.
It is designed to support pharmacists in their interactions with patients. The role and responsibilities of pharmacists vary across jurisdictions. Users must ensure compliance with relevant national laws and professional codes, including national drug regulations, data privacy, and professional and ethical conduct.
David O’Meara with his pharmacy team at Pharmacy Plus Birr
¤7.9m PEACEPLUS
Funded Project
The Co-operation and Working Together (CAWT) Partnership has launched its ¤7.9 million PEACEPLUS-funded Early Intervention Support Youth Hubs (EASY) project.
The cross border EASY project is aimed at providing early interventio n support to 9,000 children, young people and families living in the border area with social, emotional or behavioural issues.
The project is supported by PEACEPLUS, a programme managed by the Special EU Programmes Body (SEUPB).
Launched in Armagh City, EASY will provide high quality and targeted early intervention and supports to children and young people who present with neurodevelopmental type conditions, or who have been recently diagnosed.
Such interventions and supports will be provided within local communities and in partnership with voluntary and community organisations.
Overall, the project is intended to improve the timeliness, quality and experience of the support available to children and young people presenting with neurodevelopmental conditions and behaviours, and their families, whilst also building service capacity.
Through a cross-border collaborative approach to the development and implementation of the project, it offers a unique opportunity for both jurisdictions to share and co-operate to support children, young people and families living in the border area.
Stakeholders attending the launch event included health and social care professional and leaders, children’s services and government representatives.
Minister for Health Jennifer Carroll MacNeill TD said, "I am delighted to support the launch of the Early Intervention Support Youth Hubs project, as part of the PEACEPLUS programme which will support up to 9,000 children, young people and their families in availing of appropriate early interventions and support in their local communities.”
She added: “I wish all involved the very best and look forward to hearing about the benefits it will deliver to thousands of children and their families over the coming years."
News Welcomed on Pharmacist Prescribing
The Pharmaceutical Society of Ireland has welcomed the evidence review published last month by the Health Research Board (HRB). The review, Effectiveness, safety, and cost-effectiveness of pharmacist prescribing, is significant in the current context and for future considerations regarding the evolving provision of care by pharmacists for the benefit of patients and the wider health system.
The evidence review was undertaken at the request of the Department of Health as a follow up to the recommendations made in 2024 by the Expert Taskforce to Support the Expansion of the Role of Pharmacy.
Speaking about the publication of the HRB review, Joanne Kissane, Chief Officer and Registrar of the PSI, said,
“I welcome the evidence and findings presented today within this
HRB review. As a former member of the Department of Health’s Expert Taskforce to Support the Expansion of the Role of Pharmacy and as regulator of pharmacists and pharmacies, it is important that we assess the benefits and impacts of change within the healthcare system, including for pharmacy, to ensure there is patient and health system benefit.”
“This review provides a positive evidence base about the
effectiveness, safety and costeffectiveness of pharmacists as prescribers at a time when pharmacist role expansion is being progressed. The PSI is currently involved in implementing and supporting changes in how healthcare will be provided through pharmacies, and we will support further policy initiatives, such as realising the benefits of pharmacist prescribing into the future, as part of our regulatory role.”
Landmark Study on Women’s Health
Researchers at University College Cork (UCC) want to hear from women experiencing chronic health conditions such as endometriosis, migraine, postural orthostatic tachycardia syndrome (POTS), premenstrual dysphoric disorder (PMDD), and mast cell activation syndrome (MCAS).
Pictured are Dr Sarah Foley and Jenny Cooney-Quane, UCC School of Applied Psychology
Launched recently, the research will explore issues including diagnostic delays, patient–doctor interactions, ranging from symptom dismissal to supportive engagement, and how women use symptom-tracking apps to document and share their experiences with healthcare professionals, and responses to that data.
Delays in diagnosis are welldocumented across women’s health. Internationally, endometriosis takes an average of nine years to diagnose, while POTS can take five. Conditions such as PMDD, MCAS, and less common migraine subtypes remain under-recognised despite their disabling impact. These conditions often overlap with one another, as well as with neurodivergence and connective tissue disorders like Ehlers-Danlos Syndromes, and may emerge or worsen after COVID-19 infection, creating complex healthcare needs that are poorly understood and managed in current clinical practice.
Many patients report feeling disbelieved or having their
symptoms minimised, a phenomenon often described as “medical gaslighting.” This contributes to years-long diagnostic delays. The study will examine both negative and positive healthcare experiences, including moments of validation and support.
“Too often, we hear patients speak about delays in diagnosis, and the barriers that contribute to them, such as symptom dismissal, minimisation, or normalisation. We want to hear about these experiences, as well as good patient–doctor interactions, so that we can learn from both and improve women’s healthcare,” Jenny Cooney-Quane, lead researcher on the project and
Research Associate in UCC School of Applied Psychology, said.
The study will also investigate how patients use symptom-tracking apps to record symptoms and identify patterns, and how doctors respond to this patient-generated data in relation to diagnosis, treatment, and communication.
The study acknowledges that non-binary individuals and trans men may also be affected by these health conditions, often facing additional diagnostic challenges. The survey is designed to ensure their experiences are represented. In doing so, the research aims to deliver findings that are relevant and meaningful to all groups affected.
Mapping Pharmacy Services
Community pharmacists are amongst the most accessible and trusted healthcare professionals in Europe, often serving as the first point of contact with the healthcare system for millions of patients each day.
“With supportive regulation, sustainable financing, and full integration into care pathways, pharmacists are already keeping people healthy, delivering services closer to home, and increasing the capacity of health systems”
At an event held in the European Parliament, co-hosted by MEP Michalis Hadjipantela (EPP) and MEP Vytenis Andriukaitis (S&D), and alongside the launch of the new Report on Pharmacy Services in Europe, the Pharmaceutical Group of the European Union (PGEU) highlights how expanding pharmacists’ scope of practice can transform healthcare delivery, ensuring patient-centred and sustainable care is provided closer to where people live.
Dispensing medicines is the foundation of pharmacy, and it is now complemented by an enhanced range of patientfocused services. Across Europe, pharmacists deliver vaccinations, promote health, conduct early screenings, manage chronic diseases, perform medication reviews, and provide digital health support, among other essential services that enhance patient experience and support adherence to treatments. These services have been shown to improve health outcomes, reduce
hospitalisations, and reinforce the resilience of healthcare systems, particularly in underserved and rural communities. The COVID-19 pandemic further reinforced their vital role, with pharmacies ensuring continuity of care, administering millions of vaccines, and offering trusted public health guidance in a situation where the healthcare system was strained and overburdened.
PGEU President Clare Fitzell said, “Europe’s 160,000 community pharmacies and over half a million pharmacists are a cornerstone of healthcare. With supportive regulation, sustainable financing, and full integration into care pathways, pharmacists are already keeping people healthy, delivering services closer to home, and increasing the capacity of health systems. Our report sets out a practical roadmap to build on this success and expand these benefits to patients in every community.”
Pharmacy services have already demonstrated their value, and with
Clare Fitzell, PGEU President
more supportive legal frameworks, fair remuneration models, and better digital health integration, their full potential can be realised. To advance the implementation, development, and recognition of pharmacy services across Europe, PGEU calls for:
• A strategic policy shift: recognising community pharmacies as essential partners in delivering peoplecentred, sustainable healthcare and empowering them through supportive regulation, appropriate investment, and systemic integration.
• Regulatory reforms: expand pharmacists’ scope of practice according to competency areas and remove barriers to service provision.
• Sustainable financing: ensure appropriate and consistent remuneration for pharmacy services to reflect their clinical and public health contributions.
• Workforce planning: strengthen education, leadership, and ongoing professional development.
• Crisis preparedness: fully integrate pharmacies into national public health response frameworks.
• Access and equity: strengthen pharmacies’ role in reducing health inequities by ensuring their presence in underserved areas and enabling access to specialty medicines, supporting territorial cohesion.
• Antimicrobial stewardship: enable pharmacies to take a proactive role in infection control and antibiotic use.
The outcomes of the PGEU Event on Shaping the Future of Pharmacy Services in Europe demonstrated that policymakers, health professionals and patients are ready to align priorities and advance the implementation and development of new and expanded pharmacy services across the continent.
Turn to page 22 for a full report on how this impacts pharmacists in Ireland.
Funding for Drugs & Health Services
The Minister for Public Health, Wellbeing and the National Drugs Strategy Jennifer Murnane O’Connor has announced additional ¤11 million in recurring funding for drugs and inclusion health services in Budget 2026.
The allocation includes ¤4 million for service enhancement measures and will address regional disparities in availability of drug and inclusion health services, with a strong focus on the provision of services in disadvantaged and rural areas. It also aims to enhance prevention measures, including through early intervention measures to improve child health and wellbeing.
Highlights include:
• enhanced capacity in drug services for under-served populations, including residential treatment and early intervention for young people
• strategic workforce development plan for staff working in drug services across all six health regions
• expansion of health services for people who are homeless, including national in-reach care and case management for those in emergency accommodation and interventions for women at risk of homelessness
• access to the medication Buprenorphine, enabling treatment of an additional 200 people with opioid dependence
• expansion of the innovative Brighter Beginnings programme for Traveller child health to two new health regions
• provision of additional health supports for refugees and migrants
An allocation of ¤100,000 will support a hospital monitoring system for drug overdose. This system will help the HSE to identify non-fatal and fatal drug overdoses at a faster pace, and issue risk communications and emergency plans as appropriate. This funding will also provide interventions for participants in the Dublin drug treatment court, which will aim to increase engagement and support those who have more complex issues to successfully complete the programme.
The end of erectile problems? Touch wood.
Available over the counter. No prescription required. Always read the leaflet. Available in a 4 or 8 pack.
ABBREVIATED PRESCRIBING INFORMATION
Product Name: Sidena 50 mg Tablets.
Composition: Each tablet contains, 50 mg sildena l (as citrate) .
Description: Light blue, round, slightly dotted tablets. Cross breaking notch on one side and marked ‘50’ on the other side. Can be divided into equal quarters. (Only two quarters of the 50 mg is covered by posology).
Indication(s): Treatment of men with erectile dysfunction, which is the inability to achieve or maintain a penile erection su cient for satisfactory sexual performance.
Dosage: Adults and elderly: 50 mg taken as needed approximately one hour before sexual activity. Dose may be decreased to 25 mg. Max dose: 50mg once daily. Impaired renal and hepatic function: Sildena l clearance is reduced in hepatic and severe renal impairment. Consider a dose of 25 mg. Dose may be increased step-wise to 50 mg if tolerated. Children and adolescents below 18 years of age: Contraindicated. Use in patients using other medicines: Starting dose of 25 mg with CYP3A4 inhibitors (not advised to use with ritonavir). To minimise postural hypotension in patients receiving and alpha-blocker, stabilise patient rst on the alpha blocker and use a starting dose of 25 mg sildena l. Contraindications: Hypersensitivity to sildena l or any of the excipients. Concomitant with ritonavir, nitric oxide donors or nitrates in any form, guanylate cyclase stimulators e.g. riociguat. In patients that sexual activity is inadvisable (e.g. severe cardiovascular disorders such as a recent (6 months) acute myocardial infarction (AMI) or stroke, unstable angina or severe cardiac failure). Refer these patients to a doctor. Patients with loss of vision in one eye due to NAION. Known hereditary degenerative retinal disorders. Severe hepatic impairment. Hypotension. Anatomical deformation of the penis. Not intended if no erectile dysfunction. Women. Warnings and Precautions for Use: First diagnose erectile dysfunction and determine potential underlying causes (e.g. hypertension, diabetes mellitus, hypercholesterolaemia or cardiovascular disease), before considering pharmacological treatment. Consider the cardiovascular status of patients, since there is a degree of cardiac risk associated with sexual activity. Serious cardiovascular events, including myocardial infarction, unstable angina, sudden cardiac death, ventricular arrhythmia, cerebrovascular haemorrhage, transient ischaemic attack, hypertension and hypotension have been reported post-marketing in temporal association with the use of sildena l. Most, but not all, of these patients had pre-existing cardiovascular risk factors. Sildena l has vasodilator properties, resulting in mild and transient decreases in blood pressure. Caution: Patients with anatomical deformation of the penis (such as angulation, cavernosal brosis or Peyronie’s disease), or in patients who have conditions which may predispose them to priapism (such as sickle cell anaemia, multiple myeloma or leukaemia). Advise patients that in case of priapism, prolonged erections (longer than 4 hours) or sudden visual defect, they should stop taking sildena l and consult a physician immediately. Administer to patients with bleeding disorders or active peptic ulceration only after careful bene t-risk assessment, as there is no safety information available. Interactions: See SPC for detailed information. Inhibitors of the cytochrome P450 (CYP) isoforms 3A4 (major route) and 2C9 (minor route) isoenzymes such as CYP3A4 inhibitors: Itraconazole, ketoconazole, erythromycin, cimetidine, HIV protease inhibitor saquinavir: May reduce sildena l clearance and increase sildena l plasma levels. Consider a starting dose of 25 mg. Strong CYP3A4 inducers e.g. rifampicin may increase sildena l clearance and decrease sildena l plasma concentrations. Grapefruit juice: May give rise to modest increases in plasma levels of sildena l. Nicorandil (Hybrid of potassium channel activator and nitrate): Due to the nitrate component it has the potential to have serious interaction with sildena l. Sildena l potentiates the hypotensive e ect of nitrates. Alpha blocker: Concomitant administration of sildena l may lead to symptomatic hypotension in a few susceptible individuals. Patients should be hemodynamically stable on alpha-blocker therapy prior to initiating sildena l treatment. Sildena l potentiates the antiaggregatory e ect of sodium nitroprusside in vitro. Not recommended in patients with a history of bleeding disorders or active peptic ulceration. Not recommended to use with other pulmonary arterial hypertension treatment containing sildena l. Caution when sildena l is initiated in patients treated with sacubitril/valsartan. May result in a increase of bosentan availability. Ability to Drive and Use Machinery: Minor in uence, dizziness and altered vision were reported. Patients should be aware of how they react to sildena l before driving or using machinery. Undesirable E ects: Very common: Headache. Common: Dizziness, visual disorders, visual colour distortion, vision blurred, ushing, hot ush, nasal congestion, nausea, dyspepsia. See SPC for more adverse e ects.
Marketing Authorisation Holder: Rowex Ltd, Bantry, Co. Cork. Marketing Authorisation Number: PA 0711/170/002. Further information and SPC are available from: Rowex Ltd., Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417
E-mail: rowex@rowa-pharma.ie
Legal Category: Not subject to medical prescription. Date of Preparation: Jan 2024
of preparation: (10-24) CCF: 26643
Minister Defends Move to Limit Blister Pack Funding Under New Pharmacy Agreement
Minister for Health Jennifer Carroll MacNeill TD has rejected claims that the Government’s new Community Pharmacy Agreement will remove funding for blister packs, insisting that phased dispensing remains in place but that new controls are being introduced to ensure it is used only for specific high-risk medicines.
The clarification came in response to a Dáil question from Deputy Pat the Cope Gallagher TD, who warned that the withdrawal of HSE funding for pharmacy-prepared blister packs could have “serious implications for elderly patients, particularly those living alone.”
In her written reply, the Minister stated that “The Community Pharmacy Agreement 2025 does not remove phased dispensing,” emphasising that patient safety was the driving factor behind the new framework.
Phased dispensing — the supply of a medicine in instalments rather than as a full monthly supply — was introduced in 1996 to protect patients at risk of medication misadventure with certain high-risk medicines. Pharmacists receive an additional fee when dispensing in phases under the General Medical Services (GMS) scheme.
In contrast, Monitored Dosing Systems (MDS) — commonly known as blister packs — are a separate organisational aid that allows doses to be arranged according to a patient’s schedule. The Minister noted that “the State has never agreed to fund Monitored Dosing Systems.”
Over time, she said, a practice had developed where pharmacies claimed phased dispensing fees for the preparation of blister packs — an approach that “was never intended by the State.”
While acknowledging that MDS packs “may have a role for some
patients,” the Minister pointed to limited and equivocal evidence supporting their use, citing an assessment by the National Centre for Pharmacoeconomics (NCPE).
Under the Community Pharmacy Agreement 2025, which takes effect in January 2026, phased dispensing under Reason 1 (at a physician’s request) and Reason 4 (where a patient is incapable of managing their own medicines) will be restricted to a defined list of high-risk drug classes:
• Psychotropics
• Opioids
• Codeine
• Pregabalin and gabapentin
The Minister said the move is designed to target limited resources where they are most needed.
“By focusing phased dispensing reimbursement on the medication categories on the approved list, payments can be targeted to medicines with the highest risk or potential for misuse,” she said.
“The introduction of improved controls around phased dispensing is being done in a way which puts patient safety first and allows the State to repurpose ¤20 million of funding to implement new patientcentred services.”
Pharmacies will retain the option to provide Monitored Dosing Systems privately, charging patients directly if they wish to continue receiving medicines in that format.
Deputy Gallagher’s intervention reflects wider concern in the pharmacy and patient community that restricting reimbursement could affect older people and those with complex medication regimens. Many community pharmacists argue that MDS blister packs are a proven adherence tool, particularly for patients with cognitive decline or who live alone.
While the Minister’s reply reinforces that phased dispensing is not being abolished, pharmacy groups are likely to seek further clarification on how the new rules will apply in practice and whether exceptions will be made for vulnerable patients whose adherence depends on blister pack support.
With the new Community Pharmacy Agreement promising a “patient-centred reinvestment” of ¤20 million, the profession will be watching closely to see how those savings are channelled — and whether the intended safety and efficiency benefits materialise for patients on the ground.
Medicines Supply and Pricing
The Minister for Health Jennifer Carroll MacNeill has announced the commencement of discussions between the State and Irish Pharmaceutical Healthcare Association (IPHA) on the Framework Agreements on the Supply and Pricing of Medicines.
These discussions will aid the development of a new multiannual Agreement which supports the financial sustainability of medicines and improves access to innovative new medicines for patients.
The commencement of formal talks follows extensive preliminary engagement between the Department of Health, Department of Public Expenditure, Infrastructure, Public Service Reform and Digitalisation, the Health Service Executive (HSE) and IPHA.
Minister Carroll MacNeill said, “I am pleased that these formal talks have commenced. This longstanding relationship has been an important one, particularly for patients in Ireland, contributing towards a sustainable supply of innovative medicines.
"We remain committed to supporting timely access to new and innovative medicines. This is underpinned by the continued collaboration between the State and the pharmaceutical industry on our shared objectives of reaching decisions on applications within the context of existing legislation for the benefit of patients.
“I look forward to continuing to work in partnership with the pharmaceutical industry to realise our shared ambition for enhanced access and affordability of medicines in Ireland.”
The State has entered into agreements with the pharmaceutical industry since the 1970s, bringing certainty and stability to the supply and pricing of medicines.
The 2021-2025 Agreement with the Irish Pharmaceutical Healthcare Association was signed in December 2021. A parallel Agreement with Medicines for Ireland (MFI) was also signed in 2021. The State will separately negotiate with MFI on a potential successor Agreement in due course.
Budgets 2021 to 2025 provided ¤158 million for new medicines.
Deputy Pat the Cope Gallagher TD
Record Budget Marks a Turning Point — or Another Test of Delivery Budget 2026:
What It Means for Community Pharmacy
The Government’s Budget 2026 sets a new record for health spending — €27.4 billion, a €1.5 billion (6.2%) increase on 2025. Ministers describe the package as a “performance-led investment” designed to improve access, modernise care, and strengthen delivery at every level of the health system.
For community pharmacists, the record allocation signals both opportunity and scrutiny. While the Budget includes new investment in medicines and workforce expansion, sector leaders warn that the practical delivery of care in communities will depend on resolving chronic issues around funding, staffing, and service integration.
“This is a budget about smarter delivery, not just higher spend,” Minister for Health Jennifer Carroll MacNeill TD said. “We are asking every part of the health system — especially primary and community care — to demonstrate measurable impact.”
A Performance-Led Model for Local Care Delivery Budget 2026 formally ties funding to performance — with all six Health Regions gaining more autonomy to direct spending according to local needs. For community pharmacy, this regionalisation could finally enable
locally commissioned pharmacy services aligned with GP and primary-care networks.
The Department of Health says the approach continues the Sláintecare shift toward care “closer to home,” integrating pharmacy, general practice, and community nursing under shared access and outcome metrics.
Digital enablement is central: the rollout of eHealth, shared care records, and e-prescribing is now linked to budgetary accountability. Pharmacy leaders view this as essential to expanding pharmacists’ clinical role in areas such as chronic-disease management, vaccination, and medicines optimisation.
Key Budget Figures at a Glance
Focus on Access, Prevention and Workforce
The Budget’s four pillars — equity of access, safety and prevention, capacity and reform, and productivity/value — have clear implications for community pharmacy.
Expanded investment in the Primary Care Reimbursement Service (PCRS), including ¤30 million for new medicines, underpins both patient access and pharmacy viability. Yet workforce pressures persist. The Pharmaceutical Society of Ireland (PSI) has warned of mounting shortages across the pharmacy workforce and called for structured planning to sustain community services.
While the addition of 3,300 new HSE staff will strengthen system capacity, pharmacy organisations
Minister for Health Jennifer Carroll
note that community settings need dedicated funding for pharmacist expansion, not just broader healthservice headcount.
Community Pharmacy: The New Front Line
Community pharmacists increasingly act as firstcontact clinicians — delivering vaccinations, emergency contraception, and medication reviews. Budget 2026’s emphasis on performance-led, seven-day access could open the door to extended pharmacy opening hours and new service contracts, but only if reimbursement and staffing models evolve accordingly.
The Irish Pharmacy Union (IPU) welcomed the Budget’s “commitment to primary care,” but cautioned that community pharmacies “cannot deliver extended services on historic fees.” Rising operating costs, medicine shortages, and delayed payments continue to undermine viability, especially in rural areas.
“Without a sustainable funding model, the pharmacy network risks erosion — precisely when it’s needed most,” an IPU spokesperson said.
Medicines, Innovation and the PCRS
The ¤217 million PCRS medicines allocation, including ¤30 million for new therapies, has been well received by the sector. The Irish Pharmaceutical Healthcare Association (IPHA) says it should enable reimbursement of up to
32 innovative medicines in 2026, benefiting roughly 6,000 patients across cancer, cardiovascular disease, diabetes, and rare conditions.
Faster access to new medicines strengthens the role of community pharmacists in adherence support, patient education, and pharmacovigilance. The Minister’s confirmation that the statutory 180-day reimbursement timeline will be enforced under the Health Act 2013 is also seen as a major step toward predictability and patient access.
However, ongoing medicine shortages remain a major operational headache. Pharmacists report daily challenges sourcing stock, managing substitutions, and explaining supply gaps to patients — all of which consume clinical time and erode public confidence.
Older Persons, Home Support and Chronic Care
The ¤215 million boost for older persons’ services and 26.7 million funded home-support hours point to an ageing-in-place strategy that relies heavily on local pharmacies. Community pharmacists are central to polypharmacy review, falls prevention, and adherence monitoring — yet few structured programmes currently fund these interventions. Pharmacy leaders argue that redirecting even a fraction of the home-care budget toward pharmacist-led medication management could deliver measurable savings and safety improvements.
Public and Preventive Health: A Growing Role
The Budget’s ¤11 million for public and inclusion health expands national prevention campaigns on youth vaping, obesity, and sexual health. Pharmacists, with their accessibility and public-trust advantage, are expected to play a visible role in delivering these initiatives.
Expanded vaccination services, health-screening pilots, and participation in smoking-cessation programmes are all anticipated, though details on remuneration are pending. The IPU has urged Government to establish a formal Community Pharmacy Services Framework to ensure consistent funding and quality standards nationwide.
The Frontline Reaction: Optimism Tempered by Caution
While the biopharma industry and Department of Health highlight investment and innovation, frontline community pharmacists remain cautious.
Key concerns include:
• Lack of a long-term funding agreement for professional services.
• Persistent workforce shortages, particularly in rural and commuter-belt areas.
• Medicine-supply fragility, with substitutions now routine.
• Need for clarity on expanded scope, including prescribing and independent supply models.
At the same time, there is optimism that the regionalised, data-driven approach will finally reward performance and encourage pharmacist-led innovation — from minor-ailment management to chronic-disease support.
Looking Ahead to 2027
For community pharmacy, Budget 2026 is a crossroads: it recognises the sector’s frontline value but tests the State’s ability to fund and deliver on that recognition.
Key indicators to watch:
• Implementation of new community-pharmacy service contracts.
• Workforce and training investment aligned with PSI recommendations.
• Progress toward e-prescribing and digital integration.
• Delivery of the 180-day reimbursement timeline for new medicines.
• Supply-chain resilience and shortage mitigation.
If achieved, these measures could cement community pharmacy as a cornerstone of integrated primary care. If not, another year may pass with ambitions outpacing the resources to realise them.
“Pharmacists are ready to do more,” one Dublin contractor said. “The question is whether the system is ready to let us.”
What It Means for Community Pharmacists
Opportunities
• Increased PCRS and new-medicine funding.
• Potential expansion of pharmacy-based clinical services under Sláintecare.
• Greater integration with primary care teams and digital systems.
• Growing public-health role through vaccination and prevention campaigns.
Challenges
• No clear framework for expanded service remuneration.
• Ongoing staff and medicine shortages.
• Administrative complexity under regional performance models.
• Rising operational costs and recruitment difficulties.
Europe’s Pharmacy Vision: What It Means for Irish Pharmacists
New European data show just how far community pharmacy has evolved — and how much more it could do in Ireland if policy keeps pace.
Across Europe, community pharmacists are transforming from medicine dispensers to frontline health partners. The Pharmaceutical Group of the European Union (PGEU)’s Report on Pharmacy Services in Europe captures that shift in clear numbers: in 33 countries, an average of 26 distinct pharmacy services are now formally recognised, spanning vaccination, chronic-disease management, screening, digital health, and casemanagement programmes.
It’s a powerful reminder that pharmacy is no longer a secondary access point. With more than half a million pharmacists delivering four billion patient interactions annually, Europe’s community pharmacies have become a cornerstone of primary care. For Ireland — where contractual reform, workforce strain, and scope expansion are all under debate — the message is timely and unambiguous: the profession’s future lies in clinical service delivery.
From Dispensing to Delivering Care
The PGEU report shows how European pharmacists are moving well beyond the counter.
Services such as medicine-use reviews, structured adherence support, disease screening, and pharmacist-led vaccination are not pilot concepts but standard practice across much of the continent.
These roles build on the trust and accessibility that have always defined the profession.
Ireland’s own pharmacies already perform elements of this model: flu and COVID-19 vaccination, emergency contraception, smoking cessation, and supervised dosing. But compared with European peers, the scope and consistency remain limited. The PGEU findings highlight the need to move from ad-hoc initiatives to a structured, nationally funded clinical-services framework.
Removing the Barriers
The report is candid about what still holds pharmacies back: outdated legislation, uneven reimbursement, and patchy digital integration. Pharmacists in many countries can’t yet renew prescriptions, deprescribe, or fully access shared health records — the same constraints Irish pharmacists face.
The European data provide reassurance that these are safe, evidence-based extensions that improve access without compromising clinical governance. Where countries have implemented them, results show higher patient satisfaction and reduced GP workload — two outcomes Ireland urgently needs.
Funding the Future
Sustainable remuneration is the thread running through the report’s policy recommendations. Dispensing remains core, but it can no longer be the sole source of income for pharmacies expected to deliver preventive and clinical care.
The PGEU urges governments to pay for the value pharmacies
President of PGEU Claire Fitzell with MEP Michalis Hadjipantela (EPP) and MEP Vytenis Andriukaitis (S&D)
create, not just the boxes they supply. That includes funding for adherence programmes, screening, vaccinations, and counselling. Without this shift, services risk becoming “optional extras” offered only by pharmacies that can afford them — deepening health inequality.
For Ireland, where the new Community Pharmacy Agreement is reshaping reimbursement, the European position is instructive. If policymakers want pharmacists to deliver on access and prevention goals, the contract must recognise professional time, clinical responsibility, and outcome impact, not just dispensing volume.
Digital Readiness and Workforce Planning
The report also pushes digital transformation and workforce investment to the top of the European agenda. It calls for pharmacists to have read-andwrite access to shared electronic health records, participation in the EU’s digital-health framework, and training in AI-supported care tools.
For Irish pharmacists, digital integration remains a gap. Electronic prescribing and interoperable health records are still incomplete, limiting collaboration and data-driven care. PGEU’s message is clear: the pharmacy of the future is connected — and pharmacists must be part of the system design, not passive users.
Workforce planning is another European imperative. The report warns that without structured national strategies for education, leadership, and continuing development, the sector will struggle to meet growing demand. This echoes the Pharmaceutical Society of Ireland’s Workforce Intelligence Report, which has already highlighted recruitment pressures and the need for new career pathways.
Ireland in the European Picture Ireland performs strongly on accessibility — almost every community has a pharmacy within walking distance — but
less so on service diversity. Many EU counterparts now reimburse medicine-use reviews, structured adherence support, and minorailment consultations. The Irish system, by contrast, still relies heavily on fee-for-supply rather than fee-for-care.
By aligning with the European roadmap, Ireland could unlock new opportunities for pharmacists to manage chronic conditions, deliver local prevention programmes, and contribute to antimicrobial stewardship. These aren’t futuristic ideas; they’re already everyday practice in countries such as Portugal, France, and the Netherlands.
The Irish Government’s emphasis on moving care “closer to home” under Sláintecare aligns perfectly with this direction — but achieving it requires policy follow-through: legislative reform, service commissioning, and sustained investment.
A Call to Action
The PGEU concludes that community pharmacists are essential partners in peoplecentred, sustainable healthcare — but only if policy and funding frameworks evolve accordingly. That conclusion applies squarely to Ireland.
Pharmacists here have proven their value during COVID-19 and in daily front-line service. The challenge now is to ensure that value is recognised systematically, not episodically. The European experience shows that when pharmacists are empowered, patients gain faster access, health systems save money, and communities become more resilient.
As one European policy observer put it:
“Pharmacy isn’t a back-office function anymore — it’s the front door to care.”
For Irish pharmacists, that means embracing the profession’s clinical future while demanding the structures that make it possible: fair remuneration, full digital integration, and a scope of practice that reflects both training and trust.
If Ireland can align ambition with action, its pharmacists won’t just match Europe’s best practice — they’ll help define it.
With phased dispensing fees gone, now is the time to make huge savings off your MDS labour & consumable costs with a Tosho Xana & Pouch Inspector solution!
A MONTH’S SUPPLY OF MEDICATION CAN BE PACKED AND CHECKED IN UNDER 3 MINUTES!
Fed up with slow, costly, manual MDS production?
The manual method of filling MDS trays is both time consuming and labour intensive. JW Pharmacy Solutions offer a total automated solution, which includes: automated de-blistering, automated tablet packing, automated checking and compliance, with seamless integration to your dispensing software.
MANUAL TRAY FILLING:
100 patients per month – labour costs = €100,000 per annum
(1.5 Technicians and 0.4 Pharmacist per month)
200 patients per month – labour costs = €150,000 per annum
(2 Technicians and 0.7 Pharmacist per month)
Tosho and Pouch Inspector Solution:
100 patients per month – labour & machine costs = €40,000 per annum
(0.1 Technician and 0.15 Pharmacist per month)
200 patients per month – labour & machine costs = €60,000 per annum
(0.2 Technician and 0.25 Pharmacist per month)
Consumables savings - €1.50 per month per patient
TOTAL SAVINGS (with Tosho Xana and Pouch Inspector Solution)
100 patients per month; Saving = €60,000+ per annum
200 patients per month; Saving = €90,000+ per annum
Please Note: These figures have been verified by existing Tosho and Pouch Inspector owners!
JW Pharmacy Solutions Ltd
Unit 1a Balmoral Industrial Estate, Kells Road, Navan, County Meath
M: +44 7557 508940 E: johnny@jwpsireland.com
United Drug Elements: Your Trusted Partner for Exempt Medicine Products
At United Drug, we know how important it is for pharmacists to have timely access to medicines that may not be available through regular distribution channels. That is why we created United Drug Elements – a dedicated service for the safe, efficient and reliable supply of Exempt Medicine Products (EMPs).
What is Elements?
United Drug Elements is the specialist sourcing and supply service for unlicensed medicines and pharmaceutical products. Whether due to shortages, discontinuations or unavailability in Ireland, we ensure pharmacies have access to the medicines their patients need.
Our team manages the sourcing, storage and delivery of EMPs in line with HPRA guidelines, giving pharmacists confidence in both the process and the product. Stocked lines are available for same-day delivery, while emergency products can often be turned around in less than 48 hours.
More than a supplier – a partner Like pharmacists, United Drug puts the patient at the centre of everything we do. That philosophy underpins our work in Elements.
Our dedicated EMP Sourcing Team works closely with pharmacists to locate and supply the right products as quickly as possible. We know every request matters, so our team is always available to support with sourcing queries, product searches or advice on quality guidelines.
This partnership approach is backed by practical benefits:
• Safe and secure sourcing under HPRA regulations
• Fast turnaround times, including same-day delivery on stocked lines
• Live stock visibility on UDW.ie
• Simple ordering of non-stocked lines via email, online or phone
• Ongoing investment in technology to make ordering easier
Proactive Sourcing You Can Rely On
Our EMP team actively monitors the HPRA shortages list each week. Where a medicine is at risk of shortage or discontinuation, we move quickly to identify and source alternatives. New EMP listings are added to our system each month, with a focus on Irish alternatives where possible to avoid customs delays and reduce lead times.
This proactive approach ensures patients are not left without essential medication and pharmacists can focus on providing care with peace of mind.
Ordering Through Elements
Ordering EMPs has never been simpler. Through UDW.ie, you can:
• Access the full list of EMP products with live stock visibility
• Request non-stocked lines quickly and easily
• View alternative unlicensed options for unavailable licensed stock
• Manage invoices and credits directly through the portal
Always Here to Help
Our Customer Care team is available on a dedicated phone line (01 463 2410) to support with sourcing queries or EMP quality guidelines. With United Drug Elements, you have a trusted partner that understands the urgency, complexity and responsibility of sourcing unlicensed medicines.
At United Drug, we are committed to providing best-in-class service, safe supply and reliable support so that you can continue to deliver the best care to your patients.
PHX Ireland: Recognising People Awards 2025
At PHX Ireland, people are at the heart of everything they do. The team are a vibrant, energetic community driven by teammates who go above and beyond to support customers, patients, and one another. On Thursday, 11 September 2025, they came together in the beautiful surroundings of the Mansion House, Dublin, to celebrate exactly that at the Recognising People Awards 2025.
This annual programme is a cornerstone of PHX Ireland culture, shining a spotlight on the outstanding contributions, dedication, and values of teammates across the PHX Ireland network, which includes McCabes Pharmacy, United Drug, TCP Homecare, and PHX Ireland.
The awards are based on the core values, Customer Focused, Quality Driven, Collaborative, Ambitious, and Innovative, and are designed to honour those who embody these principles every day. With over 550 nominations submitted across our teams, and 90 finalists chosen across nine categories, this year’s celebration was a true reflection of the pride and passion that exists across PHX Ireland.
Awards were presented by members of the Senior Leadership Team, who expressed genuine admiration and pride as they celebrated the achievements of teammates. Guests were also treated to inspiring opening and closing addresses from CEO, Paul Reilly, framing the night with words of encouragement and appreciation.
The teams from PHX Ireland celebrating at the Recognising People Awards
Market Leader in the sourcing and supply of unlicensed medicines
Ireland's largest portfolio of sourced unlicensed medicines
If it’s not on the list, it’s on the way! products ready to order
We estimate that there were 100 pharmacy sector transactions over the 36-month review period from H2 2022 through to H1 2025. Fitzgerald Power advised on 44 of these transactions.
We estimate that there were 100 pharmacy sector transactions over the 36-month review period from H2 2022 through to H1 2025. Fitzgerald Power advised on 44 of these transactions.
In the below table we have analysed the transactions over the review period based on annual State dispensing fees.
Confidence, consolidation and the changing face of ownership in Ireland’s community pharmacy sector
TRANSACTIONS BY SIZE
In the below table we have analysed the transactions over the review period based on annual State dispensing fees.
After a subdued 2024, the Irish pharmacy M&A market has regained its footing. According to new data from Fitzgerald Power’s Irish Pharmacy Sector M&A Review H1 2025, 17 pharmacies changed hands in the first half of the year — nearly double the nine recorded in the previous six months. Spread across a three-year rolling period, activity now averages around 100 transactions since 2022, confirming that the market has settled into a pattern of measured but consistent dealmaking.
quality of earnings, operational strength and regional opportunity
Transactions: Bigger, Smarter, More Regional
We estimate that there were 100 pharmacy sector transactions over the 36-month review period from H2 2022 through to H1 2025. Fitzgerald Power advised on 44 of these transactions.
TRANSACTIONS BY SIZE
For pharmacy owners and would-be buyers, the numbers tell a story of steady recovery, renewed confidence, and cautious professionalism. Interest rates are easing, access to finance is improving, and the new Community Pharmacy Agreement promises to reshape how pharmacies are valued. Yet this is no return to boom-era exuberance: the focus has shifted firmly toward
“The Irish pharmacy market remains active, but it’s a more strategic kind of activity,” says one sector analyst familiar with the data. “Buyers are asking harder questions about sustainability, and sellers are coming to market better prepared.”
Across the three-year review window (Q3 2022 – Q2 2025), Fitzgerald Power estimates around 100 single-unit pharmacy transactions nationwide. The firm advised on 44 of those, providing one of the clearest windows into valuation trends and buyer behaviour available in the sector.
The data shows a distinct upward drift in deal quality. Pharmacies earning annual State dispensing fees of ¤250 000 or more have dominated transactions every year. Mid-range deals (¤175 000–¤249 000) are gaining ground, while smaller pharmacies under ¤175 000 are gradually disappearing from the M&A radar. It’s a sign of consolidation around scale and stability: pharmacies with stronger
Pharmacies receiving state fees ≥ €250K accounted for the majority of transactions every year over our review period. Mid-range deals (€175K–€249K) have grown, while smaller transactions (€100K–€174K) and low-value deals (<€100K) have declined, highlighting a clear shift toward higher-value deals in the sector.
In the below table we have analysed the transactions over the review period based on annual State dispensing fees.
TRANSACTIONS BY SIZE
TRANSACTIONS BY OWNERSHIP TYPE
Pharmacies receiving state fees ≥ €250K accounted for the majority of transactions every year over our review period. Mid-range deals (€175K–€249K) have grown, while smaller transactions (€100K–€174K) and low-value deals (<€100K) have declined, highlighting a clear shift toward higher-value deals in the sector.
The majority of transactions involved the sale of independently owned pharmacies. Over the review period, the proportion of corporate group pharmacies sold increased, while the share of symbol group pharmacies disposed of declined. Transactions involving indigenous group pharmacies remained relatively stable, showing only minor fluctuations across the periods.
TRANSACTIONS BY OWNERSHIP TYPE
The majority of transactions involved the sale of independently owned pharmacies. Over the review period, the proportion of corporate group pharmacies sold increased, while the share of symbol group pharmacies disposed of declined. Transactions involving indigenous group pharmacies remained relatively stable, showing only minor fluctuations across the periods.
Pharmacies receiving state fees ≥ €250K accounted for the majority of transactions every year over our review period. Mid-range deals (€175K–€249K) have grown, while smaller transactions (€100K–€174K) and low-value deals (<€100K) have declined, highlighting a clear shift toward higher-value deals in the sector.
TRANSACTIONS BY OWNERSHIP TYPE
TRANSACTIONS BY LOCATION
The majority of transactions involved the sale of independently owned pharmacies. Over the review period, the proportion of corporate group pharmacies sold increased, while the share of symbol group pharmacies disposed of declined. Transactions involving indigenous group pharmacies remained relatively stable, showing only minor fluctuations across the periods.
Over the past three-year rolling period, Leinster (excluding Dublin) experienced a significant increase in deal activity, rising from 22% to 38% in the latest period, making it the most active region. Munster also showed consistent growth, with its share increasing from 24% to 31%. In contrast, Connacht/Ulster’s share fell from 24% to 15%, reflecting a slowdown in transactions. Dublin recorded the sharpest decline, dropping from 32% in H2’23–H1’24 to 15% in H2’24–H1’25.
TRANSACTIONS BY LOCATION
TRANSACTIONS BY LOCATION
Over the past three-year rolling period, Leinster (excluding Dublin) experienced a significant increase in deal activity, rising from 22% to 38% in the latest period, making it the most active region. Munster also showed consistent growth, with its share increasing from 24% to 31%. In contrast, Connacht/Ulster’s share fell from 24% to 15%, reflecting a slowdown in transactions. Dublin recorded the sharpest decline, dropping from 32% in H2’23–H1’24
State income streams, higher prescription volumes and more diversified revenue are now the most attractive assets.
Regional balance re-emerges
The most active region for deals in the latest period is Leinster (excluding Dublin), which now accounts for 38% of all transactions — up sharply from 22% a year earlier. Munster follows with 31%, continuing its steady rise. By contrast, Dublin’s share of deals has almost halved, from 32% in 2023–24 to just 15% in the most recent cycle.
The picture in Connacht/Ulster is also quieter, dropping to 15%.
These shifts suggest that the centre of gravity in pharmacy ownership is moving outwards — toward regional hubs and commuter towns where growth potential, property affordability and staffing stability may outweigh citycentre turnover.
“Regional buyers are driving the market,” one broker notes. “They’re often pharmacists who know their communities, see an opportunity to expand locally and want to build something sustainable.”
• Mid-tier stores (¤1 m – ¤1.5 m) averaged 4.93 ×
• Upper-mid (¤1.5 m – ¤2 m) achieved 5.13 ×
• The largest cohort, those above ¤2 million, reached an impressive 5.67 ×
These gradients highlight the premium attached to scale — not only higher profitability but also operational depth, stronger management teams and more diversified income.
Regional differentials
While valuations were broadly consistent nationwide, Dublin still leads with an average multiple of 5.28 ×, influenced by several highvalue transactions in larger stores.
Leinster (excluding Dublin) follows at 5.05 ×, Munster at 4.85 ×, and Connacht/Ulster at 4.64 ×
Crucially, these regional spreads are narrowing compared with earlier years, another sign of market maturity and the levelling effect of national reimbursement models.
What drives value now
5.17X
transactions shows a nuanced market structure.
Independent operators completed 26 purchases, while pharmacy groups (defined as owners of six or more outlets) accounted for 18.
The headline difference lies in deal size and valuation.
26
4.75X
with reduced upfront capital. These arrangements bridge the gap between employee and entrepreneur, often facilitated by groups seeking motivated managing partners.
Valuations: Stability Amid Transition
VALUATION MULTIPLES
• Independent buyers paid an average 4.75 × EBITDA.
• Groups paid a higher 5.17 × EBITDA.
We have estimated the valuation multiple achieved on each transaction for which we have visibility by comparing the maintainable EBITDA presented in information memorandum to the actual consideration paid (before the working capital adjustment).
If there’s one headline number for 2025, it’s 4.92 × EBITDA — the average multiple achieved across Fitzgerald Power’s 44 transactions. That figure is almost identical to the 4.91 × recorded in the previous rolling period, demonstrating a market that has found equilibrium.
VALUATION MULTIPLES
With interest rates trending downward and the new Community Pharmacy Agreement introducing reimbursement changes, valuers expect closer scrutiny of each pharmacy’s quality of future earnings. Buyers and lenders alike want clarity on how sustainable profitability will be under the revised funding regime.
Groups generally target higherrevenue pharmacies — five of the ten pharmacies with turnover above ¤2 million went to group acquirers — reflecting their appetite for scale efficiencies and centralised management.
Interest-rate reductions have made financing more accessible, while lenders have grown comfortable with pharmacy’s low-risk profile. The result: a new generation of “operator-owners” bringing fresh energy to local pharmacies, often supported by group resources but maintaining independent ethos.
We have estimated the valuation multiple achieved on each transaction for which we have visibility by comparing the maintainable EBITDA presented in information memorandum to the actual consideration paid (before the working capital adjustment).
Hybrid deals on the rise
The average multiple achieved over the three-year review period to end of H1 2025 was 4.92X, which was very similar to the 2024 three-year rolling average of 4.91X. We analysed the multiple achieved by turnover bracket and as expected, the average multiple increased in line with the increase in the size of the pharmacy, in revenue terms.
Size matters
Valuation multiples rise predictably with pharmacy turnover.
EBITDA is still the anchor metric, but elements such as clinical service delivery, digital integration, and workforce stability are beginning to influence deal pricing.
“We’re seeing a more collaborative ownership model,” notes a senior advisor. “It’s no longer just big groups versus lone independents — it’s partnerships built around capability and community presence.”
• Pharmacies under ¤1 million turnover averaged 3.69 × EBITDA.
Buyers: Independent Spirit Meets Corporate Scale
The average multiple achieved over the three-year review period to end of H1 2025 was 4.92X, which was very similar to the 2024 three-year rolling average of 4.91X. We analysed the multiple achieved by turnover bracket and as expected, the average multiple increased in line with the increase in the size of the pharmacy, in revenue terms.
Fitzgerald Power’s analysis of 44
A defining feature of 2025 is the growth of hybrid ownership structures — partnerships or deferred-equity models that allow pharmacists to step onto the ownership ladder
Valuations were largely consistent across the country with transactions in Dublin achieving the highest average valuation multiple at 5.28. It should be noted that 5 of the 10 >€2m turnover transactions were in the Dublin region, which has impacted the average earnings multiple achieved in this region.
Valuations were largely consistent across the country with transactions in Dublin achieving the highest average valuation multiple at 5.28. It should be noted that 5 of the 10 >€2m turnover transactions were in the Dublin region, which has impacted the average earnings multiple achieved in this region.
The Market Picture: A Sector Holding Steady
Despite ongoing consolidation, the total number of community pharmacies in Ireland remains remarkably stable.
According to PSI data cited in the report, there were 1 913 pharmacies at the start of 2023 and 1 908 by Q2 2025. Over that time, there were 69 openings and 66 closures, leaving a near-netzero change.
This equilibrium reflects a mature, saturated market where growth comes primarily through acquisition rather than new openings. Barriers to entry — capital costs, location saturation, and workforce pressures — remain high, while local demand dynamics keep closures limited.
For the profession, this stability is double-edged: it signals resilience, but also underscores the need for innovation in service delivery, diversification, and digital engagement to maintain margins.
Outlook: Confidence Returns — with Caution
Looking ahead to the second half of 2025, Fitzgerald Power anticipates continued momentum in deal activity, driven by easing interest rates and improved financing conditions.
Mergers and rationalisations
A notable recent trend involves “proximity mergers” — where smaller units are acquired by nearby pharmacies and integrated to create a single, more efficient operation. This approach maintains service continuity for patients while improving business sustainability. Expect to see more of these rationalisations as owners seek efficiency without reducing community access.
Impact
of the new Community Pharmacy Agreement
Announced in September 2025, the new Agreement will reshape reimbursement structures and service delivery expectations. Its ultimate impact on valuations remains to be seen, but early analysis suggests greater
emphasis on clinical services and outcome-based payments.
In valuation and due diligence exercises, earnings quality — not just headline profitability — will become a primary focus. Pharmacies demonstrating diversified income from vaccination, minor-ailment schemes, or digital health services may command premium valuations in future transactions.
Economic undercurrents
While macroeconomic headwinds — inflationary cost pressures, wage expectations, and supplychain challenges — continue to test operators, the combination of lower borrowing costs and steady consumer demand is supporting optimism across the sector.
The general consensus: 2025 marks a transition from uncertainty to cautious confidence.
What It Means for Pharmacy Owners
For independent pharmacy owners, the current environment represents both an opportunity and a test.
Thinking of selling?
Transaction multiples remain robust, but buyers are more discriminating. Owners considering exit should focus on:
• Demonstrating stable dispensing volumes and wellmanaged operating costs.
• Ensuring compliance, governance and HR structures are up to date.
• Highlighting community reputation and patient-service quality — qualitative factors increasingly valued in due diligence.
A well-prepared pharmacy can still achieve strong valuations, particularly if it offers scale or location advantages. However, expectations must remain realistic: the era of automatic premium pricing is over.
Thinking of buying?
For aspiring owners, especially pharmacists seeking their first purchase, the window is open wider than it has been for several years.
Hybrid and partnership models can lower entry barriers, and lenders are receptive to applicants with solid professional backgrounds and detailed business plans.
Still, prudence is essential: the most successful acquisitions are those grounded in realistic growth projections, strong local market knowledge and disciplined management of working capital.
The Bigger Picture: Professionalism Over Speculation
The data paints a portrait of a sector defined not by volatility, but by measured professionalism. The average valuation multiple may have plateaued, but that stability is itself a sign of maturity. Buyers are sophisticated, sellers are better advised, and the market operates with transparency unimaginable a decade ago.
The Irish Pharmacy Sector M&A Review 2025 shows a community that values sustainable growth over quick wins — a reflection of how far the profession has evolved from the frenetic expansion years of the early 2000s.
For the public, this means continuity of care; for pharmacists, it means a business environment where long-term stewardship is finally being rewarded.
“The pharmacy market has entered a new era,” concludes one adviser. “It’s less about how many pharmacies you own, and more about how well they perform and integrate into the wider healthcare system.”
Looking to 2026: The Shape of What’s Next
As Ireland’s health system continues to regionalise under Sláintecare, community pharmacy will remain central to local healthcare delivery. The next wave of M&A will likely align with service-based growth — pharmacies positioned to deliver vaccinations, diagnostics, and chronic-disease management are expected to attract premium investor interest.
Meanwhile, the anticipated continuation of low interest rates should sustain transaction activity, though valuations may edge toward greater differentiation based on quality of earnings.
In essence, pharmacy ownership in Ireland is consolidating around capability. Scale matters, but so does professionalism, data quality, and the ability to adapt to evolving healthcare models.
Final Word
Ireland’s pharmacy sector has weathered economic uncertainty, reimbursement reform and demographic change with quiet resilience. The H1 2025 M&A data confirm a market that is neither overheated nor stagnant — a market defined by confidence tempered with discipline.
For pharmacists contemplating their next move — whether expansion, partnership or succession — the message is clear:
The opportunity is real, but preparation is everything.
Masters of Pharmacy Programme
A new Master’s of Pharmacy (MPharm) Degree Programme at South East Technological University (SETU) has been accredited by the PSI – the Pharmacy Regulator. SETU intends to offer the MPharm Programme from next September 2026 at its Waterford campus.
Dr Aisling Croke (MPSI), Lecturer in Pharmacy; Dr Claire Lennon, Head of Department of Pharmacy; Sarah Brown (MPSI); and Dearbhla Walsh (MPSI), both Lecturers in Pharmacy
This is the third new pharmacy programme accredited this year by the PSI. It brings to six the number of MPharm courses that will be available from 2026 to people wishing to study pharmacy in Ireland.
Having been engaged with universities towards accreditation over the past two years, the Council of the PSI, the pharmacy regulator’s governing board, was pleased to accredit the SETU programme at its meeting on 2 October*.
This new pharmacy programme is established following the Government commitment to funding for expanded healthcare places, including the creation of three new MPharm Programmes. The MPharm provides the qualification necessary for registration to practise as a pharmacist and is a five-year integrated programme that incorporates clinical and other experiential learning placements.
Speaking about the accreditation of the new programme, PSI Registrar and Chief Officer, Joanne Kissane, said, “Congratulations to all those involved in establishing the new programme at South East Technological University.
The PSI has been pleased to support the expansion of pharmacy programmes through our accreditation role since first proposed by Government through the Higher Education Authority (HEA) in 2023. Approval of this new MPharm Programme is positive for SETU, the southeast region, and for students wishing to study pharmacy within Ireland.”
“The availability of a greater number of student places is significant for those interested in this field of study, for the future provision of patient care, and for our evolving healthcare services."
"Today’s announcement is another positive milestone for our ongoing work with the Department of Health and many other stakeholders in relation to workforce planning for pharmacy and for the range of healthcare
services and industries where pharmacists can contribute their expertise.
“Our role as the pharmacy regulator is to maintain and support patient safety and public trust in pharmacy. This includes accrediting and approving educational programmes for pharmacy and for setting the accreditation standards that must be met on an ongoing basis by the approved pharmacy programme providers. Our aim is to ensure that future pharmacists are equipped to meet their professional and clinical obligations, the needs of patients and the health system.”
The President of SETU, Professor Veronica Campbell, added, “Accreditation of our MPharm programme represents a major step for SETU in expanding healthcare education and training in Ireland. Our provision of the programme will ensure that students across the southeast can pursue their studies regionally. More broadly, it allows our university to have a direct impact on the development of pharmacy in healthcare, community, and industry settings. The programme supports the need for expansion of the national pharmacy
workforce, and the establishment of our new Department of Pharmacy directly responds to these national, regional, and university imperatives. It also builds on SETU’s existing strengths in pharmaceutical science, bioscience, nursing and healthcare, teaching and research. I would like to acknowledge and thank the HEA and the Department of Further and Higher Education, Research, Innovation, and Science (DHERIS) for their support in bringing the MPharm programme to fruition."
Dr Claire Lennon, Head of the Department of Pharmacy at SETU, commented, “Our multidisciplinary cross-campus MPharm development team at SETU is very proud to have received Pharmaceutical Society of Ireland accreditation. The team has worked extremely hard to develop an innovative and impactful, futurefocused MPharm programme. Pivotal to programme development has also been the collaborative input and support of our pharmacy professional advisory committee, and stakeholders from community, hospital, and industry pharmacy settings across the southeast. This will ensure graduates meet the requirements of modern pharmacy
practice and the skills needs of the sector, all the while maintaining a patient-centred focus. We look forward to welcoming our first group of 40 students to the programme in 2026.”
Commending the availability of the new pharmacy programme, the Minister for Health, Jennifer Carroll McNeill, said, “I extend my sincere congratulations to South East Technological University on the successful accreditation of its Masters in Pharmacy programme. This innovative programme will provide students in the South East with the opportunity to pursue a career in pharmacy closer to home and reflects the Government’s strategic investment in regional education and our commitment to expanding access to high-quality healthcare training across all regions of the country.
"I look forward to seeing the first group of students begin their journey in pharmacy education in Waterford from September 2026 and to the lasting impact they will have on patient care and public health across Ireland.”
Prospective students for the new MPharm Programme are encouraged to communicate with the relevant universities directly.
One Seamless System: Integrate your EPOS and dispensary systems for smarter pharmacy workflow
DispenSense, launched by Navi Group, - the first fully-cloud based PMR product to be launched in the Irish pharmacy market - uses the latest, state-of-the-art software technologies which are future-proofed to address the challenges facing a pharmacist today and into the future, while also offering superior flexibility and operational efficiencies.
The incorporation of state-of-the-art technologies ensures that DispenSense is not just a software solution; it’s a catalyst for positive change and digital transformation within the pharmacy landscape. This cuttingedge software, designed by pharmacists and technicians, boasts unrivalled features and modules striving to make dispensing reliable, safe, and efficient, while empowering teams to overcome everyday challenges and maximise their focus on patient care.
TillSense is Navi Group’s latest and most advanced EPOS solution, designed specifically for pharmacies based on feedback we have received from our network of 600+ independent pharmacies. For many years, the pharmacy sector has required innovation and a POS system that can cater to the needs of a constantly growing industry. TillSense provides the necessary flexibility, innovation, and tools to manage your pharmacy business effectively and efficiently, centred around improved ordering integrations, pricing and stock management, and reporting.
Integration
With Navi’s goal of “making pharmacy easier,” we knew it was crucial for our two systems –EPOS & dispensary – to “speak” to each other, making everyday life in the pharmacy even more efficient.
Integrating a pharmacy EPOS system with dispensary software (PMR or pharmacy management system) delivers major operational, financial, and customer service advantages by uniting retail and clinical workflows.
Key Benefits
1. Enhanced Workflow Efficiency
Integration removes the need to constantly switch between systems or physical locations, enabling pharmacists to check prescription statuses, update records, or process payments
directly from the counter. This reduces waiting times and duplicates of effort across systems.
2. Enhanced Patient Safety
Linked systems share real-time patient and prescription data, allowing automatic verification of patient information, dispensing warnings, and alerts for potential interactions or errors before completion of sales or handover.
3. Connecting prescription and OTC sales
All sales of prescription medications through the EPOS system will be linked to the respective patient’s prescription in DispenSense. This allows visibility in BI for both prescription and non-prescription products sold together.
4. Real-Time Inventory Synchronisation
Unified systems maintain synchronisation between OTC and prescription stock. This ensures accurate stock counts, automatic reordering, and real-time visibility of fastor slow-moving items, helping minimise overstocking or shortages.
5. Basket Analysis and Cross-Selling Opportunities
BI tools will provide insights into the OTC products sold alongside prescription medicines. When a prescription medicine is scanned, the system will suggest relevant OTC products that could be cross-sold, enhancing customer service and increasing sales.
6. Better Customer and Patient Experience
Pharmacists can provide faster, more personalised service, instantly confirm prescription readiness, and manage transactions without leaving the patient waiting.
7. Compliance and Audit Readiness
Because all sales and prescription events are logged in one system, audit trails are easier to maintain and retrieve, supporting compliance with pharmacy regulations and facilitating insurance or HSE claim validation.
8. Cost and Space Savings
Modern integrated systems consolidate hardware (shared terminals and printers), eliminate redundant software licences, and reduce maintenance costs. They also streamline printing of shelf-edge labels, claim forms, and patient receipts from one interface. Navi
Group is a software solutions provider –any hardware is provided at cost price, with no mark up.
9. Business Growth Potential
With cross-system data, pharmacies can better identify profitable product ranges, apply targeted promotions, and plan services more effectively. Integration supports future technology adoption, including automated dispensing robots. Built with BI and automation at the core, this integration ensures long-term scalability.
In essence, integrating pharmacy EPOS and dispensary systems like TillSense and DispenSense unifies operational, clinical, and retail functions—saving time, improving accuracy, and elevating both patient and business outcomes.
Coming soon
Our upcoming Script Finder feature will enhance the tracking and storage of prescription bags in the pharmacy. The benefits of this feature include:
1. Prescription Tracking and Storage
o Track stock levels of prescriptions stored in bags ready for collection.
o Highlight prescriptions not collected by patients after a set period, prompting their return to stock.
2. Multiple Storage Locations
o Ability to track prescriptions stored across multiple locations (e.g., fridge, drawer).
To learn more about this integration, our individual systems or to book a demo, get in touch at dispensense.ie or by email at hello@dispensense.ie.
DispenSense interface
TillSense interface
Smarter Safety: How AI Uses Data to Prevent Dispensing Errors in Irish Pharmacies
Dispensing errors are one of the most critical risks in community pharmacy. While most are caught before they reach the patient, even near misses can reveal valuable lessons. Every mistake, no matter how small, is an opportunity to improve systems, protect patients, and reduce long-term costs to both pharmacies and the wider healthcare system.
At Taskgo AI, we’re building Ireland’s first intelligent tool to help pharmacies take control of this risk — turning errors and complaints into actionable insights that improve patient safety, boost compliance, and enhance operational efficiency.
AI Oversight for Safer Dispensing
Our latest AI-powered system is designed to help pharmacy teams easily report dispensing errors, near misses, and patient complaints. Staff simply enter the details into a secure digital log, which then automatically notifies the superintendent pharmacist. This immediate alert system ensures transparency, real-time oversight, and the ability to take swift corrective action.
But our tool goes much further than traditional reporting. As more entries are logged, Taskgo AI learns from the data. It identifies the most frequent types of errors, the times of year they happen most, and the contributing factors behind them. For example, if a particular type of error increases every December, a pharmacy can prepare ahead of time — adjusting staffing, reviewing SOPs, or offering refresher training.
Business Intelligence Meets Patient Safety
Using integrated business intelligence dashboards, the system gives superintendents and owners a clear overview of SOP compliance, recurring risk factors, and key safety trends. Rather than trawling through
Written by Adam Esa, Superintendent Pharmacist
About the Author: Adam Esa is a superintendent pharmacist in Ireland and the director of Taskgo AI. He has previously founded and exited multiple health tech ventures, including a pharmacy-focused healthtech education company.
paper logs or spreadsheets, pharmacy leaders can now access real-time insights to make informed decisions about training, processes, and risk management. This technology not only supports better compliance with pharmacy regulations, but also reduces the financial impact of dispensing issues — from loss of stock to reputational damage and potential legal claims.
Building a Smarter, Safer Pharmacy Network
Looking to the future, our vision is to connect as many pharmacies as possible into a shared learning network. By pooling anonymised data, we can identify nationwide patterns in pharmacy errors, better understand the pressures on frontline staff, and share solutions more effectively.
We also aim to collaborate with regulatory boards and representative unions to ensure that this data supports national improvements — not just in safety, but in how pharmacies are supported and resourced.
As our AI system continues to learn, we’re training it to
Call for Pharmacy Placements
understand how pharmacists respond to specific types of errors. This will allow it to suggest action points in the future, such as offering tailored SOP updates, risk alerts, or training modules — helping pharmacists make safer decisions in real time.
The Cost of Inaction
Dispensing errors can have serious consequences — from minor patient inconvenience to lifethreatening outcomes. But even when no harm is caused, these mistakes carry a cost: wasted medication, lost time, patient dissatisfaction, and potential legal implications. More importantly, repeated errors without intervention put both patient trust and professional credibility at risk.
By turning isolated incidents into structured, learnable data, Taskgo AI helps pharmacies shift
from reactive problem-solving to proactive safety management. It’s a smarter way to protect patients, reduce risk, and build a culture of continuous improvement.
Learn
Learn More
To find out how your pharmacy can AI, visit www.digitalpharmacy.ai and
To find out how your pharmacy can reduce dispensing errors and improve compliance using AI, visit www.digitalpharmacy.ai and request a free demo today.
APPEL are now accepting expressions of interest for the 2026 4th-year pharmacy placements, running from 31st August to 18th December 2026
About the Author
These placements are a vital part of our students’ journey toward professional practice. In their 4th year, students can complete placements across a wide range of settings; from community and hospital pharmacy to industry and innovative, role-emerging areas of practice. By hosting a student, you will have the opportunity to:
• Support the next generation of pharmacists
• Contribute to your own CPD through mentoring and supervision
• Strengthen your organisation’s talent pipeline
• Share your expertise and shape the future of the profession
Register your interest by completing this short form here, by 14th November 2025.
If you have any questions or would like further details, please don’t hesitate to get in touch with eoi@appel.ie
Adam Esa is a superintendent pharmacist previously founded and exited multiple healthtech education company.
Boots Ireland – Recycling Champions
Boots Ireland has been announced as winner of the Repak Business Recycling Champion Award at the Repak Resource Awards 2025, recognising their ongoing commitment to reducing waste and driving sustainable change.
The win comes as Boots Ireland celebrate another major milestone, 1 million products scanned through their Recycle at Boots scheme.
Available in 54 stores nationwide, Recycle at Boots makes it easier for customers to return beauty, health, wellness, and dental empties that can’t be recycled at home. It’s a simple way to make a big difference - turning empties into opportunities, with customers earning ¤5 worth of Advantage Card points when they recycle five qualifying items and spend ¤10 in store.
This recognition reflects their ambition to be trusted for generations to come, making a positive impact not just within their stores, but in their communities and for the planet.
A spokesperson said, “Thank you to Repak and sponsors ERP Ireland, James Burgess, Yvonne Holmes for the recognition and to all our colleagues and customers helping us build a more sustainable future.”
IIOP Mentoring Programme – Applications Open
The Irish Institute of Pharmacy (IIOP) Mentoring Programme is for pharmacists, by pharmacists. Pharmacists from across the profession are invited to apply for the flexible programme running from December to May 2026. Applications are open for mentors and mentees until Friday, 7 November.
What’s involved?
The aim of the IIOP Mentoring Programme is to empower pharmacists to take control of their professional development and to realise the benefits of reflective practice. Practically, this means pairing pharmacists with
a pharmacist mentor to support them with their development. Our programme is flexible by nature with orientation training and ongoing support provided by the programme team.
The programme will run for 4-6 months between December 2025 and May 2026. Previous mentoring pairs reported meeting for 60 minutes virtually or in person every 3-4 weeks, outside of work, with some time spent on preparation and reflection in between meetings. Who can apply?
Mentees
Applications are open to all pharmacists across the profession, at any stage of your career and in any practice area.
This is an opportunity to access to your own personal mentor who is there to support you in your development. Mentee orientation training will take place online on Monday 24 November.
Mentors
Applications for mentors are open to all pharmacists who have completed the IIOP Mentorship Skills Training. Have you completed this training and want to put your skills into practice? Would you like to support a fellow pharmacist with their development? Are you looking to develop your mentoring skills further? Training and support will be provided. Mentor orientation training will take place online on Tuesday 25 November.
First Endometriosis Framework
The Minister for Health, Jennifer Carroll MacNeill, TD, has launched the National Framework for the Management of Endometriosis in Ireland, marking an important milestone in the evolution of women’s healthcare in Ireland.
Developed by the Health Service Executive’s (HSE) National Women and Infants Health Programme (NWIHP), the framework reflects the voices of patient advocates and aims to transform how endometriosis is recognised and treated across the country. Central to the Model of Care is the principle of presumed diagnosis, proposing that a woman presenting with symptoms should be treated on the presumption that she has endometriosis.
The care pathway spans primary care to secondary care and complex tertiary care. Moderate cases will be treated in five regional specialist centres. Complex cases will be referred to two supra-regional centres in Tallaght University Hospital and Cork University Maternity Hospital.
In addition to the launch of the Framework, Minister Carroll MacNeill has mandated several actions to accelerate access to care for women affected by this debilitating condition.
• The HSE will increase the number of surgeries over the coming months and will carry out more than 100 additional surgeries for women waiting for treatment across all regions.
• An Endometriosis Advisory Group has been established.
• To improve education and training, international endometriosis experts will be invited to collaborate and engage with our clinicians to improve treatment options, build expertise and share learnings.
• The HSE will be communicating with all GPs, consultants and other clinicians to raise awareness of endometriosis in their clinical assessments.
• A national awareness campaign will also be developed around menstrual health, including endometriosis, early next year.
Pictured at the ceremony are Maeve McNamara and Louise O’Brien, ESG Managers, accepting the award on behalf of Boots Ireland
Scabies, Head Lice and Pubic Lice in Males: An Overview for
Community Pharmacists
Ireland has seen a marked rise in scabies outbreaks since 2023. The Health Protection Surveillance Centre (HPSC) reported 26–27 outbreaks in 2023 versus nine in 2022; in 2024 the figure rose again to 51 outbreaks across a range of congregate settings (nursing homes, residential institutions and households). Although individual scabies cases aren’t notifiable, the outbreak trend is clear and relevant to community practice.
Scabies (Sarcoptes scabiei var. hominis)
Clinical picture in men: intensely pruritic papules/burrows, itch worse at night; common sites include finger webs, wrists, axillae, waistline, buttocks and genitals. In men you may see nodular scabies on the scrotum/penis, and outbreaks linked to close-contact sports, crowded housing, dorms/ prisons, and sexual networks (any sexual orientation). Post-treatment itch may persist for 2–4 weeks.
First-line treatment & logistics:
• Permethrin 5% dermal cream applied to the whole body (including neck, scalp and face if indicated—beards too) and washed off after 8–12 hours; repeat in 7 days. Treat all household and close/ sexual contacts simultaneously regardless of symptoms. Launder clothing/bedding at ≥50 °C (or seal 72 h). These steps break reinfestation cycles that commonly derail treatment.
• For treatment-resistant cases, crusted scabies, or where rapid control is needed, GP/specialist may consider oral ivermectin (off-label; Rx only in Ireland). Coordinate counselling on adherence and repeat dosing.
Pharmacist tips (male-specific):
• Remind patients to apply under fingernails, around genitalia and in body hair (beard, chest, pubic). Shaving is not required.
• Clarify post-scabetic itch ≠ treatment failure; consider non-sedating antihistamines/ emollients and safety-netting for persistent lesions or secondary infection.
• If a customer mentions institutional residence, team sport changing rooms, or multiple contacts, prompt them to notify managers/partners and to treat contacts together.
When to refer/flag: infants, immunocompromised patients, suspected crusted scabies, widespread bacterial superinfection, and failure after correctly executed two-dose permethrin (consider dermatologist or public health liaison).
2) Head Lice
(Pediculus humanus capitis)
Who and how: Head lice are most common in school-age children, but adult men can be affected— particularly fathers/caregivers, men living in shared accommodation, and contact sports participants. Transmission is almost always head-to-head contact, not fomites.
First-line options in Ireland:
• Wet combing with a fine-tooth (NIT) comb every 3–4 days for at least 2 weeks, continuing until no lice are seen for three consecutive sessions. Demonstrate technique; good lighting is key.
• Physical-mode topical products (e.g., 4% dimeticone, or isopropyl myristate/ cyclomethicone formulations) are widely used; they act by occluding/dehydrating lice rather than neurotoxicity, helping sidestep resistance. Follow manufacturer timings exactly and repeat to target hatching eggs. (HSE guidance emphasises correct application and repetition; avoid routine “preventive” use of medicated products.)
Pharmacist tips (male-specific):
• Check beards and eyebrows only if symptoms/transfer are suspected; head lice prefer scalp hair but can occasionally be found elsewhere.
• Reassure: lice affect clean and unwashed hair alike; avoid stigma with dads and teenage boys who may delay help-seeking.
• Screen all household members and coordinate treatment on the same day to reduce ping-pong transmission. Provide return-towork/sport advice (no exclusion needed after treatment if live lice are cleared).
When to refer/flag: suspected treatment failure after two properly executed cycles (consider alternative product class and check combing technique), secondary infection, or eyelash involvement (risk of blepharitis— medical review).
Framing for men: Pubic lice are an STI-associated ectoparasite transmitted via close body/ sexual contact; they infest coarse hair—pubic, perianal, thigh, chest, axillary, and sometimes beard hair. Eyelash infestation (phthiriasis palpebrarum) requires medical review.
Symptoms & signs: pruritus, worse at night; excoriations; skyblue maculae (maculae ceruleae) may be seen in lighter skin; visible lice/nits attached to hair shafts.
OTC treatment & partner management:
• Treat with OTC pediculicides (cream/shampoo/lotion per pack instructions) and repeat after 3–7 days. Critically, treat all sexual partners/close contacts at the same time and avoid sexual contact until everyone has completed treatment and is clear. Shaving is not required. Offer nit combing for egg removal and laundering advice for underwear/bedding.
• Because pubic lice signal intimate contact, signpost men to free STI testing and HIV/ syphilis screening, and discuss condom use. Where eyelashes are involved or topical treatments can’t be used safely near eyes, refer to GP/ophthalmology.
Pharmacist tips (male-specific):
• Normalise the conversation (“many people experience this; it’s treatable”).
• Remind men with beards/chest hair to apply product to all infested coarse hair areas, not just the pubic region.
• Provide a discreet checklist bag: treatment, fine-tooth comb, emollient for itch, and written partner-notification guidance. Quick counselling contrasts at the counter
• Scabies: whole-body permethrin 5% (repeat in 7 days); treat all contacts simultaneously; manage post-treatment itch; escalate suspected crusted scabies.
• Head lice: wet combing rigorously; or physical-mode lotions with correct timing and repeat; check/coordinate household.
• Pubic lice: treat patient and partners together; repeat in 3–7 days; STI screen and avoid sex until clear; shave not required.
Final word for teams
With scabies outbreaks increasing in Ireland and seasonal head-lice spikes common in households and teams, pharmacy-led early recognition, clear instructions, and whole-contact management make the difference between cure and revolving-door reinfestation. Equip staff to ask the right questions, demonstrate application/comb techniques, and safety-net confidently—especially for male customers who may present late or feel awkward discussing intimate sites. The result is faster resolution for patients, fewer returns, and better infection control in the community.
3) Pubic Lice (Pthirus pubis; “crabs”)
Bringing It All Together: The Holistic Men’s Health Zone
How community pharmacies can become the go-to destination for men’s wellbeing, grooming, and self-care
For too long, men’s health has been defined narrowly — by crisis moments rather than ongoing care. Many men still only enter a healthcare setting when prompted by a partner, or when a problem becomes too severe to ignore. But attitudes are changing, and community pharmacies are perfectly positioned to lead that change.
By integrating traditional health promotion with personal care, wellbeing, and male grooming, pharmacies can create a holistic “Men’s Health Zone” — a visible, engaging space where men feel comfortable seeking advice, learning about prevention, and discovering products that support their overall wellbeing.
Why Men’s Health Belongs at the Front of the Pharmacy
Despite clear progress in awareness, men remain underrepresented in preventive healthcare. Research consistently shows that men are less likely to visit their GP, discuss emotional concerns, or engage in screening programmes. At the same time, they’re increasingly investing in their personal appearance and fitness.
This creates a natural overlap between health and grooming — an intersection that community pharmacies can harness. By aligning the messaging around self-care, confidence, and performance, rather than illness or deficiency, pharmacists can make health engagement more relatable to male audiences.
A well-designed Men’s Health Zone can act as both a retail driver and a public health platform — merging skincare, sexual health, supplements, and screening services under one cohesive theme.
Understanding the Modern Male Health Consumer
Today’s male customer is informed, image-conscious, and time-poor. He expects convenient access to solutions, clear information, and a shopping experience that feels relevant — not intimidating.
Three broad consumer profiles are typically seen in pharmacies:
1. The Proactive Self-Care Enthusiast:
Usually aged 25–45, this group actively seeks products to support energy, fitness, and appearance. They’re interested in supplements, skincare, and tech-based health tracking.
2. The Health Maintenance Group:
Men aged 40–60 often start thinking about heart health, prostate care, and lifestyle balance. They want practical, trustworthy guidance and may welcome discreet advice from a pharmacist.
3. The Reluctant Visitor:
Many older men or those unfamiliar with pharmacy services only come in when something is wrong — perhaps an infection, pain issue, or erectile dysfunction. For this group, privacy, sensitivity, and encouragement are key.
Understanding these mindsets allows pharmacists to design store layouts and conversations that meet men where they are — not where we assume they should be.
Designing the Men’s Health Zone
A “Men’s Health Zone” doesn’t need to be large — but it does need to be intentional, visible, and coherent. Even a single wall bay or front-of-store feature can send a clear message that the pharmacy welcomes and supports male customers.
1. Strategic Location
Place the section near other high-traffic areas such as the counter, the grooming section, or the health supplements aisle. Avoid positioning it deep within the beauty or female skincare zones, which can deter men from browsing.
Where space allows, an end-cap or stand-alone gondola branded “Men’s Health & Grooming” can make a strong first impression.
2. Visual Identity
Design the area with muted, professional tones — charcoal, navy, forest green, or metallic accents — to contrast with brighter wellness or beauty aisles. Clean signage such as “Men’s Health Starts Here” or “Look Good. Feel Strong. Stay Well.” is inviting without being medicalised.
3. Product Grouping
Organise products into four logical pillars:
• Grooming & Skincare: Shaving, beard care, moisturisers, sunscreen, and sensitive skin solutions.
• Energy & Vitality: Multivitamins, protein supplements, sleep aids, and fatigue remedies.
• Sexual & Reproductive Health: Condoms, lubricants, fertility supplements, and discreet erectile dysfunction information.
• Preventative Health: Prostate support, heart and cholesterol supplements, joint care, and screening services.
Each pillar reflects a stage in the self-care journey — from looking good, to feeling energised, to long-term wellbeing.
Merchandising with Purpose
Effective merchandising turns information into inspiration. The Men’s Health Zone should tell a clear story: men can look after their health confidently, easily, and without embarrassment.
Use of Space
Keep displays clean and minimal. Men are often task-oriented shoppers; cluttered shelves or overcomplicated ranges can discourage browsing. Instead, offer good-better-best product tiers in each category — for example, a pharmacy-brand moisturiser, a mid-range everyday option, and a premium item.
Cross-Merchandising Opportunities
• Position beard oils next to razors or trimmers.
• Place vitamins for energy beside protein powders.
• Pair heart health supplements near blood pressure monitors.
• Display SPF creams alongside skincare products and sunburn treatments.
Cross-merchandising not only boosts sales but reinforces the link
between external appearance and internal wellbeing.
Seasonal and Awareness Campaigns
• Movember: Focus on men’s mental health, prostate awareness, and moustache care products.
• Father’s Day: Offer curated gift bundles that combine skincare, fragrance, and supplements.
• Men’s Health Week (June): Highlight screenings, weight checks, and heart health advice.
• Summer: Emphasise SPF and travel-friendly grooming products.
Rotate displays every few months to keep the section fresh and relevant.
Staff Engagement and Training
Even the most beautiful display will underperform without confident staff engagement. Many men are hesitant to ask about health issues, so pharmacy teams must lead the conversation subtly and supportively.
Building Confidence
Train staff to recognise openings for discussion:
• A customer buying shaving products may be open to advice on moisturisers or sun protection.
• Someone requesting multivitamins might benefit from guidance on fatigue, sleep, or stress.
• A repeat purchaser of pain relief could be a candidate for joint care or physiotherapy referral.
Encourage short, friendly questions — “How’s that working for you?” or “Are you looking for something for daily use or for travel?” — to open dialogue without intruding.
Education
Provide staff with quick-reference sheets or supplier training on men’s health categories. Key talking points include:
• Recognising signs of low mood or burnout.
• Awareness of skin sensitivity and beard irritation.
• Understanding supplements for vitality and stress.
• Knowing when to refer to the pharmacist for more sensitive topics.
An informed, confident team transforms the Men’s Health Zone from a retail area into an extension of clinical care.
Pharmacist-Led Services: From Product to Practice
The real power of the Men’s Health Zone lies in connecting front-ofstore engagement with pharmacyled clinical services.
Pharmacists can use this space to signpost or directly deliver interventions such as:
• Blood pressure and cholesterol checks.
• Diabetes risk assessments.
• Weight management consultations.
• Smoking cessation programmes.
• Sleep and fatigue support.
• Erectile dysfunction and hair loss advice.
When presented as part of a broader self-care offering, these services feel natural rather than clinical. For example, a poster reading “Tired all the time? Ask about our Energy & Sleep Check” can normalise health checks for men who might otherwise never book an appointment.
Pharmacists can also collaborate with local GPs, sports clubs, or workplaces to deliver outreach sessions — bringing the Men’s Health Zone concept into the community.
Digital Integration: Reaching Men Where They Are
Men’s health engagement doesn’t stop at the store door. Digital tools can extend the pharmacy’s presence and build loyalty.
• Social Media: Post short, factual tips about men’s
26 Men’s Health: Holistic Care
skincare, heart health, or stress management. Keep language positive and performancebased (“How to stay sharp and energised”) rather than medical.
• Email Newsletters: Segment male customers and send seasonal advice (e.g., “Summer Skin Protection for Men” or “Top 3 Supplements for Energy”).
• QR Codes: Add them to shelf talkers or product stands linking to online pharmacist videos or articles on men’s health topics.
• Online Booking: Make it easy to book health checks or consultations directly via the pharmacy’s website.
Digital engagement complements in-store messaging and positions the pharmacy as a modern, supportive health partner.
Privacy and Sensitivity
Privacy remains a major barrier for male health engagement. Many men fear embarrassment or stigma when discussing intimate or emotional issues. Pharmacies can counter this by:
• Using discreet signage — e.g. “Confidential Men’s Health Advice Available Here.”
• Training staff to offer follow-up discussions in private rather than at the counter.
Some pharmacies even use neutral language like “Performance and Energy Checks” rather than “Erectile Dysfunction Services” to reduce discomfort while still prompting meaningful engagement.
Case Study: Bringing It Together in Practice
A Dublin-based independent pharmacy recently introduced a “Men’s Health & Grooming Zone” near its entrance. The team reallocated one gondola from general cosmetics, using clean navy branding and a clear sign reading “Men’s Health Starts Here.”
The display included shaving and skincare essentials, vitamins for energy and immunity, prostate and joint health supplements, and discreet signposting to services such as blood pressure checks and ED advice.
Staff received a short training session from the superintendent pharmacist on conversation openers and red flags.
Within three months, the pharmacy recorded:
• A 40% increase in sales of maletargeted vitamins and skincare.
• Doubling of blood pressure check appointments.
• A noticeable rise in male customers attending for private consultations.
This success underscores that when pharmacies make men feel welcome — not targeted — they respond with trust and engagement.
Language Matters: Framing the Conversation
Men respond better to language that focuses on function, strength, and performance, rather than illness or vulnerability.
Instead of “Prevent heart disease,” try:
➡️ “Keep your energy strong and your heart healthy.”
Instead of “Manage stress,” try:
➡️ “Stay focused and sleep better.”
Instead of “Get checked for prostate issues,” try:
➡️ “Take control of your long-term health.”
Simple linguistic shifts can dramatically change how men perceive healthcare conversations.
Measuring Success
A holistic Men’s Health Zone should deliver results across both health outcomes and business performance. Pharmacies can monitor:
• Product sales by category (e.g., male skincare, supplements).
• Uptake of health checks and services by male customers.
• Customer feedback or repeat visits.
• Engagement with digital or social media campaigns.
Tracking progress ensures the initiative remains fresh, data-driven, and aligned with customer needs.
Conclusion: A Modern Approach to Men’s Wellbeing
1. Clear Identity
Top 10 Components of a Successful Men’s Health Zone
Use signage that’s confident and approachable — “Men’s Health & Grooming” or “Look Good. Feel Well.” Avoid overly clinical language.
2. Strategic Placement
Locate near high-traffic areas or front-of-store, not hidden beside cosmetics. Visibility equals engagement.
3. Smart Segmentation
Group products under clear themes:
• Grooming & Skincare
• Vitality & Energy
• Sexual & Reproductive Health
• Preventative Care & Supplements
4. Keep It Simple
Men are goal-oriented shoppers. Offer clear choices — everyday, premium, and pharmacy-trusted options.
5. Cross-Merchandising
Link categories: beard oil beside trimmers, sunscreen beside moisturisers, vitamins near energy drinks or protein.
6. Seasonal Refresh
Plan themed updates for Movember, Father’s Day, summer skincare, or Men’s Health Week. Rotate displays every quarter.
7. Staff Confidence
Train the whole team to discuss products comfortably. Encourage short, friendly questions that open conversations.
8. Link to Services
Promote pharmacist-led checks for blood pressure, cholesterol, sleep, or fatigue alongside front-of-store displays.
9. Subtle Privacy Cues
Use signage for private consultations and discreet packaging for sensitive products like ED treatments or fertility aids.
10. Positive Messaging
Focus on performance and wellbeing: “Stay strong.” “Keep your energy high.” “Feel your best.” — not illness or decline.
Quick Win Ideas
• Add a QR code linking to your pharmacy’s men’s health services.
• Offer free blood pressure checks during Men’s Health Week.
• Partner with a local gym or barber for cross-promotion.
• Display “Pharmacist Recommended” tags for credibility.
Key Takeaway
A Men’s Health Zone doesn’t just sell products — it builds relationships. When men feel comfortable in your pharmacy, they return for advice, trust your recommendations, and become loyal customers for life.
The OTC & Retail Pharmacy Product Awards 2026
Enter Your Products Now
Entries are now open for the 2026 OTC & Retail Pharmacy Product Awards, celebrating innovation, quality, and excellence across Ireland’s pharmacy sector.
Entries are accepted on a first-come, first-served basis, with a maximum of five entries per category, so early submission is essential. The entry fee is €799, and participants must provide 30 sample products or dummy packs by 23rd January 2026 to complete their entry.
For category details, entry forms, or any queries, please contact Robyn Maginnis at robynmaginnis@ipn.ie.
Don’t miss your chance to showcase your brand’s innovation and commitment to pharmacy — enter today and be part of Ireland’s premier OTC awards.
How to protect your family during Tummy Bug Season
Electrolyte for hydration* Gut-Friendly Bacteria
At certain times of the year, there is an increase in tummy bugs and viruses. While symptoms include nausea, diarrhoea and vomiting, the highly contagious norovirus is one of the most common stomach infections.
There is nothing worse than a vomiting bug or diarrhoea. In some cases, you can have a fever and muscle aches as well.
MyPro DiaCare is a solution, which is suitable for the whole family, from the age of 3 years.
MyPro DiaCare is a unique food supplement for Children and Adults su ering from diarrhoea, fever or other conditions which can cause loss of body fluids.
MyPro DiaCare is a scientifically balanced blend of glucose electrolyte, minerals and and GutFriendly Bacteria (Lactobacillus Rhamnosus GG).
Contains:
• Magnesium which contributes to electrolyte balance.
• Chloride which contributes to normal digestion by production of hydrochloric acid in the stomach.
• *Carbohydrate electrolyte solution which enhances the absorption of water during physical exercise
Choose MyPro DiaCare
MyPro DiaCare’s unique dual chambered sachet allows for two-in-one benefits:
1 Contains Electrolytes which tackles the problem of dehydration.
Oral rehydration therapy (ORT) is recommended as first-line therapy for both mildly and moderately dehydration.
2 Contains a Gut-Friendly Bacteria which helps to swiftly restore the gut to normal.
Probiotics act faster than bacteria: e ectively colonises the gut within 5-7 days, outnumbers pathogenic species. (National Institutes of Health O ce of Dietary Supplements).
Probiotics are more durable than bacteria: both in antibiotic environment and with gastric acid.
More about our Gut-Friendly Bacteria (Lactobacillus Rhamnosus GG)
• Clinical trials show people taking Lactobacillus Rhamnosus GG are protected against bacterial infections.
• Increased adherence of beneficial bacteria results in reduced diarrhoea-causing bacterial numbers in the GI tract. Therefore, Lactobacillus is e ective in both the treatment and prevention of diarrhoea.
• Lactobacillus Rhamnosus GG provides immune support in the gastrointestinal tract.
• Repopulates natural gut bacteria.
• Restores normal acidic pH of the stomach.
• The lactic acid facilitates other organic acids and bacteriocins to reduce counts of diarrhoea causing bacteria.
Recover Well This Tummy Bug Season
Electrolyte for hydration*
Electrolytes to rehydrate and replace essential minerals
Gut-Friendly Bacteria
Gut friendly bacteria to help restore balance in the digestive system
Suitable for the whole family from aged 3+
Now available in Orange and Berry flavours
*Carbohydrate electrolyte solution which enhances the absorption of water during physical exercise.
Suitable for Age 3+ years
MyPro DiaCare is a ZEON Healthcare Brand.
Men’s Health: Hormonal Health
Behind the Counter: Opening the Conversation on Men’s Hormonal Health
By Chantal Alexander
Across Ireland, pharmacists are hearing quiet admissions from men who stop at the counter a little longer than usual. They might mention feeling tired all the time, struggling with energy, or that things “just aren’t the same anymore.” These brief exchanges, handled with care, can uncover something important. While menopause is widely recognised and supported, the male version of hormonal change, sometimes referred to as andropause or testosterone deficiency, is often misunderstood or ignored.
Many men do not realise that hormonal changes can affect them too. Others are reluctant to talk about it. That silence means community pharmacists are often the first to notice patterns. Regular customers might show signs of low mood or fatigue, or they may quietly mention issues that suggest hormonal imbalance. Recognising these subtle cues can open the door to better support and early intervention.
Dr Emmett Byrne, a GP and men’s health specialist in Bray, says that awareness starts at community level. “The three lead symptoms I see are low libido, loss of early morning erections, and erectile dysfunction. Fatigue and anxiety are also common,” he explains. “Pharmacists are ideally placed to notice repeat complaints. They are trusted, and they see men who might never make a doctor’s appointment.”
Research suggests that around one in ten men over fifty in Ireland has low testosterone, but very few are aware of it. Many also live with obesity, diabetes, or high blood pressure, which can lower hormone levels further. These are patient’s pharmacists see every day. When a man repeatedly mentions tiredness or poor motivation, a simple question such as “Have you spoken to your GP about this?” can lead to real action.
A simple question at the counter can start a life-changing conversation.
A diagnosis of testosterone deficiency requires proper medical assessment. Testing involves two early morning blood tests, usually between seven and 11 am, after fasting. The GP will also check other hormones to find out what is driving the change. Results are only meaningful when combined with symptoms and clinical history. Community pharmacists can explain this process clearly and discourage men from using unregulated online products that promise quick fixes.
Lifestyle changes are often the first step. Exercise, better sleep, losing excess weight, and reducing alcohol intake can make a measurable difference. Dr Byrne notes that many men see improvements without any medication. “Once weight, sleep, and stress are under control, testosterone often rises naturally,” he says. “It is about addressing the whole person, not just the numbers.”
When testosterone replacement therapy is appropriate, pharmacists play a key role in
ensuring safety. Transdermal gels and patches are common in Ireland and need to be applied carefully to avoid skin contact with others. Pharmacists can demonstrate proper application, explain storage, and ensure the patient understands the monitoring schedule. Regular checks for testosterone levels, blood pressure, blood count, cholesterol, and prostate health are essential.
Consultant Urologist Dr John Sullivan of St James’s Hospital in Dublin cautions against taking shortcuts. “There is a lot of online testosterone-prescribing, and it is unsafe,” he says. “A man showing symptoms must be properly assessed and followed up by a doctor.” Pharmacists can help enforce this message and protect patients who may be tempted by online advertisements for hormone products.
The conversation does not need to be complicated. Simple, open language works best. One pharmacist in Cork explains, “If you can normalise the topic, they’ll talk. It’s not about embarrassment. It’s about health.” Creating an approachable environment within the pharmacy, and offering private consultations when needed, helps men feel comfortable raising personal issues.
Community pharmacies are well suited to lead this kind of engagement. Men already visit
their local pharmacy more often than their GP, and these visits present real opportunities for early health intervention. Campaigns like Men’s Health Week can help spark conversations, with posters, leaflets, or staff-led discussions that encourage men to ask questions about their wellbeing.
Pharmacists can also support broader men’s health checks by offering services such as blood pressure screening, weight management advice, and lifestyle counselling. These simple interventions often highlight underlying conditions that may contribute to hormonal imbalance. By approaching men’s hormonal health as part of overall wellbeing, pharmacists can ensure that conversations are natural, not clinical.
As Ireland’s understanding of men’s health evolves, community pharmacists have an important part to play. They are the bridge between uncertainty and informed care, between online misinformation and genuine medical support. Each small conversation can build awareness, confidence, and healthier futures for men across the country.
Men’s hormonal health may not yet have the same visibility as menopause, but that is changing. Pharmacists are in the right place, at the right time, to lead the shift.
References avalable on request
Dr Emmett Byrne, a GP and men’s health specialist in Bray
“Pharmacists are trusted and accessible. We can ask the questions men often avoid, and that is where better care begins.”
Breaking the Silence: How Irish Pharmacies are Leading the Fight Against Erectile Dysfunction
I have worked in pharmacy in Ireland as a qualified pharmacist since 2016 and my experience shows that Erectile Dysfunction (ED) is widespread but frequently concealed by stigma. As community pharmacists we witness the brief, discreet request for a box Viagra Connect or Cialis reveals much more than a single symptom. ED is frequently the first clinical signal of underlying cardiovascular, metabolic, or mental-health problems, and the pharmacist’s role is to safely recognise that signal and steer men toward comprehensive GP review.
There is opportunity for Irish community pharmacists to normalise the discussion about ED especially in the consultation room where we can offer discreet, evidence-based care that not only addresses the presenting issue but also initiates a conversation about men’s wider health.
Prevalence, Impact, and Clinical Significance in Ireland
Erectile dysfunction is defined as the persistent inability to achieve or maintain an erection sufficient for satisfactory sexual performance. (Marita P. McCabe, et al., 2016) (Lowery-Lehnen, 2025) While precise population-based prevalence data from Ireland are limited market research conducted on behalf of Viatris on erectile dysfunction in Irish men, it was identified that 1 in 3 experience ED regularly. (Viatris, 2025) It is difficult to obtain accurate values for the true prevalence of erectile dysfunction however, as many patients fail to seek medical attention, and many clinicians are reluctant to ask patients about their sexual health. (Norton, 2022)
ED significantly impacts quality of life, relationships, and
psychological wellbeing. Among men, the most prevalent sexual problems and the corresponding percentages of those who were bothered by them were difficulty in achieving or maintaining an erection (37% and 90%, respectively), lack of interest in sex (28% and 65%), climaxing too quickly (28% and 71%), anxiety about performance (27% and 75%), and inability to climax (20% and 73%). (Tessler Lindau, et al., 2007)
ED is not merely a lifestyle issue; it is a strong and early predictor of significant systemic disease. Irish clinical consensus highlights the strong association between ED and:
• Advancing age: Sexual activity significantly declines with age, and ED incidence rises due to comorbidities and other factors.
(Marita P. McCabe, et al., 2016)
• Cardiovascular Disease: ED is closely tied to endothelial dysfunction and atherosclerotic risk, making it an important early marker for cardiovascular disease (CVD) and metabolic syndrome. A cardiac assessment is strongly
Written by Frank Olden, Hickey’s Pharmacy, Cork
warranted in men presenting with ED. (Wayne, 2007)
• Diabetes: The prevalence of ED is significantly higher in men with diabetes, and they often experience its onset earlier than non-diabetic men (Walsh, et al., 2017)
Pharmacy as a Pivotal Access Point
Irish-specific context reveals that pharmacies are the most accessed health professionals, with 51% of the adult population have visited a pharmacy in the past week, equating to 118 million visits per annum. (Union, 2025) This high level of public access makes the pharmacy a natural, trusted first touchpoint for men who might otherwise avoid care for a stigmatised condition like ED.
Pharmacists in Ireland are ideally placed to support men with ED through:
1. First Contact and Screening: ED requests offer a unique opportunity to screen for unmanaged or undiagnosed conditions. The structured consultation for over-thecounter (OTC) supply of
Call for Judges: OTC & Retail Pharmacy Product Awards 2026
As a judge for the OTC & Retail Pharmacy Product Awards 2026, you will play a crucial role in evaluating and selecting the most outstanding Over-the-Counter Pharmacy Products in Ireland. Your expertise and insights will help us identify products that have made significant contributions to the field, whether through technological advancements, patient care improvements, or other remarkable achievements.
Here are some key details about the judging process and requirements:
Judging Process:
• The judging process will be conducted remotely.
• Finalists’ Products will be posted to each judge giving you the opportunity to try, test and evaluate.
• Each judge will be assigned specific product categories.
• Judges will review product submissions, provide scores, and offer constructive feedback.
Requirements:
• Pharmacists, Buyers and Owners.
• A commitment to fairness, impartiality, and confidentiality.
• Availability to review and evaluate product submissions during the judging period.
If you are interested in becoming a judge for the OTC & Retail Pharmacy Product Awards 2026, please email with your name, contact information to robynmaginnis@ipn.ie
34 Men’s Health: Erectile Dysfunction
• Underlying Disease: The pharmacist ensure that the patient’s focus on a ED medication does not mask undiagnosed or poorly managed hypertension, diabetes, or depressive illness, reinforcing the need for GP review and investigation. (Walsh, et al., 2017)
• Mental Health Integration:
The consultation provides an opportunity to gently enquire about mood, anxiety, and relationship strain.
Practical Guidance for Pharmacy-Led Consultations
Pharmacy-led consultations for erectile dysfunction (ED) should adopt a structured, people-centred approach that reflects both Irish CPD guidance and international best practice as outlined by the International Pharmaceutical Federation (FIP):
1. Discretion and EmpathyPharmacists should create a private, welcoming environment for sensitive discussions. The use of open-ended, nonjudgmental questions helps explore the onset, severity, and psychosocial context of ED. This approach fosters trust and encourages men to disclose concerns that may otherwise remain hidden.
2. Risk Screening and Red Flags - Pharmacists must assess for underlying health risks, including cardiovascular symptoms (e.g., chest pain, syncope), diabetes, hypertension, and psychological distress. Screening should include a review of medical history and current medications, especially contraindicated agents like nitrates. As mentioned ED may be an early marker of systemic disease, making this step critical for timely referral.
3. Counselling and Follow-Up
Provide clear guidance on the safe use of phosphodiesterase type 5 inhibitors (PDE5Is), including common side effects such as headache and flushing. Reinforce the importance of GP follow-up within six months to investigate potential comorbidities. Pharmacists should also support lifestyle changes—such as tobacco cessation, stress management, and weight control—that enhance treatment outcomes.
4. Documentation and Safety-Netting - Maintain a comprehensive record of each consultation, including assessment findings, advice given, and any decisions not to supply medication. This ensures
continuity of care, supports audit requirements, and protects patient safety. Structured documentation also facilitates interprofessional collaboration and reinforces the pharmacist’s clinical role.
Conclusion
ED is not merely an isolated sexual function issue; it is a clinically rich entry point into men’s cardiovascular and mental health. Irish pharmacies, by virtue of their unparalleled access, established trust, and mandated structured consultation, are leading the fight against the stigma surrounding ED. By safely and rigorously delivering OTC supply, integrating brief health interventions, and ensuring timely medical referral, pharmacists transform a discreet counter request into a powerful opportunity for prevention, early detection, and better long-term health outcomes for men in Ireland.
Bibliography
Lowery-Lehnen, T., 2025. www.irishpharmacist.ie. [Online] Available at: https://irishpharmacist.ie/ clinical/in-focus/erectile-dysfunction/ Marita P. McCabe, P. et al., 2016. Definitions of Sexual Dysfunctions in Women and Men: A Consensus Statement From the Fourth International Consultation on Sexual Medicine 2015. The Journal of Sexual Medicine, pp. 135-143.
Norton, D., 2022. Hospital Professional News. [Online] Available at: https://hospitalprofessionalnews. ie/2022/08/03/management-oferectile-dysfunction-in-ireland/ Nunes da Cunha, I., 2025. fip.org. [Online]
Available at: https://www.fip.org/ file/6226 [Accessed 16 October 2025]. T., L.-L., 2025. [Online] Available at: https://irishpharmacist.ie/ clinical/in-focus/erectile-dysfunction/ Tessler Lindau, S. et al., 2007. A Study of Sexuality and Health among Older Adults in the United States. New England Journal of Medicine, pp. 762-774.
Union, I. P., 2025. www.ipu.ie. [Online] Available at: https://ipu.ie/ communication/major-surveyconfirms-strong-public-support-forexpanding-pharmacy-services-inireland/ [Accessed 16 October 2025].
Viatris, 2025. [Online]
Available at: https://www. viagraconnect.ie/en-ie/what-iserectile-dysfunction
Walsh, C., Murphy, A. W. & O’Shea, B., 2017. 'Improving the detection and management of type 2 diabetes in general practice in Ireland: a review of current practice and future priorities'. Irish Journal of Medical Science, 1(186), pp. 263-270..
Wayne, M., 2007. Cardiovascular disease and erectile dysfunction. Journal of modern pharmacy, 14.7(38).
Men’s Health: Prostate Cancer
PSA for proactive prostate health management
Every year, 620 men in Ireland die from prostate cancer. Most of those deaths could be prevented with awareness and early detection.
Unfortunately, a lot of men avoid or delay speaking to their GP about Prostate health because they assume that it will lead to something awkward and invasive.
What they don’t realise is that the first step in being proactive about your prostate health is much simpler than that. Early detection can start as a simple PSA blood test.
Prostate cancer is the most common male cancer in Ireland. Around 4,067 men are diagnosed annually in Ireland. 1 in 6 people born with a prostate will be diagnosed in their lifetime with rates of prostate cancer higher in black men with 1 in 4 getting diagnosed with prostate cancer. Men are two and a half times more likely to get prostate cancer if their father or brother had it. Inherited genes especially BRCA 2, being overweight or obese can also be risk factors to be aware of.
However, prostate cancer responds well to treatment and, if detected early, it can be treated successfully. With early detection, over 93% of men survive.
Like many other forms of cancer, these survival rates are all dependant on when the cancer is detected. Early detection saves lives allowing for better treatment options that will include a noninvasive Active Surveillance plan if suitable and can ensure a more straightforward cancer journey – and most importantly improve survival outcomes and quality of life.
The Marie Keating Foundation is urging men to take charge of their prostate health by talking to their GP about a simple PSA blood test once they turn 50 — or from 45 if there’s a family history of prostate or breast cancer.
A PSA or prostate-specific antigen test is a simple blood test that monitors possible changes in your prostate which may need further investigations and follow up. By having regular PSA levels checked as instructed by your GP or Urologist, it can help to detect prostate problems or cancer in its earliest stages, even if you are experiencing no symptoms.
Prostate cancer is often asymptomatic, meaning there are no obvious changes or signs that something might not be right with your body. This is why open and honest communication between men, and their GPs is so vital and why we urge you to ask about that important PSA blood test.
We want men to feel confident speaking openly about prostate health, recognising the signs and symptoms if they are present, and starting that important conversation with their GP. A PSA test is quick, non-invasive, and takes less than five minutes — but it could be the first step in prioritising your prostate health.
Signs and symptoms to be aware of
Dysuria – difficulty and pain passing urine.
Written by Helen Forristal, Director of Nursing, Marie Keating Foundation
Urgency – difficult to postpone passing urine.
Frequency – going to the toilet more frequently than before.
Nocturia – getting up more than twice a night to pass urine.
Hesitancy – taking time to get going when passing urine.
Flow – has become weak or intermittent.
Incomplete emptying – feeling that the bladder has not emptied.
Blood – present in the urine.
Less common symptoms include:
• Trouble having or keeping an erection.
• Lower back pain or pain in hips or upper thighs.
It is important to note that the prostate enlarges with age. It wraps around the urethra (waterpipe) and this enlargement (benign prostatic hyperplasia –BPH) can cause bladder outlet obstruction which can lead to the above symptoms. BPH is more common than prostate cancer, but the conditions may exist together. BPH is not cancerous but can be troublesome.
Do not wait for signs and symptoms to present before taking action, as Prostate Cancer is very often symptom free, particularly in its early stages. If you do however have urinary symptoms speak to your GP, it could be for a variety of reasons not necessarily prostate cancer, but the sooner you address
it, the better the outcome. Get proactive for peace of mind and more positive treatment paths when issues are detected early. If you experience any of the listed symptoms your GP will determine the severity of your symptoms and examine your prostate gland. Examination involves a digital rectal examination (DRE) where the prostate is examined and felt by the doctor by using a finger in the back passage. The examination itself will be quick and painless, and will assess the size, texture and consistency of the gland and look for any irregularities.
If discovered early, prostate cancer can be treated successfully.
In closing, we urge you to Stand Up for Your Prostate.
All men, but especially those whose father, brother or grandfather has or had prostate cancer, need to engage in conversations earlier because we know that early cancer detection from the age of 40- 45 years of age onwards can save lives. A simple prostate blood test, the PSA, is the best way to assess your risk.
For more information on the Marie Keating Foundations Stand Up for Your Prostate 2025 campaign go to mariekeating.ie
Men's Health
Men’s Mental Health in Ireland
One in every four people in Ireland will experience a mental health condition during their lifetime; with depression being the most common occurring in one in ten of us.1 Factors like stress, loneliness, financial struggle, alcohol/ substance misuse as well as the psychological impacts of major life events (eg - parenthood/ separation/ retirement) contributing to this. The likelihood of dying from suicide is four times higher for men.2 Men are also less likely to seek support or engage in services due to unique challenges that discourage them.3 These include societal expectations of stoicism, self-reliance and perceived gender norms.2
Mental health literacy which describes someone’s knowledge and beliefs around mental health has been found to be significantly lower in men.4 Men may believe asking for help is an admission of failure or weakness (it can actually be a sign of strength).5 Men may worry how they will be perceived by family, friends or neighbours and fear judgement by others if they seek help. Despite significant efforts and campaigns to improve this, considerable stigma still exists around mental health. Men also hold more stigmatising attitudes in this respect.3
The National Men’s Action Plan (2024) which superseded the National Men’s Health Policy identifies isolation, access to services (especially in rural areas) and a lack of awareness of available resources and supports as barriers to men’s mental health.2
Although women have higher rates of suicidal ideation, selfharm and suicide attempts, men have substantially higher rates of completed suicide. Of the 512 deaths by suicide in Ireland in 2021 78.3% were men and men aged between 45 to 49 were the highest cohort of all suicides (9.4%).6 Men also have an increased likelihood of dying by suicide from more lethal methods (eg - hanging, carbonmonoxide poisoning or firearms).2
Written by Patrick J McGee; Advanced Specialist PharmacistMental Health, Beaumont Hospital
Sub groups of men at increased risk of poor mental health include the unemployed, homeless, prisoners, LGBTQI+, veterans, ethnic minorities and men with existing mental illness.7 In the traveller community where masculinity is fostered and celebrated men are even less likely to seek support.2 There exists an even greater stigma and cultural sensitivity around mental health and suicide within this group.2, 8 In people with autism suicidality is common (66%) and people with ADHD are five times more likely to attempt suicide.9, 10
Another at risk group of men are the farming community; the majority of whom are selfemployed males. Irish farmers can experience a higher level of mental health issues and suicide due to factors such as the isolative nature of farming and the reduced opportunities for social interaction.11 Farmers are often faced with significant financial pressures and have considerable responsibilities to both their farms and their families and often prioritise the interests of their farms over their own health.11
Community Pharmacist Role
Pharmacists are highly educated, readily accessible and trusted healthcare professionals who are well placed to support men’s mental health, especially for the harder to reach groups like rural farmers and travellers. Such men may be less inclined to make an appointment with their GP but may prefer a less formal chat with their pharmacist. They are likely to visit their local pharmacy more regularly than a GP and this presents opportunities for engagement.
Contact and Rapport
Building good relationships with male patients allows pharmacists more opportunities to make positive interventions around wellness and mental
health. Pharmacists should be aware of early warning signs of mental health deterioration or psychological distress, such as subtle changes in appearance (reduced self-care, weight changes) or behaviour (excessively talkative/ less talkative/ overly pessimistic/ withdrawn) or changes in activity levels. Asking patients about and taking an interest in a patient’s mental wellbeing is a positive intervention. Asking how they are doing or how their medication is going is a simple conversation opener. In fostering open conversations it is important to be supportive and nonjudgemental, to ask questions, to listen and to signpost if necessary. Offering privacy to male patients (in the consultation room) may encourage men who are reluctant to engage. Early intervention is one of the key factors in suicide prevention and if concerned someone is thinking about suicide it is important to ask them clearly, directly and sensitively.
Stigma
Pharmacists have a role in challenging mental health stigma by creating a supportive environment that promotes positive mental health and emotional wellbeing. Pharmacists should challenge stigmatizing attitudes (eg - people’s views or sensationalised media headlines) around mental health and promote open conversations around mental wellbeing among customers, patients and staff. Improved public knowledge around mental health will reduce the negative attitudes held by society and enable more men with mental health challenges to seek support. There are large gaps in mental health literacy in Ireland and especially among men.4 Pharmacists can be proactive within their community by engaging in positive mental health initiatives and awareness campaigns (egholding a pharmacy event for world mental health day).
Medications
Pharmacists also clearly have important roles in managing patients’ medications by providing
information and counselling and giving advice on minimising and managing side-effects of medications for mental health. They are also well placed for monitoring and advising on patients’ physical health (especially for patients on medication that cause metabolic side-effects like weight gain or increased lipids/ glucose such as antipsychotics). Pharmacists (and patients) can access the HSE’s subscription to the “Choice and Medication” service. This is an invaluable resource containing detailed information, fact sheets and printable leaflets covering all mental health medications and mental illnesses for patients with a range of literacy levels in multiple languages. www. choiceandmedication.org/ireland Vigilance
Pharmacists have responsibility in monitoring and restricting the sale of drugs with potential for abuse or harm. These include laxatives, codeine containing products and cough and cold remedies. They should also be vigilant to repeated purchases of products containing paracetamol which may indicate self-harm/ suicide intent. Another intervention may be to follow up with patients where there may be non-compliance and to liaise with their GP/ CMHT (Community Mental Health Team) where there is an obvious mental health deterioration.
Continued Professional Development
To ensure pharmacists can support men with mental health challenges they may require upskilling in the area. Mental health first aid is an excellent course that can be undertaken by all pharmacy staff. It is an evidence based, early intervention training programme that teaches people the signs and symptoms of common mental health disorders and how to provide relief, support and signposting. It is a paid course provided by a range of institutions in Ireland (St John of God; Redcross; MHFA Ireland). There are also many accredited CPD
resources for pharmacists wishing to build expertise and confidence in this area. These include:
Mental Health First Aid www.mhfaireland.ie; www.stjohnofgodhospital.ie
Irish Institute of Pharmacy (IIOP): e-learning and webinars IIOP Mental Health and Wellbeing Resource Hub www.iiop.ie
IPU Academy: e-learning and live courses www.ipuacademy.ie
Choice and Medication www.choiceandmedication.org/ ireland
National Office for Suicide Prevention www.hse.ie/eng/ services/list/4/mental-healthservices/nosp/
Connecting for Life - Ireland’s national suicide reduction strategy 2015 to 2020 www.hse.ie/eng/services/ list/4/mental-health-services/ connecting-for-life/nationalstrategy-to-reduce-suicide/
Signposting
It is important to be aware of the resources available to men and encourage them to seek support when necessary. Requesting and displaying highly visible leaflets/ posters/ signage from signposting resources is also beneficial.
Men’s Sheds – Community based groups where men gather to share skills, work on projects, and socialize. Open to men of all ages. www.menssheds.ie
HSE Mental Health –Information on common difficulties and self-help tips. www.yourmentalhealth.ie
Mental Health Ireland – Charity dedicated to promoting mental health and supporting people with mental health challenges. www.mentalhealthireland.ie
Sheds for Life – Health promotion programme for supporting physical, mental and social wellbeing of Irish Men’s Sheds members. www. menssheds.ie/sheds-for-life/
Men’s Aid (formerly AMEN) –For men experiencing domestic violence. www.mensaid.ie
Samaritans – Provide a dedicated confidential emotional support helpline for anyone in distress or despair. www.samaritans.ie
Aware – Provide support and information for people who experience depression or bipolar illness and their families. www.aware.ie
Pieta House – Provide free, professional support for people experiencing suicidal thoughts, self-harm or who are bereaved by suicide. www.pieta.ie
Text About it – Anonymous HSE funded SMS/ WhatsApp service for people requiring mental health support. www.text50808.ie
HSE Drugs and Alcohol Helpline – Confidential service providing support, information and available services. www.hse. ie/eng/services/list/5/addiction/ drugshivhelpline/
Drug and Alcohol Information and Support – Education, Training, Information, Support and Treatment and Rehabilitation Services. www.drugs.ie
Alcoholics Anonymous –Fellowship where alcoholics help each other and reach out to others struggling with alcoholism. www.alcoholicsanonymous.ie
Gamblers Anonymous –Fellowship where people help each other recover from gambling addiction. www.gamblersanonymous.ie
Grow – Provide community based, peer support groups and deliver mental health programmes within the community and workplace. www.grow.ie
Shine – Support and education for individuals, families and communities impacted by mental illness and stigma. www.shine.ie
Bodywhys – Support organisation for people with eating disorders. www.bodywhys.ie
Lighthouse – Holistic support to constriction community on emotional, physical and financial wellbeing. www.lighthousecharoty.org
HUGG – Support organisation for people bereaved by suicide. www.hugg.ie
CAIRDE – Programme to enhance knowledge of mental health issues and reduce stigma in the construction industry. www.hsa.ie/eng/your_industry/ construction
First Fortnight – Arts based mental health charity that challenges mental health stigma and promotes mental wellbeing. Arts festival held every January. www.firstfortnight.ie
Practitioner Mental Health Matters Programme –Confidential service for health professionals. www.practitionerhealth.ie
Traveller Counselling Service –Counselling service for members of the travelling community. www.travellercounselling.ie
In a crisis situation where there is imminent concern then contacting a relative or referring to the GP or emergency services is appropriate. References available on request
Men's Health - News
¤2m for New Counselling Supports for Men
The Minister for Mental Health, Mary Butler, has announced €2 million in funding to provide access to a suite of new talk therapies and counselling supports specifically tailored for men. Access to the services began from September 2025.
This initiative is embedded within Ireland’s approach to mental health policy implementation. Sharing the Vision – A Mental Health Policy for Everyone, and Connecting for Life, Ireland’s national strategy for suicide prevention, clearly state that talk therapies should be considered a first-line treatment option for most
people who experience mental health difficulties.
This recurring funding is allocated from Budget 2025 as part of an integrated series of initiatives led by the Minister to ensure people with mental health difficulties are able to access the appropriate range of supports, from mental
health promotion and prevention, through to specialist services and clinical programmes.
The funding is targeted at assisting with stigma reduction and to actively encourage men who otherwise would not usually avail of counselling to seek help with their mental health, to
assist men in accessing mental health services, and to provide much-needed support for men experiencing a mental health crisis.
The funding will provide over 15,000 free counselling sessions to men and establish accessible supports over the phone and in-person.
Groundbreaking Research Helping Infertile Men Conceive
Over the past few decades, male reproductive health has seen a concerning decline, with infertility emerging as a growing global challenge. As awareness increases, so too does the need for safe, effective, and evidence-based solutions to support male fertility.
Pillar Healthcare, a leader in reproductive health innovation, is announcing the launch of a new clinical research project focused on male infertility and the efficacy of its nutritional supplement, pre-Conceive. This landmark study aims to evaluate the supplement's impact on key male fertility parameters including sperm count, motility, morphology, and overall seminal health. This study is designed to expand upon their original, pioneering research that first demonstrated the clinical potential of pre-Conceive in supporting male reproductive health.
Male factor infertility contributes to approximately 50% of infertility cases worldwide, yet it remains critically under-researched and underserved. Pillar Healthcare is taking decisive action to address this gap through this clinical study, continuing to demonstrate the efficacy of pre-Conceive in relation to male factor infertility.
“With this research, we intend to firmly re-establish pre-Conceive as an evidence-backed solution for men facing fertility challenges; putting scientifically grounded support back in their hands. We believe and have demonstrated that nutrition plays a fundamental
role in reproductive health,” said Mark Whitney of Pillar Healthcare, “and this research aims to provide more clinical evidence that preConceive can make a measurable difference for men who are trying to conceive.”
pre-Conceive is a comprehensive, scientifically formulated nutritional blend specifically developed to support reproductive health. In preConceive’s previous independent study, the results demonstrated significant improvements across multiple parameters associated with male fertility, in just ninety days! Founded in 2012, with the goal of addressing rising infertility rates, pre-Conceive was launched into the European market. Over the past decade, pre-Conceive has supported thousands of people to conceive and have healthy children.
This new clinical study will build on that foundation with a dedicated focus on male-specific outcomes, aiming to deliver robust clinical data that underscores the efficacy of pre-Conceive as a frontline,
Stakeholder Briefing
non-invasive fertility support option for men.
Men interested in participating in the study, particularly those with a prior diagnosis of infertility, are encouraged to visit www.preconceive.co.uk or contact Pillar Healthcare directly at study@preconceive.co.uk to learn more.
For more information about pre-Conceive and Pillar Healthcare’s ongoing commitment to fertility research, please visit www.preconceive.co.uk
The Pharmaceutical Managers’ Institute (PMI) are hosting Dr Lesley Tilson, Deputy Head with the NCPE for a breakfast briefing on November 20th. During her talk, Lesley will discuss Healthcare Cost Effectiveness and will give an outline of the trends and observations in reimbursement across the industry along with policy updates from the NCPE.
This will be an essential stakeholder briefing for anyone involved with market access, commercial or external relationship management aspects in their organisations.
The briefing takes place from 7.30-9.30am at the Clayton Hotel, Liffey Valley Dublin. Members can visit www.thepmi.com and non-members can contact the office to book on: 01-2352310
Male Grooming
Unlocking a High-Growth Category for Community Pharmacy
Once considered a niche market, male grooming has evolved into one of the most dynamic and profitable sectors within personal care. From skincare and beard maintenance to men’s wellness supplements and fragrances, male grooming now represents a diverse, fast-moving category that continues to attract new customers and product innovation.
For community pharmacists, this trend presents a clear opportunity. Pharmacies already enjoy high levels of consumer trust, making them ideal destinations for advicedriven retail. By refining category layout, in-store visibility, and team engagement, pharmacies can successfully capture a greater share of this lucrative market.
Understanding the Male Grooming Market
The modern male grooming market has shifted far beyond traditional shaving products. Men of all ages are investing more in their personal appearance, health, and hygiene — and expect easy access to high-quality, credible products.
According to industry analysts, the global men’s grooming market is projected to exceed $115 billion by 2028, with skincare, beard care, and hair styling products among the fastest-growing segments. In Ireland and the UK, the growth has been driven by lifestyle changes, social media influence, and the increasing normalisation of male self-care.
Where once male grooming was confined to aftershave and razor blades, today’s consumer is exploring moisturisers, anti-ageing serums, exfoliating cleansers, beard oils, hair styling clays, and wellness supplements. The lines between health and beauty are blurring, placing pharmacies in a prime position to serve this evolving demand.
Who Is the Male Grooming Customer?
Understanding customer motivation is the first step in designing an effective merchandising and service strategy.
Broadly, the male grooming shopper falls into three main groups:
1. Traditionalists – often 40+, these men focus on shaving, deodorant, and basic skincare. They value trusted brands, practicality, and ease of use.
2. Modern Groomers – typically 20–40 years old, they’re interested in skincare, hair styling, and beard maintenance. They’re more brand-conscious and influenced by social media and professional appearance.
3. Gift Buyers – partners, family, and friends buying male grooming sets, fragrances, or luxury shaving kits, particularly around Father’s Day, Christmas, and Valentine’s Day.
Pharmacies can tailor promotions and merchandising to appeal to each group. For instance, Father’s Day displays can combine premium shaving sets and skincare gift boxes, while a year-round shelf can emphasise affordable everyday essentials for men.
Pharmacy Advantages: Trust, Advice, and Accessibility
Community pharmacies have several built-in strengths that can differentiate them from supermarkets or online retailers:
• Health Expertise: Pharmacists can advise on sensitive skin, acne, eczema, or beard irritation — common barriers to product use.
• Credibility: Men are often cautious about experimenting with new skincare or
• Convenience: Pharmacies are easily accessible, offering both over-the-counter products and professional guidance in one visit.
These advantages make pharmacies ideal for introducing men to tailored grooming routines and cross-selling relevant healthcare products, such as sunscreen, supplements for hair and skin health, or fragrance-free options for sensitive skin.
Product Segmentation: Building the Right Range
Successful male grooming merchandising starts with smart range selection. The category can be divided into five clear segments:
1. Shaving and Beard Care –razors, blades, shaving foams and gels, beard oils, trimmers, and aftershave balms.
2. Skincare – facial cleansers, moisturisers, exfoliators, serums, and anti-ageing products formulated for men.
3. Haircare and Styling –shampoos, conditioners, styling gels, clays, pomades, and scalp treatments.
4. Fragrance and Body Care –deodorants, body washes, and signature scents.
5. Men’s Wellness and Supplements – hair loss prevention, vitamins for skin and nails, energy boosters, and testosterone support.
A well-curated range doesn’t need to be vast; instead, it should balance trusted pharmacy brands (e.g. Nivea Men, L’Oréal Men Expert, Bulldog) with a few premium or niche products to attract gift buyers and younger shoppers.
Merchandising Strategies: Making the Category Stand Out
1. Location and Layout
Visibility is crucial. Many pharmacies still position male grooming in low-traffic corners or near women’s beauty aisles, where male shoppers may feel out of place.
Men's Health - Grooming
Instead, consider creating a distinct male grooming zone — ideally near the entrance, men’s health products, or fragrance displays.
A dedicated end bay or branded gondola signals that this is a space for men, encouraging browsing. Clear signage such as “Men’s Grooming – Shave, Style, Skincare” works well.
2. Visual Appeal
Use darker tones like charcoal, navy, or metallic accents for shelf headers and signage — these convey a masculine aesthetic that contrasts well with brighter cosmetics sections.
Display products vertically by category (e.g. shave → skincare → hair → fragrance), and ensure pricing and product information are clear. Keep the section uncluttered — men shop differently from women and are often goal-oriented, preferring clarity over variety.
3. Seasonal Focus
Plan seasonal refreshes around key male gifting times:
Starts Within” above grooming products could direct customers to supplements for skin, hair, and nail health.
Front-of-Store Engagement: Turning Browsers into Buyers
Pharmacy teams play a vital role in converting casual interest into sales. Here are some practical, achievable tips:
1. Use the Counter Space Wisely
Counter displays can feature highmargin impulse products such as beard oils, small travel grooming kits, or moisturisers. Compact point-of-sale (POS) units with bold visuals work well.
2. Empower the Team
Many pharmacy teams are more familiar with female skincare, so training is key. Encourage staff to test male grooming products themselves or use brand training materials to learn about key ingredients (e.g., charcoal, hyaluronic acid, caffeine).
Confidence in discussing these products helps overcome the barrier many male customers feel when asking for advice.
3. Sampling and Mini Sizes
Small testers or sachets of shaving gels, moisturisers, and beard oils allow men to try products risk-free. Sampling drives brand trust and repeat purchase.
4. In-Store Events
• Father’s Day – gift sets, premium grooming kits, and fragrance bundles.
• Christmas – pre-wrapped gift options and limited editions.
• Summer – travel-size grooming kits and SPF skincare.
Seasonal displays help maintain freshness and encourage repeat visits.
4. Cross-Merchandising Opportunities
Strategic cross-merchandising can boost average basket size. Pair related categories, such as:
• Beard oil beside beard trimmers.
• Moisturiser beside razor blades or shaving gel.
• Shampoo beside hair supplements.
• Aftershave beside men’s fragrance testers.
You can also link male grooming with men’s health. For example, a sign reading “Healthy Skin
This hybrid approach builds brand consistency and helps pharmacies compete with online retailers.
Common Mistakes to Avoid
• Neglecting range depth: Avoid relying solely on shaving products; include skincare and wellness lines.
• Over-cluttering shelves: A small, well-organised range with clear signage is more effective than a crowded display.
• Gender-neutral confusion: Avoid placing male grooming items within generic “unisex” skincare areas; men often want clear cues that the products are designed for them.
• Lack of staff knowledge: Uninformed recommendations can lose sales; ensure ongoing team training.
Measuring Success
Success in the male grooming category isn’t just about volume sales. Consider these performance indicators:
• Increased male footfall in frontof-store areas.
• Uptake of cross-category sales (e.g. supplements and skincare).
• Repeat purchases of male grooming products.
• Seasonal spikes linked to instore promotions.
A “Men’s Grooming Week” tied to Father’s Day or Movember can create buzz. Offer mini skincare consultations, beard care demonstrations, or discounts on male fragrances.
5. Leverage Local Partnerships
Work with local barbers or gyms to display flyers, share samples, or run small co-promotions. This builds credibility and attracts new footfall.
Digital and Cross-Channel Opportunities
While pharmacies excel in physical engagement, integrating digital touchpoints enhances visibility.
• Use the pharmacy’s social media to post product highlights, seasonal promotions, or skincare tips for men.
• Offer click-and-collect for male grooming gift sets.
• Include QR codes on displays linking to online advice from pharmacists on skincare or shaving tips.
Tracking these metrics helps refine displays, reallocate shelf space, and identify which brands or price points work best.
Conclusion: A Small Space with Big Potential
Male grooming offers one of the strongest growth opportunities for community pharmacies seeking to enhance their front-of-store performance. By leveraging pharmacists’ unique credibility, refining merchandising, and engaging customers with confident recommendations, pharmacies can transform what was once a small shelf of razors into a profitable, dynamic destination category.
The key lies in visibility, education, and consistency. When the male grooming section looks and feels like an intentional part of the pharmacy — not an afterthought — customers respond with curiosity, trust, and loyalty.
In a competitive retail landscape, a well-merchandised and advice-led male grooming offer can set your pharmacy apart, one clean shave and confident smile at a time.
60 Second Summary
Coughs, colds and flu remain among the most common respiratory illnesses seen in Irish pharmacies, particularly during the autumn and winter seasons.
While all are viral infections and cannot be cured by antibiotics, pharmacists play a crucial role in guiding patients on effective symptom relief, self-care, and prevention. Typical cold symptoms develop gradually and are usually confined to the head and sinuses, whereas influenza strikes suddenly, causing fever, muscle pain and extreme fatigue that can confine sufferers to bed for several days.
Pharmacy advice is essential in ensuring the safe use of over-the-counter medicines. Decongestants, antihistamines, painkillers and cough preparations must be selected carefully, especially for patients with conditions such as hypertension, asthma or gastric ulcers. In children, most coughs and colds are viral and selflimiting; the HPRA recommends avoiding cough and cold preparations in under-sixes, instead focusing on fluids, rest and saline nasal drops.
Influenza continues to pose serious risks for vulnerable groups including older adults, pregnant women, those with chronic illness and children. The 2025/26 flu vaccine, incorporating updated viral strains, remains the most effective protection and is free for at-risk groups under the HSE. Vaccination uptake in Ireland has increased steadily in recent years, helping to reduce flu-related hospitalisations and deaths. With pharmacists positioned at the forefront of winter health services, patient education, vaccination and early intervention continue to be key strategies for minimising illness and maintaining community wellbeing.
Written by Eamonn Brady, MPSI
41 CPD: Cough, Cold and Flus
Eamonn is the Supervising Pharmacist and Owner of Whelehan’s Pharmacy’s, Pearse Street and Clonmore, Mullingar
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the 4 previous steps, log and record your findings.
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author. Sponsor has no editorial oversight of the CPD programmes included in these modules.
Coughs, Cold and Flus
Cold or influenza (flu) are caused by viruses so have no cure, but the symptoms can be relieved by over-the-counter remedies. These symptoms include runny/blocked nose, sneezing/coughing, aches and pains, high temperature and sore throat. The flu comes on suddenly, whereas a cold develops over several hours.
Flu is a much more 'hard hitting' illness than a cold and will usually leave the sufferer confined to bed for a few days (more about flu symptoms later in this article). The symptoms of a cold, while unpleasant, usually allow the sufferer to continue his or her normal daily activities; though with COVID-19 in our community, COVID-19 must be considered a possibility too. Symptoms of a cold are generally confined to the head, while a patient with the flu will feel sick all over. The treatment for both colds and flu is similar. Colds and flu symptoms generally last a maximum of 7 days and need no specific treatment other than painkillers for aches, pains and temperature and simple measures such as decongestant rubs or vaporisers. Antibiotics are of no benefit as both colds and flu are caused by viruses.
• Sneezing is treated by an antihistamine.
• Cough may be due to irritation or to post-nasal drip. An expectorant mixture can help.
• Headaches are due to inflammation of the sinuses and nasal passages, and muscular or joint pain is common - this will need a painkiller.
• Sinus pain worsens on leaning forward or lying down and may develop into an infection.
• High temperature is more common in the flu than with a cold - paracetamol is very useful to bring down high temperature.
• Sore throat is usually the first sign of a cold, and one of the common OTC sore throat lozenges will help.
Precautions
Many cold and flu remedies contain several drugs, so anyone on prescription medication should speak to the pharmacist. Anyone who is pregnant, has heart disease or lung disease or very young or old should also be seen by the pharmacist.
So, for example, if someone suffers from hypertension it is best to avoid many cold and flu remedies which contain decongestants as these products tend to raise blood pressure.
Asthmatics and people with stomach complaints such as stomach ulcers should avoid products which contain aspirin and Non-Steroidal Anti-inflammatories (NSAIDs) like ibuprofen. This is because aspirin and NSAIDs can trigger asthma attacks in some asthmatics and irritate stomach ulcers. There are a vast number of preparations available for the treatment of cold and flu symptoms, some of which are combination preparations and may be capable of treating many symptoms at once.
COUGH
Essentially, there are two main types of cough — dry and chesty. During a cold, a cough is often triggered by nasal drip irritating the back of the throat. Chesty coughs occur when mucus (also called phlegm or catarrh) builds up in the airways; coughing helps the body clear this mucus. Chesty cough mixtures containing expectorants such as guaifenesin or carbocisteine help to loosen and thin the mucus, making it easier to expel. Some formulations also include sedative ingredients to support sleep when coughing is troublesome at night, and sugar-free options are available for people with diabetes.
42 CPD: Cough, Cold and Flus
codeine derivatives and are available in both drowsy and non-drowsy forms.
In addition to these conventional preparations, some patients may prefer herbal or medical-devicebased remedies that act by coating and soothing the throat and upper airways, providing relief from both dry and chesty coughs irrespective of cause. These products work through physical or demulcent mechanisms rather than pharmacological suppression and can be suitable for adults and children seeking a more natural approach.
When to see the doctor?
Patients should see their GP if they experience any of the following symptoms with cough as it can be a sign of more serious conditions (e.g.) COPD, Cancer:
• Phlegm, which is green, yellow, or rusty colour*
• Coughing up blood
• Cough lasting longer than two weeks
• Shortness of breath
• Chest pain on breathing or coughing
• Unexpected loss of weight
• Regular nighttime cough
• Harsh barking cough in children (croup)
• Whooping sound when breathing in after a fit of coughing (whooping cough)
*The meaning of different colours of phlegm: green phlegm means a bacterial infection; yellow phlegm means a viral infection; brown or reddish phlegm can mean the presence of blood (serious sign) and clear phlegm means no infection.
Self Help for coughs
Stop smoking
If determined to continue smoking, at least stop for the duration of the cough. This gives the lungs an opportunity to try to clear the infection. When stopping smoking, coughing more for a few weeks is common as the lungs clear the tar that coated the lungs while smoking.
Steam inhalations
Steam inhalations can be useful, particularly in productive (chesty) coughs. Simply putting hot
steaming water (not boiling) in a basin, putting a towel over one’s head and inhaling the steam can accelerate the clearing of catarrh. The steam helps to liquefy lung secretions, and the warm, moist air is comforting. Adding a little eucalyptus to the steaming water is a favourite of some people.
Increase fluid intake
Maintaining a good fluid intake helps to hydrate the lungs. Hot drinks like hot lemon and honey provide a soothing and comforting effect.
Could the cough be due to blood pressure medication?
A type of blood pressure medication can cause a persistent dry cough in some people. The class of drug that causes this cough is ACE inhibitors. Examples include ramipril, perindopril, and lisinopril. About 10 to 15% of people who use this class of blood pressure medication experience a dry cough. The incidence of cough appears to be higher in women. It is a persistent dry cough which is worse when lying down and generally does not start for 24 hours after starting an ACE inhibitor. If the dry cough occurs, the doctor will need to change to another drug. (e.g., To an angiotensin 2 inhibitor). The cough will subside once the ACE inhibitor is stopped.
Coughs in children
Coughs are more common during school term and are caused by common viruses which are commonly passed from child to child in school. While rarely serious, coughs and colds are an inconvenience and lead to many missed school days. Some prevention tips help prevent coughs and colds. Examples include ensuring children wash their hands regularly and properly, especially after touching their nose or mouth and before handling food. Teach them to always sneeze and cough into tissues to prevent spreading infection. Sharing cups and utensils is a common way to spread colds and flu. Chesty coughs are especially common during school terms. Antibiotic is rarely needed. Only 20% of chest infections are bacterial so antibiotics are ineffective in most cases.
Guidelines for coughs and colds remedies for children
Guidelines introduced by the Health Products Regulatory
Authority (HPRA) in 2011 restrict the sale of pharmacological cough and cold medicines (those containing ingredients such as cough suppressants, decongestants, or antihistamines) for children under six years of age.
This decision was not based on specific safety concerns, but on the recognition that most coughs and colds in young children are self-limiting and that there is limited evidence of benefit from these active medicines in this age group.
As a result, pharmacies should not recommend or sell traditional cough suppressants, decongestants, or antihistamines to children under six.
For these children, supportive measures remain first line — rest, plenty of fluids, and simple comfort strategies such as saline nasal drops or sprays, and paracetamol or ibuprofen liquids when required for fever or discomfort.
However, non-pharmacological cough remedies such as medicaldevice-based or demulcent preparations, indicated from one year of age, may also be considered.
These products act by coating and soothing the throat and upper airways, helping to reduce irritation and ease coughing without relying on systemic drug action. They can provide gentle symptomatic relief where appropriate parental reassurance and advice are also given.
For children aged six years and over, a range of over-the-counter (OTC) options are available, but no single product has proven superior. Pharmacists should always check age-appropriate doses and advise parents that most coughs and colds resolve within one to two weeks without antibiotics, since over 80% are viral in origin.
Prevention
As so many different viruses can cause the common cold, there is no vaccination against it. Some prevention tips are:
• Wash hands regularly and properly, most importantly after touching nose or mouth and before handling food.
• Always sneeze and cough into tissues prevent spreading infection.
• Do not share cups or kitchen utensils with others. Use own cup, plates, and cutlery.
TO RELIEVE ANY COUGH
INFLUENZA (FLU)
Influenza (flu) is a highly infectious acute respiratory illness caused by the influenza virus. It can affect people of any age. The seasonal flu vaccine (flu jab) protects against a number of strains of flu virus.
According to the World Health Organisation (WHO) recommendations for the 2025/26 Northern Hemisphere influenza season, the following strains are included in the vaccines distributed in Ireland and across Europe. These updates aim to provide optimal protection against the influenza viruses expected to circulate during the 2025/26 flu season.
The recommended strains for the 2025/26 vaccine are:
• A/Croatia/10136RV/2023 (H3N2) like virus (for egg-based vaccines).
• A/District of Columbia/27/2023 (H3N2) like virus (for cell culture- or recombinant-based vaccines).
• B/Austria/1359417/2021 (B/ Victoria lineage) like virus (for both vaccine types).
• B/Phuket/3073/2013 (B/ Yamagata lineage) like virus –included only in quadrivalent vaccines, though many programmes now use trivalent formulations due to low B/ Yamagata circulation.
Source: World Health Organisation (WHO). Recommended composition of influenza virus vaccines for use in the 2025–2026 Northern Hemisphere influenza season (published February 2025). These recommendations are adopted by the European Medicines Agency (EMA) and the Health Service Executive (HSE) in Ireland.
Flu vaccination is available through GP surgeries, local pharmacies, and some workplaces.
Symptoms of Flu
Symptoms of flu include sudden fever, chills, headache, muscle pain, sore throat, non-productive
Illustration
1 – Differences between common cold, influenza, and COVID-19
Side-by-side comparison of the three most common viral respiratory illnesses seen in community pharmacy settings. It highlights how onset, symptoms, and duration differ among the common cold, influenza, and COVID-19.
Feature Common cold Influenza (Flu) COVID-19
Onset
Gradual (1–2 days)
Sudden (hours) Variable (2–10 days)
Main cause Rhinoviruses, coronaviruses Influenza A & B viruses SARS-CoV-2 virus
Fever Rare, mild if present Common, high (38–40 °C) Common, variable
Aches & pains
Fatigue / weakness
Mild Often severe Can be severe
Mild Prominent Frequent, prolonged
Nasal congestion / runny nose Very common Sometimes Sometimes
Cough Mild, dry
Common, dry
Common, persistent
Loss of taste/smell Occasional Rare Common early symptom
Vaccination available No Annual flu vaccine COVID-19 booster
Illustration 1 – Differences between common cold, influenza, and COVID-19
Side-by-side comparison of the three most common viral respiratory illnesses seen in community pharmacy settings. It highlights how onset, symptoms, and duration differ among the common cold, influenza, and COVID-19.
dry cough, exhaustion, and weakness. Flu characteristically causes a temperature of 38 to 40° C that lasts 3-4 days.
Difference between cold and flu?
A cold will develop slowly over a few days with symptoms like a sore throat and a blocked or runny nose. The symptoms of flu hit suddenly and severely with symptoms like fever and muscle aches. Flu hits like a brick. Often people suffering from a bad cold wrongly believe they have flu. Flu causes extreme exhaustion, muscle aches, severe sweats and leaves the person so weak they will not be able to get out of bed. Work and other normal routines are not possible with flu.
Complications of flu
Most people recover from flu in 2-7 days, but in some it can last for up to two or three weeks. Flu can be severe and can cause serious illness and death, especially in the very young and in the elderly. Serious respiratory complications can develop, including pneumonia and bronchitis. Older people and those with certain chronic medical conditions are at particular risk of these complications. Pregnant women and women up to six weeks after giving birth have also been found to be at increased risk of the complications of flu. 80 to 90% of reported deaths from influenza occur in the elderly, mainly from bacterial pneumonia (200 deaths per year in Ireland up to 2020 but has reduced since), but also from the underlying disease.
Those considered more “at-risk” from flu:
Some people are more at risk of getting complications if they catch flu. People can get the HSE flu vaccine for free if:
• 60 years of age and over
• a healthcare worker
• pregnant (at any stage of pregnancy)
• children aged 2 to 17 years
• adult or child aged 6 months or older at increased risk for flurelated complications including:
Illustration 2 – Trend in confirmed influenza cases in Ireland (2015–2025)
chronic respiratory disease (including COPD, cystic fibrosis, moderate or severe asthma, bronchopulmonary dysplasia)
chronic neurological disease (including multiple sclerosis, hereditary and degenerative disorders of the central nervous system)
diabetes mellitus and other metabolic disorders, including inherited metabolic disorders
haemoglobinopathies
National trend in confirmed influenza cases in Ireland from 2015 to 2025. The data reflects how influenza activity dropped dramatically during the COVID-19 pandemic and has gradually returned to pre-pandemic levels in recent years.
Illustration 2 – Trend in confirmed influenza cases in Ireland (2015–2025)
National trend in confirmed influenza cases in Ireland from 2015 to 2025. The data reflects how influenza activity dropped dramatically during the COVID-19 pandemic and has gradually returned to pre-pandemic levels in recent years.
Impact of flu
ow influenza vaccination rates in Ireland have improved since 2019, alongside reductions in flu related hospitalisations and deaths. It also highlights the growing impact of public health initiatives such as pharmacy vaccination programmes and nasal spray use in children.
Illustration 3 – Impact of flu vaccination in Ireland (2019–2025)
44 CPD: Cough, Cold and Flus
How influenza vaccination rates in Ireland have improved since 2019, alongside reductions in flurelated hospitalisations and deaths. It also highlights the growing impact of public health initiatives such as pharmacy vaccination programmes and nasal spray use in children.
References
Illustration 3 – Impact of flu vaccination in Ireland (2019–2025)
How influenza vaccination rates in Ireland have improved since 2019, alongside reductions in flu-related hospitalisations and deaths. It also highlights the growing impact of public health initiatives such as pharmacy vaccination programmes and nasal spray use in children.
• Health Service Executive (HSE). Influenza (Flu) Vaccine Information for 2024/25 Season. Dublin: HSE, 2025.
• Health Products Regulatory Authority (HPRA). Guidelines on Cough and Cold Medicines for Children. Dublin: HPRA, 2023.
o body mass index (BMI) ≥ 40 kg/m2 (morbid obesity)
o immunosuppression due to disease or treatment (including treatment for cancer)
• Household contacts of people aged 60 years and over
the better, as it takes about two weeks to achieve full protection.
• National Immunisation Advisory Committee (NIAC). Immunisation Guidelines for Ireland. 13th Edition, 2024.
• Household contacts of pregnant women
Flu vaccine side effects
• World Health Organisation (WHO). Influenza (Seasonal) Fact Sheet. Updated 2024.
to get severe complications of flu. Children who are sick with flu miss days in crèche, childcare and school. They also miss out on their usual activities such as hobbies and sports. Children aged 2 to 17 can now get the nasal flu vaccine for free. The flu vaccine will help protect a child against flu and reduce the spread of flu to others. For example, their brothers and sisters, parents, and grandparents.
• UK National Institute for Health and Care Excellence (NICE). Cough (Acute): Antimicrobial Prescribing [NG120]. London: NICE, 2025 (updated).
o children with moderate to severe neurodevelopmental disorders such as cerebral palsy
• Household contacts of children aged 2 to 17 years
• UK National Institute for Health and Care Excellence (NICE). Influenza – Seasonal: Vaccination [NG103]. London: NICE, 2023.
• Household contacts of healthcare workers
• Household contacts of carers
o children on long-term aspirin therapy
o those with any condition that can compromise respiratory function (e.g. spinal cord injury, seizure disorder or other neuromuscular disorder), especially those attending special schools or day centres
o children or adults with Down syndrome
• live in a nursing home or other long-term care facility
• In regular contact with pigs, poultry or waterfowl should get the flu vaccine
Household contacts and eligibility
Not all household contacts are eligible for the free flu vaccine. The National Immunisation Advisory Committee (NIAC) recommends the flu vaccine only for household contacts of people with certain long-term medical conditions or of people with Down syndrome.
The following household contacts are not recommended for the free flu vaccine through the HSE programme unless they are in a risk group themselves:
If a household contact is not in a recommended risk group themselves, they cannot avail of the free flu vaccine via the HSE programme and would need to source the flu vaccine privately if they choose to get vaccinated. The flu vaccine is not free for medical card or doctor visit card holders unless they are part of the “at-risk” groups above.
Flu vaccines available for the 2025/26 season - This season, there are two different types of flu vaccine being offered to different groups:
• Live Attenuated Influenza Vaccine (LAIV) – nasal spray for children aged 2 to 17 years.
• Inactivated Influenza Vaccine (IIV) – injectable vaccine for all other eligible groups, including children (aged 2 to 17) with contraindications to LAIV.
There may be a mild fever and aching muscles for a couple of days after having the vaccine. The arm where the vaccine was given may also be a bit sore. Serious side-effects of the flu vaccine are very rare.
For children receiving the nasal spray:
• The vaccine is given as a spray in each nostril – not by injection.
• Most children need only 1 dose each year.
• Some children with chronic heart or lung conditions may need 2 doses, 4 weeks apart, if they have never had a flu vaccine before.
• Common side effects: runny or blocked nose, headache, muscle aches, mild fever can be treated with paracetamol or ibuprofen.
• Aspirin or any medicine containing aspirin should never be given to children unless prescribed by a doctor (risk of Reye syndrome).
• There is no risk of catching flu from the nasal spray – the virus is too weak to cause infection.
Flu vaccine and COVID-19 booster
The vaccine is given as a single spray in each nostril of the child's nose. The child can breathe normally while getting the vaccine. There is no need to take a deep breath or sniff. The vaccine is not painful and is absorbed quickly. It will work even if the child has a runny nose, sneezes, or blows their nose after the vaccination. Most children need only 1 dose of the vaccine each year. Some children with chronic health conditions like chronic heart or lung conditions may need 2 doses. The doses are given 4 weeks apart for these high-risk children if they have never had a flu vaccine.
Side effects of the nasal flu vaccine
The most common side effects are mild and include:
• a runny or blocked nose
• headache
• muscle aches
• Vaxigrip Tetra – Sanofi Pasteur Pharmacies must buy vaccines privately for those who pay. The earlier a patient gets vaccinated,
The flu vaccine and the COVID-19 booster are separate vaccines. Both can be administered at the same time if eligible for a COVID-19 booster dose.
Flu vaccine for children
Broncho Group New KV Strip ad for CPD HIRES.pdf 1 24/10/2025 14:37
Children are more likely than adults
TO RELIEVE ANY COUGH
Some children get a fever (temperature) after the vaccine. It is usually mild and goes away on its own. If the child has a fever or a headache, paracetamol or ibuprofen can help. Aspirin, or any medicines that contains aspirin, should never be given to children unless prescribed by a doctor (due to risk of Reye syndrome). This is especially important in the 4 weeks after getting the flu vaccine. Serious side effects such as a severe allergic reaction are rare. There is no evidence of catching flu from the nasal flu spray.
References available on request
RELIEVE COUGH USED TO ANY
*Broncho 5in1 and Bronchostop Junior. Associated with a cold. ^Bronchostop Syrup and Bronchostop Pastilles. Based on traditional use only. Buttercup Bronchostop Cough Syrup contains thyme herb extract and marshmallow root extract. A traditional herbal medicinal product for the relief of coughs, such as chesty coughs and dry, tickly, irritating coughs and catarrh, exclusively based upon long-standing use as a traditional remedy. Adults and children over 12 years: 15ml every 4 hours, 4 times per day. Max 6 doses (90ml) per day. Max dose should not be exceeded. To be taken 30 to 60 minutes before or after intake of other medicines. Not recommended for children under 12 years. To be administered undiluted or diluted in water or warm tea. Seek medical advice if symptoms persist after 7 days or if dyspnoea, fever or purulent sputum occurs. Contraindications:
Hypersensitivity to marshmallow root, thyme, to other members of the Lamiaceae family or to any of the excipients. Warnings and precautions: Asthmatics and atopic patients should consult a doctor before using the medicine. Contains E218 and E216 that may cause allergic reactions (possibly delayed). Patients with HFI, glucose-galactose malabsorption or sucrase-isomaltase insu ciency should not take the medicine. The additive e ect of concomitantly administered products containing fructose (or sorbitol) and dietary intake of fructose (or sorbitol) should be considered. Pregnancy and lactation: Not recommended. Side e ects: pruritus, rash, urticaria, angioedema, anaphylactic reaction, oral mucosal blistering, abdominal pain, diarrhoea, nausea, vomiting, dyspnoea, exacerbation of asthma. Product not subject to medical prescription. TR 2006/001/001.TR Holder: Kwizda Pharma GmbH, E ngergasse 21, A-1160 Vienna, Austria. Date of preparation: Feb 2023. SPC: https://www.medicines.ie/medicin es/buttercup-bronchostop-cough-syrup-31510/spc Buttercup Bronchostop Cough Pastilles contain thyme herb extract. A traditional herbal medicinal product for the relief of coughs, such as chesty coughs and dry, tickly, irritating coughs and catarrh, exclusively based upon long-standing use as a traditional remedy. Adults and children over 12 years: 1 – 2 pastilles every 4 hours. Max dose 12 pastilles per day. Not recommended for children under 12 years. Seek medical advice if symptoms persist after 7 days or if dyspnoea, fever or purulent sputum occurs. Contraindications: Hypersensitivity thyme, or to any of the excipients. Warnings and precautions: Asthmatics and atopic patients should consult a doctor before using the medicine. Contains E1519 that may cause allergic reactions (possibly delayed). Patients with HFI should not take the medicine. The additive e ect of concomitantly administered products containing fructose (or sorbitol) and dietary intake of fructose (or sorbitol) should be considered. Pregnancy and lactation: Not recommended. Side e ects: pruritus, rash, urticaria, angioedema, anaphylactic reaction, oral mucosal blistering, abdominal pain, diarrhoea, nausea, vomiting, dyspnoea, exacerbation of asthma. Product not subject to medical prescription. TR 2006/001/002. TR Holder: Kwizda Pharma GmbH, E ngergasse 21, A-1160 Vienna, Austria. Date of preparation: Feb 2023. SPC: https://www.medicines.ie/medicin es/buttercup-bronchostop-berry-flavour-cough-pastilles-31509/spc Broncho Junior is a medical device according to Directive 93/42/EEC, used to relieve any cough (dry & chesty) associated with a cold for children from 1 year. Children under 3 years of age should consult with a doctor to exclude more serious diseases being present. Use in children under 1 year of age is not recommended. Children aged 1 year and above: 5ml up to 3 times daily. Children 2 to 3 years: 5ml up to 4 times daily. Children 4 to 5 years: 7.5ml up to 4 times daily. Children 6 to 11 years: 15 ml up to 4 times daily. Always read the Instructions for Use. Date of preparation: 04/2022. Broncho 5 in 1 Multi-Symptom Action Syrup is a medical device according to Directive 93/42/EEC, used for the relief of any cough (dry & chesty) associated with a cold, as well as sore throat due to common cold, associated hoarseness, and dryness of the throat. Adults and adolescents from 12 years of age: 15ml up to 3 times daily. Not recommended for children under 12 years. Date of preparation: Feb 2023. MAT-10976
Nutrition in Children
Vitamins, minerals and supplements (VMS) have always been an important category in the pharmacy with various benefits for not only adults but children of all ages from birth right up to the elderly.
Vitamins and minerals are important for healthy growth and development in children. Children who eat a well-balanced diet usually do not need a vitamin or mineral supplement. However, some children are at risk for deficiencies and may need a supplement.
Important Considerations
Parents should strive for a wellrounded diet to ensure their child meets the daily recommended vitamin and mineral intakes. A balanced diet includes dairy or dairy alternatives, fruits and vegetables, whole grains and protein foods such as poultry, fish, eggs, nuts and legumes including beans and lentils. While all vitamins and minerals are important for growth and development, some are especially critical for children. It is generally recommended that all children aged 6 months to 5 years are given vitamin supplements containing vitamins A, C and D every day. Babies who are having more than 500ml (about a pint) of infant formula a day should not be given vitamin supplements. This is because formula is fortified with vitamins A, C and D and other nutrients. Vitamin D
Vitamin D, the sunshine vitamin, is a very powerful immune modulator which means it helps our immune system to work properly. While we’re all topped up over the summer, these stores will only last for 30 to 60 days. Indeed, the World Health Organisation advice is to get 5 to 15 minutes of casual sun exposure to hands, face and arms two to three times a week during the summer months.
We are unable, however, to make Vitamin D effectively from November to March and as a result, it is important to eat Vitamin D rich foods, such as eggs, oily fish including salmon, mackerel and trout, and fortified foods.
The Food Safety Authority of Ireland recommends that food, including supplements needs to deliver 10ug (400IU) of Vitamin D per day for everyone over 5 years of age. 100g of salmon, for example, provides 8ug, one egg provides 2ug and a 200ml glass of fortified milk provides 4ug. If consumption of these foods is sporadic, it would be a good idea to supplement over the winter months with a vitamin D spray, drops or tablet.
Fish Oils
Omega-3s are fatty acids that are important to many aspects of health, including foetal development, brain function, heart health, and immunity.
They’re considered essential fatty acids because your body cannot produce them on its own and needs to obtain them from food. The three main types are alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). ALA is present in a variety of plant foods, including nuts, such as walnuts, and seeds, such as ground flaxseed, chia seed and pumpkin seeds. Meanwhile, EPA and DHA occur naturally in fatty fish, such as salmon, mackerel, and tuna, and are widely available in supplements.
Studies have shown a possible link between Omega-3 fatty acids and reduced asthma risk in
children, brain development and mood modulation. In addition, the anti-inflammatory effect of Omega 3 has been studied widely. Ensuring that children are eating oily fish at least twice per week ensures that they can benefit from this essential nutrient.
Probiotics
If you think about it, our digestive tract is effectively ‘the outside’, so our digestive system plays a very important role in keeping bacteria, yeasts and viruses, that we inadvertently consume, away from the rest of our body.
If the gut lining is the castle wall, our ‘good’ bacteria, along with our immune system, are the soldiers at the gate.
Not only do our ‘good bacteria’ help our digestive system to clear out the waste every day, they also ‘feed’ the cells in our gut, helping the gut lining stay healthy so that it can do its job and keep any pathogens out. They also crowd out any bad bacteria and create an acidic environment that is more favourable to their own growth. A virtuous cycle.
Fibre
Interestingly, a way to increase your ‘good’ bacteria is to give them the food that they particularly like; fibre. By including a range of different coloured fruit and vegetables in their diet, or even hidden in tomato sauces or smoothies, you can help to feed their good bacteria.
Start the academic year by printing off an ‘Eat a Rainbow’ chart and start ticking off all the different colour fruits and vegetables you eat per day, no matter how small a piece it is. Incorporating a variety into smoothies, or hidden vegetable sauces, is a great way to boost your ‘good’ bacteria.
Fibre is also found in beans, legumes, lentils, nuts, seeds and wholegrains.
Iron Deficiency
Recent studies found that half of Irish 2-year-olds have low levels of iron. Almost 1 in 10 suffer from anaemia because of this.
Anaemia is a condition in which the amount of red blood cells in the body is decreased below normal for a child's age. It can make the child appear pale in colour and feel cranky, tired, or weak. The most common causes of anaemia, such as iron deficiency, are generally easy to treat, especially when it is detected early.
Because rapid growth is a potential cause of the condition, the first year of life and adolescence are two age groups where infants and children are especially prone to anaemia. At the bottom of the page is a table illustrating how much daily iron a child should have each day. What are the common signs and symptoms of anaemia?
• Pale or sallow (yellow) skin
• Pale cheeks and lips
• Lining of the eyelids and the nail beds may look less pink than normal
• Irritability
• Mild weakness
• Tiring easily, napping more frequently
Red meat is the best source of iron. Children should be offered this 3 times a week. Beef, lamb, pork and poultry are good sources of iron. Iron supplements are also available, especially for those children who may be vegetarian, vegan, following a plant-based diet or when their iron is very low.
Capasal Therapeutic Shampoo
Salicylic acid removes scales, distilled coal tar relieves itching, and coconut oil softens and moisturises the scalp
Uses: As a shampoo in the treatment of dry, scaly scalp conditions such as seborrhoeic eczema, seborrhoeic dermatitis, pityriasis capitis, psoriasis and cradle cap in children. It may also be used to remove previous scalp applications.
Contra-indications, warnings, side e ects etc: Please refer to SPC for full details before prescribing. Do not use if sensitive to any of the ingredients. In case of irritation or if there is no improvement a er 4 weeks, or the condition is aggravated, discontinue treatment. Keep away from the eyes. Keep out of the reach of children.
Use in pregnancy: avoid use during rst trimester.
Package quantities, trade prices and MA number: 100ml bottle €3.78, 250ml bottle €7.30, PA23128/008/001.
Legal category: Supply through pharmacy only.
Date of preparation: June 2024. ‘Capasal’ is a trademark.
Directions: Adults, children and the elderly: Use as a shampoo, once or twice weekly until the condition improves. Therea er, occasional use may be necessary. Wet the hair thoroughly. Massage a small amount of the shampoo into the scalp, leaving on for a few minutes. Remove as much lather as possible with the hands, before rinsing out thoroughly under running water. Repeat if necessary.
Further information is available from: Dermal Laboratories (Ireland) Ltd, Head O ce Tatmore Place, Gosmore, Hitchin, Herts, SG4 7QR, UK.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Dermal.
Prescribing information www.dermal.ie
Reckitt: Driving Innovation in Everyday Health
At Reckitt, our brand’s purpose & commitment is driving product innovation, designed to support the needs of our consumer. Our focus is superior efficacy, without losing sight of sustainability. Our heritage brands operate in 4 different categories. Household (Finish & Vanish), Intimate Wellness (Durex), Germ Protection (Dettol) and Self Care (Nurofen).
Globally, Reckitt is a purposeled consumer health company committed to protecting, healing and nurturing in the pursuit of a cleaner, healthier world.1 With a culture built on integrity, sciencedriven innovation, and care for communities, we strive to deliver solutions that empower people to take control of their wellbeing.2
Pharmacists are increasingly the first point of contact for healthcare in Ireland,3 making our mission more relevant than ever: to partner with pharmacists and healthcare professionals to expand access, support self-care, and help deliver trusted relief.
Putting Everyday Care in People’s Hands
In recent years, the strain on general practice in Ireland has become more acute. A recent report4 projects that, due to population growth, ageing demographics, and increased complexity, Ireland will need up to 943 to 1,211 additional general practitioners (GPs) by 2040 just to maintain current consultation rates.
Meanwhile, the GP workforce is under pressure: many GPs are approaching retirement age, recruitment is difficult in rural and single-doctor practices, and the
supply of new doctors has not kept pace with demand.5
At the same time, public expectation of timely primary care is rising. According to Irish Pharmacy Union (IPU) research,6 77% of people report having to wait longer for GP appointments than in the past.
All of this underscores a shift: safe, effective over-the-counter (OTC) options are not just convenience - they are an essential part of community health, especially when GP access is challenging.
Reckitt’s Trusted Portfolio
Our consumers and pharmacists know and trust several Reckitt brands:
Nurofen:7 Effective pain relief for many aliments from headache to dental pain, period pain and many more.
Gaviscon:8 trusted digestive, heartburn and reflux relief.
Lemsip and Strepsils:9 classic household names during the cold and flu season.
Nuromol: A New Alternative in OTC Pain Relief
To meet evolving needs, Reckitt has launched Nuromol in
Ireland - a dual-action analgesic combining ibuprofen and paracetamol in one formulation.10
Evidence shows that fixeddose combinations of ibuprofen and paracetamol provide more effective pain relief than standard paracetamol or ibuprofen alone.
Clinical trials of ibuprofen 400 mg + paracetamol 1000 mg showed significantly greater total pain relief and pain intensity scores compared to singleagent regimens ibuprofen or paracetamol alone.11
Clinical evidence confirms the combination achieves faster onset and longer duration of pain relief compared to standard OTC painkillers alone.12
Together, these findings reveal that Nuromol is an effective painkiller and especially suitable for pain which has not been relieved by ibuprofen or paracetamol alone while offering a good safety profile.
This October: Spreading Awareness
From October 2025, Reckitt will roll out a nationwide campaign across Ireland targeting both consumers and healthcare professionals. The objective: to make clear that Nuromol is now
available, to explain how it works, and when it is appropriate to recommend it. We will support pharmacies with educational materials, in-store tools, and training to help ensure that pharmacists are confident and empowered to advise and recommend Nuromol where appropriate.
Innovation Built on Proven Track Record
Innovation is part of Reckitt’s DNA. In Ireland, Nurofen Rapid Relief continues to be the leading OTC pain relief brand,13 demonstrating our long-term commitment to advancing science and supporting pharmacy-led care.
Nuromol builds on this legacy: a next-generation product designed to meet real patient needs and help strengthen the role of pharmacy in everyday healthcare.
Reckitt remains steadfast in our purpose: to protect, heal and nurture, and to partner with pharmacists in delivering better health outcomes. As we look ahead, we are committed to continuing investment in science, sustainable practices, and the collaborative relationships that make everyday care accessible across Ireland.
Matthew List-Rose, Managing Director or General Manager, Reckitt Ireland says, “At Reckitt, we build on a heritage of trusted brands. With Nurofen, Gaviscon, Lemsip and Strepsils, we already deliver recognisable relief to consumers across Ireland. Now, with Nuromol, we are offering a next-generation pain solution - one that helps deliver more effective, faster and more lasting relief compared with standard painkillers like ibuprofen and paracetamol alone. By working closely with healthcare professionals including pharmacists, we aim to empower people to manage pain more effectively and reduce strain on general practice. Together, we can make everyday health better for everyone.”
For more information on Reckitt and its portfolio, visit reckitt.com.
Full prescribing information on Reckitt's medicinal products available at www.medicines.ie References available on request
Integrating Exercise into Cancer Care: The PERCS Approach to Personalised Rehabilitation in Ireland
Written by Dr Emer Guinan, Associate Professor in Cancer Rehabilitation and Survivorship, Trinity College Dublin and Dr Marie Tierney, Research Fellow, Trinity College Dublin
Exercise Oncology: Evidence and Application
Exercise is increasingly recognised as a critical component of cancer care. Research over the past two decades has shown that regular, tailored physical activity can reduce cancer-related fatigue, preserve muscle mass, improve cardiovascular and psychological health, particularly anxiety and depression, and enhance overall quality of life. In June 2025, the results of the landmark CHALLENGE trial were published, which demonstrated for the first time through a definitive randomised clinical trial, that exercise both reduced recurrence and improved survival in patients who had completed adjuvant chemotherapy for resected colon cancer.1
The CHALLENGE trial results add to the compelling body of clinical trials demonstrating the significant benefits of exercise for people living with and beyond cancer. Accordingly, international expert organisations such as the American College of Sports Medicine and the Clinical Oncology Society of Australia highlight and recommend that exercise should be considered a standard part of cancer treatment and recovery. However, despite this clear evidence base, access to safe, structured and individualised exercise rehabilitation remains limited across many health systems, including Ireland’s.
The Challenge in Ireland
Over 200,000 people are living with and beyond cancer in Ireland, and with improved diagnostics and treatment options, this number will continue to grow. More people than ever are living for longer after diagnosis, often managing the long-term effects of treatment. While we have made great strides with survivorship programmes, and psycho-oncology services nationally, more needs to be done to develop cancer rehabilitation and exercise pathways.
Research has shown that while many cancer survivors are motivated to become more active after treatment, they face multiple barriers. These include the limited availability of suitable supervised programmes, inconsistent referral pathways and uncertainty among clinicians about how and where to refer patients safely. For health professionals, competing clinical demands and the absence of clear, system-wide structures often
make appropriate exercise referral difficult to prioritise. The gap between what we know about the benefits of exercise and what we do in practice represents both a challenge and a timely opportunity for the Irish health system.
2. Structured referral pathways that link patients to appropriate levels of exercise support based on clinical need and current exercise behaviours
1. Routine screening for exercise needs and safety concerns as part of oncology assessments
Integrating Exercise into Routine Cancer Care: The PERCS Programme
3. Collaboration between hospital and community services to ensure sustainable access
2. Structured referral pathways that link patients to appropriate levels of exercise based on clinical need and current exercise behaviours
3. Collaboration between hospital and community services to ensure sustainable
Integrating exercise into cancer care requires more than simply increasing awareness. It requires a coordinated multidisciplinary approach that embeds exercise as part of the patient’s pathway from diagnosis through survivorship.
Successful models internationally typically include three key components:
1. Routine screening for exercise needs and safety concerns as part of oncology or survivorship assessments
This tiered structure approach ensures that people who have more complex, high-level needs can receive specialist rehabilitation, while others can be safely supported through community-based programmes or self-management guidance.
This tiered structure approach ensures that people who have more complex, highreceive specialist rehabilitation, while others can be safely supported through community programmes or self-management guidance.
In Ireland, the Personalised Exercise Rehabilitation in Cancer Survivorship (PERCS) developed at Trinity College Dublin, was created as a model that could work in the (Figure 1). The system begins with a brief assessment of medical history, comorbidities levels, as well as functional tests. Two simple questions guide the triage, which leads of exercise support. In PERCS 1.0, funded by the Irish Cancer Society in partnership Cancer Control Programme through the Research Grant COV21GUI, pilot work at St showed that this provided a practical, scalable way to ensure that people are directed level of exercise support based on their needs and safety 2,3. It supports integration, efficiency ensuring that exercise is not dependent on where a person lives or receives
In Ireland, the Personalised Exercise Rehabilitation in Cancer Survivorship (PERCS) programme, developed at Trinity College Dublin, was created as a model that could work in the Irish context (Figure 1). The system begins with a brief assessment of medical history, comorbidities and activity
Dr Emer Guinan
Dr Marie Tierney
levels, as well as functional tests. Two simple questions guide the triage, which leads to three levels of exercise support. In PERCS 1.0, funded by the Irish Cancer Society in partnership with the National Cancer Control Programme through the Research Grant COV21GUI, pilot work at St James Hospital showed that this provided a practical, scalable way to ensure that people are directed to the right level of exercise support based on their needs and safety.2,3 It supports integration, safety and efficiency ensuring that exercise is not dependent on where a person lives or receives care.
Implementation of the pilot project was supported by a website, created with patients and healthcare professionals, to provide exercise advice, sample programmes and videos, and a national service directory to identify the existing cancer rehabilitation and exercise services around Ireland. The website, www. cancerrehabilitation.ie is currently being updated as part of the ongoing PERCS programme.
Physiotherapists and exercise professionals can add to the service directly by contacting percs@tcd.ie
Building on this earlier pilot work, PERCS 2.0 is a Health Research Board (HRB) Investigator-Led Project grant (ILP-HSR-2024-011) focused on developing a costeffective national implementation strategy for exercise rehabilitation in cancer survivorship. The project is led by researchers, clinicians, exercise professionals, policymakers and people impacted by cancer. One of our first actions is to understand the barriers and facilitators to integrating exercise into cancer care in different settings around Ireland, and from different stakeholder perspectives through focus group discussions. If you are interested in learning more about or participating in the focus groups, please contact the team at percs@tcd.ie.
Hospital professionals have a crucial role in advancing the exercise in cancer care agenda. Simple actions, such as initiating conversations about exercise,
identifying suitable patients for referral or engaging with local community programmes, can make a significant difference. As awareness grows and systems like PERCS become established, oncology teams will have clearer pathways and stronger partnerships with community exercise providers. The result will be a more coordinated, person-centred approach to survivorship care.
Exercise is not an optional extra in cancer care. It is a clinically effective, evidence-informed intervention that supports recovery, enhances wellbeing and improves long-term outcomes for people living with and beyond cancer. Ireland now has an opportunity to move from evidence to action. Through collaboration across the health system, we can ensure that every person diagnosed with cancer has access to safe, effective exercise rehabilitation. For general queries or to engage more broadly with the PERCS 2.0 project, please contact percs@tcd.ie.
References
1. Courneya KS, Meyerhardt JA, O’Connell MJ, et al. Structured exercise after adjuvant chemotherapy for colon cancer. N Engl J Med. 2025;393(1):13–25. https://doi.org/10.1056/ NEJMoa2502760
2. Brennan L, Sheill G, Collier S, et al. Personalised exercise rehabilitation in cancer survivorship: Findings from a triage and referral feasibility study. J Cancer Surviv. 2024. https://doi.org/10.1007/s11764024-01684-2
3. Brennan L, Kennedy M, Grehan S, Connolly H, Sheill G, Donohoe CL, Guinan E. Patient experiences of participating in a cancer rehabilitation triage and referral system in the Irish healthcare system. J Cancer Surviv. 2025 Mar 27. https:// doi.org/10.1007/s11764-02501785-6
New report highlights only 3 of 28 targets met in National Cancer Strategy News
The Irish Cancer Society has launched new figures that highlight only 3 of 28 defined targets have been met in the National Cancer Strategy. With Ireland’s cancer mortality rate the third highest in Western Europe, the Society has warned that things will get worse unless increased investment is provided in budget 2026.
The Irish Cancer Society’s NCS Scorecard highlights performance against the 28 defined targets in the National Cancer Strategy in 2024 and 2025.
Of these targets only 3 have been met. 14 have not been met; 7 have no data available; 1 is considered unlikely to meet its 2026 target given its current trajectory, and 3 have a 2026 deadline which cannot yet be assessed.
CEO, Averil Power said, “One in two of us will get cancer in our lifetime. When we do, we deserve to be given the best possible chance of surviving the disease. But as the National Cancer Strategy Scorecard highlights, target waiting times for vital cancer tests and treatment are not being met. As a result, our cancer death rate is the 3rd highest in Western Europe.
“The National Cancer Strategy was launched in 2017 and will expire in 2026. As we head into the final year of the Strategy, it's clear most targets are not being met. That will only change if Government
provides additional investment in the National Cancer Strategy in next week’s budget.”
Professor John Kennedy, Chair of the last National Cancer Strategy, added, “We are deeply concerned about the impact lack of investment in the National Cancer Strategy is having on people with cancer in Ireland. The fact of the matter is that patients are being let down.
“Without Government investment in cancer services, staff, and infrastructure, it is cancer patients who continue to pay a too high price. Budget 2026 must prioritise the National Cancer Strategy, with ringfenced new recurrent development funding for the National Cancer Control Programme of at least ¤20 million each year. The huge challenges posed by the combination of a growing and increasingly aged population along with ever more complex, expensive and effective therapy, can only be addressed by coherent planning for, and multiannual funding of, the next
Professor John Kennedy, Chair of the last National Cancer Strategy
National Cancer Strategy over its lifetime.”
The Irish Cancer Society is calling for increased investment in Budget 2026 towards cancer staff, buildings, and equipment to ensure target waiting times are met. Specifically:
• Provide sufficient investment in staff, buildings, and equipment to enable targets of the current National Cancer Strategy to be met
• Plan and resource the next National Cancer Strategy
• Improve the availability of data to support transparency and decision-making.
What is Cervical Cancer?
Cervical cancer is cancer that starts in the cells of the cervix. The cervix is the lower part of the womb (uterus), also called the neck of the womb. Cervical cancer usually develops slowly over time.1
What causes cervical cancer?
Most cases of cervical cancer (at least 9 in 10) are caused by the human papillomavirus (HPV). HPV can cause cells in the cervix to become abnormal. These abnormal cells can develop into cervical cancer over time. It usually takes 15 to 20 years for abnormal cells to become cancer but rarely it can develop quicker.
If you have HPV, the following can increase your risk of getting cervical cancer:
• smoking - if you smoke you are twice as likely to develop cervical cancer.
• having a weakened immune system
• being sexually active in your early teens
• if your birth mother took the hormonal drug diethylstilbesterol (DES) while pregnant with you2
What is HPV?
HPV is very common. At least 80% of people will get a HPV infection in their life. There are at least 100 different types of HPV and around 14 types are considered high risk for cervical cancer. time. You can get HPV by having vaginal, anal, or oral sex with someone who has the virus. It is also spread through close skin to skin contact, usually during sexual activity. Most HPV infections cause no symptoms and resolve spontaneously.3
Written by Bernie Carter, Assistant Director of Nursing, Marie Keating Foundation
Screening age:
All eligible women and people with a cervix will now be screened up to the age of 65 instead of age 60. The number of years between your screening tests changes depending on your age.
People with a cervix age 25 to 29 are screened every 3 years. You are screened more often than people over 30 because you are more likely to have HPV.
People with a cervix age 30 to 65 are screened every 5 years from age 30 to 65.
o HPV found in repeat test then a Colposcopy will be scheduled
• HPV found and abnormal cell changes found
o Scheduled for a Colposcopy
• Inadequate or unsatisfactory sample
o Issue with the sample, repeat test in around 3 month
o If 3 inadequate results in a row you will be referred for a colposcopy8
What are the symptoms of cervical cancer?
Not everyone diagnosed with cervical cancer will have symptoms. That's why it's important to attend for regular cervical screening. The most common symptoms include:
• unusual vaginal bleeding
• pain or discomfort during sex.
• vaginal discharge
• pain in the area between the hip bones (pelvis)
If you have any of these symptoms, see your GP. Don't panic as many of those symptoms can be caused by other conditions which are not cancer. 4
What is HPV cervical screening?
HPV cervical screening is a new way of cervical screening which was introduced in Ireland in 2020. It has replaced the previous screening test known as ‘The Smear.’ This type of screening has already been introduced in Australia, England, and Wales.
HPV cervical screening:
• is a better way of cervical screening
• prevents more cancers
• taken in the same way as the smear
• if your sample tests positive for HPV, this same sample will then be checked for abnormal cells (pre-cancerous)
• It is important to note that precancerous cells are not cancer
If you have never had a cervical screening test, you can ask any registered GP or clinic for a free cervical screening test up to age 65.
Is 5 years a big gap between screening?
It is safe to wait for 5 years between screening tests if you do not have a HPV infection.
This is because:
• your risk of developing cell changes is very low
• a test showing that you do not have a HPV infection is more reliable than a test finding normal cells
In most cases, it takes 15 to 20 years for a HPV infection to develop into cervical cancer.7
HPV Cervical Screening Results:
You'll usually get your results by letter within 4 weeks of your screening test.
There are 14 high-risk types of HPV that can cause cervical cancer. Cervical screening looks to see if you have any of these. It does not tell us which HPV type, or how many types, were found.
Your results may say:
• HPV not found
o Next Cervical Screening in 3 or 5 years depending on your age
• HPV found and no abnormal cell changes found
o Repeat test in 12 months
o No HPV present then return to screening every 3 or 5 years
Please speak to your GP for further explanations on the results of your cervical screening.
Irelands plan to eliminate cervical cancer:
Ireland is on target to eliminate cervical cancer by 2040. A global initiative led by the World Health Organisation (WHO). Elimination does not mean eradication of cervical cancer. Elimination is defined as less than 4 cases of cervical cancer per 100,000.5
Cervical cancer is highly preventable and highly curable if caught early. Nearly all cervical cancers could be prevented by HPV vaccination, routine HPV cervical screening, and effective treatment of high grade abnormal cervical disease.6
To achieve elimination Ireland must meet the following targets:
• 90% of girls vaccinated against HPV by age 15
• 70% of women screened by age 35 and again by age 45
• 90% of people identified with cervical disease treated
The HSE’s Cervical Cancer Elimination Strategy Group are working closely together to help make this a reality. We can do this through HPV vaccination, HPV cervical screening and effective treatment of high grade abnormal cervical disease
Visit the Marie Keating Foundation at www.mariekeating.ie for more information about cervical cancer, other types of gynaecological cancer, specific cancer types, cancer prevention, and our support services.
References available on request
Promotional material for Irish HCPs only. Full Prescribing Information and Adverse Events information available at the bottom of the page.
START AN IMPACTFUL CONVERSATION WITH PATIENTS ABOUT HUMAN PAPILLOMAVIRUS (HPV) VACCINATION.
Gardasil 9 is indicated for active immunisation of individuals from the age of 9 years against the following HPV diseases:
• Premalignant lesions and cancers affecting the cervix, vulva, vagina and anus caused by vaccine HPV types.1
• Genital warts (Condyloma acuminata) caused by specific HPV types.1
HPV infections can occur in most sexually active people in their lifetime. Models consistently estimate that at least 30% of disease-causal infections occurred after age 26.2,3,4,5 Not all cervical, vulvar, vaginal, and anal cancers are caused by HPV.
Safety statement
In Gardasil 9 clinical trials adverse events were mostly mild to moderate. The most common reactions were injection-site reactions (84.8%) and headache (13.2%). Only 0.1% discontinued due to adverse events. Safety was consistent across age groups and when co-administered with other vaccines. Post-marketing data confirm the established safety profile.1
for use from the age of 9 years for the prevention of premalignant lesions and cancers affecting the cervix, vulva, vagina and anus caused by vaccine HPV-types and genital warts (condyloma acuminata) caused by specific HPV types. The indication is based on the demonstration of efficacy of Gardasil 9 in males and females 16 to 26 years of age and on the demonstration of immunogenicity of Gardasil 9 in children and adolescents aged 9 to 15 years. The use of Gardasil 9 should be in accordance with official recommendations. DOSAGE AND ADMINISTRATION Individuals 9 to and including 14 years of age at time of first injection: Gardasil 9 can be administered according to a 2-dose schedule. The second dose should be administered between 5 and 13 months after the first dose. If the second vaccine dose is administered earlier than 5 months after the first dose, a third dose should always be administered. Gardasil 9 can be administered according to a 3-dose (0, 2, 6 months) schedule. The second dose should be administered at least one month after the first dose and the third dose should be administered at least 3 months after the second dose. All three doses should be given within a 1-year period. Individuals 15 years of age and older at time of first injection: Gardasil 9 should be administered according to a 3-dose (0, 2, 6 months) schedule. The second dose should be administered at least one month after the first dose and the third dose should be administered at least 3 months after the second dose. All three doses should be given within a 1-year period. It is recommended that individuals who receive a first dose of Gardasil 9 complete the vaccination course with Gardasil 9. The need for a booster dose has not been established. Studies using a mixed regimen (interchangeability) of HPV vaccines were not performed for Gardasil 9. Subjects previously vaccinated with a 3-dose regimen of quadrivalent HPV types 6, 11, 16, and 18 vaccine (Gardasil or Silgard), hereafter referred to as qHPV vaccine, may receive 3 doses of Gardasil 9. The use of Gardasil 9 should be in accordance with official recommendations. Paediatric population (children <9 years of age): The safety and efficacy of Gardasil 9 in children below 9 years of age have not been established. No data are available. The vaccine should be administered by intramuscular injection. The preferred site is the deltoid area of the upper arm or in the higher anterolateral area of the thigh. Gardasil 9 must not be injected intravascularly, subcutaneously or intradermally. The vaccine should not be mixed in the same syringe with any other vaccines and solution. CONTRAINDICATIONS Hypersensitivity to any component of the vaccine including active substances and/or excipients. Individuals with hypersensitivity after previous administration of Gardasil 9 or Gardasil /Silgard should not receive Gardasil 9. PRECAUTIONS AND WARNINGS In order to improve traceability of biological medicinal products, the name and batch number of the administered product should be clearly recorded. The decision to vaccinate an individual should take into account the risk for previous HPV exposure and potential benefit from vaccination. As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of rare anaphylactic reactions following the administration of the vaccine. The vaccine should be given with caution to individuals with thrombocytopaenia or any coagulation disorder because bleeding may occur following an intramuscular administration in these individuals. Syncope, sometimes associated with falling, can occur before or after vaccination with Gardasil 9 as a psychogenic response to the needle injection. Vaccinees should be observed for approximately 15 minutes after vaccination; procedures should be in place to avoid injury from faints. Vaccination should be postponed in individuals suffering from an acute severe febrile illness. However, the presence of a minor infection, such as a mild upper respiratory tract infection or low-grade fever, is not a contraindication for immunisation. As with any vaccine, vaccination with Gardasil 9 may not result in protection in all vaccine recipients. Gardasil 9 will only protect against diseases that are caused by HPV types targeted by the vaccine. The vaccine is for prophylactic use only and has no effect on active HPV infections or established clinical disease. The vaccine has not been shown to have a therapeutic effect and is not indicated for treatment of cervical, vulvar, vaginal and anal cancer, high-grade cervical, vulvar, vaginal and anal dysplastic lesions or genital warts. It is also not intended to prevent progression of other established HPV-related
Scan the QR code below for more Gardasil 9 resources on msdconnect.ie
or efficacy data to support interchangeability of Gardasil 9 with bivalent or quadrivalent HPV vaccines. FERTILITY,
AND LACTATION There are insufficient data to recommend use of Gardasil 9 during pregnancy; therefore vaccination
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie Adverse events should also be reported to MSD (Tel: 01-299 8700)
References
1. Gardasil 9 SPC. Accessed October 2025 at: Gardasil 9 suspension for injection in a pre-filled syringe | SPC medicines.ie
2. Estimating the Age of Disease-causal HPV Infection Based on the Natural History of CIN2+ Among Females in Canada. Cherif A1, You X1, Hillhouse E2, Stone R2, Murphy B2, Baluni G3, Yadav M3, Gotarkar S3, Reuschenbach M4, Chen YT1, Cook J3, Roberts C1, Franco EL5. IPVC 2024
3. Estimating the Age of Acquisition of Disease-causing HPV Infection for CIN2+ in England Kayla Engelbrecht1, Xuedan You2, Dionysios Ntais, Olga Ovcinnikova1, Alhaji Cherif2. IPVC 2024
4. Prabhu, V.S., et al., Median Age at HPV Infection Among Women in the United States: A Model-Based Analysis Informed by Real-world Data. Open Forum Infect Dis, 2021. 8(7): p. ofab111.
5. Burger, E.A., et al., Age of Acquiring Causal Human Papillomavirus (HPV) Infections: Leveraging Simulation Models to Explore the Natural History of HPV- induced Cervical Cancer. Clin Infect Dis, 2017. 65(6): p. 893–899.
6. Ipsos Veracity Index 2024. (2024). Accessed October 2025 at HYPERLINK “https://www.ipsos.com/sites/default/files/ct/news/documents/2024-09/%20Ipsos%20BandA%20%20Veracity%20Index%202024.pdf”https://www.ipsos.com/sites/default/files/ct/news/documents/2024-09/ Ipsos%20BandA%20%20Veracity%20Index%202024.pdf
7. HIQA. NIAC – Chapter 10 Human Papillomavirus. Accessed October 2025 at: https://www.hiqa.ie/sites/default/files/NIAC/Immunisation_Guidelines/Chapter_10_Human_Papillomavirus.pdf
Red Oak North, South County Business Park, Leopardstown, Dublin D18 X5K7 Ireland
Image for illustration purposes.
What’s New in Smoking Cessation
Smoking cessation continues to be one of the most high-impact public health interventions — and for community pharmacy teams, the evolving landscape brings fresh opportunities and responsibilities. In this article we look at what’s new in smoking cessation management and how pharmacy teams can step confidently into the evolving role.
1. Evolving service models in community pharmacy
Community pharmacies are now firmly part of the stop-smoking pathway, offering more than overthe-counter support. The NHS Community Pharmacy Smoking Cessation Service (SCS) was commissioned as an advanced service from March 2022, enabling community pharmacies to deliver structured smoking-cessation programmes. Community Pharmacy England+1
Key updates for 2025 include allowing suitably trained pharmacy staff (not only pharmacists but also pharmacy technicians) to deliver the service and supply via Patient Group Directions (PGDs) for medications such as Varenicline and Cytisine. Community Pharmacy England
For pharmacy teams this means: more flexibility in staffing, clearer service-contracts, and a more embedded role in referrals from secondary care. For example, hospitals can refer patients into community pharmacy to continue their quit attempt after discharge. NHS England+1
Tip: Ensure your team has a designated smoking-cessation lead, appropriate SOPs, and that training (e.g., via the National Centre for Smoking Cessation and Training [NCSCT]) is up to date. The 2023 Standard Treatment Programme for pharmacy teams is available. NCSCT
2. New medications and pharmacotherapy options
The pharmacotherapy toolkit for tobacco-dependence is growing, and pharmacy teams need to be aware of the changes.
Varenicline
Varenicline has returned to the UK market after supply disruption and is being promoted as a highly effective quitting aid: a daily pill that reduces cravings and blocks nicotine’s reward in the brain. NHS England+1
The latest guideline by National Institute for Health and Care Excellence (NICE) (NG209) now includes recommendations on varenicline use and extends to broader settings. NICE
What this means for pharmacy teams: With PGDs enabling supply in some settings, you may directly support initiation of varenicline (or
liaise with prescribers). Monitoring for side-effects, counselling and follow-up remain critical.
Cytisine
Cytisine is gaining recognition: the NICE guideline NG209 now includes updated recommendations for its use. NICE
It is a partial agonist at nicotinic receptors (similar model to varenicline) and has costeffective potential. World Health Organisation+1
Pharmacy teams should keep abreast of its licensing status, supply chains and local formulary inclusion.
Combination NRT and e-cigarettes
Combination nicotine replacement therapy (NRT) — for example, patch + fast-acting form (gum, spray) — remains first-line. nhs.uk+1
Meanwhile, the role of e-cigarettes (vapes) supported by a pharmacy intervention has been explored: a study in England found for every 20 people given an e-cigarette via pharmacy support, six quit smoking at 4-week follow up. PMC
While e-cigarettes are not formally first-line medication, pharmacy teams should be ready to advise objectively on their role (benefits, risks, regulation) and integrate into a broader cessation plan. The WHO now recommends cytisine, varenicline, NRT and bupropion over no treatment. World Health Organisation
Tip: When counselling, emphasise combinations of behavioural support + pharmacotherapy give the best quit rates. American Academy of Family Physicians+1
3. Behavioural support, consultation quality and equity
Pharmacy teams are more than dispensers: your role in behavioural support, follow-up and tailored interventions is now central.
The NCSCT Standard Treatment Programme (STP) for pharmacy SCS (2023) emphasises inclusive practice: explicitly including people with serious mental illness (SMI), screening for medications etc. NCSCT
Key consultation steps remain: ask, advise, act; assessing dependence, readiness to quit, providing relevant pharmacotherapy and scheduling
follow-up (4-week, 12-week reviews). NCSCT+1
Pharmacy teams must ensure:
• Every smoker is identified (brief advice is opportunistic).
• Tailored plan is made (which aid, how long, what support).
• Follow-up is consistent (relapse prevention, ongoing contact).
Equity-wise: smokers from disadvantaged groups or with mental health conditions often need more support; pharmacy teams can make a difference.
4. Implementation considerations in pharmacy practice
Here are some practical implementation points for pharmacy teams:
• Training and competence: Ensure relevant staff (including pharmacy technicians) are trained and certified as stop-smoking practitioners.
• Standard Operating Procedures (SOPs): Update your SOPs to reflect the latest service specification (see PSNC Briefing 008/22). Community Pharmacy England
• Staff mix: With the expanded service, trained technicians or other suitably competent staff may deliver parts of the service under supervision; this offers flexibility. Community Pharmacy England
• Patient pathways and referrals: Make hand-offs smooth: for example, from hospital to community pharmacy via the SCS. Check whether your pharmacy is registered and set up for referrals. NHS England
• Medication supply and PGDs: Check local agreements around PGDs for varenicline/cytisine and ensure governance is in place. NCSCT+1
• Record-keeping and follow-up: Track quit date, medication used, dual NRT combinations, relapse triggers, reviews at 4 and 12 weeks. The STP outlines timelines. NCSCT
• Patient engagement: Use motivational language, address barriers (stress, social cues),
offer repeated support rather than one-off advice.
5. The future: what’s on the horizon
Looking ahead, a few trends to watch:
• New pharmacotherapies beyond nicotinic mechanisms are in development (non-nicotinic agents, vaccines, etc.). PubMed
• Precision-tailored interventions: adapting interventions according to individual responses is being evaluated (though a 2023 study suggested multiple pharmacotherapy adaptations may not yield major gains).
JAMA Network
• Digital and remote delivery: pharmacy-supported remote consultations (for prescribing varenicline) have shown promise. PMC
• Stronger focus on healthinequalities: the newest NICE guideline NG209 emphasises support for people not ready to quit, and addressing uptake among young people. NICE Pharmacy teams should remain alert and agile — being part of this evolving landscape will maximise your role in delivering successful quit outcomes.
6. Key messages for the pharmacy team
• The stop-smoking service in community pharmacy is more structured and integrated than ever — being ready and competent is essential.
• Pharmacotherapy options are richer: varenicline, cytisine and combination NRTs are important tools; pharmacy teams must familiarise themselves.
• Behavioural support remains vital: medication alone is rarely sufficient — follow-up, counselling and personalised support increase success.
• Implementation matters: training, SOPs, referral infrastructures, PGDs and record-keeping are all key enablers.
• Stay current: monitor emerging evidence, service-spec changes, new medications and policy updates.
Kind and effective for the whole family
Zarbee’s Cough and Sore Throat Syrups are medical devices to relieve any cough, dry or chesty. Zarbee’s Lozenges are food supplements and should not be used as a substitute for a varied balanced diet. Vitamin C and Zinc contribute to the normal function of the immune system. Cough & Sore Throat Syrups from 2 years. Cooling Throat & Immune Support Lozenges from 6 years.
Recognition Award for Dr Fleming
Congratulations to Dr Aoife Fleming, who has been awarded the 2025 University College Cork Staff Recognition Award for Leadership in recognition of her outstanding contributions to leadership at UCC.
Dr Fleming has consistently exemplified excellence and leadership throughout her career. She currently serves as Director of the MPharm Programme and Vice Head for Interprofessional Learning (IPL) in the College of Medicine and Health. A clinical pharmacist and academic, she has led major initiatives that strengthen collaboration across health disciplines and enhance the quality of healthcare education.
Among her many leadership highlights are:
• Championing Interprofessional Learning at UCC: A passionate advocate for IPL for over a decade, Dr Fleming has introduced transformative learning experiences and has chaired the All-Ireland Interprofessional Healthcare Challenge (AIPEC) at UCC since 2019.
• National Recognition: Aoife led the UCC AIPEC student team to victory in 2025 in the All Island final. AIPEC won 'Best Collaboration Project' and 'Overall Excellence' at the Irish
McLernons Pharmacy Event
Professor John O’Halloran, President of University College Cork; Dr Aoife Fleming, recipient of the 2025 UCC Staff Recognition Award for Leadership; and Professor Helen Whelton, Head of the College of Medicine & Health, UCC
Tallaght Go Green
Staff at Tallaght University Hospital (TUH) are playing their part in helping to reduce greenhouse gas emissions by switching to environmentally friendly inhalers. Their ‘greener inhaler’ project focused on reducing greenhouse gases from inhalers at TUH and making green inhaler prescribing a hospital policy.
Education Awards, as featured in The Irish Times.
• Enhancing pharmacy-led research and education: Dr Fleming has led numerous impactful initiatives, including the recent publication of the 'Patient & Healthcare Staff Stories Project: Experiences of Sepsis, Infection & Antimicrobial Resistance (AMR)', commissioned by the Department of Health.
Dr Fleming is widely respected for her professionalism, creativity, and dedication. Her impact is felt across UCC and beyond, making her a truly deserving recipient of this leadership award.
The team at McLernons recently welcomed customers in Munster to 'Building A Profitable Future with McLernons' in Rochestown Park Hotel in Cork on Thursday 4th September.
The event, which was oversubscribed, provided updates on the latest versions of our market-leading MPS Dispensing and Retail community pharmacy software solutions.
Experts Martin Lethbridge, WatchGuard, Leigh Quilty, Fitzgerald Power and Brian Battles, Pharmacy Success gave a series of presentations on cyber security, the financial landscape for community pharmacy, and increasing revenue and maximising profitability.
The McLernons team have been delighted with the positive response from customers for these three over-subscribed events and plan to host more over the coming months.
The project involved educating both prescribers and patients on the impact inhalers have in terms of CO2 emissions, adding Green Prescribing information to the Hospital’s Audit Medicines Guide and switching to a greener version of the hospital’s most commonly prescribed inhaler. The doctors choose the right inhaler for the right patient, with the lowest carbon footprint possible and dispose of them correctly.
Supported by the HSE’s Spark Innovation Programme, the team at TUH was awarded the best sustainable waste management project at the HSE’s Annual Climate Conference recently. The Spark Programme encourages healthcare workers to develop solutions to improve our health service.
Inhaler emissions were audited between 01/03/2024 and 31/12/2024 to assess policy change compared to the same period in 2023.
The audit results show:
• Total emissions fell from 91.5t to 75.9t CO2e
• Monthly emissions from inhalers fell by 22.8%
• Emissions from salbutamol inhalers fell from 77.7t to 58.2t CO2e
Commenting on the award, Dr Deirdre Fitzgerald, Respiratory (Pleural Medicine) and Integrated Care, TUH, said, “As clinicians, we have a responsibility, not only to deliver the highest standard of care, but to do so in a way that protects the future of our patients and the planet. This initiative is a testament to what is possible when innovation meets environmental stewardship.
“By changing our prescribing habits, we have shown at TUH that sustainability and clinical excellence are not competing priorities; they are complementary pillars of our hospital strategy.”
GETS TO WORK FAST TO SOOTHE YOUR COUGH
BENYLIN NON-DROWSY CHESTY COUGHS: Composition: Each 5 mls contains 100 mg guaifenesin and 1.1 mg levomenthol Clear red syrup having a characteristic odour. Indications: The symptomatic relief of productive cough. Dosage: Adults and children over 12 years: Two 5 ml spoonfuls four times a day. Children under 12 years: Not recommended. The Elderly: As for adults. Hepatic/renal dysfunction: Experience with the use of this product suggests that normal adult dosage is appropriate for mild to moderate dysfunction. Caution should be exercised in severe hepatic and severe renal impairment. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Special warnings and precautions for use: Should be not used for persistent or chronic cough, such as occurs with asthma, or where cough is accompanied by excessive secretions, unless directed by a physician. Caution should be exercised when using the product in the presence of severe renal or severe hepatic impairment. This medicinal product contains3.5 g glucose per 5ml, 1 g of sucrose per 5ml and 6.75mg invert sugar per 5ml. This should be taken into account in patients with diabetes mellitus. Patients with rare hereditary problems of fructose intolerance, glucose galactose malabsorption or sucrose-isomaltase insufficiency should not take this medicine. This medicine contains 197 mg of alcohol ethanol) in each 5 ml dose. The amount in a 5 ml dose of this medicine is equivalent to less than 5 ml beer 2ml wine. The small amount of alcohol in this medicine will not have any noticeable effects. This medicine contains Ponceau 4R (E124) which may cause allergic reactions. This medicine contains 16.42 mg sodium per 5 ml equivalent to 0.82% of the WHO recommended maximum daily intake of 2 g sodium for an adult. This medicine contains 1.07mg propylene glycol in each 5ml dose.This medicine contains 20mg sodium benzoate per 5ml dose. Should not be used in children under the age of 12 years. Undesirable effects: Immune system Disorders Not known Hypersensitivity (including Pruritus and Urticaria) Gastrointestinal Disorders Not known Abdominal pain upper, Diarrhoea, Nausea, Vomiting Skin and Subcutaneous Tissue Disorders Not known Rash. MA holder: JNTL Consumer Health I (Ireland) Ltd. Block 5, Hight Street, Tallaght, Dublin 24, Ireland. PA number: PA23490/007/001. Product not subject to medical prescription. Supply through non- pharmacy outlets and pharmacies. Full prescribing information available upon request. Date of revision of text: March 2024
BENYLIN NON DROWSY DRY COUGHS SYRUP: Syrup Composition: Dextromethorphan hydrobromide 7.5mg/5ml. Each 5 ml of Benylin Non Drowsy for Dry Coughs Syrup also contains: Sorbitol solution (70%) E420: 325mg, Sucrose 1625mg, Glucose 2380mg, Sodium 4.4mg, Ethanol (96% v/v) 0.311ml. Pharmaceutical form: Syrup. A clear amber coloured syrup with a characteristic smell of peaches. Indications: BENYLIN Non Drowsy for Dry Coughs is indicated for the relief of non-productive irritating cough. Dosage: Adults and children 12 years and over: Oral. 15mg (10 ml syrup) 3-4 times a day. maximum daily dose: 40 ml syrup. Children under 12 years: This product is contraindicated in children under the age of 12 years. Hepatic dysfunction: Due to the extensive hepatic metabolism of dextromethorphan, caution should be exercised in the presence of hepatic impairment. Contraindications: This product is contraindicated in individuals with known hypersensitivity to dextromethorphan or to any of the excipients. Dextromethorphan should not be used in patients taking monoamine oxidase inhibitors (MAOIs), or within 14 days of stopping MAOI treatment (see section 4.5). There is a risk of serotonin syndrome with the concomitant use of dextromethorphan and MAOIs and the concomitant use of these medications may cause a rise in blood pressure and/ or hypertensive crisis. This product is contraindicated in patients taking serotonin reuptake inhibitors (SSRIs). Dextromethorphan, should not be given to patients in, or at risk of developing respiratory failure. Benylin Non-Drowsy Dry Coughs, Syrup is contraindicated for use in children under 12 years of age. Special warnings and special precautions for use: Patients with the following conditions should not use this product, unless directed by a physician: acute or chronic asthma, a persistent or chronic cough such as occurs with chronic bronchitis or emphysema, or where cough is accompanied by excessive secretions. Cases of dextromethorphan abuse and dependence have been reported. Caution is particularly recommended for adolescents and young adults as well as in patients with a history of drug abuse or use of psychoactive substances. Use of dextromethorphan with alcohol or other CNS depressants may increase the effects on the CNS and cause toxicity in relatively smaller doses. While taking this product, patients should be advised to avoid alcoholic drinks and consult a healthcare professional prior to taking with central nervous system depressants. Serotonin Syndrome: Serotonergic effects, including the development of a potentially life-threatening serotonin syndrome, have been reported for dextromethorphan with concomitant administration of serotonergic agents, such as selective serotonin re-uptake inhibitors (SSRIs), drugs which impair metabolism of serotonin (including monoamine oxidase inhibitors (MAOIs)) and CYP2D6 inhibitors. Serotonin syndrome may include mental-status changes, autonomic instability, neuromuscular abnormalities, and/or gastrointestinal symptoms. If serotonin syndrome is suspected, treatment with Benylin Dry Coughs Syrup should be discontinued. Dextromethorphan is metabolised by hepatic cytochrome P450 2D6. The activity of this enzyme is genetically determined. About 10% of the general population are poor metabolisers of CYP2D6. Poor metabolisers and patients with concomitant use of CYP2D6 inhibitors may experience exaggerated and/or prolonged effects of dextromethorphan. Caution should therefore be exercised in patients who are slow metabolizers of CYP2D6 or use CYP2D6 inhibitors. This product should be used with caution in atopic children due to histamine release. This product contains sucrose, glucose, and invert sugar. This should be taken into account in patients with diabetes mellitus. Patients with rare hereditary problems of fructose intolerance, glucose-galactose malabsorption or sucrase-isomaltase insufficiency should not take this product. Sorbitol: This medicine contains 650 mg sorbitol in each 10 ml dose. The additive effect of concomitantly administered products containing sorbitol (or fructose) and dietary intake of sorbitol (or fructose) should be taken into account. The content of sorbitol in medicinal products for oral use may affect the bioavailability of other medicinal products for oral use administered concomitantly. Patients with hereditary fructose intolerance (HFI) should not take/be given this medicinal product. This medicine contains 472 mg of alcohol (ethanol) in each 10 ml dose. The amount in a 10 ml dose of this medicine is equivalent to less than 12 ml beer or 5 ml wine. The small amount of alcohol in this medicine will not have any noticeable effects. This medicine contains 42 mg benzoate salt in each 10 ml dose. This medicine contains 5.43 mg propylene glycol in each 10 ml dose. This medicine contains less than 1 mmol sodium (23 mg) per 10 ml dose, that is to say essentially ‘sodium-free’. Patients who are taking other medication including cough and cold medicines and / or who are under the care of a physician, should consult their doctor / pharmacist before taking this product. Undesirable effects: Adverse drug reactions (ADRs) identified during post-marketing experience with Dextromethorphan are included below. The frequencies are provided according to the following convention: Very common ≥1/10, Common ≥1/100 and < 1/10, Uncommon≥1/1,000 and <1/100, Rare ≥1/10,000, <1/1,000, Very rare <1/10,000, Not known (cannot be estimated from the available data). Psychiatric Disorders - Rare - Confusional state. Not known – Agitation, Insomnia, Nervous System Disorders: Not known – Dizziness, Psychomotor hyperactivity, Seizure. Somnolence. Respiratory,Thoracic and Mediastinal Disorders: Rare – Bronchoconstriction, Dyspnoea Gastrointestinal Disorders: Not known - Abdominal pain, Diarrhoea, Nausea, Vomiting. Skin and Subcutaneous Tissue Disorders: Not known - Angioedema Pruritus, Rash, Urticaria. PA Number: PA PA23490/010/001. MAH: JNTL Consumer Health I (Ireland) Ltd. Block 5, Hight Street, Tallaght, Dublin 24, Ireland. Date of revision of text: March 2024. Product not subject to medical prescription. Supply through pharmacies only. Full prescribing information available upon request. BENYLIN MUCUS COUGH MENTHOL: Composition: This product contains 20 mg guaifenesin in each ml (100mg in 5ml). Indications: To help loosen phlegm and thin bronchial secretions associated with productive cough, for use in adults and adolescents over 12 years. Dosage: Adults and adolescents over 12 years: For oral administration: 10 ml (200mg guaifenesin) 4 times a day. Maximum daily dose: 40ml (800mg guaifenesin). Paediatric population: The safety and efficacy of Benylin Mucus Cough Menthol in children aged under 12 years have not yet been established. The Elderly: As per adults. Hepatic/ renal impairment: Caution should be exercised in severe hepatic and severe renal impairment. If cough persists for more than 7 days, tends to recur, or is accompanied by a fever, rash, or persistent headache, a physician should be consulted. Contraindications: Hypersensitivity to active substance or to any of the excipients. Special warnings and precautions for use: This product should not be used for persistent or chronic cough, such as occurs with asthma, or where cough is accompanied by excessive secretions, unless directed by a physician. A persistent cough may be a sign of a serious condition. If cough persists for more than 7 days, tends to recur, or is accompanied by a fever, rash, or persistent headache, a physician should be consulted. Caution should be exercised when using the product in the presence of severe renal or severe hepatic impairment. The concomitant use of cough suppressants is not recommended. This medicinal product contains 10mg of benzoate salt in each 10ml dose. This medicinal product may contain very trace amounts of glucose. Patients with rare glucose galactose malabsorption should not take this medicine. This medicinal product contains 381 mg of alcohol (ethanol) in each 10 ml dose which is equivalent to 38.1 mg/ml. The amount in 10 ml of this medicine is equivalent to 9.5 ml beer or 3.8 ml wine. The small amount of alcohol in this medicine will not have any noticeable effects. This product contains Ponceau 4R (E124) red colouring which may cause allergic reactions. This medicinal product contains less than 1 mmol sodium (23 mg) per 10 ml dose, that is to say essentially ‘sodium-free’. This medicinal product contains 2003.5 mg propylene glycol in each 10 ml dose. While propylene glycol has not been shown to cause reproductive or developmental toxicity in animals or humans, it may reach the foetus and was found in milk. As a consequence, administration of propylene glycol to pregnant or lactating patients should be considered on a case by case basis. Medical monitoring is required in patients with impaired renal or hepatic functions because various adverse events attributed to propylene glycol have been reported such as renal dysfunction (acute tubular necrosis), acute renal failure and liver dysfunction. This medicinal product contains macrogol glycerol hydroxystearate 40. It may cause stomach upset and diarrhoea. Undesirable effects: Immune System Disorder: Not Known - Hypersensitivity reactions including pruritus and urticaria, Rash, Anaphylactic reaction. Gastrointestinal Disorders: Not Known -Gastrointestinal discomfort, nausea and vomiting. MAH: JNTL Consumer Health I (Ireland) Ltd, Block 5, High Street, Tallaght, Dublin 24, Ireland. MA Number: PA23490/040/001. Date of revision: May 2025 Product not subject to medical prescription. Supply through non-pharmacy outlets and pharmacies. Full prescribing information available upon request from JNTL Consumer Health I (Ireland) Ltd.
Ireland’s Fragility Fracture Crisis
New national data from the Irish Fracture Liaison Service has exposed significant shortcomings in Ireland’s ability to prevent and manage fragility fractures –injuries that signal underlying bone weakness and dramatically increase the risk of further, often life-changing fractures.
The fourth Irish Fracture Liaison Service Database (FLSDB) Report highlights both encouraging improvements in the quality of care for those who can access services and serious inequities in early identification, treatment and access nationwide.
Fragility fractures cost the HSE an estimated ¤464 million annually, and with Ireland’s ageing population, this figure is set to rise sharply without decisive action
Professor Frances Dockery, co-chair of the national Fracture Liaison Service Database, said, “A fracture, even if minor, is an important opportunity to examine bone health and so prevent major fractures ahead such as hip and spine, maintain independence and reduce unnecessary hospital admissions.
“Ireland has adopted a proven model of care that can do this, through Fracture Liaison Services, but we need to make it available to everyone and avoid missed opportunities to prevent future fractures.”
Significant regional inequities
The report analysed the experiences of 3,335 patients who sustained low-trauma ‘fragility’ fractures in 2024 across ten of
Ireland’s sixteen adult trauma hospitals. It found that two HSE regions, the Midwest and South-West, managed no patients through a Fracture Liaison Service, while coverage in other regions varied from 12% in HSE Dublin and South-East to around 25% in Dublin and Midlands and HSE North/North-West. Nationally, 84% of non-hip fragility fractures still do not receive gold-standard preventative care.
This inconsistency means that access to fracture prevention remains a postcode lottery, with large parts of the country lacking any structured fracture liaison service.
A proven model
Fragility fractures are often the first warning sign of osteoporosis, doubling the risk of subsequent hip fractures. The consequences for patients can be severe, including loss of independence and reduced quality of life.
At a time when the Minister for Health has set a ¤633 million savings target across the health service for 2025, this approach represents a clinically proven, cost-effective solution to reduce avoidable admissions and free up hospital capacity
World Stroke Day
To mark World Stroke Day which took place last month on 29th October, the HSE is urging everyone to know the signs of stroke and the importance of seeking treatment as soon as symptoms appear. Strokes are a medical emergency, and urgent treatment is essential.
A stroke can happen at any time. It is the third leading cause of death in Ireland and the leading cause of acquired adult neurological disability. Over 90,000 people live with the effects of stroke in Ireland, and it is estimated that there will be a 58% increase in incidents of stroke over the next 10 years.
An easy way to be aware of the signs of stroke is to remember the established acronym, F.A.S.T:
• Face – Has the face drooped or become weak on one side?
• Arm – Has an arm become suddenly weak or clumsy on one side?
• Speech – Has speech suddenly become slurred or confused in nature?
International experience shows what is possible. New Zealand’s national FLS strategy, backed by targeted investment, now captures more than 70% of patients presenting with fragility fractures and has saved an estimated 57,000 hospital bed days over five years.
Mr Tom McCarthy, Joint Clinical Lead, National Clinical Programme for Trauma and Orthopaedic Surgery, added, “Ireland has an opportunity to achieve similar impact by expanding and standardising its services. We must expand FLS coverage across all regions and address regional disparities to guarantee equitable access.”
The National Clinical Programme in Trauma and Orthopaedic Surgery is a strategic initiative between RCSI and the HSE. The programme aims to design and implement change initiatives to improve and standardise the quality of care and access for all patients in a cost-effective manner.
The programme established the national Fracture Liaison Service in 2018 with the goal of reducing the number of preventable fractures in the country.
• Time – Time to act FAST: phone 999 or 112 for an ambulance immediately.
There have also been significant advancements in stroke recovery in Ireland. Today, the HSE will publish a new report, Early Supported Discharge (ESD) for Stroke 2022 to 2023. Early Supported Discharge is an initiative in which stroke survivors can have therapy, social work and nursing support at home so that they can leave the hospital earlier. This allows patients to be more independent and are more likely to avoid longterm residential care. ESD also improves bed capacity across stroke units, with more than 800 stroke survivors benefiting from the initiative in 2023. On average, 22% of stroke survivors are discharged with ESD.
There have also been significant advancements in stroke recovery in Ireland. The HSE has published a new report, Early Supported Discharge (ESD) for Stroke 2022 to 2023. This allows patients to be more independent and are more likely to avoid long-term residential care. ESD also improves bed capacity across stroke units, with more than 800 stroke survivors benefiting from the initiative in 2023. On average, 22% of stroke survivors are discharged with ESD.
Call for papers: make your contribution to Irish Pharmacy News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to editor
In-depth review articles critique fundamental concepts, issues, and problems that define a field of research or practice and support advanced practitioners as well as aspiring early-year pharmacists.
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients with the aim to improving pharmacy practice.
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions.
Ketamine in Depression: What the Latest Evidence Means —
and Where Pharmacists Fit In
Researchers from Trinity College, St Patrick’s Mental Health Services, and Queen’s University Belfast, Ireland, have investigated the use of twice-weekly ketamine infusions as an add-on treatment for inpatients with serious depression.
Findings from a randomised and blinded clinical trial investigating repeated ketamine infusions for treating depression have revealed no extra benefit for ketamine when added to standard care for people admitted to hospital for depression. The paper is published in JAMA Psychiatry.
The KARMA-Dep (2) Trial involved researchers from St Patrick’s Mental Health Services, Trinity College Dublin, and Queen’s University Belfast, Ireland. It was sponsored by Trinity College Dublin and led by Professor Declan McLoughlin, Research Professor of Psychiatry at Trinity College Dublin and Consultant Psychiatrist at St Patrick’s Mental Health Services.
Depression has been recognised by the World Health Organization
as a leading cause of disability globally. According to the Health Research Board’s most recent report, there were 15,631 adult admissions to psychiatric services in Ireland in 2023. Similar to previous years, depressive disorders accounted for the highest proportion — around 24% — of all admissions.
Studies show that about 30% of people with depression do not respond sufficiently to conventional antidepressants, which mostly target monoamine neurotransmitters such as serotonin, dopamine, and noradrenaline. There is thus a need for new treatments. One such novel treatment is the dissociative anaesthetic ketamine, when given intravenously in low
sub-anaesthetic doses. Ketamine works differently to other antidepressants and is believed to mediate its effects in the brain through the chemical messenger glutamate.
Single infusions of ketamine have been reported to produce rapid antidepressant effects, but these typically disappear within days. Nonetheless, ketamine is increasingly being adopted as an off-label treatment for depression even though the supporting evidence remains limited. One possibility is that repeated ketamine infusions may have a more sustained benefit. However, this has so far been evaluated in only a small number of trials that have used an adequate control condition to mask ketamine’s
obvious dissociative effects, such as altered consciousness and perception.
KARMA-Dep 2 was designed to assess antidepressant efficacy, safety, cost-effectiveness, and quality of life during and after serial ketamine infusions compared to a psychoactive comparator drug, midazolam. Trial participants were randomised to receive up to eight infusions of either ketamine or midazolam, given over four weeks, alongside usual inpatient care.
Key Findings
• There was no significant difference between the ketamine and midazolam groups at the end of the treatment course on the primary depression outcome (Montgomery–Åsberg Depression Rating Scale).
• There was no difference on patient-rated scales (QIDSSR-16).
• No significant differences were found for secondary cognitive, economic, or quality-of-life outcomes.
• Despite efforts to maintain blinding, most patients and raters correctly guessed treatment allocation, potentially inflating placebo effects.
Speaking about the findings, Professor McLoughlin commented, “Our initial hypothesis was that repeated ketamine infusions for people hospitalised with depression would improve mood outcomes. However, we found this not to be the case. Under rigorous clinical trial conditions, adjunctive ketamine provided no additional benefit to routine inpatient care during the initial treatment phase or the six-month follow-up period.”
Lead author Dr Ana Jelovac added, “Our trial highlights the importance of reporting the success, or lack thereof, of blinding in clinical trials… Such problems can lead to enhanced placebo effects and skewed trial results that can overinflate real treatment effects.”
The Community Pharmacy Role in Managing Depression
While hospital research continues to explore innovative treatments like ketamine, the everyday management of depression happens largely in primary care — and community pharmacists are increasingly recognised as vital partners in that continuum of care.
Depression is one of the most common conditions pharmacists encounter indirectly — through antidepressant dispensing, conversations with patients about side effects, or queries from concerned family members. Given the scale of the challenge in Ireland, where one in ten
Professor Declan McLoughlin, Research Professor of Psychiatry at Trinity College Dublin
adults experience depression at any given time, the pharmacy’s position as a trusted, accessible healthcare touchpoint makes it an essential part of both prevention and management.
1. Early Identification and Signposting
Pharmacists are often the first professionals to notice subtle signs of low mood, withdrawal, or poor self-care in patients they see regularly. Through sensitive questioning and supportive communication, pharmacists can help identify individuals who may need help and encourage timely GP review or mental health referral.
Simple interventions — such as asking about sleep, appetite, and medication adherence — can open the door to conversations that might not otherwise happen. In rural or underserved areas, this proactive role can be especially valuable, reducing barriers to helpseeking.
2. Supporting Safe and Effective Medication Use
Antidepressants remain the mainstay of depression treatment, yet adherence is notoriously low, with up to 50% of patients discontinuing within three months. Pharmacists play a key role in:
• Educating patients about expected timelines for response (often several weeks).
• Managing expectations and reinforcing adherence through regular follow-up.
• Providing reassurance about transient side effects and when to seek help.
• Identifying and resolving drug–drug interactions (e.g., SSRIs with NSAIDs or triptans).
• Advising on safe use of overthe-counter medicines and complementary therapies.
These daily, informal interactions help improve persistence and outcomes, often preventing unnecessary medication switching or escalation.
3. Managing Side Effects and Physical Health
Depression rarely occurs in isolation. Many patients live with chronic diseases such as diabetes, cardiovascular illness, or chronic pain — conditions that can both contribute to and worsen depression.
Community pharmacists can monitor for antidepressantinduced adverse effects (e.g., weight changes, gastrointestinal upset, sexual dysfunction) and liaise with prescribers when dose adjustments or alternative therapies may be appropriate. They can also support monitoring of blood pressure, weight, or metabolic risk, especially in patients taking long-term antipsychotic augmentation.
4. Collaborative Care and Continuity
Pharmacists are integral to the multidisciplinary team model promoted in the Sláintecare framework. By maintaining open communication with GPs, psychologists, and mental health nurses, pharmacists can support continuity of care — particularly during medication initiation, dose changes, or transitions between inpatient and community settings.
Pharmacy’s role in medicines reconciliation after discharge is crucial for patients leaving psychiatric hospitals, where medication regimens are often complex. A clear understanding of what was prescribed and why reduces duplication, omission, and confusion that can lead to relapse.
5. Reducing Stigma and Building Trust
Because pharmacy spaces are local and familiar, they offer a non-stigmatising environment where patients can talk about mental health without formal referral. Pharmacists who use empathetic, non-judgmental language and maintain confidentiality can normalise helpseeking and counter myths about antidepressant use or addiction. Participating in or promoting initiatives such as #SeeChange Green Ribbon Month or World Mental Health Day reinforces pharmacy’s position as an ally in mental health advocacy.
6. Public Health and Preventive Roles
Depression prevention increasingly overlaps with public health priorities such as sleep
hygiene, smoking cessation, alcohol moderation, and chronic disease management — all areas where pharmacists already engage with patients.
Pharmacists can also play a part in suicide prevention awareness, knowing local crisis pathways and being prepared to signpost individuals to emergency or support services if risk is disclosed. Even brief, compassionate interactions can make a measurable difference.
7. Innovation and Digital Health
As Ireland moves toward e-prescribing and digital integration, pharmacists will have more opportunities to support mental health management through remote follow-up, digital adherence monitoring, and electronic communication with care teams.
Emerging pharmacy-based digital platforms may allow automated reminders, side-effect tracking, or teleconsultations — helping sustain engagement between appointments and reducing isolation.
8. Policy and Training Imperatives
The PGEU’s Report on Pharmacy Services in Europe (2025) explicitly calls for expanding pharmacists’ role in chronic disease and mental health management. For Ireland, this means embedding mental health as a core service competency in future community pharmacy frameworks and ensuring appropriate remuneration.
Enhanced training in psychological first aid, motivational interviewing, and suicide awareness could empower pharmacists to provide safe, confident support without stepping beyond their clinical remit.
Looking Ahead
The KARMA-Dep trial’s findings remind us that no single intervention — whether pharmacological or experimental — will solve depression. Effective management depends on continuity, compassion, and collaboration, values already at the heart of community pharmacy practice.
As Ireland reimagines its primarycare landscape, community pharmacists have the opportunity to become central partners in mental health care — improving adherence, promoting wellbeing, and ensuring that people living with depression are never left to manage alone.
The next frontier in depression management may not lie in a new molecule, but in better connection — and community pharmacy is uniquely placed to provide it.
Topic Team Training – Sleep Disorders
Following on from the October issue Continuing Professional Development on the Pharmacy Role in Sleep Disorders, this 5-Minute Learning Module is designed to enhance the community pharmacy team understanding and ask further questions as to how you can support and advise patients.
After completing this team session, pharmacy staff should be able to: Recognise the main types of sleep disorders seen in community practice; Offer safe, evidence-based self-care advice and understand when referral is required; Review medicines that may worsen or improve sleep and, Support responsible use, monitoring, and deprescribing of hypnotics.
A community pharmacy environment that fosters teamwork ensures high levels of consumer satisfaction. This series of articles is designed for you to use as guide to assist your team in focusing on meeting ongoing CPD targets and to identify any training needs in order to keep the knowledge and skills of you and your team up to date.
The below information, considerations and checklist provide support to enable you to run a team training session and identify opportunities for learning within the topic of Sleep Disorders.
Sleep is a universal human need— vital for physical and mental wellbeing. Yet around one in three adults in Ireland reports poor sleep, and up to 45% of people globally will experience a sleep
Consider:
disorder during their lifetime. The impact is wide-ranging: fatigue, reduced work performance, higher accident risk, and links with chronic illness and mental health conditions.
Contributing factors
Lifestyle: caffeine, alcohol, nicotine, irregular schedules, screen time before bed.
Demographic: older age, women (especially during pregnancy and menopause), shift work.
Encourage staff to consider these factors when engaging with patients.
Non-Pharmacological Management
Behavioural approaches remain the first-line strategy for managing sleep disorders and should be reinforced during every pharmacy consultation. Good sleep hygiene forms the foundation of effective sleep health. Patients should be encouraged to keep consistent
Am I/my team aware of the licensed indications, maximum recommended duration of treatment, doses and age limitations for OTC products used for the various types of sleep disorders?
Am I/my team aware of the medicines that can cause some sleep disorders, such as insomnia?
bedtimes and wake times, even on weekends, to help stabilise their body clock. They should avoid caffeine, alcohol, and nicotine later in the day, as these can all interfere with sleep onset and quality. Limiting exposure to electronic screens before bedtime is also important, since the blue light emitted by phones, tablets, and televisions can suppress melatonin and delay sleep. Creating a restful environment is essential: bedrooms should be kept cool, quiet, and dark, and used only for sleep or intimacy. Regular physical activity can promote better sleep, but it is best scheduled earlier in the day rather than close to bedtime.
Cognitive Behavioural Therapy for Insomnia (CBT-I) is regarded as the gold standard treatment for chronic insomnia. It focuses on the thoughts and behaviours that perpetuate poor sleep, using techniques such as stimulus control, sleep restriction, and cognitive restructuring. Increasingly, digital CBT-I programmes and mobile applications make this therapy more accessible, and pharmacists are well placed to signpost patients towards reputable, evidence-based platforms.
Pharmacological Options
Benzodiazepines such as temazepam and the related “Z-drugs” zopiclone and zolpidem can be effective for short periods. Melatonin may be useful in circadian rhythm disorders but should be initiated by a GP to ensure appropriate dosing
Key Points:
Ensure the pharmacy team knows to be sensitive in dealing with customers who may feel vulnerable as a result of insomnia
Ensure pharmacy staff understand the function and importance of sleep and what effect a lack of sleep has on overall health
Ensure we are all aware of how much sleep is enough for different groups of people
Promote training and education as to the types of sleep disorders and their possible causes
Educate the pharmacy team on how OTC treatments, including herbal remedies, differ
and timing. Over-the-counter sedating antihistamines may also provide short-term relief of sleep difficulties for some individuals. In RLS, dopamine agonists like ropinirole or pramipexole and gabapentinoids such as gabapentin or pregabalin may be prescribed, while iron supplementation is essential when ferritin levels fall below 75 µg/L. Treatment for obstructive sleep apnoea, such as continuous positive airway pressure (CPAP) or wake-promoting agents, should remain under specialist supervision. Pharmacy teams should always emphasise correct use, appropriate duration, and safety precautions—especially regarding alcohol intake and driving impairment.
Pharmacist-Led Actions
Community pharmacists play a central role in identifying, advising, and supporting patients with sleep problems. They should use brief, structured screening tools such as the Epworth Sleepiness Scale for OSA or the Insomnia Severity Index to help assess symptoms and guide advice. During medication reviews, pharmacists should remain alert for medicines that may contribute to insomnia, suggest safer alternatives where possible, and optimise timing of doses to reduce disruption to sleep. When dispensing hypnotics, pharmacists must reinforce shortterm use, monitor for side effects, and discuss dependency risks.
Appropriate referral is important — patients with persistent insomnia, suspected OSA, or underlying mental health issues should be directed to their GP for assessment, with specialist sleep clinics such as those in Beaumont, Tallaght, Cork, or Galway providing further diagnostic support.
Actions:
Ensure support staff understand the following key points:
The common causes of insomnia, including lifestyle issues, medication and conditions that can cause sleep issues
How to spot sleep disorders and insomnia in both colleagues and customers to get them the help they need
The benefits and limitations of OTC medicines
The importance of good sleep hygiene for everyone
IREL AND’S No.1
Sl eep A Id BRAND
CLINICALLY PROVEN
CAN H
E
LP YOU GET A GOOD NIGHT’S SLEEP
*Based on IQVIA sales data MAT 05/2025. Nytol One-A-Night 50 mg Tablets contains diphenhydramine hydrochloride. A symptomatic aid to the relief of temporary sleep disturbance in adults. Adults: One tablet to be taken 20 minutes before going to bed, or as directed by a physician. Do not exceed the maximum dose of one tablet in 24 hours. Elderly patients or patients with liver or kidney problems should consult their doctor before taking this medicine. Children under 18 years: Not recommended. The product should not be taken for more than 7 days without consulting a doctor. Contraindications: hypersensitivity to the active substance or to any of the excipients, stenosing peptic ulcer, pyloroduodenal obstruction, phaeochromocytoma, known acquired or congenital QT interval prolongation, known risk factors for QT interval prolongation. Special warnings and precautions: pregnancy/lactation, renal and hepatic impairment, myasthenia gravis, epilepsy or seizure disorders, narrow-angle glaucoma, prostatic hypertrophy, urinary retention, asthma, bronchitis, COPD. Patients should be advised to promptly report any cardiac symptoms. Tolerance and / or dependence may develop with continuous use. Do not take for more than 7 consecutive nights without consulting a doctor. Should not be used in patients currently receiving MAO inhibitors (MAOI) or patients who have received treatment with MAOIs within the last two weeks. Use in the elderly should be avoided. Avoid concomitant use of alcohol or other antihistamine-containing preparations. Do not drive or operate machines. Cases of abuse and dependence were reported in adolescents or young adults for recreational use and/or in patients with psychiatric dis-orders and/or history of abuse disorders. Contains lactose. May suppress the cutaneous histamine response to allergen extracts and should be stopped several days before skin testing. Interactions: Alcohol, CNS depressants, MAO inhibitors, anticholinergic drugs (e.g. atropine, tricyclic antidepressants), metoprolol and venlafaxine, CYP2D6 inhibitors, Class Ia and Class III anti-arrhythmics. Side effects: dry mouth, fatigue, sedation, drowsiness, disturbance in attention, unsteadiness, dizziness, thrombocytopenia, hypersensitivity reactions, confusion, paradoxical excitation, convulsions, headache, paraesthesia, dyskinesias, blurred vision, tachycardia, palpitations, thickening of bronchial secretions, gastrointestinal disturbance, muscle twitching, urinary difficulty, urinary retention. Product not subject to medical prescription. PA1186/016/001. MAH: Chefaro Ireland DAC. The Sharp Building. Hogan Place. Dublin 2. Ireland. Date of preparation: Nov. 2023. SPC: https://www.medicines.ie/medicines/nytol-one-a-night-50-mg-tablets-34889/spc MAT-10247
Pharmacy Views on VTE
Venous thromboembolism (VTE) remains one of the leading causes of maternal mortality worldwide, despite being largely preventable with timely risk assessment and prophylaxis. In Ireland, national initiatives such as the recently launched Eve Protocol are driving standardisation and raising awareness of VTE prevention across hospital and community settings.
At the National Maternity Hospital, Áine Toher, Deputy Pharmacist Executive Manager, has combined her expertise in clinical pharmacy, informatics, and education with a personal passion shaped by family experience to champion safer prescribing, electronic risk assessment, and multidisciplinary collaboration in women’s health. We spoke with Áine about her role, her motivations, and the continuing challenges in preventing VTE.
Can you share your role and how you came to specialise in thrombosis/VTE?
I am the Deputy Pharmacist Executive Manager in The National Maternity Hospital (NMH), with a special interest in venous thromboembolism (VTE) prevention, especially in the context of women's* health. I am passionate about raising awareness of VTE risk factors among patients, the public and healthcare staff as well as the potential for standardisation of measures to aid VTE prevention for all patients.
I am also a member of the Dublin South East VTE Service Review Group and part of the Clinical Advisory Group to the National Clinical Programme for VTE (NCPVTE)
There has been a long established haematology service, VTE prevention programme and maternal medicines clinic in the NMH. I work alongside the haematologist and haematology specialist midwife to review the VTE risk assessments, optimise low molecular weight heparin (LMWH) prescribing and providing patient and staff education.
With the introduction to the NMH of the National Maternal and Newborn Clinical Management System (MN-CMS) Electronic Health Record (EHR), as part of my role in informatics, I worked with the MN-CMS National Meds Team to develop and introduce NMH specific packages (care plans) which promote safe LMWH prescribing for our obstetric and gynecology patients.
I also collaborated with the haematology and MNCMS teams to introduce to the EHR - NMH specific electronic VTE risk
assessment forms to replace the paper versions.
In conjunction with the Dublin South East VTE Service Review Group, I coordinate the ongoing collection, analysis and presentation of NMH data to the hospital and DSE hospital group on VTE risk assessment and prophylaxis using an electronic VTE audit application.
What inspired your interest in clotting disorders and hospital care?
I have a professional and personal interest in the prevention, diagnosis and management of VTE as well as the follow-up care provided to patients.
My family has a history of thromboembolic disease. My father experienced and was treated for an unprovoked DVT in his 20s. There was very little follow-up at the time and he subsequently developed what is now known as post-thrombotic syndrome, it didn’t hold him back and managed symptoms with exercise and tubigrib when his leg was swollen. I also have had first-hand experience attending a haematology service, sourcing and self-administrating a LMWH during the postnatal period and the value of aftercare follow-up as well as discussion regarding contraceptive choices.
All of this has influenced my clinical awareness and the importance of the patient perspective and voice when designing models of care.
Early in my career, when I first qualified, there was a case that deeply impacted me. A young mother with three small children, was in the rehabilitation ward after suffering a postpartum stroke
secondary to a thrombotic event and was unable to hold her new baby due to the neurological deficits. Witnessing the emotional and physical toll on the young woman and her family was heartbreaking. It reinforced the importance of recognising and managing VTE risk, especially in pregnancy and the postpartum period.
What are the biggest challenges hospitals face in diagnosing and managing VTE that can impact on patient care?
I am aware that working in a specialised maternity hospital with a long established haematology, VTE prevention service and access to an electronic healthcare record is a position of privilege. Therefore, VTE is likely to be considered in those who present with symptoms and/or risk factors. We are linked with St Vincent’s University Hospital and all patients with suspected VTE
are transferred without delay for screening and diagnosis.
However, it is important to note that VTE remains one of the leading causes of maternal mortality worldwide. Thrombosis and thromboembolism was reported to be the leading cause of maternal death in the 2025 MBRRACE-UK report which looks at the care of 643 women who died during or up to one year after pregnancy in the UK and Ireland (2021-2023).
VTE prevention is key but it is also a challenge as there are different risk assessment tools available. This can contribute to inconsistent or incomplete use across specialities.
Patients can have overlapping risk factors which makes assessment difficult e.g. surgery, cancer, immobility, age, family history, pregnancy, weight changes. For younger patients, VTE risk
assessment may be overlooked despite risk factors such as oral contraceptives or smoking etc.
If an initial assessment is not carried out, it can be difficult to reassess risk if there is a change in clinical status.
Prophylaxis guidelines usually include mechanical and/or pharmacological options. If risk assessments are missed or incomplete or bleeding risks present concerns, this can result in inappropriate prophylaxis choices, incorrect doses as well as gaps or delays in prophylaxis.
Diagnostic challenges may be present in all patient groups as VTE symptoms can overlap with other conditions and pregnancy symptoms e.g. breathlessness, fatigue, leg pain and swelling.
Diagnostic tests and tools may have limitations depending on the patient cohort, availability of out of hours diagnostic imaging, balancing the radiation and contrast risks for pregnant patients and for those with renal failure.
Management
Compression stocking sizes may not be available for those at extremes of body weight and intermittent pneumatic compression devices may not be available or suitable.
Pharmacological anticoagulation choices may vary and considerations must be made depending on the treatment group. Other factors to consider are, for example, renal function, cancer, drug interactions, contraindications, dose adjustment, treatment durations, bleeding risk and monitoring.
Therapeutic choices remain limited in pregnancy as warfarin is teratogenic and DOACs have limited evidence of safety, therefore they are not recommended in pregnancy or breastfeeding. This leaves LMWH as the main option with unfractionated heparin (UFH) reserved for emergency use or in high-risk cases during labour and delivery. Education and planning for staff and patients regarding timing of doses around labour, delivery and anaesthesia is important to prevent bleeding or thrombosis.
Transitions of care
Risk can occur if there is no clear documentation in patient notes
and/or if communication is not effective between teams and patients; especially when patients move between settings and on discharge. As a result, missed doses, incorrect continuation/ stopping of anticoagulants, risk of VTE recurrence or bleeding can increase, poor adherence, and patients may not be followed-up.
Adherence to prophylaxis, especially on discharge, can be difficult to assess if follow-up is not scheduled.
Daily subcutaneous injections can be painful and intimidating for patients and this can impact compliance, particularly if LMWH is the only choice e.g. in pregnancy and postpartum.
Staffing and resources
Adequate staffing, resources, creation and maintenance of posts including succession planning, especially in specialised areas like haematology and VTE stewardship are essential components for safe provision and continuity of care. Not all Irish hospitals have a multidisciplinary VTE team to provide ownership or accountability for VTE-related services. This could potentially lead to delayed implementation and compliance with guidelines and national recommendations and therefore pose a risk for patient safety.
Staff shortages, loss of expertise if posts are not replaced and gaps in staff training and education can lead to missed assessments, delays in prophylaxis, incorrect dosing, contraindications and inappropriate treatment decisions. Challenges can also arise if there is limited time and staff experience with providing patient information, especially before discharge. Other challenges to consider are language, literacy and health literacy barriers.
Adequate pharmacy staffing is important as pharmacists play a critical role in optimising safe and effective anticoagulant use. They collaborate on guideline development, provide staff and patients with education, support accurate risk assessment and optimise prescribing and dosing (especially in high-risk groups).
At discharge, pharmacists help to ensure continuity of care through medication review, prevention of error and communication with community pharmacies and GPs. Their involvement in quality improvements, informatics and
audits further strengthens VTE safety protocols and reduces preventable harm.
Are there common misconceptions about VTE among staff or patients?
Although staff awareness of VTE in the NMH is good, misconceptions regarding VTE can still exist and can impact care.
Common ones are:
Those requiring surgery or having a C-section are at risk while young people are low-risk,
Anticoagulation must be avoided if there is a bleeding risk and in pregnancy/breastfeeding,
If the patient is mobile or once they are mobile post-surgery, they don’t need prophylaxis and
Risk stops at discharge.
Patients often link blood clots to long flights and older people, but may not be aware of other risk factors. Commonly patients are familiar with leg swelling and pain as symptoms but can attribute signs and symptoms like fatigue, swelling and breathlessness to pregnancy or other health conditions. Concerns regarding harm to the baby if taking medication are common.
VTE prevention and management is collaboration across a wide variety best outcomes. Doctors, nurses, midwives, diagnostic imaging teams, physiotherapists informatics, quality and safety teams play. Multidisciplinary teamwork with guidelines, reduces errors an improves be considered as part of the team and (‘Making Every Contact Count), leading adherence to treatment.
reduces errors an improves safety. Patients and their families should always be considered as part of the team and included in any decisions related to their care (‘Making Every Contact Count), leading to increased trust, understanding and adherence to treatment.
New prevention protocols and systemic changes most needed in Ireland to reduce VTE-related harm?
New prevention protocols and systemic changes related harm?
The National Clinical Programme for VTE (NCP-VTE) provides governance for the prevention, diagnosis, management and long term care of VTE in hospitals and community settings.
The National Clinical Programme for VTE (NCP diagnosis, management and long term care
In reality, clear guidelines with optimisation of education for staff and patients is important as VTE risk is multifactorial and clots can present silently or with mild symptoms. Due to the complexities of individual VTE risk and in order to balance clot risk and bleeding risk, assessment, prophylaxis and treatment should be individualised. Individualisation of care can also help maximise understanding and adherence especially at transitions of care.
The recent launch of the National Clinical Guideline Eve Protocol, named in memory of Eve Cleary framework for best practice in prevention, patient education
The recent launch of the National Clinical Guideline on Venous Thromboembolism (NCG-VTE) Eve Protocol, named in memory of Eve Cleary who tragically died due to VTE, provides a framework for best practice in prevention, assessment, diagnosis, treatment, recovery and patient education
Contributing to this guideline as part of the family representatives was a rewarding experience.
Contributing to this guideline as part of the multidisciplinary team, including patient and family representatives was a rewarding experience.
What role do multidisciplinary teams play in preventing and managing VTE?
VTE prevention and management is complex and requires clear communication and collaboration across a wide variety of disciplines and teams to ensure best practice and best outcomes. Doctors, nurses, midwives, haematologists, pharmacists, radiologists, diagnostic imaging teams, physiotherapists, occupational therapists, administration, informatics, quality and safety teams as well as, patients and families, all have roles to play. Multidisciplinary teamwork with shared responsibility improves compliance with guidelines,
National Clinical Guideline on Venous Thromboembolism (NCG-VTE)
Eve Protocol
https://www2.healthservice.hse.ie/ files/534/
68 Ask the Expert: VTE
Systemic changes are needed to ensure the Eve’s Protocol is implemented nationwide to improve care and reduce VTE-related harm. Changes needed include:
Mandating the establishment of thromboprophylaxis policy and use of standardised VTE risk assessment tools at key time points in hospitals e.g. admission, post-surgery, postpartum and if the patient condition changes.
Investing in VTE stewardship roles (pharmacists, nurses/ midwives) and VTE multidisciplinary teams, including IT, in hospitals. Implementing change takes time. Therefore, investing in local champions and teams with protected time, resources and responsibility for oversight and compliance is essential for sustainability of service.
Launching National education and awareness campaigns for healthcare workers and staff.
Raise awareness of the signs and symptoms of clots, risk factors, prophylaxis and treatment options.
Provide plain language and consistent education, patient information leaflets and training materials to patients. Translations into other languages is hugely beneficial (e.g. the blood clot alert cards).
Provide education modules on VTE in all healthcare undergraduate courses
Strengthen standardised surveillance and audit locally and nationally.
Robust reporting identifies trends over time and allows targeted intervention
Without consistent data it is hard to identify areas of concern or track improvements.
Digitalising VTE risk assessments and tools. Provide resources to allow EHR integration of VTE risk assessments. Develop digital clinical decision support packages for safe prescribing and administration.
Progression of the Health Digital for Care Framework 2030 to improve care and
safety across services through introduction of the:
National Shared Care record and
Electronic Health Record availability and functionality in all hospital settings
Balancing our digital health footprint with the provision of safe healthcare while minimising climate impact.
The Dublin South East hospital group are at the forefront of implementation with many of the recommendations are already being acted upon in the hospitals within the group.
It has an established and active multidisciplinary VTE service review group with patient representation to highlight and discuss key priorities for patients.
Audit and feedback relating to VTE risk assessment and prophylaxis using an electronic VTE audit application is promoted and used to track and monitor trends in;
percentage of admitted patients with documented VTE risk assessment;
percentage of adherence to guidelines;
percentage of patients receiving appropriate prophylaxis.
The numbers of hospital acquired thromboses are also collated.
The introduction of the National Maternal and Newborn Clinical Management System (MNCMS), enhanced collaboration, standardization and safety in obstetric and neonatal care across the 5 sites that are currently live. The National meds team of informatics pharmacists in conjunction with clinical
pharmacists working in the live sites have helped to digitalise local VTE risk assessments. Clinical decision support tools and packages have been developed to enhance safe monitoring and prescribing of anticoagulation.
Three practical actions hospital teams can take right now to improve VTE care.
a. Prioritise VTE risk assessment completion (on paper or as part of an EHR) at all key time points e.g. admission, post-surgery, postpartum and if the patient condition changes
b. Establish clear links between VTE risk assessment and mechanical and/ or pharmacological prophylaxis. Include guidance for dose recommendations and treatment duration on the paper drug kardex or embedded with decision support and alerts/ triggers in the EHR for safety. Facilitate pharmacists and nurses/midwives in the regular review of VTE risk assessment completion and appropriate prescribing of prophylaxis.
c. Design and implement staff and patient education and awareness programs using patient information leaflets from the National Clinical Programme for VTE, the Irish Heart Foundation and World Thrombosis Day resources. Provide plain language and consistent education and training materials to patients at discharge relating to VTE risks, management and administration of medication at home. ‘Make Every Contact Count’ for better health, safety and chronic disease prevention.
Footnote: *including those who identify as women and all those who may not identify as female but share female biology and experience*
National clinical guideline on vte (ncg-vte): Supplementary appendix
Protect, Rejuvenate. Lubricate with LubriSyn HA
Lubrisyn HA was developed by renowned specialist Dr. Steve Allday. He knew the power of bio-identical HA. He developed LubriSyn HA, the first bio-identical HA supplement, natural, safe and effective.
• Bio-identical Hyaluronic Acid – identical to the HA the body makes.
why does synovial decline?
• High Molecular Weight HA (HMW-HA), the body’s natural HA.
The Source of HA
What your customer needs to know
LubriSyn HA+
Highest quality HA.
High Molecular Weight HA.
Cutting edge innovation. Patented BioFermentation derived HA Vegan.
What other brands wont tell you!
Other Brands
Low quality degraded HA.
Low molecular weight / fragmented HA.
Extracted using chemicals, from chicken and shark cartilage.
LubriSyn HA is distributed in Ireland by McCormack Distribution.
“LubriSyn HA is the highest quality pure HA. We are focused on caring for our customers with trusted quality products, and clinical information”
Jim McCormack, Pharmacist Premium, Natural, Hyaluronic Acid Joint Supplement. and easy to take, doesn’t interact with other medications.
Molecular Weight HA produced by our fragmented low molecular weight causes inflammation.
GRAPE FLAVOUR
weight HA protects against ageing, and joint disease. fluid provides lubrication, viscosity the joint.
fluid contains a lot of HMW-HA.
taking LubrisynHA since just before works, it’s like the WD-40 I have in the struggling, especially with my right hip. far less active now without it. “ Martin Hoban, 74, Active Gardener
The only liquid Bio-identical HA supplement Rapidly absorbed, highly effective.
High Purity, High Quality.
Powder form, capsules or tablets.
Full of impurities (chemicalS and proteins). Easily manufactured.
Cheap degraded HA.
70 Ask the Expert: Diabetes
Diabetes in Pregnancy
We spoke with Ciara Coveney, Advanced Midwife Practitioner in Diabetes in Pregnancy, about the realities of hospital care, common misconceptions, and the opportunities ahead for Irish maternity services.
Ciara Coveney works as an Advanced Midwife Practitioner specialising in Diabetes in Pregnancy. Her decision to enter this field stemmed from seeing first-hand how tailored, expert-led care can transform outcomes for both women and their babies.
“Pregnancy is already a huge journey,” she explains. “When diabetes is added, it brings extra challenges that can feel overwhelming. What drew me in was the opportunity to combine advanced clinical decision-making with the heart of midwifery — supporting women, giving them clear information, and helping them feel more confident. That blend of specialist expertise and personalised support can truly change outcomes.”
Different challenges in Type 1 and Type 2 diabetes
In hospital practice, the challenges of supporting women with Type 1 and Type 2 diabetes diverge significantly.
For Type 1 diabetes, the complexity lies in the constant adjustments required. “Insulin sensitivity shifts dynamically during pregnancy,” Ciara says, “so frequent dose changes are essential. Technology such as hybrid closed-loop pumps and continuous glucose monitors (CGMs) help enormously, but they still require extensive expertise to interpret and manage safely.”
Women with Type 1 diabetes may also present with advanced comorbidities such as renal or retinal disease, hypertension, or vascular complications, requiring close collaboration across specialties. Some will also need input from maternal–fetal medicine experts, something Ciara feels
Ciara Coveney
fortunate to have access through the specialist obstetricians on the diabetes in pregnancy team.
For Type 2 diabetes, the picture is often different. Many women enter pregnancy with limited prior engagement with specialist teams or pre-conception care. “They may be on multiple agents not suitable for pregnancy, requiring a rapid transition to safer alternatives. Add to this the high burden of comorbidities such as obesity and hypertension, and it can feel overwhelming for women early on in pregnancy,” Ciara notes. Encouragingly, she highlights the role of chronic disease hubs in creating better pathways and earlier specialist input for these women.
Day-to-day realities for women Regardless of type, diabetes in pregnancy means frequent monitoring, multiple hospital visits, and ongoing adjustments to care. “For women who are used to independently managing their diabetes, the intensity of hospital-based care can feel disempowering,” Ciara says.
Technology plays a role in alleviating some of this burden, particularly CGMs and pumps that reduce the need for constant finger-pricking or manual dose adjustments. “We hope that in the near future, technology will be made more widely available to women with Type 2 diabetes too,” she adds.
The team works hard to streamline care and ensure women feel listened to and involved in decisions. “Pregnancy changes the landscape of diabetes care,” Ciara reflects. “Our job is not just to monitor closely, but to make sure women still feel empowered and supported.”
Misconceptions that persist
Ciara regularly encounters myths that can undermine care.
• That all types of diabetes are essentially the same. “In reality, Type 1, Type 2, and gestational diabetes require very different approaches,” she stresses.
• That technology alone is the answer. “Insulin pumps and CGMs are fantastic tools, but they don’t solve everything — they still need
education, expertise, and active engagement from women and staff alike.”
• That poor control is simply a matter of lifestyle. “There’s stigma attached to diabetes, and assumptions about personal choices. But in pregnancy, hormonal changes make management uniquely complex. Women are often working incredibly hard, and part of my role is to challenge those misconceptions and make sure women feel supported, not judged.”
“CGMs provide real-time feedback, reducing the burden of fingerpricks and giving us a much clearer picture of glucose patterns,” she explains. “Insulin pumps and hybrid closed-loop systems allow for more precise insulin delivery and adapt to the rapid changes that happen in pregnancy. They play a vital role in maintaining the tight glycaemic control needed for fetal growth and development.”
Digital platforms that share data remotely are also changing how maternity teams work. “Women can upload glucose readings from home, and we can adjust treatment without needing an in-person visit. That’s a huge step forward in reducing the burden of frequent hospital appointments.”
This shift towards proactive, rather than reactive, care means complications can be avoided, interventions made earlier, and women feel more confident day to day.
The most exciting advances, Ciara says, are in technology. Hybrid closed-loop systems are showing strong evidence for safe use in pregnancy, helping to achieve tighter glucose control while reducing hypoglycaemia risk.
Another important area is screening and prevention of complications. Retinal screening has been strengthened, with a pregnancyspecific pathway launched by Ireland’s Diabetic RetinaScreen programme. “The ability to detect and intervene earlier in diabetic retinopathy is a huge step forward in protecting women’s long-term health,” she notes.
“What excites me most,” Ciara adds, “is that these advances aren’t just about hitting glucose targets — they’re about supporting women to feel safer, more confident, and less burdened during such a critical time.”
The power of the multidisciplinary team
Ciara emphasises that diabetes in pregnancy is never just about glucose control. “It impacts midwifery, obstetrics, fetal growth, mental health, and long-term maternal wellbeing,” she explains.
“The strength of the multidisciplinary approach is that it reduces silos, gives women confidence through joined-up thinking, and improves both maternal and neonatal outcomes.”
Building a stronger system in Ireland
For Ciara, the priorities are clear: workforce, technology, and integration.
• Workforce: “We need more specialist staff across all disciplines, not just in tertiary centres, so every woman has equitable access to expertise.”
• Technology: Expanding CGMs, pumps, and digital platforms to become standard in pregnancy care.
• Integration: Stronger pathways between maternity hospitals, GPs, and community teams. She is currently contributing to the update of the national guideline for diabetes in pregnancy, being written with multidisciplinary stakeholders. A key aim is to align with the Diabetes in Pregnancy: A Model of Care for Ireland launched in February 2024.
Three steps hospitals can take now
Ciara identifies three immediate actions maternity hospitals can take to improve care for women with diabetes in pregnancy:
1. Strengthen multidisciplinary teams with adequate specialist midwifery, obstetric, endocrinology, and dietetic support.
2. Embed technology into routine care, making CGMs and datasharing platforms standard for women with pre-existing diabetes.
3. Improve integration with GPs and community teams to prevent women from falling through the cracks.
“These are achievable steps,” Ciara says. “While we work towards national implementation of guidelines and models of care, hospitals can act now to make a difference.”
Conception Care
Pregnancy and Contraception Care in Pharmacy
Pre-Pregnancy & Fertility
Just over a third of couples will conceive in the first month of trying, while for others it can be a much longer road, with factors such as age, general health and reproductive health affecting how long it takes.
Around 1 in 6 couples in Ireland may experience issues with fertility.
The growing demands of a modern lifestyle are having a significant impact on our nutritional health. Stress, anxiety, lack of sleep, dieting and poor nutrition all impact the bodies ability to absorb the nutrition needed to optimise reproductive health.
Improving nutrition and lifestyle for as little as three months before trying to conceive can make a noticeable difference to both genders as both the male and female reproductive systems need adequate nutritional support to contribute to sperm and egg quality.
Factors Affecting Fertility
Age: For women, the most fertile period is in their mid-twenties and fertility starts to decrease after the age of 35.For men, sperm is strongest in their mid-twenties and starts to decrease after the age of 40.
Smoking: Smoking can affect fertility in both men and women, it can affect the chances of conceiving for women and sperm quality in men.
Weight: A body mass index (BMI) of 30 or over is known to reduce fertility in men and women. While, for women, being underweight (BMI less than 18) can also affect ovulation.
Alcohol: For women planning to get pregnant, the HSE recommend the safest approach is not to drink alcohol at all. While for men drinking too much alcohol can affect the quality of sperm.
Stress: Stress can affect your relationship and cause a loss of
sex drive. In severe cases, stress may also affect ovulation and sperm production.
Diet & Lifestyle: The HSE recommends all women begin taking folic acid at least 3 months before conception. There are number of other vitamins, minerals and amino acids that are known to be beneficial to the reproductive system, however it can be difficult to get all of these nutrients in the diet in today’s busy world. This is where supplements can help, by providing extra support needed to support good pre-conception health.
How Do Fertility Supplements Work?
Supplements can help to correct nutritional deficiencies associated with the reproductive cycle by supplying the raw materials needed to support the reproductive system so it can function optimally.
For Women: Supplements can support the nutritional needs of the female reproductive system.
Getting the environment right and developing good quality egg cells are key factors when trying for a baby.
Nutrients play an important role in the development of the egg, womb and the hormonal system. Each month, the reproductive and hormonal cycle develop an egg cell, prepare the womb and a myriad of other processes have to be performed to create the right fertile balance.
Egg quality can be enhanced if it is released into a healthy nutritious environment. Fostering a good diet and ensuring that you are taking the essential nutrients can positively effect the health of your eggs and subsequently the developing foetus.
For Men: Men have to produce between 40 and 300 million sperm cells to be fertile. This is an intensive process and the energy involved in creating these cells is significant. Getting the environment right and developing
72 Conception Care
good quality sperm cells are key factors when trying for a baby. A deficiency in any nutrient may have an impact on male fertility. Improvements to both sperm quality and quantity can be made in as little as 3 months.
Key Nutrients for Conception
Look for a combination of Folic Acid, Vitamins, Minerals, Amino Acids, CO-Q10 & Omega 3 DHA.
Folic acid contributes to normal maternal tissue growth during pregnancy. The HSE recommends all women begin taking 400ug folic acid at least 3 months before conception.
Mineralsincluding Calcium, Magnesium, Iron, Zinc, Copper (gluconate), Manganese, Selenium, Chromium, Molybdenum, Iodine, Boron, are essential for both male and female reproductive health. Minerals work together creating a synergy. Multiple mineral deficiencies are common amongst many women particularly those who have been using hormonal contraception.
Vitamins are vital for the production of energy in the body. Sufficient energy production is required for reproductive health. Key reproductive vitamins are: Beta Carotene, Vitamin B1 (Thiamin), Vitamin B2 (Riboflavin), Vitamin B3 (Niacin), Vitamin B5 (pantothenic acid), Vitamin B6 (Pyridoxine), Folic acid, Inositol, Biotin, Vitamin C, Vitamin D, Vitamin E, Vitamin K1.
Amino acids are the building blocks of proteins necessary for growth and repair in the body. Look for: L'Arginine, L'Carnitine, L'Citruline, L'Glutamine, N-AcetylL-cysteine, Glycine, Taurine.
Antioxidantssuch as Co-Q10 are important for reproduction. CoQ10 is a powerful antioxidant and energy power house. It is present in the membrane of almost every cell in the body.
Omega 3 DHA contributes to the maintenance of normal brain function and vision. During pregnancy, essential fatty acids are important to the baby’s brain and eye development.
Pharmacy teams have the unique role as accessible healthcare providers to optimise preconception health, such as in screening tobacco and alcohol use, in offering advice on preconception risk factors and current medication use.
Heartburn and Indigestion
Many women suffer from both heartburn (acid reflux) and indigestion during pregnancy and it tends to become more common as the pregnancy progresses. In fact, by the third trimester nearly three quarters of pregnant women can suffer from heartburn.
There are two main reasons why heartburn and, to a lesser extent, indigestion are common at this time:
1. The surge in the hormone progesterone causes muscles to relax. This includes the sphincter (ring of muscle) at the entrance to the stomach. When this relaxes, stomach acids are able to travel back up into the oesophagus (food pipe) causing heartburn.
2. During the latter stages of pregnancy symptoms can also be caused by the baby physically putting pressure on the woman's digestive tract.
Although harmless to the baby, heartburn and indigestion can be painful and uncomfortable for expectant mothers and pharmacists can advise patients that eating a healthy diet and sitting and/or sleeping in a more upright position can help ease heartburn and indigestion.
Fatigue
Fatigue is an early sign of
pregnancy which nearly all women experience in the first trimester that can begin weeks after conception and implantation. It typically gets better around the start of the second trimester and returns in the third trimester, though it varies from pregnancy to pregnancy.
A number of tips to give expectant mums include:
1. Get enough rest. Advising a patient to start by going to bed earlier, and take naps during the day when they can. Even a 15-minute catnap can make a difference.
2. Stay hydrated. Cutting back on caffeine, and making sure plenty of water is consumed. If frequent urination is keeping a patient up at night, suggest drinking less water a few hours before bedtime and making up for it during the day.
3. Exercising regularly. Getting at least 20-30 minutes of moderate activity, such as walking can also help a patient feel less fatigued and that they have more energy.
Morning Sickness
Despite its name, can happen any time of day or night. It’s also extremely common affecting over 80% of mums-to-be.
Although it’s not known exactly what causes expectant mums to feel nauseous, it’s most likely that the feelings of nausea are all down to hormones, particularly Beta hCG, although it is thought that it can be due to a lack of vitamin B6, too.
There are several techniques that although have not been scientifically proved to work, have been frequently noted as helping subside the nausea symptoms for pregnant women.
1. Eating little and often, 6 meals a day.
2. Avoiding food with lots of sugar or saturated fats – such as sweets, chocolate and red meat.
3. Avoiding “trigger” foods or smells that make a patient feel sick.
4. Trying food or drinks that contain ginger.
5. Wearing acupressure bands throughout the day.
Sciatica and Muscular Back Pain
As many as 98% women will suffer from muscular back pain at some stage during their pregnancy. The pain is caused by the additional weight and changes in the body during pregnancy; hormonal
changes can cause ligaments which support the spine to become loose, which puts more pressure on the lower back. There are a number of suggestions pharmacists can make to alleviate symptoms:
1. Use a warm compress on the area where pain is being experienced.
2. Placing a pillow between the legs to better align the pelvis and take some pressure off the sciatic nerve.
3. Strengthen the core and reduce inflammation with pelvic tilts and kegel exercises.
4. Use a cold compress to provide cooling relief for back pain.
Medication taking whilst pregnant
As 50% of pregnancies are unplanned, a woman often discovers she is pregnant while already taking a medication and visits a pharmacy which is easily accessible, to enquire if she has harmed her baby by this action.
Whilst studies show there may be a lack of adequate information regarding use of certain medications during pregnancy, it has been suggested that pharmacists should be able to integrate available information with their medication expertise, to make appropriate individual risk/ benefit decisions. This requires active engagement with pregnant women, rather than automatically referring them to their physician.
The trimester of the pregnancy often plays an important part in whether medications can be taken, for example Some medicines can be dangerous to take in the first three months but safe in the second or third, or vice versa.
Current recommendations are that women should take 400mcg folic acid daily from before pregnancy until the end of the first trimester, and 10mcg vitamin D daily throughout pregnancy and while breastfeeding.
The role of folic acid in reducing the risk of neural tube defects and the value of vitamin D supplements in building bone formation in babies is well supported. Expectant mothers can therefore be reassured that it is not necessary to invest in expensive multivitamin supplements, and that eating a good balanced diet during pregnancy, along with folic acid and vitamin D supplements, should be all that is required to ensure the best possible health outcomes for both themselves and their unborn child.
Myocardial Infarction
most frequent category, involving mechanisms where the coronary arteries myocardial ischaemia despite the absence of flow-limiting atherosclerotic
Myocardial Infarction with Non-Obstructive Coronary Artery Disease: review of diagnosis and management approach
Common aetiologies include:
Written by Dr. Muslim Madhag (Cardiology Registrar), Dr Ross O’Grady
Dr Muslim Madhag
Dr Ross O’Grady
(Cardiology SPR) and Dr. Samer Arnous (Consultant Cardiologist)
Plaque rupture or erosion (most common)
Coronary artery spasm
Coronary embolism
• Coronary artery spasm
Spontaneous coronary artery dissection (SCAD) — further classified into three by angiographic morphology: (8)
• Spontaneous coronary artery dissection (SCAD) — further classified into three types by angiographic morphology:8
Type 1: Classic appearance of longitudinal radiolucent flap with contrast staining.
Coronary thrombosis
Myocardial bridging
Dr Ross O’Grady
Introduction
Cardiovascular disease remains the leading cause of mortality among both men and women worldwide. In Ireland, acute coronary syndrome (ACS) accounts for approximately 6,000 hospital admissions annually.1
Between 5% and 15% of patients diagnosed with myocardial infarction (MI) have nonobstructive coronary arteries on invasive angiography—typically defined as <50% diameter stenosis in a major epicardial vessel. This clinical entity is termed myocardial infarction with nonobstructive coronary arteries (MINOCA) and remains common yet often underrecognised.2,3
Dr S Arnous Dr S Arnous
o Type 1: Classic appearance of longitudinal radiolucent flap with contrast staining.
Type 2: Long, diffuse, smooth tubular narrowing with abrupt calibre change.
Type 3: Focal, tubular stenoses mimicking atherosclerosis.
magnetic resonance (CMR), and provide aetiologyspecific management principles with key evidence where available. We also highlight prognosis and followup considerations, including rehabilitation and psychosocial support.
Classification of MINOCA
MINOCA encompasses a heterogeneous group of conditions and can be broadly classified into two categories based on whether the underlying mechanism is coronary or noncoronary in origin.3
1. NonCoronary MINOCA
(a) NonCardiac causes
• Cardiac trauma
• Cardiotoxicity (e.g., chemotherapy)
2. Coronary MINOCA
This is the most frequent category, involving mechanisms where the coronary arteries contribute to myocardial ischaemia despite the absence of flowlimiting atherosclerotic stenosis. Common aetiologies include:
• Plaque rupture or erosion (most common)
o Type 2: Long, diffuse, smooth tubular narrowing with abrupt calibre change.
o Type 3: Focal, tubular stenoses mimicking atherosclerosis.
• Coronary embolism
• Coronary thrombosis
• Myocardial bridging
Figure 1. Invasive coronary angiogram showing SCAD of the mid left circumflex artery with an intimal flap
Dr S Arnous
MINOCA is a working diagnosis made in patients who present with clinical features of ACS and a rise/fall in cardiac troponin consistent with acute myocardial injury, in whom coronary angiography does not demonstrate obstructive coronary artery disease (CAD). Compared with MI due to obstructive CAD (MICAD), patients with MINOCA are more often women and tend to have fewer traditional cardiovascular risk factors.2,3
These conditions cause myocardial injury via supply–demand imbalance rather than direct coronary pathology, sometimes labelled Type 2 MI. Common examples include:
Invasive coronary angiogram showing SCAD left circumflex artery with an intimal flap.
• Sepsis
• Pulmonary embolism (PE)
• Severe anaemia
• Acute respiratory failure
(b) Cardiac, noncoronary causes
Scope of this review. We summarise the contemporary classification of MINOCA (coronary and noncoronary causes), outline a practical diagnostic pathway integrating invasive angiography, intracoronary imaging and physiology, and cardiac
These conditions directly injure the myocardium without obstructive CAD, leading to troponin elevation. Key examples:
• Myocarditis
• Cardiomyopathies
• Takotsubo (stressinduced) cardiomyopathy
Dr. Muslim Madhag
Dr Ross O’Grady
Dr. Samer Arnous
74 Myocardial Infarction
Diagnostic Approach
Clinical Assessment
Diagnosis begins with a thorough history and examination. Certain features may point toward specific aetiologies—for example, ACS after exertion in young women may suggest SCAD; a history of illicit drug use raises suspicion of coronary vasospasm; and chest pain following intense emotional or physical stress may indicate Takotsubo cardiomyopathy.
Initial Investigations
The cornerstone investigation in diagnosing patients with MINOCA is invasive coronary angiography. Prior to angiography, baseline laboratory and bedside tests should be performed to guide differential diagnosis.
• Transthoracic echocardiography to assess left ventricular systolic function and wallmotion abnormalities
Invasive Coronary Angiography
Invasive coronary angiography remains central to the evaluation of suspected MINOCA. A meticulous, framebyframe review of angiographic images is essential, as subtle findings such as plaque rupture, small thrombus, or SCAD may otherwise be missed.
When the angiographic appearance is uncertain or atypical:
• Intracoronary imaging with optical coherence tomography (OCT) or intravascular ultrasound (IVUS) can clarify the presence of plaque disruption
or SCAD. Given the procedural risks, these modalities should be reserved for situations where angiography alone is inconclusive.
• Intracoronary pharmacological testing: Administration of intraarterial glyceryl trinitrate can relieve vasospasm, aiding diagnostic accuracy.
• Coronary physiology: In patients where microvascular dysfunction is suspected, physiological indices may be measured. Abnormal values are defined as coronary flow reserve (CFR) <2.0 and/or index of microvascular resistance (IMR) ≥25.
• Left ventriculography: Injection of contrast into the left ventricular cavity can reveal characteristic wallmotion abnormalities consistent with Takotsubo syndrome, such as apical ballooning.
Cardiac Magnetic Resonance (CMR)
CMR offers detailed myocardial tissue characterisation, enabling differentiation between myocarditis, Takotsubo syndrome, infarction, and other cardiomyopathies. It can demonstrate oedema, inflammation, fibrosis, and scar, while also providing accurate functional assessment. CMR is therefore recommended in all patients with a working diagnosis of MINOCA, ideally within two weeks of presentation to maximise diagnostic yield.4 Delays in access may significantly reduce sensitivity, particularly for detecting transient conditions such as myocarditis or Takotsubo cardiomyopathy.
Diagnostic algorithm for Patients with working diagnosis of MINOCA. By Sykes R, Doherty D, Mangion K, Morrow A, Berry C. What an Interventionalist Needs to Know About MI with Non-obstructive Coronary Arteries. Interventional Cardiology Review 2021;16:e10. https://doi. org/10.15420/icr.2021.10
algorithm for Patients with working diagnosis of MINOCA. By Sykes R, Doherty D, Mangion K, Morrow A, Berry C. What an Interventionalist Needs to Know About MI with Non- obstructive Coronary Arteries. Interventional Cardiology Review 2021;16:e10. https://doi.org/10.15420/icr.2021.10
Figure 2
Figure 2: Diagnostic algorithm for patients with MINOCA4
Figure 1 Diagnostic
Integrated Imaging Strategy
A multimodality approach— incorporating invasive angiography, intracoronary imaging, coronary physiology, and CMR—can identify a specific aetiology in up to 85% of patients initially labelled with MINOCA.2,4 The choice and sequence of tests should be individualised according to clinical presentation and haemodynamic stability, balancing diagnostic benefit against the risk of iatrogenic complications. A rigid, onesizefitsall pathway is not appropriate; investigations should be tailored to the patient’s clinical context.
Management
General Principles
Management of MINOCA should be guided by the underlying aetiology whenever identified. In the absence of large-scale randomised controlled trials, current recommendations rely primarily on observational data and expert consensus.4,5
Secondary prevention strategies, modelled on those used in obstructive MI, are often considered beneficial—especially when plaque rupture or erosion is suspected. These typically include highintensity statins, ACE inhibitors or ARBs, betablockers, and appropriate antiplatelet therapy.
AetiologySpecific Management
• Plaque rupture or erosion: Treat as for atherosclerotic ACS, with dual antiplatelet therapy (DAPT) for 12 months followed by lifelong single antiplatelet therapy, highdose statins, betablockers, and ACE inhibitors/ARBs.4
• Spontaneous coronary artery dissection (SCAD): Conservative management is preferred, as >70% of lesions heal spontaneously within weeks to months (7). Revascularisation with PCI or CABG should be considered only in highrisk scenarios such as left main stem involvement, persistent ischaemia, malignant arrhythmia,
or haemodynamic compromise. Medical therapy generally includes betablockers and aspirin; statins and ACE inhibitors may be added, and a second antiplatelet agent can be considered in selected patients.7,9
• Coronary vasospasm: Calcium channel blockers are firstline therapy, often in combination with nitrates if tolerated. Avoid precipitants such as cocaine and sympathomimetic drugs.
• Microvascular dysfunction: Antianginal therapy (betablockers, calcium channel blockers, nitrates, ranolazine) is the mainstay, with lifestyle modification and riskfactor control.
• Takotsubo cardiomyopathy: Supportive therapy is indicated, often with betablockers and ACE inhibitors. Management should follow ESC heart failure guidance if LV dysfunction is significant.
• Myocarditis or cardiomyopathies: Treatment should follow diseasespecific guidelines, with supportive heart failure therapy where appropriate.
Heart Failure and Secondary Prevention
Patients who develop LV dysfunction should be managed according to ESC heart failure guidelines, with optimisation of guidelinedirected therapy and followup in a specialist heart failure service. All MINOCA patients should be referred to a structured cardiac rehabilitation programme.
Prognosis
Compared with MI due to obstructive CAD (MICAD), patients with MINOCA generally have a more favourable prognosis. Nevertheless, their risk of major adverse cardiovascular events (MACE) remains significantly higher than that of the general population. (2) Prognosis varies according to underlying aetiology—for example, SCAD typically carries a good
PMI Annual Charity Lunch
mediumterm outlook with vessel healing, whereas myocarditis or microvascular dysfunction may be associated with recurrent symptoms. Importantly, MINOCA patients remain at risk of recurrent MI, heart failure, and arrhythmia, underscoring the need for close followup and secondary prevention.
Psychological sequelae— including anxiety, depression, and posttraumatic stress disorder—are not uncommon after MINOCA. Timely referral for screening, counselling, and rehabilitation services should therefore be integrated into holistic care.8
Conclusion
MINOCA represents a heterogeneous clinical syndrome encompassing a wide range of coronary and noncoronary pathologies. It should be regarded as a provisional working diagnosis, prompting thorough investigation to establish the precise mechanism of myocardial injury. A multimodality diagnostic pathway—combining angiography, intracoronary imaging and physiology, and CMR—can clarify the underlying cause in most cases.
Management must be tailored to the identified aetiology, with secondary prevention applied judiciously. While outcomes are generally better than for MICAD, MINOCA still confers a substantial risk of adverse events compared to the general population. Ongoing research and clinical trials are needed to refine treatment strategies and improve prognosis.
References
1. Shannon J. Heart attack audit shows need for new cardiovascular strategy. Irish Heart Foundation. Available at: https://irishheart. ie/news/heart-attack-audit-shows-need-for-new-cardiovascular-strategy (Accessed March 2025).
2. Bakhshi H, Gibson CM. MINOCA: Myocardial infarction with nonobstructive coronary artery disease. Am Heart J Plus Cardiol
The PMI Annual Charity Lunch takes place this year on December 11th from 12-4pm in the Dublin Royal Convention Centre, Dublin.
This much-loved annual event is a perennial highlight of the PMI events calendar; bringing members, colleagues and guests together for an afternoon of good food, great company and the opportunity to support an amazing charity.
This year the PMI are proud to support Make-A-Wish Ireland, an incredible organisation that grants life-changing wishes to children living with life-threatening illnesses. Make-A-Wish has granted over 3,350 unique wishes to date. More than just experiences, each wish creates treasured memories and gives children and their families hope, joy and precious moments together.
Don’t miss this opportunity to connect and celebrate all while supporting an incredible cause. Tables of 10 and 12 are available and sell out quickly each year – secure yours today by contacting the PMI office or visiting www.thepmi.com
Res Pract. 2023;33:100312. doi:10.1016/j.ahjo.2023.100312.
3. Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44:3720–3826. doi:10.1093/eurheartj/ehad191.
4. Sykes R, Doherty D, Mangion K, Morrow A, Berry C. What an interventionalist needs to know about MI with nonobstructive coronary arteries. Interv Cardiol Rev. 2021;16:e10. doi:10.15420/ icr.2021.10.
5. Montone RA, Caffè A, Yasumura K, Kini A. Routine diagnosis of ANOCA/INOCA: pros and cons. EuroIntervention. 2025;21:e293–e295. doi:10.4244/EIJ-E-24-00072.
6. Lindahl B, Baron T, Erlinge D, Hadziosmanovic N, Nordenskjöld A, Gard A, Jernberg T. Medical therapy for secondary prevention and longterm outcome in patients with myocardial infarction with nonobstructive coronary artery disease. Circulation. 2017;135:1481–1489. doi:10.1161/CIRCULATIONAHA.116.026336.
7. Khiatah B, Jazayeri S, Yamamoto N, Burt T, Frugoli A, Brooke DL. Cardiovascular disease in women: A review of spontaneous coronary artery dissection. Medicine (Baltimore). 2022;101(38):e30433. doi:10.1097/ MD.0000000000030433.
8. Krittanawong C, Gulati R, Eitzman D, Jneid H. Revascularisation in patients with spontaneous coronary artery dissection: Where are we now? J Am Heart Assoc. 2021;10(13):e018551. doi:10.1161/JAHA.120.018551.
9. Tweet MS, Kok SN, Hayes SN. Spontaneous coronary artery dissection in women: What is known and what is yet to be understood. Clin Cardiol. 2018;41:203–210. doi:10.1002/clc.22909.
¤28M Programme to Deliver Next Generation Cancer Care
Minister for Further and Higher Education, Research, Innovation and Science, James Lawless TD, launched Phase 2 of Ireland’s leading and largest ever cancer research programme, Precision Oncology Ireland (POI).
Siobhan Gaynor, Advanced Cancer Patient Council member and patient researcher; Prof Donal Brenan, UCD Professor of Gynae-Oncology, Consultant Gynaecological Oncologist at the Mater Hospital, and Deputy-Director of POI; Prof Walter Kolch, Director of Precision Oncology Ireland and Systems Biology Ireland (based at UCD); Dr Siobhan Roche, Director of Science for the Economy, Taighde Éireann–Research Ireland; Prof Kate Robson Brown, UCD Vice-President for Research, Innovation and Impact. Photo credit: Angela Halpin, photographer
POI is a cancer research consortium dedicated to advancing personalised cancer research and care. Its mission is to develop tailored diagnostic and therapeutic solutions using cuttingedge technologies and data, ensuring every patient receives the right treatment at the right time. The programme is an ambitious and unique strategic partnership model, co-funded through Research Ireland, industry and the
not-for-profit sector, coordinated by the Systems Biology Ireland centre based at University College Dublin (UCD), which is led by Professor Walter Kolch.
Minister Lawless said: “Breakthroughs in cancer research are most likely when clinicians, scientists, industry leaders, patients, charities and other stakeholders come together with a shared purpose. The first phase of Precision Oncology Ireland stands
as proof that strong, sustained collaboration can unlock innovation and accelerate transformative solutions. I congratulate the team on the advances made to date and wish them every success as they embark on this next phase of funded research.”
Professor Walter Kolch said, “Research is the engine behind new medicines. POI-2 is all about linking top notch cancer research to clinical translation. This includes the development of advanced computer simulations of the disease, so that we can design the best diagnostic and treatment approaches for each individual patient.”
UCD Professor of GynaeOncology, Consultant Gynaecological Oncologist at the Mater Hospital, and DeputyDirector of POI, Professor Donal
Brennan said: “The first phase of this programme delivered significant achievements. We now aim to strengthen collaboration with clinical partners and move towards embedding research within standard cancer care, so that patients and society across Ireland – and beyond – can benefit from improved outcomes, enhanced healthcare innovation, and more sustainable delivery of cancer services.”
The first phase of POI established a pioneering cross-sector collaborative model, bringing together academics, industry partners, charities, and patients. Dr Diarmuid O’Brien, CEO, Research Ireland, said: “The highly-impactful Precision Oncology Ireland strategic partnership is enabling breakthroughs in cancer
Adex Gel has been shown to improve atopic eczema from moderate to mild in 2 weeks without corticosteroids1
Adex Gel also improved:
Quality of life1
Total eczema area2
Redness2
Dryness2
Sleeplessness2
Itch2
Specially formulated with a high level of oils (30%) and an ancillary anti-inflammatory, nicotinamide (4%) which is a form of vitamin B3, to help reduce inflammation
Recommended for use as long as necessary, all over the body including on the face, hands and flexures.
Available at your local pharmacy. For patients aged 1 year+
Scan the QR code for more trial information
Adex Gel does not contain corticosteroids
Product name: Adex™ Gel. Key ingredients: Isopropyl myristate 15%, liquid paraffin 15%, nicotinamide 4%. Uses: Highly moisturising and protective emollient with an ancillary anti-inflammatory medicinal substance for the treatment and routine management of dry and inflamed skin conditions such as mild to moderate atopic dermatitis, various forms of eczema, contact dermatitis and psoriasis. Package sizes: 100g tube and 500g pump pack. Further information is available from: Dermal Laboratories Ltd, Tatmore Place, Gosmore, Hitchin, Herts, SG4 7QR, UK. ‘Adex’ is a trademark. SCORAD, SCORing Atopic Dermatitis. CDLQI, Children’s Dermatology Life Quality Index.
References: 1. Gallagher J. et al. Evaluation of an Emollient with Nicotinamide in Managing Moderate Atopic Eczema in Paediatric Patients: A RealWorld GP Study. Data presented at the European Academy of Dermatology and Venereology (EADV) Spring Symposium, May 2025, Prague, Czech Republic. 2. Gallagher J. et al. Impact of an Emollient Containing Nicotinamide on Moderate Atopic Eczema and Quality of Life in Paediatric Patients. Data presented at the European Academy of Dermatology and Venereology (EADV) Spring Symposium, May 2025, Prague, Czech Republic.
Adverse Events/Incidents should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse Events/Incidents should also be reported to Dermal.
Scan for Adex Gel essential information and adverse event/ incident reporting.
“The challenge has moved to focus on quality of life needs as well as the need for more real-world data to be gathered to better inform service delivery and hopefully improve our care. In addition, we are hoping to better educate the public and the health service about the realities of living with an advanced cancer diagnosis.”
biology, supporting the development of new treatments, training the next generation of researchers, nurturing biotech start-ups, and strengthening critical research infrastructure.
“This programme has built a unified community that is creating a lasting impact on how we approach cancer research in Ireland. Phase 2, now, represents a substantial increase in investment, scale and ambition, as we work to deliver the next generation of cancer care.”
Patient advocate and researcher Siobhan Gaynor supports the launch of POI-2. Siobhan lives with advanced breast cancer which is a life-limiting disease. She volunteers on several cancer research committees and conducted a survey via Cancer Trials Ireland in 2023 to capture never beforeseen input from stage IV cancer patients. Her research was
Professor Walter Kolch, Director of Precision Oncology Ireland and Systems Biology Ireland (based at UCD)
POI-2 will build on the success of Phase 1 by deepening interdisciplinarity through stronger clinical engagement, broadening scientific scope and infrastructure, enhancing patient and public involvement, expanding training opportunities, and fostering collaboration across the cancer research and healthcare communities from the outset.
UCD Vice-President for Research, Innovation and Impact, Professor Kate Robson Brown said: “The launch of POI-2 marks a pivotal step in realising our collective strategic vision to advance precision medicine, accelerate interdisciplinary collaboration, and harness the transformative power of AI and digital technologies. Most importantly, it reflects our unwavering commitment to translating groundbreaking research into tangible improvements in patient care and outcomes. This programme exemplifies the future of healthcare research and innovation and we are proud to be at the forefront.”
New report highlights only three of 28 targets met in National Cancer Strategy
The Irish Cancer Society has launched new figures that highlight only three of 28 defined targets have been met in the National Cancer Strategy. With Ireland’s cancer mortality rate the third highest in Western Europe, the Society has warned that things will get worse unless increased investment is provided in budget 2026.
The Irish Cancer Society’s NCS Scorecard highlights performance against the 28 defined targets in the National Cancer Strategy in 2024 and 2025.
Of these targets only three have been met. 14 have not been met; seven have no data available; 1 is considered unlikely to meet its 2026 target given its current trajectory, and three have a 2026 deadline which cannot yet be assessed.
CEO, Averil Power said, “One in two of us will get cancer in our lifetime. When we do, we deserve to be given the best possible chance of surviving the disease. But as the National Cancer Strategy Scorecard highlights, target waiting times for vital cancer tests and treatment are not being met. As a result, our cancer death rate is the third highest in Western Europe.
“The National Cancer Strategy was launched in 2017 and will expire in 2026. As we head into the final year of the Strategy, it's clear most targets are not being met. That will only change if Government provides additional investment in the National Cancer Strategy in next week’s budget.”
awarded the Irish Cancer Society Public and Patient Involvement (PPI) project of the year in 2025.
Following the survey, Siobhan was also behind the creation of an Advanced Cancer Patients Council, which ensures dissemination of the survey results and campaigns for changes in Irish advanced cancer care by patients and for patients.
Speaking at the launch, Siobhan said: “Most Stage IV cancers are incurable, although thanks to science and research, we are now living longer. The challenge has moved to focus on quality-of-life needs as well as the need for more real-world data to be gathered to better inform service delivery and hopefully improve our care. In addition, we are hoping to better educate the public and the health service about the realities of living with an advanced cancer diagnosis.”
Professor John Kennedy, Chair of the last National Cancer Strategy, said, “We are deeply concerned about the impact lack of investment in the National Cancer Strategy is having on people with cancer in Ireland. The fact of the matter is that patients are being let down. “Without Government investment in cancer services, staff, and infrastructure, it is cancer patients who continue to pay a too high price. Budget 2026 must prioritise the National Cancer Strategy, with ringfenced new recurrent development funding for the National Cancer Control Programme of at least ¤20 million each year. The huge challenges posed by the combination of a growing and increasingly aged population along with ever more complex, expensive and effective therapy, can only be addressed by coherent planning for, and multiannual funding of, the next National Cancer Strategy over its lifetime.”
The Irish Cancer Society is calling for increased investment in Budget 2026 towards cancer staff, buildings, and equipment to ensure target waiting times are met. Specifically:
• Provide sufficient investment in staff, buildings, and equipment to enable targets of the current National Cancer Strategy to be met.
• Plan and resource the next National Cancer Strategy.
• Improve the availability of data to support transparency and decision-making.
NEW BREAST HEALTH PROGRAMME FOR FÓRSA MEMBERS LAUNCHES NATIONWIDE
Cornmarket Group Financial Services Ltd., in partnership with Fórsa and Breast Cancer Ireland, this week officially launched a twoyear breast health awareness and education programme at Fórsa HQ, Nerney’s Court, Dublin.
The programme, which began on a trial basis in July 2025, will now be rolled out to Fórsa workplaces nationwide in a phased regional approach. Delivered by Breast Cancer Ireland’s Outreach Coordinator and breast cancer survivor, Juliette O’Connell, the initiative will provide 88,000 Fórsa members with complimentary practical, engaging presentations on breast health, and the importance of early detection, along with information on the 8 signs and symptoms of breast cancer to be aware of.
Juliette, herself a breast cancer survivor, with lived experience of the disease, will travel to Fórsa workplaces across Ireland in a distinctive pink Breast Cancer Ireland branded car to deliver these education and awareness sessions in person, whilst Fórsa members can also access presentations online. Sessions can be arranged at any time during the working day, making the programme as accessible, as possible, to all programme participants.
This initiative is being delivered to Fórsa members in partnership with Cornmarket Group Financial Services Ltd., and their longstanding partner Breast Cancer Ireland, making vital health education available directly to union members.
Clodagh Ruddy, Cornmarket Group Financial Services Ltd, Aisling Hurley, CEO of Breast Cancer Ireland and Julie Flood, Fórsa Senior Vice President
Clodagh Ruddy, speaking on behalf of Cornmarket Group Financial Services Ltd., said at the launch “Early detection of breast cancer can save lives and the programme’s main focus is about driving awareness. The effect of this programme in the short and longer term will be hugely significant and has the potential to really make a difference to the lives of Fórsa members and their colleagues. Cornmarket is proud to partner with Breast Cancer Ireland and Forsa on this important new initiative, and to build on our existing relationship with Ireland’s leading breast cancer charity”
Aisling Hurley, CEO of Breast Cancer Ireland, added:
“We’re delighted to partner with Cornmarket Group Financial Services and Fórsa to extend the reach of our breast health awareness programme nationwide. We are ever so grateful for this support of the work that we do. Juliette’s personal experience and expertise help bring the importance of early detection to life, empowering people with the knowledge to take action. Together, we can improve survival rates and support research that changes outcomes for future generations – and indeed become the generation that ends breast cancer once and for all”
Julie Flood, Fórsa Senior Vice President added “We at Fórsa are delighted and proud to launch our breast cancer awareness campaign in conjunction with Breast Cancer Ireland and Cornmarket. Raising awareness in workplaces is an extremely important step in assisting early detection and in turn, saving lives. Our campaign will educate our members about risk factors and symptoms, encourage selfexamination, promote regular screenings and help to dispel myths about breast cancer. Breast cancer is the second most common factor affecting women.
Statistics show one in seven women in Ireland will be diagnosed with breast cancer in their lifetime.”
Fórsa members who wish to arrange a presentation in their workplace can do so by emailing forsa@bciresearch.ie
HIQA PUBLISHES REVIEW ON THE DESIGN AND DELIVERY OF URGENT AND EMERGENCY HEALTHCARE SERVICES IN HSE MID WEST
The Health Information and Quality Authority (HIQA) has published its independent Review to inform decision-making on the design and delivery of urgent and emergency healthcare services in HSE Mid West.
Commenting on the publication of the Review, HIQA’s Director of Healthcare Regulation, Sean Egan, said: “This Review was prompted by significant concerns for patient safety in HSE Mid West, which have remained the utmost priority informing the advice provided to the Minister for Health. This Review was delivered with the support of a number of organisations and individuals, including patients and their families, whom HIQA wishes to thank for their contributions.”
Dr Máirín Ryan, Director of Health Technology Assessment and Deputy CEO at HIQA said: “HIQA also wishes to acknowledge the significant work undertaken by the Economic and Social Research Institute (ESRI) at the request of the Department of Health in relation to future bed requirements for the Mid West, which informed HIQA’s advice.”
Dr Ryan continued: “HIQA found that the core issue impacting urgent and emergency healthcare delivery in HSE Mid West is the significant inpatient bed capacity deficit relative to demand from patients presenting with more serious or complex care needs. This is intensified by an evergrowing demand for services, which will continue into the future as highlighted by the ESRI projections for the period up to 2040. The current situation caused by the demand-capacity gap at University Hospital Limerick (UHL) and across HSE Mid West, presents a risk to patient safety.”
HIQA’s advice highlighted an immediate need for action and investment to address current risks to patient safety in the shortest timeframe and safest way possible. The solution must also have regard for the ESRI projected capacity requirements to 2040.
HIQA has presented the Minister for Health with three options for how this might be achieved. These include the expansion of capacity at UHL on the Dooradoyle site
(Option A); the extension of the UHL hospital campus to include a second site in close proximity under a shared governance and resourcing model (Option B); and the development of a Model 3 hospital in HSE Mid West, providing a second emergency department (ED) for the region (Option C).
HIQA is of the view that Options A or B will likely yield the required inpatient capacity in the Mid West within a shorter timeframe, thereby addressing the immediate risk to patient safety. Option C may have the potential to meet longer-term bed requirements, but would be least capable of addressing immediate capacity deficits, while being associated with the longest lead times. Given that the ESRI projections span a wide range in terms of additional beds required, it will be important to ensure that decisions made around the future design and delivery of urgent and emergency healthcare services enable flexibility in how services are planned and developed. It is essential that there is ongoing monitoring of actual demand for services relative to the ESRI capacity projections, to support timely decision-making.
HIQA’s Director of Healthcare Regulation, Sean Egan, continued: “In working to progress any of these options, HIQA recommends the development of a comprehensive strategic plan. This should remain focused on addressing the safety concerns which prompted this Review, while having regard to the future demographic and policy considerations. Ongoing communication and engagement with the people of the Mid West will also be crucial to its delivery.”
HIV IRELAND CALLS ON GOVERNMENT TO PUBLISH A NATIONAL ACTION PLAN TO END NEW TRANSMISSIONS OF HIV BY 2030
HIV Ireland is urging the Government to honour its Programme for Government pledge to publish a National HIV Action Plan, warning that without clear timelines and accountability, Ireland risks falling short of its goal to end new HIV transmissions by 2030. The call comes ahead of the HIV Ireland and Fast Track Cities UK & Ireland National HIV Conference, Towards a National Action Plan for HIV in Ireland, which takes place today at the Aisling Hotel in Dublin. HIV Ireland Executive Director Stephen O’Hare said “We have the knowledge and tools to end new HIV transmissions. What we need now is political will and leadership. A National HIV Action Plan, informed by both clinical and community expertise, with
80 Clinical Profiles
specific targets and oversight, is the only way Ireland can meet its UNAIDS commitment to end new transmissions by 2030.”
The landmark conference brings together leading experts from Ireland and the UK including UCD’s Centre for Experimental Pathogen and Host Research led by Infectious disease specialist Prof Patrick Mallon, Sussexbased Irish Clinical Professor and Consultant in HIV Medicine & Sexual Health Prof Yvonne Gilleece and UK Government advisor on HIV and chair of the HIV Action Plan Implementation Group for England Prof Kevin Fenton as well as people living with HIV and advocates. The conference aims to share best practice and effective initiatives on prevention, testing, and combatting HIV related stigma to focus on turning the government’s promise into action.
In June, Ireland published an updated National Sexual Health Strategy 2025-2035. The Strategy commits to developing a HIV Action plan and HIV Model of Care. A similar plan is in place in England, which was published in 2021.
Speaking of the success of the National HIV Plans in England, Scotland and Wales Prof Yvonne Gilleece said “The experience across the UK demonstrates how a structured, evidence-based plan can lead to measurable improvements in HIV prevention and treatment outcomes. Developing a similar framework in Ireland is critical if the stated goal of ending new transmissions by 2030 is to be realised.”
Prof Patrick Mallon said “In recent decades, advances in testing, treatment and prevention have substantially changed the trajectory of HIV in Ireland. Of the new cases identified this year, fewer than 200 will constitute new transmissions. Ending new transmissions by 2030 is not insurmountable, but only if we redouble our efforts now.”
Rebecca Tallon de Havilland is an advocate living with HIV. Speaking on the Government’s commitment to better support people living with HIV, she said “When I was first diagnosed, I thought my life would be defined by HIV. Over time, with treatment and the right support, I’ve learned that it doesn’t have to be that way. Living well with HIV is possible and it’s important that the right supports are in place.”
The conference is supported by Gilead Sciences and Viiv (GSK) and represents a milestone moment for HIV advocacy in Ireland and a critical opportunity to ensure the Government fulfils its promise to end new HIV transmissions by 2030.
MICROSOFT DRAGON COPILOT HAS LAUNCHED IN IRELAND
Dragon Copilot brings together the trusted natural language voice dictation capabilities of Dragon Medical One (DMO) with the ambient listening capabilities of Dragon Ambient eXperience (DAX) Copilot, fine-tuned generative AI and healthcare-adapted safeguards. Part of Microsoft for Healthcare, Dragon Copilot is built on a secure modern architecture that enables organisations to deliver enhanced experiences and outcomes across care settings for clinicians and patients alike.
More than 200 clinicians with a wide range of medical disciplines across seven healthcare organisations, in the UK and Ireland, tested Dragon Copilot as part of a private preview programme that involved over 10,000 consultations.
In September, The Department of Finance published a long-term demographic outlook projecting sustained ageing trends over the next four decades. Meanwhile, the HSE’s "Medical Workforce Analysis Report 2024-2025" outlines workforce retention challenges. These national challenges mirror broader European trends; according to the OECD’s “Health at a Glance: Europe 2024 – State of Health in the EU Cycle” the EU faces a health workforce deficit that stems from an ageing population, impacting both patients and the health workforce, as well as difficult working conditions that are contributing to staff burnout and retention challenges. The report notes that technologies, such as AI, will be essential to augment the health workforce’s productivity and ability to focus more on patient care.
Recognising the pressing challenges facing Ireland’s healthcare—including an ageing population, workforce shortages, and persistent waiting lists— “Dragon Copilot is helping to reshape how clinicians manage time-consuming administrative tasks, such as documentation, referrals, and after-visit summaries, freeing up valuable time for patient care,” said Ciara Perciavalle, Head of Health at Microsoft Ireland.
“By streamlining workflows and integrating seamlessly with electronic patient records (EPR), Dragon Copilot not only enhances operational efficiency, but also supports clinician well-being, retention, and patient experiences. As Ireland continues to address growing demand and resource constraints, solutions like Dragon Copilot are vital in building more resilient and compassionate healthcare for the future.”
In a recent Microsoft commissioned report, 40 percent of patients surveyed reported having a consultation where they felt the clinician was too focused on the screen to provide their full attention. With the clinician-patient experience serving as the heart of high-quality care, AI solutions like Dragon Copilot offer practitioners a solution that helps improve human connection by reducing administrative tasks and facilitating more personalised care with enhanced data-driven insights.
Dr Peter-Marc Fortune, Paediatric Intensive Care Physician and Chief Medical Information Officer at the Manchester University NHS Foundation Trust, agrees that clinical AI assistants like Dragon Copilot “should reduce the burden of ensuring that [clinicians are] capturing everything, so they can actually focus on the interaction with the patient. [Consultations now feel more] face-to-face… like would have happened in the GP surgery 20 years ago, before everybody had PCs on their desk. The most important thing is to develop a relationship with a patient.”
STRIKING PORTRAIT BASED ON EXTENSIVE IRISH RESEARCH, REVEALS THE LIVED EXPERIENCE OF CHRONIC SPONTANEOUS URTICARIA
A unique piece of art, developed through a partnership with an Irish researcher and artist, was created to increase awareness and understanding of Chronic Spontaneous Urticaria (CSU), a debilitating chronic autoimmune condition. The portrait, "A Shared Canvas: The Untold Stories of Urticaria", will be on display at the Royal College of Physicians today. CSU, characterised by spontaneous hives, uncontrolled
itching and unpredictable episodes of disfiguring swelling of the skin can significantly impact the quality of life of those affected, causing physical discomfort and emotional distress.1 It is estimated that 1 in 100 people in Ireland suffer from chronic spontaneous urticaria.2,3 For the majority of these, they can be treated with over-the-counter antihistamines if diagnosed correctly. However, even with antihistamine treatment, the literature indicates that up to 9000 patients in Ireland could have uncontrolled symptoms.
At the heart of the event in the RCPI is the unveiling of a striking portrait by artist Valentina Vittorio. This isn't just any painting; it is a co-designed artwork, deeply informed by extensive Irish patient research conducted by PhD student Jennifer Donnelly from the RCSI. The research, based on in-depth patient interviews, uncovered the often-invisible psychosocial and emotional burdens of living with uncontrolled flares of hives, including profound loneliness, isolation, a devastating loss of identity, burning sensations and relentless sleep deprivation.
"Chronic Spontaneous Urticaria is a condition under recognised in public discourse. Our research over the past few years has highlighted the raw, often hidden, emotional toll including the loneliness, the isolation, the burning sensation that goes beyond the skin" said Jennifer Donnelly, PhD student, RCSI. "I had so many text documents of quotes and interviews, but it was Artist Valentina Vittorio who took on the task of translating these perspectives into her artwork.”
“Turning the different experiences of individuals living with CSU into a visual form was really moving and challenging " Artist Valentina Vittorio explained. "The feedback from the patients was that I should focus on the themes of loneliness, isolation and that intense burning sensation. These were challenging to put into art, but it helped to have this input and direction. I aimed to create one portrait to represent all the different emotions and experiences. I hope it helps others better understand the unseen side of this condition."
Speaking about the symptoms, Professor Niall Conlon, Consultant Clinical Immunologist, St James’s Hospital and Senior Clinical Lecturer, Trinity College Dublin, said: "The uncontrolled itch from CSU substantially impacts quality of life, disrupting sleep and interrupting daily activities. This condition disrupts relationships, sleep, work, school and mental wellbeing. Around the world, patients often feel unable to
Ciara Perciavalle, Head of Health at Microsoft Ireland
participate fully in society due to the unpredictability and discomfort of urticaria. It is not only a medical issue but a significant barrier to living a full and confident life. The global burden of this disease must be recognised and addressed with urgency.”
Agron Hasani, Country Head of Medical Affairs and Chief Medical Officer at Novartis Ireland said: "At Novartis, our purpose is to reimagine medicine to improve and extend people's lives. Raising awareness of this research ‘A Shared Canvas: The Untold Stories of Urticaria' underscores our commitment to the CSU community. It is important to work alongside health care practitioners and patient advocates to address the unmet needs and ultimately improve the lives of those affected by this challenging condition."
Ireland is home to a designated UCARE Centre at St James’s Hospital in Dublin, focused on improving management and research for urticaria patients.
#ChronicSpontaneousUrticaria
#UDAYYourJourney
#UnmetNeedInHives #UDAY2025
#CSU
CHANELLE PHARMA ANNOUNCES THREE STRATEGIC APPOINTMENTS TO BOARD
OF DIRECTORS
Chanelle Pharma (“Chanelle”), Ireland’s largest indigenous pharmaceutical company and a leading manufacturer of generic pharmaceuticals for human and animal health, today announced the appointment of Steven Mahoney, Rafik Amrane, and Jean Hoffman to its Board of Directors, effective immediately.
Steven, Rafik, and Jean will bring decades of global leadership experience across healthcare, manufacturing, and entrepreneurship, further strengthening Chanelle’s governance framework and supporting the company’s ambitious growth in both veterinary and human health markets.
Carsten Hellmann, Chair of the Board at Chanelle Pharma, said: “Steven, Rafik, and Jean each bring unique perspectives and decades of global leadership, especially in the Animal Health space. Their broad international experience will deepen the Board’s strategic insight and strengthen
A unique piece of art, developed through a partnership with an Irish researcher and artist, was created to increase awareness and understanding of Chronic Spontaneous Urticaria (CSU), a debilitating chronic autoimmune condition. The portrait, "A Shared Canvas: The Untold Stories of Urticaria", will be on display at the Royal College of Physicians today. Pictured were Susanne O'Reilly Head Communications & Patient Advocacy , researcher Jennifer Donnelly, PhD Scholar at the RCSI with artist Valentina Vittorio, Lisa Bashorum, Senior Patient Advocacy Manager and Prof Niall Conlon, Consultant immunologist St James's Hospital. Picture Jason Clarke
our ability to building a strong Chanelle platform.”
Angelo Gatto, CEO and Board Member of Chanelle Pharma, added: “The addition of these distinguished professionals brings to Chanelle world-class expertise that will help us scale faster, innovate smarter, and deepen our impact across global markets. Their vast knowledge and experience will be instrumental as we continue our growth journey.”
Steven Mahoney is a seasoned healthcare executive with 35 years’ experience. He spent most of his career at Merial where he held key leadership roles across Asia Pacific, the U.S. and Latin
America focusing on regional strategy, commercial operations, and integration. His expertise in managing complex global teams and driving growth in regulated markets aligns directly with Chanelle’s international ambitions. Rafik Amrane currently leads Global Operations at Opella, a 5 Billion Euro turnover HealthCare company, overseeing Manufacturing, Supply Chain and Quality across 13 manufacturing sites, 140 CMOs and more than 5,000 professionals worldwide. His background includes transformational leadership roles at Toyota, Merial and Sanofi, bringing deep operational insight and a strong track record in driving manufacturing excellence and supply chain innovation. Rafik has also led large scale performance transformation in various industries at McKinsey & Co.
Jean Hoffman is an accomplished entrepreneur and board director who has successfully built and exited two healthcare companies, including Putney Inc., a leading U.S. generic veterinary pharmaceutical firm acquired for $200 million. Jean’s expertise spans portfolio strategy, commercial growth and governance, providing Chanelle with valuable experience in scaling high-growth businesses.
ST
PATRICK’S
MENTAL HEALTH SERVICES
MARKS 20 YEARS OF SERVICE USER ADVOCACY THIS WORLD MENTAL HEALTH DAY
This World Mental Health Day, St Patrick’s Mental Health Services is celebrating 20 years of structured service user engagement via its Service Users and Supporters (SUAS) Council, with a campaign focused on one clear message:
Steven Mahoney, Rafik Amrane, and Jean Hoffman
82 Clinical Profiles
Lived experiences must be central to the design and delivery of mental healthcare services.
Established in 2005 as the Patient and Carers Council, today’s Service User and Supporters Council has always been led by the voices of people with lived experience. Its members, all experts by experience, advocate on behalf of service users to shape and improve the care provided at St Patrick’s Mental Health Services. SUAS now stands as a cornerstone of the organisation’s commitment to involving service users in the planning, management and evaluation of their treatment and support.
With over 30 members contributing their time and expertise over the last 20 years, SUAS Council members have:
• Provided invaluable insights into clinical care and evidence-based research.
• Championed the voices of fellow service users.
• Helped raise awareness about mental health at a national level.
Speaking about the crucial role of service user engagement, Paul Gilligan, CEO, St Patrick’s Mental Health Services said: “This year, as we celebrate 20 years of structured service user involvement at St Patrick’s Mental Health Services, we recognise and commend the invaluable role that SUAS has in shaping and improving services. The commitment and insight of our Council members has not only influenced how we deliver care here in St Patrick’s, but has also helped to challenge stigma, inform national policy and drive meaningful change.
The work of SUAS is a powerful reminder of the importance of lived experience in building services that are effective and grounded in human rights. As we look ahead, we do so with renewed determination to deepen this impact and ensure the voices of service users continues to guide everything we do.”
At an event to celebrate the 20th anniversary of SUAS, and in the lead up to World Mental Health Day 2025, current and former Council members, staff, supporters and partners of St Patrick’s Mental Health Services came together to reflect on 20 years of SUAS’ impact and its key achievements, such as:
• Improving care experiences:
- From playing a key role in redesigning the inpatient admission process to introducing peer-led hospital tours and talks, SUAS has consistently worked
to ensure service users feel supported from the very first point of contact.
• Shaping staff learning and support:
- Initiatives such as the Caring with Respect eLearning module and the Carers and Supporters Information Guide have helped staff and families better understand and respond to service users’ perspectives and needs.
• Driving innovation in digital health and service development:
- SUAS play a central role in consultations on new digital initiatives at St Patrick’s, including the launch of the eSwift electronic health record and Ireland’s first online service user portal, Your Portal.
• Influencing policy and challenging stigma nationally:
- The Council has contributed to policy reform, including collaborating with Amnesty International on capacity legislation; providing input to St Patrick’s advocacy submissions process; engaging in national campaigns and media interviews; and earning recognition from the Mental Health Commission for its impact on service quality
Speaking at the 20th anniversary event, Chris Miley, Chair of the Service User and Supporters Council at St Patrick’s Mental Health Services, said: “Involving those with lived experiences in the development and delivery of mental health services is key to providing care and treatment that is effective, responsive and person-centred.
As experts by experience, our perspectives and insights are crucial to informing approaches to care that truly respond to the needs and rights of service users. I have been proud to work alongside my peers on SUAS over the last several years to advance meaningful participation, and I look forward to what the future will bring as we continue to champion the service user voice and advocate for positive change across the mental healthcare system.”
Since SUAS was launched 20 years ago, St Patrick’s has continued to expand opportunities for service user involvement. Today, service users contribute through the Service User Advisory Network, which now has more than 100 members getting involved in a range of service improvement initiatives and strategic projects; the Family Carers and Supporters Network; the Remote Care Advisory Forum, which shapes
digital health initiatives and improves remote access to care; and the Academic Institute Steering Committee, where service users guide research priorities.
HPRA
HEALTH WARNING
An ongoing investigation by the Health Products Regulatory Authority (HPRA) and Revenue’s Customs Service has identified a small consignment of counterfeit tirzepatide injection pens that have been found to contain insulin and could pose a serious health risk for consumers. The HPRA is advising members of the public to only source prescription medicines from a registered pharmacy using a valid prescription to ensure they are accessing legitimate authorised medicinal products. The consignment detained, which included falsified pens, was sourced online and originated from outside Europe. Laboratory tests confirm that two of the pens contain insulin instead of tirzepatide, posing a serious risk to unsuspecting users due to the possible onset of severe hypoglycaemia upon administration.
Tirzepatide is a manufactured peptide designed to help manage type 2 diabetes and support weight loss. The counterfeit products appear similar to the authorised form of tirzepatide, branded as Mounjaro®
Hypoglycaemia occurs when blood sugar levels, also called blood glucose levels, drop too low. It must be treated quickly to stop it getting worse. Symptoms of low blood sugar can include feeling hungry, feeling dizzy, sweating, shaking, heart palpitations, changes in vision and feeling confused. More severe symptoms include extreme drowsiness, seizures and loss of consciousness. If left untreated, severe low blood sugar can be life-threatening.
The HPRA advises anyone who suspects they may have used any falsified tirzepatide or other GLP-1 type product, and who are experiencing symptoms of hypoglycaemia, to seek medical attention immediately.
The HPRA confirms that, to date, no reports of harm have been received in connection with this issue, nor is there evidence that these particular counterfeit products have reached end users. It continues to work closely with Revenue’s Customs Service, whose decisive action in this case successfully intercepted the falsified pens and prevented their entry into the country via the postal system.
As recently as September, the HPRA confirmed that it detained almost 400,000 units of illegal medicines in first half of 2025. It reminds the public that purchasing prescription medicines from unregulated sources means you can't be sure what you're getting. These products may be unsafe, ineffective, or fake – and could seriously harm your health.
ST JOHN OF GOD RESEARCH FOUNDATION OPENS DEDICATED PSYCHOSIS RESEARCH CENTRE
The St John of God Research Foundation (SJOG Research) announces the opening this week of a new Centre dedicated specifically to Psychosis Research. The newly established St John of God Psychosis Research Centre builds on the organisation’s respected heritage of supporting those with mental ill health.
With up to 45,000 people affected by psychosis at any one time in Ireland, the SJOG Psychosis Research Centre will aim to harness research activity and coordinate efforts across all of St John of God (SJOG) group and to offer the opportunity to strengthen collaborations nationally with other leading specialists in the area. The research outputs will inform the delivery of psychosis treatment across all relevant SJOG services and support its policies and advocacy programmes to develop improved mental health services.
A key initiative of the SJOG Psychosis Research Centre will be Patient and Public Involvement (PPI) meaning people with lived experience will be actively involved in the planning, conducting, and sharing of research findings. Conor Gavin, who has been recruited as the Psychosis Research Centre Co-Ordinator has himself lived experience in this area and is looking forward to bringing it to bear in the development of the Centre.
“As a person with my own lived experience of psychosis, I am thrilled to be a part of this new initiative in St John of God. It’s inspiring to see the work that has been done over the last number of decades to strive for better outcomes in this area of mental health. My motivation always stems from my own personal experience, and I often ask: ‘What would have worked for me?’ when I approach research questions. I am hugely excited to work with St John of God Research Foundation, researchers and clinicians alongside others with lived experience to help bring this project to fruition.”
SJOG has provided services in Ireland for those with mental
has informed international services and policies.
Professor Mary Clarke, Consultant Psychiatrist , St John of God DETECT Service said:
OXYGENCARE EXPANDS DIGITAL HEALTHCARE OFFERING WITH MEDANETS
ill-health for nearly 150 years and research began over 40 years ago. The SJOG Research was incorporated in 2011 to solidify SJOG commitment to research.
Dr Lesley O’Hara, CEO SJOG Research said,
We are incredibly proud to support the establishment of the St John of God Psychosis Research Centre. Our organisation has a long-standing reputation as leaders in this field of research, and we welcome the opportunity to extend our expertise to include research across the life span, and with disability and minority groups. A central focus of the new Centre is the person with psychosis, and their family. They will have the opportunity to shape the strategy, ensuring the research conducted is truly reflective of what is important to the people we support.
Collaboration has always been a key part of SJOG with many international researchers in psychosis spending time training in St John of God in Ireland. The SJOG Early Intervention in Psychosis (EIP) Service known as ‘DETECT’ was founded in 2005 and was the first of its kind in Ireland. It has continued to provide opportunities for building alliances across the globe and it
The St John of God Psychosis Research Centre builds on a strong legacy of clinical research in psychosis, grounded in the collaboration of clinicians, researchers, and the lived experience of individuals with psychosis and their families. We are excited by the opportunity to bring diverse areas of expertise together and to learn from one another, fostering a culture of shared purpose, curiosity and respect, in pursuit of better outcomes for individuals with psychosis. We are committed to translating research into better care, from early detection and intervention to long-term recovery.
The research evidencing and acting on early intervention programmes and initiatives is a step in better care for people.
In addition, the SJOG Psychosis Research Centre will provide research training, with a focus on supporting people to be leaders in this field. It goes further to support the full health service development and improvement cycle for psychosis, from research to policy and from implementation to evaluation.
Uniquely, the SJOG group of companies delivers services but also funds and carries out research on mental ill-health, implements its research findings into policy and practice, and builds clinical services based on the evidence.
impression made by their team further solidified our confidence in this partnership. It seems we are a natural fit in both values and working style.”
For over 30 years, OxygenCare has been transforming digital healthcare through clinical systems and working with innovative products and solutions throughout Ireland. The Medanets integrated nursing app supports point-of-care documentation and immediate access to key patient data, making it a natural fit with OxygenCare’s digital portfolio.
Combining OxygenCare’s connectivity solutions with Medanets' mobile solutions can provide significant added value both to organisations already using an electronic health record (EHR) and to hospitals beginning their digital journey.
OxygenCare is delighted to announce the introduction of the Medanets integrated Point of Care Nursing app to its ever-expanding Digital Healthcare solutions portfolio. The collaboration brings together two companies with a shared vision for improving patient care through innovative digital healthcare solutions.
Stephen Nicholson, Digital Health Manager, OxygenCare, explains: “Medanets simplifies nursing routines, supports decision making, complements and integrates with EHR systems, and releases time to care for patients.’ The CE and MDR certified app was developed in collaboration with healthcare professionals.
OxygenCare is a multi-awardwinning, family-owned business with over 50 years supporting healthcare throughout the island of Ireland.
“Their dedicated digital health team and prior experience in delivering complex ICU and anaesthesia systems make them an ideal partner for us,” says Medanets CEO Juha-Matti Ranta. “On top of that, their deep market knowledge and the
“We can offer healthcare providers a fast-track way to modernise operations, even in settings where an EHR is not yet in place. For instance, Medanets supports "lightweight IT" approaches such as sending PDFs directly to a document archive—a direct impactful step forward in digital empowerment,” Ranta explains.
Maurice Moran, Managing Director of OxygenCare, adds: “This Medanets offering complements our portfolio, and we see strong market potential. Together, we are currently conducting exploratory efforts in the market to identify opportunities and tailor our approach to local needs. Through this new partnership, all care phases can be managed digitally through a single provider. This partnership marks a promising step toward improving healthcare outcomes in Ireland and underscores the strength of collaboration in driving innovation forward."
Conor Gavin, Psychosis Research Centre Co-Ordinator, Professor Mary Clarke, Consultant Psychiatrist, SJOG DETECT,Lesley O’Hara, CEO SJOG Research Foundation.
Photo: Aidan Oliver
Pictured left to right: Stephen Nicholson, Digital Health Manager, OxygenCare; and Maurice Moran, Managing Director, OxygenCare
Unlock easy glucose monitoring1.
With the FreeStyle Libre 2 system, your patients get minute-to-minute glucose readings to help them manage diabetes more confidently.2
The FreeStyle Libre 2 system provides accurate glucose monitoring.3 Excellent 14-day accuracy.3
Reduces HbA1c compared with SMBG.4–6
Increases Time in Range by over 2 hours a day compared with SMBG in T1D.5
Living life as a full-time mother, surf instructor, dance teacher, and diabetes coach is a whirlwind of constant movement and energy. For me, this busy lifestyle demands a proactive way to manage my diabetes. That’s where diabetes technology comes into play. My FreeStyle Libre 2 system offers the support, confidence, and convenience I need to keep moving forward in my life with diabetes. Erin Dolan
Scan the QR code to find out how you can help your patients achieve better outcomes today1,4-6