THIS ISSUE: NEWS: Importance of Funding New Medicines Page 5
CONFERENCE: Irish College of Ophthalmologists Page 8
FEATURE: Migraine Care in Ireland Page 13
GUIDLINES: New Guidelines on Hypertension Page 19
GENETICS: The Role of the Genetic Counsellor Page 24 CPD: Non-Small Cell Lung Cancer Page 33
PHARMACY: AntipsychoticInduced Weight Gain Research Page 45
PREVENT
THE DISRUPTION OF MIGRAINE1
The only oral once-daily calcitonin gene-related peptide (CGRP) receptor antagonist for both episodic and chronic migraine patients1,2
Tablet not actual size.
Typical characteristics of migraine are headache of unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity and association with nausea and/or photophobia and phonophobia.3
ABBREVIATED PRESCRIBING INFORMATION. AQUIPTA®▼ (atogepant) 10 mg tablets; 60 mg tablets. Please refer to the Summary of Product Characteristics (SmPC) before prescribing.
PRESENTATION: Each tablet contains: 10 mg atogepant in 10 mg tablet, 60 mg atogepant in 60 mg tablet. INDICATION: Prophylaxis of migraine in adults who have at least 4 migraine days per month. DOSAGE AND ADMINISTRATION: The recommended dose is 60 mg taken orally once daily with or without meals; swallowed whole and not split, crushed or chewed. Missed dose to be taken as soon as it is remembered. If forgotten for an entire day, missed dose to be skipped and next dose taken as scheduled. Dose Modification: The recommended dosage of atogepant with concomitant use of strong CYP3A4 inhibitors or strong OATP inhibitors is 10 mg once daily. Special Populations: Elderly (≥65 years): No dose adjustment of atogepant is needed in elderly patients. Renal impairment: In patients with severe renal impairment (creatinine clearance [CLcr] 15-29 mL/ min), and in patients with end-stage renal disease (ESRD) (CLcr <15 mL/min), the recommended dosage of atogepant is 10 mg once daily. For patients with ESRD undergoing intermittent dialysis, atogepant should preferably be taken after dialysis. No dose adjustment is recommended for patients with mild or moderate renal impairment. Hepatic impairment: Avoid use of atogepant in patients with severe hepatic impairment. No dose adjustment is recommended for patients with mild or moderate hepatic impairment. Paediatric Population: The safety and efficacy of atogepant in children (< 18 years of age) have not yet been established. CONTRAINDICATIONS: Hypersensitivity to active substance or any of the excipients. SPECIAL WARNINGS AND PRECAUTIONS: Atogepant 60 mg tablets contain 31.5 mg sodium per tablet; this is equivalent to 1.6% of the WHO recommended maximum daily intake of 2 g sodium for an adult. Atogepant 10 mg tablets contain less than 1 mmol sodium (23 mg) per dose, that is to say essentially ‘sodium-free’. Atogepant has no or negligible influence on the ability to drive and use machines. However, if affected by somnolence, patients should exercise caution before driving or using machinery. FERTILITY, PREGNANCY AND LACTATION: Pregnancy: Atogepant is not recommended during pregnancy and in women of childbearing
potential not using contraception. Breast-feeding: It is unknown whether atogepant is excreted in human milk. A decision must be made whether to discontinue breast-feeding or to discontinue/ abstain from therapy taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman. Fertility: No human data on the effect of atogepant on fertility are available. Animal studies showed no impact on female and male fertility with atogepant treatment. UNDESIRABLE EFFECTS: Common (≥ 1/100 to <1/10): Decreased appetite, nausea, constipation, fatigue/somnolence, weight decreased. Refer to Section 4.8 of the SmPC for details of other side effects, and for further information.
▼ This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance; website: www.hpra.ie.
LEGAL CATEGORY: POM (S1B). MARKETING AUTHORISATION NUMBERS: EU/1/23/1750/001 AQUIPTA 10 mg tablets in blisters, in cartons of 28 tablets; EU/1/23/1750/003 AQUIPTA 60 mg tablets in blisters, in cartons of 28 tablets. MARKETING AUTHORISATION HOLDER: AbbVie Deutschland GmbH & Co. KG, Knollstrasse, 67061 Ludwigshafen, Germany. Further information is available on request from: AbbVie Limited, 14 Riverwalk, Citywest Business Campus, Dublin 24. DATE OF REVISION: October 2023. PI/1750/001.
References: 1. AQUIPTA® Summary of Product Characteristics, available at www.medicines.ie. 2. Morena-Ajona D, et al. J Clin Med. 2022;11(6):1656. 3. Ferrari MD, et al. Nat Rev Dis Primers. 2022;8(1):2.
Contents Foreword
Medical Workforce Intelligence Report published by Medical Council P4
Hospital waiting lists continue to increase P6
ICO Host Annual Conference
New Head of School of Pharmacy at RCSI P11
Updated Guidelines on elevated blood pressure and hypertension
The role of the Genetic Counsellor
School of Pharmacy AntipsychoticInduced Weight Gain Research
Editor
In one of our leading new stories, we detail how, ahead of Budget 2025, the Irish Pharmaceutical Healthcare Association (IPHA) has reiterated the importance of funding new medicines which are an integral and vital part of our healthcare system.
REGULARS
Feature: Interstitial Lung Disease P20
CPD: Non-Small Cell Lung Cancer P33
Feature: Sepsis P44
Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only. All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
It is estimated that an allocation in the order of ¤25 million in new development funding for new medicines in 2025 is required to allow patients in Ireland access to these new lifeenhancing treatments.
IPHA Chief Executive Oliver O’Connor said “We believe that there needs to be a clear policy to plan for and fund the continuous flow of life-enhancing new medicines in 2025 and over multiple years.” Turn to page 5 to read the full story.
Meanwhile, it’s not good news from the latest figures published by the National Treatment Purchase Fund (NTPF) which confirm that targets to reduce waiting lists by 6% this year are increasingly unlikely to be met, according to the Irish Hospital Consultants Association (IHCA).
The IHCA has warned that the decision to cancel essential elective surgeries, endoscopies and outpatient appointments for an indefinite period in hospitals across the Mid-West will exacerbate wait times for patients in the region and could have severe knock-on consequences for health outcomes.
IHCA President Professor Gabrielle Colleran said, “The latest waiting lists figures have confirmed what many patients in this country already knew far too well; that the Government’s Action Plans have failed to significantly reduce waiting lists, despite millions being spent on the initiatives.” You can read more about this on page 6.
In other news on page 45, we carry a full report on a qualitative study from researchers within the Pharmacy Department of St Patrick’s Mental Health Services and the School of Pharmacy in University College Cork. This has revealed the urgent need for tailored guidelines in managing antipsychotic-induced weight gain, as findings highlight the gaps between current guidelines and practices and the needs of those taking antipsychotics.
Speaking about the study, Lead Researcher and Senior Pharmacist at St Patrick’s Mental Health Services, Ita Fitzgerald said: “Findings have shown that the lack of available management guidance for antipsychotic-induced weight gain remains a challenge for clinicians, with currently endorsed approaches neither being fit-for-purpose or aligned with the experiences and needs of those prescribed antipsychotics and who experience unwanted weight gain.”
The Medical Council has published its 2023 Medical Workforce Intelligence Report.
The report presents an analysis of data on doctors who have retained their place on the Medical Council’s medical register in 2023. It focuses on the clinically active medical workforce in Ireland, presenting quantitative analysis of demographics and divisional status, and details on employment and practise such as self-reported role, medical discipline and specialty, and working hours.
The report ‘Spotlights’ several specialty cohorts, including Non-Consultant Hospital Doctors (NCHDs), General Practitioners, discipline of Medicine, Surgery, and Hospital Consultants. It highlights that a substantial proportion of doctors are close
to retirement age and working in contravention of the European Working Times Directive (EWTD).
The data analysed and presented aims to inform future workforce planning, training, and education requirements to support the delivery of timely and high-quality care to patients.
Later this year, the Medical Council will publish a second report focusing on doctors who left and also those who joined the Register in 2023.
Key Highlights
• Of the 24,794 doctors who retained their registration in 2023, 19,328(78%) selfreported that they were clinically active in Ireland, all, or some of the time in 2023. A small proportion of doctors
did not answer this question and as such this may slightly underestimate the true number.
• Half (50.2%) of clinically active doctors working in Ireland were on the Specialist Division of the Register, 16.1% were on the Trainee Specialist Division; and 33.0% were on the General Division of the Register.
• In 2023, over a quarter (26.6%) of clinically active doctors working in Ireland self-reported working more than 48 hours a week on average, and a further 32.6% self-reported working between 40 – 48 hours per week.
• 53% (10,251) of clinically active doctors in Ireland were male, and 47% (9,077) were female.
• In 2023, 8,234 doctors worked as NCHDs, with just under half
Women in Leadership
in training (48.6%), while the remainder were not in training (51.4%).
• From those NCHDs not in training, the top three countries in which doctors obtained their qualifications were Pakistan (26.7%), Ireland (22.1%), and Sudan (18.5%)
Commenting on the report, Medical Council President, Dr Suzanne Crowe said, “We’re pleased to present this report, which is the first of two reports analysing our registration data to be published this year.
“Our data highlights Ireland’s high reliance on international medical graduates (IMGs). It’s important that Ireland remains an attractive place for doctors and their families to stay and work here long-term. Our report cites research which states that lack of progression opportunities, fear of de-skilling, quality of training, excessive work hours and poor working conditions are among reasons why doctors seek to leave Ireland.
“As the National Taskforce on the NCHD Workforce has stated previously, quality training and proper induction for IMGs is essential for both patient care and for doctor wellbeing. Medical workforce shortages in Ireland highlight the need for greater support to ensure we retain doctors and incentivise them to practise medicine in Ireland.
“I would encourage all doctors on the Register to contribute to the data in this report by completing the questions posed during the registration and retention process with the Medical Council. In doing so, doctors can support planning for an effective and well-resourced medical workforce in the future”, Dr Crowe added.
The Pharmaceutical Managers’ Institute final Women in Leadership event of 2024 takes place on 16th October at Kingswood House Hotel, Dublin. They will host Averil Power, CEO with the Irish Cancer Society as the guest speaker. Averil is currently leads one of the best known patient advocacy groups in the country, having previously held the role of CEO in the Asthma Society. Prior patient advocacy, Averil was heavily involved in politics, having been employed as a political adviser by Minister Mary Hanafin in the Departments of Tourism, Social and Family Affairs and Education.
Dr Suzanne Crowe, President, Irish Medical Council
New Medicines Funding Urgency
Ahead of Budget 2025, the Irish Pharmaceutical Healthcare Association (IPHA), which represents the international research-based biopharmaceutical industry, reiterates the importance of funding new medicines which are an integral and vital part of our healthcare system.
Advances in medical development are steadily growing. To ensure that patients in Ireland can access these therapeutic advances, it is vital that a direct allocation for new medicines is provided for again in 2025 as was done in 2021, 2022, 2023 and eventually in 2024.
For 2025, IPHA members expect to make applications for reimbursement for 36 medicines which, according to most recent estimates, would benefit as many as 3,700 patients in Ireland. These medicines would improve the standard of care for patients
suffering from a number of diseases such as cancer – breast cancer, leukaemia, prostate cancer, multiple myeloma and others – Alzheimer’s, stroke, women’s health conditions, migraine, dermatitis, asthma, ulcerative colitis, type 2 diabetes and liver disease. Along with benefitting thousands of patients, these life-enhancing medicines will also positively impact the lives of their families and carers.
It is estimated that an allocation in the order of ¤25 million in new development funding for new medicines in 2025 is required to allow patients in Ireland access to these new lifeenhancing treatments.
Budget 2024 initially allocated zero funding for new medicines. Thankfully, this decision was reversed by the Government last December with ¤20 million
The PSI Launches New Website at www.psi.ie
The Pharmacy Regulator has launched a new website that can be visited at www.psi.ie As part of its extended Corporate Strategy 2021-2024, the new website supports the PSI’s commitment to engage in a broad and accessible manner with patients, the public and registrants and to communicate clearly and consistently with stakeholders that include the Department of Health, HSE, other public bodies, regulators and the media.
The new website is mobile responsive and user-friendly with improved accessibility and design. It hosts the registers for pharmacies, pharmacists, pharmaceutical assistants, and the Internet Supply List which are searchable from the homepage. The PSI’s website redevelopment project also supports its commitment as a public body to becoming a digital-first regulator. Underway at the PSI, is a digital transformation programme ‘Better Ways of Working’ that is bringing numerous benefits to the organisation and its registrants and is delivering effective and efficient digital services to members of the public, supported by well-
designed, reliable and robust technology solutions.
“Effective and clear communication and engagement with our stakeholders including the public is central to our remit as the pharmacy regulator,” said Joanne Kissane, Registrar and Chief Officer, PSI – The Pharmacy Regulator. “The new website is created on a modern scalable digital platform and the innovative approach we’ve taken will help us to build even greater awareness of our role, so that the public can be informed of the standards they can expect from pharmacists and pharmacies. As our primary communication channel, the new website will serve us well into the future as we look to support enhanced and expanded pharmacy services and pharmacy regulations in Ireland.”
The new website delivers an intuitive layout, enhanced search functionality and utilises multimedia in a seamless and engaging way. It also features imagery from pharmacies across Ireland and from within the PSI offices, which were specially commissioned to give an accurate and authentic representation of modern pharmacy services and pharmacy regulation in Ireland.
allocated for new medicines and a further ¤10 million to be made available through savings. As a consequence, by 1st July 2024, 20 new medicines – both IPHA (13) and non-IPHA (7) – have already been reimbursed by the HSE. Current data indicates that at least 700 patients and their families and carers are benefitting from 15 of those new medicines. Further positive reimbursement decisions this year should benefit several thousand patients more.
IPHA Chief Executive Oliver O’Connor said “We believe that there needs to be a clear policy to plan for and fund the continuous flow of life-enhancing new medicines in 2025 and over multiple years. Efficiencies are both possible and desirable to make the medicines spend sustainable but alone they cannot provide sufficient funding for the
uptake of new medicines. Annual new developments Exchequer funding remains a necessity.”
“IPHA member companies are actively delivering significant savings to the State on an annual basis via the Framework Agreement we agreed in 2021 and which expires in September 2025, within the Budget year now being considered. This Agreement has delivered more than ¤400m in savings in its first two years of implementation, well above the anticipated overall savings of between ¤600-¤700 million for the full four-year period. We remain ready and willing to partner with the Government to achieve certainty for clinicians and patients and to work with the HSE to bring newly-authorised medicines to the Irish healthcare system as quickly as possible.”
Hospital Waiting Lists on Course to Increase
“The IHCA believes the Government must work towards a serious reduction in waiting times for patients, aiming for a six-week maximum wait. But without addressing the very obvious shortages of hospital beds, theatres, diagnostic and other facilities, together with filling the 850 Consultant posts that are vacant or filled on a temporary basis, the Government will not address the core problems facing our public hospitals and these lengthening waiting lists.”
New figures published by the National Treatment Purchase Fund (NTPF) confirm that targets to reduce waiting lists by 6% this year are increasingly unlikely to be met, according to the Irish Hospital Consultants Association (IHCA).
The IHCA warned that the decision to cancel essential elective surgeries, endoscopies and outpatient appointments for an indefinite period in hospitals across the Mid-West will exacerbate wait times for patients in the region and could have severe knock-on consequences for health outcomes.
According to a new trend analysis carried out by the Association, more than 74,700
people could be added to the three main waiting lists this year if current trends continue – an increase of 11% compared with the start of the year.
The Department of Health and HSE had targeted a reduction of 39,300 by the end of December, which it is now almost certain to miss, with a total for the three main waiting lists potentially reaching 746,000 by year end.
Under these projections, waiting lists for outpatient appointments, inpatient and day case treatment and gastrointestinal (GI) endoscopies could potentially end the year 114,000 (18%) above the Government’s reduction targets for 2024. This projected
increase would dwarf the modest reductions in waiting lists of 4% (29,800) and 3% (18,800) achieved in 2022 and 2023 respectively, undermining what little progress was made.
The figures also show that instead of an expected reduction of around 22,900 by this point in the year, almost 40,800 additional people have been added to these three main waiting lists – a 63,700 shortfall.2 This is because demand continues to outstrip limited supply, which is impacting on the health service’s ability to deliver care.
Likewise, the outpatient waiting list has increased by 37,400 so far in 2024 to 599,458, with inpatient and day case waiting lists up by more than 2,300 (+3%) to 88,063. Adding these to the 24,670 awaiting a GI scope and the over 200,800 on a myriad of other ‘hidden lists’ for planned procedures and suspensions, brings the total NTPF waiting list figure to a record 913,000.
The Association has urged the Government to take the necessary actions to follow through on their promises to significantly increase public hospital capacity, including the opening of 3,000 additional hospital beds, surgical hubs and elective hospitals already announced by the Minister for
IHCA President, Professor Gabrielle Colleran
Health, in order to address these unacceptable waiting lists.
It also expressed concern over the HSE’s ability to hire the required admin support staff and multidisciplinary team members given that the latest pay and numbers strategy shows vacancies up to the end of 2023 have been effectively suppressed. Consultants fear that the failure to fill these posts will cause a loss of productivity and may result in patient safety issues.
Commenting on today’s waiting list figures from the NTPF, IHCA President Professor Gabrielle Colleran said, “The latest waiting lists figures have confirmed what many patients in this country already knew far too well; that the Government’s Action Plans have failed to significantly reduce waiting lists, despite millions being spent on the initiatives. In fact, it seems likely 2024 will see significant increases, in a stark reversal of the modest reductions achieved over the past two years. A radical rethink is long overdue.
“It is extremely disappointing to see the HSE in the Mid-West this week switching off services by cancelling essential elective surgeries, endoscopies and outpatient appointments for an indefinite period as the ‘solution’ to the overcrowding problems in the Emergency Department at University Hospital Limerick. This should not be the ‘go-to solution’ for management, as it only undermines our commitment to care for already vulnerable patients, increases waiting lists and may lead to poorer health outcomes. Patients in Limerick and elsewhere deserve better.
“The IHCA believes the Government must work towards a serious reduction in waiting times for patients, aiming for a six-week maximum wait. But without addressing the very obvious shortages of hospital beds, theatres, diagnostic and other facilities, together with filling the 850 Consultant posts that are vacant or filled on a temporary basis, the Government will not address the core problems facing our public hospitals and these lengthening waiting lists.”
Youth Mental Health in Crisis
New research reveals an "unprecedented" mental health crisis among young people, with calls to make the matter an “international health priority".
Intergenerational inequality, unregulated social media, insecure employment and the climate crisis are driving a global surge in mental ill health among youth, (opens in a new window)according to a new study published in The Lancet Psychiatry Journal.
Evidence suggests that in many countries, the mental health of young people has been declining over the past two decades, and changes in many societies are increasing mental ill health.
The report was released by Orygen - Australia’s Centre of Excellence in Youth Mental Health -following
years of extensive research and was developed by an international team of researchers, including (opens in a new window)Professor Barbara Dooley, Dean of Graduate Studies & Deputy Registrar at University College Dublin.
Professor Patrick McGorry, lead author of the report and Executive Director of Orygen, the new study is a “major step” towards the recognition of youth mental health as an “international health priority”.
According to the research, mental illness accounts for 45% of the overall burden of disease in individuals aged 10-24 years globally.
It also found the need for mental health support for this age bracket has risen by 50% in the last two decades.
Speaking on (opens in a new window)RTÉ Radio One’s Drivetime, Professor Dooley said there was an urgent need to address the driving factors behind the growth in mental ill health and improve mental health treatments for young people as mental illnesses have their peak onset at age 15 years.
“Some of the things we think are really important in terms of what young people are exposed to versus to past generations are a lot more complex.
“A couple of generations ago reaching adulthood physically was a key thing but now the number one issue young people are going to encounter is a mental health one.
Pat Smullen Chair in Pancreatic Cancer
Professor Grainne O’Kane has been appointed as the inaugural Pat Smullen Chair in Pancreatic Cancer at University College Dublin.
The new position aims to act as an anchor for pancreatic research in Ireland, with the ambition of creating a global centre of excellence for the treatment and research of this form of cancer, which has one of the poorest outcomes.
The new role will receive ¤900,000 over the next five years from Cancer Trials Ireland’s Pat Smullen Pancreatic Cancer Fund, and will allow Professor O’Kane to divide her time between clinical work as a treating physician at St Vincent’s University Hospital, the national surgical centre for pancreatic cancer, and research work at UCD School of Medicine.
Matching funding will be provided for the role by the HSE National Cancer Control Programme (NCCP).
“A diagnosis of pancreatic cancer can be quite devastating as its one of the most difficult cancers to treat, however we are learning more and more every day,” said Professor O’Kane.
“Research has contributed to this. This cancer has also come with two big challenges beyond
“When we look at data over 20 years ago, we can see a step change in the number of young people experiencing mental health and mental health difficulties.”
Early intervention is crucial to stymie rates of premature death, disability and lost potential, all of which have escalated over the past two decades, she added.
“We need to invest in the mental health of young people at a time when it will make an impact, so we need to think about early intervention because we do know if these difficulties persist over time, they can stay with someone throughout their entire lives. If there is intervention early on, we can change that journey… not just in Ireland, but globally we need a lot more investment."
science and medicine: People are not as aware of pancreatic cancer, compared to other cancers and despite being one of the most lethal cancers, it does not receive the same funding or attention as other cancers.”
According to the Irish Cancer Society, over 600 people are diagnosed with pancreatic cancer each year in Ireland. Unfortunately, the disease is biologically complex and challenging to treat and study.
The tumour microenvironment in pancreatic cancer creates a
particularly hostile barrier that shields the tumour, making it challenging for treatments to reach and effectively target cancer cells.
In addition, pancreatic cancer has one of the highest mortality rates among cancers due to its rapid progression and aggressive nature, with the disease often only being detected at an advanced stage.
Global developments in pancreatic research are promising according to Professor Ray McDermott, Vice Clinical Lead for Cancer Trials Ireland, who said “with the
Pat Smullen Chair in Pancreatic Cancer now in place, Ireland is in a strong position to attract trials using new agents that better target this mutation. Hopefully we will see patients benefitting from these trials soon.”
Professor Grainne O’Kane, inaugural Pat Smullen Chair in Pancreatic Cancer
Conference
ICO Host Annual Conference 2024
The Irish College of Ophthalmologists hosted their Annual Conference 2024 at the Knockranny House Hotel in Westport, Co Mayo from Wednesday 15th to Friday 17th May. Over 200 ophthalmologists gathered for the three-day scientific conference to hear the latest clinical and scientific developments in the speciality from eye experts at home and abroad.
Key symposia at this year’s conference focused on Vision and Strabismus, Orbit and Socket, and Sustainability in Ophthalmology.
Among the keynote guest speakers, the College was delighted to welcome Mr Ian Marsh, Consultant Ophthalmic Surgeon at the Liverpool University Hospital NHS Trust and Dr Arvind Chandna, Consultant Paediatric Ophthalmologist at Alder Hey Children’s Hospital, Liverpool and Senior Clinician Scientist at Smith Kettlewell Eye Research Institute, San Francisco to present at the Vision and Strabismus symposium, alongside Ms Kathryn McCreery, Consultant Ophthalmic Surgeon at Children’s Health Ireland at Crumlin Hospital.
In her talk, Ms McCreery discussed difficult paediatric ophthalmology and strabismus consultations including drop administration in children, evaluation of the child with autism and delivering bad news. The management of strabismus surgery complications
and the informed consent process in paediatric and adult strabismus surgery was also discussed, with an emphasis on effective communication with children, their parents and adults in advance of undergoing strabismus surgery.
Mr Ian Marsh currently runs a comprehensive strabismus service mainly for adults but also including more complex children squint at Liverpool University Hospital NHS Trust in Liverpool and spoke to delegates about decoding the process of strabismus management. Recent developments have included the introduction of Bupivacaine injections to permanently straighten eyes, the use of inferior medial rectus plication in near exotropia and since the Covid pandemic, a regular video clinic and a monthly local anaesthetic squint list.
Dr Arvind Chandna delivered a comprehensive talk on Cerebral Visual Impairment and a structured approach to managing the condition beyond visual acuity.
Dr Chandna conducts research programmes dealing with significant gaps in clinical and scientific knowledge of common childhood eye conditions with poor management outcomes, investigating them in collaboration with SKERI’s vision scientists. His talk outlined this investigation of visual brain neuroscience and oculomotor behaviour using eye tracking, photorefraction,
Former international rugby player, Ian McKinley, is pictured during his keynote speech ‘SCNF - Second Chances Never Forget’ at the Irish College of Ophthalmologists ‘Eye Care in Focus 2023’ Conference on Tuesday September 19, The Gibson Hotel Dublin
psychophysics and visually evoked brain potentials in childhood eye disease.
Mr Manoj Parulekar, Consultant Ophthalmic Surgeon at the Birmingham Women’s and Children’s NHS Foundation Trust and Oxford University Hospitals NHS Trust and Professor Geoffrey Rose, Consultant Orbital, Lacrimal and Plastic Reconstructive Surgeon at Moorfields Eye Hospital, London were guest speakers at the Orbit and Socket symposium. Mr Tim Fulcher, Consultant Ophthalmic Surgeon at the Mater Misericordiae University Hospital Dublin chaired and presented on the management of socket complications at this session.
Mr Parulekar outlined the clinical assessment, differential diagnosis and management of benign and malignant lesions of the paediatric orbit. He contributes to the paediatric ophthalmology service at the Birmingham Women’s and Children’s Hospital, the largest women’s and children’s hospitals in Europe, where he treats a wide range of childhood eye conditions including strabismus, paediatric cataracts and glaucoma, oculoplastics and neuro-ophthalmology, ocular oncology, and external eye diseases. He has special expertise in the treatment of eye cancers in children and is a consultant ophthalmologist to the Birmingham National Retinoblastoma Unit, the largest nationally designated retinoblastoma center in the UK. Mr Parulekar contributes to the ocular motility service (squints and complex eye movement disorders), and the neuro-ophthalmology service at the Oxford University Hospital where he provides a supra-regional service to Oxfordshire, Buckinghamshire, Berkshire and Wiltshire.
Prof Geoffrey E. Rose, Honorary Consultant Ophthalmic Surgeon, Moorfields Eye Hospital, and Senior Research Fellow of the Biomedical Research Centre at the Institute of Ophthalmology, London, gave a detailed presentation on ‘Managing the Removal of an Eye’ at the Orbit and Socket symposium. In his talk, he discussed the problems that can occur with socket management and the alternatives to eye removal, the patient consent process and challenges which can occur as a result of “over promise” by the physician. Prof Rose addressed the mechanics of eye removal and how to manage (largely by prevention) the volume deficiency that would otherwise arise from the removal of the globe.
It was a great honour for the College to invite Professor Rose to deliver the Annual Mooney Lecture at the 2024 ICO Conference, which he presented on the evening of Wednesday 15th May.
Prof Rose’s lecture entitled “Trends in rehabilitation of patients with thyroid eye disease” considered what thyroid eye disease means, in practical terms, to the patient and the mechanism of the disease in terms of the underlying inflammatory mechanism, and the biomechanics of the condition. Prof Rose outlined the historical treatment of thyroid eye disease in patients, up to the modern day advances and the changes in treatment approaches. Four decades ago, changes in treatment were largely directed to improving surgical techniques to allow a better restoration of function and appearance, with less injury to neighbouring tissues. Early immunosuppressive regimes were based on various regimes for systemic corticosteroids, either oral or intravenous (and occasionally intraorbital administration). More recently, the immune response has been mollified with monoclonal antibodies directed against the inflammatory mediators or cells and over the last 20 years, it has been shown that changes in thyroid eye disease appear to be produced through an immune activation of the TSH-receptor and IGF1-receptors.
On the final day of the conference, a dedicated symposium on Sustainability in Ophthalmology welcomed experts from both home and overseas to share their knowledge on ways to minimise the carbon footprint of the
speciality and plan for the future from both an environmental and sustainable practice perspective. Healthcare is a notable contributor to greenhouse gas emissions, accounting for an estimated 5% of total emissions globally. The ophthalmic field, like many others in healthcare, has a significant environmental footprint. From the disposal of single-use instruments to the energy consumption of diagnostic equipment, the impact is significant.
Miss Radhika Rampat, Consultant Ophthalmic Surgeon at the Royal Free London NHS Trust outlined the sustainability in the ophthalmology journey so far of the American European Congress Of Ophthalmic Surgery - Green Working Group, examining “How can I act locally and share globally”. She examined what has been achieved to date in eye clinics and theatres locally and internationally in the efforts to reduce the carbon footprint in the specialty. Miss Rampat is the co-chair of AECOS Green Working Group.
Ireland is among the major healthcare emitters per capita internationally. The ICO welcomed Dr Philip Crowley, National Director of Strategy and Research and HSE National Lead for Climate Change who spoke to delegates about the HSE Climate Action Strategy 2023-2050 being adopted to reduce emissions and protect population health in the Irish healthcare system.
The strategy is one of the first national health service climate strategies globally, and Dr Crowley outlined the progress on implementation of its target to achieve net-zero emissions for the
PIctured at the Irish College of Ophthalmologists ‘Eye Care in Focus 2023’ Conference, The Gibson Hotel, Tuesday 19 September:
(L-R) keynote speakers at the Glaucoma clinical education session Dr Robert Harper, Optometrist, Manchester Royal Eye Hospital and Honorary Professor of Optometry, School of Health Sciences, University of Manchester; Dr Margaret Morgan, Consultant Medical Ophthalmologist, CHO 7 and Royal Victoria Eye and Ear Hospital, Dublin; Ms Elaine Brennan; Clinical Nurse Specialist, Glaucoma Clinic, Beaumont Hospital Eye Department with ICO President, Mr John Doris
HSE by 2050, the relevant actions for ophthalmology practice and the work to mobilise health service staff.
Dr Emilie Mahon, RCSI Ophthalmology Clinical Tutor at the Royal Victoria Eye and Ear Hospital, outlined the findings of her research on the ecological impact of phacoemulsification cataract surgery where she examined the single-use items consumption and the results concerning the carbon footprint of cataract surgery in the Eye and Ear Hospital.
Mr Arthur Cummings, Consultant Ophthalmologist at the Wellington Eye Clinic in Dublin looked at the practice side of sustainability
in ophthalmology in light of the growing burden of ophthalmic needs building globally while the number of ophthalmologists is decreasing.
Mr Cummings highlighted the need for the specialty to become more efficient and effective while the shortage of ophthalmologists is addressed. His talk reviewed three areas that can help achieve greater efficacy and efficiency, namely system design, artificial intelligence and the role of the allied health professional team in leading to improvements in making ophthalmic practice sustainable.
Workshop sessions, paper and poster presentations and the European Society of Ophthalmology (SOE) Lecture 2024 presented by Mr Michéal O’Rourke, Royal Victoria Eye and Ear Hospital, St James’s Hospital and Children’s Health Ireland at Crumlin, Dublin on the topic of Paediatric Oculoplastics also featured on the three day conference programme.
The Barbara Knox Medal for Best Paper was awarded to Dr Shane
O’Regan for his paper entitled “Eyes on Spina Bifida: A TwoDecade Retrospective Exploration of Ophthalmic Manifestations in Paediatric Patients at Temple Street Children’s University Hospital, Dublin.”
The William Wilde Medal for Best Poster was awarded to Dr Patrick Murtagh for his poster “Uveal Melanoma Patients Treated with Iodine Plaque versus Ruthenium Plaque versus Proton Beam Radiation: A Ten-Year Review.”
Dr Murtagh was presented with his medal by Professor Brendan Kelly, Consultant Psychiatrist, Tallaght University Hospital, Dublin and Professor of Psychiatry at Trinity College Dublin who shared with the audience his insights on human behaviours and reactions to perceived challenges in his fascinating talk on “Pandemics in Ireland, and Lessons Learned from Covid (If Any)”
Prof Kelly’s recently published book ‘Resilience: Lessons from Sir William Wilde on Life After Covid’ reflects on the pandemic in Ireland and what we might learn as a society and as individuals from the experience.
Former international rugby player, Ian McKinley is pictured with Mr John Doris, President, Irish College of Ophthalmologists (ICO) and Ms Janice Brady, Consultant Ophthalmic Surgeon, University Hospital Waterford at the ICO ‘Eye Care in Focus 2023’ Conference on Tuesday September 19, The Gibson Hotel Dublin
The ICO announced the publication of its Annual Report for 2023 at the conference in Westport. The ICO is a registered Irish charity. The organisation is committed to the advancement and improvement of eye health and patient safety and works to protect, enhance and promote the highest standards in the delivery of eye care
The Annual Report 2023 outlines the activities undertaken by the College and finances for that year.
New Blood Test for Alzheimer’s Disease
Trinity researchers have examined the effectiveness of a new blood test which could change the way Alzheimer’s Disease is identified. The blood test (plasma p-tau217) detects the presence of ‘amyloid plaques’ that build up in the brain of people with Alzheimer’s Disease. In the Alzheimer’s brain, abnormal levels of this naturally occurring protein clump together to form plaques that disrupt normal cell function.
Research just published in the leading international journal Alzheimer’s Research & Therapy outlines a study undertaken in the Institute of Memory & Cognition at Tallaght University Hospital (TUH) which could change the way Alzheimer’s Disease is detected.
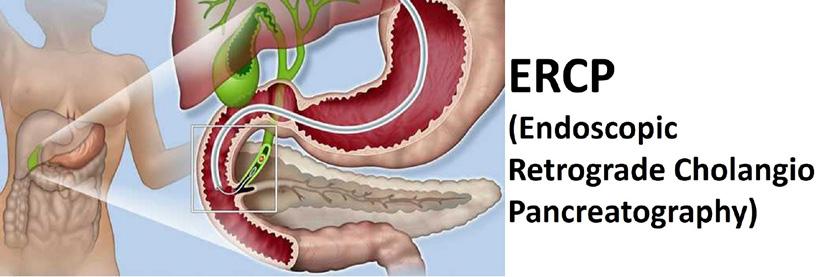
Researchers wanted to know if a simple blood test would be easier and more accurate than a lumbar puncture (spinal tap), which currently is the only method to detect amyloid plaques. The lumbar puncture is invasive,
and scans are limited in their availability. The use of blood tests has clear advantages over both of these methods being less invasive, more straightforward for patients, easier to scale up and less costly.
Using samples from the biobank at the TUH Institute of Memory and Cognition, study lead, Dr Adam Dyer, examined the performance of the new blood test. Adam is a Geriatric Medicine Trainee at Tallaght University Hospital and Medical Gerontology, Trinity College Dublin. Patients who are undergoing a diagnostic lumbar puncture for the detection of Alzheimer’s disease at TUH opt to donate cerebrospinal fluid and blood samples for future research. This is crucial in examining the performance of these new blood tests in real-world clinical cohorts.
The research examined how well the new blood test performed in detecting the same proteins (in particular “amyloid” protein) that are looked for in
cerebrospinal fluid in samples from the existing biobank
The potential for significant change in detection
Overall, the blood test was more than 90pc as accurate as the outcome from lumbar punctures. Different blood test cut-off values were then examined and it was found that if - theoretically - the blood test was used in the future, over half of lumbar punctures could be avoided.
This has significant implications in terms of invasiveness, length of time to a diagnosis and also may reduce cost. Lumbar punctures are safe and well-tolerated as diagnostic procedures, however a small number of individuals may experience side-effects such as post lumbar-puncture headache.
Commenting on the research
Dr. Dyer said, “This study found that blood tests such as plasma
p-tau217 demonstrate excellent performance to detect the changes that are characteristic of Alzheimer’s disease. In the future, clinical use of these blood tests may enable us to avoid invasive tests such as lumbar punctures in over half of individuals who currently have these procedures performed”. This research is one of a handful in the world to assess this in ‘real-world’ clinical cohorts and the first Irish study to examine the performance of these blood tests.”
Moving forward, the next step in this research is to examine if the performance of these blood tests can be matched in diagnostic laboratories. This would mean that patients referred can hopefully have a blood test in the first instance, and that those who clearly have a negative or positive result could avoiding the need for diagnostic lumbar puncture.
New Appointment at Johnson & Johnson
Johnson & Johnson Innovative Medicine has appointed Michaela Hagenhofer as General Manager of its commercial operations for Ireland. Michaela will be responsible for leading all aspects of the commercial business in Ireland, focused on driving sustainable business growth
through enhanced access to innovative therapies.
Michaela brings a wealth of experience to her new role, having previously served as Commercial Director for Specialty Care at J&J Innovative Medicine in Austria. During her tenure, she achieved
consistent business growth across key therapeutic areas including immunology, central nervous system, and cardiopulmonary therapies, driven by a customercentric approach and a commitment to talent development. She has dedicated her career to date to the pharmaceutical industry, having previously worked for Takeda, AbbVie and Merck in roles with increased responsibility across many therapy areas including haematology, oncology and gastroenterology.
Johnson & Johnson Innovative Medicine innovates with purpose to lead where medicine is going. Its ambition is to tackle the toughest health challenges, where
patient need is highest. Currently, its research and development are focused on the areas of oncology, immunology, neuroscience, cardiopulmonary and speciality ophthalmology, with a commitment to changing the standard of care including evaluation of new medicines and therapeutic interventions that are personalised for optimised clinical outcomes.
Based in Dublin, Michaela is enthusiastic about the opportunities that lie ahead. Commenting on her appointment, Michaela said, “Taking on the role of General Manager for Johnson & Johnson Innovative Medicine Commercial Operations Ireland is an exciting next chapter in my career. As a business, we are committed to leading where medicine is going, identifying the patients with the highest unmet needs and developing increasingly personalised care for specific subsets of patients. I am committed to continuing to collaborate with our talented team in Ireland to seek timely access to these innovative treatments, working in partnership with the Government, patient groups, the health service, academia and the wider industry to make a tangible difference in the lives of people, health systems and society here.”
Michaela Hagenhofer
School of Pharmacy Appoints new Head
RCSI University of Medicine and Health Sciences has announced the appointment of Professor Helena Kelly as Head of its School of Pharmacy and Biomolecular Sciences.
Professor Kelly succeeds Professor Tracy Robson who was recently appointed Deputy Vice-Chancellor for Academic Affairs at the University. She will lead the School of Pharmacy and Biomolecular Sciences in its ambition to be recognised internationally as a leading centre for pharmacy education, research and innovation.
Professor Kelly’s research focusses on the use of delivery platforms in translational research applications. She has been a Principal Investigator and deputy co-ordinator in two EU consortia, where she led on the formulation of hydrogel delivery platforms for minimally invasive delivery clinical applications. She is the inventor of ChemoGel, a novel patented thermoresponsive hydrogel platform for intratumoral drug delivery, the development of which has been funded through the Enterprise Ireland Commercialisation Fund. In 2023, this technology was spun out into a company ‘OncoLize’ of which Professor Kelly is a co-founder and which is seeking to translate this technology platform to the clinic.
She has been closely involved in RCSI's growing collaboration
Professor Helena Kelly RCSI
with Soochow University in China and has been involved in Erasmus+ exchange programmes and Government of Ireland mobility programmes with Soochow University.
Accepting her role as Head of School, Professor Helena Kelly said: “My vision for the School of Pharmacy and Biomolecular Sciences is for it to evolve into a larger, more successful and more international School while maintaining the outstanding student experience and high quality of programme delivery for which we are known. In a very
competitive environment, I will lead the School in identifying and attracting new student cohorts and in recruiting and retaining the highest calibre of staff”.
“I look forward working with my colleagues in the School to further enhance the impact of our research which spans across the translational spectrum from drug discovery and delivery, through to population health and healthcare education research, reflecting RCSI’s strategic goal of innovating for a healthier future, along with our commitment to the UN Sustainable Development Goals”.
The RCSI School of Pharmacy and Biomolecular Sciences is focused on delivering world-class, patient-centred and fully integrated teaching and research. In recent years, the School secured ¤11.3 million in educational funding, including a significant award (¤7.8 million) from the Higher Education Authority under the Human Capital Initiative, Pillar 3. The School has also significantly grown student numbers on RCSI’s flagship MPharm programme (from a year 1 intake of 66 students in 2019 to a year 1 intake of 92 students in 2023; growing to 125 in September 2024).
Greater Progression needed for Pharmacy
Greater progression across the pharmacy profession is needed in order to address challenges such as inequitable healthcare access, medicines shortages, antimicrobial resistance, and substandard and falsified medicines, Mr Paul Sinclair, president of the International Pharmaceutical Federation (FIP), said today in his opening address at FIP’s 82nd World Congress of Pharmacy and Pharmaceutical Sciences.
Mr Sinclair also highlighted a need for innovation in pharmacy to address public health challenges and disparities, citing pharmacybased vaccination as an example of an innovative approach that has had high impact. He said:
“Innovation is not just beneficial — it’s essential. Innovating pharmacy enhances patient care, improves therapeutic outcomes, addresses the dynamic challenges of health care, and propels the profession forward.”
The FIP president said that the application of three principles — integrity, performance and passion — would help facilitate the advancement of the profession. He explained:
• “Integrity in our actions will help grow our reputation as accessible and reliable experts in medicines and as healthcare professionals, and will reinforce collaborations.”
• “Advancement of our profession to its full capability requires performance. This means consistently demonstrating expertise, commitment and ethical conduct in professional activities. It means applying best practices.”
• “Our passion as pharmaceutical scientists, pharmacy educators and practitioners drives our advocacy work to expand our scopes of practice and to deliver the best possible health outcomes for our communities.”
Mr Sinclair said that FIP’s passion for pharmacy had led it to create its “Think Health, Think Pharmacy” campaign to
advance the profession, and urged pharmacists from around the world to support it. “Through this campaign, we’re raising awareness of the importance of pharmacies, and of pharmacists themselves, as an underutilised resource in the primary healthcare space, with the potential to deliver more for healthcare systems. . . . We want everyone to think about pharmacy when they think about their health. We want policymakers to think about universal pharmacy coverage when they think about universal health coverage. Promoting our professional identity will facilitate more pharmacy services with benefits for our communities,” he said.
A LIFE IN MOTION
BEGINS WITH LESS MIGRAINE TM
Maintain a life in motion with only 4 injection days per year *1
• Flexible quarterly and monthly dosing1
• Rapid† and long-acting‡ efficacy1,2
• Safety profile comparable to placebo3,4
To find out more, get in touch with an AJOVY® representative
AJOVY® is indicated for prophylaxis of migraine in adults who have at least 4 migraine days per month1
*Based on the quarterly dosing regimen1 †In Phase III pivotal studies, fewer migraine days were seen with AJOVY® vs placebo as early as Week 1 (p<0.0001)1 ‡Long-acting defined as efficacy over 12 months and is based on data for patients treated with AJOVY® in the HALO extension study (n=1,890)2
Please refer to the Summary of Product Characteristics (SmPC) for full details of Prescribing Information.
Ajovy® (fremanezumab) 225mg Solution for Injection in Pre-filled syringe and Ajovy® (fremanezumab) 225mg Solution for Injection in Pre-filled Pen Abbreviated Prescribing Information. Presentation: Fremanezumab 225mg solution for injection in pre-filled syringe. Fremanezumab 225mg solution for injection in pre-filled pen. Indications: For prophylaxis of migraine in adults who have at least 4 migraine days per month. Dosage and administration: The treatment should be initiated by a physician experienced in the diagnosis and treatment of migraine. Ajovy is for subcutaneous injection only and can be injected into areas of the abdomen, thigh, or upper arm that are not tender, bruised, red, or indurated. For multiple injections, injection sites should be alternated. Patients may self-inject if instructed in subcutaneous self-injection technique by a healthcare professional. Adults: Two dosing options are available: Monthly dosing: 225mg once monthly. Quarterly dosing: 675mg every three months. When switching dosing regimens, the first dose of the new regimen should be administered on the next scheduled dosing date of the prior regimen. The treatment benefit should be assessed within 3 months after initiation of treatment. Evaluation of the need to continue treatment is recommended regularly thereafter. Missed dose: The indicated dose
should resume as soon as possible, a double dose must not be administered to make up for a missed dose. Children: No data are available. Elderly: Limited data available. Based on the results of population pharmacokinetic analysis, no dose adjustment is required. Renal impairment: No dose adjustment is required. No data in severe renal impairment. Hepatic impairment: No dose adjustment is required. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Precautions and warnings: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Anaphylactic reactions have been reported rarely with fremanezumab. Most reactions have occurred within 24 hours of administration although some reactions have been delayed. Patients should be warned about the symptoms associated with hypersensitivity reactions. If a serious hypersensitivity reaction occurs, initiate appropriate therapy and do not continue treatment with fremanezumab. No safety data are available in patients with certain major cardiovascular diseases. Interactions: No formal clinical drug interaction studies have been performed. Pregnancy and lactation: It is preferable to avoid the use of Ajovy during pregnancy as a precautionary measure. A risk to the breast-fed child cannot be excluded. A decision must be made whether to continue Ajovy therapy while breast-feeding. Effects on ability to
drive and use machines: No influence on the ability to drive and use machines. Adverse reactions: Anaphylactic reaction, hypersensitivity reactions such as rash, pruritus, urticaria and swelling. Very Common: Injection site pain, injection site induration and injection site erythema. Common: Injection site pruritus. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: It is recommended that the patient be monitored for any signs or symptoms of adverse effects and given appropriate symptomatic treatment if necessary. Legal category: POM. Marketing Authorisation Number: EU/1/19/1358/001004. Marketing Authorisation Holder: Teva GmbH, Graf-Arco-Str. 3, 89079 Ulm, Germany. Job Code: MED-IE-00076. Date of Preparation: November 2023.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
References:
1. AJOVY® Summary of Product Characteristics. Teva Pharmaceuticals Ireland. 2. Goadsby PJ et al. Neurology 2020; 95(18): e2487–e2499. 3. Dodick DW et al. JAMA 2018; 319(19): 1999–2008. 4. Silberstein SD et al. N Engl J Med 2017; 377(22): 2113–2122.
Migraine Care in Ireland
Over a billion people live with migraine worldwide, across all cultures, world regions and socioeconomic statuses, including over 700,000 in Ireland based on the current population. It is the 2nd leading cause of disability worldwide and accounts for more disability than any other neurological disorder, according to the Lancet Burden of Disease Study 2016.1 Migraine and other headache disorders are estimated by WHO to be the second leading cause of years lived with disability worldwide, the first for women under fifty years of age.2 A migraine attack is considered to be one of the most disabling experiences that a human being can have.3
It is believed that only a small percentage of individuals living with headache disorders ever come forward to receive care, making it largely a silent and invisible illness. Patients who live with headache disorders are recognised as being a heavily stigmatised and misunderstood group, perhaps the most stigmatised patient group of all (Shapiro et at 2024,4 Migraine has historically been chronically under researched, underfunded, misunderstood, minimised and dismissed across broader society, within healthcare and within patients themselves through internalised stigma. Stigmatisation itself is recognised as a driver in the chronic underfunding and under researching of headache care. The experience of stigma has been shown to play a significant role in the exacerbation of chronic pain.5
Thankfully, there is something of a culture shift in migraine care. More research into and awareness of the condition and its manifestations alongside newly developed treatments are hopefully improving the quality of life of the many who live with the daily, often unnoticed challenges of the condition. This article hopes to explore how impactful changes can be made within the healthcare setting.
What is Migraine?
Migraine is understood now to be a disorder of nerve activity in the brain. When an attack is triggered, it causes a wide range of different symptoms and disabling experiences to the individual. Migraine is classified into episodic and chronic migraine, depending on the number of days per month a person experiences migraine symptoms. Typically, a migraine
attack lasts 4-72 hrs untreated and manifests with symptoms such as a one-sided pulsating headache of moderate to severe intensity, aggravated or causing avoidance of physical activity, nausea, vomiting, photophobia and phonophobia. (ICHD3, 6). It is a highly individualised condition however with an extremely broad range of other symptoms and manifestations, however. There are many subtypes with individual features. Some subtypes include migraine with aura, vestibular migraine, hemiplegic migraine, retinal migraine, menstrual migraine. It is helpful to be aware of other types of primary headache conditions, including New Daily Persistent Headache, Cluster Headache and Tension-Type Headache. These are conditions experienced by individuals with whom we regularly interact at Migraine Ireland.
People who live with a headache disorder are at risk of developing complex complications such as secondary headache condition known as Medication Overuse Headache. Correct, informed management of headache conditions is essential to protect patients.
Migraine Burden
The burden of disability that comes with living with migraine is often not fully understood by society. Individuals can live with highly debilitating, pain, focal disturbances, nausea and vomiting, aphasia, dizziness, mobility issues and much more, depending on their diagnosis. Hemiplegic migraine for example can cause temporary paralysis of the face and limbs on one side of the body. In some cases, more commonly in the older populations, migraine symptoms can present without headache at all. Symptoms that are often overlooked yet carry significant quality of life issues include the pre and postdrome stages, where following an attack patients can be left for days with lingering symptoms such as exhaustion and brain fog. There is also what is known as inter-ictal burden of headache. This is the burden of living with the fear of the next attack. This burden can significantly impact a person’s quality of life, decision making and ability to live independently and interact with society.
Migraine is often described as an invisible or hidden disability. Many living with this condition live lives punctuated by stigma,
Written by Naomi Thornton, Migraine Association of Ireland
misunderstanding and silent suffering. Much of this stems from societal legacy issues, for example, migraine has had an historic association as disease of women. This association has had a heavy hand in the chronic stigmatisation of the condition, and all that stems from this stigma. It is well documented that societal pressures on men have obstructed men from coming forward for help early in relation to their health concerns overall. This can put men at risk of developing more complex and severe manifestations of headache conditions before they come forward for help, which often require more complicated treatment and management.
Individuals living with migraine are at increased risk of social isolation and misunderstanding and discrimination in the workplace or at school or college. The largely invisible nature of the condition and its symptoms, coupled with fact that the term “migraine” is generally synonymous in daily society, with a bad headache attack, has caused many to manage the condition silently, alone and misunderstood, managing a silent burden that is even at times, unbeknownst to themselves. Individuals living with migraine are at risk of the socioeconomic dangers that come with disability. Building the awareness needed through education at all levels, healthcare practitioner - patient interactions, within healthcare itself and across broader public, societal and cultural spheres is paramount.
Migraine Care In Ireland
The patient who is concerned about headache symptoms, usually starts their journey by visiting their GP Practice or Emergency Department. Migraine can, and is often, managed at Primary Care level, often a specialist referral is needed too. Community pharmacists are crucial resources for migraine management in the community.
In recent years, migraine and headache care in Ireland has significantly improved. There are now several specialist headache clinics in the Dublin area, clinics in Cork and Galway, Limerick and more. There are a growing number of Consultant Neurologist Headache Specialists, Clinical Nurse Specialists and Psychologists providing specialist headache care within the hospital settings. Sometimes these clinics aren’t well known. Contacting your neurology department a finding out what resources are available within your clinical setting could prove a valuable resource to patients and to staff members.
Diagnosis can be lengthy, and usually involves a detailed history and patient diary keeping. Treatment depends on the history, diagnosis and circumstances of the patient, there are a range of acute and preventative treatments, including advanced treatments. Patient support with lifestyle management, understanding of their condition and how it manifests, and getting to understand “triggers” are all part of the process. Specialist physiotherapy, cognitive
Migraine
behavioural therapy, acupuncture are also recognised as supportive options for migraine care.
When Migraine Is Diagnosed
Often times a patient receives their diagnosis of migraine in hospital. Patients may have presented with what can be frightening symptoms. A series of investigations is carried to determine the cause and rule out life threatening conditions before the diagnoses is given. Understandably, there can be some initial relief experienced by both the patient themselves and their healthcare team, once more sinister or acutely threatening causes of their symptoms have been ruled out.
At Migraine Ireland, we frequently receive calls from patients who have been newly diagnosed with migraine after being hospitalised with their symptoms. Patients are often left reeling from a rollercoaster journey from hospital. Having for perhaps the first time experienced the scary and debilitating symptoms of migraine, the fear and trauma of having gone through the process of ruling out life threatening conditions, followed then perhaps by initial feelings of surprise and relief from receiving a diagnosis of migraine, only to be then faced with the gravity of being diagnosed with a complex, debilitating neurological condition, can be extremely confusing and hard to process the
meaning of the experience and new diagnosis for many reasons.
Healthcare professionals are in an optimum position to significantly impact patient’s quality of life and outcome, and ability to cope. Providing education at this crucial stage can have a long-lasting positive effect. Resourcing patients in understanding, and preparing to manage their condition once discharged, empowers patients and makes a meaningful impact on a person’s ability to cope and quality of life, both of which have been shown to improve patient outcomes, and reduce the impact of symptoms.
Some examples of patient education could include, but are not limited to
- building an understanding of migraine as a condition within the patient
- explaining terms and developing understanding of terms such as episodic and chronic migraine
- the patient’s particular migraine condition and what this may mean for them, for example migraine without/ with aura, hemiplegic migraine, vestibular migraine.
- Skill building, such as informed diary keeping, lifestyle and trigger knowledge in a sense that empowers the patient.
- Navigation and signposting for multi-disciplinary follow up care
- Establishing the importance of GP and community pharmacy relationships
- Awareness of risks that the migraine community may face on their journey such as stigmatisation, social isolation, workplace challenges and supports that are available, such as Migraine Ireland, Disability Federation of Ireland, HSE Living Well Course, Social Prescribing.
Hopes For the Future
With greater awareness, understanding and knowledge, there is hope that the quality of life and disease burden of individuals living with migraine can be improved. Thankfully, in many cases, the condition is treatable when managed effectively. Healthcare professionals, both in the hospital setting and elsewhere are placed within a unique opportunity to make long lasting meaningful impacts into the lives of many who are often overlooked. We at Migraine Ireland wish to thank you profoundly for your interest in this patient cohort and remain at your disposal for any support whatsoever that we can provide.
References
1. Global Burden of Disease Study 2016 (GBD 2016) Data Resources | GHDx (healthdata.org)
2. Vos T, Allen C, Arora M. Global regional and national incidence prevalence and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–602.
3. Silver, Nick (2018) Migraine - a comprehensive guide (thewaltoncentre.nhs.uk)
4. Shapiro et al 2024 MigraineRelated Stigma and Its Relationship to Disability, Interictal Burden, and Quality of Life | Neurology
5. Parikh et al Stigma and Migraine: Developing Effective Interventions | Current Pain and Headache Reports (springer.com)
6. 1. Migraine - ICHD-3
7. Hämel et al How do nurses support chronically ill clients’ participation and self-management in primary care? A cross-country qualitative study | BMC Primary Care | Full Text (biomedcentral.com)
8. Benkel et al Living with a chronic disease: A quantitative study of the views of patients with a chronic disease on the change in their life situation - Inger Benkel, Maria Arnby, Ulla Molander, 2020 (sagepub.com)
A LIFE IN MOTION
BEGINS WITH LESS MIGRAINE TM
Maintain a life in motion with only 4 injection days per year *1
• Flexible quarterly and monthly dosing1
• Rapid† and long-acting‡ efficacy1,2
• Safety profile comparable to placebo3,4
To find out more, get in touch with an AJOVY® representative
AJOVY® is indicated for prophylaxis of migraine in adults who have at least 4 migraine days per month1
*Based on the quarterly dosing regimen1 †In Phase III pivotal studies, fewer migraine days were seen with AJOVY® vs placebo as early as Week 1 (p<0.0001)1 ‡Long-acting defined as efficacy over 12 months and is based on data for patients treated with AJOVY® in the HALO extension study (n=1,890)2
Please refer to the Summary of Product Characteristics (SmPC) for full details of Prescribing Information.
Ajovy® (fremanezumab) 225mg Solution for Injection in Pre-filled syringe and Ajovy® (fremanezumab) 225mg Solution for Injection in Pre-filled Pen Abbreviated Prescribing Information. Presentation: Fremanezumab 225mg solution for injection in pre-filled syringe. Fremanezumab 225mg solution for injection in pre-filled pen. Indications: For prophylaxis of migraine in adults who have at least 4 migraine days per month. Dosage and administration: The treatment should be initiated by a physician experienced in the diagnosis and treatment of migraine. Ajovy is for subcutaneous injection only and can be injected into areas of the abdomen, thigh, or upper arm that are not tender, bruised, red, or indurated. For multiple injections, injection sites should be alternated. Patients may self-inject if instructed in subcutaneous self-injection technique by a healthcare professional. Adults: Two dosing options are available: Monthly dosing: 225mg once monthly. Quarterly dosing: 675mg every three months. When switching dosing regimens, the first dose of the new regimen should be administered on the next scheduled dosing date of the prior regimen. The treatment benefit should be assessed within 3 months after initiation of treatment. Evaluation of the need to continue treatment is recommended regularly thereafter. Missed dose: The indicated dose
should resume as soon as possible, a double dose must not be administered to make up for a missed dose. Children: No data are available. Elderly: Limited data available. Based on the results of population pharmacokinetic analysis, no dose adjustment is required. Renal impairment: No dose adjustment is required. No data in severe renal impairment. Hepatic impairment: No dose adjustment is required. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Precautions and warnings: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Anaphylactic reactions have been reported rarely with fremanezumab. Most reactions have occurred within 24 hours of administration although some reactions have been delayed. Patients should be warned about the symptoms associated with hypersensitivity reactions. If a serious hypersensitivity reaction occurs, initiate appropriate therapy and do not continue treatment with fremanezumab. No safety data are available in patients with certain major cardiovascular diseases. Interactions: No formal clinical drug interaction studies have been performed. Pregnancy and lactation: It is preferable to avoid the use of Ajovy during pregnancy as a precautionary measure. A risk to the breast-fed child cannot be excluded. A decision must be made whether to continue Ajovy therapy while breast-feeding. Effects on ability to
drive and use machines: No influence on the ability to drive and use machines. Adverse reactions: Anaphylactic reaction, hypersensitivity reactions such as rash, pruritus, urticaria and swelling. Very Common: Injection site pain, injection site induration and injection site erythema. Common: Injection site pruritus. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: It is recommended that the patient be monitored for any signs or symptoms of adverse effects and given appropriate symptomatic treatment if necessary. Legal category: POM. Marketing Authorisation Number: EU/1/19/1358/001004. Marketing Authorisation Holder: Teva GmbH, Graf-Arco-Str. 3, 89079 Ulm, Germany. Job Code: MED-IE-00076. Date of Preparation: November 2023.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
References:
1. AJOVY® Summary of Product Characteristics. Teva Pharmaceuticals Ireland. 2. Goadsby PJ et al. Neurology 2020; 95(18): e2487–e2499. 3. Dodick DW et al. JAMA 2018; 319(19): 1999–2008. 4. Silberstein SD et al. N Engl J Med 2017; 377(22): 2113–2122.
Supporting Women to Love Their Hearts
September is Irish Heart Month, and this year the focus is on ‘Her Heart Matters’ – A campaign highlighting the importance of women’s heart health, particularly in midlife.
Community pharmacy is at the ‘heart’ of women’s health and there is a plethora of support and advice pharmacy teams can give. Already helping millions of women every day, pharmacies have a unique role to play during this important campaign.
In recent years, there has been a welcome focus in the national conversation around women’s health issues, be it reproductive health, menopause, or cancer screening. However, there has been a glaring gap. One in four women dies from heart disease and stroke each year – the same as men and, incredibly, six times more than die from breast cancer. That’s over 4,000 mothers, daughters and sisters each year in Ireland. There is a false belief that cardiovascular disease (CVD) is a man’s disease but there are many female-specific factors that affect a woman’s risk, including menopause and hypertensive disorders of pregnancy. However, the good news is that 80% of premature heart disease and stroke is preventable through healthy lifestyles.
But too many women aren’t aware of these facts and many health professionals are also missing these important messages.
According to the Lancet Women and Cardiovascular Disease Commission, heart disease and stroke in women has been under-researched, underdiagnosed and under-treated.
• under-researched (women have been left out of clinical trials)
• under-diagnosed (women often present with more unusual signs of CVD and can receive an incorrect diagnosis. Rather than the classic version of a heart attack where someone is seen clutching their chest, the symptoms of a heart attack in women can be quite vague making it hard to diagnose. They can include nausea, tiredness, shortness of breath, back pain or tightness in the jaw rather than the more familiar scenario of a crushing pain in the chest that shoots down one arm).
• under-treated (women can be under-treated or treatment can be delayed if they are under-diagnosed. Many treatments are made for men and not adequately researched in women).
There are a number of advice points pharmacy teams can employ to help women take better care of their heart health.
Mindset
Getting into the right frame of mind is essential for change. Women need to feel ready and have clear, powerful reasons for making a change. As part of the Her Heart Matters campaign, the Irish Heart Foundation has created a free Self-Care and Wellbeing Journal to support women to reflect on their lifestyle habits and prepare for meaningful change.
Stress
While stress is a normal part of life, it can be negative when it starts to impact day to day tasks. Many women are juggling multiple demands, and this can be particularly challenging during menopause. Advise them to try to keep a regular sleep routine, be physically active and stay connected to friends and family. If they are struggling, they should contact their GP.
Physical Activity
Regular physical activity is one of the greatest tools for preventing heart disease and stroke as well as helping to reduce some menopause symptoms. Getting at least 150 minutes a week of moderate-intensity activity is recommended for good health. This can be broken down into three 10 minute sessions. They should try to add muscle-strengthening exercises too.
Nourishing your Heart
Research shows that a Mediterranean-style diet can help to reduce heart disease and stroke and help manage menopause symptoms. Like the Irish Food Pyramid, a Mediterranean-style
diet is based around fruit and vegetables, whole grains, beans and other pulses, nuts, and seeds. It includes some olive oil, fish, seafood, and poultry, and is low in sugar, salt, processed foods, and red meat.
Start the Conversation
Be part of the movement of women and men who want to see change and protect all women from one of Ireland’s biggest killers. Talk with your sisters, mothers, daughters, and friends, share the campaign with them, and empower them to make changes.
What can women do?
Diet can play a major role in modifying the risk for CVD, women should focus on what they can add to their diets to make it more heart healthy.
One of the most important things is to focus on following a consistent healthy dietary pattern, one in line with the Mediterranean style of eating. This contains protein sources mainly from plants, nuts, fish, or alternative sources of omega-3 fatty acids; fat mostly from unsaturated plant sources; carbohydrates primarily from whole grains; at least five to seven servings of fruits and vegetables per day; and moderate dairy consumption.
Omega-3 fatty acids are polyunsaturated fats that are beneficial for heart health. Eicosapentaenoic acid (EPA), docosahexaenoic acids (DHA) and alpha-linolenic acid (ALA) are the three main omega-3 fats. As a group, omega-3’s lower blood triglyceride levels, slow the growth of plaque in arteries and have a slight effect on lowering blood pressure. EPA and DHA are found mainly in oily fish and should be consumed once or twice per week. ALA needs to be converted
from ALA to EPA and DHA, but this happens at very slow rates, which means ALA food sources like flaxseed, olive oil, walnuts and avocado need to be consumed daily. Women who completely avoid these food sources or have raised triglyceride levels may benefit from omega-3 supplements with EPA and DHA, 200 to 500mg a day of combined EPA and DHA.
Saturated fats coming from fatty meats, butter, lard, palm oil and coconut oil, as well as cakes, biscuits, pies and pastries need to be reduced to prevent the elevation of LDL levels, which promote plaque build-up in the arteries. Ideally less than 10% of total daily calories should come from saturated fat.
The Role of CoQ10
CoQ10, also known as coenzyme Q10, is a naturally occurring nutrient found in every cell of our bodies. It’s a vital component of our cellular machinery, playing a key role in the production of energy. This compound is synthesised within our cells’ powerhouses, the mitochondria, where it aids in the creation of adenosine triphosphate (ATP), the primary energy source for our cells. CoQ10, a vitamin-like compound, has been linked to potential benefits for heart health. It’s been studied for its potential to improve conditions such as heart failure, atherosclerosis, and coronary artery disease. The high energy requirements of cardiac cells make them particularly susceptible to low levels of CoQ10, which is where supplementation may come into play.
Research suggests that CoQ10 may support heart health by reducing oxidative stress, a factor that can contribute to heart disease. It’s also been found to potentially aid recovery after heart attacks, easing symptoms of heart failure, and helping to regulate blood pressure.
GO BEYOND LOWERING LDL-C
ADD ON TO REDUCE CV RISK
When statins* and ezetimibe are not enough, add on once daily oral Bempedoic Acid earlier, to help your patients go even further.1,2Δ
* Concomitant use with simvastatin >40 mg daily is contraindicated; please refer to the relevant SmPC for more information.1,2
Δ NILEMDO® and NUSTENDI® are indicated in adults with established, or at high risk for, ASCVD to reduce CV risk by lowering LDL-C levels, as an adjunct to correction of other risk factors, who are on maximally-tolerated statins, or statin-intolerant, or statin-contraindicated with or without ezetimibe or not adequately controlled with ezetimibe treatment.1,2
▼These medicinal products are subject to additional monitoring. This will allow quick identification of new safety information. Refer to Summary of Product Characteristics (SmPC) prior to prescribing.
Presentation: Each Nilemdo film-coated tablet contains 180 mg bempedoic acid. Each Nustendi filmcoated tablet contains 180 mg of bempedoic acid and 10 mg of ezetimibe. Indications: Hypercholesterolaemia and mixed dyslipidaemia: Nilemdo/Nustendi are indicated in adults with primary hypercholesterolaemia (heterozygous familial and non-familial) or mixed dyslipidaemia as an adjunct to diet: In combination with a statin (Nilemdo: or statin with other lipid-lowering therapies) in patients unable to reach LDL-C goals with the maximum tolerated dose of a statin; alone or in combination with other lipid-lowering therapies in patients who are statin-intolerant, or for whom a statin is contraindicated (Nustendi: and are unable to reach LDL-C goals with ezetimibe alone). Cardiovascular disease: In adults with established or at high risk for atherosclerotic cardiovascular disease to reduce cardiovascular risk by lowering LDL-C levels, as an adjunct to correction of other risk factors: in patients on a maximum tolerated dose of a statin and not adequately controlled with additional ezetimibe or, in patients who are either statin-intolerant, or for whom a statin is contraindicated (Nustendi in patients already being treated with the combination of bempedoic acid and ezetimibe as separate tablets with or without statin.) Posology and method of administration: The recommended dose is one tablet of 180 mg Nilemdo or 180 mg/10 mg Nustendi taken once daily, with or without food. Tablet should be swallowed whole. Concomitant simvastatin therapy: When Nilemdo/Nustendi are co-administered with simvastatin, simvastatin dose should be limited to 20 mg daily (or 40 mg daily for patients with severe hypercholesterolaemia and high risk for cardiovascular complications, who have not achieved their treatment goals on lower doses and when the benefits are expected to outweigh the potential risks). Coadministration with bile acid sequestrants: Dosing of Nustendi should occur either at least 2 hours before or at least 4 hours after administration of a bile acid sequestrant. Patients with renal impairment: No dose adjustment is necessary when Nilemdo/Nustendi is administered in patients with mild or moderate renal impairment. Additional monitoring for adverse reactions may be warranted in patients with severe renal impairment and patients with end-stage renal disease (ESRD) on dialysis when Nustendi is administered. Patients with hepatic impairment: No dose adjustment is necessary when Nilemdo/Nustendi is administered in patients with mild hepatic impairment (Child-Pugh A). Treatment with Nustendi is not recommended in patients with moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic impairment due to the unknown effects of the increased exposure to ezetimibe. Contraindications: Hypersensitivity to the active substance or any of the excipients (see SmPC); pregnancy; breast-feeding; concomitant use with simvastatin > 40 mg daily. When Nustendi is co-administered with statin in patients with active liver disease or unexplained persistent elevations in serum transaminases; when Nustendi is co-administered with a statin, consult the SmPC for that particular statin therapy. Warnings and precautions: Potential risk of myopathy with concomitant statins: Bempedoic acid increases plasma concentrations of statins. Patients receiving Nilemdo and a statin should be monitored for adverse reactions that are associated with high doses of statins. Statins occasionally cause myopathy. In rare cases, myopathy may take the form of rhabdomyolysis with or without acute renal failure secondary to myoglobinuria and can lead to fatality. In post marketing experience with ezetimibe, very rare cases of myopathy and rhabdomyolysis were reported. Most patients who developed rhabdomyolysis were taking a statin with ezetimibe. Patients receiving Nilemdo/Nustendi and a statin should be advised of the potential increased risk of myopathy and told to report promptly any unexplained muscle pain, tenderness, or weakness. If such symptoms occur, a lower maximum dose of the same statin or an alternative statin, or discontinuation of Nilemdo/Nustendi and initiation of an alternative lipid-lowering therapy should be considered under close monitoring of lipid levels and adverse reactions. If myopathy is confirmed by creatine phosphokinase (CPK) > 10× upper limit of normal (ULN), immediately discontinue Nilemdo/ Nustendi and any statin. Doses of simvastatin > 40 mg should not be used with Nilemdo/Nustendi. Increased serum uric acid: Bempedoic acid may raise serum uric acid due to inhibition of renal tubular OAT2 and may cause or exacerbate hyperuricaemia and precipitate gout in
patients with history of gout or predisposed to gout. Discontinue Nilemdo/Nustendi if hyperuricaemia accompanied with symptoms of gout appear. Elevated liver enzymes: Liver function tests should be performed at initiation of therapy. Discontinue Nilemdo/Nustendi if increase in transaminases > 3× ULN persists. Renal impairment: Additional monitoring for adverse reactions may be warranted in patients with severe renal impairment (eGFR < 30 mL/min/1.73 m2) or patients with ESRD on dialysis. Hepatic impairment: Periodic liver function tests should be considered for patients with severe hepatic impairment (Child-Pugh C) taking Nilemdo. Nustendi is not recommended in moderate to severe hepatic impairment (Child-Pugh B and C) due to unknown effects of increased exposure to ezetimibe. Fibrates: If cholelithiasis is suspected in a patient receiving Nustendi and fenofibrate, gallbladder investigations are indicated, and therapy should be discontinued. Ciclosporin: Caution when initiating Nustendi in the setting of ciclosporin. Ciclosporin concentrations should be monitored. Anticoagulants: Appropriately monitor INR if Nustendi is added to warfarin, other coumarin anticoagulants, or fluindione. Contraception: Women of childbearing potential must use effective contraception during treatment. Patients should be advised to stop Nilemdo/ Nustendi before stopping contraceptive measures if planning to become pregnant. Excipients: Patients with rare hereditary problems of galactose intolerance, total lactase deficiency, or glucose-galactose malabsorption should not take Nilemdo/Nustendi as it contains lactose. Patients at high risk of cardiovascular disease: Evidence for the use of the fixed combination medicinal product of bempedoic acid with ezetimibe in patients at high risk of cardiovascular disease is only available for the lipid-lowering effect in absence of any cardiovascular risk reduction estimation for ezetimibe in primary prevention patients. Driving and use of machines: Nustendi has minor influence on ability to drive and use machines. Dizziness has been reported. Interaction with other medicinal products: Refer to SmPC for full information on interactions. Adverse reactions: Nilemdo: Common (≥ 1/100 to < 1/10): Glomerular filtration rate decreased, anaemia, gout, hyperuricaemia (includes blood uric acid increased), AST increased, pain in extremity. Uncommon (≥ 1/1,000 to < 1/100): weight decreased, haemoglobin decreased, ALT increased, liver function test increased, blood creatinine increased, blood urea increased, Consult Nilemdo SmPC in relation to other adverse reactions. Nustendi: Common (≥ 1/100 to < 1/10): Glomerular filtration rate decreased, anaemia, decreased haemoglobin, hyperuricaemia (includes uric acid increased), decreased appetite, dizziness, headache, hypertension, cough, constipation diarrhoea, abdominal pain, nausea, dry mouth, flatulence, gastritis, liver function test increased (includes liver function test abnormal), back pain, muscle spasms, myalgia, pain in extremity, arthralgia, blood creatinine increased, fatigue, asthenia, gout, AST increased (for bempedoic acid), blood CPK increased. Uncommon (≥ 1/1,000 to < 1/100): weight decreased, ALT increased, blood urea increased, hot flush, dyspepsia, gastrooesophageal reflux disease, AST increased (for ezetimibe), GGT increased, pruritus (with statin), neck pain, muscular weakness (with statin), chest pain, pain, oedema peripheral (with statin). Frequency not known: Thrombocytopaenia, hypersensitivity (including rash, urticaria, anaphylaxis, angio-oedema), depression, paraesthesia (with statin), dyspnoea, pancreatitis, hepatitis, cholelithiasis, cholecystitis, erythema multiform, myopathy / rhabdomyolysis. Consult Nustendi SmPC in relation to other adverse reactions. Legal Classification: POM. Package quantity, marketing authorisation (MA) number: Nilemdo 28 tablets: EU/1/20/1425/002. Nustendi 28 tablets: EU/1/20/1424/002. MA Holder: Daiichi Sankyo Europe GmbH, Zielstattstrasse 48, 81379 Munich, Germany. Further information available on request from Daiichi Sankyo Ireland Ltd. D09 YF97. Telephone: (01) 489 3000. Fax: (01) 489 3033. Email: medinfo@daiichi-sankyo.ie Date of Preparation: May 2024 JOB ID: IE/BIL/05/24/0004
▼ These medicinal products are subject to additional monitoring. This will allow quick identification of new safety information. Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events or a product complaint about a Daiichi Sankyo medicine can also be directly reported to Daiichi Sankyo Ireland Ltd. D09 YF97 by telephone: +353 (1) 4893000
New Implant to Power Healing
A research team at RCSI University of Medicine and Health Sciences has developed a new implant that conveys electrical signals and may have the potential to encourage nerve cell (neuron) repair after spinal cord injury.
Details of the implant and how it performs in lab experiments have just been published in the Journal Materials Today
“To date, it has been extremely difficult to promote the regrowth of neurons after spinal cord injury which is a major obstacle in the development of successful treatments for such debilitating injuries,” explains Professor Fergal O’Brien, Deputy Vice Chancellor for Research and Innovation, Professor of Bioengineering and Regenerative Medicine at RCSI and Head of RCSI’s Tissue Engineering Research
Group (TERG). “Our research here represents a promising new approach which may have potential for the treatment of spinal cord injuries.”
Spinal cord injury is a devastating and often paralysing condition. One person suffers a spinal cord injury every week in Ireland, and there are over 2,300 individuals and families living with spinal cord injury across Ireland. After injury, the long axonal projections of nerve cells are cut and 'die-back' from the injury site, and at the same time a lesion or gap forms at the wound site that prevents their regrowth necessary to restore function.
To address this complex problem, the research team at RCSI’s TERG and the SFI Advanced Materials and Bioengineering Research (AMBER) Centre at Trinity College
Professor Fergal O’Brien, Deputy Vice Chancelllor for Research and Innovation and Professor of Bioengineering and Regenerative Medicine at RCSI and Head of RCSI’s Tissue Engineering Research Group (TERG)
Dublin developed an implantable, electroconductive 3D-printed scaffold that can be placed directly into the injury site, bridging the gap.
Professor O’Brien, who is also Deputy Director of AMBER sees the implant as a new approach “Bridging the lesion with an electroconductive biomaterial designed to mimic the structure of the spinal cord, combined with the application of electrical stimulation, may help injured neurons regrow their axons and reconnect to restore function,” he said, adding that, “No such platform exists to date.”
Promising results
When electrical stimulation is applied to the implant, it can convey that electrical signal to boost the regrowth of the injured axons. At the same time, the scaffolding and channels of the implant are designed to act as a bridge and direct the axons to grow back in the correct formation.
When the researchers put the implant to the test in the lab, they saw promising results.
¤180m Hole in Cancer Funding
The Irish Cancer Society has launched it's Budget 2025 Submission, urging the Government to stop underfunding the National Cancer Strategy. This call for investment in the National Cancer Strategy is supported by the two main representative bodies for cancer doctors in Ireland, the Irish Society of Medical Oncologists (ISMO) and the Irish Society of Radiation Oncologists (ISRO).
According to the HSE, the National Cancer Control Programme’s
annual budget for implementation of the National Cancer Strategy should have increased incrementally over the past 8 years to be ¤110m higher in 2024 than in 2016. The actual incremental increase has only been ¤65m. As a result, the cumulative loss of investment in cancer services from 2017 to 2024 is almost ¤180m.
Due to this underfunding:
• screening has not been expanded as planned;
• target waiting times for cancer are not being met;
• cancer surgeries are frequently delayed;
• investment in infrastructure is lacking;
• radiotherapy services are operating below capacity;
• clinical trials are falling far short of target; and
• access to new medicines is much slower in Ireland than in other European countries.
“We could see that when we applied electrical stimulation for a week to neurons growing on this scaffold, they developed long healthy extensions called neurites. In the body, this kind of growth would be a key step towards repair and recovery after an injury,” said Liam Leahy, first author of the study and a PhD candidate at RCSI.
Guiding the research
The RCSI and AMBER researchers teamed up with the Irish Rugby Football Union Charitable Trust (IRFU-CT) on the project and brought together a spinal cord injury advisory group to oversee and guide the research. That group included clinicians, individuals living with spinal cord injury and Public and Patient Involvement (PPI) researchers.
“This advisory group provided valuable insight into the realities of spinal cord injuries and potential treatment strategies,” says Leahy. Through regular meetings as well as laboratory visits, the advisory group helped guide the work from its inception to the current publication and led to two separate publications on the role of Public and Patient Involvement in preclinical research.”
The implant project was supported by the Irish Rugby Football Union Charitable Trust, the Science Foundation Ireland Advanced Materials and Bioengineering Research (AMBER) Centre, the Irish Research Council and the research findings were recently presented at the TERMIS World Congress in Seattle, Washington, USA.
CEO, Averil Power said, “In the latest year for which comparable data is available, Ireland’s cancer mortality rate was the third highest in Western Europe. Ireland is a leader in many areas. We should not be a laggard in cancer care.
"Budget 2025 must prioritise the National Cancer Strategy, with ringfenced new recurrent development funding for the National Cancer Control Programme of at least ¤20 million.”
New Hypertension Guidelines
The European Society of Cardiology (ESC) has released updated guidelines on the management of elevated blood pressure and hypertension to better identify people at risk of heart attack and stroke.
The new guidelines include a new category of Elevated Blood Pressure, more ambitious and intensive treatment targets, and, for the first time, recommendations on the use of renal denervation to treat various forms of hypertension.
The guidelines have been produced by an international panel of experts, including co-chairpersons, Professor Bill McEvoy of University of Galway, and Professor Rhian Touyz of McGill University, Canada.
This is the first time that an Irish academic has led a major European clinical practice guideline on the treatment of elevated blood pressure and hypertension, which has potential implications for more than 700 million Europeans.
Professor McEvoy is also first author on the principal results paper for the INTERASPIRE research study which is being published in the European Heart Journal and coincides with the ESC Congress in London today, Friday August 30th, the world’s largest gathering of cardiovascular professionals.
In the INTERASPIRE global study, 61% of participants with heart disease did not have their blood pressure controlled.
Professor McEvoy’s dual roles as co-Chair of the ESC Guidelines and co-principal investigator on INTERASPIRE are closely connected. His work in the creation of the guidelines establishes evidence-based care standards, while his leadership in INTERASPIRE provides realworld data on blood pressure management in coronary disease patients worldwide and his work on this study bridges the gap between ideal clinical practices and actual global outcomes.
Key takeaways from the updated ESC guidelines on hypertension:
• A new systolic blood pressure (BP) treatment target range of 120-129 mmHg for most patients receiving BP lowering medication.
By placing the emphasis on an intensive treatment target as the first step in managing most patients, and only opting out of this
target in select circumstances or when treatment is not tolerated by the patient, these 2024 guidelines represent a paradigm shift from previous European guidelines. The guidelines also provide pragmatic recommendations to pursue a BP that is ‘as low as reasonably achievable’ in patients who are unable to tolerate or who opt out of the intensive treatment target.
• The definition of hypertension remains BP ≥140/90 mmHg, however, the guidelines introduce a new category of 'Elevated Blood Pressure' which is defined as a BP 120-139/7089 mmHg. More patients at risk of heart attack and stroke will be identified by the new category.
• The new 'Elevated Blood Pressure' category is introduced to facilitate consideration of more intensive blood pressure treatment targets among people at increased risk for cardiovascular disease.
• The updated guidelines introduce recommendations for new lifestyle options to help lower BP, such as new guidance on exercise and potassium supplementation.
• For the first time the ESC Hypertension Guidelines provide recommendations of the use of renal denervation to treat hypertension.
Elevated blood pressure and hypertension are by far the most common and important risk factors for heart attack and stroke (otherwise known as cardiovascular disease). As many as 45% of European adults have hypertension.
The new 2024 ESC Guidelines are designed to get more patients to an evidence-based blood pressure treatment target and to increase the eligibility for blood pressure lowering medications to match the best current evidence from clinical trials.
They also provide numerous pragmatic recommendations to avoid patients becoming symptomatic from overtreatment.
Professor McEvoy, Professor of Preventive Cardiology at University of Galway and Medical and Research Director of NIPC, said, “The new category of Elevated Blood Pressure recognises that people do not go from normal BP to hypertensive overnight.
“It is in most cases a steady gradient of change, and different subgroups of patients - for
Professor Bill McEvoy, University of Galway. Credit: Aengus McMahon
example those at a higher risk of developing cardiovascular disease such as people living with diabetes - could benefit from more intensive treatment before their blood pressure reaches the traditional threshold of hypertension.”
Professor Rhian Touyz of McGill University, Canada, added, “The risks associated with increased blood pressure, start at systolic blood pressure levels even below 120 mmHg.”
In another major change, the 2024 ESC Guidelines introduce a new systolic BP treatment target range of 120-129 mmHg for most patients receiving BPlowering medication, with the important proviso that the new target requires that treatment is well tolerated. The 2024 ESC Guidelines also provide pragmatic recommendations on a systolic BP target 'as low as reasonably achievable' (known as the ALARA principle) in frail and older people and in those not tolerating the primary treatment target of 120129 mmHg. The guidelines focus more on ‘frailty’ of individuals rather than chronological age.
Professor McEvoy said: “This change is driven by new trial evidence confirming that more intensive BP treatment targets reduce CVD outcomes across a broad spectrum of eligible patients.”
This new systolic BP treatment target of 120-129 represents a paradigm shift from prior European guidelines, including the 2018 ESC/ESH Hypertension guidelines, the 2021 ESC Prevention Guidelines, and the 2023 ESH Hypertension guidelines.
Specifically, whereas prior guidelines generally recommended patients be treated to a BP <140/90 mmHg in the first instance and only thereafter be considered for treatment to <130/80 mmHg (a 2-step approach) the new 2024 guidelines recommend that most patients be treated to a systolic BP of 120-129 mmHg in the first instance (those who cannot tolerate this target can have it relaxed).
In part to accommodate this new more intensive systolic blood pressure treatment target range, the 2024 ESC Guidelines provide stronger recommendations than prior guidelines for the use of out-of-office blood pressure measurements (including
ambulatory BP monitors and validated home BP monitors).
The 2024 Guidelines also, for the first time, make recommendations on the use of renal denervation for treatment of hypertension. Due to lack of evidence regarding cardiovascular outcomes benefit, the guidelines do not recommend this medical procedure as first line treatment, and nor is it recommended for patients with highly impaired renal function, (eGFR <40 mL/min/1.73 m2) or secondary causes of hypertension. On renal denervation, the guidelines say: “To reduce BP, and if performed at a mediumto-high volume centre, catheterbased renal denervation may be considered for patients with resistant hypertension who have BP that is uncontrolled despite a three BP-lowering drug combination (including a thiazide or thiazide-like diuretic), and who express a preference to undergo renal denervation after a shared risk-benefit discussion and multidisciplinary assessment.”
Professor Touyz explained, “These evidence-based recommendations provide guidance for clinicians and their patients on the use of this important new technology. However, it must be stressed that this procedure needs to be undertaken in a centre where there is expertise and experience.”
The ESC Guidelines also update dietary advice on sodium and potassium intake and further emphasise the importance of lifestyle modifications for patients in a range of different circumstances and stages of CVD and chronic kidney disease.
The Guidelines also highlight the importance of sex and gender differences in hypertension and integrate this throughout the document, rather than as a separate section, as in most other guidelines.
Lung Disease
Interstitial Lung Disease – An update from the Irish Lung Fibrosis Association
Then…
A fascinating set of photographs in the British Museum’s Egyptology section describes how tissue from ancient mummies were studied with modern microscopic and analytical techniques. Lung tissue from one mummy showed histological evidence of lung fibrosis providing evidence that this condition has been around since ancient times, yet only in relatively recent times has research and investment in the study of lung fibrosis experienced exceptional growth.
And now…
Lung fibrosis, also known as Interstitial lung diseases (ILD), is an umbrella term for a heterogenous group over 200 types of lung diseases characterised by the process of abnormal tissue repair with resultant disruption and destruction of the lung architecture by scar tissue formation (fibrosis). The most prevalent ILD is idiopathic pulmonary fibrosis (IPF) – a diagnosis of exclusion when all other known ILDs have been ruled out. IPF is a severe, progressive lung disease characterised by breathlessness, hypoxemia, dry and non-productive cough, fatigue, and ultimately respiratory failure. Lung fibrosis is a devastating diagnosis that causes significant physical, mental, and financial burden to patients and their caregivers.1 Psychological distress can develop when lung fibrosis impacts on patients’ abilities to engage in normal activities of daily living and the associated deterioration in quality of life.
Written by Nicola Cassidy, Director of the Irish Lung Fibrosis Association
ILD is thought to affect around 5,000 patients in Ireland. This figure is extrapolated from international prevalence data as the lack of a disease registry means there are no direct data currently collected in Ireland. This omission will have significant implications for planning and service delivery for the healthcare system going forward as the incidence and prevalence of lung fibrosis are likely to rise with an ageing population. The median survival time from diagnosis is 3-5 years which is worse than many cancers, yet awareness of this serious, life-limiting condition is poor among healthcare professionals and the public.
The cause and pathogenesis of ILD is poorly understood but there has been remarkable progress in our understanding of the disease pathogenesis and treatment options over the last 10-15 years. Risk factors include male gender, aged >60 years, previous history of smoking, connective tissue disease, occupational exposure to dusts, mould, birds and other organic matter, industrial agents, radiation. Exposure to certain medications including nitrofurantoin and amiodarone may be significant in certain cases. Familial lung fibrosis is a well-recognised entity, and inherited genes likely influence the risk of developing ILD in up to 20% of individuals.2
During the Covid-19 pandemic, ILD patients were deemed to be extremely medically vulnerable because of their underlying respiratory health and were prioritised for vaccination.
International studies revealed the stark fact that 50% of lung fibrosis patients admitted to hospital with Covid-19 died.3 Given the pulmonary complications associated with severe covid-19 infection, it was expected that an increase in ILD cases might emerge due to the pandemic. Early data in a recent study has suggested an increased incidence but longitudinal data is needed to understand the emerging impact.4
Diagnosing ILD can be difficult with many patients experiencing long delays as the symptoms are quite non-specific. Many patients are initially misdiagnosed with more common respiratory conditions such as Chronic Obstructive Pulmonary Disease (COPD) and asthma, and congestive cardiac failure (CCF). A thorough medical history should be conducted considering the presenting symptoms, timeline of symptom onset and nature of progression, comorbidities, occupational history, hobbies and pastimes, family medical history, and current and past medical therapies. On physical examination the presence of signs like finger clubbing and crackles on chest examination are significant. General Practitioners should have a high index of suspicion and include ILD on the list of differential diagnoses in patients presenting with worsening respiratory symptoms despite antibiotic therapy, recurrent pneumonia, and chronic unresolving, nonproductive cough. In the first incidence investigations like chest X-Ray and possibly CT Thorax and pulmonary function tests should be requested. Patients with abnormal finding or a worrisome or unexplained presentation should be referred to a respiratory consultant for further assessment. In cases of suspected ILD this would ideally be to an ILD Specialist Centre.
A specialist review will include a high-resolution CT scan of the thorax-this is a key study in the diagnosis of all ILDs. Pulmonary function tests are used to quantify any physiological abnormalities in the size or function of the lungs. Blood tests including a full biochemistry panel with immunological and rheumatological profiles are also needed.
An accurate and timely diagnosis requires a multidisciplinary team approach involving radiologists and respiratory
clinicians supported by pathologists, rheumatologists, and cardiothoracic surgeons. There is no cure for lung fibrosis, but anti-fibrotic medications (Nintedanib and Pirfenidone) have been shown to slow the rate of disease progression. A significant percentage of patients may not tolerate these due to side effects or other contra-indications. Hence continued research and drug development in this area is crucial. Lung transplantation can provide longer term survival for some individuals, but it is available only to a small number of patients who meet strict health criteria. Supportive therapies including pulmonary rehabilitation and targeted exercise are key components of the treatment for all patients with ILD and ideally should be universally available. Similarly, access to supplemental oxygen therapy is important for certain patients. Respiratory clinical nurse specialists, palliative care professionals and allied healthcare professionals particularly physiotherapists, dietitians, social workers play an essential role in supporting patients but there is evidence that ILD patients frequently have poor access to these healthcare professionals.5
The Irish Lung Fibrosis Association (ILFA) is a patient organisation founded in 2002 to support individuals with lung fibrosis and their families, and to promote research and education in lung fibrosis. Over the years, ILFA has experienced an exceptional increase in demand for our support services, advocacy activities, and educational opportunities. ILFA is firmly established as a leading lung fibrosis patient organisation in the national and international respiratory community and was a founding member of the European Union Pulmonary Fibrosis Federation (EUPFF).
The National Patient Charter for Idiopathic Pulmonary Fibrosis was developed by ILFA in collaboration with key stakeholders in 2015 to ensure that lung fibrosis patients have
1. Early and accurate diagnosis with multi-disciplinary team input.
2. Clear and concise information about PF in plain language.
3. Access to appropriate medicines and oxygen therapy.
4. Early referral to pulmonary rehabilitation and exercise programmes.
5. Early referral to the National Lung Transplant Unit for lung transplant assessment, with a minimal emphasis on age.
6. Access to social, practical and emotional supports.6
Today, unfortunately, the vast majority of ILD patients are still forced to fight a battle on two fronts – against the progression of their disease, and against an inequitable ‘healthcare system’ that denies them access to the care they need. Equitable healthcare as was envisioned in Sláintecare for ILD patients can only be realised through the establishment of a Clinical Care Programme. While ILFA works toward this goal, there are interim priorities that ILFA have requested the Irish Government fund. These priorities include access to pulmonary rehabilitation, tax rebates to offset increased electricity costs, the establishment of an ILD patient registry, and resourcing the Clinical Care Pathway.
September is Pulmonary Fibrosis Awareness Month, an international global campaign that aims to raise awareness of lung fibrosis. In Europe, the campaign is led by the EUPFF in association with its member organisations including ILFA. The theme for the 2024 campaign is “Oxygen is a fundamental human right”. This theme aligns with ILFA’s work ensuring that patients must be spared financial hardship and having to make agonising health choices if they cannot afford to purchase and run oxygen via electricity due to high costs. We want all patients to receive supplemental oxygen for free under the Drug Payment Scheme eliminating the cumbersome payment and reimbursement system currently in operation. Patients should also be entitled to an automatic tax rebate on their electricity costs. ILFA is also working with other patient organisations to ensure that the new home oxygen contracted introduced by the HSE Community
Funded Schemes, Service Improvement Programme is efficient, fit for purpose, and patient centred. Oxygen is lifepreserving and patients requiring supplemental oxygen should have the right to breathe easier.
If you are involved in the care of ILD patients, please refer them to the Irish Lung Fibrosis Association where they can access information, resources, and peer support through our network. www.ilfa.ie
References
1. Impact of pulmonary fibrosis on the lives of patients and carers in Ireland in 2022. Nicola Cassidy, Daniel Sheahan, Gemma O'Dowd, Lindsay Brown, Colin Edwards, Katherine O'Reilly. European Respiratory Journal 2023, 62 (suppl 67).
2. The Genetic Landscape of Familial Pulmonary Fibrosis. Qi Liu, Yuan Zhou Joy D. Cogan, Daphne B. Mitchell et al. Am J
Respir Crit Care Med 2023, Vol 207, Iss 10, pp 1345–1357.
3. Drake TM, Docherty AB, Harrison EM et al. Outcome of Hospitalization for COVID-19 in Patients with Interstitial Lung Disease. An International Multicenter Study. Am J Respir Crit Care Med. 2020, 202(12):1656-1665.
4. Post-COVID-19 pulmonary fibrosis: An ongoing concern. Nuha Nasser Alrajhi. Ann Thorac Med. 2023, 18(4): 173–181.
5. Access to Specialist and Multidisciplinary Healthcare for Pulmonary Fibrosis. N. Cassidy N, Sheahan D, Fox L, Brown L, Galvin L, Cassidy E, O’Dowd G, O’Reilly KMA. Ir Med J;2022; 115 (9):672.
6. The National Patient Charter for Idiopathic Pulmonary Fibrosis (2015). https://ilfa.ie/ wp-content/uploads/2021/10/ ILFA_CharterBooklet_lores-1.pdf
Treatment of Acute Coronary Syndrome1
2.5 mg
Product subject to medical prescription which may not be renewed (A)
fondaparinux sodium
The Only Selective & Synthetic Factor Xa Inhibitor Injectable Anticoagulant Licensed for Use in Adults1
Reference: 1. Arixtra® 2.5 mg/0.5 ml solution for injection, pre-filled syringe. Summary of Product Characteristics (SmPC). Available at: www.medicines.ie. Last accessed: August 2024.
ABBREVIATED PRESCRIBING INFORMATION
Arixtra (fondaparinux sodium) 2.5 mg/0.5 ml solution for injection, pre-filled syringe
Please refer to Summary of Product Characteristics (SmPC) before prescribing Indications, Dosage and Administration:
Indications:
Prevention of Venous Thromboembolic Events (VTE) in adults undergoing major orthopaedic surgery of the lower limbs such as hip fracture, major knee surgery or hip replacement surgery. Prevention of Venous Thromboembolic Events (VTE) in adults undergoing abdominal surgery who are judged to be at high risk of thromboembolic complications, such as patients undergoing abdominal cancer surgery. Prevention of Venous Thromboembolic Events (VTE) in adult medical patients who are judged to be at high risk for VTE and who are immobilised due to acute illness such as cardiac insu ciency and/or acute respiratory disorders, and/or acute infectious or inflammatory disease.
Treatment of unstable angina or non-ST segment elevation myocardial infarction (UA/NSTEMI) in adults for whom urgent (<120 mins) invasive management (PCI) is not indicated. Treatment of ST segment elevation myocardial infarction (STEMI) in adults who are managed with thrombolytics or who initially are to receive no other form of reperfusion therapy. Treatment of adults with acute symptomatic spontaneous superficial-vein thrombosis of the lower limbs without concomitant deep-vein thrombosis.
Dosage
Patients undergoing major orthopaedic or abdominal surgery: The recommended dose of fondaparinux is 2.5 mg once daily administered post-operatively by subcutaneous injection. The initial dose should be given 6 hours following surgical closure provided that haemostasis has been established. Treatment should be continued until the risk of venous thromboembolism has diminished, usually until the patient is ambulant, at least 5 to 9 days after surgery.
Medical patients who are at high risk for thromboembolic complications based on an individual risk assessment: The recommended dose of fondaparinux is 2.5 mg once daily administered by subcutaneous injection. A treatment duration of 6-14 days has been clinically studied in medical patients.
Treatment of unstable angina/non-ST segment elevation myocardial infarction (UA/NSTEMI): The recommended dose of fondaparinux is 2.5 mg once daily, administered by subcutaneous injection. Treatment should be initiated as soon as possible following diagnosis and continued for up to a maximum of 8 days or until hospital discharge if that occurs earlier. If a patient is to undergo percutaneous coronary intervention (PCI), unfractionated heparin (UFH) as per standard practice should be administered during PCI, taking into account the
patient’s potential risk of bleeding, including the time since the last dose of fondaparinux, the timing of restarting subcutaneous fondaparinux after sheath removal should be based on clinical judgment. In the pivotal UA/NSTEMI clinical trial, treatment with fondaparinux was restarted no earlier than 2 hours after sheath removal.
Treatment of ST segment elevation myocardial infarction (STEMI): The recommended dose of fondaparinux is 2.5 mg once daily. The first dose of fondaparinux is administered intravenously and subsequent doses are administered by subcutaneous injection. Treatment should be initiated as soon as possible following diagnosis and continued for up to a maximum of 8 days or until hospital discharge if that occurs earlier. If a patient is to undergo non-primary PCI, unfractionated heparin (UFH) as per standard practice should be administered during PCI, taking into account the patient’s potential risk of bleeding, including the time since the last dose of fondaparinux. The timing of restarting subcutaneous fondaparinux after sheath removal should be based on clinical judgment. In the pivotal STEMI clinical trial, treatment with fondaparinux was restarted no earlier than 3 hours after sheath removal.
Patients who are to undergo coronary artery bypass graft (CABG) surgery: In STEMI or UA/NSTEMI patients who are to undergo coronary artery bypass graft (CABG) surgery, fondaparinux where possible, should not be given during the 24 hours before surgery and may be restarted 48 hours post-operatively.
Treatment of superficial-vein thrombosis: The recommended dose of fondaparinux is 2.5 mg once daily, administered by subcutaneous injection. Patients eligible for fondaparinux 2.5 mg treatment should have acute, symptomatic, isolated, spontaneous superficial-vein thrombosis of the lower limbs, at least 5 cm long and documented by ultrasonographic investigation or other objective methods. Treatment should be initiated as soon as possible following diagnosis and after exclusion of concomitant DVT or superficial-vein thrombosis within 3 cm from the sapheno-femoral junction. Treatment should be continued for a minimum of 30 days and up to a maximum of 45 days in patients at high risk of thromboembolic complications. Patients could be recommended to self-inject the product when they are judged willing and able to do so. Physicians should provide clear instructions for self-injection. Patients who are to undergo surgery or other invasive procedures: In superficial vein thrombosis patients who are to undergo surgery or other invasive procedures, fondaparinux, where possible, should not be given during the 24 hours before surgery. Fondaparinux may be restarted at least 6 hours post-operatively provided haemostasis has been achieved.
Special populations: Prevention of VTE following Surgery: In patients undergoing surgery, timing of the first fondaparinux injection requires strict adherence in patients ≥75 years, and/or with body weight <50 kg and/or with renal impairment with creatinine clearance ranging between 20 to 50 ml/min. The first fondaparinux administration should be given not earlier than 6 hours following surgical closure. The injection should not be given unless haemostasis has been established.
Renal impairment:
Prophylaxis of VTE - Fondaparinux should not be used in patients with creatinine clearance <20 ml/min. The dose should be reduced to 1.5 mg once daily in patients with creatinine clearance in the range of 20 to 50 ml/min. No dosage reduction is required for patients with mild renal impairment (creatinine clearance >50 ml/min). Treatment of UA/NSTEMI and STEMI - Fondaparinux should not be used in patients with creatinine clearance <20 ml/min. No dosage reduction is required for patients with creatinine clearance >20 ml/min.
Treatment of superficial-vein thrombosis - Fondaparinux should not be used in patients with creatinine clearance <20 ml/min. The dose should be reduced to 1.5 mg once daily in patients with creatinine clearance in the range of 20 to 50 ml/min. No dosage reduction is required for patients with mild renal impairment (creatinine clearance >50 ml/min).
Hepatic impairment:
Prevention of VTE and Treatment of UA/NSTEMI and STEMI - No dosing adjustment is necessary in patients with either mild or moderate hepatic impairment. In patients with severe hepatic impairment, fondaparinux should be used with care as this patient group has not been studied. Treatment of superficial-vein thrombosis - The safety and e cacy of fondaparinux in patients with severe hepatic impairment has not been studied, therefore fondaparinux is not recommended for use in these patients.
Paediatric population - Fondaparinux is not recommended for use in children below 17 years of age due to a lack of data on safety and e cacy.
Low body weight: Prevention of VTE and Treatment of UA/NSTEMI and STEMIPatients with body weight <50 kg are at increased risk of bleeding. Elimination of fondaparinux decreases with weight. Fondaparinux should be used with caution in these patients. Treatment of superficial-vein thrombosis - The safety and e cacy of fondaparinux in patients with body weight less than 50 kg has not been studied, therefore fondaparinux is not recommended for use in these patients.
Administration
Subcutaneous administration: Fondaparinux is administered by deep subcutaneous injection while the patient is lying down. Sites of administration should alternate between the left and the right anterolateral and left and right posterolateral abdominal wall. To avoid the loss of medicinal product when using the pre-filled syringe do not expel the air bubble from the syringe before the injection. The whole length of the needle should be inserted perpendicularly into a skin fold held between the thumb and the forefinger; the skin fold should be held throughout the injection.
Intravenous administration (first dose in patients with STEMI only) Intravenous administration should be through an existing intravenous line either directly or using a small volume (25 or 50 ml) 0.9% saline minibag. To avoid the loss of medicinal product when using the pre-filled syringe do not expel the air bubble from the syringe before the injection. The intravenous tubing should be well flushed with saline after injection to ensure that all of the medicinal product is administered. If administered via a minibag, the infusion should be given over 1 to 2 minutes.
Presentation: Solution for injection
Contraindications:
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1.
Active clinically significant bleeding.
Acute bacterial endocarditis.
Severe renal impairment defined by creatinine clearance < 20 ml/min.
Warnings and precautions:
Fondaparinux is intended for subcutaneous use only. Do not administer intramuscularly.
There is limited experience from treatment with fondaparinux in haemodynamically unstable patients and no experience in patients requiring thrombolysis, embolectomy or insertion of a vena cava filter.
Haemorrhage: Fondaparinux should be used with caution in patients who have an increased risk of haemorrhage, such as those with congenital or acquired bleeding disorders (e.g. platelet count <50,000/mm3), active ulcerative gastrointestinal disease and recent intracranial haemorrhage or shortly after brain, spinal or ophthalmic surgery and in special patient groups. As for other anticoagulants, fondaparinux should be used with caution in patients who have undergone recent surgery (<3 days) and only once surgical haemostasis has been established.
(For prevention of VTE) Agents that may enhance the risk of haemorrhage should not be administered concomitantly with fondaparinux. These agents include desirudin, fibrinolytic agents, GP IIb/IIIa receptor antagonists, heparin, heparinoids, or Low Molecular Weight Heparin (LMWH). When required, concomitant therapy with vitamin K antagonist should be administered. Other antiplatelet medicinal products (acetylsalicylic acid, dipyridamole, sulfinpyrazone, ticlopidine or clopidogrel), and NSAIDs should be used with caution. If co-administration is essential, close monitoring is necessary.
For treatment of UA/NSTEMI, STEMI and superficial-vein thrombosis: Fondaparinux should be used with caution in patients who are being treated concomitantly with other agents that increase the risk of haemorrhage (such as GPIIb/IIIa inhibitors or thrombolytics).
PCI and risk of guiding catheter thrombus: In STEMI patients undergoing primary PCI, the use of fondaparinux prior to and during PCI is not recommended. Similarly, in UA/NSTEMI patients with life threatening conditions that require urgent revascularisation, the use of fondaparinux prior to and during PCI is not recommended. These are patients with refractory or recurrent angina associated with dynamic ST deviation, heart failure, life-threatening arrhythmias or haemodynamic instability.
In UA/NSTEMI and STEMI patients undergoing non-primary PCI: the use of fondaparinux as the sole anticoagulant during PCI is not recommended due to an increased risk of guiding catheter thrombus. Therefore adjunctive UFH should be used during non-primary PCI according to standard practice.
Patients with superficial-vein thrombosis: Presence of superficial-vein thrombosis greater than 3 cm from the sapheno-femoral junction should be confirmed and concomitant DVT should be excluded by compression ultrasound or objective methods prior to initiating treatment of fondaparinux.
anaesthesia or spinal puncture. The risk of these rare events may be higher with post-operative use of indwelling epidural catheters or the concomitant use of other medicinal products a ecting haemostasis.
Spinal/Epidural anaesthesia:
In patients undergoing major orthopaedic surgery, epidural or spinal haematomas that may result in long-term or permanent paralysis cannot be excluded with the concurrent use of fondaparinux and spinal/epidural
Elderly patients: The elderly population is at increased risk of bleeding. As renal function is generally decreasing with age, elderly patients may show reduced elimination and increased exposure of fondaparinux. Fondaparinux should be used with caution in elderly patients.
Low body weight: Prevention of VTE and Treatment of UA/NSTEMI and STEMI - Patients with body weight <50 kg are at increased risk of bleeding. Fondaparinux should be used with caution at a daily dose of 5 mg in this population. Elimination of fondaparinux decreases with weight. Fondaparinux should be used with caution in these patients.
Treatment of superficial-vein thrombosis - Fondaparinux is not recommended for treatment of superficial-vein thrombosis in patients with body weight less than 50 kg.
Renal impairment: Fondaparinux is known to be mainly excreted by the kidney. Prophylaxis of VTE - Patients with creatinine clearance <50 ml/min are at increased risk of bleeding and VTE and should be treated with caution. For the treatment of UA/NSTEMI and STEMI- there are limited clinical data available on the use of fondaparinux 2.5 mg once daily in patients with creatinine between 20 and 30 ml/min. Therefore, the physician should determine if the benefit of treatment outweighs the risk. For treatment of superficial-vein thrombosis - Fondaparinux should not be used in patients with creatinine clearance <20 ml/min. The dose should be reduced to 1.5 mg once daily in patients with creatinine clearance in the range of 20 to 50 ml/min.
Severe hepatic impairment: Prevention of VTE and Treatment of UA/NSTEMI and STEMI - Dosing adjustment of fondaparinux is not necessary. However, the use of fondaparinux should be considered with caution because of an increased risk of bleeding due to a deficiency of coagulation factors in patients with severe hepatic impairment.
Treatment of superficial-vein thrombosis - Fondaparinux is not recommended for the treatment of superficial-vein thrombosis in these patients.
Heparin Induced Thrombocytopenia: Fondaparinux should be used with caution in patients with a history of HIT.
Latex Allergy: The needle shield of the pre-filled syringe may contain dry natural latex rubber that has the potential to cause allergic reactions in latex sensitive individuals.
Interactions with other medicinal products and other forms of interaction: Bleeding risk is increased with concomitant administration of fondaparinux and agents that may enhance the risk of haemorrhage. In clinical studies performed with fondaparinux, oral anticoagulants (warfarin) did not interact with the pharmacokinetics of fondaparinux; at the 10 mg dose used in the interaction studies, fondaparinux did not influence the anticoagulation monitoring (INR) activity of warfarin. Platelet inhibitors (acetylsalicylic acid), NSAIDs (piroxicam) and digoxin did not interact with the pharmacokinetics of fondaparinux. At the 10 mg dose used in the interaction studies, fondaparinux did not influence the bleeding time under acetylsalicylic acid or piroxicam treatment, nor the pharmacokinetics of digoxin at steady state.
If follow-up treatment is to be initiated with heparin or LMWH, the first injection should, as a general rule, be given one day after the last fondaparinux injection. If follow up treatment with a Vitamin K antagonist is required, treatment with fondaparinux should be continued until the target INR value has been reached.
Fertility, pregnancy and lactation:
Pregnancy: No clinical data on exposed pregnancies are available. Animal studies are insu cient with respect to e ects on pregnancy, embryo/foetal development, parturition and postnatal development because of limited exposure. Fondaparinux should not be prescribed to pregnant women unless clearly necessary.
Breast-feeding: Fondaparinux is excreted in rat milk but it is not known whether fondaparinux is excreted in human milk. Breast-feeding is not recommended during treatment with fondaparinux. Oral absorption by the child is however unlikely.
Fertility: There are no data available on the e ect of fondaparinux on human fertility. Animal studies do not show any e ect on fertility.
Undesirable effects:
Serious adverse reactions reported with fondaparinux are bleeding complications (various sites including rare cases of intracranial/intracerebral and retroperitoneal bleedings). Fondaparinux should be used with caution in patients who have an increased risk of haemorrhage.
Very common (≥1/10): None. Common (≥1/100, <1/10): anaemia, post-operative haemorrhage, uterovaginal haemorrhage, haemoptysis, haematuria, haematoma, gingival bleeding, purpura, epistaxis, gastrointestinal bleeding, hemarthrosis, ocular bleeding, bruise.
For details of uncommon, rare and very rarely reported adverse events and those of unknown frequency, see SmPC.
Reporting of adverse reactions:
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Website: www.hpra.ie. Adverse reactions/events should also be reported to the marketing authorisation holder at the email address: pv.ireland@viatris.com or phone 0044(0)8001218267.
Legal Category: Product subject to prescription which may not be renewed (A).
Full prescribing information available on request from: Viatris, Dublin 17. Email: enquiry.ire@viatris.com
Date of Revision of Abbreviated Prescribing Information: 27 Feb 2024
Reference Number: IE--AbPI-Arixtra-2.5mg-v003
Genetics
The Role of the Genetic Counsellor
Written by Megan Berkeley, Pre-registration Genetic Counsellor, Department of Clinical Genetics, CHI at Crumlin; Dr Shauna Quinn; Lynsey Marriott, Pre-registration Genetic Counsellor, Department of Clinical Genetics, CHI at Crumlin
Genetic Counsellors are a specialised group of healthcare professionals trained in genomic medicine and counselling skills. The role involves supporting individuals and their families to understand and adapt to a diagnosis of a genetic condition, facilitate the genetic testing process, and guide ongoing care according to a patient’s specific needs. Genetic counsellors can offer a unique perspective as advocates for individuals under their direct care as well as for those in the wider family, which can involve managing highly complex situations and ethical challenges.
Genetic counsellors have traditionally worked as part of a Clinical Genetics service, alongside Clinical Geneticists, Scientists, other Healthcare Professionals, and Administrative Staff. In recent years, increased genetic testing is being offered in non-genetics specialities, known as “mainstreaming”, which is changing how patients and clinicians encounter information about genetic risks and the implications of inherited conditions. Genetic counsellors are therefore taking on more specialised roles in a range of settings, including oncology, cardiology, and prenatal care, as well as promoting education of the workforce to ensure patients are being provided with accurate information and appropriate support at each stage of their healthcare journey.
Key skills and expertise
Genetic counsellors must have a wide-ranging and detailed knowledge about genetic medicine to ensure patients are fully informed of their options for genetic testing, family planning, screening, management, and communication to relatives about genetic conditions. Skilful communication is therefore central to the role, alongside the capability to highly tailor explanations to the individual’s background and personal circumstances. Counselling skills are a key aspect of this, as genetic counsellors must interpret how potentially challenging information is landing with a patient, and explore how they will cope with the impact of a diagnosis or a genetic test result. Alongside relevant medical and family history information, genetic counsellors factor in how psychosocial factors and interpersonal relationships could affect a patient’s outcomes, and use a person-centred, holistic approach to support them in making the right decision for themselves at the right time with regards to their health and wellbeing.
Training Pathways
Genetic Counsellor
Most genetic counsellors have scientific backgrounds following completion of an undergraduate degree related to molecular biology, however some originally trained as nurses or other
professions. Aspiring genetic counsellors require specialist training to develop the unique knowledge and skills of the role, either through a Masters degree or the 3-year Scientist Training Programme run by NHS England. There is currently no accredited MSc course offered in Ireland, so practising genetic counsellors here have completed their qualifications and much of their training abroad. Different countries have different professional registration requirements, but typically following the training course, individuals will work in a pre-registered role to ensure they meet the necessary competencies to practice autonomously, which encompass comprehensive patient care, multidisciplinary working, education, and service improvement. Genetic counsellors make up a relatively small group of clinicians, but the potentially wide-reaching nature of the role emphasises the need for consistently high standards which centre patient safety, particularly as genomic medicine becomes more closely integrated with the wider healthcare service.
Clinical Geneticist
Clinical Geneticists are medically trained Doctors who are involved in the diagnosis and management of rare & non-rare inherited disorders and birth defects. Clinical Geneticists estimate genetic risk and assist with genetic counselling of family members. With the constantly evolving role, Clinical Geneticists have adapted to be an information resource for other medical specialists and generally work in multidisciplinary regional genetic centres, in close collaboration with laboratory scientists, clinical co-workers and academic colleagues. Furthermore, Clinical Geneticists have an important role in mainstream clinician and public education regarding ethical issues that arise from new developments in the clinical application of genetic knowledge.
All Clinical Geneticist must have completed either an undergraduate or postgraduate medical degree. In Ireland, aspiring Clinical Geneticists typically pursue postgraduate basic specialist
training in medicial/paediatric or other specialty training to obtain the certificate of completion. Successful attainment of the relevant examinations is required. Following this, it is possible to apply for the Clinical Genetics higher specialist training programme. This is a four year programme for full time specialty training in core clinical genetics and biochemical genetics. The first two years of training must be undertaken in Ireland before completing any research or out of year programme experience. Research and out of programme experience is recommended and will contribute up to 12 months towards the completion of training. The training scheme promotes a basic understanding and training in genetics embracing clinical, laboratory and theoretical work. During the four years, one must meet the required competencies and assessments to ensure satisfactory completion of specialist training. There is a European exam that all trainees are encouraged to complete prior to finishing.
What type of referrals do we triage?
We triage referrals for >10,000 single gene disorders e.g. Cystic Fibrosis, Duchenne Muscular Dystrophy and Fragile X Syndrome. Referrals for childhood developmental delay, chromosome disorders, hereditary cancer, inherited cardiac conditions, metabolic disorders and neurological disorders are also assessed. We receive referrals for family members where there is a known causative variant or genetic alteration in the family, and patients who are seeking a genetic diagnosis.
Genetic counselling referrals can be roughly grouped into the specialisms of cancer, general and prenatal. Cancer referrals include those with a personal history or strong family history of cancer. General referrals relate to a variety of disorders including cardiac conditions, metabolic disorders and neurological disorders. Referrals can be for patients seeking a genetic test for a known condition in the family but are unaffected at the time of referral.
Megan Berkeley
Lynsey Marriott
This is termed predictive genetic testing. Referrals can be for patients trying to identify a genetic cause for their own diagnosis, for example if there was an inherited component to their breast cancer diagnosis. Diagnostic testing may be offered to such patients to try and identify a genetic cause for their diagnosis and provide individual risk estimates. We also receive referrals for prenatal genetic testing for patients who wish to know the genetic status of their pregnancy when there is a known genetic disorder in the family. Other referrals relate to people seeking genetic counselling regarding reproductive information when a genetic condition is known in the family.
When a referral comes in to the department we usually check if we have seen other members of the family for the same condition. In this way we can link referrals for family members which can give us a detailed understanding of the family history and what members of the wider family may require genetic testing or screening advice.
What should I expect in a genetic counselling appointment?
During the 45 minute appointment a genetic counsellor will first discuss the patient’s personal medical history. A three-generation family tree will then be drawn up to capture relevant family history. Drawing a family tree is a valuable tool to help identify markers of a possible inherited condition and unravel potential modes of inheritance. The genetic counsellor will then discuss the indication for genetic testing, the genes for which testing would be offered, their associated risks, possible screening recommendations onward referrals. Genetic counsellors talk through the implications of genetic test results. For instance, if a genetic change is identified then other family members may be at risk and could seek a referral for genetic counselling for an individualised assessment. Genetic counsellors explore patient’s feelings around genetic testing and its implications. Genetic counsellors are uniquely skilled to help patients understand genetic information, its implications and the benefits and limitations of available testing. The potential intergenerational impact of genetic testing means it can have personal, familial and psychosocial implications for patients.
Genetic testing is done by taking a blood sample from which DNA is extracted. Samples can be analysed for a single gene or a
number of genes associated with a condition, which is termed a panel test. Genetic testing has advanced dramatically in recent years. For instance, genetic testing has now expanded to a panel of 9 genes for hereditary breast cancer, compared to only testing BRCA1 and BRCA2 genes previously.
Patients are offered a follow-up appointment to discuss the results of their genetic test. Results for panel tests can take 3-6 months to be finalised and single gene tests can take 3-4 months. During a results appointment genetic counsellors give personalised risk information to patients based on the combination of their family history and genetic test result. They can also provide advice regarding family planning, screening, for example frequency of mammograms, and other health checks.
What is the difference between an appointment with a Clinical Geneticist and a Genetic Counsellor?
Genetic counsellors and clinical geneticists work in collaboration but have differing backgrounds and roles within the Department of Clinical Genetics. Clinical Geneticists are Doctors with specialised training in medical genetics and have expertise in the diagnosis and treatment of genetic conditions. A major differences between Clinical Geneticists and Genetic Counsellors, are that Clinical Geneticists examine, clinically diagnose, co-ordinate medical investigations, and integrate the results of clinical presentation and investigations to identify a diagnosis, whereas genetic counsellors do not.
Referrals can be made to a Clinical Geneticist in our department for a variety of reasons. Examples include foetal abnormalities, a child with congenital malformation(s) or learning difficulties associated with other problems or a family history, which may be due to an undiagnosed genetic condition. Other common referrals are for children with a known inherited condition or congenital abnormality where parents want information regarding the condition and recurrence risks, and a pregnant person or couple who have received an abnormal test result and want to discuss their options and gain greater understanding of the results. During an appointment with a Clinical Geneticist, they will take a detailed medical and family history, complete a physical examination and may take clinical photographs. Clinical Geneticists can order genetic tests such as trio exomes, arrays, karyotyping, panel tests and single gene tests.
The future of genetic counselling
The Department of Clinical Genetics at Children’s Health Ireland, Crumlin serves the entire country and provides a national genetic counselling and clinical genetics service. The National Strategy for Accelerating Genetic and Genomic Medicine in Ireland was launched in December 2022 and outlines actions to develop the service in Ireland. It highlights that genetic counselling is under-resourced compared to international standards. Only 25 genetic counsellors are practising in Ireland, which is approximately only one for every 200,000 people. The move at a national level to increase the numbers of genetic counsellors
is a welcomed development in an area of healthcare that has been under resourced and underfunded to date.
Currently genetic counsellors register and gain accreditation through the Genetic Counsellor Registration Board, which is a UK accreditation body. The national strategy supports the recognition of genetic counsellors by CORU, a regulator for a variety of health professions in Ireland, and the greater inclusion of genetics into the curriculum for healthcare professionals. These improvements will support the expansion of knowledge of genetic counselling through improved education and recognition via national professional accreditation. A primary aim of the strategy is to have increased integration of genetics into other departments to improve access to genetic testing and the specialist input of Genetic Counsellors across the country. There are currently four genetic counsellors embedded in specialist clinics, two in the National Centre for Inherited Cardiac Diseases, another in the National Centre for Inherited Metabolic Disorders and the third in The National Maternity Hospital. The expansion of the embedding of genetic counsellors into specialist clinics and multidisciplinary care teams will improve the timely access to genetic testing, support for interpretation of results and clinical decision making. Genetic counselling is a rapidly developing field with exciting prospects as regards specialisation and career development. The future of genetic counselling is bright for the upcoming generation of medical professionals in Ireland.
Colitis
Ulcerative colitis (UC) Explained
Ulcerative colitis (UC) is a chronic idiopathic inflammatory bowel disease (IBD) indicated by continuous inflammation of the colon's mucosal lining, and often accompanied by ulcers and bleeding. The inflammation typically begins in the rectum and extends proximally. Unlike Crohn's disease, which can affect any part of the gastrointestinal tract, UC is confined to the colon and rectum. While the exact cause remains unknown, UC is thought to arise from an abnormal immune response to intestinal microbiota in genetically predisposed people.
UC is classified based on the extent of inflammation and its location within the colon:
• Ulcerative Proctitis: Inflammation is confined to the rectum.
• Proctosigmoiditis: Inflammation involves the rectum and sigmoid colon.
• Left-Sided Colitis: Inflammation extends from the rectum through the sigmoid and descending colon.
• Pancolitis: Inflammation affects the entire colon, often leading to severe symptoms such as bloody diarrhea, abdominal cramps, pain, fatigue, and significant weight loss.
Epidemiology/Global prevalence
UC is the most common form of IBD globally, with a higher prevalence in developed countries, such as North America and Western Europe. This lifelong disorder impacts both physical
and mental health, and there is no known cure. The most severe form, fulminant ulcerative colitis, is rare but can lead to life-threatening complications.
Clinical Presentation
The clinical manifestations of UC vary according to the severity and location of inflammation. The hallmark symptom is bloody diarrhoea, and is often accompanied by urgency, abdominal pain, and tenesmus. Symptoms range from mild, with intermittent rectal bleeding and minimal systemic involvement, to severe, with frequent bloody stools, intense abdominal pain, fever, and weight loss, and typically develop over time.
Approximately 25% of UC patients experience extraintestinal manifestations (EIMs), which can involve the skin, joints, eyes, and liver.
Etiology
The exact cause of ulcerative colitis remains unknown but encompasses multiple factors including genetics, environmental factors, abnormal immune responses, and microbial interactions. A person who has a first-degree family member with UC is four times more likely to develop it than the general population.
Diagnosis
Diagnosing UC involves excluding other conditions such as Crohn's disease through blood tests, stool analysis, and imaging studies.
Written by Dr Rahim Khan, Consultant Gastroenterologist and Advanced Endoscopist at Mater Private Network, Dublin
Management and Treatment
Treatment of UC is tailored to the severity and extent of the disease, incorporating both pharmacological and surgical approaches:
• Aminosalicylates (5-ASA): First-line treatment for mild to moderate UC.
• Corticosteroids: Used to induce remission in moderate to severe cases but are not suitable for long-term use due to their side effect profile.
• Immunomodulators: Drugs like azathioprine, 6-mercaptopurine, or methotrexate are used to suppress the immune response and maintain remission.
• Small Molecule Inhibitors: Janus Kinase (JAK) inhibitors help manage inflammation by targeting specific signalling pathways.
• Surgery: typically 15-30% of UC patients will require surgery, with proctocolectomy and ileal pouch-anal anastomosis (IPAA) being the main curative procedure. In cases where IPAA is not feasible, a permanent ileostomy may be necessary.
• Biologics and Biosimilars: recent studies have shown biological agents and their biosimilar equivalents to be effective in treating moderate to
severe UC, with TNF inhibitors, integrin inhibitors, and IL-12/23 inhibitors targeting key proteins involved in the inflammatory process. They are particularly promising for patients who do not respond to conventional medical treatment.
Complications
UC, if unmanaged, can lead to several serious complications, including:
• Anaemia due to significant blood loss
• Severe dehydration
• Toxic megacolon
• Perforated colon
• Thrombosis
• Inflammation of the skin, joints, and eyes
• Increased risk of colon cancer
• Osteoporosis
• Primary sclerosing cholangitis, liver scarring due to inflammation
• Growth inhibition in affected children
Life-long management
Regular monitoring of disease activity and response to treatments is critical in UC management. Screening for complications, such as colorectal cancer, is essential, and patients living severe colitis for 8 to 10 years should undergo surveillance colonoscopy at regular intervals as per guidelines to identify high risk lesions/polyps and remove them in timely manner.
Crohn’s Disease
Crohn’s Disease: An Experience of 2 IBD Centres
Written by Ciarán McDonald1, MSc, Hilary Kerr, MRCPI, Eimear Gibbons2, MRCPI, Tincymol Lukose, BSc1, Danny Cheriyan, MD1, Gavin Harewood, MD1, Stephen Patchett, MD1, Aoibhlinn O’Toole, MD1, Orlaith Kelly, PhD2 and Karen Boland, PhD1
1Department of Gastroenterology, Beaumont Hospital, RCSI Hospital Group, Dublin
2Department of Gastroenterology, James Connolly Hospital, RCSI Hospital Group, Dublin
Patients with moderate to severe Crohn’s disease (CD) often require biologic therapy for induction and maintenance of remission. Antitumor necrosis factor alpha (anti-TNF-α) agents have been the mainstay of biologic therapy for the past 25 years1 and are associated with significantly improved disease-related outcomes and quality of life.2,3 Anti-TNF therapy is not without risk, with well documented potential adverse outcomes that need to be considered upon commencement of treatment.4-9 Furthermore, approximately 20% to 50% of patients will experience loss of response to anti-TNF therapy at 12 months.10-12 An additional 60% of this primary cohort who fail initial anti-TNF therapy will achieve long-term remission on second line anti-TNF therapy.13,14 The need for alternative
therapeutic pathways and biologic classes in the management of refractory Crohn’s disease has led to approval of alternative therapeutic targets. Ustekinumab is a human monoclonal antibody with a favorable safety profile15,16 that binds the p40 subunit of interleukin (IL)-12 and IL-23, thus neutralizing their pro-inflammatory effects on the gastrointestinal mucosa.17 Ustekinumab has become established as a viable treatment option for patients with moderate to severe CD following the landmark UNITI-1, UNITI-2, and IM-UNITI studies,18 along with patients with moderate to severe UC as demonstrated in the UNIFI19 trial.
With the advent of the STRIDE-I20 guidance in 2015 and the implementation of “treat to target” for all biologic and biosimilar drugs, therapeutic drug monitoring
(TDM) has played an ever increasingly important role in the IBD armamentarium. Maintaining higher trough concentrations of anti-TNF biologics in the absence of anti-drug antibodies is associated with achieving clinical and endoscopic response and a greater likelihood of achieving clinical remission.21,22 Similar data regarding potential benefits of drug-level monitoring of ustekinumab in the context of Crohn’s disease are lacking for patients who have had an initial response. This is of particular interest in regions and countries where access to escalated or higher than standard dosing is restricted for financial reasons, and clinicians are asked to provide additional data to support higher doses of ustekinumab or dose escalation in patients achieving response but not remission.
Our aims are to determine whether a threshold maintenance serum concentration for patients with Crohn’s disease is associated with mucosal healing, and whether higher drug levels are associated with increased likelihood of mucosal response or healing.
Methods
Study Design and Recruitment
This was a dual-center retrospective observational study of patients on maintenance dose ustekinumab for management of CD between 2016 and 2021. The study was approved by the local research ethics board at each site. Patients were identified from the cohort of confirmed patients with CD at Beaumont Hospital and Connolly Hospital Blanchardstown, which both operate as tertiary IBD centers in Ireland. Patients
Crohn’s Disease
included were 18 years and older with a histologically confirmed diagnosis of Crohn’s disease and who were on maintenance ustekinumab, defined as having received induction dose (subcutaneous or intravenous) and at least 2 further subcutaneous (maintenance) doses of ustekinumab for a combined minimum treatment duration of 24 weeks. Patients with ulcerative colitis (UC) and inflammatory bowel disease unspecified (IBD-U) were excluded, as were patients with insufficient monitoring data for fecal calprotectin level (FC), endoscopy, and ustekinumab serum trough levels.
Data Collection
Patients were identified from prospectively maintained treatment databases. A comprehensive chart review was carried out at both sites. Patient demographics were recorded including age, gender, family history of IBD, smoking status, disease phenotype, and age of diagnosis. In addition, Montreal-classified23 disease distribution, medication history was noted, and disease activity at the time of ustekinumab induction was recorded using both the endoscopic assessment score via the Simplified Endoscopic Scoring for Crohn’s Disease (SESCD) and fecal calprotectin level. Similar indices of disease
monitoring approximate to time of ustekinumab trough level analysis were repeated. Mucosal response (MR) was defined as ≥50% reduction in FC and/or ≥50% reduction in global SES-CD score. Mucosal healing (MH) was defined as FC ≤150 µg/mL and/or global SES-CD score ≤5.
Ustekinumab Serum Through Level Assays
Patients on maintenance dose subcutaneous ustekinumab having received a minimum of 3 doses (inclusive of induction dose) for management of active luminal or perianal IBD were included in this study. The minimum treatment period evaluated was accordingly 24 weeks. Serum trough levels were drawn during maintenance therapy during a 48-hour window before the patient’s next ustekinumab dose. A drug-tolerant ELISA assay was employed to record trough concentrations and antibody titres.
Statistical Analysis
Quantitative data were analyzed using median and standard deviation (SD) values with 95% confidence intervals. The Kruskal-Wallis test was used to determine differences between responders and nonresponders to ustekinumab. Using GraphPad Prism, logistic regression was used to determine sensitivity and
specificity of levels predicting mucosal response. Receiver operating characteristic (ROC) curve analysis was used to calculate area under the curve (AUC) as a means of assessing performance of serum ustekinumab concentration predicting mucosal healing. A P value of < .05 was deemed to be statistically significant.
Results
Demographics of Cohort
We identified a total of 72 patients on maintenance ustekinumab across both centers, with 47 patients included in the final analysis after applying selection criteria. Patients with insufficient data measuring disease activity (n = 19) were excluded, as were patients with ulcerative colitis (n = 4) or inflammatory bowel disease unspecified (n = 2). The median age of the cohort was 40 years (21-78 years). The majority were female (66%) and had histologically confirmed CD (100%, n = 47). This was a predominantly treatment-refractory cohort with complex disease, as evidenced by the fact that 89.4% were anti-TNFexperienced; and 79% of patients had a stricturing or penetrating disease phenotype. Ustekinumab serum trough levels were obtained after a minimum of 3 doses, and median time from blood draw to
disease assessment with either FC or endoscopy was 1 month (range 0-13 months). Standardization of time to endoscopy from serum assay was limited by access to endoscopy in the context of the coronavirus disease 2019 (COVID-19) pandemic. The median time from induction of ustekinumab to trough levels was 14 months (range 5-44 months).
In our patient group, 63.8% (n = 30 of 47) achieved mucosal healing, with a further 10 patients (85.1%, n = 40 of 47) achieving at least MR during maintenance therapy with ustekinumab. These response rates are striking considering that a high proportion of the overall cohort (n = 42 of 47) had previous primary or secondary loss of response to at least 1 anti-TNF therapy along with some failing further biologic agents. When biologic-naïve patients are excluded (n = 5), this represents an overall mucosal response rate in the anti-TNF-experienced group of 92.9% (n = 39 of 42). This proportion reflects patients who remained on ustekinumab after induction, with a minimum of 3 doses received.
Thirty-nine patients received standard first intravenous dose (6 mg/kg) as outlined in the UNITI trial,18 and another 8 patients received this as a subcutaneous dose due to regional restrictions at
Uzpruvo® is currently not approved for the ulcerative colitis indication (since the originator still has exclusivity for this indication).
PFS - pre-filled syringe. *Stelara®; †29 vs 27-gauge needle of the reference product, Stelara®1,3; ††Plunger stopper made of bromobutyl rubber. 1. Uzpruvo® SmPC (Feb. 2024); 2. Feldman SR et al. Expert Opin Biol Ther. 2023;23(3):253-60. DOI: 10.1080/14712598.2023.2235263; 3. Stelara® PI (Aug. 2022).
UZPRUVO 45 & 90 mg SOLUTION FOR INJECTION IN PRE-FILLED SYRINGE
This medicinal product is subject to additional monitoring.
Uzpruvo 45 mg: Each pre-filled syringe contains 45 mg ustekinumab in 0.5 mL. Uzpruvo 90 mg: Each pre-filled syringe contains 90 mg ustekinumab in 1 mL. Ustekinumab is a fully human IgG1κ monoclonal antibody to interleukin (IL)-12/23 produced in a murine myeloma cell line using recombinant DNA technology. Presentation: Pre-filled glass syringe. Indications: Uzpruvo is indicated for the treatment of plaque psoriasis, paediatric plaque psoriasis, psoriatic arthritis (PsA) and Crohn’s disease. Dosage: Uzpruvo is intended for use under the guidance and supervision of physicians experienced in the diagnosis and treatment of conditions for which Uzpruvo is indicated. Refer to Summary of Product Characteristics. Method of administration: Subcutaneous injection. Contraindications: Hypersensitivity to the active substance or to any of the excipients listed in section 6.1. Clinically important, active infection. Warnings and precautions: In order to improve the traceability of biological medicinal products, the name and batch number of the administered product should be clearly recorded. Ustekinumab may have the potential to increase the risk of infections and reactivate latent infections. Patients should be instructed to seek medical advice if signs or symptoms suggestive of an infection occur. If a patient develops a serious infection, the patient should be closely monitored and Uzpruvo should not be administered until the infection resolves. Immunosuppressants like ustekinumab have the potential to increase the risk of malignancy. Serious hypersensitivity reactions have been reported in the postmarketing setting, in some cases several days after treatment. Cases of allergic alveolitis, eosinophilic pneumonia, and non-infectious organising pneumonia have been reported during post-approval use of ustekinumab. Risk factors for cardiovascular disease should be regularly assessed during treatment with ustekinumab. It is recommended that live viral or live bacterial vaccines (such as Bacillus of Calmette and Guérin (BCG)) should not be given concurrently with Uzpruvo. Caution should be exercised when considering concomitant use of other immunosuppressants and Uzpruvo or when transitioning from other immunosuppressive biologics. It is not known whether ustekinumab may affect allergy immunotherapy. In patients with psoriasis, exfoliative dermatitis has been reported following ustekinumab treatment. Cases of lupus-related conditions have been reported in patients treated with Ustekinumab. Because there is a higher incidence of infections in the elderly population in general, caution should be used in treating the
elderly. Interactions: Live vaccines should not be given concurrently with Uzpruvo. In psoriasis studies, the safety and efficacy of ustekinumab in combination with immunosuppressants, including biologics, or phototherapy have not been evaluated. In psoriatic arthritis studies, concomitant MTX use did not appear to influence the safety or efficacy of ustekinumab. In Crohn’s disease and ulcerative colitis studies, concomitant use of immunosuppressants or corticosteroids did not appear to influence the safety or efficacy of Ustekinumab. Fertility, pregnancy and lactation: Women of childbearing potential should use effective methods of contraception during treatment and for at least 15 weeks after treatment. There are no adequate data from the use of ustekinumab in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonic/foetal development, parturition or postnatal development. As a precautionary measure, it is preferable to avoid the use of Uzpruvo in pregnancy. Limited data from published literature suggests that ustekinumab is excreted in human breast milk in very small amounts. Because of the potential for adverse reactions in nursing infants from ustekinumab, a decision on whether to discontinue breast-feeding during treatment and up to 15 weeks after treatment or to discontinue therapy with Uzpruvo must be made taking into account the benefit of breast-feeding to the child and the benefit of Uzpruvo therapy to the woman. The effect of ustekinumab on human fertility has not been evaluated. Driving and operation of machinery: Uzpruvo has no or negligible influence on the ability to drive and use machines. Undesirable effects: Upper respiratory tract infection, nasopharyngitis, sinusitis, dizziness, headache, oropharyngeal pain, diarrhoea, nausea, vomiting, pruritus, back pain, myalgia, arthralgia, fatigue, injection site erythema, injection site pain. Refer to Summary of Product Characteristics for other adverse effects. Adverse reactions should be reported via HPRA Pharmacovigilance, website: www.hpra.ie. Pack size: 1 pre-filled syringe. A copy of the Summary of Product Characteristics is available upon request or go to www.clonmelhealthcare.ie. Marketing authorisation holder: STADA Arzneimittel AG, Stadastrasse 2-18, 61118 Bad Vilbel, Germany. Marketing authorisation number: EU/1/23/1784/001,004. Medicinal product subject to restricted medical prescription. Date last revised: February 2024.
Date prepared: July 2024. 2024/ADV/UZP/131H
Crohn’s Disease
the time in funding of intravenous ustekinumab. Maintenance ustekinumab doses were variable, reflecting the study status as an observational retrospective review of physician practice preferences. Most patients (59.6%) were maintained on 90 mg of every 8 weeks. Over one-third of patients (n = 18, 38.3%) were on higher than standard dosing of 90 mg every 8 weeks. Some patients were dose-escalated to 180 mg of ustekinumab every 8 weeks (n = 1) or up to the highest prescribed dose in the patient cohort of 180 mg every 4 weeks (n = 9), due to disease burden and physician preference. Seventy percent (n = 7 of 10) of patients on higher dosing of 180 mg 8 and 4 weekly had achieved MH, with 100% demonstrating MR. In addition, the mean serum trough level in these 10 patients was higher (16.4 µg/mL) than patients on standard dosing of 90 mg 8-weekly (3.5 µg/mL). Similar dose-related effects on rate of MH were not seen when patients on 90 mg
of ustekinumab 90 mg 8 weekly were compared with those on 90 mg 4 weekly (P > .05). One patient was prescribed dual biologic therapy with ustekinumab and infliximab, whereas 19.1% (n = 9) of patients were treated with concurrent immunomodulator therapy using azathioprine (n = 4), 6-mercaptopurine (n = 3), and methotrexate (n = 2). These immunomodulators combined with ustekinumab did not influence ustekinumab serum trough levels and had no significant impact on likelihood of achieving mucosal healing (P = .4). Furthermore, no antidrug antibodies were detected in patient samples included despite use of a drug tolerant assay.
In Crohn’s Disease, Maintenance Trough Ustekinumab Levels >2.3 µg/mL Were Associated with Mucosal Healing
Studies of anti-TNF biologic drugs have identified that target serum trough levels associated with mucosal healing differ based
on underlying patient phenotype such as UC vs CD24-26 or perianal vs luminal disease.27,28 Patients with CD were chosen as a distinct population to observe in this study, as there was an insufficient number of patients with confirmed UC/IBDU (n = 5) to power this analysis; and these were excluded from this study. Patients with mucosal healing (n = 30) had significantly higher mean ustekinumab levels (5.7 µg/ mL, SD 6.4) compared with those with no response (1.1 µg/mL, SD 0.52; n = 7, P < .0001, Figure 1). Furthermore, higher mean trough ustekinumab levels (5.1 µg/mL, SD 6.1) were noted in patients with any mucosal response (n = 40) compared with nonresponse (1.1 µg/mL, SD 0.52; n = 7, P < .0001).
We did not identify a trend towards higher mean serum ustekinumab levels in patients with perianal disease who achieved mucosal healing compared with patients with exclusively luminal disease, although the sample size may limit comparisons in this subpopulation.
Relationship between serum through levels and mucosal healing or response in patients in Chron’s disease. A, Mean through serum ustekinumab levels with standard deviation in patients who had achieved mucosal healing (n = 30), mucosal response (n = 40) or nonresponse (n = 7). B, Curve constructed from a probabilistic model determining specificity and sensitivity of a trough level >2.3 to predict mucosal healing in Crohn’s disease patients on maintenance ustekinumab therapy with an area under the curve of 0.95. *P < .001.
Our probabilistic model constructed after logistic regression identified that serum ustekinumab trough levels greater than 2.3 µg/mL were 10.7 times more likely to be associated with MH (100% sensitivity; 95% CI, 71.5% to 100%; 90.6% specificity) and were 10.5 times more likely to achieve MR (100% sensitivity; 95% CI, 71.5% to 100%; 90.5% specificity) compared with nonresponse.
Figure 1. Relationship between serum through levels and mucosal healing or response in patients in Chron’s disease. A, Mean through serum ustekinumab levels with standard deviation in patients who had achieved mucosal healing (n = 30), mucosal response (n = 40) or nonresponse (n = 7). B, Curve constructed from a probabilistic model determining specificity and sensitivity of a trough level >2.3 to predict mucosal healing in Crohn’s disease patients on maintenance ustekinumab therapy with an area under the curve of 0.95. *P < .001.
Inflamm Bowel Dis, Volume 30, Issue 3, March 2024, Pages 423–428, https://doi.org/10.1093/ibd/izad073 The content of this slide may be subject to copyright: please see the slide notes for details.
Discussion
Studies indicate that 10% to 30% of patients with IBD have no initial response to anti-TNF therapy, and over 50% of those who do will lose response over time (secondary loss of response).26 Previously, research has indicated that serum concentration of anti-TNF biologic therapies is dose proportionate; this suggest an association between serum anti-TNF concentration level or neutralizing antibodies and objective endoscopic mucosal response.29,30 There are numerous studies reporting target trough levels of infliximab,31 adalimumab,32 and golimumab22 to achieve MH and some data investigating relationship between trough levels and outcomes with vedolizumab, an anti-integrin therapy.33 In contrast, there are few data supporting a correlation between serum ustekinumab levels and MH. The STARDUST randomized control trial34 is studying standard of care compared with treat-totarget ustekinumab therapy and has reported preliminary data at 1-year showing superiority of treat-to-target approaching achieving endoscopic response. The aim of this study was to determine whether dose escalation and higher ustekinumab levels may benefit patients with Crohn’s who have not achieved mucosal healing. In our observational cohort of patients with CD on maintenance ustekinumab, 63.8% of patients (n = 30 of 47) had achieved MH at time of level assay, and 85.1% (n = 40 of 47) had achieved at least MR. Seven patients in total exhibited nonresponse to ustekinumab dosing at the time of analysis. Our patient cohort was largely biologic-experienced, and a high proportion of patients with CD exhibited advanced luminal disease with stricturing or penetrating disease behaviour.
Previously published data has demonstrated that week-6 ustekinumab serum trough levels are associated with a change in surrogate biochemical markers of disease activity.35 A recent single-center prospective study36 in France involving 49 patients with CD on maintenance ustekinumab reported a mean serum ustekinumab serum trough concentration of 1.88 ± 1.40 µg/ mL. There was no statistically significant difference reported in ustekinumab serum trough levels in patients with or without clinical, radiological, or endoscopic response to ustekinumab (P > .11). In contrast, another
observational study37 of 62 nonresponders to anti-TNF therapy who then received subcutaneous ustekinumab induction reported that ustekinumab serum trough levels of 4.5 µg/mL at 26 weeks or later were associated with reduction in biomarkers and endoscopic response (67% sensitivity, 70% specificity; AUC, 0.67). In our study cohort, we report that an ustekinumab serum trough level greater than 2.3 µg/mL in patients with CD is associated with mucosal healing (SESCD 0-5 or FC ≤150 µg/L), with sensitivity of 100% and specificity of 92.5% and a likelihood ratio of 13.3 (Figure 1B). Overall, mean serum ustekinumab trough levels in patients with mucosal healing or response compared with nonresponse were higher (P < .0001, Figure 1A).
There were no antidrug antibodies detected in the cohort, supporting speculation that the likelihood of developing anti-ustekinumab antibodies is less overall when compared with the traditionally observed rate of auto-antibody formation among patients who are maintained on TNF-α inhibitors.38 These data point to some potential benefit in using serum trough levels of ustekinumab to determine true nonresponse rather than insufficient dosing in patients who have not responded to ustekinumab. A further analysis of target levels or relationship between serum levels and MH in UC is also needed. However, we could not power this statistical analysis largely due to wider use of anti-integrin therapy and small molecule therapy as second- and third-line treatment options in this group at our centers. This reflects physician preference in some cases but also the financial restrictions around ustekinumab prescribing regionally. All decisions around ustekinumab dosing were at the discretion of the treating physician. A significant proportion of patients included in this study received higher than standard dosing. The most common reasons for change of dose frequency included patients who had achieved a clinical response but not remission, persistent endoscopic disease activity with improvement from baseline, and patients with aggressive perianal or penetrating disease who had previously required dose escalation of other biologic agents. The latter group, which was a minority, often received higher doses or shortened frequency from induction.
Moreover, only 45.3% of patients in the UNITI-1 study18 had a history of 1 anti-TNF treatment failure in comparison with 89.4% of our cohort. Induction strategies have comparable clinical response rates whether administered intravenously or subcutaneously.39 The UNITI 1, 2, and IM-UNITI studies18 and current approvals have led to current standard induction dosing for ustekinumab (6 mg/kg ustekinumab intravenously followed by 90 mg subcutaneously every 8 weeks). Pharmacokinetic analysis of ustekinumab in CD shows an association between higher serum ustekinumab concentrations and normalization of inflammatory biomarkers that are unaffected by prior biologic or immunomodulator use.40 A previous observational cohort study demonstrated that dose escalation to ustekinumab 4-weekly achieved clinical response in 61.1% of patients,41 and this influenced treatment strategies in our study where patients who required dose escalation were escalated to 6 (n = 4) and 4 (n = 12) weekly regimens. A further 9 patients in the 4 weekly cohort progressed to a maximum dose of 180 mg, with a mucosal healing rate of 66.6% (n = 6) with at least mucosal response seen in 100% (n = 9) of this subgroup. Despite patients on escalated doses of 180 mg of ustekinumab 4-weekly and 8-weekly having significantly higher ustekinumab serum trough concentrations recorded, there was no statistically significant correlation between all higher ustekinumab doses including 90 mg 4-weekly and high trough levels, despite increased rates of mucosal healing. This may point to higher nonimmune-mediated drug clearance associated with greater inflammatory burden of patients for whom physicians may elect to use higher doses in response to disease therapy.42
There were no adverse events (AEs) or side effects recorded for patients with high trough levels or who were maintained on a higher dose of ustekinumab or shorter frequency of drug administration. This finding is consistent with data published on higher serum trough levels in other biologic classes.43 Interestingly, we did not see any additional benefit to the use of combination therapy with immunomodulators or correlation between immunomodulator use and higher serum ustekinumab levels. This may relate to the lack of antibodies noted on the drug assay or point to differing
pharmacokinetics between biologic classes and supports previously published data showing minimal, if any, benefit to combination therapy with ustekinumab.44 Our data on serum trough ustekinumab levels associated with mucosal healing or response in a predominantly treatment-experienced patient cohort may support the use of dose escalation or reduction in treatment interval in order to achieve mucosal healing in patients. This is particularly noteworthy for jurisdictions such as Ireland where reimbursement is limited to 90 mg doses every 8 weeks in many regions. Cost burdens associated with Crohn’s disease are influenced by biologic status due to higher frequency of admissions and outpatient visits.45 Despite this, there are hidden and overt financial barriers to biologic use and dose escalation of biologics for patients with Crohn’s disease.
This study contributes to the literature on the potential role or utility of serum ustekinumab levels within the overall therapeutic drug monitoring landscape informing bespoke treatment strategies of biologics for patients. These data identifying an association between serum ustekinumab levels and mucosal healing, particularly in CD, may support the use of proactive therapeutic drug monitoring to determine whether optimal dose regimes have been prescribed to increase likelihood of mucosal response.
Limitations of this study include the study’s retrospective design, the low number of biologic-naïve patients, the impact on timing to drug monitoring (largely due to timing of introduction of drug assay to our institutions), and the variable dosing regimens utilized, reflecting physician preference in this observational study. Strengths include its status as a dual-center study and the complex nature of disease detailed in this treatmentexperienced cohort. This dualcenter study associates higher ustekinumab serum trough levels with mucosal healing and mucosal response in patients with CD who are predominantly experienced with anti-TNF. Further prospective studies are required to correlate target maintenance trough levels and the optimal time to dose escalate to improve patient outcomes, as well as the potential impact of dual biologic therapy.
References available on request
The Use of AI in Pharma Production
Artificial Intelligence can be used to make drug production more efficient, economical, and sustainable, according to the international research team behind a groundbreaking new collaboration.
Scientists from University College Cork (UCC) with academic and industry leaders from Ireland and the United States are part of a new initiative named ‘InTeleCat’,
which aims to accelerate the development of pharmaceuticals.
The team, lead by Dr Ger McGlacken of UCC’s School of Chemistry, is comprised of experts in the fields of catalysis, computational chemistry, and data science.
Dr McGlacken said, “The optimisation of chemical structures for a desired clinical effect is a very expensive and
Dr Ger McGlacken
time-consuming process. In this project we will use high throughput screening and Artificial Intelligence (AI) to dramatically accelerate future pharma campaigns. This is the future of drug optimisation and very much part of the UCC ambition through Future Pharmaceuticals”.
The primary goal of InTeleCat is to leverage Machine Learning (ML) and Artificial Intelligence (AI) to optimise and predict catalytic processes that are critical in the pharmaceutical industry. This initiative aims to significantly reduce the time and cost required to identify the best route to a desired Active Pharmaceutical
Ingredient (API) and to predict which APIs are suitable for specific reaction conditions.
The project has been mobilised by funding of $120,000 from the University of Notre Dame through a Naughton Fellowship, supported by the SSPC (The Science Foundation Ireland (SFI) Research Centre for Pharmaceuticals) and represents a significant step forward in the pursuit of innovative and efficient solutions for the pharmaceutical sector.
Scott A. Frank, Associate Vice President, Eli Lilly said: “Eli Lilly is looking forward to collaborating with the McGlacken group at UCC in cooperation with the University of Notre Dame, and the University of California, Los Angeles. This is a very exciting project which will leverage our high throughput experimental capabilities in Indianapolis to carry out thousands of reactions in a single day, building data platforms which will be used with machine learning and AI to sort data. It is our firm position that this is the future of drug development and will accelerate rapid identification of ideal chemical processes”.
New Model of Care for Paediatric General Surgery
A new model of care for the sustainable delivery of paediatric general surgery in Ireland will be launched by the National Clinical Programme in Surgery (NCPS) and the National Clinical Programme for Paediatrics and Neonatology (NCPP&N).
The model was developed as part of a collaboration between the Health Service Executive (HSE), the Royal College of Surgeons in Ireland (RCSI), the Royal College of Physicians of Ireland (RCPI) and a national network of hospitals providing surgical care for children supported by Children’s Health Ireland.
Paediatric General Surgery: A model of care for Ireland 2024, announced at RCSI, outlines a comprehensive framework to enhance surgical services for children close to where they live, ensuring access to a high standard of surgical care with clear oversight and governance.
The new model addresses the growing challenges faced by the paediatric surgical community, including the increasing specialisation of surgical practices and the recruitment of general surgeons who can deliver paediatric care. Without intervention, these challenges could impact access to local or regional general paediatric surgical care for children in the future.
The model of care sets out recommendations on how service improvements in the provision of general paediatric surgery could be achieved with the designation of both regional paediatric surgical facilities and local paediatric surgical facilities, outlining operative procedures appropriate for each site.
The framework aligns with the Sláintecare principles of treating patients closer to home, whenever possible. Complex surgeries will continue to be delivered through Children’s Health Ireland in Dublin.
Dr Ciara Martin, National Clinical Advisor and Group lead for Children and Young People, HSE said: “Having a networked approach to surgical care, that is underpinned by national standards and supported training and education for the teams of nurses and doctors delivering care in all of our national hospitals is important. It is important for those delivering care to children and young people and even more so it means that patients and their families can be confident of the care they receive wherever and whenever they need it”
The key principles of the model of care are:
• A national network of hospitals provides safe surgical care for children supported by Children’s Health Ireland
• Children and families benefit from being able to access appropriate elective and acute surgery close to home regional
general paediatric surgeons decide where surgeries will be delivered, i.e.:
o Children who require transfer to Children’s Health Ireland (CHI) in Dublin are transferred in a timely and safe manner with senior surgeons regionally and in CHI coordinating the transfer.
o Acute surgery for children provided locally occurs in an appropriate environment.
• RCSI incorporates appropriate paediatric surgical experience within the general surgery training programme supporting general paediatric surgery workforce planning for the regional and local general surgery paediatric units.
• An audit and peer review process are developed to assure the quality and safety of care.
60 Second Summary
Use of immune checkpoint inhibitors (ICIs) for cancer have resulted in significant improvements in the survival for patients with advanced non-small cell lung cancer (NSCLC). Given this success, recent studies have proposed investigating the use of ICIs +/- chemotherapy in the adjuvant or neoadjuvant settings for patients with resectable disease.
In this article, we will provide a historical context and background to the adjuvant and neoadjuvant treatment of NSCLC. We will summarize key data exploring patient outcomes, biomarker analyses and future directions for perioperative studies utilising ICIs or ICI-based combinations for patients with resectable NSCLC. Finally, we will provide a summary of the current state of the art care in resectable NSCLC.
Non-small cell lung cancer (NSCLC) is the leading cause of cancer related mortality worldwide with an estimated 1.8 million lung cancer deaths in 2020.1 Unfortunately, the majority of patients (60 – 70%) present with late stage disease and treatment is not delivered with curative intent. The scientific rationale for an adjuvant approach is that it minimises time to surgical resection and can be used to treat micrometastatic disease which is not identifiable on standard clinical imaging.
There have been 2 seminal studies exploring the potential benefit of adjuvant ICI in NSCLC, IMPower010 & PEARLS. We will explore relevant clinical and scientific questions that emerge from these data which we will explore with two critical questions. There is mounting evidence that immunotherapy has activity in the perioperative setting for patients with resectable NSCLC.
The decision as to whether pursue a neoadjuvant or adjuvant approach will likely be influenced by patient values & preferences aswell as clinical, radiological and pathological factors.
Continued
AUTHOR: David O Reilly1, 2, Jarushka Naidoo1,2,
1. Beaumont RCSI Cancer Centre, Beaumont Hospital, Beaumont Road, Dublin
2. RCSI University of Health Sciences, Dublin, Ireland
Correspondence: Dr David O Reilly, davidoreilly22@rcsi.com
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings.
Published by HPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author. MSD has no editorial oversight of the CPD programmes included in these modules
Neoadjuvant versus adjuvant immunotherapy in resectable NSCLC: Which approach is best?
Introduction
Non-small cell lung cancer (NSCLC) is the leading cause of cancer related mortality worldwide with an estimated 1.8 million lung cancer deaths in 2020.1 Unfortunately, the majority of patients (60 – 70%) present with late stage disease and treatment is not delivered with curative intent.2 For patients with NSCLC, the majority of patients with early stage disease will ultimately relapse and die from lung cancer.3 For patients with stage I disease, only 58 – 73% of patients are likely to be cured.3 NSCLC poses a significant challenge whereby our ‘curative’ treatments are uncommonly curative. The established standard of care for patients in the adjuvant setting is the use of platinum-based chemotherapy.4 This confers modest benefit, estimated to be in the region of 5-6%.5 Immune checkpoint inhibitors (ICI), mainly targeting Programmed Death Ligand 1 (PD-1 or PDL1) or Cytotoxic T Lymphocyte Associated Protein– 4 (CTLA-4), have transformed outcomes for advanced solid organ malignancies particularly in diseases such as melanoma, NSCLC and renal cell carcinoma.6 This has resulted in long-term survival (>5 years) for a subset of patients with these malignancies. More recently, there
has been studies investigating the use of ICIs in early-stage disease (adjuvant or neoadjuvant) for disease such as melanoma, NSCLC and renal cell carcinoma.
The successes with ICIs in the metastatic setting have encouraged the exploration of these treatments in the neoadjuvant and adjuvant settings. Herein, we will summarise the current standard of care in the perioperative management of resectable NSCLC. We will review the scientific rationale, clinical data and explore critical questions in the area of adjuvant and neoadjuvant therapy. Finally, we will discuss the advantages and disadvantages of each approach.
Adjuvant Therapy in NSCLC
The scientific rationale for an adjuvant approach is that it minimises time to surgical resection and can be used to treat micrometastatic disease which is not identifiable on standard clinical imaging.7 In addition, resection of cancers allow for complete pathological staging which can guide the appropriateness of adjuvant therapy.
Since the 1970’s, clinical investigators have been investigating the role of platinumbased chemotherapy following surgical resection of NSCLC and
its role in reducing the risk of recurrence for patients with early stage disease. These studies were evaluated in a landmark meta-analysis, published in the British Medical Journal in 1995, which demonstrated modest but statistically significant improvements in overall survival (OS). Across all stages, there was a 5.4 % improvement in OS for patients who received adjuvant platinum-based chemotherapy.4 Adjuvant platinumbased chemotherapy should be considered for patients with resected high-risk stage IB-IIIA NSCLC.8 However, there has been no improvement upon this modest benefit until recent years.
A landmark phase III study (See Table 1), the MAGRIT study, was published in 2014 which investigated the immunotherapeutic vaccine MAGE-A3 in the adjuvant setting for patients with Stage IB-IIIA NSCLC.9 Unfortunately, this study (n = 2312) resulted in no significant improvements in DFS (disease free survival 60.5 months in the investigational arm and 57.9 months in the control arm, Hazard Ratio [HR] 1.02, p = 0.74). This disappointing result was the most recent adjuvant study until ICIs proved efficacy in the metastatic setting and have recently been investigated in the adjuvant setting.
David O Reilly Jarushka Naidoo
34 CPD 111: LUNG CANCER
Name
MAGRIT
Vansteenkiste et al
Lancet
Oncology 2016
IMPower010
Felip et al
NEJM 2021
PEARL
Pas Arez et al
ESMO Virtual Plenary 2022
III 2312 MAGE-A3 cancer immunotherapeutic *13 doses
Stage IB – IIIA -
III 1280 Adjuvant atezolizumab * 1 year versus placebo
III 1177 Adjuvant pembrolizumab * 1 year versus placebo
Stage IB – IIIA
ALK/EGFR + (140/1280)
Stage IB – IIIA with PD-L1 > 1%
EGFR No 434 (37%)
EGFR Yes 73 (7%)
EGFR Unknown 670 (57%)
DFS 60.5 mo (Tx arm) versus 57.9 mo (Placebo)
PD-L1+ with stage II-IIIA
DFS: HR 0.66
PD-L1+ with stage I – IIIA
DFS: HR 0.79
ITT DFS: HR 0.81
ITT DFS of 53.6 mo versus 42 mo (HR 0.76)
The clinical development of this approach provides a roadmap for the development of neoadjuvant treatment for patients with NSCLC. In the NATCH trial, neoadjuvant treatment was equivalent to adjuvant treatment for patients with resectable NSCLC in terms of survival outcomes.13 Five year survival in the neoadjuvant and adjuvant arms respectively in this study was 38.3% and 36.6%. However, only 66.2% of patients in the adjuvant arm completed chemotherapy as opposed to 97% in the neoadjuvant arm. Neoadjuvant chemotherapy is a treatment option in this setting and would be commonly utilised for patients with stage IIIA – IIIB resectable disease.
There have been 2 seminal studies exploring the potential benefit of adjuvant ICI in NSCLC, IMPower010 & PEARLS. We will explore relevant clinical and scientific questions that emerge from these data which we will explore with two critical questions. In the IMPower010 study (n=1280), adjuvant atezolizumab for 1 year was compared to best-supportive care for patients with resected stage IB to IIIA NSCLC.10 With 32.2 months of follow-up, patients with PD-L1 >1% and stage II – IIIA disease had an improved DFS (HR 0.66, CI = 0.50 – 0.88) and benefit was also seen in all comers with stage IB – IIIA disease (0.79, CI = 0.64 – 0.96). In the ITT population, a less clear effect was seen with a HR for DFS of 0.81 (CI = 0.67 –0.99). Those whose tumors had a PD-L1 >50% appeared to benefit the most with a HR of 0.43 (CI = 0.27 – 0.68). Serious adverse events were uncommon with 53 or 11% of patients suffering from a Grade 3 or 4 adverse event in the atezolizumab arm. In the PEARLS study (n=1177), adjuvant pembrolizumab was investigated versus placebo for patients with completely resected early stage NSCLC.11 Chemotherapy was not mandated in the PEARLS study. DFS was significantly improved in the pembrolizumab arm for allcomers (Median of 53.6 mo versus
42 mo, HR 0.76, P = 0.0014). Unlike in the IMPower010 study, the preliminary HR of 0.82 (CI 0.57 – 1.18, p =0.14) would suggest the effect was not greater in the PD-L1 >50% population. Similarly, OS data was immature at the time of presentation of this initial data.
Both of these studies have similar designs including staging of eligible patients, mechanism of action of treatment (PD-L1 versus PD-1), stratification factors (PDL1), duration of therapy (1 year) and outcomes measures (DFS). Both studies suggest significant activity of PD-L1/PD-1 inhibition in the adjuvant setting (HR for DFS of 0.81 for atezolizumab in ITT & 0.76 for pembrolizumab). While both studies demonstrate a DFS benefit in the adjuvant setting – they have conflicting subgroup results. In the IMPower010 study, patients with a high PD-L1 appeared to obtain the majority of the benefit for adjuvant treatment. In the PEARLS study however, the PD-L1 positive population did not derive the most benefit. There is not an obvious explanation for these differences but they may become apparent in updated survival analyses. The European Medicines Agency (EMA) has licensed adjuvant atezolizumab for patients with PDL1 >50% only whereas the Food and Drug Administration (FDA) has licensed for the intention to treat population. Looking to the future,
it remains unclear if adjuvant treatments in clinical practice will require routine PD-L1 testing. Interestingly, the rates of grade 3 or 4 adverse events were three times higher (34 % versus 11%) in patients in the investigational arm of the IMPower010 study compared to the PEARLS study.
In addition to the above studies, there are ongoing randomised phase III studies investigating nivolumab (ANVIL) and durvalumab (AEGEAN) in similar settings to IMpower010 and PEARLS.12
Neoadjuvant Therapy in NSCLC
Neoadjuvant therapy has several clinical and scientific advantages. Systemic therapy is delivered early, thus increasing the chance of treatment of micrometastatic disease. Furthermore, it provides an in vivo test of drug sensitivity, enhanced tissue availability for translational research and increased tolerance of therapy in the pre-surgery setting as demonstrated in the NATCH trial.13
Neoadjuvant therapy allows for the addition of new agents with the use of pCR as a surrogate endpoint response. For example in triple negative breast cancer, there have been advances in the neoadjuvant setting with evidence for the addition of carboplatin and more recently pembrolizumab.14,15 The combination of up to 5 drugs in the neoadjuvant setting has resulted in pCR rates in the region of 60%. Nonetheless, a significant minority of patients have residual disease and these patients are at the highest risk of relapse. In the setting of residual disease, olaparib (BRCA mutant) or capecitabine are considered standards of care.16–18
There are 12 studies published to date (See Table 2) which have investigated neoadjuvant ICI without the addition of chemotherapy for patients with resectable NSCLC (Stage IIIA). The majority of these studies (10 of 12) investigated the use of neoadjuvant ICI alone without any postoperative treatment. All of the studies utilised a PD-1 or PD-L1 inhibitor namely nivolumab, durvalumab, pembrozliumab, atezolizumab, or sintilimab. All of the studies allowed the inclusion of patients with stage I – IIIA disease, with some studies stipulating eligibility requiring at least stage IB disease.
Nivolumab monotherapy
Three studies to date have investigated the use of nivolumab +/- ipilimumab for patients with resectable NSCLC. Two of these studies utilised a single arm study design to investigate single agent nivolumab given for 2 cycles (3 mg/kg, 2 weeks apart) prior to lung resection for stage I – IIIA NSCLC (19,20). Both of these studies involved small numbers (n=20, n = 21) and both demonstrated an MPR rate of 45% for all eligible participants. In the third study, NEOSTAR, authors randomised 44 patients with stage IA – IIIA NSCLC to nivolumab (3 doses q 2 weekly) versus nivolumab (3 doses q 2 weekly) + ipilimumab (1 dose).21 In the nivolumab arm, 5/23 (22%) patients had an MPR. In the nivolumab + ipilimumab arm, 8/21 (38%) had an MPR.
In the study by Bott et al, the median time from first treatment to surgery was 33 days (Range =
17-43).19 There was no operative mortality. The most common postoperative complication was atrial arrhythmia (6/20, 30%) with a total of 10/20 (50%) patients having a postoperative complication.19 In the NEOSTAR study, adverse events were consistent with previous experience (G3 or higher = 13% in monotherapy arm & 10% in combination arm).
In one of the studies investigating nivolumab monotherapy, tumour mutational burden was associated with an increased likelihood of response to therapy but PDL1 status was not.20 Authors discovered that pre-treatment PD-L1 expression (but not post treatment) was associated with increased likelihood of an MPR. They discovered that combination treatment was also associated with greater frequencies of effector, tissue-resident memory and effector memory T cells. Finally, increased levels of gut Ruminococcus and Akkermansia spp was associated with enhanced response to combination therapy.
In summary, nivolumab has been associated with MPR rates of between 22 – 45% and 38% when combined with ipilimumab in the neoadjuvant setting. To date, no new safety signals have emerged in the study of these investigational agents and no clear biomarkers have been identified to predict response.
Pembrolizumab monotherapy
Pembrolizumab monotherapy has been investigated in three early phase studies (n = 10 to date for patients with resectable NSCLC.22–24 The NEOMUN study (n = 15) included patients with more advanced disease – stage II – IIIA. The MK3475 -223 study (n=30) included earlier stage patients – I – II. Finally, the TOP 1501 study (n = 10) included those with stage IB – IIIA disease. In the TOP 1501, four cycles of pembrolizumab were planned post-operatively. For patients who received 2 doses of pembrolizumab (200 mg q 3 weekly), the MPR in these studies were 40 % (MK3475 -223), 26 % (NEOMUN), 28% (TOP 1501). In these three studies, no new safety signals emerged and there was no suggestion that neoadjuvant ICI
Name
NCT02904954
Aktori et al Journal of Thoracic Oncology
MK3475-223
Bar et al JCO 2019
NEOSTAR
Study Cascone et al Nature 2021
Forde et al, NEJM 2018
Goa et al Journal of Thoracic Oncology 2020
LCMC3
Kwiatkowski et al JCO 2019
NEOMUN Study Eichhorn et al BMC Cancer, 2019
Bott et al Thoracic Lung Cancer, 2019
IoNESCO Study Wislez et al Annals of Oncology, 2020
TOP 1501
Tong et al Journal of Thoracic Cardiovascular Surgery
NEOCOAST Annals of Oncology Spicer et al
is associated with increased risk of perioperative morbidity or mortality.
In these studies, no tumour related biomarkers were associated with an increased likelihood of MPR at the time of surgery. However, in the MK3475 – 223 study, they discovered that patients with an MPR had a longer time to surgery compared to those without. In the NEOMUN study, four patients had a PET detected clinical response prior to surgery with the same four patients going on to have an MPR at the time of surgery.
In summary, pembrolizumab was associated with significant activity
Treatment
Neoadjuvant: 1.Durvaluamb *2 vs 2.Durvalumab *2+ SBRT
in the neoadjuvant setting in three small studies investigating primarily two doses given prior to therapy. Similar to what we observed in patients receiving nivolumab, MPR rates ranged between 26% and 40% and safety and feasibility was demonstrated in this treatment setting.
Other monotherapy therapy studies targeting PD-1/PD-L1
Three further monotherapy studies have explored the use of durvalumab (IONESCA), sintilimab (SINTIL) and atezolizumab (LCM3) respectively for patients with stage I – IIIA NSCLC(25–27). Albeit using different agents
in these studies, all patients received 3 – 4 weeks of neoadjuvant treatment prior to surgical resection. For these studies, the sample sizes were n = 46 (IONESCA), n = 40 (SINTIL) and n = 180 (LCM3). For participants receiving sintilimab, 15/37 (40.5%) achieved an MPR of which 6/40 (16.2%) had a complete pathological response. In the LCM3 study, in patients without EGFR/ALK mutations who underwent surgery, the major pathologic response rate was 21% and the pathologic complete response rate was 7%. Unfortunately, the IONESCA study was stopped early due to
36 CPD 111: LUNG CANCER
an unexpected high mortality rate with 4/43 patients dying in the 90 day postoperative period. For participants that were enrolled and went on to have surgery, the median residual viable tumour was 37%.
Similar to findings in the NEOMUN study, there was a strong correlation between reduction in preoperative SUV following neoadjuvant sintilimab and pathological regression at the time of surgery (p <0.000001). In the same study, there was a weak correlation between PD-L1 expression in stromal cells and pathological regression (p = 0.04)
While the excess deaths in the IONESCA study are a cause of concern, the cause of deaths was not of conditions typically associated with ICI toxicity and it is very plausible that these may have been an unfortunate coincidence. The pathological regression seen in these further monotherapy studies once again demonstrated activity for this approach in the monotherapy setting. With 5 different drugs being assessed in the monotherapy setting, a challenge for clinicians is identifying which agent, if any, may be preferentially used.
Chemo-immunotherapy studies
Finally, and most importantly, we will explore randomised phase III
studies of perioperative chemoimmunotherapy in resectable NSCLC. These are the studies which are likely to have the greatest impact on clinical practice in next 3-5 years.
To date, seven randomised studies have presented results which have investigated ICIs +/- chemotherapy for patients with resectable NSCLC(28–34). This data is summarised in Figure 1 including study design, enrolled patients and efficacy outcomes. All of these studies included perioperative ICI except for CHECKMATE-816 which include just three cycles of neoadjuvant nivolumab and chemotherapy only. In summary, all studies demonstrated significantly improved MPR, pCR, EFS and OS benefit with the addition of ICI to chemotherapy. In these studies, six PD-(L)1 inhibitors were studied including nivolumab, pembrolizumab, durvalumab, atezolizumab, tiseleizumab and toripalimab. All of these studies have demonstrated that neoadjuvant PD-(L)1 inhibition is associated with a significant improvement in EFS ranging with HR ranging from 0.4 – 0.67. To date, the KEYNOTE-671 study is the only study to have demonstrated a significant improvement in OS with a HR of 0.72. Neodjvuant nivolumab (CHECKMATE816 regimen) is approved in the US and Europe
with the European Medicines Agency limiting the licensing of nivolumab to those with a PD-L1 score >1%. Pembrolizumab has been approved in the perioperative setting in the US while it remains pending in Europe.
In summary, there is significant evidence of efficacy of chemotherapy + PD-(L)1 inhibition for patients with resectable NSCLC with randomised data suggesting an improved pCR, event free survival and overall survival. It is apparent that a neoadjuvant approach with PD-L1 inhibition is superior to chemotherapy alone. Given the extensive data, it would appear that neoadjuvant/perioperative therapy is likely to be preferred over adjuvant by most clinicians.
Discussion
There is mounting evidence that immunotherapy has activity in the perioperative setting for patients with resectable NSCLC. Pembrolizumab and ateolizumab have demonstrated improved DFS in phase III studies in the adjuvant setting for patients whose tumours harbouring a PD-L1 score >1%, with a similar magnitude of benefit. Nivolumab in combination with chemotherapy has demonstrated impressive antitumour activity and an event free survival benefit in the neoadjuvant setting. To date, adjuvant atezolizumab
and neoadjuvant nivolumab + chemotherapy have been approved by the FDA.
The decision as to whether pursue a neoadjuvant or adjuvant approach will likely be influenced by patient values & preferences aswell as clinical, radiological and pathological factors. Factors favouring a neoadjuvant approach would include higher stage of disease (particularly stage IIIA), ALK/EGFR negative and an ECOG of 0/1. Factors favouring an adjuvant approach would include high PD-L1 (particularly >50%) and an unknown ALK/EGFR status.
If we are guided by the clinical development pathway of neoadjuvant therapies in breast cancer, the combination of neoadjuvant chemo + ICI in conjunction with therapy escalation/de-escalation based on pathological response may result in incremental improvements towards best outcomes. However, until that treatment paradigm is established, decisions regarding neoadjuvant and adjuvant approaches must be made in a collaborative manner between patients and clinicians to ensure that therapy results in the best oncological outcome while taking into account individual patient and clinical factors.
References available on request
Figure 1 - Overview of phase III neoadjuvant chemotherapy + immunotherapy studies for patients with resectable non-small cell lung cancer
KEYTRUDA: multiple treatment options for patients with mNSCLC1 (pembrolizumab)
1st line Combination* Therapy2
1st line Combination** Therapy 3 SQUAMOUS
1st line*** Monotherapy4
AND SQUAMOUS
* KEYTRUDA, in combination with pemetrexed and platinum chemotherapy, is indicated for the first-line treatment of metastatic non-squamous
** KEYTRUDA, in combination with carboplatin and either paclitaxel or nab-paclitaxel, is indicated for the first-line treatment of metastatic squamous
*** KEYTRUDA, as monotherapy, is indicated for the first-line treatment of metastatic non-small cell lung carcinoma (NSCLC) in
KEYTRUDA® (pembrolizumab)
ABRIDGED PRODUCT INFORMATION Refer to Summary of Product Characteristics before prescribing. PRESENTATION KEYTRUDA 25 mg/mL:
One vial of 4 mL of concentrate contains 100 mg of pembrolizumab. INDICATIONS • KEYTRUDA as monotherapy is indicated for the treatment of adults and adolescents aged 12 years and older with advanced (unresectable or metastatic) melanoma. • KEYTRUDA as monotherapy is indicated for the adjuvant treatment of adults and adolescents aged 12 years and older with Stage IIB, IIC or III melanoma and who have undergone complete resection. • KEYTRUDA, in combination with platinum-containing chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment, is indicated for the treatment of resectable non-small cell lung carcinoma at high risk of recurrence in adults. • KEYTRUDA as monotherapy is indicated for the adjuvant treatment of adults with non-small cell lung carcinoma who are at high risk of recurrence following complete resection and platinum-based chemotherapy. • KEYTRUDA as monotherapy is indicated for the first-line treatment of metastatic non-small cell lung carcinoma (NSCLC) in adults whose tumours express PD-L1 with a ≥50% tumour proportion score (TPS) with no EGFR or ALK positive tumour mutations. • KEYTRUDA, in combination with pemetrexed and platinum chemotherapy, is indicated for the first-line treatment of metastatic non-squamous NSCLC in adults whose tumours have no EGFR or ALK positive mutations. • KEYTRUDA, in combination with carboplatin and either paclitaxel or nab-paclitaxel, is indicated for the first-line treatment of metastatic squamous NSCLC in adults. • KEYTRUDA as monotherapy is indicated for the treatment of locally advanced or metastatic NSCLC in adults whose tumours express PD-L1 with a ≥1% TPS and who have received at least one prior chemotherapy regimen. Patients with EGFR or ALK positive tumour mutations should also have received targeted therapy before receiving KEYTRUDA. • KEYTRUDA as monotherapy is indicated for the treatment of adult and paediatric patients aged 3 years and older with relapsed or refractory classical Hodgkin lymphoma (cHL) who have failed autologous stem cell transplant (ASCT) or following at least two prior therapies when ASCT is not a treatment option. • KEYTRUDA as monotherapy is indicated for the treatment of locally advanced or metastatic urothelial carcinoma in adults who have received prior platinum-containing chemotherapy. • KEYTRUDA as monotherapy is indicated for the treatment of locally advanced or metastatic urothelial carcinoma in adults who are not eligible for cisplatin-containing chemotherapy and whose tumours express PD L1 with a combined positive score (CPS) ≥ 10. • KEYTRUDA as monotherapy or in combination with platinum and 5-fluorouracil (5-FU) chemotherapy, is indicated for the first-line treatment of metastatic or unresectable recurrent head and neck squamous cell carcinoma (HNSCC) in adults whose tumours express PD-L1 with a CPS ≥ 1. • KEYTRUDA as monotherapy is indicated for the treatment of recurrent or metastatic HNSCC in adults whose tumours express PD-L1 with a ≥ 50% TPS and progressing on or after platinum-containing chemotherapy. • KEYTRUDA, in combination with axitinib, is indicated for the first-line treatment of advanced renal cell carcinoma (RCC) in adults. • KEYTRUDA, in combination with lenvatinib, is indicated for the first line treatment of advanced renal cell carcinoma in adults. • KEYTRUDA as monotherapy is indicated for the adjuvant treatment of adults with renal cell carcinoma at increased risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions. Microsatellite instability high (MSI-H) or mismatch repair deficient (dMMR) cancers. Colorectal cancer (CRC) • KEYTRUDA as monotherapy is indicated for adults with MSI-H or dMMR colorectal cancer in the following settings: - first line treatment of metastatic colorectal cancer. - treatment of unresectable or metastatic colorectal cancer after previous fluoropyrimidine-based combination therapy. Non-colorectal cancers • KEYTRUDA as monotherapy is indicated for the treatment of the following MSI-H or dMMR tumours in adults with (a) advanced or recurrent endometrial carcinoma, who have disease progression on or following prior treatment with a platinum-containing therapy in any setting and who are not candidates for curative surgery or radiation, (b) unresectable or metastatic gastric, small intestine, or biliary cancer, who have disease progression on or following at least one prior therapy. • KEYTRUDA, in combination with platinum and fluoropyrimidine based chemotherapy, is indicated for the first-line treatment of locally advanced unresectable or metastatic carcinoma of the oesophagus in adults whose tumours express PD-L1 with a CPS ≥ 10. • KEYTRUDA, in combination with chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment after surgery, is indicated for the treatment of adults with locally advanced, or early-stage triple-negative breast cancer at high risk of recurrence. • KEYTRUDA, in combination with chemotherapy, is indicated for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumours express PD L1 with a CPS ≥ 10 and who have not received prior chemotherapy for metastatic disease. • KEYTRUDA, in combination with lenvatinib, is indicated for the treatment of advanced or recurrent endometrial carcinoma in adults who have disease progression on or following prior treatment with a platinum containing therapy in any setting and who are not candidates for curative surgery or radiation. • KEYTRUDA, in combination with chemotherapy with or without bevacizumab, is indicated for the treatment of persistent, recurrent, or metastatic cervical cancer in adults whose tumours express PD-L1 with a CPS ≥ 1. • KEYTRUDA, in combination with trastuzumab, fluoropyrimidine and platinum-containing chemotherapy, is indicated for the first-line treatment of locally advanced unresectable or metastatic HER2-positive gastric or gastro-oesophageal junction adenocarcinoma in adults whose tumours express PD-L1 with a CPS ≥ 1. • KEYTRUDA, in combination with fluoropyrimidine and platinum-containing chemotherapy, is indicated for the first-line treatment of locally advanced unresectable or metastatic HER2-negative gastric or gastro-oesophageal junction adenocarcinoma in adults whose tumours express PD-L1 with a CPS ≥ 1. • KEYTRUDA, in combination with gemcitabine and cisplatin, is indicated for the first-line treatment of locally advanced unresectable or metastatic biliary tract carcinoma in adults. DOSAGE AND ADMINISTRATION See SmPC for full details. Therapy must be initiated and supervised by specialist physicians experienced in the treatment of cancer. The recommended dose of KEYTRUDA in adults is either 200 mg every 3 weeks or 400 mg every 6 weeks administered as an intravenous infusion over 30 minutes. The recommended dose of KEYTRUDA as monotherapy in paediatric patients aged 3 years and older with cHL or patients aged 12 years and older with melanoma is 2 mg/kg bodyweight (up to a maximum of 200 mg), every 3 weeks administered as an intravenous infusion over 30 minutes. For use in combination, see the Summary of Product Characteristics (SmPC) for the concomitant therapies. KEYTRUDA must not be administered as an intravenous push or bolus injection. When administering KEYTRUDA as part of a combination with intravenous chemotherapy, KEYTRUDA should be administered first. Treat patients until disease progression or unacceptable toxicity (and up to maximum duration of therapy if specified for an indication). For the adjuvant treatment of melanoma, NSCLC, or RCC, KEYTRUDA should be administered until disease recurrence, unacceptable toxicity, or for a duration of up to one year. Refer to the SmPC for dosing in neoadjuvant and adjuvant treatment of resectable NSCLC and neoadjuvant and adjuvant treatment of locally advanced, or early stage triple-negative breast cancer at high risk of recurrence. KEYTRUDA, as monotherapy or as combination therapy, should be permanently discontinued (a) For Grade 4 toxicity except for: endocrinopathies that are controlled with replacement hormones; or haematological toxicity, only in patients with cHL in which
References 1. KEYTRUDA Summary of Product Characteristics available at www.medicines.ie.
2. Gandhi L, et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N Engl J Med. 2018;378:2078-2092.
Sarcoma
Immunotherapy in Sarcoma: Current Data and Promising Strategies
Written by Georgina E. Wood, MD, PhD1, Christian Meyer, MD2, Florent Petitprez, PhD3, and Sandra P. D'Angelo, MD4
1University College Hospital of London, London, United Kingdom
2Johns Hopkins, Baltimore, MD
3The University of Edinburgh, Edinburgh, Scotland
4Memorial Sloan Kettering Cancer Center, New York, NY
Immune Checkpoint Inhibitors
ICIs regulate inhibitory signals to T cells such as cytotoxic T-cell lymphocyte-4 (CTLA-4) and the PD-1/PD-L1 axis and have demonstrated efficacy as both monotherapy or combinatorial therapy. This led to US Food and Drug Administration (FDA) treatment approval of >50 solid tumors, mismatch repair (MMR)–deficient tumors, and tumors with a high TMB.5 Several trials have shown some success of ICIs in STS. The SARC028 phase II clinical trial was the first to demonstrate efficacy of pembrolizumab (PD-1 inhibitor) in patients with either STS (undifferentiated pleomorphic sarcoma [UPS], dedifferentiated liposarcoma [DDLPS], leiomyosarcoma [LMS], synovial sarcoma [SS]) or BS (Ewing’s Sarcoma [ES], osteosarcoma [OS], chondrosarcoma [CS]). The objective response rate (ORR) in STS was 18%, with best responses seen in UPS (4 of 10) and DDLPS (2 of 10).6 The ORR for BS was a disappointing 5%.6 SARC028 expansion cohort analysis confirmed the clinical activity of pembrolizumab in UPS, with an ORR of 23%, but was lower in DDLPS with an ORR of 10%.7
The AcSE phase II trial illustrated the heterogeneity of responses to pembrolizumab in rare sarcoma subtypes, with alveolar soft part sarcoma (ASPS) and SMARCA4deficient sarcoma or malignant rhabdoid tumor showing partial responses (PRs) of 50% and 25%, respectively.8 Two complete responses (CR) were seen in patients with ASPS and epithelioid sarcoma.8
However, BSs have fared poorly with ICIs. SARC28 had an ORR of 5% in ES, OS, and CS subtypes.6 The PROMO trial
recapitulated the disappointing results for pembrolizumab with 12 patients with OS having no clinical benefit with early stoppage of the trial.9 Similarly, a pediatric phase I/II trial of pembrolizumab in melanoma, PD-L1–positive solid tumors (primarily ES and OS), and lymphoma demonstrated a PR in 3 of 33 patients with sarcoma.10
Exploration of other ICI monotherapies, including the PD-1 inhibitor nivolumab or the CTLA-4 inhibitor ipilimumab, has proved to be less fruitful.11-15 The nivolumab monotherapy arm in the Alliance trial registered only a 5% response rate and was not pursued further.
An observational study of patients with sarcoma treated with ICIs identified responses enriched
in patients with ASPS,16 leading to prospective studies demonstrating a benefit of PD-1/ PD-L1 inhibition in this histologic subtype.8 17-20 Atezolizumab demonstrated excellent results in ASPS achieving durable responses in one third of patients,21 leading to its FDA approval in this rare subtype. However, this success was not replicated in the general sarcoma population in the iMATRIX phase I/II trial of atezolizumab. Forty patients with pediatric BS + STS were treated, with only six achieving stable disease and no objective responses.22
As monotherapeutic ICIs have proved to be largely unsuccessful
for most patients with sarcoma, the efficacy of the dual checkpoint blockade and other combinations has been evaluated in the phase II Alliance trial, in those patients treated with nivolumab and ipilimumab, the ORR was 16%, and responses were seen in LMS, myxofibrosarcoma (MFS), UPS, and angiosarcoma.14 An expansion cohort revealed an ORR of 14% for the dual checkpoint blockade in patients with UPS and DDLPS. The phase II DART trial confirmed efficacy of the nivolumab/ipilimumab combination in angiosarcoma with an ORR of 25%, 23 and the phase II durvalumab + tremelimumab trial demonstrated similar histologyspecific activity patterns as other studies with best responses in
ASPS.24 Results of the phase III RAR-Immune study exploring the efficacy of nivolumab and ipilimumab in sarcomas are eagerly anticipated (ClinicalTrials. gov identifier: NCT04741438).
The recent pilot study of bempegaldesleukin with nivolumab in patients with metastatic sarcoma similarly showed the highest ORR in angiosarcoma + UPS, with CD8+ T-cell infiltrates and PD-1 expression correlating with improved ORR.25
This was echoed in a retrospective analysis of 88 patients with metastatic STS receiving pembrolizumab, nivolumab, ipilimumab, or a combination of them, which showed greater responses to immunotherapy in UPS and LMS.26
Combination with Local Therapy
Local treatment with radiotherapy (RT) can generate tumorassociated antigens (TAAs) that enhance the immunogenicity of tumors with low TMB, increasing their sensitivity to ICIs in a T-cell–dependent manner.27 28 Trials in the neoadjuvant setting have shown very promising results of RT in combination with ICIs with significant efficacy in UPS.29-31
Isolated limb infusion (ILI) is the local administration of highdose chemotherapy used to treat STS of the extremities.32 A successful case report of two patients with recurrent MFS with tumor regression after ILI with pembrolizumab33 led to a phase II trial investigating this combination (ClinicalTrials.gov identifier: NCT04332874).
Talimogene laherparepvec (T-VEC), an oncolytic viral immunotherapy, delivered via intratumoral injection, is approved for metastatic melanoma.34 A phase II trial demonstrated an ORR of 35% and a median duration of response of 56.1 weeks in patients with advanced sarcoma when given in combination with pembrolizumab, with responses seen in patients who had received a previous checkpoint blockade.35 36
Combination with Systemic Therapies
Evidence shows that combining ICIs with chemotherapy has increased efficacy in STS. With anthracycline chemotherapy as the backbone of treatment for many sarcoma histotypes, two clinical trials evaluating the synergistic efficacy of doxorubicin with
pembrolizumab had promising results. The Pollack study showed an ORR of 19%, which is similar to pembrolizumab or doxorubicin alone6; however, median progression free survival (mPFS) and median overall survival (mOS) were favorable at 8.1 months and 27 months, respectively.37 The Livingstone study showed an enhanced ORR of 36.7%; however, improvement in mPFS and mOS was modest (5.7 months + 17 months).
38
Responses were preferentially seen in UPS (4 of 4) and LMS (4 of 10).
38
The Phase II PEMBROSARC trial assessed the combination of pembrolizumab and metronomic cyclophosphamide in gastrointestinal stromal tumors (GIST), LMS, UPS, and other sarcomas.39 A recent update of this study demonstrated a best response of PR for nine patients (five DDLPS, three epithelioid, one LMS).40 This study included only 15 patients with OS with best responses of PR in 6% (1 of 15 patients). There was no correlation between PD-L1 expression and response in this cohort.41
A retrospective analysis demonstrated that trabectedin with nivolumab is safe and effective in STS,42 corroborated by the recent NiTraSarc trial.43 Subsequently, trabectedin has shown clinical activity including some CRs
in combination with ICIs— ipilimumab/nivolumab (SAINT trial)44 (87.3% disease control rate [DCR], ORR, 19.5%). Other combinations did not show an synergistic effect of trabectedin with avelumab (ORR, 13%)45 or durvalumab (ORR, 7%).46 The combinations were safe with tolerable toxicity profiles, with the majority of treatment-related grade 3-5 events being attributable to trabectedin45 including two cases of fatal febrile neutropenia.46
The combination of ICI with tyrosine kinase inhibitors (TKIs) has also been evaluated.
Patients with advanced sarcoma in the phase II ImmunoSarc trial received sunitinib and nivolumab, with tolerable toxicity, and the ORR was 22% with an 18-month overall survival of 100% for patients with a PR (ASPS [n = 2], angiosarcoma [n = 1], extraskeletal myxoid CS [n = 1], SS [n = 1]).47 CR was observed in one patient with angiosarcoma.
Pembrolizumab with axitinib in STS demonstrated clinical benefit in 73% of patients with ASPS; the PR rate was 54.5% and 18% with SD, leading to an expansion cohort in this histotype.19 The ORR was only 9.5% in patients without ASPS, with a clinical benefit rate of 42.9%.19 A pilot study of pembrolizumab with lenvatinib has also shown promise with PR in OS, malignant peripheral nerve sheath tumor, angiosarcoma, and SS.48
Significant responses were seen in a phase II study of nivolumab with cabozantinib in patients with advanced angiosarcoma (Alliance A091902) with an ORR of 59% including two CRs, and mOS was not reached.49
These histotype-specific responses have been emphasized by studies in GIST (dasatinib + ipilimumab)50 and BS,51 52 showing no significant benefit of ICI with TKIs. No immunomodulatory effect of treatment has been noted in these trials.
Interestingly, a meta-analysis of STS showed higher responses for the combination of TKIs with anti–CTLA-4 for ASPS, whereas best responses were seen for the combination of anti–PD-1 and anti–CTLA-4 with chemotherapy in UPS.53 Overall, grade 3-5 toxicity ranged from 7% to 76%. Combinations with chemotherapy led to substantial hematologic toxicity (absolute risk [AR], 0.74 [95% CI, 0.60 to 0.85]), with TKI combinations being more manageable (AR, 0.18 [95% CI, 0.11 to 0.27]).53
Adoptive Cell Therapy
Engineered T-Cell Receptor Therapy
T-cell receptor (TCR)–based adoptive cell therapy (ACT) is a method of targeting TAAs. Sarcomas express higher
Sarcoma
than normal levels of TAAs called cancer testis antigens (CTA), particularly SS and myxoid/round cell liposarcoma (MRCLS).40,41 CTAs expressed by sarcomas include NYESO-1, MAGE, GAGE, and fetal acetylcholine receptors.42
In 2011, the first clinical trial of engineered TCR therapy for sarcoma evaluated the efficacy of autologous NY-ESO-1–specific TCRs with high-dose interleukin-2 (IL-2) in HLA-A*021 patients with refractory SS. Preliminary analysis showed RECIST PRs in four of six patients.54
Long-term follow-up of this study found that 11 of 18 patients with SS (61%) who received anti–NYESO-1 T cells responded, with one patient achieving a CR.55
Subsequently, a phase I study of the NY-ESO-1–targeting SPEAR TCR treated HLA-A*021 patients with advanced SS, after a lymphodepleting regimen of fludarabine and cyclophosphamide.56 An ORR of 50% (6 of 12 patients) was demonstrated, with one CR. Correlative analyses found postinfusion expansion with persistence of polyfunctional selfgenerating pools of SPEAR T cells (Ny-ESO-1c259T) for at least 6 months in vivo.56
Patients treated with dosereduced lymphodepletion regimens saw lower ORRs. Furthermore, fludarabine also seems to be necessary, as has been demonstrated in hematologic malignancies.57 NY-ESO-1–specific TCR therapy for MRCLS has also been investigated and demonstrated ORR with 20% and 40% reduction in two cohorts, one with low-dose chemotherapy and the other with standard-dose chemotherapy, respectively.58
ADP-A2M4 SPEAR TCRs directed against MAGE-A4 have shown similar promise. An ORR of 25% was observed in an initial phase I study in advanced solid tumors with all PRs of 44% in patients with SS.59 The subsequent pivotal Spearhead study in patients with advanced SS or MRCLS showed an ORR of 39% in patients.60
Chimeric Antigen Receptor T-Cell Therapy
CAR T cells have emerged as effective therapies in multiple hematologic malignancies, resulting in FDA approvals.61 Progress in solid tumors has been challenging, but signals have
been identified in patients with sarcoma. Taking advantage of lower-level human epidermal growth factor receptor 2 (HER2) expression in sarcomas, a phase I/ II clinical trial using HER2-specific CAR T cells primarily in patients with OS revealed a median OS of 10.3 months.62 HER2-CAR T cells were found in some tumor samples tested at resection with one patient at 90% necrosis.62 Further evaluation of this therapy in 10 patients with sarcomas produced an overall survival of 60% at one year with one CR in OS and another in RMS.63
Other CAR T-cell trial targets recruiting in sarcoma include GD2 (ClinicalTrials.gov identifiers: NCT03373097, NCT05080790), which demonstrated promise in diffuse midline gliomas and glioblastoma64,65 and EGFR+/– CD19 in the STRIvE-01 study, with 3 of 11 patients demonstrating mixed responses at early dose levels.66
Tumor-Infiltrating Lymphocyte Therapies
TIL therapy is now FDA-approved for melanoma.67 There is an ongoing phase I trial assessing the feasibility of TIL treatment in adolescent and young adult patients with STS (ClinicalTrials. gov identifier: NCT04052334), after positive preclinical investigation.68
Cancer Vaccines Targeting CTAs
Cancer vaccines aim to elicit an adaptive antitumor immune response, promoting both cellular and humoral immunities.
One patient with ES was treated with intratumoral (pubis) Pexa-Vec, a replication-competent vaccinia virus, achieving stable disease at 22 days post-treatment with evidence of the treatment effect on imaging.69 However, the disease elsewhere progressed.
A vaccine using a dendritic cell NY-ESO-1–expressing lentivirus, LV305, induced T-cell and antibody responses to NY-ESO-1, but the ORR in patients with sarcoma was 4.2%.70
In combination with ipilimumab, an NY-ESO-1 dendritic cell vaccine administered with autologous NY-ESO-1–targeting T cells had an overall 90-day ORR of 20% (2 of 10 patients, one with a CR).71 Notably, the addition of ipilimumab had no apparent clinical benefit.
The heterologous vaccine, CMB305, attempted to improve response rates by adding a TLR-4
agonist to NY-ESO-1. Phase 1b evidence suggested that this was a good vehicle for SS and MRCLS with a DCR of 61.9%.72 73
However, the phase II study of CMB305 with atezolizumab had progression-free and overall survivals similar to published data for standard chemotherapy.74
Experience with NY-ESO-1 vaccines in STS has been disappointing, with ORRs at best equivalent to standard-of-care chemotherapy. Although a durable response was seen in one patient, this patient also received ACT, raising the question of whether ACT rather than vaccination led to the excellent response.
A substantial subset of STS is driven by pathognomonic fusion events. These fusion events generate chimeric proteins (TAAs) that are immunogenic and often serve as oncogenic drivers.75 Targeting these fusion-derived neoantigens has proven to be successful in other tumor types.76,77 In STS, targeting fusion-derived TAAs with the peptide-pulsed dendritic cell vaccine approach have to date not had clinically meaningful responses.78-80
Tumor Necrosis Factor-α Family Pathway Targeting
Identification of the tumor necrosis factor (TNF)-α ligand pathways as a means of selectively affecting apoptosis in tumor cells generated enthusiasm for developing compounds targeting receptors to family members. These efforts were stymied largely due to early hepatotoxicity and lack of potency.81 However, development of a third-generation functional mimic of TNF-related apoptosis-inducing ligand (TRAIL), INBRX-109, which binds to death receptor 5 (DR5) triggering its clustering, generated exciting early data in the CS cohort in a phase I trial.82 INBRX-109 administration resulted in an 87% DCR, with durability exceeding 180 days. The progression-free survival (PFS) in the study was 7.6 months with a 6-month PFS rate of 58%. These phase I data have led to an ongoing registration trial in conventional CS (ClinicalTrials.gov identifier: NCT03715933).
In addition, a separate ongoing trial (ClinicalTrials. gov identifier: NCT03715933) evaluates the drug in two other sarcoma subtypes, ES- and SDHdeficient GIST. Previous work in ES identified DR5 on the surface
of primary tissue samples,83 and that in GIST identified DR5 on cell lines.84 The trial combines INBRX-109 with temozolomide and irinotecan in refractory ES while providing it alone for patients with SDH-deficient GIST.
Altering the TME
The TME generates barriers to immune recognition and activation through different mechanisms. Newer studies targeting this immunosuppressive landscape attack different signaling molecules supporting immune downregulation. Tumorassociated macrophages (TAMs), which differentiate from myeloid derived suppressor cells (MDSCs), promote growth of cancer cells by releasing angiogenic factors improving delivery of oxygen and fuel while simultaneously secreting immunosuppressive cytokines.85 Colony stimulating factor 1 receptor (CSF1R) engagement drives differentiation of precursor myeloid cells into immune dampening M2 macrophages within the TME. Strategies used to block CSF1R signaling include small-molecule intracellular inhibitors of receptor signaling and extracellular inhibitory antibodies against either the CSF1 ligand or the receptor itself.86 A phase I clinical trial investigated the small-molecule inhibitor DCC-3014 in conjunction with avelumab in patients with metastatic sarcoma revealing decreased circulating MDSCs and stable disease in three of 13 patients (ClinicalTrials.gov identifier: NCT04242238).
A second novel target supporting tumor growth in the TME is CD73. Sarcomas express high levels of CD73 on their cell surface, and this pervasive nucleotidase converts adenosine monophosphate to extracellular adenosine. Adenosine signaling into tumor cells can increase metastatic potential, whereas binding to receptor on immune cells downregulates T cell, natural killer (NK) cell, and macrophage function.87,88 Clinical trials are attempting to overcome the inhibitory environment of the TME by interfering with adenosine. A phase II study is evaluating a targeted inhibitor of CD73, oleclumab, with durvalumab in various sarcomas subtypes.89 Furthermore, a second study is evaluating an oral adenosine antagonist, etrumadenant, in combination with the PD-1 inhibitor, zimberelimab in DDLPS (ClinicalTrials.gov identifier: NCT05886634).
Another widely expressed transmembrane protein contributing to immunosuppression in the TME is CD47. This molecule binds a variety of proteins including signal regulatory protein family members, integrins, and thrombospondin, among others.90 Its engagement through cognate ligands on macrophages prevents phagocytosis of cells. Tumor cells expressing CD47 thus blunt the effectiveness of macrophages in the TME. CD47 is expressed in OS and a variety of STSs.91 92 The blockade of CD47 in preclinical models increased phagocytosis of cancer cells and diminished metastatic disease.91 93 A phase I/II clinical trial combining ontorpacept, a soluble fusion decoy receptor for CD47 with doxorubicin in advanced LMS, has shown clinical activity with a DCR of 80%.94
Biomarkers of Response to Immunotherapy in Soft Tissue Sarcoma
Efficacy in Different Sarcoma Histotypes
Clinical trials for ICIs that included all STS histotypes have usually been considered to be disappointing, with response rates around 15% only,6 7 14 95 and a meta-analysis of phase II clinical trial evidenced an overall 15.1% response rate to PD-1/PD-L1
inhibitors.96 However, substantial differences in response rates have been observed between histologies. In particular, UPSs have been reported to exhibit a stronger response rate than LPS,6 7 15 37 LMS,6 12 37 or SS.6 The most responsive histotype to ICIs (PD-1/PD-L1 and/or CTLA-4 inhibition) is the rare ASPS with much higher response rates than any other histotypes, over 35%.14 18 19 24 95 However, given the overall low response rate across the most common histotypes, there is still a need for crosshistotype or histotype-agnostic biomarkers of response to ICIs.
Relevance of Pan-Cancer
Biomarkers for Soft Tissue Sarcoma
Tumor Mutational Burden
TMB is a measure of the number of mutations in the exome of a tumor. In many solid tumor types, there have been reports of stronger response rates to the PD-1 blockade in patients with tumors, exhibiting a high TMB as noted in the KEYNOTE-158 pan-cancer study.97 This study, and the subsequent FDA approval, uses a threshold of 10 mutations per megabase (Mb) to distinguish between TMB-high and TMB-low tumors. However, the majority of soft tissue sarcoma tumors bear a very low TMB, with a median below three mutations per Mb.3,98,99 Only
Importantly, STSs with MMRd still have a lower TMB than most nonsarcoma MMRd tumors.104 Therefore, MMRd and MSI have a limited applicability as biomarkers for immunotherapy in STS.
PD-1 Expression
2% of STSs are classified as TMBhigh,99 making TMB an impractical biomarker for STS.
Interestingly, some histologies have higher frequencies of TMB-high tumors, notably angiosarcoma.99 100 In the Angiosarcoma Project, it was reported that angiosarcoma of the head and scalp had a higher TMB (20.7 mutations/Mb) than other angiosarcomas (2.8 mutations/Mb).101 Two patients with angiosarcoma of the head and scalp received and benefited from the PD-1 blockade, whereas there was no clinical benefit for the three patients with angiosarcomas of other locations. While these numbers are too low to draw a conclusion on the association between TMB and response to immunotherapy, they indicate that further studies would be required.
Mismatch Repair Deficiency and Microsatellite Instability
Mismatch repair deficiency (MMRd) in tumors is associated with higher TMB and can result in microsatellite instability (MSI). MMRd is associated with higher response rates to the PD-1 blockade.102 However, MMRd and MSI remain rare in STS, representing only 1% of tumors.103 Notable exceptions are pleomorphic RMS and embryonal RMS, which exhibit high MMRd frequency.
The expression of PD-L1 by cancer or immune cells is commonly regarded as a potential TME biomarker of enhanced response to PD-1/PD-L1 inhibitors and is approved as a biomarker by the FDA and the EMA.105,106 In STS, there have been reports on strong variability of PD-L1 expression between histotypes and between tumors.107-109 Correlative analysis of the SARC028 study revealed that PD-L1 expression on both tumor and immune cells was stronger in responders to the PD-1 blockade.4 This association was not reported in OS.41 Moreover, previous treatment such as RT can influence levels of PD-L1 expression.110 Collectively, these results indicate that PD-L1 could be a valuable biomarker for immunotherapy in STS, but further studies are required.
TMEs and Response to Immune Checkpoint Inhibitors in
STS
The cellular composition of tumors reveals not only malignant cells, but virtually all immune cell types can be present, along with fibroblasts and endothelial cells. These diverse cellular populations, engaging in strong interactions, are together referred to as TME. In many different cancer types, it has been shown that the composition of the TME is strongly connected to either response or resistance to ICI.111
B Cells and TLS
An in-depth transcriptomic-based characterization of the TME in soft tissue sarcoma allowed us to establish an immune classification into five Sarcoma Immune Classes (SIC).112 Three classes, A, C and E had distinct immune profiles: immune desert, highly vascularized and immune high, respectively. Immune-high SIC E was associated with a longer patient survival, and B cells were found to be the key determinant of patient survival. One of the hallmarks of SIC E tumors is the presence of TLSs. TLSs are lymph node–like aggregates of lymphocytes located in the tumor or in close proximity, and mature TLSs exhibit a functional germinal center.113 They can perform a large
Sarcoma
range of function, such as priming and activation of an antitumor immune response.114 They have been shown to increase patient survival in many different malignancies115 and can be viewed as part of a local cancer immune cycle.116
SIC E tumors had a much higher response rate to pembrolizumab than tumors from any other SIC, and no responder was identified in immune-low SIC A.112 TLSs as potential biomarkers for immunotherapy were simultaneously reported in melanoma117,118 and kidney cancer,118 which suggests that this could have a broader applicability. A pan-cancer study, including STS, concluded that mature TLSs presenting a germinal center were predictive of response to ICI, independent of PD-L1 expression.119 To validate these findings, the PEMBROSARC trial39 was conducted on another cohort enrolled on the basis of the presence of TLS in their tumors and treated with pembrolizumab and low-dose cyclophosphamide.40 This study reported in the TLS+ cohort an ORR of 30%, substantially higher than the 2.4% ORR in the allcomer cohort. Within TLS+ tumors, response was found to be associated with a lower density of regulatory T cells and a higher infiltration of plasma cells, fully differentiated B cells specialized in antibody production.40 This was reminiscent of similar results in clear-cell renal cell carcinoma120 and non–small cell lung cancer.121 In line with these results, a recent study combining durvalumab and pazopanib showed an improved PFS with a higher presence of B cells.122
CD8+ T Cells
The presence of potentially cytotoxic CD8+ T cells has been associated with increased response to ICI in different cancer types.111 123 The correlative study of SARC028 reported a higher infiltration of responding tumors by CD8+ T cells.4 Further analyses of this data set revealed that this association between CD8+ T cells and response was increased in tumors with a high neoantigen burden, a trend that was not visible when combining CD8+ T cells and TMB, suggesting that neoantigen load could play a higher predictive role.124
In a trial combining the oncolytic immunotherapy T-VEC with PD-1 inhibition by pembrolizumab, it
was reported that the presence of CD8+ T cells at the tumor periphery before treatment was associated with response.35 In a trial of IL-2 pathway agonist bempegaldesleukin in combination with anti–PD-1 nivolumab, a correlation between response and CD8+ T cells infiltrates, and PD-1 expression was also noted, while hedgehog pathway expression correlated with treatment resistance.25 Immune hot tumors (enriched in T cells, B cells, and NK cells) are enriched in responders to various ICI combinations.125 Interestingly, this class of immune hot tumors also correlated with expression of transposable elements and epigenetic regulators.
Other TME Markers
TAMs are an expanding field, and many therapeutic strategies have been designed to target them.126-128 Their role in relation to immunotherapy in STS has, however, been only scarcely studied. The correlative study of the SARC028 study reports an increased presence of macrophages in tumors responding to pembrolizumab.4 Larger studies are needed to assess the potential of tumor-associated macrophages to be used as biomarkers for immunotherapy.
A recent study indicates a correlation between immunerelated adverse events and survival in patients with sarcoma treated with ICIs.129 The tumors of patients having undergone immune-related adverse events were found to have a higher infiltration by dendritic cells, CD8+ T cells, and regulatory T cells. Others inflammatory indexes have been highlighted as indicators of prognosis or response to therapy, for example, low lymphocyte-to-monocyte ratio.130
Conclusions and Future Directions
BS and STS remains a devastating diagnosis with poor prognosis in advanced disease, and although treatment options are expanding, durable responses remain elusive with the checkpoint blockade. Recent efforts have demonstrated that some STSs are indeed immunogenic and immunotherapy may play a role in their management. Although overall responses to ICIs in STS are not high, there is histologyspecific activity. Enhanced immune characterization of these ICIsensitive tumors will help to guide
treatment strategies. Observation of divergent responses emphasizes the need for histologyspecific approaches, which should be incorporated into clinical trial design, along with correlative studies to identify predictive biomarkers.
Results in BS have been more disappointing, the checkpoint blockade is essentially ineffective, and exploration of alternative immunotherapeutic options is needed.
Given the TME of sarcomas, it is likely that most histologic subtypes will require a multimodality approach to induce effective antitumor immunity. In alignment with this, improvements in ORRs have been achieved through combinatorial approaches with RT or other systemic treatments.
Equally, ACT therapies such as TCR-based therapy targeting CTAs have demonstrated impressive response rates in patients with advanced SS and MRCLPS although most of those patients who respond ultimately experience recurrence of disease. Moving forward, understanding the primary and acquired mechanisms of resistance in these patients will be important to enhance the treatment strategy. Extending inclusion for TCR-based therapies by developing technologies to enable removal of human leukocyte antigen (HLA) restriction and broadening identification of TAAs will also be advantageous.
In light of the excellent responses seen with engineered TCR approaches in STS, where dendritic cell vaccines targeting the same antigen have been disappointing, further exploration of the role for TCR-based therapy targeting fusion-derived neoantigens is warranted.
Clinical Implications
At this time, atezolizumab for ASPS remains the only FDA approval with the checkpoint blockade in sarcoma. While access to pembrolizumab or nivolumab remains an option in the United States through the National Comprehensive Cancer Network (NCCN) compendium listing for angiosarcoma, UPS, and DDLPS, there is a pressing need to define biomarkers of response/resistance even in these subtypes—thereby highlighting need to explore efficacy of these agents in the context of clinical trials. Further international
studies will also increase global access to these agents. Since the efficacy of the monotherapy checkpoint blockade remains limited to a few histologies, combinatorial strategies will likely take precedence while thoughtfully balancing the risks/benefits of these approaches. The addition of ipilimumab likely does’ not warrant the increased toxicities as noted in the Alliance expansion cohorts in UPS/DDLPS.
Clinical trials must continue to be conducted in histology-specific cohorts, and the collection of tissue on these studies is extremely important. While TLS is the most promising biomarker to date, selection by TLS still only yielded a 30% response rate to the checkpoint blockade. Ultimately, a panel of biomarkers will likely be needed to guide practitioners.
Novel checkpoints such as those targeting lymphocyte activation gene 3 (LAG-3) can be considered in sarcoma. Furthermore, identifying drugs that can modulate the presence of regulatory T cells and myeloid derived suppressor cells is also relevant in sarcoma. Currently, there are limited compounds that can effectively target these pathways. Novel bispecific fusion proteins targeting immunooncology pathways causing downregulation of CD80, upregulation of IL2, and activation of NK cells are in active clinical trials.
In the setting of adoptive cell therapy, TCR targeting MAGEA-4 (afami-cel) is under review at the FDA. This may become the second ACT approved for solid tumors, which would highlight another area of progress but underline the pressing need to expand applicability to other HLA subtypes. In addition, identifying mechanisms of resistance, that is, loss of antigen expression, decreased antigen-presenting machinery, which will guide the field moving forward. After the approval of lifileucel in ICIrefractory melanoma, this is a provocative avenue to consider in sarcoma as well.
While there has been some progress in the field, many questions remain unanswered. Multi-institutional collaborations (for both clinical trials and correlative efforts) are critical for the advancements that are desperately needed in this field.
References available on request
Understanding ERCP
What is ERCP?
ERCP, otherwise known as Endoscopic Retrograde Cholangiopancreatography, is a minimally invasive advanced therapeutic endoscopic procedure that is used to diagnose and treat conditions that affect the bile ducts, liver, gallbladder and pancreas by using an endoscope. Most commonly this includes bile duct stones or bile duct blockages, (strictures) which may or may not require stenting, diagnosing and treating bile duct cancers, and pancreatic cancers. It is also useful in the management of surgical complications from gallbladder surgery, for example an injury to bile ducts during gallbladder surgery. It is performed using an endoscope which passes through the oesophagus and the stomach and reaches the second part of the duodenum (small bowel).
Due to my interest and subspecialization in advanced GI endoscopy and HPB (Hepatopancreatic biliary) medicine, Mater Private Network in Dublin is one of the two private hospitals in Dublin providing ERCP as a service on a full-time basis. Procedures are carried out under my supervision, supported by an excellent team of nurses, technicians and administrative staff.
Who needs an ERCP?
One of the most common signs and/or symptoms that will result in patients needing an ERCP is the development of jaundice (with or without pain), along with blood tests (liver tests and Bilirubin raised) and scans (either ultrasound CT and or MRI) that show a bile duct stone or a stricture (benign or malignant) within the bile ducts, or a mass from pancreatic head pressing on the bile ducts and resulting in jaundice.
Written by Dr Rahim Khan, Consultant Gastroenterologist and Advanced Endoscopist at Mater Private Network, Dublin
Historically, cases such as this were treated with either open surgery or a laparoscopic procedure. In some scenarios, it would have resulted in death if the patient was not fit for surgery, especially in the case of elderly patients. But ERCP has no age limit and can be performed at any age; it can be life-saving in the case of sepsis in the bile ducts and liver due to such blockages.
ERCP is most commonly performed while patients are under light sedation. The exception are patients who cannot tolerate the procedure under sedation, in which case, general anaesthesia is given instead. The procedure is carried out in the main operating theatre or an endoscopy suite.
What is the recovery time?
The recovery time following an ERCP is just two hours, providing there are no complications. For most patients, this is a day case procedure, meaning they will come from home and are discharged on the same day with after care advice. Patients who already have an advanced diagnosis, i.e. cancer or infection in the bile ducts from bile duct stone(s), may be kept in hospital and the procedure is done while they are an inpatient.
What are the side effects & risks?
As with every medical procedure or medication, there may be
some side effects. ERCP also comes with some risks and complications, however, the risk of complication is <5% in the vast majority of cases, and can range from 5%-20% depending on case by case basis depending on other co-morbidities. We discuss complications and risks carefully with each patient to identify which category they fall into, depending on their case.
On rare occasions patients may require a short hospital stay with medications +/- antibiotics or pain relief if complications occur. The most common complication is post ERCP pancreatitis (PEP). This is an inflammation (swelling) of the pancreas after ERCP as the pancreas and its pancreatic duct lies very close to the bile duct. The pancreatic duct (PD) opens through the same channel into the small bowel in almost every individual (with some exceptions). Due to the invasive nature of this procedure, internal bleeding can happen but most of the time the
bleeding stops itself. If it requires endoscopic treatment, this will be done by the consultant during the procedure. In extremely rare cases it may require surgery to stop the bleeding.
Conclusion
ERCP offers transformative care for patients with digestive ailments, providing potential cures for several GI diseases. It allows patients to receive treatment on the same day, avoiding the need for traditional laparoscopic surgical procedures and extended hospital stays. This minimally invasive approach significantly reduces recovery times and associated risks. In addition to ERCP, Mater Private Network will soon offer Video Capsule Endoscopy, further enhancing our specialised gastroenterology services in 2024. We are excited to enhance our patients' quality of life and demonstrate our commitment to advanced, innovative treatments for better patient outcomes.
Patients can be referred for ERCP by gastroenterologists, ED consultants, radiologists, general surgeons, and GPs. The procedure is covered by most major private health insurers.
To learn more about the procedure, please visit - https:// www.materprivate.ie/ourservices/digestive-diseases/ endoscopic-retrogradecholangiopancreatography-(ercp)
Sepsis
Diagnosing Sepsis in The Emergency Department Setting
Sepsis is a potentially life-threatening dysregulated (exaggerated and abnormal) response to infection, causing body organ damage. Sepsis can damage organs such as the heart, brain, kidneys, lungs, and liver. Consequently, sepsis is a potentially life-threatening complication of an infection. Sepsis is a global public health challenge and a leading cause of preventable death, with about 20% of all deaths worldwide associated with sepsis. Meanwhile, most hospital deaths in Ireland, like many other developed countries, are associated with an infection or sepsis.
Sepsis occurs when, for unclear reasons, the body’s response to an infection injures its tissues, causing significant damage to vital organs such as the heart, brain, kidneys, lungs, and liver. In sepsis, substances (mediators) into the bloodstream to fight an infection trigger inflammation in the whole body. This inflammation can trigger a cascade of changes that can damage many organ systems in the body, causing them to fail. If sepsis progresses to septic shock, blood pressure dramatically drops, which may lead to death.
Prompt identification and treatment are vital to improve a patient’s chances of survival and reduce their likelihood of death and longterm or permanent disability. It is in that context that the emergency department (ED) has a critical role in preventing death and long-term disability in patients presenting to a hospital with sepsis because the ED is the entry point of many patients with sepsis admitted to the hospital. However, unlike other common time-sensitive medical emergencies treated in an ED that require relatively expensive drugs and infrastructure, such as acute myocardial infarction (AMI [heart attacks]) and acute strokes, the treatment of sepsis, if diagnosed early, before shock sets in, is cheaper because it usually requires relatively inexpensive drugs and equipment. Early
Written by Professor Abel Wakai, MD FRCEM, Consultant in Emergency Medicine, Beaumont Hospital Dublin 9
sepsis treatment involves quickly administering an appropriate antibiotic(s), ensuring oxygenated blood flow supports intravenous fluids and, if feasible, controlling the source of the sepsis (surgically or non-surgically.
If early sepsis treatment is simple and cheap, why is sepsis still a deadly global public health challenge? From an ED perspective, the main reasons that sepsis still kills so many people are the non-specific (and subtle) way sepsis can present in the ED and the lack of a reliable gold standard test for promptly diagnosing sepsis. Sepsis can be especially hard to spot in babies, young children, pregnancy, people with a compromised immune system, dementia, a learning disability or difficulty communicating (e.g. due to a speech or language impairment). Even when sepsis progresses to septic shock, more than 30% of patients still present with vague and non-specific symptoms such as fatigue and weakness. The Sepsis Alliance, a leading United States (US) sepsis organisation, has a helpful acronym called TIME for patients, patient carers, the general public and healthcare professionals when it comes to identifying the symptoms of sepsis; the T stands for Temperature (higher or lower than normal); the I stands for Infection (may have symptoms of an infection); M stands for Mental decline (confused, sleepy, difficult to rouse) and E stands for Extremely ill (severe pain, discomfort, shortness of breath).
In the ED setting, the lack of a reliable test for diagnosing sepsis leads to variability in sepsis treatment, patient outcomes and healthcare costs. Other timesensitive medical emergencies treated in EDs, such as AMI and acute strokes, have objective (gold standard) and reliable tests to diagnose them immediately. For AMI, all that is frequently required is the patient’s symptoms and a relatively simple test, an electrocardiogram (ECG), for objective diagnosis and initiation of treatment. In the case of acute stroke, all that is frequently required is the patient’s symptoms, physical signs, and an appropriate neuroimaging study (e.g., computed tomography [CT] or magnetic resonance imaging [MRI] scan of the brain) for objective diagnosis and initiation of treatment. The ECG, in the case of AMI, and the appropriate neuroimaging study, in the case of acute stroke, provide visual evidence of the diagnosis that avoids subjective interpretation
of the patient’s symptoms. Similar objective and reliable tests to diagnose AMI and strokes are not available for ED patients with sepsis; there is no objective and reliable single test result to tell an ED nurse or doctor a patient has sepsis. Instead, we currently base the diagnosis of sepsis on searching for evidence of damage to body tissues and organs (heart, brain, kidneys, lungs, and liver) in a patient with an infection. In a patient with a suspected or presumed infection, ED nurses and doctors can find evidence of damage to body tissues and organs at the bedside (such as an acutely altered mental state and high respiratory rate) and from the results of blood tests (such as abnormal white cell count, renal and liver function tests).
It is intuitively logical that the absence of a gold standard diagnostic test for sepsis is a significant contributory factor for delayed diagnosis, misdiagnosis and death currently associated with sepsis. However, since the first National Clinical Effectiveness Committee National Clinical Guideline for Sepsis in Ireland was published in 2014 after the Health Service Executive (HSE) established the National Clinical Programme (NCP) for Sepsis, the early recognition and evidencebased management of sepsis has demonstrably improved. For example, the 2021 National Sepsis Report published in March 2023 revealed a 22.3%% reduction in age-adjusted mortality from sepsis/ septic shock since 2011 in Ireland. This reduction in age-adjusted mortality from sepsis/septic shock since 2011 in Ireland is attributable to the development and implementation of the Sepsis Management for Adults (including maternity)
National Clinical Guideline and the National Implementation Plan for implementing the International Guidelines for the Management of Septic Shock & Sepsis-Associated Organ Dysfunction in Children which provide a standardised approach to the recognition and management of sepsis. The increased awareness and action of healthcare professionals were the key drivers behind these improvements in the care of patients with sepsis and the associated reduction in age-adjusted mortality.
Regarding the current challenges in diagnosing sepsis in the ED setting posed by the absence of a gold standard diagnostic test for sepsis, omics provide hope for overcoming this problem. Omics is a new term that describes the exciting and innovative field of large-scale, data-rich biology. Omics research aims to collectively characterise and quantify the pools of biological molecules that translate into the structure, function, and dynamics of an organism or organisms. Current advances in omics research provide
hope that, in future, we may have a simple finger-stick blood test based on sepsis blood biomarkers (short for biological markers), like current finger-stick glucose monitoring for people with diabetes. The availability of such a simple finger-stick blood test may make ED sepsis screening and diagnosis as accessible and accurate as current diabetes screening and diagnosis. Machine learning and artificial intelligence (AI) provide another source of hope in overcoming the diagnostic challenge of sepsis. Proof-of-concept research shows AI algorithms have the potential to predict sepsis hours before its onset. While several AI-powered sepsis diagnosis algorithms are under development, this technology may still have some time away from routine clinical use. However, the United States Food and Drug Administration (FDA) approved the first AI-powered sepsis diagnostic tool earlier this year. The tool uses 22 different parameters like temperature, heart rate and laboratory test results to help clinicians assess a patient's sepsis risk; the tool then generates an overall risk score and four categories that correlate to a patient's risk of deterioration. Despite FDA approval of the AI-powered sepsis diagnostic tool, scientifically valid clinical validation is pending. Combining machine learning, AI, and omics research can potentially improve the timeliness and accuracy of ED sepsis diagnosis in future. Until then, we must rely on ED healthcare professionals' knowledge of sepsis and their actions in the fight against it. ED healthcare nurses and doctors should promptly approach each ED patient with an infection with the mindset that they have sepsis until proven otherwise, using the national sepsis guideline's sepsis screening form to metaphorically sniff out those with sepsis among the over one million patients who attend EDs in Ireland annually.
Ultimately, to meaningfully tackle sepsis as a global public health challenge, the truism that prevention is better than cure is highly relevant. The HSE’s National Sepsis Outcome Report 2021 states that prevention is the most effective way to reduce sepsis mortality. These preventative measures include sanitation, personal hygiene, healthy eating, moderate exercise, breastfeeding, avoiding unnecessary antibiotics, and vaccination for vaccine-preventable infections. The report also highlights that during the COVID-19 pandemic, we have learned of the benefit of good infection prevention and control measures, including social distancing, mask-wearing and handwashing. We should not forget the lessons learned from the COVID-19 pandemic if we are to reduce the societal burden of sepsis significantly.
References Available on request
School of Pharmacy Antipsychotic-Induced Weight Gain Research
A qualitative study from researchers within the Pharmacy Department of St Patrick’s Mental Health Services and the School of Pharmacy in University College Cork has revealed the urgent need for tailored guidelines in managing antipsychotic-induced weight gain, as findings highlight the gaps between current guidelines and practices and the needs of those taking antipsychotics.
The study, Informing the development of antipsychoticinduced weight gain management guidance: patient experiences and preferences - a qualitative descriptive study, which was published in BJPsych Open on 1 August 2024, explores how patients with lived experiences of antipsychotic-induced weight gain (AIWG) perceive and manage this challenging side-effect.
Clinically significant weight gain has been linked to almost all antipsychotic medications, prescribing of which extends to many mental health difficulties beyond psychosis, and is usually seen within weeks of starting treatment.
Managing weight gain effectively in patients with mental health difficulties who are taking antipsychotics is crucial to ensuring their physical health is maintained. However, while limited international guidance exists, management recommendations for clinicians largely replicates recommendations for population level weight management practices, with self-led ‘lifestyle changes’ given prominence, and the use of additional medications to reduce antipsychotic-induced appetite increases considered only when other options have proven ineffective.
The development of available management recommendations has largely been informed by the expert opinion of guideline development groups, with no or minimal representation of the voice of lived experience. This study was the first of its kind to explore the management preferences of patients with experience in managing weight gain from antipsychotics and to compare this with current management algorithms informing clinicians’ practice.
A diverse range of people (n = 17) with experiences of mild to severe antipsychotic-induced weight gain and mental health
Professor
Laura Sahm, Head of Clinical Pharmacy Practice at UCC and Senior Pharmacist at St Patrick’s Mental Health Services, Ita Fitzgerald
difficulties including schizophrenia, bipolar affective disorder and major depressive disorder were interviewed regarding:
• Their experiences of managing AIWG
• The acceptability, feasibility, and transferability of current management algorithms and the interventions contained within (both pharmacological and non-pharmacological)
• How patient-centred management practices can be realised within Irish healthcare settings.
Speaking about the study, Lead Researcher and Senior Pharmacist at St Patrick’s Mental Health Services, Ita Fitzgerald said: “Findings have shown that the lack of available management guidance for antipsychotic-induced weight gain remains a challenge for clinicians, with currently endorsed approaches neither being fitfor-purpose or aligned with the experiences and needs of those prescribed antipsychotics and who experience unwanted weight gain.
“This study provides guidance and recommendations for ways in which a proactive, individualised, holistic, and collaborative approach to AIWG management can be practically realised both within guidelines and services. It is hoped that the publication of this study will mark a significant step towards empowering and supporting clinicians to manage the complex side effect of antipsychotic-induced weight gain in a way that is most responsive to the needs of the individual patient.”
Key Findings
1. Patient preferences for management differ significantly from that advocated for in management guidelines: Patients with AIWG
describe current management guidelines as overly simplistic and lacking the flexibility required for management to be tailored towards their needs. The standardised, stepwise approach, universally recommended and focusing primarily on the use of lifestyle changes, does not reflect the realities of managing overweight or obesity caused by antipsychotics.
2. Behavioural changes are often insufficient: Many participants reported that lifestyle changes alone were insufficient to manage AIWG. Continued recommendations from clinicians to implement lifestyle changes could worsen feelings of isolation and internalised stigma, while also reducing the likelihood of seeking help in future due to fear of stigma.
3. Individualised approaches are key: Participants emphasised that AIWG is a unique cause of weight gain and as such, requires an equally distinctive approach to management. Recommendations for management of AIWG must recognise diversity among individuals and allow for interventions to be tailored towards risk of living with overweight or obesity, individual physical and mental health capabilities and patients’ treatment preferences.
4. Need for early use of pharmacological interventions: Study participants advocated for the earlier use of pharmacological interventions, such as metformin, especially for those who are severely ill at the onset of antipsychotic treatment, have a personal or family history of living with obesity, or where appetite increases following starting an antipsychotic are severe.
Professor Laura Sahm, co-author of the study and Head of Clinical Pharmacy Practice at UCC, said: “This study represents a crucial step in recognising the importance of a patient-centred and patient-informed approach to combat antipsychoticinduced weight gain. By working collaboratively, patients and prescribers can adopt a strategy that aligns best with their shared and agreed goals of therapy.”
Based on the experiences of participants, the study recommends that current guidelines are expanded to include preventive measures and early interventions tailored to individual patient needs and risks. The study recommendations also put forward ways in which the four tenets of patient-centred management (proactive, individualised, holistic and collaborative approaches) can be enacted both within guidelines and psychiatric services.
VTE Risk
VTE Risk Assessment and Prevention in Pregnancy
Written by Ellen O'Rourke1, Rehman Faryal1, Marc Blondon2, Saskia Middeldorp3, Fionnuala Ní Áinle4,5,6
1Mater Misericordiae University Hospital, Dublin, Ireland
2Division of Angiology and Hemostasis, Geneva University Hospitals and Faculty of Medicine, Geneva, Switzerland
3Department of Internal Medicine, Radboud University Medical Center, Nijmegen, The Netherlands
4Rotunda Hospital, Dublin, Ireland
5Royal College of Surgeons in Ireland, Ireland
6School of Medicine, University College, Dublin, Ireland
Venous thromboembolism (VTE) comprises deep vein thrombosis (DVT) and pulmonary embolism (PE). Despite improvements in care pathways for pregnant people, VTE is still a leading cause of death in pregnancy and in the postpartum period.1 During 2014 to 2016, VTE was listed as the leading cause of direct maternal death (defined as death from a cause arising directly from pregnancy) in the United Kingdom and Ireland, at 1.39 (95% confidence interval [CI]: 0.95–1.96) per 100,000 pregnancies.2 A maternal death due to PE has tragic and wide-reaching consequences for the mother's family, friends, and society. VTE can also result in lifelong physical and psychological impairment.3
VTE risk increases during pregnancy and reaches a peak in the early postpartum period. The pooled incidence rate of VTE in a systematic review restricted to studies in which VTE cases were validated was reported to be 118 (95% CI: 101–137) per 100,000 person-years during the antepartum period and 424 (95% CI: 238–755) per 100,000 personyears during the postpartum period.4 Superficial venous thrombosis (SVT) is also common during pregnancy and postpartum and, while it is a manifestation
of VTE, is also a strong risk factor for pregnancy-associated DVT. A nationwide cohort study including data from Danish registries was published recently.5
Among 1,276,046 deliveries, 710 diagnoses of lower extremity SVT were reported during pregnancy and up to 12 weeks postpartum (0.6 per 1,000 person-years [95% CI: 0.5–0.6]). Among 211 people with and without antepartum SVT, 22 (10.4%) and 25 (11.8%), respectively, were diagnosed with DVT (hazard ratio [HR]: 83.3 [95% CI: 46.3–149.7]).
What causes this pregnancyrelated increase in VTE risk?
Reported underlying mechanisms include pelvic venous compression by the pregnant uterus, hormoneand uterus-related venous stasis, compression of the left iliac vein by the right iliac artery, and changes in procoagulant and anticoagulant pathways along with fibrinolytic mechanisms.6,7,8,9 For example, plasma endogenous thrombin potential (a marker of prothrombotic potential) and plasminogen activator inhibitor-1 levels (markers of fibrinolytic activity) are significantly higher in pregnant people than in nonpregnant controls.8,9 In pregnancy, platelets also undergo morphological changes and
platelet activation is increased.10 When they are activated, platelets release many signalling factors, known as the platelet releasate,11 which plays crucial roles in wound healing, hemostasis, and inflammation.12 Intriguingly, maternal platelet releasate contents differ in pregnant people compared with nonpregnant people. In a recent Irish study, 18 healthy pregnant and 13 nonpregnant platelet releasate were analyzed using comparative label-free quantitative proteomic profiling and the differences were characterised.13 Sixty-nine PR proteins were differentially released, and it was possible to discriminate between pregnant and nonpregnant people in the case of 11 PR proteins. It remains to be determined whether this change in platelet releasate contents contributes to pregnancyassociated VTE risk.
In this review, we provide an update on the recent evidence of known VTE risk factors in pregnancy, the frequency of these risk factors, and evidence-based prevention of VTE in people with prior VTE, anchoring to recently published randomized controlled trial (RCT) data. We outline knowledge gaps and current approaches to VTE prevention in the postpartum period, including ongoing pilot trials. Finally, we review recently published registry data on the incidence and prognosis of superficial vein thrombosis during pregnancy and the postpartum period.
VTE Risk Factors in Pregnancy
The higher pregnancy-associated VTE baseline risk can be increased by additional characteristics that can preexist or present during pregnancy or in the peripartum period.6,14,15,16,17,18,19,20,21 This is why it is so crucial to carry out a VTE risk assessment at various time points in pregnancy, repeating this risk assessment postpartum or if risk factors change.22 Risk
factors can relate to personal characteristics (age, body mass index [BMI], smoking), previous medical history (history of VTE, inflammatory disease), or current pregnancy (preeclampsia, preterm delivery, mode of delivery). They can be classified according to their strength of association with VTE: very strong (e.g., personal history of VTE), strong (e.g., emergency cesarean delivery, morbid obesity), and weak (e.g., age ≥35 years). Literature pertaining to the strength of risk factors, in terms of their odds ratios (ORs) for VTE, has been summarized by the authors in detail in previous reviews.6,23,24
How Frequently and When Do Pregnancy-Associated VTE Risk Factors Occur?
The relationship between VTE risk variables and the risk of pregnancy-associated VTE varies; however, we now know that, certainly when assessed in the postpartum period, these risk factors are multiple and common ([Table 1]).25 According to a recently published cross-sectional study of prospectively collected data from 21,019 sequential postpartum VTE risk assessments completed over a 3-year period in the Rotunda Hospital, Dublin, Ireland, the most frequent VTE risk factors related to maternal characteristics and delivery characteristics included overweight status and obesity (36%), age ≥ 35 years (35%), and cesarean delivery (32%).25 In total, 78% of people had at least one VTE risk factor, and 40% of them had several risk factors (two or more). The crucial necessity of doing a VTE risk assessment after delivery is shown by the fact that in 19% of people, all VTE risk factors occurred during delivery or in the postpartum period (and were not present prior to this peripartum time).25
Thrombophilia
People with hereditary and acquired thrombophilia are more
Ellen O'Rourke
Fionnuala Ní Áinle
Table 1 Prevalence of postpartum VTE risk factors among people delivering an infant >24 weeks’ gestation and undergoing VTE risk assessment between January 2015 and December 2017 in a single center
likely to experience pregnancyassociated VTE than people without these disorders, especially if they also have a family history of VTE.26,27,28,29 The reported increase in pregnancy-associated VTE risk varies significantly between studies and by thrombophilia type. The acceptable threshold for starting thromboprophylaxis during pregnancy, according to experts from the American Society of Hematology's (ASH) guidelines panel, is approximately 2%.26 In some thrombophilias, the absolute risk of VTE during pregnancy does not appear to cross this threshold, while it does in others. For instance, in a pooled analysis of published cohort studies including thrombophilic women with a family history of VTE reported in the 2018 ASH guideline, an absolute risk of 0.5% (95% CI: 0.06–1.21%) was estimated.26 This is not surprising, given the results of a more general case control study including 437 first-degree relatives of 112 symptomatic heterozygous factor V Leiden (FVL) mutation carriers (and 30 relatives of 6 homozygous FVL carriers) reported annual VTE incidences of 0.45% (95% CI: 0.28–0.61%) in FVL mutation–positive relatives of propositi who were heterozygous FVL carriers and 0.10% (CI: 0.02–0.19%) in those
who did not have the mutation (relative risk [RR]: 4.2 [CI: 1.8–9.9]).30 Notably, 30% of VTE events were associated with pregnancy or use of oral contraceptives.
However, among people whose past incident was triggered by a significant transitory nonhormonal VTE risk factor, the chance of VTE recurrence during pregnancy was predicted to be 1.0% (95% CI: 1.9–5.7%).7
VTE is much more likely to occur in pregnant people with a personal history of VTE16,31 than in those without a history of VTE. The reported absolute risk in the absence of thromboprophylaxis is estimated at 2 to 6% in the antepartum32,33,34 and 6 to 8% in the postpartum period,31,33,34 and it appears to be highest for people with an unprovoked or a hormonerelated VTE in these cases. In comparison to people who had an unprovoked or nonhormonal transient risk factor–provoked event, people with a history of a VTE event in the presence of oral hormonal contraceptive use or pregnancy experienced a higher VTE recurrence rate during pregnancy (although this finding did not reach statistical significance).33,34 In addition, a sizable retrospective cohort study found that people with pregnancy-associated VTE had a greater risk of recurrence during a future pregnancy than people with unprovoked VTE (4.5 vs. 2.7%; RR: 1.7; 95% CI: 1.0–2.8).35
Although the frequency and risk of individual VTE risk factors has been characterized in multiple observational studies, an important knowledge gap still exists surrounding the duration of the increased risk and the interaction of VTE risk factors with each other, which requires a high statistical power and thus very large sample sizes.
The possibility that individual risk factors impact the risk of postpartum VTE for different durations would have clinical implications, but this has not been investigated thoroughly. One large United Kingdom retrospective cohort has suggested that people who are obese, with preeclampsia, infection, or those with cesarean delivery have persistently elevated risks for 6 weeks, while the risk of those with postpartum hemorrhage (PPH) or preterm birth was only elevated for 3 weeks after
With regard to the combination of risk factors, a Norwegian hospitalbased case control study offered an intriguing perspective. In total, 559 people with objectively confirmed VTE during pregnancy or the postpartum period and 1,229 controls were enrolled in this study.15 Some risk factors exhibited additive interaction (as seen with the combination of assisted reproductive technology [ART] with multiple pregnancy and emergency cesarean section [CS] with infection), while others appeared to act as multipliers. For example, adjusted ORs of antepartum immobilization in people with BMI of <25 and ≥25 kg/m2 were 7.7 (95% CI: 3.2–19.0) and 62.3 (95% CI: 11.5–337.6), respectively. We view these findings as exploratory, given the wide confidence intervals around these possible interactions and the possibility of selection bias in this study.
Understanding how these VTE risk variables affect absolute pregnancy-associated VTE in particular is crucial. A risk prediction model for postpartum VTE was derived and externally
VTE Risk
Table 2 Estimated proportion of people recommended postpartum thromboprophylaxis according to international guidelines
expertopinionratherthanhigh-qualitydata. The confl ictingdangersanddiffi cultiesofpharmaceuticalthromboprophylaxis,whichareratherprevalent50 andinclude bleeding,bruising,skinresponses,pain,possibleincreased woundcomplications,51 and,inmanyjurisdictions,signifi cant
Total( N ¼ 21,019)Caesareandelivery ( n ¼ 6,717) Vaginaldelivery ( n ¼ 14,302) n %(95%CI) n %(95%CI) n %(95%CI)
validated, utilizing data from 433,353 deliveries in the United Kingdom Clinical Practice Research Datalink linked to Hospital Episode Statistics. In total, 662,387 deliveries in Swedish datasets were used to externally validate this model. The strongest VTE predictors in the final multivariable model were emergency CS, stillbirth, varicose veins, preeclampsia/ eclampsia, infection, and medical comorbidities. The model performed reasonably well in predicting postpartum VTE with a C statistic of 0.70 (95% CI: 0.67–0.73) in the United Kingdom cohort and 0.73 (95% CI: 0.71–0.75) in the Swedish cohort.20 Limitations of this tool lie in possible bias from misclassification of VTE events and of risk factors in both development and validation efforts, the fact that it should not be used for people with thrombophilia, and that very few people have predicted postpartum VTE risks greater than 0.2 to 1%.
Reducing the Risk of VTE in Pregnancy
Two VTE prevention strategies are expected to be most effective: the prevention of postpartum VTE among people with risk factors, as the incidence of pregnancy-associated VTE peaks in the 3 weeks after delivery, and
the prevention of pregnancyassociated VTE among people with a prior VTE, who have the greatest risk.
However, answering the question “Does pharmacological thromboprophylaxis reduce the risk of pregnancy-associated VTE?” has proven to be difficult.
In fact, a 2014 Cochrane review's authors came to the conclusion that “there is insufficient evidence on which to base recommendations for thromboprophylaxis during pregnancy (and that) large scale, high-quality randomised [sic] trials of currently used interventions are warranted.”
37 The same conclusions arise from a recent (2023) systematic review and meta-analysis, stating that the existing literature is insufficient.38
VTE Risk Reduction in People with Prior VTE
The multicenter, multinational academic Highlow RCT was published in 2022 and tested the risk–benefit of two doses of low-molecular-weight heparin (LMWH) during pregnancy and the postpartum period in women at high risk of VTE.39 This RCT included 1,110 pregnant people aged ≥18 years and ≤14 weeks' gestation with a history of prior objectively confirmed VTE (either unprovoked/provoked by a
hormonal-/pregnancy-related risk factor). Nine countries took part in the study with 70 sites in total. People were randomized to weight-adjusted intermediatedose or fixed low-dose LMWH. No significant difference was observed in the primary efficacy outcome of objectively confirmed, adjudicated VTE up to 6 weeks postpartum. The primary outcome was reported in 3 and 2% of people in the low- and intermediate-dose groups, respectively (RR: 0.69 [95% CI: 0.32–1.47]; p = 0.33). There was also no significant difference between the groups in the primary safety outcome, major bleeding (RR: 1.16 [95% CI: 0.65–2.09]). Based on this study, low-dose LMWH is appropriate for prevention of recurrent VTE in pregnancy, although the risk of VTE despite prophylaxis is not negligible. Interestingly, antepartum VTE was numerically similar in both study arms (1% in both), whereas postpartum VTE recurrence was more frequent in those receiving low-dose LMWH compared with intermediate-dose LMWH (2 and 1%, respectively). While this suggests the hypothesis that intermediate-dose LMWH may be more favorable after delivery or in the late third trimester, this finding is exploratory and needs confirmation in future randomised controlled studies.
Pregnancy-Associated VTE Risk Reduction in People with Multiple, Common VTE Risk Factors
Following the publication of data from the Highlow study,39 we now have high-quality data to support optimal management of pregnant people who have a personal prior VTE history. However, this risk factor is thankfully uncommon among the entire pregnant population (0.5% [95% CI: 0.5–0.7%] of all people recruited to a recent large observational study25). Wide variations in worldwide guideline recommendations,22,26,40,41,42 as well as heated debate,43,44 demonstrate the important information gap that still exists about the best method for pregnancy-associated VTE prevention in people with more prevalent VTE risk factors. It is noteworthy that the 2018 ASH guideline panel26 emphasised critical research requirements, including a desire for greater evidence on the absolute VTE risk in people with combinations of known risk factors, and that the balance of thrombosis and bleeding risk remains uncertain.
A multicenter study conducted by the STRATHEGE investigators of the French INNOVTE Network evaluated the rates of pregnancyassociated VTE and placental
vascular complications before and after a risk scoring system was put in place to identify antenatal and postpartum thromboprophylaxis techniques in 2,085 people with major VTE risk factors. Before and after the application of risk score–driven prophylaxis, vascular incidents (pregnancy-associated VTE including SVT and placental vascular complications) occurred in 190 (19.2%) and 140 (13%) cases, respectively (RR: 0.68 [95% CI: 0.55; 0.83]), with an associated increase of low-dose LMWH use during pregnancy and puerperium from 59 to 71%. In addition, there was a decrease in the incidence of pregnancyassociated DVT (RR: 0.30 [95% CI: 0.14; 0.67]), mainly driven by a reduction of antepartum SVT. PPH was noted in 3.2% of people prior to implementation and 4.5% afterward (RR: 1.38 [95% CI: 0.89; 2.13]; p = 0.15).45 These findings are encouraging, with improved outcomes following a risk score and a greater use of LMWH, but given the lack of randomization these cannot be interpreted as causal and definite.
Postpartum Prevention
Conducting RCTs for people with (in this case, postpartum) VTE risk factors can prove to be quite difficult, as the PROSPER investigators' experience has shown.46,47 To ascertain the viability of carrying out a fullscale multicenter trial, Rodger et al conducted a multinational, double-blind pilot RCT comparing LMWH for 21 days with placebo injections in postpartum people at high VTE risk.46 In six centers, recruiting for a mean of 6.3 months, with a recruitment rate of 0.7 per site per month and just 25 (6.6%) of the 378 eligible people being randomised, the authors came to the conclusion that a double-blind RCT design for this intervention was not practical in North America. The feasibility of a randomized, open-label trial contrasting 10 days of LMWH medication with no treatment for postpartum thromboprophylaxis in people at risk of VTE was investigated in a second pilot study by the same team.47 With a recruitment rate of 0.9 per center each month, only 37 of the 343 eligible people were randomized throughout 4.9 months. According to the authors, “poor recruitment is a frequent and significant threat to the completion of RCTs, especially notable in the peripartum population.” As a result, guideline recommendations are currently primarily based on expert opinion rather than high-quality data.22,26,41,48,49 The conflicting dangers and difficulties of pharmaceutical thromboprophylaxis, which
are rather prevalent50 and include bleeding, bruising, skin responses, pain, possible increased wound complications,51 and, in many jurisdictions, significant out-of-pocket costs, can make this highly challenging for health care professionals.
Surprisingly, the difficulty of conducting trials of postpartum thromboprophylaxis contrasts with the views and preferences of people. Very recently, in the “PREFER-Postpartum” study, we elicited the desire for postpartum thromboprophylaxis among 122 pregnant/postpartum people in Geneva and Paris. Using structured interviews, most people favored receiving shortterm postpartum prophylaxis with LMWH, even at low projected risks of postpartum VTE (0.1%). This result was somewhat sensitive to the bleeding risk associated with the drugs and varied substantially across people. Hence, while postpartum people are reluctant to participate in clinical trials, most value measures to prevent postpartum VTE.52
The lack of strong evidence for the risk–benefit of LMWH has led to extremely varying guidance and clinical practice. We recently conducted an analysis of prospectively collected Irish data from 21,019 continuous comprehensive postpartum VTE risk assessments, applying the recommendations of representative international guidelines, and calculating the percentage of people who would have received a recommendation for postpartum thromboprophylaxis under each guideline.25 This analysis was done to reflect the lack of data.
According to the recommendations from the American College of Obstetricians and Gynecologists (ACOG)53 and the Royal College of Obstetricians and Gynaecologists (RCOG)22 of the United Kingdom ([Table 2]), the percentage of people who would have received a recommendation for postpartum thromboprophylaxis ranged from 7 to 37%. A similar range from 9 to 40% was found in a similar work from Switzerland.54
We foresee different strategies to improve the evidence on postpartum thromboprophylaxis. The first is to test an oral drug to prevent postpartum VTE to eliminate the burden of subcutaneous injections. Unfortunately, the excretion of oral direct anticoagulants in maternal milk greatly limits their use.55 Low-dose aspirin has some effect on VTE prevention, albeit weak.56,57 This is the focus of the Postpartum Aspirin to Reduce Thromboembolism Undue Morbidity (PARTUM) pilot trial, assessing the feasibility of
randomizing people with some risk factors for postpartum VTE to 6 weeks of aspirin or placebo (NCT04153760). A second strategy is to infer the risk–benefit of LMWH from observational studies, but this is very challenging. Large sample sizes with varying prevalences of LMWH are required for the somewhat rare VTE outcome, with a need to limit VTE misclassification and to adjust for many confounding variables, with the persisting possibility of residual confounding. Retrospective before/ after evaluations of protocols for postpartum VTE prevention in individual large hospitals have remained underpowered to detect differences in clinical outcomes.58
A third strategy is to challenge the perception that a large-scale postpartum VTE is unfeasible.
The Postpartum Heparin Against Venous Thromboembolism (PPHEP) pilot trial in Geneva has recently shown that one out of four people was willing to participate in a pragmatic, open-label trial of 10 days of LMWH after delivery, with a promising recruitment rate, contrasting with previously pessimistic results in North America.52
We hope that this effort will be followed by a practice-changing randomized clinical trial to finally guide practice for postpartum thromboprophylaxis. While awaiting future data, how should we handle postpartum VTE prevention? There is agreement that people without any risk factors should not receive postpartum LMWH and that people at high risk (prior VTE, see below, or strong thrombophilia) should be administered LMWH. The clinical equipoise concerns people with some risk factors for VTE, usually in combination, where the evidence is insufficient. Here, hospital-based recommendations based on local preferences and individual shared decision-making are the only advisable processes at this time.
Conclusions
VTE is the leading cause of maternal mortality in developed countries. The pathophysiology of derangements in hemostasis during pregnancy are well described, at both the patient and molecular levels. Despite this, there remains a paucity of highquality data surrounding optimal VTE prevention strategies for pregnant people. This lack of data is multifactorial, but it can largely be attributed to poor recruitment rates—particularly in the crucial postpartum period—as well as the fact that pregnant people are frequently excluded from clinical research studies. Encouragingly, recent efforts demonstrate that while postpartum people are
reluctant to participate in clinical trials, they strongly value the prevention of postpartum VTE, and that the feasibility of a postpartum thromboprophylaxis trial is better than previously believed.48
At present, two prevention strategies prevail: preventing postpartum VTE among people with risk factors and preventing pregnancy-associated VTE among people with a prior VTE. Risk assessment is a fundamental component in combating pregnancy-associated VTE, and it is crucial to carry out a risk assessment at various points throughout pregnancy. It is important to classify risk factors by their strength of association with VTE. Even in thrombophilia, the indication for pharmacological VTE prophylaxis depends on the subtype. It is intriguing to consider the conjecture that risk factors in combination can exhibit additive or exponential interactions.16 Similarly, the possibility that individual risk factors may impact the risk of postpartum VTE for different durations adds uncertainty to the optimum duration of postpartum thromboprophylaxis. Although highly susceptible to bias, a recently developed risk prediction model was shown to successfully distinguish between postpartum people with and without VTE. This is an exciting potential avenue in the pursuit of pregnancyassociated VTE prevention.
At present, strategies for prevention of pregnancyassociated VTE are based on expert opinion or observational data. Astonishingly, there is still insufficient evidence to confirm that pharmacological thromboprophylaxis reduces the risk of pregnancy-associated VTE.35 Thankfully recent trials have aimed to bridge this knowledge gap and following the publication of data from the Highlow study,39 we now have high-quality data to support optimal management of pregnant people who have a history of VTE. However, a question remains regarding the optimal dose in the postpartum period.
While the Highlow study succeeded in answering a critical clinical question, the evidence is still lacking for the vast majority of pregnant people who do not have the risk factor of prior VTE. Despite the fundamental challenges in conducting RCTs with pregnant people, we are optimistic that the recent phenomenal efforts will translate into clinical guidance. In the interim, individual risk assessments and shared decisionmaking remain the best practice.
Environment & Health
Trees and Health in a Changing World
ENVIRONMENTAL OVERVIEW
Background
I was thinking about climate change and whether there was any place for the medical profession (world-wide) to advocate for the people. I was looking for some up-to date article on the subject to try to briefly put into perspective the size of the problem, and whether the threats that have been expounded are real, and thus likely to make people die (like diseases that we try to prevent and treat). Well in a case of nearly perfect timing, the Guardian, not known for disinformation, in May, published an article where they had asked 380 top climate scientists what they felt about the future, and to be honest, it made scary reading. The climate crisis is already causing profound damage as the average global temperature has reached about 1.2C above the pre-industrial average over the last 4 years. Of the respondents 77% believe that global temperatures will reach at least 2.5C above preindustrial levels, and 44% believe that it will be more than 3C. Only 6% believe that the 1.5C limit (UN climate summit Paris 2015) will be achieved. A few pointers on these observations. Even just 1C of heating has supercharged the planets extreme weather, delivering searing heatwaves that would have been otherwise impossible. A world hotter by 2.5-3C takes us into truly unchartered territory, with everything from 2 billion people being pushed outside humanity’s climate niche, to Cities like Rio, Miami, Shanghai and the Hague ending up below sea level. “It is the greatest threat humanity has faced with the potential to wreck our social fabric and way of life. It has the potential to kill millions, if not billions, through starvation, war over resources, and displacement – none of us will be unaffected by the devastation”. Climate tipping
Written by Dr David Mulcahy, Consultant Cardiologist MD FRCPI FESC
points, where a tiny temperature rise tips crucial parts of the climate system into collapse, such as the Greenland Ice-sheet, the Amazon rain-forest, and key Atlantic currents, have also come into play. “Most people do not realise how big these risks are”.
So I (like the rest of the more than 19,000 practicing physicians in Ireland in 2023) am spending much of my life trying to improve the lot of my patients but I am beginning to feel that we have a very significant health issue here with climate change which, by and large, we are assiduously avoiding. I am aware that, as governments come and go, it is difficult for them to commit to often unpopular longterm strategies when their jobs are “on the line” after 4-5 years. So, as it seems climate change is a major health issue (clearly more of a one than many of the diseases that we successfully treat) perhaps the (global) medical profession should take climate change as a vital new disease to attempt to treat, either with personal actions or with lobbying as a way of advocating for our (8 billion) “patients”.
Action we can take
So, in Ireland, what can we do? Well, we can always encourage our government to do better, and to support initiatives which reduce our reliance on fossil fuels (Banks worldwide have apparently given
almost 7 Trillion dollars to fossil fuel firms since the Paris Accord). We can join the ranks of people who don’t ignore those who advocate for “green” initiatives, while questioning those who use “green” initiatives purely for money-making purposes, but who make no positive contribution to climate change. We can take personal action to try to
make even tiny contributions in mitigating against climate change, and while knowing that, whatever we do in Ireland is not going to change the global situation directly, it may generate a global effect (A la our cigarette ban), which might then lead to greater benefits. With these musings in mind – let's talk about trees!
1. Trees are the best way of increasing Carbon trapping
2. Planting trees is enormously helpful when trying to protect our natural world and increase biodiversity
3. Ireland has one of the lowest levels of afforestation in Europe (approx. 11.5%) with most trees being non-native conifers
Trees. We just take them for granted. They are everywhere They have been in Ireland for eons. We live in the emerald Isle. We are inundated with trees – are we not ? Forest upon forest of – aah but they are dark green – imported from North America in the 1800’s, the Sitka Spruce now accounts for over half the tree population in
With photography by Martin Blake, Bailey and Blake Video productions
Figure 1 Figure 1: Commercial Spruce Forest, County Wicklow
and indeed most of the native tree planting done over this period has been done by private individuals over the past 40 years.
on
Ireland, with over 70% of all trees in Ireland composed of conifers. Great for investors and good for building, they have marched through the Irish landscape, killing all below them (ecological dead zone) (Figure 1); but a good investment, and very important for building etc. But why would
we worry, there are stacks of native trees in Ireland, are there not; everything from giant Oak to beautiful Irish Cherries. No !. Unfortunately Ireland is one of the least afforested countries in Europe, ranking 40thin 2020, at about 11.35% of land forested, and ahead of the Netherlands, Malta, Iceland and Monaco (Figure 2). Ireland has lost almost all of its native forests, with just 2% of the country being covered by native broadleaf trees. With it are going all the things, both plant and animal, that would have lived
in those native “hotels” (Figure 3). While most of Ireland was covered in trees 6000 years ago (80% coverage), by the end of the 19th Century only 1% of the country was forested, representing almost total destruction of our woodlands and forests, and resulting from multiple factors, ranging from mobile sawmills touring around the country, the destruction of anything standing in the way of the rush to increase agricultural land, to, understandably, tree felling for wood to keep the home fire burning. For a long time outside agencies were held responsible for the loss of the native tree, one of the emeralds of our Isle, but in the over 100 years where we have been able to directly impact on this issue ourselves, little has been done to address the loss of such a vital cog in our natural world,
Government incentives in the past have only tended to aggravate the problem of afforestation in Ireland. Grants were available to plant forests, but once forests were planted, that land could not be used for any other purpose again into the future (described as a “negative nudge” for landowners). Furthermore the grants were only for 15-20 years, and so this provided a strong financial incentive to plant fast-growing non-native species, which when harvested would disturb wildlife, release carbon, damage water quality, and leave the landscape “scarred”. It is argued that if we really wanted people to grow native forests (predominantly slow growing) there should be a subsidy to reflect long-term ecosystem support, and subsidies should of course also reflect the value of any action as a public good.
Figure 2
Figure 3: Native Oak Forest at Tomnafinnoge, County Wicklow
Figure 4: Benefits of Urban Mini-forests
Figure 4 Benefits of Urban mini-forests
Environment & Health
Example of 2000 Tree native miniforest planted December 2022 (Tinturn Abbey) and photgraphed 19 months later.
How do you get the public on board?
change. Trees hugely benefit wildlife, and trees improve physical and mental health (Figure 4).
Figure 5: Example of 2000 Tree native miniforest planted December 2022 (Tinturn Abbey) and photgraphed 19 months later
But what does any of that matter to people, especially as many don’t really feel any personal responsibility for the protection of nature and the environment, and as we continue to strive for the inexorable expansion of the human’s world. Are trees actually any use for humans, and indeed do they have any health benefits. Well, yes actually, they do. To mention a few, trees help clean our air. Trees help reduce noise. Trees help reduce storm water and run-off. Trees provide cooling. Trees help clean our drinking water. Trees provide us with oxygen. Trees increase our property values and apparently help reduce crime. Trees help us save energy. Trees help us reduce the effects of climate
Private individuals and communities need to “seize the moment” to address the afforestation issue for the benefit of our environment, and to attempt to mitigate, in whatever small way, against climate change. Most importantly we need to think about our birds, our bees, our insects and our wildlife, none of which we can afford to lose, but who we have given scant regard to. As of 2022, 63% of Irelands bird species are in serious trouble. More than half of Irelands bee species have undergone substantial declines since the 1980’s, in part due to loss of the natural abundance of flora due to increased land use, and habitat destruction.
Insectageddon is probably an exaggeration, but it is suggested that there is a loss of insect biomass at a rate of 2.5% per annum in some cases.
Example of 2000 Tree native miniforest planted December 2022 (Tinturn Abbey) and photgraphed 19 months later.
How do we move forwards together?
So what can we do ? well we have set up a community driven programme, the 100 million tree project (www.100milliontreeproject. ie), with the aim of planting 100 million native trees in a 10 year period. We call it community driven because we need philanthropists to help us pay for the trees; we need the tree growers to upscale, knowing that we will buy their native trees, and that they don’t have to be exported (or imported); we need Forestry services to upscale on tree planters to deal
with the exponential increase in tree planting over time, and most importantly we need people, and institutions to give of their land for the benefit of all, so that native trees can be grown – these of course would be their trees, their mini-forests, with no restriction to future use of the land, while hoping of course that the forest would be allowed to flourish with all the attendant benefits, from birdsong to the buzzing of bees, pleasures often absent in our modern world. And how much land would have to be used ? A quarter acre would allow the planting of 2500 native trees of 14-15 different varieties, with everything from Oak to Alder and Birch to Hawthorne, Scots pine to Irish Cherry, Rowan to Hazel to Holly and many more. The intensive planting (Miyawaki method, also referred to as crowdforesting), allows for rapid growth, increased density, increased biodiversity, and the development of a very rapid carbon sink. Evidence suggests that trees prefer being planted close together, and do well when species are mixed in close quarters. Finally, maintenance is simple with occasional trampling down of weeds for the first couple of years, and then the rapidly growing forests look after themselves. The
Examples of 10 different miniforest sites planted December 2022 to March 2024 at:
Fairyhouse racecourse
Tintern Abbey
Glenstal Abbey
Powerscourt Estate
Ballymun kickhams GAA
IDA Site Athlone
Figure 6: Examples of 10 different miniforest sites planted December 2022 to March 2024 at:
Fairyhouse racecourse
Tintern Abbey
Glenstal Abbey
Powerscourt Estate
Ballymun kickhams GAA
IDA Site Athlone
Ballybritt Racecourse Galway
Bride Street Church Wexford
Waterford Airport
University College Dublin
Ballybritt Racecourse Galway
Bride Street Church Wexford
Waterford Airport
University College Dublin
argument over what type of trees to plant on the 450,000 hectares of land needing to be planted if the government wishes to achieve its aim of 18% of Ireland covered in forestry by 2050 should be mute – if most of this land needs to be planted with fast growing sitka forests in order to protect the building and manufacturing industry into the future, then more land should be made available for native tree planting, thus protecting the wood production for building while significantly increasing our afforestation and biodiversity, and eliminating substantial penalties for failing to achieve our environmental goals. In the meantime, we, the people, should be doing as much as we can ourselves.
In our “trial” year (Nov 22 – Apr 23 (bare-root planting season)) we developed a comprehensive website and planted just over 20,000 native trees in 18 different sites throughout the country, funded by an Irish Philanthropist living in the US, (figure 5) and in our first “full” planting season (Nov 23- May24) we planted just over 200,000 native trees in 83 different sites, funded almost entirely by Uniphar. Most of the sites were of a 1/4 acre size with 2500 native trees being planted
in each one. A few landowners wanted more than one 1/4 acre site (up to 3 in one case). Unlike many countries where the soil is not rich, and requires preparation prior to planting, Ireland should be an ideal climate for tree planting, and preparation simply involves ploughing the site, and rotivating it to loosen the soil to about 8 inches so that the saplings can be easily (and quickly) planted, and this also gives tree saplings an early breathing space where they don’t have to contend with grass or weeds. If there are rabbits or hares around then appropriate fencing will be required, and of course if there are deer, then deer fencing is essential. While this (fencing) requires some expenditure, it will be well worth it when your own native forest is flourishing. A normal mini-forest should take a few hours to plant with proper preparation and professional planters (also provided) (Figure) The benefits of mini-forests are not simply confined to the actual planting of thousands of small areas of carbon capture and biodiversity. Intense planting means that the forests will be impenetrable to natures biggest threat, the human, after a couple of years: Because only 1 native tree
is a conifer, excellent undergrowth areas of biodiversity can develop within the mini-forests; Also having 40,000 miniforests (100,000,000 trees) means that destructive forest fires are not a worry (Canada lost 4 times the total tree stock of Ireland last summer in extensive forest fires). Finally it is likely that little or none of the 10,000 acres used to intensively plant the 100 million trees would have been considered for tree planting under any national plan, as it almost entirely consists of small allotments of private land. To plant a similar number of native trees with “normal” planting of 1000 trees per acre, 100,000 acres of land would need to be acquired. Thus the contribution of the 100 million tree project should be very much a win-win situation for both citizens and state.
In summary
So, if the medical profession in Ireland decided to get stuck into tree planting, as part of our overall management of the “health of the nation”, and say 500 (5%) had a site to turn into a native mini-forest, or knew someone who had one, this would add 500 new areas of biodiversity and 1,250,000 native trees, with all the attendant benefits of same
(at 5 to 8 years you can assume that 1.25 million trees will be sequestering about 17,500 tonnes of Carbon per year). All that is needed is a quarter acre of land and we will supply and plant a 2500 tree native mini-forest for you (or you and your friends can plant or help plant it). At present we have enough philanthropic support to plant 550,000 native trees for the upcoming (2024 –25) season, and over 120 people or institutions have prebooked mini-forests. If people choose, they can pay for a 2500 tree native mini-forest (works out as 2 euro/ tree), and we will video the whole project for them: any money left from the tree growers and tree planters goes back into the system to pay for future trees. As mentioned before, if we can get a commitment to significant funding, we can commit to supporting our tree growers, who will be able to expand their growth and supply of native trees, thereby reducing and, hopefully eventually eliminating, the requirement to import native species from abroad. Ideally government should support our tree growers to exponentially expand their productivity.
Do we believe that climate change is, as they would say in the movies, an existential threat to mankind. If we do, let us as Doctors, Nurses and allied Professionals get more generally involved in treating it – a good way to help treat would be to plant, or support the planting of trees, while also setting an example for all our colleagues internationally.
Atopic Dermatitis
EACCI Task Force Report
A systematic review and meta-analysis of nutritional and dietary interventions in randomized controlled trials for skin symptoms in children with atopic dermatitis and without food allergy: An EAACI task force report
Written by Emilia Vassilopoulou, Anna Comotti, Nikolaos Douladiris, George N. Konstantinou, Torsten Zuberbier, Ilaria Alberti, Carlo Agostoni, Roberto Berni Canani, Ioana Corina Bocsan, Antonio Corsello, Valentina De Cosmi, Gavriela Feketea, Kirsi Laitinen, Alessandra Mazzocchi, Nicola A. Monzani, Nikolaos G. Papadopoulos, Diego G. Peroni, Constantinos Pitsios, Franziska Roth-Walter, Isabel Skypala, Sophia Tsabouri, Abdoulie K. Baldeh, Liam O'Mahony, Carina Venter, Gregorio Paolo Milani
Atopic dermatitis (AD) is a chronic, recurrent inflammatory skin disorder characterized by skin dryness, intense pruritus.1, 2 The onset of AD is usually during childhood, and it affects 15%–30% of children.3 4 About 5%–10% of adults suffer from AD, 25% of which are adult-onset cases.4 5 Pathophysiology of AD is characterized by skin barrier impairment, due to defects in the stratum corneum (SC), an abnormal inflammatory immune response and skin microbial dysbiosis.6, 7
The skin barrier impairment in AD applies to the thinner epidermis, with defective lipid and protein composition and function, leading to poor hydration, increased trans-epidermal water loss (TEWL) and increased permeability to microbes, irritants, and allergens.8
Non evidence-based food restriction practices, poor diet quality, and impaired growth are common in children with AD.911 Disease severity is associated with poorer quality of life (QoL), affecting mental health.12-14
The management of AD focuses on: (a) minimization of the underlying inflammation, both locally and systemically, with corticosteroids, topical calcineurin inhibitors, and immunosuppressive and/or immunomodulating drugs in the most severe cases, in order to treat the AD and modify the impairment of the skin barrier, (b) restoration of the skin barrier, mainly through the use of moisturizers, and (c) identification of aggravating factors, and education of the patient and the family on how to avoid them, in order to alleviate the symptoms and improve the patient’s QoL.15-17
Several studies have indicated that long-term “Western” dietary patterns rich in processed food, fat and sugar, lead to dysregulation of the Th1/Th2 balance, favoring the Th2 inflammatory pathway,18 as confirmed by a recent meta-analysis by Li
and colleagues.19 Conversely, traditional dietary patterns, rich in natural products, such as the Mediterranean diet (MedDiet)20 and the Korean diet,21 are considered to be protective of AD, due to their high content of antioxidants, fibers and “good fat” sources, such as olive oil and fish oil, although the relevant research findings are inconsistent.22, 23
In infants and young children, elimination diets have been suggested as a treatment of AD. These diets mainly involved the avoidance of common allergens, such as milk and egg.24 25 Older children, adolescents and adults often follow exclusion diets, or attempt elimination diets, or use special health food preparations without the guidance of a physician. In order to improve their eczema, they minimize (following an “exclusion diet”) or completely eliminate several foods or food groups.21 Nosrati and colleagues reported in their survey that 68% of the AD patients excluded processed foods, 53.6% white flour products, 49% gluten and 35% nightshades, while they increased consumption of leafy vegetables (84%), fish (80%), and fruit (78%).26
Dietary interventions have been investigated in a wide range of studies, but the published results from randomized clinical trials (RCTs) of dietary interventions in patients with AD have not provided clear conclusions. To date, such trials have focused mainly on interventions with a wide range of dietary supplements, including fish oil, and vitamins D and E, but the interpretation of the results are limited due to low sample
sizes and methodological issues.27-29 Intervention studies with probiotics in some cases appeared promising.30 The positive effect is probably linked to an improvement and rebalancing of the skin microbiota through the gut-skin axis.31 32 However, the study population is often mixed, with some participants being food allergic or sensitized to several food allergens affecting food avoidance.
A systematic review and meta‐analysis of nutritional and dietary interventions in randomized skin symptoms in children with atopic dermatitis and without food allergy: An EAACI
A systematic review and meta‐analysis of nutritional and dietary interventions in randomized controlled skin symptoms in children with atopic dermatitis and without food allergy: An EAACI task force report
A systematic review and metaanalysis of nutritional and dietary interventions in randomized controlled trials for skin symptoms in children with atopic dermatitis and without food allergy: An EAACI task force report
Allergy, Volume: 79, Issue: 7, Pages: 1708-1724, First published: 23 May 2024, DOI: (10.1111/all.16160)
Allergy, Volume: 79, Issue: 7, Pages: 1708-1724, First published: 23 May 2024, DOI: (10.1111/all.16160)
Call for papers: make your contribution to Hospital
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
Atopic Dermatitis
A systematic review and meta‐analysis of nutritional and dietary interventions in randomized controlled trials for skin symptoms in children with atopic dermatitis and without food allergy: An EAACI task force report
Allergy, Volume: 79, Issue: 7, Pages: 1708-1724, First published: 23 May 2024, DOI: (10.1111/all.16160)
A systematic review and metaanalysis of nutritional and dietary interventions in randomized controlled trials for skin symptoms in children with atopic dermatitis and without food allergy: An EAACI task force report
“vitamin” OR “macronutrient” OR “micronutrient.”
The complete search strategy of the three databases is included in the Supporting Information. The reference lists of the retrieved articles and relevant articles were manually screened for further publications for inclusion.
Methods
Literature search
Due to the scarcity of comprehensive and reliable evidence for drafting a position or guideline paper on nutritional and dietary interventions for skin symptoms in children affected by AD without food allergy, we aimed to evaluate and summarize available data on this topic. To fulfill this task force’s primary objective, a systematic review and meta-analysis was conducted.
This study was performed according to the Cochrane Handbook for Systematic Reviews Interventions and the statement by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses group (PRISMA). The study was registered in the international prospective register of systematic reviews (PROSPERO) (code CRD42022328702).
A literature search was conducted on May 23, 2022 and updated on January 30, 2024, inPubMed, Embase and Web of Science databases, using the following Medical Subject Heading (MeSH) terms and text words in the queries: “atopic eczema” OR “atopic dermatitis” AND “diet” OR “nutrition” OR “supplement” OR “probiotics” OR “prebiotics” OR
A meta-analysis was performed when at least three studies assessed the same nutrient intervention (independent of the dose or duration of the intervention), and provided an improvement of the AD SCORAD severity score, where available.
Inclusion criteria
A systematic review and meta‐analysis of nutritional and dietary interventions in randomized controlled trials for skin symptoms in children with atopic dermatitis and without food allergy: An EAACI task force report
Allergy, Volume: 79, Issue: 7, Pages: 1708-1724, First published: 23 May 2024, DOI: (10.1111/all.16160)
The eligible studies were RCTs in children and adolescents with AD without food allergy, treated with: (a) a dietary modification; (b) a nutritional supplement (vitamins, mineral supplements, probiotics, prebiotics, symbiotics, and/or postbiotics); (c) at least one dietary intervention and at least one nutritional supplement. Furthermore, only trials evaluating the effects of interventions on skin clinical manifestations assessed by SCORAD or equivalent scores, regardless of the use of adjunctive topical anti-inflammatory treatment (e.g., corticosteroids, calcineurin inhibitors, phosphodiesterase inhibitors), were considered. Participants of any race were eligible for inclusion in the study.
Exclusion criteria
Descriptive studies or systematic reviews and meta-analyses, letters, case reports, studies involving elimination diets and
A systematic review and metaanalysis of nutritional and dietary interventions in randomized controlled trials for skin symptoms in children with atopic dermatitis and without food allergy: An EAACI task force report
studies reported AD related to specific food allergens in children and adolescents were excluded Studies evaluating the effect of elimination diets on the culprit food on the AD of food-allergic individuals were excluded. However, all nutritional supplementation studies were eligible independently of the sensitization profile of the examined subjects.
Studies on adults, animals (nonhuman) studies, ex vivo, and in vitro studies were also excluded.
Results
The PRISMA diagram for study search was used for article selection. The flow chart shown in Figure 1 depicts the process by which the relevant studies were retrieved from the databases, assessed, and selected, or excluded. In total, 27 studies met the criteria for inclusion in the review, 20 of which focused on probiotics/synbiotics, and 7 on other forms of supplementation.
Vitamin D
Four RCTs have investigated supplementation with vitamin D (cholecalciferol) in infants and children with AD, at various dosages, ranging from 1000 to 5000 IU per day.39-42 Three studies reported significant (daily dose: 1000 IU,39 5000 IU,41 1600 IU42 vitD3 in a fat soluble drop) and one nonsignificant (1000 IU40 vitD3 in a cellulose capsule) improvement in AD symptoms in children taking vitamin D, in comparison with those taking a placebo (Table 1).
Primrose oil
One study supplemented evening primrose oil in children with AD at two different dosages, 320 mg and 160 mg, for 8 weeks. Significant improvement in symptoms was reported in the high-dose group.43
Dietary modifications
In one study of infants with AD,44 conventional cow’s milk formula (CMF) was replaced by a partially hydrolyzed whey and casein formula (phCMF) in the intervention group. An improved SCORAD was reported in the group of infants receiving phCMF compared to the control group that received CMF (Table 1).
Prebiotics
One study, which investigated the supplementation of fructooligosaccharides, such as kestose, in infants with AD for 12 weeks, reported a significant improvement in SCORAD scores compared to infants in a placebo group that received maltose45 (Table 1).
Meta-analysis was not conducted on the data derived from the above seven studies. Although four of the studies pertained to Vitamin D, the variety of the outcome measures did not permit a meta-analysis. Probiotics/synbiotics/postbiotic
Twenty RCTs focusing on probiotics alone or in the form of synbiotics (probiotics with prebiotics) or postbiotics in a variety of combinations, have been included in the metaanalysis (Table 2). Seven of these were relevant to the use of L. rhamnosus, two of which reported a significant reduction in the SCORAD, compared to placebo,49 54 three reported no effect, either when L. rhamnosus was used alone51 or mixed with other Lactobacillus species50 or with prebiotics.55 56 63
Six studies have used other Lactobacillus strains,46, 53, 57, 58, 61 out of which five have reported a statistically significant benefit in comparison to the administration of placebo, while one64 reported no difference.
A study used a mixture of various Lactobacillus strains, reporting a beneficial effect.60 In three studies various Lactobacillus strains were combined with prebiotics (synbiotics),47 52 62 and two of these studies demonstrated no effect, while one did.62 Two studies used a mixture of Lactobacillus with other probiotics, with one study also including a prebiotic. Both reported benefit in comparison to the placebo.65 66
Two studies that used probiotics other than Lactobacillus, reported either no significant benefit59 or only a borderline significant effect.48
Three studies43 51 53 utilized postbiotics, resulting in a significant reduction compared to the placebo. However, when compared to live cells,51, 53 no significant benefits were observed.
Discussion
This systematic review, to the best of our knowledge, is the first to investigate the effect of dietary interventions, including dietary modifications and food supplements, in children with AD without food allergy. It included 27 RCTs of interventions that aimed to improve AD symptoms, as evaluated using the SCORAD score or another scoring system converted to SCORAD when possible. Gut microbiota modification, to date, appears to have attracted the major interest of researchers, with 20
RCTs involving intervention with probiotics and postbiotics alone or in combination with prebiotics.
Our meta-analysis of the 20 studies, including 1387 infants or children with AD, showed that supplementation with probiotics may benefit SCORAD outcomes, regardless of the race of the population under study.
Probiotics are live organisms, that when administered in sufficient amounts, modulate the intestinal microbiome and confer several health benefits on the host, including enhancing immune function by improving the integrity of the intestinal barrier.68 69 Dysbiosis in AD has been thoroughly characterized70 and various trials explored the effectiveness of pre and postbiotics in reducing the allergic phenomena and the severity of AD.17 71-73
In our meta-analysis, we observed a trend toward a higher effect when: (a) the intervention period is longer than 12 weeks, (b) the children are older than 36 months of age at inclusion to the study, (c) probiotics other than L. rhamnosus are used, and (d) probiotics are used in combination with prebiotics, in the form of synbiotics.
The age group of children with AD, for use of probiotic supplementation has gained the attention of several studies, but the results have been contradictory. A meta-analysis published in 2017 by Huang and colleagues on the efficacy of probiotics in 1070 children and adolescents with AD aged ≤18 years, concluded that the benefit was higher in children older than 12 months.74 The lower efficacy of probiotics in infants aged under 1 year was further supported by the metaanalyses conducted by Jiang and colleagues75 and Husein-El Ahmed and colleagues,76 but the authors reported a high degree of diversity among the studies with participants aged <1 year. In contrast, Zhao and colleagues77 supported that supplementation in infants under 1 year might be more effective. In our systematic review, we detected improved SCORAD scores as an effect of administration of probiotics throughout childhood, but with a more pronounced effect in children aged older than 36 months. Recent research describes the first 1000 days of life as the optimum window for preventive interventions impacting the microbial colonization.78 The trend toward a better therapeutic response, though, after the third year of life is possibly indicative of the slow transformation of the
gut microbiota in infants from a “maternal-like,” taxonomically and functionally, state during the first 2 years of life79 toward an adultlike state during the age period 3–5 years.80 This more effective response might also be an indication of the parallel ongoing maturation of the skin81 and the immune system.82
An important factor affecting the efficacy of the probiotics is the duration of treatment, but differences were observed among the studies. We observed that a period of administration of more than 12 weeks might benefit the SCORAD outcomes, but the differences in this outcome did not reach statistical significance. The data of Jiang and colleagues supported the theory that the benefit might increase after 8 weeks of supplementation, but, again, not to a significant degree.75 Conversely, Zhao and colleagues in their metaanalysis including infants aged ≤36 months of age with moderateto-severe AD symptoms, a supplementation of preparations containing Lactobacillus given for periods of <8 weeks is significantly more effective.77 However, our study encompassed a wider age range, including older children. It is possible that a more extended period of probiotic administration may be required for enhanced effectiveness, but further investigation is necessary in the future.
Some studies concluded that the response to probiotic supplementation might be determined by the phylogenetic characteristics of the populations investigated,83 as they observed a significant reduction in SCORAD scores in Asian, but no effect in European participants.74 This observation was not supported by our meta-analysis, as no difference in effect was demonstrated between Asian and European participants.
Many researchers used L. rhamnosus for their interventions, but we determined no higher effectiveness in its capacity to reduce the SCORAD score in children with AD, in comparison to other probiotics or other Lactobacillus strains. On the contrary, we observed a nonsignificant trend towards greater effectiveness of other strains of Lactobacillus or other probiotics used in interventions to treat AD. Our findings are thus in accordance with Huang and colleagues, whose data supported that L. rhamnosus is not effective for improvement of SCORAD scores in children with AD, but that a significant benefit may be provided by L. fermentum, L. salivarius, and a mixture of
Atopic Dermatitis
different Lactobacillus strains.74 Jiang and colleagues also reported an apparent but nonsignificant, beneficial effect on AD outcomes when mixed strains are administered in comparison to single-strain probiotics.75
Prebiotics are non-digestible food compounds that are fermented by intestinal microbiota to produce metabolites such as short-chain fatty acids and are potentially able to confer health benefits to the host.84 To examine the theory that probiotics might function better when combined with prebiotics85 86 we compared outcomes from studies using synbiotics and those using probiotics only. In line with the meta-analysis of Chang and colleagues that supported the greater effect of synbiotic supplementation, in comparison to the probiotics alone, after the first year of life, we identified a nonsignificant trend in favour of synbiotics. As such, the use of prebiotics to enhance commensal bacterial growth, microbiome diversity, and the overall health of the host,87 is still unclear due to the limited number of studies in infants and children,45 thus no clear outcomes are permitted.
Postbiotics are defined as a preparation of inanimate microorganisms and/or their components that confer a health benefit on the host.
88 They refer to the metabolites or byproducts produced by probiotics as they carry out their actions in the gut, often through processes like fermentation.89 Postbiotics present promising alternatives to probiotics, as they mitigate the risk associated with using live microbial strains.88 In the case of AD it has been hypothesized that postbiotics influence the molecular composition of enterocytes, leading to the closure of the intestinal barrier and providing antibacterial activity.
89 The systematic review and metaanalysis of Carol et al. which included 9 RCTs with postbiotics in a total of 793 children with AD, concluded that there was low-certainty evidence regarding the therapeutic effectiveness of Lactobacillus paracasei GM080.69 Similarly, we were unable to identify significant beneficial effects of postbiotics in our metanalysis.
Furthermore, despite the substantial variation in the doses employed for gut microbiota manipulation, ranging from 109 to 1010 CFU/day, no significant differences were observed in
their effectiveness concerning SCORAD outcomes. This finding is consistent with a recent meta-analysis conducted by Xue et al., encompassing 1000 patients AD, which concluded that the probiotic’s benefit persists irrespective of the quantity used.71
Vitamin D, which acts like a pleiotropic hormone, has been suggested to benefit skin immunity, barrier function, and inflammation due to its capacity to regulate the proliferation and differentiation of keratinocytes.90 91 Furthermore, vitamin D demonstrates pluripotent effects on functions within the adaptive immune system, including the activation of T-cells and maturation of dendritic cells.92, 93 Vitamin D was used in four RCTs in infants and children and provided consistent benefit, regardless of the dose, when used in a fat-soluble matrix,39 41 42 but not when used in a water-soluble (cellulose) capsule.40 In addition, a meta-analysis conducted by Kim and colleagues supported vitamin D supplementation in the treatment of AD in adults.94 Future research should take into consideration the baseline serum vitamin D levels of the population under study.95, 96
Among the hypotheses on the pathogenesis of AD is a deficiency of essential fatty acids in the skin.29 97 Fatty acid levels have a direct impact on the impairment or repair of the functioning of the epidermal barrier. Therefore it is considered important to maintain optimal levels of monounsaturated fatty acids (MUFA) and an equilibrium of omega-3 and omega-6 fatty acids for the synthesis of long-chain fatty acids, specifically C20 eicosanoic and C22 docosahexaenoic acids, as well as the subsequent formation of bioactive lipids like prostaglandins.97-99 Evening primrose oil, extracted from the flowering plant Oenothera biennis, is rich (8%–10%) in gammalinolenic acid (GLA), an Ω-6 fatty acid, offering an anti-inflammatory action.100 Supplementation of evening primrose oil in children was shown to improved SCORAD outcomes in a single RCT.43 Fatty acids, and especially omega-3 fatty acids, have been used for the prevention of AD in RCTs, but their use in the treatment of AD has been limited and applied in adults.20, 101
Finally, information on the possible benefits of dietary modifications for the management of AD during infancy or childhood is scarce. Most relevant studies
focused on food elimination and highlighted the fact that these should be considered carefully and applied under strict indications, as such dietary manipulation may increase the risk of both nutritional deficiencies and the future presentation of food allergy.24, 25, 102 Only one study was identified in the current study: partially hydrolyzed cow’s milk (phCMF) infant formula showed a favorable effect as compare to conventional cow’s milk formula.44
Our systematic review and metaanalysis had certain limitations. First, the effect size on the minimal clinically important difference (MCID) of SCORAD was lower than 8.7, which indicates inadequate clinical responsiveness of the intervention.103 Nevertheless, probiotics supplementation could be used as an add-on therapy to the maintenance therapy consisting of emollients and gentle skin care.
It may also be regarded as an adjunctive therapy to decrease the frequency of using antiinflammatory topical agents, systemic anti-inflammatory or immunosuppressive treatments, and other biologicals, which are often effective but costly104 However, further exploration is needed to confirm this potential benefit. Second, although we attempted to minimize heterogeneity and publication bias in the meta-analysis, significant heterogeneity among the RCTs remained evident. We were able, however, to detect the most influential outliers, after the removal of which, heterogeneity became moderate with a stable effect size. Differences in intervention methods (single, or mixture of probiotic strains, or combined with prebiotics or postbiotics and dosage), duration of intervention, and study population (race, age), contributed to the heterogeneity. The low number of studies in the various sub-group analyses performed reduced the confidence associated with the data interpretation and increased the heterogeneity and publication bias. Finally, for the same reason, we could not draw robust conclusions as to which probiotic strain or strains, or which synbiotic should be given to children with AD, at which age, and for how long, in order to lower SCORAD score maximally. In the past, the different species used in the interventions were collectively categorized under the genus of Lactobacillus. However, recent advancements in nomenclature have led to their dispersion into
new classifications.105 Only one of the included studies adopted the updated nomenclature, while we retained the terminology originally employed in the original articles. Moreover, we could not conduct meta-analysis of the data from the relevant studies with vitamin D in children, because of the different, and non-comparable, ways of describing the outcomes. Another aspect which was not covered in the meta-analysis are studies where potential factors commonly omitted by patients were investigated by exposure studies. One example is the dietary avoidance of sugar based on the belief that it might provoke AD signs. Although the short-term effect of sugar was excluded in a DBPC trial,106 the long-term effect on skin microbiome has not been studied yet, and cannot be excluded as the sugar dose influences the gut microbiota synthesis.107
Conclusions
The results of this systematic review and meta-analysis highlight the intensive efforts of the research community to find dietary means to alleviate the symptoms of AD in children without FA. To date, vitamin D, and probiotics have been more extensively examined, and both show promise in moderating skin symptoms as measured by SCORAD or an equivalent measurement.
From our meta-analysis on the use of probiotics, a consistent trend was revealed regarding the alleviation of AD symptoms in children without food allergy, the mechanisms likely being the manipulation of gut microbiota with probiotics, with subsequent eubiosis. Regarding the appropriate age for intervention and its optimal duration, it is apparent that adequately powered RCTs, involving stratified populations and specific interventions and using standardized measures will be needed to draw firm conclusions about the species of probiotics and the prebiotics to be combined, dosages, and treatment periods, and at which age of life the greatest efficacy will be achieved. Alternatively, with such a multifactorial disease and with such a multitargeted intervention, we might need to proceed by designing studies where we should use the “-omics” (transcriptomics, proteomics, and metabolomics) in order to acquire knowledge of an etiological interaction and a significant outcome.
LYPRINOL JOINT SUPPORT IS BACK IN STOCK ! NOW ALSO AVAILABLE IN 180 CAPSULE BOTTLES!
• The world’s leading Joint Support Supplement
• Lyprinol contains over 30 x Omega3’s and an amazing 91 x different Fatty Acids
• No fishy taste or after taste
• No known side effects, no allergic reactions
• Easy to swallow capsules
• No blood thinning
• Safe to take long term for all the family
“Lyprinol is the most powerful marine oil available. It is far superior to conventional pharmaceuticals, vegetable based Omega 3 oils and fish oils” Dr Georges M. Halpern, M.D., PH.D
Available from all major wholesalers now!
HEAR FROM EPILEPSY EXPERTS THIS SEPTEMBER!
September will be a busy month for the epilepsy community in Ireland, with two major events set to take place at the Gibson Hotel, Dublin!
First, the Irish Epilepsy League (IEL) will be hosting their annual Expert Day on Friday September 20th. The Irish Epilepsy League
are the Irish chapter of the International League Against Epilepsy. Their membership is made up of epilepsy healthcare professionals, scientists and researchers working in or investigating epilepsy in Ireland.
The Expert Day is an annual event organised by the IEL, specifically targeted at healthcare professionals and researchers working in epilepsy, but the event is also open to all healthcare professionals who may want to learn more about the condition and hear from experts working within the field of epilepsy.
The full agenda for the IELs Expert Day is as follows:
• 09.00 - Opening remarks and ILAE update - Dr. Peter Widdess-Walsh, President IEL
• 09.10 - Update from Epilepsy Ireland - Peter Murphy, CEO, Epilepsy Ireland
• 09.20 - Epilepsy nursing update – TBA
• 09.30 - John Kirker lecture
- The first epileptic seizure: Prof Tony Marson, The Walton Centre NHS Foundation Trust
• 10.30 - Break – tea/coffee and pastries
• 10.50 - Paediatric epilepsy surgery update: Dr. Sophia Varadkar, Great Ormond Street London
• 11.45 - How to order genetic tests for epilepsy: Prof Norman Delanty, Beaumont Hospital
• 12.30 - Lunch
• 13.30 - John Lynch Memorial Lecture - A mirror on social attitude: how epilepsy is depicted in film and literatureProf. Simon Shorvon, UCL/ Queen Square
• 14.30 - Debate – Folic acid 5mg (high dose) should be given to all women of childbearing age; For: Dr.Tudor Munteanu, Our Lady’s Hospital Drogheda; Against: Dr. Elisabeth Doran, St. James Hospital
• 16.00 - Concluding remarks –Dr. Peter Widdess-Walsh
If you are interested in attending the Irish Epilepsy League’s Expert Day, you can do so by registering via Eventbrite. The cost of attending is ¤20 for nonconsultant and ¤50 for consultants. Registration closes on the 12th of September. The link to the registration page is below or scan the QR code alongside this article! https://bit.ly/IELED24
Following the conclusion of the Irish Epilepsy League Expert Day, Epilepsy Ireland will be hosting their National Conference at the Gibson the following day on Saturday September 21st. Epilepsy Ireland are the national organisation representing people with epilepsy and their families and are the Irish chapter of the International Bureau for Epilepsy.
While the Irish Epilepsy League’s Expert Day is targeted solely at Health Care Professionals, Epilepsy Ireland’s conference is patient-focused and sees people with epilepsy and their families from across Ireland attending, aiming to learn more about clinical developments and research in epilepsy. The conference also acts as an opportunity for people with epilepsy to meet with others in a similar situation to themselves. It is also open to allied Health Care Professionals, those working in education or any interested professional.
The full agenda for the conference is as follows:
• 9:00 – 10:00: Registration
• 10:00 – 10:05: Welcome and official opening
• 10:05 – 10:45: Dr Sophia Varadkar – Developments in diagnosis and treatment of complex childhood epilepsies
• 10:45 – 11:20: Professor Tony Marson – The First Epileptic Seizure
• 11:20 – 11:35: Questions and Answers for first two speakers
• 11:35 – 11:50 – Movement Break
• 11:50 – 12:30 - Dr Cristina Ruedell Reschke, Royal College of Surgeons in Ireland –Circadian Rhythms and epilepsy and sleep hygiene
• 12:30 – 1:00 – Epilepsy Ireland Updates and Volunteer of the Year awards presentation
• 1:00 – 2:15 - Lunch
• 2:15 – 2:50 – Registered Advanced Nurse Practitioner in Epilepsy, Sinéad Murphy –Women with epilepsy, the need to knows!
• 2:50 – 3:25 – Professor David Henshall, FutureNeuro –Epilepsy in dogs as a way to trial a new gene therapy.
• 3:25 – 4:00 – Dr Aoife Morrin, Dublin City University – AI, seizure scents and dogs!
• 4:00 – 5:00 – Epilepsy Community Meet-Up!
If you are interested in attending Epilepsy Ireland’s National Conference, tickets are available at the cost of ¤45 (including a two-course lunch) and can be purchased on Epilepsy Ireland’s website Epilepsy Ireland National Conference or by scanning on the QR code alongside this article.
Commenting on the busy September for the epilepsy community in Ireland, Epilepsy Ireland Advocacy & Communications Manager Paddy McGeoghegan said, “This year is the first year where we have our National Conference directly after the Irish Epilepsy League Conference – and it has allowed us to collaborate with our colleagues in the IEL to have international speakers attend both – seen by the fact Prof Tony Marson and Dr. Sophia Varadkar are speaking at both the patient and professional conferences. Hopefully this will be something that we will see replicated in the years ahead!
“We’re really looking forward to both conferences and would encourage HCPs with an interest in epilepsy to come to either or both to hear from experts working in the field! We hope to see you there!”
NOW also in 180 Caps Bottles
Standard 60 Caps Box
Clinical R&D
CORMICA‘S LABORATORY, MET ACHIEVES FIRST-TIME FDA INSPECTION SUCCESS
Cormica, as a global leader in comprehensive microbiological, analytical and physical testing services, upholds a commitment to quality across all its world renown laboratories. Our accreditations include Good Manufacturing Practice (GMP), Good Laboratory Practice (GLP), ISO 17025, and recognitions from leading regulatory bodies such as the Medicines and Healthcare products Regulatory Agency (MHRA), the US Food and Drug Administration (FDA), and the United Kingdom Accreditation Service (UKAS). These certifications validate our dedication to excellence, enabling us to support clients in launching and releasing their products safely and rapidly worldwide.
MET (Medical Engineering Technologies Ltd), a Cormica laboratory, is dedicated to delivering world-class Combination Device, Medical Device and Pharmaceutical testing services. MET’s capabilities include performance, verification, validation, ageing, transit, packaging testing and analytical chemistry with a keen interest in extractables and leachables. By upholding the highest standards of quality and safety, we ensure that products meet rigorous safety and efficacy standards, maintaining their integrity from development through to market release.
We are excited to announce that MET, has successfully passed its first FDA inspection. The inspection, which took place in April, focused on batch release testing after MET was named on a client’s submission. The result of this rigorous examination was NAI (No Actions Indicated), a significant achievement for our team.
“Passing our first FDA inspection with no actions indicated is a testament to the hard work and dedication of our team.
We have worked tirelessly to adhere to GMP principles, and this achievement validates our commitment to quality and excellence,” said Naomi Allkins, Quality Assurance Manager.
The positive outcomes from both the FDA inspection and the UKAS audit underscore MET’s position as a trusted and reliable partner in the field of pharmaceutical and medical device testing. These achievements demonstrate our capability to meet and exceed regulatory standards, providing our clients with the confidence that their products are tested with the utmost precision and care.
“This significant achievement by MET highlights the strength and commitment of our entire organisation to quality and regulatory compliance. It reinforces our mission to improve patients’ lives by providing comprehensive testing services that enable our clients to launch and release their products safely and rapidly,” said Mark Hammond, CEO of Cormica.
SARCLISA INDUCTION TREATMENT DEMONSTRATED SIGNIFICANTLY IMPROVED PROGRESSION-FREE SURVIVAL IN PATIENTS WITH NEWLY DIAGNOSED MULTIPLE MYELOMA ELIGIBLE FOR TRANSPLANT
New results from the two-part, double-randomized, German-
speaking Myeloma Multicenter Group (GMMG)-HD7 phase 3 study shows that Sarclisa (isatuximab) in combination with lenalidomide, bortezomib, and dexamethasone (RVd) during induction therapy in transplant-eligible, newly diagnosed multiple myeloma (NDMM) significantly prolonged progression-free survival (PFS) from first randomization, resulting in a statistically significant and clinically meaningful reduction in disease progression or death, compared to RVd induction regardless of the maintenance regimen. Full results will be submitted for presentation at a forthcoming medical meeting.
Hartmut Goldschmidt, MD, President of GMMG, Professor of Medicine at the Heidelberg University Hospital (UKHD), Germany and principal investigator of the study says, “Successful induction therapy is one of the most critical components to reduce the relapse or recurrence risk in patients with newly diagnosed multiple myeloma. While we observed this investigational combination showed improved minimal residual disease negativity rates in the bone marrow, indicating potentially deeper responses after induction, further follow-up was needed to better understand how this translated to long-term outcomes. These data provide evidence that the Isa-RVd regimen potentially improves progressionfree survival in the frontline, transplant-eligible population and supports the potential of this quadruplet to become a new standard-of-care induction regimen in this treatment setting.”
GMMG-HD7 is one of six phase 3 studies to report positive results for Sarclisa in patients with multiple myeloma, which includes four positive readouts of a Sarclisabased quadruplet in the frontline setting. The most recent included results from the IMROZ phase 3 study evaluating the investigational use of Sarclisa with VRd versus VRd for patients with transplantineligible NDMM, demonstrating a statistically significant and clinically meaningful improvement in PFS and a higher proportion of patients with minimal residual disease (MRD) negativity.
In December 2021, Sanofi and GMMG shared the results from part one, which met the primary endpoint of MRD negativity after induction therapy and before transplant in NDMM patients. The GMMG-initiated study is being conducted in close collaboration with Sanofi based on jointly defined research. Sanofi provided financial support to GMMG for this study. The use of Sarclisa in combination
with RVd is investigational and has not been evaluated by any regulatory authority.
While considered a rare disease, MM is the second most common hematologic malignancy,1 with more than 180,000 new diagnoses of MM worldwide yearly.2 Despite available treatments, MM remains an incurable malignancy in most patients with an estimated 61% five-year survival rate for newly diagnosed patients.3 Since MM does not have a cure, most patients will relapse. Relapsed MM is the term for when the cancer returns after treatment or a period of remission. Refractory MM refers to when the cancer does not respond or no longer responds to therapy.
GILEAD’S TWICEYEARLY LENACAPAVIR
DEMONSTRATED 100% EFFICACY AND SUPERIORITY TO DAILY TRUVADA® FOR HIV PREVENTION
Gilead Sciences, Inc. (Nasdaq: GILD) has announced topline results from an interim analysis of its pivotal, Phase 3 PURPOSE 1 trial indicating that the company’s twice-yearly injectable HIV-1 capsid inhibitor, lenacapavir, demonstrated 100% efficacy for the investigational use of HIV prevention in cisgender women.
PURPOSE 1 met its key efficacy endpoints of superiority of twiceyearly lenacapavir to once-daily oral Truvada® (emtricitabine 200mg and tenofovir disoproxil fumarate 300mg; F/TDF) and background HIV incidence (bHIV). Based on these results, the independent Data Monitoring Committee (DMC) recommended that Gilead stop the blinded phase of the trial and offer open-label lenacapavir to all participants.
“With zero infections and 100% efficacy, twice-yearly lenacapavir has demonstrated its potential as an important new tool to help prevent HIV infections,” said Merdad Parsey, MD, PhD, Chief Medical Officer, Gilead Sciences. “We look forward to additional results from the ongoing PURPOSE clinical program and continuing toward our goal of helping to end the HIV epidemic for everyone, everywhere.”
These are the first data generated from Gilead’s landmark PURPOSE program, which is the most comprehensive and diverse HIV prevention trial program ever conducted. The PURPOSE program comprises five HIV prevention trials around the world that are focused on innovation in science, trial design, community engagement and health equity.
Mark Hammond, CEO, Cormica
Topline PURPOSE 1 data
PURPOSE 1, a Phase 3, doubleblind, randomized study, is evaluating the safety and efficacy of twice-yearly, subcutaneous lenacapavir for pre-exposure prophylaxis (PrEP) and oncedaily oral Descovy® (emtricitabine 200mg and tenofovir alafenamide 25mg; F/TAF) in more than 5,300 cisgender women and adolescent girls aged 16-25 across 25 sites in South Africa and three sites in Uganda. The drugs are being tested in parallel, with one group receiving twice-yearly lenacapavir and one group taking once-daily oral Descovy. Additionally, a third group was assigned once-daily oral Truvada. Study participants were randomized in a 2:2:1 ratio to lenacapavir, Descovy and Truvada, respectively. Because effective PrEP options already exist, there is broad consensus in the PrEP field that a placebo group would be unethical; thus, the trial used bHIV as the primary comparator and Truvada as a secondary comparator.
There were 0 incident cases of HIV infection among 2,134 women in the lenacapavir group (incidence 0.00 per 100 person-years). There were 16 incident cases among 1,068 women in the Truvada group (incidence 1.69 per 100 personyears). The results demonstrated superiority of twice-yearly lenacapavir over bHIV (primary endpoint, incidence 2.41 per 100 person-years) and superiority of twice-yearly lenacapavir over once-daily Truvada (secondary endpoint), with p<0.0001 for both endpoints. In the trial, lenacapavir was generally well-tolerated and no significant or new safety concerns were identified.
HIV incidence in the Descovy group was numerically similar (39 incident cases among 2,136 women, incidence 2.02 per 100 person-years) to that in the Truvada group and was not statistically superior to bHIV. Previous clinical trials among cisgender women have commonly found challenges with adherence to daily oral pills for PrEP, and adherence analyses for Descovy and Truvada from PURPOSE 1 are ongoing. In the trial, both Descovy and Truvada were generally well-tolerated and no new safety concerns were identified.
More detailed data from PURPOSE 1 will be presented at a future conference.
“Twice-yearly lenacapavir for PrEP, if approved, could provide a critical new choice for HIV prevention that fits into the lives of many people who could benefit from PrEP around the world—especially cisgender women,” said Linda-Gail
Bekker, MBChB, DTM&H, DCH, FCP(SA), PhD, Director of the Desmond Tutu HIV Center at the University of Cape Town, South Africa, and past President of the International AIDS Society. “While we know traditional HIV prevention options are highly effective when taken as prescribed, twiceyearly lenacapavir for PrEP could help address the stigma and discrimination some people may face when taking or storing oral PrEP pills, as well as potentially help increase PrEP adherence and persistence given its twice-yearly dosing schedule.”
The use of lenacapavir and the use of Descovy for the prevention of HIV in cisgender women are investigational and have not been determined to be safe or efficacious and are not approved anywhere globally.
ADULT PATIENTS IN IRELAND WITH ADVANCED NONSMALL LUNG CELL CANCER WITH METEX14 SKIPPING ALTERATIONS TO BENEFIT FROM ACCESS TO TREATMENT AS HSE REIMBURSES MERCK’S TEPMETKO® (TEPOTINIB) AS ORAL MET INHIBITOR SECONDLINE TREATMENT OPTION
Merck, a leading science and technology company, has today announced that the HSE has approved TEPMETKO® (tepotinib) for reimbursement in Ireland, for the second-line treatment of adult patients with advanced non-small cell lung cancer (NSCLC) harbouring mesenchymal-epithelial transition factor gene (MET) exon 14 (METex14) skipping alterations.
Tepotinib is the first and only oral MET inhibitor to be reimbursed in Ireland for the second-line treatment of adult patients with advanced NSCLC harbouring METex14 skipping alterations, and was previously only available for use on the NHS in England, Wales, Scotland and Northern Ireland.
Roisin Molloy, Managing Director of Merck Healthcare in Ireland, said, “This is an important step forward for targeted treatments in Ireland and it is fantastic news that the HSE has reimbursed tepotinib. There are a myriad of lung cancer types and we know that patients with METex14 skipping mutations suffer from poorer survival rates. Cancer treatments are thankfully evolving to personalise and target these specific variations. Every new reimbursement for a targeted treatment will be a game-changer for certain sets of patients who previously felt less hope than others with existing treatment options.”
Dr Stuart Hill, Medical Director of Merck Healthcare UK and Ireland,
said, “We know from working with healthcare professionals in oncology for many years that this particular variation of lung cancer brings a whole host of challenges and uncertainties for patients. It is brilliant that research is diversifying to start to target the wide spectrum of aggressive lung cancers. With tepotinib, a crucial next step will be ensuring that when patients initially present with lung cancer symptoms, they are able to easily access genomic testing to find out if this treatment might benefit them.”
Professor Stephen Finn, Consultant Pathologist, said, “Nonsmall cell lung cancer is a difficult disease to treat, but those who have METex14 skipping mutations sadly suffer from lower chances of progression-free survival than others. It is therefore very welcome news to have tepotinib made newly available to treat these patients in the second line and provide a targeted therapy. Studies have shown that it has clear benefits for eligible patients who are facing the challenges posed by this aggressive type of lung cancer. With the various mutations that lung cancer patients can develop, using targeted treatment and developing our genomics offer will be an important step forward for improving our personalised treatment offer to cancer patients in Ireland.”
NSCLCs with MET alterations are generally associated with poorer clinical prognosis compared to NSCLCs without MET alterations, with a lower median overall survival observed. The presence of these genetic alterations has been recognised as an important therapeutic target for personalised treatment, which can be identified via a tissue and/or blood sample. Targeted treatments, like tepotinib, require genomic testing to determine which patients are eligible. To enable advanced genomic testing, in 2022 HSE launched the National Strategy for Accelerating Genetic and Genomic Medicine in Ireland. The model will allow the HSE to develop a genomics service that improves health outcomes, reduces cost of care and fuels scientific innovation and discovery.
NEW HSE GUIDELINE TO SUPPORT PEOPLE DIAGNOSED WITH SKIN CANCER
A new guideline launched by the HSE National Cancer Control Programme, aims to support patients who have been diagnosed with melanoma skin cancer. Around 1,100 people are diagnosed with melanoma each year in Ireland, which has become more common in recent years.
The guideline will help provide information for treatment planning for people with melanoma. It will also help catch any recurrence or relapse early, leading to earlier treatments and interventions. It was developed in consultation with oncology patients, doctors, nurses and researchers. It aims to improve the quality of clinical care for patients and improve patient experience
Melanoma cancer patients and members of the Guideline Development Group, Kay Curtin, and Miriam Staunton said: “It was great to be involved in the process of creating the guidelines we felt the patient voice was heard. Melanoma Cancer guidelines are essential as they give patients an ability to advocate for themselves and help ensure consistency across Irelands cancer centres.”
Benefits to patients include:
• Provides information for treatment planning
• Catch a recurrence/ relapse early
• Reassurance that you are being monitored based on the best current evidence
Dr Sinéad Field, Consultant Dermatologist and Chair the clinical guideline development group, said: “Melanoma is on the increase in Ireland and while it is more common in people over 50, you can get it at any age. The new National Clinical Guideline for Radiological Staging and Surveillance of Patients with Cutaneous Melanoma will support people who are undergoing or have had treatment. Staging scans help to determine if a patient’s cancer has spread or is likely to spread to other parts of the body, or recur. This knowledge is useful as it provides an opportunity to optimise the patient’s treatment plan. Surveillance of patients after they have finished their treatment is to check for a recurrence or relapse of their cancer. This is useful as it provides an early opportunity for treatment.”
Dr Eve O’Toole, Head of Evidence and Quality Hub in the NCCP, said: “The purpose of the guideline is to provide evidence-based recommendations on the staging and surveillance of patients with cutaneous melanoma through the integration of the best research evidence with clinical expertise, patient values and experiences. Knowing what is happening now and what will be happening next can provide reassurance to patients that an optimum plan for them is in place. The guideline describes what tests patients should have and for how long surveillance should continue.”
62 Clinical R&D
CLONMEL HEALTHCARE LAUNCH UZPRUVO® (USTEKINUMAB) – THE FIRST APPROVED USTEKINUMAB BIOSIMILAR IN IRELAND
Clonmel Healthcare are delighted to announce the introduction of Uzpruvo®, the new Ustekinumab biosimilar. Uzpruvo® will be marketed from July 22nd 2024, upon expiry of patent protection of the active ingredient of the reference biological medicine.
Uzpruvo® 45mg and 90mg solution for injection in pre-filled syringe are indicated for the treatment of Plaque Psoriasis, Paediatric Plaque Psoriasis, Psoriatic Arthritis and Crohn’s Disease1. Uzpruvo® is currently not approved for the treatment of ulcerative colitis indication (since the originator still has exclusivity for this indication).
Uzpruvo® offers patients a wide variety of benefits:
• European manufacturing1 and supply chain*
• Equivalent efficacy, safety and immunogenicity to the reference product**2
• Cost-effective option enabling improved access to ustekinumab treatment
Donagh O’Leary, General Manager said “Clonmel Healthcare
UZPRUVO 45 & 90 mg SOLUTION FOR INJECTION IN PRE-FILLED SYRINGE
continues to grow and strengthen its portfolio of biosimilar medicines, which now spans several therapeutic areas including rheumatology, gastroenterology dermatology and oncology. We remain steadfastly committed to bringing a comprehensive range of biosimilar medicines to the market, thereby increasing access for patients, physicians and pharmacists to affordable medicines and treatments. We are delighted to contribute to the ongoing savings to the Irish healthcare system and supporting patient needs”.
*Supply chain is constantly being optimised and manufacturing location is subject to change.
**Stelara®. + 29 v 27-guage needle of the reference product, Stelara® ++ Plunger stopper made of bromobutyl rubber.
1 Uzpruvo® SmPC (Feb. 2024).
2 Feldman SR et al. Expert Opin Biol Ther. 2023;23(3);253-60. DOI: 10. 1080/14712598.2023.2235263;
3 Stelara® PI (Aug. 2022).
APC MICROBIOME IRELAND WELCOMES DR. SEBASTIAN SCHMIDT AS A NEW PRINCIPAL INVESTIGATOR
APC Microbiome Ireland (APC), a world-leading SFI Research Centre based at University College Cork (UCC), is proud to announce the appointment of Dr. Sebastian Schmidt, an outstanding computational biologist with a global reputation for pioneering advancements in microbiome data analysis, as a new Principal Investigator.
Previously based in the prestigious European Molecular Biology Laboratory (EMBL) in Heidelberg, Dr. Schmidt brings to APC an exceptional background in computational biology, focusing on the development of cuttingedge tools to analyse complex microbiome data. His innovative work has already made significant impacts on the field, including contributions to two seminal papers recently published in the leading international scientific journals Cell and Nature. As part of the UCC Futures Food, Microbiome & Health recruitment drive, Dr. Schmidt will also serve as a lecturer in microbiome and health affiliated with the UCC School of Medicine.
With nearly a decade of experience in microbiome research, Dr. Schmidt has explored fundamental questions of microbial ecology and evolution, while also engaging in applied work, such as discovering predictive microbiome signatures of diseases. His expertise in integrating large datasets to address new challenges in microbiome science has led to the development of several influential computational tools and resources.
Reflecting on his appointment, Dr. Schmidt stated, “APC and UCC have one of the longest and most distinguished histories in modern microbiome research. I am thrilled to join such a highly stimulating environment, surrounded by worldleading researchers in the field. I look forward to building a team here and working on fascinating research questions relevant to the global challenges of our time.”
A Future of Cutting-Edge Research
Dr. Schmidt’s appointment signals high ambition on the part of the APC as it continues to strengthen
its position as a global leader in microbiome research. His focus on developing cutting-edge computational tools and resources that push the boundaries of microbiome science will undoubtedly play a crucial role in advancing the APC’s research and strategic goals.
Welcoming Dr. Schmidt, APC Director Prof. Paul Ross, noted that “Dr. Schmidt’s expertise in computational biology, particularly in large-scale data analysis and tool development will hugely contribute to our capacity for microbiome research. We are excited to see the innovations and breakthroughs that will emerge from his work here at APC.”
Dr. Schmidt will initially focus his research at APC on the intricate interactions between diet and the gut microbiome. He aims to develop computational models that predict how dietary changes impact the microbiome at an individual level, with the ultimate goal of creating dietary interventions that can modulate the gut microbiome to improve health and wellbeing.
TEPKINLY® (EPCORITAMAB) RECEIVES SECOND EUROPEAN COMMISSION APPROVAL FOR THE TREATMENT OF ADULTS WITH RELAPSED/REFRACTORY FOLLICULAR LYMPHOMA
Genmab A/S (Nasdaq: GMAB) has announced that the European Commission (EC) has granted conditional marketing authorization for TEPKINLY® (epcoritamab) as a monotherapy for the treatment of adult patients with relapsed or refractory (R/R) follicular lymphoma (FL) after two or more lines of systemic therapy. TEPKINLY is the first and only subcutaneous T-cell engaging bispecific antibody approved for the treatment of this patient population in the European Union (EU), as well as the European Economic Area (EEA) countries (Iceland, Liechtenstein, Norway) and Northern Ireland.
New APC PI Dr Sebastian Schmidt pictured with APC Director Prof Paul Ross and COO Dr Brendan Curran
“Follicular lymphoma can be challenging to treat and today’s approval of TEPKINLY for the treatment of relapsed/refractory follicular lymphoma after two or more lines of systemic therapy marks an important milestone for patients in the European Union who are in need of more options offering a balance of meaningful efficacy and favorable safety,” said Jan van de Winkel, Ph.D., President and Chief Executive Officer of Genmab. “Alongside our partner AbbVie, we are committed to exploring the continued development of epcoritamab as a potential core therapy across B-cell malignancies.”
FL is typically a slow-growing form of Hodgkin’s lymphoma (NHL) that arises from B-cell lymphocytes. FL is the second most common form of NHL overall, accounting for 20-30 percent of all NHL cases, and represents 10-20 percent of all lymphomas in the Western world.i FL is considered incurable, and there is no standard of care treatment for third-line or later FL.i,ii Patients who achieve remission also often experience relapse.iii,iv,v
The conditional marketing authorization is supported by data from the Phase 1/2 EPCORE® NHL-1 clinical trial: an open-label, multi-cohort, multicenter, singlearm trial that evaluated TEPKINLY as monotherapy in patients with R/R FL after two or more lines of prior systemic therapy. Patients included in the study were refractory to both anti-CD20 monoclonal antibody therapy and an alkylating agent (70% having double refractory disease), patients who were refractory to last prior treatment (82%), and patients whose disease progressed within two years of initiating first systemic therapy (52%). The results published in the Lancet Haematology showed that patients treated with TEPKINLY (n=128) had an overall response rate (ORR) of 83% and a complete response (CR) rate of 63%. At a median follow-up of 16.2 months, the median duration of response was 21.4 months (13.7, NR). Duration of complete response (DOCR) was not reached.
The study included a planned separate optimization cohort, which evaluated 86 patients with the recommended 3-stepup doses for cytokine release syndrome (CRS) mitigation. Hospitalization was not mandatory in the cycle 1 optimization cohort. With the optimized regimen, 40% of patients experienced Grade 1 CRS and 9% experienced Grade 2 (no Grade 3 or higher CRS were reported). No immune effector cellassociated neurotoxicity syndrome
(ICANS) cases were reported in this cohort.
The safety profile of epcoritamab in the pivotal cohort was similar to reports of epcoritamab monotherapy in the pivotal EPCORE NHL-1 diffuse large B-cell lymphoma (DLBCL) cohort. In the pooled safety population (n=382), the most common adverse reactions (≥ 20%) with TEPKINLY were CRS, injection site reactions, fatigue, viral infection, neutropenia, musculoskeletal pain, pyrexia, and diarrhea. The most frequent serious adverse reaction (≥ 10%) was cytokine release syndrome (34%). Fourteen patients (3.7%) experienced a fatal adverse reaction (pneumonia in 9 (2.4%) patients, viral infection in 4 (1.0%) patients, and ICANS in 1 (0.3%) patient.
“The approval of epcoritamab by the European Commission is a promising update for the lymphoma community,” said Kate Rogers, CEO of the Follicular Lymphoma Foundation. “Given that relapsed or refractory follicular lymphoma can be a very challenging form of cancer to treat, especially in later lines of therapy, it is critical that patients and physicians have additional options when it comes to treating this type of cancer.”
IRELAND’S FIRST ASIAM ACCREDITED AUTISMFRIENDLY CAMHS AT LUCENA CLINIC
St John of God Community Mental Health Services (CAMHS) at Lucena Clinic, a leading provider of mental health services for young people, today announces its formal accreditation as the first mental health service in Ireland to be recognised as autism-friendly by AsIAm.
This prestigious recognition underscores the service’s commitment to provide all young people with inclusive, compassionate, and supportive care. The accreditation, awarded by AsIAm, is testament to the service’s ongoing dedication to fostering an environment where all those attending feel respected, understood, and valued.
Community Mental Health Services is specifically a mental health service and not an autism service but at least 50% of young people who attend may also have a cooccurring diagnosis of autism or other neurodivergence. Therefore, the service needs to show leadership in neuroaffirmative practices. This new accreditation reflects the continuing efforts to integrate best practice and promote a culture of acceptance and understanding.
This project is funded by a ¤200k grant from the St John of God Foundation’s “Better Life” Programme. It encompasses six key components: a sensory and environmental audit, an evaluation of written communication, consultation with service users, staff training, a roadmap report, and a blueprint for creating an autistic and neurodivergentfriendly environment in other service settings.
In consultation with the autistic and wider neurodivergent community, this project seeks to extend the renowned St John of God hospitality to neurodivergent service users and their families and to improve the experience and engagement of all those involved in the service.
The project also involved partnering with ADHD Ireland, who contributed with consultation and by delivering staff training. The National Adult Literacy Agency (NALA) collaborated by reviewing communication documents to award the Plain English mark, as well as training staff. The project team at Community Mental Health Services will continue to work closely with these organisations to ensure universal accessibility best practice.
The neurodiversity movement highlights the life-long and positive aspects of naturally occurring cognitive ‘differences’ such as creativity and passions as opposed to a focus on developmental deficits.
CORK HOSPITAL TRANSLATES CRUCIAL PATIENT INFORMATION INTO SIX LANGUAGES
A Cork hospital has begun translating complex health information into six different languages in a project which organisers say should be replicated nationwide.
Cork University Hospital Charity is funding the unique initiative at CUH to reflect the growing number of foreign national patients presenting at its breast radiology department.
Crucial patient care information is now available in Arabic, Lithuanian, Polish, Romanian, Ukrainian and Russian.
The pamphlets will explain in their native language what a mammogram, ultrasound or biopsy involves, risk factors to be aware of, breast symptoms and lifestyle advice.
“It will have a widespread impact. The information is there, not only for these patients, but for other patients into the future,” said Advanced Nurse Practitioner Susan Walsh of the Rapid Access Breast Service at CUH.
“Because we have so many nationalities residing in Ireland, it should be in all hospitals and part of the standard of care to provide information in as easy-tounderstand language as possible.”
Patient care information has already been produced in four different languages by the Breast Family History Service at CUH.
Most of the 5,500 new patients seen every year at the hospital’s symptomatic breast clinic will be further referred to the radiology department for diagnostic scans.
CUH collaborated on the translation project with the National Adult Literacy Agency (NALA), which helps remove barriers to people with literacy difficulties.
Census data from 2022 shows that the number of non-Irish citizens living in this country stands at almost 632,000 (12%) and to address the communications gap, a multi-disciplinary team from the breast radiology department set about reviewing patient letters and information.
The documentation was reviewed and edited over several months with NALA and achieved the ‘plain English’ mark before being translated into the six languages based on Census figures and the most frequently requested translators in the breast service.
The next step is transferring the common information onto an online platform.
“A lot of information is given to patients at these clinics and the main purpose is that what we provide to them is easily understood, regardless of nationality,” said Ms Walsh.