With 1,600 people working across five sites in Ireland, Viatris provides access to medicines, develops innovative solutions and improves healthcare for patients.
IN THIS ISSUE: Irish Medical Council publish new Sanctions Guide MEDICINES: Addressing the Growing issue of Medicine Shortages
CONFERENCE: National Stroke Conference Tipperary Exploring Pharmacy Career Choices Making Communities Epilepsy Aware Annual Meeting Advancing Brain
Call for papers: make your contribution to Hospital
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
Contents Foreword
Mater Private Network to participate in NAVIGATE-PF study P4
IPHA calls for reform of clinical trials process P6
Medicines for Ireland unveils Manifesto for Europe P9
National Stroke Conference P12
Breakthrough development for Barrett’s Oesophagus P18
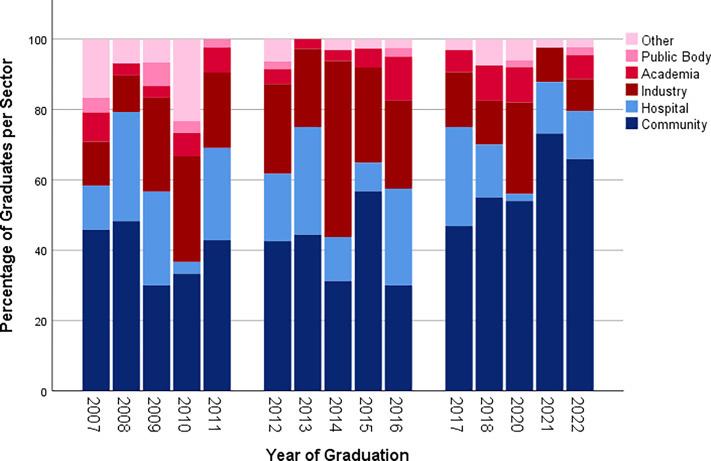
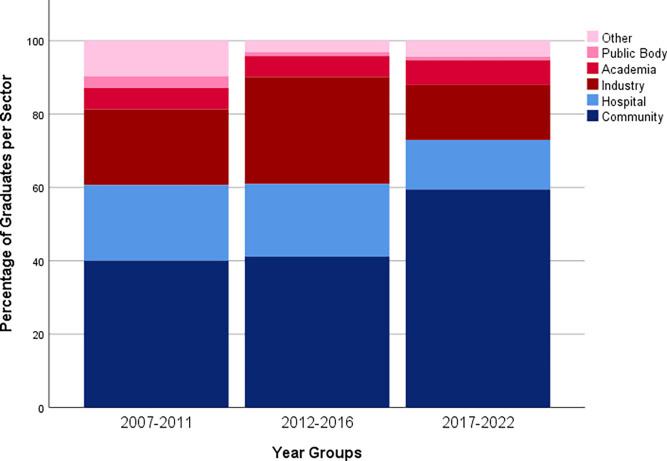
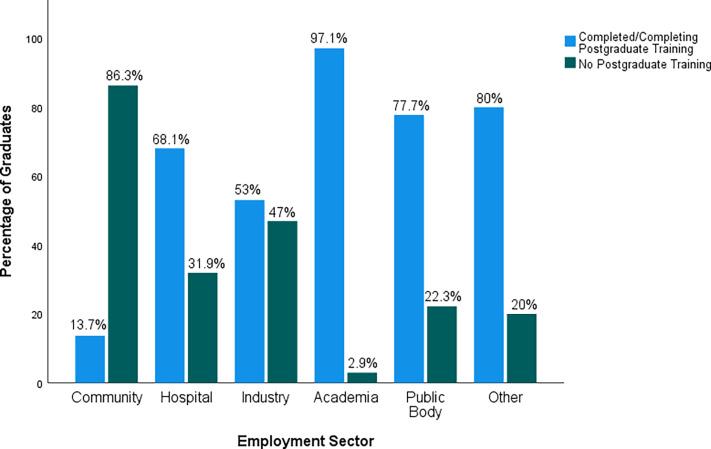
Exploring career choices of pharmacy graduates P19
REGULARS
Feature: Gynaecological Cancer P29
CPD: DXA Meeting P33
Haematology: Haematology Oncology Podcast P40
Feature: Multiple Sclerosis P42
Feature: Urothelial Cancer P50
P60
Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only. All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
In one of our lead news stories this month, it has been revealed that Ireland is attracting fewer clinical trials than some European countries with similar populations and economic performances, according to a report by the Irish Pharmaceutical Healthcare Association (IPHA), the representative body for the researchbased biopharmaceutical industry.
The 2024 IPHA Clinical Trials Performance Report, which captures data across 10 years (2014 to 2023), saw Ireland attracting fewer all-industry sponsored interventional clinical trials than Finland and Denmark Dr Rebecca Cramp whose populations and economic wealth are similar to ours. Of 2,411 interventional clinical trials carried out in the three countries across the 10 years, 19% were conducted in Ireland (460) compared to 27% in Finland (661) and 54% in Denmark (1,290).
Turn to page 6 to read more about this.
On page 8 Medicines for Ireland (MFI), the leading representative body for the generic, biosimilar, and value added medicines industry, is highlighting the urgent need for action to address the increasing medicine shortages affecting the Irish population. A recent Red C survey reveals a concerning trend: 1 in 5 (20%) of individuals have been personally affected by medicine shortages in the past two years.
Additionally, 22% report that family members or friends have been impacted totalling 38% of the population either directly or indirectly experiencing the consequences of these shortages. Commenting on the Red C survey results, Chair of Medicines for Ireland Paul Neill said, “The growing scarcity of essential medicines is more than an inconvenience; it’s a barrier to health and well-being. With 38% of those surveyed expressing that shortages have impacted them or someone close to them, it is a clear and urgent signal that our healthcare system faces a crisis that requires immediate action.”
A major National Conference on Stroke, hosted by the South Tipperary Stroke Communication Group, took place at the Cashel Palace Hotel, Cashel, Co. Tipperary, on Monday May 20th. The Conference, which attracted around 200 people, heard from professionals and stroke survivors and included demonstrations on developments in the area of innovations for persons with spinal cord injury, stroke, multiple sclerosis and other neurological conditions. Full details on this conference can be read on page 12.
Meanwhile, an estimated 450,000 people in Ireland have asthma and, according to a recent patient survey, concerning numbers are experiencing persistent symptoms that may indicate their asthma is uncontrolled. In response, this World Asthma Day, the Asthma Society of Ireland is launching a campaign to empower people with asthma to recognise the signs and symptoms of uncontrolled asthma and when to seek medical help. Turn to page 24 for the full story.
I hope you enjoy the issue.
Hospital Pharmacists Manifesto
Hospital pharmacists are pivotal in ensuring medication management and safety across hospital settings, bridging inpatient and out-patient services to support seamless transitions within the healthcare system.
Recognizing their crucial role, the European Association of Hospital Pharmacists (EAHP) has released its 2024 European Parliament Elections Manifesto, highlighting five critical topics for the upcoming legislative cycle:
1. Addressing Medicines and Medical Devices Shortages
The 2023 Shortages Survey Report of the EAHP showed that 95% of European hospital pharmacists still experience medicine shortages and 61% reported that the unavailability of medical devices is a problem in their hospital.
2. Tackling Antimicrobial Resistance
Hospital pharmacists are gatekeepers to the use of antimicrobials. However, the utilization of their expertise through the establishment of antimicrobial stewardship teams is far from being routine in European hospitals.
3. Investing in the Healthcare Workforce
Promoting the expansion of pharmacy education capacities and effectively fostering professional mobility is paramount to mitigating shortages in the hospital pharmacy workforce, where member states that have more professionals could easily allow them to work in a member state that needs more professionals.
4. Improving Medication Safety
Due to their expertise in allmedicines-related processes, hospital pharmacists are responsible for medicines and treatment outcomes optimisation. Their invaluable contributions to multidisciplinary teams in ensuring patients’ compliance with their therapies are also essential
5. Prioritizing Health on the Public Agenda
EAHP believes that coordination and communication are essential to safeguard that the trinity of Accessibility, Availability and Affordability of healthcare systems is managed in a balanced way.
These priorities, say EAHP, are essential for enhancing patient outcomes and ensuring a resilient healthcare system.
Prestigious Selection for Mater Private Network
Mater Private Network has been selected as one of only three centres worldwide and the only centre in Ireland to participate in the prestigious NAVIGATEPF clinical study, led by Boston Scientific. This recognition highlights Mater Private Network's status as one of the most acknowledged atrial fibrillation (AFib) centres in Europe.
The prospective, single-arm, openlabel, multi-centre NAVIGATE-PF study began at the Dublin site from last month, marking a significant step in Mater Private Network's involvement in pioneering medical research. AFib is the most common irregular heart rhythm, which significantly reduces the quality of life and life expectancy of patients. An estimated 8 million patients live with this condition in Europe.
Professpr Gábor Széplaki, Head of Cardiac Electrophysiology at Mater Private Network, expressed his enthusiasm for the project, "We are honoured to participate in this groundbreaking study, which will be another milestone in our journey to transform the way arrhythmias are treated globally. This initiative represents a significant stride towards integrating advanced cardiac mapping with ablation technology, aiming to elevate the standard of care for our patients with atrial fibrillation. As a centre of excellence in cardiac electrophysiology, we are committed to contributing to research that may significantly improve patient outcomes. As early adaptors of the most advanced technologies we are hoping to deliver safe and efficient therapies to the wider patient populations, including elderly patients living with atrial fibrillation."
Mater Private Network’s CVRI research team involved in the study: Heta Jigar Panchal, Professor Gábor Széplaki and Fionnuala Duffy
Medical Council Publish Sanctions Guide
The Medical Council has published its new Sanctions Guidance, which comes into effect immediately.
In cases where a complaint about a doctor is deemed serious enough to be referred to the Medical Council’s Fitness to Practise Committee, an inquiry may take place. At a Fitness to Practise inquiry, both parties are given the opportunity to present their case before the Medical Council’s Fitness to Practise Committee, and should there be a finding by the Committee that a doctor’s fitness to practise is impaired, the Medical Council must then decide the appropriate sanction(s) to impose, this new Sanctions Guidance is designed to assist the Council in making this decision.
The Medical Council believes that it is important to be as transparent
as possible, and that the new Sanctions Guidance will also be of assistance to the medical profession, their representatives, and members of the public. The document covers:
• the purpose of sanctions;
• the approach taken to sanctions;
• factors to be considered when deciding on sanctions;
• cases which may result in a more serious sanction being imposed.
The Medical Council may revise its Sanctions Guidance as and when it determines necessary.
Dr Suzanne Crowe, President, Medical Council added “One of the important statutory functions placed on the Medical Council is determining a doctor’s fitness to
Dr Suzanne Crowe, President, Irish Medical Council
practise following the investigation of a complaint and Fitness to Practise Inquiry. We’re very much aware of the difficulties that can be involved in going through the Fitness to Practise process for both doctors and complainants.
“The publication of this guidance today increases the transparency around decision-making processes of the Council when it comes to sanctioning a doctor. Indemnifiers are there for doctors to engage with for support, guidance, and representation throughout the Fitness to Practise inquiry process, which is complex and legalistic.”
Government Announces New Beds by 2031
The Government has announced around 3,000 new hospital beds which would be equivalent to “six large hospitals”. Minister for Health Stephen Donnelly said the measure was a “gamechanger” and called it “the largest planned expansion of public hospital beds in many decades”.
Commenting, the Irish Hospital Consultants Association said they ‘remain cautious.’ “In April 2023, the IHCA cautiously welcomed the Minister for Health’s announcement of a rapid build programme to open 1,500 additional public hospital beds across 15 acute public hospital sites. However, over a year on from this and we have yet to see any of these beds come on stream. We
now seek clarification as to how the 1,541 beds due by the end of 2028 and the 2,997 beds due by 2031 announced today differ from those already promised in 2023, and urge the Government to provide the promised ¤1 billion capital budget to open these beds as indicated without delay.
“Additionally, the figure of 3,000 beds falls well short of the needs which will face the country by 2031. That the Minister is publicly acknowledging that our bed capacity is way behind what is needed is notable in and of itself.
“The urgency of expanding hospital capacity is further reinforced by the Minister’s acknowledgement that the 2018 Capacity Review – which proposed
an increase of just 2,600 acute public beds by 2031 – “lowballed” the hospital capacity needs. In the 6 years since the 2018 Capacity Review and National Development Plan, which committed to open 260 hospital beds per annum, only 1,182 additional beds have been added. This is almost a quarter (23%) behind the commitment.
“In addition, just two of the promised six national surgical hubs are likely to be open by the end of year, with the four elective hospitals not due to receive their first patients before 2027 at the earliest.
“While announcements of new hospital beds may be politically expedient in a year in which elections grow closer, it does nothing to address the chronic
capacity shortages which are preventing the delivery of timely care across the country. At some point, the Government is going to need to start delivering on their promises to deliver, rather than kicking the can down the road, while the problem continues to grow.
“To fully address the chronic lack of capacity, Government must stay focused on delivering the required beds, to reduce our bed occupancy rates, which are among the highest in the developed world at 95%, address the increased numbers of admitted patients being treated on trolleys, and reduce the cancellation of appointments and waiting lists.”
Reform Needed in Irish Clinical Trials
Ireland is attracting fewer clinical trials than some European countries with similar populations and economic performances, according to a report by the Irish Pharmaceutical Healthcare Association (IPHA), the representative body for the research-based biopharmaceutical industry.
The 2024 IPHA Clinical Trials Performance Report, which captures data across 10 years (2014 to 2023), saw Ireland attracting fewer all-industry sponsored interventional clinical trials than Finland and Denmark
Dr Rebecca Cramp
whose populations and economic wealth are similar to ours.
Of 2,411 interventional clinical trials carried out in the three countries across the 10 years, 19% were conducted in Ireland (460) compared to 27% in Finland (661) and 54% in Denmark (1,290).
Clinical trials are used to evaluate the safety and effectiveness of medicines including vaccines. A strong clinical trial infrastructure gives patients access to sometimes life-saving treatments.
The Report shows that IPHA member companies sponsored or collaborated in 292 out of 460 listed all-industry sponsored interventional clinical trials during this period. Most (68%) of these interventional clinical trials were in Phase III. Cancer accounted for just over half of all IPHA member-sponsored interventional clinical trials with other therapy areas such as gastroenterology, immunology and endocrinology accounting for 21%.
However, in Ireland there has been a decrease of over 40% in the number of all-industry sponsored interventional clinical trials taking place in 2022 compared to 2021, and a similar trajectory is evident for 2023.
Dr Rebecca Cramp, Director of Code and Regulatory Affairs at IPHA, said reforms are needed in the clinical trials process in Ireland and, if we get them right, more patients will benefit from breakthrough innovation in medicines.
“Healthcare providers in Irish hospitals and academic institutions have shown that they have the ability to drive world-class research. We believe that Ireland can play a leading role in the provision of clinical trials in Europe. However, this can only be achieved through a predictable, transparent and efficient clinical research system which is necessary to attract more clinical trials. Patients in Ireland deserve a strong clinical research infrastructure to provide access to sometimes life-saving treatments.”
To accelerate the conduct of clinical trials and increase the number of them carried out in Ireland, IPHA has already developed a new standardised Clinical Trial Agreement between the site and the Sponsor. The Model Clinical Trial Agreement, or mCTA, which
is a first for Ireland, is an efficiency initiative, which can reduce delays, cut costs, increase standardisation and enable the faster commencement of more clinical trials – all aimed at significantly improving patient outcomes.
However, further collaboration by all stakeholders including the Government, hospitals, academic institutions and industry is required to reform the clinical trial process and help accelerate new medicines’ development, thereby raising standards of care for patients in Ireland. IPHA continues to urge for this reform through the following five steps:
1. Provide standardised clinical trial start-up requirements (including Data Protection Impact Assessments) and timelines for hospitals;
2. Designate specific clinical trial signatories in each hospital and a standard, timely sign-off process;
3. Appoint one permanent clinical research nurse post for each teaching hospital;
4. Ring-fence clinical trial funding and working time for multidisciplinary research; and,
5. Protect dedicated clinical research time.
Revolutionising Surgical Navigation for Cancer
A groundbreaking development by researchers at Tyndall National Institute and Microelectronics Circuits Centre Ireland (MCCI), based at University College Cork (UCC), is set to
transform surgical navigation.
In a significant breakthrough, researchers have developed the first sensor-on-a-chip for magnetic tracking in surgery and other image-guided interventions.
This development accelerates a move away from reliance on harmful radiation imaging (x-rays) towards a safer, more precise approach to navigating medical instruments within the body.
Traditional image-guided interventions often use x-rays for navigation of instruments. However, a pioneering technology known as ‘magnetic tracking’ is revolutionising clinical practice by minimising the dependency on x-rays, while accelerating the use of surgical robotics and image-guidance.
Magnetic tracking uses lowfrequency magnetic fields, similar
to everyday devices like electric motors and radios, to precisely detect the position of tiny sensors inside the patient. However, existing sensors are complex to manufacture, they are expensive, and are extremely delicate.
Preliminary results published in the IEEE Transactions on Biomedical Circuits journal report tracking accuracy of less than a millimetre, making the new sensor the most accurate on-chip sensor to date for navigating instruments inside the body.
Researchers were able to demonstrate the use of the chip for tracking instruments inside the lungs, an important application for effective targeting and treatment of diseases like lung cancer, which is the leading cause of global cancer incidence and mortality (source: ncbi.nlm.gov).
The sensor is manufactured using standard silicon chip technology resulting in a simplified manufacturing process. Silicon chips are cost-effective at scale allowing the technology to be manufactured at a fraction of the cost of existing medical sensor technology. Silicon chips are also easily integrated with the latest flexible circuits, making assembly quick and reliable.
Pádraig Cantillon-Murphy, Professor of Biomedical Engineering at Tyndall and UCC, who led the research team, said: “This represents the culmination of 10 years development of magnetic tracking technology at Tyndall and UCC. I'm immensely proud of the team's achievements over that time and we look forward to translating this technology to clinical applications where it can make a significant difference in patient outcomes.”
Professor Pádraig Cantillon-Murphy and Researcher Manish Srivastava
The Medicines Management Programme
(MMP) recommends Tetridar ® as a Best Value Medicine (BVM) for teriparatide on the High Tech Arrangement.
Tetridar ®
20 micrograms /80 microlitres
Solution for Injection in pre-filled pen teriparatide
Indications
Tetridar® is indicated in adults. Tetr:dar 20 rn1crog
teriparatide ra_ms/BO microlitres cton npt •"'°Pe
Subcutaneous use
Treatment of osteoporosis in postmenopausal women and in men at increased risk of fracture. In postmenopausal women, a significant reduction in the incidence of vertebral and non-vertebral fractures but not hip fractures has been demonstrated.
Treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk for fracture.
Further information available from the SmPC available at HPRA.ie Tetridar® (teriparatide) 20 micrograms/SO microlitres Solution for Injection in pre-filled pen Abbreviated Prescribing Information.
Presentation: Each dose of 80 microlitres contains 20 micrograms of teriparatide. One pre-filled pen of 2.4 ml contains 600 micrograms of teriparatide (corresponding to 250 micrograms per ml).
Indications: Tetridar is indicated in adults for the treatment of osteoporosis in postmenopausal women and in men at increased risk of fracture. In postmenopausal women a significant reduction in the incidence of vertebral and non-vertebral fractures but not hip fractures has been demonstrated.
Treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk for fracture. Dosage and administration: The recommended dose of Tetridar is 20 micrograms administered once daily. The maximum total duration of treatment with Tetridar should be 24 months and the 24-month course of teriparatide should not be repeated over a patient's lifetime. Patients should receive supplemental calcium and vitamin D supplements if dietary intake is inadequate. Following cessation of teriparatide therapy, patients may be continued on other osteoporosis therapies. Adults: Teriparatide should be administered once daily by subcutaneous injection in the thigh or abdomen. Patients must be trained to use the proper injection techniques and correct use of the pen. Until further clinical data become available, the recommended treatment time of 24 months should not be exceeded. Children: The safety and efficacy of teriparatide in children and adolescents less than 18 years has not been established. Teriparatide should not be used in paediatric patients or young adults with open epiphyses. Elderly: No dosage adjustment required. Renal impairment: Teriparatide must not be used in patients with severe renal impairment. In patients with moderate renal impairment, teriparatide should be used with caution. No special caution is required for patients with mild renal impairment. Hepatic impairment: teriparatide should be used with caution in hepatically impaired patients, as no data are available. Contraindications: Hypersensitivity to the active substance or to any of the excipients, Pregnancy and breast-feeding, Pre-existing hypercalcaemia, Severe renal impairment, Metabolic bone diseases (including hyperparathyroidism and Paget's disease of the bone) other than primary osteoporosis or glucorticoid-induced osteoporosis, Unexplained elevations of alkaline phosphatase, Prior external beam or implant radiation therapy to the skeleton, Patients with skeletal malignancies or bone metastases should be excluded from treatment with teriparatide. Precautions and warnings: In normocalcaemic patients, slight and transient elevations of serum calcium concentrations have been observed following teriparatide injection. Serum calcium concentrations reach a maximum between 4 and 6 hours and return to baseline by 16 to 24 hours after each dose of teriparatide. Blood samples for serum calcium measurements should be taken at least 16 hours after the most recent Tetridar injection. Tetridar may cause small increases in urinary calcium excretion. Tetridar has not been studied in patients with active urolithiasis, therefore should be used in caution in patients with active or recent urolithiasis due to potential exacerbation of this condition. In short-term clinical studies with teriparatide, isolated episodes of transient orthostatic hypotension were observed. Typically, an event began within 4 hours of dosing and spontaneously resolved within a few minutes to a few hours. When transient orthostatic hypotension occurred, it happened within the first several doses. Experience in the younger adult population, including
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67ESAO, Ireland.
Further information is available on request or in the SmPC. Product Information also available on the HPRA website. Prescription Only Medicine.
premenopausal women, is limited. Treatment should only be initiated if the benefit clearly outweighs risks in this population. Interactions: In a study of 15 healthy subjects administered digoxin daily to steady state, a single teriparatide dose did not alter the cardiac effect of digoxin. However, sporadic case reports have suggested that hypercalcaemia may predispose patients to digitalis toxicity. Because teriparatide transiently increases serum calcium, teriparatide should be used with caution in patients taking digitalis. Teriparatide has been evaluated in pharmacodynamic interaction studies with hydrochlorothiazide. No clinically significant interactions were noted. Co-administration of raloxifene or hormone replacement therapy with teriparatide did not alter the effects of teriparatide on serum or urine calcium or on clinical adverse events. Pregnancy and lactation: Women of childbearing potential should use effective methods of contraception during use of Tetridar. If pregnancy occurs, Tetridar should be discontinued. Tetridar is contraindicated for use during pregnancy and breastfeeding. It is not known whether teriparatide is excreted in human milk. Animal studies have shown reproductive toxicity. The effect of teriparatide on human foetal development has not been studied. The potential risk for humans is unknown. Effects on ability to drive and use machines: Tetridar has no or negligible influence on the ability to drive and use machines. Transient, orthostatic hypotension or dizziness was observed in some patients. These patients should refrain from driving or the use of machines until symptoms have subsided. Adverse reactions: Anaphylaxis, serious cases of back pain have been reported within minutes of the injection, syncope, hiatus hernia, nephrolithiasis, renal failure and renal impairment. Very Common: pain in limb; Common: anaemia, hypercholesterolaemia, depression, dizziness, headache, sciatica, vertigo, palpitations, hypotension, dyspnoea, nausea, vomiting, gastroesophageal reflux disease, sweating increased, muscle cramps, fatigue, chest pain, asthenia, mild and transient injection site events, including pain, swelling, erythema, localised bruising, pruritus and minor bleeding at injection site. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: The effects of overdose that might be expected include delayed hypercalcaemia and risk of orthostatic hypotension, nausea, vomiting, dizziness, and headache. No fatalities associated with overdose have been reported. There is no specific antidote for Tetridar. Treatment of suspected overdose should include transitory discontinuation of Tetridar, monitoring of serum calcium, and implementation of appropriate supportive measures, such as hydration. Legal category: Medicinal product subject to medical prescription. Marketing Authorisation Number: PA1986/053/001. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00060. Date of Preparation: May 2022.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Date of Preparation: December 2023
Job Code: GEN-IE-00054
Freephone: 1800 - 201 700
Email: info@teva.ie
Patients Protected by Pharmacist Positive Work in Addressing Medicine Shortages
The problem of medicine shortages remains high, with a latest IPU annual survey revealing that every pharmacy in Ireland has been challenged by medicine shortages in the past four months. The Irish Pharmacy Union (IPU) has said this highlights the need to expedite the planned introduction of a serious shortage protocol under the Health Miscellaneous Bill for all molecules in short supply, and ensure that the legislation will be flexible enough to find solutions for patients.
In the 12 month The IPU Medicine Shortage Survey found that all pharmacists have experienced medicine shortages in the last 4 months with a considerable 57% (60% in 2023) of pharmacies experiencing more than 40 medicine shortages in that period.
Among the key findings of the Irish Pharmacy Union’s (IPU) Medicine Shortage Survey are:
1. 84% of pharmacists expect this problem to increase over the next 12 months.
2. Irish community pharmacists are spending over 4 hours 37 minutes per week managing medicine shortages, work that often goes unnoticed and not recompensed.
3. 62% believe that allocations imposed by manufacturers is the leading cause of medicine shortages.
Medicine shortages can have a serious impact on patients and their families according to Clare
Vice Chair of Medicines for Ireland, Deirdre Kelly
Fitzell, IPU’s Head of Strategic Policy. “Behind each medicine that is in short supply are patients who need them for their health and wellbeing. Medications in short supply this year have included certain steroid creams used to treat eczema, ADHD medication and Ozempic. Medicine availability issues have potential to impact medical conditions and can create considerable stress and inconvenience to patients.
“Pharmacists are highly experienced and work with prescribers to source alternatives where required. However, this process is often time consuming for healthcare providers and takes too long for patients.
The amount of time spent by pharmacies on dealing with shortages has increased significantly since 2018. The average pharmacist spends 4 hours 37 minutes per week dealing with shortages, in 2018, 5-10 hours per month was more typical.
“There is no expectation that this problem will improve in the next year with 84% of pharmacists surveyed predicting it will get worse”, Ms Fitzell said. “This is a global problem and therefore we must look at what Ireland can control and implement this rapidly. In particular, moves to introduce a Serious Shortage Protocol must be expedited to ensure effective use of healthcare professional resource.”
The Health Miscellaneous Provisions Bill 2024 is currently before the Oireachtas. This will
allow the Minister for Health to introduce a scheme where pharmacists can appropriate substitute medicines for patients without needing to revert to the prescribing doctor. “This should dramatically speed up the process for both pharmacists and prescribers and crucially will ensure that patients get appropriate medicines quicker.”
Concluding, Ms Fitzell said, “Medicine shortages are a growing and significant problem. The focus in Ireland should be to address what is in our own control and how we can best support patients. There are very obvious and beneficial proposals that can be introduced, and the patients of Ireland cannot afford for these to be delayed any longer.”
Meanwhile, Medicines for Ireland (MFI), the leading representative body for the generic, biosimilar, and value added medicines industry, is highlighting the urgent need for action to address the increasing medicine shortages affecting the Irish population.
A recent Red C survey reveals a concerning trend: 1 in 5 (20%) of individuals have been personally affected by medicine shortages in the past two years. Additionally, 22% report that family members or friends have been impacted totalling 38% of the population either directly or indirectly experiencing the consequences of these shortages.
Commenting on the Red C survey results, Chair of Medicines for Ireland Paul Neill said, “The growing scarcity of essential medicines is more than an inconvenience; it’s a barrier to health and well-being. With 38% of those surveyed expressing that shortages have impacted them or someone close to them, it is a clear and urgent signal that our healthcare system faces a crisis that requires immediate action.”
The impact is felt across various medical treatments, with pain relief medication shortages affecting nearly 2 in 5 (37%) of those impacted. Other areas, such as respiratory, gastroenterology, and rheumatology treatments, also face significant challenges.
Medicines for Ireland, a solutionsfocused organisation, is proposing
a multifaceted approach to address these shortages:
• Implement dynamic pricing policies that encourage competition.
• Policies that incentivise the use of generic medicines, ensuring access to affordable, high-quality, and essential medications.
• Evolve the best-value biologics (BVB) process to ensure the sustainability of best-value medicines and best-value biologics.
• Create a streamlined regulatory and reimbursement pathway for value-added medicines, allowing for medicine repurposing and aligning Ireland with other leading European nations.
Mr Neill emphasises, “There is no single simple solution to addressing the challenges leading to medicine shortages, but we have detailed the solutions that MFI and our members believe can address these challenges in our five-year vision, Looking forward: Building the framework for a sustainable generic, biosimilar and value-added medicines industry in Ireland. By adopting these solutions, we can mitigate the impact of shortages and ensure a robust supply of medicines for all who need them.
“By encouraging the use of generic, biosimilar and value added medicines, we can alleviate the strain on our healthcare system. It’s not just about cost savings; it’s about ensuring that every patient has access to the medicines they need when they need them. Establishing a sustainable pathway for biosimilar medicines and a streamlined regulatory process for valueadded medicines are critical steps towards a more resilient healthcare system.”
Vice Chair of Medicines for Ireland Deirdre Kelly commented, “Patients are often left waiting, revisiting pharmacies, or accepting alternatives. This is not the standard of care we strive for in Ireland. This data shows that nearly half (49%) of the population recognises the worsening of this issue over the past two years.”
Medicines for Ireland unveils its Manifesto for Europe
Suppliers of generic, biosimilar, and value-added medicines call for reform of EU pharmaceutical laws to ensure equitable access to treatments for all patients.
Increased penetration of generic, biosimilar, and value-added medicines will be critical to enhancing treatment accessibility for patients, while managing the healthcare spend of EU member states. That’s the message from Medicines for Ireland (MFI) to European election candidates in its ‘Manifesto for Europe’ setting out the association’s key European policy asks.
In its manifesto MFI is calling for:
1. Equitable access to essential medicines through the introduction of pro-competitive measures that ensure early entry of generic, biosimilar, and value-added medicines into the Irish market.
2. Safeguarding of Europe’s pharmaceutical production through the adoption of a Critical Medicines Act to bolster manufacturing competitiveness, mitigate supply risks, and support investments in cutting-edge, sustainable manufacturing technologies and workforce upskilling.
3. The establishment of a contemporary regulatory framework to keep pace with scientific and technological progress by fast-tracking digital and regulatory efficiency measures within new EU pharmaceutical legislation.
4. Promotion of healthcare innovation through the introduction of legislative measures that reward innovation while ensuring affordability.
Commenting, Chair of MFI, Paul Neill said: “Access, affordability, and availability are central to our future vision of healthcare in Ireland and must be championed in Europe by our new cohort of Irish MEPs. Pro-competitive measures in EU pharmaceutical and intellectual property legislation, need to act as a key enabler to facilitating earlier entry of generic, biosimilar, and value-added medicines in the Irish market. Under the direction of the 10th European Parliament, we urgently need to see EU pharmaceutical laws reformed to drive greater competition, and
of MFI, Paul Neill
support investment in affordable off-patent innovation.
“A shift in policy thinking is also required to secure availability of medicines for patients which is a challenge members states, including Ireland continue to grapple with. Fostering timely competition and sustainable uptake of generic, biosimilar, and value-added medicines would significantly help shape a future where shortages are an exception rather than the norm. Furthermore, we would like to see the adoption of a Critical Medicines Act to promote open strategic autonomy in healthcare and restore medicines manufacturing competitiveness across Europe. This in turn would reduce dependency risks for essential medicines, also easing pressures on supply.”
MFI has continuously advocated for legislative reforms that guarantee every patient in Ireland and across Europe has access to the essential medicines they need. The associations policy asks, aim to secure a regulatory environment that keeps pace with science and technology evolution, ensuring Irish patients have early access to new medical innovations.
Commenting, Vice-Chair of MFI, Deirdre Kelly said: “The forthcoming European elections hold significant weight in shaping the future of health policy in Europe, a factor that directly influences the levels of shortages Irish patients endure. Irish MEPs will play a pivotal role in the future policy development and implementation that impacts national health systems and the well-being of citizens in Ireland and across Europe.
“As part of this, we need to see fast-tracking of digital and regulatory efficiency measures within new EU pharmaceutical legislation, recognising the urgency of modern healthcare needs. We are calling on Irish MEPs to pursue measures that enable regulatory flexibility to prevent shortages, including spearheading the swift adoption of Electronic Product Information Leaflets (EPIL). This goes hand in hand with the establishment of a viable shortage prevention and mitigation policy.”
Ms Kelly concluded: “In reforming EU pharmaceutical legislation we want the bolar clause exemption to be explicit on facilitating any activities that need to be undertaken to allow generic or biosimilar medicines launch
immediately after the expiry of an originator patent. Furthermore, the definition of repurposed medicines needs to be expanded beyond new indicators to include value-added medicines. These issues are of utmost importance for health systems to realise increased value from their medicine spend and to broaden patient access to medicines.”
MFI’s ‘Manifesto for Ireland’ asks align with those made by its European sister association Medicines for Europe (MFE), which will host its 30th Anniversary Annual Conference in Dublin from 12th – 13th June. The themes of the upcoming conference resonate with the pillars of MFI’s manifesto, focusing on access to medicines, innovation, and sustainable healthcare solutions. The conference will serve as a platform to further these discussions, fostering collaboration and progress towards a healthier Europe.
MFI member companies include Accord Healthcare, Celltrion Healthcare, Clonmel Healthcare, Consilient Health, Fannin, Fresenius Kabi, Pinewood Healthcare, Sandoz trading as Rowex, Teva, and Viatris.
Chair
Calls for Better Access to Mental Health for the Young Leading Psychiatrist says wider mental health services essential
for young people post-Covid
A leading Consultant Child and Adolescent Psychiatrist says children and young people need better access to mental health services, particularly within their own communities.
Irish trained Dr Elaine Lockhart, who is the Chair of the Royal College of Psychiatrists Child and Adolescent Faculty based in Scotland, says she has seen a worsening in children’s mental health which has been exacerbated by Covid-19 and its associated lockdowns.
Speaking in a new video as part of the Irish Hospital Consultants Association’s (IHCA) Care Can’t Wait campaign, Dr Lockhart says she has witnessed a surge in referrals and an increase in very sick young people, particularly those with eating disorders, selfharm and suicidality. These referral patterns have also been observed in Ireland.
Latest figures from the Department of Health confirm that there
were 3,759 children on the Child and Adolescent Mental Health Services (CAMHS) waiting lists at the end of December 2023. While this is a reduction from the record high of around 4,400 recoded last year, it is still an increase of approximately 6% (+203) since the end of 2021 and almost a twothirds increase (+1,432 or 62%) in the CAMHS waiting list compared with pre-pandemic levels at the start of 2020.
Consultants say that the difficulty in filling permanent Consultant Psychiatry posts and growing hospital and mental health capacity deficits against increases in demand are the root causes of the unacceptably long waiting lists. New data released to the IHCA under the Freedom of Information Act confirms that 156 (28%) of the 548 approved permanent Consultant Psychiatry posts in Ireland were either vacant or filled on a temporary or agency basis on 1 March 2024. This consisted of 52
totally vacant posts, 28 posts filled by agency staff, a further 74 posts filled on a temporary/locum basis and two posts of ‘unknown’ status which are likely vacant. In Child & Adolescent Psychiatry, more than a third of approved permanent Consultant posts (44 posts or 35%) were either vacant or filled on a temporary basis at the end of 2023.
Dr Lockhart, a UCD graduate currently practising as a Consultant Psychiatrist with the Greater Glasgow and Clyde Learning Disability CAMHS team, says that it is imperative specialist mental health services are in place for the most unwell children, given the surge in referrals of children with eating disorders, self-harm and suicidality.
However, the former clinical advisor to the Scottish government also stresses that children and young people require access to services in their communities,
including getting support and advice within a school setting.
“What we were seeing before Covid was an increase in social inequality which can be toxic for children’s mental health. And although social media can be real force for good, vulnerable children can be really harmed by being online. So, things were getting worse before Covid.
“But then the lockdowns really removed children from their usual routine, structure and predictability. They couldn’t meet friends and access activities and that triggered quite an increase in those seeking care. That was something we hadn’t seen before.
“While specialist mental health services must be in place for those who are most unwell, what many children are looking for and require is access to services where they can get advice in schools and community settings,” said Dr Lockhart.
New Research on Heart Health Investigations
Consultant Cardiologist Dr Richard Armstrong at Blackrock Health
New data has shown that the top reasons why people seek heart health investigations are chest pain at 51%, palpitations caused by possible heart arrhythmia at 30% and heart failure at 10%, according to 2023 admission data from Blackrock Health’s Rapid Cardiac Care Service which is available at Blackrock Clinic, Galway Clinic and Hermitage Clinic. Further research
conducted by Blackrock Health last year also showed that 77% of people have experienced one of the symptoms associated with one of these conditions yet almost 20% of people did not take any action regarding their symptoms.
On the back of this data, Consultant Cardiologist Dr Richard Armstrong at Blackrock Health is striving to drive awareness of the most commonly experienced heart health conditions and importantly when to seek medical attention.
Starting with chest pain, Dr Richard Armstrong said, “Heartrelated chest pain can vary significantly in terms of severity, from quite subtle or a mild discomfort through to crushing or searing pain. A more severe pain should spark an immediate call to 999 to attend the nearest emergency department in case you are experiencing a heart attack, but we know that more milder chest pain can often be put down to other less serious health concerns by the person experiencing it. Chest pain should always spark action to
seek medical attention as there are many conditions related to the heart that should be investigated to ensure the symptom is not masking something more sinister.”
Dr Armstrong focused on the area of palpitations caused by a heart arrhythmia as the second most common reason for presenting at the Rapid Cardiac Care Service, “Palpitations can vary in experience from feeling as though the heart beats too fast or slow, or the sensation that the heart is skipping beats. It’s important to seek medical attention if you experience a change in your heartbeat as you might have an underlying heart health issue that needs early intervention and management to reduce longerterm damage.”
Heart failure has a very distinct set of symptoms that many wouldn’t associate with a heart condition so awareness of these is important to incite action to seek medical attention. Speaking about heart failure, Dr Armstrong advised, “Heart failure, despite the name, does not mean that your heart
stops working entirely but it is an early warning sign of wider heart disease that needs early intervention and management. Distinct symptoms of heart failure include shortness of breath, swelling in the legs, ankles and feet and very rapid weight gain from fluid build-up. These symptoms occur because the heart muscle is not working as it should to adequately pump blood around your body causing the blood to back-up. Failing to diagnose heart failure can be life-threatening and can lead to a multitude of other heart health problems, so early diagnosis is key.”
Blackrock Health operates a Rapid Cardiac Care service which provides swift access to its team of cardiology specialists across its three hospitals, Blackrock Clinic, Galway Clinic and Hermitage Clinic, for cardiac patient care, with or without a GP referral. This service provides fast and expert medical care to patients with worrying, acute cardiac symptoms such as chest pain, dizziness, shortness of breath or a racing pulse rate.
The Medicines Management Programme (MMP)
recommends Lonquex® (Lipegfilgrastim) as a Best-Value Biological (BVB) Medicine for the long-acting granulocyte-colony stimulating factors on the High Tech Arrangement.
Prescribing Lonquex ® will lead to significant savings for the health service.
Lonquex ®
6 mg solution for injection pre-filled syringe (Lipegfilgrastim)
Indications
,c® 6 r119 L ollque njection . n for I ge so1ut10. I d svrin . pre-fil e 1n 'rTlLipe9f·1grast1 •
• Lonquex is indicated in adults for the reduction in the duration of neutropenia and the incidence of febrile neutropenia in patients treated with cytotoxic chemotherapy for malignancy (with the exception of chronic myeloid leukaemia and myelodysplastic syndrome).
Further information available from the SmPC available at HPRA.ie Lonquex® (lipegfilgrastim) 6mg solution for injection Abbreviated Prescribing Information
Presentation: Lipegfilgrastim 6mg solution for injection in 0.6ml pre-filled syringe. Indications: Reduction in the duration of neutropenia and the incidence of febrile neutropenia in adult patients treated with cytotoxic chemotherapy for malignancy (with the exception of chronic myeloid leukaemia and myelodysplastic syndromes). Dosage and administration: Lonquex treatment should be initiated and supervised by physicians experienced in oncology or haematology. Adults and Children 2 years and older (weighing� 45kg): 6mg of Lonquex for each chemotherapy cycle, approximately 24 hours after cytotoxic chemotherapy. Elderly: No relevant age-related difference with regards to safety or efficacy. Impaired renaVhepatic function: The pharmacokinetic profile is not expected to be affected. However, no recommendation on a posology can be made. Children less than 2 years: No data available. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Precautions and warnings: Not to be used to increase the dose of cytotoxic chemotherapy beyond established dosage regimens. Patients hypersensitive to G-CSF or derivatives are at risk of hypersensitivity reactions to lipegfilgrastim. Regular monitoring of the platelet count and haematocrit is recommended since lipegfilgrastim does not preclude thrombocytopenia and anaemia caused by myelosuppressive chemotherapy. Leukocytosis may occur; therefore a white blood cell count should be performed at regular intervals during therapy owing to the clinical effects of lipegfilgrastim and the potential for leukocytosis. Increased haematopoietic activity of the bone marrow in response to growth factor therapy has been associated with transient positive bone-imaging findings. Not to be used in patients with chronic myeloid leukaemia, myelodysplastic syndromes or secondary acute myeloid leukaemia. Spleen size should be carefully monitored since frequent asymptomatic cases of splenomegaly and infrequent cases of splenic rupture, including fatal cases, have been reported. Patients with a recent history of pulmonary infiltrates or pneumonia may be at higher risk of pulmonary adverse reactions. Physicians should exercise caution when administering Lonquex in patients with sickle cell anaemia, since sickle cell crisis has been associated with the use of G-CSF in these types of patients. Hypokalaemia may occur; therefore serum K+ levels should be carefully monitored and K+ substituted if necessary, in patients at risk of hypokalaemia. Not to be used in patients with rare hereditary problems of fructose intolerance since Lonquex contains sorbitol. During post-marketing, capillary leak syndrome has been reported after administration of G CSF or derivatives and is characterised by hypotension, hypoalbuminaemia, oedema and haemoconcentration. Patients who develop symptoms of Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67ESAO, Ireland.
Further information is available on request or in the SmPC. Product Information also available on the HPRA website. Prescription Only Medicine.
capillary leak syndrome should be closely monitored and receive standard symptomatic treatment, which may include a need for intensive care. This has generally occurred in patients suffering advanced malignant disease, having sepsis, taking multiple chemotherapy medications or undergoing apheresis. Glomerulonephritis has been reported in patients receiving filgrastim, lenograstim or pegfilgrastim. Generally, events of glomerulonephritis resolved after dose reduction or withdrawal of filgrastim, lenograstim and or pegfilgrastim. Urinalysis monitoring is recommended. Interactions: Concomitant use of lipegfilgrastim with any chemotherapeutic medicinal product has not been evaluated in patients. In animal models, concomitant administration of G-CSF and 5-fluorouracil (5-FU) or other antimetabolites has been shown to potentiate myelosuppression. The safety and efficacy of Lonquex in patients receiving chemotherapy for delayed myelosuppression has not been evaluated. The potential for interaction with lithium, which also promotes the release of neutrophils, has not been specifically investigated. Pregnancy and lactation: Not recommended in pregnancy or whilst breastfeeding. No data available with regards to fertility. Effects on ability to drive and use machines: No or negligible influence on the ability to drive and use machines. Adverse reactions: Serious: Leukocytosis, hypersensitivity reactions, pulmonary adverse reactions including haemorrhage, glomerulonephritis. Capillary leak syndrome, which can be life-threatening, has been reported in post-marketing experience and aortitis. Very common: Musculoskeletal pain, nausea. Common: Thrombocytopenia, hypokalaemia, headache, skin reactions, chest pain, haemoptysis. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: In the case of overdose, white blood cell and platelet counts should be performed regularly, and spleen size should be carefully monitored. Legal Category: POM. Marketing Authorisation Number: EU/1/13/856/001-002. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031 GA Haarlem, Netherlands. Job Code: MED-IE-00061. Date of Preparation: August 2022.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Date of Preparation: May 2024
Job Code: LQX-IE-00006
Freephone: 1800 - 201 700
Email: info@teva.ie
National Stroke Conference calls for more support for Patient Services
A major National Conference on Stroke, hosted by the South Tipperary Stroke Communication Group, took place at the Cashel Palace Hotel, Cashel, Co. Tipperary, on Monday May 20th. The Conference, which attracted around 200 people, heard from professionals and stroke survivors and included demonstrations on developments in the area of innovations for persons with spinal cord injury, stroke, multiple sclerosis and other neurological conditions. At the outset, Cathaoirleach of the Municipal District, Cllr. Declan Burgess, welcomed all the delegates and the speakers to the 'City of the Kings'. Delegates had travelled from as far away as Coleraine in Northern Ireland, from Dublin, Mayo, Carlow and from several other parts of the country.
As one of the organisers and a stroke survivor, I had the great pleasure of opening the Conference. Speaking at the Conference I said that it was an opportunity for experts, practitioners, researchers, and advocates from across the nation, to discuss the pressing health challenge of stroke. "Stroke, with its profound impact on individuals, families, and communities, demands our collective attention and concerted efforts. This conference serves as a platform for sharing knowledge, fostering collaboration, and advancing innovative solutions in stroke prevention, treatment, and rehabilitation. At this Conference we will engage in enlightening discussions, explore research driven initiatives, and exchange invaluable insights that will shape the future landscape of stroke care in our country. Today is an
Martin Quinn opens the National Conference on Stroke at the Cashel Palace Hotel
Professor Joe Harbison addresses the National Conference on Stroke at the Cashel Palace
Chris Macey of the Irish Heart Foundation speaking to delegates at the National Conference on Stroke at the Cashel Palace Hotel
"Stroke, with its profound impact on individuals, families, and communities, demands our collective attention and concerted efforts. This conference serves as a platform for sharing knowledge, fostering collaboration, and advancing innovative solutions in stroke prevention, treatment, and rehabilitation”
opportunity to discuss awareness, access to quality care, the needs of patients and carers, and how we can make meaningful strides towards reducing the burden of
stroke on our society" were my opening remarks.
One of the keynote speakers was Professor Joe Harbison,
Associate Professor and Head of Discipline of Medical Gerontology in Trinity College Dublin & Stroke Physician in St James’s Hospital in Dublin and Clinical Lead of the Irish National Audit of Stroke. Professor Harbison gave a very insightful presentation on data from hospitals around the country in relation to stroke, and he highlighted some of the key messages from the Irish National Audit of Stroke. The Professor also gave a presentation on Atrial Fibrillation and he took questions from the floor on several different aspects of stroke.
Chris Macey, Director of Advocacy and Patient Support at the Irish Heart Foundation, was another speaker at the Conference and he highlighted the current funding challenges facing the Irish Heart Foundation. "The Irish Heart Foundation is running a national support service for the biggest patient group in the country. Out of a total cost of ¤1.24 million a year to operate the service, it is receiving just ¤130,000 a year in statutory funding. This represents funding averaging less than ¤19 a head to deliver a pathway of professional support to people currently in the service, with often complex support needs. Any patients here today who have benefited from these services, know what the impact of losing them would be to individual lives, and on a wider scale across the country. The Irish Heart Foundation has been making up the shortfall by running down its reserves, and we are extremely concerned that we cannot guarantee the continuation of all of our services beyond the end of 2024. This is very worrying and must be addressed by the Government as a matter of urgency" said Chris.
Ronan Langan, Clinical Lead of the DCU Exoskeleton Programme, delivered a hugely interesting presentation, which included a
demonstration of the Exoskeleton. The Exoskeleton programme is physiotherapist led service allowing persons with reduced mobility due to paralysis, access to the ekso bionics exoskeleton, Ekso GT to allow them to complete sessions of supported walking facilitated by a trained handler. The programme is designed to deliver an array of benefits that regular walking in an exoskeleton provides for persons with spinal cord injury, stroke, multiple sclerosis and other neurological conditions.
Other speakers at the Conference included young stroke survivors Heidi Kingston and Darren Creaven. Young mother Heidi, gave an emotional testimony of suffering a stroke in December 2021. "I was an active and adventurous 32 year-old. I convinced myself that I was having a headache, a hormonal headache or maybe a side-effect of medication I took for the headache. Along with the headache I had numbness and tingling from my right side, from my neck all the way to my foot, and I had darkened peripheral vision. I was visiting family in New Jersey with my husband from our home in Galway, and only went to hospital following a phone call with my GP. It was there that he and I learned I had had a stroke. I was in complete shock" said Heidi. Actor Darren Creaven from Galway explained that he suffered a stroke almost 7 years ago when he was visiting family in Clonmel, Co. Tipperary. "I suffered a bleed in my brain which caused me to lose all movement on my left side. I was taken to Tipperary University Hospital and later transferred to Cork University Hospital before going to Galway University Hospital and finally to the National Rehabilitation Hospital for rehab. Though I still have some deficits I have made a great recovery and am bac acting once again" said Darren.
There was a lively and engaging question and answer session during the Conference and there was also a musical treat for attendees with performances from Aoife O'Farrell of the Rockwell Music Academy.
Young
Tea/Coffee and some treats were served by the wonderful staff at the Cashel Palace Hotel with one attendee remarking that they were "treated like Royalty". The Conference was supported financially by TASK Community Care and Home Instead Ireland and financial and technical support was provided by the Tipperary Volunteer Centre. In excess of 20 stands were in attendance with a wide range of information available.
Ronan Langan of the DCU Exoskeleton Programme speaking at the National Stroke Conference at the Cashel Palace Hotel
mother and stroke survivor, Heidi Kingston, speaking at the National Conference on Stroke at the Cashel Palace
Paediatric Fever
Acute Paediatric Fever Advice: ‘Fever is mostly one of the Good Guys’
Written by Karl Kavanagh1, Diarmaid Semple2, Michael Barrett1,3
1Department of Paediatric Emergency Medicine, Children’s Health Ireland at Crumlin, Dublin 12
2Pharmacy Department, Children’s Health Ireland at Crumlin, Dublin 12
3Women’s and Children’s Health, School of Medicine, University College Dublin
Dr Karl Kavanagh
What is a fever?
Fever is a common symptom that can incite fear and worry in many parents. In practice, it is one of the most frequent reasons for health care attendance.1
A fever is a binary entity, it is a temperature of greater than or equal to 38.0°C. There has been a shift away from the concept of a “low grade” fever. In Ireland there is much variation in the knowledge on what is the actual definition of a fever.2, 3 Remember that an error with the definition can cause much confusion and unnecessary worry. If this is not clarified, this can sometimes expose the patient to an unnecessary medical visit and all that ensues.
Temperature-taking
There is a vast array of products to assess temperature, however some are more accurate than others. In the <1yr old population, an axillary thermometer is recommended, whereas at older ages a digital ear probe is both fast and accurate.4 Infrared thermometers, glass thermometers and forehead strips should be discouraged as they are less reliable. Again, a falsely positive temperature could
result in children, in the interest of safety, being subjected to several potentially unnecessary investigations (e.g. Lumbar puncture, vascular access etc).
For the parent in the middle of the night, who can’t recall where the thermometer is, we have a natural gauge quite literally at our fingertips. Tactile assessment of temperature has been shown to be a sensitive measurement, though it is the least accurate way in terms of establishing a definitive quantity. Palpation of the chest and back is preferred to the forehead.
Common Questions to be addressed
Q. Fever is dangerous?
Answer: No. Fever is the body’s natural response to infections. It represents immune response activation and an indicator of an illness. The presence of a fever in of itself doesn’t require treatment with antipyretics. Observational trials in humans suggest a survival benefit from fever. The heat of fever augments the performance of immune cells, induces stress on pathogens and infected cells directly, and combines with other stressors to provide a nonspecific immune defence.
Q. Does the height of fever indicate the severity of illness?
Answer: False. A worry for parents is the upper limit of the temperature. While it is natural to assume a proportional severity to the degree of temperature, there is in fact no correlation between the temperature height and how ill the patient is. A child could be critically unwell with a temperature of 38.1°C, whereas another child could develop a 40°C fever and only experience a mild illness.5
Q. Is a failure to respond to antipyretics an indicator of severity of illness?
Answer: In a similar vein, the fact that a temperature does not resolve with antipyretics does not indicate a more severe illness. A child could have a consistent temperature for hours despite antipyretics and have a mild viral illness.
Q. How long is too long to have a fever?
Answer: Parents often worry about the duration of a fever. It is recommended that a child with a daily fever for 5 consecutive days seek medical attention. These patients have a higher incidence of serious bacterial infection and warrant a clinical assessment. In
cases where antibiotics have been prescribed and indicated, it would be typical for the fever to resolve within 2-3 days of commencing antibiotic therapy. A fever that has not resolved after this duration of treatment would also be another indication for medical review.
Q. Will the fever cause a seizure?
Answer: This quite often leads to the discussion surrounding febrile convulsions and fevers. It is true that febrile convulsions occur in the setting of a febrile illness, however the risk of convulsion is not just related to fever. Rather, it is the genetic component that is a greater factor in the development of febrile convulsions. Indeed, teaching would discourage parents from actively avoiding temperatures to prevent convulsions, as the fever itself does not cause harm to the child.
Q. What should I look out for?
Answer: The important aspect to recognise in each acute febrile episode is the overall clinical condition of the child. Are they dehydrated, lethargic, poorly responsive, tolerant of oral intake or have a non-blanching rash? These are far more sensitive markers of severity of illness in the context of a fever.
Q. Does my child have sepsis?
Answer: One should always be vigilant for sepsis. As per the HSE, sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection. Fever in isolation does not automatically translate to sepsis, and few infections will develop into sepsis. There is no single test that detects sepsis, but as we will outline below it is the constellation of symptoms in the setting of an infection that invokes the diagnosis of sepsis. If you are concerned your child has sepsis, medical attention should be sought. It is always an important question to ask in the setting of fever.
For a public video resource see the following HSE Sepsis Public Awareness information: Sepsis Awareness by Health Service
Diarmaid Semple
Professor Michael Barrett
1: Infographic with educational video on fever (QR Code) from the Department of Emergency Medicine, Children’s Health Ireland at Crumlin.
• Convulsion
• Cold to touch despite the temperature
Executive (HSE) Ireland; Available from Youtube HSE Ireland
• The appearance of poor skin perfusio
Paediatric Sepsis Awareness
(http://www.youtube.com/ watch?v=U0yqqkxsn_8 and https://www.hse.ie/eng/about/ who/nqpsd/qps-improvement/ sepsis.html).
In these situations, it is recommended that the parent seeks urgent medical attention
There is one further scenario in which we would encourage parents to seek medical attention and that is:
When to be more concerned and seek help
As mentioned above, there are times when a fever is cause for greater concern. This is when there is:
• If their parental instinct tells them something is wrong
• The presence of a bruising rash that does not go away when pressed
• Convulsion
• Cold to touch despite the temperature
Parents have a great sense of their concern should never be disregarded regarded as key information to inform the situation
• The appearance of poor skin perfusion
In these situations, it is recommended that the parent seeks urgent medical attention.6
There are several groups of children that are at higher risk of infection, and these can present differently A higher degree of caution is required. These include those with disabilities cognitive impairment or communicative Children that have these conditions susceptible to infections such as pneumonia or urinary tract infections. compounded by factors such as immobility dependence potential source of infection Communication can be an issue, and their symptoms in ways that are only recognised by a carer and underappreciated by clinical staff This underpins the need for the parent’s (or caregiver’s) input as they know the child well and are familiar with the nuances of their
There is one further scenario in which we would encourage parents to seek medical attention and that is:
A low threshold is reserved for or immune systems are compromised they don’t mount the same response to infection. associated with these conditions could potentially be life , and prompt investigation and treatment is mandated under these circumstances
• If their parental instinct tells them something is seriously wrong
The final types of patients that we would consider “at risk” newborn and young infant.
Small baby rules (6 months and younger)
Parents have a great sense of their child; their concern should never be disregarded and should be regarded as key information to inform the situation.
At risk populations:
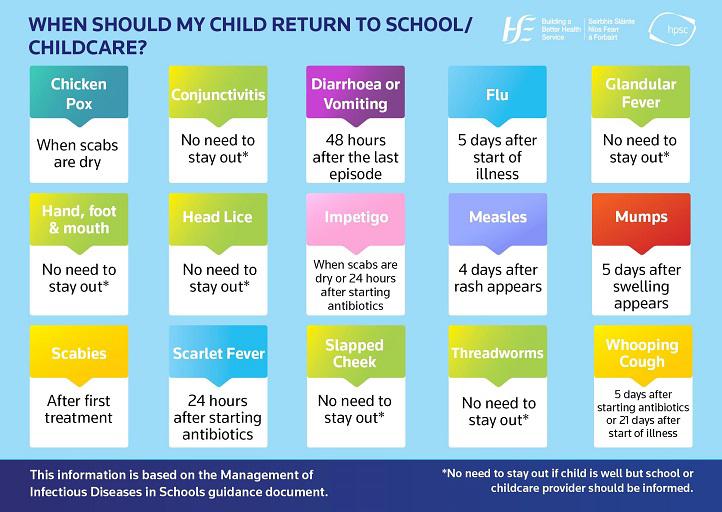
2: When should my child return to school/childcare advice for parents when their child develops symptoms of some of the common childhood illnesses about whether their child should stay out of school or childcare
The above advice pertains to children older than 6 months of age. Babies younger than six months are a special population that require a different approach when it comes to fevers. Febrile babies require more investigation than their older counterparts.
There are several groups of children that are at higher risk of infection, and these can present differently. A higher degree of caution is required. These include those with disabilities with cognitive impairment or communicative difficulties. Children that have these conditions are more susceptible to infections such as pneumonia or urinary tract
• Baby 0-3 months old develop a fever ≥38.0°C
• Baby 3-6 months old develop a fever >39.0°C
infections. These vulnerabilities are compounded by factors such as immobility or medical device dependence which can be another potential source of infection to consider. Communication can be an issue, and the child may convey their symptoms in ways that are only recognised by a carer and underappreciated by clinical staff. This underpins the need for the parent’s (or caregiver’s) input as they know the child well and are familiar with the nuances of their behaviours.7
Current HSE guidance would recommend medical attention be sought if:
A low threshold is reserved for those that are immunocompromised or neutropenic.8 As their immune systems are compromised, they don’t mount the same response to infection. A fever associated with these conditions could potentially be life-threatening, and prompt investigation and treatment is mandated under these circumstances.9
The final types of patients that we would consider “at risk” are the newborn and young infant.
Small baby rules (6 months and younger)
The above advice pertains to children older than 6 months of age. Babies younger than six months are a special population that require a different approach when it comes to fevers. Febrile babies require more investigation
This is recommended even if temperature is the only symptom present. This caution stems from a cautious approach and the baby’s inability to naturally fight some infections and incomplete vaccination status.
Table 1: Concerning symptoms associated with serious illness in infants < 6 months
Difficult to wake
Bulging fontanelle
Vomiting
Excessively sleeping
Poor feeding
Irritable
Abnormal or high-pitched crying
Floppy or poor tone
Breathing difficulties
Table 1: Concerning symptoms associated with serious illness in infants < 6 months
Figure
Figure
Figure 1: Infographic with educational video on fever (QR Code) from the Department of Emergency Medicine, Children’s Health Ireland at Crumlin
Paediatric Fever
than their older counterparts.
References:
Current HSE guidance would recommend medical attention be sought if:
Figure 2: When should my child return to school/childcare advice for parents when their child develops symptoms of some of the common childhood illnesses about whether their child should stay out of school or childcare
References
1. Poirier MP, Collins EP, McGuire E. Fever phobia: a survey of caregivers of children seen in a pediatric emergency department. Clin Pediatr (Phila). 2010;49(6):530-4.
2. Lynch CJ, Kuhar M, Blackburn C, Barrett MJ. Fever education for caregivers in the emergency room (The FEVER study)–an interventional trial. Pediatric Research. 2024.
3. Kelly M, Sahm LJ, Shiely F, O’Sullivan R, McGillicuddy A, McCarthy S. Parental knowledge, attitudes and beliefs regarding fever in children: an interview study. BMC Public Health. 2016;16(1):540.
• Ibuprofen should be avoided in chickenpox unless clinician advised.
• Baby 0-3 months old develop a fever ≥38.0°C
4. Apa H, Gözmen S, Bayram N, Çatkoğlu A, Devrim F, Karaarslan U, et al. Clinical accuracy of tympanic thermometer and noncontact infrared skin thermometer in pediatric practice: an alternative for axillary digital thermometer. Pediatr Emerg Care. 2013;29(9):992-7.
1. Poirier MP, Collins EP, McGuire E. Fever phobia: a survey of caregivers of children seen in a pediatric emergency department. Clin Pediatr (Phila). 2010;49(6):530-4.
• Baby 3-6 months old develop a fever >39.0°C
This is recommended even if temperature is the only symptom present. This caution stems from a cautious approach and the baby’s inability to naturally fight some infections and incomplete vaccination status.
The instinct may be to strip clothes off and actively cool the patient, but this can cause shivering, and shivering can lead to an increase in temperature through movement. If the child is dressed comfortably, layers can be gradually removed if overheating. The importance of fluids cannot be understated. Dehydration compounds illness and has a detrimental effect on children. It is vital to anticipate this.
• It is important to maintain adequate hydration in the setting of ibuprofen use. If a child is not maintaining full oral intake then ibuprofen use should be limited to 3 days.
5. Wrotek S, LeGrand EK, Dzialuk A, Alcock J. Let fever do its job: The meaning of fever in the pandemic era. Evol Med Public Health. 2021;9(1):26-35.
2. Lynch CJ, Kuhar M, Blackburn C, Barrett MJ. Fever education for caregivers in the emergency room (The FEVER study)–an interventional trial. Pediatric Research. 2024.
6. Health Service Executive Ireland. High temperature - fever in children 2021 [Available from: https://www2.hse.ie/ conditions/high-temperature/.]
3. Kelly M, Sahm LJ, Shiely F, O’Sullivan R, McGillicuddy A, McCarthy S. Parental knowledge, attitudes and beliefs regarding fever in children: an interview study. BMC Public Health. 2016;16(1):540.
Vaccine-associated Temperatures:
Please note that HSE weight-based dosing guides for ibuprofen and paracetamol (www.hse.ie) are derived from Irish College of General Practitioners General Practitioner Quick Reference Guide for Antipyretic Prescribing and are intended for use by prescribers only.11
7. Barbi E, Marzuillo P, Neri E, Naviglio S, Krauss BS. Fever in Children: Pearls and Pitfalls. Children (Basel). 2017;4(9).
4. Apa H, Gözmen S, Bayram N, Çatkoğlu A, Devrim F, Karaarslan U, et al. Clinical accuracy of tympanic thermometer and noncontact infrared skin thermometer in pediatric practice: an alternative for axillary digital thermometer. Pediatr Emerg Care. 2013;29(9):992-7.
Further Advice Supports
8. Haslam DB, McKinney JS. Chapter 229. Fever and Infection in the Immunocompromised Patient. In: Rudolph CD, Rudolph AM, Lister GE, First LR, Gershon AA, editors. Rudolph's Pediatrics, 22e. New York, NY: The McGraw-Hill Companies; 2011.
5. Wrotek S, LeGrand EK, Dzialuk A, Alcock J. Let fever do its job: The meaning of fever in the pandemic era. Evol Med Public Health. 2021;9(1):26-35.
Fever may occur in the first 48hrs after routine vaccine administration, and parents can be reassured that these particular fevers are normal in the absence of other concerning symptoms (Table 1).10 If a baby continued to have fevers beyond this timeframe, this would be abnormal and should be investigated further.
Temperature Management
9. Vedi A, Pennington V, O'Meara M, Stark K, Senner A, Hunstead P, et al. Management of fever and neutropenia in children with cancer. Support Care Cancer. 2015;23(7):2079-87.
6. Health Service Executive Ireland. High temperature - fever in children 2021 [Available from: https://www2.hse.ie/conditions/high-temperature/.]
7. Barbi E, Marzuillo P, Neri E, Naviglio S, Krauss BS. Fever in Children: Pearls and Pitfalls. Children (Basel). 2017;4(9).
There are numerous traditional methods of managing a fever, but the tried and tested means are:
The most common first port of call for a temperature is an antipyretic such as paracetamol or ibuprofen. These are effective medications in reducing temperatures, though their use needs to be reasoned. As already discussed, the fact of having a temperature has little impact on the severity of the illness, and as such antipyretics play little part in improving the clinical condition. Whereas they are an effective means of improving the child’s comfort and wellbeing. Oftentimes, when we have a fever, we can be quite miserable, with aches and pains, and being somewhat off form. It is in these circumstances that antipyretics are endorsed. In the young >6month old children that lack the ability to convey their displeasure, this can be represented as excessive “crankiness”.
10. Health Service Executive Ireland. After Immunisation. 2022.
11. Health Service Executive Ireland. Prescribing for Children 2022 [Available from: https://www.hse.ie/eng/services/ list/2/gp/antibiotic-prescribing/ prescribing-for-children/.]
8. Haslam DB, McKinney JS. Chapter 229. Fever and Infection in the Immunocompromised Patient. In: Rudolph CD, Rudolph AM, Lister GE, First LR, Gershon AA, editors. Rudolph's Pediatrics, 22e. New York, NY: The McGraw-Hill Companies; 2011.
9. Vedi A, Pennington V, O'Meara M, Stark K, Senner A, Hunstead P, et al. Management of fever and neutropenia in children with cancer. Support Care Cancer. 2015;23(7):2079-87.
• Dress comfortably
It is important to note:
10. Health Service Executive Ireland. After Immunisation. 2022.
• Avoid fans/open windows or cold compresses
• Paracetamol should be given 4-6 hourly as required and never more than 4 times per day
• Treat aches or pains
• Ensure the child is drinking plenty of fluids.
12. Health Service Executive. My Child: 0 to 2 years Expert advice for every step. 5th Edition. Health Service Executive; 2021 [cited 2024 Feb 28]. [Available from: https://assets.hse.ie/media/ documents/My_Child_0_to_2_years_ book_QIxabfB.pdf]
11. Health Service Executive Ireland. Prescribing for Children 2022 [Available from: https://www.hse.ie/eng/services/list/2/gp/antibiotic-prescribing/prescribing-for-children/.]
• Ibuprofen should be given 6-8 hourly as required and never more than 3 times per day.
Finally, any time parents are in a medical setting with their child, it is often a time of high-stress and low-retention. One should be sure to provide written advice (e.g. digital resources) on the management and caveats of fevers, in order to allow the parent time to absorb the information or use it at their leisure. A broad sweep of expert advice for children 0-2 years is available from HSE MYCHILD.ie resources.12 Other innovative methods such as infographics or short videos explaining the fever process have been proven to be of value and should be considered (Fig. 1).2 Also attached is an infographic advising the appropriate timeframes for returning to school/childcare after different infections/symptoms from the Health Protection Surveillance Centre (Fig. 2).13
12. Health Service Executive. My Child: 0 to 2 years Expert advice for every step. 5th Edition. Health Service Executive; 2021 [cited 2024 Feb 28]. [Available from: https://assets.hse.ie/media/documents/My_Child_0_to_2_years_book_QIxabfB.pdf]
13. Health Protection Surveillance Centre. When should my child return to school/childcare [Available from: https:// www.hpsc.ie/a-z/lifestages/childcare/ whenshouldmychildreturntoschoolchildcare/ ]
New research on gut microbes and allergies in newborns
Lockdowns imposed during the COVID-19 pandemic had an impact on the gut microbiome development of babies born during these periods according to new research from RCSI University of Medicine and Health Sciences, Children’s Health Ireland and APC Microbiome Ireland (APC), a world-leading SFI Research Centre based in University College Cork.
Our gut microbiome, an ecosystem of microbes that live in our digestive tract, plays an essential role in human health. The study, published in Allergy, is the first to specifically explore the gut health of newborns in the pandemic. It revealed significant differences in the microbiome development of babies born during lockdown periods when compared to prepandemic babies. Babies born during lockdown also had lower than expected rates of allergic conditions, such as food allergies. The findings highlighted gut health benefits for ‘pandemic babies’ arising from the unique environment of lockdown, including lower rates of infection and consequent antibiotic use, and increased duration of breastfeeding. The newborns were found to have more of the beneficial microbes acquired after birth from their mother. These maternal microbes could be playing a protective role against allergic diseases.
Professor Jonathan Hourihane, Head of the Department of Paediatrics at RCSI and Consultant Paediatrician at Children’s Health Ireland Temple Street, who is joint senior author of the study, commented on the
Professor Jonathan Hourihane, Head of the Department of Paediatrics at RCSI
research’s implications: “This study offers a new perspective on the impact of social isolation in early life on the gut microbiome. Notably, the lower allergy rates among newborns during the lockdown could highlight the impact of lifestyle and environmental factors, such as frequent antibiotic use, on the rise of allergic diseases.
“We hope to re-examine these children when they are five years old to see if there are longerterm impacts of these interesting changes in early gut microbiome.”
Early life exposures
Professor Liam O’Mahony, Principal Investigator at APC Microbiome Ireland and Professor of Immunology at University College Cork, is joint senior author. He added: “While we all start life sterile, communities of beneficial microbes that inhabit our gut develop over the first years of life. We took the opportunity to study microbiome development in infants raised during the early COVID-19 era when strict social distancing restrictions were in
Waiting List Plan
Minister for Health Stephen Donnelly has published the 2024 Waiting List Action Plan (WLAP). Total funding of ¤360 million has been provided for the WLAP this year and the WLAP sets out 19 actions across three themes, namely Delivering Capacity, Reforming Scheduled Care, and Enabling Scheduled Care Reform.
The 2024 Plan builds on progress achieved in 2021, 2022 and 2023 as part of the multi-annual WLAP approach, initiated by Minister Donnelly to sustainably reduce
and reform hospital waiting lists and waiting times, and to move closer to achieving the Sláintecare maximum wait times.
This year’s Plan encompasses four overarching targets to reduce both waiting list numbers and also the time that people wait for their care, namely:
• Sláintecare Time Targetsreducing the number of patients breaching the Sláintecare Time Targets (as of year-end 2023) by 10%
• Patients Waiting Over three
place, as the complexity of early life exposures was reduced and this facilitated a more accurate identification of the key early life exposures. Prior to this study it has been difficult to fully determine the relative contribution of these multiple environmental exposures and dietary factors on early-life microbiome development.
“One fascinating outcome is that due to reduced human exposures and protection from infection, only 17% of infants required an antibiotic by one year of age, which correlated with higher levels of beneficial bacteria such as bifidobacteria. The study has provided a rich repository of data, which we will continue to analyse and investigate in the future.”
The researchers from RCSI, CHI and APC Microbiome Ireland analysed fecal samples from 351 babies born in the first three months of the pandemic, comparing these with prepandemic cohorts. The former
were part of the CORAL (Impact of CoronaVirus Pandemic on Allergic and Autoimmune Dysregulation in Infants Born During Lockdown) project. Online questionnaires were used to collect information on diet, home environment and health. Stool samples were collected at six, 12 and 24 months and allergy testing was performed at 12 and 24 months.
'Association between Gut Microbiota Development and Allergy in Infants Born during Pandemic-Related Social Distancing Restrictions' was carried out in collaboration with University College Cork, University of Helsinki, University of Colorado, Karolinska Institute Stockholm, Children’s Health Ireland, Rotunda Hospital and The Coombe Hospital.
The CORAL study was supported by the Temple Street Hospital Foundation in Dublin, Ireland and the Clemens von Pirquet Foundation in Geneva, Switzerland.
years – reducing the number of patients waiting over 3 years or at risk of being over 3 years by 90%
• National Service Plan (NSP) Maximum Wait Time targets - increasing the proportion of patients who are waiting less than the NSP maximum wait time targets to 90%
• Waiting List Volume - reducing the overall waiting list volume by almost 6% by year-end
It is important that these targets are contextualised based on
projected activity rates for 2024. In 2023, the overall removals target was exceeded by 5%, with over 1.74 million patients removed from hospital waiting lists. The 2024 WLAP expects to remove even more patients this year and is projecting that over 1.81 million patients will be removed from hospital waiting lists by the end of December 2024.
However, the rate of additions to the waiting list in 2024 is also projected to further increase beyond the levels experienced last year.
Breakthrough Research Development for Barrett’s Oesophagus
Ahead of World Barrett’s Oesophagus Day which took place last month, researchers behind the recently established Breakthrough Cancer Research AllCaNOesophageal Network have announced they are working on a new treatment at the bench which aims to target inflammation in people with Barrett’s oesophagus, a condition affecting the food pipe.
Barrett's Oesophagus is characterised by a transformation in the cells lining the oesophagus due to exposure to acid reflux and various stressors, which can increase the risk of these cells becoming more damaged and possibly turning cancerous over time. People with Barrett’s oesophagus can progress to 2 stages, either dysplasia (abnormal cells/not cancer) or oesophageal cancer.
Traditionally, patients with Barrett's that have progressed to dysplasia undergo procedures such as ablation therapy to remove damaged tissue or abnormal cells. This thermal approach needs to be carefully
applied to avoid damaging the muscles and some post-procedure complications can occur. Following patient consent, Prof. Jacintha O’Sullivan’s team in collaboration with Mirai Medical (Declan Soden, CEO), are examining in the lab if treating Barrett’s disease patient tissue with electroporation can reduce inflammation and alter immune cell biology. This technique utilises pulses of electricity to target affected cells while preserving healthy tissue, potentially revolutionising care for individuals with this condition. This technology is non-thermal and doesn’t destroy the underlying healthy tissue. As the number of Barrett’s patients are increasing, this innovative treatment may represent a paradigm shift in early intervention and prevention of oesophageal cancer.
This innovative work is part of the Breakthrough Cancer Research AllCaN-Oesophageal network, a unique network of scientist, clinicians, industry partners and patient groups on the island of Ireland, focused on accelerating discoveries across
the oesophageal cancer patient journey from cancer prevention, diagnosis, treatment, and survivorship. Breakthrough Cancer Research has allocated ¤1 million in funding, with co-support from industry and other charities such as the Oesophageal Cancer Fund and CROSS, to deliver impact for people with Barrett’s and Oesophageal cancer.
Commenting on the new research, Dr Declan Soden, CEO of Mirai Medical, expressed enthusiasm for the collaboration, stating, "Our partnership with AllCaN marks a significant step towards advancing treatment options for Barrett’s Oesophagus patients. By leveraging cutting-edge technologies, we aim to mitigate inflammation and improve patient outcomes."
Orla Dolan CEO of Breakthrough Cancer Research said, "We have championed the potential of electroporation for many years which has progressed clinical trials in colorectal cancer, fostered the development of groundbreaking tools like the EndoVE®
Lorraine Smith, PhD Student and Professor Jacintha O’Sullivan, Trinity St. James’s Cancer Institute
device to deliver electroporation, and have seen the transformative impact it can have on the treatment of skin cancer. It's truly exciting to witness this technology now being harnessed to prevent cancers from developing."
Speaking about his own experience Peter Browne (Public Patient Involvement Rep) said,
“Because I was identified as having Barrett’s Oesophagus, I was fortunate to have been closely monitored and caught at a very early stage as a result. The medical team was able to act on changes before things became even more serious. I think this research is so important for patients as the AllCaNOesophageal team are exploring so many ways to identify those most at risk of progressing and ways to halt it.”
For more information about the Breakthrough Cancer Research AllCaN-Oesophageal Network, please visit www. breakthroughcancerresearch.ie/ allcan.
Exploring career choices of pharmacy graduates over 15 years: A cross-sectional evaluation
Written by Katie L. Fitzpatrick, Evin A. Allen, Brendan T. Griffin, Joseph P. O'Shea, Kieran Dalton, Harriet Bennett-Lenane University College Cork, Cavanagh Pharmacy Building, College Road, Cork, Ireland
The pharmacy profession has evolved over time and continually adapted to the needs of society and the everchanging healthcare system. 1,2 Within clinical settings, this has comprised a more patient-centred, rather than a product-orientated role, as provision of patient counselling, drug monitoring, and advanced practices have led to improved treatment outcomes for patients.1,3 In 1997, the World Health Organisation (WHO) introduced the concept of the ‘7-star pharmacist’2,4,5, which detailed the roles which pharmacists should perform – namely: ‘caregiver’, ‘communicator’, ‘decision-maker’, ‘manager’, ‘teacher’, ‘lifelong learner’, and ‘leader’. Later, three additional roles were added, including ‘researcher’, ‘entrepreneur’, and ‘agent of positive change’, resulting in the ‘ten-star pharmacist’.6,7 Owing to the diversity and transferability of many of these roles, pharmacy graduates, now more than ever, appear fully equipped to work in multidisciplinary roles across both patient and non-patientfacing settings.
Increased recognition of the highly educated pharmacy graduate workforce across the wider employment landscape has significantly expanded graduate career prospects. The broad set of technical skills and expertise obtained through a pharmacy degree enables graduates to thrive professionally within both an integrated healthcare sector and the global employment marketplace.8 Typically, careers outside of the clinically focused or “patientfacing” settings of community or hospital pharmacy have been associated with a career within pharmaceutical manufacturing. However, increasingly diverse employment opportunities are now also arising in other nonconventional “non-patient facing” settings, such as drug regulatory authorities, academia, public bodies, consulting, and beyond. This has resulted in an increase in varied employment prospects for pharmacy graduates in different areas like never before - thus providing a golden
opportunity for pharmacists to diversify their career paths and professional aspirations. While these nonconventional opportunities are certainly welcomed, the increasing numbers of pharmacists employed in nonpatient facing sectors has meant a decrease in the proportion of pharmacy graduates choosing employment in patient-facing roles, of which pharmacists are the only healthcare professionals licensed to hold. This has resulted in an increased global demand and significant international pressures on the patient-facing pharmacy workforce worldwide. A 2021 report by the International Pharmaceutical Federation (FIP) raised concerns over access to pharmacists,9 while their 2018 report also anticipated increasing capacity challenges in the future, predicting a 40% growth of the global pharmacy workforce over the next 15 years.10,11 Similarly, the World Health Organisation estimates a projected shortfall of 10 million health workers by 2030.12 Therefore, considering continued pressures on the patient-facing workforce and the ever-evolving pharmacy landscape, it appears pertinent to create more accurate predictors of where pharmacy graduates are working. In doing so, helping to create increasingly accurate projections of workforce capacity to inform pharmacy workforce models.
Numerous international studies have examined career intentions or aspirations of pharmacy students, including countries such as Australia,13 Jordan,14 Malaysia,15 Northern Ireland,16 Nigeria,17 Qatar,18 S audi Arabia,19,20 Sudan,2 and the United States of America (USA).21, 22, 23, 24, 25 While a previous study did examine the career choices of pharmacy graduates in the early career stage (<3 years post-graduation) in Japan,26 the authors believe the present study is novel as it provides the first cross-sectional analysis of pharmacy graduate career paths over a 15-year time frame. Furthermore, given the current landscape of patientfacing workforce capacity problems internationally, the everwidening graduate employment
opportunities, and apparent paucity of robust European data, this study presents a timely opportunity to investigate the career paths of graduates from a pharmacy training programme in Ireland.
Using an online survey and publicly accessible Linkedin® profile data, this study primarily aimed to provide an overview of the career paths of pharmacy graduates from University College Cork (UCC) School of Pharmacy since its establishment in 2004. Secondary aims included identifying the proportions of graduates per employment sector across both patient-facing and non-patient-facing roles, those who have completed post-graduate education, along with graduate satisfaction with the pharmacy programme and their chosen career paths. This research should help inform key stakeholders of trends in Irish trained pharmacy graduate employment over the past fifteen years, guide strategic development of pharmacy programmes and future policy-making, while also informing current pharmacy students of potential employment opportunities through data-driven analysis of graduate career paths
Methods
Study context
First established in 2024, UCC School of Pharmacy is currently one of only three schools in the Republic of Ireland (ROI) accredited by the Pharmaceutical Society of Ireland (PSI) and entry to the UCC undergraduate pharmacy programme is competitive. A pharmacy degree is unique in delivering both a healthcare and pharmaceutical science curriculum, providing students with a strong education in the main areas of pharmaceutical chemistry, biochemistry, pharmaceutics, sterile manufacturing, microbiology, pharmacology, and clinical pharmacy practice.
Prior to 2015, ROI pharmacy students undertook a ‘4 year plus 1 year’ pharmacy programme: a 4 years Bachelor’s degree in UCC plus a 1 year Masters. The final year comprised a 1-year work placement (with a minimum
of 6 months in a patient-facing setting) and academic modules completed via the Royal College of Surgeons in Ireland. Since 2015, all incoming pharmacy students undertake an integrated five-year Master of Pharmacy (MPharm) degree, all completed with UCC. Students undertake a 4-month experiential work placement in the fourth year in either a patient-facing setting or a non-patient facing (such as in pharmaceutical industry, academia, or a public body etc.).
Study design and participants
The population eligible for inclusion were graduates of UCC pharmacy programmes (BPharm and MPharm) from 2007 to 2022 (n = 798). As student contact email information becomes inaccessible upon graduation from UCC, this study utilised two approaches to collect data on graduates’ career paths: an online survey and analysis of publicly accessible information from Linkedin® profiles. Ethics approval for this study was granted by UCC›s Social Research Ethics Committee. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement was used to guide study reporting.27
Data collection
Survey design
The survey (Supplementary Material 1) was created based on previous literature2,3,13,14,22 by the research team, consisting of pharmacist academics based in UCC, some of whom are current students or previously graduated from UCC›s pharmacy programme. The survey used a combination of multiple-choice questions, yes/no questions, and Likert-scale ratings. Participant names and year of graduation were required to avoid duplication of graduates during the crosscheck process described below. An information sheet preceding the survey highlighted that any identifying information would be removed prior to data analysis
Survey distribution
School of Pharmacy staff contacted one class representative
Pharmacy
from each graduating year from 2007 to 2022 with whom they had a professional or personal connection via email, phone, or social media between the 15th of May and 25th of June 2023 (date of survey closure). To ensure consistency representatives were contacted using a pre-determined body of text containing the study aims. They were also provided with a participant information sheet and asked to distribute the online survey link via email, phone, or social media. The survey link was also posted to the “UCC Pharmacy Alumni” Linkedin® page on the 9th of June. Participation was voluntary and participants could withdraw from the survey up until the point of data submission. Efforts to maximise the response rate involved a reminder message sent to the class representatives two weeks after initial contact. Data was extracted from the survey platform (Microsoft® Forms, Microsoft Office, 2016).
LinkedIn® profiles and PSI register
Publicly accessible LinkedIn® profile information of graduates was searched online. Information like that obtained from the online survey was collected (current role, employment sector, and postgraduate training enrolment/ completion). Graduates who were currently undertaking postgraduate education were classified similarly to those who had completed postgraduate education. Finally, the PSI register of registered pharmacists was used to attain graduates’ registration status (which is required to legally practise as a pharmacist in ROI).
Data analysis
A valid survey response was achieved when a participant clicked ‘submit’ at the end of the survey. Three duplicate responses from one participant were identified, deemed invalid, and removed. All survey questions were answered by all respondents (i.e., no incomplete surveys). Graduate LinkedIn® profile information was cross-checked with the survey responses to avoid any duplication. The final information was imputed into a master Microsoft® Excel (Microsoft Office 2016) spreadsheet. Any discrepancies between LinkedIn® information and survey answers were resolved on a case-by-case basis.
Data remediation was performed both manually and using Microsoft® Excel (Microsoft Office 2016) functions to reduce the chance of human error, and thereafter analysed using descriptive and inferential statistics in Statistical Package for Social Sciences (SPSS), Version 27. Chi-squared (χ2) tests were conducted to examine the association between graduate demographics and their responses. As part of the analysis on time since graduation, the year groups were categorised into 2007–2011, 2012–2016, and 2017–2022 cohorts representing those 0–5, 6–10, and 11–15 years after graduation. Post-hoc analysis was conducted using the z-test to compare column proportions; adjustment for multiple testing using the Bonferroni method was also performed.
Results
Since the inception of the school of pharmacy, there have been 798 graduates over a 15-year period; in this study, data from 556 of these were obtained (69.7%). This included 203 valid survey responses (25.4%), 148 of whom had a corresponding LinkedIn® profile (18.6%), with data from LinkedIn® only from 353 graduates (44.2%) (Supplementary Material 2). Over 90% (92.1%) of graduates are currently named on the PSI pharmacy regulator list of registered pharmacists. Entering on this register and maintaining registration to practice as a pharmacist in Ireland was more commonly observed (χ2 = 9.59, df = 2, p < 0.05) for those who graduated in the last 5 years (2017–2022) at 96.6% versus those from the years 2012–2016 (90.1%) and 2007–2011 (88.5%) - highlighting an attrition rate of deregistering as time from pharmacy graduation increases.
Patient-facing versus non-patient-facing roles
Approximately two thirds (n = 362; 65.4%) of graduates were working primarily in pharmacy-based patient-facing roles at the time of the study i.e., in community or hospital pharmacy settings (Fig. 1). The percentage working in patient-facing settings ranged from 79.5% for 2022 graduates to 36.7% for 2010 graduates (Fig. 2). Factors which appeared to affect differences in patient-facing employment prevalence are seen in Table 1 (year of graduation, PSI registration status).
Women were significantly more likely to be working in a hospital pharmacy setting compared to men (20.9% versus 10.2%; p < 0.05), whereas a significantly higher proportion of men were working in academia (12% versus 3.6%; p < 0.05).
Patient-facing roles
A higher proportion (χ2 = 18.94, df = 2, p < 0.05) of 2017–2022 graduates were primarily employed in community pharmacy (59.4%) versus 2012–2016 (41.1%) and 2007–2011 (39.5%) graduates (Fig. 3). Table 2 shows that the variety of community pharmacy roles included pharmacy owner, superintendent pharmacist, supervising pharmacist, support pharmacist, locum pharmacist, and pharmacy manager. Practising as a locum pharmacist was more prevalent among the 2017–2022 cohort of community pharmacists (25.2%) versus those in the 2012–2016 (12.8%) and 2007–2011 (6.5%) groups (χ2 = 11.66, df = 2, p < 0.05). Of those not primarily working in community pharmacy at the time of the study, 61.1% had previously worked full time as a pharmacist in community pharmacy. At the time of the study, 17.7% of graduates were primarily working in hospital pharmacy, where roles included basic grade hospital pharmacist, senior hospital pharmacist, and chief hospital pharmacist; these roles refer to different grades of pharmacist within the ROI hospital system. Of these graduates working in hospital pharmacy, 65.2% had previously
1. Total percentage of pharmacy graduates per employment sector (n = 554).
Fig.
worked full time as a pharmacist in community pharmacy.
Non-patient-facing roles
Of the 192 graduates (34.7%) working in non-patient-facing pharmacy roles, the highest proportion (62.2%) worked in the pharmaceutical industry (21.5% of total). There were a wide variety of roles in industry-based graduates, as displayed in Table 2. A higher proportion of 2012–2016 graduates (29.2%) were employed in the pharmaceutical industry
versus the 2007–2011 (20.7%) and 2017–2022 (15.5%) respectively (χ2 = 12.06, df = 2, p < 0.05).
Most graduates in pharmaceutical industry were PSI registered (85.7%). Working primarily in academia, a public body, or another workplace collectively accounted for the remaining 13.1% of graduates. Of graduates primarily working in academia, 81.8% were working in ROI.
Postgraduate education
Postgraduate education up-
take and related demographics (including year of graduation and PSI registration status) are shown in Table 1 and Fig. 4. Over twofifths (43.1%) of graduates had either completed a postgraduate degree since their pharmacy graduation or were undertaking one at the time of the study. Of these, 38.4% undertook a postgraduate degree in UCC. Over one fifth of these have undertaken a Doctor of Philosophy (PhD) (n = 49; 22.0%).
Fig. 2. Percentage of pharmacy graduates per employment sector in each graduating year from 2007 to 2022. Blue shades represent patient-facing pharmacy roles, whereas red shades represent non-patient-facing roles (n = 554)
Other than a PhD, the range of postgraduate degrees undertaken by graduates included: Master of Science (38.1%), Postgraduate Diploma (17.5%), Postgraduate Certificate (8.7%), Postgraduate Entry Medicine (7.6%) Master of Business Administration (2.2%). Of those who undertook a Master of Science programme, 41.2% did so in clinical pharmacy or hospital pharmacy. No substantial difference was seen between men (45.8%) and women (41.9%) in undertaking postgraduate degrees (Table 1). Graduates not PSI registered displayed a higher prefer-
Fig. 3. Visual representation of the grouped analysis of graduate career sectors (i.e. 2007–2011, 2012–2016, and 2017–2022).
2017–2022 graduates were significantly more likely (p < 0.05) to be in a patient-facing role versus 2007–2011 and 2012–2016 graduates (n = 554).
Pharmacy
ence (χ2 = 9.31, df = 1, p < 0.05) to undertake postgraduate degrees (65.1%) versus PSI-registered graduates (41.1%). Higher numbers of graduates primarily in non-patient-facing roles (
χ2 = 67.62, df = 1, p < 0.05) had undertaken a postgraduate degree (66.5%) versus those primarily in patient-facing roles (29.3%).
Within patient-facing roles, a higher proportion (χ2 = 95.89, df = 1, p < 0.05) of graduates working in hospital pharmacy have undertaken postgraduate degrees (68.1%) versus graduates in community pharmacy (13.7%). As seen in Fig. 4, graduates primarily working in community pharmacy represented the lowest rate in undertaking postgraduate degrees, which was lower (χ2 = 150.22, df = 1, p < 0.05) than graduates primarily working in other sectors (65.2%). Graduates primarily working in hospital pharmacy (68.1%) (χ2 = 29.94, df = 1, p < 0.05) or the pharmaceutical industry (53.0%) (χ2 = 6.01, df = 1, p < 0.05) displayed a higher prevalence for completing/ undertaking a postgraduate degree compared to others.
Discussion
The study findings provide a unique insight into trends in career pathways of pharmacy graduates over a 15-year period. Results will be of interest to pharmacy educators, potential employers, policymakers, and prospective students alike. While international pharmacy education structures may differ from Ireland, the roles filled by pharmacists are often
generalisable across regions. Thus, this research provides a universal mechanism to track career progression and may be used to inform improved methods of pharmacy workforce capacity prediction. Considering the diverse employment opportunities increasingly available to pharmacy graduates, rebalanced workforce analyses which account for nonconventional and emerging pharmacy career paths will provide a truer representation of the workforce available to the patient-facing pharmacy sector. The timing of future pharmacy workforce planning analyses by educators or regulators is also significant according to results obtained in this study. Here, approximately twothirds of graduates (65.4%) were primarily working in patient-facing settings (community or hospital pharmacy). However, differences in preferences for patient-facing versus non-patient facing settings, as well as likelihood of registration with the Irish pharmacist regulator, between graduates when grouped ≤5 years graduated versus graduated >5 years were identified. In line with previous findings that the median time for pharmacists to change their primary practice setting is seven years post qualification,28 this study suggests to obtain a more reflective estimate of long-term practice setting choices, future pharmacy workforce analyses involving data collection from graduates should be undertaken >5 years post-graduation. By this period, it is more likely that graduates will have chosen their long-term practice setting, thereby providing educators and regulators
Fig. 4. Percentage of graduates per employment sector who have completed/are completing postgraduate training versus those who have not undertaken any postgraduate training (n = 518)
with increasingly accurate patientfacing workforce data to fulfil the global demand.
Within patient-facing settings, nearly half of the graduates (47.7%) worked in community pharmacy at the time of the study. A career as a community pharmacist is considered a respected career choice in Ireland, as ‘local pharmacists’ have been found the most trusted group of professionals by the Irish public.29 During their pharmacy education, it is common for students to be heavily exposed to community practice due to weekend work or experiential placement, which may influence career choices.30 Accordingly, this higher preference for community pharmacy seen in this study is in line with previous studies of pharmacy students› career intentions and preferences where higher preferences for this sector were also seen in Australia (50.42%),13 Northern Ireland (57%),16 and USA (50.9%).23 However, despite this prevalence rate, trends of decreased preference for working primarily in community pharmacy as time post-graduation progressed were observed in this study. Our findings also highlighted the greater appeal of locum community pharmacist positions for newer graduates. Within the Irish pharmacy context, these results align with a previous workforce survey finding that preference for locum work decreases with age, as 52% of pharmacists surveyed aged <35 years had worked as locum pharmacists, while this dropped
to 25% in those >46 years.28 Such positions offer perceived advantages like less responsibility, improved remuneration, and flexible hours, while the wide availability of locum positions upon graduation may be attractive to newer graduates.28 In comparison, further from graduation, those in community roles appear to have switched to more classical fixed roles of supervising pharmacist, superintendent pharmacist, or pharmacy owner.31
This apparent trend of graduates beginning their careers in community pharmacy but migrating away from this sector over time is reinforced by our finding that 61.1% of graduates not primarily working in community pharmacy had previously held a full-time community pharmacy role. This aligns to previous findings that 1 in 5 pharmacists in Ireland have changed their primary practice area since registration, where the biggest reason for changing was ‘looking for enhanced professional satisfaction’.28 A recent Irish qualitative study of pharmacists identified six categories affecting community pharmacy retention in Ireland based on the views of 23 interviewees. These included working conditions, limited career fulfilment, and professional progression opportunities.31 Similar themes were also highlighted in a similar Northern Irish qualitative study,32 as well as in a recent Irish workforce survey of 1272 PSI registered pharmacists (September 2023). There, 70% of respondents in community pharmacy strongly agreed that job stress is a feature of the role and 73% had experienced burnout.33 Within the Irish pharmacy context, these reports arise in the backdrop of significant workforce capacity shortages in the community pharmacy sector. Previous research in 2022 found that 57% of pharmacist respondents were ‘concerned’ or ‘extremely concerned’ about the patient-facing workforce capacity issues28, where a heavy reliance on the transient locum pharmacist workforce and high prevalence of vacancies nationwide were also
highlighted. Meanwhile, a 2023 PSI workforce survey has worryingly revealed that over one quarter of respondents (27%) intend to leave the profession.33
Reasoning why almost two thirds of those in hospital pharmacy previously worked in community pharmacy is likely multifaceted related to the factors negatively affecting community retention in addition to a combination of skill utilisation, specialisation potential, and job security factors.8,12,27 More broadly speaking, factors influencing primary practice choice setting by pharmacists are varied and have also previous been explored internationally.15,23,34, 35, 36 In relation to community pharmacy however, while graduates in community expressed lower career path satisfaction ratings versus those in other sectors, it must be remembered that overall satisfaction in the sector was still very positive (78.8%). Furthermore, the ability of students to move career sector can also be seen as a positive reflection of the wide applicability of the skillset attained through a degree in pharmacy. Recommendations recently highlighted by the Irish pharmacy regulator and beyond33,37 aim to initiate the process of addressing concerns among community pharmacists and incentivise more graduates to remain in community pharmacy settings long-term.
In this study, the proportion of graduates primarily in non-patient-facing settings lies at greater than one third (34.6%), where almost 20% of these have relinquished their ability to be named on the PSI register of registered pharmacists. This substantial proportion of graduates occupying non-patient facing roles, highlights the significant current underestimation of the non-patient-facing cohort according to Irish pharmacy regulator statistics, which stand at only 10.4% (i.e., three times lower, as of November 2023). Therefore, our findings highlight discrepancies associated with the use of this register as a predictor of pharmacist career paths, most definitely in this cohort of graduates. In reality, the present study’s results are more comparable to statistics from Scandinavia, where the percentage of pharmacists in non-patient-facing roles in Sweden and Denmark have risen to 50% or more.30,38 While multifaceted, one reason for this increase could be due to higher career path satisfaction, as found in this study. Furthermore, as previously mentioned, Irish pharmacy students are now also being exposed to more non-patientfacing placement opportunities at an earlier stage in their education.
Over one fifth of Irish pharmacy graduates (21.5%) were primarily working in the pharmaceutical industry at the time of the study. This may have been aided by the fact that Ireland represents one of the leading locations for pharmaceutical industry in Europe.39 The proximity of many pharmaceutical employment may in some way account for the large proportion of pharmacy graduates working in this sector, while the pharmacy degree also remains sole degree which meets all criteria to act as a ‘Qualified Person’ in the European pharmaceutical industry.40 Furthermore, pharmacy represents a clinical and pharmaceutical science degree, and as a result pharmacy graduates represent a unique cohort of students, attractive to potential industry employers and equipped with real world communication skills developed through clinical practice. This draw to the pharmaceutical industry for Irish graduates can be contrasted to other countries, such as Saudi Arabia,19 Sudan2 and Malaysia15 where the percentage of undergraduate pharmacy students that wished to pursue a role in industry ranged from 7%19 to 17.8%15. The importance of proximity to pharmaceutical companies was also previously highlighted in a Nigerian study, where a significantly higher percentage of students in a Nigerian university situated in a highly industrialised environment (36.5%) chose industry as their career preference versus other Nigerian universities (22.5% and 20% respectively)17
In terms of postgraduate education, completion or undertaking of such was less prevalent among those in patientfacing versus non-patient-facing roles. However, stark differences were seen in undertaking a postgraduate degree between those in community (13.1%) and hospital pharmacy (68.1%). These differences were echoed in a workforce survey where 34% of respondents in community had undertaken additional formal higher education compared to 86% of respondents in hospital.33 Such differences could be linked to the fact that experiential learning and standard continuous professional development (CPD) are more commonly crucial elements of community pharmacy skills enhancement, while no postgraduate education is required to progress to more senior roles in the sector. The relevance of micro-credentials versus traditional postgraduate qualifications may also need to be considered. Comparatively, undertaking a clinical pharmacy master›s degree
is a common desirable criterion of progression for hospital-based pharmacists in Ireland (albeit not essential), and is at times even funded by the employer. For non-patient-facing roles, a possible explanation behind the high rates of postgraduate study uptake may be that these graduates are competing with non-pharmacists for employment. Depending on the sector, they may either require a postgraduate qualification or perhaps be financially supported by an employer to undertake studies to upskill and aid progression to more senior positions. This in turn may aid pharmacist retention within these sectors due to clear career progression opportunities. This is further supported by 2018 research which revealed that nearly half (45%) of pharmacists in industry roles believed that postgraduate education is essential for such roles.30 It was suggested that responses may have been influenced by the individual›s own entry pathway to pharmaceutical industry, as 22% of those respondents entered nonpatient-facing settings following a postgraduate qualification.
Along with overall high career path satisfaction, high satisfaction rates with the pharmacy training programme among graduates from all career sectors highlights the applicability of the programme to support varied career pathways over a 15-year period since the school’s inception. The variance in career sectors across all graduating years also suggests that changes to the MPharm degree have not limited nor dissuaded Irish Pharmacy graduates from taking up employment across varied sectors. Moving forward, this study provides capacity to inform potential strategic adjustments to the delivery of the pharmacy programme to meet the needs and skillsets of the graduates’ prospective employment sectors, while also providing useful information to prospective and current pharmacy students and associated employers. The advantages of more precise mechanisms for maintaining contact with graduates and tracking career progression by universities was also highlighted.
Regarding study strengths and limitations, it is recognised that 30% of graduates were not accounted for in this study and data is representative of one pharmacy training programme. Secondly, at the time of data collection, graduates who were currently undertaking postgraduate education were classified similarly to those who had completed postgraduate education, as exact timing of programme completion was not available from
LinkedIn® profiles. It is recognised that this method of data collection does not facilitate a quantitative comparison of those undertaking versus those who have completed a postgraduate degree. It is also not possible to say that all LinkedIn® data was up to date, as some users may have been more frequent users of the platform than others. While the use of two data collection methods allowed for a greater number of graduate data to be identified, this meant the survey was not anonymous and may have influenced answers provided. It is also acknowledged that this study is limited by providing p-values above or below the 0.05 level, rather than reporting specific values. However, this study provides an impetus for potential further research comparing results to those obtained both internationally and across other pharmacy training programmes in Ireland.
Conclusion
This study has successfully analysed career paths of pharmacy graduates from a school of pharmacy over a 15-year period. Impacts of this research include the revelation that although nearly two thirds of graduates currently occupy patient-facing roles, this proportion has decreased as time from graduation increased. Consequently, future workforce capacity data collection initiatives may be optimised by considering the growing non-patient-facing pharmacy workforce and undertaking analyses of graduate career choice at least >5 years post-graduation. Then, a more precise estimate of graduates occupying the patient-facing workforce in the long term will likely be achieved. In this study graduates in non-patient facing roles were shown to display a higher degree of career path satisfaction along with higher rates of postgraduate degrees versus graduates in community pharmacy. This study indicates that future research should more closely examine the motivators for pharmacy graduates in choosing a given career sector. Given the increasingly multimorbid ageing population, while the increasingly diverse professional opportunities for pharmacists are welcomed, it is vital that we have sufficient pharmacists in patient-facing roles to provide pharmaceutical care. The present study demonstrates the importance of evaluating pharmacist career paths and represents a springboard for further research to inform future pharmacist workforce planning worldwide to avoid potentially significant implications of shortages in patient-facing pharmacy workforce.
New Survey shows Alarming Asthma Concerns
An estimated 450,000 people in Ireland have asthma and, according to a recent patient survey, concerning numbers are experiencing persistent symptoms that may indicate their asthma is uncontrolled. In response, this World Asthma Day, the Asthma Society of Ireland is launching a campaign to empower people with asthma to recognise the signs and symptoms of uncontrolled asthma and when to seek medical help.
The Asthma Society is also joining the global call on healthcare professionals, led by the Global Initiative for Asthma (GINA), to increase their awareness of the continuing avoidable morbidity and mortality from asthma. According to CSO figures, 81 asthma deaths were registered in 2022. The majority of asthma deaths are believed to be preventable. By following up-to-date guidelines and published evidence on effective asthma management, healthcare professionals will ensure that they are equipped to provide reliable information and optimal treatment for their patients. Despite significant advances in asthma care over recent years, key challenges persist. These include missed or mis-diagnoses, underuse of anti-inflammatory inhaled corticosteroid inhalers, over-reliance on short-acting beta2–agonist (SABA) inhalers and oral corticosteroids, and poor recognition of patients requiring specialist assessment and further management.
In a recent Asthma Society survey of 1,205 asthma patients and their carers,
• Over half (51%) of those surveyed reported that they or their child had had an asthma attack in the last year, and nearly one quarter (24%) had an attack in the previous month.
• Almost one-quarter (24%) of adults and children have used their reliever/rescue inhaler at least once daily.
• 43% of people surveyed had taken steroid tablets at least twice in the past year, with onefifth (20%) having taken them more than three times.
• 74% said they or their child’s sleep had been disturbed by asthma in the past year.
The survey also found that almost a quarter (24%) of respondents felt that healthcare providers did not take asthma seriously.
If left untreated, uncontrolled asthma can lead to decreased quality of life, asthma attacks, and even fatalities. Recognising the urgent need for action, the Asthma Society of Ireland encourages individuals to speak to their healthcare provider for an initial or updated assessment and urges healthcare professionals to reexamine their treatment protocols for patients.
In addition to providing helpful educational resources for patients, the campaign will highlight the importance of implementing a personalised asthma action plan under the guidance of a GP and working closely with their primary healthcare physician to develop comprehensive strategies to
control their asthma symptoms, reduce the risk of exacerbations, and improve their overall quality of life.
The Asthma Society of Ireland also provides a range of free self-management education services and resources to help people manage their asthma in between consultations with healthcare providers, which can be accessed via asthma.ie. There is also an e-referral system in place for healthcare professionals to refer their patients to the Asthma Society’s free nurse-led Adviceline and WhatsApp messaging service.
"Knowledge is power when it comes to managing asthma effectively," said Eilis Ní Chaithnía, CEO of the Asthma Society of Ireland. “Our campaign is supporting people to recognise the signs and symptoms of uncontrolled asthma and when to seek medical help. Worryingly, however, according to our recent patient survey, almost a quarter (24%) of the 1,205 respondents say that healthcare providers do not take asthma seriously.
Asthma is a complex disease that can be challenging to manage effectively. Patients need confidence in their diagnosis, treatment and their healthcare professional. While patient education and professional education in asthma are time consuming in an already overburdened healthcare service, they are integral to achieving optimal quality of life and health outcomes.”
Professor Marcus Butler, Consultant Respiratory Physician at St Vincent's Hospital and Medical Director of the Asthma Society, highlights the role of healthcare professionals in
supporting self-management saying, “Our findings released today indicate a high prevalence of potentially uncontrolled asthma in the Irish asthma population. Asthma is a chronic condition, but there is no room for complacency—managing asthma requires a combined effort, and we, as healthcare professionals, have an important role to play. This is why education by and for healthcare professionals is crucial—we need to keep up to date with the latest clinical guidelines and ensure our patients have the required support, information, and treatment.”
Professor Butler continued, “Adherence to asthma medications is only about 30%. This is due to a number of factors including cost and a lack of education about their uses, correct mode of delivery and potential side effects. Up-to-date knowledge of the various asthma treatments is crucial for healthcare professionals and patients to support shared decision making.”
“Through our regular webinars featuring expert speakers, our asthma management resources, and our free nurse-led patient services, the Asthma Society empowers patients, carers and healthcare professionals through education. All of its supports and services are governed by its Medical Advisory Group, of which I am a member. I’d recommend referring asthma patients to these services via our e-referral system for self-management support between consultations.”
Professor Marcus Butler
ONOURS Hospital Professional 2024
The Hospital Professional Honours will take place on Saturday, 14th September 2024 in the Radisson Blu Hotel, Dublin.
Haematology Project of the Year
Young Hospital Pharmacist of the Year
Galapagos Biotech Ltd, an Alfasigma company, Multidisciplinary Team of the Year
Fresenius Kabi Innovation in Aseptic Compounding
Medisource Hospital Pharmacy Technician of the Year
Grünenthal Advancing the Standard of Care in Pain Management
Athlone Pharmaceuticals Hospital Pharmacy Team of the Year
Excellence in Respiratory
Viatris Excellence in Cardiovascular Initiative
Pharmasource Hospital Pharmacist of the Year
MSD Excellence in Oncology Initiative
MedFind Solutions Innovation and Service Development
Excellence in Patient Safety
GSK ViiV Infectious Diseases Project of Year
Consultant-Led Team of the Year
Crohn’s & Colitis
Crohn’s & Colitis Ireland Releases Survey Results of 1,400 People with IBD
Ahead of World Inflammatory Bowel Disease (IBD) Day which took place on May 19, Crohn’s and Colitis Ireland has released the results of a survey of almost 1,400 people with IBD.
There are approximately 40,000 people living with IBD in Ireland, with the two most common types being Crohn’s disease and ulcerative colitis. IBD causes inflammation, swelling and ulceration of the intestines, with the most common symptoms being urgent and frequent bowel motions, sometimes with blood, diarrhoea, and stomach cramps.
On World IBD Day (May 19), Crohn’s and Colitis Ireland celebrated their 40th anniversary by hosted a conference in the Kingsley Hotel, Cork city, with talks on dating and relationships, and on eating well with IBD.
Comprehensive Survey
The research survey of people with IBD was undertaken by Crohn’s and Colitis Ireland between February and March 2024. Amongst the key findings were:
• Getting diagnosed. One in seven (14%) had to wait more than a year between being referred to hospital and getting diagnosed. Separately, almost half (47%) had to go to A&E with symptoms before being diagnosed with IBD
• Symptoms. When it comes to the worst symptom of IBD, a quarter of respondents (28%) noted abdominal pain and cramping, followed by a similar number for diarrhoea (26%), and one in five (20%) identifying fatigue and tiredness. On their worst day, one in two (50%)
would visit the bathroom more than ten times, while two in five (45%) had found it hard to cope with IBD over the past year on a consistent basis
• Flare-ups. One in two (52%) had experienced a flare of their IBD in the previous 12 months, with three-quarters (75%) of these having two or more flares. A substantial number had to attend hospital because of their flare
• Stigma. One in three (35%) had experienced stigma or unfair treatment because of their IBD in the past 12 months
• Facilities. An overwhelming majority of respondents (86%) believe shops/public spaces should do more to support people with IBD, with access to a toilet top of the list
• Costs. One in two (53%) respondents estimated the annual cost of medications, GP and hospital visits to be in excess of ¤1,000, with three in five (62%) saying the cost of treating their IBD is a financial burden in their life. It is worth noting that IBD is not currently covered under the Long-Term Illness Scheme
Two-thirds (65%) of those surveyed were in full or parttime employment. Of these respondents, the following findings were noted:
• Disclosing a diagnosis. Almost four in five (77%) say their boss knows about their IBD diagnosis, while one in four (23%) had not disclosed their diagnosis. Four in five (82%) had also disclosed their diagnosis to colleagues
is Amy Kelly, COO and Bruno Lucas Board Chair
Celebrating the 40th anniversary of Crohn’s and Colitis Ireland
Disappointing Findings
For Professor Aoibhlinn O’Toole, consultant gastroenterologist at Beaumont Hospital, much work needs to be done to enhance access to diagnostics, improve symptom control and provide proper financial supports to patients.
She said, “The survey findings around delays in diagnosis, as well as emergency presentation to access diagnostics, are very disappointing. Specifically, 47 per cent were diagnosed following attendance at the ED, with symptoms likely reflecting patients with more severe disease that can present as a medical emergency, such as acute severe colitis, bowel obstruction or a peri-anal abscess. However, I suspect also that for some patients, there was no alternative to access care except via the emergency room. The figure of 14 per cent waiting for more than a year to get diagnosed is also unsatisfactory and we must strive to improve referral pathways and access to diagnostics such as imaging, endoscopy and calprotectin stool tests for patients with suspected IBD.
“Almost half (45 per cent) reported difficulty coping with symptoms, which points to a significant number of patients struggling with disease control and poor quality of life, and this needs to be addressed. Overall, these results highlight massive delays in accessing care, a large cohort of patients living with poorly controlled symptoms, as well as having to deal with stigma, financial and occupational stress.
Clearly much work needs to be undertaken to improve disease control and quality of life for patients living with IBD in Ireland, as well as recognising IBD as a long-term illness in terms of State financial support.”
Unnecessary Stress
Amy Kelly, Chief Operations Officer at Crohn’s & Colitis Ireland added, "People living with inflammatory bowel disease, also known as IBD, know only too well that it is more than just managing physical symptoms; it's about navigating a plethora of emotional and financial challenges too. Our survey shows that patients are shouldering a heavy financial burden, with many spending over ¤1,000 annually on medications, GP visits, and hospital care. This financial strain adds an additional layer of stress to an already very difficult situation. We know that IBD is a long-term illness but, inexplicably, it continues to be excluded from the Long-Term Illness Scheme. This needs to change urgently so that patients receive the financial support that they desperately need.
“The survey also showed the challenges faced by people with IBD in getting diagnosed, coping with distressing symptoms and flare-ups, and experiencing stigma. We need to ensure uniformity of access to specialised healthcare professionals such as dietitians and psychologists in addressing the needs of people with IBD. These professionals offer invaluable guidance in navigating dietary restrictions, managing flare-ups, and coping with the psychological impact of chronic illness. We need to see more compassion and support for those grappling with the challenges of IBD but, most of all, we need to see action.”
There is currently no cure for IBD, but early diagnosis and treatment can help to stabilise the disease and provide a normal quality of life. For more information on the supports and services offered by Crohn’s and Colitis Ireland, call the Support Line on 01 531 2983 (Mon/Wed/Fri, 9.30am to 12.30pm) or visit www.crohnscolitis.ie.
Pictured
With all the benefits you expect from an adalimumab biosimilar, and more
Patient friendly:
Citrate-free and concentrated formula with a 50% lower injectable volume* to reduce pain following injection1,2
Experienced:
European production supported by over 20 years of biosimilars experience**
Flexible:
Two subcutaneous administration options
The new adalimumab biosimilar from CLONMEL
ABBREVIATED PRESCRIBING INFORMATION. Hukyndra 40 mg solution for injection in pre-filled syringe. One 0.4 ml single dose pre-filled syringe contains 40 mg adalimumab. Hukyndra 40 mg solution for injection in pre-filled pen. One 0.4 ml single dose pre-filled pen contains 40 mg adalimumab. Indications: 1) Rheumatoid arthritis 2) Juvenile idiopathic arthritis 3) Axial spondyloarthritis 4) Psoriatic arthritis 5) Psoriasis 6) Paediatric plaque psoriasis 7) Hidradenitis suppurativa (HS) 8) Crohn’s disease 9) Paediatric Crohn’s disease 10) Ulcerative colitis 11) Paediatric ulcerative colitis 12) Uveitis 13) Paediatric uveitis. Dosage: Refer to Summary of Product Characteristics. Method of administration: Hukyndra is administered by subcutaneous injection. Full instructions for use are provided in the package leaflet. Hukyndra is only available as 40 mg pre-filled syringe and 40 mg pre-filled pen. Thus, it is not possible to administer Hukyndra to patients that require less than a full 40 mg dose. If an alternate dose is required, other adalimumab products offering such an option should be used. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Active tuberculosis or other severe infections such as sepsis, and opportunistic infections. Moderate to severe heart failure (NYHA class III/IV). Warnings and precautions: Infections (Serious infections, Tuberculosis, Other opportunistic infections), Hepatitis B reactivation, Neurological events, Allergic reactions, Immunosuppression, Malignancies and lymphoproliferative disorders, Haematologic reactions, Vaccinations, Congestive heart failure, Autoimmune processes, Concurrent administration of biologic DMARDS or TNF-antagonists, Surgery, Small bowel obstruction, Elderly and Paediatric population. Interactions: Refer to Summary of Product Characteristics. Fertility, pregnancy and lactation: Women of childbearing potential should consider the use of adequate contraception to prevent pregnancy and continue its use for at least five months after the last Hukyndra treatment. Hukyndra should only be used during pregnancy if clearly needed. Hukyndra can be used during breast-feeding. Driving and operation of machinery: Hukyndra may have a minor influence on the ability to drive and use machines. Vertigo and visual impairment may occur following administration of Hukyndra. Undesirable effects: Very common: Respiratory tract infections (including lower and upper respiratory tract infection, pneumonia, sinusitis, pharyngitis, nasopharyngitis and pneumonia herpes viral), Leukopenia (including neutropenia and agranulocytosis), Anaemia, Lipids increased, Headache, Abdominal pain, Nausea and vomiting, Elevated liver enzymes, Rash (including exfoliative rash), Musculoskeletal pain, Injection site reaction (including injection site erythema). A copy of the SmPC is available upon request or go to www.clonmelhealthcare.ie Pack size: Hukyndra 40 mg solution for injection in pre-filled syringe - 2 pre-filled syringes + 2 alcohol pads, Hukyndra 40 mg solution for injection in pre-filled pen - 2 pre-filled pens + 2 alcohol pads. Marketing authorisation holder: STADA Arzneimittel AG, Stadastrasse 2-18, 61118 Bad Vilbel, Germany. Marketing authorisation numbers: EU/1/21/1589/002, EU/1/21/1589/005. Distributed by Clonmel Healthcare Ltd. Medicinal product subject to medical prescription. Date last revised: December 2021. 2023/ADV/HUK/130H. Date of Preparation: May 2023.
*When compared with Humira®. For example, 0.4 mL instead of 0.8 mL for a Hukyndra® 40 mg dose. **STADA founded Bioceuticals Arzneimittel AG in 2000. 1. Hukyndra® SmPC (Jan. 2022). 2. Nash P et al. Rheumatol Ther 2016;3:257–270. 3. Best-value biological medicines https://www.hse.ie/eng/about/who/cspd/ncps/medicines-management/best-value-medicines/best-valuebiological-medicines/
http://biosimilars.stada
School of Pharmacy Host HSRPP Conference
The School of Pharmacy at University College Cork recently hosted the 30th Health Services Research and Pharmacy Practice (HSRPP) Conference on 25-26 April 2024 in Cork, the theme of which was 'Sustainable Development in Healthcare' The conference attracted over 110 national and international delegates from over 15 countries across a range of disciplines, bringing together leading experts in the areas of health services and pharmacy research, as well as pharmacy practice and education.
Professor Stephen Byrne, Deputy President and Registrar of UCC, opened proceedings, acknowledging the rich and impactful history of the HSRPP conference, while also emphasising UCC’s commitment to sustainability. The conference
co-chairs, Dr Suzanne McCarthy and Dr Kieran Dalton, outlined the main goal of the conference – to provide a forum to share ideas, innovations, and best practices aimed at enhancing developing sustainability in healthcare. Through keynote speakers, workshops, oral presentations, and poster presentations, we had a packed programme exploring innovative strategies to ensure sustainable healthcare delivery with the patient at the centre of our efforts.
The conference’s exciting line-up of keynote speakers included:
• Barry Melia, Principal Pharmacist at Public Health Scotland: ‘Environmental Sustainability – A public health perspective’.
• Carmel Hughes, Professor of Primary Care Pharmacy at the School of Pharmacy, Queen’s
University Belfast: ‘Move fast and break things: Efficiency and sustainability in development and implementation of interventions focusing on medicines use in older people’.
• Debi Bhattacharya, Professor of Behavioural Medicine at the University of Leicester: ‘Embracing the diversity of research methodology to develop interventions’.
Several engaging and informative workshops were delivered during the conference on topics such as: sustainability, exploratory research, human factors, public and patient engagement, and health literacy.
Oral Presentations
1st Prize: Ita Fitzgerald
2nd Prize: Frank Moriarty and Maria Donovan (Joint)
Calls for All-Ireland Cancer Institute
An Tánaiste Micheál Martin has called for an All-Island Cancer Institute, stating initiatives such as the (opens in a new window) All-Island Cancer Research Institute (AICRI), a partnership of 10 universities which UCD coleads, has shown a cross-border approach to cancer can deliver better outcomes for patients.
Citing the hugely successful ‘Ireland-Northern Ireland-US National Cancer Institute Cancer Consortium’, which celebrates its 25th anniversary this year, the Tánaiste said he favoured the establishment of an All-Island Cancer Institute while speaking at the inaugural Joint EuroAmerican Forum on Cancer at Farmleigh House.
Echoing the sentiment, (opens in a new window)Professor William Gallagher, Professor of
Cancer Biology at UCD School of Biomolecular and Biomedical Sciences, and co-lead of AICRI, said he “wholeheartedly agree with the Tánaiste’s call for an All-Island Cancer Institute”.
“Our work in AICRI has demonstrated the benefit of working together on a crossborder basis. Projects such as AICRIstart, funded through the Shared Island-funded North South Research Programme, emphasise the importance of collaborative research. Critical areas of all-island partnership should encompass cancer biobanking, crossborder cancer clinical trials, and survivorship research.”
Support for All-Island Cancer Institute was also raised by Professor Deirdre Heenan, Ulster University, and Professor Mark Lawler, Queen’s University Belfast
An Tánaiste Micheál Martin, Professor Alberto Costa, Special Advisor to EU Health Commissioner Stella Kyriakides and CEO of the European School of Oncology, Professor Mark Lawler, Professor of Digital Health at Queen’s University Belfast and Co-Lead of AICRI
and Co-Lead of AICRI at the forum, as they jointly launched the ‘Cancer Knows No Borders – an all-island blueprint for cancer research and care’ at the conference.
“Our data are compelling, demonstrating how the quality of research increases with cross-
3rd Prize: Darren Walsh
Poster Presentations
1st Prize: Sarah Wilson and Aisling McGowan (Joint)
3rd Prize: Rosemary Lim
Speaking after the event, Dr Suzanne McCarthy and Dr Kieran Dalton said, “We would like to sincerely thank the HSRPP Conference steering committee, Pharmacy Research UK, our esteemed speakers, workshop leaders, sponsors (including Fáilte Ireland and UCC), the dedicated team at the School of Pharmacy, including our postgraduate students who were wonderful conference ambassadors, and all attendees who contributed to making HSRPP 2024 a great success.”
border collaboration, coupled with the evidence linking quality research to better care and improved outcomes for patients,” said Professor Lawler.
“We firmly believe that a dataenabled patient-centred All-Island Cancer Institute would deliver unparalleled benefits for the health and wealth of our societies North and South. Cancer Knows No Borders, neither should we.”
Doctor Julie Gralow, Chief Medical Officer of the American Society for Clinical Oncology (ASCO), who with Professor Lawler was Scientific CoChair of the Forum concurred.
“These two days of discourse and debate have firmly embedded the concept of enhanced transatlantic cooperation as a means of delivering research-enabled enhanced cancer care on the island of Ireland. An All-Island Cancer Institute would be the logical next step.”
Professor Heenan added: “We aim to bring together the combined strengths of cancer researchers, clinicians, academics, and service users across the island of Ireland to create a blueprint to tackle this common enemy.
“This is an opportune time to redouble our efforts to significantly improve services and outcomes for cancer patients throughout this island.”
An Tánaiste Micheál Martin
The Irish Network for Gynaecological Oncology: Giving a Voice to Gynaecological Cancers in Ireland
New research carried out in April 2024 amongst adult women in Ireland, has highlighted that four out of five are not confident to recognise the symptoms of ovarian cancer. The study was commissioned by the Irish Network for Gynaecological Oncology (INGO) (https://isgo.ie/ irish-network-for-gynaecologicaloncology/) to mark World Ovarian Cancer Day on Wednesday 8th May 2024. The INGO is a voluntary group of over thirty of Ireland’s foremost gynaecological cancer campaigners, researchers and patient advocates whose aim is to raise awareness of gynaecological cancers across the Island of Ireland. The group are part of an international effort for 2 major awareness events annually; World Ovarian Cancer Day on May 8th and World Gynaecological Oncology Day on September 20th.
Unfortunately, more than three quarters of patients with ovarian cancer are diagnosed when the disease is at a late stage. This is partly due to the vagueness of symptoms and similarity with other conditions such as irritable bowel syndrome, and in some cases, symptoms may not always be obvious or present at all.
The INGO run an annual campaign to raise awareness of the symptoms of ovarian cancer and encourage women to contact and explain their symptoms to their GP if they are worried, as
early diagnosis can save lives. The campaign emphasises the BEAT symptoms:
• Bloating that is persistent and doesn’t come and go
• Eating less and feeling full more quickly
• Abdominal and pelvic pain you feel most days
• Toilet changes in urination or bowel habits
The clear message is that if a woman experiences any of these symptoms for three weeks or more, she should contact her GP.
The INGO partnered with Brazilian street artist Brutto who created an impressive mural on Grafton Street on May 4th 2024 depicting BEAT messaging, which was widely shared on social media and educated passersby on ovarian cancer symptoms.
Several notable landmarks across the country lit up in teal, World Ovarian Cancer Day’s official colour, on the 8th of May, including Leinster House in Dublin, the Titanic Museum Belfast and City Hall in Cork.
Annually, approximately 400 women are diagnosed with ovarian cancer, and almost 300 women die from this disease in the Republic of Ireland (National Cancer Registry Ireland). In Northern Ireland, almost 300 are
Written by Dr Sharon O’Toole, Trinity College Dublin and Co-ordinator of the INGO, on behalf of the Irish Network for Gynaecological Oncology
diagnosed and 128 women die (Northern Ireland Cancer Registry). Ovarian cancer is the fourth leading cause of cancer death in women in Ireland, after lung, breast, and colorectal cancer.
There is no standard screening test to pick up ovarian cancer in women who don’t have symptoms. Early diagnosis can significantly improve survival – 88% of patients diagnosed with stage one ovarian cancer are alive five years after diagnosis compared to 17% with stage four ovarian cancer.
The campaign also sought to dispel the myth that cervical screening detects ovarian cancer. The research showed that one in three mistakenly believe that CervicalCheck Screening Programme checks for all five gynaecological cancers (ovarian, cervical, uterine, vulva and vaginal). It is important for women to understand that cervical screening only checks whether a woman is at risk of having cervical cancer and no other cancer type.
The INGO will continue to highlight gynaecological cancers and are working with key stakeholders in an effort
to improve on the current low awareness levels of symptoms.
On September 20th, World Gynaecological Oncology Day, the INGO will focus their message on all five gynaecological cancers.
The Irish Network for Gynaecological Oncology (INGO) Members
ARC Cancer Support Centres, Dublin; Answers for Cancer Podcast team; Breakthrough Cancer Research; Cancer Care West; Cancer Trials Ireland; CERVIVA; Circle of Friends Cancer Support Centre; Coombe Hospital, Dublin; Cork ARC Cancer Support; Cork Cancer Care Centre; East Galway and Midlands Cancer Support Centre; Emer Casey Foundation; Irish Cancer Society; Irish Society of Gynaecological Oncology; Karen Fenton Ovarian Cancer Fund; Lynch Syndrome Ireland; Marie Keating Foundation; Mater Hospital Dublin; National Cancer Control Programme; National Immunisation Office; National Women’s Council of Ireland; OvaCare; Hive Cancer Support, Derry; Purple House Cancer Support; Queens, Belfast; Sláinte an Chláir; Sligo Cancer Support; SOCK; Swell Fermanagh Cancer Survivorship Group; St. James’s Hospital Foundation (GynaeCancerCare); Trinity College Dublin; Trinity St. James’s Cancer Institute; University College Cork; University College Dublin School of Medicine; University College Dublin Gynaecological Oncology Group and 221+ CervicalCheck Patient Support Group.
For more information, please visit: www.thisisGO.ie www.isgo.ie
Melanoma Forum
Irish Melanoma Forum Annual Meeting
The Irish Melanoma Forum held its 12th Annual Scientific Meeting recently in the O’Reilly Hall at University College Dublin. There was a stellar line-up of speakers including Professor James Larkin, Consultant Medical Oncologist at The Royal Marsden, NHS Foundation Trust who spoke about ‘Finally prime time for cellular therapy in melanoma?’ and Dr Garrett O’Connell, SpR in Dermatology with South Infirmary Victoria University hospital who gave a talk entitled, ‘Variation in the practice of wide local excision for melanoma in Ireland and the United Kingdom.’
Below are pictured some of those who attended. The July issue of Hospital Professional News will have full coverage of this Meeting.
1. Dr Deirdre Muray; Kay Curtin and Dr Triona McCarthy.
2. Reconstruction surgeon Ms Deirdre Jones and reconstriuction surgeon Mr Jack Woods
3. Dr Sarah McLoughlin and Prof Breandán Kennedy
4. Dr Emily Taylor and Dr Cristina Casalou
5. Louise Fleming, Skin Cancer Clinical Nurse Specialist and Dr Ronan Brady
6. Dr Andrea Corry and Mr Jeremy Bond, Consultant Plastic Surgeon
7. Dr Paula Calvert, Prof Shirley Potter and Dr Ned Quirke
8. Roisin Costigan, School of Medicine, UCD, Mary Walsh, Radiology Dept. Mater Hosp and Kelsy O'Donnell, Skin Cancer CNS, Mater Hosp. All Photos courtesy of Brendan Lyon
Start Strong Go Long
Deep and durable relief across psoriatic disease
Tremfya 100 mg solution for injection in pre-filled pen PRESCRIBING INFORMATION. ACTIVE INGREDIENT(S): Guselkumab. Please refer to Summary of Product Characteristics (SmPC) before prescribing. INDICATION(S): Treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy. Treatment of active psoriatic arthritis in adult patients, alone or in combination with methotrexate, who have had an inadequate response or have been intolerant to a prior disease-modifying antirheumatic drug (DMARD) therapy. DOSAGE & ADMINISTRATION: For use under guidance/supervision of physician experienced in diagnosis and treatment of conditions for which Tremfya is indicated. Subcutaneous injection. Avoid areas showing psoriasis. Adults: For both indications, 100 mg at weeks 0 and 4, followed by maintenance dose every 8 weeks. In the case of psoriatic arthritis, for patients at high risk for joint damage according to clinical judgement, consider a dose of 100 mg every 4 weeks. Consider discontinuation if no response after 16 weeks of treatment for plaque psoriasis and 24 weeks for psoriatic arthritis. Children: No data available in children/adolescents <18 years. Elderly: No dose adjustment required, limited information in subjects aged ≥ 65 years, very limited information > 75 years. Renal & Hepatic impairment: Not studied. CONTRAINDICATIONS: Serious hypersensitivity to active substance or excipients; clinically important, active infection. SPECIAL WARNINGS & PRECAUTIONS: Infections: Potential to increase risk. If signs/ symptoms of clinically important chronic/acute infection occur, monitor closely and discontinue Tremfya until resolved. Tuberculosis: Evaluate patients for TB pre-treatment; monitor for signs/ symptoms of active TB during and after treatment. Consider anti-TB therapy prior to Tremfya if past history of latent/active TB and adequate treatment course not confirmed. Serious hypersensitivity reaction: Includes anaphylaxis. Some serious hypersensitivity reactions occurred several days after treatment and included urticaria and dyspnoea. If occurs, discontinue Tremfya immediately and initiate appropriate therapy. Hepatic Transaminase Elevations: An increased incidence of liver enzyme elevations has been observed in patients treated with Tremfya q4w compared to patients treated with Tremfya q8w or placebo. When prescribing Tremfya q4w in psoriatic arthritis, consider evaluating liver enzymes at baseline and thereafter according to routine patient management. If increases in ALT or AST are observed and drug-induced liver injury is suspected, Tremfya should be temporarily interrupted until this diagnosis is excluded. Immunisations: Consider completing all appropriate immunisations prior to Tremfya. Do not use live vaccines concurrently with Tremfya; no data available; before live vaccination, withhold Tremfya for at least 12 weeks and resume at least 2 weeks after vaccination. SIDE EFFECTS: Very common: Respiratory tract infection. Common: headache, diarrhoea, arthralgia, injection site reactions, transaminases increased. Other side effects: hypersensitivity, anaphylaxis, rash, herpes simplex infections, neutrophil count decreased. Refer to
SmPC for other side effects. LEGAL CATEGORY: Prescription Only Medicine (POM). PRESENTATIONS, PACK SIZES, MARKETING AUTHORISATION NUMBER(S): Pre-filled pen, X1, EU/1/17/1234/002. MARKETING AUTHORISATION HOLDER: Janssen-Cilag International NV, Turnhoutseweg 30, B-2340 Beerse, Belgium. FURTHER INFORMATION IS AVAILABLE FROM: Janssen Sciences Ireland UC, Barnahely, Ringaskiddy, IRL - Co. Cork, P43 FA46. Prescribing information last revised: July 2022. Adverse events should be reported. Healthcare professionals are asked to report any suspected adverse events via: HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events should also be reported to Janssen Sciences Ireland UC on 1800 709 122 or at dsafety@its.jnj.com.
References: 1. Reich K. et al., Five-year maintenance of clinical response and improvements in healthrelated quality of life in patients with moderate-to-severe psoriasis treated with guselkumab: results from VOYAGE 1 and VOYAGE 2. British Journal of Dermatology, 2021, June. https://doi.org/10.1111/ bjd.20568. 2. Blauvelt A, Papp KA, Griffiths CEM, et al. Efficacy and safety of guselkumab, an antiinterleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: Results from the phase III, double-blinded, placeboand active comparator-controlled VOYAGE 1 trial. J Am Acad Dermatol 2017;76:405-17. 3. Reich K, Armstrong AW, Foley P, et al. Efficacy and safety of guselkumab, an antiinterleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: Results from the phase III, double-blind, placebo and active comparator-controlled VOYAGE 2 trial. J Am Acad Dermatol. 2017;76:418-31. 4. McInnes IB, et al. Long-Term Efficacy and Safety of Guselkumab, a Monoclonal Antibody Specific to the p19 Subunit of Interleukin-23, Through Two Years: Results From a Phase III, Randomized, DoubleBlind, Placebo-Controlled Study Conducted in Biologic-Naive Patients With Active Psoriatic Arthritis. Arthritis Rheumatol. 2022 Mar;74(3):475-485. 5. Mease PJ, et al. Guselkumab in biologic-naïve patients with actives psoriatic arthritis (DISCOVER-2): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet 2020;395:1126-1136. 6. Ritchlin CT, et al. Guselkumab, an inhibitor of the IL-23p19 subunit, provides sustained improvements in signs and symptoms if active psoriatic arthritis: 1 year results of a phase III randomised study of patients who were biologic-naïve or TNFα inhibitor-experienced. RMD Open. 2021;7:e001457. 7. Deodhar A et al. Guselkumab in patients with active psoriatic arthritis who were biologic-naive or had a previously received TNFα inhibitor treatment (DISCOVER-1): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet 2020; 395:1115-1125. 8. TREMFYA® Summary of Product Characteristics, available at medicines.ie.
CP-430955 | Date of Preparation: February 2024
Epilepsy
Epilepsy Ireland – making communities
Epilepsy aware!
May 20th – May 26th marked National Epilepsy Week, bringing one of the most common neurological conditions in the country into focus. With this important week for the epilepsy community having just taken place, we invited Epilepsy Ireland – via their Advocacy & Communications Manager, Paddy McGeoghegan - to share more information with Irish Pharmacy News about the work of the organisation….
It a pleasure to be writing in this edition of Irish Pharmacy News to give community pharmacists insight about our work on the behalf of people with epilepsy and their families.
Epilepsy Ireland’s vision is to achieve a society where no person’s life is limited by epilepsy. Our Head Office is in Dublin, but like community pharmacists, we are also based in communities across Ireland – with 9 regional offices from Donegal to Cork. This strong community presence and work within communities is so important because epilepsy is a condition that affects people in all walks of life across Ireland. In fact, we estimate that over 45,000 people live with epilepsy in Ireland – making it one of the most common neurological conditions in the country.
Working towards our overall vision involves various strands of work. This includes our support and
Written by Paddy McGeoghegan, Advocacy & Communications Manager, Epilepsy Ireland
information services for people with epilepsy and their families; our training and education programmes for the wider community; our awareness and advocacy campaigns; and finally, our investment in epilepsy research. Our support and information services are much depended upon by people with epilepsy and their families. This service is delivered by our local Community Resource Officers via our regional offices, and experiences circa 20,000 contacts every year. Epilepsy is a very individual journey for those living with it and the families that support them. Our services aim to support people along every step of that journey through one-toone work via the Living Well with Epilepsy ‘Toolkit’ programme, and groups events like our local/ national supports groups in addition to groups targeted at different age cohorts for e.g. Teen Time – an online group for teens to meet others living with epilepsy and discuss challenges they may be facing.
The best example of our Training and Education programmes can be seen via our Epilepsy Awareness and Administration of Buccal Midazolam (BM) training for professionals. I know many of you reading will be familiar with BM and its importance in reducing hospitalisation and reducing risk from prolonged seizures.
Every year, we train circa 3,000 professionals in the administration of BM – with the vast majority of those being teachers/SNAs supporting a child with epilepsy in the classroom.
Awareness is so important when it comes to epilepsy. Unfortunately, as mentioned, there can still be stigma and misconceptions associated with the condition. The best way to combat this is by encouraging ongoing education and in particular, encouraging people with epilepsy to speak more openly about their condition to help the public separate the myths from the facts. During National Epilepsy Week, we provided a platform and shared several personal stories of the lived experience of epilepsy; these are the most powerful tools available to us when it comes to educating the public.
Achieving positive policy changes to improve the lives of people with epilepsy is also a key area of our work. As I write this, we have just assisted Minister Heather Humphreys with the launch of a new Free Travel scheme for those medically unfit to drive for at least a year and those who have never held a license due to a long-term health condition or disability. For many years, we advocated for this scheme and are delighted to see it officially launched – with an
estimated 32,000 people set to potentially benefit. With elections on the horizon, we hope to achieve many more positive policy changes for people with epilepsy in the future.
Research can mean many things to many people, but to our community, it represents hope. Learning more about a condition which still has many unknowns can help to change the outlook for people diagnosed with epilepsy in the future. We first began investing in research in 2009, and last year, we reached the milestone of having invested a total of ¤1.5 million in Irish epilepsy research across 23 different projects.
While this has been a brief overview, I hope I have provided you with some insight into the work we do. As community pharmacists, you will engage with people with epilepsy every day – so please do encourage the people with epilepsy you meet to reach out to us for information and support. Likewise, we are also there for local communities on all thing’s epilepsy-related so if you need information, please do not hesitate to contact us on info@epilepsy.ie or by calling 014557500.
For more information on epilepsy and Epilepsy Ireland, visit www.epilepsy.ie
Some of the Epilepsy Ireland Community Resource Officer team
60 Second Summary
The recent Irish DXA Meeting themed - “Collaboration Matters” - took place at the University of Galway on May 10th and 11th with a variety of speakers from government, university staff, HIQA, China, Ireland, Taiwan, Singapore, UK, and the USA'.
The meeting was opened by Ms. Catherine Connolly. She acknowledged that Ireland has one of the highest prevalences of osteoporosis in the world and admitted that she was both startled by some of the recent figures and surprised that a national osteoporosis programme has yet to be put in place.
Mr. Fergal Lynch gave an excellent presentation on "Why Health Policy Matters" and how health policy is formed. He noted the theme of the meeting and agreed it is a critical part of the journey. He noted the Irish figures, and gave an outline of the journey for a national cancer programme and how it now delivers much better outcomes for patients but is not perfect.
Professor Gerard Boron, Tallaght University Hospital provided a brief but excellent overview of the biochemical basis of bone mineral density. He outlined the structure of bone and bone biochemistry, the factors which affect it and finished with a couple of unusual cases to highlight the clinical and biochemical assessment and some of the factors involved.
The last session of the day commenced with a presentation on the importance of the “Least significant change” (LSC) by Nurse Susan van der Kamp and what it means. In essence it is a measure of consistent, also known as the coefficient of variation with a 95% confidence interval and an important scientific step to understanding the consistency of measurements.
AUTHOR: Professor John J Carey & Dr Attracta Brennan, University of Galway
Professor John J Carey is a consultant physician in Medicine and Rheumatology, and Clinical lead in DXA, osteoporosis and fracture liaison services, at Galway University Hospitals, and Professor in Medicine at the University of Galway, Galway, Ireland.
Dr. Attracta Brennan is a lecturer in the School of Computer Science at the University of Galway. Her research interests span a number of areas, including: healthcare analytics, adaptive learning systems, game based learning, socio-technical systems to support older people, AR/VR and medical informatics.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no,
I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings.
Published by HPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author.
Collaboration Matters: Irish DXA Annual Meeting
The recent Irish DXA Meeting themed - “Collaboration Matters” - took place at the University of Galway on May 10th and 11th with a variety of speakers from government, university staff, HIQA, China, Ireland, Taiwan, Singapore, UK and the USA.
The meeting was opened by Ms. Catherine Connolly, Leas Ceann Comhairle for the Dail. In a beautiful confluence of Gaeilge and English, she gave attendees a ‘céad mile failte go Gaillimh’. She acknowledged that Ireland has one of the highest prevalences of osteoporosis in the world and admitted that she was both startled by some of the recent figures and surprised that a national osteoporosis programme has yet to be put in place. She noted this disease affects around 1 in 3 women and 1 in 4 men aged 60 years and older, resulting in approximately 50,000 fractures annually. She emphasised that if we are to impact waiting times, trolley numbers and the lives of patients with this disease, then a national programme has to be a priority.
Following the address by Ms. Connolly, a patient shared her personal experience of having osteoporosis; she gave an eloquent but heart-breaking presentation titled “my story”. She recalled how she was sent to the emergency room with fractures in her back, only to be sent home
‘because there was nothing we could do’. All she was given for the pain was Panadol! She suffered needlessly for several months, and today is no longer the person she once was. She spoke about how osteoporosis doesn’t just shatter bones, it shatters lives. Despite having other illnesses, being familiar with the healthcare system and adhering very strictly to a healthy diet, regular exercise and her prescribed medication, she still ended up with eight spinal fractures. She saw an expert who noted that it was one of the worst cases that he had ever seen. She has since listened regularly to
podcasts and, as a patient finds it difficult to accept that four things which could have benefitted her are not available in Galway for public patients:
1. Shorter waiting times for MRI and DXA scans with modern technology;
2. Access to bone turnover markers to monitor her treatment;
3. Access to a team of experts to manage her acute fracture pain;
4. Access to Romosozumab which is an excellent option for those who need it.
Saturday session: Ms. Nicola Crabtree’s Presentation on Pediatric Densitometry and Professor John J Carey
Dr Attracta Brennan
Professor John J Carey
Opening speakers: Professor Bobo Tanner, Vanderbilt University, Tennessee, USA. Past President ISCD, Committee member for Osteoporosis Essentials writing group; Mr. Lee O’Hora, Health Information and Quality Authority, Ireland; Professor Manju Chandran, Singapore General Hospital, Board Member International Osteoporosis Foundation; Professor Andrea Singer, Georgetown University, D.C., USA. Chief Medical Officer, National Bone Health Alliance, USA; Professor Wing Chan, Taipei Medical University, Taiwan, Chair Scientific Advisory Committee, ISCD; Professor John J Carey
This speaker’s eloquent presentation had a profound impact on all present.
Next, Mr. Fergal Lynch gave an excellent presentation on “Why Health Policy Matters” and how health policy is formed. He noted the theme of the meeting, agreeing that it is a critical part of the journey. He discussed the Irish statistics, and outlined the journey in the development of a national cancer programme, which now delivers much better outcomes for patients, although it is not perfect. He emphasised the importance of working together, speaking to politicians and understanding their priorities, in addition to involving patients, researchers as well as expert clinicians and health professionals. He highlighted the critical role of the patient voice in driving changes and the value of international expertise and experience in leading to change.
Mr. Lee O’Hora from HIQA followed, outlining the role of HIQA in ensuring compliance with regulations for the use of ionizing medical radiation. He gave a very clear and concise overview of the regulations, the responsibilities of those undertaking procedures and the role of HIQA He explained to the audience that he was not there to punish people but to ensure that inspected organisations had clear policies and practices in place in order to adhere to the legislation thereby protecting patients and with respect to DXA, the staff and members of the public, although this would fall under the E.P.A. in many instances. He stressed that he was very impressed overall
with the processes and the level of dedication he encountered, praising many of the excellent services which are in place. He also highlighted some concerns where further clarity is desirable with regard to legislation, policy and practice. He provided an excellent overview of what they look for during inspections, and how to prepare for one should one be forthcoming. He also stressed how they welcome active engagement, feedback and discussion to protect patients and promote safe practice.
The next session featured four international panellists answering questions about the process and significance of the Position Development Conference (PDC) of the International Society for Clinical Densitometry (ISCD). The panellists were:
1. Prof. Andrea Singer, USA, 2023 ISCD PDC Expert Panellist and medical director of the National Bone Health Alliance, USA;
2. Prof. Bobo Tanner, USA, Past-President ISCD, Writing Committee member for The ISCD Osteoporosis Essentials / Bone Densitometry Course;
3. Prof. Manju Chandram, Singapore, 2023 ISCD PDC Expert Panellist and board member of the International Osteoporosis Foundation.
4. Prof. Wing Chan, Taiwan, Chair of the ISCD Scientific Advisory Committee, dual trained as an osteoporosis physician and musculoskeletal radiologist.
These experts reviewed the PDC process from the selection of topics to be considered, the extensive reviews of the literature, the work of each team on their individual sections, the voting system to either accept, reject or reconsider the proposed position and the final day of ‘word-smithing’ to use the most appropriate language to ensure that the positions were useful to a global audience. Prof. Carey chaired the session and pointed out that most Irish people would never attend an ISCD PDC and so thanked the panellists for their insights. He also noted that some Irish people perceive these to be “American” guidelines and wondered whether the expert panel agreed or not. The panel emphasised that the teams were composed of experts from around
the world, including; Australia, Brazil, Canada, Ireland, Israel, Lebanon, Singapore and of course the USA. They also noted that the positions are as relevant globally as they are in the USA, despite differences in the availability and quality of services across the globe. Prof. Chandran highlighted that Pakistan, a country which is larger than any European country, has only one DXA centre. The experts agreed that local applicability must be considered for all official positions and that in some cases, where there is limited evidence to support or refute a position, a consensus of experts can be very helpful.
Following a short break, Mr. O’Hora again returned to the stage and gave an overview of national audit guidelines published by HIQA in the past year. While these guidelines are new and at the moment are not mandatory, they will be enforced by the end of the year with HIQA requiring every centre to actively perform audits and engage at all levels of their corporation or institution. Mr. O’Hora pointed out that further details are available on the HIQA website, which also offers an excellent overview of what auditing
entails and how it promotes and supports safe practice.
Prof. Gerard Boron from Tallaght University Hospital then delivered a brief but excellent overview of the biochemical basis of bone mineral density. He explained the structure and biochemistry of bone and the factors which affect it. He also presented a number of unusual cases to highlight the clinical and biochemical assessment in addition to some of the other factors involved. His review was welcomed by many engaged in clinical practice for a long time, who might not frequently think about some of the more fundamental biochemical and structural aspects of bone disease.
Prof. Wing Chan gave a fantastic overview of vertebral fractures, their importance and their diagnosis. He pointed out that all diagnostic methods have limitations but highlighted how a combined approach could help close the diagnostic gap. He reviewed methods such as the Genant deformity scale and the Yoshida criteria in addition to some cutting edge artificial intelligence driven solutions which are currently attracting a lot of interest.
Following this, Prof. Bobo Tanner took the audience on a journey through the diagnostic approaches used for diagnosing osteoporosis or assessing bone strength. Prof. Tanner covered everything from pre-DXA non-invasive methods,
to bone biopsy, engineering laboratories testing mechanical strength and resistance to indentation to state of the art imaging such as virtual bone biopsy and the use of CT and MRI for opportunistic screening. He discussed some of the strengths and limitations of these methods, providing a comprehensive overview of a very complex field with a brief synopsis of each method. Although DXA remains the primary tool in the Republic of Ireland for osteoporosis diagnosis, it is clear there are other options, some of which may have distinct advantages in specific situations although no one solution or alternative is ideal to date.
The session closed with two brief presentations from Irish researchers. First, Dr. Louise Horrigan from the University of Galway presented her findings on using bioimpedance to assess bone strength, noting that future work is needed to correlate these results with DXA or some other gold standard. Prof. Carey then presented the results of the HRB funded DXA-MAP project demonstrating how a new screening tool has the ability to identity healthy men and women most likely to benefit from a DXA test. This tool has the potential to reduce waste by eliminating unnecessary testing in healthy people less likely to benefit, while also identifying those most likely to have osteoporosis who should be tested.
Afternoon session: Ms. Catherine Armstrong, CNS in Osteoporosis, Galway University Hospital; Professor Sansin Tuzun, Istanbul University, Turkey, Board Member European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases; Professor Andrea Singer; Professor Manju Chandran; Dr Carmel Silke, Consultant Rheumatologist, SAOLTA Hospital Group, University of Galway Rheumatology Lead, Session Chair
The afternoon session commenced with an excellent overview of the need for, and principles of modern treatment algorithms by Prof. Andrea Singer. She highlighted a paradigm shift whereby it is now clear that those deemed at very high or imminent risk of fracture are most likely to benefit from osteoanabolic therapy. Importantly, she also pointed out that evidence now shows that such therapy has a greater impact if used before rather than after anti-resorptive therapy. Prof. Singer concluded by stating that all osteoporosis medications are effective, and that individual treatment decisions should be made in consultation with the patient taking into account their concerns, wishes and abilities.
Findings from our most recent 2022 census reveal that almost 1 in 5 residents of Ireland were born abroad. This raises the complexity of understanding medical care and assessment. Professor Manju Chandran reviewed the differences between social constructs such as ‘race’ and ‘ethnicity’ and societal norms and cultural issues. She highlighted their importance for understanding both bone mineral density and fracture risk and gave examples of where she works and resides i.e. “The little Red Dot” Singapore, which has a complex multi-ethnic society. She noted there is an ‘Irish’ community there (a ‘little green dot’) who likely differ in bone content and fracture risk compared to indigenous Asian citizens. Despite some clear scientific data, she pointed out the scientific controversies and complexities that arise, especially when considering people of ‘mixed race’ and those who are immigrants in other countries.
Professor Sansin Tuzun reviewed the principles behind the
rehabilitation of osteoporotic patients, both with and without fractures. She highlighted key elements which are often not available for Irish patients, including counselling on nutrition, core strengthening and correct posture maintenance, weightbearing exercises, adequate pain control and when needed, osteoporotic medications. She also discussed the limited evidence supporting the use of certain back braces, noting that while some may be helpful in specific circumstances, many are not and/or are too cumbersome for patients to utilise. She reviewed many of these areas which are covered in detail in a recent paper of the Rehabilitation Working Group of the International Osteoporosis Foundation.
Nurse Catherine Armstrong from Galway University Hospital emphasised the importance of DXA in fracture liaison services for patients and healthcare professionals looking after them. She explained how once patients have sustained a fracture, osteoporosis is the likely, diagnosis and DXA measurement of BMD is crucial for assessing prognosis and monitoring treatment. She pointed out that there was much more to DXA than measuring BMD; it includes vertebral fracture assessment technology which can impact management decisions. Also, it serves as another healthcare visit for patients to receive education and discuss their concerns, often helping to bridge the gap between ’what the doctor said’ and what the patient understands. The final session of the day began with a presentation by Nurse Susan van der Kamp on the importance of the “Least significant change” (LSC) and what it means. She explained that LSC is a measure of consistency, also known as the coefficient of variation with a 95% confidence interval; it is an important scientific step to understanding the consistency of measurements. She emphasised that using the manufacturer’s LSC is not recommended as it is only one of four factors that affect the true value. Random error, patient factors and the scanning health professional factors also affect the measurement, underscoring the need for a scientific approach. She pointed out that repeat DXA scans have no proven value in the absence of a known LSC for that DXA machine in that centre, and
ideally for each individual involved in scanning patients.
Ms. Ciera O’Reilly followed with a review of their experience in establishing the LSC for their centre, which is a new DXA facility for their institution. She detailed their protocol and how they used the ISCD calculation tool to generate their values. She reiterated that this metric is essential if patients are to have a follow-up scan.
Dr. Eithne Murphy then reviewed the risk of systemic and periarticular bone loss in rheumatic diseases, in particular rheumatoid arthritis. She highlighted that all rheumatic illnesses are associated with a substantially higher risk of fracture compared to the general population. She also noted that not only are these patients at greater risk of losing bone strength but they are also are at greater risk of losing muscle strength and balance due to their underlying arthritis or concomitant use of some medications such as corticosteroids. Dr. Murphy made some general recommendations to assess the bone health and fall risk of all patients with rheumatic diseases and advised consideration of whether risky treatments like corticosteroids are necessary when assessing them.
Finally, the evening finished on a lighter note when Dr. Attracta Brennan showcased Tik Tok videos created by her university students to explain why Humpty Dumpty had osteoporosis and how it affected him. Given the excellent presentations earlier in the day, which highlighted the need for clear and appropriate communication, the use of Tik Tok videos created by non-medical 20-21 year old undergraduate students was seen as an excellent way to help nonmedical individuals understand the significance of bone health. Although it was difficult to choose a winner from several outstanding videos, conference attendees awarded the top prize to a student who not only provided an excellent story outlining why poor old Humpty Dumpty ‘with bones like that never stood a chance’ accompanied by amazing graphics. Other students unpicked the biases in the nursery rhyme questioning why people thought Humpty Dumpty was an egg when he was in fact, a man with osteoporosis. A number of Tik Tok videos featured fantastic rhyming stories and graphical illustrations comparing the difference between falling with healthy bones (or egg-shells) to falling with osteoporosis
Day two commenced with a brief review of all the society’s activities and some challenging clinical cases that built on some of the principles discussed on the first day. This session prompted pertinent questions and lively discussions. Dr. Erjiang E, from China, then presented his study on the sensitivity, specificity and accuracy of DXA for diagnosing osteoporosis in Irish adults. His extensive analysis showed that there is a considerable range in these values depending on : age, gender, site of BMD measurement and site of skeletal fracture. These factors must always need to be considered when performing any test. For the first time, we have some robust Irish data from thousands of people both with and without fractures.
Next, Dr. Emerald House, Medical physics, Galway University Hospital provided an excellent pre-recorded review of ‘Diagnostic Related Levels’ (DRLs). This presentation helped attendees understand the various ionizing radiation exposures associated with DXA, how these exposures compare to the general environment and other imaging modalities, and the purpose of DRLs. Dr. House clearly explained how DLRs are
calculated, their significance and how, like LSC, they are important for understanding the ALARA principle and best practice when it comes to justification for medical ionizing radiation.
Dr. Nicola Crabtree (a lecturer in the first ISCD paediatric course 16 years ago) then reviewed some of the complexities of scanning paediatric patients. She provided some updates on current ISCD positions and practices and reviewed the complexities with some case examples. She emphasised that DXA in children is complex and should not be undertaken by those unfamiliar with the field. The performance and interpretation of these scans is more challenging than in adults in many situations, but can be extremely helpful when performed and interpreted correctly by the right people for the right reasons. She noted that some complex issues in paediatric DXA remain evolving and, similar to adult cases, have certain limitations.
The conference concluded with several workshops and discussion groups. These focussed on manufacturer specific considerations for GE and Hologic DXA systems – the two most common DXA systems in use in Ireland. Led by Irish experts: Ms. Bridie Rooney and Ms. Catherine Corry for G.E. Lunar and Ms. Susan van der Kamp for Hologic, these sessions featured lively discussions with plenty of questions and answers. They provided DXA users, who often operate in remote or single person locations, a chance to discuss any concerns or ask necessary questions. Following these, workshops run by GP and Hospital units that have already undergone HIQA inspections, helped attendees understand the inspection process, how to organise and present their working practices and standard operating procedures to help them prepare for future inspections.
Note: A booklet was provided to the attendees courtesy of the Irish DXA MAP team highlighting several key statistics related to DXA and Osteoporosis in Ireland: References: https://www.dxasoc.ie/nextmeeting
https://dxa-map.com
Advancing Brain Research and Treatment: FutureNeuro's Vision to Change the Patient Journey
Written by Prof David Henshall, Bridget Doyle, and Fiona McLoone
Brain disease is one of the biggest challenges for public health, society and the economy in Ireland. With one in three individuals affected over their lifetime, the annual burden on healthcare and welfare systems amounts to an estimated ¤30 billion. In Ireland alone, more than 800,000 people grapple with conditions impacting the brain and central nervous system, ranging from epilepsy and Amyotrophic lateral sclerosis (ALS) to Parkinson's disease, Multiple Sclerosis (MS), and acquired brain injury. More than 30% of people affected will also contend with psychiatric disorders, adding complexity to their care.
FutureNeuro, an Ireland-based interdisciplinary research centre, is committed to alleviating this burden by accelerating progress and translating innovations into real-world solutions. With a focus on improving diagnosis, developing targeted treatments, and advancing healthcare management, the Centre is committed to making tangible differences to patient outcomes. Already, FutureNeuro's research has led to transformative
interventions, including genetic testing to identify patients most suitable for life-changing therapies.
Navigating the Path Forward: FutureNeuro's Vision for the Future
As FutureNeuro embarks on its second phase, fuelled by remarkable achievements since it launched in 2017, its vision for the future remains clear - to change the patient journey. However, the
reality is that most brain diseases still lack effective treatments and diagnosis remains a prolonged process for many. Recognising the scale of the challenge ahead, the Centre has brought together the very best scientists, clinicians, and academic and industry partners. Together they will work on an integrated research programme to progress the Centre’s ambition to become a world-leading research institute that directly connects with the needs of patients and their clinicians.
An electroencephalography - or EEG cap monitoring electrical activity in the brain
Expanding the Team
FutureNeuro's integrated academic and clinical research network
To realise transformative advances, FutureNeuro, led by David Henshall, Centre Director and Professor of Molecular Physiology and Neuroscience at RCSI University of Medicine and Health Sciences, is scaling up its operations and integrating new science, talent, and expertise in brain research from prestigious institutions across Ireland, including RCSI University of Medicine and Health Sciences, Trinity College Dublin, Dublin City University, University College Dublin, University of Galway, University College Cork, Maynooth University and South
David Henshall, Centre Director
Bridget Doyle, Centre Manager
Fiona McLoone, Communications Lead
Brain Research
East Technological University. Most importantly, the Centre is integrated with a researchengaged national clinical network who collectively inform the research questions and ensure valuable access to patients and their data in order to make the research relevant and translational.
While maintaining a strong focus on epilepsy and Motor Neuron Disease (MND), FutureNeuro is broadening its impact to include neurodevelopmental disorders, multiple sclerosis, Parkinson's disease, traumatic brain injury, and their intersections with psychosis and mental health. FutureNeuro has grown their network to over thirty research leaders, their dedicated teams and new enabling infrastructure. This collective expertise will further our understanding of the mechanism of action of the brain and brain disease, enable the identification of new molecular diagnostics, neurogenetics, noncoding RNA biology, and gene therapies.
Moreover, FutureNeuro recognises the invaluable potential in cross-pollinating discoveries across different disease areas. By leveraging insights gleaned from one condition to inform research and treatments for others, the Centre aims to maximize impact and efficiency, ultimately accelerating progress towards addressing the broader spectrum of brain diseases.
New Research Frontiers: From Diagnostics to Therapy and Beyond
FutureNeuro’s research is built on three connected themes –diagnosis, therapy and digital health. The Centre is rolling out an integrated programme of work across their eight academic partners which will be complemented by collaborative projects with world-leading industry partners.
Diagnosis
This strand of the programme concentrates on discovering
genes that cause brain disease or influence how people respond to treatments. The Diagnostics Team is examining the chemistry of the blood and fluid that surrounds the brain to look for answers to causes and prognosis, recognising that errors in DNA may not always be the sole cause.
By analysing the chemistry outside brain cells, researchers can create a molecular fingerprint or profile specific to a particular brain condition. These are known as biomarkers. When combined with brain imaging, artificial intelligence, and recordings of brain activity, these biomarkers enable increasingly accurate predictions of how a brain disease will develop in an individual overtime.
Genomics is transforming the diagnosis of neurological diseases, paving the way for the emergence of precision medicine. FutureNeuro has been instrumental in incorporating genomics into clinical practice, leading to faster and more
The eight academic partner institutions
accurate diagnoses. Currently, FutureNeuro Deputy Director, Prof Gianpiero Cavalleri is co-leading an Irish consortium of partners to contribute to the ¤20M Digital Europe Call “Federated European infrastructure for genomics data”. This initiative is geared towards advancing the European 1+ Million Genomes Initiative, aiming to realise a unified platform for genomic data across Europe.
Therapeutics
FutureNeuro’s therapeutics research is organised as a pipeline, drawing on the insights from their diagnostics teams to identify to identify potential targets for future medications. A ground-breaking capability lies in the ability to generate human brain cells in the lab, allowing safer and more effective drugs to be screened for. But, to fully capitalise on the promise of genetics, however, requires gene therapy. Encouragingly, remarkable progress has been achieved; Clinical investigator Prof Orla Hardiman is trialling a number of pioneering gene therapy-based treatments for ALS in collaboration with world-leading pharmaceutical companies.
The Centre is also looking at how to safely deliver genes to precise areas of the brain, to control their activation via on/off switches and minimise potential side effects. Research extends to areas such as small noncoding RNAs and the biology of the blood-brain barrier. With a sharpened focus on accelerating clinical development and understanding the intricacies of the human brain, FutureNeuro is charting a course towards neurotherapeutics of the future.
Digital Health
In the rapidly evolving landscape of digital health, innovations are fundamentally reshaping healthcare delivery, access, and system operations. FutureNeuro's research program stands at the forefront, driven by the insights of clinicians and patients alike. Leveraging a rich data environment and cuttingedge digital technologies, they are co-designing solutions for proactive, personalised, and costeffective healthcare.
A researcher carefully uses a pipette in the lab
The Centre is laying the groundwork for a learning health system. This involves ethically integrating diverse datasets, including electronic health records and passive data from connected devices in homes. Furthermore, responsible artificial intelligence (AI) solutions aim to extract valuable insights from data, aiding clinical decision-making and continually improving patient care.
In tandem, FutureNeuro is pioneering a smartphone appbased digital therapeutic. Tailored to capture lifestyle data, it provides personalised interventions for mental well-being. Moreover, through strategic industry partnerships nurtured by programs like SFI SPOKE (EMPOWER and Precision ALS), they are advancing next-phase projects focused on health data analytics and building trust in the secondary use of data, alongside the utilisation and adoption of technologies such as artificial intelligence.
Mental Health
Mental health research is threaded throughout the new programme. In diagnostics, a significant new study is underway to look for changes in blood chemistry, aiming to identify people at risk earlier than is currently possible. In the drug development programme, researchers are targeting genes associated with psychosis while incorporating assessments for depression, anxiety, and psychosis across all drug development projects. This approach not only enhances drug efficacy but also provides insights into addressing the underlying mechanisms of mental health disorders. In the digital therapeutics program, efforts are focused on leading advancements in technologies that not only monitor but also positively intervene in brain health. This includes digital therapeutics that offer individuals greater control and continuity of care.
Rare Diseases
The Irish Government is committed to addressing rare diseases, with plans underway to create a National Rare Diseases Plan and a National Genetics and Genomics Medicine Network. FutureNeuro clinical researchers are developing patient registers for rare genomic diseases in order to stratify patients for clinical trials and be ready to implement advances in genomic medicine. Additionally, promising treatments are emerging at pre-clinical stage for epilepsy, including those for conditions like Dravet syndrome.
FutureNeuro will prioritize these often-overlooked conditions, aiming to drive progress and improve patient outcomes.
New Research Projects
FutureNeuro is already working on some remarkable projects that are taking a deep dive into the workings of the human brain. One such project involves recording patterns of electrical activity of brain cells, essentially eavesdropping on neurons and listening for when they misfire. This is possible because sometimes doctors will implant electrodes into the brains of people with treatment-resistant epilepsy to pinpoint the source of their seizures. The researchers have found a way to measure gene activity at the site of those recordings. This is helping to discover new genes that influence brain function and could hold promise for clinical decisionmaking. Like so much of the Centre’s work, this research relies on specialised scientific skills and collaboration with their dedicated clinical partners. This is only made possible by the robust framework upon which FutureNeuro is built.
Another exciting study aims to understand how to repair leaky blood vessels in the brain. In a healthy brain, blood vessels are tightly sealed, but in many neurological diseases, they become permeable. This hallmark is also associated with psychosis. By reapplying the genetic 'glue' responsible for maintaining the blood-brain barrier, researchers hope to open the doors to a completely new type of treatment.
Education, Public and Patient Engagement
A further evolution within FutureNeuro is the deeper
integration of patients within the Centre. They contribute to identifying research priorities, evaluating progress, and aid in communication with the public, funders, and policymakers, ensuring that research aligns closely with patient needs. Their Patient Panel played a key role in preparing the research strategy for FutureNeuro. The Centre is now actively developing diseasespecific patient panels that will be embedded across all areas of their research, including Parkinson's disease and MS.
Education and public engagement is another key component of their mission. The Brain Health webinar series, developed in partnership with Epilepsy Ireland, is just one example of the strategic collaborations they have undertaken to help break down barriers and make epilepsy research accessible to all. The team will also raise awareness of brain health and wellness with the wider community through an innovative education and engagement campaign called ‘My Moving Brain’, co-delivered across Ireland with patient advocacy groups and local sports partnerships as part of an SFI Discover Award. This initiative will build on their highly successful ‘Cell Explorers’ school programme that will continue to inspire the next generation of life scientists.
With over 350 engagement activities undertaken, including collaborative events with charitable organizations, enlightening workshops in schools, thoughtprovoking discussions at the Pint of Science festival, the creation of informative blogs for wider audiences, and valuable contributions to national policy, the Centre will continue to raise awareness and capture the
public's imagination, supported by a dedicated Education and Public and Patient Engagement Lead. Industry
Collaborating with industry is fundamental to the success of FutureNeuro. To date, the Leadership Team have undertaken more than 30 collaborative research projects, including partnerships with Roche, UCB, IQVIA, Novartis, Janssen, and Congenica. These include bringing new diagnostic supports to market, advancing a pipeline of new drugs through development and testing, and expanding digital health solutions to enable patients and their clinicians to co-monitor their health better than ever before. In FutureNeuro, the team will expand engagement with industry with a collective aim to advance new therapeutics and precision medicines, identify faster and more precise diagnostics tools, leverage the power of AI to accelerate discoveries based on clinical data and promote Ireland as a preferred location for early-stage clinical trials.
As FutureNeuro embarks on its mission to revolutionize brain research and treatment in Ireland, it commits not only to unravelling the complexities of brain diseases but also to leading the charge in translating these findings, paving the way for improved patient outcomes and transformative strides in healthcare.
For more information on the work of FutureNeuro go to www.futureneurocentre.ie
Haematology Oncology
The Irish Haematology Oncology Podcast: A New Learning Opportunity
Have you been featured in Hospital Professional News or published insightful research shaping the field of cancer care? The Irish Haematology Oncology Podcast wants to hear from you!
Introduction
In the ever-evolving world of cancer care, staying informed is crucial. The Irish Haematology Oncology Podcast is your go-to resource for clear, concise, and engaging discussions on the latest advancements, challenges, and best practices in treating cancer. Designed for busy healthcare professionals, this podcast offers accessible insights to enhance your knowledge and optimise patient care.
About the Podcast
Hosted by clinical cancer services pharmacist Eoin Tabb, the Irish Haematology Oncology Podcast delves into the complexities of cancer care through conversations with leading specialists in the field. The podcast welcomes a diverse range of voices, including haematology/oncology experts, pharmaceutical specialists,
Written by Eoin Tabb, Chief II Pharmacist (Clinical Cancer Services), Pharmacy Department, University Hospital Waterford
nurses, and other healthcare professionals across Ireland. These diverse perspectives offer practical knowledge and a wellrounded understanding of the cancer care landscape.
Why You Should Listen
• Stay up-to-date: The Irish Haematology Oncology Podcast is your key to keeping pace with rapidly evolving research, new drug developments, and shifts in best practices for treating cancer patients.
• Expand your knowledge: Explore a wide range of topics and gain a deeper understanding of the intricacies of cancer treatment, improving your overall expertise in the field.
• Gain practical insights: Learn directly from healthcare professionals at the forefront of patient care. Their experiences and strategies can be easily translated into your own practice.
• Contribute to CPD: Listening to the Irish Haematology Oncology Podcast aligns with your Continuing Professional Development (CPD) goals. Enhance or refresh your knowledge and gain CPD simultaneously.
• Enhanced Patient Care: The knowledge and insights you'll gain from the podcast translate directly into improved patient outcomes. Stay informed about the latest advancements and provide the highest quality of care.
Dive into the Fundamentals: Our Opening Episodes
Get ready to strengthen your knowledge base with the Irish Haematology Oncology Podcast's opening episodes! We're kicking things off by exploring core concepts that shape the world of cancer care:
• Safe Handling of SACT: Understand the critical safety risk assessments and procedures when working with Systemic Anti-Cancer Therapy (SACT), ensuring patient and healthcare provider well-being.
• Pharmacology of SACT: Delve into the mechanisms of action of different SACT drugs. Gain a deeper understanding of how they target cancer cells and their potential side effects.
• Cancer Staging: Learn the systems used to classify and stage cancers. This knowledge is essential for understanding treatment options, disease progression, and prognosis.
• Antiemetics: Explore the use of antiemetics to manage nausea and vomiting, common side effects of cancer therapy. We'll discuss different types of antiemetics and strategies to optimise their effectiveness.
• Hypersensitivity Reactions: Learn how to recognise, manage, and prevent hypersensitivity reactions to SACT. These critical skills can ensure patient safety and optimal treatment outcomes.
This is Just the Beginning!
Our opening episodes provide a solid foundation, and we hope to grow your knowledge base along with the podcast! Stay tuned for in-depth discussions on a wide range of topics, including immunotherapy, targeted therapies, supportive care, managing side effects, and much more! Subscribe now and join us as we enhance cancer care knowledge within the Irish healthcare community.
Call for Guest Participants
Have you been featured in Hospital Professional News or published insightful research shaping the field of cancer care?
The Irish Haematology Oncology Podcast wants to hear from you! We seek dedicated healthcare professionals who:
• Have published in Hospital Professional News: Delve deeper into your article, discussing your research and its broader implications for the field.
• Have publications elsewhere: Share your impactful work in haematology and oncology to reach a wider audience within the healthcare community.
• Possess specialist knowledge: Help break down complex concepts and make the field more accessible to all healthcare professionals involved in cancer care.
Become a Part of the Conversation
If you're passionate about cancer care and eager to share your expertise, reach out to us! Email irishhaemoncpodcast@gmail. com with a brief description of your background and potential discussion topics you'd like to explore.
Where to Find the Podcast
Access the Irish Haematology Oncology Podcast for free on popular platforms like:
• Spotify
• Apple Podcasts
• YouTube Music
• And wherever you get your podcasts…
Subscribe today and never miss an episode!
Let's Learn and Grow Together
The Irish Haematology Oncology Podcast is committed to empowering healthcare professionals and fostering a collaborative learning environment within the Irish healthcare community.
Important Disclaimer: This podcast is for educational purposes only. Remember, the field of cancer is always advancing, and new research may lead to changes in treatment approaches and safety protocols. Always consult with your healthcare providers for personalised guidance and discuss any information from this podcast with them. Seek information from trusted local resources for the most up-to-date recommendations.
Connections That Last
Three molecules engineered for an uninterrupted 24-hour effect, delivered via easy-to-use Ellipta device*1,2
* Fluticasone furoate and vilanterol are not licensed as monotherapies in COPD. 3
Safety information
TRELEGY Ellipta is generally well tolerated. Common adverse reactions include: headache, nasopharyngitis, influenza, upper respiratory tract infection, pneumonia, back pain, rhinitis, cough, pharyngitis and arthralgia.1 In common with other corticosteroid-containing medicines, there is an increased risk of pneumonia in patients with COPD receiving TRELEGY Ellipta.1
TRELEGY Ellipta should be used with caution in patients with unstable or life-threatening cardiovascular disease.1
References: 1. TRELEGY Ellipta SmPC, 2024. Available at www.medicines.ie. Accessed April 2024. 2. Van der Palen J et al. NPJ Prim Care Respir Med 2016; 26:16079.
Trelegy Ellipta (fluticasone furoate/umeclidinium/vilanterol [as trifenatate]) Prescribing information. Please consult the full Summary of Product Characteristics (SmPC) before prescribing.
or request a visit from a GSK representative
Trelegy Ellipta (fluticasone furoate/umeclidinium/vilanterol [as trifenatate]) inhalation powder. Each single inhalation of fluticasone furoate (FF) 100 micrograms (mcg), umeclidinium bromide (UMEC) 62.5 micrograms and vilanterol as trifenatate (VI) 25 mcg provides a delivered dose of 92 mcg FF, 55 mcg UMEC and 22 mcg VI. Indications: Maintenance treatment in adult patients with moderate to severe COPD who are not adequately treated by a combination of an inhaled corticosteroid (ICS) and a long-acting ß2-agonist (LABA) or a combination of a LABA and a long acting muscarinic antagonist. Dosage and administration: One inhalation once daily at the same time each day. Contraindications: Hypersensitivity to the active substances or to any of the excipients (lactose monohydrate & magnesium stearate). Precautions: Paradoxical bronchospasm, unstable or life-threatening cardiovascular disease or heart rhythm abnormalities, convulsive disorders or thyrotoxicosis, pulmonary tuberculosis or patients with chronic or untreated infections, narrow-angle glaucoma, urinary retention, risk factors for urinary retention, hypokalaemia, patients predisposed to low levels of serum potassium, diabetes mellitus. In patients with moderate to severe hepatic impairment patients should be monitored for systemic corticosteroid-related adverse reactions. Eye symptoms such as blurred vision may be due to underlying serious conditions such as cataract, glaucoma or central serous chorioretinopathy (CSCR); consider referral to ophthalmologist. Increased incidence of pneumonia has been observed in patients with COPD receiving inhaled corticosteroids. Risk factors for pneumonia include: current smokers, old age, patients with a history of prior pneumonia, patients with a low body mass index and severe COPD. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take Trelegy. Acute symptoms: Not for acute symptoms, use short-acting inhaled bronchodilator. Warn patients to seek medical advice if short-acting inhaled bronchodilator use increases. Therapy should not be abruptly stopped without physician supervision due to risk of symptom recurrence. Systemic effects: Systemic effects of ICSs may occur, particularly at high doses for long periods, but much less likely than with oral corticosteroids. Interactions with other medicinal products: Caution should be exercised with concurrent use of ß-blockers. Caution is advised when co-administering with strong CYP3A4 inhibitors (e.g. ketoconazole, ritonavir, cobicistat-containing products), hypokalaemic treatments or non-potassium-sparing diuretics. Co-administration with other long-acting muscarinic antagonists or long acting ß2-adrenergic agonists is not recommended. Pregnancy and breast-feeding: Experience limited. Balance risks against benefits. Side effects: Common (≥1/100 to <1/10): pneumonia, upper respiratory tract infection, bronchitis, pharyngitis, rhinitis, sinusitis, influenza, nasopharyngitis, candidiasis of mouth and throat, urinary tract infection, headache, cough, oropharyngeal pain, arthralgia, back pain. Uncommon (≥1/1,000 to <1/100): viral respiratory tract infection, dysgeusia, vision blurred, glaucoma, eye pain, supraventricular tachyarrhythmia, tachycardia, atrial fibrillation, dysphonia, dry mouth, fractures. Rare (≥1/10,000 to <1/1,000): Hypersensitivity reactions, including anaphylaxis, angioedema, urticaria, and rash, intraocular pressure increased, urinary retention, dysuria, hyperglycaemia, anxiety, tremor, palpitations and muscle spasms. Marketing Authorisation (MA) Holder: GlaxoSmithKline Trading Services Limited, 12 Riverwalk, Citywest Business Campus, Dublin 24, Ireland. MA No. [EU/1/17/1236/002]. Legal category: POM B. Last date of revision: October 2023. Code: PI-6725. Further information available on request from GlaxoSmithKline, 12 Riverwalk, Citywest Business Campus, Dublin 24. Tel: 01-4955000.
TRELEGY Ellipta was
in
with Adverse events should be reported directly to the Health Products Regulatory Authority (HPRA) on their website: www.hpra.ie. Adverse events should also be reported to GlaxoSmithKline on 1800 244 255.
Multiple Sclerosis
Delays in Multiple Sclerosis diagnosis (DIMES): protocol for a multicentre, observational study of multiple sclerosis diagnostic pathways in the United Kingdom and Republic of Ireland
Written by Ashvin Kuri1,2, David E. Henshall2,3, Daoud Chaudhry2,4, Setthasorn Zhi Yang Ooi2,5, Qiqi Zhang1, Joela Mathews6, Alison Thomson1, David Rog7, Jeremy Hobart8, Ruth Dobson1 & Neurology and Neurosurgery Interest Group (NANSIG)
1Wolfson Institute of Population Health, Queen Mary University of London, Charterhouse Square, London
2Neurology and Neurosurgery Interest Group (NANSIG), London
3Deanery of Clinical Sciences, College of Medicine & Veterinary Medicine, The University of Edinburgh
4Royal Stoke University Hospital, University Hospitals of North Midlands, Stoke-on-Trent
5Cardiff University School of Medicine, Cardiff
6Department of Neurology, Royal London Hospital, London
7Department of Neurology, Manchester Centre for Clinical Neurosciences, Salford, Manchester
8Peninsula Medical School, Faculty of Health, University of Plymouth, Plymouth
NB: The following is a brief of the original article published in BMC Neurology. The link to the full article is available at the end of this overview.
Multiple Sclerosis (MS) is a chronic progressive disabling neurological disease. It is a leading cause of non-traumatic disability in young adults worldwide.1
The therapeutic armamentarium for relapsing remitting MS consists of numerous disease modifying therapies (DMTs). Most DMTs are immunotherapies targeting the dysregulated immune system in MS, and many have shown significant impact on slowing progression and time-to-relapse in clinical trials.2, 3 Growing evidence suggests early aggressive treatment confers a better longterm prognosis for people living with MS; finding a more concrete answer to this question represents a top 10 research priority area for people with MS according to MS Society UK.4,5,6,7,8,9,10,11
Crucially, early treatment initiation in MS is predicated upon
efficient diagnostic pathways that facilitate early, accurate diagnosis.12 However, the MS diagnostic pathway is intrinsically complex. Diagnostic confirmation requires the integration of clinical history and examination (to exclude differential diagnoses), magnetic resonance imaging (MRI) findings (to identify MS lesions disseminated in space and time), and potentially laboratory findings (IgG oligoclonal bands in cerebrospinal fluid analysis).13 Logistically, the collection and amalgamation of this data in a timely manner poses a challenge. Delays in the diagnostic process will differ between healthcare systems, but may include availability of neurology outpatient appointments, long MRI waiting lists, and access to lumbar puncture services. Furthermore, the impact of the COVID pandemic on services and service recovery has posed additional challenges.14 In addition to service-level aspects, individual-level factors may play a role, for example whether individuals recognised their initial symptoms merited
medical review and/or could relate to MS. Existing literature has identified a number of factors associated with diagnostic delay in MS, including delayed MRI/ lumbar puncture,15 nature of presenting symptoms,16,17,18,19,20,21 lower educational level,17, 19, 20 older age,18, 22, 23 greater number of relapses before diagnosis,18, 22 previous misdiagnosis,18 primary progressive MS subtype,18, 19, 21 male sex,19, 24 greater distance to MS centre,19 increased comorbidity burden,25 negative family history,26 lack of awareness of MS symptoms amongst the general public or healthcare professionals (non-MS specialist diagnosing doctor),27 and lack of familiarity with the McDonald criteria.16, 27, 28 There is a need to evaluate and assess such delays in the UK healthcare system to potentially facilitate earlier treatment, identify groups at greater risk of diagnostic delay, and to help improve the overall diagnostic pathway.
This study protocol proposes a multicentre retrospective observational study of the UK
and ROI MS diagnostic pathway. DIMES involves data collection direct from clinical records, by a unique, trained, and geographically diverse network of student and junior doctor collaborators, to provide new insights that cannot be provided by contemporary databases.
Standard diagnostic service and relevant quality standards
There is no single guideline that provides a set diagnostic pathway for MS. National bodies, such as the National Institute for Health and Care Excellence (NICE), provide some guidance as to recommended standards in England. Recent position papers have employed the iterative Delphi method to develop benchmark standards, but no single position paper is considered the goldstandard in the UK.29,30,31
Through reviewing guidelines (listed in Supplement S1), position papers, and proposed standards, and consulting a
Figure 1
geographically diverse range of UK MS specialists, we developed the data dictionary (Supplement S2). Given the diagnostic journey of people with multiple sclerosis exhibits significant inter-person heterogeneity, the data dictionary allows for collection of data that deviates from a ‘typical’ diagnostic journey.
Objectives
The primary objective is to quantify the time taken for people to be diagnosed with MS in the UK and ROI using 1) time from symptoms/ signs prompting referral to neurology (as listed in referral letter or neurology clinic letters), to MS diagnosis; and 2) time from the referral to neurology for suspected MS, to MS diagnosis (Fig. 1).
The secondary objectives are:
• To characterise the diagnostic journey of people with MS in the UK and ROI, including initial/ presenting symptoms, referring specialties, investigations performed, time to completion of investigations, number of neurology appointments, functional status at diagnosis.
• To identify factors associated with diagnostic delay in the UK and ROI.
• To characterise the treatments prescribed for people with MS, including the use of DMTs and time to receipt.
• To evaluate the immediate post-diagnosis MS quality of care pathways in the UK by assessing adherence to NICE Quality Statement (QS) QS 108 Statements 1, 2 and 4, as outlined, verbatim, below.32
QS 108 guidelines
Statement 1: Adults with multiple sclerosis (MS) are given support at the time of diagnosis to understand the condition, its progression and the ways it can be managed, by the consultant neurologist making the diagnosis.
Audit Calculation: Proportion of adults with MS who are given information about MS, its progression and the ways it can be managed by the consultant neurologist at the time of diagnosis.
Statement 2: Adults with multiple sclerosis (MS) are offered a faceto-face follow-up appointment with a healthcare professional with expertise in MS, to take place within 6 weeks of diagnosis.
Audit Calculation: Proportion of adults with MS who have a faceto-face follow-up appointment with a healthcare professional with expertise in MS within 6 weeks of diagnosis.
Statement 4: Adults with multiple sclerosis (MS) who have problems with mobility or fatigue are offered support to remain physically active.
Audit Calculation: Proportion of adults with MS who are offered support to remain physically active.
Patient eligibility criteria
Inclusion criteria
We will include individuals who received a new diagnosis of MS between 1st July 2022 and 31st December 2022. This 6-month time period was selected to 1) balance data collection burden with the number of included individuals, 2) examine a period sufficiently outside the most critical influence of the COVID-19 pandemic, and 3) enable collection of post-diagnosis follow up data relating to use of DMTs and care.
Formal diagnosis by a clinician working in neurology should be clearly documented in the individual’s notes. In order to maximise case ascertainment, we will include individuals irrespective of investigations or treatments received, or the completeness/ accessibility of their clinical data. Each centre will recruit all consecutively diagnosed individuals in the specified time period. Individuals must have received their formal diagnosis (as evidenced by a letter/clinical note) from the centre, and not had their care transferred into the centre post-diagnosis (e.g., for DMT treatment). Individuals transferred out of the centre following diagnosis (e.g., for treatment at a tertiary centre) will remain eligible for inclusion.
Exclusion criteria
• We will exclude individuals with only a possible/suspected diagnosis of MS (as opposed to confirmed).
The number of people excluded following screening will be reported, including the rationale for exclusion.
Patient identification
Local teams will work with a supervising consultant at participating centres to identify all individuals meeting inclusion criteria. Additional assistance may be provided by an MS Nurse or junior doctor, and the contributions of these individuals will be acknowledged in the study. Suggested methods for identification in ordered preference include:
• 1st line: Review of locally curated lists of individuals with MS, or new diagnoses.
• 2nd line: Review of MS clinic appointments.
• 3rd line: Review of general neurology / neurology clinic appointments.
• 4th line: Review of individuals with relevant diagnostic hospital (ICD-10) or General Practice (Read Clinical Terms Version 3) code(s) (full list in Supplement S3).
Teams will be expected to report the method used for patient identification, with one method alone being sufficient. Methods based on use of MSassociated medications such as attendance at DMT infusion centres, Blueteq records or pharmacy records are not acceptable due to selection bias. Other methods of identification such as search of radiology databases for MS-related terms may be acceptable if discussed with the Steering Committee.
Recorded variables
All measures, exposures and outcomes are defined in detail, in our data dictionary (Supplement S2), including the likely sources of information from the electronic health record.
Baseline measures and exposures
Demographic variables include: age; sex; ethnicity; index of deprivation (UK centres: index of deprivation decile and rank; ROI centres: Pobal Haase Pratschke (HP) Index 2016 and description); distance from home postcode to MS centre; employment status; and smoking status.
MS variables include: family history of MS (with the degree of relatedness of relative with MS); possible prior misdiagnosis or MS mimic; date of ‘First Relevant’ referral to neurology/MS clinic and source of this referral; symptoms/ signs/abnormal investigations prompting this ‘First Relevant’ referral to neurology and date of onset; historical MS-associated symptoms/signs/abnormal investigations that precede ‘First Relevant’ referral to neurology and date of onset.
Neurology appointment and investigation variables include: date of first neurology appointment after referral (if available), and whether this neurologist had a practice focus in MS; documented follow up plan from this appointment; date of subsequent neurology appointment(s); date MRI requested, performed, and reported; MRI findings, region, use of contrast, and modality; date lumbar puncture requested, and performed; and lumbar puncture findings.
MS diagnosis variables include:
date of diagnosis and whether the diagnosing neurologist had a practice focus in MS; previous diagnosis of CIS; MS subtype; number of MS relapses at the time of diagnosis; and disability scores at diagnosis (EDSS, Timed 25-Foot Walk Time, Nine-Hole Peg Test Time at Diagnosis (right and left hands), Fatigue Severity Score, and Multiple Sclerosis Functional Composite Score).
MS treatment variables include: DMT(s) received; date of referral for DMT MDT; date of DMT MDT; date of first DMT started; administration method.
Quality measures from QS 108 include: Support at diagnosis (including specifically support to (a) understand the condition, (b) understand MS progression and (c) understand MS management); Follow up after diagnosis; and Physical activity advice.
Outcomes
Primary outcomes
The primary outcomes relate to time to diagnosis and include: 1) time from symptoms/signs prompting referral to neurology (as listed in referral letter or neurology clinic letter), to MS diagnosis; and 2) time from referral to neurology for suspected MS, to MS diagnosis. These outcomes have been selected with equal weighting of importance, as the former may be most important from a patient perspective (as disease starts, from their perspective, when they first notice symptoms), whereas the latter gives a more meaningful evaluation of the diagnostic service.
Secondary outcomes
The outcomes relating to diagnostic journey include: a) symptoms prompting referral and earliest symptoms potentially relating to MS; b) which specialties refer to neurology for diagnostic work up for MS; c) the number and results of lumbar puncture and MRI investigations performed; d) the time from request of investigation to completion and to reporting; e) the number of neurology appointments between referral for suspected MS and MS diagnosis; and f) functional status at time of diagnosis (according to various scoring systems).
The outcomes relating to MS care include: a) the prescription of DMTs including the specific agents used and time to receipt after diagnosis; and b) adherence to QS 108 Statements 1, 2 and 4 (NICE Quality Statements, 2016).
Data collection
At each centre, a team of collaborators will lead the data collection with guidance from
Multiple Sclerosis
a supervising consultant, and mandatory specific training from the study leads (Fig. 2).
Data collectors will extract information from existing clinical records onto a paper proforma (case report form (CRF)). The template for this proforma will be provided by the study steering team. These paper records will not leave hospital premises, and must be kept securely on site in a locker cabinet or similar, in accordance with Good Clinical Practice [35].
Following paper data collection, collaborators will enter data onto a standardised Microsoft Excel spreadsheet on passwordprotected NHS computers/ servers (Supplement S4). Each new individual will be assigned a ‘Record ID’ [e.g. sequentially 1–100] on the spreadsheet. For the purposes of local traceability, a separate spreadsheet will be securely kept, matching each ‘Record ID’ to local ‘Hospital Number’. This separate spreadsheet contains identifiable information, is solely for internal use at the hospital centre, and must not be shared outside of the local collaborator team. This identifiable information should be deleted at final study completion (defined as post-data validation). CRFs should be disposed of appropriately, as per local hospital protocol.
Data will be collated centrally for analysis. Individual centres will not be identified by name in study outputs, in relation to centre-level data.
This Microsoft Excel spreadsheet will be sent to the steering committee at the study-specific nhs.net email from an nhs.net (or local equivalent) email to maintain confidentiality and security of the data.
Discussion
Study approval and registration
This study will not change local routine practice and will use data obtained as part of usual care. The UK Health Research Authority (HRA) decision tool has confirmed that this study is not considered research by the NHS and does not require NHS research ethics committee approval (Supplement S6).37
The centre lead and accompanying research team at each unit are responsible for registering the study with appropriate approvals, in line with national guidelines. In the UK, this will usually be as a service evaluation study. Supervision by a local neurology consultant is required for this process, therefore it is the responsibility of the local teams to identify suitable consultants for study registration. Collaborators will be required to confirm that a local approval is in place prior to data collection.
Data governance
Data will be collected onto purpose-designed CRFs and entered into a bespoke Microsoft Excel spreadsheet at the respective centres’ password-protected hospital server. All data should be handled in accordance with local data governance policies, and all paper copies of any data should be destroyed as confidential waste within the centre, once uploaded onto the local hospital server. At the end of the data collection period, de-identified data will be transferred to the DIMES Steering Committee via a secure nhs. net encrypted email (or local equivalent), for data cleaning and analysis. For information governance, patient identifier data will be stored securely locally, but will not be sent on to the DIMES Steering Committee. No patient data will be transferred without prior local permissions.
Data will be collated, stored and analysed by the DIMES Steering Committee. Data collected during the DIMES study can be used for future analyses at the steering committee’s discretion.
Protocol dissemination
The protocol will be disseminated primarily through recruited medical student collaborators in the NANSIG network. Should local neurology units wish to view the protocol, this will be freely accessible from the DIMES study hub on the NANSIG website (www.
nansig.org). Any publications of the protocol will be advertised through social media.
Dissemination of results
Following study completion, teleconferences will be held with all collaborators to share and discuss the data analysis undertaken and the study results. Following this, results will be presented at local, regional, national, and international conferences by collaborators. A standardised PowerPoint presentation and poster will be created for this purpose. All presentations will be coordinated by the DIMES steering committee to avoid duplications and to ensure all conference regulations are fulfilled. In addition, the results will be disseminated via publication in a peer-reviewed medical journal. The study results will be reported using the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines.38
Following publication, the manuscript can be shared by collaborators with their local neurology units to discuss the study results, and to highlight the scope for areas of improvement for MS diagnosis [39]. Local teams at each neurology unit can request for their respective centre data from the steering committee following study completion.
The full article can be viewed at: www.link.springer.com/ article/10.1186/s12883-02403598-z
Figure 2
SETACOURSEFOR LONGERSURVIVAL
IN LOCALLY ADVANCED OR METASTATIC UROTHELIAL CANCER WITH PADCEV™ (ENFORTUMAB VEDOTIN) VS INVESTIGATOR-CHOICE CHEMOTHERAPY
An innovative Nectin-4–targeted treatment, PADCEV (enfortumab vedotin) extended mOS to 12.9 months in patients who previously received platinum-containing chemotherapy and a PD-1 or PD-L1 inhibitor vs investigator-choice chemotherapy (mOS, 12.9 vs 9 months; HR=0.70, 95% CI: 0.56–0.89; P=0.001).1,2
INDICATION
PADCEV (enfortumab vedotin) as monotherapy is indicated for the treatment of adult patients with LA or mUC who have previously received a platinum-containing chemotherapy and a PD-1 or PD-L1 inhibitor.1
Ireland Abbreviated Prescribing Information: PADCEV™ powder for concentrate for solution for infusion For full prescribing information refer to the Summary of Product Characteristics (SPC).
Name: PADCEV 20mg powder for concentrate for solution for infusion & PADCEV 30mg powder for concentrate for solution for infusion. Presentation: One vial of PADCEV powder for concentrate for solution for infusion contains either 20 mg or 30 mg enfortumab vedotin. After reconstitution, each ml of solution contains 10 mg of enfortumab vedotin. Enfortumab vedotin is comprised of a fully human IgG1 kappa antibody, conjugated to the microtubule-disrupting agent monomethyl auristatin E (MMAE) via a protease-cleavable maleimidocaproyl valine-citrulline linker. Indications: PADCEV as monotherapy is indicated for the treatment of adult patients with locally advanced or metastatic urothelial cancer who have previously received a platinumcontaining chemotherapy and a programmed death receptor-1 or programmed death-ligand 1 inhibitor (see section 5.1 of the SPC). Posology and method of administration: Treatment with PADCEV should be initiated and supervised by a physician experienced in the use of anti-cancer therapies. PADCEV is for intravenous use. Good venous access prior to starting treatment should be ensured (see section 4.4 of the SPC). The recommended dose of enfortumab vedotin is 1.25 mg/kg (up to a maximum of 125 mg for patients ≥100 kg). It must be administered as an intravenous infusion over 30 minutes on Days 1, 8 and 15 of a 28-day cycle until disease progression or unacceptable toxicity. It must not be administered as an intravenous push or bolus injection. For information on recommended dose reductions for adverse reactions as well as instructions on dose modifications (interruption, reduction and discontinuation) in patients experiencing adverse reactions refer to section 4.2 of the SPC. Special Populations: Elderly: No dose adjustment is necessary in patients ≥65 years of age (see section 5.2 of the SPC). Renal impairment: No dose adjustment is necessary in patients with mild [creatinine clearance (CrCL) >60-90 mL/min], moderate (CrCL 30–60 mL/min) or severe (CrCL 15–<30 mL/min) renal impairment. Enfortumab vedotin has not been evaluated in patients with end stage renal disease (CrCL <15 mL/min) (see section 5.2 of the SPC). Hepaticimpairment:No dose adjustment is necessary in patients with mild hepatic impairment [total bilirubin of 1 to 1.5 × upper limit of normal (ULN) and aspartate transaminase (AST) any, or total bilirubin ≤ ULN and AST > ULN]. Enfortumab vedotin has only been evaluated in a limited number of patients with moderate hepatic impairment and has not been evaluated in patients with severe hepatic impairment (see section 5.2 of the SPC). Paediatric population: There is no relevant use of enfortumab vedotin in the paediatric population for the indication of locally advanced or metastatic urothelial cancer. Contraindications: Hypersensitivity to the active substance or to any of the excipients listed in section 6.1 of the SPC. Special warnings and precautions for use: Traceability: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Skin reactions: Skin reactions are associated with enfortumab vedotin as a result of enfortumab vedotin binding to Nectin-4 expressed in the skin. Fever or flu-like symptoms may be the first sign of a severe skin reaction, and patients should be observed, if this occurs. Mild to moderate skin reactions, predominantly maculopapular rash, have been reported (see section 4.8 of the SPC). Severe cutaneous adverse reactions, including Stevens-Johnson syndrome (SJS) and Toxic Epidermal Necrolysis (TEN), with fatal outcome have also occurred in patients treated with enfortumab vedotin, predominantly during the first cycle of treatment. In clinical trials, the median time to onset of severe skin reactions was 0.6 months (range: 0.1 to 6.4). Patients should be monitored starting with the first cycle and throughout treatment for skin reactions. Appropriate treatment such as topical corticosteroids and antihistamines can be considered for mild to moderate skin reactions. For suspected SJS or TEN, or in case of bullous lesions onset, withhold treatment immediately and refer to specialised care; histologic confirmation, including consideration of multiple biopsies, is critical to early recognition, as diagnosis and intervention can improve prognosis. Permanently discontinue PADCEV for confirmed SJS or TEN, Grade 4 or recurrent severe skin reactions. For Grade 2 worsening, Grade 2 with fever or Grade 3 skin reactions, treatment should be withheld until Grade ≤1 and referral for specialised care should be considered. Treatment should be resumed at the same dose level or consider dose reduction by one dose level (see section 4.2 of the SPC). Pneumonitis/Interstitial Lung Disease (ILD): Severe, life-threatening or fatal pneumonitis/ILD have occurred in patients treated with enfortumab vedotin (see section 4.8 of the SPC). Monitor patients for signs and symptoms indicative of pneumonitis/ILD such as hypoxia, cough, dyspnea or interstitial infiltrates on radiologic exams. Corticosteroids should be administered for Grade ≥ 2 events (e.g., initial dose of 1-2 mg/kg/day prednisone or equivalent followed by a taper). Withhold PADCEV for Grade 2 pneumonitis/ILD and consider dose reduction. Permanently discontinue PADCEV for Grade ≥3 pneumonitis/ILD (see section 4.2 of the SPC). Hyperglycaemia: Hyperglycaemia and diabetic ketoacidosis (DKA), including fatal events, occurred in patients with and without pre- existing diabetes mellitus, treated with enfortumab vedotin (see section 4.8 of the SPC). Hyperglycaemia occurred more frequently in patients with pre-existing hyperglycaemia or a high body mass index (≥30 kg/m2). Patients with baseline HbA1c ≥8% were excluded from clinical trials. Blood glucose levels should be monitored prior to dosing and periodically throughout the course of treatment as clinically indicated in patients with or at risk for diabetes mellitus or hyperglycaemia. If blood glucose is elevated >13.9 mmol/L (>250 mg/dL), PADCEV should be withheld until blood glucose is ≤13.9 mmol/L (≤250 mg/dL) and treat as appropriate (see section 4.2 of the SPC). Peripheral neuropathy: Peripheral neuropathy, predominantly peripheral sensory neuropathy, has occurred with enfortumab vedotin, including Grade ≥3 reactions (see section 4.8 of the SPC). Patients with pre-existing peripheral neuropathy Grade ≥2 were excluded from clinical trials. Patients should be monitored for symptoms of new or worsening peripheral neuropathy as these patients may require a delay, dose reduction or discontinuation of enfortumab vedotin. PADCEV should be permanently discontinued for Grade ≥3 peripheral neuropathy (see section 4.2 of the SPC). Ocular disorders: Ocular disorders, predominantly dry eye, have occurred in patients treated with enfortumab vedotin (see section 4.8 of the SPC). Patients should be monitored for ocular disorders. Consider artificial tears for prophylaxis of dry eye and referral for ophthalmologic evaluation if ocular symptoms do not resolve or worsen. Infusion site extravasation: Skin and soft tissue injury following enfortumab vedotin administration has been observed when extravasation occurred (see section 4.8 of the SPC). Ensure good venous access prior to starting PADCEV and monitor for possible infusion site extravasation during administration. If extravasation occurs, stop the infusion and monitor for adverse reactions. Embryo-foetal toxicity and contraception: Pregnant women should be informed of the potential risk to a foetus (see sections 4.6 and 5.3 of the SPC). Females of reproductive potential should be advised to have a pregnancy test within 7 days prior to starting treatment with enfortumab vedotin, to use effective contraception during treatment and for at least 12 months after stopping treatment. Men being treated with enfortumab vedotin are advised not to father a child during treatment and for up to 9 months following the last dose of PADCEV. Effects on ability to drive and use machines: PADCEV has no or negligible influence on the ability to drive and use machines. Interactions: Formal drug-drug interaction studies with enfortumab vedotin have not been conducted. Caution is advised in case of concomitant treatment with CYP3A4 inhibitors. Patients receiving concomitant strong CYP3A4 inhibitors (e.g. boceprevir, clarithromycin, cobicistat, indinavir, itraconazole, nefazodone, nelfinavir, posaconazole, ritonavir, saquinavir, telaprevir, telithromycin, voriconazole) should be monitored more closely for signs of toxicities. Strong CYP3A4 inducers (e.g. rifampicin, carbamazepine, phenobarbital, phenytoin, St John’s wort [Hypericumperforatum]) may decrease the exposure of unconjugated MMAE with moderate effect (see section 5.2 of the SPC). Fertility, pregnancy and lactation: Women of childbearing potential/ Contraception in males and females: Refer to ‘Special warnings and precautions for use’ section above. Pregnancy: PADCEV can cause foetal harm when administered to pregnant women based upon findings from animal studies. PADCEV is not recommended during pregnancy and in women of childbearing potential not using effective contraception. Breast-feeding: Breast-feeding should be discontinued during PADCEV treatment and for at least 6 months after the last dose. Fertility: Men being treated with this medicinal product are advised to have sperm samples frozen and stored before treatment. There are no data on the effect of PADCEV on human fertility. Undesirable effects: Summary of the safety profile: The
most common adverse reactions with enfortumab vedotin were alopecia (48.8%), fatigue (46.8%), decreased appetite (44.9%), peripheral sensory neuropathy (38.7%), diarrhoea (37.6%), nausea (36%), pruritus (33.4%), dysgeusia (29.9%), anaemia (26.5%), weight decreased (23.4%), rash maculo-papular (22.9%), dry skin (21.6%), vomiting (18.4%), aspartate aminotransferase increased (15.3%), hyperglycaemia, (13.1%), dry eye (12.8%), alanine aminotransferase increased (12.1%) and rash (10.4%). The most common serious adverse reactions were diarrhoea (2%) and hyperglycaemia (2%). Nine percent of patients permanently discontinued enfortumab vedotin for adverse reactions; the most common adverse reaction (≥2%) leading to dose discontinuation was peripheral sensory neuropathy (4%). Adverse reactions leading to dose interruption occurred in 44% of patients; the most common adverse reactions (≥2%) leading to dose interruption were peripheral sensory neuropathy (15%), fatigue (7%), rash maculo-papular (4%), aspartate aminotransferase increased (4%), alanine aminotransferase increased (4%), anaemia (3%), diarrhoea (3%) and hyperglycaemia (3%). Thirty percent of patients required a dose reduction due to an adverse reaction; the most common adverse reactions (≥2%) leading to a dose reduction were peripheral sensory neuropathy (10%), fatigue (5%), rash maculo-papular (4%) and decreased appetite (2%). Summary of adverse reactions: The safety of enfortumab vedotin as monotherapy has been evaluated in 680 patients with locally advanced or metastatic urothelial cancer receiving 1.25 mg/kg on Days 1, 8 and 15 of a 28-day cycle in clinical studies. Patients were exposed to enfortumab vedotin for a median duration of 4.7 months (range: 0.3 to 34.8 months). Adverse reactions observed during clinical studies are listed in this section according to Medical Dictionary for Regulatory Activities (MedDRA) system organ classification by frequency category. Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. Frequency categories are defined as follows: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data). Blood and lymphatic system disorders: Very common: Anaemia, Not known1: Neutropenia, febrile neutropenia, neutrophil count decreased. Metabolism and nutrition disorders: Very common: Hyperglycaemia, decreased appetite. Nervous system disorders: Very common: Peripheral sensory neuropathy, dysgeusia. Common: Neuropathy peripheral, peripheral motor neuropathy, peripheral sensorimotor neuropathy, paraesthesia, hypoaesthesia, gait disturbance, muscular weakness. Uncommon: Demyelinating polyneuropathy, polyneuropathy, neurotoxicity, motor dysfunction, dysaesthesia, muscle atrophy, neuralgia, peroneal nerve palsy, sensory loss, skin burning sensation, burning sensation. Eye disorders: Very common: Dry eye. Respiratory, thoracic, and mediastinal disorders: Common: Pneumonitis. Uncommon: ILD. Gastrointestinal disorders: Very common: Diarrhoea, vomiting, nausea. Skin and subcutaneous tissue disorders: Very common: Alopecia, pruritus, rash, rash maculo-papular, dry skin. Common: Drug eruption, skin exfoliation, conjunctivitis, dermatitis bullous, blister, stomatitis, palmar-plantar erythrodysesthesia syndrome, eczema, erythaema, rash erythaematous, rash macular, rash papular, rash pruritic, rash vesicular. Uncommon: Dermatitis exfoliative generalised, erythaema multiforme, exfoliative rash, pemphigoid, rash maculovesicular, dermatitis, dermatitis allergic, dermatitis contact, intertrigo, skin irritation, stasis dermatitis, blood blister. Not known1: TEN, SJS, epidermal necrosis, symmetrical drug-related intertriginous and flexural exanthaema. General disorders and administration site conditions: Very common: Fatigue. Common: Infusion site extravasation. Investigations: Very common: Alanine aminotransferase increased, aspartate aminotransferase increased, weight decreased. 1Based on global post-marketing experience. Description of selected adverse reactions. Immunogenicity: A total of 590 patients were tested for immunogenicity to enfortumab vedotin 1.25 mg/kg; 15 patients were confirmed to be positive at baseline for anti-drug antibody (ADA), and in patients that were negative at baseline (N=575), a total of 16 (2.8%) were positive postbaseline (13 transiently and 3 persistently). Due to the limited number of patients with antibodies against PADCEV, no conclusions can be drawn concerning a potential effect of immunogenicity on efficacy, safety or pharmacokinetics. Skin reactions: In clinical studies, skin reactions occurred in 55% (375) of the 680 patients treated with enfortumab vedotin 1.25 mg/kg. Severe (Grade 3 or 4) skin reactions occurred in 13% (85) of patients and a majority of these reactions included maculo-papular rash, rash erythematous, rash or drug eruption. The median time to onset of severe skin reactions was 0.62 months (range: 0.1 to 6.4 months). Serious skin reactions occurred in 3.8% (26) of patients. In the EV-201 (N=214) clinical study, of the patients who experienced skin reactions, 75% had complete resolution and 14% had partial improvement (see section 4.4 of the SPC). Pneumonitis/ILD: In clinical studies, pneumonitis occurred in 15 (2.2%) and ILD occurred in 2 (0.3%) of the 680 patients treated with enfortumab vedotin 1.25 mg/kg. Less than 1% of patients experienced severe (Grade 3-4) pneumonitis or ILD. Pneumonitis or ILD led to discontinuation of enfortumab vedotin in 0.1% and 0.3% of patients, respectively. There were no deaths from ILD or pneumonitis. The median time to onset of any grade pneumonitis or ILD was 3.6 months (range: 0.8 to 6.0 months) and the median duration was 1.4 months (range: 0.2 to 27.5 months). Of the 17 patients who experienced pneumonitis or ILD, 6 (35.3%) had resolution of symptoms. Hyperglycaemia: In clinical studies, hyperglycaemia (blood glucose >13.9 mmol/L) occurred in 14% (98) of the 680 patients treated with enfortumab vedotin 1.25 mg/kg. Serious events of hyperglycaemia occurred in 2.2% of patients, 7% of patients developed severe (Grade 3-4) hyperglycaemia and 0.3% of patients experienced fatal events, one event each of hyperglycaemia and diabetic ketoacidosis. The incidence of Grade 3-4 hyperglycaemia increased consistently in patients with higher body mass index and in patients with higher baseline haemoglobin A1c (HbA1c). The median time to onset of hyperglycemia was 0.6 months (range: 0.1 to 20.3). In the EV-201 (N=214) clinical study, at the time of their last evaluation, 61% of patients had complete resolution, and 19% of patients had partial improvement (see section 4.4 of the SPC). Peripheral neuropathy: In clinical studies peripheral neuropathy occurred in 52% (352) of the 680 patients treated with enfortumab vedotin 1.25 mg/kg. Four percent of patients experienced severe (Grade 3-4) peripheral neuropathy including sensory and motor events. The median time to onset of Grade ≥2 was 4.6 months (range: 0.1 to 15.8). In the EV-201 (N=214) clinical study, at the time of their last evaluation, 19% of patients had complete resolution, and 39% of patients had partial improvement (see section 4.4 of the SPC). Oculardisorders:In clinical studies, 30% of patients experienced dry eye during treatment with enfortumab vedotin 1.25 mg/kg. Treatment was interrupted in 1.3% of patients and 0.1% of patients permanently discontinued treatment due to dry eye. Severe (Grade 3) dry eye only occurred in 3 patients (0.4%). The median time to onset of dry eye was 1.7 months (range: 0 to 19.1 months) (see section 4.4 of the SPC). Prescribers should consult the full SPC in relation to other adverse reactions. Overdose: There is no known antidote for overdosage with enfortumab vedotin. In case of overdosage, the patient should be closely monitored for adverse reactions, and supportive treatment should be administered as appropriate taking into consideration the half-life of 3.6 days (ADC) and 2.6 days (MMAE). Cost (excluding VAT): POA. Legal classification: S1A. Marketing Authorisation numbers: PADCEV 20 mg powder for concentrate for solution for infusion EU/1/21/1615/001 PADCEV 30 mg powder for concentrate for solution for infusion EU/1/21/1615/002. Marketing Authorisation Holders: Astellas Pharma Europe B.V. Sylviusweg 62, 2333 BE Leiden, The Netherlands. Date of Preparation of Prescribing Information: November 2023. Job Bag Number: MAT-IE-PAD-2023-00014. Further information available from: Astellas Pharma Co. Ltd., Tel.: +353 1 467 1555. For full prescribing information, refer to the SPC, which may be found at www.medicines.ie
Adverse events should be reported. For Ireland, Healthcare professionals are asked to report any suspected adverse reactions via: HPRA Pharmacovigilance, Website: www.hpra.ie or Astellas Pharma Co. Ltd. Tel: +353 1 467 1555, E-mail: irishdrugsafety@astellas.com. This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. Thehyperlinksonthispagewilltakeyoutonon-Astellaswebsites.Astellasdoesnotendorseoracceptliabilityforsitescontrolled bythird-parties.
CI – confidence interval; HR – hazard ratio; LA – locally advanced; mOS – median overall survival; mUC – metastatic urothelial carcinoma; PD-1 – programmed death-1; PD-L1 – programmed death-ligand 1
Record attendance at DICE 2024 conference focusing on improving diabetes care in Ireland
On the 22nd of May, Diabetes Ireland Conference & Exhibition (DICE) saw its largest ever attendance with over 380 healthcare professionals working in the field of diabetes attending the event held in the Croke Park Conference Centre, Dublin. Throughout the day, delegates heard from a host of national and international speakers presenting on a wide range of topics and issues, covering paediatric diabetes care, pregnancy, adult Type 1 and Type 2 diabetes care all aimed at providing delegates with new practical information to enhance their continuing professional development.
From a Type 2 diabetes perspective, delegates were updated on current and new Type 2 diabetes and obesity medications and treatments, exercise and the new model of integrated care network in primary care. There were research presentations on epidemiological research to improve diabetes care and behavioural interventions to improve long-term Type 2 diabetes self-management.
Type 2 diabetes and pregnancy was also a hot topic for discussion with presentations on providing virtual gestational diabetes care services and enhancing pre-pregnancy care and Type 2 diabetes prevention following gestational diabetes. Other topics included metformin use in women with GDM and the benefits of technology in pregnancy care for women with pregestational diabetes and outcomes of retinal screening
in women with diabetes during pregnancy. Moreover, speakers from Ireland, UK and Denmark also shared their expertise about stigma associated with diabetes in pregnancy, and technology use to enhance diabetes management in pregnancy.
Diabetes technology loomed large in relation to topics around Type 1 diabetes management. Beginning from the topic of hypoglycaemia recognition in the age of continuous glucose monitoring systems (CGM), through to the findings on technology use in people with type 1 diabetes, based on the Diabetes Ireland survey on accessing care, as well as practical advice from Professor Rob Andrews, international expert in exercise and diabetes, who provided an excellent overview of diabetes self-management tactics for exercising with type 1 diabetes.
From a paediatric diabetes perspective, delegates learned about the use of hybrid closed loop systems in children and adolescents with diabetes and how to manage family conflict and collaboration in diabetes management. Delegates were also updated on the growing issue of Type 2 diabetes in children and adolescents, the prevention and prediction of vascular complications in youths and population screening for Type 1 diabetes. There were also presentations on the adolescent experiences of school life, and a report on the transition of care from paediatric to adult diabetes care units in Ireland.
Sinead Powell (Diabetes Ireland), Kate Gajewska (Diabetes Ireland), Prof. Sean Dinneen, Prof. Edward Gregg, Dr. Patrick Divilly, Dr Tomas Griffin, Ms. Marcia Carvalho and Dr. Darren Rattigan
The Keynote Lecture was delivered by Professor Partha Kar, Type 1 Diabetes and Technology Lead, NHS England, which focused on leading change to improve access to diabetes technology and the need for collaboration of all stakeholders to improve lives of those living with diabetes. The inspiring and very well-received talk from Professor Kar was followed by a session focusing on the gaps and improvements needed in diabetes health services and care in Ireland, and updates from the HSE national clinical leads in diabetes (paediatric –Professor Michael O’Grady, adult – Professor Derek O’Keeffe), and key leads in pregnancy (Professor Fidelma Dunne), diabetes registry (Professor Sean Dinneen) plus Diabetes Ireland Wellbeing focused initiatives (Ms Sinead Powell).
The panel discussion with all the above-mentioned speakers focused on the steps required to improve diabetes care with delegates encouraged to work together with people living with diabetes calling for a National Diabetes Strategy that would see improvements in local diabetes services nationwide. Confirmation that a strategy was very much on the radar of the Minister for Health was warmly welcomed bringing some hope that continuous collaboration and strong advocacy from the diabetes community will bring better care to people living with diabetes in Ireland.
‘It was great to see so many people attending the meeting and spending their day learning from the best international and national experts in all areas of diabetes care – commented Mr Kieran O’Leary, the CEO of Diabetes Ireland. –We would like to thank all the attendees, sponsors and speakers who made this day so remarkable and brought hope for further improvements in the care and lives of people living with diabetes in Ireland. A lot of organisation goes into DICE each year and I would also like to acknowledge my colleagues for delivering the best attended DICE conference ever. Roll on DICE 2025.
Professor Michael O'Grady, Ms Sinead Powell, Professor Sean Dinneen, Dr Kate Gajewska, Prof. Derek O'Keeffe, Professor Hilary Hoey (Chairperson, Diabetes Ireland), Professor Partha Kar and Professor Fidelma Dunne
RCSI Appoints Chair of Radiology
Professor Nuala Healy has been appointed Chair of Radiology at RCSI University of Medicine and Health Sciences. In her role, Professor Healy will lead RCSI’s academic Department of Radiology while providing patient care as a consultant radiologist at Beaumont Hospital.
Professor Healy completed her undergraduate medical training at University of Galway. Following basic surgical training, she undertook a lab-based MD and was awarded a Molecular Medicine Ireland Clinician Scientist Fellowship, and she also completed a master's in clinical education at the University of Galway.
Her radiology training was undertaken at St James’ Hospital, Dublin, followed by a breast imaging fellowship at the Mater Hospital, Dublin. She moved
to Addenbrooke’s Hospital, Cambridge, UK as a clinical fellow and was subsequently appointed as a breast and oncology radiologist.
Throughout her career, Prof. Healy has had multiple educational roles – from an early foundation as clinical lecturer and anatomy demonstrator for University of Galway, to more recently as Deputy Training Programme Director for Cambridge University Hospital radiology trainees.
She is the research lead for the British Society of Breast Radiology, a trustee of Symposium Mammographicum and chair of the organising committee for the Cambridge Conference on Breast Cancer imaging. She is member of the editorial board for Cancer Imaging, where she is editor of the breast section, and a member
Professor Nuala Healy, Chair of Radiology, RCSI University of Medicine and Health Sciences
of the scientific editorial board of Insights into Imaging.
She is involved in multiple breast imaging studies, and her research interests include AI in radiology, novel techniques in breast imaging, MRI (including abbreviated breast MRI), surveillance and postoperative breast imaging, and novel ways of measuring bone health in women with a history of breast cancer.
Prof. Healy is chair of the organising committee for the Cambridge Conference on Breast Cancer Imaging. She also has a clear focus on issues around wellbeing and the contribution of role models and mentors in medicine.
Urgent Call to ‘Make Lupus Visible’
Arthritis Ireland and AstraZeneca Ireland have come together this World Lupus Day to call for people living with lupus to share their stories to increase visibility of the autoimmune condition and its impact on patients.
Lupus, also known as Systematic Lupus Erythematosus (SLE), is a complex autoimmune disease that is experienced differently by each person and causes a variety of symptoms, including skin rash, joint pain, swelling and fevers. It is an often under recognised condition that can take many years to be
diagnosed and disproportionately affects women within the 15–45-year-old age cohort.
Arthritis Ireland conducted a new survey to understand the impact of lupus and to know more about the day-to-day problems that affect those living with the disease. 90% of those surveyed indicated that lupus negatively impacts physical activity and their ability to exercise. 69% said lupus negatively impacts their family life and over 70% of those surveyed reported that the condition negatively impacts on their career, with many having
to take prolonged time off work. Respondents also indicated a negative impact on their mental health due to their disease with anxiety (57%), loneliness (45%) and depression (36%) featuring strongly.
As part of their joint initiative, Arthritis Ireland and AstraZeneca Ireland are calling on people living with lupus or who have family with the condition to share their stories online using the hashtag #makelupusvisible.
Commenting on the results of this survey, Arthritis Ireland chief executive Gráinne O’Leary said, “The results of this Arthritis Ireland survey clearly indicate the huge impact lupus has on the day-today lives of those living with the disease. As lupus predominately affects women between the ages of 15 and 45, it can have a significant impact on fertility and on family life in general. There is a financial burden as well with many patients having to take time off work. At Arthritis Ireland, we
provide support and resources for those living with lupus and through this campaign are aiming to increase awareness of the condition amongst the general public.”
In Ireland, Lupus is recognised as a relatively uncommon condition, but its exact prevalence is difficult to determine due to the complexity of its diagnosis, variability of its symptoms, and lack of official data on prevalence. There is also a large unmet need in relation to effective and targeted treatments for lupus.
Speaking to the difficulties of diagnosing lupus and the lack of dedicated treatments, Professor Gráinne Murphy, Consultant Rheumatologist from Cork University Hospital said,
“Lupus remains a challenging diagnosis to treat. While there have been significant therapeutic advances in many other immunemediated conditions, there have been many disappointments in clinical trials for SLE. In more recent times, reassuringly, there have been some positive developments in clinical research which have led to the development of a limited number of new therapies. Unfortunately, these agents are not yet widely available and equity of access remains an issue. There remains a significant need for more effective treatment options.”
Ruth Levins from Drogheda who lives with lupus and Arthritis Ireland chief executive Gráinne O’Leary
NOW AVAILABLE*
• Delivers extended durability with ~80% of patients on Q12W or Q16W treatment intervals at Year 21
• Demonstrated comparable safety profile to aflibercept over 2 years1,2 >2M DOSES globally of Dual-Pathway inhibiton, since Jan 20223
THIS MATERIAL IS INTENDED FOR HEALTHCARE PROFESSIONALS WORKING IN IRELAND ONLY.
Pharmacovigilance and adverse event reporting information can be found below. *Now available in some private health insurer settings.
Vabysmo ▼(faricimab) 120 mg/mL solution for injection (each vial contains 28.8 mg faricimab in 0.24 mL solution. This provides a usable amount to deliver a single dose of 0.05 mL solution containing 6 mg of faricimab).
▼This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. See box below for details on how to report. Therapeutic Indications: Vabysmo is indicated for the treatment of adult patients with: neovascular (wet) age-related macular degeneration (nAMD); visual impairment due to diabetic macular oedema (DME). Posology and Method of Administration: This medicinal product must be administered by a qualified physician experienced in intravitreal injections. Each vial should only be used for the treatment of a single eye. nAMD: the recommended dose is 6 mg (0.05 mL solution) administered by intravitreal injection every 4 weeks (monthly) for the first 4 doses. Thereafter, an assessment of disease activity based on anatomic and/or visual outcomes is recommended 20 and/or 24 weeks after treatment initiation so that treatment can be individualised. In patients without disease activity, administration of faricimab every 16 weeks (4 months) should be considered. In patients with disease activity, treatment every 8 weeks (2 months) or 12 weeks (3 months) should be considered. If anatomic and/or visual outcomes change, the treatment interval should be adjusted accordingly, and interval reduction should be implemented if anatomic and/or visual outcomes deteriorate. There is limited safety data on treatment intervals of 8 weeks or less between injections. Monitoring between the dosing visits should be scheduled based on the patient’s status and at the physician’s discretion, but there is no requirement for monthly monitoring between injections. DME: the recommended dose is 6 mg (0.05 mL solution) administered by intravitreal injection every 4 weeks (monthly) for the first 4 doses. Thereafter, treatment is individualised using a treat-and-extend approach. Based on the physician’s judgement of the patient’s anatomic and/or visual outcomes, the dosing interval may be extended up to every 16 weeks (4 months), in increments of up to 4 weeks. If anatomic and/or visual outcomes change, the treatment interval should be adjusted accordingly, and interval reduction should be implemented if anatomic and/or visual outcomes deteriorate. Treatment intervals shorter than 4 weeks between injections have not been studied. Monitoring
inflammation, rhegmatogenous retinal detachment, retinal tear and iatrogenic traumatic cataract. Proper aseptic injection techniques must always be used when administering Vabysmo. Patients should be instructed to report any symptoms, such as pain, loss of vision, photophobia, blurred vision, floaters, or redness, suggestive of endophthalmitis or any of the above-mentioned adverse reactions without delay, to permit prompt and appropriate management. Patients with increased frequency of injections may be at increased risk of procedural complications. Intraocular pressure increases: transient increases in intraocular pressure (IOP) have been seen within 60 minutes of intravitreal injection, including those with faricimab. Special precaution is needed in patients with poorly controlled glaucoma (do not inject Vabysmo while the IOP is ≥ 30 mmHg). In all cases, both the IOP and perfusion of the optic nerve head must be monitored and managed appropriately. Systemic effects: systemic adverse events including arterial thromboembolic events have been reported following intravitreal injection of vascular endothelial growth factor (VEGF) inhibitors and there is a theoretical risk that these may be related to VEGF inhibition. A low incidence rate of arterial thromboembolic events was observed in the faricimab clinical trials in patients with nAMD and DME. There are limited data on the safety of faricimab treatment in DME patients with high blood pressure (≥ 140/90 mmHg) and vascular disease, and in nAMD patients ≥ 85 years of age. Immunogenicity: as this is a therapeutic protein, there is a potential for immunogenicity with faricimab. Patients should be instructed to inform their physician of any signs or symptoms of intraocular inflammation such as vision loss, eye pain, increased sensitivity to light, floaters or worsening eye redness, which might be a clinical sign attributable to hypersensitivity against faricimab. Bilateral treatment: the safety and efficacy of faricimab administered in both eyes concurrently have not been studied. Bilateral treatment could cause bilateral ocular adverse reactions and/or potentially lead to an increase in systemic exposure, which could increase the risk of systemic adverse reactions. Until data for bilateral use become available, this is a theoretical risk for faricimab. Concomitant use of other anti-VEGF: there are no data available on the concomitant use of faricimab with anti-VEGF medicinal products in the same eye. Faricimab should not be administered concurrently with other anti-VEGF medicinal products (systemic or ocular). Withholding treatment: treatment should be withheld in patients with: •Rhegmatogenous retinal
For the treatment of adult patients with: neovascular (wet) age-related macular degeneration (nAMD); visual impairment due to diabetic macular oedema (DME)4
tears. RPE tears are common in nAMD patients with PED, treated with IVT anti-VEGF agents including faricimab. There was a higher rate of RPE tear in the faricimab group (2.9%) compared to aflibercept group (1.5%). The majority of events occurred during the loading phase, and were mild to moderate, without impact on vision. Populations with limited data: there is only limited experience in the treatment of nAMD patients ≥ 85 years, and DME patients with type I diabetes, patients with HbA1c over 10%, patients with high-risk proliferative diabetic retinopathy (DR), high blood pressure (≥ 140/90 mmHg) and vascular disease, sustained dosing intervals shorter than every 8 weeks (Q8W), or nAMD and DME patients with active systemic infections. There is limited safety information on sustained dosing intervals of 8 weeks or less and these may be associated with a higher risk of ocular and systemic adverse reactions, including serious adverse reactions. There is also no experience of treatment with faricimab in diabetic patients with uncontrolled hypertension. This lack of information should be considered by the physician when treating such patients. Sodium content: This medicinal product contains less than 1 mmol sodium (23 mg) per dose, that is to say essentially “sodium-free”. Interactions: No interaction studies have been performed. Based on the biotransformation and elimination of faricimab, no interactions are expected. However, faricimab should not be administered concurrently with other systemic or ocular anti-VEGF medicinal products. Fertility, Pregnancy and Lactation: Women of childbearing potential: should use effective contraception during treatment and for at least 3 months following the last intravitreal injection of faricimab. Pregnancy: there are no or limited amount of data from the use of faricimab in pregnant women. The systemic exposure to faricimab is low after ocular administration, but due to its mechanism of action (i.e. VEGF inhibition), faricimab must be regarded as potentially teratogenic and embryo-/foetotoxic. Faricimab should not be used during pregnancy unless the potential benefit outweighs the potential risk to the foetus. Breast-feeding: it is unknown whether faricimab is excreted in human milk. A risk to the breast-fed newborn/infant cannot be excluded. Vabysmo should not be used during breast-feeding. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from faricimab therapy taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman. Fertility: no effects on reproductive organs or fertility were observed in a 6-month cynomolgus monkey study with
Uncommon (≥ 1/1,000 to < 1/100): vitreous haemorrhage, ocular discomfort, eye pruritus, ocular hyperaemia, blurred vision, iritis, uveitis, iridocyclitis, vitritis, sensation of foreign body, endophthalmitis, retinal tear, conjunctival hyperaemia, procedural pain, reduced visual acuity, rhegmatogenous retinal detachment. Rare ((≥ 1/10,000 to < 1/1,000): transiently reduced visual acuity, traumatic cataract. Not known (frequency cannot be estimated from the available data): retinal vasculitis, retinal occlusive vasculitis. Refer to SmPC for full listings of adverse events. Refer to SmPC section 4.8 for instructions on reporting of suspected adverse events. Legal Category: Product subject to prescription which may not be renewed (A). Presentation(s) and Marketing Authorization Number(s): one mL of solution contains 120 mg of faricimab (EU/1/22/1683/001). Marketing Authorisation Holder: Roche Registration GmbH, Emil-Barell-Strasse 1, 79639 Grenzach-Wyhlen, Germany. Vabysmo® is a registered trademark. Further information is available from Roche Products (Ireland) Limited, 3004 Lake Drive, Citywest, Naas Road, Dublin 24. Telephone: (01) 4690700. Date of API Preparation: March 2024.
▼ This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions.
In the event of a suspected adverse reaction, please report it to: The Drug Surveillance Centre Roche Products (Ireland) Limited Telephone: (01) 4690700
Email: ireland.drug_surveillance_centre@roche.com
Or alternatively, report to: HPRA Pharmacovigilance Website: www.hpra.ie
Vabysmo® Summary of Product Characteristics [SmPC] is available on www.medicines.ie. M-IE-00001770 - based on Vabysmo SmPC dated 08 February 2024
Blood Cancer
Enfortumab Vedotin With
or Without Pembrolizumab
in
Cisplatin-Ineligible Patients With Previously Untreated
Locally Advanced or Metastatic Urothelial Cancer
Peter H. O’Donnell, MD1; Matthew I. Milowsky, MD2; Daniel P. Petrylak, MD3; Christopher J. Hoimes, DO4; Thomas W. Flaig, MD5, Nataliya Mar, MD6; Helen H. Moon, MD7; Terence W. Friedlander, MD8; Rana R. McKay, MD9; Mehmet A. Bilen, MD10; Sandy Srinivas, MD11; Earle F. Burgess, MD12; Chethan Ramamurthy, MD13; Saby George, MD14; Daniel M. Geynisman, MD15; Sergio Bracarda, MD16; Delphine Borchiellini, MD17; Lionnel Geoffrois, MD18; Jose Pablo Maroto Rey, MD19; Christiano Ferrario, MD20; Anne-Sophie Carret, MD21; Yao Yu, PhD21; Maria Guseva, MD, PharmD22; Blanca Homet Moreno, MD, PhD23; and Jonathan E. Rosenberg, MD24
RandomAssignmentandTreatment
Enrolledpatientswererandomlyassigned1:1toreceiveEV aloneorincombinationwithPembro.Randomassignment wasstratifiedbyECOGPS(0 v 1or2)andlivermetastasis (present v absent)atbaseline.EVwasadministeredatadose of1.25mgperkilogramofbodyweight(maximumtotaldose of125mg)asasingleintravenousinfusionover30minutes ondays1and8ofa3-weekcycle.Pembrowasadministered atadoseof200mgasasingleintravenousinfusionover 30minutesonday1ofa3-weekcycle.Dosemodifications andreductionswerepermittedtomanagetreatment-related adverseevents(TRAEs)asdescribedinthestudyProtocol.
The occurrence of urothelial cancer is increasing worldwide, with locally advanced or metastatic urothelial cancer (la/ mUC demonstrating an especially poor prognosis.1-4 Cisplatin-based chemotherapy is the gold standard first-line (1L) treatment in patients with la/mUC, but approxi-mately half of all patients are ineligible for 1L cisplatin-based chemotherapy because of impaired renal function, poor performance status, and other comorbidities.5-8 Carboplatin plus gemcitabine is a commonly used regimen for cisplatin-ineligible patients but has shown lower activity and poor tolerability.9-12 Other therapeutic options exist but are limited to subgroups of patients; avelumab maintenance therapy is approved for patients who have remained free from disease progression after 1L platinum-based treatment and has shown improved survival; however, only patients who do not progress after four to six cycles of 1L therapy are eligible.13,14 Singleagent PD-1/PD-L1 checkpoint inhibitors (CPIs) may be another 1L option for cisplatin-ineligible patients; however, they have become increasingly restricted to certain pop-ulations. In the United States currently, pembrolizumab (Pembro) is limited to 1L patients who are not eligible for any platinum-based chemotherapy.15-19 Additionally, approximately 60% of cisplatin-ineligible patients with la/mUC who receive 1L treatment do not receive second-line (2L) treatment.20 This underscores the need for effi-cacious and tolerable 1L therapies.
1University of Chicago, Chicago, IL - 2University of North Carolina Lineberger Comprehensive Cancer Center, Chapel Hill, NC - 3Yale Cancer Center, New Haven, CT - 4Duke Cancer Institute, Duke University, Durham, NC - 5University of Colorado Comprehensive Cancer Center, Aurora, CO 6University of California at Irvine, Irvine, CA - 7Kaiser Permanente Southern California, Riverside, CA - 8University of California at San Francisco, San Francisco, CA 9University of California at San Diego, San Diego, CA - 10Emory University Winship Cancer Institute, Atlanta, GA - 11Stanford Cancer Center, Stanford, CA 12Levine Cancer Center, Charlotte, NC - 13University of Texas Health Sciences Center at San Antonio, San Antonio, TX - 14Roswell Park Cancer Center, Buffalo, NY - 15Fox Chase Cancer Center, Temple University Health System, Philadelphia, PA - 16Azienda Ospedaliera Santa Maria di Terni, Terni, Italy 17Centre Antoine Lacassagne, Universit´eCˆote d’Azur, Nice, France 18Institut de Cancerologie de Lorraine, Vandoeuvre Les Nancy, France 19Hospital de la Santa Creu i Sant Paul, Barcelona, Spain - 20Jewish General Hospital, Montreal, Quebec, Canada - 21Seagen Inc, Bothell, WA - 22Astellas Pharma, Northbrook, IL - 23Merck & Co Inc, Rahway, NJ - 24Memorial Sloan Kettering Cancer Center, New York, NY
Enfortumab vedotin (EV), an antibody-drug conjugate (ADC), comprises a fully human monoclonal antibody specific for nectin-4 and monomethyl auristatin E (MMAE). EV delivers MMAE to cells expressing nectin-4, leading to cell cycle arrest and cell death. Pembro is an anti–PD-1 antibody that uses the PD-1 receptor as a therapeutic
target and has antitumor activity in multiple tumor types.16
EV and Pembro as individual agents have shown overall survival (OS) benefits compared with 2L or third-line treatment in patients with la/mUC.16,21,22 Preclinical data have shown that vedotin ADCs, including EV, in combination with PD-1/PD-L1 inhibitors such as
Pembro, may enhance antitumor activity relative to their respective mechanisms of action and support complimentary efficacy.23-25
In the phase Ib/II study EV-103, results from the Dose Escalation/ Cohort A demonstrated high antitumor activity and durable responses with encouraging survival and a manageable safety
Randomly assigned 1:1 (N = 151)
EV + Pembro (n = 77)
Treated (n = 76)
Patients off treatment (n = 51)
(n = 33)
(n = 12)
decision (n = 4)
decision (n = 1)
(n = 1)
Discontinued study (n = 23) Patient withdrawal of consent (n = 2)
(n = 20)
(n = 1)
(n = 73) EV monotherapy (n = 74) Patients off treatment (n = 65)
(n = 40) AE (n = 18)
Patient decision (n = 3)
Physician decision (n = 3)
Others (n = 1)
Remained on treatment (n = 25) Remained on treatment (n = 8)
profile for EV plus Pembro (EV 1 Pem-bro), providing the rationale for further evaluation.26 Randomized Cohort K is intended to provide efficacy and safety data on the treatment combination. The EV monotherapy arm was included to better understand the safety and effi-cacy of EV monotherapy in 1L cisplatin-ineligible patients. No statistical comparison between treatment arms was performed.
Here, we present the efficacy and safety results of EV-103 randomized Cohort K for cisplatinineligible patients with la/mUC treated with EV 1 Pembro or EV monotherapy in the 1L setting.
PATIENTS AND METHODS
Trial Participants
In Cohort K of the EV-103 study, eligible patients were 18 years or older with histologically documented la/mUC, including squamous differentiation or mixed cell types. Patients had an Eastern Cooperative Oncology Group performance status (ECOG PS) of 2 or less and were eligible for Pembro therapy. Patients in Cohort K were deemed ineligible for cisplatin-based chemotherapy on the basis of at least one of the following: glomerular filtration rate (GFR) <60 mL/min and ≥30 mL/min, grade ≥ 2 hearing loss, ECOG PS of 2, or New York Heart Association (NYHA) Class III heart failure. Patients with an ECOG PS of 2 met additional criteria: hemoglobin ≥ 10 g/dL, GFR ≥ 50 mL/min, and no NYHA Class III heart failure. Patients were excluded from the trial if they had any of the following: previous systemic treatment for locally ad-vanced or metastatic disease, including adjuvant/ neoadjuvant platinum-based therapy within 12 months before random assignment, previous treatment with a PD-1, PD-L1, or PD-L2 inhibitor, or any previous treatment with stimulatory or coinhibitory T-cell receptor agents, previous treatment with EV or another MMAE-based ADC, ongoing grade 2 or higher sensory or motor neuropathy, or ongoing clinically significant toxic effects associated with previous treatment, active central nervous system metastases, or uncontrolled diabetes (defined as hemoglobin A1c [HbA1c] ≥ 8% or HbA1c 7%to <8% with associated diabetes symptoms [polyuria or polydipsia] that were not otherwise explained). Full eligibility criteria are provided in the study Protocol (online only).
Random Assignment and Treatment
Enrolled patients were randomly assigned 1:1 to receive EV alone
or in combination with Pembro. Random assignment was stratified by ECOG PS (0 v 1 or 2) and liver metastasis (present v absent) at baseline. EV was administered at a dose of 1.25 mg per kilogram of body weight (maximum total dose of 125 mg) as a single intravenous infusion over 30 minutes on days 1 and 8 of a 3-week cycle. Pembro was administered at a dose of 200 mg as a single intravenous infusion over 30 minutes on day 1 of a 3-week cycle. Dose modifications and reductions were permitted to manage treatment-related adverse events (TRAEs) as described in the study Protocol.
Trial Oversight
The study was designed by the sponsors in collaboration with an advisory committee. The trial received approval from site independent institutional review boards or ethics committees and was conducted in accordance with the ethics principles of the Declaration of Helsinki and with Good Clinical Practice guidelines defined by the International Council for Harmonization. All patients provided written informed consent. The trial was sponsored by Seagen Inc (Bothell, WA), Astellas Pharma (Northbrook, IL), and Merck Sharp & Dohme LLC (Rahway, NJ). The authors vouch for the accuracy and completeness of the data and for the adherence of the trial to the Protocol.
End Points
The primary end point was confirmed objective response rate (cORR; proportion of patients with a complete or partial response) per RECIST version 1.1 by blinded independent central review (BICR). Secondary end points were cORR by investi-gator, disease control rate (DCR) by BICR and investigator assessment, duration of response (DOR) and progression-free survival (PFS) by BICR and investigator assessment, OS, and safety and tolerability of EV monotherapy and EV 1 Pembro. Exploratory end points included biomarkers of activity, including baseline PD-L1 status and nectin-4 expression.
Assessments
Investigators assessed and confirmed antitumor activity by reviewing computed tomography scans or magnetic resonance imaging with or without intravenous contrast of the chest, abdomen, and pelvis. Patients were evaluated for response assessments using the same imaging method throughout the study. Bone and brain scans were required at screening and repeated if positive at baseline and/or if clinically indicated.
Objective responses were confirmed per RECIST version 1.1, with repeat scans 4-5 weeks after a first documented response. Subsequent response assessments were timed from cycle 1 day 1 and were performed every 9 weeks (67 days) until 1 year after the first dose and then every 12 weeks (67days).
EV adverse events of special interest (AESIs) are medical concepts/composite terms used to characterise identified and potential risks for EV. AESI time-to-onset is calculated as time from the date of the first dose to the start date of the first treatment emergent event that meets the respective AESI search criteria. TRAEs were determined by the inves-tigator and assessed
for both arms. Pembro AESIs (AEOSIs), including immunemediated adverse events (AEs) and in-fusion reactions, were evaluated using previously described criteria for Pembro monotherapy.16
Treatment discontinuations were summarised according to the percentage of patients who had TRAEs leading to discontinuation of either agent, including patients who had TRAEs leading to discontinuation of EV only, Pembro only, or both. Of note, discontinuations because of each agent alone, or both, are counted by patient and are not mutually exclusive.
(43.4%). The primary disease location was the lower tract (60.5%). Visceral metastases were present in 84.2% of patients, including 17.1% with liver metastases. At baseline, 57.9% of patients had low PD-L1 expression (defined as CPS < 10) (Table 1). The median nectin-4 H-score at baseline was 262.5 (interquartile range [IQR], 200.0-297.0).
Baseline characteristics of patients in the monotherapy arm are summarized in Table 1. The median H-score at baseline was 284.0 (IQR, 240.0-298.0).
Efficacy
In patients treated with EV 1 Pembro (N 5 76), the cORR by BICR was 64.5% (95% CI, 52.7 to 75.1; 49 of 76 patients). Eight patients (10.5%) had a complete response; 41 patients (53.9%) achieved a partial response; the median time to response was 2.1 months (range, 1.1-6.6; Fig 2). A total of 97.1% of assessable patients had a reduction in their target lesions per BICR (Fig 2). The median DOR per BICR has not yet been reached; 65.4% of responders maintained a response at 12 months (Fig 3). The DCR was 86.8% (95% CI, 77.1 to 93.5; 66 of 76 patients). The PFS rate per BICR at 6 and 12 months was 73.8% and 55.1%, respectively, and the OS rate at 6 and 12 months was 88.2% and 80.7%, respectively (Fig 4). The median OS was 22.3 months (95% CI,19.09 to not achieved) with 54 (of 76) patients remaining on study for OS follow-up at the time of data cutoff (Appendix Fig A1, online only).
tumor tissue using analytically validated im-munohistochemistry (IHC) assays. Nectin-4 expression was evaluated at Q2 Solutions as described previously, and stained slides were scored by a pathologist to generate an H-score (range, 0-300).27 PD-L1 expression was assessed using the Agilent PD-L1 IHC 22C3 pharmDx assay, with stained slides scored by a pathologist to generate a PD-L1 combined positive score (CPS; low, <10; high, ≥10).
Statistical Analysis
each treatment arm. No statistical comparisons were made between treatment arms; EV monotherapy arm was included for isolation of the monotherapy contribution. Secondary end points, cORR by investigator assessment and DCR by BICR and investigator assessment, were summarised with two-sided 95% CIs using the Clopper-Pearson method. DOR and PFS by BICR and by investigator assessment and OS were analyzed using Kaplan-Meier methodology. ORR, DOR, and PFS are presented by BICR in results.
The cORR in prespecified subgroups in the combination arm (including PD-L1 expression, liver metastasis, ECOG PS, and primary disease site of origin) was consistent with overall cORR (Appendix Fig A2, online only).
Nectin-4 expression was generally high as indicated by median H-score in the combination arm, and the distribu-tion was similar between responders (median, 260.0; IQR, 200.0-297.0) and nonresponders (270.0; 155.0-300.0; Ap-pendix Fig A3, online only).
Efficacy and safety end points were assessed for all patients who received EV 1 Pembro or EV monotherapy. The sample size was based on the precision of the estimate for objective response rate (ORR) as characterised by 95% CIs. The cORR by BICR was summarized with two-sided 95% CI and calculated using the Clopper-Pearson method for
Patient Disposition and Baseline Characteristics
A total of 151 patients were randomly assigned and 149 re-ceived EV 1 Pembro (N 5 76) or EV monotherapy (N 5 73; Appendix Table A1, online only). Two patients, one in each arm, were randomly assigned but never
received corre-sponding study treatment (Fig 1). At data cutoff (June 10, 2022), 29 patients in the combination arm had discontinued treatment but remained in the study in long-term follow-up. The median follow-up on study was 14.8 months (95% CI, 12.9 to 17.3) in the combination arm and 15.0 months (95% CI, 12.7 to 17.4) in the monotherapy arm. The median duration of treatment was 9.0 months (range, 0.6-26.1) in the combination arm with patients receiving a median of 11.0 cycles (range, 1-29). The median duration of treatment was 5.5 months (range, 0.5-26.9) in the monotherapy arm with patients receiving a median of 8.0 cycles (range, 1-33).
In the combination arm, patients were predominately male (71.1%) and White (80.3%), with a median age of 71 years (range, 51-91 years). Most patients had an ECOG PS of 0 (43.4%) or 1
In the monotherapy arm, the cORR per BICR was 45.2% (95%CI, 33.5 to 57.3; 33 of 73 patients; Fig 2). The DOR was 13.2 months (range, 6.14-15.97), and the median time to response was 2.1 months (range, 1.9-15.4). The DCR was 79.5% (95% CI, 68.4 to 88.0; 58 of 73 patients). The 12-month PFS and OS were 35.8% and 70.7%, respectively (Fig 5). The cORR per BICR for prespecified subgroups can be found in Appendix Figure A2. The nectin-4 H-score
median and distribution were similar between responders and nonresponders (Appendix Fig A3).
The concordance rate of best overall response per RECIST between BICR and investigator assessments was 86.7% in the combination arm and 85.5% in the monotherapy arm.
Safety
In patients treated with the combination, the most common TRAEs were fatigue, peripheral sensory neuropathy, alopecia, and maculopapular rash; the most common grade 3 or higher event was maculopapular rash (Table 2). Eighteen (23.7%) patients experienced a serious TRAE, and three (3.9%) patients died due to a TRAE (respiratory failure, pneumonitis, and sepsis). TRAEs leading to dose interrup-tions of either EV or Pembro occurred in 68.4% of patients. TRAEs leading to discontinuation of EV and/or Pembro are listed in Table 2. The most frequently occurring TRAEs leading to discontinuation of either agent was peripheral neuropathy (nine of 76 patients, 11.8%) and of EV only was peripheral neuropathy (nine of 76 patients, 11.8%) and Pembro only was pneumonitis (three of 76 patients, 3.9%). TRAEs leading to discontinuation of both agents were peripheral motor neuropathy, myasthenia gravis, pneumonitis, and sepsis (one patient [1.3%] each).
Treatment-related EV AESIs in the combination arm were peripheral neuropathy (46 of 76 patients, 60.5%), skin reactions (51 of 76 patients, 67.1%), hyperglycemia (11 of 76 patients, 14.5%), ocular events (20 of 76 patients, 26.3%), and infusion-related reactions (three of 76 patients, 3.9%; Appendix Table A2, online only). Grade 3 or higher skin reactions, peripheral neuropathy, and hyperglycemia in the combination arm occurred in 16 of 76 (21.1%), two of 76 (2.6%), and five of 76 (6.6%) pa-tients, respectively. No serious skin reactions occurred, including no severe cutaneous adverse reaction events. One patient experienced serious peripheral neuropathy (1.3%).
FIG4. EV 1 Pembro.(A)PFSperBICR,byRECISTv1.1,OS,andmedianfollow-uptime.(B)Kaplan-MeierestimateofPFSperBICRbyRECISTv1.1. (C)Kaplan-MeierestimateofOS.PreliminarymPFSandmOSarereportedhereandareexpectedtoevolveovertime.Atthetimeofdatacutoff,54 (of76)patientsremainonstudyforOSfollow-up.BICR,blindedindependentcentralreview;EV,enfortumabvedotin;mOS,medianoverallsurvival; mPFS,medianprogression-freesurvival;OS,overallsurvival;Pembro,pembrolizumab;PFS,progression-freesurvival;v1.1,version1.1.
The most frequent Pembro treatment-emergent AEOSIs in the combination arm were severe skin reactions (21 of 76 patients, 27.6%) and hypothyroidism (10 of 76 patients, 13.2%); the most common grade 3 or higher AEOSIs were severe skin reactions (15 of 76 patients, 19.7%) and pneumonitis (four of 76 patients, 5.3%; Appendix Table A3, online only). Pembro AEOSIs associated with the use of systemic steroids are reported in the Protocol.
follow-up, which are trending similarly to median OS found in previously dis-closed Dose Escalation/Cohort A data. The safety profile of the combination was manageable and consistent with results from Cohort A of EV-103, with no new safety concerns emerging.26,35
Most skin reactions and peripheral neuropathy events were grade ≤ 2 in severity, consistent with observations in the previously reported results for EV-103 Dose Escalation/Cohort
A. Skin reactions (including the Pembro AEOSI category of severe skin reactions) and pneumonitis are an identified part of the safety profile for both EV and Pembro monotherapy and were more frequently observed in the combination arm. Higher rates of skin reactions were managed with EV treatment in-terruption, dose reduction, treatment discontinuation (EV and/or Pembro), and/or corticosteroids, as previously described.36,37 The safety results highlight theimportanceofeducatingboth health care practitioners and patients; early intervention for AEs are key components of successfully treating patients with the combination.
TRAEs and deaths in patients treated with monotherapy are summarized in Table 2. The most frequent treatment-related EV AESIs reported in patients in the monotherapy arm were peripheral neuropathy and skin reactions (Ap-pendix Table A2).
medianDORhasnotyetbeenreachedforthecombination arm.Theseresultsstandoutfromhistoricaldatafor gemcitabineandcarboplatinchemotherapyandcon firm the findingsofEV-103DoseEscalation/CohortA.These datasuggestthattheEVplusPembrocombinationrepresentsapotentialnewtherapeuticoptionasa1Lregimenfor cisplatin-ineligiblepatientswithla/mUC.
a potential new therapeutic option as a 1L regimen for cisplatinineligible patients with la/mUC.
Approximately half of all patients with la/mUC are unfit for 1L cisplatin-based chemotherapy, and limited 1L therapeutic options exist for these patients.20,28 Carboplatin plus gemcitabine is currently a standard option for cisplatin-ineligible patients but is associated with low response rate (approximately 36%-42%), short DOR (6.3-7.1 months), and relatively poor tolerability.9,29,30 In this study of cisplatin-ineligible patients with la/mUC, EV in combina-tion with Pembro showed a 64.5% overall response rate, with responses lasting beyond 1 year for 65.4% of responders, trending similarly with previously disclosed data from EV-103 Dose Escalation/Cohort A.26 Additionally, the median DOR has not yet been reached for the combination arm. These results stand out from historical data for gemcitabine and carboplatin chemotherapy and confirm the findings of EV-103 Dose Escalation/Cohort A. These data suggest that the EV plus Pembro combination repre-sents
Pembro is an US Food and Drug Administration–approved option that has shown durable responses as monotherapy but is currently restricted in the 1L setting to platinum-ineligible patients.16,19,31 Avelumab maintenance therapy has shown a survival benefit compared with observation after platinum-based chemotherapy, but it is only an option for patients who remain free from disease progression after four to six cycles of 1L platinum-based therapy. In fact, modeling data suggest that approximately half of patients with la/mUC may not be eligible for maintenance therapy.14 Despite the availability of these therapies, approximately 60% of cisplatinineligible patients with la/mUC who re-ceive 1L treatment never receive 2L treatment, likely because of early progression, tolerability, or short DORs.20 At the time of the primary analysis, the minority of patients in this study had data captured on subsequent therapies; thus this study required additional follow-up to determine whether there is any potential effect from subsequent treatments on patient outcomes.
safety profile so that a larger proportion of the cisplatinineligible population with la/mUC receives more durable therapeutic benefit. In this study, the overall re-sponse rates reported for patients in Cohort K (from ei-ther arm) numerically exceeded those reported in trials for the current standard for cisplatin-ineligible patients, gemcitabine plus carboplatin, or for PD-1/PD-L1 CPIs as monotherapies.16,17,19,32,33
A high unmet need remains for a highly efficacious 1L treatment option with rapid and durable responses and a manageable
Although the primary objective was to evaluate the efficacy and safety of the combination, the monotherapy arm was studied to characterize the activity of EV alone in this patient population. The overall response rate of patients treated with EV in the monotherapy arm was 45.2%. The monotherapy arm demonstrated a manageable safety profile, consistent with previous EV monotherapy studies.22,26,34
The ORRs observed in this study were consistent across a range of prespecified subgroups, including patients with liver metastases, and antitumor activity was seen regardless of PD-L1 status. High nectin-4 expression was observed, and the median and distribution was similar between responders and nonre-sponders. The preliminary PFS and OS results reported here are promising, and data will evolve with additional
It isimportanttonote thatthisstudy wasnotdesignedtomake statistical comparisons between arms. Similarly, although the cORR found in the EV 1 Pembro cohort is numerically higher than contemporary studies, including even cisplatin-based chemotherapy arms, the study was not designed as a direct comparison with current standardof-care regimens. This study builds on the promising results from Dose Escalation/Cohort A and further justifies the ongoing investigation of EV with Pembro in a randomized, phase III study compared with cisplatin or carboplatin plus gemcitabine in biomarker-unselected 1L patients (EV-302/KN-A39, ClinicalTrials. gov identifier: NCT04223856). EV 1 Pembro are also being evaluated in muscle invasive bladder cancer in randomized phase III trials (EV-303/KN-905, ClinicalTrials.gov identifier: NCT03924895 and EV304/KNK-B15, ClinicalTrials.gov identifier: NCT04700124).
In conclusion, in the 1L cisplatinineligible la/mUC patient population with high unmet need, EV 1 Pembro had a manageable safety profile and resulted in a high ORR with durable responses and encouraging PFS and OS results, which will evolve with follow-up. These results from Cohort K add to the previously reported re-sults from Dose Escalation/Cohort A of
this study and indicate that this combination may represent a new 1L treatment option for a patient population with high unmet need.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Disclosures provided by the authors are available with this article at DOI https://doi. org/10.1200/JCO.22.02887.
DATA SHARING STATEMENT
Deidentified patient-level trial data that underlie the results reported in this publication will be made available on a case-by-case basis to researchers who provide a methodologically sound proposal. Additional documentation may also be made available. Data availability will begin after approval of the qualified request and end 30 days after receipt of data sets. All requests can be submitted to CTDR@seagen.com and will be reviewed by an internal review committee. Please note that the data sharing policy of this clinical study’s sponsor, Seagen Inc, requires all requests for clinical trial data be reviewed to determine the qualification of the specific request. This policy is available at https:// www.seagen.com/healthcareprofessionals/clinical-data-requests and is aligned with BIO’s Principles on Clinical Trial Data Sharing (available at https://www.bio.org/ blogs/principles-clinical-trial-datasharing-reaffirm-commitment).
Report Calls for More Staff to Open Critical Care Unit
The National Office of Clinical Audit (NOCA) has published its Irish Paediatric Critical Care Audit National Report 2021-2022, highlighting the requirement for detailed workforce planning to be in place. This will safely maintain the current number of Paediatric Critical Care Unit (PCCU) beds and realise the planned increase in beds in order to open the National Children’s Hospital (NCH) Critical Care Unit in line with national standards.
This report underscores the urgency of addressing detailed workforce planning to ensure the hospital can meet its projected opening in 2025 with a fully operational 42-bed PCCU. The report reveals a 14% increase in paediatric critical care admissions in 2021 and 2022 compared to 2018, with occupancy rates at Children's Health Ireland (CHI) at Crumlin consistently exceeding 95%, far above the recommended national standard of 85%. The anticipated NCH PCCU expansion from 32 to 42 beds necessitates a comprehensive multidisciplinary workforce plan to handle increased capacity and maintain high-quality care standards.
• Neonatal Admissions: Neonates, defined as corrected age at admission of less than 29 days old, accounted for 28% of admissions at CHI Crumlin and 25% at CHI Temple Street.
• Respiratory Diagnoses: Respiratory issues made up 30% of admissions at CHI Crumlin and 39% at CHI Temple Street in 2022, up from 18% and 24% respectively in 2020. There is a predicted annual increase from October to January each year and is associated with annual respiratory syncytial virus (RSV)
outbreaks. It also correlates with a greater than 100% occupancy in both Units over the same period. This report has recommended immunisation of infants against RSV.
• Emergency Admissions: Unplanned emergency admissions comprised 67% at CHI Crumlin and 73% at CHI Temple Street in 2022. This is an increase from 60% in 2021 for CHI Crumlin
• Workforce Shortages: Staffing levels at CHI Temple Street fell below the recommended 5.5 whole-time equivalent (WTE)
nurses per bed each year from 2018-2022, averaging around 4.84 WTE in 2022.
• Critical Care Bed Days: The average annual number of bed days provided was 10,232, with an increase to 10,795 bed days in 2022.
• Mortality Rates: Crude mortality rates remained steady at 4% annually, with 75% of deaths at CHI Crumlin occurring in infants under 1 year.
• Organ Donation: In 20212022, 11 infants and children from 2 days old to 15 years
of age donated organs and/or tissue. Dedicated hospital organ donation personnel should be appointed to increase awareness of organ donation and to ensure opportunities are not missed.
• Need for Regional High Dependency Units: Developing regional Paediatric High Dependency Units (PHDUs) is recommended to support the expansion of regional paediatric surgery and to alleviate pressure on central PCCUs, as most admissions to CHI Temple Street are transfers from other hospitals.
The Experience of Anaemia and Ingesting Oral Iron Supplementation in Pregnancy: A Qualitative Study
Written by F.E O'Toole1, 2, E. Hokey1, F.M McAuliffe1,2, J.M Walsh1,2
1 UCD Perinatal Research Centre, University College Dublin, National Maternity Hospital, Dublin, Ireland
2 National Maternity Hospital, Dublin, Ireland
Highlights
• Qualitative research exploring anaemia and supplemental iron in pregnancy.
• Gastro-intestinal side-effects and forgetfulness negatively impact compliance.
• Improvement in symptoms, routine and alternate day dosing all aid compliance.
• Patient knowledge on possible negative sequelae of anaemia was limited.
Introduction
Iron deficiency anaemia is the most common haematological problem in pregnancy. It affects approximately 38 % of women in pregnancy globally. Crosssectional data from fifteen European countries gives a prevalence of iron deficiency anaemia in pregnancy of 35 %. Prevalence of iron deficiency anaemia in pregnancy from an audit encompassing 86 maternity units across the United Kingdom and Ireland was 30.4 %. It remains a common problem in Western well-nourished nations despite these countries being much less afflicted by helminths, malaria or haemolytic conditions.
Significant adverse pregnancy, maternal, foetal, neonatal and childhood outcomes are associated with iron deficiency anaemia. Maternal complications include fatigue, post-partum haemorrhage, increased risk of caesarean section, postpartum anaemia, blood transfusion, and labour induction. Infant complications include preterm birth, low birth weight infant, increased risk of stillbirth, lower Apgar scores at delivery
and increases in perinatal and neonatal mortality. Symptoms of anaemia include fatigue, breathlessness, and dizziness. Postpartum anaemia has been linked to depression, fatigue, lactation failure and early cessation of breastfeeding. Maternal anaemia has also been associated with behavioural and neurodevelopmental abnormalities in offspring.
Iron deficiency anaemia in pregnancy has a multitude of contributing causes including physiological changes and inadequate nutrient intake, rates will depend on baseline iron stores pre-conception. Women of reproductive age are at increased risk of anaemia due to menstruation. Acute blood loss can also occur from miscarriage, placental events such as abruption or praevia or recent childbirth resulting in postpartum haemorrhage. Both breastfeeding and pregnancy deplete maternal iron stores. The iron demands of pregnancy can cause an iron deficit even in iron-replete women. Insufficient dietary iron intake may compound the problem.
Iron deficiency anaemia in pregnancy can be challenging to treat. The hormonal and physiological effects of pregnancy predispose women to slowed gut transit, hemorrhoidal disease, heartburn, nausea, vomiting. Oral iron supplementation is the recommended first-line treatment and is often commenced as both a diagnostic and therapeutic trial without further investigations, as iron deficiency is commonly the underlying cause of anaemia. The commencement of oral iron in pregnancy may exacerbate pre-existing pregnancy-induced gastro-intestinal disturbances or may cause new unpleasant gastrointestinal side-effects to include nausea, vomiting, constipation, abdominal discomfort, and black stools. Advice on optimal absorption of oral iron will typically be to take in the morning, on
an empty stomach and with a source of vitamin C. Women are generally advised to increase their dietary iron and often given advice on foodstuff that may hinder absorption. Compliance with treatment can be limited secondary to side-effects, among other factors.
Rates of iron deficiency anaemia in pregnancy appear to be relatively unchanged over the past two decades, despite treatment being affordable, accessible and in theory straight-forward. The World Health Organization Global Health repository data only demonstrated a 4 % reduction over a twenty-year period to a prevalence of 37 %. The 2017 World Health Organization Global Nutrition Targets include a 50 % reduction of anemia in women of reproductive age by 2025.
There a paucity of published qualitative data from higher income countries on women’s experience of taking oral iron in pregnancy. This study was performed to examine the lived experience of ingesting supplemental oral iron to treat anaemia in pregnancy. We specifically wished to explore women’s awareness and experience of this problem both before and during pregnancy, their awareness of any potential negative sequelae of untreated anaemia, how they felt about the role of diet in its management, and what factors contributed negatively or positively to their compliance with oral iron supplementation in pregnancy. Feedback was also sought on acceptability of a proposed randomized controlled trial of daily versus alternate day oral iron for the treatment of confirmed iron deficiency anaemia in pregnancy. This project successfully answered these research questions.
Materials and methods
Recruitment for this qualitative study performed between 4th November 2021 and 17th December 2021. Ethical approval
was obtained in advance of recruitment by the National Maternity Hospital Research Ethics Committee (EC23.2021). Informed written consent from each participant was obtained in advance of an interview. Pregnant or recently pregnant women who required iron supplementation in pregnancy were invited to take part in interviews. Women were invited to participate in the study via social media channels such as on the UCD Perinatal Research Centre Twitter account and women were also approached for study participation during antenatal hospital visits. Ethically approved patient information leaflets on the study and study-specific consent forms were provided in advance of participation and an opportunity to ask questions was provided. Interviews were audio-recorded virtually or in person using the audio function in Zoom (Zoom Video Communications Inc. 2016). Interviews were then transcribed using Sonix (Sonix, Inc. San Francisco, 2021). To ensure patient confidentiality all transcripts were anonymised and allocated a unique study identifier (P1–P14) and the audio files were destroyed. Interviews were carried out by one member of the research team (FOT). This researcher was a female obstetric trainee performing research as part of an MD thesis. There was no prior relationship with any of the interviewees. Participants were provided with clear typed information regarding the study and the researcher’s background and role as part of the consent process in advance of participation. Consent forms were stored on a secure server and could not be linked to the transcripts to ensure participant confidentiality. No medical records were accessed as part of this study and participants contact details were deleted following a two-week period after the interview. Participants were offered an opportunity to review their anonymized typed transcript
Supplementation
for a two-week period after the interview. After this period, their contact details were destroyed as per the consent form and planned management of their data.
The interview took the following format: an interview tool comprising of 5 open-ended questions for semi-structured interviews was developed by the research team. Interview length varied between 14 and 17 min duration. There was scope for exploratory questions on new themes. Open-ended questions were asked of each participant surrounding their awareness of iron deficiency anaemia both before and during pregnancy, their knowledge of its symptoms and of potential sequelae, how big a role they felt diet played as part of management, and their experience of taking iron tablets in pregnancy. Factors affecting compliance with oral iron supplementation were explored. Finally, each participant was asked about how acceptable they felt participation in a randomized controlled trial of daily versus alternate day iron would be to other women. Details of what participation in the trial would involve was outlined and feedback was sought on how acceptable they felt this would be.
The anonymized transcripts were then analysed separately by two members of the research team (EH, FOT). Data saturation was felt to be reached with clear recurring themes. Individual analyses were compared, and agreement of themes and subthemes was reached through discussion. Rigour in the analytic process was ensured through review and confirmation of themes by other members of the team (FMcA, JW). Main findings
Overall, there appeared to be a varied awareness that iron deficiency could become a problem in pregnancy. Prior awareness was sometimes from previous personal experience, and often from anecdotal reports from friends or family who had previously been pregnant. Personal experience ranged from experience of anaemia as a teenager, vegetarianism, and during work-up for a history of subfertility. Often, however, it was their first pregnancy that initially highlighted the problem to them. Women described being warned of it as a potential problem more in their initial pregnancies:
P8- “I did have people telling me in the first pregnancy that I looked pale, and they were like you’re anaemic. You need to take iron. Other Mums were telling me.”
P13- “I was aware, because of all my sisters who’ve gone through pregnancy. I know it’s quite common now.”
With regards to participants’ experience of symptoms of iron deficiency anaemia in pregnancy, significant and depleting fatigue was a recurring theme. Women described it as a more severe fatigue than previously experienced:
P2- “I was absolutely exhausted and the tiredness, it’s just inexplicable if you’ve never been pregnant. It’s a completely flattening experience.”
Knowledge and awareness on the potential effects of untreated anaemia on the pregnancy and baby were limited. Participants did not demonstrate good knowledge on the potential negative consequences/sequelae for themselves in their pregnancy or afterwards in the postpartum period. Awareness and knowledge of potential foetal sequelae such as childhood iron deficiency was poor:
P8- “No actually, I don’t. I’m not aware of any of the effects in pregnancy of untreated anaemia for me in pregnancy or for the baby in the long-term.”
With regards to the lived experience of ingesting oral iron in pregnancy, the unpleasant side-effects of ingesting oral iron were a commonly recurring theme. Constipation and nausea appeared to be the most frequently described and troublesome:
P2- “It did not agree with me at all, it was absolutely horrendous to take. I got constipation, I got heartburn. It just really played havoc with my digestive system. Made me nauseous if I took it without food, it was really hard. It was really unpleasant to take.”
P12- “It helped me, but the sideeffects were horrible. It’s not nice to be constantly sick for 50 days.”
Barriers and enablers to oral iron supplementation in pregnancy were explored in this study.
Gastro-intestinal side-effects featured heavily in the interview transcripts and appeared to contribute to poor compliance with oral iron supplementation in pregnancy. Forgetfulness also negatively impacted compliance. One participant commented that the cost of a more expensive brand of iron supplementation influenced compliance. A prior experience of poorly tolerating oral iron in the past also caused hesitation with compliance.
Factors that positively affected compliance included a noticeable or anticipated improvement in fatigue with oral iron supplementation. The benefit of a routine with ingestion of oral iron was also cited as an aid in terms of assisting compliance. A fear of worsening symptoms of anaemia and a desire to avoid the risks of a blood transfusion were other factors which appeared to motivate compliance with oral iron therapy. There was also evidence that reduced dose frequency positively impacted compliance with oral iron supplementation.
Pregnancy as motivating factor recurred as a theme in analysis of the interviews. Participants felt that most women were highly motivated to do everything in their power for the best possible outcome for themselves and their baby. This effect was described as greater than any motivation for compliance with treatment outside of pregnancy.
P6- “I presume, like most women, when they’re pregnant, you just want to do the best thing for your health and the baby’s health. In more normal times… I probably wouldn’t have been as compliant, but I think being pregnant, you just want to look after yourself and the baby. So that was definitely a motivating factor.”
P2- “I didn’t object to taking them because you do take whatever you need to take. You know, whatever they tell you. They tell you; you need coal. You’re going to take the coal. Your motivation is high in pregnancy.”
In terms of the role of diet in the management of iron deficiency anaemia in pregnancy, participants’ knowledge and awareness of iron-rich foods was generally good. There also was evidence that women believed and understood that diet alone would not rectify their anaemia:
P4- “For me, dietary stuff was ineffective. I’d go for all the ironrich foods, and it was just neglible. It was just the impact was too tiny for the mountain I was trying to climb.”
Pregnancy symptoms and nausea negatively impacted appetite for some women. For some, they felt a reliance on supplementation due to this. Knowledge of facilitators and inhibitors of iron absorption was also widely good.
Themes that emerged in relation to trial acceptability included the benefit and attraction of extra supportive care in pregnancy and the time constraints women can be under. Participants highlighted the demands on women’s time
and to try to work around this for convenience for any trial participants. Pregnancy alone requires planning for regular and frequent appointments in women who have busy lives and would not otherwise require planning for regular medical appointments outside of pregnancy.
The proposed trial generally received very positive feedback with participants feeling that this was an important area of research:
P1- “I think this trial is very important and it sounds like it’s going to be very educational for women in the longer term.”
P5- “I think it’s a very interesting study. So very, very much needed… I’m happy you are working on it”
P6- “There doesn’t seem to be a particularly large burden on the participants, and I think that it would be largely acceptable.”
There were mixed responses to the acceptability of taking alternate day versus daily iron. Some women felt alternate day iron would be acceptable and potentially beneficial for that arm of the trial. However, there was doubt among some participants about the willingness of patients to accept alternate day iron over daily iron.
Main findings
Themes of awareness, compliance, the role of diet and pregnancy as a motivating factor recurred throughout our analysis. Fatigue emerged as the predominant and most troubling symptom. Knowledge and awareness of possible adverse consequences of iron deficiency anaemia in pregnancy were poor. Significant unpleasant gastrointestinal side-effects appeared to be experienced widely among interviewees and affected compliance. Factors that positively impacted compliance with oral iron supplementation included routine, a perceived or historical improvement in symptoms with supplementation, reduced dose frequency and a desire to avoid both worsening symptoms of anaemia and a blood transfusion.
Clinical significance
Awareness pre-pregnancy of iron deficiency anaemia varied in our cohort. When present, it stemmed from personal experience of friends and family and anecdotal advice. However, knowledge on symptoms and the potential need for iron supplementation in pregnancy was generally good. First pregnancy also appeared to be a time when women noticed an emphasis
from health professionals on the problem. This may possibly be explained by health providers assuming prior knowledge from previous pregnancies in multiparous women. Participants knowledge on both iron-rich diets and foodstuff that could impact iron absorption was also good. This may be due to the population in our catchment area being generally well-educated, from a higher socio-economic background and the mean age of our participants being 36. The appreciation that an iron-rich diet alone was not sufficient to rectify anaemia in pregnancy appeared to stem from personal experience of increasing dietary iron with no noticeable improvement in symptoms:
P4- “For me, dietary stuff was ineffective. I’d go for all the iron-rich foods, and it was just neglible. It was just the impact was too tiny for the mountain I was trying to climb.”
Knowledge on the possible negative sequelae of untreated iron deficiency anaemia in pregnancy however was poor. None of our participants commented on the potential for maternal complications or the negative associations including preterm birth, low-birth weight, Caesarean delivery, post-partum haemorrhage. Knowledge surrounding possible adverse outcomes for the foetus in the short and long-term were also poor. Only one participant commented on the effect maternal iron deficiency anaemia might have on the baby’s iron stores in the 6 months post-delivery.
Fatigue emerged as a pervasive and debilitating symptom women experienced with iron deficiency anaemia in pregnancy. The effects were dramatic and appeared worse than previously experienced tiredness. Significant fatigue is known to affect quality of life and increase the likelihood of depressive symptoms in pregnancy. Undetected and untreated antenatal depression is one of the strongest risk factors for postnatal depression.
The feedback on trial acceptability from our study was used to inform our design for a planned randomized controlled trial of daily versus alternate day oral iron in pregnancy. Acceptability refers to determining how well an intervention will be received by the target population and the extent to which the new intervention or its components might meet the needs of the target population and organizational setting.
It has become a key consideration in the design, evaluation and implementation of clinical trials. Positive feedback noted from this qualitative study included the benefit of extra supportive care in pregnancy and the potential to improve side-effects of oral iron for women in pregnancy. Perceived research relevance has been shown to be an important factor for clinical trial recruitment in pregnancy.
Advice on incorporating research visits with routine antenatal care and limiting extra hospital visits was used to finalise our trial protocol. Time constraints on women has been shown to be a factor affecting both recruitment and retention in clinical research trials in pregnancy.
It is useful to be aware that some participants may resist or refuse their randomized dosing regimen. Participants’ understanding that a scientific question is being answered and the nature of participation will need to be ensured prior to recruitment. Randomised trials in pregnancy face specific enrolment challenges and research in pregnancy can be limited due to an individual’s risk perception.
Altruism and a wish to contribute to scientific research has been shown to be a previous motivating factor in trial participation in pregnancy. However, key motives which have previously been identified for non-participation in clinical trials in pregnancy include a dislike for the intervention, either because of a risk of harm or due to practical considerations. Future research
Further qualitative research in this area could focus on a younger cohort and populations from lower socio-economic groups but who are still residing and receiving antenatal care in a higher income country. Purposive sampling from ethnicities more strongly affected by iron deficiency anaemia would also be of interest to ascertain if the same themes recur and if there are any cultural differences in the analyses.
Conclusion
In conclusion, women view sideeffects as a significant barrier to taking oral iron. Informing women on the important maternal and infant complications associated with iron deficiency may prove to improve compliance with oral iron treatment. Women clearly view this topic as an important research area.
Clinical R&D
IRISH REIMBURSEMENT GRANTED TO PRODUODOPA® (FOSLEVODOPA/ FOSCARBIDOPA) FOR PEOPLE LIVING WITH ADVANCED PARKINSON’S DISEASE
AbbVie has announced that the Irish health authorities have approved reimbursement of PRODUODOPA® (foslevodopa/ foscarbidopa) for the treatment of advanced levodopa-responsive Parkinson’s disease with severe motor fluctuations and hyperkinesia (excessive movement) or dyskinesia (involuntary movement) when available combinations of Parkinson medicinal products have not given satisfactory results.
This follows granting of the product authorisation for PRODUODOPA® (foslevodopa/foscarbidopa) in Ireland on 23 September 2022.1 It is a subcutaneous 24-hour infusion of levodopa-based therapy for the treatment of severe motor fluctuations in people living with advanced Parkinson’s disease whose symptoms are inadequately controlled by other therapies.1 The continuous delivery of foslevodopa/foscarbidopa provides levodopa 24-hours a day which may help patients by extending the period when symptoms are well-controlled, often referred to as “On” time. The VYAFUSER™ pump for the subcutaneous delivery of PRODUODOPA® received Conformité Européenne (CE) Mark in November 2023.
Parkinson’s disease is a chronic, progressive neurodegenerative disorder affecting approximately 6.1 million people globally. Parkinson’s disease is characterised by tremor, muscle rigidity, slowness of movement and difficulty with balance. As the disease progresses, the severity of symptoms increases , and patients tend to experience greater disability and an impaired ability to perform activities of daily living , as well as the reemergence of symptoms as standard treatment wears off. Characteristics of advanced Parkinson’s disease may include needing help with performing daily activities, increased motor fluctuations (changes in the ability to move referred to as “On-Off” times), difficulty swallowing, recurrent falls, dementia, dyskinesia (involuntary movements) and other symptoms.5
“People living with Parkinson’s disease experience daily challenges and uncertainty, especially as their disease progresses and symptoms are no longer adequately controlled” said Andres Rodrigo, General Manager of AbbVie in Ireland.7,8, 9,10 “I welcome the
availability of foslevodopa/ foscarbidopa for the therapeutic management of Parkinson’s disease in indicated patients.”
Three Studies
The authorisation was supported by three studies: the Phase 3, 12-month open label study (M15-741 study) which evaluated the long-term safety, tolerability, and efficacy of continuous subcutaneous infusion of foslevodopa/foscarbidopa , the Phase 3, 12-week study (M15736 study) which compared the efficacy and safety of foslevodopa/foscarbidopa to oral levodopa/carbidopa2, and a Phase 1 pharmacokinetic comparability study.
The most frequent adverse reactions (greater than or equal to 10 percent) were infusion site events (infusion site erythema, infusion site cellulitis, infusion site nodule, infusion site pain, infusion site oedema, infusion site reaction, and infusion site infection), hallucination, fall, and anxiety. The majority of infusion site events were non-serious, mild or moderate in severity and resolved spontaneously or with treatment.1
References available on request
BEYFORTUS REAL-WORLD EVIDENCE PUBLISHED IN THE LANCET SHOWS 82% REDUCTION IN INFANT RSV HOSPITALIZATIONS
Beyfortus reduced respiratory syncytial virus (RSV) hospitalizations by 82% (95% CI: 65.6 to 90.2) in infants under 6 months of age, compared to infants who received no RSV intervention, according to the interim results of an ongoing study published in The Lancet. These results, from the first RSV season after Beyfortus’ introduction, are part of the three-year NIRSE-GAL study conducted in Galicia, Spain under a collaborative framework with the Galician Directorate of Public Health of the Xunta de Galicia (Galician government) and Sanofi.1
The results echo real-world evidence (RWE) reported from several broad infant immunization programs across the US, Spain and France during the 2023-2024 RSV season, which add to the consistent and high efficacy seen in pivotal clinical studies with Beyfortus. Real-world evidence demonstrates if a treatment or immunization is effective in dayto-day practice, as opposed to “efficacy” determined in carefully controlled clinical trials. A favorable safety profile was observed following Beyfortus use, consistent with clinical study results.1-10
Federico Martinon Torres Head of Pediatrics, Hospital Clínico Universitario Santiago, Spain and principal investigator of NIRSEGAL study
“Galicia provides the first population-based real-world evidence of the impact of nirsevimab to prevent RSV disease in infants, showing a reduction by almost 90% in the number of hospitalizations due to this virus when compared with several previous RSV seasons. This achievement is the result of the exemplary pragmatic collaboration among scientists, industry, healthcare providers and policy makers aligned with a carefully planned roll-out of the immunization campaign, and the outstanding response of the Galician parents to this prophylaxis campaign.”
Thomas Triomphe Executive Vice President, Vaccines, Sanofi
“The scale and speed of impact seen after Beyfortus’ introduction demonstrates the strength of all-infant immunization strategies against RSV in babies. In Galicia, we saw an effectiveness of 82% in reducing RSV hospitalizations following the launch of Beyfortus, with more than 90% of eligible infants immunized. A growing body of evidence from these programs support policymakers, healthcare providers and parents who share our collective ambition to safeguard babies from RSV disease.”
NIRSE-GAL is a large, populationbased, three-year follow-up study to evaluate the effectiveness of Beyfortus following its inclusion in the Galician immunization schedule. The study aims to measure the impact of Beyfortus on hospitalizations due to RSV, all-cause lower respiratory tract disease, severe lower respiratory tract disease caused by RSV, all-cause lower respiratory tract disease hospitalizations, and all-cause hospitalizations among infants born during the RSV season, infants under 6 months of age at the start of the season, and children aged 6-24 months who are vulnerable to severe RSV disease at the start of the season.
The 2023-2024 immunization campaign ran from September 25, 2023 to March 31, 2024.1
RWE from countries with Beyfortus all-infant immunization programs in 2023-24
In addition to this new effectiveness study, evidence of the high impact following Beyfortus’ introduction has been consistently shown in several other real-world studies.
• An interim analysis of 2023-24 surveillance data published
in the US Centers for Disease Control and Prevention’s (CDC) Morbidity and Mortality Weekly Report (MMWR) shows a single dose of Beyfortus was 90% effective in preventing hospitalizations due to RSV in babies who were immunized below 8 months of age.2
• A recent draft recommendation from Haute Autorité de Santé in France reported, across six hospitals, an effectiveness of 83% against RSV-associated hospitalization in infants who received Beyfortus compared to those with no intervention.3
• In Catalonia, Spain, a study pre-printed in The Lancet showed reductions of 87.6% and 90.1% in hospital and ICU admissions for RSV, respectively, among babies born before the start of the RSV season, who were eligible to receive Beyfortus, compared to those with no intervention.4
• A pooled analysis of data from three Spanish regions, including Valencia, Murcia, and Valladolid, showed an 84.4% effectiveness in preventing hospitalizations due to RSV in infants under 9 months of age versus infants who received no intervention. The results were published in Eurosurveillance.5
• A study from Navarra, Spain published in Vaccines found an effectiveness of 88.7% in preventing hospitalizations among infants immunized at birth with Beyfortus, compared to no intervention.6
The expansion of the Beyfortus manufacturing network is progressing well and according to plan. This expansion will allow Sanofi and AstraZeneca to more than triple manufacturing capacity. Based on this, and assuming regulatory validations are delivered in due time by regulatory agencies, Sanofi and AstraZeneca are confident to meet global commitments and build inventory that can be used in future RSV seasons. In addition, the companies are producing Beyfortus well in advance of the RSV season, with the vast majority of doses planned to be available by October.
References available on request TAR-210 RESULTS SHOW 90 PERCENT RECURRENCE-FREE SURVIVAL AND 90 PERCENT COMPLETE RESPONSE IN PATIENTS WITH HIGH-RISK AND INTERMEDIATE-RISK NONMUSCLE-INVASIVE BLADDER CANCER, RESPECTIVELY
Janssen-Cilag International NV, a Johnson & Johnson company,
has announced updated results from an open-label, multicentre, multi-cohort Phase 1 study of the safety and efficacy of TAR210, an intravesical targeted releasing system designed to provide sustained, local release of erdafitinib into the bladder, in patients with non-muscle-invasive bladder cancer (NMIBC) with select FGFR alterations.1 These data were featured today in an Oral Presentation Session (Abstract #PD48-02)1 at the 2024 American Urological Association (AUA) Annual Meeting taking place 3-6 May, 2024, in San Antonio, Texas.
Results featured updated data from Cohort 1 (C1); patients with recurrent, Bacillus Calmette-Guérin (BCG)-unresponsive high-risk (HR) NMIBC (high-grade Ta/T1; papillary only) who refused or were ineligible for radical cystectomy and Cohort 3 (C3); patients with recurrent, intermediate-risk (IR) NMIBC (Ta/ T1) low-grade papillary disease left in situ as tumour marker lesions.1 First results were featured at the European Society for Medical Oncology 2023 Congress, with interim results presented at the European Association of Urology (EAU) 2024 Annual Congress.2,3
“Advancement in the treatment landscape of high or intermediaterisk non-muscle-invasive bladder cancer has remained stagnant for more than 50 years,” said Antoni Vilaseca*, M.D., Ph.D., of the Hospital Clínic de Barcelona, presenting author of the Phase 1 TAR-210 study. “Results presented today further underscore that TAR210 for the localised treatment of bladder cancer may offer a promising alternative for patients with limited treatment options.”
At the data cutoff of 22 March, 2024, 64 patients had been treated with TAR-210 across the two cohorts.1 Of the 21 patients in C1 with HR-NMIBC, the 12-month recurrence free (RF) survival rate was 90 percent (95 percent confidence interval (CI), 66-97).1 In C3, 31 patients were efficacy evaluable with 28/31 achieving a complete response (CR) rate of 90 percent (95 percent CI, 74-98).1
The most common treatmentrelated emergent adverse events (TEAEs) were Grade 1/2 lower urinary tract events.1 There were no dose-limiting toxicities and no deaths.1 Two patients (3 percent) discontinued the study due to TEAEs of low-grade urinary symptoms and two patients had serious TEAEs with pyelonephritis and sepsis or UTI (urinary tract infection) and sepsis, respectively.1
“FGFR genetic alterations are most common in NMIBC,” said Sabine Brookman-May, M.D., Vice President, Late Development
Oncology, Johnson & Johnson Innovative Medicine. “These results further support the potential of TAR-210 with quarterly administration as a bladdersparing and BCG-free treatment option, underscoring our deep commitment to pioneering novel therapies for patients who face limited treatment avenues.”
“At Johnson & Johnson, we are committed to transforming bladder cancer treatment with novel drug delivery technology and precision-based therapies,” said Henar Hevia, Senior Director, EMEA Therapeutic Area Lead, Oncology at Johnson and Johnson Innovative Medicine. “As the data continue to mature, it is encouraging to see sustained positive responses to treatment. We look forward to investigating the full potential of TAR-210 in patients with FGFR-altered non-muscle invasive bladder cancer through an ongoing and comprehensive clinical development programme.”
Europe has one of the highest rates of bladder cancer in the world4 with nearly 225,000 patients diagnosed in 2022,5 a 10 percent increase from 2020.6 NMIBC constitutes approximately 75 percent of all newly diagnosed bladder cancers.7 Currently, adjuvant intravesical immunotherapy with BCG or intravesical chemotherapy is the standard of care for patients with intermediate- and highrisk NMIBC.8 Between 30 to 40 percent of patients do not respond to BCG, facing disease recurrence or progression.9 In such scenarios of HR-NMIBC, radical cystectomy (removal of the bladder) emerges as the primary treatment option.9 This major abdominal procedure requires a urinary diversion to be created to collect and store urine.10
References available on request
URGENT CALL TO ‘MAKE LUPUS VISIBLE’ AS NEW RESEARCH SHOWS THE IMPACT THE AUTOIMMUNE DISEASE HAS ON PATIENTS’ LIVES
Arthritis Ireland and AstraZeneca Ireland came together on World Lupus Day to call for people living with lupus to share their stories to increase visibility of the autoimmune condition and its impact on patients.
Lupus, also known as Systematic Lupus Erythematosus (SLE), is a complex autoimmune disease that is experienced differently by each person and causes a variety of symptoms, including skin rash, joint pain, swelling and fevers.2 It is an often under recognised condition that can take many years to be diagnosed3 and disproportionately
affects women within the 15–45-year-old age cohort.4
Arthritis Ireland conducted a new survey to understand the impact of lupus and to know more about the day-to-day problems that affect those living with the disease. 90% of those surveyed indicated that lupus negatively impacts physical activity and their ability to exercise. 69% said lupus negatively impacts their family life and over 70% of those surveyed reported that the condition negatively impacts on their career, with many having to take prolonged time off work. Respondents also indicated a negative impact on their mental health due to their disease with anxiety (57%), loneliness (45%) and depression (36%) featuring strongly. (refer to reference 1)
As part of their joint initiative, Arthritis Ireland and AstraZeneca Ireland are calling on people living with lupus or who have family with the condition to share their stories online using the hashtag #makelupusvisible.
Commenting on the results of this survey, Arthritis Ireland chief executive Gráinne O’Leary said, “The results of this Arthritis Ireland survey clearly indicate the huge impact lupus has on the day-today lives of those living with the disease. As lupus predominately affects women between the ages of 15 and 45, it can have a significant impact on fertility and on family life in general. There is a financial burden as well with many patients having to take time off work. At Arthritis Ireland, we provide support and resources for those living with lupus and through this campaign are aiming to increase awareness of the condition amongst the general public.”
Pictured at the Butterfly House, Malahide Castle is Ruth Levins from Drogheda who lives with lupus and Arthritis Ireland chief executive Gráinne O’Leary
In Ireland, Lupus is recognised as a relatively uncommon condition, but its exact prevalence is difficult to determine due to the complexity of its diagnosis, variability of its symptoms, and lack of official data on prevalence. There is also a large unmet need in relation to effective and targeted treatments for lupus.
Speaking to the difficulties of diagnosing lupus and the lack of dedicated treatments, Professor Gráinne Murphy, Consultant Rheumatologist from Cork University Hospital said,
“Lupus remains a challenging diagnosis to treat. While there have been significant therapeutic advances in many other immunemediated conditions, there have been many disappointments in clinical trials for SLE. In more recent times, reassuringly, there have been some positive developments in clinical research which have led to the development of a limited number of new therapies. Unfortunately, these agents are not yet widely available and equity of access remains an issue. There remains a significant need for more effective treatment options.”
References available on request 78% OF CHILDREN IN LEINSTER ARE REPORTED NOT TO CONSUME THE RECOMMENDED DAILY AMOUNT OF FRUIT AND VEGETABLES EVERY DAY ACCORDING TO RESEARCH FROM VIVIO® JUNIOR
A study by innovative children’s range Vivio® Junior has revealed the concerns that parents in Leinster have around their children’s health and immunity. The research,* shows that 8 in 10 (80%) parents surveyed from Leinster claim they aim to keep their children healthy by providing them with a healthy diet / ensuring that they are eating a variety of foods, with just under half (49%)
Clinical R&D
claiming they use vitamins and supplements. Only 1 in 5 (21%) parents claim their child(ren) are consuming five portions of fruits and vegetables every day.
As the seasons change, so too do the myriad of concerns that parents have. Just over half (54%) of parents surveyed in the region claim illness is their main concern, almost half (48%) are concerned about schoolwork and keeping grades high, while just over a third (35%) listed their children socialising with peers as their biggest concern.
The research also revealed how parents of school-going children are experiencing 'lunchbox anxiety'. Over a third (37%) of parents surveyed in Leinster find it difficult to come up with new ideas for lunchboxes, with females (43%) more likely to claim they find it difficult to present new ideas on a daily basis. Inspiration for lunchboxes is most likely to come from friends (58%), social media (34%) or online recipes (26%).
Growing children need to absorb vital nutrients from their food but to do so they need to be eating enough of the right foods. The Vivio® Junior expert Clinical Nutritionist is supporting parents in providing a holistic approach to ensure that their children are prepared for the season ahead.
Éva Hill Hamilton, Clinical Nutritionist comments, “We know parents can struggle to fulfil their children’s needs of five portions of fruits and vegetables every day – just 1 in 5 parents surveyed in Leinster are managing this every day. Equally, preparing school lunches for children can pose a problem for many parents in Leinster seeking to meet those needs. Selecting colourful fresh fruit and vegetables balanced with protein and healthy fats will provide children with a spectrum of nutrients that bolsters the immune system.
To support the growth and well-being of children who are not consuming sufficient fruits and vegetables, I recommend incorporating a multivitamin tonic for extra nutrients in their diet and introducing a probiotic supplement with live bacteria. These measures can improve gut health, assist in nutrient absorption, and boost immunity. As the seasons transition and children develop colds or coughs, natural remedies that can alleviate the symptoms without suppressing them are also beneficial. Remember, coughs act as the body's innate defence mechanism to expel and safeguard against harmful substances.”
MATER PRIVATE NETWORK SELECTED AS ONE OF THREE CENTRES WORLDWIDE FOR GLOBAL AFIB STUDY
Mater Private Network has been selected as one of only three centres worldwide and the only centre in Ireland to participate in the prestigious NAVIGATEPF clinical study, led by Boston Scientific. This recognition highlights Mater Private Network's status as one of the most acknowledged atrial fibrillation (AFib) centres in Europe.
The prospective, single-arm, openlabel, multi-centre NAVIGATE-PF study will begin at the Dublin site from today, Friday 10th May, marking a significant step in Mater Private Network's involvement in pioneering medical research. AFib is the most common irregular heart rhythm, which significantly reduces the quality of life and life expectancy of patients. An estimated 8 million patients live with this condition in Europe.
The NAVIGATE-PF study will examine the FARAVIEW™ Software Module* when it is used to visualize and track the FARAWAVE™ Nav Pulsed Field Ablation (PFA) Catheter* for the treatment of patients with paroxysmal and persistent atrial fibrillation (AF). The FARAVIEW technology and the FARAWAVE Nav catheter expand the capabilities of the FARAPULSE™ PFA System through integration with the Boston Scientific cardiac mapping system. The FARAWAVE Nav PFA Catheter adds magnetic navigation capabilities to the current
Mater Private Network’s CVRI research team involved in the study: Heta Jigar Panchal, Prof. Gábor Széplaki and Fionnuala Duffy
FARAWAVE PFA catheter, enabling detailed mapping and PFA therapy within the same device.
This mapping data is visualised using the new FARAVIEW Software Module, offering a tailored mapping solution for procedures with the FARAPULSE PFA System. This will be the second generation of the novel FARAWAVE catheter as a part of the FARAPULSE PFA System, which has had extensive real-world use demonstrating safety of the system with no reports of permanent phrenic nerve palsy, pulmonary vein stenosis or oesophageal injury.
Prof. Gábor Széplaki, Head of Cardiac Electrophysiology at Mater Private Network, expressed his enthusiasm for the project: "We are honoured to participate in this groundbreaking study, which will be another milestone in our journey to transform the way arrhythmias are treated globally. This initiative represents a significant stride towards integrating advanced cardiac mapping with ablation technology, aiming to elevate the standard of care for our patients with atrial fibrillation. As a centre of excellence in cardiac electrophysiology, we are committed to contributing to research that may significantly improve patient outcomes. As early adaptors of the most advanced technologies we are hoping to deliver safe and efficient therapies to the wider patient populations, including elderly patients living with atrial fibrillation."
Mater Private Network continues to demonstrate its commitment to medical innovation and dedication to providing the latest and most effective treatments to its patients. The Electrophysiology team is offering comprehensive, multidisciplinary patient management at the Atrial Fibrillation Institute in Dublin. The network remains
focused on advancing medical science and improving the health of those it serves.
In a pulsed field cardiac ablation procedure, a catheter is guided into the heart to administer targeted non-thermal electrical fields that selectively treat heart tissue cells, while avoiding damage to nearby structures.
Mater Private Network has been one of the first centres which has adopted the groundbreaking technology and delivered >750 procedures since 2022.
LONQUEX® (LIPEGFILGRASTIM) RECOMMENDED AS A BESTVALUE BIOLOGICAL ON THE HIGH TECH ARRANGEMENT
Teva Pharmaceuticals is pleased to announce that the Medicines Management Programme (MMP) now recommends Lonquex® (lipegfilgrastim) as a Best-Value Biological (BVB) Medicine for the long-acting granulocyte-colony stimulating factors on the High Tech Arrangement. Prescribing Lonquex® will lead to significant savings for the health service.
Lonquex is indicated in adults for the reduction in the duration of neutropenia and the incidence of febrile neutropenia in patients treated with cytotoxic chemotherapy for malignancy (with the exception of chronic myeloid leukaemia and myelodysplastic syndrome).
Contact your local Teva representative, for any queries in relation to Lonquex® (Lipegfilgrastim).
Further information is available upon request or from the SmPC available at HPRA.ie. Product Information is also available on the HPRA website.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com.
Date of preparation: May 2024
Job code: LQX-IE-00005
BREAKTHROUGH AT TYNDALL REVOLUTIONISES SURGICAL NAVIGATION FOR CANCER
A groundbreaking development by researchers at Tyndall National Institute and Microelectronics Circuits Centre Ireland (MCCI), based at University College Cork (UCC), is set to transform surgical navigation. In a significant breakthrough, researchers have developed the first sensor-on-a-chip for magnetic tracking in surgery and other image-guided interventions. This development accelerates a move away from reliance on harmful radiation imaging (x-rays) towards a safer, more precise approach to navigating medical instruments within the body. Traditional image-guided interventions often use x-rays for navigation of instruments. However, a pioneering technology known as ‘magnetic tracking’ is revolutionising clinical practice by minimising the dependency on x-rays, while accelerating the use of surgical robotics and image-guidance.
Magnetic tracking uses lowfrequency magnetic fields, similar to everyday devices like electric motors and radios, to precisely detect the position of tiny sensors inside the patient. However, existing sensors are complex to manufacture, they are expensive, and are extremely delicate.
Preliminary results published in the IEEE Transactions on Biomedical Circuits journal report tracking accuracy of less than a millimetre, making the new sensor the most accurate on-chip sensor to date for navigating instruments inside the body.
Researchers were able to demonstrate the use of the chip for tracking instruments inside the lungs, an important application for effective targeting and treatment of diseases like lung cancer, which is the leading cause of global cancer incidence and mortality (source: ncbi.nlm.gov).
The sensor is manufactured using standard silicon chip technology resulting in a simplified manufacturing process. Silicon chips are cost-effective at scale allowing the technology to be manufactured at a fraction of the cost of existing medical sensor technology. Silicon chips are also easily integrated with the latest flexible circuits, making assembly quick and reliable.
Pádraig Cantillon-Murphy, Professor of Biomedical Engineering at Tyndall and UCC, who led the research team, said: “This represents the culmination of
Professor Pádraig Cantillon-Murphy and Researcher Manish Srivastava
10 years development of magnetic tracking technology at Tyndall and UCC. I'm immensely proud of the team's achievements over that time and we look forward to translating this technology to clinical applications where it can make a significant difference in patient outcomes.”
Marcus Kennedy, Professor of Medicine at Cork University Hospital and President of the Irish Thoracic Society who has been collaborating with Tyndall and UCC said: “Magnetic navigation has huge potential in helping with the diagnosis of diseases like lung cancer. Accurate and low-cost access to peripheral lung cancers via bronchoscopy provides a pathway towards not only safe and low-cost biopsy, but also endobronchial treatment of lung cancer without the need for invasive surgery. However, the high costs of robotic-assisted interventions and the cost per tracked instrument are prohibitive in most countries. This on-chip sensor could be a real game-changer for navigation in bronchoscopy and many other image-guided interventions.”
The breakthrough research was made possible through funding from the European Research Council, Science Foundation Ireland, Enterprise Ireland, and through the Microelectronics Circuit Centre Ireland (MCCI) at Tyndall.
FIRST IRISH PATIENT
IMPLANTED WITH INNOVATIVE HEART FAILURE MANAGEMENT SYSTEM FROM IRISH COMPANY FIRE1
Dublin-based FIRE1 ha announced that the first Irish patient has been successfully implanted with its
FIRE1™ System for remote heart failure monitoring. The innovative system has the potential to positively impact thousands of people living with heart failure in Ireland every year and alleviate the burden on hospital emergency rooms. The successful implantation took place at University Hospital Galway in the First in Human Clinical Investigation of the FIRE1 System in Heart Failure Patients (FUTURE-HF). The study will assess FIRE1’s novel solution to improve outcomes for those living with heart failure.
Irish medtech company FIRE1, whose CEO, Conor Hanley was recently announced as a 2024 EY Entrepreneur of the Year finalist, seeks to transform heart failure management by enabling patients to monitor and control their fluid volume themselves with a device at home, similar to how continuous glucose monitoring transformed diabetes care. Fluid overload is a classic clinical feature of heart failure, which affects approximately 90,000 Irish people and is a leading cause of hospitalisations, including high admission and readmissions rates in Ireland.
FIRE1 CEO and President, Conor Hanley said: “I am especially pleased to announce our first patient in Ireland. This represents a true clinical research success for Ireland, being one of the first systems of its nature to be developed, manufactured and now to be in a clinical trial in Ireland. It showcases Ireland's capability for groundbreaking medical innovation with the potential to change healthcare delivery globally. The FIRE1 team is steadfast in our mission to help millions of people around the world living with heart failure to get their normal lives back, but it is very special to be able to give access to people here at home. It is gratifying to see the physician interest in our novel technology. I would like to extend
my thanks on behalf of the whole FIRE1 team to the fantastic staff at UHG, and most importantly to the patients who continue to put their trust in us and participate in this important research.”
The FIRE1 sensor is implanted into the body's largest vein, located in the abdomen, known as the inferior vena cava (IVC) and works by continuously measuring the size of the IVC, giving a marker of the amount of fluid in the body. High levels can increase the risk of breathing difficulties and a build-up of fluid in the lungs which lead to an emergency hospital admission. The patient wears a belt reader around the abdomen for around a minute a day to take a reading from the sensor and the data is sent to the patient’s clinical team at the hospital. The system is designed to alert whenever the patient's condition deteriorates.
Professor of Interventional Cardiology and Translational Medicine at University Hospital Galway (UHG), Prof Faisal Sharif performed the implant. “We are delighted to bring this new, transformative technology to Ireland for the first time,” said Prof Sharif. “The procedure was very straightforward, minimally invasive and the patient was confident using the FIRE1 system and taking the readings. The data we will get from this patient will give a new window into heart failure management and has the potential to dramatically improve our understanding of this patient’s condition, and to enable proactive changes in medications that will keep them healthy and at home. We hope to implant further patients at UHG while recruitment is still active.”
Conor Hanley of FIRE1. EY EOY 2024 Finalist. Photograph by Naoise Culhane
The Medicines Management Programme
(MMP) recommends Tetridar ® as a Best Value Medicine (BVM) for teriparatide on the High Tech Arrangement.
Tetridar ®
20 micrograms /80 microlitres
Solution for Injection in pre-filled pen teriparatide
Indications
Tetridar® is indicated in adults. Tetr:dar 20 rn1crog
teriparatide ra_ms/BO microlitres cton npt •"'°Pe
Subcutaneous use
Treatment of osteoporosis in postmenopausal women and in men at increased risk of fracture. In postmenopausal women, a significant reduction in the incidence of vertebral and non-vertebral fractures but not hip fractures has been demonstrated.
Treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk for fracture.
Further information available from the SmPC available at HPRA.ie Tetridar® (teriparatide) 20 micrograms/SO microlitres Solution for Injection in pre-filled pen Abbreviated Prescribing Information.
Presentation: Each dose of 80 microlitres contains 20 micrograms of teriparatide. One pre-filled pen of 2.4 ml contains 600 micrograms of teriparatide (corresponding to 250 micrograms per ml).
Indications: Tetridar is indicated in adults for the treatment of osteoporosis in postmenopausal women and in men at increased risk of fracture. In postmenopausal women a significant reduction in the incidence of vertebral and non-vertebral fractures but not hip fractures has been demonstrated.
Treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk for fracture. Dosage and administration: The recommended dose of Tetridar is 20 micrograms administered once daily. The maximum total duration of treatment with Tetridar should be 24 months and the 24-month course of teriparatide should not be repeated over a patient's lifetime. Patients should receive supplemental calcium and vitamin D supplements if dietary intake is inadequate. Following cessation of teriparatide therapy, patients may be continued on other osteoporosis therapies. Adults: Teriparatide should be administered once daily by subcutaneous injection in the thigh or abdomen. Patients must be trained to use the proper injection techniques and correct use of the pen. Until further clinical data become available, the recommended treatment time of 24 months should not be exceeded. Children: The safety and efficacy of teriparatide in children and adolescents less than 18 years has not been established. Teriparatide should not be used in paediatric patients or young adults with open epiphyses. Elderly: No dosage adjustment required. Renal impairment: Teriparatide must not be used in patients with severe renal impairment. In patients with moderate renal impairment, teriparatide should be used with caution. No special caution is required for patients with mild renal impairment. Hepatic impairment: teriparatide should be used with caution in hepatically impaired patients, as no data are available. Contraindications: Hypersensitivity to the active substance or to any of the excipients, Pregnancy and breast-feeding, Pre-existing hypercalcaemia, Severe renal impairment, Metabolic bone diseases (including hyperparathyroidism and Paget's disease of the bone) other than primary osteoporosis or glucorticoid-induced osteoporosis, Unexplained elevations of alkaline phosphatase, Prior external beam or implant radiation therapy to the skeleton, Patients with skeletal malignancies or bone metastases should be excluded from treatment with teriparatide. Precautions and warnings: In normocalcaemic patients, slight and transient elevations of serum calcium concentrations have been observed following teriparatide injection. Serum calcium concentrations reach a maximum between 4 and 6 hours and return to baseline by 16 to 24 hours after each dose of teriparatide. Blood samples for serum calcium measurements should be taken at least 16 hours after the most recent Tetridar injection. Tetridar may cause small increases in urinary calcium excretion. Tetridar has not been studied in patients with active urolithiasis, therefore should be used in caution in patients with active or recent urolithiasis due to potential exacerbation of this condition. In short-term clinical studies with teriparatide, isolated episodes of transient orthostatic hypotension were observed. Typically, an event began within 4 hours of dosing and spontaneously resolved within a few minutes to a few hours. When transient orthostatic hypotension occurred, it happened within the first several doses. Experience in the younger adult population, including
Teva Pharmaceuticals Ireland, Digital Office Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67ESAO, Ireland.
Further information is available on request or in the SmPC. Product Information also available on the HPRA website. Prescription Only Medicine.
premenopausal women, is limited. Treatment should only be initiated if the benefit clearly outweighs risks in this population. Interactions: In a study of 15 healthy subjects administered digoxin daily to steady state, a single teriparatide dose did not alter the cardiac effect of digoxin. However, sporadic case reports have suggested that hypercalcaemia may predispose patients to digitalis toxicity. Because teriparatide transiently increases serum calcium, teriparatide should be used with caution in patients taking digitalis. Teriparatide has been evaluated in pharmacodynamic interaction studies with hydrochlorothiazide. No clinically significant interactions were noted. Co-administration of raloxifene or hormone replacement therapy with teriparatide did not alter the effects of teriparatide on serum or urine calcium or on clinical adverse events. Pregnancy and lactation: Women of childbearing potential should use effective methods of contraception during use of Tetridar. If pregnancy occurs, Tetridar should be discontinued. Tetridar is contraindicated for use during pregnancy and breastfeeding. It is not known whether teriparatide is excreted in human milk. Animal studies have shown reproductive toxicity. The effect of teriparatide on human foetal development has not been studied. The potential risk for humans is unknown. Effects on ability to drive and use machines: Tetridar has no or negligible influence on the ability to drive and use machines. Transient, orthostatic hypotension or dizziness was observed in some patients. These patients should refrain from driving or the use of machines until symptoms have subsided. Adverse reactions: Anaphylaxis, serious cases of back pain have been reported within minutes of the injection, syncope, hiatus hernia, nephrolithiasis, renal failure and renal impairment. Very Common: pain in limb; Common: anaemia, hypercholesterolaemia, depression, dizziness, headache, sciatica, vertigo, palpitations, hypotension, dyspnoea, nausea, vomiting, gastroesophageal reflux disease, sweating increased, muscle cramps, fatigue, chest pain, asthenia, mild and transient injection site events, including pain, swelling, erythema, localised bruising, pruritus and minor bleeding at injection site. Consult the Summary of Product Characteristics in relation to other side effects. Overdose: The effects of overdose that might be expected include delayed hypercalcaemia and risk of orthostatic hypotension, nausea, vomiting, dizziness, and headache. No fatalities associated with overdose have been reported. There is no specific antidote for Tetridar. Treatment of suspected overdose should include transitory discontinuation of Tetridar, monitoring of serum calcium, and implementation of appropriate supportive measures, such as hydration. Legal category: Medicinal product subject to medical prescription. Marketing Authorisation Number: PA1986/053/001. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00060. Date of Preparation: May 2022.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com