Further product information available on request from: AstraZeneca Pharmaceuticals (Ireland) DAC, College Business and Technology Park, Blanchardstown Road North, Dublin 15, Ireland. Freephone 1800 800 899.
ONDEXXYA® is a trademark(s) of the AstraZeneca group of companies. This medicinal product is subject to additional monitoring.
Veeva ID: IE-5804 Date of Preparation: January 2024
IN THIS ISSUE:
NEWS: Waiting List Plan falls at the First Hurdle Page 4
MEDICINES: Five-Year Vision published by Medicines for Ireland Page 6
PHARMACY: Personal Experiences of Hospital Pharmacy Placements Page 14
The Hospital Professional Honours will take place on Saturday, 14th September 2024 in the Radisson Blu Hotel, Dublin. Entries are now open across a number of categories including:
Haematology Project of the Year
Young Hospital Pharmacist of the Year
Galapagos Biotech Ltd, an Alfasigma company, Multidisciplinary Team of the Year
Fresenius Kabi Innovation in Aseptic Compounding
Medisource Hospital Pharmacy Technician of the Year
Grünenthal Advancing the Standard of Care in Pain Management
Athlone Pharmaceuticals Hospital Pharmacy Team of the Year
Excellence in Respiratory
Viatris Excellence in Cardiovascular Initiative
Pharmasource Hospital Pharmacist of the Year
MSD Excellence in Oncology Initiative
MedFind Solutions Innovation and Service Development
Excellence in Patient Safety
GSK ViiV Infectious Diseases Project of Year
Consultant-Led Team of the Year
Contents Foreword
New treatment shows benefits for Multiple Myeloma P5
New Five-Year vision for Medicines in Ireland P6
Almost 900,000 illegal medicines detained says HPRA P10
Clonmel Healthcare opens new Warehouse Facility P12
Annual Innovation Awards 2024 Recipients P18
Fostering connections in Mental Health P67
REGULARS
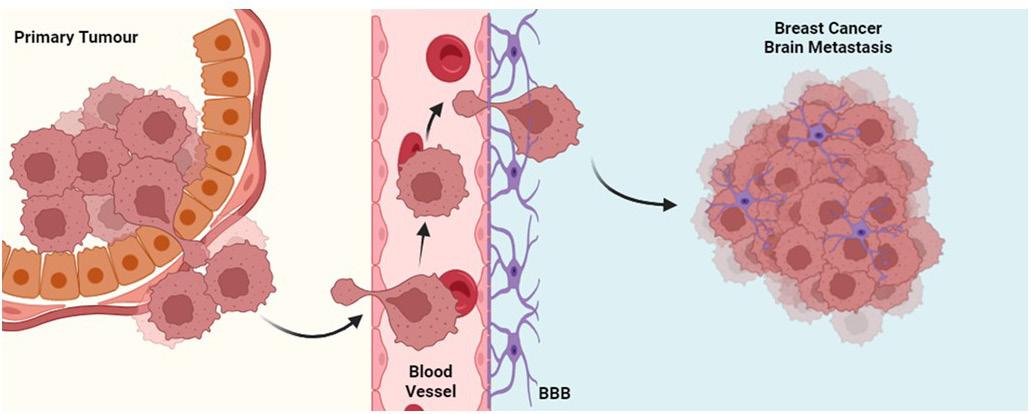
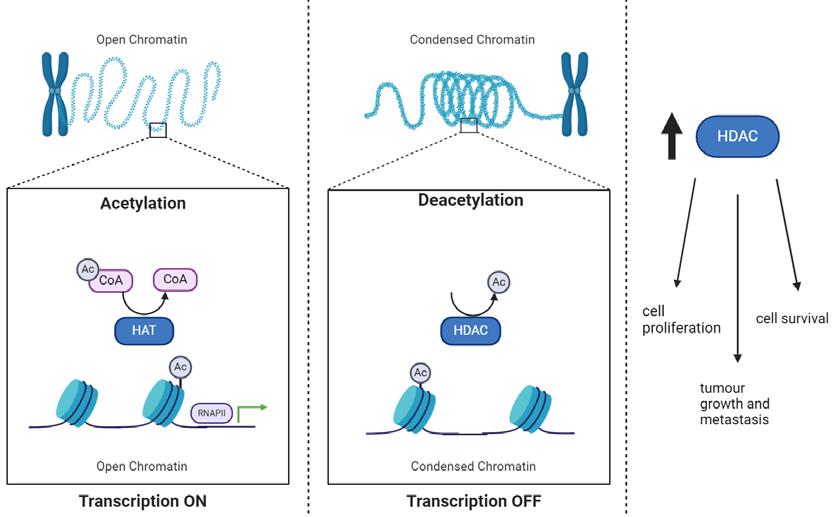
Oncology Focus: Breast Cancer Brain Metastasis P22
Oncology Focus: Merkel Cell Carcinoma P30
Editor
In one of your lead news stories this month, Medicines for Ireland (MFI) has published its new five-year vision Looking forward: Building the framework for a sustainable generic, biosimilar and value-added medicines industry in Ireland. The vision sets out MFI’s approach to address current and emerging market challenges, including demographic shifts, access to medicines, and inflationary pressures.
Chair of MFI, Paul Neill said, “It’s well documented how Ireland’s healthcare system is facing formidable challenges underscoring the urgent need for reform to ensure affordability, efficiency and sustainability for patients and the State. In the context of these challenges, the significance of a resilient and sustainable generic, biosimilar and value-added medicines industry cannot be overstated.”
You can read more about this on page 8.
CPD: Management of Joint and Muscle Pain P35
Endocrinology Focus: HIV P52
Feature: CardioStart in Tanzania P62
Hospital Professional News is a publication for Hospital Professionals and Professional educational bodies only. All rights reserved by Hospital Professional News. All material published in Hospital Professional News is copyright and no part of this magazine may be reproduced, stored in a retrieval system or transmitted in any form without written permission. IPN Communications Ltd have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
In other news on page 11, a new cross border report has found common barriers for smaller vendors in healthcare and urges an all-island shift to innovation procurement to enable SMEs and Start-ups to thrive in domestic health tech markets.
Launched last month, the ‘Buying All-Island in Healthcare – North and South’ report publishes the findings and recommendations framework of the All-Island Medtech SMEs (AIMS) initiative, delivered through a 12-month crossborder partnership of Enterprise Ireland and HSE partnership Health Innovation Hub Ireland (HIHI) and Health Innovation Research Alliance Northern Ireland (HIRANI), supported by InterTradeIreland’s Synergy programme.
SALES EXECUTIVE
Avril Boyd avril@hospitalprofessionalnews.ie
SALES & TRAINING MANAGER
Sibongile Mude s.mude@hospitalprofessionalnews.ie
CONTRIBUTORS
Marie Duffy | Grainne Warren
Amanda Tirone | Sarah King
Dr Katie Liston
Dr Maeve Crowley
Declan O’Sullivan
Professor Roisin O’Hare
Bernie Carter
Claire Doyle
Mr Diego Abril Carbonell
Miss. Aoibheann Dowd
Dr Jason McGrath
Dr Gordon Daly
Dr Damir Vareslija
Professor Leonie Young
DESIGN DIRECTOR
Ian Stoddart Design
Our Oncology Special Focus section has contributed articles from Professor Shirley Potter and Professor Des Tobin on the Irish Melanoma Forum 12th Annual Scientific Meeting, an interview with Dr Catherine O’Gorman and Ashley Lily on the first patient passport for gynaecological oncology patients and Claire Doyle discussing the incidence of Merkel Cell Carcinoma.
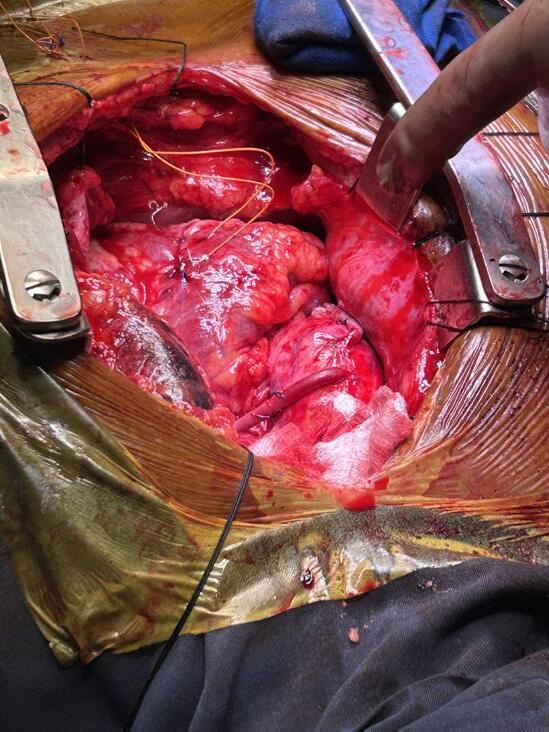
Meanwhile, on page 64, the team from CardioStart International talk about their recent trip to Jakaya Kikwete Cardiac Institute (JKCI) in Dar Es Salaam, Tanzania. The group consisted of cardiac surgeons, anaesthetists, nurses, perfusionists, cardiac sonographer, and a critical care doctor. The group travelled from the USA, Australia, and Ireland under the auspice of a charity called CardioStart International. The basic mission of CardioStart is to educate and assist local medical teams in providing heart surgery and cardiac services to adults and children in underserved regions of the world, with a vision of a world where access to cardiac care can be realized by everyone.
I hope you enjoy the issue.
Waiting List Plan falls at ‘First Hurdle’
The Irish Hospital Consultants Association (IHCA) has warned that the Government’s Waiting List Action Plan for 2024, launched just last month, has already fallen at the first hurdle, just as its previous plans have done over the past two years.
Commenting as the National Treatment Purchase Fund (NTPF) released its figures for the end
Professor Gabrielle Colleran, Vice President, Irish Hospital Consultants Association
of March, the IHCA said that the three main waiting lists for hospital appointments and treatments have increased by 24,300 (4%) in the first three months of 2024 alone. This is compared with an expected pro rata target reduction of 9,800 people by the end of March, giving a shortfall already of over 34,000.
The ¤437 million Action Plan for 2024 has set a target to reduce waiting lists for outpatient appointments and inpatient and day case treatment and procedures by 39,300 (6%) by the end of December compared with the number waiting at the start of the year. Similar Action Plans in 2022 and 2023 had set ambitious reduction targets of 18% and 10%, but only cut waiting lists by 4% and 3% respectively.
The modest decrease last year was only achieved by removing more than 129,000 people from the waiting lists without any treatment through an NTPF ‘validation programme’. This year’s projected cuts in waiting lists are again dependent on the NTPF removing more than 117,000 people without any treatment under the same administrative scheme.
Over 896,500 people were on some form of NTPF waiting list at the end of the first quarter, including numerous less publicised pre-admit, planned procedure and suspension lists, which collectively total over 200,000 for the very first time. The total number of people currently on waiting lists is an increase of almost 313,000 (54%) compared with May 2017 when Sláintecare was published.
Commenting on today’s NTPF figures, IHCA Vice President Professor Gabrielle Colleran said,
Risks of Repeating Regressive Mistakes
“The 2024 Waiting List Action Plan published by the Department of Health just two weeks ago has already fallen at the first hurdle, as did the two previous plans in 2022 and 2023. While we welcome any funding which aims to cut these unacceptably long waiting lists and allow patients access to the care they require, perhaps it is time the Government takes a different approach, if it is doing the same thing over and over again and still expecting to get different results.
“The NTPF figures released today confirm Consultants’ grave concerns that these waiting lists may take a decade or more to get under control unless the opening of long-promised additional hospital capacity is fast-tracked by the Government, and simultaneously the one in five Consultant posts vacant or filled on a temporary basis are permanently filled.”
The Irish Medical Organisation (IMO) has warned that the Department of Health risks repeating the same “regressive” mistakes of the austerity years if it plans to move away from health service investment in order to prioritise savings.
The warning follows the publication of a report by the Department of Health and the Irish Government Economic Evaluation Service into hospital activity and investment.
The IMO said that inadequate capacity and workforce staffing had a major detrimental effect on the patient journey, leading to unnecessary delays and poorer outcomes. This is exacerbated by our rising population and increased complexities of care, particularly in relation to the growing and ageing population. It added that too few doctors and consistent work pressure has led to rising rates of burnout, stress and emigration to the point where we have a recruitment and retention crisis among doctors.
Professor Matthew Sadlier, Chair of the Consultants’ Committee of the IMO, said: “It is surprising and disappointing to see this Department of Health report highlight the need for savings in the health service, especially considering similar Government policy during the recession had negative ramifications which are still being experienced to this day. The health service’s main problem is that we have neither the beds nor the doctor numbers to meet ever-growing patient demand.
“While the healthcare budget has increased in recent years, that must be seen in the context of restricted budgets for over a decade and a population that has increased beyond expectations leading to increased demand. The 2024 Budget allocated to the HSE will be challenged in terms of maintaining service levels, never mind expanding services.
“Doctors are spending increasing number of hours trying to get patients beds and support services in a timely manner and this reduces clinical patient-facing time. The vast majority of consultants are working longer hours and 84% of our NCHD colleagues report consistently working in excess of legal hours.”
New drug Combination for Multiple Myeloma
RCSI research has found that venetolax, a medication currently approved for leukaemia, has benefits for patients with multiple myeloma when used in combination with another drug. This discovery offers a new avenue of treatment options for the currently incurable disease.
Multiple myeloma (MM) is a type of blood cancer that is newly diagnosed in around 400 people in Ireland each year. Despite treatment advances in recent years, it remains incurable. The search for innovative treatment strategies is crucial, particularly for patients whose cancer is resistant to standard care.
In the new study researchers at the RCSI Department of Physiology and Medical Physics and the Beaumont RCSI Cancer Centre set out to identify complementary drugs that would enhance the efficiency of venetolax, a drug approved for use in leukaemia, for MM treatment. Although previously tested in MM, venetoclax, which blocks the function of a protein called BCL-2, was only found to be effective for a small proportion of patients.
The researchers discovered that combining venetoclax with a drug called 5-azacytidine significantly increased its effectiveness across many MM cell lines, indicating
Professor Siobhán Glavey and Professor Tríona Ní Chonghaile
a broader potential patient population that could be treated with the new combination.
“This research is a significant step in identifying more effective treatment options for multiple myeloma. By combining venetoclax and 5-azacytidine we’ve seen enhanced efficacy across a wide range of patient samples. It shows the benefits of re-evaluating existing treatments in new contexts to expand their potential.” said Professor Tríona Ní Chonghaile, Associate Professor and research lead, Department of Physiology and Medical Physics.
Professor Siobhán Glavey, Chair, RCSI Department of Pathology and Clinician Scientist, Beaumont RCSI Cancer Centre commented:
“Discovering the potential of this new drug combination is a promising development. Our next goal is to test for efficacy and safety for multiple myeloma in a clinical trial setting to bring us closer to offering a new treatment strategy for patients.”
The mechanism of how the two drugs work efficiently together was also investigated and it was shown that the combination of the two therapies was effective in patient
‘Hospital at Home’ Model in Ireland
Maynooth University’s Innovation Value Institute (IVI) have welcomed Professor Dan Lasserson, the UK’s expert in ‘Hospital at Home’ models and acute ambulatory care, who spoke on the topic of delivering acute medical care for patients at home, his experience of similar models in the UK and opportunities for such an approach in support of Ireland’s HSE services that benefit end users.
In his presentation, Prof Lasserson discussed how advances in diagnostic and monitoring technology could lead to more patients being assessed and treated without any admission to hospital if that is their choice.
Drawing on his recent research and presentation of clinical cases that he has managed at Warwick University Medical School, Prof
Lasserson also spoke about how patients with severe and complex medical problems can be given a care pathway that is personalised as well as delivering key processes of healthcare at home.
Prof Lasserson runs an acute hospital at home service from the Geriatric Medicine department at the John Radcliffe Hospital in Oxford and is a Past President of the UK Hospital at Home Society.
Prof Dan Lasseron commented: “It is a privilege to be invited by Maynooth University to give this lecture which I hope will be a catalyst for the start of the Hospital at Home journey in Ireland and I look forward to mutual learning and innovation as we look to accelerate the adoption of digital enable models of care across the Irish sea.
“A change in the health system mindset and culture, and using technology to enable a stay left, shift left of care to the home is essential to deliver personalized acute care in a future proofed healthcare pathway. “
Prof Martin Curley, Professor of Innovation at Maynooth University, added: “Shifting more care from hospital to home is one of the key Copernican shifts needed to drive a metamorphosis in our health system. Using digital technologies such as the Irish developed Blueeye hospital at home system, means patient vital signs can be better measured and managed in their homes than in ninety percent of Irish hospitals. It is positive to see the HSE looking to introduce virtual ward solutions, we just need to go faster to help
samples from different stages of cancer, even if that patient had been previously treated with chemotherapy drugs.
The research was conducted in collaboration with the Department of Haematology, Beaumont Hospital, Dublin; Department of Medical Oncology, Dana-Farber Cancer Institute, Boston; and the Department of Medicine/ Haematology, University of Galway, Galway.
solve Ireland’s Acute hospital bed occupancy problem and perhaps more importantly bring better care and a better patient experience for to all.”
As a follow on to this event, the second International Digital Health Summer School will be hosted by the Innovation Value Institute (IVI), Maynooth University, on June 26th and 27th.
Featured speakers for the Summer School will include Russ Brazell, President and Chief Executive of College of Healthcare Information Management Executives (CHIME), Robert Watt, Secretary General at the Department of Health, Prof Martin Curley, Professor of Innovation at Maynooth University and Dr Colm Henry, Chief Clinical Officer at the HSE.
Medicines for Ireland Publish New Vision
Medicines for Ireland (MFI) has published its new five-year vision Looking forward: Building the framework for a sustainable generic, biosimilar and valueadded medicines industry in Ireland. The vision sets out MFI’s approach to address current and emerging market challenges, including demographic shifts, access to medicines, and inflationary pressures.
In developing its new Vision Strategy 2024 – 2029, MFI member companies focused on three core strategic pillars:
1. Enhancing patient access and affordability through delivering a coherent framework agreement with the Department of Health and the Health Service Executive which facilitates innovation, patient centricity and value.
2. Securing a resilient and competitive supply chain ecosystem by championing local and European policies that support medication supply in Ireland.
3. Embedding industry sustainability through fostering a balanced approach to environmental practices which don’t overshadow public health benefits and accelerating the adoption of electronic patient information leaflets.
MFI’s overarching objective is to effect real change and reform around how Ireland procures and
supplies medicines, expanding patient access to affordable, lifesaving and life-enhancing treatment. Commenting on how the new strategy will allow the industry to deliver on this ambition, Chair of MFI, Paul Neill said: “It’s well documented how Ireland’s healthcare system is facing formidable challenges underscoring the urgent need for reform to ensure affordability, efficiency and sustainability for patients and the State. In the context of these challenges, the significance of a resilient and sustainable generic, biosimilar and value-added medicines industry cannot be overstated.
“This year, the Department of Health has projected that almost ¤3 billion will be spent on medicines, representing nearly ¤1 in every ¤8 spent by the State on healthcare. Health policy decision makers must recognise how increased penetration of generic, biosimilar, and value-added medicines offers significant savings to the State and the opportunity for earlier treatment interventions for more patients. This further expands the opportunity to redirect scarce resources to other areas of the healthcare system. Currently generics account for 58 per cent of all prescribed medicines in Ireland behind the European average of 70%.”
Mr Neill added: “There are several influencing factors causing Ireland to lag our European counterparts when it comes to generic penetration which must be
Pictured at the launch of the Medicines for Ireland (MFI) new five-year Vision Strategy are Chair of MFI, Paul Neill and Vice-Chair of MFI, Deirdre Kelly
addressed. These include reduced price entry point, downward only pricing structures, and lengthy timelines for price uplifts for unviable products. These factors have an overall impact on the attractiveness of the Irish market for manufacturers. To fully realise the potential of enhanced patient access and affordability through increased penetration, it is pivotal that we foster a market ecosystem which promotes fair competition and availability of medicines over the next five years.
“From the perspective of our members, key to this must be the delivery of a coherent framework agreement on the supply and pricing of medicines with the Department of Health. To help alleviate some of the pressure points faced by the industry, any new agreement must embrace tiered pricing, de-linkage from the originator price model, and automatic indexation models. As an industry body, we are committed to championing dynamic policies that support competition through balanced price control measures, aligned with demand side policies which incentivise the use of generic, biosimilar, and value-added medicines which benefit patient access and affordability.”
Established in 2016, MFI is the leading voice for the generic, biosimilar, and value-added medicines industry with its members supplying the majority of medicines to the HSE and patients
directly. Generic companies play an essential role in the supply of prescription medicines in Ireland, with eight of the top 10 companies in the total prescription market (based on volume of units) supplying generic medicines. Six of these are MFI members.
Commenting on the roll-out of the association’s five-year strategy, Vice-Chair of MFI, Deirdre Kelly said: “Our members remain steadfast in their focus on ensuring access to essential medicines in Ireland. The commitments and deliverables detailed under the three core strategic pillars in our Vision Strategy present a clear roadmap to drive patient-centric solutions that prioritise value, accessibility, and quality for patients, healthcare providers and the State. In line with the OECD’s recommendations, we are wellpositioned to support and deliver increased use of generic, biosimilar, and value-added medicines.
“Recognising the interconnected nature of healthcare delivery, policy frameworks, and economic considerations, our ambitions will only be achieved through a collective and collaborative partnership approach. Working with industry partners, we will advocate for fair policies that balance value for patients and the State with medication supply viability for the industry. We consider our Vision Strategy as a call to action. By collaborating with stakeholders, policymakers, and healthcare professionals, we can shape a future where patients receive high-quality, affordable medicines in a resilient healthcare ecosystem,” Ms Kelly concluded.
A safety barrier to medication errors
Inpatient prescriptions made legible
“This is a tried and tested product addressing the problem of prescription illegibility.”
¤11.6 million ELEVATE cerebral palsy research programme
The Tánaiste, Minister for Foreign Affairs and Minister for Defence, Micheál Martin TD, has launched a new ¤11.6 million research programme focused on cerebral palsy at University College Cork (UCC).
The programme will be led by the Irish Centre for Maternal and Child Health Research (INFANT)
Dr Jennifer Ryan, Senior Lecturer, RCSI
at UCC, partnering with RCSI University of Medicine and Health Sciences, Trinity College Dublin, and all the tertiary-level maternity hospitals in Ireland.
ELEVATE, a ground-breaking fiveyear initiative, has been funded under the Science Foundation Ireland (SFI) Strategic Partnership Programme (¤5 million), with co-funding partner the Cerebral Palsy Foundation (CPF) providing support of over ¤6 million. Dr Jennifer Ryan, Senior Lecturer at the RCSI School of Physiotherapy and Director of the CP-Life Research Centre, will lead RCSI’s involvement in the programme.
ELEVATE brings together a team of researchers and experts in early brain injury to create cutting-edge AI screening algorithms, devise
novel detection methods, explore potential new treatments, and, most importantly, actively involve cerebral palsy-affected families in ongoing trials, education, and information platforms. The programme will also see the establishment of a cerebral palsy registry in Ireland, to track the rate of the condition for the first time and enable access to the best research and clinical trials.
Launching the ELEVATE Programme, Tánaiste Micheál Martin TD said: “I'm delighted to launch this ambitious new programme, which has the potential to transform lives and reshape the landscape of cerebral palsy research and care in Ireland. The ELEVATE strategic partnership programme marks a landmark investment and milestone in the collective efforts to address what is one of the most pressing challenges in healthcare. We stand on the cusp of a new era in cerebral palsy research.”
Significant challenges
Cerebral palsy (CP) is the most common childhood-acquired, lifelong physical disability, affecting about 17 million people worldwide. There is no known cure.
It is caused by abnormal development or damage to the brain before, during, or shortly after birth. Many individuals with CP face significant and unnecessary challenges in their daily lives, including problems with movement, speech, and other body systems. An estimated 150 babies receive a CP diagnosis in Ireland each year and an estimated 3,000 children and young people and 9,500 adults are living with cerebral palsy in Ireland.
But these diagnoses are often delayed, with devastating consequences for children and their families. Early intervention and the right care pathways make a significant difference in the long-term outcomes and quality of life for people living with Cerebral Palsy.
¤36.5m investment in New Theatres at Bon Secours
Bon Secours Hospital Galway is to construct two new theatres as part of a significant ¤36.5 million investment in its services, it has been announced.
The hospital is to submit an application for planning permission to Galway City Council to construct the two new theatres, extending the Endoscopy Suite to include a fourth Endoscopy treatment room, sixteen endoscopy bays, four theatre recovery bays and fourteen surgical dayward bays.
Bon Secours Hospital Galway remains steadfast in its commitment to advancing healthcare services and expanding its facilities to better
serve the community and earlier today the Group CEO, Bill Maher and Hospital CEO, Henry Burrows announced that it is poised to embark on another phase of expansion.
Bon Secours Health System Group Chief Executive, Bill Maher, added, “Aligned with its strategic 2025 Plan and with a projected investment of ¤36.5 million, this will reinforce Bon Secours Hospital Galway's position as a premier healthcare provider in the west of Ireland, ensuring continued excellence in healthcare delivery for years to come.”
Earlier this year, the hospital unveiled its ¤1.3m investment in relocating its Minor Operating
Procedure Room and the inauguration of a state-of-theart third Endoscopy Suite. The addition of the third endoscopy suite substantially bolstered the hospital's capacity to serve patients, with the capability to now conduct an additional 4,000 scopes in 2024 alone.
Bon Secours Hospital Galway celebrated another milestone with the opening of new and upgraded facilities. Among these is a cutting-edge MRI scanner, the Magnetom Sola, representing a ¤1 million investment in advancing medical imaging capabilities. The Magnetom Sola enables more targeted and effective treatment plans while prioritising patient
comfort and safety during MRI examinations which in turn aids reduction in patient waiting times.
Also, the hospital inaugurated new theatre sterile stores and two autoclaves at a cost of ¤1.75m, further solidifying its infrastructure to support surgical procedures and maintain stringent sterilisation standards and future proofing future expansion.
In early May 2024 Bon Secours Hospital Galway will further enhance its offerings by expanding its Echocardiogram capabilities by creating a standalone Echocardiogram room. This will increase the hospital’s capacity from 10 echos per week to 5 per day.
All-Island Shift to Innovation
Dr Siobhan McGrath, Health Innovation Research Alliance Northern Ireland, Eimear Galvin, Health Innovation Hub Ireland, Prof Joann Rhodes Health Innovation Research Alliance Northern Ireland
New cross-border report finds common barriers for smaller vendors in healthcare and urges an all-island shift to innovation procurement to enable SMEs and Start-ups to thrive in domestic health tech markets.
Launched last month, the ‘Buying All-Island in Healthcare – North and South’ report publishes the findings and recommendations framework of the All-Island Medtech SMEs (AIMS) initiative, delivered through a 12-month cross-border partnership of Enterprise Ireland and HSE partnership Health Innovation Hub Ireland (HIHI) and Health Innovation Research Alliance Northern Ireland (HIRANI), supported by InterTradeIreland’s Synergy programme. This allisland collaborative initiative with SMEs and healthcare stakeholders - health sector, health industry, policy, state agency, academia and procurement - identified barriers and experienced by smaller vendors in Irish healthcare and proposed solutions.
38 stakeholder groups from health, industry, policy, state agency, academia and procurement, identified common challenges to SMEs and start-ups within the Irish (North and South) health market. New and smaller suppliers below certain revenue thresholds are not equally positioned to compete with established vendors for healthcare tenders, unfairly affected by scale and liquidity requirements. Outdated assessments for software products, lack of innovation procurement and funding for its mechanisms, limited use of dynamic purchasing systems and purchasing standards that vary widely across secondary care sites in ROI are also perceived to be prohibitive.
AIMS stakeholder workshops; expert advisory group sessions and European benchmarking informed the proposed solutions contained in the ‘AIMS Framework of recommendations for Innovation Procurement’. The framework focuses on four key areas to deliver system-wide impact that will facilitate the procurement of innovative products across the healthcare sector on the island of
Ireland from all vendors, regardless of size –
1. Budget and Mechanisms –create a protected healthcare budget for the procurement of innovation, implement EU approved mechanism
To boost innovation procurement allocate a portion of the public budget, replicating successful European exemplars. Public Procurement of Innovative solutions (PPI) is one mechanism. The public sector uses its purchasing power to act as early adopter of innovative solutions that are not yet available on largescale commercial basis. PPI can target specific healthcare challenges by seeking innovative solutions, and through a testing phase, reduce risks commonly associated with smaller vendors.
2. Review and revise procurement thresholds — hardware vs software
Tender requirements often demand high turnovers, a relic of old hardware focussed companies. This excludes smaller, innovative firms. Unlike hardware, software does not rely on costly supply chains; its main costs are licenses and setup. Software procurement
should prioritise features, capabilities, and fit with needs over financial size.
3. Increase use of Dynamic Purchasing Systems (DPS) in healthcare procurement
A DPS is a digital tool allowing qualified suppliers to join anytime to compete for contracts. In contrast to tender frameworks, which usually last four years. DPS increases small businesses access to public contracts, simplifying the process by cutting out repetitive bids.
4. Co-develop and publish education tool for SMEs navigating HSC and HSE
Developing an educational tool with HSE procurement for SMEs and start-ups will benefit small entities understanding of a multi-faceted complex process. The online tool will be co-developed, user-friendly, accessible and regularly updated to reflect any changes in regulations or best practice.
Currently, there are no Irish innovation procurement policy frameworks driving public buyer engagement with smaller vendors. This is in stark contrast to common European practice. Austria, Belgium, Finland, and the
Netherlands have specific action plans for innovation procurement. Denmark, Germany, Estonia, Greece, France and Sweden include specific objectives on innovation procurement in wider national strategies.
Dr Tanya Mulcahy, National Director Health Innovation Hub Ireland said, “While the development of innovative healthcare products by Irish and Northern Irish-based companies is something we excel at, the application and procurement of those innovations in Irish healthcare has not been realised. This report identifies some of the barriers and measures that could be implemented immediately with significant effect. The ‘Programme for Government – Our Shared Future’ identified the role public procurement can play as an instrument to support innovation and allow greater access for SMEs to public procurement. The six new Regional Health Authorities also present an opportunity to assess these recommendations and consider suitability per region.”
“The HSE is making changes to its procurement processes and has specifically identified working with HIHI in its Corporate Plan 2022-2024. The recommendations of the ‘Buying Irish in Healthcare – North and South’ report recommend priorities on which we can collaborate.
Almost 900,000 Illegal Medicines Detained
The Health Products Regulatory Authority (HPRA) has released its annual enforcement data which shows that it detained 874,945 dosage units* of falsified and other illegal medicines in 2023. Announcing the figures, the HPRA warned of the serious health dangers posed by sourcing prescription medicines online and from unauthorised sources. It states that the supply of these products into and within Ireland is illegal and stresses that consumers can have no guarantees about the safety or quality of prescription medicines they are seeking to buy outside of the regulated pharmacy setting.
In the 12 months of 2023, the most significant categories of illegal products detained included sedatives (34%), anabolic steroids (29%), erectile dysfunction medicines (10%), analgesics (5%), and Stimulants (3%). The breakdown is as follows:
• Sedative medicines – 294,145 units detained
• Anabolic steroids – 250,922 units detained
• Erectile dysfunction medicines –84,119 units detained
• Analgesic medicines – 42,307 units detained
• Stimulants – 24,530 units detained
The HPRA also continues to monitor online activity promoting prescription medicines and other substances, and routinely intervenes to disrupt this promotion. Such activity is often linked to the use of particular substances for aesthetic and body image purposes.
The following are some of the key enforcement actions taken by the HPRA in 2023:
• Two prosecution cases initiated, relating to the importation or distribution of anabolic steroids.
• 2,348 websites, e-commerce listings and/or social media pages amended or shutdown.
Grainne Power, Director of Compliance with the HPRA, expressed concern that the
FIP Impact Database
Grainne Power, Director of Compliance with the HPRA
2023 data continue to highlight the risks that individuals take when attempting to purchase prescription medicines from unauthorised suppliers.
“While we welcome a slight decrease in overall detentions this year (874,945 units in 2023 compared to 939,388 units in 2022), the data shows a concerning increase in a number of categories. Of particular note, there was a more than 20% increase in the volume of illegal anabolic steroids detained. This is continuing an upward trend observed over several years.
“We believe young men in particular may be sourcing anabolic steroids for body enhancement while being unaware of the serious health complications posed by these products. Anabolic steroids can cause serious physical and psychological health issues. The potential physical side effects alone include heart failure, liver issues, kidney damage, and infertility.
According to Ms Power, there appears to be a willingness among
some consumers to take risks in sourcing falsified medicines and unauthorised substances for what would be considered aesthetic and body image purposes.
“Whether for privacy, ease of access, cost, or simply aware that their doctor may not deem it appropriate medical use, many choose to seek out these products online and from other unregulated sources. In addition to anabolic steroids, we are also seeing a concerning upward trend in detentions of Melanotan 2, an unregulated substance promoted as a self-tanning aid, as well as botulinum toxin and online semaglutide and liraglutide products. While overall numbers remain low, as with all illegally supplied products, once consumers step outside of the regulated supply chain, they have absolutely no guarantees as to safety, quality or effectiveness. Some of these substances are not authorised for use by any regulator anywhere in the world while other products that are presented as legitimate medicines, could well be falsified or fake.”
The HPRA will initiate prosecution cases where it considers that there is a significant risk to public health or where there are persistent non-compliances. The HPRA also supports prosecutions brought by the Director of Public Prosecutions in relation to the illegal supply of medicines.
Before initiating a prosecution, the HPRA will typically engage with an offender, detain product and may formally caution the individual to ensure any illegal activity is ended.
In 2023, 14 voluntary formal cautions were issued.
A new FIP resource for evidence-based advocacy and policy engagement, the FIP Impact Database, is launched today on World Health Day. The database collates, summarises, categorises and provides analyses of FIP outputs that support the federation’s vision and mission. It also includes main areas of work, challenges, opportunities and best practices of FIP member organisations over the past decade related to improving global health through influencing practice.
The resource, hosted by the FIP Global Pharmaceutical Observatory (GPO), is currently in its testing phase. FIP is inviting its members to provide feedback here. “The database will continue to evolve into a sustainable, dynamic resource for policymakers and leaders. I invite you to explore [it] and see for yourself the wealth of information available to you and the pharmacy profession,” said FIP’s GPO director Prof. Ian Bates. The FIP Impact Database collates, summarises, categorises, and provides access to a complete range of outputs that support the Federation and its members’ vision and mission. The FIP Impact Database also includes the main work areas, innovations, and best practices of FIP member organisations over the past decade that have contributed to the advancement of pharmaceutical global health through influencing practice, education, and policy. The target audience includes pharmacists, leaders, policymakers, researchers, and members of FIP. FIP plans to expand the scope of the database by incorporating a wider range of publications that have impacted global policy formation. This database is currently in its testing phase, providing an opportunity for members to explore its features and provide feedback. Your insights are important for enhancing its functionality and user experience. Please click here to share your feedback and suggestions for improvement. For more information please contact: observatory@fip.org
The Medicine Management Programme (MMP) recommends Tetridar® as a Best Value Medicine (BVM) for
teriparatide on the High Tech Arrangement.
Indications
• Tetridar® is indicated in adults.
• Treatment of osteoporosis in postmenopausal women and in men at increased risk of fracture. In postmenopausal women, a significant reduction in the incidence of vertebral and non-vertebral fractures but not hip fractures has been demonstrated.
• Treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk for fracture.
Further information available from the SmPC available at HPRA.ie
Tetridar® (teriparatide) 20 micrograms/80 microlitres Solution for Injection in pre-filled pen
Abbreviated Prescribing Information.
Presentation: Each dose of 80 microlitres contains 20 micrograms of teriparatide. One pre-filled pen of 2.4 mL contains 600 micrograms of teriparatide (corresponding to 250 micrograms per mL).
Indications: Tetridar is indicated in adults for the treatment of osteoporosis in postmenopausal women and in men at increased risk of fracture. In postmenopausal women a significant reduction in the incidence of vertebral and non-vertebral fractures but not hip fractures has been demonstrated. Treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk for fracture. Dosage and administration: The recommended dose of Tetridar is 20 micrograms administered once daily. The maximum total duration of treatment with Tetridar should be 24 months and the 24-month course of teriparatide should not be repeated over a patient’s lifetime. Patients should receive supplemental calcium and vitamin D supplements if dietary intake is inadequate. Following cessation of teriparatide therapy, patients may be continued on other osteoporosis therapies. Adults: Teriparatide should be administered once daily by subcutaneous injection in the thigh or abdomen. Patients must be trained to use the proper injection techniques and correct use of the pen. Until further clinical data become available, the recommended treatment time of 24 months should not be exceeded. Children: The safety and e cacy of teriparatide in children and adolescents less than 18 years has not been established. Teriparatide should not be used in paediatric patients or young adults with open epiphyses. Elderly: No dosage adjustment required. Renal impairment: Teriparatide must not be used in patients with severe renal impairment. In patients with moderate renal impairment, teriparatide should be used with caution. No special caution is required for patients with mild renal impairment. Hepatic impairment: teriparatide should be used with caution in hepatically impaired patients, as no data are available. Contraindications: Hypersensitivity to the active substance or to any of the excipients, Pregnancy and breast-feeding, Pre-existing hypercalcaemia, Severe renal impairment, Metabolic bone diseases (including hyperparathyroidism and Paget’s disease of the bone) other than primary osteoporosis or glucorticoid-induced osteoporosis, Unexplained elevations of alkaline phosphatase, Prior external beam or implant radiation therapy to the skeleton, Patients with skeletal malignancies or bone metastases should be excluded from treatment with teriparatide. Precautions and warnings: In normocalcaemic patients, slight and transient elevations of serum calcium concentrations have been observed following teriparatide injection. Serum calcium concentrations reach a maximum between 4 and 6 hours and return to baseline by 16 to 24 hours after each dose of teriparatide. Blood samples for serum calcium measurements should be taken at least 16 hours after the most recent Tetridar injection. Tetridar may cause small increases in urinary calcium excretion. Tetridar has not been studied in patients with active urolithiasis, therefore should be used in caution in patients with active or recent urolithiasis due to potential exacerbation of this condition. In short-term clinical studies with teriparatide, isolated episodes of transient orthostatic hypotension were observed. Typically, an event began within 4 hours of dosing and spontaneously resolved within a few minutes to a few hours. When transient orthostatic hypotension occurred, it happened within the first several doses. Experience in the younger adult population, including
Teva Pharmaceuticals Ireland, Digital O ce Centre Swords, Suite 101 - 103, Balheary Demesne, Balheary Road, Swords, Co Dublin, K67E5AO, Ireland.
Further information is available on request or in the SmPC. Product Information also available on the HPRA website. Prescription Only Medicine.
premenopausal women, is limited. Treatment should only be initiated if the benefit clearly outweighs risks in this population. Interactions: In a study of 15 healthy subjects administered digoxin daily to steady state, a single teriparatide dose did not alter the cardiac e ect of digoxin. However, sporadic case reports have suggested that hypercalcaemia may predispose patients to digitalis toxicity. Because teriparatide transiently increases serum calcium, teriparatide should be used with caution in patients taking digitalis. Teriparatide has been evaluated in pharmacodynamic interaction studies with hydrochlorothiazide. No clinically significant interactions were noted. Co-administration of raloxifene or hormone replacement therapy with teriparatide did not alter the e ects of teriparatide on serum or urine calcium or on clinical adverse events. Pregnancy and lactation: Women of childbearing potential should use e ective methods of contraception during use of Tetridar. If pregnancy occurs, Tetridar should be discontinued. Tetridar is contraindicated for use during pregnancy and breastfeeding. It is not known whether teriparatide is excreted in human milk. Animal studies have shown reproductive toxicity. The e ect of teriparatide on human foetal development has not been studied. The potential risk for humans is unknown. E ects on ability to drive and use machines: Tetridar has no or negligible influence on the ability to drive and use machines. Transient, orthostatic hypotension or dizziness was observed in some patients. These patients should refrain from driving or the use of machines until symptoms have subsided. Adverse reactions: Anaphylaxis, serious cases of back pain have been reported within minutes of the injection, syncope, hiatus hernia, nephrolithiasis, renal failure and renal impairment. Very Common: pain in limb; Common: anaemia, hypercholesterolaemia, depression, dizziness, headache, sciatica, vertigo, palpitations, hypotension, dyspnoea, nausea, vomiting, gastroesophageal reflux disease, sweating increased, muscle cramps, fatigue, chest pain, asthenia, mild and transient injection site events, including pain, swelling, erythema, localised bruising, pruritus and minor bleeding at injection site. Consult the Summary of Product Characteristics in relation to other side e ects. Overdose: The e ects of overdose that might be expected include delayed hypercalcaemia and risk of orthostatic hypotension, nausea, vomiting, dizziness, and headache. No fatalities associated with overdose have been reported. There is no specific antidote for Tetridar. Treatment of suspected overdose should include transitory discontinuation of Tetridar, monitoring of serum calcium, and implementation of appropriate supportive measures, such as hydration. Legal category: Medicinal product subject to medical prescription. Marketing Authorisation Number: PA1986/053/001. Marketing Authorisation Holder: Teva B.V., Swensweg 5, 2031GA Haarlem, Netherlands. Job Code: MED-IE-00060. Date of Preparation: May 2022.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com
Just last month, in the presence of Mayor of Clonmel Borough District, Cllr Richie Molloy, Clonmel Healthcare, popular consumer health brand, has announced the completion of the construction of a brand new ¤3 million euro warehouse facility in Clonmel.
The 1650 square metre build, which officially opened its doors today comes after a previous extension of 1,800 square metre in 2017, and will see the increase in production potential of STADA AG pharmaceutical products through this additional distribution capacity for specialised medical products supplied to pharmacists and medical professionals across Ireland.
The construction involved an extensive renovation and extension of a building that was over 50 years old. Previously, the warehouse capacity was 3,500 pallets, yet was responsible for moving 22 million prescription drugs and over the
counter products annually - the single largest distribution of pharmaceutical products in Ireland in 2023 by volume.
With the opening of the new, larger facility, located on Waterford Road, Clonmel Healthcare expect to store 6,000 pallets of products at any one time which is a huge increase on last year, along with ensuring a much more efficient storage and distribution process.
Jim Hanlon, CEO Clonmel Healthcare said of the new warehouse, “The consumer demand for Clonmel Healthcare products has been growing incrementally year on year, so it was time we invested in the
Pictured L - R: Donagh O’Leary, Barry Fitzpatrick, Cllr. Richie Molloy (Mayor of Clonmel Borough District), Jim Hanlon, Michelle Aylward (CEO Tipperary Chamber of Commerce), Ger Roberts, Kieran Mulhall and Simon McGowan
re-sizing of our facility, in addition to our commercial office with Sale & Marketing functions in Dublin, in order to meet increased customer demands.”
Mr Hanlon added, “This is a reflection of the drivers of our business over the last number of years and a project that will provide more growth opportunities in line with our purpose of Caring for Patient’s Health as a Trusted Partner.”
“We are delighted to see this additional investment from Clonmel Healthcare at its HQ in Clonmel. Clonmel Healthcare has been a significant part of our vibrant commercial hub in Clonmel for over 50 years,” commented Mayor, Cllr. Richie Molloy.
The construction was completed by Mulcahy Construction, Clonmel, with the design and project management work carried out by local architect Kenneth Hennessy of Ailtiri Architects. The entire process saw the investment of ¤3 million and took 10 months to complete.
Established in 1970, and with over 50 years’ experience, Clonmel Healthcare now places 22 million packs of medicine into the Irish market every year, making the company one of the top suppliers in Ireland. Clonmel Healthcare launched its biosimilar division in recent years and now offers a comprehensive range of specialty products.
World Pharmacists Day 2024
“Pharmacists: Meeting global health needs” is to be the theme of World Pharmacists Day on 25 September 2024, the International Pharmaceutical Federation (FIP) has announced.
The campaign, led by the federation, is now in its 14th year. “The pharmacy profession has achieved so much in improving health and well-being. FIP’s World Pharmacists Day is an opportunity to celebrate these successes but also to advocate our profession’s value and further potential
in meeting health needs and addressing health challenges.
In many and diverse ways, every day the pharmacy profession meets health needs. The FIP World Pharmacists Day campaign is a means for the profession to celebrate and make known the contributions it makes to better health around the world. It is also an opportunity to highlight our further potential in improving global health.
Pharmacists across the world are invited to join FIP in marking
World Pharmacists Day, reminding decision-makers and the public how the role of pharmacists in meeting health needs remains crucial for building healthier communities everywhere.
“FIP’s work is aligned with the UN Sustainable Development Goals, providing key tools such as the FIP Development Goals to support the profession and facilitate progress in all countries and territories so that we can reach our full potential,” said FIP president Paul Sinclair.
World Pharmacists Day marks the
anniversary of the inception of FIP in 1912 and was adopted by the FIP Council in 2009. As such, the World Pharmacists Day campaign is led by FIP every year, with the theme chosen by the FIP Bureau.
Any reference to “World Pharmacists Day” or “World Pharmacy Week” should, therefore, include FIP.
As a service to the profession, FIP develops and offers a range of World Pharmacists Day / World Pharmacy Week campaign materials for use each year.
Pictured are Kieran Mulhall with Hugh McGovern
Pharmacy
Hospital Pharmacy Placements: Personal Experiences
Three Pharmacy students with APPEL, and their Trainers, share their placement experiences with Hospital Professional News
Laura Johnson is a 5th Year Pharmacy Student at Trinity College Dublin and is completing her final experiential learning placement in the Mater Misericordiae University Hospital (MMUH).
I chose to complete this placement in a hospital setting because I was fascinated by the diversity of specialities and services within hospital pharmacy. I was particularly eager to complete my placement in the MMUH due to the vast array of specialities that are cared for and its strong academic and research focus.
When I began placement in the MMUH, I received a timetable for my rotation through the Pharmacy services over the eight months. I had limited knowledge of what these would involve, but was excited to learn! My first rotation was within the MMUH Dispensary. This enhanced my understanding of the processes for medication supply within the MMUH and the collaboration between pharmacists and pharmacy technicians. While processing pharmacy ward requisitions, I became increasingly aware of the vitality of this service to ensure continuity of care for patients, particularly in the case of medication shortages. I especially enjoyed dispensing parenteral nutrition, and shadowing the pharmacist during the verification of clozapine prescriptions.
My next rotation was within the Medicines Information (MI) service. The key function of this service is to provide up-to-date and accurate information to healthcare professionals within the hospital. I completed UKMI workbook training across areas such as drug interactions, adverse drug reactions, and drugs in
pregnancy, breastfeeding, renal disease and liver disease. This enhanced my clinical knowledge and competence in utilising resources to address complex enquiries. I had the opportunity to promote evidence-based practice through the update of institutional guidelines on the use of direct oral anticoagulants and enteral drug administration. My involvement in producing a monograph comparison for generic substitution and processing a drug approval application increased my awareness of the role hospital pharmacists play in promoting the cost-effective use of medicines.
During my time in Clinical Pharmacy services, I have had exposure to the acute care of patients in the Emergency Department and the care of patients within specialities such as orthopaedics, cancer care and stroke services. Clinical pharmacists play a vital role in optimising the care of patients by reviewing the prescribing, monitoring and administration of medications, and performing appropriate interventions. This has enhanced my ability to apply patient-specific factors, (e.g. weight for enoxaparin dosing), for medication optimisation. I had the opportunity to attend a multidisciplinary meeting with the Frailty Intervention Team (FIT) pharmacist, and learned how health professionals collaborate to optimise the care of older people.
Over the next five months, I will experience several other Pharmacy services. My next rotation is within the Drug Safety (DS) services, which will involve reviewing medication variances and producing a medication safety alert. I will spend one month in the Aseptic Compounding service, with exposure to the preparation of chemotherapy and cancer clinical trials. I will also work within the Infectious Diseases (ID) service, which provides multidisciplinary care to patients with HIV and hepatitis C.
A key highlight of my experience on placement in the MMUH is the supportive learning environment. I attend a pharmacy journal club every Thursday, where a different pharmacist delivers an educational presentation each week. My placement in the MMUH has provided me with a variety of experiences across different Pharmacy services, and this
diversity has delivered extremely rewarding learning opportunities. I am thoroughly enjoying my placement in the MMUH, and would highly recommend a placement within hospital pharmacy to anyone with an interest in clinical pharmacy.
Ellen Holmes is Laura’s Senior Preceptor, and Senior Pharmacist, in the Mater Misericordiae University Hospital.
I qualified as a registered pharmacist back in 2019 and began working as a basic grade pharmacist in the Dispensary of the Mater Misericordiae University Hospital (MMUH). After a year of working in the Dispensary, I started training as a clinical pharmacist on the wards, where I worked mainly on the GI surgical ward and the Respiratory medical ward. After about six months, I started to work with the Satellite Infectious Diseases Pharmacy alongside my clinical pharmacy duties. There, I received training in counselling patients on their medications for
the treatment of HIV, Hepatitis C, and TB. In August 2022, I became a Senior Pharmacist when I received the position of Acting Deputy Dispensary Services Manager and have since been promoted to the permanent Deputy position. I have also just completed a Masters in Clinical Pharmacy with UCC.
Last year I was delighted to be presented with the opportunity to become a Senior Preceptor to our incoming 5th year student. Given my experience in many of the services within the Pharmacy Department, I felt I was an excellent candidate to guide the student through their placement. Having also completed a hospital-based placement for my pre-registration year in Our Lady’s Hospice, I understood the value that these placements offer students.
Patient-centred hospital placements allow the student to see and work through “realworld” scenarios with the support of an experienced team of pharmacists behind them. These opportunities are invaluable and prepare the student to manage similar challenges as qualified professionals. The range of pharmacy services that large acute hospitals provide also demonstrates the scope of practice available for newly qualified pharmacists. By allowing pharmacy students to explore specialised areas, such as MI, DS, ID and Aseptic Compounding services, students will also expand their knowledge of these areas and get an appreciation for the key role that pharmacists play within the health system.
Kate Walsh is a fifth-year pharmacy student completing her final experiential learning placement in the South Infirmary Victoria University Hospital, Cork (SIVUH).
I spent my first few weeks in the dispensary utilising the dispensing software system. This gave me a good base to learn about the patient profile in the hospital and the critical role that the Pharmacy Department plays.
I had the opportunity to extemporaneously prepare eye drops for patients in the ophthalmology ward. Wearing sterile PPE, I followed the compounding protocol to prepare antimicrobial eye drops. Utilizing a closed system approach, I ensured the sterility of the compounding process, applying the aseptic techniques that I had learned in college laboratories.
Away from the dispensary, I began a series of ward rounds, initially to complete medication reconciliations. This involves engaging with patients to accurately gather their medication histories, often contacting community pharmacies to clarify past prescriptions and address queries. The process isn't just about reconciling medications; it's about connecting the dots between a patient's medications and their health conditions, to ensure maximum patient data is available to the entire clinical team.
My responsibilities have expanded to include screening patients starting zoledronic acid treatment, an infusion aimed at slowing down bone breakdown, commonly prescribed to many of our patients with fragile bones post-fracture. Assessing their suitability for this bisphosphonate therapy involves analysing lab results, reviewing drug charts, and confirming medication history with pharmacies.
I have also helped assess patients starting anticoagulants, such as
apixaban. This involves evaluating patient parameters including renal function, and subsequently making dosage adjustments tailored to each patient.
After head and neck surgeries, many patients encounter challenges with swallowing. I was tasked with conducting assessments of medication crushability to ensure optimal administration for these individuals. This process involves consulting various sources and confirming the size of their enteral tube to ensure blockages are prevented. In instances where crushability information is absent from guidelines or the SPC, contacting the pharmaceutical company becomes essential for accurate guidance.
I often shadow my preceptor, Lydia, during her ward rounds as an antimicrobial pharmacist. This gives me a unique insight into the rationale behind each antibiotic selection. Whether it involves factors like blood brain barrier penetration or MRSA coverage, each case offers a learning opportunity.
I have participated in a variety of educational events at the hospital. I recently attended a Medical Grand Rounds session where the focus was on stroke treatment. Our monthly Lunch and Learn sessions provide a platform for interdisciplinary learning. Recent topics have ranged from vitamin D education led by dieticians to the Pharmacy Department's presentation on the evolution of anticancer drugs. Furthermore, I regularly attend student training sessions conducted by pharmacists, covering essential topics such as opioid prescribing and anticoagulation strategies. These opportunities not only broaden my knowledge but also keep me up-to-date with the latest advancements in healthcare
Currently, I'm involved in conducting the VTE audit, a task that takes me to every ward monthly to ensure doctors are diligently completing VTE assessments. VTE assessments are crucial as they assess patients for the risk of developing blood clots in veins, known as Venous Thromboembolism (VTE). A properly conducted assessment enables the doctors to determine the most appropriate anticoagulant therapy.
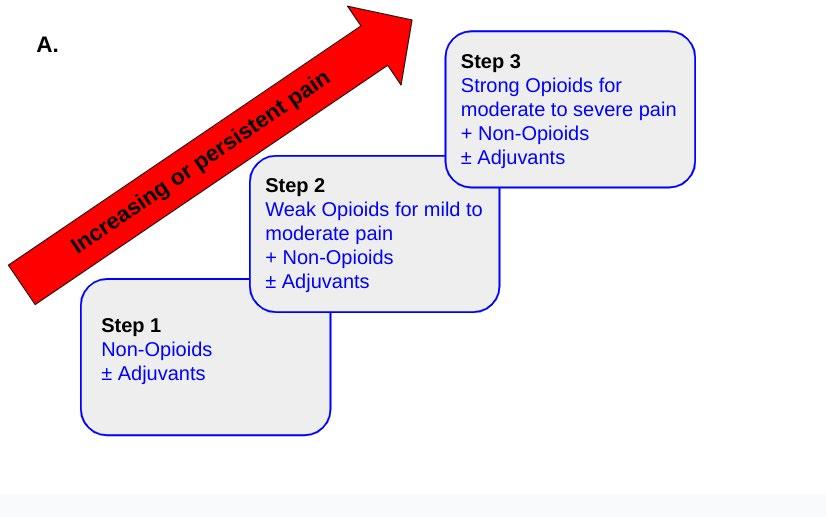
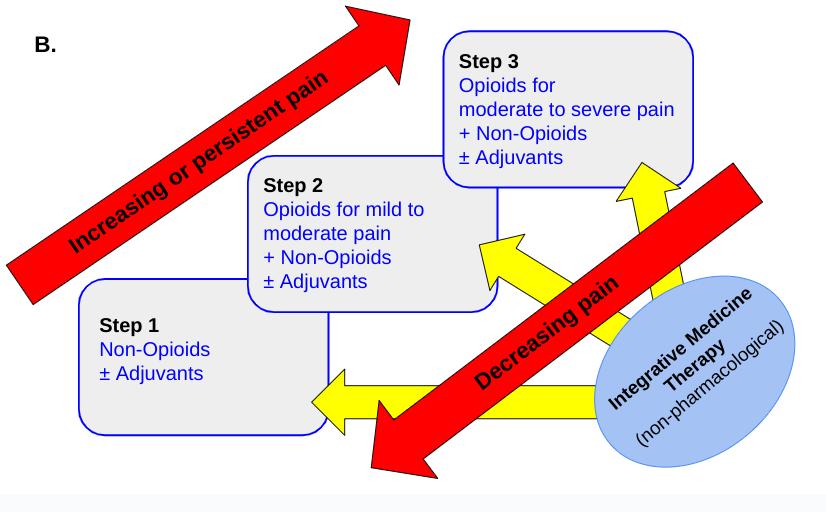
I am also working on an opioid audit, ensuring adherence to the WHO Analgesic Ladder in prescribing pain relievers. This endeavour emphasizes the importance of proper pain management protocols in enhancing patient care.
I have also worked with the oncology pharmacists. During this time, I calculated chemotherapy doses, tailored to factors such as body surface area or renal function, ensuring they aligned with dose bands. I was particularly impressed by the efficiency of the NCIS system, which is the National Cancer Information System that facilitates e-prescribing and e-administration of the cancer drugs.
I have learned so much in my first three months in the South Infirmary Victoria University Hospital. Mentoring, sharing of knowledge and continuous professional development are all part of the ethos of the student placement. The dynamic and challenging environment is firmly built around patient need and I hope that I can make my own small contribution over the remainder of my placement.
Lydia Duggan is Kate’s Senior Preceptor in South Infirmary Victoria University Hospital (SIVUH).
At SIVUH we are fortunate to be able offer both 4 and 8-month APPEL placements. Our aim is to provide a placement which allows pharmacy students to experience all that hospital pharmacy has to offer. Facilitating placements is a real team effort and planning begins well in advance of the placement start date. Training generally begins in the dispensary and our technicians ensure each student becomes comfortable with, what can be, a fast paced environment. Each preceptor will check-in with their pharmacy student regularly; placement is a collaboration and if an student has a particular preference or interest we adapt the programme to suit them. Clinical training involves shadowing ward pharmacists and includes activities such as completing medicines reconciliations, dealing with medicines information queries, attending ward rounds etc. We are part of a very inclusive
multidisciplinary team (MDT) and students have the opportunity to shadow some of these team members including nurses on medication rounds, Speech and Language Therapists performing video fluoroscopy, dieticians reviewing clinic patients and anaesthetists in theatre. Pharmacy students often say this is the most unique part of the placement and that it adds context to our role and responsibilities as clinical pharmacists. For example; after shadowing the dietician it is easier to understand why it’s important to inform the MDT if a medication, which requires a significant alteration of an enteral feed schedule, is commenced for a patient.
If possible, each pharmacy student takes part in our audit schedule and is responsible for developing or continuing an audit. Kate is currently running our venous thromboembolism audit and provides monthly feedback to both pharmacy and the MDT. Pharmacy students also complete placements in our specialist areas like oncology and med safety. By the end of each placement our students are very much part of the fabric of the pharmacy team. Every student adds something new to our department and we learn as much from them as they (hopefully!) do from us.
Lucy Moran is a 5th Year Pharmacy Student at Trinity College Dublin and is completing her final experiential learning placement in the Beacon Hospital.
Having started my experiential learning placement in the Beacon hospital in January, I have already learned so much about the potential roles of a pharmacist in the hospital setting. The Beacon, like many other hospitals, have a structured programme for their pharmacy students. Within this, the student undergoes rotations through different departments of the hospital. My Senior Preceptor is responsible for coordinating
Pharmacy
all of this and keeping a general eye on me. However, within each rotation I am allocated a mentor who is experienced in that area, and who orients me to their particular role. At the same time, I have the autonomy to manage my own workload throughout the placement.
I began my placement in the dispensary, which was imperative for learning the lay of the land. It was the best way to become familiar with the hospital environment and it gave me a chance to get to know some of the staff. I had no prior experience in a hospital, so areas like total parenteral nutrition (TPN) orders from dieticians and orders of anaesthesia for theatre were things I had never seen before. I now understand that a major part of a pharmacist's role in the dispensary is checking these items for accuracy and clinical appropriateness. However, I’ve also seen that it’s rarely ever that simple, and that all of this must also fit into the hospital system as a whole. It's about doses and quantities, but also stock levels on wards, who has ordered the medicine, and more. All of this was entirely different to my experience in community pharmacy.
I’m now finishing up my rotation in the Clinical Pharmacy office. I had the brilliant opportunity of working with somebody different every 2 weeks, starting with the Medicine’s Information Pharmacist. She gave me a host of online clinical resources to use to answer queries from the wards. This was often complex and multi-dimensional, and required a certain degree of assertiveness, confidence, and the ability to think ahead. I have learned the importance of the role, as there is rarely ever a simple answer to a complex issue which involves a unique patient each time. An example of a query I answered is how a patient should be administered their medication when they have a temporary swallowing difficulty after surgery. We accessed patient files for this, and at one point it was necessary to contact the manufacturer of a medicine for advice.
I then sat with the Antimicrobial Stewardship (AMS) Pharmacist. I went with her to ward rounds and meetings alongside the microbiology consultant. I was also shown the lab where the micro team test and evaluate samples taken from patients. The AMS pharmacist works closely with them to make sure that patients are given the antimicrobials to which the bug is most sensitive. It was demonstrated to me the profound impact this has on the safety, cost,
and protection of antibiotics in the hospital as a whole.
Now I’m working alongside my Senior Preceptor, who is the manager of Clinical Pharmacy Services and Medication Safety. Together we are working on one of the many audits I have been involved in so far. This time, the focus is on the clinical and administrative accuracy of discharge prescriptions. Audits seem to be a win-win for the preceptor and the pharmacy student. Students can allocate more time to them, whilst they also provide a great opportunity for learning. They can have a big impact, highlighting areas which need to be refined to enhance the patient experience.
In terms of what the next few months will look like for me, I have a three-week slot in the aseptics unit coming up in the summer. I’m looking forward to doing some hands-on work and understanding of compounding medicines such as chemotherapy. But first, I’m working alongside clinical pharmacists up on the wards. I’ll be regularly switching between different pharmacists and wards. I think my experience on placement so far will enable me to extract the absolute most from this experience. It’s important to have a solid understanding on how the pharmacy department works in the hospital, and I think it’s easy to underestimate the complexity of the workflow. I hope I’ll be able to make some genuine contributions!
Keira Hall is Lucy’s Senior Preceptor, and Clinical Pharmacy Services Manager, in the Beacon Hospital.
Arranging a 5th Year placement can be challenging. As a Senior Preceptor, you have a responsibility to ensure the most comprehensive experience of Hospital Pharmacy possible. This involves giving the student exposure to learn experientially within all specialities as well as some exposure to the wider hospital and multidisciplinary working.
I find working with a competency document and pre-planned timetable, with sections aligned to the broader APPEL competencies, provides a good base for the 8-month placement. Prior to the placement, the timetable is populated with the student’s specific breaks and the first parts of the placement discussed
with the relevant teams. This is followed throughout and gives clarity to all involved. Of course, it may not always be possible to stick exactly to the timetable and occasionally, there may need to be some amendments, given the nature of the areas of work but these can be easily managed provided effectively communicated to the team.
Competency-based learning is particularly effective within the dispensary and within the clinical ward rotation. Setting standards to achieve week-by-week allows the student to show progression, especially within the 10-week clinical ward block. These allow consistency regardless of which clinical pharmacist is providing the training which is also important as it allows the training resource to be shared and develops the student to be a contributory member of the team at an early stage.
Having a structured, multimodal programme allows the right person to be providing the optimal experience throughout and facilitates progression towards the end aim of developing a Pharmacist ready to practice. The programme being competency based and well defined gives me the confidence as the preceptor responsible for completing the summative assessments, to do so regardless of who delivered the individual components of the training.
Call for papers: make your contribution to Hospital Professional News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
Awards
Recipients of Annual Innovation Awards
The recipients of NovaUCD’s annual innovation awards, which highlight successes made in areas of knowledge transfer, consultancy, entrepreneurship and the promotion of an innovation culture, by members of the UCD research, innovation and entrepreneurial community, have been announced today.
A total of 7 Awards, including the main 2024 NovaUCD Innovation Award, were presented by Professor Orla Feely, President, University College Dublin (UCD) during an event held in the UCD University Club.
Professor Orla Feely, President, UCD said, “The NovaUCD Innovation Awards have become a key annual event highlighting the University’s commitment to innovation and recognise the achievements of our research, innovation and entrepreneurial communities and I congratulate all who have received this year’s Awards. I would also like to wish the Awardees future success as they continue to work towards delivering economic and societal impact in Ireland, and further afield, through their commercialisation, consultancy, entrepreneurial and innovation activities.”
The 2024 NovaUCD Innovation Award, which recognises excellence in innovation or of successes achieved in the commercialisation of UCD research, or other intellectual activity, over a number of years, was awarded to Professor Therese Kinsella, CEO and founder of ATXA Therapeutics. ATXA Therapeutics is a clinical-stage pharmaceutical company committed to the advancement of innovative, life-changing treatments for cardiopulmonary diseases.
The company was founded by Professor Kinsella, a biochemist and a leading expert in the field of prostanoid biology, in 2015 as a spin-out from the UCD School of
Pictured is Professor Therese Kinsella, CEO and founder, ATXA Therapeutics recipient of the 2024 NovaUCD Innovation Award. (Credit: Nick Bradshaw, Fotonic)
Molecular and Biomedical Science based on over 20 years of research carried out by her and her team at the UCD Conway Institute.
The company’s focus is the development of its lead candidate drug NTP42 for the treatment of Pulmonary Arterial Hypertension (PAH). PAH is a devastating disease of the lungs and heart with an urgent unmet need for new improved therapies. While the condition itself is classed as a rare or orphan disease, affecting 15-50 patients per million of the population, it carries an enormous health burden with an annual spend in excess of $8 billion globally on prescribed medicines alone in 2023.
On receiving the 2024 NovaUCD Innovation Award, Professor Therese Kinsella, CEO and Founder, ATXA Therapeutics, said, “It is indeed a great honour for me to accept this Award from UCD both personally and on behalf of everyone on the ATXA team who have been part of our success journey so far.”
ATXA Therapeutics, headquartered at the UCD Conway Institute, has raised over ¤17 million in funding (equity and grant) to date, and Professor Kinsella and ATXA have a patent estate of 16 granted patents, in Europe, USA, Canada, Japan, and Australia, with numerous others filed globally protecting their drugs out to the mid-2040s.
Among the other Awardees are Associate Professor Nan Zhang, recipient of the 2024 NovaUCD Invention of the Year Award and EpiCapture, recipient of the 2024 NovaUCD Spon-out of the Year Award.
The recipient of the 2024 NovaUCD Invention of the Year Award is Associate Professor Nan Zhang, UCD School of Mechanical and Materials Engineering. He received this Award in recognition of a patented microfluidic system and process for the formulation of nanomedicines, which was developed by him and his research team.
The invention consists of a highthroughput microfluidic system, featuring a cartridge with a uniquely designed mixing channel, coupled with a desktop machine for conducting nanoparticle
synthesis. This system is designed to accelerate formulation screening and to enhance formulation optimisation, crucial for the development of gene therapy, cell therapy, and vaccines.
EpiCapture, which is focused on developing accurate and non-invasive liquid tests for the early detection and prognostic assessment of high-grade cancers, including prostate cancer, has been named recipient of the 2024 NovaUCD Spin-out of the Year Award.
The company was co-founded in 2021 by Associate Professor Antoinette Perry, Co-Director of the UCD Cancer Biology and Therapeutics Lab, and Edward Simons, as a spin-out from the UCD School of Biology and Environmental Science.
EpiCapture-prostate, the company’s first test which is currently in development, is a novel urine DNA test to detect high grade prostate cancer. EpiCapture-prostate selectively detects high grade prostate cancer by measuring epigenetic changes at six genes in urine using a PCR platform to generate a score, indicating the likelihood that a person has high grade prostate cancer.
The initial intended use of the test is as a disease monitoring tool for patients on active surveillance,
Pictured is Associate Professor Nan Zhang, UCD School of Mechanical and Materials Engineering, recipient of the 2024 NovaUCD Invention of the Year Award. (Credit: Nick Bradshaw, Fotonic)
i.e. patients who have been diagnosed with low-risk prostate cancer, to be used repeatedly to monitor disease progression.
On receiving the 2024 NovaUCD Spin-out of the Year Award, Associate Professor Antoinette Perry, CSO and co-founder, EpiCapture, said, “We are absolutely delighted with this Award. We continue to work hard to make our prostate cancer test available to the millions of men and their clinicians who will benefit from an accurate, non-invasive test.”
The company also intends to develop a test to detect ovarian cancer where there is a significant unmet need to improve early detection to improve outcome for patients, and research has commenced on this test by Associate Professor Perry and her team.
2024 NovaUCD Consultancy of the Year Award: Professor Fiona Timmins, UCD School of School of Nursing, Midwifery and Health Systems
2024 NovaUCD Licence of the Year Award: Go Eve
2024 NovaUCD Founder of the Year Award: John Byrne, CEO and Founder, Corlytics
2024 NovaUCD Innovation Champion of the Year Award: Professor Nick Holden, UCD School of Biosystems and Food Engineering.
EpiCapture is the recipient of the 2024 NovaUCD Spin-out of the Year Award and pictured (l-r) are Edward Simons, co-founder; Associate Professor Antoinette Perry, UCD School of Biology and Environmental Science and co-founder with Kevin Tansley, CEO. (Credit: Nick Bradshaw, Fotonic)
is a weekly email updating you on stocks, new product launches and other business news, sent directly to your inbox. Or register online at https://cloud.teva-europe.com/TevaSource_Registration.
Oncology Focus Dermatology
Irish Melanoma Forum 12th Annual Meeting
The Irish Melanoma Forum 12th Annual Scientific Meeting takes places this month on Thursday 2nd May.
Hospital Professional News recently spoke to Professor Shirley Potter and Professor Des Tobin, Co-chairs of the Forum to learn more about this year’s line-up. Topics to be discussed for 2024 include clinical research in phenotypes, biomarkers and histopathology; perioperative systemic therapy in melanoma and phenotypic plasticity in melanoma.
Desmond J. Tobin is Full Professor of Dermatological Science and Director of The Charles Institute of Dermatology at the UCD School of Medicine, Dublin. He researches in basic and applied skin/hair sciences, with a focus on skin/ hair pigmentation in health and disease (incl. melanoma) and on hair growth disorders, especially alopecia areata. He is a recent past president of the British Society for Investigative Dermatology.
Professor Shirley Potter is a Consultant Plastic and Reconstructive Surgeon at the Mater Misericordiae University Hospital and Associate Clinical Professor at the UCD School of Medicine. In her clinical practice she specialises in melanoma, advanced skin cancer, and head and neck microvascular reconstruction. She supervises translational research at the
Conway Institute in UCD and is the chief investigator for Ireland for the internationally recruiting MelmarT trial investigating surgical margins in melanoma.
Professor Tobin explains, “I joined as IMF co-chair after discussion with Shirley. We both felt that there would be benefits for having clinical and basic researcher experience front and central in the IMF leadership. This was a departure from how the IMF was previously run (only clinical).”
The work of the Forum is currently largely focused on the upcoming 12th Annual Scientific Conference.
Professor Tobin adds that while this event is still largely clinical, researchers are also now joining. “Remarkably there is very little basic research on human skin cancer currently in Ireland, even less melanoma. This is largely due to poor research funding for human skin cancer research in Ireland. Money tends to be focused on animal models e.g., laboratory inbred mice and fish models.”
Professor Potter adds, “We would encourage specialists from all disciplines to get involved. Melanoma management is multidisciplinary, and therefore melanoma research should be multidisciplinary. By attending the Irish Melanoma Forum, specialists are exposed to unique insights of other disciplines and we would hope that this encourages cross collaboration in clinical and basic research.”
So where does Ireland stand in the management and treatment of melanoma compared to European counterparts? Professor Potter says, “The incidence of, and mortality from, Melanoma in Ireland ranks among the highest in Europe.
“This is largely due to the Irish fair skin type, combined with increasing sun exposure, and a historical lack of awareness of the damage that UV exposure causes. Thankfully, due to public health campaigns, awareness is improving and behaviours are starting to change. The damage is already done for a certain proportion of the population, and for this reason we are expecting what is being described as a melanoma epidemic, with incidence expected to increase exponentially up to at least 2040. This, combined with the explosion of non-melanoma skin cancer in the aging and immunosuppressed populations, will put significant strain on our already stretched health systems. Ireland unfortunately lags behind in terms of approvals for, and access to, new therapeutic options, that are available to melanoma patients internationally.
“Despite intense lobbying by advocacy groups such as the Irish Cancer Society, and Melanoma Support Ireland, inequalities in access to drugs continue to exist and Irish melanoma patients are suffering as a consequence, this needs to be urgently addressed.”
She goes on to add, “Melanoma management is in an exciting period of change. New therapeutics are coming on stream, both targeted therapies and immunotherapies and the combinations and timings which these drugs are given is changing. Drugs are being given to earlier stages of disease and drugs are being used to downsize tumour burden prior to surgery, with significant improvements in survival.
“Melanoma management is becoming more and more personalised to each individual patient, with tumours being profiled to give more information on how a given tumour might behave or respond to treatment. Melanoma patients are living longer, and the quality of life of melanoma survivors is improving. It is difficult to keep up, there is so much change, but this is a great thing for melanoma patients.”
Looking at future developments in the field, Professor Tobin notes a desire for, “A greater focus on human skin cancer basic research, especially in melanoma, in Ireland. We need to build significant capacity, including via lowering unnecessarily-restrictive ethics and bio-banking hurdles common in Ireland. Non-uveal melanoma patients are justified in questioning why most current research efforts focus on animal models (esp. mouse and fish) rather than actual human melanoma patient tissue samples.
“Checkpoint inhibitors and Neoadjuvant therapy are another 2 opportunities we are looking forward to.
“It is also hoped that Dermatology Specialists will begin to appreciate more the value of academic dermatology, which is at risk in my opinion after a period of strength over the last few decades. We need to urgently build capacity in this area.”
The 12th Annual Scientific Meeting of the Irish Melanoma Forum takes place Thursday 2nd May at University College Dublin.
Professor Shirley Potter and Professor Desmond Tobin
Obesity and Alcohol contributing to Increase in Bowel Cancer
Overweight and obesity are contributing to rising death rates from bowel cancer among people aged 25-49 years in the European Union (EU) and the UK, although death rates from this type of cancer are decreasing overall across Europe.
These findings are from a new study published in the leading cancer journal Annals of Oncology1 which predicts death rates from cancer in the EU and UK for 2024. It is the first time that an increase in bowel cancer death rates among young adults has been predicted for some EU countries, and it confirms a trend in the UK that the researchers first noted in 2021.
Researchers led by Carlo La Vecchia (MD), Professor of Medical Statistics and Epidemiology at the University of Milan (Italy), predict that the greatest increase in bowel cancer death rates among younger people will be seen in the UK where they will rise by 26% in men and nearly 39% in women in 2024 as compared to 2018. Increases will also be seen in Italy (up 1.5% in men and 2.6% in women), among Spanish and Polish men (up 5.5% and 5.9% respectively) and German women (up 7.2%).
“Key factors that contribute to the rise in bowel cancer rates among young people include overweight, obesity and related health conditions, such as high blood sugar levels and diabetes,” said Prof. La Vecchia.
“Additional reasons are increases in heavier alcohol drinking over time in central and northern Europe and the UK, and reductions in physical activity. Alcohol consumption has been linked to early onset bowel cancer, and countries where there has been a reduction in alcohol consumption, such as France and Italy, have not experienced such marked rises in death rates from this cancer. Early onset bowel cancer tends to be more aggressive, with lower survival rates, compared to bowel cancer that is diagnosed in older people.
“National governments should consider strengthening policies to encourage increased physical activity, a reduction in the number of people who are
Carlo La Vecchia (MD), Professor of Medical Statistics and Epidemiology at the University of Milan
overweight or obese, and a reduction in alcohol consumption.
“In terms of prevention, governments should consider the extension of screening for bowel cancer to younger ages, starting at ages 45 years. Screening programmes vary across Europe, but an increase in the incidence of bowel cancer among young people in the US has prompted the US Preventive Service Task Force to recommend lowering the age at which screening starts to 45 years.”
The researchers analysed cancer death rates in the EU 27 Member States2 as a whole and separately in the UK. They looked at the five most populous EU countries (France, Germany, Italy, Poland and Spain) and, individually, for stomach, intestines, pancreas, lung, breast, uterus (including cervix), ovary, prostate, bladder and leukaemias for men and women.3 Prof La Vecchia and his colleagues collected data on deaths from the World Health Organization and Eurostat databases from 1970 to 2018 for most of the EU-27 and the UK. This is the fourteenth consecutive year the researchers have published these predictions.
All cancers
In the EU-27 countries, they predict there will be a 6.5% fall in the age standardised death rates [4] for all cancers from 132 per 100,000 of the population in 2018 to 123 per 100,000 in 2024 for men, and a 4% fall from 82.5 to 79 per 100,000 among women. A total of approximately 1,270,800 people will die from the disease in the EU.
Over 36 years between 1989 and 2024, the researchers calculated the number of cancer deaths avoided, assuming that rates remained constant at the 1988 rates. They estimate that a total of 6,183,000 deaths from all cancers have been avoided in the EU
(4,244,000 in men and 1,939,000 in women), and a total of 1,325,000 in the UK (899,000 in men and 426,000 in women).
Lung cancer
Although death rates from lung cancer are falling in men, it remains the cancer with highest rates for men and women in both the EU and the UK. The researchers predict death rates in 2024 of 28 men and 13.6 women per 100,000 in the EU. This represents a 15% reduction among men since 2018, but no reduction among women. In the UK, death rates will be 19 men and 16 women per 100,000 from lung cancer, representing a 22% and 17% reduction among men and women, respectively.
Bowel cancer
In both the EU and the UK, bowel cancer is now the second biggest killer after lung cancer among men, and the third biggest killer after breast and lung cancer in women although death rates are falling, except among UK women. Among non-smokers it is the leading cause of cancer death in both sexes combined in the EU and UK.
Compared to 2018, overall death rates from bowel cancer in the EU are predicted to fall by 5% to 15 men per 100,000 in 2024, and by 9% to 8 women per 100,000. In the UK, they are predicted to fall by 3% to 14 men per 100,000 but will remain stable in women at about 10 per 100,000.
Breast cancer
Death rates continue to improve in Europe and the UK for breast cancer. In 2024, the researchers predict a fall of 6% from 14 per 100,000 women in the EU in 2018 to 13 per 100,000 in 2024, and an 11% fall from 15 to 13 per 100,000 in the UK.
Prof. Eva Negri from the University of Bologna (Italy), co-leader of the research, said: “Advances in the diagnosis of breast cancer contribute to these substantial declines in death rates, but improvements in the treatment and management of the disease are the main reasons for more people surviving.”
Pancreatic cancer
Pancreatic cancer, which is very difficult to detect or to treat successfully, is the only major cancer where no improvements in death rates are predicted for both sexes in the EU (but not the UK). It accounts for over 3% of new cancer diagnoses in Europe, but for approximately 7% of cancer deaths, and it is the fourth leading cause of death from any cancer. Death rates are predicted to rise by 1.6% and 4% among men and women respectively in the EU. Trends are better in the UK where they are predicted to fall by 7% among men and 2% among women.
References available on request
Oncology Focus Breast Cancer
Histone Deacetylase Inhibitors as a Potential Future Therapy for Breast Cancer Brain Metastasis
Written by Mr. Diego Abril Carbonell (Research Assistant), Miss. Aoibheann Dowd (Research Assistant), Dr. Jason McGrath (Postdoctoral Research Fellow), Dr. Gordon Daly (Ph.D. Researcher), Dr. Damir Vareslija (Lecturer and Principal Investigator), and Prof. Leonie Young (Professor, Scientific Director Beaumont RCSI Cancer Centre). Department of Surgery, Royal College of Surgeons in Ireland & Beaumont Hospital.
Introduction to Breast Cancer
Breast cancer (BC) stands as the most diagnosed malignancy among women, significantly impacting global health.1, 2 In 2018, it was estimated that approximately 2.1 million women were diagnosed with BC, leading to over 600,000 deaths. Alarmingly, the global incidence of this disease has been rising at an annual rate of 3.1%.2
BC’s complexity is further unravelled when categorised into five distinct subtypes. These classifications are based on the presence or absence of certain biomarkers: the oestrogen receptor, progesterone receptor, HER2, and Ki67. These subtypes include luminal A, luminal B, luminal B-like, HER2-positive, and triple-negative BC.3 The incidence and mortality rates vary significantly across these subtypes, with HER2-positive cases associated with the highest risk of death. This elevated risk is largely due to the increased likelihood of developing brain metastases.1, 3
The narrative of BC shifts between hope and despair, depending on the stage at diagnosis. When
detected early – before the cancer has spread beyond the breast – the disease is considered potentially curable. However, once the cancer has metastasized, the prognosis falls considerably. Metastatic BC, often referred to as advanced BC, is deemed incurable. It is worth noting that it is not the primary tumour but rather the metastases that are the leading cause of mortality among BC patients.1-3 This stark reality underscores the critical importance of early detection and tailored treatment strategies to combat this pervasive disease.
Breast Cancer Brain Metastasis
BC’s propensity to metastasize to the brain is notably high in HER2-positive and triple-negative subtypes, progressing through a well-defined cascade.1, 4 Initially, the process begins with the epithelial-mesenchymal transition (EMT), where epithelial cells morph into motile mesenchymal stem cells, facilitated by specific gene overexpression and downregulation that affect cell attachment and proliferation. However, not all cells undergo EMT – only a select few advance to metastasis. Following EMT, tumour cells intravasate into the bloodstream by navigating through the tumour microenvironment and crossing the endothelial barrier. The third phase involves preparing the brain environment for tumour spread by priming the
metastatic niche and breaching the blood-brain barrier (BBB). The culmination of this journey is the tumour cells’ extravasation into the brain, where they exploit the brain’s defences and proliferate (Summarised in Figure 1).3 Addressing BC involves a multidisciplinary approach, including conventional therapies like surgery, radiation, and chemotherapy, alongside emerging treatments targeting specific mechanisms like histone deacetylases (HDACs).
Histone Deacetylases
Recent research has illuminated that tumorigenesis is influenced not just by genetic mutations but significantly by epigenetic programming within cells. This revelation has elevated the study of the epigenetic landscape as a burgeoning field of research. At the core of epigenetic regulation lies histone acetylation, controlled by histone acetyltransferases (HATs) and histone deacetylases (HDACs). These enzymes play a pivotal role in gene expression: HATs enhance gene transcription by unwinding DNA, facilitating access for transcriptional machinery, whereas HDACs condense DNA, suppressing gene expression (summarised in Figure 2). Their critical involvement in gene regulation and the association of their dysregulation with various cancers, including BC, spotlight these enzymes as potential
therapeutic targets. Intervening with their function offers a way to rectify epigenetic imbalances and curb cancer-promoting gene expression. There are 18 mammalian HDAC proteins, classified into four subclasses based on sequence similarity and structural characteristics. Research has shown that several HDACs contribute to cancer progression by a range of mechanisms. Often, HDAC overexpression leads to the silencing of tumour suppressor genes, enhancing oncogenic signalling—given that histone 3 acetylation is tied to the activation of many such genes. Furthermore, aberrant HDAC activity has been linked to increased cell proliferation, survival, and invasion in lab settings, as well as to tumour growth and the spread of breast cancer in animal models (summarised in Figure 2).5, 6 HDAC inhibitors
HDAC inhibitors inhibit the activity of HDACs by blocking the binding of essential molecules like Zn2+ ions or NAD+, which are crucial for the enzymatic function of HDACs. Among these inhibitors, some target specific subtypes, such as Entinostat, which is a Class I-specific inhibitor. Notably, Entinostat received Breakthrough Therapy designation from the FDA in 2013 for the treatment of metastatic oestrogen receptorpositive BC. Conversely, panHDAC inhibitors like Vorinostat
Mr. Diego Abril Carbonell
Figure 1. Schematic representation of the metastatic cascade from the primary BC to brain metastasis.
Figure 2. The diagram illustrates the mechanism of action of both HATs and HDACs and their effect on chromatin structure and subsequently, gene transcription. Aberrant HDAC expression leads to downstream effects such as cell proliferation and survival, as well as tumour growth
and Panobinostat, which target a broader range of HDAC enzymes, have gained FDA approval for certain haematological cancers and are being explored for their potential in treating breast cancer. Despite their broader application, pan-HDAC inhibitors tend to induce more side effects, such as nausea and fatigue, driving research towards more selective HDAC inhibitors to minimize offtarget effects and toxicity.7 Various HDAC inhibitors are currently undergoing clinical trials for both haematological and solid tumours. Although HDAC inhibitors have demonstrated tolerability in clinical settings, resistance to these drugs poses a significant challenge, and they have shown limited efficacy as standalone treatments. However, when combined with other therapeutic agents, HDAC inhibitors have displayed synergistic effects that enhance efficacy, reduce toxicity, and mitigate resistance in both pre-clinical and clinical settings. Such combination therapies, involving both pan- and selective HDAC inhibitors, have been tested alongside alkylating chemotherapy, immunotherapy, and radiotherapy, showing promising results.8 This discussion will further delve into the use of HDAC inhibitors in combination with PARP inhibitors, highlighting an innovative approach to cancer therapy.
HDAC inhibition and PARP inhibition
HDAC inhibitors play a crucial role in modulating gene expression related to DNA damage repair pathways, notably homologous recombination (HR). Similarly, the enzyme ADP-ribose (poly) polymerase (PARP), involved in HR, has been targeted by PARP inhibitors, which have shown
effectiveness as anticancer treatments by blocking HR and prompting cell death. Research involving the combination of Olaparib, a PARP inhibitor, with the HDAC inhibitor Vorinostat has demonstrated that this duo significantly curtails proliferative signalling and tumour growth more effectively than when either drug is used alone, evident in
both lab settings and animal models.9, 10 This synergistic effect results in enhanced apoptosis and autophagic cell death by diminishing HR efficiency.
This combination therapy holds particular promise for treating triple-negative breast cancer (TNBC). Many TNBC cases lack BRCA1 mutations, which would typically confer sensitivity to PARP inhibitors. However, HDAC inhibition can induce a state of "BRCAness" in TNBC cells that lack BRCA1, rendering them more susceptible to PARP inhibition (summarised in Figure 3).9 "BRCAness" refers to cells exhibiting molecular features akin to those with BRCA mutations, specifically deficiencies in the HR DNA repair pathway. Clinical trials exploring the combination of Olaparib and Vorinostat for metastatic breast cancer treatment are currently in progress, highlighting the potential of this innovative approach in oncology.
Conclusion
HDAC inhibitors have great potential in the treatment of cancer, especially in combination with other promising drugs such as PARP inhibitors. With significant results in BC models, their potential in treating BCBM has yet to be explored. Continuing to investigate the potential of these drugs for that purpose will then be an important future avenue of future research.
References available on request
Figure 3. The combination of Olaparib and Vorinostat is effective due to HDAC inhibition inducing HRD in cells, making them susceptible to PARP inhibition and inducing cell death. Without HDAC inhibition, PARP inhibition is ineffective and these cancer cells survive treatment
Oncology Focus Prostate Cancer Management of Prostate Cancer
What is prostate cancer?
Prostate cancer happens when abnormal cells form and grow in the prostate gland. Most prostate cancers start in the outer gland cells of the prostate and are known as acinar adenocarcinomas. Many of these cancers grow extremely slowly and are not likely to spread but some can grow more quickly.1
Research published on April 5th, 2024 by the International Agency for Research on Cancer (IARC) together with partners in a new Lancet Commission predict that the global burden of prostate cancer is set to more than double to almost three million new cases by 2040, compared with the estimated number of cases today.2
The Prostate Gland
The prostate gland is part of the male reproductive system. It is situated at the base of the bladder and is about the size of a walnut but gets bigger as men get older. It surrounds the first part of the tube that carries urine from the bladder to the penis. This tube is called the urethra, also known as the pipework’s. The prostate gland produces a fluid that mixes with sperm (from the testicles) to make semen. It also produces a protein called the prostate specific antigen (PSA) which can be measured in the blood. Male hormones, such as testosterone, control its growth and function.3
Prostate cancer in Ireland
After non-melanoma skin cancer, prostate cancer is the most common cancer in men in Ireland. It accounts for almost one-third of all invasive cancers in men. According to the 2023 National Cancer Registry of Ireland (NCRI), an average of 3,980 people are diagnosed annually with a mortality rate of 623. Prostate cancer has a high survival rate if caught in time.
Written by Bernie Carter, Assistant Director of Nursing, Marie Keating Foundation
The five-year survival rate currently stands at 93%.4
Risk Factors for Prostate Cancer
In most cases cause is unknown. Factors that may increase the risk of developing prostate cancer include:
• Age - Prostate cancer is more common in older men. Most prostate cancers occur in men aged 50 or over.
• Ethnicity - Prostate cancer is more common in black-African men than white men. It is least common in Asian men.
• Family history - Prostate cancer is more common in men who have a father, son or brother with prostate cancer.
• Genetics - Prostate cancer is more common in men with certain genetic alteration (e.g. BRCA1 and BRCA 2 alterations) and syndromes (e.g. Lynch syndrome)
• Obesity and weight - Obesity and overweight is the second biggest preventable cause of cancer after smoking. Being overweight or obese increases your risk of metastatic or advanced prostate cancer.
Maintaining a healthy body weight, being physically active and eating a balanced diet is good for your health and may help to reduce your risk of prostate cancer.5,6,7
Symptoms of prostate cancer
Prostate cancer does not usually cause symptoms in the early stages. Most prostate cancers start in the outer part of the prostate gland. This means that to cause symptoms, the cancer needs to be big enough to press on the urethra (pipeworks) that carries urine from the bladder to the penis.
While not common, symptoms of early prostate cancer might include the following:
• Passing urine more frequently
• Getting up at night to pass urine (nocturia)
• Difficulty passing urine –this includes:
○ A weaker flow
○ Straining when starting to urinate
• Needing to rush to the toileturgency
• Less common symptoms include:
○ Blood in the urine or semen
○ Feeling of not emptying your bladder fully8
Along with the symptoms above, more advanced prostate cancer can sometimes cause other symptoms, such as:
• Trouble getting an erection (erectile dysfunction or ED)
• Pain in the hips, back (spine), chest (ribs), or other areas, from cancer that has spread to the bones
• Weakness or numbness in the legs or feet, or even loss of bladder or bowel control, from cancer in the spine pressing on the spinal cord
• Weight loss
• Feeling very tired
Most of these symptoms are more likely to be caused by something other than prostate cancer. For example, benign prostatic hyperplasia (BPH), a non-cancerous growth of the prostate.9,10
Diagnosing prostate cancer
If you have any of the symptoms above, you should contact your GP without delay to find out what is causing your symptoms:
Tests your G.P. may do include the following:
• Medical history and examination
• A blood test called a PSA test
• Digital Rectal Examination (DRE)
Prostate-specific antigen (PSA) is a protein made by cells in the prostate gland (both normal cells and cancer cells). The PSA level alone is not a reliable test to check whether a man has prostate cancer or not. Some men have prostate cancer but have a PSA level that is normal for their age while other men have a higher PSA level but do not have prostate cancer. Urinary infection or a prostate infection can also raise the PSA. If you’re due to have a PSA test don’t ejaculate or exercise heavily for 48 hours beforehand as it also affects the results.
Depending on the results of your tests, your GP may repeat your PSA in 6–12 weeks or may refer you to one of the National Cancer Control Programme (NCCP) Rapid Access Prostate Clinics where your prostate can be assessed further by a Urologist. The urologist may repeat the above tests and may take a biopsy of your prostate gland – TRUS biopsy/Trans perineal biopsy. Further tests may also be required and may include one or more of the following: MRI/ Multiparametric MRI (mpMRI)/CT Scan/Pet-CT Scan.
These tests and scans provide information about:
• the type of cell the cancer started in and where it began
• how abnormal the cells look under the microscope (the grade – known as the Gleason’s score for prostate cancer)
• the size of the cancer and whether it has spread (the stage)11
Treatment for prostate cancer
Treatment depends on the stage and grade of your cancer, size of your prostate gland and your general health.
A team of experts called the MultiDisciplinary Team (MDT) will decide on the most appropriate treatment. Sometimes no active treatment may be required, and the patient may be monitored through ‘Active surveillance’ or ‘Watchful waiting’. If active treatment is required, it may include one or combination of the following:
There are different types of prostate cancer. The most common type is adenocarcinoma of the prostate. Two types of adenocarcinomas of the prostate are Acinar adenocarcinoma and Ductal adenocarcinoma.
Other types of prostate cancer include Transitional cell carcinoma, Squamous cell carcinoma and Small cell prostate cancer.13
References available on request
Oncology Focus Gynaecological Cancer
First patient passport for gynaecological oncology patients launched by the Trinity St James’s Cancer Institute
The Trinity St James’s Cancer Institute (TSJCI) has announced the roll-out of ‘My Gynaecology Patient Passport,’ a resource for patients diagnosed with, or undergoing investigation for, gynaecological cancer which will be carried by patients throughout their cancer journey.
The first of its kind for gynaecological cancers in Ireland, the patient passport will be provided to patients being treated for ovarian, uterine, cervical, vaginal and vulval cancers during their first visit with the St James’s Hospital Gynaecology Team. The document, which is filled in collaboratively by patients and their clinicians, will include important information and visual aids related to the patient’s diagnosis and care plan, and will provide helpful resources to support patients both before and after treatment. It has been designed to allow patients to take ownership of their care and improve communication between patients, specialist healthcare teams and primary care physicians.
Prof. Catherine O’Gorman, Consultant Gynaecological Oncologist at the TSJCI, said, “We are really pleased to have developed this simple but effective document that aims to empower patients with a clearer understanding of their diagnosis and care. Importantly, clinicians and patients collaboratively fill in personalised details of diagnosis, treatment and survivorship. Patients diagnosed with gynaecological cancer can understandably be fearful and overwhelmed by the information they receive during their initial appointments. We hope that the patient passport will improve how information is absorbed and shared with family or other healthcare practitioners.”
‘My Gynaecology Patient Passport’ has been developed by the multidisciplinary team providing care to patients with gynaecological cancers at the TSJCI, as well as patients who have been diagnosed with gynaecological cancers. Noting the importance of patient involvement, Ashley Lilly, Gynaecology Oncology Advanced Nurse Practitioner, said: “The reallife experiences of patients have been crucial to the development of the gynaecology patient passport.
Throughout the process, patients have been centrally involved so that their main concerns are addressed in the passport, including those related to exercise, diet and sexual wellness.”
Clinicians at the TSJCI treat approximately 300 gynaecological cancer patients each year and, as treatments for gynaecological cancers improve, focus is turning towards cancer survivorship.
Professor John Kennedy, Clinical Professor of Oncology at Trinity College Dublin and Co-Director of the Trinity St James’s Cancer Institute said: “Given the growing number of cancer survivors in Ireland, survivorship is regarded as a distinct phase in a patient’s cancer journey. The Trinity St James’s Cancer Institute views survivorship as part of the continuum of patient care. Initiatives such as the gynaecology patient passport and our recently opened Gynae Oncology Survivorship Clinic, which caters for the holistic needs of patients, underline how important all elements of cancer care are, not just surgical, radiation or medical oncology treatments.”
The first print of ‘My Gynaecology Patient Passport’ has kindly been funded by the Crosby family in memory of their daughter and sister Niamh, who sadly died from ovarian cancer in 2016 and was cared for by the St James’s Gynaecology Team. Peter Crosby, Niamh’s father, said: “We are extremely grateful for the dedicated care Niamh received from the gynaecology team at St James’s Hospital. Throughout Niamh’s illness, the team were always on hand to answer any questions and ease concerns. We are delighted to support the first print of the patient passport which will hopefully give some comfort and reassurance to patients receiving treatment for gynaecological cancer.”
We spoke to both Prof. O’Gorman and Ashley Lilly to find out more about this important initiative. What is included in patient passport?
A lot of information is provided at initial visits to cancer care clinics, and it is well known that people will not absorb all of it. Often what we are discussing is very new to the patient, it’s out of their normal conceptual framework and with their associated anxiety it is very understandable that not all is absorbed. The passport contains more information than we can provide in clinic, but the value is more that the patient owns it. They can take it home, go through it in their own time and pace, and can share it with their family, their GP and other healthcare providers.
“It also contains a structured treatment summary part where we can say very precisely and succinctly, what the diagnosis
was, and what the treatment was and that’s going to be very useful for sharing with their family or GP or other healthcare practitioners. There is advice or recommendations for GPs, for long-term kind of care and followup as well.”
So how do they envisage this will change, or improve the care for patients? Prof. O’Gorman believes that the function is to empower patients. She adds, “It's about giving patients all of the information so they can take ownership of their care. They will know what to expect from hospital stays, what they should and shouldn't do before or after treatment, including for example easy to understand advice on pelvic floor exercises. There is advice on what to look out for and when to seek medical attention.
“We as hospital professionals are always delighted to see a
Oncology Focus Gynaecological Cancer
well-informed patient, a patient taking ownership of their health. Many survivorship issues can be appropriately dealt with by patient education and self-management at home, with signposting to relevant resources and services. This passport aims to improve just that, and hopefully will result in better survivorship care for women with gynaecological cancers, and reduce unnecessary clinic attendances at busy cancer care clinics.
“We hope to improve patients' general health after their cancer because of the recommendations around bone health or other types of screening or a healthy lifestyle after cancer or HRT after cancer.”
Ashley adds that the treatment summary page will be particularly useful. “Within the passport, there is a treatment summary page that the clinician fills out. The idea being that when the patient finishes all their appointments in hospital, they can go to their GP and say, ‘This is my diagnosis, this is what I have done. This is the
follow-up that I'm going to have.
This is the recommendations for you. I need to make sure that I've got a DEXA scan booked, I need to make sure that this is monitored.’
“Our clinicians can write in this and improve the communication between us and their GP through the patient, empowering the patient to advocate for themselves.”
Is there a plan for this initiative to be rolled-out across other hospital groups in Ireland? “We are collaborating with the NCCP to create a national Gynae working group with a view to roll-out our initiative nationally,” says Ashley.
Prof. O’Gorman adds, “We were keen to develop a passport specific in our centre so that we were able to have a little bit more information to it that would be particular to our patients. We will have to make it a little bit more generic when rolling it out nationally, and we'd be developing it with representation from all of the gynae-cancer units in Ireland.
“I think it is absolutely key that we have good engagement with the passport from healthcare providers. I believe patients will value it and engage with it more if they see their healthcare providers engaging with it. To this end we really focused on involving all of our multidisciplinary team in its design, and its evaluation. Their feedback was very valuable. It needs to be user friendly for both patient and healthcare provider if we are to achieve the levels of engagement and value that we are aiming for.”
Will there be any future editions or updates?
Ashley says, “We have tried to leave quite a lot of space for say notes or additions or other options. So if there are new clinical trials - there is space to add additional information. I suppose long-term we would like to go digital. But I think it's important that we utilise and learn from this before we go down that line.
“A hard copy version is useful given our patient population are not all IT literate, though IT literacy in our older patients is increasing over time. The next phase will be moving into digital and interactive applications or platforms,” adds Prof. O’Gorman.
Ashley continues, “We have a survivorship clinic which has just been set up as well, which goes hand in hand with the passport and is like the other end of the journey, once patients are finished treatment, we will have a consultation with them, around
six months post-diagnosis and because that's when we feel that patients are kind of just getting back on their feet. Their acute appointments and treatment and everything has been completed and that's when they feel a little bit lost.
“They are wondering who will look after them when their appointments are not as regular. People stop treating them like a patient and they are often expected to go back to their normal lives. But these women have been through such a massive ordeal . We are using a holistic needs assessment as the structure for the clinic. Therefore, it is not only about their clinical symptoms, it includes their sexual health, mental health, day-to-day living, their relationships, and their sleep. It's a more general holistic approach to make sure support is provided in all aspects of their lives.
“To conclude we would like to note, the print and design of the passport was funded by one of our patient's families. The patient unfortunately passed away but her parents are still very involved in fundraising for the service and for St James's Gynaecology Department.
They have funded the first print and design. They are an incredible family, the Crosby family, and we are very appreciative of all their efforts.”
alilly@stjames.ie
caogorman@stjames.ie
Developments in standard of care and the future of myeloma in Ireland
Myeloma is the second most common blood cancer in Ireland, with about 380 new cases diagnosed annually. In the past two decades, the myeloma population has grown from around 700 to over 2,000. Over two-thirds of patients are aged over 65.
Professor Paul Browne Consultant Haematologist, Fellow Emeritus, Trinity College Dublin
In Ireland 20 years ago, median survival from myeloma was approximately three years, and patients required conventional chemotherapy. Today, most newly diagnosed patients are offered chemotherapy-free protocols using combinations of immunomodulatory (eg. lenalidomide) and immunotherapeutic (eg. daratumumab) agents.
In 1998, the first breakthrough observed that the old drug thalidomide was effective in salvaging patients with advanced refractory myeloma. This thalidomide repurposing was based on a potential anti-angiogenic mechanism thought to be clinically relevant in myeloma.
Following initial results, a class of related immunomodulatory derivatives known as IMiDs were assessed, with lenalidomide emerging as the clinical leader in 2003. Meanwhile, a separate class of compounds (proteasome inhibitors) also demonstrated striking clinical efficacy. By 2006, the combination of IMiDs and proteasome inhibitors emerged as the backbone of myeloma therapy and remained so for the last 15 years.
Combination immunotherapy without chemotherapy
The next breakthrough was the introduction of highly effective direct immunotherapy with the monoclonal anti-CD38 antibody daratumumab, initially in the relapsed refractory setting. Sequential combination studies with daratumumab confirm that for many myeloma patients aged over 65 ineligible for high-dose chemotherapy, combination immunotherapy with daratumumab and lenalidomide plus weekly pulse dexamethasone (without conventional chemotherapy) represents the globally accepted standard of care for newly diagnosed patients. This European Medicines Agency (EMA) licensed protocol achieved a striking improvement in progression-free survival and overall survival compared to previous standards of care.
Standard of care for younger patients
More recently, combining
daratumumab with the standard IMiD/proteasome inhibitor combination has proven more effective in progression-free survival for fit patients under 70 undergoing high-dose melphalan autologous stem cell transplant.
The European Myeloma Network PERSEUS trial published in the New England Journal of Medicine shows a remarkable progressionfree survival of over 80% after three years. While demonstrating an overall survival advantage will take years, the notable responses and residual disease assessments suggest that this protocol will be rapidly adopted as the standard of care for younger patients.
Relapse innovations in immunotherapy
Despite these improvements, myeloma patients continue to experience recurrence, requiring salvage therapy. Multiple options are now available for re-inducing remission, depending on the primary treatment. The most striking development in the relapse setting has again been in immunotherapy, with bi-specific T-cell engager therapy. The first agents teclistamab and talquetamab are now licensed in Europe.
These treatments mobilise and redirect the patient’s T-cells directly to the myeloma cells targeting a relevant antigen, such as B-cell maturation antigen (BCMA). These agents are highly effective in the relapse/refractory setting, with response rates of over 65% and durable responses in patients who have undergone multiple lines of therapy. These agents could form part of highly potent immunotherapy combinations for newly diagnosed myeloma over the next few years, depending on ongoing trial results.
CAR-T: cilta-cel efficacy
Genetically modified CAR-T cell therapy, especially with the cilta-cel agent, is a potent option showing clinically relevant responses in over 60% of advanced disease patients. Currently, no survival plateau is observed.
While most patients experience disease recurrence, many still gain clinical benefit with a treatment-free interval exceeding two years. Ongoing trials, like CARTITUDE-5, explore the potential use of CAR-T cell therapy
in the upfront setting, with initial results expected in three years.
Myeloma success in Ireland
Ireland has provided timely access to novel agents and stem cell therapy according to best international practices for 20 years. Well-established cooperative care programmes and strong collaboration among myeloma medical, nursing and scientific teams have delivered optimal care to the entire population.
The National Cancer Registry of Ireland (NCRI) reveals that myeloma has seen the most significant increase in both absolute and proportional survival among all cancers in Ireland over the past two decades — a remarkable achievement. For example, overall survival has notably improved for patients aged over 65. In 2000, less than 25% of patients over 65 could expect to live over five years after a myeloma diagnosis.
NCRI data confirm that for the Irish population, the five-year survival has more than doubled (to well over 50%) in this cohort, with improved quality and quantity of life. This illustrates how a coordinated myeloma therapy programme in Ireland has been improving cancer care across a cohort that had previously been disadvantaged in terms of access to clinical innovation.
Access and cost challenges in Ireland
Breakthroughs by the Irish health service in the last 20 years relied on timely access and optimal use of newer agents according to international best practices and EMA-licensed indications. This was generally feasible until around 2015.
Today, however, rising costs of new medication, alongside delays in accessing new EMAlicensed agents/indications, may hinder further overall survival advantage in Ireland. Projected expenditure exceeds €100,000 for an active therapy programme. Adopting innovative strategies and increasing collaboration among stakeholders including the public health service, private insurance system and pharmaceutical industry ensures timely access to newer immunotherapy agents aligned with best international practice.
DARZALEX ® 20 mg/ml Concentrate for Solution for Infusion and 1800 mg Solution for Injection PRESCRIBING INFORMATION
ACTIVE INGREDIENT(S): Daratumumab
Please refer to Summary of Product Characteristics (SmPC) before prescribing.
INDICATION(S):
Newly diagnosed multiple myeloma: in combination with lenalidomide/dexamethasone or bortezomib/melphalan/ prednisone in adults, ineligible for autologous stem cell transplant; in combination with bortezomib, thalidomide and dexamethasone in adults, eligible for autologous stem cell transplant. Relapsed/ Refractory multiple myeloma: Monotherapy for adults whose prior therapy included a proteasome inhibitor and an immunomodulatory agent and who have demonstrated disease progression on last therapy. In combination with lenalidomide/ dexamethasone or bortezomib/dexamethasone in adults who have received ≥ one prior therapy. Darzalex SC: in combination with pomalidomide and dexamethasone for the treatment of adult patients with multiple myeloma who have received one prior therapy containing a proteasome inhibitor and lenalidomide and were lenalidomide-refractory, or who have received at least two prior therapies that included lenalidomide and a proteasome inhibitor and have demonstrated disease progression on or after the last therapy. AL Amyloidosis: Darzalex SC in combination with cyclophosphamide, bortezomib and dexamethasone for the treatment of adult patients with newly diagnosed systemic light chain (AL) amyloidosis.
DOSAGE & ADMINISTRATION: Administration by healthcare professional where resuscitation facilities are available, intravenous (IV) infusion or subcutaneous (SC) injection. For SC injection, resuscitation facilities required only for first dose. Adults: Recommended IV dose: 16 mg/kg body weight. Dilute with sodium chloride 0.9% solution for injection and administer by IV infusion using incremental escalation of infusion rate, only if previous infusion well-tolerated. SC dose: inject 15 mL (1 800 mg) Darzalex solution for SC injection into the subcutaneous tissue of the abdomen approximately 7.5 cm to the right or left of the navel over approximately 3-5 minutes according to dosing schedule. Patients > 120 kg, flat-dose 1 800 mg SC, efficacy not established. SC injection: no dose adjustments based on body weight recommended. Darzalex solution for SC injection should never be injected into areas where the skin is red, bruised, tender, hard or areas where there are scars, rotate injection site. During treatment with Darzalex SC injection, do not administer other medicinal products for subcutaneous use at the same site as Darzalex. Check the vial labels to ensure that the appropriate formulation (IV or SC formulation) and dose is being given as prescribed. For dose and schedule of medicinal products administered with DARZALEX, refer to SmPC 4.2 and the corresponding SmPC for other products. Administer pre- and post-injection medicinal products to reduce the risk of infusion-related reactions (IRRs). Recommended concomitant medications for management of infusion/injection-related reactions (IRRs): administer pre- IV infusion/ SC Injection medicinal products to all patients 1-3 hours prior to every infusion (corticosteroid, antipyretics and antihistamine). For SC injections, pre- medications can be given orally from the first dose. When dexamethasone is background-regimen specific corticosteroid, this dose will serve
Use DARZALEX® (daratumumab) at the earliest opportunity in multiple myeloma
DARZALEX® + Rd results in mPFS 61.9 months vs 34.4 months for Rd alone1* CP-413397 |
as pre-medication on infusion days. If dexamethasone given on infusion day, do not take additional background regimen specific corticosteroids (e.g. prednisone). Post- IV infusion/SC injection medicinal products should be administered to reduce the risk of delayed IRRs: administer oral corticosteroid. SC injections: if the patient experiences no major IRRs after the first three SC injections, post-injection corticosteroids (excluding any background regimen corticosteroids) may be discontinued. Consider short/long acting bronchodilators and inhaled corticosteroids in patients with history of chronic obstructive pulmonary disorder. IV Infusion: Any grade/severity IRRs, interrupt Darzalex immediately and manage symptoms. Re-starting Darzalex IV infusion: reduce infusion rate (refer to SmPC); Grade 4 IRRs (or third occurrence of Grade 3) – permanently discontinue. For haematological toxicity dose delay may be required to allow recovery of blood cell counts. No dose reductions of Darzalex recommended. Consider antiviral prophylaxis for prevention of herpes zoster virus reactivation.
Children: No data available. Elderly/Renal impairment/Hepatic impairment: No dose adjustments.
CONTRAINDICATIONS: Hypersensitivity to active substance or excipients.
SPECIAL WARNINGS & PRECAUTIONS: IRRs: can cause serious IRRs including anaphylactic reactions. Majority occurred following first IV infusion/SC injection. Fatal outcomes have been reported with IV infusion. IV infusion: monitor for IRRs throughout the IV infusion, continue monitoring post-IV infusion until symptoms resolve. For SC injection, median time to onset of IRRs was 3.7 hours following injection, monitor IRRs especially in the first and second SC injection. IV infusion: interrupt Darzalex for any severity IRRs. Institute medical management/supportive treatment as needed. For both IV and SC Darzalex if an anaphylactic reaction or life-threatening (Grade 4) IRR occurs, initiate appropriate emergency resuscitation immediately and discontinue Darzalex immediately and permanently. Neutropenia/Thrombocytopenia: Darzalex may increase neutropenia and thrombocytopenia induced by background therapy; monitor for infections & periodic complete blood cell counts (refer to relevant SmPCs); consider supportive care. Indirect Antiglobulin Test (Indirect Coombs Test): Daratumumab binds to CD38; may mask detection of antibodies to minor antigens; ABO and Rh blood typing not impacted. Interference may occur up to 6 months post-treatment. Type and screen patients prior to starting daratumumab; consider phenotyping; red blood cell genotyping not affected by daratumumab. Inform blood transfusion centres when appropriate. If emergency transfusion required, give non-cross-matched ABO/ RhD- compatible RBCs. Hepatitis B virus (HBV) reactivation: Fatal cases reported in patients treated with Darzalex. Perform HBV screening before initiation of treatment. Suspend treatment in patients who develop reactivation of HBV while on Darzalex. Patient’s with body weight >120 kg receiving SC injection, potential for reduced efficacy. IV infusion contains sodium. SC injection contains sorbitol.
SIDE EFFECTS: Very common: IRRs, pneumonia, bronchitis, upper respiratory tract infection, anaemia,
No new safety concerns were observed1*
*In newly diagnosed transplant-ineligible multiple myeloma patients. Median follow-up of 64.5 months1
SC only: dizziness, musculoskeletal chest pain, pruritus, injection site reactions. Other side effects: HBV reactivation (uncommon), anaphylactic reaction (rare). Refer to SmPC for other side effects.
FURTHER INFORMATION IS AVAILABLE FROM: Janssen Sciences Ireland UC, Barnahely, Ringaskiddy, IRL – Co. Cork P43 FA46 Prescribing information last revised: January 2022
Adverse events should be reported. Healthcare professionals are asked to report any suspected adverse events via: HPRA Pharmacovigilance, Website: www.hpra.ie Adverse events should also be reported to, Janssen Sciences Ireland UC on 1800 709 122 or at dsafety@its.jnj.com.
References: 1. Kumar DJ, et al. Poster presented at the 64th American Society of Hematology (ASH) Annual Meeting & Exposition. December 10–13, 2022. #4559.
Janssen Sciences Ireland UC 2023
Oncology Focus Merkel Cell Carcinoma
Incidence of Merkel Cell carcinoma in the Republic of Ireland (1994-2019)
Merkel Cell Carcinoma (MCC) is a rare aggressive neuroendocrine cutaneous malignancy most commonly observed in those over 65 years of age.1 MCC is twice as common in males compared to females and is 25 times more common in those with fair skin compared to those with darker skin.2 Solid organ transplant recipients have a 24-fold increased risk of developing MCC.3. Merkel Cell human polyomavirus (MCPyV) which is found on healthy skin has been found to contribute to 80% of MCC via integration of the virus into the host cell genome. The other 20% of cases are UV radiation induced and do not demonstrate viral genomic integration. There has been an 95% increase in incidence in MCC in the United States from 2000 to 2013 with further increases predicted.4 The aim of this study was to investigate the trends of incidence of MCC in the Republic of Ireland. The National Cancer Registry of Ireland (NCRI) collects data on all cancers diagnosed in Ireland, using the International Classification of Diseases for Oncology (version 2 1994-2004, version 3 2005-2011, version 3.1 2012-2019) to code the topography and morphology of registered tumours. The data regarding MCC diagnosis was from histopathology reports. NCRI provided data on the number of MCC diagnoses from 1994-2019 (morphology code
Table 1 detailing the ASR for both male and female patients
Written by Claire Doyle, Dermatology Department, Tallaght Hospital
M-8247/3). Age-standardised rates were calculated using the 2013 European standard population. There were 447 histologically confirmed MCC diagnosed between 1994 and 2019. 49.2% (220/447) were in males. Median age was 80 years (range 15-19 years to 95+ years). Median for males was 78 years, median for females was 82 years. On average there were 7 cases of MCC diagnosed per year between 1994 and 1998 compared to 27 cases of MCC per year diagnosed between 2015-2019 almost a quadrupling of case numbers over the course of the time period. Due to relatively small absolute numbers of MCC diagnosed we report the ASR in five-year time periods. The results are detailed below in table one and showing that the ASR of MCC has significantly increased in male patients from 1994 to 2019. In contrast, the ASR of MCC has not
significantly increased in females over the same time period despite an increase in absolute numbers. Previous literature has indicated that MCC is twice as common in males and in females2. Our cohort differed to this in that there was a slight female predominance in patients diagnosed with MCC. While the absolute numbers of MCC diagnosed in Ireland has increased in both male and female patients, the age adjusted incidence rate is increasing in males but there has not been a significant change in females. Other Northern European groups have also demonstrated both a female predominance in absolute numbers of MCC and an increase in incidence of MCC in males that was not observed in females.5 This contrasts with increases in both genders observed in the United States. Further research is needed to explain this gender discrepancy. This article adds to the data on MCC which is important for service provision and planning for dermatology, radiology, histopathology, radiation oncology and plastic surgery.
References
1. Xue, Y., & Thakuria, M. (2019). Merkel Cell Carcinoma Review. Hematology/Oncology Clinics of North America, 33(1), 39–52. doi:10.1016/j.hoc.2018.08.002
2. Agelli M, Clegg LX. Epidemiology of primary Merkel cell carcinoma in the United States. J Am Acad Dermatol 2003. https://doi. org/10.1016/S0190-9622(03) 02108-X.
3. Clarke CA, Robbins HA, Tatalovich Z, et al. Risk of Merkel cell carcinoma after solid organ transplantation. J Natl Cancer Inst 2015. https://doi.org/10.1093/ jnci/ dju382.
4. Paulson KG, Park SY, Vandeven NA et al. Merkel cell carcinoma: current US incidence and projected increases based on changing demographics. J Am Acad Dermatol 2018; 78:457–63
Table 1 detailing the ASR for both male and female patients
5. Hussain SK, Sundquist J, Hemminki K. Incidence trends of squamous cell and rare skin cancers in the Swedish national cancer registry point to calendar year and age-dependent increases. J Invest Dermatol. 2010;130:1323–8.
Oncology Focus Skin Cancer
Management of Skin cancer and Melanoma
Skin cancer in Ireland
Skin cancer is the most common cancer in Ireland. More than 11,000 cases are diagnosed annually accounting for over one-third of all cancers diagnosed, yet most skin cancers could be prevented. There are 2 main types of skin cancer: Non-melanoma skin cancer and melanoma skin cancer.
Non-melanoma skin cancer includes:
• Basal cell skin cancerthis is also called Basal Cell Carcinoma (BCC)
• Squamous cell skin cancerthis is also called Squamous Cell Carcinoma (SCC)
This is much more common but less aggressive than melanoma skin cancer. It slowly progresses over months or years.
Melanoma Skin Cancer
Melanoma is a less common but more aggressive type of skin cancer. The most common sign is the appearance of a new mole or change in an existing mole. It is more likely to spread to other parts of the body if not caught and treated early. Commonly affected areas are the trunk (chest and back) in men and the legs in women. It
has a high 5-year survival rate of 93% if caught in time.
It is important for everyone to familiarize themselves with all the moles on their skin and not only look for changes in existing moles, but also any new spots that may appear.
What changes to look out for:
A – Asymmetry - if you draw a line down the centre of your mole, is it larger on one side?
B – Border - are the borders of your mole uneven, jagged or notched?
C – Colour - has your mole changed colour over time or does it contain several different colours?
D – Diameter - is the circumference of your mole larger than the top of a rubber on a pencil (larger than 6mm – the size of a pencil rubber), although melanomas can sometimes be smaller than this.
E – Evolving - has your mole changed in height, appearance or are you experiencing any changes within or around your mole (eg. itching, bleeding, crusting)
It is important to know what is normal for you and what your normal skin looks like. If you are
Written by Bernie Carter, Assistant Director of Nursing, Marie Keating Foundation
concerned about a change in your skin, or any of the above symptoms, see your GP.
What are the risk factors?
Ultraviolet (UV) radiation
Exposure to UV radiation is the main risk factor responsible for skin cancers. It is emitted naturally from the sun and from artificial sources such as sunbeds and sun lamps.
It’s important to remember that skin damage doesn’t just happen on holiday or in hot, sunny places. The sun is often strong enough to cause damage in Ireland, even on a cloudy day.
Sunbed usage
Research shows that the type of ultraviolet light used in sunbeds (UVA) can cause all types of skin cancer. The International Agency for Research into Cancer (IARC) has classified using sunbeds as a cause of melanoma. Just one session can increase your risk of developing cancer by 20%. The risk is highest for people who use a sunbed before age 35. Sunbed use by under-18s is banned in Ireland.
melanoma is also quite common in younger people.
Family history
Your risk of melanoma is higher if you have a close relative who has had melanoma.
Genetic risk for Melanoma
Some families tend to have large numbers of moles, or moles that are unusual (atypical moles). The atypical moles tend to be an irregular shape or colour and may be larger than usual. An inherited condition called familial atypical multiple mole melanoma syndrome (FAMMM) increases your risk of melanoma.
The SunSmart Code
Skin Type
Fairer skinned people with lots of freckles and moles are more at risk. However, remember that if you have skin, you can get skin cancer.
Having lots of Moles
The more moles you have on your body, the higher your risk of melanoma, meaning you should be very careful about exposing yourself to the sun and keep an eye on all your moles particularly new moles. The majority of melanomas occur on new moles.
Birthmarks
Most birthmarks, carry no risk of developing into a cancer. A very rare type, called a giant congenital melanocytic nevus, can develop into a melanoma if it is larger than 20cm. Check all birthmarks regularly for any signs of change.
Age
The risk of melanoma increases with age. However, compared to most other cancer types,
Five steps we can take to help protect skin from the harmful effects of the sun while outdoors.
1. Seek Shade if outdoors from 11am to 3pm, when the sun is at its strongest. Always use a sunshade on a child’s buggy
2. Slip on some clothes made from close woven material that covers skin.
3. Slap on a wide brimmed hat to protect exposed skin such as face, neck, and ears from harmful rays
4. Slide on sunglasses with UV protection to shield your eyes from UV rays and protect yourself from cancer and chronic conditions such as cataracts.
5. Slop on sunscreen with an SPF of 30+ for adults and 50+ for children, with high UVA protection and water resistant. Apply regularly and thoroughly throughout the day.
Visit www.mariekeating.ie for more information and support.
New Report Highlights Need for Action on Cancer Inequalities
Responsible for 30% of deaths, cancer is the single biggest killer in Ireland, with more than 9,620 deaths a year[1]. A new report from the European Cancer Organisation (ECO) and the Irish Cancer Society highlights the state of cancer care in the country and the specific areas that require urgent attention from policymakers.
The report was launched during the Joint Euro-American Forum on Cancer at Farmleigh House in Dublin.
The data from ECO’s rapidly expanding online repository, the European Cancer Pulse, captures evidence of progress but also highlights areas that need scrutiny, particularly those around cancer inequalities.
“The data presented here as part of the European Cancer Pulse highlight the significant cancer inequalities faced by people
living in the most deprived areas of Ireland. Given our previous work, it is quite likely that the impact of Covid-19, as well as the Government’s failure to provide any new recurrent development funding for the National Cancer Strategy in 2023 or 2024 has widened this 9% survival gap even further,” said Professor Mark Lawler, Professor of Digital Health, Queen’s University Belfast, co-lead of the All Island Cancer Research Institute (AICRI) Chair of the International Cancer Benchmarking Partnership and Co-Chair, ECO Emergencies & Crises Network.
‘Our data have shown that consistency of cancer policy has resulted in better outcomes for cancer patients in Ireland when compared to the UK for example. But consistency means you have to keep on doing it. Letting up gives the advantage
Raising Concerns in Healthcare
Professor Mark Lawler, Professor of Digital Health, Queen’s University Belfast
back to cancer. The recent lack of investment in the Irish National Cancer Strategy is worrying and risks sending Ireland backwards in terms of cancer outcomes, undoing the good work of previous decades. Ireland must act now,’ he added.
Speaking at the launch, Averil Power, CEO Irish Cancer Society said, “We know that people across the country do not have equal access to cancer care and services in Ireland. Inequality between public and private patients is growing, particularly in terms of access to new medicines. The lack of Government investment in Ireland’s current National Cancer Strategy means target waiting times for cancer tests are consistently being exceeded. Those who cannot afford to go private are too often left languishing on long waiting lists, getting more anxious with each day that passes.
“It is very positive that the uptake of Ireland’s current screening programmes is higher than the EU average. However, BowelScreen has not been expanded as planned. The age groups covered by screening in Ireland are more limited than in some other European countries. Previous data has also found significant differences in screening uptake between affluent and lower income areas.
“We need to ensure that every Irish person, regardless of their background or income, has the best possible chance of surviving cancer. Without proper multiannual funding for the National Cancer Strategy, not only are Ireland’s cancer outcomes unlikely to improve but we are at serious risk of going backwards.’
Key recommendations
ECO has presented a series of recommendations from its European Cancer Manifesto for 2024 which if implemented would have significant impact, including here in Ireland. The Manifesto is endorsed by over 50 politicians across Europe, including Barry Andrews MEP, Frances Fitzgerald MEP, Cathal Crowe TD, and Stewart Dickson MLA.
Recommendations include:
• A minimum age for tobacco sales of 21 years old (‘tobacco 21’) to achieve a European tobacco-free generation
• Regular public reporting on progress on EU recommendations on cancer screening
• Initiatives to eliminate vaccinepreventable cancers caused by HPV and hepatitis B (HBV)
• Addressing the Cancer Workforce Crisis, which is a threat to health system resilience
• Legal protections for cancer survivors so that they need not declare their disease to financial service providers
Addressing sexual misconduct in healthcare and the role of whistleblowing were among the issues to be discussed during the annual RCSI medical professionalism conference, which took place as HPN was going to print.
The conference heard medical professional and patient perspectives on raising concerns in healthcare, while hearing testimonies from whistleblowers. It explored the ethical, professional and legal duty of medical professionals to raise concerns when appropriate, as well as protection for whistleblowers and the educational interventions that can encourage a culture of raising concerns.
Professor Carrie Newlands, co-lead on the Working Party on Sexual Misconduct in Surgery at the University of Surrey School of Medicine, shared insights from her work to understand sexual misconduct in healthcare.
Dr Ravi Jayaram, who was among those who raised concerns about former neonatal nurse Lucy Letby, gave an account of his experience as a whistleblower.
Stephen Teap, CervicalCheck campaigner and co-founder of 221plus, also shared his personal view on the impact of the Cervical Check scandal.
Professor Denis Harkin, Chair of Medical Professionalism at RCSI, said: “Today’s conference provides us the opportunity to emphasise the importance of raising concerns in healthcare and to learn from the lived experience of whistleblowers. These conversations are important in allowing us to reflect on how we can move forward in encouraging and supporting a culture of raising concerns.”
RCSI’s Centre for Medical Professionalism aims to provide global leadership in medical professionalism to achieve excellence in patient care and experience, caring for those who care and promoting a healthier society, through innovation in research, education and practice.
Mater Private Network’s Heart Summit Reveals Insights into Future of Cardiac Care in Ireland
Just last month in Dublin, leading European cardiologists came together to share new insights and groundbreaking advancements in cardiac patient care with Irish GPs, cardiologists and other healthcare professionals.
Mater Private Network’s inaugural Heart Summit was presented in collaboration with CVRI Dublin and the Royal College of Surgeons Ireland, and represented a unique opportunity for healthcare professionals, researchers, and stakeholders to come together and proactively shape the future of cardiovascular medicine, ultimately improving patient outcomes.
The keynote presentation was delivered by Professor Thomas Luscher, President Elect of the European Society of Cardiology. The days event saw insightful analysis around topics related to cardiac patient care, from a number of European cardiology experts. Both experts from the
Mater Private Network award winning cardiology panel, as well as speakers from further afield, including, Prof. Alan Fraiser, Dr. Maurizio Panarelli, and Prof. Borja Ibanez, shared their insights.
During the summit, dynamic discussions and interactive sessions took place on the
role of polypills in preventing cardiovascular disease, advancements in female care for coronary artery disease, and the evolving landscape of CT coronary angiography. Other highlights include discussions on recent regulatory changes in high-risk medical devices, interventions for
Back row, L-R: Dr. Noel Fitzpatrick, Prof. Jim O'Neill, Dr. Niamh Keenan, Prof. Gábor Széplaki, Dr. Magid Awadalla and Prof. Borja Ibanez
Front row, L-R: Prof Pascal McKeown, Prof. Robert Byrne and Prof. Thomas Luscher
tricuspid regurgitation and atrial fibrillation. Each presentation included an engaging Q&A session and panel discussions, with a high level of audience engagement both online and in person an indicator of the huge interest in these key aspects of cardiovascular medicine. Three key takeaways for Irish adults:
• While incidences of cardiac events are an ongoing issue globally, teams within Europe are working proactively to provide medical and technical advancements for the benefit of all.
• Treatment facilities within Ireland are amongst some of the best in the space and are constantly being improved, and when detected in time, a heart-based illness does not mean mortality.
Panel discussion with Prof. Borja Ibanez, Prof. Jim O'Neill, Dr. Maurizio Panarelli. Dr. Roger Byrne and Dr. Sarah Short
Opening the conference at The Royal College Of Surgeons, Dublin, Prof. Robert Byrne, Director of Cardiology at Mater Private Network said
“Cardiovascular disease is a leading cause of death for Irish adults and so we are particularly honoured to bring this Heart Summit to Dublin and host it on home soil. The conference is designed to educate, spur on knowledge share and inspire innovation in our field, both in medical techniques and indeed in patient care. The energy here at our Dublin City event has been infectious. At Mater Private Network, we are passionate about fostering a culture of international collaboration and continuous improvement, paving the way for the future of healthcare”
During his keynote speech at this year’s event, Prof. Thomas Lüscher, President-Elect of the European Society of Cardiology stated, “I am thrilled to have been invited to speak at Mater Private Network’s Heart Summit here in Dublin. The cardiology specialism
is unfortunately becoming more and more prevalent in the lives of patients across Europe and thus our work is more vital than ever. Together, we can increase the speed of innovation in the field and ensure better outcomes for patients and the quality of presentations and knowledge share today is the perfect example of that.”
Committed to ongoing the excellence and innovation in cardiac care in Ireland, Mater Private Network was delighted to be able to provide this educational session, not only to improve the understanding of cardiac treatment and screening options available in Ireland, but overall, to improve standards of cardiac care for all.
Full recordings of the days event will be available to view on MedCafé and on Mater Private Network’s website shortly. To learn more about Mater Private Network’s cardiac offering, and treatment options available to the public, please visit www.materprivate.ie
• No two case of cardiac disease are the same. To ensure excellence in patient care, continuous consideration, collaboration and insights are needed. Thankfully, Summits
such as today’s Dublin event are helping GPs and cardiologists across Ireland stay abreast of the information they need to know to best support their patients and communities.
Prof. Pascal McKeown, President of the Irish Cardiac Society, with Amy Carswell from the Cardiovascular Research Institute, Dublin
Prof. Robert Byrne with co-chairs Dr. Sarah Short and Dr. Louise Fitzgerald
International faculty Dr. Maurizio Panarelli, Prof. Borja Ibanez and Prof. Alan Fraser, with Prof. Robert Byrne and Dr. Róisín Colleran from Mater Private Network
Deep in thought: Dr. Maurizio Panarelili and Prof. Thomas Luscher
Dr. Jim O'Brien, Dr. Niamh Keenan, Ms. Sarah Early and Dr. Magid Awadalla
60 Second Summary
Chronic musculoskeletal pain affects about 30% of the world’s population, leading to disability, reduced quality of life, and substantial costs for healthcare systems.
AUTHOR: Donna Cosgrove, MPSI, PhD
Donna did her Pharmacy degree in RCSI, and then returned to university to pursue an interest in psychiatric conditions and treatments through a MSc in Neuropharmacology. This led to a PhD investigating the genetics of schizophrenia using data from genome-wide association studies and cognitive test data. This was followed by a postdoctoral research position in a similar area. Donna has worked in hospital, research and community pharmacy settings, and currently works as a community pharmacist in Galway, and as a clinical writer. Donna’s overall aim is to improve patient outcomes through education.
Management of Joint and Muscle Pain CPD
There are different types of pain including nociceptive, neuropathic, nociplastic, idiopathic, and mixed. Pain and nociception are different phenomena, with the experience of pain varying widely for a given type of nociception.
Since 1986, clinicians have been guided by the WHO pain ladder, although its intended use was for treating cancer pain and has certain limitations. A revised version includes additional steps for non-pharmacological, integrative health therapies; and de-escalation of pain medication. Principles of the WHO pain ladder are still used in strategies for pain management, e.g. oral dosing when possible, around the clock rather than on demand administration, and individualised therapy.
There are many drug classes used in the pharmacological management of joint and muscle pain, including simple analgesics/non steroidal analgesics, opioids, anticonvulsants, antidepressants, musculoskeletal agents, anxiolytics, and DMARDs. Nonpharmacological treatments such as cryotherapy/heat therapy can help with reducing muscle spasm.
Transcutaneous electrical nerve stimulation therapy, acupuncture, exercise, and psychological treatments are also useful add-ons for management of joint and muscle pain.
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice?
2. IDENTIFY - If the answer is no,
I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a
Introduction
According to the World Health Organisation, 20-33% of the global population has some form of chronic musculoskeletal pain, most commonly low back pain, which is the single leading cause of disability in 160 countries. Musculoskeletal impairments include over 150 diseases or conditions that affect the system, which cause impairments in the muscles, bones, joints, nerves and adjacent connective tissues, and the associated limitations in functioning (temporary or lifelong). It leads to a reduced quality of life due to the inability to enjoy daily activities or participate in society, increased drug use, high frequency of sick leave; also leading to socioeconomic problems and substantial costs for healthcare
knowledge gap - will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result? Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the
4 previous steps, log and record your findings.
Published by HPN. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published is copyright, no part of this can be used in any other publication without permission of the publishers and author. HALEON has no editorial oversight of the CPD programmes included in these modules
systems, especially rehabilitation services. The number of people living with functional limitations of this pain is increasing globally due to population growth and ageing. People with musculoskeletal conditions are also more likely to develop mental health issues.1,2 Increasing age is associated with higher risk of musculoskeletal pain (e.g. knee pain in osteoarthritis). The most common forms are:1
Chronic low back pain (30-40% of adults)
Neck pain
Osteoarthritis (OA, 43% of people over 65)
Rheumatoid arthritis
Sprained muscles
Bone fracture pain
Gout
Risk factors that have been identified for musculoskeletal pain include:
Smoking
Lower educational status
Sedentary lifestyle
Poor or limited social interactions
Low income
Insomnia or sleep disorders
Anxiety
Depression
Manual labour
Country specific information on musculoskeletal conditions can be found through the World Health Organisation (WHO) Rehabilitation Need Estimator tool (Figure 1).
Joints may be inflamed (arthritis) or painful (arthralgia). Inflammation
Joints may be inflamed (arthritis) or painful (arthralgia). Inflammation in the joints often involves warmth, swelling (due to intra-articular fluid/effusion), and less commonly, erythema. Joint pain can often have an alternative, extra articular source, like a bone or periarticular structures such as tendons, ligaments, bursae or muscles. The synovium and the joint capsule are the major sources of pain
the joint (4).
Joint and Muscle Pain
Donna Cosgrove MPSI PhD
Figure 1. WHO Rehabilitation Need Estimator Tool Information for Ireland (3).
Figure 1. WHO Rehabilitation Need Estimator Tool Information for Ireland3
36 CPD 107: MUSCLE PAIN
in the joints often involves warmth, swelling (due to intra-articular fluid/ effusion), and less commonly, erythema. Joint pain can often have an alternative, extra articular source, like a bone or periarticular structures such as tendons, ligaments, bursae or muscles. The synovium and the joint capsule are the major sources of pain within the joint.4
Polyarticular joint pain arising from within the joint can be caused by inflammation (e.g. infection, presence of urate crystals, systemic inflammatory disorders like rheumatoid arthritis). It can also be caused by mechanical disorders like OA or hypermobility syndrome. Peripheral polyarticular arthritis is more likely to be associated with systemic infection or systemic inflammatory disorder than monoarticular arthritis. Causes of acute polyarticular arthritis tend to be due to infection, a flare up of a systemic inflammatory disorder, or gout. Chronic causes include rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. OA causes non-inflammatory polyarticular pain in adults.
The Pain Experience
Pain and nociception are different phenomena. Nociception is the physiology of actual or potential tissue damage, whereas pain includes the unpleasant thoughts, emotions, and behaviours that accompany nociception.5 Pain is an “unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage”, as defined by the International Association for the Study of Pain (IASP).6 IASP stresses the importance of acknowledging that pain is always a personal experience that is influenced to varying degrees by biological, psychological, and social factors, such as life experience, and it is important that a person’s report of their pain experience is respected. Pain intensity can vary widely for a given nociception - studies of musculoskeletal injuries have actually found no association between pain intensity and degree of nociception, or injury severity. In fact, variations in pain intensity are accounted for more by measures of psychosocial factors than by measures of pathophysiology. Identifying and addressing psychosocial factors may limit persistent pain.5 Although pain usually serves an
adaptive role, it may have adverse effects on function and social and psychological well-being. Pain can be classified into nociceptive, neuropathic, nociplastic, idiopathic, or mixed type, according to the pathophysiological categories.2 In the ICD 11, there is a separate “parent code” for chronic pain which includes chronic secondary musculoskeletal pain. However, sub diagnoses can fall under multiple parent codes, including one of the pathophysiological categories above.
Nociceptive pain is the most common following tissue injury, and the most commonly implicated in musculoskeletal pain. It can be sharp, throbbing, or aching, is well localised, and has a protective function. It is a normal sensory experience. Somatic nociceptive pain originates from the skin, subcutaneous tissues and muscles. Bone pain originates from the skeleton due to bone fractures or trauma, often associated with tenderness in the overlying tissue. Visceral pain is associated with deep visceral organs, such as in appendicitis. This type of pain is poorly localised, dull, cramping pain; and can also be associated with nausea and vomiting.
Neuropathic (pathological) pain usually occurs as a result of a primary injury that results in dysfunction of the somatosensory nervous system, along the involved neural tissue or structure. It is commonly attributed to sensory changes including hypoesthesia/ hyperesthesia, hypoalgesia/ hyperalgesia, allodynia, or paresthesia. Neuropathic pain is often described as burning, shooting, electric, numbness, or pins and needles.
Mixed pain refers to both a component of continued nociceptive pain with a component of neuropathic pain.
Idiopathic pain is disproportionate to the level of tissue injury, or there is no definite cause identified. Psychological factors can influence idiopathic pain.
Nociplastic pain has recently been added by the IASP as “pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing
the pain”. It may be mistaken for central sensitisation (increased nociceptive responsiveness to stimuli from things that are not typically painful), although pathophysiology has not been fully established. Nociplastic pain is present in many different diseases such as fibromyalgia, complex regional pain syndrome, and irritable bowel syndrome.7
Donna present in many different diseases such as fibromyalgia, complex regional pain syndrome, bowel syndrome (7).
Evidence Based Recommendations for Musculoskeletal Pain Management
In terms of pharmacological treatment, healthcare professionals have been guided since 1986 by the WHO pain ladder system (Figure 2), although this pain ladder has been used more widely than its initial intended use (in cancer pain) and has its limitations. The original version was unidirectional (Figure 1A), starting with NSAIDs or paracetamol as step 1, and escalating up to weak (step 2) and strong (step 3) opioids, with
or without adjuvants, depending on the patient’s level of pain, with no plan for de-escalation.8 It has been suggested that step 2 ( use of weak opioids) be eliminated, as there is little evidence that these offer much for pain control. Instead, reduced doses of strong opioids may be more useful. Another limitation of the original pain ladder was lack of inclusion of non-pharmacological approaches into the pain treatment path. Subsequently, a fourth step has been added to the pain ladder. This integrates non-pharmacological evidence based interventions.
Evidence Based Recommendations for Musculoskeletal Pain Management
In terms of pharmacological treatment, healthcare professionals have been guided WHO pain ladder system (Figure 2), although this pain ladder has been used more intended use (in cancer pain) and has its limitations. The original version was 1A), starting with NSAIDs or paracetamol as step 1, and escalating up to weak (step 3) opioids, with or without adjuvants, depending on the patient’s level of pain, escalation (8). It has been suggested that step 2 ( use of weak opioids) be eliminated, evidence that these offer much for pain control. Instead, reduced doses of strong useful. Another limitation of the original pain ladder was lack of inclusion of approaches into the pain treatment path. Subsequently, a fourth step has been ladder. This integrates non-pharmacological evidence based interventions.
Despite limitations, there are important principles with the WHO pain ladder that can be used as part of a simple strategy for pain management (8):
I. Oral dosing of drugs whenever possible.
II. Around-the-clock rather than on-demand administration.
III. Analgesics prescribed according to pain intensity as evaluated by a pain severity scale.
Despite limitations, there are important principles with the WHO pain ladder that can be of a simple strategy for pain management (8):
V. Oral dosing of drugs whenever possible.
VI. Around-the-clock rather than on-demand administration.
VII. Analgesics prescribed according to pain intensity as evaluated by a pain severity
VIII. Individualised therapy addressing the concerns of the patient (which assumes that
Figure 2. Original (A) and Revised (B) WHO Pain Ladders
Joint and Donna Cosgrove
Figure 2. Original (A) and Revised (B) WHO Pain Ladders.
IV. Individualised therapy addressing the concerns of the patient (which assumes that there is no standardised dosage in pain treatment.) This is probably the biggest challenge in pain medicine, as the dose must be continuously adapted to the patient, to balance desired effects and possible side effects.
V. Proper medication adherence.
The updated ladder includes the introduction of integrative medicine therapies and includes a step down approach for when pain improves.
Pharmacological Pain Management
Table 1 shows many pharmacological options for pain management in musculoskeletal conditions, non opioids, opioids and adjuvants.
Paracetamol reduces prostaglandin (PG) synthesis from arachidonic acid through COX 1 and 2 inhibition, and is thought to act centrally. Due to its high tolerability and relative effectiveness, it is commonly used on its own or with NSAIDs. However, research suggests it is ineffective as monotherapy in OA.2
NSAIDs are the mainstay of treatment in OA, and should be considered in chronic lower back pain. Non-specific NSAID use is associated with the potential development of gastrointestinal (GIT), renal, and cardiovascular side effects, and patients should be educated and monitored appropriately.
COX-2 selective inhibitors (e.g. celecoxib, etoricoxib) are as effective as traditional NSAIDs for mild to moderate pain. They have fewer GIT side effects, but long term, an increased risk of cardiovascular effects, which should be taken into account when initiating. COX-2 is found in inflammatory cells, damaged tissue, synovia, endothelium and the CNS.
Topical NSAIDs (e.g. diclofenac) should be considered in chronic pain, including knee and hand OA, and those who cannot tolerate oral formulations. Topical NSAIDs should be considered before oral because of the more limited systemic exposure with topical. Due to the depth of the joint beneath the skin surface in hip OA, in this case topical NSAIDs are unlikely to be beneficial.
Table 1. Pharmacological Pain Management for Musculoskeletal Conditions2,9
Drug Type
Simple analgesics/non steroidal analgesics and antipyretics
Opioids work as agonists at mu, delta and kappa receptors in the brain, spinal cord and periphery. Respiratory depression, sedation, nausea, vomiting and constipation are the main adverse effects associated with most opioids. These are not first line therapy for chronic pain and for short to medium term treatment only in suitable patients.
Anticonvulsants (e.g. gabapentin, pregabalin, carbamazepine) are used to treat pain including neuropathic pain, spinal cord injury, shingles, fibromyalgia, and diabetic nephropathy. Gabapentinoids bind
Treatment
Paracetamol
NSAIDs (including non-selective and selective COX-2 inhibitors)
Morphine (strong)
Oxycodone (strong)
Tapentadol (μ-opioid agonist and noradrenaline reuptake inhibitor)
Buprenorphine (partial μ-opioid agonist)
Tramadol (weak, with additional 5HT and NA effects)
Codeine (weak)
Gabapentin
Pregabalin
Carbamazepine
Tricyclic antidepressants
SNRIs
Lidocaine (topical)
Baclofen
Tizanidine
Benzodiazepines
Ketamine
Clonidine
Prednisolone
Hydroxychloroquine
Methotrexate
Leflunomide
Tofacitinib
Drugs that inhibit TNF-α
IL-6 inhibitors
Drugs that inhibit of T cell co-stimulation
Drugs that cause B- cell depletion
Colchicine
Allopurinol
Febuxostat
to the alpha 2 delta subunit of the voltage gated calcium channels, reducing ion influx in hyperexcitable states. The mechanism of action of carbamazepine has not been fully elucidated.
Tricyclic antidepressants (e.g. amitriptyline, nortriptyline) demonstrate an analgesic effect separately to their effect as antidepressants, thought to be due to presynaptic reuptake inhibition of serotonin and noradrenaline.
SNRIs (e.g. duloxetine) is used to treat pain from diabetic nephropathy, fibromyalgia, OA,
and lower back pain. SSRIs (e.g. fluoxetine) can be considered in fibromyalgia, although trials show that SSRIs are usually not effective in neuropathic pain.
Musculoskeletal agents (e.g. baclofen, tizanidine) are used commonly in pain treatment. Baclofen is used as a skeletal muscle relaxant, and is a GABA agonist. Its mechanism is not fully understood, but it can inhibit synaptic reflexes at the spinal level. Tizanidine is a central alpha 2 adrenergic receptor agonist, causing muscles to relax through increased presynaptic inhibition.
38 CPD 107: MUSCLE PAIN
Anxiolytics are often used to help with anxiety associated with acute pain or fluctuations in chronic pain symptoms, but e.g. benzodiazepine treatment should be given short term. If needed for longer periods, appropriate long term treatment e.g. antidepressants should be considered.
Alpha 2 adrenergic agonist activity reduces dorsal horn neuronal activity and inhibits substance P release, leading to analgesia, sedation, and sympatholytic effects. Clonidine and tizanidine (also described above) have been used in chronic pain.
Topical lidocaine patches are used for 12 hours on, 12 hours off, and are useful in treating localised nociceptive pain, neuropathic pain, and post herpetic neuralgia.
Ketamine is a phencyclidine derivative that was developed in the 1960s as an anaesthetic agent. Its analgesic action at subanesthetic doses is thought to be mostly due to N-methyld-aspartate (NMDA) receptor antagonism in the brain and spinal cord.10 NMDA receptors have roles in learning, memory, and synaptic plasticity; but their utility as a target for pain is due to the receptor’s involvement in the amplification of pain signals, development of central sensitisation, and opioid tolerance. The evidence base for use of ketamine in pain is still quite limited. There are at least two ongoing clinical trials including a RCT of paramedic analgesia comparing ketamine and morphine in trauma (PACKMaN), and the Ketamine for Acute Pain after Trauma (KAPT) trial. An RCT comparing oral ketamine vs placebo in cancer-related neuropathic pain reported that ketamine was equivalent to placebo in this cohort, although the authors suggest that there may be subgroups of patients for whom ketamine is helpful, such as those with central sensitisation.11
There are many drugs included under the “conventional synthetic DMARDs” umbrella, for the treatment of RA. Glucocorticoids, e.g. prednisolone, are highly potent anti-inflammatory drugs. They work by general suppression of gene expression.12 Glucocorticoids bind to intracellular glucocorticoid receptors, move to the cell nucleus and reduce gene transcription of inflammatory molecules while promoting
transcription of other genes that ultimately reduce inflammation.
The mechanism of hydroxychloroquine is likely through inhibition of lysosomal antigen degradation, ultimately preventing activation of T cells and the following inflammatory responses. Hydroxychloroquine also inhibits the production of RF antibodies, and collagenase/ proteinases which directly cause cartilage breakdown. Ophthalmic toxicity is the most important side effect (4.4 - 19%).
Leflunomide interferes with cell cycle progression by inhibiting the mitochondrial enzyme involved in DNA and RNA synthesis (dihydroorotate dehydrogenase). This action inhibits the production of rapidly dividing cells, e.g. autoimmune T-cells, and the production of antibodies from B cells.13 It is also a tyrosine kinase inhibitor, which means DNA repair, apoptosis, and cell proliferation are affected. The dose-limiting side effects are liver damage, lung disease and immunosuppression.
Methotrexate is an analogue of folic acid that interferes with dihydrofolate reductase.12 This inhibits nucleotide synthesis and purine metabolism. Through this, it produces adenosine, which has direct anti-inflammatory properties. The potential side effects including hair loss, stomatitis, nausea, and hepatotoxicity are caused directly by the disruption of folate metabolism and can be prevented by folic acid supplementation.
Sulfasalazine is a prodrug of 5-ASA, and while the exact mechanism is unknown, it has been shown to have antiinflammatory, immune modulatory, and antibiotic properties. Typical side-effects of sulfasalazine include fatigue, CNS reactions, nausea, abdominal pain (dyspepsia), diarrhoea, hypersensitivity reactions, and with a lower frequency of blood dyscrasias.
Targeted Synthetic DMARDs were developed specifically to disrupt the cytokine-mediated induction of inflammation, i.e. the JAK-STAT pathway.12 Tofacitinib was the first JAK inhibitor approved.
There are four modes of action of current biological DMARDs:12
Inhibition of TNF-α or the TNF receptor: infliximab, certolizumab, adalimumab and golimumab are TNF-α neutralising antibodies. Certolizumab pegol is an
anti-TNF-α antibody fragment. Etanercept is a soluble TNF receptor that binds TNF-α
IL-6 receptor antagonism: tocilizumab
Inhibition of T cell co-stimulation by antigen presenting cells: Abatacept is the first of these agents that suppress induction of inflammation upstream of the pro-inflammatory signalling cascade.
Depletion of B cells: Rituximab decreases B cells and diminishes the activation of T cells.
Drugs that reduce uric acid include colchicine, allopurinol and febuxostat. Colchicine prevents granulocyte migration into the inflamed joint, inhibits release of glycoprotein which aggravates inflammation, and binds to the intracellular protein tubulin causing disappearance of microtubules in granulocytes, which are essential for cell function. It also limits formation of IL-1β and IL-18.14 The enzyme xanthine oxidase is responsible for conversion of hypoxanthine and xanthine into urate, and by inhibiting this enzyme, allopurinol and febuxostat prevent formation of urate.
Non-Pharmacological Treatment
A common cause of musculoskeletal pain is muscle spasm. Application of heat or cold reduces muscle shortening, caused either by direct muscle trauma or the underlying neurological or skeletal disease.2 Evidence for many of these modalities is sparse because there are no large clinical trials in this area.
Cryotherapy reduces haemorrhage, vasodilation, local inflammation and oedema production, and pain perception. PRICE (protection, rest, ice, compression, elevation) is an approach often employed for e.g. acute sports injuries, as well as more chronic conditions.
Application of heat causes increased collagen extensibility, blood flow, metabolic rate, and resolution of inflammation in subacute and chronic conditions. Heat application in combination with stretching reduces muscle contraction, joint stiffness, and chronic inflammatory diseases, ultimately leading to pain reduction and increased range and function. Heat raises the pain threshold and reduces muscle excitability.
Transcutaneous electrical nerve stimulation therapy (TENS) is based on the “gate control
theory” of pain, where preferential activation of A beta fibres inhibits the transmission of painful impulses. There is support for its use in OA and neuropathic pain, and it has been used to manage postoperative pain, complex regional pain syndrome, phantom limb pain, peripheral nerve injury, and during pregnancy and labour. Acupuncture is considered to be an invasive procedure due to the insertion of thin metal needles into specific areas of the body, and requires a professional practitioner. There is no evidence that acupuncture is more effective than NSAIDs in some pain conditions. However, it may be helpful for some types of pain including back or neck pain, knee pain associated with OA, and postoperative pain. It may also help relieve joint pain associated with the use of aromatase inhibitors.
Therapeutic exercise, e.g. passive movements, active assisted exercises, active exercises, stretching, relaxation exercises, can be useful when combined with other pain management modalities. Initial treatment of musculoskeletal pain includes immobilisation, compression, and cryotherapy. Acute muscle injuries may cause contraction or shortening of the muscles as a protective mechanism, so when pain reduces enough, the injured region should be gradually mobilised. If the contraction/ shortening becomes chronic, this causes further pain.
Psychological factors can impact the experience of pain, and can be helped with treatments including cognitive behavioural therapy, explanation, reassurance, stress reduction or counselling.
Conclusion
Joint and muscle pain includes a large variety of conditions with different causes and treatment trajectories that are a significant burden on patients, society and healthcare resources. Pharmacological treatment is often prescribed and can provide substantial relief. However, depending on the treatment, it may be associated with risks, and not all patients respond adequately. Non pharmacological treatment should be incorporated where appropriate, with patient care involving shared decision making. References available on request
Endorcrinology Focus Diabetes
The
IRELAnD
study - investigating the role of early low-dose aspirin in diabetes mellitus: a
Written by: Catherine Finnegan PhD1, Patrick Dicker MSc1, Denisa Asandei MPhil1, Mary Higgins MD2, Neil O'Gorman MD3, Mairead O’ Riordan MRCOG4, Fidelma Dunne PhD5, Geraldine Gaffney MD5, Christine Newman MD5, Fionnuala McAuliffe FRCOG2, Vineta Ciprike MD6, Elena Fernandez MS7, Fergal D. Malone MD1, Fionnuala M. Breathnach MD1
1RCSI Fetal Centre, Rotunda Hospital, Dublin, Ireland (PhD Finnegan, MSc Dicker, MPhil Asandei, MD Breathnach and MD Malone)
2UCD Perinatal Research Centre, University College Dublin, National Maternity Hospital, Dublin, Ireland (MD Higgins and FRCOG McAuliffe)
3Coombe Women and Infants University Hospital, Dublin, Ireland (MD O'Gorman)
4Infant Research Centre, Department of Obstetrics and Gynaecology, University College Cork, Cork, Ireland (MRCOG O’ Riordan)
5University College Hospital Galway, Galway, Ireland (PhD Dunne, MD Gaffney, and MD Newman)
6Our Lady of Lourdes Hospital, Drogheda, Ireland (MD Ciprike)
7Rotunda Hospital, Dublin, Ireland (MS Fernandez)
Introduction
A global increase in the prevalence of type 1 (T1DM) and type 2 diabetes mellitus (T2DM) has been observed over the last 3 decades, with 1% of all pregnancies being complicated by pregestational diabetes mellitus (PGDM).1,2 When compared with women with normal glycemic control, women with PGDM have consistently higher rates of serious obstetrical and perinatal complications, which renders PGDM one of the highest-risk medical disorders of pregnancy.3,4 Placental dysfunction, manifesting as preeclampsia, preterm delivery, and growth restriction, is one example of the increased obstetrical risk in this population. Preeclampsia, a multisystem disorder characterized by elevated blood pressure and proteinuria during pregnancy, occurs more commonly in pregnancies complicated by PGDM. The repercussions of this intricate disorder manifest with greater intensity in this population, which accounts for much of the heightened risk of adverse perinatal outcome associated with PGDM. Rates of preeclampsia in women with PGDM range from 20% to 54% in those with microvascular disease and resultant nephropathy.5,6
A UK–based population study of pregnancies complicated by PGDM reported preterm delivery rates of 43% and 23% for T1DM and T2DM, respectively.7 Placentamediated growth restriction is observed in 9% to 24% of PGDM pregnancies.8,9 Aspirin has been investigated for the prevention of preeclampsia, yielding inconsistent results.10, 11, 12 The conflicting reports on aspirin effectiveness in the prevention of preeclampsia may reflect heterogeneity in the selection of trial participants, including inconsistency in the definition of “high-risk pregnancy,” disparate study design, inconsistent dosing regimens, gestational age at initiation of aspirin, and nonuniformity in the definition of preeclampsia. Where aspirin has been shown to reduce the incidence of preeclampsia in certain at-risk groups, its benefits are most pronounced when started before 16 weeks of gestation.13 Aspirin is acceptable and has been shown to be cost-effective in the prevention of preeclampsia in low-risk women.14,15
Importantly, women with PGDM have typically been underrepresented in studies evaluating the impact of aspirin. Two notable studies that included women with PGDM failed to demonstrate a beneficial effect
of aspirin in risk modification for this population.11,12 The ASPRE trial reported a 62% reduction in preterm preeclampsia among women deemed high-risk by firsttrimester ultrasound and biomarker evaluation.10 However, <7% of those recruited had PGDM. Professional guidelines increasingly recommend considering low-dose aspirin for individuals with PGDM because of its reported positive impact on perinatal outcomes in similar high-risk groups.16, 17, 18 However, the consensus-based guidance (Grade E recommendation by the American Diabetes Association16) raises uncertainty about the shared pathophysiological mechanisms for placental dysfunction or preeclampsia among diverse at-risk groups. It remains unclear whether the clinical benefits observed in one group will be replicated in others given that manifestations of preeclampsia may represent a final common pathway influenced by various pathophysiological determinants. We therefore designed a doubleblinded, randomized, placebocontrolled trial of 150-mg aspirin, initiated in the first trimester, to determine its effect on perinatal outcome in pregnancies complicated by PGDM.
Materials and Methods
A phase 3 multicenter randomized double-blinded placebo-controlled trial of daily low-dose 150-mg aspirin initiated between 11+0 and 13+6 weeks’ gestation and continued until 36 weeks’ gestation was designed. Participants had a background history of prepregnancy T1DM or T2DM of at least 6-month duration, and a singleton viable intrauterine pregnancy. Women with a background of cardiovascular disease, diabetic nephropathy, or hypertension were excluded, as were those for whom aspirin was already recommended on the basis of other risk factors such as earlyonset preeclampsia in a previous pregnancy or multifetal gestation. The study was conducted at 6 university-affiliated perinatology centers across Ireland.
After screening and consent procedures, a computer-generated randomization system assigned study participants to aspirin or placebo groups. Participants were prescribed low-dose 150-mg aspirin or matched placebo to be taken once daily (night-time dosing), initiated between 11+0 and 13+6 weeks of gestation. Treatment commenced after a satisfactory first-trimester assessment, which included
Endorcrinology Focus Diabetes
follow-up
sonographic confirmation of fetal cardiac activity, followed by 4-weekly clinical review visits including blood draws for renal profile, with quantification of microalbuminuria. Once a gestational age of 36 weeks was reached, medication was discontinued and weekly study visits took place until birth.
Participants took the medication once daily at night with water. Trial staff checked returned medication for discrepancies at dispensing, and discussed noncompliance during study visits. Noncompliance, defined as taking <80% of prescribed medication, resulted in trial withdrawal.
The primary outcome was a composite clinical measure of placental dysfunction that included preeclampsia (newonset hypertension after 20 weeks’ gestation and new-onset proteinuria or maternal organ dysfunction19), preterm birth at <34 weeks, birthweight <10th centile,20 or perinatal mortality. Secondary outcome measures included mode of delivery, neonatal unit admission, and determination of glycemic control including insulin requirements and glycosylated hemoglobin (HbA1c) across gestation.
Owing to the variation in insulin regimens among study participants (basal bolus regimens and insulin
pumps), insulin dosing in units per kilogram of body weight was calculated at each visit to facilitate comparison. HbA1c was measured at screening, once per trimester, and at any other time point in accordance with clinical need.
The planned study sample size was determined on the basis of a composite outcome of placental dysfunction consisting of preeclampsia, preterm delivery at <34 weeks’ gestation, low birthweight <10th centile, and perinatal mortality. The expected rate of the baseline composite outcome of placental dysfunction was assumed to be 30% (20% preeclampsia plus 50% of other outcomes, due to coincidental outcomes). A total sample size of 566 was required to achieve a 35% reduction in the composite outcome, assuming a 5% type I error and 80% statistical power.21 However, because of a lower than anticipated recruitment rate during the COVID-19 pandemic, 134 patients were recruited and the primary outcome was therefore underpowered, with a retrospective power calculation of 64%.
The database was anonymized, encrypted, and stored in accordance with data protection law.
Treatment groups were analyzed by intention-to-treat analysis, with all randomized patients included
in the composite outcome measure. Data were centrally managed using ClinInfo (ClinInfo, Lyon, France) and analyzed using SAS 9.4 (SAS Institute, Cary, NC). The 2 treatment groups were compared using t tests or chi-square tests, as required, and longitudinal data were compared using a repeated-measures analysis. A P value <.05 was considered statistically significant.
The trial protocol21 was reviewed and approved by the National Ethics Committee (EudraCT number 2018-000770-29), and the trial was registered prospectively on ClinicalTrials.gov (identifier: NCT03574909).
An independent monitor was assigned to visit the recruiting sites periodically to validate compliance with the protocol according to good clinical practice principles, the maintenance of the trial-related records, and the extensiveness and accuracy of a proportion of case report form entries relative to source data. The study's clinical trial governance was meticulously managed by the Trial Steering Committee (TSC), Trial Management Group (TMG), and Data and Safety Monitoring Board (DSMB). The TSC, consisting of key stakeholders and experts, provided strategic oversight and guidance, ensuring adherence to protocol and ethical considerations. The TMG
handled day-to-day management, fostering communication and coordination among study sites. The independent DSMB monitored safety data, enhancing the overall integrity and reliability of trial results. This collaborative governance structure established a robust and ethical framework for the trial's successful execution.
Results
In total, 437 women were screened for recruitment across 6 centers between February 2020 and September 2022. A total of 191 patients met the eligibility criteria for study inclusion, and 134 women were recruited. Figure 1 displays the screening, randomization, and follow-up study population. Reaching the target sample size was limited by the impact of the COVID-19 pandemic. Baseline characteristics were similar between treatment groups.
The composite primary outcome was observed in 25% of the aspirin group and in 21% of the placebo group. No statistically significant distinctions were observed between the treatment groups in the composite primary outcome nor in any of its individual components. The mean gestational age at delivery was 37.3 weeks (range 23-40 weeks of gestation), and there was an overall cesarean birth rate of 70% in the study population. There was no significant difference between
Figure 1. Study population: screening, randomization, and
A, Trends in insulin use in units/kg by treatment group. B, Trends in HbA1c levels across gestation by treatment group.
HbA1c, hemoglobin A1c.
study groups for any listed secondary outcome nor for any pre-specified indicator of perinatal or neonatal morbidity. The median birthweight centile according to the Fetal Medicine Foundation growth centile standards was 94th (range, 73rd–98th) in the aspirintreated group and 82nd (range, 60th–98th) in the placebo group (P=.126).
Glycemic control
To adjust premeal insulin levels, 55% of participants used a fixed-dosing regimen and 27% used carbohydrate counting. In total, 18% of participants used continuous subcutaneous insulin infusion therapy. Participants in the aspirin group had a mean dose of insulin of 0.7 units/kg at screening (SD, 0.3), increasing throughout pregnancy to a mean of 1.1 units/kg (SD, 0.6) at 38 weeks, and decreasing to a mean of 0.5 units/kg (SD, 0.3) at 6 weeks postpartum. The placebo group had a mean dose of 0.7 units/kg
at baseline (SD, 0.4), increasing throughout pregnancy to 1.3 units/ kg at 38 weeks (SD, 0.4). The postnatal dose in the placebo group decreased to a mean of 0.6 units/kg (SD, 0.4).
The mean change in insulin dose throughout pregnancy from baseline was calculated for each participant. The temporal change in insulin requirements between groups was statistically significant (P=.002). Insulin dosing in the aspirin group was notable for a mean increase in dose of 83% by 37 weeks (SD, 135), whereas those in the placebo group had escalating doses from an earlier gestation, reaching a mean increase in dose by 181% in the same period (SD, 353) (Figure 2, A). Improved HbA1c levels throughout pregnancy were observed in the study cohort (Figure 2, B), with a more marked mean decrease in HbA1c in the aspirin group of 5 mmol/mol (SD, 7.4 mmol/mol) and mean decrease in the placebo group
of 3.2 mmol/mol (SD, 7.4 mmol/ mol). This observed trend toward more favorable HbA1c levels in the aspirin group did not reach statistical significance (P=.222). Women with T1DM had a more marked mean decrease in HbA1c of 4.4 mmol/mol (SD, 7.0 mmol/ mol), and those with T2DM a mean decrease of 3.3 mmol/mol (SD, 9.8 mmol/mol) (P=.021).
In a repeated-measures analysis of insulin use, we sought to determine if adverse perinatal outcome (fetal growth restriction, stillbirth, preeclampsia, or preterm delivery, or a composite of these) was associated with greater insulin requirements, in both an unadjusted and adjusted analysis for baseline insulin use (Figure 3). The analysis was performed for all participants and for T1DM patients alone. Stillbirth and fetal growth restriction were not modeled because of the small numbers of events. Adverse perinatal outcome was associated with higher insulin requirements, most notably
among women with T1DM (+0.13 insulin/kg [P=.0002] for placental dysfunction, +0.08 insulin/kg [P=.0075] for preeclampsia, and +0.23 insulin/kg [P=.011] for preterm delivery, over the course of pregnancy). The analysis of all participants (ie, including T2DM) also showed similar elevated levels in insulin requirements among those with adverse outcomes, but with less statistical significance. Principal findings
Although the trial was ultimately insufficiently powered to examine the composite primary outcome, the secondary observation of highly significant differences in glycemic control deserves close scrutiny. The aspirin group had an increase of 28% in insulin dosing from screening to 20 weeks, whereas the placebo group required more than double that increase in the same time period. By 37 weeks’ gestation, the statistically significant difference in insulin requirements between study groups was more
Figure 2. Glycemic control data
Endorcrinology Focus Diabetes
Figure 3. Adverse perinatal outcome and changes in insulin requirements across gestation (*) Adjusted analysis: adjusted for baseline insulin use. (**) Placental dysfunction: composite outcome of any of the following: preeclampsia, preterm birth <34 weeks of gestation, fetal growth restriction <10th percentile, or stillbirth
marked, with an 83% increase in the aspirin group and a 181% increase in insulin dosing in the placebo group.
Results in the context of what is known
The magnitude of perinatal risk associated with PGDM pregnancies exceeds that of any other commonly observed medical complication in pregnancy. In recognition of the stark disparity in perinatal outcomes reported in this population, the St. Vincent Declaration of 1989 established a goal of achieving pregnancy outcomes in women with PGDM similar to those of the nondiabetic population.23 More than 30 years later, the aspirations of the St. Vincent Declaration have not been realized,24 with the prevalence of congenital abnormality, preeclampsia, preterm birth, and perinatal mortality being far in excess of that observed in women with normal glucose tolerance.25, 26, 27 Despite advances in glucose sensing and insulin delivery technology in recent years,28 rates of fetal macrosomia, birth trauma, and cesarean delivery remain much higher in women with PGDM compared with the background population.29,30 Furthermore, although advances in diabetes technology offer
many advantages, the associated costs preclude widespread use, particularly in resource-limited settings, where T2DM prevalence is rising.
Low-dose aspirin has been investigated for the prevention of preeclampsia and placental dysfunction for many years, with over 40,000 women recruited to randomized trials to date.31 The rationale for using aspirin to optimize placental function is based on its inhibitory effect on thromboxane production. However, evidence that aspirin influences biochemical, biophysical, and ultrasound markers of placental disease in low-risk women is sparse.32,33 Paradoxically, however, the highrisk nature of PGDM has led to exclusion of women with diabetes mellitus from many clinical trials,34,35 and thus there is a paucity of evidence to support the use of aspirin in this cohort.
Nonetheless, current guidance advocating for the consideration of aspirin treatment in PGDM pregnancies may have diminished the clinical equipoise required to recruit a sufficient number of participants for this study. Among screened patients deemed ineligible for study participation, 40 of 206 (19%) were already
on aspirin therapy. It is further plausible that the group that declined participation did so in favor of opting for aspirin. Recruitment was further impacted by the COVID-19 pandemic, which had the effect of limiting in-person hospital attendance, resulting in diminished opportunities for trial recruitment.
Clinical implications
Our data suggest that women using aspirin therapy during pregnancy require lower insulin dosing to attain normoglycemia. This observation suggests enhanced glycemic regulation linked to aspirin use. Nevertheless, the degree to which this reduction in insulin requirements signifies an ameliorated metabolic or vascular environment for the fetus remains uncertain. More specifically, the extent to which these findings should be considered to indicate a beneficial effect must be closely examined. Although decreasing insulin doses in pregnancy have previously been associated with worse neonatal outcome, and are considered to potentially reflect placental dysfunction,36,37 the most important determinant of optimal pregnancy outcome in the setting of PGDM is tight glycemic control.38 Our study supports the well-recognized
association between higher insulin requirements and adverse perinatal outcome, such that the clearly demonstrated lesser escalation of insulin requirements among aspirin-treated women could be considered to indicate a beneficial effect of aspirin on perinatal outcome. Importantly, the benefit of aspirin among PGDM patients may be independent of any effect on platelet aggregation or endothelial dysfunction, but rather may depend on an effect on glycemic regulation.
The observation that aspirin reduces the incidence of glycosuria in patients with diabetes mellitus was first reported in 1957.39 Subsequently, Hundal et al40 also showed that hepatic glucose production was reduced, and an improvement in insulin-stimulated peripheral glucose uptake was observed in nonpregnant individuals with diabetes mellitus taking aspirin.40 Those with poor glycemic control have been shown to have higher baseline platelet activity and incomplete suppression of platelet activity.41, 42, 43 Furthermore, patients taking aspirin with higher levels of HbA1c demonstrate higher rates of aspirin resistance compared with those with lower HbA1c levels.44 However, no genetic signatures associated with reduced platelet response to aspirin in pregnancy have been described to date.45 Therefore, better glycemic control is known to result in improved platelet suppression and improved responsiveness to aspirin,
whereas aspirin itself appears to result in improved metrics of glycemic control (reduced insulin requirements and lower levels of HbA1c), thereby indicating a potentially beneficial effect of aspirin on diabetes mellitus–related morbidity.
In a secondary analysis of the Maternal-Fetal Medicine Units Network trial on aspirin for preeclampsia prevention, the association between HbA1c and thromboxane B2 levels was examined.44 Higher HbA1c levels correlated with increased thromboxane B2 before randomization (r=0.67; P<.05). Pregnancies with rising HbA1c had higher incomplete thromboxane B2 compared with those with decreasing levels (69.2% vs 18.1%; P=.02). The authors concluded that low-dose aspirin positively affects glycemic control, which is corroborated by findings from our study.
Although the exclusion of women with established diabetes mellitus–related microvascular disease may
explain the lower than anticipated preeclampsia incidence in this study (overall incidence of 14%), preterm birth before 34 weeks was observed in 5% of the study cohort, and the stillbirth rate was 2.4%. The observed persistence of these perinatal complications in a selected population of women with “nonvascular”
PGDM indicates a degree of perinatal risk that may be independent of the prothrombotic state of pregnancy and merits continued attention to alternative mechanisms underpinning adverse perinatal outcomes in this group. Importantly, improved glycemic control in the aspirin-treated group was not accompanied by lesser degrees of macrosomia.
Strengths and limitations
This study is notable for several strengths. The trial demonstrated high overall acceptability among participants, as indicated by the minimal number of withdrawals. Five of 6 withdrawals were at the request of the trial monitor during site visits, citing low compliance
with the study medication. Among the remaining participants, compliance with study medication and adherence to the study schedule were high, and complete outcome data were ascertained for 99%. However, because of a lower than anticipated recruitment rate during the COVID-19 pandemic, 134 patients were recruited and the primary outcome was therefore underpowered.
Research implications
Cord C-peptide levels may have yielded supporting evidence of improved glycemic control among aspirin-treated participants. However, procurement of cord samples was not included in the study schedule. A subset of participants provided serial serum samples at prespecified time periods throughout gestation, and interrogation of these samples for additional markers of glycemic control and for evaluation of thromboxane B2 levels is planned.
Conclusions
Despite showing no difference in the primary outcome (a composite measure of placental dysfunction), aspirin use in pregnancy among women with PGDM was associated with a significant reduction in insulin requirements and improvement in glycemic control when compared with placebo. A beneficial effect of aspirin therapy for PGDM pregnancies may be independent of its antiplatelet effect. Given the importance of optimal glycemic control for successful PGDM pregnancy outcomes, it is important to consider initiation of aspirin therapy at the earliest opportunity, potentially in advance of conception. Future studies should investigate the potential benefits of preconception initiation of aspirin therapy and continuing it until term, including the possibility of reducing the risk of hyperglycemia-related teratogenesis.
References available on request
Endocrinology News
Diabetes Ireland Donegal Branch challenges the Taoiseach Simon Harris
On the 18th of April, a statement from Paul Gillespie, Chairperson of the Donegal Branch of Diabetes Ireland to the Taoiseach Simon Harris TD was highlighted by Mr Padraig MacLochlainn (TD) in the Dail. Mr Gillespie was highlighting the critical situation in Letterkenny University Hospital (LUH) in Donegal and the severe under-resourcing of the hospital diabetes unit.
Mr Gillespie outlined that along with other Donegal committee members, they had met Mr Simon Harris when he was the Minister for Health in 2016 and again twice in 2017, where Mr Harris had then outlined ‘that radical changes for future diabetes care nationally were on the way’ and promised he would ‘look into the current staffing levels for diabetes care in LUH’ to limit the long waiting lists at that time (10 months for the first appointment, and 20+ months for the review appointment in 2017). Mr Harris was instrumental in developing the Advance Nurse Practitioner (ANP) posts nationwide for all care paths. Based on the number of people with diabetes receiving care in LUH, of the three ANP’s needed, only one ANP was ever appointed and only
in the paediatric diabetes team. HSE and Saolta group continue to ignore the crisis in adult diabetes care services in LUH.
As recently highlighted by the Donegal Branch of Diabetes Ireland, the situation in LUH in 2024 is even worse than it was 7 years ago when the current Taoiseach was Minister for Health and promised major positive changes. Despite our meetings with four successive Ministers of Health over the past 12 years, resources have deteriorated to such a level for Type 1 Diabetes care in LUH that we are concerned that patient safety of care is now beyond critical –wrote Mr. Gillespie.
According to Mr Gillespie, “There are currently NO Consultant Endocrinologists (3 vacant posts), which have led to recall waiting lists now over 36 months in some cases, whereas the HSE guideline is that people with Type 1 diabetes should be seen by an endocrinologist every 6 months. There are NO Advanced Nurse Practitioners in Adult Diabetes (2 posts never approved by HSE), which led to the inability to provide structured diabetes education
and access to insulin pump therapy, there are NO Podiatrists (2 Vacant posts), NO Paediatric Endocrinologist (never put in place by Saolta despite more than 160 children living with Type 1 Diabetes across Donegal), NO Psychologists, NO Shared Centre of Excellence for Children between LUH & Sligo University Hospital, despite the initial plans to share a centre due to the geographical isolation of LUH, and large population in Donegal. And there is still NO access to adult insulin pump start therapy due to a severe shortage in Endocrinologists for over 10 years now and no adult ANP role.
“This serious under resourcing will lead to poor patient outcomes, increased hospital admissions and huge increase in the number of people suffering with the many side effects of chronic or frequent hypo- and hyperglycaemia, due to lack of support from multidisciplinary diabetes team, and frequent (bi-annual) and regular appointments.
Diabetes Ireland recently wrote to the Minister for Health Mr Stephen Donnelly, TD, to highlight the critical situation in Donegal
and asked for his immediate intervention to set up an emergency plan to put some sort of extra support into LUH in the short term as a matter of urgency.
“Without a diabetes register and no epidemiological data, we don’t accurately know how many families live with diabetes, but we know from the last census that the Donegal population is now over 167,000. As the nationally estimated prevalence rate of diabetes is 6%, it can be assumed that more than 10,000 people live with diabetes in Donegal, with approximately 1,000 of those with Type 1 diabetes. Despite that, the resources in LUH are very limited which has led to very long waiting lists, no access to insulin pump therapy and limits access to diabetes education or other technologies (e.g. Continuous Glucose Monitoring), which the HSE acknowledge as gold standard for diabetes management, as it will improve patient outcomes (including quality of life), reduce the risk of developing more serious long-term diabetes related complications and prevent costly hospital admissions, interventions and hospitalisation.”
Endorcrinology Focus Tooth Loss/Diabetes
Tooth loss is associated with prevalent diabetes and incident diabetes in a longitudinal study of adults in Ireland
Written by Amara Naseer1, 2, Christine Mc Garrigle2,3, Jacinta McLoughlin1, 2, Brian O'Connell1, 2
1Dublin Dental University Hospital
2Trinity College Dublin, Dublin
3The Irish Longitudinal Study on Ageing (TILDA)
It is estimated that oral diseases affect nearly 3.5 billion people worldwide and many share common risk factors with other major non-communicable diseases.1-3 The relationship between oral health and systemic health conditions has been investigated for many years and the importance of this relationship has been endorsed by the World Health Organization (WHO).3-6 Some oral health and systemic health conditions not only share common risk factors and risk indicators, but there are also pathophysiological connections between the oral cavity and the body systems in both healthy and diseased situations.3, 7, 8 The inter-relationship between oral health and systemic disease needs further research to establish the nature of these relationships; in particular, whether they are associations or causative.9-11 The relationship between oral health and systemic health conditions may be more apparent in older adults. Chronic diseases are more common as people age; apart from the pathophysiological links and common risk factors between chronic diseases and oral health status, the medicines used to manage different chronic diseases can lead to poor oral health, as hyposalivation is a side effect of many of them.
Tooth loss is a basic indicator of oral health and represents the cumulative effect of oral disease and dental treatment.12 Studies have reported on the relationship between periodontal health, tooth loss and diabetes.13-22 Globally, diabetes mellitus is a widespread disease with complications that lead to poor quality of life and reduced longevity. In 2014, the WHO reported that worldwide 422 million people
suffered from diabetes and this figure is projected to increase to 439 million (affecting 10% of adults) by 2030.23 The WHO has reported that diabetes is the 9th most common cause of death (an increase of 70% since 2000) and is responsible for the largest rise in male deaths, with an 80% increase since 2000.23
There are three possible mechanisms behind the link between periodontal disease and diabetes: (i) an interrelationship between periodontitis and diabetes caused by systemic inflammation and poor glycaemic control, which leads to increased tooth loss,17, 24-26 (ii) eating habits
TABLE 1. TILDA criteria used to classify adults with diabetes.
in a person with fewer teeth that can lead them to develop diabetes,27-30 (iii) common risk factors exist for diabetes, periodontitis and tooth loss.8, 31, 32
However, it is not clear to what extent diabetes contributes to periodontal disease and subsequent tooth loss in a particular population and how much the prevention and control of diabetes (and periodontal disease) would reduce tooth loss. This may depend on a range of local factors, such as the prevalence of other dental diseases, access to dental treatment and the influence of other common risk factors (diet, smoking, oral hygiene). In this
TABLE 1. TILDA criteria used to classify adults with diabetes.
Diabetes Self-reported
Undiagnosed diabetes
No diabetes
Prediabetes Objectively measured
Incident diabetes Self-reported
context, firstly, a cross-sectional study was conducted to evaluate the relationship between tooth loss, periodontal status and diabetes, after controlling for both general health and socio-economic factors, among communitydwelling adults aged 50 years and over in Ireland. Secondly, the study investigated the longitudinal associations of tooth loss and periodontal status with incident diabetes over a 4-year follow-up.
Materials and Methods
An observational study was carried out, based on data from The Irish Longitudinal Study on Ageing (TILDA) Wave 3 to Wave 5. The
Self-reported doctor diagnosed diabetes in TILDA Wave 3
Taking diabetic medications (oral hypoglycaemic or insulin) Wave 3
HbA1c ≥ 48 nmol/mol in Wave 3 and no self-reported diabetes or no use of diabetic medications (oral hypoglycaemic or insulin) in Wave 3
No self-reported diabetes in Wave 3, no record of taking diabetic medications and HbA1c <48 nmol/mol in Wave 3.
HbA1c ≥ 38 nmol/mol and <48 nmol in Wave 3 and no selfreported diabetes or no use of diabetic medications (oral hypoglycaemic or insulin)
Self-reported doctor diagnosed diabetes in TILDA Wave 4–Wave 5 and no previous diagnosis/or use of diabetic medication Wave 1–Wave 3
For the analysis, the number of teeth was divided into three categories (edentate, 1–19 teeth, 20 or more teeth). These categories were used because they included the worst case (edentate adults) and adults with 20 or more teeth, which is the recommended WHO target for retention
methods used for TILDA data collection and details about the TILDA cohort have been reported previously.33 In line with the WHO criteria, missing teeth were recorded as missing due to caries, except missing third molar teeth or where there was a clear indication and history of teeth missing due to trauma or orthodontic extractions.34 CPITN on index teeth was used for the periodontal examination, the mouth was divided into sextants and the highest (worst) score on the index teeth (1.6/1.6, 1.1, 2.6/2.7, 3.6/3.7, 3.1 and 4.6/4.7) in each sextant was recorded as the sextant score. The scores were no disease (H), bleeding on examination (B), supra or subgingival calculus present (C), pocket depth up to 4–5 mm (P1), pocket depth > 6 mm (P2) and if no
teeth were present in a sextant/ unable to record (X).
In 2014–2015, from the TILDA Wave 3 cohort (n = 6618) who completed the Computer-Assisted Personal Interview (CAPI) and SelfCompleted Questionnaire (SCQ), 4256 participants underwent a health assessment. Of those who completed the health assessment, 3111 respondents were invited to have an oral health assessment; 2539 (81.6%) agreed to the assessment. Respondents aged less than 50 years (n = 31) and those with incomplete assessments (n = 4) were omitted from the sample. The final oral health sample consisted of 2504 respondents aged 50 years and over.
The examination criteria used in this study were the same as those
TABLE 2. Multinomial regression analysis of diabetes and pre-diabetes at Wave 3 associated with the number of teeth in Wave 3 (Base-edentate and dentate, n = 1958).
used in previous national Irish oral health surveys and similar to those recommended by the WHO.34, 35 Further details of methods used for oral health assessment study are reported elsewhere.36
Self-reported data from TILDA Waves 3–5, and clinically measured data from Wave 3 were used to determine the presence of diabetes. Table 1 shows the criteria for reporting a respondent as having diabetes. Diagnosed diabetes was defined using selfreported doctors' diagnoses and medication data. The American Diabetic Association provides a cut-off value of HbA1c ≥ 48 nmol/ mol, as undiagnosed diabetes. Glycated haemoglobin (HbA1c) analysis was used to identify undiagnosed and pre-diabetes.
TABLE 2. Multinomial regression analysis of diabetes and pre-diabetes at Wave 3 associated with the number of teeth in Wave 3 (Base-edentate and dentate, n = 1958).
Relationship of diabetes with number of teeth (Reference value no diabetes)
Diabetes status associated with edentulism (n = 232) and 1–19 teeth (n = 831) compared to (base) 20 or more teeth (n = 1295)
HbA1c provides an individual estimate of glycaemic control over the previous 8–12 weeks and is an accepted method to diagnose diabetes and pre-diabetes.37 Incident diabetes between Wave 3 and Wave 5 was estimated based on self-reported newly diagnosed diabetes in Wave 4 and Wave 5, from those with no previously diagnosed diabetes based on the question ‘Did a doctor diagnose you with diabetes or high blood sugar since your last interview?’
For the analysis, the number of teeth was divided into three categories (edentate, 1–19 teeth, 20 or more teeth). These categories were used because they included the worst case (edentate adults) and adults with 20 or more teeth, which is the recommended WHO target for retention of teeth among older adults.38-41 For periodontal status, the Community Periodontal Index of Treatment Need on index teeth was used.36 Periodontal status was collected only for those who had teeth and was categorized as 0, No disease, healthy (CPITN score 0); 1, bleeding & calculus (CPITN score 1 and 2) and 2, shallow and deep pockets (CPITN score 3 and 4).
Model 1
Model 2 controlling for demographics
Model 3 controlling for demographics and behaviours
• Note: Number of teeth is a dependent variable, and pre-diabetes, diabetes, demographic and behavioural factors are independent variables. Model 1 univariate; Model 2 adjusted for demographics: age, sex, educational attainment, area of residence; Model 3 adjusted for demographics and health behaviours: smoking status and BMI.
• Abbreviation: PR, prevalence ratio.
• Note: Number of teeth is a dependent variable, and pre-diabetes, diabetes, demographic and behavioural factors are independent variables. Model 1 univariate; Model 2 adjusted for demographics: age, sex, educational attainment, area of residence; Model 3 adjusted for demographics and health behaviours: smoking status and BMI.
• Abbreviation: PR, prevalence ratio.
Diabetes was the independent variable. Directed acyclic graphs (DAG), shown in Figures S1–S4, were used to clarify the study questions, explicitly identify assumptions of temporality and determine a minimally sufficient set of covariates for the models, derived from the literature and the accepted evidence about the relationship between diabetes, tooth loss and periodontal health. Included as categorical variables were age group (single year), gender (male and female), education (three categories; primary or no education, secondary, and third-level or higher), area of residence (three categories; Dublin city or county, another town or city and rural area), BMI (three categories; normal 18.5–24.9, overweight 25.0–29.9 and obese ≥30.0) and smoker (three categories; never, former and current) (see Supplementary Data for detailed descriptions of the oral health assessment and definition of variables).
The analysis was completed in two stages based on the DAGs. First, the study estimated the cross-sectional association of diabetes at Wave 3 and number of teeth (Figure S1) and periodontal status (Figure S2) at Wave 3. As the dependent variable was categorical, multinomial regression analysis was used. Second, to
TABLE 3. Multinomial regression analysis of diabetes and prediabetes associated with periodontal status (Base-dentate, n = 2121) at Wave 3. investigate the bi-directionality of the relationship, the study estimated the association between the number of teeth at Wave 3 (Figure S3) and periodontal status (Figure S4) with incident diabetes between Wave 4 and 5. The study repeated the analyses with periodontal status as the outcome variable. STATA software (Stata 15.1 Stata Corp LLC) was used for data analysis.
Results
The respondents were categorized according to the number of teeth present; (i) edentate (n = 249), (ii) 1–19 teeth (n = 895) and (iii) ≥20 teeth (n = 1360). Among the study sample with HbA1c results (n = 2358), 8.4% (n = 198) of the adults were determined to have diabetes according to the criteria defined in Table 1 and a further 12.2% had pre-diabetes.42
Table 2 shows that adults with both pre-diabetes and diabetes at Wave 3 were at higher risk of being edentate (p = .001) and having 1–19 teeth (p < .001) relative to having ≥20 teeth. After controlling for covariates- age, gender, education, area of residence, BMI and smoking, adults with diabetes remained at higher risk of being edentate (p = .004) relative to having 20 or more teeth (Table 2).
Regression analysis in Table 3 shows that there was no evidence of an association of either prediabetes or diabetes at Wave 3 with periodontal disease status. By including an oral health assessment in the main TILDA study, this project was able to access a large sample of TILDA respondents and their systemic health data, such as longitudinal data on diabetes and socioeconomic and behavioural covariates. This study adds to the literature as a large nationally representative cohort of older adults that included an objective measure of tooth loss, periodontal disease and diabetes. Furthermore, it represents a cohort of older adults who only had access to basic dental care, for example, extractions, rather than preventive and restorative care which are accessible to younger adults nowadays.
Endorcrinology Focus
Tooth Loss/Diabetes
TABLE 3. Multinomial regression analysis of diabetes and pre-diabetes associated with periodontal status (Base-dentate, n = 2121) at Wave 3. Relationship of diabetes with periodontal status (Reference value no diabetes)
Diabetes status associated with bleeding and calculus (n = 793) and shallow and deep pockets (n = 1273) compared to healthy periodontium (n = 131) as the base.
Bleeding and calculus Shallow and deep pockets
Model 1
Model 2 controlling for demographics
Model 3 controlling for demographics and behaviours
• Note: Periodontal status is the dependent variable, and pre-diabetes, diabetes, demographic and behavioural factors are independent variables. Model 1 univariate; Model 2 adjusted for demographics: age, sex, educational attainment, area of residence; Model 3 adjusted for demographics and health behaviours: smoking status and BMI.
• Abbreviation: PR, prevalence ratio.
• Note: Periodontal status is the dependent variable, and pre-diabetes, diabetes, demographic and behavioural factors are independent variables. Model 1 univariate; Model 2 adjusted for demographics: age, sex, educational attainment, area of residence; Model 3 adjusted for demographics and health behaviours: smoking status and BMI.
• Abbreviation: PR, prevalence ratio.
The data showed that a reduced number of teeth was associated with the presence of diabetes; this relationship remained after controlling for demographics and health behaviours. These findings are consistent with other research, which also found a relationship between diabetes and tooth loss.16-18, 43, 44 Similar findings were seen in a crosssectional evaluation of the relationship between self-reported data on tooth loss and selfreported diabetes, among adults aged 54 years and over in the complete TILDA Wave 3 sample (n = 6425).20 Both self-reported and objectively measured missing teeth in the TILDA samples included tooth loss for any reason. It would be preferable if tooth loss due to periodontal disease only could be identified to
fully understand any relationship with diabetes.
Many investigators have described a relationship between periodontal disease and diabetes.11, 13, 24-26, 45, 46 A recent meta-analysis suggests that severe periodontitis may have a strong influence on incident diabetes,47 but this study did not find such a relationship, which could possibly be due to the method by which periodontal status was assessed. The use of CPITN on index teeth is not designed to comprehensively record the presence and severity of periodontal disease. A full periodontal charting (bleeding on probing, measurement of loss of attachment and tooth mobility) of all remaining teeth would be a better assessment of periodontal
disease. This CPITN index was used in Wave 3 because it is a simple and reliable way to assess broad treatment needs, and because of the limitations of time for the oral health assessments. There is evidence to show that glycaemic control plays an important role in the relationship between diabetes and the severity of periodontal disease. It is not known whether the sample in this study had good glycaemic control, to the extent that it might have limited the impact of diabetes on tooth loss. Alternatively, as periodontal disease is a precursor to tooth loss, and the study only measured periodontal disease in those with teeth, a cohort with less tooth loss may be necessary to evaluate this association. Another reason for not finding any relationship between periodontal
Call for papers: make your contribution to Hospital Professional News
Articles
Research Papers
Reviews
Programme Descriptions
Reports
Case Reports
Letters to Editor
Support fellow hospital professionals as well as aspiring junior professionals and early-year hospital pharmacists
Practice reports share innovations on any area of practice, including delivering clinical services, pharmacy administration, or new approaches to inform and engage with patients
Perspective articles focus on a specific field or discipline and discuss current advances or future directions, and may include original data as well as expert insight and opinions
disease and diabetes could be the availability of only self-reported data on diabetes from TILDA wave 4 and wave 5, which was used for the evaluation of this relationship. Self-reporting of diabetes might have underestimated the diabetes incidence because adults with poor health literacy may not be aware of the symptoms or risks of diabetes. However, in the TILDA cohort underdiagnosis of diabetes was found to be low (0.9%) and was associated with area of residence and medical cost cover.42 Among the adults who were classified as diabetic (n = 536), 10 respondents had Type 1 diabetes, while the remaining respondents had Type 2 diabetes. For this reason, it was not possible to evaluate the relationship of Type 1 and Type 2 diabetes separately with oral health. Our findings support the bi-directional relationship between tooth loss and incident diabetes, and the study found that having fewer than 20 teeth was associated with an incident diagnosis of diabetes over a 4-year follow-up, supporting findings from other studies.48-50
In this study, the oldest age group was at higher risk of tooth loss for any reason, but diabetes was a risk indicator for tooth loss following adjustment for age. The clinical significance of
Endorcrinology Focus
Tooth Loss/Diabetes
this relationship needs further investigation because, as reported by Haworth and colleagues, the reasons for tooth loss in older adults are difficult to determine.51 TILDA is a longitudinal study which provides an opportunity to follow these people over time. Important aspects of such a follow-up might be whether the people with diabetes continue to lose teeth and whether they receive regular dental care and the effect of that care.
Controlling for socio-demographic factors in this study does not rule out other factors affecting tooth loss, such as lack of access to dental care, and lack of knowledge of oral health care in the early part of the respondents' lives. There has been an increased awareness of oral health among all sociodemographic groups in Ireland, and dental care has become more accessible and affordable over the lifetime of people in this study. Data from the first Irish national survey of adult oral health (1989–1990) reported that tooth loss was higher among adults with low incomes who were entitled to statefunded dental care, which was limited to episodic care including extractions, removable dentures and simple restorations for caries, but very little periodontal care.52
At that time, a much higher level of edentulousness in females was also reported, which indicates that socioeconomic or access to care issues were factors.52 However, this gender discrepancy has reduced over time in Ireland.36
In Ireland, a new national oral health policy (Smile agus Sláinte) was launched in 2019 which focuses on oral health care over the life course, rather than providing items of episodic care.53 This approach will be expected to improve periodontal health and retention of natural teeth. Monitoring the oral health status of the oldest age groups in populations is essential for planning and delivering oral health programmes, though a dental assessment can be a challenge for some older people with impairment, loss of cognitive function and poorer general health. A limitation of this study was that it did not include adults living in institutional care, who are more likely to have significant systemic or cognitive decline. There is a need to develop simplified oral health assessments that can allow a range of healthcare workers to collect key basic data on oral health status in all older adults.
A further limitation of this study was that only one oral health
assessment was carried out so a cross-lagged panel model to determine bi-directional associations between tooth loss and diabetes was not possible. To mitigate this limitation, and to attempt to investigate the potential bi-directionality of the relationships, we completed a second analysis and estimated the association of tooth loss at Wave 3 with incident diagnoses of diabetes between Wave 4 and 5.
Conclusions
This study found that diabetes was associated with being edentate and having fewer than 20 teeth among adults aged 50 years and over in Ireland, but no association was found with periodontal status, possibly due to the high number of extractions in this population. Furthermore, having fewer than 20 teeth was associated with a higher incident diagnosis of diabetes over 4 years. The analysis controlled for age and socio-economic status, and all respondents were ambulant and not in residential care. In the TILDA study, there is an opportunity to monitor tooth loss on a longitudinal basis which may give an indication of the value of tooth loss as a simple indicator of oral health.
References available on request
Setting a New Standard for Patient-Centred Care
Minister for Health, Stephen Donnelly T.D. has visited a new Respiratory Pulmonary Function Testing (PFT) Lab in the Integrated Care Hub, Bray on Friday 19th April to tour the facility and meet with staff and patients. Martina Queally, the recently appointed Regional Executive Officer for HSE Dublin and South East was also in attendance.
The Integrated Care Hub, Bray was the first of its kind to be opened by Minister Donnelly T.D. in 2022. The Hub delivers a range of Chronic Disease and Older Persons specialist services in the community under the HSE’s Enhanced Community Care (ECC Programme) – a Sláintecare initiative which helps reduce dependence on a hospital-central model of care.
The new Pulmonary Function Testing (PFT) Lab in the Bray Hub aims to further integrate hospital and community respiratory care in order to provide patients in Wicklow with advanced diagnostics and streamlined healthcare pathways. Under this new service, GP’s in the area can refer patients directly for pulmonary testing in the community, reducing waiting lists for respiratory consultants in hospitals and allowing patients to be tested faster and closer to home.
During his visit, Minister Donnelly T.D. discussed how the service sets a new standard for patient-centred care: “Diagnostic services in community settings offer increased efficiencies in service delivery as
well as a better experience for patients who can complete their diagnostic tests and meet the clinical team in the same visit, close to their home. This innovative service sets a new standard for patient-centred care. It also serves as a model for effective collaboration and integration within the healthcare service”.
The local Respiratory team collaborated with colleagues in St. Vincent’s University Hospital (SVUH) to establish a network link between SVUH, St Michael's Hospital Dún Laoghaire and the Hub’s IT systems. This means that results from the PFT Lab in Bray can be accessed remotely by hospital consultants who review the test findings and provide a comprehensive report to the GP.
Onward referrals to members of the Respiratory Integrated Care (RIC) team can then also be arranged, if required.
The service first commenced in June 2023 in SVUH and St Michael’s Hospital and it has been in operation in Bray since January. To date, 333 patients have been assessed. 32% of patients who were referred for testing haven’t required further input by the clinical team, while 37% of patients were referred onto a Respiratory Clinical Nurse Specialist (CNS) in the community. Combined this means that 69% did not require referral to a respiratory consultant, assuring consultant capacity and hospital waiting lists are optimised.
Launches New Packaging Design
for the right patient, at the right time
OTEZLA is the simple oral choice for your adult patients with moderate to severe psoriasis or active psoriatic arthritis1
• Long-term safety and efficacy profile spanning 5 years in psoriasis (PsO) and psoriatic arthritis (PsA)1,2
• Improved quality of life sustained up to 5 years1,2
• No laboratory pre-screening or ongoing drug-specific monitoring1
• No label warning against use with live vaccines1
• 9-hour half-life, rapid clearance1
OTEZLA is an intracellular PDE4 inhibitor with demonstrated efficacy in high-impact areas, which can improve your patient’s quality of life1–7
OTEZLA® (apremilast) 10mg, 20mg and 30mg film coated-tablets Brief Prescribing Information Refer to the Summary of Product Characteristics (SPC) before prescribing Further information is available upon request
Presentation: 10mg, 20mg and 30mg film coated-tablets.
Indications: Psoriatic arthritis: OTEZLA, alone or in combination with Disease Modifying Antirheumatic Drugs (DMARDs), is indicated for the treatment of active psoriatic arthritis (PsA) in adult patients who have had an inadequate response or who have been intolerant to a prior DMARD therapy. Psoriasis: OTEZLA is indicated for the treatment of moderate to severe chronic plaque psoriasis in adult patients who failed to respond to or who have a contraindication to, or are intolerant to other systemic therapy including ciclosporine, methotrexate or psoralen and ultraviolet-A light (PUVA).
Dosage and administration: Treatment with OTEZLA should be initiated by specialists experienced in the diagnosis and treatment of psoriasis or psoriatic arthritis. The recommended dose of OTEZLA is 30mg twice daily taken orally in the AM and PM, approximately 12 hours apart, with no food restrictions. The film-coated tablets should be swallowed whole. An initial dose titration is required per the following schedule: Day 1: 10mg in the AM; Day 2: 10mg in the AM and 10 mg in the PM; Day 3: 10mg in the AM and 20mg in the PM; Day 4: 20mg in the AM and 20mg
in the PM; Day 5: 20mg in the AM and 30mg in the PM; Day 6 and thereafter: 30mg twice daily in the AM and PM. No re-titration is required after initial titration. If patients miss a dose, the next dose should be taken as soon as possible. If it is close to the time for their next dose, the missed dose should not be taken and the next dose should be taken at the regular time.
Patients with severe renal impairment: The dose of OTEZLA should be reduced to 30mg once daily in patients with severe renal impairment (creatinine clearance of less than 30mL per minute estimated by the Cockcroft-Gault equation). For initial dose titration in this group, it is recommended that OTEZLA is titrated using only the AM doses and the PM doses be skipped. Paediatric population: The safety and efficacy of OTEZLA in children aged 0 to 17 years have not been established. No data is available.
Contraindications: Hypersensitivity to the active substance(s) or to any of the excipients. OTEZLA is contraindicated in pregnancy. Pregnancy should be excluded before treatment can be initiated.
Special warnings and precautions: Diarrhoea, nausea and vomiting: Severe diarrhoea, nausea, and vomiting associated with the use of OTEZLA have been reported. Most events occurred within the first few weeks of treatment. In some cases, patients were hospitalized. Patients 65 years of age or older may be at a higher risk of complications. Discontinuation of treatment may be
necessary. Psychiatric disorders: OTEZLA is associated with an increased risk of psychiatric disorders such as insomnia and depression. Instances of suicidal ideation and behaviour, including suicide, have been observed in patients with or without history of depression. The risks and benefits of starting or continuing treatment with OTEZLA should be carefully assessed if patients report previous or existing psychiatric symptoms or if concomitant treatment with other medicinal products likely to cause psychiatric events is intended. Patients and caregivers should be instructed to notify the prescriber of any changes in behaviour or mood and of any suicidal ideation. If patients suffered from new or worsening psychiatric symptoms, or suicidal ideation or suicidal attempt is identified, it is recommended to discontinue treatment with OTEZLA. Severe renal impairment: See dosage and administration section. Underweight patients: OTEZLA may cause weight loss. Patients who are underweight at the start of treatment should have their body weight monitored regularly. In the event of unexplained and clinically significant weight loss, these patients should be evaluated by a medical practitioner and discontinuation of treatment should be considered. Lactose content: Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicinal product.
Interactions: Co-administration of strong cytochrome P450
3A4 (CYP3A4) enzyme inducer, rifampicin, resulted in a reduction of systemic exposure of OTEZLA, which may result in a loss of efficacy of OTEZLA. Therefore, the use of strong CYP3A4 enzyme inducers (e.g. rifampicin, phenobarbital, carbamazepine, phenytoin and St. John’s Wort) with OTEZLA is not recommended. In clinical studies, OTEZLA has been administered concomitantly with topical therapy (including corticosteroids, coal tar shampoo and salicylic acid scalp preparations) and UVB phototherapy. OTEZLA can be co-administered with a potent CYP3A4 inhibitor such as ketoconazole, as well as with methotrexate in psoriatic arthritis patients and with oral contraceptives.
Pregnancy, lactation and fertility: Women of childbearing potential should use an effective method of contraception to prevent pregnancy during treatment. OTEZLA should not be used during breast-feeding. No fertility data is available in humans.
Undesirable effects: Psychiatric disorders: In clinical studies and post-marketing experience, uncommon cases of suicidal ideation and behaviour, were reported, while completed suicide was reported post-marketing. The most commonly reported adverse reactions with OTEZLA in these indications are gastrointestinal (GI) disorders including diarrhoea (15.7%) and nausea (13.9%). These GI adverse reactions generally occurred within the first 2 weeks of treatment and usually resolved within 4 weeks.
Images depict fictional patients.
Adverse reactions reported in the psoriatic arthritis and/ or psoriasis clinical trial programme and post marketing experience include: very common (≥1/10) diarrhoea*, nausea*; common (≥1/100 to <1/10) bronchitis, upper respiratory tract infection, nasopharyngitis*, decreased appetite*, insomnia, depression, migraine*, tension headache*, headache*, cough, vomiting*, dyspepsia, frequent bowel movements, upper abdominal pain*, gastroesophageal reflux disease, back pain*, fatigue; uncommon (≥1/1,000 to <1/100) hypersensitivity, suicidal ideation and behaviour, gastrointestinal haemorrhage, rash, urticaria, weight loss; not known (cannot be estimated from the available data) angioedema. *At least one of these adverse reactions was reported as serious. Please consult the SPC for a full description of undesirable events.
Pharmaceutical Precautions: Do not store above 30ºC. Legal category: POM. Presentation and Marketing Authorisation Numbers: Initiation pack containing 27 film coated tablets (4 x 10mg, 4 x 20mg, 19 x 30mg)EU/1/14/981/001; 30mg film coated tablets in a pack size of 56 tablets - EU/1/14/981/002. Marketing Authorisation Holder: Amgen Europe B.V. Minervum 7061, 4817 ZK Breda, The Netherlands. Further information is available from Amgen Ireland Limited, 21 Northwood Court, Santry, Dublin D09 TX31. OTEZLA is a trademark owned or licensed by Amgen Inc., its subsidiaries, or affiliates. Date of preparation: April 2020 (Ref: IE-OTZ-2000019).
Adverse reactions/events should be reported to the Health Products Regulatory Authority (HPRA) using the available methods via www.hpra.ie. Adverse events should also be reported to Amgen Limited on +44 (0)1223 436441.
Inhibition of HIV-1 release by ADAM metalloproteinase inhibitors
Written by Joanna Ireland1, Jason Segura1, Genbin Shi2, Julianna Buchwald1, Gwynne Roth1, Thomas Juncheng Shen1, Ruipeng Wang1, Xinhua Ji2, Elizabeth R. Fischer3, Susan Moir4, Tae-Wook Chun4 and Peter D. Sun1*
1Laboratory of Immunogenetics, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Rockville, MD, United States
2Center for Structural Biology, National Cancer Institute, National Institutes of Health, Frederick, MD, United States
3Electron Microscopy Unit, Research Technology Branch, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Hamilton, MT, United States
4Laboratory of Immunoregulation, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD, United States
HIV infection remains a public health threat with over 38 million infected people worldwide.1 Currently, the use of antiretroviral therapy (ART) remains the most effective treatment against HIV-1 infection (Martin and Siliciano, 2016). Although ART effectively controls plasma viremia in infected individuals, it is not sufficient to eradicate the virus. As a consequence, plasma viremia rebounds upon withdraw of ART in the majority of infected individuals (Eisinger and Fauci, 2018). This inability of ART to eliminate HIV in infected individuals has been attributed to the persistence of viral reservoirs that resist the antiviral treatment (Huang et al., 2018; Sengupta and Siliciano, 2018). The compounds present in ART comprise inhibitors that target the viral entry, reverse transcription, host integration, and virion maturation (De Miguel et al., 2018; Ribera, 2018). There is currently no compound that targets HIV-1 viral release. Over the years, intense efforts have been directed at the development of effective vaccines against HIV-1, resulting in a greater understanding of antibody mediated anti-viral responses and a large collection of highly potent neutralizing antibodies (Escolano et al., 2017; Bar-On et al., 2018). However, finding a protective anti-HIV vaccine remains elusive (Bar et al., 2016; Sneller et al., 2017; Andrabi et al., 2018; Gao et al., 2018; Mendoza et al., 2018; Chun et al., 2019).
We previously showed that in addition to CD4 and chemokine receptors, HIV utilizes glycan
Figure 1. Inhibition of CD62L shedding as detected by ELISA assays. (A,B) CD62L shedding and TNFα release from either PHA or anti-CD3 stimulated CD4 T cells. Both soluble CD62L and TNFα released to supernatant were detected by ELISA (R&D systems). Blank, NT and control designate no cells, no treatment, and isotype control treatment, respectively. (C–F) Anti-CD3 stimulated (C–E) or unstimulated (F) PBMC were treated with indicated inhibitor compounds for 6 (C,E) or 24 (D,F) hours, respectively. Effect of serine-, cysteine-, aspartyl-protease inhibitors (C), MMP inhibitors (D) as well as titration of MMP inhibitors (E) to the shedding of CD62L from stimulated PBMC. (F) Shedding of CD62L from unstimulated PBMC (F) in the presence of titrating amount of indicated ADAM inhibitors. All statistical analysis were performed using student’s t-test between DMSO and inhibitor treated experiments. Unless indicated with p-values, most treatment did not result in significant differences in the shedding of CD62L. P-values are * < 0.05, ** < 0.01, *** < 0.001, **** < 0.0001.
receptors, such as Siglec and L-selectin/CD62L, on target cells as adhesion receptors to facilitate efficient viral attachment and entry (Zou et al., 2011; Kononchik et al., 2018). CD62L-mediated binding to viral envelope glycans underscores preferential replication of HIV-1 in central memory CD4 T cells. Interestingly, HIV-1 infected CD4 T cells downregulated their CD62L expressions. CD62L functions to provide adhesion for lymphocyte trafficking (Von Andrian et al., 1993; Stein et al., 1999), and is a marker for central memory T
cells (Sallusto et al., 2004). Upon activation or under inflammation, CD62L is known to be cleaved by cell surface transmembrane proteases, named ADAM (A disintegrin and metalloproteinase) (Le Gall et al., 2009; Wang et al., 2010). ADAM family enzymes, also known as α-secretases, are responsible for ectodomain shedding of diverse cell surface proteins, including growth factors, cytokines, receptors and adhesion molecules (Edwards et al., 2008; Saftig and Reiss, 2011). Similar to members of
matrix metalloproteinase (MMP), the catalytic activities of ADAM proteases are Zn-dependent and can be inhibited by hydroxamic acid-based Zn-chelators, such as BB-94 (Batimastat) (Parsons et al., 1997; Kapp et al., 2012). This paradoxical role of CD62L, while facilitating the viral entry but detrimental to the viral exit, is best illustrated by manipulating CD62L expression in HIV-1 permissive CEM T cells. Transfection of CD62L boosted the viral infection of CEM T cells, but also resulted in the infection more sensitive
Figure 2. Inhibition of ADAM10 and 17 proteolytic activities using a kinetic enzymatic cleavage assay. (A) Kinetic cleavage of a fluorogenic TNF-α substrate peptide ES003 by recombinant ADAM10 or 17 (R&D systems, Inc) in the presence and absence of 2 μM BB-94. In the presence of BB-94, the kinetic ES003 cleavage curves by ADAM10 and 17 are indistinguishable from that of ES003-only curve without the enzyme. (B,C) Inhibition of ADAM17 (B) or ADAM10 (C) cleavage of ES003 by various compounds at 2 μM concentration. All statistics are calculated between no inhibitor and respective inhibitor data sets using multiple t-tests with p-values indicated above their data. The data are a representative of two repeated experiments. (D,E) Inhibition of ADAM10 (D) and ADAM17 (E) enzymatic activities by titrating amount of BB-94, GI254023X, prinomastat, and 14mb. The compound concentrations are indicated on the x-axis. The enzymatic activities measured at 4-h time point of the reactions are normalized against zero compound condition and plotted on the y-axis. The inhibition curves are fitted with non-linear regression with inhibition constants (Ki) for each compound listed in Table 2 (F) Enzymatic cleavage of a fluorogenic CD62L peptide by recombinant ADAM10 or 17. The CD62L cleavage curves in the presence of 2 μM BB-94 are indistinguishable with that of fluorogenic peptide CD62L-only without the enzyme. (G,H) Inhibition of ADAM10 cleavage of CD62L substrate peptide by various compounds at 2 μM concentration. (I) Inhibition of ADAM10 cleavage of CD62L by titrating amount of 14mb. P-values are ****<0.0001.
to BB-94 inhibition compared to the untransfected cells. On the other hand, knocking down of endogenous CD62L reduced the viral infection, but also resulted in the loss of BB-94 inhibition to the infection (Kononchik et al., 2018). This intricate role of CD62L expression and shedding in HIV-1 infection highlights the importance of ADAM metalloproteinases in the viral transmission. The shedding of CD62L in infected CD4 T cells further depended on HIV-1 Nef induced host caspases activation as inhibition of caspases blocked L-selectin shedding and impeded the viral release (Segura et al., 2023). However, the sheddases responsible for HIV-induced CD62L shedding and the mechanism linking CD62L shedding to viral release are yet to be established (Kononchik et al., 2018). In the current study, we attempted to screen compounds that effectively inhibit CD62L shedding and HIV-1 infection, and we investigated the molecular mechanism linking CD62L shedding and HIV-1 viral release. These findings support a therapeutic approach targeting the HIV-1 viral release.
Results
L-selectin/CD62L shedding on PBMC depends on zinc metalloproteinases
L-selectin/CD62L is a marker for central memory T cells and promotes the homing of T cells to lymph nodes (Von Andrian et al., 1993; Sallusto et al., 2004). We previously showed that L-selectin shedding facilitated HIV-1 release (Kononchik et al., 2018). However, the proteases responsible for the viral-induced CD62L shedding remain to be defined. CD62L shedding is mainly studied in the context of neutrophil activation and has been shown to involve ADAM10 and ADAM17 metalloproteinases (Le Gall et al., 2009; Wang et al., 2010; Saftig and Reiss, 2011). Like neutrophils, activated CD4 T cells shed CD62L and release TNFα that can be detected by ELISA (Figures 1A,B). The release of both TNFα and soluble CD62L were inhibited by batimastat (BB94), a matrix metalloproteinase inhibitor that inhibits both ADAM10 and 17 (Saftig and Reiss, 2011), suggesting the involvement of ADAM enzymes in the shedding of CD62L on CD4 lymphocytes. To further characterize the enzymes responsible for T cell shedding of CD62L and thus facilitate the design of protease specific inhibitors as potential antiviral reagents, we measured shedding
of CD62L by ELISA in the presence of various protease inhibitors. As T cells express other proteases (Kido et al., 1990), we systematically evaluated the inhibition of CD62L shedding in both anti-CD3
Endorcrinology Focus HIV
stimulated and non-stimulated cell cultures by serine-, cysteine-, aspartyl-proteases as well as metalloproteinases inhibitors. Stimulated or unstimulated peripheral blood mononuclear
cells (PBMC) were treated with inhibitors specific against various proteases for 6–24 h. None of the serine-, cysteine-, or aspartylprotease inhibitors affected the release of soluble CD62L from
Figure 3. Effect of MMP inhibitors to HIV-1 infection of PBMC. (A) Bar diagram showing the inhibition of R5 tropic HIV-1BAL infection by MMP and ADAM10/17 inhibitors. All compounds were at 100 μM concentration except GI254023X which was at 250 μM. The infection is measured by percentage of intracellular p24 staining of CD3+ T cells as shown in the panel (B) of the figure. (B) FACS analyses of HIV-1 induced loss of CD4 and CD62L in infected CD4 T cells in the presence of 100 μM BB-94, 80 μM prinomastat, 100 μM DMDP or control DMSO. Left panel shows the viral infection levels by intracellular p24 staining (% p24+ population) in CD3+ cells. The p24+ (middle panel) and p24 (right panel) CD3+ populations are further separated by CD62L and CD4 expressions. The quadrant corresponding to CD4 /CD62L cells is highlighted in red box in the p24+ populations. (C) Bar diagram showing the accumulation of CD4 /CD62L population in HIV-1 infected cells in the presence of various inhibitors. (D) Correlation between CD62L shedding and HIV-1 infection in the presence of various compounds. The x-axis represents the CD62L shedding level detected from each compound normalized against that of DMSO. The y-axis represents the relative infection level in the presence of individual compounds with respect to DMSO. A linear regression resulted a straight line with r-square for linearity goodness of fit being 0.6947 and a p-value of <0.0001 when compared to null hypothesis (no correlation). (E) Comparison in inhibition of R5 and X4 tropic HIV-1 infections of PBMC by BB-94 and prinomastat. The PBMC for the infections were from the same donor. All compounds were used at the same concentrations as in panel (A). Unless indicated with p-values, the treatments did not result in significant differences from their controls. P-values are *<0.05, ** <0.01, *** <0.001.
either stimulated or naïve PBMC (Figure 1C; Table 1). We then evaluated ~20 additional known inhibitors of Zn-dependent metalloproteinases for their ability to inhibit CD62L shedding from stimulated PBMC. Most of the metalloproteinase inhibitors did not inhibit CD62L shedding, except TAPI-2, GM6001, GI254023X, BB-94 and prinomastat (Figure 1D; Le Gall et al., 2009; MollerHackbarth et al., 2013; Woods and Padmanabhan, 2013). These compounds target Zn-dependent metalloproteinases and are known to inhibit ADAM10 and 17 (Parsons et al., 1997; Hooper and Turner, 2002; Woods and Padmanabhan, 2013). Further dose titration of these compounds showed that the reductions in CD62L shedding from both stimulated and unstimulated T cells were dependent on the inhibitor doses with minimum cytotoxicity between 20–100 μM compound concentrations (Figures 1E,F;). Interestingly, 3,4-dichloroisocouman (or 3,4-dichloro for short), a serine protease inhibitor enhanced CD62L shedding and this shedding enhancement was blocked by BB94 (Figure 1E).
Inhibition of ADAM10 and 17 enzymatic activities by L-selectin shedding inhibitors
To address the potency and specificity of CD62L shedding inhibitors against ADAM10 and 17, we carried out an enzymatic cleavage assay using recombinant ADAM10 and 17 to cleave a fluorogenic TNF-α substrate in the presence of 2 μM individual compounds (Figures 2A–C;). While the broad specificity metalloprotease inhibitors BB-94 and prinomastat inhibited both ADAM10 and 17, an MMP-1 specific inhibitor, Dichloromethylenediphosphonic acid disodium salt (DMDP) inhibited neither ADAM10 nor 17 enzymatic activities, consistent with DMDP’s lack of CD62L shedding inhibition (Figures 2B,C;). As expected, GI254023X, a ADAM10 specific compound, preferentially inhibited the enzymatic activity of ADAM10 compared to ADAM17 (Figures 2B–E;). In addition, we also synthesized two 3-Clphenylpyrrolidine tartrate diamide analogs, 14 m and 15, that were developed specifically against ADAM17 to further investigate the involvement of ADAM17 in HIV infection (Li et al., 2010). Compounds 14 m and 15 differ only by one methyl-group. The chemical synthesis resulted in 2
racemic isomers for compound 14 m (14ma and 14mb) and 4 racemic isomers for compound 15 (15a, b, c, d). Between the two compound 14 m isomers, 14mb exhibited better inhibition to both ADAM10 and ADAM17 enzymatic cleavage of the fluorogenic peptide. In contrast, the best of compound 15 isomers, 15b, only marginally inhibited the enzymatic cleavage. Further titration inhibition resulted in inhibition constants (Ki) for BB-94 of 18 nM against both ADAM17 and 10, for prinomastat of 48 nM and 2 nM against ADAM17 and 10, respectively, and 0.5–1.1 μM for 14mb against ADAM17 and 10, respectively (Figures 2D,E).
We then examined ADAM10 and 17 cleavage of a fluorogenic CD62L peptide substrate. While ADAM17 cleaved TNF-α peptide better than ADAM10 (Figure 2A), the enzymes showed reverse activities against CD62L (Figure 2F), suggesting ADAM10 may be more effective in shedding of CD62L than ADAM17. Similar to the cleavage of TNF-α peptide, BB-94, GI254023X and prinomastat but not DMDP completely suppressed ADAM10 cleavage of CD62L at 2 μM compound concentration (Figure 2G). In comparison, the tartratebased compounds (14ma, mb, 15a,b,c,d) were significantly less potent in inhibiting ADAM10 (Figure 2H), with the best inhibitory compound, 14mb, displaying a Ki of 1.6 μM against ADAM10 cleavage of CD62L (Figure 2I; Inhibition of HIV-1 infection requires suppressing both ADAM10 and 17
To investigate the contribution of individual ADAM to HIV-1
infection, we infected CD8depleted PBMC with a replication competent R5 tropic HIV-1BAL in the presence of either ADAM10 or 17 specific or broad specificity inhibitors and analyzed the intracellular p24 levels on day 7 of post infections (Figure 3). Both BB-94 and prinomastat, inhibited HIV-1BAL infections without significant impact to cell viabilities (Figures 3A,B;). As GI254023X distinguished ADAM10 and 17 enzymatic activities (Figures 2D,E), we investigated the effect of their specific inhibition to HIV-1 infection using either GI254023X or TAPI-0, a known ADAM17 inhibitor. In comparison, individual ADAM10 and 17 inhibitor, GI254023X and TAPI-0, respectively, fail to significantly suppress the viral infections, suggesting the involvement of both ADAM10 and 17 in HIV-1 infections. Importantly, DMDP, an MMP-1 inhibitor that did not inhibit ADAM10 and 17 enzymatic activities nor CD62L shedding (Figures 1E, 2B,C), failed to inhibit HIV-1BAL infections (Figures 3A,B). To address the mechanistic connection between ADAM-mediated CD62L shedding and HIV-1 infection, we examined the loss of CD62L expression in infected (p24+) T cells and its dependence on ADAM inhibitions. Upon infection, HIV-1 down regulated cell surface expression of CD62L, as evident from the preferential accumulation of CD4 and CD62L double negative T cells in the p24+ compared to the p24 populations or uninfected samples (Figure 3B; Kononchik et al., 2018). The presence of BB-94 or prinomastat reduced the accumulation of infected CD4 / CD62L T cells in the R5 HIV-1 infections, suggesting the loss of CD62L expression in infected T
cells is ADAM dependent. Similar to their lack of inhibitions to the p24 levels, the individual ADAM10 or 17 inhibitors, GI254023X or TAPI-0, respectively, did not inhibit the accumulation of CD4 / CD62L T cells compared to BB94 and prinomastat (Figure 3C), consistent with the involvement of both ADAM10 and 17 in downregulation of CD62L. Importantly, the MMP-1 inhibitor, DMDP, failed to prevent the loss of CD62L on HIV-1BAL infected cells (Figures 3B,C). Indeed, the effect of these inhibitors to HIV-1BAL infection correlated with their ability to inhibit CD62L shedding (Figure 3D). Interestingly, when cells were treated with BB-94 on day 3 and 5 after the initiation of the infection, the compound showed a progressive reduction in its inhibition. This is likely due to the presence of multi-round replications of HIV-1BAL during the experiment (Murray et al., 2011). In addition, a serine protease inhibitor, 3,4-dichloroisocouman, significantly increased soluble CD62L concentration in treated media compared to the control (Figure 1E;). The compound, however, did not enhance HIV-1 infection, suggesting either the viral-induced CD62L shedding is sufficient for its release or 3,4-dichloroisocouman did not affect CD62L shedding but merely reduced the degradation of soluble CD62L in treated cell culture supernatant. To address if X4 tropic HIV-1 infection also depended on CD62L shedding, we infected CD8-depleted PBMC with a replication competent X4 tropic HIV-1LAI or the R5 tropic HIV-1BAL in the presence of BB-94 or prinomastat. Both compounds inhibited the X4 tropic HIV-1LAI infections similar to
their inhibitions to the R5 tropic HIV-1BAL (Figure 3E), suggesting ADAM10 and 17 are also involved in X4 tropic HIV-1 infections.
Although 3-Cl-phenylpyrrolidine tartrate diamide analogs were developed as ADAM17 inhibitors, two of the isoforms,14mb and 15b inhibited ADAM10 and 17 enzymatic activities at 2–10 μM concentrations (Figure 2;). They are 50–100 times less potent compared to 20–50 nM concentrations of BB-94 and prinomastat. Despite with dual ADAM inhibitory specificities, 14mb only partially inhibited HIV1BAL infection of PBMC and the loss of CD62L expression from some donors (Figures 4A,B;). When 14mb and 15b failed to inhibit HIV-1 infection of PBMC, they also failed to suppress CD62L shedding (Figure 4C), suggesting both potency and broad specificity are needed to suppress HIV-1 infection. Consistently, those tartrate analogs failed to inhibit ADAM10 digestion of CD62L, including 14ma, 15a,b,c, also failed to suppress HIV1BAL infection (Figures 2H, 4A). Together, our data showed that both R5 and X4 HIV-1 infections as well as the loss of CD62L expression on infected T cells are inhibited by broad spectrum metalloproteinase inhibitors, suggesting HIV-1 infections depend on ADAM-mediated shedding of CD62L.
BB-94 inhibited transient upregulation of ADAM10 and 17 expressions during HIV-1 infections
To characterize the effect of ADAM inhibition on HIV infection, we performed transcriptome analysis by high throughput RNAseq using
Figure 4
Endorcrinology Focus HIV
Figure 5. Inhibition of viral release from HIV-1 patient derived CD4 T cells in the presence of 50 μM of indicated compounds or DMSO. The results from day 2 (solid line) and 4 (dash line) samples are displayed on the same graphs organized by the compounds. The statistical analyses were performed based on percentage inhibitions using student’s t-test between DMSO and inhibitor treated experiments
Illumina platform (Novogene Co. Ltd.) on HIV-1BAL infected with and without BB-94 treatment as well as uninfected CD4 T cells on day 6 post infection. Pathway analysis on differentially expressed genes performed using iDEP based on top 400 up- and 400 downregulated genes showed that HIV-1 infection (samples B1 and B2) significantly up-regulated genes in type I interferon pathway and down-regulated those involved in cell cycle pathways compared to the uninfected (U1 and U2) samples (Sx et al., 2018;). This upregulation in type I interferon genes is not observed in the presence of BB-94. However, BB-94 alone does not suppress the transcription of type I interferon pathway genes, suggesting the lack of type I interferon gene upregulation in the BB-94 treated infection is primarily due to the reduction of viral infections in the presence of BB-94. In contrast to genes in type I interferon pathway, HIV-1 infections (B1 and B2) significantly downregulated the cell cycle pathway compared to the uninfected samples (U1 and U2). Interestingly, BB-94 alone decreased slightly the expressions of cell cycle genes without HIV-1 infection. Thus, BB-94 does
not counter the viral infection in neither interferon nor cell cycle genes, suggesting the antiviral effect of BB-94 is not through regulating the expressions of the two major signaling pathways but rather through its inhibition to the enzymatic activity of metalloproteinases.
Human CD4 T cells express multiple members of ADAM family genes in addition to ADAM10 and 17. The higher expression of ADAM10 than 17 on CD4 T cells suggests ADAM10 contributes more to HIV infection than ADAM17. The expressions of ADAM8, 15 and 19 are also significant on CD4 T cells. The presence of all five ADAMs was confirmed by western blot analysis using antibodies specific to the extracellular domain of individual ADAMs. Interestingly, while transcriptomic analysis showed no significant differences in ADAM mRNA levels among infected with or without BB-94 and uninfected samples on day 6 of the infection, western blot analysis showed a marginal increase of ADAM10 and 17 in day 3 infected samples . To further address if HIV-1 infection resulted in a transient increase in ADAM expressions, we used RTPCR to quantify ADAM9, 10 and 17
mRNA in infected and uninfected cells from both day 3 and 6 post infection. Indeed, HIV-1BAL infection elevated all three ADAM mRNA levels compared to the uninfected samples only on day 3 but not day 6 of post infections. Their increase was not observed in the presence of BB-94 on both day 3 and 6 of infected samples. Thus, HIV-1 infection induced transient expressions of ADAM10 and 17 in the infected cells.
BB-94 treatment increased budding virion tethering and suppressed ex vivo HIV-1 release
While CD62L shedding inhibitors suppressed HIV-1 viral infection and deficient budding virions were observed in the presence of BB-94 (Kononchik et al., 2018), it is not clear of the molecular mechanism linking CD62L to HIV-1 release. Recent evidence showed that the viral infection-induced CD62L shedding requires caspase activation and inhibition of caspases impeded the viral release (Segura et al., 2023). CD62L is a C-type lectin receptor capable of binding to HIV-1 envelope glycans (Kononchik et al., 2018). While this glycan binding enhanced viral attachment and entry, it may tether budding virions from release when
CD62L shedding is prevented. To visualize CD62L-mediated virion tethering, we labeled X4 tropic HIV-1LAI infected cells in the presence and absence of BB-94 with immunogold particlelabeled anti-CD62L on day 6 of the infection and examined the budding virions using transmission electron microscope (TEM). The CD62L labeling produced fewer than 50 gold-particles/cell to minimize non-specific labeling in the infected and uninfected cells. While the majority of immunogold particles labeled cell surface CD62L that were not associated with HIV-1 virions, many immunogold particles (25% of the total gold particles) were observed in contact with HIV-1 virions, illustrating the presence of virionassociated CD62L. We further separated the virion-associated immunogold particles into two categories, the ones tethered to budding virions on cell surface (non-cleaved CD62L, indicated by red arrows) and the ones bound to detached virions from cells (cleaved CD62L, indicated by blue arrows). The two categories represent cell surface and shed CD62L. A survey of ~100 TEM images each from the DMSO and BB-94 treated HIV-1 infections
showed the fraction of the virionassociated immunogold particles varied between the budding and released virions in DMSO versus BB-94 treated infections. In the absence of BB-94, the fraction of budding virion associated gold-particles (45%, red arrows) is slightly less than that bound to the released virions (55%, blue arrows). In the presence of BB-94, however, the fraction of CD62Ltethered virions increased to 79% while those on released virions decreased to 21%. Namely, the ratio of CD62L-tethered budding versus released virions increased from 1:1 to 4:1 in favor of cell surface tethering in the presence of BB-94. Many virions appeared in small aggregates tethered to cell membranes . The increase in CD62L-tethered budding virions in the presence of BB-94 illustrates the hindrance of cell surface CD62L to the release of budding virions and supports importance of CD62L shedding in HIV-1 viral release.
To investigate if CD62L shedding inhibitors affected viral release in clinical specimens, we stimulated CD4 T cells from six HIV-1 infected individuals with anti-CD3 antibody in the presence of BB-94, 14 MB, GM6001 or prinomastat and measured the level of virionassociated HIV RNA released on day 2 and 4 post stimulation. The results showed that BB-94 inhibited the viral release from all individuals’ CD4 T cells (Figure 5), resulting in 2–50 fold reductions in released virion-associated RNA (5). Prinomastat and GM6001 inhibited viral release in a portion of the samples, whereas 14mb fail to inhibit the viral release. It is worth noting that BB-94 was more effective in inhibiting the viral release in individuals with lower viral loads (Figure 5). Together, the results showed that HIV-1 viral release can be inhibited by the most potent metalloprotease inhibitor, suggesting an optimum therapy to inhibit HIV-1 viral release is in conjunction with the existing ART therapy.
Discussion
Our recent work showed L-selectin (CD62L) bound HIV-1 envelope glycan and functions as a viral attachment receptor (Kononchik et al., 2018). Upon infection, however, HIV-1 induces the shedding of CD62L resulting in a near complete loss of the receptor in infected T cells. This viral induced shedding of CD62L appears mediated by ADAM metalloproteinases as BB-94 inhibited the receptor shedding. Importantly, inhibition of CD62L shedding also inhibited the viral infection, suggesting the attachment receptor impedes viral release. This paradoxical function of CD62L in HIV-1 infection, facilitating the viral entry but detrimental to viral release, reveals a new therapeutic opportunity to target the viral release using compounds suppressing viral-induced CD62L shedding. In efforts to identify anti-HIV release compounds, we systematically examined the involvement of serine, cysteine, aspartyl-proteases, and Znmetalloproteinases in CD62L shedding on human lymphocytes using various protease inhibitors. Those compounds inhibited CD62L shedding and suppressed both R5 and X4 tropic HIV-1 infection. They represent a new class of anti-HIV reagents that do not overlap with the current ART compounds. Interestingly, broad specificity inhibitors, such as BB94, and prinomastat, consistently suppressed the viral infection better than ADAM17 or ADAM 10 specific inhibitors. As CD4 T cells express multiple ADAMs, including ADAM8, 10, 15, 17, and 19, we cannot rule out the involvement of additional ADAMs in HIV infection. Interestingly, the expressions of ADAM10 and 17 were upregulated on day 3 but returned to the uninfected levels on day 6, suggesting that the shedding of CD62L needs to occur prior to HIV-1 release from the infected cells. Mechanistically, inhibition of CD62L shedding by BB-94 resulted in more budding virions tethering
Exploring Pharma Masterclass
on cell surface by CD62L, thus, impeding the viral release. Conceptually, it is less intuitive to understand why inhibition of adhesion receptor CD62L shedding did not result in an increased viral infection. We think the key resides in which cells shed CD62L and hence are subject of shedding inhibition. Since CD62L downregulation occurred in HIV infected p24+ but not p24- cells as evidenced in an increase of CD4-/ CD62L- cells in p24+ but not p24populations nor in the uninfected samples, thus CD62L shedding is primarily induced by the viral infection. Further, the shedding of CD62L is induced through an HIV Nef-dependent apoptotic caspase activation (Segura et al., 2023). As a result, BB-94 primarily inhibited the shedding of CD62L in infected T cells. Namely, shedding inhibition will likely not affect CD62L expression in uninfected cells and thus would not affect viral entry. It is worth noting that cell-to-cell transfer represents a major route for HIV transmission. While we did not investigate the current compounds in their ability to inhibit HIV infection in a cell-tocell transfer infection mode, our earlier study showed that BB-94 effectively suppressed HIV cell-tocell transfer infections (Kononchik et al., 2018). The inhibition of viral release in a cell-to-cell transfer infection is counter intuitive as viral release to the media is not required for virus cell-to-cell transmissions. It is possible that inhibition of CD62L shedding results in not only tethered virions but also intrinsically deficient virions on budding cells, such as the presence of aggregated virions in BB-94 treated samples.
Finally, the involvement of multiple ADAMs is consistent with our observation that single specificity ADAM inhibitors alone, such as potent ADAM17 inhibitor 14mb or ADAM10 inhibitor GI254023X, were less effective than broad specificity inhibitor BB-94 in suppressing
The Pharmaceutical Managers’ Institute is holding a Masterclass on Exploring Pharma: From Drug Discovery to Dispensing on June 13th 2024. This one day masterclass is designed as an overview to the industry and will provide excellent learnings and a wealth of information – regardless of your length of time in the industry! It’s ideal for those new to roles, those moving to another area of their organisation or simply those who wish to round out their knowledge of the industry and the journey a drug takes all the way from discovery to being dispensed in a retail pharmacy.
As the masterclass will include a tour of Uniphar’s warehouse in Citywest, numbers for this masterclass will be strictly limited – so an early reservation of your seat is advised!
The event takes place from 9.30am-4.30pm and you can find more details by visiting www.thepmi.com
HIV-1 infection. However, due to its broad specificity, BB-94 may have unintended consequences in vivo by suppressing metalloproteinases unrelated to HIV release but are involved in normal cellular function (Abel et al., 2004; Wetzel et al., 2017; Schlomann et al., 2019). It is conceivable that the use of a combination of highly potent ADAM isoform specific inhibitors may be more effective in suppressing HIV-1 release than the use of a broad-spectrum inhibitor. With the exception of ADAM10 and 17, however, highly potent isoform specific inhibitors are not available for other ADAMs.
In summary, broad specificity ADAM metalloprotease inhibitors, such as BB-94 and prinomastat, are effective inhibitors of HIV-1 infection through inhibition of CD62L shedding and the viral release. Both ADAM10 and 17 can cleave CD62L for shedding and both appeared to be involved in HIV-1 infection as the single specificity inhibitors generally failed to suppress the viral infection. These CD62L shedding inhibitors constitute a new class of antiHIV compounds. Mechanistically, inhibition of CD62L shedding resulted in increased receptor tethering of budding virions on CD4 T cells, thus impeding their release. Finally, CD62L shedding inhibitors, in particular BB-94, suppressed HIV-1 release from patient-derived CD4 T cells, demonstrating their potential therapeutic benefit. Importantly, the host regulation to HIV-1 viral release brings novel cellular targets for potential anti-retroviral therapy. As the current ART regiments are insufficient to eradicate the virus, it is intriguing to speculate on the combination of ART with viral release inhibition may bring additional therapeutic benefits since these metalloproteinase inhibitors do not overlap with existing ART compounds in their antiviral activities.
References available on request
Endorcrinology Focus AI Focus
Human-artificial intelligence interaction in gastrointestinal endoscopy
Written by John R Campion, Donal B O'Connor, Conor Lahiff John R Campion and Conor Lahiff
John R Campion, Conor Lahiff, Department of Gastroenterology, Mater Misericordiae University Hospital, Dublin
John R Campion, Conor Lahiff, School of Medicine, University College Dublin
Donal B O'Connor, Department of Surgery, Trinity College Dublin, Dublin
Artificial intelligence (AI) encompasses a wide variety of applications for sophisticated computer algorithms that use large volumes of data to perform tasks traditionally thought to require human intelligence.1 There is a growing list of current and proposed applications for AI in medicine, including direct patient interaction with AI chatbots to answer patient queries, analysis of a large amount of disparate data to predict disease diagnosis and course, and interpretation of images from radiological investigations.2-4 In gastroenterology, potential clinical applications span from use of domain-specific large-language models (LLMs) in the triage of specialist referrals to prediction of early-stage pancreatic cancer before it becomes overtly visible on imaging.5,6 Following the development of convolutional neural networks (CNNs) for computer-aided detection and diagnosis of pathology in the fields of radiology and dermatology, gastrointestinal (GI) endoscopy became an area of early research into applications of CNNs in medicine.7-10 Among the most promising initial applications of AI in GI endoscopy were computeraided detection (CADe) and computer-aided diagnosis (CADx) of premalignant polyps during colonoscopy using machine learning (ML) systems.11,12 These
applications were prioritised in an effort to improve adenoma detection rate (ADR) and to differentiate premalignant polyps from those without malignant potential, with the attendant possibility of reducing incidence of colorectal cancer (CRC) and reducing costs and complications associated with unnecessary polypectomy.13,14 Additional applications have developed rapidly to include detection and diagnosis of other pathology in upper and lower GI endoscopy, capsule endoscopy and biliary endoscopy. There has also been initial exploratory use of LLMs to aid decision-making on management of early CRCs and patient-facing applications to determine adequacy of bowel preparation prior to colonoscopy.15-19 While initial results on colorectal polyp CADe showed impressive improvements in key metrics of colonoscopy quality,20 some subsequent
real-world studies showed more modest effects or even no effect, and noted an increased rate of unnecessary resection of nonneoplastic polyps.21-23 It is possible that factors involved in real-world human-AI interaction (HAII) are a driver of such differences between experimental and real-world results.24 More than most other advances in medical science, successful implementation of AI platforms will depend not solely on the technical success and technical efficacy of the platform, but equally on the ability of the technology to interact with its human operators.25 There was early adoption of CADe technology in the field of breast radiology, based on experimental evidence of benefit.26 Analysis of real-world data from those systems later showed that early iterations contributed to greater resource utilisation due to false positives and increased additional radiological investigations.27 It is
an important lesson for application of AI in GI endoscopy, that effectiveness of AI platforms and their impact on patient outcomes can only be properly assessed in real-world settings. Despite the high speed of progress in development and roll-out of new applications for AI in GI endoscopy, the real-world effects of AI on clinician decision-making remain underexplored.28 Multiple factors can affect HAII at each phase of the development and deployment of an AI platform (Figure 1). Areas of interest in the interaction between humans and AI in GI endoscopy, which will be explored in this review, include: (1) Human design choices in creation of AI platforms and their user interfaces; (2) Regulatory processes and interventions for new AI platforms; (3) Human factors influencing user interaction with AI platforms; and (4) Clinician and patient attitudes toward individual platforms and AI broadly.
Growth in use of information and computer technologies in the 1980s led to recognition of the importance of studying the relationship between humans and these new technologies.29 The field of human–computer interaction (HCI) sought to investigate social and psychological aspects of interactions that would influence the acceptability and utility of these new technologies.30 Humans interacted with early computers by inputting code via keyboard, but as humans’ methods of interacting with technology have become more sophisticated, the influences on and impact of HCI have also become more complex.31 Ease of use is recognised as an important driver of uptake of new technological products or platforms.32 Psychological aspects of HCI were extensively explored in the pre-AI era. The ‘computers are social actors’ (CASA) theory held that, because psychological mechanisms evolve over centuries rather than decades, the human brain reflexively treats any entity with human-like abilities as human.29,33 Recent work has queried the durability of the CASA effect, and suggested that the human brain’s treatment of interactive technology as human may relate more to a technology’s relative novelty than to its existence.34 Whether human operators innately regard new technologies as tools or as other humans has significant ramifications for how the presence of AI may affect human performance. A key question with regard to technological development in any sector is that of function allocation i.e. deciding which roles should be performed by the human and which by the technology. AI has led to a rapidly burgeoning cadre of tasks that can be performed by technology, with an everdiminishing number of tasks the sole preserve of humans.29 Since the conception of AI, there has been disagreement between researchers on what the aim of AI should be; to replace human labour or to augment human performance. The prevailing view on this has changed from one position to the other frequently in the intervening period.35 At the current juncture, it appears that the decision will be made by the speed at which the technology can be developed, rather than by specific ethical considerations. A contrast between HCI and HAII is seen in the view by the former that computers and new technologies should be assistive, whereas the latter field recognises that AI has the possibility to replace human
efforts entirely in some instances, so-called agential AI.36
Algorithm Design and Interface Design
CADe and CADx platforms based on CNNs are created by training the programme on large volumes of data e.g. images and videos with a defined diagnosis, allowing the programme to learn patterns in the images that are suggestive of the presence of pathology or of the specific diagnosis of interest.37 Design of CADe and CADx systems requires the selection, curation and annotation of a large number of images of relevant pathology, to use as ‘ground truth’ for training and testing of the algorithm, while design of LLMs require large volumes of text data. Selection and curation of such image or text data represents the first point of contact between humans and the AI platform. There are several ways in which human decisions on training and design can influence the long-term operation of the AI platform. The functioning of the AI platform after its creation and the mechanism by which it arrives at its decisions are both opaque, with the processes being described as a ‘black box’.38 The possibility of building biases into the platform’s functioning makes selection of the best possible training database imperative, as unintended consequences of biased training data have been shown in other applications to have negative consequences on health outcomes for patients from minority groups.39 Difficulties can arise due to a number of problems with the training dataset, giving rise to different types of selection bias. When a CADe algorithm is trained using images from prior colonoscopies, those images are typically compressed and altered in the process of saving them to a database. The compression may introduce artefact and alter the value of the image for the CNN’s learning. It may also cause changes to the image that are imperceptible to the human but integrated into the algorithm’s processing. Choosing images that are too idealised may lead the algorithm to be poor at detecting pathology that deviates from archetypal descriptions.40 There is also concern that if a CNN is trained on data that comes from homogenous Western populations in the most developed countries, this may weaken the algorithm’s ability to give appropriate advice in racially diverse groups.41 An unbalanced dataset with too many instances of pathology and not enough images without pathology may skew the algorithm causing
decreased specificity. The larger the number of images used to train the algorithm, the better the system can be expected to perform.42 When the algorithm encounters, in real-world use, images outside what it encountered in the training set, it is more likely to flag those images as pathology.40 A novel methodology to train a CADe algorithm that involves training the platform by teaching it to read images in a similar fashion to an expert clinician, has recently been described.43 Design of the user interface is an important factor in optimising CADe/CADx performance. Design features that minimise additional cognitive burden and make alarms and advice coherent can result in synergistic effects. Conversely, poorly-designed platforms may increase the risk of automation bias, discussed later.44 The effect of presenting, alongside a CADx bounding box, additional data regarding the algorithm’s confidence in the given diagnosis, may alter the endoscopist’s trust in the AI advice and influence their likelihood to endorse the same diagnosis.45,46
Precise definitions and classifications for medical device software and AI systems differ between jurisdictions but in general AI or ML-based tools or algorithms when used for diagnostic or therapeutic purposes, including applications for GI endoscopy, will meet the definition of a medical device and should be appropriately developed and evaluated before they are approved for clinical use in accordance with the relevant regional regulation.47 Similarly, clinical research including pilot studies to generate the clinical data required to validate and appraise novel and uncertified AI tools in endoscopy should be performed in accordance with applicable regulatory and ethical requirements. To facilitate new and potentially beneficial advancements while protecting patients, regulation and scrutiny should be proportionate to the risk of the software and it is recognised that regulation of AI systems as medical devices is challenging and this is not unique to GI applications.48 The intended use of the AI and not simply the technology is a critical determinant of risk so for example CADx for malignancy diagnosis would generally fall into a higher risk category and require sufficient evidence and evaluation to support its use. Other important principles influencing risk evaluation include transparency, explainability, interpretability and control of
bias. In CADe in GI endoscopy this includes the ability of the clinician user to detect erroneous output information compared to so called ‘Blackbox’ algorithmbased interpretations. While many AI and ML applications have been approved, some experts have questioned the ability of currently emerging LLM products to meet these principles and GI clinicians must consider the evidence base and reliability of such devices for clinical practice use.49 Outside of basic regulation and licensing, clinicians and health systems trialling or implementing AI in GI endoscopy practice have a responsibility to ensure the applications (whether diagnostic or therapeutic) have a sufficient evidence base and the clinical data supporting algorithms for example is reliable and representative for the intended use patient population.
Human Factors influencing User Interaction with AI
Analysis of the interaction between humans and AI platforms in GI endoscopy can be informed by a human factors approach, examining how human work interacts with work systems.50 Human factors theories help to study and optimise components of work systems to allow human workers to get the most from the system.25 Human factors research also recognises that there are several cognitive biases that can affect human interaction with AI.51 Some of the cognitive biases that are most relevant to applications of AI in GI endoscopy are discussed below.
Automation bias
Automation bias refers to the human propensity to disengage cognitively from tasks that are assigned for execution or support by an external technology, usually resulting in decreased situational awareness.52 The potential for negative outcomes due to automation bias has been explored through a human factors paradigm in healthcare and other settings requiring high levels of accuracy.50,52 In the example of AI in GI endoscopy, automation bias may manifest as an over-reliance on a CADe or CADx platform to rapidly detect and diagnose all pathology encountered during the endoscopic procedure.46
The use of automated decision support systems that are presumed to be highly accurate can lead to an over-reliance on the part of users, which may manifest as bias or as complacency. Automation complacency may manifest
with the endoscopist paying less attention to the presence of on-screen pathology during endoscopy, due to an assumption that the software will detect any pathology that appears.53
This reduced vigilance, whereby the user becomes dependent on the software to shoulder the detection burden, can result in reduced human detection of pathology.54,55 Second, the user can become progressively more confident in the AI platform’s performance, to the point where they over-rely on its advice against their own correct judgement.56,57
Studies of mammography and histology showed concerning overreliance of clinicians on incorrect AI advice labelling cancers as benign.57 The complexity of verifying that the AI platform is performing appropriately impacts on the degree of automation bias that arises in a given task.44 In endoscopy, the ease of that verification task may vary depending on the endoscopist’s experience, where the complexity of verification is higher for non-expert endoscopists than for experts.
It is important that users of AI platforms are educated on the limitations of the individual platform. The latency of the system i.e. the time difference between pathology appearing on-screen and recognition of the pathology
Endorcrinology Focus AI Focus
by the computer system is typically as short as 0.2 s in the current generation of CADe platforms.37 The cumulative time taken for the platform to identify the pathology, activate the alarm and for the user to register the alarm may be significantly longer, however.
A related cognitive bias is anchoring bias, which posits that when presented with external advice, humans tend to adjust insufficiently from that advice toward their own opinion, in reaching their decision.58 It has been suggested that this insufficient adjustment is due to a trade-off between the accuracy required in the decision and the time required to fully consider the difference between the external advice and one’s own opinion.59 Taking longer to consider a decision may be an effective mitigation against anchoring bias.51
In real-time CADe-assisted endoscopy, however, the rapidity of decisions is an important factor in the efficiency of the procedure. In CADx applications, the effect of AI may be synergistic for both expert and non-expert endoscopists.46 A study that reached this conclusion advised endoscopists to treat advice from CADx as that from a colleague, weighing it against how accurate it usually is compared to the endoscopist. A simple adjustment to reduce automation bias may involve decreasing the
prominence of alarms on screen.60 More comprehensive strategies to mitigate automation bias could aim to decrease cognitive load on the endoscopist, instigate thorough training on use of the specific AI platform, address explainability and transparency of decision making and design adaptive user interfaces.44,52,61
False positives and alarm fatigue
False positives are of significant interest in CADe, as they may negatively affect the efficiency and economy of endoscopic procedures.62 A false positive may prolong the procedure as the endoscopist reviews the highlighted area.63
It may also add to the cost of the procedure by increasing use of implements e.g. forceps/ snares and raising the number of normal tissue samples submitted for processing and pathologic analysis.64 In colonoscopy, a CADe false positive may be caused by a normal colonic fold, other normal anatomy (e.g. the ileocaecal valve), a non-polypoid abnormality e.g. a diverticulum, or luminal contents.63 In commercially-available CADe systems, false positives in colonoscopy may occur in a ratio to true positives as high as 25:1.63
The incidence of false positives during colonoscopy has been reported to range from 0.071 to 27 alarms per colonoscopy, depending heavily on the definition used.11
Whereas some studies defined a false positive as any activation of a bounding box, others defined it as an activation that resulted in resection of normal tissue.
Most studies examined the incidence of false positives only during withdrawal, as the CADe system was typically only active during withdrawal. In real world practice, however, the CADe platform is often active during both insertion and withdrawal, likely leading to more false positives than in the reported experimental studies. False positive alarms may be categorised according to the amount of time the endoscopist spends examining the area involved in the false positive alarm: mild (< 1 s), moderate (1-3 s) or severe (> 3 s).63
While most false positives in the published studies did not result in additional examination time, the endoscopists involved in those studies were experts, so may have been more easily able to dismiss false alarms than non-expert endoscopists. Alarm fatigue is a well-described phenomenon whereby the repetitive activation of visual or audio alarms causes diminished, delayed or absent response in the user over time.65
Alarms have the potential to add to cognitive burden on the endoscopist, increasing fatigue and negatively impacting performance.66 While the amount of time taken to examine the site of each false alarm is low in published studies, the effect of repeated activations (at a rate of 2.4 +/- 1.2 false positive alarms per minute of withdrawal time) on endoscopist fatigue and possibly on algorithm aversion remains to be elucidated.63 The frequency of alarms may be addressed by altering the confidence level of the CADe i.e. decreasing the sensitivity of the platform, though this would need to be balanced against the resulting risks of decreased sensitivity. AI may also provide part of the solution for this problem, through development of CADe platforms with better accuracy and through filtering technology that uses generative learning to suppress false positives in realworld use.67 Another approach may be to increase the latency of output, so that activations of the bounding box of less than one second duration, which are almost always spurious, are suppressed and do not trigger an alarm. Alarm fatigue may also be reduced by minimising the alarm stimulus e.g. visual alarm without audio alarm, or altering the prominence or display of the bounding box.
Algorithm aversion
The ‘CASA’ phenomenon, discussed earlier, was a cornerstone of early HCI research. More recent research has shown that the way humans interact with technology is more nuanced than simply treating a new technology as they would another human.
There are multiple influences on how humans interact with technology and how they use or discard advice given by technology, though the interaction of these factors is poorly understood.68,69 Several studies have shown that a human user is likely to judge an AI algorithm more harshly for a mistake in advice than they would judge another human.
This results in the user being substantially more likely to disregard the algorithm’s future advice, a phenomenon known as algorithm aversion.70 In contrast to automation bias, algorithm aversion suggests that once a human user notices the imperfect nature of the algorithm advising them, their adherence to the algorithm’s future suggestions decreases, causing under-reliance on the AI system.
71
More recent work suggests that there are many factors affecting whether a user develops algorithm aversion, and durability of the phenomenon; these may include the individual endoscopist’s expertise, attitudes to AI and expectations of the system. Experts may be more likely to reduce their adherence to AI advice after a false alarm than nonexperts, even when later advice is correct.72,73 In the CADe setting, where the platform alerts for many more false positives than true positives, the impact of algorithm aversion may be important. A systematic review of the factors influencing algorithm aversion identified incorrect expectations of the algorithm, control of decision making and external incentives as significant contributors.55
With respect to AI in GI endoscopy, these factors may provide a framework for research on the human and AI platform variables that affect the propensity of a user to develop algorithm aversion.
Learning effect and deskilling The effect of CADe and CADx platforms on an endoscopist’s learning and on their development of skills essential to performance of endoscopy is uncertain. Several studies have shown that CADe may improve a trainee’s ADR to close to that of an expert, providing additional safety and
reducing the adenoma miss rate.74 It is not clear, however, whether this improved performance produces a persistent learning effect or whether it may bring about dependence of trainees on the CADe platform. There is some evidence that the ability of such platforms to draw a trainee endoscopist’s eye to a polyp and to give advice on the likely histologic type of the polyp may improve the trainee’s recognition and diagnosis of such lesions.46
Evidence from non-endoscopic applications of AI show that the potential for non-expert clinicians and female clinicians to over-estimate the reliability of an AI platform raises concerns for poor training outcomes and for inequitable distribution of performance benefits.68 Interestingly, providing an explanation for its decision does not appear to improve the application of AI for training. In explainable AI platforms that showed the user how it had arrived at its advice, trainees were more likely to accept the advice, even when it was incorrect, than if no explanation was given, the socalled ‘white box paradox’.75
Visual gaze pattern (VGP) is an important metric in vigilance tasks including detection of pathology during endoscopy, with substantial differences between VGPs of experts and those of non-experts.66,76-78 Analysis of the VGP of endoscopists with high ADRs showed a positive correlation with VGPs that tracked the periphery of the bowel wall and the periphery of the screen in a ‘bottom U’ configuration during colonoscopy.76,79 The repeated attraction of the endoscopist’s attention to a bounding box on screen may serve to embed alterations in the endoscopist’s VGP, which have been posited to have a negative effect on an endoscopist’s attainment of expertise in polyp detection in colonoscopy.80 In the eye-tracking experiment, endoscopists’ gaze patterns focused more on the centre of the screen when using CADe, reducing their likelihood of detecting pathology peripherally.
Clinician and Patient Attitudes to AI
The quality of HAII depends to a significant degree on the attitudes of users and patients toward the technology. Levels of trust in technology generally, and in AI technologies specifically, are heterogenous across groups of clinicians and groups of patients.81 They depend on many factors including personal, professional,
organisational and broader cultural considerations.82 Research and speculation on the role of AI platforms have occupied increasing amounts of space in the endoscopy literature.
The promise of AI in revolutionising patient care and administrative burden have been much-vaunted in academic literature and in popular media, leading to high levels of awareness of AI among the general population, but low levels of knowledge on specific applications.83 Knowledge of AI is seen to correlate with a positive perception of the benefits of AI, and perhaps an underestimation of its risks.84
Surveys of the attitudes of gastroenterologists and other endoscopists in the United States and the United Kingdom show a high degree of optimism on the potential role of AI to improve quality of care for patients.85 They also support development of guidelines for use of AI devices86 and endorse concerns that CADe technology will create operator dependence on the technology.87 Patient attitudes toward AI algorithms making decisions or offering advice appear more cautious.88 When used as a tool by their clinician, patients perceive benefit in AI in specific settings including cancer diagnosis and treatment planning.89 Patient attitudes to use of AI in GI endoscopy require further research.
Conclusion
In many of its current applications, AI marks a fundamental transition from technology as a tool to technology as a team member. Research is required to define what skills clinicians will need to optimally leverage AI technologies and to apply AI advice with adequate discrimination. It will then be necessary to decide how best to teach these skills from undergraduate to expert endoscopist level. While there are regulatory pathways for appropriate trialling and development of AI software applications, guidance for clinical evidence requirements is lacking for medical AI software in general and not limited to software devices in GI endoscopy. Frameworks for design and reporting of trials involving AI are therefore to be welcomed.90
Uniform definitions of variables (e.g. false positive) are needed for research and reporting of realworld performance of AI platforms. Several professional societies have published opinions on priority areas for future research on AI in GI endoscopy.91,92 These opinions
place a notable emphasis on technical outcomes, rather than on outcomes related to human interaction or patient-centred endpoints. It can be expected that priorities will need to be updated and redefined by professional societies frequently, as new technologies emerge.
The medical community and professional societies should lead the way in defining the research agendas for AI platforms including the clinical evidence base required for their validation, adoption into clinical practice and continuous appraisal, while ensuring that patient priorities, human factors and real-world evidence are prioritised.93 Priorities for research on HAII in GI endoscopy should include factors predicting individual clinician variations in utility of AI and the effect of AI use on trainees’ development of core competencies for endoscopy.94
A HAII focus in platform development may give rise to AI that learns how best to interact with each clinician based on their performance and use style, and adapts accordingly. Complementarity may be enhanced by prioritising study of human interaction with novel AI platforms that can perform tasks at which human clinicians are poor e.g. measurement of polyps or other pathology, measurement/ estimation of the percentage of the stomach/colon visualised during a colonoscopy.95
HAII will be a key determinant of the success or failure of individual applications of AI. It is therefore essential to optimise interface elements, as clinician frustration with poorly-designed platforms now may have a negative impact on later engagement and uptake.96 The rapid development and implementation of AI platforms in GI endoscopy and elsewhere in medicine has been performed while studying mainly technical outcomes in idealised settings.
This trend of adopting a technology-first approach expects clinicians and patients to adapt to the AI platforms, and risks taking insufficient account of human preferences and cognitive biases.50 Reorienting the focus toward development of human-centred AI and incorporating the study of human interaction at each stage of a new platform’s development, while aligning to appropriate regulation and governance, may allow creation of AI that is more user-friendly, more effective, safer and better value.90
References available on request
CardioStart International Trip to Tanzania
Written by Grainne Warren - Grainne Warren, a cardiothoracic intensive care nurse at Galway University Hospital for 5 years, holds postgraduate degrees in intensive care nursing and clinical trials.
Amanda Tirone - Amanda Tirone, with seven years as a registered nurse in intensive care and a forthcoming Master’s in Cardiovascular Perfusion from Thomas Jefferson University, is graduating as a Certified Clinical Perfusionist in Norfolk, Virginia.
Sarah King - With eight years as a Registered Diagnostic Cardiac Sonographer and ongoing studies for a Master’s in Healthcare Informatics, Sarah King is currently on assignment as a travel sonographer in California with Aya Healthcare.
Introduction
Between March 9th and 16th, an international group of volunteers visited Jakaya Kikwete Cardiac Institute (JKCI) in Dar Es Salaam, Tanzania. The group consisted of cardiac surgeons, anaesthetists, nurses, perfusionists, cardiac sonographer, and a critical care doctor. The group travelled from the USA, Australia, and Ireland under the auspice of a charity called CardioStart International. The basic mission of CardioStart is to educate and assist local medical teams in providing heart surgery and cardiac services to adults and children in underserved regions of the world, with a vision of a world where access to cardiac care can be realized by everyone. The following article will discuss the personal and professional experience of intensive care nursing, perfusion and cardiac sonography gained during this mission.
United Republic of Tanzania is the largest country in East Africa with a population of over 65 million people (United Nations, 2022). Even though Tanzania is one of the most politically stable African nations, it is an impoverished country, with over 25 million of the
population surviving on less than 2 USD per day (World Bank Open Data, 2020).
The hospital that CardioStart International is linked with, known locally as JKCI, is the only available cardiac surgery centre in the country. It is a government owned hospital which accepts patients from all over Tanzania and surrounding countries, from regional referral and designated hospitals, for cardiovascular intervention. On average they cater for 700 outpatient appointments per week and have over 100 inpatients at any given time. There are three operating rooms, an eight bedded adult intensive care unit, a paediatric intensive care unit, and several floors of inpatient wards. This was the fifth visit made by CardioStart to the hospital.
Intensive Care Experience
The main observation I made in my time in intensive care in JKCI, was that teamwork was abundant. The severe lack of resources extended to every consumable item you can imagine, including all medications, dressings, syringes, needles, monitors, infusion pumps etc. However, this did not affect the primal desire within nurses and medics which is to improve
the patient experience and outcomes. Despite having very minimal supplies, the intensive care staff were extremely attentive, excellent advocates for their patients, and quick to point out their observations to the medical staff. I was positively surprised at the lack of negative hierarchy that exists, everyone was listened to respectfully and discussions were open and transparent.
One element of postoperative cardiac surgery care which is central to practise in the developed world, is the idea of “fast track extubation” (Wong et al, 2016). There are multifaceted benefits associated with this concept, including reduced length of stay in ICU. Whilst on this mission, I was initially surprised to see that both pain relief and sedation were given reactively to patients, via bolus injection. It is routine in intensive care practise to provide these medications via a continuous infusion pump during the first hours post-surgery. However, there was discernible positives associated with the methods witnessed in JKCI. The primary reason for giving a PRN bolus of medications in this context was a simple lack of infusion pumps. A maximum of three pumps were available for each bedspace, these were usually administering inotropes or vasopressors for cardiovascular support. By administering only bolus of sedatives, the nurses were highly attuned to the patients’ needs and communicated continuously with them in a calm and professional manner, in order to maintain endotracheal tube tolerance. This made it likely that the patients were suitable for extubation at a very early stage postoperatively. An aspect of holistic patient care which was accommodated
throughout the patient’s journey was open visiting of family members. The visitors were made to feel welcome, encouraged to be involved in the basic care of their relative and kept updated to their condition with little prompting. This had the added effect of reducing anxiety for the patient in ICU, during a lifechanging experience for them.
Physiotherapy is a very important element to the recovery process following cardiac surgery. The physiotherapy offered to the patients, was as good as any developed country. The physiotherapist was calm, patient, and took a long time to go through the exercises with each patient. There was a good flow and routine to their practise, and this culminated in early mobilisation where suitable.
Naturally there were some areas of ICU care that needed some polishing, that was the purpose of the mission after all. It’s important to acknowledge that the hospital functions in the absence of charitable input for most of the year. It was obvious though that the staff were very receptive to learning and the nurses had questions about every aspect of care that they were providing, and how this is carried out in Western hospitals. Didactic training was given over the course of the week, in many different subjects. Advanced physical assessment such as chest auscultation, perfusion status, neurological assessment and skin assessment skills were practised. Methods of assessing fluid responsiveness was a subject of great interest to the staff, as there is no access to advanced haemodynamic monitoring or point of care testing for lactate. Thus, passive leg raises, central venous pressure monitoring and mixed venous gas exchange were employed instead. This highlighted a resourcefulness and willingness to learn in the staff which was unlike anything I had witnessed.
CardioStart group photo
ONOURS Hospital Professional 2024
The Hospital Professional Honours will take place on Saturday, 14th September 2024 in the Radisson Blu Hotel, Dublin. Entries are now open across a number of categories including:
Haematology Project of the Year
Young Hospital Pharmacist of the Year
Galapagos Biotech Ltd, an Alfasigma company, Multidisciplinary Team of the Year
Fresenius Kabi Innovation in Aseptic Compounding
Medisource Hospital Pharmacy Technician of the Year
Grünenthal Advancing the Standard of Care in Pain Management
Athlone Pharmaceuticals Hospital Pharmacy Team of the Year
Excellence in Respiratory
Viatris Excellence in Cardiovascular Initiative
Pharmasource Hospital Pharmacist of the Year
MSD Excellence in Oncology Initiative
MedFind Solutions Innovation and Service Development
Excellence in Patient Safety
GSK ViiV Infectious Diseases Project of Year
Consultant-Led Team of the Year
The impact of the mission overall was obvious for the patients, several underwent coronary artery bypass grafting and others had repair of secundum atrial septal defect. The impact for the patients is that they can now go back to their daily lives in comfort. The impact on the volunteers is perhaps even more great. From a personal point of view, witnessing healthcare workers succeed and excel in such hardship was a privilege. The care provided was genuinely the best possible, within the resource constraints of a severely underserved environment. Staff were kind, inclusive and communicative. It was truly amazing to see how they do so much with so little.
Perfusion Experience
When you hear the word “luxury” your mind will wander to a mansion set back in the woods, the front seat of a Lamborghini throttling around curves on the side of a cliff in a faraway country, or to a fantastical land with birds and animals of bright colours. Never would your mind conjure up an image of an operating room with minimal supplies in a hospital regularly combating the heat and humidity of the typical weather of East Africa. For the people of Dar
Es Salaam, Tanzania, arriving at Jakaya Kikwete Cardiac Institute (JKCI) for heart surgery is a luxury that most in the surrounding areas cannot afford.
The first day in the operating room was approached with caution, as there were bound to be barriers. As with any developing country, there are deficits of both supplies and medications; fortunately, the mission team was able to travel with a small mountain of suitcases filled with donated supplies and medications, even those that were expiring, which were so gratefully used. Despite the varying countries and years of experience that the team brought to the table, the eclectic combination of equipment, ventilators, and cardiopulmonary bypass machines forced a sense of teamwork to navigate and troubleshoot each machine.
It is important to recognize that the JKCI team has been functioning to the best of their ability prior to the mission team coming in. However, the team was able to help perform necessary complex cases, provide much needed supplies, and instil further knowledge on more
efficient techniques and even more evidence-based approaches that can enhance both their future cases and outcomes. For example, employing vacuum to the cardiopulmonary bypass machine was not in the routine wheelhouse of the JKCI perfusion team. On complex cases, vacuum is an essential component to ensure adequate venous drainage and a bloodless, motionless field for the surgeon. Perfusionists of the mission team were able to rig together a useful vacuum system for these cases as well as MacGyver together and introduce the idea of a recirculation-priming combination line. This line typically serves to recirculate air and fluid from the oxygenator, transfuse fluids, medications, and blood, and to remove blood or fluid from the circuit and displace it to empty fluid bags in the setting of volume overload as to avoid pressurizing the reservoir.
Another vital component of cardiac surgery that was harnessed is cardioplegia. This is used to stop the heart and provide myocardial protection during cardiac surgery while using the cardiopulmonary
bypass machine. The CardioStart mission team was able to provide a researched formula and education on how to make cardioplegia each day including dosing, shelf-life, and crystalloid alternatives to be used. This helped to combat previous complications with ineffective cardioplegia administration, unknown dosages, and a lack of supplies. This equally instilled a sense of independence with the ability to constitute their own cardioplegia for each case. Coupled with this came the education on haemodilution and effective interventions and methods to prevent and combat this as it can lead to unnecessary post-operative complications and risks of volume overloading and requiring blood transfusions both intraoperatively and postoperatively.
As is easily imagined, the language barrier was one of the largest hurdles as this ranged from languages spoken, to what device was used, to protocols and anticipation of next steps. However, all these fears were quickly dissipated by the hospitality that was extended by the local team. The operating room staff at JKCI was not only welcoming but encouraged the Cardiostart medical mission team’s involvement and input. Both the local and traveling teams
Amanda and Grainne in OT
CABG
understood that communication (and candy) would be their biggest ally and used this to their advantage to create a cohesive, seamless team. One of the most enlightening attributes of the team at JKCI was their sense of comradery with their local team and visitors alike. This continued even through the longest case of the week- a partial arch replacement, Bentall procedure, and coronary artery bypass graft (CABG) which included a 13-hour cardiopulmonary bypass run. Throughout this procedure the team did not lose their spirit nor their dedication to the patient, even far into the night. As the hands of the clock passed into a new day, team members would alleviate others so that they could rest, snack, or grab a fresh bottle of Coca-Cola. The support, encouragement, perseverance, and devotedness that was felt so strongly is something that we can only hope to emulate in the future. While this procedure was the longest and most complex, there were a variety of additional procedures performed. These included atrial septal defect
(ASD) repair, CABG, aortic valve replacement, and a combination of these procedures. Unfortunately, JKCI had seen a recent reduction in cardiac procedures performed due to an interruption in supplies. Considering this, the impact of the visiting mission team will be felt for months to come as they will be able to perform more cardiac surgery cases with the donated cannulas, tubing, sutures, valves, grafts, tools, and medications that the team was able to supply. This trip has provided a sense of pure appreciation- both for what we have, and for what amazing things the local team is able to accomplish with the tools and equipment at their disposal. However, the privilege of joining this team was held in the hearts of the CardioStart medical mission team. Needless to say, this newly formed team definitely has the beat!
Cardiac Sonography Experience
Tanzania has a limited supply of resources, high rates of HIV/AIDS, pneumonia, malaria, and maternal and child deaths. Additionally, Tanzanians have some of the lowest rates of global access to medical professionals. This is due to low medical school output, outmigration due to poor compensation, and adverse working conditions. HIV/AIDS has increased demand for skilled health workers but reduced their availability. An urban-rural imbalance also exists, with more staff in urban centres. To
improve productivity, solutions include improved management measures, local-specific training, strengthening enabling factors like equipment and skills, and introducing financial incentives to increase workers' efforts. Rheumatic heart disease is still prevalent in Tanzania. Rheumatic heart disease affects 40.5 million people globally, with up to 80 million having asymptomatic cases. Despite almost eradicated in developed countries, rheumatic heart disease continues to affect children and young adults in sub-Saharan African countries like Tanzania. Tanzania also has a severe shortage of specially trained medical professionals. To ensure improved access and improved medical care, their health infrastructure needs to be improved.
During my two-day echo clinic, I was able to examine 39 patients with cardiac ultrasound. I found that 16 of these patients (roughly 38%) had abnormal cardiac findings on their echocardiogram. They desperately need an advanced training curriculum specifically geared towards echocardiography. Every cardiac illness assessment and treatment revolves around echocardiography, or "echo." Ultrasound waves are used to create a moving image of the heart during an echocardiogram. The inherent benefits of this technology— sound waves are painless and
Amanda leading perfusion in OT
Sarah carrying out echo at the Outreach clinic
safe, and portable devices offer convenience and quick, repeatable results—allow its application to spread far beyond conventional medical settings. Numerous kinds of cardiac disease can be identified by an echocardiogram. Among them are congenital heart disease, cardiomyopathy, infective endocarditis, valvular disease, and pericardial disease. Additionally, an echo can reveal changes in the heart that can indicate an aneurysm in the aorta, thrombi, or a tumour of the heart. Notwithstanding any possible benefits, echocardiography requires training and ongoing professional development to be used safely in any healthcare context. The risk of patients being harmed by unskilled personnel utilizing subpar equipment is considerable and must be reduced in the absence of a strong certification, accreditation, and revalidation procedure.
Hypertension was another finding that was seen frequently with the patients I examined. In urban Tanzania, hypertension is said to be the most common cause of heart disease. Reportedly, most patients do not receive treatment prior to echocardiography and most have advanced stages of cardiac disease. To identify
Grainne grabbing a few coca colas
and treat heart failure and hypertension in urban Africa, there is an immediate need for greater infrastructure, knowledge, and awareness.
Taking all of this into account, the chance to use your skills where they are most needed can be one of the most fulfilling parts of participating in a medical mission trip. In addition to being a great opportunity, it was an honour. When I went to Tanzania, I was joined by other professionals who shared my enthusiasm for medicine, empathy for others, awareness of the global community, and a sense of adventure. My fellow volunteers encouraged me, tested me, and some will end up as lifelong friends.
Conclusion
The aim of this article is twofold: to delineate the profound experience of participating in a medical mission and to ignite a passion for such endeavours among our peers. While acknowledging the challenges—both logistical and financial—the accrued learning is immeasurable. From the point of view of personal and professional development, it is invaluable. Reflecting on the impact of our efforts, we recognize that the true value lies not only in the
lives touched but also in the transformative journey it ignites within ourselves. Beyond the operating room, outreach clinics, and the intensive care unit, the lessons learned in empathy, collaboration, and resilience reverberate far beyond the borders of any country. May this narrative serve as a testament to the power of compassionate action and the enduring spirit of humanity.
Acknowledgements
All of the equipment which was donated to JKCI during this trip was very kindly donated by medical companies and hospitals in the volunteer’s localities. We would like to thank the following for their continuing support:
• Ciara Power, Aerogen for the donation of Aerogen Pro controllers
• Damien McCann, LivaNova for the donation of perfusion supplies
• Denis Coakley, Vygon for the donation arterial line catheters
• Deirdre Kileen & Marion Grady, Galway University Hospital for the donation of PPE
• Mary Maguire, biomedical engineering Galway University Hospital for the donation of expired ICU equipment
• Keystone Perfusion for the donation of perfusion supplies
• Thomas Jefferson University Hospital for the donation of perfusion supplies
• Cooper University Hospital for the donation of perfusion supplies
For more information on volunteering: grainne.warren@hse.ie
Reference list
“CDC Global Health - Tanzania.” 2019. 2019. https://www.cdc.gov/ globalhealth/countries/tanzania/ default.htm.
Galson, Sophie W., Msafiri Pesambili, Joao Ricardo Nickenig Vissoci, Preeti Manavalan, Julian T. Hertz, Gloria Temu, Catherine
A. Staton, and John W. Stanifer. 2023. “Hypertension in an Emergency Department Population in Moshi, Tanzania; a Qualitative Study of Barriers to Hypertension Control.” Edited by Anna Prenestini. PLOS ONE 18, no. 1 (January): e0279377. https://doi. org/10.1371/journal.pone.0279377. Kazahura, Parvina Titus, Theophylly L. Mushi, Pedro Pallangyo, Mohamed Janabi, Rodrick Kisenge, Mazen Albaghdadi, Naizihijwa Majani, and Edward Kija. 2021. “Prevalence and Risk Factors for Subclinical Rheumatic Heart Disease among Primary School Children in Dar Es Salaam, Tanzania: A Community Based Cross-Sectional Study.” BMC Cardiovascular Disorders 21, no. 1 (December). https://doi. org/10.1186/s12872-021-02377-9.
Munga, Michael A, and Ottar Mæstad. 2009. “Measuring Inequalities in the Distribution of Health Workers: The Case of Tanzania.” Human Resources for Health 7, no. 1 (January). https:// doi.org/10.1186/1478-4491-7-4.
Ou, Zejin, Danfeng Yu, Yuanhao Liang, Jinhua Wu, Huan He, Yongzhi Li, Wenqiao He, Yuhan Gao, Fei Wu, and Qing Chen. 2022. “Global Burden of Rheumatic Heart Disease: Trends from 1990 to 2019.” Arthritis Research & Therapy 24, no. 1 (June). https://doi.org/10.1186/ s13075-022-02829-3.
Raphael, Dominick M., Laurine Roos, Victor Myovela, Elisante Mchomvu, Jabir Namamba, Said Kilindimo, Winfrid Gingo, et al. 2018. “Heart Diseases and Echocardiography in Rural Tanzania: Occurrence, Characteristics, and Etiologies of Underappreciated Cardiac Pathologies.” PLoS ONE 13, no. 12 (December). https://doi. org/10.1371/journal.pone.0208931.
United Nations, Department of Economic and Social Affairs, Population Division (2022). World Population Prospects 2022: Data Sources. Available online at: [https://population.un.org/wpp/]
Wong WT, Lai VK, Chee YE, Lee A. Fast-track cardiac care for adult cardiac surgical patients. Cochrane Database Syst Rev. 2016 Sep 12;9(9):CD003587. doi: 10.1002/14651858.CD003587. pub3. PMID: 27616189; PMCID: PMC6457798.
World Bank Open Data (2020) Poverty & Equity Brief, SubSaharan Africa, Tanzania. Available online at: [https:// databankfiles.worldbank.org/ public/ddpext_download/ poverty/33EF03BB-9722-4AE2ABC7-AA2972D68AFE/Global_ POVEQ_TZA.pdf]
Mental Health
‘Hello, How Are You?’: Fostering real connections and mental health support in communities
In an era characterised by the frantic pace of modern life and the prevalence of digital communication, genuine human connection can sometimes feel like a scarce commodity. Mental Health Ireland’s mission is to promote and enhance mental health and wellbeing and to create a culture where we are all respected and supported, especially when our mental health is challenged. Our current campaign is called Hello, How Are You? and is about connecting with those around us and engaging in open conversations about mental health. It’s about asking the question, ‘How Are You?’ with meaning, and really listening to the response.
The campaign emerges as a reminder of the profound impact that simple acts of kindness can have on mental well-being. Rooted in the belief that meaningful conversations can change lives, this initiative seeks to destigmatise mental health while fostering a culture of support and understanding.
The essence of the campaign lies in a simple question: "How Are You?" Yet, it's not just about the words; it's about the intention behind them. It's about genuinely caring about the answer and being present to listen. By encouraging individuals, communities, workplaces, friends, and families to engage in open dialogue, the campaign aims to create a ripple effect of empathy and support.
Since its inception, the "Hello, How Are You?" campaign has
Written by Marie Duffy, PR & Communications Officer with Mental Health Ireland
gained momentum across Ireland. From distributing conversation cards and bookmarks to facilitating workshops and discussions, Mental Health Ireland has been instrumental in promoting mental well-being through meaningful connections. By distributing 300,000 conversation cards to people in 2023 alone, the campaign has sparked conversations and challenged societal attitudes towards mental health.
At the heart of the campaign is the recognition that loneliness often accompanies mental distress. By nurturing connections and support networks, individuals can combat feelings of isolation and find solace in human connection. This emphasis on community
and belonging underscores the importance of reaching out and checking in on one another, especially during challenging times. Engaging in meaningful conversations always doesn't require expertise; it requires empathy and sincerity. Mental Health Ireland offers a simple yet effective framework—the HELLO Steps—to guide these interactions:
• Hello: Extend an invitation to chat, respecting the person's readiness to engage. Remember that It’s ok if they say no as they may not be ready to talk. If they say yes, then find a quiet spot to talk. Bear in mind that now might not be the right time to talk and they might take you up on your invitation another time.
• Engage: Foster an open dialogue by asking openended questions and actively listening. Engage with the person by making eye contact with them or whatever feels most comfortable. Be open as possible to the conversation. It helps to ask open ended questions that don’t require yes or no answers. Phrases like ‘Could you tell me more?’ ‘How does that make you feel?’, ‘What has helped before?’ may be useful. When we begin a conversation, it’s only the tip of the iceberg and it might take time to get to a deeper answer. You might get an automatic response of I’m ok or I’m fine. That’s perfectly ok. It takes time to build up trust. This takes us onto the next step
• Listen: Demonstrate empathy through both words and body language, creating a safe space for expression. Use words and body language that lets the person know that you are listening. Remember you aren’t expected to have all the answers.
• Learn: Seek to understand the person's perspective and validate their experiences. Try to look at things from the other person’s perspective. Ask what has worked in the past. Trust that the person is the expert on themselves and what works for them.
• Options: Empower the individual to explore their options and access support services if needed.
By following these steps, anyone can play a vital role in supporting others' mental well-being. It's about being present, showing compassion, and recognising that small gestures can have a profound impact on someone's life.
In a society where mental health concerns are often met with silence or stigma, initiatives like "Hello, How Are You?" aim to offer something different. They remind us that by fostering connection and empathy, we can create communities where everyone feels respected, supported, and valued. So, the next time you ask someone, "How Are You?", remember, it's more than just a question—it's an opportunity to really listen and meet people where they’re at.
EAHP Congress
An update from the 28th Congress of the EAHP
The European Association of Hospital Pharmacy (EAHP) 28th Congress was held in Bordeaux, France this year, 20th – 22nd March. The Congress theme was “Sustainable healthcare; opportunities and strategies”, and attracted hospital pharmacists from almost every country in Europe. Congress attendees were welcomed to beautiful Bordeaux with unseasonable sunny weather, and characteristically exceptional gastronomic delights, during every break period of the 3 day conference. The EAHP scientific committee curated a fantastic programme this year, brimming with interesting and compelling sessions from a broad range of speakers.
The three keynote speeches covered a breadth of considerations when planning and executing a more environmentally sustainable healthcare system across our home countries. Pedro Facon, a Belgian public health manager, opened the conference by asking us to reengineer our healthcare systems in order to embed a sustainable approach within our “greening” of pharmacy.
On the second day, Peter Morgan, the Head of Medicines Net Zero for NHS England, and founding member of PharmacyDeclares®, and environmental activist group of pharmacists and pharmacy technicians who have been leading much of the strides towards sustainable medicines use in the UK. Pete’s passionate and compelling speech on the impact of climate change on human health challenged to confront the very real impact of climate change on our daily lives. He said “Our world needs climate action on all fronts; everything, everywhere, all
at once”. He described the impact on climate related environmental changes on the increase in chronic disease such as cardiovascular disease and mental health, and the inevitable increase in medication use that this will bring – which will ultimately lead to ever increasing amounts of medication in our water supply. Pete challenged us in the audience to future proof our healthcare systems – to think differently – and to keep looking for better ways of protecting our world for the generations who follow.
The final keynote speech, closing the conference, was delivered by Clare Howard, the Clinical Lead for the National Polypharmacy programme in England. Clare described her award winning work supporting healthcare professionals to address the public health crisis of over-prescribing in our patients. She uses Action Learning sets to support teams to identify gaps in their own learning, and practice, and how to apply these to support safe and appropriate deprescribing. Clare shared the bespoke tools she uses to support healthcare professionals to ensure that their approach is patient centred and sustainable, even in very complex multi-morbid patients. Her practical approach resonated with the audience, and she made everyone wonder why we weren’t already doing everything she suggested already.
But the conference was more than the keynotes – the programme offered a myriad of seminars, workshops and interactive sessions, as well as an enormous poster area – where the work of researchers spanning from student pharmacists to imminent professors of pharmacy was
Written by Professor Roisín O'Hare BSc (hons) MSc DPharm FHEA FPSNI(IP) FFRPS FRPS
NI Lead Clinical Education Pharmacist
Cardiology Pharmacist, Southern Health and Social Care Trust, N Ireland
Hon. Professor of Pharmacy Practice, Queens University Belfast
Immediate Past President, Guild of Healthcare Pharmacy
showcased. Attendees could engage in the conference by presenting their original research, QI projects, good practice initiatives and prizes were awarded to both poster and oral presenters for their innovative work and compelling presentations.
I delivered an interactive session titled “Moving forward with digital clinical education… when ward-based training is not an option” during the congress. Unfortunately, as my co-presenter was unwell, this was a solo performance! The third United Nations Sustainable Development Goal (SDG) goal focusses on Good Health and wellbeing for all by 2030, reflecting the global shortage, and unequal distribution, of healthcare professionals across low, middle and high income countries. One way to increase access to a competent healthcare workforce, is to redesign and reimagine how we deliver our health care education. The session described for attendees what digital learning is, and how common strategies such as Computer-aided Instruction (CAI), virtual patients / virtual reality, as well as Serious Gaming and Human Patient Simulation (HPS).
I shared our experiences with a hybrid approach to our Experiential Learning programme in hospitals in Northern Ireland, and how digital strategies can be used to support Pharmacists in practice to develop their mentoring, and teaching skills, as well as support students to prepare for learning in practice. In our experience, a structured hybrid preparation course for students, with digital and live elements, can support learners to develop confidence in clinical skills in a simulated environment before applying their learning to “real”
patients in practice. Attendees shared their experiences, and key takeaways included when to use which tool, and how to incorporate digital strategies meaningfully into clinical teaching, in order to demonstrate enhanced learning and importantly, improved outcomes for patients.
Aoife Fleming, Senior Lecturer in Clinical Pharmacy at University College Cork and Jelle Tichelaar, Professor of Clinical Pharmacology in Amsterdam University Medical Centre led an inspired session – sharing their real world experiences of how to make interprofessional learning for healthcare professionals work for everyone; students, healthcare teams, managers and most importantly for patient’s care.
For me, a real highlight of the conference was the Aural Apothecary’s podcast. For those of you who are unfamiliar, the Aural Apothecaries (www. theauralapothecary.com), Jamie, Gimmo and Steve the Chemist, offer a light-hearted – yet authentic – look at our practice as pharmacists, and challenge those they interview to choose a number of items which will define both memorable moments in their careers as well as what drives them as a professional pharmacists. During lunch on the second day of the Congress, we were treated to Roberto Fontini (former President of EAHP, and key champion of the EAHP statements) sharing his “Memory inducing medicine” as heparin, due to the death of a close friend, early in his career, from heparin induced thrombocytopenia, which inspired Roberto’s career in pharmacovigilance. The second guest was Beatriz Torroba, a
hospital pharmacist from Madrid, who described how challenging the repeated poor prescribing of docetaxel by a junior dr in her unit led her to meet her now husband….he is now a much better prescriber we are told!
During the congress, the EAHP Environmental sustainability working group, led by co-chairs Barry Melia, Principal Pharmacist in Public Health Scotland and Min Na Eii, Greener NHS Chief Sustainability Officer’s Clinical Fellow – launched their paper on the roles hospital teams can do, to be published later this month. Attendees were challenged to “do one thing” in their personal and also in their professional life, that would make a difference to a more sustainable system, and importantly, to find a way to measure it – and keep striving for a better future, for all of us.
At the end of the Congress, the Chair of the EAHP Scientific Committee, Prof Thomas De Rijdt, announced that the 29th EAHP Congress will take place in Copenhagen, Denmark next March with a theme of “Person centred pharmacy – navigating digital health”. Will you be there?
EAHP Congress
Possibly confused Reflections on an EAHP Seminar
After une petite IT glitch in le matrix the session “Compounding without frontiers, cooperation over country borders” commenced with Professor Koch outlining some of her research in the area of Therapeutic Drug Monitoring (TDM) and Model
Informed Precision Dosing (MIPD) and the benefits of collaborating with other global experts. TDM and MIPD are tools to allow personalised dosing/pharmaceutical care which is a holy grail of clinical pharmacists. Apart from the
Written by Declan P O’Sullivan, Head of Pharmacy, Cherry Orchard Hospital
Declan O’Sullivan has over 30 years experience as a Pharmacist. He is a member of the HPAI Executive and a delegate to the EAHP General Assembly. He has also been an internal auditor to the EAHP.
clinical benefits of optimal dosing to match the unique physiology and biochemistry of a patient there are also financial and sustainability benefits too. Instead of one (or repeated) doses for every patient, as recommended by the manufacturer/ SmPC, tailored doses can result in less medication being administered for the same benefit and a reduced side-effects burden. This can mean increased patient access to rare and/or expensive medications and financial savings. Brilliant! you say, why aren’t we all using TDM? Well, interestingly, the good professor also shared with us two studies that showed no benefits in primary and secondary outcomes between patients treated sans TDM (apart from adjustments for eGFR) and those who were. Some of the details can be found in the Dolphin Trial conducted in the Netherlands). However, collaboration came to the rescue. Other experts and researchers were able to contribute to the discussion and it seems there are important benefits to be obtained in subsets of the patients involved in the study. Professor Koch indicated that larger studies are required to verify the benefits of TDM and MIPD. TDM, According to the professor TDM may become more easily accessible to clinical pharmacists as there are now biosensors for medicines that could simplify the sampling/
analytical aspect of TDM but further validation of the benefits of expanded TDM services is required. Professor Koch also spoke about the EU’s ambition “to create new knowledge and scientific evidence and to codesign new solutions and support their transfer and scale-up across countries and regions while also fostering capacity building.” (EU text and my italics). Interested parties can also liaise directly with the professors university at COST.bEU.PREPAREDNESS@ ERASMUSMC.NL
The professor at the outset, it should be noted, protested that she was not a compounder but a collaborator but her esteemed co-presenter Professor Pascal Odou was an exquisite compounder. The author waited with bated breath to hear of his daring exploits in the field of compounding and based on the EUs desire for cross-border collaboration I was anticipating a geopharmaceutical gallop across Europe. Professor Odou did not disappoint. He recounted that during the pandemic stocks of cistracurium injections ran critically low. However he knew a “guy”. Actually it was a Belgian pharmaceutical broker who could supply him with the API. The Professor’s hospital pharmacy in Lille (France), had manufacturing facilities that could
produce ampoules. Normally it was authorised to do small batch manufacturing but during the crisis the ministry of health approved the production of much larger batches (tens of thousands instead of some hundreds). Obviously this necessitated the procurement of a large quantities of ampoules. So off to the Spanish border we go (for reasons not disclosed) and the professor gets his supply of ampoules and the manufacture of vital cistracurium amps commences. All the rigorous tests and standards of GMP were complied with and the pharmacy in Lille produced about 60,000 ampoules, if my memory is correct. So many units in fact that there was a surplus. The professors Belgian colleagues (some only 30km away) wondered if they could have some. The professor was willing and ran it by the French authorities who said Non! You can import but you can’t export. Vive la bureaucracy !! Well at least he knew he could import, that has to count for something. Well.. encore Non!
The beleaguered professor has an automated anticancer compounding device that has a very specific palate when it comes to water. As you can imagine my fatigued reader, said water became unavailable. The resourceful professor found out that an alternative supply of water was produced by a French company. Magnifique! you cry, the patients are not inconvenienced. Unfortunately for the professor the water was produced and licensed for the Belgian market only. The same authorities as before, deemed it unsuitable for French patients because it was not marketed in France. The professor is not taking that lying down and we await developments. In defence of the French officials, their counterparts in Belgian also hindered a cross-border initiative that the professor described, on the basis that Belgians don’t cross the border for healthcare!
Professor Odou believes that the EU should authorise pharmacists to exchange goods. (And this would seem to echo the EU THCS initiative). He also believes there is a need for a compendia that would harmonise compounding practises. This presumably would simplify cross-border transfers, if authorised.
Please do not hold Professor Kock or Professor Odou to account on the basis of these meagre scribblings. Other people’s recollections may be more accurate!
Anticoagulants
Anticoagulation therapy in the context of women’s health
Written by Dr Katie Liston Haematology Specialist Registrar in Haematology and Dr Maeve Crowley Consultant Haematologist, Cork University Hospital
Background: Anticoagulants are frequently prescribed medications. In Ireland, direct oral anticoagulants are the anticoagulants of choice in most cases but vitamin K antagonists still have a vital role to play, especially in the management of patients with metallic heart valves and antiphospholipid syndrome. Anticoagulants remain high risk medications (https://ipu.ie/wpcontent/uploads/2022/03/highrisk-medicines.pdf). Women face specific and evolving bleeding and thrombotic challenges throughout their lives (Figure 1.)
anaemia was iron deficiency (www. who.int/news-room/fact-sheets/ detail/anaemia). During this period, women have an increased requirement for iron in the form of menstruation and pregnancy. Iron supplementation outside of dietary sources is not always easy to tolerate so once you become iron deficient, it can be difficult to resolve. This is important in the context of anticoagulation as if you know menstruating women are commonly anaemic at baseline, putting on a treatment that leads to increased and prolonged bleeding is only likely to make things worse.
Anticoagulation therapy in the context of women’s health
Women and Iron deficiency:
Written by Dr Katie Liston Haematology Specialist Registrar in Haematology and Dr Maeve Crowley Consultant Haematologist, Cork University Hospital
The WHO estimate that ~half a billion women worldwide aged 15-49 are anaemic. In 2019 30% of non-pregnant women and 37%of pregnant women in this age group were anaemic and the most common cause of this
Heavy menstrual bleeding (HMB): HMB is common and can be caused by structural issues (e.g. polyps, leiomyomas, malignancy or adenomyosis) or non-structural issues (e.g. anovulatory cycles, medications, coagulopathy); (Samuelson Bannow B et al. Res Pract Thromb Haemost. 2021 Aug). Consequences of HMB include iron deficiency +/- anaemia, impaired quality of life, missing school/work, missed doses of anticoagulation due to fear of HMB and missing out on social activities and sport. A 2015 European survey (Fraser IS et al. Int J Gynaecol Obstet. 2015 Mar) found that ~27% of the women surveyed had experienced 2 or more HMB symptoms in the previous year; 46% of these women had never consulted a physician about it. 7% of the respondents completed an extended survey – 63% of these
Background: Anticoagulants are frequently prescribed medications. In Ireland, direct oral anticoagulants are the anticoagulants of choice in most cases but vitamin K antagonists still have a vital role to play, especially in the management of patients with metallic heart valves and antiphospholipid syndrome. Anticoagulants remain high risk medications (https://ipu.ie/wpcontent/uploads/2022/03/high-risk-medicines.pdf). Women face specific and evolving bleeding and thrombotic challenges throughout their lives (Figure 1.)
women had been diagnosed with iron deficiency or iron deficiency anaemia but only 46% had been prescribed supplementation. To identify menstrual problems, it’s important to know what is normal. A normal cycle length is 21-35 days with each cycle lasting 2-7 days and a median blood loss of 57ml/cycle. HMB is a loss of > 80mls/cycle or excessive menstrual blood loss that interferes with a woman’s physical, social, emotional, or material quality of life. It is important to identify if a woman has an underlying menstral disorder prior to starting them on anticoagulation as we know that anticoagulation is likely to make things worse. About 2/3 of women on anticoagulation experience heavy menstrual bleeding and almost ¾ of women on rivaroxaban (De Crem N et al. Thromb Res. 2015 Oct).
Table 1. Clinical Features of Heavy Menstrual Bleeding
Changing sanitary products more than every 2 hours or requiring double protection
Leaking or soaking through clothing or needing to change sanitary products overnight
Periods lasting >7 days
Passing clots >2.8cm (1.1 inch)
When trying to assess if a women has an underlying menstrual disorder, Table 1 contains some things to ask women about.
Starting a menstruating women on anticoagulation: It is good practice to try to address 4 issues when starting a menstruating women on anticoagulation. (Figure 2.)
This is particularly important if a patient is going to be on indefinite anticoagulation. If a women has underlying menstrual disorders, they may need further investigations such as imaging or a review by a gynaecologist or haematologist. Different anticoagulants have different risk of menorrhagia so agent choice is important. If a women has always had HMB and sinister causes have been out-ruled, it is better to consider measures early to
Figure 1. Bleeding and Thrombotic Challenges Faced by Women. HRT=Hormone Replacement Therapy.
Figure 1. Bleeding and Thrombotic Challenges Faced by Women. HRT=Hormone Replacement Therapy.
Starting a menstruating women on anticoagulation: It is good practice to try to address 4 issues when starting a menstruating women on anticoagulation. (Figure 2.)
to ask about as they also have an antiplatelet effect. It may not be possible to stop these medications but at least you can flag that the patient may be at a higher risk for bleeding and counsel them regarding this.
Figure 2. Issues to address when starting a menstruating women on anticoagulation. HMB = Heavy Menstrual Bleeding.
Figure 2. Issues to address when starting a menstruating women on anticoagulation. HMB = Heavy Menstrual Bleeding.
This is particularly important if a patient is going to be on indefinite anticoagulation. If a women has underlying menstrual disorders, they may need further investigations such as imaging or a review by a gynaecologist or haematologist. Different anticoagulants have different risk of menorrhagia so agent choice is important. If a women has always had HMB and sinister causes have been out-ruled, it is better to consider measures early to ameliorate the issue rather than risk the woman
ameliorate the issue rather than risk the woman experiencing significant bleeding. Ensuring that women are iron replete is vital as you are lowering their bleeding threshold so you want to ensure they have some reserve. In general, a multifaceted approach works best.
(Patel JP et al. Res Pract Thromb Haemost. 2023). The ongoing randomized MEDEA (Hamulyák EN et al. Res Pract Thromb Haemost. 2020 Dec) study will hopefully provide further evidence to guide agent choice in the future.
Hormonal therapy: The combined oral contraceptive pill (COCP) is associated with an increased risk of venous thrombosis. Women are prescribed it for many reasons, including contraception, HMB, acne, endometriosis, polycystic ovarian syndrome, dysmenorrhoea, cycle regulation. It is important to find out what the indication for the COCP was when you are considering if it should continue or be changed to an alternative. Whatever their indication, it is reassuring the note that if a women is on therapeutic anticoagulation, then their risk of recurrent VTE appears similar if they are on oestrogen containing therapies or no hormonal therapy (Martinelli I et al. Blood. 2016 Mar). Therefore, if a woman is remaining on anticoagulation, they can stay on the COCP but if they are stopping anticoagulation, an alternative needs to be found. Different modalities have different levels of efficacy in terms of contraception thrombosis risk and amenorrhoea rates (DeLoughery E et al. Hematology Am Soc Hematol Educ Program. 2022 Dec). Exploring these factors allows clinicians to counsel women about the most appropriate modality for them.
experiencing significant bleeding. Ensuring that women are iron replete is vital as you are lowering their bleeding threshold so you want to ensure they have some reserve. In general, a multifaceted approach works best.
Anticoagulant choice: Rivaroxaban appears to be associated with the highest rates of menorrhagia, when compared with apixaban, dabigatran or warfarin (Samuelson Bannow B et al. Res Pract Thromb Haemost. 2021) – see Table 2. Quality of life is also differently impacted
Concurrent medications: It is important to review a patients regular medications to look for drug-drug interactions as well as those that may increase the bleeding risk. Co-prescription of antiplatelet agents increases the risk of bleeding. The prescription of an anticoagulant may negate the need for an antiplatelet agent. Selective Serotonin Reuptake Inhibitors (SSRIs) are commonly prescribed antidepressant medications. Many of the haemostatic functions of platelets are mediated through serotonin so SSRIs potentially can make the haemostatic function of platelets less effective and increase the bleeding risk (Ann Med. 2022 Dec). Over the counter medications such as non-steroidal anti-inflammatory drugs (NSAIDs) are also important
Tranexamic acid (TXA): TXA is an antifibrinolytic agent which stops the breakdown of clots. A Danish historical prospective cohort study attempted to estimate the risk of thrombosis in women aged 15-49, not on anticoagulation with a standard risk of thrombosis. They looked at data on 2 million women followed for 13.8 million person years. The incidence of venous thrombosis appeared to be increased but the number of women who needed
Anticoagulant choice: Rivaroxaban appears to be associated with the highest rates of menorrhagia, when compared with apixaban, dabigatran or warfarin (Samuelson Bannow B et al. Res Pract Thromb Haemost. 2021) – see Table 2 Quality of life is also differently impacted (Patel JP et al Res Pract Thromb Haemost. 2023). The ongoing randomized MEDEA (Hamulyák EN et al. Res Pract Thromb Haemost. 2020 Dec) study will hopefully provide further evidence to guide agent choice in the future.
Table 2. Relative risk of Heavy Menstrual Bleeding by choice of Anticoagulant.
Anticoagulant
to get a 5 day course of TXA to cause harm was >78,000 (Meaidi A et al. EClinicalMedicine. 2021). There was no increased risk of thrombosis in the high risk patients recruited to the CRASH2 and WOMAN studies which is reassuring. It is frequently used in the prevention and management of bleeding in patients with bleeding disorders. It is not well studied in patients with thrombosis or on anticoagulation. A survey of clinicians’ prescribing habits showed that there is often a reluctance to use it in the acute setting, with 1/3 of those surveyed never prescribing it in the first 3 months and 46% very concerned with the risk of progression or recurrence. (Abdulrehman J et al. Thromb Res. 2024 Jan).
Conclusion: It’s important to be both frank and open when starting a woman on anticoagulation. Heavy Menstrual Bleeding is common, especially in woman on anticoagulation. Women are often reluctant to talk about it without prompting. Discussing where they are at present in terms of menstruation and their past experiences will help you predict how they will be on anticaogulation. If they are anaemic or iron deficient, this is a good time to address it.
Anticoagulation stewardship is an emerging movement focusing on the appropriate use of anticoagulants, which persist in being high risk medications despite the availability of newer agents. Choosing the correct agent, following consideration of patient and disease factors, at the correct dose, for an appropriate duration should ensure maximum efficacy with the minimal amount of harm.
Educational resource: The team in Kings College hospital have developed a short educational video for patients entitled ‘anticoagulants and your periods’ which is freely available on youtube https: //youtu.be/ kAIirzFVFKc?si=IrSfQUGvygKQcZDS When
uterine
*statistically significant , P<0.01. CRNMB= Clinically Relevant Non-Major Bleeding. MB=Major Bleeding. Adapted from ‘Management of heavy menstrual bleeding on anticoagulation’ Samuelson Bannow B. Hematology Am Soc Hematol Educ Program. 2020 Dec
*statistically significant , P<0.01. CRNMB= Clinically Relevant Non-Major Bleeding. MB=Major Bleeding. Adapted from ‘Management of heavy menstrual bleeding on anticoagulation’ Samuelson Bannow B. Hematology Am Soc Hematol Educ Program. 2020 Dec
Concurrent medications: It is important to review a patients regular medications to look for drugdrug interactions as well as those that may increase the bleeding risk. Co-prescription of antiplatelet agents increases the risk of bleeding. The prescription of an anticoagulant may negate the need for an antiplatelet agent. Selective Serotonin Reuptake Inhibitors (SSRIs) are commonly prescribed
Vitamin D
Rickets Types and Treatment with Vitamin D and Analogues
Written by: Giacomo Biasucci1,2,*, Valentina Donini3 andGiuseppe Cannalire1
1Pediatrics and Neonatology Unit, University of Parma, Gugliemo da Saliceto Hospital, 29121 Piacenza, Italy
2Department of Medicine and Surgery, University of Parma, 43121 Parma, Italy
3Unit of Pediatrics, Department of Medicine and Surgery, University of Parma, 43121 Parma, Italy
Rickets is a developmental bone disease characterized by reduced or absent endochondral calcification of growth cartilage, resulting in deformation and reduced mineralization of newly formed bone tissue. Rickets classification is mainly based on mineral deficiency and is conventionally defined as calcipenic or phosphopenic.1 The clinical presentation is heterogeneous and depends on the age of onset and pathogenesis; indications may include arch deformities of the legs, short stature, and joint enlargement. The disorder can be caused by nutritional deficiencies or genetic defects. Although prevalence has decreased in the last two centuries worldwide, rickets remains an important public health concern and a preventable cause of global morbidity and even mortality, especially in developing countries.2 Prevention is only possible for nutritional rickets, i.e., through dietary supplementation with vitamin D and calcium or enrichment with calcium and vitamin D, alone or in combination with exposure to sunlight. In children aged between 0 and 6 months and 6 and 12 months, the required calcium intake is 200 and 260 mg/day, respectively. In children over 1 year of age, an adequate dose of calcium is 500 mg/day. In addition, all infants should receive 400 IU/ day of vitamin D supplementation throughout the first year of life, regardless of their feeding mode. Thereafter, children with a history of symptomatic vitamin D deficiency and those with risk factors that may reduce the synthesis or intake of vitamin D are candidates for supplementation.3 However, in the absence of these predisposing conditions, children not receiving vitamin D supplementation are not obvious candidates for suffering from nutritional rickets. The aim of this paper is to summarize and highlight, while including information for generalist physicians, current knowledge
on the role of vitamin D and its metabolites, as well as that of new monoclonal therapies, in the treatment of different types of rickets.
2. Materials and Methods
A non-systematic review of the literature was performed to search for and select the most up-to-date papers on rickets classification and treatment recommendations worldwide. The terms “rickets” and “classification”, “ergocalciferol”, “cholecalciferol”, “FGF23”, “Burosumab”, “osteoporosis”, “bone health”, and “rickets” and “treatment” were searched for in papers published on PubMed from 2003 to 2023 using the MeSH database. Only reviews, consensus documents, guidelines, recommendations on conventional treatments, and/or RCTs or phase 3 trials focusing on novel therapies were considered; additionally, only papers written in English were selected. A total of 44 papers were chosen and are referred to in this manuscript.
3. Vitamin D
The two main forms of vitamin D are ergocalciferol (vitamin D2), which is synthesized by the irradiation of ergosterol in yeast and fungi and then ingested by humans through diet, and cholecalciferol (vitamin D3) generated from 7-dehydrocholesterol, which is present in the plasma membrane of keratinocytes by means of skin exposure to ultraviolet irradiation. Dietary vitamin D2 begins its absorption cycle in the stomach, where pepsin breaks down the protein fraction, and continues in the duodenum, where other digestive enzymes further contribute to the release of vitamin D from the food matrix. Moreover, bile acids initiate mixed micelles containing fat-soluble substances for emulsification and synthesis; these molecules are then absorbed by enterocytes to be
firstly released into the lymphatic circulation and then into the blood stream. With regard to vitamin D3 absorption, it is firstly delivered from the keratinocyte plasma membrane to the extracellular space and then into the systemic circulation. Like steroid hormones, vitamin D is transported in the blood stream by being bound to vitamin D-binding protein (vDBP), which acts as a regulator of total and free circulating vitamin D metabolite concentrations.
Both dietary and endogenous vitamin D must be activated. The first step is the hepatic conversion of both vitamins D2 and D3 into their 25-hydroxylated form, calcifediol (25(OH)D2 and D3, respectively), which is carried out by liver microsomal cytochrome P450 2R1 (CYP2R1). The second step of vitamin D activation is the renal conversion of 25(OH)D2 and D3 into their biologically active form, calcitriol (1,25(OH)2D2 and D3, respectively), by kidney CYP27B1. The effects of vitamin D are mediated by a nuclear VDR receptor, which, after entering the cell, heterodimerizes with the retinoic acid X-receptor and interacts with specific DNA sequences known as vitamin D response elements (VDREs); then, it may activate or repress DNA transcription, which is crucial for bone metabolism and calcium uptake.4
The key function of vitamin D is to optimize intestinal absorption of calcium and phosphorus for proper formation of the bone mineral matrix.5 Serum 25(OH) D is a negative acute-phase reactant which has implications for acute and chronic inflammatory diseases; it is an unreliable biomarker of vitamin D status after an acute inflammatory insult. Hypovitaminosis D may be the consequence rather than the cause of chronic inflammatory diseases.6
Renal calcitriol synthesis is crucial for mineral homeostasis as well as for bone metabolism; this process
is tightly regulated in humans. Indeed, calcitriol may inhibit CYP27B1, whereas parathyroid hormone (PTH), whose activity is stimulated by hypocalcemia, activates it, resulting in increased calcitriol production. Nevertheless, in a form of negative feedback, calcitriol suppresses PTH release by upregulating calcium-sensitive receptors and increasing serum calcium concentrations. Direct inhibition of PTH release by the calcitriol/VDR complex has also been demonstrated. The other regulatory signaling pathway is due to fibroblast growth factor 23 (FGF23), which is synthesized by osteoblasts and osteocytes; in this pathway, vitamin D metabolism is modulated based on serum phosphate concentrations. In cases of hyperphosphatemia, FGF23 and its cofactor α-khloto stimulate kidney phosphate excretion, inhibiting CYP27B1 and increasing CYP24A1 expression, thus lowering serum calcitriol concentrations. In turn, calcitriol promotes FGF23 expression.4
Vitamin D Deficiency
Vitamin D deficiency affects more than one billion people worldwide. There has probably been an excessive use of vitamin D testing, which has resulted in an apparent increase in “deficient” children, while diagnosis rates of rickets are only slightly increasing. This slight increase could be attributable to several reasons, including population migration, poverty, and reduced sunlight exposure due to lifestyle factors. Although 1,25(OH)2D is the active form, 25(OH)D is the generally accepted indicator of vitamin D status. To date, circulating 1,25(OH)2D concentrations have received relatively little attention (except in patients with chronic kidney disease) due to its short half-life and significantly lower concentration when compared to circulating 25(OH) vitamin D. Furthermore, immunological tests of vitamin D2 (derived
from supplements and food sources) concentrations may suffer from interference biases. Another confounding factor is that most vitamin D supplements contain ergocalciferol and not cholecalciferol. From analytical point of view, this may affect laboratory results, as immunoassays tend to detect cholecalciferol better than ergocalciferol, thus possibly over-estimating hypovitaminosis D conditions.
When assessed, deficiency rickets, either due to nutritional deficit or to insufficient sunlight exposure, may be associated with many chronic and acute diseases, including childhood dental caries, pre-eclampsia, cancer, type 2 diabetes, autoimmune diseases, cardiovascular diseases, and neurological disorders.7 As such, this form of rickets representing a major public health concern.
be used, with the serum vitamin D dosage being checked 6–8 days after starting supplementation. For children under 10 years of age, calcifediol supplementation is not recommended. In people aged from 4 to 65 years of age, vitamin D supplementation is only recommended in those who do not have sufficient exposure to sunlight. However, from the age of 65, there is a reduction in the effectiveness of vitamin D skin synthesis, so year-round supplementation is recommended in all individuals.8,9,10
factors. Although 1,25(OH)2D is the active form, 25(OH)D is the generally accepted indicator of vitamin D status. To date, circulating 1,25(OH)2D concentrations have received relatively little attention (except in patients with chronic kidney disease) due to its short half-life and significantly lower concentration when compared to circulating 25(OH) vitamin D.
Furthermore, immunological tests of vitamin D2 (derived from supplements and food sources) concentrations may suffer from interference biases. Another confounding factor is that most vitamin D supplements contain ergocalciferol and not cholecalciferol. From analytical point of view, this may affect laboratory results, as immunoassays tend to detect cholecalciferol better than ergocalciferol, thus possibly over-estimating hypovitaminosis D conditions.
Vitamin D status is usually defined as follows: deficiency, with a serum value lower than 20 ng/mL (<50 nmol/L); suboptimal concentration, with a serum value between 20–30 ng/mL (50–75 nmol/L); and optimal concentration, with a serum value between 30–50 ng/mL (75–125 nmol/L).
Vitamin D deficiency in the general population can be prevented by cholecalciferol supplementation, which should be customized according to age, body weight, sun exposure, eating habits, and lifestyle (Table 1).8
Based on renal phosphate loss rate, these forms may be further subdivided into three main groups: (1) hypophosphatemic rickets, attributed to hyperparathyroidism and vitamin D deficiency and which includes acquired or congenital pathological conditions of hypovitaminosis D; (2) FGF23mediated hypophosphatemic rickets, which includes congenital syndromes and acquired forms; and (3) hypophosphatemic rickets, attributed to non-FGF23-mediated intrinsic kidney defects. In the latter group, acquired or genetic forms are differentiated, but both may resemble renal Fanconi syndrome.14
Finally, those rickets forms associated with organ disease generally result from a congenital or acquired failure of the organs involved in the regulation of the vitamin D metabolism, i.e., intestine, liver, and kidney.
Clinical Manifestation and Radiologic Features
When assessed, deficiency rickets, either due to nutritional deficit or to insufficient sunlight exposure, may be associated with many chronic and acute diseases, including childhood dental caries, pre-eclampsia, cancer, type 2 diabetes, autoimmune diseases, cardiovascular diseases, and neurological disorders [7]. As such, this form of rickets representing a major public health concern.
Vitamin D status is usually defined as follows: deficiency, with a serum value lower than 20 ng/mL (<50 nmol/L); suboptimal concentration, with a serum value between 20–30 ng/mL (50–75 nmol/L); and optimal concentration, with a serum value between 30–50 ng/mL (75–125 nmol/L).
1,α-hydroxylase synthesis, whereas vitamin D-dependent rickets type 1B is caused by hepatic 25-hydroxylase deficiency. Vitamin D-dependent rickets type 2 is characterized by a peripheral resistance to 1,25(OH)2D; these forms might be caused by abnormalities in the vitamin D receptor (VDR) (type 2A) or impaired vitamin D receptor function (type 2B). Both are characterized by extremely high circulating 1,25(OH)2D concentrations (3–30-fold higher than the norm).10 Type 2 may be associated with the presence of alopecia in about 50% of patients. These patients commonly display more severe typical clinical features compared to those who do not have alopecia.12 Recently, a new form of vitamin D-dependent rickets (type 3), characterized by increased vitamin D degradation, has been discovered. Unlike the recessively inherited type 1 and type 2, this form is transmitted as an autosomal dominant character and may be identified by an activating mutation in the gene coding for P450-dependent enzyme CYP3A4. This enzyme is involved in the hepatic inactivation of some compounds, including the two most important vitamin D metabolites, 25OHD and 1,25(OH)2D, which are converted into more polar and inactive products13 (Table 2).
Vitamin D deficiency in the general population can be prevented by cholecalciferol supplementation, which should be customized according to age, body weight, sun exposure, eating habits, and lifestyle (Table 1) [8].
Table 1. Rickets prevention by vitamin D supplementation
Table 1. Rickets prevention by vitamin D supplementation.
Age Dose IU
0–3 months 400/die
1–3 years 600/die
4–10 years * 600–1000/die
11–18 years * 1000–2000/die
19–65 years * 1000–2000/die
65–75 years 1000–2000/die
>75 years 2000–4000/die
Available epidemiological data in Italy show a high prevalence of hypovitaminosis D during the entire pediatric age, but mostly in adolescence. It has emerged that the vitamin D status of newborns is influenced by maternal ethnicity and prophylaxis during pregnancy, while the season in which vitamin D testing is carried out, ethnicity, BMI, and sunlight exposure are major determinants in infants and children. The Italian national consensus document, issued by the main Italian pediatric scientific societies, highlights the extraskeletal functions of vitamin D, underlining its beneficial role not only for bone health but also in the prevention of non-skeletal diseases. The recommendations reinforce the need to ensure adequate circulating vitamin D concentrations throughout the pediatric age. Hence, vitamin D supplementation is recommended for all newborns in the first year of life, regardless of the type of diet and, subsequently, based on the presence of risk factors.11
Types of Rickets
Rickets classification is usually defined as calcipenic or phosphopenic, based on the main mineral deficiency.1
Calcipenic rickets is mainly due to a lack of calcium, combined with low vitamin D availability or function. Therefore, calcipenic rickets may be due to reduced calcium intake or, more frequently, hypovitaminosis D secondary to insufficient sun exposure, low intake, or malabsorption.
From an etiopathogenetic perspective, hypophosphatemic rickets can be subdivided into forms based on reduced phosphate intake or excessive renal phosphate loss, which are associated with hypophosphaturia and hyperphosphaturia, respectively. Nutritional phosphate deficiency rickets results from inadequate intestinal phosphate intake or absorption and is often found in breastfed, extremely preterm babies that are not receiving adequate phosphate supplementation.
Table 2. Causes of calcipenic rickets
Table 2. Causes of calcipenic rickets.
The classic signs of rickets are related to non-mineralized osteoid tissue buildup in growth cartilages, which is manifested by the appearance of the so called “rachitic cuff” at limb extremities, the typical thorax “rachitic rosary”, which occurs due to the widening of the chondro-costal junctions, and Harrison’s furrow, caused by an indentation of the lower part of the thorax at the point of insertion of the diaphragm muscle. In the lower limbs, as infants start to walk, the femur, tibia, and fibula may bow in varus, but valgus knees or “blow-out” deformities are also possible. Other clinical features include craniotabes, occipital platybasia, craniosynostosis, prominence of the frontal bosses with caput quadratum, and delayed fontanel closure. Scoliosis, and/or dorsolumbar kyphosis may occur and develop in the spine; in severe cases, deformities of the spine,
Calcipenic Rickets Causes
* In persons who sunbathe with bare forearms and legs for 30–45 min between 10 a.m. and 3 p.m. without sunscreen from May until June, supplementation is not necessary, even though it is recommended and safe. In people who do not fulfill these criteria, supplementation is recommended throughout the year [8].
* In persons who sunbathe with bare forearms and legs for 30–45 min between 10 a.m. and 3 p.m. without sunscreen from May until June, supplementation is not necessary, even though it is recommended and safe. In people who do not fulfill these criteria, supplementation is recommended throughout the year.8
Nutritional rickets is the most widespread form of rickets in the world, with an increasing incidence even in Western countries. Vitamin D deficiency is a pandemic in Europe, especially in winter, with a much higher incidence in darkskinned subjects.8,9
Nutritional rickets
Congenital defects of action of Vitamin D
Calcium deficiency
Vitamin D deficiency
Vitamin D dependent rickets type 1A
Vitamin D dependent rickets type 1B
Vitamin D dependent rickets type 2A
Vitamin D dependent rickets type 2B
Vitamin D dependent rickets type 3
Cholecalciferol is the preferred form of vitamin D supplementation at any age. From 11 years of age, if a good rise in serum vitamin D concentrations is not achieved with cholecalciferol, calcifediol may
Cholecalciferol is the preferred form of vitamin D supplementation at any age. From 11 years of age, if a good rise in serum vitamin D concentrations is not achieved with cholecalciferol, calcifediol may be used, with the serum vitamin D dosage being checked 6–8 days after starting supplementation. For children under 10 years of age, calcifediol supplementation is not recommended. In people aged from 4 to 65 years of age, vitamin D supplementation is only recommended in those who do not have sufficient exposure to sunlight. However, from the age of 65, there is a reduction in the effectiveness of vitamin D skin synthesis, so year-round supplementation is recommended in all individuals [8,9,10].
Vitamin D-dependent genetic rickets is due to a mutation in genes coding for the enzymes involved in vitamin D activation steps and is mainly characterized by hypocalcemia and secondary hyperparathyroidism. Vitamin D-dependent rickets type 1A is due to deficiency in renal
Acquired vitamin D deficiency
Available epidemiological data in Italy show a high prevalence of hypovitaminosis D during the entire pediatric age, but mostly in adolescence. It has emerged that the vitamin D status of newborns is influenced by maternal ethnicity and prophylaxis during pregnancy, while the season in
Hepatic insufficiency
Renal insufficiency
Malabsorption
Drugs
Hyperparathyroidism
From an etiopathogenetic perspective, hypophosphatemic rickets can be subdivided based on reduced phosphate intake or excessive renal phosphate loss, which are hypophosphaturia and hyperphosphaturia, respectively. Nutritional phosphate deficiency
Vitamin D
pelvis, and lower limbs may lead to short stature.15
In nutritional rickets, delayed tooth eruption (e.g., absence of incisors beyond 10 months and/or absence of molars beyond 18 months of age) or enamel hypoplasia may be evident, resulting in increased susceptibility to caries, even in the permanent teeth.
Extra skeletal manifestations include muscle hypotonia, bone pain,14 increased frequency of respiratory infections, hypochromic anemia, hypocalcemia, which may be asymptomatic, latent (positivity of Chvostek and Trousseau signs), or symptomatic, with acute onset and seizures,16 and dilated cardiomyopathy, that may lead to heart failure or even death.17
Moreover, in above 51% of patients with X-linked hypophosphatemic (XLH) rickets, dental and periodontal lesions, especially abscesses with gingival fistulas, have been reported, even in the absence of traumas and/or caries. Such lesions are most common in the canine and incisor teeth.18,19 In adulthood, patients with XLH may develop osteomalacia, enthesopathy, degenerative joint processes, and dental or periodontal changes with recurrent periapical abscesses that may lead to premature edentulousness.20
Besides the above-mentioned clinical features, radiological signs of rickets are detectable at the level of rapidly growing bones, such as the radius, ulna, distal femur, and proximal and distal tibia. Metaphyseal enlargement, delayed appearance of the ossification centers, osteopenia, cortical thinning of the long bones, osteomalacia, and greenwood fractures are the most commonly found radiological features.12
The Rickets Severity Score (RSS)21 is a useful scoring method to assess rickets severity by means of bilateral wrist and knee radiographs, based on the degree of fraying and concavity of the metaphysis, and on the proportion of growth cartilage affected.
Diagnostic Approach to Suspected Rickets
If rickets is suspected, the evaluation of specific biochemical parameters, such as serum calcium, phosphate, alkaline phosphatase (ALP), PTH, and vitamin D metabolites, is mandatory for a diagnosis.12
In all types of rickets, a peculiar biochemical feature, albeit not a pathognomonic, is the presence of increased serum ALP, which is more relevant in calcipenic than in phosphopenic rickets.22 ALP assessment also helps identify diseases that may mimic rickets,
such as hypophosphatasia, which is characterized by low serum ALP concentrations. Decreased ALP activity leads to the accumulation of pyridoxal 5′-phosphate (PLP), inorganic pyrophosphate (PPi), and phosphoethanolamine. Impairment in PLP dephosphorylation induces seizures, while PPi accumulation inhibits bone mineralization. Consequent clinical manifestations may include rickets-like bone changes, bone demineralization, fragility fractures, reduced muscular strength, chest deformity, pulmonary hypoplasia, nephrolithiasis, nephrocalcinosis, and chondrocalcinosis. Treatment relies on enzyme replacement therapy. The use of ALP to determine disease activity has been proven to be useful in monitoringtherapeutic treatment.23
Serum calcium concentrations may be reduced in cases of severe vitamin D deficiency and in genetically determined vitamin D defective hydroxylation.
Phosphate concentrations are reduced in hypophosphatemic rickets, as well as in more severe forms of nutritional vitamin D deficiency rickets, where they reflect secondary hyperparathyroidism.
PTH concentrations are increased in forms with hypocalcemia, being normal or just slightly increased in hypophosphatemic rickets; rare exceptions include the X-linked recessive form and the one with hypercalciuria.12,24
The concentration of 25(OH) vitamin D reflects the body’s vitamin D reserves and is usually decreased in case of deficiency. Recently, there was global consensus on setting 30 ng/mL as the cutoff serum concentration for vitamin D deficiency in nutritional rickets.3 The risk of rickets increases with decreasing serum vitamin D concentrations and is particularly high below 10 ng/mL, even in the presence of adequate Ca intake. Most children with vitamin D deficiency rickets have serum 25(OH)D concentrations below 10 ng/mL, and usually even below 5 ng/mL.25
Treatment
Rickets therapy is based on vitamin D and calcium supplementation, plus phosphate when necessary. In conditions of malabsorption/ malnutrition, combined vitamin D and calcium treatment is mandatory, whereas dietary calcium intake may be sufficient in cases of rickets secondary to metabolic disorders, even though vitamin D supplementation remains fundamental. Treatment with vitamin D in rickets due to calcium deficiency has also been hypothesized. Although the first studies on this topic were
based on drugs containing both vitamin D and calcium, due to a lack of evidence, it is conceivable that supplementing vitamin D with calcium may not always be necessary and may also increase the risk of side effects such as nephrocalcinosis and kidney stones.25
8.1. Nutritional Rickets due to Vitamin D Deficiency
Early treatment of this form of rickets is based on the combined administration of vitamin D and calcium salts.26 Calcium salts dose (30–75 mg/kg, 2–3 times per day) varies according to body weight. In case of symptomatic hypocalcemia, intravenous administration of 5–20 mg/kg of calcium salts (calcium gluconate 10%) every 4–6 h, with careful electrocardiographic (ECG) monitoring, is indicated. The dose of vitamin D to be supplemented is tailored according to the patient’s age.27
It has been claimed that this approach improves therapeutical compliance in patients who are reluctant to adhere to the daily dose intake, besides being easier to apply. As for potential concerns about the safety of large single doses, hypercalcemia and/or hypercalciuria has been seldom reported as a side effect; in a Turkish study on nutritional rickets, only 8 out of 56 children aged 3–36 months, two of whom were receiving 300,000 IU and six 600,000 IU, developed hypercalcemia.28 Another study carried out in India, comparing single oral doses of 300,000 vs. 600,000 IU of vitamin D3 in 76 children aged 6 months to 5 years with nutritional rickets, reported the occurrence of hypercalcemia in only five children (two in the 300,000 IU and three in the 600,000 IU group).29
With regard to the mode of administration, the oral route should be preferred; indeed, a study carried out on an adult population showed that orally delivered vitamin D led to higher serum 25(OH)vitamin D concentrations after 3 and 6 months compared to intramuscular administration.30 Though vitamin D2 and D3 have been considered equally active for many years, current knowledge indicates that vitamin D2 efficacy is less than a third of that of vitamin D3.31 Studies have also demonstrated that daily vitamin D2 and vitamin D3 intakes are equally effective, whereas vitamin D3 should be recommended in case of a single dose treatment due to its longer half-life. The chemical structures of ergocalciferol and cholecalciferol are similar but not identical; vitamin D3 has a double bond and an additional methyl group on the side chain, and it is supposed that
its different structure may identify cholecalciferol as the preferred substrate in different steps of the vitamin D metabolism pathway. There are data suggesting that differences in the side chains of the two forms of vitamin D directly influence the hepatic vitamin D hydroxylation rate, with vitamin D3 thought to be the preferred substrate for hepatic 25-hydroxylase.30 Vitamin D3 and its metabolites also have a higher affinity to vitamin D binding protein compared to vitamin D2. In addition to these metabolic differences between the two forms of vitamin D, vitamin D3 degradation requires an additional step compared to vitamin D2, suggesting a higher degradation rate for vitamin D2 than for vitamin D3.24,31
Vitamin D treatment is recommended for at least 12 weeks, though some children may require longer treatment duration. At the end of the treatment period, maintenance therapy with different doses (400–1000 IU/day) according to age is recommended.32
Conclusions
Vitamin D is crucial for bone development and homeostasis throughout life. Its supplementation, even in the prenatal period, is crucial for the prevention of nutritional rickets; it also plays a key role in the treatment of vitamin D-dependent genetic rickets. Several vitamin D formulations are commercially available for the treatment of the different forms of rickets.
The choice of the form of vitamin D, as well as of an active metabolite, should be made according to the underlying defect in vitamin D metabolism that inhibits its adequate absorption, synthesis, or transport. In cases of vitamin D-dependent genetic rickets, supplementation with metabolites downstream of the genetic defect is strongly recommended to ensure that an adequate phospho–calcium balance is achieved.
In XLH rickets, therapy with the monoclonal antibody Burosumab has shown excellent results in terms of improved growth, increased serum phosphate and vitamin D concentrations, and decreased circulating ALP values, which are reliable markers of disease status. Despite its evident efficacy, Burosumab use is currently hampered by its high cost; moreover, there are no studies to date on its longterm effects or on its effects on disabling conditions in adulthood (e.g., enthesopathies, osteoarthritis, spinal stenosis).
References available on request
Medical Workforce Intelligence Report 2022 Data and insights on women in medicine in Ireland
On International Women’s Dayrecently, the Medical Council published its 2022 Workforce Intelligence report. The report analyses and presents data provided by doctors on the Medical Council’s medical register (the ‘Register’). Its data reveals the growing number of female doctors registering with the Medical Council for the first time. It also provides insights from doctors as to why they chose to withdraw from the Register in 2022.
This includes doctors who have registered for the first time or retained registration with the Medical Council, and those who have voluntarily withdrawn from the Register throughout 2022.
The number of doctors on the Register has been increasing year on year, with the number of young female doctors having risen steadily over the past decade.
This year’s International Women’s Day theme is #InspireInclusion, and encourages everyone to recognise the unique perspectives and contributions of women from all walks of life. It calls on those involved to break down barriers, challenge stereotypes, and create environments where all women are valued and respected.
2022 Key Highlights
• First Time Registered Doctors:
o 3,008 doctors registered with the Medical Council for the first time in 2022, compared with 2,605 in the previous year, representing a 15% increase, between 2021 and 2022.
o Over half (52.6%) of doctors registering for the first time in 2022 were male, and 47.4% were female.
o Notably, the ratio of females to males is greater in the
Dr Suzanne Crowe, President, Irish Medical Council
youngest cohort of doctors, aged 24 and younger (45% male vs 55% female).
o Furthermore, 71.2% of doctors registering for the first time obtained their qualifications abroad.
• Doctors Retaining Registration:
o 18,839 (81.5%) doctors who renewed their registration with the Medical Council were clinically active in Ireland, all or some of the time in 2022.
o In 2022, 46.8% of clinically active doctors in Ireland were female, while 53.2% were male. The distribution of males and females was split more evenly in younger cohorts, whereas the majority of older doctors are male. Over half (51.7%) of clinically active doctors working in Ireland were on the Specialist Division of the Register, 16.3% of doctors were on the Trainee Specialist Division; and 31.2% were on the General Division of the Register.
o In 2022, over a quarter of clinically active doctors working in Ireland selfreported working more than 48 hours a week on average.
In 2022, 1,341 doctors, of whom 593 were female, voluntarily withdrew their registration with the Medical Council. Among doctors who completed the voluntary withdrawal survey, 45.9% offered detailed explanations on the reasons for withdrawing their registration. A number of workrelated issues were cited, including
DICE 2024 is the premier Irish conference dedicated to diabetes care and research, tailored for healthcare professionals working with people living with diabetes.
limited career progression and training opportunities, poor working conditions, personal or family reasons, plans to practise abroad, and other reasons such as registration requirements and the emergency response to COVID-19 coming to an end.
President of the Medical Council, Dr Suzanne Crowe said, “As the world collectively celebrates International Women's Day, I’m glad to see a rising number of women in medicine in Ireland, particularly those aged 24 and under. In 1994, women made up just 30% of the medical Register. Now, 30 years later, we are nearly at a 50/50 split male to female, with the numbers of female doctors in the younger age cohorts outpacing male doctors.
“Over the years, there has been a significant increase in the representation of women within the medical profession, reflecting a positive shift towards greater gender diversity and inclusivity in healthcare.
This year's event promises practical and research-focused sessions across specific streams (adult, paediatric, pregnancy) featuring renowned Irish and international speakers.
Location: Croke Park Conference Centre, Drumcondra, Dublin 3 D03 P6K7, Dublin
Date and time: Wed, May 22, 2024 8:30 AM - 3:50 PM BT
“One of the key elements of Inspire Inclusion is promoting diversity in leadership and decision-making positions. Women, especially those belonging to underrepresented groups, continue to face barriers when seeking leadership roles.
“Today, I’m also reflecting on the contributions of the women who tirelessly advocate for patients and vulnerable people in Ireland. Today, we celebrate their dedication, compassion, and commitment to making a positive difference in the lives of others. Women can bring a unique understanding of women’s health issues, paving the way for change in medicine, and helping other patients to feel safe and heard.”
Ms Jantze Cotter, Executive Director, Regulatory Policy and Standards, Medical Council, added, “We must do all in our power to retain our highly skilled medical workforce. A key aspect of this is organisations working together, using data, knowledge, and resources to focus efforts and produce tangible actions.”
Clinical R&D
BLACKROCK HEALTH APPOINTS NEW DIRECTOR OF NURSING
Blackrock Health, combining Hermitage, Blackrock, Galway and Limerick Clinics, has announced the appointment of Evonne Healy as Director of Nursing, effective immediately. Ms Healy will be based in Blackrock Clinic.
Ms Healy has held a number of senior nursing positions in Ireland during her career, most recently as Directorate Nurse Manager in Tallaght University Hospital. Prior to this, she held the role of Interim Director of Nursing there, having moved from her role as Director of Nursing of The Royal Hospital in Donnybrook in 2020.
Commenting on the appointment, James O'Donoghue, CEO of Blackrock Clinic said: “On behalf of the team at Blackrock Health, I am delighted to welcome Evonne Healy into her new role as Director of Nursing. She has a proven track record in leadership developed throughout her extensive career in public and private hospitals. With a keen interest in patient and staff engagement, Evonne is a great addition to our senior leadership and will support our nursing teams to continue to deliver best in class care for our patients.”
Ms Healy holds a Post Graduate Diploma in Specialist Nursing (Renal) from Trinity College Dublin, a Post Graduate Certificate in Human Factors in Patient Safety, and a Master of Science Degree in Healthcare Management from the Royal College of Surgeons in Ireland. She completed her nursing training in Meath Hospital, Dublin.
To find out more about the full range of services available at Blackrock Health, visit https:// www.blackrockhealth.com/.
JOHNSON & JOHNSON RECEIVES POSITIVE CHMP OPINION FOR RYBREVANT® (AMIVANTAMAB) IN COMBINATION WITH CHEMOTHERAPY FOR THE FIRST-LINE TREATMENT OF PATIENTS WITH ADVANCED NON-SMALL CELL LUNG CANCER WITH ACTIVATING EGFR EXON 20 INSERTION MUTATIONS
This positive CHMP opinion establishes amivantamab as a new option, and the first fully-human EGFR-MET bispecific antibody, in the first-line treatment of EGFR exon 20 insertion-mutated NSCLC.
The recommendation is supported by data from the Phase 3 PAPILLON study, which showed amivantamab plus chemotherapy significantly improved progressionfree survival in adult patients, versus chemotherapy alone.1
BEERSE, BELGIUM , April 26, 2024 (GLOBE NEWSWIRE) -- JanssenCilag International NV, a Johnson & Johnson company, today announced that the Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency (EMA) has recommended the approval of RYBREVANT® (amivantamab) in combination with chemotherapy (carboplatin and pemetrexed) for the first-line treatment of adult patients with advanced non-small cell lung cancer (NSCLC) with activating epidermal growth factor receptor (EGFR) exon 20 insertion mutations.
"The PAPILLON study results represent an important advancement in the EGFR exon 20 insertion NSCLC treatment landscape, demonstrating significantly improved progressionfree survival with first-line amivantamab plus chemotherapy, versus chemotherapy alone,” said trial investigator Professor Nicolas Girard, Head of Medical Oncology, Institut Curie, and Professor of Thoracic Oncology and Respiratory Medicine at the Paris Saclay University, France.* “Notably, we observed improvements in functional status and reduction in lung cancerrelated symptoms, underscoring the potential of this regimen to redefine standards of care for these patients, offering hope for improved quality of life and patient-relevant treatment outcomes."
An urgent need exists for innovative treatments in NSCLC, particularly for patients with EGFR exon 20 insertion driver mutations, due to the significant disease burden.2 EGFR exon 20 insertion mutations are the third most common activating EGFR mutation and are associated with real-world five-year overall survival rates
as low as 8%.2 This reinforces the critical demand for targeted therapeutic approaches, tailored to address the unique complexities of EGFR exon 20 insertion mutations, aiming to substantially improve patient survival and quality of life outcomes.
“Lung cancer remains the leading cause of cancer-related mortality in Europe. As patients living with EGFR exon 20 insertion-mutated NSCLC face a particularly poor prognosis, the need for innovative combinations in the frontline setting is vital,” said Henar Hevia, Senior Director, EMEA Therapeutic Area Lead, Oncology, Johnson & Johnson Innovative Medicine.
“At Johnson & Johnson, we are dedicated to the development and delivery of novel, targeted therapies aimed to address specific disease pathways, with the ultimate goal of ensuring each patient receives the right treatment at the right time."
The PAPILLON study met its primary endpoint, demonstrating a statistically significant and clinically meaningful improvement in progression-free survival (PFS; as measured by blinded independent central review [BICR]) in patients receiving amivantamab in combination with chemotherapy, versus chemotherapy alone (hazard ratio [HR]=0.395; 95 percent confidence interval [CI], 0.30–0.53; P<0.0001).1,3 An interim overall survival (OS) analysis showed a favourable trend for patients treated with amivantamab plus chemotherapy, compared to those treated with chemotherapy alone (HR=0.675; 95 percent CI, 0.42–1.09; P=0.106).1,3 The combination of amivantamab and chemotherapy demonstrated a safety profile consistent with the safety profiles of the individual agents, with low rates of treatment-related discontinuations (7 percent).1,3 The rates of overall adverse events (AEs) and AEs leading to death were comparable between both treatment arms.3
The rate of Grade ≥3 AEs was higher with amivantamab and chemotherapy, compared to chemotherapy alone (75 percent vs. 54 percent).3 Serious AEs (SAEs) occurred in 37 percent of patients with amivantamab and chemotherapy, compared to 31 percent with chemotherapy alone.3 EGFR and MET-related AEs were increased with amivantamabchemotherapy (primarily grade 1-2).3 Chemotherapy-associated haematologic and gastro-intestinal toxicities were comparable, except for neutropenia, which was transient.3 Pneumonitis was reported in three percent of patients in the amivantamabchemotherapy arm.3
“Today’s positive opinion represents the culmination of years of work and our team’s commitment to the lung cancer community. We will continue to focus on redefining treatment paradigms, starting from the very first line of therapy, with a goal of improving survival rates and overall patient outcomes.” said Kiran Patel, M.D., Vice President, Clinical Development, Solid Tumours, Johnson & Johnson Research & Development, LLC. “Through our extensive research and development efforts, we are pioneering novel approaches and targeting key pathways implicated in lung cancer progression, with the ultimate goal of transforming clinical outcomes for patients with EGFR-mutated NSCLC.”
MEDICAL
MICROWAVE TREATMENT TRANSFORMATIVE FOR IRISH CLINICS
A leading podiatrist and business owner who has completed nearly 1000 treatments using a revolutionary new medical device has hailed its potential as the future of treating painful skin lesions
Having adopted Emblation’s Swift® device, Dublin-based podiatrist Joseph Egan revealed that it has become the most effective form of treatment in his three clinics across Ireland.
Designed by global medical microwave leader Emblation, Swift is an innovative form of treatment that uses targeted bursts of microwaves to treat warts and verrucae.
Joseph, who is the owner and director of MyFeet, explained that he was convinced to implement the device into his clinic after seeing promising research on its resultsand has since reaped the benefits of its highly effective treatment.
Joseph said: “We are seeing hugely positive results for patients across our clinics. I’ve been really impressed with how effective treatment with the device has been.
“When you compare this against more traditional forms of treatment such as cryotherapy or treating with salicylic acid, the difference is night and day.
“For us, it’s been a positive step change, leading to a much easier process. Using Swift means we don’t have to provide protective padding or dressings and they don’t need regularly changed.
“Additionally, patients aren’t having to go through persistent pain every week that they otherwise would if they went down other routes like cryotherapy, acid or invasive surgery.”
Evonne Healy, Director of Nursing, Blackrock Health
Unlike other traditional treatments, Swift utilises revolutionary microwave technology, targeting the tissue with a highly controlled dose of energy, with research showing that the treatment has an efficacy rate of up to 86.4% on verrucae.
Over 345,000 treatments have been performed across the world and the innovative microwave technology is undergoing trials as a treatment for conditions such as fungal nail, facial acne and melanoma.
Speaking about the future of treatments, Joseph added: “In my opinion Swift is currently the most effective form of treatment clinicians can provide for their patients when it comes to warts and verrucae.
“The research is what convinced us to start using it and it’s been an excellent decision from both a patient care and business standpoint and we’ve not looked back since.
“From a business perspective, we recouped what we paid for the device in three to four months, which is a massive bonus.
From the get-go, we’ve wanted to improve our treatments for customers and Swift® has managed to do that –almost instantly.”
Emblation founders Gary Beale and Eamon McErlean, who first crossed paths during their postgraduate studies at HeriotWatt University in Edinburgh, jointly established the company.
Speaking on Joseph’s feedback, Chief Commercial Officer, Jonathan Williams said: “It’s obviously incredibly encouraging and motivating to hear such positive feedback about Swift.
“The treatment has proved to be a real game changer when it comes to patients’ quality of life, and we’re still very early into our journey in Ireland. We’re happy
Swift® has had such an impact for Joseph and most importantly his patients and we can’t wait to continue to grow Swift’s presence across the country.”
In 2021, the firm experienced a significant injection of capital when Apposite Capital, a London-based specialist in healthcare, invested an eight-figure sum.
This financial boost propelled the firm's rapid global expansion, resulting in the acquisition of a distribution company to form Emblation Inc.
This financial injection also paved the way for the establishment of new Emblation subsidiaries in Canada and Germany, in addition to their expansion into more than 20 other countries.
This financial boost tripled the company's workforce necessitating larger office space. Emblation has now moved into their state-of-the-art headquarters £4m headquarters in Stirling.
SLIGO UNIVERSITY HOSPITAL AWARDED ITS SECOND AN TAISCE GREEN FLAG
Sligo University Hospital (SUH) has been awarded its second ‘Green Flag’ after a successful recertification audit by An Taisce.
The internationally recognised ‘Green Flag’ was awarded following a rigorous assessment process and recognises the commitment of hospital management and staff, HSE Estates, the NUI Galway Medical Academy and the hospital’s Green Campus Committee in developing the hospital as a healthcare facility that delivers high quality care, improved public health and wellbeing in an environmentally responsible and sustainable way.
The hospital has participated in the An Taisce Green Campus Programme since 2016 and was awarded its first Green flag in
2020 following the successful implementation of a number of sustainable initiatives.
Martin Casserly, Environmental and Waste Co-ordinator at SUH said: “This second green flag has been awarded in recognition of SUH’s commitment to a sustainable health care system and greener campus.
“Sligo University Hospital has implemented a number of successful initiatives to date relating to Energy, Waste, Water and Biodiversity. Such initiatives have included the phase out of single use cups from the canteen, a tap replacement programme to reduce water wastage, the installation of an onsite food composting unit to compost hospital generated food waste and the creation of the SUH Garden project to preserve and enhance Biodiversity on campus.”
Deirdre O’Carroll, An Taisce Green Campus Programme Manager said: “I would like to congratulate Sligo University Hospital Green Campus Committee on achievements to date culminating in the award of a first green flag in 2020. Sligo University Hospital is to be greatly commended for its leadership in being one of the first hospitals to achieve and maintain a green flag.
“Your work in this area sets an example for other sites to follow. The involvement of local community groups shows the potential of community partnership projects to be highly impactful and significant in the sustainable development and wellbeing of the hospital campus and wider community.”
Grainne McCann, Hospital Manager at SUH said: “The green campus programme very much compliments the HSE’s Climate Action Strategy and Decarbonisation Roadmap. We have a good Green Campus Committee in place here in Sligo University Hospital made up of both management and nonmanagement personnel as well as personnel from HSE Estates.
“Many of these initiatives would not be as successful if it wasn’t for the buy in and support from our staff, patients and visitors, this support is very much appreciated. We are delighted to be awarded our second Green Flag in recognition of the efforts of all involved and to keep us motivated on our sustainability journey.”
Martin Casserly, Environmental and Waste Co-ordinator; Ann Marie McGovern, Catering Manager; and Georgina Kilcoyne, Assistant General Manager, Sligo University Hospital
Clinical R&D
COMMEMORATING A QUARTER CENTURY OF PIONEERING
SCIENCE: ASTRAZENECA'S 25YEAR MILESTONE
Dublin, Ireland (8th April 2024). Today heralds a significant milestone for AstraZeneca as it celebrates the 25th anniversary of the merger of Swedish Astra AB and UK-based Zeneca Group PLC in 1999. The merger catalysed the company’s growth into a global leader in pharmaceuticals and biotechnology.
AstraZeneca in Ireland celebrated this landmark occasion at its Blanchardstown headquarters with a panel discussion focusing on the company’s future growth and developments. Speakers included Alex Wilkes, Country President, AstraZeneca Ireland Marketing Company; Ruth March, Senior Vice President, Precision Medicine; Shane Doyle, Senior Vice President, Head of Operations & Sustainability for Alexion, AstraZeneca Rare Disease Unit and Jon-Paul Sherlock, API Commercialisation Site Lead.
Their forward-looking perspectives offered a glimpse into the exciting prospects that lie ahead for AstraZeneca and its ongoing commitment to its operations in Ireland.
Speaking at the event, Alex Wilkes said, “As we reflect on the past 25 years since the AstraZeneca merger, we celebrate innovation and excellence in science that resonates across the globe. I am immensely proud of the role our Irish operations play in our global success. The commitment, expertise, and innovative spirit of our team in
Ireland are instrumental in driving our mission forward. Here's to celebrating our achievements, and the brighter horizons that lie ahead as we continue to forge the path of medical breakthroughs and transforming patient care for people society and planet."
In the last quarter of the century, AstraZeneca has effectively harnessed science to develop ground-breaking treatments in areas including oncology, immunology, renal and metabolic diseases, and respiratory and cardiac health. In Ireland AstraZeneca and Alexion, AstraZeneca Rare Disease, employs over 1,200 people across two sites in Dublin and Athlone. AstraZeneca in Ireland provides medicines that treat more than 200,000 patients.
Globally AstraZeneca now employs over 83,000 people in 16 countries delivering therapies to patients in 130 countries worldwide.
BLACKROCK HEALTH INVESTS ¤10 MILLION INTO ENHANCED RADIOTHERAPY CARE
Blackrock Health, combining Hermitage, Blackrock, Galway and Limerick Clinics, has invested ¤10 million in two ne w radiotherapy machines. The announcement marks a significant development in cancer care services across the two sites. The first machine is now fully operational in Galway Clinic and the second will be in operation in Hermitage Clinic later this year.
The Elekta Versa HD linear accelerators are designed to deliver highly precise radiation therapy to tumours, while sparing surrounding healthy tissue. The
Elekta Versa HD uses advanced technologies like IGRT (image guided radiation therapy), IMRT (intensity modulated radiation therapy and VMAT (volumetric modulated radiation therapy) to improve accuracy and effectiveness of the treatments provided. The introduction of surface guided radiation therapy (VisionRT) in both hospitals will further improve the patient experience by eliminating the necessity for permanent marks on the patient’s skin. The versatility of the Elekta Versa HD will allow several treatment techniques, including conventional radiotherapy, stereotactic body radiotherapy (SBRT) and stereotactic radiosurgery (SRS) which will allow our teams flexibility to tailor treatment plans to offer the very best care for our patients.
Dr Joseph Martin, Consultant Radiation Oncologist in Blackrock Health Galway Clinic added: “At Blackrock Health, we are committed to delivering best-inclass care for our patients. With the incidence of cancer expected to more than double in men and to almost double in women by 2045[i], investment in oncology services to enable more precise and personalised treatment is crucial. We are delighted to have commenced offering treatment with the new machine in Galway, ensuring patients have access to the latest technology.”
The investment will enhance quality of care for patients, including a reduction in treatment time. The new machine has the capability to reduce treatment time from 20-25 minutes down to 6-7 minutes on average. This will significantly benefit patients who are required to wear facial mask coverings during treatment or are required to have a full bladder for treatment.
Brid Carroll, Radiotherapy Services Manager in Blackrock Health Hermitage Clinic added: “The new radiotherapy Linacs will enhance treatment options for oncology patients, offering reduced treatment times and increased precision in our treatments. The advanced technology allows us to deliver higher doses of radiation to tumours, while sparing surrounding normal tissue. This not only makes the treatment more effective, but also reduces side effects, therefore improving overall quality of life for our patients. The reduction in treatment time will also allow us to treat more patients, as well as improve the comfort for those receiving treatment. For our staff in the department, (radiation therapists, medical physicists and medics), this new technology will allow us to continue to develop the service for the benefit of our patients.”
WELCOME FOR THE NATIONAL CHILDREN’S RESEARCH CENTRE (NCRC) INTO CHI
Children’s Health Ireland (CHI) has announced the welcoming of the National Children’s Research Centre (NCRC) into CHI. This very welcome milestone will enable us to further enhance our ability to bring care, education and research excellence to the bedside and foster optimal therapies for children in Ireland and beyond.
The NCRC has been based on the CHI at Crumlin campus, working closely with CHI researchers and supported for many years by the Children’s Health Foundation, our fundraising partner. The Centre has worked to promote children’s health research and to improve child health outcomes across Ireland through investment in cutting-edge facilities, grant awarding and research leadership.
As of today, the NCRC is now incorporated into Children’s Health Ireland. This brings its functions, staff and facilities - including state-of-the-art research labs and critically important biosample processing and storage facilities - under the CHI umbrella. The incorporation of NCRC into CHI will allow us to take advantage of the experience and expertise of the NCRC team and to drive the integration of basic science, clinical and translational research and grant expertise. This integrated research environment will ensure that the research we do across CHI continues to be high-quality, focused on patients and families and internationally competitive.
Paul McNally, Director of Research and Innovation, Children’s Health Ireland, said:
“Throughout the last 5 years, our teams in Children’s Health Ireland have worked hard to coordinate, integrate and modernise the previously separate research structures and supports across CHI sites. This next step in our development program incorporates cutting-edge translational, basic science and grant functions into CHI, and promises to transform our ability to deliver improved health outcomes for children.”
This co-ordinated CHI research infrastructure, alongside innovation and education, falls under the remit of the Paediatric Academic Health Science Centre (PAHSC) – the new structure that sees CHI and its 4 Dublin university partners, Dublin City University (DCU), RCSI University of Medicine and Health Sciences, Trinity College Dublin (TCD) and University College Dublin (UCD), formally partnering together to advance academic child health across our campuses.
Alex Wilkes, Country President, AstraZeneca Ireland Marketing Company; Ruth March, Senior Vice President, Precision Medicine; Shane Doyle, Senior Vice President, Head of Operations & Sustainability for Alexion, AstraZeneca Rare Disease Unit and Jon-Paul Sherlock, API Commercialisation Site Lead.
The PAHSC is part of a wider network of academic child health across Ireland that is currently in development and promises to see Ireland as a key player in advancing child health internationally.
‘PATIENT COMMUNICATIONS
PASSPORT’ INITIATIVE
Portiuncula University Hospital (PUH) and Community Healthcare West (Galway, Mayo and Roscommon) are delighted to introduce the new ‘Getting to know what matters to me’ Communication Passport for people living with dementia.
The communications passport is a resource designed to reduce communication barriers and enhance the overall experience for people with dementia who utilise both hospital and community services. It can also be adapted to suit any individual who has difficulty communicating.
National and international research confirms that admission to an acute hospital can be distressing and disorientating for a person living with dementia and is often associated with a decline in their cognitive ability and levels of functioning.
The Dementia Quality Improvement Committee at Portiuncula University Hospital implemented the initiative in response to recommendations outlined in the Irish National Audit of Dementia Care in Acute Hospitals Report. The aim of the passport is to assist an individual who is receiving professional care and is unable to effectively disclose information about themselves,
especially if they have special requirements or preferences.
The person, along with their family or carers, are asked to record information in the communications passport that will help them communicate, such as their personal history, likes and dislikes, important people or places in their lives, and normal routines and abilities.
The passport is a valuable tool for patients transitioning from one care environment to another and meeting new people. It should travel with the person and be available for use when the person is experiencing any episode of care.
Speaking about the new Patient Communications Passport, Paula Noone, Assistant Director of Nursing, Dementia Quality Improvement, Saolta Group said, “The passport immediately indicates whether a patient has any communication difficulties.
“It will allow healthcare staff to see, at a glance, some of the critical information that they may have difficulty obtaining, as well as assist them understand how to effectively engage with the patient they are seeing.
“We want to make sure that all our patients are as comfortable as possible while in a healthcare setting and the passport is another tool to assist with that,” added Paula.
"Having a resource like this will help all staff to immediately identify the memories, the habits, routines, and symbols that are important to the person,” explains John Brennan, Dementia
Passport clinical caption: from left, Angela Donnellan, Senior Staff Nurse, St Joseph’s Ward, PUH; Sharon Donoghue, Patient Advice Liaison Service Coordinator, PUH; Emily McElroy, Clinical Nurse Manager 2, St Joseph’s ward, PUH; Paula Noone, Assistant Director of Nursing, Dementia Quality Improvement, Saolta Group; John Brennan, Dementia Coordinator, Community Healthcare West; Paula Daly, Clinical Nurse Manager 1, St Joseph’s ward, PUH; Anita Blake, Senior Occupational Therapist, PUH; Siobhan Coen, Senior Occupational Therapist, PUH and Maura O Connell, Assistant Director of Nursing, Medical Division, PUH
Coordinator for Community Healthcare West.
“The person will feel valued and included, especially when interacting with new people and going through inevitable care transitions.”
James Keane, Hospital Manager said, “This new initiative aims to provide person-centered and compassionate integrated care, while also promoting the delivery of safer healthcare. Having greater supports in place like the passport, will greatly enhance the care we provide to patients who have difficulty communicating.
“Ensuring we have processes to assist in meeting the needs of our patients is a priority for the hospital.”
SAOLTA UNIVERSITY CANCER NETWORK PROGRESSES TO NEXT STAGE OF EUROPEAN ACCREDITATION
Saolta University Cancer Network are delighted to have progressed to the next stage of accreditation with the Organisation of European Cancer Institutes (OECI).
The OECI Accreditation and Designation programme is considered internationally as the gold standard for cancer care. It focuses on enabling a complete quality system for cancer diagnosis, care, education and research.
OECI is an organisation of European cancer centres founded in 1979 to provide patients equal access to high quality cancer care through cooperation and knowledge exchange.
By participating in this prestigious accreditation process
the Saolta University Cancer Network has committed to ongoing quality improvement in cancer care through research, innovation, partnership and patient empowerment.
The Saolta cancer programme provides a wide range of cancer services to a population of 830,000 people across the west and northwest. In line with the national model of care (a hub and spoke model), complex care is located at University Hospital Galway with satellite centres delivering care closer to home in Letterkenny University Hospital, Sligo University Hospital, Mayo University Hospital and Portiuncula University Hospital.
The network is a clinical academic partnership between the Saolta University Healthcare Group and the University of Galway and is aligned with the strategic priorities of the National Cancer Strategy (2017-2026).
In 2021, the Saolta University Cancer Network became a member of the OECI with a view to becoming an European accredited cancer network to quality assure the cancer programme within region. Following membership and preliminary designation screening by the OECI, the Saolta University Cancer Network undertook an extensive self-assessment process against the OECI standards with a completed submission delivered in February 2024.
This was approved by the OECI Accreditation and Designation (A&D) Board, and will result in a peer review visit scheduled for May 2024.
Dr Manvydas Varzgalis, Consultant Breast Surgeon, LUH; Tony Canavan, Regional Executive Officer, HSE West and North West; Professor Maccon Keane, Associate Clinical Director of the Network, GUH Saolta Cancer MCAN / Consultant Medical Oncologist; Geraldine Cooley, General Manager Saolta Cancer MCAN; Professor Michael Kerin, Director Saolta Cancer MCAN; Olive Gallagher, Director of Nursing, Saolta Cancer MCAN; Dr Joseph Martin, Associate Clinical Director of the Network, GUH Saolta Cancer MCAN / Consultant Radiation Oncologist; Dr Gerry O’Dowd, Associate Clinical Director of the Network, LUH Saolta Cancer MCAN / Consultant Histopathologist; and Dr Andrew Hodgson, Associate Clinical Director of the Network, SUH Saolta Cancer MCAN / Consultant Haematologist
Clinical R&D
The peer review will include site visits by a European independent panel of experts who assess all elements the cancer programme in our hospitals. Any recommendations for quality improvement as a result of the review will be our focus over the next period, with a decision expected in November 2024 on our status as a fully accredited OECI Cancer Centre.
Professor Michael Kerin, Director of Saolta University Cancer Network welcomed the progress saying, “Our vision is to create a centre of excellence delivering the highest international standards in cancer treatment, research and education across our network and the OECI accreditation process will enable us to deliver patient centred cancer care at the highest standards internationally.”
Tony Canavan, Regional Executive Officer, HSE West and North West welcomed the progress adding: "The provision of integrated cancer care for the population of our region is a priority and I want to commend the team for the focus and determination they have shown in making this a reality for the people we serve."
POSITIVE RUBY PHASE III DATA SHOW POTENTIAL FOR DOSTARLIMAB COMBINATIONS IN MORE PATIENTS WITH PRIMARY ADVANCED OR RECURRENT ENDOMETRIAL CANCER
GSK plc (LSE/NYSE: GSK) has announced statistically significant and clinically meaningful overall survival (OS) results from Part 1 and progression-free survival (PFS) results from Part 2 of the RUBY/ ENGOT- EN6/GOG3031/NSGO phase III trial in adult patients with primary advanced or recurrent endometrial cancer. This data was presented in a late-breaking plenary session at the Society of Gynecologic Oncology 2024 Annual Meeting on Women’s Cancer (16-18 March).
The goal of the RUBY phase III trial programme is to evaluate which patients with primary advanced or recurrent endometrial cancer could potentially benefit from treatment with dostarlimab plus chemotherapy, with or without the addition of niraparib maintenance. Part 1 of the RUBY phase III trial is investigating dostarlimab plus standard-of-care chemotherapy (carboplatin-paclitaxel) followed by dostarlimab compared to chemotherapy plus placebo followed by placebo. Part 2 of the RUBY phase III trial is evaluating dostarlimab plus standard-of-care chemotherapy, followed by dostarlimab plus niraparib as maintenance therapy compared to chemotherapy plus
placebo followed by placebo. The safety and tolerability profiles of dostarlimab plus carboplatinpaclitaxel and dostarlimab plus carboplatin-paclitaxel followed by dostarlimab plus niraparib were generally consistent with the known safety profiles of the individual medicines.
Previous data showed a statistically significant and clinically meaningful improvement in PFS with dostarlimab plus chemotherapy versus chemotherapy alone in frontline mismatch repair deficient (dMMR)/ microsatellite instability- high (MSI-H) primary advanced or recurrent endometrial cancer.1 These data led to regulatory approvals for this patient population in the US, EU and certain other countries. Data presented shows additional potential benefit of dostarlimab plus chemotherapy, with or without the addition of niraparib, in the overall population of patients with primary advanced or recurrent endometrial cancer, including patients with mismatch repair proficient (MMRp)/microsatellite stable (MSS) tumours, for which there are currently no approved immuno-therapy-based regimens.
RUBY Part 1: a statistically significant and clinically meaningful improvement in OS was observed for dostarlimab plus chemotherapy versus placebo plus chemotherapy, meeting a primary endpoint of the study.2
Dostarlimab plus chemotherapy versus chemotherapy alone showed:
In the overall population:
• a statistically significant reduction in the risk of death by 31% (Hazard Ratio [HR]: 0.69; [95% CI: 0.539– 0.890])
• a clinically meaningful improvement of 16.4 months in median OS (44.6 months vs 28.2 months)
In a prespecified exploratory analysis of the MMRp/MSS population:
• a clinically meaningful trend in reduced risk of death by 21% (HR: 0.79; [95% CI: 0.602–1.044])
• a clinically meaningful improvement of seven months in median OS (34.0 months vs 27.0 months)
In RUBY Part 1, grade 3 or higher and serious treatment-emergent adverse events (AEs) were approximately 12% higher in the dostarlimab plus carboplatinpaclitaxel arm (treatment arm) compared with the placebo plus carboplatin-paclitaxel arm (control arm). The nature and types
of immune-related AEs in the dostarlimab plus chemotherapy safety profile were consistent with the mechanism of action of dostarlimab and similar to those reported for other PD-(L)1 inhibitors. In the trial, 40.7% of participants in the treatment arm and 16.3% of participants in the control arm had immune-related AEs assessed by the investigator as related to dostarlimab or placebo, respectively. Discontinuation of dostarlimab or placebo due to a treatment-emergent AE occurred in 19.1% of patients in the treatment arm and 8.1% of patients in the control arm.
RUBY Part 2: addition of niraparib to dostarlimab in maintenance setting significantly improved PFS in first-line primary advanced or recurrent endometrial cancer compared to chemotherapy alone, meeting the primary endpoint of the trial.3
Dostarlimab plus chemotherapy followed by dostarlimab plus niraparib compared to placebo plus chemotherapy followed by placebo showed:
In the overall population:
• a statistically significant reduction in the risk of disease progression or death by 40% (HR: 0.60 [95% CI: 0.43–0.82])
• a clinically meaningful improvement of 6.2 months in median PFS (14.5 months vs 8.3 months)
In the MMRp/MSS population:
• a statistically significant reduction in the risk of disease progression or death by 37% (HR: 0.63 [95% CI: 0.44–0.91])
• a clinically meaningful improvement of 6.0 months in median PFS (14.3 months vs 8.3 months)
In RUBY Part 2, grade 3 or higher and serious treatment-emergent AEs were approximately 36% and 24% higher, respectively, in the dostarlimab plus chemotherapy followed by dostarlimab plus niraparib arm (treatment arm) compared with the placebo plus chemotherapy followed by placebo arm (control arm). In the trial, 36.6% of participants in the treatment arm and 6.3% of participants in the control arm had immune-related AEs assessed by the investigator as related to dostarlimab or placebo, respectively. No cases of myelodysplastic syndrome/ acute myeloid leukaemia were reported; other secondary primary malignancies occurred in 1 patient each in both treatment arms. Discontinuation of dostarlimab or placebo due to a TEAE occurred in 24.1% of patients in the treatment arm and 5.2% of patients in the
control arm. Discontinuation of niraparib or placebo due to a treatment- emergent AE occurred in 15.7% of patients in the treatment arm and 4.2% of patients in the control arm.
¤36.5M INVESTMENT STRENGTHENS BON SECOURS' ONGOING DEDICATION TO ADVANCED HEALTHCARE IN IRELAND
Bon Secours Hospital Galway is to construct two new theatres as part of a significant ¤36.5 million investment in its services, it has been announced.
The hospital is to submit an application for planning permission to Galway City Council to construct the two new theatres, extending the Endoscopy Suite to include a fourth Endoscopy treatment room, sixteen endoscopy bays, four theatre recovery bays and fourteen surgical dayward bays.
Bon Secours Hospital Galway remains steadfast in its commitment to advancing healthcare services and expanding its facilities to better serve the community and earlier today the Group CEO, Bill Maher and Hospital CEO, Henry Burrows announced that it is poised to embark on another phase of expansion.
Bon Secours Health System Group Chief Executive, Bill Maher, added, “Aligned with its strategic 2025 Plan and with a projected investment of ¤36.5 million, this will reinforce Bon Secours Hospital Galway's position as a premier healthcare provider in the west of Ireland, ensuring continued excellence in healthcare delivery for years to come.”
Earlier this year, the hospital unveiled its ¤1.3m investment in relocating its Minor Operating Procedure Room and the inauguration of a state-of-theart third Endoscopy Suite. The addition of the third endoscopy suite substantially bolstered the hospital's capacity to serve patients, with the capability to now conduct an additional 4,000 scopes in 2024 alone.
Bon Secours Hospital Galway today celebrated another milestone with the opening of new and upgraded facilities. Among these is a cutting-edge MRI scanner, the Magnetom Sola, representing a ¤1 million investment in advancing medical imaging capabilities. The Magnetom Sola enables more targeted and effective treatment plans while prioritising patient comfort and safety during MRI examinations which in turn aids reduction in patient waiting times.
TETRIDAR® (TERIPARATIDE) RECOMMENDED AS A BEST VALUE MEDICINE FOR TERIPARATIDE ON THE HIGH TECH ARRANGEMENT
Teva Pharmaceuticals is pleased to announce that the Medicines Management Programme (MMP) now recommends Tetridar® as a Best Value Medicine (BVM) for teriparatide on the High Tech Arrangement.
Tetridar® is indicated in adults for the treatment of osteoporosis in postmenopausal women and in men at increased risk of fracture. In postmenopausal women, a significant reduction in the incidence of vertebral and non-vertebral fractures but not hip fractures have been demonstrated. Tetridar® is also indicated in adults for the treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk for fracture.
Contact Collin Botha, Customer Solutions Manager, Teva, for any queries in relation to Tetridar® (teriparatide) at collin.botha@teva.ie or 087 668 5876.
Further information is available upon request or from the SmPC available at HPRA.ie. Product Information is also available on the HPRA website.
Adverse events should be reported. Reporting forms and information can be found at www.hpra.ie. Adverse events should also be reported to Teva UK Limited on +44 (0) 207 540 7117 or medinfo@tevauk.com.
Date of preparation: April 2024
Job code: TERI-IE-00053
SANDOZ FULLY LAUNCHES IN IRELAND WITH PLANS TO GROW BIOSIMILARS BUSINESS
Following a 30-year joint venture, Sandoz, the world’s
largest generics and biosimilars company, has acquired full ownership of Rowex.
Rowex has been operating in Bantry, Co. Cork, since 1993 and is one of the leading players in the Irish OTC and generics market.
Sandoz will invest in the business with the aim of becoming a topthree off-patent medicine company in Ireland by 2028. The largest growth driver will be the launch of biosimilars, cost-effective copies of biologic medicines.
Sandoz was the first company to launch a biosimilar in 2006, and has significant expertise in marketing eight biosimilars as well as having a further 25 in development making the company the global leader in this area. Recent large-scale investments include a new $400m biosimilars development hub in Slovenia as well as a new partnership with Just EvoTech for biosimilar development and commercial manufacturing.
In recent years the HSE medicines budget has increased from ¤1.3 billion in 2012 to ¤3.2 billion last year and current spending being deemed “not sustainable” by the Department of Health . Greater uptake of generic and biosimilar medicines, which are below the European average, could help bring spending back to affordable levels.
Biosimilar competition has emerged through the Best Value Biologic initiative, with particular success in three medicines delivering an estimated savings of ¤22.7m in 2020 alone. With a recently expanded list of 14 biologic medicines covered by the BVB programme, there is a significant opportunity for the Irish healthcare system to unlock savings and open up access for Irish patients.
Sandoz, trading as Rowex, will continue to be based in Bantry
but with an expanding fieldbased workforce, including a new biosimilars sales team. This is in addition to shared business support functions from the Sandoz UK operation, which will help accelerate growth through shared expertise and resource.
Joe Keane, Head of Operations for Sandoz in Ireland, said “We are delighted that, after a long and fruitful partnership through the Rowex joint venture, Sandoz has made the positive step to invest in the future growth of a leading Irish business. We are excited to bring more of Sandoz’s leading portfolio to Ireland, in particular its leading pipeline of biosimilars which offer a huge savings opportunity for the Irish healthcare system.”
NEW 48-WEEK FREXALIMAB PHASE 2 DATA SUPPORT POTENTIAL FOR HIGH SUSTAINED EFFICACY IN MULTIPLE SCLEROSIS
Sanofi’s CD40L antibody, frexalimab, demonstrated sustained reduction of disease activity and favorable tolerability after nearly one year in participants with relapsing multiple sclerosis. These data will be presented today at the American Academy of Neurology (AAN) 2024 Annual Meeting in Denver, Colorado, US. Results from the 12-week doubleblind study period were previously published in The New England Journal of Medicine.
Patrick Vermersch, MD, PhD University of Lille, CHU Lille, France said, “These 48-week data showed that treatment with frexalimab resulted in further decreases in the number of lesions and a sustained reduction in disease activity. The preliminary clinical results are promising with a very low annual relapse rate. This strengthens the rationale for targeting CD40L in MS and supports further development of frexalimab as a potential highefficacy therapy in relapsing MS.”
From the initial 12-week doubleblind period, 97% (125/129) of study participants entered the open-label extension (OLE) of the phase 2 study. Of all participants receiving frexalimab, both on high- and low-dose regimens and participants who switched from placebo at the start of the open-label extension period (week 12), 87% (112/129) remained in the study at the 48-week cut-off. During the OLE, participants in the high- (n=50) and low-dose (n=49) arms continued to receive frexalimab 1200 mg intravenously every four weeks, or frexalimab 300 mg subcutaneously every two
weeks, respectively, while those initially receiving placebo switched to the aforementioned high or low dose frexalimab treatment arms (n=12 and n=14, respectively).
Erik Wallström, MD, PhD Global Head of Neurology Development, Sanofi added “Frexalimab represents a novel potential firstin-class treatment mechanism in multiple sclerosis designed to tackle the aspects of this disease where unmet medical needs still exist. We are applying our deep expertise to address the full spectrum of neuroinflammation and neurodegeneration to improve the lives of people living with multiple sclerosis.”
Results of the phase 2 OLE at week 48 showed:
• 96% of patients who continued receiving high-dose frexalimab and 87% of those who continued receiving low-dose frexalimab were free of Gd+ T1 lesions at week 48, respectively. Additionally, among patients who switched from placebo to high and low-dose frexalimab at the start of the OLE at week 12, declines were seen at Week 24, and 90% and 92% were free of Gd+ T1 lesions at week 48, respectively.
• The number of Gd+ T1-lesions (mean [SD]) remained low in participants who continued receiving frexalimab (high dose: 0.0 [0.2]; low dose: 0.2 [0.5]) and continued to decline in those who switched from placebo to frexalimab at week 12 (high dose: 0.2 [0.6]; low dose: 0.1 [0.3]).
• Number of and volume change of new or enlarging Gd+ T2-lesions remained low for all frexalimab treatment groups through week 48, and lymphocyte counts remained stable.
• Participants who continued receiving high-dose frexalimab experienced a low annualized relapse rate (ARR) of 0.04 (95% CI: 0.01, 0.18) over the 48-week treatment period with 96% being free of relapses. ARR in the initial low-dose arm was 0.22, and ARR in patients who switched to high and low-dose frexalimab were 0.09 and 0.40, respectively, through week 48.
Frexalimab was generally welltolerated through week 48. The most common adverse events (≥10%) amongst all subgroups of patients receiving frexalimab during OLE until cut-off at week 48 from baseline were nasopharyngitis (n=14 [11%]), headache (n=14 [11%]) and COVID-19 (n=13 [10%]).
For patients taking apixaban or rivaroxaban with life-threatening or uncontrolled bleed
RELY ON THE ONLY ANTIDOTE TO SHUT OFF FXa INHIBITOR ACTIVITY1-3,*
INDICATION
For adult patients treated with a direct FXa inhibitor (apixaban or rivaroxaban) when reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding.1
ONDEXXYA (andexanet alfa) is the Only Approved Antidote to Shut-off FXa inhibitor Activity1-3
Rapid Reverses FXa inhibition within 2 minutes after bolus1,†
Effective 93% decrease in FXa inhibitor activity in patients receiving apixaban (-93.3%, 95% CI: -94%; -93%)‡ and rivaroxaban (-94.1%, 95% CI: -95%; -93%)1
Consistent 79% of patients had excellent or good haemostatic efficacy at 12 hours (N=296)1,§ 79% of 169 patients taking apixaban and 80% of 127 patients taking rivaroxaban.1
Adverse events in ONDEXXYA-treated patients were non-serious and non-severe.5,II No thromboembolic events or serious or severe adverse events were observed. The most common side effects were mild to moderate infusion-related reactions .1,¶
*In ANNEXA-A (n=31) and ANNEXA-R (n=39), randomised, double-blind, placebo-controlled studies conducted in healthy older volunteers (aged 50-75 years), ONDEXXYA bolus followed by continuous infusion was associated with a 92% (apixaban-treated subjects) and 97% reduction (rivaroxaban-treated subjects) in anti-FXa activity from baseline to nadir for low- and high-dose, respectively (P<0.0001). In these clinical trials no serious or severe adverse reactions were reported. The most frequently observed adverse reactions were mild or moderate infusion-related reactions. Refer to Summary of Product Characteristics for full safety profile.1,5; †And sustained throughout the 2-hour IV infusion in older, healthy volunteers1; ‡From baseline to nadir1; §Excellent ICH haemostasis: ≤20% increase in volume compared with baseline at both 1 and 12 hours; Good ICH haemostasis: ≤35% increase compared with baseline at 12 hours; Excellent GI haemostasis: Less than 10% decrease in corrected haemoglobin and haematocrit at 12 hours compared with baseline; Good GI haemostasis: ≤20% decrease (correction done by subtracting 1 g/dL from the haemoglobin or 3% from the haematocrit for each unit of packed red blood cells given) and ≤2 units of coagulation intervention required6; IIPooled safety in older, healthy volunteers; ¶PCC is not indicated to treat patients with FXa-inhibitor–related bleeding. Characterised by a range of symptoms, including flushing, feeling hot, dysgeusia, cough, and shortness of breath.1
1. Ondexxya. Summary of product characteristics. 2. Kcentra. Summary of product characteristics. 3. Praxbind. Summary of product characteristics. 4. Siegal DM, et al. N Engl J Med. 2015;373(25):2413-2424 5. Connolly SJ, et al. N Engl J Med 2016;375(12):1131-1141.
Abridged Prescribing Information
200 mg POWDER FOR SOLUTION FOR INFUSION (andexanet alfa)
Consult Summary of Product Characteristics before prescribing.
Indication: ONDEXXYA is indicated for adult patients treated with a direct factor Xa (FXa) inhibitor (apixaban or rivaroxaban) when reversal of anticoagulation is needed due to lifethreatening or uncontrolled bleeding. Presentation: Powder in a 20 mL vial (Type I glass) with a stopper (butyl rubber). Pack size of four vials. Dosage and Administration: Restricted to hospital use only. Andexanet alfa is administered as an intravenous bolus at a target rate of approximately 30 mg/min over 15 minutes (low dose) or 30 minutes (high dose), followed by administration of a continuous infusion of 4 mg/min (low dose) or 8 mg/min (high dose) for 120 minutes. Reversal of apixaban/rivaroxaban: The recommended dose regimen of Ondexxya is based on the dose of apixaban/rivaroxaban the patient is taking at the time of anticoagulation reversal, as well as on the time since the patient’slast dose of apixaban. Measurement of baseline anti-FXa-level should support the clinical decision of starting treatment (if level is available in an acceptable time frame). Refer to SmPCfor recommended dose of Ondexxya based on the last dose of apixaban/rivaroxaban. Restarting antithrombotic therapy: Following administration of Ondexxya and cessation of a major bleed, re-anticoagulation should be considered to prevent thrombotic events due to the patient’s underlying medical condition. Antithrombotic therapy can be re-initiated as soon as medically indicated following treatment if the patient is clinically stable and adequate haemostasis has been achieved. Medical judgement should balance the benefits of anticoagulation with the risks of re-bleeding. Elderly: No dose adjustment is required in elderly patients (aged ≥ 65 years). Renal impairment: The effect of renal impairment on andexanet alfa exposure levels has not been evaluated. Based on the existing data on clearance, no dose adjustment is recommended. Hepatic impairment: Based on the existing data on clearance of andexanet alfa, no dose adjustment is recommended. The safety and efficacy have not been studied in patients with hepatic impairment. Paediatric population: The safety and efficacy of andexanet alfa in children and adolescents have not been established. No data are available. Refer to SmPC for instructions on reconstitution of the medicinal product before administration. Contraindications: Hypersensitivity to the active substance or to any other ingredients. Known allergic reaction to hamster proteins. Refer to SmPC for a full list of excipients. Warnings and Precautions: Limitations of use: Andexanet alfa is not suitable for pretreatment of urgent surgery. Use for edoxaban- or enoxaparin-reversal is not recommended due to lack of data. Andexanet alfa will not reverse the effects of non-FXa inhibitors. Thrombotic events: Thrombotic events have been reported following treatment with andexanet alfa. Patients being treated with FXa inhibitor therapy have underlying disease states that predispose them to thrombotic events. Reversing FXa inhibitor therapy exposes patients to the thrombotic risk of their underlying disease. In addition, independent pro-coagulant effect of andexanet alfa, mediated by inhibition of tissue factor pathway inhibitor (TFPI), has been demonstrated, which may pose a risk of developing thrombosis. Duration of this effect in bleeding patients is not known. Laboratory parameters such as anti- FXa activity, endogenous thrombotic potential (ETP), or markers of thrombosis might not be reliable for guidance. To reduce this risk, resumption of anticoagulant therapy should be considered as soon as medically appropriate after completion of treatment. Use of andexanet alfa in conjunction with other supportive measures: Andexanet alfa can be used in conjunction with standard haemostatic supportive measures, which should be considered as medically appropriate. Interaction with heparin: Use of andexanet prior to heparinization e.g. during surgery should be avoided as andexanet causes unresponsiveness to heparin. Use of andexanet as an antidote for heparin or low-molecular weight heparin has not been evaluated and is not recommended. Infusion-related reactions: In case of mild or moderate infusion reactions, careful observation may be sufficient. For moderate symptoms, consideration may be given to a brief interruption or slowing of the infusion with resumption of the infusion after symptoms subside. Diphenhydramine may be administered. Drug Interactions: No interaction studies with andexanet alfa have been performed. Pregnancy and Lactation: There are no data from the use of andexanet alfa in pregnant women. Andexanet alfa is not recommended during pregnancy or in women of childbearing potential not using contraception. It is unknown whether andexanet alfa is excreted in human milk. A risk to newborns/infants cannot be excluded. Breast-feeding should be discontinued during treatment with andexanet alfa. There are no data on the effects of andexanet alfa on human fertility Ability to Drive and Use Machines: Andexanet alfa has no or negligible influence on the ability to drive and use machines. Undesirable Events: Consult SmPC for full list of side effects, including those reported in healthy patients. Frequency in patients with major bleeds: Common (> 1/100 to < 1/10): cerebrovascular accident, ischaemic stroke, acute myocardial infarction, myocardial infarction, deep vein thrombosis, pulmonary embolism, pyrexia. Uncommon (≥ 1/1,000 to < 1/100): cerebral infarction, transient ischaemic attack, cardiac arrest, iliac artery occlusion, infusion related reactiona a reported signs/symptoms (rigors, chills, hypertension, oxygen desaturation, agitation and confusion) were transient and mild to moderate in severity. Legal Category: Product subject to prescription which may not be renewed (A). Marketing Authorisation Number: EU/1/18/1345/001 Marketing Authorisation Holder: AstraZeneca AB, SE-151 85, Södertälje, Sweden. Further product information available on request from: AstraZeneca Pharmaceuticals (Ireland) DAC, College Business and Technology Park, Blanchardstown Road North, Dublin 15, Ireland. Freephone 1800 800 899. ONDEXXYA® is a trademark(s) of the AstraZeneca group of companies. Date of API preparation: 02/2023 Veeva ID: IE-4783