• Esthetic-Functional Interceptive Treatment in a Patient with Dental Agenesis and Trauma: Case Report
Table of Contents
Editor
Rob Pasch, DDS, MSc, IBO
Mississauga, Ontario, Canada
E-mail: paschrob@rogers.com
Managing Editor
Allison Hester
8305 Pennwood Dr. Sherwood, AR 72120
E-mail: allisonhijo@gmail.com
Consultants
Adrian Palencar, ON, Canada
Michel Champagne, QC, Canada
Dany Robert, QC, Canada
Scott J. Manning, USA
Mike Lowry, AB, Canada
Edmund Liem, BC, Canada
Yosh Jefferson, NJ, USA
G Dave Singh, CO, USA
Monika Tyszkowski, IL, USA
William Buckley, OH, USA
International Journal of Orthodontics, copyright 2020 (ISSN #1539-1450). Published quarterly (March, June, September, December) by International Association for Orthodontics, 750 North Lincoln Memorial Drive, #422, Milwaukee, WI 53202 as a membership benefit. All statements of opinion and of supposed fact are published on the authority of the writer under whose name they appear and are not to be regarded as views of the IAO. Printed in the USA. Periodical postage paid at Milwaukee, WI and additional mailing offices. Subscription for member $15 (dues allocation) annually; $40 U.S. non-member; $60 foreign. Postmaster: Send address changes and all correspondence to: International Journal of Orthodontics 750 North Lincoln Memorial Drive, #422 Milwaukee, WI, USA 53202 Phone 414-272-2757, Fax 414-272-2754
E-mail: worldheadquarters@iaortho.org
International Journal for Orthodontics (IJO) readers can receive one hour of continuing education (CE) for each issue. The IJO is a critical piece of the International Association for Orthodontics (IAO) mission. The journal uses practice management, studies, and case base articles to: “To promote the study and disseminate the knowledge of the cause, control, treatment and prevention of malocclusion of the teeth and any possible resulting dysfunction, such as dysfunction of the temporomandibular joint.” For CE credit, please read the articles found in this issue of the IJO. Then scan the QR code below. Fill out and submit the required quiz and evaluation. Once accepted by the IAO, the CE credit will automatically be recorded in the users profile. IAO Members dues must be paid in full to receive CE credit. As the IJO and accompanying CE credit is included with IAO membership, there is no cancelation or refund for the IJO subscription.
International Journal of Orthodontics
Treatment Changes With Forsus FRD in Developing Skeletal Class III Malocclusion: A Pilot Study, by Dr. Sanjeev Datana and Dr. Shiv Shankar Agarwal
Nine Keys of Ideal Functional Occlusion 2024, by Dr. Kenneth U. Lau, Dr, Hanna Szekely, and Dr. Rob Pasch
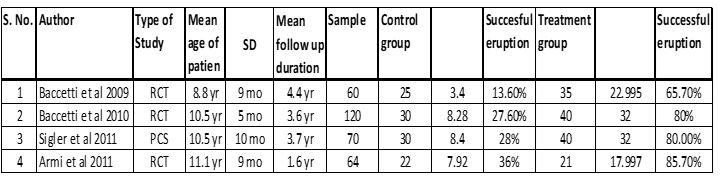
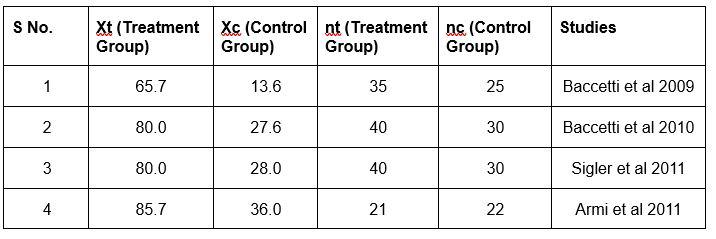
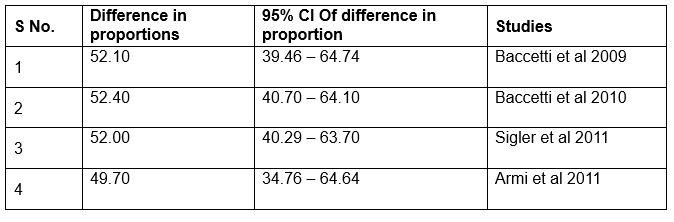
Correlation of Early Maxillary Expansion with Eruption of Palatally Impacted Maxillary Canines: A Systematic Review And Meta Analysis, Dr. Amit Antil, Dr.Saugat Ray, Dr. Prasanna Kumar MP, and Dr. Amrit Thapa
Guided Corticopuncture Associated with Microimplant-Assisted Rapid Palatal Expansion (MARPE): Planning Variables, Dr. Cristiane Barros André, Gustavo de Andrade Jacquier, Dr. Fábio Dupart Nascimento, and Bruno de Paula Machado Pasqua
Esthetic-Functional Interceptive Treatment in a Patient with Dental Agenesis and Trauma: Case Report, by Raquel Souza dos Santos Marques, Liziane Monique de Souza Cardoso. Jéssica Roberta Bispo da Silva, Gabriela Mancia de Gutierrez, Anna Paula Nigri, and Luciana Duarte Caldas
Writer’s Guidelines
Editorial, by Dr. Rob Pasch, DDS MSc IBO, Editor
Dr. Skip Truitt: Taking the Mission Beyond the Association
Growing Beautiful Teeth Chapters 9-10: Key to Health `
Practice Management Tips: The Unspoken Truth about Dental Profits, by Scott J Manning, MBA; Founder, Dental Success Today
OPINION: Diagnosis and Treatment of Maxillo-Mandibular Retrusion, Dr. Phillip Witherspoon, DDS
Tips from the Experienced: The Utlity Arch Part IV, by Dr. Adrian J. Palencar, MUDr, MAGD, IBO, FADI, FPFA, FICD
Author Guidelines
MANUSCRIPT SUBMISSION
Manuscripts are to be submitted electronically at www. editorialmanager.com/iaortho. If the manuscript is written in a language other than English, the author(s) must submit an English translation. The author may also submit a copy in his or her native language that will published in the online version only with a mention in the printed issue that the article is available online in his or her own language. The manuscript must be original and submitted exclusively to IJO.
The Journal invites authors to submit:
• Clinical reports
• Technique articles
• Review articles
• Case reports
MANUSCRIPT FORMAT
Abstract. Must include a short abstract no more than 50 words that describe the significance of the article.
Keywords. Must include keywords to help categorize the article.
Length. Manuscript should be no longer than 15 doublespaced pages, excluding figures and illustrations.
Tooth Numbering. The numbering of teeth should be international numbering. (US numbering can be added and put in parentheses.)
Non-English Manuscripts. Authors are encouraged to submit the manuscript in languages other than English for posting on the IAO website. A mention will be added to the English version published in the International Journal of Orthodontics, directing readers online for other translations.
Illustrations. Images must be available electronically as separate files. High quality digital images must be presented in one of the following formats: .tiff, .eps,.jpg, or .pdf with resolution of a minimum 300 dpi. Images must not be embedded in software programs such as Word or Power Point. The names on the digital files for photo/illustration files should match the manuscript reference. For example, if manuscript copy references Figure 1, electronic file should be titled Figure 1.jpg. No more than 16 photographs, figures, & illustrations are recommended; if greater than 16, IJO has the right to select and limit the number if necessary. Figures must be clearly referenced as to their placement in the manuscript. Brief captions for the figures, identified by number, must be provided. All images must be titled. Radiographs must be of superior quality.
References. References must be included and authors are responsible for the accuracy of references. Manuscripts without them will be returned. Cite references in the text as endnotes and number them consecutively. Citations must be referenced in the following style:
Periodical:
1. Sim JM, Jefferson Y, Dillingham SE, & Keller DC. Diagnosing an orthodontic patient using three different analyses. IJO 1990; 1(4):101-106.
Book:
2. Fonder AC. The Dental Physician. 2nd ed. Rock Falls, IL; Medical Dental Arts; 1985:25-82.
World Wide Web site:
3. Health Care Financing Administration. 1996 statistics at a glance. Available at: http://www.hcfa.gov/stats/stathili.htm”. Accessed Dec. 2, 1996.
Products: Any products mentioned in the manuscript should be footnoted disclosing the company name and address.*
*XYZ Orthodontic Co., 123 Main St., Los Angeles, CA 90000.
REVIEW AND EDITING PROCESS
Editor. Articles will initially be reviewed by the editor. If author fails to adhere to the guidelines set forth, manuscript will be returned to the author for revision and correction.
Peer review. Articles in IJO are subject to an anonymous peer review process. Reviews may take up to eight weeks to complete.
Decision. Once the reviewing consultants have completed their critiques, the editor examines their comments and makes a decision to accept, accept with minor revisions, revise and resubmit, or reject.
Editing. IJO reserves the right to edit manuscript for conciseness, clarity, and stylistic consistency. The author has final approval before publication.
Questons? Contact Managing Editor, Allison Hester at allisonhijo@gmail.com, 501-517-1620.
AUTHOR RESPONSIBILITIES
Copyright transfer. IAO holds the copyright for all editorial content published in the journal. All accepted manuscripts become the permanent property of the IAO, and may not be published elsewhere in full or in part, in print or electronically, without written permission from the IAO.
Reprint permission. The author is responsible for obtaining written permission from the publisher, or the person or agency holding the copyright for any material that is reproduced from a published source.
Consent forms. Any patient clearly identified in the article must sign a form indicating his or her consent to be depicted in the article. It is the author’s responsibility to confirm consent. Author’s photo and bio. The author(s) must submit a headshot (preferably professional) and current biographical sketch. If author holds a teaching position, the title, department, and school should be included. Any position or relationship with a dental manufacturer must be identified. The sketch should include rank or title and station of authors who are in federal service, and should be limited to 60 words or less.
Conflict of interest. The author will identify any conflicts of interest upon submission of any articles.
REPRINTS
The International Journal of Orthodontics provides the corresponding author a final electronic copy of the Journal in which the article appears as well as an electronic copy (.pdf) of the pages where the article appears. Requests for individual reprints of the article should be directed to Chris McKay, IAO, 414-272-2757 or at chris@iaortho.org.
Patients have a right to privacy that should not be infringed without informed consent. Identifying information, including patients’ names, initials, or hospital numbers, should not be published in written descriptions, photographs, and pedigrees unless the information is essential for scientific purposes and the patient (or parent/guardian) gives written informed consent for publication. Informed consent for this purpose requires that a patient who is identifiable be shown the manuscript to be published. Authors should identify Individuals who provide writing assistance and disclose the funding source for this assistance. Identifying details should be omitted if they are not essential. Complete anonymity is difficult to achieve, however, and informed consent should be obtained if there is any doubt. For example, masking the eye region in photographs of patients is inadequate protection of anonymity. If identifying characteristics are altered to protect anonymity, such as in genetic pedigrees, authors should provide assurance that alterations do not distort scientific meaning and editors should so note. (Source: International Committee of Medical Journal Editors (“Uniform Requirements for Manuscripts Submitted to Biomedical Journals”), February 2006).
Editorial
Dear colleagues, Autumn is here, and with it the Thanksgiving holiday, where families and friends gather and share the company of each other, good food, and the creation of memories.
Personally, this time of year is one where I reflect on the lessons learned over the past year, courses taken, new techniques gleaned, new colleagues met, and pearls I have learned. The articles in the International Journal for Orthodontics are part of this journey. I, and the Managing Editor, Ms Allison Hester, take pride in selecting articles that will keep you on the cutting edge of orthodontic knowledge for your professional development, and evolving patient care.
This educational relationship is valued by all IAO members, it doesn’t matter if the IAO relationship is just starting or has been there forever. Education is something to be thankful for, because if not for education we would still be living in caves. However, education is not something to be lorded over others to trump them, or coerce them into poor choices. Rather education should be used to help and guide others to improve their clinical skills, improve patient care, and safeguard our associations. So, it follows that the more education you have, the more understanding you should be to the plight of your colleagues that have been less educated, and help them attain the same level that you occupy.
We all stand on the shoulders of the ones who went before us, the more education we can bestow on our colleagues the further we will be able see. The IAO as an organization prides itself on educating its members, and electing executives who can, and will abide by their vows to uphold the IAO values, to guide this organization.
It is with great pleasure that we present this current edition of the IJO to you for your enjoyment and continued education. As such, we wish everyone an enjoyable read of the journal this Autumn, I look forward to communicating with you should you have comments, complaints or suggestions. Thank you to Ms Allison Hester, our managing editor, for her invaluable role in completing this good looking journal.
I have a request to all who read this, and ask you to please help each other to write and submit articles or case reports to the journal. For the journal is YOUR journal and, you can make it reflect what is important to you today, and in doing so making the journal better for everyone now, and in the future. Also send the journal to your friends and share the knowledge.
It is a very good feeling to see your name in print, besides your patients will appreciate it as well.
Yours for accredited GP orthodontic education and better patient care.
I remain Respectfully
Dr. Rob Pasch DDS MSc IBO General Practitioner. Summer 2024.
Dr. Rob Pasch Editor
Dr. Skip Truitt
June 15, 1943September 8, 2024
Dr. Skip Truitt: Taking the Mission Beyond the Association
Dr. John Wellington Truitt, better known as Dr. Skip Truitt, graduated Summa Cum Laude from Baylor University with his DDS in 1967. Dr. Truitt’s career spanned seven decades. He was still teaching orthodontics to dentists around the world in 2024. His last lecture for the association, “Treating Children with Airway Obstruction & Blocked Eustachian Tubes,” was given at this year’s Annual Meeting in Sitges, Spain. He dedicated a lifetime to the same mission the IAO was built to serve.
Dr. Truitt did not take long to establish himself as a leader in general practitioner orthodontics. This can be seen by the numerous awards and honors he started earning just a few years after obtaining his DDS.
• American Academy of Gnathological Orthopedics Annual Meeting 1974 , Ft Worth, TX, USA
• American Academy of Gnathological Orthopedics 1981 Lexington, Kentucky, USA
• Functional Appliances – The Woodside Approach 1982, Indiana University Purdue University
• AAGO Award 1984, Boston, Massachusetts, USA
• American Equilibration Society 1988
• Presidential Merit Award – American Academy of Gnathological Orthopedics 1986, Puerto Vallarta, Jalisco, Mexico
• AAGO Seattle 1986, Seattle, Washington, USA
• Certificate of Merit – Implants & Orthodontics 1987, San Antio, Texas, USA
• 2011 IAO Annual Meeting – Integrating Maxillofacial Orthopedics & TMD Therapy into Your Practice 2011, Scottsdale, Arizona, USA
• 2013 IAO Annual Meeting – Invisible Orthopedics & Orthodontics 2013, Universal City, California, USA
• 2024 IAO Annual Meeting – Treating Children with Airway Obstruction, and Blocked Eustachian Tubes, Barcelona, Spain
Furthermore, In 1978, just over a decade after graduating from Baylor University, he founded the Clinical Foundation of Orthopedics, Orthodontics, & TMD (CFOO). This institute was devoted to providing general dentists with the latest education in orthopedics, orthodontics, & TMD. Dr. Truitt and CFOO cover a wide range of treatment education, including:
• Maxillofacial Orthopedics & Orthodontics
• Straight Wire Therapy
• Advanced Orthopedic Therapy
• Advanced Maxillo Facial Orthopedics
• Practical TMJ Therapy
Dr. Truitt was committed to providing general dentists with a well-rounded knowledge base that could serve the most patients. He realized that many areas were underserved for orthodontics and related treatments. Dr. Truitt saw this as an international concern. As such, he provided regular courses in North America, Europe, Asia, and Australia.
Dr. Truitt’s dedication to teaching general dentists orthodontics aligned perfectly with the IAO. As such, he joined the organization in 1978. Dr. Truitt was a dedicated member for forty-nine years. During this time, he was awarded the Fellowship and Senior Instructor certifications. He was also President of the Southwest Section for many years. However, Dr. Truitt served the IAO in a greater capacity than awards and titles could capture. He helped build upon the association’s greatest asset, the members. Dr. Truitt always had a place for the IAO at all his meetings. Furthermore, he endorsed the association, and his students listened. They joined the organization in groups. As many of his students joined the IAO, they began to find themselves in leadership positions. They have left a lasting impact on the organization. Without Dr. Truitt’s introduction to orthodontics and the association, the IAO may have lost many influential leaders.
Many factors led to Dr. Truitt’s success as a teacher and leader in the IAO. First, his own commitment to learning orthopedics, orthodontics, and TMD. Dr. Truitt was dedicated to staying on top of all the latest breakthroughs in the field. Dr. Truitt also belonged to multiple groups committed to disseminating knowledge. These include:
• The American Dental Association, 1967 – Present
• The Texas Dental Association, 1967 – Present
• The Academy of General Dentistry, 1972 – Present
• The International Association of Orthodontics, 1978 – Present
• The American Orthodontics Society, 1980 – Present
• The American Association of Functional Orthopedics, 1982 – Present
• The Australian Association of Orthopedics & Orthodontics, 1986 – Present
Dr. Truitt’s membership in these different organizations is a sign of dedication to orthodontics and the knowledge he could obtain.
Maybe the greatest factor in Dr. Truitt’s success as a teacher was his own humility. He was devoted to providing accurate orthodontic education, not promoting his name. As such, he invited many speakers to participate in his courses. He helped build a mass base of knowledge that many contributed to. He understood that together, himself and the perspectives of those he invited could enrich the learning experience beyond his own ability. The quality of education was more important to Dr. Truitt than being recognized as the ultimate authority in orthopedics, orthodontics, and TMD.
It is an impossible challenge to summarize Dr. Truitt’s life. In his eighty-one years, he experienced and touched more lives around him than can be captured by the written word. Instead of attempting to encapsulate Dr. Truitt’s influence on the world around him, the IAO hopes the above information will help highlight his legacy with this organization. However, the association recognizes that the true impact of his life will be felt by those whom he held most dearest to his heart. The IAO would like to recognize those that he leaves behind.
Dr. Truitt is survived by his wife Dr. Livier Carreon-Truitt, his son John W. Truitt III and wife Ashley of Durango, Colorado, his grandson Nash Truitt, his daughter Lara Watkins-Truitt of London, UK, his sister Linda Truitt-Hawkins and her husband Larry of Rockport Texas, his nephew Josh P. Wilson and his wife Angela of Rockport, Texas.
Treatment Changes With Forsus FRD in Developing Skeletal Class III Malocclusion: A Pilot Study
by Dr. Sanjeev Datana and Dr. Shiv Shankar Agarwal
AUTHORS
Dr. Sanjeev Datana
MDS, Associate Professor (Orthodontics)
Dept of Dental Surgery & Oral Health Sciences, Pune
Dr. Shiv Shankar Agarwal
MDS, Classified Specialist (Orthodontics)
Dept of Dental Surgery & Oral Health Sciences, Pune
Abstract:
Background:Management of developing skeletal Class III malocclusion is one of the most challenging clinical conditions and has been an area of concern among researchers. Depending upon the underlying etiology, different protocols have been proposed and a variety of removable functional appliances have been developed. However, patient cooperation is of utmost concern with these removable functional appliances.
Methods: Forsus fatigue resistance device (FFRD) is a contemporary modality for the management of developing skeletal Class II malocclusion, the same appliance has been used in reverse fashion to manage the developing skeletal Class III malocclusion.
Results: The results of the study highlight the various changes brought out by the appliance in the correction of Class III malocclusion. The skeletal corrections achieved were statistically significant at point A to N vertical and Wit’s, confirming the maxillary forward growth. The reduction in overjet (mean correction of 4.03mm), was a total effect of both skeletal and dental effects, there was a forward movement of the maxilla along with proclination of maxillary incisor and retroclination of mandibular incisors. An improvement in the profile of the patients was achieved with a more harmonious relation of lips to the aesthetic line.
Conclusion: Forward movement of the maxilla was noted with a very minimal skeletal effect on the mandible. Hence, it can be used as an appliance for correction of developing skeletal Class III malocclusion (maxillary hypoplasia), especially among patients where compliance with removable appliances is questionable. Improvement in the profile of the patients along with improvement in the reverse overjet was achieved.
Keywords: Class III malocclusion, Forsus FRD, Skeletal changes, Dental changes Conflict of Interest: None
Introduction:
Treatment of skeletal Class III malocclusion has been attempted at different ages including early treatment to correct the skeletal discrepancy at a young age, it may avoid (or reduce the quantum of) surgical intervention and also the associated morbidity. Although the timing of early intervention is crucial in the management of developing skeletal Class III, there exist differences among the researchers on the same. Some authors advocated initiation of treatment at an age before 10 years to achieve more orthopedic effects1-4 while others think that age of the patient has minimal influence on treatment.5,6 The advocates of early treatment think that it provides a conducive environment for complete expression of growth (especially if the underlying etiology is maxillary deficiency). The commonly employed appliances include Protraction facemask, FR-3, Reverse twin block, Bionator, Chin cup, or mandibular headgear. Among various appliances listed above, face-mask therapy is the most commonly used modality for correction of developing Class III with maxillary deficiency and chin cup therapy for the prognathic mandible. Although the effectiveness of face-mask has been proved in short-term results, the long-term results of the same are questionable.7 The face-mask therapy has a protractive effect on the maxilla with orthopedic forces applied directly to the bone or through a splint to the dentition, at the same time it restricts the forward growth of the mandible along with redirecting it to more vertical than horizontal. The limited duration of appliance wear and compliance associated with appliance wear are the two main constraints with this therapy.
*This article has been peer reviewed
All the appliances used in literature for correction of developing skeletal Class III malocclusion are removable appliances only. Compliance associated with appliance wear is the main restricting factor for the success of these appliances. Researchers are more interested in an appliance with minimal or no compliance associated with its usage. Forsus Fatigue Resistant Device (FRD) is a fixed functional appliance developed primarily for the correction of skeletal Class II malocclusion to reduce the compliance factor associated with the treatment.8 Forsus appliance works with a principal push mechanism, a forward thrust to the mandible against the maxillary dentition to stimulate the mandibular growth.9 A recent study.10 has used the Forsus appliance in reverse fashion (opposite to its function for correction of skeletal Class II malocclusion) thereby producing a forward thrust on maxillary bone and maxillary dentition and at the same time a restrictive effect on mandibular bone and mandibular dentition. However, to the best of the knowledge of the authors, there is limited published literature on the Forsus as mentioned above for correction of Class III malocclusion. The published literature has a limited mention of the effect of Forsus on skeletal/dental structures and changes in soft tissue & upper airway used for management of developing skeletal Class III malocclusion. Hence, the present prospective study was designed to study the effect of Forsus in the correction of developing Class III malocclusion.
Materials & Method
The present prospective clinical study was planned and executed at the Department of Orthodontics and Dentofacial Orthopedics of a tertiary care government hospital. The sample consisted of patients who reported to the Outpatient department for orthodontic correction with developing skeletal Class III malocclusion, age 12-14 years, both genders included. The inclusion /exclusion criteria for the patients selected wereInclusion criteria
1. Developing skeletal Class III malocclusion (ANB 0⁰ to - 4⁰)
2. Maxillary deficiency with SNA <78⁰
3. Angle Class III molar/ super Class I relation with or without anterior crossbite
4. Minimal or no crowding in maxillary mandibular anterior
5. Permanent dentition with no missing teeth (except 3rd molars)
6. Patients with CVMI stage 3
Exclusion Criteria
1. Systemic condition affecting growth and development of jaws
2. History of orthodontic treatment
3. Syndromic cases including patients with Cleft lip & palate
4. Patients with compromised periodontal health.
The study was reviewed and approved by Institutional Ethical Committee and the study was registered with Clinical Trials Registry - India (CTRI) with registration no -CTRI/2019/08/020942 dt 28 Aug 2019. All participants of the study have explained the nature & scope of the study and written informed consent was obtained from each participant before initiation of treatment. Being a pilot project, a sample size of 10 patients was decided in consultation with the statistician of the institute.
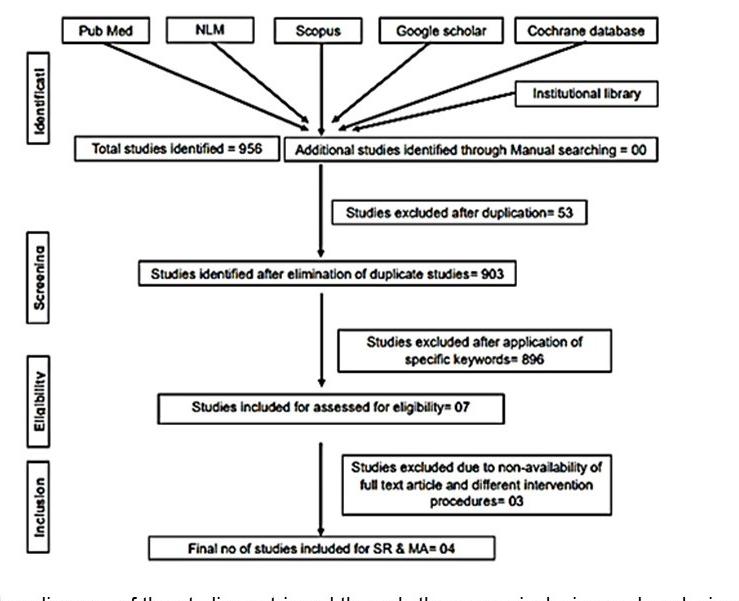
Standard orthodontic pretreatment records (T0) were obtained (Figure 1). The same operator obtained the lateral cephalogram and OPG using the same machine. The lateral cephalograms were traced manually with the standard technique by a single
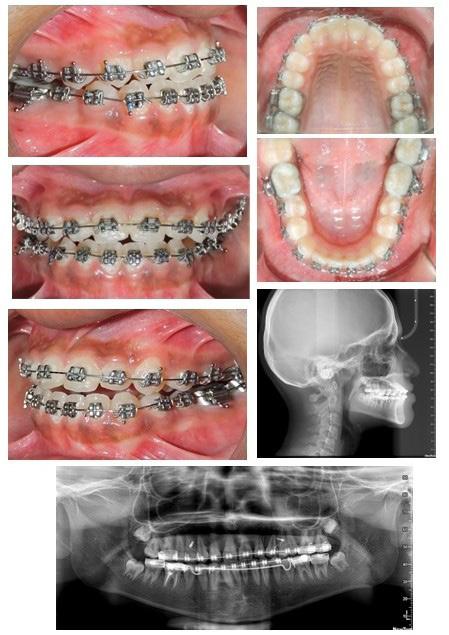
investigator and a total of 06 skeletal, 11 dental, and 03 soft tissue parameters were measured. Selected patients were also subjected to Acoustic pharyngometry (AP) for a three-dimensional evaluation of the upper airway. Fixed orthodontic appliance (022” MBT PEA) was bonded on both maxillary and mandibular arch, with banding of first & second molars. A standard wire sequence was followed till the full slot engagement with SS wire (19 X 25”) was achieved. A complete set of records were made to register the beginning of the fixed functional phase (T1) (Figure 2). Forsus appliance (FFRD) was fitted for each patient, push rod hooked on the archwire between canine and 1st premolar in the maxillary arch and distal end of open coil spring connected with the ‘L’ pin to the 1st mandibular molar. Maxillary and mandibular components of the Forsus FRD were connected to provide a forward thrush to the maxilla and a backward thrust to the mandible during the closure of the mouth (Figure 3). The functional phase with Forsus FRD continued till the desired objectives were achieved i.e., achieving positive overjet as well as satisfactory improvement in soft tissue profile.
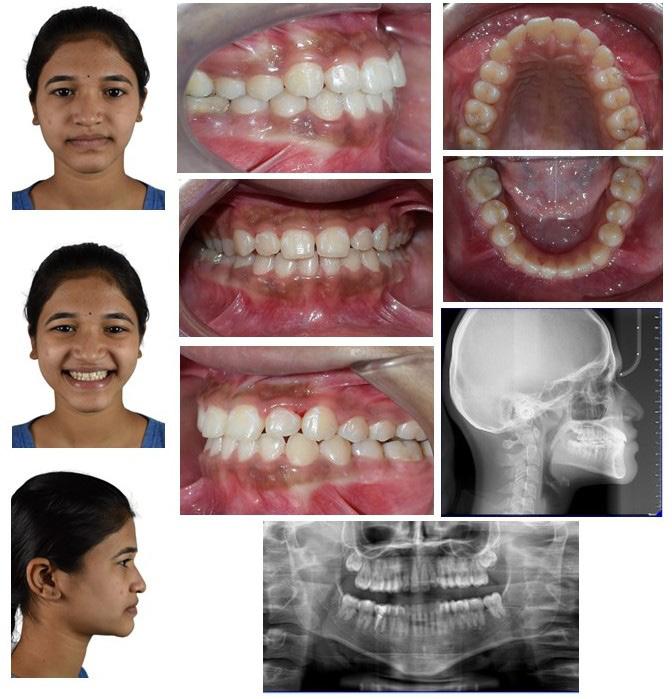
To enhance the skeletal effects of the Forsus appliance, the indirect anchorage was obtained using TADs (temporary anchorage devices), placed in the maxillary arch, distal to canine. Post-functional records were made after the removal of Forsus FRD (T2) (Figure 4). Fixed orthodontic therapy continued to settle the occlusion and patients were debonded (Figure 5).
Figure 1:Pre-treatment Orthodontic records
Results
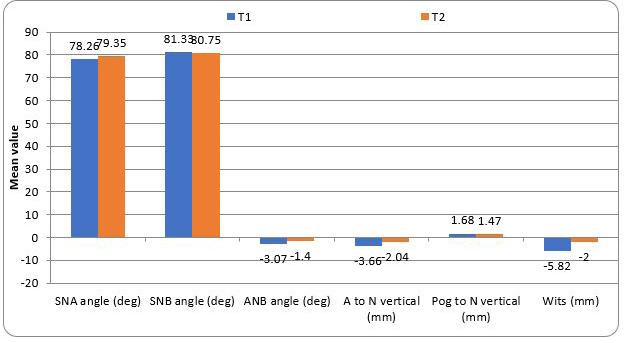
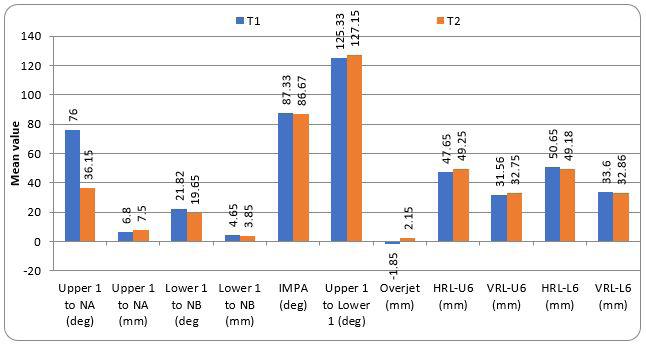
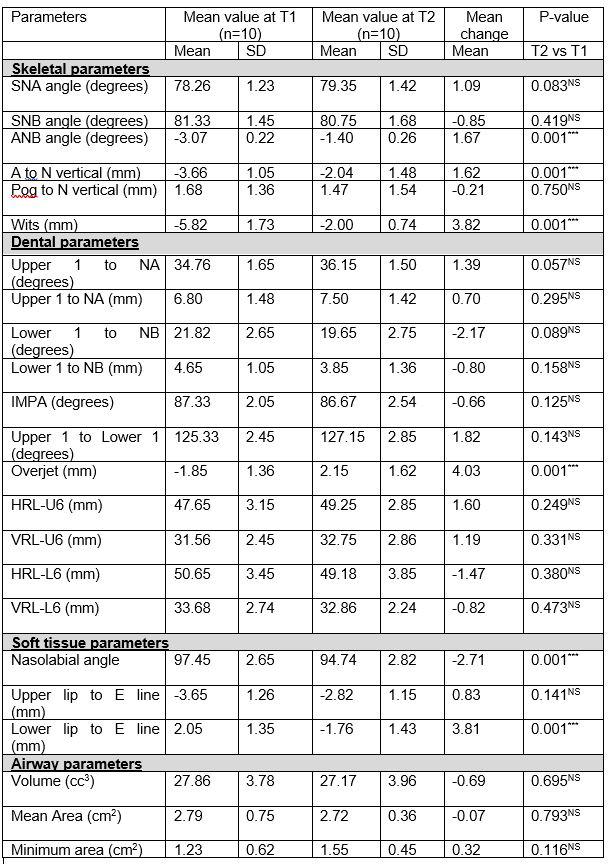
In the present study, 10 patients (06 female and 04 male) were enrolled, mean age of 13.2 years (range 12.6 to 13.9 yrs) at the time of Forsus appliance insertion. Six skeletal cephalometric parameters, three angular, and three linear parameters were evaluated for changes following Forsus therapy. The mean change in the skeletal parameters is tabulated in Table 1 and presented in Figure 6. The mean change in one angular (ANB angle) and two linear parameters (A to N vertical and Wits) were statistically significant (P-value<0.05 for all). However, for other skeletal parameters, the results were non-significant. Eleven dental parameters, seven linear parameters, and four angular parameters were studied to quantify the changes produced by the Forsus therapy. The mean changes observed are tabulated in Table 1 and presented in Figure 7. The mean change in overjet was statistically significant (P-value<0.05), while for all other dental parameters the change noticed was statistically not significant.
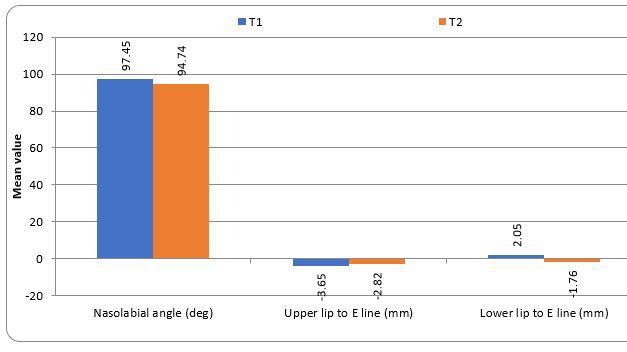
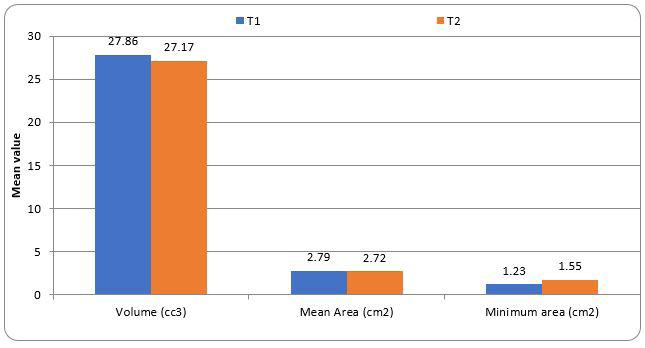
Three soft tissue parameters, one angular and two linear parameters were studied to determine the effect of reverse Forsus on soft tissues. The mean changes have been tabulated in Table 1 and presented in Fiugure 8. The mean change in the Nasolabial angle and lower line to the E line was statistically significant (P-value<0.05 for both) while the mean change in the Upper lip to the E line was not statistically significant. Three parameters were evaluated to quantify the changes in airway following Forsus therapy i.e., volume, mean area, and minimum area, the mean of the parameters studied was not statistically significant at T2 compared to the mean at T1. The mean changes are tabulated in Table 1 and presented in Figure 9.
Figure 2: Pre-functional Orthodontic records
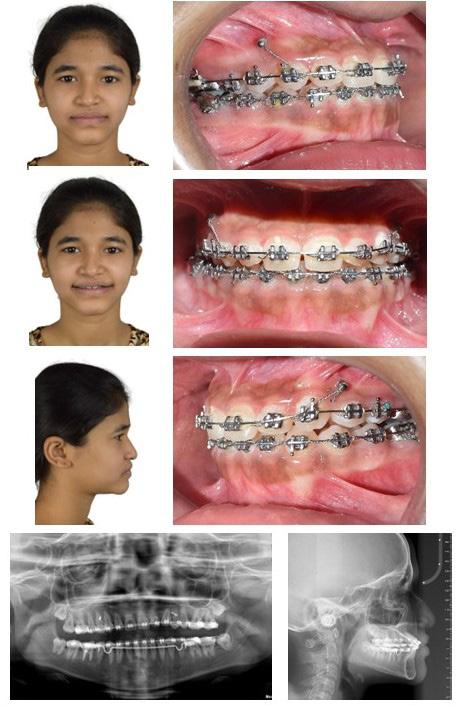
Figure 4: Post functional orthodontic records
Figure 5: Post-treatment Orthodontic records
Figure 3: Forsus appliance in situ
DISCUSSION
Management of skeletal Class III malocclusion is one of the most challenging clinical conditions in orthodontics.11 Among the various etiological factors, hereditary along with local environmental conditions are considered to play an important role.12, 13
Management of developing skeletal Class III malocclusion has been an area of concern among researchers and a challenge among clinicians.10. Intervention at an early age for developing skeletal Class III malocclusion has been recommended by various authors to improve the psychological development of an individual, correct the functional abnormality (if any), and make the growth pattern more favorable.1,4,14 Different protocols have been proposed, depending upon the underlying etiology of developing Class III (maxillary hypoplasia or mandibular prognathism). Protraction headgear/ reverse pull headgear or Face mask therapy15 is commonly advised for patients with maxillary hypoplasia, also removable functional appliances like Frankel III16 and Reverse twin-block17 is used for developing Class III. Individuals with mandibular prognathism may be prescribed chin cup therapy.18,19 Presently, the commonly used procedure for the management of developing skeletal Class III malocclusion (maxillary hypoplasia) includes the application of Rapid Maxillary Expansion (RME) along with a facemask20, 21 however, the efficiency of therapy and stability of the results achieved needs to be studied.22
Patient cooperation is of utmost importance for the successful outcome of any functional therapy, especially with a removable appliance. Commonly employed methods for correction of developing skeletal Class III malocclusion interfere with the day-to-day life of an individual and may be unesthetic and uncomfortable at times. These inherent problems associated with removable appliances may compromise the results expected and have led to the introduction of fixed-function appliances (FFA), reducing the compliance of the patients.
Forsus fatigue resistance device (FFRD) is an established contemporary modality for the management of skeletal Class II malocclusion among adolescent and literature support the effect of FFRD on the management of skeletal Class II patients.23 However, there are limited studies available in the literature who has used FFRD in the reverse fashion to manage the developing skeletal Class III malocclusion. The only previous study [10] on the subject concluded that there was a maxillary forward growth, confirmed by the statistically significant increase in SNA angle. In the present study although the change in SNA angle was not statistically significant, however, the mean change in point A to N vertical and Wits were statistically significant (P-value<0.05), confirming the maxillary forward growth.
In the present study, there was a significant reduction in the amount of negative overjet (mean correction of 4.03mm), the patients improved from negative overjet (-1.85mm) to positive overjet (2.15mm). The improvement in overjet is the total effect of both skeletal and dental effects, there was a forward movement of the maxilla along with proclination of maxillary incisor and retroclination of mandibular incisors. These observations are in line with the previous study10 where authors have confirmed a statistically significant reduction in overjet with mini-screw anchored inverted Forsus FRD.
There has been an improvement in the profile of the patients
Figure 8: Distribution of mean Soft tissue parameters at T1 and T2 time
Figure 6: Distribution of mean Skeletal parameters at T1 and T2 time
Figure 7: Distribution of mean Dental parameters at T1 and T2 time
Figure 9: Distribution of mean airway parameters at T1 and T2 time
with a more harmonious relation of lips to the aesthetic line, the mean change in the upper lip was 0.83mm (statistically nonsignificant) whereas the mean change in lower lip relation to the aesthetic line was 3.81mm (P-value 0.001). The results of the present study are in agreement with the previous study where improvement of profile resulted from improved line relation to the aesthetic line.
The Forsus appliance has resulted in positive overjet and overbite incisor relation, optimal intercuspation with Class I molar relation, and an improved functional environment. All these factors contribute toward the maintenance of the results obtained and prevent relapse. The compliance and comfort associated with the Forsus appliance have been satisfactory and no patient complained of any problem during the treatment. However, few
problems related to hygiene maintenance (brushing) and wide mouth opening (yawning) were reported. No patient reported Temporomandibular Dysfunction (TMD). Literature documents that the established modalities for the management of skeletal Class III (Chin cup and Face mask) used orthopedic forces and are not considered a risk to develop TMD.24,25 Since the force applied by Forsus are less as compared to these appliances, it is assumed that it may not develop any TMD.
Limitations
Being a pilot study, the sample size of the present study was small. Larger sample size with a multicentric study would have greater clinical significance. The results obtained need to be observed for their long-term stability. Although no patient
Table 1:The means and distributions of shear bond strengths in the different study groups
complained of any TMJ problems, it should be evaluated for any deleterious change during and after treatment.
The study results need to be analyzed with randomized clinical trials, where other established modalities of correction of skeletal Class III malocclusion should be compared with this newer modality along with the control.
Conclusion
The treatment of developing malocclusion with removable appliances is highly dependent on compliance from the young patients. It is established that cooperation during treatment is a key factor in the success of orthodontic treatment. Forsus appliance, being fixed functional appliance the compliance factor is being taken care of. Within the scope of the present study following conclusions can be made:
• Forsus appliance is effective in the management of patients with developing skeletal Class III malocclusion with maxillary hypoplasia. Forward movement of the maxilla has been noted with a very minimal skeletal effect on the mandible.
• Forsus appliance can be used as an appliance for correction of developing skeletal Class III malocclusion (maxillary hypoplasia), especially among patients where compliance with removable appliances is questionable.
• Significant improvement in the profile of the patients has been achieved, resulting from improvement in the position of the upper and lower lip.
• Improvement in the reverse overjet was achieved, a positive relation was the total of the correction achieved in both skeletal and dental parameters.
• The changes in airway parameters studied were non-significant.
References
1. Baccetti T, Tollaro I. A retrospective comparison of functional appliance treatment of Class III malocclusions in the deciduous dentitions. Eur J Orthod. 1998;20:309-17.
2. Kim JH, Viana MA, Graber TM, Omerza FF, BeGole EA. The effectiveness of protraction face mask therapy: A meta-analysis. Am J Orthod Dentofacial Orrthop. 1999;115:675-85.
3. Battagel JM, Orton HS. A comparative study of the effects of customized facemask therapy or headgear to the lower arch on developing Class III face. Eur J Orthod. 1995;17:467-82.
4. Campbell PM. The dilemma of Class III treatment. Angle Orthod. 1983;53:175-91.
5. Kapust AJ, Sinclair PM, Turley PK. Cephalometric effects of face mask/ expansion therapy in Class III children: A comparison of three age groups. Am J Orthod Dentofacial Orhthop. 1998;113:204-12.
6. Atalay Z, Tortop T. Dentofacial effects of a modified tendem traction bow appliance. Eur J Orthod. 2010;32:655-61.
7. Watkinson S, Harrison JE, Furness S, Worthington HV. Orthodontic treatment for prominent lower front teeth (Class III malocclusion) in children. Cochrane Database Syst Rev. 2013;(9):CD003451.
8. Papadopoulos MA. Orthodontic treatment of the Class II non-compliant patient: Current principles and techniques. 2nd ed. Mosby, 2006: p9-11.
9. Panigrahi P, Vineeth V. Biomechanical effects of fixed functional appliance on craniofacial structures. Angle Orthod. 2009;79:668-75.
10. Eissaa O, ElShennawy M, Gaballah S, ElMehy G, El-Bialy T. Treatment of Class III malocclusion using miniscrew-anchored inverted Forsus FRD:
11. Martina R, D’Antò V, De Simone V, Galeotti A, Rongo R, Franchi L. Cephalometric outcomes of a new orthopaedic appliance for Class III malocclusion treatment. Eur J Orthod, (2019), doi:10.1093/ejo/cjz037.
12. Litton SF, Ackermann LV, Isaacson RJ, Shapiro BL. A genetic study of Class III malocclusion. Am J Orthod. 1970;58:565-77.
13. Rokosi T, Schilli W. Class III anomalies: A coordinated approach to skeletal, dental, and soft tissue problems. J Oral Surg. 1981;39:860-70.
14. Joondeph D. Early orthodontic treatment. Am J Orthod Dentofacial Orthop. 1993;104:199-200.
15. De Clerck H, Cevidanes L, Baccetti T. Dentofacial effects of boneanchored maxillary protraction: a controlled study of consecutively treated class III patients. Am J Orthod Dentofacial Orthop. 2010;138(5):577–81.
16. Loh MK, Kerr WJ. The function regulator III: effects and indications for use. Br J Orthod. 1985;12(3):153–7.
17. Kidner G, DiBiase A, DiBiase D. Class III twin blocks: A case series. J Orthod. 2003;30(3):197–201.
18. Thilander B. Chin-cap treatment for angle class 3 malocclusion. Rep Congr Eur Orthod Soc. 1965;41:311–27.
19. Sugawara J, Asano T, Endo N, Mitani H. Long-term effects of chincap therapy on skeletal profile in mandibular prognathism. Am J Orthod Dentofacial Orthop. 1990;98(2):127–33.
20. Baccetti T, Franchi L, McNamara Jr J A. Treatment and posttreatment craniofacial changes after rapid maxillary expansion and facemask therapy. Am J Orthod Dentofac Orthop. 2000;1189(4):404–13.
21. Smyth RSD, Ryan FS. Early treatment of class III malocclusion with facemask. Evid Based Dent. 2017;18(4):107-8.
22. Rongo R, D’Antò V, Bucci R, Polito I, Martina R, Michelotti A. Skeletal and dental effects of Class III orthopaedic treatment: A systematic review and meta‐analysis. J Oral Rehabil. 2017;44(7):545–62.
23. Franchi L, Alvetro L, Giuntini V, Masucci C, Defraia E, Baccetti T. Effectiveness of comprehensive fixed appliance treatment used with the Forsus fatigue resistant device in Class II patients. Angle Orthod 2011;81:678-83.
24. Zurfluh MA, Kloukos D, Patcas R, Eliades T. Effect of chin-cup treatment on the temporomandibular joint: a systematic review. Eur J Orthod. 2015;37(3):314–24.
25. Huang X, Cen X, Liu J. Effect of protraction facemask on the temporomandibular joint: a systematic review. BMC Oral Health. 2018;18(38):1-12.
Growing Beautiful Teeth Chapter 9: Key to Health
Estie Bav is an active member and senior instructor of IAO. She graduated BDSc from the University of Western Australia, and practises in her own private family dental surgery in Melbourne Australia. In November 2018 she published her first book titled “Growing Beautiful Teeth,” primarily targeting parents, grandparents, teachers or any child health carer to look out for early signs of dental growth issues. It informs the unaware the importance and impact of teeth and jaw on other areas of health such as breathing, sleep, posture, and even behaviour.
Currently the dental profession tends to “supervise and wait” for growth issues to become complex and expensive to correct….”
“My concern is that most parents miss out on basic and important dento-facial growth information until too late.”
The book was designed to be a helpful resource for your patient to read, and for introducing the subject to younger dentists and allied health professionals who may not be familiar with the teeth-occlusion-airway-TMJ-sleep paradigm.
Her message is to get involved with a child’s dento-facialairway development early.
Growing Beautiful Teeth is available from any major online booksellers, or at
• www.drestiebav.com
• www.growingbeautifulteeth.com
She can be reached at estie@drestiebav.com
How my book can be helpful….
It takes time to educate parents on the benefits of treating dental growth issues early and explaining what signs we look for. In writing this book in simple language I hope to bring an awareness to the larger parent community, which will in turn save my dental colleagues chairside time. This book would be a helpful resource for the waiting room, and for introducing the concept to younger colleagues joining your practice.
IAs I studied my notes collected from past seminars and courses over the years, and as I searched my ever-growing collection of books, I rediscovered an amazing book which I must share with the reader. This book called The Breath of Life or Mal-respiration and its Effects Upon the Enjoyments and Life of Man (also titled Shut Your Mouth and Save Your Life) was written in the mid-1800s by American author George Catlin (1796-1872).
Catlin was by profession a lawyer and a portrait painter. Later in life, he travelled in the western plains of North and South America to live with, paint and study the Native American Indian tribes in their natural communities and habitat. He apparently visited 150 tribes, a total of about two million natives. Thus, he had an opportunity to observe and compare the way of life, especially in the area of health and diseases, of the Native Americans with that of the population from his own background.
At that time, he was aware that the average life span in the so-called ‘civilised’ communities he came from was less than one-fifth of the expected life of 70 years (3 scores plus 10), and the prevalence of infant mortality was high.
He was astonished to learn that by contrast the various tribal natives covering a large span of the America continent were altogether a much healthier people despite their more basic living conditions.
There was no parallel to the rate of child mortality that was seen in the civilised world.
There were less premature deaths, and significantly less incidences of mental and physical ‘deformities’ as they were known then.
He became curious as to why the difference existed, and what was causing the breakdown of health and the magnitude of diseases in the ‘civilised’ world but not in the other. He searched for answers by observation and talking with the natives.
First, he observed that the natives’ diet consisted mainly of locally wild-caught fish, buffalo meat, venison, maize and vegetables.
After years of observation, he concluded that the cause of ill health amongst his own civilised people was quite simply a neglect to secure a good night’s sleep, supported by proper breathing through the nose. He wrote that quiet and natural sleep is the physician and the restorer of mankind and animals.
He noted how a native mother at the end of a breastfeed would lower the infant to sleep and be sure to press its lips together to keep the mouth closed. By contrast, he observed that most children in more civilised communities inside their sanitised homes comforted by heating and cooling, in fact slept with their mouth open.
Catlin, in the mid-1800s, had said that nature has given us such a sophisticated organ as the nose to ensure that air is well purified before it reaches our lung, yet man is so unwise to not use the nose but instead the mouth, to breathe According to George Catlin keeping the mouth closed when breathing is the key to health.
I highly recommend this short book which contains interesting illustrations drawn by the author himself.
Chapter 10
I believe that we can realistically look forward to a future where everyone has amazing teeth, gorgeously bright smiles with great looking faces, balanced occlusion that keeps the TMJs healthy, and broad jaws that do not constrain the tongue – a future where everyone breathes well, sleeps well, and lives a life free of chronic pain.
People will be happier as there will be less suffering from dental and other related chronic health issues. Paying the dentist’s bill will take on a different meaning and may not be such dirty words. It would be a future with a much shorter queue for medical and hospital care, and the budget for dental and medical health can be greatly reduced.
I hope that the reader can see the big picture that I do and that it begins with paying early attention to guiding your child’s dentofacial growth in the right direction.
I think we may also need a paradigm shift at our teaching institutions. We need our university and dental schools to educate dental undergraduates on the wider paradigm of dental health care and its broader integrative links to other health professionals. Education is the key, not just for the health professionals but also for the community at large at all levels. Parents, grandparents, carers and extended family attending to a child need to work together in an integrative manner, and consider the paradigm discussed in this book.
The body is not compartmentalised into isolated parts. Quite the contrary, nature is awesome at creating this amazing body of ours that consists of many physiology systems which all connect and work together perfectly. We need to understand how the function or dysfunction of one system can affect the others and attempt to address the root cause of a dysfunction for a positive outcome for the whole body rather than just treating the isolated symptoms.
All health professionals from various disciplines need to embrace the paradigm shift and work together more closely for the benefit of the patient’s well-being.
We also need the health funds to take part in this paradigm shift. Restorative treatments are still preferential for claiming
benefits. Health benefit payouts for preventative therapy including health education have always been appalling or non-existent. This must change. They must be prepared to support the professionals and their clients, the fund members, and pay benefits for fees charged for time well spent by professionals in educating patients. Unless we make the change, nothing will change.
Epilogue
The longer I have been in practice, the stronger my conclusion that a typical dentist’s routine of helping to repair broken down teeth or restore hopeless occlusion is too much hard work. It is very challenging for the dentist, very costly for the patient and often yields only a compromised result. It is not the optimal way of going about improving dental health. There has to be a better way, and there is a better way. Therefore, I decided it was time I shared my thoughts.
As I began to write this book, I came to realise, and panicked somewhat, that I cannot condense every bit of what I have learned over the decades of clinical practice and continuing education into a book of this size. It has been a challenge to decide which bit of knowledge would be the most essential and useful in relation to growing beautiful teeth. I hope that I managed to explain with just the right amount of detail to make the points clear enough so as not to confuse.
This book can serve as a beginner’s guide to growing beautiful teeth for one’s child. Much more is now available out there on the internet. I am hoping that once parents understand the simple but essential basics as discussed in this book, they can research further to expand their knowledge on this interesting subject of dentofacial growth.
The steps to take are simple but it takes dedication and courage to do it differently. Do not wait to see how far a problem will pan out and hope that someone can fix it later. The change from a fix-it-later attitude to nipping-it-at-the-buds, to nurture growth and mitigate the problem is the paradigm shift that both the parents and the professionals need to strive for.
Unless we make the change, nothing will change.
Nine Keys of Ideal Functional Occlusion 2024
by Dr. Kenneth U. Lau, Dr, Hanna Szekely, and Dr. Rob Pasch
AUTHORS
Dr. Kenneth U. Lau
DDS, Indiana University School of Dentistry. Dr. Lau has achieved many credentials for his work in Orthodontics, Cephalometric, TMD, 3-D imaging, and Software Development.His approach to diagnosing and treating Orthodontic and TMJ pain problems is a comprehensive, evidence-based diagnosis that explains the cause of the complex problems of orthodontics, TMD, and OSA. Treatment must balance the function of occlusion, jaw muscles, and jaw joints. The treatment protocol is to treat the problems’ cause and not just the symptoms. Oral facial dysfunction is best defined as dysfunction of the Teeth-Muscles-Jaw joint complex. He developed the 9 keys to a successful Occlusal Treatment Protocol.
Dr. Olna Hanna Szekely DDES, Universitatea de Medicina si Farmacie, Targu Mures, Romania; DMD Boston University Awarded membership in the prestigious Alpha Omega Society during her study years. IAO Diplomate and Certified Instructor; Member of ADA and ISDS.
Dr. Rob Pasch General Dental Practitioner, Queens University and Toronto Faculty of Dentistry 1982. Dr. Pasch has always been interested in pursuing his orthodontic education. He graduated from the Orthodontic mini residency at University of Toronto, earned his International Board of Orthodontic Diplomate Status, and is a Masters in Special Orthodontics from the University of Duisburg-Essen.
Abstract:
I ntroduction : Integrity without knowledge is weak and useless, and knowledge without integrity is dangerous and dreadful. Samuel Johnson (September 18, 1709 – December 13, 1874)
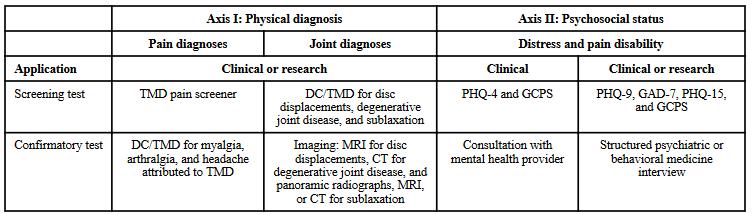
“In 1992, a paper published by the S. F. Dworkin group defined the criteria for TMD diagnosis as Research Diagnostic Criteria / TMD (RDC/TMD). Subsequently, in 2014, the group redefined RDC/TMD Diagnostic Criteria / TMD (DC/TMD).“1 (See Table 1.)
“Axis I covers the physical diagnosis, which includes pain and tm joint diagnosis. Pain diagnosis involved the screening test and confirmatory test of myalgia, arthralgia, and headache. T.M. Joint diagnosis involves the screening test for disc displacement, degenerative joint disease, and subluxation. The confirmatory test will use MRI for disc displacement, C.T. for degenerative joint disease, and panoramic radiographs, MRI, or C.T. for subluxation.
Axis II covers distress and pain disability. The screening test uses the Patient Health Questionnaire-4 (PHQ-4) and Graded Chronic Pain Scale (GCPS) for clinical evaluation. For research purposes, the forms Patient Health Questionnaire-9 (PHQ9), Generalized Anxiety Disorder-7 (GAD-7), and Patient Health Questionnaire-15 (PHQ-15).
Confirmatory tests will use consultation with a mental health professional.”1
“The occlusion covered by Costen, Ramfjord, Guichet, Farrar & McCarty, Gelb, and Williamson & Lundquist is absent
in the Axis I diagnostic criteria. Further literature search discovered that a group of professors, researchers, and academic professionals, like Zicher (1949), Schwartz (1959), Laskin (1969), Posselt (1971), Geering (1974), Rugh & Solberg (1975), Solberg (1979), ADA President’s Conference (1983), Rugh, Barghi & Drago (1984), Zarb & Carlsson (1979), Von Korff (1988), Seligman & Pullinger (1989), Dworkin & LeResche (1992), Zarb, Carlsson, Sessle & Mohl (1994), and Okeson (1996 and later editions) found no evidence for occlusion problem contributed to TMD problems.”2
Further, in “2020, Greene et al. described that the Third Pathway is based on the assumption that signs and symptoms of TMD are due to a “bad” relationship between the mandible and skull, leading to a variety of irreversible occlusal or surgical corrective treatments. The third pathway does not follow the many medically oriented conservative/surgical Two-Pathway models for the diagnosis and treat TMD within a biopsychosocial model of pain. TMD diagnosis and treatment is a third pathway that should be eliminated.”3 This third pathway seems to follow the Axis I diagnostic criteria philosophy. These overwhelming research papers indicated that occlusion does not contribute to TMD problems. One wonders why not. No one can dispute that the condyle and the teeth (Occlusion) are genetically and physically connected. They are one and one only and cannot be separated when discussing how one affected another. Meanwhile, arguing differently with the above-listed group of professors, researchers, and academic
Table 1: Dworkin’s Table 1 Patient Health Questionnaire-4 (PHQ-4), Graded Chronic Pain Scale (GCPS), Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7), Patient Health Questionnaire-15 (PHQ-15).
professionals can be difficult. However, as Samuel Johnson stated in 1709, integrity without knowledge is weak and useless, and knowledge without integrity is dangerous and dreadful. Samuel Johnson (September 18, 1709 – December 13, 1874) This paper aims to search the literature further to verify that occlusion problems can contribute to TMD problems.
Method: This paper searches the literature to verify that occlusion problems can contribute to TMD problems. Diagnosis of occlusion problems is necessary to help resolve the TMD problems.
Result: Occlusion problems contribute to TMD problems. Splint Therapy is an ideal conservative TMD problem relief for TMD patients by following the Ricketts A-Position, Andrew’s six keys of occlusion, Ramford/Ash Occlusion with cuspid and no lateral excursive interference.
Conclusion: Summation of all literature review, Splint Therapy is an ideal conservative TMD problem relief for TMD patients by following the Ricketts A-Position, Andrew’s six keys of occlusion, Ramford/Ash Occlusion with cuspid and no lateral excursive interference.
Ricketts’ A Position must be the starting point of all occlusion treatments, whether Orthodontic, TMD, or Full-mouth reconstruction. Dental treatments must have Ricketts, A Position TM Joint space for the disc to function as the condyle rotates and translates with the support of the T.M. Disc.
This Nine Keys must be included in all branches of dental protocol, especially for TMD treatment. It is not as simplistic as described by Greene et al.; following the medical two-pathway model with medications, minor surgical procedures, and nonsteroidal anti-inflammatory drugs can not solve the functional problem of occlusion.
More case studies should be published in totality based on Ricketts’ A Position, Andrew’s six keys, Cuspids guides, and No Lateral Excursive Interferences occlusion function (The Nine Keys for Successful Occlusal Treatments) and not in piecemeal.
Keywords: Occlusion, Ricketts A-Position, Andrew’s six keys of occlusion, Ramford/Ash Occlusion cuspid function, no lateral excursive interference
Introduction:
In a paper, Treating Temporomandibular Disorders in the 21st Century: Can We Finally Eliminate the Third Pathway, published in 2020, the authors suggest that “Traditional orthopedic therapy relies on a Two Pathway approach involving conservative or surgical treatments. However, over the course of the 20th century, some members of the dental community have created another way of approaching these disorders- referred to in this paper as the Third Pathway-based on the assumption that signs and symptoms of TMD are due to a “bad” relationship between the mandible and skull, leading to a variety of irreversible occlusal or surgical corrective treatments. The paper further stated that these studies have shown that TMD comprises another domain of orthopedic illness that requires a medically oriented approach for good outcomes while avoiding the irreversible aspects of the Third Pathway.”1
What is the Third Pathway?
“The “Third Pathway” is based on three assumptions: 1. The mandible-to-skull relationship at the condylar level may not be “good” (also described as misaligned, malpositioned, acquired, nonideal, suboptimal, etc.).
2. This relationship can be analyzed by a variety of so-called “diagnostic” methods, ranging from pushing on the chin to measurements using sophisticated electronic devices. 3. If the existing jaw relationship is deemed to be “bad,” then it can be improved by a variety of irreversible dental techniques, ranging from occlusal adjustments to orthognathic surgery.”3
“Why Did the Dental Profession Create a Third Pathway? Establishing a Diagnosis. Since no other branch of the medical profession has proposed a malpositioning-repositioning approach to diagnosing or treating other human joint disorders, it would be expected that the TMJ has some unique features that make it possible, and even attractive, to analyze TMD patients in such a framework. The most obvious anatomical feature is the fact that no other joint has a definitive stopping mechanism external to the joint structures that require the joint to move into a specific position upon “seating” of the opposing parts. This “stop” occurs when the maxillary and mandibular teeth (which are located several inches away from the TMJs) meet in maximum intercuspation (MIP). In healthy dentate patents, teeth meet in a precise and repeatable manner, and this event will determine with great precision and repeatability where the mandibular condyle will end up relative to the skull when the mouth is fully closed.”3
The authors pointed out that the dental profession approached the wrong concept in diagnosis. As a result, “The Third Pathway has three major problems in dealing with dental methods.
1. The Third Pathway method includes diagnostic assessments of occlusal, skeletal, and TMJ relationships as likely factors in the etiologies of various TMD conditions, leading to a variety of bitechanging and jaw-repositioning therapies. It is based on concepts and procedures that are unique to the dental profession and the TMJ because no other branch of orthopedic medicine utilizes such assessments or treatments for other body joints.
2. The study was concerned that The Third Pathway method provided irreversible dental treatments, but the conservative/ surgical treatment model (Two-Pathway approach) to diagnose and treat TMD is recommended.
3. The dental and medical professions began to converge on the issues surrounding the management of TMD as another orthopedic pain management area that requires a medically oriented approach for good outcomes while avoiding the irreversible aspects of the Third Pathway.”3
“The authors’ analysis assumes that “it is clear that this Third Pathway is a unique and artificial conceptual creation arising from the dental profession based on a biologic and mechanical viewpoint that deserves to be challenged, and it is time to abandon this approach as we move forward in the TMD field.”3 The whole article seems contradictory. One discussion is that the dental profession provides irreversible procedures, yet the medical profession is okay with providing an irreversible conservative/surgical treatment model (Two-pathway approach).
Just because other orthopedic medicine branches are ignorant of the uniqueness of Dental TMD treatment based on Angle, Andrew, Ramford, Ash, Posselt, and Travell, the authors of “Treating Temporomandibular Disorders in the 21st Century Can We Finally Eliminate the Third Pathway?”3 have no justification to suggest the “Can We Finally Eliminate the Third Pathway.”3
The paper suggested that “TMD have been distinguished by a history of controversies going back nearly 100 years that continue to have a pernicious effect on the practice of caring
for such patients”1 and “the medical Two Pathway approach is correct, and the dental Third Pathway approach should be eliminated because it has become progressively clear that the Third Pathway is a unique and artificial conceptual creation of the dental profession.”3
The 100 + year history of the dental profession deals with the principle of Andrews’ six keys and Ramford and Ash’s Occlusion. The medical profession’s Two-Pathway model to diagnose and treat TMD cannot accomplish the same as Andrew, Ramford, and Ash. It is not practical to apply the dental approach in treating a physical problem with the medical prescription of anti-inflammatory steroids or a surgical approach to a physical problem of the T.M. Joint. Yes, anti-inflammatory steroids can help the damage done by the physical effect of the posterior and or superior compression of the condyle to the fossa.
Suppose the vertical dimension of Occlusion is reduced with a compressed T.M. Joint space. In that case, the disc may displaced medial-anteriorly when the condyle is pushed backward by the masseter and medial pterygoid muscles. “The disc is displaced medially because the superior head of the lateral pterygoid muscle attachment is from the pterygoid process plate with forward traction of the disc medially. It is active when the mandible is closing. The disc can only be displaced medial-anteriorly, and the condyle head is forced against the fossa plat. The disc p pops forward medial-anteriorly and stretches the retrodical tissue. Repetitive popping will eventually weaken the retrodiscal tissue, and it will not be able to pop back into place. Many MRI studies support that compressed T.M. Joint space resulted in disc displacement and osteoarthritic changes. Numerous MRI studies recorded morphological manifestations of TMJ dysfunction (disk displacement, effusion, osteoarthritis) that were associated with the presence of symptoms of TMJ dysfunction. Gender did not correlate with disk displacement, osteoarthritis, or effusion of TMJ. Osteoarthritis was more common in the older population, and effusion was more common in the younger age group. Many studies also confirmed the importance of clinical examination and MRI in diagnosing TMJ dysfunction and, consequently, selecting the most appropriate therapy.”9-20 Another MRI study shows that TMD patient’s closed mouth images have a higher incidence of tm disc displacement.Imanimoghaddam, M. et al. two and three-dimensional studies showed that patients in more advanced TMD stages show decreased condyle height.22 MRI studies proved that compression of T.M. Joint Space correlates with disk displacement, osteoarthritis, or effusion of TMJ, and reduced condylar size. “Many treatments with prosthodontics and orthodontics successfully decompress the compressed T.M. Joint space and reduce joint noise and pain. One article reviewed over 4,500 studies that show that conservative occlusal splint therapy is one of the ideal treatment methods.”23-29
T.M. Joint compression and relief with occlusal splint therapy is a success, but studies also show the success and only a conservative reversible treatment. The problem is that the treatment is segmental and only for symptom relief. Treatment must meet the goal of Ricketts’ A-position, Ramfjord occlusion, Posselt’s Envelope of Motion, and Andrew’s six Keys of ideal Occlusion. There are nine basic keys to ideal occlusion.
Ideal Occlusion must start with the tm joint in Ricketts’ A Position, and the mandible will have a complete movement within the Envelope of Function. The optimal result after TMD
treatment can meet the goal of Ricketts’ A-position, Ramfjord occlusion, Posselt’s Envelope of Motion, and Andrew’s six Keys of ideal Occlusion.
By the coherence theory of truth or the correspondence theory of truth, one cannot deny the writing of Angle, Andrew, Ramford, Ash, Posselt, and Travell. After all things are considered, from the point of functional occlusal, the first thing to consider is the well-established Orthodontic Standard of ideal Occlusion based on Andrew’s Six Keys. “Andrew’s Six Keys are defined as proper angulation (tip), proper inclination (torque), super Class I molar position, flat curve of spee, no rotations, and no spaces.”6 The Andrew 6 keys address the appearance of teeth which are lined up in Angle Class I. Andrew 6 keys do not address the demand for function, occlusal terminal seating, and stabilization. Andrew 6 keys combined with Ricketts’ A-position, Ramfjord, Ash Occlusion, and Ulf Posselt’s Envelope of Motion is the functional occlusion for correctly diagnosing and treating TMD problems. The foregoing places the Axis/Atlas relationshipin the ideal position.
What is an ideal functional occlusion?
Occlusion deals with how the muscles, teeth, mandibular and maxilla bone in vertical, horizontal, and sagittal movements respond to the demands of physiologically balanced functions.
Ramfjord and Ash started the discussion of Occlusion with the Masticatory Muscles. “The rest position of occlusion is when the resting length of masticatory muscles is in the minimal tonic contraction to maintain the posture and to overcome the force of gravity.”4 Based on the resting length of the masticatory muscle, the ideal Occlusion should be discussed physically and functionally in the following sequence:
1. Ulf Posselt’s Envelope of Motion supported by Ricketts’ A-position;
2. Occlusion meets Andrew’s six keys,
3. Functionally, the occlusion supports Cuspid Rise, and 4. Functionally, the occlusion has no Lateral Excursive Interference. These four criteria are the nine keys of ideal functional occlusion in any occlusal treatment, especially in TMD treatments.
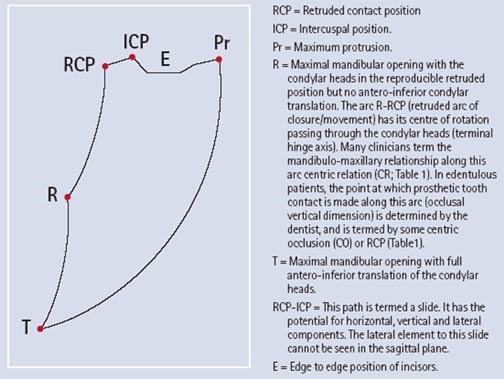
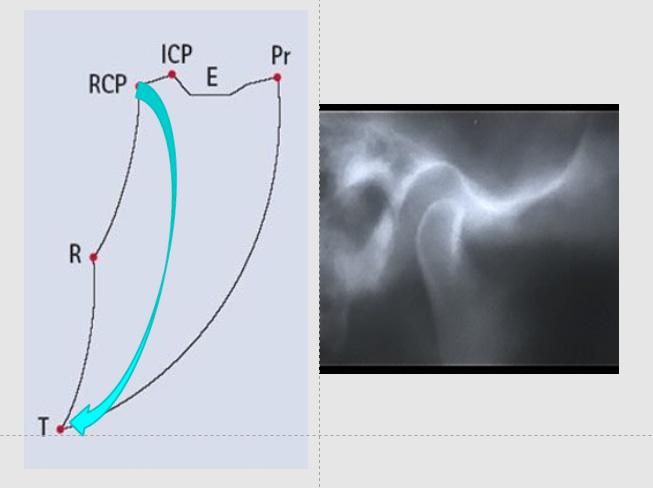
1. “Ulf Posselt’s Envelope of Motion 1952 (Envelope of Function (Border Movement)) was developed before the availability of Dental cone beam computed tomography (CBCT). It can describe the mandibular movement in relation to the maxilla. The various mandibular movement points can be updated to meet today’s added information.” (See Figure 1.)
RCP = Retruded contact position.
ICP = Intercuspal position.
RCP – ICP = This path is termed a slide. It has the potential for horizontal, vertical, and lateral components. The lateral element to this slide cannot be seen in the sagittal plane. (Condyle movement within Ricketts’ A position). (If there is no Ricketts’ A position, the Movement will be limited) or (with disc damage or displacement).
E = Edge-to-edge position of incisors.
Pr = Maximum protrusion.
R = Maximal mandibular opening with the condyle in the most Retruded position.
(R will vary depending on Ricketts’ A position) (If there is disc displacement and no tm joint space, the Maximum Opening will be limited.)
T = Maximal mandibular opening with full anterior-inferior translation of the condylar head.
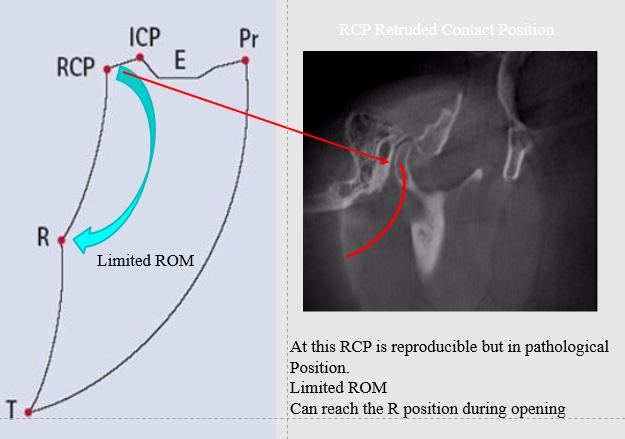
Ulf Posselt’s Envelope of Motion can have two possible border
movements based on whether there is Ricketts’ A position or no Ricketts’ A position.
For example:
1. RCP = With a healthy T.M. Joint complex and the disc supported in Ricketts’ A Position, the disc will support the terminal hinge axis rotation and translation without disc displacement. The mandible can open to the T position. (See Figure 2.)
With an unhealthy T.M. Joint complex, the disc is not supported in Ricketts’ A Position. During the terminal hinge axis rotation and translation, disc displacement can happen. The condyle can be pushed posteriorly and superiorly with or without popping noise. “If an adequate disc position does not support the occlusion, the surgical procedure will fail.” 8
RCP – ICP slide may be no more than the condyle moving within the tm joint space (Ricketts’ A Position). (Figure 3.)
2. Ricketts’ A-position of the condyle position is the best starting point.
“The definition for Ricketts’ A-position is for the tm joint space to have enough space for the function of the tm disc during rotation and translation.”5
3. Andrew’s six points are more logical when discussing the tm joint function when the condyle is in Ricketts’ A Position.
“Andrew’s six Keys are defined as Class I molar position, proper angulation (tip), proper inclination (torque), flat curve of spee, no rotations, and no space.
a.Interarch Relation (Class I molar):
• The distal surface of the distal marginal ridge of the upper first permanent molar contacts and occludes with the mesial surface of the mesial marginal ridge of the lower second molar.
• The mesiobuccal cusp of the upper first permanent molar falls within the groove between the mesial and middle cusps of the lower first permanent molar. The mesio-lingual cusp of the upper first molar seats in the central fossa of the lower first.
• The premolars enjoy a cusp-embrasure relationship buccally and a cusp fossa relationship lingually.
• Maxillary Canine has a cusp-embrasure relationship with Mandibular Canine & 1st Premolar. The cusp tip is slightly mesial to embrasure. Maxillary Incisors overlap Mandibular Incisors & midlines of arches match.”6
b. “Crown Angulation:
• Crown angulation (tip) Facial Axis of the Clinical Crown (FACC) Best viewed from the labial or buccal perspective. For all teeth except molars, it is located at the mid developmental ridge that runs vertically and is the most prominent portion in the central area of the labial or buccal surface. The facial axis of molar crowns is identified by the dominant vertical groove on the buccal surface.
• Crown angulation (tip). Viewed from a mesial or distal perspective, the FACC is represented by a line that is parallel to the middle development ridge (or with molars, the dominant groove) and tangent to the middle of the clinical crown on the labial or buccal surface
• Crown angulation (tip) refers to angulation (or tip) of the long axis of the crown, not to angulation of the long axis of the entire tooth.
• Crown Angulation or Crown tip. The degree of crown tip is the angle formed by the FACC and a line perpendicular to the occlusal plane. A “+ reading” occurs when the gingival portion of the FACC is distal to the incisal portion. A “- reading” when
Figure 1: Ulf Posselt’s Envelope of Motion 1952 (Envelope of Function (Border Movement)
Figure 2: T opening in Ricketts’ A Position w disc support
Figure 3: Opening in Ricketts’ A Position w disc support
the gingival portion of the FACC is mesial to the incisal portion.
• Crown angulation (tip): Each normal model had a distal inclination of the gingival portion of each crown. It varied with each tooth type, but within each type, the tip pattern was consistent from individual to individual.
• Crown angulation (tip) Normal Occlusion depends upon the proper distal crown tip, especially of the upper anterior teeth ( longest crowns). The degree of the tip of incisors determines the amount of M.D. space they consume & has a considerable effect on post. occlusion, as well as anterior esthetics.”6 c. “Crown Inclination:
• Crown inclination angle formed by a line which bears 90°to the occlusal plane and FACC (as viewed from the mesial or distal). A + reading is given if the gingival portion of the tangent line (or of the crown) is lingual to the incisal portion, A - reading is recorded when the gingival portion of the tangent line (or of the crown) is labial to the incisal portion.
• ANTERIOR CROWN INCLINATION. In upper incisors + crown inclination. In lower incisors - crown inclination, the average inter-incisal crown angle - is 174°.
• Properly inclined anterior crowns contribute to normal overbite and posterior Occlusion; when too straight up and down, they lose their functional harmony and overeruption results.
• If the inclination of the anterior crowns is not sufficient, space, in treated cases, is often incorrectly blamed on tooth size discrepancy.
• POSTERIOR CROWN INCLINATION— UPPER. A minus crown inclination for each crown from the U canine through the U-2nd PM. A slightly more negative crown inclination existed in the U-1st & 2nd molars.
• POSTERIOR CROWN INCLINATION— LOWER. A progressively greater “minus” crown inclination existed from the lower canines through the lower second molars.
• As the anterior portion of an upper rectangular arch wire is lingually torqued, a proportional amount of mesial tip of the anterior crowns occurs. The ratio is approximately 4:1. For every 4°of lingual crown torque; there is 1 ° of mesial convergence of the gingival portion of the central and lateral crowns.”6
d. “Rotation:
• Teeth should be free of undesirable rotations. Rotated molars would occupy more space than normal, creating a situation where they are unreceptive to normal occlusion.”6
e. “Tight Contacts:
• Contact points should be tight (no spaces). Persons who have genuine tooth-size discrepancies pose special problems.
• Serious tooth-size discrepancies should be corrected with jackets or crowns so the orthodontist will not have to close spaces at the expense of good Occlusion.”6
f. “Flat Curve of Spee:
• Occlusal plane (Curve of Spee), depth of curve of Spee ranges from flat plane to slight concave surface (0- 2.5 mm). A flat plane should be a treatment goal as a form of over-treatment. There is a natural tendency for the curve of Spee to deepen with time.
• The lower jaw’s downward and forward growth is sometimes faster and continues longer than the upper jaw. This causes the Lower Anterior teeth to be forced back and up, crowded lower anterior teeth and /or a deeper overbite and deeper curve of Spee.
• At the molar end of the lower dentition, the 3rd molars are pushing forward, even after growth has stopped, creating essentially the same results. If the Lower Anterior teeth can be held until after growth has stopped, and the 3rd molar threat has been eliminated by eruption or extraction, All should remain stable, assuming that treatment has otherwise been proper.” 6
• Intercuspation of teeth is best when the plane of Occlusion is relatively flat. There is a tendency for the c.o.s to deepen after treatment.
• Treatment of the plane of Occlusion until it is somewhat flat or reversed to allow for this tendency.
• A deep curve of Spee results in a more contained area for the Upper teeth, making normal Occlusion impossible. Only the Upper1st Premolar is properly intercuspally placed. The remaining upper teeth, Anterior and posterior to the 1st PM, are progressively in error.
• A reverse C of S is an extreme form of overtreatment, allowing excessive space for each tooth to be intercuspal placed.”6
4. Canine guidance:
“Canine guidance was defined by Thornton as the disocclusion of all the teeth by the contact of unilateral maxillary and mandibular canines in lateral excursion movement. It is also known as canine-protected occlusion, mutually protected occlusion, canine disocclusion, canine-lift, and canine rise. The canine-protected Occlusion theory is attributed to Nagao, Shaw, and D. Amico. It is based on the fact that canines are the most appropriate teeth to guide mandibular excursion for several reasons. The canines have a good crown-root ratio that tolerates high occlusal forces. Canines provide high proprioception. The shape of the Canine’s palatal surface is concave and suitable for guiding lateral movements. Canine guidance is often considered the ideal lateral guidance scheme because it will immediately disclude posterior teeth in excursions. Canine-protected Occlusion reduces the chances of temporomandibular dysfunction since it reduces lateral tooth contact and the possibility of interfering contacts. Consequently, the chance of muscular dysfunction is reduced.”33-37
Electromyography (EMG) studies and intraoral bite splint studies have shown that canine rise occlusion leads to more reductions in masticatory muscle activity compared to the group function occlusion [2]; therefore, it is worth considering that Canine- protected Occlusion is far less likely to be associated with occlusal interference on the nonworking side.38
5. No Lateral Excursive Interference:
Figure 4: Ricketts A-Position
“During maximum interdigitation (MI), Lingual Cusps of Mx Molar and Bicuspid contact the lower Mn occlusal fossa and interproximal embrasures to maintain the centric stop. The process sets the occlusal vertical dimension of the face (p 68).”4 Greene et al. describe the process as seating the bite.
“When the centric stop is in RCP position with adequate joint space to allow proper disc movement (Ricketts’ A Position), the buccal incline of the lingual cusp of the maxilla first molar will contact the lingual incline of the mandibular buccal cusp. This motion guides the mandible into the centric stop.”4 When the centric stop occlusion meets all the requirements of Adrew’s six keys and with Canine guidance, there will be no posterior teeth interference during lateral excursive movements.
“When the centric stop is in RCP position with inadequate joint space to allow proper disc movement (Compressed tm joint space), it may not meet all the requirements of Adrew’s six keys, and if there is not adequate Cuspid Rise in disclussion, there will be posterior teeth interference during lateral excursive movements. If posterior teeth interference exists during lateral excursive movements, the temporalis muscle and the sling muscles cannot rest, resulting in myogenic pains. As far back as 1958, Granger, E . R. wrote that there can be no doubt that a definite relationship exists between occlusal disharmony and traumatic temporomandibular joint arthritis, with or without muscle tendon pain. Any myogenic pains that occur will more likely come from oral-facial muscles. “4, 34
Discussion
Mishra et al. “The purpose of orthotic jaw appliance therapy is to reduce TMJ-related pain, increase range of motion, and improve joint function. The exact mechanism of action of these devices is unknown. It is suggested that orthotic occlusal device therapy may alter the TMJ mechanics and increase joint mobility, enhance patient awareness of oral parafunctional behaviors, disrupt neuromuscular that determines TMJ-fossa relationships, and protect teeth and restorations from jaw clenching, causing potential fracture or attrition of dentition.”39,40
Mishra’s description of orthotic jaw appliance therapy follows all the explanations of how ideal occlusion should be. By the coherence theory of truth or the correspondence theory of truth, one cannot deny the writing of Angle, Andrew, Ramford, Ash, Posselt, and Travell. Besides the well-established authors mentioned above, thousands of articles have been published in peer-reviewed journals over the past 100 years. The Third Pathway mentioned by Greene et al. is a total fabrication and ignorance of facts proven by Angle, Andrew, Ricketts, Ramford, Ash, Posselt, Travell, and thousands of others. The dental profession must ignore Greene’s proposal to “Finally Eliminate the Third Pathway.”3 The Two-Pathway approach of orthopedic medicine branches with conservative surgical procedures and prescriptions is ignorant of the uniqueness of the human complex Occlusion. That surgical procedure may not work because, as Montgomery M. et al. described, “after disc surgery, the condyle position was unchanged in 86% of the joints imaged at an average of two years following surgery. Although TMJ disc repositioning surgery significantly improved pain and dysfunction in TMJ surgery patients, the improvement in disc position was not maintained in most subjects following surgery.”8
Occlusion/TMD problems are not separate issues. It is a
one-and-totally connected issue and must be treated as one and only one. Call it the Third Pathway or any other terms; Functional Occlusion must follow the “coherence theory of truth or the correspondence theory of truth”41 based on the writing of Angle, Andrew, Ricketts, Ramford, Ash, Posselt, and Travell. If there is a lack of T.M. Joint Space, occlusion splint therapy is the most conservative protocol to establish and maintain Ricketts’ A Position. The splint therapy diagnosis and treatment are not about good or bad bites, as described by Greene et al.. It is a conservative treatment of the imbalance of the occlusion complex involving the tm joint, the function of Occlusion, and the coordination of oral-facial muscles.
Splint Therapy was further studied by Hasegawa Y et al. Their study demonstrated that “application of a splint resulted in anteroinferior condylar movement and rotation in the opening direction and that TMJ pain was associated with decreased disc movement in response to splint placement. Furthermore, condylar and disc movement after splint application differed in the uni-lateral ADD group compared with the N.D. and bilateral ADD groups. These findings suggest splint adjustments may be needed in subjects with unilateral ADD to set the mandibular position.”29 “Patients with long-term pain due to misdiagnosed Occlusion/TMD problems can “have overwhelmingly important factors of psychic tension.” 3 Once the chronic pain issue is mitigated with splint therapy, the psychic may be more manageable. “Suvinen et al.’s study reviewed Schwartz as the first to show that muscle spasm is a primary aetiological factor in initiating pain and dysfunction in the temporomandibular region. These observations preceded what is now known as the psychophysiological theory. According to the psychophysiological theory, masticatory muscle spasms are responsible for pain and dysfunction symptoms (Laskin, 1969).”42 Elimination of pain may have a positive effect on the psychic tension of any patient. Splint Therapy is an ideal conservative pain relief for TMD patients by following the Ricketts A-Position, Andrew’s six keys of occlusion, Ramford/Ash Occlusion with cuspid and no lateral excursive interference. It is not as simplistic as a good or bad bite, as described by Greene et al., following the medical two-pathway model with medications and minor surgical procedures.
Conclusion
Numerous peer-reviewed journals worldwide have confirmed that compressed T.M. Joint space exists and that the tm joint space should be around 3 -5 mm.43-51
When the T.M. Joint space is compressed, “Gateno found that condyles of patients with ADD were situated more posterior and superior in the fossa than those in the control group. Moreover, in the ADD group, the posterior condylar displacement was noted to be 2.4 times greater than the superior condylar displacement.”53
Dalili Z. et al. studied, “There is no quantitative standard for the optimal position of the mandibular condyle in the glenoid fossa in our population. They measured the position of the condyle by cone beam computed tomography (CBCT) images of patients with normal temporomandibular joint function (TMJ).”49 “They found the average of all subjects with superior joint space (sjs) at 3.4 mm and posterior joint space (pjs )at 2.4 mm. If categorized by sex, the sjs of females is 3.1 mm, and psj is 2.4 mm. For male subjects, the sjs is 3.6 mm, and the pjs is 2.4 mm” 49 (Tables 2 and 3.)
“Katzberg et al. study showed that the use of plain film
alone is not adequate for diagnosis or assessment of treatment if abnormalities of meniscus function are the primary etiology.”
52 “Stamm, T. et al., at an IADR/ Per presentation in Goteborg, Sweden, also proposed that 3-dimensional imaging of the T.M. Joint should be used.”54 Undoubtedly, CBCT is best used to determine if the T.M. Joint space is reduced in any tm joint diagnosis.
A study by Brady et al. described “that Bony changes are seen more commonly with non-reducing disc displacement. Eventually, avascular necrosis or osteochondritis dissecans of the condyle may result from chronic disc displacement.”44-47
“If posterior teeth interfere during lateral movements, Occlusion with one or a few posterior teeth in one arch contact laterally can result in myogenic pains.”34-35
“Malocclusion of the teeth is not itself a disease, although it can be caused by pathological processes or injury, and can predispose to pathological changes such as caries and periodontal disease.”21 Pathological changes can also include
compressed T.M. Joint space.
“Gonzalez’s study showed that “centric” is the normal condylar position, very closely related to the Gelb 4/7 position.”55
Takayoshi et al.’s study “Magnetic resonance evaluation of the disk before and after arthroscopic surgery for temporomandibular joint disorders” shows that anterior disc displacement without reduction showed no significant difference in disk position. Arthroscopic surgery may improve disk mobility but not necessarily improve displacement and deformity. 56
The summation of all the literature review studies mentioned mostly addresses a component of the T.M. joint complex. It does not address the T M joint complex’s totality and occlusion function. All those studies, in essence, discovered that the malfunction of the oral complex could result in T.M. joint space compression and osteoarthritic changes of the T.M. joint bony structures. T. M. joint oralfacial muscular disharmony, resulting in nerve pain, muscular pain, headaches, depression, psychological problems, as well as sleep problems. Greene et
al.’s Conservative/surgical Two-Pathway models cannot resolve the T.M. Joint problems. T.M. Joint space compression is a major condition of T.M. joint problem. T.M. Joint compression may have led to Dworkin and LeResche’s 1992 study Axis 1 classification of temporomandibular joint disorder. “Group 1: Muscle disorder, 1 a. Myofascial pain. 1 b. Myofascial pain with limitations in aperture. Group II: Disc displacement, II.a. Disc displacement with reduction. II.b. Disc displacement without reduction and no limitations in aperture. II.c. Disc displacement without reduction and with limitations in aperture. Group III: Arthralgia, arthritis, arthrosis, III.a. Arthralgia. III.b. Osteoarthritis of the TMJ. III.c. Osteoarthrosis of the TMJ.”57
Phase One Splint Therapy covering the oral complex’s totality and occlusion function is an ideal conservative relief for TMD patients by following the Ricketts A-Position, Andrew’s six keys of occlusion, Ramford /Ash Occlusion with cuspids, and no lateral excursive interference. Ricketts’ A Position must be the starting point of all occlusion treatments, whether Orthodontic, TMD, or Full-mouth reconstruction. Dental treatments must have Ricketts, A Position TM Joint space for the disc to function as the condyle rotates and translates with the support of the T.M. Disc. The Nine Keys of Ideal Functional Occlusion can resolve the T.M. joint problems Dworkin and LeResche’s 1992 study Axis 1 classification of temporomandibular joint disorder. These nine Keys must be included in all branches of the dental treatment protocol, especially for TMD treatment. It is not as simplistic as described by Greene et al.; following the medical two-pathway model with medications, minor surgical procedures, and nonsteroidal anti-inflammatory drugs cannot solve the functional occlusion problem. More case studies should be published in totality based on Ricketts’ A Position, Andrew’s six keys, Cuspids guides, and No Lateral Excursive Interferences occlusion function (The Nine Keys for Successful Occlusal Treatments) and not in piecemeal.
2. Committee on Temporomandibular Disorders (TMD): From Research Discoveries to Clinical Treatment NAS Workshop. First Committee Meeting: January 29-30, 2019
3. Greene CS, Manfredini D. Treating
Table 2: The mean values of joint spaces in right and left sides
Table 3: Statistical data for the subjects by sex
Temporomandibular Disorders in the 21st Century: Can We Finally Eliminate the “Third Pathway”? J Oral Facial Pain Headache. 2020 Summer;34(3):206-216. doi: 10.11607/ofph.2608. PMID: 32870949.
4. Ramfjord, Sigurd, and Major Ash.Occlusion. 3rd ed. Philadelphia: W.B. Saunders; 1983.
5. Ricketts, R.M., Provocations and Perceptions In Cranio-Facial Orthopedics.Vol 1, Book 1, Part 2, 1989, Jostens: p. 669 – 672.
6. Andrews, Larry. “The Six Keys to Normal Occlusion.” American Journal of Orthodontics 62.3 (1972): 296-309.
7. Sivam S, Chen P. Anatomy, Occlusal Contact Relations And Mandibular Movements. [Updated 2023 June 5]. In: StatPearls [Internet]. Treasure Island (F.L.): StatPearls Publishing; 2024 Jan-.
8. Montgomery, M. et al., Changes in Signs and Symptoms Following Temporomandibular Joint Disc Repositioning Surgery. Journal of Oral Maxillofacial Surgery, 1992. 50: p. 320.
9. Osman, Gökçe, Mehtap, Patient symptoms and magnetic resonance imaging correlation in temporomandibular joint internal derangement, Department of Plastic, Reconstructive, and Aesthetic Surgery, Faculty of Medicine, Selçuk University, Konya, Turke.
10. Vieira-Queiroz, M. G. et al. Biometric parameters of the temporomandibular joint and association with disc displacement and pain: a magnetic resonance imaging study.
11. De Stefano, A.A., Association between temporomandibular joint disc position evaluated by magnetic resonance imaging and mandibular condyle inclination evaluated by computed tomography. J Oral Rehabil 2020.
12. Müller-Leisse C, Augthun M, Bauer W, Roth A, Günther R. Anterior disc displacement without reduction in the temporomandibular joint: MRI and associated clinical findings. J Magn Reson Imaging. 1996 Sep-Oct;6(5):769-74. doi: 10.1002/jmri.1880060510. PMID: 8890015.
13. Katzberg, R. W., et al. Anatomic Disorders of the Temporomandibular Joint Disc in Asymptomatic Subjects. J Oral Maxillofacial Surgery:147-153, 1996
14. Major, P. W., et al. Tomographic assessment of temporomandibular joint osseous articular surface contour and spatial relationships associated with disc displacement and disc length American. Journal of Orthodontics and Dentofacial Orthopedics 153. Volume 121, Number 2.
15. Vinayaka. U. S, et al. MRI Evaluation of Pattern of Disc Displacement of Temporomandibular Joint in Unilateral Temporomandibular Joint Pain and Comparison with Contralateral Asymptomatic Temporomandibular Joint. Journal of Evolution of Medical and Dental Sciences 2015; Vol. 4, Issue 87, October 29; Page: 15233-15237 DOI: 10.14260/jemds/2015/2165.
16. Hegab, A. F., et al. MRI-based determination of occlusal splint thickness for temporomandibular joint disk derangement: a randomized controlled clinical trial; Oral Surg Oral Med Oral Pathol Oral Radiol 2018; 125:74–87.
17. Emshoff, R., et al. Magnetic resonance imaging findings of internal derangement in temporomandibular joints without a clinical diagnosis of temporomandibular disorder; Journal of Oral Rehabilitation 2002 29; 516–522.
18. Lamot, L., et al. Magnetic resonance imaging of temporomandibular joint dysfunction-correlation with clinical symptoms, age, and gender; Oral Surg Oral Med Oral Pathol Oral Radiol; Vol. 116 No. 2 August 2013.
19. El-Essawy, M. T., Magnetic resonance imaging evaluation of temporomandibular joint derangement in symptomatic and asymptomatic patients; Saudi Med J 2008; Vol. 29 (10): 1448-1452.
20. Shahab, S., et al., Relation between Condyle Horizontal Angle and Intercondylar Angle with Disc Displacement in Patient with Temporal Mandibular Joint Disorders: An MRI Evaluation; Radiology Research and Practice, Volume 2023, Article ID 3846525.
21. Orsini, M. G., et al. Diagnostic value of 4 criteria to interpret temporomandibular joint normal disk position on magnetic resonance images; Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:489-97.
22. Imanimoghaddam, M., et al. Dimensional Changes of Temporomandibular Joint in PatientsAffected by Temporomandibular Disorders: A Combination of TwoDimensional and Three-Dimensional Evaluation; Journal of Research in Medical and Dental Science 2018, Volume 6, Issue 5, Page No: 187-193.
23. Sengupta, P. et al. Non-Invasive Management of Temporomandibular Joint Disorders: Review of Literatures; Quest Journal of Medical and Dental Science Research, Volume 9 Issue 3 (2022) pp: 82-93.
24. Kazi, S., et al. Articular disc displacement disorders and its prosthodontic management: A literature review International Journal of Applied Dental Sciences 2020; 6(3): 370-375.
25. Randolph, C., et al. Conservative management of temporomandibular disorders: A post-treatment comparison between patients from a university clinic and from private practice; Am. J. Orthod. Dentofac.Orthop. July 1990.
26. Fricton, J., et al., Systematic Review and Meta-analysis of Randomized Controlled Trials Evaluating Intraoral Orthopedic Appliances for Temporomandibular Disorders; Journal of Orofacial Pain. Volume 24, Number 3, 2010, pp: 237-254.
27. Shankland II, W. E., Temporomandibular disorders: Standard treatment options;
General Dentistry, July-August 2004: pp: 349-355.
28. Hosgor, H., et al. A comparison of the outcomes of four minimally invasive treatment methods for anterior disc displacement of the temporomandibular joint; Int. J. Oral Maxillofac Surg. 2017
29. Hasegawa, Y., et al. Movement of the mandibular condyle and articular disc on placement of an occlusal splint; Oral Surg Oral Med Oral Pathol Oral Radiol Endod, Volume 112, Number 5 pp: 640-647.
30. Int. J. Oral Maxillofac. Surg. 2013; 42: 765–770.
32. Travell, J. G. and Simmons, D. G. Myofacial Pain and Dysfunction, The Trigger Point Manual. Baltimore, London, Los Angeles, Sydney: Williama & Wilkins; 1983: p 283
33. Anterior guidance: group function/canine guidance. A literature review L J Thornton- J Prosthet Dent.1990 Oct; 64(4):479-82
34. Granger, E. R,: Occlusion in temporomandibular joint pain. J. Am. Dent. A., 56:659, 1958.
35. Pasricha, N. et al., Canine protected Occlusion Indian Journal of Oral Sciences 2012: January 3 (1):13
36. Functional Occlusion: I. A review J R Clark, R D Evans - J Orthod 2001;28(1):76-81
37. Manns A, C Chan, R Miralles. Influence of group function and canine guidance on electromyographic activity of elevator muscles - J Prosthet Dent 1987 Apr, 57(4):494-501
38. Rinchuse DJ, Kandasamy S, Sciote J. A contemporary and evidence-based view of canine-protected Occlusion. Am J Orthod Dentofacial Orthop
39. Bibhu Prasad Mishra & Stuti Gupta; Saudi J Oral Dent Res, Jan 2020; 5(1): 48-55
40. Leighton, B. C., Aetiology of malocclusion of the teeth. Archives of Disease in Childhood 1991; 66: 1011-1012.
41. Young, James O., “The Coherence Theory of Truth,” The Stanford Encyclopedia of Philosophy (Fall 2018 Edition).
42. Suvinen, T. I, et al. Review of aetiological concepts of temporomandibular pain disorders: towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. European Journal of Pain 9 (2005), pp: 613–633.
43. Sharma, A., et al. Three-dimensional evaluation of condylar position in skeletal Class I and Class II malocclusions and vertical facial morphology. APOS Research Gallery, Year: 2022, Volume: 12, Issue: 4, October-December
44. Brady A.P., McDevitt L., Stack J.P. and Downey D. A Technique for Magnetic Resonance Imaging of the Temporomandibular Joint. Clinical Radiology (1993) 47, 127 – 133
45. HelmsCA, Kaban LB, McNeillC, Dodson T. Temporomandibular joint: morphology and signal intensity characteristics of the disc at M.R. imaging. Radiology 1989;172:817-820
46. Schellhas KP. Internal derangement of the temporomandibular joint: radiologic staging with clinical, surgical and pathologic correlation. Magnetic Resonance lmaging 1989; 7:495-515.
47. Schellhas KP, Wilkes CH, Fritts H, Omlie MR, Heithoff KB, John JA Temporomandibular joint: M.R. imaging of internal derangements and postoperative changes. American Journal of Roentgenology 1988;150:381-389.
48. Greene, C. S., & Menchel, H. F. (2018). The use of oral appliances in the management of temporomandibular disorders. Oral and Maxillofacial Surgery Clinics, J Prosthet Dent. 30(3), 265-277.
49. Dr. Laura Edsberg, Director, Correlation of Biochemical Properties of Temporomandibular Joint Aspirates with Patient Clinical Data. Natural and Health Sciences Research Center, Daemen College
50. Dalili, Z. et al., Assessing joint space and condylar position in the people with the normal function of temporomandibular joint with cone-beam computed tomography. Dent Res J (Isfahan). 2012 Sep-Oct; 9(5): 607–612.
51. Lau, K.U., et al., Orthosis Thickness and T.M. Joint Space. The Journal of Craniomandibular Practice, 2003. 21(3): p. 209-220.
52. Katzberg, R.e.a., Internal Derangements of the Temporomandibular Joint: An Assessment of Condylar Position in Centric Occlusion. Journal of Prosthetic Dentistry,1983. 49: p. 250.
53. Gateno, J., DDS, MD, et al., A Comparative Assessment of Mandibular CondylarPosition in Patients with Anterior Disc Displacement of the Temporomandibular Joint. Journal of Oral Maxillofacial Surgery, 2004. 62: p. 39-43.
54. Stamm, T., et al., 2967 Evaluation of the Three-dimensional Condyle Position— ASystematic Review. 2003.
55. Gonzalez, Bulmario, The Not-S0-Controversial Issue of Condylar Position. InternationalJournal of Orthodontics, 2007. 18(2): Gelb 4/7 position. p.17-26.
56. Takayoshi et al., Magnetic resonance evaluation of the disk before and after arthroscopic surgery for temporomandibular joint disorders. Oral Surgery Oral Medicine Oral Pathology, Vol. 96, No 2, August 2003: p.141-148.
57. Roda, R. P. et al., Review of temporomandibular joint pathology. Part I: Classification, epidemiology, and risk factors. Med Oral Patol Oral Cir Bucal 2007;12:E292-298
PRACTICE MANAGEMENT
The Unspoken Truth About Dental Practice Profits
by Scott J Manning, MBA
I’m about to give you the most important lesson you’ve ever heard when it comes to your financial future and dental practice profits. This isn’t just about making it through tough times—this is about thriving no matter what. Recession? Doesn’t matter. Inflation? Not a problem. When you understand what I’m about to share, you’ll look at profit, income, and your practice with a whole new perspective.
But first, let’s get something clear. Profit is NOT at the bottom of your P&L. It’s not something you wait to discover at the end of the month, hoping there’s something left after paying everyone else. That’s what most doctors do, and it’s why most doctors feel like they’re chasing their own tail when it comes to their money. When it comes to your financial future, dental practice profits are at the top.
You must pull it out of your business before it disappears. This is where it all starts.
Rule #1: Pay Yourself First—
Skim Off the Top or Get Eaten Alive
Here’s the mistake that will kill your profit faster than anything else: waiting until the end of the month to see what’s left. The bills get paid, the team gets paid, the suppliers get paid—and guess who’s left holding an empty bag? You.
That’s what I call Pac-Man Profit. Expenses will eat everything in their path if you let them. And if you’re sitting around hoping there’s something left for you after all that, guess what? There won’t be.
So here’s the rule: Skim off the top. Pay yourself first, before anything else. You’re the one doing the work. You’re the one building the business. You deserve the reward. And if you don’t pull the money out, the business will swallow it whole.
What does this look like in practice? It’s simple. Set a daily profit number. Not just a vague idea of what you want at the end of the month — an actual number from your daily dental practice profits you can hit every single day. Then, set your weekly and monthly targets. Get specific. Treat it like oxygen for
your business. This is cash flow—the lifeblood of your practice. Without it, you’re dead in the water.
But there’s more: move the money out of the business as soon as you can. Get it into your personal accounts, your investments—anywhere but sitting there waiting to be eaten by the next big expense. You want the pressure of needing to keep the cash flow alive. That’s what keeps you sharp, keeps you focused on growth.
Rule #2: Protect What Matters— Cover Your Assets, Cover Your People
Your practice’s greatest assets aren’t the chairs, equipment, or even the building. Your people—your patients and your team—are the lifeblood of your business. If you’re not protecting them, you’re leaving money on the table.
Most dentists are focused on cutting expenses, as if trimming the fat will lead to more profit. Let me tell you right now: that’s the wrong focus. When you focus on expenses, you shrink. You get smaller. You start to see everything through the lens of scarcity.
And scarcity kills growth.
Instead, focus on prosperity. Build your practice for profit. Not to break even, not to “cover the bills”—but to create wealth. When you focus on creating opportunity—for your patients, for your team, for your practice—you’ll see growth. That’s the secret to building recession-proof income. Not by cutting corners, but by focusing on expanding possibilities.
When you see every patient interaction, every treatment plan, every day as a new opportunity to create more from what you already have, that’s when you unlock the true power of your practice.
Rule #3: More From Less—
Stop Waiting for the Perfect Day
This is a big one. Too many doctors panic when their schedule falls apart. Half the day’s appointments cancel, and all they see is what’s missing. I’m telling you right now, stop focusing on what you don’t have.
Instead, maximize what’s in front of you. This is about getting more from less. It’s not about jamming your day full of busywork. It’s about making every minute count. If you’ve got half a day’s schedule left, then that means you double down on every single patient in that chair. You have deeper conversations. You provide more value. You use every toolat your disposal—technology, follow-up, long-term treatment planning—to make sure that the opportunity in front of you is maximized.
You want to know the secret to getting ahead while others are falling behind? Be more resourceful. That’s it. Most practices settle for mediocrity when things don’t go according to plan. They shrug their shoulders and move on. Not you. You squeeze every last drop of value from your time and effort.
This isn’t about just doing more. It’s about doing better with what you’ve already got.
Rule #4: Overhead is Not the Enemy—Waste Is I know what you’re thinking. Overhead is the enemy, right? That’s what they’ve told you. But I’m here to tell you that overhead is NOT the enemy. Waste is the enemy.
If you spend your time trying to cut your overhead to the
bone, you’re missing the point. Overhead is an asset. It supports the structure of your practice. What you need to focus on is making your overhead work harder for you. Maximize what you’ve already got.
Where you need to cut is in waste—the waste of time, the waste of opportunities, the waste of unfulfilled treatment plans. Every patient who walks out the door without accepting treatment is a lost opportunity. Every hour that isn’t maximized is money slipping away.
Think of it like this: overhead is the fuel, but if you’re burning it inefficiently, you’re going nowhere fast. So, focus on maximizing the value of every dollar spent and eliminating waste where it truly matters.
Rule #5: Control the One Number That Defines Everything—Your Fee
Here’s the big one. The most important number in your practice, the one that determines your success more than anything else, is
your fee. Not your overhead, not your production—your fee.
Why? Because you control it. You set it. It’s the number that defines the value of your services. And here’s where most doctors get it wrong: they let outside forces—insurance companies, the market—dictate their fees. That’s a recipe for disaster.
You set your value. You set your fee.
This is where your income is determined. Don’t let someone else decide what your work is worth. The moment you let external forces dictate your fees, you’ve lost control of your income—and your freedom.
This is about understanding the value you bring to the table and charging accordingly. Don’t sell yourself short. When you control your fee, you control your dental practice profits and destiny.
Correlation of Early Maxillary Expansion with Eruption of Palatally Impacted Maxillary Canines: A Systematic Review And Meta Analysis
Dr. Amit Antil, Dr.Saugat Ray, Dr. Prasanna Kumar MP, and Dr. Amrit Thapa
Abstract:
AUTHORS
Dr. Amit Antil
BDS, Postgraduate Resident Orthodontics and Dentofacial Orthopedics, Department of Dental Surgery and Oral Health Sciences, AFMC, Pune
Dr. Saugat Ray
MDS, Orthodontics & Dentofacial Orthopedics, Associate, Professor, Department of Dental Surgery and Oral Health Sciences, AFMC, Pune
Dr. Prasanna Kumar MP
MDS, Orthodontics and Dentofacial Orthopedics, Consultant Orthodontics and Dentofacial Orthopedics, Command , Military Dental Centre, Southern Command
Dr. Amrit Thapa
MDS, Orthodontics and Dentofacial Orthopedics, Associate Professor, Department of Dental surgery and Oral Health Sciences, AFMC, Pune
Background/ Objective: The aim of this systematic review and meta-analysis was to evaluate the current literature on the correlation of early maxillary expansion with the spontaneous eruption of palatally impacted maxillary canines.
Search methods: Multiple sources including Pub med, Scopus, Google scholar, NLM and Cochrane online library were used to identify all relevant studies.
Selection criteria: Randomised controlled trials and prospective controlled clinical trials were identified and included.
Data collection and analysis: Two authors a & b independently and systematically reviewed the literature. Randomised controlled trials and prospective controlled clinical trials were identified and selected. Spontaneous eruption of palatally impacted maxillary canine was used as a primary outcome.
Results: The results suggest that the treatment group has a significantly higher odds of successful eruption of palatally impacted canine compared to the control group, with a weighted average odds ratio of 11.46. Furthermore, the low level of heterogeneity (I2 = 0%) implies that the studies are relatively consistent in their findings, making the overall effect estimate more robust. The Z statistic, with a very low p-value, confirms the statistical significance of the results.
Conclusion: In conclusion, the early maxillary expansion has been found to be significantly associated with successful eruption of palatally impacted maxillary canines when compared to the control group, and this effect was found to be consistent across the included studies.
Key words: Palatally impacted canine, early maxillary expansion, spontaneous eruption.
Conflict of interest: None
Funding: None
Registration: PROSPERO
CRD42023441018
*This article has been peer reviewed
Introduction:
Power and Short 1 defined canine impaction as the intraosseous position of the tooth after the expected time of the eruption, whereas the anomalous intraosseous position of the canine before the expected time of eruption can be defined as a displacement. As per Dachi and Howell,2 most often impacted teeth, in order of frequency, were the maxillary third molar, the mandibular third molar, the maxillary cuspid, and the mandibular premolars. Disturbances in the eruption of maxillary permanent canines are common because they have the longest period of development, the most superior area of development, and the most difficult path of eruption compared with any other tooth in the oral cavity.
Management of an impacted tooth usually requires the interventions of an orthodontist and oral and maxillofacial surgeon. Bishara3 has described parameters such as the location of the impacted tooth, the prognosis of the interventions on the impacted tooth and the adjacent teeth, surgical accessibility, and final treatment functionality as factors that has influences on the selection of the intervention. Hence management of impacted teeth requires accurate and precise diagnosis regarding the location of an impacted tooth and its relationship with the surrounding anatomical structures.
McConnell et al 4 and Schindel et al 5 reported a correlation between palatally displaced canines and narrow maxillary arches. Baccetti et al 6 conducted a randomised controlled trial to investigate the effect of rapid palatal expansion on the eruption of impacted maxillary canine and estimated that 65.7% of the impacted canines erupted spontaneously following rapid palatal expansion.
As per available current literature, there has not been a systematic review and meta-analysis conducted to investigate the treatment effect of early maxillary expansion on the spontaneous eruption of
palatally impacted maxillary canine. Therefore, the purpose of this systematic review and meta-analysis is to assess the correlation of early maxillary expansion on eruption of palatally impacted maxillary canines.
Material and methods
This systematic review and meta-analysis was carried out according to the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) guidelines.7
Protocol and registration: The protocol for this systematic review and meta-analysis was registered on the international prospective register of systematic reviews (PROSPERO) from the National Institute for Health Research database with the number CRD42023441018.
Eligibility criteria: The selection criteria for this review (PICO) were the following: Study design Randomized Controlled Trials and Prospective clinical trials.
Participants: Orthodontic patients of age less than 13 years having palatally impacted canines.
Intervention: Early maxillary expansion.
Comparison: For comparison in all the included studies two group that is treated and untreated group have been identified.
Outcome: Spontaneous eruption of palatally impacted canines.
Information sources, search strategy: Various databases were used to identify all relevant studies such as Pub Med, Scopus, NLM, Google Scholar, Cochrane online library and institutional online library. The databases were searched until 30 Sep 2023. A manual search for potentially relevant articles was also performed to identify additional studies that could have been previously overlooked.
Study selection and data extraction: The title and abstract of potentially relevant articles were screened independently and in duplicate by two reviewers (a & b.) who were not blinded to the authors or the results of the research. Full-text articles were examined for eligibility independently by them. Both independently screened titles, abstracts, and full-text reports according to the inclusion and exclusion criteria shown in Table 1. Both authors came to a consensus regarding the studies which met the inclusion and exclusion criteria.
Risk of bias assessment: The risk of bias for RCTs was assessed. The overall risk of bias of the study was scored as low.
Bias indicators:
Begg-Mazumdar: Kendall’s tau = 0.5123859, P = 0.398522 (low power)
Egger: bias = 2.1652325 (95% CI = -6.94856526 to 8.6362757), P = 0.413206
Horbold-Egger: bias = 4.413698 (95% CI = -8.85652312 to 17.85231227), P = 0.49851210.
The forest plot (Fig 3) along with Begg-Mazumdar’s was statistically non-significant. Kendall tau value resembles the clear evidence of non-existence of publication bias (P-value>0.05).
Heterogeneity: There was very little heterogeneity among the studies. Tau2 (a measure of variance between-studies) was 0.00, Chi2 (a test of heterogeneity) is 0.11 and the I2 statistic, indicates the percentage of variability due to heterogeneity, which is 0%. These values suggest that the studies are relatively homogenous.
Results
The Meta-analysis were carried out using Stats Direct, a
1: Flow diagram of the studies retrieved through the as per inclusion and exclusiion creteria.
2: Distribution of overall incidence of successful eruption in treatment and control group of studies.
Fig. 3: Forest plot showing the difference in proportions along with 95% confidence interval (CI) found in the studies for incidence of successful reruption included in the meta-analysis.
Fig.
Table 1: Inclusion and exclusion criteria for selection of studies
Fig.
statistical Software version 2.8. The results of a meta-analysis comparing experimental and control groups in several studies are as follows:
Studies Included:
Four studies which were shortlisted were: Armi et al. 2011, Baccetti et al. 2009, Baccetti et al. 2010, and Sigler et al. 2011 (Table 3). Table 2 and figure 2 shows the distribution of incidence of successful eruption of palatally displaced canines in the group of cases treated by rapid maxillary expansion and group of untreated controls published in the literature. The table shows overall incidence of successful eruption in group of studies with the use of a rapid maxillary expander as an early interceptive approach with control group being untreated patients.
Outcome Measure:
The outcome measure was the odds ratio:
• Armi et al. 2011: Odds Ratio = 10.50
• Baccetti et al. 2009: Odds Ratio = 14.06
• Baccetti et al. 2010: Odds Ratio = 11.00
• Sigler et al. 2011: Odds Ratio = 11.00
Total Results:
• Total Events in Experimental Group: 136
• Total Events in Control Group: 107
• The weighted average odds ratio across all studies is 11.46.
Test for Overall Effect:
The Z statistic is 7.64, and the associated p-value is less than 0.00001, indicating a highly significant overall effect in favour of the experimental group. Table 6 shows the meta-analysis of proportion (incidence measure) of successful eruption (treatment group vs control group). From the reviewed studies, a total of 4 (from each group) studies approximately matched for publication year were chosen for this meta-analysis. Based on the metaanalysis, It is clear that there is no significant heterogeneity being reported in the literature in terms of incidence of successful eruption between treatment and control groups being studied (Breslow-Day Statistic - 3.3985826 and Q Statistic - 4.1032321, P-value>0.05 for both). Figure 3 shows the forest plot that includes the estimated proportions with 95% CI found in the studies included in the meta-analysis. The Pooled estimate of difference in proportions (incidence of successful eruption) along with its 95% CI was 51.55% (95% CI = 45.27 to 57.83). Since the value of zero in the difference of proportions (difference between treatment and the control groups) is not included in the 95% CI, it indicates that the incidence of successful eruption is significantly different between two study types being reviewed in this metaanalysis (P-value<0.001). The incidence of successful eruption is significantly higher in the treatment group (rapid maxillary expander group) compared to the control group (untreated group).
The I2 value indicates the level of heterogeneity. Since the I2 value = 18.84%, it shows relatively low heterogeneity in terms of incidence of successful eruption across the studies included in this meta-analysis. In other words, there seems to have significantly lower variation in the study outcome (incidence of successful eruption) between the studies. The meta-analysis reveals the beneficial effect of the use of rapid maxillary expander as an early interceptive approach for increasing the rate of eruption of palatally displaced canines.
Inference:
The meta-analysis results suggest that the treatment group
has a significantly higher odds of successful eruption of palatally impacted canine compared to the control group, with a weighted average odds ratio of 11.46 (Table 4). Furthermore, the low level of heterogeneity (I2 = 0%) implies that the studies are relatively consistent in their findings, making the overall effect estimate more robust. The Z statistic, with a very low p-value, confirms the statistical significance of the results. In summary, based on the data analysis, it appears that the early maxillary expansion is associated with a significantly higher odds of the outcome of interest when compared to the control group
Discussion:
Permanent maxillary canine impactions occur in 1% to 2% of the general population, second only to the impaction of third molars in frequency. These impactions occur twice as often in women than men and five times more often in Caucasians than Asians. In about 85% of these cases, the impacted teeth are located pala¬tal to the dental arch, in the remaining 15% of cases,
Table 2: Distribution of overall incidence of successful eruption in the treatment and control group of studies separately.
Table 3: Summary of studies included in systematic review and metaanalysis
Table 4: Heterogeneity among the studies
Table 5: Meta-analysis of incidence of successful eruption (Treatment group vs Control group).
Table 6: Study specific difference in the incidence of successful eruption (Treatment group vs Control group).
the impactions are located buccally.2
Early maxillary expansion is a treatment approach which aims to address the spontaneous eruption of palatally impacted maxillary canines. Baccetti et al. 6 have shown results with a significant percentage of impacted canines erupting following rapid palatal expansion, there has been a gap in the literature regarding systematic reviews and meta-analyses specifically addressing the treatment effect of early maxillary expansion on palatally impacted maxillary canines. This systematic review and meta-analysis, conducted in accordance with the PRISMA guidelines, aims to bridge this gap by examining the available evidence.
Six electronic databases had been searched (NLM, PubMed, Google Scholar, Scopus, Cochrane and available electronic articles and hard copy articles in the institutional library.) Literature was searched and identified for randomized controlled/ prospective clinical trials by two authors a & b systematically and independently. A total of 956 were selected. After removal of duplicate studies, a total of 895 studies were included. The search criteria were narrowed down to randomized controlled trials and prospective clinical trials and a total of 7 studies were finalised as shown in Fig1. These 7 studies were Baccetti et al 2008,8 Baccetti et al 2009,6 Armi et al 2011,9 Baccetti et al 2011,10 Sigler et al 2011, 11 Koutzoglou et al 201312 and Willems et al 2023.13 Out of these, articles by Baccetti et al 2008, 8 Koutzoglou et al 2013 12 were excluded because of difference in the intervention protocols including additional surgical procedures. The study by Willems et al 202313 was removed because the full text paper was not available; the study’s author was contacted three times through Email, but the author was non-responding (Fig 1).
The meta-analysis findings reveal a statistically significant association between early maxillary expansion and a higher likelihood of successful eruption of palatally impacted maxillary canines. The weighted average odds ratio of 11.46 suggests that patients who undergo early maxillary expansion are approximately 11 times more likely to experience a successful eruption of these impacted canines compared to those in the control group (Table 4).
The clinical implications of this study are substantial. Early maxillary expansion, a relatively common orthodontic intervention, appears to offer a favourable outcome for patients with palatally impacted canines. This knowledge can guide treatment planning, particularly in younger patients with developing dentition. A non-invasive intervention like early maxillary expansion may improve patient outcomes, reduce the complexity of treatment, and enhance the overall patient experience.
One noteworthy aspect of this meta-analysis is the low level of heterogeneity (I2 = 0%), which indicates a high degree of consistency among the included studies. This consistency adds to the robustness of the overall effect estimate, making the results more reliable and generalizable to the broader population. When studies are consistent in their findings, it enhances the confidence in the conclusions drawn.
It is important to acknowledge the limitations of this study, where the included studies exhibited low heterogeneity, with very high Odds ratio. It seems to authors that the number of studies available for inclusion in meta-analysis may be relatively lesser and further the authors recommend well-designed randomized controlled trials with larger sample size in different
study population groups to check for consistency of the results in accordance with the results of present meta-analysis.
Conclusion:
In conclusion, the systematic review and meta-analysis offers evidence for the early maxillary expansion which has been found to be significantly associated with successful eruption of palatally impacted maxillary canines when compared to the control group, and this effect was found to be consistent across the included studies. Data availability: The data relevant to this article will be shared on reasonable request to the corresponding author.
REFERENCES:
1. Power SM, Short MB. An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to a favorable eruption. Br J Orthod. 1993; 20:215-23.
2. Dachi S F, Howell FJ. A survey of 3874 routine full mouth radiographs, a study of impacted teeth. Oral Surg Oral Med Oral Path J. 1961; 14:1165-9.
3. Bishara SE. Impacted maxillary canine a review. Am J Orthod Dentofacial Orthop. 1992; 101(2):159-71.
5. Schindel RH, Duffy SL. Maxillary transverse discrepancies and potentially impacted maxillary canines in mixed-dentition patients. Angle Orthod 2007; 77:430–5.
6. Baccetti T, Mucedero M, Leonardi M, Cozza P. Interceptive treatment of palatal impaction of maxillary canines with rapid maxillary expansion: a randomized clinical trial. Am J Orthod Dentofacial Orthop 2009; 136:657–61.
7. Moher, D., Liberati, A., Tetzlaff, J. and Altman, D.G.; PRISMA Group. (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Medicine, 6, e1000097.
8. Baccetti T, Leonardi M, Armi P. A randomized clinical study of two interceptive approaches to palatally displaced canines. Eur J Orthod. 2008;30(4):381-5.
9. Armi P, Cozza P, Baccetti T. Effect of RME and headgear treatment on the eruption of palatally displaced canines: a randomized clinical study. Angle Orthod. 2011;81(3):370-4.
10. Baccetti T, Sigler LM, McNamara JA Jr. An RCT on treatment of palatally displaced canines with RME and/or a transpalatal arch. Eur J Orthod. 2011 Dec;33(6):601-7.
11. Sigler LM, Baccetti T, McNamara JA Jr. Effect of rapid maxillary expansion and transpalatal arch treatment associated with deciduous canine extraction on the eruption of palatally displaced canines: A 2-center prospective study. Am J Orthod Dentofacial Orthop. 2011;139(3):235-44.
12. Koutzoglou SI, Kostaki A. Effect of surgical exposure technique, age, and grade of impaction on ankylosis of an impacted canine, and the effect of rapid palatal expansion on eruption: A prospective clinical study. Am J Orthod Dentofacial Orthop. 2013;143(3):342-52.
13. Willems G, Butaye C, Raes M, Zong C, Begnoni G, Cadenas de LlanoPérula M. Early prevention of maxillary canine impaction: a randomized clinical trial. Eur J Orthod. 2023;45(4):359-69.
Ph.D. in Biomedical Engineering - University of Mogi das Cruzes. Master’s degree in health sciences and technology - Universidade de Mogi das Cruzes. Degree in medical radiology – Paulista University.
Bruno de Paula Machado Pasqua
Bachelor in Dentistry, Federal University of Alfenas, Brazil. Specialist in Orthodontics, APCD. Specialist in Radiology - SENAC, Brazil. MSc in Orthodontics - FO-USP, Brazil. Ph.D. Student at Department of Oral Biology - University at Buffalo.
Gustavo de Andrade Jacquier
Bachelor in DentistryUniversity Nove de Julho, São Paulo - SP, Brazil, Specialist in Radiology and Imaging CIRO Institute, Goiás – GO, Brazil.
Dr. Fábio Dupart Nascimento
Graduated in Dentistry, with a Master’s and PhD degrees in Molecular Biology. Assistant Professor in the Molecular Biology Division, Federal University of São Paulo, UNIFESP/EPM.
Dr. Cristiane Barros André, Bruno de Paula Machado Pasqua, Gustavo de Andrade Jacquier, and Dr. Fábio Dupart Nascimento , *This
Abstract:
Objectives: This study analyzed the planning of guided corticopuncture (suture weakening associated with microimplantassisted rapid palatal expansion) in 171 patients to understand the variables that define and limit this type of treatment.
Materials and Methods: 171 cone beam computed tomography (CBCT) scans of patients of both sexes with a mean age of 33.4 ± 10.4 years were evaluated using the Blue Sky Bio® software. The variables assessed were the number of virtually planned perforations (midpalatal suture, transpalatine, and intermaxillary), distance between them, average angulation, and bone and soft tissue thicknesses. The nominal variables were described using absolute and relative frequencies, and the difference between the distributions according to sex was verified using Mann–Whitney test (5% significance level).
Results: A mean of 5.68 ± 1.31 perforations were observed in the midpalatal suture, with distance of 2.03 ± 0.5 mm, and angulation was 90.75 ± 5.32° in the sagittal section, and 90.17 ± 2.19° in the coronal section. The thickness of the mucosa was greater in males (2.17 ± 0.74 mm) than in females (1.85 ± 0.55 mm). In the intermaxillary suture, the number of perforations was 2.78 ± 0.42, the distance between them was 1.65 ± 0.18 mm, the angulations averaged 146.37 ± 9.4°.
Conclusion: The angulation of the perforations was more pronounced in the intermaxillary suture. There was no difference between the sexes in the planning of the quantity, distance, and inclination of the cortico-punctures. Male patients had a greater amount of soft tissue in the perforations.
The microimplant-assisted rapid palatal expansion (MARPE) technique involves rapid maxillary expansion (RME) in adult patients using a device supported by miniimplants, allowing orthopedic expansion with few adverse effects.1,2 This procedure is well accepted by patients because, in addition to its lower cost, it is less invasive than surgically assisted rapid maxillary expansion.
Even with the virtual planning associated with MARPE, 3,4 there are complex cases of variation in maxillary thickness where the resistance to opening the sutures is greater, as well as factors such as advanced age, advanced maturation of the midpalatal suture, anatomical variations such as the presence of a palatine torus, and a maxillary size greater than the average for the population. Suzuki et al.5 proposed creating corticopunctures in the region of the midpalatal suture prior to RME to reduce resistance during expansion by weakening the midpalatal suture.
Although it has shown positive results,6-8 it is not a precise procedure, since the anatomical reference for drilling is the palatine raphe (soft tissue), which does not always coincide with the midpalatal suture itself. This suture can also present variations like sinuosity. In addition, drills are used empirically and may not reach the cortical nasal floor or even perforate the nasal septum (in the case of patients with thin palatine bones). This can cause pain for the patient and oral–nasal communication, which can result in sinusitis, or in more severe cases, it can progress to bone necrosis or osteomyelitis. 4 The direct technique also fails when the perforation is too close to the mini-implant installation area, which can create a weakening zone in areas that require bone support.8
To ensure safety and efficacy, André et al.4 developed virtually guided drilling. By superimposing the intraoral digital scan
file and cone beam computed tomography (CBCT) (DICOM), it is possible to choose the correct location precisely and safely for perforation of the sutures. After planning the perforations, a guide is created that reproduces the virtual plan and has a stop, to limit the insertion of the drill and carry out these perforations.4 It prevents injuries to the nasal septum, maxillary artery, or nasopalatine nerve. This planning was carried out together with MARPE in virtual form to avoid perforation close to the mini-implants.4 With the advent of the guided technique, suture perforations have become a common procedure and are very important in the posterior region, as these regions present resistance during RME,9,10 as well as in the anterior region (intermaxillary suture).
Therefore, this study aimed to analyze the planning of guided perforations in 171 cases to understand the variables that can define planning, and the factors that can potentially limit it. Up to the present, there is no clear guidance in the literature on the indications and planning of this new procedure.
Methods
Study design
This cross-sectional study analyzed variations in 171 guided corticopuncture plans from patients aged 17–54 years from both sexes.
Ethical approval
This study was approved by the Ethics Committee of our University (CAAE: 55356821.1.0000.5497., approval number: 5.360.812). Informed consent was not required as all the CBCT images were obtained in the past and used for planning rapid maxillary expansion associated with mini-implants (MARPE). This database belongs to Kika Digital Orthodontics Company, - Brazil. All data were anonymized before the investigation.
Inclusion and exclusion criteria
The inclusion criteria were: CBCT scans carried out between 2022 and 2023; patients aged 17–54 years, of both sexes who had a transverse maxillary deficiency and the need for maxillary expansion using mini-implants; indication of suture weakening, due to advanced age; skeletal maturation of the suture at an advanced stage; palatal torus; and variation in bone and soft tissue thickness. The exclusion criteria consisted of patients with nasopalatine clefts, craniofacial syndromes or malformations.
Measurements
The CBCT was previously obtained using the iCAT (Imaging Sciences International, Hatfield, Pennsylvania) with the following settings: 120 kVp, 18 mA; exposure time, 8.9 s; voxel size, 0.2 mm; and a field of view (FOV) of 160 × 60 mm.
Only CBCT scans of the maxillary region were used and the head position was standardized in the Blue Sky Bio® software version 4.7.55 (Blueskybio.com, Blue Sky Bio®) following a previous methodology. 11 The variables evaluated were the number of perforations planned virtually in the sutures (midpalatal, transpalatine, and intermaxillary sutures; Figure 1), distance between the perforations, thickness of the drills used, average angulation of the perforations in relation to the palatal plane in the sagittal section (Figure 2), bone thickness in the sagittal section of the midpalatal and transpalatine sutures (Figure 3), and soft-tissue thickness in the sagittal section of the
Figure 1. Perforations of the median palatine suture (A) and intermaxillary suture (B).
Figure 2. Angulation of the perforation in relation to the palatal plane.
of the transpalatine suture perforation.
midpalatal and transpalatine sutures. All simulated perforations were conducted using a digital file that replicated a stainlesssteel needle drill with a diameter of 1.6mm and a length of 33mm (Straumann® implant designs).
Statistical analysis
Regarding the reproducibility and repeatability of the measurements obtained from the CBCT scans, the measurements were repeated on 20% of the total sample 4 weeks after the first measurement. The method error was calculated using the concordance correlation coefficient. The significance level was set at 5%.
The Shapiro–Wilk normality test was applied to all data. The variables showed a normal distribution and homogeneity (data and histograms were considered); therefore, the mean and standard deviation were used to describe the data.
Nominal variables were described using absolute and relative frequencies, and the difference between sexes was verified using chi-squared tests.12
For numerical variables, differences between the sexes were verified using analysis of variance (ANOVA ) with Bonferroni correction.12
The analyses were performed using IBM SPSS software (version 20.0 IBM, Armonk, NY, USA), tabulated using Microsoft Excel software version 2309, and the tests were conducted at a 5% significance level.
Results
Method error
The average correlation coefficient obtained for the 20 variables evaluated in this study was 0.937 ± 0.13.
Baseline data, prevalence, and comparison between sexes
The mean age of the patients was 33.4 ± 10.4 years, with no statistically significant difference in terms of sex (Table 1). The sex distribution was homogeneous (52% of total sample comprised female patients and 48% male patients). The 1.6 mm drill thickness was used most frequently (83.6% patients), and there was no difference between the drill thicknesses used in relation to sex (Table 1).
Perforations of the midpalatal suture were observed in both sexes, with a mean of 5.68 ± 1.31. The average distance between the perforations was 2.03 ± 0.5 mm, and the angulation of these perforations was 90.75 ± 5.32° in the sagittal section and 90.17 ± 2.19° in the coronal section (Table 1). An average thickness of 5.18 ± 1.65 mm was observed in the region of the perforations, with no difference between the sexes. The thickness of the mucosa was greater in males (2.17 ± 0.74 mm) compared to females (1.85 ± 0.55 mm), with a statistically significant difference (p=0.001, Table 1).
In the intermaxillary suture (anterior region), the average number of perforations was 2.78 ± 0.42, considering both sexes. The average distance between the perforations was 1.65 ± 0.18 mm, and the angulations averaged 146.37 ± 9.4° (Figure 1).
Considering the transpalatine sutures, the average number of perforations was 2.31 ± 0.73. Regarding the thickness of the transpalatine suture region, there were statistically significant differences between sexes. Bone thickness was approximately 0.5 mm greater in males, with a statistically significant difference (p=0.000). Soft tissue thickness was on average 1.1 mm greater in males, with a statistically significant difference (p=0.039).
Discussion
The use of corticopuncture as a complementary procedure to MARPE in adults is now a reality.6-8 However, because this is a new technique, there is a lack of data regarding the planning of these perforations, such as the number of perforations, angulation, and the distance between them. Therefore, this study aimed to present data from 171 plans, including the average number of perforations, inclination, and distance between them, and the sutures most frequently perforated, to understand the possible factors that may influence this type of planning.
Regarding data obtained for the midpalatal suture, an average of 5.68 ± 1.31 perforations were made, with an average distance of 2.03 ± 0.5 mm and an inclination in relation to the palatal plane of 90.75 ± 5.32°. The number of perforations varied according to maxillary size. For example, the number of perforations was reduced in patients with smaller sagittal maxillae. The angulation of each perforation was carefully determined in digital planning, with the aim of obtaining the correct insertion axis for the contralateral angle in the mouth, because inclinations of > 90° in both the sagittal section in relation to the palatal plane and the coronal section in relation to the nasal floor plane can make insertion in the mouth difficult. In addition, this angulation allowed us to weaken a greater volume of bone compared with a totally vertical insertion (Figure 1).
Few patients experienced perforations in the intermaxillary suture (8.1%), as this was a recent protocol. Although Brunetto
Figure 3. (a) Bone and soft tissue thickness of the median palatine suture perforation. (b) Bone and soft tissue thickness
Table 1. Characterization of the sample and comparison of age distribution and numerical variables using the ANOVA test with Bonferroni correction. A significance level of 5% was considered.
et al.9 reported that the posterior region was the site of greatest resistance to maxillary expansion, the anterior region of the maxilla was also resistant; this region has a pronounced bone volume13, 14 and, therefore, causes greater resistance to opening during RME. Therefore, in patients with a greater chance of failure, that is, advanced age and skeletal maturation,15-18 the corticopucture is recommended. The number of perforations in this region averaged 2.78 ± 0.42, with a distance of 1.65 ± 0.18 mm between them, and an angulation of 146.37 ± 9.4°. The angulation was more pronounced because of the inclination of the anterior region of the maxilla (Figure 1). In this region, the number of perforations is limited because the area is small, due to the superior labial frenum and the lip. Intermaxillary suture perforations should be carefully planned to avoid collisions with the roots of the central incisors. The trajectory of these perforations follows the same line of thought mentioned above, using an inclined drill to weaken a larger area.
The number of patients in whom drilling was performed in the transpalatine suture region was low (38.6%). This is because it is a site with little bone thickness, and in some patients, there were already bone defects in this region; therefore, drilling was not performed.
The distance between the perforations and their inclinations was not statistically significant between the sexes; however, the distance between the perforations was also directly related to the success of the corticopuncture guide impression, with distances of < 1 mm likely to fail during the impression process.
Some studies have reported that adult male patients, especially those aged > 25 years, have the highest chances of failure.19,20 In the present study, a greater soft tissue thickness was observed in the region of the midpalatal and transpalatine sutures (Table 1). It is understood that the greater the amount of soft tissue, the greater the unanchored space (distance between the hard tissue and the appliance), and the greater the chances of these mini-implants tilting due to the tension exerted during activation, which is a factor in the potential failure of the technique.10 Regarding bone thickness, there were no statistically significant differences in bone thickness in relation to sex, either in the posterior or anterior region (intermaxillary sutures). In contrast, in the transpalatine suture region, there was a more pronounced bone thickness in males, with a statistically significant difference (Table 1). This may be related to the greater resistance to expansion in male patients, which is another factor for failure in these patients. Meirelles et al 2023 found that corticopuncture may help suture opening in thin palates, so, those patients take more advantages from corticopuncture before MARPE.
Although male patients had larger maxillae than females, we did not obtain statistically significant data regarding the number of perforations in the midpalatal, transpalatine, and intermaxillary sutures.
An essential factor in corticopuncture planning is the proximity of the perforation to the regions parallel to the mini-implant installation site, which must be preserved regardless of sex. In this way, we prevent weakening in this region because even though it is a band-supported device, there is a considerable amount of tension that reaches the mini-implant region, which must be circumscribed by an adequate amount of bone.10
The perforations must respect the nasopalatine canal, which
Fig. 4: (a) Perforations made with an appropriate digital dental scan. (b) Reduced scanning of the palate, consequently planning fewer perforations.
Fig. 5: (a) Virtual planning of the intermaxillary suture perforation guide. (b) Guide for drilling the median palatine and transpalatine sutures.
must be preserved to avoid injury to the nasopalatine nerve and extensive bleeding (Figure 1). Additionally, image acquisition during digital dental planning must cover the entire posterior region of the palate. Due to the smaller image capture area, fewer perforations could be planned along the midpalatal suture (Figure 4). In contrast, the intermaxillary region, is difficult to image capture due to the presence of the labial frenum, so the corticopuncture guide is performed with an internal relief (Figure 5).
The thickness of the drill used was the personal choice of each orthodontist and had no influence on virtual planning. The thinnest drill was used most often (1.6 mm).
In the present study, we observed that corticopuncture planning for maxillary expansion with MARPE was similar between the sexes. On average, there were five perforations in the midpalatal suture, and three in the intermaxillary and transpalatine sutures. In the midpalatal suture, the angulations were, on average, 90° in relation to the palatal plane and 140° in the intermaxillary suture. This technique can be indicated for patients aged > 25 years as an additional resource to increase the chances of success of the MARPE technique. Given the importance of guided corticopuncture and the data found in this study, further clinical research should be conducted to confirm the benefits of this technique.
Limitations and Generalizability
The primary limitation of this study was its cross-sectional design. The use of retrospective data collection may have introduced bias. To mitigate the selection bias, all tomography scans that met the inclusion criteria were included.
Conclusion
- According to the evaluation of 171 corticopuncture plans from patients with an average age of 33.4 ± 10.4 years, we observed several perforations: 5.68 ± 1.31 in the midpalatal suture, 2.78 ± 0.42 in the intermaxillary suture, and 2.31 ± 0.73 in the transpalatine suture.
- The distance between the perforations was, on average: 2.03 ± 0.5 mm at the midpalatal suture and 1.65 ± 0.18 mm at the intermaxillary suture.
- The angulation of the perforations varied according to the region, with greater angulation in the intermaxillary suture region.
- There was no difference between the sexes in planning the quantity, distance, and inclination of cortical punctures.
- Male patients had a greater amount of soft tissue in the perforated region, which may be related to higher failure rates (greater distance from the mini-implant ring to the hard tissue).
References
1. Celenk-Koca T, Erdinc AE, Hazar S, Harris L, English JD, Akyalcin S. Evaluation of miniscrew-supported rapid maxillary expansion in adolescents: A prospective randomized clinical trial. Angle Orthod. 2018;88:702–9. https://doi. org/10.2319/011518-42.1
2. Choi EA, Lee KJ, Choi SH, Jung HD, Ahn HJ, Deguchi T, et al. Skeletal and dentoalveolar effects of miniscrew-assisted rapid palatal expansion based on the length of the miniscrew: A randomized clinical trial. Angle Orthod. 2023;93:390–7. https://doi.org/10.2319/072322-512.1
3. André CB [MARPE guide]: from consolidation to technique evolution. Journal of Clin Orthod: JCO;19; 2020, p. 00–0
4. André CB, Pasqua BPM, Rino-Neto J, Dupart FN. Surgical digitally guided planning for the mini-screw assisted rapid palatal expansion (MARPE) and suture perforation: MARPE guide [Online first]. IntechOpen. https://doi.org/10.5772/ intechopen.100226; 2021
5. Suzuki SS, Garcez AS, Reese PO, Suzuki H, Ribeiro MS, Moon W. Effects of corticopuncture (CP) and low-level laser therapy (LLLT) on the rate of tooth movement and root resorption in rats using micro-CT evaluation. Lasers Med Sci. 2018;33:811–21. https://doi.org/10.1007/s10103-017-2421-5
6. Bud ES, Bică CI, Păcurar M, Vaida P, Vlasa A, Martha K, et al. Observational study regarding possible side effects of miniscrew-assisted rapid palatal expander (MARPE) with or without the use of corticopuncture therapy. Biology (Basel). 2021;10:187. https://doi.org/10.3390/biology10030187, PMID: 33802266, PMCID: PMC8001817
7. Meirelles CM, Ferreira RM, Suzuki H, Oliveira CB, Souza de Jesus A, Garcez AS, et al. Analysis of factors associated with the success of microimplant-assisted rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2023;164:67–77. https://doi. org/10.1016/j.ajodo.2022.10.029
8. André CB. Guided surgical digital planning for suture cortical perforation: Cortex Guide. J Clin Orthod. 2022;21:74–85
9. Brunetto DP, Sant’Anna EF, Machado AW, Moon W. Non-surgical treatment of transverse deficiency in adults using microimplant-assisted rapid palatal expansion (MARPE). Dental Press J Orthod. 2017;22:110–25. https://doi.org/10.1590/21776709.22.1.110-125.sar
10. André CB, Rino-Neto J, Iared W, Pasqua BPM, Nascimento FD. Stress distribution and displacement of three different types of micro-implant assisted rapid maxillary expansion (MARME): A three-dimensional finite element study. Prog Orthod. 2021;22:20. https://doi.org/10.1186/s40510-021-00357-5
11. Pasqua BPM, André CB, Paiva JB, Tarraf NE, Wilmes B, Rino‐Neto J. Dentoskeletal changes due to rapid maxillary expansion in growing patients with tooth‐borne and tooth‐bone‐borne expanders: A randomized clinical trial. Orthod Craniofac Res. 2022;25:476–84. https://doi.org/10.1111/ocr.12559
12. Kirkwood BR, Sterne JAC. Essential medical statistics. 2nd ed. MA: Blackwell Publishing Science, p. 502; 2006
13. Wilmes B, Ludwig B, Vasudavan S, Nienkemper M, Drescher D. The T-zone: Median vs. paramedian insertion of palatal mini-implants. J Clin Orthod. 2016;50:543–51
14. Becker K, Unland J, Wilmes B, Tarraf NE, Drescher D. Is there an ideal insertion angle and position for orthodontic mini-implants in the anterior palate? A CBCT study in humans. Am J Orthod Dentofacial Orthop. 2019 Set;156:345–54. https:// doi.org/10.1016/j.ajodo.2018.09.019
15. Jesus AS, Oliveira CB, Murata WH, Suzuki SS, Santos-Pinto AD. Would midpalatal suture characteristics help to predict the success rate of miniscrew-assisted rapid palatal expansion? Am J Orthod Dentofacial Orthop. 2021;160:363–73. https:// doi.org/10.1016/j.ajodo.2020.04.035. Epub 2021 Jun 24. PMID: 34175160
16. Salmoria I, de Souza EC, Furtado A, Franzini CM, Custodio W. Dentoskeletal changes and their correlations after micro-implant-assisted palatal expansion (MARPE) in adults with advanced midpalatal suture ossification. Clin Oral Investig. 2022;26:3021–31. https://doi.org/10.1007/s00784-021-04284-x. Epub 2021 Nov 13. PMID: 34773143
17. Oliveira CB, Ayub P, Angelieri F, Murata WH, Suzuki SS, Ravelli DB, et al. Evaluation of factors related to the success of miniscrew-assisted rapid palatal expansion. Angle Orthod. 2021;91:187–94. https://doi.org/10.2319/051420-436.1, PMID: 33351888, PMCID: PMC8028491
18. Winsauer H, Walter A, Katsaros C, Ploder O. Success and complication rate of miniscrew assisted non-surgical palatal expansion in adults – A consecutive study using a novel force-controlled polycyclic activation protocol. Head Face Med. 2021;17:50. https://doi.org/10.1186/s13005-021-00301-2, PMID: 34895287, PMCID: PMC8665552
19. Jia H, Zhuang L, Zhang N, Bian Y, Li S. Age-dependent effects of transverse maxillary deficiency treated by microimplant-assisted rapid palatal expansion: A prospective cone-beam computed tomography study. Am J Orthod Dentofacial Orthop. 2022;161:557–73. https://doi.org/10.1016/j.ajodo.2020.10.029. Epub 2021 Dec 11. PMID: 34903419
20. Jeon JY, Choi SH, Chung CJ, Lee KJ. The success and effectiveness of miniscrewassisted rapid palatal expansion are age- and sex-dependent. Clin Oral Investig. 2022;26:2993–3003. https://doi.org/10.1007/s00784-021-04281-0. Epub 2021 Nov 25. PMID: 34821980, PMCID: PMC8898235
Diagnosis and Treatment of Maxillo-Mandibular Retrusion
Dr. Phillip Witherspoon, DDS
Having noted that for some that the nighttime problems of many patients are mainly eliminated with a mandibular advancement appliance, which is then removed in the waking hours. Therefore, it seemed very logical that the mandible was retruded ; and, since the “daytime occlusion” was restored with removal of the appliance, it seemed apparent that the maxilla must also be retruded. Therefore, by repositioning the maxilla properly, the mandible can then be retained in the relation which restored a competent airway; and, life-time night-time mandibular advancement appliances would not be necessary.
There is an overwhelming number of dental practitioners who believe that there are only 3 skeletal relationships: Class 1 has the mandible properly related to the maxilla, class 2 has the mandible retruded, and class 3 has the mandible protruded. The assumes that the maxilla is always properly related to the base of the skull so that the only variation is from the mandibular relation. IT IS NOT!
The most probable cause of this discrepancy is mouth breathing during the early years when the maxilla depends on the presence of the tongue for lateral and anterior development during the sleeping hours. Therefore, one can have a nice Class 1 dental with both maxilla and mandible retruded; and, both need to be addressed during treatment.
There is a short article enclosed which deals with this. Since the article by McNamara defines where a normally developed maxilla should be, treatment can be delivered which eliminates the use of the night-time appliance. I do not think that this should be considered definitive treatment for all cases of sleep disorders as there may be some which should be addressed by medical practitioners in the field. This orthodontic treatment should be considered “occlusal correction”.
McNamara’s studies in this area were published in the early 1980’s. The one which I had, but cannot find among my many articles foljows growth of a youngster from roughly 7 to 20, and has a ceph taken yearly which shows a properly developing individual with “A” point in a very constant relation to the base of the skull.
For many years the dental community has adhered to the standard of there being 3 classes of skeletal and dental relationships with the unfortunate result that many assume that the two relationships are identical. This scenario gives rise to
problems which are overlooked Qy clinicians since they assume that the dental relationship (Andrews) mirrors, or Is the same, as the skeletal relationship. This is not the case.
There are many studies and reports on growth and development analyzing many possible variables; and, it would appear that many of them occur in cases of abnormal development. McNamara noted that many of them occur in adjustments in respiratory function.1,2
Normal development of the maxilla is dependent upon there being a patent airway so that the tongue rests behind the upper incisors; and, as the tongue grows, there is an accompanying pressure on the dental arches, anteriorly and laterally, resulting in growth of the arches in those directions.3
McNamara also noted that, in a well developed face, 1,2 “A”point lies on a line from Nasion (“N” point) perpendicular to the Frankfort Horizontal plane throughout development. If there is an .impediment to normal respiration (i.e. asthma, allergies, etc.), the individual is forced to open the mouth to breathe adequately, thereby removing the impetus for growth of the maxilla and resulting in a maxilla which is shorter than normal and more narrow (often seen as cross-bite), and creating a new set of skeletal relationships with the 3 dental (Andrews) relations, each requiring different treatment than the ones where the maxilla is properly situated.
When the maxilla is retruded (short of the normal position) the mandible will also be retruded to the same extent as the maxilla if there is a Class I Andrews relationship of the dentition, and, even more so if there is a Class II Andrews relation. Since the tongue is attached to the mandible and is the anterior wall of the airway, the airway will be compromised to the extent of the mandibular retrusion and often times require the individual to breathe through the mouth.
The lateral cephalometric X-ray is a profile view of the head and neck to primarily assess the relationship of the .maxilla and mandible to the base of the skull, and to each other; and some dental relations can be observed.
The clinician should also note the status of the cervical spine. In cases of mandibular retrusion, the normal curvature of the cervical spine is lost and becomes straight. This creates excessive stress on the musculature of the neck and upper back, resulting in many head and neck complaints. There have also been many cases of complaints which have been attributed to a probable Vagal referral.
Treating mandibular retrusion in a patient with the maxilla properly situated to the base of the cranium requires only mandibular advancement, orthopedically, not “surgically;” but, treatment of the patient with maxillary deficiency requires also the development of the maxilla with orthopedic appliances, such as the Schwarz and or saggital. This allows for the proper amount of advancement of the mandible which will then result in the restoration of the cervical lordosis and resolution of the attendant symptoms.
The symptoms often mentioned are generally those associated with referral from the neck and shoulders to the head and neck area; but, the Vagal referrals can involve the heart, stomach and intestines (arrhythmias, GERD, and IBS).
There is a situation of both retrusion of the mandible and maxilla with there being a Class 1 dental relation. The diagnosis associated with this has been Class I skeletal. There will exist mandibular retrusion as noted from from the loss of the cervical lordosis; and, since there is a Class I dental (Andrews), the maxilla is also retruded to achieve this. There often will be cross-bite indicating that the patient was a mouth-breather (and probably still is), which puts the tongue in the floor of the mouth and fails to achieve lateral maxillary growth as well as the deficiency of anterior growth.
This condition does not have a “classification” since there is only 3 skeletal classifications, evidently assuming that the maxilla is ALWAYS at the same point with respect to the base of the cranium, which, obviously, it is not.
Early detection of this problem would be of great benefit; and, it can be. Clinicians treating children should inform the parents of the condition, especially if the child has a cross-bite. The parents observation of the child mouth-breating while asleep should make treatment easier, with better results. Clinicians treating orthodontically, specialists or not, should note the position of “A” point (relative to Nasion perpendicular) throughout treatment and also the cervical spine.
REFERENCES
1. 1.McNamara, James A. Jr. “Influence of Respiratory Pattern on Craniofacial Growth” The Angle Orthodonticst Vol. 51, No. 4 October 1981 pp. 269-300
2. McNamara. James A. Jr. “Components of Class II malocclusion in Childred 8-10 Years of Age The Angle Orthodontist Vol. 51 July 1981 pp 177-202
3. Cooper, B.C. “Nasorespiratory Function and Orofaciat Development” Otolaryngological Clinics of North America April 1989 22(2):413-441
Fig. 1 Point A to nasion perpendicular. Fmnkfort horizontal plane is constructed using ana_tomic porion and orbitalc. A perpendicular is then erected from Frankfort plane to nas1on and extended downward pasl point A. The distance is measured from point A to the !1asion pe1·pcndicula1·; in this illustration point A lies on the perpendicular, so the distance JS zero.
Esthetic-Functional Interceptive Treatment in a Patient with Dental Agenesis and Trauma: Case Report
by Raquel Souza dos Santos Marques, Liziane Monique de Souza Cardoso. Jéssica Roberta Bispo da Silva, Gabriela Mancia de Gutierrez, Anna Paula Nigri, and Luciana Duarte Caldas
AUTHORS
Raquel Souza dos Santos Marques
Specialist in Pediatric Dentistry, CIA; MSc in Pediatric Dentistry, Araraquara-UNESP; PhD resident in Dentistry, Federal University of Sergipe (UFS) , Sergipe, Brazil.
Liziane Monique de Souza Cardoso
Specialist in Pediatric Dentistry, CIA; MSc resident in DentistryHealth Sciences Applied Program, Federal University of Sergipe (UFS) Campus Lagarto, Sergipe, Brazil.
Jéssica Roberta Bispo da Silva Specialist in Pediatric Dentistry, Centro Integrado de Aperfeiçoamento (CIA), (Integrated Improvement Center), Sergipe, Brazil.
Gabriela Mancia de Gutierrez
Specialist in Pediatric Dentistry, USP; MSc in Dentistry, UFS; PhD resident in Pediatric Dentistry, Department of Pedodontics, Cruzeiro do Sul University (UNICSUL), São Paulo, Brazil.
Anna Paula Nigri Specialist in Orthodontics, Federal University of Rio de Janeiro (UFRJ), Brazil; MSc in Dentistry (Orthodontics), UFRJ, Rio de Janeiro, Brazil.
Luciana Duarte Caldas Specialist in Orthodontics, UFBA; MSc in Orthodontics, UFS; PhD in Dentistry (Orthodontics); Postdoc, UFRJ; Federal University of Sergipe, Brazil
Abstract
Tooth loss is one of the factors that most frequently leads guardians seeking pediatric dentistry treatment. The aim of this study was to report a clinical case of dental agenesis with dental trauma in the deciduous dentition, its clinical and psychosocial repercussions and the treatment performed. A five-year-old girl was diagnosed with agenesis of tooth 52, trauma to tooth 51 and maxillary atresia. In an orthodontic approach, the treatment plan consisted of constructing a Haas-type expander associated with an esthetic-functional space maintaining device. The esthetic functional interceptive treatment made it possible to improve the format of the arch, functions of respiration, speech and the esthetics of the smile.
Keywords: Pediatric dentistry; Esthetics; Space maintenance, orthodontic.
Conflict of Interest: None
Introduction
Tooth loss, whether due to trauma, dental caries or congenital absence, is one of the factors that most frequently leads to parents and/or guardians seeking pediatric dentistry treatment, since these absences negatively influence the function and esthetics of the smile in childhood.1 Among the factors responsible for missing teeth are both congenital and local factors.
As regards congenital factors, agenesis - considered a dental anomaly of number, defined by the absence of one or more teeth - is the type that most frequently affects human dentition.2 Its etiology is multifactorial, and includes environmental factors, endocrine, systemic and genetic disorders.3,4 Dental agenesis is uncommon in deciduous dentition and affects only about 0.5 to 0.9% of the population.5,6
In the deciduous dentition, trauma is one of the main reasons for early loss of teeth, and occurs even more commonly in early childhood.7,8 Other factors, such as the high rate of violence and range of sports practices, have contributed to further increase this prevalence.9
The aim of this study was to report a clinical case of dental agenesis with dental trauma in the deciduous dentition, its clinical and psychosocial repercussions, as well as the esthetic-functional treatment performed.
Case description and Results
The patient, a girl, leukoderma, five years and five months old, together with her legal guardian, were referred for treatment to the specialist clinic in Pediatric Dentistry at the Integrated Center for Improvement, located in Aracaju - Se. On clinical examination of the face, the child was found to have a convex profile, mesiofacial pattern and asymmetry of the chin (Fig. 1).
During intraoral clinical examination, absence of the maxillary right lateral incisor was observed, associated with a thick upper labial frenulum that caused an extensive diastema between the maxillary central incisors. Moreover, the patient had the habit of interposing the lower lip into the region of this diastema. In addition, maxillary atresia, Class I relationship of left canines and Class II of right canines were also observed. On analyzing the terminal planes of deciduous second molars, it was possible to verify the existence of a vertical terminal plane on the left side and a distal step on the right.10 (Fig. 1).
In the radiographic images, we found agenesis of tooth 52 and consequently, agenesis of tooth 12, in addition to microdontia of tooth 22 (Fig. 2A) IThe complete occlusal radiograph of the maxilla showed that the palatal suture was not yet consolidated (Fig. 2B).
In lateral teleradiography, mandibular retrognathism and unfavorable oropharyngeal airway space were observed (Fig. 2C).Therefore, with the purpose of improving the shape of the maxillary dental arch, and consequently, allow mandibular displacement, rapid
*This article has been peer reviewed
maxillary expansion (RME) with a modified Haas-type expander was planned.11 However, a few days after the initial examinations, the guardian reported that the child had fallen from her own height, resulting in trauma of tooth 51. The patient was evaluated and extensive resorption of the buccal bone plate (alveolysis), with mobility grade III was found, making it necessary to extract the mentioned tooth (Fig. 3A).
In view of the occurrence and need to extract tooth 51, the guardian reported an influence on the child’s quality of life and socialization, now resulting from the unfavorable smile esthetics. Therefore, the proposal was to associate an esthetic-functional space maintainer with the expander previously planned.
Initially, orthodontic bands on teeth 55 and 65 were selected, maxillary transfer molding was performed and the modified Haas appliance was constructed. During the plastic phase of the acrylic resin, a tube was attached, into which to fit the wire12 that would contain two teeth made of composite resin in shade A1B, mounted in a clasp, in harmony with the size , color and shape of the other teeth in the patient’s arch. It was also necessary to make an artificial gingiva of acrylic resin to improve esthetics (Figs. 3B and 3C).
After inserting the device, RME using the protocol: ¼ turn activation every 12 hours, for eight days, was performed. On conclusion of maxillary arch expansion, final adjustments were made by relining of the esthetic-functional space maintainer to ensure a better result. The diastema between the central incisors was maintained due to the presence of the thick upper labial frenulum (Fig. 4).
Figure 1: Initial facial and intraoral
Figure 2: Initial radiographic images: (A) Panoramic radiography, (B) Complete occlusal radiography of the maxilla, and (C) Teleradiography of the profile.
Figure 3: (A) Intraoral condition after trauma to the tooth. 51 – side and front views and view after performing extraction, (B) Fabrication of modified Haas expander with the stock teeth mounted on clasps. (C) Intraoral images after activating the expander.
Figure 4: (A) Images of the face and smile before and (B) after insertion of the esthetic-functional orthodontic appliance.
Discussion
Congenital absence of deciduous teeth is an uncommon finding; however, when it occurs, it is more prevalent in maxillary lateral incisors, as occurred in the case reported. The etiology of tooth agenesis is multifactorial and can be influenced by genetic, environmental and systemic factors. In the majority of cases, tooth agenesis is considered a hereditary condition that is transmitted by recessive or dominant genes.13,14
The literature, however, reports that tooth agenesis can also be caused by environmental factors such as exposure to toxic substances and inadequate nutritional factors during fetal development. 4 Some studies have suggested a relationship between dental agenesis and endocrine disorders, such as hypothyroidism, Turner syndrome and ectodermal dysplasia. 15 These conditions may affect tooth development by causing changes in the number and shape of teeth.4 In the case reported, the child was referred to an endocrinologist to investigate its association with an endocrine cause, however, no changes were reported. The child’s mother did, however, report that she did not have a maxillary right lateral incisor, which suggested a genetic explanation for the etiology of the case here discussed.
In addition to agenesis of the deciduous tooth and absence of formation of the permanent tooth, on the panoramic radiograph, microdontia of the homologous tooth was observed (tooth 22) (Fig. 2A). This is in agreement with several studies that have pointed out a strong relationship between agenesis of deciduous teeth and changes in the number of the permanent teeth, such as agenesis and supernumerary teeth.16,17 Furthermore, other authors have also pointed out the relationship between agenesis and delays in eruption, reduction in size of the crowns of permanent teeth (microdontia),18 impacted deciduous teeth and conoid lateral incisors.19,20
Radiographically, as the patient presented an unfavorable oropharyngeal airway space, the treatment with RME contributed not only to improve the shape of the dental arch, allowing spontaneous mandibular advancement, but also to improve her respiratory function, since the increase in nasal cross-sectional area leads to a decrease in nasal resistance, thereby increasing airflow.21
The installation of esthetic functional space maintainers can restore esthetics, and consequently, increase the child’s self-esteem, in addition to improving mastication and phonetic functions.22 Therefore, diagnosis and early intervention in cases of loss of deciduous teeth are fundamental steps to preventing damage to the physical, and particularly to the psychosocial health of the child.
Conclusions
The esthetic functional interceptive treatment in this patient made it possible to improve not only the format of the arch, but also the functions of respiration, speech and the esthetics of the smile. This was demonstrated to be an effective treatment in a case of early tooth losses associated with occlusal problems.
References
1 Rocha DTB, Gaia PBR, Topolski F, Mattos CFP, Borges SW, Moro A. Tratamento ortodôntico em paciente com agenesia de incisivos laterais e desvio de linha média superior e inferior – relato de caso. Orthodontic Science and Practice. 2019;12: 76–85.
2 Costa AMG, Trevizan M, Matsumoto MAN, da Silva RAB, da Silva LAB, Horta KC, et al. Association between Tooth Agenesis and Skeletal Malocclusions. Journal of Oral and Maxillofacial Research. 2017;8(2).
3 Iyer NS, Trager L, Gaughan J, Akoto S, Cardonick E. Paediatric dental outcomes among children exposed to chemotherapy in utero. International Journal of Paediatric Dentistry. 2022;32: 116–122.
4 Coster PJ, Marks LA, Martens LC, Huysseune A. Dental agenesis: genetic and clinical perspectives. Journal of Oral Pathology & Medicine. 2008;38: 1–17.
5 Kolenc Fusé FJ. Agenesias dentarias: en busca de las alteraciones genéticas responsables de la falta de desarrollo. Medicina Oral, Patología Oral y Cirugía Bucal. 2004; 9: 385–395.
6 Neville BW. Patologia Oral e maxilofacial. 4th ed. Elsevier. Rio de Janeiro. 2016.
7 Petti S, Glendor U, Andersson L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Dental Traumatology. 2018;34: 71–86.
8 Jorge KO, Moysés SJ, e Ferreira EF, Ramos-Jorge ML, de Araújo Zarzar PMP. Prevalence and factors associated to dental trauma in infants 1-3 years of age. Dental Traumatology. 2009;25: 185–189.
9 Moura JA de, Silva AKXG da, Campos THG, Alencar Filho AV. Atenção odontopediatrica voltada para o traumatismo na dentição da criança. Research, Society and Development. 2022;11: 1-12.
10 Baume L. Physiological tooth migration and its significance for the development of occlusion. Journal of Dental Research. 1950;29: 123–132.
11 Haas AJ. The Treatment Of Maxillary Deficiency By Opening The Midpalatal Suture. Angle Orthodontist. 1965;35: 200–217.
12 Caldas LD, Nigri AP, de Souza MMG. Inserting Auxiliary Springs into the Acrylic of Rapid Palatal Expanders. Journal of Clinical Orthodontics. 2019;53: 355–356.13 Ravi V, Murashima-Suginami A, Kiso H, Tokita Y, Huang CL, Bessho K, et al. Advances in tooth agenesis and tooth regeneration. Regenerative Therapy. 2023;22: 160–168.
14 Letra A. Rethinking the Genetic Etiology of Nonsyndromic Tooth Agenesis. Current Osteoporosis Reports. 2022;20: 389–397.
15 Al-Ani AH, Antoun JS, Thomson WM, Merriman TR, Farella M. Hypodontia: An Update on Its Etiology, Classification, and Clinical Management. BioMed Research International. 2017;2017: 1–9.
16 Schonberger S, Kadry R, Shapira Y, Finkelstein T. Permanent Tooth Agenesis and Associated Dental Anomalies among Orthodontically Treated Children. Children. 2023;10: 596-609.
17 Davis PJ, Darvell BW. Congenitally missing permanent mandibular incisors and their association with missing primary teeth in the Southern Chinese (Hong Kong). Community Dentistry and Oral Epidemiology. 1993;21: 162–164.
18 Gungor AY, Turkkahraman H. Tooth sizes in nonsyndromic hypodontia patients. The Angle Orthodontist. 2013;83: 16-21.
19 Gomes RR, da Fonseca JAC, Paula LM, Faber J, Acevedo AC. Prevalence of hypodontia in orthodontic patients in Brasilia, Brazil. The European Journal of Orthodontics. 2010;32: 302–306.
20 Larmour CJ, Mossey PA, Thind BS, Forgie AH, Stirrups DR. Hypodontia--a retrospective review of prevalence and etiology. Part I. Quintessence international. 2005;36: 263–270.
21 Caldas LD, Takeshita WM, Machado AW, Bittencourt MAV. Effect of rapid maxillary expansion on nasal cavity assessed with cone-beam computed tomography. Dental Press Journal of Orthodontics. 2020;25: 39–45.
22 Volpato LE, Crivelli AS, Oliveira ET, Nobreza AM, Rosa A. Rehabilitation with Esthetic Functional Fixed Space Maintainer: A Report of Two Cases. International Journal of Clinical Pediatric Dentistry. 2021;14: 315–318.
TIPS FROM THE EXPERIENCED
The Utility Arch, Part 1V
By Dr. Adrian J. Palencar, MUDr, MAGD, IBO, FADI, FPFA, FICD
Utility Arches activated in sagittal plane.
1. Extrusive - Retrusive: after the Passive Utility Arch is fabricated, it should be inserted into the maxillary or mandibular tubes, to evaluate the parallelism and the tip of the molars. The 30° - 45° tip-forward (gable bend, “V” pointing apically) in front of the molar tubes precipitates:
a) Small extrusion and lingual moment (up-righting) on the incisors
b) Large intrusion and mesial moment (tipping) on the molars, this renders the dental arch shorter, the arch wire should be annealed and bent-back (cinch) distally to the molar tube.
Also, there should be about 15° - 20° toe-in bent in front of the maxillary molar tubes (not in the mandible), to disto-rotate the molars. The amount of the applied force should be measured with the Gram gage (do not exceed 70 grams).
2. Extrusive - Protrusive, the bends are the same, however, follow the protocol of the Protrusive Utility arch.
The author very seldom constructed and placed Extrusive Utility Arch because it shortens the dental arch. The obvious application would be a case with an anterior open bite with excessive spacing.
References
1) Rondeau Seminars, Level I, Session 3; 136 – 161
2) Journal of Clinical Orthodontics, Volume LVI, Number 12; 716 – 724
3) Palencar A. J., Case Finishing and Mechanics, 152 – 156