Celebrating 35 years: defying boundaries, redefining possibilities
A publication of the International Myeloma Foundation
Celebrating 35 Years: Defying Boundaries, Redefining Possibilities
Celebrating 35 years: defying boundaries, redefining possibilities
Celebrating 35 Years: Defying Boundaries, Redefining Possibilities

Read about the key takeaways from the 2025 Summit of the IMF International Myeloma Working Group (IMWG) and the annual meeting of the American Society of Clinical Oncology (ASCO) and the European Hematology Association (EHA)
PAGE 5
ALSO IN THIS EDITION: Lynozyfic™ (linvoseltamab-gcpt), a new bispecific antibody, is approved by the U.S. Food and Drug Administration (FDA) for the treatment of relapsed or refractory myeloma
PAGE 3
Dear Friends,
When I joined the International Myeloma Foundation (IMF) in April 2006, after more than two decades in the pharmaceutical industry, I already knew this organization was something extraordinary. I had worked alongside the IMF for years in my previous role and saw firsthand its unwavering commitment to changing the landscape of myeloma – from advancing research to transforming patient care. Even then, it was clear that the IMF was more than a foundation; it was a movement defined by compassion, strategy, and innovation.
For nearly 20 years now, I have had the honor of helping lead this organization and drive our mission forward: to improve the quality of life of myeloma patients while working toward prevention and a cure. Our vision is a world where every myeloma patient can live life to the fullest, unburdened by the disease. This vision feels closer each day because of the passionate and purposeful work we do together.
Since its founding in 1990, the IMF has been unlike any other organization in the field, uniting the core pillars of Research, Education, Support, and Advocacy into one integrated approach. This holistic model remains the foundation of our work and continues to set us apart. We are not only meeting critical needs – we are anticipating them. Thirty-five years later, the IMF is a global hub for everyone touched by myeloma: individuals living with the disease, their loved ones, healthcare providers, scientific innovators, and partners around the world dedicated to healing and hope.
Our strength lies in our ability to build bridges – across disciplines, across cultures, and across borders. Myeloma doesn’t stop at geographic or demographic boundaries, and neither do we. Through programs like the IMF Global Myeloma Action Network (GMAN), the IMF Asian Myeloma Network (AMN), and our expanding IMF Latin American Myeloma Network (LAMN), we are meeting patients where they are, ensuring that support, education, and access to care reach every corner of the world.
The IMF stands at the intersection of scientific excellence and the patient experience. We lead with both data and empathy – amplifying the voices of those living with myeloma while driving forward the research that shapes
their future. As the convenor of the International Myeloma Working Group (IMWG) – a coalition of more than 350 leading myeloma researchers worldwide, and in close collaboration with over 150 patient support groups across the U.S., we connect the world’s top scientific minds with the real-world challenges faced by patients every day. This unique position is our strength: advancing cutting-edge science while walking alongside patients through one of life’s most difficult journeys.

Our global leadership in myeloma is rooted in action. From shaping clinical research to empowering patient communities, our impact is both broad and deep. We evaluate every new initiative with a critical eye: Will this make a meaningful difference in someone’s life? If the answer is yes, we pursue it with everything we have.
Every program we launch, every partnership we build, is driven by one goal: improving outcomes for myeloma patients, wherever they live and however they experience this disease. We are committed to reaching underserved communities, amplifying diverse voices, and ensuring that no one faces myeloma alone.
At the IMF, we never settle for the status quo. We are constantly raising the bar, expanding our reach, and embracing innovation. Together, we deliver real solutions that make a lasting difference. This level of collaboration and impact is unmatched in the field of myeloma.
Thank you for being part of this journey with us. Together, we are turning hope into progress – and progress into lasting change.

Diane Moran, RN, MA, EdM Interim Chief Executive Officer Senior Vice President, Strategic Planning
On July 2, 2025, the U.S. Food and Drug Administration (FDA) granted accelerated approval of Lynozyfic™ (linvoseltamab-gcpt), a new bispecific antibody for the treatment of adult patients with relapsed or refractory multiple myeloma (RRMM) who have received at least 4 prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody.
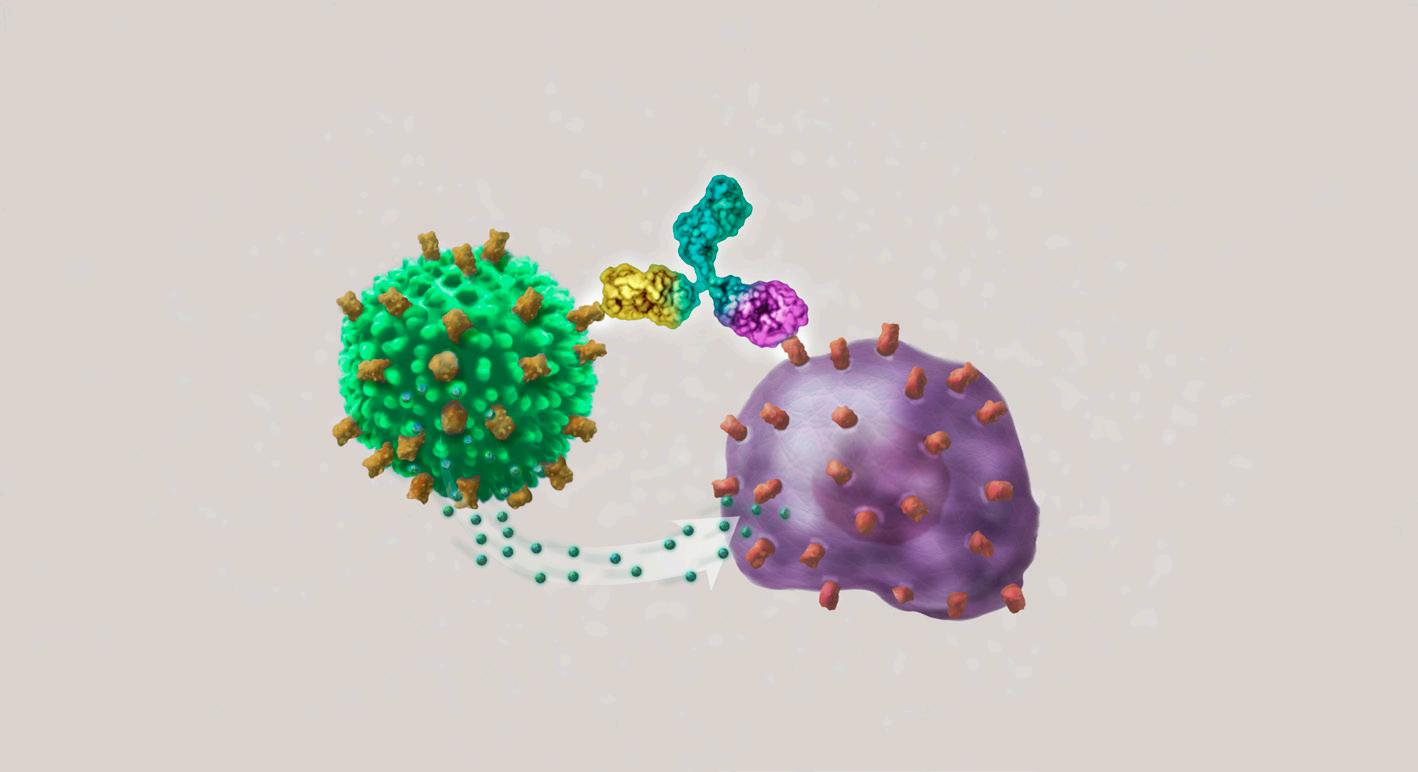
Immunotherapy is treatment that engages the patient’s own immune system to attack their myeloma. Bispecific antibody therapies use two (“bi”) arms to attach to a patient’s cells. One arm attaches to a myeloma cell, while the other arm attaches to a local immune cell. Bispecific antibodies are a dual threat to myeloma.
Lynozyfic is a bispecific antibody that binds to B-cell maturation antigen (BCMA) on the surface of myeloma cells and to CD3 on the patient’s T cells, bringing these cells together and stimulating the T cells to kill the myeloma cells. The FDA approval of Lynozyfic expands the treatment options available to patients with RRMM.
Dr. Joshua Richter and Dr. Sundar Jagannath are leading investigators of linvoseltamab in the LINKER-MM1 clinical trial, a phase I/II study of monotherapy in 282 patients with triple-class RRMM. This interview reflects their experience and opinions. For precise Lynozyfic prescribing information, please visit regeneron.com/downloads/lynozyfic_fpi.pdf
Dr. Richter, what has been your experience with Lynozyfic?
In myeloma, we always strive for increased response rates and lower side effect rates. The FDA approval is based on data from the LINKER-MM1 phase I/II clinical trial of 117 patients treated with 200 mg of Lynozyfic. The median age was 70 years, 39% had high-risk cytogenetics, and 28% had penta-refractory disease.
At a median follow-up of 14.3 months, the overall response rate (ORR) was 71%, with 50% achieving complete response (CR) or better. In 104 patients treated with 50 mg at a median follow-up of 7.4 months, the ORR was 48%, with 21% achieving CR or better. Lynozyfic 200 mg induced deep and durable responses in heav ily pre-treated patients with RRMM. The median duration of response (DoR) was 29.4 months.
Lynozyfic is given through an intra venous (IV) infusion. After a “step-up” dosing schedule that is designed
to help lower the risk of side effects, the protocol is to receive Lynozyfic once-a-week for 11 doses, then every other week for 5 doses. After these doses, the doctor will assess response to treatment and determine if the patient should continue the every-other-week schedule or receive Lynozyfic once every 4 weeks instead. The doctor will also determine how long the treatment should continue.

Joshua Richter, MD
Associate Professor of Medicine, Tisch Cancer Institute
Director of Multiple Myeloma, Blavatnik Family Chelsea Medical Center
Mount Sinai Health System New York, NY
There are a number of previously FDA-approved bispecific therapies for patients with RRMM, and the response rates with Lynozyfic are a little bit higher, but it is difficult to compare bispecifics drug-to-drug due to differences in clinical trial protocols and patient populations. However, I can address some of the advantageous features of Lynozyfic. The step-up dosing with Lynozyfic is in many ways easier on the patient. With other bispecifics, the step-up doses are 48 to 72 hours apart, so patients can be hospitalized for 5 to 9 days. With Lynozyfic, the patient may be admitted for 24 hours to receive their first dose. Then, a week later, the patient may be admitted for another 24 hours… or not.
The National Comprehensive Cancer Network (NCCN) guidelines allow us to give prophylactic tocilizumab prior to admin
(continues on next page)
Lynozy c binds to CD3 on the surface of the T cell
Lynozy c (BCMAxCD3)
Lynozy c binds to BCMA on the myeloma cell surface


T cell receptor (TCR) BCMA tumor-speci c antigen on the surface of the myeloma cell


Lynozy c activates the T cell to release cytotoxic granules that kill the myeloma cell
Sundar Jagannath, MD Professor of Medicine, Tisch Cancer Institute Network Director, Center of Excellence for Multiple Myeloma Mount Sinai Health System New York, NY

I am excited that linvoseltamab, a new bispecific antibody, has been approved by the FDA for the treatment of advanced relapsed multiple myeloma. This is another important milestone toward curing myeloma. In my experience, linvoseltamab has an impressive response rate of 70% that was durable and meaningful to patients. Even the myeloma tumor with high-risk genetics responded equally well.
While CRS is common to all bispecific antibodies, it was generally milder and easily manageable. Neurologic side effects were uncommon and reversed quickly with management.
What stands out for linvoseltamab is that the dosing is tailored to response; this is patient-friendly, with less side effects without compromising the efficacy.
adverse events later. My plan is to give tocilizumab as an out-patient prophylactic, then give the first dose of Lynozyfic and admit the patient to hospital for 24 hours. After that, no more in-patient admission.
We give Lynozyfic once-monthly because it’s better tolerated and patients prefer the increased comfort. As part of the Lynozyfic clinical trial design, patients who had partial response (PR) or better at 200mg were switched to once-monthly dosing. Although the other FDA-approved bispecifics may also be reduced to being given once-monthly, those clinical trials were not designed to properly evaluate monthly administration.
The most common adverse events included cytokine release syndrome (CRS), neutropenia, and anemia. Immune effector cell-associated neurotoxicity syndrome (ICANS) occurred in 7.7% of patients. Infections were reported in 74.4% of patients, with the frequency and severity declining over time.
In myeloma, we always strive for increased response rates and lower side effect rates.
But let’s differentiate the early side effects and the late side effects. When immunotherapies make our immune system too active, patients can develop CRS or ICANS, but the Lynozyfic step-up dosing schedule reduces the risk. In addition, patients are pre-treated with tocilizumab and monitored after their infusions. At the first sign of CRS, supportive care is administered based on CRS severity, and Lynozyfic may be interrupted or discontinued.
Longer-term side effects are things like low blood counts and infection, because when we kill bad immune cells (myeloma cells), we can also kill some good immune cells. One way to deal with potential infections is to stay up to date with vaccinations. Another is using preventive medicines against known infections. We also administer monthly intravenous immunoglobulin (IVIG), to give people healthy antibodies until their own system is able to fight off infection.
Bispecific antibodies and CAR T-cell therapies both use the patient’s own immune systems to attack their myeloma. CAR T-cell therapy requires a patient’s own T cells to be collected, genetically engineered, and multiplied in a lab before being re-infused into the patient to attack myeloma.
If I see a new patient today, it may take a minimum of 2 to 3 months before the CAR T-cell therapy is ready to be infused into that patient. Bispecifics are an “off-the-shelf” product that’s ready to be used right away, and patient comfort is greater because we don’t have to do the harvesting and the re-infusion.
In the United States, around 80% of myeloma is treated in the community, not in myeloma centers like the one I work in. And the reality is that CAR T-cell therapy is complicated, so not every facility can offer access to it. But everyone anywhere could theoretically get a bispecific. To me, one of the wonders of bispecifics is that patients who may be too frail or too sick to get a transplant or a CAR T-cell therapy might be able to get a bispecific, an extremely effective next-generation therapy. The ability to respond in an instant to whatever the myeloma throws at us is an advantage over lengthy preparations. MT
Lynozyfic is available through a Risk Evaluation and Mitigation Strategy (REMS) program, required by the FDA for treatments that may have serious safety concerns. REMS programs support the use of such treatments and help ensure that the potential benefits outweigh the risks.
Patients who are prescribed Lynozyfic will receive a Patient Wallet Card that summarizes the signs and symptoms of problems that may occur with treatment. Patients who develop any of the signs and symptoms listed on the Lynozyfic Patient Wallet Card must pursue medical help immediately.
Lynozyfic Surround™, a support program offered by Regeneron, provides financial and educational resources to help patients throughout their treatment journey with Lynozyfic. Call 1.844.746.4363 and visit regeneron.com for more information.
By Dr. Joseph Mikhael IMF Chief Medical Officer
Every year, three annual events that take place in quick succession hold a special significance for the researchers and clinicians working in the field of myeloma. The 2025 annual meeting of the American Society of Clinical Oncology (ASCO), the largest gathering of cancer specialists in the world with 45,000 doctors attending, took place from May 30 through June 3 in Chicago, IL. The 2025 Summit of the IMF International Myeloma Working Group (IMWG), which brought together approximately 100 of the more than 360 global experts in myeloma, took place June 10-12 in Milan, Italy. The 2025 annual congress of the European Hematology Association (EHA) took place June 12–15, also in Milan, attracting 18,000 doctors from all areas of hematology. It is impossible to cover in detail all that transpired during these three important events in the pages of Myeloma Today. In this article, I aim to summarize for you the selected takeaways that hold the greatest impact for patients with myeloma. For more in-depth information, please visit myeloma.org and view the videos archived at videos.myeloma.org.
The Iceland Screens, Treats, or Prevents Multiple Myeloma (iStopMM) clinical trial of early detection and prevention is a massive project that is educating us about the feasibility and usefulness of screening. Age, genetics, and family history have been shown to be important factors in all screening programs, and we should expect the same in myeloma, especially as it is twice as common in patients of African descent. In the next 2 years, the iStopMM study will likely answer the key question of whether screening for myeloma saves lives, and we are all eager to see the data.
SMM is an asymptomatic precursor to active myeloma. Discussed at the IMWG Summit, the 20-2-20 model defines high-risk smoldering multiple myeloma (HR SMM) as having at least two of the following: 20% plasma cells in the bone marrow, a monoclonal

spike (M-spike) of at least 2 g/dL, and a free light chain ratio of involved-to-uninvolved light chains being greater than 20. This model helps place SMM along the spectrum of myeloma, though definitions are still evolving.
The AQUILA clinical trial presented at the annual meeting of the American Society of Hematology (ASH) in December 2024 compared early treatment with Darzalex® (daratumumab) to close observation of patients with HR SMM. After 5 years, 63% of treated patients had not progressed, while 40% in the observation group progressed to active myeloma. Monitoring had a median time to progression of around 3 years, which wasn’t yet reached in the treatment arm.
The AQUILA study was critical to proving that we can delay the progression to active myeloma and even improve patient survival with 3 years of Darzalex. While early intervention may delay progression, it does not necessarily prevent active myeloma. Since there is no FDA-approved treatment for HR SMM, patients should consider clinical trials and discuss this with their doctors. Currently, enrollment is open for studies of drugs approved for active myeloma, as well as studies with curable intent. Ultimately, the best strategy combines the patient’s perspective with clear data to guide truly individualized care.
There is consensus among experts that no clinical trials are needed for low-risk SMM. For intermediate-risk SMM, there is a need for studies of innovative approaches to intercepting the evolution to myeloma. Ongoing research to identify risk factors at baseline may move patients with HR SMM to an early myeloma category.
Treatment of patients with newly diagnosed multiple myeloma (NDMM) was addressed in three key studies.
The PERSEUS clinical trial has truly changed the way we treat NDMM by demonstrating that “triplet” (3-drug) combination therapies are less effective than “quadruplet” (4-drug) combinations in patients who are proceeding to autologous stem cell
(continues on next page)


IMWG, ASCO, AND EHA – CONTINUED FROM PAGE 5
transplantation (ASCT). Specifically, this year’s data from ASCO and EHA showed that the combination of Darzalex + Velcade® (bortezomib) + Revlimid® (lenalidomide) + dexamethasone [DVRd] plus ASCT and dual maintenance with Darzalex + Revlimid (D-R) resulted in extraordinary outcomes for patients. More than half of the DVRd patients attained minimal residual disease (MRD)-negativity for more than 2 years.
The MIDAS clinical trial studied the quadruplet therapy of Sarclisa® (isatuximab) + Kyprolis® (carfilzomib) + Revlimid + dexamethasone [Isa-KRd]. After this quadruplet induction, patients who were MRD-negative received a less intense therapy than patients who were MRD-positive. It’s too early for a final conclusion, but it’s clear that MRD will guide more therapy with time. In the interim, we’re already seeing that patients who achieved MRD-negativity may not need ASCT at all, but we need more time to see if this MRD results holds up for progression-free survival (PFS) before we stop doing transplants for patients who achieve MRD negativity with induction. For patients who are MRD-positive, it appears that there is no more need of tandem transplants (two transplants in a row). We’re looking forward to the more mature data that will be reported from this clinical trial.
The GMMG-CONCEPT clinical trial focused on patients with highrisk multiple myeloma (HRMM). About 20% of newly diagnosed patients have HRMM. Historically, it has been challenging to treat these patients as they tend to relapse quickly. The more intense 4-drug regimen of Isa-KRd, then ASCT, is followed with continuing the 4-drug therapy, but eventually dropping the steroid dexamethasone from the protocol and giving patients Isa-KR. The outcomes were much better than what we’ve previously seen with HRMM and may signify the benefit of a more intense therapy approach for high-risk disease.
In conclusion, quadruplet combinations have become the most effective therapy we can offer in the NDMM setting, making them the new standard of care. We’re moving toward dual-maintenance therapy with Darzalex + Revlimid [D-R], which provides the best sustained MRD. We might begin using MRD-guided approaches in the very near future.

Although new approaches to the treatment of NDMM are producing excellent results for many patients, giving them their longest remissions, myeloma is a disease that typically relapses.
Studies of patients who have had 1 to 3 prior lines of therapy included the drug belantamab mafodotin, which was previously approved by the U.S. Federal Drug Administration (FDA), then removed from the market. There are 2 important studies with belantamab, DREAMM-7 and DREAMM-8. Patients in one of the studies had 3 years of remission on average!
DREAMM-7 combined belantamab + Velcade + dexamethasone [BVd], demonstrating PFS and a trend to an overall survival (OS) advantage. DREAMM-8 combined belantamab + Pomalyst® (pomalidomide) + dexamethasone [BPd], demonstrating a significantly longer median PFS (mPFS). We hope to have belantamab back in the clinic very soon as it is an easily delivered and highly effective treatment.
There was an interesting study of delivering Sarclisa. Historically, it has been given as an intravenous (IV) infusion. The new form of subcutaneous (in-the-skin) delivery is a device called on-body injector (OBI). It sticks to the skin, and a tiny needle pushes Sarclisa into the skin over about 12-13 minutes. Isa OBI had a similar safety profile to Isa IV, and patients appreciated the OBI method, which might mean that patients could receive it at home in the future.
A series of studies focused on the early relapse setting for bispecific antibodies, “off-the-shelf” drugs that are currently used in late relapse. Having more options for patients in early relapse to be treated with these highly effective therapies is a very positive sign.
Treatments for patients who have had at least 4 prior lines of therapy are the focus of a number of amazing clinical trials. Below is an overview of just a few areas of study.
Standard of care CAR T-cell therapy is emerging as the most effective treatment of relapsed myeloma, even in heavily pretreated patients. Arguably the most impactful and exciting


of all the abstracts presented at ASCO and EHA meetings was the long-term follow-up of the CARTITUDE-1 clinical trial. Study patients received Carvykti® (cilta-cel) as a onetime CAR T-cell infusion. Remarkably, 33% of patients who received Carvykti are still completely disease-free 5 years later. I’m not saying that these patients are cured, but this unprecedented outcome does raise the question of how do we define cure in myeloma?
Novel CAR T-cell therapy is another exciting area of research in late relapse is the development of new CAR T-cell therapies. In particular, a drug called anitocabtagene autoleucel (anito-cel) has a different design than the previous CAR T-cell therapies, and seems to have just as high a rate of response as previous CAR T-cell therapies but with fewer neurological side effects.
Bispecific antibodies have two arms; one arm of the drug binds to the myeloma cell while the other arm binds to a T cell. The RedirecTT-1 clinical trial studied the combination of two bispecific therapies, Tecvayli® (teclistamab) and Talvey® (talquetamab), giving them together to patients whose myeloma has historically been very difficult to treat and control. Patients with extramedullary disease (EMD) have myeloma outside of the bone. Remarkably, when the RedirecTT-1 study combined these two bispecific therapies to treat EMD, the response rate was more than 80%, something we’ve not seen before in myeloma. This approach could give us a great option to treat EMD.
Please note that a new bispecific antibody was approved by the FDA in July 2025. You can read more about Lynozyfic™ (linvoseltamab-gcpt) immunotherapy on page 4 of this edition of Myeloma Today.
Trispecific antibodies
Trispecific antibodies have two arms that bind to the myeloma cell while the third arm binds to a T cell. This allows the drug to be even more precise than bispecific antibodies. Studies of trispecifics have demonstrated strong response rates, with fewer side effects than with bispecifics. This might mean that we will be able to deliver more effective and safer therapies in the near future.
The BCMA-GPRC5D trispecific antobody has demonstrated strong efficacy and significantly less toxicity than a combination of drugs. It has the potential to supplant sequential use of bispecific antibodies.
The BCMA-CD38 trispecific antibody also has impressive efficacy and tolerability and may confer another option for late relapse of myeloma.
High-risk multiple myeloma (HRMM) remains challenging to treat, requiring an intense approach with sustained MRD as the goal. A consensus on the definition of HRMM is an essential step toward risk-stratified therapeutic approaches and clinical trials that are focused on patients with HRMM.
Members of the IMWG and the International Myeloma Society (IMS) have now reached consensus on how to define HRMM and recommend the use of this definition in all clinical trials going forward, as well as in clinical practice. Based on the new definition, the HRMM subset of patients represent approximately 20% of NDMM patients.
All of the above-noted developments will lead to new and more effective treatment options for patients with myeloma. The IMF continues to drive forward our mission of improving the quality of life of myeloma patients while working toward prevention and a cure. Our vision is a world where every myeloma patient can live life to the fullest, unburdened by the disease. MT
Stay informed about the key developments in the field of myeloma! Sign up at subscribe.myeloma.org for our quarterly journal Myeloma Today and weekly e-newsletter Myeloma Minute and contact the IMF InfoLine with your myeloma-related questions and concerns. Phone lines are open 9 a.m. to 4 p.m. (Pacific) Monday through Thursday and 9 a.m. to 2 p.m. on Friday at 1.800.452.CURE in the U.S. and Canada and 1.818.487.7455 worldwide. You can also email InfoLine@myeloma.org , or visit mmsm.link/infoline to schedule a convenient time to talk with an IMF InfoLine Coordinator..

S. Vincent Rajkumar, MD IMF Chairperson of the Board
The International Myeloma Foundation (IMF) and the International Myeloma Working Group (IMWG) are proud to announce the 2025 recipients of the Robert A. Kyle Lifetime Achievement Award and the Brian G.M. Durie Outstanding Achievement Award. Every year during the IMWG Summit, two researchers who have made significant contributions in the field of myeloma are honored with these awards. This year’s awards ceremony was held on June 10 during the 16th annual IMWG Summit in Milan, Italy.
The Robert A. Kyle Lifetime Achievement Award and Brian G.M. Durie Outstanding Achievement Award are prestigious IMWG recognitions, and I was honored to be part of the IMF Scientific Advisory Board awards committee with Dr. Philippe Moreau (University Hospital of Nantes, Nantes, France), Dr. Nikhil Munshi (Dana-Farber Cancer Institute, Boston, MA), and Dr. Jesús San Miguel (University of Navarra, Pamplona, Spain).
The Robert A. Kyle Lifetime Achievement Award recognizes individuals whose work has resulted in significant advances in research, treatment, and care of patients with myeloma. Dr. Kyle (Mayo Clinic, Rochester, MN) is a world-renowned myeloma expert whose groundbreaking work led to the discovery of significant hematologic entities, such as monoclonal gammopathy of undetermined significance (MGUS) and smoldering multiple myeloma (SMM).
The recipient of the 2025 Robert A. Kyle Lifetime Achievement Award is Dr. Sagar Lonial, internationally recognized as a leading authority in myeloma treatment and research. He is Chair and Professor at the Department of Hematology and Medical Oncology of Emory University School of Medicine in Atlanta, GA. Dr. Lonial is also Chief Medical Officer of the Winship Cancer Institute of Emory University. He serves as co-chair of the National Cancer Institute (NCI) Myeloma Committee, as a board member of the IMF Scientific Advisory Board, and as co-chair of the Multiple Myeloma Research Foundation (MMRF) Scientific Advisory Board.
Dr. Lonial is the myeloma editor for Clinical Lymphoma and Myeloma, an Associate Editor for the JCO Journal of Oncology Practice, and a former section editor for Cancer Dr. Lonial is also an ad hoc reviewer for Blood, Cancer Research, Clinical Cancer Research, Haematologica, Leukemia, and other journals, and has authored or co-authored over 400 papers and abstracts.
Dr. Lonial has worked in the field of immunotherapy and cancer. He has spent time developing the B-cell malignancy program with respect to novel targeted agents in laboratory models as well as early clinical trials. His previous laboratory work focused on evaluating the impact of purified dendritic cell subsets on the nature of immune responses against antigen. Most recently, Dr. Lonial has focused on combinations of novel agents as therapy for myeloma and lymphoma.
His notable accolades include the Celgene Young Investigator Award, the Indo American Cancer Association (IACA) Lifetime Achievement Award, and the COMy Multiple Myeloma Excellence Award for Clinical Science. He is also a Giants of Cancer Care inductee and currently holds the Anne and Bernard Gray Family Chair in Cancer.
“Dr. Kyle is such a giant in the myeloma field, to have my name spoken with the award that recognizes all his contributions is such an honor. I am very proud of our team at Emory and Winship for doing important work to improve outcomes for myeloma patients and for helping provide options to our patients,” said Dr. Lonial about receiving this award.
I am delighted that Dr. Lonial is awarded the prestigious Robert A. Kyle Lifetime Achievement Award. It is a recognition of Dr. Lonial’s immense and significant life-long contributions to myeloma treatment and research, including the development of several new drugs for the disease. He also built a world-class myeloma program at the Winship Cancer Institute in Atlanta, and in the process has mentored numerous scientists in the field. I am also confident that under his leadership, the myeloma community can be assured that the pursuit of a cure for myeloma is of the highest priority.
The Brian G.M. Durie Outstanding Achievement Award recognizes excellent achievements in myeloma research. Dr. Durie is the former IMF Chief Scientific Officer, IMWG Chairman, leader of the IMF’s Black Swan Research Initiative® (BSRI®), Professor of Medicine, Hematologist-Oncologist, and recipient of the 2019 Honorary Doctorate for Scientific Excellence from the Vrije Universiteit Brussel.
The recipient of the 2025 Brian G.M. Durie Outstanding Achievement Award is Dr. Sonja Zweegman, Head of the Department of Hematology and Vice Chair of the Cancer Center Amsterdam UMC in the Netherlands. She is chairman of the Dutch HOVON Myeloma Working Group. Dr. Zweegman’s clinical research focuses on optimizing treatment of myeloma patients, particularly for the vulnerable and older populations.

She is a principal investigator of numerous national and international clinical trials involving the elderly and aiming to personalize treatment approaches based on the degree of frailty. To this end, her work explores whether functional geriatric assessments and biological indicators of frailty – such as (immune)senescence and sarcopenia – can more accurately predict treatment feasibility and outcomes.
Dr. Zweegman co-leads the Amsterdam UMC Myeloma Translational Research Group, which is embedded within the Department of Haematology and bridges laboratory research with clinical care. Her translational efforts are dedicated to advancing immune-based therapies for multiple myeloma. These include elucidating the mechanisms of action of immunotherapeutics and investigating the biological underpinnings of treatment resistance.
To improve outcomes in patients with resistant disease, she is actively involved in the development of innovative immunotherapeutic strategies, including novel CAR T-cell therapies, designed to overcome immune escape and therapeutic resistance. Dr. Zweegman has co-authored over 350 peer-reviewed publications and contributed to several book chapters.
She is actively engaged in initiatives to improve healthcare delivery and access to treatment for individuals with hematological malignancies. As chair of the HOVON Myeloma Working Group and the Echelons in Haematological Care Working Group, she oversees the development of treatment guidelines, care centralization, and regional consultation networks aimed at improving both quality and equity of access.
A major theme throughout her work is improving quality of life for patients with myeloma by optimizing treatment efficacy and by reducing toxicity, preserving functional independence, and aligning care with patient values. Dr. Zweegman co-leads the Quality of Life Working Group within the IMWG, where she leads international efforts to incorporate patient-reported outcomes into research and clinical practice.
She is co-chair of the Membership Committee of the International Myeloma Society (IMS), where she fosters connections among hematologists worldwide to advance the Society’s mission of improving care for patients with myeloma across diverse healthcare systems.

Dr. Zweegman is a dedicated educator who provides educational outreach nationally and internationally, sharing knowledge with hematologists, the patient community, and the broader public to improve understanding and management of myeloma.
“It’s a real honor to receive this award, especially as it carries the name that marked my very first steps into the world of myeloma –Brian G.M. Durie. His work helped shape the way we treat this disease, and those early steps brought me into a passionate and warm community. It is a community deeply committed to improving both the length and quality of life for people living with myeloma –recognizing their strength, while never losing sight of their vulnerability,” said Dr. Zweegman.
“Research is something we can only do together, and that’s why this award truly belongs to all the researchers in HOVON, the international myeloma community, the patients I’ve worked with, and to my ‘scientific family’ in Amsterdam UMC-Cancer Center on our shared journey toward longer and better lives for myeloma patients,” she further stated.
Dr. Zweegman’s commitment to clinical research aimed at optimizing treatments for vulnerable and elderly myeloma patients is truly remarkable and highly deserving of the Brian G.M. Durie Outstanding Achievement Award. Her co-leadership of the Amsterdam UMC Myeloma Translational Research Group fills the gap between laboratory research and clinical care. Her dedication to improving the quality of life of myeloma patients is one of the top qualities we look for in a Brian G.M. Durie Outstanding Achievement Awardee. Her body of work all points to the IMF’s vision: A world where every myeloma patient can live life to the fullest, unburdened by the disease.

The entire IMF team, led by Interim CEO and Senior Vice President of Strategic Planning Diane Moran, joins me in extending the warmest congratulations to the 2025 IMWG Award recipients. On behalf of the myeloma community we serve, we express our profound appreciation to Dr. Lonial and to Dr. Zweegman, two outstanding myeloma researchers! MT
Carrie Bellerive, BS, RN, BMTCN® Memorial Sloan Kettering Cancer Center
Kevin Brigle, PhD, ANP VCU Massey Comprehensive Cancer Center
Donna D. Catamero, ANP-BC, OCN®, CCRC Mount Sinai Health System
Beth Faiman, PhD, MSN, APN-BC, AOCN®, BMTCN®, FAAN, FAPO Cleveland Clinic Taussig Cancer Institute
Elizabeth Finley-Oliver, MSN, ARNP, AGNP-BC H. Lee Moffitt Cancer Center & Research Institute
Charise Gleason, MSN, NP-BC, AOCNP® Winship Cancer Institute of Emory University
Michaela Hillengass, RN, ACSM-CPT Roswell Park Comprehensive Cancer Center
Lisa Hwa Christenson, APRN, DNP, CNP Mayo Clinic–College of Medicine
Tracy King, PhD, MN, RN Royal Prince Alfred Hospital, Australia
Rebecca Lu, MSN, FNP-C MD Anderson Cancer Center
Patricia A. Mangan, RN, MSN, APRN-BC Abramson Cancer Center
Ann McNeill, RN, MSN, APN John Theurer Cancer Center at HMH
Teresa Miceli, RN, BSN, OCN® Mayo Clinic–College of Medicine
Kimberly Noonan, DNP, ANP-BC, AOCN®, FAAN Dana-Farber Cancer Institute
Amy Pierre, RN, MSN, ANP-BC Memorial Sloan Kettering Cancer Center
Tiffany Richards, PhD, ANP-BC, AOCNP® MD Anderson Cancer Center
Sandra Rome, RN, MN, AOCN®, CNS Cedars-Sinai Medical Center
Mary Steinbach, DNP, APRN Huntsman Cancer Institute
Joseph D. Tariman, PhD, MBA, ANP-BC, FAAN Rutgers University
Daniel Verina, DNP, RN, ACNP-BC Mount Sinai Medical Center
By Diane Moran IMF Interim Chief Executive Officer Senior Vice President, Strategic Planning
The International Myeloma Foundation (IMF) Nurse Leadership Board (NLB) presented their 18th consecutive symposium at the 50th annual Oncology Nursing Society (ONS) Congress on April 10, 2025. The symposium, “Case Studies for Nurses: Treatment Updates and Patient Care Insights in Multiple Myeloma,” brought together approximately 600 nurses from across the United States to learn from the NLB’s expert myeloma nurses at the ONS meeting in Denver, Colorado.
Dr. Beth Faiman (Cleveland Clinic Taussig Cancer Institute, OH) chaired the symposium, which interwove patient case studies with the latest research and nursing best practices. She emphasized that quadruplet (4-drug) therapy is now the standard of care for nearly all newly diagnosed myeloma patients. This approach combines an anti-CD38 monoclonal antibody, either Darzalex® (daratumumab) or Sarclisa® (isatuximab), with the proteasome inhibitor Velcade® (bortezomib), the immunomodulatory drug Revlimid® (lenalidomide), and the steroid dexamethasone. “Evidence clearly shows that quadruplet regimens produce deeper responses than triplet regimens, with higher rates of minimal residual disease (MRD)-negativity. Typically, patients who achieve MRD-negativity have better long-term outcomes,” noted Dr. Faiman.
Dr. Tiffany Richards (MD Anderson Cancer Center, TX) presented a case study highlighting significant disparities in myeloma care. Black Americans have twice the rate of myeloma and MGUS (a precancerous

(left-to-right) Tiffany Richards, PhD, ANP-BC, Donna Catamero, ANP-BC, OCN, Mary Steinbach, DNP, APRN Beth Faiman, PhD, MSN, APRN-BC, AOCN®, BMTCN®, FAAN,
condition that can progress to myeloma) compared to White Americans. Black Americans are less likely to receive the latest treatments, autologous stem cell transplant, or participate in clinical trials. “Nurses are crucial to reducing disparities,” said Dr. Richards. “By advocating for each patient, ensuring access to the latest treatments, clinical trials, and supportive care, we can help each patient achieve their best possible outcome.” Research suggests when treated equally, Black Americans can achieve equal or better survival rates, possibly because as a group, they tend to have lower-risk myeloma.
Donna Catamero (Mount Sinai Health System, NY) discussed treatment of relapsed myeloma, including CAR T-cell therapy. “Patients with myeloma are living longer than ever, many surviving 10+ years after diagnosis. This is particularly true for younger patients with standard-risk disease,” said Catamero. She explained that CAR T-cell therapy is a promising option for many relapsed patients, with the two
(continues on page 17)

By Dr. Joseph Mikhael IMF Chief Medical Officer
The process of developing a new drug for patients with myeloma takes years of effort and millions of dollars. First, a target for the therapy is identified in the laboratory. Next, researchers confirm the anticancer activity of the drug in laboratory and in animal studies. Based on what we learn, medical research studies called “clinical trials” are designed to determine the safety, dosing, and effectiveness of the drug being investigated. A clinical trial of a new drug or a new combination therapy engages volunteers to test the new treatment. For a patient with myeloma, there are numerous benefits to participation in a clinical trial, including early access to new therapy and the knowledge that you are making a significant contribution to the myeloma world –present and future.
All patients of all races and ethnicities should be able to benefit from clinical trials. Notably, diverse patient representation in clinical trials is required to ensure that the outcomes are applicable to all patients. However, there has been a historical underrepresentation of critical groups of patients in clinical trials in cancer – and especially in myeloma. In the United States, approximately 20% of all myeloma patients are of African descent, but most clinical trials have fewer than 5% representation from this community – the numbers are even lower in pivotal clinical trials that lead to drug approval. Only 1% of all patients in clinical trials of FDA-approved CAR T-cell therapies were African American.
Reasons for this are extensive, including systemic racism, lack of trust in the healthcare system, reduced access to healthcare, the social determinants of health, culturally insensitive care, restrictive inclusion criteria for clinical trials, a lack of logistical support for patients, and more. Mortality is twice as high in African American myeloma patients when compared to White patients. The reasons for this are as extensive as those listed above and include delayed diagnosis and access to novel therapies and stem cell transplants, as well as to clinical trials.
The IMF is the leader in health equity efforts in myeloma. The IMF M-Power program has had a profound impact, reaching thousands in the effort to reduce the disparities of myeloma. We have worked in churches, fraternities, medical clinics, community centers and other places to raise awareness of myeloma and its impact on the African American community. We have educated thousands of primary care providers about myeloma, both online and in person. We have also developed an extensive strategy with medical students, nurses, and others to provide accessible, culturally sensitive care to underserved populations.

The goal of the IMF Diversity in Clinical Trials Program is to reduce health inequities in myeloma by ensuring informed and equitable access to clinical trials for previously marginalized communities. With input from our African American Patient Advocacy Panel, we selected five myeloma patients from historically underrepresented groups who have participated in clinical trials along with one care partner to take part in our first Diversity in Clinical Trials Academy. These patients received expert training to become clinical trial ambassadors and effectively relate their personal stories in order to help educate others about clinical trial participation. As “citizen scientists” these patients are now equipped to contribute to the myeloma community in a unique way; they bring credibility to underrepresented communities and provide a forum of discussion that would otherwise not be possible. MT
The IMF has partnered with SparkCures, a personalized service that takes complex criteria and delivers results that match your unique clinical trial needs and preferences. Visit myeloma.org/sparkcures for more information or to schedule a one-on-one call with a SparkCures clinical trial navigator. In addition, you can contact the IMF InfoLine at 1.818.487.7455 or infoline@myeloma.org , or schedule a time to talk with an IMF InfoLine Coordinator at mmsm.link/infoline

CLINICAL TRIALS QUESTIONS ANSWERED
More than 50 advocacy leaders from 40 countries convened for the 2025 Summit of the Global Myeloma Action Network (GMAN) held June 6–8 in Milan, Italy. As the international advocacy arm of the International Myeloma Foundation (IMF), GMAN collaborates with patient groups, healthcare professionals, industry leaders, and other global partners to raise awareness of myeloma, improve access to early diagnosis and essential medications, and strengthen the capabilities of its member organizations.
GMAN has created a dynamic forum for exchanging knowledge, showcasing innovative patient support initiatives, and discussing the latest advancements in myeloma care. At the annual GMAN Summit, participants also explore the latest developments in the regulatory environment and the pressing need to expand equitable access to life-saving treatments worldwide.
Serdar Erdogan (IMF Director of GMAN, Europe & Middle East Patient Programs) opened the 2025 Summit with a warm welcome to foster an engaging, collaborative atmosphere from the outset. Next, Martine Elias (Executive Director, Myeloma Canada) led the presentation of GMAN’s revised mission: building organizational capacity, raising global awareness, and improving access to care for myeloma patients.
Martine also introduced a flexible branding strategy designed to unify the global myeloma community while maintaining local personalization and relevance. Martine proposed the launch of a global awareness initiative in 2026 – Myeloma Action Day – and participants brainstormed how to bring this vision to life in their countries and regions.
Dr. Joseph Mikhael (IMF Chief Medical Officer and Professor, City of Hope Cancer Center) and Dr. Francesca Gay (University of Torino) led separate presentations that comprehensively covered the broad range of key medical topics in myeloma. To learn more, we invite you to read Dr. Joe’s article in this edition of Myeloma Today.
Mira Armour (Mijelom CRO) moderated a lively panel discussion on the power of patient advocacy in influencing research, policy, and access to treatment. Panelists included Dr. Mikhael, Dr. Gay, Christine Battistini (President, IMF Latin America and President, Instituto Espaço de Vida), Jungsook Park (South Korea), and Martine Elias. Felice Bombaci (Gruppi AIL Pazienti) joined the meeting virtually from Lecce, Italy. Panelists agreed that while international collaboration is essential, solutions must be tailored to local realities.
Global access strategist, Neil Grubert, gave a presenta tion exploring disparities in access to innovative therapies, evolving health technology assessment (HTA) systems, and future-facing models
for oncology and rare disease access. Drawing largely from the European experience, he emphasized that “HTA is becoming more complex and nuanced, with profound global implications,” while also pointing to international collaboration, real-world evidence, and managed entry agreements as critical levers for reform. He highlighted the European Union (EU) Joint Clinical Assessment as the biggest development in international HTA history, and also spotlighted Germany’s AMNOG system as a global model for rapid access. In contrast, England’s NICE system acts as a gatekeeper with slower uptake, despite strong evaluation frameworks. On access disparities, Grubert cited a PhRMA study showing 85% of new drugs launched and reimbursed in the U.S. versus significant delays elsewhere that average 27 months across G20 countries and a further 19 months for public reimbursement. Time to access is even longer in Central and Eastern Europe.
Mimi Choon-Quinones (IMF Senior VP, Global Advocacy Access, Policy & Research) delivered an in-depth update on the integration of MRD into HTA and its alignment with the EU’s Critical Medicines Act (CMA). The Population, Intervention, Comparator(s), Outcome(s), and Settings/Study Design framework, with input from both patients and clinicians, aims to systematically define the key elements needed to evaluate MRD-guided interventions in myeloma through the lenses of clinical effectiveness, patient experience data, and health system impact.
Andreas Kouroumalis (Scientific Officer, European Medicines Agency) provided a comprehensive overview of the regulatory framework guiding the approval of myeloma therapies in the EU. The centralized procedure allows pharmaceutical companies to submit a single application for marketing authorization valid across all 27 EU member states plus Iceland, Liechtenstein, and Norway. This process leverages a network of experts to ensure consistent and rigorous evaluation. While the standard review timeline is approximately a year, accelerated pathways are available for products addressing high unmet medical needs, including in myeloma. Dr. Kouroumalis noted the importance of patient participation in

A poster session was part of the GMAN Summit for the first time, highlighting the unique unmet needs faced by myeloma communities in different countries. Each poster represented a country’s perspective, showcasing ongoing work, research, and advocacy efforts while fostering vibrant discussion among attendees. The session included posters from Canada, Croatia, Czechia, Denmark, Norway, and Portugal.
Hayley Beer (Lead, Stakeholder Engagement and Advocacy) reported on the success of a program developed by Myeloma Australia to train eligible patients and care partners to administer subcutaneous therapies. Myeloma is the most expensive cancer to treat in Australia, and this program proved to be effective at improving the patient experience while relieving pressure on healthcare resources.
Michelle Oana (Chief Mission Officer, Myeloma Canada) addressed longstanding barriers to clinical trial participation. In 2024, Myeloma Canada convened a forum that brought together patients, researchers, industry partners, nurses, regulators, and nonprofits to collaboratively identify solutions. The consensus outcome was the concept of a preclinical trial navigation service, later formalized as Phase 0. “There are a lot of services and resources that exist,” Oana noted, “but nobody knows where to find them.”
In a follow-up summit held in March 2025, participants were tasked with designing a viable, scalable, and sustainable version of the Phase 0 model, working within existing healthcare structures without altering trial protocols or locations. The proposed solution includes a pilot project in myeloma to launch in early 2026, externally managed and potentially funded through industry and other partners. The long-term goal is to institutionalize this service within Canada and create a model adaptable for international adoption.
Eric Battini (Association Française des Malades du Myélome Multiple, AF3M) presented Hemavie, a nurse-led telephone support program designed to assist patients with myeloma and care partners throughout the treatment journey. Launched in 2016 with support from Celgene, Hemavie is now backed by Bristol Myers Squibb, Menarini-Stemline, Pfizer, and Sanofi. Hemavie offers personalized, nurse-initiated support. The program was developed in response to a critical insight: “99% of the time, patients experience the disease at home,” where access to immediate reassurance, guidance, and psychological support is often lacking.
An external qualitative study found that patients who participated in Hemavie felt more confident, less anxious, and better prepared for clinical consultations, with one key takeaway being the importance of the nurse’s “kindness, confidence, support, and advice.” Over 600 patients and caregivers benefited from the program by the end of 2024. AF3M views Hemavie as a proven, scalable approach to empowering patients and fulfilling its mission to help them become “actors of their life with myeloma.”
Diane Moran (IMF Interim CEO and Senior VP of Strategic Planning) gave the first presentation on Day 2 of the GMAN Summit, sharing heartfelt reflections on her nearly 20 years at the IMF.
“I am incredibly humbled to be here with all of you – the most courageous of the courageous,” she said, recalling her emotional first experience at a Support Group Leaders Summit. “How could these people, who at that time didn’t have the kind of medications we have now, and were demonstrably ill – how could they give their energy to others? It was overwhelming.”
Diane provided a powerful overview of the IMF’s 35-year history and emphasized the IMF’s strategic priorities: creating a globally connected patient experience, expanding real-world data collection, and advancing impactful research. “GMAN is the cornerstone of how we create a global connected patient experience,” she said. Launched in 2013, GMAN now includes 50 organizations across 46 countries, working together to expand capacity, improve access, and strengthen advocacy. GMAN supports tangible, local impact. Diane’s presentation concluded by celebrating the power of global collaboration and reaffirming the shared commitment to expanding access to lifesaving treatments, fostering connection, and driving innovation in the fight against myeloma.
The GMAN Susie Novis Durie Grants, which are awarded annually to patient advocacy organizations, help sustain projects that address the unique needs of myeloma patients in their respective countries, while also enhancing their capacity building efforts. At the Summit, the 2024 recipients reported on their projects in Croatia, Denmark, Israel, and Romania. The 2025 grants were awarded to Armenia, Kenya, Poland, and Serbia.
Another highlight of the GMAN Summit was a panel discussion focused on building effective partnerships between patient organizations and the pharmaceutical industry. This session was inspired by strong interest from the 2024 Summit, where many attendees expressed the need for practical guidance on collaborating with industry stakeholders. The conversation emphasized the importance of aligning goals early in the collaboration process. Ultimately, the session reinforced that successful partnerships between the pharmaceutical industry and patient communities are rooted in trust, transparency, and shared purpose.
The closing remarks by Mira Armour concluded with a powerful reminder of both the unprecedented progress in myeloma treatment and the stark disparities that remain across the globe. Mira’s remarks emphasized the importance of GMAN “uniting myeloma patient advocates and building on shared knowledge.” The themes of the 2025 GMAN Summit – awareness, access, and capacity building – were reflected in every session.
Uniting myeloma advocates from across the world, the IMF thanks all the 2025 GMAN Summit participants for traveling from near and far to join us in Italy, and we look forward to the 2026 GMAN Summit in Stockholm, Sweden. MT
By Sylvia Dsouza IMF Vice President, Development
Anyone who had the fortune to meet John O’Dwyer would be instantly struck by the power of his intellect and insight. If you were lucky enough to get to know John, you would learn the depth and breadth of his devotion as a husband, parent, grandparent, and philanthropist. For the myeloma community, John was a tireless champion. As a two-term member of the IMF Board of Directors, John was a visionary. His commitment to the IMF and to a brighter future for all who are touched by myeloma is a legacy of lasting impact.
On April 27, 2025, after living with myeloma for 18 years, John passed away surrounded by his family and friends. I knew and worked with John since I joined the IMF, and as the sadness of his loss continues, I honor his legacy and celebrate the gifts that John shared with his loved ones and with the myeloma community. John epitomized the IMF vision of a world where every myeloma patient can live life to the fullest, unburdened by the disease.
At the beginning of John’s myeloma journey, he and his wife, Dorothy, visited their first IMF Patient & Family Seminar in Irving, Texas. Dorothy remembers the experience as overwhelming, “So much information! Our heads were spinning.” John’s immediate reaction was to get down to working on making a difference –his altruism was always rooted in taking action. As Dorothy put it, “John has always inspired me. No matter the task – work, family, myeloma, golf, or vacations – when John decided to do something, he gave it 100%. (Except for beach vacations – John only liked sand in a trap on the golf course.)”
John quickly connected with the IMF’s leadership and soon became an integral member of the IMF Board of Directors, serving his first term from 2010 to 2016, and beginning his second

John O’Dwyer
term in 2024. John was instrumental in funding and launching the IMF Black Swan Research Initiative® (BSRI®), the ambitious plan to finance and establish research to achieve a cure for myeloma. The BSRI aimed to construct and standardize methods for assessment of the lowest levels of myeloma after best treatment. Minimal residual disease (MRD) testing is now becoming the recognized endpoint in myeloma clinical trials.
“It was natural that John would help the search for a cure,” says Dorothy. “He said that he knew the cure wouldn’t be there in time for him, but that it will help the generations of children and grandchildren.” John also brought awareness and visibility to myeloma and to the IMF. He funded a multi-award-winning documentary about the IMF’s inaugural Iceland Cycling Expedition (ICE) in 2024. He supported the IMF’s 2024 Gala. His contributions to the IMF that benefited the myeloma community are countless.

As a father, John equally inspired his children. His daughter Maureen recalled Parents’ Weekend during her freshman year at the University of Texas (UT): “My parents and I went to a game: UT vs. SMU (Southern Methodist University). Sitting in a sea of burnt orange, we cheered for the horns – my dad thinking he was funny making the ‘I love you’ hand sign instead of the Texas Horns. At one point, the refs called a questionable play in UT’s favor. The stadium erupted with cheers, but my dad started yelling at the refs that they made the WRONG call. He stood tall in a crowd of thousands, voicing support for the opposing team because he believed it was the right thing to do.”
John O’Dwyer Jr. added, “Dad challenged us to always be willing to try something new and to look at it as an adventure, and he followed his own advice. When we were living in Germany, we had traveled to France for vacation. He knew that I was interested in WWII history. One morning, Dad and I got up early and went to the Beaches of Normandy. We watched the fog roll in off the ocean. We did not say a word… we didn’t have to.”
His daughter Eileen recalls, “Dad’s resilience and spirit were felt by all. Growing up, I knew my dad was dedicated to his work, but he made sure to make time for family. He coached my softball, basketball, and coed soccer teams. He attempted to help me understand fractions (even though there were lots of tears). Family trips throughout Europe are some of my favorite memories.”
Michael said this about his Dad’s essence: “I heard about my dad’s athletic prowess growing up – that he played collegiate hockey, he played tennis, he golfed. But any time he tried to play basketball or football with John or me, he always managed to pull a muscle within a couple of plays. He had a big heart. When I needed him, he was right there to love, support, and help me. That was Dad.”
With these memories, the IMF, too, can say “That was John.” As IMF Chairperson of the Board Dr. S. Vincent Rajkumar shared, “John’s countless contributions to the IMF established him as a pillar of the myeloma community. John loved the IMF, and we miss him deeply.” IMF Interim CEO and Senior VP of Strategic Planning Diane Moran added, “John was a steadfast and loyal friend and supporter of the IMF for nearly two decades. His fight to advance science and research to find a cure for myeloma was very personal as he faced the disease himself for 18 years. John supported the IMF as a visionary and as a leader. He will be deeply missed, and the IMF will honor his memory by doubling-down on our mission to improve the lives of myeloma patients while working toward prevention and a cure.”
I am also deeply thankful to John for everything he did for the IMF and for the myeloma community. In my entire career of service in the nonprofit sector, I have never met or known anyone like John, a person so intensely dedicated to a cause and steadfast in his support. I am honored to have met him, to have known him, to have worked alongside him toward envisioning a world free of myeloma. I miss him, but I will carry his vision in my heart. John’s legacy lives on in our daily work and commitment.

Dorothy & John O’Dwyer
And the O’Dwyer Family still feels there is more to do. Dorothy said, “Honestly, I feel like I haven’t done enough! As a myeloma advocate and supporter, I’ve learned – and John stressed this whenever he could – that you have to be an advocate for YOUR health. Get up to date on the latest protocols, learn about and support the research, stay current on the disease and challenge your doctors. Be forthcoming about how the treatment is impacting you and how it is also impacting your family and friends.”
When asked what she wished more people knew and understood about myeloma, Dorothy said, “It’s an underfunded area of research that needs more financial support. When John was diagnosed 18 years ago, myeloma was an ‘old person’s disease.’ But John was only 55, and people are being diagnosed with myeloma at younger and younger ages. We need to fund the research to understand why and to help people have a better quality of life as they live with this disease.”
The IMF is grateful for and bolstered by John O’Dwyer’s legacy, his children’s memories, and Dorothy’s wishes to continue our important work to improve the quality of life of myeloma patients while working toward prevention and a cure. MT
Transformative gifts to the IMF are an investment in our mission and vision, and effective solutions that advance myeloma research and care for patients. To discuss potential philanthropic engagement with the IMF, please contact Sylvia Dsouza (IMF Vice President, Development) at sdsouza@myeloma.org or 1.310.947.4126.
By Danielle Doheny IMF Director, Public Policy & Advocacy
When cancer policy is debated in Washington, the spotlight often shines brightest on diseases with the highest levels of public awareness, such as breast, lung, and colorectal cancers. These cancers have been the focus of many awareness campaigns and a steady stream of funding is addressing the needs of those communities. But for patients living with lesser-known cancers like myeloma, the path is markedly different.
Although myeloma is the second most common blood cancer in the United States, it doesn’t get the same attention, recognition, or funding. Federal research funding and access policies have followed visibility. Despite tremendous scientific momentum in the field of myeloma, the relative lack of visibility means that myeloma can be overlooked in critical conversations about policy on local, state, and federal levels.
The current myeloma treatment paradigm offers hope to patients like never before, yet many still face challenges with insurance barriers, delays in care, and drug access policies that don’t reflect the realities of living with a disease that changes over time.
Since the founding of the International Myeloma Foundation (IMF), we have actively and consistently advocated on behalf of the myeloma community. The IMF has prioritized changing the narrative. We are ensuring that patients and their care partners are not only part of the conversation, but also help to shape the conversation. Last year, the IMF launched our first U.S. Patient Master Class to train and equip myeloma advocates, brought patients to Capitol Hill to meet with lawmakers directly, and partnered with coalition allies to elevate the unique needs of the myeloma community in national policy debates.
IMF Advocacy Master Class graduates are representing the IMF and the myeloma community on Capitol Hill in partnership with Patients Rising. The goal is to help shape policies that improve the quality of life and treatment options for patients navigating illnesses like myeloma. The efforts of the IMF advocates are focused on advancing key policy priorities including:
1. Supporting increased funding for medical research,
2. Expanding access to telehealth services, and
3. Improving access to medications through legislation such as the Cancer Drug Parity Act.
This is making an impact. Policymakers are listening. We’re seeing growing recognition on Capitol Hill, where numerous members of Congress have publicly shared their own myeloma diagnoses. That kind of honesty and visibility helps break down stigma, build urgency, and create space for more thoughtful policymaking.

We’ve also seen real momentum around patient-centered policy, from efforts to modernize clinical trials and preserve telehealth access to legislation that targets barriers like “step therapy” and prior authorization. These wins don’t happen overnight, but they are happening. The IMF is fighting to make myeloma top-of-mind in policy circles, and the outlook is improving thanks to the courage, commitment, and advocacy of the myeloma community.
Rare cancers aren’t rare to the people living with them. As a family member of a patient, I know this firsthand. Cancers like myeloma are deeply personal and deeply felt. Myeloma patients deserve policies that reflect their reality. Thanks to the voices of patients and their care partners being elevated, the movement of myeloma advocacy is growing nationwide. Myeloma advocates refuse to stay silent and invisible, and the IMF is helping to build a system that sees them and serves them.
The IMF recognizes the power of grassroots advocacy to drive policy changes that benefit patients with myeloma, and we invite you to join us by emailing advocacy@myeloma.org. There are many ways to get involved, including sharing your story, sending an email to your representatives, advocating for policy change, and supporting education efforts. The more advocates stand with us, the more we can advance the policy narrative. Every voice matters. Your voice matters. MT
Visit advocacy.myeloma.org to learn more about our activities and subscribe to the IMF Advocacy Newsletter at subscribe.myeloma.org.
FDA-approved CAR T-cell products now available after only 1 or 2 prior lines of therapy. She noted that the CAR-T process requires coordination between the patient’s local oncology practice and the center that performs the CAR T-cell therapy. Many patients find their first relapse harder than their initial diagnosis. “Patients who experience long remissions begin to think they won’t ever relapse, so when they do, it’s a huge shock. Nurses are essential for supporting patients through this difficult transition and navigating complex treatment options like CAR-T,” noted Catamero.
Mary Steinbach (Huntsman Cancer Institute, UT) focused on immunotherapies for myeloma. “Bispecific antibodies act as a bridge between T-cells and myeloma cells, allowing a patient’s own immune system to target the cancer,” explained Steinbach. “Three bispecifics are currently FDA-approved. Tecvayli® (teclistamab) and Elrexfio®(elranatamab) target BCMA on the myeloma cells, and Talvey® (talquetamab) targets GPRC5D.” These therapies require special management approaches, with possible side effects like cytokine release syndrome (CRS), neurotoxicity, and infection being important considerations. GPRC5D-targeted treatments carry the possibility of skin, nail, and oral side effects that require proactive management, but patients typically find these manageable.
The NLB symposium also covered therapies in development, including new CAR T-cell therapies, bispecific antibodies, antibody-drug conjugates (ADCs), and CELMoDs (cereblon E3 ligase modulators). “We have so many new drugs in development and expect new approvals of myeloma drugs in 2025,” said Dr. Faiman. “Through sharing stories of our patients and highlighting the latest research, we aim to empower oncology nurses to engage and educate each patient and their care partners, reduce disparities, and enhance shared decision-making. We want every patient to achieve their best possible outcomes.” These advances give patients and their families new reasons to be hopeful about future treatment options.
Beginning on July 1, a video of the NLB symposium is available at IMF-ONS.myeloma.org for a period of 6 months. MT
Visit nlb.myeloma.org to learn how the NLB is improving the nursing care and self-care of patients with myeloma via publications, symposia, multimedia, and research.



Shared experiences help to better understand the myeloma journey. Support groups empower patients and care partners with information, insight, and hope. The IMF provides educational guidance to a network of more than 160 myeloma-specific groups. We are pleased to introduce six newly formed myeloma support groups:
California (meets virtually)
City of Hope Myeloma Community Connection
Florida (meets virtually)
Multiple Myeloma Support Group in Sebring
Maine (meets virtually)
The Wicked Good Southern Maine
Myeloma Support Group
Nebraska (meets virtually)
Omaha Myeloma Care Group
South Dakota (meets in person)
The Black Hills Myeloma Networking Group
Special Interest Group (meets virtually)
Veterans with Myeloma
For more information, please contact the IMF Support Group Team at sgteam@myeloma.org or visit support.myeloma.org.
Founders
Brian D. Novis • Susie Durie • Brian G.M. Durie, MD
Board of Directors
Chairperson S. Vincent Rajkumar, MD
Christine Battistini
Loraine Alterman Boyle
Martine Elias, MSc
George T. Hayum
Jason Katz
Benson Klein, JD
Andrew Kuzneski, III
Sagar Lonial, MD
Nikhil Munshi, MD
Charles Newman, MS
Kent Oliver
Poornima Parameswaran, PhD
Matthew Robinson, MBA
Sanjay Singh
Maria Whitman, MBA
IMF Executive Team
Diane Moran
Interim Chief Executive Officer
Senior Vice President, Strategic Planning
Peter Anton Vice President, Marketing
Sylvia Dsouza Vice President, Development
Joseph R. Mikhael, MD Chief Medical Officer
IMF Team
Elizabeth Ableson Administrative Assistant, Human Resources
Betty Arevalo Inventory Control Manager
Becky Bosley Director, Support Groups
Brittnay Brandon Senior Meetings Coordinator
Michelle Carroll Director, Prospect Development
Lisette Contreras Administrative Assistant, Meetings & Events
Danielle Doheny Director, Public Policy & Advocacy
Jon Fitzpatrick Senior Manager, Meetings & Events
Esther Garnica Administrative Assistant, Operations
Simona Grace Director, Development
Sherrie Guerrero Senior Director, Human Resources
Paul Hewitt Coordinator, InfoLine
Kevin Huynh Coordinator, Tech Solutions
Katie Ives Meeting & Project Coordinator
Marya Kazakova
Senior Director, Editor-in-Chief, Publications
Missy Klepetar Coordinator, InfoLine
Sapna Kumar Marketing Strategist
Lisa Paik
Executive Vice President, Research & Operations
Jennifer Scarne Chief Financial Officer
Robin Tuohy Vice President, Patient Support
Phil Lange Director, Accounting
Jason London
Senior Manager, Marketing & Communications
Marquela Nastri Grants Specialist
Jim Needham
Publication Design
Meghan O’Connor
Meeting & Project Manager, Content & Communications
Selma Plascencia Senior Director, Operations
Joy Riznikove
Database Administrator
Cecilia Romero Project & Technology Manager, Support Groups
Miko Santos Senior Manager, Tech Solutions
Narmeen Shammami
Senior Research Project Coordinator
Brando Sordoni
Senior Associate, Accounting & Distribution
Rafi Stephan Senior Administrative Support
Daria Tabota Associate, Marketing & Communications
Joi Tisdale
Project Manager
Jennifer Wieworka Director, Support Groups
Sandy Wilkes
Grants Manager
Yara William Associate Director, Support Groups
International Myeloma Foundation
4400
Studio City, CA 91604 USA
myeloma.org
800.452.CURE
Change Service Requested
myeloma.org