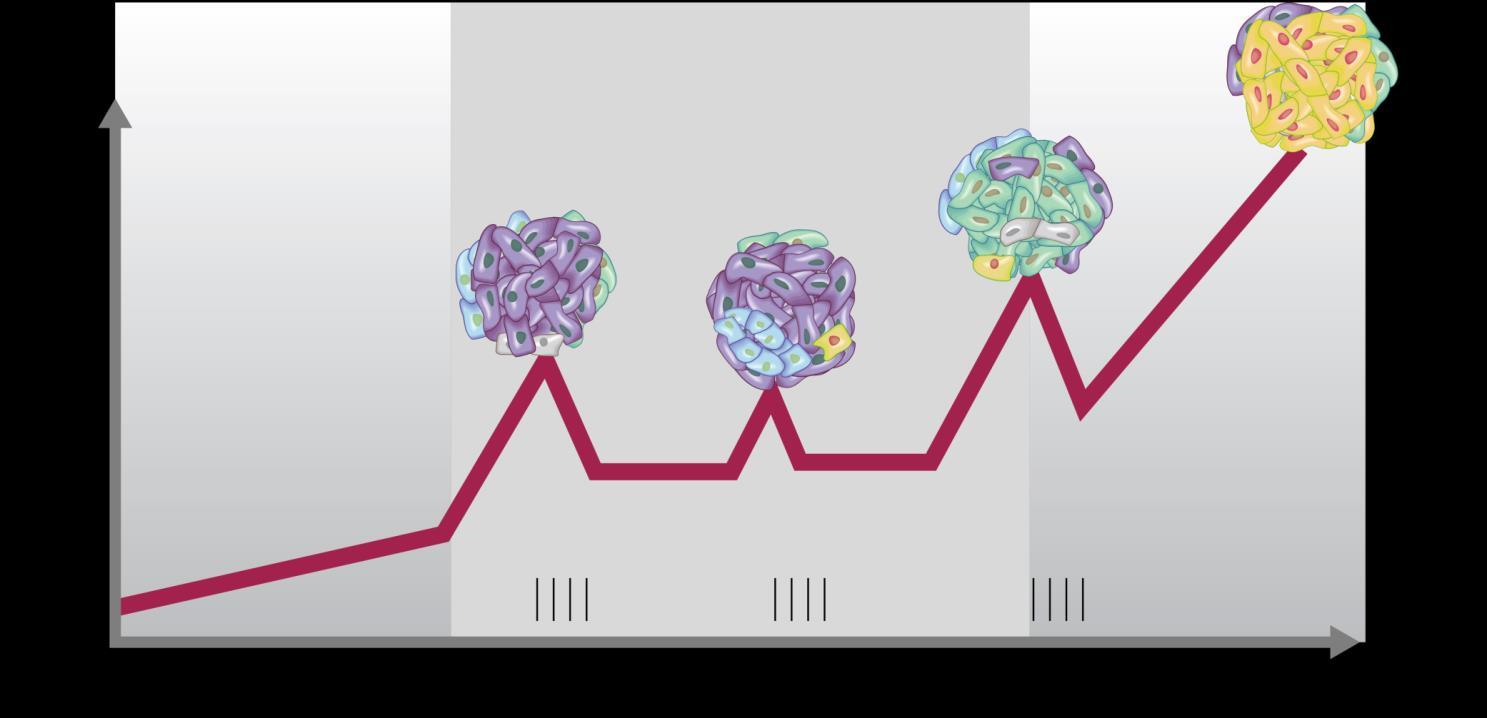
Typically the most durable remissions occur earlier in the disease course
So, we want to use the best possible therapies before the disease becomes more resistant Therapies tend to have a greater effect earlier in the disease course...
3. Typically use CAR-T Cell Therapy, Bispecific
Antibodies or Triplets
As will be discussed today, options for relapsed myeloma have grown and these three approaches have the best outcomes
This has to be balanced with patient characteristics and preferences – so other options (like doublets) can be considered
4-6. Consider Patient, Disease and Treatment Factors
over Two Decades: A Real-World Experience from a Medium-Level Hospital. Cancers (Basel). 2025Feb 25;17(5):793
Ortega-Vida E, et al.
Myeloma
WHY?
Linvoseltamab
IMiDs
▪ Key Drugs
▪ Thalidomide
▪ Lenalidomide
▪ Pomalidomide
▪ Cereblon inhibitors
▪ Route of Administration
▪ All oral
Mechanism of Action:
▪ Common Toxicities
▪ VTE
▪ Appropriate ppx
▪ Rash
▪ Teratogenicity (REMS)
▪ Cytopenias
•Modulate cereblon → degradation of Ikaros/Aiolos transcription factors
•Enhances T-cell and NK-cell activity
•Anti-angiogenic and direct tumoricidal effect
1.Mechanisms of lenalidomide sensitivity and resistance
2.Martinez-Høyer, Sergio et al.
3.Experimental Hematology, Volume 91, 22 - 31
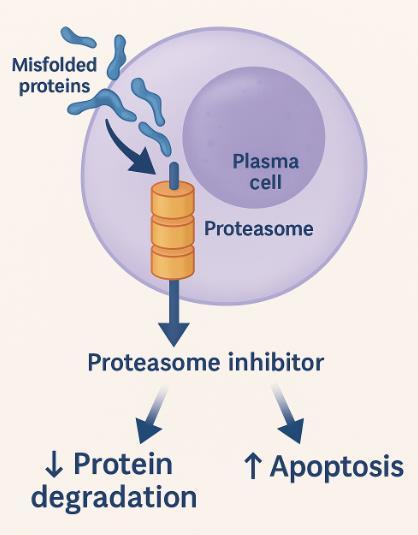
Proteosome Inhibitors
▪ Key Drugs
▪ Bortezomib (SC or IV)
▪ Carfilzomib (IV)
▪ Ixazomib (oral)
Common Toxicities
▪ Neuropathy
▪ Cardiac toxicity
▪ Heart failure
▪ Hypertension
▪ GI Upset
▪ Viral Reactivation (shingles)
. Velcade® PI 2017; b. Kyprolis® PI 2018; c. Ninlaro® PI 2016;
Drug classes- monoclonal antibodies
▪ Anti-CD38
▪ Daratumumab (IV or SC)
▪ Isatuximab (IV)
▪ Anti SLAMF7
▪ Elotuzumab (IV)
▪ Common Toxicities
▪ Infusion related reaction
▪ Infection
▪ Cytopenias
▪ Interference with blood typing
Gozzetti, et al. (2022). Anti CD38 monoclonal antibodies for multiple myeloma treatment. Human Vaccines & Immunotherapeutics. 18. 1-9. 10.1080/21645515.2022.2052658.
Drug classes- miscellaneous
Selinexor
Selective inhibitor of Nuclear
Export Inhibitor (SINE)
Blocks XPO1 leads to apoptosis
Side effects
Nausea, anorexia, weight loss
Fatigue, anorexia
Hyponatremia, thrombocytopenia
Venetoclax
BCL-2 inhibitor
Induces apoptosis
Used in high BCL-2 expressors (t11;14) Side effects
Cytopenias
GI upset
TLS possible
Cytoxan
Alkylator
Cross-links DNA to prevent replication
Side effects
Myelosuppression
Nasuea, fatigue
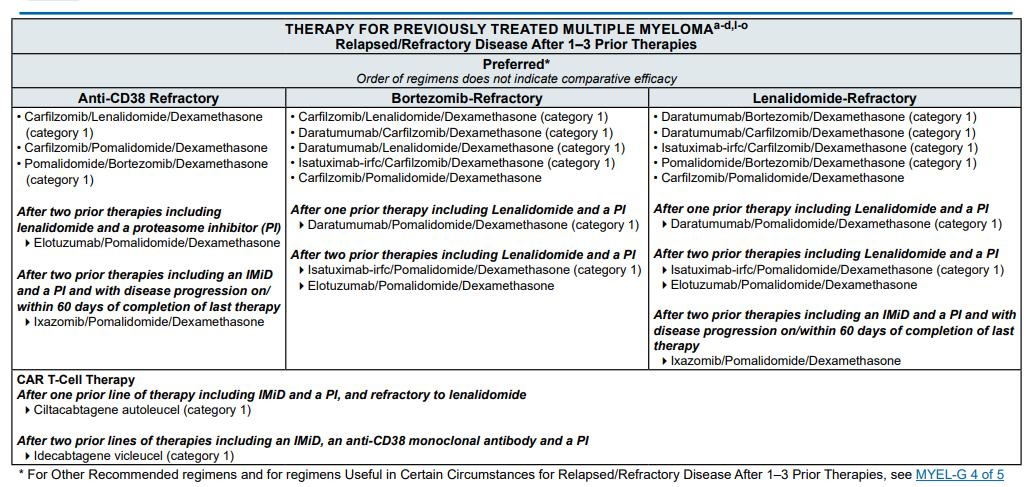
Treatment options in 1-3 prior lines
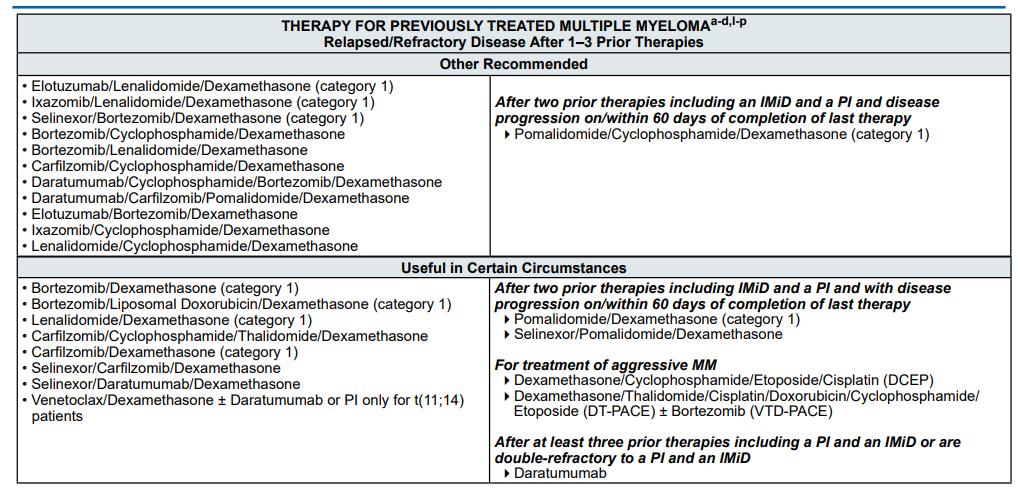
More options 1-3 prior lines
Fitting it all together
Patient Considerations
▪ What are they willing to do?
▪ Get a port?
▪ Risks of side effects?
▪ How far away from cancer center?
▪ How often are they travelling
▪ Socioeconomic factors?
▪ What is the support system?
▪ Financial considerations
▪ Mobility
▪ How hard is it to get to center?
▪ How often will they need additional testing?
▪ Toxicities
▪ Residual toxicities
▪ Neuropathy?
▪ Comorbidities
▪ Contribution to toxicity risk
▪ Ability to moderate toxicity risks
▪ VTE ppx, infection ppx
▪ General tolerability
▪ Historic experience
▪ Tolerance for toxicity
Disease Determinants
▪ What were prior therapies?
▪ How long did they last?
▪ What are the doses?
▪ How much time has elapsed since other prior therapies?
▪ What is the pace of relapse?
▪ Rapid versus gradual?
▪ Extramedullary disease? Bone disease?
▪ Risk stratification or new chromosomal mutations?
▪ Targetable mutations? T(11;14)?
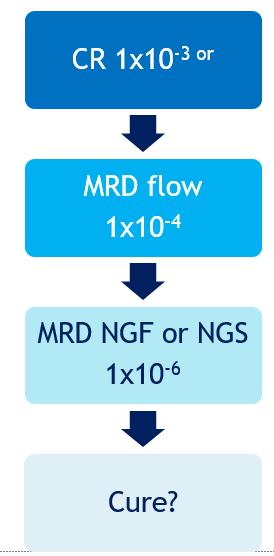
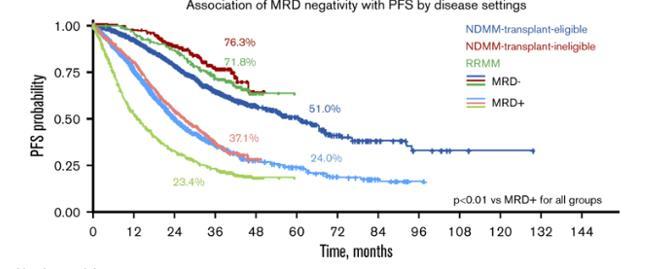
Goal of therapy- Minimal Residual Disease
Goals of therapy
Nikhil C. Munshi, et al; A large meta-analysis establishes the role of MRD negativity in long-term survival outcomes in patients with multiple myeloma. Blood Adv 2020; 4 (23): 5988–5999
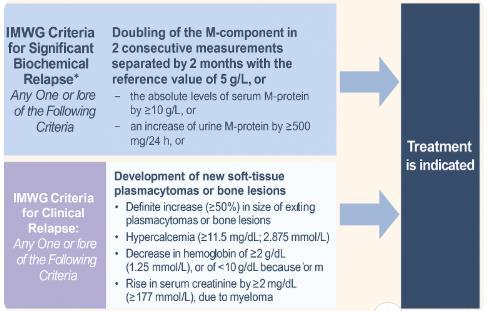
Treatment by Relapse Type
Biochemical Relapse
▪ Loss of MRD-
▪ Increase in FLC or M-protein without symptoms
▪ Treatment options:
▪ Observation
▪ Retreatment
▪ Increase Doses of Medication
▪ Complete change in therapy
▪ Refractory to drug is < 6mos since treatment
Symptomatic Disease
▪ CRAB criteria relapse
▪ Treatment indicated
▪ Triplets preferred over doublets
▪ Change in class of medications
▪ High risk relapse
▪ Relapse within 2 years of initial therapy when post ASCT and on maintenance
▪ Relapse within 18 months for non-ASCT patients
▪ New 1q gain/ amplification or del(17p)/TP53 mutation
▪ Extramedullary disease or circulating plasma cells
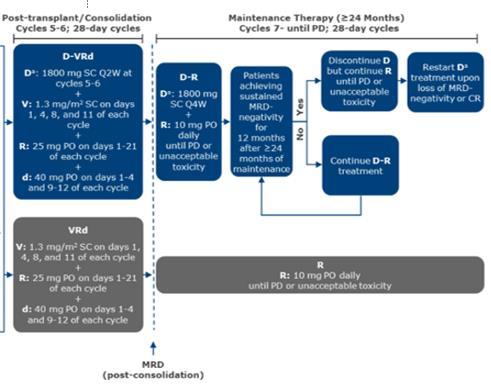
Treating MRD relapse
Perseus Trial
Remnant Trial
•Sonneveld P (presenter). Primary results of Phase 3 PERSEUS Trial. ASH 2023 Session LBA-1 International Myeloma Foundation.
•Rasmussen A-M, Askeland FB, Schjesvold F. The Next Step for MRD in Myeloma? Treating MRD Relapse … REMNANT Study. Hemato. 2020;1(2):36-48
Predator-MRD trial
Daratumumab
Doublet vs Triplet
Bottom line: triplet is better than a doublet at relapse
[a] DVd vs Vd ≥ 1, 2 498 84 vs 63 16.9 vs 7.1, HR = 0.31 (.24-.39) 49.6 vs 38.5, HR= 0.74 (.59.92) BOSTON[b] SVd vs Vd 1 to 3 402 76 vs 62 13.9 vs 9.5, HR= 0.7 (.53-.93)
[d] DKd vs Kd 1 to 3, 2 466 84 vs 73 28.6 vs 15.2, HR = .45-.78) 50.8 vs 43.6, HR=.78 (.6-1.03) IKEMA[e] IsaKd vs Kd 1 to 3, 2 302 87 vs 84 35.7 Vs 19.2, HR=0.59 (.45-.78)
▪ *Experimental vs control, respectively; †Only 10% of patients had prior Len exposure. a. Stewart AK, et al. N Engl J Med. 2015;372:142-152; b. Dimopoulos MA, et al. Lancet Oncol. 2016;17:27-38; c. Moreau P, et al. N Engl J Med. 2016;374:1621-1634; d. Lonial S, et al. N Engl J Med. 2015;373:621-631; e. Dimopoulos MA, et al. N Engl J Med. 2016;375:1319-1331; f. Palumbo A, et al. N Engl J Med. 2016;375:754-766; g. San Miguel JF, et al. Lancet Oncol. 2014;15:1195-1206; h. Siegel DS, et al. J Clin Oncol. 2018;36:728-734.
Doublet vs Triplet
Bottom line: triplet is better than a doublet at relapse
a. Dimopoulos MA, et al. J Clin Oncol. 2023;41(3):568-578.
b. Meletios A. Dimopoulos; Subcutaneous Daratumumab Plus Pomalidomide and Dexamethasone (D-Pd) Versus Pomalidomide and Dexamethasone (Pd) Alone in Patients with Relapsed or Refractory Multiple Myeloma (RRMM): Overall Survival Results from the Phase 3 Apollo Study. Blood 2022; 140 (Supplement 1): 7272–7274
c. Attal M, et al. Lancet. 2019;394:209-2107. Richardson PG, et al. IMS 2022. Abstract OAB-052
d. Sonneveld P, et al. MC. Carfilzomib, Pomalidomide, and Dexamethasone As Second-line Therapy for Lenalidomide-refractory Multiple Myeloma. Hemasphere. 2022 Sep 30;6(10):e786
e. Oral selinexor, pomalidomide, and dexamethasone (XPd) at recommended phase 2 dose in relapsed refractory multiple myeloma (MM).Darrell White, et al.Journal of Clinical Oncology 2021 39:15_suppl, 8018-8018
Recent Phase 3 Trials
Bottom line: triplet is better than a doublet at relapse
▪ Chari A, et al. Oral Selinexor-Dexamethasone for Triple-Class Refractory Multiple Myeloma. N Engl J Med. 2019 Aug 22;381(8):727-738. doi: 10.1056/NEJMoa1903455. Weisel K, J. Pomalidomide and Low-Dose Dexamethasone Improves Health-Related Quality of Life and Prolongs Time to Worsening in Relapsed/Refractory Patients With Multiple Myeloma Enrolled in the MM-003 Randomized Phase III Trial. Clin Lymphoma Myeloma Leuk. 2015 Sep;15(9):519-30. doi: 10.1016/j.clml.2015.05.007. Epub 2015 Jun 6. Alsina M,. A phase I single-agent study of twice-weekly consecutive-day dosing of the proteasome inhibitor carfilzomib in patients with relapsed or refractory multiple myeloma or lymphoma. Clin Cancer Res. 2012 Sep 1;18(17):4830-40
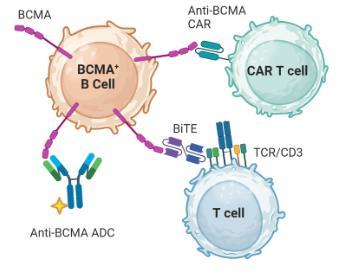
BCMA
▪ B cell maturation antigen
▪ Regulates B cell development and survival
▪ Is a cleaved and soluble protein that can circulate in the bloodstream
▪ Therapeutic target
▪ Car-T (minimal discussion)
▪ BiTEs
▪ ADC
FDA-Approved BCMA-Targeted CAR T-Cell Therapies
Inclusion
Cilta-cel: CARTITUDE-11-3 Ide-cel: KarMMa4,5
≥3 prior LOT (triple-class exposed), or double refractory to PI and IMiD, and received an anti-CD38 mAb with PD 12 months of last LOT
≥3 prior LOT, prior anti-BCMA therapy excluded
1. Martin T, et al. J Clin Oncol. 2022;41:1265-1274. 2. Lin Y, et al. ASCO 2023. Abstract 8009. 3. Munshi N, et al. EHA 2023. Abstract S202. 4. Munshi NC, et al. N Engl J Med. 2021;384(8):705-716. 5. Anderson LA, et al. ASCO 2021. Abstract 8016. No head-to-head studies have been conducted and direct comparisons cannot be made between these studies.
▪ Stands for G-protein-coupled receptor, class C, group 5, member D. It’s an orphan 7transmembrane receptor (no known ligand). It’s exact normal function remains unclear, though may be related to retinoid signaling.
▪ Highly expressed on plasma cells
▪ Higher expression in SMM, MM and aggressive MM versus healthy plasma cells
▪ Plasma cell survival is not dependent on GPRC5D expression
▪ Low expression on healthy tissues
▪ Not expressed on other hematopoietic cells or organ tissues, expressed on keratinized cells like hair follicles and filiform papillae of the tongue
RRMM with ≥1 prior LOT, PD during or after most recent therapy, no prior anti-BCMA, not refractory to or intolerant of Dara or Bort
RRMM with ≥1 prior LOT including Len, PD during or after most recent therapy, no prior anti-BCMA or Pom, not refractory to or intolerant of Bort
No head-to-head studies have been conducted and direct comparisons cannot be made between these studies.
a On November 22, 2022, GSK announced the initiation of the withdrawal of the US marketing authorization for [Belamaf].
The US FDA withdrew the US license to manufacture [Belamaf] on February 6, 2023.
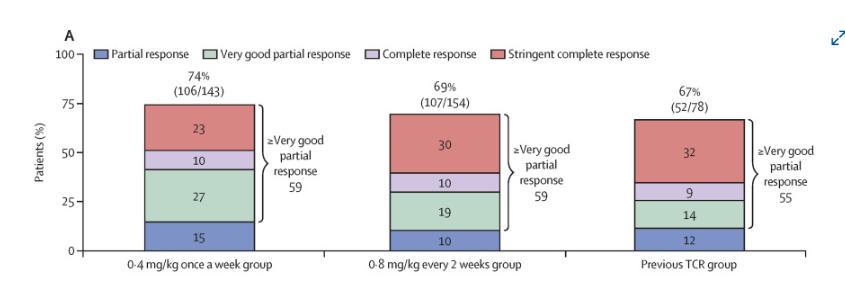
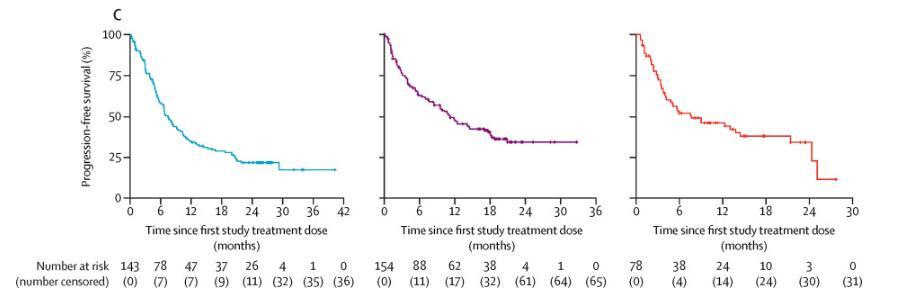
1. Mateos MV, et al. ASCO 2024. Abstracts 7503 and 439572. 2. Mateos MV, et al. EHA 2024. Abstract S214. 3. Trudel S, et al. ASCO 2024. Abstract LBA105.
4. Dimopoulos M, et al. EHA 2024. Abstract LB3440.
Belantamab Mafodotin in RRMM: Visual Acuity
Bilateral Worsening of BCVA in Patients With Normal Baseline With BVd
or
Follow-up ended with event ongoing, n/N (%)
No head-to-head studies have been conducted and direct comparisons cannot be made between these studies.
or
a Only patients with baseline visual acuity of 20/50 or better in 1 eye with on-study worsening to 20/50 or 20/200 in each eye at the same visit. b Improved: no longer 20/50 (or 20/200) or worse in both eyes.. c One event resolved to normal baseline after 57 days, while for the other event, patient follow-up ended prior to resolution; median N/A.
1. Mateos MV, et al. ASCO 2024. Abstracts 7503 and 439572. 2. Mateos MV, et al. EHA 2024. Abstract S214. 3. Trudel S, et al. ASCO 2024. Abstract LBA105.
4. Dimopoulos M, et al. EHA 2024. Abstract LB3440.
Emerging strategies
▪ Non-immune therapies
▪ Cereblon inhibitors
▪ Novel strategies
▪ More BiTE and Car-T targets
▪ Allo car
▪ NK cell targets
▪ Novel Car targets (CD38)
▪ Novel targets
▪ FcRH5 (cevostamab)
▪ Novel combinations
▪ MajesTEC-3 (teclistamab + daratumumab)
▪ Novel combinations of targets
▪ Anti-BCMA/GPRC5D bispecific CAR T
▪ Novel dosing strategies
▪ Less frequent dosing
▪ Maintenance
How to put it all together?
▪ Clinical Trials pave the way for advances
▪ There is no 1 strategy for relapsed MM and treatment must be tailored to the patient
▪ Triplets are better than doublets
▪ Novel therapies are becoming game changers and raise the bar for new drug approvals
▪ We’re still learning how best to use the drugs, in whom to use what, and how to sequence
▪ We need better predictors, better toxicity management
▪ More drugs = more options = greater responsibility for shared-decision making
Conclusion
▪ Relapsed MM
▪ Different flavors
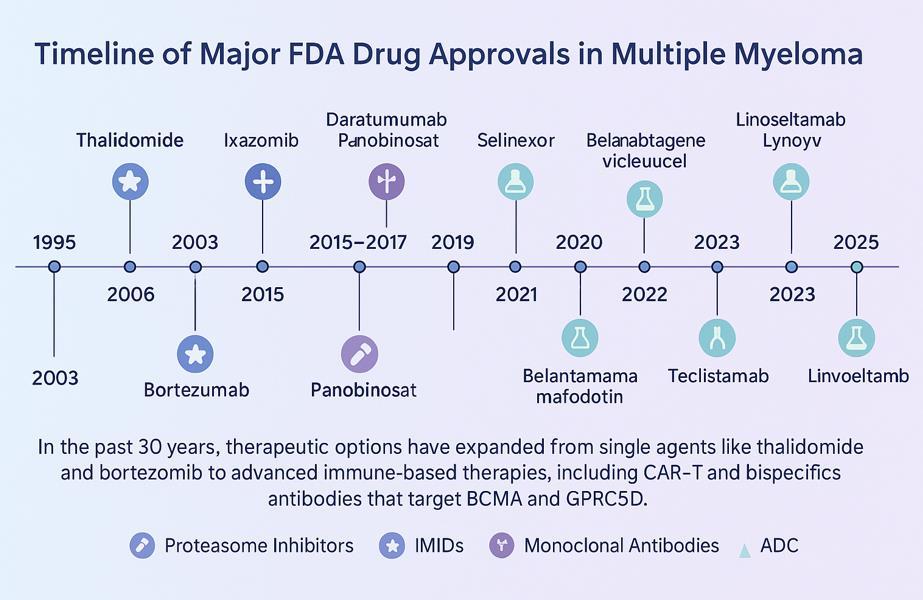
▪ Advances in the treatment of multiple myeloma
▪ New drugs
▪ Better outcomes
▪ Treatment Options
▪ Many regimens to choose from
▪ Considerations in Treatment Selection
▪ Patient characteristics
▪ Disease characteristics
▪ Goal of Therapy
▪ MRD negativity
▪ Later Lines of Therapy
▪ BCMA
▪ GPRC5D
▪ Emerging Therapies
▪ New drugs
▪ Better understanding of current drugs
▪ Better sequencing and choice
BREAK
CAR-T YOU’RE IN THE DRIVERS SEAT
YI LIN, MD, PHD
MAYO CLINIC, ROCHESTER
CAR-T: You are in the Driver’s Seat
Yi Lin, MD, PhD
Professor of Medicine
Division of Hematology; Division of Experimental Pathology
Co-Chair, Experimental and Novel Therapeutics Disease Group
Leader, Cell, Gene and Virotherapy Disease Team
Enterprise Deputy Director, Cancer Regenerative Biotherapeutics
All above funding made to the institution. No personal compensation.
Objectives
• Deciding when to drive the CAR?
• Efficacy/toxicities; am I fit enough to get CAR-T
• When: line of therapy
• How to get onto the journey for best chance of success?
• Commercial/trial CAR-T is right for me? Referral, working with local and CART center
• Prior treatment exposure for collection, disease management during CAR-T manufacturing
• How to nagivate the treatment journey
• Acute treatment management (recent FDA changes on REMS/PI)
• Intermediate toxicities
• Long term toxicities and recovery
Presenter: Yi Lin, M.D.Ph.D.
Myeloma current treatment landscape in U.S.
2nd Line 3rd Line 4th Line
• Selection Based on Response to Prior Therapy
• Changes between PI & IMiDs classes and or next generation
Teclistamab: BCMA BSAb
Talquetamab: GPRC5D BSAb
Elranatamab: BCMA BSAb
Linvoseltamab: BCMA BSAb
Backbone of major regimens: Proteasome inhibitor (PI), Immune modulatory drug (IMiD)
With and without CD38 antibodies
CAR-T is the only FDA approved therapy for myeloma given as a one-time treatment with no maintenance.
Ciltacabtagene autoleucel (CARVYKTI)
Idecabtagene vicleucel (ABECMA)
Elotuzumab (CS1 antibody) combinations
Selinexor/Bortezomib/DEX
Presenter: Yi Lin, M.D.Ph.D.
FDAApproved CAR-T Indications
Ide-Cel KarMMA-11 & KarMMa-32 Cilta-Cel
3 &
4 CAR Construct
scFv (murine)
co-signaling
After 2 or more lines of therapies
Indication
Exposure to proteasome inhibitor, IMiDs, anti-CD38 mAb
2 VHH domains (llama)
co-signaling
After 1 or more lines of therapy
Exposure to proteasome inhibitor, IMiD
Refractory to lenalidomide CAR-T Dose** 300 – 460* x 10^6 cells 0.5 – 1.0 x 10^6 cells/kg (max 1 x 10^8 cells total) Lymphodepletion
-4, -3
2.
study tested 150 – 450x10^6 CAR-T fixed dose. 300-460X10^6 fixed CAR-T cells is the FDA approved dose. ** For FDA approved CAR-T, final treatment dose is dependent on manufacturing capability of collected cells from the patients.
Presenter: Yi Lin, M.D.Ph.D.
Munshi N et al NEJM 2021.
Rodriguez-Otero P et al. NEJM 2023. 3. Berdeja J et al. Lancet 2021. 4. San Miguel J., et al NEJM 2023.
U.S. Standard of Care CAR-T Experiences
KarMMa-11 N = 128 Ide-cel RWE2 N = 211 Ide-cel CIBMTR3 N = 821
Ineligibility conditions for registration studies
ineligible 28% organ dysfunction 7% PCL, POEMS, amyloid, non-secretory MM 8% history of CNS pathology 6% prior alloSCT
77% Clinically significant comorbidity
18% prior BCMA therapy
%
The data presented are provided for ease of viewing information from multiple trials. Direct comparison between trials is not intended and should not be inferred. Ide-cel and cilta-cel are approved for patients with RRMM after ≥ 4 (FDA) or ≥ 3 (EMA) prior therapies including an IMiD® agent, a PI, and an anti-CD38mAb and who have demonstrated diseaseprogression on thelast therapy (EMA).
1. Munshi N et al. NEJM 2021. 2. Hansen DK, et al. J Clin Oncol 2023;41:2087–2097; 3. Sidana S. et al. ASH 2023.
Presenter: Yi Lin, M.D.Ph.D.
U.S. Standard of Care CAR-T Experiences
Ineligibility conditions for registration studies
* Median follow-up 5.8 months. Clinical response will continue to deepen over time. Longer follow-up is needed to identify best clinical response and PFS.
1. Berdejas J et al. Lancet 2021. 2. Martin T et al. JCO 2023. 3. Lin Y et al. ASCO 2023. 4. Hansen DK, et al. J Clin Oncol 2023;41(16 Suppl). Abstract 8012; Hansen DK et al. JCO 2024.
Presenter: Yi Lin, M.D.Ph.D.
Cilta-cel
Is there an age cutoff for CAR-T therapy?
• Resilience or functional frailty is more important than biologic age
• Patients up to age 78 in myeloma registration studies
• No age-associated difference in registration trial clinical response1–2
• RWE in older patients with ide-cel3 and cilta-cel4
CARTITUDE-1
subgroup analysis5
KarMMa subgroup analysis6
Overall median PFS (95% CI) was 8.8 months (5.6–11.6) and in:
65 years: 8.6 months (4.9–12.2)
70 years: 10.2 months (3.1–12.3)
The data presented are provided for ease of viewing information from multiple trials. Direct comparison between trials is not intended and should not be inferred. Ide-cel and cilta-cel are approved for patients with RRMM after ≥ 4 (FDA) or ≥ 3 (EMA) prior therapies including an IMiD agent, a PI, and an anti-CD38 mAb and who have demonstrated disease progression on the last therapy (EMA).
CI, confidence interval; PFS, progression-free survival; PR, partial response; VGPR, very good PR. 1. Munshi NC, et al. N Engl J Med 2021;384:705-716; 2. Berdeja JG, et al. Lancet 2021;398:314-324; 3. Hansen DK, et al. J Clin Oncol 2023;41:2087-2097; 4. Hansen DK et al. J Clin Oncol 2023;41(Suppl 16). Abstract 8012; 5. Jakubowiak AJ, et al. Blood 2021;138(Suppl 1). Abstract 3938; 6. Berdeja JG, et al. Blood 2020;136(Suppl 1): Abstract 1367; 7. Usmani SZ, et al. Clin Lymphoma Myeloma Leuk 2022;S410-S411.
Presenter: Yi Lin, M.D.Ph.D.
What about the impact of kidney dysfunction on CAR-T outcome?
US MM Immunotherapy Consortium RWE Ide-cel
• Among 211 patients, 13% had renal insufficiency (CrCl < 50mL/min), 1 patient on dialysis
• No additional worsening of renal function post CAR T cell therapy
• No difference seen in
– CRS incidence or severity
– ICANS incidence or severity
– Infections rate
– Cytopenia at month 3
– CRR or PFS
PFS following ide-cel CAR T cell therapy in patients with MM based on renal function at baseline
CrCl 50 mL/min, N = 183, median PFS: 8.1 months
CrCl < 50 mL/min, N = 28, median PFS: 6.5 months
P = 0.6
Time from CAR T cell infusion (months)
Ide-cel is approved for patients with RRMM after ≥ 4 (FDA) or ≥ 3 (EMA) prior therapies including an IMiD agent, a PI, and an anti-CD38 mAb and who have demonstrated disease progression on the last therapy (EMA).
CrCl, creatinine clearance; CRR, complete response rate; US, United States. Sidana S, et al. Blood 2022;140:10377–10379.
Presenter: Yi Lin, M.D.Ph.D.
How soon should I consider getting CAR-T?
Presenter: Yi Lin, M.D.Ph.D.
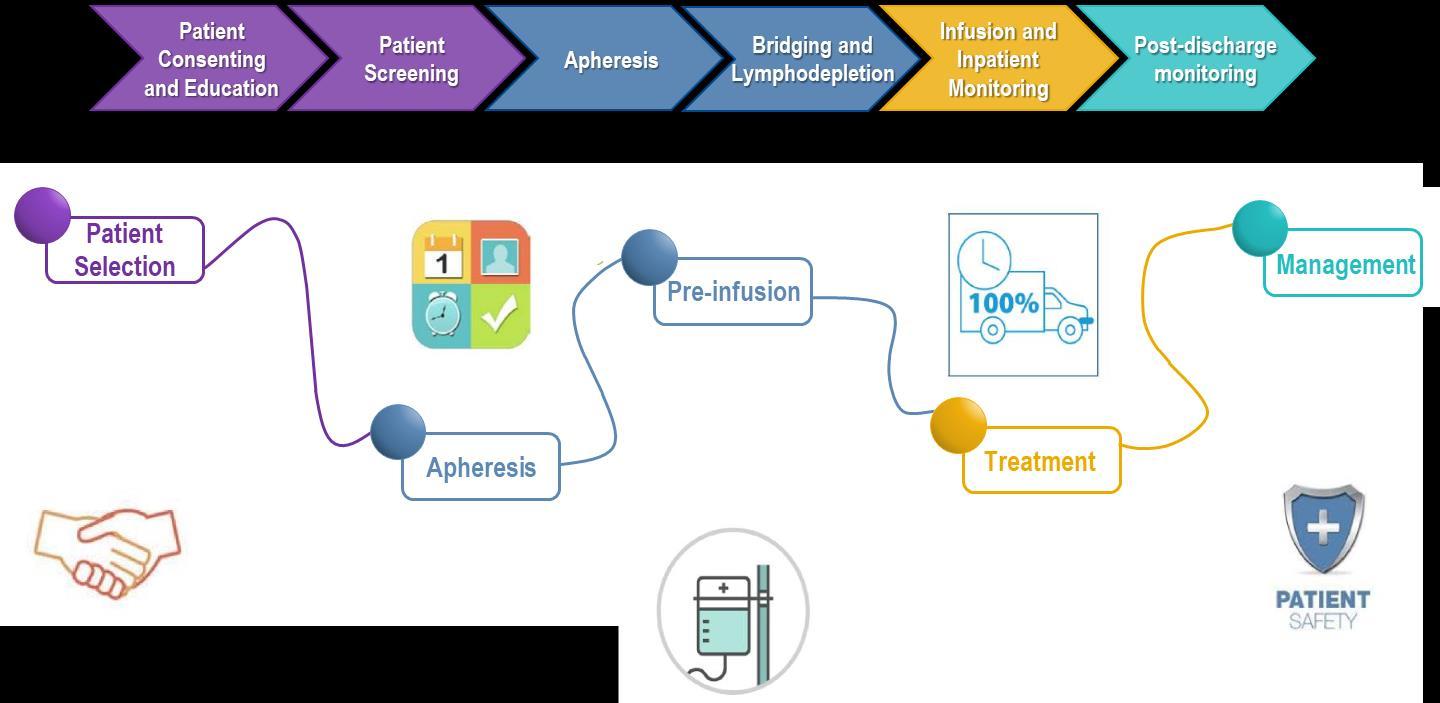
CAR-T therapy patient journey
Potential delay with insurance approval
1. Screening
• Local/primary hematologist refer patient for evaluation
• Coordination of salvage treatment
2. Evaluation
• Full eligibility assessment
4. Bridging
• Patient may return home for monitoring or bridging treatment while their CAR T cells are manufactured
• Average time 1 month
Often done together in 1 visit if possible. Average 1-2 weeks.
3. Cell collection
Early referral and close collaboration between the CAR T cell therapy center and home hematologist team is key!
• Close communication with CAR T cell therapy team
6. Ongoing monitoring
• Done by local/primary hematologist
• CAR T cell therapy team available for guidance
5. Post-infusion monitoring
• Typically for 1 month post CAR T cell infusion
Plan
to stay at CAR T cell therapy center
4. Chemo + CAR T cell infusion
• Typically 2-3 days of evaluation, 5 days of treatment
Adapted from Mayo Clinic Kern Center for Innovation
Presenter: Yi Lin, M.D.Ph.D.
Bispecific antibody and other BCMA targeting treatment before CAR-T can decrease efficacy
Sequencing type of therapy can impact outcome. Consider eligible patients for CAR-T first.
RWE Ide-Cel after
BCMA Targeted Therapy1
Cilta-Cel after
BCMA Targeted Therapy2
Overall response rate
aPercentages may not sum appropriately due to rounding.
Presenter: Yi Lin, M.D.Ph.D.
How
do I get on the CAR-T journey?
Presenter: Yi Lin, M.D.Ph.D.
Getting to CAR-T dosing
• Early referral and coordination with CAR-T center
• Streamline CAR-T eligibility testing and insurance authorization
• Plan the most recent salvage treatment if possible, avoid drugs that are toxic to T cells s.a. bendamustine
• Plan stopping time of recent treatment to allow adequate washout time for cell collection with minimum delay
• Collection of white blood cells for CAR-T manufacturing
• Usually a half day collection procedure
• Unlike stem cell collection, no mobilizing drugs are given ahead of time
• Reduce myeloma disease burden during CAR-T manufacturing, if possible
• Reduce the likelihood of more severe side-effects of CAR-T
• In earlier line of therapy, may be able to change to another regimen not yet given
Presenter: Yi Lin, M.D.Ph.D.
Talquetamab use during CAR-T manufacturing
US MM Immunotherapy Consortium
• 77 subjects received Talquetamab during bridging (median 5 prior lines of Tx)
• 40/67 (60%) of patients observed complete resolution of Talq related toxicities
• CAR-T post infusion toxicities appears comparable to prior SOC
• CRS 72%, Gr 3/4 3%
• ICANS 10%, Gr 3/4 2%
• Infections 27%
• Cytopenia Gr 3/4 10%
• CN VII palsy 1.5%
Dhakal B et al. ASH 2024,
How to navigate the CAR-T journey?
Presenter: Yi Lin, M.D.Ph.D.
Current SOC CAR-T is an individualized therapy requiring multi-disciplinary
care
Apheresis Unit
Collect white blood cells
Chemotherapy infusion followed by CAR-T cell infusion
May occur within hours but generally appears within days or weeks
Coincides with maximal T-cell expansion
Redrawn from: Kochenderfer, J. N. & Rosenberg, S. A. (2013) Nat. Rev. Clin. Oncol. Lee DW et al.
Cytokine Release Syndrome (CRS)
• CRS is a condition resulting from the release of cytokines from activated CAR T cells, as well as bystander immune cells
• CRS can be a sign of CAR T cell activities
• Often correlate with tumor burden
• Not required for tumor clinical response
• FDA approved CRS management
• Tocilizumab is first line
• Steroid is second line
• Current management is based on clinical symptoms, not lab values
• Management continue to evolve
Types of Neurologic Toxicity
Acute
• Concurrent with CRS and high fevers
• Result of elevated cytokines
• Common; some degree of neurotoxicity occurs in nearly all CAR T patients
• Symptoms include decreased attention, confusion, disorientation, delirium and ataxia
Cerebral Edema
• Rare
• Idiosyncratic
• Rapid acute onset
• Requires immediate ICU transfer and intervention
• May be fatal within 1-2 days
Delayed
Usually onset in later part of month 1 to month 6
• IEC-cranial nerve palsies
• Can be one-sided or two-sided
• IEC-Parkinsonism
• Earliest signs and symptoms may include decreased conversation, less facial emotion, changes in walking gait, new tremor, difficulty getting out of chair
• IEC-Guillain Barre Syndrome
• New onset severe backpain, paralysis
Each type of neurological toxicity is likely due to different manifestations of CAR T therapy (different underlying physiologies), responds to different mechanisms, and has a different likelihood of reversibility
IEC-associated enterocolitis
Case Report after Cilta-Cel
Presenter: Yi Lin, M.D.Ph.D.
US MM Immunotherapy Consortium
• 14 cases across 10 U.S. Centers (2-4%)
• 13 cilta-cel; 1 ide-cel
• Likely not BCMA specific, 3 case reports with CD19 CAR-T
• Median time to onset 79 (22-210) days
• Median duration 76 (17-113) days
• Response to steroid (4/10); infliximab (3/6); vedolizumab (1/3)
• 1 pt refractory to infliximab found to have CD4 lymphoproliferative disorder; responded to cyclosporin
• 5 deaths due to colitis or infection complications
• Important to escalate treatment early and monitor for C. Diff and CMV
Fortuna G et al. BCJ 2024.
Ozdermilini G et al. NEJM 2024.
Etiologies of cytopenia post CAR-T therapy
Infection
Disease
CAR T cell therapy/BMT
Potential etiologies
Early cytopenia (< 30 days)
LD chemotherapy
Prolonged cytopenia (30–90 days) Late cytopenia (> 90 days)
Infections
Immune-mediated HSC suppression
IEC-HS(rapidly rising ferritin, fever, organ dysfunction)
Primary disease relapse (evaluate for lineage switch)
Secondary marrow neoplasm
Immune-mediated mature blood cell destruction
LGL clone
TA-TMA (patients with antecedent BMT)
BMT, bone marrow transplant; HSC, hematopoietic stem cell; IEC-HS, immune effector cell-associated hemophagocytic lymphohistiocytosis-like syndrome; LGL, large granular lymphocyte; TA-TMA, transplant-associated thrombotic microangiopathy. Jain T, et al Blood 2023;141:2460-2469.
Presenter: Yi Lin, M.D.Ph.D.
Management of post CAR-T therapy cytopenia
Evaluations
Management
Month 1
Grade ≥ 3 cytopenia can be common depending on cytopenia prior to CAR T cell therapy and CRS severity
Rule out persistent or recurrent inflammation:
• CRP, ferritin, bone marrow biopsy
Rule out nutritional deficiencies:
• Iron studies, pernicious anemia eval, copper, zinc
Rule out infection:
• PCR for CMV, EBV, parvovirus B19, HHV6
• If IEC-HS identified, consider anakinra, add steroid if refractory
– Escalate immunosuppressive agents if refractory
• If nutritional deficiencies or infections identified, treat as appropriate
• Continue blood count monitoring and transfusion support
• Variable success with growth factor and thrombopoietin mimetics
Month 3
Anticipate cytopenia improvement to grade ≤ 2
Rule out nutritional deficiencies and infections as above if not tested earlier
Rule out persistent or recurrent inflammation:
• CRP, ferritin
Rule out MDS, t-MN
• BM biopsy with cytogenetic testing
• Antibacterial prophylaxis should be given during prolonged neutropenia
• If MDS and t-MN are ruled out, consider stem cell boost in patients with grade 3 or higher cytopenia and who have stem cells available
• Antifungal prophylaxis should be given in month 1 post CAR T cell therapy and continued if patient is receiving chronic immunosuppressive medications
• Antiviral prophylaxis and PJP prophylaxis should be continued until CD4 T cells count is persistently > 200 (this can take 1 year or longer)
• Prophylactic IVIG, 400 mg/kg IV, should be given monthly for IgG < 400 mg/dL, or for patients with IgG < 600 mg/dL and have frequent infections
BM, bone marrow; IgG, immunoglobin G; IV, intravenous; IVIG, IV immunoglobulin; MDS, myelodysplastic syndromes; PJP, Pneumocystis jirovecii pneumonia; t-MN, therapy-related myeloid neoplasm. Jain T, et al. Blood 2023;141:2460-2469. Adapted from mSMART.org.
Presenter: Yi Lin, M.D.Ph.D.
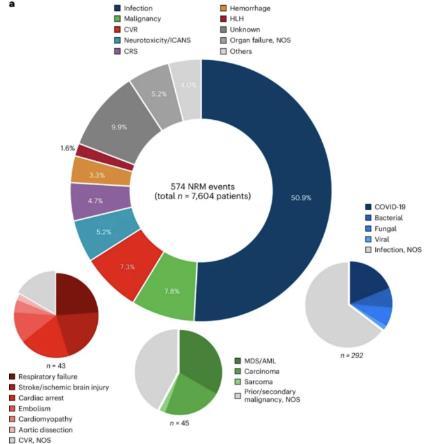
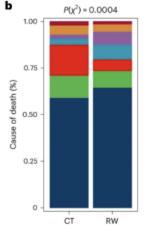
Infections is the most common cause of deaths not related to disease
relapse after CAR-T
• Meta-analysis of 5,589 patients who received CAR-T in clinical trials and standard of care practice.
New agents or regimens in clinical trials are possible options
CAR T-Cell Therapy: Patients’ own T-cells
Engineered to Target Myeloma Cells
Ask for a referral to CAR T-cell center as soon as it is possible as next treatment option (ie, before relapse)
Manufacturing takes ≈ 4 to 6 weeks
Bridging therapy may be needed
T-Cell Collection
No driving for 8 weeks
• Away from home
• Some in hospital stay
• Care partner needed
• Side effect management
• CRS, ICANS
• Low blood counts
• Fatigue and fever
• Some patients need ongoing transfusion support
Who Is Eligible for CAR T-cell Therapy?
AT RELAPSE
CAR T-cell therapies may be appropriate for patients with RRMM and …
Specific criteria may vary depending on CAR T-cell therapy center
CAR = chimeric antigen receptor; CrCl = creatinine clearance; ECOG = Eastern Cooperative Oncology Group; PS = performance status; RRMM = relapsed/refractory multiple myeloma; Abramson, JS, et al. Am Soc Clin Oncol Educ Book. 2019;39:446-453. YakoubAgha I, et al. Haematologica. 2020;105(2):297-316.
✓ Ide-Cel approved for 2 or more prior lines of therapy
✓ Cilta-Cel approved for 1 or more lines of therapy
✓ ECOG PS: 0-2
✓ Adequate organ function
– CrCl > 30 mL/min (dose reduce for fludarabine with CrCL 30-70)
✓ Ability to tolerate lymphodepleting chemotherapy, CAR T-cell therapy process, and potential toxicities
✓ No active or serious infections (ie, fungal, bacterial, viral)
✓ Sufficient social support
– Caregiver support before, during, and after therapy
– Multiple travel and housing support systems
Clinical trials are always an option. They have their own criteria for who is eligible.
Bispecific Antibodies
• Different bispecific antibodies have differences in efficacy, side effects
– Available after 4 prior lines of therapy (or clinical trial)
– About 7 in 10 patients respond
– Off-the-shelf treatment; no waiting for engineering cells
– CRS and neurotoxicity
– Risk of infection
• BCMA target: greater potential for infection
– Tecvayli® (teclistamab)
– Elrexfio ® (elranatamab)
BISPECIFIC ANTIBODIES
– Lynozyfic (linvoseltamab)
• GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss
– Talvey ® (talquetamab)
Practical Approach to the Treatment of Patients With Relapsed
Myeloma
Disease-Related Factors
• Duration of response to initial therapy
• High-risk vs low-risk status
• Molecular relapse vs symptomatic relapse
• Other medical conditions or frailty
Treatment-Related Factors
• Previous/Current therapy exposure and response (relapsed vs refractory)
• Toxicity/Tolerability of the previous regimen
• Mode of administration (ie, PO or IV)
• Cost and convenience (out-of-pocket co-pays for IV vs PO)
Patient and Caregiver’s Roles in Shared Decision Making
Ask questions (write them down in advance of visit)
• What are my treatment options?
• What are the pros and cons of each option? Efficacy? Side effects? Administration? Insurance nuances?
• Are there treatments that wouldn’t be a good option for me? Why?
Express your desire to participate in the treatment decisions
• I want to make sure the treatment we chose is the best option for me
• I want to be sure we a choosing the best therapy for my husband/wife
Ask for time (if needed/ appropriate)
• There is a lot to think about. Can I/we have some time to consider the options?
• Ask for information you can consider at home
• Note: if medical emergency/high risk, may not be appropriate
Spring Into Managing Side Effects
Infection Can Be Serious for People With Myeloma
[P]reventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
As recommended by your healthcare team:
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
Consider GCSF 2 or 3 times/wk (or as frequently as needed) to maintain ANC > 1000 cells/μL, bacterial/ fungal prophylaxis, and maintain treatment dose intensity
Some people receiving BCMA-targeting therapies have experienced infections that are less common like CMV, PJP and fungal infections
CAR T and Bispecific Antibodies: Unique Side Effects
CRS is a common but often mild & manageable side effect
CAR = chimeric antigen receptor; CRS = cytokine release syndrome. Oluwole OO, Davila ML. J Leukoc Biol. 2016;100:1265-1272. June CH, et al. Science. 2018;359:1361-1365. Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Brudno JN, Kochenderfer JN. Blood Rev. 2019:34:45-55. Shimabukuro-Vornhagen, et al. J Immunother Cancer. 2018;6:56. Lee DW, et al. Biol Blood Marrow Transplant. 2019;25:625-638.
CAR T and Bispecific Antibodies: Unique Side Effects
Management of Oral Side Effects related to GPRC5d Targeted Regimens
Dry Mouth
Taste Changes
OTC dry mouth rinse, gel, spray are recommended. Advise patients to avoid hot beverages. Initiate anti-fungal therapy for oral thrush
Dental Care
Dexamethasone oral solutions “swish and spit” have been tried but with no proven benefit yet. Sour citrus or candies before meals are also recommended.
Attention to oral hygiene.
Regular dental cleaning and evaluation. Close monitoring for ONJ, oral cancer and dental caries
Weight Management
Dietary modifications with small bites, eating upright, and sips with food can help manage symptoms.
Some medications lead to weight gain, others to weight loss.
Dry mouth leads to taste changes which can lead to anorexia.
Meet with a Nutritionist
Consider diet changes, supplements
Monitor weight
Education and emotional support are key strategies to manage oral toxicities.
Dysphagia
Catamero D, Purcell K, Ray C, et al. Presented at the 20th International Myeloma Society (IMS) Annual Meeting Nurse Symposium; September 27–30, 2023; Athens, Greece.
Skin and Nail Side Effects
Possible side effect to some treatments and supportive care medications
Skin Rash:
• Prevent dry skin; apply lotion
• Report changes to your care team
• Medication interruption or alternative, as needed
• Steroids:
– Topical for grades 1-2,
– Systemic and topical for Grade 3
• Antihistamines, as needed
Nail Changes:
• Keep your nails short and clean. Watch for “catching and tearing”
• Apply a heavy moisturizer like Vaseline or salve. Wear cotton hand coverings to bed
• A nail hardener may help with thinning
• Tell the team if you have signs of a fungal infection, like thickened or discolored nails
Photos: Mount Sinai Hospital, NY, NY
GI Symptoms: Prevention & Management
Fluid intake can help with both diarrhea and constipation and helps kidney function
Diarrhea may be caused by medications and supplements
• Laxatives, antacids with magnesium
• Antibiotics, antidepressants, other (check with provider, pharmacist)
Tell your healthcare provider about any new bone or chronic pain that is not adequately controlled
Peripheral Neuropathy Management
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e. diabetes).
– Avoid certain medications when possible (eg, NSAIDs), dose adjust as needed
• Treatment
– Treatment for myeloma
– Hydration
– Dialysis
Many myeloma patients will experience kidney issues at some point; protecting your kidney function early and over time is important
Let the Sun Shine In
98.8%
Fatigue
Fatigue is the most reported symptom.
Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression
Often, people do not share these symptoms with their providers. Talk to your provider about symptoms that are not well controlled or if you have thoughts of self-harm.
Anxiety
>35% of patients
Depression
≈25% of patients
Summer of Success
Cultivate A Care Network
• Multiple studies demonstrate that strong social ties are associated with
– Increased longevity including people with cancer
– Improved adherence to medical treatment leading to improved health outcomes
– Lower risk of cardiovascular diseases
– Increased sense of purpose & life satisfaction
– Improved mood and happiness
– Reduced stress and anxiety
– Enhanced resilience
Martino J, et al. Am J of Lifestyle Med. 2015;11(6):466-475. Yang YC, et al. Proc Natl Acad Sci U S A. 2016;113(3):578-583.
Pinquart M and Duberstein PR. Crit Rev Oncol Hematol. 2010; 75(2):122–137.
• Strategies for enhancing social connection
– Deepen existing relationships with family, friends, and loved ones
– Build new relationships by participating in a support group, joining clubs or organizations, or volunteering
Tip: Start with small steps outside your comfort zone. Call a loved one you haven’t spoken to in a while.
Invite a person you’d like to know better for lunch, coffee, or a walk.
Hetherington C. Healthnews.
https://healthnews.com/longevity/healthspan/social-connection-andlongevity/#:~:text=Research%20consistently%20demonstrates%20tha t%20people,of%20fulfillment%20in%20your%20life. Accessed Feb 1 2024.
Enjoy Life’s Bounty
Harvest Good Health
Have a Primary Care Provider & Have Recommended Health Screenings
• Blood pressure
• Cholesterol
• Cardiovascular disease
• Diabetes
• Colonoscopy
• Women specific: mammography, pap smear
• Men specific: prostate
• Vision
• Hearing
• Dermatologic evaluation
• Dental checkups & cleaning
Develop & maintain healthy behaviors
• Good nutrition
• Regular activity
• Quit tobacco use
• Sufficient Sleep (next slide)
An ounce of prevention is worth a pound of cure. Benjamin Franklin
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56. Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.
FACULTY ROUNDTABLE:
DEMYSTIFYING CLINICAL TRIALS
Q&A WITH PANEL
Workshop Video Replay & Slides
As follow up to today's workshop, we will have the speaker slides and a video replay available.
These will be provided to you shortly after the workshop concludes and posted to our website under “IMF Videos”
We Want to Hear From You
Feedback Survey
At the close of the meeting a feedback survey will pop up.
This will also be emailed to you shortly after the workshop.
Please take a moment to complete this survey.
Thank you to our speakers & our sponsors!
OUR VISION: A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
IMF Core Values:
These are the core values we bring to accomplishing our mission each day.
Patient Centric
The patient experience is the focus of everything we do. Every interaction is an opportunity to establish a personal connection built on care and compassion which is the basis for continued support.
Respect All
As a team, we value honesty and transparency while creating a culture of mutual respect. We foster a myeloma community built on sincerity, authenticity, and kindness.
Excellence and Innovation
We value accountability, personal responsibility, and a steadfast commitment to excellence. We respect the legacy and reputation of our organization while seeking new solutions and advancements to improve outcomes, quality of life, and access to the best available resources for everyone impacted by myeloma.
Honor differences
We recognize each team member's skills and talents through collaboration and cooperation. Our programs aim to celebrate and support the diversity of our patients and their communities.