


• 7% of new HIV diagnoses are due to injection drug use1
• A person without HIV has a 1 in 160 chance of getting HIV every time they share a needle with a person with HIV2
• Sharing syringes in the second riskiest behavior for acquiring HIV3
• SUD may increase the risk of getting HIV through sex due to increased likelihood of higher-risk sexual behaviors3
• Although all-cause death rates have declined in PWH, deaths related to substance use in PWH have not declined, and in fact have increased 7% in women4
1. Centers for Disease Control and Prevention (CDC). https://www.cdc.gov/hiv/data-research/facts-stats/index.html; 2. Medical News Today. https://www.medicalnewstoday.com/articles/324052#survival -outside-the-body; 3. HIVinfo.nih.gov. https://hivinfo.nih.gov/understanding-hiv/fact-sheets/hiv-and-substance-use; 4. Trickey A, et al. Lancet HIV. 2024;11(3):e176-e185.
• Large range of estimated prevalence of SUD in PWH1
– 7 academic medical centers showed 48% of PWH had an SUD
• 6.5× greater than in the general population
• Other studies have found high rates broken out by substance2

https://www.cdc.gov/hiv/data-research/facts-stats/index.html.
Who should be tested?1
• CDC: All adults and teens (range 13-64 years) should be tested at least once in routine health care
• All pregnant persons
• Tested at least once a year (some as often as every 3 months):
– MSM or transgender individuals
– PWID who share equipment
– People engaging in survival sex
– Incarcerated individuals
– Individuals with a current STI, hepatitis, or TB
– Partner with HIV or ≥1 partner since last HIV test
– People having sex without condoms
• Perform opt-out testing
• Normalize testing for all patients
• The CDC recommends initial testing with an FDA-approved Ag/Ab assay; no oral tests
CDC, Centers for Disease Control and Prevention; FDA, US Food and Drug Administration; MSM, men who have sex with men; PWID, people who inject drugs; STI, sexually transmitted infection; TB, tuberculosis. 1. CDC. https://www.cdc.gov/hiv/testing/?CDC_AAref_Val=https://www.cdc.gov/hiv/basics/hiv-testing/getting-tested.html; 2. CDC. https://www.cdc.gov/hivnexus/hcp/diagnosis-testing/; 3. Huynh K, Kahwaji CI. HIV testing. In: StatPearls [Internet]. StatPearls Publishing; 2025-. https://www.ncbi.nlm.nih.gov/books/NBK482145/.
• Multiple tests available1
– Most detect only HIV Ab
– Only 1 approved rapid POC test detects both Ab and Ag2
• There are fingerstick test options and, though not recommended, there are oral tests available1
• Results within a few minutes1
• Must send for confirmatory testing3

• Fourth-generation HIV tests that detect both Ag and Ab are recommended by the CDC and are confirmatory for HIV3,4
– Fourth-generation test can be positive only 2 to 3 weeks after exposure
– Third-generation tests detect only Ab, which appear after Ag
• Positive HIV tests must be reported to the health department5
POC, point of care.
1. CDC. https://www.cdc.gov/hivpartners/php/hiv-testing/index.html; 2. US Food and Drug Administration (FDA). https://www.fda.gov/vaccines-blood-biologics/approved-bloodproducts/determine-hiv-12-agab-combo; 3. CDC. https://www.cdc.gov/hivnexus/hcp/diagnosis-testing/index.html; 4. Huynh K, Kahwaji CI. HIV testing. In: StatPearls [Internet]; 2025-. https://www.ncbi.nlm.nih.gov/books/NBK482145/; 5. National Alliance of State and Territorial AIDS Directors (NASTAD). https:/ /nastad.org/sites/default/files/2024-03/PDF-ReportingRequirements-for-Negative-HIV-and-Hepatitis-C-Test-Results.pdf.


People whose HIV tests are positive enter primary care and are offered effective treatment and supportive services to achieve and maintain viral suppression.
SSP, syringe services program.

CDC. https://stacks.cdc.gov/view/cdc/129024/cdc_129024_DS1.pdf.
PrEP is a comprehensive set of services to reduce risk of HIV infection
• 4 FDA-approved medications for PrEP1,2
– May only be used in persons without HIV
• Comprehensive services include1:
– Regular HIV screening
– Regular STI screening
– Safer sex + risk-reduction counseling
Refer any patient interested in PrEP to a provider who can prescribe PrEP if your center cannot do so.
• Available medication options for PrEP1,2:
Oral daily tenofovir disoproxil fumarate/emtricitabine (TDF/FTC; Truvada® ); available in generic
Oral daily tenofovir alafenamide/emtricitabine (TAF/FTC; Descovy® ); not for use in people at risk of HIV through vaginal receptive sex
Cabotegravir long-acting injectable (CAB LAI; Apretude® ) every 2 months
Lenacapavir long-acting injectable (LEN LAI; Yeztugo® ) every 6 months
CDC. https://www.cdc.gov/hivnexus/hcp/prep/index.html; 2. HIV.gov. https://www.hiv.gov/hiv-basics/hiv-prevention/using-hiv-medication-to-reduce-risk/pre-exposure-prophylaxis.
• Chemsex has been linked to increased risk of HIV transmission1
– High-risk behavior, higher rates of unprotected sex, potential for increased number of partners
• Survival sex increases risk of HIV transmission2
– Inconsistent condom use, greater number of partners, increased frequency of sharing injection equipment, limited disclosure of sex work and injection drug use to health care providers
• Increasing patient knowledge about risks, prioritizing harm reduction, increasing HIV testing, increasing wraparound services, and providing mental health counseling can reduce risk of HIV transmission1,3
• PEP can be taken if a person is concerned about potential HIV exposure within the last 72 hours4
PEP, postexposure prophylaxis.
1. Pozo-Herce PD, et al. Healthcare. 2024;12(14):1411; 2. Ogden SN, et al. Int J Drug Policy. 2021;96:103285; 3. Arrington-Sanders R, et al. J Adolesc Health. 2022;70(2):275-281; 4. HIVinfo.nih.gov. https://hivinfo.nih.gov/understanding-hiv/fact-sheets/post-exposure-prophylaxis-pep.
• nPEP (nonoccupational postexposure prophylaxis) is the use of antiretroviral medication after a very recent potential exposure to HIV, to prevent infection
– Medication must be started within 72 hours of possible exposure, ideally within 24
– Test for HIV prior to initiating nPEP
– Patient should follow up with the prescribing clinician within 72 hours
– Medication is taken daily for 28 days, after which a discussion can be had about transition to PrEP
– Continue HIV/STI testing
– Usually covered by insurance (or patient assistance program on an urgent basis)
Negative HIV test: offer prevention tools (PrEP, condoms, harm reduction, and supportive services) to stay HIV negative
CDC. https://www.cdc.gov/hivpartners/php/hiv-testing/index.html.
• Life expectancy nearly equal between people with and people without HIV, as long as PWH are virally suppressed1
• People diagnosed today have a longer life expectancy vs those diagnosed many years ago2
• More likely to die of non–HIV-related illnesses than of HIV2
• Risk of earlier comorbidity onset with
U=U, or undetectable=untransmittable, means that if a patient does not have a detectable HIV viral load, HIV cannot be transmitted to another person through sex.
Human Services (DHHS). https://clinicalinfo.hiv.gov/en/guidelines/hiv -clinical-guidelines-adult-and-adolescent-arv/initiation-antiretroviral-therapy.
• Initiating ART as soon as patients are diagnosed helps them become virally suppressed more quickly1
• It is impossible to transmit HIV to sexual partners when virally suppressed (U=U)1
– Can provide a sense of relief to patients to know they cannot transmit HIV sexually
– Patients’ partners may want to take PrEP, at least until the patient is virally suppressed
• Adherence to ART and appointments is critical2
– Missing appointments has been linked to increased risk of mortality
Patients can begin ART regardless of drug use or MOUD. 1
MOUD, medication for opioid use disorder.
1. DHHS. https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/initiation-antiretroviral-therapy; 2. Mugavero MJ, et al. Clin Infect Dis. 2014;59(10):1471-1479.
• Ask open-ended questions about current knowledge level and any factors that can affect adherence1
• Promote patient empowerment and use positive reinforcement1
• Consider putting patient in touch with other PWH to listen to their experience1
• Provide educational materials at the appropriate literacy level1
• Acknowledge and address competing priorities1
• Combine education with other interventions, such as providing community resources2
1. DHHS. https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/adherence-continuum-care; 2. Pugh LE, et al. J Infect Public Health. 2022;15(10):1053-1060.
• Immediate initiation of an ART regimen, typically within 7 days of diagnosis, preferably the same day
– Patient must be ready and not have evidence of opportunistic infection
• Improves the likelihood of linkage to care and likelihood of and time to viral suppression
• Potential to improve survival and longitudinal engagement in care
Gandhi RT, et al. JAMA. 2025;333(7):609-628.

• More-rapid viral suppression
• More-rapid CD4 improvement
• Reduces time of transmissibility (U=U)
• Improves care engagement and retention
• Patients want to know they are being treated and clinicians are taking their HIV seriously; improved peace of mind
• Helps reduce stigma faster
DHHS. https://clinicalinfo.hiv.gov/en/guidelines/hiv -clinical-guidelines-adult-and-adolescent-arv/initiation-antiretroviral-therapy.
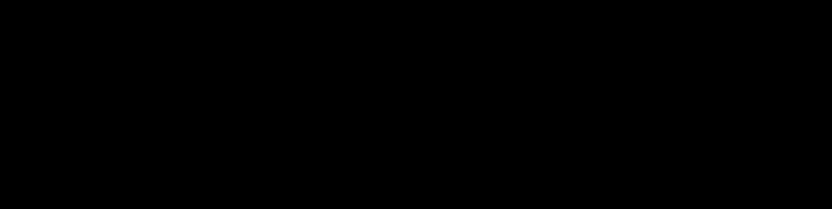
Rates of Within-Couple HIV Transmission Following Viral Suppression, per 100 Couple-Years of Follow-Up


Between September 15, 2010, and July 31, 2017, 972 MSM couples were enrolled, of whom 782 provided 1593 eligible couple -years of follow-up, with a

Rapid ART is safe and highly effective for all patients, regardless of comorbid conditions and nearly every other medication.
DHHS. https://clinicalinfo.hiv.gov/en/guidelines/hiv -clinical-guidelines-adult-and-adolescent-arv/initiation-antiretroviral-therapy?view=full; Gandhi RT, et al. JAMA. 2025;333(7):609-628.
• Everyone is eligible for rapid ART (with very rare exceptions)1
– Patients with certain infections, such as cryptococcal or TB meningitis, should delay ART initiation
– Patient does not want to start ART
• Benefits of rapid ART have been seen in patients1-4:
– Experiencing homelessness or unstable housing
– With SUD
– With mental illness
– Who are unemployed
1. DHHS. https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/initiation-antiretroviral-therapy?view=full; 2. Pilcher CD, et al. J Acquir Immune Defic Syndr. 2017;74(1):44-51; 3. Halperin J, et al. AIDS Patient Care STDS. 2018;32(2):39-41; 4. Colasanti J, et al. Open Forum Infect Dis. 2018;5(6):ofy104.

HIV Ag/Ab test
• BIC/TAF/FTC (Biktarvy®)1,2 – 1 pill, taken once per day
• DTG (Tivicay) + TDF/FTC (Truvada®) or TAF/FTC (Descovy®)1,2 – 2 pills, taken once per day
BIC, bictegravir; DTG, dolutegravir.
1. DHHS. https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv/what-start-initial-combination-regimens-antiretroviral-naive?view=full;
2. Gandhi RT, et al. JAMA. 2025;333(7):609-628.

DHHS. https://clinicalinfo.hiv.gov/en/guidelines/hiv -clinical-guidelines-adult-and-adolescent-arv/drug-interactions-insti?view=full.
• Intersectional stigma: interrelated, compounding impact of experiencing multiple stigmas at the same time1
– People with SUD have many potential sources of stigma outside SUD itself: unemployed, unhoused, race, gender, sexuality, HIV, previous incarceration2
• Can increase rates of anxiety and depression1
• Often associated with reduced rates of viral suppression or ART adherence, increased substance use, and reduced health care utilization3
• May be more prevalent among women than men3
1. Hook K, et al. AIDS Behav. 2023;27(2):431-442; 2. Dittrich D, Shomerus G. Intersectional stigma in substance use disorders. In: Shomerus G, Corrigan P, eds. The Stigma of Substance Use Disorders. Cambridge University Press; 2022; 3. Vetrova MV, et al. AIDS Behav. 2021;25(9):2815-2826.

They look at us like junkies, but you know what? This junkie right here bleeds the way you bleed, has feelings the way you have feelings, loves the way you love, hates the way you hate, holds grudges the way you hold grudges. [Health care providers] are so judgmental that they would literally come out and speak about you behind your back.

I mean, they accused me of using [drugs] while I was in the hospital. I was like, ‘How would I even…’ I don’t know. I didn’t even want to get into that. I transferred to another hospital right after that.

I caught scabies going to that shelter… so I used to tell the doctor. He tried to say it was the coke [cocaine]. No, the coke don’t get me like that. I’ve been doing coke for many years. Ever since I went to the shelter that’s when this rash started happening. He’s like ‘No, it can’t be. There’s no such thing.…’ But ever since then, I lost a little confidence in doctors, to be honest.

I just did a walk-in and when I met the doctor, everything was fine. As soon as I took off my coat for her to see, that was it. She went from being super nice, referring me here, to okay, maybe you should go to the emergency room…the whole entire face changed, the smile, the whole mood.
• Train staff on recognizing sources and signs of stigma
– Can work to address judgmental attitudes or increase understanding of patients’ experiences
• Provide community education
• Individual or group counseling or peer support
– Success has been reported with including an emotional regulation component
• Consider using stigma or stigma-related scales to identify internalized and externalized stigma
– Keeping It Together 10-item scale, HIV Stigma Index 2.0 scale, HIV Shame Inventory
Lancaster KE, et al. Curr HIV/AIDS Rep. 2022;19(5):301-311.
Ask open-ended questions to understand a patient’s adherence challenges, life circumstances, and previous experiences in health care that may negatively affect adherence

q What’s been going on with you?
q What are some things that make it challenging to come to the clinic or SUD center?
q How is everything at home?
q What has your experience been with previous clinicians or center staff?

q What has a clinician or staff member done that has made you lose trust?
q What type of support system do you have?
• Examples of personal bias:
– Assuming the partner’s gender
– Assuming married couples are monogamous
– Assuming that someone does not need HIV, STI, or HBV/HCV testing
– Assuming some people don’t need a sexual history taken
– Assuming someone who uses drugs or is experiencing homelessness can’t adhere to medication
• Addressing personal bias:
– Ascertain the number and gender of current sexual partners
– Discuss sexual history, current sexual practices, and other risk factors with all patients
– Ask all patients for their preferred pronouns and gender identity
– Discuss or provide support services for any patient in need
CDC. https://www.cdc.gov/hivnexus/hcp/sexual-history/index.html.
• Using clinically accurate and medically appropriate language matters1,2
• Stigma and stereotypes can impede solutions that will reduce HIV transmission2
• Person-first language can reduce stigma, increase patient willingness to seek treatment, reduce negative provider perceptions of PWH or those seeking PrEP, and improve care3-5
– Use “a person experiencing homelessness” instead of “homeless person”
– Use “a person who uses drugs” instead of “addict”
– Use “a person with HIV” instead of “HIV infected”
1. Botticelli MP, Koh HK. JAMA. 2016;316(13):1361-1362; 2. United States Interagency Council on Homelessness. https://www.usich.gov/news-events/news/peopleexperience-homelessness-they-arent-defined-it; 3. Goddu AP, et al. J Gen Intern Med. 2018;33(5):685-691; 4. National Institute on Drug Abuse. https://nida.nih.gov/nidamedmedical-health-professionals/health-professions-education/words-matter-terms-to-use-avoid-when-talking-about-addiction#; 5. CDC. https://www.cdc.gov/healthcommunication/php/toolkit/preferred-terms.html?CDC_AAref_Val=https://www.cdc.gov/healthcommunication/Preferred_Terms.html.
Individual trauma results from an event that is experienced by an individual that leaves a long-term negative effect on the individual’s functioning and well-being. It can be experienced by a person or an entire population.

• Safety (physical and psychological)
• Trustworthiness and transparency
• Peer support (from individuals with lived experiences of trauma)
• Collaboration and mutuality
• Empowerment, voice, and choice
• Cultural, historical, and gender issues
One of the most important changes when incorporating TIC is shifting the question from “What’s wrong with you?” to “What happened to you?”
TIC, trauma-informed care. Substance Abuse and Mental Health Services Administration (SAMHSA). SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. HHS Publication No. (SMA) 14-4884. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014.
Organization that is unaware of or ignorant to the impacts of trauma on clients and staff
Recognition and naming of trauma and toxic stress, and opportunities for resilience among clients and staff
Staff have foundational knowledge of NEAR science, trauma-informed principles, and recognize signs and symptoms of trauma
Organization fully integrates knowledge about trauma and resilience into trauma policies, procedures, and practices
Organization actively realizes, recognizes, responds to, and resists retraumatization of staff and clients
NEAR, neurobiology, epigenetics, adverse childhood experiences, and resilience. NASTAD. https://targethiv.org/sites/default/files/media/documents/2023 -01/Trauma-Informed-Approaches-Toolkit-2022_NASTAD.pdf.
Organization actively centers resilience and healing, for both clients and staff
q Create a space of physical and emotional safety
q Focus on respect and connection
q Reduce power differences by creating partnership and using shared decision-making
q Use person-first language
q Validate a patient’s strengths and understand past coping mechanisms
q Incorporate peers into your center or practice
q Work to mitigate personal stereotypes or biases NASTAD.
https://targethiv.org/sites/default/files/media/documents/2023 -01/Trauma-Informed-Approaches-Toolkit-2022_NASTAD.pdf.




























FHI360. https://www.fhi360.org/wp-content/uploads/drupal/documents/resource-linkages-peer-navigation-facilitators-guide.pdf.
• Managing SUD has wide-ranging effects, and SUD centers can play a role in ensuring linkage to and retention in care

• Welcoming and nonstigmatizing1,2
• Participates in harm reduction, including providing MOUD3
• Uses a peer navigator or person with lived experience1
• Collaborates with external partners, including SUD centers, shelters, or mental health services1
• Has low barriers to care1,2:
– Flexible clinic hours, no penalty for missed appointments, colocated care
• Can provide incentives or necessities, such as showers and clothing1,2
1. Dombrowski JC, et al. Clin Infect Dis. 2023;77(2):252-257; 2. Hickey MD, et al. J Infect Dis. 2022;226(suppl 3):S353-S362; 3. Korthuis PT, et al. Addiction. 2017;112(6):1036-1044.
• Assist patients with appointments for wraparound services1
• Build support networks through shared backgrounds and community knowledge1,2
• Encourage medication adherence1
• Provide support throughout treatment pathways2
• Make multiple peer navigator training modules available that incorporate perspectives from various initiatives3-5
– Implementation guidelines, SOPs, client flow algorithms, reference documents

SOP, standard operating procedure.


1. San Francisco Department of Public Health. https://www.sfcommunityhealth.org/program/hhome; 2. Jugnarain DV, et al. J Viral Hepat. 2022;29(1):43-51; 3. FHI360. https://www.fhi360.org/sites/default/files/media/documents/resource-linkages-peer-navigation-facilitators-guide.pdf; 4. AIDS Education & Training Center (AETC) Program. https://aidsetc.org/resource/community-health-worker-training-resources; 5. NMAC. https://www.nmac.org/capacity -building/hiv-prep-navigation-program/.
• Peer navigators (anyone with a close understanding of the community served) interacted for an average of 11 days over 6 months per patient
• Peer navigators most often provided coaching and education, emotional support, and appointment reminders
• Most contact (63%) was virtual (phone, text, social media, or email)
– If in person, 72% occurred at the program site
• Assess center’s readiness for a peer navigator program1
• Identify intended roles for the peer navigator1
• Decide where peer navigators fit in the clinic workflow1
• Look for a peer navigator who2:
– Can act as an educator, facilitator, coach, advocate, and community resource
– Is committed to meeting center goals, accountable to the community, tolerant of others’ ideas and behaviors
– Can maintain confidentiality, boundaries, and ethics
1. Health Resources and Services Administration Ryan White HIV/AIDS Program. https://targethiv.org/sites/default/files/media/documents/202303/CQII_Peer_Navigator_IG_final_Jan2023.pdf; 2. FHI360. https://www.fhi360.org/wp-content/uploads/drupal/documents/resource-linkages-peer-navigation-facilitators-guide.pdf.
• Adherence is improved when competing priorities are addressed1
• Community partners can help encourage retention in care and medication adherence2
• Utilize existing community partner relationships and collaborate with other clinicians to identify relationships2,3
1. Palacio-Vieira J, et al. BMC Public Health. 2021;21(1):1596; 2. Jones MD, et al. PLoS One. 2023;18(1):e0276852;
Broz D, et al. Am J Prev Med. 2021;61(5 suppl 1):S118-S129.
N=27 patients received initial HIV care at the IDEA clinic, then after 6 months transitioned to HIV care at a traditional cli nic, including Ryan White–funded clinics. Patients had access to peer navigation and medication management for the 12 months of the study.
Plesons M, et al. Ann Med. 2025;57(1):2461670.
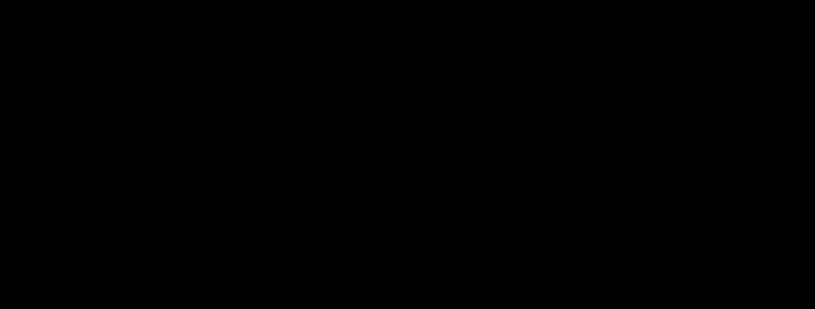
• Estimated prevalence of being virally suppressed was 19% higher at 90 days
• Using prior event rate ratio to account for unmeasured confounders, prevalence of viral suppression was 8% higher
– Increase in prevalence from 61% to 66%
– Among patients not on ART at buprenorphine initiation, the prevalence of viral suppression was 31%
N=279 adults with HIV from the Johns Hopkins HIV Clinical Cohort who initiated buprenorphine between 2002 to 2017 were identi fied using medical records. These patients were matched to 2422 patients who did not initiate buprenorphine.
Kim J, et al. Clin Infect Dis. 2021;73(11):1951-1956.
Walk-in access
Removes central barrier
• All visits available without scheduled appointments
Integrated care team with case managers
Incentives
Low-barrier care philosophy
Multisector coordination
Addresses social needs
Commitment to rapid modification
Provides tangible reward and helps address immediate needs
Adapts care goals to reflect individual needs
Coordinates services with other agencies
• Case managers get to know patients as individuals
• Low caseload case management support
• Nonmedical case management
• Streamlined care and shortened visits
• Harm reduction approach to SUD
• Minimizing the number of medications, where possible
• Minimizing specialty referrals as clinic takes a larger role
• Creating specialty network willing to see patients on a walk-in basis
• Housing agencies
• Jail release planners
• Adherence support programs
• SUD treatment programs
• Behavioral health programs
Requires continual improvements to optimize care
Dombrowski JC, et al. Clin Infect Dis. 2023;77(2):252-257.
• Iterative improvements based on experience
• Patient and staff feedback incorporated
• Able to abandon plans that don’t work
• Acceptance that policies require flexibility on case-by-case basis
• Examine enablers of and barriers to integrated service access
– Competing priorities, challenges in social determinants of health, previous experience accessing health care, support and peer navigators, convenience
• Clinician knowledge and skills in both HIV and SUD treatment
• Good patient-clinician relationship
• Patient engagement between appointments
• Designated member to be the “champion” for their center
. 2022;79(5):618-639.
• Acknowledge financial barriers, including insurance, reimbursement challenges, and patient out-of-pocket costs
• Have a referral system in place, case management, counseling, appointment reminders, medication administration, and monitoring protocols
• Address stigma

• Federal and state policies, legislation, and funding that support care integration are the foundation that will make colocated care possible
• HIV and SUD treaters can work with advocacy organizations
• Testimonials can be given at the local, state, or federal level
• HIV is a chronic disease, and patients can live a normal life
• Rapid ART will help achieve viral suppression in a timely manner and can be initiated in nearly every patient
• Patients should be educated about U=U
• PWH and SUD face stigma from numerous directions, and treaters and staff should be educated about addressing stigma
• Linking with low barrier to care HIV clinics will improve linkage to and retention in care
• Colocated services can improve both HIV and SUD outcomes