Odze, Robert D, and John R Goldblum. Odze and Goldblum’s Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas. Fourth edition. Philadelphia, PA: Elsevier, 2023. p1360.
Liver tissue processing
• Immunohistochemistry:
• Viral antigens : HBsAg, HBcAg, HDV, HCV
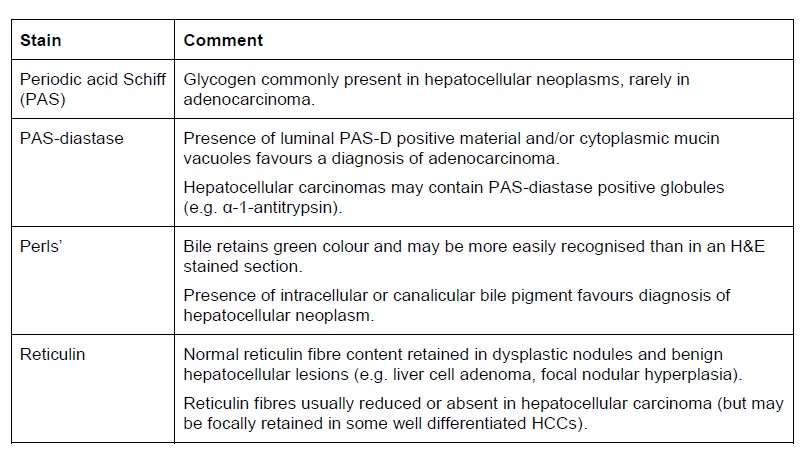
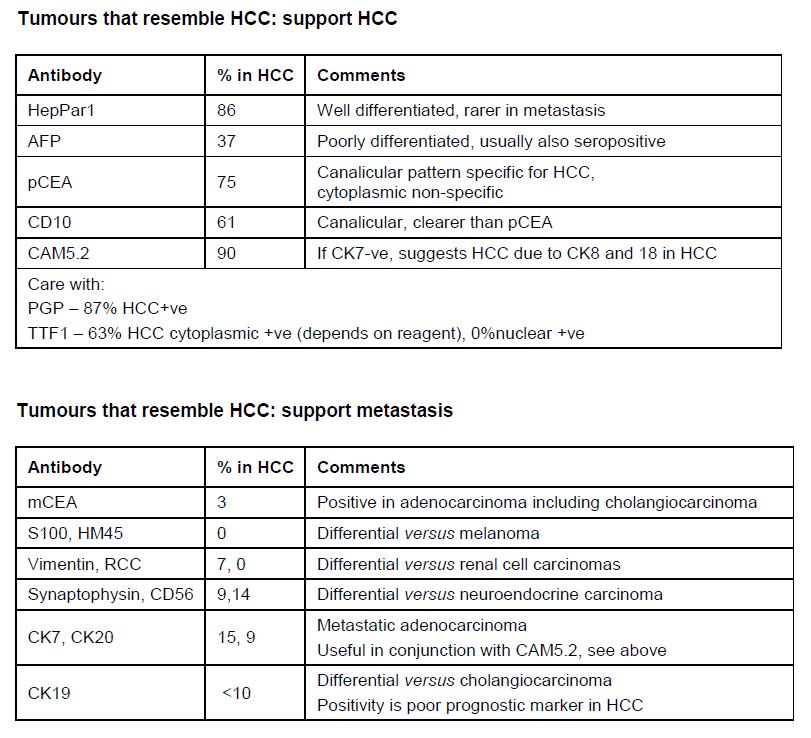
• ID and classification of tumours: HepPar1, AFP, p and mCEA, Glypican-3, Glutamine synthetase, MOC-31, CKs, CD68, SAA
• Storage and hereditary disease: α1-antitrypsin, fibrinogen
Odze, Robert D, and John R Goldblum. Odze and Goldblum’s Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas. Fourth edition. Philadelphia, PA: Elsevier, 2023. p1360.
Hepatitis B antigens
Hepatitis - risks
• Following a single hollow needle stick innoculum :-
• HIV – 0.9 %
• Hep B – 30 %
• Hep C – 3 %
• Wearing gloves reduces risk by x 10 – 100
• Mucous membrane or broken skin splashrisk is 0.09% for HIV, higher for Hep B
Liver
tissue processing
• Electron microscopy: storage diseases
• Molecular studies:
• In Situ Hybridisation: Viruses
• PCR: ID micro-oragnisms
• Laser capture microdissection
• Gene array analysis
Odze, Robert D, and John R Goldblum. Odze and Goldblum’s Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas. Fourth edition. Philadelphia, PA: Elsevier, 2023. p1360.
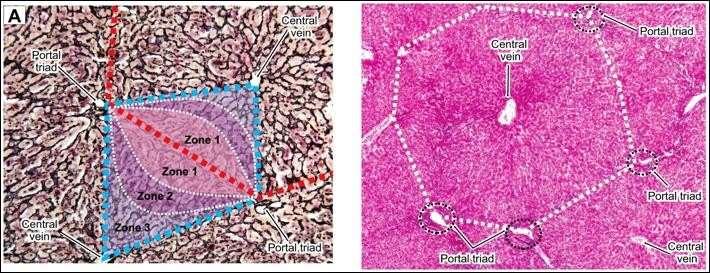
Normal liver anatomy & histology
Approach to liver disease
• Medical liver biopsy:
• Hepatitis: confirm diagnosis of chronic hepatitis, assess inflammatory (grade) and fibrosis (stage)
• Identify background pathology, may be cause (virus, alcohol)
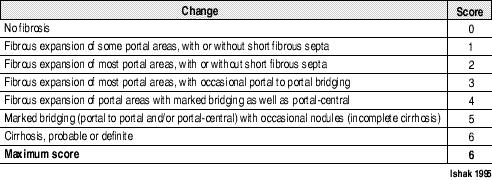
Ischak scoring in hepatitis
Patterns of liver injury
• Cholestatic
• Hepatocellular necrosis
• Fatty liver disease
• Fibrosis and cirrhosis
• Granulomas
• Vascular lesions
• Neoplasms
Kumar, Vinay, Abul K Abbas, and Jon C Aster. Robbins & Cotran Pathologic Basis of Disease. Tenth edition. Philadelphia, PA: Elsevier, 2021. p836.
Hepatobiliary topics
• Infectious disorders
• Auto-immune hepatitis
• Drug- and toxininduced liver injury
• Fatty liver disease
• Inherited liver disease
• Cholestatic disease
• Circulatory disorders
• Hepatic disease associated with pregnancy
• Nodules and tumours
• Gallbladder: stones, -it is, carcinoma
Kumar, Vinay, Abul K Abbas, and Jon C Aster. Robbins & Cotran Pathologic Basis of Disease. Tenth edition. Philadelphia, PA: Elsevier, 2021. p836.
Infectious disorders
• Hepatitis viruses (table and key concepts in Robbins): type of virus, route, incubation period, frequency of chronic liver disease, diagnosis
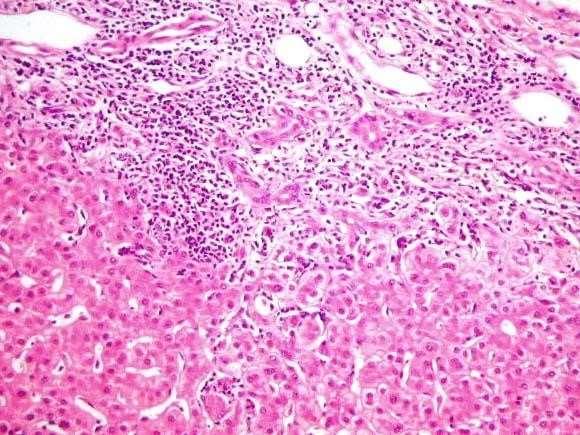
• Morphologic features of acute and chronic hepatitis
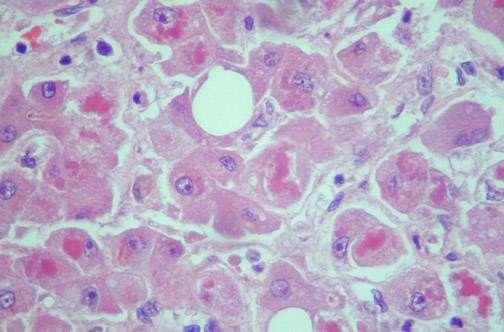
• Chronic hep B: ground-glass appearance, IHC
• Chronic hep C: prom lymphoid aggregates/follicles in portal tracts, steatosis (genotype 3), bile duct injury
• Other infections: hydatid cyst, schistosomiasis, TB
Kumar, Vinay, Abul K Abbas, and Jon C Aster. Robbins & Cotran Pathologic Basis of Disease. Tenth edition. Philadelphia, PA: Elsevier, 2021. p836.
Drug- and toxin-induced liver injury
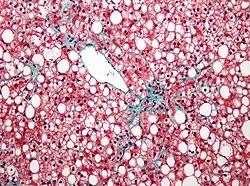
• Alcoholic liver disease
• Steatosis
• Alcoholic steato-hepatitis
• Fibrosis
Kumar, Vinay, Abul K Abbas, and Jon C Aster. Robbins & Cotran Pathologic Basis of Disease. Tenth edition. Philadelphia, PA: Elsevier, 2021. p843
Inherited liver disease
• Haemochromatosis
• Wilson disease
• α1-antitrypsin
Cholestatic disease
• PBC: Middle ages female, granulomas and lymphocytic infiltrates in portal tract
• PSC: Assoc with IBD more UC, less CD
Circulatory disorders
• Impaired blood flow into and through the liver
• Hepatic venous outflow obstruction
• Passive congestion and centrilobular necrosis
• Autopsy
• Clinical scenario
Hepatic disease associated with
pregnancy
• Pre-eclampsia and eclampsia
• Acute fatty liver of pregnancy
• Intrahepatic cholestasis of pregnancy
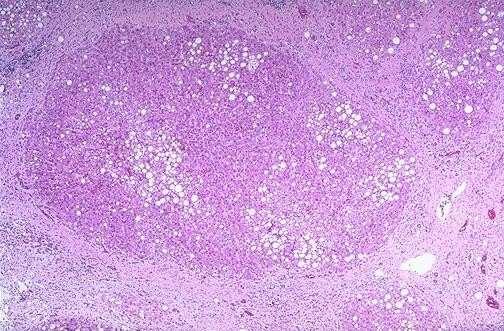
Hepatic nodules and tumours
• Focal nodular hyperplasia
• Nodular regenerative hyperplasia
• Cirrhosis
• Adenoma
• Hepatocellular carcinoma
• Metastasis
Gallbladder: stones, -it is, carcinoma
• Cholelithiasis
• Cholcystitis
• Gallbladder carcinoma:
• Porcelain gallbladder
Paediatric hepatobiliary pathology
• Neonatal cholestasis:
• Extrahepatic biliary atresia
• Reye’s syndrome
• Cystic fibrosis
• Structural anomalies of the biliary tree
• Choledochal cyst
• Fibropolycystic disease
Pancreas
• Non neoplastic cysts
– Pseudocysts
– Lymphoepithelial cysts
– Retention cysts
– Enterogenous cysts
– Parasitic cysts
– Endometrial cysts
• Neoplastic cysts
– Serous cystic neoplasm
– Mucinous cystic neoplasm
– Intraductal mucinous neoplasm
– Solid-cystic pseudopapillary neoplasm
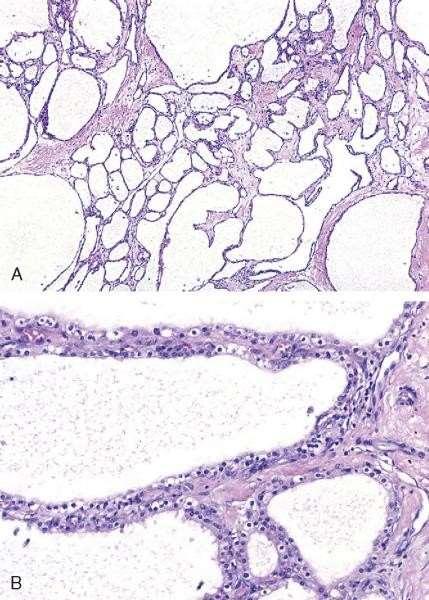
Serous cystadenoma
• Most common type of cystic
• Body, tail
• Predominantly in females
neoplasm
Serous cystadenoma
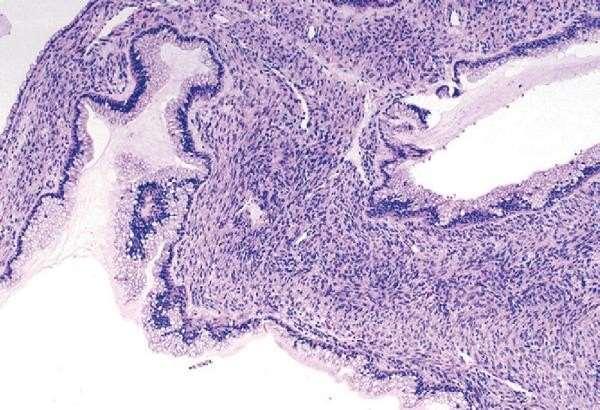
Mucinous cystadenoma
• Macrocystic
• Almost exclusively in females
• Tail
• Pathology: mucinous glands and ovarianlike stroma
Mucinous cystadenoma
EMQ
• Match the findings of liver biopsy with the correct diagnosis.
• A IVDU, interface hepatitis, orcein granules in hepatocytes
• Answer: Hepatitis B
• B Female with biopsy showing numerous plasma cells within the portal tracts
• Answer: Autoimmune hepatitis
EMQ
• C Middle aged female with biopsy showing granulomas and lymphocytic infiltrates in portal tract
• Answer: Primary biliary cirrhosis
• D Man with history of alcohol excess. Macro and microvesicular steatosis and Mallory bodies
• Answer: Alcoholic hepatitis
EMQ
• E Young patient with cirrhosis and diabetes. PERLs positive material in hepatocytes.
• Answer: Haemochromatosis
MCQ
• A 32 year old intravenous drug user is admitted to hospital with jaundice. An ultrasound demonstrates a cirrhotic liver.
• Identify the most likely cause.
• A Hepatitis B
• B Hepatitis C
• C HIV
• D Budd Chiari syndrome
• E Idiopathic
• (What is alcohol was in there?)
MCQ
• A 3 month old boy presents with progressive jaundice and pale stool. A liver biopsy shows ductular proliferation with accumulation of bile in the hepatocytes.
• Identify the most likely diagnosis.
• A Cholelithiasis
• B Hirschsprungs disease
• C Biliary atresia
• D Primary sclerosing cholangiitis
• E Primary biliary cirrhosis
MCQ
• A 52 year old alcohol dependent male is found dead at home. At autopsy he has a fatty liver but no cause of death is found. Toxicology shows a blood alcohol level of zero but elevated butyric acid levels.
• Identify the correct cause of death
• A Gastrointestinal haemorrhage
• B Cirrhosis of the liver
• C Alcohol related ketoacidosis
• D Acute intoxication of alcohol
• E Aspiration pneumonia
MCQ
• A 3 year old child presents with a febrile illness. They are prescribed aspirin. They represent 6 days later with liver failure.
• Identify the most likely change seen on liver biopsy.
• A Fatty change
• B Centrilobular necrosis
• C Ductular proliferation and bile accumulation
• D Interface hepatitis
• E Cirrhosis
MCQ
• GIST IHC
• Colorectal TNM staging
• Cystic fibrosis gene product – Chloride channel
• Zones of liver
• IVDU with varices - ?test (Hep C)
• Suspicious of GIST – CD117 negative ?other IHC (DOG1 or CD34)
MCQ
• Baby born to type 1 diabetic mother becomes hypoglycaemic soon after birth.
Why?
– Islets continue to produce increased insulin
• Child with recurrent chest infection and failure to thrive. Diagnosis?