Tumours most commonly but not uniquely encountered in the head and neck
Sinonasal tract
Head and Neck
Minimum Datasets / cancer questions
Oral cavity / hypopharynx / larynx
Question 1
Special stains / immunos
Q1: Identify the special stain / immunochemical antibody which would aid in diagnosis for each case:
CD1a CD45
S-100 DPAS
CD68 p16
Synaptophysin EBV ISH
Ziehl Neelson GFAP
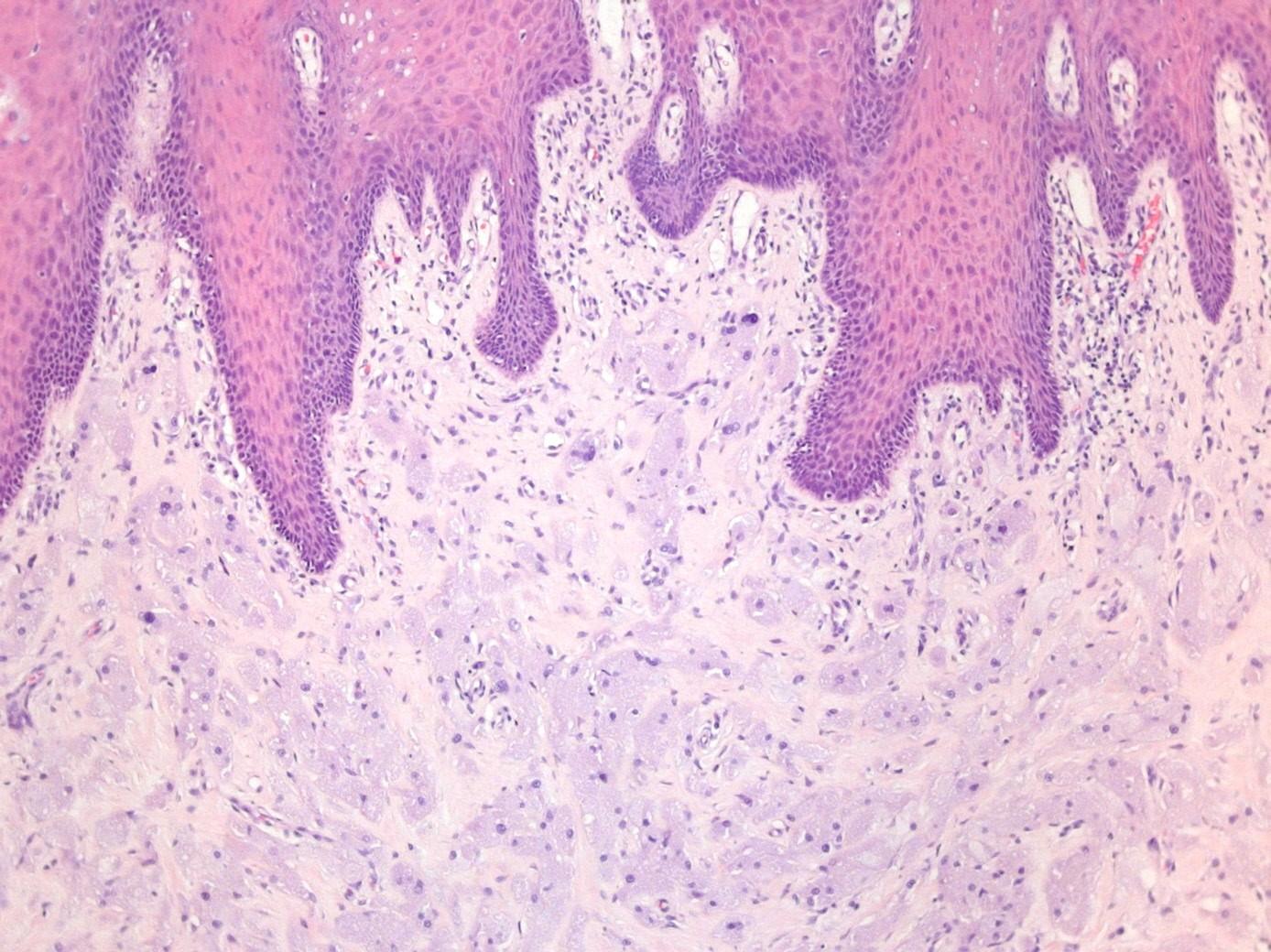
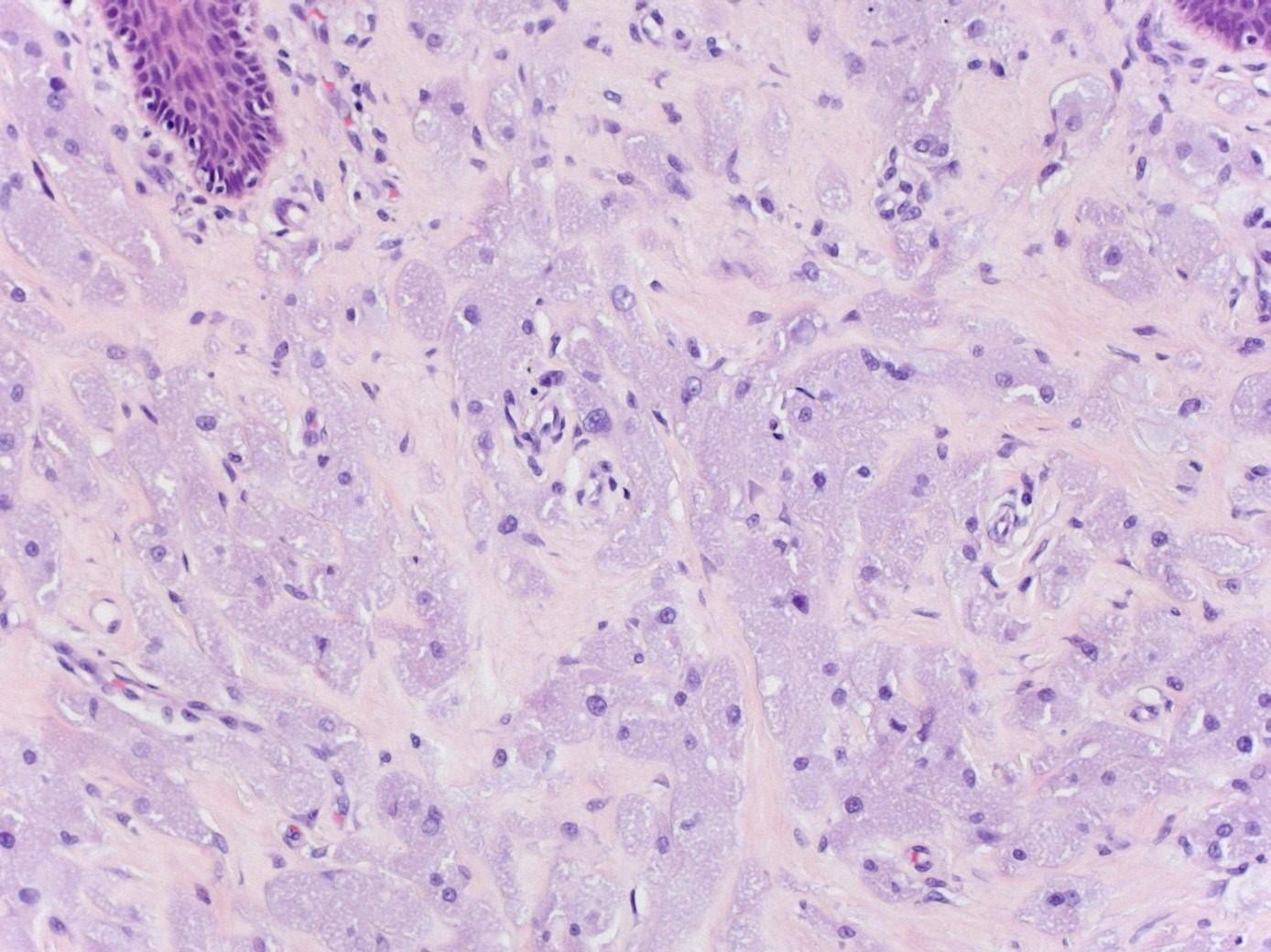
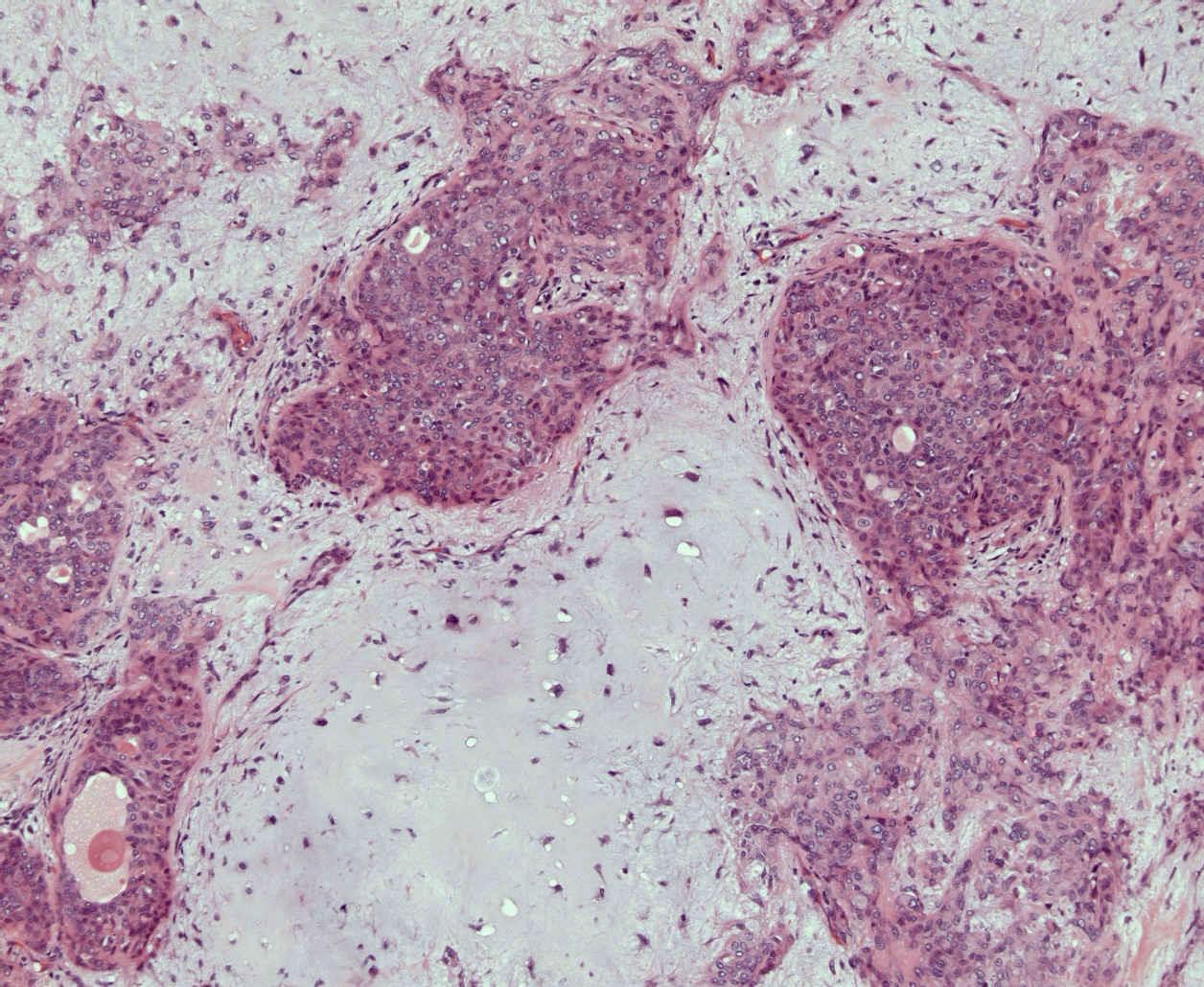
1. A 37 year old female presents with a polyp on the tongue which is excised. The H and E stained section shows sheets of plump polygonal cells with abundant eosinophilic granular cytoplasm filling the lamina propria.
Options:
CD1a CD45
S-100 DPAS
CD68 p16
Synaptophysin EBV ISH
Ziehl Neelson GFAP
Granular cell tumour
Differential diagnosis of lumps and bumps on tongue
Fibroepithelial polyp
Chronic oral candidiasis Viral wart
Minor salivary gland tumour
SCC
Granular cell tumour
Granular cell tumour
Previous names include granular cell myoblastoma
Most common non-epithelial benign tumour
50% of Head and Neck Cases
Tongue, larynx
Schwannian origin S100 positive
Granular cell tumour
Infiltrative growth pattern
Eccentric small bland nuclei
Abundant granular cytoplasm
Indistinct cell boundaries
Pseudoepitheliomatous hyperplasia
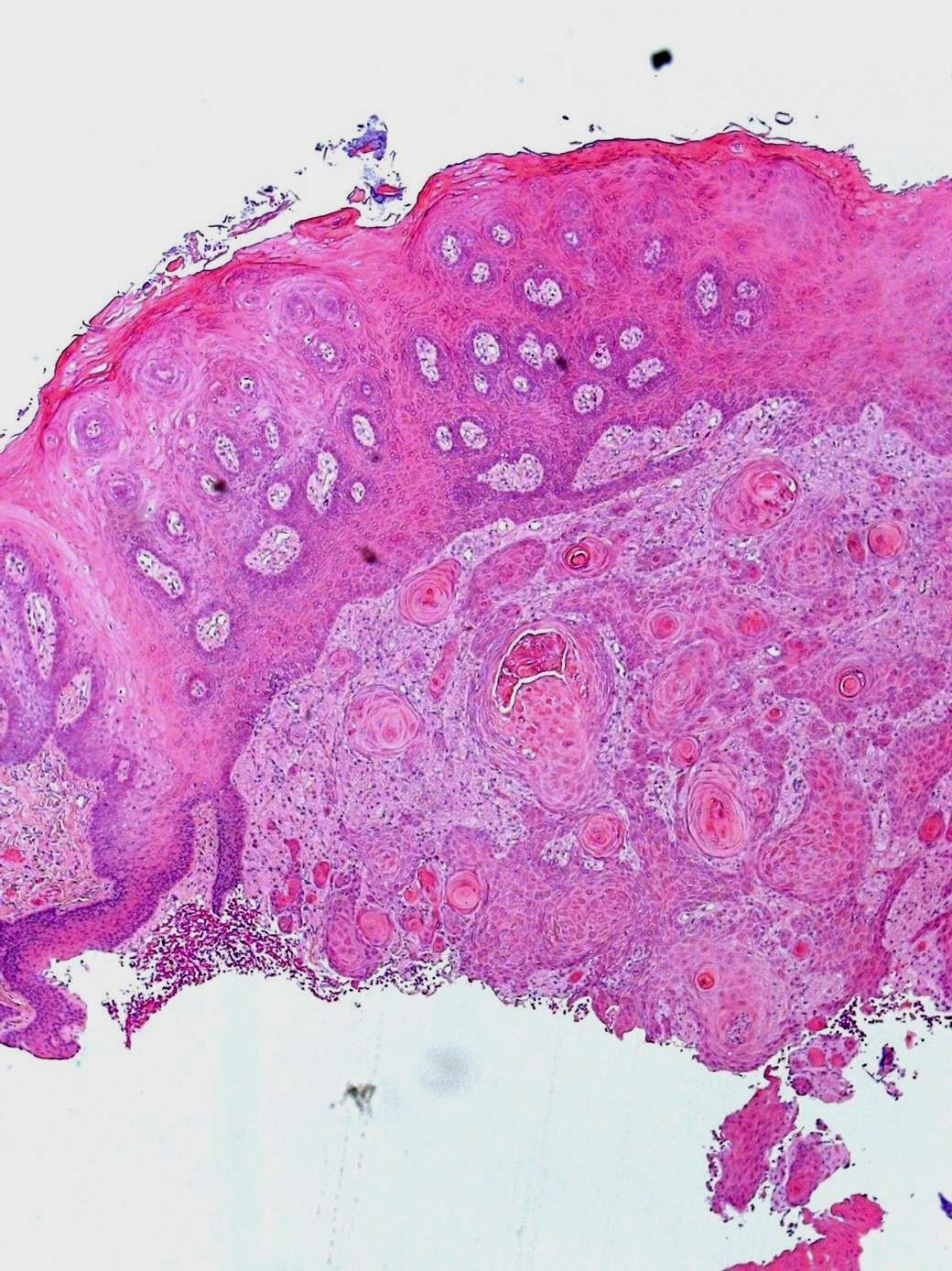
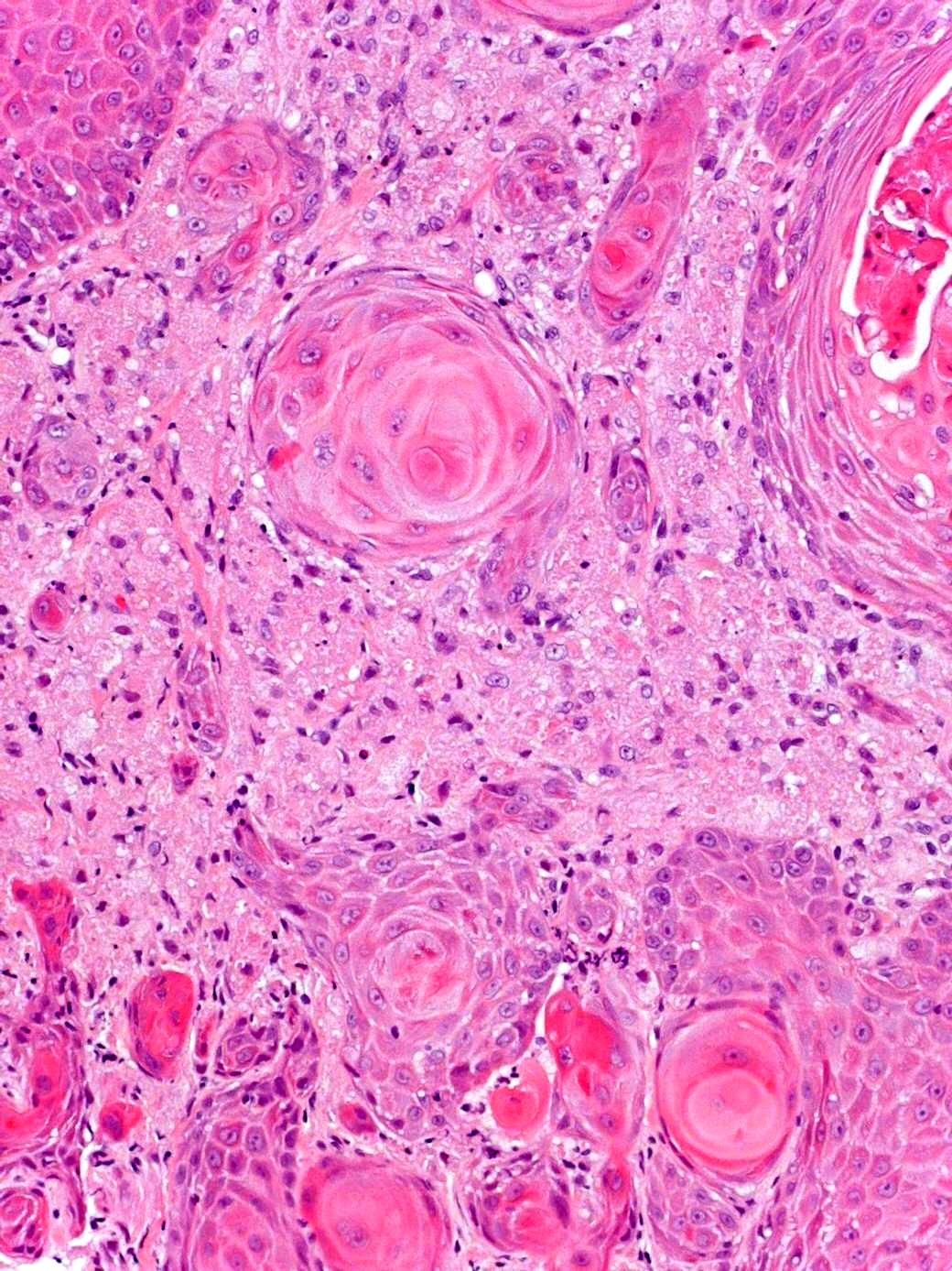
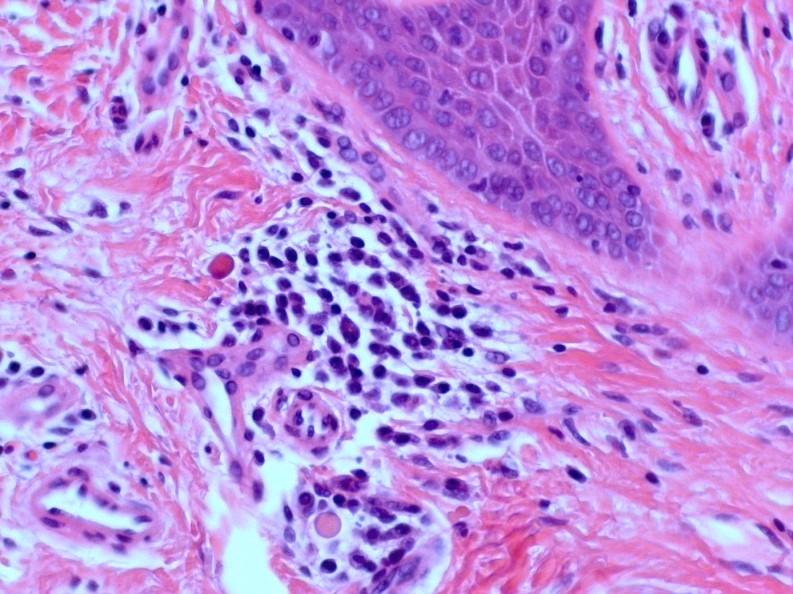
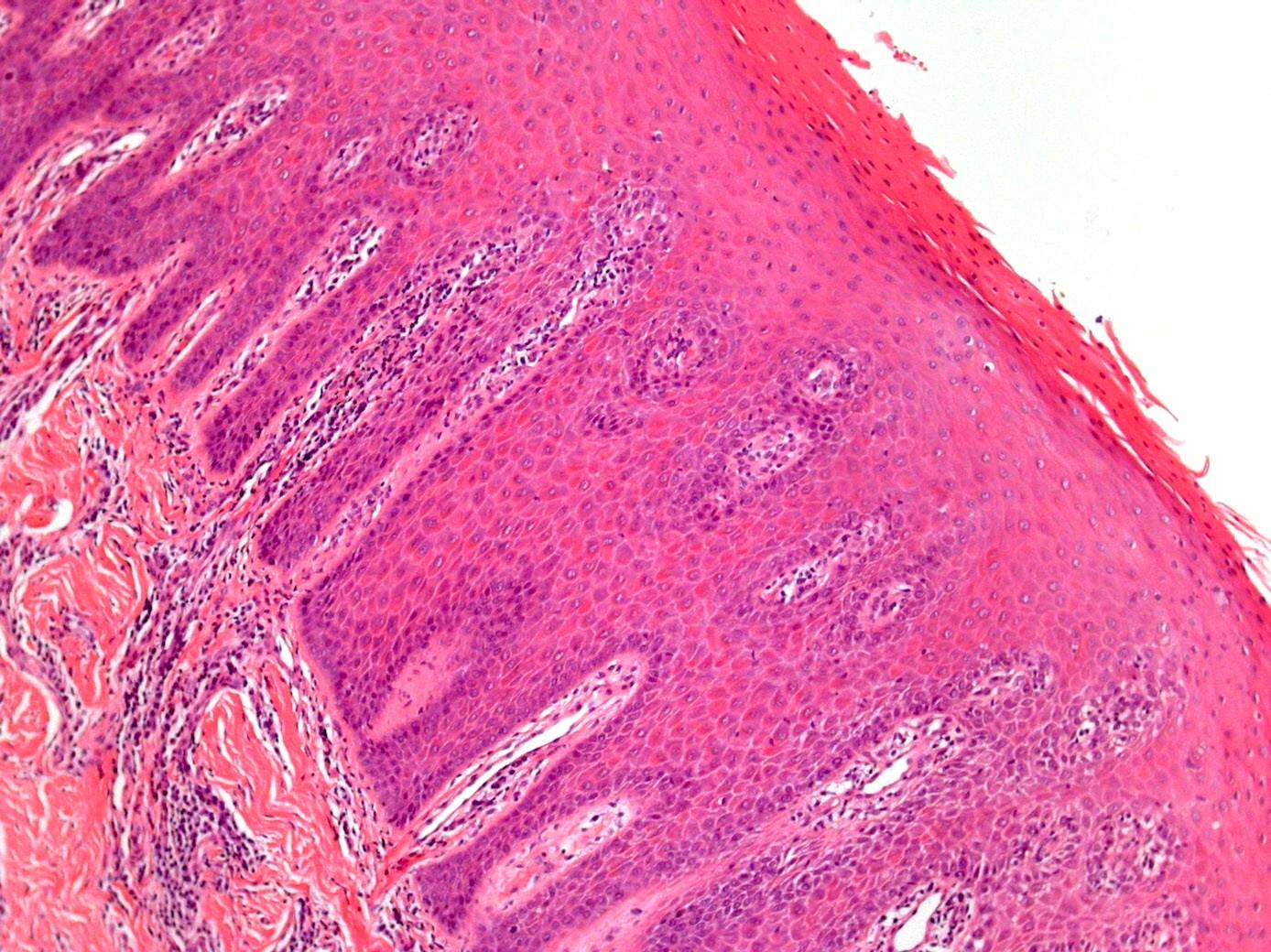
2. A 75 year old female undergoes incisional biopsy of a mixed red and white plaque on the tongue. There is some irregular pseudoepitheliomatous hyperplasia of the epithelium and mild atypia. Aggregates of neutrophils are readily detected in the surface parakeratin.
Options:
CD1a CD45
S-100 DPAS
CD68 p16
Synaptophysin EBV ISH
Ziehl Neelson GFAP
Pseudooepitheliomatous hyperplasia
Chronic hyperplastic candidiasis
Psoriasiform hyperplasia
Plasma cells
Neutrophilic microabscesses
PAS or PASD to look for hyphae
Usually some reactive keratinocyte atypia and often overcalled dysplasia
PAS
Similar appearances seen in benign migratory stomatitis aka geographic tongue
No candida will be found
Psoriasiform hyperplasia
+++ neutrophilic abscesses
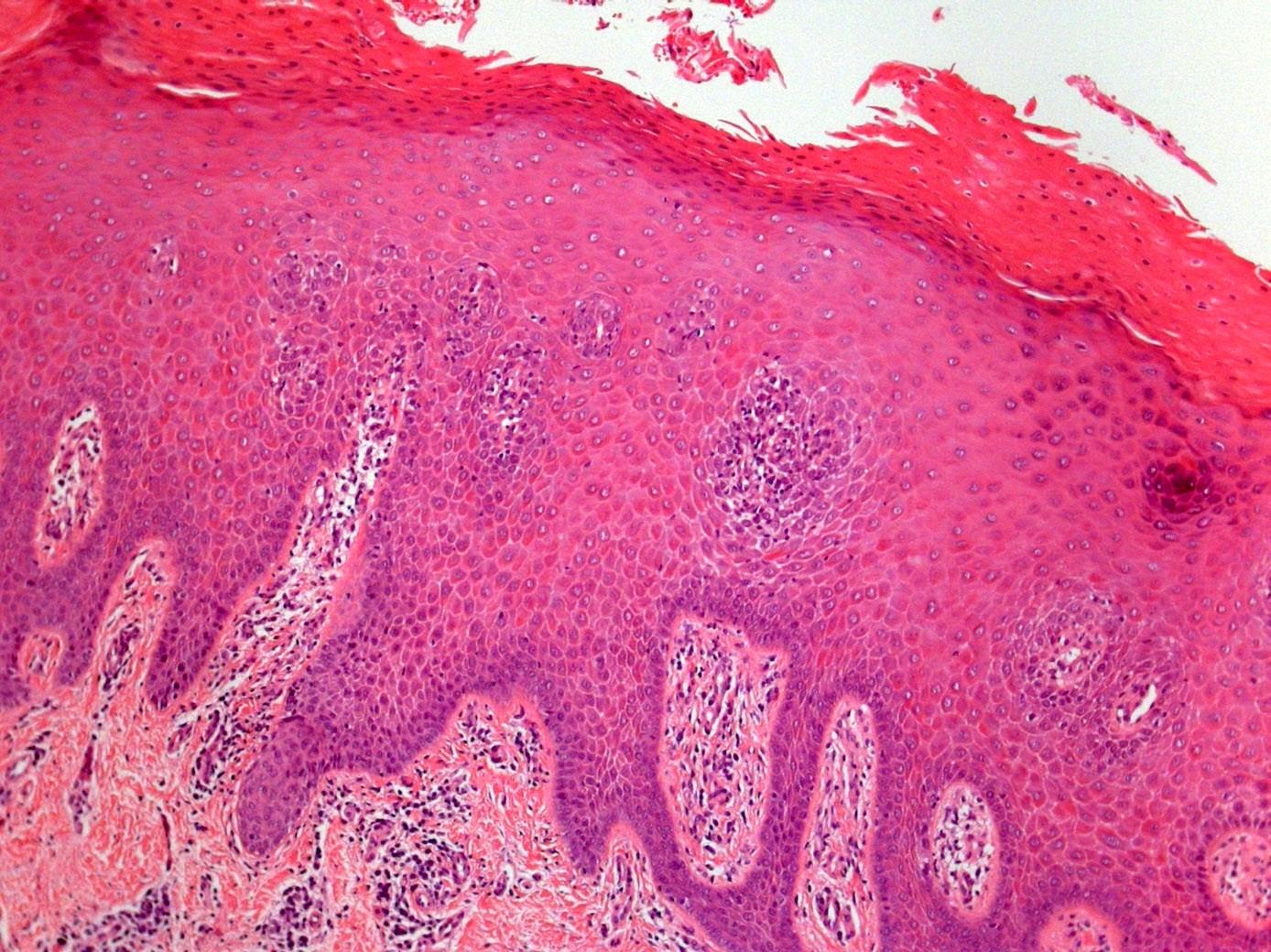
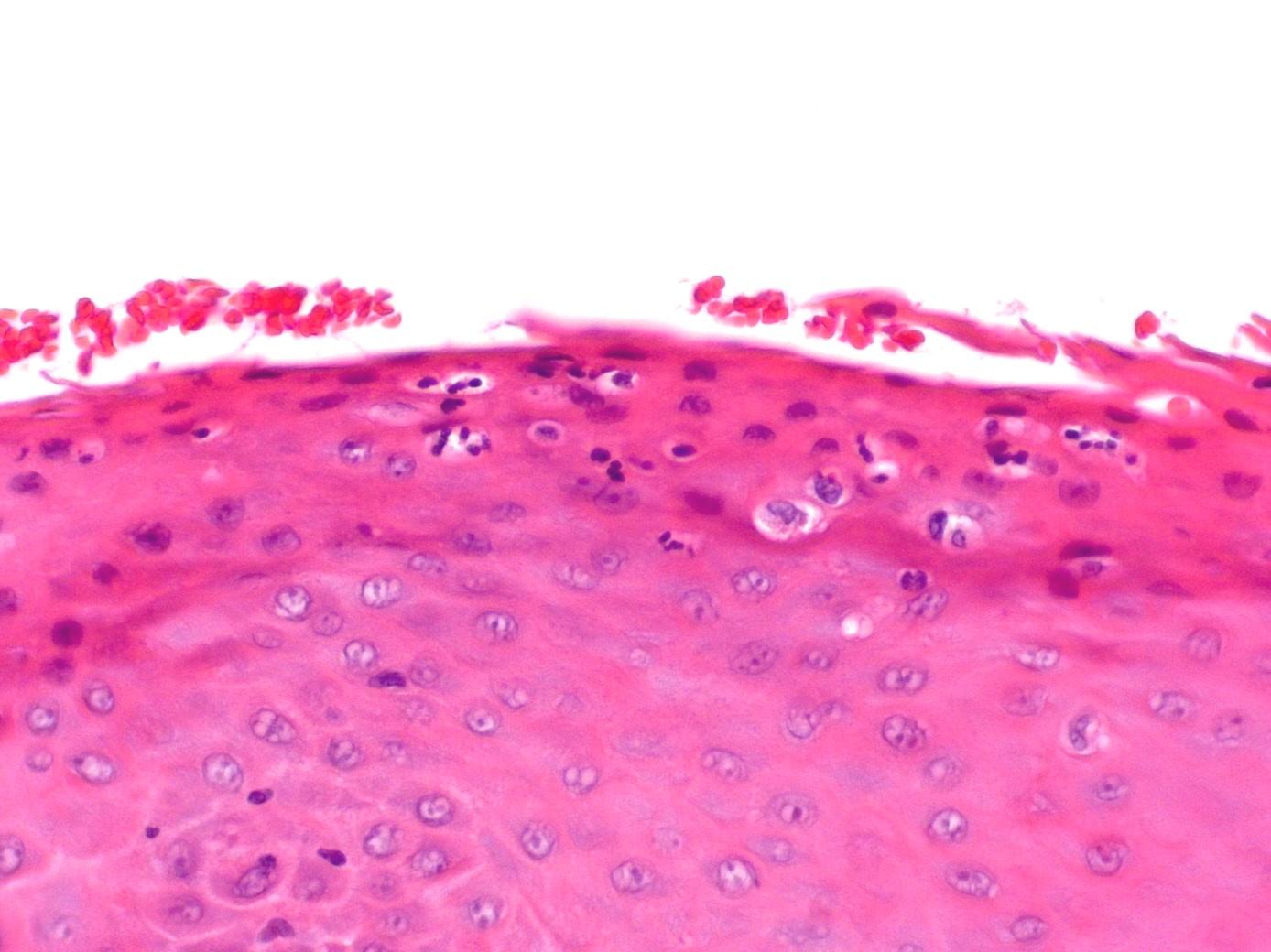
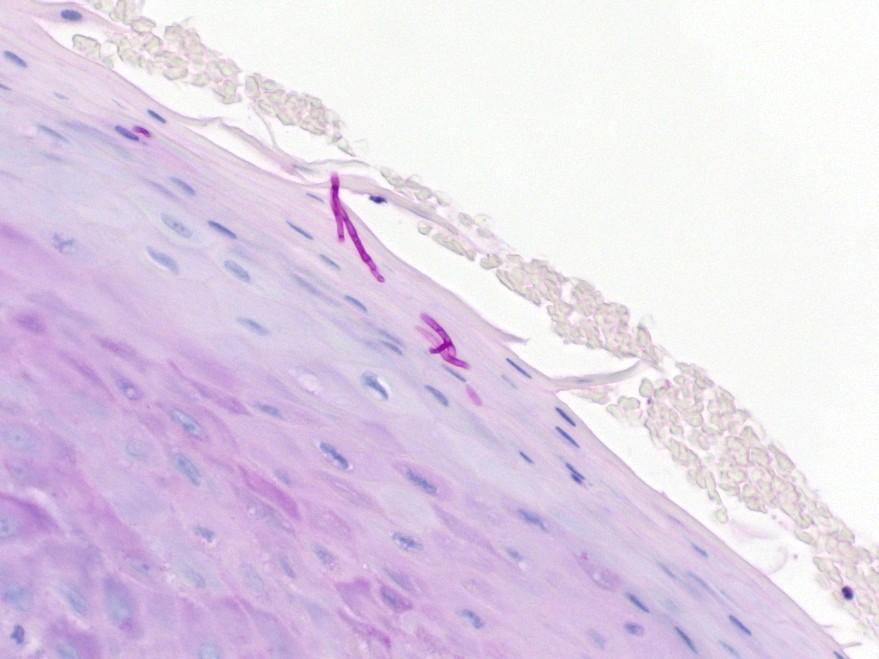
3. A 30 year old male undergoes biopsy of a white patch on the lateral border of the tongue. Histological examination shows parakeratosis and a band-like layer of cells with clear cytoplasm in the upper stratum spinosum.
Options:
CD1a CD45
S-100 DPAS
CD68 p16
Synaptophysin EBV ISH
Ziehl Neelson GFAP
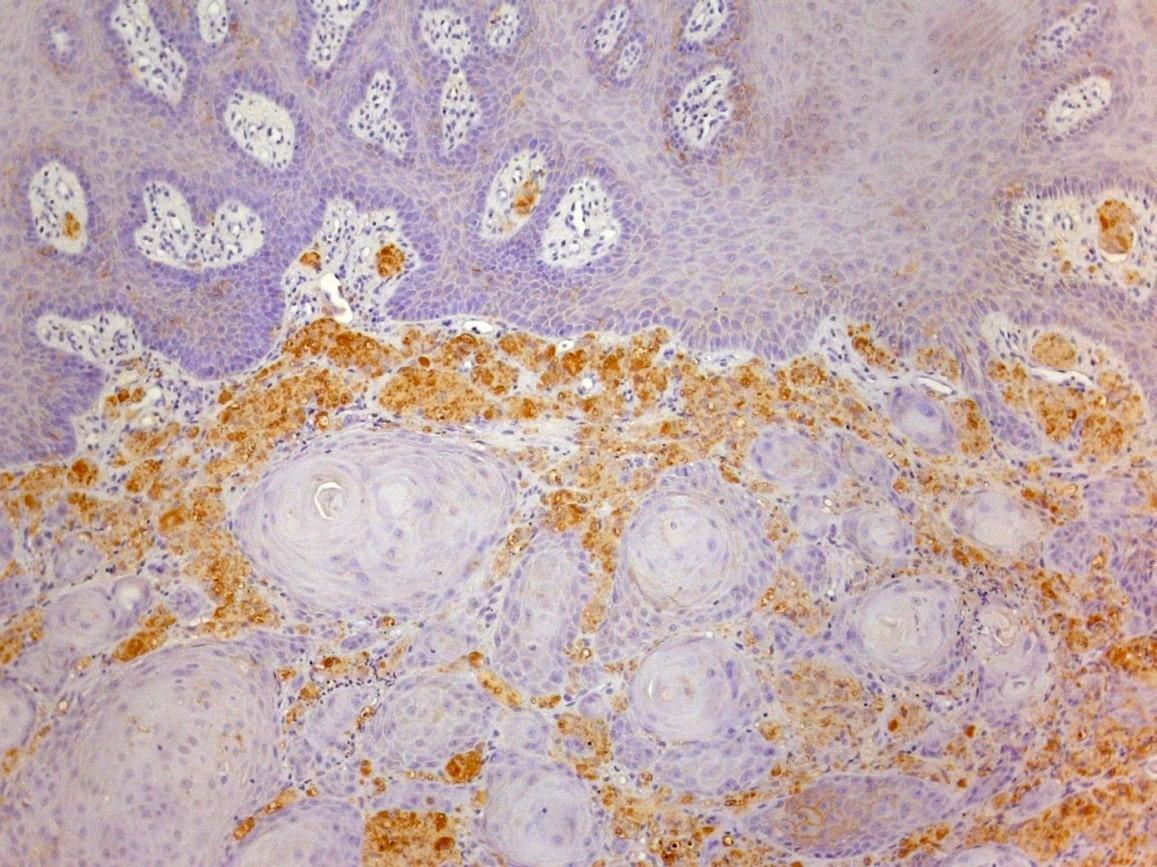
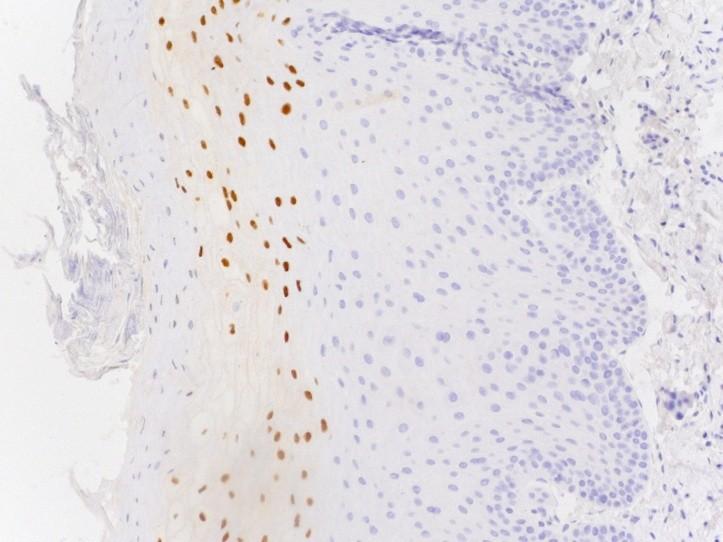
Hairy leukoplakia
Classical histological appearances
Often candida +++ but lack of inflammation
Band of clear cells classical
Should confirm diagnosis by EBV immuno’ or ISH
Pathognomonic of HIV
4. A 45 year old oriental male presents with an enlarged cervical lymph node and on pan-endoscopy is found to have a mass in the nasopharynx.
5. An 8 year old male presents with premature loosening of deciduous molars on the lower left side and an osteolytic lesion is seen on plain X-ray. Curettings show sheets of mononuclear cells with oval nuclei admixed with clusters of eosinophils.
Options:
CD1a CD45
S-100 DPAS
CD68 p16
Synaptophysin EBV ISH
Ziehl Neelson GFAP
Langerhan’s cell histiocytosis
Childhood mainly
Head and Neck: middle ear and jaw
Osteolytic punched out lesions
Unifocal, multifocal
Oval reniform nuclei with grooves or folds
Eosinophils
CD1a (also S-100 positive)
DD: other histiocytic proliferations, HL
Question 2
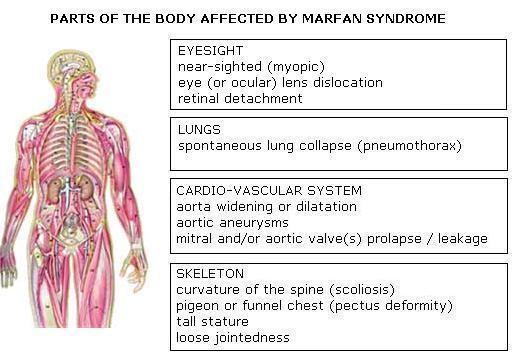
Syndromes
Many syndromes present with signs in the head and neck region. Match the syndrome to the clinical description:
Neurofibromatosis type 2
Fanconi’s anaemia
Gardners syndrome
Down’s syndrome
Albrights syndrome (McCune-Albright)
Osteogenesis imperfecta
Gorlin Goltz syndrome
MEN2b
Cowdens syndrome
Plummer-Vinson syndrome
1. A 21 year old male who on a routine dental X-ray was found to have bilateral multilocular jaw cysts and also on further examination, a pearly plaque with central telangiectasia on the forehead
Neurofibromatosis type 2
Fanconi’s anaemia
Gardners syndrome
Down’s syndrome
Albrights syndrome (McCune-Albright)
Osteogenesis imperfecta
Gorlin Goltz syndrome
MEN2b
Cowdens syndrome
Plummer-Vinson syndrome
Odontogenic keratocyst
Officially now a tumour (WHO 2005)
In syndrome: multiple and earlier onset than sporadic and greater tendency to recur
Is the only odontogenic cyst to keratinize
Basal cell palisading and corrugated surface typical
Satellite and daughter cysts more prevalent in syndromic patients
2. A 60 year old female with long standing dysphagia and anaemia undergoes pharyngo-laryngectomy for a post-cricoid (hypopharyngeal) squamous cell carcinoma
Neurofibromatosis type 2
Fanconi’s anaemia
Gardners syndrome
Down’s syndrome
Albrights syndrome (McCune-Albright)
Osteogenesis imperfecta
Gorlin Goltz syndrome
MEN2b
Cowdens syndrome
Plummer-Vinson syndrome
Soft tissue in continuity ND
Upper aerodigestive tract SCC
Mostly associated with alcohol / tobacco
Nasopharyngeal already mentioned
Small proportion of patients never smokers and little to moderate alcohol intake
Fanconi anaemia
Other inherited disorders of DNA repair
Check it’s not pseudoepitheliomatous hyperplasia in a v young patient!!!
Plummer Vinson associated with post-cricoid ca (30-70% at this site have syndrome)
3. An 8 year old boy with multiple mucosal polyps especially around the lips and a fixed thyroid mass which is reported as probably malignant on cytology
Neurofibromatosis type 2
Fanconi’s anaemia
Gardners syndrome
Down’s syndrome
Albrights syndrome (McCune-Albright)
Osteogenesis imperfecta
Gorlin Goltz syndrome
MEN2b
Cowdens syndrome
Plummer-Vinson syndrome
MEN 2b
Adrenal phaeochromocytoma
Medullary carcinoma of thyroid
Multiple mucosal neuromas
Marfanoid bodies
AD –RET mutation
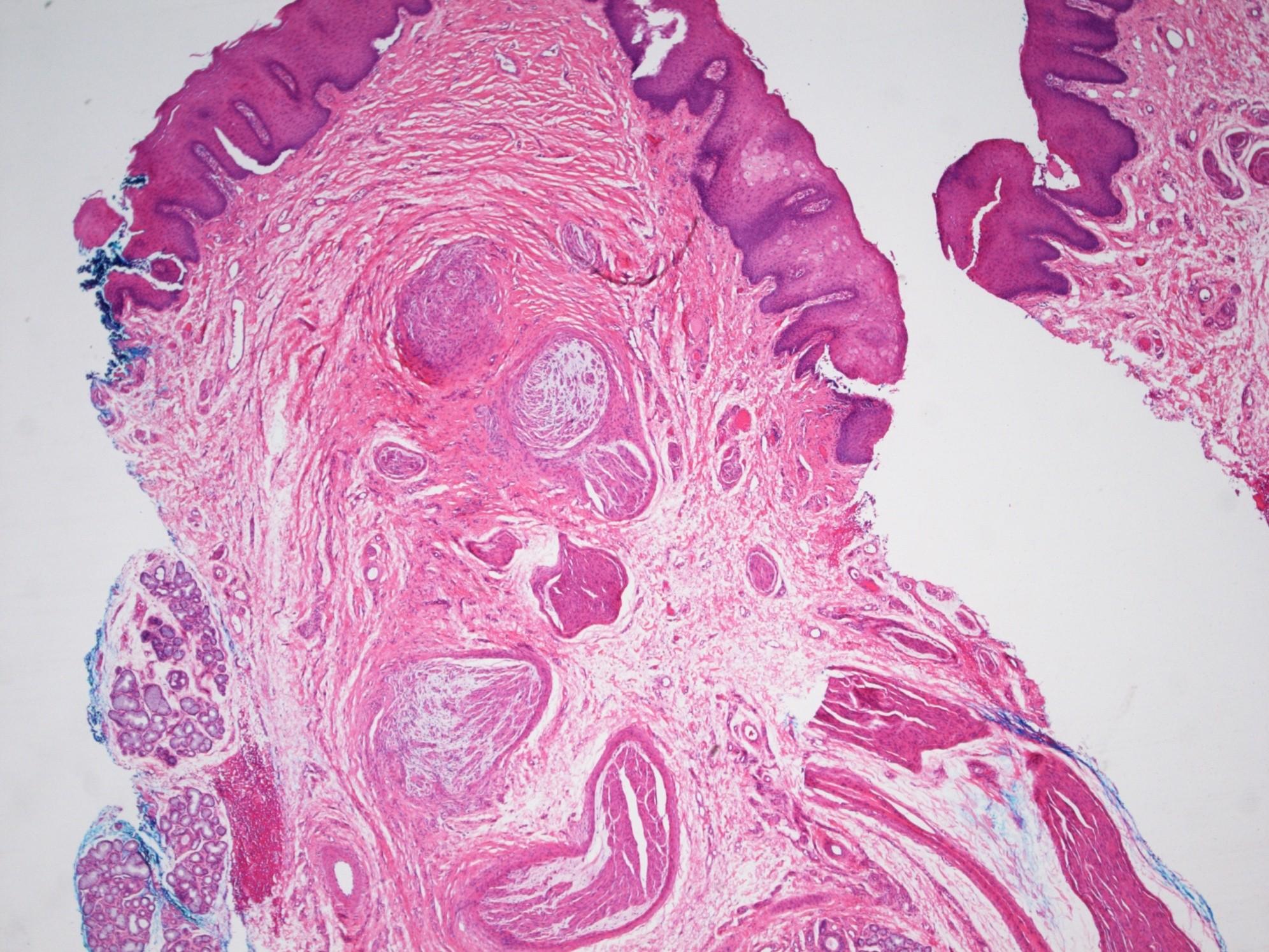
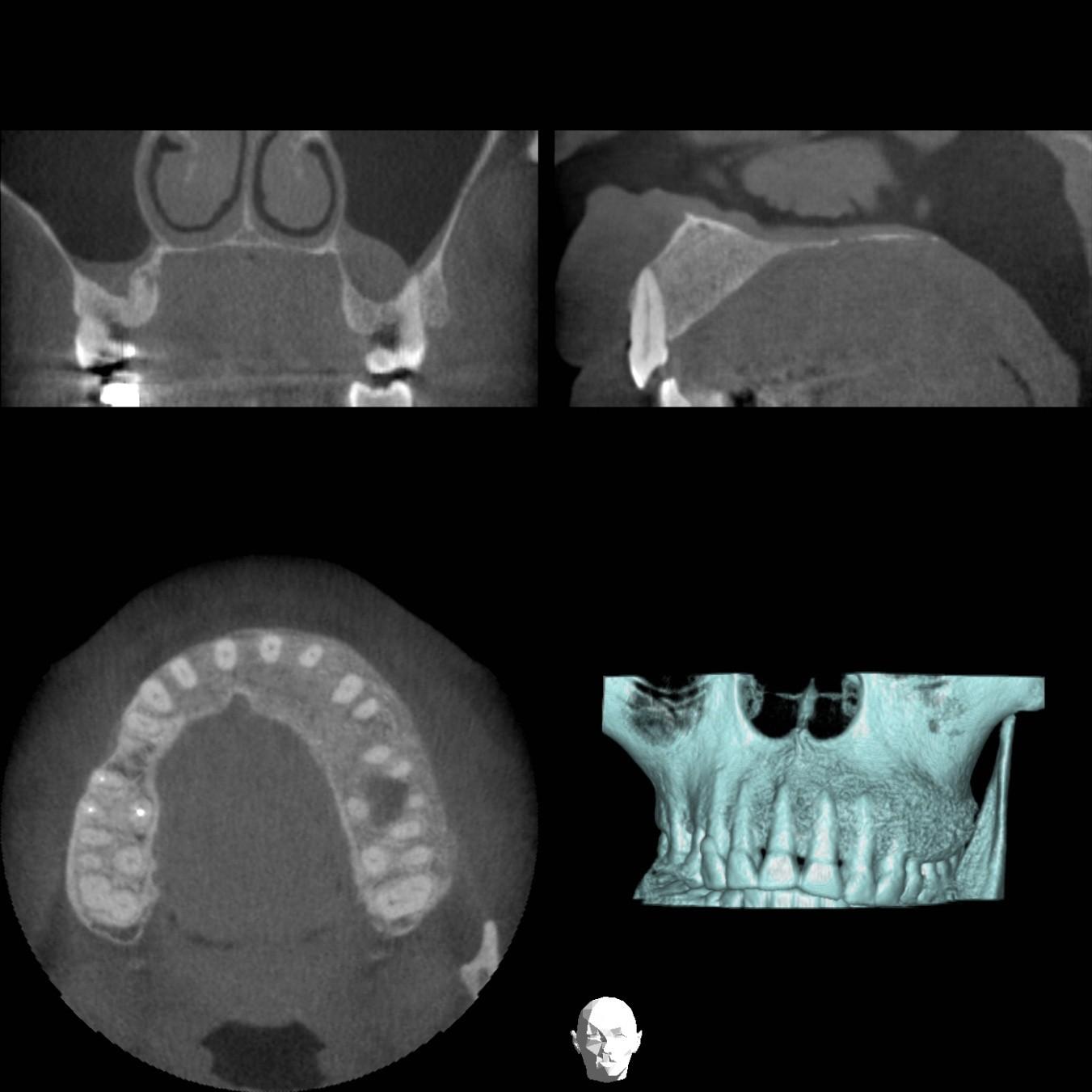
4. A 9 year old female with pigmented skin lesions, early onset of puberty and a painless unilateral swelling of the maxilla along with radiological abnormalities of the ribs and right femur.
Neurofibromatosis type 2
Fanconi’s anaemia
Gardners syndrome
Down’s syndrome
Albrights syndrome (McCune-Albright)
Osteogenesis imperfecta
Gorlin Goltz syndrome
MEN2b
Cowdens syndrome
Plummer-Vinson syndrome
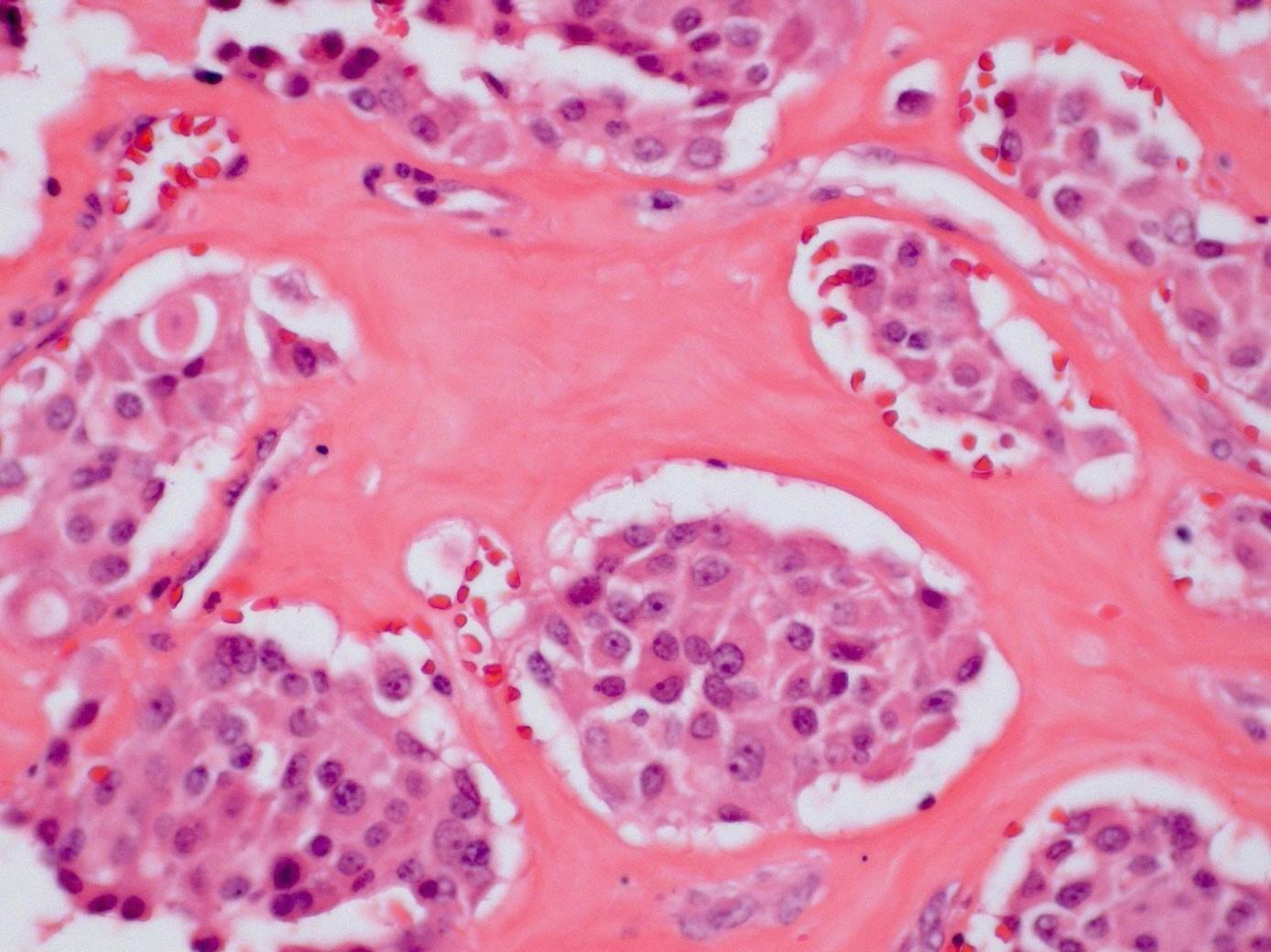
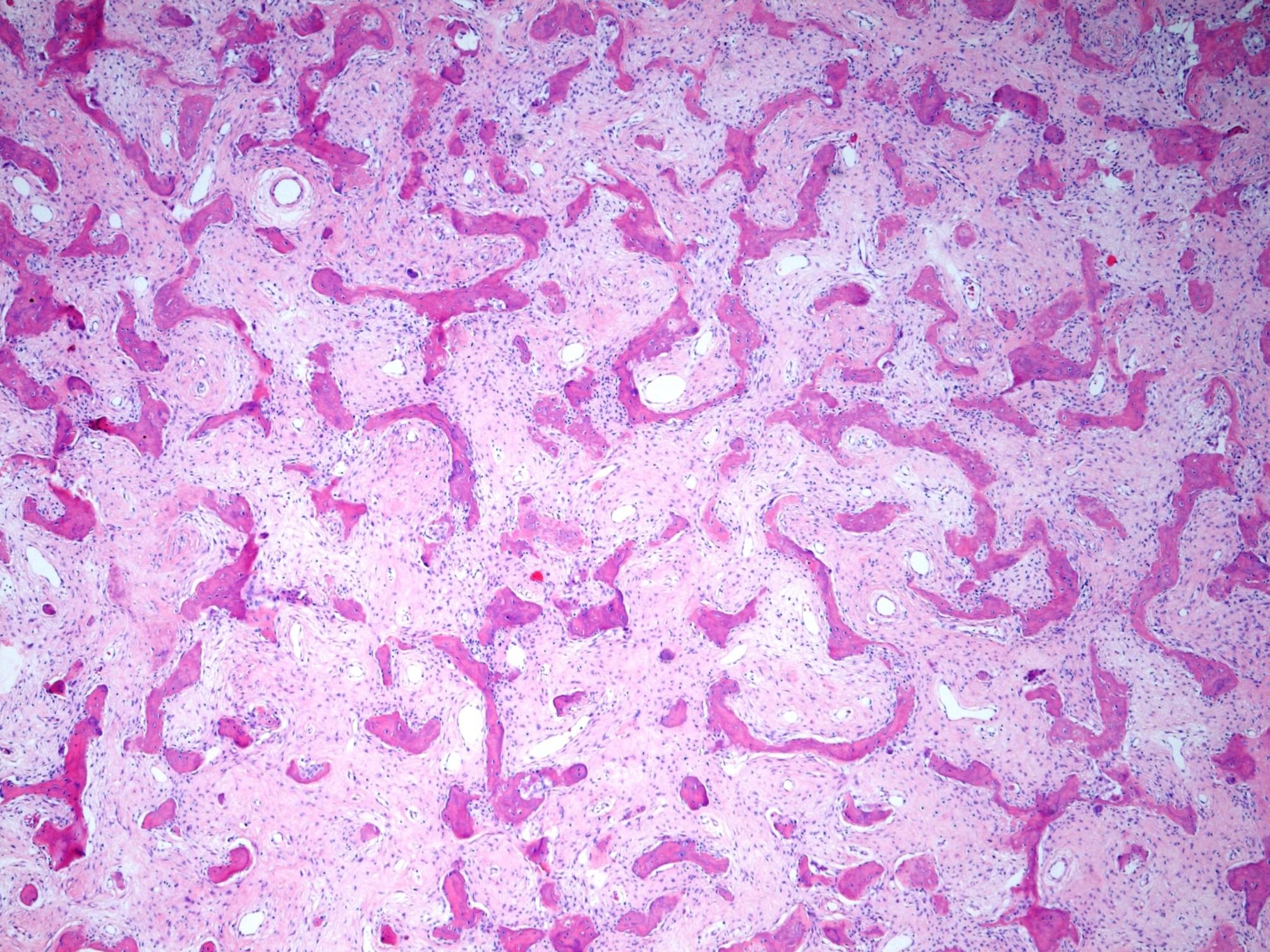
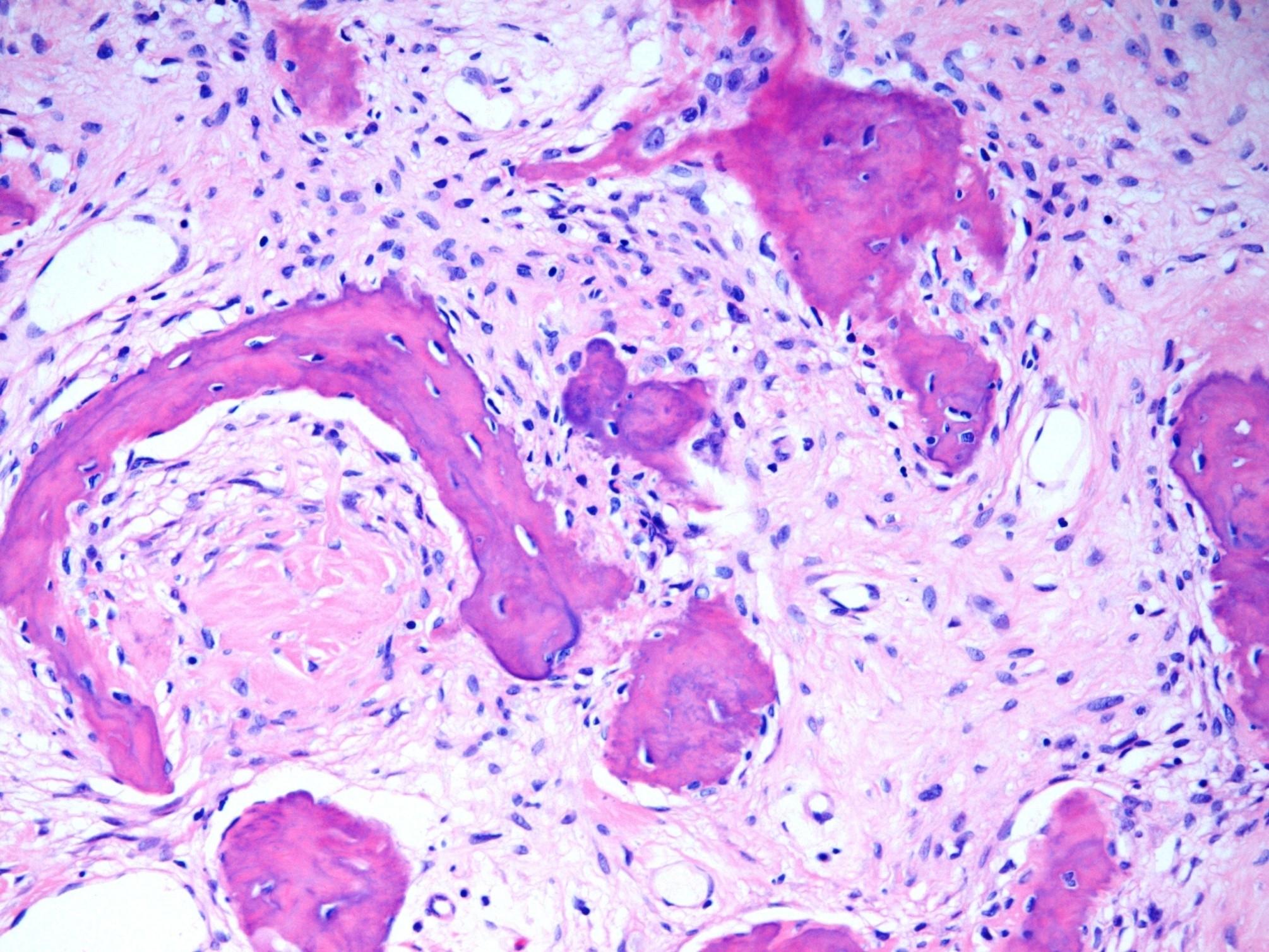
Albright’s syndrome / fibrous dysplasia
Expansion and replacement of bone by cellular fibroblastic tissue in which irregular trabeculae of woven bone are deposited
Tend to lack osteoblastic rimming and lesional bone merges with adjacent normal bone
Tumours most commonly but not uniquely encountered in the head and neck
Tumours most commonly (but not uniquely) encountered in the head and neck
Granular cell tumour
Adenomatoid odontogenic tumour
Adenoid cystic carcinoma
Acinic cell carcinoma
Squamous cell carcinoma
Ameloblastoma
Myoepithelioma
Polymorphous low grade adenocarcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
1. A 36 year old female with a multilocular radiolucency of the left body of mandible. Histology shows islands of epithelium composed of loosely cohesive cells centrally with peripheral palisading and reverse polarity
Granular cell tumour
Adenomatoid odontogenic tumour
Adenoid cystic carcinoma
Acinic cell carcinoma
Squamous cell carcinoma
Ameloblastoma
Myoepithelioma
Polymorphous low grade adenocarcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
Ameloblastoma
Most common odontogenic tumour (exc odontoma which is hamartomatous)
Wide age range
Benign but locally aggressive
Classical histological appearances
Peripheral palisading
Reverse polarity
Central stellate reticulum-like cells
Stellate reticulum like cells
like cells
Ameloblast
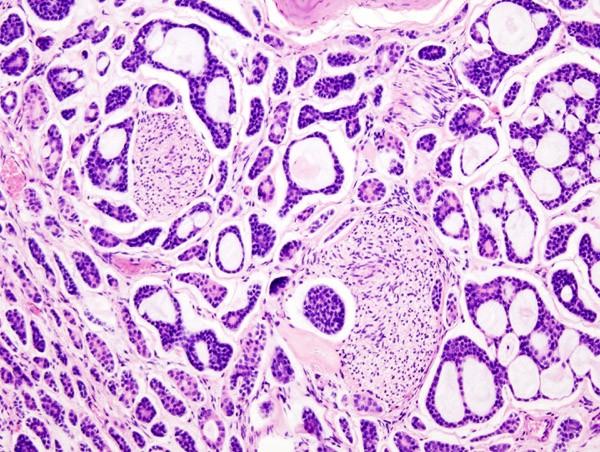
2. A 45 year old male has a biopsy of the floor of mouth swelling which consists of cribriform islands of angular basaloid cells arranged around gland like spaces filled with homogenous eosinophilic or basophilic material.
Granular cell tumour
Adenomatoid odontogenic tumour
Adenoid cystic carcinoma
Acinic cell carcinoma
Squamous cell carcinoma
Ameloblastoma
Myoepithelioma
Polymorphous low grade adenocarcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
Adenoid cystic carcinoma
Wide age range
Slow growing with tendency for perineural spread
Tubular, cribriform and solid patterns
2 cell populations: ductal cells and abluminal myoepithelial cells
Cytologically bland, angular and dense chromatin
Adenoid cystic carcinoma
Cribriform pattern: multiple punched out holes “pseudocysts”
Contain dense eosinophilic basement membrane-like material or bluish mucopolysaccharides
Perineural invasion +++
5 yr survival good, 20 yrs <10%
Lung metastases seen later in course
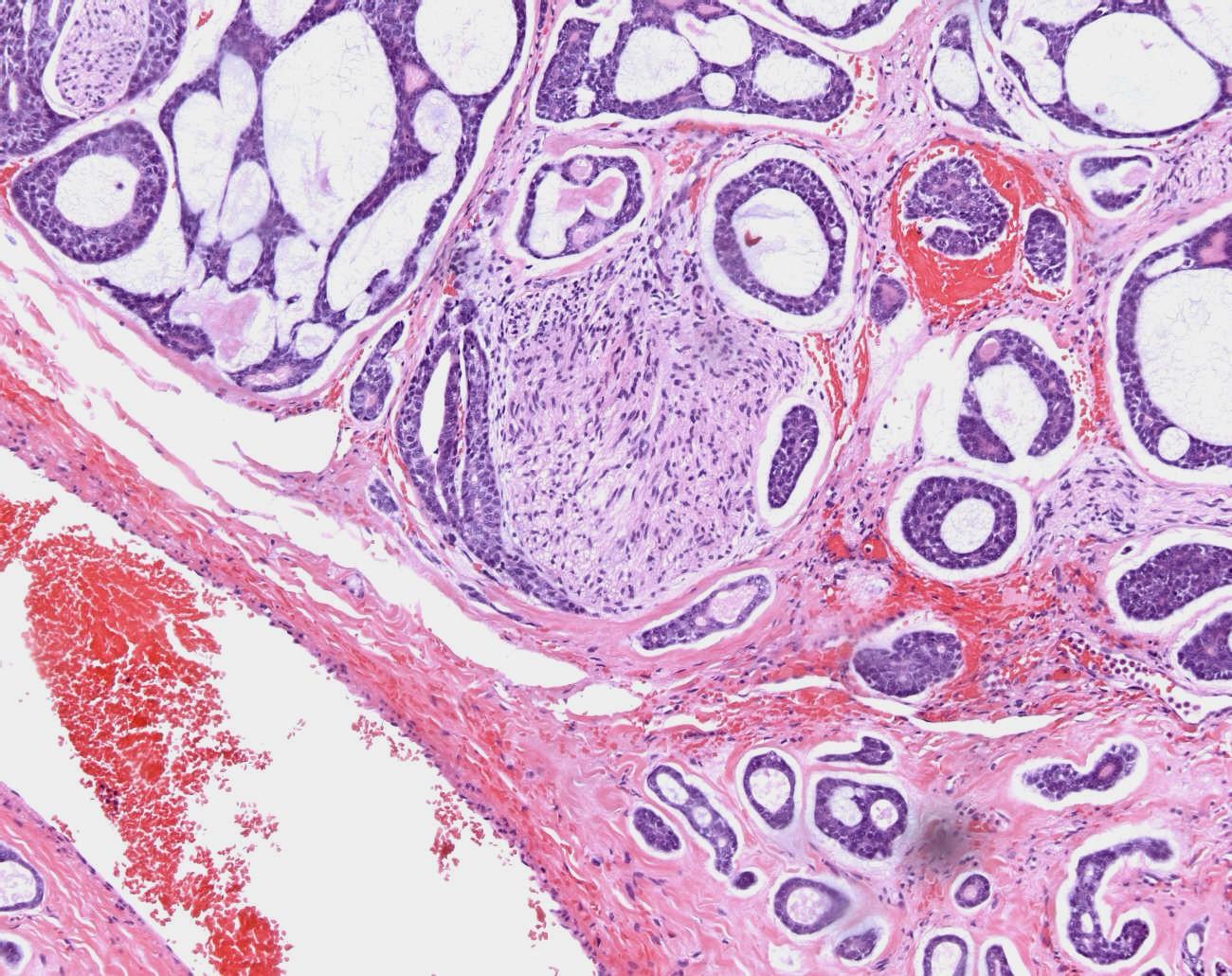
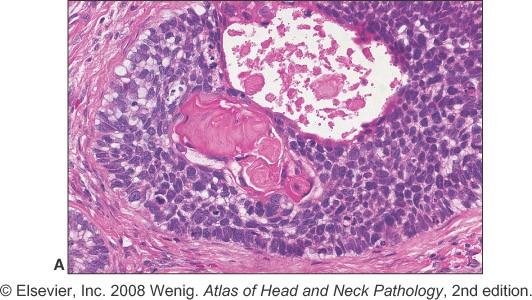
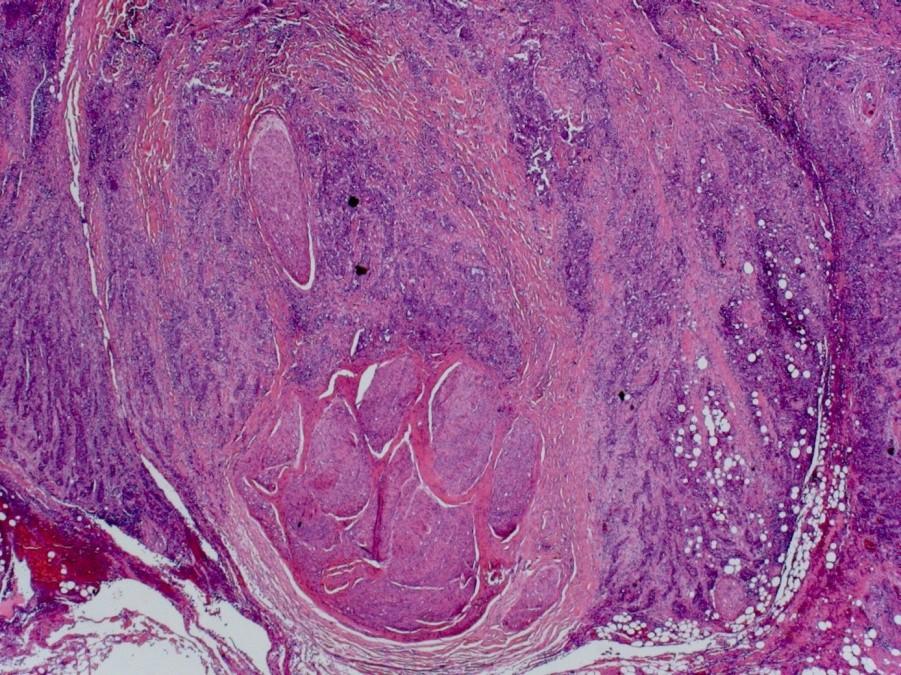
3. A palatal biopsy from a 15 year old female showing lobular islands of cytologically bland polygonal cells with distinct cell boundaries admixed with scattered mucous / goblet cells.
Granular cell tumour
Adenomatoid odontogenic tumour
Adenoid cystic carcinoma
Acinic cell carcinoma
Squamous cell carcinoma
Ameloblastoma
Myoepithelioma
Polymorphous low grade adenocarcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
Mucoepidermoid carcinoma
Wide age range and most common malignant salivary gland tumour in
adolescents and children
3 types of cells
Epidermoid cells
Mucous cells
Intermediate cells
Clear cells
Mucoepidermoid carcinoma
Grading
Cystic change
Necrosis
Neural invasion
Anaplasia
>4 mitoses / 10 hpf
Mucoepidermoid carcinoma
Low grade can be well circumscribed
Often a nesting pattern
Sometimes lymphoid stroma
4. A multinodular submandibular tumour which has rather variable appearances including cellular areas containing ductal structures, sheets and strands of hyaline plasmacytoid cells, all embedded in a loose myxoid stroma.
Granular cell tumour
Adenomatoid odontogenic tumour
Adenoid cystic carcinoma
Acinic cell carcinoma
Squamous cell carcinoma
Ameloblastoma
Myoepithelioma
Polymorphous low grade adenocarcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
Pleomorphic adenoma
Pleomorphic refers to variety of cells and architectural patterns not to cytomorphology
The most common benign tumour
Tumours of minor glands can be non or poorly encapsulated
Ductal / luminal cells and abluminal myoepithelial population
Myoepithelial population often most prominent
Pleomorphic adenoma
Myoepithelial cells
Hyaline plasmacytoid
Clear
Spindled
Epithelioid
Pleomorphic adenoma
Stroma
Myxoid
Chondroid
Hyalinised
Fibrous
(Bone)
Pleomorphic adenoma
Bosselated multinodular growth
Malignant transformation
CHONDROID
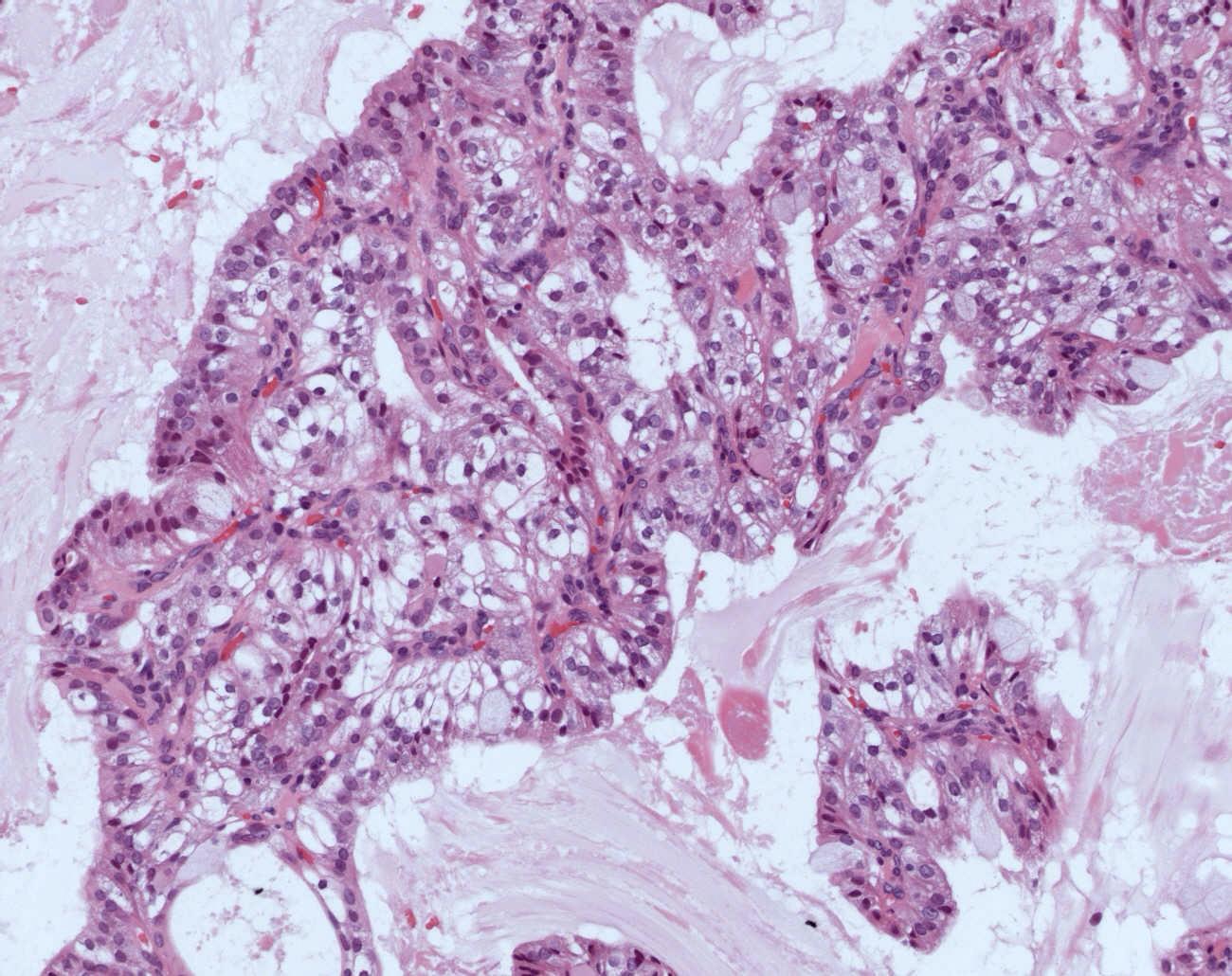
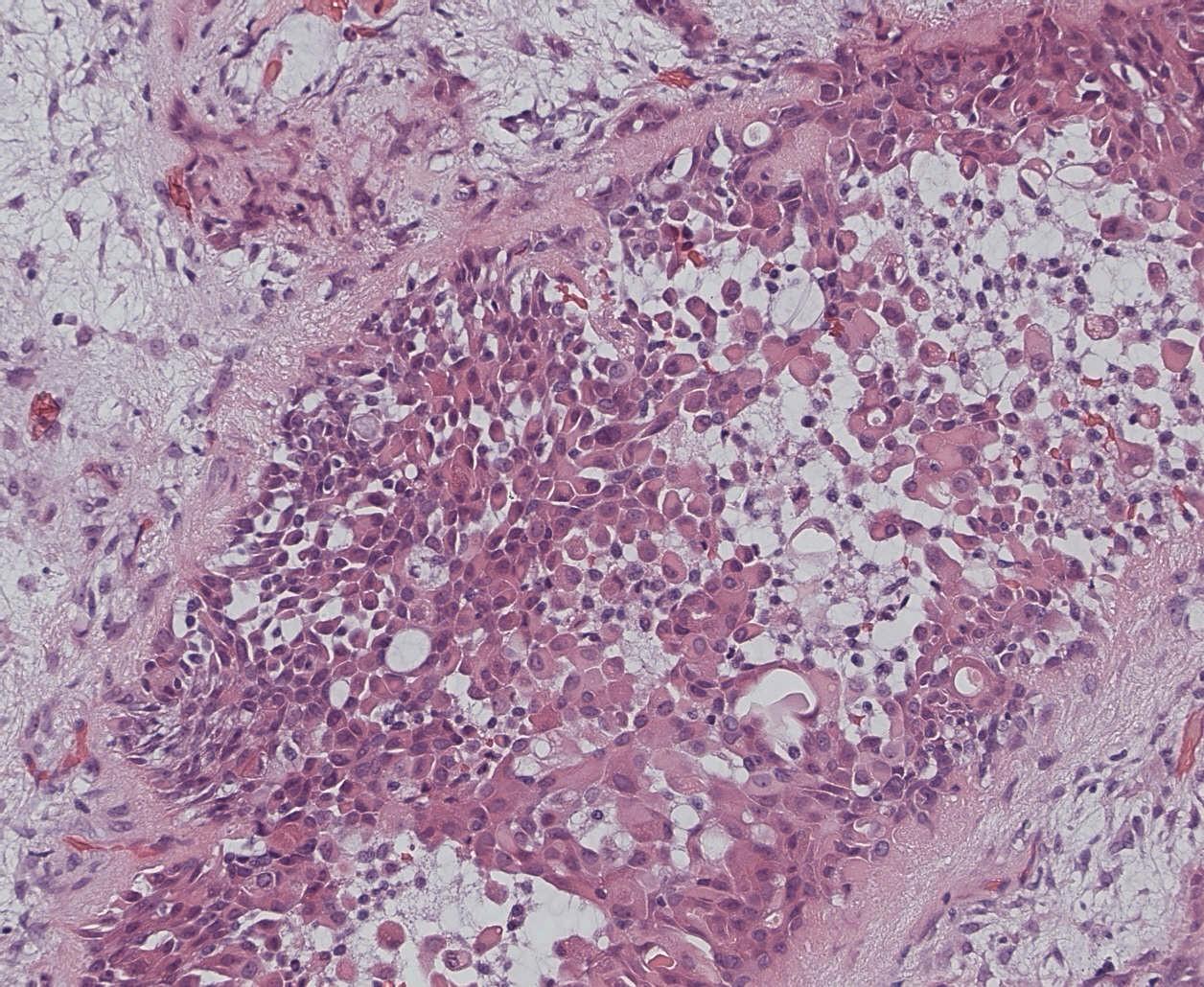
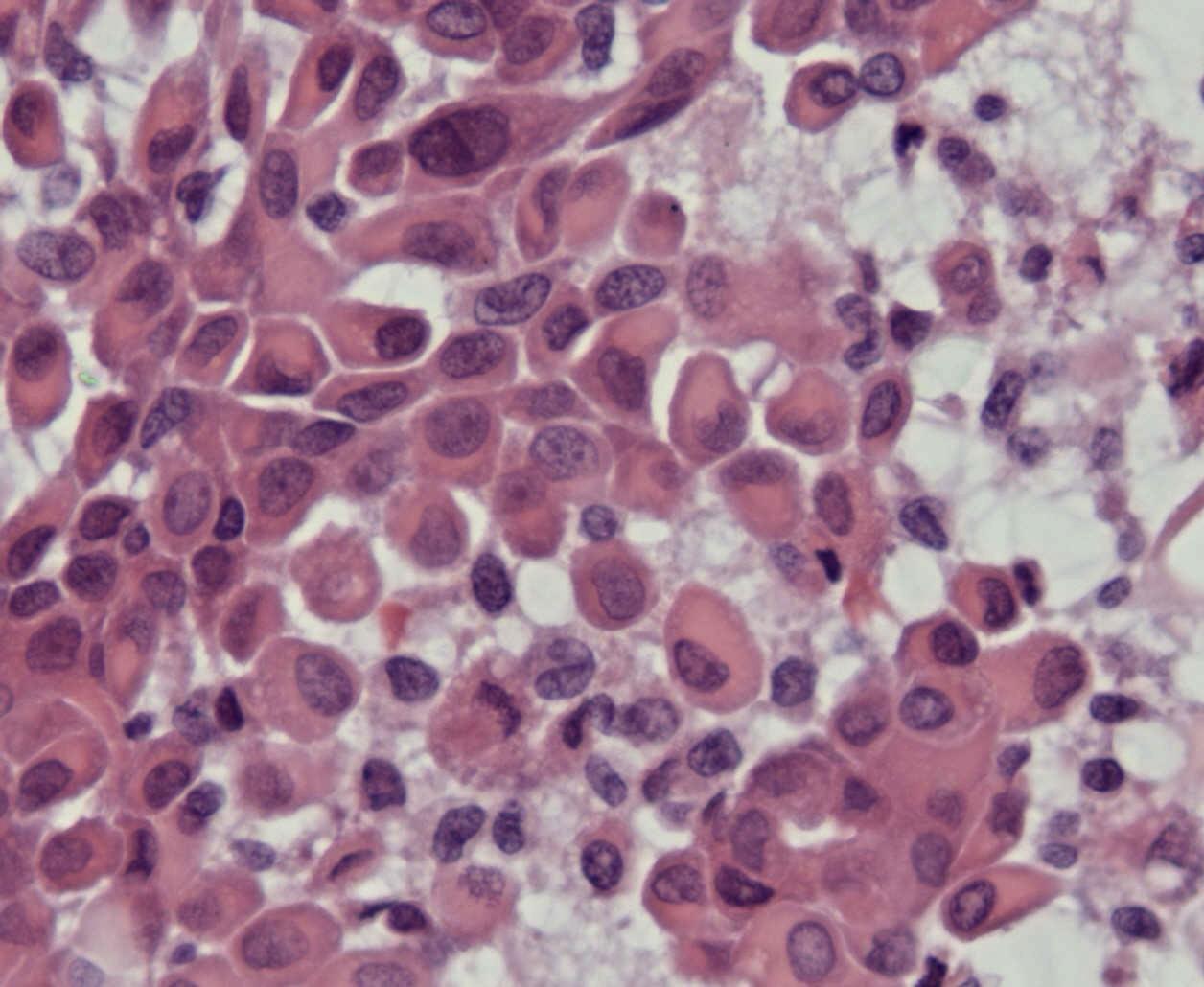
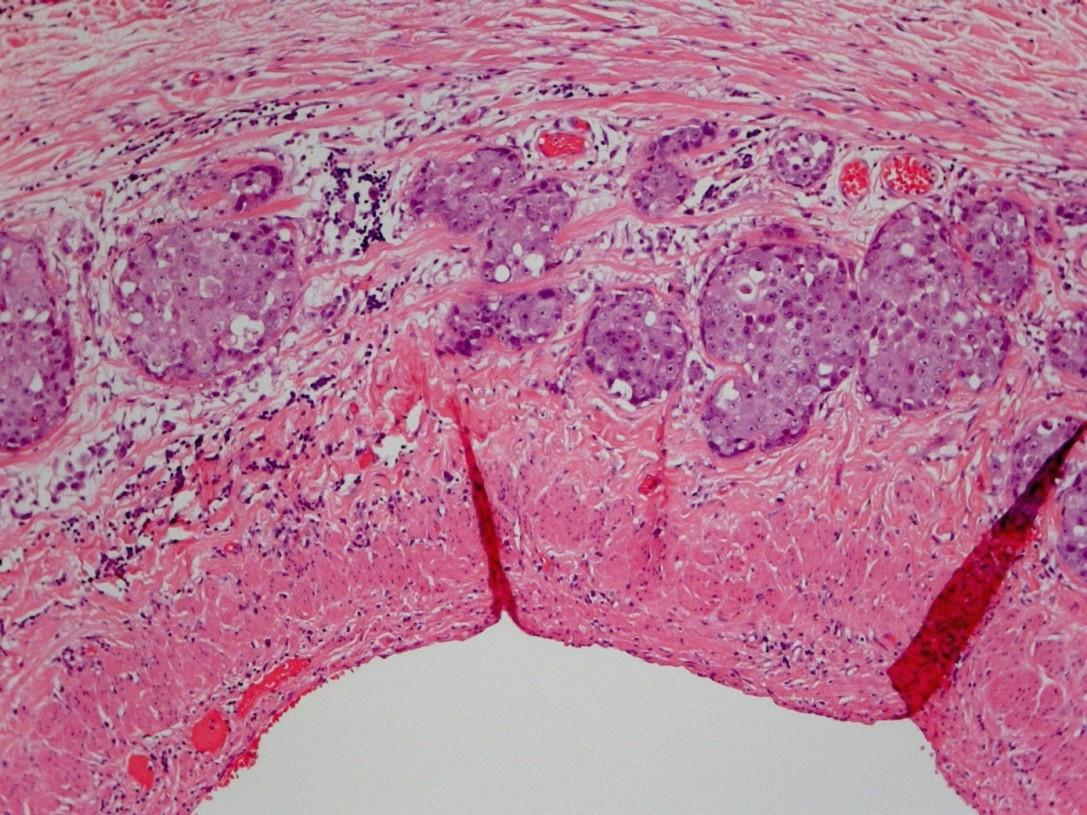
5. A well defined parotid gland tumour, reported as probably benign by the radiologist, composed of sheets of plump cells with voluminous basophilic granular cytoplasm with a smaller population of clear cells and focal areas of papillary cystic architectural change
Granular cell tumour
Adenomatoid odontogenic tumour
Adenoid cystic carcinoma
Acinic cell carcinoma
Squamous cell carcinoma
Ameloblastoma
Myoepithelioma
Polymorphous low grade adenocarcinoma
Mucoepidermoid carcinoma
Pleomorphic adenoma
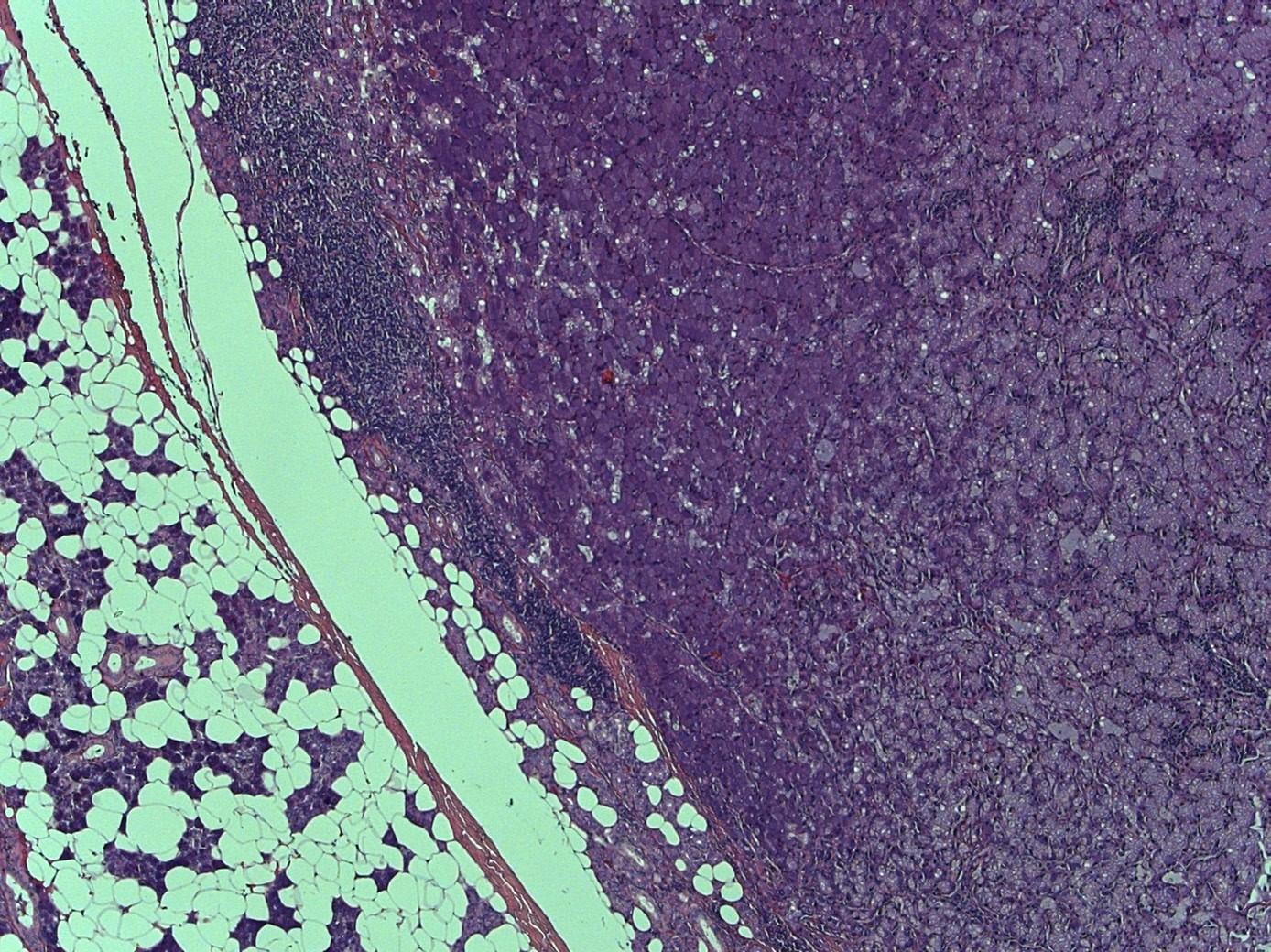
Acinic cell carcinoma
90% parotid
Low grade tumour, usually fairly well circumscribed
Lymphoid stroma
Variable histological appearances and rarity account for difficult in diagnosis in many cases
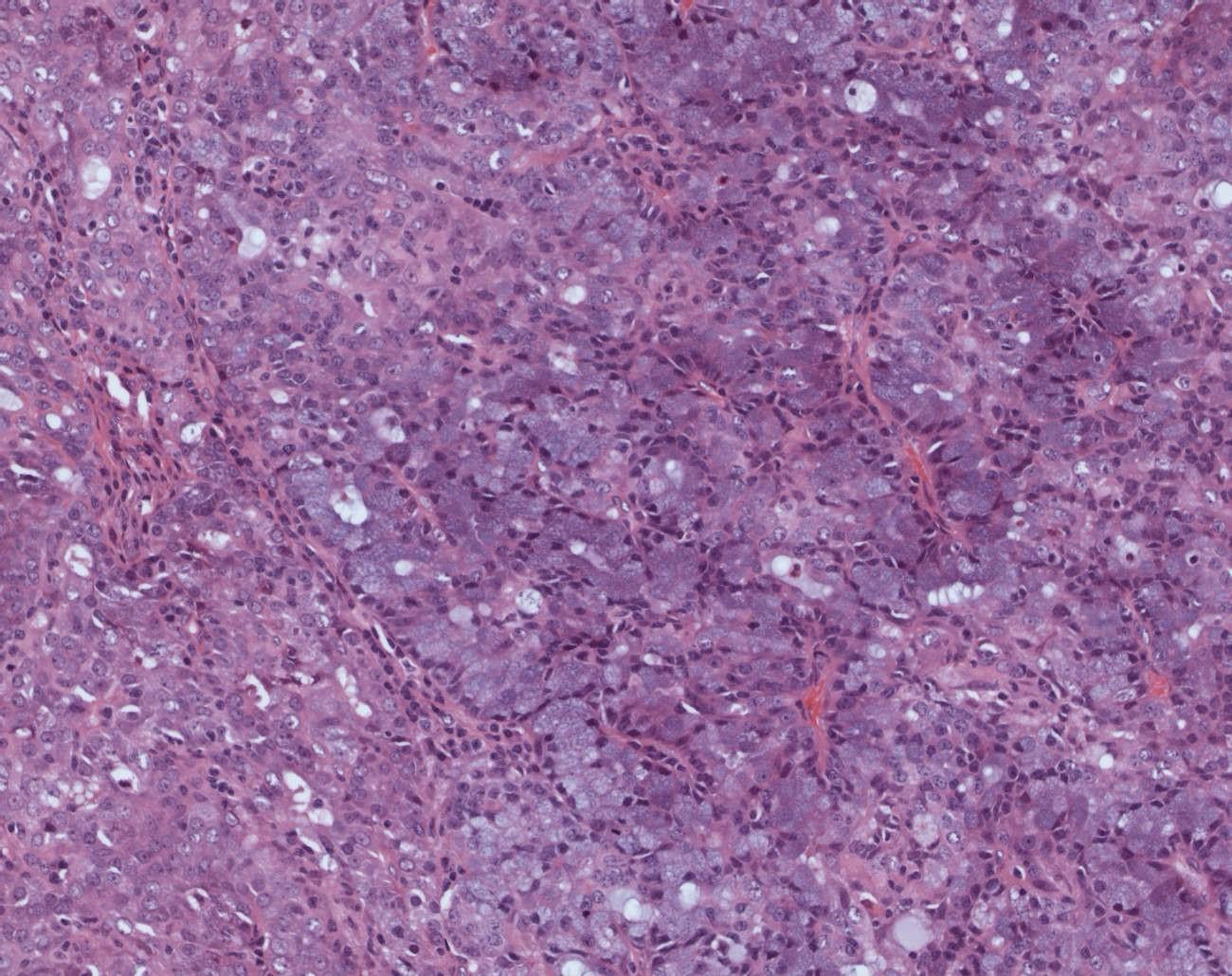
Acinic cell carcinoma
In it’s simplest form
Sheets of large polygonal cells with abundant granular basophilic cytoplasm, small eccentric nuclei with even chromatin pattern
Often nested organoid pattern
Acinic cell carcinoma
Other cell
types
Clear cells
Non-specific glandular cells
Hobnail cells
Vacuolated
Architectural arrangements
Solid
Papillary cystic
Microcystic
Follicular
Question 4
Sinonasal tract
Sinonasal lesions: select one of the following:
Tuberculosis
Wegener’s granulomatosis
Capillary haemangioma
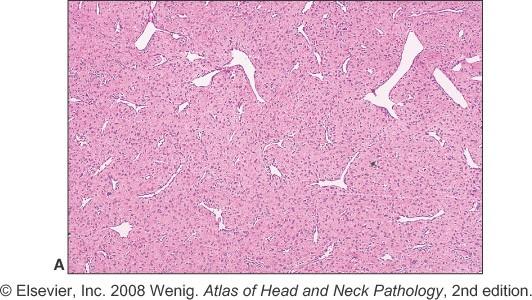
Nasopharyngeal angiofibroma
Haemangiopericytoma
Malignant melanoma
Intestinal type adenocarcinoma
Mucocele
NK/T cell lymphoma
Sinonasal undifferentiated carcinoma
Olfactory neuroblastoma
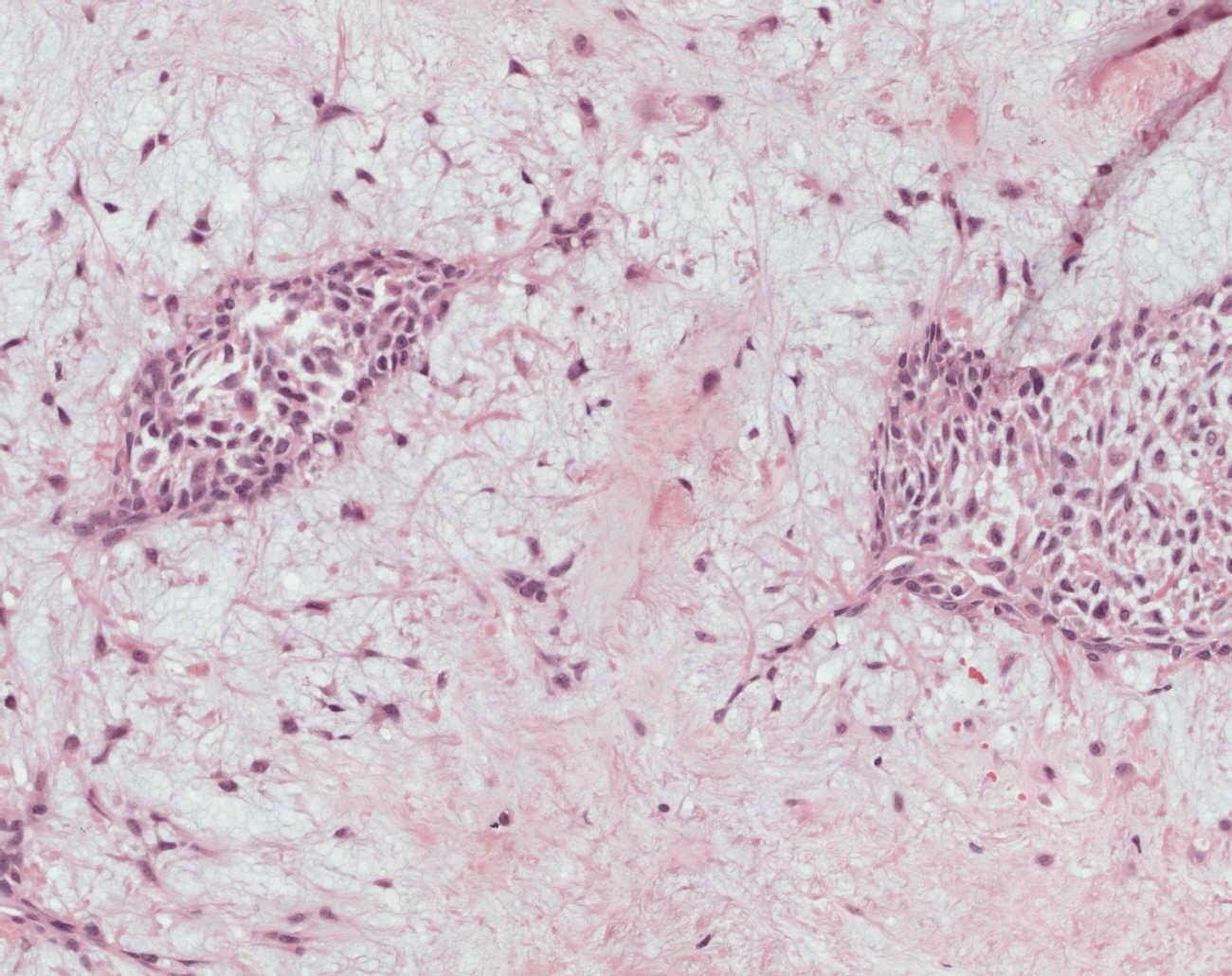
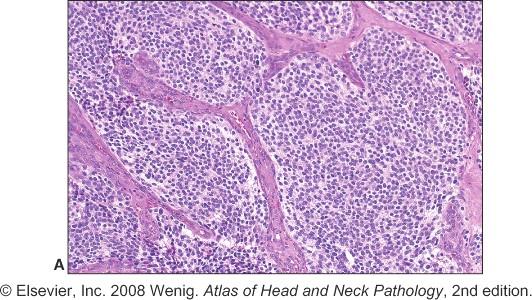
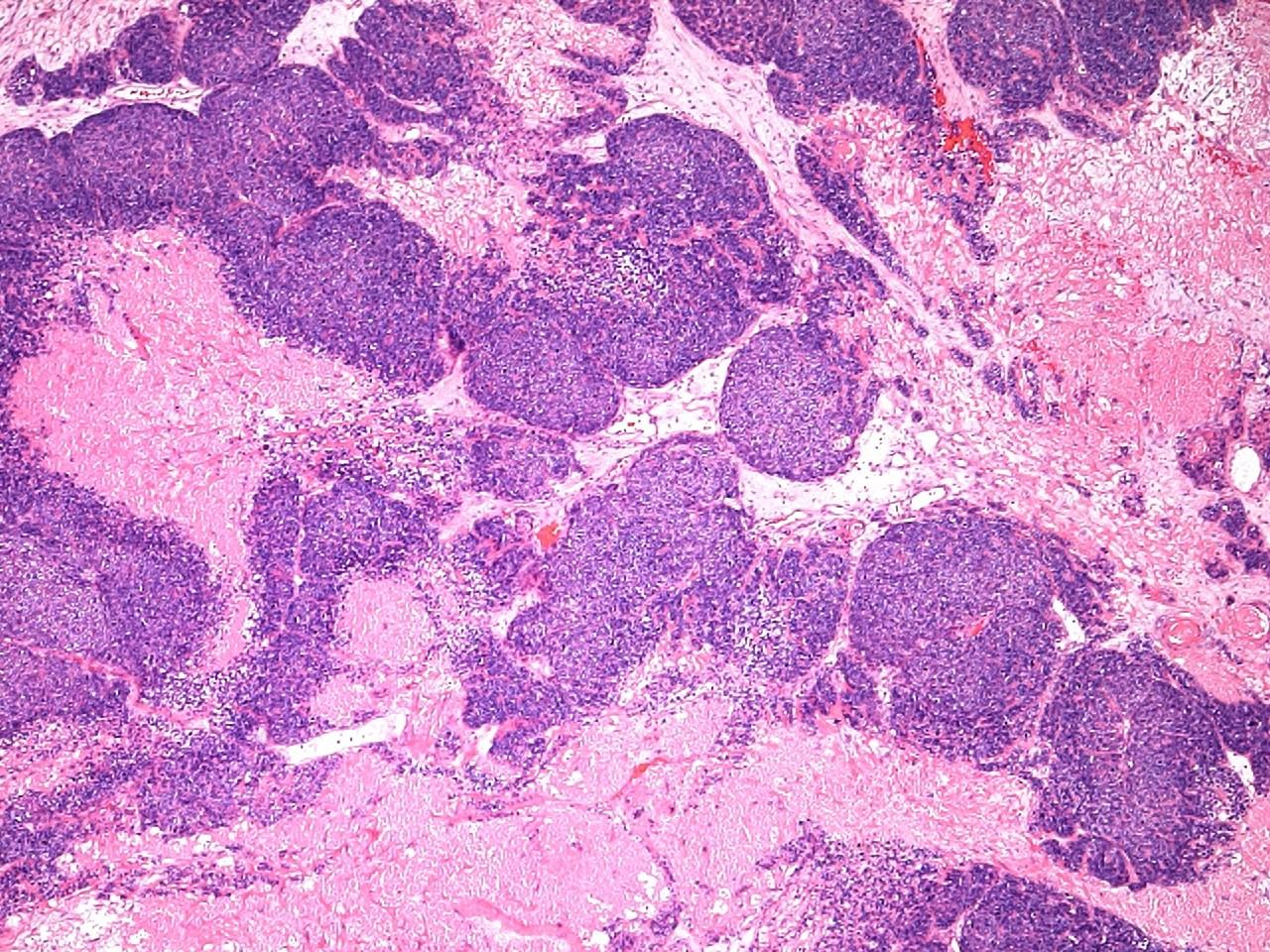
1. A 50 year old female with a polypoid mass in the roof of the nasal fossa comprising lobular sheets of small blue round cells embedded in a fibrillary background and with occasional rosettes.
Tuberculosis
Wegener’s granulomatosis
Capillary haemangioma
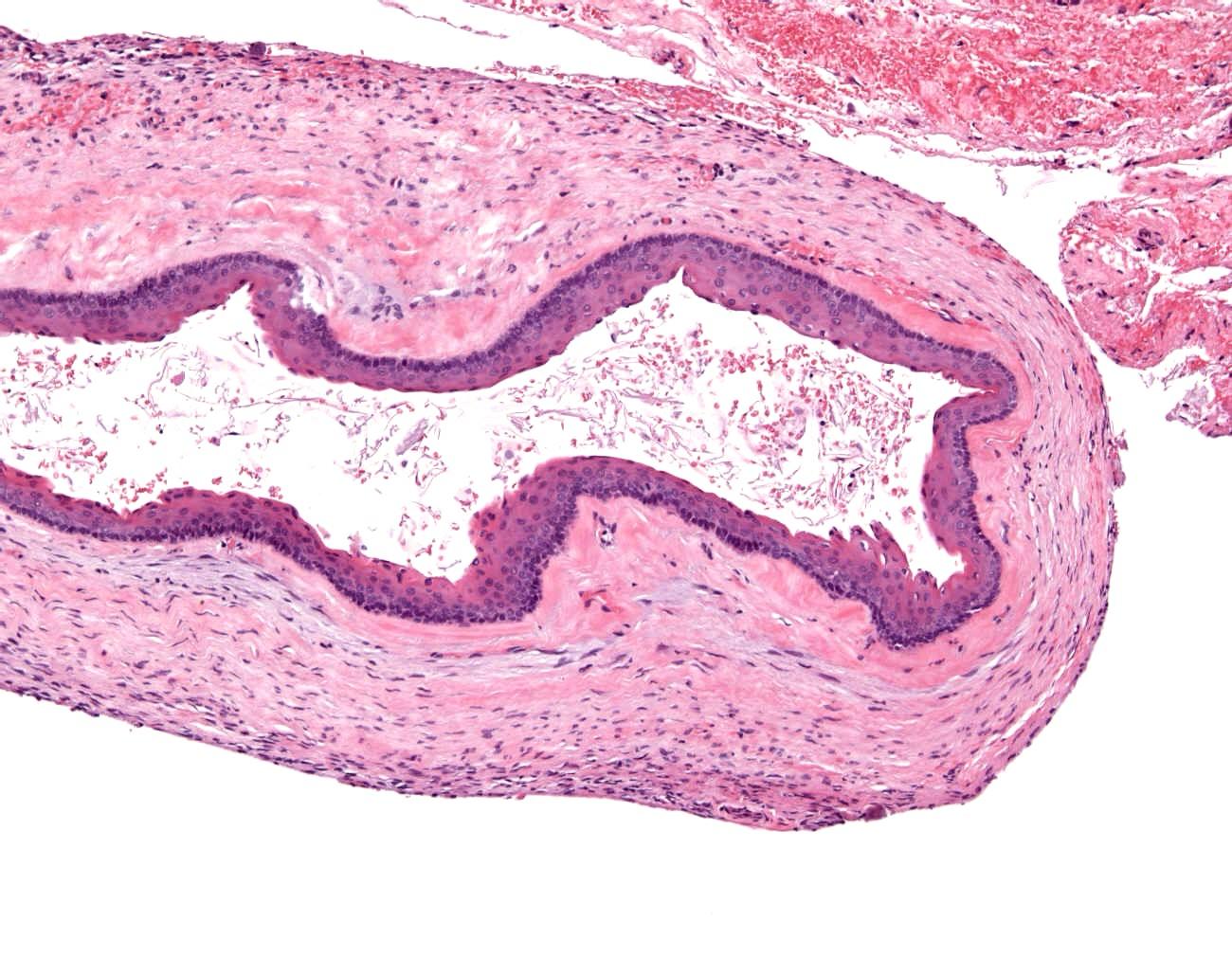
Nasopharyngeal angiofibroma
Haemangiopericytoma
Malignant melanoma
Intestinal type adenocarcinoma
Mucocele
NK/T cell lymphoma
Sinonasal undifferentiated carcinoma
Olfactory neuroblastoma
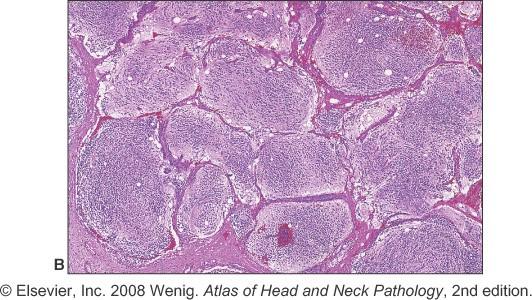
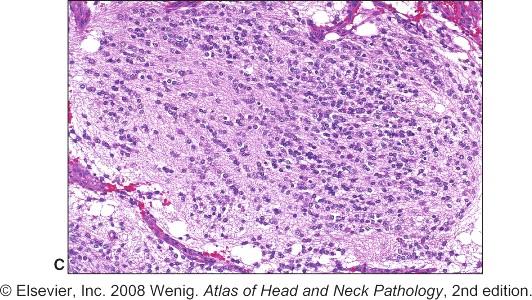
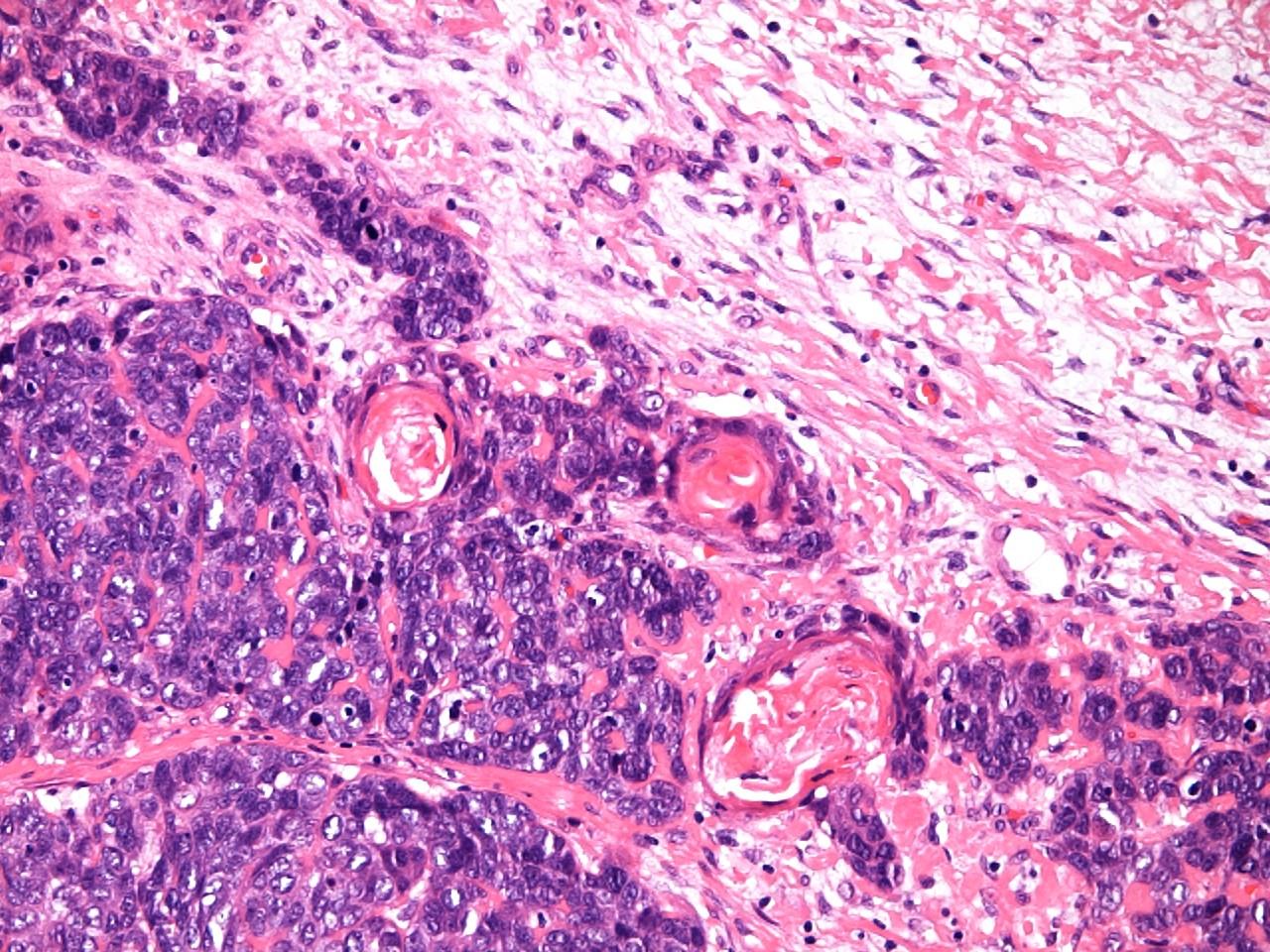
Olfactory neuroblastoma
3rd – 4th decade
Lobules of small blue round cells
60-70% have a fibrillary stroma
Rosettes: Homer - Wright or Flexner –Wintersteiner
Neuroendocrine markers +
Cytokeratins –
S-100 scattered + cells at periphery of lobules
Olfactory neuroblastoma
Differential diagnosis
Small cell carcinoma
SNUC
Rhabdomyosarcoma
ES / PNET
Melanoma
Lymphoma
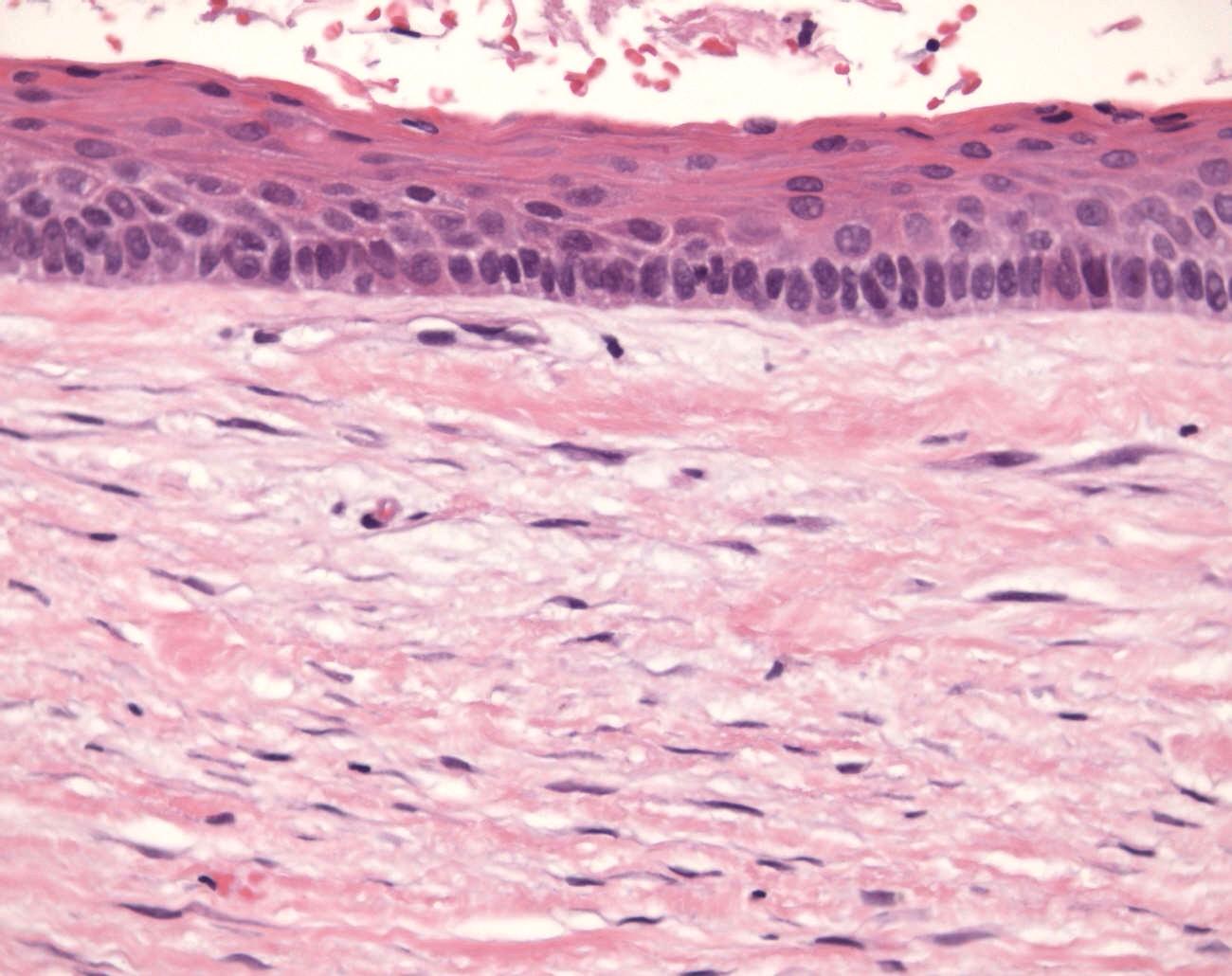
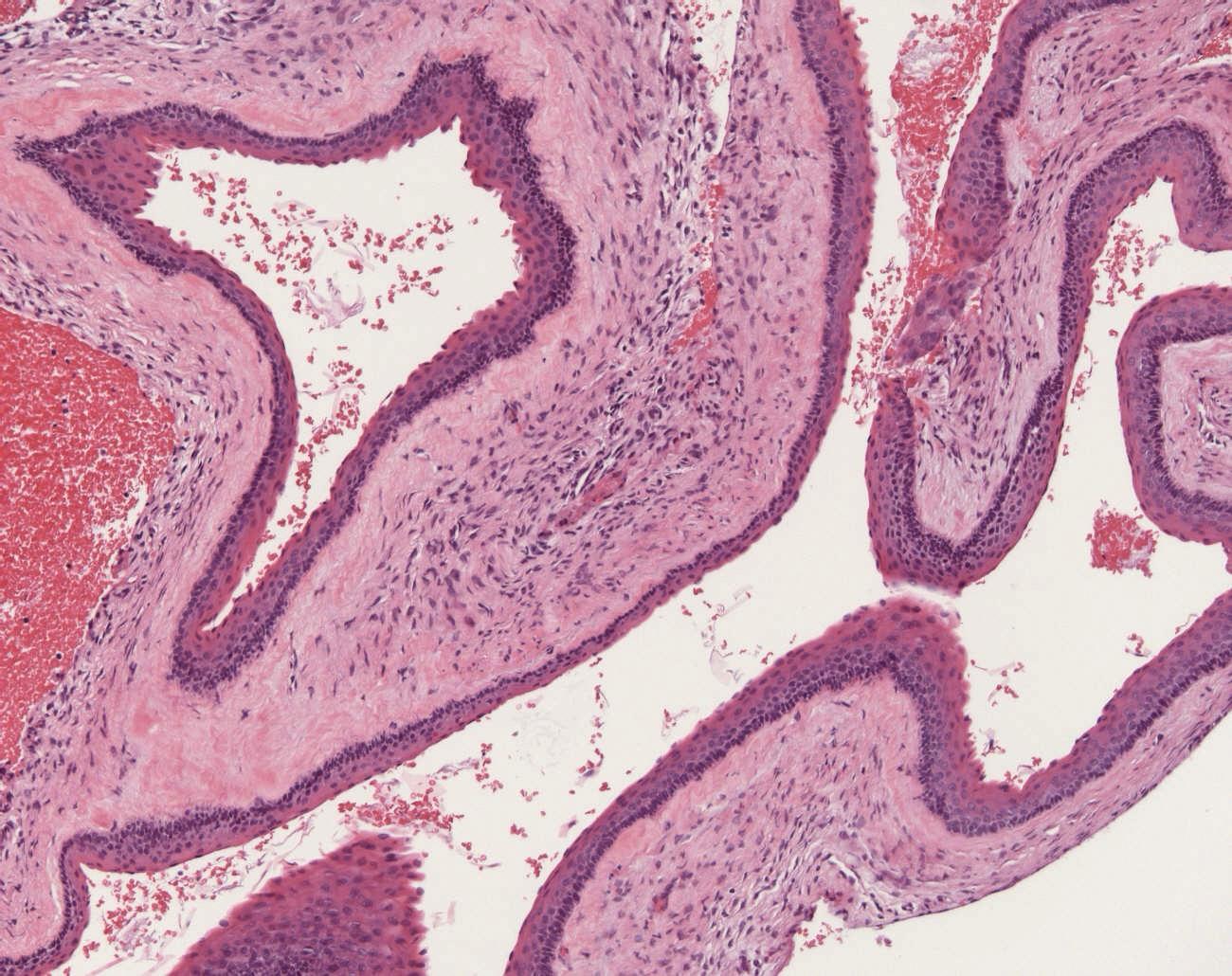
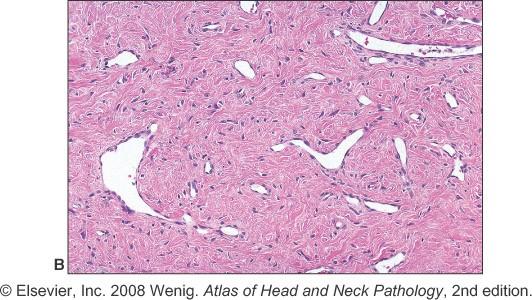
2. A 14 year old male also with a polypoid mass in the roof of the nasal fossa composed of variable sized vessels embedded in a variably cellular and collagenised fibroblastic stroma with stellate shaped fibroblasts a notable feature
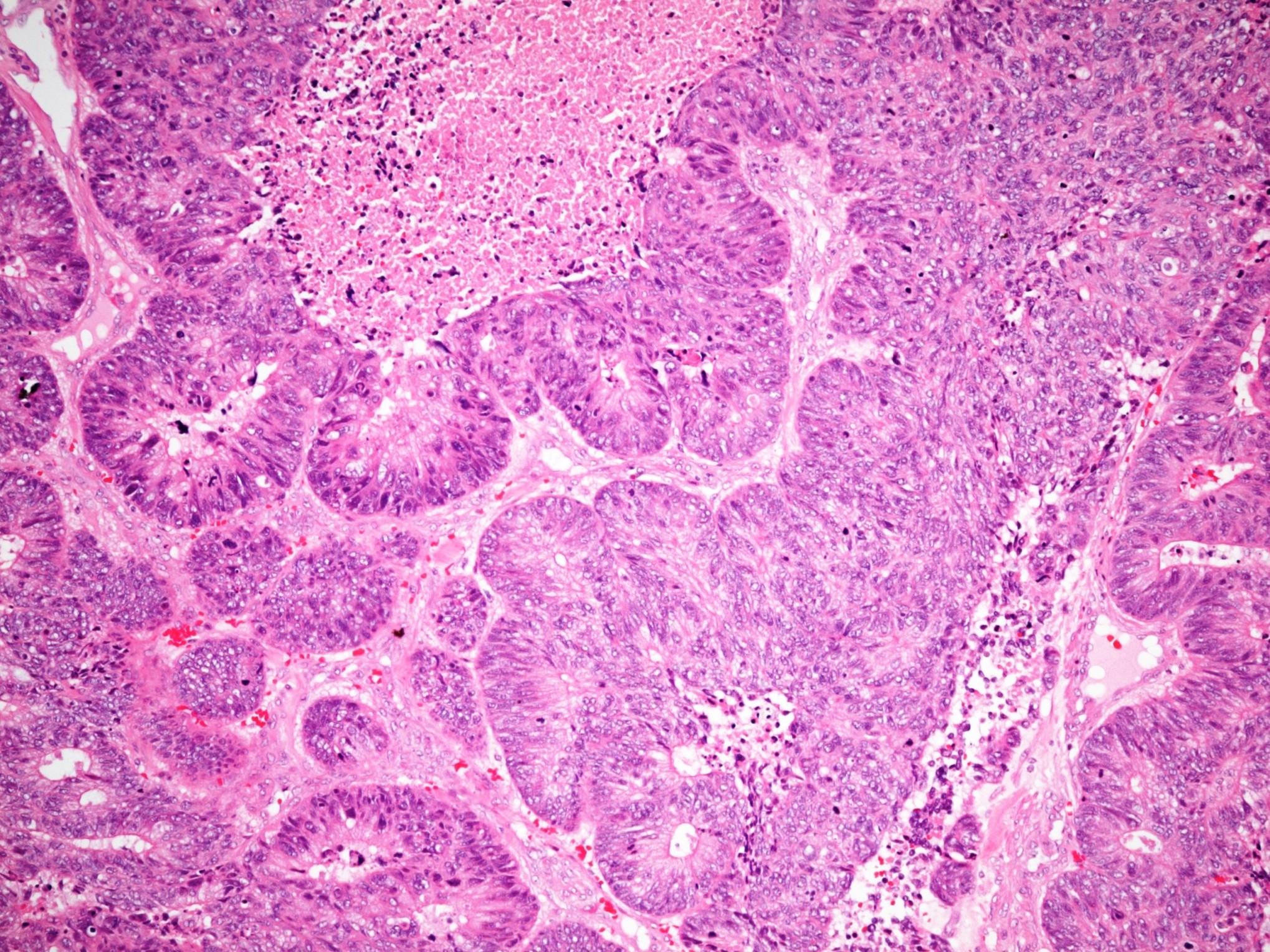
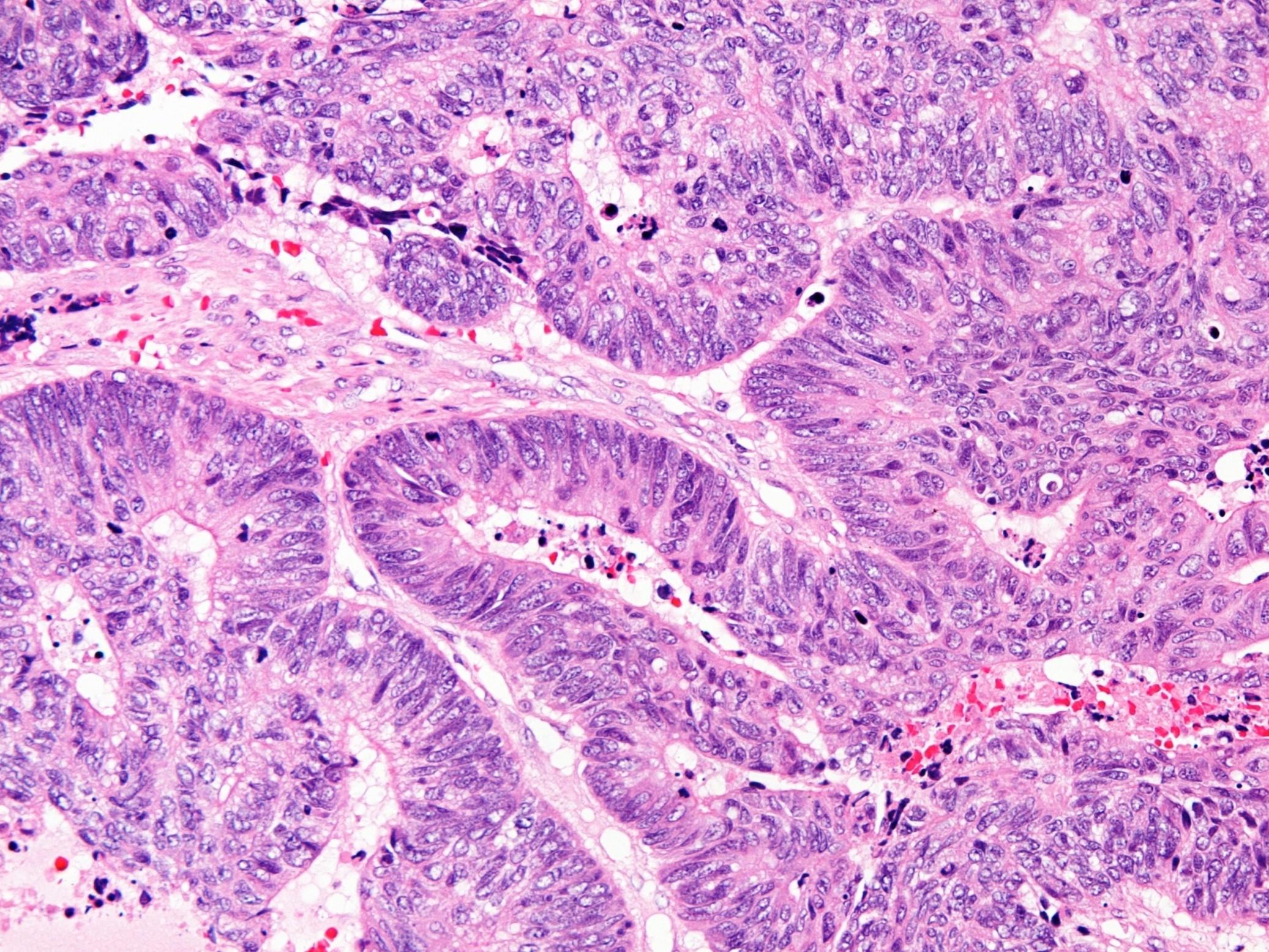
3. A 57 year old carpenter presents with nasal discharge and obstruction. Curettings comprise mucinous material containing glandular structures and papillary strands of columnar cells showing cytological atypia and frequent mitoses
Tuberculosis
Wegener’s granulomatosis
Capillary haemangioma
Nasopharyngeal angiofibroma
Haemangiopericytoma
Malignant melanoma
Intestinal type adenocarcinoma
Mucocele
NK/T cell lymphoma
Sinonasal undifferentiated carcinoma
Olfactory neuroblastoma
Intestinal type adenocarcinoma
Classification of sinonasal malignancy Keratinising squamous cell carcinoma
Intestinal type adenocarcinoma Malignant melanoma
ITAC
Aetiological factors: occupational wood and nickel workers
Well differentiated looks virtually like normal colonic mucosa
Papillary-tubular patterns, back to back glands with atypia
Essentially range of features seen in colonic adenoca
CK7+/- CK20 + can be CDX2 positive
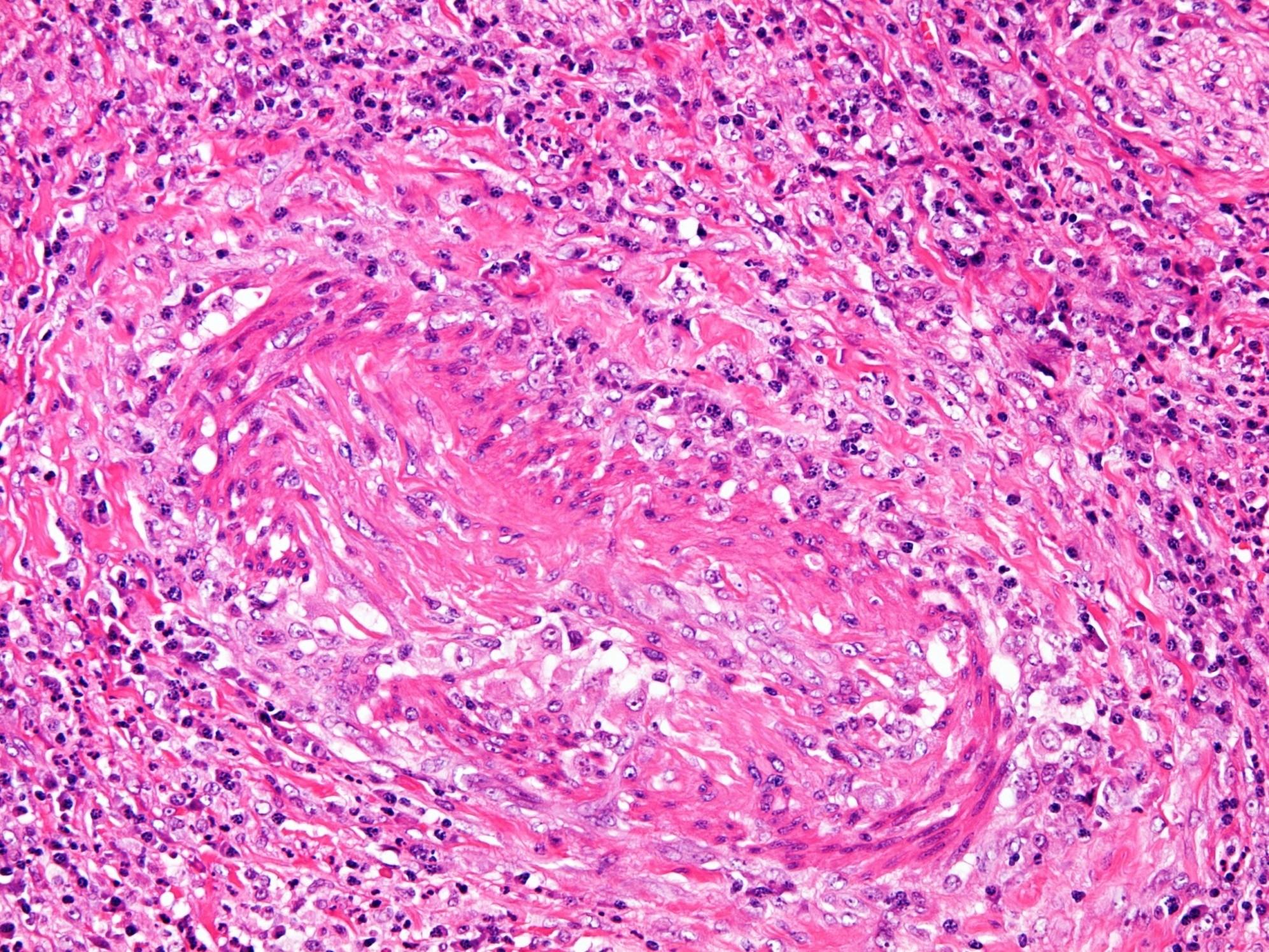
4. Crusting and ulceration of the nasal septum, altered renal function in a 39 year old female. A biopsy from the nasal cavity is largely necrotic but in viable areas, some non-caseating granulomata containing multinucleated giant cells are seen.
Tuberculosis
Wegener’s granulomatosis
Capillary haemangioma
Nasopharyngeal angiofibroma
Haemangiopericytoma
Malignant melanoma
Intestinal type adenocarcinoma
Mucocele
NK/T cell lymphoma
Sinonasal undifferentiated carcinoma
Olfactory neuroblastoma
Wegener’s granulomatosis
Systemic vasculitis and necrotising granulomatosis
Upper and lower respiratory tracts and kidneys cANCA positive
Triad
Necrosis
Vasculitis
Granulomatosis
Wegener’s granulomatosis
Mixed acute on chronic inflammation with neutrophilic microabscesses
Eosinophils
Giant cells unassociated with granulomas
Geographic necrosis
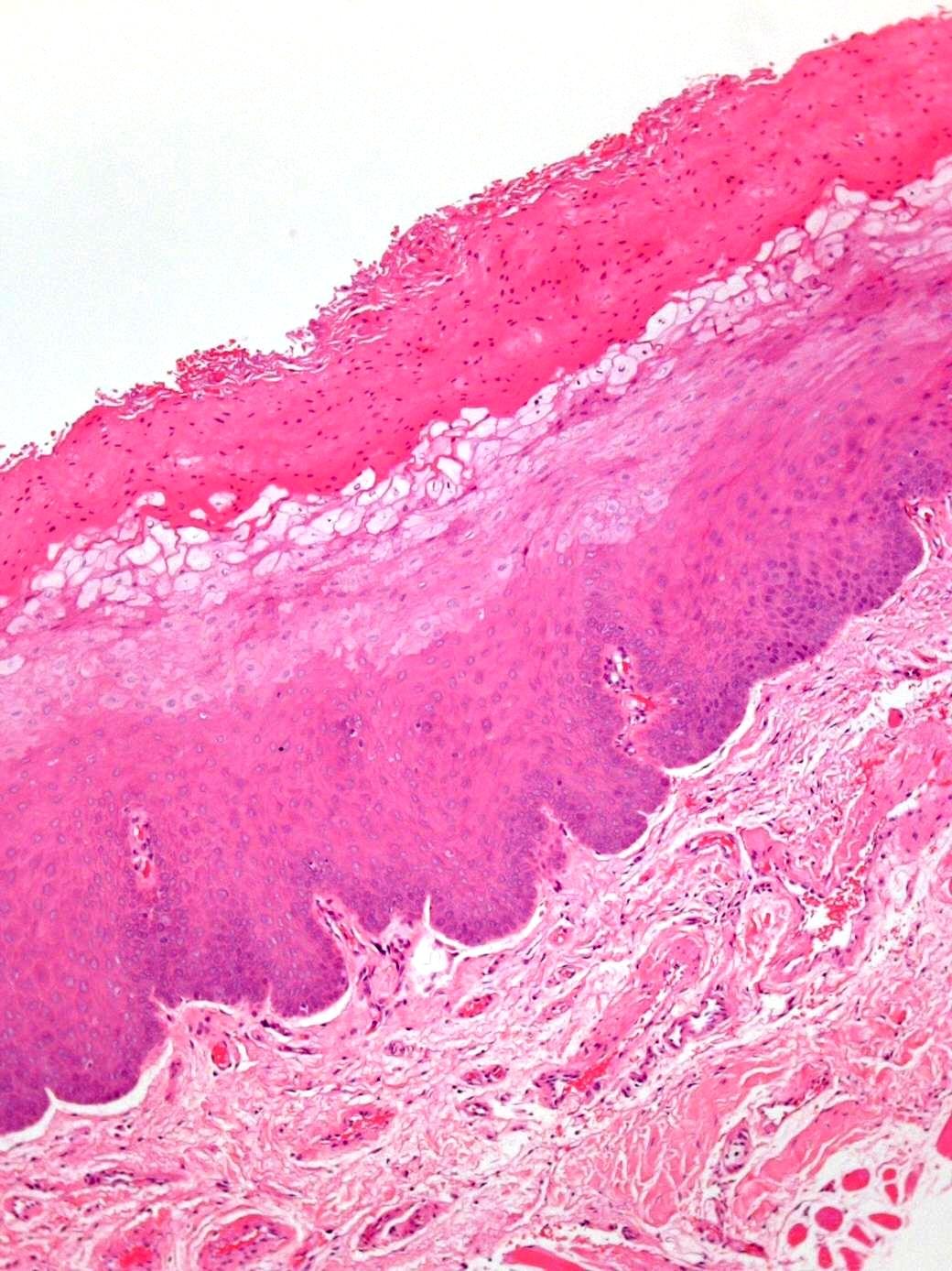
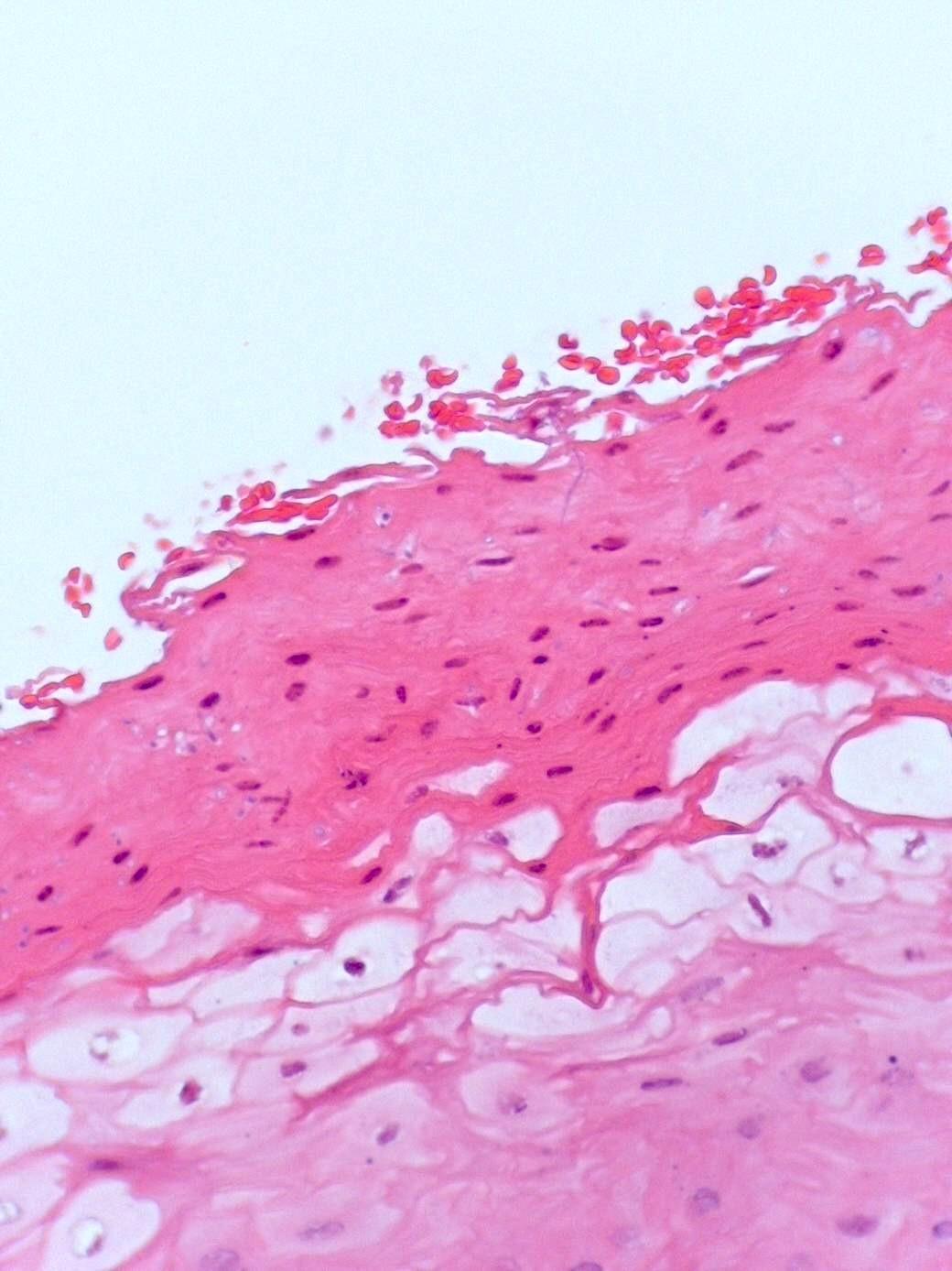
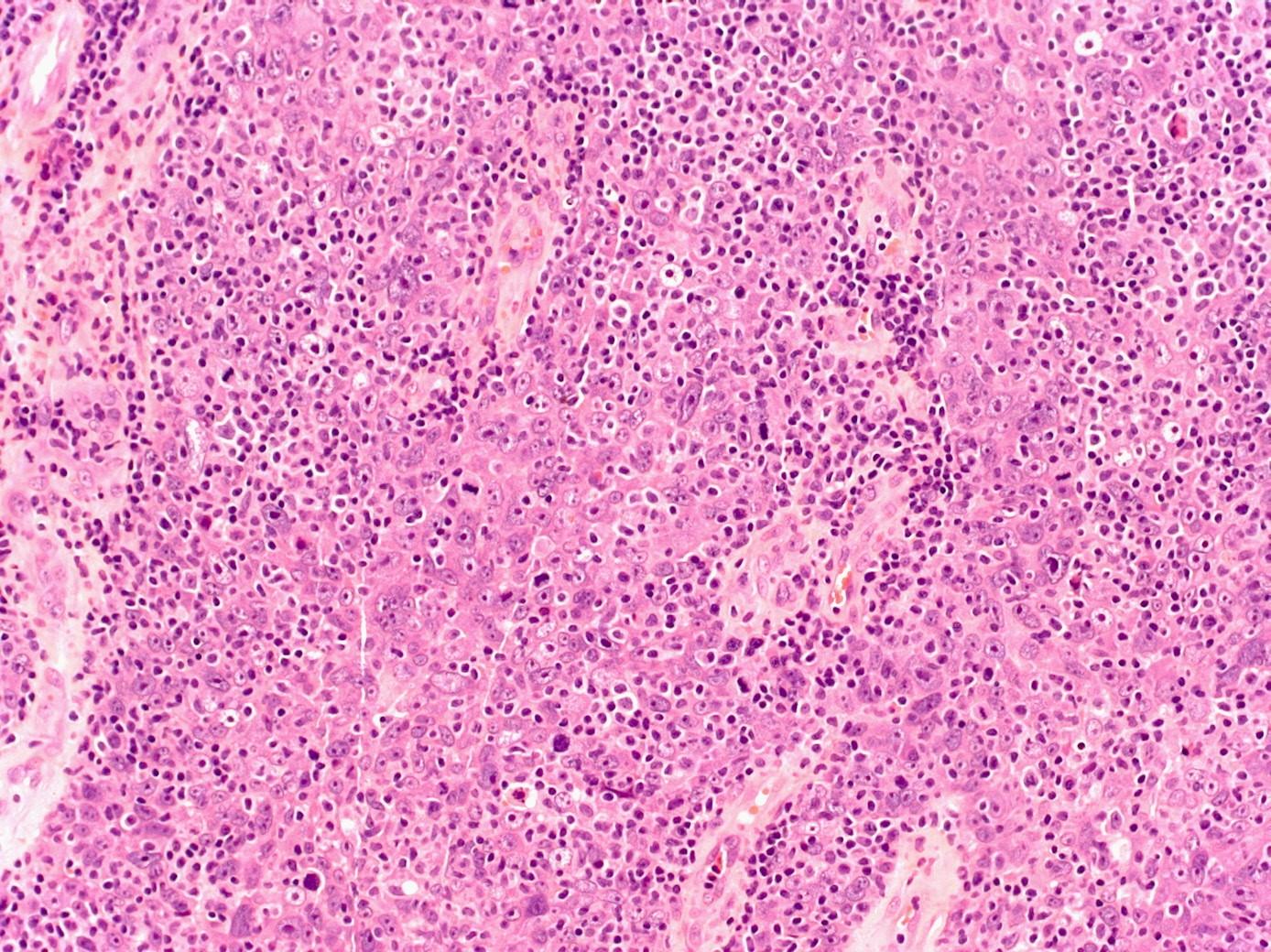
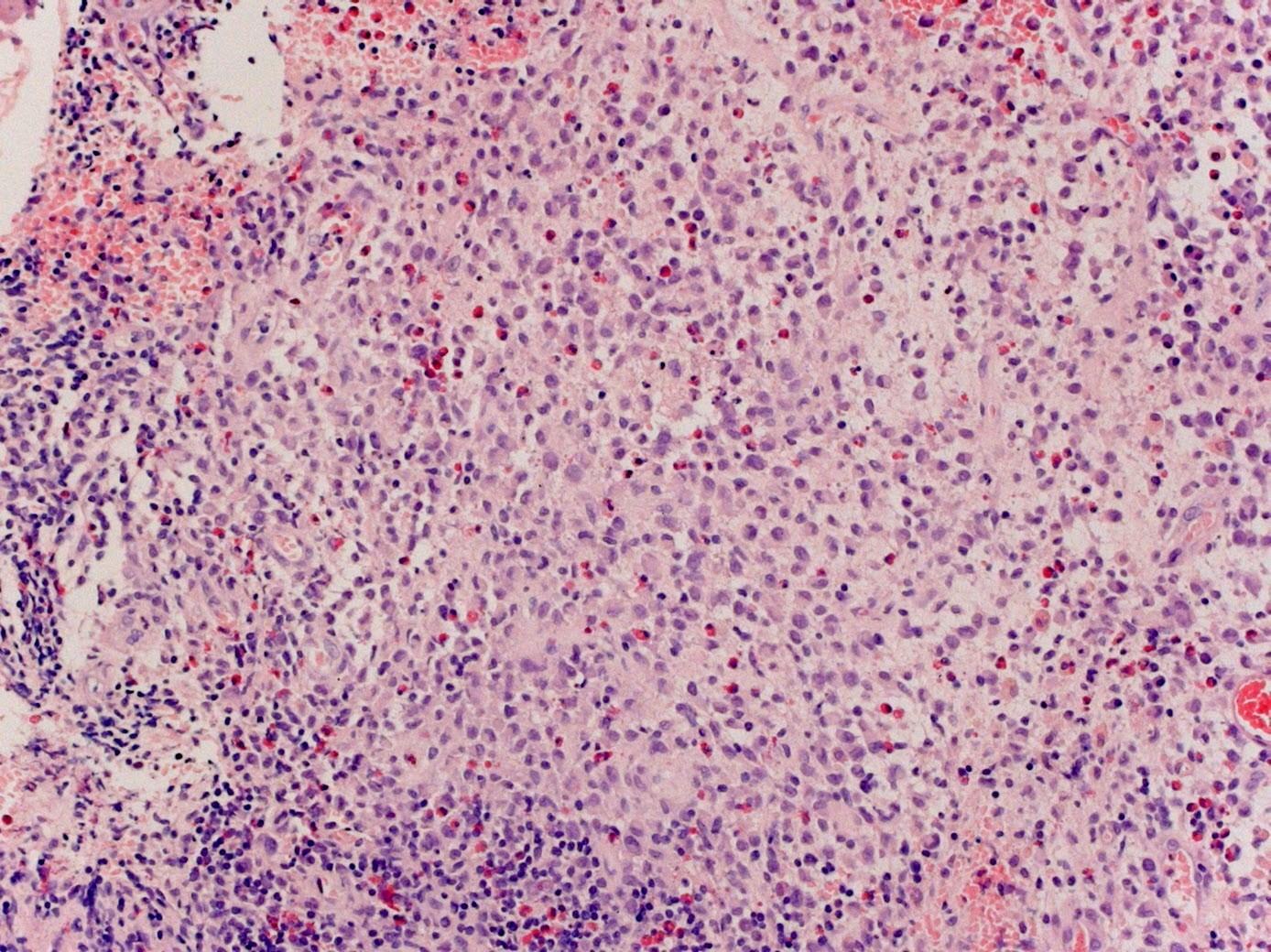
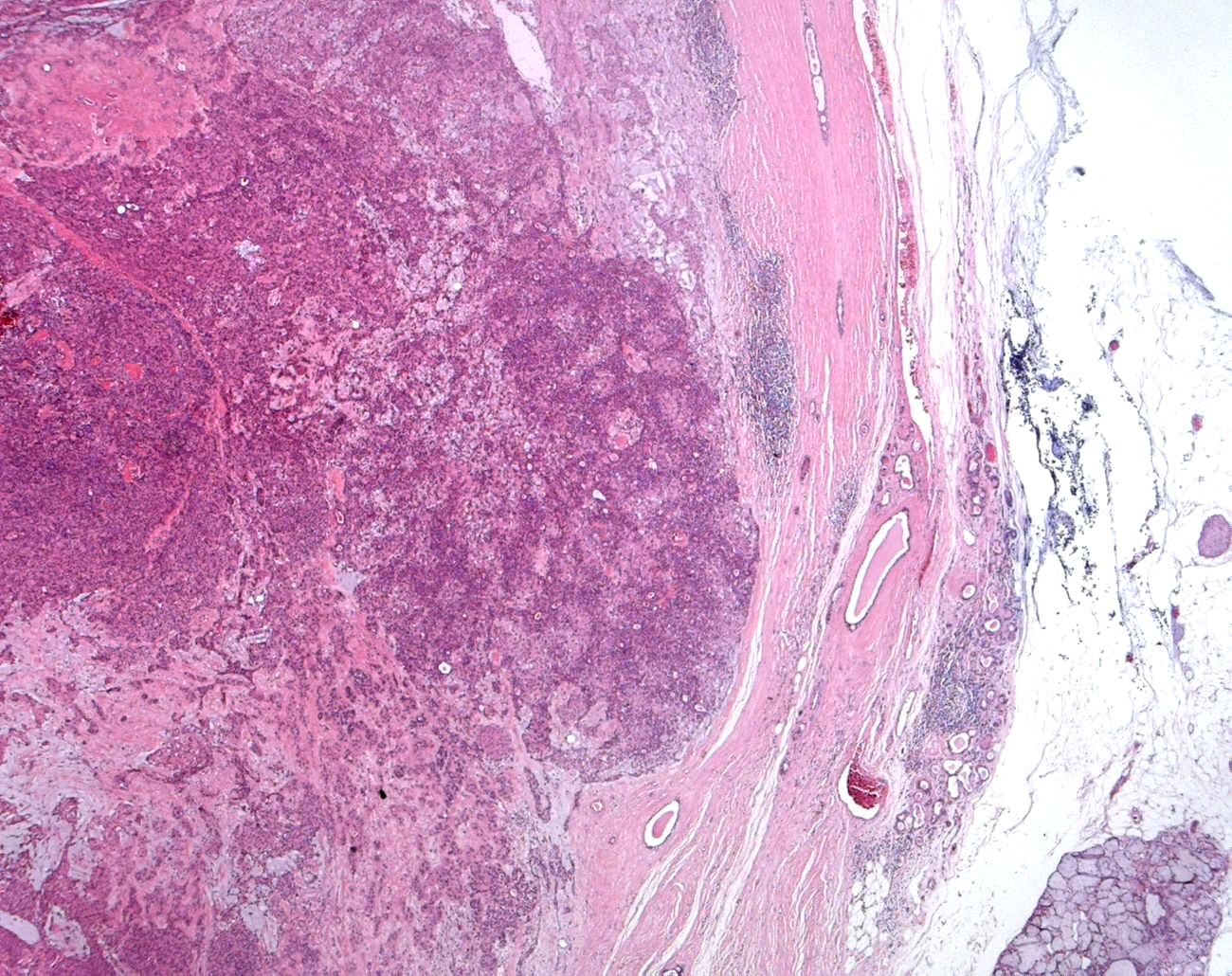
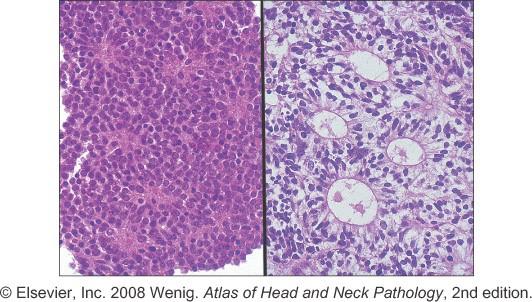
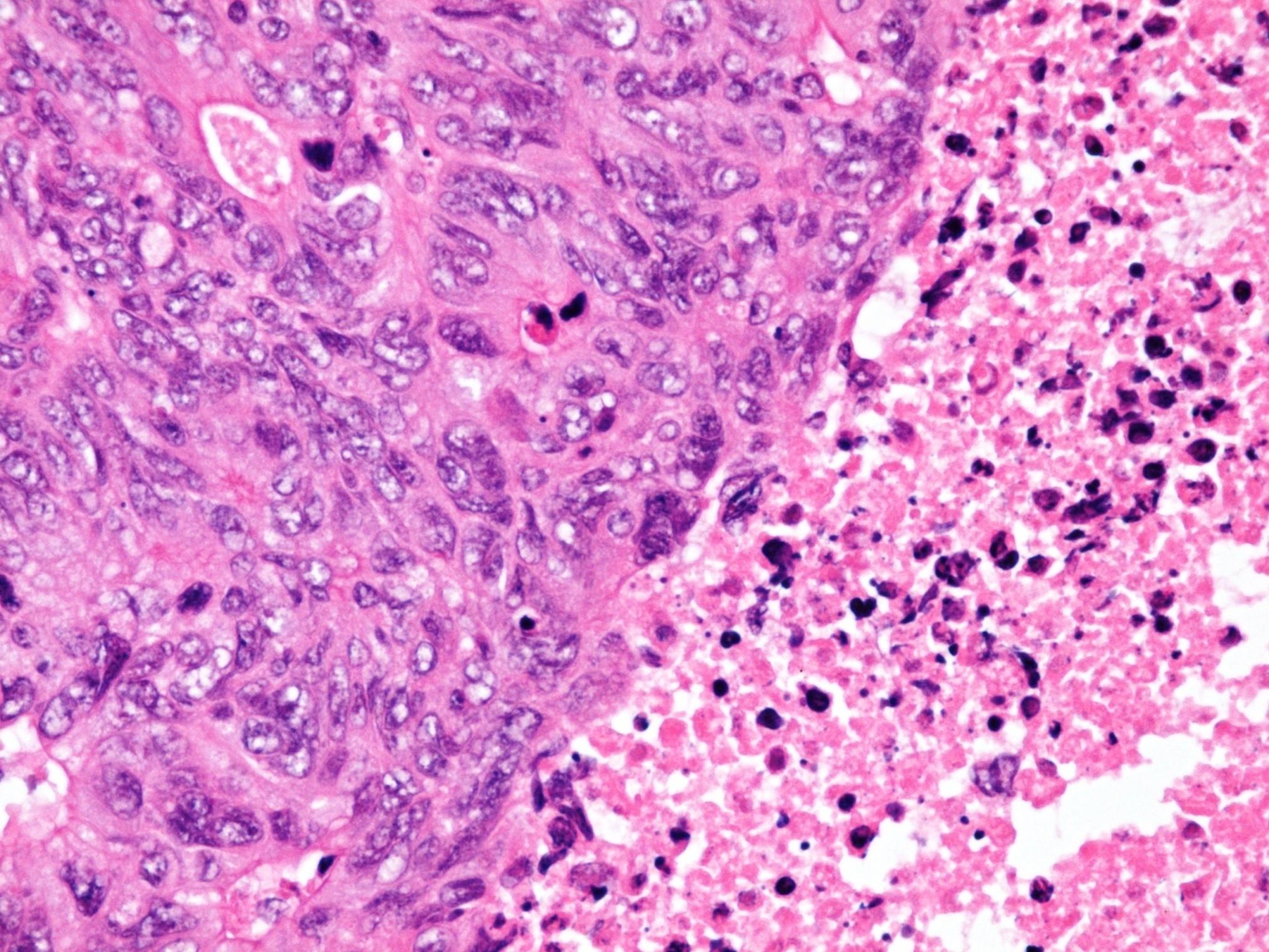
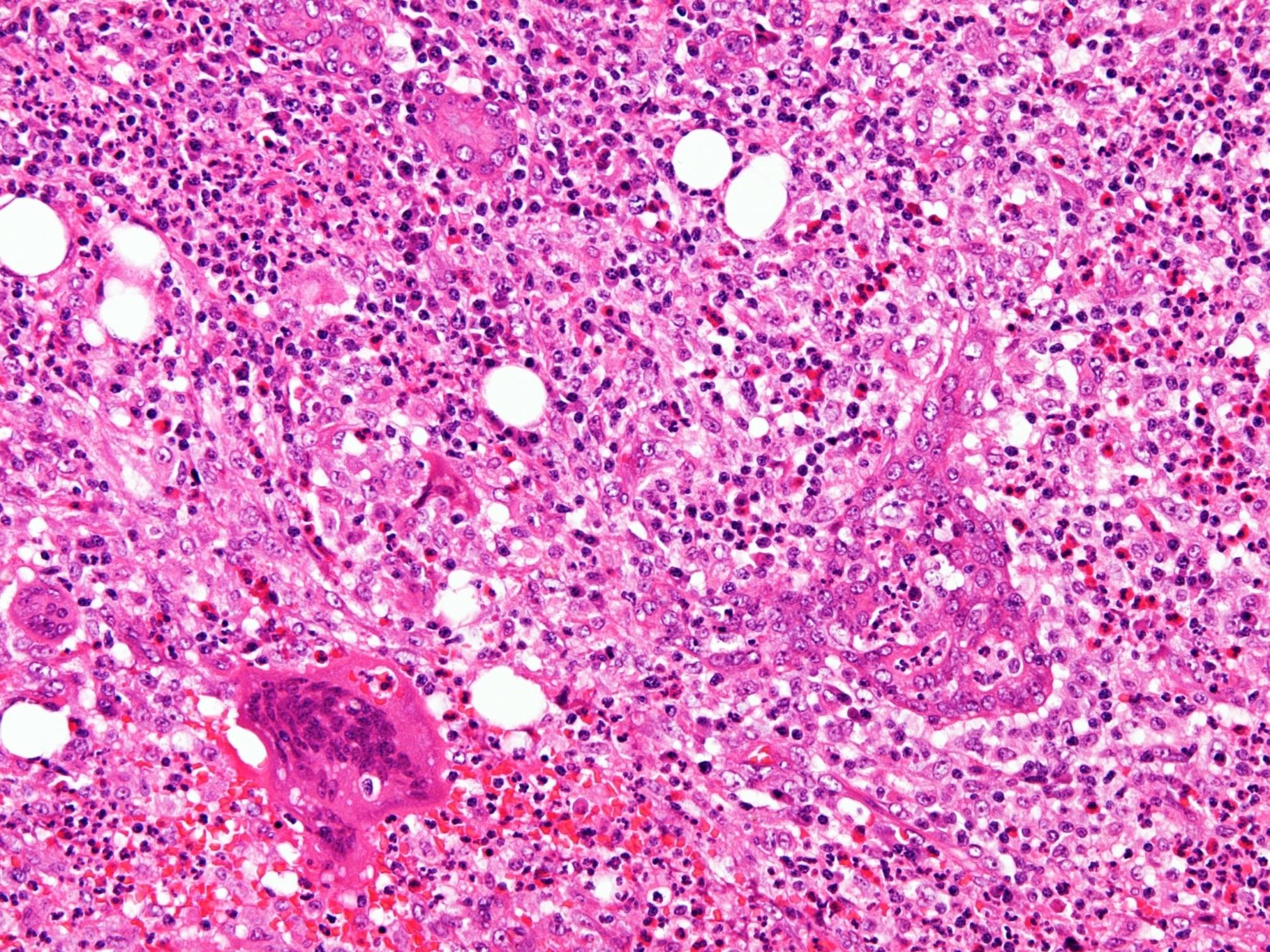
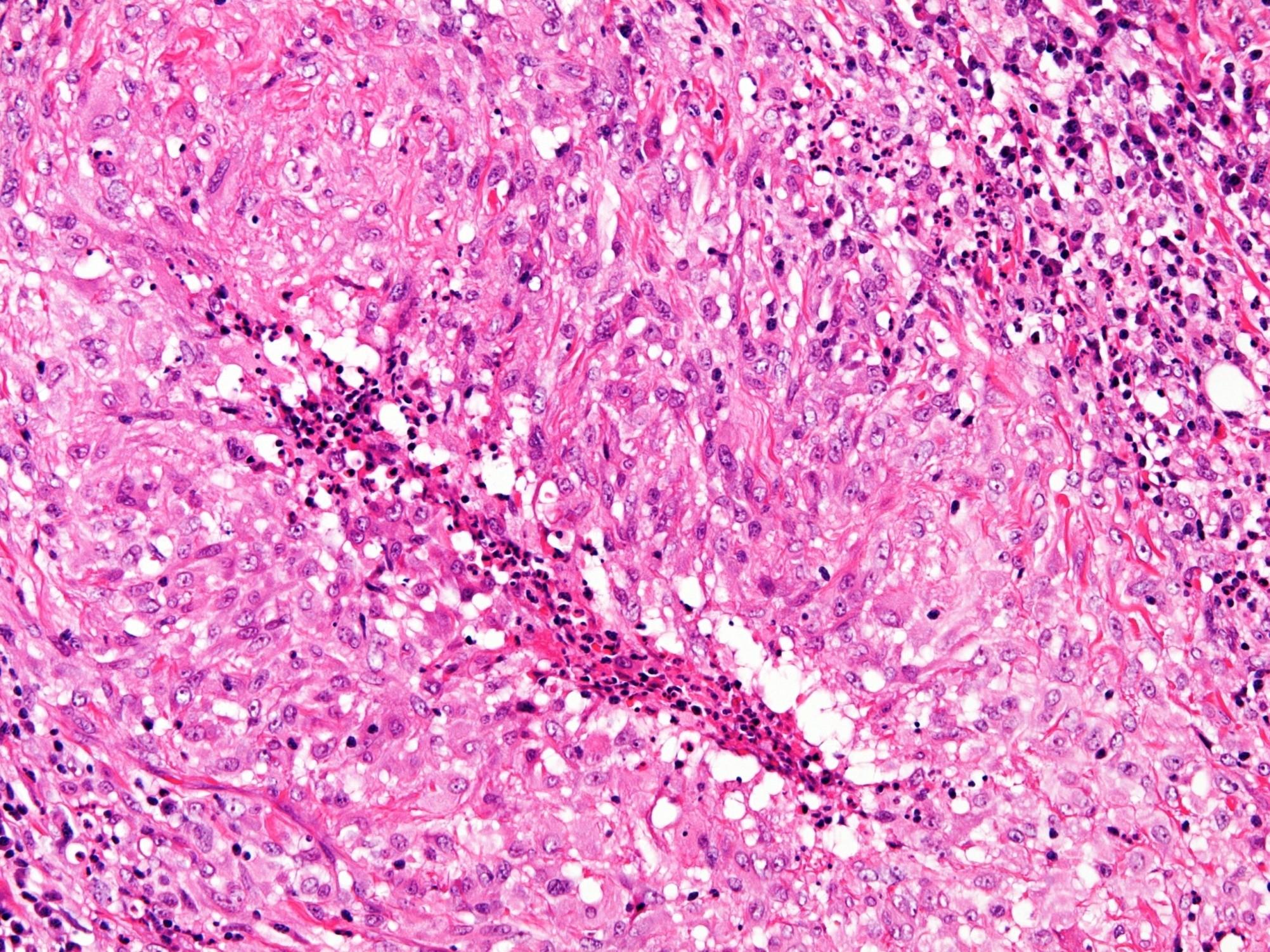
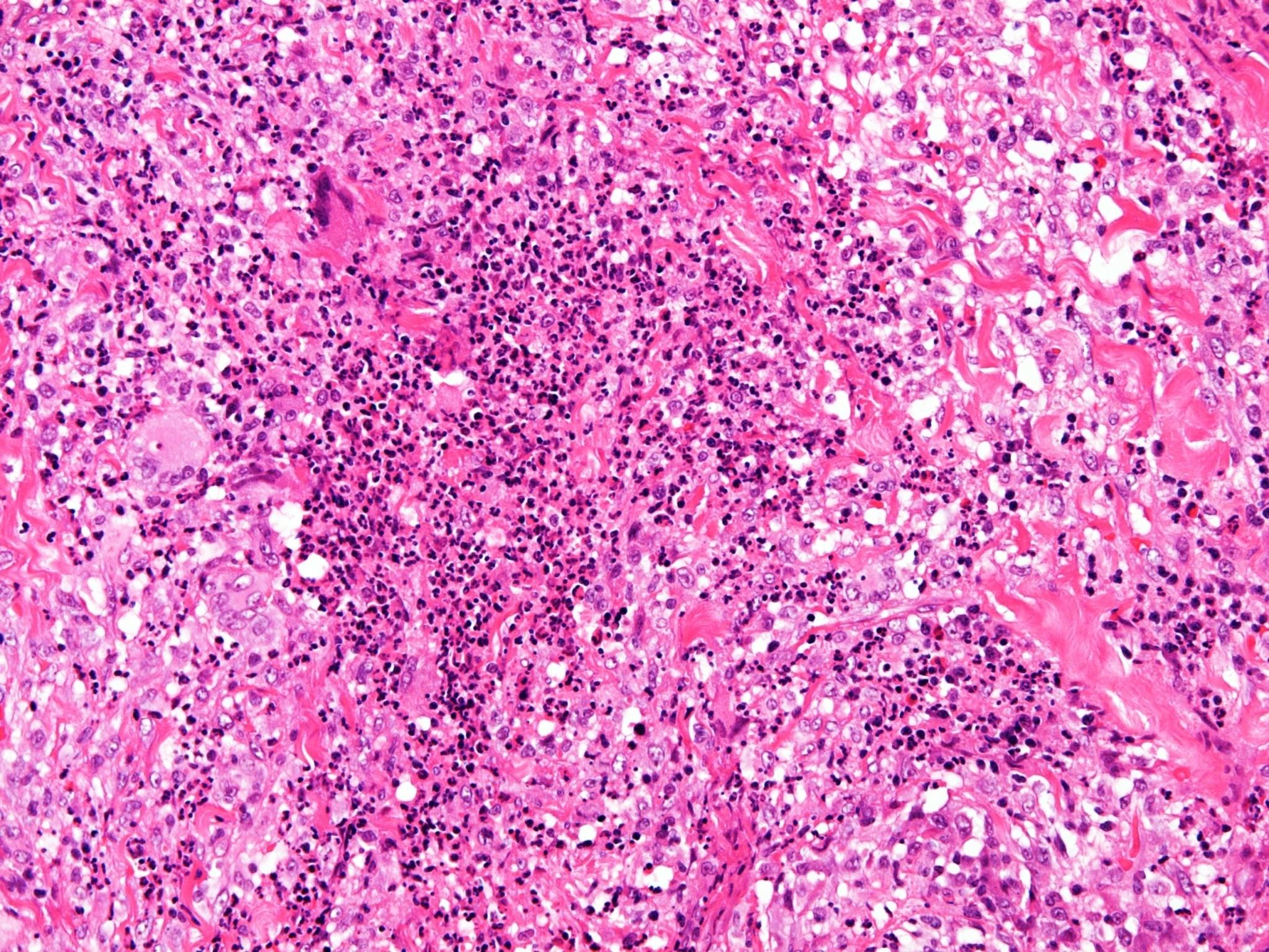
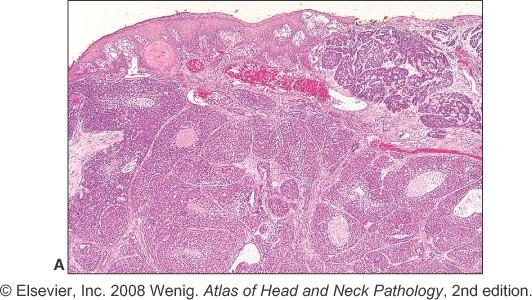
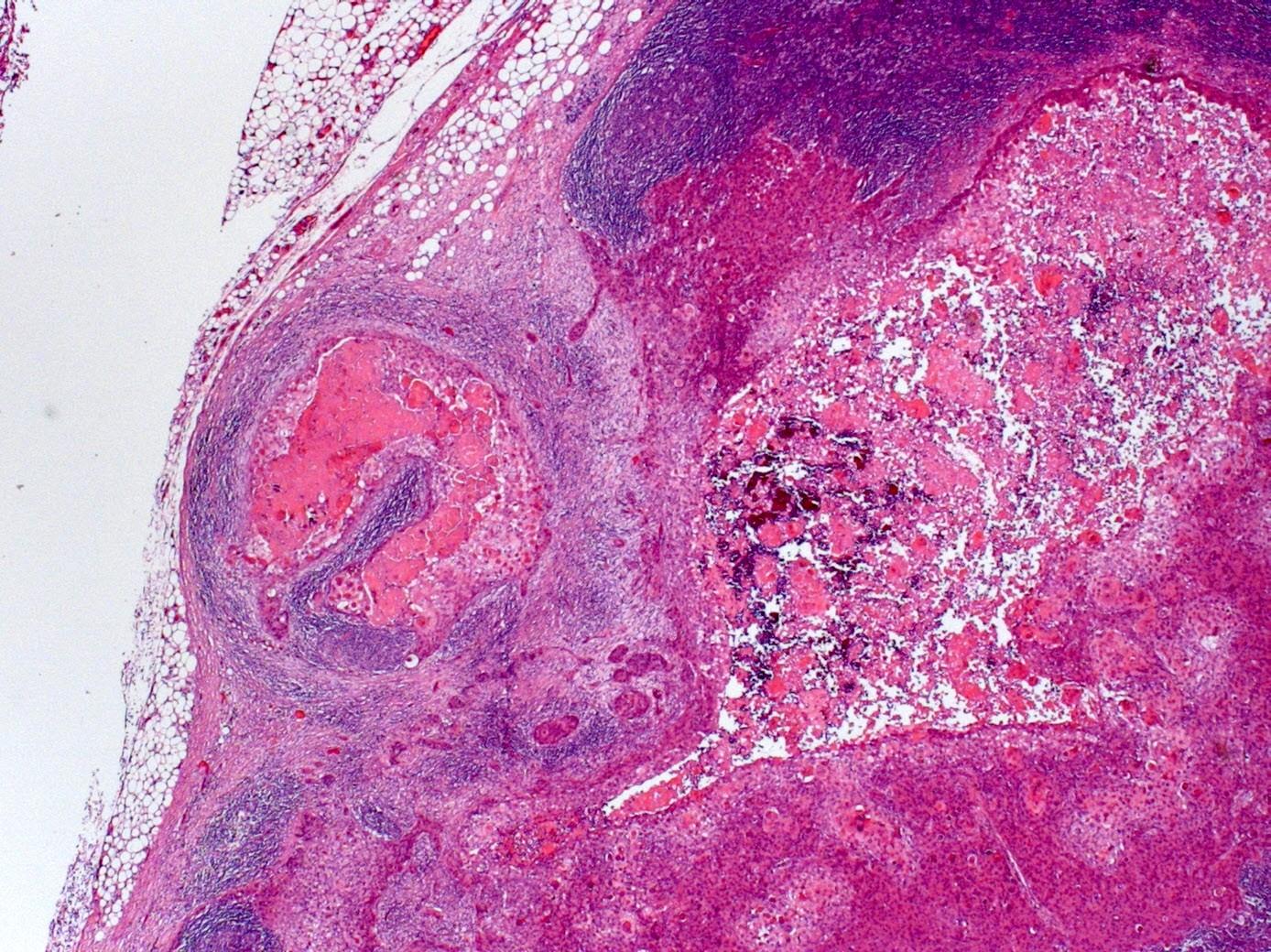
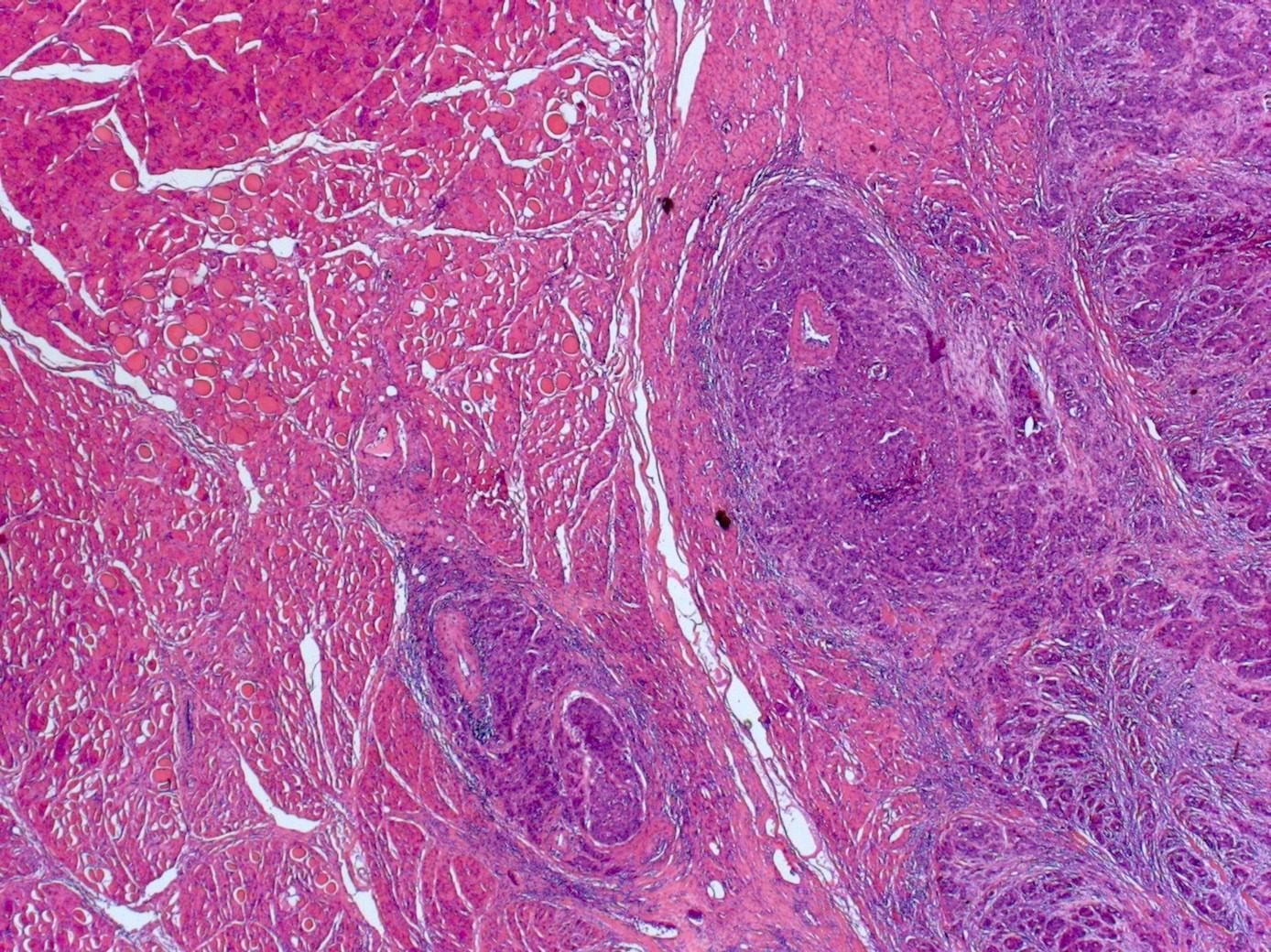
5. A 52 year old male also with crusting and ulceration of the nasal mucosa but with no other systemic symptoms. The biopsy shows geographic ulceration with sheets of small, medium and large cells present in viable areas which frequently invade vessel walls.
Tuberculosis
Wegener’s granulomatosis
Capillary haemangioma
Nasopharyngeal angiofibroma
Haemangiopericytoma
Malignant melanoma
Intestinal type adenocarcinoma
Mucocele
NK/T cell lymphoma
Sinonasal undifferentiated carcinoma
Olfactory neuroblastoma
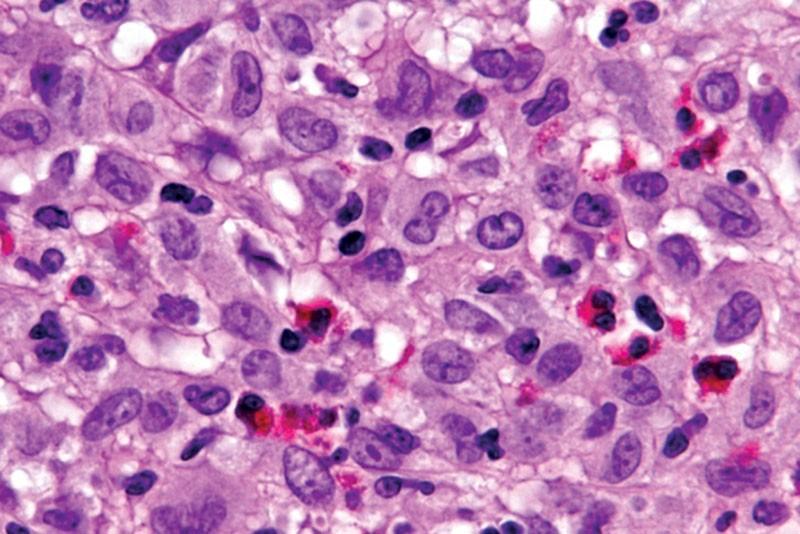
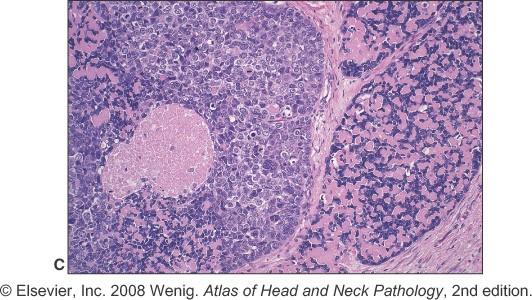
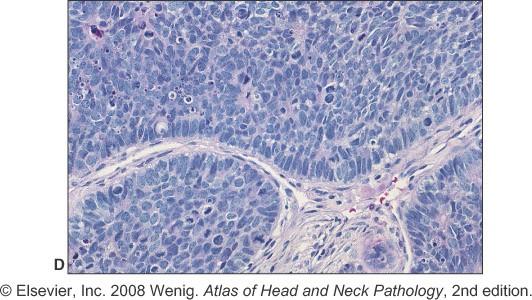
Sinonasal NK/T cell lymphoma
Broad morphological spectrum
Polymorphic with atypical lymphoid cells
Plus background of other cells (neuts eos)
Pale to clear cytoplasm
Angioinvasion
Geographic necrosis
CD56, variable for T cell markers (CD2)
EBV related
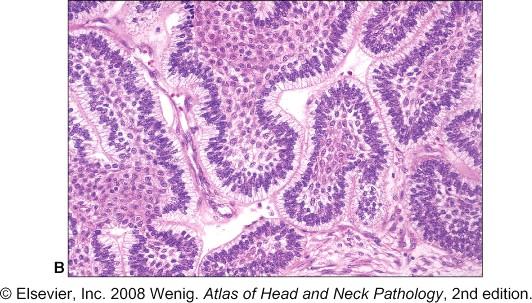
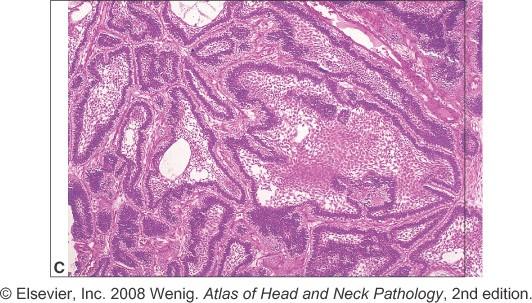
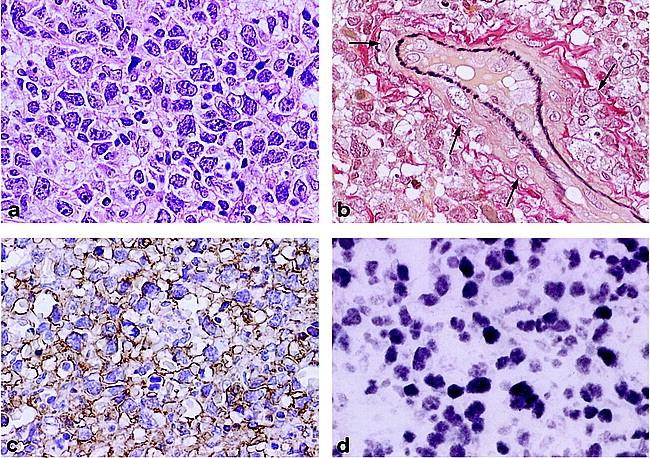
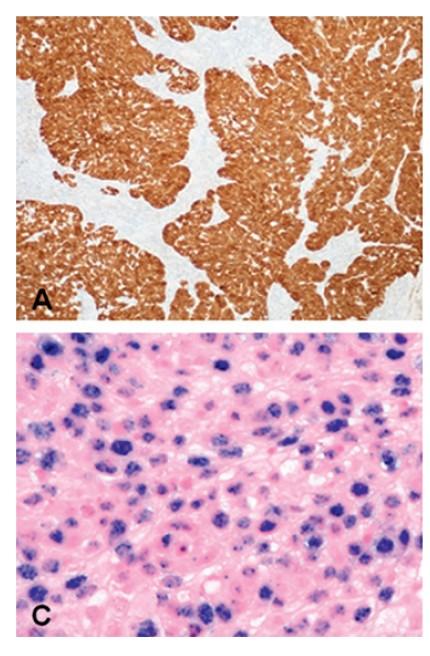
a, Proliferation of small to large, pleomorphic lymphoma cells
b, Lymphoma cells are invading a vein (arrows)
d, Expression of EBER1 in nuclei of lymphoma cells (EBER in situ hybridization,) Biopsy findings for the nasopharynx prior to radiotherapy.
c, Positive reactions for UCHL-1 are evident on the cytoplasmic membranes of lymphoma cells
Questions 5-10
Head and Neck
Minimum Datasets / cancer questions
Question 5
Lymph nodes lying deep to sternocleidomastoid at a level bounded superiorly by omohyoid muscle and inferiorly by the clavicle are located in anatomical level
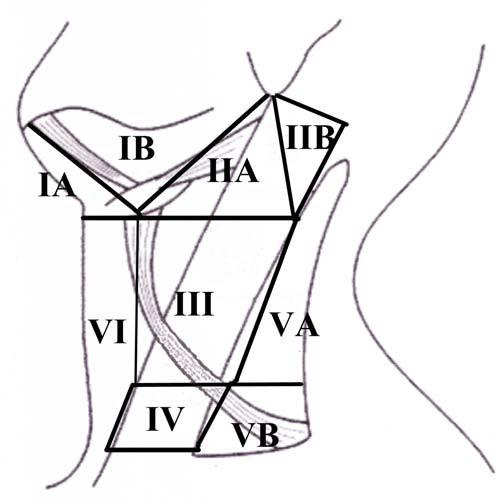
Terminology of node groups
Six major anatomical groups (levels) of lymph nodes are described.
Level I: nodes of the submandibular and submental triangles.
Levels II, III and IV: nodes of the upper, middle, and lower jugular chain. These nodes lie deep to the upper, middle and lower thirds of the sternocleidomastoid muscle respectively. The point at which the omohyoid muscle crosses deep to the sternocleidomastoid muscle is a useful landmark separating levels III and IV.
Level IV extends from the omohyoid muscle to the clavicle.
Level V: nodes of the posterior triangle, behind the posterior border of the sternocleidomastoid muscle.
Level VI: nodes of the anterior compartment, around the midline visceral structures of the neck from the hyoid bone to the suprasternal notch.
Imaging studies may subclassify node levels II and V.
It is not suggested that this should be part of routine pathological practice but if separate groups are submitted, e.g. IIA and IIB, this should be noted in the pathology report.
Lymph nodes lying deep to sternocleidomastoid at a level bounded superiorly by omohyoid muscle and inferiorly by the clavicle are located in anatomical level
Question 6
A tumour resected from the postero-lateral part of the tongue is seen to be composed of lobules of atypical cells with a high n:c ratio showing peripheral palisading, a thickened basement membrane and focal evidence of keratinisation. Cystic spaces containing mucoid material are seen and there is high grade dysplasia of the surface epithelium. There is also comedo type necrosis within larger islands. This is a:
A tumour resected from the postero-lateral part of the tongue is seen to be composed of lobules of atypical cells with a high n:c ratio showing peripheral palisading, a thickened basement membrane and focal evidence of keratinisation. Cystic spaces containing mucoid material are seen and there is high grade dysplasia of the surface epithelium. There is also comedo type necrosis within larger islands. This is a:
A resected squamous cell carcinoma of mandibular alveolus with a diameter of 22mm and depth of 7mm shows superficial erosion of the cortex of the mandible but not full thickness loss of cortical plate. This is most appropriately graded:
A resected squamous cell carcinoma of mandibular alveolus with a diameter of 22mm and depth of 7mm shows superficial erosion of the cortex of the mandible but not full thickness loss of cortical plate. This is most appropriately graded:
Question 8
Which of the following statements is true:
High risk HPV can cause squamous cell carcinoma at any site in the head and neck
HPV associated tumours are well differentiated
HPV associated tumours have a better prognosis and are more sensitive to non surgical therapy than nonHPV tumours
HPV is a rare cause of head and neck cancer
HPV associated tumours present with large primaries and rarely metastasize to cervical lymph nodes
HPV associated SCC almost exclusively in oropharynx i.e. tonsil
and base of tongue
NASAL CAVITY
PARANASAL SINUSES
ORAL CAVITY
NASOPHARYNX
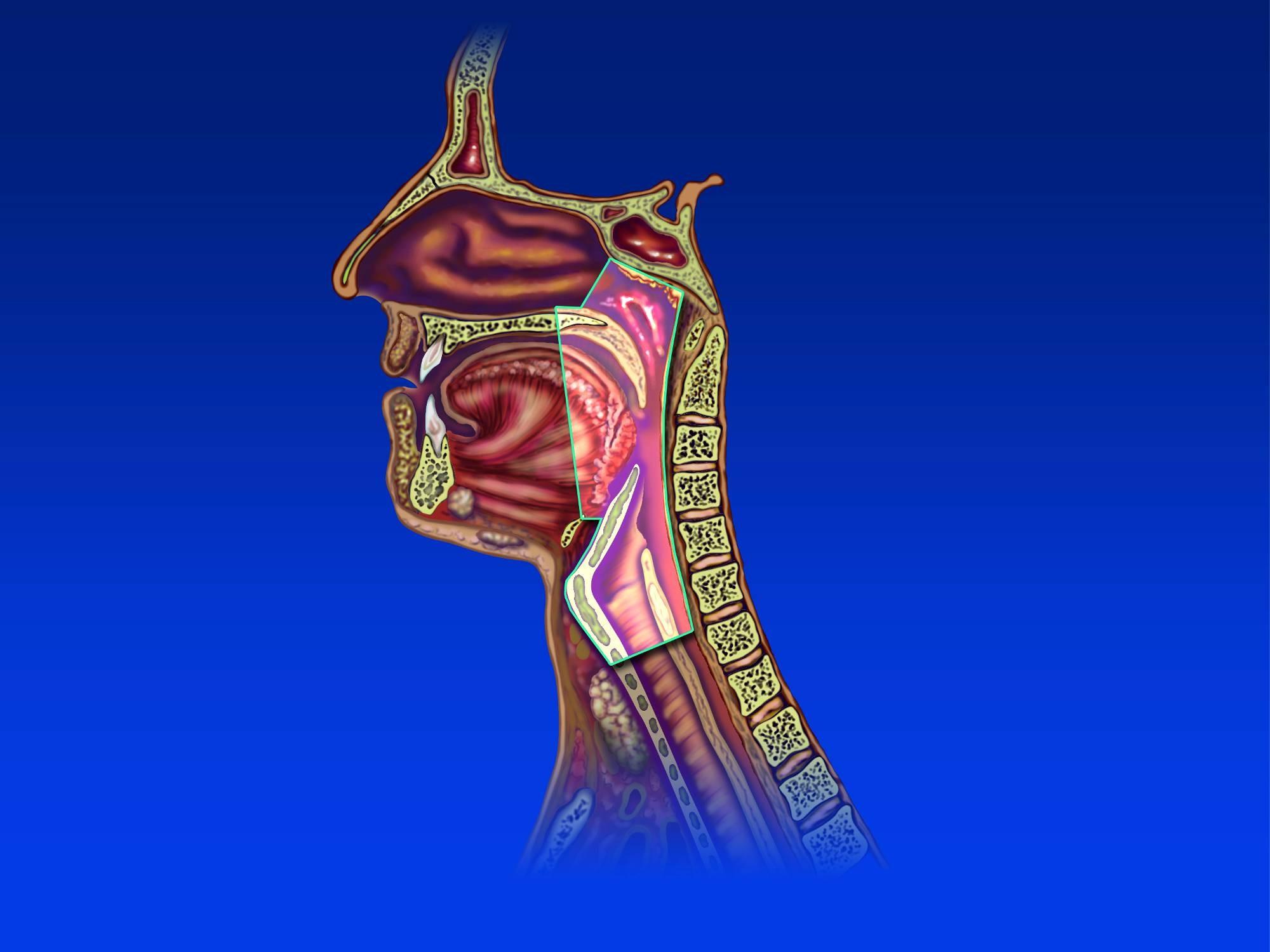
OROPHARYNX PHARYNX
HYPOPHARYNX
SALIVARY GLANDS
LARYNX
OESOPHAGUS
TRACHEA
Oropharyngeal
ca
As a proportion of H&N ca (US)
1973 – 18%
2004 – 31%
Oropharyngeal carcinoma
Incidence of tonsil cancer England
1997 n=281
2007 n=703
Oropharyngeal SCC
HPV as an aetiological agent first proposed in 1983
HPV + oropharyngeal ca is a different entity
Patient demographics and clinical presentation
Histological grading
Response to chemoradiotherapy
Clinical outcome
HPV 16
Oropharyngeal SCC
Thought currently that around 60% of oropharyngeal SCC are HPV associated
Other head and neck sites?
3% oral cavity
Detection of virus does not prove it is biologically relevant
HPV oropharyngeal carcinoma
Oral cavity ca ↓ 1.85% per year 19732004 (US)
Oropharyngeal ca ↑ 2-3% per year
Demographics
A decade younger than non-HPV SCC (50’s)
Especially males
Often non, ex or minimal smokers and low to moderate alcohol intake
Presentation more often with neck lump rather than primary lesion
Histological grading
For all cancer sites general principle in pathology that poorer differentiation associated with worse outcome
Poorly differentiated / basaloid SCC
Poorly differentiated basaloid SCC
Oral cavity / hypopharynx / larynx
HPV negative and poorer prognosis than conventional SCC
Oropharyngeal
If HPV associated, radiosensitive and much better prognosis
Basaloid squamous cell carcinoma of upper aerodigestive tract: a single squamous cell carcinoma subtype of two distinct entities hiding under one histologic pattern. Woolgar et al Eur Arch Otolaryngol 2011
Response
to chemo and radiotherapy
More radio and chemo sensitive than non-HPV tumours
Apoptosis / cell cycle inhibition pathways intact but switched off
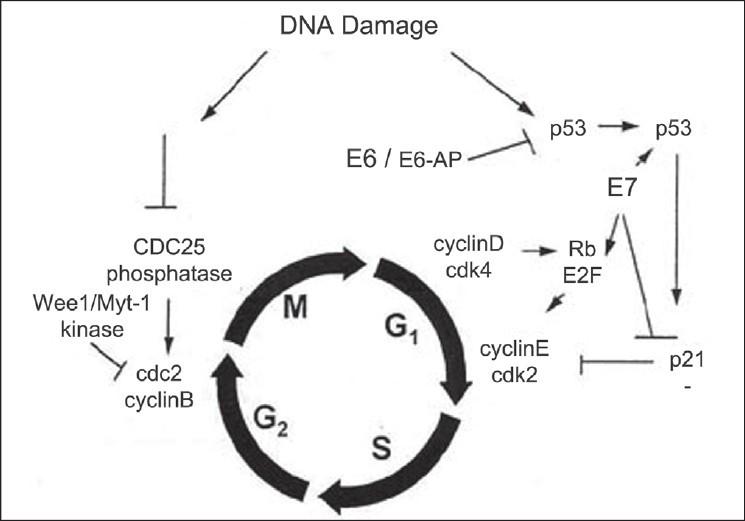
Molecular basis of HPV ca
Viral protein E6 inactivates p53
Viral protein E7 inactivates Rb
Rb normally held in a complex with E2F
E2F when free triggers cell cycle
Methods of testing
If positive HPV ISH or PCR (or both)
Survival data
5 year survival data
80-85% HPV +
30-35% HPV –
Independent of the treatment
HPV + tobacco users – negative effect on the prognosis
Which of the following statements is true:
High risk HPV can cause squamous cell carcinoma at any site in the head and neck
HPV associated tumours are well differentiated
HPV associated tumours have a better prognosis and are more sensitive to non surgical therapy than nonHPV tumours
HPV is a rare cause of head and neck cancer
HPV associated tumours present with large primaries and rarely metastasize to cervical lymph nodes
Question 9
A patient underwent bilateral selective neck dissections at the same time as removal of a floor of mouth SCC. Pathological assessment found 4 positive LNs on the right, largest 35mm and one on the left, diameter 10mm. The pathological stage is:
pN1(mi) Micrometastasis (2 mm or less) only, in single node
pN1 Metastasis in single ipsilateral node 30 mm or less in diameter
pN2(mi) Micrometastasis (2 mm or less) only, in multiple or bilateral nodes
pN2a Metastasis in single ipsilateral node 31–60 mm diameter
pN2b Metastasis in multiple ipsilateral nodes <61 mm diameter
pN2c Metastasis in bilateral or contralateral lymph nodes, none more than 60 mm in
greatest dimension
pN3 Metastasis in lymph node more than 60 mm diameter.
A patient underwent bilateral selective neck dissections at the same time as removal of a floor of mouth SCC. Pathological assessment found 4 positive LNs on the right, largest 35mm and one on the left, diameter 10mm. The pathological stage is:
Nodal staging
For nasopharyngeal primary carcinomas:
pN1 Unilateral metastasis <61 mm above the supraclavicular fossa and/or unilateral or
bilateral retropharyngeal metastases
pN2 Bilateral metastases <61 mm above the supraclavicular fossa
pN3 Metastasis in nodes >60 mm or in supraclavicular fossa
pN3a > 60 mm in dimension
pN3b Extension in the supraclavicular fossa.
Question 10
Which of these statements is true for oral SCC:
Perineural invasion does not influence prognosis
ECS is an important prognosticator and presence implies an aggressive tumour and poor prognosis
pT staging is based purely on size criteria
A cohesive pattern of invasion is associated with a
poor
prognosis
Microscopic ECS
Macroscopic ECS
Macro ECS – nerves and vessels
Importance of microscopic ECS
Which of these statements is true for oral
SCC:
Perineural invasion does not influence prognosis
ECS is an important prognosticator and presence implies an aggressive tumour and poor prognosis
pT staging is based purely on size criteria
A cohesive pattern of invasion is associated with a poor prognosis