
DEPARTMENT OF CAREER AND TECHNICAL EDUCATION HEALTH SCIENCE PROGRAMS
A health report, including a physical, is essential before the school district will admit any applicant to a Health Science Education program which involves clinical training/patient contact, because it shows evidence that the person can meet the demands of the occupation and adjust to them without hazard to self and to the patient/client.
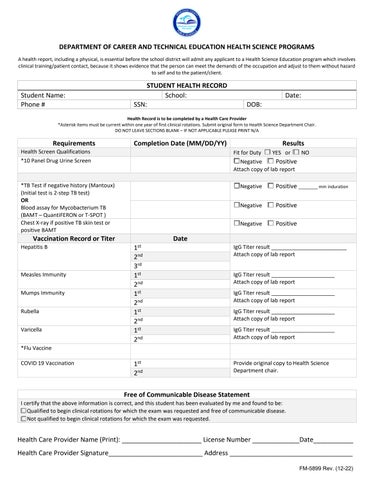
STUDENT HEALTH RECORD
Student Name: School: Date:
Phone # SSN:
Health Record is to be completed by a Health Care Provider
*Asterisk items must be current within one year of first clinical rotations. Submit original form to Health Science Department Chair. DO NOT LEAVE SECTIONS BLANK – IF NOT APPLICABLE PLEASE PRINT N/A
Requirements Completion
Health Screen Qualifications
*10 Panel Drug Urine Screen
*TB Test if negative history (Mantoux) (Initial test is 2-step TB test) OR
Blood assay for Mycobacterium TB (BAMT – QuantiFERON or T-SPOT )
Chest X-ray if positive TB skin test or positive BAMT
Vaccination Record or Titer
Hepatitis B
copy of lab report
*Flu Vaccine
COVID 19 Vaccination
Free of Communicable Disease Statement
I certify that the above information is correct, and this student has been evaluated by me and found to be:
☐Qualified to begin clinical rotations for which the exam was requested and free of communicable disease.
☐Not qualified to begin clinical rotations for which the exam was requested.
Health Care Provider Name (Print):
Health Care Provider Signature__________________________
Certification of Applicant - To be reviewed and completed by applicant
I hereby certify to the best of my knowledge; I have no mental impairments or physical illness which could interfere with the general performance of functions assigned to me as a health care provider.
I understand that I must submit a medical clearance from an obstetrician if I am pregnant or become pregnant during my training program.
Name of Applicant: _____________________________________________________________________________________
Signature: ____________________________________________________________________________________________
Parent Signature (If applicable): ___________________________________________________________________________
Date: ________________________________________________________________________________________________