

CareSource is a proud sponsor of both the Institute for Relational Health and The Family Justice Journal

CareSource is a proud sponsor of both the Institute for Relational Health and The Family Justice Journal
008 What Policy Can Make Possible
Jerry Milner & David Kelly
Directors of the Family Justice Group Foreword
010 Shrounda Selivanoff
Social Service Manager at the Washington State Office of Public Defense Parent Representation Program Introduction
032 In Brief
The Role of Congress in Improving the Child Welfare System
Representative Judy Chu
U.S. Representative for California’s 28th Congressional District
034
Supporting Tribal Families Act
Representative Don Bacon
U.S. Representative for Nebraska’s 2nd Congressional District
My Perspective
060 Alexandria Ware Founder of Culture Creations Inc.
012
Features Reimagining How Cases End and Families Evolve
Shrounda Selivanoff
Social Service Manager at the Washington State Office of Public Defense Parent Representation Program
Tara Urs
Special Counsel for Civil Policy And Practice at The King County Department of Public Defense
016 Universal, Unconditional Cash Prescriptions Address Perinatal Poverty to Reduce Child Maltreatment
Alison Dickson, MD, MPH
Resident in Preventive Medicine Residency Program at the University of Michigan School of Public Health
Teagen Medlin
Mother of three young children, a resident of Flint Michigan, and a participant in the Rx Kids Program
Luke Shaefer, PhD
Co-Director of Rx Kids & Professor of Social Justice and Social Policy at the Ford School of Public Policy at the University of Michigan
Mona Hanna-Attisha, MD, MPH
Co-Director of Rx Kids & Director of the Michigan State University-Hurley Children’s Hospital Pediatric Public Health Initiative
024 Fund Kinship Caregivers to Help Keep Families Together, Not Separate Them
Josh Gupta-Kagan
Clinical Professor of Law at Columbia Law School
064 Kathleen Creamer, J.D.
Managing Attorney, Family Advocacy Unit
Community Legal Services of Philadelphia A Better Way
036 Yven Destin
038 Reducing Family Surveillance to Improve Child Well-Being
Anna Arons
Assistant Professor of Law, St. John’s University
School of Law & Impact Project Director, Family Defense Clinic, NYU School of Law
Features, continued
044 Policies of Compassion: Supporting the Health and Safety of LGBTQ+ youth and their families
Kristen Weber
Senior Director of Child Welfare at the National Center for Youth Law
Vida Khavar
Clinical Director at Family Builders
Bill Bettencourt
Senior Fellow with the Center for the Study of Social Policy
050 Ushering in Mandated Support for U.S. Educators
Chelsea Prax, MPH CPH
Director of AFT Children’s Health and Well-Being
054 Advancing Early Relational Health Policy in Support of Next Generation Flourishing
David W. Willis, MD
Founder, Nurture Connection
Cailin O’Connor
Senior Associate of Center for the Study of Social Policy
Artwork
030 System vs. Growth
Tia Humphrey


Kevin Burdick
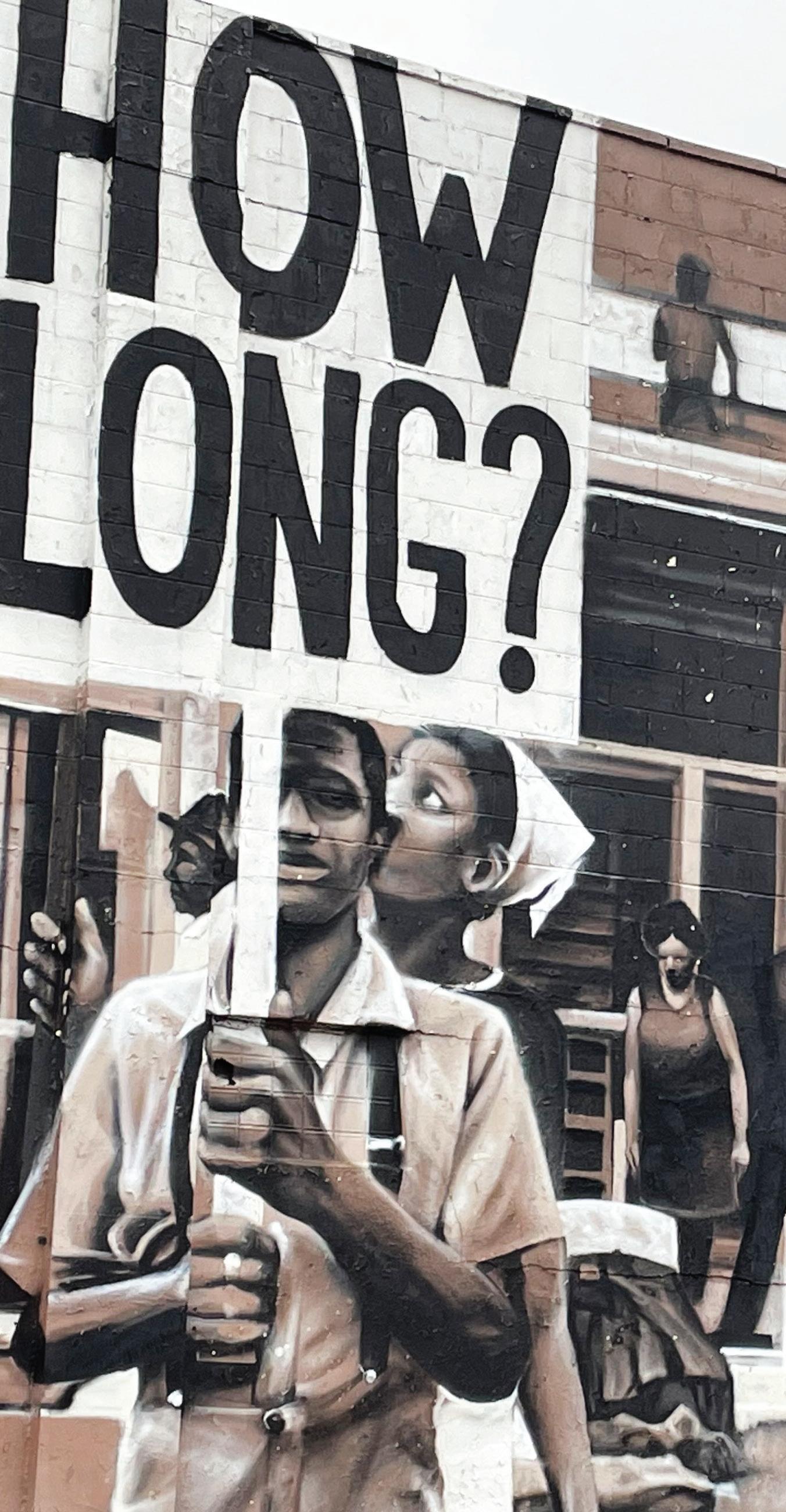
Born 1985 in Flint Mi., then raised in Fenton Mi. I First attended Mott Community College, were I studied basic art. At this point I realized that Art would be my profession. I was later accepted to the Art Institute of Pittsburgh where I studied Animation and Illustration.
After school I started experimenting with different mediums, including Airbrushing and Aerosol. I was first given the opportunity to airbrush professionally at T-Rods in Flint Mi and later partnered with Psycho Customs in Bay City Mi. In the last few years, my focus has been on aerosol murals. Although airbrushing made up the foundation of my art career, aerosol art is becoming the creative outlet and freedom every artist seeks. After years of trial and error I now feel that I can provide high quality artwork to a wide range of clients and programs.
www.scrapsdesigns.com
Christopher Baker-Scott
Executive Director & Founder SUN Scholars, Inc.
Angelique Day, Ph.D., MSW
University of Washington Seattle
Associate Professor
Faculty Affiliate of the Indigenous Wellness Research Institute
Director of federal policy for Partners for Our Children
April Lee
Director of Client Voice
Community Legal Services of Philadelphia
Dr. Melissa T. Merrick
President and CEO
Prevent Child Abuse America
Jey Rajaraman
Associate Director, Center on Children and the Law, American Bar Association
Former Chief Counsel, Legal Services of New Jersey
Vivek Sankaran
Clinical Professor of Law, University of Michigan, Michigan Law
Shrounda Selivanoff
Social Services Manager
Washington State Office of Public Defense Parents Representation Program
Victor E. Sims, MBA, CDP
Senior Associate Family Well-Being Strategy Group
The Annie E. Casey Foundation
Paul Vincent, MSW
Former Alabama Child Welfare Director Consultant and Court Monitor
Justin Abbasi
Co-Founder, Harbor Scholars: A Dwight Hall Program at Yale
Laura W. Boyd, Ph.D.
Owner and CEO, Policy & Performance Consultants, Inc.
Angela Olivia Burton, Esq.
Co-Convenor, Repeal CAPTA Workgroup
Melissa D. Carter, J.D.
Clinical Professor of Law, Emory Law
Kimberly A. Cluff, J.D.
MPA Candidate 2022, Goldman School of Public Policy
Kathleen Creamer, J.D.
Managing Attorney, Family Advocacy Unit Community Legal Services of Philadelphia
Angelique Day, Ph.D., MSW
Associate Professor, Faculty Affiliate of the Indigenous Wellness Research Center
Director of Federal Policy for Partners for Our Children School of Social Work, University of Washington Seattle
Adjunct Faculty, Evans School of Public Policy and Governance
Yven Destin, Ph.D.
Educator and Independent Researcher of Race and Ethnic Relations
Paul Dilorenzo, ACSW, MLSP
National Child Welfare Consultant
J. Bart Klika, MSW, Ph.D.
Chief Research Officer, Prevent Child Abuse America
Heidi Mcintosh
Chief Operating Officer, National Association of Social Workers
Kimberly M. Offutt, Th.D.
National Director of Family Support and Engagement Bethany Christian Services
Jessica Pryce, Ph.D., MSW
Research Professor College of Social Work Florida State University
Mark Testa, Ph.D.
Distinguished Professor Emeritus, University of North Carolina, Chapel Hill
Elizabeth Wendel, MSW, LSW
Co-Founder, Pale Blue International Consultant, Family Well-Being and Mental Health Systems
Shereen White, J.D. Director of Advocacy & Policy, Children’s Rights
Cheri Williams, MS Founder and Chief Co-Creator at CO-3
The Family Justice Group is grateful for the financial sponsorship of this issue of the Family Justice Journal by the Institute for Relational Health (IRH) at CareSource. We are happy to advance the work of the IRH in promoting relational health for families, children, youth and communities, particularly those impacted by our child welfare, juvenile justice and mental health systems and individuals with disabilities. We believe that discussing and bringing to light the harms of disconnection are necessary acknowledgements of the critical importance of relational health in all our lives.

Jerry Milner
Chief
Co-Director of the Family Justice Group

Editor
- in
David Kelly
Chief
Co-Director of the Family Justice Group

Design Director
Ann T. Dinh Design Consultant
Jerry Milner & David Kelly
Policy matters. Those who write and implement it have profound impacts on the daily lives of families, especially families struggling with poverty and other difficult societal conditions. People facing adversity most typically know what would help them. The problem is we seldom ask. If we take the time to ask, their insights would be instructive. Yet, meaningful inclusion of impacted individuals---real people whose lives have and will be most affected---in policymaking remains woefully inadequate. Too often, it’s a superficial exercise, tantamount to review and comment or a request to lend voices to premade solutions.
It should be no surprise then that there is a stark contrast between current child welfare policy and what families say would help. Where we could have a proactive, streamlined approach that addresses stated familial needs, we instead have a tangled web of laws and funding schemes that limit how and when we can help and fail to address root causes. This results in families not getting what they need, communities being undervalued and deep, enduring health, social, economic, and racial disparities. It also tills fertile ground to pit child safety against family support and other dangerous false dichotomies.
But despite all of this, there are clear pathways that can lead us in a much more humane, effective and efficient manner to keep families, communities and tribes strong and together.
In this issue of the Family Justice Journal, contributors offer compelling, common-sense solutions that are based on what impacted people say would be most helpful and grounded in additional sources of evidence. While perspectives vary, they are united in doing right by fellow human beings. Taken together, these policy recommendations propel a critical shift toward strengthening and supporting families, promoting and preserving vital relationships and thinking more broadly about permanency. The ideas shared should spark further thinking and lend support to additional legislative changes that recognize the centrality of our relationships to our health, prosperity and self-determination.
A young native woman passionately detailing the impact of child welfare practice on her community . . .
A grandmother raising her grandson to honor, know and love his father despite circumstances that keep them apart and ultimately preserving his memory after death…
Objective academics who have methodically studied policy, the outcomes it produces and the negative impact on parents, caregivers and children . . .
A pediatrician who sees daily the direct health impacts of poverty on children and their parents and how modest, short-term financial support can change their trajectories…
An educator who wants to get help to families instead of having them investigated for poverty . . .
Members of Congress who put aside partisanship to promote and sustain tribal family unity . . .
A young woman who experienced foster care speaking to the healing power of restorative justice …
Respected researchers demonstrating the impact of early relational health on child development and long-term well-being…
When perspectives such as these shape policy, it can lead to much better outcomes and experiences. They can inspire lawmakers from different sides of the aisle to jointly support policies that meet familial needs, prevent the trauma of unnecessary separation, and position children for success in life. It can lead to innovative, sensible use of public funding to prevent economic hardship, future dependence and more expensive interventions down the road. It can reduce the likelihood that harmful intergenerational cycles will continue, and it can provide prescriptions of hope.
Policy can be a tool for recognizing it is our relationships that make us human and our connections to community and culture that bind us together, lift us up and sustain us through life’s adversities. Policy can and should help ensure that this knowledge guides our work.
With something so important we cannot allow catchwords and phrases to divide us and take center stage over concrete, family-informed actions that will yield better results. It’s the impact on families that should matter most, not the name of the effort or the words used to describe it. Moreover, reliance on popular language also risks leading us to think we’ve done more than we’ve really done.
Likewise, we should not confine ourselves to relying on a singular model of evidence to justify meeting the most fundamental needs of all human beings, positioning people for success and helping them avoid child welfare entanglement.
So how, then, can policy create changes that go beyond tweaking a harmful system and truly strengthen families and communities? By directly addressing the issues that parents and caregivers most commonly raise.
• By implementing policy definitions that de-link poverty and neglect. We should not treat neglect the same as abuse. There must be a different approach. If money can fix the problem, provide money to meet the need, rather than 12 months of therapy that still won’t pay the rent or buy the food.
• By funding support for families who otherwise become vulnerable to separation. Ensure that existing programs, such as TANF, actually support families and are no longer misdirected to things that do not. Also, invest in the financial ability of new parents to meet their children’s needs when they are most likely to be unemployed and in need of assistance.
• By implementing policy that reserves the most intensive child welfare interventions for the most egregious circumstances. Restrict hotline reporting to situations where children are being harmed and fund alternate ways to get help to families who simply need help.
• By implementing policies that require active efforts to keep families safely together before family separation becomes an option. Fund community-based family supports, raise the bar for removing children, eliminate arbitrary negotiated timelines for permanently terminating children’s rights to their parents, and provide more funding for family support than for foster care and adoption.
• By swiftly passing H.R. 3461, the Strengthening Tribal Families Act, and expanding flexibilities for traditional tribal healing, wellness and caregiving practices across all title iv-e and iv-b programs and funding. Indigenous wisdom and cultural practices should be recognized as equally as valuable as western approaches and treated with the same respect.
• By requiring new child welfare policies to be sanctioned by families impacted by child welfare. Change the policymaking process itself to ensure that the voices of youth and parents carry the heaviest weight in determining the direction of change.
• By funding communities more and State removal agencies less. The community must be the face of family support. If we direct all the CAPTA funding, most of the title IV-B funding, and flex title IV-E funding to permit community funding, policy can make an unprecedented impact.
In these times of ever deepening divisions, othering, and wars of words, it’s parents, caregivers and children that suffer when resources are weaponized or harmful status quo orientations maintained. We can rise above the tendency to craft policy that doles out punishment and places limitations on worthiness. We can choose to see and be guided by our common humanity. And, when we do, we will all feel and be more human.
SHROUNDA SELIVANOFF
Social Services Manager
Washington State Office of Public Defense
Parents Representation Program




In January, as I finished giving testimony in our state legislature, the chair of the committee spoke up. She knew the dependency case involving my grandson had just ended. “Congratulations,” she said, “on finalizing the adoption of your grandson.”
“No,” I replied, “it wasn’t adoption, it was a guardianship.” And I thanked her for her work on HB 1747, a 2022 law that requires a court to rule out a guardianship before they can terminate parental rights.
Because of that legislation, which I had strongly advocated for, I was able to convince our state agency to allow me to resolve my grandson’s case with a guardianship rather than terminating the parental rights of my son Alexei. I was able to avoid adopting my grandson, which would have erased Alexei from the official record of his own son’s life.
In the hearing room in Olympia, I reflected on that legislator’s comments. I understood her confusion.
For so long in this system, success has meant finality, and finality has meant adoption
But what I couldn’t possibly have understood in that moment, however, was how much more the idea of “finality” would soon mean to me. The next day I learned that Alexei was shot and killed by the Tacoma Sheriff ’s Department while he was running away from a traffic stop. My world ended then. There are no words for it. I cannot make sense of the loss of my son, and I will not try to do that now.
But in this pain, I see this work of “child welfare” differently. It is clearer to me now that the current setup is for “finality,” this idea that things need to be concluded. That we can wash our hands of someone and believe we have done something good.
The United States does a lot of erasing: it erases people from their communities, from their connections, from their families. A central part of the American story is the legacy of erasing the
bodies and identities of Black people. Adoption, too, is an erasure; it erases parents from their child’s birth certificate and replaces them with new parents.
I could have never known that an event would happen that would remove my son’s presence from my life and from his son’s life. But if we had not passed HB 1747, if I had instead adopted my grandson, there would be a sickening feeling every time I looked at his birth certificate. I would have been reminded that I colluded to erase my family’s history—my own son. It is a disgusting proposition. Future generations need to know that my son’s life mattered—that he was here.
Thinking about HB 1747, I feel a small amount of peace and some serious unrest. I’m grateful that my son lived his last days knowing that he had rights. And he was grateful to know that I cared enough to fight for him. I think about the frustration, the misunderstandings, and the volatility that I experienced along the way. It was all necessary to keep us intact.
Through this process, I have come to believe that, more than the legal truth, there is a spiritual truth at work in what we do in this system. A child is born with far more than legal rights; a child has a birthright: to their ancestors, to their history, to the legacy of their people. The law can’t change Creation.
As my son returns back to his spirit, part of his legacy lives on in his child. It is for me to teach my grandson and to help him understand that his life is an offering to the ancestors, to respect all that was sacrificed for him to have what he has today.
When I think about the legacy my grandson has inherited, I think about my ancestors who endured the unthinkable. They fought, and they built, and they planned, and they believed that—one day— this would be different. Part of the legacy, for me, is teaching our children how much was sacrificed for them to have a life that wasn’t built on enslavement, a place where they can prosper. I want to share with my grandson the strength of his ancestors.
But I must also help him understand how, even today, none of this is designed for his advancement. So much of the world he will walk through has been designed for his demise. That is also part of our story.
In this system of “child welfare,” we can—we must—move closer to the beauty of Creation, to appreciate and love the people who have been
brought into our lives. And we must move away from the false belief that the law can design, deconstruct, or dismantle what has already been put in place by God. Our ancestors ask us to be in light, to truly love and be there for one another. From the start of my grandson’s case, I wanted him to be with his parents. I’ll never forget the day that I sat on that phone and listened to the state terminate his mother’s rights, with no attorney present, with no cross examination, no accountability. As I protested in that hearing the judge said, “be quiet,” and “our business is terminating her parental rights; your care and concern has no place here.” My care and concern had no place there.
Because of HB 1747, however, my grandson’s mother’s name remains on his birth certificate today. Since the case ended with a guardianship, there was no adoption, and there was no change to the birth certificate. My grandson has a mom and a dad, aunts and uncles, grandparents. He has a birthright to those people—that’s his lineage, that’s his legacy. I don’t want to be a part of changing that, I want to be a part of supporting that. Care and concern should always have a place.
Often in adoption finality is not just about severing ties in the legal sense, it severs connections in the physical and emotional and familial sense, and by doing that it removes spaces and options for healing. But life has many unknowns. Actually, it’s all unknowns. Closing doors, trying to securely lock them, leaves folks locked in just as much as it locks others out. As people age, we gather wisdom and experiences, and we change. Finality leaves no place for reconciliation, reconsideration, or healing.
The adoption story, which values finality, relies on an assumption: that everyone lived happily ever after. Yet, I believe that assumption hurts everyone involved. It fails parents who live with the wounds of termination for the rest of their lives. But it also fails the caregiver, who must live up to an impossible ideal. And it fails the child, who must perform a part in a fairy tale, without the freedom to acknowledge the challenges of real life.
On the other hand, HB 1747 recognizes something fundamentally true: even if the system wants “closure,” families are evolving; they don’t reach an end. Families and people are always in a state of change: messy, complicated, joyful change. If we leave the door open to change, we can welcome healing. But if we lock the doors, we deny ourselves the beauty of one another.



SHROUNDA SELIVANOFF
Social Services Manager
Washington State Office of Public Defense
Parents Representation Program
TARA URS
Special Counsel for Civil Policy & Practice at The King County Department of Public Defense




Shrounda Selivanoff is the Social Service Manager at the Washington State Office of Public Defense Parent Representation Program. She brings a fierce and passionate voice advocating for systemic change for parents and their children involved with the child welfare system. She was previously involved with the child welfare system. Through life challenges, she has persevered. She continues to learn more about the child welfare system from the perspective of a kinship caregiver to her grandson.
Shrounda’s child welfare experience birthed an advocate seeking to destigmatize parents and elevate the need for our society to value families’ diversity and uniqueness. Shrounda’s work is focused on centering parents’ perspectives to support their families.
Shrounda relentlessly pursues policy and system change toward preserving and strengthening families with a North Star, empowering and valuing parents as partners, and keeping families together. She keenly understands the power and impact of preserving families and the critical need for individual and collective transformation.










Tara Urs, special counsel for civil policy and practice at the King County Department of Public Defense. Tara has led the department’s efforts to transform dependency law in the state, drawing on our attorneys’ expertise to challenge a system that harms children and families and disproportionately harms Black and Indigenous families.
She has testified countless times in the state legislature, argued before the state Supreme Court, including In re Dependency of ZJG and In re Matter of KW, and authored numerous amicus briefs on key appellate cases. Before joining DPD’s management team, she practiced family defense at The Defender Association Division and, prior to that, worked as a staff attorney at the Brooklyn Family Defense Project.
Tara received her BA from Wesleyan University and her JD from New York University School of Law, where she was an Arthur Garfield Hays Civil Liberties Fellow and winner of the John Perry Prize for Civil Liberties and Civil Rights. She clerked for Judge Deborah A. Batts, U.S. District Judge for the Southern District of New York.
1 Richard Powers, The Overstory, pg. 115 (2018).
2 Sandra White Hawk, Generation After Generation We Are Coming Home, Outsiders Within: Writing on Transracial Adoption (2006), 291 (“The very things that I was to be ‘saved from’ – poverty, abuse, and alcoholism – were thrust onto me by life’s natural unfolding. My adoptive father died as a result of a farm accident when I was six.”)
3 Susan Devan Harness, Bitterroot: A Salish Memoir of Transracial Adoption (2018), 333 (“Yes, parents lost us as adoptees, but we have lost our entire family, entire tribes, who could have helped us navigate the dangerous waters we crossed, in ways our adoptive families could not. We needed them in our lives.”).
4 The legislative history of the bill (substitute house bill 1747, which passed in 2022) can be found on the Washington State Legislature website: https:// app.leg.wa.gov/ illsummary?BillNumber =1747&Initiative = false&Year=2021.
5 RCW 13.34.138(2) (a).
6 The dependency case can continue past age 18 if the youth elects to participate in extended foster care. RCW 13.34.030(6).
7 Washington has two different forms of guardianship, either of which can end a dependency case. One form of guardianship is a family law order pursuant to RCW 11.130 that
is available to any non-parent seeking legal custody of a child, and the other is a “dependency guardianship” pursuant to RCW 13.36 that is only available as a resolution of a dependency case. Between the two options, a guardianship under RCW 11.130 is easier to reverse if a parent comes forward later. A guardianship pursuant to RCW 13.36 can only be reversed on a showing of a substantial change in circumstances in the life of the child or the guardian (not the parent). However, both forms can be easily reversed on the agreement of all parties.
8 RCW 13.34.145(5)(a) (vii), (7)(b).
9 RCW 13.34.180(1)(f).
10 RCW 13.36.090, Laws of 2023, ch. 221, § 1(1), (ESB 5124).
11 Id. § 1(2).
12 RCW 11.130.215; RCW 13.36.050; RCW 74.13.062. Not addressed here, but equally important, are the many recent federal and state statutory and regulatory changes intended to facilitate kinship licensing. Laws of 2021, ch. 211, § 9 (E2SHB 1227) (requiring DCYF to create an initial license procedure during the period of emergency out-of-home placement and report about licensure to the court); 88 FR 66700 (federal regulatory changes to facilitate kinship licensure). A foster care license is a requirement for a guardian to receive GAP (or EGAP); historically very few relatives in Washington have been licensed, but the state is trying to improve.
As certain as weather coming from the west, the things people know for sure will change. There is no knowing for a fact. The only dependable things are humility and looking.1
At the conclusion of a dependency case, no one can know what any parent and child will need from each other in years to come, what they have to offer each other, or how they will change. It is hubris to think otherwise. Even when a court cannot agree to return a child home, no one can predict whether the caregiver will someday fall on hard times and need the support of the parent2 or whether the child will need the comfort of someone who has overcome the challenges they are facing.3
In Washington state, we have been reimagining how to end dependency cases, recognizing that change is inevitable. We envision a legal system that embraces growth, belonging, and family connections—a system that always wants to leave the door to healing open. Therefore, we have been working on ways to shift our practice towards ending cases with reversible legal orders, like guardianships, rather than supposedly permanent orders like adoption.
Of course, our ultimate goal is to ensure that families and extended families receive the support they need so that children are never removed, and families can go through hard times relying on one another, without state oversight, control, or oppression. But while we work to create such a world, in the meantime, we believe “child welfare” systems can do less harm by reimagining how cases end.
In our state, a dependency case does not end unless a child has been returned home to a parent for six months,5 the child ages out of the system,6 an order of guardianship is entered,7 or a parent’s rights are terminated and an adoption is finalized. Here— like the rest of the country, thankfully—most cases resolve with children being returned home.
But also like the rest of the country, the second most common outcome in Washington is adoption.
Hopefully, that is about to change. Because of new legislation championed by Rep. Lillian Ortiz-Self and supported by the Keeping Families Together coalition, our state must now prioritize resolving cases with a guardianship, instead of defaulting to termination and adoption.
These statutory changes have taken three forms: 1) changing the practice of permanency planning, 2) changing the law of termination, and 3) creating financial benefits and supports for guardians.
First, HB 1747 made changes to the permanency planning process in dependency cases, creating a new basis for a court to find “good cause” not to order our state agency to file a termination petition when “the department has not yet met with the caregiver for the child to discuss guardianship as an alternative to adoption or the court has determined that guardianship is an appropriate permanent plan.” 8
Second, the law made changes to the legal standard for terminating parental rights. Now, before terminating,
“the court must consider the efforts taken by the department to support a guardianship and whether a guardianship is available as a permanent option for the child.” 9
Third, the legislature has made a series of substantive changes to the benefits available to guardians to provide financial support for guardianship under the Guardianship Assistance Program (GAP). The legislature has made changes to 1) allow guardianship subsidies for non-relative guardians10, 2) ensure that (as with adoption subsidies) guardians can receive an ongoing financial subsidy even if the parent’s dependency case is not eligible for federal reimbursement11, and 3) allow subsidies for guardians of dependent children who enter minor guardianship using either form of state guardianship order.12
Even more significantly, the legislature has made financial benefits available to guardians that are not available as adoption subsidies, thereby encouraging guardianship over adoption. Unlike those who adopt, those who enter guardianships for dependent children under the age of 16 can
receive an ongoing financial subsidy—extended guardianship assistance payments (EGAP)—until the young person is 21 years of age, provided they are complying with some requirements.13 Adoption subsidies for children adopted under the age of 16 end at age 18.14
But as we look to prioritize guardianship, there are also questions we still need to answer. For example, although any child who is part of the guardianship assistance program also qualifies for state funded health insurance, some caregivers have questions about whether children in guardianships can be added to the guardian’s private insurance. Also, because guardianship ends at age 18, we have heard questions about whether a guardian would be “next of kin” in certain medical situations after the child becomes an adult, as well as questions about how we can ensure the guardian actually provides the EGAP subsidies to the young person after age 18. Finally, courts have questioned the role the caregiver should have in deciding whether the state should pursue guardianship or termination/ adoption. Should a caregiver get to decide that the state must pursue termination?
But even beyond these questions, as we have begun implementing these statutory changes, we have seen resistance in practice. In closed-door meetings with caregivers, social workers continue to question guardianship and seed worry about the parents: what if they come back?
It is apparent, therefore, that for these statutory changes to be effective, we must do more than just change the law. We must also collectively reimagine the role of the law in the lives of families.
In 2015, Anita Fineday, the Chief Judge of the White Earth Tribal Court, wrote about her experience speaking to the Tribal elders about how they wanted their laws of adoption to be written.15 The elders “voiced two clear and seemingly conflicting messages.” First, they described their custom of taking other people’s children in: “It has always been our way to take children in,
whether they’re family members, tribal members, or children from other tribes.” On the other hand, White Earth Nation did not believe in terminating parental rights, they said: “Parents should always be able to have their children returned to their care when they are ready.”
Out of this seeming contradiction, the White Earth Nation developed a process of tribal customary adoption, a result that did not require the termination of parental rights. Further, every customary adoption includes an opportunity for contact between the parent and child. These traditions recognize the uncertainty that is an unavoidable part of life. Sometimes the community needs to help raise a child, and sometimes a parent who was not ready becomes ready again.
Yet, the mainstream American legal system has long held the opposite view, looking to prevent uncertainty by entering permanent legal orders that severed children from their parents, permanently erasing their families of origin.16 Indeed, because preventing uncertainty has been the stated goal, the law has authorized extreme measures like changing a child’s birth certificate and sealing the original to protect children in their new, “better” life.17
Yet, as it turns out, human relationships are more complicated than anything that can be captured in a legal order.
We now know, for example, that even permanent legal orders are not always permanent. More than 66,000 adoptees ended up in the foster care system between 2008 and 2020.18 Among those children, “being Black, being older at adoption, or having been diagnosed with a mental health condition all were linked to statistically significant higher odds of returning to foster care.” In Washington, we have learned that adopted children make up a significant number of children whose parents refuse to pick them up from a psychiatric hospital or a juvenile detention center.
It is now well documented that adopted people are overrepresented in mental health settings and manifest higher levels of adjustment problems compared to their non-adopted peers.19 Children who experienced adoption are about 4 times as likely to have a reported suicide attempt.20 And while some have assumed that that these difficulties were the result of the adversities adoptees experienced prior to adoption, increasingly, adopted adolescents and adults are asking us to recognize that, for them, the experience of adoption itself is an emotional trauma.21
13 Compare RCW 74.13.031(13) with RCW 74.13.031(14).
14 Id.
15 Anita Fineday, Customary Adoption at White Earth Nation, Center for Advanced Studies in Child Welfare, CW 360: Culturally Responsive Child Welfare Practice, pg. 28 (Winter 2015).
16 Gabrielle Glasser, American Baby: A Mother, A Child, and the Shadow History of Adoption (2021), pp 117-143.
17 Id. at 130-131.
18 Broken Adoptions, USA Today, May 19, 2022, https:// www.usatoday.com/ in-depth/news/ investigations/2022/ 05/19/usa-todayinvestigates-whydo-adoptions-fail/ 9721902002/. Researchers acknowledge that it is an undercount of adoptions that disrupt. Some research suggests that 10–25% of adoptions end in disruption (breakdown of the adoption before legal finalization), and at least 1% to 10% end in dissolution (breakdown after legal finalization). Child Welfare Information Gateway, Discontinuity and Disruption in Adoptions and Guardianships, U.S. Department of Health and Human Services, Administration for Children and Families, Children’s Bureau (2021), https://www. childwelfare.gov/ pubs/s-discon.
19 Susana Corral, et al., Psychological Adjustment in Adult Adoptees: A Meta-Analysis, 33 Psicothema 527 (2021) (“The outcomes most strongly influenced by adoptive status were angry emotions (hostility and anger), psychiatric care, drug abuse, and psychotic symptoms.”).
20 Margaret A. Keyes, et al., Risk of Suicide Attempt in Adopted and Nonadopted Offspring, 132 Pediatrics 639 (2013).
21 David Brodzinsky, et al., Adoption and Trauma: Risks, Recovery, and the Lived Experience of Adoption, 130 Child Abuse & Neglect 105309 (2022); see also Mindy Stern, Adoption Is Trauma. It’s Time To Talk About It., The Medium, Nov. 5, 2019; Angela Tucker, You Should Be Grateful: Stories of Race, Identity, and Transracial Adoption (2024). Also, we know that physical and sexual abuse can also occur in adoptive families. E.g. H.B.H. v. State, 192 Wn.2d 154, 160, 429 P.3d 484, 488 (2018).
22 E.g. Cassian Rawcliffe, et al., Maintaining Relationships with Birth Families After Adoption: What Are Adopted Adults’ Views?, Centre for Research on Children and Families Research Briefing, University of East Anglia (Oct. 2022), https://www. pac-uk.org/uea-andpac-uk-researchbriefing-maintainingrelationships-with-birthfamilies-after-adoptionwhat-are-adoptedadults-views/, (“It is traumatic enough to be separated from your mother without it being shrouded in secrecy.”); Sixto Cancel, I Will Never Forget That I Could Have Lived With People Who Loved Me, The New York Times, Sept. 16, 2021.
Legal systems have favored finality because lawmakers believed that children would be harmed by the possibility of knowing their families of origin, yet adopted people tell us that they have been harmed by not knowing their families of origin.22 Indeed, it has been clear for a long time that adopted young people will seek out their families of origin when they can, a process that has only gotten easier in recent years with social media and the advent of genetic testing. Legal orders that terminate a relationship can’t keep people apart if they want to know one another.
Recognizing this unavoidable uncertainty and these limits of the law can help us start reimagining. Faced with the sheer scope of what we cannot know, it may come as a relief to accept impermanence. Things will change. Whatever decisions a court makes now may need to be revisited later, a flexibility made possible by a guardianship order. We can’t predict the future and we need not pretend that we can.
We can, instead, imagine a system that adds loving people to a child’s life, that allows families to evolve, without attempting to erase any family members.
A parent who is unable to regain custody of their child within the timeframes of the dependency system will still have irreplaceable stories, traditions, memories, and love to give their child.
A child has a right to those stories, memories, traditions, and love. It is their birthright.
















ALISON DICKSON, MD, MPH
Resident in Preventive Medicine Residency Program at the University of Michigan School of Public Health
Dr. Dickson is a General Pediatrician who has cared for many children suffering the effects of living in poverty. She is now a resident in the Preventive Medicine Residency Program at the University of Michigan School of Public Health, where she has been able to explore public health problems like infant poverty, and upstream solutions like the Rx Kids program. She believes that by melding science with love, Rx Kids can bring real healing. ”This project was supported by the Health Resources and Services Administration
Mother of three young children, a resident of Flint Michigan, and a participant in the Rx Kids Program
Teagan Medlin is a 25 year-old mother of three young children, a resident of Flint Michigan, and a participant in the Rx Kids Program. She believes in helping and supporting others so that they can be their best selves, and in particular thinks that kids should have a chance to do that from the start. Teagan is working to become an addiction recovery counselor.)
LUKE SHAEFER, PhD
Co-Director of Rx Kids & Professor of Social Justice and Social Policy at the Ford School of Public Policy at the University of Michigan
Luke Shaefer, Ph.D. is the Co-Director of Rx Kids and the Hermann and Amalie Kohn Professor of Social Justice and Social Policy at the Ford School of Public Policy at the University of Michigan. There he directs Poverty Solutions, a U-M presidential initiative that partners with communities to find new ways to prevent and alleviate poverty. Poverty Solutions has a proven track record of collaborating on novel evidence-based policy changes in the City of Detroit, with the State of Michigan, and nationally.
Co-Director of Rx Kids & Director of the Michigan State University-Hurley Children’s Hospital Pediatric Public Health Initiative
Rx Kids is led by Mona Hanna-Attisha, MD, MPH, a pediatrician, and director of the Michigan State University-Hurley Children’s Hospital Pediatric Public Health Initiative. A nationally recognized child health researcher and advocate, Dr. Hanna-Attisha launched the community-partnered initiative in response to the Flint water crisis to improve outcomes for kids. She is also the Associate Dean for Public Health and C. S. Mott Endowed Professor of Public Health at Michigan State University College of Human Medicine.
“This project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant D3349085, “Preventive Medicine Residency”, as part of an annual award totaling $400,000. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred.”
Teagan’s infant daughter Audrina reclines in a pink bouncy seat, a pink pacifier resting on her full, round belly. Teagan coos and chatters at her, coaxing brief intermittent smiles with a one-way conversation. “Hi, my baby. What’s the matter? Do you need a burp? Do you see mama? Who’s a good girl?” They are both glowing in the dawn of their parent-child relationship. And Teagan is excited to share that her 5- and 3-year-old children are also returning to her in four days, the first time that the family of four will be united.
Teagan experienced a period of active addiction during the pandemic. Financially dependent on the children’s father and cut off from other social support, she could not escape the substances he brought home. “It spiraled,” she says. “I needed him for the financials. If I could have separated, I could have kept [the baby] safe and healthy by myself.” At six months of age, Child Protective Services placed her second child with the first. “It broke me to lose them. I stopped caring if I lived or died because I thought I’d never get them back. And when I was done visiting them, my son would cry and cry. He never knew if he’d see me again.” Without a consistent address, a wardrobe, or transportation, she had trouble finding the employment she would need to become independent, and her addiction worsened. “I was at my lowest, in abandoned housing, on the streets. And everything that was supposed to help me just made me feel worse.” It took almost dying until she realized she “was put on this earth for two reasons,” Teagan says. “To be a mom, and to make it through active addiction so that I could be a recovery coach.”
Now living in recovery housing with her newborn, Teagan qualifies for monthly cash prescriptions as the mother of a Flint newborn through a new universal and unconditional program called RxKids. Sober for one year and two weeks and able to demonstrate her new income to the court, her first two children are returning to her next week. Through RxKids, she purchased a pack-and-play and a bouncy chair, clothes for each child, and ageappropriate toys. She bought diapers, wipes, pullups, “all the hygiene stuff they need, plus I picked
out bunk beds for the older two that I’m going to get.” The cash also allows Teagan the time to pursue job training as a recovery coach. When this assistance ends after Audrina’s first year, “I’m going to have some long-term stability for my family. I’m getting my license, my job… a trailer in the school district I know is best for them. This program changed my life .”
The child welfare system’s efforts to support children’s needs and strengthen families has complex effects on relational health between parent and child. For Teagan and other parents, the effect of separations in a system that focuses sharply on violence, abuse, and mental health disorders but doesn’t adequately address the complex factors linked to them—including economic challenges— can be emotionally shaming and functionally devastating. As the system strives for a holistic approach that prioritizes relational health, one area for focus is the financial support of parents struggling to meet their children’s needs. Most child welfare involvement is neglect, and most neglect is poverty, and babies are at highest risk. But evidence does exist that bolstering family financial security can improve child health outcomes and reduce child abuse and neglect referrals to better support whole, safe families.
Maltreatment is mostly neglect. In the US, one in three US children will experience a CPS investigation for child abuse or neglect (CAN) in their lifetime1. Although abuse and neglect are often conflated, most of the maltreatment revealed by those investigations is categorized as neglect. In the most recent National Child Abuse and Neglect Data Systems (NCANDS) report, 76% of statereported CAN referrals were for neglect2
Most neglect happens to kids in families with very low income. Eighty-five percent of the children referred for child maltreatment come from among the 37% of US children living below 200% of the federal poverty line2. Not only is the association between poverty and CAN referrals clear, but the relationship is also increasingly believed to be a causal one. A large review of 90 recent studies examining poverty and child maltreatment from 13 developed countries found strong and growing evidence for a contributory causal relationship between poverty and CAN. This review noted with clarity that the impacts of poverty on CAN are large in scale, and influenced significantly by the depth and duration of poverty3
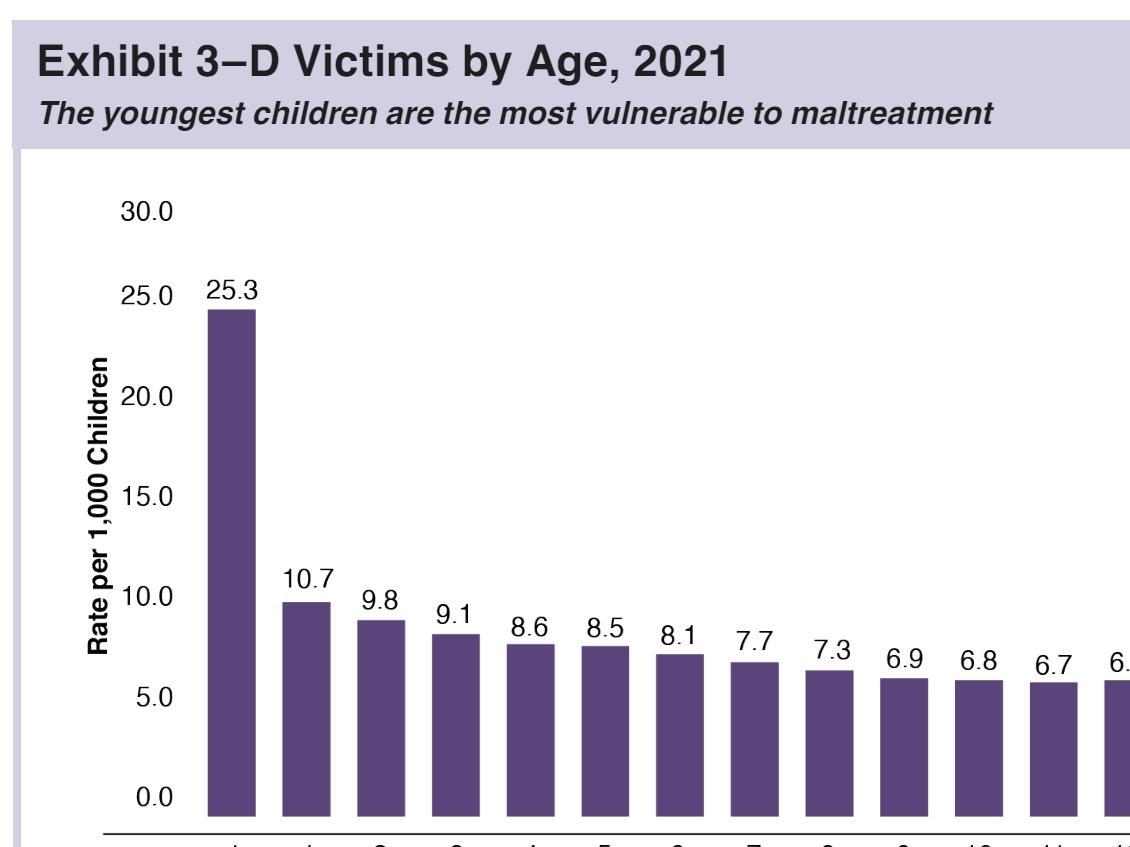
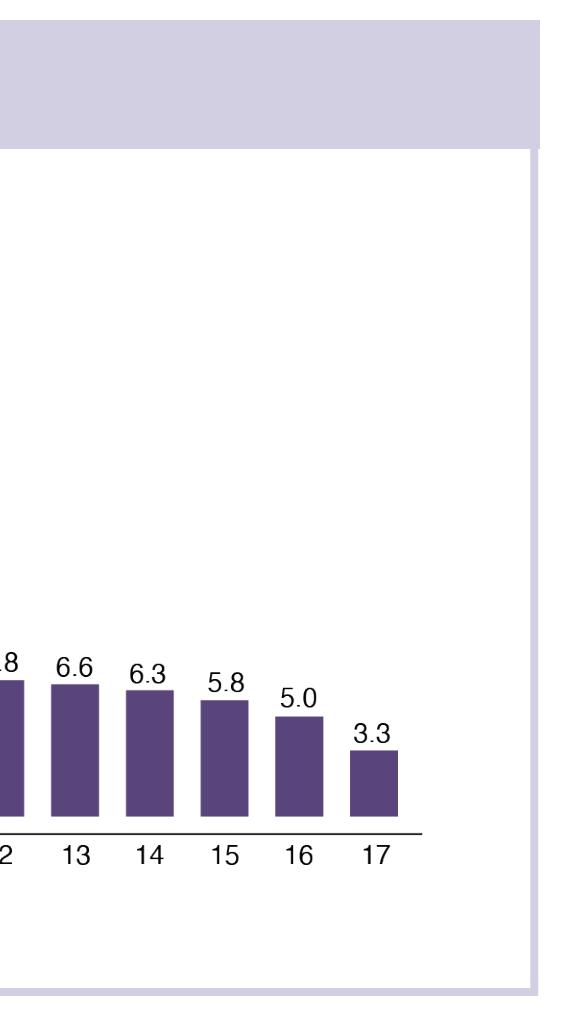
Babies are at highest risk of CAN. The riskiest period for CAN is the first year, when 25 in every 1,000 infants are victimized2. This is shown in Figure 1, drawn from the most recent NCANDS report. The rate of maltreatment in infants is more than twice that of any other year of childhood. It falls steeply after infancy, to around 11 per 1,000 children in the second year, and fewer again each subsequent year. But the effects often endure or grow. The breadth and persistence of maltreatment consequences, combined with the cost of investigation and management of cases, creates a large economic burden estimated by the CDC at $400 billion annually4
Poverty solutions are evidence-based CAN

Public Health Initiative, with RxKids co-director Luke Shaefer, Professor of Social Justice and Social Policy at the Ford School of Public Policy at the University of Michigan, where he directs UM’s Poverty Solutions Initiative. The RxKids program also partners with the Greater Flint Health Coalition and cash administrator GiveDirectly. Described as a “prescription for health, hope and opportunity,” it has three critical characteristics that are likely to support relational health by reducing child maltreatment:
1. The program begins prenatally and lasts through the infant’s first year.
2. Income support is provided throughout the period: $1500 in the third trimester, and $500 per month after birth.
solutions. Researchers have long proposed that the synergy between social protection and child protection should be strengthened5. Both the type and the quantity of economic insecurities impacted child maltreatment. Certain insecurities are reliable predictors of future CAN, including housing instability, material hardship, and income losses6. It is no surprise then to find evidence that socioeconomic interventions can reduce exposure to abuse and neglect; the strongest evidence is for housing, cash transfers, and income supplementation7. A review of evidence within the US suggests that in particular, increasing family income can reduce the rate of children in foster care8.
RxKids is an answer to infant poverty and its consequences for families in Flint, Michigan. RxKids is led by Mona Hanna-Attisha MD, MPH, a pediatrician, and director of the Michigan State University-Hurley Children’s Hospital Pediatric
3. The cash is unconditional, and eligibility is universal for pregnant moms in the city.
Perinatal Timing: RxKids is committed to supporting families prenatally (before birth) and through infancy. This timing is likely to reduce maltreatment because it addresses a period of greatest economic vulnerability, it is an evidence-based period to support other child health outcomes, it is a period of critical development for the child, and it is the best time to prevent CAN.
The perinatal period includes a poverty spike that can be addressed through social policy. Income loss (due to reduced labor market participation and lack of paid family leave) combined with increased costs (of childbirth and childcare) in the months surrounding childbirth make the perinatal period an economically vulnerable one for U.S. mothers and newborns9. There is an approximate 10% drop in gross US Household income perinatally, as shown in Figure 2 from the Washington Center for Equitable Growth10. This is particularly true for single mothers living without other adults, but it is significantly impacted even when accounting for income from unrelated household members, nearcash public programs, and tax credits11. Stanczyk et al found that the decline in income-to-needs ratios begins three months prior to birth, nadirs in the first and second months of the infant’s life (at 34% lower than pre-pregnancy baseline), and does not recover in the child’s first year. The impacts of income loss and childbirth costs cause the poverty
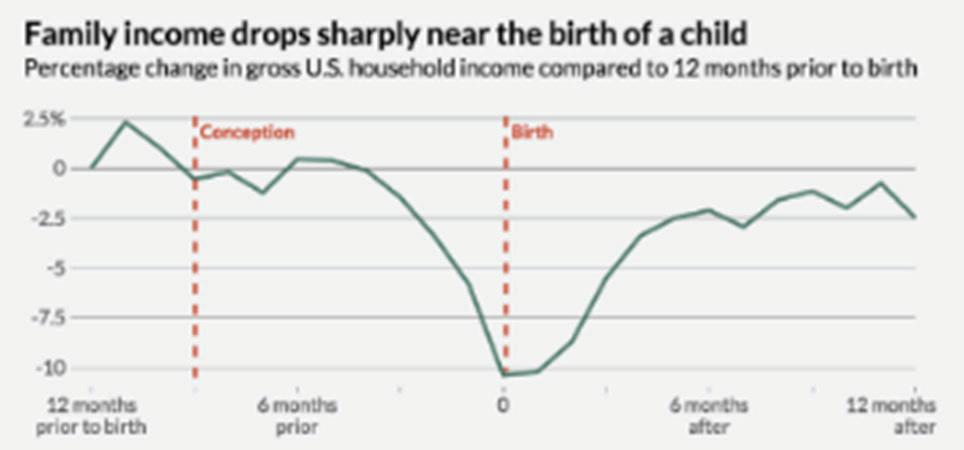
FIGURE 2
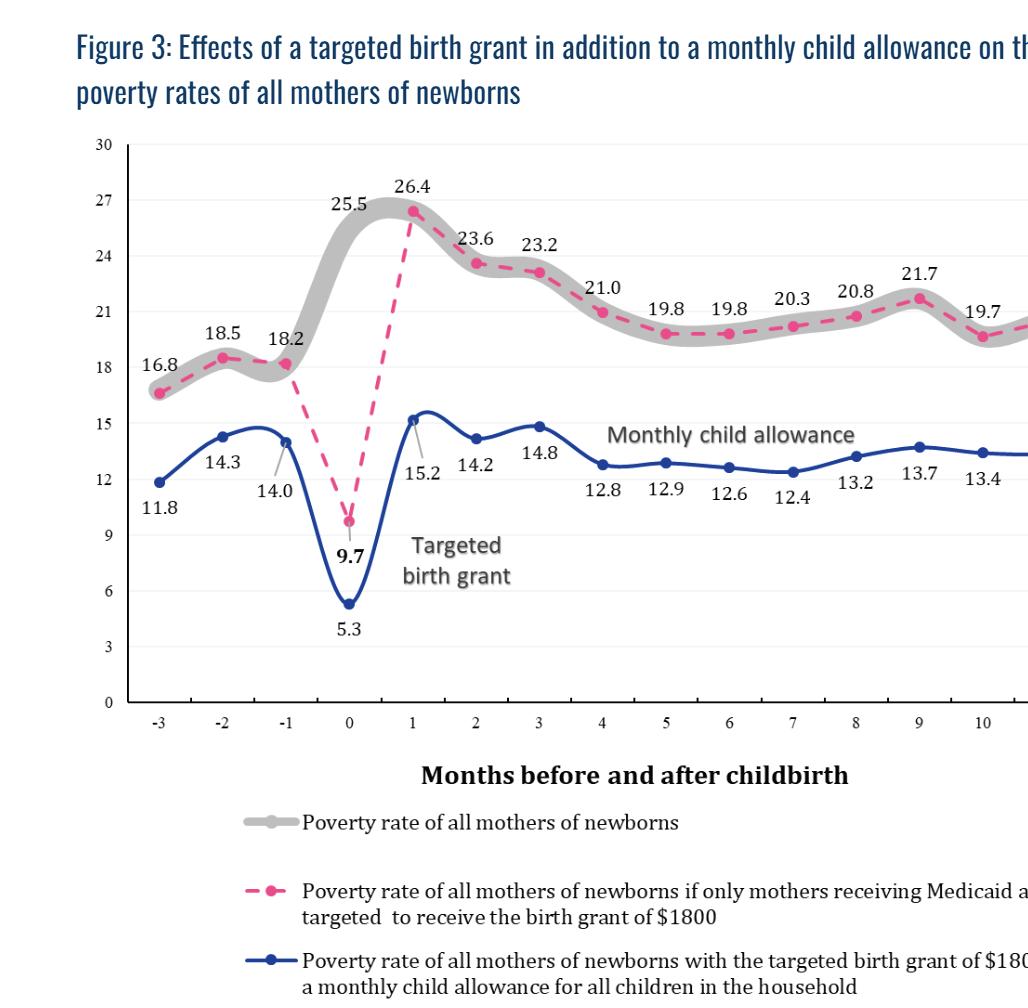
rate among all mothers to spike from 18% in the month prior to birth, to 26% in the month after birth12. The extent to which this occurs varies with birth parity and race and ethnicity: firsttime Black and Hispanic mothers are particularly affected, with 40% of Black and Hispanic mothers experiencing poverty around birth13. Modeling shown in Figure 3 by the Columbia University Center for Poverty and Social Policy shows that a perinatal cash transfer (such as that provided by RxKids) can eliminate that spike, reverse it, and, with small monthly child allowances, cut poverty rates by around 40%12
Prenatal income support works for other child health outcomes. The prenatal period is a good target for income-related interventions aiming to improve health outcomes for children through healthier pregnancies and early development. The same mechanisms that make cash transfers effective in reducing child maltreatment (namely increased family investment and decreased stress, discussed below) can be expected to function similarly in the prenatal period. Some studied prenatal interventions are inkind support (such as Food Stamps and WIC programs), or changes in policy affecting income in the prenatal period (such as the US Earned-Income Tax Credit). Literature has also examined true cash transfer programs, including conditional programs in Brazil, Uruguay, Mexico, and the UK, and unconditional cash transfer programs in Spain, South Korea, Canada, Nepal, and Alaska.
Many studies examine the impact of prenatal cash or near-cash exposures on the outcome of birth weight (which is associated with infant mortality risk, developmental problems in childhood, and even adult health problems14), finding that birth weight is positively affected by cash and near-
cash transfers15-30. Prenatal support can also lead to a reduction in prematurity18,21,23,27, and improved Apgar scores (a measure of newborn transition to life outside the uterus)18,22 Cash or near-cash transfers have been noted to positively impact parental reports of wellbeing31, breastfeeding status, vaccinations at age 1year, and developmental delays at Kindergarten32. Some studies have extended the period of observation into adulthood, finding a positive effect on years of education, income, and adult chronic disease33, along with adult neighborhood quality, economic self-sufficiency, and decreased likelihood of incarceration34
Particularly relevant to researchers working on unconditional cash transfer programs in developed countries, a number of recent, large studies in Canada23,32, Spain20, South Korea28 and the UK21, find positive effects of prenatal unconditional (or in the case of the UK, essentially unconditional) cash transfers on birth and child health outcomes. In Spain, the effects were even found to extend to children pre-conception, when their mothers received the benefit for an older sibling well ahead of gestating subsequent children whose birthweight rose20
The prenatal period is a developmentally critical one. The period from conception to birth is one of rapid cell division and differentiation, setting the stage
3

for the complex structure and functioning of the human body. Maternal stress, poor nutrition, and exposure to toxins can have profound adverse effects on fetal development. These effects may impact growth, brain and behavioral development, and gene expressions that will affect the newborn through childhood and can even cause adult-onset diseases35. There is no part of gestation which is not considered critical for some organ system, and the entire length of gestation is considered critical for the development of the fetal brain and spinal cord36,37. Because this is a time of critical growth and development, maltreatment in this period may lead to lifelong health consequences in addition to suffering, illness, injury, and death1
Ties between the prenatal environment and outcomes are not limited to physical health domains. Research from Johns Hopkins University ties economic resources at birth to socioeconomic conditions in adulthood over a 25-year study period of 800 children38. The authors suggest that interventions preceding this stage have the potential to disrupt a “long shadow” cast upon adult socioeconomic outcomes by low economic resources at birth. Studies of the effects of access to additional prenatal support are confirming: access results in long-term benefits on human capital indices, economic self-sufficiency, adult neighborhood quality, and the likelihood of incarceration33,34.
The prenatal period is the right time for primary prevention. The primary prevention of child maltreatment is medically, socially, ethically, and economically superior to secondary and tertiary interventions. The high incidence of negative outcomes in the infant’s first year shown in Figure 1 makes this period too late for interventions to prevent child maltreatment. Effective primary prevention efforts should be in place before maltreatment occurs, and that means before birth.
Generous income support: Research leverages experimental and quasi-experimental methods to explore poverty solutions as a strategy for primary prevention of child maltreatment. Quasi-experimental studies in the US are often built around policy changes to examine impacts of income fluctuation in affected populations. Cash-transfer programs, on the other hand, have been studied internationally and in the US, using observational studies and randomized trials. Cash transfers may be conditional (on participation in healthcare or employment, for example) or unconditional. They may also be targeted to specific populations, or universal (such as the Alaska Permanent Fund Dividend distributed among all
state residents). Transfer amount, frequency, and duration varies widely in the programs reviewed in the literature.
In the US, quasi-experimental studies link child abuse and neglect data to changes in the minimum wage, Earned-income Tax Credits (EITC), Child Tax Credits, and Temporary Assistance for Needy Families (TANF). These consistently demonstrate a reduction in abuse and neglect of children, with similar effects on maltreatment reduction hovering around 10% following a typical $1000 tax credit, or even from smaller amounts39-46
For instance, a $1000 EITC increase led to an 8-10% decrease in CPS involvement among singlemother low-income families in one study42 and reduced child maltreatment by 3%, and reduced days spent in foster care by 22.4%, according to a current working paper46. This same dollar amount in per-child tax refunds led to a 5% decrease in maltreatment reports in the week of and four weeks following receipt41. In another study, an EITC expansion decreased foster care entry by 7.4% per year47. In Wisconsin, a randomized controlled trial showed that even $100 of additional child support income to mothers receiving TANF benefits reduced screened-in child maltreatment reports by 10% in the following two years45. There are also studies of a generous EITC reducing Emergency Department visits for maltreatment44,48.
Studies of income instability show the same relationship between income and CAN. In one such study, children in Wisconsin whose families’ earnings dropped by 30% had an increased likelihood of CPS involvement around 18%49, and an additional increase in involvement of 15% for each additional drop in income. However, the same study showed that accessing supplemental income to offset the negative income shock can buffer against the risk of CPS involvement, particularly for families with children under 5 years old.
Universally, unconditionally given: Authors in the fields of poverty research and child welfare have long appealed for nuanced, non-coercive, and nondiscriminatory programming50,51. RxKids participation requires only proof of identification, pregnancy and/or childbirth, and residency in the city of Flint. The program’s universality and unconditionality convey potent values of dignity, trust, agency, love, empowerment, freedom, and autonomy. Universality normalizes receiving the aid and helps people to feel seen and supported by a broad village of supporters. With no other strings attached to RxKids cash prescriptions, the program shows that it is trusting families with
how to best care for their children. Moms like Teagan feel warmly welcomed by this low-burden, destigmatized approach: “Other programs are so complicated enough to where you want to give up, so they don’t have to help you. It makes me feel uncomfortable and judged, and like they don’t care. You want to give up, but you need the help, so you keep trying but it makes you feel really bad while you do it. Like you’re less than. RxKids, they want you to succeed.”
In Flint, this unconditionality is designed to uplift the dignity of every person who benefits, but it is also evidence-based. Means-tested programs and those conditional on employment do not reach all families in need. RxKids is expected to have nearly 100% penetrance, which can amplify the effects on child welfare outcomes. Reduced CPS involvement and increased family stability are strongly linked to universal, unconditional cash. In a working paper from the National Bureau for Economic Research, additional universal, unconditional cash transfers of $1000 from the Alaska Permanent Fund were associated with a 10% drop in the likelihood of referral to CPS, a lower likelihood of mother moving since the child’s birth, and a greater likelihood that a child is still living with their mother at age three52. On the other hand, conditional cash transfers requiring participants to work, attend appointments, or meet certain other criteria have shown mixed results. In Nepal, programs that were conditional on use of healthcare services had a positive effect on infant mortality, but programs conditional on work participation did not yield any positive effects53. In Delaware, increases in child neglect were demonstrated among those randomly assigned to a 1990s welfare reform program with strict work requirements and sanctions54
The scientific literature discusses several mechanisms by which income support may reduce child abuse and neglect. Among these, increased family investment and decreased parental stress top the list8,46,47,52. Universal, unconditional cash plays an important role in both mechanisms, making the process low stress for families and empowering them to determine how best to provide for their family’s unique circumstances. “It makes me feel confident, like I can do my job as a mom. I’m calmer,” Teagan says. For her, RxKids cash buys proper hygiene supplies and safe baby equipment. It supports her reunification with her two older children, her ability to pursue job training, and her plan for housing stability. A working paper evaluating New York’s Baby’s First Years unconditional cash transfer program shows that the transfers led to increased spending on child-specific goods and mothers’ early-learning
activities with their infants55. But every family can use the cash in the way they need. For some moms, the money covers rent, food, buys more time to bond with their baby before returning to work, or provides reliable transportation to work.
These aspects of the program may amount to more than individual and family effects. Researchers think that universal, unconditional payments can also boost civic engagement and community pride. Being trusted with the cash and respected while she accesses it helps Teagan feel “…excited. It makes me feel hopeful for the whole city of Flint. There are good people here and this program is something that can lift them up. They can get the chance they need, and the kids have a chance right from the beginning.”
Addressing poverty prioritizes the primary prevention of CAN, and it can be done with dignity, simplicity, and a sound scientific basis. It can even be rooted in love, a long-known component of quality health outcomes56. RxKids sets an example for poverty solutions that impact child welfare outcomes and create the conditions in which children and their parents can flourish together. Many pediatricians have called RxKids a dream come true, and many mothers, including Teagan, have called it life changing. Teagan has four days until her kids return: “I had a trial with them all last weekend, and it was awesome. They were all over me, just so much loving and snuggling. It was so, so good .”
1. Schneider W, Bullinger LR, Raissian KM. How does the minimum wage affect child maltreatment and parenting behaviors? An analysis of the mechanisms. Review of Economics of the Household 2022;20(4):11191154. DOI: 10.1007/s11150-021-09590-7.
2. Administration for Children and Families. Child Maltreatment 2021. U.S. Department of Health & Human Services, 2023. (https:// www.acf.hhs.gov/cb/data-research/childmaltreatment.).
3. Bywaters P, Skinner G, Cooper A, Kennedy E, Malik A. The relationship between poverty and child abuse and neglect: New evidence. London: Nuffield Foundation 2022.
4. Peterson C, Florence C, Klevens J. The economic burden of child maltreatment in the United
States, 2015. Child abuse & neglect 2018;86:178-183.
5. Abu-Hamad B, Jones N, Pereznieto P. Tackling children’s economic and psychosocial vulnerabilities synergistically: How well is the Palestinian National Cash Transfer Programme serving Gazan children? Children and Youth Services Review 2014;47:121-135. DOI: https://doi.org/10.1016/j.childyouth.2014.09.009.
6. Skinner GCM, Bywaters PWB, Kennedy E. A review of the relationship between poverty and child abuse and neglect: Insights from scoping reviews, systematic reviews and meta-analyses. Child Abuse Review 2023;32(2):e2795. DOI: https://doi.org/10.1002/ car.2795.
7. Courtin E, Allchin E, Ding AJ, Layte R. The Role of Socioeconomic Interventions in Reducing Exposure to Adverse Childhood Experiences: a Systematic Review. Current Epidemiology Reports 2019;6(4):423-441. DOI: 10.1007/s40471-019-00216-2.
8. Wood S, Scourfield J, Stabler L, et al. How might changes to family income affect the likelihood of children being in out-of-home care? Evidence from a realist and qualitative rapid evidence assessment of interventions. Children and Youth Services Review 2022;143:106685. DOI: https://doi.org/10.1016/j. childyouth.2022.106685.
9. Marti-Castaner M, Pavlenko T, Engel R, et al. Poverty after Birth: How Mothers Experience and Navigate US Safety Net Programs to Address Family Needs. Journal of Child and Family Studies 2022;31(8):2248-2265.
10. Stanczyk A. The Dynamics of Household Economic Circumstances Around a Birth. Washington Center for Equitable Growth working papers 2016 (https://equitablegrowth.org/wp-content/ uploads/2016/09/10042016-WP-income-volatilityaround-birth.pdf).
11. Stanczyk AB. The dynamics of US household economic circumstances around a birth. Demography 2020;57(4):1271-1296.
12. Hamilton C, David Harris, Christopher Wimer, Sara Kimberlin, Sophie Collyer, and Irwin Garfinkel. The case for a federal birth grant: a plan to reduce poverty for newborns and their families. Poverty and Social Policy Brief. Center on Poverty and Social Policy, Columbia University, 2023. (1) (povertycenter.columbia.edu/ publication/case-for-federal-birth-grant).
13. Hamilton C, Sariscsany L, Waldfogel J, Wimer C. Experiences of Poverty Around the Time of a Birth: A Research Note. Demography 2023;60(4):965-976. DOI: 10.1215/00703370-10837403.
14. Wilcox AJ. On the importance—and the unimportance— of birthweight. International Journal of Epidemiology 2001;30(6):1233-1241. DOI: 10.1093/ije/30.6.1233.
15. Barber SL, Gertler PJ. The impact of Mexico’s conditional cash transfer programme, Oportunidades, on birthweight. Tropical Medicine & International Health 2008;13(11):1405-1414.
16. Strully KW, Rehkopf DH, Xuan Z. Effects of prenatal poverty on infant health: state earned income tax
credits and birth weight. American sociological review 2010;75(4):534-562.
17. Almond D, Hoynes HW, Schanzenbach DW. Inside the war on poverty: The impact of food stamps on birth outcomes. The review of economics and statistics 2011;93(2):387-403.
18. Hoynes H, Miller D, Simon D. Income, the earned income tax credit, and infant health. American Economic Journal: Economic Policy 2015;7(1):172-211.
19. Amarante V, Manacorda M, Miguel E, Vigorito A. Do cash transfers improve birth outcomes? Evidence from matched vital statistics, and program and social security data. American Economic Journal: Economic Policy 2016;8(2):1-43.
20. González L, Trommlerová S. Cash transfers before pregnancy and infant health. Journal of Health Economics 2022;83:102622. DOI: https://doi. org/10.1016/j.jhealeco.2022. 102622.
21. Reader M. The infant health effects of starting universal child benefits in pregnancy: Evidence from England and Wales. Journal of Health Economics 2023;89:102751. DOI: https://doi.org/10.1016/j.jhealeco. 2023. 102 751.
22. Chung W, Ha H, Kim B. MONEY TRANSFER AND BIRTH WEIGHT: EVIDENCE FROM THE ALASKA PERMANENT FUND DIVIDEND. Economic Inquiry 2016;54(1):576-590. DOI: https://doi.org/10.1111/ ecin.12235.
23. Brownell MD, Chartier MJ, Nickel NC, et al. Unconditional Prenatal Income Supplement and Birth Outcomes. Pediatrics 2016;137(6). DOI: 10.1542/ peds.2015-2992.
24. Kehrer BH, Wolin CM. Impact of income maintenance on low birth weight: evidence from the Gary Experiment. Journal of Human resources 1979:434-462.
25. Bruckner TA, Rehkopf DH, Catalano RA. Income Gains and Very Low-Weight Birth among Low-Income Black Mothers in California. Biodemography and Social Biology 2013;59(2):141-156. DOI: 10.1080/ 19485565.2013.833802.
26. Hamad R, Rehkopf DH. Poverty, Pregnancy, and Birth Outcomes: A Study of the Earned Income Tax Credit. Paediatr Perinat Epidemiol 2015;29(5):444-52. (In eng). DOI: 10.1111/ppe.12211.
27. Lucas ADP, de Oliveira Ferreira M, Lucas TDP, Salari P. The intergenerational relationship between conditional cash transfers and newborn health. BMC Public Health 2022;22(1):201. (In eng). DOI: 10.1186/s12889-02212565-7.
28. Jung H. Can Universal Cash Transfer Save Newborns’ Birth Weight During the Pandemic? Population Research and Policy Review 2023;42(1):4. DOI: 10.1007/s11113023-09759-1.
29. Falcão IR, Ribeiro-Silva RdC, Fiaccone RL, et al. Participation in Conditional Cash Transfer Program During Pregnancy and Birth Weight–Related Outcomes. JAMA Network Open 2023;6(11):e2344691-e2344691. DOI: 10.1001/jamanetworkopen.2023.44691.
30. Blakeney EL, Herting JR, Zierler BK, Bekemeier B. The effect of women, infant, and children (WIC) services on birth weight before and during the 2007-2009 great recession in Washington state and Florida: a pooled cross-sectional time series analysis. BMC Pregnancy Childbirth 2020;20(1):252. (In eng). DOI: 10.1186/ s12884-020-02937-5.
31. East CN. The effect of food stamps on children’s health: Evidence from immigrants’ changing eligibility. Journal of Human Resources 2020;55(2):387-427.
32. Enns JE, Nickel NC, Chartier M, et al. An unconditional prenatal income supplement is associated with improved birth and early childhood outcomes among First Nations children in Manitoba, Canada: a population-based cohort study. BMC Pregnancy Childbirth 2021;21(1):312. (In eng). DOI: 10.1186/s12884-021-03782-w.
33. Hoynes H, Schanzenbach DW, Almond D. Long-run impacts of childhood access to the safety net. American Economic Review 2016;106(4):903-934.
34. Bailey MJ, Hoynes HW, Rossin-Slater M, Walker R. Is the social safety net a long-term investment? Largescale evidence from the food stamps program. National Bureau of Economic Research, 2020.
35. Fifer WP, Monk CE, Grose-Fifer J. Prenatal Development and Risk. Blackwell Handbook of Infant Development2004:505-542.
36. Moore KL, Persaud T. Clinically oriented embryology. The developing human 1993;10.
37. National Institutes of Health. Mother to Baby Fact Sheet: Critical Periods of Development. National Library of Medicine. (https://www.ncbi.nlm.nih.gov/ books/NBK582659/).
38. Alexander K, Entwisle D, Olson L. The Long Shadow: Family Background, Disadvantaged Urban Youth, and the Transition to Adulthood: Russell Sage Foundation, 2014.
39. Maguire-Jack K, Johnson-Motoyama M, Parmenter S. A scoping review of economic supports for working parents: The relationship of TANF, child care subsidy, SNAP, and EITC to child maltreatment. Aggression and Violent Behavior 2022;65:101639. DOI: https://doi. org/10.1016/j.avb.2021.101639.
40. Spencer RA, Livingston MD, Komro KA, Sroczynski N, Rentmeester ST, Woods-Jaeger B. Association between Temporary Assistance for Needy Families (TANF) and child maltreatment among a cohort of fragile families. Child Abuse Negl 2021;120:105186. (In eng). DOI: 10.1016/j.chiabu.2021.105186.
41. Kovski NL, Hill HD, Mooney SJ, Rivara FP, Morgan ER, Rowhani-Rahbar A. Association of StateLevel Earned Income Tax Credits With Rates of Reported Child Maltreatment, 2004–2017. Child Maltreatment 2022;27(3):325-333. DOI: 10.1177/1077559520987302.
42. Berger LM, Font SA, Slack KS, Waldfogel J. Income and Child Maltreatment in Unmarried Families: Evidence from the Earned Income Tax Credit. Rev Econ Househ 2017;15(4):1345-1372. (In eng). DOI: 10.1007/
s11150-016-9346-9.
43. Raissian KM, Bullinger LR. Money matters: Does the minimum wage affect child maltreatment rates? Children and youth services review 2017;72:60-70.
44. Klevens J, Schmidt B, Luo F, Xu L, Ports KA, Lee RD. Effect of the Earned Income Tax Credit on Hospital Admissions for Pediatric Abusive Head Trauma, 19952013. Public Health Reports (1974-) 2017;132(4):505511. (https://www-jstor-org.proxy.lib.umich.edu/ stable/26374155).
45. Cancian M, Yang M-Y, Slack KS. The Effect of Additional Child Support Income on the Risk of Child Maltreatment. Social Service Review 2013;87(3):417437. DOI: 10.1086/671929.
46. Rittenhouse K. Income and Child Maltreatment: Evidence from a Discontinuity in Tax Benefits 2023. DOI: http://dx.doi.org/10.2139/ssrn.4349231.
47. Biehl AM, Hill B. Foster care and the earned income tax credit. Review of Economics of the Household 2018;16(3):661-680. DOI: 10.1007/s11150-017-93811.
48. Bullinger LR, Boy A. Association of Expanded Child Tax Credit Payments With Child Abuse and Neglect Emergency Department Visits. JAMA Network Open 2023;6(2):e2255639-e2255639. DOI: 10.1001/ jamanetworkopen.2022.55639.
49. Cai JY. Economic instability and child maltreatment risk: Evidence from state administrative data. Child Abuse & Neglect 2022;130:105213. DOI: https://doi. org/10.1016/j.chiabu.2021.105213.
50. Pelton LH. Separating coercion from provision in child welfare: Preventive supports should be accessible without conditions attached. Child Abuse Negl 2016;51:427-34. (In eng). DOI: 10.1016/j.chiabu.2015.08.007.
51. Roelen K. Sticks or carrots? Conditional cash transfers and their effect on child abuse and neglect: researchers observe both benefits and harms of CCT programs. Child Abuse Negl 2014;38(3):372-82. (In eng). DOI: 10.1016/j.chiabu.2014.01.014.
52. Bullinger LR, Packham A, Raissian KM. Effects of Universal and Unconditional Cash Transfers on Child Abuse and Neglect. NBER Working Papers 31733 2023.
53. Siddiqi A, Rajaram A, Miller SP. Do cash transfer programmes yield better health in the first year of life? A systematic review linking low-income/middle-income and high-income contexts. Archives of Disease in Childhood 2018;103(10):920-926.
54. Fein DJ, Lee WS. The impacts of welfare reform on child maltreatment in Delaware. Children and Youth Services Review 2003. DOI: https://doi.org/10.1016/S01907409(02)00267-0.
55. Gennetian LA, Duncan G, Fox NA, et al. Unconditional Cash and Family Investments in Infants: Evidence from a Large-Scale Cash Transfer Experiment in the U.S. Res Sq 2023 (In eng). DOI: 10.21203/rs.3.rs-2507540/v1.
56. Best M, Neuhauser D. Avedis Donabedian: father of quality assurance and poet. BMJ Quality & Safety 2004;13(6):472-473
JOSH GUPTA-KAGAN Clinical Professor of Law Columbia Law School

Josh Gupta-Kagan is a Clinical Professor of Law at Columbia Law School, where he founded and directs the Family Defense Clinic. He and his students represent parents in New York Family Court neglect cases and administrative proceedings regarding the abuse and neglect system. He is the author of over 30 academic articles on the legal systems affecting families and children.
Money impacts relationships. And when the money involved is a foster care subsidy to kinship caregivers, it can drive a wedge in relationships between parents and kinship caregivers that should be strengthened, not strained. Unfortunately, foster care funding incentivizes the “relational disruption”1 endemic to foster care, when it should instead support family members coming together to support each other and their children.
In contrast, Medicaid funding has increasingly supported family members taking care of each other and can provide child welfare with a model for funding family caregiving without disrupting relationships and without even requiring a family court or foster care case.
Consider a mother who lives with her aunt, and they both struggle to make ends meet. The aunt helps the mother take care of her infant child since she has a mental illness and sometimes uses illegal drugs. Her drug use increased following an assault by her ex-boyfriend. The child protective service (CPS) agency learns that the mother has left the child at home with the aunt for days and
*I suggest only that some version of this scenario happens frequently, not that the mother has neglected the child or that removing the child from his mother is appropriate or legal.
† In practice, some families find workarounds. For instance, I have worked on cases in which adoptions or guardianships are granted even though a parent visits their child at the adoptive parent or guardian’s home nearly daily, and the CPS agency and court would exercise some willful blindness of the situation. If a parent eventually moves in with the kinship caregiver, that can create the best of all worlds: the financial support without the parentchild separation. The fact that families must resort to workarounds, however, demonstrates a problem with the existing funding structure, not that the present structure is working.
has even brought the child with her while she uses drugs. Concerned for the child’s safety, the CPS agency convinces the family court to authorize it to remove the child from his mother’s legal and physical custody on an emergency basis.* The CPS agency then describes kinship foster care to the aunt: she can apply for a kinship foster care license, keep the child with her, and get a monthly stipend from the state that will go a long way towards making ends meet.
But that kinship foster payment comes with a catch: the aunt has to keep the mother out of the home. The aunt is frustrated with her niece but is also worried about the impact of CPS’s position; without a place to stay, her niece’s drug use could worsen, and accessing mental health treatment could be harder. And what kind of system pays you to keep a loved one away? Regardless, the aunt feels she has no real choice. She says yes, and soon is receiving a monthly stipend, while being drafted to enforce the CPS agency and family court’s rules that prevent her niece from living with her.
In this family–a simplified composite of families encountered in my career as a lawyer in the family regulation system, and which represent some significant portion of the more than 120,000 children in kinship foster care on any given day2 –the aunt is an essential support to the mother. Any intervention should support both the kinship caregiver and the parent, so they can continue to take care of the child and each other together. Instead, foster care funding rules incentivize, and even demand, damage to these relationships.
When a CPS agency places a child in any foster home (including a kinship foster home), it must pay that caregiver “foster care maintenance payments.”3 By law, these payments must cover “food, clothing, shelter, daily supervision, school supplies, a child’s personal incidentals,” and more,4 and the law has long prohibited CPS agencies from discriminating against licensed kinship caregivers.5
Those payments are significant and tax-free. In New York (where I teach and practice), the family regulation system pays foster parents up to $1,282.53 per child per month, and up to $1,123 per month in lower-cost upstate counties.6 In Texas, the minimum licensed foster family payment is $812.10 per month.7 In Florida, it is $517.94 for young children and $621.77 for teens.8 In Wisconsin, the minimum rates range from $441 to $572.9 These payments are more than families received from the now-expired COVID-era expanded child tax credit (up to $300 per month per child),10 more than the average SNAP benefit (under
$300 per month per person11), and hundreds of dollars greater than the per child amount of TANF benefits parents and other caregivers can receive.12
Those payments make a tremendous difference for kinship caregivers. Kinship caregivers, like parents who face family regulation system involvement, are disproportionately poor.13 It is the rare person for whom an extra $500 or $1,000 a month would not make a big difference. These payments quickly become an important lifeline.
Those payments follow federal rules–the federal government spends more than $8 billion per year, more than 40% of all foster care expenditures,14 and so states follow federal restrictions. And federal rules require a kin caregiver to keep the parent at an arm’s length: they condition federal funding support for a kinship caregiver who “provides 24hour substitute care for children placed away from their parents or other caretakers.”15
This funding law thus creates a rigid binary: either children live with their parents, or they live with someone else. Living with both while getting a kinship foster care payment is not possible.† That rule drives a wedge between parents and trusted family members or friends. The kinship caregiver could help both the child and the parent, but the family regulation system requires them to push the parent away.
Imposing that binary on a range of family structures and dynamics makes little sense. In the vast majority of situations, any danger from a parent living in the home is limited, and can be mitigated by the parent living with a supportive family member. Cases rarely involve parents who intentionally abuse children. Far more frequently, cases involve “neglect,” which often means family regulation agencies and family courts are concerned about a parent’s substance use, mental illness, exposure to domestic violence, or some similar concern;16 a complete separation from a parent is often unnecessary.
This financial wedge between family members imposes real harm. It cuts parents off from people who have been or could be significant supports to them, and thus hurts parents’ efforts to reunify with their children.
One particularly harmful result occurs when the family regulation system makes parents homeless
by insisting that they live apart from kinship caregivers. For instance, Elizabeth Brico described how she was staying with her in-laws when she was accused of leaving her children home alone; the system let her children stay with her in-laws, but insisted that she move out.17 This action makes no sense in light of the allegation; even if she had left her children alone (Brico denies the allegation), the solution would be to have more adults around her children, not fewer. Like most neglect allegations, the allegation against Brico does not mean that she is a clear and present danger who needs to be kept away.
Another harm is how the financial payments can change complex family relationships. Kinship caregivers and parents can have fraught relationships, full of love and support, but also frustration and distrust. When kinship caregivers start receiving money on condition that they keep children away from parents, that can push a conflicted caregiver to take a more adversarial posture towards the parent and can expand parents’ feelings of distrust in the kinship caregiver.
This financial wedge can also extend a child’s time in state custody. Consider parents who are homeless but otherwise able to reunify, and whose children are in kinship foster care.‡ An obvious potential solution exists: the parent could move in with the kinship caregiver. But this step would come at a cost, as the kinship caregiver would have to give up the foster care subsidy, even though she is going to continue providing support to the child and his parent. Some in our example aunt’s situation–and many agencies and family courts reviewing that situation–will prefer the status quo, which keeps the money coming. Consequently, this also keeps the parent and child separated.
The financial wedge creates perverse incentives to keep children in kinship foster care rather than reunify. Consider families that use kinship foster payments to get important services for children, such as a non-Medicaid therapist, a private school, or some other service for the child. Reunifying parent and child would result in losing whatever it is that the foster care subsidies paid for, and parents must choose between seeking reunification with their children but losing those services, versus keeping those services and remaining involved, but not living with, their children.
The absurdity of this situation should be obvious. This system is supposed to keep parents and children together, and help parents rehabilitate and reunify as soon as possible. The system-induced separation from kinship caregivers spites these
goals. These separations harm parents–causing and exacerbating depression and increasing the risk of both mental and physical health problems, as Professor Shanta Trevedi has catalogued18 – making it even more difficult to address any challenges the parent already has.
What if the government provided funding to support a trusted family member or friend to help a parent without requiring that person to push a parent away? The parent and kin could work together to keep the child safe, and the financial help would support their relationship with each other and with the child. The funding would prevent the need for a more invasive step: the family separations inherent in foster care.
While foster care funding laws currently prohibit such a step, other complex legal systems provide a model for how financial support can help take care of individuals and support strong relationships.
In particular, consider a growing trend in state Medicaid systems: paying family members to provide home health assistance to disabled or elderly family members. This funding became more common during the COVID-19 pandemic as states sought to keep people out of nursing homes and faced staffing shortages for home health aides. Facing these incentives, at least 37 states used COVID-era funding flexibility to expand ways to pay kinship caregivers to help take care of elderly and disabled family members.19 That expanded kinship caregiving funding has remained, even as COVID has receded, with 30 states making some form of this Medicaid funding permanent.20
This funding can make a tremendous difference for families. Fundamentally, it enables family members to take care of each other, strengthening family relationships through “the intimacy of daily association” (to borrow a Supreme Court phrase).21
In Medicaid jargon, it is a “consumer-directed” funding stream, meaning the money flows to the
‡ Housing concerns frequently delay reunification. But they are not valid reasons to do so, as I have argued elsewhere. Josh Gupta-Kagan, Distinguishing Family Poverty from Child Neglect, 109 IOWA L. REV. __, __ (2024).
kinship caregiver chosen by the person needing assistance.22 It could avoid the need for anyone to even open a family court or foster care case. And it saves the state money by paying kinship caregivers to help take care of family members in their homes, thus reducing the need for more restrictive and more expensive options, such as nursing homes.23
There is another element of Medicaid funding that has long supported keeping families together. For many years, Medicaid would pay for parents to place children with severe needs in residential treatment centers, but not to provide care at home. That created a perverse incentive for parents to separate their own families and place their children in institutions. Congress addressed the problem by creating what are known as Katie Beckett waivers (named after a child whose parents resisted placing her in a residential facility). Those waivers allowed Medicaid agencies to pay for these children’s care at home, keeping families together and avoiding institutional placements.24
The same rationale that supports Medicaid’s kinship caregiver funding rules applies when the threat of custody in the foster care system looms. Both help avoid the more invasive and expensive options that separate families, whether that is a nursing home or foster care. Both support the choices that many families would make if they were free of financial pressures: keep families intact, avoid institutions, and support family members taking care of each other.
Yet the two systems treat kinship caregivers differently. When a parent with a disability needs help taking care of herself, many states’ Medicaid programs will pay a kinship caregiver to help take care of her. But if that same parent needs help taking care of her child and the family regulation system is involved, the foster care system will only pay the same kinship caregiver if she kicks the parent to the curb.
The Medicaid funding provides a model for a more supportive funding structure when parents need help from family members or kin. Medicaid funding provides highly valuable funds without conditioning them on separating parents from their children and from adult supports. Rather, the funding supports all the family members working together to help the parent address whatever challenges they face.
To be clear, funding kinship caregivers should not substitute for increasing direct financial support directly to parents. The evidence of the benefit of such aid is large and growing.25 Funding kinship caregivers who help keep families together remains important in its own right.
Though the family regulation system has resisted dramatic change, some recent foster care funding reforms suggest an opening for some positive changes. Title IV-E now provides foster care maintenance payments for children “placed with a parent who is in a licensed residential family-based treatment facility for substance abuse.”26 And, when a teenager in foster care is also a parent, Title IV-E has long provided foster care maintenance payments to support the foster home’s care for both the foster teenager and her child, with the child remaining in his parent’s legal and physical custody.27 Both situations are limited exceptions to the requirement that states place children away from parents.28 Separately, the Children’s Bureau has now authorized states to create separate licensing standards for kinship foster homes without jeopardizing federal funding.29
Policy makers should put the ideas behind these two reforms together.
When a parent seeks help from a kinship caregiver–or when the state seeks to enlist that kinship caregiver to provide help–the state should support their relationship by providing funding to keep them together, supporting each other and safely raising a child.
Legally, states should exempt kinship caregivers from the requirement that foster parents keep parents out of their home. And the federal government should permit states to do so without losing federal funding.
Such a change to foster care funding would be a marked improvement. They would represent a change in mindset in family regulation cases by providing meaningful support without punitive steps or unnecessary mandates. But the Medicaid funding streams show the path towards more dramatic change: funding kinship caregivers to help children and their parents, by avoiding the wedge that the foster care system places between parents and kinship caregivers. Using Medicaid funding also permits families to access these funds without going through CPS agencies, and thus avoiding the coercion, surveillance, and legal risk inherent in that system. And Medicaid funding allows CPS agencies to refer parents and kinship caregivers to Medicaid funding, without further CPS or family court surveillance or regulation required.
This path is particularly clear for parents with disabilities. The most frequently used Medicaid kinship caregiving waivers are for people with intellectual disabilities,30 and focusing on that population provides a strong analogy to the family regulation system.§ Parents with disabilities are significantly overrepresented in the family regulation system–accounting for nearly one in five children in foster care–and disparities regarding parents with intellectual disabilities are particularly large.31 Focusing on this population would address longstanding concerns about the family regulation system’s treatment of parents with disabilities, which are legion, and well beyond the scope of this short article.32 A crucial gap in support for parents with disabilities is the absence of governmental programs to help parents with disabilities care for their children.33 The National Council for Disability even called on Medicaid authorities to expand funding to help parents with disabilities raise their children.34
Scholars and advocates for people with disabilities have also provided essential insight applicable to all families, regardless of disability. Parents may seek and even need help raising their children. But that does not mean that they are unfit parents who are threats to their children or should be separated from them. Unfortunately, the family regulation system often sees a disabled parent’s request for assistance as a confession of unsuitability to parent. As Professor Sarah Lorr writes, reformers must “rebut the myth of independence by identifying that the need for support is evidence of a parent’s humanity, not their unfitness.”35 When a parent with a disability both identifies a need for assistance and a kinship caregiver to provide that assistance,
Medicaid should pay that kinship caregiver to help that parent and keep the family together, and thus provide the support that is sometimes needed without involving the family regulation system at all.
1 Sixto Cancel, The Need for Belonging: Relational Permanency in Child Welfare, FAMILY JUSTICE JOURNAL 24 (Winter 2023).
2 The federal Children’s Bureau reported 123,294 children living in kinship foster care on September 30, 2022, 34% of all children in foster care on that date. U.S. Dep’t of Health and Human Services, Children’s Bureau, The AFCARS Report, Preliminary FY 2022 Estimates as of May 9, 2023 – No. 30, https://www.acf.hhs.gov/sites/ default/files/documents/cb/afcars-report-30.pdf (hereinafter “AFCARS Report”).
3 “Foster care maintenance payments” is the statutory term in Title IV-E of the Social Security Act. 42 U.S.C. § 672. For an excellent critique of Title IV-E funding more broadly, see Richard Wexler, You Get What You Pay For: The Federal Government Should Stop Paying for Foster Care, FAMILY INTEGRITY & JUSTICE QUARTERLY, vol 1: Issue 3, at 56 (summer 2022).
4 42 U.S.C. § 675(4)(A).
5 Miller v. Youakim, 440 U.S. 125 (1979).
6 N.Y. Office of Children and Family Services, Maximum State Aid Rates for Foster Boarding Home Payments and Adoption Subsidies 2023-24 Rate Year (July 1, 2023, through March 31, 2024), https:// ocfs.ny.gov/main/rates/assets/docs/rates/fc-b/FCBoard-Rates-2023Jul01-2024Mar31.pdf.
7 Calculated based on a $27.07 minimum daily rate. Texas Department of Family and Protective Services, 24-Hour Residential Child Care Reimbursement Rates, https://www.dfps.texas. gov/Doing_Business/Purchased_Client_Services/ Residential_Child_Care_Contracts/Rates/default. asp.
8 Florida Department of Children and Families, Implementation of Chapter 2022-68, Laws of Florida (Senate Bill 7034) (July 1, 2022), https:// www.myflfamilies.com/sites/default/files/202305/20220701-Memo_Implementation_of_ SB7034.pdf.
9 Wisconsin Department of Children and Families, Understanding the Uniform Foster Care Rate, Effective
§ New public funding streams often begin with limited pilot programs, and a pilot could focus on parents with disabilities. Such a pilot could borrow from existing definitions of disabilities to determine eligibility, which may make administering a pilot easier.
January 1, 2024 - December 31, 2025, https://dcf. wisconsin.gov/files/publications/pdf/0142.pdf.
10 Zachary Parolin, Elizabeth Ananat, Sophie Collyer, Megan Curran, and Christopher Wimer, The Effects of the Monthly and Lump-Sum Child Tax Credit Payments on Food and Housing Hardship, 113 AEA PAPERS AND PROCEEDINGS 406. 406 (2023).
11 Center for Budget and Policy Priorities, A Quick Guide to SNAP Eligibility and Benefits (2023), https://www.cbpp.org/research/food-assistance/aquick-guide-to-snap-eligibility-and-benefits
12 TANF rates vary by state. In Texas, a child-only TANF grant is $121 (compared to more than $800 for foster parents). Texas Department of Health and Human Services, TANF Cash Help, https:// www.hhs.texas.gov/services/financial/cash/tanfcash-help. In New York, for example, benefits are higher, but still far less than the foster care rates noted above. N.Y. Office of Temporary and Disability Assistance, Temporary Assistance (TA), Frequently Asked Questions, How much do recipients receive? https://otda.ny.gov/programs/temporaryassistance/faqs.asp.
13 Christina McClurg Riehl & Tara Shuman, Children Placed in Kinship Care: Recommended Policy Changes to Provide Adequate Support for Kinship Families, 39 CHILD LEGAL RTS. J. 101, 109, 111 (2019).
14 Kristina Rosinky, Megan Fischer, & Maggie Haas, Child Trends, Child Welfare Financing SFY 2020: A survey of federal, state, and local expenditures (2023), https://cms.childtrends.org/wp-content/ uploads/2023/04/ChildWelfareFinancingReport_ ChildTrends_May2023.pdf
15 42 U.S.C. § 672(c)(1)(A)(ii)(II) (emphasis added). Physical and sexual abuse combined accounted for only 15% of all entries into foster care. AFCARS Report, supra note 2, at 3. CPS agencies reported that “neglect” was the reason for parent-child separations in 62% of cases. Id.
16 Elizabeth Brico, To “Protect” My Kids, the State Made Me Homeless, Rewire News Group, July 31, 2020, https://rewirenewsgroup.com/2020/07/31/ to-protect-my-kids-the-state-made-me-homeless/; DOROTHY ROBERTS, TORN APART: HOW THE CHILD WELFARE SYSTEM DESTROYS BLACK FAMILIES – AND HOW ABOLITION CAN BUILD A SAFER WORLD 68-69 (2022).
17 Shanta Trevedi, “Am I still a parent?: The Child Welfare System’s Devastating Effects on Parents (on file with author), abstract available at https:// papers.ssrn.com/sol3/papers.cfm?abstract_ id=4715550.
18 Alice Burns, Maiss Mohamed, & Molly O’Malley Watts, Kaiser Family Foundation, Pandemic-Era Changes to Medicaid Home-and Community-Based Services (HCBS): A Closer Look at Family Caregiver Policies (2023).
19 Id.
20 Smith v. Org. of Foster Families for Equality and Reform, 431 U.S. 816, 844 (1977).
21 Salom Teshale, Wendy Fox-Grage, & Kitty Purington, Administration for Community Living, Paying Family Caregivers through Medicaid Consumer-Directed Programs: State Opportunities and Innovations 3 (2021).
23 Id. at 3.
24 For a more detailed description, see Catalyst Center, Boston University School of Public Health, The TEFRA Medicaid State Plan Option and Katie Beckett Waiver for Children – Making It Possible to Care for Children with Significant Disabilities at Home (2016), https://ciswh.org/wp-content/ uploads/2016/07/TEFRA.pdf.
25 Gupta-Kagan, Distinguishing Family Poverty from Child Neglect, supra, at __ - __ (summarizing research).
26 42 U.S.C. 672(j)(1) (emphasis added). Congress added this provision in 2018, as part of the same compromise that included the Family First Act. Bipartisan Budget Act of 2018, Pub. L. 115-123, § 50712, codified at 42 U.S.C. § 672(j).
27 42 U.S.C. § 675(4)(B).
28 Unfortunately, the law still requires the child to be in the state’s legal custody, an unnecessary barrier that has kept use of this funding limited. U.S. Dep’t of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Human Services Policy, How some states use title IV-E foster care funding for family-based facilities that treat substance use disorders 2 (2021).
29 Children’s Bureau, Separate Licensing or Approval Standards for Relative or Kinship Foster Family Homes, 88 Fed. Reg. 66700 (2023), codified at 45 C.F.R. § 1355.20 (“Agencies may establish one set of foster family home licensing or approval standards for all relative or kinship foster family homes that are different from the set of standards used to license or approve all non-relative foster family homes.”).
30 Burns, Mohamed, & O’Malley Watts, supra.
31 Robyn Powell, Parents and Children with Disabilities in CHILD WELFARE LAW AND PRACTICE: REPRESENTING CHILDREN, PARENTS, AND AGENCIES IN NEGLECT, ABUSE, AND DEPENDENCY CASES 4TH ED. 113, 12021 (Josh Gupta-Kagan, LaShanda Taylor Adams, Melissa Dorris Carter, Kristen Pisani-Jacques, Vivek S. Sankaran Eds. 2022).
32 For a comprehensive summary, see National Council on Disability, Rocking the Cradle: Ensuring the Rights of Parents with Disabilities and Their Children (2012).
33 Id. at 25.
34 Id.
35 Sarah Lorr, Disabling Families, 76 STAN. L. REV. __, around FNs 313-17 (forthcoming 2024).




Tia Humphrey is a former foster youth having been aged out for two years now. She has a master’s degree that she uses to advocate for current and former foster youth and empower others to share their testimonies. She partnered with Kentucky Youth Advocates and two contractors to create 6 canvases illustrating her time in and out of the system.

16 years old – After being placed with a friend of the family, Tia encountered additional physical abuse. Unable to be hidden from the school system, Tia was again removed from the home. At this point, Tia experienced homelessness; and from the labels given to Tia from the previous art, she was deemed too dangerous, making it difficult to find a home. This resulted in a failed adoption and Tia’s placement back into foster care.

18 years old – After three years back in the system, Tia has flourished with her new foster family. After getting a job, and graduating high school, Tia is ready to start her new journey as an adult at the University of Louisville.

21 years old – At 21 years old and beyond, Tia has graduated from UofL with both her Bachelors and Masters degree. She bought her house on her 21st birthday and has found her forever home with a support system to aid in her healing journey.
REPRESENTATIVE JUDY CHU
Judy Chu represents the 28th congressional district of California in the U.S. House of Representatives.

I’ve been passionate about protecting youth in our foster system since my days in the California Assembly when I sponsored legislation to protect LGBTQ+ foster youth from discrimination, to keep foster care siblings together, and to increase the age of eligibility for transitional housing from age 21 to age 24. And I have been proud to continue this work in Congress as a longtime member of the Congressional Foster Youth Caucus and as a
member of the Ways and Means Committee, which has jurisdiction over the child welfare system and family support programs.
Over the years and through events like the Foster Youth Shadow Day, I have had the opportunity to meet with bright and wonderful young people from my district and across the country to better understand the challenges that they face every day and witness firsthand the amazing resilience and promise they show. Through this program, I have met incredible young people like Alejandra, a member of the First Nations Ojibwe-Cree tribe, who advocated for a stronger Indian Child Welfare Act to me in my office last year.
Also last year, I was approached by Chairman Martin of the Morongo tribe in Southern California, who was concerned about California’s alarmingly and disproportionately high rate of Native children entering the child welfare system. They are 4.5 times more likely to enter care than their non-Native counterparts. He also expressed to me that these children are also more likely to be placed outside of their own communities, away from their tribal and cultural connections.
Their advocacy was so meaningful, and I have been working on this Congress to safeguard the cultural and familial connections of tribal children who come into contact with the child welfare system. That is why I introduced a bipartisan bill along with Rep. Don Bacon of Nebraska, H.R. 3461, the Strengthening Tribal Families Act, to assist state child welfare agencies in implementing federal protections for tribal children by strengthening the
relationships between state child welfare agencies and the courts. The bill directs Health and Human Services to assess state strengths and areas for improvement in implementing federal standards as established under the Indian Child Welfare Act of 1978.
Additionally, I have heard directly from foster youth that aging out of the foster care system brings serious challenges—including difficulties accessing healthcare, housing, transportation, and higher education. To respond to this, 28 states, the District of Columbia, and nine Tribes have already extended Title IV-E foster care for youth beyond age 18. The impacts of these programs last a lifetime. One study found that 21-year-olds who’ve spent time in extended care are 2.7 times less likely to have experienced homelessness, 3 times more likely to be enrolled in school, and 1.4 times more likely to receive educational aid. But not all state agencies have opted to extend this support— meaning too many foster youth lose supportive services as soon as they turn 18.

So, building on years of research that shows that extending supports and programming into the first few years of adulthood can make a clear, positive difference in the lives of young people Rep. Erin Houchin of Indiana and I have introduced the bipartisan H.R. 7010, the Increasing
Access to Foster Care Through Age 21 Act. The passage of this legislation would provide a financial incentive for all states to extend foster care beyond age 18, thereby helping more foster youth around the country complete schooling, apply to jobs, manage a home, and make informed health care decisions.
Our nation’s future depends on us improving our child welfare systems, protecting children’s rights, and giving them a path to success. I’ll always be an unyielding partner in that fight.
REPRESENTATIVE DON BACON-R
U.S. Congressman Representing Nebraska’s 2nd District

In the intricate world of child welfare, ensuring the emotional connections and stability within families is crucial. It’s all about strengthening the bonds between children and their families, creating a sense of belonging and support that’s vital for everyone’s well-being. But it’s tough, especially for Indigenous communities who’ve faced historical traumas and unfair treatment within the system.
But there’s hope on the horizon with the Supporting Tribal Families Act. It’s a game-changer, focusing on preserving cultural heritage, community ties, and family relationships within the child welfare system. This law isn’t just about following the rules laid out in the Indian Child Welfare Act; it’s about really understanding and addressing the deeper issues facing tribal communities. At its core, the Supporting Tribal Families Act respects the rights of Indigenous communities to make their own decisions and keep their cultural identity strong. It gives tribes more
say in child welfare matters, aiming to right past wrongs and empower communities to shape their own futures.
One big thing this Act does is prioritize keeping families together whenever possible. It recognizes how important it is for kids to stay with their families for their emotional well-being. So, it pushes for support services, interventions, and resources that fit with each community’s culture and values.
The Act stresses the need for child welfare practices that understand and respect different cultures. It wants to bridge the gap between Western ways of doing things and Indigenous beliefs, making sure interventions are appropriate and honor tribal traditions. And it’s not just about laws; it’s about teamwork. The Act encourages better communication and teamwork between tribal nations, federal agencies, and state governments. Together, they can create a more united and responsive child welfare system that meets the unique needs of Indigenous communities.
But it’s not just about rules and systems; it’s about healing too. The Act calls for approaches that understand the lasting effects of past traumas and focus on healing and resilience for kids and families going through tough times.
So, in the end, the Supporting Tribal Families Act is a big step towards making sure Indigenous kids and families get the support they need in the child welfare system. By respecting cultural sovereignty, keeping families together, and focusing on healing, it’s setting the stage for a more fair and caring approach to child welfare for years to come. It’s a promise to nurture the connections that bind us all together as we work towards a future where every child feels loved and supported.
Principal Winkie thought he cried
A song in the latchkey of life on behalf of sleepDeprived youth, only to sound off placing working black mothers under lock and key.
WeeWillie“CryingattheLock”(LockHerUp!)
ANNA ARONS
Assistant Professor of Law, St. John’s University School of Law Impact Project Director, Family Defense Clinic, NYU School of Law

Anna Arons is an Assistant Professor of Law at St. John’s University School of Law and the Impact Project Director of the NYU School of Law Family Defense Clinic. She studies the government's regulation of families and the intersection of parental rights and identity along dimensions including race, poverty, and gender.
“We need eyes in the home.” This mantra of the child welfare system reflects an ethos of surveillance as protection: the idea that the state must closely watch families—more specifically, poor families and Black, Native, and Latinx families—to protect children. This ethos demands that we believe that the greatest risk that children from marginalized families face is their own parents, and not the political choices and deep-rooted inequities that have deprived families of access to food, housing, healthcare, quality schools, childcare, and material support.
The failure of surveillance as a means to achieve child well-being lays bare the falsity of that belief. To start, surveillance itself imperils children’s wellbeing. It threatens children’s sense of security, invades their privacy and their parents’ privacy, and leaves families in an ongoing state of precarity. Nor is the harm of surveillance neatly contained within family units; it bleeds out into entire communities, across generations. Further, a growing body of evidence demonstrates that the harms of surveillance are not counterbalanced by its benefits because pervasive state surveillance does not
1 The numbers in this paragraph are drawn from CHILDS.’ BUREAU, U.S. DEP’T OF HEALTH & HUM. SERVS., CHILD MALTREATMENT 2022 xv (2024).
2 See generally Kelley Fong, Child Welfare Involvement and Contexts of Poverty: The Role of Parental Adversities, Social Networks, and Social Services, 72 CHILD. & YOUTH SERV. REV. 5, 6 (2017) (describing poor families’ heightened exposure to mandated reporters); KELLEY FONG, INVESTIGATING FAMILIES 41-45 (2023) (describing mothers’ wariness of reporters).
3 I describe the intrusiveness of child welfare investigations at greater length in an earlier work, where I include citations to state statutes, regulations, and policy manuals and parents’ first-person accounts supporting the description here. See Anna Arons, The Empty Promise of the Fourth Amendment in the Family Regulation System, 100 WASH. U. L. REV. 1057, 1069-74 (2023).
4 Some states do have alternative “noninvestigative” responses for some low-level allegations. However, in many jurisdictions, even those “noninvestigative” responses bring about similar levels of surveillance. See, e.g., Soledad A. McGrath, Differential Response in Child Protection Services: Perpetuating the Illusion of Voluntariness, 42 U. MEM. L. REV. 629 (2012); Jane Walfogel, “The Future of Child Protection Revisited,” in CHILD WELFARE RESEARCH: ADVANCES FOR PRACTICE AND POLICY 235-41 (Duncan Lindsey and Aron Shlonsky, eds., 2008).
5 As one illustration of the thinness of “consent” in investigations, a recent class action lawsuit in New York alleges that caseworkers’ tactics, including threatening family separations and describing searches as mandatory, are so coercive as to render parents’ “consent” involuntary. See Complaint, Gould v. City of New York, No. 24-CV-1263 (E.D.N.Y.), filed Feb. 20, 2024.
6 KELLEY FONG, INVESTIGATING FAMILIES 13-14 (2023).
7 Id. at 37-45
8 IBr. for the Child at 25, In the Matter of Sapphire W., No. 2023-10606 (N.Y. App. Div., 2d Dept. 2024).
9 Id.
10 Id.
11 Hyunil Kim, Christopher Wildeman, Melissa JonsonReid & Brett Drake, Lifetime Prevalence of Investigating Child Maltreatment Among US Children, 107 AM. J. PUB. HEALTH 274, 277 (2017)
12 CHILDS.’ BUREAU, U.S. DEP’T OF HEALTH & HUM. SERVS., CHILD WELFARE PRACTICE TO ADDRESS RACIAL DISPROPORTIONALITY AND DISPARITY 2–3 (2021)
13 Kelley Fong, Child Welfare Involvement and Contexts of Poverty: The Role of Parental Adversities, Social Networks, and Social Services, 72 CHILD. & YOUTH SERV. REV. 5, 5–6 (2017)
keep children any safer than they would be in its absence: children are just as safe with the state’s eyes out of their homes. What actually protects children is ensuring that families’ needs are met at a societal level—shifting our collective political choices to address deep-rooted inequities—rather than surveilling and penalizing individual families.
I begin by briefly describing the role that surveillance typically plays in the child welfare system and the damage this surveillance can wreak. Next, I lay out the evidence that this intensive surveillance does not actually protect children. Finally, I describe an alternate approach to child safety, rooted in meeting all families’ needs proactively and on a societal level.
In a typical year, state family regulation agencies receive upwards of four million reports of child neglect or abuse, concerning more than seven million children.1 The vast majority of reporters express concerns of neglect—easily conflated with poverty—rather than physical or sexual abuse. About half of reports are immediately “screened out” and closed without referral for further investigation. The other half, more than two million reports annually, are referred for investigation. All told, less than ten percent of initial reports are ultimately substantiated after investigation. Fewer still result in family separations. Yet investigations alone—even investigations that do not substantiate any allegations or lead to further state intervention on families’ lives—are intrusive, upsetting, and traumatizing for families. (So, too, is the constant surveillance families experience under the lens of mandated reporters, though that is beyond the scope of this article.2)
Nearly every report referred for investigation results in state agents entering and searching families’ homes.3 Most states take a one-sizefits-all approach to investigations and require the same sort of comprehensive investigation for every report.4 Caseworkers assess everything from the home’s physical condition, to the food, provisions, and clothing the family has on hand, to more nebulous considerations like the climate of the neighborhood. In doing so, caseworkers look through refrigerators, kitchen cupboards, and medicine cabinets, and peer into closets and under beds. Beyond their searches of the home, caseworkers demand to speak to children privately and seek to perform “body checks” with children stripping down to their underwear. After these initial “evaluations,” workers return periodically
until an investigation is closed—and even if an investigation is closed and unsubstantiated, child protective agencies may still keep “eyes in the home” by referring families for ongoing preventive services. Parents face immense pressure to consent to caseworkers’ intrusions. Not only can workers credibly tell parents that “non-compliance” will be held against them during investigations and in court, but all of these interactions take place as the specter of family separation looms large.5
Its negative effects are long felt by parents, children, and communities. As sociologist Kelley Fong recently described in an exhaustively researched study, the experience of living under the ever-present threat of surveillance—by mandated reporters and by child welfare agencies—can leave mothers in a constant state of “precarity”: a sense that “state agents can take their children and there isn’t much that they can do to stop it.”6 This, in turn, contributes to parental stress and depression and can lead parents to withdraw or be wary of social supports and potentially helpful services for fear of future reports.7 Children are harmed directly, too. Summarizing decades of research, attorneys for children in the child welfare system recently wrote, “Children of all ages . . . suffer when they witness a parent’s anxiety, humiliation, distress, or loss of autonomy,” and lose trust in their own security and their own parents’ ability to protect them.8 “Ironically, the very home visits designed to ensure children’s safety at the hands of their caregivers can cause them great harm.”9
This harm is widespread and unevenly distributed. More than a third of children in the United States will experience a child welfare investigation over the course of their childhood. For Black children, that number is even higher: a Black child is more likely to experience an investigation than not.11 Native children and, in some parts of the country, Latinx children are also overrepresented in investigations.12 And across the country, investigations focus almost exclusively on poor families.13 Having seen the intrusiveness of child welfare surveillance, the harm it wreaks, and its sprawling and disproportionate focus, we might at least hope that its benefits outweigh its harms. Yet the next section shows the limits of surveillance’s efficacy.
The “eyes in the home” ethos of child welfare is so prevalent that many in the field see surveillance as inevitable, obvious, and necessary. The absence of surveillance is presumed to present a grave risk to marginalized children—making any proposed reductions in surveillance a nonstarter for many in the field.14 This is why the COVID-19 era proved a rich data source: risk aversion gave way to an international emergency that forced the child welfare apparatus to pull back in almost every conceivable way. Mandated reporters retreated, caseworkers conducted fewer evaluations inside families’ homes, and family courts constrained their operations. The sky did not fall. Child abuse and neglect did not skyrocket. The massive surveillance system, it seems, is not necessary. Nor is it sufficient—for what children protection from, often, is not their own parents but rather from a society that does not tend to their needs and their growth.
In 2022, I closely studied the effects of the 2020 COVID-19 shutdown on child welfare in New York City.15 In March 2020, New York City’s vast child welfare system came to a grinding halt, as in short order, schools were closed, caseworkers were instructed to conduct investigations remotely if possible, and the city’s family court limited the types of cases that it would hear to only those seeking to remove children from their parents’ care, rather than those seeking court-ordered supervision. With children no longer under the surveillance of mandated reporters in schools, reports of child maltreatment dropped by 40 percent, as did the number of investigations. The number of family separations dropped even more dramatically, by nearly 50 percent. These numbers are not a surprise: this drop in surveillance and intervention is exactly what many commenters said would lead to a “pandemic of child abuse.” Instead, the surprise is what happened amid this dramatic decrease in state surveillance: New York’s children stayed just as safe from maltreatment at the hands of their parents. This is clear by any number of metrics.
First, there was no increase in the rate of child abuse. Reports of child abuse resulting in injuries requiring medical care—let alone child fatalities— make up a thankfully small minority of the total number of reports of child maltreatment. However, these types of incidents not only drive child welfare policy, but also are more likely to result in medical attention and less likely to evade detection, even during the COVID-19 shutdown. Yet the number
of investigations related to child fatalities dropped in the initial shutdown period and the city’s child welfare agency commissioner later reported that the city had not experienced any changes in emergency department admissions patterns.
Second, once the city crawled back to normalcy and children were once more under the eyes of mandated reporters, there was no apparent “rebound effect” in the number of reports. While the number of reports and investigations rose to near pre-COVID-19 levels, there was no increase in the number of reports or investigations to compensate for any sustained period of underreporting
Finally, and relatedly, there was no change in the rate of substantiation for reports once the child welfare apparatus was back in force. Had mandated reporters returned to their surveillance positions and reported an influx of valid concerns from a previously unreported backlog, the rate of substantiation would have been higher. As the city’s child welfare agency commissioner himself acknowledged, there were no indications of “undetected charges” of child maltreatment.
These numbers paint a picture of stable child safety even with a decrease of state surveillance—and thus a picture of oversurveillance and overintervention prior to the pullback. In the years since my initial study, its findings have been confirmed in New York City16 and more broadly.17 Examples outside the COVID-19 case study, too, reveal that reductions in state surveillance and family separation do not increase child neglect or abuse.18 Further upstream, research shows that mandated reporting does not have any effect on detecting abuse.19 So we see: children do not need to be separated from their families, nor does the state need to ceaselessly surveil parents to maintain the status quo for child well-being. But families deserve more than the status quo.20 As the next section describes, by shifting away from surveillance, we can ensure better childhoods for more children and better lives for more families.
The “eyes in the home” model of child protection is an individualistic one. It focuses narrowly on the shortcomings of individual parents, subjecting those identified as risky or dangerous to intensive surveillance and intervention. “Risk” and “danger,” in turn, are racialized, gendered, and classed concepts. This model is ineffectual at ensuring child well-being—but it is convenient for society
14 Richard Wexler, COVID-19 Surfaces Child Welfare’s Ugly Biases About Race, Class, YOUTH TODAY, April 8, 2020 (collecting sources predicting child welfare crisis as a result of pullback of state surveillance).
15 This section draws from Anna Arons, An Unintended Abolition: Family Regulation During the Covid-19 Crisis, 11 COLUM. J. RACE & L. 1 (2022).
16 Melissa Friedman and Daniella Rohr, Reducing Family Separations in New York City: The Covid-19 Experiment and a Call for Change, 123 COLUM. L.R. F. 52 (2023).
17 See, e.g., Kristine Campbell, et al, Child Abuse Prevention in a Pandemic—A Natural Experiment in Social Welfare Policy, 177 JAMA PEDIATRICS 1263 (2023); Robert Sege and Allison Stephens, Child Physical Abuse Did Not Increase During the Pandemic, 176 JAMA PEDIATRICS 339 (2021).
18 See, e.g., Melissa Carter, Christopher Church & Vivek Sankaran, A Quiet Revolution: How Judicial Discipline Essentially Eliminated Foster Care and Nearly Went Unnoticed, 12 COLUM. J. RACE & L. no. 1 (2022) (describing dramatic decrease in foster placements in New Orleans spearheaded by a family court judge and absence of negative impact on child safety); Richard Wexler, Connecticut Losing the Gutsiest Leader in Child Welfare, HARTFORD COURANT (Dec. 6, 2018) (describing child welfare commissioner’s efforts to reduce unannounced home searches and absence of negative impact on child safety).
19 See, e.g., Grace Ho, et al, Universal Mandatory Reporting Policies and the Odds of Identifying Child Abuse, 107 Amer. J. Pub. Health 709 (2017).
20 Cara Baldari, Fact Sheet: U.S. Child Poverty Has Significantly Increased, FIRST FOCUS ON CHILDREN (Sept. 18, 2023) (noting a doubling in child poverty in a one-year period); Institute of Medicine, National Research Council, Social Trends and Child Maltreatment Trends, in Child Maltreatment Research, Policy, and Practice For The Next Decade: Workshop Summary (2012) (“Many sources of data point to a substantial reduction in the incidence of child physical and sexual abuse, but not neglect, over the past two decades.”).
21 https://www.cbpp. org/press/statements/ in-pandemics-secondyear-governmentpolicies-helped-drivechild-poverty-rate-to-a
22 NAT’L ACAD. OF SCI., ENG. & MED., A ROADMAP TO REDUCING CHILD POVERTY 89 (2019).
23 Danilo Trisi, Government’s Pandemic Response Turned a Would-Be Poverty Surge Into a Record Poverty Decline, CTR. ON BUDGET AND POLICY PRIORITIES (2023) (collecting studies).
24 Nicole L. Kovski, Heather D. Hill, Stephen J. Mooney, Frederick P. Rivara & Ali Rowhani-Rahbar, Short-Term Effects of Tax Credits on Rates of Child Maltreatment Reports in the United States, PEDIATRICS, July 2022, at 1, 5.
writ large, as it is a model that absolves society of its collective responsibility to protect children and safeguard their welfare in favor of blaming individual parents.
What if society embraced that collective responsibility instead? Instead of surveilling families after receiving reports of maltreatment, the government might instead address the conditions that give rise to reports of maltreatment proactively. Those conditions include everything from a lack of access to material support and housing, to failing schools, to inaccessible or insufficient mental and physical healthcare and substance use services. By providing all families with the resources and support they need outside any system of surveillance, the government could immediately reduce the incidence of child maltreatment directly associated with conditions of poverty and lack of access to care. More expansively, children raised in such conditions would themselves be better positioned to care for future generations, reducing more serious types of maltreatment down the line. This is a multigenerational vision—but there are concrete steps that we can take now to realize it, both in terms of tending to families’ needs outside the child welfare system and reducing family surveillance.
The COVID era serves, yet again, as an illustrative proof-of-concept of how we might increase child safety by meeting families’ material needs. In the same period that the government reduced its surveillance of families, it increased financial entitlements for families. Stimulus payments, increased unemployment benefits, and the expanded Child Tax Credit represented an unprecedented transfer of funds from the government to families without strings attached and without increased surveillance—and that transfer resulted in an equally unprecedented drop in child poverty and increase in health coverage.21
A decrease in child poverty is a boon for child safety: “The weight of the causal evidence indicates that income poverty itself causes negative child outcomes.”22 Outside the COVID example, income assistance programs have been linked with “healthier birthweights, lower stress for mothers (measured by reduced stress hormone levels in the women’s bloodstream), better nutrition in childhood, higher scores on reading and math tests and other measures of school performance, more high school completion, higher rates of college entry, and better health in adulthood.”23 It is not surprising, then, that increases in government assistance are associated with decreases in reports of child maltreatment.24
As we support families proactively and broadly outside the child welfare system, we must also move to reduce family surveillance.25 There are opportunities to do this at virtually every step of the child welfare system. First, we can “narrow the front door” by reducing the number of reports. Narrowing vague and broad definitions of “neglect” and reducing mandated reporting will save millions of families from the trauma of reports and investigations. Research shows that high rates of reporting can be counterproductive for child safety, not just because investigations cause trauma but because overreporting takes up system resources.26 Second, agencies must narrow investigations. Rather than taking a “one size fits all” approach to investigations, agencies must search families’ homes only when evidence in the home is relevant to the underlying allegations and only to the extent necessary for the investigation. I use “must” to underline an important point: too often ignored in the child welfare system, the Fourth Amendment itself demands these constraints. Recent litigation seeks to enforce the Fourth Amendment in New York City’s child welfare investigations27 —but jurisdictions need not wait for litigation. Legislatures can narrow agencies’ statutory authority and eliminate requirements for “home evaluations” for every investigation. Agency administrators can train caseworkers on constitutional obligations and retrain them away from coercive tactics.28 And legislatures and agencies alike can mandate that caseworkers inform parents of their rights, increasing families’ autonomy and empowerment during investigations. Finally, provision of wellresourced and well-trained counsel to parents during investigations and during court proceedings would reduce surveillance by increasing families’ awareness of their rights and by allowing counsel to remind family court judges of the statutory and constitutional constraints on family surveillance.
By delinking care and surveillance, we can improve child wellbeing and reduce trauma to families, immediately and intergenerationally.
Conclusion
Putting eyes in the home—sending government agents to investigate and surveil millions of families each year—has proved a costly and ineffective means of protecting children. Indeed, considering that the vast majority of allegations are ultimately unsubstantiated, it is fair to say that this approach has harmed more children and more families than it has helped. Our goal now must be to take eyes out of the home and move from an individualistic and reactive to a collective and expansive approach to child welfare, in order to better protect children, their families, and their communities. Taking eyes out of the home will require a fundamental shift in assumptions. Rather than presume that poor parents and Black, Latinx, and Native parents are deficient and require state surveillance, we must start from the premise that these parents want and know what is best for their children.
25 I describe these proposals at greater length in Anna Arons, The Empty Promise of the Fourth Amendment in the Family Regulation System, 100 WASH. U. L. REV. 1057, 1121-35 (2023).
26 Casey Foundation, Can decreasing unwarranted reports to child protection agencies improve outcomes for children and families? (Aug. 2020), https://www. casey.org/a2aunwarranted-reports/.
27 Gould v. City of New York, No. 24-CV1263 (E.D.N.Y.).
It is up to us, as a society, to ensure that all parents are provided the resources to create the lives they dream of for their children.
28 A reporter interviewing caseworkers in New York City found that they had not been trained on the Fourth Amendment but had been trained to use coercive tactics. Eli Hager, Police Need Warrants to Search Homes. Child Welfare Agents Almost Never Get One., PRO PUBLICA (Oct. 13, 2022).





Senior Director of Child Welfare at the National Center for Youth Law
Kristen Weber is Senior Director of Child Welfare at the National Center for Youth Law (NCYL) where she leads NCYL’s efforts to transform child welfare systems so that children and youth are safer and can heal and thrive in their families and communities. She has worked on a variety of federal and state research, technical assistance, and reform efforts focused on improving outcomes for children and youth of color and LGBTQ+ youth involved in child welfare systems. In 2020, she helped create and launch the upEND movement, an effort focused on abolishing the current child welfare system and building many different alternatives that will support the safety, care, and healing of children and youth.
Clinical Director at Family Builders
Vida Khavar is a licensed Marriage and Family therapist who has 25+ years’ experience in child welfare. She has assisted many organizations in developing programs that serve children and families. Vida was a consultant for the federal project: RISE, which aimed at improving the lives of LGBTQ+ youth in foster care in Los Angeles County. She is currently the Clinical Director at Family Builders. As such, she collaborates with the California Department of Social Services in developing and implementing affirming policies and practices for LGBTQ+ children in foster care. Vida also leads the Youth Acceptance Project & provides her clinical expertise and training in several jurisdictions throughout the country.
Senior Fellow with the Center for the Study of Social Policy
Bill Bettencourt has over 40 years of experience working on system reform in a variety of roles: as the Child Welfare Director in San Francisco, a Program Officer with the Stuart Foundation, a Senior Consultant with the Annie E. Casey Family to Family Initiative, as Senior Advisor to upEND Movement and currently as a Senior Fellow with the Center for the Study of Social Policy (CSSP) in Washington D.C.
1 See the Search Institute’s research on the importance of developmental relationships. https:// searchinstitute.org/
2 Matarese, M., Greeno, E. and Betsinger, A. (2017). Youth with Diverse Sexual Orientation, Gender Identity and Expression in Child Welfare: A Review of Best Practices. Baltimore, MD: Institute for Innovation & Implementation, University of Maryland School of Social Work. (Matarese et al, 2017).
3 Substance Abuse and Mental Health Services Administration. (2014). A Practitioner’s Resource Guide: Helping Families to Support Their LGBT Children. HHS Publication No. PEP14LGBTKIDS. Rockville, MD: Substance Abuse and Mental Health Services Administration. (SAMSHA, 2014).
4 Travers, R, Bauer, G, Pyne, J, Bradley, K, Gale, L, Papdimitriou, M. (October 2, 2012). Impacts of Strong Parental Support on Trans Youth: A report prepared for Children’s Aid Society of Toronto and Delisle Youth Services. TransPULSE Project. https:// transpulseproject. ca/wp-content/ uploads/2012/10/ Impacts-of-StrongParental-Support-forTrans-Youth-vFINAL.pdf
5 SAMSHA (2014).
6 Robinson, B. A., Stone, A. L., & Webb, J. M. (2023). Aunties, Aunts, and Tías: The Forgotten Othermother Supporting and Housing LGBTQ Youth. Socius, 9. https:// doi.org/ 10.1177/ 23780231231217827
7 Leung E, KasselGomez G, Sullivan S, Murahara F, Flanagan T. (2022). Social Support in Schools and Related Outcomes for LGBTQ youth: A Scoping Review. Discov Educ. 1(1):18. doi: 10.1007/s44217022-00016-9. Epub 2022 Nov 14. PMID: 36407890; PMCID: PMC9662773. https://pubmed. ncbi.nlm.nih. gov/36407890/
8 In June 2023, the Human Rights Campaign issued a state of emergency for LGBTQ+ individuals in the United States given the increasingly harsh and discriminatory laws against LGBTQ+ people. https://www. hrc.org/campaigns/ national-state-ofemergency-for-lgbtqamericans
9 For a discussion of the paradox of increasing rights and increasing violence and discrimination of LGBTQ+ youth see Paris, F. and Miller, Claire C. (June 3,2023). What It’s Like to Be a Queer Teenager in America Today, The New York Times. https:// www.nytimes. com/interactive/ 2023/06/03/ upshot/up-lgbtq-teens. html
10 See the legislative analysis and tracking work of trans activist Erin Reed at https:// www.erininthemorning. com/ and Movement Advancement Project’s Equality Maps at https://www.lgbtmap. org/equality-maps
11 Meckler, L., Natanson, H., and Harden, J.D. (March 12, 2024). In states with laws targeting LGBTQ issues, school hate crimes quadrupled. https:// www.washingtonpost. com/education/ 2024/03/12/schoollgbtq-hate-crimesincidents/
Youth is a dynamic and exciting time of identity exploration and development, including discernment of one’s gender identity and sexual orientation. Youth grow best when connected to and supported by their family and others who care about and love them. Youth need affirming social connections and supportive opportunities to try new things, make mistakes, and grow from these experiences.1 However, not all youth get the support and love they need, and lesbian, gay, bisexual, transgender, queer, intersex, two-spirited youth, and youth who are gender expansive (LGBTQ+) are especially vulnerable to rejection, discrimination, and violence. While social inclusion for LGBTQ+ youth has largely increased, our respective and collaborative work over decades has shown us the unrelenting oppressive experiences faced by LGBTQ+ youth, especially youth of color. We also know that, despite these negative experiences, LGBTQ+ youth survive and even thrive because of strong relationships with their parents, extended family, peers, and community members. Policies can support or undermine the lives and relationships of LGBTQ+ youth. Currently, an increasing number of state policies are heightening oppressive environments for LGBTQ+ youth and weaponizing public systems— such as the child welfare system—against them. It is paramount that we work collectively to eliminate laws and policies that hurt LGBTQ+ youth and discriminate against them and instead find avenues to encourage and offer community-based help and ensure they are affirmed and safe from harm when involved with child welfare systems.
Our society lacks robust help for parents, especially basic concrete supports such as cash aid, housing, childcare, and transportation, as well as more tailored supports including help with navigating adolescent development, safe and enriching recreational opportunities for youth, and supports that address youth or parent mental health challenges and substance use disorders. Some parents also need help understanding and supporting the identity development of their child, particularly around sexual orientation and gender identity and expression (SOGIE). Lack of help for family rejection of a child’s SOGIE is a significant contributing factor to the disproportionate number of LGBTQ+ youth in child welfare and juvenile justice systems and to the mental health and well-being of these youth.2 Yet we know that there are nonjudgmental interventions for parents that “meet families where they are” and can help move families to acceptance and reconciliation.3
We know that supporting family relationships is critical and has a positive impact on the health and well-being of LGBTQ+ youth, specifically teens; those who felt supported by their parents regarding their gender identity were 93 percent less likely to attempt suicide than youth who did not perceive parents as supportive.4 Parental support is a protective factor for LGBTQ+ youth.5 Affirming experiences with relatives such as grandparents, aunts, uncles, or cousins also contribute to the stability and well-being of LGBTQ+ youth.6 Additionally, we know from youth themselves that their peer relationships—especially in schools— can help support them as they navigate the rejecting and discriminatory actions of adults.7 The challenge is that what we know works isn’t consistently supported by our laws and policies.
Further, while strong relationships are critical, the larger socio-political environment also influences the safety and well-being of youth. The United States, particularly in certain states and communities, is violent and unsafe for many people, including LGBTQ+ people.8 The everyday experiences of violence and degradation are part of the legacy of white supremacy in our culture and our laws. This legacy promotes a hierarchical ideology based on race, ethnicity, class, ability, sexual orientation, and gender identity. Supporting the health of LGBTQ+ youth, especially now in this increasingly violent context, requires supporting the family system, but also requires tackling the larger environment that allows for abuse, discrimination, oppression, and violence. From outlawing same sex relationships, to declaring queerness as a mental health disorder, to police raids of gay bars, to the large number of murdered trans women of color, there has been a long history of attacking the very being of LGBTQ+ individuals and thus the safety of youth in their developmental journey.
Despite this history of harm, LGBTQ+ youth are publicly coming out earlier and pushing against oppressive and reductive ideas of gender and sexuality. When gender is not static or reductive, when it is interpreted as a social construct and can be fluid, this can be unsettling to social hierarchy. As LGBTQ+ rights and equality have been recognized and, in many places, increased, so has the violent backlash.9 Some states are escalating harsh policy efforts that attack the identity development of LGBTQ+ youth and undermine their relationships with their families and communities.10 LGBTQ+ youth who live in states with anti-LGBTQ+ laws and rhetoric are more at risk of bullying in schools.11 The impact of this bullying is devastating and even has resulted in death.12 Further, LGTBQ+
youth who are Black, brown, or Indigenous can experience compounding forms of discrimination and oppression.
The Trevor Project’s 2022 National Survey on LGBTQ Youth Mental Health of 34,000 youth ages 13-24 provides a clarion call for the necessity to support LGBTQ+ youth and work to address family rejection, societal discrimination, and violence. Data from this survey show that:
• 24% of youth came out before age 13.
• 45% of LGBTQ considered suicide in the last year; 14% attempted suicide.
• 36% of LGBTQ youth reported that they have been physically threatened or harmed due to either their sexual orientation or gender identity; 31% of LGBTQ youth reported that they have been physically threatened or harmed due to their sexual orientation; 46% of LGBTQ youth who came out before age 13 reported being physically threatened or harmed due to their SOGIE.
• Nearly 2 in 5 LGBTQ youth reported living in a community that is somewhat or very unaccepting of LGBTQ people.
• Fewer than 1 in 3 transgender or gender nonbinary youth perceived their homes to be gender-affirming.
• LGBTQ youth who found their school to be LGBTQ-affirming reported lower rates of attempting suicide.
• LGBTQ youth who live in a community that is accepting of LGBTQ people reported significantly lower rates of attempting suicide than those who do not.13
LGBTQ+ youth are being driven into child welfare systems by policies that endanger them in their homes and communities, and they are being harmed in foster systems. Data show child welfare systems decrease the safety and well-being of LGBTQ+ and gender expansive youth.14 Only in the last decade have child welfare systems even recognized that LGBTQ+ youth are disproportionately present within their systems.15 The Biden Administration noted that child welfare involvement for LGBTQ+ youth is an independent risk factor; simply being both queer and in the system puts these youth at heightened risk of poor life outcomes, independent of any maltreatment or other trauma experienced.16
We can change the conditions that contribute to these bleak outcomes and create conditions where LGBTQ+ youth are supported in the context of their families.
Much has been written about the harms and limitations of the child welfare/family policing system and its problematic orientation to punish, control, and separate families.17 Reform efforts have been limited in scope and have lacked sustainability. Ultimately, we believe that the current child welfare system should be abolished—meaning the current system dismantled and many different alternatives should be built and used to support the safety, care, and healing of youth.18 However, we are not willing to abandon youth who are currently experiencing child welfare/family policing interventions. Thus, we advocate for policy solutions that end drivers into the child welfare system and mitigate harmful family policing system interventions and practices. We work to implement what is known to support those currently involved in family policing systems and promote innovating and building many different alternative and community-based, nonpunitive supports for youth and their families.
Many policies create harm and exert social control and punishment over LGBTQ+ youth and their families and interfere with identity formation. Some policies also undermine rather than support family connection and integrity and create precarious social conditions that jeopardize the safety of youth. It is the synergy of each separate harmful policy that creates an atmosphere of violence and rejection for LGBTQ+ youth. These policies impact so many aspects of a youth’s everyday life experience—from schools to sports and recreation, medical care, mental and behavioral health care, child welfare to juvenile justice. There are too many anti-LGBTQ+ youth policy efforts to enumerate,19 but below we look at two harmful efforts that seek to expand the child welfare system/family policing system20 into the lives of LGBTQ+ youth that must be dismantled.
First, there are growing and troubling policy efforts to require child welfare systems to intervene in families seeking gender affirming care for their youth. Most notably, the Attorney General of Texas21 has a policy directive requiring child protection agencies to investigate families seeking medically necessary health care for trans youth, with other states (like Wyoming) introducing bills that would consider gender affirming care against the best interest of youth, with custody and child protection implications.22
Second, jurisdictions are passing laws affecting local school policies, not only restricting
12 In February 2024, a non-binary student, Nex Benedict, committed suicide after a school bullying incident in Oklahoma. This death is a result not just of bullying but of the larger political context of anti-LGBTQ+ legislation in the state and public statements by the State School Superintendent declaring that trans students were a “threat” in schools, institutionalizing fear and hate and in effect legitimizing the bullying of these youth. Retrieved from: https:// www.independent. co.uk/news/ world/americas/ nex-benedictoklahoma-ossawanon-binary-b2500209. html?utm_ source=substack&utm_ medium=email
13 The Trevor Project 2022 National Survey on LGBTQ Youth Mental Health, https://www. thetrevorproject. org/survey-2022/ assets/static/ trevor01_2022survey_ final.pdf
14 Survey data about the experiences of LGBTQ+ youth have been collected in a small number of jurisdictions including Los Angeles, New York City, Allegheny County, PA, and Cuyahoga County, OH. For a published study, see Wilson, B., Cooper, K., Kastanis, A. & Nezhad, S. (2014). Sexual and Gender Minority Youth in Foster care: Assessing Disproportionality and Disparities in Los Angeles. Los Angeles: The Williams Institute, UCLA School of Law.
15 Research has found that transgender youth represent 5.6 percent of youth in the foster system, but only 2.25 percent of youth in the general population. Wilson, B., Cooper, K., Kastanis, A. & Nezhad, S. (2014). Sexual and Gender
Minority Youth in Foster care: Assessing Disproportionality and Disparities in Los Angeles. Los Angeles: The Williams Institute, UCLA School of Law.
16 Safe and Appropriate Foster Care Placement Requirements for Titles IV-E and IV-B, 88 FR 66752. (September 28, 2023). The proposed federal rule (finalized in April 2024) states: “Being in foster care also appears to be an independent risk factor for LGBTQI+ youth: a 2020 survey found that “LGBTQ youth who reported having been in foster care had three times greater odds of reporting a pastyear suicide attempt compared to those who had not.”
17 Kristen Weber and Bill Bettencourt help found the upEND movement that calls for abolishing the child welfare system and building new ways of caring for one another. For more information and resources that discuss the problems of the child welfare system see www. upendmovement.org.
18 For more detail on our thinking and position see Weber, K. and Bettencourt, B. (July 2022) Different year, different jurisdiction, but the same findings: Reforming isn’t enough. Columbia Law Journal.
19 For up-to-date tracking of antiLGBTQ+ legislative efforts in the United States see the Movement Advancement Project Equality maps at https://www.lgbtmap. org/equality-maps
20 We use the child welfare system and family policing system interchangeably. Advocates, including those with lived experience, refer to child welfare or child
curriculum but also in some places requiring school personnel to “forcibly out” youth to their parents without the consent of the youth.23 Some of these policies suggest that concerns about forced outings of LGBTQ+ children to their parents should be reported to child welfare systems. This undermines trust of youth with the school personnel, weakens their connection to school, can lead to truancy, and can discourage youth from seeking support in school.
Weaponizing child welfare systems against families is wrong and dangerous. Child welfare systems are a blunt intervention with a limited array of options available to work with families and the threat of permanent family separation. Both investigations and placement in the foster system are destabilizing and traumatic events that undermine relational health and have the potential for harmful generational repercussions with disproportionate impact on Black and Indigenous families. Part of the solution to supporting LGBTQ+ youth and their families must include dismantling harmful policies like these that are based on punishment and promote fear.
Beginning in 2014, we worked on the getREAL (Recognize.Engage.Affirm.Love) initiative to support LGBTQ+ youth in their families and improve their experiences when in the foster system. We found that there are ways that child welfare systems can change to be safer and less discriminatory towards LGBTQ+ youth and their families. In 2021, we published key lessons learned and implications for policy and practice.24 We identified that:
• Anonymous data must be repeatedly collected from youth about their SOGIE and used to ensure equity in services, resources, and outcomes.
• Policies can support the accountability of child welfare systems for meaningfully helping youth and families through both ensuring youth know their rights and through mechanisms to enforce those rights, such as through Foster Youth Bill of Rights, Youth Ombudspeople, and peer support programs, to name a few.
• To be effective and relevant, policies must be developed with LGBTQ+ youth and those community partners who have expertise in working with LGBTQ+ youth and who listen to and can be guided by Black, Latine,
and/or Indigenous LGBTQ+ youth who are disproportionately involved in child welfare services.25
In 2023, the National SOGIE Center commissioned a national scan of child welfare policies focused on serving LGBTQ+ youth policies and identified essential elements of inclusive policies including: delineating nondiscrimination protections, developing disclosure and confidentiality protocols about a youth’s SOGIE, having data collection and safeguards for that data, ensuring affirming mental health and medical care access, and providing policy guidance to workers for affirming family engagement.26
Finally, anti-discrimination policy efforts must be intersectional and honor, respect, and affirm all the identities LGBTQ+ youth embody, including race, ethnicity, ability, immigration status, and more. LGBTQ+ youth of color, who make up at least 60 percent of LGBTQ+ youth in child welfare and 85 percent of LGBTQ+ youth in juvenile justice,27 are the most discriminated and overrepresented populations in systems of care.
Yet we offer these policy suggestions with the deep understanding that a reformist rather than a more revolutionary approach to child welfare will ultimately sustain an inherently unjust system designed to separate children and families. The child welfare system is not able to consistently help and ensure good outcomes for all families, despite years of efforts and significant financial investment. To truly help LGBTQ+ youth, policies must promote radical investment in nonpunitive, meaningful family and community supports.
3. Promote policies that support family integrity and limit child welfare involvement.
Policies can support innovative programs that help families heal together. The Youth Acceptance Project (YAP), a clinical intervention developed by Family Builders in Oakland, California, is one of the programs which has shown that, with concrete information, specific SOGIE-related support, and guidance, parents can affirm and support their LGBTQ+ and gender expansive children. YAP was developed to support children and youth in, or at risk of entering, the child welfare system. YAP efforts have shown that families can remain intact, and families previously separated can be reunified. YAP uses a trauma-informed, psycho-educational model, grounded in cultural humility, to address the misinformation, resistance, fear, and grief that
families often struggle with. The intervention is based on research that documents the impact and harm that families may create when they are not accepting of their child’s SOGIE .28 The YAP outcome is that families become accepting and affirming of their LGBTQ+ children. The intervention reduces the time that children spend in the foster system, reunites children with their families, and, in many cases, prevents separation in the first place. Importantly, YAP providers lean into religion, ethnicity, and race to fully understand the families they are working with. Those parts of the family’s identity are honored and integrated in the work. Caregivers often experience complex emotions in response to their child’s SOGIE, and YAP providers support families in identifying their core beliefs and feelings about LGBTQ+ identities and help them work through related emotions.
A recent preliminary study on YAP showed statistically significant improvements in LGBTQ+ youth feeling safe at home. The same study also found that LGBTQ+ youth whose families are served by YAP show significant improvement in self-esteem, reduction in self-harm, and improvements in caregivers’ affirming behavior.29 The study showed statistically significant improvement in placement stabilization, as well as families affirming their children’s gender expression, pronouns, chosen names, seeking gender affirming medical care and advocating at school for their LGBTQ+ children. The well-being of youth showed significant increase as measured by statements like “I feel positive about my future”, “I do not have thought of killing myself, “My caregiver uses the name and pronouns I want them to use”, “my caregiver stands up for me in our community”. We know that policies that support innovative and effective programs like YAP decrease expensive and harmful foster system involvement and increase safety and stability for youth.
Policies also must recognize the importance of connections to extended families for LGBTQ+ youth. Another element of the YAP is to engage other family members— kin or fictive—in the work that is being done with the family. When YAP providers meet LGBTQ+ youth, one of the questions asked is whether the youth has someone in their family who is supportive of them. The supportive adults identified are often aunts and grandparents. These family members play a vital role in helping parents become more accepting of their LGBTQ+ youth. Parents often listen to their siblings or their own parents when they redirect them from treating their LGBTQ+ youth poorly. In the article “Aunties, Aunts, and Tías: The Forgotten Othermother Supporting and Housing LGBTQ Youth” the authors highlight the importance of other
parental figures, particularly “othermothers” or “aunties” who are often nonparental relatives who provide an array of emotional support to a family by educating parents, answering questions, reminding parents of the love they have for their child and sometimes even providing housing to their LGBTQ+ family members.30
4. Innovate and create new supportive policies that help families stay connected and keep youth safe
Supporting LGBTQ+ youth and their families requires a strong web of many different strategies, including basic supports that alleviate the stress of parenting—such as economic supports, housing, recreational opportunities, childcare, etc. Policy changes will vary depending on the political environments of different states and counties. However, developing and passing some type of broad supportive policies is achievable everywhere. The increased risks of poor outcomes faced by LGBTQ+ youth are not inherent to their identities, but stem from the stresses of prejudice, discrimination, rejection, and mistreatment they experience. Policies can act to reduce harms from schools and community members, can support timely access to confidential health and mental health care, and can support youth agency as they engage in the personal and developmentally appropriate SOGIE journey. Radical investment is needed in these types of policies. Overall, when designing supportive policies for LGBTQ+ youth, these policies should:
• be respectful of youth and their parents and work to support their relationship and bond,
• not punish parents or youth for seeking health care or mental health care,
• guard against discrimination,
• recognize and correct for historic and current racial and ethnic disparities, and
• foster larger affirming environments in schools and communities, recognizing that sexual and identity development is a critical part of the journey of youth.
Ultimately, we are working to render the need for child welfare interventions obsolete because there are robust community-based, nonpunitive ways of supporting the safety and connection of youth and their families.
protection systems as family policing systems because of their experiences of surveillance, regulation, and punishment.
21 For more information see https:// lambdalegal.org/ case/pflag-v-abbott/
22 https://www. erininthemorning. com/p/wyoming-billcould-take-trans-kids
23 https://www. lgbtmap.org/equalitymaps/youth/forced_ outing
24 Weber, K. and Bettencourt, B. (May 2021). Welcoming, Affirming, Supporting: Child Welfare Systems Must Honor the WHOLE Child. Center for the Study of Social Policy. Available here: https://cssp.org/ resource/welcomingaffirming-supporting/
25 Weber, K. and Bettencourt, B. (May 2021).
26 https://sogiecenter. org/national-sogiecenter-policy-practicescan/
27 Wilson, B. et al. (2017). “Disproportionality and Disparities among Sexual Minority Youth in Custody,” Journal of Youth & Adolescence; Irvine, A. and Canfield, A. “Reflections on New National Data on LGBQ/GNCT Youth In the Justice System.” (2018). LGBTQ Policy Journal, Harvard Kennedy School; Conron, K. J. and Wilson, B. D. M. (Eds.) (2019). A Research Agenda to Reduce System Involvement and Promote Positive Outcomes with LGBTQ Youth of Color Impacted by the Child Welfare and Juvenile Justice Systems. Los Angeles, CA: The Williams Institute.
28 See Materese, M. et al (2017). Also, early research that influenced the development of YAP was conducted by Dr. Caitlyn Ryan and colleagues in 2009, Family Rejection as a Predictor of Negative Health Outcomes in White and Latino Lesbian, Gay and Bisexual Youth Adults, Pediatrics Vol 123, 1. Subsequent research with additional populations of children and youth continue to show the impact of parental rejection of the health and well-being of LGBTQ+ youth, for a review of some relevant research and Newcomb, M. et al (2019) The Influence of Families on LGBGTQ Youth Health: A Call to Action for Innovation in Research and Intervention Development. https:// www.ncbi.nlm.nih. gov/pmc/articles/ PMC6551980/
29 Irvine-Baker, A., Jacobs-Allen, S. (2024) Youth Acceptance Project Interim Evaluation Report. Unpublished report.
30 Robinson, B. A., Stone, A. L., & Webb, J. M. (2023). Aunties, Aunts, and Tías: The Forgotten Othermother Supporting and Housing LGBTQ Youth. Journal of the American Sociological Association.
31 Baldoni, J., Plank, L. and Health, J. (Hosts). (2022). The Man Enough Podcast. ALOK: The Urgent Need for Compassion https://manenough. com/podcast/
32 Youth Acceptance Project Data Dashboard Retrieved from:https:// sogiecenter.org/ wp-content/ uploads/2023/03/ Youth-AcceptanceProject-DataDashboard.pdf
There is no singular formula or approach to supporting LGBTQ+ youth, particularly those involved in child welfare systems. Support must be multifaceted and consider both the strengths and the sociopolitical environment of different communities. However, what is uniform is that transformative work must promote compassion. Within the YAP approach, the phrase “Compassion versus understanding”31 is often used, as one does not have to understand someone to have compassion for them. This phrase was coined by nonbinary writer/poet/artist Alok Vaid-Menon, and it summarizes the work YAP providers exult when they work with LGBTQ+ youth and with the families who struggle to accept their LGBTQ+ youth. Families need compassion just as much as their LGBTQ+ youth do. As a society we can and
must create more compassion to support LGBTQ+ youth and their families. Change is possible. The words of youth participating in YAP say it best: “...I think the biggest thing was her [YAP provider] working with my parents and working with me. Because me and my family, we were in a bad, bad situation. So I mean, considering I never thought that our relationship would be back to normal again, there was so many issues in the family that it shocks me to think like, ‘Wow, therapists actually do help and help you bring family back together.’ … At that time, I didn’t care about my family because I just felt so betrayed, but she helped me open my eyes and realized like, ‘You need your family.’ … I think the most impactful was her helping me find myself to improve my family relationship.”32

‘You need your family.’ … I think the most impactful was her helping me find myself to improve my family relationship
CHELSEA PRAX, MPH CPH Director of AFT Children’s Health and Well-Being

Chelsea Prax, MPH CPH, is a Black mother of two beautiful Black children, and directs AFT Children’s Health and Well-Being. Prax’s work supports affiliates to address union members’ priorities. Her recent research, advocacy, strategic partnership, and technical assistance includes
• Coordinating graduate-level professional learning on evidence-based, universal traumainformed practices;
• Advising the development of a national, equity-centered framework for supporting youth who use substances in schools;
• Leading the national “Grief-Sensitive Educator” project to increase access to training and supportive resources on best practices to support bereaved students; and
• Constituency organizing among specialized instructional support personnel.
Educators enter their professions to help children thrive. Especially in well-resourced schools, they are uniquely poised to collaborate with families and effectively intervene with meaningful support. Indeed, this is the most effective way to prevent child abuse.1 2 3 But today’s policy environments push educators away from supporting children and families. Mandatory reporting complicates relationships at school, asking educators to align more with an absent, abstract bureaucracy than the people in front of them.4 Mandatory reporting can fundamentally interfere with effective family engagement and drive away the very families educators intend to help.5 6 Mandatory reporting can even deter students from disclosing abuse or attending school.7 States must make support for children and families the easy default, transforming educators from mandatory reporters to mandated supporters.
1 Fortson, B., Klevens, J., Merrick, M., Gilbert, L., & Alexander, S. (2016). Preventing Child Abuse and Neglect: A Technical Package for Policy, Norm, and Programmatic Activities. Atlanta: National Center for Injury Prevention and Control, U.S. Centers for Disease Control and Prevention. Retrieved from https://www.cdc. gov/violenceprevention/pdf/canprevention-technical-package.pdf
2 Klevens, J., Barnett, S., Florence, C., & Moore, D. (2015). Exploring policies for the reduction of child physical abuse and neglect. Child Abuse & Neglect, 40, 1-11. doi:10.1016/j.chiabu.2014.07.013
3 Livny, K., & Katz, C. (2016). Schools, Families, and the Prevention of Child Maltreatment: Lessons That Can Be Learned from a Literature Review. Trauma, Violence, & Abuse 19(2), 148-158. doi:10.1177/ 1524838016650186
4 Waldo, L. (2024, February 7). Community Collaboration: Reimagining Mandated Reporting with Julie Ahnen, Laura Glaub and Marc Seidl. Overloaded, Season 2, 10. Wisconsin. Retrieved from https://overloaded-understandingneglect.simplecast.com/episodes/ community-collaborationreimagining-mandated-reportingwith-julie-ahnen-laura-glaub-andmarc-seidl
5 Share My Lesson. (2023, June 22). Mandated Support in Education. Retrieved from https:// sharemylesson.com/webinars/ mandated-support-education
6 Perez-Darby, S. (2023, October 30). Back to School Safely: Educators and the work to end mandatory reporting. Retrieved from https://www.youtube.com/ watch?v= YHRqw2cD3ZU
7 Lawson, D., & Niven, B. (2015). The Impact of Mandatory Reporting Legislation on New Zealand Secondary School Students’ Attitudes Towards Disclosure of Child Abuse. International Journal of Children’s Rights, 23, 491-528. Retrieved from https://papers.ssrn.com/sol3/ papers.cfm?abstract_id=2983571
8 JMACForFamilies. (2024). Mandated Supporting. Retrieved from JMACForFamilies: https:// jmacforfamilies.org/mandatedsupporting
9 Shalaby, C. (2017). Troublemakers: Lessons in Freedom from Young Children at School. New York: The New Press.
10 Prax, C. (2023). Mandated Support in Education. Washington, DC: AFT. Retrieved from AFT: https://www.aft.org/sites/default/ files/media/documents/2023/ Mandated_Support_in_ Education2023_DIGITALverson.pdf
11 American Federation of Teachers. (2017). Educator Quality of Worklife: Executive Summary. Washington. Retrieved from http://bit.ly/2zyQVID
12 American Federation of Teachers. (2015). Educator Quality of Worklife: Executive Summary. Washington. Retrieved from http://bit.ly/2b3uuxx
13 Steiner, E. D., & Woo, A. (2021). Job-Related Stress Threatens the Teacher Supply: Findings from the 2021 State of the U.S. Teacher Survey. Santa Monica: RAND Corporation. Retrieved from https:// www.rand.org/pubs/research_ reports/RRA1108-1.html
14 Steiner, E. D., Doan, S., Woo, A., Gittens, A. D., Lawrence, R. A., Berdie, L., . . Schwartz, H. L. (2022). Restoring Teacher and Principal Well-Being is an Essential Step for Rebuilding Schools. Arlington: RAND Corporation. Retrieved from https:// www.rand.org/content/dam/rand/ pubs/research_reports/RRA1100/ RRA1108-4/RAND_RRA1108-4.pdf
15 Yu, X., Sun, C., Sun, B., Yuan, X., Ding, F., & Zhang, M. (. (2022). The Cost of Caring: Compassion
Fatigue is a Special Form of Teacher Burnout. Sustainability, 14(10), 6071. doi:https://doi.org/10.3390/ su14106071
16 Lawson, H. A., Caringi, J. C., Gottfried, R., Bride, B. E., & Hydon, S. P. (2019). Educators’ Secondary Traumatic Stress, Children’s Trauma, and the Need for Trauma Literacy. Harvard Educational Review, 89(3), 421-447. doi:10.17763/1943-504589.3.421
17 McMahon, S., Anderman, E., Astor, R., Espelage, D., Martinez, A., Reddy, L., & Worrell, F. (2022). Violence Against Educators and School Personnel: Crisis During COVID. Washington, DC: American Psychological Association. Retrieved from https://www.apa.org/ education-career/k12/violenceeducators.pdf
18 Ollison, J. (2019). Improving Teacher Retention By Addressing Teachers’ Compassion Fatigue. University of the Pacific Theses and Dissertations. Retrieved from https:// scholarlycommons.pacific.edu/ uop_etds/3602
19 AFT. (2022). Here Today, Gone Tomorrow? What America Must Do to Attract and Retain the Educators and School Staff Our Students Need. Washington, DC. Retrieved from https://www.aft.org/sites/ default/files/media/2022/ taskforcereport0722.pdf
20 Proeschold-Bell, R.J., Sohail, M.M., Huynh, H., Baghdady, A., Vann, V., et. al. (2021). Teacher Well-Being: Findings from a Scoping Literature Review and Case Studies in Cambodia, Kenya, and Qatar. Durham: Duke University. Retrieved from https://www.wise-qatar.org/ app/uploads/ 2021/11/2021wiserr4-report-web-version.pdf.
21 U. S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2024). Child Maltreatment 2022. Washington, DC. Retrieved from https://www.acf. hhs.gov/cb/data-research/childmaltreatment
22 Alvarez, K., Donohue, B., Carpenter, A., Romero, V., Allen, D., & Cross, C. (2010). Development and Preliminary Evaluation of a Training Method to Assist Professionals in Reporting Suspected Child Maltreatment. Child Maltreatment, 15(3). doi:https://doi.org/10.1177/ 1077559510365535
23 McTavish, J., Kimber, M., Devries, K., Colombini, M., MacGregor, J., Wathen, C., . MacMillan, H. (2017). Mandated reporters’ experiences with reporting child maltreatment: a meta-synthesis of qualitative studies. BMJ Open, 2017(7), e013942. doi:doi: 10.1136/ bmjopen-2016-013942
24 Reddy, J; Williams-Isom, A; Putnam, Hornstein, E. (2022). Racial Sensitivity Training: An Inadequate Solution to Systemic Racial Disparities in Child Protective Systems. Child Abuse & Neglect, 128. doi:https://doi. org/10.1016/j.chiabu.2022.105584
25 Ho, G., Gross, D., & Bettencourt, A. (2017). Universal Mandatory Reporting Policies and the Odds of Identifying Child Physical Abuse. American Journal of Public Health, 107(5), 709-716. Retrieved from https://sci-hub.st/10.2105/ ajph.2017.303667
26 Chalk, R., & King, P. (Eds.). (1998). Violence in Families: Assessing Prevention and Treatment Programs. Washington, DC: National Academies Press. Retrieved from https://nap.nationalacademies.org/ read/5285/chapter/1
27 Collin-Vézina, D. (2020). Students Affected by Maltreatment. In E. Rossen, Supporting and Educating Traumatized Students (pp. 253-276). New York: Oxford University Press.
“Mandated support,” a term coined by JMACforFamilies, is an invitation to move with and towards freedom.8
When I speak of a child’s right to freedom, I mean that by virtue of being human, she is endowed with the unassailable right not to have any part of her personhood assaulted or stolen. A free person can expect to be seen and treated as a full human being, free from any threats to her identity, to her cultural values and know-how, to her safety and health, and to her language and land. A free person retains her power, her right to self-determination, her opportunity to flourish, her ability to love and to be loved. And her capacity for hope. A free person recognizes when she or others are being treated as less than fully human. And a free person embraces both her right and her duty to struggle against such treatment and to organize with others to do the same as a solidary community.”
– Carla Shalaby 9
Mandated supporters use trauma-informed practices in everyday interactions and build relationships based on honesty, trust, and shared decision-making. Mandated supporters elevate universal public health approaches, such as by proactively communicating to all families about summer meal sites and embedding health information about the effects of violence into direct instruction. Mandated supporters understand multi-tiered systems of support and match interventions to student needs, such as collaborating with specialized instructional support personnel – including school nurses, social workers, psychologists, and counselors – when new information about a child’s risk emerges. Mandated supporters prioritize family bonds, communicate openly with caregivers about concerns, and compassionately navigate challenges. Mandated supporters promote social justice and confront systemic oppression with bold freedom dreaming, and transformative unity, such as through bargaining for the common good with their unions, and school-based programs that center the marginalized.10 Thomas Stinson, a school nurse, beautifully explains an example of when he acted
as a mandated supporter and leveraged his unionnegotiated home visiting project to collaborate with a family for a student’s well-being.5
I was informed by one of our attendance clerks that they were going to refer one of our families for truancy. I asked, “Did anybody talk with the family about this –? Why they missed over thirty days?”
The answers were, “We’re busy. We reached out. We couldn’t get a hold of them. We tried texting them. We tried emails.”
I said, “Let me see if I can get reach out first before we do this because we don’t want to just turn people into truancy programs.” I was able to contact them, and I was honest, “I’m the school nurse and I’m concerned about what’s going on with your son. I was wondering if we could connect?”
They were awesome! “Absolutely, you can come out to our house.”
The home visit was heartbreaking; I learned that the student was diagnosed with cancer. The family was barely making it, barely holding on. The last thing they cared about was attendance or calling the school to let them know. They were going to doctor appointments, there was a language barrier. The least thing they were worried about was trying to get him to school. They were worried about chemo treatment, being sick every day. As we talked more and more, I said, “I’m here to help you. If it’s possible, I could talk to the doctor. I could excuse these absences and we could talk about how we can help this young man in school.”
Once we got the diagnosis and we knew what was going on, we were able to set up a homebound teacher. He turned around. Here was a student who was not doing anything, not engaged, because he was trying to recover. Now the parents were all about it. They felt valued; they felt heard. I felt great!
Initially, I was disappointed, thinking, “How could this happen?” But quickly we just said, “Let’s focus on this.” I keep thinking to myself, “What if I wouldn’t have made that call? What if I didn’t make that choice?” Collaboration and communication is critical when we’re trying to figure out ways to support our families.
Stinson left his decades-long position in schools shortly after this presentation. Too many educators find schools to be hostile work environments and leave the profession. Compared to other U.S. workers, educators are more likely to be bullied, harassed, and threatened at work.11 Educators also report more job-related stress and symptoms of depression, and worse general and mental health than other U.S. workers.12 13 14 They struggle with widespread compassion fatigue and secondary traumatic stress.15 16 Crisis events and systemic oppression, such as racism and ableism, exacerbate daily stressors.17 Deeply understanding and consistently confronting the myriad forms of violence that affront their and their students’ human dignity exhausts today’s educators.18 Today’s U.S. education workforce faces burnout, high turnover, and unstable school cultures. Policymakers must address educator well-being by attending to structural issues like school climate, working conditions, and compensation.19 20
Rather than preparing educators to effectively address violence, states designate educators as mandatory reporters. The reporting framework expects educators to wait for signs of tragedy, quickly submit observations to CPS, and delegate all further decisions. Educators make over one million calls per year to CPS, but their hopes of activating real solutions for children and families are usually misplaced. CPS substantiates just eight percent of educators’ calls and most reported families receive no support.21
Policymakers can invest in training to better prepare educators to confront violence. The best training for mandatory reporters helps educators identify child maltreatment, understand reporting requirements and procedures, and learn strategies for involving caregivers in the reporting process. It also covers information about consultation with colleagues and CPS.22 23 As mandatory reporters, educators must be equipped to undertake decisions with thoughtful ethical frameworks, such as those established by their professional associations. Furthermore, training about reporting should include
• Frank accounting for the role of bias in observations and assessments;
• Serious discussion of the consequences of CPS involvement for children and families, including its harms;
• Honest attention to CPS substantiation and service delivery rates; and
• Locally relevant, actionable information about effective supports for students and families.
It is irresponsible to limit ideas for improving educator training to a focus on mandatory reporting, which may not be an effective intervention for child abuse at all.23 24 25 26 High-quality professional learning on violence prevention must do more than provoke educators to activate another government agency; it should elevate educators’ opportunities to serve directly support children and families, and build capacity, including to
• Regulate emotions and practice boundaries for self-care;
• Establish and maintain consistent routines that include authentic student choice;
• Eradicate shame and punishment from behavior change models;
• Foster positive peer engagement; and
• Analyze and critique power, including in interpersonal and institutional relationships.27
To address abuse, educators prioritize direct support and assistance to students.28 Likewise, students who face violence understand that caring, connected educators are more effective than policing agents.29 Policymakers can play a key role in supporting protective bonds at schools by facilitating the necessary networking, iterative relationship building, and collaboration that ground crucial interventions.
High-quality violence prevention programming in schools comprises more than individual educator
28 Kraft, L., & Eriksson, U.-B. (2014). The School Nurse’s Ability to Detect and Support Abused Children: A Trust-Creating Process. The Journal of School Nursing, 31(5), 353-362. doi:10.1177/ 1059840514550483
29 Wilcox, P., Tillyer, M., & Fisher, B. (2009). Gendered Opportunity? School-Based Adolescent Victimization. Journal of Research in Crime and Deliquency 46(2), 245-269. doi:10.1177/ 0022427808330875
30 Darling-Hammond, L., Flook, L., Cook-Harvey, C., Barron, B., & Osher, D. (2019). Implications for the educational practice of the science of learning and development. Applied Developmental Science, 24(2), 97-140. doi:10.1080/10888691.2 018.1537791
31 Giles, W., Hunt, H., Lewallen, T., Potts-Datema, W., & Slade, S. (2014). Whole School, Whole Community, Whole Chld. Washington, DC: U.S. Centers for Disease Control and Prevention; ASCD. Retrieved from https://www.cdc.gov/ healthyschools/wscc/WSCCmodel_ update_508tagged.pdf
32 Yule, K., Houston, J., & Grych, J. (2019). Resilience in Children Exposed to Violence: A Metaanalysis of Protective Factors Across Ecological Contexts. Clinical Child & Family Psychology Review, 22(3), 406-431. doi:https://doi. org/10.1007/s10567-019-00293-1
33 Cook, E., & Black, P. (2020). Effective Implementation and Evaluation of Trauma-Informed Schools. In E. Rossen, Supporting and Educating Traumatized Students: A Guide for School-Based Personnel (pp. 373-395). New York: Oxford University Press.
34 Venet, A. (2021). Equity-Centered Trauma Informed Education. New York: W. W. Norton & Company, Inc.
35 Partnership for the Future of Learning. (n.d.). Community Schools Playbook. Washington, DC. Retrieved from https://communityschools. futureforlearning.org/assets/ downloads/community-schoolsplaybook.pdf
36 National Center for Community Schools. (2023). Building Community Schools: A Guide for Action. Washington, DC. Retrieved from https://www.nccs.org/wp-content/ uploads/2021/10/NCCS_ BuildingCommunitySchools.pdf
37 Piepzna-Samarasinha, L. (2020). Care Work: Dreaming Disability Justice. Vancouver: Arsenal Pulp Press.
38 Healthy Students, Promising Futures. (2023). School Medicaid Expansion: How (and How Many) States Have Taken Action to Increase School Health Access and Funding. Chicago: Healthy Schools Campaign. Retrieved from https:// healthystudentspromisingfutures.org/ wp-content/uploads/2023/10/ Status-of-School-MedicaidExpansion_-How-and-How-ManyStates-Have-Taken-Action-toIncrease-School-Health-Access-andFunding.pdf
39 Venkateswaran, N., Laird, J., Robles, J., & Jeffries, J. (2018). Parent Teacher Home Visits Implementation Study. Berkeley: RTI International. Retrieved from https://pthvp.org/ wp-content/uploads/2022/03/ parent-teacher-home-visitsimplementation-study.pdf
40 Tang, J. (2022). Boston teachers contract lays groundwork for success. Boston: CommonWealth Beacon. Retrieved from https:// commonwealthbeacon.org/ uncategorized/boston-schoolscontract-lays-groundwork-forsuccess/
41 Meiners, E., & Tolliver, C. (2016). Refusing to be Complicit in our Prison Nation: Teachers Rethinking Mandated Reporting. Radical Teacher, 106(Fall 2016), 106-114. Retrieved from https://radicalteacher.
library.pitt.edu/ojs/radicalteacher/ article/view/286/225
42 Fong, K. (2023). Investigating Families: Motherhood in the Shadow of Child Protective Services. Princeton: Princeton University Press.
43 Movement for Family Power. (2023). Survival Until Revolution: Mandatory Reporting, AntiBlackness and Education. Retrieved from https://www. movementforfamilypower.org/ survival-until-revolution-zine
44 Roe v Hesperia Unified School District, E075092 (Court of Appeals of California, Fourth District, Division Two October 12, 2022). Retrieved from https://www.leagle.com/ decision/incaco20221012024
45 Meier v Salem-Keizer School District, A155836 (Court of Appeals of Oregon March 22, 2017).
46 People v Davis, E034765 (Court of Appeal of California, Fourth District, Division Two February 18, 2005). Retrieved from https://casetext.com/ case/people-v-davis-1262
47 Labor Arbitration Decision, 126 BNA LA 620 (Clatsop County).
48 Labor Arbitration Decision, Orange County Public Schools, 09 (0521)57084-3 (127 BNA LA 737).
49 Labor Arbitration Decision, 148115AAA (2013).
50 Washington State Legislature. (2024). § RCW.26.44.032 - Legal defense of a public employee. Retrieved from https://app. leg.wa.gov/RCW/default. aspx?cite=26.44.032.
51 Bellingham School District No. 501 Board of Directors. (2022, December 14). Resolution No. 28-22. Washington. Retrieved from https://go.boarddocs. com/wa/bsdwa/Board.nsf/ files/CM2PZE642F2C/$file/ Resolution%2028-22.pdf
52 Baughman, C., Coles, T., Feinberg, J., & Newton, H. (2021). The Surveillance Tentacles of the Child Welfare System. Columbia Journal of Race and Law, 11(3), 501-532. Retrieved from https://journals. library.columbia.edu/index.php/cjrl/ article/view/8743/4502
53 Detlaff, A., Weber, K., Pendleton, M., Boyd, R., Bettencourt, B., & Burton, L. (2020). It is not a broken system, it is a system that needs to be broken: the upEND movement to abolish the child welfare system. Journal of Public Child Welfare, 14(5), 500-517. Retrieved from https://www.tandfonline.com/ doi/full/10.1080/15548732.202 0.1814542
54 Sedlak, A., Heaton, L., & Evans, M. (2022). Trends in Child Abuse Reporting. In R. Krugman, & J. Korbin (Eds.), Handbook of Child Maltreatment (Vol. 14). Springer, Cham. doi:https:// doi.org/10.1007/978-3-03082479-2_1
55 Sankaran, V., Church, C., & Mitchell, M. (2019). A Cure Worse Than the Disease? The Impact of Removal on Children and Their Families. Marquette Law Review, 102(4), 1163-94. Retrieved from https://repository. law.umich.edu/cgi/viewcontent. cgi?article=3055&context=articles
56 Merkel-Holguin, L., Drury, I., Gibley-Reed, C., Lara, A., Jihad, M., Grint, K., & Marlowe, K. (2022). Structures of Oppression in the U.S. Child Welfare System: Reflections on Administrative Barriers to Equity. Societies, 12(26). Retrieved from https://www.mdpi.com/20754698/12/1/26/pdf
57 Arons, A. (2022). An Unintended Abolition: Family Regulation During the Covid-19 Crisis. Columbia Journal of Race and Law, 12(1), 1-28. Retrieved from https://journals. library.columbia.edu/index.php/cjrl/ article/view/9149/4976
practice. Robust learning environments set educators up for success and attend to the whole child. They surround students with many things: positive relationships; constructive curriculum, teaching, and assessment approaches; direct social and emotional support; and multi-tiered systems of academic, health, and social supports.30 31 Tiered systems that support the whole child can take a variety of forms and models. Trauma-informed schools wrap evidence-based strategies around students, staff, and families to attend to the pervasive effects of toxic stress and adversity.32 33 34 Full-service community schools leverage democratic governance and strategic partnerships among an expansive set of stakeholders to provide care-full supports where they are easy for students and families to access.35 36 37 Robust school Medicaid reimbursement models sustain student health delivery, as well as good jobs for specialized instructional support personnel who provide and coordinate health services.38 Parentteacher home visiting projects establish and maintain deep, meaningful connections between schools and families.39 Strong educator unions creatively strategize simultaneous solutions and enshrine local commitments as institutional responsibilities.40
Skilled educators in well-resourced schools are essential to effective prevention of violence against children. Policymakers must also consider how to “ignite cultural shifts to reduce violence.”41 States goad educators into reporting: they offer protection if reports are unsubstantiated and threaten punishment, including jail time and excessive fines, if educators do not report.41 42 Educators are encouraged to misunderstand and downplay their power as reporters, imagining that they are activating an agency that will cradle students with solutions and compassion.6 41 43
States can strike educators from statutory lists of mandatory reporters. This would not eliminate hotlines or the state’s relationship to federal requirements under the Child Abuse Prevention and Treatment Act (CAPTA). It would not necessarily stop educators from making reports. Making educators permissive reporters would signal that a state believes struggling families merit public employees’ support, as opposed to surveillance. It would remove the threat of punishment and elevate educators’ professional judgment about the best ways to intervene when they observe students in need.
Alternatively, states that maintain educators as mandatory reporters can expand the menu of intervention options to include support. For
instance, directly referring a family to a not-forprofit organization that provides material resources could be listed in a statute as an equivalent way to fulfill the requirement to intervene. Such states should also require local educational agencies to communicate with families in plain language about what mandatory reporting laws mean for school personnel, such as practical limits to confidentiality around multiple types of disclosure, as well as about families’ rights when engaging CPS.
Imagine that another educator in Thomas Stinson’s school had reported the family to truancy court. When multiple mandatory reporters reach different conclusions about the same child or family, the educator who did not report may have their judgment called into question and be investigated against the standard of “reasonable suspicion.” In these cases, arbitrators assume the worst of parents, inflexibly interpret statutes despite educators’ credible testimony, and reject substantive arguments, citing the common refrain, “When in doubt, report.”44
Such operationalization of “reasonable suspicion” has a chilling effect on educators’ pursuit of effective violence prevention strategies.
States can better protect educators who act in good faith for children and families. The state of Washington offers a foundation on which to build. When a public employee’s judgment as a mandatory reporter is disputed, and the employee can show they were not reckless, the statute requires employers to cover such an employees’ legal fees.50 51 States could go further by requiring LEAs to support educators unless it can find evidence of an employee acting negligently.
Students deserve educators who are prepared to do more than wait for signs of tragedy before acting. The system isn’t working – for educators, kids and families, or CPS – and we can change it.52
A smaller child welfare system will not endanger children but protect them. 58 U.S. policymakers must take up the serious work of liberation and radically reorient child protective services systems to achieve children’s well-being with their families. Start with empowering educators to nurture students as mandated supporters.








DAVID W. WILLIS, MD Founder, Nurture Connection
David W Willis, MD, FAAP serves as a Senior Fellow at the Center for the Study of Social Policy and a national expert in pediatrics, early childhood systems, and early relational health. At CSSP, he leads the Nurture Connection social movement to advance early relational health at the growing intersection of child health transformation and resilient community building in partnerships with families and a social justice commitment. He also is the current Co-Chair of National Academy of Sciences, Engineering and Medicine’s Forum on Children’s Wellbeing. Dr. Willis previously served as the Inaugural Executive Director of the Perigee Fund, the Division Director of Home Visiting and Early Childhood Systems at HRSA during the Obama Administration, and an early brain and child development clinician and leader in Oregon and the American Academy of Pediatrics. He currently lives in Vancouver, WA.
CAILIN O’CONNOR
Senior Associate of Center for the Study of Social Policy
Cailin O’Connor is a Senior Associate at the Center for the Study of Social Policy, where she works to promote better outcomes for young children and their families, with a focus on promoting the protective factors that children, families, and communities need to thrive. Cailin’s work has addressed a wide range of issues, including positive and adverse childhood experiences, resilience, early childhood system building, family support, early relational health, and child abuse and neglect prevention. She is a graduate of Macalester College, and holds a master’s degree in Human Development and Family Studies and a graduate certificate in Prevention and Intervention Science from the University of Wisconsin-Madison.
Child and family advocates are pushing to rethink the narrative of how young children and families develop and thrive, and the role of policies, systems and service providers in supporting healthy development. A focus on safe, stable, and nurturing relationships (SSNRs) can buffer adversity, promote resilience, and build Early Relational Health (ERH). A growing movement promoting ERH seeks to transform the child health care system towards better supporting families, alongside other aligned early childhood systems and services, by centering foundational relationships and relational healing for babies, toddlers, and their parents and closest caregivers. Providers in the ERH workforce—a broad term inclusive of pediatricians, nurses, family support specialists, and other medical staff, as well as home visitors, doulas, early care and education providers, and community health workers—can create the context for thriving when they center families’ needs and voices, recognize and bolster family strengths, support families to improve ERH, and understand relationships to be a vital sign of health for young children. In this article, we will share our growing understanding of the power of ERH for growth and healing, and what ERH can contribute across the early childhood ecosystem to the movement for family justice, particularly through health system transformation, policy change, and civil society.
The child health care system sees over 95% of the nation’s infants and young children with their families, providing well-child care, immunizations, and preventative services. Yet, traditionally, child health providers have the dual, conflicted role of promoting health and well-being for all children, while also being mandatory reporters when they have concerns for child abuse or neglect. They must work to support families with resources, encouragement, and skill building, while remaining in the power position of judging the adequacy of caregiving and nurturance for children’s wellbeing, more notably when a family faces economic hardship, adversity, and ongoing stress. Often, lacking referral sources, community resources, and solutions, providers act on their own biases and mindsets that these observed challenges reflect the family’s own failings and inadequacies, rather than structural racism, persistent poverty, recalcitrant social policies that maintain disparities, and generational patterns of adversity.
ERH is a state of emotional well-being that grows from emotional connection between babies and
toddlers and their parents and caregivers. When they experience strong, positive, and nurturing relationships with each other, ERH is foundational to children’s healthy growth and development, as well as their parents’ and caregivers’ sense of competence, connection, and overall well-being. These strong and enduring relationships also help protect the family from the harmful effects of stress, and the challenges of adversity. ERH brings together decades of family and community wisdom, practice, and research across the fields of infant and early childhood mental health, child development, social-emotional development, neurobiology, and physiology, among others. It can be woven into and help broaden current approaches to early childhood programs, practices, and policies, and is foundational to a reimagined civil society that supports healthy development for all children and families, healing from adversity, and a renewed complex web of meaningful social connections.
Nurture Connection, established in 2023, is a national impact network that partners with families and communities to accelerate ERH for social change. This initiative has galvanized a network of early childhood leaders, champions, organizations, and families to ensure that every community and all systems support and promote ERH. Beyond “business as usual,” the mission of Nurture Connection is to co-design with families social and practice changes that advance equity by recognizing the dignity and strengths of all families, the importance of individuals’ and communities’ social, cultural, political, ecological, and spiritual identities, and the sharing of power for meaningful policy and practice change. We know that parents and caregivers understand that positive relational connections with their children matter, and we know that social, racial, cultural, and economic injustices and challenges can overload families and their own goals for ensuring relational health. Because of many generational structural barriers, persistent racist policies, and the lack of policies designed to help families and communities thrive, Nurture Connection works to advance ERH and an anti-racist and equitable agenda across programs, policies, research, teaching, and communities, coled and developed in partnership with families.
ERH can be a valuable tool for re-imagining the ways that a civil society can ensure that all children, families, and communities are safe and thriving. Civil society is more than civic organizations and charities; it is made up of all the human relationships that shape our lives, in families, neighborhoods and communal places of work, learning, and leisure. By strengthening the
“We are ushering in a new era of narrowing the door to the child welfare system, instead focusing on empowering families with the upstream resources they need to remain intact,”
Acting
Commissioner Suzanne Miles-Gustave New York Office of Child and Families Services September 2023
health of these relationships lifting up children and families, expanding upstream supportive and prevention activities, and shifting the perspective of early childhood professionals, ERH has a role to play in “narrowing the front door of child welfare.”
Particularly when professionals are mandated reporters of child maltreatment, an imbalance of power creates and reinforces barriers between families and those who are supposed to support them. Helping physicians and others in the ERH workforce to see themselves as supporters before reporters, building in access to more communitybased supports, increasing families’ access to racially and culturally concordant providers, and promoting a strengths-based approach to families can all contribute to fewer families ever having contact with the child welfare system. At the same time, educating the child welfare workforce about the essential importance of ERH—how to recognize it in families and the importance of promoting, maintaining, and preserving those bonds—can contribute to the drive toward fewer removals, greater reliance on kinship placements, and earlier reunifications, particularly for the youngest children caught up in that system. Building trust, hope, and healing with all families remains a predominant ERH principle.1
In the longer term, aligned with the upEND Movement, ERH can also be a driver for abolishing the existing child welfare system, which was built on a model of surveillance and separation and is more accurately described as a family policing system. An ERH view focuses on dismantling persistent oppressive systems and redressing the harm they have done, particularly to Black and Indigenous families and communities. Driving this narrative change are many intersecting forces:
• Our society’s social justice and racial reckoning of recent years.
• The growing acknowledgement of our nation’s historical structural and institutional racism that perpetuates child, family, and community disparities.
• The inextricable links between racism, poverty, neglect, and child welfare system involvement.
• The shift of focus from adverse childhood experiences to the protective power of mitigating positive experiences.
• The expanding scientific understandings of human development, trauma, healing, and resilience.
• The overarching recognition of the power of relationships that mitigate adversity and drive future well-being.
• An emerging vision of a shared humanity that seeks the flourishing for all, in the face of larger existential threats.
Our minds, hearts, and souls are now wide open to grieve ongoing lost individual developmental potentials, to be outraged to human suffering from societal oppression, and to embrace strategic, disruptive, and movement-making efforts to right these wrongs. Enter the transformative power of nurturing relationships.
Recent trends in community pediatrics—including the growing awareness of social determinants of health and root causes of racial disparities, the early childhood foundations of life course health, and the power of positive experiences and protective factors—are challenging pediatric practice to find new ways to partner with challenged families and communities for improving family and child wellbeing.
The Black Lives Matter movement and the growing acknowledgement of structural racism and its impact on child and family health and well-being was brought to the American Academy of Pediatrics (AAP), resulting in the release of a groundbreaking policy statement in 2019 entitled “The Impact of Racism on Child and Adolescent Health.”2 The policy makes explicit the evidence that supports the continued negative impact of racism on health and well-being through implicit and explicit biases, institutional structures, and interpersonal relationships. Racism is seen as a core social determinant that robs the health and well-being of many poor and marginalized children and families,
1 Harper Browne, C., Li, J., O’Connor, C., Russo, J.E. & Willis, D.W. (2024). Putting Principles into Action: Building an Early Relational Health Ecosystem: Center for the Study of Social Policy and Nurture Connection. https:// nurtureconnection. org/resource/earlyrelational-healthecosystem/
2 Trent M, Dooley DG, Dougé J. The Impact of Racism on Child and Adolescent Health. Pediatrics. 2019; 144(2):e20191765. doi:10.1542/ peds.2019-1765
3 Garner, A., Yogman, M., Committee on Psychosocial Aspects of Child and Family Health, Section on Developmental and Behavioral Pediatrics, & Council on Early Child. (2021). Preventing Childhood Toxic Stress: Partnering With Families and Communities to Promote Relational Health. Pediatrics, 148(2), e2021052582. https://doi. org/10.1542/ peds.2021-052582
and gives rise to these health inequities, not as a result of individual behavioral choices nor genetic predisposition, but rather caused by economic, political, and social conditions—especially racism. All of these forces generate stress, and as they create greater burdens for families, their relationships and well-being may suffer. This policy statement has now challenged pediatricians to examine and acknowledge their own biases and transform their practices, policies, and research by attending to the racist determinants of known disparities in health and development. Practices are increasingly engaging the lived-experienced voices of the families and communities they serve to begin their own equity journey in partnership.
Then, in 2021, the AAP also released a related and likewise seminal policy statement, “Preventing Childhood Toxic Stress: Partnering with Families and Communities to Promote Relational Health.”3 The first sentence of the statement begins by declaring:
By focusing on the safe, stable, and nurturing relationships (SSNRs) that buffer adversity and build resilience, pediatric care is on the cusp of a paradigm shift that could reprioritize clinical activities, rewrite research agendas, and realign our collective advocacy.
They note that SSNRs are biological necessities for all children because of the power of relational health not only to mitigate childhood toxic stress, but also to build resilience needed to cope with future adversity. Going beyond prevailing practices that are trauma-informed and strength-based, this landmark policy statement calls for partnering with families and communities with a focus on relational health, not only for promotion and prevention, but also to address the continuum of intervention needs that result from trauma and toxic stress. Hence, this policy statement brings a public health approach, a population health view, and a resilience building mindset beyond just identifying adverse childhood experiences and toxic stress. Focusing on the power of nurturing relationships, the authors call for the future to be focused on ensuring the development of thriving children, building resilience in face of adversity, and attending to relational interventions for healing and recovery when trauma experiences arise. This second policy statement has resulted in greater attention to health equity across early childhood systems, in partnership with families and communities, for greater population thriving, attending to those communities and families with the greatest needs.
Nurture Connection seeks to change the narrative for the thriving of young children to one that knows the dignity and strength of all families and the love they have for their children. Far too often, families face overwhelming stress from the burdens and barriers arising from structural racism and ongoing poverty, reinforced by policy. The early childhood workforce, especially those of similar races or ethnicities, lived experiences, or communities as the families they serve, know of the complexity of daily challenges. They are often sympathetic to those impacted by the absence of material goods (food, shelter, and safety) that lead to breaking points for some families, manifested in mental health disorders, substance abuse, and child neglect and maltreatment. Many early childhood system leaders understand the root causes of families’ suffering, and no longer can accept a view that blames families for their own challenges. Rather, they know the positive impacts of expanding culturally congruent care, narrative relational healing, and a service system that places emphasis on love and dignity. The racial and health justice movement has spurred, too, a growing literature on relational healing, family and community resilience, positive childhood
experiences, and family leadership driving innovation and transformation within pediatrics and public health.4 As the power of relationships for growth and healing is recognized, thought leaders are emphasizing the capacity of the relational health workforce to address equity, prevention, social networks, decreased disparities, and community building.5 An emphasis on advancing policy to grow and support the relational health workforce is also gaining traction.
5
Relational care coordinators
Family development specialists
Family service workers
Community health workers
Home visitors
Family coaches
Promotores
Doulas
Family navigators
The ERH policy agenda aims to create safe, stable, and nurturing relationships and environments for young children in the context of their cultural traditions and communities.6 It aims to advance the development of policies and programs that reduce the stressors and remove the structural barriers (e.g., limited time, income, racist discrimination, safety) that can make it more difficult for parents to develop strong foundational relationships with their infants and toddlers, and hence has implications for advancing prevention efforts to support families who face the greatest challenges. The high-level goals of the ERH policy agenda are to:
• Aim to advance equity in design, implementation, and practice of all policies.
• Support family economic security and mobility for multi-generation success, including paid family leave, child tax credits or allowances, and assistance to address insufficient food, housing, income, and other concrete needs.
• Train the providers serving families in ERH principles and best practices, including infant
nd early childhood mental health (IECMH) informed, relational, strengths-based, and anti-racist approaches.
• Scale up and sustain evidence-based interventions and community system innovations that promote ERH. Currently available interventions have not been taken to scale, largely due to lack of sustainable public funding.
• Develop a diverse and well-trained relational workforce to support ERH, including community health workers, doulas, home visitors, physicians, nurses, child care providers, and others.
• Advance high performing medical homes using team-based, family-driven approaches, with relational care coordination.
• Increase access to IECMH services, including promotion, prevention, and treatment for parents, infants, and young children together. Too often mental health conditions among children birth to three and their caregivers have been left unaddressed by mental health care systems largely oriented to adolescents and adults with serious disorders and substance use problems.
• Strengthen early childhood systems, with linkages and coordination among health, family support, early care and education, home visiting, early intervention, mental health, housing, child welfare, and other services and informal supports. While no single early childhood system is defined by US public policy, the opportunity exists for all levels of government to support more comprehensive systems approaches.
Each of these policy priorities, individually, advance the well-being of families. Taken together, they begin to create greater opportunities for true ecosystem change to advance thriving.7 Specifically, advancing team-based care in pediatrics, now called the “high performing medical home,” offers opportunities to advance ERH, offer upstream support to families with the greatest needs, and contribute toward the concepts of “mandatory supporting” for child health care. It expands the use of advanced team-based care models for relational care coordination and effective referral, connection, and follow-up with other community resources. Evidence-based models such as Healthy Steps or DULCE utilize an early childhood development expert or community health worker as part of the medical home team and have shown promise to reduce harsh punishments and child welfare involvement.8, 9 The future of child health care that is team-based offers new opportunities for supporting families’ capacities to thrive.
4 Trent M, Dooley DG, Dougé J, AAP Section on Adolescent Health, AAP Council on Community Pediatrics, AAP Committee on Adolescence. The Impact of Racism on Child and Adolescent Health. Pediatrics. 2019’ 114(2):e20191765.
5 Bruner C, with commentaries from Willis D, Hayes M, Bethell C, Dworkin P, Houshyar S and Gallion J, Johnson, K and Bailey, M (March 2021). Building A Relational Health Workforce for Young Children: A Framework for Improving Child Well-Being. InCK Marks Working Paper Series. No. 7. InCK Marks Initiative: Des Moines, IA. www. inckmarks.org
6 Nurture Connection. (2023). Policy Change to Promote Early Relational Health. Center for the Study of Social Policy and Nurture Connection. https:// nurtureconnection. org/resource/policychange-to-promoteearly-relational-health/
7 Johnson, K., Nagle, G., Willis, D. (2023). State Leadership and Policy Action to Advance Early Relational Health. Nurture Connection. https:// nurtureconnection.org/ resource/policy-earlyrelational-health/.
8 Guyer B, Barth, M., Bishai, D., Caughy, M., Clark, B., Burkom, D., Genevro, J., Grason, H., Hou, W., Huang, K.Y., Hughart, N., Jones, A.S., McLearn, K.T., Miller, T., Minkovitz, C., Scharfstein, D., Stacy, H., Strobino, D., Szanton, E., and Tang, C. Healthy Steps: The first three years: The Healthy Steps for Young Children Program National Evaluation. 2003.
9 Sege R, Preer G, Morton SJ, et al. Medical-Legal Strategies to Improve Infant Health Care: A Randomized Trial. Pediatrics. 2015;136(1):97106. doi:10.1542/ peds.2014-2955
10 Little, M.,(2024).
Relational Social Policy: A proposal for Public Sector Reform. Ratio, London. https:// ratio.org.uk/writing/ relational-socialpolicy-a-proposal-forpublic-sector-reform/
A next generation of population health and wellbeing and thriving families will require significant public service reform, starting with the civil society.10 The civil society has enormous power, if harnessed with a view toward child and family thriving. We believe that bringing the meaning,
“We must remember the work of anti-racism is lifelong and begins with action in everyday moments, [yet, strug�ling] to find the next steps to truly practice antiracism in an inherently racist society”.8
LaShyra T. Nolan, MS
value and importance of ERH to this sector may catalyze a much deeper and more effective social change for all families, rather than continuing to just advance public services and policy investments alone. As civil society is broad and provides the foundations for health and well-being, Nurture Connection broadens and spreads the principles of ERH to parents, families, and communities. Public spaces, such as churches, libraries, and parks, allow many opportunities for conversation, relational interactions, and meaningful engagements. In addition, conversations across civil society are the currency of lived experience, and, in essence, the “laboratory of experience” in which challenges are posed, questions asked, and new realities are shaped and named. Given the increasing focus in our society on loneliness, belonging, and connections, civil society is increasingly recognizing and seeking to address this greatest of challenges, in support of the thriving of all. The growth of natural and spontaneous social supports as was noted during the pandemic in so many communities, represents the opportunities for the future. Focusing on nurturing early relationships, ERH, and social connections, in addition to policy and service change for all families, brings hope and encouragement for the thriving of all. Hope springs eternal within a relational civil society.
https://cssp.org/resource/policy-change-to-promote-erh/ https://nurtureconnection.org/resource/policy-change-to-promote-early-relational-health/
ALEXANDRIA WARE
Foster Care Alumna and Founder, Culture Creations, Inc.

Alexandria, an alumna of foster care, founded Culture Creations Inc. to support individuals with similar experiences. She leveraged her journey to empower fellow alums through access, opportunities, and community, aiming to transform negative statistics into positive outcomes. With a commitment to change foster care narratives, Alexandria works tirelessly to provide resources and love, drawing from her challenges in navigating a predominantly white foster care system while striving to connect others with their culture and potential.
Justice is indivisible. You can’t decide who gets civil rights and who doesn’t.
– Angela Davis
Eight years ago, a pivotal conversation between my biological mother and me unfolded, shedding light on the deep-seated wounds caused by her actions during my time in the child welfare system, often called the family policing system. Prior interactions had been superficial, clouded by my smoldering anger and her apparent inability to comprehend the pain she had inflicted. But this dialogue diverged from the norm, allowing me to confront the hurt she inflicted head-on.
The memory of that day remains etched in my mind. I ventured into her room, shared by my nieces, and broached the subject by inquiring about my father’s identity. Her response - an unsure account that he resided somewhere in Wichita, and she couldn’t recall his name - sent waves of frustration through me. How could she not remember a crucial detail like that? This query led us down a path of reckoning, delving into the circumstances that had led to my siblings and me becoming entangled in the child welfare system.
A shocking revelation emerged during our dialogue. My mother didn’t surrender us to the system willingly; she had been investigated and labeled an “unfit parent.” This disclosure exposed the tangled roots of her actions. Unearthing her past involvement in the child welfare system cast her in a new light for me. Rather than an indifferent figure, I began to see her as a product of a system that had perpetuated harm across generations - a system that had failed to provide her the support and care she needed.
Yet, a pivotal moment arose when I confronted her about why I and my siblings hadn’t been deemed worthy of her fight to retain our rights. Why had she relinquished my brother’s and my rights while preserving those of my sisters? Her response was unexpected - a simple yet powerful assertion that she believed the system could offer us a better life than she could at that time. This moment of vulnerability shattered my preconceived notions of her motives. I realized she wasn’t heartless; she was caught in a cycle of harm perpetuated by societal systems and personal struggles.
This encounter marked my introduction to restorative and transformative justice concepts, although I lacked the terminology to articulate it then. Only later, during a job interview with a local organization, I gained the language to express these ideas. I share my story through this journal to advocate for innovative justice solutions, such as restorative justice, transformative justice, and asset-based community development models within the family policing system. This entails a profound shift in focus - prioritizing justice, healing, and community involvement during the experiences of young individuals and families navigating this flawed system.
Acknowledging the inherent flaws of the family policing system is crucial. It inflicts substantial harm on youth and families, tearing them from their familiar environments, often steeped in racial disparities. The emotional impact of such sudden disruptions can’t be understated - imagine being plucked from school by authorities, given mere seconds to gather belongings. This system also perpetuates racial inequality, disproportionately affecting black and brown youth. Moreover, it sows the seeds of distrust by coercing young individuals into doubting their families’ love.
Recognizing these systemic flaws prompts the question of how to repair the damage wrought. Repairing relationships within families, communities, and oneself is essential. While the family policing system might seem impenetrable, avenues like transformative justice and restorative circles offer pathways toward healing. Embracing community care over individual self-care can provide the support needed to confront these challenges.
Transformative and restorative justice strategies should be at the forefront of reform efforts. The punitive nature of the family policing system necessitates a paradigm shift. Empowering communities to lead the way, rather than relying on a punitive system, can foster lasting change. This shift requires reimagining solutions that curtail system entry except in cases of severe abuse.
Ultimately, the aim is not to police families but to have institutions that champion justice, healing, and community well-being. I will spotlight the potential of transformative justice and similar models to reshape a system marred by harm, uniting families, communities, and individuals in a shared journey toward restoration.
In a world where stories unfold, where lives interweave with struggles and hopes, there’s a
chapter that speaks of a mother, a survivor. This story is a glimpse into the cracks and crevices of a system meant to protect yet often leaves wounds unseen.
My mother, a product of a system touted as “wonderful,” emerged from the foster care embrace into a world devoid of support, connections, or a nurturing community to lean on. She stood on the precipice of adulthood but without the tools to navigate it. The tale of her journey, a journey that twisted and turned within the confines of a bureaucratic labyrinth, is one we’ll explore another day.
Can we genuinely expect someone molded by a system to understand how to nurture children? She had traversed the labyrinthine corridors of the system her entire life. But why was she never seen as an individual? Why was she reduced to a mere case number, her worth measured by the checkboxes she had to tick off to reunite with her children? I know that child welfare caseloads are heavy, time a rare commodity, and the extra mile a luxury. But isn’t it time to change this?
To forge a path from a system centered on child safety to one that embraces family well-being, we must tread that extra mile for each family. We should morph the foster care system into a nurturing ground for families and youth. Let me implore you to join hands with fellow advocates and challenge the norms. Ask more than just the routine questions. Dare to veer away from the savior narrative. Ask about their strengths and their dreams.
Such inquiries unravel the tapestry of our families and youth, showcasing the strengths they’ve held close to their hearts. Life’s journey is riddled with obstacles for all, but for those in poverty, the hurdles are met with prejudice and a savior complex. The most humane response is to ask, to listen, to understand. This stance, one of patience and grace, reminds us that each individual is, in fact, human.
Had someone asked, my mother would have shared her tapestry of talents – a masterful cook, a devotee, a church and community servant, a firebrand of passion, an artist of humor, and a whisperer to newborns. She painted her life with these colors, yet they remained unspoken. She wrestled with poverty’s grip and fought the shadows of her past trauma. She may not have been an epitome of motherhood to the mandated observer who penned her story, but she’s the reason I stand tall today.
She whispered resilience into my ears, igniting my spirit to stand for justice and fight for what’s right. As the sun sets on her tale, it rises on a plea for a paradigm shift before judgment is cast, before the Department of Children and Families steps in. Peel back the layers and uncover the complexities. Treat them as individuals, for their stories are rich and nuanced.
Imagine a world where communities are not traumatized by the systems meant to safeguard them. Envision a world where healing takes precedence over hurt. This transformation beckons us, waiting for us to grasp it firmly by the hand. Asset-Based Community Development (ABCD) stands at the threshold, a beacon of hope. It’s about forging trust, lending an ear, and believing that the answers lie within the very heart of the community.
My journey with ABCD, ignited by The Neighboring Movement, reshaped how I approached families, youth, and communities. In a world of learning conversations, hidden gems are discovered, bonds are forged, and bridges are built. And in these moments, there’s a shift, a connection that speaks to the soul. I’ve walked in their shoes and beside them, and I invite you to embark upon a journey like mine.
What do you know so deeply that you could teach it with your eyes closed? What skills do you possess that can build, create, and mend? If you could birth any endeavor, what would it be? What passion fuels your heart and propels you into action? Reflect on the moments that sculpted you, the events that pushed you to grow.
It is time to halt the trauma cycle and mend the fractures within families, youth, and communities. The narrative is shifting, and the focus is changing. Let’s turn the page and write a tale of transformation, where the system becomes a source of healing, where stories are heard and understood.
Transformative justice isn’t just an approach; it’s a profound shift in how we think about healing harm. It’s about looking beyond the surface, recognizing that behind every act of harm lies a web of causes—things like inequality, oppression, and those deep-seated norms that keep violence alive. It’s a call not just to punish but to understand, to heal at the roots. This approach brings everyone into the fold, stressing that we all have a stake in addressing harm. It makes sure those who’ve been hurt are at the heart of the process, prioritizing their healing and
giving them a say in how things unfold. It’s about rallying the community, harnessing our collective power to make decisions, spark dialogues, and build a network of support that can prevent harm before it happens.
It’s a stark contrast to traditional justice, which often just focuses on punishing the person who caused harm without really addressing the bigger picture or the needs of those who were hurt. While traditional justice seeks quick fixes, transformative justice plays the long game, aiming for deep and lasting change.
Restorative justice walks a similar path, aiming to heal the wounds caused by harm. It brings together the victim, the offender, and the wider community, creating a space where everyone can work through the aftermath together. The goal is to repair the damage, empower the victim, hold the offender accountable in a way that fosters understanding and growth and involve the community in a supportive role.
The beauty of restorative justice lies in its outcomes—victims feel heard and supported, offenders grasp the true impact of their actions and are given a chance to make amends, and the cycle of harm is broken, leading to safer, more connected communities.
These approaches, transformative and restorative justice, are about building bridges, not walls. They’re about tapping into the strength of our communities, recognizing that everyone deserves a chance to heal, to change, and to be understood. They challenge us to look beyond punishment and towards a future where healing and justice walk hand in hand. And just like Asset-Based Community Development (ABCD) underscores the importance of focusing on what’s already strong within our communities, these justice models remind us that the key to lasting change lies in harnessing our collective power, in believing in the possibility of transformation, and in the power of healing together.




For additional information, please visit: https://nurturingrelationalhealth.my.canva.site/

KATHLEEN CREAMER, J.D.
Managing Attorney, Family Advocacy Unit
Community Legal Services of Philadelphia
Writing on Behalf of United Family Advocates

Kathleen Creamer is Managing Attorney of the Family Advocacy Unit at Community Legal Services of Philadelphia. United Family Advocates (UFA) is a bipartisan coalition of child and family advocates who seek policy solutions to create a more compassionate and just approach to child welfare that focuses on supporting rather than separating families.
Lately when I’ve given trainings to child welfare professionals, I’ve asked participants to share one benefit they receive from having lifelong connections with their own families. The answers are diverse and resonant: “A belief in my ability to persevere.” “A sense that I belong to a story bigger than me.” “Having people in my life who’ve known me at every age.” “The recipe for my grandmother’s Sunday sauce.” I’ve loved every answer I’ve heard to this question, because each reminds me of the ways that our families indelibly shape us at every point in our lives.
Yet when I look at child welfare practice, it seems that what we hold most dear in our own lives has become disposable in the lives of the families we serve. In the name of getting children “permanency,” child welfare policy is designed to take away family relationships from children at every turn: first by placing them in homes away from their mothers and fathers, then moving them from place to place, and then severing them permanently from their entire family tree by terminating parental rights.
Permanency of family love, permanency of identity, and permanency of ancestry are things we take away from children and parents relentlessly. In America each year, 50,000 families experience termination of parental rights. That’s 50,000 families who lose their right to know each other as family. That’s 50,000 children who lose their ties to their parents, their siblings, their cousins, their grandparents. That’s 50,000 parents who endure the unbearable grief of losing a child. And we cannot ignore that this injury is meted with particularly brutal force against Black families, who are more than twice as likely as White families to experience termination of parental rights.
What I know for sure is that it doesn’t have to be this way. The Adoption and Safe Families Act (ASFA) is now 26 years old, and it is well past time for us to find a new way to serve families. Advocates and impacted families across the country, including many of us working with United Family Advocates, are dreaming about legal changes we can make that would center lifelong family connection as the North Star of the child welfare system.
In federal law, we could raise the legal standard for family separation, protecting more children from unnecessary foster placements. We could prioritize and financially incentivize goals like reunification, guardianship, and custody with a relative, making the termination of parental rights our leastpreferred outcome. We could eliminate arbitrary timelines. We could move from “reasonable” to “active” efforts to reunify families. We could support the enactment of the 21st Century Children and Families Act, which takes crucial first steps to stem the harm of ASFA.
Make no mistake: the time is now to repeal ASFA and to end the harm it perpetuates. As the child welfare profession reckons with racial injustice and the intergenerational harm of policies that tear apart families, we can no longer be complicit in the mass destruction of family ties. We must commit ourselves to protecting for children and families what we hold most dear in our own lives.


The FJJ features original artwork, poems, and other visual and audio works that speak to the experiences of impacted individuals, community art projects, and art works for social justice in every issue of the journal, including the front cover. If you have a creative expression you would like considered for inclusion in a future issue, please write to info@thefamilyjusticegroup.org
Subscribe to the FJJ here