Jorn Schattenberg shares highlights from UEG Week 2025
Article:
Association Between Ultraprocessed Food Consumption and Depression in Adults
10 Review of United European Gastroenterology (UEG) Week 2025, 4th-7th October 2025
Congress Features
24 What’s New in Ulcerative Colitis? Helena Bradbury
28 Microbiome Modulation: Translating Function into Clinical Practice
Aleksandra Zurowska
Abstract Reviews
33 AI-BUS: AI Bowel Ultrasound System
Ruiz-Molsgaard J et al.
35 Targeted Versus Population-Based Screening as a Primary Preventive Approach Towards Gastric Cancer: Interim Results of the Irish Experience
Deane C et al.
37 Abstract Highlights
Congress Interview
47 Jörn Schattenberg
Interviews
51 Catherine Stedman
53 Dame Parveen Kumar
Articles
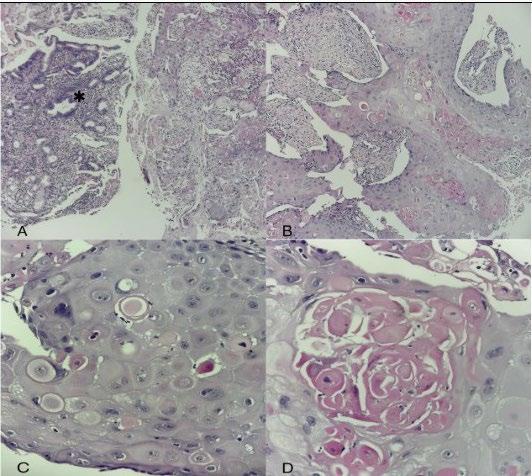
59 Primary Squamous Cell Carcinoma of the Gallbladder with Hepatic Invasion: A Case Report
Belrhali I et al.
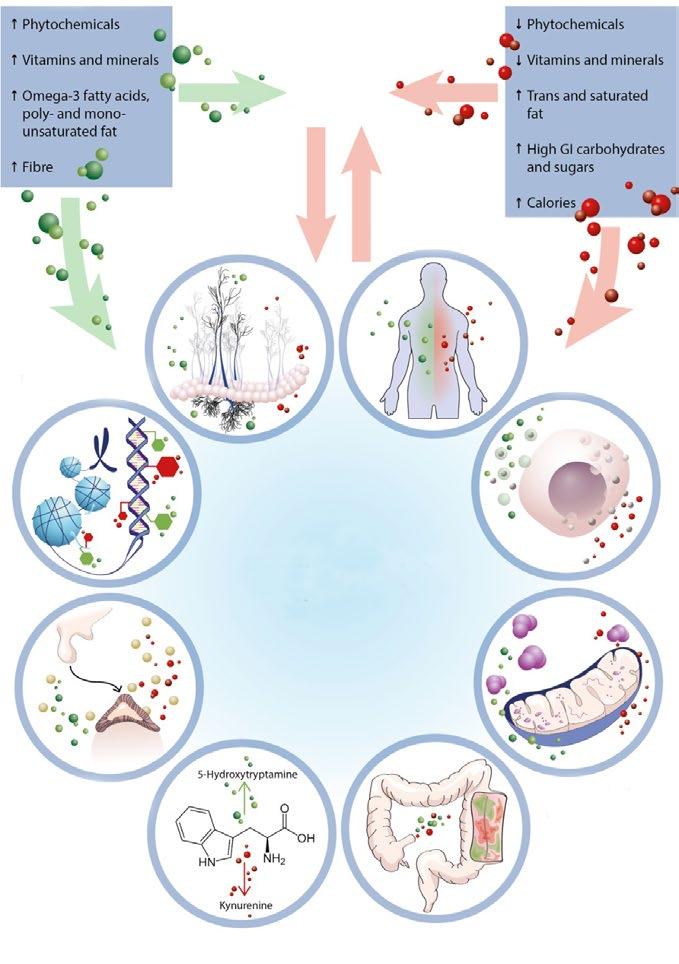
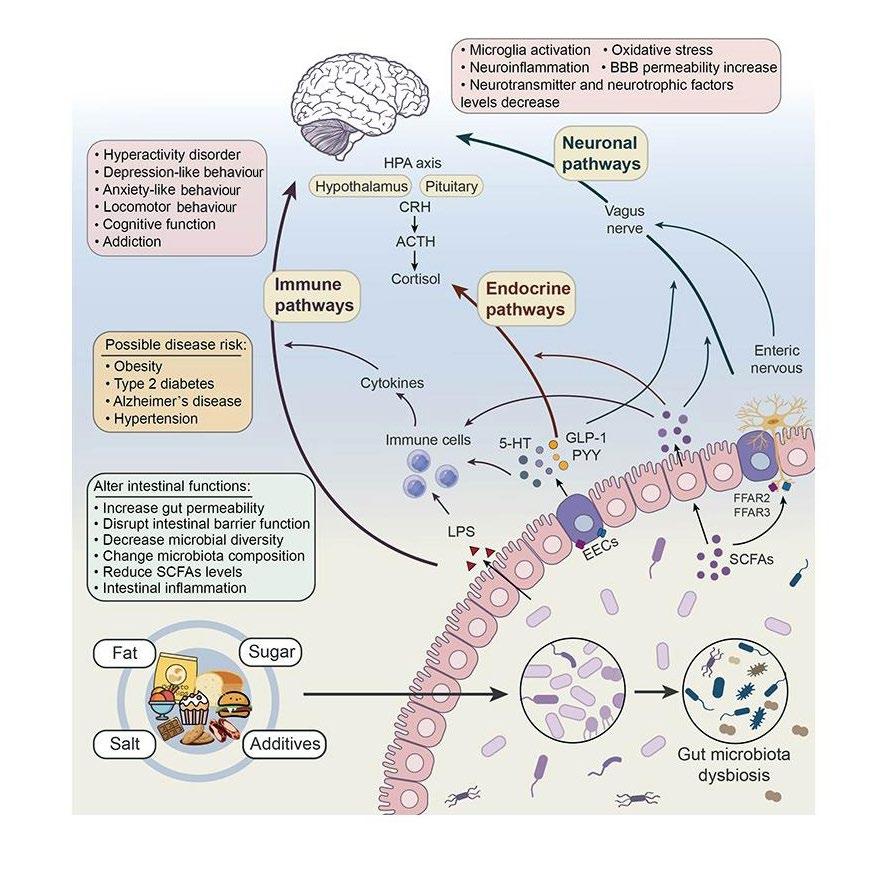
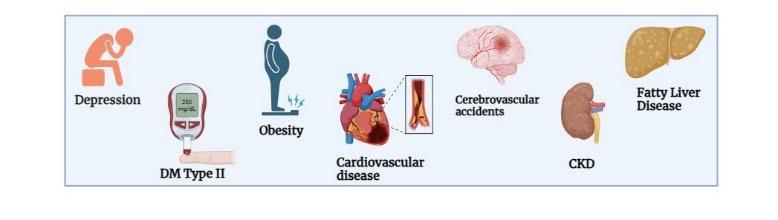
64 Association Between Ultra-Processed Food Consumption and Risk of Developing Depression in Adults: A Systematic Review
Karim S et al. 10
A notable point of pride came from the record number of abstract submissions, with over 4,000 abstracts, and the expansion of moderated poster sessions"
Editorial Board
Editor-in-Chief
Prof Sorin Barbu
“Iuliu Hațieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania
President of the Romanian Pancreatic Club since 2007, Councillor in the Executive Committee of the European Federation –International Society for Digestive Surgery (EFISDS), and member of the UEG Public Affairs Committee and the European Pancreatic Club since 2002.
Prof Dan Dumitrascu
"Iuliu Hațieganu" University of Medicine and Pharmacy, Romania
Dr Oliver Grundmann
University of Florida, USA
Dr Hasan Haboubi
Swansea University, UK
Dr Waseem Hamoudi
Royal Hospital, Jordan
Prof Christoph Gubler
Stadtspital Zürich, Switzerland
Dr Devika Kapuria
Washington University, USA
Dr Panagiotis Kasapidis
Central Clinic of Athens, Greece
Prof Milan Lukáš
Charles University, Czechia
Dr Venkata Pawan Kumar
Lekharaju
Wirral University Teaching Hospital NHS
Prof Najib Haboubi
Spire Hospital, UK
Aims and Scope
EMJ Gastroenterology is an open access, peer-reviewed eJournal committed to publishing the highest quality medical research concerning all aspects of digestive system function and disease to help advance development of this field.
The journal is published annually, six weeks after the United European Gastroenterology (UEG) Week, providing the latest developments in the field, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as indepth features on congress sessions. The journal also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Gastroenterology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. The journal is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
EMJ Gastroenterology endeavours to increase knowledge, stimulate discussion, and contribute to a better understanding of digestive system disorders. Our focus is on research that is relevant to all healthcare professionals. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of coming trends affecting clinical practice in gastroenterology.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central® .
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication
Launch Date: 2012
Frequency: Yearly Online ISSN: 2054-6203
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (UEG Week 2025) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Berlin, Germany, the location of UEG Week 2025.
Niamh Holmes, Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey White
Senior Designers
Tamara Kondolomo, Owen Silcox
Creative Artworker
Dillon Benn Grove
Designers
Shanjok Gurung, Fabio van Paris
Junior Designer
Helena Spicer
Head of Marketing
Stephanie Corbett
Business Unit Lead
Max Roy
Chief Executive Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chairman
Spencer Gore
Welcome
Dear Readers,
We are delighted to welcome you to the 2025 issue of EMJ Gastroenterology, which brings you a summary of the latest advancements and key highlights from this year’s United European Gastroenterology (UEG) Week, which was held in Berlin, Germany.
With topics such as the association between obesity and digestive diseases, the gut microbiome, and early cancer detection being of major relevance to the field in 2025, it was encouraging to see the congress include a 3-day summit on digestive disease mechanisms where delegates could gain insights into cutting-edge frontiers in basic and translational research.
Our review of the congress provides coverage of these pertinent topics, plus abstracts on gastric cancer prevention and inflammatory bowel disease updates, and a feature exploring the potential role of faecal microbiota transplant for irritable bowel syndrome. Plus, we are proud to present an exclusive interview with Scientific Committee Chair-Elect, Jörn Schattenberg, who discusses the role of GLP-1 agonists beyond obesity and diabetes and his priorities for shaping the future of UEG meetings.
Among our peer reviewed content, you will find a review evaluating gastrointestinal disease-associated depression, and an interesting case report underscoring the urgent need for improved diagnosis and treatment options for primary gallbladder squamous cell carcinoma, a rare and aggressive malignancy associated with poor prognosis.
We would like to take this opportunity to thank the Editorial Board, as well as the authors, peer reviewers, and interviewees for their invaluable contributions and expertise in bringing this issue to life. We hope you enjoy reading and can take away useful insights for your own clinical practice.
Contact us
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
It is my pleasure to introduce the latest edition of EMJ Gastroenterology, which brings together an exciting collection of original research, clinical insights, and expert perspectives from across the field. This issue highlights pioneering work in gastrointestinal science and practice, with a particular spotlight on developments presented at this year’s United European Gastroenterology (UEG) Week, held in Berlin, Germany, between 4th–7th October 2025.
Our peer-reviewed section features a systematic review examining the association between ultra-processed food consumption and the risk of developing depression in adults, offering timely insights into the gut–brain axis and lifestyle-driven disease.
Additionally, two feature articles in this issue are inspired directly by cutting-edge sessions at UEG Week 2025, exploring key advances in ulcerative colitis and the microbiome. Together, they highlight emerging evidence, evolving therapeutic strategies, and future directions that continue to shape personalised gastroenterology care.
In addition, we present two congress abstracts and exclusive interviews with global leaders in the field. From our coverage of UEG Week, we are delighted
to feature insights from Jörn Schattenberg, who reflects on progress and future priorities in hepatology and metabolic liver disease. We are also privileged to include conversations with Catherine Stedman and Dame Parveen Kumar, both of whom share invaluable perspectives on clinical practice, research trajectories, and leadership in gastroenterology.
Two feature articles in this issue are inspired directly by cuttingedge sessions at UEG Week 2025, exploring key advances in ulcerative colitis and the microbiome
I extend my sincere appreciation to all authors, reviewers, and Editorial Board members whose dedication and expertise have shaped this edition. I hope that you find the content stimulating and impactful, and that it supports you in advancing excellence in gastroenterology research and patient care.
Sorin Barbu
"Iuliu
Hațieganu"
University of Medicine and Pharmacy, Cluj-Napoca, Romania
UEG 2025
A notable point of pride came from the record number of abstract submissions, with over 4,000 abstracts, and the expansion of moderated poster sessions
Review of United European Gastroenterology (UEG) Week 2025 Congress Review
THIS YEAR, the United European Gastroenterology (UEG) Week
opened in the historical city of Berlin, Germany, welcoming close to 12,000 delegates on site and online for a week of cutting-edge science, rich education, and purposeful debate. Berlin’s blend of history and innovation proved a fitting backdrop for a meeting defined by momentum, innovation, interdisciplinarity, and a clear-eyed focus on the future of digestive health.
The opening ceremony set an energetic tone, featuring two key themes chosen by the Scientific Committee to showcase where gastroenterology is advancing the fastest: 1) getting clinical research right through precision in design, execution, and interpretation; and 2) ‘digestive disease mechanisms’, a “mini-keynote style” programme hosted in the New York room intended to bring basic scientists and clinicians together to accelerate discussions and genuine bench-to-bedside translation. Delegates were encouraged to embrace this opportunity for collaboration and learn each other’s languages, challenge assumptions, and chase the paradigm shifts already brewing. A notable point of pride came from the record number of abstract submissions, with over 4,000 abstracts, and the expansion of moderated poster sessions. The congress also saw a notable increase in attendees from Asia and the USA.
As the medical world increasingly diverts more focus to the accurate dissemination of medical information online, one of the standout plenary moments came from a keynote speech on fake news on social
media delivered by Wendi LeBrett, UCLA Health, Los Angeles, California, USA. With over half of adults now turning to social media platforms such as TikTok (Los Angeles, California, USA) and Instagram (Meta Platforms, Menlo Park, California, USA) for health advice, delegates were urged to meet the public where they are, pairing scientific rigour with engaging formats, and embedding ethical, transparent communication into everyday practice.
The opening ceremony set an energetic tone, featuring two key themes to showcase where gastroenterology is advancing the fastest
Beyond the science, UEG showcased its community pillars. Attendees were invited to explore the ‘Young GI’ and ‘Women in GI’ programmes, connect in the UEG Community Hub, and engage with year-
round education through Gutflix and the newly popular Gut Guide, which proved to be the must-grab resource of the week.
As always, UEG Week balanced serious discussions with shared celebration, inviting delegates to continue conversations at the
glamorous UEG Night and, more importantly, carry collaborations home.
EMJ was delighted to be a part of this year’s meeting and looks forward to returning for the next UEG Week taking place in Barcelona, Spain, in 2026.
Westernised Diets Fuel Colon Cancer Through Sulfate-Reducing Gut Bacteria
RESEARCH presented at UEG Week 2025 revealed how Westernised diets, which are rich in fat and sugar but low in fibre, can accelerate colon cancer development by reshaping the gut microbiome, specifically by promoting the growth of hydrogen sulfide (H₂S)producing Desulfovibrio bacteria.1
Keidel and colleagues investigated the connection between diet, gut microbes, and tumour formation in murine models of activating transcription factor 6 (ATF6)driven colon cancer. ATF6, a key regulator of the endoplasmic reticulum stress response, has previously been linked to colorectal cancer onset in humans. In mouse models engineered to express activated ATF6 in intestinal epithelial cells, the researchers explored how dietary composition influences tumour development.
Over a 7-week period, mice were fed either a control chow diet or a Westernised highlard (HL) diet enriched in fat and sugar, and depleted in fermentable fibre. The HL diet not only increased tumour burden in genetically susceptible mice, but also induced de novo tumourigenesis in animals that would otherwise remain tumour-free.
Attempts to counteract these effects by adding fibre or reducing fat content failed to protect against the HLinduced tumourigenic phenotype. Deep metagenomic sequencing and metabolomic analyses revealed that the HL diet markedly altered the gut microbial landscape, leading to a selective expansion of the Desulfovibrio species, a family of sulfatereducing bacteria known for producing H₂S, a compound that can damage DNA and intestinal tissues.
To confirm the causal role of the microbiota, the researchers transferred gut bacteria from HL-fed mice into germfree counterparts, which was sufficient to trigger tumour formation even in the absence of direct dietary exposure. Supplementing the Westernised diet with bismuth subsalicylate, an H₂S scavenger, dramatically reshaped the microbiota and prevented tumour development in previously susceptible mice.
The findings provide direct mechanistic evidence that dietinduced shifts in the microbiome, particularly the enrichment of H₂Sproducing bacteria, can drive colon cancer progression
The findings provide direct mechanistic evidence that diet-induced shifts in the microbiome, particularly the enrichment of H₂S-producing bacteria, can drive colon cancer progression. The study underscores the critical role of diet–microbiome interactions in colorectal carcinogenesis and points towards microbial H₂S as a potential therapeutic target in dietassociated colon cancer.
Stopping Anti-TNF Therapy in Early Crohn’s Disease May Risk Relapse
RESULTS from a prospective multicentre study by the Groupe d’Étude Thérapeutique des Affections Inflammatoires du Tube Digestif (GETAID) network suggest that discontinuing anti-TNF therapy, even in patients with early Crohn’s disease (CD) who achieve deep remission, may lead to loss of disease control. The findings, presented at UEG Week 2025, reinforce the importance of sustained biologic therapy to maintain long-term remission and prevent disease progression.2
CD is a chronic inflammatory condition that can cause cumulative intestinal damage if not tightly controlled. Early intervention with biologic agents such as adalimumab has been shown to improve outcomes, but the optimal treatment duration once remission is achieved remains uncertain.
This prospective cohort study evaluated whether adalimumab could be safely discontinued after 12 months in adults with early, biologic-naïve CD who achieved both clinical and biomarker remission at 6 months, and deep remission at 1 year. Among 171 patients treated across multiple centres, 22.2% (38 patients) achieved deep remission at 12 months. Of those who stopped treatment, only 22.6% (7/31) maintained deep remission 1 year after withdrawal, corresponding to just 4% of the
total cohort remaining in deep remission 2 years after starting adalimumab.
The median time to relapse after stopping therapy was 14 months, and no reliable predictive factors for sustained remission were identified. Importantly, no serious adverse events were reported during the study period.
These results, representing the first prospective trial to assess biologic withdrawal in early CD, suggest that discontinuing anti-TNF therapy, even after prolonged remission, carries a substantial risk of disease relapse. The findings highlight the continued need for ongoing maintenance therapy and careful long-term monitoring to preserve deep remission and prevent irreversible disease progression.
22.6 %
Of those who stopped treatment, only 22.6% (7/31) maintained deep remission 1 year after withdrawal
Reassuring Early Data on JAK Inhibitor Use in Pregnancy
A GLOBAL, multicentre study has found no increased risk of adverse pregnancy or infant outcomes among women with inflammatory bowel disease (IBD) exposed to JAK inhibitors (JAKi) during pregnancy. The results, presented at UEG Week 2025, offer preliminary reassurance for clinicians managing disease in expectant mothers.3
JAKis such as tofacitinib, upadacitinib, and filgotinib are increasingly used for moderate-to-severe IBD, but have raised safety concerns due to their ability to cross the placenta via passive diffusion or active extracellular transport from early pregnancy. Limited evidence has made it difficult to counsel patients on potential risks regarding pregnancy outcomes, infant infections, childhood development, and vaccine responses. To address this knowledge gap, investigators from 21 centres across 15 countries conducted a retrospective observational study within the European Crohn's and Colitis Organisation (ECCO) COllaborative Network For Exceptionally Rare case reports (CONFER), assessing pregnancy, maternal, and infant outcomes following in utero JAKi exposure.
Among 43 JAKi-exposed pregnancies, 39.5% were unplanned and 51.2% had active disease at conception. One in five women (18.6%) initiated JAKis during pregnancy. Overall, eight pregnancies ended in abortion, including three spontaneous and five induced, with two terminations driven by concerns about JAKi safety. Of the 35 ongoing pregnancies, 26 were exposed to tofacitinib, eight to upadacitinib, and one to filgotinib. Two-thirds of participants continued JAKi therapy throughout pregnancy. Disease flare was observed in nearly two-thirds of those who discontinued treatment in the first or second trimester, underscoring the risk of withdrawal. Maternal complications were infrequent: no cases of preeclampsia or thromboembolism were reported, and premature rupture of membranes occurred in three cases.
Among 35 live births, only one infant was preterm, and no congenital abnormalities were observed. Three newborns were small for gestational age, and one had a transiently low Appearance, Pulse,
Grimace, Activity, and Respiration (Apgar) score. One-third of mothers continued JAKi therapy while breastfeeding, and most infants followed standard vaccination schedules. Importantly, no adverse effects were reported after live or inactivated vaccines, and no malignancies were detected during follow-up.
This study provides encouraging early evidence that JAKi exposure during pregnancy does not increase risk for poor maternal or infant outcomes in women with IBD. Larger prospective studies are warranted to confirm long-term safety and inform treatment guidelines.
Study Supports Guselkumab as Next Step for Biologic-Resistant Crohn’s Disease
GUSELKUMAB, a selective IL-23p19 inhibitor, is under investigation as a treatment option for patients with moderately-to-severely active Crohn’s disease (CD). New information presented at UEG Week 2025 from the GALAXI 1 (Phase IIb) and GALAXI 2/3 (Phase III) long-term extension studies showed that patients who received ustekinumab and showed inadequate treatment response were eligible to switch to guselkumab without intravenous induction. The key finding from this analysis is that more than half of these patients achieved clinical remission within 16 weeks following the treatment switch.4
Participants in the long-term extension were initially treated with ustekinumab 90 mg subcutaneously every 8 weeks. Those who failed to achieve a clinical response (defined as a Crohn’s Disease Activity Index [CDAI] reduction of ≥100 points from baseline or CDAI <150) or who had a CDAI of ≥220 between Weeks 52 and 80 were eligible to switch to guselkumab 200 mg subcutaneously every 4 weeks. Clinical efficacy was assessed 16 weeks postswitch, while endoscopic outcomes and safety were evaluated at Week 96.
More than half of these patients achieved clinical remission within 16 weeks following the treatment switch
Of 80 patients who switched to guselkumab, 75 were included in the efficacy analysis. The mean age was 35.2 years, 64.0% were male, and 60.0% had prior inadequate response or intolerance to biologics. Sixteen weeks after switching to guselkumab, 61.3% of patients achieved clinical response and 52.0% achieved clinical remission. Endoscopic response and remission at Week 96 (around 1 year after the treatment switch) were seen in 49.3% and 30.7% of patients, respectively. These outcomes were similar to those observed in patients treated with guselkumab from the start of the trial. The safety profile was
Sixteen weeks after switching to guselkumab,
of patients achieved clinical response and
favourable, with 62.5% experiencing at least one adverse event, 7.5% reporting serious adverse events, and no serious infections reported during the follow-up period.
These findings suggest that guselkumab may be a viable therapeutic option for patients with CD who fail to respond adequately to ustekinumab, even without an initial intravenous induction phase. However, the study’s limitations include its non-randomised design, limited sample size, and the absence of a comparator arm, which may affect generalisability. In clinical practice, these results offer potential reassurance when considering therapeutic sequencing in biologic-experienced patients with CD.
Endoscopic Stenting as First-Line Therapy for Complex Benign Upper
Gastrointestinal Disorders
A STUDY presented at UEG Week 2025 reports that endoscopic placement of double-bump antimigratory Niti-S™ Beta-2™ EKxxxxFNT2 (TaeWoong Medical Industries, Gimpo-si, South Korea) oesophageal covered stents is an effective surgery-sparing treatment for complex benign upper gastrointestinal conditions.5
Endoscopic stenting has emerged as a viable alternative to surgery for benign upper gastrointestinal pathological conditions, particularly in patients with refractory strictures or post-surgical transmural defects. Niti-S™ Beta-2™ EKxxxxFNT2 oesophageal covered stents were developed to address these conditions, with design features aimed at minimising stent migration and tissue embedment. This study aimed to assess the safety and efficacy of these stents in a cohort of patients with complex benign gastrointestinal disorders.
A monocentric retrospective analysis was conducted on prospectively collected data of patients undergoing EKxxxxFNT2 placement for benign indications between January 2019–December 2024. Demographic, anthropometric, clinical, and technical variables were evaluated alongside safety and efficacy outcomes. A total of 32 patients were included: 17 patients were male (53.1%), the median age was 63 years, and 25 patients (78.1%) had post-surgical conditions. Indications for stent placement comprised leakage in 16 cases (50%), stricture or compression in eight (25%), and fistula in eight (25%).
The most frequently applied stent was the 24x200 mm EKxxxxFNT2 (16/32; 50%). Technical success was achieved in all procedures, with no periprocedural adverse events recorded. Stent migration occurred in four cases (12.5%). Median time to oral refeeding was 4 days (interquartile range: 2.0–10.0), and median stent dwell time was 34 days (interquartile range: 17.3–41.5). Three patients (9.4%) died before stent removal. Overall clinical success was achieved in 26 patients (81.3%), while anastomotic leakage was significantly more common among the unsuccessful cases (5/6, 83.3% versus 7/26, 26.9%; p=0.0012). Two cases (8%) of stenosis relapse were successfully managed endoscopically.
In conclusion, Niti-S™ Beta-2™ EKxxxxFNT2 oesophageal covered stents are effective interventions for complex benign upper gastrointestinal disorders, demonstrating high technical and clinical success rates. These findings support their use in clinical practice as a surgery-sparing strategy, particularly for post-surgical defects and refractory strictures. Future considerations include continued optimisation of stent dwell time and close monitoring of leakage cases to further improve outcomes.
Prior Clarithromycin Use Linked to Lower Helicobacter pylori Treatment Success
A LARGE European registry study, presented at UEG Week 2025, has found that previous macrolide consumption, especially clarithromycin, reduces the success rates of first-line Helicobacter pylori eradication therapies, underscoring the need to tailor antibiotic regimens based on local resistance trends.6
This study, conducted across 23 countries using data from the European Registry on H. pylori Management (Hp-EuReg), aimed to quantify how prior community macrolide use affects eradication success in treatmentnaïve patients. Researchers performed a retrospective, multicentre, ecological analysis including 27,549 treatment-naïve patients with linked macrolide consumption data spanning 2013–2022. Macrolide use, expressed as defined daily doses per 1,000 inhabitants per day, was obtained from the European Surveillance of Antimicrobial Consumption Network (ESAC-Net). The team identified the key variables to be first-line clarithromycin-based treatments, therapy duration (7, 10, 14 days), proton pump inhibitor dose (low, standard, high), compliance (>90%), and clarithromycin consumption. Using multivariate logistic regression and hierarchical models, investigators evaluated the relationship between national macrolide use and treatment outcomes.
Higher population-level macrolide use within the preceding 8 years was associated with lower H. pylori eradication rates, with the strongest effect observed for exposure within 4 years before treatment. The success of clarithromycin-containing regimens, including triple therapies with amoxicillin or metronidazole, and some bismuth-quadruple combinations, declined progressively as macrolide consumption increased. Eradication effectiveness fell from 93% to 82% when clarithromycin use occurred 2 years prior to treatment. The negative impact waned after approximately 5 years, suggesting partial recovery of antibiotic susceptibility over time.
These findings confirm that prior clarithromycin exposure in the community undermines the efficacy of first-line clarithromycin-based H. pylori therapies, although these effects decreased after 5 years.
New Highly Selective Salt-Inducible Kinase 3 Inhibitor Shows Promise for Inflammatory Bowel Disease
A NOVEL therapeutic candidate, O3R-5671, has shown strong potential to improve outcomes for patients with inflammatory bowel disease (IBD) by targeting multiple inflammatory pathways while minimising safety concerns seen with earlier drug classes. The findings were presented at UEG Week 2025, marking an important advance in the development of next-generation oral therapies for autoimmune diseases.7
Current IBD treatments are constrained by modest remission rates and loss of response over time. While biologic combinations can enhance efficacy, they often require complex dosing schedules. JAK inhibitors act on multiple cytokine pathways but are limited by safety issues. Researchers have, therefore, turned to saltinducible kinases (SIK), key regulators of immune signalling, as a promising new target.
Through structure-based drug design, researchers developed O3R-5671, a highly potent and selective SIK3 inhibitor with minimal off-target activity against SIK1, SIK2, or other human kinases. In laboratory assays, O3R-5671 inhibited proinflammatory cytokines TNFα, IL-12, and IL-23, while promoting the release of the anti-inflammatory cytokine IL-10.
In animal studies, O3R-5671 demonstrated dose-dependent efficacy in two independent models of IBD, as well as models of psoriasis and psoriatic arthritis. Pharmacokinetic profiling suggested a flat and predictable exposure profile suitable for sustained SIK3 inhibition in humans. Importantly, 6-week good laboratory practice toxicology studies in rats and dogs established no observed adverse effect levels, which supports safe human dosing with a large safety margin.
The compound’s selectivity for SIK3, sparing of SIK1 and SIK2, and broad cytokine inhibition profile suggest that O3R-5671 could offer ‘best-in-class’ potential for treating IBD and related autoimmune diseases. A first-in-human clinical trial is now underway to assess its safety, pharmacokinetics, and effects on immune biomarkers.
In laboratory assays, O3R-5671 inhibited proinflammatory cytokines TNFα, IL-12, and IL-23
Researchers have turned to salt-inducible kinases (SIK), key regulators of immune signalling, as a promising new target
Gut Mycobiome Biomarkers Predict Immunochemotherapy Response in Oesophageal Cancer
NEW research presented at UEG Week 2025 has demonstrated that gut fungal profiles can accurately predict patient responses to neoadjuvant immunochemotherapy in oesophageal squamous cell carcinoma (ESCC).8
ESCC continues to present poor survival outcomes despite advances in multimodal care. Variability in responses to neoadjuvant immunochemotherapy highlights the urgent need for reliable predictive biomarkers. While the influence of bacteria on immunotherapy has been widely examined, the potential contribution of the gut mycobiome remains unclear.
Internal transcribed spacer 2 sequencing was used to assess fungal diversity, composition, and co-occurrence networks
This study analysed 136 faecal samples from 68 patients with ESCC, including pre- and post-neoadjuvant immunochemotherapy specimens, alongside 19 samples from healthy controls. Tumour regression grade (TRG) scores classified patients as responders (n=26) or non-responders (n=42). Internal transcribed spacer 2 sequencing was used to assess fungal diversity, composition, and co-occurrence networks. The Boruta algorithm selected fungal biomarkers for machine learning model development using a multilayer perceptron framework with five-fold cross-validation. Mouse xenograft models were further employed to explore functional mycobiome–immune relationships through faecal microbiota transplantation and targeted fungal manipulation.
The results revealed that patients with ESCC exhibited pronounced mycobiome dysbiosis, with reduced fungal diversity and distinct compositional patterns versus controls. Responders displayed higher baseline diversity and enrichment of Meyerozyma, Candida boidinii, and Trichosporon dermatis, while nonresponders showed dominance of pathogenic Candida and Saccharomyces species. Network analyses indicated greater co-occurrence stability in responders. The final machine learning model achieved area under the curve values of 90.2% (training) and 91.9% (test). In vivo, mice receiving responder-derived faecal microbiota transplantation had reduced tumour growth and increased cluster of differentiation (CD)8+ T cell infiltration. Candida boidinii supplementation enhanced anti-programmed death (PD)-1 effects, while Saccharomyces depletion sensitised tumours to treatment.
These findings highlight the gut mycobiome as a potent biomarker of immunochemotherapy response and a modifiable therapeutic target in ESCC. Integrating fungal profiling into clinical decision-making could improve response prediction, enable personalised treatment planning, and support microbiome-based adjuvant strategies to boost immunotherapy outcomes in future practice.
AI Scoring Uncovers the Benefits of Personalised Infliximab Dosing in Acute Severe Ulcerative Colitis
AT UEG WEEK 2025, Krisztina Barbara Gecse, Amsterdam University Medical Center, the Netherlands, presented compelling findings from a post-hoc analysis of the TITRATE study, revealing that therapeutic drug monitoring-based personalised infliximab (IFX) dosing achieves better outcomes than standard treatment in patients with acute severe ulcerative colitis, a result made evident through the use of AIassisted endoscopy scoring.9
In this prospective, multicentre trial, adults with steroid-refractory acute severe ulcerative colitis were randomised 1:1 to standard dosing (SD) or personalised dosing (PD) guided by predefined serum IFX levels using a Bayesian pharmacokinetic algorithm (iDose®, Baysient, Fort Myers, Florida, USA). The dosing targets were >28 μg/mL during the first 4 weeks and >15 μg/mL between Days 29–42. The primary endpoint combined clinical and endoscopic response at Day 42, initially evaluated by expert readers and later by the AI-based DovaVision™ (Dova Health Intelligence, Vancouver, Canada) ulcerative colitis tool.
Among 48 patients enrolled (23 PD and 25 SD), baseline characteristics were comparable. By Day 42, patients in the PD arm had received a higher cumulative IFX dose (median 18.4 mg/kg versus 13.8 mg/ kg in SD). While human readers reported no statistically significant difference in response (57% PD versus 44% SD), AI
analysis detected a marked advantage for personalised dosing (74% PD versus 32% SD; p=0.0047). PD also showed superior clinical response at Day 42 (91% versus 64%; p=0.039) and higher remission rates at Day 182. Endoscopic remission at Day 182 was significantly greater with PD when scored by AI (52% PD versus 20% SD; p=0.0337).
Serious adverse events occurred in 9% of PD patients compared with 20% of SD patients, without new safety concerns.
This analysis represents the first inflammatory bowel disease study where an AI system identified a significant treatment benefit missed by expert reviewers. The findings underscore the promise of AIassisted endoscopic evaluation in clinical research and the clinical superiority of therapeutic drug monitoring-guided, personalised IFX dosing in acute severe ulcerative colitis.
Real-World Patients Often Ineligible for Inflammatory Bowel Disease Clinical Trials
A COLLABORATIVE Italian-American study presented by Federica Di Vincenzo, Fondazione Policlinico Universitario “A. Gemelli” IRCCS, Rome, Italy, at UEG Week 2025 revealed a significant gap between clinical trial eligibility and real-world practice in inflammatory bowel disease (IBD) treatment.10
The findings highlight how current RCT criteria may exclude the majority of patients seen in daily care, raising concerns about the generalisability of trial results.
The prospective, observational study analysed 166 patients with IBD (69 with ulcerative colitis [UC] and 97 with Crohn’s disease [CD]) eligible for new advanced therapies across two tertiary referral centres
Modern treatment strategies in IBD aim for mucosal healing, prevention of complications, and improved quality of life, as defined by the Selecting Therapeutic Targets in Real-world IBD: Diagnosis and Evaluation (STRIDE) II initiative. However, while advanced therapies have transformed disease management, up to half of patients with IBD fail to respond to available options, creating a pressing need for new drugs. The challenge, Di Vincenzo’s team noted, is that many of these therapies are evaluated in trials with stringent inclusion criteria that do not reflect the diversity of realworld patients.
The prospective, observational study analysed 166 patients with IBD (69 with ulcerative colitis [UC] and 97 with Crohn’s disease [CD]) eligible for new advanced therapies across two tertiary referral centres: the Gemelli Hospital in Rome, Italy, and the University of Miami’s Crohn’s & Colitis Center, Florida, USA. Each patient was systematically screened against the inclusion and exclusion criteria of actively recruiting Phase IIb and III clinical trials.
The results showed that only 23% of patients with UC and 10% of patients with CD met the eligibility criteria for at least one RCT. The most frequent reasons for exclusion in UC included Modified Mayo scores outside the required range, absence of bowel urgency, and recent corticosteroid or 5-aminosalicylic acid use. In CD, the main limiting factors were Crohn's Disease Activity Index (CDAI) scores outside the range of 220–450, low stool frequency, and the presence of complications such as strictures or fistulas.
According to Di Vincenzo, these findings reveal that many patients initiating biologic or small molecule therapy in clinical practice do so for radiologic or post-operative disease activity, rather than for meeting specific clinical score thresholds used in trials.
The study concludes that current IBD clinical trial criteria are too restrictive, particularly for CD, and should be revised to better represent real-world populations. Broadening eligibility would enhance the external validity of future trials and ensure that advances in IBD therapy truly reflect the patients treated in clinical practice.
Modern treatment strategies in IBD aim for mucosal healing, prevention of complications, and improved quality of life
References
1. Keidel I et al. Westernized diets exacerbate tumorigenesis by expanding H2S-producing desulfovibrio in murine models of AFT6-driven colon cancer. Abstract OP041. UEG Week, 4-7 October, 2025.
2. Caron B et al. Changing the course of Crohn’s disease with an early use of adalimumab: the cure study from the GETAID. Abstract OP002. UEG Week, 4-7 October, 2025.
3. Julsgaard M et al. Pregnancy and infant outcomes following in utero exposure to JAK inhibitors in women with inflammatory bowel disease: a global multicenter cohort study. Abstract OP003. UEG Week, 4-7 October, 2025.
4. Afzali A et al. Efficacy and safety of subcutaneous guselkumab rescue therapy in patients with moderately to severely active Crohn’s disease and
inadequate response to ustekinumab: results from GALAXI 1, 2, & 3 longterm extension. Abstract OP005. UEG Week, 4-7 October, 2025.
5. Gallo C et al. Endoscopic stenting for benign upper gastrointestinal conditions: safety and efficacy profile of a fully covered double-bump antimigratory stent. Abstract OP022. UEG Week, 4-7 October, 2025.
6. Nyssen OP et al. Long-term effect of macrolide consumption on Helicobacter pylori eradication treatments: data from the European Registry on H. pylori management (HPEUREG). Abstract OP026. UEG Week, 4-7 October, 2025.
7. Kolb F et al. Discovery of a novel, selective SIK3 inhibitor for the treatment of ulcerative colitis, Crohn’s diseases and other autoimmune diseases. Abstract LB08. UEG Week, 4-7 October, 2025.
8. Liu L et al. Gut mycobiome signatures predict neoadjuvant immunochemotherapy response in esophageal squamous cell carcinoma: a machine learning approach with experimental validation. Abstract OP040. UEG Week, 4-7 October, 2025.
9. Gecse KB et al. Artificial intelligence endoscopy scoring demonstrates that TDM-based infliximab doseintensification is superior to standard dosing in patients with acute severe ulcerative colitis: a post-hoc analysis of the titrate study. Abstract LB10. UEG Week, 4-7 October, 2025.
10. Di Vincenzo F et al. Real-life vs clinical trial access to biological therapy: findings from an Italian-American study on inflammatory bowel disease. Abstract OP004. UEG Week, 4-7 October, 2025.
AT THE 2025 United European Gastroenterology (UEG) Week held in Berlin, Germany, an informative session explored emerging approaches for the management of ulcerative colitis (UC), ranging from surgical interventions to updated treatment guidelines and novel therapeutics. It highlighted research on appendectomy as a potential treatment, updated clinical guidelines in the management of paediatric ulcerative colitis care, and the evolving use of combination therapies to enhance patient outcomes.
APPENDECTOMY: THE SOLUTION FOR ULCERATIVE COLITIS?
Eva Visser, Amsterdam University Medical Center, the Netherlands, first discussed appendectomy as a potential solution to UC. She began by exploring the history of the association between the appendix and UC, which was first described in a 1987 study reporting a lower appendectomy rate in patients with UC compared with healthy controls. What causes this association? To answer, Visser explored several theories; it could act as a reservoir to re-establish commensal bacteria or serve an immunological function as it contains lymphoid tissue. When these processes become dysregulated, as hypothesised by Visser, it can be the primary site for UC.
Following on, she posed the question of “whether an appendectomy can actually alter the disease course in ulcerative colitis.”
The ACCURE trial,1 an international RCT, looked to evaluate the clinical effectiveness of laparoscopic appendectomy in maintaining remission in patients with UC. Patients aged >18 years with UC who were in complete remission were randomised to an appendectomy and standard therapy, or standard therapy alone. Interestingly, the results demonstrated that an appendectomy was superior at maintaining remission at 1 year. The relapse rate was 36.4% in the appendectomy arm compared to 56.1% in the control arm.1
After observing an inverse relationship between appendectomies and the development of UC, researchers next sought to determine whether this association also extended to patients with active disease. The PASSION trial2 was an observational study that assessed patients with therapy-refractory UC referred for proctocolectomy, who were invited to undergo laparoscopic appendectomy first. The findings showed that after 12 months, nine patients (30%) had lasting clinical response, of whom five (17%) were in endoscopic remission.2
Finally, moving away from observational studies, Visser drew attention to COSTA (Visser E et al., unpublished data), the first controlled, multi-centre, patient-preference, international cohort trial. It comprised 116 patients with biologic-exposed, active UC, and looked to evaluate the efficacy of laparoscopic appendectomy in inducing remission compared with JAK inhibitor therapy in patients with active UC who failed biologic therapy. The results showed that 32.8% (22/67) of patients in the appendectomy group achieved remission at 12 months without therapy failure compared to 12.2% (6/49) in the JAK inhibitor group. As highlighted, these results showed that appendectomy was not only feasible and well-tolerated, but also effective in this hard-to-treat, biologic-exposed population (Visser E et al., unpublished data).
PAEDIATRIC ULCERATIVE COLITIS
Patrick van Rheenen, University Medical Center Groningen, the Netherlands, took the stage to share the updated guidelines for paediatric UC. He began by emphasising the importance of inflammatory bowel disease specialists having a thorough understanding of paediatric UC, as the disease is often more extensive in children. This understanding also provides crucial insight into treatment pathways before transition to adult care, and highlights the limited number of therapies currently approved for this patient population. Examples of treatment options include infliximab, adalimumab, vedolizumab, ustekinumab, and tofacitinib. However, as noted, the approval process for these therapies can take many years, with infliximab requiring 6 years, adalimumab 9 years, and several others still awaiting full approval.
Referring to the 2025 clinical guidelines,3,4 he first outlined the methodology used to ensure that they were accurate and comprehensive. This approach included the formulation of population, intervention, comparison, and outcome (PICO) frameworks; a standardised literature search; three online voting rounds; a face-to-face consensus meeting; and acceptance of statements achieving at least 80% agreement.
What has changed since the previous set of guidelines? Released in 2016, the last guidelines drew on the management of ambulatory UC and acute severe UC. Ambulatory UC is comparably more moderate than acute severe, with a Paediatric Ulcerative Colitis Activity Index (PUCAI) score of 10–60, compared to ≥65 for acute severe UC. van Rheenen emphasised that the treatment for mild-tomoderate UC has largely not changed since the 2016 guidelines, with changes only noticeable in relation to the management of severe disease or those requiring more than conventional therapy. The updated guidelines highlighted higher dosing of infliximab for both ambulatory and acute severe colitis, the importance of therapeutic drug monitoring with anti-TNFs, the use of other advanced therapies, the emerging role of intestinal ultrasounds, and the sequencing of new treatments in advanced severe UC.
The updated guidelines highlighted higher dosing of infliximab for both ambulatory and acute severe colitis
On the first change, in relation to higher dosing of infliximab and proactive therapeutic drug monitoring, van Rheenen explained that, for ambulatory UC, in
most cases there is 10 mg/dose at Weeks 0, 2, and 6, followed by 10 mg/kg every 4–8 weeks for maintenance. These are required to provide the best chance of reaching the desired clinical and endoscopic outcome. For uncomplicated UC, there is recommended therapeutic drug monitoring before the fourth infliximab infusion, and therapeutic drug monitoring before the third infliximab infusion for when increased infliximab clearance is expected.
What does therapeutic drug monitoring really mean in practice? There is a range known as the ‘target through’, which means maintaining the lowest concentration of a therapeutic drug in a patient’s bloodstream to achieve the best clinical outcome. For instance, in uncomplicated UC, the target through is ≥25 mg/kg at Week 2, ≥15 mg/kg at Week 6, and 8–10 mg/kg at Week 14. The new updated clinical guidelines recommend that, for uncomplicated UC, you monitor the target through levels at Week 14 to ensure that they are not above the target range of 8–10 mg/kg. Similarly, for patients where the drug is leaving the body at a faster rate, known as increased infliximab clearance, the recommendation is to monitor the target through levels at Week 6.
Subsequently, van Rheenen guided the audience through the recommended treatment sequence for paediatric acute severe UC. On Day 1, if the PUCAI score is ≥65 points, the first-line treatment recommendation is methylprednisone. At Day 3, if the PUCAI score is ≥45 points, it is advised to transfer the patient to a referral paediatric inflammatory bowel disease centre. Finally, at Day 5, if the PUCAI score is ≥65 points, it is advised to begin the second-line treatment; infliximab, cyclosporin, or tacrolimus. van Rheenen elaborated that infliximab is recommended as the preferred second-line rescue therapy: 10 mg/kg/dose at Weeks 0, 1, and 3, followed by 10 mg/kg every 2–4 weeks. Tacrolimus or cyclosporin can be used as alternative second-line drugs, particularly in the event of infliximab failure.
To close, van Rheenen spoke on the extrapolation strategy. This is a concept suggesting that, when a drug is approved
for adolescents (>12 years; >40 kg), it should also be given to children (2–12 years; <40 kg), as the pharmacokinetics between children and adolescents are consistently similar.
COMBINING THERAPIES IN ULCERATVE COLITIS
Joana Torres, Hospital Beatriz Ângelo, Loures, Portugal, explored the possibility of combining treatment strategies for UC. She highlighted that despite the increase in available therapies, efficacy rates have plateaued, with under 50% of patients achieving clinical remission at 1 year. 5
Torres explained the rationale for combination therapies, noting that monotherapy achieves limited remission rates and that targeting multiple pathways increases the likelihood of capturing responders. She added that sequentially used biologics often lose effectiveness, and that early combination therapy in UC may delay the development of anti-drug antibodies or escape mechanisms, thereby improving the durability of response.
Monotherapy achieves limited remission rates and targeting multiple pathways increases the likelihood of capturing responders
How should one select the therapies to combine? Torres focused on advanced combination therapies, defined as the use of two targeted agents: either two biologics or a biologic paired with a small molecule. She emphasised that therapy selection should prioritise complementary, nonoverlapping mechanisms of action while maintaining optimal safety profiles.
However, as Torres stressed, it is not only the choice of therapies that matters, but also the timing of their administration and the ongoing monitoring of the patient. For example, during induction therapy, the two drugs can be administered using an addon, simultaneous, or sequential induction
approach. Similarly, for maintenance, strategies may include withdrawing the first biologic, continuing both biologics, and maintaining biologic one with short, intermittent courses of the second therapy.
Torres noted that, unlike in other disease areas such as breast, lung, or colorectal cancer, advanced combination therapy in UC remains largely opportunistic and empirical. She spoke on the VEGA trial,6 a Phase II, proof-of-concept trial that published its results in 2023. It aimed to assess whether guselkumab plus golimumab combination therapy was more effective for UC than monotherapy. Ultimately, it showed that combination therapy outperformed monotherapy, where 59/71 (83%) patients in the combination therapy group had achieved clinical response compared with 44/72 (61%) patients in the golimumab monotherapy group.6
To conclude, Torres recommended the early induction of advanced combination therapies to prevent therapeutic resistance,
emphasising that this should be carried out in specialised centres with the resources for adequate patient monitoring. Looking ahead, she highlighted the potential of bispecific antibodies and nanobodies, which can target two pathways simultaneously, unlike current combination therapies that are administered separately. She also noted the promise of innovative clinical trial designs, such as platform trials, which allow multiple treatments to be tested simultaneously against a shared placebo group.
CONCLUSION
Overall, this session highlighted how rapidly the treatment landscape for UC is evolving, with innovation spanning surgery, paediatric management, and advanced therapeutic combinations. Together, these insights pointed towards a more personalised and multidisciplinary approach to improving long-term outcomes for patients living with this complex disease.
She also noted the promise of innovative clinical trial designs, such as platform trials, which allow multiple treatments to be tested simultaneously against a shared placebo group
References
1. The ACCURE Study Group. Appendicectomy plus standard medical therapy versus standard medical therapy alone for maintenance of remission in ulcerative colitis (ACCURE): a pragmatic, openlabel, international, randomised trial. Lancet Gastroenterol Hepatol. 2025;10(6):550-61.
2. Sahami S et al. Appendectomy for therapy-refractory ulcerative colitis results in pathological improvement of colonic inflammation: short-term results of the PASSION study. J Crohns Colitis. 2019;13(2):165-71.
3. Wine E et al. Management of paediatric ulcerative colitis, part 1: ambulatory care-an updated evidence-based consensus guideline from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition and the European Crohn's and Colitis Organisation. J Pediatr Gastroenterol Nutr. 2025;81(3):765-815.
4. Assa A et al. Management of paediatric ulcerative colitis, part 2: acute severe colitis-an updated evidence-based consensus guideline from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition and the European Crohn's and Colitis Organization. J Pediatr Gastroenterol Nutr. 2025;81(3):816-51.
5. Danese S et al. The future of drug development for inflammatory bowel disease: the need to ACT (advanced combination treatment). Gut. 2022;71(12):2380-7.
6. Feagan BG et al. Guselkumab plus golimumab combination therapy versus guselkumab or golimumab monotherapy in patients with ulcerative colitis (VEGA): a randomised, double-blind, controlled, phase 2, proof-of-concept trial. Lancet Gastroenterol Hepatol. 2023;8(4): 307-20.
Microbiome Modulation: Translating Function into Clinical Practice
AN ENLIGHTENING session delivered at the annual United European Gastroenterology (UEG) Week 2025, held in Berlin, Germany, brought together leading experts to explore the functional outputs of the gut microbiome, the real-world value of probiotics, and faecal microbiota transplantation in irritable bowel syndrome (IBS).
SPECIFIC FUNCTIONS OF THE GUT MICROBIOTA
Kicking off the session, Marius Vital, Institute of Medical Microbiology and Hospital Epidemiology, Hannover Medical School, Germany, argued that microbiome science and clinical translation progress faster when priorities shift to functionality over taxonomy. He listed Escherichia coli as an example of this. Despite being classified as a single species, its strains differ significantly in function, with some existing as harmless commensals and others serving as pathogens. Vital stated that this is a fundamental flaw of a namebased approach in microbiome research, and suggested that understanding the gut microbiota through the lens of functionality reveals a more accurate depiction of health and disease.
Central to Vital’s talk was the concept of short-chain fatty acids (SCFA), such as acetate, propionate, and butyrate. These are the main energy products of anaerobic bacterial fermentation in the colon and are essential to maintaining intestinal health, with butyrate serving as a primary energy source for epithelial cells and playing crucial roles in preserving barrier integrity and suppressing inflammation. However, he noted that “not all SCFAs are created equal,” stressing that their distinct chemical properties and receptor targets mean that their effects on the host are diverse.
Vital then illustrated how the gut’s anaerobic environment forces bacteria to rely on fermentation, which, in healthy individuals, generates tens of grams of SCFAs daily, although most are rapidly consumed before reaching circulation. This discrepancy means that stool and plasma measurements tell different stories; therefore, the choice of sampling site must match the biological question.
Vital then moved to introducing the systems biology and in vitro cultivation models that his team uses to explore how diet and microbial composition shape SCFA output. Their findings show that prebiotic substrates, such as inulin and resistant starch, boost butyrate production; yet, responses differ markedly between individuals.1 Those with a microbiota low in Ruminococcus species, for example, respond better to inulin than to resistant starch. This, Vital argued, reinforces the need for personalised nutrition strategies guided by functional profiling.
The gut’s anaerobic environment forces bacteria to rely on fermentation
He also warned that, while dietary fibres are widely considered beneficial, they can backfire in inflammatory conditions such as ulcerative colitis. Undegraded fibres may act as antigens, activating innate immune receptors and worsening inflammation. To mitigate this, his group now tests fibre degradability ex vivo before clinical application.
Concluding his talk, Vital urged the field to move beyond descriptive microbiome studies towards mechanistic, functioncentric models that integrate genomics, metabolomics, and patient stratification to deliver targeted, safe, and rational microbiome-based therapies.
SHOULD WE GIVE PROBIOTICS A CHANCE? FOR WHAT?
Continuing the session, Vanessa StadlbauerKöllner, Department of Gastroenterology and Hepatology, Medical University of Graz, Austria, shifted the focus from mechanisms to clinical application, exploring how probiotics can, and sometimes cannot, translate microbiome science into patient benefit. She reminded the audience that probiotics are defined as live microorganisms, which, when administered in adequate amounts, create a health benefit for the host. However, despite decades of research and a proliferation of products on the market, clinical evidence remains mixed and context specific.
Probiotics should not be prescribed as a uniform therapy, but rather as targeted interventions
Stadlbauer-Köllner then moved on to examining the data behind three of the most common probiotic indications: acute gastroenteritis in children, IBS, and antibiotic-associated diarrhoea. She continued to explain that in paediatric gastroenteritis, meta-analyses have consistently shown a modest (roughly 1 day) reduction in diarrhoea duration.2 However, interpretation varies across guidelines. While German guidelines suggest that probiotics may be considered, the UK’s National Institute for Health and Care Excellence (NICE) guidelines advise against routine use, and the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) recommends only a handful of well-studied strains. She noted that “the same evidence base can lead to three completely different conclusions.”
Turning to IBS, she explained that while probiotics have demonstrated symptom improvement in some trials, results remain heterogeneous. Effectiveness depends heavily on strain, dose, and patient subgroup, reflecting the complex interplay between microbial function, immune modulation, and intestinal barrier activity. Probiotics should not be prescribed as a uniform therapy, but rather as targeted interventions, with clinicians setting realistic expectations and clear stop-criteria, she explained.
Moving on to antibiotic-associated diarrhoea, Stadlbauer-Köllner explained that Cochrane data and meta-regression analyses show a risk reduction of up to 60%, but only when probiotics are started within 48 hours of initiating antibiotic therapy.3 When given later, the protective effect disappears. This timing nuance, she explained, also clarifies why studies administering probiotics after antibiotic courses, such as the trial by Suez et al.,4 found delayed microbial recovery rather than benefit. In clinical reality, prevention and restoration are distinct goals.
Stadlbauer-Köllner concluded her talk by acknowledging practical barriers: limited reimbursement, variable product regulation, and inconsistent strain availability across Europe. Nonetheless, she argued that the evidence supports probiotic use in select contexts, provided clinicians “treat the strain as seriously as a drug,” know when to start it, and ensure that patients understand both the limitations and potential of this accessible form of microbiome modulation.
PROPOSING FAECAL MICROBIAL TRANSFER FOR IRRITABLE BOWEL SYNDROME?
Concluding the session, Reetta Satokari, Faculty of Medicine, University of Helsinki, Finland, addressed one of the field’s most debated questions: can faecal microbiota transplantation (FMT) be justified for IBS?
Satokari explained that while FMT has proven highly effective for recurrent Clostridioides difficile infection, evidence in IBS remains inconsistent and uncertain. She further explained that a recent metaanalysis by Lo et al.5 found no significant difference between FMT and placebo for primary symptom outcomes, with only a small signal in trials using endoscopic delivery: a finding too fragile to guide clinical practice.
Satokari then discussed the ongoing debate over donor engraftment, the process by which transplanted microbes colonise the recipient’s gut. She explained that some studies, such as the one by Ianiro
et al.,6 suggest that greater donor strain engraftment predicts clinical success. However, others, such as Schmidt et al.,7 find that symptoms either improve or fail to improve, independently of colonisation.
Presenting data from her own IBS cohort, Satokari showed that recipients’ microbiota became strikingly donor-like after transplantation, particularly through the expansion of Prevotella species, and that these compositional and functional shifts persisted for up to a year. Yet, intriguingly, symptom scores did not correlate with engraftment or microbial diversity. She concluded that: “Engraftment may be necessary for change, but it is not sufficient for relief.”
This disconnect, she explained, underscores the complexity of IBS as a disorder of gut–brain interaction, where microbial, immune, and psychological factors converge. Satokari suggested that better patient stratification, such as targeting post-infectious IBS, may reveal subgroups who are more likely to respond. Combining FMT with dietary modulation or behavioural interventions could also enhance outcomes by aligning microbial and metabolic environments.
Despite enthusiasm, Satokari cautioned against the routine clinical use of FMT for IBS under current protocols, recommending it only as compassionate therapy in refractory cases and within structured follow-up frameworks. She emphasised that the field must now focus on identifying “super donors,” refining dosing strategies, and designing trials that capture not just microbial change but meaningful clinical improvement. Her closing message was pragmatic: the gut ecosystem can be reshaped, but transforming microbial success into patient relief remains the next, and most urgent, frontier.
The gut ecosystem can be reshaped, but transforming microbial success into patient relief remains the next, and most urgent, frontier
References
1. Van-Wehle T, Vital M. Investigating the response of the butyrate production potential to major fibers in dietary intervention studies. NPJ Biofilms Microbiomes. 2024;10(1):63.
2. Salari P et al. A meta-analysis and systematic review on the effect of probiotics in acute diarrhea. Inflamm Allergy Drug Targets. 2012;11(1):3-14.
3. Goldenberg JZ et al. Probiotics for the prevention of Clostridium difficileassociated diarrhea in adults and
4. Suez J et al. Post-antibiotic gut mucosal microbiome reconstitution is impaired by probiotics and improved by autologous FMT. Cell. 2018;174(6):1406-23.e16.
5. Lo SW et al. Clinical efficacy and safety of faecal microbiota transplantation in the treatment of irritable bowel syndrome: a systematic review, metaanalysis and trial sequential analysis. Eur J Med Res. 2025;DOI:10.1186/ s40001-024-02046-5.
6. Ianiro G et al. Variability of strain engraftment and predictability of microbiome composition after fecal microbiota transplantation across different diseases. Nat Med. 2022;28(9):1913-23.
7. Schmidt TSB et al. Drivers and determinants of strain dynamics following fecal microbiota transplantation. Nat Med. 2022;DOI: 10.1038/s41591-022-01913-0.
UEG 2025
Abstract Reviews
Drawing on insights presented at the United European Gastroenterology (UEG) Week 2025, these abstract reviews showcase the latest advances shaping the field of gastroenterology.
AI-BUS: AI Bowel Ultrasound System
Authors: Jonatan Ruiz-Molsgaard,1,2 *Jakob
Karrer,1,2 Bobby Lo,2 Bjørn Leth Møller,1 Gorm
Roager Madsen,2 Johan Fremberg Ilvemark,3
Klaus Theede,2 Johan Burisch,2 Bulat Ibragimov,1 Trine Boysen2
1. University of Copenhagen, Denmark
2. Gastro Unit, Medical Section, Hvidovre Hospital, Denmark
3. Gastroenterology Department, Herlev University Hospital, Denmark
*Correspondence to jakob.hestbjerg.karrer@regionh.dk
Disclosure: Ilvemark has received research grants from Takeda, Janssen, Abbvie, ParaTech, the Danish Research Council, and the Capital Region of Denmark; and speakers fee from Takeda. Burisch has received grants from AbbVie, Janssen-Cilag, MSD, Takeda, Tillots Pharma, Bristol Myers Squibb, and Novo Nordisk Foundation, outside of the submitted work; and personal fees from AbbVie, Janssen-Cilag, Celgene, MSD, Pfizer, Takeda, Tillots Pharma, Bristol Myers Squibb, Samsung Bioepis, Pharmacosmos, Ferring, Galapagos, Eli Lilly, Dr Falk Pharma, Celltrion, Zealand Pharma, and Orion Pharma, outside of the submitted work. The other authors have declared no conflicts of interests.
Inflammatory bowel disease requires close monitoring to detect flare-ups early and guide treatment.1,2 While endoscopy is the gold standard, it is invasive, costly, and uncomfortable.1,2 Intestinal ultrasound (IUS) is a non-invasive alternative with a strong correlation to endoscopic findings, especially bowel wall thickness (BWT), which is a marker of disease activity.3 Nevertheless, IUS remains limited due to operator dependence and a steep learning curve.4
AI has improved consistency in other domains (e.g., endoscopic evaluation), but its application to IUS in inflammatory bowel disease remains underexplored. Prior models lack interpretability, require manual image cropping, or are trained on ideal, selected data, limiting clinical use.5,6
The authors aim to develop a deep-learning model that automatically identifies and paints the bowel wall, measuring BWT directly from raw, clinical IUS images.7
MATERIALS AND METHODS
A training dataset of 570 images from 144 IUS videos, as well as a testing dataset of 55 images from 55 separate exams, were created. All images were extracted from previously performed IUS examinations reflecting real-world variation, including, for example, unclear boundaries and artefacts.
All images were annotated by International Bowel Ultrasound Group (IBUS) certified experts, including outline paintings of the inner and outer bowel wall and two BWT measurements.
The AI consisted of a combination of convolutional neural networks and other image processing algorithms.
Evaluation included BWT error against the expert mean, classification accuracy using the standard IBUS 3 mm threshold,3 and a leave-one-out comparison with individual doctors.
RESULTS
The model produced predictions on 54/55 test images, and deviated from the gold standard mean by 0.98 mm (SD: 1.10 mm) per image on the regression task. The average distance to expert-defined bounds was 0.44 mm (SD: 0.89 mm), with 59% of predictions staying inside this range (Figure 1).
For classification (using a 3 mm threshold), the model reached an accuracy of 0.77, a sensitivity of 0.69, a specificity of 0.94, and a Cohen’s Kappa of 0.56.
In the leave-one-out analysis, expert performance ranged from 0.89–0.93 accuracy and 0.79–0.83 Kappa. Depending on which expert was excluded from the gold standard, the model achieved 0.74–0.80 accuracy and 0.49–0.60 Kappa. Experts stayed within expert-defined bounds in
Figure 1: A box plot representing the measurements of the experts (green boxes) against the predicted bowel wall thickness (purple).
Mean is shown in gold. Background represents classification outcome. BWT: bowel wall thickness.
72–81% of cases, while the model did so in 46–55%.
CONCLUSION
Clinically, the model performed well. An error of 0.5–1.0 mm is negligible in practice and matches typical variation in manual measurements. Many real-world test images had BWT values near the 3 mm threshold, so small deviations led to misclassifications. In practice, a 2.5 mm reading could still raise concerns based on symptoms.3
While the system alone cannot provide expert-level BWT measurements, it could provide assistance to experts as well as non-expert and junior doctors, especially in locating the bowel, which is an essential part of IUS.
The model works on unprocessed clinical data, with the only selection criteria being that there is an identifiable bowel segment, measurable by an IBUS-certified doctor, allowing the images to reflect realistic conditions.
In summary, the authors developed an AI model that identifies the bowel and measures BWT with acceptable accuracy. The authors have already started the
process of collecting video data to extend the AI’s functionality to a fully clinical setting.
References
1. Torres J et al. Crohn’s disease. Lancet. 2017;389(10080):1741-55.
2. Ungaro R et al. Ulcerative colitis. Lancet. 2017;389(10080):1756-70.
3. Novak KL et al. Expert consensus on optimal acquisition and development of the International Bowel Ultrasound Segmental Activity Score [IBUSSAS]: a reliability and inter-rater variability study on intestinal ultrasonography in Crohn’s disease. J Crohns Colitis. 2021;15(4):609-16.
4. Bove L et al. Understanding the learning curve of intestinal ultrasound in inflammatory bowel disease: a comparative study between novice, regular, and expert. Clin Res Hepatol Gastroenterol. 2025;49(3):102548.
5. Kumaralingam L et al. Artificial intelligence-assisted approach to assessing bowel wall thickness in pediatric inflammatory bowel disease using intestinal ultrasound images. J Crohns Colitis. 2025;19(4):jjaf037.
6. Carter D et al. Automatized detection of Crohn’s disease in intestinal ultrasound using convolutional neural network. Inflamm Bowel Dis. 2023;29(12):1901-6.
Targeted Versus Population-Based Screening as a Primary Preventive Approach Towards Gastric Cancer: Interim Results of the Irish Experience
Authors: *Charlene Deane,1,2 Ana McKiernan,2
Donal Bailey,3 Colm Ó Sé,3 Dean Murray,3,4 Fiona O'Connor,3 Tom Branigan,5,6 Anthony Corcoran,5,6 Marcis Leja,7 Tatiana Kofol,8 Bojan Tepes,9 Orlaith Kelly,1,4 Colm O'Morain2,10
1. Department of Gastroenterology, Connolly Hospital, Dublin, Ireland
2. Beacon Hospital Research Institute, Dublin, Ireland
3. Irish College of General Practitioners, Dublin, Ireland
4. Royal College of Surgeons in Ireland, Dublin, Ireland
5. Royal College of Physicians of Ireland, Dublin, Ireland
6. Irish Defence Force, Dublin, Ireland
7. University of Latvia, Digestive Diseases Centre GASTRO, Riga, Latvia
8. National Institute of Public Health, Ljubljana, Slovenia
9. Diagnostični Center Rogaška, Rogaška Slatina, Slovenia
10. Faculty of Health Sciences, Trinity College Dublin, Ireland
*Correspondence to Charlene.deane@beaconhospital.ie
Disclosure: Deane has received an EU4Health grant (grant number: 101101252). McKiernan, Kofol, Leja, and Tepes have received a grant from the European Commission (EU4HEALTH - TOGAS). The other authors have declared no conflicts of interest. Richen Medical Science Ltd. provided the 13-C UBT equipment for the targeted group in this study.
Europe’s Beating Cancer Plan calls for the development of a gastric cancer screening strategy in Europe. The TOwards GAstric cancer Screening (TOGAS) consortium was established to explore the feasibility of gastric cancer screening approaches within Europe. One key method involves the detection and eradication of Helicobacter pylori, the leading causative agent of
gastric cancer. However, not all regions are affected in the same way.1 In Western Europe, infection and cancer rates are higher among males, smokers, and individuals of lower socioeconomic status, which are groups that tend to engage less with preventive health services.2,3
This pilot study aimed to determine whether targeted screening in high-risk occupational settings improves participation and outcomes compared to population-based screening via general practice invitations. Key outcome measures included response rate, prevalence of the infection, and treatment effectiveness.4
MATERIALS AND METHODS
This prospective pilot study recruited individuals aged 30–34 years from January 2024–March 2025. Participants were invited either through general practices (general population group [GPG]) or through two occupational screening programmes (targeted group [TG]) representing higherrisk, male-dominated workforces: the Irish Defence Forces and the Construction Workers Health Trust, Dublin, Ireland. Exclusion criteria included prior H. pylori treatment or gastrectomy. All participants underwent serologic screening (H. pylori IgG antibody). The TG was offered initial on-site screening at their workplace, while the GPG attended a local hospital. All seropositive individuals were offered confirmatory 13-C urea breath testing (UBT) in a local hospital. Confirmed cases were offered a 10-day regimen of bismuth subcitrate/metronidazole/ tetracycline with esomeprazole 40 mg twice a day. Eradication was assessed ≥6 weeks post-treatment. Response rates, demographics, infection prevalence, and treatment outcomes were analysed using Mann–Whitney U and Chi-squared tests (significance: p<0.05).
RESULTS
A total of 3,030 individuals were invited for screening: 2,824 in the GPG, and 206 in the TG. Key demographics and risk factors of each group are shown in Table 1. The invitation response and participation rates were significantly higher in the TG versus the GPG (invitation response: 31% versus 14%; p<0.001; participation rate: 30% versus 14%; p <0.00). H. pylori seroprevalence rates were similar between groups: 18% (11/60) in the TG and 19% (64/333) in the GPG (p<0.70). Confirmatory 13-C UBT was completed in 91% (10/11) of those who tested positive in the TG and 98% (63/64) of those who tested positive in the GPG. Overall, ‘true’ prevalence rates based on serology and confirmatory 13-C UBT results were 10% (6/59) in the TG versus 14%
(44/325) in the GPG (p=0.47). Treatment adherence exceeded 90% in both groups, with 100% adherence in the TG and 90% in the GPG. Among those who completed post-treatment testing (n=37), eradication was achieved in 100% of the TG (2/2) and 89% of the GPG (31/35).
CONCLUSION
Targeted occupational screening in highrisk populations demonstrated superior response and engagement rates compared to general practice-based screening. These early results suggest that this approach may be a more effective and resourceconscious strategy in low-to-intermediate risk countries, and merit further evaluation in broader implementation efforts.
1: Demographics, risk factors, and participation rate broken down by group.
H. pylori: Helicobacter pylori; NS: non-significant.
References
1. Lou L et al. Sex difference in incidence of gastric cancer: an international comparative study based on the Global Burden of Disease Study 2017. BMJ Open. 2020;10(1):e033323.
2. Teo CH et al. Barriers and facilitators to health screening in men: a systematic review. Soc Sci Med. 2016;165:168-76.
3. Salmani H et al. The impact of mobile health on cancer screening: a systematic review. Cancer Inform. 2020;19:1176935120954191.
4. Deane C et al. Targeted versus population-based screening as a primary preventive approach towards gastric cancer: interim results of the Irish experience. UEG Journal. 2025;13(S8):68.
The following highlights spotlight the latest advances in gastroenterology, featuring studies and insights presented at this year’s United European Gastroenterology (UEG) Week 2025. From innovative AI techniques and microbiome research to emerging therapies for ulcerative colitis and irritable bowel disease, these summaries capture the most cutting-edge developments and conversations shaping the field today.
AI System Enhances Colorectal Biopsy Quality Control by Detecting Key Histological Artifacts
RESEARCH presented at UEG Week 2025 demonstrated a new AI system that has been developed to improve the quality control of colorectal biopsy samples by automatically identifying histological artefacts such as tissue fragmentation, haemorrhage, and excess muscularis mucosa (MM).1
These artefacts, common in colorectal pinch biopsies, can obscure or distort microscopic features essential for accurate diagnosis of inflammatory bowel disease (IBD). While existing digital pathology tools focus primarily on detecting laboratory or staining errors, they often fail to assess these structural features that directly impact slide adequacy and diagnostic confidence. The proposed deep learning approach aims to bridge this gap, streamlining both sample quality assessment and the histopathologist’s evaluation process.
The research team trained convolutional neural network segmentation models on haematoxylin and eosin-stained whole slide images from 52 manually annotated colorectal biopsies. Using a human-inthe-loop training strategy, they generated over 5,000 image–annotation pairs for MM and nearly 4,000 for blood, applying data augmentations and custom postprocessing to refine accuracy. The UNet++ model achieved robust differentiation between MM and blood, which often share overlapping visual characteristics under the microscope.
In validation across 129 patients with IBD, the AI model demonstrated strong performance in segmenting key tissue components. Quantitative analysis revealed that MM occupied an average of 11.6%±10.9% of biopsy section area across 594 whole slide images, while blood was primarily distributed in the lamina propria. A tissue fragmentation score was also introduced and applied to 317 biopsies, successfully identifying damaged or degraded tissue regions that could compromise interpretation.
Importantly, the MM model provided visual cues for assessing biopsy orientation and crypt shortfall, while the blood model helped detect sampling-related injury.
Overall, the study demonstrated that AI-driven tissue evaluation can offer a more comprehensive and objective approach to pathology quality control. By flagging suboptimal samples and quantifying structural artefacts often overlooked by conventional QC systems, the tool has potential applications in guiding re-cuts, improving standardisation across laboratories, and enhancing diagnostic accuracy in IBD and other colorectal conditions.
129 patients
In validation across the AI model demonstrated strong performance in segmenting key tissue components with
Consensus Reached on Ultrasound Use After Crohn’s Surgery
INTESTINAL ultrasound (IUS) is increasingly recognised as a non-invasive method for monitoring inflammatory bowel disease, but its role in detecting postoperative recurrence of Crohn’s disease has been uncertain. A new international consensus presented at UEG Week 2025 has now outlined clear recommendations for its clinical use following surgery.2
An international panel of 16 experts, including gastroenterologists, surgeons, radiologists, and methodologists, used the modified RAND–University of California Los Angeles (UCLA) appropriateness method to develop these guidelines. A systematic literature review informed the creation of 122 statements on when, where, and how IUS should be applied after surgery.
Experts rated each statement on a nine-point scale for appropriateness in two rounds of anonymous voting. Results were discussed in videoconferences and finalised at an in-person meeting. The process focused on evaluating the anastomosis, neoterminal ileum (NTI), and adjacent segments after ileocaecal resection.
Experts rated each statement on a nine-point scale for appropriateness in two rounds of anonymous voting
Ultimately, 80% of the statements were judged appropriate with agreement. Findings in the NTI and its inlet were considered most reflective of disease recurrence. The panel agreed that IUS should not be performed within 4 weeks of surgery, as healing changes could mimic inflammation.
The full anastomotic complex, including colonic and ileal blind ends and the NTI inlet, should be assessed when visible. Parameters such as bowel wall thickness, stratification, Doppler vascularity, mesenteric fat, lymphadenopathy, peristalsis, and strictures were all endorsed as relevant markers of recurrence.
The recommendations also advise that IUS assessments be performed by trained sonographers, without bowel purge or intravenous contrast, and that visibility and image quality be documented clearly.
This consensus provides the first internationally guided framework for using IUS to assess postoperative Crohn’s disease recurrence. By standardising sonographic parameters and timing, the guidance aims to improve diagnostic accuracy and consistency in postoperative disease monitoring across centres.
Umbilical Cord Mesenchymal Stem Cells for Gut Immune Disorders
THE RESULTS of a recent study, presented at UEG Week 2025, have demonstrated the therapeutic potential of mesenchymal stem cells (MSC) in various immune-mediated gastrointestinal conditions.3
MSCs are known to influence immune tolerance, particularly through the induction of regulatory T cells (Tregs). However, their clinical effectiveness has historically varied between disorders, prompting the need to clarify when and how MSCs work best.
A large meta-analysis incorporating 79 clinical trials involving 4,710 patients with steroid-refractory graft-versus-host disease (GVHD) compared outcomes based on the source of MSCs, treatment timing, and disease severity. The findings showed that umbilical cord-derived MSCs provided notably improved 1-year survival rates compared with bone marrow-derived MSCs (76% versus 47%). Early administration, particularly within 48 hours of diagnosis, was associated with the strongest therapeutic responses, especially in paediatric patients.
To explore relevance beyond GVHD, the study also assessed MSCs in a preclinical model of inflammatory bowel disease (IBD). In a murine model of chemically induced colitis, treatment with human umbilical cord-derived MSCs led to a 67% reduction in disease severity and a 3.2-fold increase in colonic Foxp3+ Treg cells.
Further analysis demonstrated that priming MSCs with IFN-γ before administration amplified their immunosuppressive activity, driven by increased expression of IDO and PGE2, two molecules central to immune regulation.
The findings suggest that the success of MSC therapy is highly condition-specific and depends on three crucial factors: the source of MSCs, the timing of administration, and whether the cells are primed for enhanced immunomodulatory function. In particular, umbilical cord-derived MSCs appear well suited for both acute GVHD and inflammatory bowel disease when delivered early and after inflammatory priming. These results support the development of Phase II clinical trials to evaluate IFN-γ-primed umbilical cord MSCs in immune-mediated gastrointestinal conditions.
The findings showed that umbilical cord-derived MSCs provided notably improved
compared with bone marrow-derived MSCs (76% versus 47%) 1-year survival rates
New Evidence Supports Mirikizumab for Resistant Ulcerative Colitis
NEW real-world data from Spanish hospitals have revealed encouraging short-term effectiveness and safety of mirikizumab (MIRI) in ulcerative colitis (UC) care. The study, presented at UEG Week 2025, strengthens confidence that this biologic can benefit patients even outside clinical trial settings.4
Researchers aimed to verify whether the success of MIRI in pivotal LUCENT trials could be replicated in daily clinical practice. They analysed data from the ENEIDA registry, focusing on adults with UC who had not undergone colectomy and who were given MIRI as part of their treatment. Disease activity was measured using the partial Mayo score (pMS), with clinical remission defined as a pMS of 2 or less, no subscore above 1, and no rectal bleeding at Weeks 8 and 12.
The study included 171 patients from 43 hospitals across Spain, with a mean age of 49.5 years and a median disease duration of 128 months. Of these, 54% were male and 62% had extensive colitis. Most participants had received prior advanced therapies: 89% anti-TNF, 69% vedolizumab, 54% ustekinumab, and 40% JAK inhibitors. At baseline, the median pMS was 5 (interquartile range: 4–7) and faecal calprotectin 557 µg/g (interquartile range: 120–1,000).
After starting MIRI 300 mg intravenously every 4 weeks, clinical response and remission at Week 8 were 44% and 26%, respectively, increasing to 45% and 30% by Week 12. Patients exposed to only one mechanism of action (MoA) had notably higher remission rates (65%) than those exposed to two (25%) or more (27%) MoAs (p=0.04, p=0.02). Faecal calprotectin significantly dropped to 160 µg/g at Week 12 (p=0.001). Hospitalisation and colectomy rates were low (5.8% and 1.7%), and adverse events occurred in 10% of patients, with only one serious case.
These findings suggest that MIRI is both effective and well tolerated in real-world UC management, particularly for patients with limited prior exposure to advanced therapies. Continued long-term monitoring will help confirm sustained efficacy and further define its place in treatment algorithms.
Faecal calprotectin significantly dropped to 160 µg/g at Week 12 (p=0.001)
Nationwide Trends Show Increased Low-Grade Dysplasia in Inflammatory Bowel Disease
A RECENT study, presented at UEG Week 2025, has highlighted new nationwide evidence on temporal trends in dysplasia among individuals living with inflammatory bowel disease (IBD).5
Low-grade dysplasia has long been recognised as a precursor to more advanced neoplastic change, including high-grade dysplasia and colorectal cancer. However, how incidence rates of dysplasia have evolved over time in real-world clinical populations has remained unclear.
This Danish nationwide cohort study analysed healthcare registry data spanning 1990–2022, covering more than three decades of IBD care. Age-adjusted annual incidence rates of IBD-related dysplasia were calculated, and incidence rate ratios were estimated using a Poisson approximation. Importantly, figures were weighted to reflect the national age distribution as of 2022, ensuring contemporary relevance.
The key finding was a significant increase in low-grade dysplasia incidence rates over time, particularly after the introduction of Denmark’s national colorectal cancer screening programme in 2014. This rise did not coincide with a proportional increase in high-grade dysplasia or colorectal cancer incidence, which have remained generally stable or plateaued.
These trends carry meaningful clinical implications. Increased detection of lowgrade dysplasia may reflect improvements in endoscopic surveillance quality, greater awareness of dysplasia risk among clinicians, and the broader adoption of chromoendoscopy and high-definition imaging. Simultaneously, stable rates of advanced disease may indicate earlier intervention and more proactive monitoring in IBD management pathways.
For gastroenterologists and IBD specialists, these findings reinforce the importance of consistent surveillance, careful histological assessment, and timely multidisciplinary discussion when low-grade dysplasia is identified. They also suggest that screening and surveillance strategies may be succeeding in identifying dysplasia earlier, potentially preventing progression to cancer.
As dysplasia surveillance techniques continue to evolve, findings such as these support ongoing refinement of clinical pathways to reduce long-term colorectal cancer risk in IBD.
The key finding was a significant increase in low-grade dysplasia incidence rates over time
For gastroenterologists and IBD specialists, these findings reinforce the importance of consistent surveillance
Study Reveals Diagnostic Gaps Between Men and Women in Inflammatory Bowel Disease
NEW research, presented at UEG Week 2025, has revealed that women with inflammatory bowel disease (IBD) are facing significantly longer waits for diagnosis than men. The study highlights that women are also more likely to receive a misdiagnosis, revealing persistent sex-based disparities in IBD care.6
IBD, which includes Crohn’s disease (CD) and ulcerative colitis (UC), affects people of all sexes, but differences in how men and women experience the diagnostic process have rarely been examined systematically. This large-scale analysis sought to uncover potential sex-specific differences in symptom onset, reporting, and the time taken to receive an accurate diagnosis.
The interim analysis drew on data from 1,180 individuals with IBD (770 women and 410 men) across 42 centres in Germany. Participants completed an online survey capturing demographic information, disease characteristics, and details about the diagnostic timeline. All participants were aged 18 or older and had a confirmed diagnosis of UC or CD for at least 3 months.
The analysis showed no significant differences between men and women in the median time to first physician consultation for either CD or UC. For CD, the median time was 3 months in both women (interquartile range [IQR]: 1–12) and men (IQR: 0.5–10; p=0.567).
For UC, women had a median of 2 months (IQR: 0.8–5) and men 1.3 months (IQR: 0.5–4; p=0.091). Similarly, the time from consultation to referral did not differ between sexes. However, women
experienced a significantly longer median time from symptom onset to final diagnosis compared with men ([CD: women, 12 months (IQR: 5–48); men, 6.5 months (IQR: 2.5–24); p=0.002]; [UC: women, 5 months (IQR: 2–14.5); men, 3 months (IQR: 1.3–8); p=0.006]). Misdiagnosis was also more common among women (40.4%) than men (34.4%; p=0.044). Furthermore, symptom profiles varied: women with CD were more likely to present with diarrhoea, nausea, or arthralgia, while women with UC more often reported fever or abdominal pain.
The findings highlight the need for heightened clinical awareness of sex-related differences in IBD presentation and diagnostic experiences. Recognising these variations could help clinicians shorten diagnostic delays and reduce misdiagnosis rates, improving outcomes for women with IBD.
The interim analysis drew on data from with
1,180 individuals
IBD
(770 women and 410 men) across 42 centres in Germany
Upadacitinib Demonstrates Favourable Safety and Efficacy in Liver Transplant Recipients with Ulcerative Colitis
AN OBSERVATIONAL study presented at UEG Week 2025 has provided encouraging evidence that upadacitinib, a selective JAK1 inhibitor, may be a safe and effective treatment for inflammatory bowel disease (IBD) in patients who have previously undergone liver transplantation for primary sclerosing cholangitis (PSC).7
PSC is a chronic, progressive liver disease strongly linked to IBD, particularly ulcerative colitis (UC), and orthotopic liver transplantation remains the standard treatment for advanced cases. However, managing IBD after transplantation poses a unique clinical challenge due to the limited evidence available on the safety and efficacy of newer therapies such as JAK inhibitors in this population.
The study evaluated five patients (three women and two men) with UC and a history of liver transplantation due to PSC. The median age was 30 years, with an average of 7 years since orthotopic liver transplantation and 12 years since UC diagnosis. Two patients had confirmed recurrence of PSC, reflected by elevated liver function tests. All participants had previously failed biologic therapy with vedolizumab, and one had also failed infliximab treatment.
Upadacitinib was administered at an induction dose of 45 mg daily for 3 months, followed by maintenance therapy of either 30 mg or 45 mg daily. Patients were followed for a median period of 9 months. Corticosteroid therapy was continued in most cases, typically with low-dose prednisolone.
During treatment, all patients showed clinical improvement, with the partial Mayo score dropping from a median of six to two. Endoscopic follow-up confirmed mucosal healing or improvement in nearly all cases. Notably, no significant changes in liver function tests or tacrolimus levels were observed, suggesting that upadacitinib did not interfere with transplant management or immunosuppressive therapy.
Adverse effects were mild and manageable, including acne, upper respiratory tract infections, cytomegalovirus colitis, and a mild case of COVID-19. Importantly, no serious infections or graft-related complications were reported.
These findings indicate that upadacitinib may offer a viable therapeutic option for patients with refractory IBD following liver transplantation, where treatment choices are often limited by safety concerns. Although larger studies are needed to confirm long-term outcomes, this early experience suggests that JAK1 inhibition could safely control intestinal inflammation without compromising liver graft stability or immunosuppressive balance.
Severe Endoscopic Findings Predict
Corticosteroid Failure in Acute Severe Colitis
A RETROSPECTIVE study, presented at UEG Week 2025, shed new light on the predictors of corticosteroid treatment failure in patients with acute severe colitis (ASC), a life-threatening complication of inflammatory bowel disease (IBD).8
ACS represents one of the most critical emergencies in IBD, demanding rapid diagnosis and management. While intravenous corticosteroids remain the first-line treatment, approximately one-third of patients fail to respond and require alternative therapies such as infliximab, cyclosporine, or surgery.
The study included 45 adult patients with IBD complicated by ASC, as defined by the Truelove and Witts criteria and a Lichtiger score greater than 10. The average patient age was 37.9 years, with a slight female predominance. Notably, ASC was the initial presentation of IBD in nearly one-third of patients. Almost half of the cohort exhibited severe endoscopic findings at admission, reinforcing the high-risk nature of the condition.
Following intravenous corticosteroid therapy with hydrocortisone hemisuccinate, 64.5% of patients achieved a clinical response, while 24.4% required second-line therapy, either cyclosporine or infliximab. Five patients (11.1%) required subtotal colectomy due to corticosteroid failure.
Univariate analysis revealed several clinical and laboratory factors linked to poor steroid response, including male sex, absence of
extraintestinal manifestations, higher stool frequency at baseline, persistent high Lichtiger scores, elevated white blood cell counts, and raised C-reactive protein levels. However, multivariate analysis identified only one independent predictor: persistent severe endoscopic findings after 3–5 days of corticosteroid therapy (odds ratio: 42.2; p=0.028).
Following intravenous corticosteroid therapy, 64.5% of patients achieved a clinical response, while 24.4% required second-line therapy
These findings suggest that early follow-up endoscopy plays a crucial role in guiding treatment decisions for ASC. Patients showing ongoing endoscopic evidence of severe inflammation after several days of corticosteroid therapy are highly unlikely to respond and should be transitioned promptly to second-line medical or surgical management.
This study reinforces the need for proactive, individualised care strategies and highlights endoscopic monitoring as a valuable tool for improving outcomes in acute IBD flares.
References
1. Li R et al. AI models for QC and non-mucosal feature detection in histological pinch biopsies of inflammatory bowel disease. Poster. UEG Week, 4-7 October, 2025.
2. Novak LK et al. Use of intestinal ultrasound to assess for postoperative recurrence in Crohn’s disease: an international RAND/UCLA appropriateness study. Poster MP537. UEG Week, 4-7 October, 2025.
3. Li Y et al. Unlocking the dual potential of mesenchymal stem cells: from steroid refractory GVHD to inflammatory bowel disease. Poster. UEG Week, 4-7 October, 2025.
4. Gutiérrez-Casbas A et al. Shortterm effectiveness and safety of mirikizumab in ulcerative colitis: real-world evidence from the ENEIDA registry of GETECCU. Poster MP784. UEG Week, 4-7 October, 2025.
5. Andersen JW et al. Temporal trends in dysplasia among IBD patients: nationwide evidence of increasing low-grade dysplasia incidence rate amidst plateauing advanced disease in Denmark. Poster MP655. UEG Week, 4-7 October, 2025.
6. Kuhn L et al. Uncovering sex differences in the diagnostic journey of patients with inflammatory bowel disease – interim analysis of
7. Drastich P et al. Upadacitinib in the treatment of ulcerative colitis after liver transplantation for primary sclerosing cholangitis - a case series. Poster. UEG Week, 4-7 October, 2025.
8. Louati C et al. Prevalence of acute severe colitis in patients with inflammatory bowel disease: evaluation and factors associated with treatment failure. Poster. UEG Week, 4-7 October, 2025.
Congress Interview
EMJ had the pleasure of speaking with Jörn Schattenberg, Chair Elect of the Scientific Committee at the United European Gastroenterology (UEG), who shared his insights on emerging advances in metabolicassociated liver disease (MASLD), liver fibrosis diagnostics, and novel biomarker development, along with his vision for the future of UEG’s scientific agenda.
Featuring: Jörn Schattenberg
Jörn Schattenberg
Professor of Medicine and Director, Department of Medicine II, Saarland University Medical Center and Saarland University, Homburg, Germany
Q1To start, could you briefly share the key messages from your presentation on glucagon-like peptide-1 (GLP-1) agonists beyond diabetes and obesity?
It’s an exciting time for metabolic dysfunction-associated steatotic liver disease (MASLD). It’s one of the key drivers of end-stage liver disease. These patients develop cirrhosis, decompensation, and cancer. While not all patients progress that far, we have a very high prevalence of metabolic liver disease, formerly known as fatty liver, and a subgroup develop severe liver disease.
The biggest trial we’ve seen is the ESSENCE trial, which explored the effect of semaglutide at the obesity dose (2.4 mg) on improving liver histology. After 72 weeks of treatment, inflammation in the liver resolved, and fibrosis improved. These are very encouraging data. These patients typically lose around 10% of their body weight, slightly less than in obesity trials, but still significant. There’s no GLP-1 receptor in the liver, so the benefits likely come from metabolic improvement and weight loss.
We opened the Congress with a postgraduate course attended by over 5,000 participants, covering the full spectrum of gastroenterology
In my presentation, I revisited the available data on incretins. This class of drugs stimulates GLP-1 and sometimes other receptors, such as glucagon and gastric inhibitory polypeptide, producing beneficial effects on the liver. They are typically used in diabetes and obesity and show robust effects, but based on the combination of receptors they target, there can also be liver-specific benefits.
There are also drugs that target both GLP-1 and glucagon receptors. Glucagon receptors are found directly on liver cells. For example, survodutide, currently in Phase III trials, and pemvidutide, another dual agonist, have shown improved liver histology in published Phase II studies. These drugs are now being tested for outcomes beyond histology, such as clinical endpoints.
Another drug I discussed was retatrutide. The companies developing these agents have recently announced large outcome
trials enrolling patients even without liver biopsies. This reflects the growing recognition of MASLD as a relevant and prevalent disease. We now use biomarker tests to identify patients with more advanced disease and enrol them in incretin-based clinical trials.
In the same session, my colleague Frank Tacke (Charité – Universitätsmedizin, Berlin, Germany) presented data on the only currently approved drug for metabolic dysfunction-associated steatohepatitis with fibrosis, resmetirom. Interestingly, this drug improves liver phenotype even in the absence of weight loss.
Q2
Could you tell us briefly about your other United European Gastroenterology (UEG) Week sessions?
We opened the Congress with a postgraduate course attended by over 5,000 participants, covering the full
spectrum of gastroenterology. I was involved in the liver section, focusing on non-invasive testing and the shift away from biopsies now that we have effective drugs.
Day 2 featured the opening plenary, with presentations on liver regeneration and innovative therapies. I also presented data on primary biliary cholangitis, a rare liver disease affecting around 90% women that is linked to bile duct inflammation and severe itching. A new second-line therapy was recently approved for patients who don’t respond to first-line treatment, which is a major advancement.
There’s a lot happening in both common and rare liver diseases, and even in primary biliary cholangitis, we’re learning more about how sex hormones influence disease biology. It’s an exciting time for hepatology research.
Q3 Much of your research centres around metabolic liver disease. What emerging evidence suggests that GLP-1-based therapies could benefit patients with MASLD and metabolic dysfunctionassociated steatohepatitis?
There’s now a growing body of high-quality evidence from interventional, placebo-controlled, randomised trials: the highest level of evidence we have. The ESSENCE trial is the leading one published so far, and several Phase III trials are ongoing, building on promising Phase II studies.
Data from trials using tirzepatide, which is approved for diabetes and obesity, and survodutide, also show liver benefits. Beyond trials, registry studies comparing patients on GLP-1 therapy versus those not on it suggest fewer liver-related events in the GLP-1 group. These are observational, not randomised, so we can’t prove
The benefits of GLP-1 agonists extend beyond metabolic improvement; they affect overall behaviour and lifestyle
causality, but the association is strong, especially in large registries involving up to 300,000 patients.
Interestingly, GLP-1 drugs also appear to modulate behaviours like alcohol and nicotine use and even gambling or cravings for substances such as marijuana. These effects are mediated through the central nervous system, reducing cravings. So, the benefits of GLP-1 agonists extend beyond metabolic improvement; they affect overall behaviour and lifestyle.
However, these drugs work only as long as patients take them. Once treatment stops, weight regain often follows, and that regained weight tends to be fat, not muscle. So, I always discuss long-term therapy, access, and cost with my patients.
In Germany, for example, the obesity-dose semaglutide used for liver disease isn’t covered by healthcare providers. Patients must pay out of pocket, which can cost several hundred EUR per month. In the USA, only about 30% of patients remain on the drug after 1 year due to affordability and access issues. For liver disease, we often use the higher obesity dose, so cost is a major barrier.
Q4 What is actually causing the liver benefits in patients taking GLP-1 agonists?
Weight loss is the primary factor. Even a 5% reduction helps reduce liver fat, and a 10% loss can reverse fibrosis. However, there are also weight loss-independent effects. In my presentation, I showed a mediation analysis demonstrating that some improvements in liver histology occur even in patients who lose little weight.
This suggests that other mechanisms, like changes in adipose tissue, adiponectin, leptin, or metabolic markers such as fibroblast growth factor 21(FGF21), also play a role. In fact, there are FGF21 analogues in development showing early evidence of cirrhosis regression. So, GLP-1 agonists may have both direct and indirect liver-protective effects.
Q5 As GLP-1 therapies expand beyond diabetes and obesity, what challenges do you foresee in bringing these treatments into everyday hepatology and gastroenterology practice?
The first challenge is awareness. Liver disease is a key part of the metabolic injury caused by obesity and diabetes, alongside cardiac and renal complications. It’s part of what we now call the cardiokidney-liver-metabolic disease spectrum.
We also need to combat the stigma that still surrounds liver disease. Many patients with metabolic or other non-alcoholrelated liver diseases are wrongly labelled as alcoholics. Awareness among physicians, patients, and the public is essential to changing that perception.
Q6 You recently became the UEG Scientific Committee Chair-Elect. What are your priorities for this role, and how do you hope to shape the scientific direction of future UEG meetings?
Yes, I was very excited about being elected. The Scientific Committee is already planning for UEG Week 2026 in Barcelona, Spain, and my main goals are to involve the next generation of gastroenterologists and scientists, strengthen cross-disciplinary collaboration, and highlight metabolic diseases as key drivers of health issues across gastroenterology.
We’re working to connect earlycareer clinicians and researchers through initiatives such as the Rising Star Awards and UEG Fellowships, ensuring that they can engage with the society and contribute to shaping the field’s future. Another priority is to foster collaboration between different specialties (those working in areas like inflammatory bowel disease, liver disease, pancreatic disorders, and nutrition) so that we approach gastroenterology in a truly integrated way.
Liver disease is a key part of the metabolic injury caused by obesity and diabetes
I also want to bring greater attention to metabolic diseases, which are becoming increasingly common across our field. These conditions are linked not only to liver disease but also to the pancreas and colon, with rising rates of early-onset colon cancer in younger patients with obesity or diabetes. Screening programmes may need to adapt to reflect this shift. UEG’s strength lies in its breadth, and I want to use that to drive more awareness and innovation in these interconnected areas.
Q7 Are there any sessions at UEG Week that particularly interest you or that you’d recommend attending?
It’s the totality of the sessions that makes UEG Week special. This year, we introduced the Digestive Disease Meetings (DDM) Summit, which focuses on basic science, the foundation for developing new therapies and diagnostics.
The hands-on training sessions are another highlight. We offer live-streamed endoscopy demonstrations and practical sessions where participants can use simulators and work in multidisciplinary teams.
We’re also seeing a rise in original research, including Phase III trial data presented for the first time. Increasing the number and visibility of these studies will be a major goal moving forwards.
Q8
What are the main themes or take-home messages you’d like attendees to bring home from this year’s UEG Week?
That UEG is a vibrant, interconnected community where clinicians and scientists collaborate across disciplines. Early-career researchers can learn from senior clinicians about the most pressing clinical problems, while clinicians gain insight into emerging mechanisms from basic science.
We hope attendees leave with updated guidelines, awareness of new treatments, improved clinical skills, and stronger professional networks across Europe and beyond. All sessions are recorded and available through the UEG community platform, which helps keep the knowledge accessible.
Q9 Finally, what’s next for you in your research?
My current research focuses on developing new drugs and diagnostics for metabolic liver disease, preventing cancer and cirrhosis decompensation, and replacing liver biopsy with noninvasive biomarkers.
We’re involved in several largescale Phase III trials following 5,000–6,000 patients to assess whether these treatments can actually improve clinical outcomes, not just lab values or histology. I’m very excited to contribute to these studies. This is exactly what our patients need.
That UEG is a vibrant, interconnected community where clinicians and scientists collaborate across disciplines
Interviews
EMJ had the pleasure of interviewing Catherine Stedman and Dame Parveen Kumar, two distinguished leaders in gastroenterology. Stedman offers expert insights into autoimmune liver diseases, discussing diagnostic challenges and current therapeutic approaches. Kumar reflects on her remarkable career dedicated to advancing medical education and patient-centered care, highlighting the evolving landscape of gastroenterology training and clinical practice.
Featuring: Catherine Stedman, Dame Parveen Kumar
Catherine Stedman
Clinical Director of Gastroenterology, Christchurch; Clinical Professor of Medicine, University of Otago, Christchurch, New Zealand; Past President, New Zealand Society of Gastroenterology
Q1 What initially sparked your interest in gastroenterology and hepatology, and what motivates you to continue working in this field today?
I love the huge variety in the specialty, including the balance of inpatient and outpatient work, acute and routine endoscopy procedures, and also the complexity and challenge of managing difficult liver patients.
which prolongs life and averts the need for liver transplantation in many people.
Q3 From a pharmacology perspective, what lessons can we apply from hepatitis C drug development to other areas of gastroenterology or hepatology?
Hepatitis C is now an easily curable disease with a short course of tablets, rather than a negative diagnosis with stigma attached
Q2 You’ve contributed significantly to the development of hepatitis C therapies. What do you see as the most important breakthroughs in hepatitis C virus treatment during your career?
The most important breakthrough is the development of a highly effective, well-tolerated oral antiviral therapy that cures almost everyone with hepatitis C. Another major advancement has been being able to safely treat and cure people with more advanced liver disease from hepatitis C,
One of the key strategies we found was to look outside our own speciality and see how the approach to other viruses had evolved effectively. In the case of hepatitis C, we specifically learned from HIV management strategies, and this led to major progress. For other areas of gastroenterology or hepatology, I think we need to look at successful approaches to other diseases that might have similar pathogenic factors, and be willing to consider treatment strategies that are similar.
The next big therapeutic breakthrough is the development of effective drugs to treat metabolic dysfunction associated steatotic liver disease
Q4 In your clinical practice, what changes have you observed in the way patients with hepatitis C are diagnosed, managed, and supported over the past decade?
There have been many changes over the past decade. Hepatitis C is now diagnosed by a wide range of healthcare professionals and even peer workers, with the initial diagnosis now often being through a point-of-care test rather than a venesection. This testing now often occurs in the community, and most treatment also occurs in the community setting rather than specialist hospital practice.
I think one huge change is how I communicate with people regarding a new diagnosis of hepatitis C. I now tell them that this is a very positive diagnosis for the cause of their liver disease, as hepatitis C is now an easily curable disease with a short course of tablets, rather than a negative diagnosis with stigma attached.
Q5 Are there particular barriers in New Zealand, or globally, that still hinder access to life-saving hepatitis C treatments?
I think that the persistence of some older perceptions and stigma among healthcare
professionals, and even patients themselves, acts as a significant barrier to patients receiving appropriate testing for hepatitis C. Because some people are not perceived to be ‘at risk’, they are sometimes not offered appropriate diagnostic testing, and as a result, their access to treatment is delayed.
Q6
Beyond hepatitis C, where do you see the next big therapeutic breakthroughs in the field?
Within hepatology, I think the next big therapeutic breakthrough is the development of effective drugs to treat metabolic dysfunction associated steatotic liver disease. There has been a huge unmet need in this area for decades, and it is fantastic to now see therapy that is effective, even if it is not quite the cure that we have for hepatitis C. Some of the newer approaches to hepatitis B are also exciting and hold great promise for achieving a functional cure.
Q7
You were the first female gastroenterologist to become a professor of medicine in New Zealand. What did that milestone mean to you personally, and what impact has it had on the field?
It has been a great honour to become the first female gastroenterologist to become a professor of medicine in my country. As a younger woman, I never really expected this to happen, as I was simply focused on trying to meet the unmet clinical need in my day-today medical practice and find solutions for my patients, as well as balancing this with my family and personal life. The promotion to professor has given me a sense of recognition for my work and has also made it easier for
me to take up other leadership opportunities, such as President of the New Zealand Society of Gastroenterology (NZSG). I really hope that this will make it easier for younger women to consider an academic medical career and see it as something that is achievable for them to do as well.
Q8 What advice would you give to young women pursuing careers in gastroenterology or academic medicine?
Gastroenterology is a wonderful specialty, and I think that academic medicine offers a degree of flexibility and reward that is greater than a career focused solely on clinical medicine. Combining academic and clinical medicine certainly increases the pressures and challenges of life at certain times, but it is highly rewarding, improves patient care outcomes, and works surprisingly well in the earlier phase of life with a young family.
Dame Parveen Kumar
Emerita Professor of Medicine and Education, Barts and The London School of Medicine and Dentistry, Queen Mary University
of London, UK
I do join women-only societies to help support younger women, as they still face challenges such as bullying, harassment, being passed over for promotions, and the gender pay gap
Q1What first sparked your interest in gastroenterology and where did you train?
Why gastroenterology? For me, gastroenterology is one of the best specialties because of its breadth of interests. It involves the whole of the gastrointestinal tract, as well as the liver, gallbladder, and pancreas. Gastroenterology is fascinating. It covers a huge range of scientific disciplines, for example, biochemistry, enzymology, hormones, intestinal transport, through to the clinical study of major diseases. It also has the practical aspects such as endoscopy and endoscopic procedures. I started in gastroenterology over 50 years ago, and a lot has changed since then. When I began, it was a relatively new specialty, and there was just one ‘gastroenterologist’, a generalist who did everything. Not all hospitals even had one. Now, there are several gastroenterologists in every hospital, often sub-specialising in different aspects of the field, for example, coeliac disease, inflammatory bowel disease, and endoscopy, while hepatology has become a speciality in its own right.
There were very few places to train when I started. The gastroenterology unit at St Bartholomew's Hospital, London, UK, which was started by Anthony Dawson, Consultant Physician at St Bartholomew’s Hospital, was one where you were ‘invited’ to join, rather than ‘apply’, and I was one of the lucky ones. However, I was the only female for about 20 years! Dawson was an amazing clinician and researcher. He
built up a huge team, along with Michael Clark, Senior Lecturer in Medicine at St Bartholomew’s Hospital Medical College, consisting of about 16–18 research registrars and clinicians.
The training involved rotating through different aspects of becoming a gastroenterologist and general physician. We had periods in general medicine (with acute medical admissions), ward work, endoscopy, and 3–6-month research blocks. After 4 or 5 years, one ended up as both a well-trained physician, and a good gastroenterologist. During this time, we all also completed an MD in our particular area of research interest. In those days, MDs were preferable to PhDs for clinical doctors who were also doing research, although some, like myself, went down the academic route and became professors, as well as medical consultants.
Q2You began your research career focusing on small bowel disease. How did understanding of coeliac disease evolve during the course of your career?
It has changed enormously. I chose coeliac disease because I was interested in immunology. However, my research turned out to include much more, including genetics and histology (spending hours at the microscope examining self-stained specimens), as well as intestinal transport studies using self-made intestinal perfusion tubes. Those were the early days, and one had to be innovative and find ways of conducting experiments within the limits of the knowledge and technology available at that time.
For example, the technique of immunofluorescence was just emerging. I remember seeing something ‘glowing’ on my histological slides and thinking that it was artefact produced by my ineptitude at staining! However, it turned out that I had been looking at the antireticulin antibody, which was later described by someone else. It was important at that time, as it became a serological marker used to diagnose coeliac disease.
Coeliac disease has an interesting history. It was once called ‘Idiopathic steatorrhoea’, meaning ‘fatty stools’, as the cause was not known. Going back to the 2nd Century AD, Aretaeus of Cappadocia described a clinical scenario that may well have represented coeliac disease as we understand it today. However, it was not until 1888 that Samuel Gee gave the first accurate clinical description at St Bartholomew's Hospital (I held an international conference at St Bartholomew's in 1988 to celebrate this centenary). Later, in 1950, Willem-Karel Dicke demonstrated that gluten in the diet caused the intestinal damage. In 1956, the first preoral jejunal biopsy was performed, and the structural defect was subsequently described fully. Previously, the loss of villi in the small intestine on a patient with coeliac disease had only been observed in surgical specimens.
Our understanding of coeliac disease has therefore evolved completely, from recognising it as a disorder of the small bowel to now being able to delineate
exactly what occurs at a molecular level.
Coeliac disease has a multifactorial genesis. It is immunogenetic, with the human leukocyte antigen (HLA) DQ2 (and HLA DQ8, among others) marker present in the majority of patients. This haplotype is also associated with other autoimmune conditions, such as thyroid disease and Type 1 diabetes, which are therefore often seen in patients with coeliac disease. A related skin condition called dermatitis herpetiformis, is an intensely itchy, blistering rash that affects mainly extensor surfaces and shares the same gluten-dependent enteropathy and HLA associations. A glutenfree diet helps both conditions.
Q3How did you diagnose and investigate coeliac disease then and now?
Initially, diagnosis is based on clinical presentation. As the condition affects the small bowel, patients mainly present with symptoms of malabsorption. These include fatigue, weight loss, mouth ulcers, diarrhoea, and nutritional deficiencies, causing, for example, iron or vitamin B12 deficiency anaemia. In my earlier days, patients often presented looking emaciated and very ill, with severe anaemia, torrential diarrhoea, and, in some cases, bone fractures. Nowadays, however, they are often diagnosed with only minor symptoms. There are some long-term complications, for example, affecting bone (osteopenia and osteomalacia) and, very rarely, cancer.
As in adults, children used to present looking extremely ill, with failure of growth, weight loss, a protuberant abdomen, and thin limbs. Thankfully, this is now very rare, as children are identified much earlier with minor symptoms, thanks to the availability of reliable diagnostic tests.
Diagnostic tests include serology and small bowel biopsy. Serological testing has advanced rapidly. The measurement of tissue transglutaminase, particularly tissue transglutaminase 2 IgA, allows non-invasive diagnosis, making a duodenal biopsy almost redundant except in difficult cases.
In the 1960s and 1970s, before endoscopy became available, we used a ‘Crosby capsule’ to take a ‘biopsy’. We would pass a tube down the oesophagus, through the stomach and pylorus, into the second part of the duodenum. The capsule had a tiny internal blade and a rubber diaphragm. Suction with a syringe drew mucosa into an aperture, triggering the blade, and this captured a sample of the lining of the mucosa. We used to pull the tube out of the mouth and examine it under a dissecting microscope, prior to histology! Today, we just use endoscopy, which allows for multiple biopsies to be taken easily, rendering the Crosby capsule redundant. Histologically, the villi of the epithelial cells lining of the small intestine are blunted or completely atrophied.
Since its publication, the book has sold millions of copies and I have been invited around the world to teach, examine, and lecture
Dietary management is the mainstay of treatment. It is much easier nowadays, as products in supermarkets are labelled as gluten-free with the Coeliac society’s crossed-grain’ symbol.
Q4
Were you often the only woman on the team?
Yes! I was the only medically qualified woman on the gastrointestinal medical team for about 20 years. Now, thankfully, there are many more women in medicine, and medical schools have significantly increased their intakes of female students. Some men often argue against having more women as they say it reduces the work force, but many men also leave medicine, so retention is a broader issue than just gender. However, we must support women to have time off to have a family and then return to work.
In the days when there were very few women, I used to avoid joining women’s societies because I felt we should all be equal, despite gender. Now, I do join womenonly societies to help support younger women, as they still face challenges such as bullying, harassment, being passed over for
promotions, and the gender pay gap continues to persist. A very sad situation in this century. Surgery, in particular, remains markedly underrepresented by women.
Q5 Can you tell us about the major advances in gastroenterology during your career?
There have been many advances over the years with better technology, diagnostic tests, imaging, and drug therapies. Endoscopy has been transformative. Imaging has evolved massively, with newer imaging techniques including CT and MRI, and their application to specific invasive procedures. Serological diagnostics have vastly improved, some using immunological advances. Therapies using monoclonal drugs and targeted treatment have changed the treatment scenario!
Disease-wise, I believe that the discovery of Helicobacter pylori was revolutionary. We used to measure gastric acid endlessly, thinking this was the cause of gastric and duodenal ulcers, and then along came this bacterium. Its discovery story
was serendipitous, rather like the discovery of penicillin by Alexander Fleming. Helicobacter pylori was discovered by Robin Warren and Barry Marshall, who were later awarded the Nobel Prize for their work.
Inflammatory bowel disease is another area that has seen major advances, as monoclonal antibodies have vastly changed outcomes for Crohn’s disease and ulcerative colitis. In hepatology, we initially had classified hepatitis A, then hepatitis B (often via intravenous exposure), and for years we had a hepatitis which we called ‘non-A non-B’ or ‘posttransfusion’ hepatitis. This was eventually called hepatitis C once the virus had been isolated. Screening for hepatitis C in blood donations therefore came in quite late. Sadly, both hepatitis B and C can progress to chronic liver disease and cancer. Treatment looked bleak, until appropriate antivirals arrived in the last decade or so. I remember a colleague who had built his whole career and reputation on hepatitis C virus research saying, halfjokingly, that a ‘cure’ had ‘ruined’ his research agenda. I told him to pick another bug!
Q6
In 1999, I was invited and then interviewed to be a founding Non-Executive Director of NICE, a new special health authority set up by the then Secretary of State for Health
You developed the first MSc in gastroenterology in the UK. What was the reason behind creating this programme, and how has it evolved over time?
As a junior, I thought it would be wonderful to have an MSc in gastroenterology. It took me ages to design the programme, as I wanted to provide a strong foundation of basic sciences, including genetics, statistics, and an approach to critical appraisal, to shape our future researchers. This was followed by clinical modules and a research project lasting about 8–10 weeks, leading to a dissertation and viva. It worked well. We’ve had students from all over the world, and some have continued on to do PhDs. We also run it online, which is useful for those not in London, though I still think face-to-face interaction is invaluable for communication skills.
I have always recommended an intercalated degree to all medical students as they progress through their training. It gives them an extra understanding of research methodology and technology, which can be extremely helpful for their future careers. We now have many medical students undertaking an intercalated MSc in Gastroenterology at Queen Mary University of London, UK.
Q7 Many students consider your book, Kumar and Clark’s Clinical Medicine,1 their ‘bible’. What was your motivation for creating it?
As a student, the medical texts in the then medical textbooks were
verbose, vague, and unfocused. This made it very difficult to understand and learn medicine. I always thought I would like to write a definite textbook but didn’t think I would ever do it.
I was stimulated to rethink this when, as a research registrar, a letter arrived from some authors asking me to write a gastroenterology chapter for their new book. My supervisor for my post-graduate thesis, Mike Clark, was very against this and tried to dissuade me. He told me to write up my unwritten papers for research I had already done. However, as I persisted in wanting to write the requested chapter, Mike gave up and said he would help me write a textbook. I phoned a publisher I had previously written for and was amazed that they wanted to see me immediately to discuss this! Clearly there was a need for a good medical textbook!
We wrote obsessively, every lunchtime, weekend, and holiday, for about 2.5 years. We were told it would take us about 4–5 years. The early chapters were written by colleagues from St Bartholomew's Hospital. We standardised the format: bullet points, clear diagrams, algorithms, and tables, but only where the evidence supported them. We rewrote every chapter, making it easier to read and well formatted. We used short sentences consisting of one noun and one verb, to avoid ambiguity. This made it accessible for everyone to read, including those reading it around the world, where English wasn’t their first language. We gave most of the
royalties away to the contributing authors and various charities. Since its publication, the book has sold millions of copies and I have been invited around the world to teach, examine, and lecture. People tell me that the book has helped educate generations of young doctors.
When we started writing the book it was in pre-internet times! I cannot now imagine a time before internet now, as it is so easy to get the latest information. We used to fill our car boots with books and journals from the St Bartholomew’s medical school library on Friday evenings with the promise that they would be back on the library shells by Monday mornings 8 am. As it was a new book, we researched every symptom and fact, as errors are often transmitted from book to book, and sketched diagrams on envelopes for the illustrators, spending hours refining new algorithms and tables. The internet made a huge difference, but the workload didn’t change much! Mike and I worked on it for nine editions over more than 35 years. New editors have now taken the task for later editions, but we still read the chapters and proofs.
The success of the textbook, however, was not without its challenges. We faced the daunting task of keeping abreast with the rapid evolution of medical knowledge and practice. We updated the editions to reflect the latest evidence-based guidelines and advances. To ensure that the book remained relevant and comprehensive required ongoing
I have also been asked to officially review the standards of education and research in different countries. This ensures an equivalence of standards across the world
advent of the UK joining the EU, these tasks were later taken on by the European centralisation of licensing through the European Medicines Agency (EMA), a situation that had to change again with Brexit.
their international side of charity work. I was on their charities, including the BMA Foundation, and later chaired BMA Giving.
collaboration with a growing team of contributors, each bringing new insights from their specialties. Despite the hard work, the positive feedback from students and clinicians worldwide has been immensely rewarding and has reinforced my belief in the value of accessible, well-structured medical education resources.
Q8You’ve also held prominent leadership positions, from the National Institute for Health and Care Excellence (NICE) to the Royal Society of Medicine (RSM) and the British Medical Association (BMA). Could you tell us a bit more about your work with these organisations?
Before NICE, I served on the Medicines Commission UK, for about 12 years, as Commissioner, then Vice-Chairman, and for the last few years as Chairman. The Medicines Commission for the UK was the top national committee for medicines, established under the Medicines Act of 1959. Other committees scrutinised data, while we were tasked with appeals and decisions on what medicines could go public, be sold over the counter, or become prescriptiononly. It was a lot of work but enormously interesting. With the
In 1999, I was invited and then interviewed to be a founding Non-Executive Director of NICE, a new special health authority set up by the then Secretary of State for Health, Frank Dobson, UK Department of Health and Social Care, London, UK, and chaired by Sir Michael Rawlins, then Professor of Clinical Pharmacology at the University of Newcastle upon Tyne, UK. The Medicines Commission focused on the ‘safety, quality, and efficacy’ of drugs, whilst NICE focused on ‘clinical and cost-effectiveness’, in other words how well a treatment works and whether it represents value and is affordable. We had to decide how much we were prepared to spend per patient for a given benefit. It was complex but vital, as everything cannot be affordable within limited budgets.
I have been privileged to serve as President of several organisations, including the British Medical Association (BMA), the Royal Society of Medicine (RSM), The Royal Medical Benevolent Fund (RMBF), and the Medical Women’s Federation (MWF). Each brought different tasks and areas of expertise but taught me a great deal about leadership, new aspects of medicine, and medical politics.
The BMA had both a trade union and a professional side. My time as President was mainly spent on the professional side with education and research (through the Board of Science, which I later chaired after serving as President), holding conferences, meetings, and participating on
The RSM is a wonderful institution; it’s the one place you meet everyone across specialties. It’s educational, collegiate, and fun, with in-person and online meetings and lecturers covering a wide range of topics. The RSM has many speciality sections. Its educational output is immense. One of the themes for my presidency at the RSM was climate change. We started advocacy work on this in the UK, covering all aspects of climate change and pushing the ‘Greener NHS’ agenda.
The RMBF is the only charity dedicated to doctors, supporting those in distress due to medical or financial difficulties. It was an eye-opener for me to discover how many of our colleagues were struggling and living in devastating circumstances. It really is a wonderful charity and does excellent work in helping doctors and supporting them in their return to work.
The MWF is a charity supporting women in medicine and helping them to advance in their careers, as they remain grossly underrepresented in many specialties. I was honoured to serve as President in its 100th year.
I also serve on other committees and charity boards. I am an Ambassador to the UK Health Alliance on Climate Change (UKHACC), which has over 60 members, including medical colleges and paramedical groups. By advocating with one voice, the Alliance holds greater influence.
Lastly, my career would not have been possible without the incredible encouragement and support of my late husband, David Leaver, and my wonderful family
My research and our textbook book Clinical Medicine, 1 which is used across the world, have allowed me the privilege to travel the world to teach, lecture and examine. With the Royal College of Physicians, I examined for the MRCP (the Membership of the Royal College of Physicians diploma) for many years, and with my medical school, I examined both postgraduate and undergraduate degrees at medical schools abroad. I have also been asked to officially review the standards of education and research in different countries. This ensures an equivalence of standards across the world for both.
It is always a great pleasure to meet colleagues overseas and exchange ideas. Through some of my charitable work, I have visited low-income countries and raised money to set up libraries and hospital wards. I have also supported the twinning of schools
Reference
1. Kumar P, Clark M. Kumar and Clark’s Clinical Medicine (2025) 11th edition, Edinburgh: Elsevier.
and the exchange of ideas between institutions. People are just as passionate about medicine and education all over the world, as we are! However, I am now, of course, conscious of my carbon footprint and conduct as much as possible online rather than travelling overseas.
I have recently finished coediting with Babulal Sethia, then Consultant Paediatric Cardiothoracic Surgeon at the Royal Brompton Hospital, London, UK, a global health book co-authored with three colleagues and a large network of contributors.
The idea began at the RSM some years ago, when I came across a group of medical students chatting enthusiastically after a talk on global health. I joined them and said: “Why don’t we write a book?,” and then corrected myself and said I had a better idea: “Why
don’t you write it?” We eventually gathered around 160 medical student contributors from across the world, representing more than two dozen countries.
I co-edited the book with Sethia, who shares my enthusiasm for tackling climate change problems and shaping the future of healthcare.
I have been extremely fortunate in my career and am most grateful to all who have trained me and helped me along the way. I have met many amazing and inspirational people to whom I am deeply indebted. As doctors, we all learn from our patients, and I certainly learned most of my medicine from them, so I would like to thank them enormously. Lastly, my career would not have been possible without the incredible encouragement and support of my late husband, David Leaver, and my wonderful family.
Primary Squamous Cell Carcinoma of the Gallbladder with Hepatic Invasion: A Case Report
Authors: *Intissar Belrhali,1,2 Hind El Yacoubi,1,2 Saad Assila,2,3 Youssef Mahdi,2,3 Basma El Khannoussi,2,3 Hind Mrabti,1,2 Hassan Errihani1,2
1. Oncology Department, National Institute of Oncology Rabat, Morocco
2. Faculty of Medicine and Pharmacy, Mohamed V University of Rabat, Morocco
3. Pathology Department, National Institute of Oncology, Rabat, Morocco
*Correspondence to intissarbelrhali90@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Background: Primary squamous cell carcinoma (SCC) of the gallbladder is a rare, aggressive malignancy with poor prognosis.
Case Presentation: The authors report the case of a 52-year-old woman who presented with cholestatic jaundice and was diagnosed with unresectable gallbladder SCC invading the liver. Despite palliative chemotherapy and haemostatic radiotherapy, her condition deteriorated, and she died 6 months after diagnosis.
Conclusion: This case underscores the aggressive nature and limited treatment options of gallbladder SCC.
Key Points
1. Primary squamous cell carcinoma of the gallbladder is an uncommon and aggressive malignancy, often diagnosed at an advanced, unresectable stage due to its nonspecific clinical and imaging presentation.
2. This case highlights the diagnostic challenge of gallbladder squamous cell carcinoma mimicking a hepatic abscess, emphasising the need to consider malignancy when imaging reveals atypical hepatic lesions contiguous with the gallbladder.
3. Early recognition is crucial, as surgical resection remains the only curative option. Palliative chemotherapy and radiotherapy offer limited benefit in unresectable cases, underscoring the poor overall prognosis.
INTRODUCTION
Primary squamous cell carcinoma (SCC) of the gallbladder is a rare histological subtype, accounting for less than 3% of all gallbladder malignancies.1 Unlike the more common adenocarcinomas, gallbladder SCCs are composed entirely of squamous cells without glandular differentiation.2 Their origin remains debated, though chronic inflammation due to gallstones, infections, or anomalous pancreaticobiliary junctions is believed to play a key role in the metaplastic transformation of the epithelium.1,2
Large-scale analyses have shown a clear female predominance, with a median age of onset between 55–65 years.1 In a systematic review by Takahashi et al.,3 and a population-based study of 1,084 cases by Ayabe et al.,1 most patients presented with locally advanced or unresectable disease at diagnosis, reflecting the tumour’s aggressive biological behaviour and poor prognosis.
This tumour type is known for its rapid local invasion into adjacent hepatic and peritoneal tissues and its poor response to systemic therapy.1,3,4 Because of its rarity, there is no standardised treatment, and most data arise from isolated case reports or small case series.1,4
Here, the authors present a case of primary SCC of the gallbladder with hepatic invasion. Beyond its rarity, this case illustrates the diagnostic pitfalls that may occur when initial imaging findings mimic a hepatic abscess. It also emphasises the importance of considering this entity in the differential diagnosis of gallbladder masses with hepatic involvement in order to improve early recognition and management.
CASE PRESENTATION
A 52-year-old woman (gravida two and para two) with no relevant past medical history presented with a 2-month history of cholestatic jaundice and generalised fatigue. Initial abdominal ultrasonography revealed a distended gallbladder with thickened walls, gallstones, and a
hypoechoic lesion in the adjacent hepatic parenchyma, initially suggestive of an inflammatory process or hepatic abscess.
Contrast-enhanced CT of the abdomen demonstrated a hypodense lesion in liver segment IV contiguous with the gallbladder wall, associated with pericholecystic inflammation and multiple gallstones. The findings were initially interpreted as a hepatic abscess secondary to acute cholecystitis.
Magnetic resonance
cholangiopancreatography subsequently revealed an irregular gallbladder mass invading the hepatic hilum and portal vein, causing intrahepatic biliary dilatation. No distant metastases were detected on chest CT.
Endoscopic sphincterotomy was performed to relieve biliary obstruction. A duodenal biopsy revealed a well-differentiated, keratinising SCC infiltrating the mucosa. Immunohistochemical staining confirmed the squamous differentiation, showing positivity for p63 and cytokeratin (CK)5/6, and negativity for CK7, thereby excluding a poorly differentiated adenocarcinoma. The histopathological features of the tumour are illustrated in Figure 1
Owing to extensive local invasion, the tumour was deemed unresectable, and palliative chemotherapy with gemcitabine and cisplatin was initiated. During the third chemotherapy cycle, the patient’s performance status declined to WHO Grade 2, with asthenia, vomiting, Grade 1 anorexia, renal impairment, and microcytic hypochromic anaemia.
She was later hospitalised for haematemesis and rectal bleeding. Upper gastrointestinal endoscopy revealed tumour infiltration of the duodenum and biliary tract, confirming disease progression. Haemostatic radiotherapy was delivered, leading to temporary symptomatic relief. The patient’s condition progressively deteriorated, and she died approximately 6 months after diagnosis.
Representative micrographs of the tumour showing solid masses infiltrating the duodenal mucosa (A). Tumour cells are large and polygonal with prominent hyperchromatic nuclei and abundant eosinophilic cytoplasm, displaying squamous differentiation including intercellular bridges (B, C). Keratin maturation is evidenced by keratin globules (D) (haematoxylin-eosin stain; magnifications: A, B: x100; C, D: x400).
DISCUSSION
SCC of the gallbladder remains a diagnostic and therapeutic challenge due to its rarity, lack of specific symptoms, and aggressive clinical course. While adenocarcinomas account for the vast majority of gallbladder cancers, SCCs exhibit a more infiltrative growth pattern with a stronger propensity for hepatic and vascular invasion.1 These characteristics often make curative resection impossible at the time of diagnosis, as observed in the authors’ patient.
Imaging findings are usually non-specific, and SCC may initially mimic other benign or inflammatory hepatobiliary conditions, such as hepatic abscesses or xanthogranulomatous cholecystitis. In the authors’ case, the lesion was initially interpreted as a hepatic abscess on CT, delaying definitive diagnosis until magnetic resonance cholangiopancreatography and histopathological confirmation were obtained. Similar diagnostic pitfalls have been described in previous reports, emphasising the need for heightened awareness among radiologists and clinicians when evaluating atypical hepatic lesions adjacent to the gallbladder.1
Figure 1: Histologic features of gallbladder squamous cell carcinoma.
Histopathological examination remains the cornerstone of diagnosis, characterised by keratinisation, intercellular bridges, and keratin pearls. Immunohistochemistry is useful to confirm squamous differentiation (p63+, CK5/6+) and exclude poorly differentiated adenocarcinoma (CK7–).5
Treatment strategies for SCC of the gallbladder are not standardised. Radical surgery offers the only potential for cure, but most cases are diagnosed at an unresectable stage. For inoperable disease, platinum-based chemotherapy (gemcitabine–cisplatin) and radiotherapy may provide palliative benefit, although evidence remains limited and largely extrapolated from biliary tract adenocarcinoma trials.4,6
Several retrospective and population-based studies have confirmed the aggressive nature of SCC of the gallbladder. In a systematic review by Takahashi et al.,3 more than 80% of patients presented with locally advanced or metastatic disease, and median survival rarely exceeded 6 months. Similarly, Ayabe et al.1 analysed 1,084 cases
and reported poorer survival outcomes compared to adenocarcinomas, highlighting the urgent need for early detection.
A comparative overview of previously published series and case reports is summarised in Table 1. These studies consistently demonstrate the rarity and aggressiveness of primary SCC of the gallbladder. The majority of patients are diagnosed at an unresectable stage and have dismal outcomes despite surgery or combined treatment modalities.1,3
Compared with the authors’ case, which was initially misdiagnosed as a hepatic abscess, most reported cases presented as locally advanced masses with jaundice or abdominal pain. This comparison further underscores the diagnostic challenge and the need for clinical vigilance when interpreting atypical hepatobiliary imaging findings.
The present case contributes to the existing literature by illustrating a locally advanced SCC of the gallbladder initially misdiagnosed as a hepatic abscess,
review:
Overview of radiotherapy role; limited impact in advanced gallbladder carcinoma
Illustrates diagnostic pitfall (misinterpreted as hepatic abscess)
Table 1: Comparative summary of published cases of primary squamous cell carcinoma of the gallbladder.
thereby underscoring the diagnostic challenges associated with this rare entity. The educational value of this report lies in raising clinical awareness of this aggressive histologic subtype and promoting early consideration of SCC in the differential diagnosis of gallbladder masses with hepatic invasion.
Further research is warranted to better understand the molecular pathogenesis of SCC of the gallbladder and to identify potential therapeutic targets that could improve prognosis in this devastating disease.
References
1. Ayabe RI et al. Gallbladder squamous cell carcinoma: an analysis of 1084 cases from the National Cancer Database. J Surg Oncol. 2020;122(4):716-22.
Primary SCC of the gallbladder is a rare and aggressive malignancy with poor prognosis and no standardised treatment. This case highlights the importance of maintaining a high index of suspicion when imaging findings mimic benign hepatobiliary conditions such as hepatic abscess. Early recognition is crucial, as surgery remains the only potential curative option.
Beyond its rarity, this report aims to raise clinical awareness of this unusual histologic subtype and to emphasise the need for multidisciplinary collaboration in improving diagnostic accuracy and optimising patient management.
3. Takahashi H et al. Systematic review of squamous cell carcinoma of the gallbladder. Am J Surg. 2022;224(3):863-8.
4. Houry S et al. Irradiation therapy for gallbladder carcinoma: recent advances. J Hepatobiliary Pancreat Surg. 2001;8(6):518-24.
5. Adsay NV, Basturk O, “Gallbladder carcinoma,” WHO Classification of
Tumours Editorial Board (eds.), WHO Classification of Tumours: Digestive System Tumours (2019) 5ᵗʰ edition, Lyon: International Agency for Research on Cancer (IARC), pp.266-73.
6. Valle JW et al. New horizons for precision medicine in biliary tract cancers. Cancer Discov. 2017;7(9):943-62.
Association Between Ultra-Processed Food Consumption and Risk of Developing Depression in Adults: A Systematic Review
Authors: *Saba Karim,1 Aaliya Shah Alam,1 Aqsa Syed2
1. Karachi Medical & Dental College (KMDC), Pakistan
2. Loralai Medical College, Pakistan
*Correspondence to sabakrm0@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: The authors would like to thank Sahar Rameez, founder of SHAWPakistan, for her thorough guidance for this research.
Received: 02.05.25
Accepted: 03.11.25
Keywords: Depression, mental health, microbiota-gut–brain axis, NOVA classification, ultra-processed food (UPF) consumption, Western diet.
Objective: This systematic review aims to evaluate the relationship between ultra-processed food (UPF) consumption and the incidence of depression among adults. It focuses on the effects of dietary intake of UPF, characterised by high levels of additives and low nutritional value, on mental health outcomes.
Method: Following the Population, Intervention, Comparator, and Outcome (PICO) framework, the population was defined as adults, the intervention as UPF consumption, and the outcome as the risk of depression. A comprehensive search was conducted across six electronic databases: PubMed, PubMed Central, Cochrane, Google Scholar, PLOS One, and ScienceDirect, adhering to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies published from 2019–2023 were selected based on predefined inclusion and exclusion criteria. Duplicate entries were removed using Endnote™ (Clarivate, London, UK), and data extraction was standardised using Covidence (Veritas Health Innovation Ltd, Melbourne, Australia). The quality of the studies was assessed using the Critical Appraisal Skills Program checklist.
Results: Nine studies with a combined sample of 79,701 participants were included. UPF consumption showed a consistent positive association with depression. Cohort studies reported that individuals in the highest UPF intake category had a 20–50% higher risk of developing depressive symptoms (e.g., hazard ratio: 1.22–1.52; 95% CI: 1.10–1.68). Mechanistically, findings highlighted UPF-induced gut dysbiosis, neuroinflammation, and disrupted neurotransmission as potential mediators.
Conclusions and Relevance: This systematic review concludes that increased UPF consumption is significantly associated with a higher risk of depression among adults. These results highlight the necessity of public health campaigns to lower UPF consumption and encourage better eating habits. Clinicians and policymakers should consider these associations when developing dietary guidelines and interventions to improve mental health outcomes.
Key Points
1. This systematic review examined the association between ultra-processed food (UPF) consumption and the risk of depression in adults, analysing nine studies with a total of 79,701 participants.
2. Individuals with higher UPF intake demonstrated a 20–50% greater risk of developing depressive symptoms (hazard ratio: 1.22–1.52; 95% CI: 1.10–1.68).
3. The findings emphasise the need for public health strategies that reduce UPF consumption and integrate dietary guidance into mental health prevention efforts.
INTRODUCTION
Depression, also known as major depressive disorder (MDD), is marked by a loss of interest or pleasure in activities and persistent feelings of sadness and hopelessness.1 The condition affects around 280 million people globally, including 3.8% of adults and 5.7% of those over 60 years of age.1
Depression is a significant factor in the link between low nutritional quality and mental health issues, contributing to declines in quality of life and early mortality.2 Although anxiety and depression are common chronic conditions, there are no evidence-based primary prevention and treatment options based on dietary adaptation in psychiatry, which modulates biological processes.3 There is a study showing that, despite significant advancements in psychotherapy and pharmacotherapy, they only prevent half of the illness load, and only one in three mood disorders respond well to traditional treatment.4 This indicates the need for additional approaches to both prevent and cure mental diseases.
Research from nutritional psychiatry suggests that dietary quality can moderate the risk of mental diseases like depression and anxiety, which are positively correlated with unhealthy, high-fat, sugar-rich diets.5 Monteiro et al.6 introduced the NOVA method for classifying foods, which divides foods into four classes according to industrial processing. This system considers biological, physical, and chemical techniques used in food production, including additives. The groups are unprocessed; processed culinary
ingredients; processed foods containing salt, oil, sugar, or other substances; and ultra-processed foods (UPF), which are primarily or entirely derived from food and additives.6 The NOVA classification system, widely used in nutritional research, is debated for its functionality and robustness, but its widespread implementation enhances comparability and accessibility.
‘Ultra-processed’ refers to ready-to-eat products made entirely or primarily from industrial materials and additives, with high profitability.7 These are becoming more popular worldwide, and consumption of these foods has been linked to internalising symptoms, anxiety, mental illnesses, and depression.3 The introduction of refined carbohydrates in the Western world in the second half of the 20th century led to industrialised foods, which has been linked to insulin resistance, cognitive decline, and dementia, potentially promoting insulinrelated cognitive impairment.8
METHODOLOGY
Data Collection and Search Strategy
With the help of the supervisor, the authors formulated a search strategy, which was used to begin the systematic review in March 2023. PubMed, PubMed Central, Cochrane, Google Scholar, PLOS One, and ScienceDirect were all searched for relevant material. The following methodology was used to carry out the search strategy.
Establishing keywords and key terms
Keywords and key terms were identified in searching the identified databases for
“ultra-processed foods,” “ultra processed food,” “mental disorder,” “common mental disorder,” “mood disorder,” “depres,” and “anxie.” The search terms were combined using Boolean operators, which were helpful for consolidating and refining particular search terms (Supplementary File 1).
Eligibility Criteria
Following the identification of search phrases, the authors used more search filters to focus the search and facilitate the finding of pertinent articles. The following criteria were used to select studies for this analysis: 1) quantitative observational studies (cohort, case-control, or crosssectional); 2) persons above the age of 18 years; 3) English-language publications; and 4) within the previous 5 years. Excluded studies were 1) non-observational study designs (e.g., reviews, commentaries, editorials, interventional trials, and animal studies; 2) those with population under the age of 18 years; 3) those carried out prior to the last 5 years; or 4) those that used COVID-19 as a factor.
Selection Process
After applying screening filters for inclusion eligibility and conducting the final search, the researchers used ‘AND;’ to integrate all of the thoughts to further enhance the search results. The remaining articles were imported into Endnote™ (Clarivate, London, UK) and were screened for duplicates. All the investigators collectively screened every article. The relevant articles were sought for retrieval and then the full text of the articles was scrutinised individually for eligibility.
Data Extraction and Synthesis
The final articles were uploaded into Covidence software for data extraction purposes.9-17 Each investigator reviewed three articles primarily as well as six articles primarily reviewed by other investigators using Covidence (Appendix 1). The following data was extracted from the included articles: study ID, title, lead author, contact details, country of study, aim of study, study design, year of publication, study funding, conflict of interests, population,
inclusion and exclusion criteria, method of recruitment, total number of participants, baseline characteristics (age, female %, BMI, frequency), relation of food, and impact on mental health. Critical appraisal was done using the Critical Appraisal Skills Programme checklist tool.
Data Analysis Strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Supplementary File 2) and the ‘best fit’ framework synthesis were used to analyse the data. The best fit framework consists of the following steps: systematically finding pertinent primary research studies; using a search strategy to find relevant publications; extracting data based on quality-related characteristics; conducting framework analysis on the evidence; and creating a new framework made up of a new and old theme backed by the evidence. The key study additionally took advantage of the primary articles that were chosen from the scanning search and developed a comprehensive search strategy that included relevant keywords and therapeutic topics.
In the analysis, the authors employed two approaches, Eertmans, Baeyens, and Van Den Bergh’s model and the microbiotagut–brain axis theory, as complementary frameworks to achieve the study’s aims. Eertmans, Baeyens, and Van Den Bergh18 presented the model of food intake and choice, highlighting a number of variables that affect eating habits. One of the internal variables is the sensory characteristics of eating. Information, the social setting, and the physical surroundings are some examples of external variables. The connections between these variables, food preferences, and eating habits are shaped by processes like social learning, Pavlovian conditioning, and simple exposure. As they are convenient (long-lasting, ready-to-eat, or heatable), hyper-palatable (incredibly delicious), highly profitable (low-cost ingredients), and made to replace all other food groups with the help of eye-catching packaging and aggressive marketing, these highly processed food products are therefore preferred over other healthier food items.
The microbiota-gut–brain axis theory (Figure 1) is used to validate the critical role that the gut microbiota plays in the twoway communication between the gut and the brain.19 It is possible that gut microbes influence neural development, modify neurotransmission, and change behaviour, all of which could contribute to the aetiology and/or progression of a number
of neurological, neuropsychiatric, and neurodevelopmental disorders. While the authors primarily used existing frameworks, they remained open to emerging themes and developing new framework components where necessary. Thus, combining the two theories establishes the connection of increased incidence of depression in high UPF consumers.
Epigenetic change
Neurogenesis Inflammation
DEPRESSION
HPA axis (dys)function
Tryptophan-Kynurenine metabolism
Oxidative Stress
Mitochondrial (dys)function
Gut microbiota
The diagram illustrates the pathways linked to depression, with conflicting eating trends affecting consumption. Green arrows indicate helpful modulation, while red arrows suggest potentially harmful ones.
The studies were chosen by screening the titles and abstracts, after which each possibly relevant full-length article was evaluated separately. Research that didn’t fit the requirements was eliminated. The initial search yielded 110 articles. Eleven duplicate articles were removed and 99 articles were subjected to screening for titles and abstracts. Eighty-three were not related and therefore excluded, and the remaining 16 articles were sought for retrieval. Two
articles could not ultimately be retrieved, so the other 14 articles were assessed for eligibility. Five articles were then eliminated because of the following reasons: they discussed mental health disorders other than depression, and the study design was incorrect. Overall, nine articles were included in this review. The PRISMA flowchart illustrates the details of the selection (Figure 2).20
Study Characteristics
Ultimately, 79,701 participants from nine qualifying studies were included in the review.
Figure 2: Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram illustrating the process of study identification, screening, eligibility assessment, and inclusion in the systematic review.
Records identified from Databases (n=6)
PubMed: 25 results
Google Scholar: 45 results
Cochrane Library: Six results
ScienceDirect: 13 results
PubMed Central: Six results
PLOS One: 15 results
Records screened (n=99)
Reports sought for retrieval (n=16)
Records removed before screening:
• Duplicate records removed (n=11)
Adapted from Page et al.20
Reports assessed for eligibility (n=14)
Records excluded (n=83):
• Title and abstract not related
Reports not retrieved (n=2)
Records excluded:
• Reason 1 (n=4): Mental health disorder other than depression
• Reason 2 (n=1): Incorrect study design
Studies included in review (n=9)
The range of sample sizes was 152–23,299 individuals. The included studies explored the connections between depression and UPF consumption. A total of five cohort and four cross-sectional designed studies were included. Eligible studies were conducted in Spain, the USA, Italy, France, Canada, South Korea, Australia, and London, UK. These studies included adult participants. The ages ranged from 20s to 60s. Some participants were recruited voluntarily (four studies), some were clinic patients (two studies), and others were recruited from social media campaigns (one study), university websites (one study), and surveys (one study).
Diet information was collected via a food frequency questionnaire in five studies12-16 and the Canadian Diet History Questionnaire II (C-DHQ II) by one study,10 while dietary recall interviews were used in two studies and a web-based dietary record platform was used by another.9,11,17 In four investigations, the Patient Health Questionnaire-9 (PHQ-9) was used to measure depressive symptoms,9-11,15 and the Center for Epidemiological Studies Depression (CES-D) Scale was used in three studies.14,16,17 The Kessler Psychological Distress (K10) scale was utilised in one study and the remaining study used the clinical diagnosis of depression.12,13
The characteristics of the nine included studies are summarised in Supplementary Table 1. These studies varied in design, sample size, and geographic distribution, but consistently assessed UPF consumption using the NOVA classification. Depression outcomes were measured using validated screening tools. Most cohort studies demonstrated longitudinal associations, while cross-sectional studies highlighted concurrent relationships between higher UPF intake and depressive symptoms. More detail can be found in Appendix 1.
Quality Assessment
Using the Critical Appraisal Skills Programme checklist, all included studies were critically appraised for methodological rigour, clarity of objectives, validity of results, and relevance to the review question (Supplementary File 1).
Among the nine included studies, five were rated high quality, three moderate quality, and one low quality due to limitations in confounder adjustment and participant selection. Most studies demonstrated clear aims, appropriate study designs, and valid outcome measures. Common methodological strengths included the use of validated dietary assessment tools (e.g., food frequency questionnaires) and standardised depression screening scales (e.g., PHQ-9, CES-D).
However, several cross-sectional studies showed limited generalisability due to selfreported dietary data and potential recall bias. Overall, the evidence base was judged to be of moderate-to-high quality, providing reasonable confidence in the observed association between UPF consumption and depression risk (Supplementary Table 2).
DISCUSSION
A comprehensive analysis of the relationship between eating UPFs and the risk of depression was carried out. The review correlated papers with an evolving framework, which combined Eertmans, Baeyens, and Van Den Bergh’s model with the microbiota-gut–brain axis theory. The bidirectional approach ensured a theoretically sound and empirically supported framework. The review synthesised findings from relevant papers, identifying areas of agreement and disagreement, to develop a nuanced understanding of how UPF consumption correlates with depression risk.
According to a recent study, an increased risk of depression is linked to higher UPF intake, especially in artificial sweeteners and beverages. Purinergic transmission in the brain may be triggered by artificial sweeteners, and this could contribute to the aetiopathogenesis of depression, according to recent experimental findings.21 UPF food additives, like emulsifiers and artificial sweeteners, can cause biochemical alterations linked to mental illness symptoms, including reduced glucose tolerance, inflammatory mediators, oxidative stress, neuroinflammation, and changes
in neurotrophic growth factor expression (Figure 3).22 According to European prospective cohort studies, people with high added sugars, high glycaemic index, and deficient nutrients are at an increased risk of developing anxiety and depression.23
Ultra-Processed Food
As mentioned earlier, food items are divided into four classes using the NOVA classification system. UPF, which is produced using materials that have been extracted from food, food ingredients, or intentionally synthesised from food substrates or organic sources, makes up the fourth category.24 UPFs are produced using ingredients that are either cosmetic additives that make the finished product palatable or hyper-palatable, or compounds that have no or very little culinary use. These ingredients can either offer pleasing sensory qualities or mask undesired sensory qualities caused by ingredients, methods, or packaging. Colours, emulsifiers, salts, sweeteners, thickeners, flavours, taste enhancers, and anti-foaming agents are a few types of cosmetic additives.25
The consumption of visually appealing food in middle-income Asian nations is increasing due to urbanisation, labour market trends, and rising earnings. This is driven by the need for convenience foods as economies develop. Chronic diseases can result from a diet high in fat, cholesterol, sugar, processed carbs, and low in fibre and polyunsaturated fatty acids, combined with a more sedentary lifestyle (Figure 4).26 Studies show that increased use of UPFs in rich and middleincome nations is linked to negative health outcomes due to their poor nutritional profile, increased glycaemic load, and decreased gut–brain satiety signalling.27
The cohabitation of undernutrition and overweight, obesity, and diet-related noncommunicable diseases is known as the double burden of malnutrition, and it has become a problem in many nations.22 UPF causes alterations in the physical properties of food through processing, carcinogen contamination, industrial food additives, dysbiosis of the gut microflora, increased
intestinal permeability, inflammation, and endocrine disruption from chemical plasticisers used in food packaging.27
Microbiota-Gut–Brain Axis
The gut microbiota in the intestines profoundly regulates human physiology, including digestion, metabolism, and immunity, and has a strong link with nervous system diseases. Diet contributes significantly in altering the composition of gut microbiota, which either promotes or restricts the growth of specific species and results in an imbalance referred to as dysbiosis. The gut–brain-microbiota axis is a two-way communication between the enteric and central nervous systems (CNS) that links digestive processes to the brain’s emotional and cognitive centres.28 Thus, the CNS can control gastrointestinal function, and the gut can control emotional activity in the CNS. Studies show that the gut microbiota of depressed individuals significantly differs from that of healthy individuals. From the existing data, the authors can conclude that intestinal bacteria can react with the nervous system and result in depression (Figure 3).28-30
Impact on Neuropsychiatry
Around 53% of individuals who consumed UPF many times a day experienced distress or battling their mental health compared to only 18% of those who seldom or never consumed UPF, representing a threefold increase.31 The mood and cognitive dysfunction components of neuropsychiatric illnesses have historically been linked to a dysregulation of neurotransmitters such as glutamate, serotonin, norepinephrine, and dopamine.32 Recent studies have explored the biosynthesis of gut microbiome-derived neurotransmitters, including γ-aminobutyric acid (GABA), serotonin, dopamine, and norepinephrine, which may affect the stability of the HPA axis.33 A greater number of research suggests a reciprocal relationship between the gut bacteria and the hypothalamic-pituitary-adrenal (HPA) axis. Because of how it affects cortisol release, the HPA axis is important in the pathophysiology of depression. Patients with MDD had considerably higher cortisol levels
Figure 3: Ultra-processed food induced gut dysbiosis and its effect on the brain.22
than healthy volunteers. Elevated cortisol levels have been shown to affect verbal and working memory, which lowers depressionrelated cognitive function. It has been demonstrated that the hippocampus, whose volume is markedly diminished in MDD, oversees the HPA axis and neurogenesis.34
Other Associations
A lot of studies have shown that excessive use of UPF is linked to increased risk of developing health issues, such as Type 2 diabetes, obesity, cancer, heart
and brain disease, cognitive decline, chronic renal disease, and death from all causes. According to the meta-analysis, for every 10% increase in total UPF consumption there is a 12% (95% CI: 10–13%) increased risk of developing Type 2 diabetes secondary to insulin resistance, obesity, and systemic inflammation.35 Overconsumption of UPF can cause inflammation, cardiometabolic problems, and chronic noncommunicable illnesses including diabetes, obesity, heart disease, and cancer, including pancreatic, breast, and colorectal cancers.36,37 There is a strong
association between these conditions.38 A substantial correlation exists between UPF and the gut–brain axis. Reduced hippocampal size, which is connected to obesity, diabetes, hypertension, and poor diet, is linked to reduced neuroplasticity and cognitive impairment.39 Due to severe pathophysiological reasons, overuse of UPFs might harm the kidneys and raise the risk of chronic kidney disease related to advanced glycation end products found in UPFs.40 UPF consumption has been linked to the development of non-alcoholic fatty liver disease by low quality dietary fat, low quality of carbohydrates, and dietary components promoting dysbiosis and leaky gut syndrome (Figure 4).41 A sub analysis conducted by DeVito G, Sheean P using a large European cohort also revealed that UPF consumption was significantly and positively associated with head and neck cancer (hazard ratio [HR]: 1.21; 95% CI: 1.15–1.35), oesophageal
The search was limited to studies that only explored the risk of developing depression in UPF consumers. This review focused on studies from 2019–2023 to reflect recent evidence regarding the NOVA classification. However, this limited scope might overlook earlier foundational studies and some nonindexed publications. The review also only utilised six databases, omitting Embase, PsycINFO, and Scopus, which could lead to selection bias. Future reviews should aim to include a wider range of databases and longer timeframes for a more thorough synthesis. Secondly, the study aimed to provide in-depth insights into consumers’ experiences and perceptions through qualitative studies. Systematic reviews were excluded to avoid duplication, and the
Liver
UPF consumption and associated comorbid UPF consumption is characterised by lower dietary quality, unhealthy fats, added sugar, salt, artificial sweeteners, and food additives, which results in an increased risk for diabetes, obesity, cardiovascular disease, cerebrovascular accidents, non-alcoholic fatty liver disease, and CKD.
Figure 4: Health risks linked to ultra-processed food consumption.
authors focused on studies from the last 5 years to include the most recent information in this rapidly evolving field. Thirdly, all the articles that did not use NOVA classification were excluded. Finally, to eliminate the difficulties that can arise from translation, all of the papers chosen for this study were published in English.
CONCLUSION
In conclusion, data that is currently published in the literature affirm that having a diet high in UPFs increases the chance of developing depression. This association remains significant even after adjusting for potential confounders. Consumption of UPF is linked to a decline in diet quality, with negative correlations with fibre and protein and positive correlations with sugar,
References
1. World Health Organization (WHO). Depressive disorder (depression). Available at: https://www.who.int/newsroom/fact-sheets/detail/depression. Last accessed: 4 May 2024.
2. van Zoonen K et al. Preventing the onset of major depressive disorder: a meta-analytic review of psychological interventions. Int J Epidemiol. 2014;43(2):318-29.
3. Jacka FN et al. Association of western and traditional diets with depression and anxiety in women. Am J Psychiatry. 2010;167(3):305-11.
4. Lassale C et al. Healthy dietary indices and risk of depressive outcomes: a systematic review and meta-analysis of observational studies. Mol Psychiatry. 2019;24(7):965-86.
5. Marx W et al. Nutritional psychiatry: the present state of the evidence. Proc Nutr Soc. 2017;76(4):427-36.
6. Monteiro CA et al. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018;21(1):5-17.
7. Monteiro CA et al. Ultra-processed products are becoming dominant in the global food system. Obes Rev. 2013;14(S2):21-8.
8. Guillou L et al. Chronic refined carbohydrate consumption measured by glycemic load and variation in cognitive performance in healthy people. Pers Individ Dif. 2023;206:112138.
fat, and saturated fat. The authors’ findings point to a potential relationship between UPF consumption and risk of developing depression. However, considering the limitations of the NOVA classification system and the complex, multi-cause nature of depression, it is critical to take into account other contributing factors such as genetics, environment, and lifestyle.
These results have important ramifications for public health, particularly for food policymakers who ought to discourage the use of UPF and encourage the consumption of fresh, less processed foods. More practical dietary recommendations should be developed by concentrating on how ultra processing alters the characteristics of whole meals and how these foods impact the gut microbiota.
9. Zheng L et al. Ultra-processed food is positively associated with depressive symptoms among United States adults. Front Nutr. 2020;7:600449.
10. Sen A et al. The role of ultra-processed food consumption and depression on type 2 diabetes incidence: a prospective community study in Quebec, Canada. Public Health Nutr. 2023;26(11):2294-303.
11. Lee S, Choi M. Ultra-processed food intakes are associated with depression in the general population: the Korea national health and nutrition examination survey. Nutrients. 2023;15(9):2169.
12. Lane MM et al. High ultra-processed food consumption is associated with elevated psychological distress as an indicator of depression in adults from the Melbourne Collaborative Cohort Study. J Affect Disord. 2023;335:57-66.
13. Gómez-Donoso C et al. Ultraprocessed food consumption and the incidence of depression in a Mediterranean cohort: the SUN Project. Eur J Nutr. 2020;59(3):1093-103.
14. Godos J et al. Ultra-processed food consumption and depressive symptoms in a Mediterranean cohort. Nutrients. 2023;15(3):504.
15. Contreras-Rodriguez O et al. Consumption of ultra-processed foods is associated with depression, mesocorticolimbic volume, and inflammation. J Affect Disord. 2023;335:340-8.
16. Arshad H et al. Association between ultra-processed foods and recurrence of depressive symptoms: the Whitehall II cohort study. Nutr Neurosci. 2024;27(1):42-54.
17. Adjibade M et al. Prospective association between ultra-processed food consumption and incident depressive symptoms in the French NutriNet-Santé cohort. BMC Med. 2019;17(1):78.
18. Chen PJ, Antonelli M. Conceptual models of food choice: influential factors related to foods, individual differences, and society. Foods. 2020;9(12):1898.
19. Marx W et al. Diet and depression: exploring the biological mechanisms of action. Mol Psychiatry. 2021;26(1):13450.
20. Page MJ et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
21. Samuthpongtorn C et al. Consumption of ultraprocessed food and risk of depression. JAMA Netw Open. 2023;6(9):e2334770.
22. Song Z et al. Effects of ultra-processed foods on the microbiota-gut-brain axis: the bread-and-butter issue. Food Res Int. 2023;167(112730):112730.
23. Hecht EM et al. Cross-sectional examination of ultra-processed food consumption and adverse mental health symptoms. Public Health Nutr. 2022;25(11):3225-34.
24. Monteiro CA et al. Ultra-processed foods: what they are and how to identify them. Public Health Nutr. 2019;22(5):936-41.
25. Popkin BM, Ng SW. The nutrition transition to a stage of high obesity and noncommunicable disease prevalence dominated by ultra‐processed foods is not inevitable. Obes Rev. 2022;23(1):e13366.
26. Baker P et al. Ultra‐processed foods and the nutrition transition: global, regional and national trends, food systems transformations and political economy drivers. Obes Rev. 2020;21(12):e13126.
27. Popkin BM et al. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet. 2020;395(10217):65-74.
28. Stilling RM et al. Microbial genes, brain & behaviour – epigenetic regulation of the gut–brain axis. Genes Brain Behav. 2014;13(1):69-86.
29. Li N et al. Fecal microbiota transplantation from chronic unpredictable mild stress mice donors affects anxiety-like and depression-like behavior in recipient mice via the gut microbiota-inflammation-brain axis. Stress. 2019;22(5):592-602.
30. Zheng P et al. Gut microbiome remodeling induces depressive-
like behaviors through a pathway mediated by the host’s metabolism. Mol Psychiatry. 2016;21(6):786-96.
31. Sapien Labs. Ultra-processed food consumption and mental wellbeing outcomes. 2023. Available at: https://sapienlabs.org/wp-content/ uploads/2023/09/Sapien_ProcessedFood-Rapid-Report_2023-2.pdf. Last accessed: 4 May 2024.
32. Muscaritoli M. The impact of nutrients on mental health and well-being: insights from the literature. Front Nutr. 2021;8:656290.
33. Nedic Erjavec G et al. Depression: biological markers and treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2021;105:110139.
34. Mikulska J et al. HPA axis in the pathomechanism of depression and schizophrenia: new therapeutic strategies based on its participation. Brain Sci. 2021;11(10):1298.
35. Chen Z et al. Ultra-processed food consumption and risk of type 2 diabetes: three large prospective U.S. cohort studies. Diabetes Care. 2023;46(7):1335-44.
36. Moradi S et al. Ultra-processed food consumption and adult obesity risk: a systematic review and dose-response meta-analysis. Crit Rev Food Sci Nutr. 2023;63(2):249-60.
37. Mesas AE et al. Increased consumption of ultra-processed food is associated with poor mental health in a nationally representative sample of adolescent students in Brazil. Nutrients. 2022;14(24):5207.
38. Isaksen IM, Dankel SN. Ultra-processed food consumption and cancer risk: a systematic review and meta-analysis. Clin Nutr. 2023;42(6):919-28.
39. Cardoso R et al. Association between ultra-processed food consumption and cognitive performance in US older adults: a cross-sectional analysis of the NHANES 2011–2014. Eur J Nutr. 2022;61(8):3975-85.
40. Avesani CM et al. Ultraprocessed foods and chronic kidney disease— double trouble. Clin Kidney J. 2023;16(11):1723-36.
41. Hägele FA et al. Ultra-processed food consumption and the risk of nonalcoholic fatty liver disease—what are the proposed mechanisms? Explor Dig Dis. 2023;1(1):133-48.
42. DeVito G, Sheean P. A scoping review of ultra-processed food consumption and cancer risk: implications for public health, registered dietitian nutritionists and other healthcare professionals. Nutr Cancer. 2025;DOI: 10.1080/01635581.2025.2572122.