Simplified Practical Approach to Percutaneous Coronary Intervention for Bifurcation Lesions: Bridging Complexity and Clarity
Exclusive ESC insights from an interview with ESC President Thomas F. Lüscher Interviews:
Congress
10 Review of the European Society of Cardiology (ESC) Congress 2025, 29th August–1st September 2025
Congress Features
24 What’s New in Heart Failure? Highlights and Insights from ESC 2025
Han Naung Tun
28 ESC Congress Update on ESC/EACTS 2025 Valvular Heart Disease Guidelines: Establishing the Present and Designing the Future for the Therapy of the Aortic Valve
Pyrpyris N et al.
32 New ESC Guidelines: Redefining Holistic Care in Cardiology
Ada Enesco
Poster Review
37 Aficamten versus Metoprolol in Obstructive Hypertrophic Cardiomyopathy: Recent Analyses of the MAPLE-HCM Trial
Abstract Reviews
45 A Web-Based Application for Acute Coronary Syndrome Mortality Risk Prediction Using Explainable AI and Chatbot Integration in the Asian Population
Kasim SS et al.
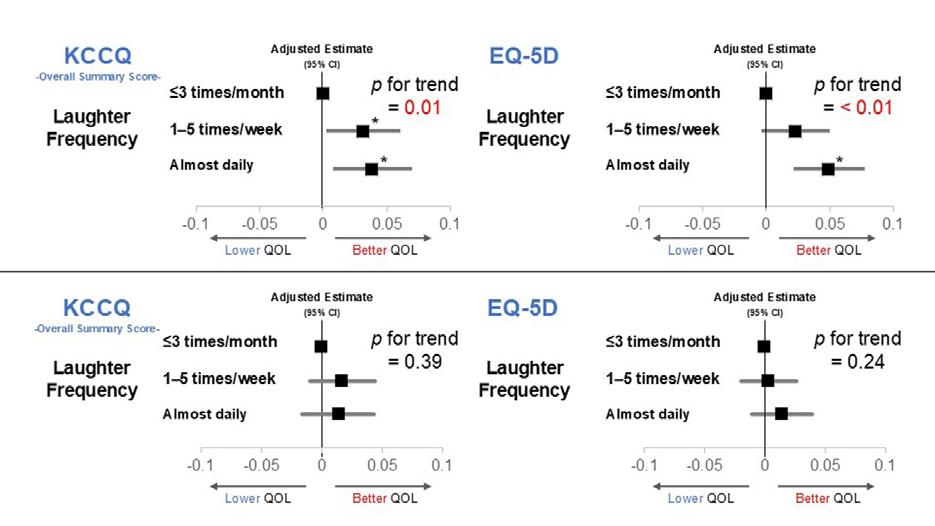
47 Association Between the Frequency of Laughter, Cardiovascular Event Risk, and Quality of Life in Asymptomatic Patients Attending a Cardiology Outpatient Clinic
Saito M et al.
49 Efficacy and Safety of Prolonged Edoxaban Treatment for Patients with Gastrointestinal Cancer Who Have Isolated Distal Deep Vein Thrombosis: Insight from the ONCO DVT Study
Yamashita Y et al.
51 Accelerometry-Defined Physical Activity and Quality of Life in Hypertrophic Cardiomyopathy
Schoonvelde SAC et al.
54 Impact of Pregnancy on Mortality in Dilated Cardiomyopathy: Immediate and 12-Month Postpartum Outcomes – Data from the InCor Registry
Avila MS et al.
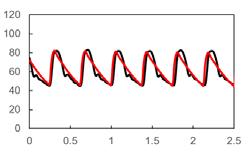
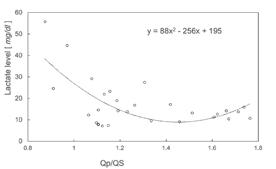
56 Optimal Pulmonary-to-Systemic Flow Ratio in the Paediatric ICU: Insights from a Series of Patient-Specific Norwood Circulation Computational Fluid Dynamics Models
Sughimoto K et al.
58 Sex-Specific Effects of Oestrogen in Takotsubo Syndrome: Protective in Females, Detrimental in Males
Zulfaj E et al.
60 Preoperative Baseline Troponin as a Predictor of Major Adverse Cardiac Events Following Kidney Transplantation in Patients with End-Stage Kidney Disease
Ardehali A et al.
63 Deep Learning-Based Approach to Emergency Department Chest Pain Risk Stratification by ECG
Parsa S et al.
Congress Interviews
65 Thomas F. Lüscher
69 Florian A. Wenzl
Interviews
72 Novel Cardiac Sarcomere Modulator, EDG-7500, in Hypertrophic Cardiomyopathy: Evaluating New Phase II Data from CIRRUS-HCM
82 Cathleen Biga
86 Christopher M. Kramer
88 David E. Winchester
90 Nancy Sweitzer
Features
95 Financial Toxicity: An Overlooked Driver of Heart Failure Risk in the USA
Tun HN
98 Sodium Glucose Co-transporter-2 Inhibitors in Heart Failure: Why the Elderly are Missing Out
Rehman MA et al.
Articles
102 Editor's Pick: Simplified Practical Approach to Percutaneous Coronary Intervention for Bifurcation Lesions: Bridging Complexity and Clarity
Kassier A et al.
112 Unrepaired Tetralogy of Fallot with Pulmonary Atresia and Major Aorto-pulmonary Collateral Arteries in Pregnancy: A Case Report
Ndale EK et al.
121 Renal Angioplasty and Stenting for Atherosclerotic Renal Artery Stenosis: Current Landscape and Future Directions
Dempsey E et al.
Editorial Board
Editor-in-Chief
Prof Çetin Erol
Department of Cardiology, School of Medicine, Ufuk University, Ankara, Türkiye
Professor Çetin Erol is a distinguished cardiologist currently serving in the Department of Cardiology at the School of Medicine, Ufuk University, Ankara, Türkiye. With extensive expertise in cardiovascular medicine, he has contributed significantly to the advancement of clinical cardiology and cardiovascular research through his roles in national and international cardiology societies and his extensive publication record in peer-reviewed journals.
Dr Andy Wai Kwong Chan
Andy Wai Kwong Chan Heart Centre, Hong Kong
Dr Carl J. Pepine
University of Florida, USA
Prof Denilson Campos de Albuquerque
Prof Uwe Nixdorff
European Prevention Center, Germany
Dr Han Naung Tun
Larner College of Medicine's University of Vermont, USA
Dr Constantine E. Kosmas
Lipid Clinic, National and Kapodistrian University of Athens, Greece
Dr Nicholas Kipshidze
Cardiovascular Research Foundation, USA
Dr Ronald J. Krone
Washington University School of Medicine, USA
Dr Carl J. Lavie
John Ochsner Heart & Vascular Institute, Ochsner Medical Center, USA
Pedro Ernesto University Hospital, State University of Rio de Janeiro, Brazil
Dr Sazzli Kasim
Universiti Teknologi MARA, Malaysia
Prof Khai Pham Gia
Bach Mai Hospital, Vietnam
Dr Sanjog Kalra University of Toronto, Canada
Dr Amandeep Goyal
University of Kansas Medical Center, USA
Prof Dr Rainer Wessely
Center for Cardiovascular Medicine (CIKA), Germany
Prof Stephen Lee
University of Hong Kong, Hong Kong
Dr Harish Ramakrishna Mayo Clinic, USA
Aims and Scope
EMJ Cardiology is an open-access, peer-reviewed eJournal, committed to helping elevate the quality of healthcare in cardiology and to contribute in advancing the development of this field by informing healthcare professionals on all aspects of cardiovascular disease.
The journal is published annually, six weeks after the European Society of Cardiology (ESC) Congress, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. The journal also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This content undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Cardiology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. EMJ Cardiology is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
EMJ Cardiology endeavours to increase knowledge, stimulate discussion, and contribute to a better understanding of cardiology. Our focus is on research that is relevant to all healthcare professionals. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of coming trends affecting clinical practice in cardiology.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
• A team of internal and independent medical writers.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with a member of the Editorial Board if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®.
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication Launch Date: 2013 Frequency: Yearly Online ISSN: 2054-3174
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (ESC 2025) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Madrid, Spain, the location of ESC 2025.
ECG, BP, SpO2, ABI and more, united in one device for an integrated, clutter-free care.
EFFORTLESS DATA FLOW
Results are automatically stored and synced with the EHR for easy and secure collaboration.
FASTER ASSESSMENTS
Automated measurements speed up workflows and reduce diagnostic delays.
With MESI mTABLET, we save 5 minutes on every ECG – thanks to automated documentation and seamless EHR integration.
Philip Heiden St Paul’s Surgery & Adelaide Medical Centre, United Kingdom
Ready to bring simplicity to cardiology?
BOOK A DEMO
Managing Editor
Darcy Richards
Copy Editors
Noémie Fouarge, Sarah Jahncke, Aranii Nagarajah
Editorial Leads
Helena Bradbury, Ada Enesco
Editorial Co-ordinators
Jenna Lorge, Bertie Pearcey
Editorial Assistants
Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey White
Senior Designers
Owen Silcox, Tamara Kondolomo
Creative Artworker Dillon Benn Grove
Designers
Shanjok Gurung, Fabio van Paris
Junior Designer
Helena Spicer
Head of Marketing
Stephanie Corbett
Business Unit Lead
Kelly Byrne
Chief Executive Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chairman
Spencer Gore
Welcome
Dear Readers,
We are delighted to welcome you to the 2025 issue of EMJ Cardiology, showcasing key highlights from the European Society of Cardiology (ESC) Congress 2025, which took place in Madrid, Spain.
To celebrate an impressive 75 years of the ESC, this event put the spotlight on the role of cardiovascular disease from a global health perspective and explored the value of crossborder collaboration. The programme featured a plethora of cutting-edge research, as well as great debates, guideline updates, symposia, and clinical cases. Within this issue, you will discover some of the pivotal developments presented over the course of the Congress, and dive deeper into the latest heart failure and valvular heart disease insights through expert-led congress features.
Additionally, you can learn about the ESC’s progress on securing EU support for a cardiovascular health plan, as well as other ESC initiatives, in our exclusive interview with ESC President, Thomas Lüscher.
Among our peer-reviewed content is a thought-provoking feature that discusses financial toxicity as an emerging concern for heart failure care, plus an enlightening review article covering the current state of play for renal angioplasty and stenting in atherosclerotic renal artery stenosis, and the knowledge gaps that need to be addressed to improve patient outcomes.
We would like to take this opportunity to thank our Editorial Board, authors, peer reviewers, and interviewees who have contributed to the publication of this issue. Your input has been invaluable. We hope you enjoy reading and find valuable insights for your daily practice!
Contact us
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
It is with great pleasure that I introduce the 2025 edition of EMJ Cardiology. This year’s issue features insights from the European Society of Cardiology (ESC) Congress 2025, held in Madrid, Spain, alongside peer-reviewed research, expert interviews, and more.
This year’s Congress celebrated 75 years of ESC with the World Heart Federation (WHF) Congress, and brought together leading minds in cardiology from across the globe, fostering interdisciplinary collaboration and presenting the latest advances in clinical and basic science. A particular highlight was the attendance of the King of Spain, who made an excellent speech on the fourth day of Congress. The overarching theme of 'Cardiology Beyond Borders', with a spotlight on 'Global Health', shaped the Congress programme, with sessions highlighting the most pressing challenges in global cardiology. With an emphasis on political advocacy, a major highlight of the ESC Congress 2025 was the unveiling of five new clinical guidelines on valvular heart disease, myocarditis and pericarditis, cardiovascular disease and pregnancy, dyslipidaemias, and mental health and cardiovascular disease.
This year’s edition of EMJ Cardiology further delves into the theme of global health, with feature articles that explore financial toxicity as a driver of heart failure risk and disparities in the use of sodium-glucose co-transporter-2 inhibitors in elderly populations.
Alongside this, our curated collection of abstracts showcases exciting developments in the field, with topics ranging from AI-based mortality risk prediction in acute coronary syndrome, to the use of accelerometry in hypertrophic cardiomyopathy.
Complementing the Congress coverage, EMJ Cardiology features conversations with several of today’s most influential cardiologists. In particular, we are delighted to include an interview with the ESC President Thomas Lüscher. Additionally, EMJ spoke to Nancy Sweitzer, Cathleen Biga, Christopher M. Kramer, David E. Winchester, and Florian Wenzl.
This year's edition of EMJ Cardiology delves into the theme of global health
Thank you to all contributors, reviewers, and our Editorial Board, as well as all the staff. We hope you find this edition informative and inspiring as we look forward to ESC 2026 in Munich, Germany.
Çetin Erol
Department of Cardiology, School of Medicine, Ufuk University, Ankara, Türkiye
ESC 2025
A major highlight of the ESC Congress 2025 was the unveiling of five new clinical guidelines
Review of the European Society of Cardiology (ESC) Congress 2025 Congress Review
THE EUROPEAN Society of Cardiology (ESC) celebrated a landmark moment this year, marking its 75th anniversary at the ESC Congress 2025, held in Madrid, Spain. In collaboration with the World Congress of Cardiology (WCC), the event brought together cardiologists, researchers, policymakers, and allied professionals. Uniting the global community to push the boundaries of cardiovascular disease within the evolving global health landscape, this year’s Congress explored 'Cardiology Beyond Borders' with a spotlight on 'Global Health'.
With three-quarters of a century dedicated to advancing cardiovascular science and improving patient care, the ESC President, Thomas F. Lüscher, took the opportunity at the inaugural session to reflect on the history of the ESC. He explained that in 1950, the ESC was founded to bring together the diverse national cardiac societies of Europe under a single umbrella organisation. Now, the ESC has grown into a global community that encompasses 58 national cardiac societies, 49 affiliated societies, seven sub-specialty associations, 15 working groups, and seven councils.
This year’s Congress provided an indepth look at the latest and greatest in cardiovascular medicine, cuttingedge science, bold ideas, practical breakthroughs, and stimulating debates. With a clear emphasis on making change at the policy level, a major highlight of the ESC Congress 2025 was the unveiling of five new clinical guidelines, designed to translate cutting-edge science into practice. Tomasz Guzik, The University of
Edinburgh, UK, highlighted the importance of these guidelines, which cover valvular heart disease, myocarditis and pericarditis, dyslipidaemias, and cardiovascular disease and pregnancy. He also noted that for the first time, there would be evidencebased recommendations on the crucial link between mental health and cardiovascular disease, which will “change your clinics on Tuesday morning when you go back to your hospitals.” Guzik further emphasised the importance of the spotlight on global health, as cardiovascular disease is universal, yet its global burden is unequal. He explained that this is why the ESC has partnered with the World Heart Federation (WHF) to advance cardiovascular health worldwide, whilst addressing regional needs.
Another key aspect of the Congress that Guzik highlighted was the Hot Line sessions, which presented 40 major clinical trials, representing new therapies and evaluating standards of care. These sessions were complemented by 29 trial discussions and 28 late-breaking science
sessions, offering insights into therapies, standards of care, and innovations from around the world. Furthermore, this year’s Congress welcomed 1,900 speakers from 85 countries and nearly 5,000 abstracts presented by researchers representing 108 nations. The Research Gateway featured 145 oral abstract sessions, 442 moderated e-posters, and 116 clinical case presentations, ensuring that even earlycareer scientists had a platform to share their work.
The Programme Committee curated multiple scientific tracks to meet the needs of the diverse global audience, with ‘New Horizons’ to showcase breakthroughs in new therapies, sessions on AI to highlight real-world algorithms ready for clinical application, clinical evidence sessions to translate trial data into day-to-day practice, and sessions on cardiometabolic medicine exploring the links between cardiology and obesity, diabetes, hypertension, sleep disorders, and anaemia. New initiatives, such as ePoster Rounds and Fireside Chats, further enriched the Congress, allowing attendees to engage in small, interactive discussions with leaders of cardiology: a reminder, as Guzik noted, that “science is about people as much as it is about data.”
The inaugural session also celebrated excellence and leadership in the field with the prestigious ESC Gold Medals. Lars Køber, University of Copenhagen, Denmark, was honoured for his pioneering work in the diagnosis and treatment of heart failure. Roxana Mehran, Icahn School of Medicine at Mount Sinai, New York, USA, was recognised for advancing interventional cardiology and championing gender equality in medicine. Ulrich Sigwart, University of Geneva, Switzerland, a trailblazer
in interventional cardiology, received the award for his role in designing and implanting one of the first self-expanding intracoronary stents. The ESC President’s Awards were also presented to Panos Vardas, University of Crete, Greece, and Béla Merkely, Semmelweis University Heart and Vascular Center, Budapest, Hungary, in recognition of their transformative contributions to both cardiology and society at large.
Concluding the inaugural session with his Presidential Lecture, Lüscher outlined a vision for the future of ESC as it enters a new era. He reflected on the Society’s legacy while confronting today’s most pressing challenges: environmental hazards, the obesity pandemic, and an ageing society. He called for stronger political advocacy, noting the ESC’s growing influence at the EU level, urging that medicine must be combined with politics in order to make sustained change. Looking ahead, he identified five major opportunities that will define the next chapter of ESC: AI and digital tools; expanding new subspecialties like cardio-oncology and cardiometabolic care; building registries and real-world evidence to guide policy and practice; investing in career development, mentoring, and training for young professionals; and strengthening global collaboration. Together, these pillars will guide the community toward ‘better science, stronger careers, and healthier patients’.
Read on for key insights into this year’s Congress, and don’t miss our coverage of ESC Congress 2026, which will be held in Munich, Germany, from 28ᵗʰ–31ˢᵗ August 2026.
Baxdrostat Lowers Blood Pressure in Uncontrolled and Resistant Hypertension
BAXDROSTAT 1 mg or 2 mg once daily significantly reduced systolic blood pressure in patients with uncontrolled or resistant hypertension, according to results of the Phase III BaxHTN trial presented during a Hot Line session at the ESC Congress 2025.1
Despite the widespread use of multiple antihypertensive drugs, many patients fail to achieve adequate blood pressure control, leaving them at increased cardiovascular risk. Uncontrolled hypertension refers to blood pressure that remains above target despite at least two medications, whereas resistant hypertension persists despite three or more agents, including a diuretic. Aldosterone is recognised as a key driver of hypertension, and the selective aldosterone synthase inhibitor baxdrostat has been developed to target this pathway with improved precision.
The BaxHTN trial was conducted across 214 international sites and included 796 patients randomised to receive baxdrostat 1 mg, baxdrostat 2 mg, or placebo once daily for 12 weeks. In total, 27% had uncontrolled hypertension and 73% had resistant hypertension, and at baseline, mean seated systolic and diastolic blood pressure were 149 and 85 mmHg, respectively, with a median number of three antihypertensive drugs.
At 12 weeks, the placebo-adjusted reductions in seated systolic pressure were 8.7 mmHg with 1 mg and 9.8 mmHg with 2 mg (both p<0.0001). Ambulatory 24-hour systolic pressure fell by 16.9 mmHg, and night-time values by 11.7 mmHg, with the 2 mg dose. Control rates <130 mmHg systolic were achieved in 39.4% with baxdrostat 1 mg, 40% with 2 mg, and 18.7% with placebo.
At the end of the 8-week randomised withdrawal phase, discontinuation of baxdrostat led to a systolic rise of 1.4 mmHg, compared with a further reduction of 3.7 mmHg in those maintained on therapy
At the end of the 8-week randomised withdrawal phase, discontinuation of baxdrostat led to a systolic rise of 1.4 mmHg
for 32 weeks (p=0.0016). Adverse events were uncommon, with serious events in <4% of patients, and hyperkalaemia leading to discontinuation in <2% of patients.
These findings support the role of aldosterone synthase inhibition in the management of hard-to-control hypertension. Baxdrostat was welltolerated and delivered clinically meaningful reductions in systolic blood pressure beyond standard therapy. Future research will focus on long-term safety, cardiovascular outcomes, and integration into treatment pathways.
These findings support the role of aldosterone synthase inhibition in the management of hard-tocontrol hypertension
Are β-Blockers Recommended After Myocardial Infarction?
LATE-BREAKING findings from the REBOOT trial, presented at the ESC Congress 2025, suggest that β-blockers may no longer be necessary for many patients recovering from myocardial infarction (MI) with preserved left ventricular ejection fraction (LVEF).2 However, results from the BETAMI and DANBLOCK trials support the use of β-blockers after MI, showing that long-term use significantly reduced all-cause mortality and major adverse cardiovascular events in patients with MI and preserved or mildly reduced LVEF. These contrasting findings add to the complexities of this area of ongoing debate.3
Current guidelines recommending β-blockers after MI without left ventricular systolic dysfunction are based on older trials conducted before routine reperfusion, invasive care, complete revascularisation, and modern pharmacologic therapy became standard. To re-evaluate their relevance, investigators in Spain and Italy conducted the REBOOT trial. This was an open-label,
randomised trial comparing β-blocker therapy with no β-blocker therapy in patients hospitalised with acute MI (with or without ST-segment elevation) and LVEF >40%.
The primary endpoint was a composite of death from any cause, reinfarction, or hospitalisation for heart failure.
Based on these results, the REBOOT trial suggests that routine β-blocker therapy may offer little benefit for patients with preserved LVEF in the contemporary treatment era
Of 8,438 patients analysed, 4,243 received β-blockers and 4,262 received no β-blocker therapy. Over a median follow-up of 3.7 years, the primary outcome occurred in 316 patients in the β-blocker group (22.5 events per 1,000 patient-years) versus 307 patients in the no-β-blocker group (21.7 events per 1,000 patient-years; hazard ratio [HR]: 1.04; 95% CI: 0.89–1.22; p=0.63).
Individual components of the outcome were also similar: death from any cause occurred in 161 versus 153 patients (11.2 versus 10.5 events per 1,000 patient-years; HR: 1.06; 95% CI: 0.85–1.33), reinfarction in 143 versus 143 patients (10.2 versus 10.1 events per 1,000 patient-years; HR: 1.01; 95% CI: 0.80–1.27), and hospitalisation for heart failure in 39 versus 44 patients (2.7 versus 3.0 events per 1,000 patient-years; HR: 0.89;
95% CI: 0.58–1.38). No significant differences in safety outcomes were observed.
Based on these results, the REBOOT trial suggests that routine β-blocker therapy may offer little benefit for patients with preserved LVEF in the contemporary treatment era. These findings could prompt a re-evaluation of guideline recommendations and influence post-MI management strategies.
However, opposing results from the BETAMI trial in Norway and the DANBLOCK trial in Denmark were also presented at the congress. Whilst β-blockers are strongly recommended in the management of MI with reduced LVEF, their benefit in patients with preserved or mildly reduced function (40% or higher) is unclear. These two trials were conducted to address this gap and to evaluate the efficacy of β-blocker therapy in contemporary clinical practice. The combined programme randomised 5,574 patients with recent MI, LVEF of at least 40%, and no clinical heart failure to receive long-term β-blocker therapy or no β-blocker therapy. The primary endpoint was a composite of all-cause mortality, new MI, unplanned coronary revascularisation, ischaemic stroke, heart failure, or malignant ventricular arrhythmias.
After a median follow-up of 3.5 years, the primary endpoint occurred in 14.2% of patients assigned to β-blockers and 16.3%
of those without therapy (HR: 0.85; 95% CI: 0.75–0.98; p=0.027). The incidence of new MI was lower with β-blockers (5.0% versus 6.7%; HR: 0.73; 95% CI: 0.59–0.92). All-cause mortality was similar between groups (4.2% versus 4.4%), as were the risks of stroke, heart failure, and arrhythmia, although event numbers for individual endpoints were relatively low. Safety outcomes were favourable, with serious adverse events infrequent and comparable between groups.
Of 8,438 patients analysed, 4,243 received β-blockers and 4,262 received no β-blocker therapy.
These findings support the continued clinical relevance of β-blocker therapy for secondary prevention following MI in patients with preserved or mildly reduced left ventricular function. In particular, the reduction in recurrent infarction highlights an important therapeutic benefit despite contemporary advances in acute and long-term care. Further pooled analyses, including meta-analyses of patients with mildly reduced ejection fraction, will help to refine patient selection.
Routine Breath Test for Helicobacter Pylori Not Recommended Post-heart Attack
A MAJOR Swedish clinical trial, presented at the ESC Congress 2025, has investigated whether routinely screening patients for Helicobacter pylori infection after an MI could help reduce the risk of upper gastrointestinal bleeding, a frequent complication following heart attacks.4
16.8 events per 1,000 person-years
Among patients in the screening group, the incidence rate was 16.8 events per 1,000 person-years
The study, which involved 18,466 patients admitted across 35 hospitals, tested the impact of adding a urea breath test for H. pylori to standard post-infarction care. Participants were randomly assigned by hospital clusters to either a year of routine screening or a year of usual care, with a short washout period before switching approaches. Patients were followed for a median of 1.9 years, and the primary outcome measured was the rate of upper gastrointestinal bleeding.
The findings showed that routine screening did not significantly lower bleeding events overall. Among patients in the screening group, the incidence rate was 16.8 events per 1,000 person-years, compared with 19.2 events per 1,000 person-years in the usual care group. This translated to a rate ratio of 0.90, a difference that did not reach statistical significance. Of those screened, 70% underwent testing, and nearly a quarter tested positive for H. pylori.
Interestingly, subgroup analyses suggested that some patients at higher risk, particularly those with anaemia, may benefit from screening. For individuals with moderate-to-severe anaemia, the risk of bleeding was notably reduced. However, these analyses were not adjusted for multiple comparisons, meaning the results should be interpreted with caution.
Overall, the trial concluded that routine H. pylori screening in all patients with MI cannot be recommended. While the potential benefit for high-risk subgroups warrants further investigation, the broad use of such testing does not appear to meaningfully reduce bleeding risk in this population.
Patients were followed for a median of 1.9 years, and the primary outcome measured was the rate of upper gastrointestinal bleeding
Olezarsen Significantly Lowers Triglycerides in Patients at High Cardiovascular Risk
OLEZARSEN, an investigational RNA-based therapy, presented at the ESC Congress 2025, has been shown to markedly lower triglyceride levels in patients with elevated cardiovascular risk, addressing an unmet clinical need for more effective treatments.5
Led by Brian Bergmark from the TIMI Study Group, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA, the ESSENCE-TIMI
73b trial was a placebo-controlled, doubleblind Phase III trial conducted at 160 sites in North America and Europe. Despite advances in lipid-lowering therapies, many patients continue to face residual cardiovascular risk driven by elevated triglycerides. The trial tested olezarsen, a novel medicine targeting the mRNA of apolipoprotein C-III (apo-CIII), which inhibits triglyceride clearance.
At 160 sites across North America and Europe, 1,349 patients with moderate hypertriglyceridaemia (triglycerides: 150–499 mg/dL) were enrolled, all with an established diagnosis of atherosclerotic cardiovascular or increased risk due to diabetes and older age (≥55 years). Participants were randomised to olezarsen 50 mg (n=254), olezarsen 80 mg (n=766), or placebo (n=329) given every 4 weeks via subcutaneous injection for 12 months. The primary endpoint was the percentage change from baseline to triglyceride levels at 6 months compared with placebo.
The findings were striking. At 6 months, olezarsen reduced triglyceride levels: the placebo-adjusted least-squares mean difference in percentage change from baseline was –58.4 percentage points for olezarsen 50 mg and –60.6 percentage points for olezarsen 80 mg (both p<0.001 versus placebo). Conversely, in the placebo group, 12.5% of patients had triglyceride levels <150 mg/dL at 6 months, compared with 85.0% of patients receiving olezarsen 50 mg, and 88.7% receiving olezarsen 80 mg (p<0.001 for both).
These results were similar at the 12-month mark, showing reductions to be greater in the groups receiving olezarsen compared to placebo groups (20.6%, 82.8%, and 85.0% for placebo, olezarsen 50 mg, and olezarsen 80 mg, respectively; p<0.001 for both versus placebo).
Reductions were also seen in other atherogenic lipoproteins, including remnant cholesterol and apolipoprotein B (apoB), but without impact on low-density lipoprotein cholesterol. Importantly, treatment was generally safe and well-tolerated, with adverse events consistent across groups.
RESULTS from the POTCAST trial, presented at the ESC Congress 2025, found that actively increasing plasma potassium concentrations to the mid-to-high normal range significantly reduced arrhythmic events, hospitalisations, and mortality risk compared with standard care.6
These findings support the hypothesis that higher-normal potassium levels confer anti-arrhythmic protection in patients at elevated risk of ventricular arrhythmias with implantable cardioverter defibrillators (ICD).
The benefit was largely driven by reductions in appropriate ICD therapies (15.3% versus 20.3%; HR: 0.75; 95% CI: 0.57–0.80) and unplanned arrhythmia-related hospitalisations (6.7% versus 10.7%; HR: 0.63; 95% CI: 0.28–0.64)
The open-label RCT enrolled 1,200 patients across three Danish centres. Participants had an ICD or cardiac resynchronisation therapy defibrillator, and a baseline potassium concentration ≤4.3 mmol/L. Key exclusion criteria were advanced renal impairment (estimated glomerular filtration rate: <30 mL/min/1.73 m2) and pregnancy.
Patients were randomised 1:1 to a strategy aiming to raise potassium to 4.5–5.0 mmol/L via dietary counselling, potassium supplements, and/or mineralocorticoid
receptor antagonists, or to standard care. The primary endpoint was a composite of sustained ventricular tachycardia (>125 beats per minute for >30 seconds), appropriate ICD therapy, unplanned hospitalisation (>24 hours) for arrhythmia or heart failure, and all-cause mortality. Median follow-up was 39.6 months.
Results showed a baseline mean potassium level of 4.01 mmol/L. At 6 months, levels increased to 4.36 mmol/L in the intervention group versus 4.05 mmol/L in controls. The primary endpoint occurred in 22.7% of patients in the treatment arm compared to 29.2% of controls (HR: 0.76; 95% CI: 0.61–0.95; p=0.015).
The benefit was largely driven by reductions in appropriate ICD therapies (15.3% versus 20.3%; HR: 0.75; 95% CI: 0.57–0.80) and unplanned arrhythmia-related hospitalisations (6.7% versus 10.7%; HR: 0.63; 95% CI: 0.28–0.64). Hospitalisation for heart failure (3.5% versus 5.5%) and all-cause mortality (5.7% versus 6.8%) were numerically lower in the intervention group, though not statistically significant.
Safety outcomes were reassuring, with comparable rates of hyperkalaemia- or hypokalaemia-related hospitalisations (1% in both groups). Overall, 29.5% of patients in the treatment group and 33.2% of controls experienced the combined outcome of unplanned hospitalisation and death (HR: 0.88; 95% CI: 0.72–1.08).
The investigators concluded that raising plasma potassium into the mid-to-high normal range represents an inexpensive and widely accessible adjunctive strategy for patients with ICDs and a high risk of ventricular arrhythmias.
Mavacamten Falls Short in Non-obstructive Hypertrophic Cardiomyopathy Trial
NEW DATA from the ODYSSEY-HCM
trial, presented at the ESC Congress 2025, challenge the potential role of mavacamten in patients with non-obstructive hypertrophic cardiomyopathy (HCM), showing limited impact on exercise capacity or symptoms.7
While mavacamten is approved for obstructive HCM, where it improves outflow tract obstruction, exercise tolerance, and quality of life, its benefits in non-obstructive HCM have remained uncertain. To evaluate this, investigators conducted a Phase III, international, double-blind, placebocontrolled trial in adults with symptomatic non-obstructive HCM. Participants were randomised 1:1 to mavacamten (starting at 5 mg/day, titrated up to 15 mg/day based on LVEF) or placebo with sham dose adjustments for 48 weeks. The co-primary endpoints were the change from baseline to Week 48 in peak O2 uptake and the Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS).
A total of 580 patients were enrolled (289 mavacamten, 291 placebo; mean age: 56 years; 46% women). Over 48 weeks, peak O2 uptake increased by 0.52 mL/kg/min (95% CI: 0.09–0.95) in the mavacamten arm versus 0.05 mL/kg/min (95% CI: –0.38–0.47) with placebo, for a betweengroup difference of 0.47 mL/kg/min (95% CI: –0.03–0.98; p=0.07). KCCQ-CSS improved by 13.1 points (95% CI: 10.7–15.5) with mavacamten versus 10.4 points (95% CI: 8.0–12.8) for placebo, yielding a between-group difference of 2.7 points (95% CI: –0.1–5.6; p=0.06). Adverse effects, including reductions in ejection fraction and treatment interruptions, were more common in the mavacamten group.
The findings suggest that mavacamten does not meaningfully improve functional capacity or patient-reported symptoms in non-obstructive HCM. Clinicians should interpret these results cautiously, and the study emphasises the ongoing need for effective therapies in this challenging patient population.
While mavacamten is approved for obstructive HCM, its benefits in non-obstructive HCM have remained uncertain
Initiation of Sodium-Glucose Co-transporter-2 Inhibitors in Patients Hospitalised for Heart Failure
STARTING sodium-glucose co-transporter-2 inhibitors (SGLT2i) during hospitalisation for heart failure (HF) appears beneficial, according to late-breaking data from the DAPA ACT HF-TIMI 68 trial and a supporting meta-analysis presented at the ESC Congress 2025.8
All-cause mortality was numerically lower with dapagliflozin (3.0% versus 4.5%; HR: 0.66; 95% CI: 0.43–1.00)
DAPA ACT HF-TIMI 68 was a double-blind, placebo-controlled trial conducted at 210 sites in the USA, Canada, Poland, Hungary, and Czechia. A total of 2,401 patients (median age: 69 years; 33.9% women) hospitalised with HF and signs of fluid overload were randomised to dapagliflozin 10 mg daily or placebo, initiated between 24 hours and 14 days after admission.
The primary endpoint, which was a composite of cardiovascular death or worsening HF within 2 months, occurred in 10.9% of patients in the dapagliflozin group and 12.7% in the placebo group (HR: 0.86; 95% CI: 0.68–1.08; p=0.20). Rates of cardiovascular death (2.5% versus 3.1%) and worsening HF events (9.4% versus 10.3%) were not significantly different.
All-cause mortality was numerically lower with dapagliflozin (3.0% versus 4.5%; HR: 0.66; 95% CI: 0.43–1.00). Safety outcomes were consistent with the known profile of SGLT2is, with slightly higher rates of hypotension (3.6% versus 2.2%) and renal events (5.9% versus 4.7%) in the dapagliflozin arm.
A pre-specified meta-analysis pooling DAPA ACT HF-TIMI 68 with two other in-hospital initiation trials (empagliflozin and sotagliflozin; n=3,527) demonstrated significant benefits. SGLT2i initiation reduced cardiovascular death or worsening HF (HR: 0.71; 95% CI: 0.54–0.93; p=0.012) and all-cause mortality (HR: 0.57; 95% CI: 0.41–0.80; p=0.001).
Dual Antiplatelet Therapy Offers No Benefit Over Aspirin Alone After Coronary Artery Bypass Grafting
DUAL antiplatelet therapy (DAPT) with ticagrelor and aspirin does not provide additional protection against major cardiovascular events after coronary artery bypass grafting (CABG) compared with aspirin alone, and it significantly increases bleeding risk, according to results of the TACSI trial, presented at the ESC Congress 2025.9
Led by Anders Jeppsson from Sahlgrenska University Hospital, Gothenburg, Sweden, the TACSI trial was an investigator-initiated pragmatic, open-label, registry-based trial. Current ESC Guidelines recommend DAPT for patients with acute coronary syndrome undergoing CABG, but this is largely based on data extrapolated from non-CABG trials.
To address the evidence gap, TACSI enrolled 2,201 patients across 22 cardiothoracic surgery centres in Sweden, Denmark, Norway, Finland, and Iceland. Patients undergoing their first isolated CABG were randomised to either DAPT (ticagrelor 90 mg twice daily plus aspirin 75 mg once daily) or aspirin only (75–160 mg daily according to local protocols) for 12 months.
At 12 months, the primary endpoint of major adverse cardiovascular events, including all-cause death, MI, stroke, or repeat revascularisation, occurred in 4.8% of patients receiving DAPT and 4.6% of patients on aspirin alone (HR: 1.09; 95% CI: 0.74–1.60; log rank p=0.77).
This demonstrated no significant benefit of DAPT for event prevention. However, the incidence of major bleeding was more than doubled with DAPT compared to the aspirin group (9.1% versus 6.4%; HR: 1.45; 95% CI: 1.07–1.97).
Patients undergoing their first isolated CABG were randomised to either DAPT or aspirin only for 12 months
Prospective Validation of an AI Stethoscope for Early Cardiovascular Disease Detection
AN AI-enabled stethoscope can accurately detect heart failure with reduced ejection fraction (HFrEF), atrial fibrillation, and valvular heart disease, according to a prospective multicentre study presented at the ESC Congress 2025.10
The AI stethoscope demonstrated high specificity (>93%) for detecting at least moderate valvular heart disease at the pulmonic position >93 %
Heart failure, atrial fibrillation, and valvular heart disease are all frequently diagnosed at advanced stages, often following emergency hospital admission, despite being conditions where earlier intervention is associated with improved outcomes. Therefore, researchers sought to determine if the use of digital stethoscopes augmented with AI has the potential to improve early detection of these conditions during routine clinical examinations.
In this observational, multicentre study, 1,378 adult patients undergoing transthoracic echocardiography at three UK centres were prospectively recruited. Each patient received a 15-second examination with the AI-enabled stethoscope, which simultaneously captured single-lead ECG and phonocardiogram waveforms from four auscultation positions (aortic, pulmonary, tricuspid, and mitral). These were analysed using AI algorithms developed for the detection of HFrEF, atrial fibrillation, and structural murmurs.
For HFrEF, defined as reduced LVEF ≤40%, the AI stethoscope achieved an area under the curve of 0.87 (95% CI: 0.84–0.90), with sensitivity of 83% and specificity of 76%.
For moderate or severe aortic stenosis, performance was also robust, with an area under the curve of 0.81 (95% CI: 0.76–0.86), sensitivity of 61%, and specificity of 85%.
The AI stethoscope demonstrated high specificity (>93%) for detecting at least moderate valvular heart disease at the pulmonic position, and detection of atrial fibrillation demonstrated a sensitivity of 84% and specificity of 93%.
These results indicate that an AI-enabled stethoscope can provide accurate detection of HFrEF, atrial fibrillation, and clinically significant aortic stenosis in routine settings. Integration into primary care could support earlier diagnosis, streamlined workflows, and timely initiation of treatment, with potential to reduce late presentations and associated complications.
References
1. Williams B et al. BaxHTN - efficacy and safety of the aldosterone synthase inhibitor baxdrostat in patients with uncontrolled or resistant hypertension. ESC Congress, 29 August-1 September, 2025.
2. Ibanez B. REBOOT-CNIC: betablockers after infarction with LVEF greater than 40%. ESC Congress, 29 August-1 September, 2025.
3. Atar D et al. BETAMI-DANBLOCK trial: randomised discontinuation of beta-blockers after myocardial infarction. ESC Congress, 29 August-1 September, 2025.
4. Hofmann R et al. Helicobacter pylori screening after acute myocardial
5. Bergmark B et al. Olezarsen in patients with hypertriglyceridemia at high cardiovascular risk: the ESSENCE-TIMI 73b trial. ESC Congress, 29 August-1 September, 2025.
6. Jons C, Bndgaard H. Increasing potassium levels improve outcomes in patients at high risk of ventricular arrhythmia. ESC Congress, 29 August-1 September, 2025.
7. Desai M. ODYSSEY-HCM: mavacamten in nHCM. ESC Congress, 29 August-1 September, 2025.
8. Berg D et al. Evidence appears supportive for the initiation of SGLT2 inhibitors in patients hospitalised for heart failure. ESC Congress, 29 August-1 September, 2025.
9. Anders Jeppsson et al. TACSI: dual or single antiplatelet therapy after CABG in patients with acute coronary syndrome. ESC Congress, 29 August-1 September, 2025.
10. Bachtiger P et al. Quick and easy multi-pathology cardiovascular disease detection with an artificial intelligence-enabled stethoscope: multi-centre prospective validation study in secondary care. ESC Congress, 29 August-1 September, 2025.
What’s New in Heart Failure? Highlights and Insights from ESC 2025
Author: *Han Naung Tun1,2
1. Geisel School of Medicine at Dartmouth College, Hanover, New Hampshire, USA
2. Department of Medical Science, Northeastern University, Bouvé College of Clinical and Health Science, Boston, Massachusetts, USA *Correspondence to Han.Naung.Tun@dartmouth.edu
Disclosure: The author has declared no conflicts of interest.
NEW late breaking trials in heart failure (HF) continue to refine therapy in patients with heart failure with reduced ejection fraction (HFrEF) and post-myocardial infarction (MI). DIGIT-HF,1 BETAMI-DANBLOCK,2 REBOOT-CNIC,3 VICTOR,4 and DAPA ACT HF-TIMI 685 are some studies presenting novel evidence on pharmacological therapy optimisation, including digitoxin, β-blockers, vericiguat, and sodium glucose co-transporter-2 (SGLT2) inhibitors. These studies highlight the strategic use of traditional and innovative therapies, taking patient-specific traits, comorbidities, and time of intervention into account. Interpretation of these studies proves critical for optimisation of benefits and guiding patient-specific HF management.
DIGITOXIN
AS ADD-ON THERAPY IN HEART FAILURE WITH REDUCED EJECTION FRACTION: INSIGHTS FROM DIGIT-HF
The DIGIT-HF trial1 demonstrated that digoxin lowered hospitalisation for HF, but not mortality. As a result of this, a Class 2b recommendation was included in the 2022 USA guidelines for HF for symptomatic patients with HFrEF, despite being on guideline-directed medical therapy. This refers to treatments recommended by major HF guidelines to improve survival, reduce hospitalisations, and relieve symptoms. These typically include angiotensinconverting enzyme inhibitors, angiotensin II receptor blockers or angiotensin receptorneprilysin inhibitors (ARNI), β-blockers, mineralocorticoid receptor antagonists, SGLT2 inhibitors, and device therapy when
indicated. The DIGIT-HF trial randomised digitoxin (0.07 mg/day, dose titrated for serum levels 8–18 ng/mL) versus placebo in 1,212 patients with chronic HF, with a left ventricular EF <40%. Individuals were mainly New York Heart Association (NYHA) Class III, and most had optimal therapy: β-blocker in 93%, mineralocorticoid receptor antagonist in 76%, ARNI in 40%, SGLT2 inhibitor in 20%, and implantable cardioverter defibrillator in 64%.1
The all-cause mortality or hospitalisation for HF endpoint was reached at a median follow-up of approximately 40 months in 39.5% of those treated with digitoxin compared to 44.1% in the placebo arm (P=0.03). Individual component effects favoured outcomes but did not reach statistical significance. Gender- or outcome-component inconsistency did not
exist, as opposed to digitoxin.1 The sideeffects were more frequent with digitoxin (4.7% versus 2.8%), primarily ventricular arrhythmias (approximately equal to 3%). Interestingly, it is preferred for use in patients with renal disease because it is not concentrated by enterohepatic clearance.
β-BLOCKERS AFTER MYOCARDIAL INFARCTION WITHOUT HEART FAILURE: INSIGHTS FROM BETAMIDANBLOCK AND REBOOT-CNIC
Even ‘old drugs’ like digitoxin can add meaningful benefit in modern HFrEF care
Further trial interpretation is limited as the DIGIT-HF trial was stopped early when funds ran out, and it included only 55% of target population. Fewer events than expected and later addition of ARNI and SGLT2 inhibitors may have diluted intergroup contrasts. Event curves diverged early, but became superimposed in long-term follow-up, and this is best explained by fewer late events. This study stated that digitoxin lowered the composite endpoint in advanced HFrEF by a modest amount, thus endorsing future potential adjuvant use in patients not optimally controlled by guideline-directed medical therapy. This trial highlights that even ‘old drugs’ like digitoxin can add meaningful benefit in modern HFrEF care, and I am excited to see data from the upcoming DECISION trial on digoxin.6
Two large contemporary trials provided new data about the long-debated post-MI β-blocker role in the context of preserved or mildly reduced ejection fraction (EF). The BETAMI-DANBLOCK trial,2 a collaborative study of Norwegian and Danish centres recruiting 5,574 patients (mean age 63; 21% females), found that β-blocker therapy decreased the composite of death, MI, revascularisation, stroke, HF, or arrhythmias at a median of 3.5 years (14.2% versus 16.3%; HR: 0.85; 95% CI: 0.75–0.98). Benefit was principally due to fewer repeated MIs with a suggestion of a larger effect in subjects with mildly impaired EF (40–49%).2
In comparison with the larger REBOOTCNIC trial3 of 8,438 patients with acute coronary syndromes (mean age: 61 years; 19% women) which was randomised in Spain and Italy and found no overall benefit in outcomes at a median of 3.7 years (22.5% versus 21.7%; HR: 1.04; 95% CI: 0.89–1.22), subgroup results did suggest the potential for harm in women with normal EF, and highlighted the relevance of sex-adjusted analyses.3
Altogether, these trials highlight that standard long-term β-blockade therapy is probably not useful in all patients
with a normal EF post-MI.2,3 Instead, the suggestion of benefit in those with mildly impaired EF and the troublesome sex differences require more fine-grained therapy tailored at the patient level.
The primary endpoint was a composite of cardiovascular death or HF hospitalisation, which occurred in 18.0% of the vericiguat group versus 19.1% in the placebo group
INSIGHTS FROM THE VICTOR TRIAL AND POOL ANALYSES OF VICTORIA AND VICTOR
Vericiguat, an oral soluble guanylate cyclase stimulator, restores impaired nitric oxide signalling, a hallmark of HFrEF. While the VICTORIA trial established its benefit in patients with recent worsening
HF, the VICTOR trial explored its role in a broader ambulatory population without recent HF hospitalisation.4
This Phase III, double-blind, placebocontrolled study enrolled 6,105 adults with HFrEF (left ventricular EF ≤40%, NYHA Class II–IV) across 616 centres in 42 countries.4 Patients were on optimised guidelinedirected medical therapy and had no recent HF decompensation. Participants were randomised 1:1 to vericiguat (target dose 10 mg) or placebo, with a median followup of 18.5 months. The primary endpoint was a composite of cardiovascular death or HF hospitalisation, which occurred in 18.0% of the vericiguat group versus 19.1% in the placebo group (HR: 0.93; 95% CI: 0.83–1.04; P=0.22). While HF hospitalisation was not significantly reduced (11.4% versus 11.9%; HR: 0.95), cardiovascular death was lower with vericiguat (9.6% versus 11.3%; HR: 0.83), translating into a reduction in all-cause mortality (12.3% versus 14.4%; HR: 0.84). Benefits were consistent across prespecified subgroups, and serious adverse events were similar between groups. Additional pooled analyses of VICTORIA and VICTOR, as well as prespecified mortality outcomes, were presented at the ESC Congress 2025.7
EARLY SODIUM-GLUCOSE CO-TRANSPORTER-2 INHIBITOR THERAPY IN HOSPITALISED HEART FAILURE: DAPA ACT HF-TIMI 68 INSIGHTS
Hospitalisation for HF continues to be a significant cardiovascular burden with high short- and long-term morbidity and mortality. Although disease-modifying therapies are the norm in chronic HF, the issue of safely initiating therapy during hospitalisation has been underexamined, with particular reference to the SGLT2 inhibitors. DAPA ACT HF-TIMI 685 attempted to fill the void with a trial of whether early in-hospital initiation of dapagliflozin would decrease cardiovascular death or worsening HF in individuals hospitalised for HF.
These trials highlight that standard long-term β-blockade therapy is probably not useful in all patients with a normal EF post-MI
This double-blind, placebo-controlled study enrolled 2,401 patients across 210 sites in the USA, Canada, and Europe. Participants were randomised within a median of 3.6 days after admission to either dapagliflozin 10 mg daily or placebo. Over the first 2 months, the primary endpoint occurred in
References
1. Bavendiek U et al.; DIGIT-HF Study Group. Digitoxin in patients with heart failure and reduced ejection fraction.
N Engl J Med. 2025;DOI:10.1056/ NEJMoa2415471.
2. Munkhaugen J et al.; BETAMI–DANBLOCK Investigators. Betablockers after myocardial infarction in patients without heart failure. N Engl J Med. 2025;DOI:10.1056/ NEJMoa2505985.
3. Ibanez B et al.; REBOOT-CNIC Investigators. Beta-blockers after
10.9% of patients treated with dapagliflozin versus 12.7% with placebo (HR: 0.86; 95% CI: 0.68–1.08; P=0.20). Cardiovascular death and worsening HF individually also trended favourably, and all-cause mortality was numerically lower with dapagliflozin (3.0% versus 4.5%; HR: 0.66).5 Safety signals were reassuring, with only modest differences in hypotension and renal events.5 From a clinical viewpoint, the results support a proactive approach: why delay therapies that could significantly decrease early risk until the time of hospital discharge? Hospitalisation could very well turn out to be the best opportunity to finetune HF care.
SUMMARY AND TAKEAWAYS
Digitoxin reduces hospitalisations modestly in advanced HFrEF, and may be added to standard therapy. New trials in post-MI care and in HF provide valuable lessons in patient prognoses. Long-term β-blockade in preserved EF patients postMI is not helpful in all cases, but patients with a mildly depressed EF may benefit, with sex-related responses. Vericiguat reduces cardiovascular death modestly and is well tolerated, and early start of SGLT2 inhibitors, like dapagliflozin, in HF hospitalisation is safe and reduces early risk, highlighting proactive therapy. These studies illustrate the need for proper selection of therapy, early therapy, and use of established and novel agents to maximise benefit of therapies for HF.
myocardial infarction without reduced ejection fraction. N Engl J Med. 2025;DOI:10.1056/NEJMoa2504735.
4. Butler J et al. Vericiguat and mortality in heart failure and reduced ejection fraction: the VICTOR trial. Eur Heart J. 2025;DOI:10.1093/eurheartj/ehaf655.
5. Berg DD et al.; DAPA ACT HFTIMI 68 Trial Committees and Investigators. Dapagliflozin in patients hospitalized for heart failure: primary results of the DAPA ACT HF-TIMI 68 randomized clinical trial and meta-analysis of sodiumglucose cotransporter-2 inhibitors
in patients hospitalized for heart failure. Circulation. 2025;DOI:10.1161/ CIRCULATIONAHA.125.076575.
6. van Veldhuisen DJ et al. Efficacy and safety of low-dose digoxin in patients with heart failure. Rationale and design of the DECISION trial. Eur J Heart Fail. 2024;26(10):2223-30.
7. Rossello X et al. β blockers after myocardial infarction with mildly reduced ejection fraction: an individual patient data meta-analysis of randomized controlled trials. Lancet. 2025;DOI:10.1016/S01406736(25)01592-2.
ESC Congress Update on ESC/EACTS 2025 Valvular Heart Disease Guidelines: Establishing the Present and Designing the Future for the Therapy of the Aortic Valve
AT THIS YEAR’S European Society of Cardiology (ESC) Congress held in Madrid, Spain, more than 40,000 participants shared updates over a full 4-day programme. Several new guidelines were presented, aiming to provide timely recommendations that assist clinical decision-making in everyday practice. In this context, the much-awaited update on the guidelines for the management of valvular heart disease was announced,1 which was jointly endorsed by ESC and the European Association for Cardiothoracic Surgery (EACTS), and included several updates from older versions, as well as a total of 28 new recommendations. This feature aims to summarise the most important updates in the aortic valve interventions.
AORTIC STENOSIS UPDATES
The most discussed recommendation change in aortic stenosis (AS) intervention is the change of the age cut-off for performing transcatheter aortic valve implantation (TAVI), which has been reduced from 75 to 70 years old. Specifically, the guidelines provide a Class I recommendation with level of evidence A for performing TAVI in patients 70 years or older with tricuspid aortic valves, if the anatomy is suitable and transfemoral artery access is feasible.1 This update results from recent data comparing TAVI and surgery in lower-risk patients, which have increasingly included patients younger than 75 years old, such as the DEDICATE-DZHK6, NOTION-2,
and Evolut Low Risk study, where the mean age ranged from 72–74 years old.2-4 In the absence of randomised data in individuals younger than 70, the recommendation for surgery in these patients remains unchanged. The lowering of the age cutoff for TAVI reflects the increasing number of younger individuals being treated with TAVI. However, it is met with scepticism, especially considering that the longest, to date, follow-up for TAVI comes mostly from the NOTION trial 10-year followup.5 Although in this study, major clinical outcomes were not different at 10 years, while the risk of severe bioprosthetic structural valve deterioration was lower in TAVI, the long-term risk for bioprosthetic failure in TAVI is not extensively known, which could impact treatment selection,
especially in younger patients. Moreover, the clinical entity of the bicuspid valve is related to a lower level of recommendation for TAVI, and only high surgical risk patients with suitable anatomy (another point of ongoing debate) can be assigned to transcatheter therapy. As longer-term data and a more thorough understanding of bioprosthetic valve degeneration in TAVI patients are needed, this updated recommendation is an important step towards reflecting and implementing trial findings in clinical practice, and allows for more comprehensive discussions and individualised care within heart team decision-making.
The lowering of the age cut-off for TAVI reflects the increasing number of younger individuals being treated with TAVI
Another important update concerns interventions on patients with asymptomatic severe AS, where guidelines suggest that aortic intervention should be considered as an alternative to watchful waiting in patients at low procedural risk and with a left ventricular ejection fraction (LVEF) ≥50%, with a Class IIa recommendation. Randomised data
on early intervention are scarce and conflicting, with the EARLY-TAVR trial6 documenting a significant reduction of the primary endpoint (all-cause mortality, stroke, or unplanned hospitalisation associated with pre-emptive intervention), mostly driven by the large number of ‘watchful-waiting’ patients crossing to TAVI due to symptoms or adverse events at 6 months (22.6%). On the other hand, the EVoLVeD study7 reported no reduction of all-cause death or unplanned AS-related hospitalisation compared with clinical surveillance, despite being underpowered. Importantly, a meta-analysis of available randomised studies showed a significant reduction in rehospitalisation and stroke, but not mortality.8 Based on the aforementioned data, the provided Class IIa recommendation suggests early intervention as an alternative to
22.6 %
Mostly driven by the large number of watchful-waiting patients crossing to TAVI due to symptoms or adverse events at 6 months (22.6%)
The development of new, dedicated devices has been shown to mitigate this increased risk
close patient surveillance, which could be particularly attractive in situations where rigorous follow-up is not feasible, in order to avoid future events. However, considering the heterogeneity and low number of available randomised studies, further data that could support an increase in the level of recommendation for early intervention in this setting are necessary and awaited in the near future.
AORTIC REGURGITATION UPDATES
Significant insights have also been provided for aortic regurgitation (AR), where the guidelines provide a Class IIb recommendation for performing TAVI in symptomatic patients who are ineligible for surgery and have suitable anatomy. In the setting of AR, surgery remains the cornerstone of treatment. However, recent studies may support the use of TAVI, although the data are still early. As the guidelines note, selection of a
dedicated valve is more appropriate, considering the increased risk for valve migration and residual AR seen with nondedicated devices. The development of new, dedicated devices has been shown to mitigate this increased risk, as shown in the ALIGN-AR study.9 However, the authors note an increased new pacemaker implantation risk with dedicated devices (reaching 24%), which is an important consideration needing further aetiological clarification in future studies.
UPDATES REGARDING URGENT TRANSCATHETER AORTIC VALVE IMPLANTATION AND SEX DIFFERENCES
Finally, for the first time, urgent TAVI as well as sex differences have been discussed in the guidelines. Despite the fact that no specific recommendations are made, the guidelines note the use of TAVI in patients with AS-related cardiogenic shock, which
An increased new pacemaker implantation risk with dedicated devices (reaching 24%)
%
For the first time, urgent TAVI as well as sex differences have been discussed in the guidelines
has shown better results than balloon aortic valvuloplasty, which can be used as a bridge to more definitive treatment in decompensated AS. For AR, the guideline committee notes that surgery remains the standard, as only case reports have performed TAVI in acute AR. For females, the authors highlight the differences in both diagnosis (less and later referral of women to cardiology clinics and different cut-offs to define flow limitation) and intervention, particularly highlighting the results of the RHEIA trial, which showed that TAVI compared to surgery in female patients is superior in regard to the composite endpoint of death, stroke, or rehospitalisation at 1 year, mostly driven by reductions in rehospitalisation rates.10 Noting and discussing special phenotypes of valvular heart disease is of utmost importance for guiding clinical management, and the inclusion of such considerations in the new guidelines is certainly a step towards more individualised, evidencebased care.
References
1. Praz F et al.; ESC/EACTS Scientific Document Group. 2025 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2025;DOI:10.1093/eurheartj/ehaf194.
2. Blankenberg S et al.; DEDICATE-DZHK6 Trial Investigators. Transcatheter or surgical treatment of aorticvalve stenosis. N Engl J Med. 2024;390(17):1572-83.
3. Jørgensen TH et al.; NOTION-2 investigators. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45(37):3804-14.
CONCLUDING REMARKS
As 23 years have passed from the first TAVI, and whilst important knowledge has been gathered through the years, helping to tailor and improve the intervention, there are still several unknowns and gaps in knowledge in aortic interventions. The 2025 ESC/EACTS Guidelines on Valvular Heart Disease provide an important framework for guiding treatment in everyday practice, offering an updated perspective guided by the latest evidence. As research efforts continue in the coming years, the new guidelines act as the basis towards establishing a standard of care, advancing treatment options, and exploring new indications for less studied patient phenotypes that could further enhance patient outcomes in the future.
4. Popma JJ et al.; Evolut Low Risk Trial Investigators. Transcatheter aortic-valve replacement with a selfexpanding valve in low-risk patients. N Engl J Med. 2019;380(18):1706-15.
5. Thyregod HGH et al. Transcatheter or surgical aortic valve implantation: 10year outcomes of the NOTION trial. Eur Heart J. 2024;45(13):1116-24.
6. Généreux P et al.; EARLY TAVR Trial Investigators. Transcatheter aorticvalve replacement for asymptomatic severe aortic stenosis. N Engl J Med. 2025;392(3):217-27.
7. Loganath K et al.; EVOLVED investigators. Early intervention in patients with asymptomatic severe
aortic stenosis and myocardial fibrosis: the EVOLVED randomized clinical trial. JAMA. 2025;333(3):213-21.
8. Généreux P et al. Aortic valve replacement vs clinical surveillance in asymptomatic severe aortic stenosis. J Am Coll Cardiol. 2025;85(9):912-22.
9. Vahl TP et al. Transcatheter aortic valve implantation in patients with high-risk symptomatic native aortic regurgitation (ALIGN-AR): a prospective, multicentre, single-arm study. Lancet. 2024;403(10435):1451-9.
10. Tchetche D et al. Transcatheter vs. surgical aortic valve replacement in women: the RHEIA trial. Eur Heart J. 2025;46(22):2079-88.
New ESC Guidelines: Redefining Holistic Care in Cardiology
LANDMARK guideline updates and consensus statements were unveiled at the European Society of Cardiology (ESC) Congress 2025 in Madrid, Spain, reshaping the way cardiologists approach patient care. From myocarditis to mental health, dyslipidaemias, pregnancy, and valvular disease, the new recommendations share common themes: multimodality imaging, genetic insights, psychosocial factors, and patient-centred, multidisciplinary decision-making. Together, they mark a shift towards more precise, integrated, and holistic cardiovascular care.
MYOCARDITIS AND PERICARDITIS
The first European joint guidelines on myocarditis and pericarditis1 mark a significant step forward in unifying the management of these overlapping conditions. A new umbrella term, inflammatory myopericardial syndrome (IMPS), has been introduced to highlight their shared aetiologies and anatomical contiguity. The overlap is clinically important: up to 30% of patients with pericarditis show troponin elevation, indicating myocardial involvement, while cardiac MRI (CMR) in myocarditis often reveals pericardial effusion. Recognition of red flags, such as flu-like prodromes, ECG changes, and multimodality imaging findings, can aid risk stratification and help identify patients at higher risk of recurrence.
The guidelines introduce presentationdriven flowcharts, tailored to chest pain, arrhythmias, or heart failure, providing stepby-step pathways from diagnosis through therapy. A paradigm shift is evident in the reliance on multimodality imaging: ECG and echocardiography remain cornerstones, but CMR has emerged as the definitive, non-invasive tool to confirm myocarditis, distinguishing between reversible and irreversible changes while identifying inflammation, oedema, and fibrosis. By
contrast, endomyocardial biopsy now has a narrower role, reserved for intermediateto high-risk patients where histology may guide treatment decisions.
Genetics is increasingly recognised as a determinant of disease trajectory, whether involving a single episode, recurrence, or multiple relapses. This supports selective genetic screening, particularly in patients with autoimmune or inflammatory overlap. Management has become more tailored: personalised exercise recommendations replace blanket restrictions, advocating cessation of training or exertion for at least 1 month until remission in both athletes and non-athletes.
Therapeutic strategies are similarly nuanced. Anti-inflammatory therapy is first-line in uncomplicated cases, escalating to aetiology-directed treatments in more complex disease, while immunosuppressants are not routinely
CMR has emerged as the definitive, non-invasive tool to confirm myocarditis
recommended in acute myocarditis with preserved ejection fraction. For pericarditis and IMPS, combination therapy with corticosteroids, non-steroidal antiinflammatory drugs, and colchicine is encouraged before progressing to biologics. Anti-IL-1 agents are reserved for refractory inflammatory phenotypes.
At the heart of the recommendations is the IMPS multidisciplinary team, bringing together expertise in imaging, surgery, pathology, and clinical management to optimise outcomes for this heterogeneous and often challenging group of patients.
DYSLIPIDAEMIAS
The 2025 ESC/European Atherosclerosis Society (EAS) updated guidelines on dyslipidaemias2 introduce important updates in cardiovascular risk assessment and lipid-lowering strategies. For risk estimation, the traditional Systematic COronary Risk Evaluation (SCORE) system has been replaced by SCORE2, which calculates 10-year risk of both fatal and non-fatal atherosclerotic cardiovascular
disease in apparently healthy individuals. Risk assessment is further refined by incorporating subclinical coronary atherosclerosis as a modifier, in addition to elevated coronary calcium scores. A new set of clinical risk modifiers, including demographic and clinical factors alongside biomarkers such as elevated high-sensitivity C-reactive protein and lipoprotein(a), has also been introduced. Notably, lipoprotein(a) >50 mg/dL is now recognised as a cardiovascular risk-enhancing factor in all adults.
Treatment targets for low-density lipoprotein cholesterol (LDL-C) remain unchanged, but a new 'extreme risk' category has been added, with a recommended target LDL-C threshold of <1.0 mmol/L. In terms of therapy, statins remain first-line, but new agents expand the treatment landscape. Bempedoic acid is recommended for patients unable to tolerate statins, while evinacumab is highlighted for those with homozygous familial hypercholesterolaemia refractory to standard therapies. Lipid-lowering therapy should be intensified during acute coronary syndrome hospitalisation: for patients
already on therapy, treatment is escalated; for treatment-naïve patients, initiation with high-intensity statin plus ezetimibe is advised.
For hypertriglyceridaemia, high-dose icosapent ethyl (rather than general polyunsaturated fatty acid supplementation) is now specifically recommended alongside statins in high-risk patients. Volanesorsen may be considered for severe familial chylomicronaemia syndrome. The guidelines also broaden statin use to special populations, recommending therapy for all people with HIV aged ≥40 years, regardless of LDL-C, and for patients with cancer at high risk of chemotherapy-related cardiotoxicity. Finally, the use of dietary supplements lacking proven LDL-lowering efficacy is discouraged.
CARDIOVASCULAR DISEASE AND PREGNANCY
The 2025 ESC guidelines on cardiovascular disease (CVD) and pregnancy3 reflect an important shift in focus from managing CVD during pregnancy only, to addressing women’s health from preconception and pregnancy through delivery, postpartum,
and long-term outcomes. Central to the recommendations is the Pregnancy Heart Team, which ensures coordinated care and shared decision-making throughout this journey.
Risk stratification remains key, with the modified WHO (mWHO) 2.0 classification providing a more refined framework. Categories have been expanded to include arrhythmias and cardiomyopathies, with more nuanced risk estimates. Women in mWHO II–III and IV categories require Pregnancy Heart Team involvement. Notably, Class IV is no longer an absolute contraindication to pregnancy; instead, expert counselling and recognition of women’s autonomy are emphasised.
Delivery planning is clarified, with vaginal delivery recommended for most women with CVD, supported by stronger evidence than in prior guidelines. A new flowchart outlines the management of urgent delivery in women receiving anticoagulation. Beyond pregnancy, a dedicated chapter highlights the need for long-term cardiovascular risk assessment in women with adverse pregnancy outcomes, together with lifestyle counselling to reduce future risk.
Several clinical management updates are included. Pre-pregnancy aortic root surgery is now recommended based not only on clinical history but also genetic variants and patient preference. Genetic counselling is also advised in peripartum cardiomyopathy. Women with pulmonary arterial hypertension require clear contraceptive advice, as several targeted therapies, including endothelin receptor antagonists, riociguat, and selexipag, are contraindicated in pregnancy. In suspected postpartum venous thromboembolism, diagnostic imaging should not be withheld, including CT scans.
Specific recommendations address cardiomyopathies and arrhythmias, including the use of β-blockers in long QT syndrome. Practical clinical scenarios are also embedded: for example, chest pain in pregnancy should be investigated as in non-pregnant patients, but with heightened awareness of pregnancy-specific causes such as pulmonary embolism, acute aortic syndromes, and spontaneous coronary artery dissection. In cardiac arrest, standard management also applies, supplemented by pregnancy-specific measures such as left uterine displacement, intravenous access above the diaphragm, and reassurance that no drugs should be withheld due to teratogenicity concerns.
CARDIOVASCULAR DISEASE AND MENTAL HEALTH
The first ESC Clinical Consensus Statement on mental health and cardiovascular disease4 represents a landmark, developed with the same rigorous process as formal guidelines and incorporating both patient perspectives and clinical case scenarios. It recognises mental health as a continuum, from optimal wellbeing, through conditions and disorders, to severe mental illness, and emphasises the multidirectional links between CVD and mental health. People with depression are 50% more likely to experience myocardial infarction, while up to one in three patients with established CVD live with anxiety, depression, or posttraumatic stress disorder, particularly women and younger patients. When CVD
and mental health conditions co-exist, the risk of adverse outcomes and mortality rises sharply. Psychosocial stress is now also recognised as an independent risk factor, and support for informal caregivers is also highlighted.
To address these challenges, the statement calls for Psycho-Cardio teams embedded in both hospital and outpatient cardiovascular services, integrating mental health professionals with primary and social care. A practical framework, the list of ACTIVE principles (Acknowledge, Check, Tools, Implement, Venture, Evaluate), is recommended to support mental health within cardiovascular practice.
50 %
People with depression are 50% more likely to experience myocardial infarction, while up to one in three patients with established CVD live with anxiety, depression, or post-traumatic stress disorder
Routine screening is advised, beginning with a brief two-item questionnaire and followed, if positive, by validated tools such as the General Anxiety Disorder-7 (GAD7) scale or Patient Health Questionnaire-9 (PHQ-9). Screening should occur after a new diagnosis or cardiovascular event, at annual follow-up, and whenever prompted by clinical judgement.
Management follows a stepped care model. Non-pharmacological approaches form the foundation, including improved communication, psycho-education, social prescribing, lifestyle interventions, and psychological therapies such as cognitive behavioural therapy or exposure therapy. Pharmacological treatment is reserved for moderate-to-severe cases and must be guided by mental health specialists. Overuse of anxiolytics and sedatives is discouraged; antidepressants may be
considered for depression and anxiety, but in heart failure are reserved for severe depression only.
Finally, special attention is paid to severe mental illness, often underdiagnosed and stigmatised, but the treatment of which reduces CVD risk. Given the metabolic and arrhythmic side effects of many antipsychotics, recommendations include monitoring cholesterol, glucose, and QTc intervals, with clear thresholds for discontinuation. Finally, sex, gender, and age-specific factors are addressed, acknowledging higher risks in women, challenges for transgender patients, and the burden of mental health conditions in older populations with comorbidities.
VALVULAR HEART DISEASE
The 2025 ESC/European Association for Cardio-Thoracic Surgery (EACTS) Guidelines for the management of valvular heart disease (VHD),5 developed by a 25-member task force including two patients with VHD, emphasise a patientcentred, shared decision-making approach underpinned by regional Heart Valve Networks and dedicated Heart Teams. These teams, made up of cardiologists, surgeons, interventionalists, and imaging specialists, ensure that complex cases are managed in high-volume expert centres, reflecting the robust relationship between procedural volume and outcomes. Clear communication with patients, referring cardiologists, and general practitioners is central to this model of care.
A major theme is the central role of multimodality imaging in diagnosis, risk stratification, and procedural planning. Transthoracic and transoesophageal
References
1. Schulz-Menger J et al. 2025 ESC Guidelines for the management of myocarditis and pericarditis. Eur Heart J. 2025;DOI:10.1093/eurheartj/ ehaf192.
2. Mach F et al. 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2025;DOI:10.1093/eurheartj/ ehaf190.
Across all lesions, management now balances symptom burden, cardiac damage, procedural risk, and lifetime planning
echocardiography, cardiac CT, and CMR provide complementary insights into valve anatomy, left ventricular (LV) volumes and function, and aortic dimensions. CT is now particularly emphasised for assessing coronary artery disease ahead of intervention.
Imaging directly informs treatment strategy: in aortic regurgitation, LV volumes and aortic root geometry guide surgical repair or replacement; in aortic stenosis, an integrated assessment of gradients, valve area, calcification, and LV function defines severity and determines suitability for surgery or transcatheter aortic valve implantation; and in mitral and tricuspid disease, 3D echocardiography and CMR enhance quantification, mechanism identification, and procedural planning.
The guidelines also extend recommendations to complex and subspecialty populations, including patients with cancer, prior radiation, cardiogenic shock, acute heart failure, and mixed valvular disease, alongside sexspecific considerations. Across all lesions, management now balances symptom burden, cardiac damage, procedural risk, and lifetime planning with multimodality imaging and structured Heart Teams at the centre of contemporary VHD care.
3. De Backer J et al. 2025 ESC Guidelines for the management of cardiovascular disease and pregnancy. Eur Heart J. 2025;DOI:10.1093/eurheartj/ehaf193.
4. Bueno H et al. 2025 ESC Clinical Consensus Statement on mental health and cardiovascular disease. Eur Heart J. 2025;DOI:10.1093/eurheartj/ ehaf191.
5. Praz F et al. 2025 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2025;DOI:10.1093/eurheartj/ehaf194.
Aficamten versus Metoprolol in Obstructive Hypertrophic Cardiomyopathy: Recent Analyses of the MAPLE-HCM Trial
These poster presentations took place between 29th August–1st September 2025 as part of the European Society of Cardiology (ESC) Congress in conjunction with the World Congress of Cardiology (WCC) held in Madrid, Spain
Support: The publication of this article was supported via a hands-off educational grant from Cytokinetics.
Presenters: Pablo Garcia-Pavia,1,2 Sheila Hegde3,4
1. Inherited Cardiac Diseases and Heart Failure Unit, Department of Cardiology, Hospital Universitario Puerta de Hierro, Madrid, Spain
2. Centro Nacional de Investigaciones Cardiovasculares (CNIC), Madrid, Spain
3. University of Texas, Southwestern Medical Centre, Dallas, USA
4. Brigham and Women's Hospital, Boston, Massachusetts, USA
Disclosure: Garcia-Pavia has received speaker fees from BMS; and consulting fees from Alexion, BioMarin, BMS, Cytokinetics, Edgewise Therapeutics, Lexeo Therapeutics, and Rocket Pharmaceuticals. Hegde has received advisory board fees from Cytokinetics; and fees for core lab services from Cytokinetics and BMS, with payment to the institution.
Acknowledgements: Writing assistance was provided by Rachel Danks, RSD Medical Communications Ltd, Lydbrook, UK.
Disclaimer: Aficamten is an investigational agent and is not approved for use by the US Food & Drug Administration (FDA) or European Medicines Agency (EMA).
This article is based on presentations of a late breaking clinical trial at the European Society of Cardiology (ESC) Congress in conjunction with the World Congress of Cardiology (WCC), which took place between 29th August–1st September 2025 in Madrid, Spain. The presentations described analyses of MAPLE-HCM, a Phase III, headto-head, comparative efficacy and safety study evaluating aficamten versus metoprolol as monotherapy in adults with symptomatic obstructive hypertrophic cardiomyopathy
(oHCM). Pablo Garcia-Pavia, Hospital Universitario Puerta de Hierro, Madrid; and Centro Nacional de Investigaciones Cardiovasculares (CNIC), Madrid, Spain, presented the primary and secondary outcomes of MAPLE-HCM, showing that 24 weeks of aficamten led to significant and clinically meaningful improvements in exercise capacity, symptoms, left ventricular outflow tract (LVOT) gradient after the Valsalva manoeuvre, N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels, and structural cardiac remodelling. By contrast, metoprolol led to a reduction in the exercise capacity of these patients and, despite demonstrating on-target haemodynamic effects, failed to reduce LVOT gradients either at rest or following the Valsalva manoeuvre. Sheila Hegde, University of Texas, Southwestern Medical Centre, Dallas, USA; and Brigham and Women's Hospital, Boston, Massachusetts, USA, presented further substantial improvements in multiple measures of cardiac structure and function with aficamten versus metoprolol. Overall, MAPLE-HCM data highlight the superior efficacy of aficamten over metoprolol, while maintaining an acceptable safety profile. These results strengthen the positioning of aficamten as monotherapy or potential first-line therapy for patients with symptomatic oHCM.
Background
oHCM is characterised by a hypercontractile left ventricle, myocardial hypertrophy, and LVOT obstruction, resulting in limiting symptoms and reduced exercise capacity.1,2
Aficamten, an investigational, next-inclass cardiac myosin inhibitor, has been developed to target the underlying pathophysiology of oHCM by reducing myocardial hypercontractility.2,3 Clinical studies have demonstrated that, when administered to patients with symptomatic oHCM despite standard-of-care therapy, aficamten has consistently been associated with an improvement in exercise capacity,2,3 a reduction in symptom burden,4 a normalisation of LVOT gradients,3,5 a decreased eligibility for septal reduction therapy,3 improvements in cardiac biomarkers,6 and favourable effects on cardiac structure and function.5,7
By contrast, β-blockers, despite having served as the cornerstone of therapy for symptomatic oHCM for almost 6 decades, are supported by limited high-quality evidence. The most recent ESC (2023)8 and American College of Cardiology (ACC)/ American Heart Association (AHA; 2024)9 guidelines continue to recommend nonvasodilating β-blockers as first-line therapy, despite the absence of robust comparative trials.
The MAPLE-HCM trial was conducted to evaluate the efficacy and safety of aficamten as monotherapy in comparison with metoprolol in patients with symptomatic oHCM.10,11
MAPLE-HCM: Overview and Key Findings
Study Design
MAPLE-HCM was an international, doubleblind, double-dummy Phase III trial (Figure 1). Participants, aged 18–85 years with newly diagnosed or chronic oHCM, were randomly assigned to receive aficamten plus placebo or metoprolol plus placebo.10,11 Doses of metoprolol were uptitrated in 50 mg increments from 50 to 200 mg, while aficamten doses were titrated in 5 mg increments from 5 to 20 mg, guided by echocardiographic and clinical parameters.10,11 Patients on pre-existing therapy underwent a 2-week washout prior to screening.10,11
The primary endpoint was the change from baseline to Week 24 in peak O2 uptake, as assessed during exercise testing. Secondary endpoints included an improvement from baseline to Week 24 of at least one New York Heart Association (NYHA) functional class, and a change
*Metoprolol doses were uptitrated in 50 mg increments from 50–200 mg. Aficamten doses were uptitrated in 5 mg increments from 5–20 mg. Dose adjustment was based on site echo and vital signs.
Adapted from Garcia-Pavia P et al.10
CPET: cardiopulmonary exercise testing; D: day; KCCQ: Kansas City Cardiomyopathy Questionnaire; KCCQ-CSS: Kansas City Cardiomyopathy Questionnaire Clinical Summary Score; LVEF: left ventricular ejection fraction; LVOT: left ventricular outflow tract; NT-proBNP: N-terminal pro-B-type natriuretic peptide; NYHA: New York Heart Association; oHCM: obstructive hypertrophic cardiomyopathy; pVO₂: peak oxygen uptake; SoC: standard of care; SV: screening visit; W: week.
from baseline to Week 24 in the Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS), NT-proBNP level, LVOT gradient after the Valsalva manoeuvre, and left ventricular mass index.10,11 Safety endpoints included a left ventricular ejection fraction (LVEF) <50%.11
Baseline Characteristics
In total, 175 patients were randomised.11 Overall, baseline characteristics reflected a milder phenotype compared with prior cardiac myosin inhibitor studies, including SEQUOIA-HCM.4 Hypertension was more prevalent in the aficamten group compared with metoprolol (61.4% versus 37.9% of patients, respectively).10
The majority of participants tolerated higher doses of the study medications, with 63% of patients randomised to metoprolol achieving doses of 150–200 mg, while 76% of those
assigned to aficamten were maintained on doses of 15–20 mg.11 Haemodynamic effects reflected the expected pharmacology of the treatments, with a decrease in heart rate and systolic blood pressure of approximately 6 bpm and approximately 6 mmHg, respectively, by Week 24 among patients receiving metoprolol. No significant change in heart rate and a modest increase in systolic blood pressure (approximately 5 mmHg) was observed with aficamten.10
Primary Endpoint
Over the 24-week treatment period, patients treated with metoprolol experienced a reduction in peak O2 uptake of 1.2 (95% CI: 0.8–1.7) mL/kg/min, compared with a mean increase of 1.1 (95% CI: 0.5–1.7) mL/kg/min among patients treated with aficamten.10,11 The least squares mean (LSM) difference between groups was 2.3 (95% CI: 1.5–3.1) mL/kg/min, which
Figure 1: MAPLE-HCM study design.
Mean (95% CI) Resting LVOT Gradient (mmHg)
2: Secondary endpoints: change in left ventricular outflow tract obstruction at Week 24.
Resting LVOT gradient Valsalva LVOT gradient
The grey dashed lines indicate the thresholds for resting (30 mmHg, left panel) and post-Valsalva (50 mmHg, right panel) LVOT gradient for oHCM.
Adapted from Garcia-Pavia P et al.10
BL: baseline; LSM: least squares mean; LVOT: left ventricular outflow tract; oHCM: obstructive hypertrophic cardiomyopathy.
exceeds the clinically relevant threshold of 1.0 mL/kg/min commonly applied in practice.10,11 This benefit was consistent across all pre-specified subgroups.10,11
Secondary Endpoints
Patients receiving aficamten showed greater improvements in all secondary endpoints (p<0.01 for all) except for left ventricular mass index.11 At Week 24, a total of 51% of patients in the aficamten arm demonstrated an improvement by at least one NYHA class compared with 26% in the metoprolol group (p<0.001).10,11 Moreover, 40% of patients in the aficamten group were asymptomatic (NYHA Class I) by study end, compared with only 9% in the metoprolol arm.10 Quality of life, as assessed by KCCQ-CSS, improved in both treatment groups, but the magnitude of benefit (LSM difference) was seven points greater with aficamten by Week 24 versus metoprolol (p=0.002).10
Haemodynamic differences between the two groups were particularly striking. No
improvement in resting or Valsalva LVOT gradients was observed with metoprolol, despite a significant reduction in heart rate and blood pressure.10 In contrast, aficamten produced a rapid and profound reduction in LVOT gradients, with mean values falling below the range generally associated with relief of obstruction (clinically relevant threshold) by the study end (Figure 2).10,11
Favourable changes in biomarkers and structural indices were also observed. At Week 24, aficamten significantly decreased the NT-proBNP level, while this parameter remained elevated in the metoprolol group (81% reduction at Week 24 versus metoprolol; p<0.0001).10 Similar findings were reported for left atrial volume index, with an LSM difference of 7 mL/m2 in favour of aficamten versus metoprolol (p<0.0001) at Week 24.
Safety
Treatment with aficamten was well tolerated. Serious adverse events occurred in seven patients (8%) on aficamten and six patients (7%) receiving metoprolol. Three
Figure
patients discontinued metoprolol due to adverse events, compared with one patient in the aficamten group. Dose reduction was required in 26 patients on metoprolol and in only four patients on aficamten.10,11 By Week 24, 10 patients were unable to tolerate metoprolol, and one patient was not able to tolerate aficamten.
Consistent with its mechanism of action, aficamten was associated with a modest reduction in LVEF (LSM betweengroup difference of −4.2 percentage points [95% CI: −5.3 to -3.1] at Week 24).11 However, values remained within the normal range for almost all participants; only one aficamten-treated patient had an ejection fraction <50%, and this individual remained asymptomatic without signs of heart failure.10,11
In summary, aficamten demonstrated superiority over metoprolol for the primary and multiple secondary endpoints, with clinically meaningful improvements
in exercise capacity, symptoms, haemodynamics, and biomarkers, while maintaining an acceptable safety profile.10,11
Effect of Aficamten Compared with Metoprolol on Cardiac Structure and Function in Symptomatic Obstructive Hypertrophic Cardiomyopathy
A separate pre-specified analysis, presented by Hegde, further evaluated cardiac structural and functional parameters among patients in the MAPLE-HCM trial.
As described by Garcia-Pavia, resting and Valsalva LVOT gradients declined significantly with aficamten, while remaining unchanged with metoprolol. LVEF decreased modestly in the aficamten group (approximately 5%) but remained well above the normal threshold (≥50%), reflecting a reduction in hypercontractility without the development of systolic dysfunction.10-12 In addition, patients
Treatment-corrected difference (95% CI) is adjusted for baseline echo measure, treatment, exercise mode (bicycle vs treadmill), and stratification by time of diagnosis (recent [Group 1] vs chronic [Group 2]) with corresponding p values at 24 weeks.
Horizontal dashed lines represent thresholds for gradients and normal values for LVEF.
Adapted from Hegde SM et al.12
GCS: global circumferential strain; GLS: global longitudinal strain; LV: left ventricular; LVEF: left ventricular ejection fraction; vs: versus.
Figure 3: Systolic function and strain.
treated with aficamten demonstrated a significant advantage in global circumferential strain and longitudinal strain, with betweengroup differences of −2.5% (95% CI: −3.7to -1.3) and −1.8% (95% CI: −1.8 to -0.5), respectively, while remaining within the normal range (Figure 3).12
Regarding structural remodelling, maximal wall thickness and inferolateral wall thickness declined modestly in the aficamten group compared with metoprolol (−1.0 mm [95% CI: −1.8 to -0.20] and −0.8 mm [95% CI: −1.5 to-0.0], respectively). In addition, the left ventricular end systolic volume index increased by 1.6 mL/m2 (95% CI: 0.7–2.5) in the aficamten group compared with metoprolol.12
Improved diastolic function was also observed following treatment with aficamten compared with metoprolol, as demonstrated by statistically significant improvements in left atrial volume index, as well as ratios of early mitral inflow velocity and septal and lateral mitral annular early diastolic velocity.12
Systolic anterior motion (SAM) of the mitral valve, a hallmark of oHCM, was present in most participants at baseline (83% metoprolol and 84% aficamten patients). After 24 weeks, aficamten significantly reduced the prevalence and severity of SAM compared with metoprolol (odds ratio [OR] versus metoprolol for SAM: 0.20 [95% CI: 0.08–0.52]; OR for SAM plus septal contact: 0.09 [95% CI: 0.04–0.24] at Week 24). Parallel improvements were observed in mitral regurgitation severity, whereby the proportion of patients in the aficamten group with moderate or severe regurgitation reduced from 39% at baseline to 25% at Week 24 (OR versus metoprolol: 2.49 [95% CI: 1.38–4.51] at Week 24).12
References
1. Maron BJ. Clinical course and management of hypertrophic cardiomyopathy. N Engl J Med. 2018;379(7):655-68.
2. Lee MMY et al. Aficamten and cardiopulmonary exercise test performance: a substudy of the
Overall, these findings demonstrated that, as well as improving exercise capacity and symptoms, aficamten achieved significant improvement in multiple measures of cardiac structure and function compared with metoprolol. The benefits of aficamten were evident as early as Week 2 after treatment initiation. Although there was a modest decline in measures of left ventricular systolic function with aficamten, all values remained within the normal range, reflecting reduced hypercontractility. Surprisingly, LVOT gradients were not effectively lowered with metoprolol despite physiologic evidence of adequate β-blockade.
Conclusion
The MAPLE-HCM trial provides the first head-to-head comparison of aficamten and metoprolol in symptomatic oHCM. Across both efficacy and structural endpoints, aficamten consistently demonstrated superiority, with significant and clinically meaningful improvements in exercise capacity, symptom burden, haemodynamic parameters, biomarkers, and cardiac structure.10-12 The safety profile was favourable, with only modest reductions in LVEF observed, which remained within normal limits.
Despite the historical reliance on β-blockers as first-line therapy for oHCM, the results of MAPLE-HCM indicate that aficamten may represent a more effective alternative, directly targeting the underlying pathophysiology of the disease. These data extend prior evidence and support the use of aficamten as a monotherapy or potential first-line therapeutic option in patients with oHCM, with potential implications for future treatment guidelines.13
3. Maron MS et al. Aficamten for symptomatic obstructive hypertrophic cardiomyopathy. N Engl J Med. 2024;390(20):1849-61.
4. Sherrod CF 4th et al. Effect of aficamten on health status outcomes in obstructive hypertrophic cardiomyopathy: results from SEQUOIA-HCM. J Am Coll Cardiol. 2024;84(19):1773-85.
5. Hegde SM et al. Impact of aficamten on echocardiographic cardiac structure and function in symptomatic obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol.
6. Coats CJ et al. Cardiac biomarkers and effects of aficamten in obstructive hypertrophic cardiomyopathy: the SEQUOIA-HCM trial. Eur Heart J. 2024;45(42):4464-78.
7. Masri A et al. Effect of aficamten on cardiac structure and function in obstructive hypertrophic cardiomyopathy: SEQUOIA-HCM CMR substudy. J Am Coll Cardiol. 2024;84(19):1806-17.
8. Arbelo E et al. 2023 ESC guidelines for the management of cardiomyopathies. Eur Heart J. 2023;44(37):3503-626.
9. Ommen SR et al. 2024 AHA/ACC/ AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology joint committee on clinical practice guidelines. Circulation. 2024;149(23):e1239-311.
10. Garcia-Pavia P et al. MAPLE-HCM: aficamten vs metoprolol in obstructive HCM. Presentation. ESC Congress, 29 August-1 September, 2025.
11. Garcia-Pavia P et al. Aficamten or metoprolol monotherapy for obstructive hypertrophic cardiomyopathy. N Engl J Med. 2025;393(10):949-60.
12. Hegde SM et al. Effect of aficamten compared with metoprolol on cardiac structure and function in symptomatic obstructive hypertrophic cardiomyopathy: a prespecified analysis of MAPLE-HCM. Presentation. ESC Congress, 29 August-1 September, 2025.
13. Ambardekar AV. Expanding the role of myosin inhibition in hypertrophic cardiomyopathy - a tale of two conditions. N Engl J Med. 2025;393(10):1026-8.
ESC 2025
Abstract Reviews
Drawing on key findings presented at ESC 2025, the following abstract reviews spotlight the latest advancements in cardiology. Authored by the presenters themselves, topics include AI-based risk prediction, accelerometry in hypertrophic cardiomyopathy, and sexspecific effects of oestrogen in takotsubo syndrome.
A Web-Based Application for Acute Coronary Syndrome Mortality Risk Prediction Using Explainable AI and Chatbot Integration in the Asian Population
Authors: *Sazzli Shahlan Kasim,1 Lim Bing Feng,2
Sorayya Malek,2 Raja Ezman Faridz Raja Shariff,3 Khairul Shafiq Ibrahim,3 Ahmad Firdaus Zakaria,3 Ahmad Bakhtiar Md Radzi3
1. Cardiovascular Advancement and Research Excellence (CARE) Institute, Universiti Teknologi MARA, Selangor, Malaysia
2. Faculty of Science, Bioinformatics Division, Institute of Biological Sciences, University of Malaya, Kuala Lumpur, Malaysia
3. Faculty of Medicine, Cardiology Department, Universiti Teknologi MARA (UiTM), Sungai Buloh Campus, Malaysia
*Correspondence to sazzlikasim@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements: This work was supported by the Higher Institution Centre of Excellence (HICoE) research grant (600-RMC/MOHE HICoE CARE-I 5/3 [01/2025]) awarded to the Cardiovascular Advancement and Research Excellence Institute (CARE Institute), Universiti Teknologi MARA, Selangor, Malaysia.
ST-elevation myocardial infarction (STEMI) is a leading cause of mortality, with significant variations in risk profiles among the Asian population. Traditional risk scores, such as the Thrombolysis in Myocardial Infarction (TIMI) score, were developed based on Western cohorts and have limited predictive accuracy for Asian patients. Machine learning models have shown superior performance but remain underutilised due to a lack of accessible and interpretable tools.
PURPOSE
This study aims to develop a web-based application that integrates ensemble learning, explainable AI, and a chatbot for STEMI mortality risk prediction.1 The system provides transparent assessments, enhancing clinical decision-making for Asian healthcare providers.
METHODS
A dataset of 42,348 STEMI cases (2006–2019) from the National Cardiovascular Disease Database (NCVD) registry with 54 clinical features was used. Data preprocessing included handling missing values, outlier detection, and feature normalisation. Feature selection was performed using recursive feature elimination and expert input.
Ensemble models, including random forest, gradient boosting, XGBoost, and stack ensemble, were trained and validated using 10-fold cross-validation. SHapley Additive exPlanations (SHAP) provided interpretability of model predictions, with a user-friendly interface displaying summary plots and individual risk factor explanations.
A chatbot, powered by a fine-tuned large language model, was developed for realtime guidance. The chatbot was localised with region-specific clinical guidelines, terminology, and frequently asked questions to improve usability for Asian healthcare providers. The LangChain framework (LangChain, Inc., San Francisco, California, USA) facilitated seamless knowledge retrieval, enhancing chatbot interactions.
A prospective data collection feature enabled continuous model validation and refinement by incorporating new patient data over time.
RESULTS
The ensemble models outperformed traditional risk scoring methods, achieving an area under the curve score of 0.96, a recall score of 0.89, and a precision of 0.61 for in-hospital mortality prediction, compared to the TIMI risk score (area under the curve: 0.81). SHAP analysis identified key predictors, providing interpretable insights into risk stratification. The chatbot improved accessibility, offering real-time assistance for clinicians in risk assessment. The prospective data collection feature ensured ongoing model updates, maintaining predictive accuracy and clinical relevance.
CONCLUSION
This study presents a web-based STEMI risk prediction tool that integrates ensemble learning, explainable AI, and a chatbot, tailored for the Asian population. The system enhances predictive accuracy, interpretability, and usability, bridging the gap between advanced machine learning models and clinical practice. By combining AI-driven risk assessment with a userfriendly interface, this tool provides a scalable solution for improving STEMI outcomes in Asian healthcare settings.
Reference
1. Kasim SS et al. A web-based application for ACS mortality risk prediction using explainable AI and chatbot integration in the Asian population. Abstract. ESC Congress, 29 August-1 September, 2025.
Association Between the Frequency of Laughter, Cardiovascular Event Risk, and Quality of Life in Asymptomatic Patients Attending a Cardiology Outpatient Clinic
1. Department of Cardiology, Kitaishikai Hospital, Ehime, Japan
2. Department of Cardiology, Pulmonology, Hypertension and Nephrology, Ehime University Graduate School of Medicine, Japan
*Correspondence to saito0321jp@yahoo.co.jp
Disclosure: The authors have declared no conflicts of interest related to this work.
Acknowledgements: The authors would like to thank Mayu Ninomiya, Natsumi Ichii, Rumi Taniguchi, Ayako Kinoshita, Keiko Furuno, Kiyomi Mukai, Keiko Ogura, and Mamoru Morino for their assistance in compiling the survey data.
Keywords: Cardiovascular event risk, crosssectional study, Japanese, laughter, quality of life (QOL).
Negative emotions, particularly depression, are known to increase cardiovascular disease risk and reduce quality of life (QOL). By contrast, positive emotions such as laughter may have beneficial effects on vascular function and psychological wellbeing. Epidemiological and experimental studies have suggested that frequent laughter may reduce stress hormone levels, improve endothelial function, and promote healthy behaviours.1-5 However, the relationship between laughter frequency, cardiovascular risk, and QOL has not been comprehensively examined in stable cardiac populations. This cross-sectional study investigated these associations in asymptomatic patients attending a cardiology outpatient clinic.6
METHODS
A survey of asymptomatic patients attending a cardiology outpatient clinic between April 2023–March 2024 was performed. Patients with a clinical frailty scale score of ≥3, a history of hospitalisation, or an inability to complete the questionnaire were excluded. Laughter frequency was assessed using a threepoint scale (almost daily, 1–5 times a week, and 1–3 times a month). The relationship between laughter frequency and cardiovascular event risk (assessed using the Suita score as a surrogate marker), along with QOL measures (Kansas City Cardiomyopathy Questionnaire [KCCW] overall summary score and EuroQol-5 Dimension [EQ-5D]) were analysed.
RESULTS
Overall, 611 patients (median age: 71 years; 65% male) were included. Laughter frequency was significantly higher in women than in men (daily laughter: 41% versus 28%; p<0.01). Although no significant association was found between laughter frequency and cardiovascular event risk, a higher laughter frequency was positively associated with both QOL measures. After adjusting for age, sex, grip strength, B-type natriuretic peptide, Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) score, smoking, exercise habits, gardening habits, pet ownership, and bathing habits, the association with improved QOL remained significant (Figure 1A). However, the strength of this association was attenuated after further adjustment for the depression indicator (Patient Health Questionnaire-2 [PHQ-2] score; Figure 1B).
CONCLUSION
The self-reported frequency of laughter was not associated with cardiovascular event risk, but showed a positive association with QOL. This association was attenuated after accounting for depression, which signifies
partial mediation by mental health factors. Promoting laughter may serve as a simple, nonpharmacological approach to improve the QOL of patients with asymptomatic cardiac conditions, particularly through its effect on mental well-being.
Figure 1: Multivariable analysis of laughter frequency and quality of life (Kansas City Cardiomyopathy Questionnaire and EuroQol-5 Dimension).
*p<0.05; p for trend indicates the significance of trends across laughter frequency categories.
A) Adjusted for age, sex, grip strength, BNP, MAGGIC score, smoking, exercise habits, gardening habits, pet ownership, and bathing habits. B) A+adjustment for PHQ-2 (depression indicator).
BNP: B-type natriuretic peptide; EQ-5D: EuroQol-5 Dimension; KCCQ: Kansas City Cardiomyopathy Questionnaire; MAGGIC: Meta-analysis Global Group in Chronic Heart Failure; PHQ-2: Patient Health Questionnaire-2; QOL: quality of life.
References
1. Sakurada K et al. Associations of frequency of laughter with risk of all-cause mortality and cardiovascular disease incidence in a general population: findings from the Yamagata Study. J Epidemiol. 2020;30:188-93.
2. Hayashi K et al. Laughter is the best medicine? A cross-sectional study of cardiovascular disease among older Japanese adults. J Epidemiol. 2016;26(10):546-52.
3. Sugawara J et al. Effect of mirthful laughter on vascular function. Am J Cardiol. 2010;106(6):856-9.
4. Kramer CK, Leitao CB. Laughter as medicine: a systematic review and meta-analysis of interventional studies evaluating the impact of spontaneous laughter on cortisol levels. PLoS One. 2023;18(5):e0286260.
5. Vlachopoulos C et al. Divergent effects of laughter and mental stress on arterial stiffness and central hemodynamics. Psychosom Med. 2009;71(4):44653.
6. Saito M et al. Association between the frequency of laughter and cardiovascular event risk and quality of life in asymptomatic patients attending a cardiology outpatient clinic. Abstract. ESC Congress, 29 August-1 September, 2025.
Efficacy and Safety of Prolonged Edoxaban Treatment for Patients with Gastrointestinal Cancer Who Have Isolated Distal Deep Vein
1. Graduate School of Medicine, Kyoto University, Japan
2. Division of Cardiology, Shizuoka Cancer Center, Japan
3. Division of Vascular Surgery, Department of Surgery, Tohoku University Hospital, Sendai, Japan
4. Division of Cardiology, Osaka General Medical Center, Japan
5. Department of Cardiology, Tokyo Women's Medical University, Japan
6. Department of Cardiology and Nephrology, Mie University Graduate School of Medicine, Tsu, Japan
7. Department of Onco-Cardiology, Osaka International Cancer Institute, Japan
8. Division of Cardiovascular Medicine, Toho University Ohashi Medical Center, Tokyo, Japan
9. Division of General Internal Medicine, Department of Internal Medicine, Kobe University Graduate School of Medicine, Japan
10. Department of Cardiovascular Medicine, Graduate School of Medical Sciences, Kumamoto University, Japan
11. Department of Internal Medicine, Division of Medical Oncology and Respiratory Medicine, Shimane University Faculty of Medicine, Izumo, Japan
12. Department of Cardiovascular Medicine, National Cancer Center Hospital, Tokyo, Japan
13. Department of Obstetrics and Gynecology, Faculty of Medicine, University of Tsukuba, Japan
14. Department of Cardiovascular Surgery, Kyorin University, Tokyo, Japan
15. Division of Cardiology, Department of Internal Medicine, St. Marianna University School of Medicine, Kawasaki, Japan
*Correspondence to yyamashi@kuhp.kyoto-u.ac.jp
Disclosure: Yamashita has received payment for lectures from Bayer Healthcare, Bristol Myers Squibb, Pfizer, and Daiichi-Sankyo; and grants from Bayer Healthcare and Daiichi-Sankyo. Nishimoto has received payment for lectures from Bayer Healthcare, Bristol Myers Squibb, Pfizer, and Daiichi-Sankyo. Ogihara has received payment for lectures from Bayer Healthcare, Bristol Myers Squibb, Pfizer, and Daiichi-Sankyo; and research funds from Bayer Healthcare and Daiichi-Sankyo. Ikeda has received payment for lectures from Bayer Healthcare, Bristol Myers Squibb, and Daiichi-Sankyo. Tsubata has received payment for lectures from AstraZeneca, Chugai Pharmaceutical, Bristol Myers Squibb, Kyowa Kirin, Pfizer, Taiho Pharmaceutical, Takeda Pharmaceutical, and Daiichi-Sankyo; and grant support from Daiichi-Sankyo, AstraZeneca, and OnoPharmaceutical. The other authors have declared no conflicts of interest.
Keywords: Anticoagulant, cancer, cardio-oncology, deep vein thrombosis (DVT), edoxaban.
Patients with gastrointestinal (GI) cancer could be at high risk of bleeding with anticoagulation therapy involving direct oral anticoagulants. The ONCO DVT study1 revealed that 12-month edoxaban treatment for patients with cancer and isolated distal deep vein thrombosis (DVT) reduced the composite outcome of symptomatic recurrent venous thromboembolism (VTE) or VTE-related death compared with 3-month edoxaban treatment. However, whether these results are applicable to patients with GI cancer has been uncertain.
The purpose of this post-hoc subgroup analysis was to evaluate the efficacy and safety of 12-month edoxaban treatment for patients with GI cancer.2
METHODS
The ONCO DVT study was an RCT that randomly assigned patients with cancer and isolated distal DVT to receive either 12-month or 3-month edoxaban treatment in a 1:1 ratio and evaluated clinical outcomes at 12 months. In the current study, 601 patients were stratified into GI cancer (N=102) and non-GI cancer (N=499) subgroups. GI cancer was defined as oesophageal, gastric, duodenal, small intestine, caecal, or colon cancer. The primary endpoint was a composite outcome of symptomatic recurrent VTE or VTErelated death at 12 months. The major secondary endpoint was major bleeding at 12 months.
RESULTS
Patients with GI cancer were older (73.4 years versus 70.3 years; p=0.004) and there was a higher proportion of men (38% versus 26%; p=0.01) compared with those without. There was no significant difference in body weight, symptoms at baseline, site of thrombus, or dosing of edoxaban between the two subgroups. There was also no significant difference in cancer status including metastatic disease. In the GI cancer subgroup, the primary endpoint did not occur in the 12-month edoxaban group, and occurred in 3/53 (5.7%) patients in the 3-month edoxaban group. In the nonGI cancer subgroup, the primary endpoint occurred in 3/247 (1.3%) patients in the
12-month edoxaban group, and in 19/252 (7.5%) patients in the 3-month edoxaban group (odds ratio [OR]: 0.15; 95% CI: 0.04–0.45). There was no significant interaction in the primary endpoint (interaction p=0.38). In the GI cancer subgroup, the major secondary endpoint occurred in 3/49 (6.1%) patients in the 12-month edoxaban group, and in 4/53 (7.6%) patients in the 3-month edoxaban group (OR: 0.80; 95% CI: 0.15–3.81). In the non-GI cancer subgroup, the major secondary endpoint occurred in 25/247 (10.1%) patients in the 12-month edoxaban group, and in 18/252 (7.1%) patients in the 3-month edoxaban group (OR: 1.46; 95% CI: 0.78–2.79). There was also no significant interaction in the major secondary endpoint (interaction p=0.48).
CONCLUSION
In patients with cancer-associated isolated distal DVT, those with GI cancer did not show signals of an increased risk of major bleeding with prolonged anticoagulation therapy of edoxaban.
References
1. Daiichi Sankyo Co, Ltd. Optimal duration of anticoagulation therapy for isolated distal deep vein thrombosis in patients with cancer study (ONCO DVT). NCT03895502. https://clinicaltrials.gov/ study/NCT03895502.
2. Yamashita Y et al. Efficacy and safety of prolonged edoxaban treatment for gastrointestinal cancer patients with isolated distal deep vein thrombosis: insight from the ONCO DVT study. Abstract. ESC Congress, 29 August-1 September, 2025.
Accelerometry-Defined Physical Activity and Quality of Life in Hypertrophic Cardiomyopathy
Authors: *Stephan A.C. Schoonvelde,1 Peter-Paul Zwetsloot,1,2 Alexander Hirsch,1,3 Arend F.L. Schinkel,1 Christian Knackstedt,4 Tjeerd Germans,5 Marjon A. van Slegtenhorst,6 Judith M.A. Verhagen,6 Rudolf A. de Boer,1 Michelle Michels1
1. Department of Cardiology, Cardiovascular Institute, Thorax Center, Erasmus MC, Rotterdam, the Netherlands
2. Netherlands Heart Institute, Utrecht, the Netherlands
3. Department of Radiology and Nuclear Medicine, Erasmus MC, Rotterdam, the Netherlands
4. Department of Cardiology and Cardiovascular Research Institute Maastricht (CARIM), Maastricht University Medical Centre, the Netherlands
5. Department of Cardiology, Noordwest Ziekenhuisgroep, Alkmaar, the Netherlands
6. Department of Clinical Genetics, Erasmus University Medical Center, Rotterdam, the Netherlands
*Correspondence to s.schoonvelde@erasmusmc.nl
Disclosure: Zwetsloot has received partial funding through the Dutch Heart Foundation Public Private Partnership Grant (CARMA, grant: 01-003-2022-0358), with payments to the institution; and consulting fees from Bayer, Alnylam, and Bristol Myers Squibb, with payments to the institution. Hirsch has received research grants from GE Healthcare, with payments to the institution; consultancy fees from GE Healthcare, with payments to the institution; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from GE Healthcare, Bayer, and Bristol Myers Squibb, with payments to the institution; and has participated on a data safety monitoring board or advisory board for Medis Medical Imaging Systems. Knackstedt has received research grants from Pfizer, Philips/TomTec Imaging, and AstraZeneca, with payments to the institution; consulting fees from Pfizer, Philips/TomTec Imaging, and AstraZeneca; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Pfizer, Novartis, Biomarin, Bristol Myers Squibb, and Alnylam; and has participated on a data safety monitoring board or advisory board for Pfizer, Philips/TomTec Imaging, Novartis, Biomarin, Bristol Myers Squibb, and Alnylam. de Boer has received grants from AstraZeneca, Abbott, Bristol Myers Squibb, Cardior Pharmaceuticals, Novo Nordisk, and Roche, with payments to the institution; consulting fees from AstraZeneca, Abbott, Bristol Myers Squibb, Cardior Pharmaceuticals, Novo Nordisk, and Roche, with pay-
ments to the institution; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Abbott, AstraZeneca, Bristol Myers Squibb, Cardior Pharmaceuticals, Novo Nordisk, and Roche, with payments to the institution; and support for attending meetings and/or travel from Abbott, Cardior Pharmaceuticals, and Novo Nordisk, with payments to the author. Michels has received a research grant from Bristol Myers Squibb, with payments to the institution; consultancy fees from Cytokinetics, with payments to the institution; and payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Bristol Myers Squibb and Pfizer. The other authors have declared no conflicts of interest.
Acknowledgements: The authors thank Lisette de Vogel for logistical support with accelerometer provision.
Keywords: Accelerometry, exercise, hypertrophic cardiomyopathy (HCM), obstruction, quality of life (QoL), sedentariness, step count.
Patients with hypertrophic cardiomyopathy (HCM) frequently reduce physical activity due to concerns about sudden cardiac death, though evidence for these restrictions is limited.1,2 Most data on activity in HCM rely on patient-reported measures, with little objective quantification or phenotype-specific analysis.3
METHODS
In this multicentre Dutch study,4 accelerometry was used to measure 7-day physical activity in 203 patients with HCM and 37 genotype-positive, phenotypenegative (G+/P–) relatives. G+/P– relatives were considered healthy controls. The primary outcomes were daily steps, time spent in moderate-to-vigorous physical activity, and sedentariness. Quality of life (QoL) was assessed using the Kansas City Cardiomyopathy Questionnaire (KCCQ)
A B
A) Distribution of MVPA (min/day) in 30-minute increments. B) Distribution of sedentary behaviour (%/day) for participants who are G+ phenotype-negative and participants who have hypertrophic cardiomyopathy. G+: genotype-positive; MVPA: moderate-to-vigorous physical activity.
and the EuroQoL 5-dimension 5-level (EuroQoL-5D-5L) questionnaire. Subgroup analyses included symptomatic versus asymptomatic, obstructive versus non-obstructive, BMI groups, and medication use.
RESULTS
Physical activity in patients with HCM was significantly decreased. Patients with HCM walked fewer steps per day (5,254 versus 6,573). Furthermore, as displayed in Figure 1, these patients engaged in less moderateto-vigorous physical activity (3.4% versus 4.5% of the day), and were more sedentary (>80% of waking hours: 61% versus 35%) compared with G+/P– individuals (all p<0.01). Patients who were symptomatic and those with left ventricular outflow tract obstruction had the lowest activity. While patients who were asymptomatic and non-obstructive were as physically active as healthy controls, strikingly, even patients who were asymptomatic and obstructive showed markedly reduced
activity, comparable to individuals who were symptomatic. Obesity and the use of cardiac medications, particularly β-blockers, were associated with significant reductions in physical activity.5,6
Daily steps correlated with QoL, with every 250 step/day increase being associated with a 2.15-point higher KCCQ score, and every 1,000 step/day increase with a 0.05-point higher EQ-5D-5L score (both p<0.001). All associations remained significant after adjustment for age and sex. Lastly, more than half of patients recalled receiving previous exercise guidance from their cardiologist, and most reduced their activity as a consequence. However, objective activity measured with accelerometry did not differ between those who restricted their activity versus those who did not.
Figure 1: Physical activity and sedentariness.
CONCLUSION
This is the largest multicentre accelerometry-based analysis in HCM that included G+/P– controls. Patients with HCM are substantially less active and more sedentary, especially if symptomatic, obstructive, or obese. Even modest increases in step counts were linked to clinically meaningful QoL improvements.7 These findings underline the need for individualised, phenotype-informed exercise counselling and careful reconsideration of restrictive advice, and support the integration of wearable data into clinical care and clinical trials.8-11
References
1. Arbelo E et al. 2023 ESC guidelines for the management of cardiomyopathies. Eur Heart J. 2023;44:3503-26.
2. Ommen SR et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2020;76:e159-240.
3. Sweeting J et al. Physical activity in hypertrophic cardiomyopathy: prevalence of inactivity and barriers. Open Heart. 2016;3:e000484.
4. Schoonvelde et al. Physical activity measured by accelerometry in hypertrophic cardiomyopathy: findings from the AFFECT-HCM study. ESC Congress, 29 August-1 September, 2025.
5. Olivotto I et al. Obesity and its association to phenotype and clinical course in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2013;62:44957.
6. Kwon S et al. Association of physical activity with all-cause and cardiovascular mortality in 7666 adults with hypertrophic cardiomyopathy (HCM): more physical activity is better. Br J Sports Med. 2021;55:1034-40.
7. Spertus JA et al. Interpreting the kansas city cardiomyopathy questionnaire in clinical trials and clinical care: JACC state-of-the-art review. J Am Coll Cardiol. 2020;76:2379-90.
8. Saberi S et al. Effect of moderate-intensity exercise training on peak oxygen consumption in patients with hypertrophic cardiomyopathy: a randomized clinical trial. JAMA. 2017;317:1349-57.
9. Gudmundsdottir HL et al. Exercise training in patients with hypertrophic cardiomyopathy without left ventricular outflow tract obstruction: a randomized clinical trial. Circulation. 2025;151: 132-44.
10. Basu J et al. High intensity exercise programme in patients with hypertrophic cardiomyopathy: a randomized trial. Eur Heart J. 2025;46:1803-15.
11. Gati S, Sharma S. Exercise prescription in individuals with hypertrophic cardiomyopathy: what clinicians need to know. Heart. 2022;108:1930-7.
Impact of Pregnancy on Mortality in Dilated Cardiomyopathy: Immediate and 12-Month Postpartum Outcomes –
Authors: *Mônica Samuel Avila,1 Fernando Bacal,1 Fabio Fernandes,1 Flavio Tarasoutchi,1 Walkiria Samuel Avila1
1. Heart Institute (InCor), Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, Brazil
*Correspondence to mo_avila@hotmail.com
Disclosure: The authors have declared no conflicts of interest.
Pregnant women with dilated cardiomyopathy (DCM) face high risks of complications and maternal death due to haemodynamic overload, withdrawal of teratogenic but essential therapies, and limited treatment options during pregnancy.1,2
The purpose of this study was to evaluate maternal and fetal outcomes in women with DCM during pregnancy and up to 12 months postpartum across different aetiologies, and identify predictors of maternal death.3
Data from the InCor Registry
METHODS
The prospective cohort of women with confirmed DCM were enrolled in the InCor Pregnancy and Heart Disease Registry for over 10 years. All received standardised cardio-obstetric care. Left ventricular ejection fraction (LVEF) was assessed using echocardiography, and brain natriuretic peptide was evaluated when available. Treatment during pregnancy included β-blockers, hydralazine, diuretics, nitrates, enoxaparin, and hospitalisation when needed. Guideline-directed therapy was resumed postpartum. Outcomes included maternal (heart failure, arrhythmias, thromboembolism, death) and obstetric/ fetal complications. Logistic regression identified predictors of maternal mortality.
RESULTS
Among 983 registry patients (2013–2023), 90 had DCM. Cardiomyopathy aetiologies were peripartum (32), idiopathic (21), myocarditis (15), Chagas disease (11), and others (11). Maternal complications occurred in 51.1% during pregnancy, 36.0% in the early postpartum period (up to 6 weeks after delivery), and 38.6% in the late postpartum period (from 6 weeks–12 months after delivery; Table 1). All nine maternal deaths
Table 1: Main clinical complications by follow-up period.
(10%) occurred postpartum, mostly due to heart failure, at a mean of 8.8±3.1 months (Figure 1). Caesarean section was performed in 75% of patients, with 10.0% fetal loss and 33.8% prematurity. Mean birth weight was 2,606 g. LVEF improved from 32% at diagnosis to 39% during pregnancy and 42% at 12 months postpartum. Lower LVEF (odds ratio: 0.87; p=0.006) and prior thromboembolism (odds ratio: 15.5; p=0.017) were independent predictors of death.
CONCLUSION
Pregnancy in women with DCM was associated with high morbidity and late mortality. Reduced LVEF and a history of thromboembolism were independent predictors of maternal death.
References
1. Kotit S, Yacoub M. Cardiovascular adverse events in pregnancy: a global perspective. Glob Cardiol Sci Pract. 2021;2021(1):e202105.
2. DeFilippis EM et al. Cardio-obstetrics and heart failure: JACC: heart failure state-of-the-art review. JACC Heart Fail. 2023;11(9):1165-80.
3. Samuel WA et al. Impact of pregnancy on mortality in dilated cardiomyopathy. Immediate and 12- months postpartum outcomes. Data from the InCor Registry. Abstract. ESC Congress, 29 August-1 September, 2025.
Figure 1: Incidence of maternal outcomes: complications and mortality.
Optimal Pulmonary-to-Systemic Flow Ratio in the Paediatric ICU: Insights from a Series of Patient-Specific Norwood Circulation Computational Fluid Dynamics Models
2. Chukyo Hospital, Nagoya, Japan *Correspondence to ksughimoto@gmail.com
Disclosure: Sughimoto, Kasai, Koda, Maeda, Miki, T. Sakurai, H. Sakurai, and Liu have received grant support from the Tateisi Science and Technology Foundation, with payment to Chiba University.
Acknowledgements: The authors would like to thank the Tateisi Science and Technology Foundation for the grant support.
The Norwood procedure for hypoplastic left heart syndrome is one of the most complex neonatal surgeries. Even after technically successful repair, patients remain vulnerable to haemodynamic instability, which can compromise survival and long-term outcomes. Traditionally, clinicians empirically target a pulmonary-tosystemic flow ratio (Qp/Qs) of 1.0 to achieve balance between systemic and pulmonary circulations. However, the true optimal Qp/ Qs in the early post-operative period has not been determined.1
This study developed patient-specific computational fluid dynamics (CFD) models of the Norwood circulation using perioperative clinical data. By integrating lactate levels as a marker of haemodynamic stability, the authors aimed to define the optimal Qp/Qs and clarify underlying physiological mechanisms in the immediate post-operative period.2
METHODS
Three neonates (all female; median age: 34 days [range: 30–41 days]; median weight: 2.6 kg [range: 2.5–2.7 kg]) who underwent the Norwood procedure were analysed (Figure 1). Patient-specific, 0–1-dimensional lumped parameter CFD models3 were generated using radial artery pressure waveforms, O2 saturation, and lactate measurements. Models were reconstructed at 30 post-operative blood-draw time points by minimising the difference between observed and simulated waveforms with a gradient descent algorithm. Qp/Qs and associated haemodynamic parameters were then calculated at each time point. Correlations between lactate levels, elapsed time, and haemodynamic indices were examined.4
RESULTS
Model accuracy was high, with agreement rates of 96.0±2.5% for mean arterial pressure and 97.0±2.3% for arterial O2 saturation. Over time, pulmonary vascular resistance decreased (correlation coefficient [R]=–0.488) and pulmonary arterial compliance increased (R=0.350), reflecting natural post-operative adaptation. Importantly, declining lactate levels correlated with reduced pulmonary vascular resistance (R=0.609) and improved pulmonary arterial compliance (R=–0.296). Simultaneously, right ventricular active elastance decreased (R=0.299), indicating lower ventricular afterload and improved ventricular efficiency.
The lowest lactate concentrations coincided with a Qp/Qs of 1.45, not 1.0. This finding suggests that slightly higher pulmonary flow relative to systemic flow is associated with the most stable haemodynamics in the early post-operative Norwood circulation.
Re-approximation by Gradient
method post-Norwood (RV to PA conduit ) in PICU
Minimise the differences between actual and pt-specific model More
CFD: computational fluid dynamics; CT,puaI: total pulmonary artery compliance index; CT,svI: total systemic venous compliance index; D: days; ervaI: right ventricle active elastance index; PA: pulmonary artery; PICU: paediatric ICU; pt: patient; Qp/Qs: pulmonary-to-systemic flow ratio; RT,pvbI: total pulmonary vascular resistance index; RV: right ventricle.
CONCLUSION
The authors successfully developed patientspecific CFD models capable of simulating Norwood haemodynamics by integrating routine physiological and biochemical data. These models provide a quantitative insight into dynamic cardiovascular adaptation after surgery, and reveal that lactate, a readily available biomarker, strongly reflects changes in vascular resistance, compliance, and ventricular function.
Most importantly, the authors’ findings showed that a ratio closer to 1.45 is associated with the most favourable balance between systemic and pulmonary circulations in the immediate post-operative period.
This study demonstrates the potential of patient-specific CFD modelling as a decision support tool in congenital heart surgery. By linking computational haemodynamic
analysis with simple biological markers such as lactate, clinicians may refine post-operative management, individualise targets, and improve stability for vulnerable neonates after the Norwood procedure.
References
1. Photiadis J et al. Optimal pulmonary to systemic blood flow ratio for best hemodynamic status and outcome early after Norwood operation. Eur J Cardiothorac Surg. 2006;29(4):551-6.
2. Sughimoto K et al. Optimal pulmonary-to-systemic flow ratio in the paediatric intensive care unit: insights from a series of patient-specific Norwood circulation computational fluid dynamics models. Abstract 82463. ESC Congress, 29 August-1 September, 2025.
3. Sughimoto K et al. Assessment of cardiovascular function by combining clinical data with a computational model of the cardiovascular system. J Thorac Cardiovasc Surg. 2013;145(5):1367-72.
4. Sughimoto K et al. Machine learning predicts blood lactate levels in children after cardiac surgery in paediatric ICU. Cardiol Young. 2023;33(3):388-95.
Figure 1: Flow of the research work.
Sex-Specific Effects of Oestrogen in Takotsubo Syndrome: Protective in Females, Detrimental in Males
Authors: *Ermir Zulfaj,1 Amirali Nejat,1 Maryna Karasnikova,1 Tetiana Pylova,1 Elin Wrångemyr,1 Anna Karin Norlén,2 Ahmed Elmahdy,1 Aaron Espinosa,1 Abhishek Jha,1 Abdulhussain Haamid,3 Karin Horkeby,4,5 Marie Lagerquist,4,5 Åsa Tivesten,1,6 Björn Redfors,1,7 Elmir Omerovic1,7
1. Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Sweden
2. Department of Clinical Chemistry, Sahlgrenska University Hospital, Gothenburg, Sweden
3. Core Facilities - Experimental Biomedicine, Sahlgrenska Academy, University of Gothenburg, Sweden
4. Department of Internal Medicine and Clinical Nutrition, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Sweden
5. Osteoporosis Centre, Centre for Bone and Arthritis Research, Sahlgrenska Academy, University of Gothenburg, Sweden
6. Department of Endocrinology, Sahlgrenska University Hospital, Gothenburg, Sweden
7. Department of Cardiology, Sahlgrenska University Hospital, Gothenburg, Sweden
*Correspondence to ermir.zulfaj@gu.se
Disclosure: This study was funded by the Swedish Research Council (2020-02592), the Swedish Heart and Lung Foundation (20200826), and the Swedish state under the agreement between the Swedish government and the country councils (ALF-agreement, ALFGBG-966521). The authors have declared no other conflicts of interest.
Keywords: Oestrogen, sex differences, stress, Takotsubo syndrome (TS).
Takotsubo syndrome (TS) is characterised by transient regional wall-motion abnormalities manifesting as apical ballooning on imaging following acute stress.1,2 Sex differences in TS prevalence are well-documented, with a marked preponderance among postmenopausal women.3 Oestrogen deprivation is believed to play a facilitating role. Using a highfidelity rat model of TS,4,5 the authors aimed to investigate the relationship between oestrogen and stress-induced apical ballooning in female and male rats.6
METHODS
Study 1 examined 24 oophorectomised female rats receiving daily subcutaneous 17β-oestradiol injections (0–72.9 µg) for 3 weeks before TS induction. Study 2 randomised 32 orchiectomised male rats to receive subcutaneous oestrogen supplementation (54.3 µg daily for 3 weeks) or vehicle (MIGLYOL® 812 N [IOI Oleo GmbH, Hamburg, Germany]). TS was induced in all animals via isoprenaline infusion (1 mg/kg over 15 minutes), and blood samples were taken prior to induction for the analysis of sex hormones using high-sensitive gas chromatographytandem mass spectrometry. Using high-resolution echocardiography, left ventricular akinesia index (LVAI) was measured to quantify the extent of regional wall-motion abnormalities.
RESULTS
In Study 1, oestrogen demonstrated an exponential dose-dependent protective effect against TS in females, with higher plasma levels correlating with reduced LVAI (correlation coefficient: –0.564; p=0.006). In contrast, Study 2 demonstrated that oestrogen supplementation in males significantly increased TS severity (p=0.022) and incidence of apical thrombus formation (22% versus 0% in controls; p=0.002), and showed a trend towards increased mortality (p=0.100) due to earlyphase arrhythmias. Combined analysis revealed an increased TS susceptibility in female rats after adjusting for sex hormone differences (coefficient for male sex: –7.85; p=0.022), and a significant sex-specific effect of oestrogen supplementation (interaction: p<0.001), with protective effects in females but detrimental effects in males.
DISCUSSION
TS has long been described as a 'woman's disease', and differences in sex hormones, mainly oestrogen, have been considered the main cause. The authors' investigations reveal that oestrogen's role is more complex than previously thought. Their findings provide strong evidence for the protective role of oestrogen in females; however, it paradoxically increases TS severity in male rats. This distinct, sex-specific response to oestrogen suggests that additional mechanisms beyond simple hormone levels contribute to the sex differences observed in patients with TS. This sex-specific response to oestrogen helps explain why, despite men having lower oestrogen levels throughout life, they don't show the same TS susceptibility as postmenopausal women.
CONCLUSION
Oestrogen attenuates stress-induced regional wall-motion abnormalities in a dosedependent manner in oophorectomised female rats, while increasing them in orchiectomised male rats.
References
1. Ghadri JR et al. International expert consensus document on Takotsubo syndrome (part I): clinical characteristics, diagnostic criteria, and pathophysiology. Eur Heart J. 2018;39(22):2032-46.
2. Omerovic E et al. Pathophysiology of Takotsubo syndrome - a joint scientific statement from the Heart Failure Association Takotsubo Syndrome Study Group and Myocardial Function Working Group of the European Society of Cardiology - part 1: overview and the central role for catecholamines and sympathetic nervous system. Eur J Heart Fail. 2022;24(2):257-73.
3. Omerovic E et al. Pathophysiology of Takotsubo syndrome - a joint scientific statement from the Heart Failure Association Takotsubo Syndrome Study Group and Myocardial Function Working Group of the European Society of Cardiologypart 2: vascular pathophysiology, gender and sex hormones, genetics, chronic cardiovascular problems and clinical implications. Eur J Heart Fail. 2022;24(2):274-86.
4. Zulfaj E et al. Development of a small animal model replicating core characteristics of Takotsubo syndrome in humans. Eur Heart J Open. 2024;4(4):oeae048.
5. Zulfaj E et al. Temperature and repeated catecholamine surges modulate regional wall motion abnormalities in a rodent Takotsubo syndrome model. Sci Rep. 2025;15:3876.
6. Zulfaj E et al. Sex-specific effects of oestrogen in Takotsubo syndrome: protective in females, detrimental in males. Abstract. ESC Congress, 29 August-1 September, 2025.
Preoperative Baseline Troponin as a Predictor of Major Adverse Cardiac Events Following
Kidney Transplantation in Patients with End-Stage Kidney Disease
1. Division of Cardiology, The University of British Columbia, Vancouver, Canada
2. Division of Nephrology, The University of British Columbia, Vancouver, Canada
*Correspondence to arya774@student.ubc.ca
Disclosure: The authors have declared no conflicts of interest. This research did not receive any designated funding from public, commercial, or not-for-profit entities.
Cardiac biomarkers, such as troponins, are indicative of myocardial damage and can be detected in circulation. Not only are they frequently elevated following non-cardiac surgery, but clinically silent troponin elevations are associated with mortality and adverse cardiac events. As such, many patients are evaluated for myocardial injury after non-cardiac surgery, defined as one or more post-operative troponin measurements exceeding the 99th percentile upper reference limit of normal within 30 days of surgery.1 Ischaemic features, such as clinical symptoms or ischaemic electrocardiographic findings, are not required for the diagnosis of myocardial injury after non-cardiac surgery.1,2 However, patients with end-stage kidney disease (ESKD) present a unique challenge, as they often have elevated baseline troponin levels prior to surgery in the absence of myocardial ischaemia. As such, clinicians are not able to reliably interpret postoperative troponin measurements in patients with ESKD following non-cardiac
surgery. Given that cardiovascular disease and its associated complications remain the leading cause of death in kidney transplant (KT) recipients with a functioning kidney allograft,3 it is imperative that the authors reflect on current pre-KT cardiac risk assessment practices. To date, no studies have examined the utility of baseline troponin levels in patients with ESKD as a tool to risk-stratify patients prior to KT. This study aims to evaluate the association between pre-transplant baseline troponin levels and the incidence of major adverse cardiac events (MACE) in the year following KT.4
METHODS
This is a retrospective cohort study at a tertiary care centre in Vancouver, Canada, consisting of 261 patients with ESKD and cardiovascular disease referred for assessment prior to KT between January 2013–January 2024. The primary endpoint was MACE in the year following KT, defined as all-cause death, non-fatal myocardial infarction, non-fatal stroke, coronary revascularisation, heart failure hospitalisation, or cardiac arrest. Patients undergoing multiorgan transplantation or lacking baseline troponin measurements were excluded.
RESULTS
Of the 261 patients referred, 153 (59%) had a KT, 83 (32%) died pre-KT, and 25 (9%) were removed from the transplant programme (Figure 1). Among the 153 patients who received a transplant, 136 met the inclusion criteria. Of these, 24 patients (18%) experienced MACE within 1 year of KT. Elevated baseline troponin levels, defined as exceeding the 99th percentile upper reference limit of normal,
Figure 1: Flowchart of patients with end-stage kidney disease referred to the authors’ clinic during the study period.
261 patients with ESKD referred for cardiac clearance
83 patients passed away pre-transplant
93 patients (68%) with elevated baseline troponin
153 patients received a kidney transplant
21 patients (22.6%) with MACE within 1 year of transplant
136 patients met study criteria
25 patient files closed by the transplant programme
43 patients (32%) with non-elevated baseline troponin
3 patients (7.0%) with MACE within 1 year of transplant
KT recipients meeting study criteria are differentiated by elevated versus non-elevated baseline troponin.
were present in 93 patients (68%), while 43 (32%) had non-elevated troponin levels. Pre-KT demographics and comorbidities were comparable between the two groups. MACE in the year following KT was more prevalent in patients with elevated baseline troponin levels (22.6% versus 7.0%; p=0.026). Additionally, among those who developed MACE, baseline troponin levels were markedly greater (4.2 times versus 3.2 times the upper reference limit; p=0.048). Elevated troponin was associated with a nearly four-fold increased risk of MACE within 1 year of KT (odds ratio: 3.9; 95% CI: 1.1–13.8; p=0.036).
CONCLUSION
Among patients with ESKD and cardiovascular disease, elevated baseline troponins were predictive of MACE in the year following KT. The authors' study demonstrates the potential for baseline troponin measurements to enhance current, pre-KT cardiac risk stratification practices and act as an objective indicator of postoperative morbidity and mortality risk. However, further evaluation with longterm studies and larger cohorts remains necessary to validate the clinical utility of baseline troponin levels in risk stratifying patients with ESKD for adverse outcomes such as MACE following KT.
References
1. Rangaswami J et al. Cardiovascular disease in the kidney transplant recipient: epidemiology, diagnosis and management strategies. Nephrol Dial Transplant. 2019;34(5):760-73.
2. Botto F et al. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120(3):564-78.
3. Devereaux PJ, Szczeklik W. Myocardial injury after non-cardiac surgery: diagnosis and management. Eur Heart J. 2019;41(32):3083-91.
4. Ramanathan K et al. Preoperative baseline troponin as a predictor of major adverse cardiac events following kidney transplantation in patients with end-stage kidney disease. Abstract. ESC Congress, 29 August-1 September, 2025.
Deep Learning-Based Approach to Emergency Department Chest Pain Risk Stratification by ECG
Authors: Shyon Parsa,1 J. Weston Hughes,2 Guson Kang,3 James Zou,4 Albert J. Rogers,5 Sanjiv Narayan,5 Euan Ashley,5 *Marco Perez5
1. Department of Medicine, Stanford University School of Medicine, California, USA
2. Department of Biomedical Informatics, Columbia University Irving Medical Center, New York, USA
3. Interventional Cardiology Section, Division of Cardiovascular Medicine, Department of Medicine, Stanford University School of Medicine, California, USA
4. Department of Biomedical Data Science, Stanford University School of Medicine, California, USA
5. Division of Cardiovascular Medicine and Cardiovascular Institute, Stanford University School of Medicine, California, USA *Correspondence to mvperez@stanford.edu
Disclosure: Ashley has received royalties or licences from Personalis, Svexa, Swift Bio, Deepcell, and Saturnus Bio; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Illumina, Oxford Nanopore, Cellsonics, Pacific Biosciences, and Cache; held leadership or fiduciary roles in boards, societies, committees, and advocacy groups, with AstraZeneca, Pacific Biosciences, Parameter Health, Dexcom, and Candela; and holds stock or stock options in Personalis, AstraZeneca, and Pacific Biosciences. Rogers has received grants from the National Institutes of Health (NIH; K23 HL166977) and the American Heart Association (AHA) Career Development Award (23CDA933663), with payment to the author; and consulting fees from WearLinq Inc, EBR Systems, and YorLabs Inc. The other authors have declared no conflicts of interest.
Chest pain is among the most common reasons for presentation to the emergency department, yet identifying patients at the highest short-term risk remains a clinical challenge.1,2 Conventional triage tools rely on clinical variables and troponin assays, but these have limited sensitivity at the time
of arrival.3 Recent advances in deep learning applied to ECGs have demonstrated the ability to detect arrhythmias, structural heart disease, and prevalent atherosclerotic cardiovascular disease, but their application to acute chest pain risk stratification has been less studied.4-6 The authors evaluated whether a convolutional neural network (CNN)-derived ECG risk score could improve the prediction of nearterm cardiovascular mortality in patients presenting with chest pain.
MATERIALS AND METHODS
This retrospective cohort study leveraged over 1.5 million ECGs recorded at Stanford, California, USA, between 2005–2019. After exclusions for low-quality tracings, missing troponin, and non-chest pain presentations, the final study cohort comprised 22,590 adults presenting with chest pain. Raw waveform data from 12-lead ECGs were used to train and validate a CNN model to generate a continuous ECG risk score (ECG-Risk). Outcomes were ascertained from electronic health records and the Social Security Death Index (SSDI). The primary endpoint was 30-day all-cause mortality, while secondary endpoints included 365-day mortality and a composite of 30-day cardiovascular mortality or revascularisation (percutaneous coronary intervention or coronary artery bypass grafting). Multivariable logistic regression models incorporated ECG-Risk alongside age, troponin, race, blood pressure, hyperlipidaemia, diabetes, prior myocardial infarction, and smoking status. Model discrimination was assessed with the area under the receiver-operating characteristic curve, and improvements were evaluated with DeLong testing and reclassification indices.
RESULTS
In the overall cohort (median age: 55 years; 52% female), the 30-day mortality
1: Area under the receiver operating characteristic curve comparison for baseline risk model versus ECG-based risk estimator model.
rate was 1.4%. ECG-Risk was strongly associated with short-term mortality in both unadjusted analysis (odds ratio [OR]: 3.74; 95% CI: 2.91–4.82) and adjusted models (OR: 3.47; 95% CI: 2.66–4.54). Notably, no 30-day deaths occurred in patients with an ECG-Risk below –1.25, suggesting potential utility as a rule-out threshold. Incorporation of ECG-Risk significantly improved prediction beyond traditional clinical variables and troponin (area under the receiver-operating characteristic curve: 0.80 versus 0.75 for baseline model; p<0.05), and net reclassification analyses confirmed incremental prognostic value (Figure 1). ECG-Risk also predicted secondary endpoints, including higher 365-day mortality (adjusted OR: 2.03; 95% CI: 1.80–2.30) and the 30-day mortality/ revascularisation composite (adjusted OR: 2.43; 95% CI: 2.17–2.72). Importantly, ECGRisk was not correlated with troponin levels (p>0.05), highlighting its ability to capture independent prognostic information.
CONCLUSION
These findings suggest that a CNN-derived ECG risk score meaningfully improves shortterm risk prediction in patients presenting with chest pain, offering additive value
to existing triage models. The absence of events among patients with very low scores highlights its potential role in early rule-out strategies, while its independence from troponin indicates complementary clinical utility. Once validated prospectively, this tool could enable earlier and more precise decision-making in the emergency department, ultimately improving outcomes for patients with acute chest pain.
References
1. Parsa S et al. Deep-learning based approach to ED chest pain risk stratification by ECG. Abstract. ESC Congress, 29 August-1 September, 2025.
2. Backus BE et al. Risk scores for patients with chest pain: evaluation in the emergency department. Curr Cardiol Rev. 2011;7(1):2-8.
3. Boone S, Peacock WF. Contemporary biomarker strategies for patients with chest pain. Rev Cardiovasc Med. 2022;23(5):157.
4. Hughes JW et al. A deep learning-based electrocardiogram risk score for long term cardiovascular death and disease. NPJ Digit Med. 2023;6(1):169.
5. Attia ZI et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: a retrospective analysis of outcome prediction. Lancet. 2019;394(10201):861-7.
6. Goto S et al. Multinational federated learning approach to train ECG and echocardiogram models for hypertrophic cardiomyopathy detection. Circulation. 2022;146(10):755-69.
Figure
Model
Congress Interviews
In these exclusive interviews, Thomas F. Lüscher (ESC President) and Florian A. Wenzl (member of the ESC Digital Cardiology and Artificial Intelligence Committee) discuss ESC’s 75th anniversary, its global impact, and future priorities. They highlight cardiology’s evolution, advances in AI and precision medicine, novel biomarkers, and new congress initiatives, showcasing how ESC leadership is driving collaboration, innovation, and cardiovascular health worldwide.
Featuring: Thomas F. Lüscher and Florian A. Wenzl
Thomas F. Lüscher
Director of Research, Education, and Development and Consulting Cardiologist, Royal Brompton & Harefield Hospital Trust; Professor of Cardiology, Imperial College London, UK; Director of the Center for Molecular Cardiology, University of Zurich, Switzerland; President, European Society of Cardiology (ESC)
The ESC today consists of seven associations, seven councils, and 15 working groups
This year, you celebrated 75 years of the European Society of Cardiology (ESC), with this year’s overarching theme of Cardiology Beyond Borders and a spotlight on Global Health. How has global collaboration in cardiology evolved over the past 75 years?
First of all, the pioneers started the ESC 75 years ago. These were mainly colleagues from Sweden, France, Germany, and the UK, so it was a relatively smaller group of people. Remember, at the time, Europe was divided, and the Iron Curtain was in place, so it was a rather small society: a club of friends, as I called it in my article.1 Now we really are an institution, and we have 48 national cardiac societies as members. The ESC today consists of seven associations, seven councils, and 15 working groups. We have more than 100,000 members. So, it's been a fantastic growth.
We are also very proud of what our members have achieved over the years. European physicians
and scientists developed the first pacemaker, performed the first coronary angioplasty, implanted the first stent, introduced ablation of atrial fibrillation, performed the first catheter-based pulmonary valve replacement, and the first aortic valve replacement. And then, of course, many drugs have been invented in Europe, and echocardiography was invented in Sweden and has become the work horse of cardiology worldwide. Godfrey Hounsfield, a British electrical engineer, developed CT, so Europe has made a fantastic contribution to cardiology. That's why I published the President’s lecture, ‘Shaping the future on a solid tradition’.2
Q2
When we spoke this time last year, you mentioned a desire to expand ESC collaboration with societies in Northern Africa, the Middle East, and Eurasia. What steps have been taken so far?
We took the newer societies that emerged after the fall of the Iron Curtain and beyond into the ESC,
but we have to further help them with education and research options. And so, I created three task forces. For North Africa and the Middle East, the task force is run by a friend from Egypt: Magdy Abdelhamid, Kasr Alainy School of Medicine, Cairo, Egypt. Then, one task force for Eastern societies, for example, Poland, Serbia, and Hungary, among others, is run by Petar Seferović, University Clinical Center of Serbia, Belgrade, Serbia. The third task force involving Eurasia is run by Robert Gil, National Medical Institute of the Ministry of Internal Affairs, Warsaw, Poland. We did a survey to ask them what they expect from the ESC, and what the ESC could do for them. As an immediate action, we provided 45 travel grants for young colleagues aged ≤40 years who had an abstract accepted at our Annual Congress in Madrid this August. We would also like to expand on this further and consider observerships for fellows. So, we're working on that to really help these National Cardiac Societies develop their practice and research further, because in these countries, access to care is still suboptimal for many procedures. Transcatheter aortic valve implantation, as an example, is massively less accessible in
these countries compared with richer ones.
Q3
Exploring the theme of global health, what do you believe to be the top three health challenges in global cardiology today, and how might your answer change if I asked you again in 5 years?
Currently, I think the top three health problems we face are, first of all, pollution. Climate change affects the cardiovascular system, and many people are exposed to environmental hazards; this applies very much to developing countries. For instance, in New Delhi, India, the air quality is very poor. It used to be very poor in Beijing, China, too, but it has improved a bit. We're also exposed to environmental hazards, such as noise and light, which interfere with the circadian rhythm.
The second big problem is the obesity pandemic and the cardiometabolic changes in different organs, such as the pancreas, muscle, liver, and kidneys. This is extremely important, as it can eventually lead to heart failure, whether with preserved or reduced ejection fraction, and also myocardial
infarction, stroke, and premature cardiovascular death. We have brought this all together through the European Alliance for Cardiovascular Health (EACH), involving all the societies working on these different organs, to implement a cardiovascular health plan at the European level, and hopefully also secure proper finances for it in the near future.
The third problem is prevalent in more affluent societies, and that's the ageing population. For instance, the age distribution in the UK compared to Egypt differs massively. We have many more elderly people, whereas in Egypt, the age distribution is still like a pyramid, with most individuals being in the younger age range. As we know, cardiovascular diseases are massively age dependent. So, in spite of all the progress we made, we will see more patients with cardiovascular disease, because those aged >70 years, even >90 years, are growing rapidly. I think these are the three major topics that we have to address.
In 5 years, I think the environmental hazards will still be a problem, and this is a huge political issue. Accordingly, the ESC is addressing this at the
European Commission level. Europe, of course, had the green policy, but it has not evolved as we expected, particularly now, because of the military confrontations we are currently facing. Plastic is also a very important problem. It enters our body and eventually ends up in our arteries. The Geneva conference on plastic waste unfortunately was not successful, as there are still many countries opposing the major changes required to reduce environmental hazards. The ESC has a task force on that issue, and we are trying to move things forwards at the European level as much as possible. The obesity pandemic will still be a severe problem in 5 years. I think, with new drugs, we have tools at hand to massively reduce not only body weight, but the cardiovascular complications associated with obesity. The question still remains there: can we use this to get people back to a normal weight, or do they have to take this for
life like antihypertensives or lipid-lowering drugs? That's a big issue still under discussion. And regarding age, there's a lot of research on how to intervene with age-promoting molecular pathways. I think ageing will be the next disease, and there's a lot of progress on how to interfere with the underlying pathways that eventually determine whether or not you have risk factors for atherosclerosis, whether environmental or organic in nature.
Q4
Has the ESC made progress towards securing EU support for a cardiovascular health plan, as you hoped last year?
On the 3rd of December 2024, it was announced by the 27 Ministers of Health of the European Union, under the leadership of the then Hungarian Health Minister, Péter Takács, that cardiovascular conditions would be made a priority. We then met several times with the
newly elected Commissioner of Health, Olivér Várhelyi. We met with members of Parliament, and also with officials of the Direction de la Santé of the European Union. We talked extensively with them about the major topics that should be considered for research and prevention. I also gave a lecture to the person responsible for writing this plan, and we sent additional advice to them by email. We had a glimpse of the plan, and I think it looks pretty good. Of course, the key issue is whether sufficient funding is allocated. In the last mandate, cancer got 4 billion EUR. If we get 3 billion EUR, especially in the context of the increased military spending required, we would be happy, and we hope this will be the case. Horizon Europe is also an important factor. Initially, there were plans to cut its funding, but the budget has now been doubled for Horizon Europe calls for grants. This is significant not only for the EU, but also for the UK and Switzerland, who have agreements in place allowing
We had over 33,000 participants, and more physicians among them than ever before
them to participate in such calls. Overall, this looks very promising, and we will see what the calls are when they open next year; hopefully many are focused on cardiovascular diseases, AI, and so on.
Q5
You also noted digital cardiology, particularly AI and machine learning, as your top priority for your presidency. What progress has the ESC made in this area over the past year?
First of all, we developed the ESC Chat in record time. This is an AI-enhanced tool that uses large language models to integrate all valid ESC guidelines in one place. You can ask questions and receive an immediate answer. The ESC Chat is now available online, and people can search for it on the ESC platform or via Google, download it, and start using it. I felt that reading these huge guideline documents was just not feasible for physicians, not even for me. That is why we developed this tool, which we presented to the global community at the Annual ESC Congress in Madrid, Spain this August. We are also now using AI to support the evidence base for guidelines currently in production. Moreover, from the 21st–22nd November 2025, in Berlin, Germany, we will hold the first ESC Digital Cardiology & AI Summit. The final project is to develop an AI-enhanced digital twin app to act as a mentor for patients after myocardial infarction, helping to optimise secondary prevention according to current guidelines.
References
Q6
Reflecting on your first congress as President, what has been the most surprising part of the role?
I was surprised and delighted to see that we had over 33,000 participants, and more physicians among them than ever before. This made it the most successful Congress, with 167 countries participating. Also, because we were in Madrid, Spain, we had more participants from Latin America, with 2,800 attending this year. We're delighted that the ESC is now secured as the first-line society in cardiovascular medicine worldwide. We also had fantastic hotlines, and we really made a huge impact in the medical literature with this Congress. People were really happy, and I received lots of compliments; our post-event survey revealed an 86% satisfaction rate from participants. And, of course, we also had the King of Spain at a fantastic closing session. Initially, I was a bit concerned about whether we would have enough people attending, but the auditorium, with 3,500 seats, was packed. People were even standing, which was a very nice way to close such a succes sful Congress.
Q7
Looking to the year ahead, what ESC initiatives are you most looking forward to developing further?
The most important historical decision we have taken recently is that we will no longer leave all interventional cardiology activities exclusively to PCR (Paris Course
1. Lüscher TF. From a club of friends to an institution: past successes and future challenges for the European Society of Cardiology. Eur Heart J. 2024;45(36):3303-5.
on Revascularization). Instead, the ESC, with the European Association of Percutaneous Cardiac Intervention (EAPCI), will organise its own Congress. The first EAPCI Interventional Summit will take place in Munich, Germany, from the 19th–20th February next year. We want to expand our interventional educational offer of the EAPCI association, and we feel that we have a different profile from PCR. We are more academic. We will integrate interventional cardiology with heart failure, the association of rhythm disorders and prevention, so that we are more integrative than other courses, which mainly focus on the technical aspects of intervention itself. We will do this together with many other societies, including Transcatheter Cardiovascular Therapeutics (TCT), the European Association of CardioThoracic Surgery (EACTS), and hopefully PCR as well. We're also discussing a collaboration with the International Society of Heart and Lung Transplantation (ISHLT). This will truly make it an interventional networked event. Our strength is science, and we will thus foster science. We also publish all Interventional Cardiology guidelines, and we have a new journal, so we're well placed to develop this further over the next 5 years. We hope to make this a successful congress as well, and are very excited about this new strategy. There's such a huge interventional community; even in our own database, there are 76,000 colleagues with an interest in interventional cardiology. Thus, there is room for everybody.
2. Lüscher TF. Shaping the future on a solid tradition. Eur Heart J. 2025;DOI:10.1093/eurheartj/ehaf693.
Florian A. Wenzl
Center for Molecular Cardiology, University of Zurich, Switzerland; NHS England, London, UK; Department of Cardiovascular Sciences, University of Leicester, UK; Department of Clinical Sciences, Karolinska Institute, Stockholm, Sweden
Q1 You developed the machine learning-based Global Registry of Acute Coronary Events (GRACE) 3.0 score for early risk stratification in nonST-elevation acute coronary syndrome. How does this model improve upon traditional risk scores?
GRACE 3.0 represents the next evolution of the GRACE score, bringing AI methods into one of the most widely used risk tools in cardiology. It was trained and externally validated on data from hundreds of thousands of patients from multiple countries, which gives it a very strong evidence base. Unlike traditional risk scores, GRACE 3.0 captures complex and non-linear relationships that conventional approaches often miss. Another key improvement is that GRACE 3.0 is sex-specific and tailored specifically for patients with non-ST-elevation acute coronary syndrome, rather than being applied more broadly across the acute coronary syndrome population. We made it available online,1 and it is now becoming increasingly integrated into international guidelines.2,3
Q2
What stood out is that AI is no longer an abstract future: it is the present
At this year’s European Society of Cardiology (ESC) Congress, you co-chaired the Late-Breaking Clinical Science session on AI-driven cardiovascular biomarkers and clinical decisions. What were the most important take-home messages for clinicians from this session?
What stood out is that AI is no longer an abstract future: it is the present. We also saw very clearly that technological innovation
is a key driver of progress in healthcare, and that the current landscape is changing rapidly. Thus, I think we, as a society, need to go where the puck will be, not where it has been in the past, meaning we should position ourselves where the field is heading. And perhaps the most important message was that integrating AI into daily practice has huge potential to improve the way we deliver care and implement prevention strategies.
Q3 In your opinion, what are the main barriers to implementing AI-based tools in everyday clinical practice?
There are still many hurdles. From a data science perspective, it starts with challenges around creating workable, reliable data objects, and then there are all the important regulatory questions around data safety, privacy, and legal accountability. But perhaps the biggest gap at the moment is evidence. Many AI tools currently available have not been externally validated, and very few are supported by trial-level evidence. Until we close that gap, clinicians will understandably be hesitant to adopt them more broadly.
Q4 You also co-chaired a session on precision diagnostics. Can you briefly explain why the shift towards precision therapy in cardiology is so critical?
This was a vibrant session that I had the pleasure of co-chairing with Anja Hennemuth from Charité – Universitätsmedizin Berlin, Germany. For decades, cardiology has largely been guided
by the average treatment effect. While this approach has served us well in many ways, it does not fully reflect clinical reality. A given therapy might be highly effective for some individuals, but less beneficial or even harmful for others. Recognising this heterogeneity in treatment effects is crucial. Moreover, we are now at a point where we have remarkable tools, such as gene editing, small interfering RNAs, and monoclonal antibodies, that enable us to target disease mechanisms much more precisely. Together, these advances create the basis for truly individualised care in the future.
Q5
In your presentation, you showed that gut microbiota-derived imidazole propionate predicts cardiometabolic risk in patients with coronary artery disease. How might this novel biomarker guide the development of new therapeutic targets?
This is a very exciting area. Mechanistic studies published recently have shown how imidazole propionate drives atherosclerosis by modulating innate immune cells and endothelial cells, leading to inflammatory activation.4,5 Our recent study, presented at the
This really puts the gut–heart axis back on the map in residual risk management
ESC Congress, brought those findings into the clinical space by showing that this metabolite is a non-traditional cardiovascular risk factor that independently predicts adverse outcomes beyond established determinants of risk.6 This really puts the gut–heart axis back on the map in residual risk management. Targeting either imidazole propionate production or its signalling pathway could open up new opportunities for personalised secondary prevention strategies.
Q6
As a member of the ESC Digital Cardiology and Artificial Intelligence (DCAI) Committee, what are the committee’s top priorities in using digital innovation to advance the ESC Strategic Plan?
The ESC has made a strong commitment to making European
healthcare AI-ready. Under the leadership of Folkert Asselbergs, University College London, UK, our committee is working on several fronts. We are looking at how to harmonise datasets across Europe, build federated learning infrastructures, and establish a robust evaluation framework to ensure that AI is both trustworthy and useful. Education is another top priority. The committee is currently developing a curriculum framework for digital cardiology and AI and, for the first time, has launched a dedicated congress on AI: the ESC Digital & AI Summit.7
Q7 Looking ahead, what do you hope to achieve, both in research and within the ESC, before next year’s Congress?
In research, we are currently working on several projects aimed at refining cardiovascular risk prediction and participating in ongoing RCTs exploring new translational treatment strategies. Within the ESC, I have the privilege of working as part of the big data group, where our goals are to launch a phenotype library and establish a network of centres of excellence in big data. This will help foster international collaboration and accelerate progress in the field.
References
1. Global Registry of Acute Coronary Events Score 3.0. Available at: https:// www.grace-3.com/. Last accessed: 17 June 2025.
2. Wenzl FA, Lüscher TF. Application of a sex-specific GRACE score in practice - authors' reply. Lancet. 2023;401(10370):23.
3. Brieger D et al.; other members of the Heart Foundation working group. National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: comprehensive
Australian clinical guideline for diagnosing and managing acute coronary syndromes 2025. Heart Lung Circ. 2025;34(4):309-97.
4. Mastrangelo A et al. Imidazole propionate is a driver and therapeutic target in atherosclerosis. Nature. 2025;645(8079):254-61.
5. Nageswaran V et al. Gut microbial metabolite imidazole propionate impairs endothelial cell function and promotes the development of atherosclerosis. Arterioscler Thromb Vasc Biol. 2025;45(5):823-39.
6. Wenzl FA et al. Gut microbiotaderived imidazole propionate predicts cardiometabolic risk in patients with coronary artery disease. Eur Heart J. 2025;DOI:10.1093/eurheartj/ehaf661.
7. European Society of Cardiology (ESC). ESC Digital & AI Summit 2025. 2025. Available at:https://www.escardio.org/ Congresses-Events/ESC-Digital-AISummit?gad_source=1&gad_campaign id=22487213011&gbraid=0AAAAAD4V Fqb9Lk2eYeb7x-AL0u-XCSMNt&gclid= EAIaIQobChMInaCnrevejwMVYpGDBx 3HThmtEAAYAiAAEgL0zfD_BwE#. Last accessed: 17 September 2025.
Novel Cardiac Sarcomere Modulator, EDG-7500, in Hypertrophic Cardiomyopathy: Evaluating New
Interviewees:
Phase II Data from CIRRUS-HCM
Michelle Michels,1 Perry Elliott2,3
1. Erasmus MC Center of Expertise for Inherited Cardiovascular Diseases, Rotterdam, the Netherlands
2. Centre for Heart Muscle Disease, University College London (UCL), UK
3. Inherited Cardiovascular Disease Unit, Barts Heart Centre, St Bartholomew's Hospital, London, UK
Support: The publication of this article was funded by Edgewise Therapeutics.
Disclosure: Michels has received a research grant from Bristol Myers Squibb; and consultancy and speaker fees from Bristol Myers Squibb, Cytokinetics, Alnylam, and Bayer. Elliott has received consultancy and speaker fees from Bristol Myers Squibb, Pfizer, Cytokinetics, Amicus, Forbion, Solid, AstraZeneca, and Affinia.
Acknowledgements: Medical writing assistance was provided by Juliet George, Chester, UK.
Disclaimer: The opinions in this article belong solely to the named interviewees. The content of the article was authored independently and does not reflect the opinions of Edgewise Therapeutics. EDG-7500 is currently an investigational compound and is not approved for clinical use, with safety and efficacy not yet established.
Hypertrophic cardiomyopathy (HCM) is an inherited disease characterised by thickening of the left ventricular wall, which can lead to symptoms such as fatigue, exertional dyspnoea, and an increased risk of sudden cardiac death. The approval of the first targeted therapy (mavacamten, a cardiac myosin inhibitor [CMI]) to treat obstructive HCM (oHCM) has been a significant advance. However, there are still
many therapeutic unmet needs, crucially the lack of an approved treatment for nonobstructive HCM (nHCM). Additionally, CMIs can cause decreases in LVEF that necessitates a resource-intensive dose-titration process. EDG-7500, a novel, selective cardiac sarcomere modulator, is currently in development for the treatment of HCM, and data from the 4-week portion of the Phase II CIRRUS-HCM study of EDG-7500 were presented at the Annual Meeting of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC) in May 2025. During the interviews conducted for the European Medical Journal (EMJ) in June 2025, the significance of these new data was discussed by Michelle Michels, Director of the Erasmus MC Center of Expertise for Inherited Cardiovascular Diseases, Rotterdam, the Netherlands; and Perry Elliott, Director of the Institute of Cardiovascular Science, University College London (UCL), and consultant cardiologist at St Bartholomew’s Hospital, London, UK.
The experts reviewed the clinical findings of CIRRUS-HCM, highlighting key elements including diastolic benefits and preservation of systolic function, as well as mechanistic features and practicalities, which have the potential to differentiate EDG-7500 from current targeted therapies.
THE DEVELOPING TREATMENT LANDSCAPE
HCM is an inherited condition in which hypercontractility of the heart muscle leads to thickening of the left ventricular wall, diastolic and systolic dysfunction, reduced cardiac output, and myocardial ischaemia. Better understanding of HCM at the molecular level has allowed the development of therapies that target the actin–myosin interaction in the cardiac sarcomere to address the underlying hypercontractility. CMIs were the first class of targeted therapies for the treatment of HCM, followed by the first-in-class cardiac sarcomere modulator, EDG-7500, now in development, with the most recent clinical data released from the Phase II CIRRUS-HCM study. In this interview article, cardiology specialists Michelle Michels and Perry Elliott review these latest clinical findings for EDG-7500 and consider the potential role for this novel targeted agent within the field of HCM management.
Michels began by outlining some of the difficulties inherent in treating HCM: “It is a complex condition, with a highly variable presentation, from both a clinical and a genetic standpoint. The phenotypes range from [asymptomatic] carriers of a pathogenic, or likely pathogenic, DNA variant without any hypertrophy, to extreme left ventricular hypertrophy, and patients
presenting primarily with heart failure. So that’s the big challenge: it’s one disease with one name, but it comes with many different faces.”
HCM is classified as being either obstructive or non-obstructive, depending on the presence of left ventricular outflow tract (LVOT) obstruction at rest or with provocation. Elliott clarified, “Many people with HCM have limiting symptoms of chest pain, breathlessness, and fatigue. In the majority, symptoms are caused by LVOT obstruction.” As noted above, this results from the thickened left ventricular wall and the phenomenon of systolic anterior motion of the mitral valve, in which the valve is driven forward in ventricular systole such that it touches the septum and blocks the outflow of the heart. Elliot explained that patients with nHCM do not have LVOT obstruction, but these patients may still experience symptoms caused by a stiffened heart muscle and progressive heart failure. He added, that some complications are common to both forms of HCM, including a raised risk of atrial and ventricular arrhythmias. “The major preoccupation of doctors and patients alike over the past 50 years has been that the condition is associated with sudden cardiac death. However, with better risk stratification and protective technology (implantable cardiovascular defibrillators), sudden cardiac death is now quite a rare event,” he
said. Consequently, the focus has turned toward diastolic dysfunction, an areas where other therapies have not been as successful.
Summarising the traditional symptomatic treatment approach to HCM, Elliott remarked, “Historically, management for HCM started with drugs that target LVOT obstruction by reducing the contractility of the heart: beta blockers, calcium antagonists, and the anti-arrhythmic drug disopyramide. These drugs can be effective, but we now recognise that many patients don’t respond, or the side effects are very unpleasant and not much has changed until very recently.” However, even with the advent of targeted therapy in the form of CMIs, the experts agreed that the treatment options for non-obstructive disease remain limited. Michels clarified, “We currently lack sufficient medical options to treat patients with nHCM and to relieve them from their symptoms, compared with oHCM, where we not only have medications but also invasive treatment options [to reduce the thickening/ obstruction in the heart wall].”1,2
The Targeted Treatment Approach
The arrival of CMIs has been an important advance in the treatment of HCM, with mavacamten currently approved to treat oHCM,3,4 and aficamten awaiting approval.5 Considering the pros and cons of CMIs, Michels commented, “I think the big advantage is that [mavacamten] is the first targeted HCM treatment, and there are robust, placebo-controlled trials. In experienced hands, it’s safe, and [its] efficacy is good. However, a drawback is the extensive patient follow-up, including echocardiography to monitor the [potential drop in] left ventricular ejection fraction (LVEF),3,4 which is a challenge with the current pressure on healthcare systems and resources. It also means we can’t use CMIs in patients who already have a reduced LVEF.” The underlying cause of this effect on LVEF is the potent inhibitory action of the CMIs on the cardiac sarcomere. As Elliott explained, “The CMIs are targeting one of the fundamental molecular mechanisms of the disease. If you look at what’s happening at a cellular level in HCM, the cells are
contracting more forcefully than is normal, and the consequence is that it increases the energy requirements of the heart, leading to the secondary phenomenon of hypertrophy. So, it was reasoned that if the hypercontractile phenotype could be reduced at a molecular level, it might reduce the drive to hypertrophy. However, the major Achilles heel of the CMIs is that their effect on contractility is very potent. What you don’t want to do is overshoot, reduce the contraction, and risk precipitating heart failure. This is why we have to monitor the contractile function of the heart, the LVEF, with each dose increment. It means that the intensity and frequency of monitoring when you’re starting CMIs is much greater than for any other existing drugs [for the treatment of HCM].” Michels added, “Another drawback is that [mavacamten] is only proven effective in patients with oHCM. We’ve been disappointed and, to a certain level, also surprised that the topline results from the Phase III ODYSSEY-HCM trial [mavacamten in nHCM; NCT05582395] turned out negative recently.”6
EDG-7500
Against the background of this first wave of targeted therapies, EDG-7500 is a novel, oral, selective cardiac sarcomere modulator, which has been specifically designed to reduce the speed and force of early systole, and improve myocardial relaxation in early diastole, without impacting systolic function.7 It is being developed for the treatment of both oHCM and nHCM. Elliott explained how the modulatory effect of EDG-7500 is potentially different from the inhibitory action of the CMIs, and that this could translate into clinical distinctions: “Like the CMIs, EDG-7500 is working on the contractile function of the heart at the sarcomere level, but what it seems to do is [...] reduce the velocity at the beginning of contraction, which is when the mitral valve starts to push forwards [leading to systolic anterior motion and obstruction in the LVOT]. So, it affects contractility, but only in that early part of contraction. The other thing it seems to do is improve diastolic function, which is an important target in HCM, and also has the potential to reduce
LVOT obstruction without compromising LVEF to the same degree as CMIs.” Michels shared her thoughts on this novel drug: “While the CMIs inhibit the myosin head, EDG-7500 slows the rate of actin–myosin engagement and also speeds up the rate of disengagement [during diastole], so diastolic parameters may also be improved, and hopefully we won’t see the drop in LVEF.”
CIRRUS-HCM
CIRRUS-HCM (NCT06347159) is a Phase II, multi-part, open-label cohort trial8,9 that has provided the first inpatient data for EDG-7500 in HCM. Consistent with preclinical and Phase I study findings in healthy volunteers,7,10,11 CIRRUS-HCM (Part A) showed that a single oral dose of EDG7500 in patients with oHCM was associated with robust reductions in LVOT gradient and N-terminal pro-B-type natriuretic peptide (NT-proBNP), without meaningful changes in LVEF.7 Newly released data from CIRRUSHCM (Parts B and C) on the safety and efficacy of multiple (once-daily) oral doses of 50 or 100 mg of EDG-7500 over 4 weeks in patient cohorts with oHCM and nHCM, were presented at the Annual Meeting of the HFA of the ESC in May 2025. Michels and Elliott gave their considered reactions to these findings.
Looking at the study design and patient population of CIRRUS-HCM, the experts favoured the inclusion of oHCM and nHCM cohorts within the same study. They also remarked on the unusual (for HCM) predominance of female patients in both cohorts (oHCM: 71%; nHCM: 58%), and the high rate of hypertension in the oHCM cohort (65%) at baseline.5,12,13
Efficacy Data
In CIRRUS-HCM, early effects on diastolic function with EDG-7500, as well as improvements in quality-of-life measures (Kansas City Cardiomyopathy Questionnaire-Overall/Clinical Summary Scores [KCCQ-OSS/CSS]), were key findings in the oHCM cohort (n=17). Michels remarked, “There is a really quick response. Already at Week 1, you see improvement
[from baseline] in LVOT gradient, a drop in NT-proBNP (Figure 1), and also an increase in e’ velocity, which is a diastolic parameter. I think that is impressive. Then at 4 weeks, 89% of the patients [in the 100 mg group] had large/very large improvements in KCCQ-CSS (≥10 points; Figure 2) and 78% had improved their New York Heart Association (NYHA) functional class, which is also a quick response. We know from mavacamten, which has a longer half-life,3,4 that it takes a little bit longer to see these results.”5,12 Elliott’s impressions were also cautiously positive: “It’s a small number of patients, but it’s shown that the drug can reduce LVOT obstruction, both at rest and with Valsalva provocation, and there were reductions in NT-proBNP, which is a very sensitive marker for myocardial strain. So, in that respect, these effects are all very similar to the effects of CMIs.”
Echoing Michels’ observations, Elliott also highlighted the magnitude of improvement in quality-of-life score with EDG-7500 in the oHCM cohort.
In the nHCM cohort (n=12), Michels again noted the rapid and robust effects on NTproBNP (Figure 1) and e’ velocity, already apparent at Week 1. Elliott described the reduction in NT-proBNP an improvement in diastolic parameters as “reducing one of the fundamental problems in nonobstructive disease,” and explained the significance of the improvements in quality of life seen in both cohorts: “On the KCCQ, a 5-point change is generally regarded as being clinically meaningful. With the CMIs, we see 10–15-point changes [in oHCM], which is pretty dramatic, but in the EDG-7500 data, we see even more change, around 20 points [in KCCQ-CSS for oHCM; 22 points for nHCM; 100 mg groups], which is huge. You certainly wouldn’t see that magnitude of change in heart failure trials with conventional drugs.” Michels was in agreement: “If you look at the obstructive cohort, you see a really impressive improvement in KCCQ-CSS (Figure 2), with 22% of patients [in the 100 mg group] even showing an improvement of ≥20 points. For the nHCM cohort, it’s a little bit more of a mixed bag: some patients respond extremely well, almost 38% [in the combined 50/100 mg groups
Figure 1: Change from baseline in N-terminal pro-B-type natriuretic peptide with EDG-7500 treatment (CIRRUSHCM).
at Wk4 vs Baseline, both dose groups
Study Visit
A) Obstructive hypertrophic cardiomyopathy. B) Non-obstructive hypertrophic cardiomyopathy.
*Two participants at Week 4.
Data are mean±SEM.
EOS: end of study; NS: non-significant; SEM: standard error of mean; vs: versus; Wk: week.
have improvements of ≥20 points], but then 25% have just small improvements [of ≥5–10 points], but these are still clinically meaningful improvements. We physicians worry about prognosis and the long term, while patients just want to feel better, at least at the start. So, I was impressed by the KCCQ data.”
Summarising their thoughts on the CIRRUSHCM efficacy data, the experts said that EDG-7500 appeared at least as effective as the CMIs in oHCM, producing similar improvements but with a potentially sooner response. As for nHCM, Michels remarked, “We have just learned that the Phase III ODYSSEY-HCM trial of mavacamten is negative in nHCM6 and we are awaiting
Figure 2: Change from baseline in patient-reported health status (Kansas City Cardiomyopathy QuestionnaireClinical Summary Score) with EDG-7500 treatment (CIRRUS-HCM).
Very Large Improvements of ≥20 Points
Worsened ≤–5 Points
Very Large Improvements of ≥20 Points
Large Improvements of ≥10–20 Points
89% With Clinical Improvements
Large Improvements of ≥10–20 Points
88% With Clinical Improvements
A) Obstructive hypertrophic cardiomyopathy* B) Non-obstructive hypertrophic cardiomyopathy†
*100 mg treatment group.
†Combined 50 mg and 100 mg treatment groups.
the results of the Phase III ACACIA-HCM study of aficamten.14 The aficamten Phase II data look promising (REDWOOD-HCM),15 but I think we have to be careful, because we also thought that the Phase II data for mavacamten looked promising.”16 Consequently, Michels emphasised the importance of the study findings for EDG7500 in the non-obstructive cohort of CIRRUS-HCM.
Left Ventricular Ejection Fraction Preservation
As noted above, systolic dysfunction leading to reductions in LVEF has been described with the CMIs, making LVEF a key outcome of interest for EDG-7500. “In all drugs that modulate the actin–myosin interaction, we’re afraid of drops in LVEF,” said Michels, “but no meaningful reductions in LVEF were reported in CIRRUS-HCM (Figure 3), and also no LVEF below 50%. That’s very reassuring, although we need to take into account that we are looking at small patient numbers, so it needs to be proven in a larger cohort.” Elliott added that
Study Visit
*Two participants at Week 4.
Data are mean±SEM.
EOS: end of study; LVEF: left ventricular ejection fraction; SEM: standard error of mean; Wk: week.
there was no evidence of an LVEF doseexposure relationship, and suggested that the preservation of LVEF “may be an even greater discriminant from the CMIs in non-obstructive disease.”
Alongside the important safety implications of LVEF preservation observed with EDG7500, the experts were keen to emphasise the potential practical benefits of a treatment that requires no LVEF monitoring. “It would be a major advantage for patients first, but also for the healthcare system,”
said Michels, with Elliott adding, “At the moment, there are significant restrictions on centres that are allowed to prescribe CMIs. We also have to follow tight protocols for regular monitoring, and there’s no doubt in my mind that this is limiting access to the CMIs, certainly within the UK, but I think in many other European systems as well. We’re having to set up services specifically for the tight up-titration and monitoring of people treated with CMIs, which is a challenge. If we had a drug which we could start and then see the patient at realistic intervals
A) Obstructive hypertrophic cardiomyopathy. B) Non-obstructive hypertrophic cardiomyopathy.
Figure 3: Change from baseline in left ventricular ejection fraction during treatment with EDG-7500 (CIRRUS-HCM).
without having to worry about safety echocardiograms, I think that would be a huge step forward.”
Adverse Events
Overall, the experts found EDG-7500 to be generally well tolerated in CIRRUS-HCM in the combined oHCM and nHCM cohorts. The lack of any meaningful reduction in LVEF was viewed as a key differentiating safety outcome (see above), the adverse event profile was largely as expected. Michels noted that, similar to the CMIs, the most common treatment-emergent event was dizziness [27.6%; 8/29 patients], which was mainly mild and transient, and that atrial fibrillation (AF) was reported by 13.8% [4/29 patients]. Elliott commented, “The rate of AF was much higher than seen in the pivotal trials with CMIs,5,12,13,17,18 but this is where small patient numbers are really important. Unfortunately, there were a couple of patients who probably shouldn’t have been included in CIRRUS-HCM. For example, one had mitral valve stenosis, which is a disease where the incidence of AF is very high. I think a fairer comparison would be with the Phase II trials of CMIs; for example, PIONEER-HCM with mavacamten, where the rate of AF was actually very similar to this (27%).19 Obviously, the only way of answering this is through more data, but I’m not particularly concerned by the AF rate at this stage.” Michels added, “There’s been a lot of debate about AF in HCM patients treated with CMIs,20,21 and whether these drugs are increasing the risk of AF, or if we’re just looking at the high prevalence of AF in HCM patients. I don’t think the case is closed on that.”
LOOKING AHEAD
Although cautious about drawing conclusions from Phase II data with small patient numbers (and noting that Part D of CIRRUS-HCM is ongoing), Michels and Elliott were optimistic about the prospects for EDG-7500 and reflected on its future development in HCM. “The next step is obviously a Phase III trial,” said Elliott, “and the best outcome would be that it replicates the results of the Phase
II study, so that we’ll have a drug that is safe and capable of reducing obstruction and improving symptoms in obstructive and non-obstructive disease. Then the fundamental question will be, is this better than the CMIs? In an ideal world, we’d like to compare them head-to-head, but I don’t think that’s going to happen. So, the debate will then be around tolerability. Another difference is that the only licensed CMI (mavacamten) has a lot of drug interactions,3,4 and is metabolised in the liver, so if you carry a particular genetic variant in one of your liver enzyme systems, then you have to limit the dose. You don’t have to do that for aficamten18 and, as I understand it, it wouldn’t be an issue with EDG-7500 either. In essence, I think it’s going to be efficacy, safety, [and] impact on quality of life, and if these seem to be better than the CMIs, then EDG-7500 will have the edge. If I were being highly optimistic, I would say that the promise of EDG-7500 is that we could treat obstruction without the worrying side effect of low ejection fraction, and we may have something which is more effective in non-obstructive disease.”
Michels concurred, expressing that the big opportunity for EDG-7500 lies in nHCM, where the “playing field is completely open”.
A profile of favourable efficacy with no meaningful impact on LVEF could broaden the population for targeted treatments in HCM without the practical drawback of frequent monitoring visits. As the experts discussed earlier, the need for frequent monitoring and tightly regulated up-titration at an expert medical centre currently limits patient access to mavacamten, so a treatment that could be safely administered beyond Centres of Excellence would favour patient accessibility. Drug–drug interactions and dosing frequency were cited as further important considerations for any emerging treatment, although Elliott observed that there may be a ‘trade-off’ between dosing frequency and feeling better, with the difference between once- or twice-daily dosing becoming less significant to patients if the treatment ‘transforms their lives’.
In addition, the experts advocated the benefits of a simple dose titration scheme and noted that intra-patient dose titration for EDG-7500 would be explored in the
ongoing CIRRUS-HCM study, with longerterm data expected. Elliott commented, “A more granular dosing regime, adding a lower and a higher dose, would allow us to find the ‘sweet spot’ in efficacy for EDG7500. This would, ultimately, give us more flexibility in the use of the drug, should clinical findings be positive.”
CONCLUSION
In conclusion, Michels commented, “I think mavacamten, the first of the CMIs, was already a really sophisticated drug, and it’s very promising that there are new
References
1. Arbelo E et al.; ESC Scientific Document Group. 2023 ESC Guidelines for the management of cardiomyopathies. Eur Heart J. 2023;44(37):3503-626.
2. Ommen SR et al. 2024 AHA/ACC/ AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology Joint Committee on clinical practice guidelines. Circulation. 2024;149(23):e1239-311.
3. Bristol Myers Squibb. Camzyos® prescribing information. 2025. Available at: https://packageinserts. bms.com/pi/pi_camzyos.pdf. Last accessed: 6 June 2025.
4. Bristol Myers Squibb. Camzyos® summary of product characteristics. 2025. Available at: https://www.ema. europa.eu/en/documents/productinformation/camzyos-epar-productinformation_en.pdf. Last accessed: 6 June 2025.
5. Desai MY et al. Mavacamten in patients with hypertrophic cardiomyopathy referred for septal reduction: week 56 results from the VALOR-HCM randomized clinical trial. JAMA Cardiol. 2023;8(10):968-77.
6. Bristol Myers Squibb. Bristol Myers Squibb provides update on phase 3 ODYSSEY-HCM trial. 2025. Available at: https://news.bms.com/news/ corporate-financial/2025/BristolMyers-Squibb-Provides-Update-onPhase-3-ODYSSEY-HCM-Trial/default. aspx. Last accessed: 6 June 2025.
7. Dufton C et al. EDG-7500, a first-inclass cardiac sarcomere modulator, demonstrates favorable tolerability, safety, and pharmacokinetics in healthy adults and patients with
drugs coming onto the market that could be even smarter.” Elliott shared this sense of optimism: “The past 5 years have seen such a rapid pace of development in new therapies for people with HCM. We have one new class of drugs (CMIs), and here we are exploring another class. Already, the companies are developing a second wave of drugs, which may tidy up some of the sideeffect profiles. This is also occurring in the context of exciting approaches around gene therapy; for example, trying to treat the underlying cause of the disease. So, I think there are a lot of reasons to be optimistic about the future for people with HCM.”
hypertrophic cardiomyopathy. Presented at: Global CVCT Forum, 9-11 December, 2024.
8. Edgewise Therapeutics, Inc. Edgewise Therapeutics announces positive top-line results from Phase 2 CIRRUS-HCM four-week trial of EDG-7500 in hypertrophic cardiomyopathy (HCM). Available at: https://investors.edgewisetx. com/news/news-details/2025/ Edgewise-Therapeutics-AnnouncesPositive-Top-Line-Results-fromPhase-2-CIRRUS-HCM-Four-WeekTrial-of-EDG-7500-in-HypertrophicCardiomyopathy-HCM/default.aspx. Last accessed: 9 June 2025.
9. Edgewise Therapeutics, Inc. A study of EDG-7500 in adults with hypertrophic cardiomyopathy (CIRRUS-HCM). NCT06347159. https://clinicaltrials.gov/study/ NCT06347159.
10. Kaplan J et al. EDG-002, a novel targeted sarcomere regulator preserves intrinsic myosin-motor function, blunts hypercontractility and eliminates LVOT obstruction in cats with hypertrophic cardiomyopathy: in vitro and in vivo evidence. J Am Coll Cardiol. 2023;81(Suppl 8):349.
11. Del Rio CL et al. Cardiac effects of EDG-7500, a novel cardiac sarcomere regulator: in vitro and in vivo evidence for slowing isovolumic contraction and improved ventricular compliance. Circulation. 2023;148(Suppl 1):A15822.
12. Olivotto I et al. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2020;396(10253):759-69.
13. Maron MS et al.; SEQUOIA-HCM
Investigators. Aficamten for symptomatic obstructive hypertrophic cardiomyopathy. N Engl J Med. 2024;390(20):1849-61.
14. Cytokinetics®. Cytokinetics announces start of ACACIA-HCM, a pivotal phase 3 clinical trial of aficamten in patients with symptomatic non-obstructive hypertrophic cardiomyopathy in patients with symptomatic non-obstructive hypertrophic cardiomyopathy. 2023. Available at: https://ir.cytokinetics.com/pressreleases/press-release-details/2023/ Cytokinetics-Announces-Start-ofACACIA-HCM-a-Pivotal-Phase3-Clinical-Trial-of-Aficamtenin-Patients-With-SymptomaticNon-Obstructive-Hypertrophic-Cardiomyopathy-09-06-2023/default. aspx. Last accessed: 17 August 2025.
15. Masri A et al.; REDWOOD-HCM Investigators. Efficacy and safety of aficamten in symptomatic nonobstructive hypertrophic cardiomyopathy: results from the REDWOOD-HCM trial, cohort 4. J Card Fail. 2024;30(11):1439-48.
16. Ho CY et al. Evaluation of mavacamten in symptomatic patients with nonobstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2020;75(21):2649-60.
17. Davis BJ et al. Safety and efficacy of mavacamten and aficamten in patients with hypertrophic cardiomyopathy. J Am Heart Assoc. 2025;14(6):e038758.
18. Coats CJ et al.; SEQUOIA‐HCM Investigators. Dosing and safety profile of aficamten in symptomatic obstructive hypertrophic cardiomyopathy: results from SEQUOIA-HCM. J Am Heart Assoc. 2024;13(15):e035993.
19. Masri A et al. Long-term safety and efficacy of mavacamten in symptomatic obstructive hypertrophic cardiomyopathy: interim results of the PIONEER-OLE Study. J Am Heart Assoc. 2024;13(8):e030607.
20. Weissler-Snir A et al. Atrial fibrillation in hypertrophic cardiomyopathy. ACC Adv. 2024;3(9):101210.
21. Sikand N et al. Current management of hypertrophic cardiomyopathy. BMJ. 2025;389:e077274. FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Interviews
EMJ had the privilege to speak with four pioneering figures in cardiology: Cathleen Biga, Christopher M. Kramer, David E. Winchester, and Nancy Sweitzer. Cathleen Biga, Immediate Past-President of the American College of Cardiology (ACC), reflects on advancing team-based cardiovascular care and leadership beyond traditional roles. Christopher M. Kramer, ACC President, highlights breakthroughs in imaging biomarkers and AI in cardiac MRI. David E. Winchester, ACC Secretary and Board of Governors Chair, discusses innovations in imaging, high-sensitivity troponin, and advocacy for equitable care. Finally, Nancy Sweitzer, Director of Clinical Research, Division of Cardiology, Washington University School of Medicine, St Louis, Missouri, USA, shares insights on sex differences in heart failure, trial inclusivity, and the promise of digital health and precision medicine.
Featuring: Cathleen Biga, Christopher M. Kramer, David E. Winchester, and Nancy Sweitzer
Cathleen Biga
Immediate Past-President, American College of Cardiology (ACC); President and CEO, Cardiovascular Management of Illinois, USA
Q1You made history as the American College of Cardiology (ACC)’s first nonphysician president. With over 40 years of experience as a nurse, service line director, hospital vice president, and CEO, what perspective did you bring that might have differed from previous physician presidents?
I think what we have discovered post-COVID-19 is that cardiology is a team sport and caring for today’s patient population requires every member of the team. One of the highlights of my career was being with our patients, but as I moved into administration, I
My advice is: don't assume anything's impossible, because it probably isn't
realised that in order to take care of that full continuum of patients, we really need everybody. It isn't just our nurses and our advanced practice nurses, but our pharmacists, dietitians, technicians, vascular techs, echo techs, electrophysiology lab techs, and catheterisation lab techs are all very important as well. That was probably the one perspective that was very different and needed to be embraced, especially for our international colleagues. I think I was well received, and it was remarkable to really have that message heard. We're seeing the difference, with Clara Inés Saldarriaga Giraldo becoming president of the Colombian Society of Cardiology and Cardiovascular Surgery. I applaud the college for their vision. They certainly do walk the talk, as we say in the USA, and it's been an incredible honour to
represent them. As leaders, we may be at the top for a while, but it's our duty and our responsibility to reach down and raise others to that same stature as they go through their careers.
Q2 What advice would you give to nurses and other healthcare professionals aspiring to transition into business or leadership roles in healthcare, especially in environments traditionally dominated by physicians?
My career was in a non-academic setting, and when the thought of presidency bubbled in my head, the first person I asked was an academic physician. I figured if I was going to get pushback from anybody, it was going to be my academic colleagues, but his immediate answer was: “Amazing.” When I asked a second person, she didn't hesitate. She said: “The time is right. The time is now. The time is for all of us to realise that
we each bring a different skill set.” When I talked to nurses, I said to them: you can do anything, and there isn't really a glass ceiling. The key is to be confident in yourself, to know what you know, and more importantly, what you don't know. And for what you don't know, surround yourself with people who are smarter than you and can help. My advice is: don't assume anything's impossible, because it probably isn't. And whatever you do, keep your true North.
Q3
Equitable access to cardiovascular care was a recurring theme in your term as ACC President. What strategies have proven most effective in reducing disparities and ensuring that all patients receive highquality care?
The reasons for these disparities are a little different across the globe. In the USA, many of our family practice internal medicine
physicians have become hospitalists, and the funnel for entry-level, basic cardiovascular care has gotten very tight. There are a lot of baby-boomers who are ageing, and the issue is that preventative cardiology does not seem to be a priority in our current healthcare systems. It started with COVID-19, but we never recovered for a lot of other socioeconomic and environmental reasons. To address these gaps, we need advanced practice nurses functioning within their scope of practice and we need physician-led teams. The number one thing is to get the access, followed by equity. This is where we need to focus on women and underrepresented minorities. Everybody presents differently, and you're not going to understand that in a 15-minute office visit. We need to have clinics in the communities where our patients live and not make it difficult for them to get to us. Healthcare deserts persist in the
USA and across the globe, and I think that team-based care is one of the ways we can ensure that our patients always have access to care.
Q4
You’ve highlighted the importance of nonclinical competencies, such as emotional intelligence, for future healthcare leaders. What nonclinical competencies do you believe are the most essential for healthcare professionals to master in order to guarantee high-quality, equitable cardiovascular care?
It's really about how to live, if you think about it. Developing these non-clinical competencies will also make you a better person, husband, wife, or friend. Some of the most important nonclinical competencies include diversity and inclusion, veracity, truthfulness, and authenticity. When you look in the mirror, you need to see the same individual that others see. Many
people don't, and sometimes, as physicians go through school, they forget that they are just human beings. A leader should understand their strengths and weaknesses. In the USA, diversity and inclusion are all sort of red words right now. But the reality is that we need teams that understand the cultures of our patients in order to treat everybody equally. Leaders cannot have personal agendas.
People think you can't learn leadership, but you absolutely can. This is why the college, and I think the European Society of Cardiology (ESC) as well, is looking into embedding nonclinical competencies into our training programmes. It's critical that we turn out great clinical individuals. If people are just good in the lab or at reading echocardiograms or MRIs, that's great, but we need a little bit more than that. We need to understand what makes up those non-clinical competencies and ensure that
we have taught those well. We all have biases, but you have to recognise them in order to be able to function. I don't want physicians to read spreadsheets, or manage finances, but if they want to run a good heart failure clinic, they've got to understand the finances that go along with that. It's a total package, clinical and non-clinical.
Q5
As CEO of Cardiovascular Management of Illinois, USA, you led the creation of an advanced practice providerled Heart Function Clinic that integrates cardiologists with endocrinologists, obstetricians, pharmacists, nutritionists, and nursing staff. What lessons have you learned from this model that could be applied in other health systems?
Watching the evolution of cardiology has been amazing and heartwarming, but also a little scary. When I first started, you were a cardiologist and
We have to remember that only 20% of a patient’s outcome is due to the clinical component, while 80% is based on environmental factors
then you could become an interventional cardiologist or a non-invasive cardiologist. Now, we are sub-specialised within the sub-specialisation. Heart failure, cardio-obstetrics, cardiometabolic diseases, atrial fibrillation; so many subspecialty work groups require our colleagues from other specialties. If we're really going to treat pulmonary hypertension, we need both pulmonary and cardiology. This is where dyad leadership comes in, including both a physician and their administrative colleague. It's great when the administrative colleague has some clinical background, but I've seen dyad leadership work either way, because each has their own skill set.
We were on the cutting edge, but we've got a few things to learn from our colleagues. An estimated 80% of the world will be in atrial fibrillation at some point, which is not a good statistic. How do we fix that? In my opinion, through a multidisciplinary clinic. To ease the patient, they should not have to manage five separate appointments. Who will organise all of that? Who's orchestrating the plan of care for that patient? We have to remember that only 20% of a patient’s outcome is due to the clinical component, while 80% is based on environmental factors: where they live, who
they live with, their finances, and their educational level. If patients don't understand why they're taking four pills for heart failure, they'll stop taking them. So, it has to be a team-based approach, applied in an economically viable methodology. If we can teach them to take their blood pressure, weigh themselves, and then give them a diuretic in a heart failure clinic, we could save thousands of dollars by not having them sit in an emergency room for 4 hours. The endgame to all of this should be centred around the patient.
Q6
AI and quality metrics are becoming increasingly important in cardiovascular care delivery. How can healthcare leaders ensure that these tools enhance, rather than replace, the human elements of patient care?
The proper implementation of AI is critical, because we need human beings to ensure the ethical utilisation of AI. It is an amazing tool, and it can help us treat patients much better and quicker. But while it can process far more than our human brain can, it can never replace that human touch. The implementation of AI helps our physicians and other care providers to be efficient and not waste time in front of a computer. Our human eye can only see so much, so these tools can help enhance our imaging interpretation. When it comes to machine learning, it needs that human being to make sure it's learning correctly. We can't get so used to it that we automatically trust it; we still need our human brain to interact with it. I was just at a conference with one of the largest robotic open-heart centres in the country, and it was absolutely fascinating to watch the robot, but we've got to remember that it has a human
being behind it. We need AI to help us deliver care, but it needs to be done in such a way that our healthcare leaders can ensure they're being used appropriately.
Christopher M. Kramer
George A. Beller MD/Lantheus Medical Imaging Distinguished Professor of Cardiovascular Medicine, University of Virginia Health, Charlottesville, USA; President, American College of Cardiology (ACC)
Q1 Your career spans cardiovascular imaging, hypertrophic cardiomyopathy research, and American College of Cardiology (ACC) leadership. What first drew you to cardiovascular imaging as a focus for your research and clinical practice?
When I was a medical chief resident at the University of Pennsylvania, Philadelphia, USA, Nathaniel Reichek gave Medical Grand Rounds on cardiac MRI. I was enthralled and thought, “I want to do that.” Two years later, I began research on cardiovascular magnetic resonance (CMR) with Reichek as one of my two main mentors, and the rest is history.
Q2 You co-led the National Institutes of Health (NIH)-funded, 44-site Hypertrophic Cardiomyopathy Registry (HCMR) study aimed at improving risk prediction in hypertrophic cardiomyopathy (HCM). What are the most notable findings so far?
We are finalising event adjudication and hope to report the findings of a predictive model for the primary outcome composite endpoint in early 2026. Our paper in 2019, based on baseline findings from the 2,750 recruited patients, demonstrated two main subgroups: 40% or so who were sarcomere mutationpositive and had reverse curvature
We have a lot to learn about how novel cardiac myosin inhibitors affect these imaging biomarkers
morphology, more scar, and less outflow tract obstruction; and 45% or so who were sarcomere mutation-negative, with an isolated basal septal hypertrophy subtype, little to no scar, and more outflow tract obstruction.1 These subgroups may have very different outcomes.
Q3 Your recent work has highlighted novel imaging biomarkers in HCM, including myofibrillar disarray and microvascular dysfunction. What might these findings mean for future therapies?
We have a lot to learn about how novel cardiac myosin inhibitors affect these imaging biomarkers.
Q4 How are advanced imaging techniques, such as quantitative myocardial perfusion and magnetic resonance biomarkers, being applied in clinical practice to guide care for HCM or peripheral arterial disease (PAD)?
I have devoted my career to developing new imaging biomarkers in different disease states. Microvascular ischaemia, identified by quantitative perfusion in HCM, is likely a marker for subsequent scar development.
Q5 What new insights from imaging studies of PAD, particularly regarding microvascular dysfunction, could influence the design of clinical trials or patient monitoring strategies?
In PAD, arterial spin labelling of calf muscle perfusion is an emerging biomarker for the testing of novel therapies to improve
blood flow to muscle and improve exercise ability, which is often limited in these patients.
Q6
As AI continues to evolve, which applications in CMR imaging do you see as most promising for advancing patient care?
AI is impacting every aspect of CMR, from speeding up and improving image acquisition to image segmentation, image analysis, making specific diagnoses, and reporting.
Q7
As ACC President, which initiatives excite you most, and are there imagingfocused projects or policy efforts you are leading?
We are laser-focused on member engagement and demonstrating member value. Also, advocacy is a huge emphasis given recent changes in Washington D.C., USA, and potential effects on physician
reimbursement. We advocate on behalf of all members, not just imagers, but imaging is certainly near and dear to my heart.
Reference
1. Neubauer S et al. Distinct subgroups in hypertrophic cardiomyopathy in the NHLBI HCM registry. J Am Coll Cardiol. 2019;74(19):2333-45.
Arterial spin labelling of calf muscle perfusion is an emerging biomarker for the testing of novel therapies
David E. Winchester
Department of Medicine and Radiology, University of Florida College of Medicine, Gainesville; Assistant Chief of Cardiology, Malcom Randall Veterans Affairs Medical Center, Gainesville, Florida; Senior Medical Adviser, Office of Integrated Veterans Care, Veterans Health Administration, Washington D.C; Secretary and Board of Governors Chair, American College of Cardiology (ACC), USA
Disclaimer: Winchester’s responses do not represent the opinions of the federal government of the USA; the University of Florida, Gainesville; the State of Florida; or the American College of Cardiology (ACC), USA.
Q1 Your expertise spans echocardiography, nuclear cardiology, and cardiac CT. In your opinion, what recent advances in these imaging modalities have had the biggest impact on diagnostic accuracy and patient care?
The technology that I use most frequently is coronary flow reserve combined with PET perfusion imaging and coronary artery calcium scoring. I am fortunate enough to have this technology at my primary site of practice, and I feel like it makes a substantial difference in being a comprehensive functional and anatomic assessment for coronary artery disease and ischaemia in my patients. In the world of cardiac CT, we have seen major advancements in flow reserve and plaque analysis. However, I think I am most excited about the wider adoption of photoncounting CT to improve our spatial resolution. Advances in echocardiography also hold promise for earlier detection of cardiac structural disease and a better understanding of the complex dynamics of myocardial contraction and relaxation that contribute to the syndrome of heart failure.
to populations presenting with chest pain in the emergency department. Many of these scores have failed to substantially improve accuracy compared to the comprehensive history and physical examination of a skilled clinician. The advent of high-sensitivity cardiac troponin (hs-cTn) assays, however, has provided a substantial advance, particularly in identifying low-risk patients within this population.
Q3 Based on your work with hs-cTnT, what insights have emerged regarding its safety and efficacy for rapid risk assessment and rule-out strategies in acute coronary syndrome?
Many cardiovascular professionals primarily see patients with elevated troponin levels. They often do not see the numerous patients with low or undetectable troponin levels who can be safely discharged from the emergency department after an abbreviated stay. The data show that these patients are very unlikely to suffer a major cardiac event within the next 30 days. These are the patients for whom hs-cTnT makes a difference, allowing clinicians to discharge them with a high degree of confidence.
I am most excited about the wider adoption of photoncounting CT to improve our spatial resolution
Q2 Your research has examined the application of risk scores for chest pain evaluation in the emergency department. What do recent findings from your work suggest about the effectiveness of these scores in identifying low-risk patients and reducing unnecessary testing?
Over the decades, numerous risk scores have been applied
Q4
Chest pain decision units have become an important strategy for safely triaging patients with a lowto-intermediate risk. Based on your research, what are the key elements that make these units most effective?
First and foremost is an institutional commitment to providing the resources for these
units. This includes adequate staffing and a multidisciplinary, collaborative approach among emergency medicine, hospital medicine, laboratory medicine, and cardiovascular medicine, where frontline clinicians are not only informed of the process for triaging patients with a low-tointermediate risk, but are also invested in and see that process succeed. After that, the specifics of how the unit and its clinical protocols are run can be flexible and adapt to the needs of the patient population, clinical staff, institution, and community.
Q5 How do you see AI changing the evaluation of chest pain in the emergency department? Are there specific AI applications you find particularly promising based on current evidence?
I recently reviewed an unpublished manuscript on this very question, which demonstrated that a machine learning model could outperform established risk scores, such as the History, ECG, Risk factors, and Troponin (HEART) score. The investigators accomplished this by including >50 additional clinical variables,
which would be impractical for a frontline clinician to memorise or manually input into a risk calculator. When these models can be easily implemented into clinical workflows and electronic medical record systems, they may hold promise for enhancing the accuracy of our clinical assessments.
Q6
As Lead Author of the American College of Cardiology (ACC)’s 2023
Appropriate Use Criteria for Imaging in Chronic Coronary Disease, what were some of the most significant updates you championed?
The most important change we made to the Appropriate Use Criteria for Imaging in Chronic Coronary Disease was the inclusion of a column to suggest deferred testing. This was very deliberately added to demonstrate to clinicians that there are clinical scenarios where it may be appropriate to perform a test, but it may also be appropriate not to perform any testing. I was glad to see how this was reflected by the rating panel. Our document was developed around the same time as the multisociety guidelines
for the management of chest pain, and we were on the same page about eliminating the term ‘atypical chest pain’. Overall, I was very satisfied with our efforts to simplify the document and to make it more applicable to daily clinical care.
Q7 As Chair of the ACC Board of Governors and Secretary of the Board of Trustees, how do you engage with chapter leaders across the USA, Canada, Mexico, and the USA health services to ensure cohesive advocacy and educational strategies that reflect the diverse needs of these regions?
Service in these roles has been incredibly rewarding, and it has been my privilege to routinely engage with cardiology leaders from across the USA and the world. We have regular meetings for both the entire Board of Governors and our steering committee, which are diverse and represent a broad array of leaders' backgrounds and experiences.
Q8 In October 2025, you’ll take part in the 2025 ACC Legislative Conference, where cardiovascular professionals from across the USA will meet with policymakers. What are the most pressing issues you hope to highlight during this year’s discussions?
One of the most important areas of advocacy for us has always been adequate access to care for our patients. This is under threat from a wide variety of challenges, including regulations that are not in the best interests of patients and practices, such as prior authorisation.
Nancy Sweitzer
Professor of Medicine, Division of Cardiology; Vice-Chair of Clinical Research, Department of Medicine; Associate Director, Institute for Clinical and Translational Sciences; Director of Clinical Research, Division of Cardiology, Washington University School of Medicine, St Louis, Missouri, USA
Q1Most of your career has been devoted to understanding heart failure. What initially drew you to this complex area, and how has the field evolved since you began your work?
I’ve been in the field for a long time. What first drew me to cardiology, and then to heart failure, was the ability to treat people and make them feel better. As a medical student, I remember diuresing dozens of pounds of fluid off a few patients in a week; I loved seeing them feel so much better at the end, and that was before we had today’s modern, effective therapies.
I’ve now been involved in trials for 25 years, and watching new therapies improve both the quality and duration of life has been incredibly gratifying. I always say I have the best job in the world. We care for people in shock, people who are dying, people who are critically ill, and we have tools that can save their lives. But we also build long-term relationships with patients over years, even decades, helping them to feel better, stabilise their disease, and achieve their goals. It’s the best of both worlds: the acute, exciting care of cardiology, and the longterm, meaningful connections with patients.
A normal ejection fraction in women may be different from that in men, but we don’t know because it hasn’t been studied
Q2
Recent research has shown that heart failure with preserved ejection fraction (HFpEF) disproportionately affects women. How should this influence both trial design and therapeutic strategies?
It’s very interesting. I think that normal cardiovascular function in women is quite different from that of men, and we haven’t studied or fully appreciated that. One of my favourite studies, by Susan Cheng, Cedars-Sinai Medical Center, Los Angeles, California, USA, and colleagues in California, USA, looked at blood pressure and cardiovascular risk.1,2 For men, a blood pressure of 120/80 seems normal. For women, the ‘normal’ level is probably much lower. Women with a blood pressure between 100 and 110 already have increased cardiovascular risk, yet we still treat them when they reach 120/80, which may actually be a high blood pressure for many women.
Similarly, I think a normal ejection fraction in women may be different from that in men, but we don’t know because it hasn’t been studied. I’m very interested in learning what is truly normal for women across the lifespan. That may help explain why women disproportionately develop HFpEF. Part of it is longevity, as it’s a disease of ageing, but I suspect there’s more to it.
I know people criticise the underenrolment of women in trials, but I think we’ve done reasonably well. Women are less likely to participate in research for complex reasons tied to their lives. Still, reduced ejection fraction trials usually enrol 30–40% women, which matches the prevalence. For
preserved ejection fraction trials, if you take an ejection fraction ≥50, enrolment is typically 45–60% women. That may be a bit low, but it’s still solid representation.
I would love to see more women in trials. Companies sometimes say, ‘we provide childcare’, but women in their 70s with heart failure don’t need childcare, they need husband care. Many are caregivers not just for children, but for spouses and family. That burden makes trial participation difficult, especially with heart failure. We need innovative ways to lower those burdens while still learning what we need to know.
I’m hopeful about the future. We now have effective therapies for HFpEF that reduce hospitalisations. Over the course of my career, I’d like to say that I’ve developed many interesting hypotheses, most of which I’ve disproved. But that’s science: slowly, steadily, we discover what does work.
It’s also important to talk about awareness. When women are diagnosed with heart disease, they’re often shocked to learn that it’s the number one killer of women. That’s because women don’t talk about it. Women with breast cancer share their diagnosis; everyone knows. But women with heart failure keep it quiet. Part of that is due to the stigma that heart disease is the result of bad habits. However, age is the biggest risk factor, and none of us can avoid ageing. I hope that we can relieve some of the shame and encourage women to talk about heart disease, thereby raising awareness and increasing research participation.
Q3 As a leader in clinical trials in heart failure, how do you see socioeconomic status influencing both trial design and outcomes? Are we doing enough to ensure inclusivity and real-world applicability in large heart failure trials?
The short answer is no; we’re not doing enough. Socioeconomic
status affects everything. If you have food or housing insecurity, the last thing you can do is participate in voluntary research. Yet cardiovascular risk disproportionately affects people with socioeconomic disadvantages, and we need more resources devoted to that problem.
I practice in St. Louis, Missouri, USA, a city with a troubled history around race and inequity. We’ve done well enrolling minority and some disadvantaged patients in trials, but the truly disadvantaged, those facing multiple insecurities, can’t participate. They simply don’t have the capacity. Is it the pharmaceutical industry’s job to solve that? No. Society has to solve it. Unfortunately, we’re not solving it right now in the USA.
Q4 Left ventricular ejection fraction has long been the cornerstone for diagnosing and classifying heart failure, yet it captures only part of the disease spectrum. How can advances in imaging techniques overcome the current limitations?
Ejection fraction is a very crude measure, but understanding systolic function and cardiac performance in a more sophisticated way is helping us. At the European Society of Cardiology (ESC), we’ve seen exciting science around global longitudinal strain as a marker of subclinical systolic dysfunction. Many patients who have HFpEF, for example, have subclinical systolic dysfunction.
Some of my early studies showed that, while these patients look normal at rest, the heart can’t mount the increase in cardiac output it needs under stress. Stress testing with sophisticated cardiac
assessments done in settings of exercise or pharmacological stress can unmask this, but these assessments are not routinely done. Imaging is getting better, and we’re better at diagnosing subclinical systolic dysfunction, but I’m still waiting for a study that enrols people with abnormal strain and uses improvements as an endpoint, ideally coupled with heart failure events. Whether the FDA or other regulators will accept improvements in strain as an endpoint, I don’t know, but we need more data.
In HFpEF especially, you can have a small ventricular cavity with a thick wall. That gives you a normal ejection fraction, yet very abnormal contractility. Strain may be the best way to show that there is systolic dysfunction, even though we call it a ‘normal ejection fraction’.
Q5A significant portion of your research has focused on cardiogenic shock, and last year you published a paper on the impact of mental health on cardiovascular outcomes. What can clinicians do to ensure more holistic patient care for these patients?
I’ve been trying to study cognitive function in heart failure, but our funding agencies aren’t optimally
set up for multidisciplinary work, so it’s hard to find reviewers with the breadth to evaluate it.
One of the reasons I chose to focus on heart failure is because we care for the whole patient. We’re cardiologists, but also internists, and we like it that way. When a patient isn’t thriving, we look for all the reasons and use the resources available, because heart failure is expensive for health systems, and that gives us leverage. However, there aren’t enough mental health services anywhere in the world. Depression and anxiety are very common in heart failure.
When caring for patients, I try to optimally treat all barriers to ideal health, try to get every affected system treated optimally, but that often means my patients have ≥6 doctors. In the USA, with our fragmented care, that’s overwhelming. A general practitioner with 10-minute visits can’t manage heart failure alongside six comorbidities. Our systems simply aren’t set up to care for ageing patients with multiple chronic diseases. Over the next two decades, as populations age, this is going to explode, and I don’t think any health system is prepared.
Is there any short-term solution for this, or does systemic change need to happen?
Systemic change is needed. Unfortunately, the first thing that will happen is that patients won’t do well. I hope the 10-minute visit goes away. In the USA, there are some moves towards allowing 30-minute visits if you’re managing a complex chronic disease, but the payments still don’t match procedures like stents or ablations. The incentives are skewed. Hopefully, as the burden of disease grows, public health leaders will recognise that reactive care isn’t sustainable.
Q6
At ESC 2025, you chaired the session, ‘Heart–brain–kidney axis and beyond in heart failure’. Can you tell us more about this fascinating topic and the key take-home message?
It was a really interesting session. We kept coming back to the chicken-and-egg questions: is the heart making the kidney worse, or is the kidney making the heart worse? Is the heart driving brain decline? Is malnutrition making heart failure worse?
In today’s omics world, we drill down to cells and molecules. However, I’m a physiologist at
heart, and physiology is about how systems interact: kidneys and heart, brain and arteries, heart and metabolism, etc. Is it abnormal haemodynamics leading to cognitive decline? Is it inflammation? We have to address these questions at a systems level.
It’s an exciting time. Take the glucagon-like peptide-1 (GLP-1) agonists: they reduce inflammation, improve heart failure, and also cause weight loss. But is it the weight loss that matters, or the anti-inflammatory effect, or both? These drugs, developed for other purposes, have become natural experiments that are helping us learn. The session today featured young scientists with excellent data who are slowly chipping away at these complex problems.
Q7
Precision medicine and digital health are rapidly influencing cardiovascular care. What do you see as the most promising emerging tools for improving outcomes in heart failure?
There’s still a lot of work to do. In HFpEF, we don’t fully understand the disease. It’s likely not purely cardiac, but systemic, maybe in part due to accelerated ageing. In some patients, it’s driven by obesity or metabolic issues, and in others, by hypertension or subclinical systolic dysfunction.
Over the last decade, there have been a lot of efforts around phenotyping patients and tailoring treatment. But I’m not convinced that we’ve truly defined the mechanistic phenotypes yet. Trials are now being designed around specific phenotypes of HFpEF, but we haven’t shown whether that leads to improved outcomes.
Nonetheless, it will be fascinating to see where this research trajectory goes. As I’ve said before, much of my career has been built on great hypotheses, many of them disproved. We may find that some of the phenotypes that we’re targeting aren’t the right ones, but that’s the scientific process.
Digital health is also very exciting. People are collecting more health data than ever, though right now it tends to be healthy people. It will be interesting when patients with chronic diseases start generating that data, which we can then interrogate and learn from. Even at this meeting, I uploaded an app that can estimate my risk of systolic dysfunction with an Apple Watch (Apple, Cupertino, California, USA) ECG. With AI, wearables, and apps, we’ll have enormous opportunities for earlier and easier diagnosis. But again, it comes back to socioeconomic disparities. These tools tend to reach higher socioeconomic groups. The challenge is making sure that digital strategies reach the populations who need them most. That’s a big societal issue we still need to solve.
Q8You’ve dedicated a lot of time to mentoring and training young cardiologists. What advice would you give to those entering the field?
At this stage, my greatest satisfaction comes from helping young cardiologists and physicians build careers in clinical research. Those of us in clinical practice see unmet needs most clearly. We’re well-positioned to ask the right questions, then develop the skills and tools to design studies, gather data, and move the field forward. One question leads to another: it’s self-perpetuating.
As a journal editor, the papers I love are those with a clear hypothesis, good data, and a compelling story, whether the hypothesis is supported or unsupported by the data. That kind of science leads to more questions, more clues, and more studies: work that points the way forward.
For me, I’ve always kept both parts of my career alive: patient care and research. I love medicine and I love my patients, but I’m never happier than when I’m diving into new data and seeing what clues they hold. That’s the excitement I try to pass on to young people: stay curious, ask great questions, and keep both the science and the patient at the centre of it all.
References
1. Ji H et al. Sex differences in blood pressure associations with cardiovascular outcomes. Circulation. 2021;143(7):761-3.
2. Ji H et al. Sex differences in blood pressure trajectories over the life course. JAMA Cardiol. 2020;5(3): 19-26.
Financial Toxicity: An Overlooked Driver of Heart Failure Risk in the USA
Author: *Han Naung Tun1,2
1. Larner College of Medicine, University of Vermont, Burlington, USA
2. Boeve College of Health Sciences, Northeastern University, Boston, Massachusetts, USA
*Correspondence to tun.h@northeastern.edu
Disclosure: The author has declared no conflicts of interest.
Received: 21.11.24
Accepted: 04.03.25
Keywords: Cardiovascular outcomes, cost-related medication nonadherence, economic burden, health disparities, quality of life.
Heart failure is responsible not only for high morbidity and mortality, but also for significant out-of-pocket expenses for patients, which are increasingly being identified as an important determinant of health.1 In 2018, one in seven families in the USA who had a member with heart failure spent over 20% of their income on care, with low-income families facing an even greater burden.2 These costs, which include insurance premiums and medication expenses, contribute to what is known as “financial toxicity,” which has several medical consequences due to financial distress. This can result in delayed care, medication non-adherence, and psychological strain on patients, with impacts on overall health. Financial toxicity in the care of heart failure is emerging as a concern, as high costs related to treatment, medications, and hospital stays are placing a burden on patients and their families. The economic cost of heart failure has likely increased since 2018 because of inflation in healthcare expenses, new treatment guidelines, and the financial effects of the COVID-19 pandemic.3 All these factors have disproportionately impacted those with lower socioeconomic status, further widening the gap in access to care and
outcomes. A study of 3,386 patients with acute decompensated heart failure found that those with severe perceived economic burden had significantly higher mortality rates and a poorer heart failurespecific health status than those with little perceived economic burden; this refers to the subjective financial strain experienced by patients, often influenced by out-ofpocket expenses relative to their household income.4 Patients with heart failure can face enormous financial burdens due to high medication costs, particularly with newer treatments that include sacubitril/ valsartan, dapagliflozin, and empagliflozin. The investigators from China suggested that perceived economic burden might be useful in assessing risk and guiding quality improvement efforts in heart failure care.4
Both the USA and China may have considerable difficulties with out-of-pocket expenses for chronic illnesses such as heart failure, leading to non-adherence to treatment and poorer health outcomes, especially for low-income groups. Yet there are also profound differences: in China, healthcare access is largely based on geographic location, with the countryside frequently lacking any access to specialist care, whereas in the USA, it is largely based on the type of insurance one possesses, with Medicare and Medicaid recipients
experiencing different obstacles than the privately insured.4 In addition, China’s drug pricing policy is centralised and generally leads to lower-priced drugs, while market-based USA pricing leads to greater variability of affordability. Such structural differences highlight the need for countrylevel studies to tackle the distinctive problem of financial toxicity among USA patients with heart failure.4,5
Another study examined the financial toxicities associated with newer cardiovascular therapies, particularly angiotensin receptor-neprilysin inhibitors, exploring how high, out-of-pocket costs impede medication adherence despite superior therapeutic benefits. The researchers have stressed the need for honest patient-provider discussions about cost, and systemic reforms in healthcare that would reduce financial obstacles and improve access to care.6 Low-income families were disproportionately affected, with a fourfold increase in risk of high financial burden, and a fourteenfold increase in risk of catastrophic financial burden when compared to middle/high-income families.7 As such, patients with heart failure, and their families, frequently incur substantial out-of-pocket healthcare expenses, leading to significant financial strain. Additionally, Sukumar S et al.8 stated that, in caring for family members with heart failure, 14% of families reported a high financial burden, and 5% reported a catastrophic financial burden, both of which were driven primarily by medication costs and health insurance premiums. Financial toxicity in heart failure care is notably affected by regional disparities in the USA. Medicaid expansion under the Affordable Care Act has exacerbated disparities, with patients in expansion states experiencing improved access to financial support and medications, while those in non-expansion states face increased outof-pocket expenses. In the USA, states that expanded Medicaid experienced a far smaller increase in cardiovascular death rates among middle-aged adults, illustrating the potential for Medicaid expansion to reduce health disparities, especially in rural communities where limited access to healthcare and economic pressure further compound disparities in care.9
It has been reported in the literature that such interventions can reduce outof-pocket expenses and save money for hospital systems.8,10 There are pharmaceutical company copay assistance programs, but many are limited by factors such as insurance type and income thresholds. For example, the savings program for empagliflozin requires that patients have commercial insurance, while assistance for sacubitril/valsartan is subject to household income limits.
MITIGATING FINANCIAL TOXICITY IN HEART FAILURE CARE
Addressing financial toxicity in heart failure care is crucial for improving patient outcomes. Strategies include policy reforms to reduce financial strain, improvements in shared decision-making, and physician endorsement of transparent cost discussions with patients. These measures can reduce financial toxicity, improve access to guideline-directed medical treatment, and improve adherence and outcomes for patients. Therefore, future research is needed on financial toxicity in patients with heart failure, and prescription access disparities based on demographics such as age, gender, and income. Key approaches should include improving access to affordable medications through prescription assistance programs, generics, or biosimilars, and advocating for policies that lower the cost of heart failure drugs, such as angiotensin receptorneprilysin inhibitors and sodium-glucose cotransporter-2 inhibitors.10
Another important strategy is integrating financial counselling into the care process, guiding patients through the process of insurance coverage, payment plans, and community resources, while minimising the medical cost burden. Telemedicine and remote monitoring technologies provide another solution by making care more accessible and less expensive, allowing patients to manage their condition from home, thereby reducing costly hospital visits.11
Beyond these practical approaches, financial toxicity requires systemic changes
in expanding access to healthcare, reducing out-of-pocket costs, and addressing social determinants of health. Out-of-pocket costs for patients with heart failure may include insurance premiums, copays, and coinsurance, which vary significantly based on insurance type, such as commercial, Medicare, Medicaid, or lack of insurance. Removing financial barriers to care is an important part of what policymakers can
References
1. Dunlay SM et al. Contemporary strategies to manage and prevent heart failure readmissions. Circ Heart Fail. 2018;11(12):e005094.
2. Schultz WM et al. Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation. 2018;137(20):2166-78.
3. Kazi DS et al. Forecasting the economic burden of cardiovascular disease and stroke in the United States through 2050: a presidential advisory from the American heart association. Circulation. 2024;150(4):e89-101.
4. Yu Y et al. Perceived economic burden, mortality, and health status in patients with heart failure. JAMA Netw Open. 2024;7(3):e241420.
do. Of course, patient and family education about the financial aspects of heart failure is paramount. If patients are aware of potential costs, insurance options, and financial support available to them, they will be in a better position to make informed decisions. All these strategies combined will help alleviate the financial burden on patients with heart failure, improving their health overall.
5. Kaiser Family Foundation. Key facts about the uninsured population. 2022. Available at: https://www.kff. org/uninsured/issue-brief/key-factsabout-the-uninsured-population/. Last accessed 17 Feb 2025.
6. Warraich HJ et al. Financial toxicity with cardiovascular disease management: a balancing act for patients. Circ Cardiovasc Qual Outcomes. 2020;13(12):e007449.
7. Wang SY et al. Out-of-pocket annual health expenditures and financial toxicity from healthcare costs in patients with heart failure in the United States. J Am Heart Assoc. 2021;10(14):e022164.
8. Sukumar S et al. Financial toxicity of medical management of heart failure: JACC review topic of the week. J Am Coll Cardiol. 2023;81(20):2043-55.
9. Breathett K et al. Association of Medicaid expansion with cardiovascular mortality. JAMA Cardiol. 2019;4(7):671-9.
10. Kandula VA et al. A costly cure: understanding and addressing financial toxicity in cardiovascular disease health care within the domain of social determinants of health. Methodist Debakey Cardiovasc J. 2024;20(5):15-26.
11. Haleem A et al. Telemedicine for healthcare: capabilities, features, barriers, and applications. Sens Int. 2021;2:100117.
Sodium Glucose Co-transporter-2 Inhibitors in Heart Failure: Why the Elderly are Missing Out
Authors: Muhammad Abdul Rehman,1,2 Huda Jamil,3 Mansoor Awais,4 *Zubair Bashir5
1. Department of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota, USA
2. Mayo Clinic School of Graduate Medical Education, Mayo Clinic, Rochester, Minnesota, USA
3. Allama Iqbal Medical College, Lahore, Pakistan
4. King Edward Medical University, Lahore, Pakistan
5. Department of Cardiology, University of Texas Medical Branch, Galveston, USA
*Correspondence to shahid.zubair08@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Heart failure (HF) constitutes a significant disease burden in the USA. Its prevalence has doubled between 1990–2020, showing an increase in the age-standardised prevalence rate of 3.08%, largely due to improved life expectancy.1 It is a leading cause of morbidity and mortality among the elderly population (>65 years).2 Unlike other medications constituting goaldirected medical therapy (GDMT), sodiumglucose co-transporter-2 inhibitors (SGLT2i) are strongly recommended for patients with HF, regardless of HF phenotypes.3
Among patients with HF who have reduced ejection fraction, SGLT2i reduce cardiovascular (CV) mortality (hazard ratio [HR]: 0.82; 95% CI: 0.69–0.98), all-cause mortality (HR: 0.83; 95% CI: 0.71–0.97), and HF admissions (HR: 0.70; 95% CI: 0.59–0.83).4 Similar benefits have been observed in patients with HF who have preserved ejection fraction, where SGLT2i
reduced HF admissions (odds ratio: 0.71; 95% CI: 0.61–0.83) and the composite outcome of HF hospitalisation or CV mortality (HR: 0.78; 95% CI: 0.70–0.87).5 Notably, these favourable outcomes extend to elderly patients (age ≥75 years), among whom SGLT2i reduced the composite of HF hospitalisations or CV mortality (HR: 0.61; 95% CI: 0.41–0.91), as well as HF readmissions (HR: 0.61; 95% CI: 0.31–0.95).6
However, the utilisation of SGLT2i has remained suboptimal, especially in elderly patients, despite a Class IA recommendation.3,7 Although there was an increase in the utilisation of SGLT2i among Medicare beneficiaries between 2016–2019, from 0.34–0.58 per 100 person-months, its prescriptions have largely remained low,7 with only 0.13 initiations per 100 personmonths among patients with chronic HF.8
Available data suggest many barriers to the use of SGLT2i in elderly patients with HF in the USA. However, this population
may benefit the most from this medication due to its favourable effects on many comorbidities commonly seen in the elderly, such as chronic kidney disease, aortic stenosis, hypertension, and diabetes.8-10 Moreover, it may mitigate the healthcare costs associated with high mortality and morbidity rates among elderly patients with HF, which are mainly driven by recurrent HF admissions, the associated progressive frailty, and declining quality of life.11
BARRIERS TO SODIUM-GLUCOSE
CO-TRANSPORTER-2 INHIBITOR PRESCRIPTION
A common reason for avoiding prescriptions is the fear of increasing urinary tract and genital mycotic infections in elderly patients.12,13 SGLT2is promote the excretion of glucose and sodium in urine, which encourages the growth of bacterial and fungal infections.6,12,13 Moreover, natriuresis and glycosuria may lead to dehydration, which can be detrimental, especially in elderly patients.14 However, multiple studies have shown no significant difference in therapy discontinuation due to adverse effects, including urinary tract infectionrelated adverse events, between those above and below 75 years, nor between the SGLT2i and placebo groups.14,15
Interestingly, recent evidence suggests that SGLT2i has reno-protective effects among elderly patients.6 It significantly reduces the worsening of kidney function in the long term. It also mitigates the deleterious effects of loop diuretics on kidney function by increasing the tubuloglomerular feedback and maintaining fluid homeostasis.6 Zhuo et al.16 also reported a significantly lower risk of acute kidney injury with SGLT2i among the elderly (HR: 0.71 and 0.81) compared to other commonly used medications, such as glucagon-like peptide-1 agonists.16 Moreover, SGLT2i use was not associated with a significantly increased risk of the composite safety outcome (dehydration, urinary tract infection, or ischaemic stroke) compared to non-SGLT2i therapy (adjusted HR: 0.80; 95% CI: 0.49–1.29). Additionally, SGLT2i consistently demonstrated significant reductions in all-cause mortality and HF
readmissions, even after adjusting for BMI, frailty, and nutritional status, factors that often deter prescribing in elderly patients.11
Second, physician inertia plays an important role in suboptimal prescription rates.17 Many patients with HF are managed by primary care physicians (PCP) who may be more reluctant to try new medications. PCPs practising outside of metropolitan centres or away from the main academic centres may be more prone to physician inertia due to a lack of support from HF specialists. Moreover, a lack of infrastructure to keep abreast with the latest developments in pharmacopoeia, HF management, and a dearth of experience in dealing with elderly patients may contribute to the suboptimal prescription rates among elderly patients with HF.18
Third, sex disparities in the prescription of SGLT2i also lead to overall reduced utilisation of this drug.7 Elderly females have a higher prevalence of HF compared to men.19 Factors such as a lack of healthcare access, awareness of disease process, and a lack of evidence, due to underrepresentation of females in HF trials, may contribute to reduced prescription rates among women.20 In addition, women often present with atypical symptoms that may delay diagnosis and, consequently, management. Furthermore, disparities in the utilisation of HF management among Black people also manifest as decreased utilisation of HF pharmacotherapies among elderly patients. Despite a higher prevalence of HF among elderly Black people, the utilisation of HF pharmacotherapies has remained suboptimal, raising concerns for healthcare equity.21 Moreover, the Black population has a significantly higher burden of risk factors and comorbidities such as hypertension, diabetes, and chronic kidney disease that may benefit more from SGLT2i utilisation. It may also help in reducing the cost of HF management among Black patients with a significantly higher burden of comorbidities. However, several factors, such as healthcare access, suboptimal insurance coverage, low health literacy, under-representation of Black people in HF trials, and mistrust in the healthcare system,
may play a role in the underutilisation of GDMT, including SGLT2i in Black people.22
Lastly, the financial toxicity associated with HF management may jeopardise the optimisation of HF management, especially the initiation and maintenance of relatively expensive drugs like SGLT2i. Many elderly patients are on different Medicare plans with different copays and co-insurances that add to the growing financial burden of healthcare costs. The total cost of HF management, which was estimated to be 30.7 billion USD in 2012, is expected to increase to 69.8 billion USD by 2030, with significant contributions by GDMT, especially novel pharmacotherapies.23,24 The out-of-pocket costs for Medicare beneficiaries have ranged as high as 2,849 USD annually, with a significant cost reduction to 1,319 USD by excluding SGLT2i.25 The inability to afford SGLT2i or to continue the therapy would ultimately add to increasing healthcare costs in the form of hospital readmissions, increased use of healthcare services, and increased morbidity and mortality. Therefore, avoiding the utilisation of SGLT2i among elderly patients because of the cost of the medication would ultimately add to the growing healthcare costs and compromise optimal healthcare delivery for elderly patients.
FUTURE DIRECTIONS
Given their favourable profile, efforts should be made to increase the use of SGLT2is in the elderly, disregarding age as a barrier. Physician education and promotion of the benefits of these medicines among the elderly are needed. Focused seminars to educate PCPs and incorporate biannual continued medical education may give more comfort to PCPs and general cardiologists in prescribing and monitoring SGLT2i, as they stay abreast of the latest developments in HF management pharmacopoeia.17,26 Moreover, advocating for multidisciplinary team management, whether in person or via telehealth, may also optimise the utilisation of SGLT2i therapy. In addition, creating awareness among elderly patients with HF via different types of media such as social media, as well as conducting
periodic regional HF management seminars and HF awareness camps, may equip elderly patients with more information to make an informed decision after discussing with their providers. These strategies can also be adopted to achieve healthcare equity among races/ethnicities and sexes through patient and physician education. Furthermore, leveraging technologies such as telehealth may enhance access to care and facilitate the timely delivery of health services. Finally, reducing the shared costs of medications with patients may be a stepping stone to the increased adoption of HF medications. The amount of cost sharing should be determined based on the appropriate clinical and financial outcomes. One way could be to inversely link the value and benefit of the medication to the shared cost for patients. Benefit-based copayment is one such model of value-based insurance design that shares the cost of medications based on the clinical benefit they provide.27 High-value medications providing morbidity and mortality benefits, such as SGLT2i (as determined by ongoing research), are provided at lower and more affordable out-of-pocket costs to patients.28 This may address one of the barriers to increased utilisation of these novel drugs, providing better clinical outcomes and improving equity. This contrasts with the current model of cost sharing with patients, which is based on the absolute price of the medications.29
CONCLUSION
Despite robust evidence of the clinical benefits of SGLT2i, their utilisation among elderly patients with HF has remained suboptimal. Future studies are needed to develop a comprehensive framework to increase the utilisation of these life-saving drugs among this population. Such a framework should address critical barriers, including financial burdens, physician inertia, and healthcare disparities, to ensure optimal HF care delivery for older adults, who represent one of the most vulnerable segments of society.
References
1. Gu J et al. Global burden of heart failure in older adults: trends, socioeconomic inequalities, and future projections from 1990 to 2035. Eur Heart J Qual Care Clin Outcomes. 2025;DOI:10.1093/ehjqcco/qcaf047.
2. Savarese G et al. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. 2023;118(17):3272-87.
3. Tromp J et al. A systematic review and network meta-analysis of pharmacological treatment of heart failure with reduced ejection fraction. JACC Heart Fail. 2022;10(2):73-84.
4. McMurray JJV et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008.
5. Fukuta H et al. Sodium-glucose cotransporter 2 inhibitors in heart failure with preserved ejection fraction: a meta-analysis of randomized controlled trials. Int J Cardiol Heart Vasc. 2022;42:101103.
6. Amioka M et al. Long-term efficacy of SGLT2 inhibitors for elderly patients with acute decompensated heart failure: the OASIS-HF study. ESC Heart Fail. 2025;12(1):447-55.
7. Bashir Z et al. Predictors of sodium glucose co-transporter-2 inhibitor utilization in elderly heart failure patients: a real-world population-level dataset analysis. Am J Cardiol. 2025;DOI:10.1016/j. amjcard.2025.08.028.
8. Cromer SJ et al. Deficits and disparities in early uptake of glucagonlike peptide 1 receptor agonists and SGLT2i among medicare-insured adults following a new diagnosis of cardiovascular disease or heart failure. Diabetes Care. 2023;46(1):65-74.
9. Moore J et al. Factors and disparities influencing sodium-glucose cotransporter 2 inhibitors and glucagon-like peptide 1 receptor agonists initiation in the United States: a scoping review of evidence. Pharm Basel Switz. 2025;13(2):46
10. Shah T et al. Effect of sodium-glucose cotransporter-2 inhibitors on the progression of aortic stenosis. JACC Cardiovasc Interv. 2025;18(6):738-48.
11. Nakano K et al. The efficacy and safety of sodium-glucose cotransporter 2 inhibitors in patients aged over 80 years with heart failure. ESC Heart Fail. 2025;12(3):2087-97.
12. Bartolo C et al. Bittersweet: infective complications of drug-induced glycosuria in patients with diabetes mellitus on SGLT2-inhibitors: two case reports. BMC Infect Dis. 2021;21(1):284.
13. Storgaard H et al. Benefits and harms of sodium-glucose co-transporter 2 inhibitors in patients with type 2 diabetes: a systematic review and meta-analysis. PLoS One. 2016;11(11):e0166125.
14. Sinclair AJ et al. Efficacy and safety of canagliflozin in individuals aged 75 and older with type 2 diabetes mellitus: a pooled analysis. J Am Geriatr Soc. 2016;64(3):543-52.
15. Pratley RE et al. Cardiorenal outcomes, kidney function, and other safety outcomes with ertugliflozin in older adults with type 2 diabetes (VERTIS CV): secondary analyses from a randomised, double-blind trial. Lancet Healthy Longev. 2023;4(4):e143-54.
16. Zhuo M et al. SGLT2 inhibitors and the risk of acute kidney injury in older adults with type 2 diabetes. Am J Kidney Dis. 2022;79(6):858-67.e1.
17. Verhestraeten C et al. Clinical inertia in the treatment of heart failure: a major issue to tackle. Heart Fail Rev. 2021;26(6):1359-70.
18. Aujoulat I et al. Factors associated with clinical inertia: an integrative review. Adv Med Educ Pract. 2014;5:141-7.
19. Khera R et al. Contemporary epidemiology of heart failure in feefor-service medicare beneficiaries across healthcare settings. Circ Heart Fail. 2017;10(11):e004402.
20. Jin X et al. Women’s participation in cardiovascular clinical trials from 2010 to 2017. Circulation. 2020;141(7):540-8.
21. Chang PP et al. Trends in hospitalizations and survival of acute decompensated heart failure in four US communities (2005-2014): ARIC study community surveillance. Circulation. 2018;138(1):12-24.
22. Ilonze O et al. Unequitable heart failure therapy for Black, Hispanic and American-Indian patients. Card Fail Rev. 2022;8:e25.
23. Tsao CW et al. Heart disease and stroke statistics-2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93-621.
24. Bhatnagar R et al. Expenditure on heart failure in the United States: the medical expenditure panel survey 2009-2018. JACC Heart Fail. 2022;10(8):571-80.
25. Faridi KF et al. Medicare coverage and out-of-pocket costs of quadruple drug therapy for heart failure. J Am Coll Cardiol. 2022;79(25):2516-25.
26. Komajda M et al. The EuroHeart Failure Survey programme- a survey on the quality of care among patients with heart failure in Europe. Part 2: treatment. Eur Heart J. 2003;24(5):464-74.
27. Fendrick AM et al. A benefit-based copay for prescription drugs: patient contribution based on total benefits, not drug acquisition cost. Am J Manag Care. 2001;7(9):861-7.
28. Rao BR et al. Challenges related to out-of-pocket costs in heart failure management. Circ Heart Fail. 2025;18(3):e011584.
29. Heidenreich P. An underappreciated risk factor for heart failurefinancial toxicity. JAMA Netw Open. 2024;7(3):e241403.
Simplified Practical Approach to Percutaneous Coronary Intervention for Bifurcation Lesions: Bridging Complexity and Clarity
Editor's Pick
Bifurcation percutaneous coronary intervention remains one of the most debated and technically complex areas in interventional cardiology. By introducing a structured framework, this article emphasises the critical role of operator experience while providing clarity and practical guidance to navigate controversies and improve outcomes in this challenging field.
Çetin Erol Department of Cardiology, School of Medicine, Ufuk University, Ankara, Türkiye
Authors: *Adnan Kassier,1 Ahmed Elshafie,1 Almontasser Bella Kassier,1 Giorgio Medranda2
1. University of Michigan Health - Sparrow, Lansing, Michigan, USA
2. NYU Langone Hospital – Long Island, Mineola, New York, USA *Correspondence to Adnan.kassier@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Percutaneous coronary intervention (PCI) of coronary bifurcation lesions remains one of the most technically challenging procedures in interventional cardiology due to the complex anatomy and diverse lesion characteristics. These lesions account for approximately 15–25% of all PCI cases and are associated with higher rates of restenosis and adverse clinical outcomes compared to non-bifurcation lesions. Despite advancements in stent technology and procedural techniques, managing bifurcation lesions requires a tailored strategy that considers patient factors, lesion morphology, operator expertise, and outcome goals. This review introduces the Patient, Lesion, Operator, Technique, and Outcomes (PLOTO) framework, an innovative, algorithmic, and systemic approach to bifurcation PCI. Emphasis is placed on lesion assessment, including Medina classification, bifurcation angle, calcification, and imaging guidance, and the choice between provisional and two-stent strategies. Practical recommendations and evidence from contemporary studies are integrated to guide optimal procedural planning and execution, aiming to simplify complexity while enhancing clinical results.
Key Points
1. Coronary bifurcation lesions are challenging and are associated with higher rates of restenosis and stent thrombosis when compared to non-bifurcation percutaneous coronary intervention (PCI), particularly following complex procedures.
2. Simplifying the procedure as much as possible and limiting the number of implanted stents by using a stepwise provisional strategy remains the recommended strategy for the majority of bifurcation PCI.
3. In this review article, the authors propose the Patient, Lesion, Operator, Technique, and Outcomes (PLOTO) framework to approach bifurcation PCI, which focuses on the five titular components. This model aims to tailor interventions to individual patient needs and help select the most appropriate technique to optimise outcomes.
INTRODUCTION
Coronary bifurcation lesions pose a significant challenge in interventional cardiology, accounting for approximately 15–25% of all percutaneous coronary interventions (PCI).1,2 These lesions arise at arterial branching points, creating anatomical complexities that complicate intervention and increase the risk of side branch (SB) occlusion. Clinically, bifurcation lesions are associated with higher rates of restenosis and stent thrombosis when compared to non-bifurcation PCI, particularly following complex procedures.1-3
Despite the development of secondgeneration drug-eluting stents and advancements in procedural strategies, bifurcation PCI remains technically demanding due to factors such as heterogeneous plaque distribution, complex flow dynamics, and the need to preserve both main branches and SBs.4-6
Given these ongoing challenges, there is a critical need for practical, strategydriven approaches that simplify bifurcation interventions without compromising efficacy.7 Hence, this review aims to bridge complexity and clarity by offering a streamlined, real-world approach to PCI of bifurcation coronary lesions.
To facilitate a more effective and simplified approach to bifurcation PCI, the authors developed the Patient, Lesion, Operator, Technique, and Outcomes (PLOTO) framework (Figure 1), an innovative, simplified, and systemic approach that focuses on five key components.
This model emphasises a holistic view, tailoring interventions to individual patient needs and lesion characteristics, and selecting the most appropriate technique to optimise outcomes. By integrating these factors systematically, the authors aim to provide a clearer and more practical roadmap for navigating the complexities inherent in bifurcation interventions.
THE PATIENT
When approaching a bifurcation lesion, many patient-related factors should be considered, as they may affect the technique and equipment being used.8 Those factors include:
• Patient age: Operators might simplify the approach in older patients, minimising contrast and time in the catheterisation laboratory.
• Patient presentation, acute coronary syndrome versus stable ischaemic heart disease: A provisional approach might be preferred by some operators in unstable patients presenting with acute coronary syndrome with less than thrombolysis in myocardial infarction (TIMI) 3 flow. More complex techniques might be more appealing in stable patients.
• Diabetes: Patients with diabetes tend to have worse outcomes. In young people with diabetes who have left anterior descending bifurcation lesions, surgical consultation should be considered.
• Left ventricular function: Mechanical support devices may be considered in patients with left ventricular ejection fraction <35%, especially for left main (LM) or last conduit bifurcation disease.
• Medication adherence: Simple bifurcation techniques may reduce stent thrombosis risk in patients with questionable compliance.
• Bleeding risk: Minimising stent deployment may be advisable in patients with high bleeding risk needing possible interruption of antiplatelet therapy.
• Renal function: Simple techniques and reduced contrast use are preferred for patients with advanced kidney disease.
THE LESION
Definition
According to the Bifurcation Academic Research Consortium (Bif-ARC)9 and the European Bifurcation Club consensus,10 coronary bifurcation includes a coronary region consisting of three major parts: 1) the proximal main vessel; 2) the distal main vessel (DMV); and 3) the SB. The
longest and largest distal branch should be designated the DMV given the linear relationship between diameter, length, flow, and supplied myocardial mass.
Angiographically, a bifurcation lesion is defined as a coronary stenosis adjacent to and/or involving an adequate-sized SB (≥2.0 mm in reference diameter). The lesion is considered significant when its % diameter stenosis is >50% and the minimum luminal diameter in at least one of the three segments is located ≤4 mm from the point of bifurcation.9-12
Lesion Assessment
Accurate assessment of the bifurcation lesion not only dictates the selection of the ideal technique but can also influence clinical outcomes. The following four factors form the foundation of bifurcation lesion assessment.
Figure 1: The Patient, Lesion, Operator, Technique, and Outcomes (PLOTO) framework for percutaneous coronary intervention of coronary bifurcation lesions.
PLOTO
Bifurcation Approach
• Age
• Presentation
• Diabetes
• LV function
• Medication adherence
• Bleeding risk
• Renal function
• Medina classification
• Side branch
• Bifurcation angle
• Calcification
• <26 PCIs/yr
• 26–49 PCIs/yr
• 50–100 PCIs/yr
• >100 PCIs/yr
• >413 PCI/yr
- Provisional
- Two-Stent Strategies
• Culotte
• T-stenting & TAP
• Crush & mini-crush
• Double kissing
• V-stenting
• Major adverse clinical events
• Target lesion revascularization
• RESOLVE & DEFINITION Score
LV: left ventricular; PCI: percutaneous coronary interventions; PLOTO: Patient, Lesion, Operator, Technique, and Outcomes; TAP: T and small protrusion; yr: year.
Medina classification
The Medina classification13 evaluates the location of atherosclerotic disease by assigning a score of 1 to any lesion involving the proximal main vessel, DMV, or SB with ≥50% stenosis. The Medina classification is widely accepted as a universal classification for bifurcation lesions.9,14
Bif-ARC identifies ‘true’ bifurcation lesions, involving a significant (≥50%) diameter stenosis both in the main vessel and SB (i.e., Medina 1, 1, 1; 1, 0, 1; or 0, 1, 1), and ‘non-true’ lesions in all other cases. BifARC also recommends classifying the bifurcation lesions in LM and non-LM bifurcations, in addition to SB size and atherosclerotic involvement.9,15,16
Side branch
Accurate evaluation of the SB is critical in bifurcation PCI planning, as it strongly influences the choice between provisional and two-stent strategies.8,9,17 SB should be defined as ‘relevant’ if symptoms are stemming from a large amount (>10%) of ischaemic SB-related myocardium, impacting prognosis.9 Key factors include SB diameter (>2.5 mm), lesion length (>5–10 mm), ostial stenosis severity (≥70%), and TIMI flow postmain vessel intervention. Longer or heavily diseased SBs are at higher risk of occlusion, can be more challenging, and may warrant upfront two-stent techniques.18 Physiologic measurements such as fractional flow reserve and instantaneous wave-free ratio can guide the need for SB intervention after main vessel stenting.19 Intravascular imaging supports SB assessment by evaluating plaque burden and guidewire positioning in addition to post-PCI assessment.20
Bifurcation angle
Bifurcation angle plays a pivotal role in guiding PCI strategy.8,17,21,22 A wide bifurcation angle (>70°) is associated with a higher risk of SB occlusion, carinal shift, and difficulty in re-crossing the SB, favouring an upfront twostent technique. Conversely, a narrow angle (<70°, particularly <50–60°) may favour provisional stenting (PS).8,22
Calcification
Calcification significantly increases procedural complexity and is associated
with higher risks of stent under-expansion, SB compromise, and adverse clinical outcomes.8,9 It is a key feature of complex bifurcations, often necessitating advanced lesion preparation techniques and sometimes favouring a planned two-stent strategy.10,14
THE OPERATOR
Bifurcation PCI is challenging and requires many steps. Operator comfort and expertise with a chosen technique strongly influence procedural success and patient outcomes. Previous studies have shown an inverse relationship between PCI operator volume and in-hospital mortality that persisted in risk-adjusted analyses.23 Other studies also showed that PCI performed by experienced operators during complex PCI was independently associated with lower longterm risks of cardiac death.24 Specifically for LM bifurcation studies, patients who underwent LM PCI by high-volume and experienced operators had better shortand long-term prognoses.25 Therefore, Bif-ARC recommends reporting the volume of LM bifurcation PCI per year in the centre. In this article, the authors will use the same definition of experienced operators as previously applied in the paper by Fanaroff et al.23 Operators performing <50 PCIs annually are defined as low-volume operators.26 Operators performing 50–100 and >100 PCIs per year are defined as intermediate- and high-volume operators, respectively. Extreme high- and low-volume operators are defined as those performing >413 PCIs (97.5th percentile of the volume distribution) and <26 PCIs (2.5th percentile of the distribution) annually, respectively.23
THE TECHNIQUE
Simplifying the procedure as much as possible and limiting the number of implanted stents by using a stepwise provisional strategy remains the recommended strategy for the majority of true LM and non-LM bifurcation PCIs.8,10 Table 1 summarises the essential targets that should be pursued during bifurcation PCI.
Table 1: Key principles of bifurcation percutaneous coronary intervention promoted by the European Bifurcation Club.
Essential target Description
Keep the procedure simple and safe
Respect the original bifurcation anatomy and physiology and aim to reproduce it
Limit the number of stents
Do not stent the SB by default
Remember the step down in reference diameter from the proximal main vessel to the distal main vessel below the SB take-off
Limit metal overlap
Achieve sufficient stent expansion
• Choose a provisional stepwise stenting strategy
• Reconstruct the bifurcation anatomy with respect to the Finet, Murray, and Huo-Kassab laws
• Use a stepwise provisional strategy when the use of two stents is anticipated
• Implant the first stent reversely from the SB to the main branch when the SB is severely diseased
• Use kissing balloons (opens the SB and centres the carina)
• Implant a second stent only if needed (as T, TAP, or culotte)
• Consider the significance of the SB (CT scan, length, and diameter)
• Conditions supporting SB stent implantation after provisional stenting of the main vessel: 1) impaired TIMI flow in the SB; 2) significant stenosis (>70%) with angina and/or ECG changes; and 3) extensive dissection (>Type B) in the SB
• Size the first stent 1:1 to the distal main vessel reference diameter
• Choose a stent diameter for which the platform accommodates expansion to the reference diameter of the proximal main vessel
• Use of POT with balloon sized 1:1 to the proximal main vessel reference diameter
• Be aware of geographical miss during POT (avoid bottle neck configuration of the stent)
• Long segments and multiple layers of stents are associated with an increased risk of stent failure (ST and restenosis)
• Presence of multiple layers of stent struts across the SB ostium makes it more difficult to perform kissing balloon inflations
• Reduce the stent overlap in DK crush and DK culotte
• Suboptimal stent expansion correlates with stent failure (ST and restenosis)
• Stent expansion can accurately be estimated only by intracoronary imaging, but major underexpansion might be recognised by meticulous angiography revision and should be avoided
• Optimal lesion preparation before stent implantation aids stent expansion
• High-pressure, non-compliant balloon post-dilatation of all stented segments of coronary bifurcation is recommended
• Overdilate the stents by 5–10%, to compensate for recoil
• Aim for TIMI 3 flow in the main vessel and SB, and minimal residual stenosis in the stented segments (DS <10%)
• Major malapposition is associated with increased risk of major safety events, including cardiac death, MI, and ST
• Stent apposition can be accurately estimated only by intracoronary imaging, but major malapposition might be recognised by meticulous angiography revision and should be avoided
• Stent malapposition is most often present in the proximal main vessel of a coronary bifurcation lesion due to suboptimal POT (undersized balloon used for POT)
Avoid major stent malapposition
• The presence of stent malapposition in the proximal main vessel increases the risk of abluminal wiring and stent deformation during baseline and subsequent follow-up procedures
• Use a stent-enhanced view when possible
• Size the devices with respect to the vascular branching laws
• Consider using contrast puffing during balloon inflations when doubt of significant undersizing exists
Adapted from Burzotta et al.10
DK: double-kissing; DS: diameter stenosis; MI: myocardial infarction; POT: proximal optimisation technique; SB: side branch; ST: stent thrombosis; TAP: T and small protrusion; TIMI: thrombolysis in myocardial infarction.
Provisional Stenting
Provisional bifurcation stenting is the recommended default strategy for most bifurcation lesions,10,27 primarily due to its simplicity, safety profile, and efficiency. This is the preferred technique among many operators, especially low and intermediate volume operators.
The key procedural steps are (Figure 2):27-31
1. Initial guidewire placement: Wiring both myocardial bridge (MB) and SB to maintain access and procedural flexibility.
2. Main vessel preparation: Balloon predilation to assess lesion compliance and likelihood of plaque shift.
3. Main vessel stenting: Deploy drugeluting stent across SB ostium, ensuring lesion coverage without unnecessarily compromising SB.
4. Proximal optimisation technique (POT): Using a short balloon in proximal MB to improve stent apposition and facilitate SB access.
5. Assessment of SB: Angiographic and/ or physiologic assessment post-POT; intervention if compromised.
6. Rewiring and SB dilation: If needed, crossing stent struts for balloon dilation and possibly kissing balloon inflation.
7. SB stenting (if necessary): Techniques like T and small protrusion, T-stenting, or culotte depending on anatomy.
8. Final POT and kissing balloon inflation: To optimise proximal stent segment and correct malapposition.
Two-Stent Strategies
Two-stent strategies are used in coronary bifurcation lesions when the SB has significant disease, a large territory is at risk, or when provisional strategy fails.
Figure 2: Step-by-step provisional side branch stenting.
Adapted from Sawaya FJ et al.27
Multiple techniques have been developed, each tailored to specific anatomical and procedural needs:10
• Culotte: For similar branch sizes and narrow angles; stenting one branch then the other with overlap in MB.
• T-Stenting and T and small protrusion: For approximately 90° SB take-off; minimal protrusion into MB; a simple technique, but with a risk of incomplete coverage if the angle is suboptimal.
• Crush and mini-crush: SB stent crushed by MB stent, followed by kissing balloon inflation; mini-crush reduces metal layers.
• Double kissing (DK) crush: Two rounds of kissing balloon inflation to optimise stent apposition; superior outcomes in distal LM bifurcations. There have been many modifications to the crush techniques
over the years.32 The DKCRUSH-V trial showed superior outcomes of DK crush compared to PS in distal LM bifurcations (Figure 3).33
• V-stenting: Simultaneous MB and SB stenting in wide angles with short main branches; efficient but limited to short lesions.
Choosing the Best Technique
The provisional approach is recognised as the gold standard approach for the majority of bifurcation lesions.22,34 Yet, the use of two-stent implantation techniques is advised to treat selected patients with complex bifurcated lesions with relevant and significantly diseased SB.34 It is important to note that DK crush has many steps and can be challenging to perform.35 The DKCRUSH-V trial required the primary operators to have
Figure 3: Evolution of the crush technique demonstrating stent deployment and final kissing balloon inflation.
Classic crush: first iteration
Classic crush: with KBI
Mini crush: (7-F)
crush: (6-F)
crush: (6-F)
crush: (6-F)
performed ≥300 PCIs per year for 5 years, including at least 20 LM PCIs per year, and operators had to demonstrate proficiency in the DK crush technique in 3–5 cases before being allowed to enrol patients.36 Similar to chronic total occlusion interventions, there is likely a learning curve before optimal outcomes are achieved with DK crush.35
THE OUTCOMES
The clinical outcomes of the abovementioned techniques have been evaluated in several RCTs. However, the interpretation of the trials is challenging because of comparisons of different strategies and inconsistent findings.1 Overall, two-stent techniques were not significantly better than PS in terms of clinical outcomes. However, some analysis suggested that there might be benefits of a two-stent approach in selected patients with true bifurcation lesions, especially in the case of long SB lesions.1
A pairwise meta-analysis including 18 RCTs1,7,33,36-51 comparing provisional stenting versus two-stent techniques (5,022 patients) did not show any difference between the two groups regarding major adverse clinical events (MACE; odds ratio: 1.19; 95% CI: 0.90–1.58; p=0.23) or any secondary outcomes. In this analysis, significant heterogeneity was observed between the RCTs regarding MACE, myocardial infarction, and target lesion revascularisation (TLR). To reduce heterogeneity, a meta-regression, using the mean SB lesion length as a continuous covariate, was performed. This showed lower rates of the primary endpoint (MACE) associated with the two-stent technique in the RCTs that had enrolled patients with longer SB lesions (estimate of 0.06; 95% CI: 0.02–0.10; p=0.002; residual heterogeneity Q: 17.07; p value for residual heterogeneity=0.15). This effect was apparent in the RCTs with a mean studylevel SB lesion length >11 mm.1
When only RCTs enrolling patients with true bifurcations were considered,33,36,40,41,44-51 the analysis demonstrated a significant benefit from two-stent techniques in terms of MACE (OR: 1.52; 95% CI: 1.08–2.13; p=0.02), mainly driven by a higher risk of TLR following PS.1
In a network meta-analysis comparing all techniques to each other, DK crush was associated with significantly lower event rates than all other bifurcation stenting strategies regarding the primary endpoint (OR: 0.47; 95% CI: 0.36–0.62), as compared to PS, the second-best strategy in terms of MACE and TLR.1 Moreover, DK crush was related to a lower risk of myocardial infarction and stent thrombosis compared to all other techniques, except for T-stenting. However, the rate of cardiac death with DK crush was comparable to that of other bifurcation PCI techniques.1
Despite these advances, bifurcation PCI is still associated with a lower procedural success rate and worse clinical outcome compared with non-bifurcation PCI.27 Multiple risk scores have been introduced that mainly focused on lesion-related factors and the procedural techniques that determine clinical outcome. The Risk prEdiction of Side branch OccLusion in coronary bifurcation interVEntion (RESOLVE) score was established to evaluate the risk of SB occlusion.52 The Definitions and impact of complEx biFurcation lesIons on clinical outcomes after percutaNeous coronary IntervenTIOn using drug-eluting steNts (DEFINITION) criteria were designed to establish a stratification system that could guide optimal stenting strategy.53 In an analysis of 5,537 patients from the BIFURCAT registry, clinical features were predominant predictors for hard endpoints, and lesion features were predominant for predicting lesion-oriented clinical outcomes such as TLR and target vessel failure.54
CONCLUSION
This paper presents a referenced guide designed to assist interventional cardiologists in developing efficient strategies for bifurcation PCI. The proposed PLOTO framework serves as a tool to standardise decision-making and treatment planning, thereby supporting the achievement of optimal clinical outcomes. Continued research is encouraged to evaluate the long-term impact and effectiveness of implementing this methodology in clinical practice.
References
1. Bujak K et al. Clinical outcomes following different stenting techniques for coronary bifurcation lesions: a systematic review and network metaanalysis of randomised controlled trials. EuroIntervention. 2023;19(8):664-75.
2. Serruys PW et al. 5-year clinical outcomes of the ARTS II (Arterial Revascularization Therapies Study II) of the sirolimus-eluting stent in the treatment of patients with multivessel de novo coronary artery lesions. J Am Coll Cardiol. 2010;55(11):1093-101.
3. Lee JM et al. Ten-year trends in coronary bifurcation percutaneous coronary intervention: prognostic effects of patient and lesion characteristics, devices, and techniques. J Am Heart Assoc. 2021;10(18):e021632.
4. Morbiducci U et al. Atherosclerosis at arterial bifurcations: evidence for the role of haemodynamics and geometry. Thromb Haemost. 2016;115(3):484-92.
5. Nakazawa G et al. Pathological findings at bifurcation lesions: the impact of flow distribution on atherosclerosis and arterial healing after stent implantation. J Am Coll Cardiol. 2010;55(16):1679-87.
6. Davies PF et al. The atherosusceptible endothelium: endothelial phenotypes in complex haemodynamic shear stress regions in vivo. Cardiovasc Res. 2013;99(2):315-27.
7. Hildick-Smith D et al. Randomized trial of simple versus complex drug-eluting stenting for bifurcation lesions: the British Bifurcation Coronary Study: old, new, and evolving strategies. Circulation. 2010;121(10):1235-43.
8. Hildick-Smith D et al. Percutaneous coronary intervention of bifurcation lesions. EuroIntervention. 2022;18(4):e273-91.
9. Lunardi M et al. Definitions and standardized endpoints for treatment of coronary bifurcations. J Am Coll Cardiol. 2022;80(1):63-88.
10. Burzotta F et al. Percutaneous coronary intervention for bifurcation coronary lesions using optimised angiographic guidance: the 18th consensus document from the European Bifurcation Club. EuroIntervention. 2024;20(15):e915-26.
11. Ramcharitar S et al. A novel dedicated quantitative coronary analysis methodology for bifurcation lesions. EuroIntervention. 2008;3(5):553-7.
12. Louvard Y et al. Classification of coronary artery bifurcation lesions and treatments: time for a consensus! Catheter Cardiovasc Interv. 2008;71(2):175-83.
13. Medina A et al. Una clasificación simple de las lesiones coronarias en bifurcación. Rev Esp Cardiol. 2006;59(2):183.
14. Perl L et al. Prognostic significance of the Medina classification in bifurcation lesion percutaneous coronary intervention with second-generation drug-eluting stents. Heart Vessels. 2020;35(3):331-9.
15. Zimarino M et al. The impact of the extent of side branch disease on outcomes following bifurcation stenting. Catheter Cardiovasc Interv. 2020;96(1):E84-92.
16. Kassier A et al. Kissing balloon-stent technique for simple bifurcation lesions. J Clin Med. 2024;13(9):2645.
17. Hahn JY et al. Predictors and outcomes of side branch occlusion after main vessel stenting in coronary bifurcation lesions: results from the COBIS II Registry (COronary BIfurcation Stenting). J Am Coll Cardiol. 2013;62(18):1654-9.
18. Hara H et al. Impact of stent length and diameter on 10-year mortality in the SYNTAXES trial. Catheter Cardiovasc Interv. 2021;98(3):E379-87.
19. Lee HS et al. Physiological approach for coronary artery bifurcation disease: position statement by Korean, Japanese, and European bifurcation clubs. JACC Cardiovasc Interv. 2022;15(13):1297-309.
20. Gao XF et al. 3-year outcomes of the ULTIMATE trial comparing intravascular ultrasound versus angiography-guided drug-eluting stent implantation. JACC Cardiovasc Interv. 2021;14(3):247-57.
21. Zhang D, Dou K. Coronary bifurcation intervention: what role do bifurcation angles play? J Interv Cardiol. 2015;28(3):236-48.
22. Burzotta F et al. European Bifurcation Club white paper on stenting techniques for patients with bifurcated coronary artery lesions. Catheter Cardiovasc Interv. 2020;96(5):1067-79.
23. Fanaroff AC et al. Outcomes of PCI in relation to procedural characteristics and operator volumes in the United States. J Am Coll Cardiol. 2017;69(24):2913-24.
24. Choi KH et al. Prognostic impact of operator experience and IVUS guidance on long-term clinical outcomes after complex PCI. JACC Cardiovasc Interv. 2023;16(14):1746-58.
25. Xu B et al. Impact of operator experience and volume on outcomes after left main coronary artery percutaneous coronary intervention. JACC Cardiovasc Interv. 2016;9(20):2086-93.
26. Harold JG et al. ACCF/AHA/ SCAI 2013 update of the clinical competence statement on coronary artery interventional procedures: a report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians Task Force on Clinical Competence and Training (writing committee to revise the 2007 clinical competence statement on cardiac interventional procedures). J Am Coll Cardiol. 2013;62(4):357-96.
27. Sawaya FJ et al. Contemporary approach to coronary bifurcation lesion treatment. JACC Cardiovasc Interv. 2016;9(18):1861-78.
28. Darremont O et al. Technical aspects of the provisional side branch stenting strategy. EuroIntervention. 2015;11(Suppl V):V86-90.
29. Lefèvre T et al. Provisional side branch stenting for the treatment of bifurcation lesions. EuroIntervention. 2010;6(Suppl J):J65-71.
30. Vassilev D, Gil R. Clinical verification of a theory for predicting side branch stenosis after main vessel stenting in coronary bifurcation lesions. J Interv Cardiol. 2008;21(6):493-503.
31. Albiero R et al. Treatment of coronary bifurcation lesions, part I: implanting the first stent in the provisional pathway. The 16th expert consensus document of the European Bifurcation Club. EuroIntervention. 2022;18(5):e362-76.
32. Raphael CE et al. Evolution of the crush technique for bifurcation stenting. JACC Cardiovasc Interv. 2021;14(21):2315-26.
33. Chen X et al. 3-year outcomes of the DKCRUSH-V trial comparing DK crush with provisional stenting for left main bifurcation lesions. JACC Cardiovasc Interv. 2019;12(19):1927-37.
34. Neumann FJ et al. 2018 ESC/ EACTS guidelines on myocardial revascularization. EuroIntervention. 2019;14(14):1435-534.
35. Brilakis ES et al. DK-crush should become preferred strategy for treating unprotected LM bifurcation lesions: no pain, no gain. J Am Coll Cardiol. 2017;70(21):2618-20.
36. Chen SL et al. Double kissing crush versus provisional stenting for left main distal bifurcation lesions: DKCRUSH-V randomized trial. J Am Coll Cardiol. 2017;70(21):2605-17.
37. Ferenc M et al. Long-term outcomes of routine versus provisional T-stenting for de novo coronary bifurcation lesions: five-year results of the Bifurcations Bad Krozingen I study. EuroIntervention. 2015;11(8):856-9.
38. Colombo A et al. Randomized study to evaluate sirolimus-eluting stents implanted at coronary bifurcation lesions. Circulation. 2004;109(10): 1244-9.
39. Colombo A et al. Randomized study of the crush technique versus provisional side-branch stenting in true coronary bifurcations: the CACTUS (Coronary Bifurcations: Application of the Crushing Technique Using SirolimusEluting Stents) study. Circulation. 2009;119(1):71-8.
40. Hildick-Smith D et al. The European bifurcation club Left Main Coronary Stent study: a randomized comparison of stepwise provisional vs. systematic dual stenting strategies (EBC MAIN). Eur Heart J. 2021;42(37):3829-39.
41. Kumsars I et al. Randomised comparison of provisional side branch stenting versus a two-stent strategy for treatment of true coronary bifurcation lesions involving a large side branch: the Nordic-Baltic Bifurcation Study IV. Open Heart. 2020;7(1):e000947.
42. Maeng M et al. Long-term results after simple versus complex stenting of coronary artery bifurcation lesions: Nordic Bifurcation study 5-year follow-up results. J Am Coll Cardiol. 2013;62(1):30-4.
43. Kim YH et al. Randomized comparisons between different stenting approaches for bifurcation coronary lesions with
or without side branch stenosis. JACC Cardiovasc Interv. 2015;8(4):550-60.
44. Hildick-Smith D et al. The EBC TWO Study (European Bifurcation Coronary TWO): a randomized comparison of provisional T-stenting versus a systematic 2 stent culotte strategy in large caliber true bifurcations. Circ Cardiovasc Interv. 2016;9(9): e003643.
45. Lin QF et al. Choice of stenting strategy in true coronary artery bifurcation lesions. Coron Artery Dis. 2010;21(6):345-51.
46. Pan M et al. Rapamycin-eluting stents for the treatment of bifurcated coronary lesions: a randomized comparison of a simple versus complex strategy. Am Heart J. 2004;148(5):857-64.
47. Kim J et al. Optimal strategy for side branch treatment in patients with left main coronary bifurcation lesions. Rev Esp Cardiol (Engl Ed). 2021;74(8):691-9.
48. Ye F et al. The acute changes of fractional flow reserve in DK (double kissing), crush, and 1-stent technique for true bifurcation lesions. J Interv Cardiol. 2010;23(4):341-5.
49. Ye F et al. Hemodynamic changes of fractional flow reserve after double kissing crush and provisional stenting technique for true bifurcation lesions. Chin Med J (Engl). 2012;125(15): 2658-62.
50. Zhang L et al. A pilot study on culottes versus crossover single stenting for true coronary bifurcation lesions. Acta Cardiol Sin. 2016;32(4):450-9.
51. Kan J et al. 3-year outcomes after 2-stent with provisional stenting for complex bifurcation lesions defined by DEFINITION criteria. JACC Cardiovasc Interv. 2022;15(13):1310-20.
52. Dou K et al. An angiographic tool for risk prediction of side branch occlusion in coronary bifurcation intervention: the RESOLVE score system (Risk prEdiction of Side branch OccLusion in coronary bifurcation interVEntion). JACC Cardiovasc Interv. 2015;8(1 Pt A):39-46.
53. Chen SL et al. Impact of the complexity of bifurcation lesions treated with drug-eluting stents: the DEFINITION study (Definitions and impact of complEx biFurcation lesIons on clinical outcomes after percutaNeous coronary IntervenTIOn using drug-eluting steNts). JACC Cardiovasc Interv. 2014;7(11):1266-76.
54. Kang J et al. Impact of clinical and lesion features on outcomes after percutaneous coronary intervention in bifurcation lesions. JACC Asia. 2022;2(5):607-18.
Unrepaired Tetralogy of Fallot with Pulmonary Atresia and Major Aorto-pulmonary Collateral Arteries in Pregnancy: A Case Report
Authors: Eliasa K. Ndale,1,2 Sophia S. Muhali,2 Nasra Batchu,3 Rafiki N. Mjema,3,2,3 Simon C. Peter,4 Elifuraha W. Mkwizu,1,2 Adnan M. Sadiq,2,5 *Abid M. Sadiq2,4
1. Department of Internal Medicine, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
2. Faculty of Medicine, Kilimanjaro Christian Medical Centre University, Moshi, Tanzania
3. Department of Obstetrics & Gynaecology, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
4. Department of Cardiology, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
5. Department of Radiology & Imaging, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
*Correspondence to abid.physician@gmail.com
Disclosure: The authors have declared no conflicts of interest. Ethical approval was waived by the ethics committee as this is a single case report. Written informed consent was obtained from the patient for their anonymised information and any accompanying images to be published in this article.
Acknowledgements: Abid M. Sadiq is the corresponding author, who participated in the organisation and writing of the article. Ndale, Muhali, Batchu, Mjema, and Salum contributed to clinical examination, treatment, and follow-up of the patient. Peter and Adnan M. Sadiq in the radiology and imaging department read and validated the figures. Mkwizu and Abid M. Sadiq supervised work, validated the figures, and allowed the article’s publication.
Received: 18.03.25
Accepted: 27.08.25
Keywords: Cardiovascular, cyanotic congenital heart disease, major aortopulmonary collateral arteries (MAPCA), pregnancy complications, pulmonary atresia, Tanzania, tetralogy of Fallot (TOF).
Tetralogy of Fallot with pulmonary atresia and major aortopulmonary collateral arteries (MAPCA) represents the most severe variant of this congenital heart disease, with complete atresia of the pulmonary valve replacing pulmonary stenosis. Pregnancy in women with unrepaired lesions of this complexity is exceedingly rare and associated with major maternal and fetal risks. The authors report the case of an 18-year-old primigravida presenting at 31 weeks’ gestation with progressive dyspnoea, cyanosis, and peripheral oedema. Clinical evaluation and echocardiography revealed unrepaired tetralogy of Fallot with pulmonary atresia, a large ventricular septal defect, and MAPCAs. She was managed with diuretics, nitrates, antiplatelet therapy, and prophylactic heparin. Cardiac CT confirmed the diagnosis,
demonstrating absent native pulmonary arteries and a MAPCA arising from the aortic root. Despite medical stabilisation and multidisciplinary care, she required Caesarean delivery at 35 weeks for fetal distress. A live but premature infant weighing 1.1 kg was delivered; however, neonatal demise occurred on Day 3. The mother remained stable post-partum and was discharged on medical management, though she declined surgical intervention. This case highlights the profound challenges of managing pregnancy in unrepaired tetralogy of Fallot with pulmonary atresia and MAPCAs, particularly in resource-limited settings. It underscores the need for early pre-pregnancy counselling, risk stratification, and coordinated multidisciplinary care in specialised centres to improve outcomes for both mother and child.
Key Points
1. Tetralogy of Fallot with pulmonary atresia and major aorto-pulmonary collateral arteries is an exceptionally rare condition, and its occurrence during pregnancy poses significant risks to both mother and fetus.
2. In unrepaired tetralogy of Fallot, epidural or combined spinal-epidural analgesia is generally recommended, as it minimises abrupt reductions in systemic vascular resistance and helps prevent worsening of right-to-left shunting.
3. Early counselling and planning around contraception, pregnancy timing, and maternal/fetal risk are essential for women with congenital heart disease, to reduce complications and improve outcomes.
INTRODUCTION
Tetralogy of Fallot (TOF) is one of the most common forms of cyanotic congenital heart disease, characterised by right ventricular hypertrophy, an overriding aorta, a ventricular septal defect, and pulmonary stenosis. A less frequent anatomical variant occurs when pulmonary stenosis is replaced by pulmonary atresia. This form has an incidence of approximately 0.07 per 1,000 live births, accounting for up to 2.5% of all congenital heart diseases and around 20.0% of all TOF cases.1
In pulmonary atresia, the atretic pulmonary valve prevents blood flow through the right ventricular outflow tract, and pulmonary perfusion is therefore supplied via major aorto-pulmonary collateral arteries (MAPCA). The Congenital Heart Surgery Nomenclature and Database Project classifies TOF with pulmonary atresia into three subtypes according to pulmonary circulation: Type A, native pulmonary arteries present without MAPCAs; Type B, native pulmonary arteries present with MAPCAs; and Type C, MAPCAs only.1
The rarity of unrepaired TOF in pregnancy means that management strategies are not standardised and must be guided by case reports, expert opinion, and multidisciplinary collaboration. In resourcelimited settings, the challenges are compounded by delayed diagnosis, limited access to advanced imaging, and restricted availability of surgical or interventional options.
Here, the authors report a rare case of unrepaired TOF with pulmonary atresia and MAPCA Type C in an adolescent primigravida. The patient experienced a premature pregnancy complicated by maternal cyanosis and neonatal demise. This case underscores the unique challenges of managing congenital heart disease in pregnancy, particularly in lowresource contexts, and adds to the limited literature on outcomes of unrepaired TOF with pulmonary atresia in young women.
CASE PRESENTATION
An 18-year-old primigravida presented at 31 weeks’ gestation (by dates) with a 2-week history of progressive shortness of breath
(worse on minimal exertion; New York Heart Association [NYHA] Class III) associated with gradual, non-painful, bilateral lowerlimb swelling. On examination, she was conscious, afebrile, and not pale, with central and peripheral cyanosis, Grade 3 digital clubbing, and bilateral pitting oedema of the lower limbs. Her initial observations were a blood pressure of 130/78 mmHg, a heart rate of 88 beats/min, a respiratory rate of 24 breaths/min (tachypnoeic), and an arterial O2 saturation of 86% on room air by pulse oximetry.
Cardiovascular examination revealed a regular, good-volume pulse synchronous with peripheral pulses. The jugular venous pressure was raised, at 8 cm H₂O. The apex beat was displaced, and a holosystolic murmur was audible at the left lower sternal border. A respiratory examination demonstrated diffuse bilateral basal fine crackles. An abdominal examination revealed a gravid uterus with a fundal height of 32 weeks and a fetal heart rate of 136 beats/min.
Initial laboratory investigations showed a haemoglobin of 15.0 g/dL, a haematocrit of 45.0%, and a platelet count of 197x10⁹ /L. Chest radiography demonstrated cardiomegaly (Figure 1).
Electrocardiography showed features of right heart strain. Transthoracic echocardiography revealed situs solitus with laevocardia, dilated right atrium, hypertrophied right ventricle, a large inlet ventricular septal defect (20 mm) with bidirectional shunt, an overriding aorta (>85% of the conotruncal artery), and pulmonary atresia. A right aortic arch with collateral arteries arising from the aorta was noted. Left ventricular function and valvular anatomy were preserved, with minimal pericardial effusion (Figure 2).
She was started on intravenous furosemide 40 mg twice daily, oral isosorbide dinitrate 5 mg twice daily, oral acetylsalicylic acid 75 mg once daily, and subcutaneous unfractionated heparin 7,500 U twice daily. Under lead protection, a cardiac CT
Radiograph demonstrates a markedly enlarged cardiac silhouette consistent with moderate cardiomegaly. Increased pulmonary vascular markings (pulmonary plethora) are visible, suggestive of a left-to-right shunt.
Figure 1: Chest radiograph.
Echocardiography shows: A, B) situs solitus with levocardia, a dilated right atrium, a hypertrophied right ventricle, and a large inlet ventricular septal defect (20 mm) with bidirectional shunting; C) an overriding aorta involving >85% of the conotruncal artery; and D) pulmonary valve atresia (yellow arrow).
scan was performed, which confirmed TOF with a large ventricular septal defect. The pulmonary artery was not visualised, consistent with pulmonary atresia, and a MAPCA was identified arising from the sinotubular junction of the aortic root, providing alternative pulmonary blood supply (Figure 3).
The patient’s symptoms improved over the following days. A multidisciplinary team counselled her regarding maternal and fetal risks, but she and her family opted to continue with the pregnancy. She received intramuscular dexamethasone 6 mg twice daily for 48 hours to promote fetal lung maturation and was monitored closely. Follow-up laboratory tests revealed a haemoglobin of 16.5 g/dL, a haematocrit of 50.8%, and a platelet count of 171x10⁹ /L.
At 35 weeks’ gestation, due to fetal distress, a Caesarean section was performed under general anaesthesia. A live female infant weighing 1.1 kg was delivered, with Appearance, Pulse, Grimace, Activity, and Respiration (Apgar) scores of 6 and 8 at 1 and 10 minutes, respectively. The neonate was admitted to the premature unit but, unfortunately, died after 3 days. The mother remained clinically stable post-partum, and was monitored closely for 1 week without further deterioration. Counselling regarding her condition was provided prior to discharge.
At follow-up visits, additional counselling addressed future pregnancies, contraceptive options, and surgical intervention. However, the patient and her family were reluctant to proceed with surgery and chose to continue with medical management.
Figure 2: Transthoracic echocardiography.
A B C
The CT demonstrates: A) an overriding aorta with a large ventricular septal defect and absent pulmonary artery consistent with pulmonary atresia; and B, C) a MAPCA Type C arising from the sinotubular junction of the aortic root and supplying the pulmonary arteries (yellow arrow). The right atrium, left atrium, and left ventricle appear dilated.
MAPCA: major aortopulmonary collateral artery.
DISCUSSION
Unrepaired TOF that persists into adulthood is a rare occurrence, and even rarer in pregnancy. Adult patients with TOF usually present according to the severity of the underlying anatomical defects, with common manifestations including heart failure, palpitations, arrhythmias, syncope, and right ventricular dysfunction.2 Fewer than 1% of unrepaired TOF cases survive into adulthood, as early surgical repair is considered the definitive management. However, in patients with pulmonary atresia, survival may be facilitated by the development of pulmonary collaterals and the absence of additional congenital malformations.3
The burden of congenital heart disease is lower in Africa compared with highincome regions. The prevalence has been estimated as two per 1,000 live births in Africa, compared with eight and nine per 1,000 in Europe and Asia, respectively.3 The incidence of TOF with pulmonary atresia is approximately 0.7 per 100,000 live births, representing around one-fifth of all TOF cases.4 In Tanzania, the prevalence of TOF with pulmonary atresia has been reported as 1.2% of congenital heart disease cases.5 Unrepaired TOF is predominantly reported in developing countries, with a 10-year survival of less than 8%. In contrast, surgical
repair increases survival to approximately 80%.6 Factors influencing outcomes include abnormalities of the pulmonary arteries, elevated right ventricular systolic pressure, arterial O2 saturation below 85%, a haemoglobin of >20 g/dL, and haematocrit >65%.2
Disease-specific maternal cardiovascular risk assessment is best undertaken using the modified WHO classification, which remains the most widely adopted system. However, its utility is limited in low-resource settings.7 In this case, the patient was categorised as modified WHO Class III, reflecting unrepaired cyanotic congenital heart disease.
Pregnancy induces profound physiological adaptations, particularly within the cardiopulmonary system. These include an increase in maternal plasma volume by approximately 50%, erythrocyte mass by approximately 40%, and total blood volume by approximately 45% by 32 weeks’ gestation.8-10 There is also an increase in cardiac output of around 45% by 24 weeks, mediated by both stroke volume and heart rate, and facilitated by reduced afterload, though end-diastolic pressures, ejection fraction, and central and pulmonary pressures remain largely unchanged.9,10 Systemic vascular resistance decreases by approximately 30% by mid-pregnancy
Figure 3: Cardiac CT.
before rising again near term.10 Maternal serum albumin falls by about 18% at 24 weeks, lowering colloid oncotic pressure and predisposing to pulmonary oedema after crystalloid infusion.10 In normal pregnancies, mean pulmonary wedge pressure is around 7.5 mmHg, pulmonary congestion develops above 18 mmHg, and oedema typically develops after ≥28 mmHg.11,12 Respiratory adaptations include increases in tidal volume and minute ventilation by approximately 40%, and O2 consumption by approximately 15%, producing around a 25% reduction in maternal arterial partial pressure of CO2. 13,14 Maternal arterial O2 tension rises slightly due to hyperventilation and enhanced cardiac output; however, O2 saturation should remain >95% in both rest and exertion.15
In women with TOF, these physiological changes exacerbate right-to-left shunting, further lowering systemic O2 saturation and worsening hypoxaemia.10,16 Reduced cardiac reserve predisposes women to decompensation.10,17 Non-cardiac dyspnoea in patients with cyanosis may also result from the altered gas exchange and pH changes associated with the augmented right-to-left shunt during pregnancy and exercise.15,18 Maternal mortality is particularly high in those with co-existing pulmonary hypertension, even when they are in functional Class II before pregnancy. In such cases, acute increases in pulmonary vascular resistance due to haemorrhage, anaesthesia, or haemodynamic shifts can precipitate sudden death.19,20
Cardiac catheterisation remains the reference standard for defining the pulmonary arterial tree and delineating MAPCA anatomy in TOF with pulmonary atresia. It enables selective angiography of individual collaterals, assessment of segmental pulmonary perfusion, and quantification of shunt and pulmonary vascular resistance. These data are crucial in determining surgical options, such as staged or single-stage unifocalisation and suitability for a right ventricular–pulmonary artery conduit. Cardiac catheterisation can also identify collaterals supplying nonfunctional lung segments.1 In specialist
centres, catheter-based interventions may be employed to support surgical management, including coil embolisation of competing collaterals, occlusion of non-contributory high-flow MAPCAs, and balloon angioplasty or stenting of stenotic collaterals to optimise downstream perfusion.1,2
During pregnancy, diagnostic catheterisation is generally avoided unless results are expected to alter immediate management. When required, measures such as abdominal shielding, reduced fluoroscopy frame rates, collimation, and minimised exposure times are essential, with the second trimester preferred where feasible.2,6 In the authors’ patient, detailed anatomical definition was achieved using cardiac CT imaging. Invasive haemodynamic assessment was therefore deferred, in keeping with the principle that catheterisation should only be undertaken if results would significantly change management.1,6
Vaginal delivery is associated with an acute rise in cardiac output (up to 80%) due to caval decompression and the autotransfusion of blood from the contracting uterus into the maternal circulation.10 This abrupt increase in venous return elevates pulmonary blood volume and flow but usually returns to prelabour levels within an hour post-partum. By comparison, Caesarean delivery is accompanied by greater blood loss, which partially blunts this increase in venous return.13 Cardiac output peaks around 15 minutes post-partum, with maximum increments of approximately 37% under epidural anaesthesia and approximately 28% under general anaesthesia.10,20 Stroke volume and cardiac output may remain modestly elevated for up to a year postpartum, and haemodynamic responses are augmented in subsequent pregnancies. Thus, pregnancy induces a permanent remodelling of the maternal cardiovascular system.10,13
Pregnancy in unrepaired TOF is associated with serious risks, including maternal morbidity up to 65%, maternal mortality up to 15%, and adverse perinatal outcomes.21,22
Management is therefore vital to minimise complications. Haemodynamic changes in pregnancy may exacerbate right-toleft shunting, precipitating hypoxaemia, cyanosis, and increased risks of both maternal and fetal death.23 Chronic hypoxia also drives secondary polycythaemia, which contributes to hyperviscosity and thrombosis.24
Cyanotic congenital heart disease confers a complex coagulation profile. Secondary erythrocytosis and haemoconcentration elevate thrombotic risk, yet iron deficiency, thrombocytopenia, platelet dysfunction, and reduced clotting factor levels predispose to haemorrhage. Pregnancy adds another layer of hypercoagulability and plasma volume shifts, further amplifying risks of both thrombosis and bleeding during the peripartum period.2,6,7
Management strategies should therefore include: a) careful hydration with avoidance of unnecessary venesection; b) active investigation and correction of iron deficiency to reduce hyperviscosity without resorting to routine phlebotomy; c) individualised decisions on antithrombotic therapy, typically low-dose aspirin and/or prophylactic heparin, based on cyanosis, immobility, and obstetric risk; and d) multidisciplinary peripartum planning to avoid haemodynamic instability.2,7 Therapeutic phlebotomy is reserved for patients with symptomatic hyperviscosity and very high haematocrit, and should be combined with volume replacement to avoid circulatory collapse.6,7 Postpartum, early mobilisation and extended thromboprophylaxis may be appropriate, provided bleeding risk is controlled.2,7
Maternal complications in TOF include right ventricular dilatation and failure, worsening cyanosis, dyspnoea, arrhythmias, thromboembolism, aortic root dilatation, endocarditis, and maternal death. Obstetric complications include miscarriage and postpartum haemorrhage,25 while fetal complications include abortion (approximately 20%), intrauterine growth restriction (approximately 50%), prematurity (approximately 50%), and fetal loss (approximately 15%).2,26 In the authors’ case,
the neonate was premature with growth restriction and died within 3 days. Maternal cyanosis, ventricular dysfunction, and polycythaemia were the main contributory factors.26
The optimal mode of delivery is determined by balancing maternal and fetal risks. Vaginal delivery is usually preferred due to lower risks of haemorrhage, thromboembolism, infection, pulmonary congestion, and maternal death. Caesarean delivery is reserved for obstetric indications, and regional anaesthesia is generally favoured over general anaesthesia owing to better haemodynamic stability, absence of respiratory depression, and readiness for urgent operative delivery.16 Epidural or combined spinal-epidural anaesthesia reduces abrupt decreases in systemic vascular resistance and may mitigate worsening of right-to-left shunting. In contrast, general anaesthesia with intermittent positive-pressure ventilation can increase pulmonary vascular resistance and exacerbate shunting.16 If general anaesthesia is required, meticulous attention to maintaining systemic and pulmonary vascular resistance balance is crucial.2
After delivery, the prevention of haemorrhage is essential. Oxytocin remains first-line, but must be administered cautiously, as it can provoke hypotension and reflex tachycardia, thereby worsening shunting.16 Methylergometrine may be preferable for uterine tone, as it preserves systemic vascular resistance.23 Careful postpartum monitoring is imperative, especially in the first 48 hours, when cardiovascular adaptations are most pronounced.2,16
Published literature on pregnancy in TOF, spanning repaired and unrepaired anatomies, consistently demonstrates that maternal and fetal outcomes are primarily determined by cyanosis, right-sided pressures, and the presence of residual shunting. Reports already cited in this manuscript2,4,21,23,25,26 highlight the high rates of prematurity, growth restriction, and fetal loss in unrepaired TOF, with comparatively improved outcomes following surgical repair
or when maternal O2 saturation is ≥90%. Caesarean delivery is typically reserved for obstetric reasons, and regional anaesthesia is preferred when feasible, reflecting current guideline-based practice.2,7
The authors’ case echoes these themes: delayed presentation, the constraints of a resource-limited setting, and neonatal vulnerability. It contributes new insights by a) demonstrating detailed multimodality imaging consistent with TOF with pulmonary atresia and MAPCAs; b) illustrating the rationale for deferring catheterisation until post-partum; and c) outlining a pragmatic haemostatic strategy tailored to a lowresource environment. Collectively, these features extend the available evidence from sub-Saharan Africa and underscore the importance of pre-pregnancy counselling,
References
1. Ganigara M et al. Tetralogy of Fallot with pulmonary atresia: anatomy, physiology, imaging, and perioperative management. Semin Cardiothorac Vasc Anesth. 2021;25(3):208-17.
2. Thakur S et al. Challenges and outcomes of pregnancy in an uncorrected tetralogy of Fallot with pulmonary atresia and major aorta-pulmonary collateral arteries (MAPCA): a case report. Egypt Heart J. 2023;75(1):9.
3. Sadiq AM, Sadiq AM. A case of computed tomography diagnosis of truncus arteriosus type IV. Oxf Med Case Reports. 2021;2021(2):omaa144.
4. Agarwal N et al. Successful management of pregnancy in uncorrected tetralogy of Fallot with pulmonary atresia. J Obstet Gynaecol India. 2015;65(6):417-9.
5. Zuechner A et al. Spectrum of heart diseases in children presenting to a paediatric cardiac echocardiography clinic in the Lake Zone of Tanzania: a 7 years overview. BMC Cardiovasc Disord. 2019;19(1):291.
6. Sames-Dolzer E et al. Outcome of patients with tetralogy of Fallot with pulmonary atresia. Front Pediatr. 2023;10:1077863.
7. Regitz-Zagrosek V et al. 2018 ESC guidelines for the management of cardiovascular diseases during pregnancy. Eur Heart J. 2018;39(34):3165-241.
multidisciplinary care, and planned delivery in centres equipped with adult congenital cardiology and high-risk obstetric expertise.2,4,21,23,25,26
CONCLUSION
TOF with pulmonary atresia and MAPCAs is exceptionally rare, and its occurrence during pregnancy poses major challenges for both maternal and neonatal outcomes. Effective management requires early recognition, comprehensive counselling, and coordinated multidisciplinary care. Where possible, delivery should be planned in centres with specialised cardiac and neonatal expertise to optimise survival and reduce the risks of maternal and perinatal mortality.
a systematic review and metaanalysis of longitudinal studies. BMC Pregnancy Childbirth. 2019;19(1):508.
9. Sanghavi M, Rutherford JD. Cardiovascular physiology of pregnancy. Circulation. 2014;130(12):1003-8.10.
10. Canobbio MM et al. Management of pregnancy in patients with complex congenital heart disease: a scientific statement for healthcare professionals from the American Heart Association. Circulation. 2017;135(8):e50-87.
11. Zhou Q et al. Evaluation of maternal and fetal outcomes in pregnancy complicated with pulmonary arterial hypertension. Ann Palliat Med. 2021;10(2):1404-10.
12. Humbert M. et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022;43(38):3618-731.
13. Soma-Pillay P et al. Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27(2):89-94.
14. Vinturache A, "Maternal physiological changes in pregnancy," Khalil A (ed.), The Continuous Textbook of Women’s Medicine: Volume 4: Fetal Development and Maternal Adaptation (2021), London: Global Library of Women's Medicine (GLOWM).
15. Schaeffer MR et al. Impact of ageing and pregnancy on the minute ventilation/carbon dioxide production response to exercise. Eur Respir Rev. 2021;30(161):200225.
16. Ladouceur M, Nizard J. Challenges and management of pregnancy in cyanotic
17. Anthony J, Sliwa K. Decompensated heart failure in pregnancy. Card Fail Rev. 2016;2(1):20-6.
18. Naeije R et al. The physiological basis of pulmonary arterial hypertension. Eur Respir J. 2022;59(6):2102334.
19. Price LC et al. Perioperative management of patients with pulmonary hypertension undergoing non-cardiothoracic, non-obstetric surgery: a systematic review and expert consensus statement. Br J Anaesth. 2021;126(4):774-90.
20. Meng ML et al. Anesthetic care of the pregnant patient with cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2023;147(11):e657-73.
21. Veldtman GR et al. Outcomes of pregnancy in women with tetralogy of Fallot. J Am Coll Cardiol. 2004;44(1):174-80.
22. Kumari G et al. A case report on pregnancy with uncorrected tetralogy of Fallot with pulmonary hypertension managed uneventfully at a tertiary health care in India. Int J Reprod Contracept Obstet Gynecol. 2022;12(1):275-7.
23. Gomez LM et al. Pregnancy with uncorrected tetralogy of Fallot (TOF), pulmonary atresia and major aorto-pulmonary collateral arteries (MAPCA). Case Rep Perinat Med. 2018;7(1):20170053.
24. McMullin MFF et al. A guideline for the
management of specific situations in polycythaemia vera and secondary erythrocytosis: a British Society for Haematology guideline. Br J Haematol. 2019;184(2):161-75.
25. Wang K et al. Pregnancy outcomes among 31 patients with tetralogy of Fallot, a retrospective study. BMC Pregnancy Childbirth. 2019;19(1):486.
26. Garagiola ML, Thorne SA. Pregnancy considerations in tetralogy of Fallot. CJC Pediatr Congenit Heart Dis. 2023;2(6 Part A):301-13. FOR REPRINT QUERIES PLEASE CONTACT: INFO@EMJREVIEWS.COM
Renal Angioplasty and Stenting for Atherosclerotic Renal Artery Stenosis: Current Landscape and Future Directions
Authors: Ellen Dempsey,1 Cristian Deliv,1 Goran Mitreski,1-3 Limy Wong,4,5
Renal artery angioplasty and stenting remain controversial in managing atherosclerotic renal artery stenosis. Landmark trials (ASTRAL and CORAL) failed to show superiority over optimal medical therapy, yet design limitations, including the exclusion of high-risk patients, the employment of variable imaging modalities, and the utilisation of non-standardised protocols, undermined both studies and limited their applicability. Since these trials, the RADAR trial was prematurely terminated, echoing prior findings, but in a small cohort of patients. Of six major RCTs since 1998, most excluded patients with flash pulmonary oedema, refractory hypertension, or rapidly declining renal function. Meta-analyses report reduced antihypertensive burden after renal artery revascularisation, particularly in those with severe or resistant hypertension, but without clear benefit for mortality, renal function, or adverse events. Lower-level evidence from case series highlights success in select high-risk situations (recurrent pulmonary oedema, progressive renal decline, or complex anatomy). Current American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) and European Society of Cardiology (ESC) guidelines endorse revascularisation in specific contexts (Level B–C evidence). Given the limitations of past RCTs, there is a need for robust new RCTs in appropriate patient populations to conclusively determine the role of renal angioplasty and stenting in atherosclerotic renal artery stenosis.
Key Points
1. Both the ASTRAL and CORAL RCTs excluded high-risk patient cohorts (flash pulmonary oedema, refractory hypertension, rapidly declining renal function), underrepresented patients with severe renal artery stenosis (RAS), relied on variable imaging modalities for RAS diagnosis, and lacked procedural consistency, reducing broad applicability in real-world clinical practice.
2. Despite being a relatively common condition, the role of RAS revascularisation remains highly debated. Highrisk subgroups remain underrepresented in the current evidence base, with limited low-level recommendations for offering treatment from the American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) and the European Society of Cardiology (ESC) guidelines (Level B–C).
3. A robustly powered, multicentre RCT targeting severe RAS (>70% stenosis, ideally confirmed by pressure gradients and with core lab adjudication) and including patients who are high-risk with flash pulmonary oedema and rapid decline in renal function, is important to definitively assess the clinical benefit of angioplasty and stenting in RAS.
INTRODUCTION
Renal artery stenosis (RAS), which is most often atherosclerotic in aetiology (90% of cases), remains a contentious indication for endovascular therapy. Its prevalence varies from approximately 1% in mild hypertension to 14–24% in resistant hypertension,1 and it accounts for 2–5% of cases of secondary hypertension.2 In advanced chronic kidney disease (CKD) populations, rates may reach 5–22%.1 Beyond hypertension, atherosclerotic RAS contributes to flash pulmonary oedema and acute coronary syndromes.2 Fibromuscular dysplasia and rarer vasculopathies make up the remaining 10% of RAS encountered in clinical practice.1 This review outlines current evidence for renal angioplasty and stenting in atherosclerotic RAS, critically appraises landmark trials, and highlights knowledge gaps to guide future research.
KEY TRIALS IN RENAL ARTERY STENOSIS ANGIOPLASTY AND STENTING
The ASTRAL trial was a multicentre, randomised, and unblinded trial comparing angioplasty ± stenting versus medical therapy in atherosclerotic RAS (N=806).3 No difference was seen in renal function, blood pressure (BP), or survival at a median follow-up of 33.6 months. However, nearly 41% of participants had <70% stenosis, and those most likely to benefit, such as patients with flash pulmonary
oedema, refractory hypertension, or rapidly declining renal function, were largely excluded.3-6 Patient inclusion required ‘clinical uncertainty’ about benefit, undermining ‘investigator equipoise’.5,6 There was no central core laboratory to validate RAS diagnosis or severity,4,5 and imaging modalities, including digital subtraction angiography, CT, magnetic resonance angiography, and duplex renal ultrasonography, varied and lacked standardisation amongst recruitment sites. Operator technique and variability in angioplasty and stenting further compounded the lack of standardisation.7 In August 2024, long-term follow-up data (median: 56.4 months) again showed no overall advantage of revascularisation, though lower risk enrolment likely underpowered the detection of subgroup benefits, with the authors suggesting further trials in high-risk populations.6
Following this, the CORAL trial randomised 947 patients with atherosclerotic RAS and hypertension or CKD to stenting plus medical therapy versus medical therapy alone, finding no difference in major cardiovascular or renal outcomes over a median of 43 months.8 Critics note that by excluding fibromuscular dysplasia, nonischaemic CKD, and lesions unsuitable for a single stent, and by altering systolic BP targets mid-trial,9 it underrepresented the highest-risk patients. Although a modest 2 mmHg greater BP reduction was seen in the stenting arm,8 aggressive background therapy and inconsistent pressure-
gradient measurements (only 53% of the stent arm versus 34% of the medical arm) likely blunted any real-world benefit.10 Imaging modalities varied despite core laboratory oversight,7,11 and a 2023 subgroup analysis suggested improved event-free survival in those with renal function gains post-stenting.12 Together with ASTRAL’s limitations, these findings underscore the need for new RCTs targeting high-risk RAS cohorts. Table 1 summarises the key highlights of the ASTRAL and CORAL trials.
Two earlier RCTs, DRASTIC13 and STAR,14 also failed to demonstrate a clear benefit in revascularisation. In DRASTIC, primarily balloon angioplasty (without routine stenting) reduced antihypertensive use (mean of two versus three drugs), but saw high crossover (approximately 44%) from medical to angioplasty arms due to refractory hypertension. A post-hoc review found 10 patients with mild <50% stenosis, calling into question the diagnosis of renovascular hypertension15 in many participants, and thus, the conclusion
Sample size
Inclusion criteria
806 patients
RAS with clinical uncertainty about the benefit of revascularisation
Key exclusions Patients where stenting was clearly indicated
Stenosis severity
Baseline renal function
Intervention
Primary endpoint
Follow-up duration
≥50% (uncertain in many cases, no haemodynamic criteria)
Table 1: Summary of the ASTRAL and CORAL trials.3,8
Feature
ASTRAL (2009)3
CORAL (2014)8
Design
Multicentre RCT (UK-based)
Multicentre, international RCT
that angioplasty has little advantage over antihypertensive-drug therapy.13 Similarly, the STAR trial enrolled mostly moderate stenoses and excluded high-risk patients, finding no significant preservation of renal function with stenting plus medical therapy versus medical therapy alone.14,16
The HERCULES study was a single‐arm, prospective, multicentre trial of the Herculink Elite® (Abbott, Santa Clara, Illinois, USA) stent for the treatment of RAS. HERCULES enrolled 202 patients with ≥70% RAS and uncontrolled hypertension. At 9 months, the mean systolic blood pressure (SBP) decreased from 162±18 mmHg to 145±21 mmHg (p<0.0001) in 77.5% of patients, with restenosis rates of 10.5%.17 At 36 months, SBP reductions persisted (146±21 mmHg; p<0.001), with low restenosis (<10%) and periprocedural complication rates (<4%). The majority (74.3%) maintained SBP improvement, particularly those with baseline SBP ≥180 mmHg (mean: −46 mmHg).18
Although limited by its non-randomised design and predominantly White cohort, HERCULES suggests durable BP benefit
RCT, angioplasty (PTRA) versus medical therapy in hypertensive patients with RAS (N=106)
RCT, stenting + medical versus medical alone in RAS with renal dysfunction (N=140)
in severe RAS and supports the need for a rigorously controlled RCT in high‐risk patients.17
CURRENT DATA SINCE THESE TRIALS
Since CORAL,8 no new RCTs have definitively assessed revascularisation in atherosclerotic RAS. The RADAR trial19 was halted in 2017 after enrolling only 86 of the 300 planned patients with ≥70% de novo RAS. It showed no benefit of stenting plus medical therapy over medical therapy alone, but is likely to have been underpowered given the low number of participants recruited. Slow patient enrolment was likely reflective of its stringent inclusion criteria.19 Thus, the contemporary evidence base remains confined to seven trials from 1998–2014 (Table 2): EMMA,20 Scottish and Newcastle Renal Artery Stenosis Group study,21
DRASTIC,13 STAR,14 ASTRAL,3 CORAL,8 and HERCULES.17 No further major trials have been identified at the time of this review. BP: blood pressure; CKD: chronic kidney disease; CV: cardiovascular; Herculink Elite®: Abbott, Santa Clara, Illinois, USA; PTRA: percutaneous transluminal renal angioplasty; RAS: renal artery stenosis; SBP: systolic blood pressure.
No significant improvement in BP or renal function Small, underpowered; no stents; 44% crossover
No significant benefit in the preservation of renal function
Mild stenosis included; underpowered; didn't include high-risk patients 2009 ASTRAL3
RCT, stenting versus medical therapy in patients with uncertain benefit (N=806)
RCT, stenting + optimal medical therapy versus medical therapy alone in RAS with hypertension or CKD (N=947)
Single-arm, prospective study using Herculink Elite® stent in RAS with uncontrolled hypertension (N=202)
No benefit in BP, renal function, or mortality
No difference in major CV/renal outcomes, small BP benefit
Major impact on clinical practice; criticised for selection bias and inclusion of low-risk patients
High-quality design; confirmed conservative approach; underpowered for subgroups and high-risk patients
Not randomised, but included patients with severe RAS; supports the role of stenting in select patients who are hypertensive
Table 2: Timeline of key renal artery stenosis trials and studies.
Meta-analyses of ASTRAL and CORAL data suggest stenting may modestly lower BP or reduce antihypertensive requirements, especially in severe or refractory hypertension, within 2 years, but without a clear impact on mortality, renal decline, or serious adverse events.22,23 Numerous case reports24-29 and small cohort studies30 document successful outcomes in highrisk lesions excluded from these major RCTs. Early innovations, such as intraprocedural elamipretide infusion, have shown promise in improving the estimated glomerular filtration rate and lowering BP in a small Phase IIa trial,31 underpinning the potential for evolving techniques to reshape future study outcomes.
CURRENT INDICATIONS
The 2013 American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) Peripheral Artery Disease guidelines32 grade all RAS revascularisation recommendations as Level B or C evidence. The guideline suggests percutaneous angioplasty ± stenting may be considered in asymptomatic bilateral or solitary-kidney RAS with haemodynamic significance (Level C), but is unproven in asymptomatic unilateral disease. Revascularisation is supported (Level B) for progressive kidney disease, bilateral RAS, or RAS in a solitary functioning kidney.32 It is also a reasonable treatment (Level B) for recurrent pulmonary oedema, unstable angina with significant RAS, and recurrent, unexplained congestive heart failure. The 2017 ESC/ESVS Peripheral Artery Disease guidelines advise against routine revascularisation in atherosclerotic RAS (Level A) but support angioplasty ± stenting for recurrent cardiac failure or flash pulmonary oedema (Level C).33
Both ACC/AHA and ESC stress individualised clinical judgement on a case-by-case basis.
References
Case reports highlight successful interventions in high-risk scenarios such as recurrent pulmonary oedema,34 including Pickering syndrome35 and progressive renal decline.36 Such cases highlight that it would be remiss not to reiterate the criticisms of ASTRAL and CORAL and their lack of inclusion of such patients. Importantly, it should be noted that guidelines often lag behind available evidence, and indeed, both guidelines are derived from data pre-2017.
GAPS IN KNOWLEDGE
Despite extensive study, the authors lack RCT data in the highest-risk RAS subgroups: >70% stenosis or haemodynamically confirmed stenosis with pressure measurements, bilateral disease, rapidly declining renal function, and flash pulmonary oedema. HERCULES suggests promising long-term BP control and safety data in patients with severe RAS, but its findings require confirmation in a rigorously controlled trial targeting these highrisk cohorts.
CONCLUSION
More than 10 years after ASTRAL and CORAL, the role of renal angioplasty and stenting for atherosclerotic RAS remains uncertain. Existing RCTs suffer from selection bias and variable lesion grading, and they exclude patients most likely to benefit from revascularisation. However, limited evidence does exist and suggests benefit in appropriate patients (HERCULES, subgroup analysis of CORAL). There is a need for a contemporary, high-quality RCT, free of the issues above, to reach a definitive conclusion regarding renal artery revascularisation for the treatment of atherosclerotic RAS in properly defined patient populations.
1. Sarafidis PA et al. Atherosclerotic renovascular disease: a clinical practice document by the European Renal Best Practice (ERBP) board of the European Renal Association (ERA) and the Working Group Hypertension and the Kidney of the European Society of Hypertension (ESH). Nephrol Dial Transplant. 2023;38(12):2835-50.
2. Prince M et al. When and how should we revascularize patients with atherosclerotic renal artery stenosis? JACC Cardiovasc Interv. 2019;12(6):505-17.
3. Wheatley K et al.; ASTRAL Investigators. Revascularization versus medical therapy for renalartery stenosis. N Engl J Med. 2009;361(20):1953-62.
4. Sarac TP. Influence and critique of the ASTRAL and CORAL trials. Semin Vasc Surg. 2011;24(3):162-6.
5. Ritchie J et al. Contemporary management of atherosclerotic renovascular disease: before and after ASTRAL. Nephrology. 2011;16(5):457-67.
6. O’Keeffe H et al.; ASTRAL Investigators. Long term outcomes after renal revascularization for atherosclerotic renovascular disease in the ASTRAL trial. Circ Cardiovasc Interv. 2024;17(9):e013979.
7. Zhang HL et al. Renal artery stenosis: imaging options, pitfalls, and concerns. Prog Cardiovasc Dis. 2009;52(3):209-19.
8. Cooper CJ et al.; CORAL Investigators. Stenting and medical therapy for atherosclerotic renal-artery stenosis. N Engl J Med. 2014;370(1):13-22.
9. Mann SJ, Sos TA. The cardiovascular outcomes in renal atherosclerotic lesions study and the future of renal artery stenting. J Clin Hypertens (Greenwich). 2014;16(3):162-5.
10. Gafoor S et al. The CORAL trial, round 2. J Am Coll Cardiol. 2015;66(22):2495-7.
11. Rountas C et al. Imaging modalities for renal artery stenosis in suspected renovascular hypertension: prospective intraindividual comparison of color doppler US, CT angiography, GD-enhanced MR angiography, and digital substraction angiography. Ren Fail. 2007;29(3):295-302.
12. Modrall JG et al. Retrieval of renal function after renal artery stenting improves event-free survival in a subgroup analysis of the Cardiovascular Outcomes in Renal Atherosclerotic Lesions trial. J Vasc Surg. 2023;77(6):1685-92.e2.
13. van Jaarsveld BC et al. The effect of balloon angioplasty on hypertension in atherosclerotic renal-artery stenosis. N Engl J Med. 2000;342(14):1007-14.
14. Bax L et al. Stent placement in patients with atherosclerotic renal artery stenosis and impaired renal function: a randomized trial. Ann Intern Med. 2009;150(12):840-8.
15. Weinberg I, Jaff MR. Controversies surrounding renal artery intervention: making sense of the confusion. Interventional Cardiology. 2011;3(5):569.
16. Mann SJ, Sos TA. Misleading results of randomized trials: the example of renal artery stenting. J Clin Hypertens (Greenwich). 2010;12(1):1-2.
17. Jaff MR et al.; HERCULES
Investigators. Significant reduction in systolic blood pressure following renal artery stenting in patients with uncontrolled hypertension: results from the HERCULES trial. Catheter and Cardiovasc Interv. 2012;80(3):343-50.
18. Chrysant GS et al. Proper patient selection yields significant and sustained reduction in systolic blood pressure following renal artery stenting in patients with uncontrolled hypertension: long-term results from the HERCULES trial. J Clin Hypertens. 2014;16(7):497-503.
19. Zeller T et al. A randomized, multi-center, prospective study comparing best medical treatment versus best medical treatment plus renal artery stenting in patients with hemodynamically relevant atherosclerotic renal artery stenosis (RADAR) – one-year results of a prematurely terminated study. Trials. 2017;18(1):380.
20. Pappaccogli M et al. Endovascular versus medical management of atherosclerotic renovascular disease: update and emerging concepts. Hypertension. 2023;80(6):1150-61.
21. Webster J et al. Randomised comparison of percutaneous angioplasty vs continued medical therapy for hypertensive patients with atheromatous renal artery stenosis. J Hum Hypertens. 1998;12(5):329-35.
22. Chen Y et al. Use of percutaneous transluminal renal angioplasty in atherosclerotic renal artery stenosis: a systematic review and meta-analysis. J Int Med Res. 2021;49(1):0300060520983585.
23. Fujiwara T et al. Combination of medical therapy and percutaneous transluminal renal angioplasty versus medical therapy alone for patients with atherosclerotic renal artery stenosis: systematic review and meta-analysis. Hypertens Res. 2025;48(6):1870-9.
24. Vischer A et al. Renal artery intervention in the post-CORAL era - obsolete or sometimes reasonable? Dtsch Med Wochenschr. 2015;140(18):1372-5.
25. Sarafidis PA et al. To intervene or not? A man with multidrug-resistant hypertension, endovascular abdominal aneurysm repair, bilateral renal artery stenosis and end-stage renal disease salvaged with renal artery stenting. Blood Press. 2016;25(2):123-8.
26. Kuznetsov E et al. Recovery of acute renal failure following bilateral renal artery angioplasty and stenting. Clin Nephrol. 2007;68(1):32-7.
27. Chrysochou C et al. Anuric acute renal failure and pulmonary oedema: a case for urgent action. Int J Cardiol. 2009;132(1):e31-3.
28. Kane GC et al. Renal artery revascularization improves heart failure control in patients with atherosclerotic renal artery stenosis. Nephrol Dial Transplant. 2010;25(3):813-20.
29. Kanamori H et al. Improvement of renal function after opening occluded atherosclerotic renal arteries. J Invasive Cardiol. 2009;21(9):E171-4.
30. Catena C et al. Long-term renal and cardiac outcomes after stenting in patients with resistant hypertension and atherosclerotic renal artery stenosis. Kidney Blood Press Res. 2017;42(5):774-83.
31. Saad A et al. Phase 2a clinical trial of mitochondrial protection (elamipretide) during stent revascularization in patients with atherosclerotic renal artery stenosis. Circ Cardiovasc Interv. 2017;10(9):e005487.
32. Anderson JL et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/ AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(13):1425-43.
33. Aboyans V et al.; ESC Scientific Document Group. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries endorsed by: the European Stroke Organization (ESO) the task force for the diagnosis and treatment of peripheral arterial diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018;39(9):763-816.
34. Dionne AR et al. Revascularization in a time after CORAL. JACC Case Rep. 2024;29(17):102501.
35. Pelta A et al. Flash pulmonary edema in patients with renal artery stenosis -the Pickering syndrome. Blood Press. 2011;20(1):15-9.
36. Triantis G et al. Renal artery revascularization is a controversial treatment strategy for renal artery stenosis: a case series and a brief review of the current literature. Hellenic J Cardiol. 2022;65:42-8.