Receptor Agonists in Osteoarthritis: From Clinical
Promise to Preclinical Evidence
ANCA Vasculitis Presenting with Bilateral Toe Cyanosis Article
Review of the American College of Rheumatology (ACR) Convergence 2025, October 24th–29th, 2025
Glucagon-Like Peptide-1 Receptor Agonists in Osteoarthritis: From Clinical Promise to Preclinical Evidence
Alena Sofieva
Driving CAR-T Into the Future: What Are the Right B Cell Targets in Systemic Lupus Erythematosus and Beyond?
Helena Bradbury
Elena Myasoedova Mayo Clinic, Rochester, Minnesota, USA
The Cost of Complexity: Financial Toxicity in Rheumatic Disease, Cancer, and Their Intersection
Sondhi M et al.
Oral Glucocorticoid Treatment for Checkpoint Inhibitor Associated Inflammatory Arthritis Does Not Affect Progression Free Survival: A RADIOS
Methotrexate Alone or in Combination and Higher Age Impair Humoral Response Against the Recombinant Herpes Zoster Vaccine in Rheumatoid Arthritis: A Prospective, Randomized, Placebo-Controlled Trial de Medeiros-Ribeiro AC et al.
Multimodal Analysis Revealed Altered Brain Connectivity Patterns and Neuroinflammatory Processes in the Background of Difficult-To-Treat Rheumatoid Arthritis
Gunkl-Tóth L et al.
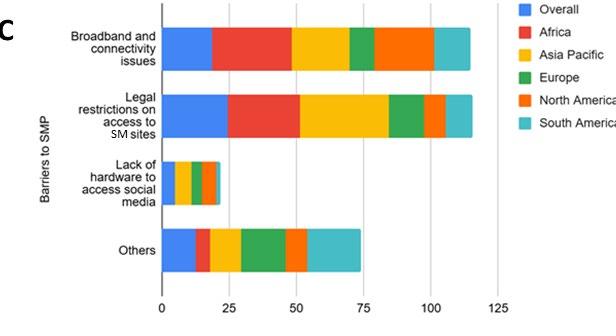
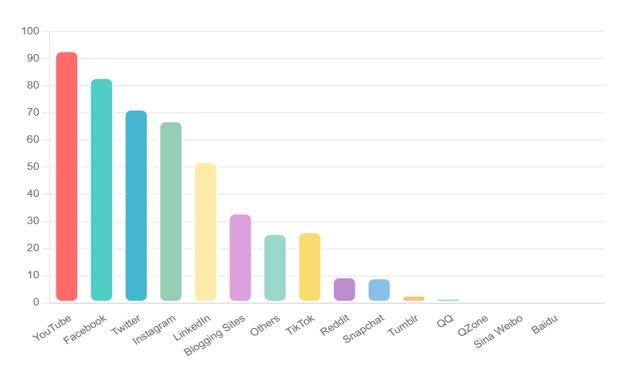
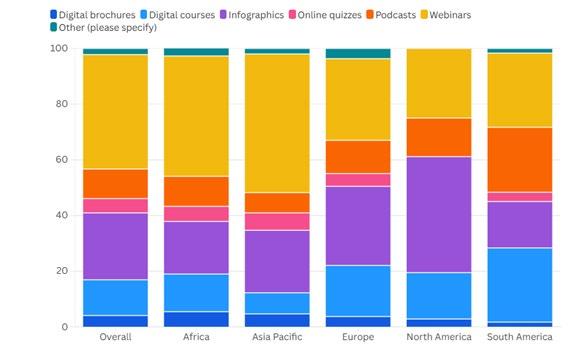
The Evolving Digital Landscape of Social Media Among Rheumatology Professionals: Results of the EULAR SoMeR Study Group Survey Gupta L et al.
58 Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis Manifesting Solely as Bilateral Toe Cyanosis: Case Report Motamedi M et al.
"The rapid expansion of artificial and augmented intelligence in healthcare was highlighted as both an opportunity and a responsibility to bear"
Editorial Board
Dr. Elena Myasoedova
Mayo Clinic Rochester, Minnesota, USA
Dr. Christine Peoples
University of Pittsburgh Medical Center, Pennsylvania, USA
Dr. Arthur Kavanaugh
University of California San Diego, California, USA
Dr. Isabelle Amigues
UnabridgedMD, Colorado, USA
Prof. Yoshiya Tanaka
University of Occupational and Environmental Health, Japan
Dr. Judith A. Smith
University of Wisconsin School of Medicine and Public Health, Wisconsin, USA
Aims and Scope
AMJ Rheumatology is an open access, peer-reviewed ejournal committed to helping elevate the quality of practices in rheumatology globally by informing healthcare professionals on the latest research in the field.
The journal is published annually, six weeks after the American College of Rheumatology (ACR) Convergence, and features highlights from this event, alongside interviews with experts in the field, reviews of abstracts presented at ACR, as well as in-depth features on sessions from this event. The journal also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the inhouse editorial team.
AMJ Rheumatology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. The journal is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
AMJ Rheumatology endeavours to increase knowledge, stimulate discussion, and contribute to a better understanding of practices in the field. Our focus is on research that is relevant to all healthcare professionals in this area. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of coming trends affecting clinical practice in rheumatology.
Further details on coverage can be found here: www.emjreviews.com/en-us/amj/.
Editorial Expertise
AMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial@americanmedicaljournal.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in AMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
AMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Indexing and Availability
AMJ and EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®
AMJ and EMJ are available through the websites of our leading partners and collaborating societies. AMJ and EMJ publications are all available via our website: www.emjreviews.com/en-us/amj/.
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
This Publication
Launch Date: 2024
Frequency: Annually Online ISSN: 2977-5868
All information obtained by AMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, AMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. AMJ is completely independent of the review event (ACR 2025) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Chicago, Illinois, the location of ACR 2025.
We provoke conversation around healthcare trends and innovation - we also create engaging educational content for healthcare professionals. Join us for regular conversations with physician & entrepreneur, Jonathan Sackier. Listen Now
Editorial Director
Andrea Charles
Vice President of Content
Anaya Malik
Managing Editor Darcy Richards
Copy Editors
Noémie Fouarge, Sarah Jahncke
Editorial Co-ordinators
Bertie Pearcey, Alena Sofieva
Editorial Leads
Helena Bradbury, Ada Enesco
Editorial Assistants
Niamh Holmes, Katrina Thornber, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey White
Designers
Shanjok Gurung, Tamara Kondolomo, Fabio van Paris, Owen Silcox, Helena Spicer
Creative Artworker
Dillon Benn Grove
Head of Marketing
Stephanie Corbett
Senior Vice President of Customer Success
Alexander Skedd
Senior Vice President of Business Development
Robert Hancox
Chief Executive Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chairman
Spencer Gore
Welcome
Dear Readers,
Welcome to this issue of AMJ Rheumatology. I am pleased to bring you a collection of content that reflects the momentum of the American College of Rheumatology (ACR) Convergence 2025 and the clinical landscape of rheumatology in 2025. From glucagonlike peptide-1 agonists to CAR-T cells, this issue captures a field reshaping rheumatologic care across metabolic, immune, and socio-economic dimensions.
Our Review of the ACR Convergence 2025 covers inflammatory arthritis, connective tissue disease, vasculitis, and emerging targeted therapies. In-depth features on the use of GLP-1 agonists in rheumatic disease and osteoarthritis, and on B cell-directed CAR-T cell therapy in systemic lupus erythematosus and related conditions, offer focused reviews on the topics that drew audiences and sparked debate at the meeting.
A series of abstracts presented at the ACR Convergence 2025 enrich the publication, covering topics such as checkpoint inhibitorassociated inflammatory arthritis, vaccine responses in rheumatoid arthritis, and social media use among rheumatology healthcare professionals. Our anti-neutrophil cytoplasmic antibody-associated vasculitis case report offers clinical learning for day-to-day practice, and our interview with key opinion leaders provides leadership perspectives on workforce, advocacy, and improving outcomes for people living with rheumatic disease.
I would like to thank the Editorial Board, contributors, reviewers, and production team for their ongoing support and contributions.
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Anaya Malik Vice President of Content
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
Foreword
Dear Colleagues,
The latest issue of AMJ Rheumatology reflects the rapidly growing landscape of rheumatic diseases. Metabolic therapies, advancing cellular approaches, and evolving models and care are reshaping what is possible for patients. We present key coverage of the American College of Rheumatology (ACR) Convergence 2025, original analyses, and peer perspectives on day-to-day clinical decision-making and long-term care.
This in-depth review of the ACR Convergence 2025 distills highlights from across the meeting, and aims to help busy rheumatologists rapidly align with the most clinically relevant developments and translate this into their own practice.
The congress features dive into therapeutic frontiers that caused great discussion and debate at the meeting: the expanding role of glucagon-like peptide-1 receptor agonists in rheumatic disease and osteoarthritis, and for whom these agents may be appropriate; and how CAR-T cell therapy could be driven into autoimmune disease. The abstract reviews shine a spotlight on the less visible dimensions of rheumatologic care, spanning the clinical, biological, social, and financial
This in-depth review of the ACR Convergence 2025 distills highlights from across the meeting to help busy rheumatologists rapidly align with the most clinically relevant developments
aspects of modern rheumatology practice. Interviews with ACR leadership showcase workforce sustainability, multidisciplinary collaboration, education efforts, and the strategic direction of the ACR.
I am grateful to the contributors, reviewers, and fellow board members for their ongoing commitment to elevating the quality of healthcare. I hope this publication will support you in patient-centered care and prompt discussion on where we will be this time next year.
Best wishes,
Elena Myasoedova Mayo Clinic, Rochester, Minnesota, USA
ACR 2025
Insights From The American College of Rheumatology Convergence 2025
The rapid expansion of artificial and augmented intelligence in healthcare was highlighted as both an opportunity and a responsibility to bear
Review of the American College of Rheumatology (ACR) Convergence 2025 Congress Review
THE AMERICAN College of Rheumatology (ACR) Convergence returned to Chicago, Illinois, USA, this year, and with it brought thousands of rheumatology healthcare professionals together at McCormick Place and online. Over 6 days, attendees engaged with over 3,000 abstracts spanning basic, translational, and clinical research, and a program brimming with plenary sessions, late-breaking data, skills courses, and interactive formats at the annual meeting “where rheumatology meets.”
In the Opening Ceremony, ACR President, William Harvey, reflected on a year eclipsed by uncertainty and change, and returned to three mission pillars that shaped both his presidency and this year’s meeting: education, research, and community. Education remains the forefront of the ACR's work. The 2025 Convergence built on this foundation with an expanded online program, traditional plenaries, an impressive Poster Hall, Meet the Professor sessions, and the Practice Innovation Summit, designed to give healthcare providers direction and strategies to move forward in the current healthcare landscape.
Since its establishment in 1985, the Foundation has invested approximately 243 million USD to support nearly 5,000 awards
Several themes running through the Opening Ceremony framed the scientific and clinical discussions that shaped the meeting. The rapid expansion of artificial and augmented intelligence in healthcare was highlighted as both an opportunity and a responsibility to bear. This set of tools can accelerate discovery, support new educational models, and streamline practice, but they must be guided to strengthen compassionate, patientcentered care for patients with rheumatic disease. The ACR President also spoke candidly and refreshingly about the spread of medical misinformation, emphasizing the community’s commitment to evidence-based practice and the role of clinicians in translating data into trusted information and maintaing transparency with patients and the public.
Research and advocacy were presented as parallel strands of the ACR’s mission. Harvey noted mounting pressures on academic
institutions, federal agencies, journals, and funding priorities that risk slowing the pace of discovery and narrowing the scope of discourse. Against this backdrop, the ACR’s Washington, D.C. office and its advocacy team have worked to ensure that the voice of rheumatology is heard in policy debates. In 2025 alone, the College issued more than 120 op-eds, letters, comments, and public statements, and during the Advocates for Arthritis event, members, interprofessional colleagues, and patients met with bipartisan lawmakers to champion sustained National Institutes of Health (NIH) funding, protect Medicare and Medicaid access, and press for pharmacy benefit manager reforms to improve affordability and access to rheumatic therapies.
The Rheumatology Research Foundation (RRF), celebrating its 40th anniversary this year, featured prominently in the
ceremony. Since its establishment in 1985, the Foundation has invested approximately 243 million USD to support nearly 5,000 awards across training, career development, and project funding. Nearly 1,000 students and residents have attended the ACR Convergence through Foundation scholarships, and the organization continues to prioritize pipeline development, with awards for investigators and implementation research that bring evidence-based care into everyday practice.
Community, workforce, and wellbeing were celebrated in the Opening Ceremony. The Association of Rheumatology Professionals (ARP) marked its 60th anniversary, and celebrated a diverse community of more than 1,600 members representing over 20 disciplines. ARP members lead innovations in telehealth, raise awareness of health disparities, and build inclusive environments
for learners and colleagues at all career stages, underscoring the holistic role of allied health professionals in delivering indispensable care.
As is tradition, the Opening Ceremony honored excellence across the rheumatology community with a series of awards. ARP awards recognized outstanding clinicians, scholars, students, and lifelong contributors, with the ARP Lifetime Achievement Award. The ACR Distinguished Fellow Awards celebrated the next generation of clinical and research leaders, and the ACR Master awards acknowledged senior members whose careers have demonstrated outstanding service to the profession. The ACR Presidential Gold Medal, the College’s highest honor, was awarded to Eric L. Matteson, Mayo Clinic, Rochester, Minnesota, USA, who has spent decades of leadership within the ACR and the RRF. His career has combined scholarship, clinical care, and reshaped understanding and management of vasculitis and rheumatoid arthritis.
The invited keynote talk focused on the people who make this possible. Tate Shanafelt, Chief Wellness Officer at Stanford University, California, USA, and a pioneer in the field of clinician wellbeing, used data from large national cohorts to explore occupational distress, burnout, and their impacts on quality of care, turnover, and workforce sustainability. Shanafelt emphasized that personal resilience and meaning in work cannot by themselves offset excessive administrative burden, electronic health record demands, and lack of true time away from clinical duties on a system-level. He recommended to “chart a course” for clinician wellbeing through organizational change, leadership accountability, and support for professional fulfilmen. This is aligned with the ACR’s broader commitment to sustain a thriving rheumatology workforce.
As the ACR Convergence 2025 continued to unfold in the theaters of McCormick Place and online, these key themes of education, research, advocacy, community, and
wellbeing were staples in conversation and debates. The following congress highlights showcase a selection of key abstracts and important data. These are practice-changing insights that demonstrate how this meeting brings the global rheumatology community together to improve the lives of people with rheumatic and musculoskeletal diseases.
Today, ARP members lead innovations in telehealth, raise awareness of health disparities, and build inclusive environments for learners and colleagues at all career stages
Earlier Kidney Biopsy May Improve Lupus Nephritis Detection
FINDINGS presented at the ACR Convergence 2025 suggest that current guidelines for kidney biopsy in systemic lupus erythematosus (SLE) may miss early, clinically significant cases of lupus nephritis (LN).1
Researchers from the Accelerating Medicines Partnership (AMP), led by Michelle Petri of Johns Hopkins University, Baltimore, Maryland, USA, found that patients with modest elevations in urine protein-tocreatinine ratio (UPCR) but other risk indicators often already have histologic evidence of LN on biopsy.
Guidelines from the ACR, European Alliance of Associations for Rheumatology (EULAR), and Kidney Disease: Improving Global Outcomes (KDIGO) currently recommend kidney biopsy in patients with SLE when UPCR is ≥0.50 g/g. However, emerging data have shown that patients with lower proteinuria may still harbor proliferative or membranous LN, conditions that can lead to irreversible renal damage if not treated early. The AMP study evaluated whether earlier biopsy could identify subclinical disease in patients at risk.
The study enrolled 28 patients with SLE without known LN whose UPCR ranged from 0.250–0.499 g/g and who had at least one additional LN predictor, such as non-White race, low complement (C3 or
C4), positive anti-double-stranded DNA antibodies, or active urine sediment. All participants had normal renal function, were on minimal corticosteroids, and had no prior immunosuppressive therapy.
Biopsy results revealed that 20 of 28 participants (69%) already had LN, including proliferative forms: six Class III and seven Class V. Two Class II, two Class III, and three Class V cases later progressed to higher UPCR levels despite treatment, indicating early but active disease at the time of biopsy. Patients with low C3 or C4 before enrolment were significantly more likely to have LN (p=0.0223 and p=0.0296, respectively). No biopsy complications were reported.
These findings challenge the current 0.50 g/g UPCR biopsy threshold, suggesting it may delay diagnosis and treatment of early LN. The AMP team’s algorithm (biopsy for UPCR 0.250–0.499 g/g plus another LN predictor) identified a high proportion of patients with meaningful renal pathology, supporting revision of current LN biopsy guidelines to promote earlier detection and intervention.
The study enrolled 28 patients with SLE without known LN whose UPCR ranged from 0.250–0.499 g/g and who had at least one additional LN predictor
These findings challenge the current 0.50 g/g UPCR biopsy threshold, suggesting it may delay diagnosis and treatment of early LN
Upadacitinib Maintains Long-Term Remission
in Giant Cell Arteritis
TWO-YEAR results from the Phase III SELECT-GCA trial, presented at the ACR Convergence 2025, show that continued treatment with upadacitinib 15 mg (UPA15) sustained remission and significantly reduced the risk of disease flare and glucocorticoid exposure in patients with giant cell arteritis (GCA). These data reinforce the long-term efficacy and safety of the JAK inhibitor as a potential treatment option for this chronic inflammatory vasculitis.2
Of the 428 patients treated in the first year, 181 entered the extension phase, and 91% completed the full 104 weeks
SELECT-GCA enrolled patients aged ≥50 years (mean age: 71 years) with active GCA, and included a 52-week randomized, placebo-controlled first phase followed by a 52-week blinded extension phase. In the initial phase, participants received UPA15, UPA7.5, or placebo alongside a glucocorticoid taper. Those who achieved at least 24 consecutive weeks of remission entered the extension phase, where participants previously on upadacitinib were rerandomized either to continue their assigned dose or switch to placebo, while the original placebo group continued the same regimen.
Of the 428 patients treated in the first year, 181 entered the extension phase, and 91% completed the full 104 weeks. Among patients originally treated with UPA15, 68.6% who continued the same dose maintained remission through 2 years, compared with only 28.6% who switched to placebo. Continuous UPA15 treatment reduced the risk of disease flare by approximately 90% from Weeks 52–104 compared with
discontinuation. Patients remaining on UPA15 also showed greater improvements across secondary endpoints, including glucocorticoid sparing, with a cumulative one-gram reduction in glucocorticoid use during the second year.
Safety findings were consistent with earlier reports. Serious treatment-emergent adverse events were less frequent in both upadacitinib groups than in the placebo group. Serious infections occurred less often with UPA15, although higher rates of herpes zoster and mild elevations in creatine kinase were observed. One venous thromboembolism occurred in a patient with pre-existing risk factors. No major cardiovascular events or deaths were reported.
In this older patient population, upadacitinib 15 mg maintained durable remission over 2 years without new safety concerns. These results further support its role as a long-term, steroid-sparing therapy for managing GCA.
GLP-1 Receptor Agonists Linked to Lower Cardiovascular Risk and Mortality in Psoriatic Arthritis
A NEW retrospective study, presented at the ACR Convergence 2025, suggests that glucagon-like-peptide-1 receptor agonists (GLP-1 RA), a class of drugs widely used for Type 2 diabetes management, may provide cardiovascular and survival benefits for patients with psoriatic arthritis (PsA). The study analyzed data from 83 large healthcare organizations worldwide, using the TriNetX database (TriNetX, LLC, Cambridge, Massachusetts, USA) to examine patient records from January 2015–December 2024.3
Researchers identified 4,104 patients with PsA taking GLP-1 RAs, including semaglutide, liraglutide, exenatide, and lixisenatide, and 86,432 patients with PsA not on these medications. Patients in the GLP-1 RA group were slightly older at diagnosis, with a mean age of 55.4±11.5 years compared to 52.6±15.1 years for the non-GLP-1 RA group. Female patients were more prevalent in the GLP-1 RA group, while males predominated in the nonuser group. White patients comprised the majority in both groups, with 80.9% of GLP-1 RA users and 73.5% of non-users.
Using 1:1 propensity score matching to balance demographics, comorbidities, and medication use, the study found that PsA patients on GLP-1 RAs had a significantly lower risk of major adverse cardiovascular events and reduced overall mortality compared with those not taking the drugs. The analysis accounted for pre-existing cardiovascular events to ensure only new events after GLP-1 RA initiation were included.
GLP-1 RAs are known for their cardiovascular, renal, and weight-loss benefits in Type 2 diabetes. Previous research has shown that weight reduction, whether through lifestyle modification or surgery, can improve disease activity in inflammatory conditions such as PsA, rheumatoid arthritis, and psoriasis.
The study suggests that GLP-1 RAs may offer dual benefits for patients with PsA by addressing both metabolic and inflammatory risk factors. The authors note that further research is needed to understand the mechanisms behind these effects and to confirm long-term outcomes. If validated, GLP-1 RAs could become a valuable adjunct therapy for PsA patients, particularly those with obesity, Type 2 diabetes, or heightened cardiovascular risk.
These findings highlight the growing interest in therapies that target both metabolic and inflammatory pathways in chronic autoimmune diseases.
LEVI-04 Reduces Bone Marrow Lesions and Symptoms in Knee Osteoarthritis
A NOVEL therapy for knee osteoarthritis (OA), presented at the ACR Convergence 2025, LEVI-04, has demonstrated significant improvements in both structural and symptomatic measures of the disease in a Phase II clinical trial. Bone marrow lesions (BML), areas of increased bone turnover, oedema, and fibrosis detectable on MRI, are a hallmark of OA and affect approximately 80% of symptomatic patients with knee OA. These lesions are associated with radiographic severity and fluctuating knee pain.4
LEVI-04 is a first-in-class p75NTRFc fusion protein that has previously shown clinically meaningful improvements in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain
LEVI-04 is a first-in-class p75NTR-Fc fusion protein that has previously shown clinically meaningful improvements in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain, function, stiffness, Patient Global Assessment (PGA), and pain on movement (Staircase-Evoked Pain Procedure [StEPP]), while maintaining a favorable safety profile. The latest analysis focused on LEVI-04’s impact on BMLs and the relationship to OA symptoms.
The study enrolled 518 participants with symptomatic knee OA (WOMAC pain ≥4/10, Kellgren-Lawrence [KL] grade ≥2) in a multicenter, randomized, doubleblind, placebo-controlled trial. Participants received either placebo or LEVI-04 (0.3, 1, or 2 mg/kg) every 4 weeks through Week 16. BMLs were measured using coronal proton density-weighted fat-suppressed MRI sequences at baseline and Week 20, with the largest lesion area per participant quantified electronically.
At baseline, 74–79% of participants had BMLs across treatment groups. By Week 20, LEVI-04 produced a significant, dosedependent reduction in both the proportion of participants with BMLs and the mean BML area (0.3 mg/kg, p<0.01; 1 mg/kg and 2 mg/ kg, p<0.001) compared with placebo. Patients with higher baseline KL grades experienced the greatest reductions. Modest but statistically significant positive correlations were observed between changes in BML area and clinical improvements, including WOMAC pain (Rho=0.21), function (Rho=0.22), stiffness (Rho=0.19), PGA (Rho=0.20), and StEPP (Rho=0.25).
These findings indicate that LEVI-04 not only reduces BMLs but also aligns with improvements in patient-reported symptoms, supporting its potential as a therapy that addresses both structural changes and symptomatic relief in knee OA.
By Week 20, LEVI-04 produced a significant, dose-dependent reduction in both the proportion of participants with BMLs and the mean BML area (0.3 mg/kg, p<0.01; 1 mg/kg and 2 mg/kg, p<0.001) compared with placebo
Revised Criteria Boost Specificity for Axial Spondyloarthritis
RESULTS from the CLASSIC study, presented at the ACR Convergence 2025, have shown a major international effort to refine diagnostic criteria for axial spondyloarthritis (axSpA).5
The study addressed limitations of the 2009 Assessment of SpondyloArthritis International Society (ASAS) criteria, which had shown sensitivity (83%) and specificity (84%) for a rheumatologist’s diagnosis, adequate but insufficient given the high prevalence of chronic back pain. The CLASSIC study aimed for higher diagnostic precision, targeting ≥75% sensitivity and ≥90% specificity.
CLASSIC enrolled 1,015 patients from 61 centers across 27 countries, all presenting with undiagnosed back pain lasting at least 3 months and starting before the age of 45 years. Comprehensive diagnostic evaluations, including centralized imaging reviews, were conducted in five stages, with Stage 5 serving as the reference standard. Using advanced regression methods such as LASSO and multivariable logistic regression, investigators identified which clinical and imaging features best predicted a confirmed axSpA diagnosis.
The findings showed that MRI of the sacroiliac joints, particularly when both active and structural lesions were present, was the strongest independent predictor of axSpA, followed by radiographic sacroiliitis. Key clinical variables included HLA-B27 positivity, inflammatory back pain, inflammatory bowel disease, acute anterior uveitis, heel enthesitis, and elevated C-reactive protein.
After consensus review by ASAS and SPARTAN members, the final revised criteria achieved 79.5% sensitivity and 90.4% specificity, surpassing the predefined targets.
These updated ASAS-SPARTAN classification criteria represent a significant advance in identifying axSpA, emphasizing imaging findings and a streamlined set of clinical features to enhance diagnostic accuracy and consistency worldwide.
Study Defines Optimal Hydroxychloroquine Range for Lupus Safety
FINDINGS from a large international analysis, presented at the ACR Convergence 2025, have refined the therapeutic range for hydroxychloroquine (HCQ) in managing systemic lupus erythematosus (SLE).6
Current guidelines recommend an HCQ dose of ≤5.0 mg/kg, yet prior data have shown up to six-times higher rates of SLE flares, often requiring hospitalization, among patients on this lower dose. Additionally, clinicians have lacked clear guidance on adjusting HCQ dosing in individuals with chronic kidney disease. This study aimed to establish blood level thresholds that balance efficacy and safety.
These results confirm and extend earlier findings that have previously defined a therapeutic HCQ range of 750–1,150 ng/mL
Researchers analyzed pooled data from 1,842 patients with SLE across five cohorts and registries spanning North America, Europe, and Asia. HCQ blood levels at baseline were compared with subsequent HCQ-related toxicity, such as retinopathy, cardiomyopathy, and myopathy, and with disease activity measured by SLEDAI-2K scores. Using
mixed regression models, the investigators identified that HCQ levels above 1,150 ng/mL were associated with a 1.9-fold higher risk of toxicity, primarily due to retinal damage. In contrast, levels below 750 ng/mL were linked to 1.4-fold higher odds of active disease, indicating insufficient therapeutic exposure.
Among patients taking ≤5 mg/kg, nearly 52% had subtherapeutic levels (<750 ng/ mL), while 18% had supratherapeutic levels (>1,150 ng/mL). Those with chronic kidney disease Stage ≥3 were particularly vulnerable, showing 2.3-fold higher odds of toxic or supratherapeutic levels, even when on guideline-recommended doses.
These results confirm and extend earlier findings that have previously defined a therapeutic HCQ range of 750–1,150 ng/mL that optimizes disease control while minimizing toxicity risk. The study emphasizes that routine HCQ blood level monitoring, rather than fixed weight-based dosing, could enable personalized treatment strategies for SLE, especially in patients with kidney impairment.
MAIT Cells Drive Inflammation and Joint Damage in Rheumatoid Arthritis
NEW research presented at the ACR Convergence 2025 identifies mucosalassociated invariant T (MAIT) cells as key contributors to inflammation and joint damage in rheumatoid arthritis (RA). The findings, from investigators at Paris University, France, and collaborating French research centers, highlight MAIT cells as both inflammatory effectors and potential therapeutic targets in RA.7
MAIT cells are innate-like T lymphocytes that recognize microbial metabolites and bridge the immune system and the microbiota. Previous studies have shown altered MAIT cell frequencies and function in autoimmune diseases, but their precise role in RA pathogenesis remained unclear.
In this study, researchers analyzed MAIT cells in blood and synovial fluid samples from 75 patients with RA and 42 healthy donors using flow cytometry and single-cell RNA sequencing. Additional experiments examined how MAIT cells interact with fibroblast-like synoviocytes in vitro, and how they affect arthritis severity in mouse models.
Circulating MAIT cells were markedly reduced in patients with RA compared with healthy donors (0.51% versus 2.7%; p<0.001) but displayed an activated and exhausted phenotype, producing high levels of IL-17 and granzyme B. In contrast, MAIT cells were enriched in the synovial fluid, particularly in early RA, and exhibited signatures of activation, exhaustion, and interferon
pathway engagement. Computational analysis indicated that plasmacytoid dendritic cells and monocytes generate chemokine gradients that recruit MAIT cells into inflamed joints.
In co-culture experiments, activated MAIT cells stimulated fibroblast-like synoviocytes to increase the production of inflammatory cytokines (IL-1β, IL-6, IL-8, MCP-1) and matrix-degrading enzymes, amplifying joint inflammation. Importantly, in two arthritis mouse models, deletion of MR1, the molecule required for MAIT cell activation, or pharmacologic blockade with Ac-6-FP, significantly reduced arthritis severity and joint destruction.
These findings reveal that MAIT cells migrate from the blood to the joints, where they fuel local inflammation and tissue damage while also expressing IL-10, suggesting a complex role in immune regulation. Modulating MAIT cell activity or migration may offer a new therapeutic avenue for RA.
0.51 %
Circulating MAIT cells were markedly reduced in patients with RA compared with healthy donors p<0.001
versus
2.7%
Urinary Tenascin C Predicts Kidney Function Loss in Lupus Nephritis
A GROUNDBREAKING study presented at the ACR Convergence 2025 identifies urinary Tenascin C as an important early predictor of kidney function loss in lupus nephritis (LN), offering a potential advance beyond traditional response markers such as proteinuria. Long-term predictors of renal decline remain limited in LN, despite kidney survival being a central therapeutic goal.8
Researchers followed 170 patients from the Accelerating Medicines Partnership cohort for up to 7.8 years. During this period, 31% experienced significant estimated glomerular filtration rate loss. Among more than 1,200 urinary proteins analyzed, Tenascin C measured at Month 3 demonstrated the strongest association with future kidney decline, with elevated levels persisting through Month 12. Other inflammatory and fibrosis-related markers, including CD163, CD206, FABP4, IL-6, and IGFBP-6, were also consistently linked to higher risk.
Single-cell RNA sequencing and spatial transcriptomics localized Tenascin C production to interstitial myofibroblasts, supporting its role in progressive renal fibrosis. Using these insights, the investigators developed an 11-protein urinary classifier capable of predicting long-term estimated glomerular filtration rate loss with high accuracy (area under the curve: 0.91 at
48 months). Notably, the model classified risk independently of proteinuria status at 1 year. It also revealed heterogeneity within response categories defined by the urine protein-to-creatinine ratio (UPCR): some UPCR responders had high-risk biomarker signatures, while some non-responders showed low-risk profiles, highlighting the limitations of relying solely on UPCR thresholds for clinical decision-making.
The study’s findings demonstrate the potential for biomarker-driven risk assessment to personalize LN management, improve trial design, and identify patients who may benefit from early treatment intensification. By monitoring ongoing profibrotic and inflammatory activity that proteinuria may miss, urinary Tenascin C and related markers could help prevent irreversible kidney damage in high-risk individuals.
Checkpoint Inhibitor-Induced Arthritis Emerges as a Unique Cell-Driven Autoimmune Disease
A STUDY presented during the Plenary Session at the ACR Convergence 2025 provides important insight into the biology of inflammatory arthritis (IA) that emerges as an immune-related adverse event (irAE) after immune checkpoint inhibitor (ICI) therapy.9
Although this arthritis often resembles rheumatoid arthritis (RA) clinically, the study demonstrates that its underlying immunology is fundamentally different, and likely driven primarily by autoreactive T cells rather than autoantibodies.
Investigators from Mayo Clinic, Rochester, Minnesota, USA, analyzed immune profiles from 163 participants, including patients with IA irAEs, ICI-treated patients with cancer without irAEs, serology-matched RA controls, and healthy volunteers. Using flow cytometry, cytokine profiling, single-cell RNA sequencing, and functional in vitro assays, the team compared immune cell phenotypes, metabolic signatures, and autoreactivity across groups.
The findings revealed that IA irAEs represent a unique autoimmune phenotype, dominated by highly cytotoxic CD8+ T cells that are more activated than those seen in ICI-treated controls. These IA-associated CD8+ T cells expressed the highest levels of effector and cytotoxic molecules, alongside elevated metabolic activity. In contrast to RA, patients with IA irAEs did not show autoantibody elevations or expansion of atypical B cell populations. RA controls displayed increased CD4/CD8 ratios, reduced regulatory T cell frequencies, and robust autoantibody responses, none of which were present in the irAE group.
CD4+ T-cell alterations further distinguished IA irAEs from RA. Patients with irAEs exhibited a striking shift toward a CXCR3-CCR6- T cell phenotype, alongside reductions in the CXCR3+CCR6+ subset, suggesting a
reprogramming of T helper cell pathways in response to ICI exposure.
Cytokine patterns also supported a T cellcentered mechanism. Patients with IA and irAEs showed elevated plasma IL-6, IL-12, and Type I IFN signatures, with in vitro experiments demonstrating that this cytokine combination promotes cytotoxic gene expression in T cells. Blocking IL-6 receptors, IL-12 or IFN-α pathways reversed these cytotoxic and metabolic phenotypes, indicating potential therapeutic targets.
Cytokine patterns also supported a T cell-centered mechanism. Patients with IA and irAEs showed elevated plasma IL-6, IL-12, and Type I IFN signatures
Together, the data suggest that inflammatory arthritis irAEs are not simply ICI-triggered RA, but rather a distinct autoimmune condition characterized by T cell hyperactivation, metabolic reprogramming, and cytokinedriven cytotoxicity, yet largely independent of traditional autoantibody mechanisms.
This work provides a more refined understanding of checkpoint inhibitorassociated arthritis and highlights pathways that may guide future treatment strategies for affected patients.
Many High-Risk Women with Osteoporosis Remain Undertreated
MORE than 85% of postmenopausal women in the USA with high or very high fracture risk remain untreated, according to a new retrospective cohort study presented at the ACR Convergence 2025. Among those who did receive therapy, more than half were treated with oral bisphosphonates, despite these not being recommended for women at very high risk in current guidelines. Only around 5% of treated women received anabolic therapies, the most effective initial treatment.10
Data from the Optum Market Clarity Bone database (Optum®, Eden Prairie, Minnesota, USA) were analyzed to identify women aged 55 years or older with osteoporosis, a prior fracture, or earlier osteoporosis therapy between 2016–2023. To be eligible, women were required to have at least 455 days of continuous insurance coverage and to have complete data on BMI and race. Those with Paget’s disease or metastatic cancer were excluded.
The study identified 41,597 women treated for postmenopausal osteoporosis. Just over half met the criteria for very high fracture risk. Among these women, 12.6% had experienced a recent fracture within the previous year, fewer than 1% had a bone mineral density T-score of −3.0 or below, and more than 38% had a FRAX® score (University of Sheffield, UK) indicating very high risk. A further 21% were classified as high risk, and around 27% as low risk.
More than 85% of postmenopausal women in the USA with high or very high fracture risk remain untreated
Oral bisphosphonates were the most frequently used medications across all patients. More than 56% of treated women received this therapy. Denosumab was prescribed for 23% and zoledronic acid for nearly 16% of participants. Despite guideline recommendations, only around 5% of treated women and 5.7% of those at very high risk received anabolic therapies, which are considered the most efficient initial treatment option for this group.
The analysis also included 318,140 untreated women (mean age: 74 years), 37% of whom had very high fracture risk and 47% high risk, with a further 15.9% classified as low risk. These findings indicate that a substantial proportion of women who could benefit from treatment remained untreated.
References
1. Petri M et al. Redefining when to biopsy the kidney in patients with SLE. Abstract 0772. ACR Convergence, October 24-29, 2025.
2. Schmidt W et al. Efficacy and safety of upadacitinib in giant cell arteritis: 2-year results from the re-randomized, double-blind SELECT-GCA Phase 3 trial. Abstract 0776. ACR Convergence, October 24-29, 2025.
3. Tsibadze N et al. Mortality and major adverse cardiac events (MACE) with GLP-1 receptor agonists in psoriatic arthritis. Abstract 0849. ACR Convergence, October 24-29, 2025.
4. Westbrook S et al. LEVI-04 significantly reduces bone marrow lesions and symptoms in knee osteoarthritis: results from a phase II RCT. Abstract 0852. ACR Convergence, October 24-29, 2025.
5. Maksymowych WP et al. The Assessments in Spondyloarthritis International Society (ASAS) and Spondyloarthritis Research and Treatment Network (SPARTAN) revised classification criteria for axial spondyloarthritis: development and validation in the classification of axial SpA inception cohort study. Abstract 0854. ACR Convergence, October 24-29, 2025.
6. Garg S et al. Defining safe hydroxychloroquine blood levels: time to switch to precision monitoring for optimized lupus care. Abstract 1722. ACR Convergence, October 24-29, 2025.
7. Lesturgie-Talarek M et al. Pathogenic role of mucosal-associated invariant T cells in rheumatoid arthritis. Abstract 1724. ACR Convergence, October 2429, 2025.
8. Lee CY et al. Urinary Tenascin C predicts kidney function loss in lupus nephritis. Abstract 0851. ACR Convergence, October 24-29, 2025.
9. Zhu X et al. Inflammatory arthritis immune related adverse events represent a unique autoimmune disease entity primarily driven by T cells, but likely not autoantibodies. Abstract 1726. ACR Convergence, October 24-29, 2025.
10. Chien HC et al. Distribution of Fracture Risk Status and Osteoporosis Treatment Use Among Postmenopausal Women with Osteoporosis in the United States. Abstract 1727. ACR Convergence, October 24-29, 2025.
Glucagon-Like Peptide-1 Receptor Agonists in Osteoarthritis: From Clinical Promise to Preclinical Evidence
THIS YEAR, at the American College of Rheumatology (ACR) Convergence 2025, a dedicated session explored whether glucagon-like peptide-1 (GLP-1) receptor agonists could represent a new therapeutic frontier in osteoarthritis (OA). Tom Appleton, The University of Western Ontario and St. Joseph’s Health Care in London, Ontario, Canada; and Francis Berenbaum, Sorbonne University, INSERM, AP-HP SaintAntoine Hospital, Paris, France, provided an integrated view of how GLP-1 biology intersects with obesity, inflammation, pain, and joint tissue protection, highlighting the potential of this drug class as a novel therapeutic option for OA.
Appleton provided a comprehensive overview of the clinical application of GLP-1 agonists in knee osteoarthritis (KOA). He outlined their potential mechanisms, reviewed emerging evidence supporting their benefits, and summarized known side effects and contraindications. He concluded by highlighting the key unanswered questions and knowledge gaps that future research must address.
In the second part of the session, Berenbaum explained the pleiotropic effects of GLP-1 and its receptors on metabolic, inflammatory, and tissue-protective pathways relevant to OA. He reviewed pre-clinical data, including findings from his own research group, and discussed how these results support GLP-1 agonists as a potential new therapeutic class for OA.
BEYOND WEIGHT LOSS:
UNCOVERING GLUCAGON-LIKE PEPTIDE-1’s JOINT
EFFECTS
GLP-1 agonists reduce the load on lower limb joints by treating obesity,1 and protect against cardiovascular diseases. This is particularly relevant given that patients with KOA experience increased cardiovascular mortality, which is considered an independent risk factor.2 Lastly, GLP-1 agonists modify both local (synovial joint) and systemic inflammation.
Groundbreaking Studies Demonstrate Benefits in Knee Osteoarthritis
Multiple studies have explored the effects of GLP-1 agonists on KOA. The first published study in 2021 showed that liraglutide induced weight loss but yielded only minimal pain improvement.3
In 2023, Zhu et al.4 reported observational data from Shanghai Sixth People’s Hospital, China, showing that, with adequate treatment duration, GLP-1 agonists may have diseasemodifying effects in patients with KOA
with comorbid Type 2 diabetes, potentially mediated by weight loss.
A large retrospective analysis of 237,043 patients with hip or knee OA, including 23,000 individuals exposed to GLP-1 agonists for at least 1 year, found that arthroplasty risk at 1 year was reduced by approximately 40% for hip replacement and 25% for knee replacement.5
The STEP-9 trial, a 68-week, double-blind, randomized study conducted across 61 sites in 11 countries, evaluated semaglutide in people with obesity (mean BMI: 40 kg/m²) and KOA with at least moderate pain.6 Semaglutide produced significantly greater weight loss (an 11–12 kg difference versus placebo) and larger improvements in pain (Western Ontario and McMaster Universities Arthritis Index [WOMAC] score: −41.7 versus −27.5). No serious adverse effects were reported. However, potential limitations included possible unblinding due to noticeable weight loss and the absence of assessments of joint structure or other pathological endpoints.
The STEP-5 trial examined the 2-year effects of semaglutide on body weight in adults who were obese or overweight with comorbidities.7 Semaglutide led to an average weight loss of 15.2% versus 2.6% with placebo. More participants on semaglutide achieved ≥5% weight loss at Week 104 (77.1% versus 34.4%). Mild-to-moderate gastrointestinal adverse events were more frequent with semaglutide (82.2% versus 53.9%). Although partial weight regain was observed after withdrawal, overall long-term efficacy remained clear.
Adverse Effects and Contraindications
Safety data from meta-analyses of semaglutide trials show that the most common adverse events are gastrointestinal, including nausea, vomiting, and constipation.8 Contraindications include medullary thyroid carcinoma, multiple endocrine neoplasia Type 2,
and pregnancy. Lean muscle mass loss occurs proportionally with weight loss, highlighting the importance of resistance exercise and adequate protein intake to preserve muscle and bone health. Cardiovascular and renal benefits have been consistently demonstrated, with lower rates of cardiovascular events observed in semaglutide-treated patients compared with placebo 8
Remaining Questions and Knowledge Gaps
There is strong evidence that synovitis drives worse outcomes in osteoarthritis, contributing to more severe and persistent pain, heightened pain sensitization, faster structural deterioration, and an increased need for joint replacement.9-13 A key unanswered question is whether GLP-1 agonists, beyond promoting weight loss, can directly target chronic synovial inflammation. Understanding their potential disease-modifying effects on the inflamed synovium is essential to determine whether these therapies could alter the trajectory of OA rather than solely improve symptoms.
Appleton highlighted several important remaining gaps in the understanding of GLP-1-based therapies for OA. It is uncertain whether their effects are similar in nonobese or less-obese populations, or whether benefits extend to other disease subtypes such as hand OA. It also remains unclear whether improvements are driven purely by biomechanical changes from weight loss or whether cardiometabolic mechanisms contribute independently, potentially offering disease-modifying effects or benefits through intra-articular delivery. Additional questions include how to mitigate lean muscle mass loss, which is important for joint stability, and whether adding glucose-dependent insulinotropic polypeptide or glucagon receptor activation could offer advantages over GLP-1 agonists on their own.
GLUCAGON-LIKE PEPTIDE-1 IN OSTEOARTHRITIS: WHAT PRECLINICAL STUDIES REVEAL
A recent groundbreaking study described a gut–joint pathway that may help explain the development of OA.14 In healthy people, the gut bacterium Clostridium bolteae converts primary bile acids into ursodeoxycholic acid, which is then conjugated into glycoursodeoxycholic acid (GUDCA). These bile acids suppress the farnesoid X receptor (FXR) in the intestine. When FXR is inhibited, intestinal stem cells generate more L-cells, which produce GLP-1. This endogenous GLP1 enters the bloodstream, reaches the joint, binds to GLP-1 receptors in joint tissue, and protects cartilage.
In patients with OA, levels of C. bolteae are reduced. Because of this, less GUDCA is produced, FXR remains activated, fewer L-cells are formed, and GLP-1 production falls. The study showed that restoring C. bolteae or giving GUDCA directly protects cartilage in a mouse OA model. Importantly, when researchers blocked the GLP-1 receptor by injecting its inhibitor into the joint, the protective effects disappeared. This indicates that the benefit depends on GLP-1 signaling itself, rather than on unrelated metabolic changes.
Furthermore, in a series of preclinical studies, GLP-1 analogues demonstrated protective effects on joint tissues across multiple OA models.14-15 Liraglutide reduced cartilage degradation more effectively than intraarticular dexamethasone, which showed no structural benefit. In human cartilage pellet cultures, GLP-1 analogues restored proteoglycan markers suppressed by IL-1β They also reduced catabolic enzyme activity and promoted anabolic matrix formation, consistent with the anti-catabolic and anabolic actions described in preclinical OA models.
Glucagon-Like Peptide-1 Analogues Reduce Pain and Fibrosis in Animal Models
Berenbaum discussed his own research in this area, where his team first demonstrated that multiple GLP-1 analogues markedly reduced pain in the monoiodoacetate mouse model. He then compared the effects of liraglutide and dexamethasone on synovitis in rat models, finding that, although inflammatory scores were similar between the two treatments, the density scores differed. In subsequent anterior cruciate ligament transection combined with medial meniscectomy rat studies, the team showed that liraglutide produced a strong antifibrotic effect, whereas dexamethasone had no measurable impact on fibrosis.
Macrophage–Fibroblast Crosstalk: A Potential New Paradigm
To begin dissecting potential cellular mechanisms within the synovium, Berenbaum’s group examined how GLP1 analogues influence innate immune and stromal cells. In synovial macrophages, liraglutide treatment shifted cells from a pro-inflammatory M1 phenotype toward an anti-inflammatory M2 state, a transition that correlated with an overall reduction in inflammatory activity. Complementing these findings, preliminary data from human synovial fibroblasts show that GLP1 stimulation reduces cytokine production and alters inflammatory gene expression, suggesting broader immunomodulatory effects across key synovial cell populations.16
Berenbaum hypothesized that the therapeutic potential of GLP-1 in OA may arise from targeting the crosstalk between macrophages and fibroblasts, which are known to drive inflammation, fibrosis, and downstream cartilage damage. This dual effect could explain why GLP-1 analogues, unlike dexamethasone, improve both synovitis and fibrosis in preclinical models.
A Potential New Osteoarthritis Therapeutic Class
Together, these findings suggest that GLP-1 receptor modulation influences multiple jointspecific pathways: reducing inflammation, preventing cartilage catabolism, promoting matrix regeneration, and modifying synovial tissue responses. These pleiotropic actions, combined with robust analgesic and antifibrotic effects, support GLP-1 analogues as a promising new therapeutic class for OA. Ongoing mechanistic studies and upcoming clinical trials will determine how these preclinical benefits translate to human disease.
CONCLUSION
The clinical and preclinical data presented at the ACR Convergence 2025 show both the therapeutic potential and the scientific complexity of GLP-1 agonists in OA. While early findings suggest significant effects on weight, pain, inflammation, and joint tissues, main mechanisms and clinical implications remain unclear. As larger and longer-term trials start to report their results, we will gain a clearer picture of whether GLP-1 agonists can ultimately modify disease progression or serve as mainly symptomatic therapies.
References
1. Karacabeyli D et al. Glucagon-like peptide-1 receptor agonists in arthritis: current insights and future directions. Nat Rev Rheumatol. 2025;21(11):671-83.
2. Hawker GA et al. All-cause mortality and serious cardiovascular events in people with hip and knee osteoarthritis: a population based cohort study. PLoS One. 2014;9(3):e91286.
3. Gudbergsen H et al. Liraglutide after diet-induced weight loss for pain and weight control in knee osteoarthritis: a randomised control trial. Am J Clin Nutr. 2021;113(2):314-23.
4. Zhu H et al. Glucagon-like peptide-1 receptor agonists as a diseasemodifying therapy for knee osteoarthritis mediated by weight loss: findings from the Shanghai Osteoarthritis Cohort. Ann Rheum Dis. 2023;82(9):1218-26.
6. Bliddal H et al. Once-weekly semaglutide in persons with obesity and knee osteoarthritis. N Engl J Med. 2024;391(17):1573-83.
7. Garvey WT et al. Two-year effects of semaglutide in adults with overweight or obesity: the STEP 5 trial. Nat Med. 2022;28(10):2083-91.
8. Kushner RF et al. Safety profile of semaglutide versus placebo in th SELECT study: a randomized controlled trial. Obesity. 2025;33(3):452-62.
9. Baker K et al. Relation of synovitis to knee pain using contrastenhanced MRIs. Ann Rheum Dis. 2010;69(10):1779-83.
10. Philpott HT et al.; WOREO Knee Study Group. Synovitis is associated with constant pain in knee osteoarthritis: a cross-sectional study of OMERACT knee ultrasound scores. J Rheumatol. 2022;49(1):89-97.
5. Porto JR et al. The impact of contemporary glucagon-like peptide-1 receptor agonists on the onset, severity, and conversion to arthroplasty in hip and knee osteoarthritis. Orthop J Sports Med. 2025;13(2):23259671241297157.
11. Neogi T et al. Association of joint inflammation with pain sensitization
in knee osteoarthritis: the multicenter osteoarthritis study. Arthritis Rheumatol. 2016;68(3):654-61.
12. Felson DT et al. Synovitis and the risk of knee osteoarthritis: the MOST Study. Osteoarthr Cartil. 2016;24(3):458-64.
13. Conaghan PG et al. Clinical and ultrasonographic predictors of joint replacement for knee osteoarthritis: results from a large, 3-year, prospective EULAR study. Ann Rheum Dis. 2010;69(4):644-7.
14. Yang Y at al. Distinct transmission sites within a synapse for strengthening and homeostasis. Sci Adv. 2025;11(15):eads5750.
15. Ciftci E et al. Anti-inflammatory and anabolic effects of liraglutide on 3D inflammatory osteoarthritic pellets of human chondrocytes. Osteoarthritis Cartil. 2024;32(Suppl 1):S113-4.
16. Meurot C et al. Liraglutide, a glucagonlike peptide 1 receptor agonist, exerts analgesic, anti-inflammatory and antidegradative actions in osteoarthritis. Sci Rep. 2022;12(1):1567.
Driving CAR-T Into the Future: What Are
the Right B Cell Targets in Systemic Lupus Erythematosus and Beyond?
THE AMERICAN College of Rheumatology (ACR) 2025 Convergence was an epicenter for discussion, collaboration, and celebration of the advancements in rheumatology. This session, ‘Driving CAR-T Into the Future: What is the Right B Cell Targets in Systemic Lupus Erythematosus and Beyond?’ was a program highlight, exploring the various B cell subsets, their role in autoimmunity, and examining novel pathways and targets that might promote the selective targeting of autoreactive B cells in autoimmune disease. It was moderated by Jeremy Tilstra, University of Pittsburgh School of Medicine, Pennsylvania, USA; and Anne Davidson, Feinstein Institute for Medical Research, Manhasset, New York, USA, and featured notable panelists including Nan Shen, Shanghai Jiao Tong University School of Medicine, China; and Inaki Sanz, Emory University School of Medicine, Atlanta, Georgia, USA.
A BACKGROUND ON CAR-T CELL THERAPY
Opening the discussion, Tilstra gave some background on the history of CAR-T cell therapy. First developed for prostate cancer in 2002, it was followed by the first CAR-T cell trial just over 10 years later in 2013, and the first FDA-approved CAR-T cell therapy in 2017. So, how are CAR-T cells manufactured? As summarized by Tilstra, T cells or natural killer cells are isolated from a patient’s blood sample, and the CAR gene, encoding the CAR receptor, is inserted inside the isolated immune cells via a vector, then expanded and infused back into the patient.
Tilstra then drew the audience’s attention to a case series published in 2024 that assessed the effect of a cluster of differentiation (CD)19 CAR-T cell therapy for three different types of autoimmune diseases: systemic lupus erythematosus (SLE), idiopathic inflammatory myositis,
and systemic sclerosis.1 The study enrolled 15 patients: eight with SLE, three with idiopathic inflammatory myositis, and four with systemic sclerosis, and administered a single infusion of CD19 CAR-T cell therapy after preconditioning with two types of chemotherapy: fludarabine and cyclophosphamide. Interestingly, after a median follow-up of 15 months, all patients achieved disease remission or major clinical response specific to their condition, allowing complete discontinuation of immunotherapy.
T cells or natural killer cells are isolated from a patient’s blood sample, and the CAR gene, encoding the CAR receptor, is inserted inside the isolated immune cells via a vector, then expanded and infused back into the patient
First developed for prostate cancer in 2002, it was followed by the first CAR-T cell trial just over 10 years later in 2013, and the first FDAapproved CAR-T cell therapy in 2017
QUESTION 1: CAN WE AND SHOULD WE CONSIDER MORE SPECIFIC B CELL TARGETS?
Tilstra then recapped the activation pathway from naïve B cells to CD27+ antibodysecreting memory B cells. Naïve B cells become activated via toll-like receptor (TLR) 7 and TLR9, with TLR9 directing activation via the germinal center; however, B cells can also become activated in the extrafollicular space. Once activated, these naïve B cells migrate to the germinal center, driven by cytokines such as IL-21 and IL-4. There, they interact with T follicular helper cells in the dark zone and undergo expansion and somatic hypermutation, generating both CD27+ memory cells and long-lived plasma cells. Although this process is well established, Tilstra highlighted growing research interest in the alternative extrafollicular pathway, where cytokines IL-12 and interferon gamma interact with activated naïve B cells to drive the production of several cell types, notably double-negative (DN)1-3, plasmablasts, and long-lived plasma cells.
Tilstra then posed an important question: “Which subset of B cells may be targeted by unique CAR-T cells?” He presented a slide illustrating the various B cell subtypes, from pro- and pre-B cells in the bone marrow to transitional, naïve, germinal centre, memory, and plasmablast populations in the periphery, spleen, and lymph nodes, and finally plasma cells back in the bone marrow. While CAR-T cell therapy commonly targets CD19 due to its widespread expression across most B cell types, Tilstra noted that CD19 expression is reduced in plasmablasts and plasma cells. CD20 is another frequently used target, but it is more restricted, as it is present only from the pre-B cell stage through to some memory B cells. CD38 is expressed across all B cell types, though its expression is variable and tends to be highest in later-stage populations. Additional targets discussed included B cell maturation antigen (BCMA) and B cell activating factor receptor.2
The question was then posed to the panellists. Sanz responded first, cautioning that much remains to be understood in this field and that this foundational knowledge is essential before refining treatment targets. He
emphasized that treatment specificity should consider not only B cell subtypes but also differences between patient populations, depending on which pathway, germinal centre or extrafollicular, is most relevant to their disease.
“Different patients are going to be different, so when we talk about which B cells, specific B cells, might be the target, I would argue that there are going to be some groups of patients for which the germinal center pathway may be a better target, or the extrafollicular pathway, and the other way around.”
Shen added that more diseasespecific context is needed, particularly in identifying the pathogenic clone in each case. He also noted that further research is required to determine whether precursor B cell populations should also be targeted. In conclusion, Shen recommended a broad approach to B cell targeting for CAR-T therapy at this stage, given current knowledge and evidence.
QUESTION 2: IF WE WERE TO BE MORE SPECIFIC, WHAT SHOULD OUR B CELL TARGETS BE? ARE THERE DIFFERENT TARGETS FOR DIFFERENT DISEASES?
Building on this, Tilstra then posed another thought-provoking question: “If we were to consider being more specific, what should our B cell targets be?” He introduced the concept of ‘precision immunotherapy’,
asking whether different diseases may require distinct targets. Tilstra suggested several cell populations for targeted CAR-T therapies, in addition to CD19 and CD20. These included 1) plasma cells using BCMA-CAR-T and anti-CD38 CAR-T; 2) autoimmune or age-associated B cells or DN2 B cells; and 3) autoreactive B cells.
Focusing on plasma cells, many autoimmune diseases are characterized by autoantibody production, with plasma cells and plasmablasts as the major producers of these autoantibodies. As Tilstra highlights, if CAR-T cell therapy becomes more targeted by B cell subtype, plasma cells would be an ideal population to pursue. For example, daratumumab, which targets CD38 expressed on plasma cells, has demonstrated efficacy in lupus nephritis.
If we were to consider being more specific, what should our B cell targets be?
When this concept was presented to the panel, Sanz urged caution, noting: “I think it is hard to think that the plasma cells alone, or the autoantibodies alone, are responsible for the entire burden of disease.” Shen agreed, adding that targeting only plasma cells may not result in a sustainable clinical remission. “If we have not eliminated upstream control and determined these very critical extrafollicular pathogenic cells, [then] we have not cut the upstream origin of these cells.”
QUESTION 3: IS THERE UTILITY IN TARGETING SPECIFIC B CELL AFFINITY POPULATIONS?
Tilstra then shifted the discussion toward whether therapy should target specific B cell populations that express known pathogenic markers. For instance, it is known that some autoimmune diseases show high levels of antibodies produced by B cells with the VH434 heavy chain segment.3 Additionally, antiSm and anti-Jo-1 are autoantibodies found mainly in SLE and polymyositis, respectively. Sanz explained that, “for those who might not be familiar with it, typically, the VH4-34 B cells are anywhere from 5–10% of all naïve cells, including in healthy people, but they are heavily central in the germinal centers, and thus, effective in lupus.” While he acknowledged the potential of targeting B cells that express known pathogenic markers, such as VH4-34, he cautioned that this approach would require selecting patients in whom the marker is not only pathogenic but also the sole pathogenic B cell population, something that is challenging to determine in practice.
ANTIBODY REPERTOIRES AFTER CAR-T CELL THERAPY
Tilstra then drew attention to two studies from 2022 and 2025. The first study demonstrated that autoantibody profiles measured using a 57-antigen microarray could reliably detect patients who will later develop SLE, identifying 53% of prediagnosis cases with high specificity (94%), highlighting their potential as early diagnostic biomarkers to prevent irreversible organ damage.4 The second study was a Phase I trial that showed that dual anti-CD19/
anti-BCMA CAR-T cell therapy was safe and highly effective in treatment-refractory SLE, inducing remission in 80% of patients and eliminating autoreactive B cell and plasma cell clones, with sustained immune reconstitution and potential long-term cure.5
CONCLUSION
The session highlighted that while CAR-T therapy targeting broad B cell populations shows strong promise in SLE and other autoimmune conditions, the future lies in refining targets based on individual disease mechanisms and pathogenic cell subsets. Continued research into B cell biology and autoantibody profiles will be crucial to advancing precision immunotherapy and improving long-term treatment outcomes.
References
1. Müller F et al. CD19 CAR T-Cell therapy in autoimmune diseasea case series with follow-up.
N Engl J Med. 2024;390(8):687-700.
2. Robinson WH et al. Cutting-edge approaches to B-cell depletion in autoimmune diseases. Front Immunol. 2024;15:1454747.
3. Bhat NM et al. VH4-34 encoded antibody in systemic lupus erythematosus: effect of isotype. J Rheumatol. 2002;29(10):2114-21.
4. Brunekreef TE et al. Microarray analysis of autoantibodies can identify future systemic lupus erythematosus patients. Hum Immunol. 2022;83(6):509-14.
5. Feng J et al. Co-infusion of CD19targeting and BCMA-targeting CAR-T cells for treatment-refractory systemic lupus erythematosus: a phase 1 trial. Nat Med. 2025;31(11):3725-36.
ACR 2025
Abstract Reviews
This collection of abstracts presented at the American College of Rheumatology (ACR) Convergence 2025 spans the clinical, biological, social, and financial aspects of modern rheumatology practice.
The Cost of Complexity: Financial Toxicity in Rheumatic Disease, Cancer, and Their Intersection
Financial toxicity (FT) is the financial burden of accessing healthcare. It is well known in cancer and increasingly seen in rheumatic disease (RD). The authors compared FT among adults with neither condition, RD only, cancer only, and both.1
MATERIALS AND METHODS
The authors used the National Health Interview Survey (NHIS), a nationally representative sample of US adults from 2019–2023. Adults were categorized by self-reported RD, including arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia, and/or cancer. FT was defined as the presence of one or more of the following: financial distress, difficulty paying bills, delayed or forgone care, cost-related medication non-adherence, and food insecurity.2 Weighted logistic regressions were used to examine associations between disease groups and FT components, adjusting
for demographics, comorbidities, and insurance status. To account for baseline differences and insurance coverage, analyses were stratified by age (<65 versus ≥65 years). Analyses were conducted in RStudio v4.4.1 (Posit, Boston, Massachusetts, USA); significance was set at p<0.05.
RESULTS
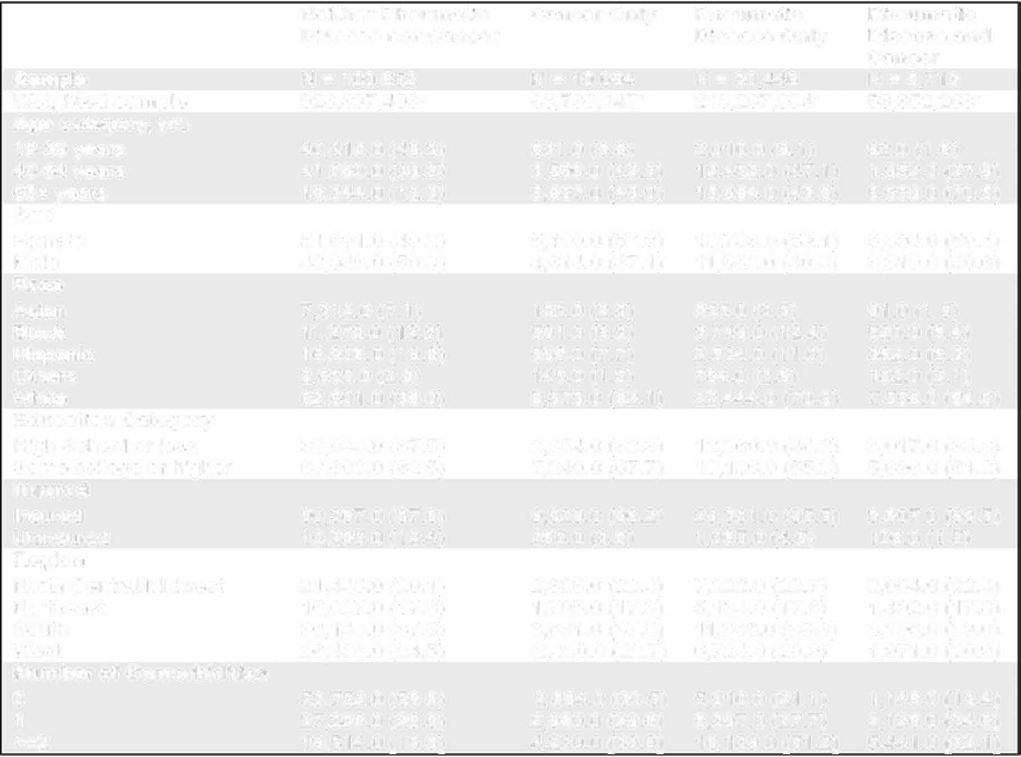
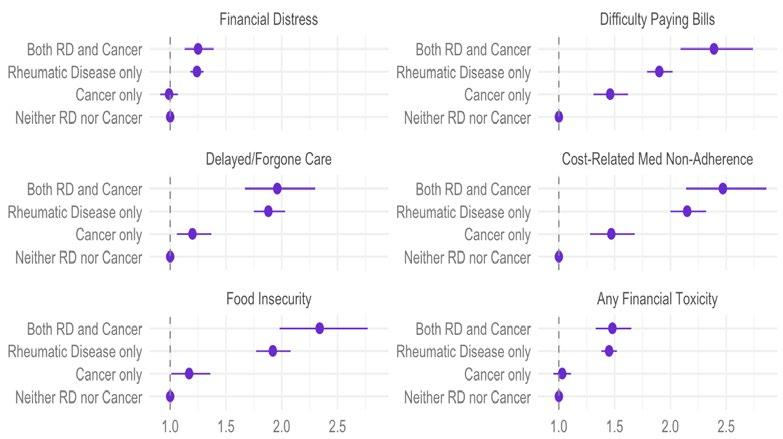
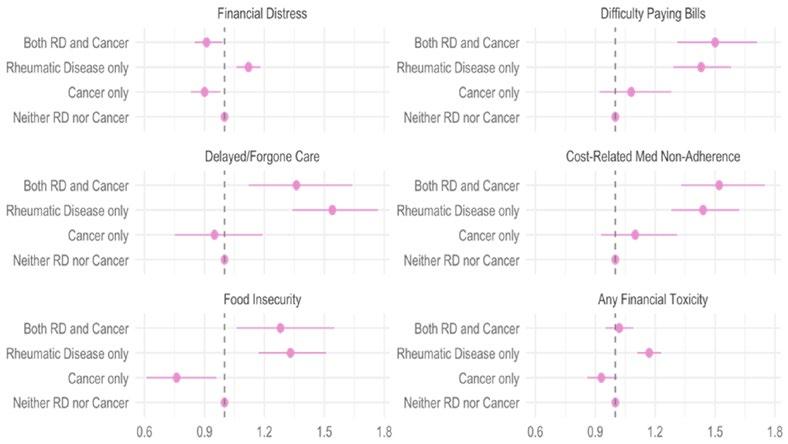
A total of 149,905 adults were included, of whom 10,094 (weighted prevalence: 6.3% [95% CI: 6.1–6.5%]) had cancer only, 30,446 (18.5% [95% CI: 18.2–18.8%]) had rheumatic disease (RD) only, and 8,713 (4.7% [95% CI: 4.6–4.9%]) had both RD and cancer. These correspond to approximately 80.5, 235.6, and 59.9 million US adults, respectively. Adults with both RD and cancer were more likely to be aged ≥65 years (70.5%) and had the highest rates of multimorbidity (62.1% with ≥2 comorbidities). Most adults across groups were female and insured, with higher educational attainment in the cancer-only and neither condition (Table 1). In adults under 65 years, FT was highest in those with RD alone (63.9%) or RD plus cancer (64.3%), compared to 54% in those without either condition. Medication non-adherence was higher in RD groups (RD only: 16.3%; RD with cancer: 19.2%). In adults over 65 years, FT was most prevalent in those with RD only (41.4%), with financial distress being highest in this group (35.1%). Among adults <65 years, compared to those with neither RD nor cancer, persons with RD alone or in combination with cancer were consistently associated with increased FT across all domains (Figure 1). Among adults ≥65 years, RD remained associated with higher odds of difficulty paying bills, cost-related medication non-adherence, and food insecurity, while cancer alone
Neither Rheumatic Cancer Only Rheumatic Disease nor Cancer Disease Only N = 100,652 N= 10,094 N = 30,446 928,897, 493
yrs: years. was not associated with increased financial toxicity and appeared protective in some domains compared to those with neither condition. The combined burden of RD and cancer conferred a similar level of risk as RD alone (Figure 2).
CONCLUSION
Among younger adults, RD had a stronger association with FT than cancer, with the highest burden seen in those with both.
Similar trends were observed among older adults, though with more modest effect sizes. While cancer may lead to shortterm high costs, RD imposes a chronic financial burden from ongoing treatment and care. Even among Medicare-insured older adults, FT persists. These findings underscore the need for RD-specific FT assessment tools and greater clinical attention to financial burden, particularly as longer life expectancy amplifies the long-term economic impact of chronic RDs.
Table 1: Baseline characteristics of adults with cancer and/or rheumatic disease from the National Health Interview Survey, 2019–2023.
Figure 1: Adjusted odds ratios for financial toxicity outcomes among younger adults (<65 years) by disease group.
RD: rheumatic disease.
Figure 2: Adjusted odds ratio for financial toxicity outcomes among older adults (≥65 years).
RD: rheumatic disease.
References
1. Sondhi M et al. The cost of complexity: financial toxicity in rheumatic disease, cancer, and their intersection. Abstract
2615. ACR Convergence, October 24-29, 2025.
2. Valero-Elizondo et al. Atherosclerotic cardiovascular disease, cancer, and
financial toxicity among adults in the United States. JACC CardioOncol. 2021;3(2):236-46.
Oral Glucocorticoid Treatment for Checkpoint
Inhibitor Associated Inflammatory Arthritis Does Not Affect Progression Free Survival: A RADIOS Registry Cohort Study
Authors: *Deanna Jannat-Khah,1 Pankti Reid,2 Maria Suarez-Almazor,3 Noha Abdel-Wahab,3 Jeffrey Sparks,4 Tawnie Braaten,5 Cassandra Calabrese,6 Alexa Meara,7 Minerva Nong,8 Kyle Ge,1 Laura Cappelli,9 Ami Shah,10 Clifton Bingham,11 Anne R. Bass1
1. Hospital For Special Surgery, New York, USA
2. University of Chicago Medical Center, Ilinois, USA
3. MD Anderson Cancer Center, Houston, Texas, USA
4. Brigham and Women's Hospital, Boston, Massachusetts, USA
5. University of Utah, Salt Lake City, USA
6. Cleveland Clinic Foundation, Cleveland Heights, Ohio, USA
7. The Ohio State University Wexner Medical Center, Columbus, USA
8. Columbia University, New York, USA
9. Johns Hopkins University School of Medicine, Baltimore, Maryland, USA
10. Johns Hopkins Rheumatology, Baltimore, Maryland, USA
11. Johns Hopkins University, Baltimore, Maryland, USA
*Correspondence to jannatkhahd@hss.edu
Disclosure: Shah has received a grant from the National Institutes of Health, with payments to his institution. Meara has received consulting fees from Abbvie, Sanofi, Astrazeneca, and Amgen; support for attending meetings from Abbvie, Sanofi, and Amgen; payments for expert testimony from Davis, Levin, and Livingston; and is a board member for the Foundation for Autoimmune Cancer Support. Cappelli has received consulting fees from Bristol Myers Squibb, Abbvie, Amgen, and Sanofi. Calabrese has received consulting fees and honoraria from Sanofi-Regeneron. Bass is treasurer for the American College of Rheumatology and Rheumatology Research Foundation. Jannat-Khan has declared a Discovery Grant to the Hospital for Special Surgery Department of Medicine; has received a travel award from the ACR/ EULAR research exchange program; participated in two data safety monitoring boards: Phase II Trial of Abaloparatide vs. Placebo in Post-Menopausal Women Receiving Initial Spinal Fusion Surgery, and Topical Epidural Steroid Usage in Patients Undergoing Posterior Lumbar Decompression: A
Randomized Control Trial; is a member of the ACR Committee on Registries and Health Information Technology (RHIT), ACR RHIT representative on the ACR Annual Meeting, and member of the ACR subcommittee on Publications and Research; and has stock in Cytodyn and Astrazeneca. Abdel-Wahab has received a grant from the National Insitutes of Health/National Institute of Allergy and Infectious Diseases; received institutional support from The University of Texas MD Anderson Cancer Center (2018–July 2025), including the Cancer Survivorship Seed Fund, Institutional Research Grant, Prioritizing Research Innovation & Mentoring Excellence Award, Division of Internal Medicine Development & Translational Science Award, Bridge Funding Award, Cyrus Scholar Award for Outstanding Clinical Research, Melanoma SPORE Career Enhancement Program Award, and the Melanoma Boat Walk Seed Fund, for research around the subject matter; has participated in advisory boards, consulted, and received honoraria from ChemoCentryx; and is a Chair of the Alliance for Clinical Trials in Oncology Immuno-Oncology Toxicity (IOTOX) Working Group & Executive Committee Member of the Alliance for Support and Prevention of Immune-Related adverse Events (ASPIRE), unpaid. Bingham has received consulting fees from Abbvie, Avalo, BMS, Eli Lilly, Janssen, Pfizer, Sanofi, and Tonix; participated on Boards for Eli Lilly; and is President Elect of the PROMIS Health Organization. Sparks has received grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Heart, Lung, and Blood Institute, Rheumatology Research Foundation, Arthritis Foundation, R. Bruce and Joan M. Mickey Research Scholar Fund, Gordon and Llura Gund Foundation, Bristol Myers Squibb, Boehringer Ingelheim, Johnson & Johnson, and Sonoma Biotherapeutics; and consulting fees from Abbvie, Amgen, Anaptys, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Fresenius Kabi, Gilead, Inova Diagnostics, Invivyd, Johnson & Johnson, Merck, MustangBio, Novartis, Optum, Pfizer, Recor, Sana, Sobi, and UCB. Suarez-Almazor has received a grant from Novartis, unrelated to this paper; and consulting fees from Syneos Health and Set Point Medical. The other authors have declared no conflicts of interest.
Immune checkpoint inhibitors (ICI) are efficacious treatments for various cancers. As approvals for ICI treatment increase for additional cancers, the prevalence of rheumatologic immune related adverse events (irAE) also grows. First-line treatment for these irAEs is glucocorticoids; however, there is a lack of standardization in dosing, tapering, and duration of treatment. There are varying results published on ICI-treated patients on the association of oral glucocorticoids on progression-free survival (PFS).1
MATERIALS AND METHODS
Data from a prospective USA multi-center rheumatic irAE cohort (RADIOS) were utilized. Inclusion criteria for this study were the following: patients enrolled since February 2023; treated with an ICI for cancer; diagnosed with ICI-inflammatory arthritis (ICI-IA), defined as inflammatory arthritis, arthralgia, or polymyalgia rheumatica; and treated with glucocorticoids. Patients with pre-existing autoimmune disease, or treatment for another irAE with glucocorticoids, were excluded. Data on demographics, cancer and cancer treatment, disease-modifying antirheumatic drugs, and glucocorticoid treatment were collected. Glucocorticoid dosage was converted to prednisone equivalents. Cumulative glucocorticoid exposure and the average daily prednisone dose was calculated at different time points and displayed in a box plot. Descriptive statistics were performed. Thirty-day landmark Kaplan-Meier plots were drawn to investigate glucocorticoid treatment and cancer progression using time from glucocorticoid initiation to radiographic
cancer progression or death (PFS). Timevarying Cox proportional hazard models were also performed using time from ICI initiation to glucocorticoid treatment. Adjusted models included the following covariates: age, irAE grade at baseline, cancer type (melanoma, non-small cell lung cancer, renal cell cancer), cancer stage, and ICI combination therapy.
RESULTS
The analytic cohort consisted of 206 patients with a mean age of 65 years (SD: 12.36), 48.5% were female, and 85.9% were White (Table 1). The most frequent cancers were melanoma (32.5%), renal cell cancer (18.4%), or non-small cell lung cancer (11.7%), and were Stage 3 (26.7%) or 4 (58.3%). Time from ICI-IA diagnosis to glucocorticoid initiation was a median of 24.5 days (interquartile range: 3–63).
Median time from glucocorticoid initiation to cancer progression was 82.5 days (interquartile range: 70–283) among the 46 patients (22.3%) who progressed. In a landmark Kaplan-Meier curve the median glucocorticoid dose in the first month of treatment was not associated with PFS (logrank p value 0.99). Similarly, using quartiles of glucocorticoid dose, there was also no association between glucocorticoid use and PFS (log rank p value 0.31). Lastly, all of the adjusted Cox models were not significant.
CONCLUSION
Using data from RADIOS, the authors found no association between glucocorticoid treatment and PFS in patients with ICIIA. Rheumatologists often prescribe glucocorticoids at lower doses than oncology guidelines recommend. These findings suggest that glucocorticoid treatment by rheumatologists for ICI-IA may not have a substantial impact on cancer outcomes.
Table 1: Demographic and cancer characteristics (N=206).
Has ICI been held for rheumatic irAE at any point since ICI start?
*Missing data: N=1 for female; N=40 for baseline irAE grade; N=17 baseline cancer stage.
1. Jannat-Khah D et al. Oral glucocorticoid treatment for checkpoint inhibitor associated inflammatory arthritis do not affect progression free survival: a RADIOS Registry cohort study. Abstract 1730. ACR Convergence, October 24-29, 2025.
Methotrexate Alone or in Combination and Higher Age Impair Humoral Response Against the Recombinant Herpes
Zoster Vaccine in Rheumatoid Arthritis: A Prospective, Randomized, Placebo-Controlled Trial
Authors: *Ana Cristina de Medeiros-Ribeiro,1 Lucas Guimarães Nolasco Farias,1 Nádia Emi Aikawa,1,2 Sandra Gofinet Pasoto,1 Léonard de Vinci Kanda Kupa,1 Carla Gonçalves Saad,1 Andrea Yuki Shimabuco,1 Karina Rossi Bonfiglioli,1 Diogo Souza Domiciano,1 André Franco,1 Ana Marli Sartori,3 Clóvis Artur Silva,1,2 Eloisa Bonfá1
1. Rheumatology Division, Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Brazil
2. Pediatric Rheumatology Unit, Instituto da Criança e do Adolescente, Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Brazil
3. Infectious Disease Department, Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Brazil
*Correspondence to ana.medeiros@hc.fm.usp.br
Disclosure: This investigator-initiated study (NCT05879419) was funded by GSK, Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; #303116/2022–6 to Pasoto; #304984/2020–5 to Silva), and Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP; #2022/12925-8 to de Medeiros-Ribeiro, Aikawa, Pasoto, Silva, and Bonfá).
The vaccine against herpes zoster (HZ), known as the recombinant zoster vaccine (RZV) is recommended by the American College of Rheumatology (ACR) and European Alliance of Associations for Rheumatology (EULAR) for individuals who are immunocompromised. Short-term observational data from rheumatoid arthritis (RA) cohorts aged ≥50 years support its overall reactogenicity and possible safety in non-randomized designs.1-3 However, the specific impact of different
immunosuppressive drugs or combinations on vaccine immunogenicity are limited to small sample sizes, hampering conclusions about the effect of specific therapies. To address these gaps, the authors conducted a large prospective RCT to evaluate safety and assess humoral and cellular immunogenicity induced by RZV in adult (≥18 years) patients with RA.4,5
MATERIALS AND METHODS
Patients were randomized to receive RZV (P1) or placebo (P2) at Day (D)0 and D42. Groups were blindly evaluated for disease activity (Clinical Disease Activity Index [CDAI], Simple Disease Activity Index [SDAI], and Disease Activity Score-28 for Rheumatoid Arthritis with CRP [DAS28-CRP]) at D0, D42, and D84 and classified as worsening disease activity at D84 according to the respective worsening disease activity criteria and the patient perception. The P2 group was vaccinated with a similar schedule at D84 and D126. Anti-gE antibody concentrations (ELISA) were assessed before first RZV dose and 6 weeks after the second dose. Pre- and post-vaccination geometric mean titers (GMT) were calculated. Cellular immunogenicity was measured at baseline and 6 weeks after full vaccination by cytometry after in vitro stimulation with gE ectodomain: frequency and number of gE-specific CD4+[2+] T cells producing at least 2/4 markers (IFN-γ, IL-2, TNF-α, and CD40 ligand) were measured in a sample of patients and controls. Adverse events were monitored for 3 months through scheduled visits and phone contacts.
RESULTS
A total of 320 patients with RA were randomized at D0: 165 in P1 and 155 in P2
(Figure 1). The groups were well balanced for age (p=0.562), sex (p=0.331), previous HZ infections (p=0.580), disease duration (p=0.838), rheumatoid factor (p=0.411), antic-cyclic citrullinated peptide antibody (p=0.456) positivity, disease modifying anti-rheumatic drugs (DMARD) distribution (p>0.05), DAS28-CPR (p=0.268), and SDAI (p=0.343). After two vaccine doses, seroconversion (96.6% versus 100%; p=0.030) and GMT (8.3 [7.2-9.5] versus 12.9 [11.5-14.5 mUI/mL]; p<0.001) were significantly reduced in patients compared to control group. No factors were associated with absence of SC (p>0.05). Linear regression corrected for pre-vaccination GMT linked older age (p=0.032), higher disease activity (p=0.042), methotrexate (MTX; p>0.001), and prednisone use
(p=0.045) with lower post vaccination GMT. The concomitant use of MTX reduced postvaccination GMT among biologic DMARD (p<0.001) users (mainly TNF inhibitor users; p=0.003) and synthetic DMARD users (p<0.001). In multivariate analysis, higher pre-vaccination GMT persisted, associated with higher post-vaccination GMT (<0.001), while older age (>60 years; p=0.033) and MTX use (p<0.001) remained associated with lower post-vaccination GMT (effect estimate ratio [95% confidence interval]: 0.761 [0.5900.981] and 0.562 [0.399–0.791], respectively). Cellular immunogenicity was measured in 42 patients with RA and 29 controls, who showed comparable responses according to the frequency (p=0.233) and number (p=0.531) of specific CD4[2+] T cells. No HZ cases occurred by Week 12. The frequencies
Figure 1: Frequencies of worsening rheumatoid arthritis disease activity at Day 42 and Day 84, 6 weeks after the first and second doses of recombinant zoster vaccine (P1)
of patients worsening disease activity were comparable between P1 (vaccine) and P2 (placebo) at D42 and D84 according to delta CDAI, delta SDAI, and DAS28-CRP worsening criteria (p>0.05 for all). No moderate/severe adverse events were observed.
CONCLUSION
This large study showed that RVZ was safe in immunosuppressed patients with RA, with no evidence of increased flare rate using validated measures. Importantly, the authors identified MTX and older age as key factors that significantly impair vaccine-induced immune response. These findings emphasize the need for drug discontinuation strategies or booster doses to optimize long-term protection.
References
1. Källmark H et al. Serologic immunogenicity and safety of herpes zoster subunit vaccine in patients with rheumatoid arthritis receiving Janus kinase inhibitors. Rheumatology (Oxford). 2024;63(7):2024-33.
2. Kojima S et al. Immunogenicity and influence on disease activity of recombinant zoster vaccine in patients with rheumatoid arthritis treated with DMARDs. RMD Open. 2024;10(1):e003902.
3. Medeiros-Ribeiro A et al. Methotrexate use and higher age impair humoral response against the recombinant herpes zoster vaccine (RZV) in rheumatoid arthritis: a prospective, randomized, placebo-controlled trial. Abstract 2682. ACR Convergence, October 24-29, 2025.
4. Kupa LVK et al. Disease safety, immunogenicity, and efficacy of recombinant herpes zoster vaccine (RZV or Shingrix) in autoimmune rheumatic diseases: launching a randomized phase 4 study. J Clin Rheumatol. 2025;31(6):e104-11.
5. Venerito V et al. Immunogenicity and safety of adjuvanted recombinant zoster vaccine in rheumatoid arthritis patients on anti-cellular biologic agents or JAK inhibitors: a prospective observational study. Int J Mol Sci. 2023;24(8):6967.
Multimodal Analysis Revealed Altered Brain Connectivity Patterns and Neuroinflammatory Processes in the Background of Difficult-To-Treat Rheumatoid Arthritis
Authors: Lilla Gunkl-Tóth,1-3 Gergely Orsi,4,5 Noémi
Császár-Nagy,6,7 Lili Duzsik,6 Gábor Mátay,6 Krisztina Csókási,8 Gábor Sütő, 9 Gábor Kumánovics,10 Szabolcs Takács,11 Zoltán Vidnyánszky,12 József Kun,1,13,14 Krisztina Takács-Lovász,1 Anett Pintér,3 Panna Királyhidi,3,15 Gellért Karvaly,16 Róbert Farkas,16 Georg Schett,16 *György Nagy,3,15,16 Zsuzsanna Helyes1,2,14
1. Department of Pharmacology and Pharmacotherapy, Medical School, University of Pécs, Hungary
2. HUN-REN–PTE Chronic Pain Research Group, Pécs, Hungary
3. Department of Rheumatology and Immunology, Semmelweis University, Budapest, Hungary
4. HUN-REN-PTE Clinical Neuroscience MR Research Group, Pécs, Hungary
5. Department of Neurology, Medical School, University of Pécs, Hungary
6. Psychosomatic Outpatient Clinic, Budapest, Hungary
7. National University of Public Services, Budapest, Hungary
8. Institute of Psychology, Faculty of Humanities and Social Sciences, University of Pécs, Hungary
9. Second Department of Medicine and Nephrology-Diabetes Centre, University of Pécs, Hungary
10. Department of Rheumatology and Immunology, Medical School, University of Pécs, Hungary
11. Károli Gáspár University, Budapest, Hungary
12. Brain Imaging Centre, Research Centre for Natural Sciences, Budapest, Hungary
13. Hungarian Centre for Genomics and Bioinformatics, Szentágothai Research Centre, University of Pécs, Hungary
14. Heart and Vascular Centre, Semmelweis University, Budapest, Hungary
15. Department of Genetics, Cell and Immunobiology, Semmelweis University, Budapest, Hungary
16. Department of Laboratory Medicine, Semmelweis University, Budapest, Hungary
17. Department of Internal Medicine 3 –Rheumatology and Clinical Immunology, Friedrich-Alexander University Erlangen Nuremberg, Germany
*Correspondence to nagy.gyorgy2@semmelweis.hu
Disclosure: Kumánovics has reported serving on the Executive Board of the Hungarian Association of Rheumatology. Sütő has reported serving on the Executive Board of the Hungarian Association of Rheumatology and the Hungarian Society of Allergology and Clinical Immunology. Schett has received honoraria from BMS, Cabaletta, Janssen, Kyverna, Miltenyi, and Novartis; and support for attending meetings from Biotest. Gunkl-Tóth has received a Richter Gedeon PhD Scholarship from the Richter Talentum Foundation; and honoraria from Abbvie. Nagy has received consulting fees from Miltenyi, AstraZeneca, and Richter; honoraria from Abbvie, Eli Lilly, Merck Sharp & Dohme, Swedish Orphan Biovitrum, GSK, Pfizer, Swixx, Amgen, UCB, Takeda, Janssen, and AstraZeneca; support for attending meetings from Biotest; is on the Executive Board of the Hungarian Association of Rheumatology; and is a congress committee member for the European Alliance of Associations for Rheumatology. The other authors have declared no conflicts of interest.
Acknowledgements: This research was funded by the Richter Gedeon Talentum Foundation through the “Richter Gedeon PhD Scholarship” awarded to Lilla Gunkl-Tóth, as well as by the National Laboratory for Drug Research and Development (RRF-2.3.1-21-2022-00015), the National Laboratory for Translational Neuroscience (RRF2.3.1-21-2022-00011), HUN-REN, NAP 3.0, OTKA K138046, GINOP-2.3.4-15-2020-00010, and GINOP-2.3.1-20-2020-00001. Project no. TKP-2021EGA-13, TKP2021-EGA-16, and TKP2021-EGA-29 were implemented with support from the National Research, Development and Innovation Fund of Hungary, financed under the TKP-2021-EGA funding scheme and provided by the Ministry of Culture, with the support Innovation of Hungary. Bioinformatics infrastructure was supported by ELIXIR Hungary. György Nagy and Zsuzsanna Helyes contributed equally to this manuscript.
Keywords: Brain imaging, central nervous system (CNS), difficult-to-treat (D2T), neuroinflammation, psychology, rheumatoid athritis (RA).
Despite recent advancements in therapy of rheumatoid arthritis (RA), approximately 5–30% of patients with RA remain symptomatic and are classified as difficult-totreat (D2T).1 Difficult-to-treat RA (D2T RA) is a complex and heterogeneous disease state with several possible contributing factors, including immunological heterogeneity, maladaptive central pain processing, the presence of comorbidities, psychological disturbances, or socioeconomic factors. However, the exact mechanisms driving this disease phenotype remain poorly understood. The authors’ study aimed to investigate the underlying factors behind the D2T condition, potentially revealing the connections between pain and inflammation with a multimodal approach.2
MATERIALS AND METHODS
A total of 31 patients with D2T RA (defined by the 2020 European Alliance of Associations for Rheumatology [EULAR] criteria), 18 patients with non-D2T RA, and 32 healthy controls were included. All participants underwent detailed clinical assessment, psychological evaluation (including in-depth interviews, standardized questionnaires, and the Rorschach test), resting-state functional MRI (fMRI) scans before and after standardized heat pain stimulation, as well as peripheral blood transcriptomic and plasma metabolomic analyses.
RESULTS
Resting-state functional MRI demonstrated significantly reduced intrinsic connectivity of the posterior cingulate cortex in RA, most pronounced in the D2T subgroup. Following acute painful stimulation, posterior cingulate cortex connectivity increased in D2T RA but decreased in non-D2T RA and healthy controls, overall suggesting alterations in the baseline and pain-related connectivity
of the default-mode network in D2T RA. Seed-based analysis of the postcentral gyrus revealed a reduction in connectivity strength across many connections within the somatosensory area, which were significantly altered after pain stimulation in all patients with RA compared to healthy controls. Fractional amplitude of low-frequency fluctuations analysis further identified reduced activity in several brain regions (e.g., lateral occipital cortex, middle frontal gyrus, medial prefrontal cortex, and frontal pole) among patients with RA, with the most significant decreases in D2T RA. Compared to non-D2T RA, D2T patients also exhibited lower fractional amplitude of low-frequency fluctuations in additional brain regions, indicating more complex alterations in pain and somatosensory processing, behavior, and cognitive functions. The authors’ psychological results also strengthened these findings by demonstrating that D2T patients are characterized by maladaptive coping strategies, reduced motivation, negative outlook, and altered cognitive control. Peripheral transcriptomic profiling identified 87 differentially expressed mRNAs (70 downregulated, 17 upregulated) in D2T RA versus non-D2T RA comparisons, many of which could be linked to processes related to neuroinflammation, synaptic plasticity, or neuronal development (e.g., NRG1, S100B, or CDK5), which was also demonstrated by functional enrichment analysis. Metabolomic profiling revealed altered amino acid and sphingolipid metabolism, further supporting the roles of inflammatory and neuronal signaling pathways in the development of D2T RA.
CONCLUSION
Overall, this integrative, multimodal approach identified mechanisms related to the central nervous system that potentially contribute to the development of D2T RA. This disease state can be characterized by altered brain connectivity patterns, characteristic psychological features, and distinct
transcriptomic and metabolomic profiles, which could provide a basis for improving patient stratification, identifying new biomarkers, and developing novel therapeutic strategies targeting central mechanisms. Furthermore, understanding and addressing these central contributors may improve outcomes for patients who are D2T.
References
1. Nagy G et al. EULAR definition of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis. 2021;80:31-5.
2. Gunkl-Tóth L et al. Multimodal analysis revealed altered brain connectivity patterns and neuroinflammatory processes in the background of difficult-to-treat rheumatoid arthritis. Abstract 2684. ACR Convergence, October 24-29, 2025.
The Evolving Digital Landscape of Social Media Among Rheumatology Professionals: Results of the EULAR SoMeR Study Group Survey
A. Sparks,5 Loreto Carmona,6 Taanya Talreja,7 Vikas
Agarwal,8 Carlos Vinicio Caballero-Uribe,9 Dzifa
Dey,10 Christopher Edwards,11 Francis Berenbaum,12 Elena Nikiphorou;13-15 on behalf of the Social Media for Rheumatology (SoMeR) Study Group
1. Department of Rheumatology, Royal Wolverhampton Hospitals NHS Trust, UK
2. School of Infection, Inflammation and Immunology, College of Medicine and Health, University of Birmingham, UK
3. Francis Crick Institute, London, UK
4. Sir H. N. Reliance Foundation Hospital and Research Centre, Mumbai, India
5. Division of Rheumatology, Inflammation, and Immunity, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts, USA
6. Instituto de Salud Musculoesquelética (INMUSC), Madrid, Spain
7. Seth G.S. Medical College and King Edward Memorial Hospital, Mumbai, India
8. Department of Clinical Immunology and Rheumatology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India
9. Department of Medicine, Hospital Universidad del Norte, Barranquilla, Colombia
10. Rheumatology Unit, Department of Medicine and Therapeutics, University of Ghana School of Medical School, College of Health Sciences, Accra, Ghana
11. Department of Rheumatology and NIHR Clinical Research Facility, University Hospital Southampton NHS Foundation Trust, UK
12. Department of Rheumatology, Sorbonne University, INSERM CRSA, AP-HP SaintAntoine hospital, Paris, France
13. Centre for Rheumatic Diseases, King’s College London, UK
14. Rheumatology Department, King's College Hospital, London, UK
15. Centre for Education, King’s College London, UK
*Correspondence to drlatikagupta@gmail.com
Disclosure: The authors have declared no conflicts of interest. The views and opinions expressed are solely those of the author and do not represent or reflect those of any affiliated institution.
Acknowledgements: The authors are grateful to all respondents for completing the questionnaire.
The authors wish to thank all members of the EULAR social media for Rheumatology (SoMeR) study group: APLAR Young Rheumatologists- Ghita Harifi, Chuanhui Xu, Emerging EULAR Network (EMEUNET): Kim Lauper, Manouk de Hooge, Africa League of Associations for Rheumatology (AFLAR): Dzifa Dey, and Pan-American League of Associations for Rheumatology (PANLAR) Joven: Wilson Bautista-Molano, Carlos Vinicio Caballero-Uribe, for their invaluable role in the data collection.
Keywords: Digital communication, digital media, social media (SM), survey.
Social media (SM) has become an indispensable tool in healthcare, providing platforms for networking and education. However, its use presents challenges, including misinformation, professional boundaries, and platform-specific limitations. Building upon the Emerging European Alliance of Associations for Rheumatology (EULAR) Network survey, the authors aimed to characterize SM utilization within rheumatology globally.1
METHODS
The EULAR study group on social media (SoMeR) convened in March 2024 with global, multiprofessional representation. A 30-item survey was designed, validated, translated into six languages, and distributed via mailing lists and SM channels (the Emerging EULAR Network, the Pan-American League of Associations for Rheumatology [PANLAR] Joven, the Africa League of Associations for Rheumatology [AFLAR], and the Asia Pacific League of Associations for Rheumatology [APLAR] Young Rheumatology). Analysis employed the Human Development Index (HDI)
and Internet Freedom Index (IFI) to assess digital divides.
RESULTS
The survey received 840 respondents, among whom 597 used SM (42.2% female; Figure 1A). SM adoption varied by region: Europe (97.3%) versus Asia-Pacific (88.6%). The top
platforms used were YouTube (Google LLC, San Bruno, California, USA), Facebook (Meta Platforms, Menlo Park, California, USA), X (formerly Twitter; X Corp, Bastrop, Texas, USA), Instagram (Meta Platforms, Menlo Park, California, USA), and LinkedIn (Microsoft, Sunnyvale, California, USA; Figure 1B). Lower HDI regions reported more connectivity issues (28.1% versus 16.7%), while higher HDI regions cited legal restrictions (24.4%; Figure 1C).
A) Worldwide distribution of respondents. B) Choice of social media platform by respondents. C) Regional barriers to the use of social media. D) Format for course on social media learning event in medicine.
SM: Social media; SMP: social media platform.
Baidu: Baidu Inc., Beijing, China; Facebook: Meta Platforms, Menlo Park, California, USA; Instagram: Meta Platforms, Menlo Park, California, USA; LinkedIn: Microsoft, Sunnyvale, California, USA; QQ: Tencent Holdings Ltd., Shenzhen, China; QZone: Tencent Holdings Ltd., Shenzhen, China; Reddit: San Francisco, California, USA; Sina Weibo: Sina Corporation, Beijing, China; Snapchat: Santa Monica, California, USA; TikTok: Los Angeles, California, USA; Tumblr: Automattic Inc., San Francisco, California, USA; Twitter (now known as X), X Corp., Bastrop, Texas, USA; YouTube, Google LLC, San Bruno, California, USA.
Figure 1: Social media use among rheumatology professionals.
IFI analysis showed that countries with restricted internet freedom paradoxically reported a higher positive impact from SM (4.04/5.00 versus 3.86/5.00; p<0.01).
Longitudinal analysis (2015–2023) revealed trends toward professional applications and away from networking functions. Respondents increasingly reported feeling overwhelmed by SM content (56.9%), particularly in South America and Africa (73.3% and 70.3%, respectively; p<0.01).
Interest in digital communication was high (83.3%), with webinars being the preferred means of learning (41.1%; Figure 1D).
Following these results, the SoMeR Study Group developed a consensus (“Declaration on the use of Social Media for Rheumatology professionals”) focusing on professional integrity, evidence-based communication, cohesive platforms, patient dignity, and inclusive engagement.2
CONCLUSION
This survey demonstrates SM’s integral role in rheumatology with significant regional variations, calling for targeted interventions addressing connectivity and legal concerns. Through strategic engagement with SM, and while upholding professionalism and scientific integrity, rheumatology’s digital presence can be transformed from isolated efforts to a cohesive global community.
References
1. Gupta L et al. The evolving digital landscape of social media among rheumatology professionals: a global analysis by the EULAR SoMeR study group. Abstract 2185. ACR Convergence, October 24-29, 2025.
2. Gupta L et al; EULAR SoMeR Study Group. Declaration on the use of social media for rheumatology professionals. RMD Open. 2025;11(3):e005917.
Congress Interviews
In these interviews, we speak with Natasha M. Ruth, Chair of the American College of Rheumatology (ACR) Division Directors Committee; and Marcy Bolster, Chair of the ACR Committee on Education. These leaders reflect on the ACR Convergence 2025 and how education is prioritized by the organization. Their perspectives offer a snapshot of how the rheumatology community is strengthening leadership and learning.
Featuring: Natasha M. Ruth and Marcy Bolster
Natasha
M. Ruth Chair, The Division Directors Committee, American College of Rheumatology (ACR); Professor of Pediatrics, Division Chief and Program Director, Medical University of South Carolina, North Charleston, USA
Q1As Chair of the American College of Rheumatology (ACR) Division Directors Committee, what are some key strategic priorities you are bringing forward this year? How do you plan to engage both pediatric and adult rheumatology division directors in advancing them?
This year, our committee is prioritizing several strategic initiatives, with particular emphasis on the Division Director Mentorship and Coaching Program. Considering the significant transformations occurring within the healthcare landscape, we, as leaders within the ACR, are presented with a valuable opportunity to assist new division directors both in adult and pediatric rheumatology through our mentoring program. Furthermore, we are equipped to address the specific needs of both novice and seasoned division directors via our coaching program.
In 2025, this initiative was refined to incorporate coaching and
ad hoc matching, allowing division directors to apply for mentorship or coaching at any point throughout the year. Matches are meticulously curated by a dedicated group of Division Director Committee members to ensure compatibility in skill sets, division types, and personal preferences. Presently, we have established seven active mentorship pairs and one coaching relationship.
Looking ahead, we aspire to broaden the reach of this program to a larger segment of our membership. We aim to provide enhanced resources through direct mentorship and coaching, as well as through our Division Director Toolkit, which includes a wealth of resources on specialized topics pertinent to managing an academic division in both adult and pediatric rheumatology. Additionally, we intend to improve our communication strategies through public relations efforts to ensure that our membership is fully aware of these valuable resources.
Q2 In your view, what have been the major challenges facing academic rheumatology divisions (adult and pediatric) that the Committee should address?
I believe that the most significant challenge we face is the rapidly evolving landscape of healthcare in recent years. We are grappling with issues related to compensation plans, work relative value units, and, crucially, research funding, all while striving to maintain a robust workforce to support our missions. These challenges are further complicated by the diminishing trust in medicine and science. Our aim is to continually support division directors as they navigate these changes by providing them with safe spaces to discuss concerns and share best practices, all with the overarching goal of delivering the highest quality care to our patients.
Q3
How is the ACR working to prepare the next generation of division chiefs and ensure smoother transitions in academic leadership roles?
Certainly, the Mentorship and Coaching Program offers valuable support to division chiefs in this area. Additionally, the Division Directors Committee organizes several Town Hall meetings throughout the year, aimed at educating and facilitating discussions on the most pressing challenges faced by division directors. Our most recent Town Hall topics included: “Budgeting and Contract Negotiations” and “Leading through Uncertain Times.” These Town Halls not only enhance communication among members but also contribute to the cultivation of a stronger community.
Q4 What emerging unmet need or clinical gap in pediatric rheumatology currently drives your own clinical and research interests?
The clinical gap in pediatric rheumatology, which informs my research interests, pertains to the health disparities affecting access to quality care for young women with lupus. These young women are at a pivotal stage in their lives, navigating the challenges of completing high school, applying for college, and developing their individual identities, all while managing a chronic disease through no fault of their own. As a researcher, my primary objective is to identify strategies to improve access to high-quality care. As a clinician, I am dedicated to instilling a sense of hope in these young women regarding their futures. I strive to empower them with the confidence necessary to succeed in their personal and professional lives.
Q5
What upcoming projects or data trends from your recent work with the Childhood Arthritis Rheumatology Research Alliance (CARRA) and the Pediatric Rheumatology Care and Outcomes Improvement Network (PR-COIN) do you think could have the most immediate implications for patients?
The CARRA Registry stands as the cornerstone of CARRA's mission, and the utilization of its extensive data to enhance diagnoses and treatments for our patients is paramount to advancing care for children with rheumatic diseases. Harnessing the potential of the registry will also pave the way for advancements in AI, data
Harnessing the potential of the registry will also pave the way for advancements in AI, data analytics, and biomarker studies in the future
analytics, and biomarker studies in the future. PR-COIN serves as an exceptional platform for institutions across North America to exchange best practices and facilitate improvements in the quality of care provided to our patients. Notably, two of our esteemed pediatric rheumatology faculty at the Medical University of South Carolina (MUSC), North Charleston, South Carolina, USA, in collaboration with Children's Healthcare of Atlanta (CHOA) and Levine Children’s Hospital in Charlotte, North Carolina, USA, are diligently working to improve the mental health of our patients by implementing a comprehensive change package focused on depression screening for those with rheumatic diseases.
Q6
Physician well-being is a significant focus in your role at MUSC. What institutional or cultural shifts are most needed to sustain fulfilment and prevent burnout, and when can this be achieved?
This year at the ACR Convergence, I had the privilege of attending Tait Schanfelt’s [Stanford Medicine, California, USA] presentation on the institutional changes required to foster a culture of wellness. As a pioneer in wellness
transformation within the healthcare sector, he eloquently delineates nine organizational strategies aimed at enhancing engagement and mitigating burnout. These strategies encompass: acknowledging and assessing the problem, leveraging the influence of leadership, developing and implementing targeted interventions, cultivating a sense of community within the workplace, wisely utilizing rewards and incentives, aligning organizational values and strengthening culture, promoting flexibility and work-life integration, providing resources to enhance resilience and selfcare, and facilitating and funding organizational science. At MUSC, I have witnessed a remarkable cultural transformation over the past 5 years. We have established an integrated center of excellence dedicated to advancing wellness within the healthcare system and increasing support for interventions that lead to professional fulfillment and a thriving workforce. I had the opportunity to contribute to a Duke Endowment Grant, a collaborative
initiative with the South Carolina Hospital Foundation, focusing on this important mission. My specific area of the grant concentrated on faculty development and enhancing mentorship. I piloted an automated mentorship software within our department, which is increasingly vital as our healthcare system expands and our workforce becomes more geographically dispersed.
Q7
Looking ahead 5–10 years, what do you most hope will change in pediatric rheumatology and what role do you personally hope to play in driving that change?
In the next 5–10 years, I hope to enhance our understanding of the diseases that afflict our patients, supported by the steadfast commitment of the outstanding science that is coming out of research organizations within our pediatric rheumatology community, such as the ACR Rheumatology Research Foundation, CARRA, and the Pediatric Rheumatology Collaborative Study Group
(PRCSG), along with the continued support of our international research partners. These entities play a crucial role in advancing the field of pediatric rheumatology. Furthermore, I hope to witness a new generation of aspiring pediatric rheumatologists drawn to our specialty. I trust that my efforts in medical education and faculty development will contribute meaningfully to this objective. I envision that the intrinsic allure of our field, the deep connections we cultivate with our patients and their families, and the camaraderie we experience among colleagues will inspire these young individuals to perceive our discipline as a pathway to a life imbued with purpose and fulfillment. I firmly believe that embracing a life driven by passion and purpose is fundamental to fostering genuine wellness.
Marcy Bolster
Chair of the American College of Rheumatology (ACR) Committee on Education; Professor of Medicine, Harvard Medical School, Boston, Massachusetts; Director of the Rheumatology Fellowship Training Program, Massachusetts General Hospital (MGH), Boston, USA
As Chair of the American College of Rheumatology (ACR)’s Committee on Education, what are the committee’s most pressing strategic priorities?
Our priorities are to provide cutting-edge research findings, enrich clinical practice, and educate our educators as we bring scientists, clinicians, educators, advanced practice providers, allied health professionals, trainees, and students together to learn and to connect.
Q2 You’ve previously said the ACR’s Committee on Education lies at the intersection of many other committees and initiatives. How do you plan to enhance connectivity among members beyond the ACR Convergence?
This is such an important question! The connectivity between attendees at Convergence is energizing. It is one of our goals to continue the education connections throughout the year. We have scheduled webinars to bring curated and impactful sessions from Convergence to be held shortly after Convergence through the first quarter of 2026. There are a limited number of these
I must admit that I am not surprised by educational gaps. Rheumatology is a rapidly evolving field
sessions to offer, and we anticipate that the curated sessions will be of high interest to those who were not able to attend Convergence, as well as to attendees who may have missed these sessions. The webinars will include live question and answer with the sessions’ speakers.
Q3 Given your prior leadership on training, workforce, and milestones, what key educational gaps in rheumatology continue to surprise you?
I must admit that I am not surprised by educational gaps. Rheumatology is a rapidly evolving field. We continue to learn through scientific discoveries being made across many disciplines, including oncology, nephrology, pulmonology, and others. The science is exploding to help improve our knowledge in disease pathogenesis, disease monitoring, and management options. I do not see that there are educational gaps, but rather that this is an exciting time to be in rheumatology.
Q4
What do you consider the most important leadership qualities for rheumatologists who aspire to move beyond clinical roles into institutional or professional society leadership, such as with the ACR?
A willingness to step forward and participate. Be a good listener. Create engagement so others want to and benefit from participation. Empower others to participate, to
take responsibility, to grow, and to lead. Foster excellence in those around you.
Q5
Looking ahead to the next ACR Convergence and beyond, what would you like the broader rheumatology community to remember about the value of lifelong education and engagement with the ACR?
ACR Convergence is where rheumatology meets! It offers highly impactful scientific content, a superb environment for meeting people who share your interests, the opportunity to network with others, and connectivity with colleagues from the US and from around the world. Convergence is a high-energy environment where people gather to learn, to connect, and to share their common interest in rheumatology.
Interview
Susan Manzi, Professor of Medicine and Chair of the Medicine Institute at Allegheny Health Network, Pittsburgh, Pennsylvania; and Director for the Lupus Foundation of America, USA, spoke to AMJ about her pioneering work in lupus research, the next frontiers in this field, and how we can expect this to impact patient outcomes.
Susan Manzi
Professor of Medicine and Chair, Medicine Institute, Allegheny Health Network, Pittsburgh, Pennsylvania, USA; Medical Director, Lupus Foundation of America
Q1Often termed “the great mimicker,” lupus presents as many things, including fatigue and rashes, to severe organ impairment. What strategies can clinicians employ to enhance early and accurate diagnosis?
I am a big believer in empowering the public with enough information to be their own advocates in their own healthcare
I always say that you have to think of lupus to diagnose it. A few facts that may help: lupus tends to impact young women (ages 15–45 years), and 90% of those living with lupus are women. Keeping in mind that it can impact men, older individuals, and children. It is four times more common in people of color (Black, Hispanic, and Native American populations). Common features include profound fatigue, rashes (often made worse with sun exposure), hair loss, joint pain (often with swelling and stiffness in the morning), chest pain due to fluid that develops around the heart and lungs (pericarditis and pleuritis), seizures and premature strokes, and heart attacks (especially in young people with no traditional risk factors). They also include kidney disease, causing potential kidney failure requiring dialysis or kidney transplant. Many
patients may also experience changes in their blood counts, low white blood cells, red blood cells, and platelets. Although some patients with lupus can have mild symptoms, many have lifethreatening conditions. Because lupus can present in so many different ways, the diagnosis can be challenging.
Q2
Your work on cell-bound complement activation products (CB-CAPs) has been trailblazing in this field. How do you envision these biomarkers transforming clinical practice in lupus diagnosis and monitoring?
One of the major issues with lupus is accurate and timely diagnosis. The sooner we can identify and treat the disease, the less likely there will be serious complications. Since lupus can go undiagnosed for years, having improved diagnostic tests to increase the likelihood of identifying those with lupus earlier is essential. Our research program has focused on developing new diagnostic tests for lupus and other autoimmune diseases. We discovered that people with lupus
have higher levels of CB-CAPs (proteins that bind to blood cells in the circulation), and that they can improve the diagnosis of lupus by nearly 33%. These tests have been licensed and commercialized by Exagen, Inc., a company in California, USA, and are now available to physicians across the country. These tests may also help physicians monitor the disease once the diagnosis is made. Since lupus can flare at times with increased periods of inflammation and activity, close monitoring to prevent or treat the flares becomes important. Our research team continues to develop new and improved blood tests to diagnose and monitor lupus.
Q3
What steps can healthcare providers take to improve awareness and care for male patients with lupus, given males may experience more severe manifestations?
Recognizing that men can get lupus is the first step. Even though most are women, when men do develop lupus, the disease tends to be more severe, with more central nervous system disease and kidney disease. We also see that men of color are more commonly impacted, but all men are at risk, particularly young men.
Q4 The Addressing Lupus Pillars for Health Advancement (ALPHA) project identified key barriers in lupus care. How can clinicians integrate the findings from this initiative to enhance patient outcomes?
Educating providers, those that deliver healthcare, doctors, advanced practice providers (APPs), nurses and patients, those seeking healthcare about lupus. You have to think of lupus to diagnose it, and having information about common features allows both the providers and the patients to
We have had more FDA-approved treatments for lupus in the past decade than we had for 60 years before that… and there are more in the pipeline
ask the question: “Could this be lupus?” I am a big believer in empowering the public with enough information to be their own advocates in their own healthcare. Ask questions and be informed.
Q5
With the approval of therapies like anifrolumab and belimumab, what are the most significant takeaways from recent clinical trials? How can clinicians integrate these into their practice, and how will these directly impact patient outcomes?
This is one of the most exciting times for those living with lupus. We have had more FDA-approved treatments for lupus in the past decade than we had for 60 years before that… and there are more in the pipeline. These new agents are also designed specifically for lupus and targeted to the immune mechanisms that are most relevant to lupus.
Q6
As Medical Director for the Lupus Foundation of America (LFA), one of your key roles has been in policy advocacy. What legislative initiatives should healthcare professionals be aware of to better support patients with lupus?
I encourage everyone to lean in and get involved with advocacy. Now more than ever we need the voices of those impacted by lupus and those of us that care for people living with lupus. One of our top priorities is supporting lupus research at the federal level. The LFA had successfully advocated for research funding earmarked for lupus through the Department of Defense years ago, which amounted to 10 million USD a year. This was a major breakthrough.
With more and more women joining the military, the number struggling with lupus had risen. A number of high-impact research initiatives were supported through this grant mechanism until this year, when the program was put on hold. This and other funding cuts threaten to slow down the pipeline of new treatments or steps toward a cure for lupus. We also need to advocate for access to treatment. We may have new biologic therapies that are highly effective, but many people cannot access or afford them. We are to change that.
We may have new biologic therapies that are highly effective, but many people cannot access or afford them
Anti-Neutrophil Cytoplasmic AntibodyAssociated Vasculitis Manifesting Solely as Bilateral Toe Cyanosis: Case Report
Authors: Melika Motamedi,1 Jadin Chahade,2 Robert Gniadecki,1 *Elaine Yacyshyn3
1. Division of Dermatology, University of Alberta, Canada
2. Faculty of Medicine and Dentistry, University of Alberta, Canada
3. Division of Rheumatology, University of Alberta, Canada
*Correspondence to eyacyshyn@ualberta.ca
Disclosure: The authors have declared no conflicts of interest.
Received: 01.28.25
Accepted: 10.7.25
Keywords: Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis, blue toe syndrome (BTS) cyanosis, proteinase 3 (PR3) autoantibody.
Introduction: Blue toe syndrome (BTS) manifests as a sudden onset of blue/violaceous discoloration on the toe that is often associated with pain. The etiology of this condition is multifactorial, but it is distinguished by its occurrence in the absence of trauma or generalized cyanosis. The differential diagnosis of BTS can include factors such as vascular obstruction, autoimmune conditions, hyperviscosity syndromes, infections, drug-induced occurrences, and vasospasm. The authors describe a case of a 71-year-old female who presented with a 2-year history of bilateral toe cyanosis and was found to have positive c-anti-neutrophil cytoplasmic antibody (ANCA) with high titer proteinase 3 (PR3; 735 mean fluorescence unit), Type III cryoglobulinemia, and positive cryofibrinogen. She had no other symptoms associated with ANCA vasculitis. Further rheumatologic workup was unremarkable, including investigations for atheroembolic disease and infections. The patient was prescribed azathioprine with near complete resolution of symptoms within 1 year.
Methods/Results: To further understand this condition, the authors performed a literature review of PubMed/Scopus/Medline using the following combination of keywords: “vasculitis” AND (“Blue” OR “purple” OR “cyanosis” OR “necrotic” AND “toe”). This search yielded only one other case of this manifestation.
Conclusion: In this report, the authors identify, to the best of their knowledge, the first documented case of PR3-ANCA vasculitis presenting with BTS as the sole and primary manifestation.
Key Points
1. The authors aim to raise awareness in the medical community about atypical presentations of ANCA-associated vasculitides, and in this case, how it can present solely as Blue Toe Syndrome.
2. The authors presented a case of a 71-year-old female with the first documented case of PR3-ANCA vasculitis presenting with Blue Toe Syndrome as the sole and primary manifestation.
3. The report highlights the importance of a careful history and physical examination, in addition to discriminatory laboratory tests as the differential diagnosis is quite broad but can present with a very similar clinical picture.
INTRODUCTION
Blue toe syndrome (BTS) presents as a sudden development of localized blue or purple discoloration of one or more toes, typically associated with tenderness.1 The phenomenon arises from diverse underlying causes and is distinguished from generalized cyanosis or trauma-related change.2 Other conditions resulting in generalized cyanosis can lead to this clinical presentation but, importantly, pedal pulses are preserved.3 When a patient presents with blue/purple toes, in keeping with the diagnosis of BTS, it is important for clinicians to perform a careful history and physical examination in addition to discriminatory laboratory tests, as the differential diagnosis is quite broad but can present with a very similar clinical picture. The differential diagnosis for BTS can be thought to encompass multiple different etiologies that include autoimmune conditions.2,4 The authors describe what appears to be the first reported occurrence of BTS serving as both the initial and exclusive manifestation of the leukocyte protein proteinase 3 (PR3)-anti-neutrophil cytoplasmic antibody(ANCA)-associated vasculitis. While ANCA-associated vasculitis often presents with palpable purpura, ulcers, and splinter hemorrhages, BTS is only occasionally part of the clinical presentation.5
CASE PRESENTATION
A 71-year-old East-Asian female presented with a 2-year history of constant bilateral cyanosis of all toes (Figure 1A-B), not
influenced by temperature changes. Her medical history was significant for deep venous thrombosis (unprovoked, left leg), dyslipidemia, hypertension, osteoporosis, baker’s cysts, osteoarthritis, and rotator cuff tendinopathy. Her family history was noncontributory. She reported minimal alcohol exposure and no history of smoking or recreational drug use. She reported a burning sensation and one episode of blistering on the right second toe (Figure 1C). These symptoms preceded the COVID-19 pandemic. She denied finger involvement, erythromelalgia, or other rashes. There were no signs of ANCA-associated vasculitis, including no constitutional symptoms, sinusitis, hemoptysis/ cough, palpable purpura, hematuria, frothy urine, or neurologic symptoms. She had tried acetylsalicylic acid 81 mg without improvement and nifedipine 30 mg with mild relief before seeking rheumatological evaluation.
Her laboratory investigations were remarkable for positive c-ANCA with a high titer PR3 of 735 mean fluorescence unit, confirmed by two separate tests (assessed via multiplex bead immunoassay). Other rheumatologic investigations, including antinuclear antibody, extractable nuclear antigens, rheumatoid factor (tested multiple times), anti-cyclic citrullinated peptide, anti-double stranded DNA, scleroderma panel, and antiphospholipid antibodies, were negative. There was no evidence of monoclonal protein on protein electrophoresis, and quantitative Ig measurements showed a low IgM level. The complement system was not evaluated. No abnormalities were noted
Figure 1: Blue toe syndrome in a patient with proteinase 3-anti-neutrophil cytoplasmic antibody vasculitis.
A B C
This figure illustrates blue toe syndrome in a patient with PR3-ANCA vasculitis, as described in the case report. (A) and (B) depict bilateral toe cyanosis, while (C) shows the blistering episode on the right second toe. All photos were taken before initiating treatment with azathioprine.
on a chest CT; specifically, there was no evidence of interstitial lung disease, and no mediastinal, hilar, or neck lymphadenopathy. Ophthalmological assessment ruled out uveitis. General chemistry parameters, including creatinine, urinalysis, C-reactive protein, creatine kinase, and coagulation profile, were within normal limits.
She was found to have Type III cryoglobulinemia and positive cryofibrinogen. Both were weakly positive, with a cryocrit <5%. Quantitative measurement in g/L was not provided by the laboratory. Hematology was consulted for a full workup of her positive cryoglobulins, which were all unremarkable. The patient denied a skin biopsy. There was no underlying connective tissue disease and no hepatitis or HIV infection. She did not have an assessment of her complement levels given the absence of clinical signs or laboratory findings indicative of underlying connective tissue disease
or cryoglobulinemic vasculitis. The patient declined a bone marrow biopsy, although she did have a low pre-test probability of underlying hematologic malignancy.
Although her disease was limited to her toes, she was eventually started on azathioprine due to concerns about developing systemic features. She was seen in follow-up after a year of being on azathioprine 75 mg with a significant decrease in cyanosis of her toes and a decrease in PR3 titer to 3.7. She was only experiencing intermittent cyanosis of the right second toe.
METHODS
For determination of prior case reports, the authors performed a review of Medline/ PubMed/Scopus using the following combination of keywords: “vasculitis”
AND (“Blue” OR “purple” OR “cyanosis” OR “necrotic” AND “toe”). The search included studies published from the database inception to December 2023. The authors also searched for other cases by reviewing the references of relevant papers. Cases were reviewed and the ones that had cyanosis of the toes, in addition to other vasculitic manifestations, were excluded. Cases with blue toes secondary to connective tissue disease, COVID-related cases, druginduced cases, and cases with ischemiarelated to arterial disease were excluded.
RESULTS
A total of 60 results were retrieved and, after removing duplicates, 25 unique results remained for the initial title and abstract screening. Of the 25 studies screened, six reports described vasculitis blue toe case reports. In these cases, two studies described BTS as the initial, but not the sole, manifestation of PR3-ANCA vasculitis.
DISCUSSION
BTS can result from numerous etiologies that produce nearly identical clinical features; however, the authors’ report describes what they believe to be the first instance of PR3-ANCA-associated vasculitis presenting exclusively with BTS and no extracutaneous manifestations. Two other published cases have described BTS as the initial sign of PR3-ANCA vasculitis; however, these instances differed as the patients progressed to have other manifestations such as mononeuritis multiplex, renal impairment, and hemorrhagic sinusitis.6,7 In contrast, the authors’ patient’s presentation remained confined to her toes, without involvement of other organs, highlighting the unusual and noteworthy nature of this case. The differential diagnosis for BTS encompasses a wide range of vascular and inflammatory conditions, including embolic, thrombotic, vasospastic, autoimmune, and drug-induced
etiologies. The authors’ differential diagnosis was guided by a systematic framework for evaluating BTS.2 In this case, the patient did have a history of a previous deep vein thrombosis, as well as risk factors such as dyslipidemia and hypertension. However, several features argued against an embolic or occlusive process: the patient’s peripheral pulses were intact, vascular imaging revealed no evidence of an occlusive disease such as atheroembolism, and there was no history of vascular procedures or endocarditis. Additionally, the patient’s lifelong nonsmoking status made thromboangiitis obliterans an unlikely diagnosis. Although the patient also had positive cryoglobulins, the authors were not suspicious of this being the culprit as these findings were not consistent with clinically significant cryoglobulinemic vasculitis. Mixed cryoglobulinemia typically correlates with temperature-dependent symptom fluctuations and elevated rheumatoid factor, neither of which were part of this clinical presentation.8 This aligns with current literature cautioning against labeling patients with low-level cryoglobulin positivity as having true cryoglobulinemic disease.9,10
After a 2-year history of constant bilateral cyanosis of all toes, the patient was started on azathioprine. To date, the patient still has no systemic features and only experiences intermittent cyanosis of the right second toe. The presence of a high-titer PR3-ANCA, confirmed on two separate occasions, in conjunction with the absence of secondary causes and marked improvement on azathioprine therapy, further corroborates the diagnosis of PR3-ANCA–associated vasculitis presenting solely as BTS.
PATIENT PERSPECTIVE
Dealing with persistent blue discoloration in my toes for 2 years has been frustrating. The burning sensation and blistering were alarming, especially since they started long before the pandemic. Despite trying medications like aspirin and nifedipine,
I found little relief. Seeking help from Dr Yacyshyn was a turning point for me.
Starting treatment with azathioprine brought me hope. After a year, I noticed significant improvement, with much less discoloration. While I still experience occasional symptoms, I’m grateful for the progress I’ve made. I’m also thankful that my experience is being shared to inform other clinicians, as it comforts me to know my journey might help others facing similar challenges.
References
1. Brown PJ et al. The purple digit: an algorithmic approach to diagnosis. Am J Clin Dermatol. 2010;11(2):103-16.
2. Motamedi M et al. A review and approach to the diagnosis of blue toe syndrome. Discov Med. 2025;DOI:10.1007/s44337025-00275-z.
3. Karmody AM. “Blue toe” syndrome: an indication for limb salvage surgery. Arch Surg. 1976;111(11):1263-8.
CONCLUSION
BTS is a cutaneous manifestation with a broad list of differential diagnoses, including vasculitis. Before the diagnosis can be made, a clinician should be suspicious of an underlying malignancy, infection, and conditions that predispose patients to an embolus or thrombus, as well as factors such as druginduced BTS. The patient case reported here also encourages clinicians to consider rare presentations of known causes of BTS.
4. O'Keeffe ST et al. Blue toe syndrome: causes and management. Arch Intern Med. 1992;152(11):2197-202.
5. Marzano AV. Cutaneous manifestations of ANCA-associated small vessels vasculitis. Clin Rev Allergy Immunol. 2017;53(3):428-38.
6. Marinchev L et al. Blue toe syndrome as the initial manifestation of ANCAassociated vasculitis. Open Med. 2013;8(5):577-9.
7. Bégon E et al. Isolated blue toe syndrome as the initial sign of Wegener granulomatosis. Am J Med. 2010;123(7):e7-8.
8. Muchtar E et al. How I treat cryoglobulinemia. Blood. 2017;129(3):289-98.
9. Dispenzieri A. Symptomatic cryoglobulinemia. Curr Treat Options Oncol. 2000;1(2):105-18.
10. Canadian Rheumatology Association. Canadian Rheumatology Association Annual Scientific Meeting. J Rheumatol. 2025;52(Suppl 2):8–124.