Prevalenceandassociationofmetabolicsyndromewith C-reactiveproteinin peopleattendingatertiarycarehospitalofNorthBengal— Debjani Laha, Ranjan Pal, Anupam Gupta, P P Pal, G Ghoshal, D S Mondal 13
Status of cold chain monitoring in primary health centres of Bangalore urban — north
— Jyothi Jadhav, Selvi Thangaraj, Thilak S A, Ranganath T S............................................................17
MyWholeheartedthankstoallIMAfraternityforelectingmeasEditorofJIMA2017. I am cent percent confident to do justice to my post. I will not only focused on evidence based excellent articles but also try to make this journal one of the best in the world (Pubmedindexwithgoodimpactfactor).FirstissueofJIMAwillbefocusedonMaternal Death.
Whymother’sdie?Itisaveryimportantissuetoallconcerned.Whetheritisduetofor delays- to seek treatment, or to reach Hospital or to start treatment by doctors or lack of transportationduetobadroadcondition.
Women are dying during their long journey of 280 days during pregnancy period without antenatal check up, investigation & treatment. Every minute of everyday a womandiesas aresultof pregnancyor childbirthsomewhereintheworld maybedueto –(a)Teenage pregnancy, physically not fit to deliver the baby leading to obstructed labor, sepsis, eclampsia and anemia, etc. (b) Due to want of blood or drug. (c) Elderly women from low socioeconomicresourcesgoingforillegalabortion.
SuchtragicpicturestillexistsinmanystatesofIndiaexcludingKerala,Mizoramandinothertwoorthree states. Maternal death reviews are not done in many states till date. No CME was held on MMR in many places. Government (State & Central) in good faith started National Rural Health Mission (NRHM) by spendingalotoffundbutnopositiveresulttopreventMMRsofar. MDG(Goal5)-Mother:cutbackbythree quarters the number of women who die when they are having babies has failed to fulfill its goal. SDG is now started to implement his own vision. The Sustainable Development Goals (SDGs), officially known as transforming our world: the 2030 Agenda for Sustainable Development is a set of seventeen inspirational “GlobalGoals”with169targetsbetweenthem.
(1) 1stpriority- Preventionofteenagepregnancy(5A)BY(a)Aware–nottomarrybefore20years,(b)Avoid pregnancy before 20 years if married early by contraception, (c) Awake – if she come with pregnancyadequate to prevent maternal complications, (d)Audit- if she dies during pregnancy, (e)Assurance–for education,employmentandhealthcareafterdelivery.
(5) Facility based maternal Death Review Format would be filled up The Medical officer (MO) who had treatedthemotherandwasindutyatthetimeofmaternalDeath.
Disclaimer
The information and opinions presented in the Journal reflect the views of the authors and not of the Journal or its Editorial Board or the Publisher Publicationdoesnotconstituteendorsementbythejournal. JIMA assumes no responsibility for the authenticity or reliability of any product, equipment, gadget or any claim by medical establishments/institutions/manufacturersoranytrainingprogrammeintheformofadvertisementsappearinginJIMAandalsodoesnotendorse orgiveanyguaranteetosuchproductsortrainingprogrammeorpromoteanysuchthingorclaimsmadesoafter — Hony Editor
4 5
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
Review Article
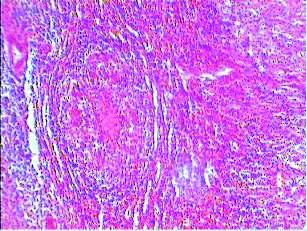
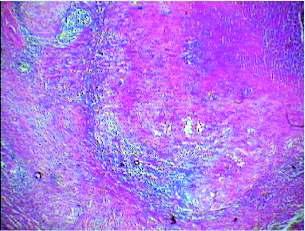
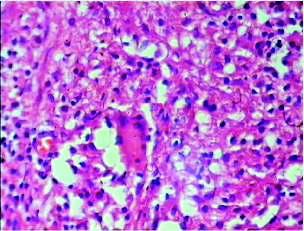
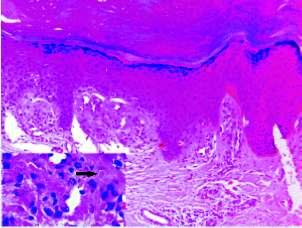
Cell
mediated immune response in children suffering from tuberculosis
1
Gaytri Koley , K C Koley
2
Tuberculosis is a serious problem in children. The objective of the study was to study the cell mediated immune response in childhood tuberculosis and its' role in prognosis if any. This was a cohort study,undertakenamong40childrenvisitingoutpatientdepartmentandagedbetween2to5yearswhowere diagnosed as tuberculosis in a tertiary care hospital setting in Delhi. Mantoux test which was used as diagnostic criteria was also taken as a marker of intact cell mediated immune (CMI). Mantoux positivity irrespectiveofsizewasthefirstin-vivoindicatorofCMI.Cytokinesreleasedfromlymphocytewereassessed in-vitro. Peripheral venous blood samples were taken and mononuclear cells were harvested. lymphocyte suspensions were prepared and lymphocyte proliferation was done in vitro after BCG stimulation. The cytokines released from these were assayed as per the genzime protocol provided with the kit. Since CMI is protectiveintuberculosisclinicalcorrelationandoutcomeofpatientsattheendof6monthswasdonetosee thecorrelationbetweenthe2testsdoneasanindicatorofCMIandtheclinicalprofileofthepatientandtosee if these tests could be used to prognosticate the case. The study revealed that children with only pulmonary tuberculosis that is a restricted disease showed a higher incidence of Mantoux positivity, as compared to children with disseminated disease. They also responded by showing a Th1 pattern of cytokine release. These children also responded well to therapy and had excellent cure rates. This shows that Mantoux test besidesbeingagooddiagnostictestalongwithcytokineresponsecanbeusedtopredictabetterprognosis inpulmonarytuberculosisinpreschoolgoingchildren.
Tuberculosis (TB) is a serious problem in children.
Globally about 2 billion people are infected with
Mycobacterium tuberculosis, 8 to 10 million of them develop active disease and 2 million die from TB 1 every year The ease with which the pathological process spreads and difficulties with disease confinement are the most characteristic features of tuberculosis in children. Thesearemainlyduetoimmaturityofbothrespiratoryand immunesystems.ProtectiveimmunityintuberculosisisT 2 cell mediated and this study was done to see a correlation between T cell response in the form of Mantoux test, cytokinesecretion,theclinicalseverityandtheoutcomeof the disease. Mantoux test is an established test in diagnosing childhood tuberculosis but its exact role in 1 prognosticatingacasehasnotbeenestablished
1MD (Ped), Associate Professor, Department of Pediatrics, PIMS MedicalCollegeHospital,Jalandhar144006
2MD (Med), Senior Adviser Department of Medicine, Military Hospital,JalandharCantt144005
MATERIALAND METHOD
This study was conducted at Army Hospital, New Delhi. Forty children aged 2-5 years diagnosed as pulmonary tuberculosis/ extra pulmonary tuberculosis/ disseminated tuberculosis visiting the paediatric outpatient department over 1 year comprised the material forthisstudy
In the absence of a gold standard for diagnosis of tuberculosis in children, the study children were diagnosed based in criteria for diagnosis of tuberculosis 3 as per Seth V and in accordance with other studies and subsequently they also satisfied the latest IAP guidelines aspertheconsensusstatementonchildhoodtuberculosis These were based on (i) essential criteria of symptoms, mainly low grade fever weight loss, and persistent cough ofmorethan2weeks(ii)animportantcriteriaofapositive chest skiagram /other site scanning (iii) presence of acidfast bacilli (AFB) in gastric aspirate/ sputum / any other tissue fluid (iv) contact with an adult TB index case (v) presence of some other supportive criteria. A thorough clinical examination was done to find the extent of the
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017 9
Thetestchildrenweredividedinto2groupsgroupA(n = 31) consisted of children with only pulmonary tuberculosis and group B (n = 9) were children with extra pulmonary as well as disseminated tuberculosis. Four of thesehadTBmeningitisand5werecasesofdisseminated TB. All the children were in category 1 as per IAP 5guidelines These children were treated with standard antituberculosis therapy (ATT) (EHRZ for 2 months followed by HR for 4 months). Their clinical profile was monitored throughout the duration of treatment and compared to their laboratory profile. Cure was declared whenthechildrenafter6monthsoftreatmentweretotally symptom free and had gained their weight, regained their appetite, the skiagrams / CT scans had resolved and there wasresolutionofallsymptomspertainingtothedisease.
To study the immune profile, two tests were done, (i) Mantoux test which is an indicator of delayed hypersensitivity, a type of CMI and ii) the cell mediated immune response in-vitro in the form of cytokines secreted by lymphocyte from the harvested mononuclear cells.Thesetestsweredonebeforestartingtreatment.The CMI was compared to the clinical profile the outcome of thediseaseattheendof6months.
Mantoux test was done on the volar aspect of left forearm using PPD of 2TU strength. The result was read between 48 hours to 72 hrs and interpreted as positive or negative. Induration more than 10 mm was taken as positive. This cut-off size was in accordance with various 5,6 otherstudies .
Ten ml of heparinised blood was collected and mononuclear cells were separated using ficoll hypaque gradient centrifugation technique. Lymphocyte cell suspensionswereprepared.BCGwasusedtostimulatethe suspension. All the samples were cultured for 3 days at 37°C. Cytokines, IFN - , IL-2 and IL-4 were assayed as pergenzimeprotocolprovidedwiththekit. The difference between the groups with continuous variables was statistically tested using Student’sttest.Phenotypicdistributions between the study groups were compared using the Chi-square test. Two tailed P values <0.05 were consideredstatisticallysignificant. Informed consent of parents was taken. The study was approved by the instituteethicscommittee.
OBSERVATIONS
Table 1 shows that 28 children in groupAareMantouxpositiveandonly3 are Mantoux negative. This shows that in restricted pulmonary disease Mantoux positivity in this study
8 diseaseandany
associatedpathology. is 88%. In group B only 3 out of 9 are Mantoux positive whereas6areMantouxnegative.Thisshowsthatinsevere disseminateddiseaseonly33%areMantouxpositive.
A significant pattern of cytokine secretion from these lymphocyteswasseen.Asseenin(Table2),amajority(26 out of 40 cases) showed increased levels of IFN – (mean level 34 ng/ml) and IL-2 (mean level 26 ng/ml). This is a Th1 response in children Five cases showed a Th2 response with predominantly IL-4 secretion (mean level 8 20 ng/ml) A third group comprising 9 out of 40 patients responded to BCG stimulation by producing all three cytokines IFN- , IL-2 and IL-4. Such a response is describedasTh0oramixedresponseandhasbeenseenin 7,8 otherstudies
Clinical correlation of the cytokine response with the clinical profile shows that of 26/40 cases responding with Th1 pattern of cytokines all had only pulmonary involvement. The next group of 5 cases which responded by producing mainly IL-4 (Th2) were all cases of disseminateddisease.Finallythethirdgroupof9children, which responded by producing all the 3 cytokines namely IFN-?,IL-2andIL-4(Th0)had4childrenofdisseminated tuberculosisand5childrenofpulmonarytuberculosis.
Table 1 — Showing Correlation between Incident of Mantoux Positivity and type of Disease
Group Noofmantouxtest Noofmantouxtest TotalNo positivecases negative test ofcases
GroupA 28 03 31
(Pulmonarydisease)
GroupB 03 06 09
(Extrapulmonary/ disseminateddisease)
Total 11 29 40
Table 2 — Showing Clinical Correlation between Cytokines Response and the Clinical Profile
Typeofdisease Group Th1 Th2 Th0 Cured
DISCUSSION
The study of cellular immune response of T cells in patients with tuberculosis is important for the understanding of the protective and pathological mechanisms in tuberculosis. A clinical correlation of severity and outcome of the disease with CMI response helps us to understand the significance of CMI in TB as also predicts the outcome of the disease on the basis of these tests. This study was done to see the correlation of Mantouxtestwith (i)thetypeofdisease (ii)thecytokine secretion by these patients as another indicator of T cell response (iii) the outcome of the disease in children aged 2to5yearswhichisaveryvulnerablepopulation.
Mantoux test is a widely used diagnostic test in children for diagnosing tuberculosis.The basis of this test is a delayed hypersensitivity reaction which is a cell mediated immune response. Here Mantoux test was used asanindicatorofanintactCMI. Thecytokineprofilewas another test to see the in-vitro response in the study group anditscorrelationtotheclinicalpatternofthediseaseand theultimateresponseintermsofcureinthesechildren.
About88%ofgroupApatientswereMantouxpositive showing that in children with a limited disease, delayed hypersensitivity reaction and CMI were unimpaired. Other various studies have also cited 70% to 91% Mantoux positivity in non-immunocompromised TB 4patients
Asignificant pattern of cytokine secretion from these lymphocytes was seen. In 84% of groupApatients that is patients with only pulmonary involvement, the cytokine assayedwereIFN- andIL-2.ThisTh1responsehasbeen shown to be the protective immune response and is 9,10 ultimately responsible for cure Five cases which showedaTh2responsewithpredominantlyIL-4secretion were all cases from group B with disseminated TB and 9,10 comprised 55% of that group .Athird group of 9 out of 40 patients responded to BCG stimulation by producing all three cytokines IFN- , IL-2 and IL-4. Such a response isdescribedasTh0oramixedresponseandhasbeenseen 7,8 in other studies .This response was seen in16% of group Aand45%ofGroupB.
Correlating the clinical severity with the Mantoux test and cytokine release reveals a very significant pattern. In group A that is patients with only pulmonary disease Mantouxpositivityis88%,Th1patternofcytokinerelease isseenin84%andclinicalcureisseenin100%signifying a very strong correlation between limited disease, intact CMIwithaTh1patternofcytokinereleaseandoutcomeof 9,10 thedisease .
In group B Mantoux positivity is 33%, Th2 pattern is seen in 55% cases, Th0 in 45% cases and clinical cure is seenin50%cases.Theaboveresultsareinagreementwith various other studies which showed that protective
immunity in tuberculosis is Th1 mediated and Th2 response is associated with increased inflammatory 10,11 response and tissue destruction This again shows that disseminated /advanced disease is associated with an impaired CMI On further clinical correlation it is seen that in group B 33% patints show a good CMI and these same patients achieve cure after 6 months. This very significantfindingtellsusthatthoughCMIisimpairedina large majority in severe tuberculosis, it is associated with 12,13 clinical cure and a good outcome can be predicted when it is intact. Hence though an impaired T cell response is seen in severe disease and is generally associated with pooreroutcomesbut50%ofthesechildrendoachievecure and these are the children who still have a fairly large amountofIFN- secretionalongwithIL-4secretion. Based on this study, prognosis of a case can be predicted. Children showing aTh1 response and Mantoux 10,11 positivityhaveabetterprognosis
REFERENCES
1 World Health Organisation — Tuberculosis Facts. Geneva: WHO,2006.
2 Banaszkiewicz A, Feleszko W — Immune mechanisms in children with tuberculosis. Pol Merkur Lekarski 2003; 15: 203-7.
4 Rigouts L — Clinical practice: diagnosis of childhood tuberculosis. Eur J Pediatr 2009;168:1285-90.
5 Amdekar YK, Singh V, Kabra SK — Consensus statement onchildhoodtuberculosis. Indian Pediatr 2010; 47:41-55.
6 Alseda M, Godoy P — Tuberculin reaction size in tuberculosis patient contacts. Arch Bronchoneumol 2007; 43:161-4.
7 Kruisbeek AM, Shevach EM — Proliferative assays for T cells.In:CouganJE,KruisbeekAM,MarguilesDH,Shevach EM,StroberWeditors.CurrentProtocolsinImmunology.Vol 3.12thed.NewYork:JohnWileyandSons,1992:1-13.
8 Orme IM, Anderson P, Boom WH — T cell response to mycobacterium tuberculosis. Inf disease 1993; 167: 148197.
9 AE, Ciftic F, Bilgic S — Peripheral immune response in pulmonarytuberculosis.ScanJImmunol2009.
10 Rook G A — Th2 cytokines in susceptibility to tuberculosis. Curr Mol Med 2007;7:327-37.
11 Al-AttiyahRJ,MustafaAS—Mycobacterialantigen-induced T helper type 1 (Th1) and Th2 reactivity of peripheral blood mononuc ear ce s rom d abetic and non-d abet c tuberculosis patients and Mycobacterium bovis bacilli calmette-guérin (BCG)-vaccinated healthy subjects. Clin Exp Immunol 2009;158:64-73.
12 Leite AL, Carvalho I, Tavares E — Tuberculosis disease : statistics of a paediatric department in the 21st century. Rev Port Pneumol 2009;15:771-82.
13 Tsuyuguchi I — Immunology of tuberculosis and cytokines. Kekkaku 1995;70:335-46.
Early neonatal morbidities in late preterm newborns in a tertiary care teaching hospital of Uttarakhand
1 2 3
Jain Anand , Jain Suchitra , Upadhyay Amar N
To compare early neonatal morbidity (within first 7 days of life) in late preterm infants with term infants. A Prospective non-interventional study. All live inborn late preterm infants (34 0/7 to 36 6/7 weeks) and term infants (37 0/7 to 41 6/7 weeks). Any of the predefined medical conditions listed in the study, resultinginpost-deliveryinpatienthospitalobservation,admission,orreadmissioninfirst7daysoflife.522 late preterm infants and 5906 term infants were included in the study (228 of total 6656 being excluded because of unsure/unreliable date of L.M.P./other causes). Number of babies having at least one of the predefined neonatal conditions was 320 (61.3%) of late preterm and 1778 (30.1%) of term nfants. (Late preterminfantswereatsignificantlyhigherriskforoverallmorbidityduetoanycause(P<0.001),respiratory morbidity (P<0.001), any ventilatory support (P=0.001), jaundice (P<0.001), hypoglycemia (P<0.001), and probable sepsis (P<0.001). The incidence of morbidities increased from 27% at 40 weeks to 37%, 45%, 58%, 61% and 73% at 38, 37, 36, 35 and 34 weeks, respectively (P<0.001). Late preterm infants are as acompared with term infants at high risk for respiratory morbidity, need of ventilation (non invasive or invasive), jaundice, hypoglycemia, sepsis, and probable sepsis. All gestations except 39 weeks were at significantly higherriskformorbidityascomparedto40weeks.
[J Indian Med Assoc 2017; 115: 10-2 & 16]
Key words : India, late preterm infants, early neonatal morbidity, outcome.
Having pregnancy that too wanted, is most pleasur-able event in the life of a lady But the long drawn period of 40 weeks, fear of ultimate
labor pains coupled with perhaps uncertain outcome isn’t sopleasurablealways.Attemptsonthepartofwomenand attendants have been there to reduce this suffering, by insistingonhavingelectiveCSandbyepassingtheprocess of normal vaginal delivery Of late, especially in affluent societiestherehasbeenastressoncuttingtheperiodof40 weeks to 34-36 weeks, by having elective CS at about 34 weeks,anditis,attimesnoteasyforobstetriciantorefuse. Therationalebehindthisis,asthebabyisalmostfree(??) ofrisksofprematuritywhytobeartheagony&theriskof continuing pregnancy for additional 4-6 weeks or so?
Besides the question that, is it truly a healthy trend , the largermatteris,thatisitreallyriskfree?
Thelatepreterminfants(34-0/7through36-6/7weeks of gestation) are physiologically less mature and have limited compensatory responses to the extra-uterine
Department of Pediatrics, VCSGGMS&RI, Government Medical College,SrinagarGarhwal,Uttarakhand246174
1MD(Paediatrics),AssociateProfessor
2MS(Obst&Gynaecol),Gynaecologist
3MD(Paediatrics),AssistantProfessor
environ
ment, compared with term infants.Although late
preterminfantsarethelargestsubgroupofpreterminfants, there has been little research on this group until recently This is mainly because of labeling them as ‘‘near-term’’, thus being looked upon as ‘‘almost mature,’’ with little 1-9 need to be concerned. Recent research has revealed a contrarytrend Whileseriousmorbiditiesarerare,thelate preterm group has 2 to 3 fold increased rates for mild to moderate morbidities such as hypothermia, hypoglycemia, and respiratory distress, poor feeding, jaundice, infection, and readmission. As the late preterm subgroup accounts for nearly 10-20% of all births, even a modest increase in any morbidity will have a huge impact on the overall health care resources.The absolute number of late preterm infants being admitted to NICUs has been 1-9 increasing worldwide. Few studies have been conducted to assess the neonatal morbidity and mortality 1-8 inlatepreterminfants.AllStudies werefromdeveloped 9 countriesandwereretrospectiveinnature. Arecentstudy istheonlystudyfromIndia(AndhraPradesh)andtheonly prospective study Our study is the only study from Uttarakhandand the 2ndinit’sbeingaprospectivestudy
MATERIALAND METHOD
This prospective non-interventional study was con
ducted at VCSGGMS& RI & Government Medical College & Attached Hemwati Nandan Bahuguna Base HospitalSrinagarGarhwal(Uttarakhand). Allliveinborn late preterm infants (34 0/7 to 36 6/7 weeks) and term infants(370/7to416/7weeks),bornbetweenJuly2008to June 2011 were eligible for enrollment in the study Infantsinwhommotherwasnotfullycertainofexactdate of LMP/dates given appeared unreliable & those with major congenital anomalies were excluded. Gestational agewasassessedbymaternallastmenstrualperiodandby ultrasoundscanwheneverrequired.
A performa mentioning infant’s particulars, risk factors, and neonatal morbidity was developed for the study Itwaspre-testedon20infantsandmodified.Anyof the following predefined medical condition resulting in post delivery inpatient hospital observation, admission or readmission in first 7 days of life: (i) Post Resuscitation care: Requirement of post-resuscitation care as per NRP 2005guidelines.(ii)Hypoglycemia:Bloodglucoseofless than 40 mg/dL. Blood sugars were monitored frequently inalllatepreterm,IUGR(intrauterinegrowthrestriction), IDM (Infant of diabetic mother) and LGA (Large for gestation, birth weight >2SD) infants. Random blood sugar estimation was also done in all symptomatic infants aspertheclinician’sdiscretion.(iii)Jaundice:only babies requiring phototherapy/exchange transfusion (PTT/ET) asperhourspecifictotalserumbiluribin(TSB)nomogram (AAP chart) were included. Criteria for 35 weeks were used for infants with 34 weeks gestation. (iv) Respiratory distress: Presence of at least 2 of the following criteria: Respiratory rate >60/min, Subcostal/intercostal recessions, Expiratory grunt/groaning, and requiring oxygen therapy. (v) Sepsis: Probable sepsis: Positive septic screen (two of the five parameters namely, TLC 3 <5000/mm or >15000/mm , band to total polymorphratioof>0.2,absoluteneutrophilcount 3 less than 1800/mm3 or >7200/mm C reactive protein >0.5mg/dL, platelets <1 lakh/mm); or Proven sepsis: Isolation of pathogens from Blood or CSF or Urine (vi) Readmission: Any readmission after post-delivery discharge from hospital.
All infants enrolled in study were followed daily till first 7 days of life for any morbidity byclinicalevaluationandreviewinghospital records. Infants who were discharged before 7 days were called for mandatory follow up evaluation in the outpatient clinic on 5th or 7th day of life. Infants who did not come for followupwerecalledontelephoneandstatus ofthebabywasenquired.Statisticalanalysis was done and P-value calculated by using chi-square Method with the help of t e s t w w w o p u s 1 2 o r g / C h iSquare_Calculator.html
OBSERVATIONS
Therewere7492deliveriesinhospitalduringthestudy period, of whom 836 were stillbirths and 228 were excluded from study due to unreliable/uncertain date of LMP/major congenital anomalies/gestation >41- 6/7 weeks. Thus the study constituted of total 6428 neonates. Of these 522 (8.12%) were late preterm and 5906 (91.88%) were term births. All included infants were followedfor7daysoflifeforoutcomes.Oncomparingthe two groups, there was appreciable difference in mean gestation, mean birth weight, appropriateness of weight forgestationalageandthemodeofdelivery(Table1).
320 (61.3%) of late preterm and 1778 (30.1%) of term infants had at least one of the neonatal morbidities requiring inpatient hospital observation, admission or readmission during the first 7 days of life. On comparing the neonatal morbidity, late preterm infants were at highly significant increased risk for overall morbidity due to causes viz respiratory morbidity, jaundice requiring PTT/ET, hypoglycemia, probable sepsis, and confirmed sepsis; and at significantly increased risk of requiring ventilatorysupport(Table2).
DISCUSSION
In the present study, 61.3% of late preterm and 30.1% of term infants had at least one neonatal morbidity requiring inpatient hospital observation, admission or
Table 1 — Baseline variables of the study population
Table 2 — Comparison of morbidity in
12 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
readmis
sion during the first 7 days of life. Neonatal study Rates in our study (61.3% & 30.1% respectively)
jaundice requiring phototherapy (47.5%) followed by respiratorymorbidity(16.4%)andhypoglycemia(12.6%) were the frequently identified morbidities in late preterm infants while neonatal jaundice requiring PTT (14.7%) was the most frequently identified morbidity in term infants. Of late preterm (43.68%) babies were born by cessarean delivery, corresponding rate being (23.25%) in term group. Compared with term infants, late preterm infantswereat2.04timeshigherriskforoverallmorbidity due to any cause, 2.93 times higher risk for respiratory morbidity 1.9timeshigherriskforventilation,3.23times higher risk for jaundice, and 2.62 times and 2.73 times higher risk for hypoglycemia and probable sepsis, respectively(Table3).
Similar to our findings, in a retrospective study1 77.8% near term infants compared with 45.3% of term infants had at least one clinical problem and nearly all clinical outcomes differed significantly between neartermandfull-termneonateviz hypoglycemia,respiratory problem, and jaundice. They found that during the initial birth hospitalization, late preterm infants were 4 times more likely than term infants to have at least one medical conditiondiagnosedand3.5timesmorelikelytohavetwo or more conditions diagnosed. In another study it was found that compared with full-term infants, late preterm delivery was independently associated with an increased risk of neonatal morbidity including respiratory distress syndrome, sepsis,
intraventricular
h e m o r r h a g e , hypoglycemia, and jaundice requiring PTT. Another study in 2006 reported that late preterm infants were 1.5 times more likely to require hospital-related care and 1.8 times more
9 also,aremoreclose tothisonlyprospectivestudy
Inourstudy,theincidenceofmorbidityincreasedfrom 27% at 39-40 weeks to 73% at 34 weeks showing an inverserelationshipwithgestationalage.Therewasan8% increasefrom38weeksto37weeks,11%increasefrom37 weeks to 36 weeks and 17% from 36 weeks to 34 weeks. The differences were highly significant statistically with rise of every single week up to 39 except for 34 to 35, & 35 to 36 weeks rise, as depicted inTable 4.With 40 weeks asreferencestandard,allgestationsexcept39weekswere at significantly higher risk for morbidity Similar findings were also reported in the study from Hyderabad in 2010. 10 Similarly the study in 2008 also concluded that clinically significantrespiratorymorbiditiesareleastcommonat3940 weeks. The mortality and morbidity having a strong Gestational Age related trend with the lowest incidences found between 38 and 40 weeks of gestation were also reportedbyastudy in2009.
Our study is among earliest prospective studies to obtain actual data on late preterm births and associated neonatalmorbiditiesfromIndiaandthefirstonlyfromthe state. Among the neonatal units, often there is as a wide variationinantenataluseofsteroids,asepsisprotocolsand management of jaundice/ respiratory distress and hence theresultsofthisstudymaybemoreapplicabletosimilar
Table 3 — Comparison of morbidity in late preterm and term ,as per their gestational ages
l i k e l y t o b e readmitted than term 6 infants.Inyetanotherstudy, newborn morbidity was 7 times more likely in late preterm compared with term infants (22% versus 3%). A 9 recent prospective study
Table 4 — Differences in the incidence of morbidity (all) as per gestational age & corresponding p values 34 weeks 35 weks 36 weeks 37 weeks 38 weeks 39 weeks 40 weeks 41 weeks
from Hyderabad in 2010(being only study done in India), found a much higher risk of neonatal morbidity viz 70.8% in late pretermscomparedto29.1% in term babies. They attributed it to be due to more precise follow-up being a hospital based prospective
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
Prevalence and association of metabolic syndrome with C-reactive protein in people attending a tertiary care hospital of North Bengal
1 2 3 4 5 6
Debjani Laha , Ranjan Pal , Anupam Gupta , P P Pal , G Ghoshal , D S Mondal
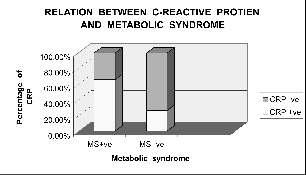
Metabolic syndrome (MS) is a constellation of several cardiovascular risk factors. It is often found to be associated with elevated C-Reactive Protein level. Compared to other established cardiovascular risk factors, CRP adds more predictive information about the possible future cardiovascular complications. The present study was carried out to enquire about the association of C-reactive protein with Metabolic Syndrome ,in persons of age group of 20-50 years and residing in the sub-himalayan region of West Bengal, using NCEP- ATP III criteria to identify MS and qualitative estimation of C-reactive protein. Sixty threesubjectswerechosenforthestudyfrompatientsattendingthegeneralMedicineOPDinNorthBengal Medical College for minor ailments. 46.1% of study population was found to be affected with MS. Amongst theMSpositivepersonnel65.5%werealsopositivewithCRP(pvalue<0.05(0.002).Theresultsuggeststhat a significant fraction of persons with MS are at risk to develop cardiovascular complications as evidenced bypresenceofhighlevelsofCRPinthesesubjects.
[J Indian Med Assoc 2017; 115: 13-6]
Key words : Metabolic syndrome, c-reactive protein.
Metabolic syndrome is defined as presence of insulin resistance in combination with at least 3 of the following conditions: Hyperglycemia,
1 Hypertension, Dyslipidaemia & Central obesity People with MS are twice as likely to die from coronary heart disease and three times as likely to have a heart attack or 2 strokecomparedwiththePeoplewithoutthesyndrome Diagnosis & management of Metabolic Syndrome is of paramount importance not only to prevent type II DM but also to abort the future vascular complications of the 3MS
The National Cholesterol Education Program- Third Adult Treatment Panel III (NCEP-ATP III) has set guidelines for clinically identifying the subjects with Metabolic Syndrome & defined them as new secondary targets for Cardiovascular risk reduction therapy Data have revealed that the plasma concentration of inflammatory mediators, such as TNF-Alfa,
Department of Physiology North Bengal Medical College, Thiknikata, WestBengal734012
MBBS,MD, AssistantProfessor
MBBS, DGO, RMO cum Clinical Tutor, Department of Obst & Gynae
MBBS,AssistantProfessor,DepartmentofPharmacology
MBBS, MD (Commun y Medicine) Assistant Professor, DepartmentofCommunityMedicine
MBBS,MedicalOfficer,EmergencyDepartment
MBBS,AssistantProfessor,DepartmentofPhysiology
Interleukin-6, CRP Fibrinogen,& Plasminogen activator inhibitor-1 are increased in insulin resistant states of 4,5 obesity & type-II diabetes mellitus Also an increase in inflammatory mediators have been shown to predict the 4,5 futuredevelopmentofobesity&type-II diabetes . Variation of plasma level of CRP can prospectively predict the risk of Myocardial Infarction. CRP level also correlates positively with the outcome of acute coronary syndrome.Acontrol trial was conducted by Tahir Ahmed Munir et al where CRPlevels increased in patients with ACS as compared to controls, and in patients of STEMI andNSTEMIascomparedtoUA .
TheuseofCRPandothernovelinflammatorymarkers may significantly add to our ability to correctly identify patients presenting with Acute Coronary Syndrome who 7 areathighriskforfuturecardiovascularevents
HSCRPhasthepotentialtoplayanimportantroleasan adjunct for global risk assessment in the primary 8 preventionofcardiovasculardisease
Inastudyamongthosewiththemetabolicsyndromeat study entry age-adjusted incidence rates of future cardiovascular events were 3.4 and 5.9 per 1000 personyears of exposure for those with baseline CRP levels less than or greater than 3.0 mg/L, respectively. Additive effects for CRP were also observed for those with 4 or 5
13
14 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
characteris different definitions of the metabolic syndrome had minimalimpactonthesefindings.
tics of the metabolic syndrome. The use of National Cholesterol Education Program – Adult TreatmentPanelIII(NCEP-ATPIII) Anythreeoffive:
These prospective data suggest that measurement of CRP adds clinically important prognostic information to themetabolicsyndrome
India is projected to have the largest number of individuals suffering from atherosclerotic cardiovascular diseasesbytheyear2020,butthenumberofdataonAsian Indians is limited. Available data suggests that the prevalence of MS in Indian general population is about 40% which is much higher than the 25% prevalence 10 quoted for the western population Indians are also found to have higher visceral obesity & waist circumference 10 compared to their body weight . There is scarcity of data on the association of C-Reactive protein and Metabolic syndrome in the eastern part of India particularly in the Sub Himalayan Bengal.The present study aims to throw lightonthis.
MATERIALSAND METHODS
ThestudyhadbeenconductedinGeneralMedicalOut Patient Department of North Bengal Medical College & Hospital, Darjeeling amongst the patient presenting with minor ailments other than the following preexisting diseases like; (a) patients with previous episodes of cardiovascular accidents, proven diabetes mellitus, CRF, hyper-urecimia (b) people who had other CRP related diseases, like , recent trauma, surgery, neoplasia , rheumatoidarthritis,SLE,thyroidrelateddisordersand(c) all pregnant & nursing mothers. The prior necessary departmental permission and ethical committee approval weretakenaccordinglyalongwithinformedconsentfrom each subjects. Data collected twice weekly at every alternate individual of 20-50 years age group attending here and fulfilling the selection criteria over a period of 6 months. Total 63 study subject of either sex were ultimately included and one year duration was taken to conduct this cross-sectional study for necessary lab. investigation,analysisandmanuscriptpreparation. Tools & Technique : A pretested, predesigned semi structured questionnaire was used for data collection.The Modified NCEP-ATP III criteria was used to define Metabolic Syndrome as shown below Fasting blood samples were drawn from the subjects on the following morning for Blood Glucose, Triglyceride estimation and HDL Cholesterol. Blood pressure was recorded as per averages of three occasions of measurement by same investigator. To measure waste circumference , measurement was taken by the help of measuring tape absolutely in the horizontal plane both antero-posterior and laterally The value recorded at the mean of the height ofexpirationandinspirationnearestto0.5cm.Forfemale subjectsafemaleattendant’spresencewasconsidered.
Abdominal obesity (waist circumference >102 cm (men) or 88 cm (women)
Plasma triglycerides > 150 mg/dl
HDL-cholesterol < 40 mg/dl (men) or < 50 mg/dl (women)
Blood pressure > 130/85 mmHg
Blood glucose > 110 mg/dl
Plasma C-reactive rotein (CRP) Estimation : As acute phase protein CRPfound in level up to 5 microgram /dl in normal individuals, This test is based on immunologic reaction between CRP as an antigen , latex particles have been coated with monospecific anti-human CRP & sensitized to detect levels greater than 6microgram/mlCRP It is a qualitative test
• Positive & Negative control are used simultaneously
Data was analyzed using SPSS (ver 14, Chicago Inc) after entering into MS Excell data sheet (Microsoft Corporation, USA). Descriptive statistics along with nonparametric test were applied where necessary at 95% confidence interval considering P value 0.05 as level of significance.
Results :
Table 1 — Relation between Metabolic Syndrome & C-Reactive Protien
MetabolicSyndrome Total Present CRPAbsent
Positive 19(65.5%) 09(26.5%) 28(44.4%)
Negative 10(34,5%) 25(73.5%) 35(55.6%)
Pearson Chi- Square test value is 9.664, df =1, p value =< 0.05 (0.002 ), so there is an obvious significance lies between Metabolic Syndrome and CReactiveprotein.
DISCUSSION
Humans have become victim of their own evolutionary success, having high caloric diet with lacking exercise. As a consequence obesity,type IIdiabetesmellitushavereached epidemic proportion. Today the biggest killers in the world are not the infectious diseases but it is the chronic afflictions such as cardiovascular diseases, obesity & diabetes. Evolving role of inflammation in obesity & 1,12 MS provide a common path physiological link between these diseases.Atherosclerosis is a low grade inflammatory disorder leading to expression of many inflammatory markers of plasma,CRPisoneofthem.
Prevalence of MS in the Asian Indian population ranges from 20-55%. This wide variation is due to the considerable heterogeneityofpopulation.
SomeauthorstriedtoestimatetheprevalenceofMSin different countries, like Third National Health and Nutrition examination Survey by Ford ES et al estimated 27.3%in USA, Ramchandran et al in 2004 found that 41.1%prevalenceinIndia.
Present study revealed 46.1% prevalence (Table 2)in patientsattendinggeneralMedicineOPDofNorthBengal Medical College. Majority of the MS positive patients belong to the age group of the 46-50 years. There was a significantrelationbetweenMS&CRPasseeninTable1, 65.5% CRP positive people also having Metabolic Syndrome,pvalue<0.05(0.002).
There were no significant variation (Pearson chi square 0.003, df 1, P>0.05) of Metabolic syndrome prevalence with CRPpositivity in this study (44.1% male &44.8%female)asshowninTable3a.
From obesity grade 2-5 (there is no people belongs to gradeIobesityinthestudy)therewasincreaseof theCRP level but statistically it is insignificant (Linear-by-Linear Association1.912, df 1, P>0.05).
Performance of the qualitative estimation of the CRP was done in the study, but quantitative estimation might help to categorize the subjects who were at immediate risk,asCRPvaluenotonlytellusabouttheprogressionof thediseasebutalsotellabouttheprognosis of thedisease. So this was a limitation of the study The study was small one involving only 63 people further study involving much larger population will be needed along with the quantitativeestimationofCRP
This can be concluded from that from the study, the prevalenceofmetabolicsyndromeisquitehighinpatients attending in General Medicine OPD. A significant corre
Table 3a — Sex wise distribution of CRP
Table 3b — Relation of Obesity Grade and CRP
lationliesbetweenMS&CRP Furtherinvestigationis needed quantitative estimation of CRP to evaluate the progressionofMS.
16 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
new millennium .Hasner H, German diabetic research institute at the Heinrich. Heine-University, Dusseldorf, Germany.Publicationtypereview:-PMID.11965519.
5 Hanefield M, Leonhardt W, Das Metabolische Syndromje, DT,Gesundh–wesenin1981; 36:545-51.
6 Munir TA, Afzal MN, Ahmed R — C-reactive protein and acute coronary syndrome: correlation with traditional risk factors,diagnosticcardiacbiomarkers,andejectionfraction. RMJ 2009;34:154-9.
7 Gavin J Blake, M Ridker — C-reactive protein and other inflammatory risk markers in acute coronary syndromes. J Am Coll Cardiol 2003;41:37-42
8 Paul M Ridker — High-Sensitivity C-Reactive Protein Potential Adjunct for Global Risk Assessment in the Primary
(Contined from page 12)
settings and may not be generalizable.Another limitation ofourstudyisthatweneitherasessedmorbiditybeyond7 days, nor long term outcomes. Results show that so presumed ‘almost mature’ (late preterms) infants have more than 2 times higher risk for overall morbidity due to anycauserelativetoterminfants.Theconcludingmessage isthatelectivecaesserian/inducedlaborat34or35weeks, hopinganalmostmature babyisnottrue.
REFERENCES
1 Wang ML, Dorer DJ, Fleming MP, Catlin EA — Clinical outcomesofnear-terminfants. Pediatrics 2004;114:372-6.
2 Raju TN, Higgins RD, Stark AR, Leveno KJ — Optimizing care and outcome for late-preterm (near-term) gestations and for late-preterm infants: a summary of the workshop sponsored by the National Institutes of Health and Human Development. Pediatrics 2006;118:1207-14.
3 Tomashek KM, Shapiro-Mendoza CK, Weiss J, Kotelchuck M, Barfield W, Evans S, et al — Early discharge among late preterm and term newborns and risk of neonatal mortality. Semin Perinatol 2006;30:61-8
4 Young PC, Glasgow TS, Xi Li, Guest-Warnick G, Stoddard GJ — Mortality of late-preterm (near-term) newborns in Utah. Pediatrics 2007;119:659-65.
5 McIntireDD,LevenoKJ—Neonatalmortalityandmorbidity rates in late preterm births compared with births at term.
Prevention of Cardiovascular Disease. Circulation 2001; 103:1813-8.
9 C-Reactive Protein, the Metabolic Syndrome, and Risk of Incident Cardiovascular Events An 8-Year Follow-Up of 14 719 Initially Healthy American Women Paul M Ridker, MD; JulieE.Buring,ScD;NancyR.Cook,ScD;NaderRifai.
10
Wechselbeziehungenzwischenlipidstoffwechselund 11 Hasson GK — atherosclerosis, & coronary artery diseases. N Engl J Med 2005; 252:1685-95.
12 Fernández-Real JM1, Ricart W — Insulin resistance and chroniccardiovascularinflammatorysyndrome. Endocr Rev 2003;24:278-301.
Original Article
Obstet Gynecol 2008;111:35-41.
6 Shapiro-Mendoza CK, Tomashek KM, Kotelchuck M, Barfield W, Weiss J, Nannini A, et al Effect of latepreterm birth and maternal medical conditions on newborn morbidityrisk. Pediatrics 2008;121:223-32.
7 Khashu M, Narayanan M, Bhargava S, Osiovich H — Perinatal outcomes associated with preterm birth at 33 to 36 weeks’ gestation: a population-based cohort study. Pediatrics 2009;123:109-13.
8 Melamed N, Klinger G, Tenenbaum-Gavish K, Herscovici T,LinderN,HodM, et al Shorttermneonataloutcomein low risk, spontaneous, singleton, late preterm deliveries. Obstet Gynecol 2009;114:253-60.
9 Jaiswal Ashish, Murki Srinivas, Gaddam Pramod, Reddy Anupama — Early Neonatal Morbidities in Late Preterm Infants. Indian Pediatrics 2011;48:607-11.
10 Yoder BA, Gordon MC, Barth WH — Late-preterm birth: Does the changing obstetr c paradigm a ter the ep dem o ogy o respiratory comp cat ons? Obstet Gynecol 2008;111:814-22.
11 Luca RD, Boulvain M, Irion O, Berner M, Pfister RE — Incidence of early neonatal mortality and morbidity after late-preterm and term cesarean delivery. Pediatrics 2009; 123:1064-71.
If you want to send your queries and receive the response on any subject from JIMA, please use the E-mail facility.
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
Status of cold chain monitoring in primary health centres of Bangalore urban — north
Jyothi Jadhav , Selvi Thangaraj
, Thilak S A , Ranganath T S
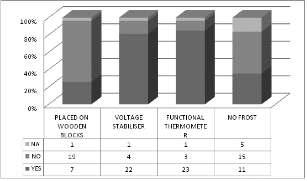
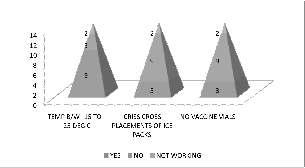
Child immunisation is among the most cost-effective ways of preventing premature child deaths. The potency of vaccines, crucial for vaccine efficacy, is dependent on effective management of the cold chain at all levels of vaccine handling. India’s immunization program is one of the largest in the world. However, full immunization coverage still stands at 61% only. Since there were gaps in immunization coverage and a situationofhighmorbidityandmortalityamongunderfivechildren,Indiadecidedtodeclaretheyear2012-13 as a year of “Intensification of Routine Immunization” for effective vaccine management. This is a cross sectionalstudyinwhich30PrimaryHealthCentresthatwereallotted,27werestudiedonimmunizationdays (Thursday). Mentors were trained and data was collected using observational checklist. Among the 27 Primary Health Centre’s studied, 1 centre didn’t have Ice line refrigerator or Deep freezer, 13 centres didn’t have deep freezer. In 22 centres, Cold Chain equipments were attached to stabilizer, 7 centres placed equipments as per standard norms, 3 centres had not maintained temperature charts, 3 centres didn’t have thermometers. Tencentresshoweddiscrepancyinrecordedtemperature.Vaccinesatthesessionsitewere in zipper pouch in vaccine carrier at 23 centres. There are a lot of weaknesses and gaps in cold chain maintenance,thusarisingthedoubtofpotency/efficacyandsafetyofvaccinesadministered.Toimprovethe situationconstantmonitoringandsupervision,periodictrainingofpersonnelisnecessary.
[J Indian Med Assoc 2017; 115: 17-20]
Key words : Cold chain equipments, immunization, supervised monitoring, vaccines.
Immunization is one of the most cost effective health investments and proven tool for controlling and
eliminating life-threatening infectious diseases (known as vaccine preventable diseases). Globally it is estimated to avert over between 2-3 million deaths each year India’simmunizationprogramisoneofthelargestin the world in terms of quantity of vaccines used, beneficiaries, number of vaccine sessions organized, the geographical spread and diversity of area. Regrettably, however, full immunization coverage in the country continuestobesub-optimal,standingatamere60%atthe 2 national level. There are many states where full immunization coverage is less than 50%. On the other hand there are states having coverage above the national level yet the coverage there is either stagnant or is declining.GovernmentofIndiaisannuallyspendingmore than 1500 crores on universal immunization program and pulse polio. Gaps in the immunization coverage result in low return on this investment, besides a situation
Department of Community Medicine, Bangalore Medical College & Research Institute,Bangalore560002
1MD,PGDHHM,AssociateProfessor
2MD,Professor
3MBBS,MD,Postgraduatestudent
4MD,Professor&Head 17
where morbidity and mortality among children continues tobeunacceptablyhigh.
Inviewoftheabove,ithasbeendecidedtodeclarethe financial year 2012-13 as the year of ‘Intensification of Routine Immunization’in which all efforts shall be made to improve full immunization cover throughout the country This declaration is in consonance with the resolution of all countries in South-East Asian region to declare 2012 as the year of “Intensification of Routine 4Immunization”
Oneofthemajoractivitiesproposedduring2012-13as the year of “Intensification of Routine Immunization” is the effective vaccine management exercise in all priority states to assess and strengthen cold chain and vaccine 4management
The cold chain is a system of storing and transporting vaccines at recommended temperatures from the point of manufacture to the point of use. The key elements of the coldchainare:
(1) Personnel-to manage vaccine storage and distribution.
(2) Equipment- to store and transport vaccines and to monitortemperature.
(3) Procedure- to ensure that vaccines are stored and 5 transportedatappropriatetemperatures
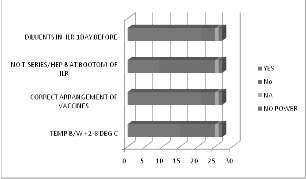
Reconstituted BCG, measles, JE vaccines are the most sensitive to heat and light. Also there is risk of contamination with staphylococcus aureus leading to ToxicShockSyndrome.Andthereforetheyshouldbeused within 4 hours of reconstitution. Hepatitis B and all T series vaccines lose their potency if frozen. Deep freezers o (DF)maintainacabinettemperaturebetween-15to-25C. Icelinedrefrigerator(ILR)maintainacabinettemperature o o between +2C to +8C and are used to store all Universal Immunization Programme (UIP) vaccines at the Primary Health Centre level (PHC). ILRs can keep vaccines safe with as little as 8 hours continuous electricity supply in a 5 24hourperiod AtPHClevel,deepfreezersareusedonly for preparation of ice packs and are not to be used for storingUIPvaccines.
InIndia,UIPwasintroducedsince1985withobjective of immunization of pregnant women with two doses of tetanus toxoid and immunization of children in their first 6 year of life against six vaccine preventable diseases. Achieving this objective depends on quality of vaccines used. To preserve its potency and safety, cold chain has to be maintained at all levels. Those involved in this to be skilled and equipped regarding condition of storage and transportationaswellastemperaturemonitoring.
In Karnataka, there has been a decline in full immunization coverage between National family health survey(NFHS)-2(60%)andNFHS-3(55%)
Reasons for poor coverage were said to be poor monitoring and lack of feedback on reported data in monthly meetings at various levels by routine immunization managers, poor usage of the standard tools to track, document and report immunized children by healthworkersatPHC/Subcentrelevel.Thereisadisarray of documentation with poor quality coverage of data, lack of effective and supportive supervision of the program, failure to assess output of the program. Realizing the need foradditionalsupportingmonitoringoftheprogram,State institute of health and Family welfare (SIHFW) in collaboration with UNICEF has developed a model by involving medical colleges for this activity. Two mentors were selected from medical colleges and were trained. Each mentor will do field visits on selected Thursdays (thrice a month) to supervise and monitor various components of routine immunization activities viz the adherencetomicroplanningforconductingimmunization session,qualityofpractices,sessionmonitoring,qualityof reports, hands on training to service providers, identificationoftrainingneeds,availabilityofequipments and supplies, maintenance of cold chain equipments and supplies, knowledge and attitude towards immunization among primary care givers, etc. Thus, here we have presented the status of cold chain monitoring which was one of the components of supportive supervision.
MATERIALSAND METHODS
It was a cross sectional study to assess the cold chain maintenance of vaccines. This study was part of program to support district health authorities by monitoring and providing supportive supervision for the immunization related activities. Bangalore district was one of the selecteddistrictsintermsofdensesturbandistrict.Alistof 30 PHCs were given by SIHFW, out of which 27 centers were studied. PHCs were visited on Thursdays (immunization day). The mentors were trained and data was collected using observational checklist to ascertain cold chain maintenance of vaccines and by related documents. Data collected were on availability of Cold Chain Equipments (CCE) and its placements, twice daily monitoring of temperature recordings and its variation on the day of the visit, presence of functional thermometer, record of power failures and periodic defrosting, periodic check of temperature Log books by facility in charge. Informationonstorageconditionsofvaccineanddiluents, its correct placement in ILR, correct placement of ice packsinDFs,presenceofanyfooditemsoranyothernonrecommendeditemsfoundinCCE andatthesessionsite, presence of vaccines in zipper bag in the vaccine carrier and written time on reconstituted BCG, measles vaccine was recorded. Collected data were coded and entered in excelsheetandanalyzedusingtrialversionofSPSS20.
RESULTS
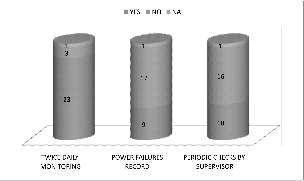
Twenty seven PHCs were included in the study One PHC (3.7%) out of 27 did not have ILR or DF, 13 PHC‘s (48.1%) out of 27 did not haveDF CCEs were attachedto electric outputs through voltage stabilizer in 22 PHC’S (81.5%) (Fig 1). Placing of ILRs and DF 10cm away from the wall or adjoining structures were in 7 PHCs (25.9%) (Fig 1). The CCEs were kept away from direct sunlight in all the centers. Temperature chart with 2 entries was maintained in 23 centers (85.2%) (Fig 2). Three of the centersdidnothavefunctionalthermometer(Fig1)where the temperature was recorded from display On the day of thevisit,discrepancyinILRtemperaturewasnotedamong 10 (37%) PHC’S (Fig 2) where the temperature was less than +2 deg c in 4 centers and more than +8 deg c in 6 centersandwithonecentrehavingpowerfluctuationfrom two days. Food articles were not present in any of the PHCs. Ice formation of more than 5mm in CCEs were found in 11 centers (40.7%) (Fig 1) and water logged ILR inonecentre,suggestiveoflackofregulardefrosting.Heat sensitive vaccines were correctly stored. Freeze sensitive vaccines were not correctly stored in 9 PHCs where they were placed at the bottom of the ILR. The power failure was present for more than 24 hours in 1 center Uninterrupted Power Supply backup was present in 3 of thecenters.Actionstakenduringthesepowerfailureswere
2 — Monitoring of temperature log books
19
—
not docu (33.3%) ice packs in DFs were not placed in criss-cross manner(Fig3). At the session site there was no shortage of any of the vaccinesorthediluents.Allthevaccineswerefoundinthe usable condition with respect to vaccine vial monitor (VVM).Thevaccinesatthesessionsitewereinthezipper pouch in vaccine carrier in 85.2% (23) (Table 1). In 15 centers (55.6%), time of reconstitution was written on reconstitutedBCGandmeaslesvials(Table1).
Flaws noticed during the monitoring of immunization session were brought to the notice of the medical officer Methods of correcting the same were discussed. The importance of ensuring that these methods were put into practice on a regular basis was emphasized to the health worker mented in 19 centres (63%) (Fig 2). In 9 centres
1 — Observation of placement of vaccines in vaccine carrier and time of reconstitution
Yes No
Vaccine
DISCUSSION
The purpose of the study was to provide supportive supervisionandmonitoringofroutineimmunization.Itisa process of helping staff to continuously improve their knowledge and skills, thus improving work performance. It is a two way communication and builds team approach thatfacilitatesproblemsolving.
One of the PHC was conducting immunization sessions without CCEs where they had to get the vaccines from mother PHC. Transporting of vaccines before and afterimmunizationsessionincreasestheriskofvaccineto lose its potency thus increasing its wastage. It was good to note that power source was permanent (UPS backup) in 11% which can be extended to other centers. Non functional thermometer (11.53%), lack of temperature monitoringcharts(11.1%)anddocumentationofirregular powersupplyisoneofthecriticalelementsinmaintaining thepotencyofvaccines.
The degree of implementation of cold chain with respect to presence of ILR was 96.3% and DF was 51.9%.The study by S Sachdeva and U Dutta showed the presence of ILR as 6.25%. Our study showed an insufficientsupervisionof59.3%whereasitwas25.9%in astudybyJeromeAteudjieu et al .Itwasnotedthatlackof temperature maintenance and monitoring was 11.1% in
18 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017 |
Fig 1 — Placement and functioning of ILR’s and DF’s
20 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
our study However,
S.Sachdeva , U Dutta, and a study by ACKNOWLEDGMENTS
Jerome Ateudjieu et al observed 71.87% and 40.7% respectively Freeze sensitive vaccines (T series and hep.B) were not correctly stored in 9(33.3%) PHCs where they were placed at the bottom of the ILR. The consequences of not keeping the vaccines at the right temperature (either heat or cold) can be disastrous. Once vaccinepotencyislost,itcannotberegained.Thisleadsto wastage of expensive vaccines. Moreover, children and women who receive such a vaccine are not protected. All o vaccines are damaged by temperatures more than +8C, whethertheyareexposedtoalotofheatinashorttimeora smallamountofheatoveralongperiod(frequentopening oflidofILR).
Various loopholes in the system have been noted from thisstudyasariskfactorforvaccinepotency Theproject experiences were used for further strengthening the immunization programme. Some intervention like constant supervision, training of professionals in charge, availabilityofcoldchaintoolsanditsmaintenanceincase ofbreakdowncanreducethegaps.Furthermore,strategies like installment of UPS, annual maintenance contract, developing thermostable vaccines could improve the vaccinepotency
CONCLUSION
There are a lot of weakness and gaps in cold chain maintenance in the country, thus arising the doubt of potency/efficacyandsafetyofvaccinesadministered.This in turn increases the cases of vaccine preventable diseases and adverse events following immunization. To improve thissituation,werecommend:
• Constant supervision of CC equipments and periodiccheckbysupervisors.
• Identify and address factors leading to failure of CCmonitoring.
• Periodic training of personnel in CC monitoring andstrengtheningtheirskills.
• Assistancetomakerepairwhennecessary
• RoutinemaintenanceofCCEs.
The author acknowledges the support and cooperation of SIHFW, Directotare of Health and Family welfare services, DME. The authors are indebted to Dr Santhosh Shirolforhisenormoussupport.
REFERENCES
1 WHO | Immunization coverage. World Health Organization; [ c i t e d 2 0 1 4 J a n 2 4 ] A v
2 National Family Health Survey [Internet]. [cited 2014 Jan 28].Availablefrom:http://www.rchiips.org/nfhs/nfhs2.shtml
3 Handbook for Vaccine & Cold Chain Handlers [Internet]. [cited 2014 Jan 24]. Available from: http://www.unicef.org/ india/Cold_chain_book_Final_(Corrected19-04-10).pdf
4 S ra egic framework for Intens ficat on of rout ne Immunisation in India [Internet]. [cited 2014 Jan 24].
Ava lable from: http: /210 212 20 93 8082/ jrhms F leUploaded By User 7 Ind a IR S ra eg c Framwork_2012_FINAL.pdf
5 Immunization handbook for medical officers. Dept of health andfamilywelfare,MoHFW,Govt.ofIndia.2009.39-72.
6 Park K — Park’s Text book Preventive & Social Medicine. 21sted2011:Jabalpur;M/sBabsaridasBhanot.404.
7 National Family Health Survey (NFHS-3) [Internet]. [cited 2014 Jan 28]. Available from http://www.rchiips.org/ nfhs/NFHS-3Data/Karnataka_report.pdf
8 Sachdeva S, Datta U. Status of vaccine cold chain maintenance in Delhi, India. Indian J Med Microbiol [serial online] 2010 [cited 2014 Jan 28];28:184-5. Available from: http://www.ijmm.org/text.asp?2010/28/2/184/62507
9 Ateudjieu J, Kenfack B, Nkontchou BW, Demanou M. Program on immunization and cold chain monitoring: the statusineighthealthdistrictsinCameroon.BMCRes.Notes [Internet]. 2013 Jan [cited 2014 Jan 24];6:101. Available from:http://www.pubmedcentral.nih.gov/articlerender.fcgi? artid=3630054&tool=pmcentrez&rendertype=abstract
We request you to send QualityArticle addressed to : Hony. Editor, Journal of IMA(JIMA), 53, Sir Nilratan Sarkar Sarani (Creek Row), Kolkata 700014
Dr.DilipKumarDutta
Dr.KakaliSen Hony Editor, JIMA Hony Secretary, JIMA
Observational Study
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
A study on knowledge, attitude and practices (KAP) regarding usage of Hydrogen Peroxide among Orthopaedic surgeons in Hyderabad,
AP
1 2 3
K
L Jagadishwar Rao , Kantilal G Jain ,Subash B
Hydrogen peroxide is familiar to most of the Orthopaedic surgeons as an over the counter preparationthatiseasilyavailableatanysupermarketaswellaspharmacy.Hydrogenperoxideisregarded as a safe antibacterial and oxidising agent by US FDA. Hydrogen peroxide is used therapeutically in a variety of different ways. Most of the surgeons use HO routinely without fully knowing the facts, some are reluctanttousefearingcomplicationsandsomerefusetodiscloseitsusage.Insuchscenario,wethoughtit isworthwhiledoingsuchastudy.
[J Indian Med Assoc 2017; 115: 21-5]
Key words : Hydrogen peroxide, questionnaire, orthopaedic surgeons.
Methods:
It is a descriptive, cross sectional and observational study The participants are about 100 Orthopaedic surgeons in tertiary care hospitals in and around Hyderabad, Andhra Pradesh. It includes teaching, non teaching and corporate hospitals. The tool of data collection is a close ended, self administered, pre tested questionnaire.
Results & Conclusions :
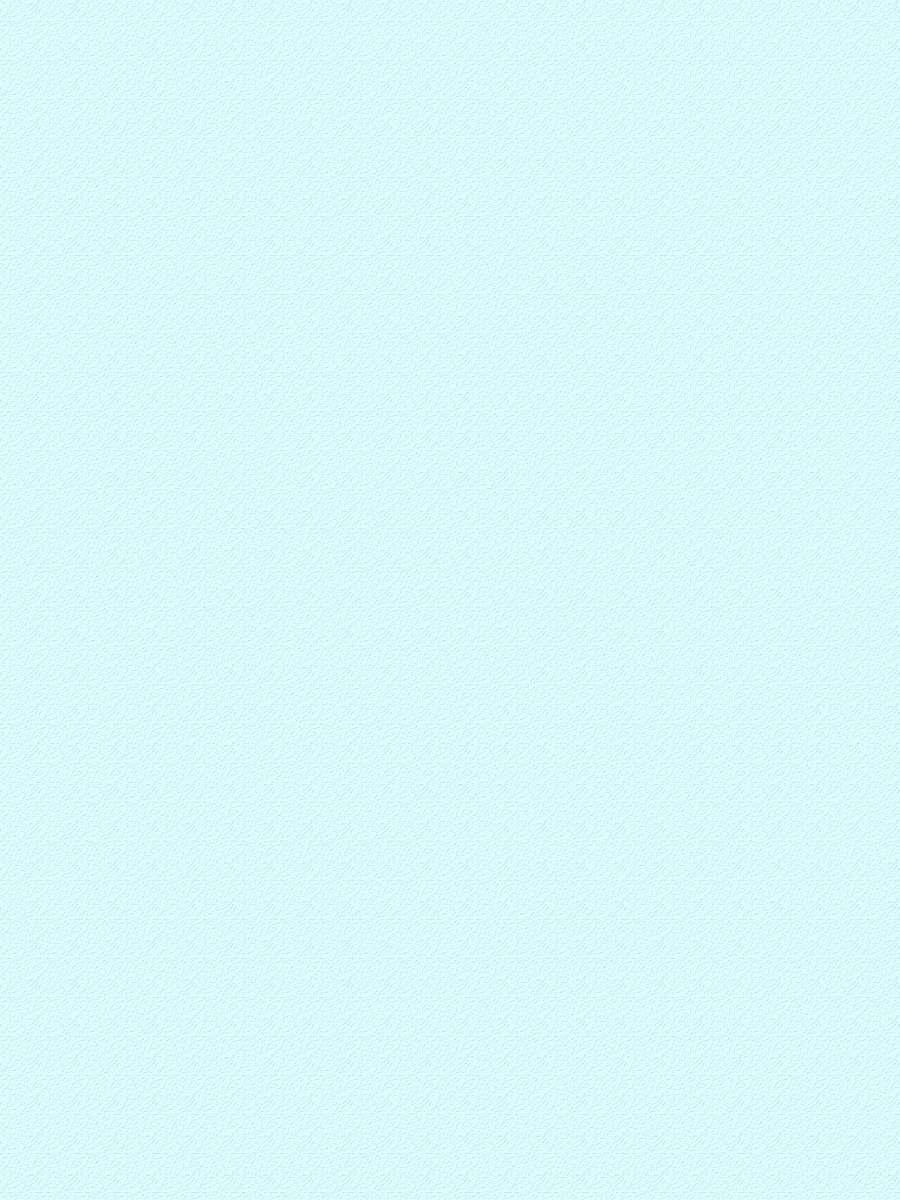
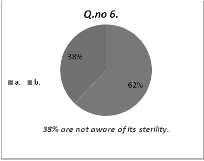
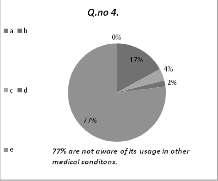
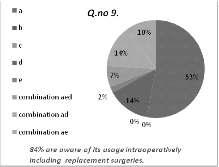
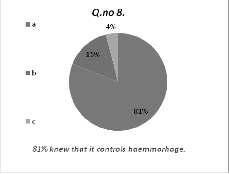
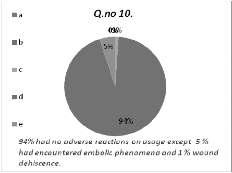
Theresultsareanalyzedaftercollectingtheresponseto the questionnaire. The data analyzed depicted by the pie diagrams. Our study revealed that the level of knowledge pertaining to questions 1,2,5,6 ranged from 62 to78%, obviously showing a majority.The level of practice pertaining to questions 3,7,8,10 was about 63% and the attitude levels pertaining to questions 4 and 9 was meager as regard to usage in medical conditions. 94% of the surgeons did not come across any untoward reactions. 6% hadencounteredcomplicationslikeembolicphenomenon, wound dehiscence, surgical emphysema in puncture wounds and anaphylaxis. The attitude to use Hydrogen Peroxide was found to be more in senior faculty members and senior Orthopaedic surgeons contrary to young and recentsurgeons.
Department of Orthopaedics, SVS Medical College, Mahabubnagar,AP 509002
MS,Professor DNB, Consultant Orthopaedic Surgeon, Sai Vani Super Speciality Hospital,Hyderabad,Telangana500029
MS, Consultant Sagar Lal Memorial Hospital, Hyderabad, Telangana500020
Introduction :
The usage of Hydrogen Peroxide looks a little anachronistic in the present scenario, wherein a lot of costly antimicrobial solutions are available. As an aficionado of Hydrogen Peroxide since 30 years, we have embarked on doing such a study on its usage, which is a cheap and easily available solution. Our interest is to highlight the usage of Hydrogen Peroxide in Orthopaedic practicefurnishinglittleknownfacts.Mostofthesurgeons are unaware of many facts pertaining to its usage as an adjunct to surgical debridement and intra operative use. Dealing with such subject in detail will certainly clear the myths and encourage its use benefiting many more patients. Our intention is to disseminate the information regarding the usage of Hydrogen Peroxide to the Orthopaedic fraternity, considering our experience of usingthissince30years.
Hydrogen Peroxide was prepared first by a chemist Thenard. Commercial name of Hydrogen Peroxide is Perhydril Hydrogen Peroxide in high concentration is usedinagriculture,chemical,foodandtextileindustriesas oxidizer,disinfectantandbleachingagent.
Properties of Hydrogen Peroxide : It is colorless, 2 odorless but not tasteless It is an unstable compound made up of two atoms of Oxygen and Hydrogen each. Anhydrous Hydrogen Peroxide is a syrupy liquid; which has a bluish tinge in thick layers. It is regarded as weak acid. Its boiling point is 152C and melting point is 0.4C. On heating it decomposes liberating oxygen. It is a very powerful oxidizing; reducing and bleaching agent thus effectively kills bacteria, virus and fungi. It is
22 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
suppliedinplasticbottles in contact with light and rough surfaces, so it used to be supplied in brown glass bottles. Of late it is supplied in opaqueplasticbottles.
Molecular structure : Hydrogen Peroxide has a nonpolar,non-linearstructure.Canbebestpicturedasoxygen atoms lying on the spine of a book, opened at an angle of o94 and the hydrogen atoms lying along each leaf of the openbook.
Strength of Hydrogen Peroxide solution : The concentration or the strength of Hydrogen Peroxide is usually expressed in terms of volume. For example 10 volume solution means that one milliliter of this solution will liberate 10 milliliters of oxygen. Strength is also expressedinweight/volume-w/v.
in3-6%strength.Itdisintegrates penetration into the deep muscles Thus there is insufficient evidence to make recommendations as regards to irrigation methods. No significant difference with respect to infection and bone healing were found by Anglen et al except for the wound healing problem. Thereforegiventheavailableevidenceitisnotpossibleto recommend any particular additive to the irrigation fluid in musculo skeletal wounds.The usage of 3% Hydrogen Peroxide intra operatively in almost all orthopedic surgeries has become a routine in our institutions. We use Hydrogen Peroxide in our hospital for conditions like open musculoskeletal wounds and fractures, intra operative use in clean wounds, joint replacement surgery, infected wounds – post op or otherwise, spine surgeries andinbonetumorsandcysts.
Commercial Hydrogen Peroxide (Perhydril) is supplied as 30% w/v and medical grade Hydrogen Peroxideissuppliedas3%w/v
Mechanism of action : Hydrogen Peroxide is nonallergenic. Hydrogen Peroxide is used for high-level 3 disinfection and sterilization. It provides hydroxyl free radicals and ions that can attack membranes, lipids, DNA and other essential cell components. The effervescence thatoccurswhenitisappliedtoopenwoundsisbecauseit reacts with the peroxidase enzymes present in blood.This reactionisexo-thermicinnature.Thisthermalinjurytothe vessels releases lipids, resulting in the formation of tissue thrombin, which in turn reduces bleeding or oozing from the wound. It also produces temporary spasm of small vessels which aids in haemostasis Hydrogen Peroxide does not act on dead tissue which can be readily observed during debridement where the effervescent action is seen only with living tissue. Dead and macerated tissues will not react with Hydrogen Peroxide because catalase is present in living tissues only. The decomposition of Hydrogen Peroxide liberates nascent oxygen, which can kill many pathogens, by damaging cell wall and cell membranes, leading to changes in the membrane permeability. All anaerobic strains of pathogens cannot surviveinthepresenceofHydrogenPeroxide.Noonecan 5,6 doubt its efficacy in treating infections topically A varietyofirrigationfluidshavebeenusedincludingwater, wine, milk, urine and vinegar since prehistoric times (biblical story God Samaritan Luke 10:33-34). Irrigation is the key component of the effort to prevent infection by decreasing bacterial load and removing foreign bodies. Copious amounts of irrigation fluids either at higher 7 pressure or otherwise is recommended by many In vitro studies by Bhandari et al showed macroscopic bone damage. Adili et al showed reduced mechanical strength of the bone in diaphysial fractures, some even sho
MATERIALSAND METHODS
The pretested questionnaire of 10 questions was prepared going through the scantily available literature and with our experience of using it since 30 years (author 1). This questionnaire was answered by 100 practicing orthopedic surgeons in and around Hyderabad, India. As regards the questions, we have classified them into knowledge based (q no. 1,2,5 & 6), practice based (q no. 3,7,8 & 10) and attitude based (q no. 4 & 9). The data collected was analyzed. Questionnaire in awareness and usageofhydrogenperoxide:
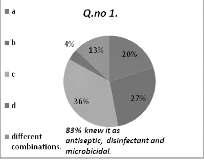
(1) You know hydrogen peroxide solution as : (a) Antiseptic, (b) disinfectant, (c) microbicidal, (d) bleachingagent.
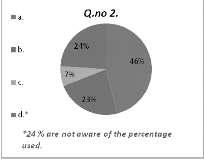
(2) Percentage of hydrogen peroxide solution commonlyused:(a) 3%, (b) 6%, (c) 30%, (d) do not know
(3) Conditions where you have used hydrogen peroxide:(a) Tidy injuries, (b) untidy injuries, (c) infectedwounds,(d)diabeticulcers,(e)others.
(4) Any other medical conditions you have tried like : (a) Pulmonary medicine, (b) bio oxidative therapy, (c) dermatology, (d)degenerativejointdisease,(e)noidea.
(8) Does it control hemorrhage : (a) Yes, (b) no, (c) notaware.
(9) Where did you use the solution: (a) Intra operatively, (b) orally, (c) nasally, (d) topically, (e) replacementsurgeries.
(10) Any untoward reactions encountered like : (a) Anaphylaxis, (b) surgical emphysema, (c) wound dehiscence,(d)nil, (e)embolicphenomenon.
‘The answers highlighted in red were presumed to be correct and considered for analyzing the responsefromthesurgeons.’
Results :
Among the hundred
Orthopaedic surgeons evaluated aftergoingthroughtheanswersto the questionnaire, the following wereobserved.
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017 23
Knowledge based indicators (Q.no’s :- 1,2,5 & 6).
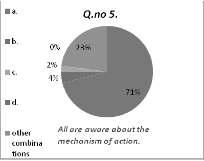
Theageofthesurgeonranges from 27 years to 81 years. The experienceofusingHO lessthan 2 10yearswasabout32%and68% had the experience of using HO for more than 10 years. Among these surgeons 61 % were from teaching hospitals and 39 % were non teaching as well as corporate set up. Analysis of knowledge based questions revealed that 83% of the surgeons knew it as antiseptic disinfectant and anti microbicidalandremainingknewit as bleaching agent, 69% were aware of its percentage of usage from 3 – 6%, 7% revealed it as 30% and 24% of the surgeons are unaware of the percentage of its use which is quiet significant. Seventy one per cent knew its mechanism of action as nascent O liberation, remaining were aware of its haemostatic and bactericidal actions
Sixtytwopercentwereaware that it is a sterile solution which can be used intra operatively, rest of them were not aware of its sterility
Analysis of attitude based questions revealed that seventy six per cent of the surgeons had no idea about its usage in medical conditions, remaining had an idea of its usage in dermatology, biooxidative therapy and degenerative joint disease
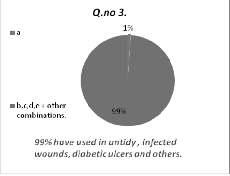
Fifty three per cent of the surgeons have used intra operatively in elective cases, 14% used topically and remaining 23% used the solution in replacement surgeries.Analysis of practice based questions revealed that 79% of the surgeons used in tidy, untidy and infected w o u n d s r e m a i n i n g
Attitude based indicators (Q.no’s :- 4&9)
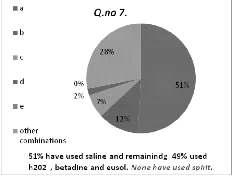
21% used in diabetic ulcers and other conditions. Regarding commonly used solutions for cleaning wounds 51% used saline, remaining have used HO, Betadine and EUSOL. None have used surgical spirit.81% have used it ashaemostaticagentandremaining19%haveneverused/ aware of it. Ninety four per cent did not come across any untoward incident which is quiet significant, 5% had embolic phenomenon which was later controlled with the help of anaesthesiologist and revived. One revealed anaphylaxis which proved fatal.
The results of the knowledge, attitudeandpracticesaredepictedinthe followingpiediagrams.
Discussion
:
Going through the responses for the questionnaire and the results, it looks a vast majority of surgeons know about the usage as an adjunct to surgical debridement and its usage in intra operative clean incised wounds
Knowledge about the percentage of hydrogen peroxide, mechanism of action looks to be well understood. Only few expressed reservations using itinviewofcomplicationslikeembolic phenomenon, wound dehiscence and surgical emphysema in punctured 9,10,11wounds The purpose of adding additives like hydrogen peroxide and
of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
Practice based indicators (Q.no’s : 3, 7, 8, 10)
povidoneiodineistokillthepathogensinthewoundsand this lessens the pathogen load that must be handled by immune system. Cell and tissue culture studies have shown that antiseptics have a concentration dependant detrimental effect on the viability and function of host cells. Wound healing and efficacy in preventing infection weretwoproblemsencounteredinevaluationofhydrogen peroxide in animal studies done by Geffery O Anglen (IBID 7). The negative effect in the study was wound dehiscence and little or no influence in controlling infection. In human studies as expressed by Anglen the usage of antiseptics in surgical wounds lowering the rate of infection, is not convincing and little or no information regarding usage of hydrogen peroxide in clean incised musculoskeletalwoundsisavailable.
Theideainusinghydrogenperoxideintraoperatively in clean musculo skeletal wounds is to show, in case of immenseoozing,bleedingfrominaccessiblesitespacking with hydrogen peroxide definitely stops the ooze and providesclearoperatingfield.
Inmajorjointreplacementsurgeries,openreductionof diaphysial fractures of long bones the usage of hydrogen peroxide is beneficial and exemplary.The area of surgical field becomes dry mainly in replacement surgeries where it is desirable for optimal cementing. This is practiced by most of the replacement surgeons who pack the femoral madullary cavity with 3% hydrogen peroxide
soakedribbongauge. In infection like osteomyelitis, diabetic foot, gangrene, post operative infections both superficial and deep hydrogen peroxide is extensively used without concomitant use of topical antibiotics, resulting in good healing. Inallthecasesofusageof hydrogen Peroxide, it is imperativetowashoffthe debris and residual hydrogen peroxide with normalsaline.
Usage of hydrogen peroxide in tumors and cysts based on the facts that it inhibits the giant cells and osteoblast metabolism in vitro, we have been using in all cystic lesions and tumors
12 likegiantcelltumor After using hydrogen peroxide extensively in all cases, since years, we have not come across the problems of wound dehiscence, wound healing nor did we encounter clinically significant 13 embolicphenomenonnorcardiacarrest
Observations :
The following were observed during the usage of hydrogenperoxide
14,15
(1)Lessbleedingandoozinginthesurgicalfield
(2)Immediateandtemporaryhypotension.
(3) Temporary changes in pulse rate, blood pressure, no change in oxygen saturation as noted by anesthesiologist.
(4) In major joint replacement surgeries medullary 16 cavitybecomesbonedrytofacilitateeasycementing
(5) By its effervescent action any small loose bony fragments are brought up in the surgical field to be removedeasily
A few case reports of embolism phenomenon while usinghydrogenperoxidewhichwerecorrectible
Absorption of suture material and decrease in tensile 17 strengthofthewoundarealsoreported .
Venous gas embolism due to hydrogen peroxide 18 irrigationinneurosurgeryasreported .
Conclusion :
Our study concludes that majority of the surgeons had good amount of knowledge about mechanism of action
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017 25
and other advantages. Only few had complications like embolicphenomenonwhichwerecontrolled.Quantitative and qualitative assessment of microscopic tissue damage after the usage was beyond the scope of this article.There were some variations in perception in using HO as regards to its toxicity, anaphylaxis during surgery in comparison with other microbicidal solutions. Difference inperceptiondependedontheexperienceofthesurgeonin usingitinvariousconditions.Ourstudyalsoshowssenior faculty members and senior Orthopaedic surgeons have more knowledge and attitude to use than the young and recent surgeons who are averse to use it.The advantage of using HO in all routine surgeries outweigh the rare complicationsanddisadvantages,whichwasexpressedby a few Inspite of the extensive knowledge of HO among 2 2 the surgeons, it is fraught with the danger of complications. Our experience of using it since 30 years shows that it can still be safe, less expensive and useful solution to be used in all Orthopaedic surgeries. Finally HO usage does not increase the risk of fatal and non fatal vascularocclusiveeventslikepulmonaryembolism,DVT, airandvenousthromboembolism.
Recommendations :
We strongly recommend the usage of HO in all 2 2 Orthopaedic surgeries as we have explained in introduction and discussion. During surgery the anesthetist must be informed about the possibility of adverse reactions like embolic phenomenon, anaphylaxis. To be watchful in using in case of puncture wounds. Special care is to be taken in using the solution in punctured wounds to avoid local surgical emphysema and compartment syndrome. It is important to wash off the debris along with the residual Hydrogen Peroxide with normal saline. To the objection that it is not a sterile solution to be used in clean incised wounds as expressed by some, this can be achieved by passing the solution through.Twenty two micron filters to make it devoid of contaminants. There is a need to understand and research about the implications of using HO in clean incised wound, as to reveal the amount of debris liberated and its detrimental effect on host tissue. We intend to extend our further study in detail about the various conditions in which we have used and the conclusions to be derived fromit.
Acknowledgements :
We thank Dr Surya Prabha MD, Professor of Social and Preventive medicine, Osmania Medical College, Hyderabad, India, for her valuable advice. All the Orthopaedic Surgeons who took part in the study. SVS Medical College, MahaboobnagarAndhra Pradesh, India. Allthefamilymembersoftheauthors.
REFERENCES
1 Textbook of chemistry, Intermediate yr. Board of Intermed ate Education 2002, Te ugu Academy Publications–preparationandpropertiesofH2O2.
2 NCERT,chemistrypart2,class11unit9 285-6.
3 h p/www a2c2 com/art c es/l fe ano2asp!p d=328ar c e text=lifejano2.
4 Hawkin FM, Campbell SE, Goldstein SA et al - H2O2 as topical haemostatic agent – Clinical Orthopaedics and Related Research 1984;186:244-8.
6 The many benefits of HO by Dr David G Williams (title –H2O2 Curse or Cure) posted Ju y 17 2003 http www educateyourself org cancer/benef s of H2O2 html.
7 Jeffrey O Anglen MD — Wound irrigation in musculoskeletal surgery – Journal of American Academy of Orthopaedic Surgeons,Vol.9, no.4July,August2001.
8 Bhandari M, Schemitsch EH, Adili A — High and low pressure lavage of contaminated fracture tibia – An in vitro study of bacterial adherence and bone damage. Journal Orthopaedics and trauma 1999;13:526-33.
9 Shukrimi A, Aminuddin CA, Azril MA — Venous gas embolism following H2O2 irrigation during debridement in osteomyelitis. Medical Journal Malaysia 2006;61:88-90
10 D Uday PK, Singh AK — Venous oxygen embolism due to H2O2 irrigation posterior fossa surgery. Department of Anaesthesia, Indira Gandhi Institute of Medical Sciences, Patna, India. Journal of Neurosurgical Anesthesia 2000; 12: 54-6.
11 HO could cause absorbable sutures to come apart –decreased tensile s rength Research rom UT Southwestern Medical Centre. Source – UT Southwestern MedicalCentre.
12 Nicholson NC, Ramp WK, Kneisl JS — HO inhibits Giant Cell Tumor and osteoblast metabolism in vitro. Department of orthopaedics, Carolina Medical Centre, Charlotte NC 28232-2861USA.
13 AJ Timperly FRCS Edin, Bracy FRCS Edin. Cardiac arrest followinguseofHO Volume4Issue4Dec1989–369-70.
14 Lichtenbaum R, deSouza AA, Jaff JJ — Intramural HO during meningioma resection. Dept neurosurgery NY, University School of Medicine NY. Neurosurgery 2006; 59: (4supplement2).
15 Potyodyl, Lottenburg L, Andersa J — Use of H2O2 for achievingdermalhaemostasisafterburnresection. Journal of Burn Care Research 2006;27:99-101.
16 Masomori, Shigemattu, Masaru Kitajama — Effect of H2O2 as artificialjoint– The Journal of Arthroplasty 2005;20:63946.
17 LineaweawerW,McMorrisS,SaucyD,HowardR—Cellular and bacter a oxicity o commonly used op ca antimicrobials. Plastic and Reconstructive Surgery 1985; 75:394.
18 Hitoshi Morikawa MD, Hiroyuki Mima MD, Hishashi Fujija — oxygen embolism due to H2O2 irrigation during cervical spine surgery – a case report. Canadian Journal Of Anesthesia 1995;42:231-3.
Observational Study
Profile of road traffic accidents from semi-urban area of Bihar
1 2 A Kumar , R R Jha
Road traffic accidents cause 1.25 million deaths throughout world. Majorities of them are young adults aged between 15 to 29 years. In India 1,42,485 people died due to RTA in 2011. The worst suffers are "vulnerable road users" pedestrians, cyclists and motorcyclists. Major risk factors for accidents are drink and drive, not using protective measures, speed, defective maintenance of vehicle, distracted driving etc. A cross-sectionstudywithconvincesamplingmethod.Combinationofinterviewmethodandhospitalrecords wasusedtogainrequiredinformation.Mostofthevictimsweremaleofyoungeragegroup.Averagestayfor major injuries was almost twice that of minor injuries. No seasonal variation in accident was noted. Alcohol was strongly associated with severity of injury sustained. Most of the accidents were reported by twowheelers. With development of country more vehicles on road and increases in road congestion thus more probability of road traffic accidents. There is an urgent need of intervention in terms of public awareness aboutroadsafetyandcomplianceofstricttrafficrules.
[J Indian Med Assoc 2017; 115: 26-7 & 30]
AKey words : RTA, severity of injury, drink and drive, Bihar. ny accident resulting due crash originating from, ter-minatingintoorinvolvingvehiclepartiallyor fully on public road is known as road traffic
accidents.Roadtrafficaccidentscause1.25milliondeaths throughoutworldwhere,90%offatalityoccursinlowand middle income countries Majorities of them are young adults aged between 15 to 29 years.As per 2012 data RTA is ninth leading cause of death worldwide, accounting 2 2.2% of all deaths RTAis not limited to mortality but 2050 million suffers non-fatal injuries leading to major disabilities.
Development in India is accompanied by major development in infrastructures and increase in vehicles. RTA in India is no exception, as by numbers of fatalities due to RTA.According to 2011 data 1, 42,485 people died 3 due RTA. These accidents involved more than 18000 people in age group of 15-24 years. Every year the numbers are increasing steadily. The worst suffers are "vulnerable road users" pedestrians, cyclists and motorcyclists. Unlike developed world in India twowheeler are more in numbers and being unstable, more venerable to accidents. RTAis matter of national concern. Majorriskfactorsforaccidentsaredrinkanddrive,nouse or improper use of protective measures like helmet/seat belts etc, speed, defective maintenance of vehicle,
Department of Community Medicine, Narayan Medical College and Hospital,Sasaram,Bihar821305
1MBBS(MAHE),MD(PSM),AssistantProfessor
2MBBS,MD(CommunityMedicine),AssistantProfessor
Theaveragelengthofstayofpatientinhospitalwas6.9 days with median stay of 3 days. Among total cases 41(41.8%) cases were admitted with major injury and 57 (58.2%) were of minor injuries. Average stay of patients with major injury was 7.5 days and with minor injury it was 3.6 days. There are various factors which is responsibleforRTA.
Time and Season Factor It was found that 70 (71.4%) of the accident occurred during day time and 28 (28.5%) during night. The difference in type of injury sustained depending upon duration of accident (Table 1) was found out to be statically insignificant where, p= 0.746103. The difference in injury depending on weather condition (Table 2) was found to statically insignificant where,p=0.08052.
Alcohol and RTA Drink and drive is major risk factor of RTA. Use of alcohol by drivers was accessed by smell of breath or other evidence like ineptitude in behavior, was considered for some evidence of alcohol consumption (Table 3) by found that there is a probability ofmajoraccidentifdriverisintoxicated.Whenchi-square wasapplieditwasfoundtobestaticallysignificantwhere, p=0.0045.
- Types of vehicle involved in RTAs (N=98)
Table 4 — Severity of injury depending upon Type of vehicle
Major Minor TwoWheeler(59)
tive of the study was to find
distracted driving etc. Objec theprofileofpatientsofRTAandtofindassociationofrisk factorswithtypeofinjurysustained.
MATERIALAND METHODS
A cross-section study was done at tertiary center of Rohtas. The hospital is situated 7 km from national highway; hence most of RTA comes to this hospital. The studywasdoneforoneyearie,January2015toDecember 2015. The subjects were enrolled using convenience sampling technique. During this period all the RTAcases admittedinthehospitalweretakenup,withonlyexclusion criteria being those who were severely sick or not willing to participate. Data was collected using pretested and predesigned questionnaire and further information was collected using hospital records. Questions accessed socio-demographic profile, type of vehicle involved, use of alcohol and severity of injury sustained The participation was voluntary Data was analyzed using Microsoftexcelsoftware.
OBSERVATION
Inthisstudy98casesweretakenupwhere79(80.6%) were males and 19 females (19.4%). The mean age of participantswas35.3years,wheremeanageofmaleswas less than females, which were 33.7 years and 42.1 yrs respectively Most of patients were from Rohtas district which was 78.5% followed byAurangabad district 20.5% andrestwerefromotherareas.
Type of vehicle and RTA Majority of RTA was reported by two wheeler (Fig 1) as its unstable ride but accident involving four wheeler reported maximum proportion of major injury (Table 4) followed by heavy vehiclesliketruck/dumper Whenchisquarewasappliedit wasfoundtostaticallysignificantwhere,p=0.012582.
DISCUSSION
RTAis a major NCD problem which claims ninth spot inleadingcauseofdeathsworldwide.InIndiathereisone 4 accident every minute Majority of victim are of younger
Table 1 — Severity of injury depending upon duration of accident
Durationofday Major Minor
Day 30 40 =0.1048
Night 11 17 DF=1
Table 2 — Severity of injury depending upon season
Season Major Minor Total
Summer 22 31 53(54.08%)
Winter 13 9 22(22.44%) =5.0385
Monsoon 6 17 23(23.46%) DF=2
Total 41 57 98(100%)
Table 3 — Severity of injury depending upon Driver's intoxication Intoxicated Major Minor
age ie, in their productive age group. In this study it was noted that mean age of victim was 35 years where 80% of them were males. Study done by Baruah and Chaliha in 2013-14atGauhati,foundalmostallinvolvedweremales with most of the in age group of 20-29 years. Similarly 6 study done by Singh et al found mean age of victim to be 30.91yearswithhighestnumberofvictiminagegroupof 20-30years.
In this study severity of injury was independent of timing of a day and season of the year. It was found to be statically insignificant. As most of patient of RTA were fromNHwhichisfourorsixlanes,sotheconditionofthe road may be the reason for this. Moreover the local traffic usesby-lanesfortheirdailycommute,leadingtodecrease 7 congestion of NH. In 2004-05 Mishra et al found peck numbers during evening and morning hours. This may be due to fact that place of study was done in city as morning andeveninghourshavehighercongestionandhencemore numberofaccidents.Moreovertheyalsonotedriseinfatal accidents in month of January This was attributed to foggyconditionofhillyarea.In2008-09Singh et al found thatmaximumaccidentswerenotedduringwinterseason. Again it may be due to dense fog during winter in 8 catchmentareaofSIMS.In2010-11Bayan et al foundthe peakinaccidentsduringnightasthestudywasdoneincity and it may be due to it to low visibility and peak hours for officecommuters.
In this study it was found that severity of injury was associated with driver intoxication. This was statically significant. Patil et al found that 29.5% of drivers who meet accident were under influence of alcohol. Similarly 2013-14 Baruah and Chaliha noted that among all fatal
(Continued on page 30) Journal of
Fig.1:
Observational Study
Knowledge of cardio-pulmonary resuscitation in medical undergraduates
The objective of the study was to evaluate the knowledge of Cardio-Pulmonary Resuscitation in medical undergraduates (final year MBBS students & Interns). The study was designed as a cross sectional questionnaire based study, conducted at a private medical institute. Data was analyzed with SPSS version 11.101. Out of 73 participants, only one scored passing percentage of > 85%. More than half of the respondents (68.49%) scored in the range of 10-18 marks. The overall performance of students as well as interns was very poor. Interns were found to be better than students (p < 0.001) in their knowledge of CPR. Conclusion: Knowledge of CPR must be one of the core topics in medical curriculum. Every medical practitionermustcompulsorilyattendacertifiedcourseinCPRforrenewaloftheirlicense.
[J Indian Med Assoc 2017;115: 28-30]
Key words : Cardiopulmonary resuscitation, knowledge of CPR, medical curriculum.
Immediate commencement of resuscitation may increase survival rate amongst victims of cardiac
arrest and Cardiopulmonary Resuscitation (CPR) is anemergencyprocedurewhichisperformedinaneffortto manually preserve intact brain function until further measures are taken to restore spontaneous blood circulationandbreathing.TheobjectiveofCPRistodelay tissuedeathandtoextendthebriefwindowofopportunity for a successful resuscitation without permanent brain damage. It may be performed both in and outside of a 1hospital The success of the first golden minute after cardiopulmonaryarrestdependsentirelyontheskillofthe personnelattemptingrescue.
CPR skills based workshops are held regularly by various medical organizations and it is also included as a one hour lecture in the medical curriculum for the final MBBS course. Medical undergraduates usually do not undergo any formal training in CPR, thus when they become interns they have no practical skills for prompt 2,3 institutionofrescueprocedures
It is no wonder then that most of our medical students feel helpless when they suddenly come across a situation of a critically ill patient. There are not many studies from India, which assess the expertise of health care professionalswhooftenassumetheroleoffirstresponders
Department of Pediatrics, NKP Salve Institute of Medical Sciences and ResearchCentreandLataMangeshkarHospital,Nagpur440019
MDAssociateProfessor
MDProfessor
MBBS,Student
MDAssistantProfessor
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017 29
Study Design : Cross sectional questionnaire based study
StatisticalAnalysiswasdonebySPSSversion11.101. Descriptive statistics and Mann Whitney U Test was applied.
Results :
There were 73 respondents, 51 (69 86%) undergraduatesand22(30.13%)interns.Auniformlylow scoring performance was observed amongst both interns and students (Table 1). Majority of students (76.5%) and 50% of interns, scored in the range of 10-18 marks (Table 2).Whilenoneoftheundergraduatestudentswasdeclared successful,onlyoneoutof22interns(4.54%)scoredmore than 85% and was declared successful (Table 3). Though the overall performance was very poor, two-sample Wilcoxon rank-sum (Mann-Whitney) test was applied to comparetheknowledgeofstudentsandinterns.Therewas asignificantdifferenceinknowledge(pvalue0.001),with internsscoringsignificantlybetter(Table4).
Discussion :
inemer
gencysituations.Thisstudywasconductedtotest
the knowledge of CPR amongst final MBBS students and Interns. Interns were included because this is the group which is posted directly in rural health centers with only the basic knowledge they acquire during their undergraduate course and in many remote areas of the country, interns may be the sole providers of health care andalsothefirstresponderstocardiacarrest.
Objective : To evaluate knowledge of CardioPulmonary Resuscitation in medical undergraduates (finalyearMBBS)&Interns.
Material & Methodology :
This study was conducted in a private teaching institute. It is a questionnaire based cross sectional study andallthefinalMBBSstudentsandinternsfromthesame year who consented to participate in the study were included The final MBBS students had already completed all their lectures at the time the study was conducted.
A prevalidated questionnaire on CPR was given to them. The questions included were based on American HeartAssociation guidelines 2010 for Cardio-Pulmonary Resuscitation.Therewere35multiplechoicequestionsin English with only one correct answer in each. Students were given 30 minutes to complete the task. Each correct answer was awarded 1 mark. There were no negative marking. The test was conducted on the spot without any prior intimation. Students who scored at least 85% were considered successful and declared as having knowledge ofCardio-PulmonaryResuscitation.
Table 2 — Distribution of participants based on range of marks
Table
CPR is a life saving skill to be acquired not just by health professionals but also general public because cardiopulmonary arrests are more common in the out of 4, 5 hospital scenario While the developed countries have devised a successful policy wherein even school children are taught CPR skills, in India even the medical curriculum does not give enough emphasis on acquiring knowledgeofCPRattheundergraduatelevel.Neitherthe Govt. of India nor Medical Council of India has made it mandatory for interns to attend a certificate course in Table 1 — Scorewise distribution of participants
CPR. Our in all interns at the beginning of their internship in which CPR is taught in a one hour session, but this remains an individual policy by institutes not mandated by any governing body In this background, the results shown in ourstudyisnotverysurprising.Infact,otherstudiesfrom 7 India have also shown similar observations The overall scores in our study were very low and all subsequent analysis is made only to compare the students and the interns. Thus the significant difference observed between the students and interns just shows that the one hour session undergone by the interns prior to participating in thisstudyprobablyhelps,thoughonlyinasmallway Such results are really disturbing because CPR is one of the fundamental emergency technique performed in medicalpractice,andlackofknowledgecanhavedreadful consequences, especially in remote health care areas where the only tool to deal with emergencies are the skills
stitute conducts orientation programme for
30 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017 in CPR in the absence of any other life saving equipments 8 ormedicalfacilities
This paper assumes greater significance in the background of a national debate on the issue of compulsory posting of interns in rural areas. This study also serves to send a strong message to policy makers to make acquisition of CPR skills a mandatory step in obtainingaMBBSdegreeeitherduringtheundergraduate course or during internship and an essential criteria for renewal of license for medical professionals especially considering the fact that already there are private organisations in India like the Indian Academy of Pediatrics, the Cardiology society etc. who have the infrastructure and manpower required to conduct such programmesacrossthewholecountry
Conclusion :
The basic knowledge of cardiopulmonary resuscitation amongst medical students is inadequate. A major revision in the medical curriculum is required to rectifytheerror Infact,knowledgeofCPRshouldbecome a ‘must know’category of topic in medical curriculum, so that all forms of evaluation must include testing this knowledge Renewal of license for all medical professionalsshouldalsomandateattendingaCPRcourse everyfewyears.
(Continued from page 27)
cases
Case Report
REFERENCES
1 Sasson C, Rogers MA, Dahl J, Kellermann AL — Predictors of survival from out-of hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes 2010;3:63-81.
2 Skinner D, Camm A, Miles S — Cardiopulmonary skills of preregistrationhouseofficers. BMJ 1985;290:1549-50.
3 Casey WF — Cardiopulmonary resuscitation: a survey amongjuniorhospitaldoctors. J RSoc Med 1984;77:921-4.
4 Sankar J, Janakiraman L, Ramesh J, Ranjith S — Impact of PALS on pediatric resuscitation Knowledge, Asian Journal of Critical Care 2007;3:18-21.
5 Zaheer H, Haque Z — Awareness about BLS (CPR) among medical students: status and requirements. Journal of Pakistan Medical Association 2009;59:57-9.
6 Chandrasekaran S, Kumar S — Awareness of basic life support among medical, dental, nursing students and doctors. Indian J Anaesth 2010;54:121-6.
7 Avabratha SK, Bhagyalakshmi K, Puranik G, Shenoy KV, RaiBS—AStudyoftheKnowledgeofResuscitationamong Interns. Al Ameen J Med Sci 2012;5:152-6.
8 Zaheer H, Haque Z — Awareness about BLS (CPR) among medical students: status and requirements. JPMA 2009; 59: 57.
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
Epidural anaesthesia for fixation of intertrochanteric fracture in a 108-year old elderly patient
Leena Goel , Pabitra Ghoshal , Rina
1 2 3 3
Cordeiro , Sambhram Shenoy
Age itself is an independent morbidity and mortality risk factor for a long list of diseases and injuries and awareness of such additional risk factors may modify our perioperative anaesthetic management in a way that will ultimately improve the postoperative outcome. Here we describe the successful anaesthetic managementinararecaseofa108yearoldfemalewithintertrochantericfractureofrightfemurbydynamic hip screw fixation. Taking into account her age and compromised cardiac function, epidural anaesthesia was planned as it had several distinct advantages over general anaesthesia in terms of an improved pulmonary and myocardial function, decreased chances of thromboembolic complications, early mobilizationandpostoperativeanalgesiathroughepiduralcatheter.
J Indian Med Assoc 2017; 115: 31-2 & 34]
Key words :Age factors, epidural anaesthesia, mortality.
Elderly patients’ still have the highest postoperative mortality and morbidity rate in the adult surgical population in spite of advancement in knowledge and
blood.Fromvariousstudiesitiswelldocumentedfactthat alcohol is one of the major risk factor for RTA. In this study most of the RTA was reported by two wheelers followed by four-wheeler. Four-wheeler and heavy vehiclehadbiggerimpactthantwo-wheeler,causingmost 9 of the major injuries to victims. Patil et al in their study found that highest number of victims were two-wheeler occupants, followed by four-wheelers. Similarly Singh et 6al foundthatmaximumnumberofcasesandcasualtywith two-wheelers.
CONCLUSION
In India, there is rapid urbanization and modernization. This development also means more number of vehicles and increases in road congestion thus more probability of road traffic accidents.The result from this study clearly indicates alcohol as major preventable factorforRTA.Italsopointsmorenumberoftwo-wheeler involvement in RTA. If strong political and public commitment supports the implementation of preventive measures like use of protective gears, following of traffic rules, good medical emergency support on highways can preventlotsofmorbidityandmortality.
REFERENCES
1 Road Traffic Injuries: WHO: May 2016. Available on http://www.who.int/mediacentre/factsheets/fs358/en/ [last accessedon02/07/16] of RTA nearly 20% of them had alcohol in their
2 Factsheet: Top 10 causes of Death: WHO: May 2014. Available on http:// www. who.int/ mediacentre/ factsheets/ fs310/en/[lastaccessedon02/07/16]
3 OGD Platform India: Ministry of Road Transport and H ghways, Government of India: Avai ab e at https://data gov n/ca alog/tota -number-road-accidentsindia[lastaccessedon15/07/16]
4 Road Accidents in India: Issues and Dimensions. Ministry of Road Transport and Highways, Government of India. Ava lab e from: http //www unescap org/ s es/defau / files/2.12.India_.pdf.
5 BaruahAM,ChalihaR—AstudyofIncidenceofAlcoholUse In Fatal Road Traffic Accidents. J Indian Acad Forensic Med 2015;37:12-5.
6 Singh R, Singh HK, Gupta SC, Kumar Y — Pattern, Severity and Circumstances of Injuries Sustained in Road Traffic Accidents:AtertiaryCareHospital-BasedStudy. IJCM 2014; 39:30-4.
7 Mishra B Sinha ND, Sukh a SK, S nha AK Epidemiological Study of Road Traffic Accident Cases from WesternNepal. IJCM 2010;35:115-9.
8 Bayan P, Bhawalkar JS, Jadhav SL, Banerjee A — Profile of non-fatal injuries due to road traffic accidents from a industrialtowninIndia. IJCIIS 2013;3:8-11.
9 Patil SS, Kakade RV, Durgawale PM, Kakade SV — Pattern of Road Traffic Injuries: A study From western Maharastra. IJCM 2008;33:56-7.
techniques of geriatric pathophysiology Preoperative clinical assessmenttodetectpatientsathighriskofpostoperativeevents, and specific intra-operative and postoperative anaesthesia management are important to minimize postoperative adverse eventsintheelderly
Among the steadily increasing population of surgical patientsaged65yearsandolder,thefastestgrowingsectionisof individuals85yearsorolder Physiological reserve is reduced and mortality becomes more common with increasing age. Cardiovascular diseases, renal disease, compromised respiratory function, neurosurgical pathology and metabolic disease are more likely in the elderly
The incidence of diabetes is up to 25% in those aged over 80 years. For improved outcome in elderly patients surgery is recommendedbetween24to36hoursafteradmission Epidural Anaesthesia and Analgesia have been demonstrated to improve postoperative outcome and alternate the physiological response to surgery In particular, significant reduction in perioperative cardiac morbidity (30%), pulmonary infections (40%), pulmonary embolism (50%), ileus (-2 days), acute renal failure (30%)andbloodloss(30%)werenoted
CASE REPORT
A108 year old female (Fig 1) was scheduled to undergo an internal fixation by dynamic hip screw for intertrochanteric fracture of right femur Patient was a known case of ischemic heart disease (IHD) since 10 years and was on tablet enalapril 5 mg, atorvastatin 20 mg and aspirin 75mg once a day, tablet betaloc 25 mg and isosorbide mononitrate 20 mg twice a day
Shealsohad for which she was started on tablet cefexime 200mg twice a day for5days.
The patient was obese and her BMI was 32.87 kg/m Her pulse rate was 86/minute regular and blood pressure 138/72 mm of Hg. She was edentulous and her haemoglobin was 9.7gm%. Total and differential counts were normal. Her random blood sugar was 92 mg%. Her renal function tests were deranged. Serialrecordingofserumcreatinineshowedacontinuousriseup to2.2mg/day PreoperativeArterialBloodGases(ABG)analysis showedpH–7.42,pCO of40.4mmofHg,pO of70.2mmofHg and 125.9 mEq/L HCO BE-1.3 mEq/L and SpO 92%. Nephrologists suggested maintaining adequate hydration. Renal ultrasoundwasnormal.Herbloodsugarlevelsandliverfunction tests were normal. Her ECG had changes suggestive of an old anterioseptal myocardial infarction. Echocardiography revealed a calcif ed aortic valve, akinesia of who e septum, hypokinesia of anterior wall, concentric left ventricular hypertrophy and LV grade-1 diastolic dysfunction with LV feverwithcoughandexpectorationsinceoneweek,
Fig 1—A108 year old patient
32 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
ejection fraction 45% Her chest X-ray showed mild emphysematous changes. Pulmonary functioned test suggested mild restrictive and obstructive changes.The patient was started on enoxaparin 40 mg subcutaneous OD which was continued in thepost-operativeperiod.Patienthaddementia. Consideringher age, medical and surgical conditions, epidural anaesthesia was planned. She was kept nil by mouth 6 hours prior to surgery and was given 5 mg of Alprazyolam the previous night. In OT intravenous access was secured with an 18 G cannula. Monitoring of pulse rate, electrocardiography, oxygen saturation, non-invasive blood pressure, urine output and temperaturewasstartedandcontinuedthroughoutthesurgery She was preloaded with 500 ml of Ringer Lactate Solution.
An 18 G Tuohy needle was inserted via a para median approach into L- L interspace using the loss of resistance technique in sitting position.An epidural catheter was inserted via the Tuohy needle and was fixed at 8cm (12 hours after the dose of enoxaparin). Test dose of 3ml 2% lignocaine with 1:200,000 epinephrine was injected. 8ml of 0.5% bupivacaine was given in a titrated manner through catheter and the block was ensured to beuptothesensorylevelofT8.
Oxygen was given by mask at 6L /min. Ephedrine was kept readyintraoperatively Meanbloodpressureof90-100mmofHg was maintained with the help of ephedrine and crystalloids. We avoided co loids in view of her altered renal status
Intraoperating blood loss was 300 ml and her urine output was 100 ml The patien remained hemodynamically stable throughout the 90 minutes procedure. After surgery the patient was shifted to the Intensive Care Unit (ICU) for monitoring.
Postoperative analgesia was given by an epidural infusion of 0.125 % Bupivacaine with Fentanyl 2mcg /ml at 2-4 ml/h. The patientwaswellpostoperativelyandshewasdischargedfromthe hospitalafteroneweek.
DISCUSSION
Management of geriatric patients can be challenging to an anaesthesiologist due to limited organ reserve, compromised organfunctionsanduniquediseasepredispositions.
Functional status can be expressed in Metabolic Equivalent ofTask(MET)levels.It’soneofthemostimportantpredictorsof perioperative outcome in elderly surgical patients. Our patient hadaMETlessthan4,ie,poorfunctionalcapacity Three factors contribute to the increased perioperative risk duetoanadvancedage.
(1) Physiological aging is accompanied by a progressive decline in resting organ function. Consequently the reserve capacity to compensate for impaired organ function, drug metabolism and added physiological demands is increasingly impaired.
(2) Ageing is associated with progressive manifestation of chronic diseases which further limits baseline function and accelerateslossoffunctionalreserveintheaffectedorgan.
(3) The increased intake of medications and altered pharmacokineticsandpharmacodynamics.
Renalbloodflowandkidneymassdecreasewithage.Muscle bulk decreases with age resulting in reduced creatinine production; hence even a modest rise in serum creatinine may represent a significant renal impairment and should be viewed cautiously Impairment of sodium handling, concentrating ability and diluting capacity predisposes elderly patients to dehydration and fluid overload Preoperative fluid replacement must be managed carefully n eld
erlypatientstopreventdevelopmentofpostoperativepulmonary oedema as a result of age related prolonged extracellular water (ECW)expansion.Comparedwith5daysforyoungpatientswith sepsis, elderly septic patients require 10 days to excrete over expanded ECW Renal functions deteriorate with age and hence urineoutputmonitoringandpulmonaryarterycatheterizationare invaluabletoguidefluidtherapyinelderlypatients
Perioperative hypothermia is more frequently pronounced and prolonged in the elderly who have compromised ability to regain norma thermoregulatory control quickly In the postoperative period for the elderly, mild hypothermia can elevate norepinephrine concentration and increase peripheral vasoconstric ion and arterial blood pressure, thereby contributing to cardiovascular ischemia and arrhythmia. It may also increase blood loss during total hip replacement procedures thereby risking wound infection, decreasing drug metabolism andprolonginghospitalization
Adverse perioperative effects on the cardiac, pulmonary, cerebral systems and cognitive functions are major concerns in caseofelderlypatients
RegionalAnaesthesia techniques attenuate the perioperative stress response improving myocardial oxygenation, reducing release of troponin T and effectively controlling unstable 10 refractory angina pectoris Epidural Anaesthesia has the ability to completely block the sympathetic response to surgery below the umbilicus and to significantly blunt the response to surgery above the umbilicus. Local epidural anaesthetics block the sympathetic response, whereas epidural opioids incompletely blockthesignal.Thisisconsistentwiththefactthatopioidsonly block the nociceptive pathways of sympathetic activation while local anaesthetics inhibit both nociceptive and non-nociceptive 11routes
Cardiac morbidity is the most common cause of death after majorsurgicalproceduresinelderly Anaesthetictechniquesthat reduce cardiac morbidity will therefore have potential for improving surgical morbidity and mortality Since perioperative excessive activation of the cardiac (T-T) sympathetic nervous system by surgical stress has been demonstrated to increase indices of myocardial oxygen demand, while inducing coronary artery vasoconstriction (decreasing supply), thus resulting in clinical correlates of myocardial ischemia such as ST segment changes,anginaandarrhythmias.ThoracicEpiduralAnaesthesia (TEA) with local anaestheticscan produce a selectivesegmental 12, 13 blockade of the cardiac sympathetic innervation (T-T)
Thoracic Epidural Anaesthesia and Analgesia (TEAA) can reduce incidence of postoperative atelectasis, pneumonia and hypoxemia. TEAA improves measurable pulmonary function by blunting spinal reflex arcs, controlling pain and increasing chest wall compliance.The use of systemic and epidural opioids is associated with a higher incidence of hypoxemic events when 14 comparedtoepiduralanalgesiawithlocalanaestheticalone
EpiduralAnaesthesia andAnalgesia (EAA) decreases blood loss during total hip ar hroplasty thereby preventing intraoperative hypertension in patients with intraoperative ischemia and results in lower incidence of reoperation for 15 inadequate tissue perfusion during vascular surgery . It also attenuatesthehypercoagulableperioperativestateanddecreases thromboembolic complications associated with surgery by blunting the sympathetic response and improving lower 16 extremitybloodflow
EAA preserves postoperative immune function by
(Contined on page 34)
Case Report
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
Placenta accreta — a multidisciplinary team approach
The management of placenta accreta is a night mare. They are at increased risk for uncontrolled haemorrhage.Thispatientwithhistoryofpreviouscaesareansection,typeIIplacentapraeviawith accreta, with complications of intra-uterine growth refardation, oligo-amnios was planned for elective classical caesarean section preceeded by prophylactic uterine artery embolisation. This case report was been presented to emphasise a "team based approach" compris ng obstetrician, neonatologist, anaesthesiologist, interventional radiologist and transfusion medicine specialist for prevention and life savingstrategiestopreventmorbidityandmortality.
J Indian Med Assoc 2017;115: 33-34]
Key words : Placenta accreta, uterine artery embolisation, multidisciplinary team approach.
Apatient with placenta accreta is at increased risk for uncon-trolled haemorrhage. The clinical and surgical management should focus on prevention and treatment
ofuncontrolledhaemorrhage.
CASE REPORT
A 29-year-old second gravida with previous caesarean section done for foetal distress 2/ years back was referred at 33weeks, 4days gestational age with the diagnosis of placenta praevia type II anterior, suspected placenta accreta, with intrauterinegrowthrefardationandoligoamniosfortertiarycare.She had regular antenatal check up. Placenta praevia with suspected placentaaccretawasdiagnosedat33weeks.
Examination — On admission she had no episodes of bleeding per vaginum or pain abdomen. Her vitals were stable, clinically she had evidence of IUGR and reduced liquor, with an estimated foetal weight of 1500g. She was administered two dosesofsteroidprophylaxis.
Investigation — Ultrasoundrevealedagestationalageof2829weeks,cephalicpresentation,placentawasanterior lowlying and the edge covering the os with increased retroplacental vascularitywithanestimatedfoetalweightof1421±213g,AFI–4.6. Her Hb was 12gm/dl%, renal and liver function tests were normal.
Management — In view of the previous cesarean section, presently with type II placenta previa with accreta, severe oligoamnios and IUGR, she was planned for elective classical caesarean section; preceeded by prophylactic uterine artery embolisation(UAE).
Earlier the interventional radiologist sited the uterine catheter under fluoroscopic guidance, followed by a classical caesarean section under general anaesthesia in catheter laboratory. Per operatively there was increased vascularity over lower uterine segment and on the bladder A baby girl was delivered as breech weighing
Department of Obstetrics & Gynaecology Sri Ramachandra University Chennai600116
MBBS,MD,DGO,Professor&HeadoftheDepartment
MBBS,DGO,DNB,MNAMS,FICS,AssociateProfessor
MBBS,MD,DGO,DICOG,DNB,AssociateProfessor
MBBS,MD,AssistantProfessor
1590g,with an APGAR of 8/10 and 9/10. The placenta was extending from the upper to the lower uterine segment (LUS) anteriorly and was partially covering the os. It was highly vascularandmanualremovalofplacenta(MRP)wasdone.There was profuse bleeding from the placental site and LUS. Hence it was decided to proceed with UAE. Left uterine artery was embolised with graded PVAparticles and gel foam and the same was repeated on the right uterine artery Post embolisation angiogramrevealedcompleteabsenceofabnormalblushandthe vascularity on either side. Patient tolerated the procedure well andtheperipheralpulsationwasfelt.
Uterus was closed in layers.Two units of packed cells were transfused intra-operatively in view of blood loss of around 1500ml. She was kept under observation in ICU for 24 hours. Postoperativeperiodwasuneventful. Sutureswereremovedon 9thpostoperativeday(POD)anddischargedon10thPOD.
DISCUSSION
A team based approach is needed for prevention and life savingstrategiestostopbleeding.Bydefinitionplacentaaccreta is abnormal placental attachment with absence of both decidua basalis and Nitabuch membrane. In placenta accreta there is superficial attachment of the trophoblastic villi to myometrium. The risk factors include prior uterine surgery, multiparity, advanced maternal age and previous uterine curettage. This patient had a previous caesarean section as the risk factor The incidenceofplacentaaccretahasclimbedfrom1:2,510in1980’s to1:533in2002and1:210in2006.Thatislikelytoberelatedto the rising caesarean section rates in the same period. After a prior caesarean section, a woman is twice as likely to develop placentaaccreta Withtheadventofultrasound,placentaaccreta can be diagnosed as early as first trimester and so caesarean section can be scheduled before labour, thereby reducing the morbidityand themortality
In Maternal Foetal Medicine Unit (MFMU) network study, the mean gestational age was 35 years unlike in our patient; where termination of pregnancy was done at 33-34 weeks itself in view of IUGR and severe oligo-amnios. Routine MRI is not required when ultrasound shows evidence of placenta accreta.
33
34 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
(1) Counseling the patient and her attendants regarding the risks, trauma to surrounding structures, treatment options, consent for hysterectomy in case of uncontrolled haemorrhage anddocumentingthesameinmedicalrecords
(2)Preparationformassivebloodtransfusion.
(3) Alerting the interventional radiology team and the vascularsurgicalteam.
(4)Preparationforstepwisedevascularisation.
InthispatientafterMRP,itwasnecessarytoproceedwiththe UAE in view of uncontrolled haemorrhage from placental site and LUS. Even though conservative management is not an option for placenta increta and percreta, it has a role in placenta accreta The post operative complications like laryngeal and pulmonary oedema, prolonged intra-operative hypotension leading to renal compromise, Sheehan’s syndrome, thromboembolism were not encountered in this patient.This is due to the pre-operative diagnosis and preparations, the prophylactic measures taken and the team approach. Such measures will
(Contined from page 32)
attenuating Concentration (MAC) of inhaled anaesthetics and minimizing the use of parenteral opioids, thus helping to maintain a 17 competent immune system It also allows better pain control with less sedation, and increase post-operative pO, all of which 18 maycontributetoimprovedpostoperativecognition
So patients undergoing major operations under EAAbenefit from improved venous blood flow, attenuation of the sympathetic response to surgery, anticoagulant properties of local anaesthetics, early mobility and lowering of MeanArterial Pressure (MAP).These advantages strongly support the use of Epidural Anaesthesia as the anaesthetic technique of choice in thepresentcase.
To facilitate early mobilization, improve recuperation and reduce morbidity with decreased hospital stay Epidural Anaesthesia should be considered as a reliable anaesthetic technique as compared to general anaesthesia for appropriate surgicalproceduresintheelderly. REFERENCES
1 F Jin, F Chung — Minimizing perioperative adverse events in the elderly. British Journal of Anaesthesia 2001; 87: 60824.
2 Weintraub HD, Kekoler Lj — Demographics of aging. In: Mcleskey CH, ed. Geriatric Anaesthesiology. Williams and Wilkins 1997;3-12.
3 Jandziol A, Griffiths R — The anaesthetic management of patients with hip fractures. British Journal of Anaesthesia CEPD Reviews 2001;1:52-5.
4 MoracaRJ,SheldonDG,ThirlbyRC—TheRoleofEpidural Anaesthesia and Analgesia in Surgical Practice. Ann Surg 2003;238:663-73.
5 Reilly DF, Mcneely MJ, Doerner D — Self-reported exercise tolerance and he r sk o ser ous per operat ve complications. Arch Intem Med 1999;159:2185-92.
6 Priebe HJ — The aged cardiovascular risk patient. British Journal of Anaesthesia 2000;85:763-78.
reduce not only the morbidity and mortality but also would preservetheuterus.
REFERENCES
1 Stafford I, Belfort MA, Placenta accrete, increta and percreta: a team based approach starts with prevention. Contemp OB/GYN 2008;52:77-82.
3 Kockerginsky YW, Mankutta D, Rojansky N — Perinatal outcome of pregnancies complicated by placenta accreta. Obstet Gynecol 2004;104:527-30.
4 Grobman WA, Gersnoviez R, Landon MD — Pregnancy outcome for women with placenta praevia in relation to the number of prior caesarean delivery. National Institute of Child health and Human Development(NICHD), MaternalFoetal Medicine unit (MFMU) network. Obstet Gynecol 2007;110:1249-55.
5 Stafford I, Belfort M — Placenta accre, increta and percreta: lifesavingstrategiestostopthebleeding. Contemp OB/GYN 2008;53:48-53.
Case Report
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
Tuberculosis of spleen : a rare case report
1 Ajithkumar C S
Twenty four years old immunocompetent male patient with fever for 6 weeks duration with left upper abdominal pain. On examination he was febrile with minimal tenderness at left hypochondral area. USS abdomen revealed the splenic abscess. CT abdomen showed multiple hypodense lesions of splenic abscess. Mantoux test was non reactive but ESR was elevated. Laparotomy done revealed the enlarged spleen with attachment to the diaphragm. Histopathology result was of caseating granuloma which was confluent consistent with tuberculosis of spleen. Tuberculous chemotherapy started with 4 drug regime. Patientwasalsogivenpneumococcalandinfluenzavaccinationinthepostoperativeperiod.
[J Indian Med Assoc 2017; 115: 35-6 & 37]
Key words : Splenic abscess, tuberculosis, splenectomy.
Clinically tuberculosis may present as pulmonary or extra pul-monary disease. Extra pulmonary tuberculosis accounts for 15% of tuberculosis. Of all the organs, lung
nonreactive.
Sputum AFBwasnegative. InChestxrayreading
9 Pederson T, Eliasen K, Henrikson E — A prospective study of mortality associated with anaesthesia and surgery: Risk indicators of mortality in hospital. Acta Anaesthesiol Scand 1990;34:176-82.
10 Glantz L, Drenger B, Gozal Y — Perioperative myocardial ischemia in cataract surgery patients: General versus local anaesthesia. Anesth Analg 2000;91:1415-9.
11 Magnusdottir H, Kimo K, Ricksten SE — High thoracic epidural anaesthesia does not inhibit sympathetic nerve activity in the lower extremities. Anaesthesiology 1999; 91: 1299-304.
12 Grass JA — The role of epidural anaesthesia and analgesia in postoperative outcome. Anaesthesiol Clin North America 2000;18:407-28.
13 Park WY, Thompson JS, Lee KK — Effect of epidural anaesthesia and analgesia on peri-operative outcome. Ann Surg2001;234:560-71.
14 Wheatley R, Somerville I, Sapsford D — Postoperative hypoxemia: comparison of extradural, M And patientcontrolledanalgesia. Br J Anaesth 1990;64:267-75.
15 Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A, et al Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: Results from anoverviewofrandomisedtrials. BMJ 2000;321:1493.
16 Muravchick S — Anaesthesia for the geriatric patient. In: Barash PG, Cu len RK, Stoe t ng RK Ed C n cal Anaesthesia. 4th ed. Philadelphia, USA: LWW; 2001: 120516.
17 deLeon – Casasola OA, Parker BM, Lema MJ — Epidural analgesia verses intravenous patient-controlled analgesia: differences in the postoperative course of cancer patients. Reg Anesth 1994;19:307-15.
18 Salomaki TE, Leppaluoto J, Laitinen JO — Epidural vs. Intravenous Fentanyl for reducing hormonal, metabolic and physiologic responses after thoracotomy. Anesthesiology 1993;79:672-9.
7 Cheng AT,PlankLD,Hill GL—Prolonged overexpansion of extracellular water in elderly patients with sepsis. Arch Surg 1998;133:745-51. the stress response, reducing the MinimumAlveolar 8 Frank SM, Higgins MS, Breslow MJ — The catecholamine, cortisol, and hemodynamic responses to mild perioperative hypothermia. A randomized clinical trial. Anesthesiology 1995;82:83-93.
is the predominantly affected organ. Involvement of spleen in tuberculosis occurs in miliary/disseminated form of the disease. However isolated splenic tuberculosis or solitary tuberculosis of spleen is very rare in immunocompetent individuals. When spleenisinvolvedasanisolatedorgan,patientmayhavemultiple hypoechoic foci less than 2 cm which may be evident on USS andmultiplehypodenselesionsinCTabdomen.Splenicabscess is a comparatively commoner stage than the solitary or nodular stage when patient seeks medical advice. Isolated splenic tuberculosis abscess is rarely suspected clinically and the diagnosisismaderetrospectively CASE REPORT
Twenty four years old immunocompetent male patient withoutanyprevioushistoryoftuberculosisor familyhistoryof tuberculosis presented with left hypochondrial pain and fever for previous 6 weeks. There was no previous history of contact with tuberculosis. Fever was of low grade with chills and rigor. There was no associated cough, sputum or dyspnea.Abdominal pain on left hypochondriac area was not associated with vomiting or diarrhoea or malena. Examination revealed a moderately built and ill nourished patient with temperature of 38.2C Respiratory system examination was within normal limits. Tenderness on deep palpation on left hypochondral area was there without any mass or hepato splenomegaly There was noascites.Bowelsounds werenormal.Othersystemswerewith in normal limits. Routine work up showed hemoglobin 14.3 grams per dl, total count 7700 cells per cmm with 66% polymorphs, lymphocytes 26%, eosinophils of 8% and ESR of 30mminthefirsthour Liver andrenalfunctiontests werewith in normal limits. Serum calcium and phosphorous were 9.3 mg per dl and 4.8 mg per dl respectively Mantoux test was
MBBS, DNB (Respiratory Diseases), FCCP (USA), Assistant Professor Department of Pulmonary Medicine, Medical College, Thrissur,Kerala68059
nothing was suggestive of tuberculosis. Ultrasonography of abdomen showed multiple hypoechoic lesion in the spleen with splenomegaly
Liver was normal and no lymphadenopathy or intra abdominalcollectionwereseen.CTabdomen revealedmultiple hypodenselesionsinthespleenconsistentwithsplenicabscess. Laparotomy was done based on these data. Intraoperatively spleen was found enlarged and found adhered to diaphragm on separation of which pus discharged from spleen. Splenectomy done and was submit ed for histopat
y examination.Tuberculous splenic abscess was identified by the pathologist and based on this 4 drug antituberculous chemotherapy was started along with other supportive treatments Patien also received post splenectomy pneumococcalandinfluenzavaccination
DISCUSSION
Isolated splenic tuberculosis is a very rare manifestation of extra pulmonary tuberculos s in immunocompetent individuals Here a young HIV negative patient with out prior history of contact with tuberculosis presented with fever and left upper abdominal pain for 6 weeks duration and he had tuberculoussplenicabscess.Splenictuberculosisisarareformof abdominal t
losis It i
lly seen in immunocompromised individuals or as a part of disseminated tuberculosis although it can also be manifested in immunocompetent individuals infrequently Spleen can be the only site of tuberculous infection (isolated splenic 4,7,8,9 12 tuberculosis) Bhansali et al in a series of 300 patients with abdominal tuberculosis did not encounter even a single case of splenic tuberculosis. Tuberculosis has been reported as a rare 11 cause of splenic abscess . On USG, splenic tuberculosis usually 17,18 presentedasmultiplesmallhypoechoiclesions andCECT(Fig 3,9,18 1) may demonstrate hypodense lesions . The reported yield of aspirationcytologyfromthespleniclesionsisvariable. Suri et al reported up to 88% sensitivity for fine needle aspiration cytology (FNAC) for diagnosing a tuberculous pathology in the 14spleen Onhistopathologicexaminationtherewillbeepithelioid granulomas composed of aggregates of epithelioid cells, lymphocytes and Langhans giant cells with variable de
36 Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017
There are 5 types of pathomorphological classifications for splenicTBincludingmiliaryTB,nodularTB,tuberculousspleen abscess, calcific TB and mixed type TB.Tuberculosis should be considered as one of the differential diagnosis in patients presenting with FUO and splenomegaly especially in areas where the disease is prevalent Splenic tuberculosis can even affect immunocompetent individuals In patients presenting withFUOandsplenomegaly whereanexactdiagnosiscouldnot be established after all possible and available investigations, splenectomy is strongly recommended for the diagnosis and further treatment. Empirical exposure to antituberculous drugs could be hazardous in these situations as it may mask a definite diagnosis later At times such patients may not respond to 13 antituberculousdrugsandrequiresplenectomysubsequently CONCLUSION
Tuberculosis should be considered in the differential diagnosis of patients presenting with FUO and splenomegaly Splenictuberculosiscanpresentinisolationwithoutextrasplenic involvement,andeveninimmunocompetentindividuals.
REFERENCES
1 Prathmesh CS, Tamhankar AP, Rege SA — Splenic TuberculosisandHIV-1infection. Lancet 2002;369:353.
2 Thomson SR, Ghimenton F — Splenic Tuberculosis. Postgrad Med J 1999;75:578.
3 Chandra S Srivas ava DN, Gandh D Splen c tuberculosis:anunusualsonographicpresentation. Int J Clin Pract 1999;53:318-9.
4 Adil A, Chikhaoui N, Ousehal A — Splenic Tuberculosis Aproposof12cases. Ann Radiol (Paris) 1995;38:403-7.
6 Ho PL, Chim CS, Yuen KY — Isolated Splenic Tuberculosis presentingwithpyrexiaofunknownorigin. Scand J Infect Dis 2000;32:700-1.
7 Sato T, Mori M, Inamatsu T — Isolated splenic tuberculosis. Nippon Ronen Igakkai Zasshi 1992;29:305-11.
8 Fernandez Miranda C, Perpina C kESSLERp, Torres N, Manion P, Dela Calle A — Hepatosplenic tuberculous abscess in a patient with polyarteritis nodosa. Am J Gastroenterol 1993;88:1297-8.
9 Sharma S, Dey AB, Agarwal N, Nagarkar KM, Gujral S — Tuberculosis : a rare cause of splenic abscess. J Assoc Physicians India 1999;47:740-1.
(Continued on page 37)
Pictorial CME
Journal of the Indian MedicalAssociation, Vol 115, No 1, JANUARY 2017 LICHEN AMYLOIDOSIS
Fig 1 — Discrete light to dark brown-colored hyperkeratotic papules over the shin of left leg
A53-year-old man presented with a 10-year history of itchy brownish skin eruptions over both shins. He gave history of scrubbing his legs with a pumice stone while bathing every day for many years. Cutaneous examination revealed multiple, 2 to 3-mm sized, ligh to dark brown-colored xerotic and hyperkeratotic papules present discretely and symmetrically over both shins, extending from the knees till dorsa of the feet (Fig 1). Rest of the body was spared. Except for the history of chronic friction and scratching due to the use of pumice stone, there was no history of preceding trauma, or any systemic symptoms. His medical and family histories were insignificant. Clinical possibilities of lichen amyloidosis, hypertrophic lichen planus, and prurigo nodularis were considered. Histopathology from skin biopsy revealed prominent hyperkeratosis, hypergranulosus epidermal hyperplasia and dermal papillae filled with multiple eosinophilic globular amyloid deposits and sparse, superficial perivascular lymphocytic infiltrate (Fig 2). On Congo red staining, the globules p r o d u c e d a p p l e - g r e e n birefringence under polarizing light, confirming them to be amyloid depos ts Laboratory investigations including complete blood count, plasma glucose,renal,hepatic,andthyroid function tests and urinalysis were normal.With the final diagnosis of lichen-variant of primary localized cutaneous amyloidosis (with secondarylichenificationduetochronicscratching),patientwas prescribed an ointment containing halobetasol (super-potent topical steroid) and 3% salicylic acid twice a day (1 month regularly followed by weekend therapy ie, twice a day on weekends with 5-day steroid free period, for 6 months),
(Continued from page 37)
10 Bhansali SK — Abdominal tuberculosis: experiences with 300cases.Am J Gastroenterol 1977;67:324-37.
11 Ho PL, Chim CS, Yuen KY — Isolated splenic tuberculosis presentingwithpyrexiaofunknownorigin. Scand J Infect Dis 2000;32:700-1.
12 WildeCC,KuehYK—Casereport:tuberculous hepatic and splenicabscess. Clin Radiol 1991;43:215-6.
13 Nayyar V, Ramakrishna B, Mathew G, Williams RR, Khanduri P — Response to antituberculous chemotherapy aftersplenectomy. J Intern Med 1993;233:81-3.
14 Suri R, Gupta S, Gupta SK, Singh K, Suri S — Ultrasound guided fine needle aspiration cytology in abdominal tuberculosis. Br J Radiol 1998;71:723-7.
Fig 2 — Histopathology revealing prominent hyperkeratosis, hypergranulosus, epidermal hyperplasia and dermal papillae filled with multiple eosinophilic globular deposits of amyloid and sparse superficial perivascular lymphocytic infiltrate (100X, hematoxylin & eosin).Arrow inside the inset (left inferior corner) points towards a prominent amyloid deposit (400X, hematoxylin & eosin)
oral acitretin 50 mg/day (6 months with monitoring of liver enzymes and serum lipids) and oral levocetrizine 5 mg at night for itching. He had marked improvement within 3 months of treatmentandremainsasymptomatictilloneyearfollow-up.
15 Fooladi AAI, Hosseini MJ, Azizi T — Splenic tuberculosis: a casereport. Int J Infect Dis 2009;13:e273-5.
16 Ozgüroðlu M, Celik AF, Demir G, Aki H, Demirelli F, MandelN, Büyükünal E, Serdengeçti S, Berkarda B — Primary splenic tuberculosis in a patient with nasal angiocentric lymphoma:mimicking metastatic tumor on abdominalCT. J Clin Gastroenterol 1999;29:96-8.
17 Porcel-MartinA,Rendon-UncetaP,Bascunana-QuirellA— Focal splenic lesions in patients with AIDS: sonographic findings. Abdom Imaging 1998;23:196-200.
18 Jain A, Sharma AK, Kar P, Chaturvedi KU — Isolated splenic tuberculosis. J Assoc Physicians India 1993; 41: 605-6.