August 2025 | Issue 59
www.neuronewsinternational.com
Featured in this issue:
First-time COATING trial data revealed
Profile Wim van Zwam
What will be the next “holy grail” in mechanical thrombectomy?
Quantanosis
page 7
page 16
page 20
page 24
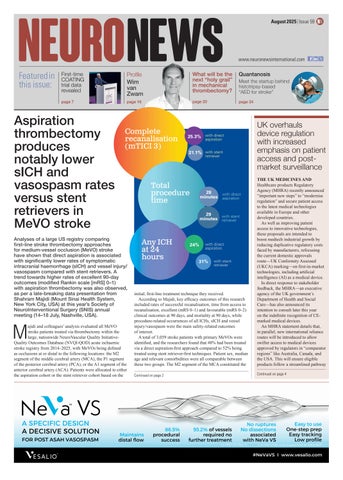
Aspiration thrombectomy produces notably lower sICH and vasospasm rates versus stent retrievers in MeVO stroke
Complete recanalisation (mTICI 3)
Analyses of a large US registry comparing first-line stroke thrombectomy approaches for medium-vessel occlusion (MeVO) stroke have shown that direct aspiration is associated with significantly lower rates of symptomatic intracranial haemorrhage (sICH) and vessel injury/ vasospasm compared with stent retrievers. A trend towards higher rates of excellent 90-day outcomes (modified Rankin scale [mRS] 0–1) with aspiration thrombectomy was also observed, as per a late-breaking data presentation from Shahram Majidi (Mount Sinai Health System, New York City, USA) at this year’s Society of NeuroInterventional Surgery (SNIS) annual meeting (14–18 July, Nashville, USA).
M
ajidi and colleagues’ analysis evaluated all MeVO stroke patients treated via thrombectomy within the large, nationwide NeuroVascular Quality InitiativeQuality Outcomes Database (NVQI-QOD) acute ischaemic stroke registry from 2014–2025, with MeVOs being defined as occlusions at or distal to the following locations: the M2 segment of the middle cerebral artery (MCA), the P1 segment of the posterior cerebral artery (PCA), or the A1 segment of the anterior cerebral artery (ACA). Patients were allocated to either the aspiration cohort or the stent retriever cohort based on the
Meet the startup behind histotripsy-based “AED for stroke”
25.3% with direct aspiration
21.1% with stent retriever
UK overhauls device regulation with increased emphasis on patient access and postmarket surveillance
initial, first-line treatment technique they received. According to Majidi, key efficacy outcomes of this research included rates of successful recanalisation, time from access to recanalisation, excellent (mRS 0–1) and favourable (mRS 0–2) clinical outcomes at 90 days, and mortality at 90 days, while procedure-related occurrences of all ICHs, sICH and vessel injury/vasospasm were the main safety-related outcomes of interest. A total of 3,059 stroke patients with primary MeVOs were identified, and the researchers found that 48% had been treated via a direct aspiration-first approach compared to 52% being treated using stent retriever-first techniques. Patient sex, median age and relevant comorbidities were all comparable between these two groups. The M2 segment of the MCA constituted the
THE UK MEDICINES AND Healthcare products Regulatory Agency (MHRA) recently announced “important new steps” to “modernise regulation” and secure patient access to the latest medical technologies available in Europe and other developed countries. As well as improving patient access to innovative technologies, these proposals are intended to boost medtech industrial growth by reducing duplicative regulatory costs faced by manufacturers, refocusing the current domestic approvals route—UK Conformity Assessed (UKCA) marking—on first-in-market technologies, including artificial intelligence (AI) as a medical device. In direct response to stakeholder feedback, the MHRA—an executive agency of the UK government’s Department of Health and Social Care—has also announced its intention to consult later this year on the indefinite recognition of CEmarked medical devices. An MHRA statement details that, in parallel, new international reliance routes will be introduced to allow swifter access to medical devices approved by regulators in “comparator regions” like Australia, Canada, and the USA. This will ensure eligible Continued productson follow page 0a streamlined pathway
Continued on page 2
Continued on page 4
Total procedure time
28 minutes
with direct aspiration
29 with stent minutes retriever
Any ICH at 24 hours
24%
with direct aspiration
31%
with stent retriever