The application of artificial intelligence (AI) is becoming an increasingly prominent topic on the agendas of key vascular meetings and the contents pages of vascular surgery journals. At this juncture, Vascular News looks at some of the recently shared research and opinion on the topic, highlighting a need for “guardrails” amid significant clinical potential.
Several papers on the emerging uses of AI in vascular surgery were presented at the recent 2025 Vascular Annual Meeting (VAM; 4–7 June, New Orleans, USA). Among these were two papers from Ben Li (University of Toronto, Toronto, Canada) and colleagues—one looked at developing an AI model to predict one-year mortality after major lower extremity amputation, the other to predict one-year successful clinical use of an arteriovenous access for haemodialysis. The team found that their two models—both of which were trained on Vascular Quality Initiative (VQI) patient data—could “very accurately predict” outcomes and performed better than logistic regression. “Having that kind of information preoperatively helps the clinician and the patient decide the best treatment plan moving forward,” Li comments, considering the clinical implications of the work.
Another paper presented at VAM 2025 looked at the use of a large language model to accurately extract aortic information from abdominal imaging reports in a large, real-world, multicentre database in San Francisco, USA. Robert Chang (Kaiser Permanente Northern California, Oakland, USA) and Colleen Flanagan (University of California, San Francisco, San Francisco, USA) led the research, which found that an opensource, foundational, or “off-the-shelf” large language model was able to extract critical information about the aorta from the imaging reports. “We did not train this model ourselves at all; we crafted and refined a prompt to extract information of interest,” Chang and Flanagan detail, speaking to Vascular News about the research. The team then used this prompt on over 16,000 imaging reports in their real-world arterial aneurysm
registry. The researchers found that the accuracy of the model, LLaMa 3.3, was over 90% overall. “We think this could support our ability to closely track AAAs [abdominal aortic aneurysms], including those found on screening and those found incidentally on non-aortic imaging studies, by automating the flagging of these patients for appropriate referral and follow-up,” Chang and Flanagan remark.
Elsewhere at VAM 2025, Justin Bader (Yale School of Medicine, New Haven, USA) presented a paper outlining the creation of a prediction model for safe contrast volume thresholds to prevent post-contrast acute kidney injury (PCAKI) after endovascular aneurysm repair (EVAR). The research team is now using AI to harness the model’s future potential. Bader explains that the team—led by Cassius Iyad Ochoa Chaar (Yale School of Medicine, New Haven, USA)—used VQI data to create a “calculator” that allows physicians to generate a recommended contrast volume to minimise PC-AKI risk by inputting 13 patient-specific variables. “It serves as a guideline for surgeons when they’re operating,” he says. The model, Bader tells Vascular News, is “working extremely well” and the team is presently collaborating with statistics experts at Yale on advanced AI and machine learning techniques to make the calculator “even more accurate”.
VAM 2025 also saw data from Prem Chand Gupta (CARE Hospitals, Hyderabad, India) and colleagues that looked at the correlation of imaging characteristics of carotid plaque with clinical and histopathological features, and the application of AI. “We found that routinely performed ultrasound by us was
Continued on page 3
First official ESVS consensus statement consolidates expert opinion on “truly novel” aTEVAR procedure
AGAINST THE BACKDROP OF
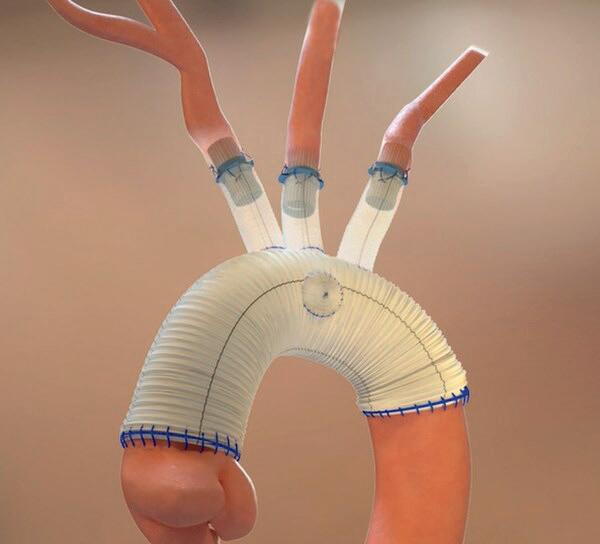
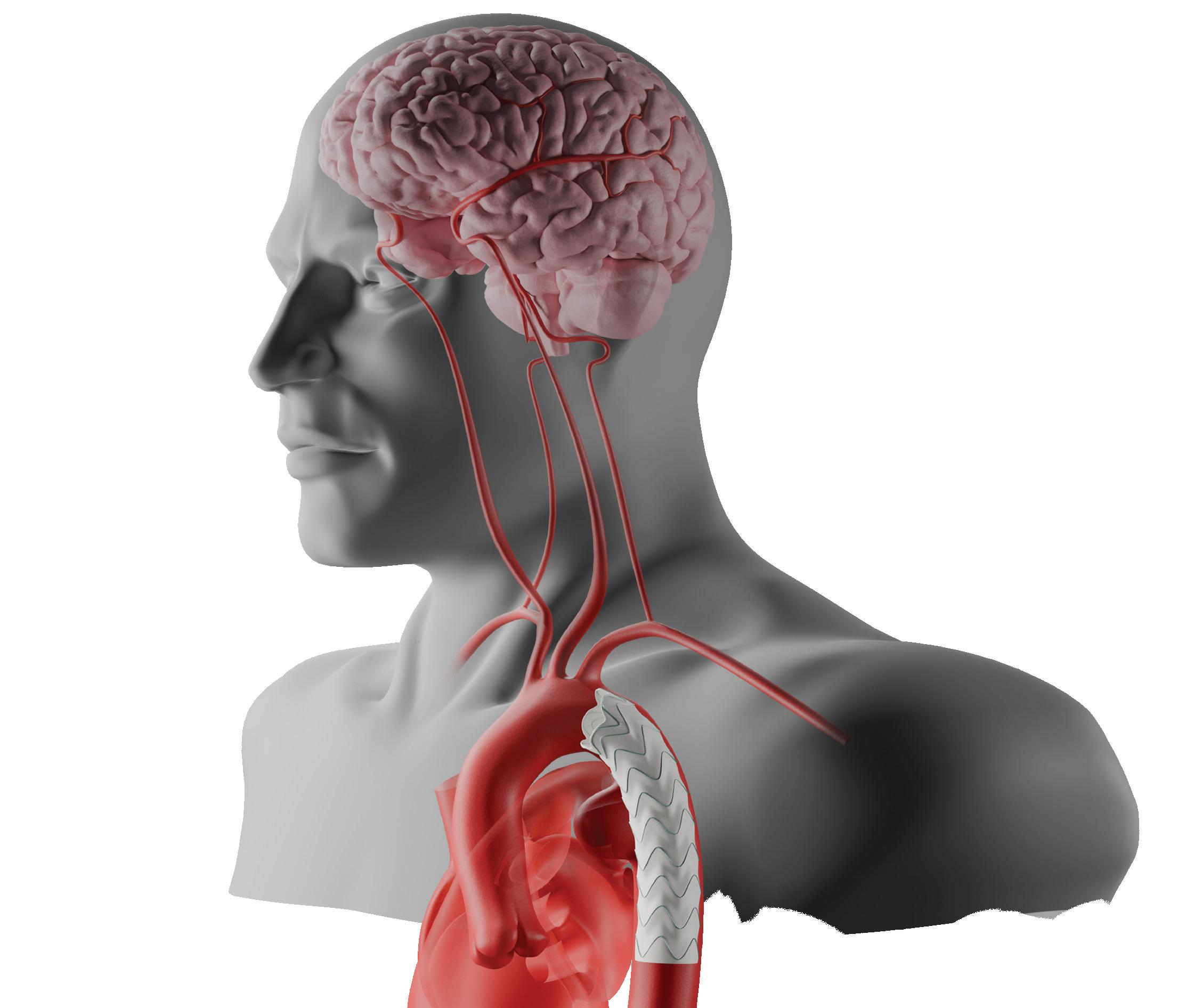
an ageing population and increasing demand for complex endovascular aortic solutions, Santi Trimarchi (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy) and a global team of experts recently authored a consensus statement on ascending thoracic endovascular aortic repair (aTEVAR).
The statement has been published as part of the new European Society for Vascular Surgery (ESVS) consensus statement programme, which aims to standardise and strengthen the process for publishing expert opinion-based recommendations in areas of clinical practice where evidence is lacking. The framework was recently formalised by Chris Twine (University of Bristol, Bristol, UK) and Anders Wanhainen (Uppsala University, Uppsala, Sweden) in the European Journal of Vascular and Endovascular Surgery (EJVES).
The aTEVAR statement includes recommendations on patient selection, procedural strategies, and postoperative management among other areas.
“By addressing key topics such as landing zones, stent graft sizing, risk assessment, and adjunctive procedures, this document aims to guide clinical practice, improve patient outcomes, and enhance procedural safety,” Trimarchi and colleagues write in the paper.
Highlighting one of the key reasons why aTEVAR was selected as a topic for the first official ESVS consensus statement, Trimarchi,
Continued on page 5
ESVS
Welcome to the September edition of Vascular News Europe
It gives me great pleasure to welcome you all to the September edition of Vascular News Europe, published to coincide with the 39th annual meeting of the European Society for Vascular Surgery (ESVS) in Istanbul, Türkiye. The ESVS annual meeting 2025 promises to be a highlight on the conference calendar.
It marks a year since I handed over the presidential reins of the ESVS, with significant sorrow but great satisfaction. I am thrilled to watch the society continue to go from strength to strength, leading the way in multidisciplinary education and training, and international evidence-based practice. I am equally thrilled to now be able to join the great team that comprise the editorial board of Vascular News Europe
Not a day passes without a reference in the news to artificial intelligence (AI). The importance of AI in vascular surgery was highlighted at the ESVS meeting last year, where the Volodos Lecture, celebrating innovation, was delivered by Alan Karthikesalingham from Google DeepMind. This was followed by a dedicated session at the Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM) in New Orleans, USA earlier this year. It is becoming clear that AI will likely transform the landscape for vascular surgery, through diagnostics, consultation, treatment algorithms and therapeutics. In this edition, we lead on where AI lands today and how it might impact the vascular future.
Another area where technology is advancing at an exciting pace, is the development of endovascular arch therapies. To provide safe and robust solutions for challenging anatomies and pathologies, adoption of these technologies demands caution. In this issue, we discuss the recently published ESVS clinical practice consensus statement on ascending thoracic endovascular aortic repair, with analysis of the new ESVS consensus statement framework.
This edition features a profile of the career of Dawn Coleman, professor of surgery and chief of the Division of Vascular and Endovascular Surgery at Duke University School of Medicine in Durham, USA, which is as inspiring as it is impressive. We also spotlight Matthew Eagleton’s recent presidential address at VAM 2025 and an article discussing the message from Linda Harris, president-elect of the SVS, to the recent Women’s Vascular Summit. In other aortic news, we cover the one-year Gore TAMBE data, presented by Mark Farber at VAM 2025, as well
as Sherene Shalhub’s Greenberg Lecture at the meeting encouraging us to “move beyond” binary aortic disease classifications and towards a novel biologically informed framework. Among several other items discussed are the ENGAGE registry 10-year outcomes, recently published in the European Journal of Vascular and Endovascular Surgery (EJVES). This study highlights the value of robust, real-world, long-term outcome data for the benefit of our patients and profession.
Regarding peripheral arterial disease, a VAM 2025 presentation from Anahita Dua is highlighted, comparing the outcome data from transcatheter arterialisation of the deep veins from the PROMISE I and II studies to real-world standard of care, suggesting the emerging modality is worth pursuing, as well as the promising midterm outcomes of Shockwave intravascular lithotripsy (IVL) in the IVLIAC registry for the treatment of calcified iliac occlusive disease, among other topics.
In the carotid field, data from the Vascular Quality Initiative (VQI) is presented, and the role of revascularisation is questioned in a highlighted publication in The Lancet Neurology of two-year interim results from ECST-2. Longer-term results are eagerly anticipated.
Regarding venous disease, there is a focus on new, evidence-based clinical practice guidelines to support the treatment of chronic venous disease from the Society for Cardiovascular Angiography and Interventions (SCAI).
Elsewhere in the issue you will find data from a phase 3 clinical trial which demonstrate promising outcomes using acellular tissue engineered vessel (ATEV; Humacyte) in arteriovenous access for patients at high risk of autologous
It is becoming clear that AI will likely transform the landscape for vascular surgery.”
arteriovenous fistula (AVF) maturation failure and an opinion piece from Adam Talbot on moral injury in vascular surgery. And while we advance our endovascular therapies, so we face increased awareness of the damaging effects of repeated exposure to ionising radiation. There is a focus on the recently published work from Gilles Soenens and colleagues on the impact of a massive open online course on radiation safety in the hybrid operating room.
I trust you find this edition of Vascular News Europe both educational and enjoyable, and I look forward to seeing many of you at ESVS 2025, in Istanbul.
IAN LOFTUS is a consultant and professor in vascular and endovascular surgery at St George’s University Hospitals NHS Foundation Trust in London, UK.
EUROPE
Editorial board: Ian Loftus, Rob Morgan, Stephen Black and Nicholas Inston | Publisher: Stephen Greenhalgh Editor: Jocelyn Hudson Jocelyn@bibamedical.com | Contributing editor: Bryan Kay | Editorial contribution: Jamie Bell, Will Date and Éva Malpass | Design: Terry Hawes, Josh Lyon and David Reekie
A five-year prospective cohort study using longitudinal registry data from two Danish population-based screening trials has found that high-dose statin use was associated with decreased abdominal aortic aneurysm (AAA) growth rates and lowered risk of undergoing repair, rupture, and death. Researchers therefore suggest high-dose statins should be “strongly considered” for patients with small AAAs. The study was recently published in Circulation by Joachim S Skovbo, Jes Sanddal Lindholt (both of Odense, Denmark) and colleagues.
For more on this story go to page 5.
n LAUNCH PAD:
In this issue’s Launch Pad column, Adam Talbot (Manchester, UK) writes about moral injury in vascular surgery, suggesting steps that could be taken to prevent it. “Vascular surgery often places surgeons in high-pressure situations where the right course of action is clear, but systemic constraints prevent its delivery,” he writes. “This dissonance is increasingly recognised as moral injury, a psychological harm distinct from burnout.”
For more on this story go to page 18.
n VASCULAR UNITY:
Society for Vascular Surgery (SVS) president-elect Linda Harris (Buffalo, USA) extolled the values of “coelevation” in her presidential address at the 7th annual Women’s Vascular Summit (2–3 May, Chicago, USA), invoking lessons on teamwork from the world of sport to argue that a united vascular specialty is greater than the sum of its parts. Harris addressed the summit as its founder and first outgoing president.
For more on this story go to page 20.
Vascular surgery meets AI
better than CT [computed tomography] angiography and MR [magnetic resonance] angiography in deciding whether the plaque was vulnerable or not,” he tells Vascular News. Gupta shares that, for asymptomatic carotid patients, it is currently unclear whether intervention should be offered or not. While guidelines suggest that patients who are asymptomatic should not be offered surgery, around one-third of the patients in Gupta and colleagues’ study who were not operated on were found to have vulnerable or soft plaque, with almost 20% of these patients going on to have a stroke within one year. “If we are able to identify soft or vulnerable plaque in asymptomatic patients, we can be more confident that operating on these patients will prevent stroke,” Gupta notes, considering his ultimate ambition for the clinical application of the team’s research.
As research dedicated to the applications of AI in vascular surgery
proliferates, so too do calls for its safe integration into the specialty.
Bader raises the issue of liability, for example, asking: “Who’s liable for a botched surgery if AI is leading it?”
This is an issue raised in a letter to the editor of the Journal of Vascular Surgery (JVS), in which Antonio V Sterpetti (Sapienza University, Rome, Italy) and colleagues state: “Recommendations made by AI should remain simple suggestions, which cannot substitute for the opinion of surgeons in a complex clinical analysis, to prevent legal controversies and to preserve the dignity of patients and vascular surgeons.” The letter was published in response to a study by Joachim Sejr Skovbo (Odense University Hospital, Odense, Denmark) and colleagues, who in JVS had previously outlined the successful development of the SHAPFire AI tool to identify AAAs at increased risk of rupture with “significantly higher” accuracy than diameter alone. In their response to the letter, Skovbo et al write that “AI recommendations should be viewed as valuable adjuncts that enhance—not substitute for—clinical expertise”, going on to stress that
vascular societies “could help facilitate the integration of AI decision-making tools while ensuring they support, rather than replace, clinical judgment”.
Amun G Hofmann (Klinik Ottakring, Vienna, Austria) also raises some of the challenges associated with integrating AI in vascular surgery in a recent letter to the editor of the European Journal of Vascular and Endovascular Surgery (EJVES). Specifically, he highlights the importance of establishing the digital infrastructure, monitoring safety and efficacy, and considering legal and ethical requirements.
AI is going to have an increasingly important role in medicine.”
Ben Li
Li tells Vascular News there is a need to ensure “guardrails” are in place before AI is deployed in healthcare. “AI is going to have an increasingly
“Critical” importance of lifelong surveillance after EVAR headlines newly published 10-year ENGAGE data
Ten-year data highlight the long-term efficacy and durability of the Endurant stent graft (Medtronic) in abdominal aortic aneurysm (AAA) patients who survived beyond five years post-enrolment in the ENGAGE registry. However, researchers also draw attention to the incidence of late events in this extended follow-up cohort, which they say underscores the need for lifelong surveillance. These findings were recently published online in the European Journal of Vascular and Endovascular Surgery (EJVES).
ENGAGE IS A MEDTRONIC-SPONSORED, observational, multicentre, non-randomised, prospective global registry designed to shed light on the long-term outcomes of endovascular aneurysm repair (EVAR). In their EJVES paper, Hence Verhagen (Erasmus University Medical Centre Rotterdam, Rotterdam, the Netherlands) and a team of coinvestigators from across Europe, the USA and Canada note that the registry will be the first to report long-term outcomes of real-world, global AAA patients with the Endurant stent graft.
Verhagen and colleagues share that inclusion criteria for the registry were “minimal” and allowed for the incorporation of patients who fell outside the instructions for use guidance. Exclusion criteria, meanwhile, were “high probability of non-adherence to follow-up requirements, or concurrent participation in another trial that could confound results”. The authors note that clinical and imaging data were continuously collected to evaluate treatment efficacy through 10 years.
cohort. The remaining 873 patients made up a nonextended follow-up cohort.
In EJVES, the authors report the continued longterm efficacy and durability of the Endurant stent graft. They share that freedom from site-reported all-cause mortality and clinical event committee (CEC)-adjudicated aneurysm-related mortality for the extended follow-up cohort was 75.7% and 97.3% through 10 years, respectively.
Furthermore, through 10 years, Verhagen et al note that each rate for freedom from aneurysm-related rupture (96.2%) and aneurysm-related interventions (71.4%) was comparable with the respective rate through the first five years.
Among several other datapoints, the authors detail that late re-interventions (n=72) were associated with type Ia endoleaks (18/72), type II endoleaks (18/72), and type Ib endoleaks, adding that, at 10 years, 64.1% of patients exhibited sac regression, 19.2% were sac stable, and 16.8% had sac expansion.
important role in medicine,” he says, before stressing that these are early days and that the “true impact” of AI in the field may not be apparent for some time to come. Chang and Flanagan agree that “caution is vital” when it comes to utilising AI tools, especially with regard to sensitive patient data, and suggest that “protocols would need to be in place to bring some of these technologies online on reasonable timelines while also balancing potential security concerns”.
Another concern, highlighted by Gupta, is whether AI could replace the surgeon altogether if combined with the power of robotics. At present, however, Gupta is “really not worried” about this possibility. “There are just too many variables which come into surgery,” he says. “It is going to be very, very difficult for AI to have enough data to be able to deal with different variables […] unless there is a human to guide it.” Instead, Gupta sees AI as an adjunct for now. “At least for the next few generations I don’t think AI is going to take over diagnostics or robotics in a way we should be concerned about,” he comments. “I think we should use it as a good tool.”
when the protocol was amended and thus the data in the extended follow-up cohort (more than five to 10 years) do not represent the full ENGAGE cohort,” they write, for example. However, the authors state that event rates in the extended and non-extended follow-up cohorts were similar from zero to five years and that the team provided baseline differences in the extended follow-up cohort “to allow readers to put outcomes in context and be transparent with any potential bias of the patient population”.
The lack of a control group was another potential drawback, Verhagen and team note. Consequently, the results “could only be indirectly compared with results from other clinical studies”. Among other limitations, the authors highlight the fact that follow-
This study was the first to demonstrate longterm performance and durability of the Endurant stent graft for aortic aneurysm treatment.”
up compliance over the more than five to 10-year period decreased due in part to challenges with data collection during the COVID-19 pandemic.
Of the 1,263 patients enrolled in the ENGAGE registry, Verhagen and colleagues state that 390 reconsented for follow-up from more than five through 10 years, constituting an extended follow-up
Verhagen and colleagues do highlight some limitations of their paper. “Potential bias was introduced as a subset of patients and sites did not reconsent from the original ENGAGE population
In the conclusion of their paper, the authors also draw attention to the fact that “this study was the first to demonstrate long-term performance and durability of the Endurant stent graft for aortic aneurysm treatment.” They also home in on the incidence of late events. “Different factors led to reintervention in the later years,” they state, noting that this supports current recommendations of lifelong surveillance.
“The authors suggest that lifelong surveillance is critical for EVAR patients due to the incidence of late events,” Verhagen and colleagues write.
AORTIC
Hence Verhagen
One-year TAMBE data highlight low mortality, importance of renal branch assessment
The four-branch Gore Excluder thoracoabdominal branch endoprosthesis (TAMBE) device demonstrated low mortality at one year with renal artery occlusion being the predominant device-related event associated with small renal arteries and pararenal aneurysms. So concluded Mark A Farber (University of North Carolina at Chapel Hill, Chapel Hill, USA) presenting the latest TAMBE data at the 2025 Vascular Annual Meeting (VAM; 4–7 June, New Orleans, USA).
DRAWING A TAKE-HOME message from the new findings— which were simultaneously published online in the Journal of Vascular Surgery (JVS)—Farber advised: “During follow-up, attention should be focused on renal branch assessment to identify patients at risk for occlusion.”
Farber was presenting one-year results from the pivotal trial of the Gore TAMBE to treat extent IV thoracoabdominal aortic aneurysms (TAAAs) and pararenal aortic aneurysms (PRAAs). Farber detailed that this prospective, non-randomised, multicentre study included 102 patients, 59 of whom had an extent IV TAAA and 43, a PRAA, adding that the mean maximum aneurysm diameter was 59.4mm.
The presenter shared that, at one year, eight patients were lost to follow-up and six patients died, specifying that one death was device-related, one was procedure-related, and four
were due to unrelated causes. He stated that, in total, 88 patients completed a follow-up visit at one year.
Moving on to key results, Farber revealed that freedom from all-cause mortality at one year was 94.1% and that target vessel occlusions occurred in 14.7% of patients. This figure included one celiac artery, one superior mesenteric artery (SMA), eight right renal and six left renal artery occlusions.
Farber continued that reintervention was attempted in six of the renal arteries and involved additional target vessel stenting in three patients, thrombolysis and embolectomy in two, and angioplasty in one. “Although branch vessel occlusion events were more common in pararenal aneurysms compared to extent IV TAAAs, this was not significant,” he said.
renal artery patency was influenced by renal artery diameter, with renal arteries of less than 5mm in diameter being three times more likely to occlude. He also noted that acute kidney injury requiring dialysis occurred in 1.96% of patients and that renal deterioration— defined as a greater than 25% decrease in glomerular filtration rate (GFR) over two consecutive visits—was 18.9% through one year. Additionally, Farber revealed that renal artery primary patency at one year was 91.8% and “nearly identical between the right and left renal arteries.” Primary patency with respect to renal arteries greater than 5mm in diameter, he continued, was 95.1%, while for those less than 5mm it was 82.5%.
Farber shared that 94.2% of target vessels were free from target vessel instability events through one year. At the individual vessel level, he noted that Kaplan-Meier estimates for freedom from target vessel instability were 99%, 97.1%, 90.8% and 89.8% for the celiac, SMA, right renal and left renal arteries, respectively.
Furthermore, Farber outlined device effectiveness data at one year, which included no major endoleaks, aortic enlargement in 5.4% of patients, and loss of device integrity in 16.3%, which he specified included wire fractures in 3.6% and compression in 12.2%. Farber reiterated that renal deterioration was seen in 18.9%, and that reintervention occurred in 15.6%.
“With respect to the reinterventions,” Farber outlined, “approximately one-quarter were major and included thrombectomy or thrombolysis in five, [and] one exploratory laparotomy for aortic bifurcation rupture to control
Sherene Shalhub (Oregon Health and Science University, Portland, USA) set out a new biologically informed framework that “captures the diverse spectrum of arterial fragility and repair outcomes across inherited and acquired aortic disease” during the Roy Greenberg Distinguished Lecture on Innovation at VAM 2025.
SHALHUB INTRODUCED THE AORTIC AND Arterial Vulnerability Spectrum (AAVS) in her talk ‘The aortic vulnerability spectrum: Reshaping the future of aortic surgery’.
Speaking to Vascular News ahead of the lecture, Shalhub noted that the AAVS was designed to address a gap between molecular and ultrastructural pathology and clinical decision-making and aims to “move beyond binary classifications” to better predict procedural durability, remodeling potential, and long-term risk.
“We always think about aortic disease in a binary manner,” Shalhub commented. “In reality, we should think of aortic disease as a spectrum, where you have some people who have extreme manifestations of the disease and then have other people with milder manifestations of the disease.” Shalhub asserts that “everybody falls somewhere
on that spectrum,” encouraging a shift in thinking to inform better patient care.
Homing in on some of the specifics of her work, Shalhub highlighted the use of ultrastructural skin biopsy analysis as a surrogate for aortic and arterial biology as “one of the most transformative innovations.” She explained: “In patients with aortic aneurysms and dissections, the skin provides a minimally invasive, accessible tissue that mirrors the extracellular matrix and connective tissue vulnerabilities found in the aorta, offering a unique window into the aorta.”
In addition, Shalhub considered how her work continues the legacy of Roy Greenberg ahead of delivering this year’s eponymously named lecture at VAM. “Dr Roy Greenberg pioneered customised endovascular solutions long before FDA [US Food and Drug Administration]-approved
bleeding.”
Minor reinterventions, the presenter continued, included treatment of target vessel stenosis in eight patients, target vessel occlusion in two and branchrelated endoleak treatment in three.
Revealing overall device performance data, Farber shared that combined device effectiveness was achieved in 60.5% and 78.7% of the pararenal and type 4 TAAAs, respectively. “This difference was mainly driven by a higher incidence of target lesion growth and branch vessel occlusion in pararenal aortic aneurysms,” the presenter commented.
In the discussion following Farber’s presentation, Wes Moore (David Geffen School of Medicine at UCLA, Los Angeles, USA) asked how the new data might weigh up to those for physician-modified endovascular grafts (PMEGs).
“It’s hard to compare those results because we’re talking about a fourbranch off-the-shelf device, and the majority of the PMEGs are probably fenestrations or laser fenestrations depending upon where you are, and so it’s hard to compare those,” Farber responded.
The presenter continued: “The important part about the manuscript is that we know that there are renal events that occur and that the goal of this manuscript is to talk about how you can help select your patients better. We have some renal events and 95% patency if you’re greater than 5mm at a year. If you have a patient who has small renal arteries, you need to think about how this might impact them since renal function is linked to survival.”
devices were widely available,” Shalhub says. “He understood that durable repair requires more than device deployment; it demands alignment between anatomy, haemodynamics, and biology. That philosophy resonates directly with AAVS, which seeks to individualise care based on biologic vulnerability, not just anatomy. AAVS can be seen as a biologic extension of Greenberg’s legacy: just as he matched devices to anatomy, we now aim to match interventions to underlying arterial biology.
“His legacy inspires today’s push toward precision vascular medicine where genotype, and substrate, guide care.”
SVS president Matthew Eagleton (Massachusetts General Hospital, Boston, USA) selected Shalhub to deliver this year’s Greenberg Lecture. Commenting on his choice of speaker, Eagleton told Vascular News: “The intent of the Greenberg Lecture was to highlight a physician who was interested in progressing the field of endovascular care through research. Dr Shalhub’s research on the genetic component of aortic disease would be very interesting to Roy. In particular, her focus on how that may affect what treatment options we offer our patients. He would love this year’s topic and to hear Dr Shalhub’s address.”
Shalhub’s introduction to the AAVS has also been published in the Journal of Vascular Surgery (JVS).
Sherene Shalhub
First official ESVS consensus statement consolidates expert opinion on “truly novel” aTEVAR procedure
Continued from page 1
speaking to Vascular News following the open-access publication of the statement in EJVES, notes a growing interest in this niche area. “The data are limited, but the observational evidence we do have shows that a large number of aortic lesions are being treated with aTEVAR,” he says. Trimarchi also highlights growing interest in aTEVAR from industry.
Behind these factors, Trimarchi continues, is an ageing population in need of new aortic technologies.
“Twenty years ago, the mean age of patients who had a type A dissection was about 70, 72 years of age; now, it’s shifting towards 80,” he points out. Trimarchi adds that with age comes fragility and that aTEVAR “offers these patients a chance”.
“Our aim was to try to give a framework to a topic that many people are discussing, and it was a chance to highlight the state of the art and figure out how we can move forward,” Trimarchi summarises.
A lack of evidence, however, necessitates caution. This is a point stressed by Twine and Jonathan R Boyle (University of Cambridge and Cambridge University Hospitals NHS Trust, Cambridge, UK) in an editorial accompanying Trimarchi and colleagues’ paper in EJVES. Speaking to Vascular News, Twine emphasises the “truly novel” nature of aTEVAR and the fact that “very few units are doing it at the moment”. With this in mind, he stresses the importance of “trying to harmonise” all aspects of care around the procedure and avoid “outlying practice” at this stage—which the consensus statement aims to achieve. “I hope the document reinforces that you can’t start doing these very difficult, novel procedures in isolation,”
AORTIC
Twine remarks, stressing that “there needs to be an experienced multidisciplinary team in place, careful patient selection and consent and ideally the use of a framework for implementation of new procedures.”
Future projects
Trimarchi and colleagues’ publication is set to be the first of many to be published within the new ESVS framework, with several other statements in the works. Due to be published in 2026 is a consensus statement from Isabelle Van Herzeele (Ghent University Hospital, Ghent, Belgium) and colleagues on the management of women vascular patients. “The consensus document on women has already become a larger document than initially anticipated,” Van Herzeele shares with Vascular News. Specifically, she notes that the paper will include several subtopics including the representation of women in vascular research, the need for a diverse healthcare staff representing the target vascular population including women, and differences in treatment outcomes and postoperative management between men and women.
Looking ahead, Van Herzeele points to some of the longer-term goals of the document. “Women are still underrepresented in vascular research and often if women are treated within a study population, sex-stratified reporting is not available, making it almost impossible to analyse the results,” she says. “Therefore, we hope that this ESVS document will ensure that women with arterial disease are not only increasingly included in prospective trials, but that sex differences are considered in the design of future trials and that sex-stratified reporting of the primary outcome is becoming the norm. This will be crucial, allowing healthcare workers to treat women with vascular disease using evidence-based medicine and have an impact in the long term on the quality of care of women with vascular disease.”
Paediatric vascular surgery will be the topic of a later consensus statement, set to be authored by Kevin Mani (Uppsala University, Uppsala, Sweden) and colleagues. Mani tells Vascular News that, while rare, paediatric vascular complications represent a “dreaded” situation
Danish study suggests patients with AAA could benefit from high-dose statin use
A five-year prospective cohort study using longitudinal registry data from two Danish population-based screening trials has found that high-dose statin use was associated with decreased abdominal aortic aneurysm (AAA) growth rates and lowered risk of undergoing repair, rupture, and death. Researchers therefore suggest high-dose statins should be “strongly considered” for patients with small AAAs.
WRITING IN CIRCULATION, authors Joachim S Skovbo (Odense University Hospital, Odense, Denmark) and colleagues state that AAAs present with high morbidity and mortality when they occasionally rupture. Multiple meta-analyses have identified both metformin and statins as potential treatments, the authors go on to note, but neither has successfully been proven to reduce AAA growth. The present study, therefore, aimed to investigate a relationship between statin use and AAA growth rates and risk of undergoing repair, rupture, or death. Skovbo and colleagues detail that the
study population included all men with screening-detected AAAs—ranging in diameter from 30–55mm—from two large, population-based screening trials: the Viborg Vascular Screening trial and the Danish Cardiovascular Screening trial, which included patients in the years 2008–2011 and 2014–2018, respectively. The authors add that the clinical database was supplemented with data from the nationwide Danish Healthcare Registries, including prescription and outcome data. In order to evaluate the risk of repair, patients were followed from inclusion until surgery, rupture, death, five-year
amongst vascular surgeons. “Our aim is that the consensus statement will be a clinically useful tool for vascular surgeons who encounter paediatric complications or acute vascular situations,” Mani says. He goes on to highlight the importance of clinicians having “basic recommendations on how to manage different situations” available, in this area and others lacking sufficient evidence to warrant guidelines. Mani also notes that part of the statement will identify areas for future research that will “hopefully establish a baseline for collaborative data collection to shed more light on remaining questions”.
Avoiding “eminence-based” surgery
Considering the new consensus statements more generally, Mani notes a key challenge in that there is a risk of moving away from evidence-based and towards “eminence-based” vascular surgery if the line between expert consensus and clinical practice guideline is blurred. However, he is confident the new framework addresses this concern. “The process of establishing the consensus group and actually doing the work of reaching a consensus for the recommendations that are provided is important,” he says, noting “there are processes in place to ensure that the group is diverse along lines of geography and discipline”.
On this point, Twine is keen to stress that one of the main reasons behind publishing an editorial outlining the new process was to be clear about the statements’ role in vascular practice and “be upfront” about what the guideline writing committee is setting out to do and why with the new statements.
Van Herzeele remarks that the consensus statements hold a distinct place in vascular research and will “hopefully bridge a gap” by providing clinically relevant recommendations for areas of clinical practice that guidelines are unable to cover.
Mani is also confident that the statements will be a positive step towards best practice in areas lacking data and consolidate practice patterns. He remarks: “I believe what the consensus framework can achieve is, to some extent, harmonisation.”
For more information, visit esvs.org/guidelines
follow-up, or 31 December 2021.
The researchers included a total of 998 aneurysmal men with a mean age of 69.5 years and a median AAA diameter of 35.4mm in the study. They report in Circulation that statin use was “significantly associated with reduced AAA growth rate,” sharing that an increase of one defined daily dose statin per day was associated with an adjusted change in growth rate of -0.22mm per year.
Additionally, Skovbo and colleagues relay that the five-year adjusted hazard ratio for undergoing repair per doubling of statin dose presented a “significantly reduced adjusted hazard ratio” of 0.82, which they note was significant after 2.5 years. “Statin use was associated with a significantly lower risk of the
composite outcome (surgery, rupture, and death) in a dose-dependent manner,” the authors continue, citing an adjusted hazard ratio of 0.83 per doubling of statin dose.
Skovbo and colleagues write that their findings were “robust” in several sensitivity analyses and conclude that high-dose statin use was associated with a dose-dependent reduction in AAA growth rates and a lower risk of undergoing repair, rupture, and death during a five-year follow-up period.
“These findings study suggest that high-dose statins may offer direct protection against AAA progression, beyond cardiovascular risk reduction alone,” Skovbo and colleagues write.
Considering the clinical implications of their work, the authors advise that, “Because of their proven cardiovascular benefits, safety profile, and costeffectiveness, high-dose statins should be strongly considered for patients with small AAAs, particularly those without contraindications.”
“Although randomised trials may be ethically challenging,” the authors continue, “further high-quality observational studies are needed to validate these findings and inform clinical guidelines.”
L-R: Joachim S Skovbo (lead author) and Jes Sanddal Lindholt (senior author)
Transcatheter arterialisation of the deep veins: Comparative analysis
probes whether emerging modality is worth pursuing
“We’re living in a new world order” when it comes to “nooption” chronic limb-threatening ischaemia (CLTI) patients, says Anahita Dua (Massachusetts General Hospital, Boston, USA). In recent years, into this arena has stepped transcatheter arterialisation of the deep veins (TADV), raising hopes of reducing amputation rates amid a rise in diabetes and other disease affecting microvascular dissemination. At the 2025 Vascular Annual Meeting (VAM; 4–7 June, New Orleans, USA), Dua put forward data from a new study comparing no-option CLTI patients enrolled in the PROMISE studies treated with TADV to a CLariTI study cohort who were treated using standard of care (SoC). So, “is TADV worth it?” she pondered. The one-year comparative data she presented seemed to provide an answer in the affirmative.
POSITIVE PROMISE I AND II data have seen TADV, also known as deep vein arterialisation (DVA), gain traction, Dua told VAM 2025, but the “real question remains,” she said. “If you’re going to do a [TADV] procedure on a patient, then go forward with all the wound care, all the phone calls, and all the pain for the next six months to try to salvage the limb, does it really lead to better wound healing, better limb salvage rates and better amputation-free survival?”
With no randomised clinical trial data
to call upon in the space to measure a difference between TADV and standard of care, Dua and colleagues compared the combined patient groups from PROMISE I and II to the real-world CLariTI group to “see whether or not limb salvage rates genuinely decrease” when the former modality is deployed.
“We did CLariTI after PROMISE, so we were able to design the study to match the PROMISE studies so that we could ensure we had matching across groups,” she explained. “As you can see, most importantly this is, again,
a real-world study, with a significant number who were Black or African American, had Rutherford 5/6, and a significant history of CKD [chronic kidney disease].” The data showed limb salvage rates of 82.2% vs. 51.3% in the TADV/PROMISE I/II group and CLariTI, respectively; and amputationfree survival (AFS) rates of 71% for TADV vs. 34.1% for standard of care.
“For wound healing, 78% of patients at one year were either fully healed or healing in the DVA group versus the standard of care,” said Dua. “Going out, because durability matters, in the patient cohort for CLariTI—we are still collecting our data, because that was after the PROMISE study—but for the PROMISE data, we are at two years now and the limb salvage rate is still
Analysis of BEST-CLI, PREVENT III reveals significant improvement in vein bypass outcomes over 20-year period
A post-hoc comparison of the BEST-CLI and PREVENT III multicentre prospective randomised controlled trials (RCTs) aimed at evaluating outcomes of vein bypass in chronic limb-threatening ischaemia (CLTI) patients over the past two decades found that they have “significantly improved” during the study period, “even amidst concerns about declining case volume and training”.
THAT WAS THE HEADLINE FINDING OF A paper presented during a Vascular and Endovascular Surgery Society (VESS) session that took place during VAM 2025, delivered by presenting author Mohamad A Hussain (Harvard Medical School, Boston, USA).
With BEST-CLI demonstrating superiority of vein bypass compared with endovascular treatment for patients with CLTI and the rise in endovascular techniques as vein bypass procedures decline, the authors sought to elucidate concerns over whether
The study included 2,114 patients who underwent vein bypass for CLTI
710 in BEST-CLI 1,404 in PREVENT III AND
open surgery can still be safely and effectively carried out.
The study included 2,114 patients who underwent vein bypass for CLTI—710 in BEST-CLI (2014–2019) and 1,404 in PREVENT III (2001–2003), with the study findings revealing that the primary outcome measure of one-year major adverse limb event (MALE) or death was lower in BEST-CLI at 21% compared with PREVENT III at 38% (adjusted hazard ration [HR], 0.50; 95% confidence interval [CI], 0.40–0.62; p<0.0001). This was an observation found to be consistent across subgroup analyses, which included comparisons between patients in which single-segment great saphenous vein was available for use and those where it was not; those who underwent a femoropopliteal bypass and those who did not; and those aged below 65 and those equal to or above 65.
Meanwhile, major reinterventions—new bypass, surgical revision, thrombectomy or endovascular intervention for graft occlusion—were also lower in BEST-CLI (7.2% vs. 18.4%; adjusted HR, 0.40; 95% CI, 0.28–0.57; p<0.0001) at one year,
78%
For wound healing, 78% of patients at one year were either fully healed or healing in the DVA group versus the standard of care
at 68%, which is excellent compared, already, to the 51% at one year for the standard of care.”
Dua concluded: “I think the data is relatively clear. Even though we don’t have an RCT [randomised controlled trial], we have an excellent matched set from CLariTI compared to patients that have DVA and it is clear that DVA does have clinical benefit in patients selected appropriately. These benefits are consistent, especially if you use the LimFlow system [Inari Medical], which is kind of like the TCAR [transcarotid artery revascularisation] of the leg in that you are able to do the same thing every time. The off-the-shelf DVA that exist—and the data around that—is very variable so that is not included in any of this.”
although rates of any reinterventions were similar (25.8% vs. 29.3%; adjusted HR, 0.90; 95% CI, 0.72–1.14; p=0.39), Hussain and colleagues discovered. The gains detected in the comparison between the two trials “are likely driven by better risk factor optimisation, refined surgical techniques and advancements in perioperative care,” Hussain told VESS, acknowledging that the need for graft surveillance and maintenance was underscored by the data showing that the overall burden of reinterventions was consistent between BEST-CLI and PREVENT III.
It’s encouraging to see that patients undergoing vein bypass surgery for CLTI are doing significantly better today than they were two decades ago.”
Speaking to Vascular News, Hussain hailed progress made over the years.
“It’s encouraging to see that patients undergoing vein bypass surgery for CLTI are doing significantly better today than they were two decades ago,” he said. “Thanks to advances in surgical techniques, medical therapy, and overall care, we’re seeing fewer amputations, fewer complications, and better survival—real progress for a population that faces serious health challenges.”
Anahita Dua
STRIDE trial analysis confirms potential impact of semaglutide on quality-of-life metrics for PAD patients with diabetes
The findings of a new analysis from the STRIDE trial, published in Diabetes Care in line with its presentation at the American Diabetes Association (ADA) 2025 scientific session (20–23 June, Chicago, USA), demonstrate the potential vascular benefits of semaglutide in patients with peripheral arterial disease (PAD) and type 2 diabetes, including improvement in symptoms, quality of life, and disease progression in patients.
STRIDE IS A PHASE 3, multinational, double-blind, randomised clinical trial conducted at 112 outpatient clinical trial sites in 20 countries in North America, Asia, and Europe. Researchers enrolled 792 patients aged 18 years and older with type 2 diabetes and PAD with intermittent claudication and reduced ankle-brachial or toe-brachial index.
Patients were randomly assigned to receive either semaglutide (n=396) or placebo (n=396) over a 52-week period to assess the impact on walking capacity, symptoms, and quality of life. The median age was 68 years, and 195 (25%) participants were female and 597 (75%) were male.
The subanalysis builds on results
previously presented at the American College of Cardiology (ACC) 2025 scientific session (29–31 March, Chicago, USA) and published in The Lancet, demonstrating that semaglutide significantly improved walking outcomes in people with PAD and diabetes, enhanced quality of life, and reduced the risk of disease progression by 54%.
At week 52, the estimated median ratio to baseline in maximum walking distance was 1.21 in the semaglutide group compared to 1.08 in the placebo group. Semaglutide was well tolerated, with no treatment-related deaths and a low rate of serious adverse events (1%), consistent with its known safety profile.
The analyses from STRIDE
These findings indicate that clinicians can now recognise semaglutide as a vascular protective medication.”
presented new and critical information on the benefits of semaglutide, which were observed independent of baseline levels of A1C, duration of diabetes, or intensity of diabetes, ADA said in a press release. The benefits were seen across all body mass index
Multicentre experience shows “promising” midterm outcomes with IVL for calcified iliac occlusive disease
Shockwave intravascular lithotripsy (IVL) “expands endovascular strategies for iliac occlusive disease and can facilitate a ‘leave nothing behind’ approach,” Stefano Fazzini (Tor Vergata University, Rome, Italy) and colleagues write in an open-access Journal of Vascular Surgery (JVS) paper highlighting midterm outcomes from the IVLIAC registry—a multicentre, retrospective study of prospectively collected data.
“CALCIUM REMAINS A CHALLENGE IN the endovascular treatment of iliac artery disease, affecting both procedural and long-term outcomes,” Fazzini tells Vascular News. He goes on to comment that the standard approach of primary stenting, “although effective, is susceptible to stent recoil and under expansion in heavily calcified vessels” and notes that extensive calcification increases the risk of ruptures, especially when high-pressure balloons or balloon-expandable stents are used.
Fazzini also stresses that “no single stent is ideal for all calcified iliac lesions,” and that unnecessary stenting, especially at the bifurcation or when covering key branches, “can be avoided”.
In light of this, Fazzini et al set out to evaluate the midterm outcomes of patients with calcified iliac lesions treated with IVL, with or without adjunctive stenting, and to propose a new algorithm guiding these different treatment strategies.
The new algorithm, Fazzini explains, is based on lesion type (stenosis versus chronic total occlusion) and intraoperative functional assessments (extravascular ultrasound and pressure gradient) to determine whether stenting is necessary. “The impact
of sonic pressure waves improves vessel compliance and luminal gain, but such modifications may not always be evident on digital subtraction angiography alone,” he says, adding that intraoperative functional assessments play a “crucial” role in determining whether IVL alone is enough.
The investigators included all consecutive patients at four centres (Rome, Milan, Negrar and Trento) who underwent treatment with the Shockwave Medical peripheral IVL system for calcified iliac arteries from February 2021 to May 2024. Indication for IVL was Rutherford category of three or above in iliac lesions with moderate-to-severe calcification and was based on the new algorithm. The primary endpoint was primary patency, with assisted primary patency, secondary patency, and freedom from iliac complications also analysed.
Fazzini and colleagues share in JVS that a total of 100 iliac arteries were treated in 86 patients. They note that chronic limb-threatening ischaemia (CLTI) was present in 55% of patients, mean target lesion length was 40.95±29.25mm with a mean stenosis of 84±10%, and 12 of the lesions were chronic total occlusions. The authors report that technical
BMI categories and regardless of the treatment with SGLT2 inhibitors.
“These findings indicate that clinicians can now recognise semaglutide as a vascular protective medication, with benefits that extend beyond lowering weight or A1C,” said senior author Subodh Verma (University of Toronto, Toronto, Canada). “The totality of data now suggest that in people with diabetes, semaglutide favourably affects the pipes [atherosclerosis], pump [heart failure], filter [kidney outcomes].
And, in patients with PAD, these new data provide robust evidence that semaglutide is a therapy to improve their function, quality of life, and progression of disease.” The study authors indicate that further research is warranted to understand whether these benefits extend to individuals with PAD who do not have diabetes.
success was 99% and that target lesions were treated with IVL alone in 77% of cases, whereas IVL plus adjunctive stenting was employed in the remaining 23% of the cases. They add that provisional stenting was performed in 11% of cases, while planned stenting was performed in 12%, and that mean residual stenosis was 14.95±14% at final angiogram. Primary patency and assisted primary patency at 24 months were 95% and 98%, respectively, while secondary patency was 100%. Primary patency showed no statistically significant difference between the IVL only and IVL plus adjunctive stenting groups.
“Shockwave IVL offers a safe and effective treatment option for calcific iliac occlusive disease,” the authors write in their conclusion. “This multicentre experience shows promising midterm results in terms of primary patency despite the very low stenting rate, preserving future treatment options.” They go on to stress that further studies are needed to confirm these findings.
Discussing the findings with Vascular News, Fazzini summarises that, in cases of severely calcified disease, “Shockwave IVL as a first-line strategy in iliac interventions allows for either the avoidance of unnecessary stenting or optimisation of stent expansion, both of which contribute to favourable midterm outcomes”.
The Society for Cardiovascular Angiography & Interventions (SCAI) has released new, evidence-based clinical practice guidelines to support the treatment of chronic venous disease (CVD).
PUBLISHED IN JSCAI WITH AN accompanying technical review, the document offers recommendations on a range of therapeutic options—from compression therapy and wound care to ablation, sclerotherapy, phlebectomy, and deep vein stenting. The Society for Vascular Medicine has endorsed the guidelines.
“These are the first SCAI guidelines focused on chronic venous disease, and they come at a time of increasing recognition of the burden it places on patients and healthcare systems,” said Robert Attaran (Yale School of Medicine, New Haven, USA), chair of the guideline writing committee and member of the SCAI Vascular Disease Council. “CVD may present with discomfort, heaviness, and swelling, but it can progress to venous ulcers that are difficult to heal and severely impair quality of life. Our recommendations aim to provide clinicians and patients with a roadmap for personalised, evidence-informed care.”
The guideline panel addressed eight
clinical scenarios, culminating in nine formal recommendations and multiple identified knowledge gaps. The guidelines provide practical insights on which patients may benefit most from conservative therapy alone and when to consider escalating to more invasive options.
The recommendations were categorised as either ‘strong’ or ‘conditional,’ depending on the certainty of the evidence and other contextual considerations, including patient values and preferences. Among the key recommendations: Compression therapy is suggested for patients with symptomatic varicose veins (conditional recommendation) and strongly recommended for patients with venous ulcers (strong recommendation).
Ablation therapy in combination with conservative management, is suggested for patients with symptomatic reflux in the great or small saphenous veins and ulcer-associated perforator vein reflux (conditional recommendations)
US FDA deems Envveno’s VenoValve “not-approvable”
THE US FOOD AND DRUG Administration (FDA) has issued a letter to Envveno Medical stating that its VenoValve technology is “notapprovable”, the company reports. The letter was issued in response to Envveno’s premarket approval (PMA) application for VenoValve—a surgical replacement venous valve for treating severe deep chronic venous insufficiency (CVI).
According to Envveno, the letter indicates that the FDA completed its review of the VenoValve PMA application and determined that it is unable to approve the PMA for the VenoValve in its current form.
“In particular, the FDA indicated that the favourable revised Venous Clinical Severity Score (rVCSS) data generated by the [SAVVE] study to show clinical improvement, together with the improvements in pain scores and venous-specific quality-of-life indicators was not sufficient on its own to determine favourability of the benefit-risk profile for the VenoValve,” the company press release reads. “Without a specific
in combination with conservative management.
Foam sclerotherapy and phlebectomy, when applied in patients without truncal vein reflux or with persistent symptoms after treatment of truncal veins, may be considered in combination with conservative therapy (conditional recommendations).
Venoplasty or stenting may offer improved quality of life and symptom relief for patients with iliocaval venous obstruction, though with low certainty of evidence (conditional recommendation). In addition to formal recommendations, the guidelines introduce two treatment algorithms, one for patients with symptomatic varicose veins and another for those with venous ulcer disease, to help guide clinical decision-making in real-world settings. The document pays close attention to patient-centred care, shared decision-making, and the potential trade-offs associated with each treatment modality, particularly in the context of comorbid conditions such as peripheral arterial disease (PAD) or prior surgical history.
These are the first SCAI guidelines focused on chronic venous disease, and they come at a time of increasing recognition of the burden it places on patients and healthcare systems.”
“These guidelines reflect SCAI’s commitment to bringing high-quality, evidence-based standards to areas where our members are increasingly practicing,” said SCAI President Srihari S Naidu (New York Medical College, New York, USA). “As interventional cardiologists take a larger role in managing chronic venous disease, a common problem affecting millions of people, these recommendations will help ensure that patient care remains both consistent and personalised. SCAI is proud to support this milestone publication and its vision of advancing patient outcomes through collaboration across disciplines, which ultimately increases the quality and quantity of patient access to muchneeded treatment options.”
Spotlight falls on CVI following US President’s diagnosis
haemodynamic measurement that correlates with patient improvement, the FDA raised concerns about bias and the possibility that clinical improvement occurred as a result of the patients being enrolled in a study.”
The FDA also focused on safety concerns which were attributed to the VenoValve open surgical procedure.
“We are obviously disappointed by the FDA’s decision. The results showed that a high percentage of the patients in the SAVVE study, who all previously failed standard-ofcare treatments, showed significant clinical improvement after receiving the VenoValve. With the VenoValve being the only difference in their care, it is hard to not attribute the improvement to the VenoValve,” said Robert Berman, Envveno’s chief executive officer. “We remain committed to the 2.5 to 3.5 million patients suffering from severe deep venous CVI in the US and who have no effective treatment options and will continue to work with the FDA on new criteria to demonstrate the safety and effectiveness of our devices.”
THE QUESTION ‘WHAT IS chronic venous insufficiency (CVI)?’ has been central to media coverage of the recent news that US President Trump has been diagnosed with the condition. Speaking to Vascular News, Kathleen Ozsvath (St Peters Health Partners, New York, USA) says this highlights a pressing need for enhanced awareness of CVI, a disease state she says is “underdiagnosed” and “not understood”.
Ozsvath notes that CVI is four times more prevalent than arterial disease. “There are a lot of people suffering from venous insufficiency who really do need help,” she says. Despite this, Ozsvath goes on to stress that knowledge of CVI eludes not just patients, but often physicians and healthcare providers too.
As a result, Ozsvath details that she often sees the most extreme form of CVI—a venous ulcer. “People really suffer with this,” she says, both on a medical and social level. “Patients are embarrassed. It looks terrible, can smell bad, and has increased risk of infection. Some patient do not have
the resources to find good physicians and centres who provide appropriate treatment.” When patients do seek help, Ozsvath notes that they often go to a provider who may not have the experience or expertise to treat the patient. “It’s a vicious cycle,” she says, and one that can be “very costly”.
Ozsvath stresses that there is “such a disparity of knowledge” among specialists when it comes to the treatment of CVI, with a key issue being data lagging behind technological developments. This, she says, “makes it harder for us to know what the best practices are and what kind of treatment options we have”. To address this, Ozsvath underlined the importance of keeping up with the latest guidelines. Patient awareness too is “extremely important” to avoid CVI resulting in a leg ulcer, according to Ozsvath. “I think I spend most of my time explaining to patients what the pathophysiology of venous disease is, why they have a problem, and what their treatment options are to help fix the problem,” she says.
Photo by Wesley Tingey on Unsplash
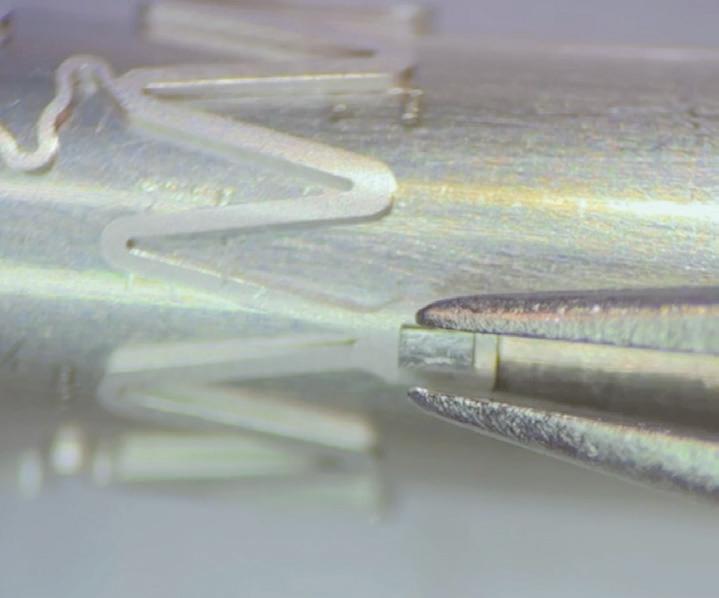
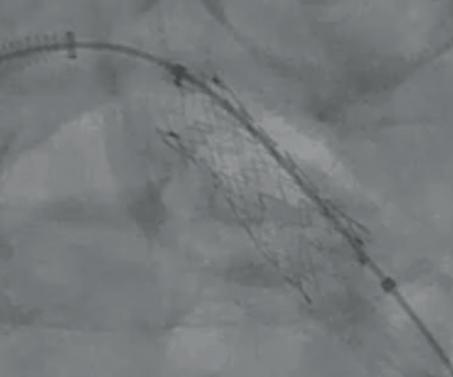
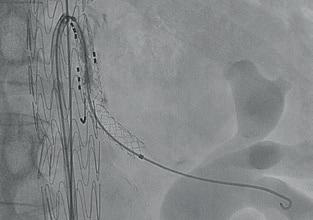
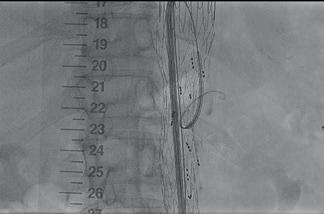
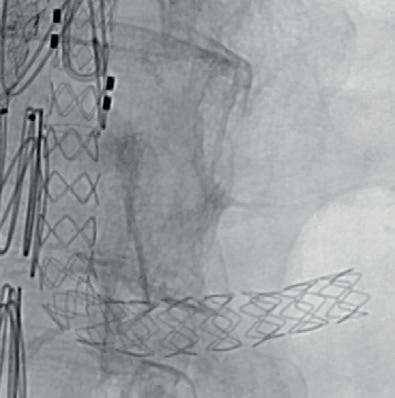
Precise implantation
Exact location and post-expansion
Not all carotid procedures are equal after patients suffer a postoperative stroke
Strokes after transfemoral carotid artery stenting (TFCAS) were “the most disabling and lethal” when compared with transcarotid artery revascularisation (TCAR) and carotid endarterectomy (CEA) in a multicentre, retrospective analysis of Vascular Quality Initiative (VQI) data using modified Rankin Scale (mRS).
THE STUDY WAS RECENTLY published in press in the Journal of Vascular Surgery (JVS) by first author Mohammed Hamouda, senior author Mahmoud B Malas (both UC San Diego, San Diego, USA) and colleagues following its initial presentation at the 2025 Vascular Annual Meeting (VAM; 4–7 June, New Orleans, USA).
The VQI database was queried from September 2016–August 2024 for patients who suffered a postoperative stroke after their carotid revascularisation procedure, with the magnitude of the event quantified using mRS 0–6, where 0 is a stroke with no symptoms and 6 is a stroke leading to
death. A severe stroke was defined as one having mRS>4.
Hamouda and colleagues found a total of 2,752 patients suffered a postoperative stroke after all three procedures. Overall, 22.5% of the postoperative strokes had mRS>4, the researchers discovered. When stratifying by procedure type, TFCAS had the highest rate of severe strokes— CEA 21.2% vs. TCAR 19.1% vs. TFCAS 30.7% (p<0.001). After adjusting for confounding variables, “there was no significant difference between TCAR and CEA in terms of odds of severe stroke, odds of a lethal stroke (mRS=6/dead) even after stratifying by symptomatic
status (p>0.05),” they report. However, TFCAS-related strokes had 75% (adjusted odds ratio [aOR] 1.75, confidence interval [CI] 1.26–2.43), p<0.001) and 45% (aOR 1.45, CI 1.05–2.00, p=0.024) increased odds of being severe compared to CEA and TCAR, respectively.
“After stratifying by symptomatic status, there was no significant difference observed in asymptomatic patients; however, symptomatic TFCAS patients had more than double the odds (aOR 2.21, CI 1.47–3.33, p<0.001) of severe strokes compared to CEA and 72% increased odds of severe stroke (aOR 1.72, CI 1.12–2.67, p=0.014) compared to TCAR patients,” Hamouda and colleagues write in JVS Likewise, risk of dying following postoperative stroke was the highest with TFCAS—“the odds being 79% and 47% higher compared to CEA and TCAR, respectively”. In terms of oneyear outcomes, patients who underwent TFCAS complicated by a stroke were at higher risk of recurrence and mortality compared to those getting a stroke after CEA, the investigators continue.
Two-year ECST-2 data published, find “no evidence”
for benefit of carotid revascularisation additional to optimised medical therapy
Recently published in The Lancet Neurology, two-year interim data from the ECST-2 trial have shown no evidence for a benefit of revascularisation in addition to optimised medical therapy (OMT) for patients with symptomatic and asymptomatic carotid stenosis of 50% or greater, with a five-year predicted stroke risk of less than 20%, in the first two years following the procedure.
SIMONE JA DONNERS (UMC UTRECHT, Utrecht, The Netherlands) and colleagues write that the results “support treating patients with asymptomatic and low- or intermediate-risk symptomatic carotid stenosis with OMT alone until further data from the five-year analysis of ECST-2 and other trials become available”.
Donners et al detail that ECST-2—or the ‘Second European carotid surgery trial’—is a multicentre, randomised trial with blinded outcome adjudication. The trial was conducted at 30 centres with stroke and carotid revascularisation expertise in Europe and Canada, recruiting patients aged 18 years or older with asymptomatic of symptomatic carotid stenosis of 50% or greater, and a five-year predicted risk of ipsilateral stroke of less than 20%. The risk of stroke was estimated using the Carotid Artery Risk (CAR) score.
The authors explain that patients were randomly assigned to either OMT alone or OMT plus revascularisation using a web-based system. The primary outcome for the analysis was a hierarchical outcome composite of: (1) periprocedural death, fatal stroke, or fatal myocardial infarction; (2) non-fatal stroke; (3) non-fatal myocardial infarction; or (4) new silent cerebral infarction on imaging.
Analysis was conducted by intention-to-treat using
the win ratio, with the authors noting that theirs was the first stroke trial to use this method to analyse a primary hierarchical outcome. The win ratio is described as follows: “Each patient in the OMT alone group was compared as a pair with each patient in the OMT plus revascularisation group, with a win declared for the patient with a better outcome within the pair (a tie was declared if neither patient in the pair had a better outcome).”
Donners and colleagues share that, between 1 March 2012 and 31 October 2019, 429 patients were assigned to OMT alone (n=215) or OMT plus revascularisation (n=214). Of these patients, one allocated to OMT alone withdrew consent within 48
The results of ECST-2 provide an important step towards more individualised treatment in patients with carotid stenosis enabled by the CAR score.”
Similarly, TFCAS-related strokes were associated with “higher hazard of death during the first year of follow-up” compared to the TCAR group, but there was no difference in ipsilateral stroke recurrence. “Finally, there was no significant difference between TCAR and CEA in any of the one-year outcomes,” they add, with strokes after CEA and TCAR in the study “of a very similar magnitude in terms of postoperative functional outcomes as well how the index stroke impacts one-year recurrence or mortality”. Concluding, Hamouda and colleagues note, “CEA exhibited the highest unadjusted strokefree survival rate” among the three procedures.
CEA exhibited the highest unadjusted strokefree survival rate.”
hours and was not considered further. The median age of the patients was 72 years, and the majority (69%) were male.
Sharing the key findings, Donners et al report that no benefit was recorded in favour of either treatment group with respect to the primary hierarchical outcome assessed two years after randomisation, with 5,228 (11.4%) wins for the OMT alone group, 5,173 (11.3%) wins for the OMT plus revascularisation group, and 35,395 (77.3%) ties between groups.
“ECST-2 is unique in comparing the efficacy of OMT alone versus OMT plus carotid revascularisation in patients with both asymptomatic carotid stenosis and symptomatic carotid stenosis at low to intermediate predicted risk of future stroke, with five-year follow-up,” the authors write in The Lancet Neurology, commenting on the value the present study adds to the literature.
In the discussion of their findings, Donners and colleagues point to certain limitations of the interim analysis. These include the relatively small number of patients included and the fact that ECST-2 is the first study to use a recalibrated CAR score. “Although event rates in ECST-2 were well within that predicted by the score,” the authors write, “its accuracy has not been independently tested.”
Donners et al go on to remark that, “The results of ECST-2 provide an important step towards more individualised treatment in patients with carotid stenosis enabled by the CAR score.” However, they do stress that the findings only apply in general to the group of patients with low- or intermediate-risk symptomatic stenosis selected using the CAR score, and to asymptomatic patients.
Looking ahead, they suggest that identifying individual patients with carotid stenosis within these groups and those excluded from the selection criteria who are most likely to benefit from or be harmed by revascularisation should be a goal of future research.
The interim two-year results from ECST-2 were first shared at the 2023 European Stroke Organisation Conference (ESOC).
Mohammed Hamouda (top) and Mahmoud B Malas
DAWN COLEMAN
It was by chance rather than design that Dawn Coleman (Durham, USA) entered a career in vascular surgery, she tells Vascular News. Her unorthodox route into the profession, however, has not hampered Coleman’s rise to several senior positions. Now professor of surgery and chief of the Division of Vascular and Endovascular Surgery at Duke University School of Medicine, Coleman here speaks about some defining moments of her professional life as well as wider trends in the field, sharing how a military background has instilled in her a commitment to service and dedication to good leadership that have been core tenets of her medical career.
Why did you choose to pursue a career in medicine and what drew you to vascular surgery?
I think everybody’s decision to pursue medicine is personal. For me, I feel lucky that I found my path towards medicine and surgery, although by no means was it linear. I don’t come from a background of physicians or professors, but I know that I had a lot more opportunity than most because of my dad’s commitment to supporting our family and allowing my brother and I to do whatever we wanted, be whatever we wanted. I felt compelled to do something that he would be proud of.
I struggled to identify an industry to pursue when I was in high school and, to be honest, I wasn’t actually sure medicine was for me. I was shy, I was afraid of blood, and I certainly didn’t meet the phenotype of what a physician looked like then.
However, I was encouraged by my dad to volunteer at the emergency department at the University of Cincinnati (Cincinnati, USA) and just found myself enamoured with the pace and the impact on human lives and it was really inspiring.
Ultimately, I made the decision to go to medical school with the plan to be an emergency medicine doctor, and I matched in emergency medicine at the University of Michigan (Ann Arbor, USA).
I had ambitious plans to pursue disaster medicine or military medicine in a vision for my future that was based on service and along the way I found surgery, and I found it serendipitously. I found it because I was exposed to the right people during formative times and I ultimately made a very rash, uncounselled decision to quit my residency and go into surgery.
I got very lucky because a lot of people took risks on me along the way to give me more opportunity. I got to stay at the University of Michigan to be a general surgery resident and from there I found my way to vascular surgery.
And so I credit my dad for pushing me towards medicine, I credit the University of Cincinnati’s emergency medicine team for harnessing that enthusiasm and allowing me a platform to get into medical school, and then I credit the Surgery Department at the University of Michigan for giving me a chance to be a general surgery resident and specifically the likes of Gilbert Upchurch, Thomas Wakefield, John Eliason and John Rectenwald for their roles in recruiting me into the vascular surgery field.
I entered medicine and vascular surgery via a super non-traditional, non-conventional route, but I look back and I don’t know that I would have done anything differently. I think that this is the best job for me. I really love it.
How has your military background influenced your surgical career?
I come from a long line of military service members and knew when I was at college that I wanted to commission. When I matched at the University of Michigan and went into emergency medicine, the first thing I did— after getting my badge and onboarding as a new intern—was find a recruiter.
I’ve had a really productive, high impact and gratifying career in the military, including three deployments for combat care and two joint training missions supporting NATO efforts. I’ve also done some things that have been really hard, but from which I’ve grown a lot. I think all these experiences have helped me to be a better human and probably a better surgeon, because we do hard things in the hospital all the time and keeping that frame of reference at the ready has been helpful.
I’ve also seen some of the best and worst leadership in the military, and I think that’s influenced how I think about leading at whatever level that has been for me.
A huge part of who I am is a service member, a soldier. I’m still active in the reserve and I appreciate that service very much.
You are currently the secretary for the Vascular and Endovascular Surgical Society (VESS). How did you get involved with the society and what does it offer?
I got lucky and fell into a role at VESS thanks to my partner and mentor at the University of Michigan, John Eliason. He was active in the society and is a past president.
I had the privilege of being put on a VESS committee early on and subsequently had the opportunity to serve at the higher levels of the society.
For me, getting engaged with VESS has offered me an unquantifiable benefit just in the human connections I’ve been able to make through enduring friendships, and I would encourage everybody to get engaged and get engaged early with the society because it’s just such a fun space.
I remember going to my first VESS meeting as a trainee and there were a few things about it that I just found so refreshing. It’s focused on early career surgeons and particularly those with academic interests, and the senior
FACT FILE
CURRENT ROLES
2023–2026: Secretary, Vascular and Endovascular Surgical Society (VESS)
2024–2026: President, Association of Program Directors in Vascular Surgery (APDVS)
2023–present: Professor of surgery, Duke University School of Medicine (Durham, USA)
2022–present: Chief, Division of Vascular and Endovascular Surgery, Duke University School of Medicine
EDUCATION AND TRAINING
2010–2012: Vascular surgery fellow, University of Michigan (Ann Arbor, USA)
2004–2010: General surgery resident, University of Michigan
2003–2004: Emergency medicine resident, University of Michigan
2003: MD, University of Cincinnati College of Medicine (Cincinnati, USA)
members are active rising leaders and are very approachable. It’s also a winter meeting and delegates like to attend for the skiing, so they will often save some of their best science for VESS, which makes the scientific programming and rigour just awesome!
What are some of your current research interests?
My paediatric work probably feels the most active to me right now in a very exciting way. Early in my time at the University of Michigan I had the opportunity to care for children and was able to learn about paediatric renovascular hypertension from Jim Stanley and John Eliason, who I worked alongside for many years.
I found additional clinical and research collaborators in this area at the University of Michigan and we still push work forward. Some of that work is in the translational scientific space with a lens towards the genotypic factors and molecular pathways that underpin the diagnosis of paediatric renovascular hypertension and understanding it better.
We’re looking now, through the support of a multidisciplinary and patient-powered collaborative, at research questions that have been prioritised by our patients and their families. We’re treating children across a spectrum of disease severity and there is a real paucity of evidence-based guidance at present.
In my opinion, treatment needs to be individualised according to a patient’s genotype, their anatomic phenotype, and the severity of their disease alongside other factors that are relevant to their own social development age. I think this collaborative will push the needle forward in really prioritising these children who have a very rare vascular disease.
What do you think are some of the biggest challenges facing vascular surgery?
There is a considerable administrative burden in vascular surgery that is growing exponentially, exhausting the workforce and eroding the patient-provider experience. Compounding that are challenges with reimbursement. These challenges, and others, threaten our workforce severely and I worry will compromise our efficacy in treating the sum of projected future vascular surgery patients.
What do you propose could be done to address these challenges?
I am of the opinion that, as a specialty, we can’t grow fast enough. We need a workforce that will be appropriately sized to care for the disease burdens we are facing.
I also think it’s important for us to acknowledge what our patients need the most, and make sure that we prioritise. At some point, I think we have to shift our logic and stop thinking about training every vascular surgeon to be exactly the same and highly skilled in all areas.
Rather, I think we should ensure that our workforce is prepared with an adequate volume of surgeons that can tackle what our patients need the most. Our patients need an adequate vascular surgery workforce, alongside interventions that target rising population threats like obesity, hypertension, gun violence and other population health threats inclusive of social determinants of health and environmental exposures.
I also think we have to be really intentional about populating gaps where there are access challenges and where we know there is an under-representation of medical care at large
and vascular surgeons specifically, particularly in rural spaces. Advocacy and intention will be required to recruit and retain vascular surgeons to serve these areas specifically.
We’ve got a beautiful integrated residency programme in the USA, but we’re graduating a number of residents who come through academic centres wanting to do academic work, which means they stay in big cities that have academic institutions. We have to train people in community and rural spaces who want to stay and serve those patients. It has to be prioritised.
And so I charge our community and our leaders, including myself, to prioritise out workforce. If we don’t do it proactively and lead it, somebody else is going to seize that opportunity and they may not offer the same commitment to comprehensive vascular care that we are dedicated to providing as vascular surgeons.
All of this requires energy, effort, and goodwill, which not everybody has its spades at the moment, and so I’m sensitive to that, but I think we have a lot of work ahead of us.
“We need a workforce that will be appropriately sized to care for the disease burdens we are facing.”
What advice would you give to someone looking to start a career in vascular surgery?
Be curious and ask questions. You’ll be a better clinician, leader, and researcher if you can stay curious, ask questions, and understand the why.
Focusing on people and focusing on relationships is also super important. It has been for me. Whether those are patients, their families, your partners, or your trainees, I think without the people part of this job, it would not be worth any of the struggle, so find the right people to serve and to work with. And the final thing I’d say is that patients always come first.
What are your hobbies and interests outside of medicine?
I’m a mother to two kids and that’s the best part of my life outside of work. I really like to cook and show love through cooking and hosting. I also enjoy country music, Italian opera, travelling and immersing myself in other cultures, and running.
Acellular tissue engineered vessel shows promise in highrisk patients on haemodialysis
Results from the CLN-PRO-V007 pivotal phase 3 clinical trial of the acellular tissue engineered vessel (ATEV; Humacyte) in arteriovenous access for patients at high risk of autologous arteriovenous fistula (AVF) maturation failure with end-stage renal disease were presented at the 2025 Vascular Annual Meeting (VAM; 4–7 June, New Orleans, USA).
THE TRIAL’S RESULTS, presented by Mohamad A Hussain (Brigham and Women’s Hospital and Harvard Medical School, Boston, USA), demonstrated the superiority of ATEV over autologous AVF in highrisk patients with end-stage kidney disease (ESKD).
CLN-PRO-V007 was a prospective, multicentre, two-arm, randomised controlled trial comparing the efficacy
and safety of ATEV and AVF in ESKD patients on haemodialysis undergoing single-stage surgical vascular access creation.
AVF is the preferred method for vascular access in haemodialysis patients as, when successful, it can reduce long-term catheter use and associated complications. However, women and patients with obesity and diabetes are at higher risk of AVF maturation failure, meaning the fistula doesn’t develop adequately for use in dialysis, often resulting in prolonged catheter dependence and increased morbidity.
ATEVs are bioengineered blood vessels grown from human vascular cells, designed to restore, replace, or enhance the function of damaged or diseased vascular tissue.
The trial enrolled a total of 242 ESKD patients, of which 110 were specified as high-risk of fistula non-
Modelling suggests early CKD screening and diagnosis could cut dialysis use
New analysis of the IMPACT CKD study suggests that targeted screening, diagnosis and improved access to care for patients with chronic kidney disease (CKD) could bring about a significant reduction in the number of patients requiring dialysis across the UK.
PRESENTED AT THE 2025 EUROPEAN Renal Association (ERA) congress (4–7 June, Vienna, Austria), the analysis by AstraZeneca modelled outcomes for the UK population over a 25-year period (2022 to 2047). It assessed the combined effect of targeted screening, diagnosis, and better access to care and recommended treatments— including annual targeted screening for patients with comorbidities and over the age of 45 combined with 75% adherence to guideline-directed medical therapy (GDMT).
IMPACT CKD is one of the first studies to examine and forecast the impact of CKD over a 25-year time horizon. It is part of AstraZeneca’s Accelerating Change Together (ACT) for CKD programme, which aims to improve understanding
maturation (defined as all individuals with a body mass index [BMI] ≥ than 30kg/m2 and having diabetes).
Humacyte previously announced positive topline results from the trial in October 2024, whereby the ATEV demonstrated superior function and patency at six and 12 months (coprimary endpoints) compared to autogenous fistula.
In the latest study ATEV was observed to have better functional patency, usability, and a comparable access-related complication profile compared to AVFs in this high-risk subgroup of patients.
The safety profile of ATEV was reported to be comparable to AVF, with similarly low rates of infections. The cohort of patients treated with ATEV had more thrombosis and stenosis events compared to AVF, however the majority were successfully treated.
Patients treated with ATEV had a lower need for maturation and surgical revision procedures compared to AVF.
“Often, we see patients who are considered high risk and in end-stage kidney failure needing
multiple interventions and autologous arteriovenous fistulas often failing,” said Hussain, the lead author of the study.
Considering ATEV’s potential, he continued: “Acellular tissue engineered vessels are a new and exciting technology in regenerative medicine that has the potential to make a great impact in how we treat a vulnerable population.”
Authors note a currently enrolling randomised control study is looking specifically at high-risk ESKD female patients across multiple centres in the USA who receive ATEV or AVFs to further analyse the effectiveness specifically in the female population. For uses other than US Food and Drug Administration (FDA) approval in the extremity vascular trauma indication, ATEV is an investigational product and has not been approved for sale by the FDA or any other regulatory agency.
Co-authors for this study include Shamik Parikh, chief medical officer of Humacyte, and Laura Niklason, chief executive officer and founder of Humacyte.
Often, we see patients who are considered high risk and in end-stage kidney failure needing multiple interventions and autologous arteriovenous fistulas often failing.”
and outcomes of CKD worldwide.
The modelling projected improvements in health, including a 45% decrease in cardiovascular (CV) events and a 3.1% decrease in death events over 25 years in the UK. These outcomes were accompanied by a 34.7% projected reduction in dialysis use over the same period in the UK, one of the most resource-intensive treatment options in CKD care.
As a result, the UK is projected to save £13.8 billion in costs related to kidney replacement therapy (KRT) over 25 years—enough to fund more than two years’ worth of all NHS obesity-related care, or to clear the entire NHS maintenance backlog for 2024.
CKD—not only to improve lives, but to build a stronger, more sustainable NHS. Earlier diagnosis and better treatment access could keep people healthier for longer, ease pressure on healthcare services, and boost net GDP contributions, adding £200 billion to the UK economy over 25 years. We believe that a five-year action plan for cardiovascular disease is needed, with a focus on CKD, to help unlock long-term gains for patients, society and the environment.”
Fiona Loud, policy director at Kidney Care UK, said: “Screening, early diagnosis and treatment can provide patients with the opportunity to manage their condition, stay well for longer and avoid the distressing and disruptive reality of dialysis. Yet, far too often, CKD is only diagnosed once it has reached a critical stage. We need to change that— and that means urgent policy action to support early detection and ensure people can access the care they need. If we act now, there is a real opportunity to improve lives and help people remain active members of their families, communities and society.”
Tom Keith-Roach, president of AstraZeneca UK, added: “It’s clear there is an urgent need to act on
Screening, early diagnosis and treatment can provide patients with the opportunity to manage their condition, stay well for longer and avoid the distressing and disruptive reality of dialysis.”
Humacyte’s acellular tissue engineered vessel
Coverage that counts: Dedicated iliac covered stent opens new chapter in treatment of complex occlusive disease
The story of iliac stenting in patients with TASC C and D lesions is one of evolution. From traditional self-expanding, bare metal stents to modern covered devices, the field has witnessed several new technologies in the course of its history, each designed to hone the treatment of complex iliac occlusive disease. A new dedicated iliac covered stent—the BeFlow (Bentley)—opens the latest chapter, promising an evidence-backed, economically sound solution. Here, one expert shares their clinical experience with the device in the context of a dynamic disease landscape, shifting practice patterns, and strict health economic parameters.
Raghu Lakshminarayan (Hull University Teaching Hospitals NHS Trust, Hull, UK) has extensive experience treating complex iliac occlusive disease. Fifteen years ago, he recalls, the placement of an uncovered self-expanding or—less frequently— balloon-expandable stent was commonplace, based on evidence showing that their use decreased the incidence of distal embolisation in occlusive disease.
Bare-metal stents were not without their limitations, however. For instance, Lakshminarayan shares that the positioning of a self-expanding stent was “quite difficult” for early operators. “There was a long learning curve in order to precisely position them,” he states. Cost was also an issue, with stenting being a more expensive option than plain balloon angioplasty.
Lakshminarayan notes that his go-to treatment algorithm has changed significantly over the past 10 to 15 years. One of the main reasons for this, he explains, is that the complexity of disease he sees on a day-to-day basis has changed over time. “The kind of disease that we used to treat 15 years back was different. We used to treat a lot of claudicants; nowadays, we’re treating severe forms of chronic limb-threatening ischaemia,” he says.
According to Lakshminarayan, the limitations of uncovered stents, combined with the increasing complexity of the disease state in question, warranted new technologies.
Covered stents have shown promise here. The COBEST trial, for example, showed that covered stents performed better than uncovered stents in TASC C and D lesions. Patency rates were 82.1% vs. 70.9% at two years, 79.9% vs. 63% at four years, and 74.7% vs. 62% at five years for covered and uncovered stents, respectively. Covered stents were also associated with fewer revascularisations for TASC C and D lesions than uncovered stents.
There is still work to be done, however, with Lakshminarayan referencing the European Society for Vascular Surgery (ESVS) guidelines to illustrate a data gap. These guidelines include a IIb recommendation for the use of covered stents in TASC C and D lesions, indicating weak or conditional evidence. “The bottom line is we still require a lot more work on this,” Lakshminarayan comments. Further data are forthcoming, with Lakshminarayan referencing the EVOCC trial in the UK as an important case in point. This randomised controlled trial will assess the clinical and cost-effectiveness of endovascular versus open revascularisation in severe aortoiliac occlusive disease. EVOCC is set to randomise 628 patients at several centres in the UK, including Lakshminarayan’s in Hull. Lakshminarayan goes on to highlight the importance of gathering further data on covered stents, particularly to demonstrate their cost-effective potential. “The major obstacle to using covered stents is cost, and what we need to demonstrate is that upfront cost might reduce reintervention rates,
BeFlow iliac covered ballonexpandable stent system
We need a lot of tools in our kit because of the increasing complexity of patients with iliac disease.”
and therefore even if you have higher costs in the beginning, in the long term the technology will be economically beneficial,” he says.
“If cost was not an issue, then I think whenever somebody was going to use a particular kind of stent, they would use consider using a covered stent,” Lakshminarayan posits. “But having said that, the evidence is still limited, and we need to gather more data.”
There are signals in the literature that future research will point to the benefits of covered stents. Lakshminarayan mentions the DISCOVER trial, for example, which looked at reintervention rates following the use of covered and uncovered stents. In this trial, freedom from reintervention was not significantly different between the two groups overall, but in a subset of patients with moderate and heavy calcification—a disease state Lakshminarayan reiterates is becoming more common—the researchers found a signal that reintervention and restenosis rates were higher in the uncovered stent group.
Lakshminarayan remarks: “If somehow we can present the upfront cost of a covered stent as
something that will deliver durability and decrease reinterventions, based on robust evidence, I think that would be very useful.”
As for Lakshminarayan’s current treatment algorithm, this focuses almost exclusively on covered stents—during the covered endovascular reconstruction of aortic bifurcation (CERAB) procedure for aortoiliac disease; for occlusive TASC C and D lesions, for fresh plaque or lesions that have been recently embolised, and for long occlusive lesions or dissections.
BeFlow, launched earlier this year at the Leipzig Interventional Course (LINC 2025; 28–30 January, Leipzig, Germany), has become a key part of this treatment algorithm.
“I have been using covered stents for complex iliac procedures for a very long time, but only for very complex (TASC C and D) cases,” he says. “Now, with the BeFlow, which gives me more liberties within my budget, I’m increasingly also using covered stents in less complex cases, because I believe in the better long-term outcomes and like the safety and delivery a covered stent gives me in relation to distal embolisations.”
BeFlow has been positioned as a dedicated iliac solution that is more economically accessible than some other covered stent options, which Lakshminarayan points out is of crucial importance in today’s healthcare environment.
“Aortoiliac disease is quite a significant component of the treatment of peripheral arterial disease, so having a stent that is positioned for treating the iliac arteries is very useful,” he says. Lakshminarayan goes on to note that BeFlow closes a gap between clinical requirements and economic needs.
Looking ahead, Lakshminarayan is of the opinion that innovation will continue in this area. “We need a lot of tools in our kit because of the increasing complexity of patients with iliac disease,” he stresses, pointing to calcium modification techniques among several other future advances.
Sharing a message to younger vascular specialists about choosing the right stent for the right lesion, Lakshminarayan homes in on the importance of a long-term solution. “A good completion angiogram is not necessarily a durable solution,” he says. “Please do keep in mind the durability of the solution over a long period of time, and try and do the best that you can to provide the patient a good long-term outcome, and in that respect, considering a covered stents is a good idea.”
Case presentation: A 55-year-old patient who presented with acute limb ischaemia due to embolisation from an iliac plaque rupture. The iliac lesion was treated successfully with a BeFlow.
Moral injury in vascular surgery: Recognising the hidden cost
Adam Talbot (Manchester, UK) writes about moral injury in vascular surgery, suggesting steps that could be taken to prevent it.
Vascular surgery often places surgeons in highpressure situations where the right course of action is clear, but systemic constraints prevent its delivery. This dissonance is increasingly recognised as moral injury, a psychological harm distinct from burnout.
The British Medical Association (BMA) defines moral distress as the experience of knowing the ethically appropriate action to take but being unable to act due to external constraints.1 When this distress becomes prolonged or is caused by serious ethical breaches, it can result in moral injury, a deeper, long-term psychological impact that erodes professional integrity and mental wellbeing. In a 2021 BMA survey of UK doctors, 78% reported experiencing moral distress, and more than 50% said the term moral injury reflected their experience. These findings spanned specialties, and they highlight a widespread challenge across the health service.
For vascular surgeons, this may arise when patients with chronic limb-threatening ischaemia (CLTI) present too late due to delays in referral or diagnostics, when urgent
revascularisation is postponed due to lack of theatre access, or when decisions are made based on bed availability rather than clinical priority. These situations are not rare; they are becoming routine.
Intraoperatively, moral distress can occur when surgeons encounter unforeseen complications or deviations from the expected course of surgery, where they are aware of the optimal intervention but lack the means or opportunity to effect it.
A surgeon might encounter an unexpected anatomic variation or an unanticipated technical complication that prevents the desired outcome. Despite following all the established protocols, the surgeon may feel a profound sense of failure, as they are aware that the result falls short of both clinical expectations and their personal standards of care.
This sense of powerlessness is particularly damaging when it occurs in the context of an emotionally charged situation such as limb loss. Surgeons, driven by a deep sense of responsibility and a commitment to achieving the best possible outcome, may experience guilt or moral distress when they are unable to fulfil the duty they perceive to the patient. These intraoperative moments, though often beyond the surgeon’s control, can lead to long-term moral injury, especially in the absence of avenues for reflection
The culture of vascular surgery, which historically values decisiveness and perfectionism, may further compound the issue. Surgeons may be less likely to speak openly about emotional distress or seek help, fearing judgment, loss of credibility, or other consequences. Over time, unaddressed moral injury can
US blood pressure guidelines bump up recommendation for renal denervation
New guidelines from the American College of Cardiology (ACC) and the American Heart Association (AHA) for the prevention and management of high blood pressure have, for the first time, added renal denervation as a treatment option for patients with resistant or uncontrolled hypertension.
PUBLISHED IN THE JOURNAL OF the American College of Cardiology (JACC), Circulation and Hypertension, the guidelines give the therapy a class IIb recommendation for patients with a systolic blood pressure of 140–180mmHg and diastolic blood pressure ≥90mmHg despite four drugs, or in patients with uncontrolled hypertension intolerant to drug escalation. All patients with hypertension who are being considered for renal denervation should be evaluated by a multidisciplinary team with expertise in resistant hypertension and in performing the technique, the guidelines state.
Renal denervation is a device-based treatment in which energy is targeted
through a catheter to the renal nerves to modulate the sympathetic signalling between the kidneys and brain to reduce blood pressure. Two devices have been approved by the US Food and Drug Administration (FDA)—the Paradise (Recor Medical) and Symplicity Spyral (Medtronic) systems—following a review of evidence from trials assessing both technologies, evidence that also contributed to the ACC/AHA guideline change. Medtronic’s Symplicity Spyral system is a minimally invasive procedure that delivers radiofrequency energy to nerves near the kidneys that can become overactive and contribute to high blood pressure, whilst the Paradise system is an ultrasound-based
contribute to low morale, detachment, depression, or even thoughts of leaving the profession altogether.
To prevent moral injury in vascular surgery, organisational change is essential, not just personal resilience. The BMA 2021 report recommends increasing staffing and resourcing, especially in key areas like CLTI, to reduce systemic delays that contribute to ethical conflict. It also calls for simplified bureaucracy, enabling faster patient pathways and clearer clinical decision-making. Equally crucial is the cultivation of an open, supportive culture. Surgeons need safe forums to voice concerns, such as Schwartz rounds or facilitated peer discussions, embedded as protected elements of job plans.2 Finally, improving access to wellbeing resources, from counselling to occupational health support, offers early psychological relief that can head off longerterm moral injury.
We cannot eliminate all pressures, but by taking moral injury seriously, and addressing it through practical methods, we can begin to protect our colleagues, our patients and the standards of care we are committed to uphold.
I would like to thank Mr R Chandrasekar for suggesting the topic of moral injury in vascular surgery. Please see ‘The Countess Technique of Vascular Anastomosis’. His innovative work in advancing vascular surgical techniques continues to inspire improvements across our specialty.
References 1. British Medical Association. (2021) Moral distress and moral injury: Recognising and tackling it for UK doctors. London: British Medical Association 2. The King’s Fund. (2025) Schwartz Center Rounds®. Insight and analysis, The King’s Fund. Available at: https://www.kingsfund.org.uk/insight-andanalysis/projects/schwartz-center-rounds (Accessed: 1 August 2025).
ADAM TALBOT is is a specialty trainee in vascular surgery based in Manchester, UK and education representative for the Rouleaux Club—the vascular trainees’ association for Great Britain and Ireland.
technology.
In July, the US Centres for Medicare & Medicaid Services (CMS) has issued its proposed National Coverage Determination (NCD) on renal denervation, recommending coverage for the therapy for the treatment of uncontrolled hypertension. A final determination is due in October.
The 2025 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults replaces guidelines from 2017 and includes new or updated recommendations for blood pressure management based on the latest scientific evidence to achieve the best health outcomes for patients.
The new guideline reflects several major changes since 2017, including use of the AHA’s PREVENT risk calculator to estimate cardiovascular disease risk. It also provides updated guidance on medication options, including the early treatment for high blood pressure to reduce the risk of cognitive decline and dementia; use of specific medications including the possible addition of newer therapies such as GLP-1 medications for some patients with high blood pressure and who are overweight or have obesity,
and recommendations for managing high blood pressure before, during and after pregnancy.
“High blood pressure is the most common and most modifiable risk factor for heart disease,” said chair of the guideline writing committee Daniel W Jones (University of Mississippi School of Medicine, Jackson, USA), who was also a member of the writing committee for the 2017 high blood pressure guideline. “By addressing individual risks earlier and offering more tailored strategies across the lifespan, the 2025 guideline aims to aid clinicians in helping more people manage their blood pressure and reduce the toll of heart disease, kidney disease, type 2 diabetes and dementia.
“This updated guideline is designed to support healthcare professionals— from primary care teams to specialists, and to all clinicians across health systems—with the diagnosis and care of people with high blood pressure. It also empowers patients with practical tools that can support their individual health needs as they manage their blood pressure, whether through lifestyle changes, medications or both,” Jones said.
Adam Talbot
Expanded indication for Gore Viabahn VBX balloon-expandable endoprosthesis as F/BEVAR bridging stent heralds “new era of standard devices”
The Gore Viabahn VBX balloon-expandable endoprosthesis (VBX stent graft) has achieved an expanded indication as a bridging stent for fenestrated and branched endovascular aneurysm repair (F/BEVAR). Providing confirmation of the device’s durability and reliability, experts believe this latest development in the evolution of bridging stent technology will instil confidence in both physicians and patients.
The VBX stent graft has been designed to offer precise delivery and support positive outcomes in a variety of complex aortic applications.
Real-world evidence from the Gore EXPAND and EMBRACE registries has confirmed the clinical performance and safety of the device as a bridging stent, with the official launch of the indication planned for this autumn.
Jacob Budtz-Lilly (Aarhus University, Aarhus, Denmark) and Martin Austermann (St FranziskusHospital Münster, Münster, Germany) were early users of the VBX stent graft. The pair recently spoke with Vascular News to share their extensive clinical experience with the device, as well as their reactions to the expanded indication.
Budtz-Lilly and Austermann first highlighted the necessity of having access to a bridging stent such as the VBX for challenging anatomy. “When you encounter a difficult vessel, that’s where you reach for a bridging stent that you know can get through it,”
Budtz-Lilly shared, noting that he started using the device “very early on” for difficult cases.
In fact, he added that the VBX stent graft has enabled his team to perform cases that would not previously have been possible. “Before we had the VBX stent graft,” he recalled, “you might have had a vessel that you weren’t able to access, weren’t able to treat.”
Austermann detailed that he has been using the VBX stent graft for several years now too, with his institution’s experience recently published in the European Journal of Vascular and Endovascular Surgery. Over the course of almost a decade, Austermann shared that he has seen his use of the device evolve, selecting it to treat an increasing variety of anatomical scenarios, including the renal arteries.
Key features
Homing in on what makes the VBX stent graft a good bridging stent, Budtz-Lilly outlined three key features: its sheath compatibility, its flexible cannulation— particularly in steep-angled take-off vessels—and its simple placement. On this last point, he elaborated: “You can place the balloon-expandable stent where you want to place it. It’s a nice feature. I know other stents can be difficult to place where you want them to.”
Austermann agreed, describing the VBX stent graft’s compatibility as its “number one feature”. He explained: “I can always manoeuvre the VBX stent graft around steep angles due to its unique design and features.”
Austermann then described how the features of the VBX stent graft represent the ongoing evolution of bridging stent technology. “If you just go back five or six years, sheath compatibility was a huge issue,” he said. “You always had to upscale the introducer sheath. We didn’t have the steerables, so you had to have massive sheaths in the groin and enlarged sheaths through those large sheaths. Cannulations
were difficult. We were really limited.”
In addition, Austermann highlighted the importance of a bridging stent being durable in order to avoid issues such as stent fractures, fatigue of the fabric, endoleaks, obstructions, and occlusions.
On fatigue resistance specifically, Austermann shared that he and his team conducted research to evaluate this aspect of the VBX stent graft in fenestrated endografting. He described that the team addressed what would happen to the stent inside the fenestration after flaring using a model involving bridging stents from several companies. The team simulated breathing movements over the equivalent of a 13-year period and, while observing “some material fatigue” over time, the stents held up well. In the VBX stent graft, specifically, Austermann reported that there was “not a single hole” at the end of the experiment, and no stent fractures.
“Our explanation is that, because of the VBX stent graft’s flexibility, the stress is absorbed outside the fenestration, so there is much less stress on the area
When you encounter a difficult vessel, that’s where you reach for a bridging stent that you know can get through it.”
Budtz-Lilly
flared inside the fenestration. All the movements created were absorbed by the rest of the stent,” Austermann told Vascular News. “If you have flexibility, if you have conformability like with the VBX stent graft, it is always an advantage.”
Austermann underlined another finding from the experiment, which was that the VBX stent graft fabric is “very, very durable”. When the VBX stent graft is flared it becomes transparent, which made Austermann and colleagues question whether it would be suitable for fenestration. To test this element of the device, he described that the team placed the fenestration in the middle of the stent and then flared the middle, putting a line with water on both sides. “Then we set it under pressure, under blood pressure let’s say, and it was completely dry on the outside. We could therefore prove that the thinness of the device is not a problem,” he reported.
An important step
For both Budtz-Lilly and Austermann, the news that the VBX stent graft now has an indication to be used on label as a bridging stent for F/BEVAR is validation of years of clinical experience and represents the start of a new chapter.
“It’s nice to see that we have real-world evidence confirming the VBX stent graft’s use,” Budtz-Lilly said. “I think these things are important. I think that’s one thing Gore has been pretty good about—their commitment to both innovation but also to going through this process of establishing real-world data to show that devices can be used.”
Austermann invoked the history of complex aortic repair to demonstrate the significance of the news in the ongoing development of bridging stent technology. “Endografts have been custom made for the last 20 years,” he stressed, going on to state that the Gore device ushers in a “new era of standard devices” for complex aortic repair.
Furthermore, Budtz-Lilly pointed out the impact the news will have on shared decision-making. “It’s important, particularly when speaking with our patients,” he remarked. “I think a lot of them know that treating complex aneurysms is relatively new, or at least that it’s an evolving and technically complicated process. To be able to say that we have a device that we’ve been using that has been confirmed, has evidence that it works, is a nice feature. It’s reassuring, both for us and for the patients.”
A VBX stent graft case involving a subacute 7cm type IV thoracoabdominal aortic anuerysm. (1) and (2) Left renal; (3) cannulation; (4) DSA; (5) and (6) VBX placement.
Jacob Budtz-Lilly
Vascular unity: “Let’s stop standing on the sidelines while others define what vascular care looks like”
MATTHEW EAGLETON (MASS GENERAL
Brigham and Harvard Medical School, Boston, USA) did not go looking for vascular surgery—it found him. His vascular journey started when his grandfather was a patient of a cardiac and vascular surgeon. That surgeon’s calm, focused demeanour sparked something in him, he told attendees during the 2025 Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM; 4–7 June, New Orleans, USA) presidential address. That encounter led Eagleton down the vascular path, from a position as a college sophomore where he was “uncertain and unfocused”. Invoking that personal journey, he used the address to make a call for the SVS to choose unity, excellence and each other to make vascular surgery’s next chapter a proud one.
“Rise
Early on, Eagleton recognised that people in the vascular community exerted incredible influence on others aspiring in the field. Take the late Roy Greenberg, an intern then, and Karl Illig, a senior resident, who were both major influences when he started out. They would go on to grapple with the future of aortic repair, as well as introduce Eagleton to invaluable future mentors such as Dick Green, and Ken Ouriel—“people who didn’t just do vascular surgery, but lived it. The intensity, the pace, the sense of urgency at times—it was a world I couldn’t turn away from,” he said.
Eagleton was convinced, even as a fourth-year medical student, that one of the great strengths of vascular surgery was in its ability to deliver longitudinal care. And the early experience of presenting his research at a regional conference opened the door to interaction with the giants in the field, like former SVS president Frank Veith. “Be prepared. Vascular surgery doesn’t hand you anything. But if you’re willing to show up, stay humble and learn fast—it gives back in ways few other fields can,” Eagleton said.
He highlighted the successes that the SVS has achieved—advocacy, reform and often “quiet” progress—but he also listed the numerous challenges,
together”: Harris urges unity in Women’s Vascular Summit presidential address
Society for Vascular Surgery (SVS) president-elect Linda Harris (University at Buffalo, Buffalo, USA) extolled the values of “coelevation” in her presidential address at the 7th annual Women’s Vascular Summit (2–3 May, Chicago, USA), invoking lessons on teamwork from the world of sport to argue that a united vascular specialty is greater than the sum of its parts.
HARRIS ADDRESSED THE summit as its founder and first outgoing president. “Dr Linda Harris has established her legacy as a trailblazer in vascular surgery on all fronts,” said incoming president Palma Shaw (Upstate Medical University, Syracuse, USA) as she introduced Harris at the meeting.
Harris’ address centred on uniting those involved in vascular care across lines of geography, sex, race and specialty. “We have to talk together, and we have to walk together,” she opined, “otherwise we will not succeed, and that goes for working with our friends across the pond, men and women, Black and white, private practice and academic, vein and artery,” emphasising also the importance of collaborating with interventional radiology and cardiology colleagues.
Focusing on the summit and its associated International Society for Women Vascular Surgeons (ISWVS)— which Harris founded in 2023 to promote education about vascular disease in women and promote women in the vascular field—the presenter paid homage to the team around her, in particular Shaw, Kathleen Ozsvath, Kellie Brown, and Joann Lohr. Harris stressed that a strong, unified
team was central not only to the creation of the summit and ISWVS, but will also be key to their longevity. “I don’t ever want an organisation or something I create to be at the best when I create it or when I’m leading,” she said. “I want it to be the best it’s been to that date, but I want it to be better when my successors come along, because otherwise I’m not succeeding.”
To ensure unity within a team, Harris proposed the concept of “co-elevation.” She explained:
“Leaning on someone does not mean you’re weak. It means you recognise your areas of weakness, and you complement them with someone else’s strengths, and they do the same for you and you rise together.”
“We will not succeed if we leave people behind,” Harris continued. “We need to encourage deliberate, intentional inclusivity and encourage people to learn their unconscious biases.”
To support her argument, Harris shared lessons to be learned from the world of sport about sacrificing personal gain for the greater good of group success. In the first of several sporting references, Harris shared the words of American football coach Vince Lombardi: “Individual
notably a heterogeneous and growing group of members that confronts the organisation. The faultlines of the struggle lie in fragmentation and disconnection.
“Our biggest internal challenge right now is fragmentation and disunity. And it’s been a problem growing over the past several years,” he noted. “We’re not just disagreeing—we’re disengaging. And that weakens us. It weakens our credibility. It weakens our voice.”
Yet, patients and purpose are always at the heart of vascular surgery, Eagleton argued. And beyond this dual bedrock, he called for a different kind of leadership, one that is layered, brave and collaborative.
“We need bridge-builders. People who can bring together our fragmented membership—who can sit in a room of differing opinions and find common ground without compromising our core values,” he said.
Vascular surgery’s relationship with other specialties has too often been defined by tension, Eagleton told attendees. And yet, the volume of vascular disease is rising fast, and “we are not enough. We can’t serve this population alone. That doesn’t mean we dilute our identity. It means we must instead lead with clarity, not defensiveness.” He added: “Let’s stop standing on the sidelines while others define what vascular care looks like. […] Because this is our house.”
commitment to a group effort is what makes a team work, a company work, and a civilisation work.”
“Other sports legends have echoed the same thing,” the presenter continued, noting that blue chip basketball player Michael Jordan has previously said that “talent wins games, but teamwork and intelligence is what wins championships”.
Harris used another basketball reference to demonstrate how individual ambition can lead to a divided, unsuccessful team. Referencing Los Angeles Lakers teammates Kobe Bryant and Shaquille O’Neal, she stated: “When they were put together, the team actually did worse because they were both ‘the guy who had to be the guy,’ and they weren’t willing to work in a united fashion. They had to be the superstar.”
“Listen to each other”
Speaking to Vascular News following her summit address, Harris homes in on the ways in which teams can unify. “I think the simplest thing that we need to do is we need to get in groups together, either virtual or real, and actually listen to each other,” she says, highlighting a current problem of individuals “digging their trenches” instead of working collaboratively.
Looking ahead, Harris notes that she intends for unity to be a key theme of her future SVS presidency, which is due to commence in 2026.
Harris will be the second woman to assume the lofty role, which she hopes will soon become a moot accolade.
Caveating her argument for unity, Harris was keen to stress that this should not be confused with uniformity, urging the audience to avoid “groupthink.” Instead, the presenter encouraged discussion of differing viewpoints as a core tenet of any successful team.
We need to encourage deliberate, intentional inclusivity and encourage people to learn their unconscious biases.”
“Obviously it’s an amazing honour,” Harris remarks, “but I want to get to a point where it’s not a unique honour because I’m a woman. It’s just an honour”.
The focus, Harris believes, must rest firmly on her skillset, and, in particular, her “ability to bring people together and to empower and to help to elevate those around [her]”.
Fostering unity, Harris posits, will allow the specialty to deal with a multitude of current and future challenges. “There are so many things that we need to deal with,” she comments, referencing artificial intelligence (AI), entrepreneurship and advocacy as just three of several key topics that the specialty “needs to work together on”.
Following the address, Harris passed the presidential torch to Shaw, who she described as the “next great leader” and one she hopes will “surpass [her] success”. “I have every belief she will,” Harris remarked in closing her address, “as will those who follow behind her.”
INTERVIEW
Linda Harris
New robotic C-arm goes “far and beyond” current technologies in endovascular treatment
Speaking to Michele Antonello (University of Padua, Padua, Italy) at the 2025 Charing Cross (CX) Symposium (23–25 April, London, UK), Nikolaos Tsilimparis (Ludwig Maximilian University Hospital, Munich, Germany) highlighted the benefits of a new robotic C-arm from Siemens Healthineers: Ciartic Move. Among several advantages, Tsilimparis underscored the system’s potential to reduce the workforce capacity needed during a procedure without compromising on image quality.
“The surgeon is in control”
One of the biggest challenges associated with a traditional C-arm, as highlighted by Antonello, is the difficulty for the whole team of manoeuvring the system into the operating room and positioning it correctly. “Everything is out of the operator’s control,” Antonello stressed, adding that these steps take up a significant amount of time for operating room staff.
“With Ciartic Move, the surgeon is in control,” Tsilimparis emphasised. He highlighted that this level of autonomy enables the operator to remain fully focused on the procedure, rather than becoming distracted by instructing staff unfamiliar with a particular C-arm on how to reposition it. In addition to streamlining workflow for the surgeon, he noted, it also saves valuable time for nurses and technicians. “That, in my opinion, is amazing,” he remarked.
departments.
Tsilimparis agreed, detailing that word spread fast in his institution—through departments ranging from orthopaedics to pulmonology and neurosurgery— about the benefits of the system. “If you are working in a setting where you need a C-arm that can be multidisciplinary and needs to move around the hospital from room A to room B to C to D, this is the perfect option,” he remarked.
Going into more detail about the system’s manoeuvrability, Tsilimparis provided an analogy for how the system works. “It resembles what we see on moon expeditions and how the robots on the moon work, which is really fascinating,” he said, underlining its ability to avoid collisions and be manoeuvred easily.
Device specifics
Homing in on some of the robotic C-arm’s key technical features, Tsilimparis highlighted a 3D computed tomography (CT) option. “It takes a little bit longer than a cone-beam CT with a mounted system,” he said, adding that combining 3D CT with an injection of contrast medium for vascular procedures might be a limitation; however, he emphasised that 3D CT without contrast to assess the condition and position of the stent graft post-implantation is “something that you can easily do”.
Additionally, Tsilimparis mentioned that Ciartic Move can store up to 12 positions and be returned to a “parking position” at the end of a procedure, both of which save the operator and operating team even more time. “No scrub nurse has to stop providing you the instruments or materials that you need,” he explained, restating that this is “all done by the operator” with a remote control from the sterile field.
“High-quality” imaging
Aside from the workforce efficiencies brought by Ciartic Move, Antonello was keen to drill down on the imaging quality of the robotic system. He stated that this is usually “very high” in the lower limbs but questioned whether similarly top-grade imaging could be achieved in areas such as the carotid arteries and thoracoabdominal cavity.
“Ciartic Move is a high-quality imaging system,” Tsilimparis responded, referencing recent software adjustments Siemens Healthineers has made on the device that have improved its imaging offering.
Referencing his own experience with the C-arm, Tsilimparis continued that he and his team have used Ciartic Move in four fenestrated, three branched, and four thoracic endovascular aortic repairs (TEVARs) so far.
Tsilimparis was keen to place the imaging capabilities of Ciartic Move in the right context among available technologies. “If you already have a dedicated hybrid operating room with a mounted imaging system for all your procedures, this may not be necessary,” he acknowledged. “However, many centres around the world still don’t have that option. In those cases—where a mobile solution like a C-arm is required—this robotic C-arm comes
I think the most important thing for me is the ability of the surgeon to have full control during the procedure.”
Nikolaos Tsilimparis
remarkably close to the performance and precision of a fixed, mounted system,” he explained.
Tsilimparis pointed out that a robotic C-arm is “still one level below” a mounted system but is “certainly one level above the regular C-arms that we know”.
“Perfect option” for multispecialty use
Closing the discussion, Antonello asked Tsilimparis to highlight the most important features of Ciartic Move that might convince colleagues to adopt the system in their institutions. “I think the most important thing for me is the ability of the surgeon to have full control during the procedure, that with a remote control you are able to take all of the positions you want, to move it up and down, just like you do with a mounted system, and that’s something that’s far and beyond all systems that are on the mobile C-arm market,” he responded.
Tsilimparis also reiterated that Ciartic Move ensures the nurses in the operating room have capacity to perform other tasks, pointing out that the acceptance rate among operating room staff is “extremely high”.
Finally, Tsilimparis underscored the quality of the imaging. He explained that this is based on traditional C-arm technologies from Siemens Healthineers, which are “known to offer some of the best imaging qualities among all the C-arms”.
Discussion then turned to the mobile nature of Ciartic Move, which allows it to be easily transported from one theatre to another. “If you have an emergency and cannot operate in your hybrid room at a particular time, you can easily go to any room and make a hybrid room with this system,” he said, emphasising that a robotic C-arm offers an institution “amazing flexibility” in terms of where and when procedures can be performed.
On this note, both Antonello and Tsilimparis mentioned how the benefits of Ciartic Move extend beyond the vascular surgery department. “Sometimes you need imaging on the first floor, sometimes on the second floor, and so I told my hospital that this device could be a great option, because you can have highquality images and move it easily,” Antonello shared, highlighting that the system can be used in vascular as well as in orthopaedic trauma, spine surgery and other
Summarising his take on where Ciartic Move fits in the wider market, Tsilimparis stressed that the system offers several benefits to the operating team when compared to the alternatives of either a mounted system or a traditional C-arm. A robotic C-arm, he explained, “is closer to a mounted system in terms of quality of movement within the operating theatre than a traditional C-arm, while at the same time has all the flexibility that we get from the C-arm”.
Ciartic Move will not replace a mounted system, Tsilimparis put forward, but instead posited that it offers a strong alternative to “put you one or two levels above what you would have if you bought a regular C-arm”.
Disclaimer: The statements by Siemens Healthineers’ customers described herein are based on results that were achieved in the customer’s unique setting. Because there is no “typical” hospital or laboratory and many variables exist (e.g., hospital size, samples mix, case mix, level of IT and/or automation adoption) there can be no guarantee that other customers will achieve the same results.
Nikolaos Tsilimparis
Michele Antonello
Ciartic Move
Radiation safety in the hybrid operating room: Online course increases knowledge but dose unaffected
The implementation of a massive open online course (MOOC) has been shown to increase radiation safety behaviour in the hybrid operating room and decrease fluoroscopy time. This and other findings— including uncertainty around the course’s ability to reduce radiation dose—were recently published online as a research letter in the European Journal of Vascular and Endovascular Surgery (EJVES).
SPEAKING TO VASCULAR NEWS, LEAD author Gilles Soenens (Ghent University Hospital, Ghent, Belgium) considers the course as it pertains to the wider context of radiation safety for vascular patients and operating room staff, sharing his opinion that “there are still a lot of questions to be answered”.
The MOOC in question is, Soenens shares, an easily accessible, interactive educational tool that is “convenient to implement at your local hospital”.
Consisting of three parts, the course involves e-learning chapters, educational videos showing both ‘good’ and ‘poor’ radiation safety behaviour, and finally a serious game section in which participants perform a simulated endovascular aneurysm repair (EVAR) procedure with a focus on radiation safety. The serious game was developed in collaboration with Surgical Science (formerly Simbionix).
Development and initial testing of the MOOC were previously published in EJVES. The course was tested in seven centres across Europe: two in each of Belgium, the UK and France, and one in Denmark. “The knowledge of participants increased 23% after completing the MOOC, which is very good,” Soenens reports, noting that this was the case for nurses, anaesthesiologists, and surgeons alike.
New medical device reporting requirements come into effect in the UK
New regulations have come into effect in the UK which place a greater emphasis on medical device manufacturers to monitor the safety and performance of their products.
THE NEW POST-MARKET Surveillance (PMS) regulations came into effect from Monday 16 June requiring device manufacturers to actively track the safety and performance of products already in use. The reforms, which are a part of a wider effort by the Medicines and Healthcare products Regulatory Agency (MHRA) to overhaul the UK’s medical device
Soenens et al then implemented the MOOC at their centre in Belgium, with this experience forming the basis of their recent EJVES research letter. “It’s a real-life implementation study, so participants were not obliged to do the course,” he explains. The researchers found that radiation safety behaviour improved after implementation of the MOOC, but they “didn’t see a lot of impact on radiation dose”. Elaborating on this latter finding, Soenens continues: “We saw that fluoroscopy time decreased, but the dose area product and cumulative air kerma remained similar.”
Despite its current limitations, Soenens describes the radiation safety course as a “big breakthrough”. He explains, focusing on its future potential: “We are convinced about the added value of the course, because—based on previous research by our group— we know that if knowledge and awareness about radiation safety increases, it will also impact positively on radiation safety behaviour and the radiation safety climate.”
Considering the course as part of a wider conversation about radiation safety in the hybrid operating room, Soenens highlights a dearth of knowledge in the field. In particular, he points out that “there is still a lack of knowledge about the impact of radiation on healthcare workers,” marking this as a key unanswered question.
Soenens underscores the dated nature of the available evidence on radiation, noting that “most research is based on survival studies of Hiroshima and Nagasaki—still”.
“There’s no new real knowledge about the increased risk of cancer, by what percentage radiation increases cancer risk, how we should optimally protect ourselves, if we should wear lead caps on our heads or protect the shins as suggested by research by the group of Bijan Modarai et al,” Soenens says. While acknowledging that some progress has been made, and new research emerges, he stresses that the answers “have not yet been found”.
Soenens also highlights unanswered questions with regard to education on radiation safety. “You have European legislation that healthcare workers should be trained adequately, but there is no definition of adequate training,” he notes. Soenens suggests that
regulatory framework, are intended to identify potential safety issues earlier and to strengthen protection for patients and the public through faster responses to incidents and emerging risks.
The reform applies to all UKCAand CE-marked devices placed on the market in Great Britain after 16 June.
This includes in vitro diagnostic devices, active implantable medical devices as well as other technologies used in a clinical setting and within the home.
Manufacturers are now required to collect and assess real-world safety and performance data; report serious incidents to the MHRA within 15 days (previously 30); submit essential communications on patient safety (Field Safety Notices) to the MHRA for review before sharing with users; and provide PMS Reports or Periodic Safety Update Reports (PSUR) within three days of request. For higher risk devices, UK approved bodies will monitor these reports ensuring these products receive a higher level of scrutiny.
“As innovation in health technologies accelerates, regulation must keep pace,” Lawrence Tallon, chief executive of
societies such as the European Society for Vascular Surgery (ESVS) should play a role here, in standardising radiation safety training. Soenens also touches on the importance of refresher courses when it comes to radiation safety. Bringing the focus back to the radiation safety course, he comments: “We have provided a course that can easily be implemented; radiation safety knowledge will increase and behaviour improve as a result, but then we still don’t know when you should do a refresher course or how to handle participants who just do it as a tick-the-box exercise and are not really interested nor committed to it.”
He admits that radiation safety remains a “difficult topic” from a training perspective because its effects are not immediately apparent. “You can get cancer in 20 years but it’s not a 1:1 causal relationship where we can say ‘it’s because you were not working with proper radiation safety protection’.”
Looking ahead, Soenens is hopeful that things are moving in the right direction. He sees the development of the 2023 ESVS clinical practice guidelines on radiation safety, for example, as an important step. As for the MOOC, Soenens notes that the work for this was underway ahead of the publication of the guidelines, but their publication certainly “fuelled extra research around this topic” and acted as a catalyst for future change. “The guidelines are great,” he says, “since they create new research questions and research itself, but will require updates as well.”
The senior author for the EJVES research letter was Isabelle Van Herzeele (Ghent University Hospital).
You have European legislation that healthcare workers should be trained adequately, but there is no definition of adequate training.”
the MHRA said. “Today’s reform is a critical step in ensuring safety standards evolve alongside this progress. By strengthening oversight of devices once they’re in use and setting clearer expectations for manufacturers, these new regulations provide a robust framework for identifying risks earlier and responding to protect patients.
“This represents an important
Manufacturers are now required to report serious incidents to the MHRA within 15 30 days days previously
milestone in our work in building a modern, responsive regulatory system—one that puts patient safety first, while also supporting innovation in life sciences and medical technologies across the UK.”
The introduction of new data analysis reporting requirements will apply to
all medical devices but are particularly valuable for improving oversight of lower-risk devices, MHRA adds. These rules will require manufacturers to regularly summarise and assess device performance over time.
As well as the reforms on medical device surveillance, the UK government has announced plans to make it easier for individuals to volunteer to participate in clinical trials. Patients will be able to sign up to participate in trials via the National Institute for Health and Care Research (NIHR) Be Part of Research service on the NHS app, where they will be able to browse and select trials best suited to their interests and needs.
Eventually this will automatically match patients with studies based on their own health data and interests, sending them push notifications to their devices about relevant trials that they may wish to sign up to participate in.
NIHR is also launching a recruitment drive to find as many volunteers for trials as possible, including those from underrepresented groups, including young people, Black people and people of South Asian heritage.
To see conference agendas, CME information, and register — scan here.
Clinical News
Aquedeon Medical receives US FDA approval to expand clinical trial of Duett vascular graft system
The US Food and Drug Administration (FDA) has approved the expansion of Aquedeon Medical’s investigational device exemption (IDE) clinical trial evaluating the Duett vascular graft system, a company press release reveals. Duett is a novel device designed to facilitate open surgical repair of aortic arch aneurysms and dissections, including hybrid procedures.
Aquedeon Medical notes that it is developing the Duett system “to address a critical need in open surgical thoracic aortic arch reconstruction, a complex and high-risk procedure typically performed during deep hypothermic circulatory arrest (DHCA) while the patient is on cardiopulmonary bypass”.
The Duett system, Aquedeon Medical shares, is engineered to “simplify and accelerate” the vascular anastomosis process, with the goal of reducing DHCA duration and re-establishing cerebral perfusion more rapidly.
hurdles in the creation of vascular access. Patients could have vascular mapping conducted in their dialysis facility, enabling a more efficient way to obtain a permanent vascular access point,” commented Varshi Broumand, interventional nephrologist at South Texas Renal Care Group (San Antonio, USA) and CANSCAN study principal investigator. “Performing the ultrasound scans during the clinic visit would make AV fistula mapping more convenient and timely and potentially avoid sending patients to additional imaging appointments.”
The VxWave ultrasound imaging system is a robotic tomographic ultrasound system specifically designed for upper limb vascular imaging— integrating advanced robotics, machine learning and ultrasound signal processing to create a 3D vascular model and detailed report that potentially provides insights into vascular access points—all at the point of care.
Aquedeon Medical launched its two-stage IDE clinical trial in 2024 to evaluate the safety and effectiveness of the Duett system. With the recent FDA approval, the study will now expand to enrol up to 90 patients across additional clinical sites in the USA.
“It is exciting that Aquedeon has received FDA approval to expand the Duett IDE study to 90 patients. Open aortic arch surgery is complex and technically demanding. The Duett technology has the potential to transform the field by providing aortic surgeons with an innovative tool to facilitate arch reconstruction and enhance care for patients with aortic disease. We look forward to continued investigation with this novel technology,” said Wilson Szeto (University of Pennsylvania, Philadelphia, USA), principal investigator of the IDE study.
Enrolment completed in CANSCAN trial of ultrasound imaging system for AVF mapping Vexev and US Renal Care have announced the successful completion of enrolment in the CANSCAN trial.
The first-of-its-kind, multicentre feasibility study enrolled 120 patients with chronic kidney disease to evaluate the use of semi-autonomous ultrasound scanning utilising the VxWave ultrasound imaging system for arteriovenous fistula (AVF) mapping in dialysis clinics.
“The VxWave ultrasound system may remove one of the biggest
trial (RCT) designed to investigate the clinical safety and effectiveness of the Auryon atherectomy system combined with standard balloon angioplasty, compared to balloon angioplasty alone, in treating infrapopliteal lesions in patients with CLTI. The primary endpoint will be evaluated using a win ratio approach, comparing the two treatment groups based on the following components in a hierarchical manner at 12 months: freedom from major amputation, freedom from clinically driven target lesion revascularisation (CD-TLR), and primary patency.
The RCT will include up to 224 patients at up to 30 sites. In parallel, a companion registry will enrol up to 1,500 additional patients who are ineligible for the RCT and are treated with the Auryon system above or below the knee.
stent restenosis (ISR) and, to date, it has been used to treat more than 100,000 patients in the USA and worldwide.
First patient enrolled in RECOVER-AV trial evaluating AngioDynamics’ AlphaVac F18 85 system for PE AngioDynamics recently announced the first patient enrolment in RECOVER-AV—a prospective, multicentre, multinational, singlearm study evaluating the AlphaVac multipurpose mechanical aspiration (MMA) F1885 system in the treatment of acute, intermediate-risk pulmonary embolism (PE).
“Validating this concept is the first step toward a future where intelligent machines can perform high-precision medical imaging without a human hand on the probe. The potential for a robotic system guided by AI [artificial intelligence], delivering real clinical value—it’s not science fiction anymore,” said Shannon Thomas, chief medical officer, Vexev. “The real excitement begins when this can change lives, not just lab results. This is a huge step forward in our mission to improve the lives of millions of people worldwide living with endstage kidney disease.”
“US Renal Care is committed to delivering innovative treatments that address the most critical needs for people living with kidney disease,” said Geoffrey A Block, associate chief medical officer and senior vice president, clinical research and medical affairs, US Renal Care. “The CANSCAN trial of the VxWave ultrasound imaging system opens the possibility of integrating semiautonomous ultrasound imaging into our workflow and improving patient outcomes, by allowing patients to receive life-saving permanent vascular access placed in the optimal location, as quickly as possible.”
First patient enrolled in AngioDynamics’ AMBITION BTK trial for CLTI
AngioDynamics has announced enrolment of the first patient in AMBITION BTK, a randomised study of the Auryon atherectomy system in patients with below-the-knee chronic limb-threatening ischaemia (CLTI).
A press release details that AMBITION BTK is a prospective, multicentre, randomised controlled
“The enrolment of the first patient in the AMBITION BTK trial is a significant milestone in our commitment to advancing clinical evidence for the treatment of below-the-knee peripheral [arterial] disease (PAD),” said Laura Piccinini, senior vice president/ general manager, Cardiovascular and International, AngioDynamics. “There is a pressing need for new treatment strategies to help patients suffering from chronic limb ischaemia, and we are proud to partner with clinicians to evaluate the Auryon system in this important setting.”
“Treatment options for belowthe-knee lesions are still limited and often depend heavily on balloon angioplasty,” said AMBITION BTK coprincipal investigator Ehrin Armstrong (Advanced Heart and Vein Center, St Helena, USA). “The Auryon laser can restore laminar flow and therefore has the potential to improve outcomes in this challenging patient population significantly.”
The first patient in the trial was treated by Anahita Dua (Massachusetts General Hospital and Harvard Medical School, Boston, USA), co-principal investigator of AMBITION BTK.
“I’m excited to perform the first patient case in the AMBITION BTK study. Patients with below-the-knee disease often face limited treatment options and poor long-term outcomes,” said Dua. “Across the world, there has been a significant increase in patients with below-the-knee (BTK) disease, which is, unfortunately, resulting in an amputation epidemic. Having new tools and techniques to restore blood flow to the foot, allowing wounds to heal, and patients to preserve both their limbs and lives, is critically important and the focus of this trial. This trial will allow us to collect high-quality, real-world data using a robust research design, helping us truly evaluate the impact of laser technology in BTK disease.”
AngioDynamics advises that the Auryon laser can be used to treat all infrainguinal lesion types, including above-the-knee (ATK), BTK, and in-
The study follows the US Food and Drug Administration (FDA) 510(k) clearance of the AlphaVac F1885 system for the treatment of PE in the USA in April 2024 and its CE-mark approval in Europe in May 2024. The RECOVERAV trial is designed to evaluate the safety and efficacy of the AlphaVac F1885 system in support of its adoption in the global market, as well as to assess long-term functional outcomes for patients following treatment.
“The first patient enrolment in the RECOVER-AV trial marks an important step forward as AngioDynamics continues to grow its global clinical presence and commitment to evidence-based care,” said Laura Piccinini, senior vice president/general manager, Cardiovascular and International.
“With AlphaVac already 510(k)-cleared in the US and CE-marked in Europe for PE, we’re investing in high-quality data focused on functional recovery and quality of life that will equip clinicians, payers, and patients with even greater confidence in the system’s safe, effective performance and help broaden access to life-saving PE treatment across Europe and the wider global
The trial is enrolling patients with confirmed acute, intermediate-risk PE at up to 20 hospital-based sites in Europe, Canada, and Hong Kong. The primary safety endpoint is the incidence of adverse events by type and seriousness through 12 months. Patients will be followed for 12 months, with functional and quality-of-life outcomes assessed at 30 days and 12 months. Additional investigations will provide a more comprehensive assessment of the long-term recovery of patients after mechanical thrombectomy with the AlphaVac MMA F1885 system.
The RECOVER-AV trial is led by co-principal investigators Erik Klok (Leiden University Medical Center, Leiden, The Netherlands) and Andrew Sharp (Mater Misericordiae Hospital and University College Dublin, Dublin, Ireland).
Duett vascular graft system
AlphaVac F1885 system
Inari Medical, now part of Stryker, launches InThrill thrombectomy system
Inari Medical—now part of Stryker— has announced the launch of its next-generation InThrill thrombectomy system.
The company stated in a recent press release that this is the first and only purpose-built small vessel and arteriovenous (AV) access thrombectomy system that can deliver fast, full luminal clot removal.
The second-generation InThrill thrombectomy system is an 8Fr over-the-wire system comprising the InThrill thrombectomy catheter and the InThrill sheath. InThrill is built upon a familiar platform, optimised to become the standard for AV access and small vessel thrombectomy.
Offering “unmatched” efficiency and clot removal, Inari notes that InThrill has distinctive features which include: increased radial force for improved luminal wall apposition for optimised clot removal; offset single open mouth to optimise clot capture and removal; internal struts for even clot distribution within the element; and a redesigned backend to streamline ergonomics and improve the user experience.
On 19 May 2025, Joshua Pinter and Anish Ghodadra of the University of Pittsburgh Medical Center (UPMC) performed the first commercial case using the new InThrill thrombectomy system. “The next generation of InThrill has made our thrombectomies more effective and consistent than ever,” said Pinter. “Inari’s dedication to building a small vessel tool has changed our paradigm of treatment for AV access thrombectomy,” added Ghodadra.
“The launch of the next-generation InThrill thrombectomy system reflects our deep commitment to solving real-world challenges in vascular care,” said Tim Lanier, president, Inari Division. “This latest innovation delivers new tools and enriches our work with physicians in the vascular space.”
First patient treated with InterVene’s Recana thrombectomy catheter system
InterVene recently announced that the first patient has been treated with its Recana thrombectomy catheter system for venous in-stent restenosis (ISR).
The company shares in a press release that Recana is the first fully integrated mechanical thrombectomy
system designed specifically to address the long-term complications of venous disease, including ISR and native vein obstructions. The case was performed at University Hospital Galway in Galway, Ireland, by interventional radiologist Gerry O’Sullivan.
“The long-term sequelae of venous obstructions, whether in-stent or native vessel, are a devastating consequence of deep venous thrombotic disease. There remains a considerable gap in effective interventional treatments for physicians and their patients living with persistent symptoms related to venous outflow obstructions,” said O’Sullivan.
“I had previously tried and failed to recanalise this patient’s vessels on four separate occasions—Recana succeeded in just one. This technology offers real promise for patients with limited treatment options.”
The case was a result of collaboration between InterVene and the University of Galway Institute of Clinical Trials.
“We are proud to see Recana become one of the first innovations to enter clinical use in Ireland through the Hypercare initiative,” said Fidelma Dunne, director of the Institute for Clinical Trials at the University of Galway. “This first-in-human procedure reflects Hypercare’s core mission to streamline the clinical trial process and accelerate patient access to breakthrough therapies.”
“This successful first-in-human procedure comes after several years of rigorous work to prove a transformative design to address a major unmet need in venous disease,” stated Jeff Elkins, chief executive officer of InterVene.
“We are proud to support Dr O’Sullivan in caring for patients suffering from the life-limiting effects of ISR. Completing this first case marks an important milestone in bringing our technology to patients affected by the long-term complications of venous disease.”
FastWave Medical secures eighth US patent for IVL portfolio
FastWave Medical has secured its eighth US patent for its electric intravascular lithotripsy (E-IVL) platform, Artero, reflecting the company’s continued innovation in developing nextgeneration solutions for peripheral arterial disease (PAD) treatment, the company reports in a press release.
“IVL has become one of my frontline tools for treating peripheral arterial disease—it’s one of the most
exciting breakthroughs we’ve seen in years,” said Constantino Pena (Miami, USA), a diagnostic and interventional radiologist at Baptist Health South Florida. “Watching companies like FastWave push the envelope and bring fresh ideas to IVL technology makes this an incredible time to be in the field. The pace of innovation is truly inspiring, and it’s patients who stand to benefit most.”
The Artero system is designed to “streamline” PAD treatment with a simplified interface that delivers circumferential sonic pressure waves at 4Hz—twice the speed of existing IVL devices, according to the company.
“Too many medical devices are designed behind closed doors with limited user feedback. We wanted to flip that around and start with the daily frustrations physicians face and build from there,” said Scott Nelson, cofounder and chief executive officer of FastWave Medical.
Cook Medical announces US launch of Zenith iliac branch device
Cook Medical has announced that its Zenith iliac branch device (ZBIS) is now commercially available in the USA with US Food and Drug Administration (FDA) approval as an endovascular treatment option for aortoiliac or iliac aneurysmal disease.
The company has also shared that first implantations of the ZBIS were performed at several centres in the USA.
According to Cook, the ZBIS—when used with the necessary additional components (Zenith AAA and a covered bridging stent)—is indicated for the endovascular treatment of patients with an aortoiliac or iliac aneurysm to preserve internal iliac arterial blood flow when the distal sealing site in the common iliac artery is insufficient for the abdominal aortic aneurysm (AAA) device alone and when the vessel morphology is suitable for repair.
“This product offers an endovascular treatment option for many patients who do not meet the criteria of other commercially available technology.
The ZBIS anatomical inclusion criteria is broader and is backed by five-year pivotal data. It’s a great addition to Cook’s portfolio of aortic devices that addresses an important patient need,” said Johnny LeBlanc, director of Cook Medical’s Aortic specialty.
Gore announces MDR expanded indication for the VBX stent graft as a bridging stent Gore has announced CE-mark approval of an expanded indication for the Gore Viabahn VBX balloon-expandable endoprosthesis (VBX stent graft) when used as a bridging stent with branched and fenestrated aortic endografts in the treatment of aortic aneurysms involving the renal and mesenteric arteries.
“This is a landmark indication for a stent graft, equipping physicians
with an on-label solution for more patients in complex pathologies,” said Luca Bertoglio (Spedali Civili Brescia, Brescia, Italy), co-ordinating investigator of the EMBRACE registry.
A total of 259 patients were enrolled in EMBRACE. Gore reports high rates of patency and freedom from endoleaks, target vessel instability and reinterventions were observed with the VBX stent graft in both branched and fenestrated endovascular aneurysm repair (BEVAR and FEVAR) cohorts at one year.
“We have studied performance in both fenestrated and branched cohorts, and the results demonstrate that we can safely and effectively treat these patients with the VBX device,” Bertoglio added.
This multicentre, retrospective and prospective registry was conducted to evaluate the clinical performance and safety of the VBX stent graft as a bridging stent. A total of 14 centres in Europe enrolled 259 patients who have had treatment with the VBX stent graft. These patients will have prospective follow-up visits up to five years after the index procedure.
“Physicians have waited some time for an approved bridging stent indication for fenestrated and branched repair. Having a CE-marked indication is very important, as it is certainly of relevance to the endovascular community and the eligible patient population,” said Mauro Gargiulo (IRCCS S Orsola Hospital and University of Bologna, Bologna, Italy), principal investigator of the EXPAND registry. “I applaud Gore for recognising the need for a CE-mark indication and for being committed to conducting such thorough and expertly run clinical studies like EXPAND and EMBRACE.”
Gore notes that the official launch is planned after summer when many European and local congresses are taking place.
The VBX stent graft, Gore details, offers precise delivery and supports positive outcomes in a variety of complex applications. The device was developed utilising the small diameter, ePTFE stent graft technology from the Gore Viabahn endoprosthesis. The VBX stent graft is available in a range of diameters from 5 to 11mm and lengths of 15, 19, 29, 39, 59 and also 79mm. It is currently the longest balloon-expandable stent graft available, according to Gore, covering a wide variety of treatment needs. The company adds that the VBX stent graft offers the largest range of diameter adjustability in a single device, with a maximum post-dilated diameter of up to 16mm with 8L or 11mm devices.
Viabahn VBX balloon expandable endoprosthesis
Fastwave Medical IVL system
Industry News
InspireMD announces US$58 million in combined financings and new addition to board of directors
InspireMD has announced that it has raised approximately US$58 million in combined gross proceeds through an equity private placement (PIPE) financing and the exercise of warrants that were triggered by the company’s recent premarket application approval (PMA) of the CGuard Prime carotid stent system by the US Food and Drug Administration (FDA).
The PIPE—with aggregate gross proceeds of US$40.1 million—was led by current investors OrbiMed and Marshall Wace, with strong participation from new and existing investors, as well as InspireMD board members. Pursuant to the securities purchase agreement, the company has agreed to issue an aggregate of 16,556,184 shares of common stock and, if applicable, prefunded warrants, at a purchase price of US$2.42 per share.
now poised to become the leader of the carotid intervention market.”
In connection with the PIPE, InspireMD has entered into a registration rights agreement pursuant to which the company will subsequently file a registration statement to register the resale of common stock purchased in the transaction and the common stock underlying the pre-funded warrants.
InspireMD currently intends to use the net proceeds from this PIPE transaction to fund its operations, including—but not limited to—sales and marketing, research and development, and working capital and other general corporate purposes.
InspireMD also recently announced the appointment of Raymond W Cohen—a businessman and entrepreneur with more than 40 years of leadership experience in medical technology—to its board of directors.
Merit Medical names
Martha Aronson as new president and CEO
Merit Medical recently announced the appointment of Martha Aronson as the company’s new president and chief executive officer (CEO), effective 3 October 2025. Fred P Lampropoulos will remain as chairman of the board, president and CEO of Merit through 3 October. Upon Aronson’s appointment, Lampropoulos will continue to serve as chairman of the board.
“I am pleased to welcome Martha to Merit,” said Lampropoulos. “I believe the company has never been in a stronger position. Martha is uniquely qualified to lead Merit into the future and drive its continued success. Her keen intellect and proven track record of empowering global teams through collaborative excellence, consistent with ‘The Merit Way,’ makes her the ideal leader for Merit’s next stage of growth. Since our founding in 1987, we have achieved significant milestones, including strong returns delivered to shareholders since our IPO on 10 May 1990. I am incredibly proud of these achievements. With Martha’s experience and capability, I look forward to supporting her vision while she charts Merit’s course forward.”
idea and building it into the incredibly successful global company that it is today. Working with the talented team at Merit, I look forward to building upon his remarkable legacy and leading the company into a future of continued excellence and innovation.”
“The board is delighted to welcome Martha to Merit,” added F Ann Millner, lead independent director.
Teleflex completes acquisition of Biotronik’s Vascular Intervention business Teleflex recently announced that is has completed the previously announced acquisition of substantially all of the Vascular Intervention business of Biotronik. The company notes in a press release that the acquisition adds a broad portfolio of therapeutic products to Teleflex’s portfolio of interventional access products.
The warrant exercise generated gross proceeds of US$17.9 million, which was triggered by the receipt of the PMA from the US FDA. This is the second tranche of warrants that were originally issued as part of the company’s milestone-based financing announced in May 2023, an InspireMD press release notes.
“This transaction accomplished several key objectives to fund our growth plan as we launch CGuard Prime into the US market,” said Marvin Slosman, chief executive officer (CEO) of InspireMD. “We fortified our shareholder base, broadened our investor reach and significantly strengthened our balance sheet, giving us the ability to rapidly expand our commercial growth. With a strong balance sheet, favourable reimbursement environment including a national coverage decision (NCD) for carotid stenting and best-in-class clinical trial data generated from our pivotal US study recently resulting in PMA approval, InspireMD is
Conference calendar
11 September
Interdisciplinary Aortic Dissection Symposium (IADS) London, UK aorticdissectionsymposium.com
13–17 September
Cardiovascular and Interventional Radiological Society of Europe (CIRSE) annual congress Barcelona, Spain cirsecongress.cirse.org
Cohen was the CEO and co-founder of sacral neuromodulation (SNM) company Axonics, which he took public in late 2018 and led through its US$3.7 billion acquisition by Boston Scientific in November 2024. Until May 2025, Cohen served as chairman of SoniVie, a company focused on a device treatment for hypertension until it was also acquired by Boston for US$600 million. In addition, Cohen serves as an independent director for Kestra Medical and Spectrum Vascular, as well as chairman of Nalu Medical and vice chairman of Tulavi.
“The CGuard Prime stent system represents a true best-in-class innovation,” Cohen commented. “Moreover, the company’s singular focus, entrepreneurial agility and deep clinical commitment uniquely positions it to penetrate and lead the US carotid stent market. I’m looking forward to sharing my experiences scaling highgrowth MedTech businesses to support Marvin and his team as they strive to execute with precision, capture market share and deliver sustained long-term value.”
23–26 September 39th European Society for Vascular Surgery (ESVS) annual meeting Istanbul, Türkiye esvs.org/events/annual-meeting/ annual-meeting-2025/
30 October–1 November Venous Symposium Europe Athens, Greece venoussymposiumeurope.com
Merit notes in a press release that Aronson has extensive experience in global healthcare. Her business management experience includes overseeing global healthcare businesses ranging in size from US$500 million to US$1 billion. She was the executive vice president and president of global healthcare for Ecolab and previously served as the senior vice president and president—North America for Hill-Rom Holdings. Prior to that, she spent nearly 20 years at Medtronic in various general management and leadership roles, both in the USA and internationally. Aronson guided and advised companies as a board director, most recently serving as a director, and formerly as chair of the board, for ConMed. She also served as a director of Methode Electronics, Clinical Innovations, Cardiovascular Systems, Beta Bionics, Hutchinson Technology, Bright Uro, and OmCare.
“I am excited to join Merit and truly honoured to take on this role,” said Aronson. “Fred has built and grown an extraordinary company over the past four decades, starting with one single
1–5 November The VEINS (Venous Endovascular Interventional Strategies) and VIVA (Vascular InterVentional Advances) Las Vegas, USA viva-foundation.org
18–22 November VEITHsymposium New York, USA veithsymposium.org
On 27 February 2025, Teleflex announced its entry into a definitive agreement to acquire substantially all of Biotronik’s Vascular Intervention business. Under the terms of the agreement, Teleflex acquired the Vascular Intervention business for a cash payment of €760 million, less certain adjustments as provided in the purchase agreement, including certain working capital not transferring and other customary adjustments.
“We are pleased to announce the completion of the acquisition of substantially all of the Vascular Intervention business of Biotronik earlier than expected,” said Liam Kelly, chairman, president and chief executive officer of Teleflex. “The acquisition will significantly enhance our global presence in the cath lab, expand our suite of innovative technologies, and improve patient care. We believe the acquisition will allow us to position this advanced coronary portfolio alongside our existing interventional business and establish our global footprint in the fast-growing peripheral intervention market. The acquired business is rooted in robust research and development, clinical expertise, and global manufacturing capabilities, which we believe will further bolster Teleflex’s innovation pipeline, and position the company to participate in the emerging potential for resorbable scaffold technologies. We will provide additional details on our second quarter earnings conference call.”
26–28 November The Vascular Societies’ Annual Scientific Meeting Hull, UK vascularsociety.org.uk/events/57/ vascular-society-annual-scientificmeeting-2025
4–5 December 14th Munich Vascular Conference (MAC) Munich, Germany mac-conference.com
4–6 December VERVE Symposium Sydney, Australia vervesymposium.com
11–13 December
Paris Vascular Insights Course (PVIC) Paris, France paris-vascular-insights.com
THE POWER OF CONFIDENCE
When confidence matters most, place your trust in the only bridging stent indicated for both fenestrated and branched endovascular aortic repairs (fEVAR and bEVAR).1
Clinically proven performance,2,3 from renowned experts in endovascular.