The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.
Implemented by: Partner:





The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.
Implemented by: Partner:
Evaluation of changes in gross motor function in children with cerebral palsy.

Dott.ssa Veronica Desanzo TNPEE
Neurorehabilitation department-
Pediatric Hospital Bambino Ges˘
Motor disturbances in CP are often accompanied by other disorders that can impact and modify both the functional picture and the prognosis in the early stages or long term.
Functional
"Failure to acquire" "Loss of function"
(Rosenbaum et al., 2006)
The development of motor behavior occurs through the progressive maturation and interaction of many systems, which organize themselves to respond increasingly adequately to the needs of the environmental context.
Progressive maturation and interaction between systems
Development of motor behavior
Environmental context

Motor learning is defined as an adaptive modification of motor behavior that leads to the stable acquisition of skills, achieved through a complex perceptual-motor-cognitive process, in search of a solution to a task that emerges from the interaction between the individual and the environment.
M.H. 1995
"It is therefore necessary to adopt a more global perspective, focused on the child in its continuous interaction with the surrounding environment and the problems it poses, within a dynamic balance between the personal resources of that child and the most appropriate (and effective) tools to activate and enhance them."
2003
The first phase in the evaluation is that of observation, related to the child's ability to interact with the environment, to formulate proposals for exploring the surrounding reality, to analyze and select information from the context that is consistent with the action plan, and to use varying strategies in different contexts.
The evaluation of the organization of the patient's adaptive functions aims both to investigate the modes of integration between the various functional systems and to the detailed analysis of a specific function.
Integration between functional systems

spontaneous movement
evaluation of gross motor skills level of psychomotor development
Both to investigate the integration methods among the various functional systems that one relies on in the detailed analysis of a specific function.





GMFM © Russell DJ, Rosenbaum PL, Cadman DT, Gowland C, Hardy S,Jarvis S ´The gross motor fuction measure: A means to evaluate the effects of physical therapyª Cdevelopmental Medicine anc ChildNeurology, 1989,31: 341-352
©

• Standardized measurement tool
• Quantitative assessment of global motor functions in children with cerebral palsy
• Useful for measuring changes in gross motor function over time
• Contributes to a qualitative observation of movement without affecting the score
• Tool based on criteria
• Practical, valid, and reliable
• Applicable in clinical and research settings
• Useful for evaluating the ability to perform a task independently without assistance.

Original items taken from a literature review and evaluations by clinical researchers at the participating centers.
Items: measurable, clinical relevance, and potential response to treatment.
In 1990, the GMFM-88 was made available as an initial version for clinical application, validated for children with CP aged 5 months to 16 years.
Absence of Gold Standard among the evaluative tools of FM
Sensitivity of the instrument
Comparison between GMFM scores
Observers 'blind'
3 observational tools:
Independent assessments on the variation in motor function formulated by
Therapists
Children with Cerebral Palsy
Validation sample
Typical development age < 5aa
Parents
recent head trauma
Subsequently validated for: Osteogenesis imperfecta, acute lymphoblastic leukemia, and Down syndrome.
Two versions
Original version with 88 items (GMFM-88).
Most recent version with 66 items (GMFM-66).
Why the 66 ITEM version?
Some limitations regarding score interpretation: Percentage score
High number of items to administer
Need to observe each item to assign a score, Score 0 and artificial reduction of the overall score.
• Initially designed and validated for children (5 months - 16 years) with cerebral palsy.
• It has been validated only for children with Cerebral Palsy.
• Validated by Russel et al. (1998) for children with Down syndrome.
• Reliable, valid, and sensitive.
• Interval scale.
• Reliable, valid, and sensitive.
• Unidimensional (items that did not fit the construct were eliminated).
• Ordinal scale.
• Item results ranked in hierarchical order of difficulty.
• Information on the difficulty of moving from one score to another within each item.
• Only with the GMAE (scoring processing program).
• Development of basic motor skills.
• Severe motor disability.
• Aids and orthotics.
• No access to the PC.
• Research applications
• Children with cognitive deficits or comprehension difficulties, NT value.
• Evaluation also with aids/orthotics.
• Evaluation without orthoses/aids.
• Provides more indications on the development of the early motor skills of the child.
• Better interpretability of scores and changes.
• Useful in the longitudinal study of the same child or in specific evaluations.
• To be used to compare changes between individuals/groups (research).
• High number of items (more time) and the necessity to administer them all to provide a score.
• Fewer items (less time) and possible score calculation even if not all items are administered.

-Children with Cerebral Palsy
-Typical development age < 5aa
-Recente trauma cranico
- Subsequently validated for: Osteogenesis imperfecta, acute lymphoblastic leukemia, and Down syndrome.
Approximately 45 to 60 minutes
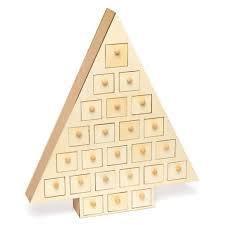
Physiotherapy gym (e.g mat, bench, toys). Access to stairs (with at least 5 steps)
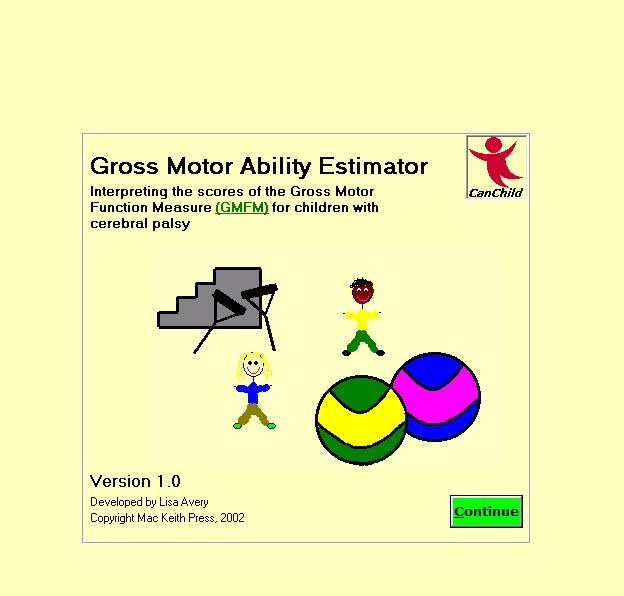
Structured in 5 dimensions:
A. Lying position and rolling (17 items)
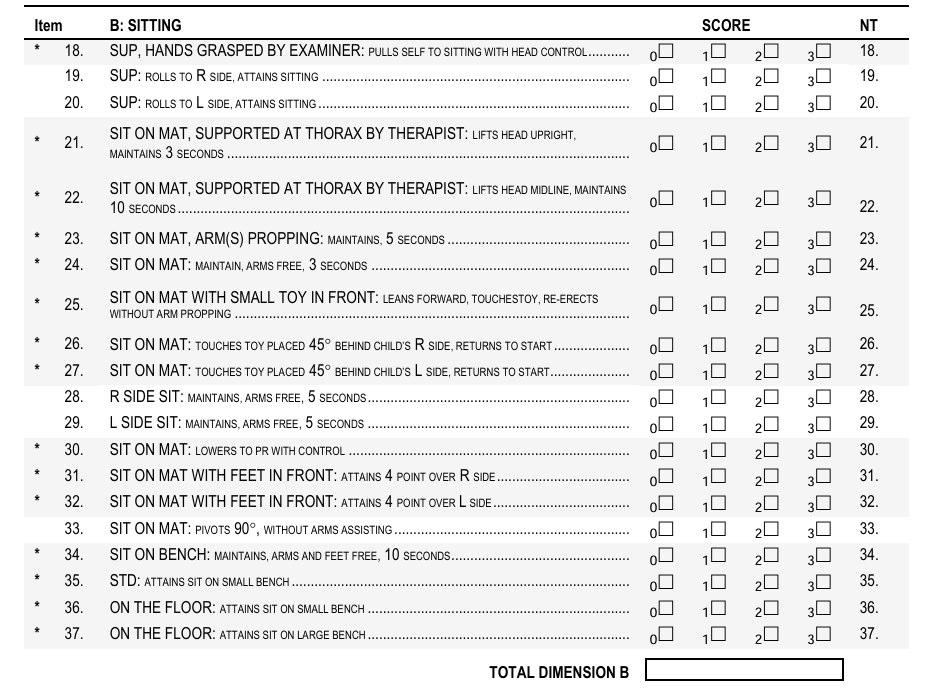
B. Sitting position (20 items)
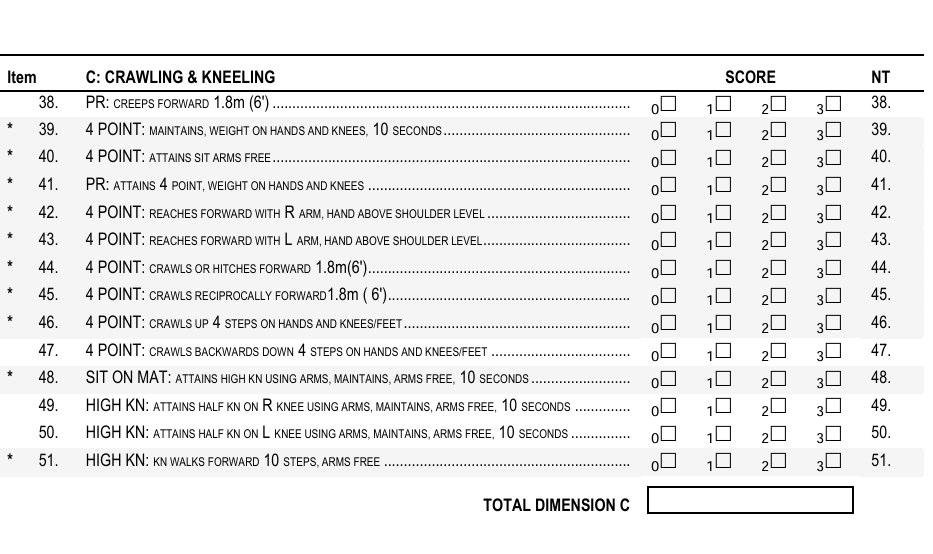
C. Crawling and kneeling (14 items)
D. Standing position (13 items)
E. Walking, running, and jumping (24 items)
For each item, the starting position is initially defined and the maximum level of function that must be achieved is subsequently described.
A maximum of three attempts are allowed per item, spontaneous execution is accepted and considered one of the three attempts
It is advisable to start from the dimension most suitable for the child
Administer the Items in the given order and complete each dimension
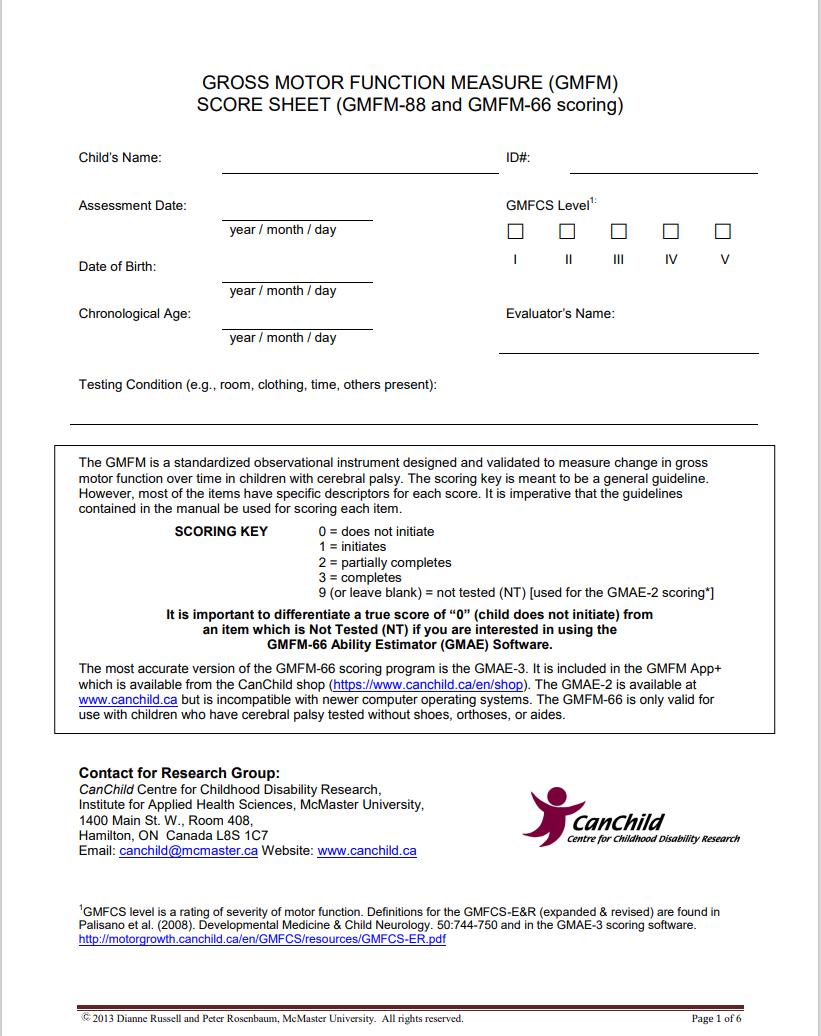
Fill in the Palisano level.
A maximum of three attempts are allowed per item, spontaneous execution is accepted and considered one of the three attempts.
The score is the best of
You can verbally encourage or demonstrate the items
It is possible to place the child in the starting position, no other interventions or facilitations are required
You can use objects or toys as incentives
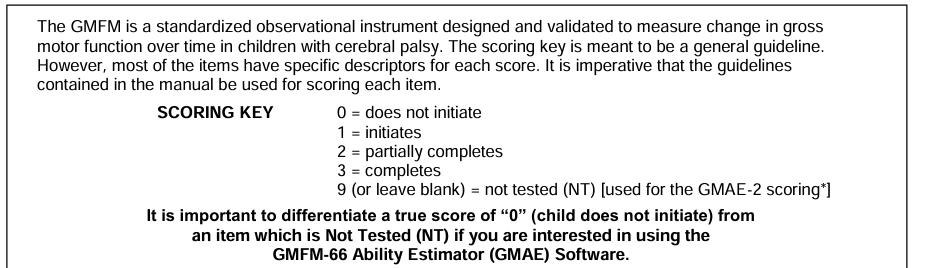
Items that the child does not attempt to perform or are omitted are classified as NT
The GMAE, or Gross Motor Ability Estimator, is a computer programme required to score the GMFM-66. This program is on CD ROM and is provided in the Gross Motor Measures (GMFM-66 and GMFM-88) User’s manual. A simple self-teaching tutorial helps new users to become familiar with the use of the GMAE.

Gross Motor Ability Estimator
GMFM © Russell DJ, Rosenbaum PL, Cadman DT, Gowland C, Hardy S,Jarvis S ´The gross motor fuction measure: A means to evaluate the effects of physical therapyª
Cdevelopmental Medicine and ChildNeurology, 1989,31: 341-352
GMFM ©
• To determine the score in a single dimension, the scores of the various items must be summed up and reported in the <Score> section. In each of the five dimensions, a percentage score is calculated.(Total dimension/maximum score) X 100
• The total score is obtained by calculating the average of the percentage scores of all dimensions.
Note: Decimal numbers should be rounded to the nearest whole number.
Dimensions most relevant for achieving the child's short-medium term goals.
Taking into account some factors:
• Current functional status.
• Age.
• Current area of interest of the child.
• Skills needed in various contexts of daily life.
• Indicate with “ⱱ” the target areas selected in the <score> sheet.
Total target score:
Sum of scores % of each dimension identified as target area/N of target area.
SELECTIVE USE OF TARGET AREAS MAY BE OF QUESTIONABLE VALIDITY FOR ASSESSING GLOBAL MOTOR CHANGE.
Work Cited
Wang, Hui-Yi, and Yi Hsin Yang. Evaluating the Responsiveness of 2 Versions of the Gross Motor Function Measure for Children With Cerebral Palsy. American Congress of Rehabilitation Medi cine and the American Academy of Physical Medicine and Rehabilitation. vol. 87, 2006, 51-6.
• It is necessary to administer version 88.
• Neutral test and subsequently with the aid/a device of interest (shoes are considered a device).
• It is not necessary to repeat the entire GMFM.
• The result corresponds to a functional change.
• The calculations for determining the score are identical to the normal evaluation.
On the back page of the score sheet, it must be indicated which aids/orthoses have been used and in what sizes.
It’s also important to consider negative aspects
• Dimension B items 35, 36, 37.
• Dimensions D/E applied at the beginning of the dimension.
• Applicable in any size.
• They must be applied at the beginning of the dimension of interest.
Scoring assignment: if the functionality changes as a result of assistive devices/orthoses, an A should be placed in the score box..

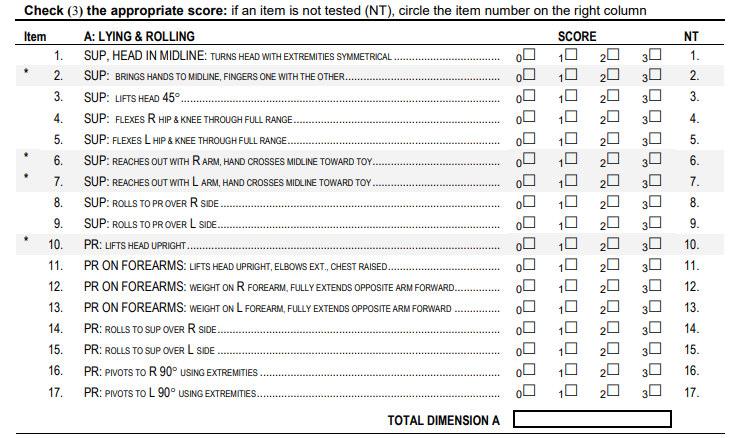
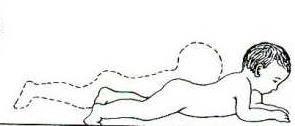
Starting position: Supine, head on midline
does not keep the head on the midline
1. Sup, head in midline: turns head with extremities symmetrical
1. Holds head on midline for 1-3 sec.
2. Keeps head on midline, rotates with asymmetric limbs
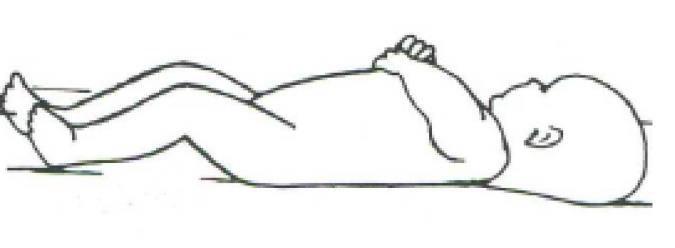
3. Rotate your head with limbs symmetrical

In the case of small children who try to grasp the object that is being proposed, the movements of the
AA.SS can be observed and the <symmetry> assessed. To assign a score of 2, the asymmetry must be evident and determined by the position of the head.
Starting position: Supine
0. does not attempt to bring hands to midline
2. Sup: brings hands to midline, fingers one with the other.
1. Try to bring hands to the midline
2. Bring hands in front of body without interclaing fingers
3. Bring hands in front of the body interclaing fingers
<Interlocked fingers> the child holds both hands together long enough to demonstrate contact between the fingertips (one finger of the hand in contact with the other is also acceptable, but contact with the hands closed in a fist is not).
Starting position: Supine
6. Reaches out R arm, hand crosses midline toward toy
0. Does not to atempt to reach the arm toward the midline
1. Try to stretch arm toward the midline
2. Extend R arm, the hands does not go beyond the midline
3. Stretches out R arm, hand goes beyond the midline in the direction of the toy
Avoid holding the contralateral arm down because it is not acceptable. For children who show a tendency to use both hands or the closest one, it can consider offering a larger toy.
Starting position:
Supine
8. Rolls to pr. Over right side
0. does not try to roll 1. Try to roll
2. Rolls partially to prone
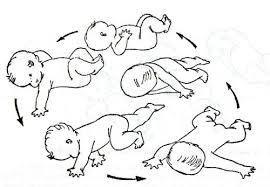
3. Rolls to pr. completely
If the child rolls completely, but the arm remains stuck under the body, it’s possible to award a score of 3.
Starting position: Prone on forearms
0. does not attempt to bear weight on the right forearm
12. Pr on forearms: weight on R forearm, fully extends opposite arm forward.
1. free the left arm, do not extend it, do not stretch it forward
2. partially extends the left arm forward

3. fully extends the left arm forward
The position of the arm that supports the weight is not fundamentally important as long as the limb is in contact with the mat and is effectively supporting the weight.



20 Item Investigates the skills of: maintaining posture, reaching for other items, and performing tasks while sitting.



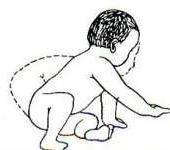

14 Item Investigate the abilities of: Adopting and/or maintaining variations of the 4-point position and kneeling; Moving forward in the prone position, on all fours, or kneeling; performing specific tasks in the 4point position.
8 Hemiparesis
Starting position: Prone
38. PR: Creeps forward 1.86 m
Creeps forward 1,8 m
Starting positions: 4 points
sit arms
0. He\She does not try
He\She tries to sit
Attains sit with the arms
Attains sit arms free
Starting position: 4 points
44. 4 point: Crawls or hitches forward
0. He\ She does not try
1. Crawls or hitches forward <60cm
2. Crawls or hitches 60150 cm
3. Crawls or hitches forward 1,8 m
"CRAWLING" moves on hands and knees; it is not necessary for arms and legs to move in an alternating pattern. "BOUNCE" moves in hops, the "rabbit hop" or "sitting on the buttocks walk" is accepted. Place the child in a 4-point position at the end of a 2.5 m mat, and it is necessary for them to maintain the posture for a few seconds.
Starting position: 4 points
46. 4 Point: Crawls up 4 steps on hands and knees\feet
0. He\She does not try 1. Crawls 1 step
2. 2-3 steps
The height of each individual step must be about 18 cm.
3. Crawls up 4 steps on hands and knees\feet
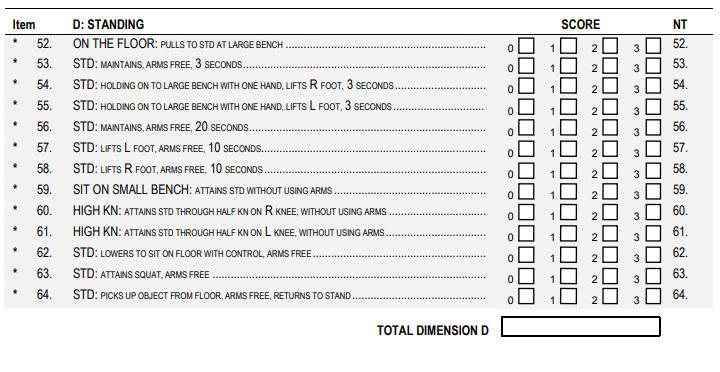


13 Items
Describe various aspects of the child's ability to:Maintain positions other than standing - Reach a standing position from different posturesPerform specific tasks from a standing position
Age: 8
Starting position: On the floor
0. He\She does not try to get up on its feet
1. He\She tries to stand up
2. He\She stands up partially
3. He\she stands up at bench
The goal is to establish the child's ability to stand up. The alignment may vary as long as the buttocks are lifted off the legs and/or the supporting surface.
Starting position: Standing
0. He\She does not mantain the position
1. He\She mantains the position mantiene, supporting with both hands
2. holds on, supporting oneself with one hand, for 3 seconds.
3. holds, without the help of the arms, for 3 seconds.
"WITHOUT THE HELP OF THE ARMS" absence of contact with any surface, weight on arms and legs. "SUPPORTING ONESELF" can oc one or both hands, refers to indicated equipment, does not include supporting oneself on a person.
Starting position:
Standing
0. . He\She does not try
STD: Holding on to large bench, with one hands lift, lift R foot, 3 second
1. supporting yourself on a bench with both hands, lift right foot, <3sec.
2. supporting yourself on a bench with both hands, lift right foot, 3 sec
3. supporting yourself on a bench with one hand, lift right foot, 3sec.
Score 3: when the child lifts one leg while supporting themselves with one hand; the child cannot score if they lift the leg with both hands and then remove one. It is requested for both sides.
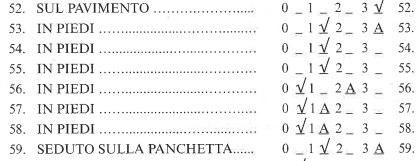
Starting position: Standing
56.
2.
1.
0.
3.
Starting position: H-kn
0. Does not try
H-kn: Attains std through half kn on R knee, without arms
1. Tries to attains
2. Attains std with the arms
3. Attains std through half kn on R knee, without arms
24 Item
Starting from the standing position, investigate the child's ability to:
- Perform different walking modes
- Perform specific tasks such as going up and down stairs or kicking a ball
- Perform different jumping modes
- Investigate the abilities to: maintain posture, reach others, and perform tasks while sitting.
When the starting position is described as 'standing', the child must begin the movement from a standing position without the help of their arms. They must not support themselves with their hands or lean on equipment. These instructions apply to items 69-83 and 86-88.
Starting position:
Standing, 2 hands on large bench
65. Cruises 5 steps to R
0. He\ She does not try 1. He\She tries to cruise, <1 step to R 2. Cruises 14 steps to R 3. Cruises 5 steps to R
EDGE OF A STEP: the lateral movement of both legs, one at a time. The child should be at one end of a bench, and can lean on their forearms or touch the equipment with other parts of their body as long as the weight is on the arms and legs (rather than on the trunk).
Starting position:
Standing, 2 hands held
Walking forward 10 steps 0. He\ She does not try
He\She tries to walk < 3 steps
He\She walks 3-9 steps
He\She walks 10 steps
ADVANCE ONE STEP: the forward movement of a leg from the lift-off to the heel contact with the ground.
CONSECUTIVE STEPS: without interruption; any pauses between steps must not exceed 2 seconds, otherwise the test must be considered concluded.
The child walks forward with their hands held by the therapist. The therapist must be in front of the child to reduce the inclination.
70. STD: walks forward 10 steps, stops, turns 180 , returns
0. 10 steps, does not stops. 1. 10 steps and stop, not turns
2. walks forward 10 steps, stops, turns 180 ,
3. Walks forward 10 step, stops, turns 180 , returns
STANDING POSITION: the child must start the movement from the standing position without the use of the arms. WITHOUT THE USE OF THE
ARMS: without interruptions; any pauses between steps must not exceed 2 seconds, otherwise the test must be considered concluded.
SCORE 3: The child walks forward, must stop and then turn around (and not turn around to then stop). There is no need to count the number of steps.
Starting position:
Standing Runs 4,5 m., stops and returns
Starting position:
Standing Runs 4,5 m., stops and returns
Starting position:
Standing
Hops on right foot 10 times in a circle with a diameter of 60 cm.


@ospedalebambinogesu
TWITTER @bambinogesu
INSTAGRAM @ospedalepediatricobambinogesu
Ospedale Pediatrico
Bambino Ges˘
Ospedale Pediatrico
Bambino Ges˘ FLICKR @ospedalebambinogesu
www.ospedalepediatricobambinogesu.it
Age: 8 Hemiparesis
Starting position:
Sitting on the mat with a little toy in front
0. does not try to stretch forward
25. Sit on mat with small toy: leans forward
1. it stretches forward but rises again
2. leans forward, touches the toy, gets back up using her arms

3. leans forward, touches the toy, gets back up without the help of the arms
Make at least one attempt to establish whether the toy is within reach of the child who has to stretch forward to grab it. For the older child, they are only asked to touch it and not to bend the opposite arm; for younger children, a larger object is needed to encourage them to use both hands.
Starting position:
Sitting on the mat
0. does not try to touch toy
26. Sit on mat: touches toy placed 45° behind child’s R side, returns to start
1. tries to stretch out the arm, does not reach back
2. stretches the arm backward but does not touch the toy or return to the starting position
3. Touch the toy placed at a 45 angle in a rearward position relative to the right side, return to the starting position.
The child should turn to the right and execution is allowed only if they touch the toy. To score 2 points, the hand must extend backward beyond the greater trochanter.
Starting position : Sitting on mat with feet in font
31. Attains 4 points over R side
0. He\She does not try
1. He\She tries to attain 4 points position
He\She partially placed on 4 points from the upper
3. He\She completes the passage
The starting position from sitting in a 'W' is not accepted, they must have their legs semi-extended or fully extended. They can load weight on their forearms or directly on their hands, but they cannot assume the prone position and then move to all fours.
Starting position: Standing
0. He\She does not try
35. STD: attains sit on small bench
1. He\She tries to sit on the bench
2. He\She partially attains sit on bench

3. He\She attains sit on bench
It is possible to sit on the bench in whichever way children prefer. To achieve a score of '1', the children must make a clear attempt. The bench should not be longer than one meter (while sitting, the child must be able to touch the floor with their feet).
Starting position: On the floor
0. He\She does not try
1. He\She tries to sit on the bench 2.
He\She partially attains sit on bench
3. He\She attains sit on bench
Establish whether the children can get up from the floor to sit on the bench. Children who attempt to lift themselves from the starting position and move towards the bench receive a score of '1'. A score of '2' should be assigned to children who are able to lift themselves to reach a standing position near the bench.