2A_Marotta_Verbal and non verbal communication-Topic 1
The project is being implemented with the support of UNICEF Ukraine and with financial support from the Government of Norway.
Implemented by: Partner:
Assessment and intervention in acquired speech, language and communication impairments
Area Clinica di Neuroscienze
Neuroriabilitazione Santa Marinella
Luigi Marotta
luigi.marotta@opbg.net
PROGRAM
Topic 1 (30 minutes)
Verbal and non-verbal communication. Language and communication deficits after other injuries.
Topic 2 (30 minutes)
Evaluation procedures and assestment tools. Receptive abilities.
Topic 3 (30 minutes)
Evaluation procedures and assestment tools. Expressive abilities.
Topic 4 (30 minutes)
Guidelines and care needs. Augmentative Alternative Communication strategies.
PROGRAM
Topic 1 (30 minutes)
Verbal and non-verbal communication. Language and communication deficits after other injuries.
Topic 2 (30 minutes)
Evaluation procedures and assestment tools. Receptive abilities.
Topic 3 (30 minutes)
Evaluation procedures and assestment tools. Expressive abilities.
Topic 4 (30 minutes)
Guidelines and care needs. Augmentative Alternative Communication strategies.
Introduction
This unit aims to equip speech therapists, as well as other therapists and caregivers, working with children with severe acquired brain injuries….
Introduction ...or spinal cord injuries and other conditions affecting language and communication skills, with the necessary knowledge and practical skills.
Introduction
These disabilities have a strong impact during early care and reintegration into daily activities.
Introduction
Our focus will therefore be on re-establishing sufficient communication skills in young patients from the time of initial admission.
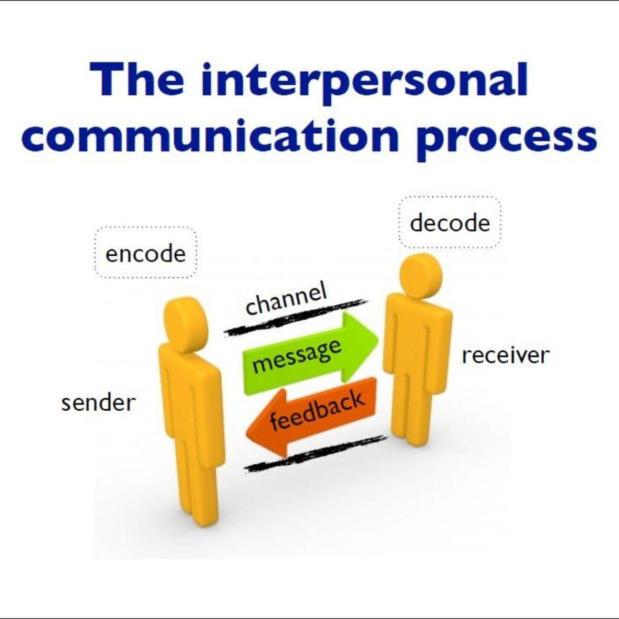
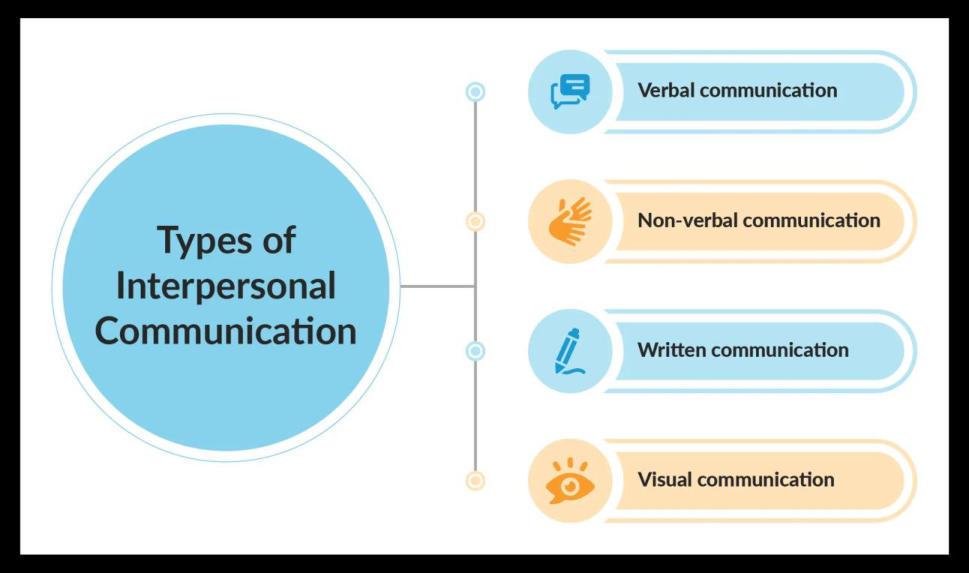
IC consists of the set of phenomena that convey the exchange of information between two or more persons, whether through verbal language or body language
Interpersonal Communication (IC)
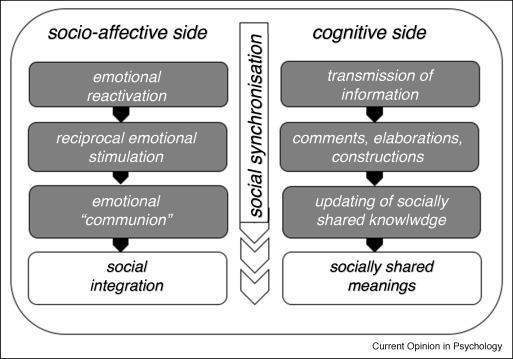
Two aspects are important in the process of interpersonal communication
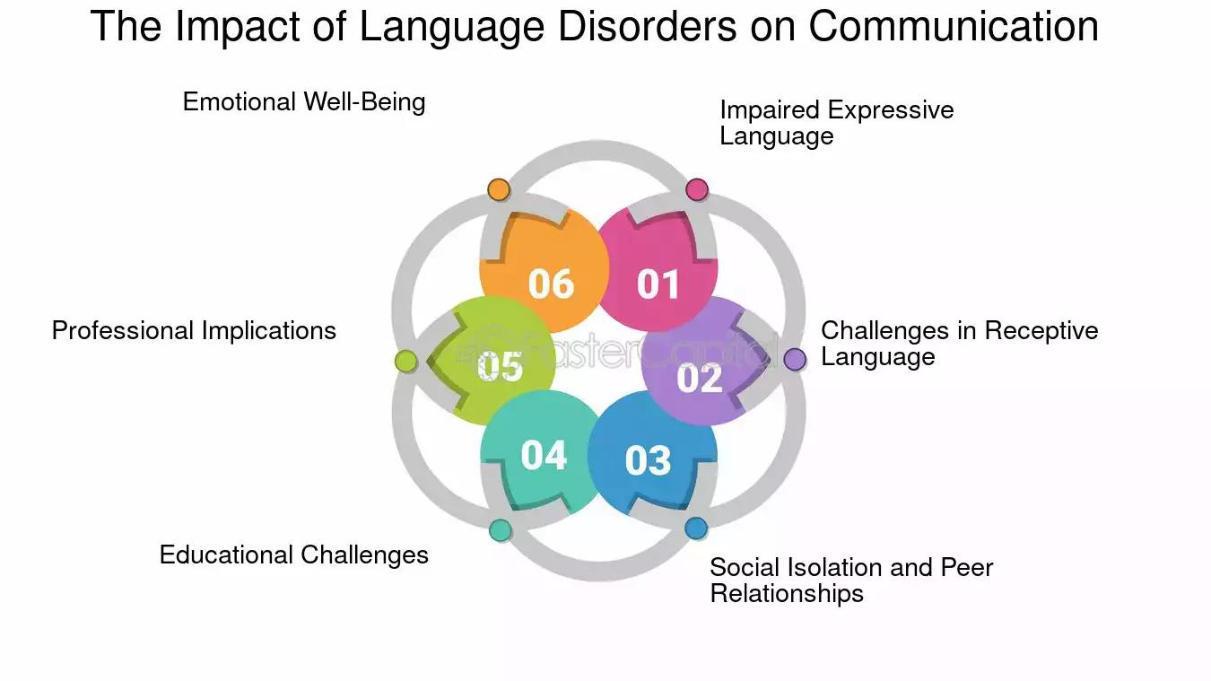
LANGUAGE AND COMMUNICATION DISORDERS
LANGUAGE AND COMMUNICATION DISORDERS
PRIMARY LANGUAGE DISORDER
in the absence of cognitive, sensory, motor, affective problems and major socio-environmental problems.
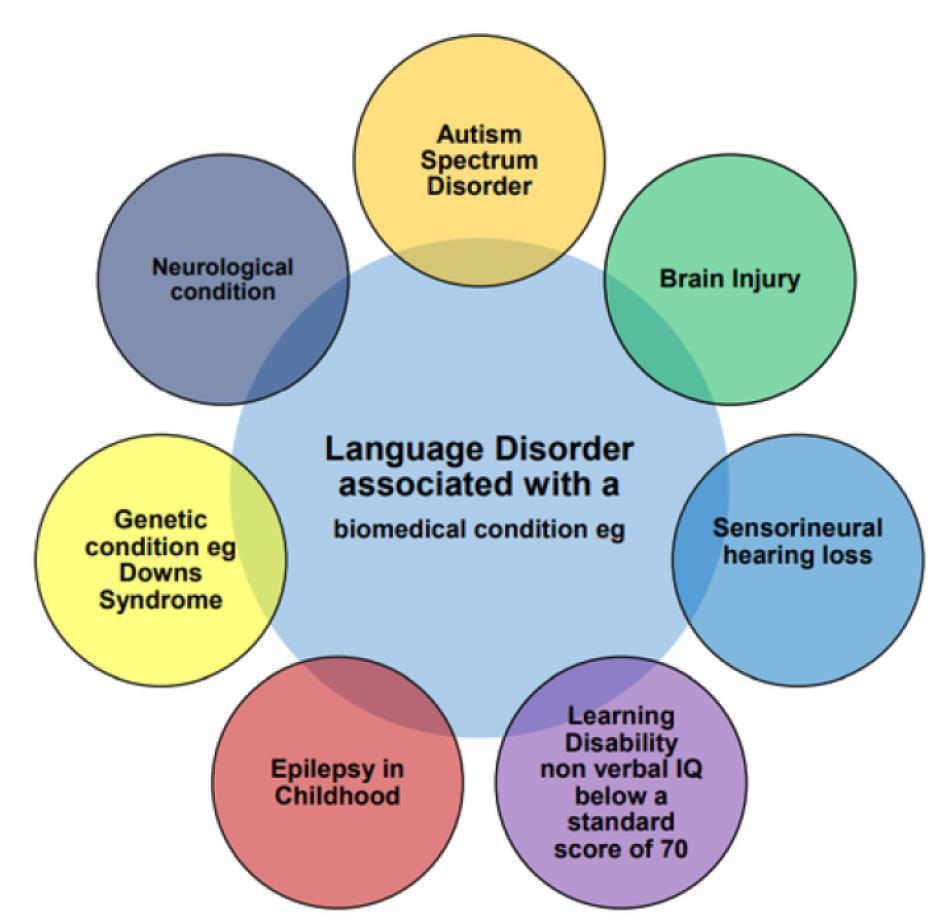
SECONDARY LANGUAGE DISORDER
In the presence of congenital and/or acquired brain damage, genetic syndromes or other pathologies
PRIMARY LANGUAGE DISORDERS
in ICD 9 may be:
COMMUNICATION
DISORDERS in DSM 5
Communication disorders represent the most frequent developmental disorders between 2 and 6 years of age. They represent a set of syndromic pictures characterised by different quality and severity difficulties in the comprehension, production and use of language.
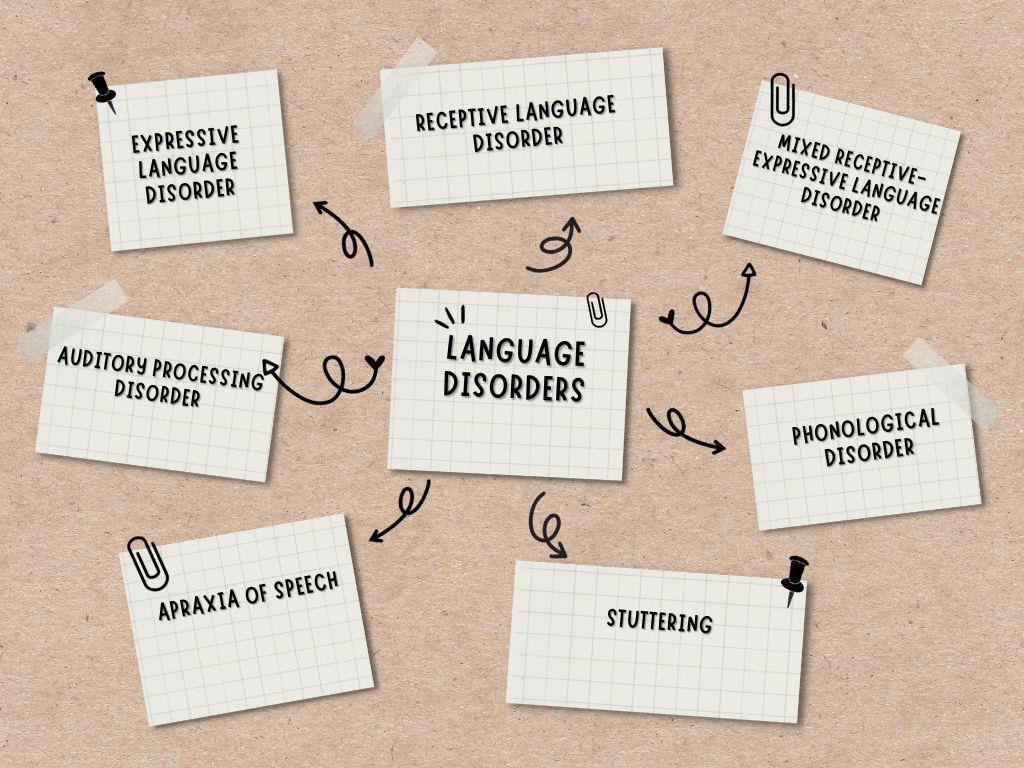
PRIMARY COMMUNICATION DISORDERS in
Language disorder
Phonetic-phonological disorder
Fluency disorder with onset in childhood
Social Communication Disorder
Communication Disorder without Specification
PRIMARY COMMUNICATION DISORDERS in DSM 5
1. Language disorder (expressive, receptive and mixed) is part of the neurodevelopmental disorders and is characterised by a delay in one or more areas of language development
This in the absence of cognitive, sensory, motor, affective problems and socio-environmental problems.
PRIMARY COMMUNICATION DISORDERS in DSM 5
2.
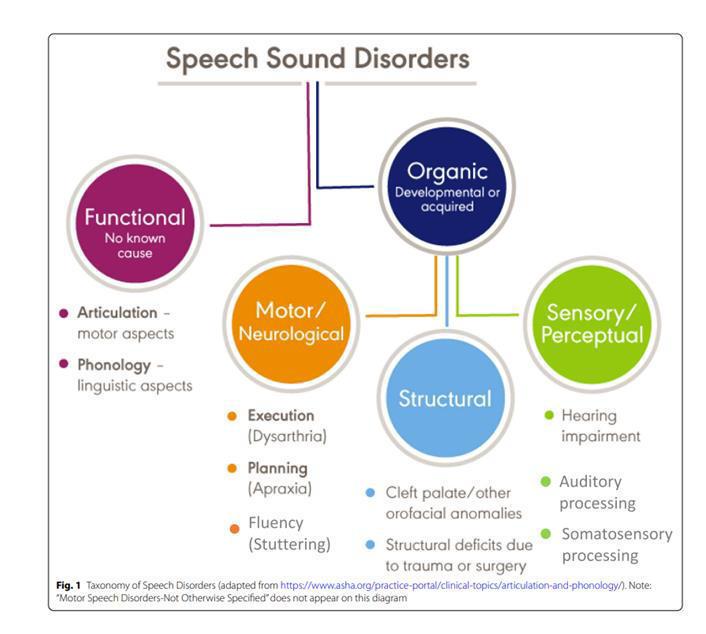
Phonetic-phonological disorder (speech and sound disorders)
They specifically describe difficulties in phono-articulatory and phonological organisational levels.
They functionally include disorders that fall under the definition of Childhood Apraxia of Speech (CAS).
We can schematise the taxonomy of speech and language disorders:
PRIMARY COMMUNICATION DISORDERS in DSM 5
3.
Fluency
disorder with
onset in childhood is commonly known as stuttering, is a speech disorder that disrupts the smooth flow of speech. It's characterized by repetitions, prolongations, or blocks of sounds, syllables, or words, and can cause anxiety and impact social interactions and academic performance.
PRIMARY COMMUNICATION DISORDERS in DSM 5
4. Social Communication Disorder (SCD)
is a neurodevelopmental condition characterized by persistent difficulties with using verbal and nonverbal communication for social purposes.
Individuals with SCD struggle to adapt their communication to different social situations, understand social cues, and engage in reciprocal social interactions.
PRIMARY COMMUNICATION DISORDERS in DSM 5
4. Social Communication Disorder (SCD)
SCD is distinct from Autism Spectrum Disorder (ASD) though some symptoms can overlap.
The key differentiator is the presence of restricted, repetitive patterns of behavior, interests, or activities (RRBs). If these RRBs are present, the diagnosis leans towards ASD; if absent, SCD is considered.
PRIMARY COMMUNICATION DISORDERS in DSM 5
5. Communication Disorder without Specification
This category is used when there's a communication impairment causing significant distress or impairment in social, occupational, or other areas of functioning, but the specific type or cause isn't clear or can't be determined.
SECONDARY DISORDER
SECONDARY DISORDER
SECONDARY DISORDER
SECONDARY DISORDER
SECONDARY DISORDER
SECONDARY DISORDER
SECONDARY DISORDER
Summary of the Rehabilitation Intervention Guidelines
Traumatic Brain Injury (TBI) in children leads to complex, evolving conditions.
Rehabilitation is crucial after acute medical care.
Goal: Restore function and improve quality of life.
While acute care focuses on medical needs, rehabilitation becomes paramount afterward.
Neuropsychological and linguistic-communicative deficits are assessed using clinical observation and standardized tests that allow for age-based comparison, correlation with brain areas, and verification of processing strategies.
Individual Rehabilitation Project (IRP)
Multidisciplinary Evaluation
Outcomes
: Complete clinical balance of patient deficits.
Definition of IRP:
Outlines primary rehabilitation objectives. Followed by detailed rehabilitation programs for each treatment area.
Early Treatment Phases
Stimulation Approach:
Brief, repeated Sessions throughout the day are more effective.
Avoid standardized 60-minute sessions.
Patient Capacity:
Short attention spans. Process limited information simultaneously.
Early Post-Acute Speech Therapy Goals
Oral Feeding Recovery: Mastication and swallowing.
Articulation of Words.
Extraverbal Communication Training (AAC; for anarthric patients).
Combine test results with informal assessments (interviews with family, teachers, therapists).
Objectives of Assessment
1. Identify Cognitive-Linguistic Profile: Strengths and weaknesses (for training and compensation).
2. Impact on Daily Activities: Determine which areas most interfere with daily life.
3. Define & Monitor Goals: Set cognitive rehabilitation goals and update based on progress.
4. Baseline & Progress: Obtain baseline indicators and measure improvements.
5. Treatment Efficacy: Demonstrate which treatments promote cognitive-linguistic improvement.
6. Personalized Learning: Identify personal thinking/learning style for customized training.
7.
Environmental
Factors:
Identify variables impacting adaptive cognitive function and learning.
Linguistic-Communicative Complications:
Dysarthria
Definition: Speech articulation disorders due to neurological lesions.
Types: Flaccid, spastic, ataxic, hypotonic/hyperkinetic (depending on lesion site).
• Acquired Stuttering: Possible after TBI (brainstem/basal ganglia damage).
• Common Presentation: Dysphonia often associated with mixed dysarthria after severe TBI.
• Rehabilitation: Challenging; simultaneous treatment of dysphonia and dysarthria.
Speech therapy for articulation often shows unsatisfactory results.
Language Deficits & Aphasia
Definition: Impaired language performance (requires baseline development, usually >2 years old).
Leading Cause: TBI is now the primary cause of aphasia in children.
Types: Children can exhibit all adult forms (e.g., Wernicke's, Broca's, anomic, conduction, transcortical).
Persistent Language Disorders & Prognosis
Recovery vs. Persistence: While recovery is often high, persistent (even subclinical) language disorders are common after severe TBI.
Long-Term Impact: Significantly influence academic performance and overall prognosis.
Learning Disabilities: Can lead to marked learning disabilities, reading, and writing disorders.
Monitoring: Systematic, long-term monitoring is crucial for early detection and intervention.
Recovery Expectation: Complete recovery from aphasic syndrome is rarely achieved.
Pragmatic Disorders
Definition: Difficulties with social use of language.
Impact on Communication:
Understanding/developing conversation topics.
Interpreting stories, metaphors, humor.
Understanding/producing gestures and facial expressions.
Prosodic difficulties.
Social Interaction: Significant difficulties in turn-taking and inhibiting inappropriate behaviors/thoughts.
Child vs. Adult Impact: More profound impact on children, affecting social interaction during personality development.
Rehabilitation Focus: Essential to include pragmatic aspects of communication in treatment.
Conclusion: Importance of Continuous Monitoring
Systematic Evaluation: Crucial for diagnosis, prognosis, and appropriate rehabilitation of language and verbal communication disorders after severe TBI.
Ongoing Monitoring: Most children do not achieve full linguistic development, so neuro-linguistic skills need continuous monitoring.
Recommended bibliography
Castelli, E., Marotta, L., Gazzellini, S., & Tarter, G. (2020). Manuale di logopedia in et‡ evolutiva. Erikson Ed.
McCabe, P., Beiting, M., Hitchcock, E. R., Maas, E., Meredith, A., Morgan, A. T., ... & Grigos, M. I. (2024). Research Priorities for Childhood Apraxia of Speech: A Long View. Journal of speech, language, and hearing research, 67(9S), 3255-3268.
Novak, I. (2014). Evidence-based diagnosis, health care, and rehabilitation for children with cerebral palsy. Journal of child neurology, 29(8), 1141-1156.
On, Z. X., Ryan, N. P., Konjarski, M., Catroppa, C., & Stargatt, R. (2022). Social cognition in paediatric traumatic brain injury: A systematic review and meta-analysis. Neuropsychology review, 1-22.
Vite che aiutano la Vita
Il presente documento Ë stato elaborato in n.xx slide da Ospedale Pediatrico Bambino Ges˘ il xxxxxx.
I contenuti sono strettamente riservati; Ë vietata la riproduzione e la divulgazione, anche solo parziale, senza il benestare scritto di Ospedale Pediatrico Bambino Ges˘.