
Allegheny County Medical Society
Allegheny County Medical Society
Allegheny County Medical Society
Editorial
• Pruning/Nothing is Promised Deval (Reshma) Paranjpe, MD, MBA, FACS
Membership
• Q&A with Matthew Simpson, MD
ACMS News
• Member Acknowledgements
ACMS News
• Specialty Group Updates
ACMS Staff: Nadine
Popovich, Melanie Mayer and Haley Thon
Medical
• Reportable Diseases 2025: Q1-Q3
Allegheny County Health Department Selected Reportable Diseases/Conditions
Jennifer Fiddner, MPH, CIC
Allegheny County Health Department
Article
• Speaking Clearly When Science Gets Cloudy
Dr. Devon Ramaeker and Dr. Michael Aziz
Article
• 20th Annual ACIC Conference A Milestone Day for Immunization Leadership (Nov. 5)

Melanie Mayer
Materia medica
• SGLT2i Showdown Which Inhibitor Steals the Spotlight?
Devon Hess, PharmD, MBA; Noopur Doshi, MD; Jason Fine, PharmD, BCPS

2025
Executive Committee and Board of Directors
President
Keith T. Kanel, MD
President-elect
Kirsten D. Lin, MD
Secretary
Richard B. Hoffmaster, MD
Treasurer
William F. Coppula, MD
Board Chair
Raymond E. Pontzer, MD
Board of Directors
Term Expires 2025
Anuradha Anand, MD
Amber Elway, DO
Mark A. Goodman, MD
Elizabeth Ungerman, MD, MS
Alexander Yu, MD
Term Expires 2026
Michael M. Aziz, MD, MPH, FACOG
Michael W. Best, MD
Micah A. Jacobs, MD, FIDSA
Kevin G. Kotar, DO
Jody Leonardo, MD
Term Expires 2027:
David J. Deitrick, DO
Sharon L. Goldstein, MD
Prerna Mewawalla, MD
Raymond J. Pan, MD
Nicole F. Velez, MD
James Latronica, DO, DFASAM
Richard B. Hoffmaster, MD
Finance
William F. Coppula, MD
Nominating
Kirsten D. Lin, MD
Women’s Committee
Prerna Mewawalla, MD & Meilin Young, MD
Managing Editor
Sara C. Hussey, MBA, CAE
ACMS Executive Director shussey@acms.org
Medical Editor
Deval (Reshma) Paranjpe, MD reshma_paranjpe@hotmail.com
Bulletin Designer
Victoria Gricks victoria@thecorcorancollective.com
2025 Bulletin Editorial Board
Richard Daffner, MD, FACR
Robert Howland, MD
Anthony Kovatch, MD
Charles E. Mount, MD, FAAD
Alexandra Johnston, DO
John P. Williams, MD
Executive Director
Sara Hussey shussey@acms.org
Vice President - Member and Association Services
Nadine M. Popovich npopovich@acms.org
Manager - Member and Association Services
Haley Thon hthon@acms.org
Operations CoordinatorACMS & ACMS Foundation
Melanie Mayer mmayer@acms.org
Manager - Operations and Finance
Elizabeth Yurkovich eyurkovich@acms.org
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
EDITORIAL/ADVERTISING
OFFICES: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212; (412) 321-5030; fax (412) 321-5323.
USPS #072920. PUBLISHER: Allegheny County Medical Society at above address.
The Bulletin of the Allegheny County Medical Society is presented as a report in accordance with ACMS Bylaws.
The Bulletin of the Allegheny County Medical Society welcomes contributions from readers, physicians, medical students, members of allied professions, spouses, etc. Items may be letters, informal clinical reports, editorials, or articles. Contributions are received with the understanding that they are not under simultaneous consideration by another publication.
Issued the third Saturday of each month. Deadline for submission of copy is the SECOND Monday preceding publication date. Periodical postage paid at Pittsburgh, PA.
Bulletin of the Allegheny County Medical Society reserves the right to edit all reader contributions for brevity, clarity and length as well as to reject any subject material submitted.
The opinions expressed in the Editorials and other opinion pieces are those of the writer and do not necessarily reflect the official policy of the Allegheny County Medical Society, the institution with which the author is affiliated, or the opinion of the Editorial Board. Advertisements do not imply sponsorship by or endorsement of the ACMS, except where noted.
Publisher reserves the right to exclude any advertisement which in its opinion does not conform to the standards of the publication. The acceptance of advertising in this publication in no way constitutes approval or endorsement of products or services by the Allegheny County Medical Society of any company or its products.
Annual subscriptions: $60
Advertising rates and information available by calling (412) 321-5030 or online at www.acms.org.
COPYRIGHT 2025: ALLEGHENY COUNTY MEDICAL SOCIETY POSTMASTER—Send address changes to: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212. ISSN: 0098-3772

By: Deval (Reshma)
MD, MBA, FACS
October is here, and the first frosts are falling. A seemingly endless hot summer has finally ended. I took in all umpteen plants from the outside deck to the warmth and safety of the indoors, along with their attendant spiders who are doubtless confused about the sudden onset of global warming. Some people say I have a green thumb because my house is filled with plants and my orchids always manage to thrive. Some people think otherwise. A dear friend with a dry sense of humor recently suggested on a beautiful day that I make sure to go outside after work, even if I just spent some time “you know, on the deck, where you kill your plants.”
He’s not wrong. This year, I started out strong, with so many plants that they looked like a emerald-clad symphony orchestra with me as their conductor, waving a 5-function sprayer for a baton. My plants were healthy and green and bursting with fruit and flowers. I enjoyed every bit of their bounty and together with the bees and hummingbirds sniffed to my heart’s content. Jasmine, plumeria, strawberries, tomatoes, lemon balm. Cilantro, sage, rosemary and thyme. Figs. Neem and curry leaf plants. Every kind of pepper imaginable.
And then life happened. Work stress, family medical issues, career shifts, all of the things that happen to all of us. As another dear friend said at dinner tonight, "nothing is promised". She was on her way to the restaurant when she had the sudden thought: I hope I make it there.
There are plants still in pots outside that withered in the long stretches of
90 degree weather when I left home too early and came home too late to water them. There are plants that I cultivated lovingly for a decade who lie dead out there because I was sick in bed for an entire week and could barely water myself.
Plants that I did not think would survive the drought have lived. Plants that I was sure would make it lie barren. Nothing is promised.
In my mad dash to bring in the plants before the frost, I follow an order that has nothing to do with size, weight, or proximity to the screen door. The plants I cannot afford to lose are rescued first. The ones that mean the most were gifts from the people I love — the plumeria and Meyer lemons from my mother, all the herbs, yes, but especially the tiny turtle holding a succulent from my father. All the plants we bought together at the nursery down the road and carried home in the car, shaking our heads and laughing.
A wildly flowering hibiscus is all that I have left of someone who meant the world to me; it lives, while he is gone. While it lives, he is still with me. Nothing is promised.
I look at the plants I’ve brought in and it’s clear that I need to debride them. I’m fairly good at debridement but have never been good at pruning and discipline. “If something shows you that it’s determined to live, you have to help it live”, says my mother, as she pots a piece of ginger that defiantly sprouted leaves in my dark kitchen. I suppose I take that to extremes. I take joy in the wild abandon of plants that send out shoots and vines, even if they turn into a glorious jungle. “Prune them! And cut
the blooms! Before your garden goes to seed!” cry the voices of reason. I know they are right, but I shudder at taking scissors to green stems.
My orchids thrive with benign neglect. I water them once a week, tell them they are beautiful, and shower them with sunshine and cold nights. And I never give up on them.
Earlier this summer another dear friend was bemoaning her blighted orchids. She’d tried everything, consulted a master gardener, but to no avail. One last treatment administered outside would be the final test. “If they survive, I’ll bring them back in.” She had had enough of the struggle and heartbreak. It was one of those “I’m barely watering myself” days. An extreme form of pruning, for people who hate pruning.
In the garden, as in life, we have to make choices. We have to prune and cut back so that the plant blooms more, grows more, redirects its energy, becomes more hardy and vigorous. We have the privilege of giving away prize cuttings to people we love to create new joy in other gardens. We have to choose what to keep and what to leave, and how to decide. Maturity is realizing that wielding the blade on a still-green stem can be an act of love, oddly enough.
I look at my life and wonder what needs to be pruned in order to grow stronger and more fruitful. What memories of old struggles need to be debrided in order to sprout new optimism and adventures? What will you prune in your own life so that you will grow stronger and more beautiful, and rediscover your own lust for life?
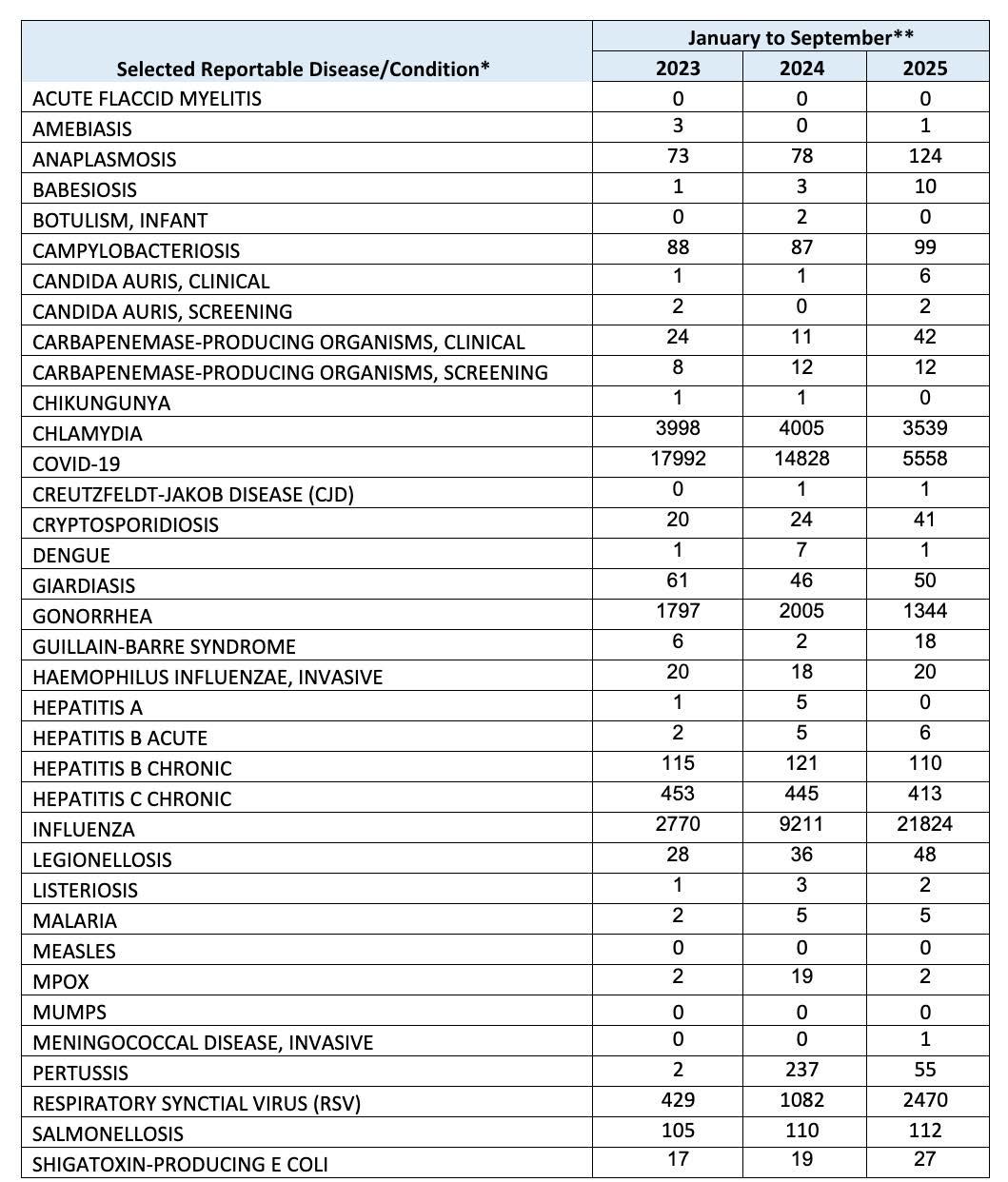
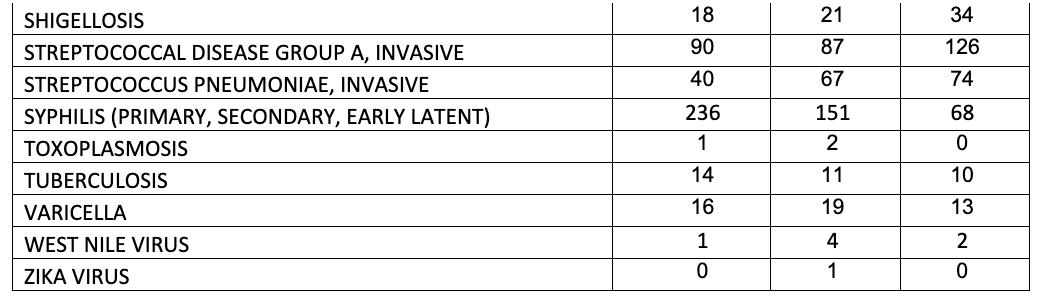
* Case classifications reflect definitions utilized by CDC Morbidity and Mortality Weekly Report. ** These counts do not reflect official case counts, as current year numbers are not yet finalized. Inaccuracies in working case counts may be due to reporting/investigation lag.
NOTE: Disease reports may be filed electronically via PA-NEDSS. To register for PA-NEDSS, go to https://www.nedss. state.pa.us/NEDSS. To report outbreaks or diseases reportable within 24 hours, please call the Health Department’s 24-hour telephone line at 412-687-2243.
For more complete surveillance information, see ACHD’s 10-year summary of reportable diseases: https://www. alleghenycounty.us/Health-Department/Resources/Data-and-Reporting/Infectious-Disease-Epidemiology/EpidemiologyReports-and-Resources.aspx.

This fall, ACMS members came together across Allegheny County to celebrate connection, compassion, and community. From our Coffee Truck visit at UPMC Passavant in recognition of National Physician Suicide Awareness Day, to the inspiring Feel Well arts collaboration with the Pittsburgh Opera, and the empowering AHN Women’s Conference, ACMS continued its mission to support physician well-being and leadership.
Our September 9 Board Meeting brought together leaders to advance the work of organized medicine, while the House of Delegates Opening Session reminded us of the strength of our collective voice in advocacy and policy.
Each moment captured here reflects the heart of our organization— physicians supporting one another, championing wellness, and strengthening the fabric of our medical community.




















Dr. Matthew Simpson, MD is a physician, medical educator, and the founder and CEO of Top MD LLC, an award-winning academic support company dedicated to empowering medical students and recent graduates, especially those from underrepresented backgrounds. Dr. Simpson completed his internal medicine residency and is currently a Pulmonary and Critical Care Fellow at Morehouse School of Medicine. Through his work with Top MD LLC, he has mentored and tutored hundreds of students nationwide, helping them excel on USMLE exams, match into competitive residencies,

and succeed in their medical careers. In addition to his educational work, Dr. Simpson is passionate about leadership, community outreach, and promoting diversity and inclusion in healthcare, earning the 40 under 40 Top Physicians award, along with the 2025 young physician, 2025 Everyday Hero Award, and 2024 Resident of the year award.
Q: CAN YOU SHARE A LITTLE ABOUT YOUR BACKGROUND AND WHAT LED YOU TO A CAREER IN MEDICINE?
A: I was born and raised in Columbus, Ohio, in a family that always valued service, perseverance, and education. My path to medicine was shaped by both personal hardships and mentors who showed me the impact a physician can have not only on patients, but on entire communities. I became the first black biochemistry major graduate at the University of Mount Union, and after completing my medical degree at the American University of Antigua, I returned to the U.S. to complete my residency training in Internal Medicine at Allegheny Health Network. I am now pursuing a fellowship in Pulmonary and Critical Care Medicine at Morehouse School of Medicine. Throughout my journey, I’ve been deeply committed to mentorship, diversity, and equity in medicine. Founding Top MD LLC allowed me to combine my passion for education with service—helping
hundreds of students, particularly those from underrepresented backgrounds, achieve their goals on licensing exams and in the residency match. What ultimately led me to medicine was a desire to give back: to treat patients with compassion, to advocate for those who are often overlooked, and to help open doors for the next generation of physicians.
Q: WHAT INSPIRED YOU TO PURSUE YOUR CURRENT SPECIALTY?
A: I was drawn to Pulmonary and Critical Care Medicine because it brings together the intellectual rigor of complex physiology with the privilege of caring for patients at their most vulnerable moments. During residency, I felt a natural pull toward the ICU— where rapid decisions, teamwork, and compassionate communication with families can directly change outcomes. The ability to bring stability and hope during moments of crisis is what solidified my commitment to this field. My academic work further deepened that interest. I have focused on research in COPD readmissions, lung disease, and ICU outcomes, which has shown me how much room there is to improve both individual patient care and health systems. This balance of bedside medicine, evidence-based research, and leadership in critical care is what excites me most. Pulmonary and Critical Care Medicine allows me not
only to treat illness in the acute setting, but also to advance prevention and education while addressing disparities in respiratory health.
Q: WHAT HAS BEEN THE MOST REWARDING ASPECT OF BEING AN ACMS MEMBER?
A: The most rewarding part of being an ACMS member has been the sense of connection and community it provides. Medicine can feel isolating at times, but ACMS creates opportunities to collaborate with colleagues, share ideas, and advocate for our patients on a larger scale. I’ve especially valued the chance to learn from other physicians’ experiences and to contribute to initiatives that promote education, equity, and improved patient care across Allegheny County.
Q: ARE THERE ANY ACMS INITIATIVES (OR PAMED INITIATIVES) OR EVENTS THAT YOU ARE PARTICULARLY PASSIONATE ABOUT?
A: I am especially passionate about ACMS and PAMED initiatives that focus on mentorship, community outreach, and promoting diversity within medicine. During residency, I saw firsthand how impactful these programs can be in supporting both physicians and the communities we serve. Initiatives that connect physicians with students from underrepresented backgrounds resonate deeply with me, because


they align with my own work through Top MD LLC and mentorship groups I’ve founded. I’m also enthusiastic about ACMS’s community health and advocacy efforts, particularly those aimed at addressing healthcare disparities and improving access to care in underserved populations. These initiatives remind us that our work extends beyond the hospital walls and that physicians have a powerful role in shaping healthier, more equitable communities.
Q: WHAT DO YOU THINK IS THE BIGGEST CHALLENGE FACING HEALTHCARE TODAY?
A: One of the biggest challenges in healthcare today is the growing gap in access and equity. While medical innovation is advancing at an incredible pace, not all patients or communities are benefiting equally. Social determinants of health—such as housing, education, food insecurity, and systemic barriers—continue to drive disparities in outcomes. As physicians, we often see patients when these inequities have already translated into advanced disease or preventable hospitalizations. Another challenge is workforce strain. From physicians to nurses and allied health professionals,
burnout and shortages are affecting the quality of care. Addressing these issues requires not only systemlevel reform but also investment in mentorship and pipeline programs to diversify and strengthen the next generation of healthcare providers. To me, meeting these challenges head-on means pairing innovation with advocacy and ensuring that compassion and equity remain central to the future of medicine.
Q: WHAT IS ONE SENTIMENT YOU'D LIKE TO SHARE WITH YOUR FELLOW ACMS MEMBERS?
A: I’d like to express gratitude for being part of such a dedicated community of physicians and healthcare leaders. Medicine can be both inspiring and challenging, and I believe our greatest strength lies in supporting one another. Whether through mentorship, advocacy, or collaboration, we have the opportunity to not only advance patient care but also uplift the next generation of physicians. My hope is that we continue fostering a culture of inclusivity, compassion, and innovation—because together, we can build a healthcare system that reflects the best of who we are and the future we want to create.



*This handout is informational only and not legal advice. Contact Quatrini Law Group for a consultation.
BRIAN PATRICK BRONSON, ESQ.
Filing a disability claim as a physician is not the same as filing one in any other profession. Medicine is divided into dozens of specialties, each with unique demands. Yet insurers often reduce “orthopedic surgeon,” “interventional pain specialist,” or “cardiac electrophysiologist” to a generic label of “physician.”
That oversimplification can make the difference between an approved claim and a denial. To protect your livelihood, approach the claim process with the same precision you bring to patient care. Three tools are especially critical: accurate job descriptions, specialty-specific language, and precise ICD-10 coding..
1. Why Job Descriptions Matter
Insurers will request a job description, but too many physicians rely on generic HR forms. These rarely reflect the true demands of your specialty.
Unhelpful: “Examines, diagnoses, and treats patients.”
Helpful: “Performs image-guided lumbar transforaminal epidural injections and spinal cord stimulator placements requiring prolonged standing, bimanual dexterity, and exposure to fluoroscopy.”
A strong physician job description should include:
• Primary procedures performed
• Frequency/duration of tasks
• Physical demands
• Cognitive demands
GENERIC HR FORMS = DENIED CLAIMS
2. Using Specialty-Specific Language
Policies define “own occupation” as the work you were performing at the time of disability. For physicians, that usually means your specialty—but only if the claim file reflects it.
Instead of: “Doctor cannot operate due to tremor.”
Use: “Loss of fine motor control prevents the performance of microsurgical tendon and nerve repairs required in hand surgery.”
Instead of: “Doctor cannot work long hours.”
Use: “Unable to maintain concentration and postural endurance necessary for
prolonged spinal fusions exceeding six hours.”
YOUR WORDS DEFINE YOUR OCCUPATION.
3. ICD-10 Codes as Specialty Evidence
ICD-10 codes can be persuasive evidence when tied directly to specialty limitations:
• Vascular surgeon: I73.9 + M62.81 Impossible to perform delicate bypass procedures
• Ophthalmologist: H53.2 Unsafe to perform microsurgical cataract or retinal procedures
• Interventional pain physician: G56.01 Loss of hand precision required for fluoroscopic needle placement
CODES TRANSFORM COMPLAINTS INTO EVIDENCE.
4. Best Practices for Physicians Filing Claims
• Draft your own job description — don’t rely solely on HR forms.
• Coordinate with treating providers to ensure specialty duties are clear.
• Use specialty terminology when describing restrictions.
• Document ICD-10 codes strategically.
• Anticipate insurer pushback and close off “transition” arguments with precision.
Thoughts
Filing a disability claim as a physician is about more than documenting illness — it’s about proving that your condition prevents you from performing the specialized duties of your occupation. A detailed job description, specialty-specific language, and precise ICD10 coding create a strong, defensible record that resists oversimplification and strengthens your claim.
The more precise and specialty-focused your documentation, the harder it is for an insurer to deny what is clear: you are no longer able to safely and effectively practice your chosen specialty.
Brian Patrick Bronson is an attorney with Quatrini Law Group. He concentrates his practice in the areas of Disability Insurance, ERISA, and Social Security Disability. Brian understands how long and short term disabilities insurances are governed by ERISA (the Employee Retirement Income Security Act of 1974), as well as how they can interact with and affect other benefits. Brian can be reached at (724) 552-2755 or bbronson@qrlegal.com.

When scientific debate becomes political theater, physicians face a difficult choice: remain silent and allow misinformation to grow—or speak out to set the record straight.
Two members of the Allegheny County Medical Society, Dr. Devon Ramaeker and Dr. Michael Aziz, both AHN Physicians, recently stepped forward to do just that, offering calm, evidence-based commentary amid national confusion surrounding new federal statements linking acetaminophen (Tylenol) use in pregnancy to autism.
A Physician’s Voice Amid Uncertainty
In a Tribune-Review article exploring shifting trust in national health authorities, Dr. Ramaeker, Division Director of Maternal-Fetal Medicine at Allegheny Health Network’s Women’s Institute, described the tension many clinicians feel when public guidance becomes politicized. “When the guidance feels inconsistent, physicians turn inward,” she said. “Patients need to rely on their medical providers to make informed decisions for them, in conjunction with them.”
She also underscored the danger of oversimplifying complex conditions like autism:
“We know that autism is likely a very complex diagnosis that has a lot of potential reasons it may occur. Simplifying it down to a single cause, risk factor, or exposure is oversimplifying the diagnosis.”
When President Trump warned pregnant women to “fight like hell” not to take Tylenol, Dr. Ramaeker countered with science, reminding readers of what every obstetrician knows:
By: Dr. Devon Ramaeker and Dr. Michael Aziz
untreated fever in early pregnancy carries real risk. “Fever itself is not a benign condition, especially in the first trimester—it can increase the risk of birth defects,” she told the Post-Gazette. Her message was clear: patients deserve accurate, measured advice, not fear-driven directives.
Science, Not Sound Bites
Dr. Aziz, a maternal-fetal medicine specialist with Allegheny Health Network, reinforced that message in interviews with CBS Pittsburgh, WTAE, and the Observer-Reporter. He pointed out that the administration’s announcement was not accompanied by any new data and emphasized the findings of a recent JAMA study involving more than 2 million children, which showed no association between prenatal acetaminophen use and autism.
“Just to clarify, there was no new scientific information that came out of the press conference,” said Dr. Aziz. “The JAMA study is the highest-quality study available—and the best study available.”
He urged that policy announcements remain rooted in established evidence and the consensus of expert organizations such as the American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM)—both of which reaffirmed that acetaminophen remains safe for use in pregnancy when indicated.
Advocacy Through Clarity
Together, Drs. Ramaeker and Aziz exemplify how physician advocacy extends beyond the exam room. Advocacy is not only about legislation,
it’s about leadership in public dialogue, where physicians’ voices can help restore reason when politics clouds science.
Their work underscores that credibility in medicine depends on intellectual honesty, humility, and the willingness to engage. As Dr. Ramaeker noted, this is a “confusing time” for patients—and that makes clear communication more important than ever.
At the Allegheny County Medical Society, we applaud our members for serving as trusted messengers and advocates for evidence-based care. When science grows cloudy, physicians must be the ones to speak clearly—for their patients, their profession, and the truth.
Dr. Devon M. Ramaeker, MD is Division Director of Maternal-Fetal Medicine at Allegheny Health Network’s Women’s Institute and a member of the Allegheny County Medical Society, as well as an elected ACMS Delegate. Her work focuses on complex pregnancies, public health communication, and improving trust in women’s healthcare.
Dr. Michael M. Aziz, MD, MPH, FACOG is Director of Fetal Echocardiography at Allegheny Perinatal Associates and serves as a member of the ACMS Board of Directors and Chair of the ACMS Delegation to the Pennsylvania Medical Society. He is an advocate for organized medicine, maternal health policy, and evidence-based physician communication.

Dr. Kanel attends National Conference
On behalf of our membership, ACMS President Dr. Keith T. Kanel attended the 2025 American Board of Medical Specialties Annual Conference, held September 17-19 at The Westin Pittsburgh. ABMS is the national convener of the 24 organizations which impart “board-certified” status on over 1 million physicians in the United States, with members including the American Board of Internal Medicine, American Board of Surgery, American Board of Family Practice, American Board of Dermatology, etc.
The theme of the 2025 conference was “Transforming Certification for Better Care”. Specialty boards came together to share strategies for updating certification standards in a rapidly changing world, touching on subjects ranging from continuing medical education to physician wellness.


After decades of dedicated service to physicians and healthcare providers, Michael Cassidy, Esq. has announced his retirement from the practice of law, effective October 31, 2025.
Mike has long been a trusted friend and advisor to the Allegheny County Medical Society, serving as legal counsel and guest of the ACMS Board of Directors for many years. His deep knowledge, thoughtful counsel, and unwavering commitment to the medical profession have left a lasting mark on our organization and the greater healthcare community.
As he transitions into retirement, Mike has worked closely with Adam Appleberry, Esq., an experienced healthcare attorney who will continue serving ACMS and its members beginning November 1, 2025. Adam
advises healthcare professionals on practice formation, employment contracts, regulatory compliance, acquisitions, and more, bringing both legal insight and real-world business experience to his work.
The ACMS extends its heartfelt gratitude to Mike for his many years of partnership and wise counsel, and we wish him all the best in his welldeserved retirement.
PAMED
Congratulations again to our 2025 Top Physicians Under 40 honorees! Several awardees from Allegheny County were recognized at a special ceremony with PAMED leadership on September 27 at DiSalvo’s Station in Latrobe. The Allegheny County Medical Society looks forward to celebrating these outstanding young physicians once again at our Distinguished Awards Program on November 13 at Acrisure Stadium.

ACMS Remembrance
David A. Blandino, MD : February 22, 1952 - September 30, 2025
The Allegheny County Medical Society (ACMS) extends its deepest condolences on the passing of Dr. David A. Blandino, a longtime member of ACMS and the Pennsylvania Medical Society (PAMED), who dedicated many years to advancing medicine and improving patient care in Western Pennsylvania. A former Chair of the Allegheny Health Network Board of Directors and recipient of the 2017 ACMS Nathaniel Bedford Primary Care Award, Dr. Blandino was known for his compassion, integrity, and unwavering commitment to the community he served. His leadership and example leave a lasting legacy within organized medicine and the broader Pittsburgh healthcare community.
ACMS President Dr. Keith Kanel noted:
“Dave Blandino was a role model for a generation of physician leaders. He showed us that there is brilliance in a well-timed smile or thoughtful word, as powerful in the boardroom as it is sitting across from a patient. He was one of a kind.”

5, 1937 - September 24, 2025
The Allegheny County Medical Society extends its condolences on the passing of Dr. Milton “Mickey” Henry Black, a devoted physician and ACMS/PAMED member for 37 years. A proud graduate of the University of Pittsburgh School of Medicine, Dr. Black dedicated his career to anesthesiology, occupational medicine, and medical education— serving at Children’s Hospital, West
Penn Hospital, and later with U.S. Steel and the U.S. Departments of Energy and Labor. A U.S. Army veteran and Bronze Star recipient, he was known for his intellect, compassion, and lifelong commitment to patient care. He is survived by his wife, Dr. Judith “Judy” Black, also a long-standing ACMS member, with whom he shared a deep dedication to the medical profession and to improving the health of the Pittsburgh community.
John Byrd, MD
Shea Ford, MD
Brionna Matt, DO
William Parks, MD
Kamal Pathak, MD
Venkata Tammana, MD
Vladimir Valakh, MD
Mofe Adeosun, MD
Sandra Alhaj, MD
Sara Chadwick, MD
Shalini Khatri, MD
Ria Mehta, MD
Sadaf Sanaullah, MD
Najya Williams, MD
Yuhua Xue, MD
Shlomo Bear
Dongwon Lee
Jamal Maloney
Yash Raka
Sarah Siddiqui
By: Melanie Mayer - ACMS/ACIC Administrator

On Wednesday, November 5, 2025, the Allegheny County Immunization Coalition (ACIC) convenes its 20th Annual Immunization Conference at the Regional Learning Alliance in Cranberry Township - a milestone year that also recognizes the 70th anniversary of Pittsburgh’s polio-vaccine breakthrough.
This full-day program brings together clinicians, public health professionals, school health leaders, pharmacists, and community partners to dig into the toughest current challenges in vaccination and vaccine confidence. The expert lineup features keynote

speaker Dr. Peter Salk on vaccine legacy and public trust, alongside sessions spanning emerging pathogens, ethics, behavioral science, and school vaccination strategy—plus a crosssector panel on building trust.
Participants can earn up to 6.25 hours of CME, CNE, CPE, and CE. This activity is planned and implemented by the University of Pittsburgh and ACIC; Pitt is jointly accredited by ACCME, ACPE, and ANCC to provide continuing education for the health care team. Credit is available for physicians (AMA PRA Category 1 Credit™), nurses, pharmacists, and social workers, with certificates of attendance provided for other professionals.
General registration is $50; complimentary student registration is available with valid student ID. Advance registration is required and closes October 30.
This year’s gathering also reflects the strengthened partnership between ACMS and ACIC—joining forces to expand vaccine education, outreach, and timely programming across Allegheny County and the region.
Whether you work in clinical care, pharmacies, schools, community health, or local government, this conference is designed to deliver practical tools, fresh evidence, and new partnerships you can put to
work immediately—while celebrating Pittsburgh’s enduring contributions to immunization. For the full agenda and speaker lineup, visit ACIC’s conference page; then secure your spot before registration closes.
ACMS Members receive a 30% discount on registration with code ACMS30.












• Compliance
• Reimbursement
• Mergers & Acquisitions
• Peer Review and Credentialing for Physicians
• Employment Contracts and Restrictive Covenants
• Tax & Employment Benefits For additional information contact any of the following attorneys at (412) 566-1212
• Mike Cassidy - Compliance; Contracts, Peer Review, Stark/AKS
• Jeremy Farrell - Labor & Employment and Commercial Litigation
• Adam Appleberry - Compliance, Credentialing, Reimbursement, and Physician Contracts
• Jerry Russo - Criminal Defense and Investigations
• Paul Welk - Mergers & Acquisitions







By: Devon Hess,
Sodium-glucose cotransporter 2 inhibitors (SGLT2i) reduce the kidney reabsorption of glucose and sodium which in turn helps with improved glycemic control, helps lower both pre-and afterload of the heart, and downregulate sympathetic activity.1 Therefore, the SGLT2i class is quite multipurpose in nature, with applications for type 2 diabetes mellitus (T2DM), chronic kidney disease (CKD), and heart failure (HF). The 2022 American Heart Association, American College of Cardiology, and Heart Failure Society of America Guideline for the Management of Heart Failure clinical practice guidelines include SGLT2i as an essential medication class in guideline-directed medical therapy (GDMT) to reduce hospitalizations for HF (HHF) in patients with HF with a reduced ejection fraction (HFrEF), HF with a mildly reduced ejection fracture (HFmrEF) and HF with a preserved ejection fracture (HFpEF).
There are currently six SGLT2i approved by the Food and Drug Administration (FDA) in the USA.1 While canagliflozin (Invokana), bexagliflozin (Brenzavvy) and ertugliflozin (Steglatro) exist, this article will focus on the two most widely studied and clinically proven SGLT2i, empagliflozin (Jardiance) and dapagliflozin (Farxiga), and one of the newest SGLT2i, sotagliflozin (Inpefa). Empagliflozin and dapagliflozin were initially approved for use by the FDA in 2014 to improve glycemic control in adult patients with T2DM.2,3 Sotagliflozin was approved for use by the FDA more recently in 2023 to reduce the risk of cardiovascular (CV) death, HHF, and urgent HF visit in adults
with HF or T2DM or CKD or other CV risk factors.4 Besides being an SGLT2i, sotagliflozin has an additional inhibition of the sodium-glucose cotransporter 1 (SGLT1i) which leads to reduced intestinal absorption of glucose and sodium, further helping overall glycemic control. The mechanism of action of sotagliflozin for cardiovascular benefits has not been established yet. All three drugs are now indicated to reduce the risk of HHF, CV death, and urgent HF visits in patients with HF or patients with T2DM, CKD or other CV risk factors.4 Empagliflozin and dapagliflozin are also approved for glycemic control in adults and pediatric patients aged 10 years and older with T2DM and to slow progression of CKD.2, 3 All three drugs have been studied in placebo-controlled clinical trials. Empagliflozin has been studied in adults with T2DM, pediatric patients aged 10-17 years with T2DM, adults with HF, and adults with CKD.2 Dapagliflozin has been studied in clinical trials in patients with T2DM in the DECLARE trial, patients with HF in DAPA-HF and DELIVER trials and patients with CKD in DAPA-CKD trial.3 Sotagliflozin has been studied in SOLOIST-WHF and SCORED trials.4
Sotagliflozin, empagliflozin, and dapagliflozin have similar safety profiles. None of these three drugs carry any black box warnings. Due to the increased risk of diabetic ketoacidosis, drugs that inhibit SGLT2 are not recommended in patients with type 1 diabetes mellitus. In patients with T2DM, dapagliflozin is not recommended when the eGFR is less than 45 mL/min/1.73 m2 and
empagliflozin is not recommended when the eGFR is less than 30 mL/ min/1.73 m2.2, 3 In clinical trials, sotagliflozin was not initiated in patients with an eGFR of less than or equal to 25 mL/min/1.73 m2 or on dialysis and was discontinued if eGFR fell to less than 15 mL/min/1.73 m2. Sotagliflozin is also not recommended in patients with moderate or severe hepatic impairment.4 Additionally, dapagliflozin, empagliflozin, and sotagliflozin are not recommended in the second or third trimesters of pregnancy or during breastfeeding.2,3,4 Urinary tract infections were noted as an adverse reaction with incidence ≥ 5% for all the three drugs. Other adverse reactions with an incidence ≥ 5% for dapagliflozin and empagliflozin included female genital mycotic infections. Additionally, dapagliflozin has a labeled incidence of ≥ 5% of patients experiencing nasopharyngitis.3 Sotagliflozin demonstrated a ≥ 5% incidence of adverse reactions including volume depletion, diarrhea, and hypoglycemia.4
In the SOLOIST-WHF study for sotagliflozin, the primary endpoint was the rate of a composite of CV death, hospitalization for HF, and urgent HF visit. The study showed a 33% risk reduction in the primary composite endpoint of CV death, hospitalization for HF, and urgent HF visit (HR=0.67 (95% CI: 0.53, 0.85), p=0.001). The number needed to treat (NNT) to prevent one CV death, hospitalization for HF, and urgent HF visit was 4.4
In the EMPEROR-Preserved trial for empagliflozin, a randomized, double-blind, parallel-group, placebo-
controlled study for HFpEF population, the primary endpoint was time to first event of CV death or HHF. Patients without T2DM had a relative risk reduction (RRR) of 22% and absolute risk reduction (ARR) of 3.0%, while patients with T2DM had RRR of 21% and ARR of 3.5%. In the EMPA-KIDNEY trial for empagliflozin in patients with CKD without T2DM, the primary endpoint was composite of sustained decrease in eGFR of ≥40% from baseline, sustained decrease in eGFR to <10 mL/ min/1.73 m2, end stage kidney disease (the initiation of maintenance dialysis or receipt of a kidney transplant), or CV or renal death. The study showed the NNT was 28 to reduce the risk of kidney disease progression and CV death in a two-year span (HR = 0.72 (95% CI: 0.640.82), p<0.0001).2
In the DAPA-CKD trial for patients with CKD taking dapagliflozin, the NNT was 19 to avoid one composite of sustained ≥ 50% eGFR decline, end stage kidney disease, or cardiovascular/renal death. The relative risk ratio for the composite endpoint was 39% (HR 0.61 95 CI: 0.51-0.72). In the DAPA-HF trial for patient HF taking dapagliflozin, the NNT was 21 to avoid one event of CV death, HHF, or urgent HF visit. The relative risk ratio for the composite endpoint was 26% with a hazard ratio of 0.74 (95% CI: 0.65-0.85, p < 0.0001). In the DECLARE trial for patients with type 2 diabetes mellitus and multiple cardiovascular risk factors or established cardiovascular disease taking dapagliflozin, the relative risk reduction for HHF was 27% (HR 0.73, 95% CI: 0.61-0.88). Even though dapagliflozin was studied for major adverse cardiovascular events (MACE), which includes CV death, myocardial infarction, or ischemic stroke, it was not FDA approved for the indication for MACE (HR, 0.93; 95% CI, 0.84-1.03).3
Empagliflozin, dapagliflozin, and sotagliflozin are only available as brand name medications, which impacts the cost of these medications. Dapagliflozin is ~$582 for 30 tablets, but the manufacturer offers a co-pay
card to the commercially insured patients to pay as low as $0 per month. Empagliflozin is ~$653 for 30 tablets, but the manufacturer offers a copay card for commercially insured patients to pay as low as $10per month. Sotagliflozin is ~$739.44 for 30 tablets and the manufacturer only offers a voucher for their first 30-day supply to be free.5
All three medications are once daily medications. Empagliflozin and dapagliflozin can be taken with or without food.2,3 The difference is that sotagliflozin is recommended to take no more than one hour prior to the first meal of the day. The initial dose of empagliflozin is 10 mg and may be increased up to 25 mg for additional glycemic control.2 The initial dose of sotagliflozin is 200 mg and may be increased to 400 mg after two weeks of tolerating the medication.4 Dapagliflozin is dosed at 10 mg daily for patients with CKD or HF. For patients with T2DM, the initial dose of dapagliflozin is 5 mg and may increase to 10 mg after four weeks of tolerating the medication.3 All three SGLT2i are recommended to be held for three to four days prior to procedures, surgeries, and events that require fasting because they may cause hypoglycemia if the patient is not able to have nutrition for a prolonged period due to a procedure or surgery.2, 3, 4
Overall, empagliflozin, dapagliflozin, and sotagliflozin are all beneficial SGLT2i and indicated to reduce the risk of HHF, CV death, and urgent HF visits in patients with HF or patients with T2DM, CKD or other CV risk factors. However, empagliflozin and dapagliflozin have been around for more than a decade and have been studied in a robust population showing great benefit for more indications than sotagliflozin.4 On the contrary, sotagliflozin was only studied in patients with T2DM, and it has been on the market for less than five years, so there is limited long-term real-world data and insurance coverage may vary and be more limited than with other SGLT2i. Empagliflozin is the
only medication with MACE reduction benefit.2 Therefore, empagliflozin could be considered the winner of the SGLT2i showdown to reduce the risk of major cardiac events and benefits in HFrEF, HFpEF, T2DM, and CKD. However, at the end of the day, the “best” choice depends on numerous factors such as specific patient comorbidities, cost, insurance coverage, individual tolerability, and specific treatment goals.
The authors and reviewers have no conflicts of interest:
Dr. Devon Hess, PharmD, MBA is a PGY1 Pharmacy Resident at UPMC St. Margaret and first year Faculty Development Fellow served as an author and can be reached at hessd5@upmc.edu.
Dr. Noopur Doshi, MD is a Faculty Development Fellow at UPMC St. Margaret and Family Medicine Faculty at UPMC served as an author and can be reached at doshin2@upmc.edu.
Dr. Jason Fine, PharmD, BCPS is a PGY2 Pharmacy Resident in Geriatrics at UPMC St. Margaret and second year Faculty Development Fellow served as editor and mentor and can be reached at jtfine18@gmail.com.
Dr. Heather Sakely, PharmD, BCPS, BCGP, the Director of Clinical Pharmacy Services and Director of the PGY2 Geriatric Pharmacy Residency served as editor and mentor for this work and can be reached at sakelyh@upmc.edu.
References:
1. DynaMed. Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors for Diabetes Mellitus. EBSCO Information Services. Accessed November 11, 2024. https://www.dynamed.com/drug-review/ sodium-glucose-cotransporter-2-sglt2-inhibitorsfor-diabetes-mellitus-1
2. JARDIANCE® [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc. 2021.
3. FARXIGA® [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2014.
4. INPEFATM [package insert]. The Woodlands, TX: Lexicon Pharmaceuticals, Inc.; 2023.
5. Inpefa, Jardiance, Farxiga. GoodRx. Available at: https://www.goodrx.com/inpefa. Accessed November 10, 2024.
By: Nadine Popovich, Melanie Mayer, and Haley Thon
Allegheny County Immunization Coalition (ACIC) — 2025-2026 ChairJenny Bender, MPH, BSN, RN, CIC: The Allegheny County Immunization Coalition invites physicians and public health professionals to engage in two meaningful opportunities this month and next.
On November 5, ACIC will host its 20th Annual Conference at the Regional Learning Alliance. This year’s theme, “Uniting for Immunity,” centers on how vaccination strengthens public health, workforce resilience, and community trust. The agenda includes Dr. Peter Salk, sessions on ethics, behavioral science, school vaccination, and a panel on rebuilding trust. ACMS members receive 30% off registration with code ACMS30. Details: www.immunizeallegheny.org/acicconference-2025
On October 24–25, ACIC will host a vaccine education table at Mission of Mercy Pittsburgh, a free dental, vision, and hearing clinic at the David L. Lawrence Convention Center. This is a chance to connect directly with patients and families, answer questions, and represent the medical community in a high-impact setting. No clinical duties required. Any amount of time is welcome. Sign up: www. immunizeallegheny.org/acic-events
ACIC membership is free and open to anyone interested in public health. Learn more: www.immunizeallegheny. org.
Southwestern Pennsylvania Chapter (ACS-SWPA) — 2025 President – Richard Fortunato, DO, FACS: The American College of Surgeons – Southwestern
Pennsylvania Chapter hosted its Annual Resident Surgical Jeopardy Competition on Thursday, October 16, 2025, at Hyde Park Steakhouse on the North Shore. Resident teams came together to test their knowledge and competed in this exciting, fast-paced event. The evening was filled with energy, camaraderie, and enthusiasm as participants showcased their surgical expertise in a Jeopardy-style format. At the end of the night, the winning team split a $500 jackpot, celebrating their victory among peers and mentors.
For any questions or membership inquiries, please contact Haley Thon, Chapter Administrator, at 412-321-5030 x105 or hthon@acms.org
Pennsylvania Geriatric Society Western Division (PAGS-WD) — 2025 President - Heather Sakely, PharmD, BCPS, BCGP: Fall Program 2025
The Pennsylvania Geriatrics Society –Western Division invites you to the 2025 Fall Program and Business Meeting on Wednesday, October 29, 2025, from 5:30 to 8:30 p.m. at the PNC Champions Club at Acrisure Stadium. The evening will begin with the Society’s final business meeting of the year, followed by an engaging panel discussion titled “From Impact to Action: Understanding Shifts in Medicare and Medicaid for Pennsylvanians.” This timely program will feature expert panelists Alex Bardakh, MPP, CAE, PLC, Senior Director of Advocacy and Strategic Partnerships for the Post-Acute and Long-Term Care Medical Association (PALTmed); Howard Degenholtz, PhD, Professor in the Department of Health
Policy & Management at the University of Pittsburgh School of Public Health and the Center for Bioethics and Health Law; Chad Worz, PharmD, BCGP, Chief Executive of the American Society of Consultant Pharmacists and boardcertified geriatric pharmacist; and Rob Maher, BS, PharmD, President and Chief Operating Officer of the Pennsylvania Pharmacists Care Network, Administrative Pharmacist, and Assistant Professor of Pharmacy Practice at Duquesne University School of Pharmacy. Together, the panel will explore the implications of the July 2025 budget bill, which is reshaping Medicare, Medicaid, and healthcare funding across Pennsylvania. Topics will include changes in post-acute, longterm, and home health services; access to care in rural and aging communities; and provider pay and reimbursement. Don’t miss this opportunity to gain valuable insight into the evolving healthcare landscape and connect with colleagues across the region. To Register: https://pagswd.org/ event-6315015
2025 Geriatrics Teacher of the Year Award – Nominations Submission Deadline is December 15th
The Society is proud to announce that nominations are now being accepted for the 2025 Geriatrics Teacher of the Year Award. This prestigious annual honor recognizes two outstanding educators, one physician and one healthcare professional, who have shown exceptional commitment to advancing geriatrics education. Award recipients are individuals who have made a lasting impact on the training and development of future geriatric professionals and
have significantly contributed to the growth of geriatrics education across the healthcare continuum. Full details, including eligibility requirements, selection criteria, and the nomination form, are available on the Society’s website at Pennsylvania Geriatrics Society - WD - Teacher of the Year.
For any questions or to join the society, please contact Haley Thon, Chapter Administrator, at 412-321-5030 x105 or hthon@acms.org .
The Pittsburgh Ophthalmology Society (POS) — 2025 President - Laurie A. Roba, MD: Pittsburgh Ophthalmology Society: 2025-2026 Monthly Meeting Series Begins | October Monthly Meeting Highlights
The Pittsburgh Ophthalmology Society (POS) held its monthly meeting on October 9, welcoming guest speaker Jordan Deaner, MD, Uveitis and Vitreoretinal Surgery, Mid Atlantic Retina, Wills Eye Hospital; Assistant Professor of Ophthalmology, Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, PA.
Dr. Deaner, a widely published clinician-scientist, has authored numerous book chapters and peer-reviewed articles focused on vitreoretinal and ocular inflammatory diseases. An active member of the American Academy of Ophthalmology and the American Society of Retina Specialists, he has presented his research nationally and internationally, including at meetings of the American Uveitis Society, The Retina Society, and others.
During the session, Dr. Deaner delivered two engaging lectures — Post-Operative Macular Edema and The Case(s) for a Combined UveitisVitreoretinal Surgeon — followed by thoughtful dialogue during the question-and-answer discussion.
In addition, Haniah Zaheer, MD, a second-year ophthalmology resident at the University of Pittsburgh Department of Ophthalmology, presented a clinical case for review and commentary by Dr. Deaner.
The POS monthly series will continue November 6 with guest speaker Christopher Teng, MD, MBA, board certified cataract and glaucoma specialist. He is a Professor and Chair of the Department of Ophthalmology and Visual Sciences. He has lectured internationally and published extensively in peer-reviewed journals. His research on the Effect of a Tight Necktie on Intraocular Pressure was recognized by Doximity as one of the top 10 ophthalmology articles of all time. His clinical and research interests include the optic nerve complex, glaucoma and anterior segment surgery, microinvasive glaucoma techniques, and advancing ophthalmic education and inclusivity.
The Society thanks Ken Cheng, MD, for arranging Dr. Teng’s visit. Online
registration begins October 20. To register visit www.pghoph.org
Society Business Updates
Membership renewal notices will be emailed to members on November 4. Practice administrators for group practices that opt for consolidated billing will receive group invoices on November 1.
Member Acknowledgement
The Society also congratulates Donald Morris, DO, on his election as President of the Pennsylvania Academy of Ophthalmology (PAO). We extend our sincere appreciation to Dr. Morris and the many POS members who contribute actively to the PAO through their leadership roles. Their dedication and advocacy continue to advance the interests of our profession and the field of ophthalmology.

