
Allegheny County Medical Society

Allegheny County Medical Society
Editorial
• Out of the Past
Deval (Reshma) Paranjpe, MD, MBA, FACS
Editorial
• Samuel Wilson, James Flagg and the Birth of an American Icon
Richard H. Daffner, MD, FACR
ACMS News
• Specialty Group Updates
ACMS Staff: Nadine
Popovich, Eileen Taylor, and Melanie Mayer
Article
• The Rise & Fall of Done Global
Timothy Lesaca, MD
Article
• Sarcoma Awareness Month
Mark Goodman, MD
ACMS News
• HIPAA's Breach Notification Rule
Adam Appleberry, Esq. & Michael Cassidy, Esq.
Article
• Radium and Vanadium in Radium City
Mark Trombetta, MD and Thomas B. Julian, MD

ACMS News
• Investment Considerations for Physicians
Chris Pfanstiel
Materia Medica
• Bexagliflozin (Brenzavvy™)
Madeline Stanko, PharmD and Drake Meaney, PharmD, BCPS

2024
Executive Committee and Board of Directors
President
Raymond E. Pontzer, MD
President-elect
Keith T. Kanel, MD
Secretary
Kirsten D. Lin, MD
Treasurer
William F. Coppula, MD
Board Chair
Matthew B. Straka, MD
Directors
Term Expires 2024
Douglas F. Clough, MD
David J. Deitrick, DO
Jan B. Madison, MD
Raymond J. Pan, MD
G. Alan Yeasted, MD, FACP
Term Expires 2025
Anuradha Anand, MD
Amber Elway, DO
Mark A. Goodman, MD
Elizabeth Ungerman, MD, MS
Alexander Yu, MD
Term Expires 2026
Michael M. Aziz, MD, MPH, FACOG
Michael W. Best, MD
Richard B. Hoffmaster, MD
Micah A. Jacobs, MD, FIDSA
Jody Leonardo, MD
G. Alan Yeasted, MD, FACP
2024 Board Committees
Bylaws
Kirsten D. Lin, MD
Finance
William Coppula, MD
Nominating
Keith T. Kanel, MD
Women’s Committee
Anu Anand, MD & Tiffany DuMont, DO
Managing Editor
Sara C. Hussey, MBA, CAE ACMS Executive Director shussey@acms.org
Medical Editor
Deval (Reshma) Paranjpe, MD reshma_paranjpe@hotmail.com
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
Term Ending 2024
Richard Daffner, MD; Anthony Kovatch, MD; Andrea Witlin, DO, PhD
Term Ending 2025
Robert Howland, MD; John Williams, MD; Alexandra Johnston, DO; Charles Mount, MD
Executive Director
Sara Hussey shussey@acms.org
Vice President - Member and Association Services
Nadine M. Popovich npopovich@acms.org
Manager - Member and Association Services
Eileen Taylor etaylor@acms.org
Operations CoordinatorACMS & ACMS Foundation Melanie Mayer mmayer@acms.org
Part-Time Controller Elizabeth Yurkovich eyurkovich@acms.org
Bulletin Designer Victoria Gricks victoria@thecorcorancollective.com
EDITORIAL/ADVERTISING
OFFICES: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212; (412) 321-5030; fax (412) 321-5323.
USPS #072920. PUBLISHER: Allegheny County Medical Society at above address.
The Bulletin of the Allegheny County Medical Society is presented as a report in accordance with ACMS Bylaws.
The Bulletin of the Allegheny County Medical Society welcomes contributions from readers, physicians, medical students, members of allied professions, spouses, etc. Items may be letters, informal clinical reports, editorials, or articles. Contributions are received with the understanding that they are not under simultaneous consideration by another publication.
Issued the third Saturday of each month. Deadline for submission of copy is the SECOND Monday preceding publication date. Periodical postage paid at Pittsburgh, PA.
Bulletin of the Allegheny County Medical Society reserves the right to edit all reader contributions for brevity, clarity and length as well as to reject any subject material submitted.
The opinions expressed in the Editorials and other opinion pieces are those of the writer and do not necessarily reflect the official policy of the Allegheny County Medical Society, the institution with which the author is affiliated, or the opinion of the Editorial Board. Advertisements do not imply sponsorship by or endorsement of the ACMS, except where noted.
Publisher reserves the right to exclude any advertisement which in its opinion does not conform to the standards of the publication. The acceptance of advertising in this publication in no way constitutes approval or endorsement of products or services by the Allegheny County Medical Society of any company or its products.
Annual subscriptions: $60
Advertising rates and information available by calling (412) 321-5030 or online at www.acms.org.
COPYRIGHT 2024: ALLEGHENY COUNTY MEDICAL SOCIETY POSTMASTER—Send address changes to: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212. ISSN: 0098-3772

By: Deval (Reshma) Paranjpe, MD, MBA, FACS
Something incredible happened this weekend.
To properly tell the story, we must regress 20-odd years. I was part of a tight knit circle of friends in college—we were all bright, loving, silly, and each on our own was an odd sock. Together, we were a bunch of sock puppets putting on a daily comedy show together— morning, noon, and night in between classes, exams, lectures, and a cappella concerts. Life was fun. We couldn’t imagine not knowing each other, let alone not talking 20 years hence. Three of us would become physicians—an oncologist, a pulmonologist, and an ophthalmologist. One would become an actuary, one a high powered New York entertainment lawyer who moonlights as an improv comic, and one would become a published poet and academic who would rise to second in command of a well-known academic institution.
The earnest actuary was in love with the pulmonologist, but her parents objected. The comic lawyer and the sweet poet had been sweethearts since elementary school, but her parents objected. The oncologist and I were just best friends, sharing every pre-med high and low.
In time, we graduated. The lawyer broke the poet’s heart, and they never spoke again. The poet’s heart was so irretrievably broken that she cut contact with everyone from college and high school in order to insulate herself from memories of him. It was the stuff of cinema, or gothic novels, or tragic French love songs. We had been really good friends, and it hurt.
The actuary and his love also
eventually broke up under the strain; he moved to Manhattan and started a job at a company he loved; she moved abroad. The oncologist and I found different loci and foci in life. I was in his wedding and helped him choose the inscription for her ring, ending up closer to his wife than to him.
And then something terrible happened. The actuary, who was far more than that—he was quickwitted and brilliant, a physics major and trumpeter with a knee-slapping, deliciously wicked sense of humor and a huge and loving heart—told the few of us who remained in the circle a secret. He had active Hepatitis C, contracted from one of multiple childhood blood transfusions for hemolytic anemia. Hep C was incurable at that time. Peg-intron was on the horizon, and he was going to try it. I put on a brave face because he put on a brave face. I hugged him and encouraged him, but in my heart from that moment had already started grieving his loss. I felt like I’d been punched in the gut—we all did--but couldn’t show it to anyone, least of all him.
He did poorly on interferon, had a liver transplant, then a postop CVA, and passed at the age when the rest of our lives were just beginning. He was often sad, and somewhat bitter towards the end, and rightly so; it was all so completely unfair. He had battled and suffered so much already in so many ways since childhood, and then to have his bright light extinguished like this—it made no sense. The grief was overwhelming for all of us.
The poet resurfaced in all her sweetness when told about his death.
For a moment, we were all reunited in grief. She relayed a dream where she saw our friend renewed. “We are given to each other only for a season,” she noted, and then promptly disappeared as if to prove it. It was losing one more friend, in another way.
Amidst the daily grind of careers, families and differing priorities, the remainder of us grew apart and lost touch. Twenty years passed. The poet’s absence was a quiet undercurrent of sadness through the years, an unfinished story. A nagging part of me fretted if I had said or done something— or committed some act of omission—to cause her absence. She deliberately constructed her life to have no online trail, and I understood and respected that, hoping she would resurface one day. Every few years, she published a beautiful volume of poetry. I bought and read each one, hoping for clues as to how she was and perhaps to what had happened.
I had given up looking, but never entirely gave up hope that my dear friend the poet would come back from exile. Our other friend could not return from the dead; perhaps she could return from the ether. And then one afternoon last week on a whim, I searched LinkedIn and found her profile. I held my breath, and sent her a message.
To my great surprise, she responded immediately and like me, was overjoyed. A two-hour FaceTime call the next day melted away decades like a glorious, surreal time warp; she had barely changed. She is happily married to a man who adores her; all is finally going right in her life. We each remembered
and shared the most minute details — neither had forgotten anything. She gave me peace, saying I’d not done anything to drive her away. She made peace in her heart with her childhood sweetheart. COVID and a challenging job made her treasure good friendships. Most of all, I was filled with joy that she finally had the love, happiness and success that she deserved after being denied for so long.
There are many different joys in this life to help counteract what sometimes seems like an endless cavalcade of worries and sorrow. I am here to tell you that getting one of your closest friends back in full Technicolor with a happy ending after twenty years of radio silence is one of the most stunning and heartfelt joys I’ve ever experienced. They say that the close friends who knew you when you are still a teenager,
before you are fully formed and beaten down by the struggles of the world, are so precious—they alone really know the inner you. Cherish those friends in your life; if you are lucky enough to have them, you can provide each other with a form of eternal youth.
Keep your good friends close, and never give up on old friends—they can return to you.










By: Richard H. Daffner, MD, FACR
July fourth is celebrated as American Independence Day to commemorate the signing of the Declaration of Independence. The day is marked by cookouts, parades, fireworks, mattress sales, and many appearances of people dressed like Uncle Sam. Two men, Samuel Wilson, and James Montgomery Flagg, born a century apart, and mostly forgotten were responsible for the creation of an American Icon, “Uncle Sam”. Who were they and what did they do?
Samuel Wilson (1766 – 1854) (Fig. 1) was born in Menotomy, MA (now Arlington, MA). As a boy, his family moved to Mason, NH. In March 1781, he joined the Continental Army, where he was assigned to guard and care for cattle. His duties also involved slaughtering and packaging meat, an occupation that 31 years later would make him famous. His military service ended in October of that year with the surrender of Lord Cornwallis at Yorktown.

In 1789, at the age of 22, Samuel and his older brother Ebenezer, age 27, relocated to Troy, NY (my hometown), where they became successful business entrepreneurs by making bricks from the exceptional clay found in the city. Many of Troy’s historic buildings were made with Wilson’s bricks. In 1793 the brothers founded Ebenezer & Samuel Wilson, which was the Wilson brothers’ introduction to the profitable meat business. Their slaughterhouse was located close to the Hudson River and the brothers took advantage of their prime location by building a dock at the foot of what is now Ferry Street. Having access to the Hudson River enabled their business to prosper.
Sam Wilson’s role during the War of 1812 resulted in what he is most known for today. “An army”, as Napoleon Bonaparte is alleged to have said, “marches on its stomach.” As American troops gathered in camps for training and equipping, the demand for a supply of meat for them had significantly increased. Secretary of War William Eustis recruited Elbert Anderson Jr. of New York City to supply all the rations necessary for the American forces in New York and New Jersey. Anderson ran advertisements looking for suppliers to meet the daunting challenge. The firm of E & S Wilson secured a contract for 2,000 barrels of pork and 3,000 barrels of beef for one year. Sam Wilson was subsequently appointed meat inspector for the U.S. Army. His duties included checking freshness and packaging, and ensuring that the barrels were built and packed according to army specifications. Each barrel was marked
"E.A.-U.S.", indicating "Elbert AndersonUnited States". Most of Wilson's meat was shipped to a local camp of 6,000 troops, where soldiers from Troy who were acquainted with Samuel Wilson made an association between Wilson and the "U.S." stamp and said, “That’s the meat from ‘Uncle Sam’”. Over time, any army property marked U.S. also became linked with Wilson's name, and "Uncle Sam" became a figure of speech to represent the United States.
Sam Wilson died in 1854, at the age of 87 years. He is buried in Oakwood Cemetery in Troy (Fig. 2). Monuments mark his birthplace in Arlington, MA, and site of burial in Troy, NY, as well as a New Hampshire historical marker at his boyhood home in Mason, NH.
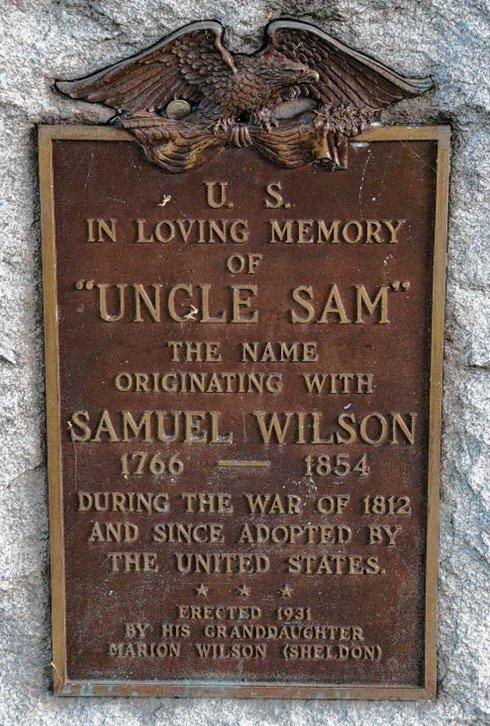
Wilson’s legacy is that he is officially recognized as “Uncle Sam”, because of an act of Congress in 1961: "Resolved by the Senate and the House of Representatives that the Congress salutes Uncle Sam Wilson of Troy, New York, as the progenitor of America's National Symbol of Uncle Sam."
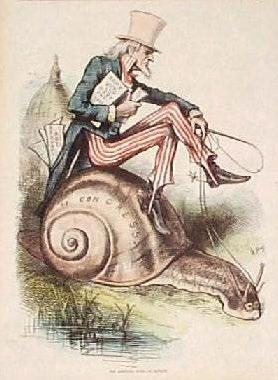
The original portrayal of Uncle Sam was a cartoon figure having long white hair, chin whiskers and dressed in a swallow-tailed coat, vest, tall hat, and striped trousers. It was first published in 1877 by political cartoonist Thomas Nast (1840 – 1902) (Fig 3), who also created the classic image we have of Santa Claus1
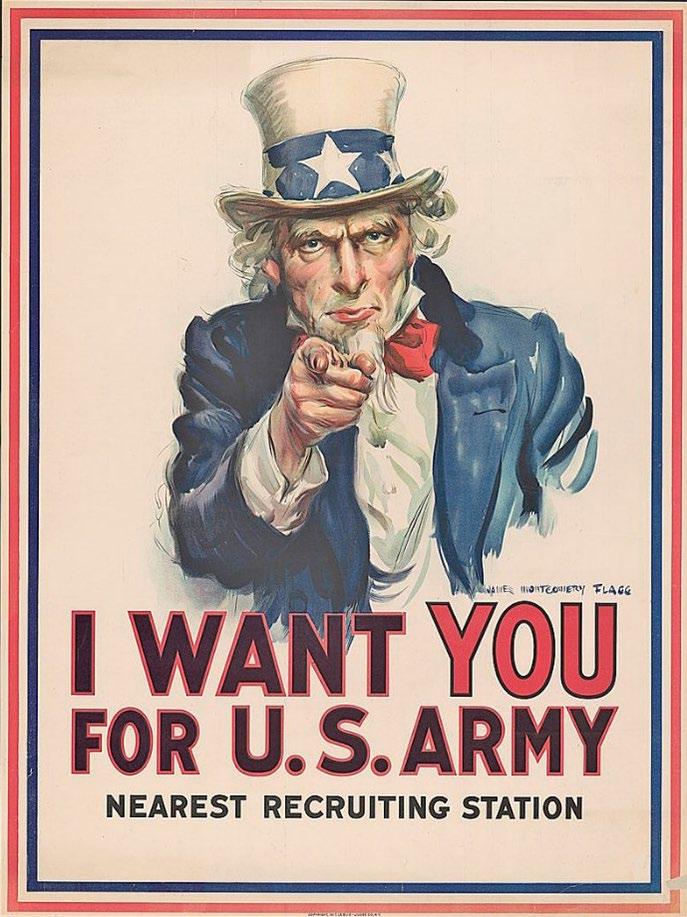
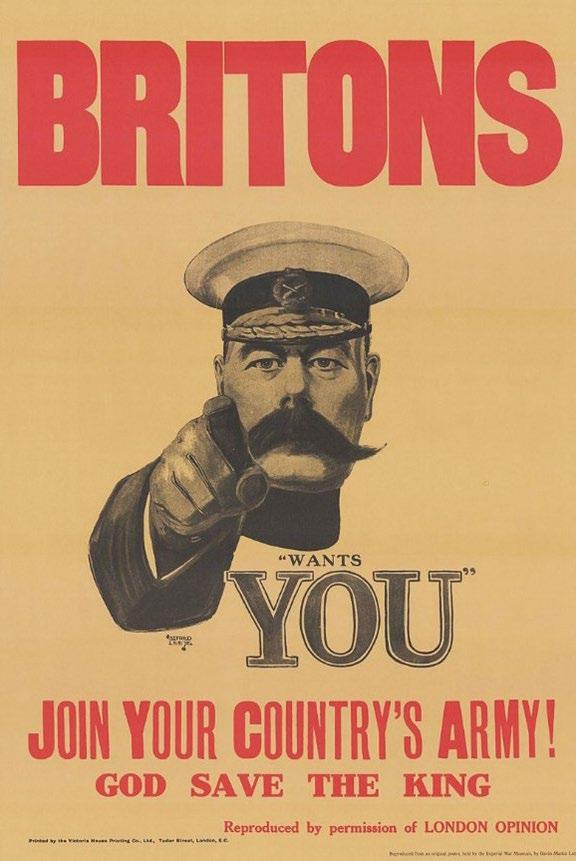
However, the iconic image of Uncle Sam was the work of American artist James Montgomery Flagg (1877 – 1960) (Fig. 4). Flagg, a native of New York, worked in media ranging from fine art painting to cartooning, but is best remembered for his political posters, particularly his 1917 poster of Uncle Sam created for United States Army recruitment during World War I (Fig. 5). Flagg used his own face (minus the whiskers) as the model for Uncle Sam’s face). He patterned his Uncle Sam poster after the 1914 British recruiting

poster by British artist Alfred Leete (1882 – 1933) showing Herbert Lord Kitchener (1850 – 1916), the Hero of Khartoum, in a similar pose (Fig. 6).
Legends have interesting beginnings. Sometimes those legends begin as the result of the work of men, who were otherwise unheralded. Have a happy and safe Fourth of July.
Reference
Daffner RH. You’re not Santa Claus. ACMS Bulletin Dec 2022, pp 12-14.
Dr. Daffner is a retired radiologist, who practiced at Allegheny General Hospital for over 30 years. He is an amateur historian.

By: Timothy Lesaca, MD — Child/Adolescent Psychiatrist at Southwestern Human Services
Statement from DEA Administrator Anne Milgram on Done Global Inc. - June 14, 2024
“The defendants in this case operated Done Global Inc., an online telehealth website that prescribed Adderall and other highly addictive medications to patients who bought a monthly subscription. The defendants allegedly preyed on Americans and put profits over patients by exploiting telemedicine rules that facilitated access to medications during the unprecedented COVID-19 public health emergency, instead of properly addressing medical needs, the defendants allegedly made millions of dollars by pushing addictive medications. In many cases, Done Global prescribed ADHD medications when they were not medically necessary. In 2022 the FDA issued a notice of shortages in prescription stimulants, including Adderall. Any diversion of Adderall and other prescription stimulant pills to persons who have no medical need only exacerbates this shortage and hurts any American with a legitimate medical need for these drugs. The DEA will continue to hold accountable anyone, including company executives, that uses telehealth platforms to put profit above patient safety.”
The recent charges against Done Global Inc.'s CEO and head doctor highlight critical issues within the burgeoning telehealth industry. Federal prosecutors allege a fraud scheme centered on providing "easy access" to Adderall and other stimulants. The Done Global Inc. case serves as a stark reminder of the potential pitfalls within the telehealth industry and might also help explain some of the supply chain issues regarding ADHD medications across the nation.
Done Global Inc., a virtual ADHD medication management company, faced investigations going back to September 2022 by the Drug Enforcement Administration. Authorities accuse Ruthia He, the founder, and David Brody, the clinical president, of fraud and distributing controlled substances without legitimate medical purpose. According to the Department of Justice, Done generated over $100 million by prescribing more than 40 million pills, often to individuals who didn't medically qualify for such treatment.
What does it say about a company when its priority shifts from patient safety to profit? The DOJ's indictment paints a troubling picture. Done allegedly used deceptive advertisements to attract individuals seeking stimulants, structured its platform to facilitate easy access to these drugs, and limited the information available to prescribers. Initial consultations lasted under 30 minutes, and an "auto-refill" function allowed for monthly prescription renewals with minimal oversight. Despite awareness of overdoses and deaths among its
members, the company continued its practices.
The case against Done reveals significant gaps in regulatory oversight. The DEA’s delayed response allowed potential abuses to continue unchecked for years. This reactive approach undermines trust in regulatory agencies and hampers efforts to ensure compliance within the telehealth industry. The temporary suspension of in-person consultation requirements during the COVID-19 pandemic, part of the Ryan Haight Act amendments, facilitated the growth of virtual behavioral health providers. However, it also created opportunities for exploitation, as seen in the Done case.
The fallout from Done’s practices extends beyond legal repercussions. The Centers for Disease Control and Prevention warns that disrupting Done’s services could impact up to 50,000 patients, exacerbating the existing shortage of ADHD medications like Adderall. This shortage, first noted by the FDA in 2022, has made it challenging for individuals with legitimate needs to access their medication. The case also casts a shadow over other digital health startups, particularly those involved in prescribing controlled substances. Retail pharmacies, wary of potential abuses, have already started rejecting prescriptions from digital providers or requiring in-person consultations. This increased scrutiny could hinder the accessibility and growth of legitimate telehealth services.
One of the most disturbing aspects of the Done case is the involvement of licensed physicians in potentially
widespread unethical practices. Physicians are bound by a code of ethics to "do no harm," yet the allegations suggest that medical professionals at Done were complicit in practices prioritizing profit over patient welfare. This complicity is not just a legal issue but a profound ethical breach that shakes the foundation of trust between patients and healthcare providers. As telehealth continues to evolve, we must learn from the Done case to regulate future similar practices. Ensuring that digital health platforms operate with integrity and prioritize patient safety will be key to their sustainable growth. Strengthening regulatory frameworks to adapt to the unique challenges of telehealth is critical. This includes updating laws to address new technologies and ensuring robust enforcement mechanisms. Developing patientcentric care models that emphasize comprehensive treatment and followup can improve outcomes and reduce the risk of misuse. Investing in research to understand the impacts of telehealth on patient care and outcomes can guide future policy decisions and improve service delivery.
Pharmacies play a crucial role in the prescription and distribution of medications. Major chains like CVS, Walgreens, and Walmart have become increasingly cautious about filling prescriptions from telehealth providers, especially for controlled
substances. Their policies often require in-person consultations to verify the legitimacy of prescriptions. This caution, while protective, also creates barriers for patients who rely on telehealth services. Balancing patient safety with accessibility remains a significant challenge.
Telehealth has transformed significantly over the past few decades. Initially limited to basic consultations via phone or video, advanced technologies now enable a broader range of services. The COVID-19 pandemic accelerated this evolution, as lockdowns and social distancing measures necessitated remote healthcare solutions. Companies like Done capitalized on this shift, offering convenient and quick access to medications and mental health services. The rapid growth of telehealth exposed vulnerabilities, particularly in the regulation of controlled substances. While virtual health services offer significant benefits, including increased accessibility and convenience, we must carefully regulate them to prevent exploitation and ensure patient safety. Any disregard for patient safety underscores a severe ethical lapse and raises questions about the responsibilities of telehealth providers in the digital age. Medical professionals involved in such schemes undermine the integrity of the medical field. Their actions not only endanger patients but also tarnish the reputation of telehealth services. The Done case serves as a
cautionary tale about the importance of maintaining ethical standards and vigilance in all forms of medical practice, including telehealth.
References
United States Department of Justice. (2024, June 13). Founder/CEO and Clinical President of Digital Health Company Arrested for $100M Adderall Distribution and Health Care Fraud Scheme. Department of Justice. Retrieved from https://www.justice.gov/opa/pr/founderceoand-clinical-president-digital-health-companyarrested-100m-adderall-distribution-and.
Tabachnick, C. (2024, June 18). Telehealth CEO charged in alleged $100 million scheme to provide Adderall. Yahoo News. Retrieved from https://news.yahoo.com/telehealth-ceo-chargedalleged-100-190416700.html.
Landi, H. (2024, June 13). Telehealth startup Done's CEO and clinical president arrested, charged with fraud. Fierce Healthcare. Retrieved from https://www.fiercehealthcare.com/healthtech/telehealth-startup-dones-ceo-and-clinicalpresident-arrested-charged-fraud.
Office of Public Affairs. (2024, June 13). Founder/ CEO and Clinical President of Digital Health Company Arrested for $100M Adderall Distribution and Health Care Fraud Scheme. United States Department of Justice. Retrieved from https:// www.justice.gov/opa/pr/founderceo-and-clinicalpresident-digital-health-company-arrested-100madderall-distribution
Centers for Disease Control and Prevention. (2024, June 20). Impact of Telehealth Fraud on ADHD Medication Supply. CDC. Retrieved from https://www.dea.gov/ documents/2024/2024-06/2024-06-14/statementdea-administrator-anne-milgram-done-global-inc

By: Mark Goodman, MD
Sarcoma education was one or two lectures during your pathology course. Hands on sarcoma education was at best hit or miss. Sarcoma awareness amongst medical professionals is not very high.
Sarcomas, malignant tumors of connective tissues, comprise 1% of all adult cancers and 18% of pediatric cancers. More than 150 sarcoma diagnoses exist, distributed over 17000 new cases each year. In the pediatric population the most common of these are osteosarcoma and Ewing’s sarcoma. Soft tissue sarcomas are more common in adults. The current survival rate for a patient with a high-grade bone sarcoma is 80% and those patients with a highgrade soft tissue sarcoma survive 65% of the time.
Over the past 40 years the above rates have shown the improvement of therapy from a 15% overall survival. New chemotherapeutic drugs have been slow to develop with tried-andtrue agents like Adriamycin, Cisplatin and methotrexate remaining the backbone of care. Immunotherapy has not proven very successful. New drug combination trials, some incorporating

novel agents are underway. Research funding is very limited due the low occurrence rate. Sarcomas are classified as “orphan disease”
Surgical excision remains a key factor in sarcoma treatment. Low grade lesions respond to wide excision with no need for adjunctive therapy. High grade lesions require a wide or radical margin of resection for local control and adjunctive systemic therapy for the risk of pulmonary metastases or recurrence. Surgical excision has gotten more precise and less destructive with the help of improved imaging. New intraoperative fluorescent dye injections may precisely outline the margins of the tumor. This promises to decrease the risk of local recurrence. Surgical reconstructive techniques have improved providing limb salvage options to over 90% of all sarcoma patients.
Sarcomas can occur at any age. In the pediatric population the 2nd decade of life is the greatest risk. For adults the 6th to 8th decades of life are the most likely times for presentation. The most common symptom is an enlarging mass, with or without pain. Night pain, which awakens the patient from sleep is a common complaint. Decreased activity and pain with activity are common findings. Tenderness about the soft tissue mass may be present. Weight loss is not often noted. Lymphatic spread is not a common event for most sarcomas. Pulmonary metastases are the greater risk. Except for families with Multiple Heritable Exostoses, there is no known genetic risk factor. A P53 genetic mutation may be a risk factor
for sarcoma growth. Environmental exposures may relate to sarcoma development, such as the ingestion of radium and the development of osteosarcoma.
Although rare, patients with sarcomas may present to any of us. Locations may vary from skull to toes. An awareness of risk will certainly facilitate early diagnosis and treatment. Pittsburgh is an internationally recognized hub for sarcoma research and treatment, so getting proper specialized care for a patient is easily done.
Pittsburgh Cure Sarcoma is growing every year, which is wonderful thing! But that growth requires people and their time. PCS is 100% a volunteer organization full of selfless humans working hard to make an impact. If you’ve been affected directly or indirectly by sarcoma, or just want to join the fight, we welcome you into our PCS family with open arms.
Visit: https://www. pittsburghcuresarcoma. org/ to learn about volunteer opportunities and events. The ACMS is a proud supporter of the annual PCS 5k Walk/Race.


The situation surrounding Change Healthcare’s ransomware attack that occurred in February has been a reminder of the sensitivity of PHI and just how diligent providers and practices must be in establishing appropriate safeguards to protect their patients’ data. By way of summary, in mid-February, Change Healthcare experienced a ransomware attack that impacted the PHI of millions of patients, resulting in chaos for providers nationwide, especially with accounts receivable and payment systems. As a result of this breach, there also stemmed a significant amount of confusion as to who is responsible for providing notification to the patients that were impacted as well as notification to the Department of Health and Human Services. Under the Breach Notification Rule, the covered entity is ultimately responsible for providing these notifications; however, given the size and complexity of Change Healthcare’s breach, these responsibilities became unclear.
In light of this complex case and related ambiguity regarding notification responsibilities, we thought it would be a perfect time to put together a summary of the Breach Notification Rule. Whether it’s a small breach where someone in your organization accidentally sent a patient’s contact information to the wrong individual or a large breach where your system has been hacked and all your patient records have potentially been exposed, the Department of Health and Human Services lays out clear guidance for your next steps.
By: Adam Appleberry, Esq. & Michael Cassidy, Esq.
Before diving into the required process following a breach, it may be helpful to discuss what is considered a breach in the first place.
Under the Breach Notification Rule, a breach has taken place when there is an unpermitted use or disclosure under the Privacy Rule that compromises the security or privacy of PHI. Whether or not a breach has occurred can be determined by a risk assessment that evaluates:
• the nature and extent of PHI involved;
• the unauthorized individual who used or gained access to the PHI;
• whether an unauthorized individual actually acquired or viewed the PHI; and
• the extent to which the covered entity or business associate reduced the PHI exposure risk.
Unless the covered entity can demonstrate that there is a low probability that the PHI has been compromised, any impermissible use or disclosure of PHI is presumed to have been a breach.
The rule does provide for three exceptions to this definition:
• If an employee or authorized individual unintentionally, but in good faith and within their scope of authority, accesses or uses the PHI;
• If the PHI is disclosed to an individual who is not authorized to access that particular individual’s PHI but is authorized to access PHI in general; or
• If the covered entity has a good faith belief that the unauthorized person to whom the PHI was
disclosed would have not been able to access or retain the information.
When a covered entity determines that a breach has occurred, the covered entity must provide notification to (1) the individual, (2) the Department of Health and Human Services, and (3) in some situations, the media.
Individual Notification
The individual must be notified without unreasonable delay but no later than 60 days following the discovery of the breach.
In the notification, the individual must be provided:
• a brief description of the breach;
• a description of the types of information that were involved in the breach;
• the steps the individual should take to protect themselves from potential harm;
• a description of what the covered entity is doing to investigate the breach; and
• contact information for the covered entity.
This notification must be provided in the form of first-class mail but can be sent via email if the individual has agreed to receive such notices electronically. In the event that the covered entity is unable to contact 10 or more individuals affected by the breach, the covered entity must substitute the individual notice by either posting the notice on its website for a minimum of 90 days or by providing the notice in the media where the affected individuals likely reside. In these instances, the covered entity must include a toll-free phone number that remains active for
at least 90 days where individuals can call to learn if their information was involved in the breach.
When a business associate is responsible for the breach, the covered entity remains the party responsible for providing notification to the individuals affected. In these situations, the business associate must notify the covered entity within 60 days.
Department of Health and Human Services Notification
The process for notifying the Secretary of the Department of Health and Human Services can be completed online on the HHS website (https:// ocrportal.hhs.gov/ocr/breach/wizard_ breach.jsf).
In breaches that affect 500 or more individuals, the Secretary must be notified without unreasonable delay
but no later than 60 days following the discovery of the breach.
In breaches that affect less than 500 individuals, the notification requirement only needs to occur annually but no later than 60 days after the end of the calendar year in which the breach is discovered.
The Department of Health and Human Services maintains a list on its website of recent HIPAA breach cases under investigation (https://ocrportal. hhs.gov/ocr/breach/breach_report.jsf).
Media Notification
In situations where 500 individuals or more are affected by a breach, the covered entity must provide notice to the prominent media outlets covering the region where the affected individuals likely reside. This notice can be provided in the form of a
press release, must include the same information as required for notifying the individuals, and must be provided without unreasonable delay but no later than 60 days following the discovery of the breach.
Conclusion
Navigating HIPAA compliance can be a confusing and burdensome task. If you’ve had a breach and are questioning what your next steps should be, or if you require guidance on safeguarding your patients’ data and aligning your practice’s procedures with HIPAA’s compliance standards, seeking the advice of a healthcare attorney is always a great place to start.


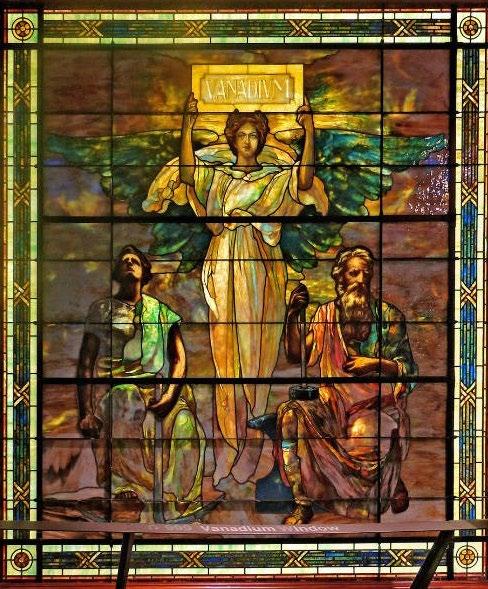
On the pages of this journal, we have previously described the importance of the Pittsburgh region and its delivery of the most precious quantity in the world at that time: one gram of radium to Madame Curie. The Standard Chemical Company, at its Canonsburg, Pa. location is where radium was extracted from carnotite which was mined then transferred from Colorado. The final processing occurred at the Vanadium Building, still located at Forbes and Meyran Avenues (later the Parkvale Savings building and now part of the University of Pittsburgh). A large and impressively beautiful stained-glass image of Freyja (aka Vanadis), Nordic god of beauty (Vanadis is the root of vanadium; named for the beautiful properties that vanadium imparts to structures) (Figure 1) was relocated from that site. This undertaking led to the opportunity for Madame Curie to continue her research. History denotes well that Madame Marie Curie was not only the first woman to win the Nobel Prize, but the first person to win two Nobel Prizes and the only person in history to win two Nobel Prizes in two different categories of science (Physics and Chemistry). She was also the first woman to be appointed as Professor at the University of Paris.
Pierre and Marie Curie discovered the first two radioactive substances identified by radioanalysis: polonium and (five months later) radium in 1898. Historically, polonium was named after Poland, the homeland of Mdme. Curie At that time, Poland was lost, having been divided by and incorporated into Russia, Austria, and Prussia in 1797. In
By: Mark Trombetta, MD & Thomas B. Julian, MD
the naming of polonium, the diminutive in size Marie Curie made a bold political statement to resurrect her beloved country. Triumphantly, this would occur during her lifetime on Armistice Day, November 11th, 1918 (now Veteran’s Day). Curie’s radium equipped “Petite Curies”, early versions of mobile x-ray and sterilization units, would be used to assist in the care of an estimated 1 million troops during World War I.
Following the discovery of radium, a rapid development of potential uses was spurred. The Standard Chemical Company, headquartered in Pittsburgh, began commercial production of radium in 1913, and this region quickly became the hotbed of American production. To ensure the project solvency, a demonstration of versatility in the use of radium would be necessary. World War I, the “Great War”, erupted and an immediate market developed. Radium was incorporated into gun sites, luminescent dials, naval and aeronautical vessel instrumentation, and compass illumination; all of which propelled the nascent industry. Standard Chemical Company rapidly achieved economic and political success. By the early 1920’s, half of the world’s radium was produced in Pittsburgh, creating America’s nuclear industry. Standard Chemical Company realized the need for standardization and calibration of radium and enlisted none other than Marie Curie to assay their radium. American standardization had begun. Almost concurrently, the extraction of radium from carnotite began in Canonsburg, Pa. Carnotite was mined in Colorado and shipped to
Canonsburg where the crude extraction process began. The final fractional crystallization would take place in the Vanadium Building and the extracted salts were stored in the rear of the vault. From there, radium was shipped all over the United States.
In 1921 Madame Curie would visit America to receive one gram of radium delivered to her by President Warren G. Harding through a grant presented on behalf of the Women and Girls of America. Radium was the most precious commodity on earth at the time. During her visit, Curie honored the workers at the Canonsburg site with a visit. She appreciated the difficult work of the men at the initial extraction site as she had done this same work in her Paris laboratory. The men were thrilled to see this world-famous scientist and to know that she so valued their work.
During her visit, William J. Holland, Director of the Carnegie Institute added a nickname to the city of Pittsburgh. Speaking in a ceremony to confer the honorary degree of Doctor of Laws on Marie Sklodowska Curie he stated: “We are in the habit of speaking of Pittsburgh as The Iron City. We sometimes call it The Steel City. It may also be justly called The Radium City.” The University of Pittsburgh concurrently conferred a similar degree on Professor Curie (a native of Poland) and a plaque was later commemorated on Allen Hall by the then Bishop of Krakow, Karol Wojtyla in 1969. Bishop Wojtyla would later become Roman Catholic Pope John Paul II (later Pope Saint John Paul II), who was instrumental in the collapse of Communism and the fall of the
Soviet Union. Bishop Wojtyla would also visit St. Stanislaus church in the Strip District in solidarity with the rich Polish culture in Pittsburgh. A kneeler used by Pope Saint John Paul II is a prized relic in the church. The Women’s Medical College of Pennsylvania (later merged with Hahnemann University into the Allegheny University of the Health Sciences) also conferred a similar degree on Professor Curie. This University now continues as Drexel University College of Medicine with Allegheny Health Network as its main clinical campus.
One of us (TBJ) was an invited speaker at a University of Paris meeting several years ago and visited the Institute Curie Hospital in Paris which is perhaps the most famous radiation clinic in the world. Attached to the Hospital is the original Curie Laboratory, now a museum. Visitation of the Curie Laboratory is a rare, limited event and reserved for very special persons. There the Curator is the final arbiter of who may visit. During the invited visit, the curator was asked If a visit was possible, and she initially declined. When she was informed by Julian’s colleague that the visitor was from Pittsburgh, the curator broke into fluent English and immediately agreed to the visitation and a personal tour was given! She well knew our local history.
Radium was widely used in watch dials, military gauges, as a fertilizer for plants, in foodstuffs, toothpaste, hair preparations and other applications until the 1960’s, when safety concerns negated its use. Commercially, radium is increasingly used in precise instruments such as optical clocks, industrial radiography, and other applications. Biologically, radium revolutionized cancer therapeutics early on, continuing to the present day.
Vanadium
By the end of the Great War, 50% of the Nation’s steel products and nearly all American vanadium was produced in Pittsburgh. The Flannery Bolt Company (the Flannery Brothers owned Standard
Chemical) developed the Tate Flexible Staybolt, which was widely adopted for steam locomotives. The company noted a possibility of improving the bolt, consulting with European engineers who suggested the incorporation of vanadium to greatly increase strength and lessen metal fatigue. Near the same time, automobile magnate, Henry Ford, was seeking a stronger and lighter metal for his Model “T” automobile. The United Steel Company was opened in Canton, Ohio and soon 50% of the steel used in the Model T was vanadium steel. Over the next few years, more than 15 million Model T automobiles were constructed and sold.
In 1911, vanadium steel from the company was used in the construction of the Panama Canal. Vanadium, the “Miracle Alloy” was supplied by United Steel for this project as well; more than 1000 tons in all. Today, vanadium is still used to strengthen steel, reducing wear and retarding corrosion. American vanadium is used in everything from surgical instruments to mechanic tools, jet engines and seamless tubing, energy storage, superconducting magnet construction, and lining for nuclear fusion reactors. Biologically, naturally occurring vanadium is essential in both plant and animal life.
In 1954, President Dwight D. Eisenhower authorized Admiral Hyman Rickover to construct a nuclear reactor power plant. A site on the Ohio River at Shippingport, Pa was identified, and, in 1957, the world’s first commercial reactor dedicated solely to peacetime usage reached full operational status at a cost of more than 70 million dollars. Over 2 billion Kilowatts of power were produced at the Shippingport Atomic Power Station until its decommissioning in 1982. Two additional nuclear reactors have replaced the original and continue producing power to this day under the name of the Beaver Valley Nuclear Generating Stations 1 and 2.
In 1937, the Westinghouse Atom
Smasher, the world’s first Van de Graaff accelerator went into operation and the era of non-military nuclear radiation research was born. These generators accelerate particles to very high clinically useful energy levels and were used for cancer therapy. They have largely been replaced by linear accelerators and proton units, although they are still essential in physics research today, especially in nuclear medicine.
Reference
1. Trombetta M: Mdme Curie: “Brilliant Scientist and her Pittsburgh Connection” Invited Editorial for the Allegheny County Medical Society Bulletin. March 2018.
2. Radium City: 1987 Documentary directed by Marie Becker Rossiter: Carole Langer Productions
3. Radium City: Joel Lubenau and Edward R Landa; online publication through the Senator John Heinz History Center
4. https://www.tour.pitt.edu/tour/ allen-hall
5. Trombetta M: Madame Maria Sklodowska Curie: Brilliant scientist, humanitarian, humble hero: Poland’s gift to the world. J Contemp Brachytherapy 2014: 6, 3:297299. milgram-done-globalinc

By: Chris Pfanstiel
Axias Wealth Advisors is a financial planning group who specializes in planning for physicians. Clients can engage with Axias in the traditional manner whereby they advise then execute upon recommendations or choose to pay a monthly subscription fee to receive their advice but not pay advisory fees nor commissions. With their deep understanding of financial planning for physicians, clients appreciate strategies and an understanding of student loans, physician-specific insurance planning, tax-sensitive investing, and more.
Physicians might consider using Separately Managed Accounts, “SMAs,” particularly when investing taxable funds. SMAs can be thought of as deconstructed mutual funds. Separate management allows direct ownership of stock or bond positions and avoids “intrafund trading,” and the corresponding taxable distribution. Additional considerations include:
SMAs may offer greater tax efficiency compared to mutual funds. Because investors have more control over individualized portfolios, they can implement tax-saving strategies such as tax-loss harvesting.
Transparency
Since each account holds stocks directly, investors can see each security and transaction clearly.
SMAs offer greater customization compared to mutual funds. Investors in SMAs can tailor their portfolio to their specific needs, preferences, and
Direct ownership can provide investors with greater control over their investments and potentially lower costs, as there are less layers between the investor and their holdings.
SMAs can accommodate a wide range of investment strategies, including those tailored to specific investment goals or risk preferences.
MEGA ROTH – TEAM HEALTH, AHN, UPMC, AND MORE
Retirement funds inside of a Roth tax shelter can be the most beneficial. Contributions to Roth accounts are post-tax dollars. Growth is tax-deferred, and withdrawals (at retirement age) are tax-free. Typically, you can utilize Roth treatment via IRAs or 401(k)s, etc.. In 2024, Roth IRA contribution limits are $7,000/year ($8,000/year if age 50 or older). In 2024, Roth 401(k) contribution limits are $23,000/year ($30,500/year if age 50 or older). There are income restrictions applied to eligibility to directly fund Roth IRAs, but families over those limits can ask professionals about Back Door Roth IRAs.
To retire comfortably, many physicians need to invest more than these limits might allow. Mega Roth can expand these limits. This strategy utilizes convertibility of post-tax qualified funds and increased contribution limits to capture significant Roth funding opportunities. The availability of this strategy is dictated by the governing plan document of your company’s retirement plan. For example, plans at AHN, Team Health, UPMC, and many other systems enable this strategy.
While the tax code limits payroll deferrals to $23,000 per employee, there’s a lesser-known limit of $69,000 (in 2024) for total contributions made by or on behalf of employees. The $69,000 includes employee pre-tax or Roth deferrals of $23,000, company contributions, and amounts physicians might contribute via post tax deferrals. If a physician contributed $23,000 (pre-tax or Roth) and received $10,000 in contributions from their hospital, there’d be room for an additional $36,000 of post-tax contributions. If a physician elects to contribute post-tax funds up to $36,000 they could also elect an in-plan Roth Conversion similar to a Back Door Roth IRA. It’s important to act quickly or to convert during down markets to reduce tax on growth of post-tax assets..
Effectively using Mega Roth allows for additional qualified deposits and lesser tax burdens in retirement. Each plan might follow different protocols, so it’s important to consult professionals. For example, Team Health allows for an automatic conversion of each post tax contribution with each pay throughout the year while UPMC allows two conversions annually.
Axias is happy to be a resource to you as you approach these complex decisions in your financial planning.
step by step we make the complex simple…. Securities and investment advisory services offered through Hornor, Townsend & Kent, LLC (HTK), Registered Investment Adviser, Member FINRA/ SIPC, 600 Dresher Road, Horsham, PA 19044. 800873-7637, www.htk.com. HTK is a wholly owned subsidiary of The Penn Mutual Life Insurance Company. Axias Wealth Advisors is unaffiliated with HTK. 6744062RG_Jun26

By: Nadine Popovich, Eileen Taylor and Melanie Mayer
Allegheny County Immunization Coalition (ACIC) — 2024 Chair - Patrick Hussey, PharmD, MBA: The Allegheny County Immunization Coalition (ACIC) is pleased to announce that Pat Hussey, MBA, PharmD, will serve as the Chair for the 2024-2025 term. The coalition also welcomes all new board members and extends a big thank you to those rolling off. The coalition recently hosted its June general membership meeting, which saw record attendance both in person and virtually. Highlights included a compelling presentation by Samantha Faulds and Dr. Diego Chaves-Gnecco on "Increasing HPV Vaccination Rates in Pediatric Primary Care," leaving attendees motivated and well-informed about current public health challenges and solutions.
Looking ahead, ACIC invites members to participate in a volunteer opportunity at the upcoming Beverly’s Babies Baldwin Baby Shower on July 24, 2024. The event will feature a vaccination education table where volunteers can contribute to community health initiatives. ACIC membership remains free and open to all healthcare professionals interested in immunization and public health, supported by grant funding to ensure inclusivity and resource accessibility. Mark your calendars for the next General Membership Meeting, scheduled for September 22, 2024. Additionally, ACIC is gearing up for its 19th Annual Conference, "Guardians of Public Health: Strengthening Vaccine Confidence," slated for November 8, 2024, at the Regional Learning Alliance in Cranberry, PA. This event promises valuable insights and
networking opportunities for healthcare professionals committed to enhancing vaccine confidence and public health outcomes.
For more details on ACIC activities, membership benefits, and upcoming events, visit www.ImmunizeAllegheny. org. Whether attending meetings in person or via Zoom, or volunteering at local outreach events, ACIC encourages all interested individuals to join in its mission of promoting immunization and public health in Allegheny County and beyond.
American College of Surgeons
Southwestern Pennsylvania Chapter (ACS-SWPA) — 2024 President –Richard Fortunato, DO, FACS: Mark your calendars for an exciting and educational event! Our annual Resident Surgical Jeopardy competition and dinner will take place on Wednesday, October 2nd at Eddie Merlots. This

event promises to be a fun and competitive way to test your surgical knowledge and network with fellow surgeons. More details will be shared soon. Stay connected and informed by visiting our website www.acs-swpa. org for the latest news and events. Please contact Eileen Taylor, Chapter Administrator, with any questions or to become a member – 412-321-5030 x105 or etaylor@acms.org.
Pennsylvania Geriatric Society Western Division (PAGS-WD) — 2024 President - Heather Sakely, PharmD, BCPS, BCGP: We are pleased to bring you the latest updates from the Pennsylvania Geriatrics Society Western Division. Our ongoing efforts to provide outstanding educational and networking opportunities for geriatric healthcare professionals continue to thrive. We are excited to announce our Fall Program, scheduled for Wednesday, November 6th. This event is an excellent opportunity to gain insights into the latest advancements in geriatric care and connect with colleagues dedicated to improving the health and well-being of older adults. Stay tuned for more details. Be sure to visit our website www. pagswd.org regularly for the latest news and updates on upcoming events. Please contact Eileen Taylor, Chapter Administrator, with any questions or to join the society – 412-321-5030 x105 or etaylor@acms.org.
The Pittsburgh Ophthalmology Society (POS) — 2024 PresidentPamela P. Rath, MD: The Pittsburgh Ophthalmology Society (POS), led by Pamela P. Rath, MD, President, along with the POS Board of Directors, is
pleased to announce the schedule for the 2024-2025 Monthly Meeting Series and Annual Meeting dates. A total of six meetings are scheduled, starting in September and concluding with the Annual Meeting on March 21, 2025. Last year’s monthly meetings averaged 62 registrants, and similar attendance is anticipated this year.
The Society will host monthly meetings as in-person events at the PNC Champions Club at Acrisure Stadium (100 Art Rooney Ave, Pittsburgh, PA 15212), centrally located on the North Side with nearby parking options. Check POS website for details.
Each meeting will commence with registration at 4:00 pm, followed by the first lecture at 4:30 pm. The agenda includes a Resident Case Presentation featuring second-year residents from the University of Pittsburgh Department of Ophthalmology: Oliver Beale, MD; Amani Davis, MD; Aidan Dmitriev, MD; Crystal Lee, MD; and Sami Melachuri, MD.
Members will receive registration details one month prior to each meeting. Registration, managed exclusively online, is required (no walk-ins, please). Please be aware a Cancellation and NoShow policy is in place.
For more information, visit the POS website (www.pghoph.org) or contact Nadine Popovich, Administrator.
The 2024-2025 monthly meetings are scheduled as follows: September 12, 2024; November 7, 2024; December 12, 2024; January 9, 2025; and February 13, 2025. Please note that there will be no meeting in October due to the American Academy of Ophthalmology Meeting scheduled for October 18-21, 2024, in Chicago, IL.
The Society is honored to host distinguished guest faculty:
• September 12: Lisa Feulner, MD, PhD, Chief Medical Officer and founder of Advanced Eye Care & Aesthetics, Hartford, CT.
• November 7: Christopher C. Glisson, DO, MS, FAAN, Medical Director, Warren Clinic Neurology | St. Francis Health System | Tulsa, OK.
• December 12: Lauren S. Blieden, MD, Associate Professor, Ophthalmology-Departmental Glaucoma | Assistant Clinical Professor, Alkek Eye Center | Cullen Eye Institute Baylor College of Medicine | Houston, TX.
• January 9: Guest speaker to be announced (check website for updates).
• February 13: Tarek Hassan, MD, Professor of Ophthalmology at Oakland University William Beaumont School of Medicine | Senior Partner and previous Director, Vitreoretinal Fellows Training Program at Associated Retinal Consultants; President, Foundation of the American Society of Retina Specialists; Immediate Past President, American Society of Retina Specialists (ASRS) Royal Oak, MI.
Contact Nadine Popovich to confirm your membership status or to inquire about an upcoming program.
By: Madeline Stanko, PharmD and Drake Meaney, PharmD, BCPS
Introduction
Bexagliflozin is a new Sodiumglucose cotransporter-2 inhibitor (SGLT2i) that is FDA-approved for type 2 diabetes mellitus (T2DM).1 SGLT2i are growing in popularity and usage in the treatment of type 2 diabetes and heart failure. Bexagliflozin is one of the two newest SGLT2i made available on the market in 2023 along with sotagliflozin (Inpefa), the first dual SGLT1/2i.2 These medications enter an already crowded SGLT2i market that includes the likes of dapagliflozin (Farxiga) and empagliflozin (Jardiance), among a few other agents. Unlike every other SGLT2i on the market, no dose titration is necessary for bexagliflozin, as all patients can be maintained on 20 mg daily, which is helpful when frequent monitoring may be more difficult. Another unique feature of bexagliflozin is that it has the potential for greater patient cost savings as compared to current options on the SGLT2i market.
The safety evaluation of bexagliflozin included risk of long-term or serious side effects caused by the drug. In one randomized, double-blind, placebocontrolled trial, using bexagliflozin as an adjunct to metformin, the percentage of patients with at least one treatment-emergent adverse events (TEAE) was 44.8% overall, 42.4% in the bexagliflozin group and 47.2% in the placebo group.3 The most commonly reported TEAEs were nasopharyngitis, UTI and inadequately controlled diabetes mellitus.3 Overall, less subjects in the bexagliflozin arm experienced serious adverse events. It would be necessary to have a head-to-head trial
of bexagliflozin and other SGLT2i to comment further on number of adverse events. More subjects in the placebo arm experienced at least one serious adverse event. Though the study did not specify the exact timeframe, at one point throughout the 24-week trial, administration was halted due to serious adverse events in both arms.
In another study evaluating bexagliflozin efficacy and safety, UTI and genital mycotic infections were more common in the bexagliflozin group compared to placebo. Otherwise, frequency of adverse events were comparable between groups.5 TEAEs were reported for 214 patients (109 [69%] bexagliflozin vs. 105 [68%] placebo). Hypoglycemia was the most common adverse event (39 [25%] bexagliflozin vs. 38 [25%] placebo), followed by diuretic effects (18 [11%] bexagliflozin vs. 5 [3%] placebo), urinary tract infections (11 [7%] bexagliflozin vs. 5 [3%] placebo) and AKI (8 [5%] bexagliflozin vs. 6 [4%] placebo). For TEAEs, descriptive statistics were used to report findings as no confidence intervals or p-values were reported. All acute kidney injury events were stage I AKI (defined by an absolute increase in serum creatinine of 0.3 mg/dL from baseline). Stage II/ III AKI (need for kidney replacement) therapy was not reported. AKI events did not lead to withdrawals. New malignancies were uncommon (3 [2%] bexagliflozin vs. 4 [3%] placebo). There were five genital mycotic infections and one amputation in the bexagliflozin arm, compared to no cases of mycotic infection or amputation in the placebo arm. There were seven falls/fractures
in the bexagliflozin group, compared to six in the placebo arm. There were two adjudicated major adverse cardiac events, both in the bexagliflozin arm.4 Of note, no patients died during the study period.
Bexagliflozin has been shown to be well-tolerated by patients in clinical trials. In the 2023 randomized control trial, the most common drug-related interactions were UTI, increased urination, and female genital mycotic infections.3,5 When used as an adjunct to metformin, the percentage of patients with at least one TEAE was 44.8% overall, 42.4% in the bexagliflozin group and 47.2% in the placebo group.3 Of the adverse events that were considered to be exposurerelated, they were in the system organ class of infections and infestations, metabolism and nutrition disorders and renal and urinary disorders. Overall, UTIs affected four subjects in the bexagliflozin arm and two subjects in the placebo arm, followed by polyuria, which affected two subjects in the bexagliflozin arm and three subjects in the placebo arm.3 An equal number of subjects withdrew from the active arm and the placebo arm due to tolerability.
Bexagliflozin was found to be effective in adults with type 2 diabetes and stage 3a/3b chronic kidney disease (CKD).3 In this 2023 study, primary outcomes were the change in glycated hemoglobin (A1c) from baseline to week 24. Secondary outcomes included systolic blood pressure (SBP), fasting plasma glucose and weight loss. The mean change in HbA1c was -1.09% (95%
CI -1.24%, -0.94%) in the bexagliflozin arm and -0.56% (-0.71%, -0.41%) in the placebo arm, a difference of -0.53% (-0.74%, -0.32%; p < .0001).3 In the 2023 trial analyzing safety and effectiveness in CKD patients, bexagliflozin lowered hemoglobin A1c by 0.37% [95% CI 0.20, 0.54]; p <0.001 compared to placebo.5 There are currently no head-to-head studies comparing bexagliflozin to other SGLT2i currently on the market. Bexagliflozin has similar A1c reduction as found in other SGLT2i trials, which tends to be around 0.5%. Further headto-head studies would be needed to confirm this.4 Furthermore, patients with CKD stage 3a (eGFR 45 to < 60) and 3b (eGFR 30 to < 45) experienced reductions in hemoglobin A1c of 0.31% (p = 0.007) and eGFR 0.43% (p = 0.002), respectively. Compared to placebo, bexagliflozin lowered body weight (1.61 kg, p < 0.001), systolic blood pressure (3.8 mmHg, p = 0.02), fasting plasma glucose (0.76 mmol/L, p = 0.003) and albuminuria (geometric mean ratio reduction of 20.1%, p = 0.03).5
Price
Due to its price, bexagliflozin is more readily available than other current SGLT2i, especially those without commercial insurance or who are not eligible for prior authorization. The retail price of bexagliflozin is $1.56 per tablet or $47.85 per month.6 This is much more affordable compared to other SGLT2i on the market and would provide a new cost-effective option. But providers would need to ensure bexagliflozin retail price is less than that a patient would pay with commercial insurance. Empagliflozin (Jardiance) and dapagliflozin (Farxiga), the two most prescribed SGLT2i on the market, retail for $23.73 and $22.61 per tablet respectively, which equates to roughly $700 per month in drug costs.7 If cost is a major factor, bexagliflozin could be considered as a first-line option for certain patients.
Simplicity
Bexagliflozin once daily 20 mg dose is optimal for patients that have trouble with pill burden, as it only needs
to be taken once a day. Compared to the other options on the market, the lack of dose titration would provide a much simpler option when initiating diabetes medications. With regard to dietary requirements, bexagliflozin can be taken in the morning without regard to food, and the effects of food on bexagliflozin pharmacokinetics are not considered clinically relevant.1 The time to peak plasma is between two and four hours. The half-life is approximately 12 hours, which is similar to that of other SGLT2i on the market. No renal adjustments are necessary until eGFR < 30 mL/min, which is a potential advantage compared to the currently marketed options that require discontinuation or dosage adjustments at GFR <45 mL/min. Although bexagliflozin is both a CYP3A4 and P-GP substrate, therapy remains simple as there is no concern for significant drugdrug interactions. Throughout clinical trials, little pharmacokinetic changes were observed when bexagliflozin was given concomitantly with other CYP inducers.1
Bottom Line
Bexagliflozin is an SGLT2i that when combined with diet and exercise as an adjunct, has been proven to impact glycemic control in adults with type 2 diabetes mellitus. It can be used alone or in combination with metformin as it has produced clinically meaningful improvement in glycemic control, estimated glomerular filtration rate and SBP when added to metformin.3 Further studies are needed to verify safety and efficacy of bexagliflozin with all other classes of medications for glycemic control. Trials reflect no evidence of significant safety concerns and adverse effects observed were minimal or undetectable.3,5 Bexagliflozin has demonstrated statistically significant reductions in A1C, body weight, systolic blood pressure, fasting plasma glucose, and albuminuria.5 The major drawback is that it does not have any head-to-head comparison data with current SGLT2i on the market comparing A1c or cardiovascular
benefit. Additionally, unlike other SGLT2i including dapagliflozin and empagliflozin, bexagliflozin has not yet been studied or approved in heart failure patients, and therefore cannot yet be recommended in heart failure.
References
1. Bexagliflozin (Brenzavvy TM) [package insert]. TheracosBio, Inc; 2023
2. Padda IS, Mahtani AU, Parmar M. SodiumGlucose Transport Protein 2 (SGLT2) Inhibitors. PubMed. Published 2022. https://www.ncbi.nlm. nih.gov/books/NBK576405/
3. Halvorsen YD, Conery AL, Lock JP, Zhou W, Freeman MW. Bexagliflozin as an adjunct to metformin for the treatment of type 2 diabetes in adults: A 24-week, randomized, double-blind, placebo-controlled trial. Diabetes, Obesity & Metabolism. 2023;25(10):2954-2962. doi: https:// doi.org/10.1111/dom.15192
4. Ozcelik S, Celik M, Vural A, Aydin B. The effect of low and high dose empagliflozin on HbA1c and lipid profile in type 2 diabetes mellitus: A real-world data. Northern Clinics of Istanbul. 2019;7(2):167-173. doi: https://doi.org/10.14744/ nci.2019.22697
5. Allegretti AS, Zhang W, Zhou W, et al. Safety and Effectiveness of Bexagliflozin in Patients With Type 2 Diabetes Mellitus and Stage 3a/3b CKD. American Journal of Kidney Diseases. 2019;74(3):328-337. doi: https://doi.org/10.1053/j. ajkd.2019.03.417
6. UpToDate. www.uptodate.com. Accessed November 19, 2023. https://www.uptodate. com/contents/bexagliflozin-drug-information ?search=bexagliflozin&source=panel_search_ result&selectedTitle=1~3&usage_type=panel&kp_ tab=drug_general&display_rank=1
7. UpToDate. www.uptodate.com. Accessed November 19, 2023. https://www.uptodate. com/contents/empagliflozin-drug-informati on?search=jardiance&source=panel_search_ result&selectedTitle=1~46&usage_type=panel&kp_ tab=drug_general&display_rank=1
Dr. Madeline Stanko is a PGY1 Pharmacy resident at UPMC St. Margaret and can be reached at stankom2@upmc.edu. Dr. Drake Meaney is a PGY2 Ambulatory Care Pharmacy resident at UPMC St. Margaret and can be reached at meaneydt@ upmc.edu. Dr. Heather Sakely, PharmD, BCPS, BCGP, the Director of Clinical Pharmacy Services and Director of the PGY2 Geriatric Pharmacy Residency served as editor and mentor for this work and can be reached at sakelyh@upmc.edu.
