Non-communicable diseases (NCDs), also known as chronic diseases, are usually of long duration and can be caused by genetic, physiological, environmental and behavioural factors, but more typically a combination thereof (WHO, 2021). Examples of NCDs include cardiovascular diseases (CVDs), cancers, chronic respiratory diseases and diabetes.
NCDs are on the rise globally. It is estimated that the global NCD burden will increase by 17% in the next 10 years with a 27% increase in Africa (Wang & Wang, 2020). Additionally, the International Diabetes Federation (2021) predicts an increase of people with Diabetes mellitus (DM) by 129% to 55 million by 2045 in Africa.
In South Africa, NCDs contribute more to the national burden of disease than communicable diseases. A Statistics South Africa Mortality Report (2017) showed a three-year trend analysis for selected main groups of underlying causes of deaths for the years 2015 to 2017. Among NCDs, diseases of the circulatory system increased in proportion from 17.8% in 2015 to 18.4% in 2017 in contrast to infectious diseases, which declined from 19.5% in 2015 to 17.6% in 2017. According to the International Diabetes Federation (2021), South Africa ranks highest, in the Africa region, with the largest increase in the number of people with DM from 1.9 million in 2011 to 4.2 million in 2021.
As the figure below shows, from 2009 onwards the percentage of deaths from NCDs (group II) exceeded that from communicable diseases (group I). This coincides with the scaling up of access to antiretroviral therapy for people living with HIV (Johnson et al., 2017). Notably, as the contribution of communicable diseases as a percentage of total deaths declined, the contribution of NCDs increased sharply. Group III in Figure 9.1 refers to external causes of mortality such as accidents, homicides and suicides. This chapter will not cover road accidents, interpersonal violence and suicides as causes of both morbidity and mortality. The rates of these ‘external causes’ are around 10% of all
deaths and show a marginal increase since 2015. This chapter will also not cover issues related to mental health as this is comprehensively covered in a separate chapter.
Figure 9.1 Percentage of deaths from various causes of mortality (STATS SA, 2021)
The major causes of death related to NCDs between 2016 and 2018 according to Statistics South Africa are: DM, cerebrovascular diseases, other forms of heart disease, and hypertension (STATS SA, 2021). These conditions may occur as co- or multi-morbidities with other NCDs or communicable diseases including HIV and AIDS and tuberculosis (TB).
The common modifiable and unmodifiable risk factors for NCDs, such as diabetes type 2, hypertension and CVD and some of the cancers are largely known. These range from genetic and metabolic factors to what have become known as ‘lifestyle factors’. However, it is clear that characterising NCDs as a lifestyle issue places the blame on the individual and absolves environmental, social and commercial issues that relate to NCDs. In addition, the term lifestyle camouflages the contribution of unhealthy behaviours, which are not only ‘voluntary’ but also associated with negative living environments that are not conducive to adopting pro-healthy behaviours. As stated by Marmot and Bell (2019, pg. 10), ‘social determinants encompass the “causes of the causes” of health inequality: the unequal conditions in which people are born, grow, live, work, and age; and the inequities in power, money, and resources that give rise to them’. The WHO (2021) has recently acknowledged the importance of the commercial determinants of health and defined the commercial determinants as activities of the private sector that can negatively or positively affect health.
The guiding documents for NCDs programmes during the 2015–2020 period were the National Strategic Plan (NSP) for the Prevention and Control of Non-Communicable Diseases (2013–2017) as well as the Strategy for the Prevention and Control of Obesity (2015–2020). The NCD Strategic Plan 2013–2017 reflected government’s response to NCDs, which contribute towards the quadruple burden of disease experienced in the country. However, implementation of the strategy was uneven and performance towards attaining targets could not be measured due to the lack of baseline data and overall ineffective surveillance of NCDs in South Africa. Given the lack of routinely collected data on NCDs through the District Health Information System (DHIS) and the infrequency with which the Demographic and Health Survey has been conducted, it has been difficult to systematically evaluate the implementation of the NSP 2013–2017. Additionally, the poor implementation revealed the negative impact of an inadequate policy cohesion within the NDoH and between other government departments and sectors.
A process to draft the follow-on NCD strategic plan was initiated in 2018 and was completed in 2021. The reasons for this document being delayed is a result of ongoing consultation with stakeholders and lack of agreement on the type of document that would make a real difference. Civil society organisations preferred that the NCD strategic plan followed the format used for the HIV, STIs (sexually transmitted infections) and TB strategic plan, which they considered was the major reason for the relative success of these programmes. The HIV, STI and TB strategic plan placed significant emphasis on human rights as well as a multisectoral approach with defined roles for different sectors. In addition, the HIV, TB and STI strategic plan is co-owned by government, organised labour, business and civil society through the South African National AIDS Council.
In order to address the growing NCD burden of disease, the 2013–2017 NCD strategic plan adopted 10 goals and targets. These are reflected in the table below.
Goal
1. Reduce relative premature mortality (under-60 years of age) from NCDs
2. Reduce tobacco use
3. Reduce per capita consumption of alcohol
4. Reduce the mean population intake of salt
5. Reduce percentage of people who are obese and/or overweight
6. Reduce prevalence of raised blood pressure through lifestyle and medication
7. Increase prevalence of physical activity (150 mins of moderate activity per week)
8. Every woman with STIs to be screened for cervical cancer
9. Increase percentage controlled for hypertension, diabetes and asthma
10. Increase the number of people screened and treated for mental disorders
Target to be reached by 2020 unless otherwise indicated
Reduce by at least 25%
Reduce by 20%
Reduce by 20%
Reduce by up to <5g per day
Reduce by 10%
Reduce by 20%
Increase by 10%
Every five years or three screens during her lifetime
Increase by 30% in sentinel sites
Increase by 30% by 2030
Like many low- and middle-income countries (LMICs), routine surveillance systems to monitor NCDs in South Africa are sub-optimal. This compromises the ability of the NDoH to fully understand the burden of disease, its determinants as well as the impact of interventions.
While NCD outcomes remain poor, the country effected a range of legislative, regulatory and policy reforms aimed at addressing modifiable risk factors, including:
• A Regulation on Trans Fats in Foodstuffs was passed in 2011 (R127). According to this Regulation, the trans-fat content of any oils and fats cannot exceed two grams per 100 grams and products with higher trans fats levels are prohibited from entering or being sold in the country.
• The Human Papilloma Virus (HPV) vaccination programme was launched in 2014 by the NDoH, in partnership with the Department of Basic Education, as part of primary prevention against cervical cancer. The aim was to target an estimated 550 000 girls in grade 4, aged 9 years and 17 000 public and special schools, before they were exposed to HPV infection.
• In line with targets of the Strategic Plan, a Regulation on reduction of sodium in 13 categories of foodstuffs that are the most common source of sodium for the majority of South Africans was passed in 2013 (R214) and amended in October 2017.
• In February 2016, South Africa became the first country on the African continent to announce plans to introduce a tax fixed at 2.1 cents per gram of the sugar content of sugar-sweetened beverages that exceeds 4g per 100ml. The tax became law in April 2017.
• Regulations regarding warning labels on alcohol products were introduced in 2007 and amended in 2017.
• The Tobacco Products Control Act, Act no. 83 of 1993. South Africa was a global leader in tobacco control until the 2000s. In 2005, South Africa ratified the World Health Organization Framework Convention on Tobacco Control (WHO FCTC). The country is therefore a signatory to the WHO FCTC, thus it has an obligation to implement the WHO FCTC. The Tobacco Products Control Act was amended in 1999, 2007 and 2008. The amendments include a ban on tobacco advertisements and smoking in public places (but permit smoking in designated smoking areas) as well as an increase in the age of sale from 16 to 18 years.
• The NDoH is currently finalising development of the Front-of-Pack (FoP) labelling regulations as a tool to simplify nutritional information for consumers, in addition to making nutritional information mandatory on most food labels, irrespective of whether a claim is made or not. The nutrients are the same as those identified by the WHO in their global strategies which aim to reduce obesity and NCDs, namely added salt, sugars and saturated fat.
South Africa was one of the first countries to introduce mandatory salt reduction regulation for processed foods. A preliminary study by Strauss-Kruger et al. (2021) found that mandatory salt reduction in processed foods lowered the salt intake in young adults by 0.82 g salt/day. Consumer appreciation of the limitation of the use of these products after the legislation came into effect was assessed by Koen et al. (2021). They
found that over three-quarters of their sample did not notice any change in the taste of products after the law come into effect. However, these authors also found that only one-third of their study participants looked at the salt content of products before purchasing, which means that much more education around salt is required.
Research shows a significant positive impact of the levy on sugar-sweetened beverages. Stacey et al. (2021) found that sugar from taxable beverages declined from 16.25 grams per capita per day to 10.63 grams per capita per day post implementation. In addition, they found that this decline was larger in low-income households relative to higher-income households – similar to findings in Mexico. Moreover, Hofman et al. (2021) cite a number of other local studies that show the impact of this levy on the consumption of sugar-sweetened beverages.
Box 1: Impact of salt and sugar legislation
Salt intake has decreased in young people by 0.82g/day after the introduction of mandatory salt regulation for processed foods.
While both low- and high-income households reduced their sugar intake from sugar-sweetened beverages, the reduction was higher for low-income households after the introduction of the levy.
Guidelines issued during 2015–2020
In addition to related existing policies, action plans, guidelines and user guides, the following have been developed since 2015.
• Framework and Strategy for Disability and Rehabilitation Services in South Africa 2015–2020
• Strategy for the Prevention and Control of Obesity in South Africa 2015–2020
• National Cancer Strategic Framework 2017–2022 (2017)
• Cervical cancer policy (2017)
• Breast cancer policy (2017)
• Updated Management of type 2 diabetes in Adults at Primary Care Level (2017)
• National Policy Framework and Strategy on Palliative Care 2017–2022 (2017)
• National User Guide on the Prevention and Treatment of Hypertension in Adults at PHC Level, 2021.
In addition, a number of health systems changes were introduced that have benefitted persons with NCDs.
• An Integrated Clinical Services Model that incorporates all chronic diseases, whether communicable or non-communicable, was introduced through the Ideal Clinic Initiative. This means that patients are seen for whatever chronic disease they have, including for multiple conditions, during the same visit. As of 2018, 97.2% of clinics had reorganised services with designated consulting areas for management of chronic conditions and had patient appointment systems for people with chronic conditions.
• NCDS were fully included in the Primary Health Care Service Package drafted in 2015. The most common NCDs have also been included into the Adult Primary Care package including asthma/COPD, screening for breast and cervical cancers, cardiovascular disease, diabetes, mental health conditions, epilepsy, and musculoskeletal disorders.
• Medicines for many patients who have controlled NCD conditions are provided through the Centralised Chronic Medicines Dispensing and Distribution (CCMDD) model.
• Training of community health workers on NCDs including on screening for hypertension and diabetes at a community level.
The case for investing in NCDs has been made globally. The WHO estimates that investing an additional 1 US dollar per person annually can save 7 million lives by 2030 in LMICs (WHO, 2021).
Investment in NCD programme implementation is channelled to the provinces and calculated through the equitable share formula as per the Division of Revenue Act and through dedicated conditional grants for oncology and mental health, as well as for NCD-related services provided at tertiary hospitals through the National Tertiary Services Grant. It is not possible to estimate how much provinces invest in NCD implementation using the equitable share as this is not itemised in provincial or facility-level budgets. In addition, the NDoH received a small allocation from the revenues raised from the health promotion levy for use to strengthen health promotion. A criticism has been that of the R3.195 billion collected in 2018 only R100 million – less than 5% of the total revenue raised – was allocated for health promotion activities (van Rensburg, 2020).
Despite some progress in the development and implementation of strategies, policies and guidelines, South Africa, like many other LMICs, is not on track to meet the Sustainable Development Goal (SDG) Target 3.4 by 2030 – which is to reduce by one-third premature mortality from NCDs through prevention and treatment and promote mental health and well-being. It is therefore not surprising that advocating for the prioritisation of NCDs globally and locally now mainly pertains to equity and human rights. People in LMICs are disproportionally affected by NCDs and the poorest and most vulnerable communities continue to be at highest risk for disease, experience greatest barriers to accessing essential health care and are experiencing the impact of the commercial determinants of health. The poor and vulnerable are less likely to appreciate the impact of commercial determinants of health, due to lack of exposure to education and the appropriate knowledge into the role of the private sector in driving unhealthy behaviours through the marketing of products such as tobacco, and increased levels of salt, sugar and trans fats in food products. This reality highlights the urgency with which SDG Target 1, to end poverty in all its forms everywhere, must be attained, in order to accelerate progress to achieve SDG Target 3.4.
Challenges experienced during the past five years relate to inadequate priority given to the co-existence of NCDs and communicable diseases such as HIV, AIDS and TB. The attention to multi-morbidities has not kept pace with the attention to detection, treatment and care as was the case with HIV and AIDS. There needs to be both high-level political support and resources to address this burden of diseases. This is an issue that civil society organisations have raised, noting that simply acknowledging the escalating burden of NCDs at political and strategic levels fails to translate into desired action on patient engagement and empowerment as well as along the entire continuum of NCD prevention and control (South African Non-Communicable Diseases Alliance and the Cancer Association of South Africa, 2021).
In addition, the importance of involving people living with NCDs in the development of strategies, policies and guidelines at global and national levels has been acknowledged from a rights perspective and has been accepted by policy-makers (Asante, 2021; WHO, 2021). In recognition, the NDoH included a number of civil society representatives to participate in the development of the NSP. This is in line with the efforts by the WHO to convene and partner with civil society organisations in policy and guideline development (WHO, 2021).
At a population level, the significant impact of the social, economic and commercial determinants of health is observed, resulting in an escalation of preventable diseases related to, for example, obesity. According to UNICEF (2019), South Africa has the largest percentage of overweight children under the age of five years and between 10 and 19 years in Eastern and Southern Africa. The South African Demographic and Health Survey (SADHS) (2019) found that a significant percentage of men and women who perceived themselves to be either underweight or of normal weight were overweight or obese. Similarly, the survey found that self-reports of diabetes and hypertension were lower than tested prevalence. Of concern is that the survey reported that among people with hypertension, 80% of women and 87% of men have uncontrolled hypertension. These results strongly suggest that awareness of the risk factors as well as NCDs is low in many communities.
Despite the NCD Declaration of the first UN High-Level Meeting on Noncommunicable Diseases held in 2011 urging all governments to commit to adopting an ‘all of government’ and ‘all of society approach’, South Africa has not established mechanisms to ensure intersectoral collaboration across government and with civil society to combat the growth of NCDs. The lack of coordinating mechanisms to enable policy cohesion and implementation between government departments and with other sectors not only perpetuates the escalating burden of NCDs, but more importantly results in lack of accountability for meeting global and national targets.
During the five-year period provinces such as Gauteng, KwaZulu-Natal, Limpopo and Mpumalanga experienced challenges with the provision of radiation oncology services due to shortage of staff and equipment breakdowns (Schutz, 2020). This was especially acute in KwaZulu-Natal, which led to a South African Human Rights Commission investigation, for example. A number of interventions were implemented to address these challenges, including procurement of equipment and the contracting of private sector oncologists to treat public sector patients. However, many challenges related to long waiting times for oncology services remain and were exacerbated by the COVID-19 pandemic (Cancer Alliance, 2020).
Box 2: Opportunities for leveraging lessons from HIV for NCDs: Lessons from KwaZulu-Natal
The approach used for the control of the HIV epidemic at municipal ward level through Ward AIDS committees, Ward-based Outreach Teams and Operation Sukuma Sakhe in KwaZulu-Natal brings together different sectors of government as a multisectoral strategy to ending the HIV epidemic as a public health threat. An integrated approach to disease control would benefit control of NCDs leveraging experiences gained using this ward-based multisectoral approach. This approach would accelerate education, screening, testing, early detection and access to care, supported by health promotion and disease prevention interventions through multisectoral structures. Potential benefits would include reducing waiting times for appropriate oncology interventions, improved access to mental health services – which in turn improves outcomes for other diseases such as for those living with HIV and other chronic diseases, prevention of end-stage kidney diseases which require dialysis or renal transplantation, and disabilities from stroke and amputations.
One of the major challenges with data on NCDs is that very little is collected routinely through the DHIS (Wandai et al., 2017). Thus, both programme planning and review of progress relies largely on survey data.
As illustrated above, by 2018 NCDs contributed almost 60% of all deaths, with communicable diseases contributing about 30% and external deaths such as accidents and suicides contributing the remainder. Between 2015 and 2018 (the most recent year for which data is available from STATS SA) the portion of deaths from NCDs increased from 55.4% to 59.3%.
The only survey data that collected data on NCDs during this period was the SADHS which reported in 2019 on data collected in 2016. While the data from the SADHS cannot be used to report about the targets in Table 9.1, it provides some idea of key indicators. The following reflects the data on selected NCDs from the SADHS (2019).
• High blood pressure was the most common self-report condition reported: women (23%) and men (13%).
• The prevalence of measured hypertension nearly doubled since 1998, from 25% to 46% among women and from 23% to 44% among men.
• The prevalence of asthma symptoms in adults was between 3% and 4% with symptoms of COPD at less than 2%.
• 13% of women and 8% of men 15 years and older had an HbA1c level of 6.5% or above, indicating that they were diabetic.
• High proportions of women (64%) and men (66%) were pre-diabetic with HbA1c levels of between 5.7% and 6.4%.
• While 5% of women and 4% of men self-reported being diabetic, 10% of women and 6% of men who were not previously diagnosed were found to be diabetic and 67% of both women and men were found to be pre-diabetic.
• While 13% of children were found to be overweight, 27% of children under five years of age were stunted with 3% wasted, and a further 6% underweight.
• Only 30% of women and 59% of men were found to be within the normal BMI range – with a significant percentage being either overweight or obese.
(There are no comparable data for 2020.)
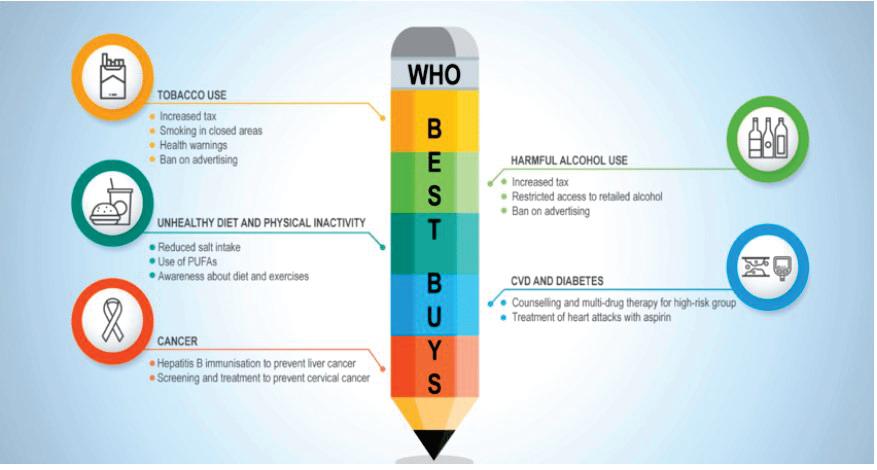
Avoidable mortality from NCDs: The WHO’s best buys
Figure 9.2 shows estimates of mortality from NCDs. These estimates suggest that the probability of premature death in both males and females will not meet global targets by 2025, although the possibility of females reaching global targets appears to be more likely.
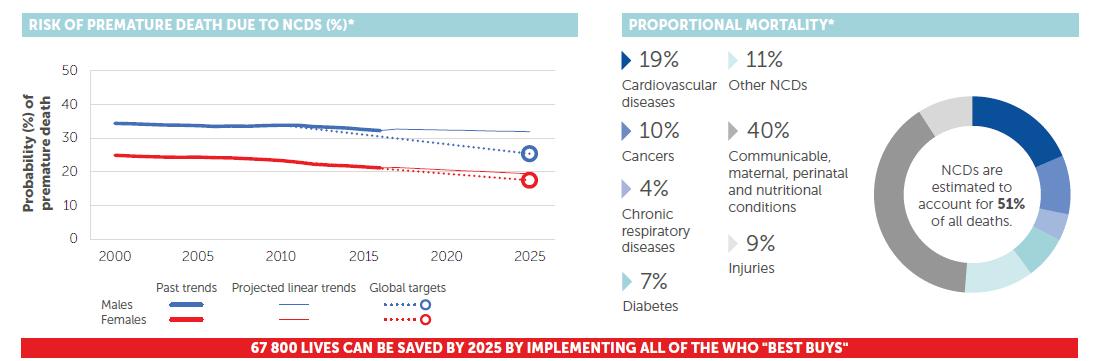
The WHO (2018) also suggests that by adopting the WHO’s best buys 67 800 deaths can be averted in the country by 2025. The best buys (Figure 9.3 below) include: reduce tobacco use, reduce harmful alcohol use, decrease unhealthy diets, increase physical activity, and focus on CVDs, diabetes and cancers.
Data on the cancer programme is largely laboratory based through the National Cancer Registry (NCR). The most recent data from the NCR is for 2018. The table below reflects the number of cancers reported by type and gender. As can be seen from Table 9.2, the most frequently reported cancers in women are: breast, cervical, basal cell carcinoma, squamous cell carcinoma, colorectal and uterus, whilst the most frequently reported male cancers are prostate, basal cell carcinoma, squamous cell carcinoma, colorectal and lung cancers. The picture has not changed over the last four years for which data is available. The quality of the data collected through the NCR depends on clinicians at facility level reporting data required against all data elements. A study at Chris Hani Baragwanath Hospital found that of 398 records of breast cancer from the hospital’s registry, all but one were matched to the NCR, giving a catchment rate of 99.75% (Ndlovu et al., 2022). Whilst this study focused on only one type of cancer and one tertiary facility, it does provide some level of assurance of the completeness of data.
Routine data on cervical cancer screening is available from the DHIS. The national target for screening is 60% which has not been reached. In 2017 the national average was 42.7% (ranging from 30.6% to 57.1%). However, this was worsened by the COVID-19 pandemic – the national average in 2020 was 39.1% (range of 18.1% to 45.9%).
Table 9.2 Most frequently reported cancers (National Cancer Registry: 2015–2018)
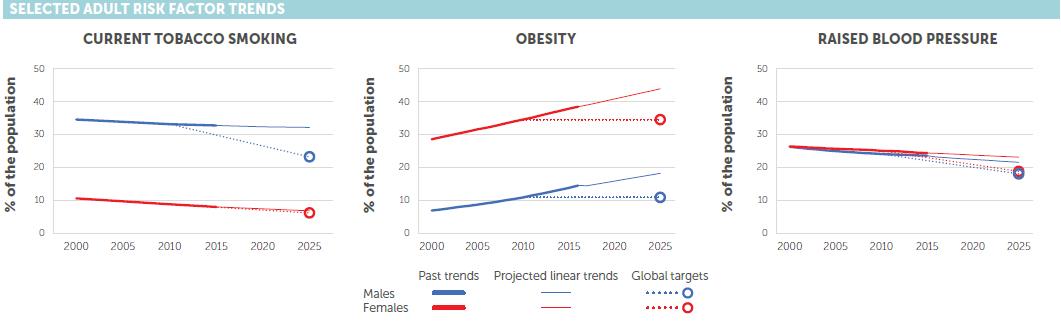
According to the SADHS (2019), 37% of men and 7% of women use tobacco products. With respect to tobacco smoking, South Africa is on track to meet global targets for females but not males (see Figure 9.4 below). According to Tobacco Tactics (2021), smoking prevalence declined from 33% in 1993 to 20% in 2017, however, the majority of the decline was in the 1990–2010 period. They also estimate that about 44 000 South Africans die annually from tobacco-related diseases.
Alcohol consumption is another major contributor to NCDs, such as cardiovascular diseases. According to the WHO (2016), consumption of pure alcohol in people over 15 years of age was 7.1 litres per person per year; however, if only those who drink alcohol were included, this increases to a staggering 29.9 litres per year. Both the WHO and others report that binge drinking especially among the poor and young people is a major issue (Marx et al., 2021).
Levels of physical inactivity are high in the country, with one report suggesting that 57.4% of the population is inactive, 14.8% are moderately active and 27.8% are very active (Mlangeni et al., 2018). South Africa’s 2018 Report Card on Physical Activity for Children and Youth suggests that the country is making insufficient progress with regard to the promotion of physical activity opportunities that are safe and accessible for the greatest number of children and adolescents (Draper et al., 2018).
According to the World Obesity Federation (2020), 21% of South African women over the age of 20 years have a BMI greater than 35kg/m2, implying severe obesity. This puts South Africa in the top 20 countries in the world with such high rates of female obesity. The Federation rates South Africa’s chance of meeting the UN global obesity targets by 2025 as ‘very poor’.
For obesity, the trajectory for both males and females is upwards and the country is not on target to meet global goals for both sexes. The country is also likely to miss the 2025 global targets on blood pressure as well
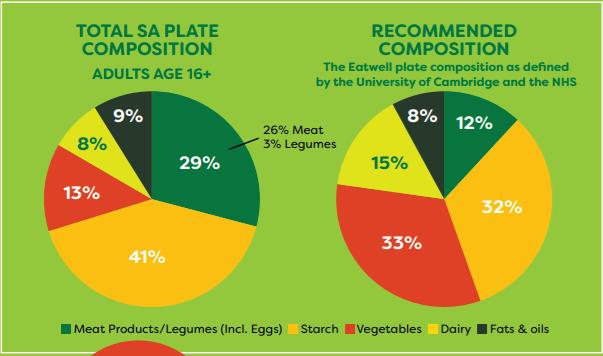
South Africa has both significant under-nutrition as well as over-nutrition (more accurately, poor eating habits). Apart from the high levels of obesity reflected above which is more severe in women than men, many children are underweight and stunted. The causes of both under- and overweight are different, with the former largely a result of poverty and food insecurity, while the causes of the latter are largely due to eating either the wrong types of food (or in the wrong combination) or eating too much and/ or inadequate physical activity.
The pandemic has exposed an intimate relationship between communicable and non-communicable diseases, placing a sharp focus on inequalities globally and in South Africa and is an important determinant in clinical outcomes. Those with comorbid NCDs were more likely to develop moderate to severe COVID-19 or die. A lack of pandemic preparedness saw disruption in health services in the process of flattening the COVID-19 pandemic curve at the early stages of the pandemic. Although lockdown regulations did not restrict access to health care facilities, access to facilities was reduced for various reasons including fear of contracting COVID-19, and reduced access to transportation or income. Consequently, screening and testing for NCDs was reduced during the pandemic, including access to treatment and assessment for disease control. The pandemic reveals significant shortcomings in the country’s response towards the prevention and control of NCDs. According to the hospital-based surveillance system, as of 10 April 2021, 231 237 COVID-19 admissions were reported from 644 facilities (393 public sector and 251 private sector) in all nine provinces of South Africa. There were 121 918 (52.7%) and 109 319 (47.3%) admissions reported in public and private sector hospitals, respectively. On multivariable analysis, factors associated with in-hospital mortality, among other, were patients having comorbid hypertension, diabetes, chronic cardiac disease, chronic renal disease, malignancy, HIV, current and past TB, and obesity.
9.6 Percentage of comorbidities among in-hospital COVID-19 deaths, by age group, South Africa (2020–2021)
The approach taken in developing the NSP was to be inclusive, involving NCD stakeholders, and to prioritise those NCDs that contributed the greatest to the burden of disease. The term NCD+ has been adopted in the NSP to signify the importance of the determinants of health (social, economic and commercial) as well as its disproportionate impact on the poor (CANSA, 2020).
The Box below illustrates the process used to develop the NSP in line with WHO guidance on the need for inclusivity and the slogan of ‘nothing about us, without us’.
Box 3: Lessons from the participatory process in developing the NSP 2022–2027
The target for South Africa in the newly adopted NSP, in compliance with the SDG Target 3.4, is to reduce, by one-third, premature mortality from NCDs+ through prevention and treatment and promote mental health and well-being by 2030. The overall aim for the NSP is to progressively improve wellness and reduce premature morbidity, disability and mortality from NCDs+ through the continuum of care across the life course.
The NSP promotes critical reforms, including the adoption of the WHO’s Integrated People-Centred Health Service (IPCHS), the development of a high-level multisectoral governance structure and the initiation of the cascading approach to NCDs. Based on the lessons learnt from the 90-90-90 cascading approach for HIV/ AIDS, the NSP outlines a similar approach for NCDs+, beginning with cascades for diabetes and hypertension. Experience in the HIV response has demonstrated that time-bound targets drive progress, promote accountability, and unite diverse stakeholders – motivating both behaviour and investments (Zuniga, 2018).
A 90/60/50 model is proposed to be applied to blood pressure and blood glucose screening treatment and monitoring as a first step to improving early detection and treatment of NCDs+.
• 90% of all people over 18 will know whether they have hypertension and/or raised blood glucose or not;
• 60% of people with raised blood pressure or blood glucose will receive intervention; and
• 50% of people receiving interventions will be controlled.
Whilst the actual implementation of the NSP lies within the remit of stakeholders that include but go beyond the NDoH, clearly defined guiding principles will be used to ensure the implementation of this NSP is underpinned by core values and principles that apply across the full burden of disease and require a robust health system. These guiding principles for action were identified as critical following a review of the Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2013–2017 and are also identified as important principles in the WHO Global Action Plan 2013–2020. The six guiding principles are described in Table 9.3.
Table 9.3 Guiding principles for the implementation of the NSP
Human Rights
Equity
Universal Health Coverage
The Bill of Rights in Chapter 2 of the Constitution lists 39 rights, apart from the right to health (Section 27) which influence the prevention and care for PLWNCDs+. These are: equality (9), dignity (10), life (11), health care, food, water and social security (27), children (28), environment (24 a) and just administrative action (33). Additionally, the constitutional values and principles governing public administration, i.e. transparency, participatory policy-making and accountability are relevant and important. This NSP aims to reinforce these rights through progressive realisation of equitable access to quality and affordable health care and interventions irrespective of ethnicity, gender, language, religion, political or health condition.
PLWNCDs+ experience significant inequities through financing, benefits packages and service delivery across the health sector. This NSP aims to raise the profile of NCDs+ as a priority in South Africa, through the prioritisation of NCDs+ from policy to service delivery and ensuring equitable access to NCD+ services for PLWNCDs+ and vulnerable populations therein.
UHC is linked to SDG Target 3.8 and the South African government’s commitment to UHC, through the delivery of NHI, is an important consideration in the formulation and delivery of this NSP. This NSP, developed during the health sector transition, and the implementation of NHI, endeavours to make its objectives align with the incremental achievement of UHC.
It must be noted that the NHI policy remains in draft form with ongoing implementation occurring in stages, many of which may occur after the expiration of this NSP.
Taking account of the structural and governance challenges that maintain siloed approaches and whilst we await the completed health sector transition, this NSP embraces the spirit of working in an integrated manner across directorates and within the health sector.
This integration occurs in various ways, including:
a) National Policy Alignment
b) Multisectoral and Multi-Stakeholder Engagement
c) Integration within the NDoH
d) Integration of Health Service Delivery
e) Integration across Health Conditions
The critical need for integration of NCDs+ with health programmes, in health systems, across levels and continuum of care, into service delivery platforms and care pathways, and across levels of government and with sectors and stakeholders is underpinned by the IPCHS framework which provides a basis for the goals within this NSP.
The Life-Course Approach
The Ottawa Charter (WHO, 1986), Alma-Ata Declaration and most recently, the IPCHS framework (WHO, 2016) all recognise the vital need to engage with and empower individuals and communities. This NSP aims to provide individuals and communities with opportunities, skills and resources as a means to participate actively and meaningfully in their health and health care in order to ensure the co-production of health espoused by the IPCHS model.
The life-course approach focuses on how multiple determinants interact to affect health throughout life and across generations. Health is considered as a dynamic continuum rather than a series of isolated health states. The approach highlights the importance of transitions (linking each stage to the next), of defining protective risk factors, of prioritising investment in health care and social determinants of health, and of gender equality and the promotion of human rights early in the life-course.
Whilst this NSP acknowledges the importance of the first 1000 days in addressing risk to the unborn child, the health status of the woman prior to conception presents a risk to both mother and baby and therefore requires monitoring throughout.
South Africa has made some progress in reducing NCDs, largely through the implementation of legislation. Legislative changes have impacted positively on several of the factors for NCDs, including those for sugar-sweetened beverages and salt. Whilst the decline in the use of tobacco products appears to have stagnated, the recent lockdowns in reaction to the COVID-19 pandemic and the ban on the sale of all tobacco and vaping products between 27 March and 17 August 2020 were found to have resulted in 9% of smokers successfully quitting (Filby et al., 2021).
While the NSP 2013–2017 included all the elements of interventions to respond to the burden of disease from NCDs, it suffered from a range of challenges. These included the lack of sufficient intersectoral collaboration as well as the means to measure progress or lack thereof and for course correction during the period 2013–2017. In addition, the hiatus between 2017 and 2020 – with no plan to guide intervention as a result of a protracted period of consultation for the drafting of the new NSP – also resulted in inadequate progress.
The COVID-19 pandemic illustrated the importance of a multi-modal approach to diseases and the need to be able to deal with patients holistically, given the range of comorbidities that patients are increasingly presenting with. Hence the importance of designing programmes and systems that place the patient/person at the centre, as described in the IPCHS Framework produced by the WHO.
The new NSP, which uses a cascade approach for diabetes and hypertension and which calls for the establishment of a coordinating mechanism similar to that for HIV and TB, holds much promise. However, unless there is high-level political support and additional funding to implement the NSP, progress in reducing the burden of NCDs in the country may be slow.
References
Asante K. The right to participate: An under-utilised component of the right to the highest attainable standard of health. BMJ. February 16, 2021 https://blogs.bmj. com/bmj/2021/02/16/the-right-to-participate-an-under-utilised-componentof-the-right-to-the-highest-attainable-standard-health/ (Accessed 24 January 2022).
Cancer Alliance (2020). Cancer Treatment Challenges During COVID-19; Letter to Minister Mkhize, 29 April 2020. https://cansa.org.za/cancer-treatment-challenges-during-covid-19/ (Accessed 12 January 2022).
CANSA (2020). Time to ACT on NCDs and Build Back Better. https://cansa.org.za/ time-to-act-on-ncds-and-build-back-better/ (Accessed 20 January 2022)
Department of Health (2013). National Strategic Plan for the Prevention and Control of Non-Communicable Diseases (2013–2017). Pretoria. https://www. iccp-portal.org/system/files/plans/South%20Africa_NCDs%20STRAT%20 PLAN%20%202013.pdf (Accessed 28 November 2021).
Filby S, van der Zee K, van Walbeek C. The temporary ban on tobacco sales in South Africa: lessons for endgame strategies. Tobacco Control. Published Online First: 20 January 2021. Doi: 10.1136/tobaccocontrol-2020-056209 (Accessed 17 January 2022)
Ganju A, Goulart A, Ray A, Majumdar A, et al. Systemic Solutions for Addressing Non-Communicable Diseases in Low-and Middle-Income Countries. Journal of Multidisciplinary Healthcare. 2020;13:693-707. 10.2147/JMDH.S252300. https://www.researchgate.net/publication/343224853_Systemic_Solutions_for_ Addressing_Non-Communicable_Diseases_in_Low-and_Middle-Income_ Countries (Accessed 6 December 2021).
Hofman K, Stacey N, Swart EC, Popkin BM, Ng SW. South Africa’s Health Promotion Levy: Excise tax findings and equity potential. Obesity Reviews. 2021;22(9). https://onlinelibrary.wiley.com/doi/epdf/10.1111/obr.13301 (Accessed 20 January 2022).
International Diabetes Federation (2021). IDF Diabetes Atlas, 10th edition. https:// diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_ Edition_2021.pdf (Accessed 12 January 2022).
Johnson LF, May MT, Dorrington RE, Cornell M, Boulle A, Egger M, Davies MA. Estimating the impact of antiretroviral treatment on adult mortality trends in South Africa: A mathematical modelling study. PLoS medicine. 2017;14(12): e1002468. https://doi.org/10.1371/journal.pmed.1002468 (Accessed 12 January 2022).
Koen N, Marais M, Smit Y, Nel D, Engelbrecht L. Sodium reduction regulations in South Africa – the consumer perspective. Journal of Consumer Science. 2021;6. Knorr. Plate of the Nation: A look at what South Africans are eating. March 2020. https://www.knorr.co.za/content/dam/unilever/knorr_world/south_africa/ print_comms_/knorr_plate_of_the_nation_report-2033974.pdf (Accessed 1 December 2021)
Marmot M, Bell R. Social determinants and non-communicable diseases: time for integrated action. BMJ. 2019;365: Suppl 1. https://www.bmj.com/content/ bmj/364/bmj.l251.full.pdf (Accessed 6 December 2021).
Marx MF, London L, Harker N, Ataguba JE. Assessing Intertemporal Socioeconomic Inequalities in Alcohol Consumption in South Africa. Front. Public Health, 11 May 2021 | https://doi.org/10.3389/fpubh.2021.606050 (Accessed 17 January 2022).
Mlangeni L, Makola L, Naidoo I, et al. Factors Associated with Physical Activity in South Africa: Evidence from a National Population Based Survey. The Open Public Health Journal. 2018. https://openpublichealthjournal.com/ VOLUME/11/PAGE/516/FULLTEXT/ (Accessed 1 December 2021).
National Department of Health, Statistics South Africa, South African Medical Research Council and ICF (2019). South Africa Demographic and Health Survey, 2016. Pretoria.
National Institute for Communicable Diseases National Cancer Registry. https:// www.nicd.ac.za/centres/national-cancer-registry/ (Accessed 3 December 2021).
Ndlovu BC, Sengayi-Muchengeti, Kellett P, Kuonza L, Cubasch H, Singh E, Chen WC. Completeness of reporting of breast cancer data in the National Pathology-Based Cancer Registry in South Africa. Journal of Registry Management. 2021;48(2).
Schutz E. Cancer care in the public sector: Are things getting better? 2020. https:// www.spotlightnsp.co.za/2020/12/08/cancer-care-in-the-public-sector-arethings-getting-better/ (Accessed 12 January 2022).
South African Non-Communicable Diseases Alliance and the Cancer Association of South Africa (2021). Communities to Act on Non-Communicable Diseases (NCDs). https://cansa.org.za/communities-to-act-on-non-communicablediseases-ncds/ (Accessed 12 January 2022).
Spotlight, 13 November 2020. https://www.spotlightnsp.co.za/2020/11/13/ finding-the-money-the-case-for-raising-the-health-promotion-levy/ (Accessed 20 January 2022).
Stacey N, Edoka I, Hofman K, Swart EC, Popkin B, Ng SW. Changes in beverage purchases following the announcement and implementation of South Africa’s Health Promotion Levy: an observational study. The Lancet Planetary Health. 2021;5(4): e200-e2008. https://www.thelancet.com/action/showPdf?pii =S2542-5196%2820%2930304-1 (Accessed 17 January 2022).
Statistics South Africa (2021). Mortality and causes of death in South Africa: Findings from death, 2018. (Accessed 3 December 2021). notificationhttps://www.statssa. gov.za/publications/P03093/P030932018.pdf (Accessed 28 November 2021).
Strauss-Kruger M, Wentzel-Viljoen E, Ware LJ, Van Zyl T, Charlton K, Schutte AE. Early evidence for the effectiveness of South Africa’s legislation on salt restriction in foods: the African-predict study. Journal of Hypertension. April 2021;39: e391e392. doi: 10.1097/01.hjh.0000749104.76735.72 9 (Accessed 17 January 2022).
Tobacco Tactics (2021). South Africa – country profile. https://tobaccotactics.org/ wiki/south-africa-country-profile/ (Accessed 17 January 2022).
UNICEF (2019). Poor diets damaging children’s health worldwide, warns UNICEF. https://www.unicef.org/southafrica/press-releases/poor-diets-damagingchildrens-health-worldwide-warns-unicef (Accessed 12 January 2022).
van Rensburg R. Finding the money: The case for raising the Health Promotion Levy. 2020.
Wandai M, Aagaard-Hansen J, Sartorius B, Hofman KJ. Available data sources for monitoring non-communicable diseases and their risk factors in South Africa. S Afr
Med J. 2017;107(4):331-337. DOI:10.7196/SAMJ.2017.v107i4.11438
Wang, Y., Wang, J. Modelling and prediction of global non-communicable diseases. BMC Public Health 20, 822 (2020). https://doi.org/10.1186/s12889-02008890-4 (Accessed 12 January 2022).
World Health Organization (1978). Declaration of Alma-Ata: International Conference on Primary Health Care, Alma-Ata, USSR, 6-12 September 1978. https://cdn.who.int/media/docs/default-source/documents/almaatadeclaration-en.pdf?sfvrsn=7b3c2167_2 (Accessed 17 January 2022).
World Health Organization (1986). Ottawa Charter for Health Promotion. https:// www.euro.who.int/__data/assets/pdf_file/0004/129532/Ottawa_Charter.pdf (Accessed 17 January 2022).
World Health Organization (2016). Framework on integrated, people-centred health services. https://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_39-en.pdf (Accessed 17 January 2022.
World Health Organization (2016). South Africa. Alcohol consumption, levels and patterns. https://www.who.int/substance_abuse/publications/global_alcohol_ report/profiles/zaf.pdf?ua=1 (Accessed 17 January 2022).
World Health Organization. (2018). Noncommunicable diseases country profiles 2018. World Health Organization. https://apps.who.int/iris/handle/10665/274512. (Accessed 1 December 2021).
World Health Organization. (2019). Global status report on alcohol and health 2018. World Health Organization. https://www.who.int/publications/i/ item/9789241565639 (Accessed 1 December 2021).
World Health Organization (2021). Commercial determinants of health: key facts. 5 November 2021. https://www.who.int/news-room/fact-sheets/detail/ commercial-determinants-of-health (Accessed 12 January 2022).
World Health Organization (2021). Investing 1 dollar per person per year could save 7 million lives in low- and lower-middle-income countries. 13 December 2021. https://www.who.int/news/item/13-12-2021-investing-1-dollar-per-personper-year-could-save-7-million-lives-in-low-and-lower-middle-income-countries (Accessed 12 January 2022).
World Obesity Federation (2020). Obesity: missing the 2025 global targets: Trends, Costs and Country Reports. https://data.worldobesity.org/publications/WOF-Missingthe-2025-Global-Targets-Report-FINAL-WEB.pdf (Accessed 17 January 2022).
World Health Organization (2021). Non-communicable diseases: key facts. https:// www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (Accessed 20 January 2022).
WHO (2021). Nothing for us, without us. Opportunities for meaningful engagement of people living with NCDs: meeting report. Geneva: World Health Organization (Accessed 24 January 2022)
Zuniga JM. UNAIDS 90-90-90—Opportunity in Every Difficulty. J Int Assoc Provid AIDS Care. 2018 Jan-Dec; 17. doi: 10.1177/2325958218809075) (Accessed 27 December 2021).