


Barry Kistnasamy, Spo M Kgalamono, Muzimkhulu Zungu, Mohamed Jeebhay, Rajen N Naidoo, Robyn Hayes Badenhorst
Occupational health in South Africa still has a fragmented policy, legal, administrative and service delivery framework. Occupational health services (OHS) are under-developed in many sectors of the economy coupled with the lack of trained occupational health personnel in the public sector and no uniform funding model for occupational health. The surveillance system for occupational injuries and diseases is non-existent and there is no reporting system across the Departments of Mineral Resources and Energy, Employment and Labour, and Health. Where data on occupational injuries and diseases is provided, it is mainly numerator data and thus difficult to interpret, compare and assess trends across sectors.
Migrant labour persists both within South Africa and cross-border with some progress on tracking and tracing workers with occupational lung diseases and ensuring their compensation payments. Informal sector workers face multiple barriers including the low wage subsistence economy and no access to OHS and other services. Class action compensation settlements for silicosis and tuberculosis (TB) in the gold mining sector were welcome developments notwithstanding the need for preventive interventions.
Some gains were made with OHS provision with specialist referral services in occupational medicine in the major metropolitan areas, expansion of the Occupational Health Information System (OHIS) in some Provincial Departments of Health (PDoHs), provision of One Stop Services for ex-mineworkers and limited health services to informal traders, use of the HealthWise tool (ILO / WHO) and incorporation of domestic workers into the compensation system. The COVID-19 pandemic, while galvanising partnerships across public and private sectors, highlighted the gaps in OHS provision especially in public sector health facilities, small and medium enterprises and the informal sector. The Department of Employment and Labour (DEL) and Department of Mineral Resources and Energy (DMRE) took the
lead on workplace interventions in COVID-19 and COVID-19 infection in workplaces was designated a compensable disease.
South Africa’s many academic institutions and professional societies play a significant role in capacity-building initiatives of the different disciplines within OHS. They assist with technical advice to government, employers and trade unions and serve on multiple governance structures. Of note is their participation in OHS initiatives across the continent and other international bodies.
Multilateral agencies such as the International Labour Organisation (ILO), the World Health Organization (WHO) and the International Social Security Association (ISSA) provide global governance and support to occupational health and safety activities at supra-regional and country levels.
South Africa’s occupational health and safety legislation is derived from Chapter 2, Section 24(a) of the Constitution of South Africa, Act 108 of 1996, which states that everyone has the right to an environment that is not harmful to their health or well-being. Section 27(2) places an obligation on the state to take reasonable legislative and other measures, within its available resources, to achieve the realisation of each of the rights in the Bill of Rights. South Africa as a member state of the WHO and ILO has ratified their conventions and adopted instruments in occupational health and safety. Occupational health and safety in South Africa is a tripartite arrangement, and is in line with the International Labour Organization Convention C144 – Tripartite Consultation Convention, 1976 (No. 144). Employers, employee representatives and government contribute on decisions that affect occupational safety and health policy, Acts, Regulations, and implementation. The Mine Health and Safety Act established the tripartite structures, namely the Mine Health and Safety Council and the Mine Qualification Authority, which are led by stakeholders. These institutions coordinate and direct research and training to improve health and safety performance of the mining industry. The Occupational Health and Safety Act (OHSA) established an Advisory Council for Occupational Health and Safety, which is also a tripartite institution. These institutions ensure that there are political, economic and social systems to influence policy and legislation on occupational health and safety (Myeni, 2020).
The legislation on occupational health and safety is progressive and enforceable. In addition, there are voluntary technical standards that, whilst not legally enforceable, are part of the health and safety management systems in many companies. However, the legislation governing occupational health is complex and spans general economic sectors and specifically mining, maritime, aviation, railway, transport and nuclear/ energy sectors. Notably, the fragmented legislative framework falls under different ministries and departments. The main pieces of legislation on occupational health and safety are in Table 11.1.
Table 11.1 Legislation on Occupational Health and Safety
Legislation
Occupational Health and Safety Act, Act No. 85 of 1993
Compensation for Occupational Injuries and Disease Act, Act No. 78 of 1973
Mine Health and Safety Act, Act No. 29 of 1996
Occupational Diseases in Mines and Works Act, Act No. 78 of 1973
Occupational health and
Administering Department
Department of Employment and Labour
Department of Mineral Resources and Energy
National Department of Health
Table 11.2 Legislation on Occupational Health and Safety for specific sectors
Legislation
National Energy Regulator Act, Act No. 47 of 1999
Railway Safety Regulator Act, Act No. 16 of 2002
South African Maritime Authority Act, Act No. 5 of 1998
Act of Civil Aviation Authority Act, Act No. 3 of 2009
National Nuclear Energy Regulator Provides for the protection of persons, property and the environment against nuclear damage in South Africa
Railway Safety Regulator Provides for safety standards and regulatory practices for the protection of persons and property
South African Maritime Authority
Safety provisions for staff on board ships, appliances and equipment
South African Civil Aviation Authority Regulates civil aviation safety and security in support of the sustainable development of the aviation industry
Health and Safety Policy
The overall policy framework for occupational health and safety is weak given the fragmentation across the three major departments governing occupational health and safety. The National Department of Health (NDoH) covered aspects of occupational health in the White Paper on National Health Insurance (NHI) but lacks the administration and funding to support occupational health initiatives. The National Institute for Occupational Health (NIOH), an agency of the NDoH, conducts research and provides education and training and specialised laboratory and clinical services in occupational health. The Medical Bureau for Occupational Diseases and the Compensation Commissioner for Occupational Diseases have narrow mandates under the Occupational Diseases in Mines and Works Act, 1973 and cover medical assessments and compensation for cardio-respiratory diseases in mineworkers. There are academic departments of occupational health at a few medical schools and nursing colleges while occupational hygiene and safety is also taught through a few universities and technical institutes. There is a programme on ergonomics at one university. The DMRE and DEL have components of their departments dealing with inspections of workplaces and enforcement under their respective health and safety Acts. In addition, the DEL has a component dealing with compensation for occupational injuries and diseases other than that covered by the NDoH.
The mining sector and major manufacturing sector companies have OHS standards that play a substantial role in occupational health and safety initiatives in the workplace. Of note is the multiplicity of ‘wellness’ services covering health promotion in the workplace that cover chronic diseases including HIV and AIDS. Some of the major trade union federations and larger unions have health and safety focal persons, but in general have not placed occupational health and safety high on the agenda in workplace interactions with management. The COVID-19 pandemic response resulted in some trade unions, especially those covering health workers, raising concerns on OHS and personal protective equipment (PPE) for workers. Various professional societies and associations are also active in occupational health and safety.
The prevention, promotion, curative, rehabilitative and compensation services are fragmented with no overall and uniform health system response. Injured workers are managed within the public and private health care systems depending on the nature and extent of their injury. Except for the system of assessments for cardio-respiratory diseases in mineworkers, there are few cases of occupational diseases reported annually. Owing to latency, many workers with occupational diseases present long after they exit the workplace and in many instances owing to a lack of education and training of health professionals, their diagnosis may not be linked to their work exposures. Injured workers are often cared for in public hospitals with no recovery of funds from the different compensation funds.
Demographic changes to the South African workforce during the period under review were marginal, largely defined by economic imperatives that occurred in the previous decade. The changes impacted on in 2020, because of the COVID-19 pandemic, have yet to be fully described, but immediate effects, such as unemployment, have already been recorded. At the end of the previous decade, economic growth in South Africa fell sharply. The impressive growth rate of 5% in 2007 gave way to almost 2% by 2009 (Organisation for Economic Co-operation and Development, 2010). Similarly, unemployment, hovering at a stable (but high) rate of 20% from 2002 through to 2007, increased to 25% by 2010 (Organisation of Economic Co-operation and Development, 2010). These economic indicators set the stage for the 2015–2020 period.
The ILO estimates that 2.78 million of the world’s 2.7 billion workers die annually from occupational accidents or diseases (International Labour Organisation, n.d.). It is estimated that a large proportion (>80%) of occupational fatalities and disease burden are due to occupational diseases. Furthermore, the economic burden of poor occupational health and safety practices is estimated to be 3.94% of global gross domestic product each year. Similarly, occupational injuries and diseases pose an enormous cost to the South African economy, individual workers, and their families. An earlier South African Demographic and Health Survey conducted over two decades ago suggested that 8.9% of adults reported staying away from work due to disease or injury related to work (Kielkowski, 2004).
Current official data on the spectrum of occupational injury and diseases in the South African workforce is incomplete, unreliable and for a large proportion of the workforce not available. The spectrum of occupational diseases is partially obtainable from the annual reports and the Occupational Diseases in Mines and Works Act. The Compensation Fund in the DEL, legally established through contributions of employers, currently covers 15 million workers employed by 1.08 million employers, which includes the Rand Mutual Association (covering mining, iron and steel) and Federated Mutual Association (covering construction) (Presentation, Milly Ruiters, Compensation Fund, ILO workshop, June 2021) in the formal sector, but excludes public sector workers (exempted employers). Compensation for occupational lung diseases is covered by the Medical Bureau for Occupational Diseases and its Compensation Commissioner administered by the NDoH.
Occupational diseases in the non-mining sector reported to the Compensation Fund by the DEL show a downward trend over the past two decades, from over 5 000/ year claims reported in 2003–4 (Adams, 2007) to less than 1 000/year over the past five years (Myeni, 2020). In the non-mining sector, TB (among health care workers), noise-induced hearing loss, diseases due to chemical agents and occupational asthma claims submitted in the 2019/20 period are shown in Table 11.3. Visibly absent from this list is post-traumatic stress disorder, dermatitis and pneumoconiosis that featured over a decade ago (Adams, 2007). Recent data from the Occupational Medicine Clinic at Groote Schuur Hospital in Cape Town indicates that occupational asthma is the most common diagnosis, followed by pneumoconiosis and work-related upper limb disorders and contact dermatitis (personal communication, S Adams, GSH, Cape Town). These trends need to be interpreted with caution in a setting of poor diagnostic capacity for occupational diseases, under-reporting of occupational diseases and overall lack of occupational health service provision in most workplaces in both the private and public sector (Jeebhay & Jacobs, 1999).
Table 11.3 Occupational diseases reported to the Compensation Fund for the non-mining sector in South Africa, 2016/17–2019/20 Occupational
COID Injuries*
Source: Myeni and Ngcobo, 2020; *probably refers to non-traumatic organ insults
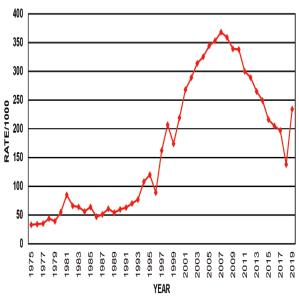
Data from the mining sector (547 847 employees in 2019) indicate that occupational lung diseases comprise the largest portion of the disease burden (70–75%). The five most frequently reported occupational diseases are pulmonary TB, noise-induced hearing loss, silicosis, and coal workers’ pneumoconiosis (see Table 11.4) (DMRE, 2019/20). The relative prevalence of occupational disease among workers in the sector is highest in the gold mining industry. The common commodity sectors reporting these outcomes are gold, platinum, chrome and coal mining. Among these diseases, TB comprised 50% of the occupational disease burden. This is also reflected in autopsy findings of miners conducted for compensation purposes where the reported rate for TB was 138/1 000 (2018). For Black miners, where the rates are extremely high, the rate increased consistently from the early 1990s and peaked at 368/1 000 in 2007, but have since declined annually to 168/1 000 in 2018, before rising again to 234/1 000 in 2019 (Figure 11.1a-b). However, the recent Masoyise report of the industry’s TB incidence was at 220/100 000 for 2020, which is below that of the general population, at 260/100 000. Silicosis rates based on autopsy results have also shown an increase particularly in the gold-mining industry, which accounts for 83% of cases (2018). Silicosis rates in Black gold miners increased over the years from 39/1 000 in 1975 and peaked at 416/1 000 in 2016, thereafter declining to 368/1 000 in 2019, while the rate in White gold miners increased from 176/1 000 in 1997 to 309/1 000 in 2019 (Figure 11.1a-b). During the year 2020, the Medical Bureau for Occupational Diseases certified 7 924 claims (47%) of 16 968 claims received (Table 11.5). The two largest components of claims certified were for TB (50%) and silicosis with/without TB (42%). A steady decline of new cases has been reported in living miners with silicosis. However, there is a risk of under-diagnosis and reporting especially in former miners. A recent study has suggested that the annually reported levels of exposure to respirable crystalline silica suggest a decline, however, the actual levels were not reported over the last few years (Brouwer, 2020). The authors concluded that there was insufficient evidence of progress towards achieving the silicosis elimination target that the country had set.
11.1 Occupational
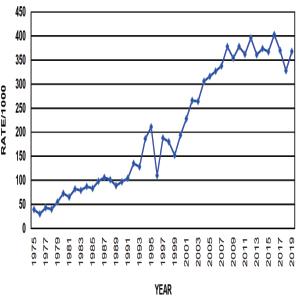
Figure 11.1b
Figures 11.1a-b. Pulmonary tuberculosis in Black miners and silicosis in Black South African gold miners at autopsy (1975–2019)
Source: Mhlongo L, Wilson K, Kgokong N, et al. Pathology Division Surveillance Report 2018. NIOH Pathology Report 1/2021
Table 11.4 Occupational diseases per commodity reported in annual medical reports by South African mines (2018 and 2019
REFORMS 2015-2020
Source: Department of Mineral Resources and Energy, Mine Health and Safety Inspectorate Annual Report 2019/20
Table 11.5 Occupational diseases reported and certified for the mining sector of South Africa (2019–2020)
Source: Andre Fourie, Office of the Compensation Commissioner for Occupational Diseases (personal communication)
Infectious diseases, COVID-19 and vulnerable occupational groups
Tuberculosis in health workers and occupational lung diseases in mining and associated industries continue to be a key priority for the NDoH (Adams, 2012/13; Grobler, 2016). This has been evident in the recent COVID-19 pandemic, which illustrated the vulnerability of the health workforce. Earlier in the epidemic, the WHO estimated that health workers accounted for up to 14% of all COVID-19 cases (WHO, 2020).
A total of 2.3% of COVID-19 hospitalisations at a national level were health care workers (HCWs) as of March 2022 (NIOH, 2022). An estimated 44 406 cases of COVID-19 were reported in the Western Cape (n=12 329), Gauteng (n=15 282) and KwaZulu-Natal (n=16 795) by mid-April 2021 in both the public and private sector. Most infections (86%) were in the public sector, which employs most HCWs in the country (Table 11.6). Among the HCWs, 11.8% experienced moderate to severe disease requiring hospitalisation and 0.9% had demised. Nurses and administrative workers were the most affected job category at all levels of the health care system (Rees, 2021). This could have been due to the large numbers of patients admitted to hospitals with limited facilities for case isolation, limited access to rapid and reliable diagnostic testing in the early stages of the outbreak, and the challenges around access to and best use of PPE (Read, 2021).
2015-2020
Table 11.6 Public sector health worker COVID-19 disease data per province (March 2020–mid August 2021)
Source: NDoH (Personal communication, Dr Nicholas Crisp, Deputy Director-General NHI, NDoH)
The impact of COVID-19 on the overall mining community mirrored the pandemic in the rest of the country. In provinces with considerable mining activity, a high proportion of community cases and fatalities emanated from the mines. Mining-related cases were concentrated in areas that are situated close to provincial borders, implying an increased interprovincial transmission risk, possibly exacerbated by work-related transmission. Occupational categories with high dust exposures such as rock drill operators in platinum and gold mining were also reported to have the most SARS-COV-2 infections (Naidoo & Jeebhay, 2020). Data is being collected on a dynamic basis to monitor the trends in other industrial sectors through the Occupational Health S urveillance System (OHSS) for COVID-19. This data reports the mortality rate among reporting workplaces as 1.5%, while 7.5% of workers had moderate to severe disease requiring hospitalisation (NIOH, 2021).
Analysis of workers’ compensation claim data for the period ending 31 March 2021 indicated that there were 20 525 claims for work-related COVID-19 submitted to the Compensation Fund. Most claimants were women workers, with a large proportion originating in the health care sector (75%). Mining contributed 23% of claims and the building industry 2.5%. Data from the Western Cape suggested that about 20% of COVID-19 claims originated from the non-health sectors such as retail, finance and transport (Jeebhay et al., 2021).
In July 2020, the DEL issued a direction on compensation for workplace-acquired COVID-19, addressing workplace-acquired COVID-19 resulting from work-related exposures, exposure to suspected or confirmed cases of COVID-19 in the workplace, or while travelling on an official trip. South Africa is one of a few countries that has taken this step of making COVID-19 infection a compensable disease.
Occupational health and safety
The patterns of occupational injuries in the country are disaggregated according to economic activity. In the non-mining sector occupational injuries have historically accounted for more than 99% of all claims submitted under the Compensation for Occupational Injuries and Diseases Act (Myeni, 2020). According to DEL reports, over a four-year period annual claims declined from 184 100 (2017/18) to 82 526 (2019/20). The largest proportion of claims originated from the more industrialised and urbanised provinces of Gauteng followed by the Western Cape. Compensation claims affecting women ranged between 40 and 45% despite 50% of the working population being women. No data is available for current injury rates, however, the rates of 42 per 1 000 workers in 2006 were 27% higher than in 1994. This suggested a worsening of occupational health and safety standards over time (Adams, 2007). Furthermore, the lack of more detailed data has resulted in an inability to identify the important sectors contributing to these injuries. As previously observed, hand injuries are the most common (Myeni, 2020). This has major implications for the rehabilitation of workers in this country since a substantial proportion are manual workers.
In the mining sector there were 2 350 occupational injuries reported in 2018, which represents an injury rate of 514 per 100 000 workers. As has been the trend over the past three decades, gold mining is the most hazardous and accounts for half of all reported fatalities (2018). Both injury and fatality rates (Figure 11.2) in mines have indicated a downward trend from 1984 and the number of injuries has halved since 2007 (Myeni, 2020; Adams, 2007). This is likely related to the contraction of the mining industry as well as improved safety measures in mines due to improved regulation of mine health and safety since the early 1990s (Jeebhay, 1999; Adams, 2007).
The number of women working in the mining sector has increased significantly in the past 15 years – from around 11 400 in 2002 to 56 691 in 2019, representing 12% of the mining workforce (2019). There has been an increase in the number of injuries involving women since entering the mining workforce (Figure 11.3). Two-thirds of these injuries are due to accidents associated with slipping and falling, material handling and being struck by objects. The Minerals Council has attributed these accidents to all forms of equipment (overalls, PPE, boots or tools) that have been designed and manufactured with men in mind (Minerals Council, 2019).
Source: Myeni and Ngcobo, 2020
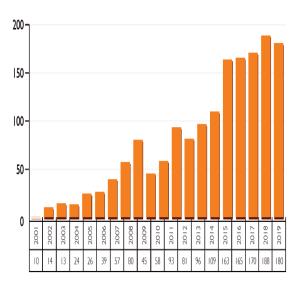
Figure11.3 Injuries reported among women in the mining industry (2001–2019)
Source: Department of Mineral Resources and Energy, Mine Health and Safety Inspectorate Annual Report 2019/20
For decades now, South Africa continues to report fragmentation, scarcity, paucity and inadequacy of the delivery of occupational health services (Kistnasamy, 1987; Zwi et al., 1988; Lowe et al., 1990; Jeebhay & Jacobs, 1999; Adams et al., 2007). This is despite, among others, the Erasmus Commission and the Abdullah report, which identified and described the gaps in OHS in South Africa (Erasmus Commission 1976; Department of Health 1996).
In South Africa, OHS is mostly delivered using one of three service delivery models, namely: 1) in-house, 2) outsourced and 3) the hybrid model. Large enterprises and the public sector, particularly the PDoHs mostly use an in-house model with multidisciplinary occupational health professionals delivering the OHS on behalf of the employer. Some enterprises use an outsourced model wherein a private entity provides OHS, often with primary health care (PHC). Some enterprises have a hybrid model where the traditional occupational health (occupational hygiene and occupational medicine) is provided in-house, and employee wellness services are outsourced (Michell, 2012; Department of Health 1996).
The ILO (International Labour Organization, 1985), WHO (World Health Organization, 1995), ICOH (International Commission on Occupational Health, 2021), SASOM (South African Society of Occupational Medicine, 2007), the South African Government (Republic of South Africa, 1993; National Department of Health, 1997; Department of Health, 1996), and peer-reviewed publications (Rantanen et al., 2017) have all defined some package of OHS. Mostly, the OHS package in these resolutions and guidelines are adaptations of the ILO Convention 161 (International Labour Organization, 1985).
OHS is intended for the prevention of sickness absenteeism, premature disability and mortality from occupational accidents and diseases, promoting health and longer working careers, work ability and better work organisation (Rantanen et al., 2017). The WHO advocates for a realistic long-term objective to provide all workers access to a competent OHS (World Health Organization, 1995). South African workers face precarious working conditions, and have been grappling with low and inadequate access to OHS for workers particularly in small and medium enterprises (SMEs) and the informal economy (Word Health Organization, 2021; Moyo et al., 2015; Moodley & Bachmann, 2002; Michell, 2012; Lwando Maki, 2019).
Over the past decade, there have been several reforms to the South African health system and occupational health legislation, which had implications for improved access and coverage with OHS. The NDoH introduced the PHC re-engineering policy (NDoH, 2010), National Public Health Institutes of South Africa Bill (Republic of South Africa, 2017) and the NHI bills (Republic of South Africa, 2021), as well as reforms at the Medical Bureau for Occupational Diseases. These reforms have and will impact OHS equity, particularly by improving demand and provision of public sector OHS. The impact is expected primarily for vulnerable workers in the informal economy, SMEs, ex-mine workers and migrant workers who are dependent on the public health system in the management of the interplay between occupational risk and access to health services and the blurred boundary between community and workplace health issues.
While there is a paucity of data, coverage and access to OHS in South Africa is reported to be between 11 and 18%, and mostly in large enterprises (Sitas et al., 1988; Jeebhay & Jacobs, 1999). However, an emphasis on vulnerable workers (informal economy, agricultural, SMEs, ex-mine and migrant workers) is needed, as workers in large enterprises (mining, banking, construction, transport, auto-industry, health sector, etc.) have reasonable access to OHS (Sitas et al., 1988; Moodley & Bachmann, 2002). Since 2015, progress in OHS health reforms has been on policy with limited implementation other than in mining. However, historically and including the past decade, numerous examples of OHS have been implemented in South Africa, including:
• Provision of referral specialist occupational medicine and hygiene services by the NIOH, University of Cape Town (UCT) and Groote Schuur Hospital, and University of KwaZulu-Natal (UKZN) Occupational and Environmental Health department.
• Provision and utilisation of a web-based comprehensive and integrated Occupational Health and Safety Information System (OHASIS) for the health sector to enter and track essential safety, health and environment indicators in the workplace, through the NIOH. OHASIS is fully implemented in the National Health Laboratory Services (NHLS), is undergoing early roll-out in Gauteng PDoH, was recently acquired by the Western Cape PDoH, and the Mpumalanga and North West PDoHs are in negotiations to acquire the system.
• The NDoH’s One Stop Services (OSS) for ex-mineworkers under the Compensation Commissioner for Occupational Diseases and the Medical Bureau for Occupational Diseases. The OSS was initially developed in 2013 to improve equitable access to Benefit Medical Examinations (BMEs) and compensation of eligible ex-mine workers with occupational diseases covered by the Occupational Diseases in Mines and Works Act 78 of 1973. This service has since been utilised as a blueprint for OHS in South Africa and the Southern African region. Occupational
• While informal economy workers are excluded from the provisions of the OHS Act, the Phephanathi Platform, an ongoing collaboration between street trader organisations working in Warwick Junction, in the inner city of Durban, South Africa, and their support organisations, Women in Informal Employment: Globalizing and Organizing, Asiye eTafuleni, and the UKZN Occupational and Environmental Health department, has attempted to link traders to various parts of the health system – local government, occupational health professionals (UKZN) and the public health system. The platform focuses on two key pieces of work – the design and roll-out of first aid stands into the markets, and attempts to institutionalise occupational health and safety for informal workers operating in urban public space (Alfers et al., 2016). While the abovementioned programme can be cited as best practice in the informal economy, most informal economy workers will never experience OHS or even standard health services.
• While there are no specified OHS requirements for domestic workers, the landmark decision by the Constitutional Court to uphold the High Court’s declaration that domestic workers were to be included in the Compensation for Occupational Injuries and Diseases Act, and as such receive compensation for occupational diseases and injuries has potential to improve OHS for domestic workers (Atrey, 2021).
• The NDoH PHC re-engineering is delivered through the Ward-Based PHC outreach team consisting of a professional nurse, health promoter, environmental health officer and community health workers. The environmental health officers can provide basic health promotion, and diseases and injury prevention information in workplaces. However, the full potential of this programme in OHS has not been realised owing to lack of conscious collaboration between District Health Services, PHC services and OHS at national, provincial and local government level (NDoH 2013, 2010).
• Implementation of the ILO and WHO-developed HealthWISE tool, to improve work conditions, performance, occupational health and safety for health workers, and the quality of health services provided. Improvements are introduced and sustained by the combined efforts of management and staff, brought together in a dedicated team. This project is led by the NIOH and adopted by the Gauteng and Mpumalanga PDoHs is implemented in selected health facilities within the two PDoHs (International Labour Organization & World Health Organization 2014; Wilcox et al., 2020).
• In the fishing industry, ‘South Africa has measures to ensure worker health on abalone and trout farms including training and annual medical examinations. Monthly OHS meetings are organised to discuss worker health. The industry often implements safety recommendations made by external consultants’ (Cavalli et al., 2019).
• The Masoyise Health Programme, the goal of which is to reduce the impact of TB, HIV, occupational lung diseases and NCDs as occupational health threats in the mining sector, is a multi-stakeholder initiative with representatives of Minerals Council member companies, trade unions (NUM, Solidarity, AMCU, UASA), government (NDoH and DMRE, the Mine Health and Safety Council, NHLS and NIOH), SABCOHA and multilateral organisations including UNAIDS, ILO and WHO. The precursor to the Masoyise Health Programme was Masoyise iTB (‘Lets Beat TB’), the aim of which was to increase counselling for HIV and screening for TB in the industry (Minerals Council South Africa, 2021).
Occupational health and safety
While tragic, the COVID-19 pandemic has thrown the spotlight on the lack of OHS and provided an opportunity for increased OHS coverage. The DEL Directions on OHS measures in workplaces included guidelines on symptom monitoring and management of workers for SARS-CoV-2 and submission of COVID-19-related health data, while the NDoH provided workplace guidelines (Department of Employment and Labour 2020; National Department of Health 2021, 2020). These instruments have led to awareness training, health promotion activities, health risk assessments, workplace screening and referral services, as well as the development of the NIOH’s OHSS for COVID-19.
South Africa still lags on OHS and overarching comprehensive occupational health and safety policy through the DEL is critical for improving equitable access and coverage with OHS. The general lack of OHS provision within the public health sector is an opportunity to adopt and implement the workers’ health interventions in PHC, and the development and/or strengthening of the occupational health units / clinics associated with medical schools / secondary-level hospitals to improve OHS coverage and access. The occupational health inspectorate should strengthen enforcement for OHS, and the informal economy and SMEs should access OHS within the public sector and where possible through the support of large enterprises. An awareness campaign on OHS rights and responsibilities should be considered on a large scale by enforcement authorities, trade unions and employers.
Occupational health professionals include occupational health doctors and nurses, occupational hygienists, environmental health professionals, workplace inspectors, employee assistance practitioners, occupational therapists, ergonomics practitioners and health and safety practitioners. These practitioners can be categorised in three broad sections, namely: those directly involved in service provision, those involved in inspections and enforcement and those involved in social protection.
The total number of certified occupational hygiene professionals is currently 836 (Southern African Institute for Occupational Hygiene). There are 404 (Myeni, 2020) occupational medicine practitioners registered with SASOM, 58 occupational medicine specialists and 1 679 occupational health nurses registered with SASOHN. According to the WHO, the ratio of 1:1 000 population is recommended as best practice. Our proportions in South Africa are very low at 1 occupational health nurse to 5 657 formal sector employees excluding agriculture. However, the doctors’ numbers are a gross under-estimation, especially for occupational medicine practitioners, as a large proportion is not affiliated with SASOM. Registration with professional bodies is voluntary, the result being that there are many more doctors practising occupational health without affiliation to SASOM. For nurses however, due to the incentive of a professional insurance cover, the numbers are a true reflection.
A large proportion of inspectors are employed by the DMRE for the mining sector and the DEL for the remaining industries. There are also other inspection agencies and regulators that perform specific inspections and are highly legislated. For example, the Railway Safety Regulator regulates the railway sector, and the National Nuclear Regulator is responsible for enforcing regulatory radiation safety standards. Currently there is approximately 1 inspector per 3 689 mining employees and 1 per
25 690 employees in the non-mining sector. This is after the recruitment of 500 inspectors in the DEL in 2019. Of note, over the past three years, more women inspectors have been employed, attempting to bridge the gender divide.
Social protection agencies such as the Medical Bureau for Occupational Diseases and the Compensation Fund together with its mutual assurances employ different cadres of professionals including administrators, nurses, doctors and occupational therapists, among others, depending on their mandate.
The majority of OHS personnel are concentrated in the private sector. Those in the public sector, although qualified as occupational health professionals, are often re-purposed for other duties that are deemed a priority in hospitals, for example, maternity services. One of the main reasons for this is poorly functioning public OHS that lacks the appropriate operational structure.
There are at least 10 different professional bodies for different categories of OHS as per Table 11.7. The direct service provision group, namely, nurses, doctors and occupational hygienists have organised themselves into professional societies.
Name of Professional Body Acronym
South African Society of Occupational Medicine
South African Society of Occupational Health Nursing Practitioners
South African Institute of Occupational Hygiene
Southern Africa Institute for Occupational Safety and Health
South African Qualifications and Certification Committee – Fire
South African Qualifications and Certification Committee – Gas
Institute for Working at Heights Professional Body
Employee Assistance Professionals Association
Ergonomics Society of South Africa
Mine Medical Professionals Association
South African Council for the Project and Construction Management Professions
SASOM
Occupational Health Doctors
SASOHN Occupational Health Nurses
SAIOH Occupational Hygiene Professionals
SAIOSH Health and Safety Professionals
SAQCC-Fire Fire Service Technicians
SAQCC-Gas Gas Practitioners
IWH
Working at Heights Professionals
EAPA Employee Assistance Practitioners
ESSA Ergonomics Practitioners
MMPA
Medical and Health Professionals in Mining Industry
SACPCMP Occupational / Construction Health and Safety Practitioners
These societies are used as a networking platform for members to engage in matters of interest and provide guidance for practice. Continuing education is often a major priority activity of societies to strengthen and promote sound occupational health knowledge and practice as well as to further professional interests of members of these societies.
Occupational
Training of occupational health professionals happens at various levels in South Africa depending on the roles that one needs to fulfil. Formal courses offered through various universities range from postgraduate diplomas to PhD. For doctors, a Fellowship qualification is offered by the Colleges of Medicine of South Africa through the University of Cape Town, University of the Witwatersrand, University of KwaZulu-Natal and Stellenbosch University. Over the past five years, the number of trained occupational medicine specialists has been increasing by an average of two specialists per year. The total of specialists trained since the speciality was gazetted in 2007 is 56 in the country, including three non-South Africans.
For nurses, various institutions offer postgraduate courses up to Masters and PhD level. It is important to note that the majority of courses are offered in the Gauteng province and none are offered in Mpumalanga, Free State, Northern Cape, Eastern Cape, Limpopo and North West.
Of note, the South African Nursing Council is currently restructuring and has drafted a new curriculum that replaces all courses with a postgraduate diploma and a BCur at NQF8 level. All institutions are in the process of being accredited and the process is rather slow, hence it will be noticed that training has been halted in institutions such as the University of the Witwatersrand. Currently, only Cape Peninsula University of Technology and Durban University of Technology have been accredited thus far for intake in the 2022 academic year of 60 and 15 students, respectively. Institutions such as the Foundation for Professional Development continue to offer short courses (e.g. audiometry, spirometry and vision screening) while awaiting accreditation for two-year courses.
Occupational hygiene consists of professionals emerging from various relevant disciplines. The majority of occupational hygienists stem from the Environmental Health stream that is still offered at a number of tertiary institutions (e.g. Tshwane University of Technology and University of Johannesburg). Many others graduated with a BSc in Physiology from universities such as the North-West and Limpopo. The North-West University recently restructured the formal training of occupational hygienists by introducing specific programmes from undergraduate to PhD level in Occupational Hygiene.
The Southern African Institute for Occupational Hygiene, being the regulatory professional body governs professional examinations that must be successfully completed to demonstrate competence at various certification levels, and continual professional development is required to ensure that occupational hygiene professionals maintain their knowledge and expertise as well as to remain up to date with new knowledge.
Other programmes for occupational hygienists are postgraduate degrees (MSc, MPH, M-Tech and PhD) offered by various universities such as Wits, UP as well as universities of technology.
Furthermore, the Wits School of Public Health has introduced new qualifications (MSc Medicine: Exposure Science & MPH Exposure and Health) which also aim to train occupational and environmental health professionals including occupational hygienists. The new qualifications begin at postgraduate level with no specific undergraduate degree to direct their academic progression. Although the qualifications aim to be specific for exposure scientists, it is however still not clear how placement of graduates will be pursued in terms of employment and career pathing.
It is important to note that South Africa also provides postgraduate occupational health training for the rest of the continent. A recent study confirms that there is still a shortage of occupational health professionals in Zambia, Lesotho, Mozambique and Malawi (Moyo, 2015).
South Africa faces multiple economic challenges such as jobless growth especially affecting young people and the need to transition to a green and climate resilient economy. The elements of an advanced industrial economy and the Fourth Industrial Revolution together with primary, secondary, tertiary and informal sectors cover important models for innovations in OHS that should ‘leave no worker’ and their families and communities behind.
Between 2015 and 2020, there was heightened awareness on occupational health and safety driven in part by occupational health professionals and trade unions. The COVID-19 pandemic exposed some of the shortcomings in occupational health and safety (especially in public health facilities) and provision of PPE. Development of a database for occupational lung diseases in mineworkers, innovations in service delivery for certain sectors of the economy and partnerships across public and private sectors and occupational health professionals in the COVID-19 workplace programme were some of the initiatives during this period. The class action settlements amounting to billions of rands for silicosis and TB allowed for introspection by the mining sector and occupational health and safety preventive interventions such as the Masoyise TB project in the mining sector. Education and training initiatives across the continent were undertaken in partnerships with occupational health professionals and institutes in different countries. The TB project in the mining sector funded by social partners raised awareness on occupational health and safety in the Southern African Development Community region using TB in current and ex-mineworkers as an entry point.
There remains a fragmented policy, governance and legislative framework for occupational health and safety. Attempts to integrate the two compensation systems failed despite substantive work over two years to develop one uniform compensation system. Surveillance data cannot be collected for occupational injuries and diseases and where available covers mainly numerator data. Thus, comparisons across sectors and monitoring of trends are not possible. The funding model for occupational health and safety is mainly driven by private sector resources especially in large companies with many sectors, including the informal sector bereft of services.
Leadership in occupational health and safety is needed and re-visiting the different commission reports and their recommendations would be an important initial step. The legal frameworks, although fragmented, can assist with driving an agenda for reform linking prevention and enforcement. Data that incorporates denominator and numerator can assist with epidemiological surveillance, the OHIS and interventions.
This chapter focused on the difficult legacy of neglect of occupational health and safety in South Africa with some innovations in service delivery. The COVID-19 pandemic provides an impetus of working together to deliver a safe and healthy workplace environment for workers.
• An approach to funding of the medical services may include the transfer of funds for medical care including rehabilitation costs to the proposed NHI fund to cover the costs of health care for occupational injuries and diseases.
• Increased investment in training should be considered to increase the numbers of trained OHS professionals to meet the needs for occupational health and safety especially in the public sector.
• Retention strategies should be developed for trained OHS professionals already in the system.
• A funding model should be developed to support OHS delivery across sectors and provide employment opportunities for occupational health and safety professionals.
Abdullah Report on Occupational Health. South Africa, 1996b.
Adams S, Ehrlich R, Quail Z, Jeebhay MF, Ismail N. Occupational health challenges facing the Department of Health: Protecting employees against tuberculosis and caring for former mineworkers with occupational health disease. South African Health Review. 2012/2013(1).
Alfers L, Xulu P, Dobson R. Promoting workplace health and safety in urban public space: reflections from Durban, South Africa. Environment and Urbanization. 2016;28: 391–404.
Anon. Women in Mining Factsheet. s.l. Mineral Council of South Africa. 2020.
Anon. World Health Organization. Prevention, identification and management of health worker infection in the context of COVID-19. 2020. [Online] [Accessed 2021].
Anon. Masoyise Health Programme Annual Report for 2020. 2021.
Atrey S. Beyond discrimination: Mahlangu and the use of intersectionality as a general theory of constitutional interpretation. International Journal of Discrimination and the Law. 2021;21(2): 168–178.
Brouwer DRD. Can the South African milestones for reducing exposure to respirable crystalline silica and silicosis be achieved and reliably monitored? Front Public Health. 2020; 8: 107.
Cavalli L, Jeebhay M, Marques F, Mitchell R, Neis B, Ngajilo D, Watterson A. Scoping global aquaculture occupational safety and health. Journal of Agromedicine. 2019; 24: 391–404.
Department of Employment and Labour. Compensation for Occupational Injuries and Diseases Act 130, s.l.: s.n. Government of South Africa. 1993.
Department of Health. Report of the Committee on Occupational Health. In: DOH (ed.). Pretoria (South Africa): Government Printers. 1996.
Department of Health, Government of South Africa, Act 33 of 2005. Nursing Act 2005
Department of Labour and Employment, Government of South Africa. COVID-19 Occupational Health and Safety Measures in Workplaces. 2020.
Department of Mineral Resources, Government of South Africa. Mine Health and Safety Act 29. 1996.
Department of Mineral Resources and Energy. Government of South Africa. Mine Health and Safety Inspectorate Annual Report 2019/20. 2020.
Erasmus Commission. The Commission of Enquiry on Occupational Health. Erasmus Commission. Pretoria (South Africa): Government Printers. 1976.
Grobler L, Mehtar S, Dheda K et al. The epidemiology of tuberculosis in health care workers in South Africa: a systematic review. BMC Health Serv Res. 2016;16: 416.
International Commission on Occupational Health. Seoul Statement on Occupational Health Services, Milano, 2021.
International Labor Organization. Health and Safety at Work. https://www.ilo.org/ global/topics/safety-and-health-at-work [Accessed Online 2021].
International Labour Organization. Convention 161 – Occupational Health Services in ILO, Geneva: 1985.
International Labour Organization and World Health Organization. HealthWISE Work Improvement in Health Services, Geneva. 2014
Occupational health and safety
Jeebhay M, Adams S, Morar R, Kolbe-Alexander TL. Health and Healthcare in the South African Workplace. South African Health Review, 13th edition. 2007;13: 103–121.
Jeebhay M, Jacobs B. Occupational health services in South Africa. In Crisp N and Ntuli A, eds. South African Health Review, 5th edition. Durban, South Africa: Health Systems Trust, 1999;19: 257–276. http://www.hst.org.za/sahr/99/chap19.htm
Kielkowski D, Rees D, Bradshaw D. Burden of Occupational Morbidity in South Africa: Two large field surveys of self-reported work-related and work-aggravated disease: research letter. South African Journal of Science. 2004;100(7).
Kgokong N, Mhlongo L, Vorajee N et al. National Institute for Occupational Health. Pathology Division Surveillance Report. 2018.
Kistnasamy MB. Occupational Health in South Africa. Dissertation, MPH, University of KwaZulu-Natal. 1987.
Lowe R, Barron P, Steyn S, Malekela L. Occupational Health and Randburg. SAMJ 1990;77: 581.
Maki L. Occupational Health Services in the South African Construction Industry: Prioritising Health. MMed, University of Pretoria. 2019.
Michell KE. Occupational Health Service Delivery in South Africa. Workplace Health & Safety. 2012: 60, 63–66.
Minerals Council South Africa. 2021. www.mineralscouncil.org.za/work/health-andsafety/masoyise-healthprogramme. [Online] [Accessed 7 June 2021].
Moodley P. Buchmann M. Inequity in Occupational Health Services for Government Hospital Workers in South Africa. Occupational Medicine. 2002: 52, 393–399.
Moyo D, Zungu M, Kgalamono S, Mwila CD. Review of Occupational Health and Safety Organization in Expanding Economies: The case of Southern Africa. Annals of Global Health. 2015: 495–502.
Myeni SS. The Profile of Occupational Health and Safety in South Africa. National Department of Employment and Labour (RSA) and the International Labour Organization. 2020.
Naidoo RJM. COVID-19 – A new burden of respiratory disease among South African miners. Curr Opin Pulm Med. 2021 Mar 1;27(2): 79–87.
National Department of Health. White Paper for the Transformation of the Health System in South Africa. Government Gazette. 1997.
National Department of Health. The Re-Engineering of Primary Health Care in South Africa. 2010.
National Department of Health. OHS within the PHC Re-engineering: The integration of occupational health services within the primary health care health system. Johannesburg, South Africa: NDoH. 2013.
National Department of Health. Guidelines for Symptom Monitoring and Management of Essential Workers for COVID-19-related infection. 2020.
National Department of Health, n.d. National Health Act 61 of 2003. Government Gazette.
National Department of Health. Guideline on the submission of COVID-19-related health data from workplaces to the National Department of Health. 2020. www. nicd.ac.za/wp-content/uploads/2020/08/Workplace-Data-SubmissionGuideline. [Online] [Accessed 20 June 2021].
National Institute for Occupational Health. OHSS Report for COVID-19 in South African workplaces for the period 1 October 2020 – 31 March 2021. 2021.
National Institute for Occupational Health. COVID-19 hospital surveillance –monthly update on hospitalized healthcare workers. Johannesburg (South Africa): NIOH / NHLS; 2022 [updated March 19, 2022; cited 2022 April 05]. Available from: https://www.nioh.ac.za/wp-content/uploads/2022/04/COVI_-HCW_ Report_week11of2022-1.pdf
Organisation of Economic Co-operation and Development. OECD Economic Surveys: South Africa 2010. 2010.
Rantanen J, Lehtinen S, Valenti A, Iavicoli S. A Global Survey on Occupational Health Services in Selected International Commission on Occupational Health (ICOH) Member Countries. BMC Public Health. 2017: 17, 787.
Read JM. Hospital-acquired SARS-CoV-2 Infection in the UK’s first COVID-19 pandemic wave. Lancet. 2021 Sep 18;398(10305): 1037–1038.
Rees K, Dunlop JL, Patel-Abrahams S, Struthers H, McIntyre JA. Primary healthcare workers at risk during COVID-19: An analysis of infections in HIV service providers in five districts of South Africa. S Afr Med J. 2021 Jan 18;111(4): 309–314.
Republic of South Africa. Medicines and Related Substances Act 101. 1965.
Republic of South Africa. Occupational Diseases in Mines and Works Act No 78. Government Gazette. 1973.
Republic of South Africa. Occupational Health and Safety Act No 85 Department of Employment and Labour. 1993: 15–16.
Republic of South Africa. National Public Health Institute of South Africa Bill. 2017. Republic of South Africa. National Health Insurance (NHI) Bill. 2021.
Sitas F, Davies J, Kielkowski D, Becklake M. Occupational Helth Services in South African Manufacturing Industries: A Pilot Survey. Am J Ind Med. 1988;14(5): 545–57.
South African Society of Occupational Medicine (SASOM). Organisational Health Services. 2017.
Wilcox E, Chimedza I, Mabhele S, Romao P, Spiegel J, Zungu M, Yassi A. Empowering Health Workers to Protect Their Own Health: A Study of Enabling Factors and Barriers to Implementing HealthWISE in Mozambique, South Africa and Zimbabwe. Int J Envron Res Public Health. 2020;17.
World Health Organization. Prevention, identification and management of health worker infection in the context of COVID-19. 2020. www.who.int/publications/i/ item/10665-336265. [Online Accessed 2021].
World Health Organization. Occupational Health. The Global Occupational Health Network [GOHNET] Newsletter, 2009 (15) [Online]. Geneva (Switzerland): WHO. 2021. Available: https://www.who.int/occupational_health/network/ gohnet_15.pdf?ua=1 [Accessed June 15 2021].
World Health Organization. Global Strategy on Occupational Health for all: the way to health at work. Recommendation of the Second Meeting of the WHO Collaborating Centres in Occupational Health, Beijing: WHO. 11–14 October 1994.
Zwi A, Fonn S, Steinbert M. Occupational Health and Safety in South Africa: The perspectives of capital, state and unions. Social Science & Medicine. 1988: 691–702.