


Peter Barron, Yogan Pillay, Keith Cloete, Steve Letsike
South Africa faces a quadruple burden of disease resulting from communicable diseases such as HIV/AIDS, tuberculosis (TB) and malaria; high rates of maternal and child mortality; non-communicable diseases (NCDs) such as hypertension and cardiovascular diseases, diabetes, cancer, mental illnesses and chronic lung diseases such as asthma; as well as injury and trauma. In this chapter there is a focus on three health issues which are used to illustrate the successes and failures of the health system’s response between 2015 and 2020. These are HIV/AIDS, TB, and maternal and child health (MCH).
For each of these three health issues relevant data are presented, painting a picture that illustrates the epidemiology and performance of the health system. Overall, between 2015 and 2019 there was an improvement in key metrics. Since 2020 we have seen the very negative impact of COVID-19 on socio-economic conditions in general, and the health system in particular, and these metrics have either stagnated or deteriorated since March 2020.
The review of progress on the response to these three health issues is complemented by two case studies. The first is the Western Cape Department of Health’s response to TB using lessons learnt from the COVID-19 response and incorporating a whole-of-society approach. The second illustrates gender issues in relation to access to health services and human rights.
South Africa faces a quadruple burden of disease resulting from communicable diseases such as HIV/AIDS, TB and malaria; high rates of maternal and child mortality for the country’s level of development; NCDs such as hypertension and cardiovascular diseases, diabetes, cancer, mental illnesses and chronic lung diseases such as asthma; as well as injury and trauma. In all these areas South Africa has a much greater burden of disease than other comparable middle-income countries. In addition, South Africa has additional structural socio-economic challenges that hamper its efforts to improve health. These include having a very inequitable society economically with one of the largest Gini coefficients in the world, large-scale unemployment and a disproportionately large, well-funded private health system that caters for a small sector of the population. The private health sector consumes around 50% of all health resources yet caters for around 15% of the population. Additionally, it distorts the distribution of scarce human resources for health with disproportionate numbers of skilled health workers in the private health sector.
South Africa has the highest number of people infected with HIV globally with more than eight million people living with HIV. In addition, South Africa is one of the 20 high burden countries for TB. These two diseases, in addition to MCH, are used to illustrate the performance of the public health sector during the period 2015 to 2020 in respect of health programmes. This is not to undermine the performance of other programmes which are equally important. For example, it has been well documented that mental health is under-resourced and this population is under-served, as noted in a separate chapter of the book.
In general, with support from its partners and funders, in particular the United States Presidential Program for AIDS Relief (Pepfar) and The Global Fund to Fight AIDS, Tuberculosis and Malaria, the public health system improved key programme metrics during the period 2015 to 2019. With the advent of COVID-19 in 2020 these subsequently either stagnated or deteriorated.
This chapter discusses these three programmes in detail and augments this with two case studies. The first highlights some of the lessons learned from the responses to the COVID-19 pandemic by the Western Cape Department of Health and how it has started to use these to improve the province’s responses to TB. The second case study illustrates particular issues related to human rights and gender equity and access to health services to marginalised communities.
During the period 2015 to 2020, South Africa had the unenviable record of continuing to be labelled a high burden country for TB by the World Health Organization (WHO), for drug-resistant TB (DR-TB) and for TB and HIV co-infection. It has contributed significantly (3.6% of the global burden) to the global numbers of both drug-sensitive and DR-TB cases. Successive WHO Global Tuberculosis reports from 2015 to 2020 paint a picture of this. 1, 2, 3, 4, 5, 6 At the end of 2019, the world as a whole, most WHO regions and many high TB burden countries were not on track to reach the 2020 milestone of reducing TB incidence by 20% from 2015 to 2020. However, South Africa was one of seven high burden countries that was on track to achieve this indicator of the End TB Strategy. During 2020 the COVID-19 epidemic had a negative impact on key aspects of the TB control programme and negatively impacted both targets and indicators. During 2016 to 2020 some real progress was made with reducing the overall burden of TB in South Africa. Figure 5.1 illustrates the decreases in the incidence of TB, the incidence of HIV-positive TB and the number of notified cases. Also, as shown in Table 5.1, the estimated number of people who died from TB fell from a high of 124 000 in 2016 to 58 000 in 2019. The number of people with DR-TB dropped by over a third from just over 20 000 in 2016 to a little over 13 000 in 2019. The estimated incidence, numbers and rates dropped steadily from 2015 onwards, but were revised upwards in 2019 as a result of the findings from the first ever TB prevalence survey conducted in South Africa in 2018. ‘Missing’ patients is one of the biggest problems facing the national TB programme and is illustrated by an analysis of the TB programme cascade conducted in 2018, as shown in Figure 5.2. There are leakages of patients at every point in the cascade, for example, with not enough patients being tested and those who are diagnosed with TB not initiated on treatment. It is important to understand who and what contributes to these leakages and ‘missing’ patients so that the appropriate interventions can be put in place.
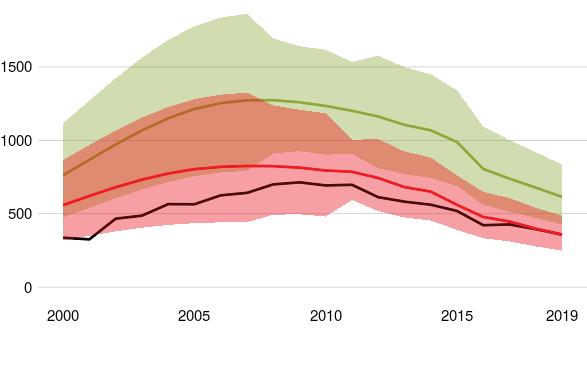
Figure 5.1 Incidence, new and relapse TB cases notified, HIV-positive TB incidence (Rate per 100 000 population per year)
Source: World Health Organization – Tuberculosis profile: South Africa 20196
Table 5.1 Key TB indicators in South Africa 2015 to 2020
Source: World Health Organization Global Tuberculosis Reports – Country Profile South Africa1,2,3,4,5,6
Source: Pren Naidoo (based on TB incidence based on National Prevalence Survey (MRC, NDoH); Accessed TB test back-calculated based on test sensitivity, assumption that 10% FN on Xpert receive culture and empiric treatment; Diagnosed based on National Health Laboratory Services (NHLS) data on case-finding (Courtesy Harry Moultrie, NICD) and National TB Report on empiric treatment; Notified and treated and treatment outcomes based on National TB Report and DR TB report (NDoH, Courtesy Sicelo Dlamini & Norbert Ndjeka); Durable cure rates based on CT data on relapse within 18 months for patients treated in 2018)
Disturbingly, 2020, the year of COVID-19, was characterised by a marked disruption of routine health services, which among other things saw a drop in the number of patients tested for TB; a decrease in the expected patients diagnosed for TB; and a drop in the numbers of patients notified and put on treatment. This is clearly illustrated in Figure 5.3. Based on data available in the routine information system, the number of symptom screenings for TB declined from 87.6 million screenings in 2019 to 70.8 million in 2020 (a 19.2% decline). The NHLS reported that the number of GeneXpert tests conducted declined by 26% between 2019 and 2020 with the percentage of positive tests declining by 18%.10,10 This had the effect of increasing the numbers of ‘missing TB’ patients across the entire TB cascade. All the patients who go ‘missing’ either die from their TB, add to the pool of TB by being chronic and infecting people in proximity to them, or else self-cure.
TB prevention has emerged as an important issue and the WHO guidance recommends TB preventive treatment for people living with HIV and household contacts. Of the 3.9 million people globally who received TB prevention treatment, 14% (509 000) were in South Africa. South Africa has also been at the forefront of innovation in TB prevention and is one of the first countries to start short course, preventive therapy through use of the new 3HP drug6. Similarly, South Africa has also been at the forefront of research into new tools, drugs and vaccines to combat TB and has been an early adopter of new drugs such as Bedaquiline in the treatment of multidrug-resistant (MDR) TB.
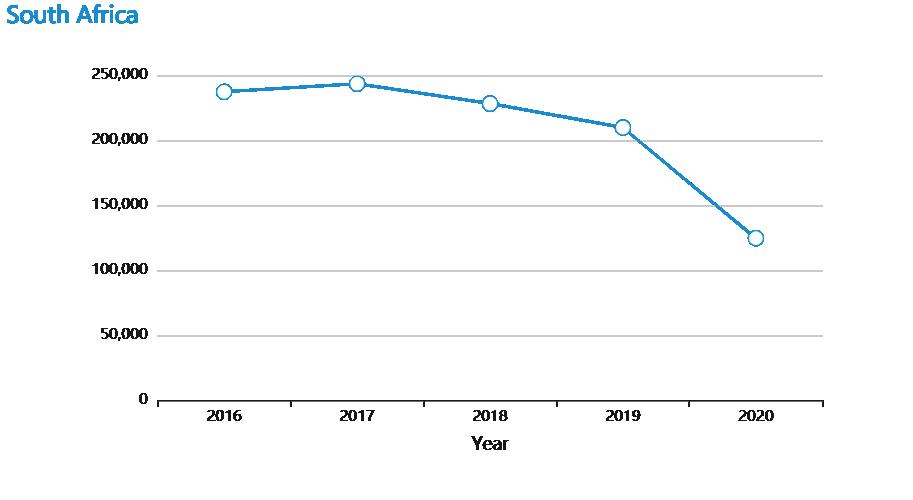
Source: World Health Organization – TB Database. Tuberculosis South Africa, provisional 20207
The Western Cape Department of Health used its lessons from its responses to the COVID-19 pandemic to strengthen its response to the significant burden of TB disease in the province. The case study highlighting the Western Cape Department of Health’s response to TB using lessons learned from COVID-19 is reflected in Box 1.
The COVID-19 pandemic resulted in significant disruptions, especially to TB services at Primary Health Care (PHC) level. GeneXpert test volumes dropped by 35% in 2020 compared to 2019, with a 40% drop at PHC facilities. GeneXpert positivity increased to 17.8% in 2020, and increased further in 2021, reaching a year-to-date average positivity of 19% by 22 August 2021. TB services were unable to recover, with 10 839 fewer TB diagnoses made in 2020, representing a 22% year-on-year reduction.
Between April 2020 and March 2021 there was a 27.2% year-on-year reduction in the number of people started on TB treatment, a 30.3% reduction in the number of people enrolled in TB treatment programmes at PHC level, and greater reductions in TB treatment initiation compared to the reduction in diagnoses, suggesting a larger treatment gap during this period. The worrying trend in these measures resulted in the launch of a provincial multisectoral emergency response plan to reduce TB, launched on 28 April 2021.3
In responding to the COVID-19 pandemic, the Western Cape Province has illustrated its ability to formulate agile, innovative and effective responses to health challenges, adopting a whole-of-society approach. Many of the lessons and innovations implemented in the response to COVID-19 have been adapted to inform the response to TB.
The Western Cape’s Emergency Response Plan for TB is centred on four focus areas:
1. Strategic communication: This includes a public-facing TB dashboard aimed at increasing public awareness.
2. Prevention of new TB infections and improving case detection: Deliberate efforts will be made to increase the uptake of TB preventative therapy amongst high-risk groups. Joint COVID-19 and TB screening is being conducted at all PHC facilities.
3. Enable early initiation of treatment and provide support to improve treatment completion rates: The province will pilot an SMS notification system, like that used for COVID-19, to inform clients of their TB test results. Other interventions in this focus area include the implementation of Urine-LAM testing as well as piloting, with the intention to expand, mobile digital X-ray services.
4. Implementing a whole-of-society response: Enhanced advocacy for socio-economic im provements, including psycho-social and nutritional support interventions for those living with TB.
The plan calls for a collective recognition amongst all stakeholders (government and civil society) that many of the social determinants that impact on the TB epidemic fall outside the scope of Departments of Health and underscores the need for an integrated and multisectoral response to addressing TB.
Box 1: Western Cape Department of Health’s COVID-19 Health Systems Lessons for TB Recovery Strategy
The COVID-19 pandemic provided fertile soil within which to innovate alternate means of approaching an infectious disease.
Community Prevention: COVID-19 provided a clear focus on increased public awareness for infection, prevention and control (IPC) measures such as mask wearing, cough etiquette and ventilation. Since both TB and COVID-19 are respiratory illnesses, the IPC measures overlap and will potentially allow for decreased stigma and increased uptake of the measures needed.
Screening: Paper-based, online and mobile screening tools proliferated during COVID-19 and allowed for patient agency in response to the pandemic. These tools offer low to no costs and help direct symptomatic patients timeously to care. Leveraging this approach for TB would provide increased passive detection of the disease with earlier treatment initiation. In addition, it may allow for combined COVID-19 and TB screening with appropriate routing of patients to care. A TB screening WhatsApp bot is already being piloted in accordance with this approach
Hotspot Identification and Response: One of the key lessons that had emerged throughout the COVID-19 pandemic was the importance of adequate, timely and accessible public data to understand the epidemic within one’s local context. This took the form of a public dashboard and has subsequently inspired the development and delivery of a first of its kind public TB dashboard in South Africa. This will allow near-real-time disease surveillance to guide programme managers to identify pitfalls within their geographic context and ensure transparency and public accountability to both citizens and the health department (https://www.westerncape.gov.za/site-page/provincial-tb-dashboard).
Testing and Tracing: COVID-19 PCR and TB Sputum GXP testing suffer similar challenges in terms of turnaround times for results. They both require the patient to be tested and return for the result after 24–48 hours. COVID-19 opened an opportunity to explore efficiencies in this process by sharing results via SMS or by a contact centre agent. Over and above this, dedicated teams were tasked to ensure telephonic contact tracing occurred to contain the spread within households. A similar strategy could be employed to ensure efficient containment of positive TB individuals as well as decreased initial lost to follow-up post sputum testing.
Virtual Case Management: The COVID-19 pandemic provided a springboard for virtual case management through telemedicine consultations. In the Western Cape, this was layered with a data-driven and risk-stratified approach to efficiently utilise clinicians to manage those most at risk of clinical deterioration. Within this project, contact centre agents were also onboarded to ensure high throughput follow-up of cases with clear red flags for escalation to the clinician team. This combination of virtual clinical and non-clinical staff supported by a risk-adjusted data-driven strategy for case identification can certainly be applied to the TB population. This will ensure a sharp directed approach to proactively manage and support patients through diagnosis, linkage to care and treatment completion.
Alternate Means of Medicine Delivery: Lastly, a by-product of restructuring the health platform in response to COVID-19 was the rapid ability to decant facilities and allow for alternate means of medicine delivery. The positive spin-off of this was reduced costs for patients to attend facilities for medication and resultant increased access for those vulnerable, with low socio-economic circumstances or too ill to attend facilities. Consideration should be given to expand this service to TB patients to gain similar benefits as those seen for chronic diseases. In addition, the delivery of chronic medication directly to patients’ homes will also potentially improve adherence to TB treatment and thus impact positively upon overall outcomes.
The Executive Director of UNAIDS, Winnie Byanyima, in the UNAIDS 2020 Annual Report15 stated that ‘the global HIV response was off track even before the COVID-19 pandemic, but the collision of COVID-19 and HIV has set it back further. The Fast-Track Targets, which expire at the end of this year, will not be achieved. Thirty-eight million people are living with HIV, with more than 12 million people waiting for life-saving HIV treatment. In 2019, 1.7 million people were newly infected with HIV and 690 000 people died from AIDSrelated illnesses’. She further stated that: ‘Ending AIDS means closing gaps and ensuring that no one is left behind. The HIV response must end inequality. If over the next five years we meet these new targets, end inequalities in HIV treatment and HIV prevention and reduce the stigma and discrimination that holds back the HIV response, the world will be well on its way to ending AIDS by 2030’.
During the past decade there has been significant progress in key indicators related to the impact of HIV in South Africa. UNAIDS country data15 shown in Figure 4.4 reflect the remarkable progress made in decreases in the annual numbers of new HIV cases and number of deaths caused by HIV between 2010 and 2019, with decreases of 53% and 61%, respectively. On the other hand, Figure 5.5 highlights the considerable way to go to achieve the 90:90:90 targets. South Africa made significant progress in reaching the first 90, viz those who are infected who know their status, and in 2019 the proportion was 92%. Of these, the proportion on antiretroviral treatment (ART) was 72%, leaving a gap of 810 000 to achieve the second 90. In terms of those who are on treatment and are viral load suppressed (the third 90), the Thembisa model (Figure 5.6) estimates that 89.7% of those on treatment were suppressed in 201918.
The Thembisa Project, a mathematical model of the South African HIV epidemic, has been the source on which the official UNAIDS estimates for South Africa are based and produced in partnership with UNAIDS and the South African Department of Health18. Tables 5.2 and 5.3 show indicators for HIV and the three 90s, respectively, for the period 2015 to 2022.
The number of new infections declined by 28.4% (from 301 837 to 216 008) during this time whilst the number of AIDS deaths dropped by 17.7% (from 86 851 to 71 435). The overall incidence rate also declined substantially from 0.87% to 0.59% in 2020. Although these are significant improvements, they are below the Sustainable Development Goal (SDG) 2030 target of ending the AIDS epidemic as well as the UNAIDS targets19 of achieving 95:95:95 by 202514. The net effect is that during the period 2015 to 2020 the number of people infected and living with HIV increased from a little over 7 million to nearly 8 million. This now chronic, lifetime infection will place a significant demand and impact on the resources of the health system for another generation. The Thembisa model predicts that by 2030 the total numbers of people living with HIV will have increased to 8.6 million, indicating a slow increase of less than 10% overall for the decade 2020 to 2030.
National health programmes
Although the prevalence numbers have been increasing, data from the Thembisa Project show that there have been notable successes with decreasing the incidence of HIV i. Recent evidence from the Thembisa model estimated an HIV incidence of 0.84% in 15–49-year-olds at the start of 2019. This represents a 62% reduction relative to 2000, and a 47% reduction relative to 2010. Although this reduction is lower than UNAIDS globally set targets of 75% reduction against the 2010 baseline, it is a significant reduction and in line with reductions seen in other countries in Southern Africa. The reduction in incidence in the period 2010 to 2019 was largely due to an increase in the scale-up of ART and condom distribution and use increase. The incidence reductions differed significantly by age and sex, with condoms having the greatest impact in youth aged 15 to 24. Overall incidence reduction was greater in men than in women. As both of these programmes have scope for further increase in scale, it is feasible to look ahead for further similar reductions in incidence over the next decade.
The impact of COVID-19 will undoubtedly amplify the challenges, and early studies provide evidence for this. In a review of routine data comparing 2020 to 2019 there is a demonstrated decrease in the number of HIV tests conducted every month in 2020 compared to similar months in 201920
Figure 5.4 Changes in HIV new infections, deaths and incidence/prevalence ratio in South Africa 2010 to 2019
Source: UNAIDS DATA 202015
Children (0-14)
Women (15+)
Men (15+)
Figure 5.5 HIV testing and treatment cascade 2019, South Africa, with gaps to the three 90s targets
Source: UNAIDS DATA 202015
Table 5.2 Key HIV indicators from 2015 to 2022, South Africa (Thembisa model)
National health programmes
(15-24 years females)
Source: Thembisa Project. Version 4.4 Downloads: National and provincial model outputs18
Table 5.3 The three 90s, South Africa, 2015 to 2022
Proportion
Source: Thembisa Project. Version 4.4 Downloads: National and provincial model outputs18
Figure 5.6 HIV tests done by month, in public health facilities, between March and December 2019 and 2020
Source: Pillay et al., South African Medical Journal 20212020
In this section, we focus on maternal and under-five mortality, pregnancy in adolescent girls as well as reproductive health services to illustrate how outcomes generally improved up to 2020. Services also improved generally over the period to 2019, but then stagnated or deteriorated with the onset of COVID-19.
During the period 2015 to 2020 the under-five mortality rate (child mortality) and the under-one mortality rate (infant mortality) both made significant improvements in 2020 after modest improvements in the previous four years. There was no change in the neonatal (under 28 days) mortality rate. This is shown in Table 5.421, which is based on the rapid mortality surveillance reports of the South African Medical Research Council, documenting mortality in the total South African population. The maternal mortality saw a steady improvement, with a decline of around one-third with an especially large decline in 2020.
The declines in child and infant mortality in 2020 can be attributed to the impact of total lockdown on both natural (decrease in pneumonia and other respiratory diseases) and also non-natural deaths (accidents). It is not obvious why maternal mortality declined by so much in 2020.
Table 5.4 Maternal and Child Mortality 2015 to 2020
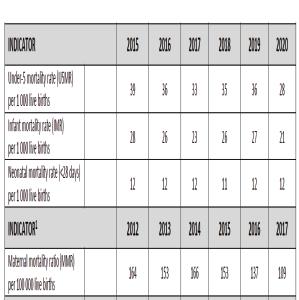
Source: Dorrington et al (2021), Rapid Mortality Surveillance Report, 2019 and 202021
The decline in maternal mortality over the last decade to 2019 is also clearly shown in Figure 5.7, which illustrates deaths in public sector institutions where more than 85% of deliveries take place.
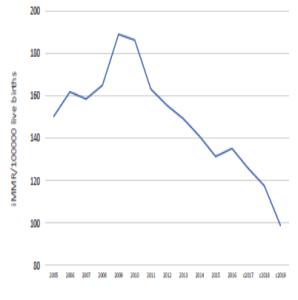
Figure 5.7 Maternal mortality in public sector institutions, South Africa 2005 to 2019
Source: Massyn et al., District Health Barometer22
However, the advent of COVID-19 in 2020 has changed the situation. An early study of routine public sector data shows that the number of maternal deaths increased by nearly 30% compared to 201924 and the institutional maternal mortality ratio increased from 90.5/100 000 live births for the period March to December 2019 to 106.8/ 100 000 for the same period in 202020. Similarly, there was a reversal in the improvement of neonatal mortality with an increase of 487 (4.8%) in the number of neonatal deaths between March and December 2019 and 2020. The institutional neonatal mortality rate increased marginally from 12.0/1 000 live births in 2019 to 12.2/1 000 in 20202020. Furthermore, routine services for essential maternal, women’s and child health, such as reproductive health services for family planning and immunisation services for childhood illnesses were severely reduced by COVID-19 in 202020
Preventing unintended pregnancies is essential for improving adolescents’ sexual and reproductive health and their social and economic well-being. Ideally pregnancies should be delayed, giving adolescent girls the opportunity to complete their schooling and be educationally, emotionally and physically ready to have children of their own. Pregnancies in this age group are important for monitoring progress towards achievement of universal access to sexual and reproductive health care services. A rise in this indicator is a cause for concern, as it indicates challenges in improving access to sexual and reproductive health care services for this vulnerable group. It also is an indicator of high-risk sex, which is a predictor of increases in sexually transmitted diseases such as chlamydia and gonorrhoea as well as HIV.
Table 5.5 shows the numbers of deliveries, terminations, delivery rates and estimated pregnancy rates by adolescent girls aged 10 to 19 years during the period 2017 to 2021. Contrary to what one would prefer from these data, which is a steady decline, there have been steady year-on-year increases in teenage pregnancies from 2017 to 2021. Part of this is due to the unavailability of routine contraceptive methods and services.
Three key issues are reflected in the routinely collected data. Firstly, there are around 4 000 deliveries each year amongst girls aged 10 to 14 years. This is statutory rape and each of these pregnancies is completely unacceptable. The increase in numbers with a nearly 50% increase in delivery rates over the period 2017 to 2020 is a shocking indictment of South African society and service delivery systems. Clearly, there has been a failure of society to protect these very young girls and their babies, with not only the health system to blame.
Secondly, there has been an overall rising trend at the national level over this time, with most provinces showing increases, with the exception of KZN, off an extremely high base. Thirdly, there is a marked difference between the urban provinces, especially Gauteng and to a lesser extent the Western Cape, having much lower proportions of teenage deliveries than more rural provinces such as Eastern Cape and KZN.
Table 5.5 Deliveries and terminations in adolescent girls aged 10–19 in the public sector, South Africa 2017/18 to 2021/22
*The numbers in 2021/22 for deliveries and terminations are for the period 1 April 2021 to 30 September 2022, a six-month period. To enable calculation of annual rates these numbers were extrapolated (doubled).
Source: Barron et al. (in press)ii
One of the ways to prevent and decrease the number of teen pregnancies is to make contraceptives readily and easily available. In Figure 5.8 below the proportion of eligible people who were using a modern contraceptive method decreased over the period 2015 to 2020. This means that they were either obtaining it through the private sector (more likely in urban areas) or simply not using contraceptives at all. The use of condoms is an ideal method for preventing not only unwanted pregnancy but also HIV and sexually transmitted infections. Successive behaviour surveys have shown that the youth generally have low condom use rates. This is a public health intervention that needs to be taken much more seriously.
During 2020, as a result of COVID-19, there was an average decrease of 5% in provision of reproductive health methods compared to 201910. This was most marked during the heavy lockdown in April, May and June of 2020.
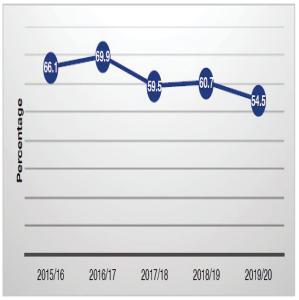
5.8 National couple year protection rate
Source: Massyn N District Health Barometer 2019/202222
The health system continues to make access difficult and is not particularly patient-centred and responsive to human dignity in general and gender differences in particular. The case study in Box 2 illustrates these issues.
The Ritshidze project (‘Saving our Lives’ in TshiVenda) is run by civil society organisations led by people living with HIV and other community activists monitoring public health clinics and the experiences of people attending these facilities for HIV and TB services. This project aims to hold the NDoH and aid agencies accountable to improve overall HIV and TB service delivery.
The reports from the project found that patients wait very long times to acquire services with an average wait of more than 4.5 hours. At least two out of five patients do not feel that the staff who attended to them are p rofessional and friendly and there were numerous reports of patients who had missed an appointment being sent to the back of the queue. Between 10 and 20% of patients interviewed said that they left the clinic without the necessary medicines because clinics were out of stock of essential medicines such as contraceptives and antiretrovirals.
The facilities also do not generally follow basic infection control guidelines to prevent the spread of infectious diseases such as tuberculosis. This is now particularly pertinent with COVID-19 as well.
There were many reports in all three of the provincial reports reviewed that the project has reported violations of people’s privacy and health care workers are treating key populations without dignity and respect. In many cases, facility staff focus on key populations’ (e.g., gay men, female sex workers) lifestyles and sexual lives, instead of on goodquality service provision.
Significant limited information gaps remain about the health status of the LGBTI+ community (the acronym LGBTI is used in some areas of the paper as a means of including the broad spectrum of sexual and gender identities and communities). This is because routine health data does not include data on the community despite the Bill of Rights guaranteeing access to health care to all regardless of sexual orientation and gender identity. The reality is that the LGBTI+ community is left behind as far as access to health services that meet their needs is concerned.
In the context of this lack of adequate services for the LGBTI+ community a number of non-governmental organisations have bridged the gap and provided dedicated health services. These include the Triangle Project, OUT and Access Chapter 2, amongst others.
However, it is important that government improves the services it provides to this community. In particular, health care workers should be better trained, appropriate services should be provided and relevant data should be routinely collected on members of the community within a rights-based approach.
During the period 2015 to 2019 there were general improvements in most of the key indicators related to HIV, TB and MCWH. However, most of the improvements were below the goals and targets set up by the SDGs, to which South Africa is a signatory. During 2020 (and up to the time of writing), there have been significant challenges posed by COVID-19, which threatens the performance of the health system and its outcomes. Not only has there been decreased access, through actual closure of facilities, lack of transport and fear of contracting COVID-19, but also the diversion of scarce resources (human and financial) towards the COVID-19 response and away from everything else, as well as declining health budgets generally, with the macro-economic environment less conducive to increasing resources for the public health sector.
The public health system as a whole has less resources to fund frontline staff (including community service doctors and nurses, as well as community health workers) who are essential for improving health programmes.
Great progress has been made in reducing the overall burden of TB in South Africa, however, this has been insufficient to reach all the targets of the End TB strategy. In addition, during 2020, as a result of COVID-19, and a reduction in access to health facilities, this has resulted in a reversal of some of the gains made in the 2015 to 2019 period.
In March 2021, a statement by the Stop TB Partnership estimated that the past 12 months have pushed back global TB progress by 12 years11. In South Africa, as in other countries, availability of health system infrastructure has been prioritised for the COVID-19 response and away from competing illnesses, including TB. Health care access has been constrained due to transport disruptions, restricted movement, reduced opening hours, depleted staffing levels, fear, and stigma. In a presentation of the 2021/22 Annual Performance Plan and Budget to the Parliamentary Committee in May 2021, the Chief Financial Officer stated that the repurposing of funds towards COVID-19 interventions meant future financial years would be difficult, with the implication that this would be to the detriment of other programmes, including TB, HIV and MCH13
There has been a range of suggestions to reverse and catch up on TB services and interventions, including using the COVID-19 crisis and not letting it go to waste.,12. These include: using COVID-19 testing to simultaneously test for TB; and using community-based and community-led responses that take diagnosis, care and support to the doors of those affected by COVID-19 and to also do contact tracing and treatment checking for TB. Other lessons from the COVID-19 response include agile decision-making involving all stakeholders, using mobile technology, real-time surveillance systems and enhanced political leadership. Finding and focussing on the missing patients including the elderly, young people and men will be vital to reduce the leakages from the TB cascade.
During the period 2015 to 2020 there were some remarkable successes, but it is clear that the work is not yet done to eliminate HIV as a public health threat. Progress towards the UNAIDS goals of 90:90:90 has been excellent and by the end of 2020 more than 92% of those infected by HIV knew their status and of those on ART treatment 89.7% were estimated to be viral load suppressed. However, of those who knew their status only 72% were on ART treatment, leaving a significant number of people (estimated at 810 000) who had either never started ART or had started but dropped out of treatment for one reason or another. The number of new infections and the number of deaths from HIV have also declined significantly over this period, with a halving of incidence between 2010 and 2019. However, these declines in incidence were below the UNAIDS and SDG goals and targets to end the HIV epidemic by 2030. HIV therefore continues to be a major epidemic in South Africa at the end of 2020 and has been clearly exacerbated by the negative effects of the COVID-19 pandemic. Given that HIV is associated with other NCDs such as diabetes and hypertension and the move to universal health coverage, it makes more and more sense for HIV to be treated as a long-term chronic disease and integrated with other conditions and programmes in a more patient-centred approach.
As with the other programmes, maternal, child and woman’s health had some successes but also experienced stagnation and deterioration associated with COVID-19. Of great concern is the inadequate uptake of contraceptives and the increasing number of adolescents becoming pregnant. This is also associated with adolescent girls being very susceptible to HIV and other sexually transmitted infections such as chlamydia and gonorrhoea, which are increasing and of epidemic proportions. There continues to be a sub-optimal use of condoms in South Africa, which has the potential to play a major role in improving outcomes for many of these challenges.
The health system continues to be negatively affected by the COVID-19 pandemic and faces a resource-constrained environment for several years. Building on the successes of the past and improving overall performance will require doing things smarter and more cost-effectively. One of the ways is to harness the power of data and improved ability to use this in the digital era. This requires greater attention to improving the quality of the data and making it available transparently and easily. Data should be packaged for the multiple users ranging from patients, community, clinicians and managers – all of whom have different needs in order to make appropriate decisions. Each disease and health programme needs to have a package of core and essential services (e.g. contraceptive services for teenage girls) that need to be available and acceptable and used by the beneficiaries of these and which need to be in place regardless of external circumstances. In other words, these need to be protected against all else and the health system needs to be resilient in doing this. In addition, as health does not come in single disease packages, health services need to be integrated so that patients can seamlessly have all their needs attended to in a patient-centred and holistic way.
References National
1. World Health Organization. (2015). Global tuberculosis report 2015, 20th ed. World Health Organization. https://apps.who.int/iris/handle/10665/191102
2. World Health Organization. (2016). Global tuberculosis report 2016. World Health Organization. https://apps.who.int/iris/handle/10665/250441
3. World Health Organization. (2017). Global tuberculosis report 2017. World Health Organization. https://www.who.int/tb/publications/global_report/gtbr2017_ main_text.pdf
4. World Health Organization. (2018). Global tuberculosis report 2018. World Health Organization. https://www.who.int/tb/publications/global_report/gtbr2018_ main_text_28Feb2019.pdf
5. World Health Organization. (2019). Global tuberculosis report 2019. World Health Organization. https://apps.who.int/iris/bitstream/hand le/10665/329368/9789241565714-eng.pdf
6. World Health Organization. (2020). Global tuberculosis report 2020 World Health Organization. https://apps.who.int/iris/bitstream/hand le/10665/336069/9789240013131-eng.pdf
7. World Health Organization (2021). Global tuberculosis database. Provisional TB case notifications in 2020. https://www.who.int/teams/global-tuberculosisprogramme/data (Accessed 5 May, 2021)
8. Pillay Y, Mvusi L, Mametja LD, Dlamini S. What did we learn from South Africa’s first-ever tuberculosis prevalence survey? S Afr Med J. 2021;111(5): 402–404. ISSN 2078-5135.
9. Van der Walt M, Moyo S. The First National TB Prevalence Survey, South Africa 2018: Short report. 2021. https://www.knowledgehub.org.za/system/files/elib downloads/2021-02/A4_SA_TPS%20Short%20 Report_10June20_Final_ highres.pdf
10. Pillay Y, Pienaar S, Barron P, Zondi T. Impact of COVID-19 on routine primary health services in South Africa. S Afr Med J [S.l.]. 2021;111(8): 714–719. ISSN 2078-5135.
11. The Stop TB Partnership. 12 months of COVID-19 eliminated 12 years of progress in the global fight against tuberculosis. March 18, 2021. http://www. stoptb.org/news/stories/2021/ns21_011.html (Accessed 8 May 2021)
12. Wingfield T, Karmadwala F, MacPherson P, Millington K, Walker N, Cuevas L, Bertel Squire S. Challenges and opportunities to end tuberculosis in the COVID-19 era. Lancet Respir Med. 2021. Published Online March 24, 2021. https://doi.org/10.1016/ S2213-2600(21)00161-2
13. TimesLive. Health services suffer as budget is prioritised to deal with COVID-19. 7 May 2021. https://www.timeslive.co.za/politics/2021-05-07-health-servicessuffer-as-budget-is-prioritised-to-deal-with-covid-19/ (Accessed 8 May 2021)
14. UNAIDS (2020). Prevailing against pandemics by putting people at the centre. Geneva. https://www.unaids.org/sites/default/files/media_asset/prevailingagainst-pandemics_en.pdf (Accessed 10 May 2021)
15. UNAIDS (2020). UNAIDS Data 2020. Geneva. https://www.unaids.org/sites/ default/files/media_asset/2020_aids-data-book_en.pdf (Accessed 10 May 2021)
16. UNAIDS (2020). COVID-19 and HIV: 1 Moment 2 Epidemics 3 Opportunities. Geneva. https://www.unaids.org/sites/default/files/media_asset/20200909_ Lessons-HIV-COVID19.pdf (Accessed 10 May 2021)
17. UNAIDS (2020). End Inequalities. End AIDS. Global AIDS Strategy 2021–2026 Geneva. https://www.unaids.org/sites/default/files/media_asset/global-AIDSstrategy-2021-2026_en.pdf (Accessed 10 May 2021)
18. Thembisa Project. Version 4.4 Downloads. National and provincial model outputs. https://www.thembisa.org/content/downloadPage/ProvOutput4_4 (Accessed 13 May 2021)
19. United Nations. Sustainable Development Goals. Goal 3: Ensure healthy lives and promote well-being for all at all ages. https://www.un.org/sustainable development/health/ (Accessed 17 May 2020)
20. Pillay Y, Pienaar S, Barron P, Zondi T. Impact of COVID-19 on routine primary healthcare services in South Africa. S Afr Med J. Published online 17 May 2021. https://doi.org/10.7196/SAMJ.2021.v111i8.15786
21. Dorrington RE, Bradshaw D, Laubscher R, Nannan N. Rapid mortality surveillance report 2019 and 2020. Cape Town: South African. Medical Research Council. 2021. https://www.samrc.ac.za/sites/default/files/files/2021-11-25/Rapid%20 Mortality%20Surveillance%20Report%202019%262020.pdf. (Accessed 15 February 2022)
22. Massyn N, Day C, Ndlovu N, Padayachee T, editors. District Health Barometer 2019/20. Durban: Health Systems Trust; December 2020. https://www.hst. org.za/publications/District%20Health%20Barometers/DHB%202019-20%20 Complete%20Book.pdf (Accessed 19 May 2021)
23. May J, Witten C, Lake L (eds) (2020). South African Child Gauge. Cape Town: Children’s Institute, University of Cape Town. http://www.ci.uct.ac.za/ sites/default/files/image_tool/images/367/Child_Gauge/South_African_ Child_Gauge_2020/ChildGauge_2020_screen_final.pdf (Accessed 17 May 2021).
24. Soma-Pillay P, Moodley J, Pattinson R, Fawcus S, Gebhardt S, Niit R. The effect of the first wave of COVID-19 on use of maternal and reproductive health services and maternal deaths in South Africa. Obstetrics and Gynaecology Forum. Published online 1 Dec, 2020. https://journals.co.za/doi/pdf/10.10520/ejc-me dog-v30-n4-a10 (Accessed 24 June 2021)
i Johnson L. Meyer-Rath G, Dorrington R et al. The effect of HIV programmes in South Africa on national HIV incidence trends, 2000-2019. JAIDS Journal of Acquired Immune Deficiency Syndromes. Publish Ahead of Print DOI: 10.1097/QAI.0000000000002927 (Accessed 13 February 2022).
ii Barron P, Subedar H, Letsoko M, Makua M, Pillay Y. Teenage births and pregnancies in South Africa 2017 to 2021 – a reflection of a troubled country: analysis of public sector data. SAMJ, in press April, 2022.