


Terence Carter, Tamlyn Roman, Wezile Chita, Gladys Bogoshi, Shrikant Peters
The health system inherited by the current government in 1994 was relatively well resourced for a middle-income country, yet there were significant inequalities present between the private and public sectors, and even within the latter the resources were skewed geographically as well as between levels of care. The performance of South Africa’s health system since the end of apartheid and the establishment of a democratic government in 1994 has been mixed. It has been argued that many good new policies were adopted, but implementation has been poor and inequitable access to hospital services remains a challenge in South Africa as a result of the two-tier health system (Michel et al., 2019). Currently there are approximately 814 hospitals in South Africa, of which 405 are in the public sector and 409 are in the private sector. The public health care facilities serve approximately 83% of the population, who are largely without medical insurance (Competition Commission, 2019).
Hospitals in particular are characterised by multiple resource requirements, processes and interactions, all of which operate within a broader health system context. All of these components require planning and coordination, and therefore sound hospital management at facility, provincial and national levels is essential.
A cascade of authorities starting from national, through provincial, to the facility level govern and manage hospitals. The National Department of Health (NDoH) is responsible for determining the strategic vision of the health system and for enacting policies to be implemented nationwide. The Provincial Department of Health (PDoH) is responsible for the implementation and oversight of service delivery at all facilities.
In 2011 the NDoH adopted the National Policy on Management of Hospitals to ensure effectiveness, efficiency and transparency in the management of public hospitals (NDoH, 2011). It provides directives for the classification of hospitals, which is based on their respective roles and functions, the size of communities served, the nature and level of their health service provision, and the hospitals’ accordance with national norms and standards.
In this classification, a hierarchical relationship exists between levels of care based on the provision of a defined package of services. Regional, tertiary, central and specialised hospitals are charged with rendering specialised tertiary and quaternary services; providing specialised referral units for other hospitals; and providing a platform for the training of health workers and research. Within each hospital, management of different functional areas is organised into functional departments. These include both clinical departments and crosscutting support service departments such as the human resource, supply chain and procurement, finance and logistics departments.
The policy also makes provision for the appointment of competent and skilled hospital managers, including the Chief Executive Officer (CEO), and calls for the development of an organisational framework for accountability to communities served, including guidelines for the establishment of hospital boards.
The national vision and policies for health are interpreted through strategic plans at national and provincial levels, which not only aim to guide implementation at a functional level, but also act to promote alignment with the requirements of a national health system by coordinating the activities of actors.
More specifically, the NDoH’s Strategic Plan outlines the strategic directions to be taken by the Department over a defined period. The overall goals for national health are embedded in the strategic plan which targets, among others, improvements in quality of care, human resources and financial management. These overarching strategies provide the direction, guidelines, norms and standards to be taken into account in provincial strategic planning for health services, and prescribes what should be done at facilities, including central hospitals where relevant. The most recent NDoH Strategic Plan 2020/21–2024/25 is grounded in strengthening the health system, with specific attention to quality improvement (QI) in the provision of care, including hospitals. While human resources for health is identified as a priority, there is limited mention in this period’s strategic plan of the requirements for improved management of hospitals.
In terms of national financing, in 2019/2020, R35 billion was spent on district hospitals alone, making up 33.8% of the total district health expenditure. Add to this that central and provincial hospital services consistently contribute more than 40% to provincial health expenditure (see Figure 7.1), hospitals absorb a significant share of overall public health expenditure (Devan et al. in District Health Barometer, 2020). The implication is that the importance of making hospital services more efficient and effective cannot be ignored, given that these institutions often constitute the largest expenditure category in the health system budget.
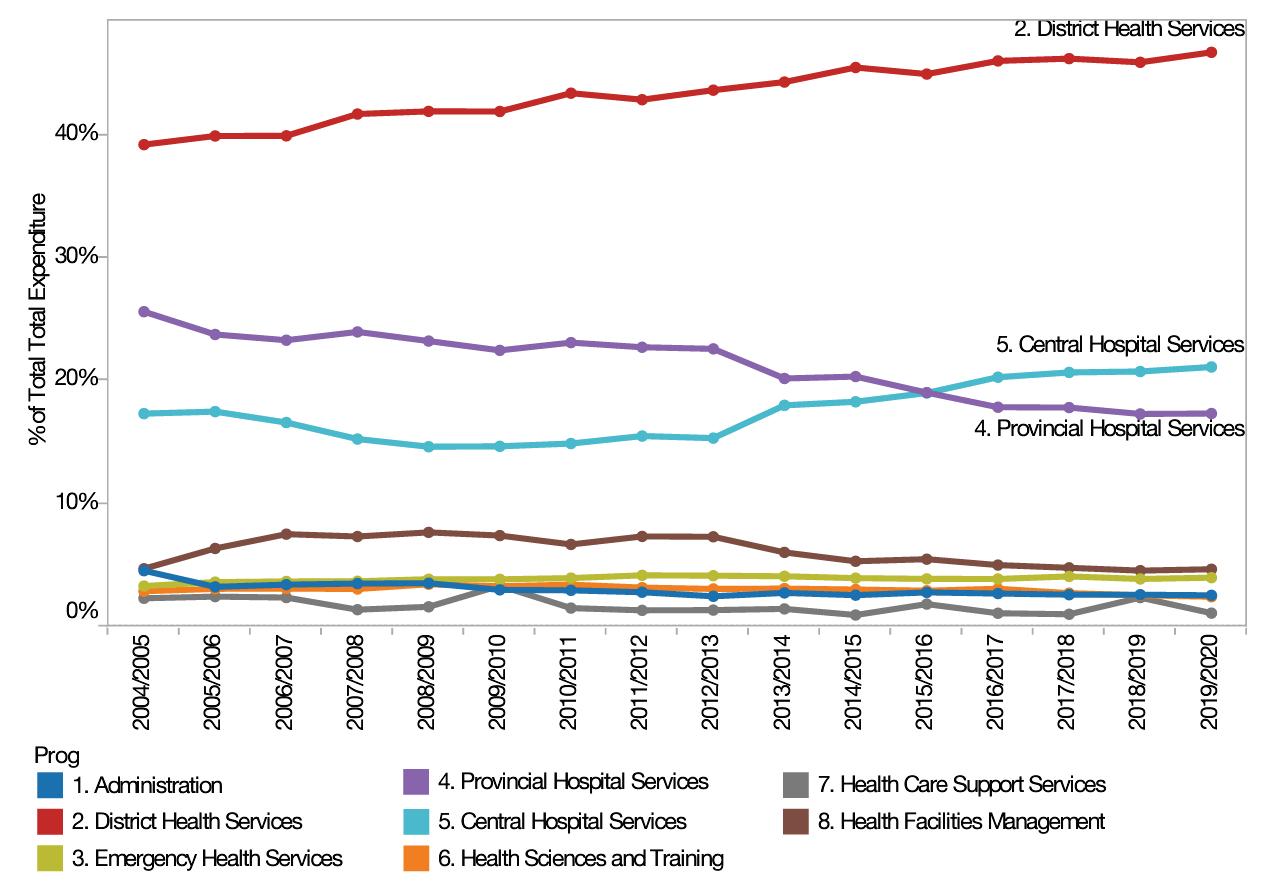
7.1 Proportion of provincial health expenditure by programme 2004/5 – 2019/20
Source: Devan et al. in District Health Barometer 2019–2020
While the national strategy for hospitals and tertiary services ascribes overall responsibility for policies and guidelines governing the management, service standards and human resources for hospitals to the national health department, provincial needs and realities dictate the resourcing and implementation of these proposals and are thus currently the mandate of the provincial health authorities.
The challenges facing the health system were acknowledged in the National Development Plan as follows: ‘The management of the health system is centralised and top-down. Poor authority, feeble accountability, the marginalisation of clinicians, and low staff morale are characteristics of the health system’ (National Planning Commission, 2010: pg. 332). These sentiments apply to all parts of the system, including the public hospital system.
In South Africa, the capacity for hospital management has been a longstanding critical area of concern (Engelbrecht & Crisp, 2010; von Holdt, Smith et al., 2010; Gilson & Daire, 2011; Doherty, 2014; GDoH, 2014).
The health system continues to face the underdevelopment of hospital services and chronic shortage of health professionals, which in turn affects the development of hospital support services in management, operations, administration, and clinical support (Barron & Padarath, 2017). The available resources to provide quality hospital services are compromised by the burden of disease, increasing demand, reducing budgets and the impact of a high medico-legal liability (Auditor-General of South Africa, 2021).
Recent research conducted on quality variability in the health care sector points to the failure of hospital boards and management in governing their establishments as a contributing factor (Brown, 2019). While issues of management and governance may not be the only shortcoming of the system, they are certainly significant contributing factors and it is argued that they should be the starting point for planned reform (Rispel, 2016).
Steward and Wolvaardt (2019) investigated hospital management and health policy in South Africa, and in the study recommended the professionalisation of hospital management, and the promotion of competency and transparency. The study further asserted that health workers must be held accountable for their actions and that hospital boards must be regulated. This was consistent with various studies that emphasise the importance of good corporate governance in the health system to ensure quality service delivery (Fusheini, Eyles, & Goudge, 2017; Govender, Proches & Kader, 2018).
1. Leadership and Management
Currently, hospital management capacity is prescribed in the context of the National Policy on the Management of Public Hospitals and the Regulations Relating to the Categories of Hospitals (Government Gazette No R; 185, 2 March 2012) as prescribed by the National Health Act 61 of 2003 (NDoH, 2011; NDoH, 2012). The regulations for the hospital management policy not only define the general categories of hospitals, but also make recommendations for their management in terms of the appropriate management structures, post levels and salary scales, as well as delegations of functions.
The regulations include guidelines for the appointment of competent and skilled managers, but explicitly define the job description and minimum requirements for appointment of the hospital CEO. The educational requirement for this position is a degree or diploma in a health-related field, with a degree or diploma in management as an added advantage, and five years of management experience in the health sector.
There are no formal competencies listed for hospital managers; instead, generic competencies for public sector management are defined in the regulations for Public Service and Administration. Their application to the role of the hospital CEO was benchmarked in a competency framework developed by the Department of Public Service and Administration (DPSA, 2008), and this formed the basis of an assessment of hospital management competencies undertaken by the Development Bank of Southern Africa, which focussed on competencies related to leadership and management, organisational responsibilities, and interpersonal engagements.
Although this assessment found that many hospital CEOs were not fit for the job, and the revised policies have since led to appointments of hospital managers who meet the minimum requirement for the post, the framework used for the detailed assessment of competencies was not formally adopted.
In June 2017, the South African NDoH released its plan for a National Health Insurance (NHI) – see Chapter on Health Financing, which is a financing system intended to facilitate better access to quality and affordable health service for all South Africans (NDoH, 2017). The NHI represents the latest step in a journey towards a
public health system that would allow the entire population to realise the right to access health care services that is embedded within the South African Constitution (RSA Constitution, 1996). This plan has been designed in response to a health system that is not without challenges and will require significant reforms to, amongst other things, the management of central hospitals.
The NHI policy gazetted in June 2017 lays out the intention to make some hospitals, including central hospitals, semi-autonomous and to allow complete decentralisation of management functions. Significant decentralisation of authority and decision-making to hospital management is envisaged within the management and governance system of the NHI. The exercise of such authority must be guided by the basic values and principles governing public administration as set out in Chapter 10 of the Constitution.
In order to make these hospitals more effective, efficient and responsive, the NHI proposes that hospital managers will have ‘full delegations and decision-making powers including control over financial management, human resources management, infrastructure and technology, as well as planning and decision-making’ (NDoH, 2017: pg. 38).
This ambitious intent of the NHI recognises that there are existing gaps in ethical and values-based leadership in South Africa, which contributes to poor quality of care through lack of accountability, corruption and fraud (South African Lancet National Commission, 2019). The prevailing management culture reflects the strong emphasis on centralisation, compliance, adherence to centrally determined processes, rigid classification of tasks, and an entrenched hierarchy (Health Ministerial Task Team, 2017).
At this time, and in response to the intentions of the NHI policy, development of a revised governance model for hospitals is in progress and, while this reform has gained much traction, there are still many questions regarding the respective governance roles of the national and provincial health departments, the accountability mechanisms that will be implemented, the financing, CEO competencies and the development of hospital performance indicators (Hendricks, Buch et al., 2015; Waterhouse, Mentor-Lalu et al., 2017).
Several lessons for management of a hospital were learned during the COVID-19 pandemic. The box below reflects some of the lessons reported by the CEO of Groote Schuur Hospital, which are applicable to any hospital both during times of crisis and for effective management on a daily basis.
Box 1 Lessons on and for Management: Personal reflections of a hospital CEO
• Caring for our staff must be a top priority:
o Creating a culture of engagement, listening to and supporting the staff
• Being adaptive and responsive
• Using Artificial Intelligence, Information Technology and Information Management to do business differently
• Maximise fiscal discipline and efficiency
• Provide leadership
• Visible leadership
• Responsive leadership
• Adaptive leadership
• Communication, Communication, Communication
Source: Dr Bhavna Patel, Hospital Annual Operational Planning Presentation, 2021
Improved accountability is often called for as an element in improving health system performance. At first glance, the notion of better accountability seems straight forward, however, it contains a high degree of complexity. For accountability to serve effectively as an organising principle for health systems reform, conceptual and analytical clarity is required.
Using an accountability lens can: a) help to generate a system-wide perspective on health sector reform, and b) identify connections among individual improvement interventions. These results can support synergistic outcomes, enhance system performance, and contribute to sustainability.
Political/democratic accountability also relates to building trust among citizens that government acts in accordance with agreed-upon standards of probity, ethics, integrity, and professional responsibility. These standards reflect national values and culture, and bring ethical, moral, and on occasion religious issues into the accountability equation at both agency and individual levels.
The governance and accountability requirements within a decentralised management framework place a greater onus of meticulous adherence and compliance to the rules and regulations related to financial management and reporting as required by the Public Finance Management Act (PFMA) and its Regulations to be followed and observed.
In this context, the hospital board will have the responsibility of an accounting authority, which must be accountable for the purposes of the PFMA. Accounting authorities must ensure that accurate books and records are kept and that financial statements and other statutory reports are prepared. In addition to obligations contained in the PFMA, the members of the hospital board will be required to carry out their fiduciary duties in accordance with the common law and to meet the same obligations as directors of private sector companies.
In addition to its fiduciary responsibilities, the hospital board also has responsibility for evaluating and improving health care quality performance, setting and oversight of strategic quality priorities, promoting leadership and culture, and ensuring effective systems and processes are in place to maintain and improve quality. Such oversight responsibilities will include a quality and safety reporting framework as well as oversight of broad strategic health care quality priorities. This implies moving beyond symbolic acknowledgement of specific planned priorities into quality planning mechanisms overseen by the governing body (Brown, 2019).
Within a complex health care environment, these fiduciary and health care quality performance oversight responsibilities will require board members to have specific training in analytic capabilities and sophistication, particularly in the evolving era of ‘big data’ (Mountford & Wakefield, 2017).
Building the capacity of members of hospital boards must therefore include the ability to analyse, understand and interpret quality and safety data, and routine morbidity reporting (Mannion et al., 2015). Quality improvement is a hospital board priority. This includes balancing a short-term focus with a long-term strategic focus on QI. Critical to achieving this is using data for improvement as well as patient and staff engagement and clinical leadership (Jones et al., 2017).
One of the foundational requirements of the NHI is to ensure health facility readiness and to improve the quality of care by establishing national norms and standards and strengthening clinical governance. However, hospitals in South Africa have faced challenges from insufficient funding, inequitable human resource distribution and poorly maintained infrastructure.
In response to these challenges, and building off of the foundation previously established through the Ideal Clinic Realisation and Maintenance (ICRM) programme (see Chapter on Quality Health Care), the NDoH has developed the Ideal Hospital Realisation and Maintenance Framework (IHRM-F) to facilitate improved quality service delivery. The framework was designed to ‘serve as a benchmark mechanism to monitor Health System Strengthening activities, to improve efficiency gains in service provision and to improve patient experiences’ (NDOH, 2018).
The definition of an ideal hospital is one with:
• Good infrastructure
• Efficient patient management administration processes
• Adequate and appropriately managed staff
• Evidence-based service delivery aligned with the defined package of service for
• that level of care
• Uses patient experience feedback for continuous QI across clinical and administrtive services
• Compliance to standards for corporate governance and accountability to the community and stakeholders.
The IHRM-F framework is based on the ICRM framework which was developed in response to the challenges to providing quality primary health care services, identified by the Office of Health Standards Compliance (OHSC) in a 2013 audit.
The OHSC was created by Parliament as an independent body charged with ensuring that the health and safety of users of all health establishments are protected. Established in terms of the National Health Amendment Act of 2013, it assesses, monitors and enforces compliance by health establishments with prescribed safety norms and standards.
The IHRM-F was designed in alignment with the standards defined by the OHSC and includes both outcome and process assessment for all functional areas of the hospital. This capacitates hospital management to identify and address comprehensive service delivery challenges and benchmark performance against a standardised assessment framework.
An Ideal Hospital Manual was developed to outline the minimum requirements for a facility and to provide detailed guidance on how to assess and satisfy these requirements. A multidisciplinary team made up of clinical, support service, diagnostic and para-clinical service representatives should be appointed every year to lead the completion of the facility assessment against the Ideal Hospital framework. Each functional departmental area in the hospital is to be scored as having achieved, partially achieved or not achieved the minimum standards required and defined by the framework. On the basis of the outcome of this assessment, a facility can then be categorised as not having achieved Ideal Hospital status, or as attaining silver, gold or platinum status. The expectation is that by identifying the areas in need of intervention, the facility management is capacitated to develop and implement a QI plan that will allow for attainment of Ideal Hospital status.
The roll-out of the IHRM-F began with implementation at district hospital level, with staggered deployment to other levels of hospital care expected to follow, but was delayed due to the COVID-19 pandemic. By the start of 2022, 42% of district hospitals nationally had conducted status self-assessments and of those that were assessed, 52% did meet the requirements for Ideal Hospital status. Of this group, 43% achieved silver status, 3% gold and 2% platinum.
The lowest performing functional areas in the assessments were infrastructure, namely, the availability of essential equipment, and operational management, including disaster and emergency preparedness. The recommendation from the NDoH is to increase the number of facilities that have completed status assessments and that PDoHs use the information generated to implement QI plans.
One of the risks of poor clinical governance and poor provision of quality clinical care is the increase in medical negligence and related litigation. There has been a proliferation of medical negligence litigation against the NDoH, leading to large payouts which have put further strain on the health budget (see Chapter on Health Financing). Medical negligence impacts on access to quality health care. The Medical Protection Society estimated that ‘the long-term average claim frequency for doctors in 2015 was around 27% higher than that in 2009’, while the amounts claimed had escalated by an average of 14% per year from 2009 to 2015 (Dhai, 2015).
At a medico-legal summit in Pretoria (9–10 March 2015), Health Minister Dr Aaron Motsoaledi described these claims as reaching ‘crisis’ level: ‘The nature of the crisis is that our country is experiencing a very sharp increase – actually an explosion in medical malpractice litigation – which is not in keeping with generally known trends of negligence or malpractice’ (Kollapen et al., 2017:3).
In a report indicating medico-legal claims paid by government in each province in South Africa (presented at the summit by the acting Chief Litigation Officer of the Department of Justice and Constitutional Development), the total amount paid out for litigation in 2015 was R498 964 916.72; the Department of Health in KwaZulu-Natal led with total claims paid amounting to R153 612 355.49 and with over 5 billion rand in pending claims against the province (Kollapen et al., 2017:16; Maphumulo & Bhengu, 2019).
In 2020–21, the provincial health departments paid out R1.76 billion for medical negligence claims, while the estimated settlement value of unpaid claims at year-end was R124.15 billion (75% of the total claims against the state). Seven provincial health departments had unpaid claims at year-end that exceeded their entire operational budget for the next year (Auditor-General of South Africa, 2019).
Following the medico-legal summit, a comprehensive strategy was developed and implemented to deal with the challenges identified. Key areas of the strategy included improving overall communication and administration, dealing with occupational stress, effective clinical governance, morbidity and mortality monitoring and clinical audits, sharing the outcomes of cases of misconducts/ malpractice, and introducinga mentoring programme in all councils.
One of the key recommendations of the Ministerial Summit was the establishment of provincial medico-legal units. Such units have now been established in seven provinces and the next step is to assess the implementation and impact of these units.
Strengthening Financial Administration and Supply Chain Management
Planning, budgeting, the award of funding and the financial management of a hospital are based on a cascade of laws, policies, auditing mechanisms and processes at both national and provincial levels, with sources of funding for PDoHs and their facilities, such as central hospitals, being both national and provincial.
At the level of the hospital, the responsibility for financial management is assigned to a financial manager, while the responsibility for managing the annual audit process lies with another manager. Annual budgets are prepared according to the Treasury guidelines for the annual performance plans for both national and provincial health departments. These plans identify the performance indicators and targets for the strategies that the facility will seek to achieve in the upcoming budget year, guide the budget, and form the basis of annual reports. Guidance on the structure of the annual performance plan, its targets and indicators and timeframes, and the planning, reporting and auditing processes are set out in the PFMA and the Treasury Regulations.
National Treasury awards every province an amount of funding called the provincial equitable share, which is a constitutionally required distribution of money from the national government to the provinces (Blecher, Kolliparna et al., 2010). It is based on a formula that aims to advance national equity.
The division of the equitable share between provinces takes into account the provinces’ need to provide basic services and therefore relates directly to the demand for education, health and welfare services (Treasury, 2016). The equitable share provided by national government to the provinces does not prescribe allocations to these service areas.
A second National Treasury allocation is made to the provinces through conditional grants earmarked for specific projects through the Division of Revenue Act No 1 of 2005 (National Treasury of RSA, 2016). Conditional grants ring-fence budgets for the provision of health services. Although there is no stipulation regarding how the funding should be distributed between organisations, the NDoH is authorised to freeze allocations when spending is slow or mismanaged (Blecher, Kolliparna et al., 2010). The conditional grants received by central hospitals include the health facility revitalisation, the national tertiary services and the health professions training and development grant. Funding for central hospitals comes from the provincial equitable share, conditional grants and provincial finances, and in theory, the pooled funding is allocated on the basis of need. Each facility submits a projected budget to the province for consideration as part of the financial cycle, but for the most part, budgets are set by historical precedent, with marginal increases allowed to compensate for inflation.
A further source of funding is facility-generated revenue from sources such as patient fees, and although these are collected at the hospital, they cannot be retained for use at that level, and have to be returned to provincial authorities.
Given the context for financing sources, in line with international trends in improving the financial management of hospitals, the approach currently being explored is to make hospital expenditure more effective and efficient. The reform will require hospitals to move away from global budgets towards case-mix-based funding (payment by activity), so that public and private commissioning agencies or purchasers can assess the volume and quality of hospital production.
This calls for more effort on the recording, coding and detailed costing of activities, requiring the following:
a. Providing funds according to a case-based formula (typically adjusted diagnosis-related groups (DRGs)) and, increasingly, tying those payments to activity and/or performance levels
b. Improving management efficiency and accountability with the implementation of cost centre management at a decentralised level
c. Revised delegations to CEOs to be consistent with the accounting of ficer system
d. Training of CEOs and hospital managers to develop capacity to execute the new delegations.
It is envisaged that hospital financial management under an NHI system will address costing, contracting, contract management, use of DRGs and ensuring audit compliance. The use of DRGs as a fee-for-service model under the NHI for costing of health care services would impose a total overarching cost charge per event, such as an admission for a cerebrovascular accident, myocardial infarction or mid-shaft femur fracture requiring operative intervention. Such charges would need to be costed based on an accurate determination of all cost inputs related to a patient’s hospital stay and would also need to factor in the variability of patient management, frequency of presentations and possible resulting economies of scale. Accurate costing is vital to mitigate the risk borne by funders and providers for variability in cost beyond the amount set for remuneration.
Medium- to long-term workforce planning and management for the whole national health system is the responsibility of the NDoH and is governed by the Human Resources for Health (HRH) strategy (NDoH, 2011) (see Chapter on Human Resources for Health). However, the PDoH is responsible for operationalising that plan, which is then implemented by the hospital.
In this respect, while the human resources plan for the hospital is determined externally and is implemented through a centralised decision process with which the hospital must comply, there is some opportunity for flexibility in human resources management at the hospital.
One major challenge is that, at present, the determination of the human resource capacity of the hospital is based on historical establishments and not on empirical data of the current need for health services. In 2009, consultants were contracted by the Gauteng Department of Health to determine an ideal staff structure for all provincial hospitals based on number of beds per hospital. To date, this organisational plan has not been updated to reflect changing demand for services and the related human resource requirement.
However, while the workforce planning for the hospital resides in the provincial authority, which also determines the staff complement and post structure for the facility, where sufficient motivation is provided based on function and purpose, and availability of budget, recommendations may be made for additional staff, or for a shift in staffing positions.
Across the national health system, there is currently a process being led by the NDoH to develop staffing norms and standards using the Workload Indicators of Staffing Need (WISN) tool (WHO, 2014). This tool determines health worker requirement by type and workload, and provides the basis for management of staff establishment. However, until the outcomes of the use of this tool have been finalised, there are no generalisable staffing norms and standards available.
The absence of such national norms and standards does not directly influence the audit practice at the hospital, as they would not inform the annual monitoring conducted by the Auditor-General, whose oversight responsibility is outlined in the section that follows and whose remit largely applies to ensuring compliance with the broad human resources policies and the regulatory mandates.
The state of many health care facilities results in ever-decreasing faith in the health care system. Millions of rands over many years have been dedicated to infrastructural improvements and maintenance (see Chapter on Infrastructure).
The HSR notes that the NDoH ‘has a health infrastructure plan, but to date the country has had neither the expertise nor adequate funding to implement the plan. In some cases, health infrastructure construction that has been successfully completed has either cost more than the initial budgeted amount or facilities have been constructed that fail to meet the need for the service required’. It also states that in most cases there is insufficient capacity for project implementation, monitoring and evaluation.
Over the next three years, R19.2 billion has been allocated to the health facility revitalisation grant and a further R4.3 billion has been allocated to the health facility revitalisation component of the NHI indirect grant. Additional allocations have been added to fund the new academic hospital in Polokwane. However, in order for provinces to access this grant, a two-year planning process is needed in which provinces are assessed and required to obtain a minimum score of 60% in order to qualify for the incentive. Only three provinces qualified in the 2019/20 financial year, these being KwaZulu-Natal, Eastern Cape and Western Cape.
South Africa continues to be plagued by a growing burden of disease, worsening social and commercial determinants of health, and an access-inequitable two-tier health care system, now compounded by the systemic disruptions imposed by the COVID-19 pandemic.
This has in turn led to a sharper diminishment of the resource envelope for funding of health care facilities in the foreseeable future. Within this difficult financial context, it is even more important to bring to fruition the initiatives aimed at defining and capacitating structures for the efficient, decentralised management of health care services.
Upon this foundation, further improvement in the quality and efficiency of health care services is predicated on an ethical leadership which gives spirit to the practice of corporate and clinical governance through continuous improvement and commitment to monitoring and evaluation of inputs, processes and outcomes.
This in turn will allow for transparent interactions with served communities, and encourage engagement with, and ownership of public health care services, to create shared resources for health generation. This will also decrease the drain on the fiscus represented by considerable medico-legal litigation, linked to poor-quality health care and a lack of trust from communities.
An overarching coordinated national commitment to quality improvement and continuous learning, both in the clinical and corporate running of health care services is required to effect the necessary changes to the system.
Auditor-General of South Africa. 2021. Consolidated General Report National and Provincial Departments. Pretoria: Auditor-General of South Africa.
Barron P, Padarath, A. Twenty years of the South African Health Review. South African Health Review. 2017(1):1-10.
Brown A. Understanding corporate governance of Health Care Quality in eight Public Hospitals in Australia. Brown BMC Health Services Research. 2019;19:725.
Competition Commission South Africa, 2019. Health Market Inquiry. Pretoria: Competition Commission of South Africa.
Conmy A. South African health care system analysis. Public Health Review. 2018;1(1).
Department of Public Enterprises. Protocol on Corporate Governance in the Public Sector. Pretoria: National Government of South Africa. 2002.
Dhai A. Medico-legal litigation: Balancing spiralling costs with fair compensation. South African Journal of Bioethics and Law. 2015;8(1):2-3.
Fetter RB, Freeman JL. Diagnosis related groups: product line management within hospitals. Academy of Management Review. 1986;11(1):41-54.
Fusheini A, Eyles J, Goudge J. The place of private care governance in the South African health care system. The International Journal of Health Planning and Management. 2018;33(4):e999-e1013.
Govender S, Proches CNG, Kader A. Examining leadership as a strategy to enhance health care service delivery in regional hospitals in South Africa. Journal of Multidisciplinary Healthcare. 2018;11:157.
Health Ministerial Task Team, 2017. Health Ministerial Task Team on Hospital Mismanagement and Poor Service Delivery – Closure Report. Pretoria: National Department of Health.
Jones L, Pomeroy L, Robert G, Burnett S, Anderson JE, Fulop NJ. How do hospital boards govern for quality improvement? A mixed methods study of 15 organisations in England. BMJ Quality & Safety. 2017;26(12):978-986.
Kollapen JJ, Carnelly M, Jaichand V, Lawrence MI. Issue Paper 33, Project 141, Medico-Legal Claims, 20 May 2017 edn., South African Law Reform Commission, Cape Town, South Africa. 2017
KPMG, 2016. The King IV Report on Corporate Governance for South Africa 2016, Institute of Directors of South Africa. Johannesburg: KPMG.
Mannion R, Davies H, Freeman T, Millar R, Jacobs R, Kasteridis P. Overseeing oversight: governance of quality and safety by hospital boards in the English NHS. Journal of Health Services Research & Policy. 2015;20(1 suppl):9-16.
Maphumulo WT, Bhengu BR. Challenges of quality improvement in the healthcare of South Africa post-apartheid: A critical review. Curationis. 2019;Jan 1;42(1):1-9.
Mountford J, Wakefield D. From stoplight reports to time series: equipping boards and leadership teams to drive better decisions. BMJ Quality & Safety. 2017;26(1):9-11.
National Department of Health, South Africa, 2009. User Guide – UPFS 2009 (version 1). South Africa: Pretoria: National Department of Health.
Office of the Presidency of the Republic of South Africa, 2018. Presidential Health Summit Report: Strengthening the South African Health System towards an integrated and unified health system. 19-20 October, 2018. Johannesburg: Birch wood Conference Centre.
Patel B. Lessons on and for Management: Personal reflections of a Hospital CEO. Hospital Annual Operational Planning Presentation. Groote Schuur Hospital, Cape Town. 2021.
South African Lancet National Commission, 2019. Confronting the right to ethical and accountable quality health care in South Africa: A Consensus Report. Pretoria: National Department of Health.
Statistics South Africa, NCD Statistics.
Stewart J, Wolvaardt G. Hospital management and health policy—a South African perspective. Journal of Hospital Management and Health Policy. 2019;3(14):1-7.