


Lungiswa Nkonki, Theodosia Adom, Carmen Sue Christian, Kholekile Malindi
Much of the premature mortality in South Africa is preventable. Given South Africa’s burden of disease, relatively mediocre health outcomes, and persistent health inequalities, addressing social determinants of health (SDH) becomes crucial to understand and address this context. We develop a hybrid framework that describes how human capital, safety, security, built environment, technology, and environmental and economic factors have influenced health outcomes in South Africa over the past five years.
Between 2015 and 2020, the South African economy struggled to achieve meaningful growth, and the economy further suffered a considerable contraction due to the COVID-19 pandemic. Despite these challenges, the government was unwavering in prioritising expenditure and investment in health care. However, the negative macroeconomic outlook and fragile state of the fiscus limits the resources available to address the challenges that hinder progress on socio-economic factors that determine health outcomes.
South Africa suffers from high inequality in health care and health outcomes, which largely stem from social protection, employment, education, housing, and infrastructure disparities. Although strides have been made post-1994 with increasing access to these basic entitlements, they are still lacking and considered poor quality. The United Nations Human Development Index for 2015 –2019 indicates that South Africa was stagnant along the dimensions of longevity, education and income.
The government provides a range of social protection programmes to cushion the vulnerable, including social grants. In 2019, almost 30% of South Africans benefited from social assistance. Furthermore, during the COVID-19 pandemic, the government increased the existing Child Support Grant. In addition, a new grant, the Special COVID-19 Social Relief of Distress (SRD), was introduced and targeted the unemployed and those not on any form of social assistance.
In 2018, South Africa implemented a sugar and beverage tax to prevent and control obesity and non-communicable diseases (NCDs). While the impact of this health promotion levy is not yet known, available evidence from observational studies suggests that the implementation has impacted product reformation, consumer choices and purchases.
Safety and security issues such as crime and substance abuse, specifically alcohol, have played an increasing role in health outcomes in South Africa, particularly mortality and morbidity linked to traumatic injuries. During the pandemic, restricted sale of alcohol resulted in a statistically significant decrease in unnatural deaths, regardless of the length of curfews. Periods where no or limited restrictions on alcohol were in place had no significant effect or resulted in significantly increased unnatural deaths. A positive impact of social cohesion on optimal health in this context is demonstrated in the recent COVID-19 vaccine roll-out in Limpopo. Despite being one of the poorest provinces in South Africa, Limpopo had the third-highest provincial vaccination rate in the country.
COVID-19 has also demonstrated the importance of technology as a determinant of health, especially literacy and internet access. Applications for employment, housing, and other assistance programmes are increasingly accessible online. As of 2020, 99.8% of the population in South Africa had access to the 3G mobile network, and almost nine in ten South African households exclusively used cellular phones in 2018.
The World Health Organization (WHO) defines SDH as: ‘the circumstances in which people are born, grow up, live, work and age, and the systems put in place to deal with illness’ (Commission on Social Determinants of Health, 2007). The recognition of the critical role of the SDH dates back to the 1940s (Kark & Cassel, 2002), and has been articulated in several ways, including the Alma-Ata Declaration (World Health Organization, 1978), WHO Commission on Health (Commission on Social Determinants of Health, 2007), United Nations Millennium Declaration in 2000, and the expanded set of 17 new Sustainable Development Goals (SDGs). These advances recognise the role of global and national political economies in creating and perpetuating health inequities – the ‘unfair and avoidable difference in health status seen within and between countries’. Some have pointed out contradictions within the SDGs and cautioned that they might not only be inadequate but could potentially be dangerous. Of concern is the failure to acknowledge that mass impoverishment is the product of extreme accumulation and overconsumption by a few, which entails processes of enclosure, extraction and exploitation along the way (Hickel, 2015).
Nationally, SDH is a cornerstone in the National Department of Health’s Primary Health Care Re-engineering Strategy and the National Development Plan (NDP). The NDP aims to eliminate poverty and reduce inequality by 2030 (National Planning Commission, 2011). The NDP is broadly aligned with the SDGs and sees national development as a process requiring a combination of increasing employment, higher incomes through productivity growth, a social wage and good-quality public services (National Planning Commission, 2011). Like the SDGs, the NDP has been criticised for its neoliberal agenda. The success of the NDP is premised on the intention to triple the size of the economy by 2030. Some have cautioned that economic growth based primarily on the extraction and export of raw materials such as minerals and agricultural products will drive unemployment, limit the social agenda and undermine decent work, including health (Scott Vera et al., 2017).
The many dimensions of poverty and vulnerability that cut across the 17 SDGs persist in South Africa despite direct government intervention to address this, including a progressive tax system, free essential and social services (electricity, water and sanitation, basic health and education), and a well-established social assistance system. At the same time, South Africa faces a quadruple disease burden, with major HIV and tuberculosis (TB) epidemics, maternal and child mortality levels higher than the global average, a growing prevalence of NCDs, and high levels of violence and injuries. Most recently, the COVID-19 pandemic has added to this burden.
Improvements in health outcomes have been observed over the past decade, and these include the availability of antiretroviral treatments that have had a dramatic impact on adult mortality and consequently increased life expectancy (Dorrington et al., 2019). Under-5 mortality rates have declined from 41 to 32 per 1 000 live births between 2012 and 2017, and infant mortality rates dropped from 27 to 23 per 1 000 live births (Goga et al., 2019). However, there remains room for improvement in this regard. Much of the premature mortality in South Africa is preventable. Given South Africa’s burden of disease, relatively mediocre health outcomes, and persistent health inequalities, addressing SDH becomes crucial to understand and address in this context.
Having reviewed multiple theoretical frameworks used to review progress on the SDH (Bradshaw, 2008; Dahlgren & Whitehead, 1991; Krieger, 2008; Scott Vera et al., 2017), our conceptual framework starts with economic growth as measured by Gross Domestic Product (GDP) (see Figure 3.1). We begin with reviewing year-on-year GDP and expenditure on health. Notwithstanding the challenges of capitalist growth as measured by GDP, we start here because both international (SDGs) and national (NDP) commitments are premised on increasing the size of the economy by 2030. Thus, looking at the public purse first is an excellent place to start, as it provides a ceiling on how much can be dedicated to improving health and well-being.
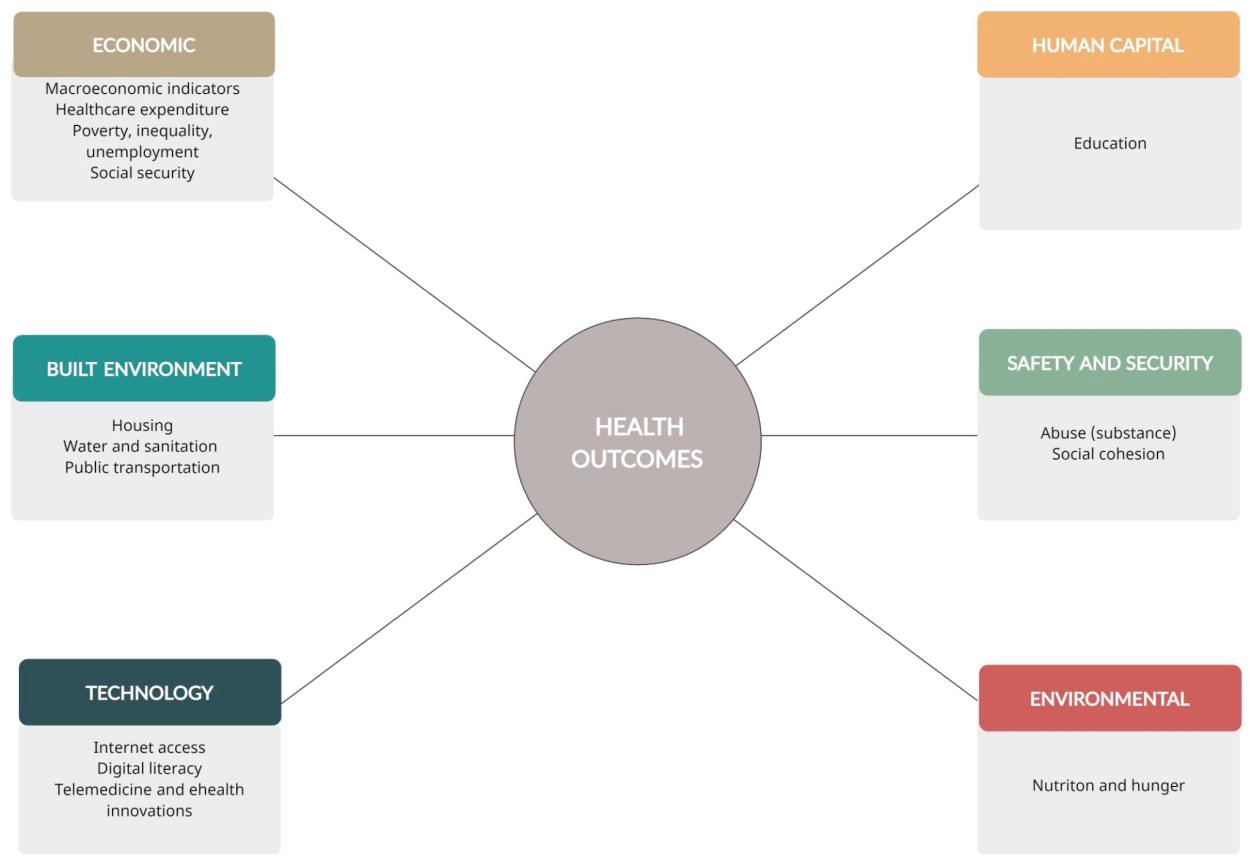
We have then clustered poverty, income inequality, education, unemployment and social security together because of their impact on human capital. Human capital has undeniable intrinsic value and consists of the knowledge, skills and health that people accumulate over their lives, and enables people to realise their potential as productive members of society. More human capital is associated with higher earnings for people, higher income for countries, and stronger community cohesion. It is a central driver of sustainable growth and poverty reduction.
We have categorised built environment factors that influence health as housing, water, sanitation, and public transportation. In addition to these environmental determinants of health, we have added accessibility of healthy foods as a social determinant of health. Nutrition-sensitive concerns to address food security and nutrition include poverty, water and sanitation, and climate change.
Social cohesion involves building shared values and communities of interpretation, reducing disparities in wealth and income, and generally enabling people to have a sense that they are engaged in a common enterprise, facing shared challenges, and that they are members of the same community. In this section, we focus on safety and security as markers of inadequate social cohesion.
The advent of COVID-19 presented numerous learning opportunities for including health in all policies. Actions developed in response to COVID-19, which adopted the SDH lens, demonstrate how different sectors worked together to produce positive health outcomes and how spheres of government worked together – connecting action across both levels and sectors. We then discuss technology and internet availability as an SDH. Technology and internet availability were not traditionally seen as SDHs; however, COVID-19 has demonstrated the importance of digital literacy and internet connectivity.
This chapter reviews South Africa’s progress, challenges and opportunities with SDH in the period from 2015–2020. We conclude with a summary of key findings and discuss recommendations for the country. It is crucial that public spending is pro-poor. In our assessment of progress in the five years under review, we pay attention to markers of vulnerability in terms of gender, rural, low-income earners and/or unemployed, very young and old, and race.
Expanding access to quality health care for all is one of the goals set by the NDP’s Vision 2030. This goal closely aligns with the SDG goal of ‘ensuring healthy lives and promoting well-being for all at all ages’ (United Nations Children’s Fund, 2020, p. 6). This close policy alignment with the SDG further cements the government’s commitment to improving health outcomes for all South Africans. Noticeable improvements in health outcomes have been achieved since the transition into democracy; these include an improved life expectancy, and declines in mortality for infants, children and women. These gains are mediocre given South Africa’s expenditure in health care. However, the gains come from a low base (due to the legacy of inequitable provision of health care services under the apartheid government) and have likely been eroded by the COVID-19 pandemic. Chapter 13, which covers the quality of care, provides more detail on the important early gains made while highlighting several actions that appear to have stalled, largely due to COVID-19.
This section reviews the social, economic and environmental determinants of health. Empirical evidence has shown that health outcomes are strongly related to socio-economic and environmental factors. Omotoso and Koch (2018) and Ataguba et al. (2016), for example, provide evidence that suggests inequalities in health outcomes are strongly associated with disparities in educational attainment, employment, social protection, housing and infrastructure, area of residence and rate of urbanisation. Consequently, tracking progress in these determinants will indicate whether strides have been made towards achieving better health outcomes for all. Another critical determinant of health outcomes is how much expenditure and investment is devoted to the health of the population. This, in turn, is dependent on the nature and extent of economic development that a country is able to achieve. Therefore, our review of progress with addressing socio-economic and environmental challenges will be preceded by a review of economic growth over the reference period as measured by annual growth in GDP and expenditure on health care.
The South African government has set an ambitious path for the growth of the economy under the NDP. The performance of the economy in the 2015–2020 reference period has been underwhelming and out of touch with the path envisioned by the NDP. Figure 3.2 shows that the economy has struggled to achieve meaningful growth and has at times endured short spells of negative growth in consecutive quarters during the reference period. With the emergence of the COVID-19 global health pandemic, the economy suffered a deep recession in 2020 that resulted in the South African economy shrinking by almost 7% compared to the previous year.
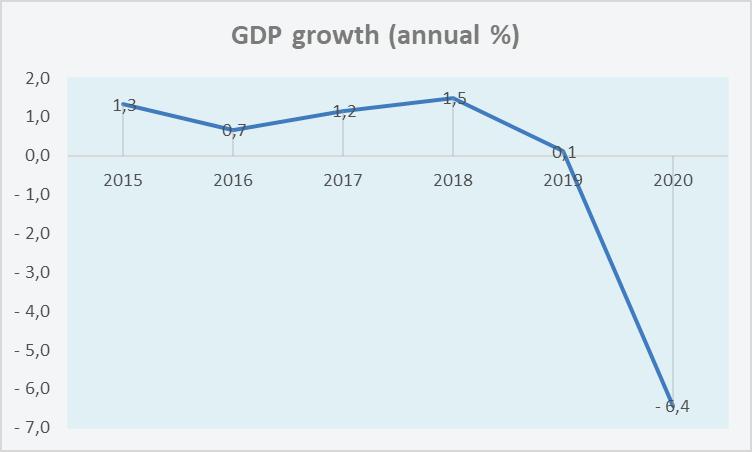
Figure 3.2 Real Gross Domestic Product 2015–2020, annual percentage change
Source: World Bank – World Development Indicators (2020)
The macroeconomic outlook during the reference period was further worsened by the sharp rise in government debt. The net loan debt as a percentage of GDP increased from 44% in 2015/16 to just over 58% in 2019/20, while the cost of servicing the debt increased from 3.1% to 4%. With the government committed to addressing the health and economic crises caused by the COVID-19 pandemic, government debt along with the debt-servicing costs are projected to increase even further, causing further strain to the fiscus (National Treasury, 2021).
The nature and extent of economic growth that a country is able to achieve sets a limit on how much expenditure and investment can be devoted to the health of the population. Despite the economy not achieving sustained growth and government debt on the rise, the government appears to be unwavering in prioritising expenditure and investment in health care. Figure 3.3 below shows a steadily rising trajectory for health care expenditure.
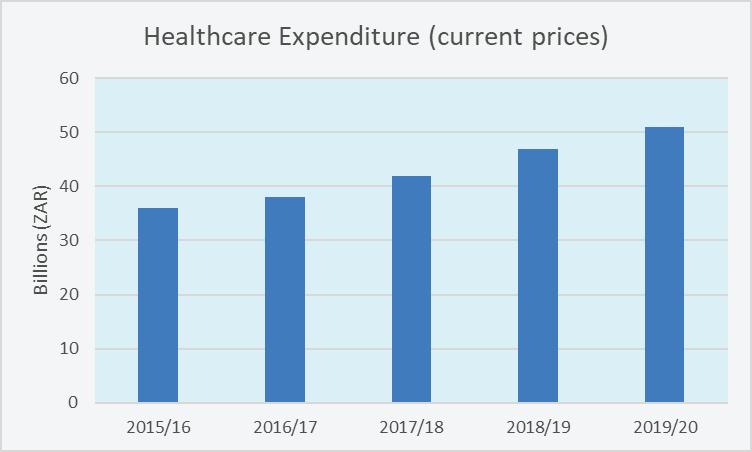
Figure 3.3 Health care expenditure 2015–16 to 2019–201
Source: National Treasury (2021)
With regard to how the budget allocation is utilised by the health department, the lion’s share of the budget is allocated to the provincial health departments. The provision of health care services in South Africa is a mandate of provinces. Since each province is tasked with the provision of health care and has some measure of autonomy in executing the task, variation in health care outcomes and quality of service between provinces is likely to appear and may, in turn, contribute to the inequality of health care outcomes in the country.
Socio-economic factors
South Africa suffers from high levels of inequality in health care and health outcomes. These inequalities reflect and largely stem from inequalities in income, labour market outcomes and access to service delivery. Ataguba et al. (2016) provide empirical evidence that identifies social protection, employment, education, housing and infrastructure as key contributors to health inequality. Some of these factors speak to the very core of human development and are captured by the Human Development Index (HDI)2
1 The expenditure values referred to in the figure are based on audited values as opposed to estimates or adjusted values.
2 Measure of human develop ment compiled by the United Nations Development Programme and published under the Human Development Report.
South Africa from 2015 to 2019. The HDI provides an assessment of South Africa’s progress on three variables (‘longevity, education, and income’) and calculates a composite score which is given as the HDI value. While South Africa’s HDI value of 0.709 for 2019 places it in the high human development category, the HDI value showed an improvement of only one percentage point between 2015 and 2019. This indicates that human development along the dimensions of longevity, education and income was stagnant. Moreover, South Africa’s HDI value was lower than the average HDI value among the group of countries in the high human category group (United Nations Development Programme, 2020).
Table 3.1 South Africa’s HDI trends (based on consistent time series data and new goalposts)
Source: United Nations Development Programme (2020)
South Africa is categorised by the World Bank as an upper-middle-income country based on its level of gross national income per capita. However, the income in the hands of South Africans is highly unequal and affords the nation the classification of one of the most unequal countries in the world. When the HDI value reported in Table 3.1 is adjusted for inequality within the three dimensions captured by the index, the HDI value falls to 0.468, representing a ‘loss in human development due to inequality’ of 34% (United Nations Development Programme, 2020, p. 4). The corresponding figure for high HDI countries that South Africa is grouped alongside (based on the unadjusted HDI value) is 17.9% (United Nations Development Programme, 2020), which illustrates South Africa’s inequality.
A recent report by Statistics South Africa (2019a) on inequality trends finds that, based on money measures, inequality has only slightly improved over the past few years. The improvement was primarily confined to the middle of the income distribution. When accounting for the sources of income inequality, the report finds that the unequal distribution of income earned from the labour market is the chief contributor, with social grants playing a significant mitigating role in the inequality gap between the poor and the rich.
To cushion the most vulnerable in the nation against social and economic hardships, the government provides a range of social protection programmes (e.g., social grants and no-fee schools). Of these programmes, social grants are arguably the most important based on the number of people reached and the resources invested. According to data from Statistics South Africa, roughly 30% of South Africans in 2019 benefited from social grants (Statistics South Africa, 2020). This figure was around 12% in 2003. Furthermore, roughly 20% of households in the country report that social grants are the primary source of income in their household (Statistics South Africa, 2020). The receipt of these grants has been linked with improvements in many outcomes at the household and individual levels, including better health outcomes (see for example Oosthuizen (2021)). Thus, these social protection programmes have an element of redistribution.
One of the Achilles’ heels of the current government is the high incidence of poverty. South Africa’s level of poverty has historically stood in sharp contrast to the country’s level of income, which places it under the category of upper-middle-income country. The most recent data on poverty trends reported by Statistics South Africa indicates that over half (55.5%) of the population were living below the upper-bound poverty line of R992 per capita per month in 2015 (Statistics South Africa, 2018b). According to the internationally comparable income poverty line of US$1.90 per day3, almost one in five (18.9%) people in the South African population in 2016 lived below this income poverty line (United Nations Development Programme, 2020). To move beyond the narrow focus on income or the lack thereof, the recent trend in the measurement of poverty augments the traditional income-based poverty statistics by adding multiple dimensions of deprivations that capture the quality of health, education and standard of living of people. Based on this measurement, roughly 6% of the South African population are multidimensionally poor (United Nations Development Programme, 2020). The lower incidence of non-income-based poverty versus income-based poverty reflects the positive impact played by social security programmes administered by the government.
3 2011 purchasing power parity.
Education is an important determinant for long-term economic development. There is increasing evidence, however, that places the emphasis on quality of education as the key policy lever in the promotion of economic development (Van der Berg et al., 2020). An analysis of key education statistics reveals that significant progress towards meeting the goals of the NDP has been achieved (Van der Berg et al., 2020). Data on high school completion, for example, indicate that educational outcomes in South Africa are at the levels that would be expected given the country’s level of income. Furthermore, data from Statistics South Africa indicates that by 2019, the Basic Education Department had been able to achieve nearly universal school attendance (96.6%) for children between the ages of 7 and 15 years old (Statistics South Africa, 2020).
While noticeable gains have been achieved in expanding access to education, ensuring quality of schooling for all still remains a key challenge. According to Van der Berg et al. (2020), the quality of schooling in South Africa is at a level below what would be expected given the country’s level of income. Lack of progress in ensuring quality schooling for all learners undermines education’s role in promoting economic development in the long term. Additionally, low quality of education can have a detrimental impact on labour market outcomes, and this may in turn lead to inferior health outcomes.
Many South Africans are without work, and this is reflected by the alarmingly high unemployment rates. According to data collected by Statistics South Africa (2015), roughly 8 million people were without work in the first quarter of 2015. Over 2 million of these unemployed individuals had given up searching for employment and were considered to be ‘discouraged work-seekers’ by Statistics South Africa. By the end of the last quarter of 2020, the number of people without work was over 10 million and those classified as ‘discouraged work-seekers’ had increased to roughly 3 million (Statistics South Africa, 2021). This represents an increase of roughly six percentage points in the official unemployment rate under the review period.
During the same period, the absorption rate (i.e., number of employed people as a fraction of the total population) fell from 43.2% in the first quarter of 2015 to 38.2% in the last quarter of 2020. This means that less than four people out of ten were employed in the last quarter of 2020 in South Africa.
The unemployment statistics quoted above were without a doubt adversely affected by the COVID-19 health pandemic that sparked a deep economic recession in 2020. However, it is also true that these unemployment statistics were at alarming levels before 2020 and had been in a negative trajectory due to an economy that had been stagnant.
With less than four people out of ten employed, this places severe strain on the resources that the government has available to address the socio-economic challenges faced by the country. This, in turn, brings into question the role of these socio-economic factors in promoting health outcomes.
This section focuses on the accessibility of healthy foods as a social determinant of health while providing insights into the food environment, food security, nutrition, and initiatives on obesity and child hunger in South Africa.
South Africa is food secure at the national level, however, there is some degree of food insecurity at the household level across the provinces, racial groups, and settlements. While in 2015, more than one in four South Africans were living at the level of food poverty, estimates by Statistics South Africa suggest that in 2017, close to 7 million South Africans and 1.7 million households experienced hunger, and a little over 10 million had inadequate access to food (Statistics South Africa, 2019b). These levels of food insecurity and hunger were reflected in the 2019 estimates (National Department of Health et al., 2019) by the South Africa Demographic and Health Survey, where more than a quarter of children under five years were stunted and 13% were overweight, while in adults aged 15 years and older, two-thirds of women and onethird of men were overweight or obese, almost half had high blood pressure, and at least 8% were diabetic.
The current South African food environment is characterised by large transnational and national food and beverage ‘Big Food’ companies that offer large varieties of healthy and unhealthy foods. In contrast, fast-food chains offer unhealthy foods (Claasen et al., 2016). One of the targets of the SDGs Goal 2 is to reduce malnutrition in all its forms, namely: undernutrition, micronutrient deficiencies, overweight or obesity, and diet-related NCDs, and this is only achievable in a supportive food environment where safe, nutritious and diverse foods are widely available and accessible in adequate quantities to contribute to the dietary requirements of the population for health and active life (Lartey et al., 2016).
Given that the NDP recognises food and nutrition security as a key element of poverty and inequality, various departments have intersectoral initiatives to promote and support food security. A number of these reforms predate the review period. For the 2015–2020 period, we focus on the Health Promotion Levy (HPL), the Child Support Grant (CSG), and the Special COVID-19 SRD grant. The HPL was introduced in 2018 to prevent and control obesity. While the impact on obesity is not yet known, available evidence from observational studies suggests that the introduction of the HPL has impacted product reformation, consumer choices and purchases (Stacey et al., 2019, 2021). A previous study in 2016 (Zembe-Mkabile et al., 2016) indicated that the existing CSG was inadequate in improving child health outcomes, particularly stunting. To mitigate the impacts of the COVID-19 pandemic on child hunger, the government increased the CSG to R300 per child in May 2020 and R500 per caregiver from June to October 2020. In addition, a new grant, the SRD, was introduced to target the unemployed as well as those who were not on any form of social support grant, and one in every three households is dependent on the grant.
The built environment plays a major role in the prevention and management of both chronic and infectious diseases. The impact of the built environment on health can be both direct – for example, by influencing the quality of an individual’s physical environment, or indirect by influencing behaviours that impact disease transmission and health (Pinter-Wollman et al., 2018). In this section, we will focus on the role that housing, water, sanitation and public transportation have played in determining health outcomes in South Africa during the period under review. (Chapter 2 takes a cursory look at waste removal, land degradation and social erosion in relation to health outcomes.) Although strides have been made post-1994 with increasing access to these basic entitlements, they are still lacking and considered to be of poor quality, as evidenced by the increasing number of protests linked to these public goods and services (Alexander, 2010; Mamokhere, 2019; Morudu, 2017; Wasserman et al., 2018).
In the South African context of urbanisation coupled with a chronic backlog of social housing (Turok & Scheba, 2019), overcrowding remains associated with poor health outcomes, particularly acute respiratory infections and gastrointestinal diseases. Survey data from a recent 11-year panel study in Johannesburg, South Africa analysed the relationship between household crowding and respiratory and gastrointestinal symptoms in two low-income communities (Nkosi et al., 2019). The study found that close to 60% of households were overcrowded by international standards4, although this level was lower compared to other African countries. Furthermore, overcrowding was associated with an increase in acute respiratory and gastrointestinal symptoms, as well as fever/chills, even when controlling for confounding variables.
The impact of inadequate water and sanitation on child health is particularly depressing in the South African context. In 2013, after the public outcry over student deaths in pit latrines at underprivileged schools, and upward pressure from civil society organisations, the Department of Basic Education (DBE) gazetted the Minimum Uniform Norms and Standards for Public School Infrastructure (Christie, 2021). However, by 2018, 19% of 23 471 (i.e. 4 460) public schools still had illegal pit latrines and 37 schools had no sanitation facilities at all (Christie, 2021). Even after a recent show of political will from government to improve the situation (brought on by the COVID-19 pandemic – described in more detail in the paragraph below), a 2021 report on water and sanitation at schools showed a lack of significant progress, with 3 297 schools still relying on pit latrines and 366 schools having no water for sanitation (South African Human Rights Commission, 2021).
The COVID-19 pandemic appeared to reignite the DBE’s commitment to their infrastructure norms and standards for public schools, which resulted in a set of non-negotiables for the reopening of schools being declared on April 29 2020, that included access to water and sanitation (pit latrines to be replaced with mobile facilities) (Parliamentary Monitoring Group, 2020). At the same time that water and sanitation featured on the list of non-negotiables for schools to reopen, the DBE also noted that 3 475 schools would require emergency water support to reopen (Christie, 2021). It took a pandemic to highlight the need for
4 The study used the UN-Habitat definition as the benchmark, i.e., when there are more than two people per room (excluding bathrooms but including kitchens and living rooms).
basic water and sanitation at schools, which they were meant to have since 2013 when the minimum norms and standards for public schools were promulgated. At the time of writing this chapter, we could not confirm whether these schools had reopened or not, and whether issues of water and sanitation had been addressed there.
The availability (or not) of transport plays an integral role in people’s ability to access essential goods and services such as health care services (Martens et al., 2012). This does not bode well for South Africa where the public transport system –which the majority of the poor and marginalised depend on – has become increasingly unreliable and costly (Maharaj, 2020). Even when transport is available, the cost thereof (direct and opportunity costs) has an impact on healthseeking behaviour (delayed care-seeking) which ultimately influences health outcomes. A 2020 study looking at access to health care in post-apartheid South Africa found that in 2009/2010, 73% of the affordability constraints to access was due to travel costs (Burger & Christian, 2020). These findings also showed an anti-poor bias, which further entrenches health inequalities. The health consequences associated with transport inefficienciesare wide-ranging: from ill-health to maternal mortality and high infant mortality rates; poor access to healthy, affordable food and essential medication; as well as transport-related traumatic injury (Litman,2002; Lucas & Jones, 2012; Pirie, 2008; Vasconcellos, 2011).
Safety and security
Safety and security have been identified as among the major determinants of health in the South African context (Scott Vera et al., 2017). This section will take a closer look at how substance abuse (specifically alcohol abuse) and social cohesion – both of which directly impact safety and security in communities –relate to health outcomes. What emerges from the recent literature is that the health of the most vulnerable in society continues to be negatively affected disproportionately by these determinants (or a lack thereof, in the case of social cohesion).
A silver lining of the COVID-19 pandemic is that it has offered us many unique learnings that otherwise would not have been possible. One such learning is the clear evidence of the harmful effects of alcohol abuse – directly and indirectly – on health outcomes. In a COVID-19 context, conditions favoured a natural experiment that showed how COVID-19 restrictions, in particular the sale of alcohol and curfews, had a major effect on the pattern of unnatural deaths in South Africa. A recent study in South Africa analysed death data over 68 weeks (January 2020 to April 2021) in relation to information on restrictions on the sale of alcohol, as well as the curfew hours (Moultrie et al., 2021). The findings were stark: During periods of complete restriction on the sale of alcohol, there was a statistically significant reduction in unnatural deaths, irrespective of the length of curfew. In fact, during times when no or limited restrictions on alcohol were in place, it had no significant effect or resulted in significantly increased unnatural deaths. While restricting the sale of alcohol is not a long-term solution and is accompanied by negative economic impacts for related industries, it is clear that alcohol-related harm needs to be addressed in South Africa. When considering the question of the trade-offs of stricter alcohol regulation in South Africa, a 2014 study estimated that the combined total tangible and intangible costs of alcohol harm to the South African economy were 10–12% of the 2009 GDP. Further analysis showed that the tangible financial cost of alcohol abuse alone was estimated at R37.9 billion, or 1.6% of the 2009
GDP (Matzopoulos et al., 2014). The study was successful in showing that the costs of alcohol-related harms were a heavy counterbalance to the economic benefits highlighted by the alcohol industry to avoid stricter regulation.
Diminishing these costs of alcohol abuse through policy interventions would, directly and indirectly, contribute to social well-being, as demonstrated by the study of the impact of COVID-19 alcohol sale prohibitions and curfews on the pattern of unnatural deaths in South Africa. At the same time, policy interventions also need to dig deeper to understand the systemic reasons behind alcohol abuse in the South African context. These studies also underscore the need for implementing evidence-based alcohol control measures. For further reading on trends in alcohol use, please refer to Chapter 2.
Evidence of the lack of social cohesion in South Africa, which may manifest as crime and violence, and how it negatively impacts health behaviours and outcomes, is well documented (Gass et al., 2010; Lamb, 2019; Lippman et al., 2018; Miller et al., 2020; Olamijuwon et al., 2018; Seedat et al., 2009; Shannon et al., 2020). In contrast, this subsection delves into a case that demonstrates how social cohesion supports optimal health. At the time of writing, Limpopo had the third-highest provincial vaccination rate (48%) (National Department of Health, 2021b) in the country despite being one of the poorest provinces in South Africa (Gateway South Africa, 2021). Social cohesion was clearly demonstrated during the recent vaccine roll-out in Limpopo. Their roll-out plan was co-designed with local churches and community leaders because communities in Limpopo trust local leaders and faith-based organisations (Burger et al., 2021). This form of social cohesion was leveraged to advance health outcomes, namely the vaccination rate, and serves as a great example of how health outcomes may be positively influenced in this context of safety and security
Coordinating responses across sectors and government levels
South Africa reported its first case of COVID-19 on March 5 2020. Within 14 days (March 5 – 19), we saw a decisive, strong leadership from the president and the significant, essential and necessary coordination between different ministries, including Education, Justice, Health, Trade and Industry, Transport, Public Works and Infrastructure, Finance, Cooperative Governance and Traditional Affairs, and International Relations and Cooperation. Within these 14 days, South Africa rapidly produced and implemented several action items (Table 3.2). This intersectoral action and coordination is something that South Africa has needed for a long time to address SDH in the country (Nkonki & Fonn, 2020). It remains to be seen whether the intersectoral coordination created as a response to COVID-19 will be fully utilised in the long term.
The literature on intersectoral collaboration suggests that success relies on a shared understanding of what can be achieved collectively and whether stakeholders can agree on mutual goals or acceptable trade-offs. COVID-19 has highlighted key policy dilemmas and trade-offs. For instance, in the case of alcohol bans, there is clear evidence that it decreased natural deaths and trauma-related hospitalisation. At the same time however, alcohol bans had a negative economic impact on the food and beverage and hospitality industry and reduced tax revenues (sin tax, company tax and VAT).
Table 3.2 List of the key actions in South Africa within the first 14 days (March 5–19) of COVID-19
Ministry List of actions taken
President Declaration of a State of Disaster in terms of section 27 of the Disaster Management Act, 2002
Health Establishment of a national hotline and WhatsApp number for the general population
Home Affairs and International Relations and Cooperation
Travel ban on foreign nationals from high-risk countries such as Italy, Iran, South Korea, Spain, Germany, the United States, the United Kingdom and China as from March 18 2020
Health Dedicated website with daily updates from the National Institute for Communicable Diseases, tests conducted, positive and negative results, information on symptoms and prevention (in local languages), list of amended regulations
Defence and Military Veterans
‘Release of resources’ by the Department of Defence, national organs of state, and institutions within national, provincial and local government
Police ‘Prevention and prohibition of gatherings.’ In this case, a gathering of 100 people was prohibited. The assembly of more than 50 persons at premises where liquor is sold and consumed was also prohibited. The Regulation also makes provision for powers of an enforcement officer to disperse a gathering, or in some cases to arrest and detain the organiser of a gathering
Trade and Industry
Health, and Justice and Correctional Services
Public Works and Infrastructure
Trade and Industry
Basic Education and Higher Education, Science and Technology
Justice and Correctional Services
Health, Police, Justice and Correctional Services
COVID-19 Block Exemption for the Health Care Sector
‘Refusal of medical examination, prophylaxis, treatment, isolation and quarantine.’ This regulation makes provision for the unlikely scenario where a person refuses to (self) quarantine or (self) isolate. The person may then be placed in isolation or quarantine for a period of 48 hours, as the case may be, pending a warrant being issued by a magistrate, on application by an enforcement officer, to perform the medical examination of a suspected or confirmed case
COVID-19 Block Exemption for the Health Care Sector
‘Places of quarantine and isolation’ by the Minister of Public Works and Infrastructure, the Members of the Executive Council in the provinces and the accounting officers of municipalities
‘Closure of schools and partial care facilities’ from March 18 2020 until April 15 2020, which period may be extended for the duration of the National State of Disaster by the cabinet member responsible
Suspension of visits for 30 days to Correctional Centres, Remand Detention Facilities, Holding Cells, Military Detention Facilities and Department of Social Development facilities, including Child and Youth Care Centres, shelters, One-Stop Centres, and Treatment Centres, which period may be extended for any period, but not beyond the duration of the National State of Disaster by the cabinet member responsible
‘Limitation on the sale, dispensing or transportation of liquor.’ In this case, all on-consumption premises selling liquor, including taverns, restaurants and clubs, must be closed with immediate effect, or must accommodate no more than 50 persons at any time: Provided that adequate space is available and that all directions in respect of hygienic conditions and limitation of exposure to persons with COVID-19 are adhered to. It is also notable that no special or events liquor licenses will be considered for approval during the duration of the National State of Disaster. Establishments will also close earlier between 18:00 and 09:00 the next morning on weekdays and Saturdays; and from 13:00 on Sundays and public holidays
Finance/ Treasury
‘Emergency Procurement Procedures’ in line with financial management legislation, regulations and instructions
President ‘Authority to issue directions.’ In this regard the president authorised the Ministers of Health, Justice and Correctional Services, Basic and Higher Education, Police, Social Development, Trade and Industry, and Transport to issue directions where needed to address, prevent and combat the spread of COVID-19 in matters falling within their respective mandates
Justice and Correctional Services
‘Offences and penalties’ for a person when found liable on conviction, to a fine or imprisonment for a period not exceeding six months, or both such fine and imprisonment
Source https://www.gov.za/Coronavirus
Intersectoral action was first proposed by the Alma-Ata Declaration (World Health Organization, 1978) and involves efforts by the health sector to collaborate with other public policy sectors to improve health outcomes, and there is consensus that it is needed to achieve health in all policies and improve health outcomes. However, translation of evidence into effective policy is a particular challenge for intersectoral policies addressing the SDH.
The literature on intersectoral collaboration suggests that success relies on a shared understanding of what can be achieved collectively and whether stakeholders can agree on mutual goals or acceptable trade-offs. The range of obstacles to effective implementation of SDH policies includes: the multifaceted nature of socio-economic factors (Exworthy, 2008), the dominance of biomedical perspective (Phillips et al., 2016), logistics surrounding intersectoral action for health, lack of ownership or territorial ownership (Skeen et al., 2010), lack of accountability (de Leeuw, 2017), limited resources and time to enable collaboration (Crichton, 2008), poor enforcement of legislative processes that demand intersectoral working, and limited dedicated resources towards integrated policy development (de Leeuw, 2017).
Studies looking at whether SDH have been applied to address population health in South Africa have had a programmatic focus. For instance, they have looked at whether and how the intersectoral approach was applied or not applied in addressing mental health (Skeen et al., 2010), child health (Okeyo et al., 2020, 2021), HIV/AIDS (Mahlangu et al., 2018), tobacco control (Sanni et al., 2018), and gender equity (Hargreaves et al., 2011).
Skeen et al. (Skeen et al., 2010) recommend that the National Department of Health (NDoH) should be a critical partner in developing the intersectoral action to achieve population health. We concur with Skeen et al., and propose that the NDoH should take a stewardship role in promoting intersectoral action in addressing social determinants of health. This recommendation is logically sound. However, several factors mitigate against this, namely, current provincial responsibilities (as outlined in the Constitution and National Health Act), equitable share allocations as well as the silo nature of budgets and accountability. Furthermore, Skeen et al. (Skeen
et al., 2010) recommended the following essential steps for achieving intersectoral collaboration, commencing with a high level of political commitment. They targeted awareness-raising to engage various sectors, using current networks between departments as a springboard and creating a communication culture between departments. They also noted that programmes should be backed by legislation and policies. Formal collaborations exist between government departments and agencies at the national, provincial and district levels. However, these collaborations were found to be more efficient at the national level compared to the provincial and local levels. In the context of this study, stakeholders recognised adequate access to essential services such as housing, education, employment, water, sanitation and transport as critical in health promotion. Aside from the lead department, other government sectors included legislations in departmental policies and plans. They recommend the active engagement of local government structures to provide insights on community-level/local issues and responses.
Mahlangu et al. (Mahlangu et al., 2018) propose mainstreaming approaches to addressing health, as it ensures sector commitments to achieve joint outcomes for national targets. At the same time, it avoids overlap and duplication of activities and functions of government and calls for vertical coordination between levels of government (national, provincial and local) within departments and horizontal coordination between departments.
Mahlangu et al. (Mahlangu et al., 2018) identified consultative engagements between different spheres of government and relevant stakeholders and communication and information sharing as factors that facilitate vertical coordination. Baum et al. (Baum et al., 2017) recommend supportive bureaucratic policy networks that include senior and mid-level staff across the sectors as means to bring about action on the SDHs. In addressing the question of how to establish supportive cross-sector spaces of engagement, cross-sector structures that promote dialogue and the negotiation of different views, e.g. interdisciplinary committees, working groups or policy networks are recommended. Consultative engagements with sub-national government stakeholders are important given that the implementation occurs at the provincial and local levels. Ideally, consultative arrangements should help clarify roles and responsibilities and support the implementation of the SDH approach to improving health outcomes. The flow of information across the different spheres with timely and established interdepartmental lines should ensure relevant, timely information to key players. Working in silos between various directorates in departments and non-synchronised reporting systems at the national level hinder vertical coordination.
There is limited evidence of horizontal collaboration and partnership between departments in practice. This is attributed to the lack of clarity of roles and responsibilities, resulting in the overlap. While platforms exist to facilitate collaboration between government departments, the lack of participation at the national and provincial levels and lack of representation of government departments across districts and local levels limit its effectiveness. Moreover, the complexities of measuring impact where contributions of departments may not be acknowledged in collaborative efforts hinder the process.
Examples of coordinated responses to COVID-19 that applied a social determinants of health lens
The COVID-19 pandemic created a context that necessitated innovation. One area of innovation that leapfrogged during this period is telemedicine, supported by the temporary relaxation of telemedicine guidelines by the Health Professions Council of South Africa (HPCSA) (Percept Actuaries and Consultants, 2020). These conditions have sparked a renewed interest in and demand for telemedicine in South Africa. While it must be stressed that telemedicine is a complimentary service in the package of care – and not a substitute – there needs to be a broader appreciation that much scope remains for the full benefits of telemedicine, i.e. increasing access to quality health care for more South Africans, to be realised. Examples of telemedicine innovations in the South African market include clinicians exchanging patient medical information via messaging apps (e.g. Signapps), telephonic/video patient consultations with health care workers (e.g. Stone Three), remote monitoring of patients (e.g. Quro), and surgeons consulting remotely on surgical procedures (eHealth Group) (Percept Actuaries and Consultants, 2020, 2021).
Another innovation during COVID-19 was alternative models for the delivery of medication in the public sector. One example of this is the home delivery of medication service that the Metropolitan Health Services in the Western Cape offered its patients during the pandemic. The innovation aimed to prevent COVID-19 amongst high-risk patients (those with comorbidities) who would be at risk of more severe disease and to decongest primary health care facilities in anticipation of the expected surge in COVID-19 cases. The innovation linked the existing chronic dispensing unit system with a community-oriented primary care approach in the Metro (Brey et al., 2020). Medication was delivered to pharmacies at local facilities as usual, but from there, a range of means was used to distribute the medication parcels to local non-profit organisations, who delivered the parcels to patients using community health workers (CHWs). Delivery models included the use of e-hailers (such as Uber), bicycles and electric scooters. The innovation lent itself to being scaled up, with 200 000 medication parcels delivered per month using 2 500 CHWs (Brey et al., 2020).
Provincial departments of health (PDoHs) across South Africa were also forced to be creative with the vaccine roll-out programmes by leveraging social capital in communities. As described in the section on Safety and Security, Limpopo’s approach of co-designing their vaccine roll-out programme with trusted local leaders resulted in a high vaccine rate relative to other provinces.
These innovations and new approaches experimented with during COVID-19 demonstrated their potential to bypass or mitigate negative SDHs such as a lack of social cohesion, costly and unreliable transport systems and the high opportunity cost of standing in long queues to access care at facilities. These lessons must be learnt and not forgotten, as well as further explored to see how best they can be leveraged to strengthen the health system.
Digital technology was not traditionally seen as an SDH. However, COVID-19 has demonstrated the importance of digital literacy and internet connectivity as capital that positively impacts health outcomes. Recently, digital literacies and internet connectivity have been called the ‘super social determinants of health’ because they address all other SDHs. For instance, applications for employment, housing, and other assistance programmes, each of which influences an individual’s health, are increasingly accessible online. In addition, digital tools and applications can support a range of health information needs such as patient portals, health trackers, remote monitoring devices, and health information communication (Sieck et al., 2021). Research suggests that tools such as health apps and patient portals can foster greater patient engagement, better support patients outside of the clinic visit, and improve health outcomes. Fundamental to the use of mobile technology in health care are internet-enabled devices, affordable broadband internet, access to digital literacy training, quality technical support, and applications and online content designed to enable and encourage self-sufficiency, participation and collaboration. Whilst technology can contribute enormously to well-being, in the absence of universal access to the necessary enabling infrastructure, it also has the potential to marginalise the poor and exacerbate inequalities.
As of 2020, 99.8% of the population in South Africa had access to the 3G mobile network. 4G/LTE coverage increased significantly from 53% in 2015 to 96.4% in 2020. This trend was accompanied by rapidly growing smartphone penetration that more than doubled to 91.2% over the four years from 2016 to 2019. In 2020, only 0.7% of the South African population had 5G coverage (See Figure 3.4).
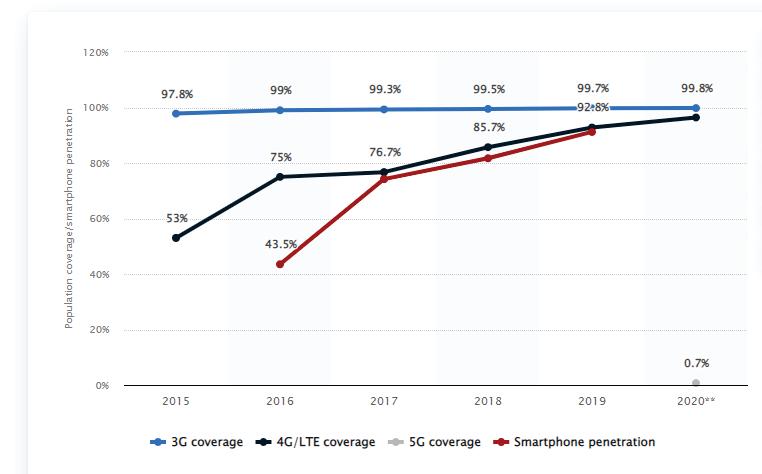
Source: https://www.statista.com/statistics/1074377/south-africa-mobile-coverage-and-smartphone-penetration/
In 2013, the South African government introduced the SA Connect programme to improve universal internet access. This programme prioritises access to free public WI-FI to the population and targets schools, clinics and other government facilities through universal, affordable and high-speed broadband access to all. Several metropolitan areas have WI-FI, while most suburban areas have fibre-optic cables. Data from the 2018 General Household Survey suggests that almost nine in ten (89.5%) South African households exclusively use cellular phones. However, only 10.4% of the population have access to the internet at home (Statistics South Africa, 2018a). Between 2019 and 2020, the number of South Africans who have access to the internet increased by over 3% (1.1 million).
We highlight two successful initiatives of digital technology (ehealth innovations) in health care in South Africa – MomConnect and the Stock Visibility System. In August 2014, the South African NDoH launched Mom Connect as a flagship initiative to strengthen maternal and infant health services and improve mortality outcomes. It is universally accessible through all mobile phones and aims to register all pregnant women, provide them with vital health information and create channels for their feedback. MomConnect has been scaled rapidly through strong government stewardship and leverage of existing technology, content and partnerships (Barron et al., 2018). In early 2019, Mom Connect had registered over 2.5 million mothers and now represents a powerful platform for real-time data collection and linkage to additional services to improve patient care. Chapter 13 provides more descriptive information on MomConnect and how it has impacted the quality of care in South Africa. At the onset of COVID-19, the Coronavirus Rapid Mobile Survey team used the Mom Connect platform to collect information from pregnant women, mothers and child pairs on access to maternal and child health services during the hard lockdown, when face-to-face interviewing was not permitted.
The Stock Visibility System (SVS) (Chapter 4 provides details on SVS) serves as an electronic stock management system on the availability of medicines at health facilities. It has been available in more than 3 000 primary health care clinics and over 300 hospitals since its inception in 2015 (National Department of Health, 2021a). In the context of COVID-19, the SVS has been widely used to monitor personal protective equipment availability in public sector hospitals and, where applicable, COVID-19 vaccine storage in health facilities. Refer to Chapter 4 on primary health care ehealth programmes for a detailed description of the SVS.
While the interventions appear to have significantly impacted the technology landscape, critical issues remain and addressing these can ensure success and consolidate the gains made. The prohibitive costs of maintaining internet connectivity, and in some cases the cost of internet-enabled devices, unequal coverage, interoperability, poor network performance – limiting internet usage and access to data, especially in resource-constrained settings, low levels of education and digital literacy, lack of social support and awareness of the applications, language, and age are significant drawbacks to the extensive application of digital technology in South Africa (Matli & Ngoepe, 2020; Petersen et al., 2020; Phokeer et al., 2016).
We have shown throughout the chapter that there is extended existing support for the SDH approach to improving health outcomes. However, translating evidence into effective policy challenges intersectoral policies addressing the SDH Formal collaborations exist between government departments and agencies at the national, provincial and district levels, however, these collaborations were found to be more efficient at the national level. The NDoH should lead the formulation and implementation of intersectoral action with a high level of active and measurable engagement of all stakeholders.
Given that collaborations between provincial- and district-level departments are less efficient, the NDoH must develop guidelines for provinces and districts on creating consultative engagements for sub-national government stakeholders, drawing on structures and processes that were developed to deal with COVID-19 and documented best practices and innovations by the PDoHs before COVID-19 and in response to COVID-19.
To improve horizontal collaboration and partnership between departments in practice, we recommend that PDoHs be the champions of consultative engagements at provincial and local levels, given that policy implementation occurs at the provincial and local levels. Ideally, consultative arrangements should help clarify roles and responsibilities and support the implementation of the SDH approach to improving health outcomes. The flow of information across the different spheres with timely and established interdepartmental lines should ensure relevant and timely information to key players.
In addressing the social determinants of health, there is a need to engage multiple stakeholders – the public sector (government), private sector and civil society, which represent the three critical stakeholders – at all stages. The interactions among the stakeholders should go beyond information sharing to cooperation, coordination or integration, which are likely to strengthen policy implementation. There is limited evidence on:
1. What the costs are (financial and human) of ensuring health in all policies;
2. How to measure and document the impact of collaborative efforts of departments to achieve social determinants of health; and
3. How policy trade-offs and goals are negotiated, and the outcomes of those negotiations communicated.
Alexander P. Rebellion of the poor: South Africa’s service delivery protests – a preliminary analysis. Review of African Political Economy. 2010;37(123): 25–40. https://doi.org/10.1080/03056241003637870
Ataguba JE-O, Day C, McIntyre D. Explaining the role of the social determinants of health on health inequality in South Africa. Global Health Action. 2016;8(1). https://doi.org/10.3402/gha.v8.28865
Barron P, Peter J, LeFevre AE, Sebidi J, Bekker M, Allen R, Parsons AN, Benjamin P, Pillay Y. Mobile health messaging service and helpdesk for South African mothers (MomConnect): History, successes and challenges. BMJ Global Health. 2018;3(Suppl 2): e000559. https://doi.org/10.1136/ bmjgh-2017-000559
Baum F, Delany-Crowe T, MacDougall C, Lawless A, van Eyk H, Williams C. Ideas, actors and institutions: Lessons from South Australian Health in All Policies on what encourages other sectors’ involvement. BMC Public Health. 2017;17(1): 811. https://doi.org/10.1186/s12889-017-4821-7
Bradshaw D. Determinants of health and their trends: Primary Health Care: In context. South African Health Review. 2008;(1): 51–69. https://doi. org/10.10520/EJC35512
Brey Z, Mash R, Goliath C, Roman D. Home delivery of medication during Coronavirus disease 2019, Cape Town, South Africa. African Journal of Primary Health Care and Family Medicine. 2020;12(1): 1–4. https://doi. org/10.4102/phcfm.v12i1.2449
Burger R, Christian C. Access to health care in post-apartheid South Africa: Availability, affordability, acceptability. Health Economics, Policy and Law. 2020;15(1): 43–55. https://doi.org/10.1017/S1744133118000300
Burger R, Maughan-Brown B, Köhler T, English R, Tameris M. A shot in the arm for South Africa—Increased openness to accepting a COVID-1789 vaccine: Evidence from NIDS- CRAM Waves 4 and 5. National Income Dynamics Study – Coronavirus Rapid Mobile Survey. 2021;31.
Christie P. The Pandemic as a Portal for Change: Pushing against the Limits of ‘Normal Schooling’ in South Africa. Education as Change. 2021;25(1): 1–21. https://doi.org/10.25159/1947-9417/8718
Claasen N, Pointer R, van der Hoeven M, Covic N. Food environments, health and nutrition in South Africa: Mapping the research and policy terrain. 2016. https://media.africaportal.org/documents/WP34_Claasen_etal_final_0.pdf Commission on Social Determinants of Health. Achieving health equity: From root causes to fair outcomes. (Commission on Social Determinants of Health). World Health Organization. 2007.
Crichton J. Changing fortunes: Analysis of fluctuating policy space for family planning in Kenya. Health Policy and Planning. 2008;23(5): 339–350. https://doi.org/10.1093/heapol/czn020
Dahlgren G, Whitehead M. Policies and strategies to promote social equity in health. Institute for Future Studies. 1991.
de Leeuw E. Engagement of Sectors Other than Health in Integrated Health Governance, Policy, and Action. Annual Review of Public Health. 2017;38(1): 329–349. https://doi.org/10.1146/annurev-publhealth-031816-044309
Dorrington R. et al. Rapid Mortality Surveillance Report 2017. Cape Town, South Africa: South African Medical Research Council. 2019. Available at: https:// www.samrc.ac.za/sites/default/files/files/2019-02-06/RapidMortality SurveillanceReport2017.pdf.
Exworthy M. Policy to tackle the social determinants of health: Using conceptual models to understand the policy process. Health Policy and Planning 2008;23(5): 318–327.
Gass JD, Stein DJ, Williams DR, Seedat S. Intimate partner violence, health behaviours, and chronic physical illness among South African women. South African Medical Journal. 2010;100(9): 582–585.
Gateway South Africa. Mapping poverty in South Africa. South Africa Gateway. (2021, June 11). https://southafrica-info.com/people/mapping-povertyin-south-africa/
Goga AE et al. Neonatal, infant and child health in South Africa: reflecting on the past towards a better future. 2019. doi:10.7196/SAMJ.2019.v109i11b.14301.
Hargreaves J, Hatcher A, Busza J, Strange V, Phetla G, Kim J, Watts C, Morison L, Porter J, Pronyk P. What happens after a trial? Replicating a cross-sectoral intervention addressing the social determinants of health: the case of the Intervention with Microfinance for AIDS and Gender Equity (IMAGE) in South Africa. Social Determinants Approaches to Public Health: From Concept to Practice. 2011;147–159.
Hickel J. The Problem with Saving the World. 2015, August 8.
Kark SL, Cassel J. The Pholela Health Centre: A Progress Report. American Journal of Public Health. 2002;92(11): 1743–1747.
Krieger N. Proximal, distal, and the politics of causation: What’s level got to do with it? American Journal of Public Health. 2008;98(2): 221–230. PubMed. https://doi.org/10.2105/AJPH.2007.111278
Lamb G. Social cohesion and violence in South Africa: Constructing a puzzle with missing pieces. Crime, Law and Social Change. 2019;72(4): 365–385. https://doi.org/10.1007/s10611-019-09828-7
Lartey A, Hemrich G, Amoroso L, Remans R, Grace D, Albert JL, Fischer CG, Garnett T. Influencing food environments for healthy diets (p. 154). Food and Agriculture Organization of the United Nations. 2016. https://cgspace.cgiar.org/bitstream/handle/10568/80578/InfluencingFood EnvironmentsForHealthyDiets.pdf?sequence=2
Lippman SA, Leslie HH, Neilands TB, Twine R, Grignon JS, MacPhail C, Morris J, Rebombo D, Sesane M, El Ayadi AM, Pettifor A, Kahn K. Context matters: Community social cohesion and health behaviors in two South African areas. Health & Place. 2018;50: 98–104. https://doi.org/10.1016/j. healthplace.2017.12.009
Litman T. Evaluating transportation equity. World Transport Policy and Practice. 2002;8(2): 50–65.
Lucas K, Jones P. Social impacts and equity issues in transport. Social Impacts and Equity Issues in Transport. 2012;21: 4–112.
Maharaj B. South African Urban Planning in the Twentieth and Twenty-First Centuries—Continuities between the Apartheid and Democratic eras? In R. R. Thakur, A. K. Dutt, S. K. Thakur, & G. M. Pomeroy (Eds.), Urban and Regional Planning and Development: 20th Century Forms and 21st Century Transformations (pp. 101–112). Springer International Publishing. 2020. https://doi.org/10.1007/978-3-030-31776-8_6
Mahlangu P, Vearey J, Goudge J. Multisectoral (in) action: Towards effective mainstreaming of HIV in public sector departments in South Africa. African Journal of AIDS Research. 2018;17(4): 301–312.
Mamokhere J. An exploration of reasons behind service delivery protests in South Africa: A case of Bolobedu South at the Greater Tzaneen Municipality. 2019. http://ulspace.ul.ac.za/handle/10386/2669
Martens K, Golub A, Robinson G. A justice-theoretic approach to the distribution of transportation benefits: Implications for transportation planning practice in the United States. Transportation Research Part A: Policy and Practice. 2012;46(4): 684–695. https://doi.org/10.1016/j.tra.2012.01.004
Matli W, Ngoepe M. Capitalizing on digital literacy skills for capacity development of people who are not in education, employment or training in South Africa. African Journal of Science, Technology, Innovation and Development. 2020;12(2): 129–139.
Matzopoulos RG, Truen S, Bowman B, Corrigall J. The cost of harmful alcohol use in South Africa. South African Medical Journal. 2014;104(2): 127–132.
Miller HN, Thornton CP, Rodney T, Thorpe RJ, Allen J. Social Cohesion in Health: A Concept Analysis. Advances in Nursing Science. 2020;43(4): 375–390. https://doi.org/10.1097/ANS.0000000000000327
Morudu HD. Service delivery protests in South African municipalities: An exploration using principal component regression and 2013 data. Cogent Social Sciences. 2017;3(1): 1329106. https://doi.org/10.1080/23311886 .2017.1329106
Moultrie TA, Dorrington RE, Laubscher R, Groenewald P, Parry CDH, Matzopoulos R, Bradshaw D. Unnatural deaths, alcohol bans and curfews: Evidence from a quasi-natural experiment during COVID-19. South African Medical Journal. 2021;111(9): 834–837. https://doi.org/10.7196/ SAMJ.2021.v111i9.15813
National Department of Health. Stock Visibility System Covid-19 Vaccine Instance Information Pack. 2021a.
https://www.google.com/search?q=National+Department+of+Health+Stock+V isibility+System+2021&rlz=1C1GCEB_enZA949ZA953&oq=National+De partment+of+Health+Stock+Visibility+System+2021&aqs=chrome..69i57.1 496j0j9&sourceid=chrome&ie=UTF-8
National Department of Health. Latest Vaccine Statistics—South Africa Corona Virus Online Portal. South Africa Corona Virus Online Portal. 2021b, December 2. https://sacoronavirus.co.za/latest-vaccine-statistics/ National Department of Health, Statistics South Africa (Stats SA), South African Medical Research, South African Medical ResearchCouncil, & ICF. 2019. South Africa Demographic and Health Survey 2016. https://dhsprogram. com/pubs/pdf/FR337/FR337.pdf
National Planning Commission. (2011). National Development Plan: Vision for 2030. Government of South Africa.
National Treasury. Estimates of National Expenditure (2019-2021) (Budget Information). 2021. http://www.treasury.gov.za/documents/national%20 budget/default.aspx
Nkonki L, Fonn S. Decisive and strong leadership and intersectoral action from South Africa in response to the COVID-19 virus. South African Medical Journal. 2020;110(5). http://www.samj.org.za/index.php/samj/ article/view/12879/9153
Nkosi V, Haman T, Naicker N, Mathee A. Overcrowding and health in two impoverished suburbs of Johannesburg, South Africa. BMC Public Health. 2019;19(1): 1358. https://doi.org/10.1186/s12889-019-7665-5
Okeyo I, Lehmann U, Schneider H. The impact of differing frames on early stages of intersectoral collaboration: The case of the First 1000 Days Initiative in the Western Cape Province. Health Research Policy and Systems. 2020;18(1): 1–14.
Okeyo I, Lehmann U, Schneider H. Policy adoption and the implementation woes of the intersectoral First 1000 Days of childhood initiative, in the Western Cape province of South Africa. International Journal of Health Policy and Management. 2021;10(7): 364–375.
Olamijuwon EO, Odimegwu CO, De Wet N. Social cohesion and self-rated health among adults in South Africa: The moderating role of race. Health & Place. 2018;51: 89–96. https://doi.org/10.1016/j. healthplace.2018.02.010
Omotoso KO, Koch SF. Assessing changes in social determinants of health inequalities in South Africa: A decomposition analysis. International Journal for Equity in Health. 2018;17(181): 13. https://doi.org/10.1186/s12939018-0885-y
Oosthuizen M. South Africa: Social Assistance Programs and Systems Review (English) (No. 164802). World Bank. 2021.
https://documents1.worldbank.org/curated/en/238611633430611402/pdf/ South-Africa-Social-Assistance-Programs-and-Systems-Review.pdf Parliamentary Monitoring Group. Schooling during COVID-19 Lockdown: Update with Deputy Minister. 2020. https://pmg.org.za/committee-meeting/30116/
Percept Actuaries and Consultants. The nurse can see you now: Reflections from the South African telemedicine market in light of Covid-19. 2020. https:// percept. co.za/wp-content/uploads/2021/02/Percept-TelehealthReport-Revisions.pdf
Percept Actuaries and Consultants. Case Notes from the Frontier: Five case studies of South African telemedicine providers. 2021. https://percept.co.za/wpcontent/uploads/2021/03/Telemedicine-Providers-Case-Study-Report.pdf
Petersen F, Brown A, Pather S, Tucker WD. Challenges for the adoption of ICT for diabetes self-management in South Africa. The Electronic Journal of Information Systems in Developing Countries. 2020;86(5): e12113. https:// doi.org/10.1002/isd2.12113
Phillips C, Fisher M, Baum F, MacDougall C, Newman L, McDermott D. To what extent do Australian child and youth health policies address the social determinants of health and health equity? A document analysis study. BMC Public Health. 2016;16(1): 512. https://doi.org/10.1186/s12889-0163187-6
Phokeer A, Densmore M, Johnson D, Feamster N. A First Look at Mobile Internet Use in Township Communities in South Africa. Proceedings of the 7th Annual Symposium on Computing for Development, 1–10. 2016. https://doi.org/10.1145/3001913.3001926
Pinter-Wollman N, Jelic A, Wells NM. The impact of the built environment on health behaviours and disease transmission in social systems. Philosophical Transactions of the Royal Society B: Biological Sciences.
2018;373(1753): 20170245. https://doi.org/10.1098/rstb.2017.0245
Pirie GH. Virtuous mobility: Moralizing vs measuring geographical mobility in Africa. Afrika Focus. 2008;22(1): 21–35. https:// doi.org/10.1163/2031356X-02201004
Sanni S, Hongoro C, Ndinda C, Wisdom JP. Assessment of the multisectoral approach to tobacco control in South Africa and Togo. 2018.
Scott V, Schaay N, Schneider H, Sanders D. Addressing social determinants of health in South Africa: The journey continues. South African Health Review. 2017;2017(1): 77–87. https://doi.org/10.10520/EJC-c80ea0402
Seedat M, Van Niekerk A, Jewkes R, Suffla S, Ratele K. Violence and injuries in South Africa: Prioritizing an agenda for prevention. The Lancet. 2009;374(9694): 1011–1022. https://doi.org/10.1016/S01406736(09)60948-X
Shannon MM, Clougherty JE, McCarthy C, Elovitz MA, Nguemeni Tiako MJ, Melly SJ, Burris HH. Neighborhood Violent Crime and Perceived Stress in Pregnancy. International Journal of Environmental Research and Public Health. 2020;17(15): 5585. https://doi.org/10.3390/ijerph17155585
Sieck CJ, Sheon A, Ancker JS, Castek J, Callahan B, Siefer A. Digital inclusion as a social determinant of health. Npj Digital Medicine. 2021;4(1): 52. https:// doi.org/10.1038/s41746-021-00413-8
Skeen S, Kleintjes S, Lund C, Petersen I, Bhana A, Flisher AJ, Health TM, Consortium, PRP. ‘Mental health is everybody’s business’: Roles for an inter sectoral approach in South Africa. International Review of Psychiatry. 2010;22(6): 611–623.
South African Human Rights Commission. Report on water and sanitation in schools. 2021. https://www.sahrc.org.za/home/21/files/Water%20 And%20Sanitation%20Report%20-%2028%20SeptemberPM.pdf
Stacey N, Edoka I, Hofman K, Swart EC, Popkin B, Ng SW. Changes in beverage purchases following the announcement and implementation of South Africa’s Health Promotion Levy: An observational study. The Lancet Planetary Health. 2021;5(4): e200–e208. https://doi.org/10.1016/ S2542-5196(20)30304-1
Stacey N, Mudara C, Ng SW, van Walbeek C, Hofman K, Edoka I. Sugar-based beverage taxes and beverage prices: Evidence from South Africa’s Health Promotion Levy. Social Science & Medicine. 2019;238: 112465.
Statistics South Africa. Quarterly Labour Force Survey—Quarter 1 (No. P0211). 2015. https://www.statssa.gov.za/publications/P0211/P02111st Quarter2015.pdf
Statistics South Africa. General Household Survey 2018. 2018a. https://www. statssa.gov.za/publications/P0318/P03182018.pdf
Statistics South Africa. Men, Women and Children: Findings of the Living Conditions Survey 2014/15 (No. 03-10-02 (2014/15); p. 65). 2018b. http://www.statssa.gov.za/publications/Report-03-10-02%20/ Report-03-10-02%202015.pdf
Statistics South Africa. Inequality Trends in South Africa: A multidimensional diagnostic of inequality (No. 03-10–19; p. 232). 2019a. https:// www.statssa.gov.za/publications/Report-03-10-19/ Report-03-10-192017.pdf
Statistics South Africa. Towards measuring the extent of food security in South Africa: An examination of hunger and food inadequacy (No. 03-00–14). 2019b. http://www.statssa.gov.za/publications/03-00-14/ 03-00-142017.pdf
Statistics South Africa. General Household Survey 2019 (No. P0318). 2020. https://www.statssa.gov.za/publications/P0318/P03182019.pdf
Statistics South Africa. Quarterly Labour Force Survey—Quarter 4 (No. P0211). 2021. http://www.statssa.gov.za/publications/P0211/P02114th Quarter2020.pdf
Turok I, Scheba A. ‘Right to the city’ and the New Urban Agenda: Learning from the right to housing. Territory, Politics, Governance. 2019;7(4): 494–510. https://doi.org/10.1080/21622671.2018.1499549
United Nations Children’s Fund. Health Budget Brief South Africa—2020. United Nations. 2020. https://www.unicef.org/southafrica/media/4616/ file/ZAF-health-budget-brief-2020.pdf
United Nations Development Programme. The next frontier: Human development and the anthropocene. Briefing note for countries on the 2020 Human Development Report—South Africa (p. 7). 2020. https://hdr.undp. org/sites/default/files/Country-Profiles/ZAF.pdf
Van der Berg S, Gustafsson M, Malindi K. Education and skills for the economy and links to labour markets in South Africa. National Planning Commission. 2020. https://www.nationalplanningcommission.org.za/assets/ Documents/Education%20and%20skills%20for%20the%20economy%20 and%20links%20to%20labour%20markets%20in%20South%20Africa.pdf
Vasconcellos EA. Equity evaluation of urban transport. Urban Transport in the Developing World. 2011. https://www.elgaronline.com/view/ed coll/9781847202055/9781847202055.00022.xml
Wasserman H, Chuma W, Bosch T. Print media coverage of service delivery protests in South Africa: A content analysis. African Studies. 2018;77(1): 145–156. https://doi.org/10.1080/00020184.2018.1426312
World Bank. World Development Indicators. 2020. https://databank.worldbank. org/source/world-development-indicators/Type/TABLE/preview/on World Health Organization. United Nations Children’s Fund. Declaration of Alma-Ata. International Conference on Primary Health Care: Alma-Ata, USSR. 1978, September 6.
Zembe-Mkabile W, Ramokolo V, Sanders D, Jackson D, Doherty T. The dynamic relationship between cash transfers and child health: Can the child support grant in South Africa make a difference to child nutrition? Public Health Nutrition. 2016;19(2): 356–362. https://doi.org/10.1017/ S1368980015001147 Social,